User login
Efficacy of Anti-Obesity Medications in Adult and Older Adult Veteran Populations
Efficacy of Anti-Obesity Medications in Adult and Older Adult Veteran Populations
The impact of obesity in the United States is significant. Between August 2021 and August 2023, the prevalence of obesity (body mass index ≥ 30) in US adults was 40.3%.1 The prevalence of obesity in adults aged 40 to 59 years was 46.4%, higher than the prevalence in adults aged 20 to 39 years (35.5%) and those aged ≥ 60 years (38.9%).1 The excess annual medical costs associated with obesity in the US are estimated at nearly $173 billion.2
The first-line treatment for obesity is lifestyle modifications, including a healthy diet and exercise. When lifestyle modifications are not enough to achieve weight-loss goals, bariatric surgery and anti-obesity medications (AOMs) are often considered. Five medications were approved for the long-term tretament of obesity by the US Food and Drug Administration (FDA) between 2021 and 2023, when this study was conducted: semaglutide (Wegovy), liraglutide (Saxenda), phentermine and topiramate, naltrexone and bupropion, and orlistat. The clinically meaningful (and commonly accepted) weight-loss target for these medications is ≥ 5% from baseline by week 12 of the maximally tolerated dose of therapy. A 5% weight loss has been shown to be clinically significant in improving cardiometabolic risk factors.3,4 These medications are intended to be used as an adjunct to healthy diet and exercise. Of note, semaglutide and liraglutide carry brand names, which are associated with different dosing for the treatment of type 2 diabetes mellitus (T2DM).
All 5 FDA-approved AOMs were available at the Veterans Affairs Sioux Falls Health Care System (VASFHCS) for the treatment of obesity at the time of the study. To qualify for an AOM, a veteran at VASFHCS must first work with a dietitian or be enrolled in the MOVE! clinic to participate in the weight management program, which focuses on dietary, exercise, and behavioral changes. At VASFHCS, AOMs are prescribed by primary care practitioners, clinical pharmacy providers, and advanced practitioners within the MOVE! program.
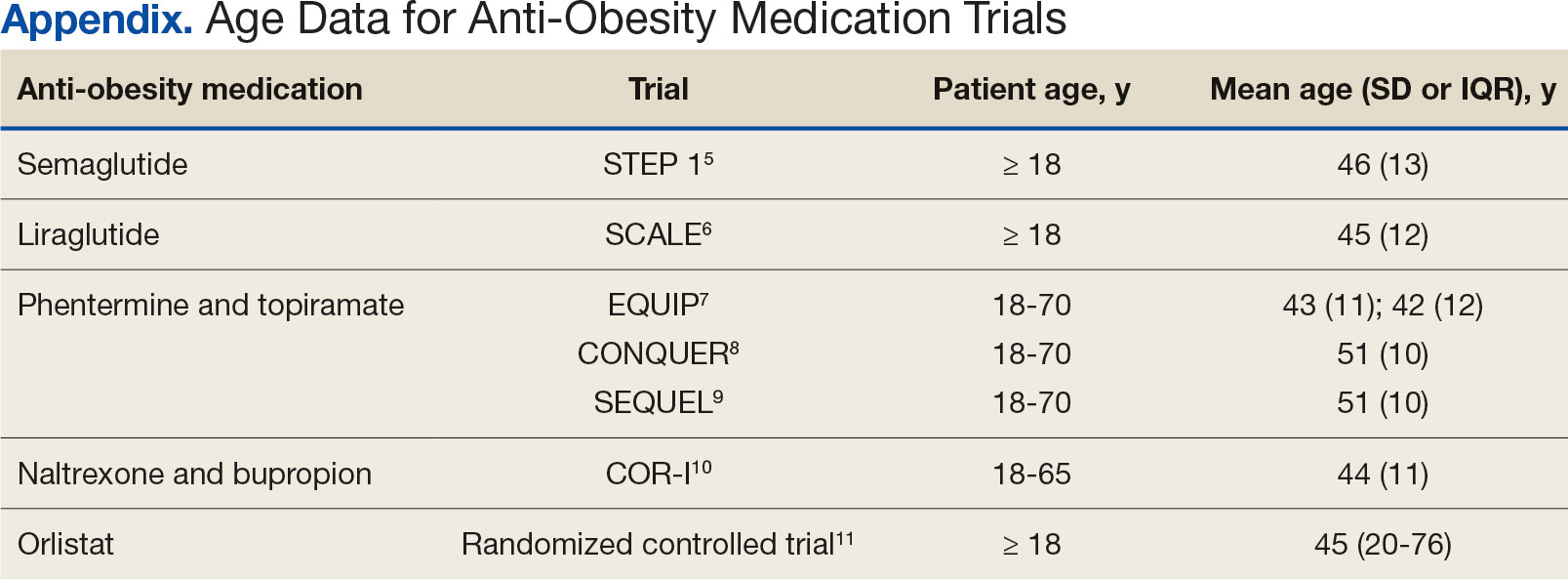
Ample data exist for the efficacy of AOMs. However, no published research has reported on AOM efficacy by age group (Appendix).5-11 While most of the AOM clinical trials included older adults, the average age of participants was typically between 40 and 50 years. It is well-known that pharmacokinetic and pharmacodynamic changes occur as age increases. Renal and hepatic clearance is reduced while the volume distribution and sensitivities to some medications may increase. 12 Although this study did not focus on specific pharmacokinetic and pharmacodynamic changes with respect to AOM, it is important to recognize that this may play a role in the efficacy and safety of AOMs in older adults.
Methods
This retrospective single-center chart review was performed using the VASFHCS Computerized Patient Record System to compare the efficacy of AOMs in older adults (aged ≥ 65 years) vs adults (aged < 65 years). The primary endpoint was the percent change in body weight from baseline to 6 and 12 months after initiation of AOM therapy in the older adult vs adult population. Secondary endpoints included changes in low-density lipoprotein (LDL), hemoglobin A1c (HbA1c), and blood pressure (BP) from baseline compared to 12 months on AOM therapy. HbA1c was assessed in patients with T2DM or prediabetes at the time of AOM initiation. Two safety endpoints were also explored to determine the incidence of medication adverse events (AEs) and subsequent discontinuation of AOM. A subset analysis was performed to determine whether there was a difference in percent change in body weight between patients in 3 age groups: 18 to 40 years, 41 to 64 years, and ≥ 65 years.
The study population included patients who were prescribed an AOM between January 1, 2021, and June 30, 2023. Patients were excluded if they did not continue AOM therapy for ≥ 6 months after initiation or if they underwent gastric bypass surgery while undergoing AOM therapy. Patients taking semaglutide (Ozempic) or liraglutide (Victoza) for both T2DM and weight loss who were eventually switched to the weight loss formulations (Wegovy or Saxenda) were included. Patients who switched between semaglutide and liraglutide for weight loss were also included. Those taking semaglutide or liraglutide solely for T2DM treatment were excluded because they are dosed differently.
Collected data included age, gender, race, weight (baseline, 6 and 12 months after initiation of AOM), metabolic laboratory values/vital signs (HbA1c, LDL, and BP at baseline and 12 months after initiation of AOM), diagnosis of T2DM or prediabetes, reported AEs associated with AOM therapy, and date of AOM initiation and discontinuation (if applicable). Baseline values were defined at the time of medication initiation or values documented within 6 months prior to medication initiation if true baseline data were not reported. If values were not recorded at months 6 and 12 after AOM initiation, values documented closest to those targets were used. Weights were used for baseline, 6-, and 12-month data unless they were unavailable due to use of virtual care modalities. In these cases, patient-reported weights were used. Patients were included in the 6-month data, but not the 12-month data, if they were taking AOMs for > 6 months but not for 12 months. If patients had been on multiple AOMs, baseline data were recorded at the start of the first medication that was used for 6 months or longer. Twelve-month data were recorded after subsequent medication change. Twelve-month metabolic laboratory values/vital signs were recorded for patients included in the study even if they did not complete ≥ 12 months of AOM therapy.
Statistical Analysis
Data from patients who were prescribed an AOM from January 2021 to June 2023 and who remained on the medication for ≥ 6 months were analyzed. Baseline characteristics were analyzed using descriptive statistics. The primary and secondary endpoints were evaluated using the t test. The safety endpoints were analyzed using descriptive statistics. An analysis of variance test was used for the subset analysis. Results with P < .05 were statistically significant.
Results
A total of 144 participants were included in this study, 116 in the adult group (aged < 65 years) and 28 in the older adult group (aged ≥ 65 years). Sixty-seven patients were excluded due to prespecified inclusion and exclusion criteria.
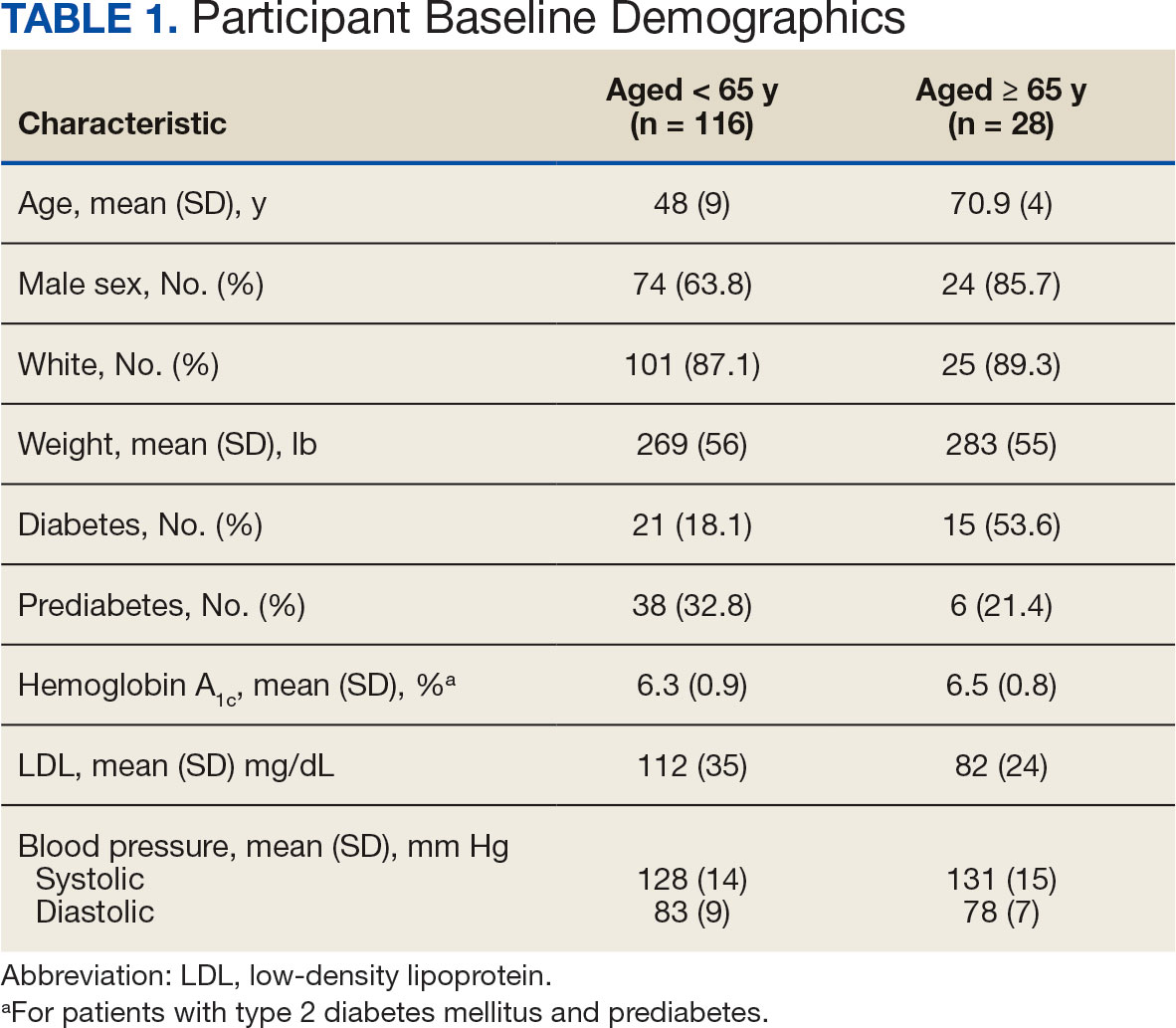
Other than the predetermined mean age differences (48 years vs 71 years), there were multiple differences in patient baseline characteristics. When comparing older adults and adults, average weight (283 lb vs 269 lb) and White race (89% vs 87%) were slightly higher in the older adult group. Also, a higher prevalence of T2DM (54% and 18%) and a lower prevalence of prediabetes (21% and 33%) was noted in the older adult group. HbA1c and BP were similar between both groups at baseline, while LDL was slightly lower in the older adult group (Table 1).
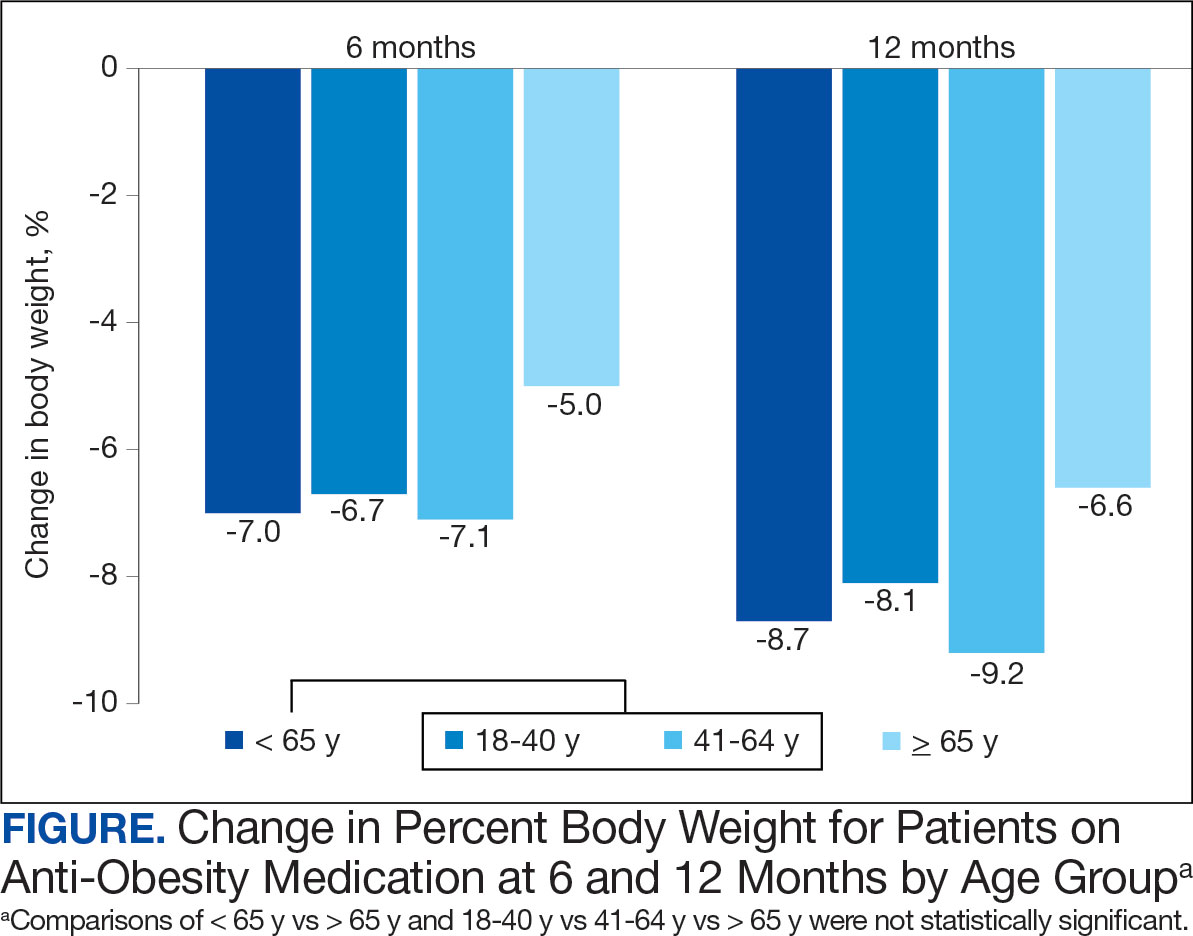
Patients in the adult group lost a mean 7.0% and 8.7% of body weight at 6 and 12 months, respectively, while the older adult group lost 5.0% and 6.6% body weight at 6 and 12 months, respectively. The difference in percent change in body weight was not statistically different at 6 (P = .08) or 12 (P = .26) months between patients in the adult group vs the older adult group or in the specific age groups (18-40 years, 41-64 years, ≥ 65 years) at 6 months (P = .24) or 12 months (P = .53) (Figure).
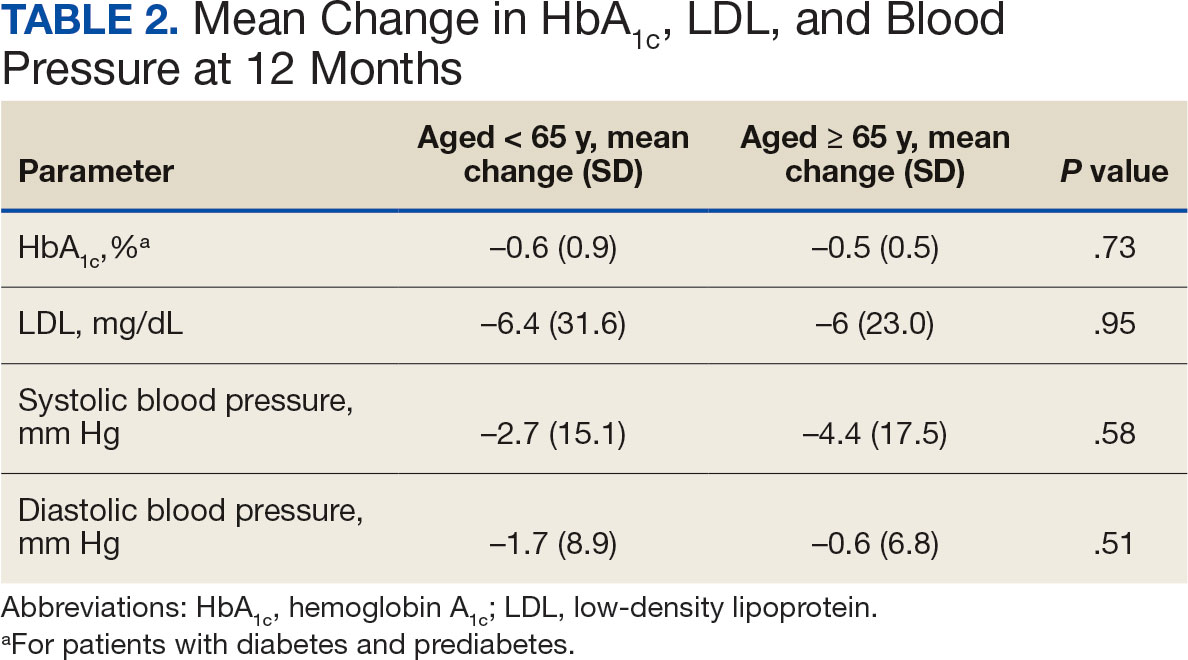
At 12 months, the difference between the adult group vs the older adult group was not statistically significant for HbA1c in patients with T2DM or prediabetes (P = .73), LDL (P = .95), systolic BP (P = .58), or diastolic BP (P = .51) (Table 2).
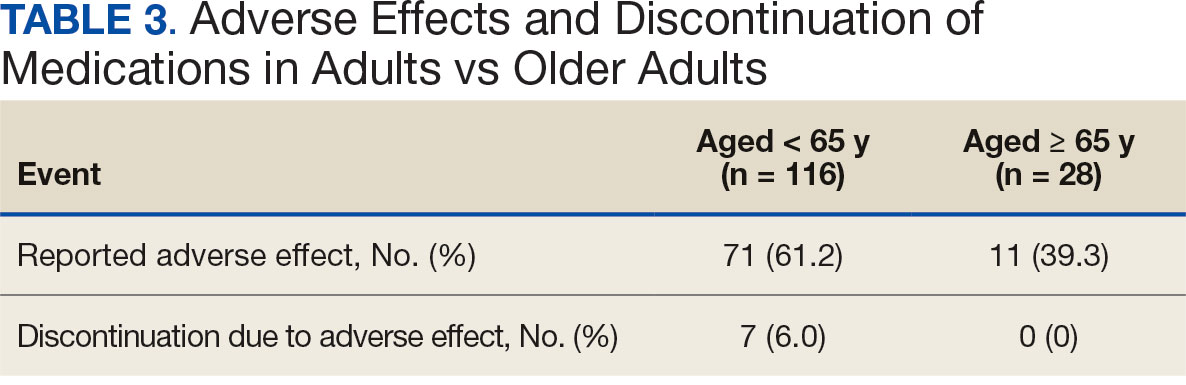
For the safety endpoint, the incidence of AEs was found to be different between groups. There were more reported AEs (61.2% vs 39.3%) and a greater increase in therapy discontinuation due to AEs (6.0% vs 0%) in the adult group compared to the older adult group (Table 3).
Discussion
Patients taking AOMs revealed no statistically significant difference in percent change in body weight at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. The subset analysis also showed no statistically significant difference in change in percent body weight between more narrowly defined age groups of 18 to 40 years, 41 to 64 years, and ≥ 65 years. This suggests that AOM may have similar efficacy for weight loss in all ages of adults.
Secondary endpoint findings showed no statistically significant difference in HbA1c (in patients with T2DM or prediabetes), LDL, or BP at 12 months between the 2 groups. Although this study did not differentiate secondary outcomes based on the individual AOM, the change in HbA1c in both groups was expected, given that 70% of the patients included in this study were taking a glucagon-like peptide-1 agonist (liraglutide and semaglutide) at some point during the study. It’s also worth noting that secondary endpoints were collected for patients who discontinued the AOM between 6 and 12 months. Therefore, the patients’ HbA1c, LDL, and BP may not have accurately reflected the change that could have been expected if they had continued AOM therapy beyond the 12-month period.
Due to the different mechanisms and range in efficacy that AOMs have in regard to weight loss, changes in all outcomes, including weight, HbA1c, LDL, and BP were expected to vary as patients were included even after switching AOM (collection of data started after ≥ 6 months on a single AOM). Switching of AOM after the first 6 months of therapy was recorded in 25% of the patients in the ≥ 65 years group and 330% of the patients in the < 65 years group.
The incidence of AEs and subsequent discontinuation of AOMs in this study was higher in the adult group. This study excluded patients who did not continue taking an AOM for at least 6 months. As a result, the incidence of AEs between the 2 groups within the first 6 months of AOM therapy remains unknown. It is possible that during the first 6 months of therapy, patients aged < 65 years were more willing to tolerate or had fewer severe AEs compared with the older adult group. It’s also possible that the smaller number of patients in the older adult group was due to increased AEs that led them to discontinue early (before completion of 6 months of therapy) and/or prescriber discomfort in using AOMs in the older adult population. In addition, because the specific medication(s) taken by patients in each group were not detailed, it is unknown whether the adult group was taking AOMs associated with a greater number of AEs.
Limitations
This was a retrospective study with a relatively small sample size. A larger sample size may have shown more precise differences between age groups and may be more representative of the general population. Additionally, data were reliant on appropriate documentation, and adherence to AOM therapy was not assessed due to the retrospective nature of this study. At times, the study relied on patient reported data points, such as weight, if a clinic weight was not available. Also, this study did not account for many potential confounding factors such as other medications taken by the patient, which can affect outcomes including weight, HbA1c, LDL, blood pressure, and AEs.
Conclusions
This retrospective study of patients taking AOMs showed no statistically significant difference in weight loss at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. A subset analysis found no statistically significant difference in change in body weight between specific age groups (18-40 years, 41-64 years, and ≥ 65 years). There was also no statistically significant difference in secondary outcomes, including change in HbA1c (in patients with T2DM or prediabetes), LDL or BP between age groups. The safety endpoints showed a higher incidence of medication AEs in the adult group, with more of these adults discontinuing therapy due to AEs. This study indicates that AOM may have similar outcomes for weight loss and metabolic laboratory values/vital sign changes between adults and older adults. Also, our findings suggest that patients aged < 65 years may experience more AEs than patients aged ≥ 65 years after ≥ 6 months of AOM therapy. Larger studies are needed to further evaluate these age-specific findings.
