User login
Follow-up care for pediatric concussions not heeded in Ontario
reported Liraz Fridman, PhD, of York University, Toronto, and associates.
In a 10-year, retrospective, population-based study, 126,654 children aged 5-18 years presented with concussions to emergency departments and physician offices in Ontario between April 1, 2003, and March 31, 2014. In 2003, 7,126 children were evaluated for a concussion, compared with 21,681 children by 2013.
Limitations to this study include that children treated by athletic therapists or chiropractors would have been missed, and that these data may not generalize across Canada or the United States, they said.
“In Ontario, the rate of follow-up care for concussions nearly tripled in both emergency departments and physician’s offices. Despite this significant improvement over time, more than two-thirds of all child and youth concussion patients still do not receive the minimum standard of care, according to accepted guidelines,” the researchers wrote, adding that the study’s findings suggest that better instructions for health care providers on management of concussion are needed.
SOURCE: Fridman L et al. J Pediatr. 2018;192:184-8
reported Liraz Fridman, PhD, of York University, Toronto, and associates.
In a 10-year, retrospective, population-based study, 126,654 children aged 5-18 years presented with concussions to emergency departments and physician offices in Ontario between April 1, 2003, and March 31, 2014. In 2003, 7,126 children were evaluated for a concussion, compared with 21,681 children by 2013.
Limitations to this study include that children treated by athletic therapists or chiropractors would have been missed, and that these data may not generalize across Canada or the United States, they said.
“In Ontario, the rate of follow-up care for concussions nearly tripled in both emergency departments and physician’s offices. Despite this significant improvement over time, more than two-thirds of all child and youth concussion patients still do not receive the minimum standard of care, according to accepted guidelines,” the researchers wrote, adding that the study’s findings suggest that better instructions for health care providers on management of concussion are needed.
SOURCE: Fridman L et al. J Pediatr. 2018;192:184-8
reported Liraz Fridman, PhD, of York University, Toronto, and associates.
In a 10-year, retrospective, population-based study, 126,654 children aged 5-18 years presented with concussions to emergency departments and physician offices in Ontario between April 1, 2003, and March 31, 2014. In 2003, 7,126 children were evaluated for a concussion, compared with 21,681 children by 2013.
Limitations to this study include that children treated by athletic therapists or chiropractors would have been missed, and that these data may not generalize across Canada or the United States, they said.
“In Ontario, the rate of follow-up care for concussions nearly tripled in both emergency departments and physician’s offices. Despite this significant improvement over time, more than two-thirds of all child and youth concussion patients still do not receive the minimum standard of care, according to accepted guidelines,” the researchers wrote, adding that the study’s findings suggest that better instructions for health care providers on management of concussion are needed.
SOURCE: Fridman L et al. J Pediatr. 2018;192:184-8
FROM THE JOURNAL OF PEDIATRICS
Variants in one gene account for 7% of juvenile myoclonic epilepsy cases
An extremely rare genetic variant that affects the maturation, migration, and death of neurons appears to be responsible for about 7% of cases of juvenile myoclonic epilepsy.
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles, and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the team wrote. “Of 34 affected nonproband family members, 5 (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, 4 (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, 4 (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
Despite the misnomer of intestinal-cell kinase, ICK “is ubiquitous and is expressed in all tissues,” senior study author Antonio Delgado-Escueta, MD, professor of neurology at UCLA, noted in an interview. He said the brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy (JME) “is very subtle, diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain. The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binging protein, has been implicated in JME. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study from the databank analyzed information from 334 families with genetic generalized epilepsies. Among these, 310 patients had adolescent-onset myoclonic seizures and polyspike waves, or had a diagnosis of JME.
The team first performed an exome-wide analysis of four affected members of a large family with genetic JME. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for JME.
A linkage analysis confirmed two candidate genes on chromosome 6p12.1. Further analyses pinpointed a single variant: K305T on the ICK gene. This was present in each of the 12 affected members and 3 unaffected members of the initial family examined. Of those affected, three had JME, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had JME (8%). Of these, nine belonged to families with other affected members. The team tested 24 ICK variants for pathogenicity and determined that 13 exerted significant JME risk, with odds ratios exceeding 5.0.
When the team looked for these 24 variants in the Genome Aggregation Database (gnomAD), the found that 12 were present but extremely rare, and 8 were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. Interestingly, that variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants accounted for 7% of the JME among the 310 cases examined.
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice under light sedation displayed muscle movements similar to human myoclonic seizures that occur upon awakening. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that those pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by a number of private and public grants from within the United States and other countries. Several authors are coholders of patents on EFHC1-based diagnostic and therapeutics that have been licensed to Athena Diagnostics. Several authors also reported receiving honoraria from various pharmaceutical companies.
SOURCE: Bailey J et al. N Engl J Med. 2018;378:1018-28
An extremely rare genetic variant that affects the maturation, migration, and death of neurons appears to be responsible for about 7% of cases of juvenile myoclonic epilepsy.
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles, and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the team wrote. “Of 34 affected nonproband family members, 5 (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, 4 (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, 4 (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
Despite the misnomer of intestinal-cell kinase, ICK “is ubiquitous and is expressed in all tissues,” senior study author Antonio Delgado-Escueta, MD, professor of neurology at UCLA, noted in an interview. He said the brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy (JME) “is very subtle, diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain. The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binging protein, has been implicated in JME. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study from the databank analyzed information from 334 families with genetic generalized epilepsies. Among these, 310 patients had adolescent-onset myoclonic seizures and polyspike waves, or had a diagnosis of JME.
The team first performed an exome-wide analysis of four affected members of a large family with genetic JME. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for JME.
A linkage analysis confirmed two candidate genes on chromosome 6p12.1. Further analyses pinpointed a single variant: K305T on the ICK gene. This was present in each of the 12 affected members and 3 unaffected members of the initial family examined. Of those affected, three had JME, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had JME (8%). Of these, nine belonged to families with other affected members. The team tested 24 ICK variants for pathogenicity and determined that 13 exerted significant JME risk, with odds ratios exceeding 5.0.
When the team looked for these 24 variants in the Genome Aggregation Database (gnomAD), the found that 12 were present but extremely rare, and 8 were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. Interestingly, that variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants accounted for 7% of the JME among the 310 cases examined.
