User login
Purpuric Lesions of the Scalp, Axillae, and Groin of an Infant
The Diagnosis: Langerhans Cell Histiocytosis
Langerhans cell histiocytosis (LCH) is a clonal proliferative disorder of Langerhans cells that can affect any organ, most commonly the skin and bones. It typically develops in children aged 1 to 3 years, with a male to female ratio of 2 to 1.1 Skin manifestations include purpuric papules, pustules, vesicles, erosions, and fissuring distributed predominantly on the scalp and flexural sites. Mucosal sites, particularly the oral mucosa, may be involved and usually present as erosions associated with underlying bone lesions.1 Langerhans cell histiocytosis should be considered in the differential diagnosis of recalcitrant diaper dermatitis in an infant, especially when there is purpura and erosions, as seen in our patient. Common conditions in infants such as cutaneous candidiasis (intense erythema with superficial erosions, peripheral scale and satellite pustules on flexural areas, potassium hydroxide microscopy revealing yeast forms and pseudohyphae) and seborrheic dermatitis (well-defined pink to red, moist, and often scaly patches favoring the folds) may be distinguished clinically from Hailey-Hailey disease (malodorous plaques with fissures and erosions favoring the folds), which is rare in infancy, and acrodermatitis enteropathica (erythema and erosions with scale-crust and desquamation on periorificial, acral, and intertriginous skin).
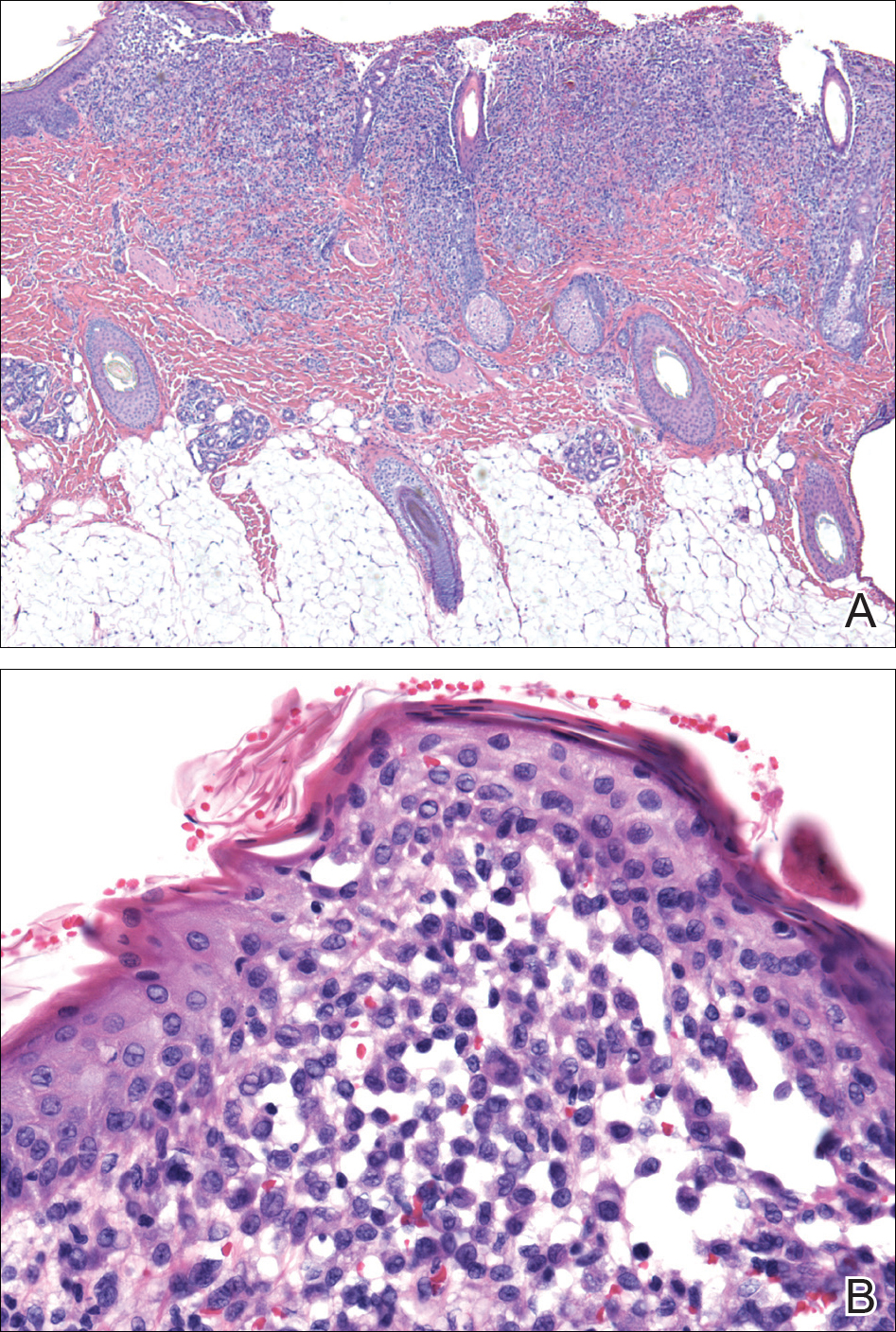
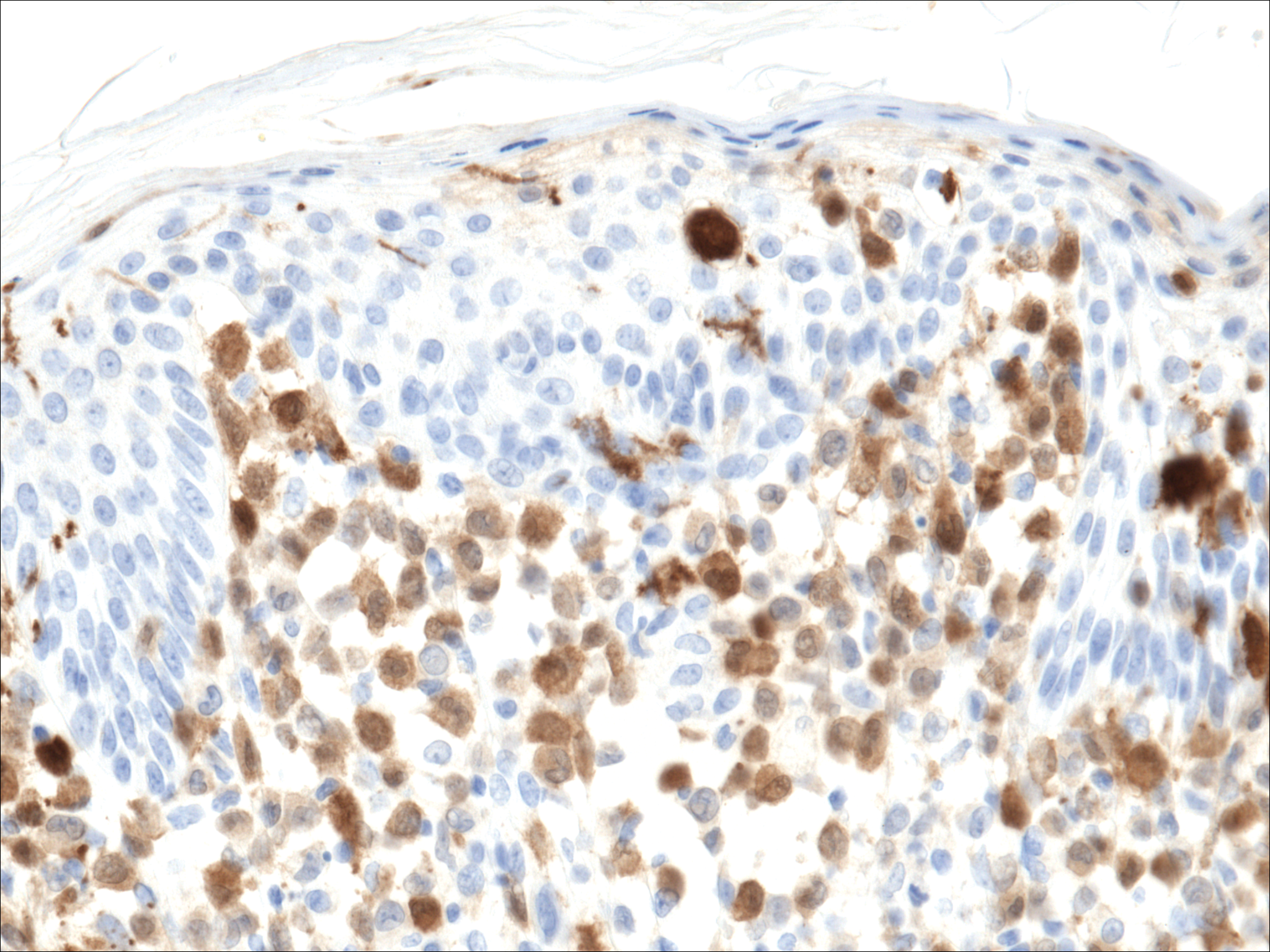
Histopathologic evaluation is instrumental in diagnosing the skin lesions of LCH. Further evaluation for systemic involvement is necessary once the diagnosis is made. Skin biopsy of the scalp and right inguinal fold revealed a wedge-shaped infiltrate of histiocytes with slightly folded nuclear contours in our patient (Figure 1). CD1a (Figure 2) and S-100 stains were markedly positive, which is characteristic of LCH. Complete blood cell count, renal function, liver function, urinalysis, and flow cytometry results were within reference range. A skeletal survey and echocardiogram were unremarkable; however, mild hepatosplenomegaly was noted on abdominal ultrasonography.
Treatment of LCH varies based on the extent of organ involvement. For isolated cutaneous disease, topical steroids, topical nitrogen mustard, phototherapy, and thalidomide may be employed.2 Multisystem disease requires chemotherapeutic agents including vinblastine and prednisone.2,3 Because more than half of patients with LCH have oncogenic BRAF V600E mutations,4 vemurafenib may have a therapeutic role in treatment. Rare case reports have documented disease response in patients with LCH and Erdheim-Chester disease.5,6
Prognosis varies based on age and extent of systemic involvement. Children younger than 2 years with multiorgan involvement have a poor prognosis (35%-55% mortality rate) compared to older children without hematopoietic, hepatosplenic, or lung involvement (100% survival rate). Additionally, response to treatment affects prognosis, as there is a 66% mortality rate in those who do not respond to treatment after 6 weeks.3 Long-term sequelae of LCH include endocrine dysfunction (ie, diabetes insipidus, growth hormone deficiencies), hearing impairment, orthopedic impairment, and neuropsychological disease; thus, multidisciplinary care often is neccessary.7
Given the multisystem involvement in our patient, he was treated with vinblastine, 6-mercaptopurine, and prednisolone with only partial and transient disease response. He was then treated with clofarabine with dramatic resolution of the mediastinal mass on follow-up positron emission tomography. The cutaneous lesions persisted and were managed with topical corticosteroids.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
- Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years [published online October 25, 2012]. Pediatr Blood Cancer. 2013;60:175-184.
- Gadner H, Grois N, Arico M, et al; Histiocyte Society. A randomized trial of treatment for multisystem Langerhans' cell histiocytosis. J Pediatr. 2001;138:728-734.
- Badalian-Very G, Vergilio JA, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923.
- Haroche J, Cohen-Aubart F, Emile JF, et al. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood. 2013;121:1495-1500.
- Charles J, Beani JC, Fiandrino G, et al. Major response to vemurafenib in patient with severe cutaneous Langerhans cell histiocytosis harboring BRAF V600E mutation. J Am Acad Dermatol. 2014;71:E97-E99.
- Martin A, Macmillan S, Murphy D, et al. Langerhans cell histiocytosis: 23 years' paediatric experience highlights severe long-term sequelae. Scott Med J. 2014;59:149-157.
The Diagnosis: Langerhans Cell Histiocytosis
Langerhans cell histiocytosis (LCH) is a clonal proliferative disorder of Langerhans cells that can affect any organ, most commonly the skin and bones. It typically develops in children aged 1 to 3 years, with a male to female ratio of 2 to 1.1 Skin manifestations include purpuric papules, pustules, vesicles, erosions, and fissuring distributed predominantly on the scalp and flexural sites. Mucosal sites, particularly the oral mucosa, may be involved and usually present as erosions associated with underlying bone lesions.1 Langerhans cell histiocytosis should be considered in the differential diagnosis of recalcitrant diaper dermatitis in an infant, especially when there is purpura and erosions, as seen in our patient. Common conditions in infants such as cutaneous candidiasis (intense erythema with superficial erosions, peripheral scale and satellite pustules on flexural areas, potassium hydroxide microscopy revealing yeast forms and pseudohyphae) and seborrheic dermatitis (well-defined pink to red, moist, and often scaly patches favoring the folds) may be distinguished clinically from Hailey-Hailey disease (malodorous plaques with fissures and erosions favoring the folds), which is rare in infancy, and acrodermatitis enteropathica (erythema and erosions with scale-crust and desquamation on periorificial, acral, and intertriginous skin).
Histopathologic evaluation is instrumental in diagnosing the skin lesions of LCH. Further evaluation for systemic involvement is necessary once the diagnosis is made. Skin biopsy of the scalp and right inguinal fold revealed a wedge-shaped infiltrate of histiocytes with slightly folded nuclear contours in our patient (Figure 1). CD1a (Figure 2) and S-100 stains were markedly positive, which is characteristic of LCH. Complete blood cell count, renal function, liver function, urinalysis, and flow cytometry results were within reference range. A skeletal survey and echocardiogram were unremarkable; however, mild hepatosplenomegaly was noted on abdominal ultrasonography.
Treatment of LCH varies based on the extent of organ involvement. For isolated cutaneous disease, topical steroids, topical nitrogen mustard, phototherapy, and thalidomide may be employed.2 Multisystem disease requires chemotherapeutic agents including vinblastine and prednisone.2,3 Because more than half of patients with LCH have oncogenic BRAF V600E mutations,4 vemurafenib may have a therapeutic role in treatment. Rare case reports have documented disease response in patients with LCH and Erdheim-Chester disease.5,6
Prognosis varies based on age and extent of systemic involvement. Children younger than 2 years with multiorgan involvement have a poor prognosis (35%-55% mortality rate) compared to older children without hematopoietic, hepatosplenic, or lung involvement (100% survival rate). Additionally, response to treatment affects prognosis, as there is a 66% mortality rate in those who do not respond to treatment after 6 weeks.3 Long-term sequelae of LCH include endocrine dysfunction (ie, diabetes insipidus, growth hormone deficiencies), hearing impairment, orthopedic impairment, and neuropsychological disease; thus, multidisciplinary care often is neccessary.7
Given the multisystem involvement in our patient, he was treated with vinblastine, 6-mercaptopurine, and prednisolone with only partial and transient disease response. He was then treated with clofarabine with dramatic resolution of the mediastinal mass on follow-up positron emission tomography. The cutaneous lesions persisted and were managed with topical corticosteroids.
The Diagnosis: Langerhans Cell Histiocytosis
Langerhans cell histiocytosis (LCH) is a clonal proliferative disorder of Langerhans cells that can affect any organ, most commonly the skin and bones. It typically develops in children aged 1 to 3 years, with a male to female ratio of 2 to 1.1 Skin manifestations include purpuric papules, pustules, vesicles, erosions, and fissuring distributed predominantly on the scalp and flexural sites. Mucosal sites, particularly the oral mucosa, may be involved and usually present as erosions associated with underlying bone lesions.1 Langerhans cell histiocytosis should be considered in the differential diagnosis of recalcitrant diaper dermatitis in an infant, especially when there is purpura and erosions, as seen in our patient. Common conditions in infants such as cutaneous candidiasis (intense erythema with superficial erosions, peripheral scale and satellite pustules on flexural areas, potassium hydroxide microscopy revealing yeast forms and pseudohyphae) and seborrheic dermatitis (well-defined pink to red, moist, and often scaly patches favoring the folds) may be distinguished clinically from Hailey-Hailey disease (malodorous plaques with fissures and erosions favoring the folds), which is rare in infancy, and acrodermatitis enteropathica (erythema and erosions with scale-crust and desquamation on periorificial, acral, and intertriginous skin).
Histopathologic evaluation is instrumental in diagnosing the skin lesions of LCH. Further evaluation for systemic involvement is necessary once the diagnosis is made. Skin biopsy of the scalp and right inguinal fold revealed a wedge-shaped infiltrate of histiocytes with slightly folded nuclear contours in our patient (Figure 1). CD1a (Figure 2) and S-100 stains were markedly positive, which is characteristic of LCH. Complete blood cell count, renal function, liver function, urinalysis, and flow cytometry results were within reference range. A skeletal survey and echocardiogram were unremarkable; however, mild hepatosplenomegaly was noted on abdominal ultrasonography.
Treatment of LCH varies based on the extent of organ involvement. For isolated cutaneous disease, topical steroids, topical nitrogen mustard, phototherapy, and thalidomide may be employed.2 Multisystem disease requires chemotherapeutic agents including vinblastine and prednisone.2,3 Because more than half of patients with LCH have oncogenic BRAF V600E mutations,4 vemurafenib may have a therapeutic role in treatment. Rare case reports have documented disease response in patients with LCH and Erdheim-Chester disease.5,6
Prognosis varies based on age and extent of systemic involvement. Children younger than 2 years with multiorgan involvement have a poor prognosis (35%-55% mortality rate) compared to older children without hematopoietic, hepatosplenic, or lung involvement (100% survival rate). Additionally, response to treatment affects prognosis, as there is a 66% mortality rate in those who do not respond to treatment after 6 weeks.3 Long-term sequelae of LCH include endocrine dysfunction (ie, diabetes insipidus, growth hormone deficiencies), hearing impairment, orthopedic impairment, and neuropsychological disease; thus, multidisciplinary care often is neccessary.7
Given the multisystem involvement in our patient, he was treated with vinblastine, 6-mercaptopurine, and prednisolone with only partial and transient disease response. He was then treated with clofarabine with dramatic resolution of the mediastinal mass on follow-up positron emission tomography. The cutaneous lesions persisted and were managed with topical corticosteroids.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
- Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years [published online October 25, 2012]. Pediatr Blood Cancer. 2013;60:175-184.
- Gadner H, Grois N, Arico M, et al; Histiocyte Society. A randomized trial of treatment for multisystem Langerhans' cell histiocytosis. J Pediatr. 2001;138:728-734.
- Badalian-Very G, Vergilio JA, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923.
- Haroche J, Cohen-Aubart F, Emile JF, et al. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood. 2013;121:1495-1500.
- Charles J, Beani JC, Fiandrino G, et al. Major response to vemurafenib in patient with severe cutaneous Langerhans cell histiocytosis harboring BRAF V600E mutation. J Am Acad Dermatol. 2014;71:E97-E99.
- Martin A, Macmillan S, Murphy D, et al. Langerhans cell histiocytosis: 23 years' paediatric experience highlights severe long-term sequelae. Scott Med J. 2014;59:149-157.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
- Haupt R, Minkov M, Astigarraga I, et al; Euro Histio Network. Langerhans cell histiocytosis (LCH): guidelines for diagnosis, clinical work‐up, and treatment for patients till the age of 18 years [published online October 25, 2012]. Pediatr Blood Cancer. 2013;60:175-184.
- Gadner H, Grois N, Arico M, et al; Histiocyte Society. A randomized trial of treatment for multisystem Langerhans' cell histiocytosis. J Pediatr. 2001;138:728-734.
- Badalian-Very G, Vergilio JA, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116:1919-1923.
- Haroche J, Cohen-Aubart F, Emile JF, et al. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood. 2013;121:1495-1500.
- Charles J, Beani JC, Fiandrino G, et al. Major response to vemurafenib in patient with severe cutaneous Langerhans cell histiocytosis harboring BRAF V600E mutation. J Am Acad Dermatol. 2014;71:E97-E99.
- Martin A, Macmillan S, Murphy D, et al. Langerhans cell histiocytosis: 23 years' paediatric experience highlights severe long-term sequelae. Scott Med J. 2014;59:149-157.

A 7-month-old boy admitted to the hospital with new-onset respiratory stridor was found to have a rash of the scalp, axillae, and groin of 1 month's duration that was unresponsive to treatment with mineral oil. Bronchoscopy revealed tracheal compression, and urgent magnetic resonance imaging of the chest demonstrated an anterior mediastinal mass. Prior to presentation, the patient was otherwise healthy with normal growth and development. On physical examination, scattered red-brown and purpuric papules with hemorrhagic crust were noted on the scalp. There were well-defined pink erosive patches and purpuric papules in the inguinal folds bilaterally and similar erosive patches in the axillae. Numerous punched out ulcerations were noted on the lower gingiva. There was no palpable lymphadenopathy. The hands, feet, penis, scrotum, and perianal area were spared. Biopsies of the skin and mediastinal mass were performed.

Predicting functional outcome after pediatric osteomyelitis
MADRID – Ninety percent of children with acute hematogenous osteomyelitis will do fine after their initial course of antibiotics and don’t require long-term follow-up; and the other 10% can be identified within the first few days of hospitalization, Lawson A. Copley, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
The tool that enables physicians to distinguish the 10% of children at high risk for severe orthopedic sequelae is a validated severity of illness score that can be determined within the first several days of hospitalization. The 0-10 score, developed by Dr. Copley and his coinvestigators (J Pediatr Orthop. 2016 Oct 12. doi: 10.1097/BPO.0000000000000879), awards points for the patient’s initial C-reactive protein level, the C-reactive protein levels on hospital days 2-3 and 4-5, the number of febrile days on antibiotic therapy, the band percentage of WBC, ICU admission, and disseminated disease such as endocarditis, septic pulmonary embolism, and deep venous thrombosis.

There is a dearth of long-term follow-up studies of pediatric osteomyelitis. To address this unmet need, he and his coinvestigators have enrolled 198 children with acute hematogenous osteomyelitis in an ongoing prospective study. All were treated with antibiotics until clinical and laboratory resolution of the infection and achievement of a normal erythrocyte sedimentation rate. All patients are being followed in a specialized multidisciplinary clinic at Texas Scottish Rite Hospital for Children directed by Dr. Copley. To date, 118 patients have been seen for their 2-year follow-up visit, which includes radiographs of the previous infection site, an orthopedic exam, and completion of the Pediatric Quality of Life Inventory and the Pediatric Outcomes Data Collection Instrument.
At follow-up, the children fell into three broad categories. Ten percent had severe radiographic and/or clinical sequelae such as limb length discrepancy, visible deformity, limited range of motion, osteonecrosis, physeal arrest, or joint destruction. Roughly 40% had complete resolution with normal function and no growth disturbance or other sequelae. And 50% had clinical resolution with a completely normal physical exam and excellent outcome measures, but minimal radiographic sequelae, mainly consisting of central physeal tenting.
“We think that they’re probably a low-risk group,” he said of that last group.
Children with severe sequelae had greater severity of illness at presentation and a more complicated course of initial therapy than those with complete resolution at 2 years of follow-up. Their mean severity of illness score was 4.9, compared with 1.8 in the 40% of children with complete resolution and 3.4 in those with mild radiographic sequelae.
In a univariate logistic regression analysis, each point increase in initial disease severity score was associated with a 20% bump in the risk of developing severe sequelae, with a predictive area under the curve of 0.67. A multivariate logistic regression analysis identified other independent predictors of severe sequelae: age below 6 years, being culture positive for methicillin-resistant Streptococcus aureus, and osteomyelitis contiguous with septic arthritis or abscess, which ultimately led to osteonecrosis and destruction. Incorporating these additional risk factors along with the initial severity of illness score improved the predictive area under the curve to 0.85.
About one-half of patients seen in the pediatric osteomyelitis clinic were bacteremic on admission, and of those, roughly half continued to be bacteremic despite antibiotic therapy. However, there was no difference in the prevalence of bacteremia between the groups with mild versus severe illness.
Asked how introduction of the severity-of-illness score has affected his surgical approach, Dr. Copley said he has become selectively more surgically aggressive.
“A lot of our children have abscesses that are pretty substantial,” he noted. “We’ve learned the hard way. I’ve been doing this for about 14 years now, and initially I used to do a lot of simple debridement of the infection. Now we’re much more extensive in our approach, so we do fewer surgeries, but those surgeries are more extensive.”
Dr. Copley reported having no financial conflicts regarding his study.
MADRID – Ninety percent of children with acute hematogenous osteomyelitis will do fine after their initial course of antibiotics and don’t require long-term follow-up; and the other 10% can be identified within the first few days of hospitalization, Lawson A. Copley, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
The tool that enables physicians to distinguish the 10% of children at high risk for severe orthopedic sequelae is a validated severity of illness score that can be determined within the first several days of hospitalization. The 0-10 score, developed by Dr. Copley and his coinvestigators (J Pediatr Orthop. 2016 Oct 12. doi: 10.1097/BPO.0000000000000879), awards points for the patient’s initial C-reactive protein level, the C-reactive protein levels on hospital days 2-3 and 4-5, the number of febrile days on antibiotic therapy, the band percentage of WBC, ICU admission, and disseminated disease such as endocarditis, septic pulmonary embolism, and deep venous thrombosis.
