User login
First-in-kind study parsed risks of central lines in children
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.

Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.
Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.
Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
AT ASH 2016
Key clinical point: Children who received peripherally inserted central catheters were at greatest risk of venous thromboembolism, while those who received tunneled lines were more likely to develop bloodstream infections.
Major finding: Venous thromboembolism occurred in 7.5% of PICC recipients and 2% of tunneled line recipients (P = .004) within 6 months after placement. CLABSI occurred in 16% of tunneled line recipients and 9% of PICC recipients (P = .005).
Data source: An observational study of 1,096 children and adolescents who received central venous catheters at three nationally recognized pediatric hospitals.
Disclosures: Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
VIDEO: SPIN tests hydroxyurea to prevent pediatric stroke in sickle cell disease
SAN DIEGO – Whether hydroxyurea can avert a first stroke in children with sickle cell disease is a question that may be answered by a soon-to-be-started trial in Nigeria.
An estimated 15,000 children with sickle cell anemia have strokes each year in Nigeria, which is considered to have the largest burden of sickle cell disease in the world. Without treatment, about half of those children will have a second stroke within 2 years.
With completion of its feasibility trial results, SPIN (Primary Stroke Prevention in Children With Sickle Cell Anemia in Nigeria) will begin to examine two doses of hydroxyurea therapy, 20 mg/kg per day and 10 mg/kg per day, to determine whether the drug can prevent a first stroke in high-risk children.
In a video interview, Najibah A. Galadanci, MBBS, MPH, of Aminu Kano (Nigeria) Teaching Hospital, discusses how SPIN is addressing the unresolved clinical issue of hydroxyurea’s risks and benefits in children, and how research in Nigeria may provide adequate patient numbers to address a wide range of clinical questions about sickle cell disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
SAN DIEGO – Whether hydroxyurea can avert a first stroke in children with sickle cell disease is a question that may be answered by a soon-to-be-started trial in Nigeria.
An estimated 15,000 children with sickle cell anemia have strokes each year in Nigeria, which is considered to have the largest burden of sickle cell disease in the world. Without treatment, about half of those children will have a second stroke within 2 years.
With completion of its feasibility trial results, SPIN (Primary Stroke Prevention in Children With Sickle Cell Anemia in Nigeria) will begin to examine two doses of hydroxyurea therapy, 20 mg/kg per day and 10 mg/kg per day, to determine whether the drug can prevent a first stroke in high-risk children.
In a video interview, Najibah A. Galadanci, MBBS, MPH, of Aminu Kano (Nigeria) Teaching Hospital, discusses how SPIN is addressing the unresolved clinical issue of hydroxyurea’s risks and benefits in children, and how research in Nigeria may provide adequate patient numbers to address a wide range of clinical questions about sickle cell disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
SAN DIEGO – Whether hydroxyurea can avert a first stroke in children with sickle cell disease is a question that may be answered by a soon-to-be-started trial in Nigeria.
An estimated 15,000 children with sickle cell anemia have strokes each year in Nigeria, which is considered to have the largest burden of sickle cell disease in the world. Without treatment, about half of those children will have a second stroke within 2 years.
With completion of its feasibility trial results, SPIN (Primary Stroke Prevention in Children With Sickle Cell Anemia in Nigeria) will begin to examine two doses of hydroxyurea therapy, 20 mg/kg per day and 10 mg/kg per day, to determine whether the drug can prevent a first stroke in high-risk children.
In a video interview, Najibah A. Galadanci, MBBS, MPH, of Aminu Kano (Nigeria) Teaching Hospital, discusses how SPIN is addressing the unresolved clinical issue of hydroxyurea’s risks and benefits in children, and how research in Nigeria may provide adequate patient numbers to address a wide range of clinical questions about sickle cell disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
AT ASH 2016

Wide variation seen in treatment of infantile spasms
HOUSTON – The types of diagnostic tests ordered and medication used for treatment of infantile spasms vary considerably, a large study of children’s hospitals showed.
“Children with infantile spasms often require extensive diagnostic work-up to determine etiology, expensive medications for treatment, and hospitalization during the initiation of certain therapies,” researchers led by Sunita N. Misra, MD, PhD, wrote in an abstract presented at the annual meeting of the American Epilepsy Society. “The common diagnostic studies and therapies have evolved over the last several decades.”
The researchers collected patient demographics, hospital length of stay, hospital admission cost, use of various diagnostic studies (such as lumbar puncture, brain MRI, and EEG), and medications used for infantile spasms (including antiepileptic drugs, corticotropin, and steroids). Cost data, calculated as a ratio of cost to charges, were collected and adjusted to 2014 dollars.
A total of 6,183 patients were included in the analysis and their average age of infantile-spasm diagnosis was 9 months. The most common diagnostic test ordered was EEG (76%), followed by brain imaging (57%), organic acids (38%), and lumbar puncture (17%). Medications were started during inpatient hospitalization in two-thirds of patients, with 33% starting on corticotropin; 29% on topiramate; and fewer than 10% of patients on an oral or intravenous steroid, zonisamide, or vigabatrin (Sabril). Use of corticotropin decreased over time, while use of oral steroids trended upwards. “We were surprised that one-third of patients did not have a medication initiated as an inpatient, given the studies showing earlier use of effective therapy has better outcomes,” Dr. Misra said in an interview in advance of the meeting.
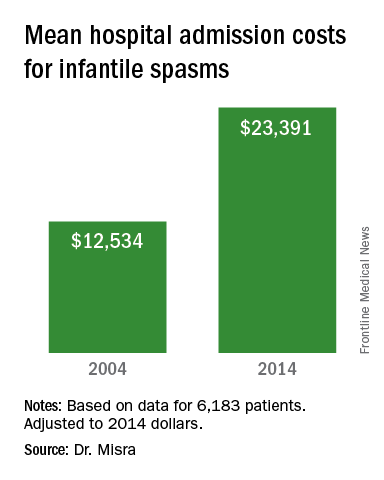
“The cost of taking care of children with infantile spasms has increased over the study period 2004-2014,” Dr. Misra said. “Although we identified a few contributors to rising cost, there are probably other factors that need to be considered in future studies.” She acknowledged certain limitations of the analysis, including its retrospective design and the fact that it only identified cost associated with the initial admission. “Several of the diagnostic studies and medications may be initiated as an outpatient, for which we do not have the data,” she said.
Dr. Misra reported having no financial disclosures.
HOUSTON – The types of diagnostic tests ordered and medication used for treatment of infantile spasms vary considerably, a large study of children’s hospitals showed.
“Children with infantile spasms often require extensive diagnostic work-up to determine etiology, expensive medications for treatment, and hospitalization during the initiation of certain therapies,” researchers led by Sunita N. Misra, MD, PhD, wrote in an abstract presented at the annual meeting of the American Epilepsy Society. “The common diagnostic studies and therapies have evolved over the last several decades.”
The researchers collected patient demographics, hospital length of stay, hospital admission cost, use of various diagnostic studies (such as lumbar puncture, brain MRI, and EEG), and medications used for infantile spasms (including antiepileptic drugs, corticotropin, and steroids). Cost data, calculated as a ratio of cost to charges, were collected and adjusted to 2014 dollars.