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice under light sedation displayed muscle movements similar to human myoclonic seizures that occur upon awakening. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that those pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by a number of private and public grants from within the United States and other countries. Several authors are coholders of patents on EFHC1-based diagnostic and therapeutics that have been licensed to Athena Diagnostics. Several authors also reported receiving honoraria from various pharmaceutical companies.
SOURCE: Bailey J et al. N Engl J Med. 2018;378:1018-28
An extremely rare genetic variant that affects the maturation, migration, and death of neurons appears to be responsible for about 7% of cases of juvenile myoclonic epilepsy.
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles, and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the team wrote. “Of 34 affected nonproband family members, 5 (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, 4 (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, 4 (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
Despite the misnomer of intestinal-cell kinase, ICK “is ubiquitous and is expressed in all tissues,” senior study author Antonio Delgado-Escueta, MD, professor of neurology at UCLA, noted in an interview. He said the brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy (JME) “is very subtle, diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain. The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binging protein, has been implicated in JME. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study from the databank analyzed information from 334 families with genetic generalized epilepsies. Among these, 310 patients had adolescent-onset myoclonic seizures and polyspike waves, or had a diagnosis of JME.
The team first performed an exome-wide analysis of four affected members of a large family with genetic JME. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for JME.
A linkage analysis confirmed two candidate genes on chromosome 6p12.1. Further analyses pinpointed a single variant: K305T on the ICK gene. This was present in each of the 12 affected members and 3 unaffected members of the initial family examined. Of those affected, three had JME, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had JME (8%). Of these, nine belonged to families with other affected members. The team tested 24 ICK variants for pathogenicity and determined that 13 exerted significant JME risk, with odds ratios exceeding 5.0.
When the team looked for these 24 variants in the Genome Aggregation Database (gnomAD), the found that 12 were present but extremely rare, and 8 were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. Interestingly, that variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants accounted for 7% of the JME among the 310 cases examined.
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice under light sedation displayed muscle movements similar to human myoclonic seizures that occur upon awakening. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that those pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by a number of private and public grants from within the United States and other countries. Several authors are coholders of patents on EFHC1-based diagnostic and therapeutics that have been licensed to Athena Diagnostics. Several authors also reported receiving honoraria from various pharmaceutical companies.
SOURCE: Bailey J et al. N Engl J Med. 2018;378:1018-28
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: ICK variants account for 7% of JME cases.
Study details: Genetic studies comprising one family and 310 epilepsy cases in a database.
Disclosures: The study was funded by a number of private and public grants from within the United States and other countries. Several authors are coholders of patents on EFHC1-based diagnostic and therapeutics that have been licensed to Athena Diagnostics. Several authors also reported receiving honoraria from various pharmaceutical companies.
Source: Bailey J et al. N Engl J Med. 2018;378:1018-28.
Vaccine priming determines teen susceptibility to pertussis
It is the initial type of pertussis vaccine given in infancy – acellular or whole cell – that primes the immune system and determines how soon adolescents become susceptible to pertussis, regardless of later acellular booster vaccination, noted the authors of a new study.
The IgG4 subclass proportion for IgG4-specific antibodies remained lower in patients who had whole-cell pertussis (wP) priming in infancy, even though they had received acellular pertussis booster vaccinations at ages 4 and 9 years, compared with patients who underwent acellular pertussis (aP) priming in infancy. This was true for all vaccine antigens, other than filamentous hemagglutinin and tetanus, 1 year after the preadolescent booster, noted researcher Saskia van der Lee of the National Institute for Public Health and the Environment, Bilthoven, The Netherlands, and her associates.
“ compared to aP-primed children, even after booster vaccinations. This is in line with epidemiological data indicating that adolescents, after aP vaccination in infancy, are more susceptible to pertussis, compared with wP-primed adolescents, though wP-primed individuals become also susceptible over time,” the researchers said.
In addition, children primed with DTwP vaccines have a more Th1-skewed response for pertussis vaccine antigens after receiving a DTap booster vaccine or clinical infection with Bordetella pertussis, whereas children primed with DTaP have a more mixed pertussis-specific Th1/Th2 response, the researchers said. So “new adjuvants that skew the immune response towards a Th1 profile are desired” for better protection against pertussis over time.
SOURCE: van der Lee S et al. Vaccine. 2018 Jan 4;36(2):220-6.
It is the initial type of pertussis vaccine given in infancy – acellular or whole cell – that primes the immune system and determines how soon adolescents become susceptible to pertussis, regardless of later acellular booster vaccination, noted the authors of a new study.
The IgG4 subclass proportion for IgG4-specific antibodies remained lower in patients who had whole-cell pertussis (wP) priming in infancy, even though they had received acellular pertussis booster vaccinations at ages 4 and 9 years, compared with patients who underwent acellular pertussis (aP) priming in infancy. This was true for all vaccine antigens, other than filamentous hemagglutinin and tetanus, 1 year after the preadolescent booster, noted researcher Saskia van der Lee of the National Institute for Public Health and the Environment, Bilthoven, The Netherlands, and her associates.
“ compared to aP-primed children, even after booster vaccinations. This is in line with epidemiological data indicating that adolescents, after aP vaccination in infancy, are more susceptible to pertussis, compared with wP-primed adolescents, though wP-primed individuals become also susceptible over time,” the researchers said.
In addition, children primed with DTwP vaccines have a more Th1-skewed response for pertussis vaccine antigens after receiving a DTap booster vaccine or clinical infection with Bordetella pertussis, whereas children primed with DTaP have a more mixed pertussis-specific Th1/Th2 response, the researchers said. So “new adjuvants that skew the immune response towards a Th1 profile are desired” for better protection against pertussis over time.
SOURCE: van der Lee S et al. Vaccine. 2018 Jan 4;36(2):220-6.
It is the initial type of pertussis vaccine given in infancy – acellular or whole cell – that primes the immune system and determines how soon adolescents become susceptible to pertussis, regardless of later acellular booster vaccination, noted the authors of a new study.
The IgG4 subclass proportion for IgG4-specific antibodies remained lower in patients who had whole-cell pertussis (wP) priming in infancy, even though they had received acellular pertussis booster vaccinations at ages 4 and 9 years, compared with patients who underwent acellular pertussis (aP) priming in infancy. This was true for all vaccine antigens, other than filamentous hemagglutinin and tetanus, 1 year after the preadolescent booster, noted researcher Saskia van der Lee of the National Institute for Public Health and the Environment, Bilthoven, The Netherlands, and her associates.
“ compared to aP-primed children, even after booster vaccinations. This is in line with epidemiological data indicating that adolescents, after aP vaccination in infancy, are more susceptible to pertussis, compared with wP-primed adolescents, though wP-primed individuals become also susceptible over time,” the researchers said.
In addition, children primed with DTwP vaccines have a more Th1-skewed response for pertussis vaccine antigens after receiving a DTap booster vaccine or clinical infection with Bordetella pertussis, whereas children primed with DTaP have a more mixed pertussis-specific Th1/Th2 response, the researchers said. So “new adjuvants that skew the immune response towards a Th1 profile are desired” for better protection against pertussis over time.
SOURCE: van der Lee S et al. Vaccine. 2018 Jan 4;36(2):220-6.
FROM VACCINE
Olopatadine/mometasone combo is safe and effective
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
ORLANDO – Twice-daily treatment with a combination of olopatadine and mometasone showed significant clinical benefit and demonstrated safety for patients with seasonal allergic rhinitis, according to the results of a phase 3 trial.
The combination, known as GSP301, is a fixed-dose nasal spray containing olopatadine, a Food and Drug Adminstration–approved antihistamine, and mometasone, an FDA-approved corticosteroid.
The combination therapy demonstrated statistically significant improvement in scores, compared with those associated with placebo (P less than .001) and olopatadine alone (P = .003). It also showed benefit when compared with mometasone alone (P = .059), Dr. Hampel reported at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Allergy Organization.
“You expect this outcome,” Dr. Hampel said in an interview. “Olopatadine is a good drug, mometasone is a good drug, so you’d expect the combination to be good, and it was.”
Dr. Hampel and his colleagues also analyzed changes in baseline scores for patients in the olopatadine group and the mometasone group and compared those changes with those seen in the placebo group. Patients in the mometasone group experienced statistically significant improvement, compared with those in the placebo group (P = .004), and patients in the olopatadine group also appeared to experienced benefit (P = .076).
Adverse events were similar across all treatment groups, although a slightly higher percentage of patients in the GSP301 group (12.9%) and olopatadine groups (12.5%) experienced adverse events, Dr. Hampel said.
Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies
SOURCE: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point: Twice-daily combination therapy improved reflective total nasal symptom scores better than either component alone.
Major finding: Combination therapy significantly improved total nasal symptom scores (P less than .001).
Study details: Phase 3, double-blind, randomized, parallel-group study of 1,180 patients aged 12 years and older with seasonal allergic rhinitis.
Disclosures: Glenmark Pharmaceuticals sponsored the study. Dr. Hampel reported funding from Glenmark Pharmaceuticals and other pharmaceutical companies.
Source: Hampel F et al. AAAAI/WAO Joint Congress, Abstract 546.
Jump-starting the day
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”

The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”
The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I’ve never been a fan of delayed school start times for high school students. The data just don’t impress me. But mostly I think delayed start times should be just one component of a broad community-wide initiative to address sleep hygiene that includes discussions about bedtimes, after-school schedules, and overuse of electronic devices. And I don’t see those discussions happening.
In most communities, delaying start times for adolescents will mean that younger children will be starting their school days earlier. Buses and drivers are finite and expensive resources that must be shared. Although I have heard it used as an argument against delayed school starts for high schoolers, an earlier start time for grade-school age children is not one of the downsides I include on my list of negatives. In fact, from my perspective, getting youngsters to school early is one of the few advantages of a delayed school start program for high school.
Underwritten by the Reebok athletic footwear manufacturer, the BOKS (Build Our Kids’ Success) program began in 2009 when a group of mothers in Massachusetts organized a before-school activity program in their local grade school (“A before-school exercise program may help children thrive,” by Gretchen Reynolds, New York Times, Feb. 14, 2018). They may have been motivated primarily by the need to survive those difficult morning hours, but clearly they weren’t alone in their concerns, and the concept has spread to include 3,000 schools worldwide.
Hoping to document the anecdotal observations of the program’s success, researchers from Harvard and the Massachusetts General Hospital surveyed children in 24 schools (“Effects of Before-School Physical Activity on Obesity Prevention and Wellness,” Am J Prev Med. 2018. Feb 12. doi: 10.1016/j.amepre.2018.01.017). Participation in the program was voluntary, and the control group consisted of children whose families chose not to participate. Those children in the before-school activity program 3 mornings per week were more likely to have lower body mass index z scores and “demonstrated improvement in their student engagement scores.” The children who participated only 2 days per week had no significant changes in their body mass index scores. However, they did demonstrate “significant improvements in positive affect and vitality/energy.”
The early-morning energy of youth is a given. The problem is that many children find themselves in home environments in which that energy is squandered or at least misdirected. School can be the environment in which that physical exuberance is allowed to run its natural course. We simply need the will to invest in what needs to be done to make it happen.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Does Fish Oil During Pregnancy Help Prevent Asthma in Kids?
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma, and she wants to know if there is anything she can do to reduce her second child’s risk for it. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 According to the CDC, 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreases the risk for atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial, by Palmer et al, which included 706 women, showed no benefit for supplementation.8 The second largest, by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR], 0.37; number needed to treat [NNT], 19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until age 3, which is around the time that asthma can be formally diagnosed—potentially leading to underreporting.8 In addition, the diagnosis of asthma was based on parent report of three episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (rate without sensitization was not reported) was 1.8% in both study groups—much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces asthma in children
This single-center, double-blind RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after age 3, persistent wheeze was termed asthma), determined based on daily diary recordings of five episodes of troublesome lung symptoms within the past six months (each lasting for at least three consecutive days); rescue use of inhaled ß2-agonists; and/or relapse after a three-month course of inhaled glucocorticoids. Secondary outcomes included reduced incidence of respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study, with 95.5% follow-up at three years and 93.1% at five. The children had scheduled pediatric visits at 1 week; at one, three, six, 12, 18, 24, 30, and 36 months; and at 4 and 5 years. They also had acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of mothers who took fish oil had a lower risk for persistent wheeze or asthma at ages 3 to 5, compared to those who received placebo (16.9% vs 23.7%; HR, 0.69; NNT, 14.7). But this effect was significant only in the children whose mothers had baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR, 0.46; NNT, 5.6). Similarly, fish oil supplementation had a greater benefit in children whose mothers had consumed the least EPA and DHA before the start of the study (18.5% vs 32.4%; HR, 0.55; NNT, 7.2).
As for the secondary outcomes, only a reduction in lower respiratory infections was associated with fish oil supplementation compared with placebo (38.8% vs 45.5%; HR, 0.77; NNT, 14.9). There was no reduction in asthma exacerbations, eczema, or risk for sensitization in the fish oil group.
WHAT’S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk for asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2,400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2,700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the US.
CAVEATS
Ideal dose? Which women to treat?
The FDA currently recommends 8 to 12 oz of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study, using 900 mg/d of fish oil, did not show a benefit, whereas there did appear to be a benefit in this study (2,400 mg/d) and the Olsen study (2,700 mg/d).1,8,9 Further research is needed to determine the optimal dosage.
The decreased risk for persistent wheeze or asthma was seen only in the children of women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r, 0.32).1 Therefore, additional screening questions to gauge fish consumption would be useful to identify women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills, additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to four additional pills per day for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[2]: 100-102).
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375(26):2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy. 2004;59(5):469-478.
3. CDC . Asthma. www.cdc.gov/asthma/most_recent_data.htm. Accessed February 1, 2018.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64(1):27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42(6):513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17(2):94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22(7): CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88(1): 167-175.
10. Helgi Library. Fish consumption per capita by country. www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed February 1, 2018.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Fed Regist. 2017;82:6571-6574.
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma, and she wants to know if there is anything she can do to reduce her second child’s risk for it. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 According to the CDC, 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreases the risk for atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial, by Palmer et al, which included 706 women, showed no benefit for supplementation.8 The second largest, by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR], 0.37; number needed to treat [NNT], 19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until age 3, which is around the time that asthma can be formally diagnosed—potentially leading to underreporting.8 In addition, the diagnosis of asthma was based on parent report of three episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (rate without sensitization was not reported) was 1.8% in both study groups—much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces asthma in children
This single-center, double-blind RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after age 3, persistent wheeze was termed asthma), determined based on daily diary recordings of five episodes of troublesome lung symptoms within the past six months (each lasting for at least three consecutive days); rescue use of inhaled ß2-agonists; and/or relapse after a three-month course of inhaled glucocorticoids. Secondary outcomes included reduced incidence of respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study, with 95.5% follow-up at three years and 93.1% at five. The children had scheduled pediatric visits at 1 week; at one, three, six, 12, 18, 24, 30, and 36 months; and at 4 and 5 years. They also had acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of mothers who took fish oil had a lower risk for persistent wheeze or asthma at ages 3 to 5, compared to those who received placebo (16.9% vs 23.7%; HR, 0.69; NNT, 14.7). But this effect was significant only in the children whose mothers had baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR, 0.46; NNT, 5.6). Similarly, fish oil supplementation had a greater benefit in children whose mothers had consumed the least EPA and DHA before the start of the study (18.5% vs 32.4%; HR, 0.55; NNT, 7.2).
As for the secondary outcomes, only a reduction in lower respiratory infections was associated with fish oil supplementation compared with placebo (38.8% vs 45.5%; HR, 0.77; NNT, 14.9). There was no reduction in asthma exacerbations, eczema, or risk for sensitization in the fish oil group.
WHAT’S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk for asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2,400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2,700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the US.
CAVEATS
Ideal dose? Which women to treat?
The FDA currently recommends 8 to 12 oz of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study, using 900 mg/d of fish oil, did not show a benefit, whereas there did appear to be a benefit in this study (2,400 mg/d) and the Olsen study (2,700 mg/d).1,8,9 Further research is needed to determine the optimal dosage.
The decreased risk for persistent wheeze or asthma was seen only in the children of women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r, 0.32).1 Therefore, additional screening questions to gauge fish consumption would be useful to identify women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills, additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to four additional pills per day for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[2]: 100-102).
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma, and she wants to know if there is anything she can do to reduce her second child’s risk for it. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 According to the CDC, 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreases the risk for atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial, by Palmer et al, which included 706 women, showed no benefit for supplementation.8 The second largest, by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR], 0.37; number needed to treat [NNT], 19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until age 3, which is around the time that asthma can be formally diagnosed—potentially leading to underreporting.8 In addition, the diagnosis of asthma was based on parent report of three episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (rate without sensitization was not reported) was 1.8% in both study groups—much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces asthma in children
This single-center, double-blind RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after age 3, persistent wheeze was termed asthma), determined based on daily diary recordings of five episodes of troublesome lung symptoms within the past six months (each lasting for at least three consecutive days); rescue use of inhaled ß2-agonists; and/or relapse after a three-month course of inhaled glucocorticoids. Secondary outcomes included reduced incidence of respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study, with 95.5% follow-up at three years and 93.1% at five. The children had scheduled pediatric visits at 1 week; at one, three, six, 12, 18, 24, 30, and 36 months; and at 4 and 5 years. They also had acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of mothers who took fish oil had a lower risk for persistent wheeze or asthma at ages 3 to 5, compared to those who received placebo (16.9% vs 23.7%; HR, 0.69; NNT, 14.7). But this effect was significant only in the children whose mothers had baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR, 0.46; NNT, 5.6). Similarly, fish oil supplementation had a greater benefit in children whose mothers had consumed the least EPA and DHA before the start of the study (18.5% vs 32.4%; HR, 0.55; NNT, 7.2).
As for the secondary outcomes, only a reduction in lower respiratory infections was associated with fish oil supplementation compared with placebo (38.8% vs 45.5%; HR, 0.77; NNT, 14.9). There was no reduction in asthma exacerbations, eczema, or risk for sensitization in the fish oil group.
WHAT’S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk for asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2,400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2,700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the US.
CAVEATS
Ideal dose? Which women to treat?
The FDA currently recommends 8 to 12 oz of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study, using 900 mg/d of fish oil, did not show a benefit, whereas there did appear to be a benefit in this study (2,400 mg/d) and the Olsen study (2,700 mg/d).1,8,9 Further research is needed to determine the optimal dosage.
The decreased risk for persistent wheeze or asthma was seen only in the children of women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r, 0.32).1 Therefore, additional screening questions to gauge fish consumption would be useful to identify women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills, additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to four additional pills per day for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[2]: 100-102).
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375(26):2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy. 2004;59(5):469-478.
3. CDC . Asthma. www.cdc.gov/asthma/most_recent_data.htm. Accessed February 1, 2018.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64(1):27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42(6):513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17(2):94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22(7): CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88(1): 167-175.
10. Helgi Library. Fish consumption per capita by country. www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed February 1, 2018.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Fed Regist. 2017;82:6571-6574.
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375(26):2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy. 2004;59(5):469-478.
3. CDC . Asthma. www.cdc.gov/asthma/most_recent_data.htm. Accessed February 1, 2018.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64(1):27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42(6):513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17(2):94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22(7): CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88(1): 167-175.
10. Helgi Library. Fish consumption per capita by country. www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed February 1, 2018.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Fed Regist. 2017;82:6571-6574.

Commonality
I grew up in a diversity-free zone. The bubble surrounding Pleasantville, New York, in the 1950s and 1960s didn’t include people of color. We were all middle-class, some upper, some lower, some blue collar, some white collar – but, all of us comfortably in the middle. The children with disabilities must have been hidden in their homes or housed in institutions. They certainly weren’t our classmates. We were spread across the broad Judeo-Christian spectrum. Who knew there were other religions?
Of course, when I left for college I entered another even less inclusive bubble that didn’t admit women.

For many years, the process that brought about this dramatic change was a fortuitous conglomeration of brush wars fought by courageous individuals and minority groups. However, in the last decade or two, the struggle for inclusion has broadened under the banner of diversity, a term once primarily used to describe evolving ecologic populations. In light of this expanding definition, it is not surprising that the American Academy of Pediatrics has begun to consider its role in promoting diversity. As reported in AAP News (Anne Hegland, March 2018) the American Academy of Pediatrics board of directors recently discussed a plan for implementing at “all levels of the Academy” the suggestions of its Task Force on Diversity and Inclusion.
The academy is in the enviable positive of having a membership that agrees in general terms where its priorities should be – the health and welfare of children. It can afford to invest some of its energies in being more inclusive. However, the United States currently is struggling to rediscover a set of priorities that its citizens can agree on. We have politicians who would rather win a battle over their adversaries than address the obvious needs of the country. And, we have journalists who prefer to feast on these battles rather than search for evidence of cooperation. This is not a time to sharpen our focus on how different we are from one another. It is time to raise another flag along side the “diversity” banner. It should read “commonality,” and remind us that while we are celebrating our differences, we must work harder to uncover the core values that we share.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I grew up in a diversity-free zone. The bubble surrounding Pleasantville, New York, in the 1950s and 1960s didn’t include people of color. We were all middle-class, some upper, some lower, some blue collar, some white collar – but, all of us comfortably in the middle. The children with disabilities must have been hidden in their homes or housed in institutions. They certainly weren’t our classmates. We were spread across the broad Judeo-Christian spectrum. Who knew there were other religions?
Of course, when I left for college I entered another even less inclusive bubble that didn’t admit women.
For many years, the process that brought about this dramatic change was a fortuitous conglomeration of brush wars fought by courageous individuals and minority groups. However, in the last decade or two, the struggle for inclusion has broadened under the banner of diversity, a term once primarily used to describe evolving ecologic populations. In light of this expanding definition, it is not surprising that the American Academy of Pediatrics has begun to consider its role in promoting diversity. As reported in AAP News (Anne Hegland, March 2018) the American Academy of Pediatrics board of directors recently discussed a plan for implementing at “all levels of the Academy” the suggestions of its Task Force on Diversity and Inclusion.
The academy is in the enviable positive of having a membership that agrees in general terms where its priorities should be – the health and welfare of children. It can afford to invest some of its energies in being more inclusive. However, the United States currently is struggling to rediscover a set of priorities that its citizens can agree on. We have politicians who would rather win a battle over their adversaries than address the obvious needs of the country. And, we have journalists who prefer to feast on these battles rather than search for evidence of cooperation. This is not a time to sharpen our focus on how different we are from one another. It is time to raise another flag along side the “diversity” banner. It should read “commonality,” and remind us that while we are celebrating our differences, we must work harder to uncover the core values that we share.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
I grew up in a diversity-free zone. The bubble surrounding Pleasantville, New York, in the 1950s and 1960s didn’t include people of color. We were all middle-class, some upper, some lower, some blue collar, some white collar – but, all of us comfortably in the middle. The children with disabilities must have been hidden in their homes or housed in institutions. They certainly weren’t our classmates. We were spread across the broad Judeo-Christian spectrum. Who knew there were other religions?
Of course, when I left for college I entered another even less inclusive bubble that didn’t admit women.
For many years, the process that brought about this dramatic change was a fortuitous conglomeration of brush wars fought by courageous individuals and minority groups. However, in the last decade or two, the struggle for inclusion has broadened under the banner of diversity, a term once primarily used to describe evolving ecologic populations. In light of this expanding definition, it is not surprising that the American Academy of Pediatrics has begun to consider its role in promoting diversity. As reported in AAP News (Anne Hegland, March 2018) the American Academy of Pediatrics board of directors recently discussed a plan for implementing at “all levels of the Academy” the suggestions of its Task Force on Diversity and Inclusion.
The academy is in the enviable positive of having a membership that agrees in general terms where its priorities should be – the health and welfare of children. It can afford to invest some of its energies in being more inclusive. However, the United States currently is struggling to rediscover a set of priorities that its citizens can agree on. We have politicians who would rather win a battle over their adversaries than address the obvious needs of the country. And, we have journalists who prefer to feast on these battles rather than search for evidence of cooperation. This is not a time to sharpen our focus on how different we are from one another. It is time to raise another flag along side the “diversity” banner. It should read “commonality,” and remind us that while we are celebrating our differences, we must work harder to uncover the core values that we share.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
New approaches needed for food allergies in minority children
ORLANDO – compared with their white counterparts, an expert said.
These ethnic groups have higher odds of food sensitization compared with whites, and an analysis of the U.S. National Mortality Database found a higher rate of food-related anaphylaxis that turned fatal more often among African-Americans than among whites, Mahboobeh Mahdavinia, MD, PhD, an allergist and immunologist at Rush University Medical Center, Chicago, said at the joint congress of the American Academy of Asthma, Allergy, and Immunology and the World Asthma Organization.
The “sadder news,” she said, is that the rate of fatal food-related anaphylaxis has been getting worse with time. Rates of fatal food-related anaphylaxis per million significantly increased in African American males from the period of 1999-2001 (.06), compared with 2008-2010 (.21) (P less than .001). Fatal anaphylaxis caused by food was significantly associated with African American race (P less than .001) (J Allergy Clin Immunol. 2014 Dec;134[6]:1318-28.e7).
“There has been a lot of research and increasing awareness about food allergy, but this has certainly not affected minorities, and they’re even dying more from these diseases,” Dr. Mahdavinia said.
Studies also have shown that African-American and Hispanic children have a higher rate of emergency department visits for food allergy, compared with white children. Dr. Mahdavinia said this might be because the severity of their allergies is worse, because they have less access to primary care, they have inferior practices at home to manage the allergies, and that higher asthma rates in these children is likely leading to worse food allergy incidents.

Compared with white children, African American children were significantly more likely to have allergy to wheat, soy, corn, fish, and shellfish (P less than .01). Compared with white children, Hispanic children were significantly more likely to have allergy to corn, fish, and shellfish (P less than .01) (J Allergy Clin Immunol Pract. 2017 Mar-Apr;5[2]:352-7.e1).
Children from low-income backgrounds, she noted, spend less on specialty outpatient care.
The difference in food allergy rates is likely linked, in part, to familial and cultural differences in childrearing, she said. African-American and Hispanic parents tend to introduce solid foods earlier, and breastfeed children at lower rates than those of white families.
Dr. Mahdavinia noted that while more affluent families are able to sidestep allergies by making a simple stop at a high-end grocer to get an allergen-free version of a food, poorer families are less able to buy these more expensive alternatives.
“The higher rate of asthma anaphylaxis observed in these minority children is concerning, especially when it’s considered in the context of the reported higher rate of fatal anaphylaxis associated food allergy in African Americans,” she said. “So there’s a tremendous need for future studies.”
ORLANDO – compared with their white counterparts, an expert said.
These ethnic groups have higher odds of food sensitization compared with whites, and an analysis of the U.S. National Mortality Database found a higher rate of food-related anaphylaxis that turned fatal more often among African-Americans than among whites, Mahboobeh Mahdavinia, MD, PhD, an allergist and immunologist at Rush University Medical Center, Chicago, said at the joint congress of the American Academy of Asthma, Allergy, and Immunology and the World Asthma Organization.
The “sadder news,” she said, is that the rate of fatal food-related anaphylaxis has been getting worse with time. Rates of fatal food-related anaphylaxis per million significantly increased in African American males from the period of 1999-2001 (.06), compared with 2008-2010 (.21) (P less than .001). Fatal anaphylaxis caused by food was significantly associated with African American race (P less than .001) (J Allergy Clin Immunol. 2014 Dec;134[6]:1318-28.e7).
“There has been a lot of research and increasing awareness about food allergy, but this has certainly not affected minorities, and they’re even dying more from these diseases,” Dr. Mahdavinia said.
Studies also have shown that African-American and Hispanic children have a higher rate of emergency department visits for food allergy, compared with white children. Dr. Mahdavinia said this might be because the severity of their allergies is worse, because they have less access to primary care, they have inferior practices at home to manage the allergies, and that higher asthma rates in these children is likely leading to worse food allergy incidents.
Compared with white children, African American children were significantly more likely to have allergy to wheat, soy, corn, fish, and shellfish (P less than .01). Compared with white children, Hispanic children were significantly more likely to have allergy to corn, fish, and shellfish (P less than .01) (J Allergy Clin Immunol Pract. 2017 Mar-Apr;5[2]:352-7.e1).
Children from low-income backgrounds, she noted, spend less on specialty outpatient care.
The difference in food allergy rates is likely linked, in part, to familial and cultural differences in childrearing, she said. African-American and Hispanic parents tend to introduce solid foods earlier, and breastfeed children at lower rates than those of white families.
Dr. Mahdavinia noted that while more affluent families are able to sidestep allergies by making a simple stop at a high-end grocer to get an allergen-free version of a food, poorer families are less able to buy these more expensive alternatives.
“The higher rate of asthma anaphylaxis observed in these minority children is concerning, especially when it’s considered in the context of the reported higher rate of fatal anaphylaxis associated food allergy in African Americans,” she said. “So there’s a tremendous need for future studies.”
ORLANDO – compared with their white counterparts, an expert said.
These ethnic groups have higher odds of food sensitization compared with whites, and an analysis of the U.S. National Mortality Database found a higher rate of food-related anaphylaxis that turned fatal more often among African-Americans than among whites, Mahboobeh Mahdavinia, MD, PhD, an allergist and immunologist at Rush University Medical Center, Chicago, said at the joint congress of the American Academy of Asthma, Allergy, and Immunology and the World Asthma Organization.
The “sadder news,” she said, is that the rate of fatal food-related anaphylaxis has been getting worse with time. Rates of fatal food-related anaphylaxis per million significantly increased in African American males from the period of 1999-2001 (.06), compared with 2008-2010 (.21) (P less than .001). Fatal anaphylaxis caused by food was significantly associated with African American race (P less than .001) (J Allergy Clin Immunol. 2014 Dec;134[6]:1318-28.e7).
“There has been a lot of research and increasing awareness about food allergy, but this has certainly not affected minorities, and they’re even dying more from these diseases,” Dr. Mahdavinia said.
Studies also have shown that African-American and Hispanic children have a higher rate of emergency department visits for food allergy, compared with white children. Dr. Mahdavinia said this might be because the severity of their allergies is worse, because they have less access to primary care, they have inferior practices at home to manage the allergies, and that higher asthma rates in these children is likely leading to worse food allergy incidents.
Compared with white children, African American children were significantly more likely to have allergy to wheat, soy, corn, fish, and shellfish (P less than .01). Compared with white children, Hispanic children were significantly more likely to have allergy to corn, fish, and shellfish (P less than .01) (J Allergy Clin Immunol Pract. 2017 Mar-Apr;5[2]:352-7.e1).
Children from low-income backgrounds, she noted, spend less on specialty outpatient care.
The difference in food allergy rates is likely linked, in part, to familial and cultural differences in childrearing, she said. African-American and Hispanic parents tend to introduce solid foods earlier, and breastfeed children at lower rates than those of white families.
Dr. Mahdavinia noted that while more affluent families are able to sidestep allergies by making a simple stop at a high-end grocer to get an allergen-free version of a food, poorer families are less able to buy these more expensive alternatives.
“The higher rate of asthma anaphylaxis observed in these minority children is concerning, especially when it’s considered in the context of the reported higher rate of fatal anaphylaxis associated food allergy in African Americans,” she said. “So there’s a tremendous need for future studies.”
EXPERT ANALYSIS FROM AAAAI/WAO JOINT CONGRESS
Is there a resilience deficit?
Even if you have never experienced a symptom of burnout, you probably have at least one colleague who has. In the last decade, collateral damage from physician burnout has earned it a place on the agenda of the American Academy of Pediatrics and most other physician organizations.
When one steps back and takes a longer view, burnout is simply a poor fit between physicians and their roles. An increasing number of physicians are finding themselves in jobs in which – for a variety of reasons – they feel uncomfortable. Eventually, the discomfort resulting from that poor fit becomes so unbearable the only solution is to change jobs or retire.
However, an article in Pediatrics entitled “Seeking professional resilience” addresses burnout from the perspective that physician vulnerability is a major contributor to the problem (Pediatrics. 2018, Feb 1. doi: 10.1542/peds.2017-2388). The author, Abby R. Rosenberg, MD, suggests that one solution to burnout is helping physicians learn how “to maintain physical and emotional well-being in the face of adversity,” that is, “resilience.”
It turns out that the recent buzz surrounding “resilience” has drawn a throng of theorists. I guess if we can have chaos theory, we can have resilience theories. Dr. Rosenberg sorts these theories into three categories based on whether they consider resilience an intrinsic trait, a process of adaptation, or an outcome. She offers an alternative description in which resilience is conceived as “a process of harnessing the resources we need to sustain well-being.” Dr. Rosenberg’s suggestions of how this harnessing process can be achieved are certainly worth reading, but I fear that most physicians threatened with burnout won’t have the time or the composure to follow her recommendations. Fifty years of watching physicians both thrive and flame out has convinced me that in most cases, resilience is an intrinsic trait gifted to the recipient at birth.
I am sure there are older physicians who believe that burnout is just another case of “they-don’t-make-’em-like-they-used-to” and would claim that young physicians just don’t have the same grit that we had a generation ago. I guess it is possible that the shift away from the owner/operator model toward one in which a physician has become a cog in the wheel of a large corporation has selected for physicians who are less resilient by nature. But I suspect that the number of resilient physicians is unchanged over the last hundred years. It is more likely that even those blessed with a resilient nature enter their training challenged by a burden of debt significantly greater than my peers and I faced 50 years ago.
The problem isn’t the resiliency deficit. Burnout is the result of a job that has evolved into one with challenges that even the more resilient physicians struggle to tolerate. Under a litigious cloud, hunched over a computer for half the day, the modern physician must struggle to find relevance in a situation in which he has relinquished control to a system that may not share his values.
Refining the selection process to find even more resilient candidates for medical school might lower the burnout rate by a point or two. However, the real answer requires a major overhaul of medical delivery system so that providers can once again feel that every hour they invest is meaningful. The privilege to practice medicine always has required sacrifices on the part of the physician. However, without a sense of purpose, these sacrifices can become intolerable.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Even if you have never experienced a symptom of burnout, you probably have at least one colleague who has. In the last decade, collateral damage from physician burnout has earned it a place on the agenda of the American Academy of Pediatrics and most other physician organizations.
When one steps back and takes a longer view, burnout is simply a poor fit between physicians and their roles. An increasing number of physicians are finding themselves in jobs in which – for a variety of reasons – they feel uncomfortable. Eventually, the discomfort resulting from that poor fit becomes so unbearable the only solution is to change jobs or retire.
However, an article in Pediatrics entitled “Seeking professional resilience” addresses burnout from the perspective that physician vulnerability is a major contributor to the problem (Pediatrics. 2018, Feb 1. doi: 10.1542/peds.2017-2388). The author, Abby R. Rosenberg, MD, suggests that one solution to burnout is helping physicians learn how “to maintain physical and emotional well-being in the face of adversity,” that is, “resilience.”
It turns out that the recent buzz surrounding “resilience” has drawn a throng of theorists. I guess if we can have chaos theory, we can have resilience theories. Dr. Rosenberg sorts these theories into three categories based on whether they consider resilience an intrinsic trait, a process of adaptation, or an outcome. She offers an alternative description in which resilience is conceived as “a process of harnessing the resources we need to sustain well-being.” Dr. Rosenberg’s suggestions of how this harnessing process can be achieved are certainly worth reading, but I fear that most physicians threatened with burnout won’t have the time or the composure to follow her recommendations. Fifty years of watching physicians both thrive and flame out has convinced me that in most cases, resilience is an intrinsic trait gifted to the recipient at birth.
I am sure there are older physicians who believe that burnout is just another case of “they-don’t-make-’em-like-they-used-to” and would claim that young physicians just don’t have the same grit that we had a generation ago. I guess it is possible that the shift away from the owner/operator model toward one in which a physician has become a cog in the wheel of a large corporation has selected for physicians who are less resilient by nature. But I suspect that the number of resilient physicians is unchanged over the last hundred years. It is more likely that even those blessed with a resilient nature enter their training challenged by a burden of debt significantly greater than my peers and I faced 50 years ago.
The problem isn’t the resiliency deficit. Burnout is the result of a job that has evolved into one with challenges that even the more resilient physicians struggle to tolerate. Under a litigious cloud, hunched over a computer for half the day, the modern physician must struggle to find relevance in a situation in which he has relinquished control to a system that may not share his values.
Refining the selection process to find even more resilient candidates for medical school might lower the burnout rate by a point or two. However, the real answer requires a major overhaul of medical delivery system so that providers can once again feel that every hour they invest is meaningful. The privilege to practice medicine always has required sacrifices on the part of the physician. However, without a sense of purpose, these sacrifices can become intolerable.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Even if you have never experienced a symptom of burnout, you probably have at least one colleague who has. In the last decade, collateral damage from physician burnout has earned it a place on the agenda of the American Academy of Pediatrics and most other physician organizations.
When one steps back and takes a longer view, burnout is simply a poor fit between physicians and their roles. An increasing number of physicians are finding themselves in jobs in which – for a variety of reasons – they feel uncomfortable. Eventually, the discomfort resulting from that poor fit becomes so unbearable the only solution is to change jobs or retire.
However, an article in Pediatrics entitled “Seeking professional resilience” addresses burnout from the perspective that physician vulnerability is a major contributor to the problem (Pediatrics. 2018, Feb 1. doi: 10.1542/peds.2017-2388). The author, Abby R. Rosenberg, MD, suggests that one solution to burnout is helping physicians learn how “to maintain physical and emotional well-being in the face of adversity,” that is, “resilience.”
It turns out that the recent buzz surrounding “resilience” has drawn a throng of theorists. I guess if we can have chaos theory, we can have resilience theories. Dr. Rosenberg sorts these theories into three categories based on whether they consider resilience an intrinsic trait, a process of adaptation, or an outcome. She offers an alternative description in which resilience is conceived as “a process of harnessing the resources we need to sustain well-being.” Dr. Rosenberg’s suggestions of how this harnessing process can be achieved are certainly worth reading, but I fear that most physicians threatened with burnout won’t have the time or the composure to follow her recommendations. Fifty years of watching physicians both thrive and flame out has convinced me that in most cases, resilience is an intrinsic trait gifted to the recipient at birth.
I am sure there are older physicians who believe that burnout is just another case of “they-don’t-make-’em-like-they-used-to” and would claim that young physicians just don’t have the same grit that we had a generation ago. I guess it is possible that the shift away from the owner/operator model toward one in which a physician has become a cog in the wheel of a large corporation has selected for physicians who are less resilient by nature. But I suspect that the number of resilient physicians is unchanged over the last hundred years. It is more likely that even those blessed with a resilient nature enter their training challenged by a burden of debt significantly greater than my peers and I faced 50 years ago.
The problem isn’t the resiliency deficit. Burnout is the result of a job that has evolved into one with challenges that even the more resilient physicians struggle to tolerate. Under a litigious cloud, hunched over a computer for half the day, the modern physician must struggle to find relevance in a situation in which he has relinquished control to a system that may not share his values.
Refining the selection process to find even more resilient candidates for medical school might lower the burnout rate by a point or two. However, the real answer requires a major overhaul of medical delivery system so that providers can once again feel that every hour they invest is meaningful. The privilege to practice medicine always has required sacrifices on the part of the physician. However, without a sense of purpose, these sacrifices can become intolerable.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Outcomes After Endoscopic Dilation of Laryngotracheal Stenosis: An Analysis of ACS-NSQIP
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1). 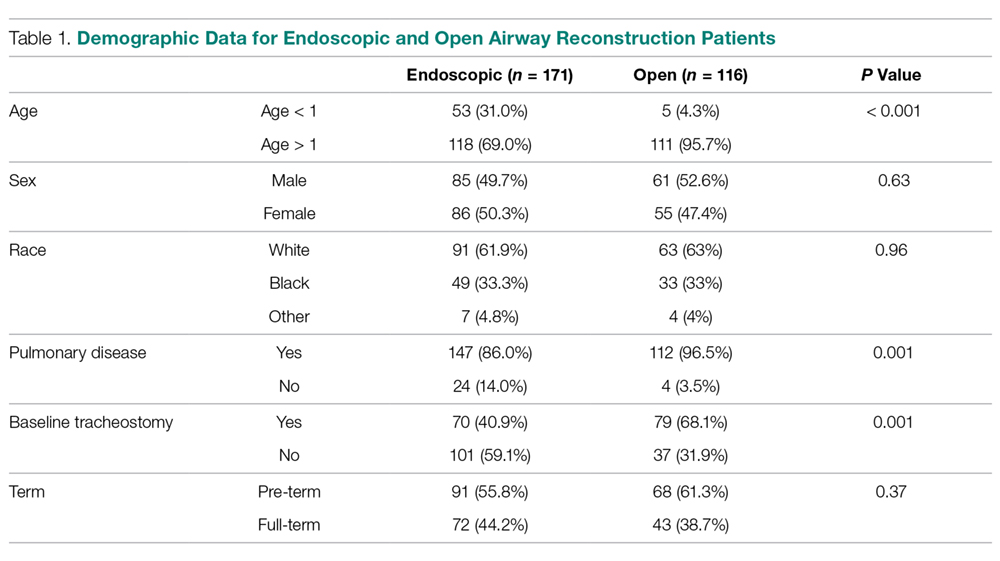
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2) 
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure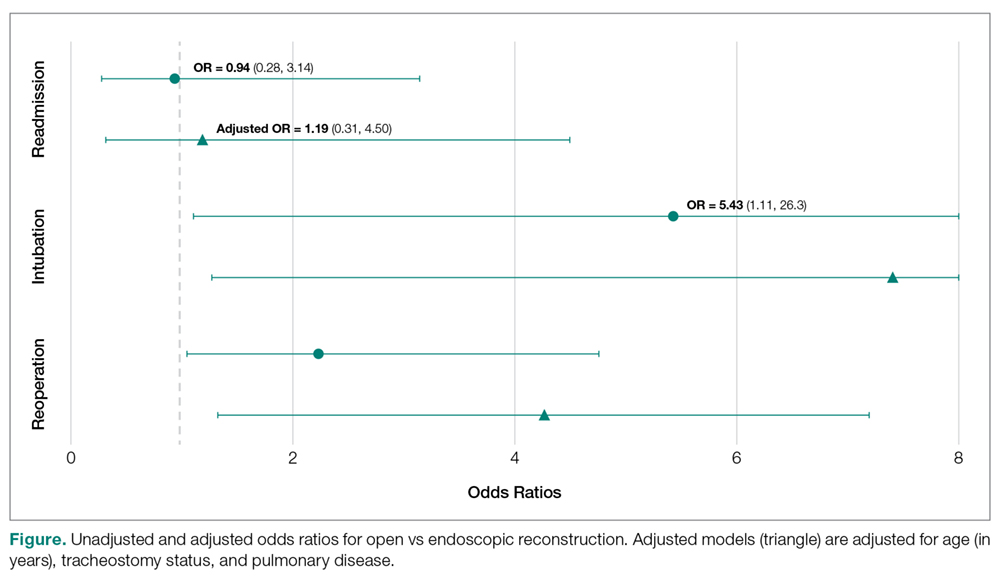
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, JLavin@luriechildrens.org.
Financial disclosures: None.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1).
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2)
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, JLavin@luriechildrens.org.
Financial disclosures: None.
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1).
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2)
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, JLavin@luriechildrens.org.
Financial disclosures: None.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.