There is a dearth of long-term follow-up studies of pediatric osteomyelitis. To address this unmet need, he and his coinvestigators have enrolled 198 children with acute hematogenous osteomyelitis in an ongoing prospective study. All were treated with antibiotics until clinical and laboratory resolution of the infection and achievement of a normal erythrocyte sedimentation rate. All patients are being followed in a specialized multidisciplinary clinic at Texas Scottish Rite Hospital for Children directed by Dr. Copley. To date, 118 patients have been seen for their 2-year follow-up visit, which includes radiographs of the previous infection site, an orthopedic exam, and completion of the Pediatric Quality of Life Inventory and the Pediatric Outcomes Data Collection Instrument.
At follow-up, the children fell into three broad categories. Ten percent had severe radiographic and/or clinical sequelae such as limb length discrepancy, visible deformity, limited range of motion, osteonecrosis, physeal arrest, or joint destruction. Roughly 40% had complete resolution with normal function and no growth disturbance or other sequelae. And 50% had clinical resolution with a completely normal physical exam and excellent outcome measures, but minimal radiographic sequelae, mainly consisting of central physeal tenting.
“We think that they’re probably a low-risk group,” he said of that last group.
Children with severe sequelae had greater severity of illness at presentation and a more complicated course of initial therapy than those with complete resolution at 2 years of follow-up. Their mean severity of illness score was 4.9, compared with 1.8 in the 40% of children with complete resolution and 3.4 in those with mild radiographic sequelae.
In a univariate logistic regression analysis, each point increase in initial disease severity score was associated with a 20% bump in the risk of developing severe sequelae, with a predictive area under the curve of 0.67. A multivariate logistic regression analysis identified other independent predictors of severe sequelae: age below 6 years, being culture positive for methicillin-resistant Streptococcus aureus, and osteomyelitis contiguous with septic arthritis or abscess, which ultimately led to osteonecrosis and destruction. Incorporating these additional risk factors along with the initial severity of illness score improved the predictive area under the curve to 0.85.
About one-half of patients seen in the pediatric osteomyelitis clinic were bacteremic on admission, and of those, roughly half continued to be bacteremic despite antibiotic therapy. However, there was no difference in the prevalence of bacteremia between the groups with mild versus severe illness.
Asked how introduction of the severity-of-illness score has affected his surgical approach, Dr. Copley said he has become selectively more surgically aggressive.
“A lot of our children have abscesses that are pretty substantial,” he noted. “We’ve learned the hard way. I’ve been doing this for about 14 years now, and initially I used to do a lot of simple debridement of the infection. Now we’re much more extensive in our approach, so we do fewer surgeries, but those surgeries are more extensive.”
Dr. Copley reported having no financial conflicts regarding his study.
MADRID – Ninety percent of children with acute hematogenous osteomyelitis will do fine after their initial course of antibiotics and don’t require long-term follow-up; and the other 10% can be identified within the first few days of hospitalization, Lawson A. Copley, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
The tool that enables physicians to distinguish the 10% of children at high risk for severe orthopedic sequelae is a validated severity of illness score that can be determined within the first several days of hospitalization. The 0-10 score, developed by Dr. Copley and his coinvestigators (J Pediatr Orthop. 2016 Oct 12. doi: 10.1097/BPO.0000000000000879), awards points for the patient’s initial C-reactive protein level, the C-reactive protein levels on hospital days 2-3 and 4-5, the number of febrile days on antibiotic therapy, the band percentage of WBC, ICU admission, and disseminated disease such as endocarditis, septic pulmonary embolism, and deep venous thrombosis.
There is a dearth of long-term follow-up studies of pediatric osteomyelitis. To address this unmet need, he and his coinvestigators have enrolled 198 children with acute hematogenous osteomyelitis in an ongoing prospective study. All were treated with antibiotics until clinical and laboratory resolution of the infection and achievement of a normal erythrocyte sedimentation rate. All patients are being followed in a specialized multidisciplinary clinic at Texas Scottish Rite Hospital for Children directed by Dr. Copley. To date, 118 patients have been seen for their 2-year follow-up visit, which includes radiographs of the previous infection site, an orthopedic exam, and completion of the Pediatric Quality of Life Inventory and the Pediatric Outcomes Data Collection Instrument.
At follow-up, the children fell into three broad categories. Ten percent had severe radiographic and/or clinical sequelae such as limb length discrepancy, visible deformity, limited range of motion, osteonecrosis, physeal arrest, or joint destruction. Roughly 40% had complete resolution with normal function and no growth disturbance or other sequelae. And 50% had clinical resolution with a completely normal physical exam and excellent outcome measures, but minimal radiographic sequelae, mainly consisting of central physeal tenting.
“We think that they’re probably a low-risk group,” he said of that last group.
Children with severe sequelae had greater severity of illness at presentation and a more complicated course of initial therapy than those with complete resolution at 2 years of follow-up. Their mean severity of illness score was 4.9, compared with 1.8 in the 40% of children with complete resolution and 3.4 in those with mild radiographic sequelae.
In a univariate logistic regression analysis, each point increase in initial disease severity score was associated with a 20% bump in the risk of developing severe sequelae, with a predictive area under the curve of 0.67. A multivariate logistic regression analysis identified other independent predictors of severe sequelae: age below 6 years, being culture positive for methicillin-resistant Streptococcus aureus, and osteomyelitis contiguous with septic arthritis or abscess, which ultimately led to osteonecrosis and destruction. Incorporating these additional risk factors along with the initial severity of illness score improved the predictive area under the curve to 0.85.
About one-half of patients seen in the pediatric osteomyelitis clinic were bacteremic on admission, and of those, roughly half continued to be bacteremic despite antibiotic therapy. However, there was no difference in the prevalence of bacteremia between the groups with mild versus severe illness.
Asked how introduction of the severity-of-illness score has affected his surgical approach, Dr. Copley said he has become selectively more surgically aggressive.
“A lot of our children have abscesses that are pretty substantial,” he noted. “We’ve learned the hard way. I’ve been doing this for about 14 years now, and initially I used to do a lot of simple debridement of the infection. Now we’re much more extensive in our approach, so we do fewer surgeries, but those surgeries are more extensive.”
Dr. Copley reported having no financial conflicts regarding his study.
AT ESPID 2017
Key clinical point:
Major finding: Ninety percent of children with acute hematogenous osteomyelitis require no long-term follow-up after their initial antibiotic therapy.
Data source: An ongoing prospective study of 118 children followed for 2 years after initial treatment of acute hematogenous osteomyelitis.
Disclosures: The study presenter reported having no financial conflicts.
Rapid lab test predicts pediatric pneumococcal pneumonia severity
MADRID – Thomsen-Friedenreich antigen activation is useful as a novel early predictor of empyema in pediatric community-acquired pneumonia, Chi-Jung Chang, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
In her retrospective study of 142 Taiwanese children and adolescents hospitalized for community-acquired pneumonia (CAP), Thomsen-Friedenreich antigen (TA) activation had 100% specificity, 100% positive predictive value, and 31% sensitivity for Streptococcus pneumoniae as the causative microorganism.
Moreover, the higher the TA activation titer, the more severe the pneumonia complications that followed, according to Dr. Chang of MacKay Children’s Hospital in Taipei, Taiwan.
The value of this lab test lies in its speed and accuracy for detection of S. pneumoniae CAP. Conventional culture methods are relatively slow and have poor sensitivity, because a child often already has been on empiric antimicrobial therapy and the culture specimen is unwittingly obtained from a sterile site, she explained.
Twenty-two of the 142 children and adolescents hospitalized for lobar CAP were TA activation positive at admission. They were considerably sicker than were the 120 patients who were TA activation negative. Their initial C-reactive protein level was 31.9 mg/dL, twice that of the negative group. Their peak CRP during the hospital stay was significantly higher as well, as was their peak WBC.
Hospital lengths of stay were longer in the TA activation–positive group. Eighteen of 22 TA activation–positive patients (82%) were admitted to the ICU for an average of 8 days, compared with 9% of the negative group.
All TA activation–positive patients had complicated pneumonia with parapneumonic effusions, empyema, necrotizing pneumonia, and/or lung abscesses, as did 36% of the negative group.
S. pneumoniae was the most common pathogen in this study of CAP. It was the responsible microbe in all 22 of the TA activation–positive patients and in 29% of the TA activation–negative ones. The most common serotype in the TA activation group was 19A, which accounted for 12 of the 22 cases. This also was the predominant serotype found in CAP across all Taiwan during the first half of this decade, when the study took place.
In a multivariate logistic regression analysis, TA activation was far and away the strongest independent predictor of empyema, with an associated 15.8-fold increased risk. The other two independent predictors – longer fever duration prior to hospitalization and a higher initial CRP level – were far less robust, according to Dr. Chang.
How TA activation works as a predictor
TA is present on the surface of erythrocytes, platelets, and glomeruli, but ordinarily it is covered by a layer of N-acetylneuraminic acid. Streptococcus pneumoniae produces circulating neuraminidases, which cleave the N-acetylneuraminic acid and expose the underlying TA. The TA then quickly becomes activated through interaction with the anti-TA antibodies, which are normally present in plasma. Once activated, the TA stays so for weeks to months.
Other neuraminidase-producing microorganisms include Clostridium perfringens, Escherichia coli, and Bacteroides.
Dr. Chang and her colleagues used the peanut lectin agglutination method in their TA activation testing.
She reported having no financial conflicts regarding her study.
MADRID – Thomsen-Friedenreich antigen activation is useful as a novel early predictor of empyema in pediatric community-acquired pneumonia, Chi-Jung Chang, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
In her retrospective study of 142 Taiwanese children and adolescents hospitalized for community-acquired pneumonia (CAP), Thomsen-Friedenreich antigen (TA) activation had 100% specificity, 100% positive predictive value, and 31% sensitivity for Streptococcus pneumoniae as the causative microorganism.
Moreover, the higher the TA activation titer, the more severe the pneumonia complications that followed, according to Dr. Chang of MacKay Children’s Hospital in Taipei, Taiwan.
The value of this lab test lies in its speed and accuracy for detection of S. pneumoniae CAP. Conventional culture methods are relatively slow and have poor sensitivity, because a child often already has been on empiric antimicrobial therapy and the culture specimen is unwittingly obtained from a sterile site, she explained.
Twenty-two of the 142 children and adolescents hospitalized for lobar CAP were TA activation positive at admission. They were considerably sicker than were the 120 patients who were TA activation negative. Their initial C-reactive protein level was 31.9 mg/dL, twice that of the negative group. Their peak CRP during the hospital stay was significantly higher as well, as was their peak WBC.
Hospital lengths of stay were longer in the TA activation–positive group. Eighteen of 22 TA activation–positive patients (82%) were admitted to the ICU for an average of 8 days, compared with 9% of the negative group.
All TA activation–positive patients had complicated pneumonia with parapneumonic effusions, empyema, necrotizing pneumonia, and/or lung abscesses, as did 36% of the negative group.
S. pneumoniae was the most common pathogen in this study of CAP. It was the responsible microbe in all 22 of the TA activation–positive patients and in 29% of the TA activation–negative ones. The most common serotype in the TA activation group was 19A, which accounted for 12 of the 22 cases. This also was the predominant serotype found in CAP across all Taiwan during the first half of this decade, when the study took place.
In a multivariate logistic regression analysis, TA activation was far and away the strongest independent predictor of empyema, with an associated 15.8-fold increased risk. The other two independent predictors – longer fever duration prior to hospitalization and a higher initial CRP level – were far less robust, according to Dr. Chang.
How TA activation works as a predictor
TA is present on the surface of erythrocytes, platelets, and glomeruli, but ordinarily it is covered by a layer of N-acetylneuraminic acid. Streptococcus pneumoniae produces circulating neuraminidases, which cleave the N-acetylneuraminic acid and expose the underlying TA. The TA then quickly becomes activated through interaction with the anti-TA antibodies, which are normally present in plasma. Once activated, the TA stays so for weeks to months.
Other neuraminidase-producing microorganisms include Clostridium perfringens, Escherichia coli, and Bacteroides.
Dr. Chang and her colleagues used the peanut lectin agglutination method in their TA activation testing.
She reported having no financial conflicts regarding her study.
MADRID – Thomsen-Friedenreich antigen activation is useful as a novel early predictor of empyema in pediatric community-acquired pneumonia, Chi-Jung Chang, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
In her retrospective study of 142 Taiwanese children and adolescents hospitalized for community-acquired pneumonia (CAP), Thomsen-Friedenreich antigen (TA) activation had 100% specificity, 100% positive predictive value, and 31% sensitivity for Streptococcus pneumoniae as the causative microorganism.