A total of 6,183 patients were included in the analysis and their average age of infantile-spasm diagnosis was 9 months. The most common diagnostic test ordered was EEG (76%), followed by brain imaging (57%), organic acids (38%), and lumbar puncture (17%). Medications were started during inpatient hospitalization in two-thirds of patients, with 33% starting on corticotropin; 29% on topiramate; and fewer than 10% of patients on an oral or intravenous steroid, zonisamide, or vigabatrin (Sabril). Use of corticotropin decreased over time, while use of oral steroids trended upwards. “We were surprised that one-third of patients did not have a medication initiated as an inpatient, given the studies showing earlier use of effective therapy has better outcomes,” Dr. Misra said in an interview in advance of the meeting.
“The cost of taking care of children with infantile spasms has increased over the study period 2004-2014,” Dr. Misra said. “Although we identified a few contributors to rising cost, there are probably other factors that need to be considered in future studies.” She acknowledged certain limitations of the analysis, including its retrospective design and the fact that it only identified cost associated with the initial admission. “Several of the diagnostic studies and medications may be initiated as an outpatient, for which we do not have the data,” she said.
Dr. Misra reported having no financial disclosures.
HOUSTON – The types of diagnostic tests ordered and medication used for treatment of infantile spasms vary considerably, a large study of children’s hospitals showed.
“Children with infantile spasms often require extensive diagnostic work-up to determine etiology, expensive medications for treatment, and hospitalization during the initiation of certain therapies,” researchers led by Sunita N. Misra, MD, PhD, wrote in an abstract presented at the annual meeting of the American Epilepsy Society. “The common diagnostic studies and therapies have evolved over the last several decades.”
The researchers collected patient demographics, hospital length of stay, hospital admission cost, use of various diagnostic studies (such as lumbar puncture, brain MRI, and EEG), and medications used for infantile spasms (including antiepileptic drugs, corticotropin, and steroids). Cost data, calculated as a ratio of cost to charges, were collected and adjusted to 2014 dollars.
A total of 6,183 patients were included in the analysis and their average age of infantile-spasm diagnosis was 9 months. The most common diagnostic test ordered was EEG (76%), followed by brain imaging (57%), organic acids (38%), and lumbar puncture (17%). Medications were started during inpatient hospitalization in two-thirds of patients, with 33% starting on corticotropin; 29% on topiramate; and fewer than 10% of patients on an oral or intravenous steroid, zonisamide, or vigabatrin (Sabril). Use of corticotropin decreased over time, while use of oral steroids trended upwards. “We were surprised that one-third of patients did not have a medication initiated as an inpatient, given the studies showing earlier use of effective therapy has better outcomes,” Dr. Misra said in an interview in advance of the meeting.
“The cost of taking care of children with infantile spasms has increased over the study period 2004-2014,” Dr. Misra said. “Although we identified a few contributors to rising cost, there are probably other factors that need to be considered in future studies.” She acknowledged certain limitations of the analysis, including its retrospective design and the fact that it only identified cost associated with the initial admission. “Several of the diagnostic studies and medications may be initiated as an outpatient, for which we do not have the data,” she said.
Dr. Misra reported having no financial disclosures.
AT AES 2016
Key clinical point:
Major finding: The most common diagnostic test ordered was EEG (76%), followed by brain imaging (57%), organic acids (38%), and lumbar puncture (17%).
Data source: Retrospective analysis of data on 6,183 patients with infantile spasms between 2004 and 2014.
Disclosures: Dr. Misra reported having no financial disclosures.
Wrist-worn system detected convulsive seizures in home setting
HOUSTON – A wrist-worn device and smartphone-based alert system worn by a patient outside of the epilepsy monitoring unit for 3 months effectively detected convulsive seizure events and minimized false alarms, results from a long-term study found.
The automated device, known as Embrace, relies on an accelerometer and electrodermal activity to detect convulsive seizures. It pairs a wrist-worn device with a smartphone-based application that provides an alert to designated caregivers when an unusual event is detected. Embrace, which is being developed by Empatica Inc., received clearance by the European Union as a medical device for convulsive seizure detection but is still under consideration by the Food and Drug Administration. Previous reports evaluating the automated detector used by Embrace have always relied on data from epilepsy monitoring units (EMUs), where it achieved sensitivity scores ranging from 92% to 100% and 0.15-2.02 false alarms per day in detecting convulsive seizures.

To find out, Dr. Picard, chief scientist at Empatica, and her associates conducted a case study of a 14-year-old patient with Dravet syndrome who was enrolled in a trial of Embrace in the outpatient setting. No data from this patient were used in training the system. The patient’s caregiver was asked to annotate the occurrence of each convulsive seizure and any activity that generated an alert. The number of false alerts was obtained by subtracting the number of correctly recognized convulsive seizures from the total alerts fired by the device. Sensitivity was the percentage of convulsive seizures that automatically triggered an alert.

“Embrace can work for patients outside the EMU, detecting events and issuing alerts through a paired smartphone to a designated caregiver. Also, for clinicians who understand machine learning, we should be clear that we used the strongest test possible: none of the patient’s data were used to train the algorithm that was used, nor was it tuned in any way special for this patient. Had we done so, the results could have possibly appeared even better. However, we chose to use this test of generalization to better get a sense of how it might work on new patients, whose data had never been seen before.”
Dr. Picard acknowledged certain limitations of the study, including the fact that it was a single case and that the patient had Dravet syndrome. She disclosed that she is a cofounder of Empatica and owns shares in the company.
HOUSTON – A wrist-worn device and smartphone-based alert system worn by a patient outside of the epilepsy monitoring unit for 3 months effectively detected convulsive seizure events and minimized false alarms, results from a long-term study found.
The automated device, known as Embrace, relies on an accelerometer and electrodermal activity to detect convulsive seizures. It pairs a wrist-worn device with a smartphone-based application that provides an alert to designated caregivers when an unusual event is detected. Embrace, which is being developed by Empatica Inc., received clearance by the European Union as a medical device for convulsive seizure detection but is still under consideration by the Food and Drug Administration. Previous reports evaluating the automated detector used by Embrace have always relied on data from epilepsy monitoring units (EMUs), where it achieved sensitivity scores ranging from 92% to 100% and 0.15-2.02 false alarms per day in detecting convulsive seizures.
To find out, Dr. Picard, chief scientist at Empatica, and her associates conducted a case study of a 14-year-old patient with Dravet syndrome who was enrolled in a trial of Embrace in the outpatient setting. No data from this patient were used in training the system. The patient’s caregiver was asked to annotate the occurrence of each convulsive seizure and any activity that generated an alert. The number of false alerts was obtained by subtracting the number of correctly recognized convulsive seizures from the total alerts fired by the device. Sensitivity was the percentage of convulsive seizures that automatically triggered an alert.
“Embrace can work for patients outside the EMU, detecting events and issuing alerts through a paired smartphone to a designated caregiver. Also, for clinicians who understand machine learning, we should be clear that we used the strongest test possible: none of the patient’s data were used to train the algorithm that was used, nor was it tuned in any way special for this patient. Had we done so, the results could have possibly appeared even better. However, we chose to use this test of generalization to better get a sense of how it might work on new patients, whose data had never been seen before.”
Dr. Picard acknowledged certain limitations of the study, including the fact that it was a single case and that the patient had Dravet syndrome. She disclosed that she is a cofounder of Empatica and owns shares in the company.
HOUSTON – A wrist-worn device and smartphone-based alert system worn by a patient outside of the epilepsy monitoring unit for 3 months effectively detected convulsive seizure events and minimized false alarms, results from a long-term study found.
The automated device, known as Embrace, relies on an accelerometer and electrodermal activity to detect convulsive seizures. It pairs a wrist-worn device with a smartphone-based application that provides an alert to designated caregivers when an unusual event is detected. Embrace, which is being developed by Empatica Inc., received clearance by the European Union as a medical device for convulsive seizure detection but is still under consideration by the Food and Drug Administration. Previous reports evaluating the automated detector used by Embrace have always relied on data from epilepsy monitoring units (EMUs), where it achieved sensitivity scores ranging from 92% to 100% and 0.15-2.02 false alarms per day in detecting convulsive seizures.
To find out, Dr. Picard, chief scientist at Empatica, and her associates conducted a case study of a 14-year-old patient with Dravet syndrome who was enrolled in a trial of Embrace in the outpatient setting. No data from this patient were used in training the system. The patient’s caregiver was asked to annotate the occurrence of each convulsive seizure and any activity that generated an alert. The number of false alerts was obtained by subtracting the number of correctly recognized convulsive seizures from the total alerts fired by the device. Sensitivity was the percentage of convulsive seizures that automatically triggered an alert.
“Embrace can work for patients outside the EMU, detecting events and issuing alerts through a paired smartphone to a designated caregiver. Also, for clinicians who understand machine learning, we should be clear that we used the strongest test possible: none of the patient’s data were used to train the algorithm that was used, nor was it tuned in any way special for this patient. Had we done so, the results could have possibly appeared even better. However, we chose to use this test of generalization to better get a sense of how it might work on new patients, whose data had never been seen before.”
Dr. Picard acknowledged certain limitations of the study, including the fact that it was a single case and that the patient had Dravet syndrome. She disclosed that she is a cofounder of Empatica and owns shares in the company.
AT AES 2016
Key clinical point:
Major finding: A device known as Embrace detected 22 of the patient’s 24 convulsive seizure events, for a sensitivity of 92% and a false-alarm rate of 0.35 false alarms per day worn.
Data source: Case study of a 14-year-old patient with Dravet syndrome who was enrolled in a trial of Embrace in the outpatient setting and used the device for 113 days.
Disclosures: Dr. Picard is a cofounder of Empatica. She also owns shares in the company.
Rate of mosaicism in parents of children with epileptic encephalopathy likely underestimated
HOUSTON – The rate of parental mosaicism in children with sporadic cases of epileptic encephalopathy and an apparent de novo mutation is believed to be at least 10%, which is much higher than previously thought.
The discovery, which was revealed with advanced genetic testing methods, underscores the need to rethink how parents of children with epileptic encephalopathy are counseled with regard to family planning, lead study author Candace T. Myers, PhD, said in an interview in advance of the annual meeting of the American Epilepsy Society. “Generally, families are counseled with a recurrence risk of 1%-3%, but we found that in 10% of our families their recurrence risk is much higher because we’re able to see the genetic mutation in either blood or saliva of an unaffected parent,” said Dr. Myers of the division of genetic medicine in the department of pediatrics at the University of Washington, Seattle. “If we’re able to detect it in either of those tissues that means that the level in their gametes is much higher than just a single cell or a handful of cells, which is usually how people think about de novo mutations. What we’re finding is that in 10% of cases these mutations happen during embryonic development of the parent.”

Dr. Myers reported that of the 109 families screened, 10 cases of low-level somatic mosaicism were identified: 6 in fathers and 4 in mothers. The fraction of mutant alleles identified ranged from 3%-25%, which are levels that would pass undetected by traditional Sanger sequencing methods. In three families where a mosaic parent was identified, there were multiple affected children. The finding “opens up more questions for families that are thinking about future pregnancies,” she said. “I think we should have more genetic counselors working with pediatric neurologists to facilitate those discussions.”
She acknowledged certain limitations of the study, including the fact that DNA samples were extracted only from blood and saliva. “If the mutation is not present or detected in those particular tissues, it is still possible for the parent to be a germline carrier,” Dr. Myers said. “The most relevant tissue type for us to be testing would be the sex cells. We’ll have to look for families to see if they’re willing to donate [those cells] for future studies.”
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Myers is supported by a postdoctoral fellowship provided by the Lennox-Gastaut Syndrome Foundation and by the American Epilepsy Society. She reported having no financial disclosures.
HOUSTON – The rate of parental mosaicism in children with sporadic cases of epileptic encephalopathy and an apparent de novo mutation is believed to be at least 10%, which is much higher than previously thought.
The discovery, which was revealed with advanced genetic testing methods, underscores the need to rethink how parents of children with epileptic encephalopathy are counseled with regard to family planning, lead study author Candace T. Myers, PhD, said in an interview in advance of the annual meeting of the American Epilepsy Society. “Generally, families are counseled with a recurrence risk of 1%-3%, but we found that in 10% of our families their recurrence risk is much higher because we’re able to see the genetic mutation in either blood or saliva of an unaffected parent,” said Dr. Myers of the division of genetic medicine in the department of pediatrics at the University of Washington, Seattle. “If we’re able to detect it in either of those tissues that means that the level in their gametes is much higher than just a single cell or a handful of cells, which is usually how people think about de novo mutations. What we’re finding is that in 10% of cases these mutations happen during embryonic development of the parent.”
Dr. Myers reported that of the 109 families screened, 10 cases of low-level somatic mosaicism were identified: 6 in fathers and 4 in mothers. The fraction of mutant alleles identified ranged from 3%-25%, which are levels that would pass undetected by traditional Sanger sequencing methods. In three families where a mosaic parent was identified, there were multiple affected children. The finding “opens up more questions for families that are thinking about future pregnancies,” she said. “I think we should have more genetic counselors working with pediatric neurologists to facilitate those discussions.”
She acknowledged certain limitations of the study, including the fact that DNA samples were extracted only from blood and saliva. “If the mutation is not present or detected in those particular tissues, it is still possible for the parent to be a germline carrier,” Dr. Myers said. “The most relevant tissue type for us to be testing would be the sex cells. We’ll have to look for families to see if they’re willing to donate [those cells] for future studies.”
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Myers is supported by a postdoctoral fellowship provided by the Lennox-Gastaut Syndrome Foundation and by the American Epilepsy Society. She reported having no financial disclosures.
HOUSTON – The rate of parental mosaicism in children with sporadic cases of epileptic encephalopathy and an apparent de novo mutation is believed to be at least 10%, which is much higher than previously thought.
The discovery, which was revealed with advanced genetic testing methods, underscores the need to rethink how parents of children with epileptic encephalopathy are counseled with regard to family planning, lead study author Candace T. Myers, PhD, said in an interview in advance of the annual meeting of the American Epilepsy Society. “Generally, families are counseled with a recurrence risk of 1%-3%, but we found that in 10% of our families their recurrence risk is much higher because we’re able to see the genetic mutation in either blood or saliva of an unaffected parent,” said Dr. Myers of the division of genetic medicine in the department of pediatrics at the University of Washington, Seattle. “If we’re able to detect it in either of those tissues that means that the level in their gametes is much higher than just a single cell or a handful of cells, which is usually how people think about de novo mutations. What we’re finding is that in 10% of cases these mutations happen during embryonic development of the parent.”
Dr. Myers reported that of the 109 families screened, 10 cases of low-level somatic mosaicism were identified: 6 in fathers and 4 in mothers. The fraction of mutant alleles identified ranged from 3%-25%, which are levels that would pass undetected by traditional Sanger sequencing methods. In three families where a mosaic parent was identified, there were multiple affected children. The finding “opens up more questions for families that are thinking about future pregnancies,” she said. “I think we should have more genetic counselors working with pediatric neurologists to facilitate those discussions.”