- Emmerich SD, Fryar CD, Stierman B, Ogden CL. Obesity and severe obesity prevalence in adults: United States, August 2021-August 2023. NCHS Data Brief No. 508. National Center for Health Statistics; 2024. Accessed December 11, 2024. https://www.cdc.gov/nchs/products/databriefs/db508.htm
- Ward ZJ, Bleich SN, Long MW, Gortmaker SL. Association of body mass index with health care expenditures in the United States by age and sex. PLoS One. 2021;16(3):e0247307. doi:10.1371/journal.pone.0247307
- Horn DB, Almandoz JP, Look M. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359-375. doi:10.1080/00325481.2022.2051366
- American Diabetes Association (ADA). Standards of care in diabetes–2023. Diabetes Care. 2023;46(suppl 1):S128- S2139. doi:10.2337/dc23-S008
- Wilding JPH, Batterham RL, Calanna S, et al. Onceweekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22. doi:10.1056/NEJMoa1411892
- Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity (Silver Spring). 2012;20(2):330-342. doi:10.1038/oby.2011.330
- Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341-1352. doi:10.1016/S0140-6736(11)60205-5
- Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308. doi:10.3945/ajcn.111.024927
- Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605. doi:10.1016/S0140-6736(10)60888-4
- Sjöström L, Rissanen A, Andersen T, et al. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group. Lancet. 1998;352(9123):167-172. doi:10.1016s0140-6736(97)11509-4
- Mangoni AA, Jackson SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x
The impact of obesity in the United States is significant. Between August 2021 and August 2023, the prevalence of obesity (body mass index ≥ 30) in US adults was 40.3%.1 The prevalence of obesity in adults aged 40 to 59 years was 46.4%, higher than the prevalence in adults aged 20 to 39 years (35.5%) and those aged ≥ 60 years (38.9%).1 The excess annual medical costs associated with obesity in the US are estimated at nearly $173 billion.2
The first-line treatment for obesity is lifestyle modifications, including a healthy diet and exercise. When lifestyle modifications are not enough to achieve weight-loss goals, bariatric surgery and anti-obesity medications (AOMs) are often considered. Five medications were approved for the long-term tretament of obesity by the US Food and Drug Administration (FDA) between 2021 and 2023, when this study was conducted: semaglutide (Wegovy), liraglutide (Saxenda), phentermine and topiramate, naltrexone and bupropion, and orlistat. The clinically meaningful (and commonly accepted) weight-loss target for these medications is ≥ 5% from baseline by week 12 of the maximally tolerated dose of therapy. A 5% weight loss has been shown to be clinically significant in improving cardiometabolic risk factors.3,4 These medications are intended to be used as an adjunct to healthy diet and exercise. Of note, semaglutide and liraglutide carry brand names, which are associated with different dosing for the treatment of type 2 diabetes mellitus (T2DM).
All 5 FDA-approved AOMs were available at the Veterans Affairs Sioux Falls Health Care System (VASFHCS) for the treatment of obesity at the time of the study. To qualify for an AOM, a veteran at VASFHCS must first work with a dietitian or be enrolled in the MOVE! clinic to participate in the weight management program, which focuses on dietary, exercise, and behavioral changes. At VASFHCS, AOMs are prescribed by primary care practitioners, clinical pharmacy providers, and advanced practitioners within the MOVE! program.
Ample data exist for the efficacy of AOMs. However, no published research has reported on AOM efficacy by age group (Appendix).5-11 While most of the AOM clinical trials included older adults, the average age of participants was typically between 40 and 50 years. It is well-known that pharmacokinetic and pharmacodynamic changes occur as age increases. Renal and hepatic clearance is reduced while the volume distribution and sensitivities to some medications may increase. 12 Although this study did not focus on specific pharmacokinetic and pharmacodynamic changes with respect to AOM, it is important to recognize that this may play a role in the efficacy and safety of AOMs in older adults.
Methods
This retrospective single-center chart review was performed using the VASFHCS Computerized Patient Record System to compare the efficacy of AOMs in older adults (aged ≥ 65 years) vs adults (aged < 65 years). The primary endpoint was the percent change in body weight from baseline to 6 and 12 months after initiation of AOM therapy in the older adult vs adult population. Secondary endpoints included changes in low-density lipoprotein (LDL), hemoglobin A1c (HbA1c), and blood pressure (BP) from baseline compared to 12 months on AOM therapy. HbA1c was assessed in patients with T2DM or prediabetes at the time of AOM initiation. Two safety endpoints were also explored to determine the incidence of medication adverse events (AEs) and subsequent discontinuation of AOM. A subset analysis was performed to determine whether there was a difference in percent change in body weight between patients in 3 age groups: 18 to 40 years, 41 to 64 years, and ≥ 65 years.
The study population included patients who were prescribed an AOM between January 1, 2021, and June 30, 2023. Patients were excluded if they did not continue AOM therapy for ≥ 6 months after initiation or if they underwent gastric bypass surgery while undergoing AOM therapy. Patients taking semaglutide (Ozempic) or liraglutide (Victoza) for both T2DM and weight loss who were eventually switched to the weight loss formulations (Wegovy or Saxenda) were included. Patients who switched between semaglutide and liraglutide for weight loss were also included. Those taking semaglutide or liraglutide solely for T2DM treatment were excluded because they are dosed differently.
Collected data included age, gender, race, weight (baseline, 6 and 12 months after initiation of AOM), metabolic laboratory values/vital signs (HbA1c, LDL, and BP at baseline and 12 months after initiation of AOM), diagnosis of T2DM or prediabetes, reported AEs associated with AOM therapy, and date of AOM initiation and discontinuation (if applicable). Baseline values were defined at the time of medication initiation or values documented within 6 months prior to medication initiation if true baseline data were not reported. If values were not recorded at months 6 and 12 after AOM initiation, values documented closest to those targets were used. Weights were used for baseline, 6-, and 12-month data unless they were unavailable due to use of virtual care modalities. In these cases, patient-reported weights were used. Patients were included in the 6-month data, but not the 12-month data, if they were taking AOMs for > 6 months but not for 12 months. If patients had been on multiple AOMs, baseline data were recorded at the start of the first medication that was used for 6 months or longer. Twelve-month data were recorded after subsequent medication change. Twelve-month metabolic laboratory values/vital signs were recorded for patients included in the study even if they did not complete ≥ 12 months of AOM therapy.
Statistical Analysis
Data from patients who were prescribed an AOM from January 2021 to June 2023 and who remained on the medication for ≥ 6 months were analyzed. Baseline characteristics were analyzed using descriptive statistics. The primary and secondary endpoints were evaluated using the t test. The safety endpoints were analyzed using descriptive statistics. An analysis of variance test was used for the subset analysis. Results with P < .05 were statistically significant.
Results
A total of 144 participants were included in this study, 116 in the adult group (aged < 65 years) and 28 in the older adult group (aged ≥ 65 years). Sixty-seven patients were excluded due to prespecified inclusion and exclusion criteria.
Other than the predetermined mean age differences (48 years vs 71 years), there were multiple differences in patient baseline characteristics. When comparing older adults and adults, average weight (283 lb vs 269 lb) and White race (89% vs 87%) were slightly higher in the older adult group. Also, a higher prevalence of T2DM (54% and 18%) and a lower prevalence of prediabetes (21% and 33%) was noted in the older adult group. HbA1c and BP were similar between both groups at baseline, while LDL was slightly lower in the older adult group (Table 1).
Patients in the adult group lost a mean 7.0% and 8.7% of body weight at 6 and 12 months, respectively, while the older adult group lost 5.0% and 6.6% body weight at 6 and 12 months, respectively. The difference in percent change in body weight was not statistically different at 6 (P = .08) or 12 (P = .26) months between patients in the adult group vs the older adult group or in the specific age groups (18-40 years, 41-64 years, ≥ 65 years) at 6 months (P = .24) or 12 months (P = .53) (Figure).
At 12 months, the difference between the adult group vs the older adult group was not statistically significant for HbA1c in patients with T2DM or prediabetes (P = .73), LDL (P = .95), systolic BP (P = .58), or diastolic BP (P = .51) (Table 2).
For the safety endpoint, the incidence of AEs was found to be different between groups. There were more reported AEs (61.2% vs 39.3%) and a greater increase in therapy discontinuation due to AEs (6.0% vs 0%) in the adult group compared to the older adult group (Table 3).
Discussion
Patients taking AOMs revealed no statistically significant difference in percent change in body weight at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. The subset analysis also showed no statistically significant difference in change in percent body weight between more narrowly defined age groups of 18 to 40 years, 41 to 64 years, and ≥ 65 years. This suggests that AOM may have similar efficacy for weight loss in all ages of adults.
Secondary endpoint findings showed no statistically significant difference in HbA1c (in patients with T2DM or prediabetes), LDL, or BP at 12 months between the 2 groups. Although this study did not differentiate secondary outcomes based on the individual AOM, the change in HbA1c in both groups was expected, given that 70% of the patients included in this study were taking a glucagon-like peptide-1 agonist (liraglutide and semaglutide) at some point during the study. It’s also worth noting that secondary endpoints were collected for patients who discontinued the AOM between 6 and 12 months. Therefore, the patients’ HbA1c, LDL, and BP may not have accurately reflected the change that could have been expected if they had continued AOM therapy beyond the 12-month period.
Due to the different mechanisms and range in efficacy that AOMs have in regard to weight loss, changes in all outcomes, including weight, HbA1c, LDL, and BP were expected to vary as patients were included even after switching AOM (collection of data started after ≥ 6 months on a single AOM). Switching of AOM after the first 6 months of therapy was recorded in 25% of the patients in the ≥ 65 years group and 330% of the patients in the < 65 years group.
The incidence of AEs and subsequent discontinuation of AOMs in this study was higher in the adult group. This study excluded patients who did not continue taking an AOM for at least 6 months. As a result, the incidence of AEs between the 2 groups within the first 6 months of AOM therapy remains unknown. It is possible that during the first 6 months of therapy, patients aged < 65 years were more willing to tolerate or had fewer severe AEs compared with the older adult group. It’s also possible that the smaller number of patients in the older adult group was due to increased AEs that led them to discontinue early (before completion of 6 months of therapy) and/or prescriber discomfort in using AOMs in the older adult population. In addition, because the specific medication(s) taken by patients in each group were not detailed, it is unknown whether the adult group was taking AOMs associated with a greater number of AEs.
Limitations
This was a retrospective study with a relatively small sample size. A larger sample size may have shown more precise differences between age groups and may be more representative of the general population. Additionally, data were reliant on appropriate documentation, and adherence to AOM therapy was not assessed due to the retrospective nature of this study. At times, the study relied on patient reported data points, such as weight, if a clinic weight was not available. Also, this study did not account for many potential confounding factors such as other medications taken by the patient, which can affect outcomes including weight, HbA1c, LDL, blood pressure, and AEs.
Conclusions
This retrospective study of patients taking AOMs showed no statistically significant difference in weight loss at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. A subset analysis found no statistically significant difference in change in body weight between specific age groups (18-40 years, 41-64 years, and ≥ 65 years). There was also no statistically significant difference in secondary outcomes, including change in HbA1c (in patients with T2DM or prediabetes), LDL or BP between age groups. The safety endpoints showed a higher incidence of medication AEs in the adult group, with more of these adults discontinuing therapy due to AEs. This study indicates that AOM may have similar outcomes for weight loss and metabolic laboratory values/vital sign changes between adults and older adults. Also, our findings suggest that patients aged < 65 years may experience more AEs than patients aged ≥ 65 years after ≥ 6 months of AOM therapy. Larger studies are needed to further evaluate these age-specific findings.
The impact of obesity in the United States is significant. Between August 2021 and August 2023, the prevalence of obesity (body mass index ≥ 30) in US adults was 40.3%.1 The prevalence of obesity in adults aged 40 to 59 years was 46.4%, higher than the prevalence in adults aged 20 to 39 years (35.5%) and those aged ≥ 60 years (38.9%).1 The excess annual medical costs associated with obesity in the US are estimated at nearly $173 billion.2
The first-line treatment for obesity is lifestyle modifications, including a healthy diet and exercise. When lifestyle modifications are not enough to achieve weight-loss goals, bariatric surgery and anti-obesity medications (AOMs) are often considered. Five medications were approved for the long-term tretament of obesity by the US Food and Drug Administration (FDA) between 2021 and 2023, when this study was conducted: semaglutide (Wegovy), liraglutide (Saxenda), phentermine and topiramate, naltrexone and bupropion, and orlistat. The clinically meaningful (and commonly accepted) weight-loss target for these medications is ≥ 5% from baseline by week 12 of the maximally tolerated dose of therapy. A 5% weight loss has been shown to be clinically significant in improving cardiometabolic risk factors.3,4 These medications are intended to be used as an adjunct to healthy diet and exercise. Of note, semaglutide and liraglutide carry brand names, which are associated with different dosing for the treatment of type 2 diabetes mellitus (T2DM).
All 5 FDA-approved AOMs were available at the Veterans Affairs Sioux Falls Health Care System (VASFHCS) for the treatment of obesity at the time of the study. To qualify for an AOM, a veteran at VASFHCS must first work with a dietitian or be enrolled in the MOVE! clinic to participate in the weight management program, which focuses on dietary, exercise, and behavioral changes. At VASFHCS, AOMs are prescribed by primary care practitioners, clinical pharmacy providers, and advanced practitioners within the MOVE! program.
Ample data exist for the efficacy of AOMs. However, no published research has reported on AOM efficacy by age group (Appendix).5-11 While most of the AOM clinical trials included older adults, the average age of participants was typically between 40 and 50 years. It is well-known that pharmacokinetic and pharmacodynamic changes occur as age increases. Renal and hepatic clearance is reduced while the volume distribution and sensitivities to some medications may increase. 12 Although this study did not focus on specific pharmacokinetic and pharmacodynamic changes with respect to AOM, it is important to recognize that this may play a role in the efficacy and safety of AOMs in older adults.
Methods
This retrospective single-center chart review was performed using the VASFHCS Computerized Patient Record System to compare the efficacy of AOMs in older adults (aged ≥ 65 years) vs adults (aged < 65 years). The primary endpoint was the percent change in body weight from baseline to 6 and 12 months after initiation of AOM therapy in the older adult vs adult population. Secondary endpoints included changes in low-density lipoprotein (LDL), hemoglobin A1c (HbA1c), and blood pressure (BP) from baseline compared to 12 months on AOM therapy. HbA1c was assessed in patients with T2DM or prediabetes at the time of AOM initiation. Two safety endpoints were also explored to determine the incidence of medication adverse events (AEs) and subsequent discontinuation of AOM. A subset analysis was performed to determine whether there was a difference in percent change in body weight between patients in 3 age groups: 18 to 40 years, 41 to 64 years, and ≥ 65 years.
The study population included patients who were prescribed an AOM between January 1, 2021, and June 30, 2023. Patients were excluded if they did not continue AOM therapy for ≥ 6 months after initiation or if they underwent gastric bypass surgery while undergoing AOM therapy. Patients taking semaglutide (Ozempic) or liraglutide (Victoza) for both T2DM and weight loss who were eventually switched to the weight loss formulations (Wegovy or Saxenda) were included. Patients who switched between semaglutide and liraglutide for weight loss were also included. Those taking semaglutide or liraglutide solely for T2DM treatment were excluded because they are dosed differently.
Collected data included age, gender, race, weight (baseline, 6 and 12 months after initiation of AOM), metabolic laboratory values/vital signs (HbA1c, LDL, and BP at baseline and 12 months after initiation of AOM), diagnosis of T2DM or prediabetes, reported AEs associated with AOM therapy, and date of AOM initiation and discontinuation (if applicable). Baseline values were defined at the time of medication initiation or values documented within 6 months prior to medication initiation if true baseline data were not reported. If values were not recorded at months 6 and 12 after AOM initiation, values documented closest to those targets were used. Weights were used for baseline, 6-, and 12-month data unless they were unavailable due to use of virtual care modalities. In these cases, patient-reported weights were used. Patients were included in the 6-month data, but not the 12-month data, if they were taking AOMs for > 6 months but not for 12 months. If patients had been on multiple AOMs, baseline data were recorded at the start of the first medication that was used for 6 months or longer. Twelve-month data were recorded after subsequent medication change. Twelve-month metabolic laboratory values/vital signs were recorded for patients included in the study even if they did not complete ≥ 12 months of AOM therapy.
Statistical Analysis
Data from patients who were prescribed an AOM from January 2021 to June 2023 and who remained on the medication for ≥ 6 months were analyzed. Baseline characteristics were analyzed using descriptive statistics. The primary and secondary endpoints were evaluated using the t test. The safety endpoints were analyzed using descriptive statistics. An analysis of variance test was used for the subset analysis. Results with P < .05 were statistically significant.
Results
A total of 144 participants were included in this study, 116 in the adult group (aged < 65 years) and 28 in the older adult group (aged ≥ 65 years). Sixty-seven patients were excluded due to prespecified inclusion and exclusion criteria.
Other than the predetermined mean age differences (48 years vs 71 years), there were multiple differences in patient baseline characteristics. When comparing older adults and adults, average weight (283 lb vs 269 lb) and White race (89% vs 87%) were slightly higher in the older adult group. Also, a higher prevalence of T2DM (54% and 18%) and a lower prevalence of prediabetes (21% and 33%) was noted in the older adult group. HbA1c and BP were similar between both groups at baseline, while LDL was slightly lower in the older adult group (Table 1).
Patients in the adult group lost a mean 7.0% and 8.7% of body weight at 6 and 12 months, respectively, while the older adult group lost 5.0% and 6.6% body weight at 6 and 12 months, respectively. The difference in percent change in body weight was not statistically different at 6 (P = .08) or 12 (P = .26) months between patients in the adult group vs the older adult group or in the specific age groups (18-40 years, 41-64 years, ≥ 65 years) at 6 months (P = .24) or 12 months (P = .53) (Figure).
At 12 months, the difference between the adult group vs the older adult group was not statistically significant for HbA1c in patients with T2DM or prediabetes (P = .73), LDL (P = .95), systolic BP (P = .58), or diastolic BP (P = .51) (Table 2).
For the safety endpoint, the incidence of AEs was found to be different between groups. There were more reported AEs (61.2% vs 39.3%) and a greater increase in therapy discontinuation due to AEs (6.0% vs 0%) in the adult group compared to the older adult group (Table 3).
Discussion
Patients taking AOMs revealed no statistically significant difference in percent change in body weight at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. The subset analysis also showed no statistically significant difference in change in percent body weight between more narrowly defined age groups of 18 to 40 years, 41 to 64 years, and ≥ 65 years. This suggests that AOM may have similar efficacy for weight loss in all ages of adults.
Secondary endpoint findings showed no statistically significant difference in HbA1c (in patients with T2DM or prediabetes), LDL, or BP at 12 months between the 2 groups. Although this study did not differentiate secondary outcomes based on the individual AOM, the change in HbA1c in both groups was expected, given that 70% of the patients included in this study were taking a glucagon-like peptide-1 agonist (liraglutide and semaglutide) at some point during the study. It’s also worth noting that secondary endpoints were collected for patients who discontinued the AOM between 6 and 12 months. Therefore, the patients’ HbA1c, LDL, and BP may not have accurately reflected the change that could have been expected if they had continued AOM therapy beyond the 12-month period.
Due to the different mechanisms and range in efficacy that AOMs have in regard to weight loss, changes in all outcomes, including weight, HbA1c, LDL, and BP were expected to vary as patients were included even after switching AOM (collection of data started after ≥ 6 months on a single AOM). Switching of AOM after the first 6 months of therapy was recorded in 25% of the patients in the ≥ 65 years group and 330% of the patients in the < 65 years group.
The incidence of AEs and subsequent discontinuation of AOMs in this study was higher in the adult group. This study excluded patients who did not continue taking an AOM for at least 6 months. As a result, the incidence of AEs between the 2 groups within the first 6 months of AOM therapy remains unknown. It is possible that during the first 6 months of therapy, patients aged < 65 years were more willing to tolerate or had fewer severe AEs compared with the older adult group. It’s also possible that the smaller number of patients in the older adult group was due to increased AEs that led them to discontinue early (before completion of 6 months of therapy) and/or prescriber discomfort in using AOMs in the older adult population. In addition, because the specific medication(s) taken by patients in each group were not detailed, it is unknown whether the adult group was taking AOMs associated with a greater number of AEs.
Limitations
This was a retrospective study with a relatively small sample size. A larger sample size may have shown more precise differences between age groups and may be more representative of the general population. Additionally, data were reliant on appropriate documentation, and adherence to AOM therapy was not assessed due to the retrospective nature of this study. At times, the study relied on patient reported data points, such as weight, if a clinic weight was not available. Also, this study did not account for many potential confounding factors such as other medications taken by the patient, which can affect outcomes including weight, HbA1c, LDL, blood pressure, and AEs.
Conclusions
This retrospective study of patients taking AOMs showed no statistically significant difference in weight loss at 6 or 12 months between adults aged < 65 years and older adults aged ≥ 65 years. A subset analysis found no statistically significant difference in change in body weight between specific age groups (18-40 years, 41-64 years, and ≥ 65 years). There was also no statistically significant difference in secondary outcomes, including change in HbA1c (in patients with T2DM or prediabetes), LDL or BP between age groups. The safety endpoints showed a higher incidence of medication AEs in the adult group, with more of these adults discontinuing therapy due to AEs. This study indicates that AOM may have similar outcomes for weight loss and metabolic laboratory values/vital sign changes between adults and older adults. Also, our findings suggest that patients aged < 65 years may experience more AEs than patients aged ≥ 65 years after ≥ 6 months of AOM therapy. Larger studies are needed to further evaluate these age-specific findings.
- Emmerich SD, Fryar CD, Stierman B, Ogden CL. Obesity and severe obesity prevalence in adults: United States, August 2021-August 2023. NCHS Data Brief No. 508. National Center for Health Statistics; 2024. Accessed December 11, 2024. https://www.cdc.gov/nchs/products/databriefs/db508.htm
- Ward ZJ, Bleich SN, Long MW, Gortmaker SL. Association of body mass index with health care expenditures in the United States by age and sex. PLoS One. 2021;16(3):e0247307. doi:10.1371/journal.pone.0247307
- Horn DB, Almandoz JP, Look M. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359-375. doi:10.1080/00325481.2022.2051366
- American Diabetes Association (ADA). Standards of care in diabetes–2023. Diabetes Care. 2023;46(suppl 1):S128- S2139. doi:10.2337/dc23-S008
- Wilding JPH, Batterham RL, Calanna S, et al. Onceweekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22. doi:10.1056/NEJMoa1411892
- Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity (Silver Spring). 2012;20(2):330-342. doi:10.1038/oby.2011.330
- Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341-1352. doi:10.1016/S0140-6736(11)60205-5
- Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308. doi:10.3945/ajcn.111.024927
- Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605. doi:10.1016/S0140-6736(10)60888-4
- Sjöström L, Rissanen A, Andersen T, et al. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group. Lancet. 1998;352(9123):167-172. doi:10.1016s0140-6736(97)11509-4
- Mangoni AA, Jackson SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x
- Emmerich SD, Fryar CD, Stierman B, Ogden CL. Obesity and severe obesity prevalence in adults: United States, August 2021-August 2023. NCHS Data Brief No. 508. National Center for Health Statistics; 2024. Accessed December 11, 2024. https://www.cdc.gov/nchs/products/databriefs/db508.htm
- Ward ZJ, Bleich SN, Long MW, Gortmaker SL. Association of body mass index with health care expenditures in the United States by age and sex. PLoS One. 2021;16(3):e0247307. doi:10.1371/journal.pone.0247307
- Horn DB, Almandoz JP, Look M. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359-375. doi:10.1080/00325481.2022.2051366
- American Diabetes Association (ADA). Standards of care in diabetes–2023. Diabetes Care. 2023;46(suppl 1):S128- S2139. doi:10.2337/dc23-S008
- Wilding JPH, Batterham RL, Calanna S, et al. Onceweekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22. doi:10.1056/NEJMoa1411892
- Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity (Silver Spring). 2012;20(2):330-342. doi:10.1038/oby.2011.330
- Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341-1352. doi:10.1016/S0140-6736(11)60205-5
- Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308. doi:10.3945/ajcn.111.024927
- Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605. doi:10.1016/S0140-6736(10)60888-4
- Sjöström L, Rissanen A, Andersen T, et al. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group. Lancet. 1998;352(9123):167-172. doi:10.1016s0140-6736(97)11509-4
- Mangoni AA, Jackson SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x
Efficacy of Anti-Obesity Medications in Adult and Older Adult Veteran Populations
Efficacy of Anti-Obesity Medications in Adult and Older Adult Veteran Populations
Quality, Not Type, of Diet Linked to Microbiome Health
new research suggested.
