User login
Placenta fails to deliver: Mother dies of hemorrhage
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
Prenatal acetaminophen exposure may affect ADHD in childhood
Prenatal exposure to acetaminophen was associated with a significantly increased risk of attention-deficit/hyperactivity–like behavioral problems, a hospital diagnosis of hyperkinetic disorder (HKD), or being on ADHD medications in children at age 7 years, based data from more than 60,000 children obtained from the national birth registry and other health registries in Denmark.
The study was published online on Feb. 24, in JAMA Pediatrics (doi:10.1001/jamapediatrics.2013.4914). The risk of ADHD-like behaviors in children at age 7 years increased by 13% among those whose mothers had used acetaminophen overall during pregnancy. When acetaminophen was used in the second and third trimesters, the risk increased by 44%, and when used during all three trimesters, the risk increased by 24%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Courtesy: Cleveland Clinic
The associations with these three outcomes were greater when acetaminophen (paracetamol) was used in more than one trimester and with increasing frequency of use (more than 20 weeks during pregnancy). Because exposure to acetaminophen is common, "these associations might explain some of the increasing incidence in HKD/ADHD, but further studies are needed," Zeyan Liew, MPH, and his coauthors concluded. Mr. Liew is with the department of epidemiology, Fielding School of Public Health, University of California, Los Angeles.
The prospective study included 64,322 live-born children and their mothers who were enrolled in the Danish National Birth Cohort during 1996-2002, and data from the national hospital, psychiatric and prescription registries. The mothers had participated in three interviews about acetaminophen use during pregnancy: at the 12th and 30th weeks of gestation, and 6 months after giving birth (28,254 women who had missed at least one of these interviews and their children were excluded).
A subgroup of approximately 41,000 women who had responded to a self-administered questionnaire (the Strengths and Difficulties Questionnaire), when their child was 7 years of age were used to evaluate ADHD-like behaviors; 55% of the women in this group had used acetaminophen at some point in their pregnancy. In the entire group of 64,322 mothers, 56% had used acetaminophen during pregnancy.
Data obtained by the investigators included parental reports of ADHD-like behaviors at age 7 years; a hospital diagnoses of HKD at or after 5 years; and use of ADHD medications, mostly Ritalin. The researchers adjusted for possible confounders, including birthweight; sex; maternal age at child’s birth; socioeconomic status; drug and alcohol use during pregnancy; mother’s self-reports of psychiatric illnesses and childhood behavioral problems; and diseases or conditions that may have prompted the mothers to have used acetaminophen.
The associations between the use of prenatal acetaminophen and the increased risks of HKD or using an ADHD medication also increased when acetaminophen was used during two or more trimesters, and a significant trend appeared with the increasing weeks of use: When used for 20 or more weeks, the risk for an diagnosis of HKD increased by 84% and the risk of having received an ADHD medication increased by 53%, the researchers noted. These results were similar "when restricting to mothers who did not report psychiatric illnesses or episodes of fever, inflammation, and infections during pregnancy," they added.

Referring to evidence from animal and human studies suggesting that acetaminophen may be an endocrine disruptor, the authors wrote: "Maternal hormones, such as sex hormones and thyroid hormones, play critical roles in regulating fetal brain development, and it is possible that acetaminophen may interrupt brain development by interfering with maternal hormones or via neurotoxicity, such as the induction of oxidative stress that can cause neuronal death."
The study strengths included the availability of different endpoints to evaluate different levels of ADHD and the use of prospective data (interviews with the mothers). But the findings were limited by the inability to evaluate the effect of dosage or number of pills, because the mothers were not able to provide this information. Despite the adjustment for confounding variables, "the possibility of unmeasured residual confounding by indication for drug use, ADHD-related genetic factors, or coexposures to other medications cannot be dismissed," the researchers said.
In an accompanying editorial, Miriam Cooper, MRCPsych, of the Institute of Psychological Medicine, Cardiff, Wales, and her associates wrote that while the study’s results are potentially important, "caution should be exercised in ascribing causation to statistical associations between prenatal risk factors and adverse outcomes" and the results "should not change practice." However, the findings should be used as a basis for future research and "underline the importance of not taking a drug’s safety during pregnancy for granted" (doi:10.1001/jamapediatrics.2013.5292).
The study was supported by the Danish Medical Council. Neither the researchers nor the editorialists had relevant financial conflicts to disclose.
There are quite a few problems with the interpretation of this cohort. Most importantly, there is potential bias by indication. For example, women who needed more acetaminophen might have had conditions that could cause the outcome, rather than the acetaminophen. In addition, the doses were not known and more than 20,000 cases were excluded for missing interviews. Therefore, it is possible that they had many more parents with ADHD, which is often a genetic condition. The acetaminophen users had more muscle and joint diseases, more infections, and more psychiatric disease-which can affect the results, independent of acetaminophen.
Dr. Gideon Koren is director of the Motherisk Program at the Hospital for Sick Children, Toronto, and professor of pediatrics, pharmacology, pharmacy, and medical genetics, at the University of Toronto. He has no relevant disclosures.
There are quite a few problems with the interpretation of this cohort. Most importantly, there is potential bias by indication. For example, women who needed more acetaminophen might have had conditions that could cause the outcome, rather than the acetaminophen. In addition, the doses were not known and more than 20,000 cases were excluded for missing interviews. Therefore, it is possible that they had many more parents with ADHD, which is often a genetic condition. The acetaminophen users had more muscle and joint diseases, more infections, and more psychiatric disease-which can affect the results, independent of acetaminophen.
Dr. Gideon Koren is director of the Motherisk Program at the Hospital for Sick Children, Toronto, and professor of pediatrics, pharmacology, pharmacy, and medical genetics, at the University of Toronto. He has no relevant disclosures.
There are quite a few problems with the interpretation of this cohort. Most importantly, there is potential bias by indication. For example, women who needed more acetaminophen might have had conditions that could cause the outcome, rather than the acetaminophen. In addition, the doses were not known and more than 20,000 cases were excluded for missing interviews. Therefore, it is possible that they had many more parents with ADHD, which is often a genetic condition. The acetaminophen users had more muscle and joint diseases, more infections, and more psychiatric disease-which can affect the results, independent of acetaminophen.
Dr. Gideon Koren is director of the Motherisk Program at the Hospital for Sick Children, Toronto, and professor of pediatrics, pharmacology, pharmacy, and medical genetics, at the University of Toronto. He has no relevant disclosures.
Prenatal exposure to acetaminophen was associated with a significantly increased risk of attention-deficit/hyperactivity–like behavioral problems, a hospital diagnosis of hyperkinetic disorder (HKD), or being on ADHD medications in children at age 7 years, based data from more than 60,000 children obtained from the national birth registry and other health registries in Denmark.
The study was published online on Feb. 24, in JAMA Pediatrics (doi:10.1001/jamapediatrics.2013.4914). The risk of ADHD-like behaviors in children at age 7 years increased by 13% among those whose mothers had used acetaminophen overall during pregnancy. When acetaminophen was used in the second and third trimesters, the risk increased by 44%, and when used during all three trimesters, the risk increased by 24%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Courtesy: Cleveland Clinic
The associations with these three outcomes were greater when acetaminophen (paracetamol) was used in more than one trimester and with increasing frequency of use (more than 20 weeks during pregnancy). Because exposure to acetaminophen is common, "these associations might explain some of the increasing incidence in HKD/ADHD, but further studies are needed," Zeyan Liew, MPH, and his coauthors concluded. Mr. Liew is with the department of epidemiology, Fielding School of Public Health, University of California, Los Angeles.
The prospective study included 64,322 live-born children and their mothers who were enrolled in the Danish National Birth Cohort during 1996-2002, and data from the national hospital, psychiatric and prescription registries. The mothers had participated in three interviews about acetaminophen use during pregnancy: at the 12th and 30th weeks of gestation, and 6 months after giving birth (28,254 women who had missed at least one of these interviews and their children were excluded).
A subgroup of approximately 41,000 women who had responded to a self-administered questionnaire (the Strengths and Difficulties Questionnaire), when their child was 7 years of age were used to evaluate ADHD-like behaviors; 55% of the women in this group had used acetaminophen at some point in their pregnancy. In the entire group of 64,322 mothers, 56% had used acetaminophen during pregnancy.
Data obtained by the investigators included parental reports of ADHD-like behaviors at age 7 years; a hospital diagnoses of HKD at or after 5 years; and use of ADHD medications, mostly Ritalin. The researchers adjusted for possible confounders, including birthweight; sex; maternal age at child’s birth; socioeconomic status; drug and alcohol use during pregnancy; mother’s self-reports of psychiatric illnesses and childhood behavioral problems; and diseases or conditions that may have prompted the mothers to have used acetaminophen.
The associations between the use of prenatal acetaminophen and the increased risks of HKD or using an ADHD medication also increased when acetaminophen was used during two or more trimesters, and a significant trend appeared with the increasing weeks of use: When used for 20 or more weeks, the risk for an diagnosis of HKD increased by 84% and the risk of having received an ADHD medication increased by 53%, the researchers noted. These results were similar "when restricting to mothers who did not report psychiatric illnesses or episodes of fever, inflammation, and infections during pregnancy," they added.
Referring to evidence from animal and human studies suggesting that acetaminophen may be an endocrine disruptor, the authors wrote: "Maternal hormones, such as sex hormones and thyroid hormones, play critical roles in regulating fetal brain development, and it is possible that acetaminophen may interrupt brain development by interfering with maternal hormones or via neurotoxicity, such as the induction of oxidative stress that can cause neuronal death."
The study strengths included the availability of different endpoints to evaluate different levels of ADHD and the use of prospective data (interviews with the mothers). But the findings were limited by the inability to evaluate the effect of dosage or number of pills, because the mothers were not able to provide this information. Despite the adjustment for confounding variables, "the possibility of unmeasured residual confounding by indication for drug use, ADHD-related genetic factors, or coexposures to other medications cannot be dismissed," the researchers said.
In an accompanying editorial, Miriam Cooper, MRCPsych, of the Institute of Psychological Medicine, Cardiff, Wales, and her associates wrote that while the study’s results are potentially important, "caution should be exercised in ascribing causation to statistical associations between prenatal risk factors and adverse outcomes" and the results "should not change practice." However, the findings should be used as a basis for future research and "underline the importance of not taking a drug’s safety during pregnancy for granted" (doi:10.1001/jamapediatrics.2013.5292).
The study was supported by the Danish Medical Council. Neither the researchers nor the editorialists had relevant financial conflicts to disclose.
Prenatal exposure to acetaminophen was associated with a significantly increased risk of attention-deficit/hyperactivity–like behavioral problems, a hospital diagnosis of hyperkinetic disorder (HKD), or being on ADHD medications in children at age 7 years, based data from more than 60,000 children obtained from the national birth registry and other health registries in Denmark.
The study was published online on Feb. 24, in JAMA Pediatrics (doi:10.1001/jamapediatrics.2013.4914). The risk of ADHD-like behaviors in children at age 7 years increased by 13% among those whose mothers had used acetaminophen overall during pregnancy. When acetaminophen was used in the second and third trimesters, the risk increased by 44%, and when used during all three trimesters, the risk increased by 24%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Courtesy: Cleveland Clinic
The associations with these three outcomes were greater when acetaminophen (paracetamol) was used in more than one trimester and with increasing frequency of use (more than 20 weeks during pregnancy). Because exposure to acetaminophen is common, "these associations might explain some of the increasing incidence in HKD/ADHD, but further studies are needed," Zeyan Liew, MPH, and his coauthors concluded. Mr. Liew is with the department of epidemiology, Fielding School of Public Health, University of California, Los Angeles.
The prospective study included 64,322 live-born children and their mothers who were enrolled in the Danish National Birth Cohort during 1996-2002, and data from the national hospital, psychiatric and prescription registries. The mothers had participated in three interviews about acetaminophen use during pregnancy: at the 12th and 30th weeks of gestation, and 6 months after giving birth (28,254 women who had missed at least one of these interviews and their children were excluded).
A subgroup of approximately 41,000 women who had responded to a self-administered questionnaire (the Strengths and Difficulties Questionnaire), when their child was 7 years of age were used to evaluate ADHD-like behaviors; 55% of the women in this group had used acetaminophen at some point in their pregnancy. In the entire group of 64,322 mothers, 56% had used acetaminophen during pregnancy.
Data obtained by the investigators included parental reports of ADHD-like behaviors at age 7 years; a hospital diagnoses of HKD at or after 5 years; and use of ADHD medications, mostly Ritalin. The researchers adjusted for possible confounders, including birthweight; sex; maternal age at child’s birth; socioeconomic status; drug and alcohol use during pregnancy; mother’s self-reports of psychiatric illnesses and childhood behavioral problems; and diseases or conditions that may have prompted the mothers to have used acetaminophen.
The associations between the use of prenatal acetaminophen and the increased risks of HKD or using an ADHD medication also increased when acetaminophen was used during two or more trimesters, and a significant trend appeared with the increasing weeks of use: When used for 20 or more weeks, the risk for an diagnosis of HKD increased by 84% and the risk of having received an ADHD medication increased by 53%, the researchers noted. These results were similar "when restricting to mothers who did not report psychiatric illnesses or episodes of fever, inflammation, and infections during pregnancy," they added.
Referring to evidence from animal and human studies suggesting that acetaminophen may be an endocrine disruptor, the authors wrote: "Maternal hormones, such as sex hormones and thyroid hormones, play critical roles in regulating fetal brain development, and it is possible that acetaminophen may interrupt brain development by interfering with maternal hormones or via neurotoxicity, such as the induction of oxidative stress that can cause neuronal death."
The study strengths included the availability of different endpoints to evaluate different levels of ADHD and the use of prospective data (interviews with the mothers). But the findings were limited by the inability to evaluate the effect of dosage or number of pills, because the mothers were not able to provide this information. Despite the adjustment for confounding variables, "the possibility of unmeasured residual confounding by indication for drug use, ADHD-related genetic factors, or coexposures to other medications cannot be dismissed," the researchers said.
In an accompanying editorial, Miriam Cooper, MRCPsych, of the Institute of Psychological Medicine, Cardiff, Wales, and her associates wrote that while the study’s results are potentially important, "caution should be exercised in ascribing causation to statistical associations between prenatal risk factors and adverse outcomes" and the results "should not change practice." However, the findings should be used as a basis for future research and "underline the importance of not taking a drug’s safety during pregnancy for granted" (doi:10.1001/jamapediatrics.2013.5292).
The study was supported by the Danish Medical Council. Neither the researchers nor the editorialists had relevant financial conflicts to disclose.
FROM JAMA
Major finding: Children exposed prenatally to acetaminophen were at a greater risk of being diagnosed with hyperkinetic disorder, having ADHD-like behaviors, or being on an ADHD medication, an association that was increased with exposure during more than one trimester and with more weeks of exposure.
Data source: A large prospective study using the Danish National Birth Cohort data and other national health registries evaluated the association between the three outcomes, and maternal use of acetaminophen, based on information obtained from the mothers of more than 64,000 children.
Disclosures: The study was supported by the Danish Medical Research Council. One of the authors was at the University of Arizona, Tucson, when she was involved in the study, but now works at Novartis Farmaceutica SA, in Barcelona.

Risk of fetal death is increased in pregnant women with pre-existing diabetes
Women who enter pregnancy with diabetes are 4.5 times more likely to experience fetal death and almost twice as likely to lose their infant in the first year of life, compared with women without diabetes, a new study shows.1
Although previous investigations have explored the link between pre-existing maternal diabetes and fetal and infant death, they have not excluded congenital anomalies as a cause of death. In this newest study, Tennant and colleagues used data from several longstanding population-based registries in the north of England to explore the link in offspring without congenital anomalies.
Details of the study
Tennant and colleagues included all normally formed singleton offspring of women with pre-existing diabetes (1,206 with type 1 diabetes and 342 with type 2 diabetes) in the North of England from 1996 to 2008 in their study. Information on these pregnancies came from the Northern Diabetes in Pregnancy Survey. The relative risks (RR) of fetal death (death of a fetus at or after 20 weeks’ gestation) and infant death (death during the first year of life) were estimated by comparing these data with population data from the Northern Perinatal Morbidity and Mortality Survey.
The RR of fetal death in pregnancies marked by preexisting diabetes was 4.56, and it was 1.86 for infant death, compared with pregnancies without diabetes. These risks did not vary between women with type 1 diabetes and those with type 2 diabetes. Other variables associated with a higher risk of fetal or infant death were glycated hemoglobin levels greater than 6.6%, prepregnancy retinopathy, and a lack of folic acid supplementation.
The prevalence of fetal death was 3% in women with preexisting diabetes, and the prevalence of infant death was 0.7%, compared with 0.7% and 0.4%, respectively, in women without diabetes.
Tennant and colleagues found no evidence that the risk of fetal and infant death associated with preexisting maternal diabetes had decreased over time, or that the relative risk of stillbirth varied by gestational age.
The average glycated hemoglobin level in the study was 7.8%. The target for glycated hemoglobin is 7% according to the American Diabetes Association (ADA) and 6.1% according to England’s National Institute for Health and Care Excellence (NICE). Tennant and colleagues estimate that the prevalence of fetal and infant death would have been about 40% lower if the women in their study had achieved either the ADA or NICE target.
Related Article: Does myoinositol supplementation reduce the rate of gestational diabetes in pregnant women with a family history of type 2 diabetes? E. Albert Reece, MD, PhD, MBA (Examining the Evidence, June 2013)
Clinical recommendations
“It’s disappointing to see so little improvement because, with the right care, most women with diabetes can—and will—have a healthy baby,” the authors commented. “Stillbirths and infant deaths are thankfully not common, but they could be even less common if all women with diabetes can be helped to achieve the best possible control of their blood glucose levels.”
“We already know that folic acid reduces the risk of certain congenital anomalies, such as spina bifida or cleft lip, which is why women with diabetes are advised to take high-dose supplements of 5 mg daily. These are available on prescription and should be taken for at least 3 months before conceiving. Our results suggest this simple action may also help to reduce the risk of stillbirth or infant death, even in babies without these conditions.”
Related Article: Does folic acid supplementation have long-term benefit to offspring? Paul L. Ogburn, Jr, MD (Examining the Evidence, January 2012)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
Reference
- Tennant PW, Glinianaia SV, Bilous RW, Rankin J, Bell R. Pre-existing diabetes, maternal glycated haemoglobin, and the risks of fetal and infant death: a population-based study. Diabetologia. 2014;57(2):285–294.
Women who enter pregnancy with diabetes are 4.5 times more likely to experience fetal death and almost twice as likely to lose their infant in the first year of life, compared with women without diabetes, a new study shows.1
Although previous investigations have explored the link between pre-existing maternal diabetes and fetal and infant death, they have not excluded congenital anomalies as a cause of death. In this newest study, Tennant and colleagues used data from several longstanding population-based registries in the north of England to explore the link in offspring without congenital anomalies.
Details of the study
Tennant and colleagues included all normally formed singleton offspring of women with pre-existing diabetes (1,206 with type 1 diabetes and 342 with type 2 diabetes) in the North of England from 1996 to 2008 in their study. Information on these pregnancies came from the Northern Diabetes in Pregnancy Survey. The relative risks (RR) of fetal death (death of a fetus at or after 20 weeks’ gestation) and infant death (death during the first year of life) were estimated by comparing these data with population data from the Northern Perinatal Morbidity and Mortality Survey.
The RR of fetal death in pregnancies marked by preexisting diabetes was 4.56, and it was 1.86 for infant death, compared with pregnancies without diabetes. These risks did not vary between women with type 1 diabetes and those with type 2 diabetes. Other variables associated with a higher risk of fetal or infant death were glycated hemoglobin levels greater than 6.6%, prepregnancy retinopathy, and a lack of folic acid supplementation.
The prevalence of fetal death was 3% in women with preexisting diabetes, and the prevalence of infant death was 0.7%, compared with 0.7% and 0.4%, respectively, in women without diabetes.
Tennant and colleagues found no evidence that the risk of fetal and infant death associated with preexisting maternal diabetes had decreased over time, or that the relative risk of stillbirth varied by gestational age.
The average glycated hemoglobin level in the study was 7.8%. The target for glycated hemoglobin is 7% according to the American Diabetes Association (ADA) and 6.1% according to England’s National Institute for Health and Care Excellence (NICE). Tennant and colleagues estimate that the prevalence of fetal and infant death would have been about 40% lower if the women in their study had achieved either the ADA or NICE target.
Related Article: Does myoinositol supplementation reduce the rate of gestational diabetes in pregnant women with a family history of type 2 diabetes? E. Albert Reece, MD, PhD, MBA (Examining the Evidence, June 2013)
Clinical recommendations
“It’s disappointing to see so little improvement because, with the right care, most women with diabetes can—and will—have a healthy baby,” the authors commented. “Stillbirths and infant deaths are thankfully not common, but they could be even less common if all women with diabetes can be helped to achieve the best possible control of their blood glucose levels.”
“We already know that folic acid reduces the risk of certain congenital anomalies, such as spina bifida or cleft lip, which is why women with diabetes are advised to take high-dose supplements of 5 mg daily. These are available on prescription and should be taken for at least 3 months before conceiving. Our results suggest this simple action may also help to reduce the risk of stillbirth or infant death, even in babies without these conditions.”
Related Article: Does folic acid supplementation have long-term benefit to offspring? Paul L. Ogburn, Jr, MD (Examining the Evidence, January 2012)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
Women who enter pregnancy with diabetes are 4.5 times more likely to experience fetal death and almost twice as likely to lose their infant in the first year of life, compared with women without diabetes, a new study shows.1
Although previous investigations have explored the link between pre-existing maternal diabetes and fetal and infant death, they have not excluded congenital anomalies as a cause of death. In this newest study, Tennant and colleagues used data from several longstanding population-based registries in the north of England to explore the link in offspring without congenital anomalies.
Details of the study
Tennant and colleagues included all normally formed singleton offspring of women with pre-existing diabetes (1,206 with type 1 diabetes and 342 with type 2 diabetes) in the North of England from 1996 to 2008 in their study. Information on these pregnancies came from the Northern Diabetes in Pregnancy Survey. The relative risks (RR) of fetal death (death of a fetus at or after 20 weeks’ gestation) and infant death (death during the first year of life) were estimated by comparing these data with population data from the Northern Perinatal Morbidity and Mortality Survey.
The RR of fetal death in pregnancies marked by preexisting diabetes was 4.56, and it was 1.86 for infant death, compared with pregnancies without diabetes. These risks did not vary between women with type 1 diabetes and those with type 2 diabetes. Other variables associated with a higher risk of fetal or infant death were glycated hemoglobin levels greater than 6.6%, prepregnancy retinopathy, and a lack of folic acid supplementation.
The prevalence of fetal death was 3% in women with preexisting diabetes, and the prevalence of infant death was 0.7%, compared with 0.7% and 0.4%, respectively, in women without diabetes.
Tennant and colleagues found no evidence that the risk of fetal and infant death associated with preexisting maternal diabetes had decreased over time, or that the relative risk of stillbirth varied by gestational age.
The average glycated hemoglobin level in the study was 7.8%. The target for glycated hemoglobin is 7% according to the American Diabetes Association (ADA) and 6.1% according to England’s National Institute for Health and Care Excellence (NICE). Tennant and colleagues estimate that the prevalence of fetal and infant death would have been about 40% lower if the women in their study had achieved either the ADA or NICE target.
Related Article: Does myoinositol supplementation reduce the rate of gestational diabetes in pregnant women with a family history of type 2 diabetes? E. Albert Reece, MD, PhD, MBA (Examining the Evidence, June 2013)
Clinical recommendations
“It’s disappointing to see so little improvement because, with the right care, most women with diabetes can—and will—have a healthy baby,” the authors commented. “Stillbirths and infant deaths are thankfully not common, but they could be even less common if all women with diabetes can be helped to achieve the best possible control of their blood glucose levels.”
“We already know that folic acid reduces the risk of certain congenital anomalies, such as spina bifida or cleft lip, which is why women with diabetes are advised to take high-dose supplements of 5 mg daily. These are available on prescription and should be taken for at least 3 months before conceiving. Our results suggest this simple action may also help to reduce the risk of stillbirth or infant death, even in babies without these conditions.”
Related Article: Does folic acid supplementation have long-term benefit to offspring? Paul L. Ogburn, Jr, MD (Examining the Evidence, January 2012)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com
Reference
- Tennant PW, Glinianaia SV, Bilous RW, Rankin J, Bell R. Pre-existing diabetes, maternal glycated haemoglobin, and the risks of fetal and infant death: a population-based study. Diabetologia. 2014;57(2):285–294.
Reference
- Tennant PW, Glinianaia SV, Bilous RW, Rankin J, Bell R. Pre-existing diabetes, maternal glycated haemoglobin, and the risks of fetal and infant death: a population-based study. Diabetologia. 2014;57(2):285–294.
Weak link found between induction and high C-section rates
NEW ORLEANS – The link between labor induction and cesarean deliveries was found to be negatively correlated, according to data presented at this year’s Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.
The findings that a woman’s odds of delivering by C-section are 30% greater (confidence interval, 1.26-1.31; P = less than .01) if she delivers at a hospital with low rates of labor induction, independent of other obstetric risk factors and hospital characteristics, were unexpected by the study’s presenter, Dr. Sarah E. Little of Brigham and Women’s Hospital in Boston. "I was quite surprised by the findings. It suggests to me that inductions themselves may not be the culprit behind the rising rate of cesarean delivery in the United States."

Dr. Little and her colleagues conducted the research to help close the gap between this commonly held belief that an overreliance on induction is at least in part responsible for why the rate of C-section deliveries performed in the United States rose from 20.7% in 1996 to 32.8% in 2011, making it the most commonly performed surgical procedure in the nation. The increased risk has not been shown in prospective trials because the control group would be women with expectant management, according to Dr. Little.
"In retrospective trials, the comparison group is often spontaneous labor, but you can’t choose to be in spontaneous labor," she said. "During expectant management, things can arise – the babies get bigger, the placentas get worse, moms can develop bleeding or preeclampsia – all of which increase the risk of cesarean section, so if you don’t take this into account, then inductions look worse."
For the study, Dr. Little and her colleagues calculated hospital rates of C-sections using the 2010 Nationwide Inpatient Sample of 813,693 deliveries at 604 hospitals. The sample was representative of roughly 20% of all American hospitals, according to Dr. Little and included women at low risk for emergency C-section, and those with no preexisting comorbidities.
The investigators classified hospital level inductions as any induction; low-risk inductions, excluding anyone with preexisting comorbidities; and elective inductions if they were performed when not medically indicated, according to Joint Commission guidelines.
Hospitals in the study were characterized according to location, number of beds, and whether they were teaching facilities. Hospitals that performed fewer than 100 C-sections or did not perform labor inductions were excluded.
The researchers then conducted unadjusted and adjusted hospital cesarean rates according to hospital induction quartile. They also conducted a logistic regression analysis across quartiles to determine the correlation between the hospital rate of induction and the individual’s risk for C-section.
Dr. Little and her team found that hospitals had an average cesarean rate of 31%, with a range of 5.1%-75.7% (mean, 30.5%); rates of labor induction varied from 0% to 50% (mean 19.1%).
Hospitals with high induction rates had lower cesarean delivery rates (Pearson, –0.18; P = less than .001), a negative correlation that held even when only low-risk C-sections and low-risk inductions were studied (Pearson –0.31; P = less than .001). Hospitals in the highest quartile of labor inductions had an average cesarean rate of 32.6%, compared with 29.7% at hospitals in the lowest quartile of inductions.
"There is wide variation in the induction rates across hospitals," said Dr. Little. "I think this speaks to the wide variation in physician practices across the U.S."
The findings were presented during a time when the society is actively encouraging physicians to think twice before inducing labor and is conducting workshops that specifically draw a connection between the two procedures. "This study provides helpful information, and is potentially reassuring to those who require labor induction, but I would continue to encourage a practice of limiting labor induction to those with an indication for delivery and no contraindication to labor," Dr. Brian Mercer, the society’s immediate past president, responded when asked about the results.
The society’s suggested protocols are outlined in the paper, "Preventing the first cesarean delivery" (Obstet. Gynecol. 2012;120:1181-93), which includes an algorithm for when to induce labor – typically, only when medically indicated, such as in the case of membrane rupture.
"I think [our study] supports the SMFM initiative as there is clearly a large variation in practice which could potentially be targeted for change," said Dr. Little. "Also, there are other downsides to labor induction – iatrogenic prematurity if done prior to 39 weeks and increased cost and resource utilization. So even if inductions don’t lead to increased cesareans directly, there are a number of reasons you might want to avoid them."
Because birth certificate data is not kept at the hospital level, the investigators used billing data from the Nationwide Inpatient Sample. "This is not perfect, as it lacks some covariates, such as parity and gestational age, but it is the best national data available currently at the hospital level," Dr. Little said. "The next step might be to look at data sets, which combine birth certificate and discharge data, or collect this data prospectively at a hospital level."
I applaud Dr. Little and her coauthors for conducting this evaluation, which highlights significant variation in the rates of induction (0%-50%), elective induction (0%-47%), and total cesarean delivery (5%-50%) between hospitals.

|
|
Induction and cesarean delivery are both important interventions that can improve outcomes for mothers and/or their baby when medically indicated. The study highlights the importance of attention to this issue, and the importance of informed decision making regarding the potential benefits and risks of intervening in an otherwise uncomplicated pregnancy.
This is a complex issue. The need for labor induction may change over time. For example, a woman with an uncomplicated pregnancy at 39 weeks may develop preeclampsia a week later, at 40 weeks, and require induction of labor. This patient would be included in the induction group rather than the noninduction group, even though a decision had previously been made not to induce electively at 39 weeks’ gestation.
While the authors found a weak association between lower hospital induction rates and higher hospital cesarean rates, they did not specifically study the rates of cesarean delivery among those being induced versus those who were allowed to labor spontaneously; especially those without medical reasons for induction or early delivery. Including women who may have required a cesarean delivery (for placenta previa, prior classical cesarean delivery, or arrest of labor) but were not induced potentially confuses the relationship, as these would not be related to whether labor was induced or not.