She acknowledged certain limitations of the study, including the fact that DNA samples were extracted only from blood and saliva. “If the mutation is not present or detected in those particular tissues, it is still possible for the parent to be a germline carrier,” Dr. Myers said. “The most relevant tissue type for us to be testing would be the sex cells. We’ll have to look for families to see if they’re willing to donate [those cells] for future studies.”
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Myers is supported by a postdoctoral fellowship provided by the Lennox-Gastaut Syndrome Foundation and by the American Epilepsy Society. She reported having no financial disclosures.
AT AES 2016
Key clinical point:
Major finding: Of 109 families screened, 10 cases of low-level somatic mosaicism were identified: 6 in fathers and 4 in mothers.
Data source: Screening of 109 families where the affected child’s epileptic encephalopathy was attributed to a substitution or small indel in 1 of 31 established epilepsy genes and reported as “de novo” by either clinical or research analysis of parental DNA.
Disclosures: The study was funded by National Institute of Neurological Disorders and Stroke. Dr. Myers is supported by a postdoctoral fellowship provided by the Lennox-Gastaut Syndrome Foundation and by the American Epilepsy Society. She reported having no financial disclosures.
Vitamin D supplementation recommended in all children, teens
SAN FRANCISCO – Vitamin D deficiency is common among children and adolescents, particularly those with chronic disease, Catherine Gordon, MD, said at the annual meeting of the American Academy of Pediatrics.
Yet the precise definition of vitamin D deficiency and the healthy threshold for vitamin D levels lack universally agreed-upon standards. Generally speaking, levels of at least 30 ng/mL (75 nmol/L) appear safe and reasonable for children with chronic disease, and additional research is confirming whether this range is appropriate for other pediatric groups as well. Although too much vitamin D can lead to hypercalcemia, vitamin D intoxication is very rare, said Dr. Gordon, director of the division of adolescents and transition medicine at the University of Cincinnati.
Severe vitamin D deficiency can lead to rickets, when bones have insufficient calcium and phosphorus levels, resulting in bone softening and weakening before growth plates close. If not treated with vitamin D and calcium supplementation, rickets becomes osteomalacia after the growth plates close.
Vitamin D deficiency rates vary by population
It’s difficult to pin down rates of vitamin D deficiency. One 2004 study of just over 300 children found nearly a quarter of them (24%) were deficient based on a threshold of levels below 15 ng/mL, and another 42% had insufficient levels, defined as 20 ng/mL or lower, but all were asymptomatic. Another 2008 study using different cut-offs found that 12% of healthy 8- to 24-month-olds were deficient, defined as levels below 20 ng/mL. Forty percent of the children had suboptimal levels below 30 ng/mL. Overall, a third of the children showed demineralization on their x-rays. While the season of the year and race/ethnicity did not emerge as predictors of vitamin D insufficiency, breastfeeding without supplementation and lack of milk consumption did.
Because the vitamin D content in human breast milk is low, breastfed infants typically develop low vitamin D levels unless they receive supplementation or plenty of exposure to sunlight. A maternal dose of 6,400 IU of vitamin D is needed for breastfed infants to reach normal vitamin D levels, Dr. Gordon said. Babies born to mothers with vitamin D deficiency have the highest risk of becoming deficient themselves, although formula-fed babies usually receive plenty through the vitamin D fortification in infant formula.
Among adolescents, obesity remains a common risk factor, and those with obesity require higher doses to correct deficiency or insufficiency. A study in the Journal of Pediatrics this year found that adult-sized teens need at least 5,000 IU of vitamin D3 a day for 8 weeks to correct deficiency. Similarly, a small 2012 study of 61 children and adolescents with inflammatory bowel disease found that supplementation of 2,000 IU of vitamin D3 daily or 50,000 IU of D2 weekly, for 6 weeks, more effectively corrected vitamin D deficiency than 2,000 IU daily of vitamin D2 without any changes to parathyroid hormone suppression.
How much to supplement
Much debate and uncertainty surround how much (if at all) healthy infants, children, and adolescents should be supplemented with vitamin D. The American Academy of Pediatrics recommends daily supplementation of 400 IU of vitamin D from birth through adolescence for all children and teens, although that’s far below the safe upper limit of vitamin D intake, Dr. Gordon said.
The health and sciences division (formerly the Institute of Medicine) of the National Academies of Sciences, Engineering, and Medicine, by contrast, recommends a daily intake of 400 IU of vitamin D for the first year of life and then 600 IU for age 1 through old age. The safe upper limits set by the health and sciences division include 1,000 IU for infants up to 6 months old, 1,500 IU for infants aged 6 months to 1 year, 2,500 IU for toddlers up to 3 years, 3,000 IU for children aged 4-8 years, and 4,000 IU for those 9 years and older.
Yet the Endocrine Society recommends a greater amount of supplementation for children at risk for vitamin D deficiency or low bone density mass: from 400 to 1,000 IU for children 1 year and younger, and 600-1,000 IU for all older children, adolescents, and adults. The Endocrine Society also cites a higher safe upper limit of 2,000 IU for infants up to 12 months and 4,000 IU for those aged 1 year and up.
Part of the discordance in these recommendations lies in what populations they are aimed at, Dr. Gordon explained. While the health and sciences division recommendations were written for healthy children and adolescents, the Endocrine Society is specifically addressing those in risk groups, such as transplant recipients, those with chronic conditions that can cause malabsorption, and those taking anticonvulsants or receiving other treatments that can threaten bone health. Among older children and adolescents, anorexia nervosa is also a risk factor for inadequate vitamin D levels.
Dr. Gordon recommended 600 IU of vitamin D daily for all healthy children and teens while noting that those in risk groups may require 1,000-2,000 IU to prevent vitamin D deficiency.
Additional concerns with inadequate vitamin D
Aside from bone mineral density and levels of 25(OH)D (25-hydroxy vitamin D) and parathyroid hormone, vitamin D insufficiency may be suspected based on several other biomarkers, including fractures or falls, intestinal calcium absorption, dental health, insulin sensitivity, beta-cell or immune functioning, respiratory disease such as wheezing or tuberculosis, and possibly hypertension.
Researchers have developed new interest in exploring whether factors during childhood and adolescence – critical years for bone acquisition – such as vitamin D levels might influence the risk for osteoporosis later in life, Dr. Gordon said.
Both males and females reach their peak bone mass and skeletal strength in their early to mid-20s and maintain these through about their mid-40s. While individuals have no control over intrinsic factors that help determine their bone mass, such as sex, family history, and ethnicity, other extrinsic factors are also bone mass determinants, including diet, body mass, a particular individual’s hormonal mix, illnesses and their treatments, physical activity level, and lifestyle choices.
Therefore, health providers should encourage patients to regularly exercise, maintain a healthy weight, eat healthfully, and take daily supplements, Dr. Gordon said. She only recommended testing 25(OH)D levels in those at risk for deficiency and/or low bone mass.
Dr. Gordon reported no relevant financial disclosures.
SAN FRANCISCO – Vitamin D deficiency is common among children and adolescents, particularly those with chronic disease, Catherine Gordon, MD, said at the annual meeting of the American Academy of Pediatrics.
Yet the precise definition of vitamin D deficiency and the healthy threshold for vitamin D levels lack universally agreed-upon standards. Generally speaking, levels of at least 30 ng/mL (75 nmol/L) appear safe and reasonable for children with chronic disease, and additional research is confirming whether this range is appropriate for other pediatric groups as well. Although too much vitamin D can lead to hypercalcemia, vitamin D intoxication is very rare, said Dr. Gordon, director of the division of adolescents and transition medicine at the University of Cincinnati.
Severe vitamin D deficiency can lead to rickets, when bones have insufficient calcium and phosphorus levels, resulting in bone softening and weakening before growth plates close. If not treated with vitamin D and calcium supplementation, rickets becomes osteomalacia after the growth plates close.
Vitamin D deficiency rates vary by population
It’s difficult to pin down rates of vitamin D deficiency. One 2004 study of just over 300 children found nearly a quarter of them (24%) were deficient based on a threshold of levels below 15 ng/mL, and another 42% had insufficient levels, defined as 20 ng/mL or lower, but all were asymptomatic. Another 2008 study using different cut-offs found that 12% of healthy 8- to 24-month-olds were deficient, defined as levels below 20 ng/mL. Forty percent of the children had suboptimal levels below 30 ng/mL. Overall, a third of the children showed demineralization on their x-rays. While the season of the year and race/ethnicity did not emerge as predictors of vitamin D insufficiency, breastfeeding without supplementation and lack of milk consumption did.
Because the vitamin D content in human breast milk is low, breastfed infants typically develop low vitamin D levels unless they receive supplementation or plenty of exposure to sunlight. A maternal dose of 6,400 IU of vitamin D is needed for breastfed infants to reach normal vitamin D levels, Dr. Gordon said. Babies born to mothers with vitamin D deficiency have the highest risk of becoming deficient themselves, although formula-fed babies usually receive plenty through the vitamin D fortification in infant formula.
Among adolescents, obesity remains a common risk factor, and those with obesity require higher doses to correct deficiency or insufficiency. A study in the Journal of Pediatrics this year found that adult-sized teens need at least 5,000 IU of vitamin D3 a day for 8 weeks to correct deficiency. Similarly, a small 2012 study of 61 children and adolescents with inflammatory bowel disease found that supplementation of 2,000 IU of vitamin D3 daily or 50,000 IU of D2 weekly, for 6 weeks, more effectively corrected vitamin D deficiency than 2,000 IU daily of vitamin D2 without any changes to parathyroid hormone suppression.
How much to supplement
Much debate and uncertainty surround how much (if at all) healthy infants, children, and adolescents should be supplemented with vitamin D. The American Academy of Pediatrics recommends daily supplementation of 400 IU of vitamin D from birth through adolescence for all children and teens, although that’s far below the safe upper limit of vitamin D intake, Dr. Gordon said.
The health and sciences division (formerly the Institute of Medicine) of the National Academies of Sciences, Engineering, and Medicine, by contrast, recommends a daily intake of 400 IU of vitamin D for the first year of life and then 600 IU for age 1 through old age. The safe upper limits set by the health and sciences division include 1,000 IU for infants up to 6 months old, 1,500 IU for infants aged 6 months to 1 year, 2,500 IU for toddlers up to 3 years, 3,000 IU for children aged 4-8 years, and 4,000 IU for those 9 years and older.
Yet the Endocrine Society recommends a greater amount of supplementation for children at risk for vitamin D deficiency or low bone density mass: from 400 to 1,000 IU for children 1 year and younger, and 600-1,000 IU for all older children, adolescents, and adults. The Endocrine Society also cites a higher safe upper limit of 2,000 IU for infants up to 12 months and 4,000 IU for those aged 1 year and up.
Part of the discordance in these recommendations lies in what populations they are aimed at, Dr. Gordon explained. While the health and sciences division recommendations were written for healthy children and adolescents, the Endocrine Society is specifically addressing those in risk groups, such as transplant recipients, those with chronic conditions that can cause malabsorption, and those taking anticonvulsants or receiving other treatments that can threaten bone health. Among older children and adolescents, anorexia nervosa is also a risk factor for inadequate vitamin D levels.
Dr. Gordon recommended 600 IU of vitamin D daily for all healthy children and teens while noting that those in risk groups may require 1,000-2,000 IU to prevent vitamin D deficiency.
Additional concerns with inadequate vitamin D
Aside from bone mineral density and levels of 25(OH)D (25-hydroxy vitamin D) and parathyroid hormone, vitamin D insufficiency may be suspected based on several other biomarkers, including fractures or falls, intestinal calcium absorption, dental health, insulin sensitivity, beta-cell or immune functioning, respiratory disease such as wheezing or tuberculosis, and possibly hypertension.
Researchers have developed new interest in exploring whether factors during childhood and adolescence – critical years for bone acquisition – such as vitamin D levels might influence the risk for osteoporosis later in life, Dr. Gordon said.
Both males and females reach their peak bone mass and skeletal strength in their early to mid-20s and maintain these through about their mid-40s. While individuals have no control over intrinsic factors that help determine their bone mass, such as sex, family history, and ethnicity, other extrinsic factors are also bone mass determinants, including diet, body mass, a particular individual’s hormonal mix, illnesses and their treatments, physical activity level, and lifestyle choices.
Therefore, health providers should encourage patients to regularly exercise, maintain a healthy weight, eat healthfully, and take daily supplements, Dr. Gordon said. She only recommended testing 25(OH)D levels in those at risk for deficiency and/or low bone mass.
Dr. Gordon reported no relevant financial disclosures.
SAN FRANCISCO – Vitamin D deficiency is common among children and adolescents, particularly those with chronic disease, Catherine Gordon, MD, said at the annual meeting of the American Academy of Pediatrics.
Yet the precise definition of vitamin D deficiency and the healthy threshold for vitamin D levels lack universally agreed-upon standards. Generally speaking, levels of at least 30 ng/mL (75 nmol/L) appear safe and reasonable for children with chronic disease, and additional research is confirming whether this range is appropriate for other pediatric groups as well. Although too much vitamin D can lead to hypercalcemia, vitamin D intoxication is very rare, said Dr. Gordon, director of the division of adolescents and transition medicine at the University of Cincinnati.
Severe vitamin D deficiency can lead to rickets, when bones have insufficient calcium and phosphorus levels, resulting in bone softening and weakening before growth plates close. If not treated with vitamin D and calcium supplementation, rickets becomes osteomalacia after the growth plates close.
Vitamin D deficiency rates vary by population
It’s difficult to pin down rates of vitamin D deficiency. One 2004 study of just over 300 children found nearly a quarter of them (24%) were deficient based on a threshold of levels below 15 ng/mL, and another 42% had insufficient levels, defined as 20 ng/mL or lower, but all were asymptomatic. Another 2008 study using different cut-offs found that 12% of healthy 8- to 24-month-olds were deficient, defined as levels below 20 ng/mL. Forty percent of the children had suboptimal levels below 30 ng/mL. Overall, a third of the children showed demineralization on their x-rays. While the season of the year and race/ethnicity did not emerge as predictors of vitamin D insufficiency, breastfeeding without supplementation and lack of milk consumption did.
Because the vitamin D content in human breast milk is low, breastfed infants typically develop low vitamin D levels unless they receive supplementation or plenty of exposure to sunlight. A maternal dose of 6,400 IU of vitamin D is needed for breastfed infants to reach normal vitamin D levels, Dr. Gordon said. Babies born to mothers with vitamin D deficiency have the highest risk of becoming deficient themselves, although formula-fed babies usually receive plenty through the vitamin D fortification in infant formula.
Among adolescents, obesity remains a common risk factor, and those with obesity require higher doses to correct deficiency or insufficiency. A study in the Journal of Pediatrics this year found that adult-sized teens need at least 5,000 IU of vitamin D3 a day for 8 weeks to correct deficiency. Similarly, a small 2012 study of 61 children and adolescents with inflammatory bowel disease found that supplementation of 2,000 IU of vitamin D3 daily or 50,000 IU of D2 weekly, for 6 weeks, more effectively corrected vitamin D deficiency than 2,000 IU daily of vitamin D2 without any changes to parathyroid hormone suppression.