For example, red meat was a strong driver of omnivore microbiomes, with corresponding signature microbes that are negatively correlated with host cardiometabolic health.
In contrast, the signature microbes found in vegans’ gut microbiomes were correlated with favorable cardiometabolic markers and were enriched in omnivores who ate more plant-based foods.
“From the viewpoint of the impact of diet on the gut microbiome, what seems to be more important is the diversity of healthy plant-based foods that are consumed,” principal author Nicola Segata, PhD, University of Trento in Italy, said in an interview. “Whether this comes within a vegan or an omnivore diet is less crucial, as long as there is no specific overconsumption of unhealthy food categories, such as red meat.”
Excluding broad categories of foods also can have consequences, he added. “For example, we saw that the exclusion of dairy fermented foods is associated with decreased presence of potentially probiotic microbes that are constitutive of such foods. Avoiding meat or dairy products does not necessarily have a positive effect if it does not come with a variety of quality plant-based products.”
The study was published online in Nature Microbiology.
Diet Tied to Microbial Signature
The researchers analyzed biological samples from 21,561 individuals across five multi-national cohorts to map how differences in diet patterns (omnivore, vegetarian, and vegan) are reflected in gut microbiomes.
They found that the three diet patterns are highly distinguishable by their microbial profiles and that each diet has corresponding unique signature microbes, including those tied to digestion of specific types of food and sometimes those derived from food itself.
The microbiomes of omnivores had an increased presence of bacteria associated with meat digestion, such as Alistipes putredinis, which is involved in protein fermentation. Omnivores also had more bacteria associated with both inflammatory bowel disease and increased colon cancer risk, such as Ruminococcus torques and Bilophila wadsworthia.
The microbiomes of vegans had an abundance of bacteria involved in fiber fermentation, such as several species of Bacteroides and Firmicutes phyla, which help produce short-chain fatty acids. These compounds have beneficial effects on gut health by reducing inflammation and helping to maintain a better homeostatic balance between an individual’s metabolism and immune system.
The main difference between vegetarians and vegans was the presence in vegetarians’ microbiomes of Streptococcus thermophilus, a bacterium found mainly in dairy products and used in the production of yogurt.
Dietary factors within each diet pattern, such as the amount of plant-based food, shape the microbiome more than the type of diet and are important for gut health, according to the authors. For example, by eating more plant-based foods, people with an omnivorous diet can bring the proportion of beneficial signature microbes in their microbiomes more in line with the levels in people who are vegan or vegetarian.
“Since our data showed that omnivores on average ingest significantly fewer healthy plant-based foods than vegetarians or vegans, optimizing the quality of omnivore diets by increasing dietary plant diversity could lead to better gut health,” they wrote.
The ultimate goal, Segata said, is “a precision nutrition approach that recommends foods based on the configuration of the microbiome of patients and of the aspects of the microbiome one wants to enhance. We are not there yet, but it is nonetheless important to know which foods are usually boosting which types of members of the gut microbiome.”
His team is currently analyzing changes in the gut microbiome induced by diet changes among thousands of participants in various cohorts.
“This is one of the next steps toward unraveling causality along the diet-microbiome-health axis, together with the cultivation of specific microbiome members of interest for potential prebiotic and probiotic strategies,” he said.
Conventional Dietary Advice for Now
The findings are consistent with those of previous studies, Jack Gilbert, MD, director of the Microbiome and Metagenomics Center at the University of California, San Diego, and president of Applied Microbiology International, Cambridge, England, said in an interview.
“Future research needs to focus on whether the gut microbial signature can predict those that develop cardiovascular disease in each cohort — ie, the n-of-1 studies, whereby a vegan develops cardiovascular disease, or a carnivore does not,” said Gilbert, who was not involved in the study.
With more data, he said, “we can also start examining these trends over time to understand what might be going on with these ‘oddballs.’ ”
“There is not much you can do with the ‘eat a healthy balanced diet’ routine,” he noted. “If I got a microbiome signature, I could potentially tell you what to eat to optimize your blood glucose trends and your lipid panels but not to handle long-term disease risk, yet. So sticking with the guideline-recommended dietary advice seems best, until we can provide more nuanced advice for the patient.
“Importantly, I would also like to see time-resolved data,” he added. “Signatures can fluctuate over time, even over days, and so collecting a few weeks of stool samples would help us to better align the microbiome signatures to clinical endpoints.”
Segata is a consultant to and receives options from ZOE. Gilbert is a member of the scientific advisory boards of Holobiome, BiomeSense, EcoBiomics Canadian Research Program, MASTER EU, Sun Genomics, and Oath; the editorial advisory board for The Scientist; and the external advisory board for the Binational Early Asthma & Microbiome Study. He is also an adviser for Bened Life.
A version of this article appeared on Medscape.com.
new research suggested.
For example, red meat was a strong driver of omnivore microbiomes, with corresponding signature microbes that are negatively correlated with host cardiometabolic health.
In contrast, the signature microbes found in vegans’ gut microbiomes were correlated with favorable cardiometabolic markers and were enriched in omnivores who ate more plant-based foods.
“From the viewpoint of the impact of diet on the gut microbiome, what seems to be more important is the diversity of healthy plant-based foods that are consumed,” principal author Nicola Segata, PhD, University of Trento in Italy, said in an interview. “Whether this comes within a vegan or an omnivore diet is less crucial, as long as there is no specific overconsumption of unhealthy food categories, such as red meat.”
Excluding broad categories of foods also can have consequences, he added. “For example, we saw that the exclusion of dairy fermented foods is associated with decreased presence of potentially probiotic microbes that are constitutive of such foods. Avoiding meat or dairy products does not necessarily have a positive effect if it does not come with a variety of quality plant-based products.”
The study was published online in Nature Microbiology.
Diet Tied to Microbial Signature
The researchers analyzed biological samples from 21,561 individuals across five multi-national cohorts to map how differences in diet patterns (omnivore, vegetarian, and vegan) are reflected in gut microbiomes.
They found that the three diet patterns are highly distinguishable by their microbial profiles and that each diet has corresponding unique signature microbes, including those tied to digestion of specific types of food and sometimes those derived from food itself.
The microbiomes of omnivores had an increased presence of bacteria associated with meat digestion, such as Alistipes putredinis, which is involved in protein fermentation. Omnivores also had more bacteria associated with both inflammatory bowel disease and increased colon cancer risk, such as Ruminococcus torques and Bilophila wadsworthia.
The microbiomes of vegans had an abundance of bacteria involved in fiber fermentation, such as several species of Bacteroides and Firmicutes phyla, which help produce short-chain fatty acids. These compounds have beneficial effects on gut health by reducing inflammation and helping to maintain a better homeostatic balance between an individual’s metabolism and immune system.
The main difference between vegetarians and vegans was the presence in vegetarians’ microbiomes of Streptococcus thermophilus, a bacterium found mainly in dairy products and used in the production of yogurt.
Dietary factors within each diet pattern, such as the amount of plant-based food, shape the microbiome more than the type of diet and are important for gut health, according to the authors. For example, by eating more plant-based foods, people with an omnivorous diet can bring the proportion of beneficial signature microbes in their microbiomes more in line with the levels in people who are vegan or vegetarian.
“Since our data showed that omnivores on average ingest significantly fewer healthy plant-based foods than vegetarians or vegans, optimizing the quality of omnivore diets by increasing dietary plant diversity could lead to better gut health,” they wrote.
The ultimate goal, Segata said, is “a precision nutrition approach that recommends foods based on the configuration of the microbiome of patients and of the aspects of the microbiome one wants to enhance. We are not there yet, but it is nonetheless important to know which foods are usually boosting which types of members of the gut microbiome.”
His team is currently analyzing changes in the gut microbiome induced by diet changes among thousands of participants in various cohorts.
“This is one of the next steps toward unraveling causality along the diet-microbiome-health axis, together with the cultivation of specific microbiome members of interest for potential prebiotic and probiotic strategies,” he said.
Conventional Dietary Advice for Now
The findings are consistent with those of previous studies, Jack Gilbert, MD, director of the Microbiome and Metagenomics Center at the University of California, San Diego, and president of Applied Microbiology International, Cambridge, England, said in an interview.
“Future research needs to focus on whether the gut microbial signature can predict those that develop cardiovascular disease in each cohort — ie, the n-of-1 studies, whereby a vegan develops cardiovascular disease, or a carnivore does not,” said Gilbert, who was not involved in the study.
With more data, he said, “we can also start examining these trends over time to understand what might be going on with these ‘oddballs.’ ”
“There is not much you can do with the ‘eat a healthy balanced diet’ routine,” he noted. “If I got a microbiome signature, I could potentially tell you what to eat to optimize your blood glucose trends and your lipid panels but not to handle long-term disease risk, yet. So sticking with the guideline-recommended dietary advice seems best, until we can provide more nuanced advice for the patient.
“Importantly, I would also like to see time-resolved data,” he added. “Signatures can fluctuate over time, even over days, and so collecting a few weeks of stool samples would help us to better align the microbiome signatures to clinical endpoints.”
Segata is a consultant to and receives options from ZOE. Gilbert is a member of the scientific advisory boards of Holobiome, BiomeSense, EcoBiomics Canadian Research Program, MASTER EU, Sun Genomics, and Oath; the editorial advisory board for The Scientist; and the external advisory board for the Binational Early Asthma & Microbiome Study. He is also an adviser for Bened Life.
A version of this article appeared on Medscape.com.
new research suggested.
For example, red meat was a strong driver of omnivore microbiomes, with corresponding signature microbes that are negatively correlated with host cardiometabolic health.
In contrast, the signature microbes found in vegans’ gut microbiomes were correlated with favorable cardiometabolic markers and were enriched in omnivores who ate more plant-based foods.
“From the viewpoint of the impact of diet on the gut microbiome, what seems to be more important is the diversity of healthy plant-based foods that are consumed,” principal author Nicola Segata, PhD, University of Trento in Italy, said in an interview. “Whether this comes within a vegan or an omnivore diet is less crucial, as long as there is no specific overconsumption of unhealthy food categories, such as red meat.”
Excluding broad categories of foods also can have consequences, he added. “For example, we saw that the exclusion of dairy fermented foods is associated with decreased presence of potentially probiotic microbes that are constitutive of such foods. Avoiding meat or dairy products does not necessarily have a positive effect if it does not come with a variety of quality plant-based products.”
The study was published online in Nature Microbiology.
Diet Tied to Microbial Signature
The researchers analyzed biological samples from 21,561 individuals across five multi-national cohorts to map how differences in diet patterns (omnivore, vegetarian, and vegan) are reflected in gut microbiomes.
They found that the three diet patterns are highly distinguishable by their microbial profiles and that each diet has corresponding unique signature microbes, including those tied to digestion of specific types of food and sometimes those derived from food itself.
The microbiomes of omnivores had an increased presence of bacteria associated with meat digestion, such as Alistipes putredinis, which is involved in protein fermentation. Omnivores also had more bacteria associated with both inflammatory bowel disease and increased colon cancer risk, such as Ruminococcus torques and Bilophila wadsworthia.
The microbiomes of vegans had an abundance of bacteria involved in fiber fermentation, such as several species of Bacteroides and Firmicutes phyla, which help produce short-chain fatty acids. These compounds have beneficial effects on gut health by reducing inflammation and helping to maintain a better homeostatic balance between an individual’s metabolism and immune system.
The main difference between vegetarians and vegans was the presence in vegetarians’ microbiomes of Streptococcus thermophilus, a bacterium found mainly in dairy products and used in the production of yogurt.
Dietary factors within each diet pattern, such as the amount of plant-based food, shape the microbiome more than the type of diet and are important for gut health, according to the authors. For example, by eating more plant-based foods, people with an omnivorous diet can bring the proportion of beneficial signature microbes in their microbiomes more in line with the levels in people who are vegan or vegetarian.
“Since our data showed that omnivores on average ingest significantly fewer healthy plant-based foods than vegetarians or vegans, optimizing the quality of omnivore diets by increasing dietary plant diversity could lead to better gut health,” they wrote.
The ultimate goal, Segata said, is “a precision nutrition approach that recommends foods based on the configuration of the microbiome of patients and of the aspects of the microbiome one wants to enhance. We are not there yet, but it is nonetheless important to know which foods are usually boosting which types of members of the gut microbiome.”
His team is currently analyzing changes in the gut microbiome induced by diet changes among thousands of participants in various cohorts.
“This is one of the next steps toward unraveling causality along the diet-microbiome-health axis, together with the cultivation of specific microbiome members of interest for potential prebiotic and probiotic strategies,” he said.
Conventional Dietary Advice for Now
The findings are consistent with those of previous studies, Jack Gilbert, MD, director of the Microbiome and Metagenomics Center at the University of California, San Diego, and president of Applied Microbiology International, Cambridge, England, said in an interview.
“Future research needs to focus on whether the gut microbial signature can predict those that develop cardiovascular disease in each cohort — ie, the n-of-1 studies, whereby a vegan develops cardiovascular disease, or a carnivore does not,” said Gilbert, who was not involved in the study.
With more data, he said, “we can also start examining these trends over time to understand what might be going on with these ‘oddballs.’ ”
“There is not much you can do with the ‘eat a healthy balanced diet’ routine,” he noted. “If I got a microbiome signature, I could potentially tell you what to eat to optimize your blood glucose trends and your lipid panels but not to handle long-term disease risk, yet. So sticking with the guideline-recommended dietary advice seems best, until we can provide more nuanced advice for the patient.
“Importantly, I would also like to see time-resolved data,” he added. “Signatures can fluctuate over time, even over days, and so collecting a few weeks of stool samples would help us to better align the microbiome signatures to clinical endpoints.”
Segata is a consultant to and receives options from ZOE. Gilbert is a member of the scientific advisory boards of Holobiome, BiomeSense, EcoBiomics Canadian Research Program, MASTER EU, Sun Genomics, and Oath; the editorial advisory board for The Scientist; and the external advisory board for the Binational Early Asthma & Microbiome Study. He is also an adviser for Bened Life.
A version of this article appeared on Medscape.com.
FROM NATURE MICROBIOLOGY
Obesity Linked with Malignant Progression of Barrett’s Esophagus
A dose-response relationship exists between body mass index (BMI) and esophageal adenocarcinoma (EAC) or high-grade dysplasia (HGD), the authors found.
“Obesity has been implicated in the pathogenesis of many reflux-related esophageal disorders such as gastroesophageal reflux disease (GERD), BE, and EAC,” said senior author Leo Alexandre, MRCP, PhD, a clinical associate professor and member of the Norwich Epidemiology Centre at the University of East Anglia and gastroenterologist with the Norfolk & Norwich University Hospital NHS Foundation Trust, both in Norwich, England.

“Guidelines advocate obesity as a criterion for targeted screening for BE in patients with chronic reflux symptoms,” he said. “While obesity is a recognized risk factor for both BE and EAC, it’s been unclear whether obesity is a risk factor for malignant progression.”
The study was published in Clinical Gastroenterology and Hepatology.
Analyzing Risk
BE, which is the only recognized precursor lesion to EAC, is associated with a 30-fold increase in the incidence of the aggressive cancer. Typically, malignant progression occurs when nondysplastic BE epithelium progresses to low-grade dysplasia (LGD) and then HGD, followed by invasive adenocarcinoma.
Current guidelines suggest that patients with BE undergo endoscopic surveillance for early detection of adenocarcinoma. However, clinical risk factors could help with risk stratification and a personalized approach to long-term BE management, the authors wrote.
Alexandre and colleagues reviewed case-control or cohort studies that reported on the effect of BMI on the progression of nondysplastic BE or LGD to EAC, HGD, or esophageal cancer (EC). Then they estimated the dose-response relationship with a two-stage dose-response meta-analysis.
Overall, 20 observational studies reported data on 38,565 adult patients, including 1684 patients who were diagnosed with EAC, HGD, or EC. The studies enrolled patients between 1976 and 2019 and were published between 2005 and 2022. Most were based in Europe or the United States, and 74.4% of participants were men.
Among 12 cohort studies with 19,223 patients who had baseline nondysplastic BE or LGD, 816 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .03%.
Among eight cohort studies with 6647 male patients who had baseline nondysplastic BE or LGD, 555 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .02%.
In addition, among 1992 female patients with baseline nondysplastic BE or LGD, 110 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .01%, which wasn’t a significant difference compared with the progression rate among male patients.
Based on meta-analyses, obesity was associated with a 4% increase in the risk for malignant progression among patients with BE (unadjusted odds ratio, 1.04; 95% CI, 1.00-1.07; P < .001).
Notably, each 5 unit increase in BMI was associated with a 6% increase in the risk of developing HGD or EAC (adjusted odds ratio, 1.06; 95% CI, 1.02-1.10; P < .001).
“Although the exact mechanisms by which obesity promotes esophageal carcinogenesis is not fully understood, several possible mechanisms may explain it,” Alexandre said. “The most obvious pathologic link is via GERD, with the mechanical effect of visceral obesity promoting the GERD directly, and the sequence of Barrett’s dysplasia to cancer indirectly. In addition, it has been demonstrated in experimental studies that gastric acid and bile acid drive malignant changes in esophageal epithelium through stimulation of proliferation, inhibition of apoptosis, and generation of free radicals.”
Considering Risk
This study highlights the importance of recognizing the association between obesity and cancer risks, said Prateek Sharma, MD, professor of medicine and director of gastrointestinal training at the University of Kansas School of Medicine, Kansas City, Kansas.

Sharma, who wasn’t involved with this study, coauthored an American Gastroenterological Association technical review on the management of BE.
“Obesity is a known risk factor for esophageal adenocarcinoma and may be a modifiable risk factor,” he said. “Showing that BMI is related to neoplastic progression in Barrett’s esophagus may impact surveillance intervals.”
Future research should look at additional obesity-related factors, such as visceral obesity and malignant progression of BE, as well as whether diet, lifestyle, and bariatric interventions can reduce the risk for progression.
“The next steps also include plugging BMI into risk scores and risk stratification models to enable targeted surveillance among high-risk groups,” Sharma said.
One of the study coauthors received funding as a National Institute for Health Research Academic clinical fellow. No other funding sources were declared. Alexandre and Sharma reported no relevant disclosures.
A version of this article appeared on Medscape.com.
A dose-response relationship exists between body mass index (BMI) and esophageal adenocarcinoma (EAC) or high-grade dysplasia (HGD), the authors found.
“Obesity has been implicated in the pathogenesis of many reflux-related esophageal disorders such as gastroesophageal reflux disease (GERD), BE, and EAC,” said senior author Leo Alexandre, MRCP, PhD, a clinical associate professor and member of the Norwich Epidemiology Centre at the University of East Anglia and gastroenterologist with the Norfolk & Norwich University Hospital NHS Foundation Trust, both in Norwich, England.
“Guidelines advocate obesity as a criterion for targeted screening for BE in patients with chronic reflux symptoms,” he said. “While obesity is a recognized risk factor for both BE and EAC, it’s been unclear whether obesity is a risk factor for malignant progression.”
The study was published in Clinical Gastroenterology and Hepatology.
Analyzing Risk
BE, which is the only recognized precursor lesion to EAC, is associated with a 30-fold increase in the incidence of the aggressive cancer. Typically, malignant progression occurs when nondysplastic BE epithelium progresses to low-grade dysplasia (LGD) and then HGD, followed by invasive adenocarcinoma.
Current guidelines suggest that patients with BE undergo endoscopic surveillance for early detection of adenocarcinoma. However, clinical risk factors could help with risk stratification and a personalized approach to long-term BE management, the authors wrote.
Alexandre and colleagues reviewed case-control or cohort studies that reported on the effect of BMI on the progression of nondysplastic BE or LGD to EAC, HGD, or esophageal cancer (EC). Then they estimated the dose-response relationship with a two-stage dose-response meta-analysis.
Overall, 20 observational studies reported data on 38,565 adult patients, including 1684 patients who were diagnosed with EAC, HGD, or EC. The studies enrolled patients between 1976 and 2019 and were published between 2005 and 2022. Most were based in Europe or the United States, and 74.4% of participants were men.
Among 12 cohort studies with 19,223 patients who had baseline nondysplastic BE or LGD, 816 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .03%.
Among eight cohort studies with 6647 male patients who had baseline nondysplastic BE or LGD, 555 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .02%.
In addition, among 1992 female patients with baseline nondysplastic BE or LGD, 110 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .01%, which wasn’t a significant difference compared with the progression rate among male patients.
Based on meta-analyses, obesity was associated with a 4% increase in the risk for malignant progression among patients with BE (unadjusted odds ratio, 1.04; 95% CI, 1.00-1.07; P < .001).
Notably, each 5 unit increase in BMI was associated with a 6% increase in the risk of developing HGD or EAC (adjusted odds ratio, 1.06; 95% CI, 1.02-1.10; P < .001).
“Although the exact mechanisms by which obesity promotes esophageal carcinogenesis is not fully understood, several possible mechanisms may explain it,” Alexandre said. “The most obvious pathologic link is via GERD, with the mechanical effect of visceral obesity promoting the GERD directly, and the sequence of Barrett’s dysplasia to cancer indirectly. In addition, it has been demonstrated in experimental studies that gastric acid and bile acid drive malignant changes in esophageal epithelium through stimulation of proliferation, inhibition of apoptosis, and generation of free radicals.”
Considering Risk
This study highlights the importance of recognizing the association between obesity and cancer risks, said Prateek Sharma, MD, professor of medicine and director of gastrointestinal training at the University of Kansas School of Medicine, Kansas City, Kansas.
Sharma, who wasn’t involved with this study, coauthored an American Gastroenterological Association technical review on the management of BE.
“Obesity is a known risk factor for esophageal adenocarcinoma and may be a modifiable risk factor,” he said. “Showing that BMI is related to neoplastic progression in Barrett’s esophagus may impact surveillance intervals.”
Future research should look at additional obesity-related factors, such as visceral obesity and malignant progression of BE, as well as whether diet, lifestyle, and bariatric interventions can reduce the risk for progression.
“The next steps also include plugging BMI into risk scores and risk stratification models to enable targeted surveillance among high-risk groups,” Sharma said.
One of the study coauthors received funding as a National Institute for Health Research Academic clinical fellow. No other funding sources were declared. Alexandre and Sharma reported no relevant disclosures.
A version of this article appeared on Medscape.com.
A dose-response relationship exists between body mass index (BMI) and esophageal adenocarcinoma (EAC) or high-grade dysplasia (HGD), the authors found.
“Obesity has been implicated in the pathogenesis of many reflux-related esophageal disorders such as gastroesophageal reflux disease (GERD), BE, and EAC,” said senior author Leo Alexandre, MRCP, PhD, a clinical associate professor and member of the Norwich Epidemiology Centre at the University of East Anglia and gastroenterologist with the Norfolk & Norwich University Hospital NHS Foundation Trust, both in Norwich, England.
“Guidelines advocate obesity as a criterion for targeted screening for BE in patients with chronic reflux symptoms,” he said. “While obesity is a recognized risk factor for both BE and EAC, it’s been unclear whether obesity is a risk factor for malignant progression.”
The study was published in Clinical Gastroenterology and Hepatology.
Analyzing Risk
BE, which is the only recognized precursor lesion to EAC, is associated with a 30-fold increase in the incidence of the aggressive cancer. Typically, malignant progression occurs when nondysplastic BE epithelium progresses to low-grade dysplasia (LGD) and then HGD, followed by invasive adenocarcinoma.
Current guidelines suggest that patients with BE undergo endoscopic surveillance for early detection of adenocarcinoma. However, clinical risk factors could help with risk stratification and a personalized approach to long-term BE management, the authors wrote.
Alexandre and colleagues reviewed case-control or cohort studies that reported on the effect of BMI on the progression of nondysplastic BE or LGD to EAC, HGD, or esophageal cancer (EC). Then they estimated the dose-response relationship with a two-stage dose-response meta-analysis.
Overall, 20 observational studies reported data on 38,565 adult patients, including 1684 patients who were diagnosed with EAC, HGD, or EC. The studies enrolled patients between 1976 and 2019 and were published between 2005 and 2022. Most were based in Europe or the United States, and 74.4% of participants were men.
Among 12 cohort studies with 19,223 patients who had baseline nondysplastic BE or LGD, 816 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .03%.
Among eight cohort studies with 6647 male patients who had baseline nondysplastic BE or LGD, 555 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .02%.
In addition, among 1992 female patients with baseline nondysplastic BE or LGD, 110 progressed to EAC, HGD, or EC. The pooled annual rate of progression was .01%, which wasn’t a significant difference compared with the progression rate among male patients.
Based on meta-analyses, obesity was associated with a 4% increase in the risk for malignant progression among patients with BE (unadjusted odds ratio, 1.04; 95% CI, 1.00-1.07; P < .001).
Notably, each 5 unit increase in BMI was associated with a 6% increase in the risk of developing HGD or EAC (adjusted odds ratio, 1.06; 95% CI, 1.02-1.10; P < .001).
“Although the exact mechanisms by which obesity promotes esophageal carcinogenesis is not fully understood, several possible mechanisms may explain it,” Alexandre said. “The most obvious pathologic link is via GERD, with the mechanical effect of visceral obesity promoting the GERD directly, and the sequence of Barrett’s dysplasia to cancer indirectly. In addition, it has been demonstrated in experimental studies that gastric acid and bile acid drive malignant changes in esophageal epithelium through stimulation of proliferation, inhibition of apoptosis, and generation of free radicals.”
Considering Risk
This study highlights the importance of recognizing the association between obesity and cancer risks, said Prateek Sharma, MD, professor of medicine and director of gastrointestinal training at the University of Kansas School of Medicine, Kansas City, Kansas.
Sharma, who wasn’t involved with this study, coauthored an American Gastroenterological Association technical review on the management of BE.
“Obesity is a known risk factor for esophageal adenocarcinoma and may be a modifiable risk factor,” he said. “Showing that BMI is related to neoplastic progression in Barrett’s esophagus may impact surveillance intervals.”
Future research should look at additional obesity-related factors, such as visceral obesity and malignant progression of BE, as well as whether diet, lifestyle, and bariatric interventions can reduce the risk for progression.
“The next steps also include plugging BMI into risk scores and risk stratification models to enable targeted surveillance among high-risk groups,” Sharma said.
One of the study coauthors received funding as a National Institute for Health Research Academic clinical fellow. No other funding sources were declared. Alexandre and Sharma reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Commission Issues ‘Radical Overhaul’ of Obesity Diagnosis
“We propose a radical overhaul of the actual diagnosis of obesity to improve global healthcare and practices and policies. The specific aims were to facilitate individualized assessment and care of people living with obesity while preserving resources by reducing overdiagnosis and unnecessary or inadequate interventions,” Professor Louise Baur, chair of Child & Adolescent Health at the University of Sydney, Australia, said during a UK Science Media Centre (SMC) news briefing.
The report calls first for a diagnosis of obesity via confirmation of excess adiposity using measures such as waist circumference or waist-to-hip ratio in addition to BMI. Next, a clinical assessment of signs and symptoms of organ dysfunction due to obesity and/or functional limitations determines whether the individual has the disease “clinical obesity,” or “preclinical obesity,” a condition of health risk but not an illness itself.
Published on January 14, 2025, in The Lancet Diabetes & Endocrinology, the document also provides broad guidance on management for the two obesity conditions, emphasizing a personalized and stigma-free approach. The Lancet Commission on Obesity comprised 56 experts in relevant fields including endocrinology, surgery, nutrition, and public health, along with people living with obesity.
The report has been endorsed by more than 75 medical organizations, including the Association of British Clinical Diabetologists, the American Association of Clinical Endocrinologists, the American Diabetes Association, the American Heart Association, the Obesity Society, the World Obesity Federation, and obesity and endocrinology societies from countries in Europe, Latin America, Asia, and South Africa.
In recent years, many in the field have found fault with the current BMI-based definition of obesity (> 30 for people of European descent or other cutoffs for specific ethnic groups), primarily because BMI alone doesn’t reflect a person’s fat vs lean mass, fat distribution, or overall health. The new definition aims to overcome these limitations, as well as settle the debate about whether obesity is a “disease.”
“We now have a clinical diagnosis for obesity, which has been lacking. ... The traditional classification based on BMI ... reflects simply whether or not there is excess adiposity, and sometimes not even precise in that regard, either…It has never been a classification that was meant to diagnose a specific illness with its own clinical characteristics in the same way we diagnose any other illness,” Commission Chair Francesco Rubino, MD, professor and chair of Metabolic and Bariatric Surgery at King’s College London, England, said in an interview.
He added, “The fact that now we have a clinical diagnosis allows recognition of the nuance that obesity is generally a risk and for some can be an illness. There are some who have risk but don’t have the illness here and now. And it’s crucially important for clinical decision-making, but also for policies to have a distinction between those two things because the treatment strategy for one and the other are substantially different.”
Asked to comment, obesity specialist Michael A. Weintraub, MD, clinical assistant professor of endocrinology at New York University Langone Health, said in an interview, “I wholeheartedly agree with modifying the definition of obesity in this more accurate way. ... There has already been a lot of talk about the fallibility of BMI and that BMI over 30 does not equal obesity. ... So a major Commission article like this I think can really move those discussions even more into the forefront and start changing practice.”
However, Weintraub added, “I think there needs to be another step here of more practical guidance on how to actually implement this ... including how to measure waist circumference and to put it into a patient flow.”
Asked to comment, obesity expert Luca Busetto, MD, associate professor of internal medicine at the Department of Medicine of the University of Padova, Italy, said in an interview that he agrees with the general concept of moving beyond BMI in defining obesity. That view was expressed in a proposed “framework” from the European Association for the Study of Obesity (EASO), for which Busetto was the lead author.
Busetto also agrees with the emphasis on the need for a complete clinical evaluation of patients to define their health status. “The precise definition of the symptoms defining clinical obesity in adults and children is extremely important, emphasizing the fact that obesity is a severe and disabling disease by itself, even without or before the occurrence of obesity-related complications,” he said.
However, he takes issue with the Commission’s designation that “preclinical” obesity is not a disease. “The critical point of disagreement for me is the message that obesity is a disease only if it is clinical or only if it presents functional impairment or clinical symptoms. This remains, in my opinion, an oversimplification, not taking into account the fact that the pathophysiological mechanisms that lead to fat accumulation and ‘adipose tissue-based chronic disease’ usually start well before the occurrence of symptoms.”
Busetto pointed to examples such as type 2 diabetes and chronic kidney disease, both of which can be asymptomatic in their early phases yet are still considered diseases at those points. “I have no problem in accepting a distinction between preclinical and clinical stages of the disease, and I like the definition of clinical obesity, but why should this imply the fact that obesity is NOT a disease since its beginning?”
The Commission does state that preclinical obesity should be addressed, mostly with preventive approaches but in some cases with more intensive management. “This is highly relevant, but the risk of an undertreatment of obesity in its asymptomatic state remains in place. This could delay appropriate management for a progressive disease that certainly should not be treated only when presenting symptoms. It would be too late,” Busetto said.
And EASO framework coauthor Gijs Goossens, PhD, professor of cardiometabolic physiology of obesity at Maastricht University Medical Centre, the Netherlands, added a concern that those with excess adiposity but lower BMI might be missed entirely, noting “Since abdominal fat accumulation better predicts chronic cardiometabolic diseases and can also be accompanied by clinical manifestations in individuals with overweight as a consequence of compromised adipose tissue function, the proposed model may lead to underdiagnosis or undertreatment in individuals with BMI 25-30 who have excess abdominal fat.”
Diagnosis and Management Beyond BMI
The Commission advises the use of BMI solely as a marker to screen for potential obesity. Those with a BMI > 40 can be assumed to have excess body fat. For others with a BMI at or near the threshold for obesity in a specific country or ethnic group or for whom there is the clinical judgment of the potential for clinical obesity, confirmation of excess or abnormal adiposity is needed by one of the following:
- At least one measurement of body size and BMI
- At least two measures of body size, regardless of BMI
- Direct body fat measurement, such as a dual-energy x-ray absorptiometry (DEXA) scan
Measurement of body size can be assessed in three ways:
- Waist circumference ≥ 102 cm for men and ≥ 88 cm for women
- Waist-to-hip ratio > 0.90 for men and > 0.50 for women
- Waist-to-height ratio > 0.50 for all.
Weintraub noted, “Telemedicine is a useful tool used by many patients and providers but may also make it challenging to accurately assess someone’s body size. Having technology like an iPhone app to measure body size would circumvent this challenge but this type of tool has not yet been validated.”
If the person does not have excess adiposity, they don’t have obesity. Those with excess adiposity do have obesity. Further assessment is then needed to establish whether the person has an illness, that is, clinical obesity, indicated by signs/symptoms of organ dysfunction, and/or limitations of daily activities. If not, they have “preclinical” obesity.
The document provides a list of 18 obesity-related organ, tissue, and body system criteria for diagnosing “clinical” obesity in adults, including upper airways (eg, apneas/hypopneas), respiratory (breathlessness), cardiovascular (hypertension, heart failure), liver (fatty liver disease with hepatic fibrosis), reproductive (polycystic ovary syndrome, hypogonadism), and metabolism (hyperglycemia, hypertriglyceridemia, low high-density lipoprotein cholesterol). A list of 13 such criteria is also provided for children. “Limitations of day-to-day activities” are included on both lists.
Management Differs by Designation
For preclinical obesity, management should focus on risk reduction and prevention of progression to clinical obesity or other obesity-related diseases. Such approaches include health counseling for weight loss or prevention of weight gain, monitoring over time, and active weight loss interventions in people at higher risk of developing clinical obesity and other obesity-related diseases.
Management for clinical obesity focuses on improvements or reversal of the organ dysfunction. The type of evidence-based treatment and management should be informed by individual risk-benefit assessments and decided via “active discussion” with the patient. Success is determined by improvement in the signs and symptoms rather than measures of weight loss.
In response to a reporter’s question at the SMC briefing about the implications for the use of weight-loss medications, Rubino noted that this wasn’t the focus of the report, but nonetheless said that this new obesity definition could help with their targeted use. “The strategy and intent by which you use the drugs is different in clinical and preclinical obesity. ... Pharmacological interventions could be used for patients with high-risk preclinical obesity, with the intent of reducing risk, but we ... would use the same medication at a different intensity, dose, and maybe in combination therapies.”
As for clinical obesity, “It could be more or less severe and could affect more than one organ, and so clinical obesity might require drugs, might require surgery, or may require, in some cases, a combination of both of them, to achieve the best possible outcomes. ... We want to make sure that the person is restoring health ... with whatever it takes.”
Rubino believes this new definition will convince the remaining clinicians who haven’t yet accepted the concept of obesity as a disease. “When they see clinical obesity, I think it will be much harder to say that a biological process that is capable of causing a dysfunction in the heart or the lungs is less of a disease than another biological process that causes similar dysfunction in the heart of the lungs. ... It’s going to be objective. Obesity is a spectrum of different situations. ... When it’s an illness, clinical obesity, it’s not a matter of if or when. It’s a matter of fact.”
There were no industrial grants or other funding for this initiative. King’s Health Partners hosted the initiative and provided logistical and personnel support to facilitate administrative work and the Delphi-like consensus-development process. Rubino declared receiving research grants from Ethicon (Johnson & Johnson), Novo Nordisk, and Medtronic; consulting fees from Morphic Medical; speaking honoraria from Medtronic, Ethicon, Novo Nordisk, Eli Lilly, and Amgen. Rubino has served (unpaid) as a member of the scientific advisory board for Keyron and a member of the data safety and monitoring board for GI Metabolic Solutions; is president of the Metabolic Health Institute (non-profit); and is the sole director of Metabolic Health International and London Metabolic and Bariatric Surgery (private practice). Baur declared serving on the scientific advisory board for Novo Nordisk (for the ACTION Teens study) and Eli Lilly and receiving speaker fees (paid to the institution) from Novo Nordisk.
A version of this article first appeared on Medscape.com.
“We propose a radical overhaul of the actual diagnosis of obesity to improve global healthcare and practices and policies. The specific aims were to facilitate individualized assessment and care of people living with obesity while preserving resources by reducing overdiagnosis and unnecessary or inadequate interventions,” Professor Louise Baur, chair of Child & Adolescent Health at the University of Sydney, Australia, said during a UK Science Media Centre (SMC) news briefing.
The report calls first for a diagnosis of obesity via confirmation of excess adiposity using measures such as waist circumference or waist-to-hip ratio in addition to BMI. Next, a clinical assessment of signs and symptoms of organ dysfunction due to obesity and/or functional limitations determines whether the individual has the disease “clinical obesity,” or “preclinical obesity,” a condition of health risk but not an illness itself.
Published on January 14, 2025, in The Lancet Diabetes & Endocrinology, the document also provides broad guidance on management for the two obesity conditions, emphasizing a personalized and stigma-free approach. The Lancet Commission on Obesity comprised 56 experts in relevant fields including endocrinology, surgery, nutrition, and public health, along with people living with obesity.
The report has been endorsed by more than 75 medical organizations, including the Association of British Clinical Diabetologists, the American Association of Clinical Endocrinologists, the American Diabetes Association, the American Heart Association, the Obesity Society, the World Obesity Federation, and obesity and endocrinology societies from countries in Europe, Latin America, Asia, and South Africa.
In recent years, many in the field have found fault with the current BMI-based definition of obesity (> 30 for people of European descent or other cutoffs for specific ethnic groups), primarily because BMI alone doesn’t reflect a person’s fat vs lean mass, fat distribution, or overall health. The new definition aims to overcome these limitations, as well as settle the debate about whether obesity is a “disease.”
“We now have a clinical diagnosis for obesity, which has been lacking. ... The traditional classification based on BMI ... reflects simply whether or not there is excess adiposity, and sometimes not even precise in that regard, either…It has never been a classification that was meant to diagnose a specific illness with its own clinical characteristics in the same way we diagnose any other illness,” Commission Chair Francesco Rubino, MD, professor and chair of Metabolic and Bariatric Surgery at King’s College London, England, said in an interview.
He added, “The fact that now we have a clinical diagnosis allows recognition of the nuance that obesity is generally a risk and for some can be an illness. There are some who have risk but don’t have the illness here and now. And it’s crucially important for clinical decision-making, but also for policies to have a distinction between those two things because the treatment strategy for one and the other are substantially different.”
Asked to comment, obesity specialist Michael A. Weintraub, MD, clinical assistant professor of endocrinology at New York University Langone Health, said in an interview, “I wholeheartedly agree with modifying the definition of obesity in this more accurate way. ... There has already been a lot of talk about the fallibility of BMI and that BMI over 30 does not equal obesity. ... So a major Commission article like this I think can really move those discussions even more into the forefront and start changing practice.”
However, Weintraub added, “I think there needs to be another step here of more practical guidance on how to actually implement this ... including how to measure waist circumference and to put it into a patient flow.”
Asked to comment, obesity expert Luca Busetto, MD, associate professor of internal medicine at the Department of Medicine of the University of Padova, Italy, said in an interview that he agrees with the general concept of moving beyond BMI in defining obesity. That view was expressed in a proposed “framework” from the European Association for the Study of Obesity (EASO), for which Busetto was the lead author.
Busetto also agrees with the emphasis on the need for a complete clinical evaluation of patients to define their health status. “The precise definition of the symptoms defining clinical obesity in adults and children is extremely important, emphasizing the fact that obesity is a severe and disabling disease by itself, even without or before the occurrence of obesity-related complications,” he said.
However, he takes issue with the Commission’s designation that “preclinical” obesity is not a disease. “The critical point of disagreement for me is the message that obesity is a disease only if it is clinical or only if it presents functional impairment or clinical symptoms. This remains, in my opinion, an oversimplification, not taking into account the fact that the pathophysiological mechanisms that lead to fat accumulation and ‘adipose tissue-based chronic disease’ usually start well before the occurrence of symptoms.”
Busetto pointed to examples such as type 2 diabetes and chronic kidney disease, both of which can be asymptomatic in their early phases yet are still considered diseases at those points. “I have no problem in accepting a distinction between preclinical and clinical stages of the disease, and I like the definition of clinical obesity, but why should this imply the fact that obesity is NOT a disease since its beginning?”
The Commission does state that preclinical obesity should be addressed, mostly with preventive approaches but in some cases with more intensive management. “This is highly relevant, but the risk of an undertreatment of obesity in its asymptomatic state remains in place. This could delay appropriate management for a progressive disease that certainly should not be treated only when presenting symptoms. It would be too late,” Busetto said.
And EASO framework coauthor Gijs Goossens, PhD, professor of cardiometabolic physiology of obesity at Maastricht University Medical Centre, the Netherlands, added a concern that those with excess adiposity but lower BMI might be missed entirely, noting “Since abdominal fat accumulation better predicts chronic cardiometabolic diseases and can also be accompanied by clinical manifestations in individuals with overweight as a consequence of compromised adipose tissue function, the proposed model may lead to underdiagnosis or undertreatment in individuals with BMI 25-30 who have excess abdominal fat.”
Diagnosis and Management Beyond BMI
The Commission advises the use of BMI solely as a marker to screen for potential obesity. Those with a BMI > 40 can be assumed to have excess body fat. For others with a BMI at or near the threshold for obesity in a specific country or ethnic group or for whom there is the clinical judgment of the potential for clinical obesity, confirmation of excess or abnormal adiposity is needed by one of the following:
- At least one measurement of body size and BMI
- At least two measures of body size, regardless of BMI
- Direct body fat measurement, such as a dual-energy x-ray absorptiometry (DEXA) scan
Measurement of body size can be assessed in three ways:
- Waist circumference ≥ 102 cm for men and ≥ 88 cm for women
- Waist-to-hip ratio > 0.90 for men and > 0.50 for women
- Waist-to-height ratio > 0.50 for all.
Weintraub noted, “Telemedicine is a useful tool used by many patients and providers but may also make it challenging to accurately assess someone’s body size. Having technology like an iPhone app to measure body size would circumvent this challenge but this type of tool has not yet been validated.”
If the person does not have excess adiposity, they don’t have obesity. Those with excess adiposity do have obesity. Further assessment is then needed to establish whether the person has an illness, that is, clinical obesity, indicated by signs/symptoms of organ dysfunction, and/or limitations of daily activities. If not, they have “preclinical” obesity.
The document provides a list of 18 obesity-related organ, tissue, and body system criteria for diagnosing “clinical” obesity in adults, including upper airways (eg, apneas/hypopneas), respiratory (breathlessness), cardiovascular (hypertension, heart failure), liver (fatty liver disease with hepatic fibrosis), reproductive (polycystic ovary syndrome, hypogonadism), and metabolism (hyperglycemia, hypertriglyceridemia, low high-density lipoprotein cholesterol). A list of 13 such criteria is also provided for children. “Limitations of day-to-day activities” are included on both lists.
Management Differs by Designation
For preclinical obesity, management should focus on risk reduction and prevention of progression to clinical obesity or other obesity-related diseases. Such approaches include health counseling for weight loss or prevention of weight gain, monitoring over time, and active weight loss interventions in people at higher risk of developing clinical obesity and other obesity-related diseases.
Management for clinical obesity focuses on improvements or reversal of the organ dysfunction. The type of evidence-based treatment and management should be informed by individual risk-benefit assessments and decided via “active discussion” with the patient. Success is determined by improvement in the signs and symptoms rather than measures of weight loss.
In response to a reporter’s question at the SMC briefing about the implications for the use of weight-loss medications, Rubino noted that this wasn’t the focus of the report, but nonetheless said that this new obesity definition could help with their targeted use. “The strategy and intent by which you use the drugs is different in clinical and preclinical obesity. ... Pharmacological interventions could be used for patients with high-risk preclinical obesity, with the intent of reducing risk, but we ... would use the same medication at a different intensity, dose, and maybe in combination therapies.”
As for clinical obesity, “It could be more or less severe and could affect more than one organ, and so clinical obesity might require drugs, might require surgery, or may require, in some cases, a combination of both of them, to achieve the best possible outcomes. ... We want to make sure that the person is restoring health ... with whatever it takes.”
Rubino believes this new definition will convince the remaining clinicians who haven’t yet accepted the concept of obesity as a disease. “When they see clinical obesity, I think it will be much harder to say that a biological process that is capable of causing a dysfunction in the heart or the lungs is less of a disease than another biological process that causes similar dysfunction in the heart of the lungs. ... It’s going to be objective. Obesity is a spectrum of different situations. ... When it’s an illness, clinical obesity, it’s not a matter of if or when. It’s a matter of fact.”
There were no industrial grants or other funding for this initiative. King’s Health Partners hosted the initiative and provided logistical and personnel support to facilitate administrative work and the Delphi-like consensus-development process. Rubino declared receiving research grants from Ethicon (Johnson & Johnson), Novo Nordisk, and Medtronic; consulting fees from Morphic Medical; speaking honoraria from Medtronic, Ethicon, Novo Nordisk, Eli Lilly, and Amgen. Rubino has served (unpaid) as a member of the scientific advisory board for Keyron and a member of the data safety and monitoring board for GI Metabolic Solutions; is president of the Metabolic Health Institute (non-profit); and is the sole director of Metabolic Health International and London Metabolic and Bariatric Surgery (private practice). Baur declared serving on the scientific advisory board for Novo Nordisk (for the ACTION Teens study) and Eli Lilly and receiving speaker fees (paid to the institution) from Novo Nordisk.
A version of this article first appeared on Medscape.com.
“We propose a radical overhaul of the actual diagnosis of obesity to improve global healthcare and practices and policies. The specific aims were to facilitate individualized assessment and care of people living with obesity while preserving resources by reducing overdiagnosis and unnecessary or inadequate interventions,” Professor Louise Baur, chair of Child & Adolescent Health at the University of Sydney, Australia, said during a UK Science Media Centre (SMC) news briefing.
The report calls first for a diagnosis of obesity via confirmation of excess adiposity using measures such as waist circumference or waist-to-hip ratio in addition to BMI. Next, a clinical assessment of signs and symptoms of organ dysfunction due to obesity and/or functional limitations determines whether the individual has the disease “clinical obesity,” or “preclinical obesity,” a condition of health risk but not an illness itself.
Published on January 14, 2025, in The Lancet Diabetes & Endocrinology, the document also provides broad guidance on management for the two obesity conditions, emphasizing a personalized and stigma-free approach. The Lancet Commission on Obesity comprised 56 experts in relevant fields including endocrinology, surgery, nutrition, and public health, along with people living with obesity.
The report has been endorsed by more than 75 medical organizations, including the Association of British Clinical Diabetologists, the American Association of Clinical Endocrinologists, the American Diabetes Association, the American Heart Association, the Obesity Society, the World Obesity Federation, and obesity and endocrinology societies from countries in Europe, Latin America, Asia, and South Africa.
In recent years, many in the field have found fault with the current BMI-based definition of obesity (> 30 for people of European descent or other cutoffs for specific ethnic groups), primarily because BMI alone doesn’t reflect a person’s fat vs lean mass, fat distribution, or overall health. The new definition aims to overcome these limitations, as well as settle the debate about whether obesity is a “disease.”
“We now have a clinical diagnosis for obesity, which has been lacking. ... The traditional classification based on BMI ... reflects simply whether or not there is excess adiposity, and sometimes not even precise in that regard, either…It has never been a classification that was meant to diagnose a specific illness with its own clinical characteristics in the same way we diagnose any other illness,” Commission Chair Francesco Rubino, MD, professor and chair of Metabolic and Bariatric Surgery at King’s College London, England, said in an interview.
