User login
Gestational Rhinitis: How Can We Manage It?
PARIS — Allergic comorbidities such as asthma and rhinitis are common among pregnant women. During the 19th French-speaking Congress of Allergology, Dario Ebode, MD, otolaryngologist and cervicofacial surgeon at Hôpital de la Conception in Marseille, France, described gestational rhinitis and detailed its management.
A Hormonal Rhinitis
The prevalence of rhinitis during pregnancy ranges from 18% to 30%, whether it is pre-existing (eg, allergic or infectious) or newly diagnosed. About half of the cases of pre-existing rhinitis worsen during pregnancy, leading to gestational rhinitis, which has a prevalence of approximately 22%.
“The latter is characterized by its onset in the 2nd or 3rd trimester, a duration of > 6 weeks, an absence of associated allergic symptoms, and complete spontaneous resolution 2-3 weeks after delivery,” said Dr. Ebode.
Uncertainties about the pathophysiology of gestational rhinitis, a “hormonal rhinitis,” remain, he added. Beta-estradiol and progesterone hormones lead to an increase in H1 histamine receptors on epithelial and endothelial cells, which promotes the migration or degranulation of eosinophils.
Management
While gestational rhinitis is benign, its symptoms can still be bothersome and can be relieved. In addition to dietary and hygienic (nasal irrigation with large volumes) measures and allergen avoidance, local treatments include nasal corticosteroids, possibly combined with antihistamines, and systemic antihistamines. “During pregnancy, nasal corticosteroids, oral antihistamines [excluding azelastine hydrochloride before 10 weeks], and ipratropium bromide are allowed,” said Dr. Ebode. Regarding sprays that combine corticosteroids and antihistamines, the combination of mometasone furoate and olopatadine is possible but not the combination of azelastine hydrochloride and fluticasone propionate before 10 weeks.
Finally, oral vasoconstrictors (which are found in many over-the-counter medications) should be avoided, as should Kenacort (triamcinolone acetonide), “which also has no place in women outside of pregnancy due to an unfavorable risk-benefit balance in rhinitis,” said Dr. Ebode. Allergen immunotherapy plans should be postponed after delivery.
Dr. Ebode reported a financial relationship with Zambon.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
PARIS — Allergic comorbidities such as asthma and rhinitis are common among pregnant women. During the 19th French-speaking Congress of Allergology, Dario Ebode, MD, otolaryngologist and cervicofacial surgeon at Hôpital de la Conception in Marseille, France, described gestational rhinitis and detailed its management.
A Hormonal Rhinitis
The prevalence of rhinitis during pregnancy ranges from 18% to 30%, whether it is pre-existing (eg, allergic or infectious) or newly diagnosed. About half of the cases of pre-existing rhinitis worsen during pregnancy, leading to gestational rhinitis, which has a prevalence of approximately 22%.
“The latter is characterized by its onset in the 2nd or 3rd trimester, a duration of > 6 weeks, an absence of associated allergic symptoms, and complete spontaneous resolution 2-3 weeks after delivery,” said Dr. Ebode.
Uncertainties about the pathophysiology of gestational rhinitis, a “hormonal rhinitis,” remain, he added. Beta-estradiol and progesterone hormones lead to an increase in H1 histamine receptors on epithelial and endothelial cells, which promotes the migration or degranulation of eosinophils.
Management
While gestational rhinitis is benign, its symptoms can still be bothersome and can be relieved. In addition to dietary and hygienic (nasal irrigation with large volumes) measures and allergen avoidance, local treatments include nasal corticosteroids, possibly combined with antihistamines, and systemic antihistamines. “During pregnancy, nasal corticosteroids, oral antihistamines [excluding azelastine hydrochloride before 10 weeks], and ipratropium bromide are allowed,” said Dr. Ebode. Regarding sprays that combine corticosteroids and antihistamines, the combination of mometasone furoate and olopatadine is possible but not the combination of azelastine hydrochloride and fluticasone propionate before 10 weeks.
Finally, oral vasoconstrictors (which are found in many over-the-counter medications) should be avoided, as should Kenacort (triamcinolone acetonide), “which also has no place in women outside of pregnancy due to an unfavorable risk-benefit balance in rhinitis,” said Dr. Ebode. Allergen immunotherapy plans should be postponed after delivery.
Dr. Ebode reported a financial relationship with Zambon.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
PARIS — Allergic comorbidities such as asthma and rhinitis are common among pregnant women. During the 19th French-speaking Congress of Allergology, Dario Ebode, MD, otolaryngologist and cervicofacial surgeon at Hôpital de la Conception in Marseille, France, described gestational rhinitis and detailed its management.
A Hormonal Rhinitis
The prevalence of rhinitis during pregnancy ranges from 18% to 30%, whether it is pre-existing (eg, allergic or infectious) or newly diagnosed. About half of the cases of pre-existing rhinitis worsen during pregnancy, leading to gestational rhinitis, which has a prevalence of approximately 22%.
“The latter is characterized by its onset in the 2nd or 3rd trimester, a duration of > 6 weeks, an absence of associated allergic symptoms, and complete spontaneous resolution 2-3 weeks after delivery,” said Dr. Ebode.
Uncertainties about the pathophysiology of gestational rhinitis, a “hormonal rhinitis,” remain, he added. Beta-estradiol and progesterone hormones lead to an increase in H1 histamine receptors on epithelial and endothelial cells, which promotes the migration or degranulation of eosinophils.
Management
While gestational rhinitis is benign, its symptoms can still be bothersome and can be relieved. In addition to dietary and hygienic (nasal irrigation with large volumes) measures and allergen avoidance, local treatments include nasal corticosteroids, possibly combined with antihistamines, and systemic antihistamines. “During pregnancy, nasal corticosteroids, oral antihistamines [excluding azelastine hydrochloride before 10 weeks], and ipratropium bromide are allowed,” said Dr. Ebode. Regarding sprays that combine corticosteroids and antihistamines, the combination of mometasone furoate and olopatadine is possible but not the combination of azelastine hydrochloride and fluticasone propionate before 10 weeks.
Finally, oral vasoconstrictors (which are found in many over-the-counter medications) should be avoided, as should Kenacort (triamcinolone acetonide), “which also has no place in women outside of pregnancy due to an unfavorable risk-benefit balance in rhinitis,” said Dr. Ebode. Allergen immunotherapy plans should be postponed after delivery.
Dr. Ebode reported a financial relationship with Zambon.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Florida Allows Doctors To Perform C-Sections Outside of Hospitals
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Risk Screening Tool Helped Identify Pregnant Patients Previously Undiagnosed With CVD
SAN FRANCISCO — More than a quarter of pregnant or postpartum patients who screened positive for cardiovascular disease ended up with a cardiovascular disease diagnosis when providers used a risk screening tool built into the electronic medical records system for all patients, according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Timely diagnosis of cardiovascular disease is critical, though challenging, since pregnancy is a state of hemodynamic stress with symptoms that are like those of cardiovascular disease, and healthcare providers may not suspect cardiovascular disease in pregnant patients with symptoms of it,” Kevin Flatley, MD, a resident ob.gyn. at Montefiore Health System and the Albert Einstein College of Medicine in New York City, told attendees at the conference. “The cardiovascular risk assessment tool proved valuable for identifying and providing individualized care for cardio-obstetric patients.”
The study senior author, Diana S. Wolfe, MD, MPH, associate division director of Maternal Fetal Medicine at Montefiore Health System and associate professor of medicine in cardiology at Albert Einstein College of Medicine, said in an interview that cardiovascular risk in Montefiore’s urban population is significant.
“Cardiovascular disease risk screening identifies true cardiac disease in this population and can change the medical management and outcome of pregnant and postpartum patients,” Dr. Wolfe said. Screening has the potential to decrease maternal morbidity and mortality in our country, she said.
Dawnette Lewis, MD, MPH, director of the Center for Maternal Health at Northwell Health and an ob.gyn. and maternal fetal medicine specialist who was not involved in the study, was impressed with the research.
“We know that cardiovascular disease is one of the leading causes of maternal mortality,” Dr. Lewis said in an interview. “It is important to have an accurate risk assessment score, so I think what is being presented in this abstract is great.” She said she’s aware that other cardio-obstetric programs across the country are also implementing cardiovascular risk assessment tools during pregnancy.
The researchers built into their electronic health records a screening algorithm developed by the California Maternal Quality Care Initiative that had been based on a retrospective review of cardiovascular maternal deaths in California from 2002 to 2006. Their study aimed to identify the true positives — those who actually had cardiovascular disease — of those determined to be at risk by the screening toolkit.
The institution’s goal was for all patients to undergo a screening risk assessment at least once during prenatal and/or postpartum visits. Patients were considered to screen positive if they had at least one symptom, at least one vital sign abnormality, and at least one risk factor, or any combination of these that added up to 4.
Symptoms in the screening tool included shortness of breath, shortness of breath while lying flat, a rapid heart rate, asthma that was unresponsive to therapy, palpitations, fainting or other loss of consciousness, and chest pain. Abnormal vital signs included a resting heart rate of 110 bpm or greater, systolic blood pressure of 140 mm Hg or higher, a respiratory rate of 24 or higher, and an oxygen saturation of 96% or lower.
Risk factors included being 40 or older, being Black, having a pre-pregnancy BMI of 35 or greater, preexisting diabetes, hypertension, substance use, and a history of cancer, chemotherapy, or chest radiation. “Current practice acknowledges that the risk factor currently included in the algorithm of self-identified as Black actually represents racism, bias, and social determinants of health, known risk factors for CVD,” Wolfe said.
Patients who screened positive underwent an echocardiogram, a cardio-obstetric consultation, and an additional work-up.
During the June 2022–September 2023 study period, 148 out of 1877 screened patients (7.9%) had a positive screen. Of these, 108 were false positives and 40 (27%) were true positives. The number of true false positives is not known because many women did not come for their workups.* The true positives mostly included patients with mild valvular disease, but about a quarter had mild, moderate, or severe ventricular dilation or hypertrophy and a little less than a quarter were positive for systolic or diastolic dysfunction.
Most (72.5%) of the 40 true-positive cases needed a multidisciplinary cardio-obstetrics team plan, and 11 patients (27.5%) needed follow-up and had multiple visits with the cardio-obstetrics team. Six of the true-positive cases (15%) “were deemed to be of higher risk for decompensation during labor and required detailed plans for intrapartum and postpartum management,” the researchers reported. Nine patients (22.5%) began new cardiovascular medications.
This research is a validation study of the current algorithm, Wolfe said, and the algorithm will be revised based on the results of the completed validation study.
“The objective is universal cardiovascular risk screening for all pregnant and postpartum persons in the US,” Wolfe said. “Once the data collection from this validation study is concluded, our goal is to disseminate a revised CVD risk screening tool that can be implemented into the electronic medical records of all institutions in our country.”
*The study partially funded by the National Institute of Child Health and Human Development award #5R21HD101783. All the authors and Dr. Lewis had no disclosures. Dr. Afshan B. Hameed of the University of California at Irvine was a partner in the study.
*This study was updated on May 30, 2024.
SAN FRANCISCO — More than a quarter of pregnant or postpartum patients who screened positive for cardiovascular disease ended up with a cardiovascular disease diagnosis when providers used a risk screening tool built into the electronic medical records system for all patients, according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Timely diagnosis of cardiovascular disease is critical, though challenging, since pregnancy is a state of hemodynamic stress with symptoms that are like those of cardiovascular disease, and healthcare providers may not suspect cardiovascular disease in pregnant patients with symptoms of it,” Kevin Flatley, MD, a resident ob.gyn. at Montefiore Health System and the Albert Einstein College of Medicine in New York City, told attendees at the conference. “The cardiovascular risk assessment tool proved valuable for identifying and providing individualized care for cardio-obstetric patients.”
The study senior author, Diana S. Wolfe, MD, MPH, associate division director of Maternal Fetal Medicine at Montefiore Health System and associate professor of medicine in cardiology at Albert Einstein College of Medicine, said in an interview that cardiovascular risk in Montefiore’s urban population is significant.
“Cardiovascular disease risk screening identifies true cardiac disease in this population and can change the medical management and outcome of pregnant and postpartum patients,” Dr. Wolfe said. Screening has the potential to decrease maternal morbidity and mortality in our country, she said.
Dawnette Lewis, MD, MPH, director of the Center for Maternal Health at Northwell Health and an ob.gyn. and maternal fetal medicine specialist who was not involved in the study, was impressed with the research.
“We know that cardiovascular disease is one of the leading causes of maternal mortality,” Dr. Lewis said in an interview. “It is important to have an accurate risk assessment score, so I think what is being presented in this abstract is great.” She said she’s aware that other cardio-obstetric programs across the country are also implementing cardiovascular risk assessment tools during pregnancy.
The researchers built into their electronic health records a screening algorithm developed by the California Maternal Quality Care Initiative that had been based on a retrospective review of cardiovascular maternal deaths in California from 2002 to 2006. Their study aimed to identify the true positives — those who actually had cardiovascular disease — of those determined to be at risk by the screening toolkit.
The institution’s goal was for all patients to undergo a screening risk assessment at least once during prenatal and/or postpartum visits. Patients were considered to screen positive if they had at least one symptom, at least one vital sign abnormality, and at least one risk factor, or any combination of these that added up to 4.
Symptoms in the screening tool included shortness of breath, shortness of breath while lying flat, a rapid heart rate, asthma that was unresponsive to therapy, palpitations, fainting or other loss of consciousness, and chest pain. Abnormal vital signs included a resting heart rate of 110 bpm or greater, systolic blood pressure of 140 mm Hg or higher, a respiratory rate of 24 or higher, and an oxygen saturation of 96% or lower.
Risk factors included being 40 or older, being Black, having a pre-pregnancy BMI of 35 or greater, preexisting diabetes, hypertension, substance use, and a history of cancer, chemotherapy, or chest radiation. “Current practice acknowledges that the risk factor currently included in the algorithm of self-identified as Black actually represents racism, bias, and social determinants of health, known risk factors for CVD,” Wolfe said.
Patients who screened positive underwent an echocardiogram, a cardio-obstetric consultation, and an additional work-up.
During the June 2022–September 2023 study period, 148 out of 1877 screened patients (7.9%) had a positive screen. Of these, 108 were false positives and 40 (27%) were true positives. The number of true false positives is not known because many women did not come for their workups.* The true positives mostly included patients with mild valvular disease, but about a quarter had mild, moderate, or severe ventricular dilation or hypertrophy and a little less than a quarter were positive for systolic or diastolic dysfunction.