How much to supplement
Much debate and uncertainty surround how much (if at all) healthy infants, children, and adolescents should be supplemented with vitamin D. The American Academy of Pediatrics recommends daily supplementation of 400 IU of vitamin D from birth through adolescence for all children and teens, although that’s far below the safe upper limit of vitamin D intake, Dr. Gordon said.
The health and sciences division (formerly the Institute of Medicine) of the National Academies of Sciences, Engineering, and Medicine, by contrast, recommends a daily intake of 400 IU of vitamin D for the first year of life and then 600 IU for age 1 through old age. The safe upper limits set by the health and sciences division include 1,000 IU for infants up to 6 months old, 1,500 IU for infants aged 6 months to 1 year, 2,500 IU for toddlers up to 3 years, 3,000 IU for children aged 4-8 years, and 4,000 IU for those 9 years and older.
Yet the Endocrine Society recommends a greater amount of supplementation for children at risk for vitamin D deficiency or low bone density mass: from 400 to 1,000 IU for children 1 year and younger, and 600-1,000 IU for all older children, adolescents, and adults. The Endocrine Society also cites a higher safe upper limit of 2,000 IU for infants up to 12 months and 4,000 IU for those aged 1 year and up.
Part of the discordance in these recommendations lies in what populations they are aimed at, Dr. Gordon explained. While the health and sciences division recommendations were written for healthy children and adolescents, the Endocrine Society is specifically addressing those in risk groups, such as transplant recipients, those with chronic conditions that can cause malabsorption, and those taking anticonvulsants or receiving other treatments that can threaten bone health. Among older children and adolescents, anorexia nervosa is also a risk factor for inadequate vitamin D levels.
Dr. Gordon recommended 600 IU of vitamin D daily for all healthy children and teens while noting that those in risk groups may require 1,000-2,000 IU to prevent vitamin D deficiency.
Additional concerns with inadequate vitamin D
Aside from bone mineral density and levels of 25(OH)D (25-hydroxy vitamin D) and parathyroid hormone, vitamin D insufficiency may be suspected based on several other biomarkers, including fractures or falls, intestinal calcium absorption, dental health, insulin sensitivity, beta-cell or immune functioning, respiratory disease such as wheezing or tuberculosis, and possibly hypertension.
Researchers have developed new interest in exploring whether factors during childhood and adolescence – critical years for bone acquisition – such as vitamin D levels might influence the risk for osteoporosis later in life, Dr. Gordon said.
Both males and females reach their peak bone mass and skeletal strength in their early to mid-20s and maintain these through about their mid-40s. While individuals have no control over intrinsic factors that help determine their bone mass, such as sex, family history, and ethnicity, other extrinsic factors are also bone mass determinants, including diet, body mass, a particular individual’s hormonal mix, illnesses and their treatments, physical activity level, and lifestyle choices.
Therefore, health providers should encourage patients to regularly exercise, maintain a healthy weight, eat healthfully, and take daily supplements, Dr. Gordon said. She only recommended testing 25(OH)D levels in those at risk for deficiency and/or low bone mass.
Dr. Gordon reported no relevant financial disclosures.
EXPERT ANALYSIS FROM AAP 16

RSV is top cause of severe respiratory disease in preterm infants
Respiratory syncytial virus is the number one virus causing severe lower respiratory disease in preterm infants, while those of younger age and those exposed to young children are at greatest risk, Eric A. F. Simões, MD, of the University of Colorado at Denver, Aurora, and his coauthors reported in the Nov. 29 edition of PLOS ONE.
“These data demonstrate that higher risk for 32 to 35 wGA [weeks gestational age] infants can be easily identified by age or birth month and significant exposure to other young children,” they wrote. “These infants would benefit from targeted efforts to prevent severe RSV disease.”

The overall rates of lower respiratory infections per 100 infant-seasons – a season being 5 months of observation from November 1 to March 31 in 2009-2010 or 2010-2011 – were 13.7 for respiratory syncytial virus (RSV), 2.9 for adenovirus, 1.7 for parainfluenza virus type 2, 1.3 for human metapneumovirus, and 0.3 for parainfluenza virus type 2 (PLoS One. 2016 Nov 29. doi: 10.1371/journal.pone.0166226).
Infants who had been exposed to young children, either through attending day care or living with non–multiple birth preschool-age siblings, had a twofold higher risk of RSV and human metapneumovirus, and a 3.3-fold greater risk of adenovirus.
The youngest infants showed the highest rate of hospitalizations with RSV: the incidence ranged from 8.2 per 100 infant season in those aged less than 1 month to 2.3 per 100 infant seasons in those aged 10 months of age. Similarly, the incidence of admission to ICU was significantly higher among younger infants.
Infants born in May, before the RSV season, had a much lower incidence of hospitalization, compared with those born in the height of RSV season in February. ICU admission rates also were higher among those born in February, compared with those born in May.
The highest overall rates of hospitalization with RSV – 19 per 100 infant-seasons – were among those born in February, and also those who were exposed to other young children.
“The current results are unique in that they provide continuous age-based risk models for outpatient and inpatient disease for infants with and without young child exposure,” wrote Dr. Simões and his coauthors.
They argued that their findings refute earlier suggestions that the rate of RSV infection in preterm infants is similar to the rate in term infants, and suggested that the limitations of their study may have even underestimated the incidence in preterm babies.
The study was supported by AstraZeneca, parent company of MedImmune. Two authors declared grant support and research funding from AstraZeneca, one author was a former employee of AstraZeneca, one author was a former employee of MedImmune and now contractor to AstraZeneca. One author was a current employee of AstraZeneca and holds stock options. Two authors also declared funding and consultancies with AbbVie.

Respiratory syncytial virus is the number one virus causing severe lower respiratory disease in preterm infants, while those of younger age and those exposed to young children are at greatest risk, Eric A. F. Simões, MD, of the University of Colorado at Denver, Aurora, and his coauthors reported in the Nov. 29 edition of PLOS ONE.
“These data demonstrate that higher risk for 32 to 35 wGA [weeks gestational age] infants can be easily identified by age or birth month and significant exposure to other young children,” they wrote. “These infants would benefit from targeted efforts to prevent severe RSV disease.”
The overall rates of lower respiratory infections per 100 infant-seasons – a season being 5 months of observation from November 1 to March 31 in 2009-2010 or 2010-2011 – were 13.7 for respiratory syncytial virus (RSV), 2.9 for adenovirus, 1.7 for parainfluenza virus type 2, 1.3 for human metapneumovirus, and 0.3 for parainfluenza virus type 2 (PLoS One. 2016 Nov 29. doi: 10.1371/journal.pone.0166226).
Infants who had been exposed to young children, either through attending day care or living with non–multiple birth preschool-age siblings, had a twofold higher risk of RSV and human metapneumovirus, and a 3.3-fold greater risk of adenovirus.
The youngest infants showed the highest rate of hospitalizations with RSV: the incidence ranged from 8.2 per 100 infant season in those aged less than 1 month to 2.3 per 100 infant seasons in those aged 10 months of age. Similarly, the incidence of admission to ICU was significantly higher among younger infants.
Infants born in May, before the RSV season, had a much lower incidence of hospitalization, compared with those born in the height of RSV season in February. ICU admission rates also were higher among those born in February, compared with those born in May.
The highest overall rates of hospitalization with RSV – 19 per 100 infant-seasons – were among those born in February, and also those who were exposed to other young children.
“The current results are unique in that they provide continuous age-based risk models for outpatient and inpatient disease for infants with and without young child exposure,” wrote Dr. Simões and his coauthors.
They argued that their findings refute earlier suggestions that the rate of RSV infection in preterm infants is similar to the rate in term infants, and suggested that the limitations of their study may have even underestimated the incidence in preterm babies.
The study was supported by AstraZeneca, parent company of MedImmune. Two authors declared grant support and research funding from AstraZeneca, one author was a former employee of AstraZeneca, one author was a former employee of MedImmune and now contractor to AstraZeneca. One author was a current employee of AstraZeneca and holds stock options. Two authors also declared funding and consultancies with AbbVie.
Respiratory syncytial virus is the number one virus causing severe lower respiratory disease in preterm infants, while those of younger age and those exposed to young children are at greatest risk, Eric A. F. Simões, MD, of the University of Colorado at Denver, Aurora, and his coauthors reported in the Nov. 29 edition of PLOS ONE.
“These data demonstrate that higher risk for 32 to 35 wGA [weeks gestational age] infants can be easily identified by age or birth month and significant exposure to other young children,” they wrote. “These infants would benefit from targeted efforts to prevent severe RSV disease.”
The overall rates of lower respiratory infections per 100 infant-seasons – a season being 5 months of observation from November 1 to March 31 in 2009-2010 or 2010-2011 – were 13.7 for respiratory syncytial virus (RSV), 2.9 for adenovirus, 1.7 for parainfluenza virus type 2, 1.3 for human metapneumovirus, and 0.3 for parainfluenza virus type 2 (PLoS One. 2016 Nov 29. doi: 10.1371/journal.pone.0166226).
Infants who had been exposed to young children, either through attending day care or living with non–multiple birth preschool-age siblings, had a twofold higher risk of RSV and human metapneumovirus, and a 3.3-fold greater risk of adenovirus.
The youngest infants showed the highest rate of hospitalizations with RSV: the incidence ranged from 8.2 per 100 infant season in those aged less than 1 month to 2.3 per 100 infant seasons in those aged 10 months of age. Similarly, the incidence of admission to ICU was significantly higher among younger infants.
Infants born in May, before the RSV season, had a much lower incidence of hospitalization, compared with those born in the height of RSV season in February. ICU admission rates also were higher among those born in February, compared with those born in May.
The highest overall rates of hospitalization with RSV – 19 per 100 infant-seasons – were among those born in February, and also those who were exposed to other young children.
“The current results are unique in that they provide continuous age-based risk models for outpatient and inpatient disease for infants with and without young child exposure,” wrote Dr. Simões and his coauthors.
They argued that their findings refute earlier suggestions that the rate of RSV infection in preterm infants is similar to the rate in term infants, and suggested that the limitations of their study may have even underestimated the incidence in preterm babies.
The study was supported by AstraZeneca, parent company of MedImmune. Two authors declared grant support and research funding from AstraZeneca, one author was a former employee of AstraZeneca, one author was a former employee of MedImmune and now contractor to AstraZeneca. One author was a current employee of AstraZeneca and holds stock options. Two authors also declared funding and consultancies with AbbVie.
FROM PLOS ONE
Key clinical point: Respiratory syncytial virus is the leading viral cause of severe lower respiratory disease in preterm infants, with those of younger age and those exposed to young children at greatest risk.
Major finding: The rates of lower respiratory infections per 100 infant-seasons were 13.7 for RSV, 2.9 for adenovirus, 1.7 for parainfluenza virus type 2, and 1.3 for human metapneumovirus.
Data source: The prospective RSV Respiratory Events Among Preterm Infants Outcomes and Risk Tracking (REPORT) study, in 1,642 preterm infants with medically attended acute respiratory illness.
Disclosures: The study was supported by AstraZeneca, parent company of MedImmune. Two authors declared grant support and research funding from AstraZeneca, one author was a former employee of AstraZeneca, and one author was a former employee of MedImmune and now contractor to AstraZeneca. One author was a current employee of AstraZeneca and holds stock options. Two authors also declared funding and consultancies with AbbVie.
Presume parents want HPV vaccines for tweens
Clinics in which providers presented human papillomavirus (HPV) vaccination as an assumed part of tween health care had a 5% increase in HPV vaccination coverage, compared with clinics that did not receive “announcement” training, based on data from a parallel-group, randomized trial of 30 pediatric and family medicine clinics in North Carolina.
Many providers hesitate to recommend HPV vaccination for 11- to 12-year-olds for a number of reasons, including lack of time and anticipation of a lengthy conversation about sex, wrote Noel T. Brewer, PhD, of the University of North Carolina, Chapel Hill, and his colleagues.
At 6 months after the training period, 17,173 children aged 11-12 years and 37,796 children aged 13-17 years were seen at the clinics. Overall, clinics that underwent announcement training increased HPV vaccine initiation for 11- and 12-year-olds by 5.4% over the control clinics. Clinics that received conversation training showed no significant increase in vaccine initiation, compared with controls. Intervention groups did not differ from the controls in terms of other ages (adolescents aged 13-17 years) or other immunization coverage, including HPV series completion, Tdap, and meningococcal vaccines.
The findings were limited by several factors, including the collection of data from a single Southeastern state that may not be generalizable to other areas, the researchers noted. The results, however, “support training providers to use announcements as an approach to address low HPV vaccination uptake in primary care clinics,” especially at the recommended ages for routine vaccination, Dr. Brewer and his associates said.
Read the full study here (Pediatrics 2016;139:e20161764. doi: 10.1542/peds.2016-1764).
Clinics in which providers presented human papillomavirus (HPV) vaccination as an assumed part of tween health care had a 5% increase in HPV vaccination coverage, compared with clinics that did not receive “announcement” training, based on data from a parallel-group, randomized trial of 30 pediatric and family medicine clinics in North Carolina.
Many providers hesitate to recommend HPV vaccination for 11- to 12-year-olds for a number of reasons, including lack of time and anticipation of a lengthy conversation about sex, wrote Noel T. Brewer, PhD, of the University of North Carolina, Chapel Hill, and his colleagues.
At 6 months after the training period, 17,173 children aged 11-12 years and 37,796 children aged 13-17 years were seen at the clinics. Overall, clinics that underwent announcement training increased HPV vaccine initiation for 11- and 12-year-olds by 5.4% over the control clinics. Clinics that received conversation training showed no significant increase in vaccine initiation, compared with controls. Intervention groups did not differ from the controls in terms of other ages (adolescents aged 13-17 years) or other immunization coverage, including HPV series completion, Tdap, and meningococcal vaccines.
The findings were limited by several factors, including the collection of data from a single Southeastern state that may not be generalizable to other areas, the researchers noted. The results, however, “support training providers to use announcements as an approach to address low HPV vaccination uptake in primary care clinics,” especially at the recommended ages for routine vaccination, Dr. Brewer and his associates said.
Read the full study here (Pediatrics 2016;139:e20161764. doi: 10.1542/peds.2016-1764).
Clinics in which providers presented human papillomavirus (HPV) vaccination as an assumed part of tween health care had a 5% increase in HPV vaccination coverage, compared with clinics that did not receive “announcement” training, based on data from a parallel-group, randomized trial of 30 pediatric and family medicine clinics in North Carolina.
Many providers hesitate to recommend HPV vaccination for 11- to 12-year-olds for a number of reasons, including lack of time and anticipation of a lengthy conversation about sex, wrote Noel T. Brewer, PhD, of the University of North Carolina, Chapel Hill, and his colleagues.
At 6 months after the training period, 17,173 children aged 11-12 years and 37,796 children aged 13-17 years were seen at the clinics. Overall, clinics that underwent announcement training increased HPV vaccine initiation for 11- and 12-year-olds by 5.4% over the control clinics. Clinics that received conversation training showed no significant increase in vaccine initiation, compared with controls. Intervention groups did not differ from the controls in terms of other ages (adolescents aged 13-17 years) or other immunization coverage, including HPV series completion, Tdap, and meningococcal vaccines.
The findings were limited by several factors, including the collection of data from a single Southeastern state that may not be generalizable to other areas, the researchers noted. The results, however, “support training providers to use announcements as an approach to address low HPV vaccination uptake in primary care clinics,” especially at the recommended ages for routine vaccination, Dr. Brewer and his associates said.
Read the full study here (Pediatrics 2016;139:e20161764. doi: 10.1542/peds.2016-1764).
FROM PEDIATRICS
VIDEO: Novel microcapsules show promise in hemophilia A with inhibitory antibodies
SAN DIEGO – Novel microcapsules loaded with factor VIII outperformed systemic factor VIII infusions in models of hemophilia A with inhibitory antibodies, Caroline E. Hansen reported at the annual meeting of the American Society of Hematology.
“This is a completely new paradigm that uses platelet biomechanics to target and deliver a drug,” said Ms. Hansen of Georgia Institute of Technology, Atlanta.
The microcapsules are designed to mechanically shield factor VIII from the immune system. When they reached a modeled site of vascular injury, they contracted and released factor VIII. Initial work showed that this approach triggered significantly more fibrin production in a developing clot than did systemic infusions of factor VIII.
Ms. Hansen had no disclosures. She discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Novel microcapsules loaded with factor VIII outperformed systemic factor VIII infusions in models of hemophilia A with inhibitory antibodies, Caroline E. Hansen reported at the annual meeting of the American Society of Hematology.
“This is a completely new paradigm that uses platelet biomechanics to target and deliver a drug,” said Ms. Hansen of Georgia Institute of Technology, Atlanta.
The microcapsules are designed to mechanically shield factor VIII from the immune system. When they reached a modeled site of vascular injury, they contracted and released factor VIII. Initial work showed that this approach triggered significantly more fibrin production in a developing clot than did systemic infusions of factor VIII.
Ms. Hansen had no disclosures. She discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Novel microcapsules loaded with factor VIII outperformed systemic factor VIII infusions in models of hemophilia A with inhibitory antibodies, Caroline E. Hansen reported at the annual meeting of the American Society of Hematology.
“This is a completely new paradigm that uses platelet biomechanics to target and deliver a drug,” said Ms. Hansen of Georgia Institute of Technology, Atlanta.
The microcapsules are designed to mechanically shield factor VIII from the immune system. When they reached a modeled site of vascular injury, they contracted and released factor VIII. Initial work showed that this approach triggered significantly more fibrin production in a developing clot than did systemic infusions of factor VIII.
Ms. Hansen had no disclosures. She discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ASH 2016
Key clinical point: Novel microcapsules loaded with factor VIII outperformed systemic factor VIII infusions in an in vitro model of hemophilia A with inhibitory antibodies.
Major finding: In an in vitro model, the microcapsules triggered 2.7 times more fibrin production than systemic treatment with factor VIII (P less than .05).
Data source: A multicenter laboratory study.
Disclosures: Ms. Hansen had no relevant financial disclosures.

Screening tool spots teens headed for substance-dependent adulthood
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
VIENNA – The creation of a simple risk score that accurately predicts which adolescents in the general population will develop persistent substance dependence as adults has been one of the highlights of the year in addiction medicine, Wim van den Brink, MD, said at the annual congress of the European College of Neuropsychopharmacology.
“These predictors are not very difficult to assess. Clinicians will be interested to know that the positive predictive value of the screen is threefold greater than the persistent prevalence rate,” noted Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
The New Zealand researchers developed what they call “a universal screening tool” by working backward in an analysis of a representative group of 1,037 individuals born in Dunedin, New Zealand, in 1972-1973 and prospectively followed to age 38 years, with a 95% study retention rate. Along the way, participants were assessed for dependence on alcohol, tobacco, cannabis, or hard drugs at ages 21, 26, 32, and 38.
Persistent substance dependence in adulthood, defined as dependence at a minimum of three of the assessments, was present in 19% of subjects.
The investigators found that the presence in childhood or adolescence of any four of nine risk factors had an area under the curve of 80% for persistent substance dependence as an adult. The sensitivity was 43%, with a 93% specificity. The positive predictive value was 60%, and the negative predictive value was 87% (Psychol Med. 2016 Mar;46[4]:877-89).
The nine risk factors are low family socioeconomic status, a family history of substance dependence, childhood depression, childhood conduct disorder, early exposure to substances, adolescent frequent alcohol use, adolescent frequent cannabis use, male gender, and adolescent frequent tobacco use.
The single least potent predictor was low family socioeconomic status, with an associated 1.73-fold increased risk. The strongest predictors were adolescent frequent tobacco use, which conferred a 5.41-fold increased risk; adolescent frequent cannabis use, with a 4.25-fold risk; and childhood conduct disorder, with a 3.2-fold increased risk.
The investigators also analyzed the screening tool’s performance in predicting a modified outcome consisting of adult persistent dependence on any of the target substances except for tobacco. The predictive power of having any four of the risk factors was similar to that found in the main analysis; however, the two strongest predictors now became adolescent frequent cannabis use, with a 9.5-fold increased risk, and childhood conduct disorder, with a relative risk of 5.42.
Regarding childhood conduct disorder as a risk factor, Dr. van den Brink said, “If you are a child with conduct disorder, your chances of becoming substance dependent in coming years is more than fivefold greater than in a child without conduct disorder.”
This raises the question of whether effective treatment of childhood conduct disorder might prevent later development of persistent substance dependence in adulthood. The answer remains unknown. Although there is no approved drug therapy for conduct disorder, methylphenidate is widely prescribed, especially in young patients with comorbid attention-deficit/hyperactivity disorder.
Several years ago a meta-analysis of 15 longitudinal studies with more than 2,500 participants concluded that stimulant therapy of childhood ADHD neither increased nor reduced the risk of subsequent substance use disorders (JAMA Psychiatry. 2013 Jul;70[7]:740-9). Prescribing physicians were happy to hear they weren’t causing iatrogenic injury, but Dr. van den Brink said he was never comfortable with the investigators’ conclusion.
“There was a lot of heterogeneity in the data, so the overall conclusion might not be the best conclusion,” he said.
He said has become more convinced of that than ever as a result of a recent randomized, double-blind, placebo-controlled MRI study of cerebral blood flow in response to methylphenidate in stimulant-naive patients with childhood or adult AHDH. The investigators found that MRIs obtained 1 week after the conclusion of 16 weeks of methylphenidate therapy showed increased blood flow in the strial and thalamic areas in the pediatric ADHD patients but not in the adults with ADHD (JAMA Psychiatry. 2016 Sep 1;73[9]:955-62).
This is evidence of an age-dependent sustained effect of methylphenidate therapy on dopamine striatal-thalamic circuitry in children that’s not related to the drug’s clinical effects, which were gone after a week off therapy. The question is, Does this effect represent neurotoxicity, or is it an expression of enhanced brain maturation? Dr. van den Brink said he suspects it’s the latter but cannot exclude the former possibility.
EXPERT ANALYSIS FROM THE ECNP CONGRESS