Dr. Brian Mercer is the immediate past president of the Society for Maternal-Fetal Medicine, and a member of its Executive Committee. He is chair of the department of obstetrics and gynecology and director of maternal-fetal medicine at Metrohealth Medical Center and professor of reproductive biology at Case Western Reserve University, Cleveland.
I applaud Dr. Little and her coauthors for conducting this evaluation, which highlights significant variation in the rates of induction (0%-50%), elective induction (0%-47%), and total cesarean delivery (5%-50%) between hospitals.
|
|
|
Induction and cesarean delivery are both important interventions that can improve outcomes for mothers and/or their baby when medically indicated. The study highlights the importance of attention to this issue, and the importance of informed decision making regarding the potential benefits and risks of intervening in an otherwise uncomplicated pregnancy.
This is a complex issue. The need for labor induction may change over time. For example, a woman with an uncomplicated pregnancy at 39 weeks may develop preeclampsia a week later, at 40 weeks, and require induction of labor. This patient would be included in the induction group rather than the noninduction group, even though a decision had previously been made not to induce electively at 39 weeks’ gestation.
While the authors found a weak association between lower hospital induction rates and higher hospital cesarean rates, they did not specifically study the rates of cesarean delivery among those being induced versus those who were allowed to labor spontaneously; especially those without medical reasons for induction or early delivery. Including women who may have required a cesarean delivery (for placenta previa, prior classical cesarean delivery, or arrest of labor) but were not induced potentially confuses the relationship, as these would not be related to whether labor was induced or not.
Dr. Brian Mercer is the immediate past president of the Society for Maternal-Fetal Medicine, and a member of its Executive Committee. He is chair of the department of obstetrics and gynecology and director of maternal-fetal medicine at Metrohealth Medical Center and professor of reproductive biology at Case Western Reserve University, Cleveland.
I applaud Dr. Little and her coauthors for conducting this evaluation, which highlights significant variation in the rates of induction (0%-50%), elective induction (0%-47%), and total cesarean delivery (5%-50%) between hospitals.
|
|
|
Induction and cesarean delivery are both important interventions that can improve outcomes for mothers and/or their baby when medically indicated. The study highlights the importance of attention to this issue, and the importance of informed decision making regarding the potential benefits and risks of intervening in an otherwise uncomplicated pregnancy.
This is a complex issue. The need for labor induction may change over time. For example, a woman with an uncomplicated pregnancy at 39 weeks may develop preeclampsia a week later, at 40 weeks, and require induction of labor. This patient would be included in the induction group rather than the noninduction group, even though a decision had previously been made not to induce electively at 39 weeks’ gestation.
While the authors found a weak association between lower hospital induction rates and higher hospital cesarean rates, they did not specifically study the rates of cesarean delivery among those being induced versus those who were allowed to labor spontaneously; especially those without medical reasons for induction or early delivery. Including women who may have required a cesarean delivery (for placenta previa, prior classical cesarean delivery, or arrest of labor) but were not induced potentially confuses the relationship, as these would not be related to whether labor was induced or not.
Dr. Brian Mercer is the immediate past president of the Society for Maternal-Fetal Medicine, and a member of its Executive Committee. He is chair of the department of obstetrics and gynecology and director of maternal-fetal medicine at Metrohealth Medical Center and professor of reproductive biology at Case Western Reserve University, Cleveland.
NEW ORLEANS – The link between labor induction and cesarean deliveries was found to be negatively correlated, according to data presented at this year’s Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.
The findings that a woman’s odds of delivering by C-section are 30% greater (confidence interval, 1.26-1.31; P = less than .01) if she delivers at a hospital with low rates of labor induction, independent of other obstetric risk factors and hospital characteristics, were unexpected by the study’s presenter, Dr. Sarah E. Little of Brigham and Women’s Hospital in Boston. "I was quite surprised by the findings. It suggests to me that inductions themselves may not be the culprit behind the rising rate of cesarean delivery in the United States."
Dr. Little and her colleagues conducted the research to help close the gap between this commonly held belief that an overreliance on induction is at least in part responsible for why the rate of C-section deliveries performed in the United States rose from 20.7% in 1996 to 32.8% in 2011, making it the most commonly performed surgical procedure in the nation. The increased risk has not been shown in prospective trials because the control group would be women with expectant management, according to Dr. Little.
"In retrospective trials, the comparison group is often spontaneous labor, but you can’t choose to be in spontaneous labor," she said. "During expectant management, things can arise – the babies get bigger, the placentas get worse, moms can develop bleeding or preeclampsia – all of which increase the risk of cesarean section, so if you don’t take this into account, then inductions look worse."
For the study, Dr. Little and her colleagues calculated hospital rates of C-sections using the 2010 Nationwide Inpatient Sample of 813,693 deliveries at 604 hospitals. The sample was representative of roughly 20% of all American hospitals, according to Dr. Little and included women at low risk for emergency C-section, and those with no preexisting comorbidities.
The investigators classified hospital level inductions as any induction; low-risk inductions, excluding anyone with preexisting comorbidities; and elective inductions if they were performed when not medically indicated, according to Joint Commission guidelines.
Hospitals in the study were characterized according to location, number of beds, and whether they were teaching facilities. Hospitals that performed fewer than 100 C-sections or did not perform labor inductions were excluded.
The researchers then conducted unadjusted and adjusted hospital cesarean rates according to hospital induction quartile. They also conducted a logistic regression analysis across quartiles to determine the correlation between the hospital rate of induction and the individual’s risk for C-section.
Dr. Little and her team found that hospitals had an average cesarean rate of 31%, with a range of 5.1%-75.7% (mean, 30.5%); rates of labor induction varied from 0% to 50% (mean 19.1%).
Hospitals with high induction rates had lower cesarean delivery rates (Pearson, –0.18; P = less than .001), a negative correlation that held even when only low-risk C-sections and low-risk inductions were studied (Pearson –0.31; P = less than .001). Hospitals in the highest quartile of labor inductions had an average cesarean rate of 32.6%, compared with 29.7% at hospitals in the lowest quartile of inductions.
"There is wide variation in the induction rates across hospitals," said Dr. Little. "I think this speaks to the wide variation in physician practices across the U.S."
The findings were presented during a time when the society is actively encouraging physicians to think twice before inducing labor and is conducting workshops that specifically draw a connection between the two procedures. "This study provides helpful information, and is potentially reassuring to those who require labor induction, but I would continue to encourage a practice of limiting labor induction to those with an indication for delivery and no contraindication to labor," Dr. Brian Mercer, the society’s immediate past president, responded when asked about the results.
The society’s suggested protocols are outlined in the paper, "Preventing the first cesarean delivery" (Obstet. Gynecol. 2012;120:1181-93), which includes an algorithm for when to induce labor – typically, only when medically indicated, such as in the case of membrane rupture.
"I think [our study] supports the SMFM initiative as there is clearly a large variation in practice which could potentially be targeted for change," said Dr. Little. "Also, there are other downsides to labor induction – iatrogenic prematurity if done prior to 39 weeks and increased cost and resource utilization. So even if inductions don’t lead to increased cesareans directly, there are a number of reasons you might want to avoid them."
Because birth certificate data is not kept at the hospital level, the investigators used billing data from the Nationwide Inpatient Sample. "This is not perfect, as it lacks some covariates, such as parity and gestational age, but it is the best national data available currently at the hospital level," Dr. Little said. "The next step might be to look at data sets, which combine birth certificate and discharge data, or collect this data prospectively at a hospital level."
NEW ORLEANS – The link between labor induction and cesarean deliveries was found to be negatively correlated, according to data presented at this year’s Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.
The findings that a woman’s odds of delivering by C-section are 30% greater (confidence interval, 1.26-1.31; P = less than .01) if she delivers at a hospital with low rates of labor induction, independent of other obstetric risk factors and hospital characteristics, were unexpected by the study’s presenter, Dr. Sarah E. Little of Brigham and Women’s Hospital in Boston. "I was quite surprised by the findings. It suggests to me that inductions themselves may not be the culprit behind the rising rate of cesarean delivery in the United States."
Dr. Little and her colleagues conducted the research to help close the gap between this commonly held belief that an overreliance on induction is at least in part responsible for why the rate of C-section deliveries performed in the United States rose from 20.7% in 1996 to 32.8% in 2011, making it the most commonly performed surgical procedure in the nation. The increased risk has not been shown in prospective trials because the control group would be women with expectant management, according to Dr. Little.
"In retrospective trials, the comparison group is often spontaneous labor, but you can’t choose to be in spontaneous labor," she said. "During expectant management, things can arise – the babies get bigger, the placentas get worse, moms can develop bleeding or preeclampsia – all of which increase the risk of cesarean section, so if you don’t take this into account, then inductions look worse."
For the study, Dr. Little and her colleagues calculated hospital rates of C-sections using the 2010 Nationwide Inpatient Sample of 813,693 deliveries at 604 hospitals. The sample was representative of roughly 20% of all American hospitals, according to Dr. Little and included women at low risk for emergency C-section, and those with no preexisting comorbidities.
The investigators classified hospital level inductions as any induction; low-risk inductions, excluding anyone with preexisting comorbidities; and elective inductions if they were performed when not medically indicated, according to Joint Commission guidelines.
Hospitals in the study were characterized according to location, number of beds, and whether they were teaching facilities. Hospitals that performed fewer than 100 C-sections or did not perform labor inductions were excluded.
The researchers then conducted unadjusted and adjusted hospital cesarean rates according to hospital induction quartile. They also conducted a logistic regression analysis across quartiles to determine the correlation between the hospital rate of induction and the individual’s risk for C-section.
Dr. Little and her team found that hospitals had an average cesarean rate of 31%, with a range of 5.1%-75.7% (mean, 30.5%); rates of labor induction varied from 0% to 50% (mean 19.1%).
Hospitals with high induction rates had lower cesarean delivery rates (Pearson, –0.18; P = less than .001), a negative correlation that held even when only low-risk C-sections and low-risk inductions were studied (Pearson –0.31; P = less than .001). Hospitals in the highest quartile of labor inductions had an average cesarean rate of 32.6%, compared with 29.7% at hospitals in the lowest quartile of inductions.
"There is wide variation in the induction rates across hospitals," said Dr. Little. "I think this speaks to the wide variation in physician practices across the U.S."
The findings were presented during a time when the society is actively encouraging physicians to think twice before inducing labor and is conducting workshops that specifically draw a connection between the two procedures. "This study provides helpful information, and is potentially reassuring to those who require labor induction, but I would continue to encourage a practice of limiting labor induction to those with an indication for delivery and no contraindication to labor," Dr. Brian Mercer, the society’s immediate past president, responded when asked about the results.
The society’s suggested protocols are outlined in the paper, "Preventing the first cesarean delivery" (Obstet. Gynecol. 2012;120:1181-93), which includes an algorithm for when to induce labor – typically, only when medically indicated, such as in the case of membrane rupture.
"I think [our study] supports the SMFM initiative as there is clearly a large variation in practice which could potentially be targeted for change," said Dr. Little. "Also, there are other downsides to labor induction – iatrogenic prematurity if done prior to 39 weeks and increased cost and resource utilization. So even if inductions don’t lead to increased cesareans directly, there are a number of reasons you might want to avoid them."
Because birth certificate data is not kept at the hospital level, the investigators used billing data from the Nationwide Inpatient Sample. "This is not perfect, as it lacks some covariates, such as parity and gestational age, but it is the best national data available currently at the hospital level," Dr. Little said. "The next step might be to look at data sets, which combine birth certificate and discharge data, or collect this data prospectively at a hospital level."
FROM THE 2014 PREGNANCY MEETING
Major finding: The mean C-section rate was 31% (5.1%-75.7%); rates of labor induction varied from 0% to 50%.
Data source: A logistic regression analysis of 813,693 deliveries at 604 hospitals using the 2010 Nationwide Inpatient Sample.
Disclosures: Dr. Little and Dr. Robinson reported they had no relevant financial disclosures.

VIDEO: Is noninvasive prenatal testing right for your patient?
NEW ORLEANS – Noninvasive prenatal testing widens the options available to patients and their physicians seeking more information than what is provided by integrated screens, but who are perhaps not willing to take the risks of invasive diagnostic testing. Dr. Mary Norton, vice chair of clinical and translational genetics and a professor of obstetrics and gynecology at the University of California, San Francisco, gives front-line obstetricians pragmatic advice for how to counsel their patients about the use of this emerging screening technology in this video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – Noninvasive prenatal testing widens the options available to patients and their physicians seeking more information than what is provided by integrated screens, but who are perhaps not willing to take the risks of invasive diagnostic testing. Dr. Mary Norton, vice chair of clinical and translational genetics and a professor of obstetrics and gynecology at the University of California, San Francisco, gives front-line obstetricians pragmatic advice for how to counsel their patients about the use of this emerging screening technology in this video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – Noninvasive prenatal testing widens the options available to patients and their physicians seeking more information than what is provided by integrated screens, but who are perhaps not willing to take the risks of invasive diagnostic testing. Dr. Mary Norton, vice chair of clinical and translational genetics and a professor of obstetrics and gynecology at the University of California, San Francisco, gives front-line obstetricians pragmatic advice for how to counsel their patients about the use of this emerging screening technology in this video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE SMFM ANNUAL MEETING

Let expectant mothers labor longer to avoid C-sections
WASHINGTON – Longer labors lead to fewer cesarean sections.
That’s according to the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine who have jointly issued the Obstetric Care Consensus guideline, urging physicians to allow women with low-risk pregnancies to remain in latent labor longer before elevating their delivery to surgical status. The report and the consensus guideline appear in the March issue of Obstetrics & Gynecology (Obstet. Gynecol. 2014;123:693-711).
"Evidence now shows that labor actually progresses slower than we thought in the past, so many women might just need a little more time to labor and deliver vaginally instead of moving to a cesarean delivery," Dr. Aaron B. Caughey, a member of ACOG’s Committee on Obstetric Practice, said in a statement.
The document calls on physicians to consider that active labor has begun at 6 cm of cervical dilation, rather than 4, and stresses that doctors should allow more time for progression of labor during the active phase. Whether a woman chooses to use an epidural should also be factored into laboring times because the analgesia can slow contractions.
Although no absolute specific time for allowing a woman to remain in the active labor phase has been determined, the document states that women who have never delivered should be given at least 3 hours to push, while women who have delivered previously should be given a minimum of 2 hours.
‘Fear and convenience’
The recommendations are specifically concerned with avoiding the primary cesarean section because more than one-third of all births in the United States are cesarean deliveries, two-thirds of which are among nulliparous women. Avoiding the first cesarean section is important, "because if the woman labors with a scar from a previous C-section, there is a risk that the uterus will rupture," SMFM president Dr. Vincenzo Berghella, director of maternal-fetal medicine at Thomas Jefferson Medical Center in Philadelphia, said in an interview. "It only happens one-half to one percent [of the time], but it can be catastrophic. The baby could even die. A lot of women, understandably, are afraid of [that]."
In addition, sometimes the procedure is medically indicated, as in the case of placenta previa or uterine rupture. However, according to the document, in most pregnancies, which are typically low risk, cesarean delivery carries with it greater overall severe morbidity and mortality risks for the mother compared with vaginal delivery: 9.2% vs. 8.6% and 2.7% vs. 0.9%, respectively.
A combination of fear of being sued for malpractice, convenience, and lack of manpower, are partially responsible for the astronomical rise in C-sections, now the most common surgical procedure performed in the United States, according to the Centers for Disease Control and Prevention.
Dr. Berghella said a scenario that plays out in a physician’s mind could run along the lines of, "You know what, maybe 99% of things are fine here, but I am just worried a little bit here. So I am just going to do a C-section just to cover my behind."
In the past, solo practitioners also were pressed in ways that today’s doctors who belong to an entire practice are not, said Dr. Berghella.
"There are many, many factors that can lead to a longer labor," Dr. Berghella said, adding it was his "hope" that the document will help doctors make decisions based on the patient and how she presents as an individual. "This is to empower doctors, and reassure everyone on the team, including that patient, that if everything is going well, there is no rush."
Redefining active labor and ‘failed’ induction
The use of alternative methods to assist with stalled labors, such as vaginally delivering the baby with forceps or vacuum, is no longer as common as it once was. So residents were taught these techniques less and less. But now Dr. Berghella and his colleagues at the college and the society are urging residency training programs to offer more training in these techniques, including with vacuum birth simulations. "It’s better to do it the first time on a simulator than to try it out on the patient and put the woman at risk. But [residents] need to learn how to do these things," he said.
Physicians also are urged in the statement to reconsider whether there is a failed induction, noting that if the maternal and fetal status allow, cesarean deliveries should be postponed up to 24 hours or longer, and that "oxytocin [should] be administered for at least 12-18 hours after membrane rupture before deeming induction a failure"
A commonly held misperception is that induction and C-section rates are positively correlated, according to the document. "That is a big, big change. The better data seem to say that if you get to 39 weeks, if you do an induction, it actually decreases the chance for a cesarean," said Dr. Berghella. "It was painted as a terrible thing, but if you do it at the right time, it is beneficial."
Into practice
Prenatal counseling should stress weight maintenance, because more than a third of women of reproductive age in the United States are obese, a factor that Dr. Berghella said contributes to the rise in C-sections. Infection risk is higher in this population, and the abundance of adipose tissues makes it harder for the baby to be delivered vaginally. "The higher your weight, the higher your chance of C-section," said Dr. Berghella.
In addition to tort reform, which the document states is "necessary" to prompt physicians to overcome their fears of being sued in case of an adverse event during vaginal delivery, Dr. Berghella said that the culture change rests on communication between office-based obstetricians, midwives, nurse practitioners, and their patients. "Doing a better job of educating women [prenatally] about labor in general, including that it can take a while, will prepare them and help avoid frustration and impatience because they will know what is going on," he said, noting that even a woman who has given birth before can have a completely different experience the next time.
Dr. Berghella said he had no relevant financial disclosures.
WASHINGTON – Longer labors lead to fewer cesarean sections.
That’s according to the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine who have jointly issued the Obstetric Care Consensus guideline, urging physicians to allow women with low-risk pregnancies to remain in latent labor longer before elevating their delivery to surgical status. The report and the consensus guideline appear in the March issue of Obstetrics & Gynecology (Obstet. Gynecol. 2014;123:693-711).
"Evidence now shows that labor actually progresses slower than we thought in the past, so many women might just need a little more time to labor and deliver vaginally instead of moving to a cesarean delivery," Dr. Aaron B. Caughey, a member of ACOG’s Committee on Obstetric Practice, said in a statement.
The document calls on physicians to consider that active labor has begun at 6 cm of cervical dilation, rather than 4, and stresses that doctors should allow more time for progression of labor during the active phase. Whether a woman chooses to use an epidural should also be factored into laboring times because the analgesia can slow contractions.
Although no absolute specific time for allowing a woman to remain in the active labor phase has been determined, the document states that women who have never delivered should be given at least 3 hours to push, while women who have delivered previously should be given a minimum of 2 hours.
‘Fear and convenience’
The recommendations are specifically concerned with avoiding the primary cesarean section because more than one-third of all births in the United States are cesarean deliveries, two-thirds of which are among nulliparous women. Avoiding the first cesarean section is important, "because if the woman labors with a scar from a previous C-section, there is a risk that the uterus will rupture," SMFM president Dr. Vincenzo Berghella, director of maternal-fetal medicine at Thomas Jefferson Medical Center in Philadelphia, said in an interview. "It only happens one-half to one percent [of the time], but it can be catastrophic. The baby could even die. A lot of women, understandably, are afraid of [that]."
In addition, sometimes the procedure is medically indicated, as in the case of placenta previa or uterine rupture. However, according to the document, in most pregnancies, which are typically low risk, cesarean delivery carries with it greater overall severe morbidity and mortality risks for the mother compared with vaginal delivery: 9.2% vs. 8.6% and 2.7% vs. 0.9%, respectively.
A combination of fear of being sued for malpractice, convenience, and lack of manpower, are partially responsible for the astronomical rise in C-sections, now the most common surgical procedure performed in the United States, according to the Centers for Disease Control and Prevention.
Dr. Berghella said a scenario that plays out in a physician’s mind could run along the lines of, "You know what, maybe 99% of things are fine here, but I am just worried a little bit here. So I am just going to do a C-section just to cover my behind."
In the past, solo practitioners also were pressed in ways that today’s doctors who belong to an entire practice are not, said Dr. Berghella.
"There are many, many factors that can lead to a longer labor," Dr. Berghella said, adding it was his "hope" that the document will help doctors make decisions based on the patient and how she presents as an individual. "This is to empower doctors, and reassure everyone on the team, including that patient, that if everything is going well, there is no rush."
Redefining active labor and ‘failed’ induction
The use of alternative methods to assist with stalled labors, such as vaginally delivering the baby with forceps or vacuum, is no longer as common as it once was. So residents were taught these techniques less and less. But now Dr. Berghella and his colleagues at the college and the society are urging residency training programs to offer more training in these techniques, including with vacuum birth simulations. "It’s better to do it the first time on a simulator than to try it out on the patient and put the woman at risk. But [residents] need to learn how to do these things," he said.
Physicians also are urged in the statement to reconsider whether there is a failed induction, noting that if the maternal and fetal status allow, cesarean deliveries should be postponed up to 24 hours or longer, and that "oxytocin [should] be administered for at least 12-18 hours after membrane rupture before deeming induction a failure"
A commonly held misperception is that induction and C-section rates are positively correlated, according to the document. "That is a big, big change. The better data seem to say that if you get to 39 weeks, if you do an induction, it actually decreases the chance for a cesarean," said Dr. Berghella. "It was painted as a terrible thing, but if you do it at the right time, it is beneficial."
Into practice
Prenatal counseling should stress weight maintenance, because more than a third of women of reproductive age in the United States are obese, a factor that Dr. Berghella said contributes to the rise in C-sections. Infection risk is higher in this population, and the abundance of adipose tissues makes it harder for the baby to be delivered vaginally. "The higher your weight, the higher your chance of C-section," said Dr. Berghella.
In addition to tort reform, which the document states is "necessary" to prompt physicians to overcome their fears of being sued in case of an adverse event during vaginal delivery, Dr. Berghella said that the culture change rests on communication between office-based obstetricians, midwives, nurse practitioners, and their patients. "Doing a better job of educating women [prenatally] about labor in general, including that it can take a while, will prepare them and help avoid frustration and impatience because they will know what is going on," he said, noting that even a woman who has given birth before can have a completely different experience the next time.
Dr. Berghella said he had no relevant financial disclosures.
WASHINGTON – Longer labors lead to fewer cesarean sections.
That’s according to the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine who have jointly issued the Obstetric Care Consensus guideline, urging physicians to allow women with low-risk pregnancies to remain in latent labor longer before elevating their delivery to surgical status. The report and the consensus guideline appear in the March issue of Obstetrics & Gynecology (Obstet. Gynecol. 2014;123:693-711).
"Evidence now shows that labor actually progresses slower than we thought in the past, so many women might just need a little more time to labor and deliver vaginally instead of moving to a cesarean delivery," Dr. Aaron B. Caughey, a member of ACOG’s Committee on Obstetric Practice, said in a statement.
The document calls on physicians to consider that active labor has begun at 6 cm of cervical dilation, rather than 4, and stresses that doctors should allow more time for progression of labor during the active phase. Whether a woman chooses to use an epidural should also be factored into laboring times because the analgesia can slow contractions.
Although no absolute specific time for allowing a woman to remain in the active labor phase has been determined, the document states that women who have never delivered should be given at least 3 hours to push, while women who have delivered previously should be given a minimum of 2 hours.
‘Fear and convenience’
The recommendations are specifically concerned with avoiding the primary cesarean section because more than one-third of all births in the United States are cesarean deliveries, two-thirds of which are among nulliparous women. Avoiding the first cesarean section is important, "because if the woman labors with a scar from a previous C-section, there is a risk that the uterus will rupture," SMFM president Dr. Vincenzo Berghella, director of maternal-fetal medicine at Thomas Jefferson Medical Center in Philadelphia, said in an interview. "It only happens one-half to one percent [of the time], but it can be catastrophic. The baby could even die. A lot of women, understandably, are afraid of [that]."
In addition, sometimes the procedure is medically indicated, as in the case of placenta previa or uterine rupture. However, according to the document, in most pregnancies, which are typically low risk, cesarean delivery carries with it greater overall severe morbidity and mortality risks for the mother compared with vaginal delivery: 9.2% vs. 8.6% and 2.7% vs. 0.9%, respectively.
A combination of fear of being sued for malpractice, convenience, and lack of manpower, are partially responsible for the astronomical rise in C-sections, now the most common surgical procedure performed in the United States, according to the Centers for Disease Control and Prevention.
Dr. Berghella said a scenario that plays out in a physician’s mind could run along the lines of, "You know what, maybe 99% of things are fine here, but I am just worried a little bit here. So I am just going to do a C-section just to cover my behind."
In the past, solo practitioners also were pressed in ways that today’s doctors who belong to an entire practice are not, said Dr. Berghella.
"There are many, many factors that can lead to a longer labor," Dr. Berghella said, adding it was his "hope" that the document will help doctors make decisions based on the patient and how she presents as an individual. "This is to empower doctors, and reassure everyone on the team, including that patient, that if everything is going well, there is no rush."
Redefining active labor and ‘failed’ induction
The use of alternative methods to assist with stalled labors, such as vaginally delivering the baby with forceps or vacuum, is no longer as common as it once was. So residents were taught these techniques less and less. But now Dr. Berghella and his colleagues at the college and the society are urging residency training programs to offer more training in these techniques, including with vacuum birth simulations. "It’s better to do it the first time on a simulator than to try it out on the patient and put the woman at risk. But [residents] need to learn how to do these things," he said.
Physicians also are urged in the statement to reconsider whether there is a failed induction, noting that if the maternal and fetal status allow, cesarean deliveries should be postponed up to 24 hours or longer, and that "oxytocin [should] be administered for at least 12-18 hours after membrane rupture before deeming induction a failure"
A commonly held misperception is that induction and C-section rates are positively correlated, according to the document. "That is a big, big change. The better data seem to say that if you get to 39 weeks, if you do an induction, it actually decreases the chance for a cesarean," said Dr. Berghella. "It was painted as a terrible thing, but if you do it at the right time, it is beneficial."
Into practice
Prenatal counseling should stress weight maintenance, because more than a third of women of reproductive age in the United States are obese, a factor that Dr. Berghella said contributes to the rise in C-sections. Infection risk is higher in this population, and the abundance of adipose tissues makes it harder for the baby to be delivered vaginally. "The higher your weight, the higher your chance of C-section," said Dr. Berghella.
In addition to tort reform, which the document states is "necessary" to prompt physicians to overcome their fears of being sued in case of an adverse event during vaginal delivery, Dr. Berghella said that the culture change rests on communication between office-based obstetricians, midwives, nurse practitioners, and their patients. "Doing a better job of educating women [prenatally] about labor in general, including that it can take a while, will prepare them and help avoid frustration and impatience because they will know what is going on," he said, noting that even a woman who has given birth before can have a completely different experience the next time.
Dr. Berghella said he had no relevant financial disclosures.
FROM OBSTETRICS & GYNECOLOGY
Study finds increased infant mortality for home births
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
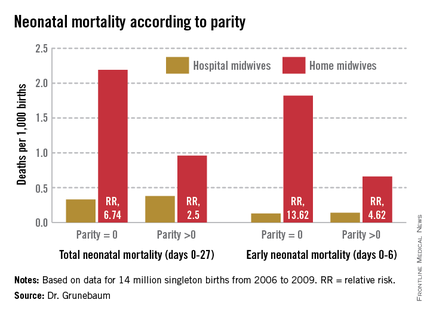
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
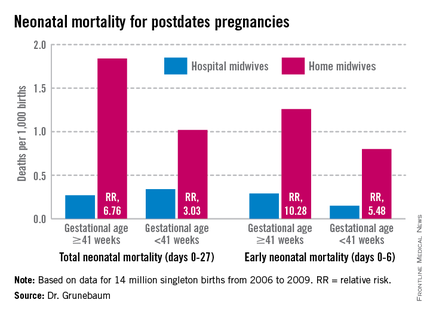
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
AT THE PREGNANCY MEETING
Major finding: Total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk.
Data source: A Centers for Disease Control and Prevention database study that looked at 14 million births from 2006 to 2009.
Disclosures: None of the sources interviewed for this story reported any financial disclosures.
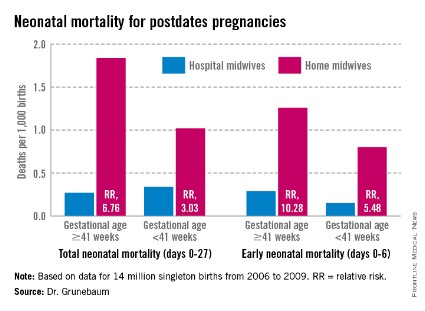
VIDEO: Tips for treating acne in breastfeeding women
WAIKOLOA, HAWAII – Acne treatment during pregnancy gets lots of attention, but no one talks about acne treatment for breastfeeding women, according to Dr. Hilary Baldwin.
She spoke with us in a video interview at the Hawaii Dermatology Seminar about how breastfeeding women can safely treat their acne.
WAIKOLOA, HAWAII – Acne treatment during pregnancy gets lots of attention, but no one talks about acne treatment for breastfeeding women, according to Dr. Hilary Baldwin.
She spoke with us in a video interview at the Hawaii Dermatology Seminar about how breastfeeding women can safely treat their acne.
WAIKOLOA, HAWAII – Acne treatment during pregnancy gets lots of attention, but no one talks about acne treatment for breastfeeding women, according to Dr. Hilary Baldwin.
She spoke with us in a video interview at the Hawaii Dermatology Seminar about how breastfeeding women can safely treat their acne.
ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

Noninvasive prenatal testing detects more than 80% of chromosomal abnormalities
NEW ORLEANS – Noninvasive prenatal testing using cell-free fetal DNA found in the maternal bloodstream detects more than 80% of the most common trisomies, including the one for Down syndrome, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Expectant mothers and their treating physicians now may have a wider range of options for balancing the risks inherent in the more invasive kinds of diagnostic testing, such as chorionic villus sampling and amniocentesis, against the desire for such tests’ near-perfect diagnostic accuracy, according to Dr. Mary Norton.
"Some of the other screening tests that we use, some of the ultrasound screens and some blood tests, have a number of false positives," the study’s presenter, Dr. Norton, vice chair of clinical and translational genetics at the University of California, San Francisco, said in an interview.

For the majority of women, the screening tests show no fetal abnormalities, but the experience can unnerve some women, who find that the test just isn’t worth the risk, said Dr. Norton. Current recommendations from the American College of Obstetricians and Gynecologists (ACOG) are that noninvasive prenatal testing (NIPT) only be offered to high-risk pregnant women as an alternative to invasive testing if integrated ultrasound/blood test screens come back positive.
While diagnostic invasive testing offers "near 100% accuracy," there is a 1 in 500 chance the woman will miscarry after having such a procedure, Dr. Norton said. NIPT, which was introduced into clinical practice in 2011, relies on a simple blood test and is typically performed during the second trimester.
"For a woman who is losing sleep with worry that her fetus may have a chromosome problem, having a test like an amniocentesis that comes back normal may allow her to enjoy the rest of her pregnancy," said Dr. Norton. "For someone whose goal is to avoid diagnostic testing at all costs, to avoid the fear of having a false positive, [NIPT] may be better to detect fewer things but to avoid false positives."
Using the California Prenatal Screening Program database from March 2009 through December 2012, Dr. Norton and her colleagues reviewed all karyotype results from invasive diagnostic tests of singleton pregnancies performed after a prenatal screen indicated possible abnormalities. In all, 26,059 results were analyzed and divided according to either the abnormalities that NIPT is currently able to detect, including nonmosaic trisomies 13, 18, and 21 and sex-chromosomal aneuploidy; or abnormalities currently undetectable by NIPT, such as mosaicism.
During the study period, more than 1.3 million women were screened, with just over 5% (68,990) screening positive for trisomy 18 or 21. Of screen-positive women, nearly 38% (26,059) assented to an invasive prenatal test; of these, 12% (2,993) came back with abnormal results. Just more than 83% (2,488) of those abnormalities were ones detectable by NIPT, while just less than 17% (511) were not. The most common abnormal result, at 53% (1,592), was trisomy 21 (Down syndrome), which has been shown to comprise more than half of all abnormalities detected prenatally.
Women aged 35-39 years composed more than a third of all women studied. While in women under age 30, NIPT misses about 22% of aneuploidies, Dr. Norton said in her presentation that in women over age 45, that number drops dramatically to 8%, largely because of the correlative risk for trisomy 18 and 21 and advanced maternal age.
She noted that one of the limitations of the study was the fact that it included only screen-positive women, and thus the study group was "enriched" for trisomy 21; hence, the results cannot be generalized to the unscreened population, which has a different rate and spectrum of fetal abnormalities.
"Our calculations are for potential detection by NIPT for the target disorders. While the sensitivity is high, it is not 100%; therefore, the overall detection for all chromosomal abnormalities will be less than the 83% we report," Dr. Norton told the audience. "In addition, only 38% of screen-positive women chose to have invasive testing, and those declining such testing might have had different risks, and therefore different outcomes."
NEW ORLEANS – Noninvasive prenatal testing using cell-free fetal DNA found in the maternal bloodstream detects more than 80% of the most common trisomies, including the one for Down syndrome, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Expectant mothers and their treating physicians now may have a wider range of options for balancing the risks inherent in the more invasive kinds of diagnostic testing, such as chorionic villus sampling and amniocentesis, against the desire for such tests’ near-perfect diagnostic accuracy, according to Dr. Mary Norton.
"Some of the other screening tests that we use, some of the ultrasound screens and some blood tests, have a number of false positives," the study’s presenter, Dr. Norton, vice chair of clinical and translational genetics at the University of California, San Francisco, said in an interview.
For the majority of women, the screening tests show no fetal abnormalities, but the experience can unnerve some women, who find that the test just isn’t worth the risk, said Dr. Norton. Current recommendations from the American College of Obstetricians and Gynecologists (ACOG) are that noninvasive prenatal testing (NIPT) only be offered to high-risk pregnant women as an alternative to invasive testing if integrated ultrasound/blood test screens come back positive.
While diagnostic invasive testing offers "near 100% accuracy," there is a 1 in 500 chance the woman will miscarry after having such a procedure, Dr. Norton said. NIPT, which was introduced into clinical practice in 2011, relies on a simple blood test and is typically performed during the second trimester.
"For a woman who is losing sleep with worry that her fetus may have a chromosome problem, having a test like an amniocentesis that comes back normal may allow her to enjoy the rest of her pregnancy," said Dr. Norton. "For someone whose goal is to avoid diagnostic testing at all costs, to avoid the fear of having a false positive, [NIPT] may be better to detect fewer things but to avoid false positives."
Using the California Prenatal Screening Program database from March 2009 through December 2012, Dr. Norton and her colleagues reviewed all karyotype results from invasive diagnostic tests of singleton pregnancies performed after a prenatal screen indicated possible abnormalities. In all, 26,059 results were analyzed and divided according to either the abnormalities that NIPT is currently able to detect, including nonmosaic trisomies 13, 18, and 21 and sex-chromosomal aneuploidy; or abnormalities currently undetectable by NIPT, such as mosaicism.
During the study period, more than 1.3 million women were screened, with just over 5% (68,990) screening positive for trisomy 18 or 21. Of screen-positive women, nearly 38% (26,059) assented to an invasive prenatal test; of these, 12% (2,993) came back with abnormal results. Just more than 83% (2,488) of those abnormalities were ones detectable by NIPT, while just less than 17% (511) were not. The most common abnormal result, at 53% (1,592), was trisomy 21 (Down syndrome), which has been shown to comprise more than half of all abnormalities detected prenatally.
Women aged 35-39 years composed more than a third of all women studied. While in women under age 30, NIPT misses about 22% of aneuploidies, Dr. Norton said in her presentation that in women over age 45, that number drops dramatically to 8%, largely because of the correlative risk for trisomy 18 and 21 and advanced maternal age.
She noted that one of the limitations of the study was the fact that it included only screen-positive women, and thus the study group was "enriched" for trisomy 21; hence, the results cannot be generalized to the unscreened population, which has a different rate and spectrum of fetal abnormalities.
"Our calculations are for potential detection by NIPT for the target disorders. While the sensitivity is high, it is not 100%; therefore, the overall detection for all chromosomal abnormalities will be less than the 83% we report," Dr. Norton told the audience. "In addition, only 38% of screen-positive women chose to have invasive testing, and those declining such testing might have had different risks, and therefore different outcomes."
NEW ORLEANS – Noninvasive prenatal testing using cell-free fetal DNA found in the maternal bloodstream detects more than 80% of the most common trisomies, including the one for Down syndrome, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Expectant mothers and their treating physicians now may have a wider range of options for balancing the risks inherent in the more invasive kinds of diagnostic testing, such as chorionic villus sampling and amniocentesis, against the desire for such tests’ near-perfect diagnostic accuracy, according to Dr. Mary Norton.
"Some of the other screening tests that we use, some of the ultrasound screens and some blood tests, have a number of false positives," the study’s presenter, Dr. Norton, vice chair of clinical and translational genetics at the University of California, San Francisco, said in an interview.
For the majority of women, the screening tests show no fetal abnormalities, but the experience can unnerve some women, who find that the test just isn’t worth the risk, said Dr. Norton. Current recommendations from the American College of Obstetricians and Gynecologists (ACOG) are that noninvasive prenatal testing (NIPT) only be offered to high-risk pregnant women as an alternative to invasive testing if integrated ultrasound/blood test screens come back positive.
While diagnostic invasive testing offers "near 100% accuracy," there is a 1 in 500 chance the woman will miscarry after having such a procedure, Dr. Norton said. NIPT, which was introduced into clinical practice in 2011, relies on a simple blood test and is typically performed during the second trimester.
"For a woman who is losing sleep with worry that her fetus may have a chromosome problem, having a test like an amniocentesis that comes back normal may allow her to enjoy the rest of her pregnancy," said Dr. Norton. "For someone whose goal is to avoid diagnostic testing at all costs, to avoid the fear of having a false positive, [NIPT] may be better to detect fewer things but to avoid false positives."
Using the California Prenatal Screening Program database from March 2009 through December 2012, Dr. Norton and her colleagues reviewed all karyotype results from invasive diagnostic tests of singleton pregnancies performed after a prenatal screen indicated possible abnormalities. In all, 26,059 results were analyzed and divided according to either the abnormalities that NIPT is currently able to detect, including nonmosaic trisomies 13, 18, and 21 and sex-chromosomal aneuploidy; or abnormalities currently undetectable by NIPT, such as mosaicism.
During the study period, more than 1.3 million women were screened, with just over 5% (68,990) screening positive for trisomy 18 or 21. Of screen-positive women, nearly 38% (26,059) assented to an invasive prenatal test; of these, 12% (2,993) came back with abnormal results. Just more than 83% (2,488) of those abnormalities were ones detectable by NIPT, while just less than 17% (511) were not. The most common abnormal result, at 53% (1,592), was trisomy 21 (Down syndrome), which has been shown to comprise more than half of all abnormalities detected prenatally.
Women aged 35-39 years composed more than a third of all women studied. While in women under age 30, NIPT misses about 22% of aneuploidies, Dr. Norton said in her presentation that in women over age 45, that number drops dramatically to 8%, largely because of the correlative risk for trisomy 18 and 21 and advanced maternal age.
She noted that one of the limitations of the study was the fact that it included only screen-positive women, and thus the study group was "enriched" for trisomy 21; hence, the results cannot be generalized to the unscreened population, which has a different rate and spectrum of fetal abnormalities.
"Our calculations are for potential detection by NIPT for the target disorders. While the sensitivity is high, it is not 100%; therefore, the overall detection for all chromosomal abnormalities will be less than the 83% we report," Dr. Norton told the audience. "In addition, only 38% of screen-positive women chose to have invasive testing, and those declining such testing might have had different risks, and therefore different outcomes."
FROM THE PREGNANCY MEETING

Preventing cardiac neonatal lupus with hydroxychloroquine
SNOWMASS, COLO. – The prospect of preventing fetal heart block from neonatal lupus by using hydroxychloroquine to treat women with systemic lupus erythematosus and other anti-Ro antibody-positive rheumatologic diseases throughout pregnancy is drawing mounting physician interest.
"I think these new data are exciting. I actually now have changed my practice as a result of these two studies. I don’t think these studies demand that everybody else change what they’re doing, but I now give hydroxychloroquine to our pregnant patients who have anti-Ro antibodies," Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Maternal anti-Ro antibodies readily transfer across the placenta starting at about week 16 of gestation. Roughly 2% of fetuses whose mothers are positive for these antibodies develop congenital complete heart block caused by inflammation at the atrioventricular node. It’s an irreversible condition with significant morbidity and even mortality.

Moreover, if the mother has previously given birth to a baby with any manifestation of neonatal lupus – even if limited to neonatal rash – the risk of congenital complete heart block in subsequent pregnancies climbs to about 15%, according to Dr. Clowse, a rheumatologist and director of the Duke Autoimmunity in Pregnancy Registry at Duke University, Durham, N.C.
She and her coinvestigators at Duke conducted one of the two studies that have led to her change in practice. It was a retrospective observational study of the recent Duke experience with pregnancies complicated by the presence of maternal anti-Ro antibodies. Twenty of the 33 subjects had systemic lupus erythematosus (SLE); most of the rest had unspecified rheumatologic disease or Sjögren’s syndrome.
Only 1 of 14 women treated with 200-400 mg/day of hydroxychloroquine throughout pregnancy had a baby with congenital heart block, while 7 of 19 pregnancies where hydroxychloroquine wasn’t prescribed resulted in this fetal cardiac disorder. This translated into an 86% relative risk reduction of fetal congenital complete heart block in hydroxychloroquine recipients (Am. J. Obstet. Gynecol. 2013;208:64.e1-7).
Dr. Clowse noted that the Duke study confirms a recent report by investigators at New York University, who searched three databases in the United States, France, and England and identified 257 pregnancies involving mothers positive for anti-Ro antibodies, all of whom had previously given birth to a child with cardiac neonatal lupus. Forty of the women were on hydroxychloroquine starting before 10 weeks of gestation and continued throughout pregnancy; the other 217 didn’t take hydroxychloroquine during the pregnancy. The incidence of recurrent neonatal congenital heart block was 7.5% in the hydroxychloroquine group, compared with 21.2% in mothers who didn’t receive the drug, for a 77% relative risk reduction (Circulation 2012;126:76-82).
The New York University researchers are in the midst of a confirmatory prospective nonrandomized study in women with a history of pregnancy complicated by fetal complete heart block who are on hydroxychloroquine in a subsequent pregnancy. But because it will probably take several more years to accumulate sufficient pregnancies to draw statistically significant conclusions, and in light of hydroxychloroquine’s favorable risk: benefit ratio in pregnancy, Dr. Clowse has decided to change her own practice.
Hydroxychloroquine is rated Pregnancy Class C by the Food and Drug Administration. It readily crosses the placenta. It has not been associated with pregnancy loss, prematurity, congenital anomalies, or any other adverse fetal effects. Dr. Clowse considers hydroxychloroquine to be the best medication for prevention of SLE flares in pregnancy.
She reported serving as a consultant to UCB.
SNOWMASS, COLO. – The prospect of preventing fetal heart block from neonatal lupus by using hydroxychloroquine to treat women with systemic lupus erythematosus and other anti-Ro antibody-positive rheumatologic diseases throughout pregnancy is drawing mounting physician interest.
"I think these new data are exciting. I actually now have changed my practice as a result of these two studies. I don’t think these studies demand that everybody else change what they’re doing, but I now give hydroxychloroquine to our pregnant patients who have anti-Ro antibodies," Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Maternal anti-Ro antibodies readily transfer across the placenta starting at about week 16 of gestation. Roughly 2% of fetuses whose mothers are positive for these antibodies develop congenital complete heart block caused by inflammation at the atrioventricular node. It’s an irreversible condition with significant morbidity and even mortality.
Moreover, if the mother has previously given birth to a baby with any manifestation of neonatal lupus – even if limited to neonatal rash – the risk of congenital complete heart block in subsequent pregnancies climbs to about 15%, according to Dr. Clowse, a rheumatologist and director of the Duke Autoimmunity in Pregnancy Registry at Duke University, Durham, N.C.
She and her coinvestigators at Duke conducted one of the two studies that have led to her change in practice. It was a retrospective observational study of the recent Duke experience with pregnancies complicated by the presence of maternal anti-Ro antibodies. Twenty of the 33 subjects had systemic lupus erythematosus (SLE); most of the rest had unspecified rheumatologic disease or Sjögren’s syndrome.
Only 1 of 14 women treated with 200-400 mg/day of hydroxychloroquine throughout pregnancy had a baby with congenital heart block, while 7 of 19 pregnancies where hydroxychloroquine wasn’t prescribed resulted in this fetal cardiac disorder. This translated into an 86% relative risk reduction of fetal congenital complete heart block in hydroxychloroquine recipients (Am. J. Obstet. Gynecol. 2013;208:64.e1-7).
Dr. Clowse noted that the Duke study confirms a recent report by investigators at New York University, who searched three databases in the United States, France, and England and identified 257 pregnancies involving mothers positive for anti-Ro antibodies, all of whom had previously given birth to a child with cardiac neonatal lupus. Forty of the women were on hydroxychloroquine starting before 10 weeks of gestation and continued throughout pregnancy; the other 217 didn’t take hydroxychloroquine during the pregnancy. The incidence of recurrent neonatal congenital heart block was 7.5% in the hydroxychloroquine group, compared with 21.2% in mothers who didn’t receive the drug, for a 77% relative risk reduction (Circulation 2012;126:76-82).
The New York University researchers are in the midst of a confirmatory prospective nonrandomized study in women with a history of pregnancy complicated by fetal complete heart block who are on hydroxychloroquine in a subsequent pregnancy. But because it will probably take several more years to accumulate sufficient pregnancies to draw statistically significant conclusions, and in light of hydroxychloroquine’s favorable risk: benefit ratio in pregnancy, Dr. Clowse has decided to change her own practice.
Hydroxychloroquine is rated Pregnancy Class C by the Food and Drug Administration. It readily crosses the placenta. It has not been associated with pregnancy loss, prematurity, congenital anomalies, or any other adverse fetal effects. Dr. Clowse considers hydroxychloroquine to be the best medication for prevention of SLE flares in pregnancy.
She reported serving as a consultant to UCB.
SNOWMASS, COLO. – The prospect of preventing fetal heart block from neonatal lupus by using hydroxychloroquine to treat women with systemic lupus erythematosus and other anti-Ro antibody-positive rheumatologic diseases throughout pregnancy is drawing mounting physician interest.
"I think these new data are exciting. I actually now have changed my practice as a result of these two studies. I don’t think these studies demand that everybody else change what they’re doing, but I now give hydroxychloroquine to our pregnant patients who have anti-Ro antibodies," Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Maternal anti-Ro antibodies readily transfer across the placenta starting at about week 16 of gestation. Roughly 2% of fetuses whose mothers are positive for these antibodies develop congenital complete heart block caused by inflammation at the atrioventricular node. It’s an irreversible condition with significant morbidity and even mortality.
Moreover, if the mother has previously given birth to a baby with any manifestation of neonatal lupus – even if limited to neonatal rash – the risk of congenital complete heart block in subsequent pregnancies climbs to about 15%, according to Dr. Clowse, a rheumatologist and director of the Duke Autoimmunity in Pregnancy Registry at Duke University, Durham, N.C.
She and her coinvestigators at Duke conducted one of the two studies that have led to her change in practice. It was a retrospective observational study of the recent Duke experience with pregnancies complicated by the presence of maternal anti-Ro antibodies. Twenty of the 33 subjects had systemic lupus erythematosus (SLE); most of the rest had unspecified rheumatologic disease or Sjögren’s syndrome.
Only 1 of 14 women treated with 200-400 mg/day of hydroxychloroquine throughout pregnancy had a baby with congenital heart block, while 7 of 19 pregnancies where hydroxychloroquine wasn’t prescribed resulted in this fetal cardiac disorder. This translated into an 86% relative risk reduction of fetal congenital complete heart block in hydroxychloroquine recipients (Am. J. Obstet. Gynecol. 2013;208:64.e1-7).
Dr. Clowse noted that the Duke study confirms a recent report by investigators at New York University, who searched three databases in the United States, France, and England and identified 257 pregnancies involving mothers positive for anti-Ro antibodies, all of whom had previously given birth to a child with cardiac neonatal lupus. Forty of the women were on hydroxychloroquine starting before 10 weeks of gestation and continued throughout pregnancy; the other 217 didn’t take hydroxychloroquine during the pregnancy. The incidence of recurrent neonatal congenital heart block was 7.5% in the hydroxychloroquine group, compared with 21.2% in mothers who didn’t receive the drug, for a 77% relative risk reduction (Circulation 2012;126:76-82).
The New York University researchers are in the midst of a confirmatory prospective nonrandomized study in women with a history of pregnancy complicated by fetal complete heart block who are on hydroxychloroquine in a subsequent pregnancy. But because it will probably take several more years to accumulate sufficient pregnancies to draw statistically significant conclusions, and in light of hydroxychloroquine’s favorable risk: benefit ratio in pregnancy, Dr. Clowse has decided to change her own practice.
Hydroxychloroquine is rated Pregnancy Class C by the Food and Drug Administration. It readily crosses the placenta. It has not been associated with pregnancy loss, prematurity, congenital anomalies, or any other adverse fetal effects. Dr. Clowse considers hydroxychloroquine to be the best medication for prevention of SLE flares in pregnancy.
She reported serving as a consultant to UCB.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