He added, “The fact that now we have a clinical diagnosis allows recognition of the nuance that obesity is generally a risk and for some can be an illness. There are some who have risk but don’t have the illness here and now. And it’s crucially important for clinical decision-making, but also for policies to have a distinction between those two things because the treatment strategy for one and the other are substantially different.”
Asked to comment, obesity specialist Michael A. Weintraub, MD, clinical assistant professor of endocrinology at New York University Langone Health, said in an interview, “I wholeheartedly agree with modifying the definition of obesity in this more accurate way. ... There has already been a lot of talk about the fallibility of BMI and that BMI over 30 does not equal obesity. ... So a major Commission article like this I think can really move those discussions even more into the forefront and start changing practice.”
However, Weintraub added, “I think there needs to be another step here of more practical guidance on how to actually implement this ... including how to measure waist circumference and to put it into a patient flow.”
Asked to comment, obesity expert Luca Busetto, MD, associate professor of internal medicine at the Department of Medicine of the University of Padova, Italy, said in an interview that he agrees with the general concept of moving beyond BMI in defining obesity. That view was expressed in a proposed “framework” from the European Association for the Study of Obesity (EASO), for which Busetto was the lead author.
Busetto also agrees with the emphasis on the need for a complete clinical evaluation of patients to define their health status. “The precise definition of the symptoms defining clinical obesity in adults and children is extremely important, emphasizing the fact that obesity is a severe and disabling disease by itself, even without or before the occurrence of obesity-related complications,” he said.
However, he takes issue with the Commission’s designation that “preclinical” obesity is not a disease. “The critical point of disagreement for me is the message that obesity is a disease only if it is clinical or only if it presents functional impairment or clinical symptoms. This remains, in my opinion, an oversimplification, not taking into account the fact that the pathophysiological mechanisms that lead to fat accumulation and ‘adipose tissue-based chronic disease’ usually start well before the occurrence of symptoms.”
Busetto pointed to examples such as type 2 diabetes and chronic kidney disease, both of which can be asymptomatic in their early phases yet are still considered diseases at those points. “I have no problem in accepting a distinction between preclinical and clinical stages of the disease, and I like the definition of clinical obesity, but why should this imply the fact that obesity is NOT a disease since its beginning?”
The Commission does state that preclinical obesity should be addressed, mostly with preventive approaches but in some cases with more intensive management. “This is highly relevant, but the risk of an undertreatment of obesity in its asymptomatic state remains in place. This could delay appropriate management for a progressive disease that certainly should not be treated only when presenting symptoms. It would be too late,” Busetto said.
And EASO framework coauthor Gijs Goossens, PhD, professor of cardiometabolic physiology of obesity at Maastricht University Medical Centre, the Netherlands, added a concern that those with excess adiposity but lower BMI might be missed entirely, noting “Since abdominal fat accumulation better predicts chronic cardiometabolic diseases and can also be accompanied by clinical manifestations in individuals with overweight as a consequence of compromised adipose tissue function, the proposed model may lead to underdiagnosis or undertreatment in individuals with BMI 25-30 who have excess abdominal fat.”
Diagnosis and Management Beyond BMI
The Commission advises the use of BMI solely as a marker to screen for potential obesity. Those with a BMI > 40 can be assumed to have excess body fat. For others with a BMI at or near the threshold for obesity in a specific country or ethnic group or for whom there is the clinical judgment of the potential for clinical obesity, confirmation of excess or abnormal adiposity is needed by one of the following:
- At least one measurement of body size and BMI
- At least two measures of body size, regardless of BMI
- Direct body fat measurement, such as a dual-energy x-ray absorptiometry (DEXA) scan
Measurement of body size can be assessed in three ways:
- Waist circumference ≥ 102 cm for men and ≥ 88 cm for women
- Waist-to-hip ratio > 0.90 for men and > 0.50 for women
- Waist-to-height ratio > 0.50 for all.
Weintraub noted, “Telemedicine is a useful tool used by many patients and providers but may also make it challenging to accurately assess someone’s body size. Having technology like an iPhone app to measure body size would circumvent this challenge but this type of tool has not yet been validated.”
If the person does not have excess adiposity, they don’t have obesity. Those with excess adiposity do have obesity. Further assessment is then needed to establish whether the person has an illness, that is, clinical obesity, indicated by signs/symptoms of organ dysfunction, and/or limitations of daily activities. If not, they have “preclinical” obesity.
The document provides a list of 18 obesity-related organ, tissue, and body system criteria for diagnosing “clinical” obesity in adults, including upper airways (eg, apneas/hypopneas), respiratory (breathlessness), cardiovascular (hypertension, heart failure), liver (fatty liver disease with hepatic fibrosis), reproductive (polycystic ovary syndrome, hypogonadism), and metabolism (hyperglycemia, hypertriglyceridemia, low high-density lipoprotein cholesterol). A list of 13 such criteria is also provided for children. “Limitations of day-to-day activities” are included on both lists.
Management Differs by Designation
For preclinical obesity, management should focus on risk reduction and prevention of progression to clinical obesity or other obesity-related diseases. Such approaches include health counseling for weight loss or prevention of weight gain, monitoring over time, and active weight loss interventions in people at higher risk of developing clinical obesity and other obesity-related diseases.
Management for clinical obesity focuses on improvements or reversal of the organ dysfunction. The type of evidence-based treatment and management should be informed by individual risk-benefit assessments and decided via “active discussion” with the patient. Success is determined by improvement in the signs and symptoms rather than measures of weight loss.
In response to a reporter’s question at the SMC briefing about the implications for the use of weight-loss medications, Rubino noted that this wasn’t the focus of the report, but nonetheless said that this new obesity definition could help with their targeted use. “The strategy and intent by which you use the drugs is different in clinical and preclinical obesity. ... Pharmacological interventions could be used for patients with high-risk preclinical obesity, with the intent of reducing risk, but we ... would use the same medication at a different intensity, dose, and maybe in combination therapies.”
As for clinical obesity, “It could be more or less severe and could affect more than one organ, and so clinical obesity might require drugs, might require surgery, or may require, in some cases, a combination of both of them, to achieve the best possible outcomes. ... We want to make sure that the person is restoring health ... with whatever it takes.”
Rubino believes this new definition will convince the remaining clinicians who haven’t yet accepted the concept of obesity as a disease. “When they see clinical obesity, I think it will be much harder to say that a biological process that is capable of causing a dysfunction in the heart or the lungs is less of a disease than another biological process that causes similar dysfunction in the heart of the lungs. ... It’s going to be objective. Obesity is a spectrum of different situations. ... When it’s an illness, clinical obesity, it’s not a matter of if or when. It’s a matter of fact.”
There were no industrial grants or other funding for this initiative. King’s Health Partners hosted the initiative and provided logistical and personnel support to facilitate administrative work and the Delphi-like consensus-development process. Rubino declared receiving research grants from Ethicon (Johnson & Johnson), Novo Nordisk, and Medtronic; consulting fees from Morphic Medical; speaking honoraria from Medtronic, Ethicon, Novo Nordisk, Eli Lilly, and Amgen. Rubino has served (unpaid) as a member of the scientific advisory board for Keyron and a member of the data safety and monitoring board for GI Metabolic Solutions; is president of the Metabolic Health Institute (non-profit); and is the sole director of Metabolic Health International and London Metabolic and Bariatric Surgery (private practice). Baur declared serving on the scientific advisory board for Novo Nordisk (for the ACTION Teens study) and Eli Lilly and receiving speaker fees (paid to the institution) from Novo Nordisk.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
New Weight Loss Drugs May Fight Obesity-Related Cancer, Too
The latest glucagon-like peptide 1 (GLP-1) receptor agonists have been heralded for their potential to not only boost weight loss and glucose control but also improve cardiovascular, gastric, hepatic, and renal values.
Throughout 2024, research has also indicated GLP-1 drugs may reduce risks for obesity-related cancer.
In a US study of more than 1.6 million patients with type 2 diabetes, cancer researchers found that patients who took a GLP-1 drug had significant risk reductions for 10 of 13 obesity-associated cancers, as compared with patients who only took insulin.
They also saw a declining risk for stomach cancer, though it wasn’t considered statistically significant, but not a reduced risk for postmenopausal breast cancer or thyroid cancer.
The associations make sense, particularly because GLP-1 drugs have unexpected effects on modulating immune functions linked to obesity-associated cancers.
“The protective effects of GLP-1s against obesity-associated cancers likely stem from multiple mechanisms,” said lead author Lindsey Wang, a medical student and research scholar at Case Western Reserve University in Cleveland.
“These drugs promote substantial weight loss, reducing obesity-related cancer risks,” she said. “They also enhance insulin sensitivity and lower insulin levels, decreasing cancer cell growth signals.”
Additional GLP-1 Studies
The Case Western team also published a study in December 2023 that found people with type 2 diabetes who took GLP-1s had a 44% lower risk for colorectal cancer than those who took insulin and a 25% lower risk than those who took metformin. The research suggested even greater risk reductions among those with overweight or obesity, with GLP-1 users having a 50% lower risk than those who took insulin and a 42% lower risk than those who took metformin.
In another recent Case Western study, both bariatric surgery and GLP-1 drugs reduced the risk for obesity-related cancers. While those who had bariatric surgery had a 22% risk reduction over 10 years, as compared with those who received no treatment, those taking GLP-1 had a 39% risk reduction.
Other studies worldwide have looked at GLP-1 drugs and tumor effects among various cancer cell lines. In a study using pancreatic cancer cell lines, GLP-1 liraglutide suppressed cancer cell growth and led to cell death. Similarly, a study using breast cancer cells found liraglutide reduced cancer cell viability and the ability for cells to migrate.
As researchers identify additional links between GLP-1s and improvements across organ systems, the knock-on effects could lead to lower cancer risks as well. For example, studies presented at The Liver Meeting in San Diego in November pointed to GLP-1s reducing fatty liver disease, which can slow the progression to liver cancer.
“Separate from obesity, having higher levels of body fat is associated with an increased risk of several forms of cancer,” said Neil Iyengar, MD, an oncologist at Memorial Sloan Kettering Cancer Center in New York City. Iyengar researches the relationship between obesity and cancer.
“I foresee that this class of drugs will revolutionize obesity and the cancer burden that comes with it, if people can get access,” he said. “This really is an exciting development.”
Ongoing GLP-1 Research
On the other hand, cancer researchers have also expressed concerns about potential associations between GLP-1s and increased cancer risks. In the obesity-associated cancer study by Case Western researchers, patients with type 2 diabetes taking a GLP-1 drug appeared to have a slightly higher risk for kidney cancer than those taking metformin.
In addition, GLP-1 studies in animals have indicated that the drugs may increase the risks for medullary thyroid cancer and pancreatic cancer. However, the data on increased risks in humans remain inconclusive, and more recent studies refute these findings.
For instance, cancer researchers in India conducted a systematic review and meta-analysis of semaglutide and cancer risks, finding that 37 randomized controlled trials and 19 real-world studies didn’t find increased risks for any cancer, including pancreatic and thyroid cancers.
In another systematic review by Brazilian researchers, 50 trials found GLP-1s didn’t increase the risk for breast cancer or benign breast neoplasms.
In 2025, new retrospective studies will show more nuanced data, especially as more patients — both with and without type 2 diabetes — take semaglutide, tirzepatide, and new GLP-1 drugs in the research pipeline.
“The holy grail has always been getting a medication to treat obesity,” said Anne McTiernan, MD, PhD, an epidemiologist and obesity researcher at the Fred Hutchinson Cancer Center in Seattle.
“There have been trials focused on these medications’ effects on diabetes and cardiovascular disease treatment, but no trials have tested their effects on cancer risk,” she said. “Usually, many years of follow-up of large numbers of patients are needed to see cancer effects of a carcinogen or cancer-preventing intervention.”
Those clinical trials are likely coming soon, she said. Researchers will need to conduct prospective clinical trials to examine the direct relationship between GLP-1 drugs and cancer risks, as well as the underlying mechanisms linked to cancer cell growth, activation of immune cells, and anti-inflammatory properties.
Because GLP-1 medications aren’t intended to be taken forever, researchers will also need to consider the associations with long-term cancer risks. Even so, weight loss and other obesity-related improvements could contribute to overall lower cancer risks in the end.
“If taking these drugs for a limited amount of time can help people lose weight and get on an exercise plan, then that’s helping lower cancer risk long-term,” said Sonali Thosani, MD, associate professor of endocrine neoplasia and hormonal disorders at the University of Texas MD Anderson Cancer Center in Houston.
“But it all comes back to someone making lifestyle changes and sticking to them, even after they stop taking the drugs,” she said. “If they can do that, then you’ll probably see a net positive for long-term cancer risks and other long-term health risks.”
A version of this article appeared on Medscape.com.
The latest glucagon-like peptide 1 (GLP-1) receptor agonists have been heralded for their potential to not only boost weight loss and glucose control but also improve cardiovascular, gastric, hepatic, and renal values.
Throughout 2024, research has also indicated GLP-1 drugs may reduce risks for obesity-related cancer.
In a US study of more than 1.6 million patients with type 2 diabetes, cancer researchers found that patients who took a GLP-1 drug had significant risk reductions for 10 of 13 obesity-associated cancers, as compared with patients who only took insulin.
They also saw a declining risk for stomach cancer, though it wasn’t considered statistically significant, but not a reduced risk for postmenopausal breast cancer or thyroid cancer.
The associations make sense, particularly because GLP-1 drugs have unexpected effects on modulating immune functions linked to obesity-associated cancers.
“The protective effects of GLP-1s against obesity-associated cancers likely stem from multiple mechanisms,” said lead author Lindsey Wang, a medical student and research scholar at Case Western Reserve University in Cleveland.
“These drugs promote substantial weight loss, reducing obesity-related cancer risks,” she said. “They also enhance insulin sensitivity and lower insulin levels, decreasing cancer cell growth signals.”
Additional GLP-1 Studies
The Case Western team also published a study in December 2023 that found people with type 2 diabetes who took GLP-1s had a 44% lower risk for colorectal cancer than those who took insulin and a 25% lower risk than those who took metformin. The research suggested even greater risk reductions among those with overweight or obesity, with GLP-1 users having a 50% lower risk than those who took insulin and a 42% lower risk than those who took metformin.
In another recent Case Western study, both bariatric surgery and GLP-1 drugs reduced the risk for obesity-related cancers. While those who had bariatric surgery had a 22% risk reduction over 10 years, as compared with those who received no treatment, those taking GLP-1 had a 39% risk reduction.
Other studies worldwide have looked at GLP-1 drugs and tumor effects among various cancer cell lines. In a study using pancreatic cancer cell lines, GLP-1 liraglutide suppressed cancer cell growth and led to cell death. Similarly, a study using breast cancer cells found liraglutide reduced cancer cell viability and the ability for cells to migrate.
As researchers identify additional links between GLP-1s and improvements across organ systems, the knock-on effects could lead to lower cancer risks as well. For example, studies presented at The Liver Meeting in San Diego in November pointed to GLP-1s reducing fatty liver disease, which can slow the progression to liver cancer.
“Separate from obesity, having higher levels of body fat is associated with an increased risk of several forms of cancer,” said Neil Iyengar, MD, an oncologist at Memorial Sloan Kettering Cancer Center in New York City. Iyengar researches the relationship between obesity and cancer.
“I foresee that this class of drugs will revolutionize obesity and the cancer burden that comes with it, if people can get access,” he said. “This really is an exciting development.”
Ongoing GLP-1 Research
On the other hand, cancer researchers have also expressed concerns about potential associations between GLP-1s and increased cancer risks. In the obesity-associated cancer study by Case Western researchers, patients with type 2 diabetes taking a GLP-1 drug appeared to have a slightly higher risk for kidney cancer than those taking metformin.
In addition, GLP-1 studies in animals have indicated that the drugs may increase the risks for medullary thyroid cancer and pancreatic cancer. However, the data on increased risks in humans remain inconclusive, and more recent studies refute these findings.
For instance, cancer researchers in India conducted a systematic review and meta-analysis of semaglutide and cancer risks, finding that 37 randomized controlled trials and 19 real-world studies didn’t find increased risks for any cancer, including pancreatic and thyroid cancers.
In another systematic review by Brazilian researchers, 50 trials found GLP-1s didn’t increase the risk for breast cancer or benign breast neoplasms.
In 2025, new retrospective studies will show more nuanced data, especially as more patients — both with and without type 2 diabetes — take semaglutide, tirzepatide, and new GLP-1 drugs in the research pipeline.
“The holy grail has always been getting a medication to treat obesity,” said Anne McTiernan, MD, PhD, an epidemiologist and obesity researcher at the Fred Hutchinson Cancer Center in Seattle.
“There have been trials focused on these medications’ effects on diabetes and cardiovascular disease treatment, but no trials have tested their effects on cancer risk,” she said. “Usually, many years of follow-up of large numbers of patients are needed to see cancer effects of a carcinogen or cancer-preventing intervention.”
Those clinical trials are likely coming soon, she said. Researchers will need to conduct prospective clinical trials to examine the direct relationship between GLP-1 drugs and cancer risks, as well as the underlying mechanisms linked to cancer cell growth, activation of immune cells, and anti-inflammatory properties.
Because GLP-1 medications aren’t intended to be taken forever, researchers will also need to consider the associations with long-term cancer risks. Even so, weight loss and other obesity-related improvements could contribute to overall lower cancer risks in the end.
“If taking these drugs for a limited amount of time can help people lose weight and get on an exercise plan, then that’s helping lower cancer risk long-term,” said Sonali Thosani, MD, associate professor of endocrine neoplasia and hormonal disorders at the University of Texas MD Anderson Cancer Center in Houston.
“But it all comes back to someone making lifestyle changes and sticking to them, even after they stop taking the drugs,” she said. “If they can do that, then you’ll probably see a net positive for long-term cancer risks and other long-term health risks.”
A version of this article appeared on Medscape.com.
The latest glucagon-like peptide 1 (GLP-1) receptor agonists have been heralded for their potential to not only boost weight loss and glucose control but also improve cardiovascular, gastric, hepatic, and renal values.
Throughout 2024, research has also indicated GLP-1 drugs may reduce risks for obesity-related cancer.
In a US study of more than 1.6 million patients with type 2 diabetes, cancer researchers found that patients who took a GLP-1 drug had significant risk reductions for 10 of 13 obesity-associated cancers, as compared with patients who only took insulin.
They also saw a declining risk for stomach cancer, though it wasn’t considered statistically significant, but not a reduced risk for postmenopausal breast cancer or thyroid cancer.
The associations make sense, particularly because GLP-1 drugs have unexpected effects on modulating immune functions linked to obesity-associated cancers.
“The protective effects of GLP-1s against obesity-associated cancers likely stem from multiple mechanisms,” said lead author Lindsey Wang, a medical student and research scholar at Case Western Reserve University in Cleveland.
“These drugs promote substantial weight loss, reducing obesity-related cancer risks,” she said. “They also enhance insulin sensitivity and lower insulin levels, decreasing cancer cell growth signals.”
Additional GLP-1 Studies
The Case Western team also published a study in December 2023 that found people with type 2 diabetes who took GLP-1s had a 44% lower risk for colorectal cancer than those who took insulin and a 25% lower risk than those who took metformin. The research suggested even greater risk reductions among those with overweight or obesity, with GLP-1 users having a 50% lower risk than those who took insulin and a 42% lower risk than those who took metformin.
In another recent Case Western study, both bariatric surgery and GLP-1 drugs reduced the risk for obesity-related cancers. While those who had bariatric surgery had a 22% risk reduction over 10 years, as compared with those who received no treatment, those taking GLP-1 had a 39% risk reduction.
Other studies worldwide have looked at GLP-1 drugs and tumor effects among various cancer cell lines. In a study using pancreatic cancer cell lines, GLP-1 liraglutide suppressed cancer cell growth and led to cell death. Similarly, a study using breast cancer cells found liraglutide reduced cancer cell viability and the ability for cells to migrate.
As researchers identify additional links between GLP-1s and improvements across organ systems, the knock-on effects could lead to lower cancer risks as well. For example, studies presented at The Liver Meeting in San Diego in November pointed to GLP-1s reducing fatty liver disease, which can slow the progression to liver cancer.
“Separate from obesity, having higher levels of body fat is associated with an increased risk of several forms of cancer,” said Neil Iyengar, MD, an oncologist at Memorial Sloan Kettering Cancer Center in New York City. Iyengar researches the relationship between obesity and cancer.
“I foresee that this class of drugs will revolutionize obesity and the cancer burden that comes with it, if people can get access,” he said. “This really is an exciting development.”
Ongoing GLP-1 Research
On the other hand, cancer researchers have also expressed concerns about potential associations between GLP-1s and increased cancer risks. In the obesity-associated cancer study by Case Western researchers, patients with type 2 diabetes taking a GLP-1 drug appeared to have a slightly higher risk for kidney cancer than those taking metformin.
In addition, GLP-1 studies in animals have indicated that the drugs may increase the risks for medullary thyroid cancer and pancreatic cancer. However, the data on increased risks in humans remain inconclusive, and more recent studies refute these findings.
For instance, cancer researchers in India conducted a systematic review and meta-analysis of semaglutide and cancer risks, finding that 37 randomized controlled trials and 19 real-world studies didn’t find increased risks for any cancer, including pancreatic and thyroid cancers.
In another systematic review by Brazilian researchers, 50 trials found GLP-1s didn’t increase the risk for breast cancer or benign breast neoplasms.
In 2025, new retrospective studies will show more nuanced data, especially as more patients — both with and without type 2 diabetes — take semaglutide, tirzepatide, and new GLP-1 drugs in the research pipeline.
“The holy grail has always been getting a medication to treat obesity,” said Anne McTiernan, MD, PhD, an epidemiologist and obesity researcher at the Fred Hutchinson Cancer Center in Seattle.
“There have been trials focused on these medications’ effects on diabetes and cardiovascular disease treatment, but no trials have tested their effects on cancer risk,” she said. “Usually, many years of follow-up of large numbers of patients are needed to see cancer effects of a carcinogen or cancer-preventing intervention.”
Those clinical trials are likely coming soon, she said. Researchers will need to conduct prospective clinical trials to examine the direct relationship between GLP-1 drugs and cancer risks, as well as the underlying mechanisms linked to cancer cell growth, activation of immune cells, and anti-inflammatory properties.
Because GLP-1 medications aren’t intended to be taken forever, researchers will also need to consider the associations with long-term cancer risks. Even so, weight loss and other obesity-related improvements could contribute to overall lower cancer risks in the end.
“If taking these drugs for a limited amount of time can help people lose weight and get on an exercise plan, then that’s helping lower cancer risk long-term,” said Sonali Thosani, MD, associate professor of endocrine neoplasia and hormonal disorders at the University of Texas MD Anderson Cancer Center in Houston.
“But it all comes back to someone making lifestyle changes and sticking to them, even after they stop taking the drugs,” she said. “If they can do that, then you’ll probably see a net positive for long-term cancer risks and other long-term health risks.”
A version of this article appeared on Medscape.com.
Nutrition, Drugs, or Bariatric Surgery: What’s the Best Approach for Sustained Weight Loss?
Given that more than 100 million US adults have obesity, including 22 million with severe obesity, physicians regularly see patients with the condition in their practices.
Fortunately, doctors have more tools than ever to help their patients. But the question remains: Which method is the safest and most effective? Is it diet and lifestyle changes, one of the recently approved anti-obesity medications (AOMs), bariatric surgery, or a combination approach?
There are no head-to-head trials comparing these three approaches, said Vanita Rahman, MD, clinic director of the Barnard Medical Center, Washington, DC, at the International Conference on Nutrition in Medicine, sponsored by the Physicians Committee for Responsible Medicine.
Instead, doctors must evaluate the merits and drawbacks of each intervention and decide with their patients which treatment is best for them, she told Medscape Medical News. When she sees patients, Rahman shares the pertinent research with them, so they are able to make an informed choice.
Looking at the Options
In her presentation at the conference, Rahman summarized the guidelines issued by the American Heart Association/American College of Cardiology/The Obesity Society for Management of Overweight and Obesity in Adults and the American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines For Medical Care of Patients with Obesity, including lifestyle changes, AOMs, and bariatric surgery (Table 1).
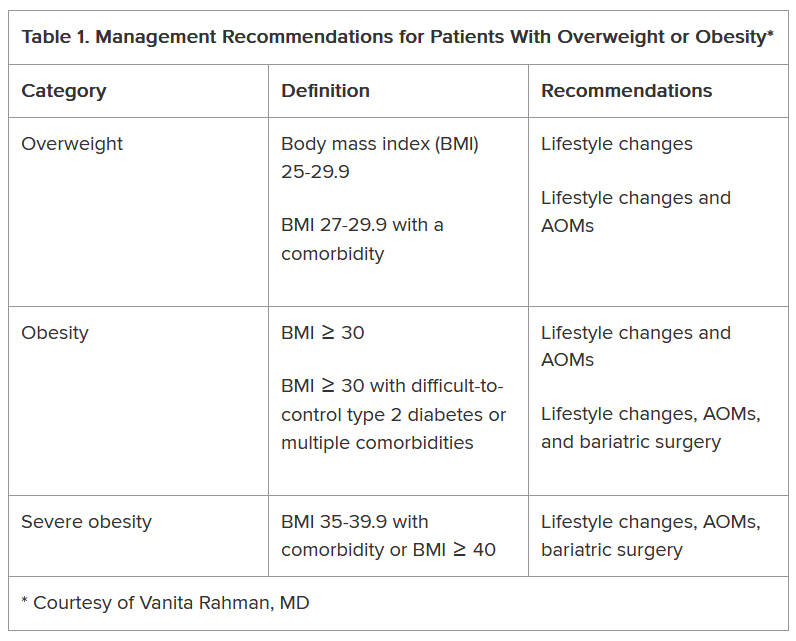
As shown, the current clinical guidelines offer recommendations that consider such factors as the patient’s BMI and presence of one or more comorbidities. Generally, they begin with lifestyle changes for people with overweight, the possibility of an AOM for those with obesity, and bariatric surgery as an option for those with severe obesity-related complications.
“In obesity, we traditionally thought the process was ‘either-or’ — either lifestyle or surgery or medication — and somehow lifestyle is better,” Sheethal Reddy, PhD, a psychologist at the Bariatric Center at Emory University Hospital Midtown, Atlanta, told Medscape Medical News.
Now physicians often use a combination of methods, but lifestyle is foundational to all of them, she said.
“If you don’t make lifestyle changes, none of the approaches will ultimately be effective,” said Reddy, who also is an assistant professor in the Division of General and GI Surgery at Emory School of Medicine, Atlanta.
Lifestyle changes don’t just involve diet and nutrition but include physical exercise.
“Being sedentary affects everything — sleep quality, appetite regulation, and metabolism. Without sufficient exercise, the body isn’t functioning well enough to have a healthy metabolism,” Reddy said.
How Durable Are the Interventions?
Although bariatric surgery has demonstrated effectiveness in helping patients lose weight, many of them regain some or most of it, Rahman said.
A systematic review and meta-analysis found weight regain in 49% of patients who underwent bariatric surgery patients, with the highest prevalence after Roux-en-Y gastric bypass.
Another study of approximately 45,000 patients who underwent bariatric surgery found differences not only in the percentage of total weight loss among Roux-en-Y gastric bypass, sleeve gastrectomy, and adjustable gastric band procedures but also in how much of that weight stayed off between 1 and 5 years following the procedure (Table 2).
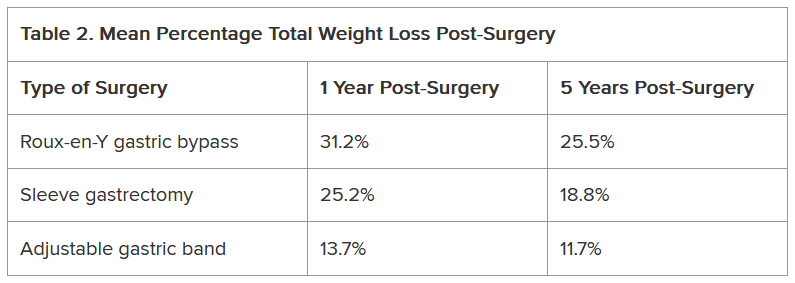
Weight regain also is a risk with AOMs, if they’re discontinued.
The STEP 1 trial tested the effectiveness of semaglutide — a glucagon-like peptide 1 (GLP-1) receptor agonist — as an adjunct to lifestyle intervention for weight loss in patients with obesity or with overweight and at least one comorbidity but not diabetes. Mean weight loss with semaglutide was 17.3% but that figure dropped 11.6 percentage points after treatment was discontinued.
Other studies also have found that patients regain weight after GLP-1 discontinuation.
Tirzepatide, a GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) combination, has shown efficacy with weight reduction, but patients experienced some weight regain upon discontinuation. In one study, patients experienced a mean weight loss of 20.9% after 36 weeks of tirzepatide. In the study’s subsequent 52-week double-blind, placebo-controlled period, patients who stopped taking the medication experienced a weight regain of 14%, whereas those who remained on the medication lost an additional 5.5% of weight.
GLP-1 and GLP-1/GIP medications do not address the factors that contribute to overweight and obesity, Rahman said. “They simply suppress the appetite; therefore, weight gain occurs after stopping them.”
Patients may stop taking anti-obesity drugs for a variety of reasons, including side effects. Rahman noted that the common side effects include nausea, vomiting, and constipation, whereas rare side effects include gastroparesis, gallbladder and biliary disease, thyroid cancer, and suicidal thoughts. GLP-1 and GLP-1/GIP medications also carry a risk for non-arteritic anterior ischemic optic neuropathy, she said.
Moreover, health insurance does not always cover these medications, which likely affects patient access to the drugs and compliance rates.
“Given the side effects and frequent lack of insurance coverage, significant questions remain about long-term safety and feasibility of these agents,” Rahman said.
What About Nutritional Approaches?
The lifestyle interventions in the semaglutide and tirzepatide studies included 500 kcal/d deficit diets, which is difficult for people to maintain, noted Rahman, who is the author of the book Simply Plant Based: Fabulous Food for a Healthy Life.
Additionally, bariatric surgery has been associated with long-term micronutrient deficiencies, including deficiencies in vitamins A, D, E, K, B1, and B12, as well as folate, iron, zinc, copper, selenium, and calcium, she said.
The best approach to food from a patient compliance standpoint and to avoid nutrient deficiencies is a whole-food, plant-based diet, Rahman said. She advocates this nutritional approach, along with physical activity, for patients regardless of whether they’ve selected lifestyle intervention alone or combined with an AOM or bariatric surgery to address obesity.
Rahman cited a 5-year heart disease study comparing an intensive lifestyle program involving a vegetarian diet, aerobic exercise, stress management training, smoking cessation, and group psychosocial support to treatment as usual. Patients in the lifestyle group lost 10.9 kg at 1 year and sustained weight loss of 5.8 kg at 5 years, whereas weight in the control group remained relatively unchanged from baseline.
She also pointed to the findings of a study of patients with obesity or with overweight and at least one comorbidity that compared standard care with a low-fat, whole-food, plant-based diet with vitamin B12 supplementation. At 6 months, mean BMI reduction was greater in the intervention group than the standard care group (−4.4 vs −0.4).
In her practice, Rahman has seen the benefits of a whole-food, plant-based diet for patients with obesity.
If people are committed to this type of dietary approach and are given the tools and resources to do it effectively, “their thinking changes, their taste buds change, and they grow to enjoy this new way of eating,” she said. “They see results, and it’s a lifestyle that can be sustained long-term.”
Addressing Drivers of Weight Gain
Patients also need help addressing the various factors that may contribute to overweight and obesity, including overconsumption of ultra-processed foods, substandard nutritional quality of restaurant foods, increasing portion sizes, distraction during eating, emotional eating, late-night eating, and cultural/traditional values surrounding food, Rahman noted.
Supatra Tovar, PsyD, RD, a clinical psychologist with a practice in Pasadena, California, agreed that identifying the reasons for weight gain is critical for treatment.
“If you’re not addressing underlying issues, such as a person’s relationship with food, behaviors around food, the tendency to mindlessly eat or emotionally eat or eat to seek comfort, the person’s weight problems won’t ultimately be fully solved by any of the three approaches — dieting, medications, or bariatric surgery,” she said.
Some of her patients “engage in extreme dieting and deprivation, and many who use medications or have had bariatric surgery hardly eat and often develop nutritional deficiencies,” said Tovar, author of the book Deprogram Diet Culture: Rethink Your Relationship with Food, Heal Your Mind, and Live a Diet-Free Life.
The key to healthy and sustained weight loss is to “become attuned to the body’s signals, learn how to honor hunger, stop eating when satisfied, and eat more healthful foods, such as fruits and vegetables, whole grains, lean proteins — especially plant-based proteins — and the body gives signals that this is what it wants,” she said.
Tovar doesn’t give her clients a specific diet or set of portions.
“I teach them to listen to their bodies,” she said. “They’ve lost significant amounts of weight and continued to keep it off because they’ve done this kind of work.”
When Lifestyle Changes Aren’t Enough
For many patients, lifestyle interventions are insufficient to address the degree of overweight and obesity and common comorbidities, said W. Timothy Garvey, MD, associate director and professor, Department of Nutrition Sciences, School of Health Professions, University of Alabama at Birmingham.
“Of course, nutritional approaches are very important, not only for weight but also for general health-related reasons,” said Garvey, lead author of the 2016 American Association of Clinical Endocrinologists obesity guidelines. “We’ve seen that the Mediterranean and some plant-based diets can prevent progression from prediabetes to diabetes and improve other parameters that reflect metabolic health.”
However, it’s “not common that patients can follow these diets, lose weight, and keep it off,” Garvey cautioned. Up to 50% of weight that’s lost through lifestyle changes is typically regained by 1-year follow-up, with almost all remaining lost weight subsequently regained in the majority of individuals because the person “has to fight against pathophysiological process that drive weight regain,” he noted.
Weight-loss medications can address these pathophysiologic processes by “addressing interactions of satiety hormones with feeding centers in the brain, suppressing the appetite, and making it easier for patients to adhere to a reduced-calorie diet.”
Garvey views the weight-loss medications in the same light as drugs for diabetes and hypertension, in that people need to keep taking them to sustain the benefit.
There’s still a role for bariatric surgery because not everyone can tolerate the AOMs or achieve sufficient weight loss.
“Patients with very high BMI who have trouble ambulating might benefit from a combination of bariatric surgery and medication,” Garvey said.
While some side effects are associated with AOMs, being an “alarmist” about them can be detrimental to patients, he warned.
Rahman and Tovar are authors of books about weight loss. Reddy reported no relevant financial relationships. Garvey is a consultant on advisory boards for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Pfizer, Fractyl Health, Alnylam Pharmaceuticals, Inogen, Zealand, Allurion, Carmot/Roche, Terns Pharmaceuticals, Neurocrine, Keros Therapeutics, and Regeneron. He is the site principal investigator for multi-centered clinical trials sponsored by his university and funded by Novo Nordisk, Eli Lilly, Epitomee, Neurovalens, and Pfizer. He serves as a consultant on the advisory board for the nonprofit Milken Foundation and is a member of the Data Monitoring Committee for phase 3 clinical trials conducted by Boehringer-Ingelheim and Eli Lilly.
A version of this article first appeared on Medscape.com.
Given that more than 100 million US adults have obesity, including 22 million with severe obesity, physicians regularly see patients with the condition in their practices.
Fortunately, doctors have more tools than ever to help their patients. But the question remains: Which method is the safest and most effective? Is it diet and lifestyle changes, one of the recently approved anti-obesity medications (AOMs), bariatric surgery, or a combination approach?
There are no head-to-head trials comparing these three approaches, said Vanita Rahman, MD, clinic director of the Barnard Medical Center, Washington, DC, at the International Conference on Nutrition in Medicine, sponsored by the Physicians Committee for Responsible Medicine.
Instead, doctors must evaluate the merits and drawbacks of each intervention and decide with their patients which treatment is best for them, she told Medscape Medical News. When she sees patients, Rahman shares the pertinent research with them, so they are able to make an informed choice.
Looking at the Options
In her presentation at the conference, Rahman summarized the guidelines issued by the American Heart Association/American College of Cardiology/The Obesity Society for Management of Overweight and Obesity in Adults and the American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines For Medical Care of Patients with Obesity, including lifestyle changes, AOMs, and bariatric surgery (Table 1).
As shown, the current clinical guidelines offer recommendations that consider such factors as the patient’s BMI and presence of one or more comorbidities. Generally, they begin with lifestyle changes for people with overweight, the possibility of an AOM for those with obesity, and bariatric surgery as an option for those with severe obesity-related complications.
“In obesity, we traditionally thought the process was ‘either-or’ — either lifestyle or surgery or medication — and somehow lifestyle is better,” Sheethal Reddy, PhD, a psychologist at the Bariatric Center at Emory University Hospital Midtown, Atlanta, told Medscape Medical News.
Now physicians often use a combination of methods, but lifestyle is foundational to all of them, she said.
“If you don’t make lifestyle changes, none of the approaches will ultimately be effective,” said Reddy, who also is an assistant professor in the Division of General and GI Surgery at Emory School of Medicine, Atlanta.
Lifestyle changes don’t just involve diet and nutrition but include physical exercise.
“Being sedentary affects everything — sleep quality, appetite regulation, and metabolism. Without sufficient exercise, the body isn’t functioning well enough to have a healthy metabolism,” Reddy said.
How Durable Are the Interventions?
Although bariatric surgery has demonstrated effectiveness in helping patients lose weight, many of them regain some or most of it, Rahman said.
A systematic review and meta-analysis found weight regain in 49% of patients who underwent bariatric surgery patients, with the highest prevalence after Roux-en-Y gastric bypass.
Another study of approximately 45,000 patients who underwent bariatric surgery found differences not only in the percentage of total weight loss among Roux-en-Y gastric bypass, sleeve gastrectomy, and adjustable gastric band procedures but also in how much of that weight stayed off between 1 and 5 years following the procedure (Table 2).
Weight regain also is a risk with AOMs, if they’re discontinued.
The STEP 1 trial tested the effectiveness of semaglutide — a glucagon-like peptide 1 (GLP-1) receptor agonist — as an adjunct to lifestyle intervention for weight loss in patients with obesity or with overweight and at least one comorbidity but not diabetes. Mean weight loss with semaglutide was 17.3% but that figure dropped 11.6 percentage points after treatment was discontinued.
Other studies also have found that patients regain weight after GLP-1 discontinuation.
Tirzepatide, a GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) combination, has shown efficacy with weight reduction, but patients experienced some weight regain upon discontinuation. In one study, patients experienced a mean weight loss of 20.9% after 36 weeks of tirzepatide. In the study’s subsequent 52-week double-blind, placebo-controlled period, patients who stopped taking the medication experienced a weight regain of 14%, whereas those who remained on the medication lost an additional 5.5% of weight.
GLP-1 and GLP-1/GIP medications do not address the factors that contribute to overweight and obesity, Rahman said. “They simply suppress the appetite; therefore, weight gain occurs after stopping them.”
Patients may stop taking anti-obesity drugs for a variety of reasons, including side effects. Rahman noted that the common side effects include nausea, vomiting, and constipation, whereas rare side effects include gastroparesis, gallbladder and biliary disease, thyroid cancer, and suicidal thoughts. GLP-1 and GLP-1/GIP medications also carry a risk for non-arteritic anterior ischemic optic neuropathy, she said.
Moreover, health insurance does not always cover these medications, which likely affects patient access to the drugs and compliance rates.
“Given the side effects and frequent lack of insurance coverage, significant questions remain about long-term safety and feasibility of these agents,” Rahman said.
What About Nutritional Approaches?
The lifestyle interventions in the semaglutide and tirzepatide studies included 500 kcal/d deficit diets, which is difficult for people to maintain, noted Rahman, who is the author of the book Simply Plant Based: Fabulous Food for a Healthy Life.
Additionally, bariatric surgery has been associated with long-term micronutrient deficiencies, including deficiencies in vitamins A, D, E, K, B1, and B12, as well as folate, iron, zinc, copper, selenium, and calcium, she said.
The best approach to food from a patient compliance standpoint and to avoid nutrient deficiencies is a whole-food, plant-based diet, Rahman said. She advocates this nutritional approach, along with physical activity, for patients regardless of whether they’ve selected lifestyle intervention alone or combined with an AOM or bariatric surgery to address obesity.
Rahman cited a 5-year heart disease study comparing an intensive lifestyle program involving a vegetarian diet, aerobic exercise, stress management training, smoking cessation, and group psychosocial support to treatment as usual. Patients in the lifestyle group lost 10.9 kg at 1 year and sustained weight loss of 5.8 kg at 5 years, whereas weight in the control group remained relatively unchanged from baseline.
She also pointed to the findings of a study of patients with obesity or with overweight and at least one comorbidity that compared standard care with a low-fat, whole-food, plant-based diet with vitamin B12 supplementation. At 6 months, mean BMI reduction was greater in the intervention group than the standard care group (−4.4 vs −0.4).
In her practice, Rahman has seen the benefits of a whole-food, plant-based diet for patients with obesity.
If people are committed to this type of dietary approach and are given the tools and resources to do it effectively, “their thinking changes, their taste buds change, and they grow to enjoy this new way of eating,” she said. “They see results, and it’s a lifestyle that can be sustained long-term.”
Addressing Drivers of Weight Gain
Patients also need help addressing the various factors that may contribute to overweight and obesity, including overconsumption of ultra-processed foods, substandard nutritional quality of restaurant foods, increasing portion sizes, distraction during eating, emotional eating, late-night eating, and cultural/traditional values surrounding food, Rahman noted.
Supatra Tovar, PsyD, RD, a clinical psychologist with a practice in Pasadena, California, agreed that identifying the reasons for weight gain is critical for treatment.
“If you’re not addressing underlying issues, such as a person’s relationship with food, behaviors around food, the tendency to mindlessly eat or emotionally eat or eat to seek comfort, the person’s weight problems won’t ultimately be fully solved by any of the three approaches — dieting, medications, or bariatric surgery,” she said.
Some of her patients “engage in extreme dieting and deprivation, and many who use medications or have had bariatric surgery hardly eat and often develop nutritional deficiencies,” said Tovar, author of the book Deprogram Diet Culture: Rethink Your Relationship with Food, Heal Your Mind, and Live a Diet-Free Life.
The key to healthy and sustained weight loss is to “become attuned to the body’s signals, learn how to honor hunger, stop eating when satisfied, and eat more healthful foods, such as fruits and vegetables, whole grains, lean proteins — especially plant-based proteins — and the body gives signals that this is what it wants,” she said.
Tovar doesn’t give her clients a specific diet or set of portions.
“I teach them to listen to their bodies,” she said. “They’ve lost significant amounts of weight and continued to keep it off because they’ve done this kind of work.”
When Lifestyle Changes Aren’t Enough
For many patients, lifestyle interventions are insufficient to address the degree of overweight and obesity and common comorbidities, said W. Timothy Garvey, MD, associate director and professor, Department of Nutrition Sciences, School of Health Professions, University of Alabama at Birmingham.
“Of course, nutritional approaches are very important, not only for weight but also for general health-related reasons,” said Garvey, lead author of the 2016 American Association of Clinical Endocrinologists obesity guidelines. “We’ve seen that the Mediterranean and some plant-based diets can prevent progression from prediabetes to diabetes and improve other parameters that reflect metabolic health.”
However, it’s “not common that patients can follow these diets, lose weight, and keep it off,” Garvey cautioned. Up to 50% of weight that’s lost through lifestyle changes is typically regained by 1-year follow-up, with almost all remaining lost weight subsequently regained in the majority of individuals because the person “has to fight against pathophysiological process that drive weight regain,” he noted.
Weight-loss medications can address these pathophysiologic processes by “addressing interactions of satiety hormones with feeding centers in the brain, suppressing the appetite, and making it easier for patients to adhere to a reduced-calorie diet.”
Garvey views the weight-loss medications in the same light as drugs for diabetes and hypertension, in that people need to keep taking them to sustain the benefit.
There’s still a role for bariatric surgery because not everyone can tolerate the AOMs or achieve sufficient weight loss.
“Patients with very high BMI who have trouble ambulating might benefit from a combination of bariatric surgery and medication,” Garvey said.
While some side effects are associated with AOMs, being an “alarmist” about them can be detrimental to patients, he warned.
Rahman and Tovar are authors of books about weight loss. Reddy reported no relevant financial relationships. Garvey is a consultant on advisory boards for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Pfizer, Fractyl Health, Alnylam Pharmaceuticals, Inogen, Zealand, Allurion, Carmot/Roche, Terns Pharmaceuticals, Neurocrine, Keros Therapeutics, and Regeneron. He is the site principal investigator for multi-centered clinical trials sponsored by his university and funded by Novo Nordisk, Eli Lilly, Epitomee, Neurovalens, and Pfizer. He serves as a consultant on the advisory board for the nonprofit Milken Foundation and is a member of the Data Monitoring Committee for phase 3 clinical trials conducted by Boehringer-Ingelheim and Eli Lilly.
A version of this article first appeared on Medscape.com.
Given that more than 100 million US adults have obesity, including 22 million with severe obesity, physicians regularly see patients with the condition in their practices.
Fortunately, doctors have more tools than ever to help their patients. But the question remains: Which method is the safest and most effective? Is it diet and lifestyle changes, one of the recently approved anti-obesity medications (AOMs), bariatric surgery, or a combination approach?
There are no head-to-head trials comparing these three approaches, said Vanita Rahman, MD, clinic director of the Barnard Medical Center, Washington, DC, at the International Conference on Nutrition in Medicine, sponsored by the Physicians Committee for Responsible Medicine.
Instead, doctors must evaluate the merits and drawbacks of each intervention and decide with their patients which treatment is best for them, she told Medscape Medical News. When she sees patients, Rahman shares the pertinent research with them, so they are able to make an informed choice.
Looking at the Options
In her presentation at the conference, Rahman summarized the guidelines issued by the American Heart Association/American College of Cardiology/The Obesity Society for Management of Overweight and Obesity in Adults and the American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines For Medical Care of Patients with Obesity, including lifestyle changes, AOMs, and bariatric surgery (Table 1).
As shown, the current clinical guidelines offer recommendations that consider such factors as the patient’s BMI and presence of one or more comorbidities. Generally, they begin with lifestyle changes for people with overweight, the possibility of an AOM for those with obesity, and bariatric surgery as an option for those with severe obesity-related complications.
“In obesity, we traditionally thought the process was ‘either-or’ — either lifestyle or surgery or medication — and somehow lifestyle is better,” Sheethal Reddy, PhD, a psychologist at the Bariatric Center at Emory University Hospital Midtown, Atlanta, told Medscape Medical News.
Now physicians often use a combination of methods, but lifestyle is foundational to all of them, she said.
“If you don’t make lifestyle changes, none of the approaches will ultimately be effective,” said Reddy, who also is an assistant professor in the Division of General and GI Surgery at Emory School of Medicine, Atlanta.
Lifestyle changes don’t just involve diet and nutrition but include physical exercise.
“Being sedentary affects everything — sleep quality, appetite regulation, and metabolism. Without sufficient exercise, the body isn’t functioning well enough to have a healthy metabolism,” Reddy said.
How Durable Are the Interventions?
Although bariatric surgery has demonstrated effectiveness in helping patients lose weight, many of them regain some or most of it, Rahman said.
A systematic review and meta-analysis found weight regain in 49% of patients who underwent bariatric surgery patients, with the highest prevalence after Roux-en-Y gastric bypass.
Another study of approximately 45,000 patients who underwent bariatric surgery found differences not only in the percentage of total weight loss among Roux-en-Y gastric bypass, sleeve gastrectomy, and adjustable gastric band procedures but also in how much of that weight stayed off between 1 and 5 years following the procedure (Table 2).
Weight regain also is a risk with AOMs, if they’re discontinued.
The STEP 1 trial tested the effectiveness of semaglutide — a glucagon-like peptide 1 (GLP-1) receptor agonist — as an adjunct to lifestyle intervention for weight loss in patients with obesity or with overweight and at least one comorbidity but not diabetes. Mean weight loss with semaglutide was 17.3% but that figure dropped 11.6 percentage points after treatment was discontinued.
Other studies also have found that patients regain weight after GLP-1 discontinuation.