Most (72.5%) of the 40 true-positive cases needed a multidisciplinary cardio-obstetrics team plan, and 11 patients (27.5%) needed follow-up and had multiple visits with the cardio-obstetrics team. Six of the true-positive cases (15%) “were deemed to be of higher risk for decompensation during labor and required detailed plans for intrapartum and postpartum management,” the researchers reported. Nine patients (22.5%) began new cardiovascular medications.
This research is a validation study of the current algorithm, Wolfe said, and the algorithm will be revised based on the results of the completed validation study.
“The objective is universal cardiovascular risk screening for all pregnant and postpartum persons in the US,” Wolfe said. “Once the data collection from this validation study is concluded, our goal is to disseminate a revised CVD risk screening tool that can be implemented into the electronic medical records of all institutions in our country.”
*The study partially funded by the National Institute of Child Health and Human Development award #5R21HD101783. All the authors and Dr. Lewis had no disclosures. Dr. Afshan B. Hameed of the University of California at Irvine was a partner in the study.
*This study was updated on May 30, 2024.
SAN FRANCISCO — More than a quarter of pregnant or postpartum patients who screened positive for cardiovascular disease ended up with a cardiovascular disease diagnosis when providers used a risk screening tool built into the electronic medical records system for all patients, according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Timely diagnosis of cardiovascular disease is critical, though challenging, since pregnancy is a state of hemodynamic stress with symptoms that are like those of cardiovascular disease, and healthcare providers may not suspect cardiovascular disease in pregnant patients with symptoms of it,” Kevin Flatley, MD, a resident ob.gyn. at Montefiore Health System and the Albert Einstein College of Medicine in New York City, told attendees at the conference. “The cardiovascular risk assessment tool proved valuable for identifying and providing individualized care for cardio-obstetric patients.”
The study senior author, Diana S. Wolfe, MD, MPH, associate division director of Maternal Fetal Medicine at Montefiore Health System and associate professor of medicine in cardiology at Albert Einstein College of Medicine, said in an interview that cardiovascular risk in Montefiore’s urban population is significant.
“Cardiovascular disease risk screening identifies true cardiac disease in this population and can change the medical management and outcome of pregnant and postpartum patients,” Dr. Wolfe said. Screening has the potential to decrease maternal morbidity and mortality in our country, she said.
Dawnette Lewis, MD, MPH, director of the Center for Maternal Health at Northwell Health and an ob.gyn. and maternal fetal medicine specialist who was not involved in the study, was impressed with the research.
“We know that cardiovascular disease is one of the leading causes of maternal mortality,” Dr. Lewis said in an interview. “It is important to have an accurate risk assessment score, so I think what is being presented in this abstract is great.” She said she’s aware that other cardio-obstetric programs across the country are also implementing cardiovascular risk assessment tools during pregnancy.
The researchers built into their electronic health records a screening algorithm developed by the California Maternal Quality Care Initiative that had been based on a retrospective review of cardiovascular maternal deaths in California from 2002 to 2006. Their study aimed to identify the true positives — those who actually had cardiovascular disease — of those determined to be at risk by the screening toolkit.
The institution’s goal was for all patients to undergo a screening risk assessment at least once during prenatal and/or postpartum visits. Patients were considered to screen positive if they had at least one symptom, at least one vital sign abnormality, and at least one risk factor, or any combination of these that added up to 4.
Symptoms in the screening tool included shortness of breath, shortness of breath while lying flat, a rapid heart rate, asthma that was unresponsive to therapy, palpitations, fainting or other loss of consciousness, and chest pain. Abnormal vital signs included a resting heart rate of 110 bpm or greater, systolic blood pressure of 140 mm Hg or higher, a respiratory rate of 24 or higher, and an oxygen saturation of 96% or lower.
Risk factors included being 40 or older, being Black, having a pre-pregnancy BMI of 35 or greater, preexisting diabetes, hypertension, substance use, and a history of cancer, chemotherapy, or chest radiation. “Current practice acknowledges that the risk factor currently included in the algorithm of self-identified as Black actually represents racism, bias, and social determinants of health, known risk factors for CVD,” Wolfe said.
Patients who screened positive underwent an echocardiogram, a cardio-obstetric consultation, and an additional work-up.
During the June 2022–September 2023 study period, 148 out of 1877 screened patients (7.9%) had a positive screen. Of these, 108 were false positives and 40 (27%) were true positives. The number of true false positives is not known because many women did not come for their workups.* The true positives mostly included patients with mild valvular disease, but about a quarter had mild, moderate, or severe ventricular dilation or hypertrophy and a little less than a quarter were positive for systolic or diastolic dysfunction.
Most (72.5%) of the 40 true-positive cases needed a multidisciplinary cardio-obstetrics team plan, and 11 patients (27.5%) needed follow-up and had multiple visits with the cardio-obstetrics team. Six of the true-positive cases (15%) “were deemed to be of higher risk for decompensation during labor and required detailed plans for intrapartum and postpartum management,” the researchers reported. Nine patients (22.5%) began new cardiovascular medications.
This research is a validation study of the current algorithm, Wolfe said, and the algorithm will be revised based on the results of the completed validation study.
“The objective is universal cardiovascular risk screening for all pregnant and postpartum persons in the US,” Wolfe said. “Once the data collection from this validation study is concluded, our goal is to disseminate a revised CVD risk screening tool that can be implemented into the electronic medical records of all institutions in our country.”
*The study partially funded by the National Institute of Child Health and Human Development award #5R21HD101783. All the authors and Dr. Lewis had no disclosures. Dr. Afshan B. Hameed of the University of California at Irvine was a partner in the study.
*This study was updated on May 30, 2024.
FROM ACOG 2024
CGM Aids in Detecting Early Gestational Diabetes
TOPLINE:
In women with gestational diabetes (GD), continuous glucose monitoring (CGM) shows elevated glycemic metrics earlier in pregnancy compared with the standard oral glucose tolerance test (OGTT).
METHODOLOGY:
- Earlier diagnosis and treatment of GDM may mitigate some perinatal risks, but the traditional OGTT at 24-28 weeks’ gestation delivers inconsistent results in early pregnancy, potentially leading to missed cases or overdiagnosis.
- This prospective noninterventional observational study conducted at two US academic-based clinical sites from June 2020 to December 2021 assessed CGM-derived glycemic patterns in 768 participants (mean age, 33 years; 77% White) enrolled prior to 17 weeks’ gestation with singleton pregnancy and an initial A1c level < 6.5%.
- Participants were encouraged to wear a blinded Dexcom G6 Pro CGM System sensor continuously until the day of delivery, with a median CGM wear duration of 67 days prior to OGTT.
- GDM was diagnosed using an OGTT conducted between 24 and 34 weeks’ gestation, which sorted women into those with GDM (n = 58) or without GDM (n = 710).
- CGM-derived glycemic patterns were compared between the participants with and without GDM.
TAKEAWAY:
- Women with GDM had a higher mean glucose (109 ± 13 vs 100 ± 8 mg/dL; P < .001) and greater glucose SD (23 ± 4 vs 19 ± 3; P < .001) than those without GDM throughout the gestational period prior to OGTT.
- Women with GDM spent lesser time in glycemic ranges of 63-140 mg/dL (87% ± 11% vs 94% ± 4%; P < .001) and 63-120 mg/dL (70% ± 17% vs 84% ± 8%; P < .001) throughout gestation than those without GDM prior to OGTT.
- The daytime and overnight mean glucose levels were higher in those with vs without GDM and attributed to increased hyperglycemia rather than decreased hypoglycemia, with those with GDM spending more time > 120 mg/dL and > 140 mg/dL and less time < 63 mg/dL and < 54 mg/dL.
- Mean glucose and percent time in the > 120 mg/dL and > 140 mg/dL ranges were higher in those with GDM as early as 13-14 weeks of gestation, which persisted at each 2-week period prior to OGTT.
IN PRACTICE:
“CGM could be used in addition to or instead of OGTT to screen individuals at risk for hyperglycemia during pregnancy, even as early as the first trimester,” the authors wrote, adding that “CGM could potentially play a pivotal role in providing timely identification of distinct glycemic patterns indicative of early dysglycemia.”
SOURCE:
The study, led by Celeste Durnwald, MD, Maternal-Fetal Medicine Research Program, Department of Obstetrics and Gynecology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, was published online in Diabetes Care.
LIMITATIONS:
To include participants with possible early GDM, the study allowed the inclusion of up to 14 days of CGM data after OGTT in the overall gestational period and up to 10 days in the first and second trimesters. A detailed analysis of glycemia at the earliest timepoint of pregnancy could not be conducted as the first trimester data were limited. The findings may not be generalizable to a population with gestational hyperglycemia, as only 58 participants were identified with GDM using OGTT.
DISCLOSURES:
The study was supported by the Leona M. and Harry B. Helmsley Charitable Trust and UnitedHealth Group. Some authors reported performing advisory work, receiving research support and consultancy fees, and being on scientific advisory boards through their employer, while several authors reported that their institution received funds on their behalf from various pharmaceutical, healthcare, and medical device companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
In women with gestational diabetes (GD), continuous glucose monitoring (CGM) shows elevated glycemic metrics earlier in pregnancy compared with the standard oral glucose tolerance test (OGTT).
METHODOLOGY:
- Earlier diagnosis and treatment of GDM may mitigate some perinatal risks, but the traditional OGTT at 24-28 weeks’ gestation delivers inconsistent results in early pregnancy, potentially leading to missed cases or overdiagnosis.
- This prospective noninterventional observational study conducted at two US academic-based clinical sites from June 2020 to December 2021 assessed CGM-derived glycemic patterns in 768 participants (mean age, 33 years; 77% White) enrolled prior to 17 weeks’ gestation with singleton pregnancy and an initial A1c level < 6.5%.
- Participants were encouraged to wear a blinded Dexcom G6 Pro CGM System sensor continuously until the day of delivery, with a median CGM wear duration of 67 days prior to OGTT.
- GDM was diagnosed using an OGTT conducted between 24 and 34 weeks’ gestation, which sorted women into those with GDM (n = 58) or without GDM (n = 710).
- CGM-derived glycemic patterns were compared between the participants with and without GDM.
TAKEAWAY:
- Women with GDM had a higher mean glucose (109 ± 13 vs 100 ± 8 mg/dL; P < .001) and greater glucose SD (23 ± 4 vs 19 ± 3; P < .001) than those without GDM throughout the gestational period prior to OGTT.
- Women with GDM spent lesser time in glycemic ranges of 63-140 mg/dL (87% ± 11% vs 94% ± 4%; P < .001) and 63-120 mg/dL (70% ± 17% vs 84% ± 8%; P < .001) throughout gestation than those without GDM prior to OGTT.
- The daytime and overnight mean glucose levels were higher in those with vs without GDM and attributed to increased hyperglycemia rather than decreased hypoglycemia, with those with GDM spending more time > 120 mg/dL and > 140 mg/dL and less time < 63 mg/dL and < 54 mg/dL.
- Mean glucose and percent time in the > 120 mg/dL and > 140 mg/dL ranges were higher in those with GDM as early as 13-14 weeks of gestation, which persisted at each 2-week period prior to OGTT.
IN PRACTICE:
“CGM could be used in addition to or instead of OGTT to screen individuals at risk for hyperglycemia during pregnancy, even as early as the first trimester,” the authors wrote, adding that “CGM could potentially play a pivotal role in providing timely identification of distinct glycemic patterns indicative of early dysglycemia.”
SOURCE:
The study, led by Celeste Durnwald, MD, Maternal-Fetal Medicine Research Program, Department of Obstetrics and Gynecology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, was published online in Diabetes Care.
LIMITATIONS:
To include participants with possible early GDM, the study allowed the inclusion of up to 14 days of CGM data after OGTT in the overall gestational period and up to 10 days in the first and second trimesters. A detailed analysis of glycemia at the earliest timepoint of pregnancy could not be conducted as the first trimester data were limited. The findings may not be generalizable to a population with gestational hyperglycemia, as only 58 participants were identified with GDM using OGTT.
DISCLOSURES:
The study was supported by the Leona M. and Harry B. Helmsley Charitable Trust and UnitedHealth Group. Some authors reported performing advisory work, receiving research support and consultancy fees, and being on scientific advisory boards through their employer, while several authors reported that their institution received funds on their behalf from various pharmaceutical, healthcare, and medical device companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
In women with gestational diabetes (GD), continuous glucose monitoring (CGM) shows elevated glycemic metrics earlier in pregnancy compared with the standard oral glucose tolerance test (OGTT).
METHODOLOGY:
- Earlier diagnosis and treatment of GDM may mitigate some perinatal risks, but the traditional OGTT at 24-28 weeks’ gestation delivers inconsistent results in early pregnancy, potentially leading to missed cases or overdiagnosis.
- This prospective noninterventional observational study conducted at two US academic-based clinical sites from June 2020 to December 2021 assessed CGM-derived glycemic patterns in 768 participants (mean age, 33 years; 77% White) enrolled prior to 17 weeks’ gestation with singleton pregnancy and an initial A1c level < 6.5%.
- Participants were encouraged to wear a blinded Dexcom G6 Pro CGM System sensor continuously until the day of delivery, with a median CGM wear duration of 67 days prior to OGTT.
- GDM was diagnosed using an OGTT conducted between 24 and 34 weeks’ gestation, which sorted women into those with GDM (n = 58) or without GDM (n = 710).
- CGM-derived glycemic patterns were compared between the participants with and without GDM.
TAKEAWAY:
- Women with GDM had a higher mean glucose (109 ± 13 vs 100 ± 8 mg/dL; P < .001) and greater glucose SD (23 ± 4 vs 19 ± 3; P < .001) than those without GDM throughout the gestational period prior to OGTT.
- Women with GDM spent lesser time in glycemic ranges of 63-140 mg/dL (87% ± 11% vs 94% ± 4%; P < .001) and 63-120 mg/dL (70% ± 17% vs 84% ± 8%; P < .001) throughout gestation than those without GDM prior to OGTT.
- The daytime and overnight mean glucose levels were higher in those with vs without GDM and attributed to increased hyperglycemia rather than decreased hypoglycemia, with those with GDM spending more time > 120 mg/dL and > 140 mg/dL and less time < 63 mg/dL and < 54 mg/dL.
- Mean glucose and percent time in the > 120 mg/dL and > 140 mg/dL ranges were higher in those with GDM as early as 13-14 weeks of gestation, which persisted at each 2-week period prior to OGTT.
IN PRACTICE:
“CGM could be used in addition to or instead of OGTT to screen individuals at risk for hyperglycemia during pregnancy, even as early as the first trimester,” the authors wrote, adding that “CGM could potentially play a pivotal role in providing timely identification of distinct glycemic patterns indicative of early dysglycemia.”
SOURCE:
The study, led by Celeste Durnwald, MD, Maternal-Fetal Medicine Research Program, Department of Obstetrics and Gynecology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, was published online in Diabetes Care.
LIMITATIONS:
To include participants with possible early GDM, the study allowed the inclusion of up to 14 days of CGM data after OGTT in the overall gestational period and up to 10 days in the first and second trimesters. A detailed analysis of glycemia at the earliest timepoint of pregnancy could not be conducted as the first trimester data were limited. The findings may not be generalizable to a population with gestational hyperglycemia, as only 58 participants were identified with GDM using OGTT.
DISCLOSURES:
The study was supported by the Leona M. and Harry B. Helmsley Charitable Trust and UnitedHealth Group. Some authors reported performing advisory work, receiving research support and consultancy fees, and being on scientific advisory boards through their employer, while several authors reported that their institution received funds on their behalf from various pharmaceutical, healthcare, and medical device companies.
A version of this article first appeared on Medscape.com.
Failed IOL Promotes Poor Maternal and Fetal Outcomes for Mothers With Diabetes
Approximately one-quarter of mothers with diabetes failed induction of labor, and this failure was associated with a range of adverse outcomes for mothers and infants, based on data from more than 2,000 individuals.
Uncontrolled diabetes remains a risk factor for cesarean delivery, Ali Alhousseini, MD, of Corewell Health East, Dearborn, Michigan, and colleagues wrote in a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
“Identifying and stratifying associated risk factors for failed induction of labor [IOL] may improve counseling and intrapartum care,” the researchers wrote in their abstract.
The researchers reviewed data from 2,172 mothers with diabetes who underwent IOL at a single university medical center between January 2013 and December 2021. They examined a range of maternal characteristics including age, ethnicity, gestational age, medical comorbidities, insulin administration, parity, and health insurance.
A total of 567 mothers with diabetes (26.1%) failed IOL and underwent cesarean delivery.
Overall, failed IOL was significantly associated with nulliparity (P = .0001), as well as preexisting diabetes compared with gestational diabetes, diabetes control with insulin, maternal essential hypertension, preeclampsia, and polyhydramnios (P = .001 for all). Other factors significantly associated with failed IOL included prenatal diagnosis of fetal growth restriction (P = .008), and placental abnormalities (P = .027).
Neonatal factors of weight, large for gestational age, head circumference, and height were not significantly associated with failed IOL (P > .05 for all).
As for neonatal outcomes, failed IOL was significantly associated with admission to neonatal intensive care unit, hyperbilirubinemia, and longer hospital stay (P = .001 for all). Failed IOL was significantly associated with lower 1-minute APGAR scores, but not with lower 5-minute APGAR scores, the researchers noted (P = .033 for 1-minute score). No association was noted between failed IOL and neonatal readmission, lower umbilical cord pH value, or maternal ethnicity.
The findings were limited by the retrospective design, but data analysis is ongoing, Dr. Alhousseini said. The researchers are continuing to assess the roles not only of optimal glucose control, but other maternal factors in improving maternal and neonatal outcomes, he said.
Data Add to Awareness of Risk Factors
The current study is important because of the increasing incidence of diabetes and the need to examine associated risk factors in pregnancy, Michael Richley, MD, a maternal fetal medicine physician at the University of Washington, Seattle, said in an interview. “The average age of onset of diabetes is becoming younger and type 2 diabetes in pregnancy is an increasingly common diagnosis,” said Dr. Richley, who was not involved in the study.
The increase in both maternal and neonatal adverse outcomes is expected given the risk factors identified in the study, said Dr. Richley. “The patients with diabetes also were sicker at baseline, with hypertensive disorders, growth restriction, and pregestational diabetes,” he noted.
The study findings support data from previous research, Dr. Richley said. The message to clinicians is that patients with diabetes not only have an increased risk of needing a cesarean delivery but also have an increased risk of poor outcomes if a cesarean delivery is needed, he said.
Although a prospective study would be useful to show causality as opposed to just an association, such a study is challenging in this patient population given the limitations of conducting research on labor and delivery, he said.
The study received no outside funding. The researchers and Dr. Richley had no financial conflicts to disclose.
Approximately one-quarter of mothers with diabetes failed induction of labor, and this failure was associated with a range of adverse outcomes for mothers and infants, based on data from more than 2,000 individuals.
Uncontrolled diabetes remains a risk factor for cesarean delivery, Ali Alhousseini, MD, of Corewell Health East, Dearborn, Michigan, and colleagues wrote in a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
“Identifying and stratifying associated risk factors for failed induction of labor [IOL] may improve counseling and intrapartum care,” the researchers wrote in their abstract.
The researchers reviewed data from 2,172 mothers with diabetes who underwent IOL at a single university medical center between January 2013 and December 2021. They examined a range of maternal characteristics including age, ethnicity, gestational age, medical comorbidities, insulin administration, parity, and health insurance.
A total of 567 mothers with diabetes (26.1%) failed IOL and underwent cesarean delivery.
Overall, failed IOL was significantly associated with nulliparity (P = .0001), as well as preexisting diabetes compared with gestational diabetes, diabetes control with insulin, maternal essential hypertension, preeclampsia, and polyhydramnios (P = .001 for all). Other factors significantly associated with failed IOL included prenatal diagnosis of fetal growth restriction (P = .008), and placental abnormalities (P = .027).
Neonatal factors of weight, large for gestational age, head circumference, and height were not significantly associated with failed IOL (P > .05 for all).
As for neonatal outcomes, failed IOL was significantly associated with admission to neonatal intensive care unit, hyperbilirubinemia, and longer hospital stay (P = .001 for all). Failed IOL was significantly associated with lower 1-minute APGAR scores, but not with lower 5-minute APGAR scores, the researchers noted (P = .033 for 1-minute score). No association was noted between failed IOL and neonatal readmission, lower umbilical cord pH value, or maternal ethnicity.
The findings were limited by the retrospective design, but data analysis is ongoing, Dr. Alhousseini said. The researchers are continuing to assess the roles not only of optimal glucose control, but other maternal factors in improving maternal and neonatal outcomes, he said.
Data Add to Awareness of Risk Factors
The current study is important because of the increasing incidence of diabetes and the need to examine associated risk factors in pregnancy, Michael Richley, MD, a maternal fetal medicine physician at the University of Washington, Seattle, said in an interview. “The average age of onset of diabetes is becoming younger and type 2 diabetes in pregnancy is an increasingly common diagnosis,” said Dr. Richley, who was not involved in the study.
The increase in both maternal and neonatal adverse outcomes is expected given the risk factors identified in the study, said Dr. Richley. “The patients with diabetes also were sicker at baseline, with hypertensive disorders, growth restriction, and pregestational diabetes,” he noted.
The study findings support data from previous research, Dr. Richley said. The message to clinicians is that patients with diabetes not only have an increased risk of needing a cesarean delivery but also have an increased risk of poor outcomes if a cesarean delivery is needed, he said.
Although a prospective study would be useful to show causality as opposed to just an association, such a study is challenging in this patient population given the limitations of conducting research on labor and delivery, he said.
The study received no outside funding. The researchers and Dr. Richley had no financial conflicts to disclose.
Approximately one-quarter of mothers with diabetes failed induction of labor, and this failure was associated with a range of adverse outcomes for mothers and infants, based on data from more than 2,000 individuals.
Uncontrolled diabetes remains a risk factor for cesarean delivery, Ali Alhousseini, MD, of Corewell Health East, Dearborn, Michigan, and colleagues wrote in a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
“Identifying and stratifying associated risk factors for failed induction of labor [IOL] may improve counseling and intrapartum care,” the researchers wrote in their abstract.
The researchers reviewed data from 2,172 mothers with diabetes who underwent IOL at a single university medical center between January 2013 and December 2021. They examined a range of maternal characteristics including age, ethnicity, gestational age, medical comorbidities, insulin administration, parity, and health insurance.
A total of 567 mothers with diabetes (26.1%) failed IOL and underwent cesarean delivery.
Overall, failed IOL was significantly associated with nulliparity (P = .0001), as well as preexisting diabetes compared with gestational diabetes, diabetes control with insulin, maternal essential hypertension, preeclampsia, and polyhydramnios (P = .001 for all). Other factors significantly associated with failed IOL included prenatal diagnosis of fetal growth restriction (P = .008), and placental abnormalities (P = .027).
Neonatal factors of weight, large for gestational age, head circumference, and height were not significantly associated with failed IOL (P > .05 for all).
As for neonatal outcomes, failed IOL was significantly associated with admission to neonatal intensive care unit, hyperbilirubinemia, and longer hospital stay (P = .001 for all). Failed IOL was significantly associated with lower 1-minute APGAR scores, but not with lower 5-minute APGAR scores, the researchers noted (P = .033 for 1-minute score). No association was noted between failed IOL and neonatal readmission, lower umbilical cord pH value, or maternal ethnicity.
The findings were limited by the retrospective design, but data analysis is ongoing, Dr. Alhousseini said. The researchers are continuing to assess the roles not only of optimal glucose control, but other maternal factors in improving maternal and neonatal outcomes, he said.
Data Add to Awareness of Risk Factors
The current study is important because of the increasing incidence of diabetes and the need to examine associated risk factors in pregnancy, Michael Richley, MD, a maternal fetal medicine physician at the University of Washington, Seattle, said in an interview. “The average age of onset of diabetes is becoming younger and type 2 diabetes in pregnancy is an increasingly common diagnosis,” said Dr. Richley, who was not involved in the study.
The increase in both maternal and neonatal adverse outcomes is expected given the risk factors identified in the study, said Dr. Richley. “The patients with diabetes also were sicker at baseline, with hypertensive disorders, growth restriction, and pregestational diabetes,” he noted.
The study findings support data from previous research, Dr. Richley said. The message to clinicians is that patients with diabetes not only have an increased risk of needing a cesarean delivery but also have an increased risk of poor outcomes if a cesarean delivery is needed, he said.
Although a prospective study would be useful to show causality as opposed to just an association, such a study is challenging in this patient population given the limitations of conducting research on labor and delivery, he said.
The study received no outside funding. The researchers and Dr. Richley had no financial conflicts to disclose.
FROM ACOG 2024
Maternal Buprenorphine Affects Fetal Breathing
Measures of fetal breathing movement were lower in fetuses of pregnant patients who received buprenorphine, compared with controls, based on data from 177 individuals.
The findings were presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists by Caroline Bulger, MD, of East Tennessee State University, Johnson City.
Pregnant patients with opioid-use disorder in the community surrounding Johnson City receive medication-assisted therapy with buprenorphine during the prenatal period, Dr. Bulger and colleagues wrote in their abstract. The current prenatal program for substance use disorder was established in 2016 based on patient requests for assistance in lowering their buprenorphine dosages during pregnancy, said senior author Martin E. Olsen, MD, also of East Tennessee State University, in an interview.
“Buprenorphine medication–assisted treatment in pregnancy is associated with long-term effects on childhood development such as smaller neonatal brains, decreased school performance, and low birth weight;” however, data on the fetal effects of buprenorphine are limited, said Dr. Olsen.
The current study was conducted to evaluate a short-term finding of the fetal effects of buprenorphine, Dr. Olsen said.
“This study was performed after obstetric sonographers at our institution noted that biophysical profile [BPP] ultrasound assessments of the fetuses of mothers on buprenorphine took longer than for other patients,” said Dr. Olsen.
The researchers conducted a retrospective chart review of 131 patients who received buprenorphine and 46 who were followed for chronic hypertension and served as high-risk controls. Patients were seen at a single institution between July 1, 2016, and June 30, 2020.
The researchers hypothesized that BPP of fetuses in patients receiving buprenorphine might be different from controls because of the effects of buprenorphine.
Overall, patients who received buprenorphine were more likely to have a fetal breathing score of zero than those who underwent a BPP for hypertension. A significant relationship emerged between buprenorphine dosage and breathing motion assessment; patients on high-dose buprenorphine were more likely than patients on low doses to have values of zero on fetal breathing motion assessment, and a chi-squared test yielded a P value of .04269.
The takeaway for clinical practice is that clinicians performing BPP ultrasounds on buprenorphine-exposed fetuses can expect that these assessments may take longer on average than assessments of other high-risk patients, said Dr. Olsen. “Additional assessment after a low BPP score is still indicated for these fetuses just as in other high-risk pregnancies,” he said.
The study was limited primarily by the retrospective design, Dr. Olsen said.
Although current treatment guidelines do not emphasize the effects of maternal buprenorphine use on fetal development, these findings support previous research showing effects of buprenorphine on fetal brain structure, the researchers wrote in their abstract. Looking ahead, “We recommend additional study on the maternal buprenorphine medication–assisted treatment dose effects for fetal and neonatal development with attention to such factors as head circumference, birth weight, achievement of developmental milestones, and school performance,” Dr. Olsen said.
“We and others have shown that the lowest effective dose of buprenorphine can lower neonatal abstinence syndrome/neonatal opioid withdrawal syndrome rates,” but data showing an impact of lowest effective dose management on long-term complications of fetal buprenorphine exposure are lacking, he noted.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Measures of fetal breathing movement were lower in fetuses of pregnant patients who received buprenorphine, compared with controls, based on data from 177 individuals.
The findings were presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists by Caroline Bulger, MD, of East Tennessee State University, Johnson City.
Pregnant patients with opioid-use disorder in the community surrounding Johnson City receive medication-assisted therapy with buprenorphine during the prenatal period, Dr. Bulger and colleagues wrote in their abstract. The current prenatal program for substance use disorder was established in 2016 based on patient requests for assistance in lowering their buprenorphine dosages during pregnancy, said senior author Martin E. Olsen, MD, also of East Tennessee State University, in an interview.
“Buprenorphine medication–assisted treatment in pregnancy is associated with long-term effects on childhood development such as smaller neonatal brains, decreased school performance, and low birth weight;” however, data on the fetal effects of buprenorphine are limited, said Dr. Olsen.
The current study was conducted to evaluate a short-term finding of the fetal effects of buprenorphine, Dr. Olsen said.
“This study was performed after obstetric sonographers at our institution noted that biophysical profile [BPP] ultrasound assessments of the fetuses of mothers on buprenorphine took longer than for other patients,” said Dr. Olsen.
The researchers conducted a retrospective chart review of 131 patients who received buprenorphine and 46 who were followed for chronic hypertension and served as high-risk controls. Patients were seen at a single institution between July 1, 2016, and June 30, 2020.
The researchers hypothesized that BPP of fetuses in patients receiving buprenorphine might be different from controls because of the effects of buprenorphine.
Overall, patients who received buprenorphine were more likely to have a fetal breathing score of zero than those who underwent a BPP for hypertension. A significant relationship emerged between buprenorphine dosage and breathing motion assessment; patients on high-dose buprenorphine were more likely than patients on low doses to have values of zero on fetal breathing motion assessment, and a chi-squared test yielded a P value of .04269.
The takeaway for clinical practice is that clinicians performing BPP ultrasounds on buprenorphine-exposed fetuses can expect that these assessments may take longer on average than assessments of other high-risk patients, said Dr. Olsen. “Additional assessment after a low BPP score is still indicated for these fetuses just as in other high-risk pregnancies,” he said.
The study was limited primarily by the retrospective design, Dr. Olsen said.
Although current treatment guidelines do not emphasize the effects of maternal buprenorphine use on fetal development, these findings support previous research showing effects of buprenorphine on fetal brain structure, the researchers wrote in their abstract. Looking ahead, “We recommend additional study on the maternal buprenorphine medication–assisted treatment dose effects for fetal and neonatal development with attention to such factors as head circumference, birth weight, achievement of developmental milestones, and school performance,” Dr. Olsen said.
“We and others have shown that the lowest effective dose of buprenorphine can lower neonatal abstinence syndrome/neonatal opioid withdrawal syndrome rates,” but data showing an impact of lowest effective dose management on long-term complications of fetal buprenorphine exposure are lacking, he noted.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Measures of fetal breathing movement were lower in fetuses of pregnant patients who received buprenorphine, compared with controls, based on data from 177 individuals.
The findings were presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists by Caroline Bulger, MD, of East Tennessee State University, Johnson City.
Pregnant patients with opioid-use disorder in the community surrounding Johnson City receive medication-assisted therapy with buprenorphine during the prenatal period, Dr. Bulger and colleagues wrote in their abstract. The current prenatal program for substance use disorder was established in 2016 based on patient requests for assistance in lowering their buprenorphine dosages during pregnancy, said senior author Martin E. Olsen, MD, also of East Tennessee State University, in an interview.
“Buprenorphine medication–assisted treatment in pregnancy is associated with long-term effects on childhood development such as smaller neonatal brains, decreased school performance, and low birth weight;” however, data on the fetal effects of buprenorphine are limited, said Dr. Olsen.
The current study was conducted to evaluate a short-term finding of the fetal effects of buprenorphine, Dr. Olsen said.
“This study was performed after obstetric sonographers at our institution noted that biophysical profile [BPP] ultrasound assessments of the fetuses of mothers on buprenorphine took longer than for other patients,” said Dr. Olsen.
The researchers conducted a retrospective chart review of 131 patients who received buprenorphine and 46 who were followed for chronic hypertension and served as high-risk controls. Patients were seen at a single institution between July 1, 2016, and June 30, 2020.
The researchers hypothesized that BPP of fetuses in patients receiving buprenorphine might be different from controls because of the effects of buprenorphine.
Overall, patients who received buprenorphine were more likely to have a fetal breathing score of zero than those who underwent a BPP for hypertension. A significant relationship emerged between buprenorphine dosage and breathing motion assessment; patients on high-dose buprenorphine were more likely than patients on low doses to have values of zero on fetal breathing motion assessment, and a chi-squared test yielded a P value of .04269.
The takeaway for clinical practice is that clinicians performing BPP ultrasounds on buprenorphine-exposed fetuses can expect that these assessments may take longer on average than assessments of other high-risk patients, said Dr. Olsen. “Additional assessment after a low BPP score is still indicated for these fetuses just as in other high-risk pregnancies,” he said.
The study was limited primarily by the retrospective design, Dr. Olsen said.
Although current treatment guidelines do not emphasize the effects of maternal buprenorphine use on fetal development, these findings support previous research showing effects of buprenorphine on fetal brain structure, the researchers wrote in their abstract. Looking ahead, “We recommend additional study on the maternal buprenorphine medication–assisted treatment dose effects for fetal and neonatal development with attention to such factors as head circumference, birth weight, achievement of developmental milestones, and school performance,” Dr. Olsen said.
“We and others have shown that the lowest effective dose of buprenorphine can lower neonatal abstinence syndrome/neonatal opioid withdrawal syndrome rates,” but data showing an impact of lowest effective dose management on long-term complications of fetal buprenorphine exposure are lacking, he noted.
The study received no outside funding. The researchers had no financial conflicts to disclose.
ACOG 2024
Most women can conceive after breast cancer treatment
The findings, presented May 23 in advance of the annual meeting of the American Society of Clinical Oncology (ASCO) represent the most comprehensive look to date at fertility outcomes following treatment for women diagnosed with breast cancer before age 40 (Abstract 1518).
Kimia Sorouri, MD, a research fellow at the Dana-Farber Cancer Center in Boston, Massachusetts, and her colleagues, looked at data from the Young Women’s Breast Cancer study, a multicenter longitudinal cohort study, for 1213 U.S. and Canadian women (74% non-Hispanic white) who were diagnosed with stages 0-III breast cancer between 2006 and 2016. None of the included patients had metastatic disease, prior hysterectomy, or prior oophorectomy at diagnosis.
During a median 11 years of follow up, 197 of the women reported attempting pregnancy. Of these, 73% reported becoming pregnant, and 65% delivered a live infant a median 4 years after cancer diagnosis. The median age at diagnosis was 32 years, and 28% opted for egg or embryo freezing to preserve fertility. Importantly, 68% received chemotherapy, which can impair fertility, with only a small percentage undergoing ovarian suppression during chemotherapy treatment.
Key predictors of pregnancy or live birth in this study were “financial comfort,” a self-reported measure defined as having money left over to spend after bills are paid (odds ratio [OR], 2.04; 95% CI 1.01-4.12; P = .047); younger age at the time of diagnosis; and undergoing fertility preservation interventions at diagnosis (OR, 2.78; 95% CI 1.29-6.00; P = .009). Chemotherapy and other treatment factors were not seen to be associated with pregnancy or birth outcomes.
“Current research that informs our understanding of the impact of breast cancer treatment on pregnancy and live birth rates is fairly limited,” Dr. Sorouri said during an online press conference announcing the findings. Quality data on fertility outcomes has been limited to studies in certain subgroups, such as women with estrogen receptor–positive breast cancers, she noted, while other studies “have short-term follow-up and critically lack prospective assessment of attempt at conception.”
The new findings show, Dr. Sorouri said, “that in this modern cohort with a heightened awareness of fertility, access to fertility preservation can help to mitigate a portion of the damage from chemotherapy and other agents. Importantly, this highlights the need for increased accessibility of fertility preservation services for women newly diagnosed with breast cancer who are interested in a future pregnancy.”
Commenting on Dr. Sorouri and colleagues’ findings, Julie Gralow, MD, a breast cancer researcher and ASCO’s chief medical officer, stressed that, while younger age at diagnosis and financial comfort were two factors outside the scope of clinical oncology practice, “we can impact fertility preservation prior to treatment.”
She called it “critical” that every patient be informed of the impact of a breast cancer diagnosis and treatment on future fertility, and that all young patients interested in future fertility be offered fertility preservation prior to beginning treatment.
Ann Partridge, MD, of Dana-Farber, said in an interview that the findings reflected a decades’ long change in approach. “Twenty years ago when we first started this cohort, people would tell women ‘you can’t get pregnant. It’s too dangerous. You won’t be able to.’ And some indeed aren’t able to, but the majority who are attempting are succeeding, especially if they preserve their eggs or embryos. So even if chemo puts you into menopause or made you subfertile, if you’ve preserved eggs or embryos, we now can mitigate that distressing effect that many cancer patients have suffered from historically. That’s the good news here.”
Nonetheless, Dr. Partridge, an oncologist and the last author of the study, noted, the results reflected success only for women actively attempting pregnancy. “Remember, we’re not including the people who didn’t attempt. There may be some who went into menopause who never banked eggs or embryos, and may never have tried because they went to a doctor who told them they’re not fertile.” Further, she said, not all insurances cover in vitro fertilization for women who have had breast cancer.
The fact that financial comfort was correlated with reproductive success, Dr. Partridge said, speaks to broader issues about access. “It may not be all about insurers. It may be to have the ability, to have the time, the education and the wherewithal to do this right — and about being with doctors who talk about it.”
Dr. Sorouri and colleagues’ study was sponsored by the Breast Cancer Research Foundation and Susan G. Komen. Several co-authors disclosed receiving speaking and/or consulting fees from pharmaceutical companies, and one reported being an employee of GlaxoSmithKline. Dr. Sorouri reported no industry funding, while Dr. Partridge reported research funding from Novartis.
The findings, presented May 23 in advance of the annual meeting of the American Society of Clinical Oncology (ASCO) represent the most comprehensive look to date at fertility outcomes following treatment for women diagnosed with breast cancer before age 40 (Abstract 1518).
Kimia Sorouri, MD, a research fellow at the Dana-Farber Cancer Center in Boston, Massachusetts, and her colleagues, looked at data from the Young Women’s Breast Cancer study, a multicenter longitudinal cohort study, for 1213 U.S. and Canadian women (74% non-Hispanic white) who were diagnosed with stages 0-III breast cancer between 2006 and 2016. None of the included patients had metastatic disease, prior hysterectomy, or prior oophorectomy at diagnosis.
During a median 11 years of follow up, 197 of the women reported attempting pregnancy. Of these, 73% reported becoming pregnant, and 65% delivered a live infant a median 4 years after cancer diagnosis. The median age at diagnosis was 32 years, and 28% opted for egg or embryo freezing to preserve fertility. Importantly, 68% received chemotherapy, which can impair fertility, with only a small percentage undergoing ovarian suppression during chemotherapy treatment.
Key predictors of pregnancy or live birth in this study were “financial comfort,” a self-reported measure defined as having money left over to spend after bills are paid (odds ratio [OR], 2.04; 95% CI 1.01-4.12; P = .047); younger age at the time of diagnosis; and undergoing fertility preservation interventions at diagnosis (OR, 2.78; 95% CI 1.29-6.00; P = .009). Chemotherapy and other treatment factors were not seen to be associated with pregnancy or birth outcomes.
“Current research that informs our understanding of the impact of breast cancer treatment on pregnancy and live birth rates is fairly limited,” Dr. Sorouri said during an online press conference announcing the findings. Quality data on fertility outcomes has been limited to studies in certain subgroups, such as women with estrogen receptor–positive breast cancers, she noted, while other studies “have short-term follow-up and critically lack prospective assessment of attempt at conception.”
The new findings show, Dr. Sorouri said, “that in this modern cohort with a heightened awareness of fertility, access to fertility preservation can help to mitigate a portion of the damage from chemotherapy and other agents. Importantly, this highlights the need for increased accessibility of fertility preservation services for women newly diagnosed with breast cancer who are interested in a future pregnancy.”
Commenting on Dr. Sorouri and colleagues’ findings, Julie Gralow, MD, a breast cancer researcher and ASCO’s chief medical officer, stressed that, while younger age at diagnosis and financial comfort were two factors outside the scope of clinical oncology practice, “we can impact fertility preservation prior to treatment.”
She called it “critical” that every patient be informed of the impact of a breast cancer diagnosis and treatment on future fertility, and that all young patients interested in future fertility be offered fertility preservation prior to beginning treatment.
Ann Partridge, MD, of Dana-Farber, said in an interview that the findings reflected a decades’ long change in approach. “Twenty years ago when we first started this cohort, people would tell women ‘you can’t get pregnant. It’s too dangerous. You won’t be able to.’ And some indeed aren’t able to, but the majority who are attempting are succeeding, especially if they preserve their eggs or embryos. So even if chemo puts you into menopause or made you subfertile, if you’ve preserved eggs or embryos, we now can mitigate that distressing effect that many cancer patients have suffered from historically. That’s the good news here.”
Nonetheless, Dr. Partridge, an oncologist and the last author of the study, noted, the results reflected success only for women actively attempting pregnancy. “Remember, we’re not including the people who didn’t attempt. There may be some who went into menopause who never banked eggs or embryos, and may never have tried because they went to a doctor who told them they’re not fertile.” Further, she said, not all insurances cover in vitro fertilization for women who have had breast cancer.
The fact that financial comfort was correlated with reproductive success, Dr. Partridge said, speaks to broader issues about access. “It may not be all about insurers. It may be to have the ability, to have the time, the education and the wherewithal to do this right — and about being with doctors who talk about it.”
Dr. Sorouri and colleagues’ study was sponsored by the Breast Cancer Research Foundation and Susan G. Komen. Several co-authors disclosed receiving speaking and/or consulting fees from pharmaceutical companies, and one reported being an employee of GlaxoSmithKline. Dr. Sorouri reported no industry funding, while Dr. Partridge reported research funding from Novartis.
The findings, presented May 23 in advance of the annual meeting of the American Society of Clinical Oncology (ASCO) represent the most comprehensive look to date at fertility outcomes following treatment for women diagnosed with breast cancer before age 40 (Abstract 1518).
Kimia Sorouri, MD, a research fellow at the Dana-Farber Cancer Center in Boston, Massachusetts, and her colleagues, looked at data from the Young Women’s Breast Cancer study, a multicenter longitudinal cohort study, for 1213 U.S. and Canadian women (74% non-Hispanic white) who were diagnosed with stages 0-III breast cancer between 2006 and 2016. None of the included patients had metastatic disease, prior hysterectomy, or prior oophorectomy at diagnosis.
During a median 11 years of follow up, 197 of the women reported attempting pregnancy. Of these, 73% reported becoming pregnant, and 65% delivered a live infant a median 4 years after cancer diagnosis. The median age at diagnosis was 32 years, and 28% opted for egg or embryo freezing to preserve fertility. Importantly, 68% received chemotherapy, which can impair fertility, with only a small percentage undergoing ovarian suppression during chemotherapy treatment.
Key predictors of pregnancy or live birth in this study were “financial comfort,” a self-reported measure defined as having money left over to spend after bills are paid (odds ratio [OR], 2.04; 95% CI 1.01-4.12; P = .047); younger age at the time of diagnosis; and undergoing fertility preservation interventions at diagnosis (OR, 2.78; 95% CI 1.29-6.00; P = .009). Chemotherapy and other treatment factors were not seen to be associated with pregnancy or birth outcomes.
“Current research that informs our understanding of the impact of breast cancer treatment on pregnancy and live birth rates is fairly limited,” Dr. Sorouri said during an online press conference announcing the findings. Quality data on fertility outcomes has been limited to studies in certain subgroups, such as women with estrogen receptor–positive breast cancers, she noted, while other studies “have short-term follow-up and critically lack prospective assessment of attempt at conception.”
The new findings show, Dr. Sorouri said, “that in this modern cohort with a heightened awareness of fertility, access to fertility preservation can help to mitigate a portion of the damage from chemotherapy and other agents. Importantly, this highlights the need for increased accessibility of fertility preservation services for women newly diagnosed with breast cancer who are interested in a future pregnancy.”
Commenting on Dr. Sorouri and colleagues’ findings, Julie Gralow, MD, a breast cancer researcher and ASCO’s chief medical officer, stressed that, while younger age at diagnosis and financial comfort were two factors outside the scope of clinical oncology practice, “we can impact fertility preservation prior to treatment.”
She called it “critical” that every patient be informed of the impact of a breast cancer diagnosis and treatment on future fertility, and that all young patients interested in future fertility be offered fertility preservation prior to beginning treatment.
Ann Partridge, MD, of Dana-Farber, said in an interview that the findings reflected a decades’ long change in approach. “Twenty years ago when we first started this cohort, people would tell women ‘you can’t get pregnant. It’s too dangerous. You won’t be able to.’ And some indeed aren’t able to, but the majority who are attempting are succeeding, especially if they preserve their eggs or embryos. So even if chemo puts you into menopause or made you subfertile, if you’ve preserved eggs or embryos, we now can mitigate that distressing effect that many cancer patients have suffered from historically. That’s the good news here.”
Nonetheless, Dr. Partridge, an oncologist and the last author of the study, noted, the results reflected success only for women actively attempting pregnancy. “Remember, we’re not including the people who didn’t attempt. There may be some who went into menopause who never banked eggs or embryos, and may never have tried because they went to a doctor who told them they’re not fertile.” Further, she said, not all insurances cover in vitro fertilization for women who have had breast cancer.
The fact that financial comfort was correlated with reproductive success, Dr. Partridge said, speaks to broader issues about access. “It may not be all about insurers. It may be to have the ability, to have the time, the education and the wherewithal to do this right — and about being with doctors who talk about it.”
Dr. Sorouri and colleagues’ study was sponsored by the Breast Cancer Research Foundation and Susan G. Komen. Several co-authors disclosed receiving speaking and/or consulting fees from pharmaceutical companies, and one reported being an employee of GlaxoSmithKline. Dr. Sorouri reported no industry funding, while Dr. Partridge reported research funding from Novartis.
FROM ASCO 2024
Fluoride, Water, and Kids’ Brains: It’s Complicated
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.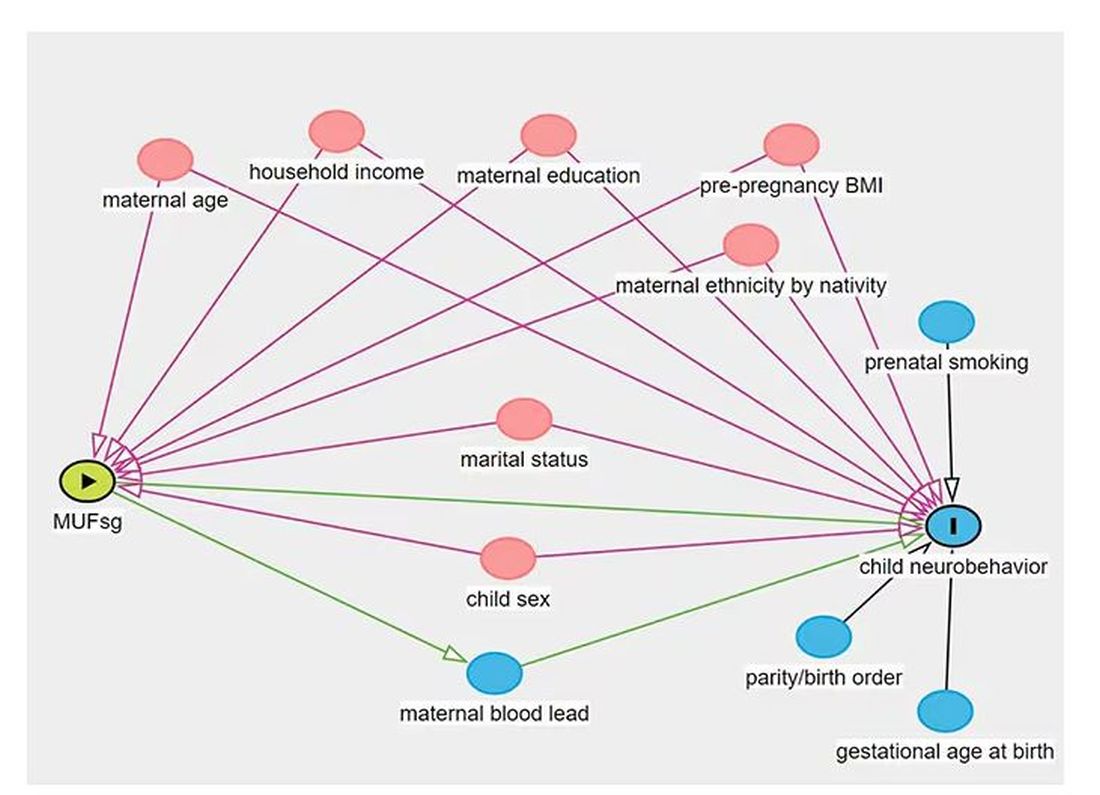
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.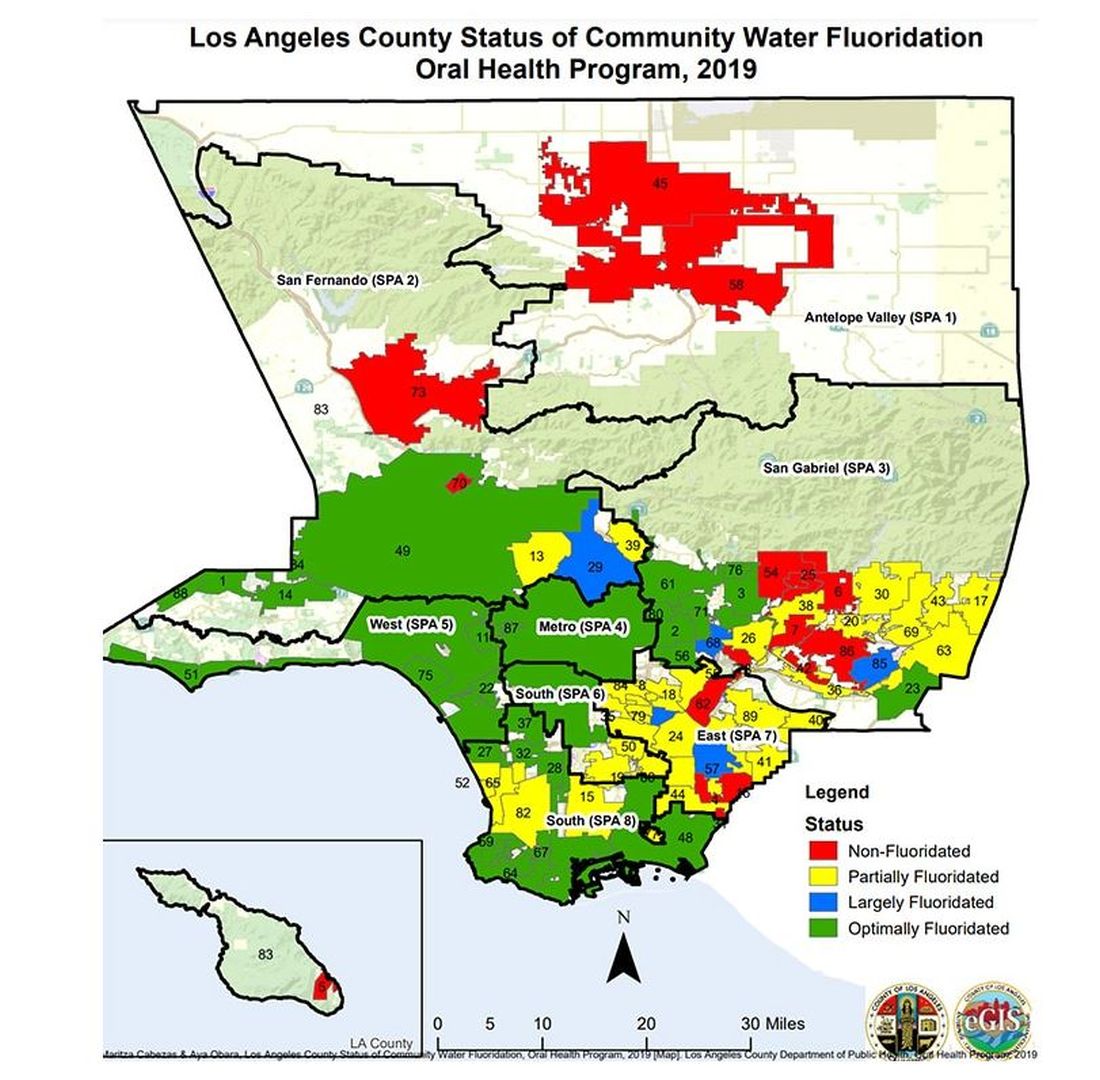
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently looked back at my folder full of these medical study commentaries, this weekly video series we call Impact Factor, and realized that I’ve been doing this for a long time. More than 400 articles, believe it or not.
I’ve learned a lot in that time — about medicine, of course — but also about how people react to certain topics. If you’ve been with me this whole time, or even for just a chunk of it, you’ll know that I tend to take a measured approach to most topics. No one study is ever truly definitive, after all. But regardless of how even-keeled I may be, there are some topics that I just know in advance are going to be a bit divisive: studies about gun control; studies about vitamin D; and, of course, studies about fluoride.
Shall We Shake This Hornet’s Nest?
The fluoridation of the US water system began in 1945 with the goal of reducing cavities in the population. The CDC named water fluoridation one of the 10 great public health achievements of the 20th century, along with such inarguable achievements as the recognition of tobacco as a health hazard.
But fluoridation has never been without its detractors. One problem is that the spectrum of beliefs about the potential harm of fluoridation is huge. On one end, you have science-based concerns such as the recognition that excessive fluoride intake can cause fluorosis and stain tooth enamel. I’ll note that the EPA regulates fluoride levels — there is a fair amount of naturally occurring fluoride in water tables around the world — to prevent this. And, of course, on the other end of the spectrum, you have beliefs that are essentially conspiracy theories: “They” add fluoride to the water supply to control us.
The challenge for me is that when one “side” of a scientific debate includes the crazy theories, it can be hard to discuss that whole spectrum, since there are those who will see evidence of any adverse fluoride effect as confirmation that the conspiracy theory is true.
I can’t help this. So I’ll just say this up front: I am about to tell you about a study that shows some potential risk from fluoride exposure. I will tell you up front that there are some significant caveats to the study that call the results into question. And I will tell you up front that no one is controlling your mind, or my mind, with fluoride; they do it with social media.
Let’s Dive Into These Shark-Infested, Fluoridated Waters
We’re talking about the study, “Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months,” which appears in JAMA Network Open.
It’s a study of 229 mother-child pairs from the Los Angeles area. The moms had their urinary fluoride level measured once before 30 weeks of gestation. A neurobehavioral battery called the Preschool Child Behavior Checklist was administered to the children at age 36 months.
The main thing you’ll hear about this study — in headlines, Facebook posts, and manifestos locked in drawers somewhere — is the primary result: A 0.68-mg/L increase in urinary fluoride in the mothers, about 25 percentile points, was associated with a doubling of the risk for neurobehavioral problems in their kids when they were 3 years old.
Yikes.
But this is not a randomized trial. Researchers didn’t randomly assign some women to have high fluoride intake and some women to have low fluoride intake. They knew that other factors that might lead to neurobehavioral problems could also lead to higher fluoride intake. They represent these factors in what’s known as a directed acyclic graph, as seen here, and account for them statistically using a regression equation.
Not represented here are neighborhood characteristics. Los Angeles does not have uniformly fluoridated water, and neurobehavioral problems in kids are strongly linked to stressors in their environments. Fluoride level could be an innocent bystander.
I’m really just describing the classic issue of correlation versus causation here, the bane of all observational research and — let’s be honest — a bit of a crutch that allows us to disregard the results of studies we don’t like, provided the study wasn’t a randomized trial.
But I have a deeper issue with this study than the old “failure to adjust for relevant confounders” thing, as important as that is.
The exposure of interest in this study is maternal urinary fluoride, as measured in a spot sample. It’s not often that I get to go deep on nephrology in this space, but let’s think about that for a second. Let’s assume for a moment that fluoride is toxic to the developing fetal brain, the main concern raised by the results of the study. How would that work? Presumably, mom would be ingesting fluoride from various sources (like the water supply), and that fluoride would get into her blood, and from her blood across the placenta to the baby’s blood, and into the baby’s brain.
Is Urinary Fluoride a Good Measure of Blood Fluoride?
It’s not great. Empirically, we have data that tell us that levels of urine fluoride are not all that similar to levels of serum fluoride. In 2014, a study investigated the correlation between urine and serum fluoride in a cohort of 60 schoolchildren and found a correlation coefficient of around 0.5.
Why isn’t urine fluoride a great proxy for serum fluoride? The most obvious reason is the urine concentration. Human urine concentration can range from about 50 mmol to 1200 mmol (a 24-fold difference) depending on hydration status. Over the course of 24 hours, for example, the amount of fluoride you put out in your urine may be fairly stable in relation to intake, but for a spot urine sample it would be wildly variable. The authors know this, of course, and so they divide the measured urine fluoride by the specific gravity of the urine to give a sort of “dilution adjusted” value. That’s what is actually used in this study. But specific gravity is, itself, an imperfect measure of how dilute the urine is.
This is something that comes up a lot in urinary biomarker research and it’s not that hard to get around. The best thing would be to just measure blood levels of fluoride. The second best option is 24-hour fluoride excretion. After that, the next best thing would be to adjust the spot concentration by other markers of urinary dilution — creatinine or osmolality — as sensitivity analyses. Any of these approaches would lend credence to the results of the study.
Urinary fluoride excretion is pH dependent. The more acidic the urine, the less fluoride is excreted. Many things — including, importantly, diet — affect urine pH. And it is not a stretch to think that diet may also affect the developing fetus. Neither urine pH nor dietary habits were accounted for in this study.
So, here we are. We have an observational study suggesting a harm that may be associated with fluoride. There may be a causal link here, in which case we need further studies to weigh the harm against the more well-established public health benefit. Or, this is all correlation — an illusion created by the limitations of observational data, and the unique challenges of estimating intake from a single urine sample. In other words, this study has something for everyone, fluoride boosters and skeptics alike. Let the arguments begin. But, if possible, leave me out of it.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Research Highlights From ESMO Breast Cancer
Among the topics the speakers addressed were breast cancer prevention, early breast cancer, advanced breast cancer, and supportive care.
In recent years, the way clinicians look at carcinogenesis in breast cancer has changed, and many new targets for potential early detection and prevention have emerged, said Suzette Delaloge, MD, of Gustave Roussy, Paris, France, in her presentation at the meeting.
Instant risk assessment at different time points could potentially intercept cancer among high-risk individuals, she said.
A study by Mikael Eriksson, PhD, and colleagues focused on external validation of the Profound AI tool to identify breast cancer risk in the general population. The researchers showed an area under the curve of 0.72 in their AI risk model, which has the potential to be clinically meaningful, although it must be prospectively validated, Dr. Delaloge said in her presentation.
She also reviewed two studies on the use of genes to further refine breast cancer risk among carriers. One of these, a prospective study presented in a session by Kelly-Anne Phillips, MD, of Peter MacCallum Cancer Center, Melbourne, Australia, used the CANRISK online risk assessment tool and validated increased breast cancer risk in BRCA1 and BRCA2 carriers, with AUCs of 0.79 and 0.78, respectively. The other study, which was by Maria Rezqallah Aron, MD, and colleagues examined polygenic scores as a way to refine breast cancer risk stratification among carriers of the ALM and PALB2 genes as well. These genes might be useful in identifying individuals who could benefit from early intervention, including surgery, Dr. Delaloge said.
Translational Research
“Preparing my talk, I felt like a kid in a candy store,” because of the amount of new translational research presented, including several studies of endocrine treatment–based approaches to therapy, said Marleen Kok, MD, of the Netherlands Cancer Institute, Amsterdam.
In her presentation, Dr. Kok highlighted findings from an analysis of patients in the monarchE study (a trial of high-risk patients) showing a consistent improvement in invasive disease-free survival for the subset of patients with germline BRCA1 and BRCA2 mutations who received abemaciclib plus endocrine therapy.
The value of tumor-infiltrating lymphocytes (TILs) on patients who are not receiving chemotherapy is important because of the focus on prognosis, and prospective trials are underway, she said.
A poster on the impact of chemotherapy and stromal tumor-infiltrating lymphocytes (sTILs) in stage I triple-negative breast cancer showed no association between chemotherapy and better outcomes regardless of sTILs in patients who did and did not receive chemotherapy, which has implications for potential treatment sparing in this population, Dr. Kok noted.
Artificial Intelligence (AI) was the subject of several posters at the meeting, and Dr. Kok identified a multisite European study of an automated HER2 scoring system as notable for its size and accuracy. In the study, the accuracy among pathologists was much higher with the assistance of AI, she said. Using AI for more complex analysis has shown success, she said.
Dr. Kok ended her talk with a poster that surveyed breast cancer patients about their understanding of their disease. The results showed that less than half (44%) of patients reported that their healthcare providers had given them enough information to learn about their breast cancer type, and less than one third could recall terminology about biomarkers; the study is important because it shows that clinicians need to do better in explaining these terms to patients, Dr. Kok said.
Early Breast Cancer
Right-sizing therapy, meaning identifying the right treatment for every patient, is a key element of new research in early breast cancer, said Erika Hamilton, MD, of the Sarah Cannon Research Institute, Nashville, Tenn.
She highlighted safety and treatment duration updates from the NATALEE study, which compared adjuvant ribociclib plus nonsteroidal aromatase inhibitor (NSAI) to NSAI alone for ER+/HER2- breast cancer. The current analysis presented at the meeting showed significant benefits with the addition of ribociclib and no evidence of new safety signals or adverse event exacerbations at 3 years, she said. Dose modifications had no significant impact on efficacy, she added.
The findings of no impact of dose reduction on efficacy in both the NATALEE and monarchE studies provide important information on whether dosage can be reduced in patients, which will increase the odds that patients will tolerate extended therapy with good outcomes and stay on their prescribed therapies, Dr. Hamilton emphasized.
The CARABELA study, a phase 2 trial of neoadjuvant letrozole plus abemaciclib vs adriamycin and cyclophosphamide (AC), showed clinically similar response rates but did not meet its endpoint for residual cancer burden (RCB) scores. These data add to results from other studies and show that it is too soon to universally replace neoadjuvant chemotherapy as first-line treatment for highly proliferative ER+ breast cancer, Dr. Hamilton said in her presentation.
Advanced Breast Cancer
Take-home messages about advanced breast cancer include growing evidence for the potential benefits of antibody drug conjugates (ADCs), said Eva Ciruelos, MD, of University Hospital, Madrid, Spain. The TROPION-BREAST01 study, a phase 3 randomized trial, showed significant and clinically meaningful improvement in progression-free survival in patients with previously treated, inoperable, or metastatic HR+/HER2- breast cancer who received datopotamab deruxtecan (Dato-DXd) compared with those who received chemotherapy.
Data from an additional safety analysis were presented at the meeting; although Dato-DXd, a trophoblast cell-surface antigen 2 (TROP2)–directed antibody-drug conjugate, was well-tolerated, it is important to remain aware of toxicities, notably oral mucositis, which occurred in 55.6% of the patients in the study across all grades, and ocular surface toxicity, which occurred in 40% of patients across all grades, Dr. Ciruelos emphasized.
Key research in the area of advanced triple-negative breast cancer included data from the IMPASSION 132 study. This study is “specifically centered on early relapsers,” a population often excluded from other trials, Dr. Ciruelos said. In this study, patients with advanced triple-negative breast cancer were randomized to chemotherapy with or without atezolizumab, and the study showed no benefits with atezolizumab for overall survival, progression-free survival, or overall response rate, she said. “This is something to work with, because this is a very refractory population,” Dr. Ciruelos noted.
New immunotherapy combinations are needed to improve survival in advanced breast cancer patients, Dr. Ciruelos said. At the meeting, researchers presented interim data from a subset of patients in the MORPHEUS-pan breast cancer trial, a phase 1B/2 study involving multiple treatment combinations in locally advanced/metastatic breast cancer patients.
The interim analysis included 18-week data from triple-negative breast cancer patients and compared outcomes for patients randomized to atezolizumab with or without sacituzumab govitecan (SG).
The study was small, with only 31 patients in the combination arm and 11 controls, but the results were promising, with an overall response rate of 76.7% in the combination arm vs 66.7% in the control arm, Dr. Ciruelos said.
Supportive Care
Key supportive care takeaways included data on pregnancy in young breast cancer survivors and the safety of vaginal estrogen therapy in breast cancer patients with genitourinary symptoms, said Anne May, MD, of the University Medical Center Utrecht, Utrecht, Netherlands.
A study previously published in JAMA including nearly 5000 BRCA carriers who were diagnosed with invasive breast cancer at age 40 years or younger showed no association between pregnancy after breast cancer and adverse maternal or fetal outcomes, and pregnancy had no significant impact on overall survival. The authors presented new data on the safety of assisted reproductive techniques (ART) based on the 543 pregnancies in the original study, at the meeting. Of these, 436 conceived naturally, and 107 used ART. After a median of 9.1 years, ART had no effect on disease-free survival compared to natural conception (hazard ratio [HR], 0.64). Based on these findings, fertility preservation should be offered to all women who receive a breast cancer diagnosis and are interested in future fertility, Dr. May said.
Conceiving after breast cancer treatment and follow-up should not be contraindicated for young BRCA carriers, she added.No trial data are available for the effects of vaginal estrogen therapy (VET) on disease-free survival in breast cancer survivors with genitourinary symptoms caused by declining estrogen levels, Dr. May said. However, researchers in France and Switzerland conducted an emulation of a hypothetical target trial using data from the French National social security system for more than 130,000 individuals. Although VET therapy had no impact on disease-free survival in most breast cancer survivors overall, it did have a negative impact in a subset of patients with HR-positive and HR-negative tumors who were treated with aromatase inhibitors. The study was hypothetical, but important because the results suggest that clinicians can safely propose VTE to patients who report genitourinary symptoms after treatment for early-stage breast cancer with tamoxifen, but VTE should be avoided in patients treated with aromatase inhibitors, Dr. May said.
Dr. Delaloge disclosed research support to her institution from AstraZeneca, MSD, Bristol Myers Squibb, Sanofi, Taiho, Novartis, European Commission, INCa, Banque des Territoires, and Fondation Philanthropia. She also disclosed honoraria to her institution from AstraZeneca, Gilead, Novartis, Elsan, Besins, Sanofi, Exact Sciences, and Lilly, as well as travel support from Novartis.
Dr. Kok disclosed research funding from AstraZeneca, Bristol Myers Squibb, Daichi, and Roche, and advisory board membership/speaker’s fees from Alderaan Biotechnology, BIONTECH, Domain Therapeutics, AstraZeneca, Daichi, Bristol Myers Squibb, Gilead, Medscape, MSD, and Roche.
Dr. Hamilton disclosed a consulting advisory role (to her institution) for Accutar Biotechology, AstraZeneca, Daiichi Sankyo, Ellipses Pharma, Entos, Forsum Pharma, Gilead Sciences, Greenwich LifeSciences, Jazz Pharmaceuticals, Lilly, Medical Pharma Services, Mersana, Novartis, Olema Pharmaceuticals, Orum Therapeutics, Roche/Genentech, Stemline Therapeutics, ands others. She also disclosed contracted research/grant support to her institution only from Abbvie, Acerta Pharma, Accutar Biotechnology , ADC Therapeutics, AKESOBIO Australia , Amgen, Aravive, ArQule, Artios, Arvinas, AstraZeneca, AtlasMedx, BeiGene, Black Diamond and others.
Dr. Ciruelos disclosed serving as an external advisor for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, and Lilly, as well as serving as a speaker for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, Lilly, and Pierre Fabre. She also disclosed travel grants from Roche, Pfizer, and AstraZeneca, and research grants from Seagen and Roche.
Dr. May had no financial conflicts to disclose.
Among the topics the speakers addressed were breast cancer prevention, early breast cancer, advanced breast cancer, and supportive care.
In recent years, the way clinicians look at carcinogenesis in breast cancer has changed, and many new targets for potential early detection and prevention have emerged, said Suzette Delaloge, MD, of Gustave Roussy, Paris, France, in her presentation at the meeting.
Instant risk assessment at different time points could potentially intercept cancer among high-risk individuals, she said.
A study by Mikael Eriksson, PhD, and colleagues focused on external validation of the Profound AI tool to identify breast cancer risk in the general population. The researchers showed an area under the curve of 0.72 in their AI risk model, which has the potential to be clinically meaningful, although it must be prospectively validated, Dr. Delaloge said in her presentation.
She also reviewed two studies on the use of genes to further refine breast cancer risk among carriers. One of these, a prospective study presented in a session by Kelly-Anne Phillips, MD, of Peter MacCallum Cancer Center, Melbourne, Australia, used the CANRISK online risk assessment tool and validated increased breast cancer risk in BRCA1 and BRCA2 carriers, with AUCs of 0.79 and 0.78, respectively. The other study, which was by Maria Rezqallah Aron, MD, and colleagues examined polygenic scores as a way to refine breast cancer risk stratification among carriers of the ALM and PALB2 genes as well. These genes might be useful in identifying individuals who could benefit from early intervention, including surgery, Dr. Delaloge said.
Translational Research
“Preparing my talk, I felt like a kid in a candy store,” because of the amount of new translational research presented, including several studies of endocrine treatment–based approaches to therapy, said Marleen Kok, MD, of the Netherlands Cancer Institute, Amsterdam.
In her presentation, Dr. Kok highlighted findings from an analysis of patients in the monarchE study (a trial of high-risk patients) showing a consistent improvement in invasive disease-free survival for the subset of patients with germline BRCA1 and BRCA2 mutations who received abemaciclib plus endocrine therapy.
The value of tumor-infiltrating lymphocytes (TILs) on patients who are not receiving chemotherapy is important because of the focus on prognosis, and prospective trials are underway, she said.
A poster on the impact of chemotherapy and stromal tumor-infiltrating lymphocytes (sTILs) in stage I triple-negative breast cancer showed no association between chemotherapy and better outcomes regardless of sTILs in patients who did and did not receive chemotherapy, which has implications for potential treatment sparing in this population, Dr. Kok noted.
Artificial Intelligence (AI) was the subject of several posters at the meeting, and Dr. Kok identified a multisite European study of an automated HER2 scoring system as notable for its size and accuracy. In the study, the accuracy among pathologists was much higher with the assistance of AI, she said. Using AI for more complex analysis has shown success, she said.
Dr. Kok ended her talk with a poster that surveyed breast cancer patients about their understanding of their disease. The results showed that less than half (44%) of patients reported that their healthcare providers had given them enough information to learn about their breast cancer type, and less than one third could recall terminology about biomarkers; the study is important because it shows that clinicians need to do better in explaining these terms to patients, Dr. Kok said.
Early Breast Cancer
Right-sizing therapy, meaning identifying the right treatment for every patient, is a key element of new research in early breast cancer, said Erika Hamilton, MD, of the Sarah Cannon Research Institute, Nashville, Tenn.
She highlighted safety and treatment duration updates from the NATALEE study, which compared adjuvant ribociclib plus nonsteroidal aromatase inhibitor (NSAI) to NSAI alone for ER+/HER2- breast cancer. The current analysis presented at the meeting showed significant benefits with the addition of ribociclib and no evidence of new safety signals or adverse event exacerbations at 3 years, she said. Dose modifications had no significant impact on efficacy, she added.
The findings of no impact of dose reduction on efficacy in both the NATALEE and monarchE studies provide important information on whether dosage can be reduced in patients, which will increase the odds that patients will tolerate extended therapy with good outcomes and stay on their prescribed therapies, Dr. Hamilton emphasized.
The CARABELA study, a phase 2 trial of neoadjuvant letrozole plus abemaciclib vs adriamycin and cyclophosphamide (AC), showed clinically similar response rates but did not meet its endpoint for residual cancer burden (RCB) scores. These data add to results from other studies and show that it is too soon to universally replace neoadjuvant chemotherapy as first-line treatment for highly proliferative ER+ breast cancer, Dr. Hamilton said in her presentation.
Advanced Breast Cancer
Take-home messages about advanced breast cancer include growing evidence for the potential benefits of antibody drug conjugates (ADCs), said Eva Ciruelos, MD, of University Hospital, Madrid, Spain. The TROPION-BREAST01 study, a phase 3 randomized trial, showed significant and clinically meaningful improvement in progression-free survival in patients with previously treated, inoperable, or metastatic HR+/HER2- breast cancer who received datopotamab deruxtecan (Dato-DXd) compared with those who received chemotherapy.
Data from an additional safety analysis were presented at the meeting; although Dato-DXd, a trophoblast cell-surface antigen 2 (TROP2)–directed antibody-drug conjugate, was well-tolerated, it is important to remain aware of toxicities, notably oral mucositis, which occurred in 55.6% of the patients in the study across all grades, and ocular surface toxicity, which occurred in 40% of patients across all grades, Dr. Ciruelos emphasized.
Key research in the area of advanced triple-negative breast cancer included data from the IMPASSION 132 study. This study is “specifically centered on early relapsers,” a population often excluded from other trials, Dr. Ciruelos said. In this study, patients with advanced triple-negative breast cancer were randomized to chemotherapy with or without atezolizumab, and the study showed no benefits with atezolizumab for overall survival, progression-free survival, or overall response rate, she said. “This is something to work with, because this is a very refractory population,” Dr. Ciruelos noted.
New immunotherapy combinations are needed to improve survival in advanced breast cancer patients, Dr. Ciruelos said. At the meeting, researchers presented interim data from a subset of patients in the MORPHEUS-pan breast cancer trial, a phase 1B/2 study involving multiple treatment combinations in locally advanced/metastatic breast cancer patients.
The interim analysis included 18-week data from triple-negative breast cancer patients and compared outcomes for patients randomized to atezolizumab with or without sacituzumab govitecan (SG).
The study was small, with only 31 patients in the combination arm and 11 controls, but the results were promising, with an overall response rate of 76.7% in the combination arm vs 66.7% in the control arm, Dr. Ciruelos said.
Supportive Care
Key supportive care takeaways included data on pregnancy in young breast cancer survivors and the safety of vaginal estrogen therapy in breast cancer patients with genitourinary symptoms, said Anne May, MD, of the University Medical Center Utrecht, Utrecht, Netherlands.
A study previously published in JAMA including nearly 5000 BRCA carriers who were diagnosed with invasive breast cancer at age 40 years or younger showed no association between pregnancy after breast cancer and adverse maternal or fetal outcomes, and pregnancy had no significant impact on overall survival. The authors presented new data on the safety of assisted reproductive techniques (ART) based on the 543 pregnancies in the original study, at the meeting. Of these, 436 conceived naturally, and 107 used ART. After a median of 9.1 years, ART had no effect on disease-free survival compared to natural conception (hazard ratio [HR], 0.64). Based on these findings, fertility preservation should be offered to all women who receive a breast cancer diagnosis and are interested in future fertility, Dr. May said.
Conceiving after breast cancer treatment and follow-up should not be contraindicated for young BRCA carriers, she added.No trial data are available for the effects of vaginal estrogen therapy (VET) on disease-free survival in breast cancer survivors with genitourinary symptoms caused by declining estrogen levels, Dr. May said. However, researchers in France and Switzerland conducted an emulation of a hypothetical target trial using data from the French National social security system for more than 130,000 individuals. Although VET therapy had no impact on disease-free survival in most breast cancer survivors overall, it did have a negative impact in a subset of patients with HR-positive and HR-negative tumors who were treated with aromatase inhibitors. The study was hypothetical, but important because the results suggest that clinicians can safely propose VTE to patients who report genitourinary symptoms after treatment for early-stage breast cancer with tamoxifen, but VTE should be avoided in patients treated with aromatase inhibitors, Dr. May said.
Dr. Delaloge disclosed research support to her institution from AstraZeneca, MSD, Bristol Myers Squibb, Sanofi, Taiho, Novartis, European Commission, INCa, Banque des Territoires, and Fondation Philanthropia. She also disclosed honoraria to her institution from AstraZeneca, Gilead, Novartis, Elsan, Besins, Sanofi, Exact Sciences, and Lilly, as well as travel support from Novartis.
Dr. Kok disclosed research funding from AstraZeneca, Bristol Myers Squibb, Daichi, and Roche, and advisory board membership/speaker’s fees from Alderaan Biotechnology, BIONTECH, Domain Therapeutics, AstraZeneca, Daichi, Bristol Myers Squibb, Gilead, Medscape, MSD, and Roche.
Dr. Hamilton disclosed a consulting advisory role (to her institution) for Accutar Biotechology, AstraZeneca, Daiichi Sankyo, Ellipses Pharma, Entos, Forsum Pharma, Gilead Sciences, Greenwich LifeSciences, Jazz Pharmaceuticals, Lilly, Medical Pharma Services, Mersana, Novartis, Olema Pharmaceuticals, Orum Therapeutics, Roche/Genentech, Stemline Therapeutics, ands others. She also disclosed contracted research/grant support to her institution only from Abbvie, Acerta Pharma, Accutar Biotechnology , ADC Therapeutics, AKESOBIO Australia , Amgen, Aravive, ArQule, Artios, Arvinas, AstraZeneca, AtlasMedx, BeiGene, Black Diamond and others.
Dr. Ciruelos disclosed serving as an external advisor for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, and Lilly, as well as serving as a speaker for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, Lilly, and Pierre Fabre. She also disclosed travel grants from Roche, Pfizer, and AstraZeneca, and research grants from Seagen and Roche.
Dr. May had no financial conflicts to disclose.
Among the topics the speakers addressed were breast cancer prevention, early breast cancer, advanced breast cancer, and supportive care.
In recent years, the way clinicians look at carcinogenesis in breast cancer has changed, and many new targets for potential early detection and prevention have emerged, said Suzette Delaloge, MD, of Gustave Roussy, Paris, France, in her presentation at the meeting.
Instant risk assessment at different time points could potentially intercept cancer among high-risk individuals, she said.
A study by Mikael Eriksson, PhD, and colleagues focused on external validation of the Profound AI tool to identify breast cancer risk in the general population. The researchers showed an area under the curve of 0.72 in their AI risk model, which has the potential to be clinically meaningful, although it must be prospectively validated, Dr. Delaloge said in her presentation.
She also reviewed two studies on the use of genes to further refine breast cancer risk among carriers. One of these, a prospective study presented in a session by Kelly-Anne Phillips, MD, of Peter MacCallum Cancer Center, Melbourne, Australia, used the CANRISK online risk assessment tool and validated increased breast cancer risk in BRCA1 and BRCA2 carriers, with AUCs of 0.79 and 0.78, respectively. The other study, which was by Maria Rezqallah Aron, MD, and colleagues examined polygenic scores as a way to refine breast cancer risk stratification among carriers of the ALM and PALB2 genes as well. These genes might be useful in identifying individuals who could benefit from early intervention, including surgery, Dr. Delaloge said.
Translational Research
“Preparing my talk, I felt like a kid in a candy store,” because of the amount of new translational research presented, including several studies of endocrine treatment–based approaches to therapy, said Marleen Kok, MD, of the Netherlands Cancer Institute, Amsterdam.
In her presentation, Dr. Kok highlighted findings from an analysis of patients in the monarchE study (a trial of high-risk patients) showing a consistent improvement in invasive disease-free survival for the subset of patients with germline BRCA1 and BRCA2 mutations who received abemaciclib plus endocrine therapy.
The value of tumor-infiltrating lymphocytes (TILs) on patients who are not receiving chemotherapy is important because of the focus on prognosis, and prospective trials are underway, she said.
A poster on the impact of chemotherapy and stromal tumor-infiltrating lymphocytes (sTILs) in stage I triple-negative breast cancer showed no association between chemotherapy and better outcomes regardless of sTILs in patients who did and did not receive chemotherapy, which has implications for potential treatment sparing in this population, Dr. Kok noted.
Artificial Intelligence (AI) was the subject of several posters at the meeting, and Dr. Kok identified a multisite European study of an automated HER2 scoring system as notable for its size and accuracy. In the study, the accuracy among pathologists was much higher with the assistance of AI, she said. Using AI for more complex analysis has shown success, she said.
Dr. Kok ended her talk with a poster that surveyed breast cancer patients about their understanding of their disease. The results showed that less than half (44%) of patients reported that their healthcare providers had given them enough information to learn about their breast cancer type, and less than one third could recall terminology about biomarkers; the study is important because it shows that clinicians need to do better in explaining these terms to patients, Dr. Kok said.
Early Breast Cancer
Right-sizing therapy, meaning identifying the right treatment for every patient, is a key element of new research in early breast cancer, said Erika Hamilton, MD, of the Sarah Cannon Research Institute, Nashville, Tenn.
She highlighted safety and treatment duration updates from the NATALEE study, which compared adjuvant ribociclib plus nonsteroidal aromatase inhibitor (NSAI) to NSAI alone for ER+/HER2- breast cancer. The current analysis presented at the meeting showed significant benefits with the addition of ribociclib and no evidence of new safety signals or adverse event exacerbations at 3 years, she said. Dose modifications had no significant impact on efficacy, she added.
The findings of no impact of dose reduction on efficacy in both the NATALEE and monarchE studies provide important information on whether dosage can be reduced in patients, which will increase the odds that patients will tolerate extended therapy with good outcomes and stay on their prescribed therapies, Dr. Hamilton emphasized.
The CARABELA study, a phase 2 trial of neoadjuvant letrozole plus abemaciclib vs adriamycin and cyclophosphamide (AC), showed clinically similar response rates but did not meet its endpoint for residual cancer burden (RCB) scores. These data add to results from other studies and show that it is too soon to universally replace neoadjuvant chemotherapy as first-line treatment for highly proliferative ER+ breast cancer, Dr. Hamilton said in her presentation.
Advanced Breast Cancer
Take-home messages about advanced breast cancer include growing evidence for the potential benefits of antibody drug conjugates (ADCs), said Eva Ciruelos, MD, of University Hospital, Madrid, Spain. The TROPION-BREAST01 study, a phase 3 randomized trial, showed significant and clinically meaningful improvement in progression-free survival in patients with previously treated, inoperable, or metastatic HR+/HER2- breast cancer who received datopotamab deruxtecan (Dato-DXd) compared with those who received chemotherapy.
Data from an additional safety analysis were presented at the meeting; although Dato-DXd, a trophoblast cell-surface antigen 2 (TROP2)–directed antibody-drug conjugate, was well-tolerated, it is important to remain aware of toxicities, notably oral mucositis, which occurred in 55.6% of the patients in the study across all grades, and ocular surface toxicity, which occurred in 40% of patients across all grades, Dr. Ciruelos emphasized.
Key research in the area of advanced triple-negative breast cancer included data from the IMPASSION 132 study. This study is “specifically centered on early relapsers,” a population often excluded from other trials, Dr. Ciruelos said. In this study, patients with advanced triple-negative breast cancer were randomized to chemotherapy with or without atezolizumab, and the study showed no benefits with atezolizumab for overall survival, progression-free survival, or overall response rate, she said. “This is something to work with, because this is a very refractory population,” Dr. Ciruelos noted.
New immunotherapy combinations are needed to improve survival in advanced breast cancer patients, Dr. Ciruelos said. At the meeting, researchers presented interim data from a subset of patients in the MORPHEUS-pan breast cancer trial, a phase 1B/2 study involving multiple treatment combinations in locally advanced/metastatic breast cancer patients.
The interim analysis included 18-week data from triple-negative breast cancer patients and compared outcomes for patients randomized to atezolizumab with or without sacituzumab govitecan (SG).
The study was small, with only 31 patients in the combination arm and 11 controls, but the results were promising, with an overall response rate of 76.7% in the combination arm vs 66.7% in the control arm, Dr. Ciruelos said.
Supportive Care
Key supportive care takeaways included data on pregnancy in young breast cancer survivors and the safety of vaginal estrogen therapy in breast cancer patients with genitourinary symptoms, said Anne May, MD, of the University Medical Center Utrecht, Utrecht, Netherlands.
A study previously published in JAMA including nearly 5000 BRCA carriers who were diagnosed with invasive breast cancer at age 40 years or younger showed no association between pregnancy after breast cancer and adverse maternal or fetal outcomes, and pregnancy had no significant impact on overall survival. The authors presented new data on the safety of assisted reproductive techniques (ART) based on the 543 pregnancies in the original study, at the meeting. Of these, 436 conceived naturally, and 107 used ART. After a median of 9.1 years, ART had no effect on disease-free survival compared to natural conception (hazard ratio [HR], 0.64). Based on these findings, fertility preservation should be offered to all women who receive a breast cancer diagnosis and are interested in future fertility, Dr. May said.
Conceiving after breast cancer treatment and follow-up should not be contraindicated for young BRCA carriers, she added.No trial data are available for the effects of vaginal estrogen therapy (VET) on disease-free survival in breast cancer survivors with genitourinary symptoms caused by declining estrogen levels, Dr. May said. However, researchers in France and Switzerland conducted an emulation of a hypothetical target trial using data from the French National social security system for more than 130,000 individuals. Although VET therapy had no impact on disease-free survival in most breast cancer survivors overall, it did have a negative impact in a subset of patients with HR-positive and HR-negative tumors who were treated with aromatase inhibitors. The study was hypothetical, but important because the results suggest that clinicians can safely propose VTE to patients who report genitourinary symptoms after treatment for early-stage breast cancer with tamoxifen, but VTE should be avoided in patients treated with aromatase inhibitors, Dr. May said.
Dr. Delaloge disclosed research support to her institution from AstraZeneca, MSD, Bristol Myers Squibb, Sanofi, Taiho, Novartis, European Commission, INCa, Banque des Territoires, and Fondation Philanthropia. She also disclosed honoraria to her institution from AstraZeneca, Gilead, Novartis, Elsan, Besins, Sanofi, Exact Sciences, and Lilly, as well as travel support from Novartis.
Dr. Kok disclosed research funding from AstraZeneca, Bristol Myers Squibb, Daichi, and Roche, and advisory board membership/speaker’s fees from Alderaan Biotechnology, BIONTECH, Domain Therapeutics, AstraZeneca, Daichi, Bristol Myers Squibb, Gilead, Medscape, MSD, and Roche.
Dr. Hamilton disclosed a consulting advisory role (to her institution) for Accutar Biotechology, AstraZeneca, Daiichi Sankyo, Ellipses Pharma, Entos, Forsum Pharma, Gilead Sciences, Greenwich LifeSciences, Jazz Pharmaceuticals, Lilly, Medical Pharma Services, Mersana, Novartis, Olema Pharmaceuticals, Orum Therapeutics, Roche/Genentech, Stemline Therapeutics, ands others. She also disclosed contracted research/grant support to her institution only from Abbvie, Acerta Pharma, Accutar Biotechnology , ADC Therapeutics, AKESOBIO Australia , Amgen, Aravive, ArQule, Artios, Arvinas, AstraZeneca, AtlasMedx, BeiGene, Black Diamond and others.
Dr. Ciruelos disclosed serving as an external advisor for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, and Lilly, as well as serving as a speaker for Roche, MSD, Gilead, AstraZeneca, Daichii Sankyo, Reveal Genomics, Pfizer, Novartis, Lilly, and Pierre Fabre. She also disclosed travel grants from Roche, Pfizer, and AstraZeneca, and research grants from Seagen and Roche.
Dr. May had no financial conflicts to disclose.
FROM ESMO BREAST CANCER 2024
Maternal Complication Risk Higher For Cesarean Deliveries With Low-Lying Placenta
SAN FRANCISCO — Patients with a low-lying placenta who underwent cesarean deliveries were at higher risk for multiple complications even if they did not have placenta previa, according to data presented at the annual meeting of the American College of Obstetricians and Gynecologists.
Rates of preterm delivery, postpartum hemorrhage, placenta accreta, and need for hysterectomy and transfusion were all significantly higher in patients with low-lying placenta than in patients without, Jacob Thomas, MD, of Advocate Aurora Health in Chicago, Illinois, and Ascension Illinois St. Alexius Medical Center in Hoffman Estates, reported at the meeting.
A low-lying placenta is defined as a placental edge less than 20 mm from the internal os but not covering it. Most studies looking at low-lying placentas, however, group them with placenta previa, making it difficult to know if there are differences in risk of adverse outcomes for those who don’t have placenta previa.
“These are not necessarily shocking findings, but it shows that even low-lying placentas have significant morbidity in and of themselves, not just when they’re lumped with placenta previas,” Dr. Thomas said in an interview. “This means, if you’re doing a C-section for a low-lying placenta, you probably want to treat it a lot like you would treat a placenta previa. You may have blood ready, whether or not you’re going to give it, and you’re going to be more prepared for those complications.”
Noting that approximately 30% of patients with low-lying placenta had preterm deliveries, Dr. Thomas added that these patients might need to be counseled differently as well. The researchers did not have data on how preterm the deliveries were — many could have been 35-37 weeks, for example — but “how you prepare those patients is different,” he said.
Breanna Bolivar, MD, MPH, an obgyn hospitalist at MAHEC Ob/Gyn Specialists in Asheville, North Carolina, said the findings confirm her experience in practice.
“Low-lying placentas are treated very similarly to placenta previas and the results seem similar to patients that have placenta previas,” Dr. Bolivar said in an interview. “In my practice, I treat patients with low-lying placenta the same as I do with placenta previa. I have the same risk factors in mind, and I prepare in the same way.”
The researchers conducted a retrospective analysis of all patients who underwent a cesarean delivery in the National Inpatient Sample from 2017 to 2019 through the Healthcare Cost and Utilization Project from the Agency for Healthcare Research and Quality. After excluding patients with placenta previa, the researchers compared outcomes among patients with ICD-10 codes for low-lying placenta to those of patients without low-lying placenta. The researchers specifically looked at preterm delivery, hemorrhage, hysterectomy, placenta accreta spectrum (PAS), sepsis, shock, disseminated intravascular coagulation, and blood transfusion.
Among 700,635 patients with cesarean deliveries in the database, 0.4% had low-lying placenta. These patients were more likely to be older, to be anemic, and to deliver at a large or urban teaching hospital. They were less likely to have public insurance or a previous cesarean.
After controlling for confounders that differed between the two populations, the researchers found a higher likelihood of all adverse maternal outcomes studied in patients with low-lying placenta (P < .05). These patients had three times greater risk for preterm delivery (adjusted odds ratio [aOR], 3.07; 95% CI, 2.81-3.35) and nearly three times greater risk for shock (aOR 2.55; 95% CI, 1.44-4.52), and transfusion (aOR, 2.56; 95% CI, 2.14-3.06).
Compared to those without low-lying placenta, risk for patients with low-lying placenta was even higher for hemorrhage (aOR, 8.87; 95% CI, 8.10-9.73), hysterectomy (aOR, 9.42; 95% CI, 7.11-12.47), and PAS (aOR, 13.41; 95% CI, 10.34-17.39).
Within the group with low-lying placenta, older patients were modestly, but significantly, more likely to have hemorrhage, hysterectomy, and PAS (aOR, 1.06 for all). The risk was more elevated and significant in patients with tobacco use for hemorrhage (aOR, 1.43), hysterectomy (aOR, 1.40), and PAS (aOR, 1.40). Patients with anemia were also significantly more likely to experience PAS (aOR, 1.34).
“Interestingly, in this population, prior cesarean was not associated with increased rates of hemorrhage or hysterectomy,” the researchers reported. The findings can also “help guide research in terms of questions for the future,” Dr. Thomas said, such as looking at complication rates for vaginal deliveries in people with low-lying placenta.
No external funding was noted, and the authors all had no disclosures. Dr. Bolivar had no disclosures.
SAN FRANCISCO — Patients with a low-lying placenta who underwent cesarean deliveries were at higher risk for multiple complications even if they did not have placenta previa, according to data presented at the annual meeting of the American College of Obstetricians and Gynecologists.
Rates of preterm delivery, postpartum hemorrhage, placenta accreta, and need for hysterectomy and transfusion were all significantly higher in patients with low-lying placenta than in patients without, Jacob Thomas, MD, of Advocate Aurora Health in Chicago, Illinois, and Ascension Illinois St. Alexius Medical Center in Hoffman Estates, reported at the meeting.
A low-lying placenta is defined as a placental edge less than 20 mm from the internal os but not covering it. Most studies looking at low-lying placentas, however, group them with placenta previa, making it difficult to know if there are differences in risk of adverse outcomes for those who don’t have placenta previa.
“These are not necessarily shocking findings, but it shows that even low-lying placentas have significant morbidity in and of themselves, not just when they’re lumped with placenta previas,” Dr. Thomas said in an interview. “This means, if you’re doing a C-section for a low-lying placenta, you probably want to treat it a lot like you would treat a placenta previa. You may have blood ready, whether or not you’re going to give it, and you’re going to be more prepared for those complications.”
Noting that approximately 30% of patients with low-lying placenta had preterm deliveries, Dr. Thomas added that these patients might need to be counseled differently as well. The researchers did not have data on how preterm the deliveries were — many could have been 35-37 weeks, for example — but “how you prepare those patients is different,” he said.
Breanna Bolivar, MD, MPH, an obgyn hospitalist at MAHEC Ob/Gyn Specialists in Asheville, North Carolina, said the findings confirm her experience in practice.
“Low-lying placentas are treated very similarly to placenta previas and the results seem similar to patients that have placenta previas,” Dr. Bolivar said in an interview. “In my practice, I treat patients with low-lying placenta the same as I do with placenta previa. I have the same risk factors in mind, and I prepare in the same way.”
The researchers conducted a retrospective analysis of all patients who underwent a cesarean delivery in the National Inpatient Sample from 2017 to 2019 through the Healthcare Cost and Utilization Project from the Agency for Healthcare Research and Quality. After excluding patients with placenta previa, the researchers compared outcomes among patients with ICD-10 codes for low-lying placenta to those of patients without low-lying placenta. The researchers specifically looked at preterm delivery, hemorrhage, hysterectomy, placenta accreta spectrum (PAS), sepsis, shock, disseminated intravascular coagulation, and blood transfusion.
Among 700,635 patients with cesarean deliveries in the database, 0.4% had low-lying placenta. These patients were more likely to be older, to be anemic, and to deliver at a large or urban teaching hospital. They were less likely to have public insurance or a previous cesarean.
After controlling for confounders that differed between the two populations, the researchers found a higher likelihood of all adverse maternal outcomes studied in patients with low-lying placenta (P < .05). These patients had three times greater risk for preterm delivery (adjusted odds ratio [aOR], 3.07; 95% CI, 2.81-3.35) and nearly three times greater risk for shock (aOR 2.55; 95% CI, 1.44-4.52), and transfusion (aOR, 2.56; 95% CI, 2.14-3.06).
Compared to those without low-lying placenta, risk for patients with low-lying placenta was even higher for hemorrhage (aOR, 8.87; 95% CI, 8.10-9.73), hysterectomy (aOR, 9.42; 95% CI, 7.11-12.47), and PAS (aOR, 13.41; 95% CI, 10.34-17.39).
Within the group with low-lying placenta, older patients were modestly, but significantly, more likely to have hemorrhage, hysterectomy, and PAS (aOR, 1.06 for all). The risk was more elevated and significant in patients with tobacco use for hemorrhage (aOR, 1.43), hysterectomy (aOR, 1.40), and PAS (aOR, 1.40). Patients with anemia were also significantly more likely to experience PAS (aOR, 1.34).
“Interestingly, in this population, prior cesarean was not associated with increased rates of hemorrhage or hysterectomy,” the researchers reported. The findings can also “help guide research in terms of questions for the future,” Dr. Thomas said, such as looking at complication rates for vaginal deliveries in people with low-lying placenta.
No external funding was noted, and the authors all had no disclosures. Dr. Bolivar had no disclosures.
SAN FRANCISCO — Patients with a low-lying placenta who underwent cesarean deliveries were at higher risk for multiple complications even if they did not have placenta previa, according to data presented at the annual meeting of the American College of Obstetricians and Gynecologists.
Rates of preterm delivery, postpartum hemorrhage, placenta accreta, and need for hysterectomy and transfusion were all significantly higher in patients with low-lying placenta than in patients without, Jacob Thomas, MD, of Advocate Aurora Health in Chicago, Illinois, and Ascension Illinois St. Alexius Medical Center in Hoffman Estates, reported at the meeting.
A low-lying placenta is defined as a placental edge less than 20 mm from the internal os but not covering it. Most studies looking at low-lying placentas, however, group them with placenta previa, making it difficult to know if there are differences in risk of adverse outcomes for those who don’t have placenta previa.
“These are not necessarily shocking findings, but it shows that even low-lying placentas have significant morbidity in and of themselves, not just when they’re lumped with placenta previas,” Dr. Thomas said in an interview. “This means, if you’re doing a C-section for a low-lying placenta, you probably want to treat it a lot like you would treat a placenta previa. You may have blood ready, whether or not you’re going to give it, and you’re going to be more prepared for those complications.”
Noting that approximately 30% of patients with low-lying placenta had preterm deliveries, Dr. Thomas added that these patients might need to be counseled differently as well. The researchers did not have data on how preterm the deliveries were — many could have been 35-37 weeks, for example — but “how you prepare those patients is different,” he said.
Breanna Bolivar, MD, MPH, an obgyn hospitalist at MAHEC Ob/Gyn Specialists in Asheville, North Carolina, said the findings confirm her experience in practice.
“Low-lying placentas are treated very similarly to placenta previas and the results seem similar to patients that have placenta previas,” Dr. Bolivar said in an interview. “In my practice, I treat patients with low-lying placenta the same as I do with placenta previa. I have the same risk factors in mind, and I prepare in the same way.”
The researchers conducted a retrospective analysis of all patients who underwent a cesarean delivery in the National Inpatient Sample from 2017 to 2019 through the Healthcare Cost and Utilization Project from the Agency for Healthcare Research and Quality. After excluding patients with placenta previa, the researchers compared outcomes among patients with ICD-10 codes for low-lying placenta to those of patients without low-lying placenta. The researchers specifically looked at preterm delivery, hemorrhage, hysterectomy, placenta accreta spectrum (PAS), sepsis, shock, disseminated intravascular coagulation, and blood transfusion.
Among 700,635 patients with cesarean deliveries in the database, 0.4% had low-lying placenta. These patients were more likely to be older, to be anemic, and to deliver at a large or urban teaching hospital. They were less likely to have public insurance or a previous cesarean.
After controlling for confounders that differed between the two populations, the researchers found a higher likelihood of all adverse maternal outcomes studied in patients with low-lying placenta (P < .05). These patients had three times greater risk for preterm delivery (adjusted odds ratio [aOR], 3.07; 95% CI, 2.81-3.35) and nearly three times greater risk for shock (aOR 2.55; 95% CI, 1.44-4.52), and transfusion (aOR, 2.56; 95% CI, 2.14-3.06).
Compared to those without low-lying placenta, risk for patients with low-lying placenta was even higher for hemorrhage (aOR, 8.87; 95% CI, 8.10-9.73), hysterectomy (aOR, 9.42; 95% CI, 7.11-12.47), and PAS (aOR, 13.41; 95% CI, 10.34-17.39).
Within the group with low-lying placenta, older patients were modestly, but significantly, more likely to have hemorrhage, hysterectomy, and PAS (aOR, 1.06 for all). The risk was more elevated and significant in patients with tobacco use for hemorrhage (aOR, 1.43), hysterectomy (aOR, 1.40), and PAS (aOR, 1.40). Patients with anemia were also significantly more likely to experience PAS (aOR, 1.34).
“Interestingly, in this population, prior cesarean was not associated with increased rates of hemorrhage or hysterectomy,” the researchers reported. The findings can also “help guide research in terms of questions for the future,” Dr. Thomas said, such as looking at complication rates for vaginal deliveries in people with low-lying placenta.
No external funding was noted, and the authors all had no disclosures. Dr. Bolivar had no disclosures.
FROM ACOG 2024