Moreover, the higher the TA activation titer, the more severe the pneumonia complications that followed, according to Dr. Chang of MacKay Children’s Hospital in Taipei, Taiwan.
The value of this lab test lies in its speed and accuracy for detection of S. pneumoniae CAP. Conventional culture methods are relatively slow and have poor sensitivity, because a child often already has been on empiric antimicrobial therapy and the culture specimen is unwittingly obtained from a sterile site, she explained.
Twenty-two of the 142 children and adolescents hospitalized for lobar CAP were TA activation positive at admission. They were considerably sicker than were the 120 patients who were TA activation negative. Their initial C-reactive protein level was 31.9 mg/dL, twice that of the negative group. Their peak CRP during the hospital stay was significantly higher as well, as was their peak WBC.
Hospital lengths of stay were longer in the TA activation–positive group. Eighteen of 22 TA activation–positive patients (82%) were admitted to the ICU for an average of 8 days, compared with 9% of the negative group.
All TA activation–positive patients had complicated pneumonia with parapneumonic effusions, empyema, necrotizing pneumonia, and/or lung abscesses, as did 36% of the negative group.
S. pneumoniae was the most common pathogen in this study of CAP. It was the responsible microbe in all 22 of the TA activation–positive patients and in 29% of the TA activation–negative ones. The most common serotype in the TA activation group was 19A, which accounted for 12 of the 22 cases. This also was the predominant serotype found in CAP across all Taiwan during the first half of this decade, when the study took place.
In a multivariate logistic regression analysis, TA activation was far and away the strongest independent predictor of empyema, with an associated 15.8-fold increased risk. The other two independent predictors – longer fever duration prior to hospitalization and a higher initial CRP level – were far less robust, according to Dr. Chang.
How TA activation works as a predictor
TA is present on the surface of erythrocytes, platelets, and glomeruli, but ordinarily it is covered by a layer of N-acetylneuraminic acid. Streptococcus pneumoniae produces circulating neuraminidases, which cleave the N-acetylneuraminic acid and expose the underlying TA. The TA then quickly becomes activated through interaction with the anti-TA antibodies, which are normally present in plasma. Once activated, the TA stays so for weeks to months.
Other neuraminidase-producing microorganisms include Clostridium perfringens, Escherichia coli, and Bacteroides.
Dr. Chang and her colleagues used the peanut lectin agglutination method in their TA activation testing.
She reported having no financial conflicts regarding her study.
AT ESPID 2017
Key clinical point:
Major finding: A positive Thomsen-Friedenreich antigen activation test in pediatric community-acquired pneumonia had 100% specificity, 100% positive predictive value, and 31% sensitivity for S. pneumoniae as the causative microorganism.
Data source: A retrospective study of 142 Taiwanese children and teens hospitalized for lobular community-acquired pneumonia.
Disclosures: The study presenter reported having no financial conflicts of interest.
CAR T cells elicit durable, potent responses in kids with EM relapse of ALL

CHICAGO—Outcomes for pediatric patients with relapsed acute lymphoblastic leukemia (ALL) are dismal, with the probability of event-free survival ranging from 15% to 70% after a first relapse to 15% to 20% after a second relapse.
“So novel therapies are obviously urgently needed,” Mala Kiran Talekar, MD, of the Children's Hospital of Philadelphia in Pennsylvania, affirmed. “And herein comes the role of CAR T cells as a breakthrough therapy for relapsed/refractory pediatric ALL.”
She presented the outcome of chimeric antigen receptor (CAR) T-cell therapy in pediatric patients with non-CNS extramedullary (EM) relapse at the ASCO 2017 Annual meeting as abstract 10507.
The investigators had drawn the patient population for this analysis from 2 CAR studies, CTL019 and CTL119.
CTL019, which had already been completed, employed a murine CAR, and CTL119 is ongoing and uses a humanized CAR.
Of the 60 patients enrolled in CTL019, 56 (93%) achieved a complete response (CR) at day 28, and 100% had a CNS remission. Their 12-month overall survival (OS) was 79%.
“[K]eep in mind, when the study first started,” Dr Talekar said, “the patient population that had been referred to us was patients who had suffered a second or greater relapse or had been refractory to forms of treatment available to them, and the majority had been refractory to multiple therapies.”
The humanized CAR study, CTL119, is divided into 2 cohorts—one with CAR-naïve patients (n=22) and the other a CAR-retreatment arm (n=15) with patients who had received previous CAR therapy and relapsed.
Dr Talekar explained that the humanized CAR was made with the intention of decreasing rejection or loss of persistence of the T cells related to murine antigenicity.
Nine patients (60%) in the CAR-retreatment arm achieved a CR at day 28, and at 6 months, 78% experienced relapse-free survival (RFS) with a median follow-up of 12 months.
All of the CAR-naïve patients achieved CR at day 28, with 86% achieving RFS at 6 months, with a median follow-up of 10 months.
ALL with EM involvement
The investigators identified 10 pediatric patients treated in the murine (n=6) or humanized (n=4) trials who had received CAR therapy for isolated extramedullary disease or for combined bone marrow extramedullary (BM/EM) relapse of ALL.
They defined EM relapse as involvement of a non-CNS site confirmed by imaging with or without pathology within 12 months of CAR T-cell infusion. After infusion, patients had diagnostic imaging performed at 1, 3, 6, 9, and 12 months.
Of the 10 patients, 5 had active EM involvement at the time of infusion, 2 had isolated EM relapse—1 with parotid and multifocal bony lesions and 1 with testis and sinus lesions—and 5 had multiple sites of EM relapse.
The patients had 2 to 4 prior ALL relapses, 2 had prior local radiation to the EM site, and all 10 had received prior bone marrow transplants.
Three patients had an MLL rearrangement, 1 had hypodiploid ALL, and 1 had trisomy 21.
Nine of the 10 patients achieved MRD-negative CR at day 28.
One patient was not evaluable because his disease progressed within 2 weeks of CAR therapy in both the bone marrow and EM site. He died 6 weeks after the infusion.
Five patients evaluated by serial imaging had objective responses. Two had no evidence of EM disease by day 28, 2 had resolution by 3 months, and 1 had continued decrease in the size of her uterine mass at 3 and 6 months. She underwent hysterectomy at 8 months with no evidence of disease on pathology.
Four patients with a prior history of skin or testicular involvement had no evidence of disease by exam at day 28.
Three of the 9 patients relapsed with CD19+ disease. One had skin/medullary involvement and died at 38 months after CAR T-cell infusion. And 2 had medullary disease: 1 died at 17 months and 1 is alive at 28 months.
The remaining 6 patients are alive and well at a median follow-up of 10 months (range, 3 – 16 months) without recurrence of disease.
The investigators therefore concluded that single agent CAR T-cell immunotherapy can induce potent and durable response in patients with EM relapse of their ALL. ![]()
CHICAGO—Outcomes for pediatric patients with relapsed acute lymphoblastic leukemia (ALL) are dismal, with the probability of event-free survival ranging from 15% to 70% after a first relapse to 15% to 20% after a second relapse.
“So novel therapies are obviously urgently needed,” Mala Kiran Talekar, MD, of the Children's Hospital of Philadelphia in Pennsylvania, affirmed. “And herein comes the role of CAR T cells as a breakthrough therapy for relapsed/refractory pediatric ALL.”
She presented the outcome of chimeric antigen receptor (CAR) T-cell therapy in pediatric patients with non-CNS extramedullary (EM) relapse at the ASCO 2017 Annual meeting as abstract 10507.
The investigators had drawn the patient population for this analysis from 2 CAR studies, CTL019 and CTL119.
CTL019, which had already been completed, employed a murine CAR, and CTL119 is ongoing and uses a humanized CAR.
Of the 60 patients enrolled in CTL019, 56 (93%) achieved a complete response (CR) at day 28, and 100% had a CNS remission. Their 12-month overall survival (OS) was 79%.
“[K]eep in mind, when the study first started,” Dr Talekar said, “the patient population that had been referred to us was patients who had suffered a second or greater relapse or had been refractory to forms of treatment available to them, and the majority had been refractory to multiple therapies.”
The humanized CAR study, CTL119, is divided into 2 cohorts—one with CAR-naïve patients (n=22) and the other a CAR-retreatment arm (n=15) with patients who had received previous CAR therapy and relapsed.
Dr Talekar explained that the humanized CAR was made with the intention of decreasing rejection or loss of persistence of the T cells related to murine antigenicity.
Nine patients (60%) in the CAR-retreatment arm achieved a CR at day 28, and at 6 months, 78% experienced relapse-free survival (RFS) with a median follow-up of 12 months.
All of the CAR-naïve patients achieved CR at day 28, with 86% achieving RFS at 6 months, with a median follow-up of 10 months.
ALL with EM involvement
The investigators identified 10 pediatric patients treated in the murine (n=6) or humanized (n=4) trials who had received CAR therapy for isolated extramedullary disease or for combined bone marrow extramedullary (BM/EM) relapse of ALL.
They defined EM relapse as involvement of a non-CNS site confirmed by imaging with or without pathology within 12 months of CAR T-cell infusion. After infusion, patients had diagnostic imaging performed at 1, 3, 6, 9, and 12 months.
Of the 10 patients, 5 had active EM involvement at the time of infusion, 2 had isolated EM relapse—1 with parotid and multifocal bony lesions and 1 with testis and sinus lesions—and 5 had multiple sites of EM relapse.
The patients had 2 to 4 prior ALL relapses, 2 had prior local radiation to the EM site, and all 10 had received prior bone marrow transplants.
Three patients had an MLL rearrangement, 1 had hypodiploid ALL, and 1 had trisomy 21.
Nine of the 10 patients achieved MRD-negative CR at day 28.
One patient was not evaluable because his disease progressed within 2 weeks of CAR therapy in both the bone marrow and EM site. He died 6 weeks after the infusion.
Five patients evaluated by serial imaging had objective responses. Two had no evidence of EM disease by day 28, 2 had resolution by 3 months, and 1 had continued decrease in the size of her uterine mass at 3 and 6 months. She underwent hysterectomy at 8 months with no evidence of disease on pathology.
Four patients with a prior history of skin or testicular involvement had no evidence of disease by exam at day 28.
Three of the 9 patients relapsed with CD19+ disease. One had skin/medullary involvement and died at 38 months after CAR T-cell infusion. And 2 had medullary disease: 1 died at 17 months and 1 is alive at 28 months.
The remaining 6 patients are alive and well at a median follow-up of 10 months (range, 3 – 16 months) without recurrence of disease.
The investigators therefore concluded that single agent CAR T-cell immunotherapy can induce potent and durable response in patients with EM relapse of their ALL. ![]()
CHICAGO—Outcomes for pediatric patients with relapsed acute lymphoblastic leukemia (ALL) are dismal, with the probability of event-free survival ranging from 15% to 70% after a first relapse to 15% to 20% after a second relapse.
“So novel therapies are obviously urgently needed,” Mala Kiran Talekar, MD, of the Children's Hospital of Philadelphia in Pennsylvania, affirmed. “And herein comes the role of CAR T cells as a breakthrough therapy for relapsed/refractory pediatric ALL.”
She presented the outcome of chimeric antigen receptor (CAR) T-cell therapy in pediatric patients with non-CNS extramedullary (EM) relapse at the ASCO 2017 Annual meeting as abstract 10507.
The investigators had drawn the patient population for this analysis from 2 CAR studies, CTL019 and CTL119.
CTL019, which had already been completed, employed a murine CAR, and CTL119 is ongoing and uses a humanized CAR.
Of the 60 patients enrolled in CTL019, 56 (93%) achieved a complete response (CR) at day 28, and 100% had a CNS remission. Their 12-month overall survival (OS) was 79%.
“[K]eep in mind, when the study first started,” Dr Talekar said, “the patient population that had been referred to us was patients who had suffered a second or greater relapse or had been refractory to forms of treatment available to them, and the majority had been refractory to multiple therapies.”
The humanized CAR study, CTL119, is divided into 2 cohorts—one with CAR-naïve patients (n=22) and the other a CAR-retreatment arm (n=15) with patients who had received previous CAR therapy and relapsed.
Dr Talekar explained that the humanized CAR was made with the intention of decreasing rejection or loss of persistence of the T cells related to murine antigenicity.
Nine patients (60%) in the CAR-retreatment arm achieved a CR at day 28, and at 6 months, 78% experienced relapse-free survival (RFS) with a median follow-up of 12 months.
All of the CAR-naïve patients achieved CR at day 28, with 86% achieving RFS at 6 months, with a median follow-up of 10 months.
ALL with EM involvement
The investigators identified 10 pediatric patients treated in the murine (n=6) or humanized (n=4) trials who had received CAR therapy for isolated extramedullary disease or for combined bone marrow extramedullary (BM/EM) relapse of ALL.
They defined EM relapse as involvement of a non-CNS site confirmed by imaging with or without pathology within 12 months of CAR T-cell infusion. After infusion, patients had diagnostic imaging performed at 1, 3, 6, 9, and 12 months.
Of the 10 patients, 5 had active EM involvement at the time of infusion, 2 had isolated EM relapse—1 with parotid and multifocal bony lesions and 1 with testis and sinus lesions—and 5 had multiple sites of EM relapse.
The patients had 2 to 4 prior ALL relapses, 2 had prior local radiation to the EM site, and all 10 had received prior bone marrow transplants.
Three patients had an MLL rearrangement, 1 had hypodiploid ALL, and 1 had trisomy 21.
Nine of the 10 patients achieved MRD-negative CR at day 28.
One patient was not evaluable because his disease progressed within 2 weeks of CAR therapy in both the bone marrow and EM site. He died 6 weeks after the infusion.
Five patients evaluated by serial imaging had objective responses. Two had no evidence of EM disease by day 28, 2 had resolution by 3 months, and 1 had continued decrease in the size of her uterine mass at 3 and 6 months. She underwent hysterectomy at 8 months with no evidence of disease on pathology.
Four patients with a prior history of skin or testicular involvement had no evidence of disease by exam at day 28.
Three of the 9 patients relapsed with CD19+ disease. One had skin/medullary involvement and died at 38 months after CAR T-cell infusion. And 2 had medullary disease: 1 died at 17 months and 1 is alive at 28 months.
The remaining 6 patients are alive and well at a median follow-up of 10 months (range, 3 – 16 months) without recurrence of disease.
The investigators therefore concluded that single agent CAR T-cell immunotherapy can induce potent and durable response in patients with EM relapse of their ALL. ![]()
Study contradicts AAP recommendations on infant room-sharing
Infants who slept in their own rooms by age 9 months slept significantly longer and better than those who continued sharing a room with their parents as recommended by the American Academy of Pediatrics, the authors of a prospective study of 279 mother-infant dyads reported June 5.
The findings “raise questions about the well-intended AAP recommendation that room-sharing should ideally occur for all infants until their first birthday,” wrote Ian M. Paul, MD, of Penn State University, Hershey, and his associates (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-0122). “Perhaps our most troubling finding was that room-sharing was associated with overnight transitions to bed-sharing, which is strongly discouraged by the AAP.”

Insufficient sleep leads to excess weight gain during infancy and sleep problems later in childhood and has negative implications for parents. “The desire to optimize infant sleep duration and consolidation, however, must be balanced with safe infant sleep,” the researchers emphasized. About 3,500 infants die annually of SIDS and other sleep-related deaths, about 90% of which occur before age 6 months. Currently, however, the AAP’s updated 2016 recommendations advise that infants sleep on a separate surface in their parents’ room for at least the first 6 months and ideally for 1 year (Pediatrics. 2016; 138:e20162938).
To examine relationships among where, how well, and how long infants slept, the researchers analyzed Brief Infant Sleep Questionnaires collected from first-time mothers of term singletons as part of the prospective, single-center Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study.
For 4-month-olds, average reported sleep duration was similar whether they slept alone or in the parental bedroom. Solo sleepers, however, had better sleep consolidation, averaging 46 more minutes of sleep at the longest stretch, compared with room sharers (P = .02). By age 9 months, infants who had slept alone by age 4 months averaged 40 more minutes of nightly sleep than room-sharers and 26 more minutes than infants who began sleeping alone after 4 months of age (P = .008). Furthermore, the average longest sleep span of early solo sleepers was 100 minutes more than that of room-sharers and 45 minutes more than that of infants who began sleeping alone between ages 4 and 9 months (P = .01).
At age 30 months, infants who had slept alone by age 9 months averaged 45 more minutes of nightly sleep than those who had shared a room (P = .004). Room-sharing at 4 months also was tied to a two-fold greater odds of having pillows, blankets, or other unsafe objects on the sleep surface, the researchers said. Together, the findings support revising the AAP recommendation until evidence conclusively supports it, they concluded.
The study’s funders included Penn State University, Hershey; Penn State Children’s Hospital; the U.S. Department of Agriculture; the Penn State Clinical and Translational Science Institute, and the National Institutes of Health/National Center for Advancing Translational Sciences. The investigators reported having no conflicts of interest.
The study by Dr. Paul and his associates is an important contribution to the literature, wrote Rachel Y. Moon, MD, and Fern R. Hauck, MD, in an accompanying editorial (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-1323). However, they said, more research is needed.
For example, it is unclear whether sleep consolidation in young infants is preferable from a physiologic perspective. “The ability to arouse is critical physiologically, and a leading hypothesis is that failure to arouse makes an infant vulnerable to SIDS,” they wrote.
Dr. Moon and Dr. Hauck also noted that the AAP’s recommendation on room-sharing without bed-sharing is based on studies conducted in England, New Zealand, and Scotland showing that room-sharing lowers the risk of SIDS, compared with solitary sleeping.
“More recent, unpublished data from the New Zealand Sudden and Unexplained Death in Infancy study show similar protection from room-sharing, with an adjusted odds ratio of 0.36 (95% confidence interval, 0.19-0.71) for room-sharing infants compared with solitary-sleeping infants (E. Mitchell, MBBS, personal communication, 2016),” they wrote. “Because none of these studies stratified the risk by infant age in months, it is difficult to determine the optimal endpoint for room-sharing.
“We strongly support more research, both about the physiology of infant sleep and arousal for room-sharing infants and about the consequences of room-sharing on parental and child sleep.”
Dr. Moon and Dr. Hauck are with the University of Virginia, Charlottesville. They had no relevant disclosures.
The study by Dr. Paul and his associates is an important contribution to the literature, wrote Rachel Y. Moon, MD, and Fern R. Hauck, MD, in an accompanying editorial (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-1323). However, they said, more research is needed.
For example, it is unclear whether sleep consolidation in young infants is preferable from a physiologic perspective. “The ability to arouse is critical physiologically, and a leading hypothesis is that failure to arouse makes an infant vulnerable to SIDS,” they wrote.
Dr. Moon and Dr. Hauck also noted that the AAP’s recommendation on room-sharing without bed-sharing is based on studies conducted in England, New Zealand, and Scotland showing that room-sharing lowers the risk of SIDS, compared with solitary sleeping.
“More recent, unpublished data from the New Zealand Sudden and Unexplained Death in Infancy study show similar protection from room-sharing, with an adjusted odds ratio of 0.36 (95% confidence interval, 0.19-0.71) for room-sharing infants compared with solitary-sleeping infants (E. Mitchell, MBBS, personal communication, 2016),” they wrote. “Because none of these studies stratified the risk by infant age in months, it is difficult to determine the optimal endpoint for room-sharing.
“We strongly support more research, both about the physiology of infant sleep and arousal for room-sharing infants and about the consequences of room-sharing on parental and child sleep.”
Dr. Moon and Dr. Hauck are with the University of Virginia, Charlottesville. They had no relevant disclosures.
The study by Dr. Paul and his associates is an important contribution to the literature, wrote Rachel Y. Moon, MD, and Fern R. Hauck, MD, in an accompanying editorial (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-1323). However, they said, more research is needed.
For example, it is unclear whether sleep consolidation in young infants is preferable from a physiologic perspective. “The ability to arouse is critical physiologically, and a leading hypothesis is that failure to arouse makes an infant vulnerable to SIDS,” they wrote.
Dr. Moon and Dr. Hauck also noted that the AAP’s recommendation on room-sharing without bed-sharing is based on studies conducted in England, New Zealand, and Scotland showing that room-sharing lowers the risk of SIDS, compared with solitary sleeping.
“More recent, unpublished data from the New Zealand Sudden and Unexplained Death in Infancy study show similar protection from room-sharing, with an adjusted odds ratio of 0.36 (95% confidence interval, 0.19-0.71) for room-sharing infants compared with solitary-sleeping infants (E. Mitchell, MBBS, personal communication, 2016),” they wrote. “Because none of these studies stratified the risk by infant age in months, it is difficult to determine the optimal endpoint for room-sharing.
“We strongly support more research, both about the physiology of infant sleep and arousal for room-sharing infants and about the consequences of room-sharing on parental and child sleep.”
Dr. Moon and Dr. Hauck are with the University of Virginia, Charlottesville. They had no relevant disclosures.
Infants who slept in their own rooms by age 9 months slept significantly longer and better than those who continued sharing a room with their parents as recommended by the American Academy of Pediatrics, the authors of a prospective study of 279 mother-infant dyads reported June 5.
The findings “raise questions about the well-intended AAP recommendation that room-sharing should ideally occur for all infants until their first birthday,” wrote Ian M. Paul, MD, of Penn State University, Hershey, and his associates (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-0122). “Perhaps our most troubling finding was that room-sharing was associated with overnight transitions to bed-sharing, which is strongly discouraged by the AAP.”
Insufficient sleep leads to excess weight gain during infancy and sleep problems later in childhood and has negative implications for parents. “The desire to optimize infant sleep duration and consolidation, however, must be balanced with safe infant sleep,” the researchers emphasized. About 3,500 infants die annually of SIDS and other sleep-related deaths, about 90% of which occur before age 6 months. Currently, however, the AAP’s updated 2016 recommendations advise that infants sleep on a separate surface in their parents’ room for at least the first 6 months and ideally for 1 year (Pediatrics. 2016; 138:e20162938).
To examine relationships among where, how well, and how long infants slept, the researchers analyzed Brief Infant Sleep Questionnaires collected from first-time mothers of term singletons as part of the prospective, single-center Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study.
For 4-month-olds, average reported sleep duration was similar whether they slept alone or in the parental bedroom. Solo sleepers, however, had better sleep consolidation, averaging 46 more minutes of sleep at the longest stretch, compared with room sharers (P = .02). By age 9 months, infants who had slept alone by age 4 months averaged 40 more minutes of nightly sleep than room-sharers and 26 more minutes than infants who began sleeping alone after 4 months of age (P = .008). Furthermore, the average longest sleep span of early solo sleepers was 100 minutes more than that of room-sharers and 45 minutes more than that of infants who began sleeping alone between ages 4 and 9 months (P = .01).
At age 30 months, infants who had slept alone by age 9 months averaged 45 more minutes of nightly sleep than those who had shared a room (P = .004). Room-sharing at 4 months also was tied to a two-fold greater odds of having pillows, blankets, or other unsafe objects on the sleep surface, the researchers said. Together, the findings support revising the AAP recommendation until evidence conclusively supports it, they concluded.
The study’s funders included Penn State University, Hershey; Penn State Children’s Hospital; the U.S. Department of Agriculture; the Penn State Clinical and Translational Science Institute, and the National Institutes of Health/National Center for Advancing Translational Sciences. The investigators reported having no conflicts of interest.
Infants who slept in their own rooms by age 9 months slept significantly longer and better than those who continued sharing a room with their parents as recommended by the American Academy of Pediatrics, the authors of a prospective study of 279 mother-infant dyads reported June 5.
The findings “raise questions about the well-intended AAP recommendation that room-sharing should ideally occur for all infants until their first birthday,” wrote Ian M. Paul, MD, of Penn State University, Hershey, and his associates (Pediatrics. 2017 Jun 5. doi: 10.1542/peds.2017-0122). “Perhaps our most troubling finding was that room-sharing was associated with overnight transitions to bed-sharing, which is strongly discouraged by the AAP.”
Insufficient sleep leads to excess weight gain during infancy and sleep problems later in childhood and has negative implications for parents. “The desire to optimize infant sleep duration and consolidation, however, must be balanced with safe infant sleep,” the researchers emphasized. About 3,500 infants die annually of SIDS and other sleep-related deaths, about 90% of which occur before age 6 months. Currently, however, the AAP’s updated 2016 recommendations advise that infants sleep on a separate surface in their parents’ room for at least the first 6 months and ideally for 1 year (Pediatrics. 2016; 138:e20162938).
To examine relationships among where, how well, and how long infants slept, the researchers analyzed Brief Infant Sleep Questionnaires collected from first-time mothers of term singletons as part of the prospective, single-center Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study.
For 4-month-olds, average reported sleep duration was similar whether they slept alone or in the parental bedroom. Solo sleepers, however, had better sleep consolidation, averaging 46 more minutes of sleep at the longest stretch, compared with room sharers (P = .02). By age 9 months, infants who had slept alone by age 4 months averaged 40 more minutes of nightly sleep than room-sharers and 26 more minutes than infants who began sleeping alone after 4 months of age (P = .008). Furthermore, the average longest sleep span of early solo sleepers was 100 minutes more than that of room-sharers and 45 minutes more than that of infants who began sleeping alone between ages 4 and 9 months (P = .01).
At age 30 months, infants who had slept alone by age 9 months averaged 45 more minutes of nightly sleep than those who had shared a room (P = .004). Room-sharing at 4 months also was tied to a two-fold greater odds of having pillows, blankets, or other unsafe objects on the sleep surface, the researchers said. Together, the findings support revising the AAP recommendation until evidence conclusively supports it, they concluded.
The study’s funders included Penn State University, Hershey; Penn State Children’s Hospital; the U.S. Department of Agriculture; the Penn State Clinical and Translational Science Institute, and the National Institutes of Health/National Center for Advancing Translational Sciences. The investigators reported having no conflicts of interest.
FROM PEDIATRICS
Key clinical point: Infants who slept in their own room by age 4 months slept significantly longer and better than those who continued sharing a room with their parents as recommended by the American Academy of Pediatrics.
Major finding: By age 9 months, infants who had slept alone by age 4 months averaged 40 more minutes of nightly sleep than room sharers and 26 more minutes than infants who began sleeping alone after 4 months of age (P = .008). Furthermore, the average longest sleep span of early solo sleepers was 100 minutes more than that of room-sharers and 45 minutes more than that of infants who began sleeping alone between ages 4 and 9 months (P = .01).
Data source: Secondary analyses of 279 mother-infant dyads from the single-center, prospective Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study.
Disclosures: The study funders included Penn State University, Hershey; Penn State Children’s Hospital; the U.S. Department of Agriculture; the Penn State Clinical and Translational Science Institute, and the National Institutes of Health/National Center for Advancing Translational Sciences. The investigators reported having no conflicts of interest.
Severe health conditions decrease among childhood cancer survivors

CHICAGO—The 15-year cumulative incidence of severe health conditions for survivors of childhood cancer has decreased over the past 30 years, from 12.7% for those diagnosed in the 1970s to 10.1% and 8.9% for those diagnosed in the 1980s and 1990s, respectively. And the decreases were greatest for patients with Wilms’ tumor and Hodgkin lymphoma (HL), followed by patients with astrocytoma, non-Hodgkin lymphoma (NHL), and acute lymphoblastic leukemia (ALL).
Investigators of the Childhood Cancer Survivor Study (CCSS) undertook a retrospective cohort analysis of children aged 0 – 14 years diagnosed with cancer between 1970 and 1999. Their goal was to determine whether cancer therapy modifications have maintained cure rates while decreasing the risk of late effects of therapy.
Todd M. Gibson, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, presented the findings at the 2017 annual meeting of the American Society for Clinical Oncology (ASCO) as abstract LBA10500.
Researchers analyzed data from 23,600 childhood cancer survivors in the CCSS who were alive 5 years after diagnosis. The patients had leukemia, lymphoma, CNS malignancies, Wilms tumor, neuroblastoma, or soft-tissue/bone sarcoma.
Dr Gibson noted that while 83% of children with a malignancy achieve a 5-year survival, more than half develop at least one severe, disabling, life-threatening health condition by age 50.
The survivors were a median age at last follow-up of 28 years (range, 5-63) and the median time since diagnosis was 21 years (range, 5-43).
The investigators found significant decreases in severe health conditions in 6 diagnostic groups:
- Wilms tumor, decreased from 13% to 5% (P<0.0001)
- HL, decreased from 18% to 11% (P<0.0001)
- Astrocytoma, decreased from 15% to 9% (P=0.004)
- NHL, decreased from 10% to 6% (P=0.04)
- ALL, decreased from 9% to 7% (P=0.002)
- Ewings sarcoma, decreased from 19% to 10% (P=0.01)
They found no reductions in subsequent severe health conditions among survivors of neuroblastoma, acute myeloid leukemia (AML), soft tissue sarcoma, or osteosarcoma.
The investigators believe the decreases were driven mainly by a reduced incidence of endocrine conditions, subsequent malignant neoplasms, gastrointestinal and neurological conditions, but not cardiac or pulmonary conditions.
They also analyzed the reduction in treatment intensities by decade for different diseases and found they correlated with the reduced incidence of serious chronic health conditions by 15 years after diagnosis.
The National Institutes of Health funded the study.
CHICAGO—The 15-year cumulative incidence of severe health conditions for survivors of childhood cancer has decreased over the past 30 years, from 12.7% for those diagnosed in the 1970s to 10.1% and 8.9% for those diagnosed in the 1980s and 1990s, respectively. And the decreases were greatest for patients with Wilms’ tumor and Hodgkin lymphoma (HL), followed by patients with astrocytoma, non-Hodgkin lymphoma (NHL), and acute lymphoblastic leukemia (ALL).
Investigators of the Childhood Cancer Survivor Study (CCSS) undertook a retrospective cohort analysis of children aged 0 – 14 years diagnosed with cancer between 1970 and 1999. Their goal was to determine whether cancer therapy modifications have maintained cure rates while decreasing the risk of late effects of therapy.
Todd M. Gibson, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, presented the findings at the 2017 annual meeting of the American Society for Clinical Oncology (ASCO) as abstract LBA10500.
Researchers analyzed data from 23,600 childhood cancer survivors in the CCSS who were alive 5 years after diagnosis. The patients had leukemia, lymphoma, CNS malignancies, Wilms tumor, neuroblastoma, or soft-tissue/bone sarcoma.
Dr Gibson noted that while 83% of children with a malignancy achieve a 5-year survival, more than half develop at least one severe, disabling, life-threatening health condition by age 50.
The survivors were a median age at last follow-up of 28 years (range, 5-63) and the median time since diagnosis was 21 years (range, 5-43).
The investigators found significant decreases in severe health conditions in 6 diagnostic groups:
- Wilms tumor, decreased from 13% to 5% (P<0.0001)
- HL, decreased from 18% to 11% (P<0.0001)
- Astrocytoma, decreased from 15% to 9% (P=0.004)
- NHL, decreased from 10% to 6% (P=0.04)
- ALL, decreased from 9% to 7% (P=0.002)
- Ewings sarcoma, decreased from 19% to 10% (P=0.01)
They found no reductions in subsequent severe health conditions among survivors of neuroblastoma, acute myeloid leukemia (AML), soft tissue sarcoma, or osteosarcoma.
The investigators believe the decreases were driven mainly by a reduced incidence of endocrine conditions, subsequent malignant neoplasms, gastrointestinal and neurological conditions, but not cardiac or pulmonary conditions.
They also analyzed the reduction in treatment intensities by decade for different diseases and found they correlated with the reduced incidence of serious chronic health conditions by 15 years after diagnosis.
The National Institutes of Health funded the study.
CHICAGO—The 15-year cumulative incidence of severe health conditions for survivors of childhood cancer has decreased over the past 30 years, from 12.7% for those diagnosed in the 1970s to 10.1% and 8.9% for those diagnosed in the 1980s and 1990s, respectively. And the decreases were greatest for patients with Wilms’ tumor and Hodgkin lymphoma (HL), followed by patients with astrocytoma, non-Hodgkin lymphoma (NHL), and acute lymphoblastic leukemia (ALL).
Investigators of the Childhood Cancer Survivor Study (CCSS) undertook a retrospective cohort analysis of children aged 0 – 14 years diagnosed with cancer between 1970 and 1999. Their goal was to determine whether cancer therapy modifications have maintained cure rates while decreasing the risk of late effects of therapy.
Todd M. Gibson, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, presented the findings at the 2017 annual meeting of the American Society for Clinical Oncology (ASCO) as abstract LBA10500.
Researchers analyzed data from 23,600 childhood cancer survivors in the CCSS who were alive 5 years after diagnosis. The patients had leukemia, lymphoma, CNS malignancies, Wilms tumor, neuroblastoma, or soft-tissue/bone sarcoma.
Dr Gibson noted that while 83% of children with a malignancy achieve a 5-year survival, more than half develop at least one severe, disabling, life-threatening health condition by age 50.
The survivors were a median age at last follow-up of 28 years (range, 5-63) and the median time since diagnosis was 21 years (range, 5-43).
The investigators found significant decreases in severe health conditions in 6 diagnostic groups:
- Wilms tumor, decreased from 13% to 5% (P<0.0001)
- HL, decreased from 18% to 11% (P<0.0001)
- Astrocytoma, decreased from 15% to 9% (P=0.004)
- NHL, decreased from 10% to 6% (P=0.04)
- ALL, decreased from 9% to 7% (P=0.002)
- Ewings sarcoma, decreased from 19% to 10% (P=0.01)
They found no reductions in subsequent severe health conditions among survivors of neuroblastoma, acute myeloid leukemia (AML), soft tissue sarcoma, or osteosarcoma.
The investigators believe the decreases were driven mainly by a reduced incidence of endocrine conditions, subsequent malignant neoplasms, gastrointestinal and neurological conditions, but not cardiac or pulmonary conditions.
They also analyzed the reduction in treatment intensities by decade for different diseases and found they correlated with the reduced incidence of serious chronic health conditions by 15 years after diagnosis.
The National Institutes of Health funded the study.
Severe health conditions decline in childhood cancer survivors
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have steadily declined, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study, funded by the National Institutes of Health.
For all childhood cancer survivors, the 15-year cumulative incidence of severe health conditions decreased from 12.7% in those diagnosed in the 1970s, to 10.1% in the 1980s, and to 8.8% among those diagnosed in the 1990s (per 10 years: hazard ratio, 0.84 [95% confidence interval, 0.80-0.89]), Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, reported at a press conference at the annual meeting of the American Society of Clinical Oncology.
The association with diagnosis decade was attenuated (HR, 0.92 [95% CI, 0.85-1.00]) when detailed treatment data were included in the model, indicating that treatment reductions mediated risk.
Changes in childhood cancer treatment protocols to reduce the intensity of therapy – along with improved screening and early detection – have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity, Dr. Gibson said.
As the data address children diagnosed over 15 years ago, it is likely that improvements since then in determining patient risk and targeting therapy might result in further incremental improvements, he said in an interview.
By cancer type, severe health problems by 15 years after diagnosis decreased from 13% to 5% among survivors of Wilms’ tumor, from 18% to 11% among survivors of Hodgkin lymphoma, from 15% to 9% among survivors of astrocytoma, from 10% to 6% among survivors of non-Hodgkin lymphoma, and from 9% to 7% among survivors of acute lymphoblastic leukemia. The conclusions are based on the incidence of severe, disabling/life-threatening, or fatal chronic health conditions (Common Terminology Criteria for Adverse Events, grades 3-5) among 5-year survivors diagnosed prior to age 21 years from 1970 through 1999.
Adjusted for sex and attained age, significant reduction in risk over time was found among survivors of Wilms tumor (HR, 0.57 [95% CI, 0.46-0.70]), Hodgkin lymphoma (HR, 0.75 [95% CI, 0.65-0.85]), astrocytoma (HR, 0.77 [95% CI, 0.64-0.92]), non-Hodgkin lymphoma (HR, 0.79 [95% CI, 0.63-0.99]), and acute lymphoblastic leukemia (HR, 0.86 [95% CI, 0.76-0.98]).
The decreases in serious health conditions were largely driven by a reduced incidence of endocrine conditions (1970s: 4.0% vs. 1990s: 1.6%; HR, 0.66 [95% CI, 0.59-0.73]) and subsequent malignant neoplasms (1970s: 2.4% vs. 1990s: 1.6%; HR, 0.85 [95% CI, 0.76-0.96]).
Gastrointestinal (HR, 0.80 [95% CI, 0.66-0.97]) and neurological conditions (HR, 0.77 [95% CI, 0.65-0.91]) also were reduced, but cardiac and pulmonary conditions were not. Changes in childhood cancer treatment protocols have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity in this population, Dr. Gibson concluded.
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have steadily declined, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study, funded by the National Institutes of Health.
For all childhood cancer survivors, the 15-year cumulative incidence of severe health conditions decreased from 12.7% in those diagnosed in the 1970s, to 10.1% in the 1980s, and to 8.8% among those diagnosed in the 1990s (per 10 years: hazard ratio, 0.84 [95% confidence interval, 0.80-0.89]), Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, reported at a press conference at the annual meeting of the American Society of Clinical Oncology.
The association with diagnosis decade was attenuated (HR, 0.92 [95% CI, 0.85-1.00]) when detailed treatment data were included in the model, indicating that treatment reductions mediated risk.
Changes in childhood cancer treatment protocols to reduce the intensity of therapy – along with improved screening and early detection – have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity, Dr. Gibson said.
As the data address children diagnosed over 15 years ago, it is likely that improvements since then in determining patient risk and targeting therapy might result in further incremental improvements, he said in an interview.
By cancer type, severe health problems by 15 years after diagnosis decreased from 13% to 5% among survivors of Wilms’ tumor, from 18% to 11% among survivors of Hodgkin lymphoma, from 15% to 9% among survivors of astrocytoma, from 10% to 6% among survivors of non-Hodgkin lymphoma, and from 9% to 7% among survivors of acute lymphoblastic leukemia. The conclusions are based on the incidence of severe, disabling/life-threatening, or fatal chronic health conditions (Common Terminology Criteria for Adverse Events, grades 3-5) among 5-year survivors diagnosed prior to age 21 years from 1970 through 1999.
Adjusted for sex and attained age, significant reduction in risk over time was found among survivors of Wilms tumor (HR, 0.57 [95% CI, 0.46-0.70]), Hodgkin lymphoma (HR, 0.75 [95% CI, 0.65-0.85]), astrocytoma (HR, 0.77 [95% CI, 0.64-0.92]), non-Hodgkin lymphoma (HR, 0.79 [95% CI, 0.63-0.99]), and acute lymphoblastic leukemia (HR, 0.86 [95% CI, 0.76-0.98]).
The decreases in serious health conditions were largely driven by a reduced incidence of endocrine conditions (1970s: 4.0% vs. 1990s: 1.6%; HR, 0.66 [95% CI, 0.59-0.73]) and subsequent malignant neoplasms (1970s: 2.4% vs. 1990s: 1.6%; HR, 0.85 [95% CI, 0.76-0.96]).
Gastrointestinal (HR, 0.80 [95% CI, 0.66-0.97]) and neurological conditions (HR, 0.77 [95% CI, 0.65-0.91]) also were reduced, but cardiac and pulmonary conditions were not. Changes in childhood cancer treatment protocols have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity in this population, Dr. Gibson concluded.
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have steadily declined, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study, funded by the National Institutes of Health.
For all childhood cancer survivors, the 15-year cumulative incidence of severe health conditions decreased from 12.7% in those diagnosed in the 1970s, to 10.1% in the 1980s, and to 8.8% among those diagnosed in the 1990s (per 10 years: hazard ratio, 0.84 [95% confidence interval, 0.80-0.89]), Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, reported at a press conference at the annual meeting of the American Society of Clinical Oncology.
The association with diagnosis decade was attenuated (HR, 0.92 [95% CI, 0.85-1.00]) when detailed treatment data were included in the model, indicating that treatment reductions mediated risk.
Changes in childhood cancer treatment protocols to reduce the intensity of therapy – along with improved screening and early detection – have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity, Dr. Gibson said.
As the data address children diagnosed over 15 years ago, it is likely that improvements since then in determining patient risk and targeting therapy might result in further incremental improvements, he said in an interview.
By cancer type, severe health problems by 15 years after diagnosis decreased from 13% to 5% among survivors of Wilms’ tumor, from 18% to 11% among survivors of Hodgkin lymphoma, from 15% to 9% among survivors of astrocytoma, from 10% to 6% among survivors of non-Hodgkin lymphoma, and from 9% to 7% among survivors of acute lymphoblastic leukemia. The conclusions are based on the incidence of severe, disabling/life-threatening, or fatal chronic health conditions (Common Terminology Criteria for Adverse Events, grades 3-5) among 5-year survivors diagnosed prior to age 21 years from 1970 through 1999.
Adjusted for sex and attained age, significant reduction in risk over time was found among survivors of Wilms tumor (HR, 0.57 [95% CI, 0.46-0.70]), Hodgkin lymphoma (HR, 0.75 [95% CI, 0.65-0.85]), astrocytoma (HR, 0.77 [95% CI, 0.64-0.92]), non-Hodgkin lymphoma (HR, 0.79 [95% CI, 0.63-0.99]), and acute lymphoblastic leukemia (HR, 0.86 [95% CI, 0.76-0.98]).
The decreases in serious health conditions were largely driven by a reduced incidence of endocrine conditions (1970s: 4.0% vs. 1990s: 1.6%; HR, 0.66 [95% CI, 0.59-0.73]) and subsequent malignant neoplasms (1970s: 2.4% vs. 1990s: 1.6%; HR, 0.85 [95% CI, 0.76-0.96]).
Gastrointestinal (HR, 0.80 [95% CI, 0.66-0.97]) and neurological conditions (HR, 0.77 [95% CI, 0.65-0.91]) also were reduced, but cardiac and pulmonary conditions were not. Changes in childhood cancer treatment protocols have not only extended lifespan for many survivors, but also have reduced the incidence of serious chronic morbidity in this population, Dr. Gibson concluded.
mdales@frontlinemedcom.com
On Twitter @maryjodales
AT ASCO 2017
Key clinical point:
Major finding: For all childhood cancer survivors, the 15-year cumulative incidence of severe health conditions decreased from 12.7% in those diagnosed in the 1970s, to 10.1% in the 1980s, and to 8.8% among those diagnosed in the 1990s (per 10 years: HR, 0.84 [95% CI, 0.80-0.89]).
Data source: An analysis of 23,600 participants in the Childhood Cancer Survivor Study.
Disclosures: The study was funded by the National Institutes of Health.
VIDEO: Childhood cancer survivors living longer with fewer severe health problems
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have been steadily declining, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study (CCSS), funded by the National Institutes of Health.
Watch our video interview with lead author Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, who reported the data at a press conference at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have been steadily declining, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study (CCSS), funded by the National Institutes of Health.
Watch our video interview with lead author Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, who reported the data at a press conference at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Severe health problems occurring 5 or more years after diagnosis of a childhood cancer have been steadily declining, based on an analysis of 23,600 participants in the Childhood Cancer Survivor Study (CCSS), funded by the National Institutes of Health.
Watch our video interview with lead author Todd M. Gibson, PhD, of St. Jude Children’s Research Hospital, Memphis, who reported the data at a press conference at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mdales@frontlinemedcom.com
On Twitter @maryjodales
AT ASCO 2017

Differences emerge in new guidelines for managing FN in kids

A multidisciplinary, international panel of experts has updated earlier clinical practice guidelines on managing fever and neutropenia (FN) in children with cancer and in those undergoing hematopoietic stem cell transplantation (HSCT). And while most of the recommendations remained unchanged from the 2012 guidelines, a few key differences emerged. The changes included addition of a 4th generation cephalosporin for empirical antifungal therapy and refinements in risk stratification for invasive fungal disease (IFD), among others.
The new guidelines were published by The International Pediatric Fever and Neutropenia Guideline Panel in the Journal of Clinical Oncology.
The recommendations were organized into 3 major sections: initial presentation, ongoing management, and empirical antifungal therapy. The guidelines panel followed procedures previously validated for creating evidence-based guidelines and used the Appraisal of Guidelines for Research & Evaluation II instrument as a framework.
For the initial presentation of FN, the panel increased the quality of evidence from low to moderate in the recommendation to obtain peripheral blood cultures concurrent with central venous catheter cultures.
In the treatment of FN, the panel added a 4th-generation cephalosporin as empirical therapy in high-risk FN.
The panel refined the IFD risk factors and decreased the quality of evidence from moderate to low. Children with acute myeloid leukemia (AML), high-risk acute lymphoblastic leukemia (ALL), relapsed acute leukemia, those undergoing allogeneic HSCT, those with prolonged neutropenia, and those receiving high-dose corticosteroids are at high risk of IFD. All others should be categorized as IFD low risk.
The panel suggested serum galactomannan not be used to guide empirical antifungal management for prolonged FN lasting 96 hours or more in high-risk IFD patients. GM does not rule out non-Aspergillus molds, and therefore high negative values provide less useful predictions. Previously, the use of galactomannan was a weak recommendation.
The panel added a new recommendation against using fungal polymerase chain reaction (PCR) testing in blood. They explained PCR testing provides poor positive predictive values and negative predictive values are not sufficiently high to be clinically useful. Also, PCR testing is not yet standardized.
Another new recommendation is the addition of imaging of the abdomen in patients without localizing signs or symptoms. Even though the ideal imaging modality is not known, ultrasound is readily available, not associated with radiation exposure, and usually does not require sedation. For these reasons, the panel said it is preferable to computed tomography or magnetic resonance imaging.
The panel also changed a previously weak recommendation to administer empirical therapy for IFD low-risk patients with prolonged FN to a weak recommendation against administering therapy for these patients.
The panel's recommendations and their rationale can be found in the JCO article.
The guidelines update was supported by meeting grants from the Canadian Institutes of Health Research and the Garron Comprehensive Cancer Centre. ![]()
A multidisciplinary, international panel of experts has updated earlier clinical practice guidelines on managing fever and neutropenia (FN) in children with cancer and in those undergoing hematopoietic stem cell transplantation (HSCT). And while most of the recommendations remained unchanged from the 2012 guidelines, a few key differences emerged. The changes included addition of a 4th generation cephalosporin for empirical antifungal therapy and refinements in risk stratification for invasive fungal disease (IFD), among others.
The new guidelines were published by The International Pediatric Fever and Neutropenia Guideline Panel in the Journal of Clinical Oncology.
The recommendations were organized into 3 major sections: initial presentation, ongoing management, and empirical antifungal therapy. The guidelines panel followed procedures previously validated for creating evidence-based guidelines and used the Appraisal of Guidelines for Research & Evaluation II instrument as a framework.
For the initial presentation of FN, the panel increased the quality of evidence from low to moderate in the recommendation to obtain peripheral blood cultures concurrent with central venous catheter cultures.
In the treatment of FN, the panel added a 4th-generation cephalosporin as empirical therapy in high-risk FN.
The panel refined the IFD risk factors and decreased the quality of evidence from moderate to low. Children with acute myeloid leukemia (AML), high-risk acute lymphoblastic leukemia (ALL), relapsed acute leukemia, those undergoing allogeneic HSCT, those with prolonged neutropenia, and those receiving high-dose corticosteroids are at high risk of IFD. All others should be categorized as IFD low risk.
The panel suggested serum galactomannan not be used to guide empirical antifungal management for prolonged FN lasting 96 hours or more in high-risk IFD patients. GM does not rule out non-Aspergillus molds, and therefore high negative values provide less useful predictions. Previously, the use of galactomannan was a weak recommendation.
The panel added a new recommendation against using fungal polymerase chain reaction (PCR) testing in blood. They explained PCR testing provides poor positive predictive values and negative predictive values are not sufficiently high to be clinically useful. Also, PCR testing is not yet standardized.
Another new recommendation is the addition of imaging of the abdomen in patients without localizing signs or symptoms. Even though the ideal imaging modality is not known, ultrasound is readily available, not associated with radiation exposure, and usually does not require sedation. For these reasons, the panel said it is preferable to computed tomography or magnetic resonance imaging.
The panel also changed a previously weak recommendation to administer empirical therapy for IFD low-risk patients with prolonged FN to a weak recommendation against administering therapy for these patients.
The panel's recommendations and their rationale can be found in the JCO article.
The guidelines update was supported by meeting grants from the Canadian Institutes of Health Research and the Garron Comprehensive Cancer Centre. ![]()
A multidisciplinary, international panel of experts has updated earlier clinical practice guidelines on managing fever and neutropenia (FN) in children with cancer and in those undergoing hematopoietic stem cell transplantation (HSCT). And while most of the recommendations remained unchanged from the 2012 guidelines, a few key differences emerged. The changes included addition of a 4th generation cephalosporin for empirical antifungal therapy and refinements in risk stratification for invasive fungal disease (IFD), among others.
The new guidelines were published by The International Pediatric Fever and Neutropenia Guideline Panel in the Journal of Clinical Oncology.
The recommendations were organized into 3 major sections: initial presentation, ongoing management, and empirical antifungal therapy. The guidelines panel followed procedures previously validated for creating evidence-based guidelines and used the Appraisal of Guidelines for Research & Evaluation II instrument as a framework.
For the initial presentation of FN, the panel increased the quality of evidence from low to moderate in the recommendation to obtain peripheral blood cultures concurrent with central venous catheter cultures.
In the treatment of FN, the panel added a 4th-generation cephalosporin as empirical therapy in high-risk FN.
The panel refined the IFD risk factors and decreased the quality of evidence from moderate to low. Children with acute myeloid leukemia (AML), high-risk acute lymphoblastic leukemia (ALL), relapsed acute leukemia, those undergoing allogeneic HSCT, those with prolonged neutropenia, and those receiving high-dose corticosteroids are at high risk of IFD. All others should be categorized as IFD low risk.
The panel suggested serum galactomannan not be used to guide empirical antifungal management for prolonged FN lasting 96 hours or more in high-risk IFD patients. GM does not rule out non-Aspergillus molds, and therefore high negative values provide less useful predictions. Previously, the use of galactomannan was a weak recommendation.
The panel added a new recommendation against using fungal polymerase chain reaction (PCR) testing in blood. They explained PCR testing provides poor positive predictive values and negative predictive values are not sufficiently high to be clinically useful. Also, PCR testing is not yet standardized.
Another new recommendation is the addition of imaging of the abdomen in patients without localizing signs or symptoms. Even though the ideal imaging modality is not known, ultrasound is readily available, not associated with radiation exposure, and usually does not require sedation. For these reasons, the panel said it is preferable to computed tomography or magnetic resonance imaging.
The panel also changed a previously weak recommendation to administer empirical therapy for IFD low-risk patients with prolonged FN to a weak recommendation against administering therapy for these patients.
The panel's recommendations and their rationale can be found in the JCO article.
The guidelines update was supported by meeting grants from the Canadian Institutes of Health Research and the Garron Comprehensive Cancer Centre. ![]()
Caffeine therapy of VLBW neonates reduces later motor impairment
SAN FRANCISCO – The 11-year follow-up results of the Caffeine for Apnea of Prematurity randomized, placebo-controlled trial has established the benefits of methylated xanthine therapy in the form of caffeine for very-low-birth-weight (VLBW) neonates in lessening the risk of motor impairment.
“The latest findings bolster the value of caffeine therapy to address apnea of prematurity in VLBW neonates. The CAP trial has provided compelling evidence for the use of caffeine even before this latest finding of improved motor function at age 11 years,” said presenter and the CAP trial’s principal investigator Barbara Schmidt, MD, of McMaster University, Hamilton, Ont.
At least 5 of every 1,000 live-born babies are very premature with a VLBW. Up of 40% die or survive with lasting disabilities. One cause of mortality or disability is apnea. Apnea can be lessened by treatment with methylxanthines such as caffeine, she noted. However, at the time the CAP trial began, it was unclear whether the therapy posed a danger by worsening the damage caused by lack of oxygen.
“Very few studies have followed more recent cohorts of very preterm infants to middle school age. Therefore, it was difficult to anticipate actual rates of functional impairment, and the possible effect of caffeine on those rates,” said Dr. Schmidt.
As reported about a decade ago, the CAP trial involving VLBW infants randomized to caffeine therapy or placebo established the short-term safety and effectiveness of the therapy in terms of reducing cerebral palsy and cognitive delay (N Engl J Med. 2007;357:1893-902).
Follow-ups at 18 months and 5 years revealed the benefits of caffeine therapy in reducing the rates of bronchopulmonary dysplasia, severe retinopathy, and neurodevelopmental disability. The present follow-up data assessed academic performance, motor function, and behavior in 1,202 children with a median age of 11 years. Of these, 602 had received caffeine therapy and 600 had been randomized to the placebo group. Data at age 11 years was available for 457 and 463 of the children randomized to caffeine therapy or placebo, respectively.
The primary outcome was functional impairment, which was indicated by at least one of poor academic performance (with at least one standard score more than two standard deviations below the mean on the Wide Range Achievement Test, 4th edition), motor impairment (percentile rank of 5 or less on the Movement Assessment Battery for Children, Second Edition), and behavior problems (Total Problem T score more than two standard deviations above the mean on the Child Behavior Checklist).
Functional impairment was evident in 145 the 457 (32%) children who had received caffeine therapy and 174 of the 463 (38%) who had not. The rates of 32% and 38% were statistically similar (P = .07). In the individual functional outcomes, the caffeine and placebo groups also were similar in terms of poor academic performance (14% vs. 13%; P = .58) and behavior (11% vs. 8%, respectively; P = .22).
However, caffeine therapy was associated with a reduced risk of motor impairment at age 11 years, compared with those in the placebo group (20% vs. 28%, respectively; odds ratio [OR], 0.66; 95% confidence interval [CI], 0.48-0.90; P = .009). The number of children needed to treat to lessen motor impairment in one child was 13 (95% CI, 8-42).
“Caffeine therapy for apnea of prematurity did not significantly reduce the combined rate of academic, motor, and behavioral impairments at age 11 years. However, caffeine therapy reduced the risk of motor impairment 11 years later,” said Dr. Schmidt. Whether caffeine therapy using higher doses or longer treatment duration is equally risk free is uncertain and further studies, which are not planned, would be needed, she said.
These 11-year follow-up findings of the CAP trial were published online in JAMA Pediatrics (2017, Apr 24. doi: 10.1001/jamapediatrics.2017.0238).
The sponsor of study was McMaster University. The study was funded by the Canadian Institutes of Health Research and the National Health and Medical Research Council of Australia. Dr. Schmidt had no relevant financial disclosures to report.
SAN FRANCISCO – The 11-year follow-up results of the Caffeine for Apnea of Prematurity randomized, placebo-controlled trial has established the benefits of methylated xanthine therapy in the form of caffeine for very-low-birth-weight (VLBW) neonates in lessening the risk of motor impairment.
“The latest findings bolster the value of caffeine therapy to address apnea of prematurity in VLBW neonates. The CAP trial has provided compelling evidence for the use of caffeine even before this latest finding of improved motor function at age 11 years,” said presenter and the CAP trial’s principal investigator Barbara Schmidt, MD, of McMaster University, Hamilton, Ont.
At least 5 of every 1,000 live-born babies are very premature with a VLBW. Up of 40% die or survive with lasting disabilities. One cause of mortality or disability is apnea. Apnea can be lessened by treatment with methylxanthines such as caffeine, she noted. However, at the time the CAP trial began, it was unclear whether the therapy posed a danger by worsening the damage caused by lack of oxygen.
“Very few studies have followed more recent cohorts of very preterm infants to middle school age. Therefore, it was difficult to anticipate actual rates of functional impairment, and the possible effect of caffeine on those rates,” said Dr. Schmidt.
As reported about a decade ago, the CAP trial involving VLBW infants randomized to caffeine therapy or placebo established the short-term safety and effectiveness of the therapy in terms of reducing cerebral palsy and cognitive delay (N Engl J Med. 2007;357:1893-902).
Follow-ups at 18 months and 5 years revealed the benefits of caffeine therapy in reducing the rates of bronchopulmonary dysplasia, severe retinopathy, and neurodevelopmental disability. The present follow-up data assessed academic performance, motor function, and behavior in 1,202 children with a median age of 11 years. Of these, 602 had received caffeine therapy and 600 had been randomized to the placebo group. Data at age 11 years was available for 457 and 463 of the children randomized to caffeine therapy or placebo, respectively.
The primary outcome was functional impairment, which was indicated by at least one of poor academic performance (with at least one standard score more than two standard deviations below the mean on the Wide Range Achievement Test, 4th edition), motor impairment (percentile rank of 5 or less on the Movement Assessment Battery for Children, Second Edition), and behavior problems (Total Problem T score more than two standard deviations above the mean on the Child Behavior Checklist).
Functional impairment was evident in 145 the 457 (32%) children who had received caffeine therapy and 174 of the 463 (38%) who had not. The rates of 32% and 38% were statistically similar (P = .07). In the individual functional outcomes, the caffeine and placebo groups also were similar in terms of poor academic performance (14% vs. 13%; P = .58) and behavior (11% vs. 8%, respectively; P = .22).
However, caffeine therapy was associated with a reduced risk of motor impairment at age 11 years, compared with those in the placebo group (20% vs. 28%, respectively; odds ratio [OR], 0.66; 95% confidence interval [CI], 0.48-0.90; P = .009). The number of children needed to treat to lessen motor impairment in one child was 13 (95% CI, 8-42).
“Caffeine therapy for apnea of prematurity did not significantly reduce the combined rate of academic, motor, and behavioral impairments at age 11 years. However, caffeine therapy reduced the risk of motor impairment 11 years later,” said Dr. Schmidt. Whether caffeine therapy using higher doses or longer treatment duration is equally risk free is uncertain and further studies, which are not planned, would be needed, she said.
These 11-year follow-up findings of the CAP trial were published online in JAMA Pediatrics (2017, Apr 24. doi: 10.1001/jamapediatrics.2017.0238).
The sponsor of study was McMaster University. The study was funded by the Canadian Institutes of Health Research and the National Health and Medical Research Council of Australia. Dr. Schmidt had no relevant financial disclosures to report.
SAN FRANCISCO – The 11-year follow-up results of the Caffeine for Apnea of Prematurity randomized, placebo-controlled trial has established the benefits of methylated xanthine therapy in the form of caffeine for very-low-birth-weight (VLBW) neonates in lessening the risk of motor impairment.
“The latest findings bolster the value of caffeine therapy to address apnea of prematurity in VLBW neonates. The CAP trial has provided compelling evidence for the use of caffeine even before this latest finding of improved motor function at age 11 years,” said presenter and the CAP trial’s principal investigator Barbara Schmidt, MD, of McMaster University, Hamilton, Ont.
At least 5 of every 1,000 live-born babies are very premature with a VLBW. Up of 40% die or survive with lasting disabilities. One cause of mortality or disability is apnea. Apnea can be lessened by treatment with methylxanthines such as caffeine, she noted. However, at the time the CAP trial began, it was unclear whether the therapy posed a danger by worsening the damage caused by lack of oxygen.
“Very few studies have followed more recent cohorts of very preterm infants to middle school age. Therefore, it was difficult to anticipate actual rates of functional impairment, and the possible effect of caffeine on those rates,” said Dr. Schmidt.
As reported about a decade ago, the CAP trial involving VLBW infants randomized to caffeine therapy or placebo established the short-term safety and effectiveness of the therapy in terms of reducing cerebral palsy and cognitive delay (N Engl J Med. 2007;357:1893-902).
Follow-ups at 18 months and 5 years revealed the benefits of caffeine therapy in reducing the rates of bronchopulmonary dysplasia, severe retinopathy, and neurodevelopmental disability. The present follow-up data assessed academic performance, motor function, and behavior in 1,202 children with a median age of 11 years. Of these, 602 had received caffeine therapy and 600 had been randomized to the placebo group. Data at age 11 years was available for 457 and 463 of the children randomized to caffeine therapy or placebo, respectively.
The primary outcome was functional impairment, which was indicated by at least one of poor academic performance (with at least one standard score more than two standard deviations below the mean on the Wide Range Achievement Test, 4th edition), motor impairment (percentile rank of 5 or less on the Movement Assessment Battery for Children, Second Edition), and behavior problems (Total Problem T score more than two standard deviations above the mean on the Child Behavior Checklist).
Functional impairment was evident in 145 the 457 (32%) children who had received caffeine therapy and 174 of the 463 (38%) who had not. The rates of 32% and 38% were statistically similar (P = .07). In the individual functional outcomes, the caffeine and placebo groups also were similar in terms of poor academic performance (14% vs. 13%; P = .58) and behavior (11% vs. 8%, respectively; P = .22).
However, caffeine therapy was associated with a reduced risk of motor impairment at age 11 years, compared with those in the placebo group (20% vs. 28%, respectively; odds ratio [OR], 0.66; 95% confidence interval [CI], 0.48-0.90; P = .009). The number of children needed to treat to lessen motor impairment in one child was 13 (95% CI, 8-42).
“Caffeine therapy for apnea of prematurity did not significantly reduce the combined rate of academic, motor, and behavioral impairments at age 11 years. However, caffeine therapy reduced the risk of motor impairment 11 years later,” said Dr. Schmidt. Whether caffeine therapy using higher doses or longer treatment duration is equally risk free is uncertain and further studies, which are not planned, would be needed, she said.
These 11-year follow-up findings of the CAP trial were published online in JAMA Pediatrics (2017, Apr 24. doi: 10.1001/jamapediatrics.2017.0238).
The sponsor of study was McMaster University. The study was funded by the Canadian Institutes of Health Research and the National Health and Medical Research Council of Australia. Dr. Schmidt had no relevant financial disclosures to report.
AT PAS 17
Key clinical point:
Major finding: At the 11-year follow-up, motor impairment was identified in 20% of those who received caffeine therapy versus 28% of those in the placebo group (P = .009).
Data source: Multicenter, randomized, placebo-controlled trial (NCT00182312).
Disclosures: The sponsor of study was McMaster University. The study was funded by the Canadian Institutes of Health Research and the National Health and Medical Research Council of Australia. Dr. Schmidt had no relevant financial disclosures to report.