Tirzepatide, a GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) combination, has shown efficacy with weight reduction, but patients experienced some weight regain upon discontinuation. In one study, patients experienced a mean weight loss of 20.9% after 36 weeks of tirzepatide. In the study’s subsequent 52-week double-blind, placebo-controlled period, patients who stopped taking the medication experienced a weight regain of 14%, whereas those who remained on the medication lost an additional 5.5% of weight.
GLP-1 and GLP-1/GIP medications do not address the factors that contribute to overweight and obesity, Rahman said. “They simply suppress the appetite; therefore, weight gain occurs after stopping them.”
Patients may stop taking anti-obesity drugs for a variety of reasons, including side effects. Rahman noted that the common side effects include nausea, vomiting, and constipation, whereas rare side effects include gastroparesis, gallbladder and biliary disease, thyroid cancer, and suicidal thoughts. GLP-1 and GLP-1/GIP medications also carry a risk for non-arteritic anterior ischemic optic neuropathy, she said.
Moreover, health insurance does not always cover these medications, which likely affects patient access to the drugs and compliance rates.
“Given the side effects and frequent lack of insurance coverage, significant questions remain about long-term safety and feasibility of these agents,” Rahman said.
What About Nutritional Approaches?
The lifestyle interventions in the semaglutide and tirzepatide studies included 500 kcal/d deficit diets, which is difficult for people to maintain, noted Rahman, who is the author of the book Simply Plant Based: Fabulous Food for a Healthy Life.
Additionally, bariatric surgery has been associated with long-term micronutrient deficiencies, including deficiencies in vitamins A, D, E, K, B1, and B12, as well as folate, iron, zinc, copper, selenium, and calcium, she said.
The best approach to food from a patient compliance standpoint and to avoid nutrient deficiencies is a whole-food, plant-based diet, Rahman said. She advocates this nutritional approach, along with physical activity, for patients regardless of whether they’ve selected lifestyle intervention alone or combined with an AOM or bariatric surgery to address obesity.
Rahman cited a 5-year heart disease study comparing an intensive lifestyle program involving a vegetarian diet, aerobic exercise, stress management training, smoking cessation, and group psychosocial support to treatment as usual. Patients in the lifestyle group lost 10.9 kg at 1 year and sustained weight loss of 5.8 kg at 5 years, whereas weight in the control group remained relatively unchanged from baseline.
She also pointed to the findings of a study of patients with obesity or with overweight and at least one comorbidity that compared standard care with a low-fat, whole-food, plant-based diet with vitamin B12 supplementation. At 6 months, mean BMI reduction was greater in the intervention group than the standard care group (−4.4 vs −0.4).
In her practice, Rahman has seen the benefits of a whole-food, plant-based diet for patients with obesity.
If people are committed to this type of dietary approach and are given the tools and resources to do it effectively, “their thinking changes, their taste buds change, and they grow to enjoy this new way of eating,” she said. “They see results, and it’s a lifestyle that can be sustained long-term.”
Addressing Drivers of Weight Gain
Patients also need help addressing the various factors that may contribute to overweight and obesity, including overconsumption of ultra-processed foods, substandard nutritional quality of restaurant foods, increasing portion sizes, distraction during eating, emotional eating, late-night eating, and cultural/traditional values surrounding food, Rahman noted.
Supatra Tovar, PsyD, RD, a clinical psychologist with a practice in Pasadena, California, agreed that identifying the reasons for weight gain is critical for treatment.
“If you’re not addressing underlying issues, such as a person’s relationship with food, behaviors around food, the tendency to mindlessly eat or emotionally eat or eat to seek comfort, the person’s weight problems won’t ultimately be fully solved by any of the three approaches — dieting, medications, or bariatric surgery,” she said.
Some of her patients “engage in extreme dieting and deprivation, and many who use medications or have had bariatric surgery hardly eat and often develop nutritional deficiencies,” said Tovar, author of the book Deprogram Diet Culture: Rethink Your Relationship with Food, Heal Your Mind, and Live a Diet-Free Life.
The key to healthy and sustained weight loss is to “become attuned to the body’s signals, learn how to honor hunger, stop eating when satisfied, and eat more healthful foods, such as fruits and vegetables, whole grains, lean proteins — especially plant-based proteins — and the body gives signals that this is what it wants,” she said.
Tovar doesn’t give her clients a specific diet or set of portions.
“I teach them to listen to their bodies,” she said. “They’ve lost significant amounts of weight and continued to keep it off because they’ve done this kind of work.”
When Lifestyle Changes Aren’t Enough
For many patients, lifestyle interventions are insufficient to address the degree of overweight and obesity and common comorbidities, said W. Timothy Garvey, MD, associate director and professor, Department of Nutrition Sciences, School of Health Professions, University of Alabama at Birmingham.
“Of course, nutritional approaches are very important, not only for weight but also for general health-related reasons,” said Garvey, lead author of the 2016 American Association of Clinical Endocrinologists obesity guidelines. “We’ve seen that the Mediterranean and some plant-based diets can prevent progression from prediabetes to diabetes and improve other parameters that reflect metabolic health.”
However, it’s “not common that patients can follow these diets, lose weight, and keep it off,” Garvey cautioned. Up to 50% of weight that’s lost through lifestyle changes is typically regained by 1-year follow-up, with almost all remaining lost weight subsequently regained in the majority of individuals because the person “has to fight against pathophysiological process that drive weight regain,” he noted.
Weight-loss medications can address these pathophysiologic processes by “addressing interactions of satiety hormones with feeding centers in the brain, suppressing the appetite, and making it easier for patients to adhere to a reduced-calorie diet.”
Garvey views the weight-loss medications in the same light as drugs for diabetes and hypertension, in that people need to keep taking them to sustain the benefit.
There’s still a role for bariatric surgery because not everyone can tolerate the AOMs or achieve sufficient weight loss.
“Patients with very high BMI who have trouble ambulating might benefit from a combination of bariatric surgery and medication,” Garvey said.
While some side effects are associated with AOMs, being an “alarmist” about them can be detrimental to patients, he warned.
Rahman and Tovar are authors of books about weight loss. Reddy reported no relevant financial relationships. Garvey is a consultant on advisory boards for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Pfizer, Fractyl Health, Alnylam Pharmaceuticals, Inogen, Zealand, Allurion, Carmot/Roche, Terns Pharmaceuticals, Neurocrine, Keros Therapeutics, and Regeneron. He is the site principal investigator for multi-centered clinical trials sponsored by his university and funded by Novo Nordisk, Eli Lilly, Epitomee, Neurovalens, and Pfizer. He serves as a consultant on the advisory board for the nonprofit Milken Foundation and is a member of the Data Monitoring Committee for phase 3 clinical trials conducted by Boehringer-Ingelheim and Eli Lilly.
A version of this article first appeared on Medscape.com.
Are Patients On GLP-1s Getting the Right Nutrients?
As the use of glucagon-like peptide 1 receptor agonists (GLP-1 RAs) continues to exponentially expand obesity treatment, concerns have arisen regarding their impact on nutrition in people who take them.
While the medications’ dampening effects on appetite result in an average weight reduction ≥ 15%, they also pose a risk for malnutrition.
“It’s important to eat a balanced diet when taking these medications,” Deena Adimoolam, MD, an endocrinologist based in New York City and a member of the national advisory committees for the Endocrine Society and the American Diabetes Association, said in an interview.
The decreased caloric intake resulting from the use of GLP-1 RAs makes it essential for patients to consume nutrient-dense foods. Clinicians can help patients achieve a healthy diet by anticipating nutrition problems, advising them on recommended target ranges of nutrient intake, and referring them for appropriate counseling.
Where to Begin
The task begins with “setting the right expectations before the patient starts treatment,” said Scott Isaacs, MD, president-elect of the American Association of Clinical Endocrinology.
To that end, it’s important to explain to patients how the medications affect appetite and how to adapt. GLP-1 RAs don’t completely turn off the appetite, and the effect at the beginning will likely be very mild, Isaacs said in an interview.
Some patients don’t notice a change for 2-3 months, although others see an effect sooner.
“Typically, people will notice that the main impact is on satiation, meaning they’ll fill up more quickly,” said Isaacs, who is an adjunct associate professor at Emory University School of Medicine, Atlanta, Georgia. “It’s important to tell them to stop eating when they feel full because eating when full can increase the side effects, such as nausea, vomiting, diarrhea, and constipation.”
A review article, written by lead author Jaime Almandoz, MD, University of Texas Southwestern Medical Center, Dallas, in Obesity offers a “5 A’s model” as a guide on how to begin discussing overweight or obesity with patients. This involves asking for permission to discuss weight and asking about food and vitamin/supplement intake; assessing the patient’s medical history and root causes of obesity, and conducting a physical examination; advising the patient regarding treatment options and reasonable expectations; agreeing on treatment and lifestyle goals; and assisting the patient to address challenges, referring them as needed to for additional support (eg, a dietitian), as well as arranging for follow-up.
Impact of GLP-1 RAs on Food Preferences
Besides reducing hunger and increasing satiety, GLP-1 RAs may affect food preferences, according to a research review published in The International Journal of Obesity. It cites a 2014 study that found that people taking GLP-1 RAs displayed decreased neuronal responses to images of food measured by functional magnetic resonance imaging in the areas of brain associated with appetite and reward. This might affect taste preferences and food intake.
Additionally, a 2023 study suggested that during the weight-loss phase of treatment (as opposed to the maintenance phase), patients may experience reduced cravings for dairy and starchy food, less desire to eat salty or spicy foods, and less difficulty controlling eating and resisting cravings.
“Altered food preferences, decreased food cravings, and reduced food intake may contribute to long-term weight loss,” according to the research review. Tailored treatments focusing on the weight maintenance phase are needed, the authors wrote.
Are Patients Vulnerable to Malnutrition?
A recent review found that total caloric intake was reduced by 16%-39% in patients taking a GLP-1 RA or dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA, but few studies evaluated the composition of these patients’ diets. Research that examines the qualitative changes in macronutrient and micronutrient intake of patients on these medications is needed, the authors wrote.
They outlined several nutritional concerns, including whether GLP-1 RA or GIP/ GLP-1 RA use could result in protein intake insufficient for maintaining muscle strength, mass, and function or in inadequate dietary quality (ie, poor intake of micronutrients, fiber, and fluid).
“Although we don’t necessarily see ‘malnutrition’ in our practice, we do see patients who lose too much weight after months and months of treatment, patients who aren’t hungry and don’t eat all day and have one big meal at the end of the day because they don’t feel like eating, and people who continue to eat unhealthy foods,” Isaacs said.
Some patients, however, have medical histories placing them at a greater risk for malnutrition. “Identification of these individuals may help prevent more serious nutritional and medical complications that might occur with decreased food intake associated with AOMs [anti-obesity medications],” Almandoz and colleagues noted in their review.
What Should Patients Eat?
Nutritional needs vary based on the patient’s age, sex, body weight, physical activity, and other factors, Almandoz and colleagues wrote. For this reason, energy intake during weight loss should be “personalized.”
The authors also recommended specific sources of the various dietary components and noted red flags signaling potential deficiencies
Nutritional needs vary based on the degree of appetite suppression in the patient, Adimoolam said. “I recommend at least two servings of fruits and vegetables daily, and drinking plenty of water throughout the day,” she added.
Protein in particular is a “key macronutrient,” and insufficient intake can lead to a variety of adverse effects, including sarcopenia — which is already a concern in individuals being treated with GLP-1 RAs. Meal replacement products (eg, shakes or bars) can supplement diets to help meet protein needs, especially if appetite is significantly reduced.
“There are definitely concerns for sarcopenia, so we have our patients taking these drugs try to eat healthy lean proteins – 100 g/d — and exercise,” Isaacs said. Exercise, including resistance training, not only improves muscle mass but also potentiates the effects of the GLP-1 RAs in patients with obesity and type 2 diabetes.
Adequate hydration is essential for patients taking GLP-1 RAs. “One of the commonly described side effects is fatigue, but there’s no biological reason why these medications should cause fatigue. My opinion is that these patients are dehydrated, and that may be causing the fatigue,” Isaacs said.
Some patients taking GLP-1 RAs lose interest in food. Isaacs regarded this as an “adverse reaction to the medication, which necessitates either stopping it altogether, changing the dose, or adjusting the diet.” There are “many different solutions, and one size doesn’t fit all,” he said.
Dietary and Behavioral Counseling
The drugs don’t necessarily motivate a person to eat healthier food, only to eat less food, Isaacs noted.
“The person might be eating low-volume but high-calorie food, such as bag of chips or a cookie instead of an apple,” Isaacs said. Patients who are losing weight “may not realize that weight loss isn’t the only important outcome. Because they’re losing weight, they think it’s okay to eat junk food.”
Patients need education and guidance about how to eat while on these medications. Most patients find counseling about meal planning helpful, he said.
Isaacs gives nutritional guidance to his patients when he prescribes a weight loss medication. “But most physicians don’t have time to offer that type of specific counseling on an ongoing basis,” he said. Isaacs refers patients requiring more detailed and long-term guidance to a dietitian.
Patients with monotonous diets of poor quality are at increased risk for nutrition deficiencies, and counseling by a registered dietitian could help improve their dietary quality.
Registered dietitians can develop a multifaceted approach not only focusing on medication management but also on customizing the patient’s diet, assisting with lifestyle adjustments, and addressing the mental health issues surrounding obesity and its management.
People seeking obesity treatment often have psychiatric conditions, psychological distress, or disordered eating patterns, and questions and concerns have emerged about how GLP-1 RA use might affect existing mental health problems. For example, if the medication suppresses the feeling of gratification a person once got from eating high-energy dense foods, that individual may “seek rewards or pleasure elsewhere, and possibly from unhealthy sources.”
Psychological issues also may emerge as a result of weight loss, so it’s helpful to take a multidisciplinary approach that includes mental health practitioners to support patients who are being treated with GLP-1 RAs. Patients taking these agents should be monitored for the emergence or worsening of psychiatric conditions, such as depression and suicidal ideation.
Achieving significant weight loss may lead to “unexpected changes” in the dynamics of patients’ relationship with others, “which can be distressing.” Clinicians should be “sensitive to patients’ social and emotional needs” and provide support or refer patients for help with coping strategies.
GLP-1 RAs have enormous potential to improve health outcomes in patients with obesity. Careful patient selection, close monitoring, and support for patients with nutrition and other lifestyle issues can increase the chances that these agents will fulfill their potential.
Isaacs declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
As the use of glucagon-like peptide 1 receptor agonists (GLP-1 RAs) continues to exponentially expand obesity treatment, concerns have arisen regarding their impact on nutrition in people who take them.
While the medications’ dampening effects on appetite result in an average weight reduction ≥ 15%, they also pose a risk for malnutrition.
“It’s important to eat a balanced diet when taking these medications,” Deena Adimoolam, MD, an endocrinologist based in New York City and a member of the national advisory committees for the Endocrine Society and the American Diabetes Association, said in an interview.
The decreased caloric intake resulting from the use of GLP-1 RAs makes it essential for patients to consume nutrient-dense foods. Clinicians can help patients achieve a healthy diet by anticipating nutrition problems, advising them on recommended target ranges of nutrient intake, and referring them for appropriate counseling.
Where to Begin
The task begins with “setting the right expectations before the patient starts treatment,” said Scott Isaacs, MD, president-elect of the American Association of Clinical Endocrinology.
To that end, it’s important to explain to patients how the medications affect appetite and how to adapt. GLP-1 RAs don’t completely turn off the appetite, and the effect at the beginning will likely be very mild, Isaacs said in an interview.
Some patients don’t notice a change for 2-3 months, although others see an effect sooner.
“Typically, people will notice that the main impact is on satiation, meaning they’ll fill up more quickly,” said Isaacs, who is an adjunct associate professor at Emory University School of Medicine, Atlanta, Georgia. “It’s important to tell them to stop eating when they feel full because eating when full can increase the side effects, such as nausea, vomiting, diarrhea, and constipation.”
A review article, written by lead author Jaime Almandoz, MD, University of Texas Southwestern Medical Center, Dallas, in Obesity offers a “5 A’s model” as a guide on how to begin discussing overweight or obesity with patients. This involves asking for permission to discuss weight and asking about food and vitamin/supplement intake; assessing the patient’s medical history and root causes of obesity, and conducting a physical examination; advising the patient regarding treatment options and reasonable expectations; agreeing on treatment and lifestyle goals; and assisting the patient to address challenges, referring them as needed to for additional support (eg, a dietitian), as well as arranging for follow-up.
Impact of GLP-1 RAs on Food Preferences
Besides reducing hunger and increasing satiety, GLP-1 RAs may affect food preferences, according to a research review published in The International Journal of Obesity. It cites a 2014 study that found that people taking GLP-1 RAs displayed decreased neuronal responses to images of food measured by functional magnetic resonance imaging in the areas of brain associated with appetite and reward. This might affect taste preferences and food intake.
Additionally, a 2023 study suggested that during the weight-loss phase of treatment (as opposed to the maintenance phase), patients may experience reduced cravings for dairy and starchy food, less desire to eat salty or spicy foods, and less difficulty controlling eating and resisting cravings.
“Altered food preferences, decreased food cravings, and reduced food intake may contribute to long-term weight loss,” according to the research review. Tailored treatments focusing on the weight maintenance phase are needed, the authors wrote.
Are Patients Vulnerable to Malnutrition?
A recent review found that total caloric intake was reduced by 16%-39% in patients taking a GLP-1 RA or dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA, but few studies evaluated the composition of these patients’ diets. Research that examines the qualitative changes in macronutrient and micronutrient intake of patients on these medications is needed, the authors wrote.
They outlined several nutritional concerns, including whether GLP-1 RA or GIP/ GLP-1 RA use could result in protein intake insufficient for maintaining muscle strength, mass, and function or in inadequate dietary quality (ie, poor intake of micronutrients, fiber, and fluid).
“Although we don’t necessarily see ‘malnutrition’ in our practice, we do see patients who lose too much weight after months and months of treatment, patients who aren’t hungry and don’t eat all day and have one big meal at the end of the day because they don’t feel like eating, and people who continue to eat unhealthy foods,” Isaacs said.
Some patients, however, have medical histories placing them at a greater risk for malnutrition. “Identification of these individuals may help prevent more serious nutritional and medical complications that might occur with decreased food intake associated with AOMs [anti-obesity medications],” Almandoz and colleagues noted in their review.
What Should Patients Eat?
Nutritional needs vary based on the patient’s age, sex, body weight, physical activity, and other factors, Almandoz and colleagues wrote. For this reason, energy intake during weight loss should be “personalized.”
The authors also recommended specific sources of the various dietary components and noted red flags signaling potential deficiencies
Nutritional needs vary based on the degree of appetite suppression in the patient, Adimoolam said. “I recommend at least two servings of fruits and vegetables daily, and drinking plenty of water throughout the day,” she added.
Protein in particular is a “key macronutrient,” and insufficient intake can lead to a variety of adverse effects, including sarcopenia — which is already a concern in individuals being treated with GLP-1 RAs. Meal replacement products (eg, shakes or bars) can supplement diets to help meet protein needs, especially if appetite is significantly reduced.
“There are definitely concerns for sarcopenia, so we have our patients taking these drugs try to eat healthy lean proteins – 100 g/d — and exercise,” Isaacs said. Exercise, including resistance training, not only improves muscle mass but also potentiates the effects of the GLP-1 RAs in patients with obesity and type 2 diabetes.
Adequate hydration is essential for patients taking GLP-1 RAs. “One of the commonly described side effects is fatigue, but there’s no biological reason why these medications should cause fatigue. My opinion is that these patients are dehydrated, and that may be causing the fatigue,” Isaacs said.
Some patients taking GLP-1 RAs lose interest in food. Isaacs regarded this as an “adverse reaction to the medication, which necessitates either stopping it altogether, changing the dose, or adjusting the diet.” There are “many different solutions, and one size doesn’t fit all,” he said.
Dietary and Behavioral Counseling
The drugs don’t necessarily motivate a person to eat healthier food, only to eat less food, Isaacs noted.
“The person might be eating low-volume but high-calorie food, such as bag of chips or a cookie instead of an apple,” Isaacs said. Patients who are losing weight “may not realize that weight loss isn’t the only important outcome. Because they’re losing weight, they think it’s okay to eat junk food.”
Patients need education and guidance about how to eat while on these medications. Most patients find counseling about meal planning helpful, he said.
Isaacs gives nutritional guidance to his patients when he prescribes a weight loss medication. “But most physicians don’t have time to offer that type of specific counseling on an ongoing basis,” he said. Isaacs refers patients requiring more detailed and long-term guidance to a dietitian.
Patients with monotonous diets of poor quality are at increased risk for nutrition deficiencies, and counseling by a registered dietitian could help improve their dietary quality.
Registered dietitians can develop a multifaceted approach not only focusing on medication management but also on customizing the patient’s diet, assisting with lifestyle adjustments, and addressing the mental health issues surrounding obesity and its management.
People seeking obesity treatment often have psychiatric conditions, psychological distress, or disordered eating patterns, and questions and concerns have emerged about how GLP-1 RA use might affect existing mental health problems. For example, if the medication suppresses the feeling of gratification a person once got from eating high-energy dense foods, that individual may “seek rewards or pleasure elsewhere, and possibly from unhealthy sources.”
Psychological issues also may emerge as a result of weight loss, so it’s helpful to take a multidisciplinary approach that includes mental health practitioners to support patients who are being treated with GLP-1 RAs. Patients taking these agents should be monitored for the emergence or worsening of psychiatric conditions, such as depression and suicidal ideation.
Achieving significant weight loss may lead to “unexpected changes” in the dynamics of patients’ relationship with others, “which can be distressing.” Clinicians should be “sensitive to patients’ social and emotional needs” and provide support or refer patients for help with coping strategies.
GLP-1 RAs have enormous potential to improve health outcomes in patients with obesity. Careful patient selection, close monitoring, and support for patients with nutrition and other lifestyle issues can increase the chances that these agents will fulfill their potential.
Isaacs declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
As the use of glucagon-like peptide 1 receptor agonists (GLP-1 RAs) continues to exponentially expand obesity treatment, concerns have arisen regarding their impact on nutrition in people who take them.
While the medications’ dampening effects on appetite result in an average weight reduction ≥ 15%, they also pose a risk for malnutrition.
“It’s important to eat a balanced diet when taking these medications,” Deena Adimoolam, MD, an endocrinologist based in New York City and a member of the national advisory committees for the Endocrine Society and the American Diabetes Association, said in an interview.
The decreased caloric intake resulting from the use of GLP-1 RAs makes it essential for patients to consume nutrient-dense foods. Clinicians can help patients achieve a healthy diet by anticipating nutrition problems, advising them on recommended target ranges of nutrient intake, and referring them for appropriate counseling.
Where to Begin
The task begins with “setting the right expectations before the patient starts treatment,” said Scott Isaacs, MD, president-elect of the American Association of Clinical Endocrinology.
To that end, it’s important to explain to patients how the medications affect appetite and how to adapt. GLP-1 RAs don’t completely turn off the appetite, and the effect at the beginning will likely be very mild, Isaacs said in an interview.
Some patients don’t notice a change for 2-3 months, although others see an effect sooner.
“Typically, people will notice that the main impact is on satiation, meaning they’ll fill up more quickly,” said Isaacs, who is an adjunct associate professor at Emory University School of Medicine, Atlanta, Georgia. “It’s important to tell them to stop eating when they feel full because eating when full can increase the side effects, such as nausea, vomiting, diarrhea, and constipation.”
A review article, written by lead author Jaime Almandoz, MD, University of Texas Southwestern Medical Center, Dallas, in Obesity offers a “5 A’s model” as a guide on how to begin discussing overweight or obesity with patients. This involves asking for permission to discuss weight and asking about food and vitamin/supplement intake; assessing the patient’s medical history and root causes of obesity, and conducting a physical examination; advising the patient regarding treatment options and reasonable expectations; agreeing on treatment and lifestyle goals; and assisting the patient to address challenges, referring them as needed to for additional support (eg, a dietitian), as well as arranging for follow-up.
Impact of GLP-1 RAs on Food Preferences
Besides reducing hunger and increasing satiety, GLP-1 RAs may affect food preferences, according to a research review published in The International Journal of Obesity. It cites a 2014 study that found that people taking GLP-1 RAs displayed decreased neuronal responses to images of food measured by functional magnetic resonance imaging in the areas of brain associated with appetite and reward. This might affect taste preferences and food intake.
Additionally, a 2023 study suggested that during the weight-loss phase of treatment (as opposed to the maintenance phase), patients may experience reduced cravings for dairy and starchy food, less desire to eat salty or spicy foods, and less difficulty controlling eating and resisting cravings.
“Altered food preferences, decreased food cravings, and reduced food intake may contribute to long-term weight loss,” according to the research review. Tailored treatments focusing on the weight maintenance phase are needed, the authors wrote.
Are Patients Vulnerable to Malnutrition?
A recent review found that total caloric intake was reduced by 16%-39% in patients taking a GLP-1 RA or dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA, but few studies evaluated the composition of these patients’ diets. Research that examines the qualitative changes in macronutrient and micronutrient intake of patients on these medications is needed, the authors wrote.
They outlined several nutritional concerns, including whether GLP-1 RA or GIP/ GLP-1 RA use could result in protein intake insufficient for maintaining muscle strength, mass, and function or in inadequate dietary quality (ie, poor intake of micronutrients, fiber, and fluid).
“Although we don’t necessarily see ‘malnutrition’ in our practice, we do see patients who lose too much weight after months and months of treatment, patients who aren’t hungry and don’t eat all day and have one big meal at the end of the day because they don’t feel like eating, and people who continue to eat unhealthy foods,” Isaacs said.
Some patients, however, have medical histories placing them at a greater risk for malnutrition. “Identification of these individuals may help prevent more serious nutritional and medical complications that might occur with decreased food intake associated with AOMs [anti-obesity medications],” Almandoz and colleagues noted in their review.
What Should Patients Eat?
Nutritional needs vary based on the patient’s age, sex, body weight, physical activity, and other factors, Almandoz and colleagues wrote. For this reason, energy intake during weight loss should be “personalized.”
The authors also recommended specific sources of the various dietary components and noted red flags signaling potential deficiencies
Nutritional needs vary based on the degree of appetite suppression in the patient, Adimoolam said. “I recommend at least two servings of fruits and vegetables daily, and drinking plenty of water throughout the day,” she added.
Protein in particular is a “key macronutrient,” and insufficient intake can lead to a variety of adverse effects, including sarcopenia — which is already a concern in individuals being treated with GLP-1 RAs. Meal replacement products (eg, shakes or bars) can supplement diets to help meet protein needs, especially if appetite is significantly reduced.
“There are definitely concerns for sarcopenia, so we have our patients taking these drugs try to eat healthy lean proteins – 100 g/d — and exercise,” Isaacs said. Exercise, including resistance training, not only improves muscle mass but also potentiates the effects of the GLP-1 RAs in patients with obesity and type 2 diabetes.
Adequate hydration is essential for patients taking GLP-1 RAs. “One of the commonly described side effects is fatigue, but there’s no biological reason why these medications should cause fatigue. My opinion is that these patients are dehydrated, and that may be causing the fatigue,” Isaacs said.
Some patients taking GLP-1 RAs lose interest in food. Isaacs regarded this as an “adverse reaction to the medication, which necessitates either stopping it altogether, changing the dose, or adjusting the diet.” There are “many different solutions, and one size doesn’t fit all,” he said.
Dietary and Behavioral Counseling
The drugs don’t necessarily motivate a person to eat healthier food, only to eat less food, Isaacs noted.
“The person might be eating low-volume but high-calorie food, such as bag of chips or a cookie instead of an apple,” Isaacs said. Patients who are losing weight “may not realize that weight loss isn’t the only important outcome. Because they’re losing weight, they think it’s okay to eat junk food.”
Patients need education and guidance about how to eat while on these medications. Most patients find counseling about meal planning helpful, he said.
Isaacs gives nutritional guidance to his patients when he prescribes a weight loss medication. “But most physicians don’t have time to offer that type of specific counseling on an ongoing basis,” he said. Isaacs refers patients requiring more detailed and long-term guidance to a dietitian.
Patients with monotonous diets of poor quality are at increased risk for nutrition deficiencies, and counseling by a registered dietitian could help improve their dietary quality.
Registered dietitians can develop a multifaceted approach not only focusing on medication management but also on customizing the patient’s diet, assisting with lifestyle adjustments, and addressing the mental health issues surrounding obesity and its management.
People seeking obesity treatment often have psychiatric conditions, psychological distress, or disordered eating patterns, and questions and concerns have emerged about how GLP-1 RA use might affect existing mental health problems. For example, if the medication suppresses the feeling of gratification a person once got from eating high-energy dense foods, that individual may “seek rewards or pleasure elsewhere, and possibly from unhealthy sources.”
Psychological issues also may emerge as a result of weight loss, so it’s helpful to take a multidisciplinary approach that includes mental health practitioners to support patients who are being treated with GLP-1 RAs. Patients taking these agents should be monitored for the emergence or worsening of psychiatric conditions, such as depression and suicidal ideation.
Achieving significant weight loss may lead to “unexpected changes” in the dynamics of patients’ relationship with others, “which can be distressing.” Clinicians should be “sensitive to patients’ social and emotional needs” and provide support or refer patients for help with coping strategies.
GLP-1 RAs have enormous potential to improve health outcomes in patients with obesity. Careful patient selection, close monitoring, and support for patients with nutrition and other lifestyle issues can increase the chances that these agents will fulfill their potential.
Isaacs declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
Can GLP-1s Reduce Alzheimer’s Disease Risk?
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
How Does End of Life Impact Diabetes Care?
TOPLINE:
Among older adults with type 2 diabetes (T2D), the use of antidiabetes medications declined in the last year before death, with notable shifts from metformin and sulfonylureas toward insulin therapy.
METHODOLOGY:
Current recommendations emphasize a more liberal approach to glycemic control in people with a high burden of comorbidities and shorter life expectancy, but little is known about the changes and discontinuation patterns of diabetes medications among older adults near the end of life.
.
All medication classes available during the study period were considered, including short-acting and long-acting insulins, metformin, sulfonylureas, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide 1 (GLP-1) receptor agonists, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and other medications.
Analysis included temporal trends in prescribing antidiabetes medications, stratified by frailty using a validated claims-based frailty index, with scores ≥ 0.30 indicating higher frailty.
Antidiabetes medication fills were assessed within 1 year before death, examining changes across three time periods: 12 to 8 months, 8 to 4 months, and 4 to 0 months before death.
TAKEAWAY:
The proportion of older patients receiving antidiabetes medications increased slightly from 71.4% in 2015 to 72.9% in 2019, with metformin showing the largest increase from 40.7% to 46.5% (standardized mean difference [SMD], −0.12) and sulfonylureas showing the largest decrease from 37.0% to 31.8% (SMD, 0.11).
The use of newer diabetes medications with cardiovascular benefits, such as GLP-1 receptor agonists and SGLT2 inhibitors, remained less common but showed increasing trends over time.
The use of any antidiabetes medication decreased from 66.1% in the 9 to 12 months before death to 60.8% in the last 4 months of life (P < .01), primarily due to the reduced use of metformin and sulfonylureas.
The use of both short-acting and long-acting insulin agents increased toward the end of life (from 28.0% to 32.9% and from 41.2% to 43.9%, respectively; both P < .001) , particularly among frailer individuals.
IN PRACTICE:
“[The study] findings underscore important implications for diabetes management in patients nearing the end of life. With ~70% of patients with T2D using at least one antidiabetes medication, there is a need to consider further de-escalation or deprescribing in this vulnerable population,” the authors wrote.
SOURCE:
The study was led by Alexander Kutz, MD, MPH, MSc, Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, and was published online in Diabetes Care.
LIMITATIONS:
The study lacked details on the reasons for changes in medication patterns, making it unclear whether these changes were due to clinical guidelines or to reduce adverse events. Moreover, the study could not capture transitions or substitutions between medications, information on the dosage data, and causes of death.
DISCLOSURES:
This study was supported by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School. Some authors reported receiving personal fees or research grants from the National Institutes of Health and other institutions and a few pharmaceutical companies. One author reported acting as a principal investigator and receiving a research grant from Boehringer-Ingelheim, unrelated to the work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Among older adults with type 2 diabetes (T2D), the use of antidiabetes medications declined in the last year before death, with notable shifts from metformin and sulfonylureas toward insulin therapy.
METHODOLOGY:
Current recommendations emphasize a more liberal approach to glycemic control in people with a high burden of comorbidities and shorter life expectancy, but little is known about the changes and discontinuation patterns of diabetes medications among older adults near the end of life.
.
All medication classes available during the study period were considered, including short-acting and long-acting insulins, metformin, sulfonylureas, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide 1 (GLP-1) receptor agonists, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and other medications.
Analysis included temporal trends in prescribing antidiabetes medications, stratified by frailty using a validated claims-based frailty index, with scores ≥ 0.30 indicating higher frailty.
Antidiabetes medication fills were assessed within 1 year before death, examining changes across three time periods: 12 to 8 months, 8 to 4 months, and 4 to 0 months before death.
TAKEAWAY:
The proportion of older patients receiving antidiabetes medications increased slightly from 71.4% in 2015 to 72.9% in 2019, with metformin showing the largest increase from 40.7% to 46.5% (standardized mean difference [SMD], −0.12) and sulfonylureas showing the largest decrease from 37.0% to 31.8% (SMD, 0.11).
The use of newer diabetes medications with cardiovascular benefits, such as GLP-1 receptor agonists and SGLT2 inhibitors, remained less common but showed increasing trends over time.
The use of any antidiabetes medication decreased from 66.1% in the 9 to 12 months before death to 60.8% in the last 4 months of life (P < .01), primarily due to the reduced use of metformin and sulfonylureas.
The use of both short-acting and long-acting insulin agents increased toward the end of life (from 28.0% to 32.9% and from 41.2% to 43.9%, respectively; both P < .001) , particularly among frailer individuals.
IN PRACTICE:
“[The study] findings underscore important implications for diabetes management in patients nearing the end of life. With ~70% of patients with T2D using at least one antidiabetes medication, there is a need to consider further de-escalation or deprescribing in this vulnerable population,” the authors wrote.
SOURCE:
The study was led by Alexander Kutz, MD, MPH, MSc, Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, and was published online in Diabetes Care.
LIMITATIONS:
The study lacked details on the reasons for changes in medication patterns, making it unclear whether these changes were due to clinical guidelines or to reduce adverse events. Moreover, the study could not capture transitions or substitutions between medications, information on the dosage data, and causes of death.
DISCLOSURES:
This study was supported by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School. Some authors reported receiving personal fees or research grants from the National Institutes of Health and other institutions and a few pharmaceutical companies. One author reported acting as a principal investigator and receiving a research grant from Boehringer-Ingelheim, unrelated to the work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Among older adults with type 2 diabetes (T2D), the use of antidiabetes medications declined in the last year before death, with notable shifts from metformin and sulfonylureas toward insulin therapy.
METHODOLOGY:
Current recommendations emphasize a more liberal approach to glycemic control in people with a high burden of comorbidities and shorter life expectancy, but little is known about the changes and discontinuation patterns of diabetes medications among older adults near the end of life.
.
All medication classes available during the study period were considered, including short-acting and long-acting insulins, metformin, sulfonylureas, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide 1 (GLP-1) receptor agonists, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and other medications.
Analysis included temporal trends in prescribing antidiabetes medications, stratified by frailty using a validated claims-based frailty index, with scores ≥ 0.30 indicating higher frailty.
Antidiabetes medication fills were assessed within 1 year before death, examining changes across three time periods: 12 to 8 months, 8 to 4 months, and 4 to 0 months before death.
TAKEAWAY:
The proportion of older patients receiving antidiabetes medications increased slightly from 71.4% in 2015 to 72.9% in 2019, with metformin showing the largest increase from 40.7% to 46.5% (standardized mean difference [SMD], −0.12) and sulfonylureas showing the largest decrease from 37.0% to 31.8% (SMD, 0.11).
The use of newer diabetes medications with cardiovascular benefits, such as GLP-1 receptor agonists and SGLT2 inhibitors, remained less common but showed increasing trends over time.
The use of any antidiabetes medication decreased from 66.1% in the 9 to 12 months before death to 60.8% in the last 4 months of life (P < .01), primarily due to the reduced use of metformin and sulfonylureas.
The use of both short-acting and long-acting insulin agents increased toward the end of life (from 28.0% to 32.9% and from 41.2% to 43.9%, respectively; both P < .001) , particularly among frailer individuals.
IN PRACTICE:
“[The study] findings underscore important implications for diabetes management in patients nearing the end of life. With ~70% of patients with T2D using at least one antidiabetes medication, there is a need to consider further de-escalation or deprescribing in this vulnerable population,” the authors wrote.
SOURCE:
The study was led by Alexander Kutz, MD, MPH, MSc, Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, and was published online in Diabetes Care.
LIMITATIONS:
The study lacked details on the reasons for changes in medication patterns, making it unclear whether these changes were due to clinical guidelines or to reduce adverse events. Moreover, the study could not capture transitions or substitutions between medications, information on the dosage data, and causes of death.
DISCLOSURES:
This study was supported by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School. Some authors reported receiving personal fees or research grants from the National Institutes of Health and other institutions and a few pharmaceutical companies. One author reported acting as a principal investigator and receiving a research grant from Boehringer-Ingelheim, unrelated to the work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Retatrutide Produces Greatest Weight Loss
A systematic review of 26 randomized controlled trials (RCTs) finds that, among glucagon-like peptide 1 (GLP-1) receptor agonists and co-agonists on the market or still being investigated, the experimental drug retatrutide (Eli Lilly) produces the greatest weight loss.
The review, conducted by researchers at McGill University, Montreal, Quebec, Canada, examined three commercially available medications in the class and nine that have not yet received regulatory approval.
In healthy adults with overweight or obesity who did not have diabetes, the highest mean reductions in relative and absolute body weight were achieved with once-weekly triple glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 and glucagon receptor agonist retatrutide, followed by the dual GIP/GLP-1 agonist tirzepatide (Eli Lilly) and lastly by the GLP-1 agonist semaglutide (Novo Nordisk), according to the authors.
The use of all the GLP-1s or co-agonist medications “led to decreased body mass index (BMI), waist circumference, SBP (systolic blood pressure), and DBP (diastolic blood pressure),” wrote the authors in Annals of Internal Medicine. All the medications had a similar safety profile.
The researchers did not find any head-to-head studies, so instead examined the results from 26 RCTs that enrolled more than 15,000 patients. Only trials with a treatment duration of at least 16 weeks were included, to ensure that patients had at least a month of a fixed dose.
Not surprisingly, the review found that, except for semaglutide, trials with “dual and triple agonists generally reported numerically greater mean weight losses than single GLP-1 agonists.”
They caution, however, against drawing conclusions about comparative efficacy, as the populations, control groups, and contexts of the various studies might not be directly comparable. All the trial enrollees also received lifestyle modification along with drug therapy or placebo, but the interventions and protocols varied across the studies.
The authors found that individuals on retatrutide (12-mg once-weekly injection) lost 22% of body weight from baseline after 48 weeks. Tirzepatide (15 mg once-weekly injection) recipients lost almost 18% of body weight after 72 weeks, while those on semaglutide (2.4-mg once-weekly injection) lost about 14% after 68 weeks. Both tirzepatide and semaglutide are commercially available.
Patients taking liraglutide (3-mg once-daily injection), also on the market, lost up to 6% of body weight after 26 weeks.
The authors also examined studies of investigational agents and reported that the greatest loss, aside from retatrutide, was with the dual glucagon/GLP-1 agonists survodutide (Boehringer Ingelheim; 6%-15%) and mazdutide (Innovent Biologics; 7%-11%).
Orforglipron (Eli Lilly), a once-daily pill, produced weight loss of 9%-15%, depending on the dose.
The study found that four investigational drugs did not produce as much weight loss: Beinaglutide (0.2-mg injection three times daily, 6%), efpeglenatide (4- to 8-mg injection once weekly, about 7%), exenatide (10-mcg injection twice daily, 5-kg change in weight), and noiiglutide (once-daily injection, 9%).
The most common adverse events for all GLP-1s were gastrointestinal (GI), such as nausea, diarrhea, constipation, and vomiting. Across all agents, 60%-80% of patients taking the medications experienced a GI adverse event, although most were transient, according to the authors. A total of 6%-26% of patients discontinued treatment as a result of a side effect.
The authors said that no serious GI disorders, such as bowel obstruction or gastroparesis, were reported in any of the 26 trials.
The review also shows that it is likely that GLP-1s would have to be used chronically to have the greatest effect, said the authors. They noted that they found that trials “with longer treatment durations demonstrate similar weight loss results to those with shorter follow-up, reinforcing the idea that continuous treatment may be required.”
One coauthor reported receiving payments or honoraria from Boehringer Ingelheim, Eli Lilly, Janssen Pharmaceuticals, and Novo Nordisk. The study was carried out independently without any grant or other funding.
A version of this article first appeared on Medscape.com.
A systematic review of 26 randomized controlled trials (RCTs) finds that, among glucagon-like peptide 1 (GLP-1) receptor agonists and co-agonists on the market or still being investigated, the experimental drug retatrutide (Eli Lilly) produces the greatest weight loss.
The review, conducted by researchers at McGill University, Montreal, Quebec, Canada, examined three commercially available medications in the class and nine that have not yet received regulatory approval.
In healthy adults with overweight or obesity who did not have diabetes, the highest mean reductions in relative and absolute body weight were achieved with once-weekly triple glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 and glucagon receptor agonist retatrutide, followed by the dual GIP/GLP-1 agonist tirzepatide (Eli Lilly) and lastly by the GLP-1 agonist semaglutide (Novo Nordisk), according to the authors.
The use of all the GLP-1s or co-agonist medications “led to decreased body mass index (BMI), waist circumference, SBP (systolic blood pressure), and DBP (diastolic blood pressure),” wrote the authors in Annals of Internal Medicine. All the medications had a similar safety profile.
The researchers did not find any head-to-head studies, so instead examined the results from 26 RCTs that enrolled more than 15,000 patients. Only trials with a treatment duration of at least 16 weeks were included, to ensure that patients had at least a month of a fixed dose.
Not surprisingly, the review found that, except for semaglutide, trials with “dual and triple agonists generally reported numerically greater mean weight losses than single GLP-1 agonists.”
They caution, however, against drawing conclusions about comparative efficacy, as the populations, control groups, and contexts of the various studies might not be directly comparable. All the trial enrollees also received lifestyle modification along with drug therapy or placebo, but the interventions and protocols varied across the studies.
The authors found that individuals on retatrutide (12-mg once-weekly injection) lost 22% of body weight from baseline after 48 weeks. Tirzepatide (15 mg once-weekly injection) recipients lost almost 18% of body weight after 72 weeks, while those on semaglutide (2.4-mg once-weekly injection) lost about 14% after 68 weeks. Both tirzepatide and semaglutide are commercially available.
Patients taking liraglutide (3-mg once-daily injection), also on the market, lost up to 6% of body weight after 26 weeks.
The authors also examined studies of investigational agents and reported that the greatest loss, aside from retatrutide, was with the dual glucagon/GLP-1 agonists survodutide (Boehringer Ingelheim; 6%-15%) and mazdutide (Innovent Biologics; 7%-11%).
Orforglipron (Eli Lilly), a once-daily pill, produced weight loss of 9%-15%, depending on the dose.
The study found that four investigational drugs did not produce as much weight loss: Beinaglutide (0.2-mg injection three times daily, 6%), efpeglenatide (4- to 8-mg injection once weekly, about 7%), exenatide (10-mcg injection twice daily, 5-kg change in weight), and noiiglutide (once-daily injection, 9%).
The most common adverse events for all GLP-1s were gastrointestinal (GI), such as nausea, diarrhea, constipation, and vomiting. Across all agents, 60%-80% of patients taking the medications experienced a GI adverse event, although most were transient, according to the authors. A total of 6%-26% of patients discontinued treatment as a result of a side effect.
The authors said that no serious GI disorders, such as bowel obstruction or gastroparesis, were reported in any of the 26 trials.
The review also shows that it is likely that GLP-1s would have to be used chronically to have the greatest effect, said the authors. They noted that they found that trials “with longer treatment durations demonstrate similar weight loss results to those with shorter follow-up, reinforcing the idea that continuous treatment may be required.”
One coauthor reported receiving payments or honoraria from Boehringer Ingelheim, Eli Lilly, Janssen Pharmaceuticals, and Novo Nordisk. The study was carried out independently without any grant or other funding.
A version of this article first appeared on Medscape.com.
A systematic review of 26 randomized controlled trials (RCTs) finds that, among glucagon-like peptide 1 (GLP-1) receptor agonists and co-agonists on the market or still being investigated, the experimental drug retatrutide (Eli Lilly) produces the greatest weight loss.
The review, conducted by researchers at McGill University, Montreal, Quebec, Canada, examined three commercially available medications in the class and nine that have not yet received regulatory approval.
In healthy adults with overweight or obesity who did not have diabetes, the highest mean reductions in relative and absolute body weight were achieved with once-weekly triple glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 and glucagon receptor agonist retatrutide, followed by the dual GIP/GLP-1 agonist tirzepatide (Eli Lilly) and lastly by the GLP-1 agonist semaglutide (Novo Nordisk), according to the authors.
The use of all the GLP-1s or co-agonist medications “led to decreased body mass index (BMI), waist circumference, SBP (systolic blood pressure), and DBP (diastolic blood pressure),” wrote the authors in Annals of Internal Medicine. All the medications had a similar safety profile.
The researchers did not find any head-to-head studies, so instead examined the results from 26 RCTs that enrolled more than 15,000 patients. Only trials with a treatment duration of at least 16 weeks were included, to ensure that patients had at least a month of a fixed dose.
Not surprisingly, the review found that, except for semaglutide, trials with “dual and triple agonists generally reported numerically greater mean weight losses than single GLP-1 agonists.”
They caution, however, against drawing conclusions about comparative efficacy, as the populations, control groups, and contexts of the various studies might not be directly comparable. All the trial enrollees also received lifestyle modification along with drug therapy or placebo, but the interventions and protocols varied across the studies.
The authors found that individuals on retatrutide (12-mg once-weekly injection) lost 22% of body weight from baseline after 48 weeks. Tirzepatide (15 mg once-weekly injection) recipients lost almost 18% of body weight after 72 weeks, while those on semaglutide (2.4-mg once-weekly injection) lost about 14% after 68 weeks. Both tirzepatide and semaglutide are commercially available.
Patients taking liraglutide (3-mg once-daily injection), also on the market, lost up to 6% of body weight after 26 weeks.
The authors also examined studies of investigational agents and reported that the greatest loss, aside from retatrutide, was with the dual glucagon/GLP-1 agonists survodutide (Boehringer Ingelheim; 6%-15%) and mazdutide (Innovent Biologics; 7%-11%).
Orforglipron (Eli Lilly), a once-daily pill, produced weight loss of 9%-15%, depending on the dose.
The study found that four investigational drugs did not produce as much weight loss: Beinaglutide (0.2-mg injection three times daily, 6%), efpeglenatide (4- to 8-mg injection once weekly, about 7%), exenatide (10-mcg injection twice daily, 5-kg change in weight), and noiiglutide (once-daily injection, 9%).
The most common adverse events for all GLP-1s were gastrointestinal (GI), such as nausea, diarrhea, constipation, and vomiting. Across all agents, 60%-80% of patients taking the medications experienced a GI adverse event, although most were transient, according to the authors. A total of 6%-26% of patients discontinued treatment as a result of a side effect.
The authors said that no serious GI disorders, such as bowel obstruction or gastroparesis, were reported in any of the 26 trials.
The review also shows that it is likely that GLP-1s would have to be used chronically to have the greatest effect, said the authors. They noted that they found that trials “with longer treatment durations demonstrate similar weight loss results to those with shorter follow-up, reinforcing the idea that continuous treatment may be required.”
One coauthor reported receiving payments or honoraria from Boehringer Ingelheim, Eli Lilly, Janssen Pharmaceuticals, and Novo Nordisk. The study was carried out independently without any grant or other funding.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE