User login
Strep infection and tics in children: new data
Group A streptococcus (GAS) infection is not associated with new-onset tic disorders in at-risk children, findings from a large prospective study show.
The results mean that if preteens present with a new-onset tic condition, “they’re unlikely to have it as a result of a group A streptococcal throat infection,” study author Anette Eleonore Schrag, MD, PhD, professor, department of clinical neuroscience, Institute of Neurology, University College London, told this news organization.
Therefore, clinicians should not automatically prescribe antibiotics for children with tics, which sometimes occurs, said Dr. Schrag.
The study was published online Feb. 2 in Neurology.
Ongoing controversy
Research shows that genetic and environmental factors contribute to chronic tic disorders (CTDs) and Tourette syndrome (TS). Prenatal exposure to maternal smoking and central nervous system (CNS) stimulants, as well as psychosocial stress, may play a role.
There has been an ongoing controversy regarding the possible role of GAS in tics, with some studies showing an association and others not showing a link. However, previous studies have been retrospective, registry based, or had limited sample size.
This new prospective study is the first in children without a tic disorder but who were at relatively high risk of developing one. The children were followed to assess development of streptococcal infections and tics, said Dr. Schrag.
The study included 259 children aged 3-10 years (mean baseline age, 6.8 years; over half female) who had a first-degree relative such as a parent or sibling with TS or CTD.
The average age at TS onset is 7 years, peaking in prevalence and severity at about 9-12 years. GAS throat infections are common in this age group.
Although study participants did not have tics themselves, they represented “an enriched group,” said Dr. Schrag. “Because they had family history, we knew they were at increased risk for developing tics.”
Participants were evaluated every 2 months, alternating between scheduled hospital visits and telephone interviews. Parents kept a weekly diary and were instructed to bring their child in for assessment if they showed any signs of tics.
The average follow-up period was 1.6 years, but some of the children were followed for up to 48 months. During the study, there were a total of 1,944 assessments, including 939 telephone interviews and 1,005 clinical visits.
More common in boys
Investigators defined tic onset as the first occurrence of any sudden, rapid, recurrent, nonrhythmic involuntary movement and/or vocalization on at least three separate days within a period of 3 weeks.
The investigators assessed GAS exposure using parameters from throat swabs, serum anti-streptolysin O titers, and anti-DNAse B titers.
They used multiple definitions and combinations of GAS exposures “to make sure we weren’t missing any association because we didn’t use the right definition,” said Dr. Schrag. She explained a definitive strep infection is not always clear-cut.
At baseline, 17.0% participants tested positive for GAS, and 78.8% tested negative. No throat swab was available from 4.2% of participants.
During follow-up, the number of confirmed positive GAS exposures was 59, 102, 125, and 138, depending on the definition.
Researchers identified 61 tic cases during the study period. There was no evidence of an association of tic onset with GAS exposure after adjusting for age, sex, and parental education level.
However, there was a strong association between tic onset and sex, with girls being 60% less likely to develop tics than boys (hazard ratio, 0.4; 95% CI, 0.2-0.7; P < .01).
This result wasn’t particularly surprising, as it’s known that more boys develop tics than girls. “We just confirmed that in a prospective way,” said Dr. Schrag.
Results from sensitivity analyses confirmed the results. This was also the case with analyses that excluded visits with missing data on GAS exposure and that further adjusted for clinical site and psychotropic medication use.
Other pathogens?
Although the results showed no association between strep and tics in this population, it does not “close the door completely” on a potential relationship, said Dr. Schrag.
“By and large, the development of tics in children is not associated with group A strep, but differences in small subgroups can never be excluded by a study like this.”
Participants in this study were part of the European Multicentre Tics in Children Studies (EMTICS), a prospective cohort study exploring the role of environmental and genetic factors in pediatric CTD. That project is also looking at immune system factors, “which might play a role in the development of chronic tic disorder and associated conditions,” said Dr. Schrag.
It’s still possible, she added, that other pathogens could play a role in tic development. “That’s going to be the subject of further analysis and future studies,” she said.
Tamara Pringsheim, MD, professor of clinical neurosciences, psychiatry, pediatrics, and community health sciences, University of Calgary (Alta.), praised the research.
“This was a well-designed study, with a large sample of 260 children followed for up to 4 years, using a standardized protocol to assess for group A streptococcal infection and new onset of tics.”
The study, which did not uncover an association between GAS exposure and tic onset, “provides high level evidence that group A streptococcal exposure is not an important risk factor for the new onset of tics in children with a family history of tic disorders.”
The study received funding from the European Union Seventh Framework Program for research technological development and demonstration. Dr. Schrag reports receiving consultancy or advisory board honoraria from Biogen, Abbvie, Bial, and Neurotechnology; research support from the National Institute of Health Research, Parkinsons UK, and the Economic and Social Research Council and the European Commission; and Royalties from Oxford University Press. Dr. Pringsheim reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Group A streptococcus (GAS) infection is not associated with new-onset tic disorders in at-risk children, findings from a large prospective study show.
The results mean that if preteens present with a new-onset tic condition, “they’re unlikely to have it as a result of a group A streptococcal throat infection,” study author Anette Eleonore Schrag, MD, PhD, professor, department of clinical neuroscience, Institute of Neurology, University College London, told this news organization.
Therefore, clinicians should not automatically prescribe antibiotics for children with tics, which sometimes occurs, said Dr. Schrag.
The study was published online Feb. 2 in Neurology.
Ongoing controversy
Research shows that genetic and environmental factors contribute to chronic tic disorders (CTDs) and Tourette syndrome (TS). Prenatal exposure to maternal smoking and central nervous system (CNS) stimulants, as well as psychosocial stress, may play a role.
There has been an ongoing controversy regarding the possible role of GAS in tics, with some studies showing an association and others not showing a link. However, previous studies have been retrospective, registry based, or had limited sample size.
This new prospective study is the first in children without a tic disorder but who were at relatively high risk of developing one. The children were followed to assess development of streptococcal infections and tics, said Dr. Schrag.
The study included 259 children aged 3-10 years (mean baseline age, 6.8 years; over half female) who had a first-degree relative such as a parent or sibling with TS or CTD.
The average age at TS onset is 7 years, peaking in prevalence and severity at about 9-12 years. GAS throat infections are common in this age group.
Although study participants did not have tics themselves, they represented “an enriched group,” said Dr. Schrag. “Because they had family history, we knew they were at increased risk for developing tics.”
Participants were evaluated every 2 months, alternating between scheduled hospital visits and telephone interviews. Parents kept a weekly diary and were instructed to bring their child in for assessment if they showed any signs of tics.
The average follow-up period was 1.6 years, but some of the children were followed for up to 48 months. During the study, there were a total of 1,944 assessments, including 939 telephone interviews and 1,005 clinical visits.
More common in boys
Investigators defined tic onset as the first occurrence of any sudden, rapid, recurrent, nonrhythmic involuntary movement and/or vocalization on at least three separate days within a period of 3 weeks.
The investigators assessed GAS exposure using parameters from throat swabs, serum anti-streptolysin O titers, and anti-DNAse B titers.
They used multiple definitions and combinations of GAS exposures “to make sure we weren’t missing any association because we didn’t use the right definition,” said Dr. Schrag. She explained a definitive strep infection is not always clear-cut.
At baseline, 17.0% participants tested positive for GAS, and 78.8% tested negative. No throat swab was available from 4.2% of participants.
During follow-up, the number of confirmed positive GAS exposures was 59, 102, 125, and 138, depending on the definition.
Researchers identified 61 tic cases during the study period. There was no evidence of an association of tic onset with GAS exposure after adjusting for age, sex, and parental education level.
However, there was a strong association between tic onset and sex, with girls being 60% less likely to develop tics than boys (hazard ratio, 0.4; 95% CI, 0.2-0.7; P < .01).
This result wasn’t particularly surprising, as it’s known that more boys develop tics than girls. “We just confirmed that in a prospective way,” said Dr. Schrag.
Results from sensitivity analyses confirmed the results. This was also the case with analyses that excluded visits with missing data on GAS exposure and that further adjusted for clinical site and psychotropic medication use.
Other pathogens?
Although the results showed no association between strep and tics in this population, it does not “close the door completely” on a potential relationship, said Dr. Schrag.
“By and large, the development of tics in children is not associated with group A strep, but differences in small subgroups can never be excluded by a study like this.”
Participants in this study were part of the European Multicentre Tics in Children Studies (EMTICS), a prospective cohort study exploring the role of environmental and genetic factors in pediatric CTD. That project is also looking at immune system factors, “which might play a role in the development of chronic tic disorder and associated conditions,” said Dr. Schrag.
It’s still possible, she added, that other pathogens could play a role in tic development. “That’s going to be the subject of further analysis and future studies,” she said.
Tamara Pringsheim, MD, professor of clinical neurosciences, psychiatry, pediatrics, and community health sciences, University of Calgary (Alta.), praised the research.
“This was a well-designed study, with a large sample of 260 children followed for up to 4 years, using a standardized protocol to assess for group A streptococcal infection and new onset of tics.”
The study, which did not uncover an association between GAS exposure and tic onset, “provides high level evidence that group A streptococcal exposure is not an important risk factor for the new onset of tics in children with a family history of tic disorders.”
The study received funding from the European Union Seventh Framework Program for research technological development and demonstration. Dr. Schrag reports receiving consultancy or advisory board honoraria from Biogen, Abbvie, Bial, and Neurotechnology; research support from the National Institute of Health Research, Parkinsons UK, and the Economic and Social Research Council and the European Commission; and Royalties from Oxford University Press. Dr. Pringsheim reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Group A streptococcus (GAS) infection is not associated with new-onset tic disorders in at-risk children, findings from a large prospective study show.
The results mean that if preteens present with a new-onset tic condition, “they’re unlikely to have it as a result of a group A streptococcal throat infection,” study author Anette Eleonore Schrag, MD, PhD, professor, department of clinical neuroscience, Institute of Neurology, University College London, told this news organization.
Therefore, clinicians should not automatically prescribe antibiotics for children with tics, which sometimes occurs, said Dr. Schrag.
The study was published online Feb. 2 in Neurology.
Ongoing controversy
Research shows that genetic and environmental factors contribute to chronic tic disorders (CTDs) and Tourette syndrome (TS). Prenatal exposure to maternal smoking and central nervous system (CNS) stimulants, as well as psychosocial stress, may play a role.
There has been an ongoing controversy regarding the possible role of GAS in tics, with some studies showing an association and others not showing a link. However, previous studies have been retrospective, registry based, or had limited sample size.
This new prospective study is the first in children without a tic disorder but who were at relatively high risk of developing one. The children were followed to assess development of streptococcal infections and tics, said Dr. Schrag.
The study included 259 children aged 3-10 years (mean baseline age, 6.8 years; over half female) who had a first-degree relative such as a parent or sibling with TS or CTD.
The average age at TS onset is 7 years, peaking in prevalence and severity at about 9-12 years. GAS throat infections are common in this age group.
Although study participants did not have tics themselves, they represented “an enriched group,” said Dr. Schrag. “Because they had family history, we knew they were at increased risk for developing tics.”
Participants were evaluated every 2 months, alternating between scheduled hospital visits and telephone interviews. Parents kept a weekly diary and were instructed to bring their child in for assessment if they showed any signs of tics.
The average follow-up period was 1.6 years, but some of the children were followed for up to 48 months. During the study, there were a total of 1,944 assessments, including 939 telephone interviews and 1,005 clinical visits.
More common in boys
Investigators defined tic onset as the first occurrence of any sudden, rapid, recurrent, nonrhythmic involuntary movement and/or vocalization on at least three separate days within a period of 3 weeks.
The investigators assessed GAS exposure using parameters from throat swabs, serum anti-streptolysin O titers, and anti-DNAse B titers.
They used multiple definitions and combinations of GAS exposures “to make sure we weren’t missing any association because we didn’t use the right definition,” said Dr. Schrag. She explained a definitive strep infection is not always clear-cut.
At baseline, 17.0% participants tested positive for GAS, and 78.8% tested negative. No throat swab was available from 4.2% of participants.
During follow-up, the number of confirmed positive GAS exposures was 59, 102, 125, and 138, depending on the definition.
Researchers identified 61 tic cases during the study period. There was no evidence of an association of tic onset with GAS exposure after adjusting for age, sex, and parental education level.
However, there was a strong association between tic onset and sex, with girls being 60% less likely to develop tics than boys (hazard ratio, 0.4; 95% CI, 0.2-0.7; P < .01).
This result wasn’t particularly surprising, as it’s known that more boys develop tics than girls. “We just confirmed that in a prospective way,” said Dr. Schrag.
Results from sensitivity analyses confirmed the results. This was also the case with analyses that excluded visits with missing data on GAS exposure and that further adjusted for clinical site and psychotropic medication use.
Other pathogens?
Although the results showed no association between strep and tics in this population, it does not “close the door completely” on a potential relationship, said Dr. Schrag.
“By and large, the development of tics in children is not associated with group A strep, but differences in small subgroups can never be excluded by a study like this.”
Participants in this study were part of the European Multicentre Tics in Children Studies (EMTICS), a prospective cohort study exploring the role of environmental and genetic factors in pediatric CTD. That project is also looking at immune system factors, “which might play a role in the development of chronic tic disorder and associated conditions,” said Dr. Schrag.
It’s still possible, she added, that other pathogens could play a role in tic development. “That’s going to be the subject of further analysis and future studies,” she said.
Tamara Pringsheim, MD, professor of clinical neurosciences, psychiatry, pediatrics, and community health sciences, University of Calgary (Alta.), praised the research.
“This was a well-designed study, with a large sample of 260 children followed for up to 4 years, using a standardized protocol to assess for group A streptococcal infection and new onset of tics.”
The study, which did not uncover an association between GAS exposure and tic onset, “provides high level evidence that group A streptococcal exposure is not an important risk factor for the new onset of tics in children with a family history of tic disorders.”
The study received funding from the European Union Seventh Framework Program for research technological development and demonstration. Dr. Schrag reports receiving consultancy or advisory board honoraria from Biogen, Abbvie, Bial, and Neurotechnology; research support from the National Institute of Health Research, Parkinsons UK, and the Economic and Social Research Council and the European Commission; and Royalties from Oxford University Press. Dr. Pringsheim reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Seniors face higher risk of other medical conditions after COVID-19
The findings of the observational study, which were published in the BMJ, show the risk of a new condition being triggered by COVID is more than twice as high in seniors, compared with younger patients. Plus, the researchers observed an even higher risk among those who were hospitalized, with nearly half (46%) of patients having developed new conditions after the acute COVID-19 infection period.
Respiratory failure with shortness of breath was the most common postacute sequela, but a wide range of heart, kidney, lung, liver, cognitive, mental health, and other conditions were diagnosed at least 3 weeks after initial infection and persisted beyond 30 days.
This is one of the first studies to specifically describe the incidence and severity of new conditions triggered by COVID-19 infection in a general sample of older adults, said study author Ken Cohen MD, FACP, executive director of translational research at Optum Labs and national senior medical director at Optum Care.
“Much of what has been published on the postacute sequelae of COVID-19 has been predominantly from a younger population, and many of the patients had been hospitalized,” Dr. Cohen noted. “This was the first study to focus on a large population of seniors, most of whom did not require hospitalization.”
Dr. Cohen and colleagues reviewed the health insurance records of more than 133,000 Medicare beneficiaries aged 65 or older who were diagnosed with COVID-19 before April 2020. They also matched individuals by age, race, sex, hospitalization status, and other factors to comparison groups without COVID-19 (one from 2020 and one from 2019), and to a group diagnosed with other lower respiratory tract viral infections before the pandemic.
Risk of developing new conditions was higher in hospitalized
After acute COVID-19 infection, 32% of seniors sought medical care for at least one new medical condition in 2020, compared with 21% of uninfected people in the same year.
The most commonly observed conditions included:
- Respiratory failure (7.55% higher risk).
- Fatigue (5.66% higher risk).
- High blood pressure (4.43% higher risk).
- Memory problems (2.63% higher risk).
- Kidney injury (2.59% higher risk).
- Mental health diagnoses (2.5% higher risk).
- Blood-clotting disorders (1.47 % higher risk).
- Heart rhythm disorders (2.9% higher risk).
The risk of developing new conditions was even higher among those 23,486 who were hospitalized in 2020. Those individuals showed a 23.6% higher risk for developing at least one new condition, compared with uninfected seniors in the same year. Also, patients older than 75 had a higher risk for neurological disorders, including dementia, encephalopathy, and memory problems. The researchers also found that respiratory failure and kidney injury were significantly more likely to affect men and Black patients.
When those who had COVID were compared with the group with other lower respiratory viral infections before the pandemic, only the risks of respiratory failure (2.39% higher), dementia (0.71% higher), and fatigue (0.18% higher) were higher.
Primary care providers can learn from these data to better evaluate and manage their geriatric patients with COVID-19 infection, said Amit Shah, MD, a geriatrician with the Mayo Clinic in Phoenix, in an interview.
“We must assess older patients who have had COVID-19 for more than just improvement from the respiratory symptoms of COVID-19 in post-COVID follow-up visits,” he said. “Older individuals with frailty have vulnerability to subsequent complications from severe illnesses and it is common to see post-illness diagnoses, such as new diagnosis of delirium; dementia; or renal, respiratory, or cardiac issues that is precipitated by the original illness. This study confirms that this is likely the case with COVID-19 as well.
“Primary care physicians should be vigilant for these complications, including attention to the rehabilitation needs of older patients with longer-term postviral fatigue from COVID-19,” Dr. Shah added.
Data predates ‘Omicron wave’
It remains uncertain whether sequelae will differ with the Omicron variant, but the findings remain applicable, Dr. Cohen said.
“We know that illness from the Omicron variant is on average less severe in those that have been vaccinated. However, throughout the Omicron wave, individuals who have not been vaccinated continue to have significant rates of serious illness and hospitalization,” he said.
“Our findings showed that serious illness with hospitalization was associated with a higher rate of sequelae. It can therefore be inferred that the rates of sequelae seen in our study would continue to occur in unvaccinated individuals who contract Omicron, but might occur less frequently in vaccinated individuals who contract Omicron and have less severe illness.”
Dr. Cohen serves as a consultant for Pfizer. Dr. Shah has disclosed no relevant financial relationships.
The findings of the observational study, which were published in the BMJ, show the risk of a new condition being triggered by COVID is more than twice as high in seniors, compared with younger patients. Plus, the researchers observed an even higher risk among those who were hospitalized, with nearly half (46%) of patients having developed new conditions after the acute COVID-19 infection period.
Respiratory failure with shortness of breath was the most common postacute sequela, but a wide range of heart, kidney, lung, liver, cognitive, mental health, and other conditions were diagnosed at least 3 weeks after initial infection and persisted beyond 30 days.
This is one of the first studies to specifically describe the incidence and severity of new conditions triggered by COVID-19 infection in a general sample of older adults, said study author Ken Cohen MD, FACP, executive director of translational research at Optum Labs and national senior medical director at Optum Care.
“Much of what has been published on the postacute sequelae of COVID-19 has been predominantly from a younger population, and many of the patients had been hospitalized,” Dr. Cohen noted. “This was the first study to focus on a large population of seniors, most of whom did not require hospitalization.”
Dr. Cohen and colleagues reviewed the health insurance records of more than 133,000 Medicare beneficiaries aged 65 or older who were diagnosed with COVID-19 before April 2020. They also matched individuals by age, race, sex, hospitalization status, and other factors to comparison groups without COVID-19 (one from 2020 and one from 2019), and to a group diagnosed with other lower respiratory tract viral infections before the pandemic.
Risk of developing new conditions was higher in hospitalized
After acute COVID-19 infection, 32% of seniors sought medical care for at least one new medical condition in 2020, compared with 21% of uninfected people in the same year.
The most commonly observed conditions included:
- Respiratory failure (7.55% higher risk).
- Fatigue (5.66% higher risk).
- High blood pressure (4.43% higher risk).
- Memory problems (2.63% higher risk).
- Kidney injury (2.59% higher risk).
- Mental health diagnoses (2.5% higher risk).
- Blood-clotting disorders (1.47 % higher risk).
- Heart rhythm disorders (2.9% higher risk).
The risk of developing new conditions was even higher among those 23,486 who were hospitalized in 2020. Those individuals showed a 23.6% higher risk for developing at least one new condition, compared with uninfected seniors in the same year. Also, patients older than 75 had a higher risk for neurological disorders, including dementia, encephalopathy, and memory problems. The researchers also found that respiratory failure and kidney injury were significantly more likely to affect men and Black patients.
When those who had COVID were compared with the group with other lower respiratory viral infections before the pandemic, only the risks of respiratory failure (2.39% higher), dementia (0.71% higher), and fatigue (0.18% higher) were higher.
Primary care providers can learn from these data to better evaluate and manage their geriatric patients with COVID-19 infection, said Amit Shah, MD, a geriatrician with the Mayo Clinic in Phoenix, in an interview.
“We must assess older patients who have had COVID-19 for more than just improvement from the respiratory symptoms of COVID-19 in post-COVID follow-up visits,” he said. “Older individuals with frailty have vulnerability to subsequent complications from severe illnesses and it is common to see post-illness diagnoses, such as new diagnosis of delirium; dementia; or renal, respiratory, or cardiac issues that is precipitated by the original illness. This study confirms that this is likely the case with COVID-19 as well.
“Primary care physicians should be vigilant for these complications, including attention to the rehabilitation needs of older patients with longer-term postviral fatigue from COVID-19,” Dr. Shah added.
Data predates ‘Omicron wave’
It remains uncertain whether sequelae will differ with the Omicron variant, but the findings remain applicable, Dr. Cohen said.
“We know that illness from the Omicron variant is on average less severe in those that have been vaccinated. However, throughout the Omicron wave, individuals who have not been vaccinated continue to have significant rates of serious illness and hospitalization,” he said.
“Our findings showed that serious illness with hospitalization was associated with a higher rate of sequelae. It can therefore be inferred that the rates of sequelae seen in our study would continue to occur in unvaccinated individuals who contract Omicron, but might occur less frequently in vaccinated individuals who contract Omicron and have less severe illness.”
Dr. Cohen serves as a consultant for Pfizer. Dr. Shah has disclosed no relevant financial relationships.
The findings of the observational study, which were published in the BMJ, show the risk of a new condition being triggered by COVID is more than twice as high in seniors, compared with younger patients. Plus, the researchers observed an even higher risk among those who were hospitalized, with nearly half (46%) of patients having developed new conditions after the acute COVID-19 infection period.
Respiratory failure with shortness of breath was the most common postacute sequela, but a wide range of heart, kidney, lung, liver, cognitive, mental health, and other conditions were diagnosed at least 3 weeks after initial infection and persisted beyond 30 days.
This is one of the first studies to specifically describe the incidence and severity of new conditions triggered by COVID-19 infection in a general sample of older adults, said study author Ken Cohen MD, FACP, executive director of translational research at Optum Labs and national senior medical director at Optum Care.
“Much of what has been published on the postacute sequelae of COVID-19 has been predominantly from a younger population, and many of the patients had been hospitalized,” Dr. Cohen noted. “This was the first study to focus on a large population of seniors, most of whom did not require hospitalization.”
Dr. Cohen and colleagues reviewed the health insurance records of more than 133,000 Medicare beneficiaries aged 65 or older who were diagnosed with COVID-19 before April 2020. They also matched individuals by age, race, sex, hospitalization status, and other factors to comparison groups without COVID-19 (one from 2020 and one from 2019), and to a group diagnosed with other lower respiratory tract viral infections before the pandemic.
Risk of developing new conditions was higher in hospitalized
After acute COVID-19 infection, 32% of seniors sought medical care for at least one new medical condition in 2020, compared with 21% of uninfected people in the same year.
The most commonly observed conditions included:
- Respiratory failure (7.55% higher risk).
- Fatigue (5.66% higher risk).
- High blood pressure (4.43% higher risk).
- Memory problems (2.63% higher risk).
- Kidney injury (2.59% higher risk).
- Mental health diagnoses (2.5% higher risk).
- Blood-clotting disorders (1.47 % higher risk).
- Heart rhythm disorders (2.9% higher risk).
The risk of developing new conditions was even higher among those 23,486 who were hospitalized in 2020. Those individuals showed a 23.6% higher risk for developing at least one new condition, compared with uninfected seniors in the same year. Also, patients older than 75 had a higher risk for neurological disorders, including dementia, encephalopathy, and memory problems. The researchers also found that respiratory failure and kidney injury were significantly more likely to affect men and Black patients.
When those who had COVID were compared with the group with other lower respiratory viral infections before the pandemic, only the risks of respiratory failure (2.39% higher), dementia (0.71% higher), and fatigue (0.18% higher) were higher.
Primary care providers can learn from these data to better evaluate and manage their geriatric patients with COVID-19 infection, said Amit Shah, MD, a geriatrician with the Mayo Clinic in Phoenix, in an interview.
“We must assess older patients who have had COVID-19 for more than just improvement from the respiratory symptoms of COVID-19 in post-COVID follow-up visits,” he said. “Older individuals with frailty have vulnerability to subsequent complications from severe illnesses and it is common to see post-illness diagnoses, such as new diagnosis of delirium; dementia; or renal, respiratory, or cardiac issues that is precipitated by the original illness. This study confirms that this is likely the case with COVID-19 as well.
“Primary care physicians should be vigilant for these complications, including attention to the rehabilitation needs of older patients with longer-term postviral fatigue from COVID-19,” Dr. Shah added.
Data predates ‘Omicron wave’
It remains uncertain whether sequelae will differ with the Omicron variant, but the findings remain applicable, Dr. Cohen said.
“We know that illness from the Omicron variant is on average less severe in those that have been vaccinated. However, throughout the Omicron wave, individuals who have not been vaccinated continue to have significant rates of serious illness and hospitalization,” he said.
“Our findings showed that serious illness with hospitalization was associated with a higher rate of sequelae. It can therefore be inferred that the rates of sequelae seen in our study would continue to occur in unvaccinated individuals who contract Omicron, but might occur less frequently in vaccinated individuals who contract Omicron and have less severe illness.”
Dr. Cohen serves as a consultant for Pfizer. Dr. Shah has disclosed no relevant financial relationships.
FROM BMJ
Chronic marijuana use linked to recurrent stroke
, new observational research suggests. “Our analysis shows young marijuana users with a history of stroke or transient ischemic attack remain at significantly high risk for future strokes,” said lead study author Akhil Jain, MD, a resident physician at Mercy Fitzgerald Hospital in Darby, Pennsylvania.
“It’s essential to raise awareness among young adults about the impact of chronic habitual use of marijuana, especially if they have established cardiovascular risk factors or previous stroke.”
The study will be presented during the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
An increasing number of jurisdictions are allowing marijuana use. To date, 18 states and the District of Columbia have legalized recreational cannabis use, the investigators noted.
Research suggests cannabis use disorder – defined as the chronic habitual use of cannabis – is more prevalent in the young adult population. But Dr. Jain said the population of marijuana users is “a changing dynamic.”
Cannabis use has been linked to an increased risk for first-time stroke or transient ischemic attack (TIA). Traditional stroke risk factors include hypertension, diabetes, and diseases related to blood vessels or blood circulation, including atherosclerosis.
Young adults might have additional stroke risk factors, such as behavioral habits like substance abuse, low physical activity, and smoking, oral contraceptives use among females, and brain infections, especially in the immunocompromised, said Dr. Jain.
Research from the American Heart Association shows stroke rates are increasing among adults 18 to 45 years of age. Each year, young adults account for up to 15% of strokes in the United States.
Prevalence and risk for recurrent stroke in patients with previous stroke or TIA in cannabis users have not been clearly established, the researchers pointed out.
A higher rate of recurrent stroke
For this new study, Dr. Jain and colleagues used data from the National Inpatient Sample from October 2015 to December 2017. They identified hospitalizations among young adults 18 to 45 years of age with a previous history of stroke or TIA.
They then grouped these patients into those with cannabis use disorder (4,690) and those without cannabis use disorder (156,700). The median age in both cohorts was 37 years.
The analysis did not include those who were considered in remission from cannabis use disorder.
Results showed that 6.9% of those with cannabis use disorder were hospitalized for a recurrent stroke, compared with 5.4% of those without cannabis use disorder (P < .001).
After adjustment for demographic factors (age, sex, race, household income), and pre-existing conditions, patients with cannabis use disorder were 48% more likely to be hospitalized for recurrent stroke than those without cannabis use disorder (odds ratio, 1.48; 95% confidence interval, 1.28-1.71; P < .001).
Compared with the group without cannabis use disorder, the cannabis use disorder group had more men (55.2% vs. 40.2%), more African American people (44.6% vs. 37.2%), and more use of tobacco (73.9% vs. 39.6%) and alcohol (16.5% vs. 3.6%). They also had a greater percentage of chronic obstructive pulmonary disease, depression, and psychoses.
But a smaller percentage of those with cannabis use disorder had hypertension (51.3% vs. 55.6%; P = .001) and diabetes (16.3% vs. 22.7%; P < .001), which is an “interesting” finding, said Dr. Jain.
“We observed that even with a lower rate of cardiovascular risk factors, after controlling for all the risk factors, we still found the cannabis users had a higher rate of recurrent stroke.”
He noted this was a retrospective study without a control group. “If both groups had comparable hypertension, then this risk might actually be more evident,” said Dr. Jain. “We need a prospective study with comparable groups.”
Living in low-income neighborhoods and in northeast and southern regions of the United States was also more common in the cannabis use disorder group.
Hypothesis-generating research
The study did not investigate the possible mechanisms by which marijuana use might increase stroke risk, but Dr. Jain speculated that these could include factors such as impaired blood vessel function, changes in blood supply, an increased tendency of blood clotting, impaired energy production in brain cells, and an imbalance between molecules that harm healthy tissue and the antioxidant defenses that neutralize them.
As cannabis use may pose a different risk for a new stroke, as opposed a previous stroke, Dr. Jain said it would be interesting to study the amount of “residual function deficit” experienced with the first stroke.
The new study represents “foundational research” upon which other research teams can build, said Dr. Jain. “Our study is hypothesis-generating research for a future prospective randomized controlled trial.”
A limitation of the study is that it did not consider the effect of various doses, duration, and forms of cannabis abuse, or use of medicinal cannabis or other drugs.
Robert L. Page II, PharmD, professor, departments of clinical pharmacy and physical medicine/rehabilitation, University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, provided a comment on this new research.
A cannabis use disorder diagnosis provides “specific criteria” with regard to chronicity of use and reflects “more of a physical and psychological dependence upon cannabis,” said Dr. Page, who chaired the writing group for the AHA 2020 cannabis and cardiovascular disease scientific statement.
He explained what sets people with cannabis use disorder apart from “run-of-the-mill” recreational cannabis users is that “these are individuals who use a cannabis product, whether it’s smoking it, vaping it, or consuming it via an edible, and are using it on a regular basis, in a chronic fashion.”
The study received no outside funding. The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
, new observational research suggests. “Our analysis shows young marijuana users with a history of stroke or transient ischemic attack remain at significantly high risk for future strokes,” said lead study author Akhil Jain, MD, a resident physician at Mercy Fitzgerald Hospital in Darby, Pennsylvania.
“It’s essential to raise awareness among young adults about the impact of chronic habitual use of marijuana, especially if they have established cardiovascular risk factors or previous stroke.”
The study will be presented during the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
An increasing number of jurisdictions are allowing marijuana use. To date, 18 states and the District of Columbia have legalized recreational cannabis use, the investigators noted.
Research suggests cannabis use disorder – defined as the chronic habitual use of cannabis – is more prevalent in the young adult population. But Dr. Jain said the population of marijuana users is “a changing dynamic.”
Cannabis use has been linked to an increased risk for first-time stroke or transient ischemic attack (TIA). Traditional stroke risk factors include hypertension, diabetes, and diseases related to blood vessels or blood circulation, including atherosclerosis.
Young adults might have additional stroke risk factors, such as behavioral habits like substance abuse, low physical activity, and smoking, oral contraceptives use among females, and brain infections, especially in the immunocompromised, said Dr. Jain.
Research from the American Heart Association shows stroke rates are increasing among adults 18 to 45 years of age. Each year, young adults account for up to 15% of strokes in the United States.
Prevalence and risk for recurrent stroke in patients with previous stroke or TIA in cannabis users have not been clearly established, the researchers pointed out.
A higher rate of recurrent stroke
For this new study, Dr. Jain and colleagues used data from the National Inpatient Sample from October 2015 to December 2017. They identified hospitalizations among young adults 18 to 45 years of age with a previous history of stroke or TIA.
They then grouped these patients into those with cannabis use disorder (4,690) and those without cannabis use disorder (156,700). The median age in both cohorts was 37 years.
The analysis did not include those who were considered in remission from cannabis use disorder.
Results showed that 6.9% of those with cannabis use disorder were hospitalized for a recurrent stroke, compared with 5.4% of those without cannabis use disorder (P < .001).
After adjustment for demographic factors (age, sex, race, household income), and pre-existing conditions, patients with cannabis use disorder were 48% more likely to be hospitalized for recurrent stroke than those without cannabis use disorder (odds ratio, 1.48; 95% confidence interval, 1.28-1.71; P < .001).
Compared with the group without cannabis use disorder, the cannabis use disorder group had more men (55.2% vs. 40.2%), more African American people (44.6% vs. 37.2%), and more use of tobacco (73.9% vs. 39.6%) and alcohol (16.5% vs. 3.6%). They also had a greater percentage of chronic obstructive pulmonary disease, depression, and psychoses.
But a smaller percentage of those with cannabis use disorder had hypertension (51.3% vs. 55.6%; P = .001) and diabetes (16.3% vs. 22.7%; P < .001), which is an “interesting” finding, said Dr. Jain.
“We observed that even with a lower rate of cardiovascular risk factors, after controlling for all the risk factors, we still found the cannabis users had a higher rate of recurrent stroke.”
He noted this was a retrospective study without a control group. “If both groups had comparable hypertension, then this risk might actually be more evident,” said Dr. Jain. “We need a prospective study with comparable groups.”
Living in low-income neighborhoods and in northeast and southern regions of the United States was also more common in the cannabis use disorder group.
Hypothesis-generating research
The study did not investigate the possible mechanisms by which marijuana use might increase stroke risk, but Dr. Jain speculated that these could include factors such as impaired blood vessel function, changes in blood supply, an increased tendency of blood clotting, impaired energy production in brain cells, and an imbalance between molecules that harm healthy tissue and the antioxidant defenses that neutralize them.
As cannabis use may pose a different risk for a new stroke, as opposed a previous stroke, Dr. Jain said it would be interesting to study the amount of “residual function deficit” experienced with the first stroke.
The new study represents “foundational research” upon which other research teams can build, said Dr. Jain. “Our study is hypothesis-generating research for a future prospective randomized controlled trial.”
A limitation of the study is that it did not consider the effect of various doses, duration, and forms of cannabis abuse, or use of medicinal cannabis or other drugs.
Robert L. Page II, PharmD, professor, departments of clinical pharmacy and physical medicine/rehabilitation, University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, provided a comment on this new research.
A cannabis use disorder diagnosis provides “specific criteria” with regard to chronicity of use and reflects “more of a physical and psychological dependence upon cannabis,” said Dr. Page, who chaired the writing group for the AHA 2020 cannabis and cardiovascular disease scientific statement.
He explained what sets people with cannabis use disorder apart from “run-of-the-mill” recreational cannabis users is that “these are individuals who use a cannabis product, whether it’s smoking it, vaping it, or consuming it via an edible, and are using it on a regular basis, in a chronic fashion.”
The study received no outside funding. The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
, new observational research suggests. “Our analysis shows young marijuana users with a history of stroke or transient ischemic attack remain at significantly high risk for future strokes,” said lead study author Akhil Jain, MD, a resident physician at Mercy Fitzgerald Hospital in Darby, Pennsylvania.
“It’s essential to raise awareness among young adults about the impact of chronic habitual use of marijuana, especially if they have established cardiovascular risk factors or previous stroke.”
The study will be presented during the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
An increasing number of jurisdictions are allowing marijuana use. To date, 18 states and the District of Columbia have legalized recreational cannabis use, the investigators noted.
Research suggests cannabis use disorder – defined as the chronic habitual use of cannabis – is more prevalent in the young adult population. But Dr. Jain said the population of marijuana users is “a changing dynamic.”
Cannabis use has been linked to an increased risk for first-time stroke or transient ischemic attack (TIA). Traditional stroke risk factors include hypertension, diabetes, and diseases related to blood vessels or blood circulation, including atherosclerosis.
Young adults might have additional stroke risk factors, such as behavioral habits like substance abuse, low physical activity, and smoking, oral contraceptives use among females, and brain infections, especially in the immunocompromised, said Dr. Jain.
Research from the American Heart Association shows stroke rates are increasing among adults 18 to 45 years of age. Each year, young adults account for up to 15% of strokes in the United States.
Prevalence and risk for recurrent stroke in patients with previous stroke or TIA in cannabis users have not been clearly established, the researchers pointed out.
A higher rate of recurrent stroke
For this new study, Dr. Jain and colleagues used data from the National Inpatient Sample from October 2015 to December 2017. They identified hospitalizations among young adults 18 to 45 years of age with a previous history of stroke or TIA.
They then grouped these patients into those with cannabis use disorder (4,690) and those without cannabis use disorder (156,700). The median age in both cohorts was 37 years.
The analysis did not include those who were considered in remission from cannabis use disorder.
Results showed that 6.9% of those with cannabis use disorder were hospitalized for a recurrent stroke, compared with 5.4% of those without cannabis use disorder (P < .001).
After adjustment for demographic factors (age, sex, race, household income), and pre-existing conditions, patients with cannabis use disorder were 48% more likely to be hospitalized for recurrent stroke than those without cannabis use disorder (odds ratio, 1.48; 95% confidence interval, 1.28-1.71; P < .001).
Compared with the group without cannabis use disorder, the cannabis use disorder group had more men (55.2% vs. 40.2%), more African American people (44.6% vs. 37.2%), and more use of tobacco (73.9% vs. 39.6%) and alcohol (16.5% vs. 3.6%). They also had a greater percentage of chronic obstructive pulmonary disease, depression, and psychoses.
But a smaller percentage of those with cannabis use disorder had hypertension (51.3% vs. 55.6%; P = .001) and diabetes (16.3% vs. 22.7%; P < .001), which is an “interesting” finding, said Dr. Jain.
“We observed that even with a lower rate of cardiovascular risk factors, after controlling for all the risk factors, we still found the cannabis users had a higher rate of recurrent stroke.”
He noted this was a retrospective study without a control group. “If both groups had comparable hypertension, then this risk might actually be more evident,” said Dr. Jain. “We need a prospective study with comparable groups.”
Living in low-income neighborhoods and in northeast and southern regions of the United States was also more common in the cannabis use disorder group.
Hypothesis-generating research
The study did not investigate the possible mechanisms by which marijuana use might increase stroke risk, but Dr. Jain speculated that these could include factors such as impaired blood vessel function, changes in blood supply, an increased tendency of blood clotting, impaired energy production in brain cells, and an imbalance between molecules that harm healthy tissue and the antioxidant defenses that neutralize them.
As cannabis use may pose a different risk for a new stroke, as opposed a previous stroke, Dr. Jain said it would be interesting to study the amount of “residual function deficit” experienced with the first stroke.
The new study represents “foundational research” upon which other research teams can build, said Dr. Jain. “Our study is hypothesis-generating research for a future prospective randomized controlled trial.”
A limitation of the study is that it did not consider the effect of various doses, duration, and forms of cannabis abuse, or use of medicinal cannabis or other drugs.
Robert L. Page II, PharmD, professor, departments of clinical pharmacy and physical medicine/rehabilitation, University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, provided a comment on this new research.
A cannabis use disorder diagnosis provides “specific criteria” with regard to chronicity of use and reflects “more of a physical and psychological dependence upon cannabis,” said Dr. Page, who chaired the writing group for the AHA 2020 cannabis and cardiovascular disease scientific statement.
He explained what sets people with cannabis use disorder apart from “run-of-the-mill” recreational cannabis users is that “these are individuals who use a cannabis product, whether it’s smoking it, vaping it, or consuming it via an edible, and are using it on a regular basis, in a chronic fashion.”
The study received no outside funding. The authors report no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM ISC 2022
Potential new neuromodulation treatment for migraines
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
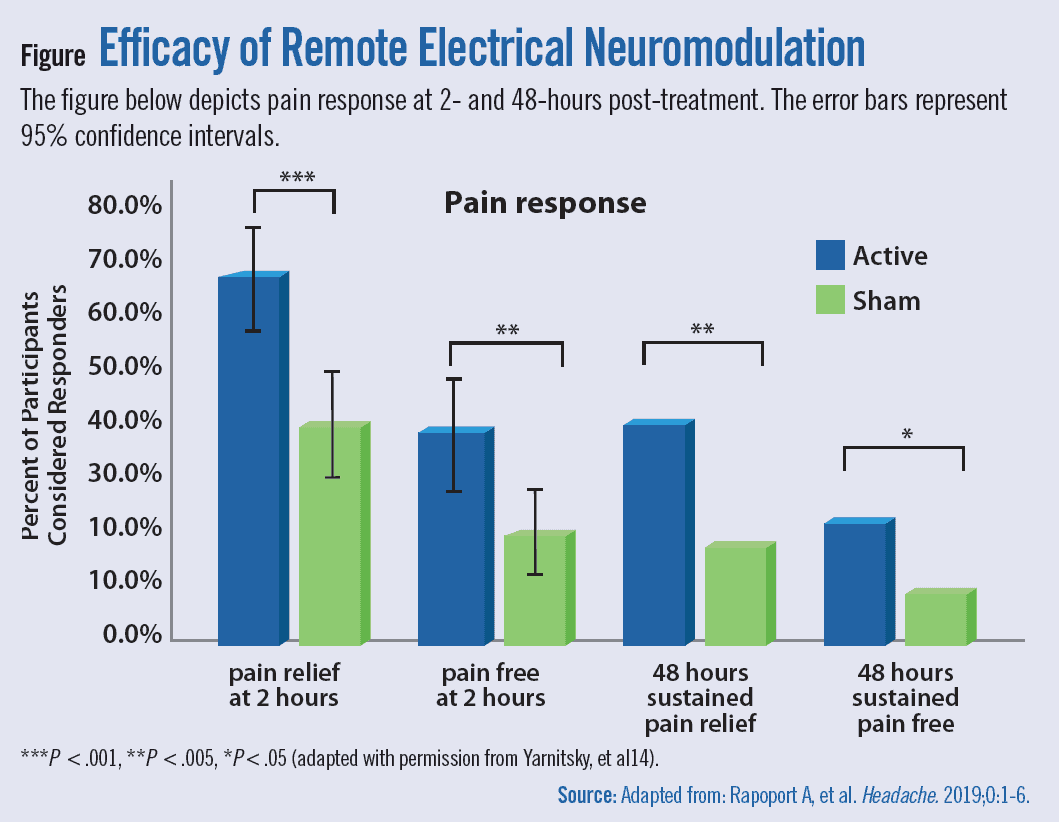
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
{kind=link}
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Motor function restored in three men after complete paralysis from spinal cord injury
(SCI), new research shows.
The study demonstrated that an epidural electrical stimulation (EES) system developed specifically for spinal cord injuries enabled three men with complete paralysis to stand, walk, cycle, swim, and move their torso within 1 day.
“Thanks to this technology, we have been able to target individuals with the most serious spinal cord injury, meaning those with clinically complete spinal cord injury, with no sensation and no movement in the legs,” Grégoire Courtine, PhD, professor of neuroscience and neurotechnology at the Swiss Federal Institute of Technology, University Hospital Lausanne (Switzerland), and the University of Lausanne, told reporters attending a press briefing.
The study was published online Feb. 7, 2022, in Nature Medicine.
More rapid, precise, effective
SCIs involve severed connections between the brain and extremities. To compensate for these lost connections, researchers have investigated stem cell therapy, brain-machine interfaces, and powered exoskeletons.
However, these approaches aren’t yet ready for prime time.
In the meantime, researchers discovered even patients with a “complete” injury may have low-functioning connections and started investigating epidural stimulators designed to treat chronic pain. Recent studies – including three published in 2018 – showed promise for these pain-related stimulators in patients with incomplete SCI.
But using such “repurposed” technology meant the electrode array was relatively narrow and short, “so we could not target all the regions of the spinal cord involving control of leg and trunk movements,” said Dr. Courtine. With the newer technology “we are much more precise, effective, and more rapid in delivering therapy.”
To develop this new approach, the researchers designed a paddle lead with an arrangement of electrodes that targets sacral, lumbar, and low-thoracic dorsal roots involved in leg and trunk movements. They also established a personalized computational framework that allows for optimal surgical placement of this paddle lead.
In addition, they developed software that renders the configuration of individualized activity–dependent stimulation programs rapid, simple, and predictable.
They tested these neurotechnologies in three men with complete sensorimotor paralysis as part of an ongoing clinical trial. The participants, aged 29, 32, and 41 years, suffered an SCI from a motor bike accident 3, 9, and 1 year before enrollment.
All three patients exhibited complete sensorimotor paralysis. They were unable to take any step, and muscles remained quiescent during these attempts.
A neurosurgeon implanted electrodes along the spinal cord of study subjects. Wires from these electrodes were connected to a neurostimulator implanted under the skin in the abdomen.
The men can select different activity-based programs from a tablet that sends signals to the implanted device.
Personalized approach
Within a single day of the surgery, the participants were able to stand, walk, cycle, swim, and control trunk movements.
“It was not perfect at the very beginning, but they could train very early on to have a more fluid gait,” said study investigator neurosurgeon Joceylyne Bloch, MD, associate professor, University of Lausanne and University Hospital Lausanne.
At this stage, not all paralyzed patients are eligible for the procedure. Dr. Bloch explained that at least 6 cm of healthy spinal cord under the lesion is needed to implant the electrodes.
“There’s a huge variability of spinal cord anatomy between individuals. That’s why it’s important to study each person individually and to have individual models in order to be precise.”
Researchers envision having “a library of electrode arrays,” added Dr. Courtine. With preoperative imaging of the individual’s spinal cord, “the neurosurgeon can select the more appropriate electrode array for that specific patient.”
Dr. Courtine noted recovery of sensation with the system differs from one individual to another. One study participant, Michel Roccati, now 30, told the briefing he feels a contraction in his muscle during the stimulation.
Currently, only individuals whose injury is more than a year old are included in the study to ensure patients have “a stable lesion” and reached “a plateau of recovery,” said Dr. Bloch. However, animal models show intervening earlier might boost the benefits.
A patient’s age can influence the outcome, as younger patients are likely in better condition and more motivated than older patients, said Dr. Bloch. However, she noted patients closing in on 50 years have responded well to the therapy.
Such stimulation systems may prove useful in treating conditions typically associated with SCI, such as hypertension and bladder control, and perhaps also in patients with Parkinson’s disease, said Dr. Courtine.
The researchers plan to conduct another study that will include a next-generation pulse generator with features that make the stimulation even more effective and user friendly. A voice recognition system could eventually be connected to the system.
“The next step is a minicomputer that you implant in the body that communicates in real time with an external iPhone,” said Dr. Courtine.
ONWARD Medical, which developed the technology, has received a breakthrough device designation from the Food and Drug Administration. The company is in discussions with the FDA to carry out a clinical trial of the device in the United States.
A ‘huge step forward’
Peter J. Grahn, PhD, assistant professor, department of physical medicine and rehabilitation and department of neurologic surgery, Mayo Clinic, Rochester, Minn., an author of one of the 2018 studies, said this technology “is a huge step forward” and “really pushes the field.”
Compared with the device used in his study that’s designed to treat neuropathic pain, this new system “is much more capable of dynamic stimulation,” said Dr. Grahn. “You can tailor the stimulation based on which area of the spinal cord you want to target during a specific function.”
There has been “a lot of hope and hype” recently around stem cells and biological molecules that were supposed to be “magic pills” to cure spinal cord dysfunction, said Dr. Grahn. “I don’t think this is one of those.”
However, he questioned the researchers’ use of the word “walking.”
“They say independent stepping or walking is restored on day 1, but the graphs show day 1 function is having over 60% of their body weight supported when they’re taking these steps,” he said.
In addition, the “big question” is how this technology can “be distilled down” into an approach “applicable across rehabilitation centers,” said Dr. Grahn.
The study was supported by numerous organizations, including ONWARD Medical. Dr. Courtine and Dr. Bloch hold various patents in relation with the present work. Dr. Courtine is a consultant with ONWARD Medical, and he and Dr. Bloch are shareholders of ONWARD Medical, a company with direct relationships with the presented work. Dr. Grahn reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(SCI), new research shows.
The study demonstrated that an epidural electrical stimulation (EES) system developed specifically for spinal cord injuries enabled three men with complete paralysis to stand, walk, cycle, swim, and move their torso within 1 day.
“Thanks to this technology, we have been able to target individuals with the most serious spinal cord injury, meaning those with clinically complete spinal cord injury, with no sensation and no movement in the legs,” Grégoire Courtine, PhD, professor of neuroscience and neurotechnology at the Swiss Federal Institute of Technology, University Hospital Lausanne (Switzerland), and the University of Lausanne, told reporters attending a press briefing.
The study was published online Feb. 7, 2022, in Nature Medicine.
More rapid, precise, effective
SCIs involve severed connections between the brain and extremities. To compensate for these lost connections, researchers have investigated stem cell therapy, brain-machine interfaces, and powered exoskeletons.
However, these approaches aren’t yet ready for prime time.
In the meantime, researchers discovered even patients with a “complete” injury may have low-functioning connections and started investigating epidural stimulators designed to treat chronic pain. Recent studies – including three published in 2018 – showed promise for these pain-related stimulators in patients with incomplete SCI.
But using such “repurposed” technology meant the electrode array was relatively narrow and short, “so we could not target all the regions of the spinal cord involving control of leg and trunk movements,” said Dr. Courtine. With the newer technology “we are much more precise, effective, and more rapid in delivering therapy.”
To develop this new approach, the researchers designed a paddle lead with an arrangement of electrodes that targets sacral, lumbar, and low-thoracic dorsal roots involved in leg and trunk movements. They also established a personalized computational framework that allows for optimal surgical placement of this paddle lead.
In addition, they developed software that renders the configuration of individualized activity–dependent stimulation programs rapid, simple, and predictable.
They tested these neurotechnologies in three men with complete sensorimotor paralysis as part of an ongoing clinical trial. The participants, aged 29, 32, and 41 years, suffered an SCI from a motor bike accident 3, 9, and 1 year before enrollment.
All three patients exhibited complete sensorimotor paralysis. They were unable to take any step, and muscles remained quiescent during these attempts.
A neurosurgeon implanted electrodes along the spinal cord of study subjects. Wires from these electrodes were connected to a neurostimulator implanted under the skin in the abdomen.
The men can select different activity-based programs from a tablet that sends signals to the implanted device.
Personalized approach
Within a single day of the surgery, the participants were able to stand, walk, cycle, swim, and control trunk movements.
“It was not perfect at the very beginning, but they could train very early on to have a more fluid gait,” said study investigator neurosurgeon Joceylyne Bloch, MD, associate professor, University of Lausanne and University Hospital Lausanne.
At this stage, not all paralyzed patients are eligible for the procedure. Dr. Bloch explained that at least 6 cm of healthy spinal cord under the lesion is needed to implant the electrodes.
“There’s a huge variability of spinal cord anatomy between individuals. That’s why it’s important to study each person individually and to have individual models in order to be precise.”
Researchers envision having “a library of electrode arrays,” added Dr. Courtine. With preoperative imaging of the individual’s spinal cord, “the neurosurgeon can select the more appropriate electrode array for that specific patient.”
Dr. Courtine noted recovery of sensation with the system differs from one individual to another. One study participant, Michel Roccati, now 30, told the briefing he feels a contraction in his muscle during the stimulation.
Currently, only individuals whose injury is more than a year old are included in the study to ensure patients have “a stable lesion” and reached “a plateau of recovery,” said Dr. Bloch. However, animal models show intervening earlier might boost the benefits.
A patient’s age can influence the outcome, as younger patients are likely in better condition and more motivated than older patients, said Dr. Bloch. However, she noted patients closing in on 50 years have responded well to the therapy.
Such stimulation systems may prove useful in treating conditions typically associated with SCI, such as hypertension and bladder control, and perhaps also in patients with Parkinson’s disease, said Dr. Courtine.
The researchers plan to conduct another study that will include a next-generation pulse generator with features that make the stimulation even more effective and user friendly. A voice recognition system could eventually be connected to the system.
“The next step is a minicomputer that you implant in the body that communicates in real time with an external iPhone,” said Dr. Courtine.
ONWARD Medical, which developed the technology, has received a breakthrough device designation from the Food and Drug Administration. The company is in discussions with the FDA to carry out a clinical trial of the device in the United States.
A ‘huge step forward’
Peter J. Grahn, PhD, assistant professor, department of physical medicine and rehabilitation and department of neurologic surgery, Mayo Clinic, Rochester, Minn., an author of one of the 2018 studies, said this technology “is a huge step forward” and “really pushes the field.”
Compared with the device used in his study that’s designed to treat neuropathic pain, this new system “is much more capable of dynamic stimulation,” said Dr. Grahn. “You can tailor the stimulation based on which area of the spinal cord you want to target during a specific function.”
There has been “a lot of hope and hype” recently around stem cells and biological molecules that were supposed to be “magic pills” to cure spinal cord dysfunction, said Dr. Grahn. “I don’t think this is one of those.”
However, he questioned the researchers’ use of the word “walking.”
“They say independent stepping or walking is restored on day 1, but the graphs show day 1 function is having over 60% of their body weight supported when they’re taking these steps,” he said.
In addition, the “big question” is how this technology can “be distilled down” into an approach “applicable across rehabilitation centers,” said Dr. Grahn.
The study was supported by numerous organizations, including ONWARD Medical. Dr. Courtine and Dr. Bloch hold various patents in relation with the present work. Dr. Courtine is a consultant with ONWARD Medical, and he and Dr. Bloch are shareholders of ONWARD Medical, a company with direct relationships with the presented work. Dr. Grahn reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(SCI), new research shows.
The study demonstrated that an epidural electrical stimulation (EES) system developed specifically for spinal cord injuries enabled three men with complete paralysis to stand, walk, cycle, swim, and move their torso within 1 day.
“Thanks to this technology, we have been able to target individuals with the most serious spinal cord injury, meaning those with clinically complete spinal cord injury, with no sensation and no movement in the legs,” Grégoire Courtine, PhD, professor of neuroscience and neurotechnology at the Swiss Federal Institute of Technology, University Hospital Lausanne (Switzerland), and the University of Lausanne, told reporters attending a press briefing.
The study was published online Feb. 7, 2022, in Nature Medicine.
More rapid, precise, effective
SCIs involve severed connections between the brain and extremities. To compensate for these lost connections, researchers have investigated stem cell therapy, brain-machine interfaces, and powered exoskeletons.
However, these approaches aren’t yet ready for prime time.
In the meantime, researchers discovered even patients with a “complete” injury may have low-functioning connections and started investigating epidural stimulators designed to treat chronic pain. Recent studies – including three published in 2018 – showed promise for these pain-related stimulators in patients with incomplete SCI.
But using such “repurposed” technology meant the electrode array was relatively narrow and short, “so we could not target all the regions of the spinal cord involving control of leg and trunk movements,” said Dr. Courtine. With the newer technology “we are much more precise, effective, and more rapid in delivering therapy.”
To develop this new approach, the researchers designed a paddle lead with an arrangement of electrodes that targets sacral, lumbar, and low-thoracic dorsal roots involved in leg and trunk movements. They also established a personalized computational framework that allows for optimal surgical placement of this paddle lead.
In addition, they developed software that renders the configuration of individualized activity–dependent stimulation programs rapid, simple, and predictable.
They tested these neurotechnologies in three men with complete sensorimotor paralysis as part of an ongoing clinical trial. The participants, aged 29, 32, and 41 years, suffered an SCI from a motor bike accident 3, 9, and 1 year before enrollment.
All three patients exhibited complete sensorimotor paralysis. They were unable to take any step, and muscles remained quiescent during these attempts.
A neurosurgeon implanted electrodes along the spinal cord of study subjects. Wires from these electrodes were connected to a neurostimulator implanted under the skin in the abdomen.
The men can select different activity-based programs from a tablet that sends signals to the implanted device.
Personalized approach
Within a single day of the surgery, the participants were able to stand, walk, cycle, swim, and control trunk movements.
“It was not perfect at the very beginning, but they could train very early on to have a more fluid gait,” said study investigator neurosurgeon Joceylyne Bloch, MD, associate professor, University of Lausanne and University Hospital Lausanne.
At this stage, not all paralyzed patients are eligible for the procedure. Dr. Bloch explained that at least 6 cm of healthy spinal cord under the lesion is needed to implant the electrodes.
“There’s a huge variability of spinal cord anatomy between individuals. That’s why it’s important to study each person individually and to have individual models in order to be precise.”
Researchers envision having “a library of electrode arrays,” added Dr. Courtine. With preoperative imaging of the individual’s spinal cord, “the neurosurgeon can select the more appropriate electrode array for that specific patient.”
Dr. Courtine noted recovery of sensation with the system differs from one individual to another. One study participant, Michel Roccati, now 30, told the briefing he feels a contraction in his muscle during the stimulation.
Currently, only individuals whose injury is more than a year old are included in the study to ensure patients have “a stable lesion” and reached “a plateau of recovery,” said Dr. Bloch. However, animal models show intervening earlier might boost the benefits.
A patient’s age can influence the outcome, as younger patients are likely in better condition and more motivated than older patients, said Dr. Bloch. However, she noted patients closing in on 50 years have responded well to the therapy.
Such stimulation systems may prove useful in treating conditions typically associated with SCI, such as hypertension and bladder control, and perhaps also in patients with Parkinson’s disease, said Dr. Courtine.
The researchers plan to conduct another study that will include a next-generation pulse generator with features that make the stimulation even more effective and user friendly. A voice recognition system could eventually be connected to the system.
“The next step is a minicomputer that you implant in the body that communicates in real time with an external iPhone,” said Dr. Courtine.
ONWARD Medical, which developed the technology, has received a breakthrough device designation from the Food and Drug Administration. The company is in discussions with the FDA to carry out a clinical trial of the device in the United States.
A ‘huge step forward’
Peter J. Grahn, PhD, assistant professor, department of physical medicine and rehabilitation and department of neurologic surgery, Mayo Clinic, Rochester, Minn., an author of one of the 2018 studies, said this technology “is a huge step forward” and “really pushes the field.”
Compared with the device used in his study that’s designed to treat neuropathic pain, this new system “is much more capable of dynamic stimulation,” said Dr. Grahn. “You can tailor the stimulation based on which area of the spinal cord you want to target during a specific function.”
There has been “a lot of hope and hype” recently around stem cells and biological molecules that were supposed to be “magic pills” to cure spinal cord dysfunction, said Dr. Grahn. “I don’t think this is one of those.”
However, he questioned the researchers’ use of the word “walking.”
“They say independent stepping or walking is restored on day 1, but the graphs show day 1 function is having over 60% of their body weight supported when they’re taking these steps,” he said.
In addition, the “big question” is how this technology can “be distilled down” into an approach “applicable across rehabilitation centers,” said Dr. Grahn.
The study was supported by numerous organizations, including ONWARD Medical. Dr. Courtine and Dr. Bloch hold various patents in relation with the present work. Dr. Courtine is a consultant with ONWARD Medical, and he and Dr. Bloch are shareholders of ONWARD Medical, a company with direct relationships with the presented work. Dr. Grahn reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
Drinking a risk factor for epilepsy?
but more research is needed before any definitive conclusions can be drawn.
Results of an updated meta-analysis are consistent with those of a previous meta-analysis but contrast with some prior cohort studies.
“Further large cohort studies of the general population are required to assert a definite causal relationship between alcohol consumption and epilepsy and to identify a potential threshold,” Yun Hak Kim, MD, PhD, departments of biomedical informatics and anatomy, Pusan (South Korea) National University, said in a press release.
The study was published online Jan. 11, 2022, in Drug and Alcohol Dependence.
Conflicting findings
Much of the research into the impact of alcohol on epilepsy risk has focused on provoked seizures related to alcohol intoxication or withdrawal, but few studies have investigated the effect of alcohol on unprovoked seizures. In addition, the research in this area has been conflicting.
A 2010 meta-analysis that included six case-control studies showed alcohol users had an increased risk of unprovoked seizure or epilepsy with a pooled relative risk of 2.19 (95% confidence interval, 1.82-2.63). This analysis also showed a dose-dependent relationship with relative risks increasing with more grams of alcohol consumed daily.
However, some recent large cohort studies showed that moderate alcohol consumption was associated with a lower risk of epilepsy.
The updated meta-analysis included eight studies – three cohort studies not included in the previous meta-analysis and five case-control studies.
The study excluded two case-control studies included in the previous meta-analysis. One of these studies used duplicated data, and the other included epilepsy patients and did not present results of subgroup analysis for patients experiencing their first seizure.
Results of the new analysis showed the pooled odds ratio for newly diagnosed epilepsy was 1.70 (95% CI, 1.16-2.49) in alcohol users versus nondrinkers.
A dose-response analysis of case-control studies carried out using the cubic spline analysis showed a significant positive dose-response relationship. A dose-response graph showed a steep increase in risk above about 150 g/day and 250 g/day of alcohol consumption.
However, a subgroup analysis showed that epilepsy risk was only found in the case-control studies. In fact, two of the three cohort studies showed that alcohol consumption was associated with a lower risk of epilepsy, although this was not significant.
Cohort studies often include more control subjects and longer follow-up periods and are less prone to bias, such as selection and recall biases, the investigators noted.
“Therefore, cohort studies usually provide a stronger association between exposure and disease than case-control studies, despite having limitations for diseases with low incidence levels,” they wrote.
More research needed
The researchers added that most case-control studies included in the new meta-analysis assessed alcohol consumption only in the 6 months prior to the onset of seizures. Research shows it usually takes heavy drinkers 5 or more years to develop repetitive unprovoked seizures.
“Considering these temporal relationships and differences in study design, alcohol may not actually increase the risk of epilepsy, as seen in our subgroup analysis for cohort studies,” the investigators wrote.
They noted that the cohort studies in the meta-analysis were variously limited to young women, elderly patients, and post–subdural hematoma patients. “This limitation makes it difficult to confirm or generalize the results of the subgroup analysis.”
To resolve this “discrepancy,” further large cohort studies of the general population over a longer period are needed, the investigators wrote.
Examining the risk of bias within studies, the authors evaluated three cohort studies as “good” quality. Of the case-control studies, they rated two as “good,” one as “fair,” and two as “poor.”
For primary prevention, an assessment of the risk of alcohol consumption in various clinical situations, such as the time relation of alcohol consumption with seizures, will be important, lead author Kyoung Nam Woo, department of neurology, Pusan National University, said in the release.
“To increase the applicability to the general population, future studies should be conducted in which the potential confounders such as age, sex, and smoking have been adjusted.”
Commenting on the study, Jacqueline French, MD, professor, New York University Comprehensive Epilepsy Center, echoed the authors in noting a number of weaknesses in the study.
The analysis was unable to exclude alcohol withdrawal seizures. Also, while some studies suggested a positive relationship, others suggested a negative relationship, she said. “The authors suggest further work is needed before a definitive determination is made, and I agree.”
The study received funding from the Medical Research Center Program, the Basic Science Research Program, and the Collaborative Genome Program for Fostering New Post-Genome Industry through a National Research Foundation of Korea grant funded by the Korean government. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
but more research is needed before any definitive conclusions can be drawn.
Results of an updated meta-analysis are consistent with those of a previous meta-analysis but contrast with some prior cohort studies.
“Further large cohort studies of the general population are required to assert a definite causal relationship between alcohol consumption and epilepsy and to identify a potential threshold,” Yun Hak Kim, MD, PhD, departments of biomedical informatics and anatomy, Pusan (South Korea) National University, said in a press release.
The study was published online Jan. 11, 2022, in Drug and Alcohol Dependence.
Conflicting findings
Much of the research into the impact of alcohol on epilepsy risk has focused on provoked seizures related to alcohol intoxication or withdrawal, but few studies have investigated the effect of alcohol on unprovoked seizures. In addition, the research in this area has been conflicting.
A 2010 meta-analysis that included six case-control studies showed alcohol users had an increased risk of unprovoked seizure or epilepsy with a pooled relative risk of 2.19 (95% confidence interval, 1.82-2.63). This analysis also showed a dose-dependent relationship with relative risks increasing with more grams of alcohol consumed daily.
However, some recent large cohort studies showed that moderate alcohol consumption was associated with a lower risk of epilepsy.
The updated meta-analysis included eight studies – three cohort studies not included in the previous meta-analysis and five case-control studies.
The study excluded two case-control studies included in the previous meta-analysis. One of these studies used duplicated data, and the other included epilepsy patients and did not present results of subgroup analysis for patients experiencing their first seizure.
Results of the new analysis showed the pooled odds ratio for newly diagnosed epilepsy was 1.70 (95% CI, 1.16-2.49) in alcohol users versus nondrinkers.
A dose-response analysis of case-control studies carried out using the cubic spline analysis showed a significant positive dose-response relationship. A dose-response graph showed a steep increase in risk above about 150 g/day and 250 g/day of alcohol consumption.
However, a subgroup analysis showed that epilepsy risk was only found in the case-control studies. In fact, two of the three cohort studies showed that alcohol consumption was associated with a lower risk of epilepsy, although this was not significant.
Cohort studies often include more control subjects and longer follow-up periods and are less prone to bias, such as selection and recall biases, the investigators noted.
“Therefore, cohort studies usually provide a stronger association between exposure and disease than case-control studies, despite having limitations for diseases with low incidence levels,” they wrote.
More research needed
The researchers added that most case-control studies included in the new meta-analysis assessed alcohol consumption only in the 6 months prior to the onset of seizures. Research shows it usually takes heavy drinkers 5 or more years to develop repetitive unprovoked seizures.
“Considering these temporal relationships and differences in study design, alcohol may not actually increase the risk of epilepsy, as seen in our subgroup analysis for cohort studies,” the investigators wrote.
They noted that the cohort studies in the meta-analysis were variously limited to young women, elderly patients, and post–subdural hematoma patients. “This limitation makes it difficult to confirm or generalize the results of the subgroup analysis.”
To resolve this “discrepancy,” further large cohort studies of the general population over a longer period are needed, the investigators wrote.
Examining the risk of bias within studies, the authors evaluated three cohort studies as “good” quality. Of the case-control studies, they rated two as “good,” one as “fair,” and two as “poor.”
For primary prevention, an assessment of the risk of alcohol consumption in various clinical situations, such as the time relation of alcohol consumption with seizures, will be important, lead author Kyoung Nam Woo, department of neurology, Pusan National University, said in the release.
“To increase the applicability to the general population, future studies should be conducted in which the potential confounders such as age, sex, and smoking have been adjusted.”
Commenting on the study, Jacqueline French, MD, professor, New York University Comprehensive Epilepsy Center, echoed the authors in noting a number of weaknesses in the study.
The analysis was unable to exclude alcohol withdrawal seizures. Also, while some studies suggested a positive relationship, others suggested a negative relationship, she said. “The authors suggest further work is needed before a definitive determination is made, and I agree.”
The study received funding from the Medical Research Center Program, the Basic Science Research Program, and the Collaborative Genome Program for Fostering New Post-Genome Industry through a National Research Foundation of Korea grant funded by the Korean government. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
but more research is needed before any definitive conclusions can be drawn.
Results of an updated meta-analysis are consistent with those of a previous meta-analysis but contrast with some prior cohort studies.
“Further large cohort studies of the general population are required to assert a definite causal relationship between alcohol consumption and epilepsy and to identify a potential threshold,” Yun Hak Kim, MD, PhD, departments of biomedical informatics and anatomy, Pusan (South Korea) National University, said in a press release.
The study was published online Jan. 11, 2022, in Drug and Alcohol Dependence.
Conflicting findings
Much of the research into the impact of alcohol on epilepsy risk has focused on provoked seizures related to alcohol intoxication or withdrawal, but few studies have investigated the effect of alcohol on unprovoked seizures. In addition, the research in this area has been conflicting.
A 2010 meta-analysis that included six case-control studies showed alcohol users had an increased risk of unprovoked seizure or epilepsy with a pooled relative risk of 2.19 (95% confidence interval, 1.82-2.63). This analysis also showed a dose-dependent relationship with relative risks increasing with more grams of alcohol consumed daily.
However, some recent large cohort studies showed that moderate alcohol consumption was associated with a lower risk of epilepsy.
The updated meta-analysis included eight studies – three cohort studies not included in the previous meta-analysis and five case-control studies.
The study excluded two case-control studies included in the previous meta-analysis. One of these studies used duplicated data, and the other included epilepsy patients and did not present results of subgroup analysis for patients experiencing their first seizure.
Results of the new analysis showed the pooled odds ratio for newly diagnosed epilepsy was 1.70 (95% CI, 1.16-2.49) in alcohol users versus nondrinkers.
A dose-response analysis of case-control studies carried out using the cubic spline analysis showed a significant positive dose-response relationship. A dose-response graph showed a steep increase in risk above about 150 g/day and 250 g/day of alcohol consumption.
However, a subgroup analysis showed that epilepsy risk was only found in the case-control studies. In fact, two of the three cohort studies showed that alcohol consumption was associated with a lower risk of epilepsy, although this was not significant.
Cohort studies often include more control subjects and longer follow-up periods and are less prone to bias, such as selection and recall biases, the investigators noted.
“Therefore, cohort studies usually provide a stronger association between exposure and disease than case-control studies, despite having limitations for diseases with low incidence levels,” they wrote.
More research needed
The researchers added that most case-control studies included in the new meta-analysis assessed alcohol consumption only in the 6 months prior to the onset of seizures. Research shows it usually takes heavy drinkers 5 or more years to develop repetitive unprovoked seizures.
“Considering these temporal relationships and differences in study design, alcohol may not actually increase the risk of epilepsy, as seen in our subgroup analysis for cohort studies,” the investigators wrote.
They noted that the cohort studies in the meta-analysis were variously limited to young women, elderly patients, and post–subdural hematoma patients. “This limitation makes it difficult to confirm or generalize the results of the subgroup analysis.”
To resolve this “discrepancy,” further large cohort studies of the general population over a longer period are needed, the investigators wrote.
Examining the risk of bias within studies, the authors evaluated three cohort studies as “good” quality. Of the case-control studies, they rated two as “good,” one as “fair,” and two as “poor.”
For primary prevention, an assessment of the risk of alcohol consumption in various clinical situations, such as the time relation of alcohol consumption with seizures, will be important, lead author Kyoung Nam Woo, department of neurology, Pusan National University, said in the release.
“To increase the applicability to the general population, future studies should be conducted in which the potential confounders such as age, sex, and smoking have been adjusted.”
Commenting on the study, Jacqueline French, MD, professor, New York University Comprehensive Epilepsy Center, echoed the authors in noting a number of weaknesses in the study.
The analysis was unable to exclude alcohol withdrawal seizures. Also, while some studies suggested a positive relationship, others suggested a negative relationship, she said. “The authors suggest further work is needed before a definitive determination is made, and I agree.”
The study received funding from the Medical Research Center Program, the Basic Science Research Program, and the Collaborative Genome Program for Fostering New Post-Genome Industry through a National Research Foundation of Korea grant funded by the Korean government. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALCOHOL DEPENDENCE
Dietary fat tied to better cognition in older adults
, new research suggests.
The study provides important “pieces of the puzzle” of the diet and cognition connection, but the results aren’t “ready for prime time,” study investigator Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, said in an interview.
“I don’t think we’re there yet when it comes to recommending supplementation to the general public,” said Dr. McIntyre, adding a larger “more compelling study” is needed.
The study was published online Jan. 14 in The American Journal of Geriatric Psychiatry.
Clinically meaningful?
Research shows that 25%-50% of community-dwelling adults aged 65-85 years have some cognitive impairment. Other evidence indicates cognition is affected by dietary fat intake.
Many lines of research show that alterations in lipid homeostasis can cause brain dysfunction, said Dr. McIntyre. “This shouldn’t surprise us because our brain is made up of protein, water, and fat.”
This new analysis used combined data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), a series of ongoing cross-sectional surveys conducted by the Centers for Disease Control and Prevention. The data are collected in two phases, an in-home face-to-face interview and a physical examination.
Researchers obtained dietary intake information through two 24-hour dietary recall interviews. Dietary information included total energy (kcal/d), intakes in grams per day (g/d) of total fat, saturated fatty acid (SFAT), monounsaturated fatty acid (MUFA), PUFA, total omega-3 and total omega-6 fatty acids, and milligrams per day (mg/d) of cholesterol.
For cognitive function, the researchers used total and delayed recall scores of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD), the animal fluency test, and the digit symbol substitution test (DSST).
The study included 2,253 adults aged 60 years and older (mean age, 69.4 years) and 51% were non-Hispanic White individuals.
After adjustment for age, sex, race/ethnicity, educational attainment, smoking status, alcohol consumption, income, and total energy, dietary intake of PUFA and omega-6 fatty acid was positively associated with DSST.
The DSST score increased about 0.06 standard deviation (SD) (about 1 score) with each SD increase in these fatty acids (8.8 g/d for PUFA and 7.9 g/d for omega-6) (P values were .02 for PUFA and .01 for omega-6).
However, it’s unclear what an improvement of 1 DSST score means clinically, said Dr. McIntyre. “The P value is significant, but how does that translate? Does this mean a person can now think more clearly or function better?”
‘Million dollar question’ remains unanswered
The fact that omega-6, considered neuroinflammatory, was associated with improved DSST score illustrates the complexity of this field, said Dr. McIntyre.
“We’re learning that when it comes to inflammation, many of the molecules in our brain that are implicated as anti-inflammatory can also be pro-inflammatory, so bad guys can be good guys and good guys can be bad guys.”
It speaks to the notion of homeostasis, he added. “Just like a seesaw; when you push this part down, that part goes up.”
The analysis showed the animal fluency score increased about 0.05 SD (around 0.3 score) with each SD (1.1 g/d) increase in dietary intake of omega-3.
There were no significant associations between other dietary fat intake and cognitive performance.
The researchers investigated the role of oxidative stress and antioxidant biomarkers (gamma glutamyl transpeptidase [GGT], bilirubin, uric acid, and vitamin D).
Cells produce oxidative radicals that are normally “mopped up” by our “innate antioxidant capability,” said Dr. McIntyre. “But in states of cognitive impairment, these oxidative stress markers accumulate and they exceed what the normal innate response is able to manage.”
The study showed GGT levels decreased with increased PUFA and omega-6 fatty acid intakes; levels of bilirubin decreased with increase in most dietary fat intakes; uric acid levels decreased with MUFA intake and omega-6/omega-3 ratio; and vitamin D levels increased with omega-3 fatty acid intake but decreased with SFAT intake.
Causal mediation analysis showed the association between dietary intake of fatty acids and DSST performance was partially mediated by GGT levels. However, Dr. McIntyre emphasized that this does not prove causality.
“The million dollar question is, is this the sole explanation for the association? In other words, is it the oxidative stress that caused the cognitive impairment and therefore correcting it improved it, or is it the case that oxidative stress is a proxy of other activities that are also taking place?”
A ‘plausible’ link
In an editorial, Candida Rebello, PhD, of the department of integrated physiology and molecular medicine at Pennington Biomedical Research Center, Baton Rouge, La., said the finding that omega-3 and omega-6 fatty acids are positively associated with cognition in older adults makes some sense.
She noted that aging is associated with an overt inflammatory phenotype, and evidence shows these fatty acids are precursors for bioactive molecules that play a role in self-limiting the acute inflammatory response.
Dr. Rebello said the positive association of omega-6 fatty acid with cognition shown in this study contrasts with the “common belief” that increasing dietary intake of these fatty acids enhances inflammation, but agreed the association is “plausible.”
She said it’s “essential” to determine “the underlying mechanisms that regulate the diverse features of inflammation and sort out the processes that protect from neuronal damage and those that contribute towards it.”
She noted the ratio of omega-6 to omega-3 is about 15:1 in the present day Western diet, as opposed to a 1:1 ratio in diets of the past. Omega-3 fatty acids are found in fish oil supplements and fatty fish like mackerel and salmon, while cereal, grains, and vegetable oil are sources of omega-6.
Attaining a measure of balance of fatty acids in the diet may be a “prudent approach,” said Dr. Rebello. “Substituting some meat entrées with fatty fish and polyunsaturated vegetable oils with monounsaturated fats such as olive oil are small changes that are likely to garner adherence.”
Dr. Rebello noted that the study used NHANES food intake data, which rely on participant self-report and so may not be accurate.
The study received funding from the MOE (Ministry of Education in China) Project of Humanities and Social Sciences and the Research Startup Fund of Southwest University. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, and AbbVie. He is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
, new research suggests.
The study provides important “pieces of the puzzle” of the diet and cognition connection, but the results aren’t “ready for prime time,” study investigator Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, said in an interview.
“I don’t think we’re there yet when it comes to recommending supplementation to the general public,” said Dr. McIntyre, adding a larger “more compelling study” is needed.
The study was published online Jan. 14 in The American Journal of Geriatric Psychiatry.
Clinically meaningful?
Research shows that 25%-50% of community-dwelling adults aged 65-85 years have some cognitive impairment. Other evidence indicates cognition is affected by dietary fat intake.
Many lines of research show that alterations in lipid homeostasis can cause brain dysfunction, said Dr. McIntyre. “This shouldn’t surprise us because our brain is made up of protein, water, and fat.”
This new analysis used combined data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), a series of ongoing cross-sectional surveys conducted by the Centers for Disease Control and Prevention. The data are collected in two phases, an in-home face-to-face interview and a physical examination.
Researchers obtained dietary intake information through two 24-hour dietary recall interviews. Dietary information included total energy (kcal/d), intakes in grams per day (g/d) of total fat, saturated fatty acid (SFAT), monounsaturated fatty acid (MUFA), PUFA, total omega-3 and total omega-6 fatty acids, and milligrams per day (mg/d) of cholesterol.
For cognitive function, the researchers used total and delayed recall scores of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD), the animal fluency test, and the digit symbol substitution test (DSST).
The study included 2,253 adults aged 60 years and older (mean age, 69.4 years) and 51% were non-Hispanic White individuals.
After adjustment for age, sex, race/ethnicity, educational attainment, smoking status, alcohol consumption, income, and total energy, dietary intake of PUFA and omega-6 fatty acid was positively associated with DSST.
The DSST score increased about 0.06 standard deviation (SD) (about 1 score) with each SD increase in these fatty acids (8.8 g/d for PUFA and 7.9 g/d for omega-6) (P values were .02 for PUFA and .01 for omega-6).
However, it’s unclear what an improvement of 1 DSST score means clinically, said Dr. McIntyre. “The P value is significant, but how does that translate? Does this mean a person can now think more clearly or function better?”
‘Million dollar question’ remains unanswered
The fact that omega-6, considered neuroinflammatory, was associated with improved DSST score illustrates the complexity of this field, said Dr. McIntyre.
“We’re learning that when it comes to inflammation, many of the molecules in our brain that are implicated as anti-inflammatory can also be pro-inflammatory, so bad guys can be good guys and good guys can be bad guys.”
It speaks to the notion of homeostasis, he added. “Just like a seesaw; when you push this part down, that part goes up.”
The analysis showed the animal fluency score increased about 0.05 SD (around 0.3 score) with each SD (1.1 g/d) increase in dietary intake of omega-3.
There were no significant associations between other dietary fat intake and cognitive performance.
The researchers investigated the role of oxidative stress and antioxidant biomarkers (gamma glutamyl transpeptidase [GGT], bilirubin, uric acid, and vitamin D).
Cells produce oxidative radicals that are normally “mopped up” by our “innate antioxidant capability,” said Dr. McIntyre. “But in states of cognitive impairment, these oxidative stress markers accumulate and they exceed what the normal innate response is able to manage.”
The study showed GGT levels decreased with increased PUFA and omega-6 fatty acid intakes; levels of bilirubin decreased with increase in most dietary fat intakes; uric acid levels decreased with MUFA intake and omega-6/omega-3 ratio; and vitamin D levels increased with omega-3 fatty acid intake but decreased with SFAT intake.
Causal mediation analysis showed the association between dietary intake of fatty acids and DSST performance was partially mediated by GGT levels. However, Dr. McIntyre emphasized that this does not prove causality.
“The million dollar question is, is this the sole explanation for the association? In other words, is it the oxidative stress that caused the cognitive impairment and therefore correcting it improved it, or is it the case that oxidative stress is a proxy of other activities that are also taking place?”
A ‘plausible’ link
In an editorial, Candida Rebello, PhD, of the department of integrated physiology and molecular medicine at Pennington Biomedical Research Center, Baton Rouge, La., said the finding that omega-3 and omega-6 fatty acids are positively associated with cognition in older adults makes some sense.
She noted that aging is associated with an overt inflammatory phenotype, and evidence shows these fatty acids are precursors for bioactive molecules that play a role in self-limiting the acute inflammatory response.
Dr. Rebello said the positive association of omega-6 fatty acid with cognition shown in this study contrasts with the “common belief” that increasing dietary intake of these fatty acids enhances inflammation, but agreed the association is “plausible.”
She said it’s “essential” to determine “the underlying mechanisms that regulate the diverse features of inflammation and sort out the processes that protect from neuronal damage and those that contribute towards it.”
She noted the ratio of omega-6 to omega-3 is about 15:1 in the present day Western diet, as opposed to a 1:1 ratio in diets of the past. Omega-3 fatty acids are found in fish oil supplements and fatty fish like mackerel and salmon, while cereal, grains, and vegetable oil are sources of omega-6.
Attaining a measure of balance of fatty acids in the diet may be a “prudent approach,” said Dr. Rebello. “Substituting some meat entrées with fatty fish and polyunsaturated vegetable oils with monounsaturated fats such as olive oil are small changes that are likely to garner adherence.”
Dr. Rebello noted that the study used NHANES food intake data, which rely on participant self-report and so may not be accurate.
The study received funding from the MOE (Ministry of Education in China) Project of Humanities and Social Sciences and the Research Startup Fund of Southwest University. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, and AbbVie. He is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
, new research suggests.
The study provides important “pieces of the puzzle” of the diet and cognition connection, but the results aren’t “ready for prime time,” study investigator Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, said in an interview.
“I don’t think we’re there yet when it comes to recommending supplementation to the general public,” said Dr. McIntyre, adding a larger “more compelling study” is needed.
The study was published online Jan. 14 in The American Journal of Geriatric Psychiatry.
Clinically meaningful?
Research shows that 25%-50% of community-dwelling adults aged 65-85 years have some cognitive impairment. Other evidence indicates cognition is affected by dietary fat intake.
Many lines of research show that alterations in lipid homeostasis can cause brain dysfunction, said Dr. McIntyre. “This shouldn’t surprise us because our brain is made up of protein, water, and fat.”
This new analysis used combined data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), a series of ongoing cross-sectional surveys conducted by the Centers for Disease Control and Prevention. The data are collected in two phases, an in-home face-to-face interview and a physical examination.
Researchers obtained dietary intake information through two 24-hour dietary recall interviews. Dietary information included total energy (kcal/d), intakes in grams per day (g/d) of total fat, saturated fatty acid (SFAT), monounsaturated fatty acid (MUFA), PUFA, total omega-3 and total omega-6 fatty acids, and milligrams per day (mg/d) of cholesterol.
For cognitive function, the researchers used total and delayed recall scores of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD), the animal fluency test, and the digit symbol substitution test (DSST).
The study included 2,253 adults aged 60 years and older (mean age, 69.4 years) and 51% were non-Hispanic White individuals.
After adjustment for age, sex, race/ethnicity, educational attainment, smoking status, alcohol consumption, income, and total energy, dietary intake of PUFA and omega-6 fatty acid was positively associated with DSST.
The DSST score increased about 0.06 standard deviation (SD) (about 1 score) with each SD increase in these fatty acids (8.8 g/d for PUFA and 7.9 g/d for omega-6) (P values were .02 for PUFA and .01 for omega-6).
However, it’s unclear what an improvement of 1 DSST score means clinically, said Dr. McIntyre. “The P value is significant, but how does that translate? Does this mean a person can now think more clearly or function better?”
‘Million dollar question’ remains unanswered
The fact that omega-6, considered neuroinflammatory, was associated with improved DSST score illustrates the complexity of this field, said Dr. McIntyre.
“We’re learning that when it comes to inflammation, many of the molecules in our brain that are implicated as anti-inflammatory can also be pro-inflammatory, so bad guys can be good guys and good guys can be bad guys.”
It speaks to the notion of homeostasis, he added. “Just like a seesaw; when you push this part down, that part goes up.”
The analysis showed the animal fluency score increased about 0.05 SD (around 0.3 score) with each SD (1.1 g/d) increase in dietary intake of omega-3.
There were no significant associations between other dietary fat intake and cognitive performance.
The researchers investigated the role of oxidative stress and antioxidant biomarkers (gamma glutamyl transpeptidase [GGT], bilirubin, uric acid, and vitamin D).
Cells produce oxidative radicals that are normally “mopped up” by our “innate antioxidant capability,” said Dr. McIntyre. “But in states of cognitive impairment, these oxidative stress markers accumulate and they exceed what the normal innate response is able to manage.”
The study showed GGT levels decreased with increased PUFA and omega-6 fatty acid intakes; levels of bilirubin decreased with increase in most dietary fat intakes; uric acid levels decreased with MUFA intake and omega-6/omega-3 ratio; and vitamin D levels increased with omega-3 fatty acid intake but decreased with SFAT intake.
Causal mediation analysis showed the association between dietary intake of fatty acids and DSST performance was partially mediated by GGT levels. However, Dr. McIntyre emphasized that this does not prove causality.
“The million dollar question is, is this the sole explanation for the association? In other words, is it the oxidative stress that caused the cognitive impairment and therefore correcting it improved it, or is it the case that oxidative stress is a proxy of other activities that are also taking place?”
A ‘plausible’ link
In an editorial, Candida Rebello, PhD, of the department of integrated physiology and molecular medicine at Pennington Biomedical Research Center, Baton Rouge, La., said the finding that omega-3 and omega-6 fatty acids are positively associated with cognition in older adults makes some sense.
She noted that aging is associated with an overt inflammatory phenotype, and evidence shows these fatty acids are precursors for bioactive molecules that play a role in self-limiting the acute inflammatory response.
Dr. Rebello said the positive association of omega-6 fatty acid with cognition shown in this study contrasts with the “common belief” that increasing dietary intake of these fatty acids enhances inflammation, but agreed the association is “plausible.”
She said it’s “essential” to determine “the underlying mechanisms that regulate the diverse features of inflammation and sort out the processes that protect from neuronal damage and those that contribute towards it.”
She noted the ratio of omega-6 to omega-3 is about 15:1 in the present day Western diet, as opposed to a 1:1 ratio in diets of the past. Omega-3 fatty acids are found in fish oil supplements and fatty fish like mackerel and salmon, while cereal, grains, and vegetable oil are sources of omega-6.
Attaining a measure of balance of fatty acids in the diet may be a “prudent approach,” said Dr. Rebello. “Substituting some meat entrées with fatty fish and polyunsaturated vegetable oils with monounsaturated fats such as olive oil are small changes that are likely to garner adherence.”
Dr. Rebello noted that the study used NHANES food intake data, which rely on participant self-report and so may not be accurate.
The study received funding from the MOE (Ministry of Education in China) Project of Humanities and Social Sciences and the Research Startup Fund of Southwest University. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, and AbbVie. He is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
AHA annual stats update highlights heart-brain connection
in its annual statistical update on heart disease and stroke.
“For several years now, the AHA and the scientific community have increasingly recognized the connections between cardiovascular health and brain health, so it was time for us to cement this into its own chapter, which we highlight as the brain health chapter,” Connie W. Tsao, MD, MPH, chair of the statistical update writing group, with Harvard Medical School, Boston, said in an AHA podcast.
“The global rate of brain disease is quickly outpacing heart disease,” Mitchell S. V. Elkind, MD, immediate past president of the AHA, added in a news release.
“The rate of deaths from Alzheimer’s disease and other dementias rose more than twice as much in the past decade compared to the rate of deaths from heart disease, and that is something we must address,” said Dr. Elkind, with Columbia University Vagelos College of Physicians and Surgeons in New York.
“It’s becoming more evident that reducing vascular disease risk factors can make a real difference in helping people live longer, healthier lives, free of heart disease and brain disease,” Dr. Elkind added.
The AHA’s Heart Disease and Stroke Statistics – 2022 Update was published online January 26 in Circulation).
The report highlights some of the research connecting heart and brain health, including the following:
- A meta-analysis of 139 studies showed that people with midlife hypertension were five times more likely to experience impairment on global cognition and about twice as likely to experience reduced executive function, dementia, and Alzheimer’s disease.
- A meta-analysis of four longitudinal studies found that the risk for dementia associated with heart failure was increased nearly twofold.
- In the large prospective Atherosclerosis Risk in Communities (ARIC) Neurocognitive Study, atrial fibrillation was associated with greater cognitive decline and dementia over 20 years.
- A meta-analysis of 10 prospective studies (including 24,801 participants) showed that coronary heart disease (CHD) was associated with a 40% increased risk of poor cognitive outcomes, including dementia, cognitive impairment, or cognitive decline.
“This new chapter on brain health was a critical one to add,” Dr. Tsao said in the news release.
“The data we’ve collected brings to light the strong correlations between heart health and brain health and makes it an easy story to tell -- what’s good for the heart is good for the brain,” Dr. Tsao added.
Along with the new chapter on brain health, the 2022 statistical update provides the latest statistics and heart disease and stroke. Among the highlights:
- Cardiovascular disease (CVD) remains the leading cause of death worldwide. In the United States in 2019, CVD, listed as the underlying cause of death, accounted for 874,613 deaths, about 2,396 deaths each day. On average, someone dies of CVD every 36 seconds.
- CVD claims more lives each year in the United States than all forms of cancer and chronic lower respiratory disease combined.
- In 2019, CHD was the leading cause (41.3%) of deaths attributable to CVD, followed by other CVD (17.3%), stroke (17.2%), hypertension (11.7%), heart failure (9.9%), and diseases of the arteries (2.8%).
- In 2019, stroke accounted for roughly 1 in every 19 deaths in the United States. On average, someone in the United States has a stroke every 40 seconds and someone dies of stroke every 3 minutes 30 seconds. When considered separately from other CVD, stroke ranks number five among all causes of death in the United States.
While the annual statistics update aims to be a contemporary update of annual heart disease and stroke statistics over the past year, it also examines trends over time, Dr. Tsao explains in the podcast.
“One noteworthy point is that we saw a decline in the rate of cardiovascular mortality over the past three decades or so until about 2010. But over the past decade now, we’re also seeing a rise in these numbers,” she said.
This could be due to rising rates of obesity, diabetes, and poor hypertension control, as well as other lifestyle behaviors, Tsao said.
Key risk factor data
Each year, the statistical update gauges the cardiovascular health of Americans by tracking seven key health factors and behaviors that increase risk for heart disease and stroke. Below is a snapshot of the latest risk factor data.
Smoking
In 2019, smoking was the leading risk factor for years of life lost to premature death and the third leading risk factor for years of life lived with disability or injury.
According to the 2020 surgeon general’s report on smoking cessation, more than 480,000 Americans die as a result of cigarette smoking, and more than 41,000 die of secondhand smoke exposure each year (roughly 1 in 5 deaths annually).
One in 7 adults are current smokers, 1 in 6 female adults are current smokers, and 1 in 5 high school students use e-cigarettes.
Physical inactivity
In 2018, 25.4% of U.S. adults did not engage in leisure-time physical activity, and only 24.0% met the 2018 Physical Activity Guidelines for Americans for both aerobic and muscle strengthening.
Among U.S. high school students in 2019, only 44.1% were physically active for 60 minutes or more on at least 5 days of the week.
Nutrition
While there is some evidence that Americans are improving their diet, fewer than 10% of U.S. adults met guidelines for whole grain, whole fruit, and nonstarchy vegetable consumption each day in 2017–2018.
Overweight/obesity
The prevalence of obesity among adults increased from 1999–2000 through 2017–2018 from 30.5% to 42.4%. Overall prevalence of obesity and severe obesity in U.S. youth 2 to 19 years of age increased from 13.9% to 19.3% and 2.6% to 6.1% between 1999–2000 and 2017–2018.
Cholesterol
Close to 94 million (38.1%) U.S. adults have total cholesterol of 200 mg/dL or higher, according to 2015–2018 data; about 28.0 million (11.5%) have total cholesterol of 240 mg/dL or higher; and 27.8% have high levels of low-density lipoprotein cholesterol (130 mg/dL or higher).
Diabetes
In 2019, 87,647 U.S. deaths were attributed to diabetes; data show that 9.8 million U.S. adults have undiagnosed diabetes, 28.2 million have diagnosed diabetes, and 113.6 million have prediabetes.
Hypertension
A total of 121.5 million (47.3%) U.S. adults have hypertension, based on 2015–2018 data. In 2019, 102,072 U.S. deaths were primarily attributable to hypertension.
This statistical update was prepared by a volunteer writing group on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Disclosures for the writing committee are listed with the original article.
A version of this article first appeared on Medscape.com.
in its annual statistical update on heart disease and stroke.
“For several years now, the AHA and the scientific community have increasingly recognized the connections between cardiovascular health and brain health, so it was time for us to cement this into its own chapter, which we highlight as the brain health chapter,” Connie W. Tsao, MD, MPH, chair of the statistical update writing group, with Harvard Medical School, Boston, said in an AHA podcast.
“The global rate of brain disease is quickly outpacing heart disease,” Mitchell S. V. Elkind, MD, immediate past president of the AHA, added in a news release.
“The rate of deaths from Alzheimer’s disease and other dementias rose more than twice as much in the past decade compared to the rate of deaths from heart disease, and that is something we must address,” said Dr. Elkind, with Columbia University Vagelos College of Physicians and Surgeons in New York.
“It’s becoming more evident that reducing vascular disease risk factors can make a real difference in helping people live longer, healthier lives, free of heart disease and brain disease,” Dr. Elkind added.
The AHA’s Heart Disease and Stroke Statistics – 2022 Update was published online January 26 in Circulation).
The report highlights some of the research connecting heart and brain health, including the following:
- A meta-analysis of 139 studies showed that people with midlife hypertension were five times more likely to experience impairment on global cognition and about twice as likely to experience reduced executive function, dementia, and Alzheimer’s disease.
- A meta-analysis of four longitudinal studies found that the risk for dementia associated with heart failure was increased nearly twofold.
- In the large prospective Atherosclerosis Risk in Communities (ARIC) Neurocognitive Study, atrial fibrillation was associated with greater cognitive decline and dementia over 20 years.
- A meta-analysis of 10 prospective studies (including 24,801 participants) showed that coronary heart disease (CHD) was associated with a 40% increased risk of poor cognitive outcomes, including dementia, cognitive impairment, or cognitive decline.
“This new chapter on brain health was a critical one to add,” Dr. Tsao said in the news release.
“The data we’ve collected brings to light the strong correlations between heart health and brain health and makes it an easy story to tell -- what’s good for the heart is good for the brain,” Dr. Tsao added.
Along with the new chapter on brain health, the 2022 statistical update provides the latest statistics and heart disease and stroke. Among the highlights:
- Cardiovascular disease (CVD) remains the leading cause of death worldwide. In the United States in 2019, CVD, listed as the underlying cause of death, accounted for 874,613 deaths, about 2,396 deaths each day. On average, someone dies of CVD every 36 seconds.
- CVD claims more lives each year in the United States than all forms of cancer and chronic lower respiratory disease combined.
- In 2019, CHD was the leading cause (41.3%) of deaths attributable to CVD, followed by other CVD (17.3%), stroke (17.2%), hypertension (11.7%), heart failure (9.9%), and diseases of the arteries (2.8%).
- In 2019, stroke accounted for roughly 1 in every 19 deaths in the United States. On average, someone in the United States has a stroke every 40 seconds and someone dies of stroke every 3 minutes 30 seconds. When considered separately from other CVD, stroke ranks number five among all causes of death in the United States.
While the annual statistics update aims to be a contemporary update of annual heart disease and stroke statistics over the past year, it also examines trends over time, Dr. Tsao explains in the podcast.
“One noteworthy point is that we saw a decline in the rate of cardiovascular mortality over the past three decades or so until about 2010. But over the past decade now, we’re also seeing a rise in these numbers,” she said.
This could be due to rising rates of obesity, diabetes, and poor hypertension control, as well as other lifestyle behaviors, Tsao said.
Key risk factor data
Each year, the statistical update gauges the cardiovascular health of Americans by tracking seven key health factors and behaviors that increase risk for heart disease and stroke. Below is a snapshot of the latest risk factor data.
Smoking
In 2019, smoking was the leading risk factor for years of life lost to premature death and the third leading risk factor for years of life lived with disability or injury.
According to the 2020 surgeon general’s report on smoking cessation, more than 480,000 Americans die as a result of cigarette smoking, and more than 41,000 die of secondhand smoke exposure each year (roughly 1 in 5 deaths annually).
One in 7 adults are current smokers, 1 in 6 female adults are current smokers, and 1 in 5 high school students use e-cigarettes.
Physical inactivity
In 2018, 25.4% of U.S. adults did not engage in leisure-time physical activity, and only 24.0% met the 2018 Physical Activity Guidelines for Americans for both aerobic and muscle strengthening.
Among U.S. high school students in 2019, only 44.1% were physically active for 60 minutes or more on at least 5 days of the week.
Nutrition
While there is some evidence that Americans are improving their diet, fewer than 10% of U.S. adults met guidelines for whole grain, whole fruit, and nonstarchy vegetable consumption each day in 2017–2018.
Overweight/obesity
The prevalence of obesity among adults increased from 1999–2000 through 2017–2018 from 30.5% to 42.4%. Overall prevalence of obesity and severe obesity in U.S. youth 2 to 19 years of age increased from 13.9% to 19.3% and 2.6% to 6.1% between 1999–2000 and 2017–2018.
Cholesterol
Close to 94 million (38.1%) U.S. adults have total cholesterol of 200 mg/dL or higher, according to 2015–2018 data; about 28.0 million (11.5%) have total cholesterol of 240 mg/dL or higher; and 27.8% have high levels of low-density lipoprotein cholesterol (130 mg/dL or higher).
Diabetes
In 2019, 87,647 U.S. deaths were attributed to diabetes; data show that 9.8 million U.S. adults have undiagnosed diabetes, 28.2 million have diagnosed diabetes, and 113.6 million have prediabetes.
Hypertension
A total of 121.5 million (47.3%) U.S. adults have hypertension, based on 2015–2018 data. In 2019, 102,072 U.S. deaths were primarily attributable to hypertension.
This statistical update was prepared by a volunteer writing group on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Disclosures for the writing committee are listed with the original article.
A version of this article first appeared on Medscape.com.
in its annual statistical update on heart disease and stroke.
“For several years now, the AHA and the scientific community have increasingly recognized the connections between cardiovascular health and brain health, so it was time for us to cement this into its own chapter, which we highlight as the brain health chapter,” Connie W. Tsao, MD, MPH, chair of the statistical update writing group, with Harvard Medical School, Boston, said in an AHA podcast.
“The global rate of brain disease is quickly outpacing heart disease,” Mitchell S. V. Elkind, MD, immediate past president of the AHA, added in a news release.
“The rate of deaths from Alzheimer’s disease and other dementias rose more than twice as much in the past decade compared to the rate of deaths from heart disease, and that is something we must address,” said Dr. Elkind, with Columbia University Vagelos College of Physicians and Surgeons in New York.
“It’s becoming more evident that reducing vascular disease risk factors can make a real difference in helping people live longer, healthier lives, free of heart disease and brain disease,” Dr. Elkind added.
The AHA’s Heart Disease and Stroke Statistics – 2022 Update was published online January 26 in Circulation).
The report highlights some of the research connecting heart and brain health, including the following:
- A meta-analysis of 139 studies showed that people with midlife hypertension were five times more likely to experience impairment on global cognition and about twice as likely to experience reduced executive function, dementia, and Alzheimer’s disease.
- A meta-analysis of four longitudinal studies found that the risk for dementia associated with heart failure was increased nearly twofold.
- In the large prospective Atherosclerosis Risk in Communities (ARIC) Neurocognitive Study, atrial fibrillation was associated with greater cognitive decline and dementia over 20 years.
- A meta-analysis of 10 prospective studies (including 24,801 participants) showed that coronary heart disease (CHD) was associated with a 40% increased risk of poor cognitive outcomes, including dementia, cognitive impairment, or cognitive decline.
“This new chapter on brain health was a critical one to add,” Dr. Tsao said in the news release.
“The data we’ve collected brings to light the strong correlations between heart health and brain health and makes it an easy story to tell -- what’s good for the heart is good for the brain,” Dr. Tsao added.
Along with the new chapter on brain health, the 2022 statistical update provides the latest statistics and heart disease and stroke. Among the highlights:
- Cardiovascular disease (CVD) remains the leading cause of death worldwide. In the United States in 2019, CVD, listed as the underlying cause of death, accounted for 874,613 deaths, about 2,396 deaths each day. On average, someone dies of CVD every 36 seconds.
- CVD claims more lives each year in the United States than all forms of cancer and chronic lower respiratory disease combined.
- In 2019, CHD was the leading cause (41.3%) of deaths attributable to CVD, followed by other CVD (17.3%), stroke (17.2%), hypertension (11.7%), heart failure (9.9%), and diseases of the arteries (2.8%).
- In 2019, stroke accounted for roughly 1 in every 19 deaths in the United States. On average, someone in the United States has a stroke every 40 seconds and someone dies of stroke every 3 minutes 30 seconds. When considered separately from other CVD, stroke ranks number five among all causes of death in the United States.
While the annual statistics update aims to be a contemporary update of annual heart disease and stroke statistics over the past year, it also examines trends over time, Dr. Tsao explains in the podcast.
“One noteworthy point is that we saw a decline in the rate of cardiovascular mortality over the past three decades or so until about 2010. But over the past decade now, we’re also seeing a rise in these numbers,” she said.
This could be due to rising rates of obesity, diabetes, and poor hypertension control, as well as other lifestyle behaviors, Tsao said.
Key risk factor data
Each year, the statistical update gauges the cardiovascular health of Americans by tracking seven key health factors and behaviors that increase risk for heart disease and stroke. Below is a snapshot of the latest risk factor data.
Smoking
In 2019, smoking was the leading risk factor for years of life lost to premature death and the third leading risk factor for years of life lived with disability or injury.
According to the 2020 surgeon general’s report on smoking cessation, more than 480,000 Americans die as a result of cigarette smoking, and more than 41,000 die of secondhand smoke exposure each year (roughly 1 in 5 deaths annually).
One in 7 adults are current smokers, 1 in 6 female adults are current smokers, and 1 in 5 high school students use e-cigarettes.
Physical inactivity
In 2018, 25.4% of U.S. adults did not engage in leisure-time physical activity, and only 24.0% met the 2018 Physical Activity Guidelines for Americans for both aerobic and muscle strengthening.
Among U.S. high school students in 2019, only 44.1% were physically active for 60 minutes or more on at least 5 days of the week.
Nutrition
While there is some evidence that Americans are improving their diet, fewer than 10% of U.S. adults met guidelines for whole grain, whole fruit, and nonstarchy vegetable consumption each day in 2017–2018.
Overweight/obesity
The prevalence of obesity among adults increased from 1999–2000 through 2017–2018 from 30.5% to 42.4%. Overall prevalence of obesity and severe obesity in U.S. youth 2 to 19 years of age increased from 13.9% to 19.3% and 2.6% to 6.1% between 1999–2000 and 2017–2018.
Cholesterol
Close to 94 million (38.1%) U.S. adults have total cholesterol of 200 mg/dL or higher, according to 2015–2018 data; about 28.0 million (11.5%) have total cholesterol of 240 mg/dL or higher; and 27.8% have high levels of low-density lipoprotein cholesterol (130 mg/dL or higher).
Diabetes
In 2019, 87,647 U.S. deaths were attributed to diabetes; data show that 9.8 million U.S. adults have undiagnosed diabetes, 28.2 million have diagnosed diabetes, and 113.6 million have prediabetes.
Hypertension
A total of 121.5 million (47.3%) U.S. adults have hypertension, based on 2015–2018 data. In 2019, 102,072 U.S. deaths were primarily attributable to hypertension.
This statistical update was prepared by a volunteer writing group on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Disclosures for the writing committee are listed with the original article.
A version of this article first appeared on Medscape.com.
Screen time in first year may raise autism risk at age 3
Boys exposed to at least 2 hours a day of screen time by 1 year of age were significantly more likely to have an autism spectrum disorder (ASD) diagnosis at 3 years, based on data from more than 80,000 children.
The World Health Organization and the American Academy of Pediatrics recommend against any screen time for infants up to 1 year of age and 18 months of age, respectively, wrote Megumi Kushima, MA, of the University of Yamanashi (Japan), and colleagues on behalf of the Japan Environment and Children’s Study Group.
The extent to which screen time duration in infancy is associated with subsequent ASD diagnosis remains unclear, the researchers said. The ongoing COVID-19 pandemic has increased screen time among children worldwide, which makes an examination of the impact of screen time on children’s health an important public health issue.
In a study published in JAMA Pediatrics, the researchers recruited pregnant women between 2011 and 2014; data were analyzed in December 2020. The final study population included 84,030 mother-child pairs. The primary exposure of screen time at 1 year of age was assessed by questionnaire, in which mothers were asked to report their number of hours they let their child watch TV or DVDs daily. Responses were none (no screen time), less than 1 hour, 1 hour or more but less than 2 hours, 2 hours or more but less than 4 hours, and 4 hours or more.
The primary outcome was ASD diagnosis at 3 years of age, and mothers were asked via questionnaire whether their 3-year-old had been diagnosed with ASD from age 2.
The study was conducted by the Japan Environment and Children’s Study Group at 15 regional centers across Japan.
Overall, 330 children had received an ASD diagnosis at age 3 years, a prevalence of 0.4%. Of these, 251 (76%) were boys, and 79 (24%) were girls. Independent of ASD, the most common response for screen time was less than 1 hour, which was reported by 27,707 mothers. The proportion of children with ASD at age 3 increased as screen time at age 1 increased, the percentages were 5.8%, 22.3%, 30.2%, and 31.7% for children with no screen time, less than 1 hour, 1 to less than 2 hours, and 2 to less than 4 hours, respectively. The percentage of children with ASD diagnoses who had 4 hours or more of daily screen time was 10%.
Logistic regression analysis showed that longer screen time at age 1 year was significantly associated with higher odds of ASD at 3 years in boys, but not in girls. The researchers controlled for variables including maternal maltreatment and children’s predisposition to ASD. Among boys, the adjusted odds ratios for screen times of less than 1 hour, 1 hour to less than 2 hours, 2 hours to less than 4 hours, and more than 4 hours were 1.38, 2.16, 3.48, and 3.02, respectively.
Screen time at age 3 years was not associated with ASD diagnosis at age 3 years, potentially “because the association with environmental factors on brain development varies with age,” the researchers noted.
The study findings were limited by several factors including the reliance on parental reports of screen time and potential for reporting bias, the researchers noted. Other limitations included the possible missed diagnoses of mild ASD cases at 3 years, and the inability to consider variables such as childcare environment, living conditions, diseases, genetics, and disabilities.
However, the results were strengthened by the large study population and examination of screen time in early childhood, they said. More research is needed to examine other factors that contribute to the association between ASD and screen time, but given the rapid increase in device use in children, “it is necessary to review its health effects on infants and control excessive screen time.”
Strong study, but some gaps appear
The study is strong in many respects, Karalyn Kinsella, MD, a pediatrician in private practice in Cheshire, Conn., said in an interview.
However, “what I am not sure they addressed is that children on the spectrum are often not entertained by basic toys and may be hard to manage behaviorally,” Dr. Kinsella said. Consequently, parents may be more inclined to offer screen time as a way to pacify children with behavioral difficulties. “Parents also may see that their children are happier interacting with devices, so they may be more apt to let them continue with screen time.We know screen time is not good for the developing brain, however; I worry that the message from this study is that screen time causes autism in boys.
“What I would have liked to know from the parents who allowed more screen time was why they were offering it,” Dr. Kinsella said. “Was it because their child was difficult behaviorally or because that is the one place that they seemed to have satisfaction? To me, that would indicate the reverse hypothesis.” That said, the study findings “remind us to counsel families about screen time, especially in the age of COVID-19. Kids are home much longer than usual, which ultimately leads to more screen time.”
The study was funded by the Japanese Ministry of Environment. The researchers had no financial conflicts to disclose. Dr. Kinsella had no financial conflicts to disclose, but serves as a member of the Pediatric News editorial advisory board.
Boys exposed to at least 2 hours a day of screen time by 1 year of age were significantly more likely to have an autism spectrum disorder (ASD) diagnosis at 3 years, based on data from more than 80,000 children.
The World Health Organization and the American Academy of Pediatrics recommend against any screen time for infants up to 1 year of age and 18 months of age, respectively, wrote Megumi Kushima, MA, of the University of Yamanashi (Japan), and colleagues on behalf of the Japan Environment and Children’s Study Group.
The extent to which screen time duration in infancy is associated with subsequent ASD diagnosis remains unclear, the researchers said. The ongoing COVID-19 pandemic has increased screen time among children worldwide, which makes an examination of the impact of screen time on children’s health an important public health issue.
In a study published in JAMA Pediatrics, the researchers recruited pregnant women between 2011 and 2014; data were analyzed in December 2020. The final study population included 84,030 mother-child pairs. The primary exposure of screen time at 1 year of age was assessed by questionnaire, in which mothers were asked to report their number of hours they let their child watch TV or DVDs daily. Responses were none (no screen time), less than 1 hour, 1 hour or more but less than 2 hours, 2 hours or more but less than 4 hours, and 4 hours or more.
The primary outcome was ASD diagnosis at 3 years of age, and mothers were asked via questionnaire whether their 3-year-old had been diagnosed with ASD from age 2.
The study was conducted by the Japan Environment and Children’s Study Group at 15 regional centers across Japan.
Overall, 330 children had received an ASD diagnosis at age 3 years, a prevalence of 0.4%. Of these, 251 (76%) were boys, and 79 (24%) were girls. Independent of ASD, the most common response for screen time was less than 1 hour, which was reported by 27,707 mothers. The proportion of children with ASD at age 3 increased as screen time at age 1 increased, the percentages were 5.8%, 22.3%, 30.2%, and 31.7% for children with no screen time, less than 1 hour, 1 to less than 2 hours, and 2 to less than 4 hours, respectively. The percentage of children with ASD diagnoses who had 4 hours or more of daily screen time was 10%.
Logistic regression analysis showed that longer screen time at age 1 year was significantly associated with higher odds of ASD at 3 years in boys, but not in girls. The researchers controlled for variables including maternal maltreatment and children’s predisposition to ASD. Among boys, the adjusted odds ratios for screen times of less than 1 hour, 1 hour to less than 2 hours, 2 hours to less than 4 hours, and more than 4 hours were 1.38, 2.16, 3.48, and 3.02, respectively.
Screen time at age 3 years was not associated with ASD diagnosis at age 3 years, potentially “because the association with environmental factors on brain development varies with age,” the researchers noted.
The study findings were limited by several factors including the reliance on parental reports of screen time and potential for reporting bias, the researchers noted. Other limitations included the possible missed diagnoses of mild ASD cases at 3 years, and the inability to consider variables such as childcare environment, living conditions, diseases, genetics, and disabilities.
However, the results were strengthened by the large study population and examination of screen time in early childhood, they said. More research is needed to examine other factors that contribute to the association between ASD and screen time, but given the rapid increase in device use in children, “it is necessary to review its health effects on infants and control excessive screen time.”
Strong study, but some gaps appear
The study is strong in many respects, Karalyn Kinsella, MD, a pediatrician in private practice in Cheshire, Conn., said in an interview.
However, “what I am not sure they addressed is that children on the spectrum are often not entertained by basic toys and may be hard to manage behaviorally,” Dr. Kinsella said. Consequently, parents may be more inclined to offer screen time as a way to pacify children with behavioral difficulties. “Parents also may see that their children are happier interacting with devices, so they may be more apt to let them continue with screen time.We know screen time is not good for the developing brain, however; I worry that the message from this study is that screen time causes autism in boys.
“What I would have liked to know from the parents who allowed more screen time was why they were offering it,” Dr. Kinsella said. “Was it because their child was difficult behaviorally or because that is the one place that they seemed to have satisfaction? To me, that would indicate the reverse hypothesis.” That said, the study findings “remind us to counsel families about screen time, especially in the age of COVID-19. Kids are home much longer than usual, which ultimately leads to more screen time.”
The study was funded by the Japanese Ministry of Environment. The researchers had no financial conflicts to disclose. Dr. Kinsella had no financial conflicts to disclose, but serves as a member of the Pediatric News editorial advisory board.
Boys exposed to at least 2 hours a day of screen time by 1 year of age were significantly more likely to have an autism spectrum disorder (ASD) diagnosis at 3 years, based on data from more than 80,000 children.
The World Health Organization and the American Academy of Pediatrics recommend against any screen time for infants up to 1 year of age and 18 months of age, respectively, wrote Megumi Kushima, MA, of the University of Yamanashi (Japan), and colleagues on behalf of the Japan Environment and Children’s Study Group.
The extent to which screen time duration in infancy is associated with subsequent ASD diagnosis remains unclear, the researchers said. The ongoing COVID-19 pandemic has increased screen time among children worldwide, which makes an examination of the impact of screen time on children’s health an important public health issue.
In a study published in JAMA Pediatrics, the researchers recruited pregnant women between 2011 and 2014; data were analyzed in December 2020. The final study population included 84,030 mother-child pairs. The primary exposure of screen time at 1 year of age was assessed by questionnaire, in which mothers were asked to report their number of hours they let their child watch TV or DVDs daily. Responses were none (no screen time), less than 1 hour, 1 hour or more but less than 2 hours, 2 hours or more but less than 4 hours, and 4 hours or more.
The primary outcome was ASD diagnosis at 3 years of age, and mothers were asked via questionnaire whether their 3-year-old had been diagnosed with ASD from age 2.
The study was conducted by the Japan Environment and Children’s Study Group at 15 regional centers across Japan.
Overall, 330 children had received an ASD diagnosis at age 3 years, a prevalence of 0.4%. Of these, 251 (76%) were boys, and 79 (24%) were girls. Independent of ASD, the most common response for screen time was less than 1 hour, which was reported by 27,707 mothers. The proportion of children with ASD at age 3 increased as screen time at age 1 increased, the percentages were 5.8%, 22.3%, 30.2%, and 31.7% for children with no screen time, less than 1 hour, 1 to less than 2 hours, and 2 to less than 4 hours, respectively. The percentage of children with ASD diagnoses who had 4 hours or more of daily screen time was 10%.
Logistic regression analysis showed that longer screen time at age 1 year was significantly associated with higher odds of ASD at 3 years in boys, but not in girls. The researchers controlled for variables including maternal maltreatment and children’s predisposition to ASD. Among boys, the adjusted odds ratios for screen times of less than 1 hour, 1 hour to less than 2 hours, 2 hours to less than 4 hours, and more than 4 hours were 1.38, 2.16, 3.48, and 3.02, respectively.
Screen time at age 3 years was not associated with ASD diagnosis at age 3 years, potentially “because the association with environmental factors on brain development varies with age,” the researchers noted.
The study findings were limited by several factors including the reliance on parental reports of screen time and potential for reporting bias, the researchers noted. Other limitations included the possible missed diagnoses of mild ASD cases at 3 years, and the inability to consider variables such as childcare environment, living conditions, diseases, genetics, and disabilities.
However, the results were strengthened by the large study population and examination of screen time in early childhood, they said. More research is needed to examine other factors that contribute to the association between ASD and screen time, but given the rapid increase in device use in children, “it is necessary to review its health effects on infants and control excessive screen time.”
Strong study, but some gaps appear
The study is strong in many respects, Karalyn Kinsella, MD, a pediatrician in private practice in Cheshire, Conn., said in an interview.
However, “what I am not sure they addressed is that children on the spectrum are often not entertained by basic toys and may be hard to manage behaviorally,” Dr. Kinsella said. Consequently, parents may be more inclined to offer screen time as a way to pacify children with behavioral difficulties. “Parents also may see that their children are happier interacting with devices, so they may be more apt to let them continue with screen time.We know screen time is not good for the developing brain, however; I worry that the message from this study is that screen time causes autism in boys.
“What I would have liked to know from the parents who allowed more screen time was why they were offering it,” Dr. Kinsella said. “Was it because their child was difficult behaviorally or because that is the one place that they seemed to have satisfaction? To me, that would indicate the reverse hypothesis.” That said, the study findings “remind us to counsel families about screen time, especially in the age of COVID-19. Kids are home much longer than usual, which ultimately leads to more screen time.”
The study was funded by the Japanese Ministry of Environment. The researchers had no financial conflicts to disclose. Dr. Kinsella had no financial conflicts to disclose, but serves as a member of the Pediatric News editorial advisory board.
FROM JAMA PEDIATRICS
Men with hypersexual disorder may have oxytocin overload
Men with hypersexual disorder showed higher levels of oxytocin in their blood than did healthy control men without the disorder, in a study with 102 participants.
Hypersexual disorder (HD) is characterized by “excessive and persistent sexual behaviors in relation to various mood states, with an impulsivity component and experienced loss of control,” John Flanagan, MD, of the Karolinska Institutet in Stockholm and colleagues wrote. Although HD is not included as a separate diagnosis in the current DSM, the similar disorder of compulsive sexual behavior is included in the ICD.
Data on the pathophysiology of HD are limited, although a previous study by corresponding author Andreas Chatzittofis, MD, and colleagues showed evidence of neuroendocrine dysregulation in men with HD, and prompted the current study to explore the possible involvement of the oxytocinergic system in HD.
In the current study, published in the Journal of Clinical Endocrinology & Metabolism, the researchers identified 64 men with HD and 38 healthy male controls. The patients were help-seeking men older than 18 years diagnosed with HD who presented to a single center in Sweden during 2013-2014. The men were included in a randomized clinical trial of cognitive-behavioral therapy for HD, and 30 of them participated in a 7-week CBT program.
Oxytocin, secreted by the pituitary gland, is known to play a role in sexual behavior, but has not been examined in HD men, the researchers said. At baseline, the mean plasma oxytocin was 31.0 pM in the HD patients, which was significantly higher than the mean 16.9 pM in healthy controls (P < .001). However, the 30 HD men who underwent CBT showed significant improvement in oxytocin levels, from a mean pretreatment level of 30.5 to a mean posttreatment level of 20.2 pM (P = .0000019).
The study findings were limited by several factors, including the lack of data on oxytocin for a wait list or control group, as well as the inability to control for confounding factors such as diet, physical activity, ethnicity, and stress, and a lack of data on sexual activity prior to oxytocin measurements, the researchers noted.
However, “although there is no clear consensus at this point, previous studies support the use of oxytocin plasma levels as a surrogate variable for [cerebrospinal fluid] oxytocin activity,” the researchers wrote in their discussion. The current study findings support the potential of oxytocin as a biomarker for HD diagnostics and also as a measure of disease severity. Larger studies to confirm the findings, especially those that exclude potential confounders, would be valuable.
Oxytocin may be treatment target
The study is important because of the lack of knowledge regarding the pathophysiology underlying hypersexual disorder, Dr. Chatzittofis of the University of Cyprus, Nicosia, said in an interview. “This is the first study to indicate a role for oxytocin’s involvement” in hypersexual disorder in men. Dr. Chatzittofis led a team in a previous study that showed an association between HD in men and dysregulation of the hypothalamic pituitary adrenal axis.

In the current study, “we discovered that men with compulsive sexual behavior disorder had higher oxytocin levels, compared with healthy men,” said Dr. Chatzittofis, adding that the take-home message for clinicians is the potential of CBT for treatment. “Cognitive-behavior therapy led to a reduction in both hypersexual behavior and oxytocin levels.” The results suggest that oxytocin plays an important role in sex addiction.
Consequently, oxytocin may be a potential drug target for future pharmacologic treatment of hypersexual disorder, he added.
The study was supported by the Swedish Research Council, the Stockholm County Council, and by a partnership between Umeå University and Västerbotten County Council. The researchers had no financial conflicts to disclose.
Men with hypersexual disorder showed higher levels of oxytocin in their blood than did healthy control men without the disorder, in a study with 102 participants.
Hypersexual disorder (HD) is characterized by “excessive and persistent sexual behaviors in relation to various mood states, with an impulsivity component and experienced loss of control,” John Flanagan, MD, of the Karolinska Institutet in Stockholm and colleagues wrote. Although HD is not included as a separate diagnosis in the current DSM, the similar disorder of compulsive sexual behavior is included in the ICD.
Data on the pathophysiology of HD are limited, although a previous study by corresponding author Andreas Chatzittofis, MD, and colleagues showed evidence of neuroendocrine dysregulation in men with HD, and prompted the current study to explore the possible involvement of the oxytocinergic system in HD.
In the current study, published in the Journal of Clinical Endocrinology & Metabolism, the researchers identified 64 men with HD and 38 healthy male controls. The patients were help-seeking men older than 18 years diagnosed with HD who presented to a single center in Sweden during 2013-2014. The men were included in a randomized clinical trial of cognitive-behavioral therapy for HD, and 30 of them participated in a 7-week CBT program.
Oxytocin, secreted by the pituitary gland, is known to play a role in sexual behavior, but has not been examined in HD men, the researchers said. At baseline, the mean plasma oxytocin was 31.0 pM in the HD patients, which was significantly higher than the mean 16.9 pM in healthy controls (P < .001). However, the 30 HD men who underwent CBT showed significant improvement in oxytocin levels, from a mean pretreatment level of 30.5 to a mean posttreatment level of 20.2 pM (P = .0000019).
The study findings were limited by several factors, including the lack of data on oxytocin for a wait list or control group, as well as the inability to control for confounding factors such as diet, physical activity, ethnicity, and stress, and a lack of data on sexual activity prior to oxytocin measurements, the researchers noted.
However, “although there is no clear consensus at this point, previous studies support the use of oxytocin plasma levels as a surrogate variable for [cerebrospinal fluid] oxytocin activity,” the researchers wrote in their discussion. The current study findings support the potential of oxytocin as a biomarker for HD diagnostics and also as a measure of disease severity. Larger studies to confirm the findings, especially those that exclude potential confounders, would be valuable.
Oxytocin may be treatment target
The study is important because of the lack of knowledge regarding the pathophysiology underlying hypersexual disorder, Dr. Chatzittofis of the University of Cyprus, Nicosia, said in an interview. “This is the first study to indicate a role for oxytocin’s involvement” in hypersexual disorder in men. Dr. Chatzittofis led a team in a previous study that showed an association between HD in men and dysregulation of the hypothalamic pituitary adrenal axis.
In the current study, “we discovered that men with compulsive sexual behavior disorder had higher oxytocin levels, compared with healthy men,” said Dr. Chatzittofis, adding that the take-home message for clinicians is the potential of CBT for treatment. “Cognitive-behavior therapy led to a reduction in both hypersexual behavior and oxytocin levels.” The results suggest that oxytocin plays an important role in sex addiction.
Consequently, oxytocin may be a potential drug target for future pharmacologic treatment of hypersexual disorder, he added.
The study was supported by the Swedish Research Council, the Stockholm County Council, and by a partnership between Umeå University and Västerbotten County Council. The researchers had no financial conflicts to disclose.
Men with hypersexual disorder showed higher levels of oxytocin in their blood than did healthy control men without the disorder, in a study with 102 participants.
Hypersexual disorder (HD) is characterized by “excessive and persistent sexual behaviors in relation to various mood states, with an impulsivity component and experienced loss of control,” John Flanagan, MD, of the Karolinska Institutet in Stockholm and colleagues wrote. Although HD is not included as a separate diagnosis in the current DSM, the similar disorder of compulsive sexual behavior is included in the ICD.
Data on the pathophysiology of HD are limited, although a previous study by corresponding author Andreas Chatzittofis, MD, and colleagues showed evidence of neuroendocrine dysregulation in men with HD, and prompted the current study to explore the possible involvement of the oxytocinergic system in HD.
In the current study, published in the Journal of Clinical Endocrinology & Metabolism, the researchers identified 64 men with HD and 38 healthy male controls. The patients were help-seeking men older than 18 years diagnosed with HD who presented to a single center in Sweden during 2013-2014. The men were included in a randomized clinical trial of cognitive-behavioral therapy for HD, and 30 of them participated in a 7-week CBT program.
Oxytocin, secreted by the pituitary gland, is known to play a role in sexual behavior, but has not been examined in HD men, the researchers said. At baseline, the mean plasma oxytocin was 31.0 pM in the HD patients, which was significantly higher than the mean 16.9 pM in healthy controls (P < .001). However, the 30 HD men who underwent CBT showed significant improvement in oxytocin levels, from a mean pretreatment level of 30.5 to a mean posttreatment level of 20.2 pM (P = .0000019).
The study findings were limited by several factors, including the lack of data on oxytocin for a wait list or control group, as well as the inability to control for confounding factors such as diet, physical activity, ethnicity, and stress, and a lack of data on sexual activity prior to oxytocin measurements, the researchers noted.
However, “although there is no clear consensus at this point, previous studies support the use of oxytocin plasma levels as a surrogate variable for [cerebrospinal fluid] oxytocin activity,” the researchers wrote in their discussion. The current study findings support the potential of oxytocin as a biomarker for HD diagnostics and also as a measure of disease severity. Larger studies to confirm the findings, especially those that exclude potential confounders, would be valuable.
Oxytocin may be treatment target
The study is important because of the lack of knowledge regarding the pathophysiology underlying hypersexual disorder, Dr. Chatzittofis of the University of Cyprus, Nicosia, said in an interview. “This is the first study to indicate a role for oxytocin’s involvement” in hypersexual disorder in men. Dr. Chatzittofis led a team in a previous study that showed an association between HD in men and dysregulation of the hypothalamic pituitary adrenal axis.
In the current study, “we discovered that men with compulsive sexual behavior disorder had higher oxytocin levels, compared with healthy men,” said Dr. Chatzittofis, adding that the take-home message for clinicians is the potential of CBT for treatment. “Cognitive-behavior therapy led to a reduction in both hypersexual behavior and oxytocin levels.” The results suggest that oxytocin plays an important role in sex addiction.
Consequently, oxytocin may be a potential drug target for future pharmacologic treatment of hypersexual disorder, he added.
The study was supported by the Swedish Research Council, the Stockholm County Council, and by a partnership between Umeå University and Västerbotten County Council. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM