User login
Desmoplastic Melanoma
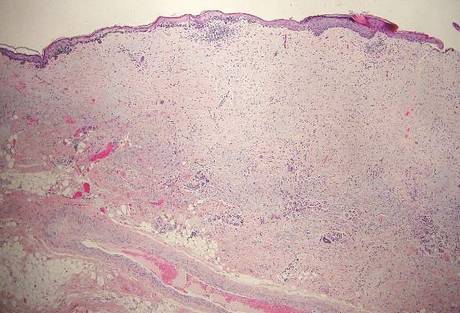
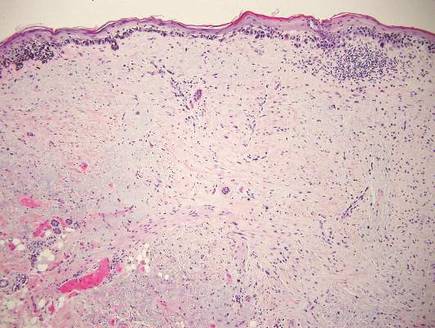
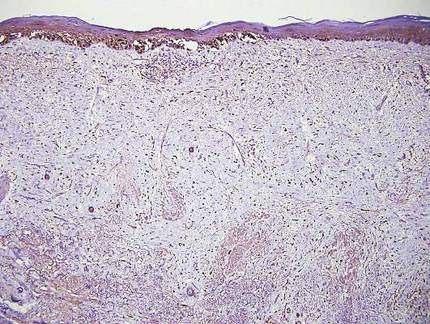
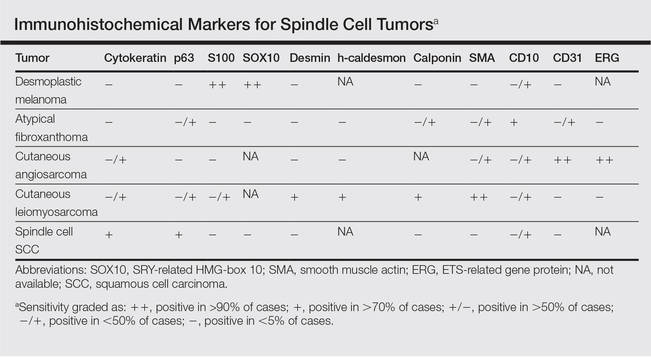
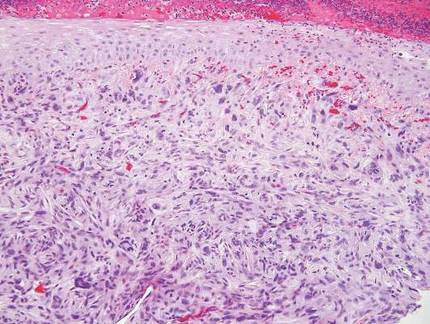
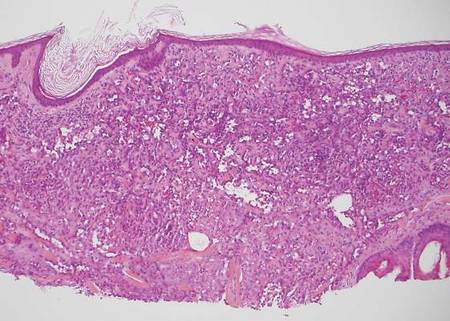
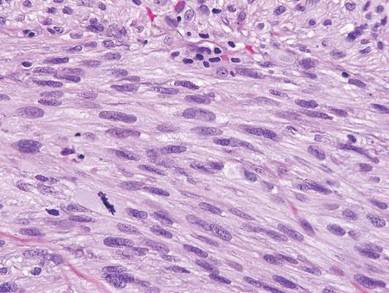
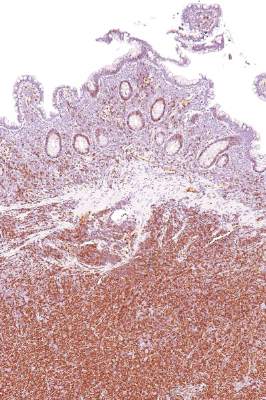
Desmoplastic melanoma, an uncommon variant of melanoma, poses a diagnostic challenge to the clinician because the tumors frequently appear as nonspecific flesh-colored or amelanotic plaques or nodules. They are more common in men than in women and are frequently found on the head and neck.1,2 Their innocuous appearance may lead to a delay in diagnosis and may explain why desmoplastic melanomas often are deeply infiltrative at the time of biopsy. Desmoplastic melanoma arises de novo in approximately one-third of cases.1 In the remainder of cases, it is seen in conjunction with overlying melanoma in situ, most commonly lentigo maligna melanoma.1 Histologically, desmoplastic melanomas are characterized by malignant spindle cells within a densely fibrotic stroma (Figure 1). Adjacent lymphoid aggregates and perineural involvement are common features,2 while pigment and atypical mitoses can be infrequent. Desmoplastic melanoma can be classified as mixed or pure based on the degree of desmoplasia and cellularity. Within mixed desmoplastic melanomas, there are areas that have histologic features of conventional melanomas while others demonstrate more typical desmoplastic characteristics. Pure desmoplastic melanoma has a higher degree of desmoplasia and fewer tumor cells than the mixed type.1 The pure subtype tends to be less aggressive and is less likely to metastasize to the lymph nodes.1 In the absence of an in situ component (Figure 2), desmoplastic melanoma may be indistinguishable from other spindle cell tumors on routine hematoxylin and eosin staining; thus, immunohistochemical staining generally is required. The most reliable stains in confirming a diagnosis of desmoplastic melanoma are S100 and SOX10 (SRY-related HMG-box 10)(Figure 3)(eTable).3
Atypical fibroxathoma typically presents as a nodule in the head and neck region or other sun-exposed areas in elderly individuals and is more commonly seen in men than in women.4 Histologically, atypical fibroxanthomas are composed of pleomorphic spindle, epithelioid, and multinucleated giant cells with numerous and atypical mitoses (Figure 4).5 Atypical fibroxanthoma is considered a diagnosis of exclusion; therefore, other dermal spindle cell tumors need to be ruled out before diagnosis can be made. Atypical fibroxanthomas generally stain negative for cytokeratin, S100, SOX10, and desmin, but in some cases there is positive focal staining for smooth muscle actin.4 Multiple immunohistochemical markers, including CD10, have shown reactivity in atypical fibroxanthomas,4 but none of these markers has a high specificity for this tumor; thus, it remains a diagnosis of exclusion.
Cutaneous angiosarcomas are aggressive tumors associated with a high mortality rate despite appropriate treatment with surgical resection and postoperative radiation treatment. They typically present as ecchymotic macules or nodules on the face or scalp of elderly patients.6,7 Ionizing radiation and chronic lymphedema are risk factors for cutaneous angiosarcoma.6 Histologically, well-differentiated cutaneous angiosarcomas are composed of irregular, anastomosing vascular channels that dissect through the dermis (Figure 5).6,7 Less well-differentiated tumors may contain spindle cells and lack obvious vascular structures; thus immunohistochemistry is essential for making the correct diagnosis in these cases. Cutaneous angiosarcomas typically stain positive for ERG (ETS-related gene) protein, CD31, CD34, and factor VIII.6,8 Unfortunately these tumors may also occasionally stain with cytokeratin, which may lead to the erroneous diagnosis of a carcinoma.6
| 
| |
| Figure 4. Pleomorphic spindle, epithelioid, and multinucleate giant cells with atypical mitoses filling the dermis in atypical fibroxanthoma (H&E, original magnification ×200). | Figure 5. Anastamosing vascular channels dissecting through collagen bundles and consuming the epidermis in cutaneous angiosarcoma (H&E, original magnification ×100). |
Cutaneous leiomyosarcoma is a smooth muscle neoplasm that arises from arrector pili muscles, genital smooth muscles, or vascular smooth muscles. It typically presents as a single plaque or nodule on the arms and legs of individuals older than 50 years of age.9 Cutaneous leiomyosarcomas can be classified as either dermal, in which at least 90% of the tumor is confined to the dermis, or subcutaneous; this distinction is important because the latter type has a higher rate of metastasis and a poorer prognosis.9 Because of this tumor’s smooth muscle derivation, well-differentiated tumors may retain features of typical smooth muscle cells, including cigar-shaped nuclei with adjacent glycogen vacuoles (Figure 6). If fascicle formation is observed, this may be an additional clue to the diagnosis. In poorly differentiated tumors, immunohistochemistry is invaluable. Leiomyosarcoma often stains positive for smooth muscle actin, muscle specific actin, h-caldesmon, desmin, and calponin.9-11
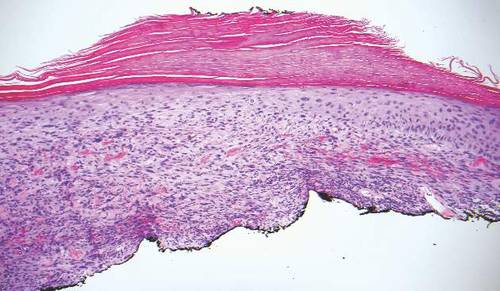
Spindle cell squamous cell carcinomas often present as ulcerated nodules on sun-exposed skin or on sites of prior ionizing radiation.2,12 Like desmoplastic melanoma, spindle cell squamous cell carcinomas are characterized by spindle cells in the dermis. Helpful diagnostic clues may include evidence of squamous differentiation, including keratin pearls or overlying actinic keratosis (Figure 7). However, actinic keratosis is common on sun-damaged skin and cannot be used to definitively confirm this diagnosis. There also may be areas of the tumor with more typical epithelioid cells that are easily identified as squamous cell carcinoma.2 Spindle cell squamous cell carcinoma stains positive for high–molecular weight cytokeratin antibodies and p63,2 which can help to differentiate it from the other spindle cell tumors in the differential.
| 
| |
| Figure 6. Spindle cells of leiomyosarcoma with cigar-shaped nuclei and adjacent glycogen vacuoles (H&E, original magnification ×600). | Figure 7. Spindle cell squamous cell carcinoma with overlying epidermal atypia that blends with the underlying dermal spindle cells (H&E, original magnification ×100). |
1. Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
2. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
3. Elston DM, Ferringer TC, Ko C, et al. Dermatopathology: Requisites in Dermatology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2014.
4. Luzar B, Calonje E. Morphological and immunohistochemical characteristics of atypical fibroxanthoma with a special emphasis on potential diagnostic pitfalls: a review. J Cutan Pathol. 2010;37:301-309.
5. Iorizzo LJ III, Brown MD. Atypical fibroxanthoma: a review of the literature. Dermatol Surg. 2011;37:146-157.
6. Luca DR. Angiosarcoma, radiation-associated angiosarcoma, and atypical vascular lesion. Arch Pathol Lab Med. 2009;133:1804-1809.
7. Mendenhall WM, Mendenhall CM, Werning JW, et al. Cutaneous angiosarcoma. Am J Oncol. 2006;29:524-528.
8. Thum C, Husain EA, Mulholland K, et al. Atypical fibroxanthoma with pseudoangiomatous features: a histological and immunohistochemical mimic of cutaneous angiosarcoma. Ann Diagn Pathol. 2013;17:502-507.
9. Bolognia JL, Jorizzo JL, Shaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
10. Hall BJ, Grossmann AH, Webber NP, et al. Atypical intradermal smooth muscle neoplasms (formerly cutaneous leiomyosarcomas): case series, immunohistochemical profile and review of the literature. Appl Immunohistochem Mol Morphol. 2013;21:132-138.
11. Perez-Montiel MD, Plaza JA, Dominguez-Malagon H, et al. Differential expression of smooth muscle myosin, smooth muscle actin, h-caldesmon, and calponin in the diagnosis of myofibroblastic and smooth muscle lesions of skin and soft tissue. Am J Dermatopathol. 2006;28:105-111.
12. Cassarino DS, DeRienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification. part one. J Cutan Pathol. 2006;33:191-205.
Desmoplastic melanoma, an uncommon variant of melanoma, poses a diagnostic challenge to the clinician because the tumors frequently appear as nonspecific flesh-colored or amelanotic plaques or nodules. They are more common in men than in women and are frequently found on the head and neck.1,2 Their innocuous appearance may lead to a delay in diagnosis and may explain why desmoplastic melanomas often are deeply infiltrative at the time of biopsy. Desmoplastic melanoma arises de novo in approximately one-third of cases.1 In the remainder of cases, it is seen in conjunction with overlying melanoma in situ, most commonly lentigo maligna melanoma.1 Histologically, desmoplastic melanomas are characterized by malignant spindle cells within a densely fibrotic stroma (Figure 1). Adjacent lymphoid aggregates and perineural involvement are common features,2 while pigment and atypical mitoses can be infrequent. Desmoplastic melanoma can be classified as mixed or pure based on the degree of desmoplasia and cellularity. Within mixed desmoplastic melanomas, there are areas that have histologic features of conventional melanomas while others demonstrate more typical desmoplastic characteristics. Pure desmoplastic melanoma has a higher degree of desmoplasia and fewer tumor cells than the mixed type.1 The pure subtype tends to be less aggressive and is less likely to metastasize to the lymph nodes.1 In the absence of an in situ component (Figure 2), desmoplastic melanoma may be indistinguishable from other spindle cell tumors on routine hematoxylin and eosin staining; thus, immunohistochemical staining generally is required. The most reliable stains in confirming a diagnosis of desmoplastic melanoma are S100 and SOX10 (SRY-related HMG-box 10)(Figure 3)(eTable).3
Atypical fibroxathoma typically presents as a nodule in the head and neck region or other sun-exposed areas in elderly individuals and is more commonly seen in men than in women.4 Histologically, atypical fibroxanthomas are composed of pleomorphic spindle, epithelioid, and multinucleated giant cells with numerous and atypical mitoses (Figure 4).5 Atypical fibroxanthoma is considered a diagnosis of exclusion; therefore, other dermal spindle cell tumors need to be ruled out before diagnosis can be made. Atypical fibroxanthomas generally stain negative for cytokeratin, S100, SOX10, and desmin, but in some cases there is positive focal staining for smooth muscle actin.4 Multiple immunohistochemical markers, including CD10, have shown reactivity in atypical fibroxanthomas,4 but none of these markers has a high specificity for this tumor; thus, it remains a diagnosis of exclusion.
Cutaneous angiosarcomas are aggressive tumors associated with a high mortality rate despite appropriate treatment with surgical resection and postoperative radiation treatment. They typically present as ecchymotic macules or nodules on the face or scalp of elderly patients.6,7 Ionizing radiation and chronic lymphedema are risk factors for cutaneous angiosarcoma.6 Histologically, well-differentiated cutaneous angiosarcomas are composed of irregular, anastomosing vascular channels that dissect through the dermis (Figure 5).6,7 Less well-differentiated tumors may contain spindle cells and lack obvious vascular structures; thus immunohistochemistry is essential for making the correct diagnosis in these cases. Cutaneous angiosarcomas typically stain positive for ERG (ETS-related gene) protein, CD31, CD34, and factor VIII.6,8 Unfortunately these tumors may also occasionally stain with cytokeratin, which may lead to the erroneous diagnosis of a carcinoma.6
|
|
| |
| Figure 4. Pleomorphic spindle, epithelioid, and multinucleate giant cells with atypical mitoses filling the dermis in atypical fibroxanthoma (H&E, original magnification ×200). | Figure 5. Anastamosing vascular channels dissecting through collagen bundles and consuming the epidermis in cutaneous angiosarcoma (H&E, original magnification ×100). |
Cutaneous leiomyosarcoma is a smooth muscle neoplasm that arises from arrector pili muscles, genital smooth muscles, or vascular smooth muscles. It typically presents as a single plaque or nodule on the arms and legs of individuals older than 50 years of age.9 Cutaneous leiomyosarcomas can be classified as either dermal, in which at least 90% of the tumor is confined to the dermis, or subcutaneous; this distinction is important because the latter type has a higher rate of metastasis and a poorer prognosis.9 Because of this tumor’s smooth muscle derivation, well-differentiated tumors may retain features of typical smooth muscle cells, including cigar-shaped nuclei with adjacent glycogen vacuoles (Figure 6). If fascicle formation is observed, this may be an additional clue to the diagnosis. In poorly differentiated tumors, immunohistochemistry is invaluable. Leiomyosarcoma often stains positive for smooth muscle actin, muscle specific actin, h-caldesmon, desmin, and calponin.9-11
Spindle cell squamous cell carcinomas often present as ulcerated nodules on sun-exposed skin or on sites of prior ionizing radiation.2,12 Like desmoplastic melanoma, spindle cell squamous cell carcinomas are characterized by spindle cells in the dermis. Helpful diagnostic clues may include evidence of squamous differentiation, including keratin pearls or overlying actinic keratosis (Figure 7). However, actinic keratosis is common on sun-damaged skin and cannot be used to definitively confirm this diagnosis. There also may be areas of the tumor with more typical epithelioid cells that are easily identified as squamous cell carcinoma.2 Spindle cell squamous cell carcinoma stains positive for high–molecular weight cytokeratin antibodies and p63,2 which can help to differentiate it from the other spindle cell tumors in the differential.
|
|
| |
| Figure 6. Spindle cells of leiomyosarcoma with cigar-shaped nuclei and adjacent glycogen vacuoles (H&E, original magnification ×600). | Figure 7. Spindle cell squamous cell carcinoma with overlying epidermal atypia that blends with the underlying dermal spindle cells (H&E, original magnification ×100). |
Desmoplastic melanoma, an uncommon variant of melanoma, poses a diagnostic challenge to the clinician because the tumors frequently appear as nonspecific flesh-colored or amelanotic plaques or nodules. They are more common in men than in women and are frequently found on the head and neck.1,2 Their innocuous appearance may lead to a delay in diagnosis and may explain why desmoplastic melanomas often are deeply infiltrative at the time of biopsy. Desmoplastic melanoma arises de novo in approximately one-third of cases.1 In the remainder of cases, it is seen in conjunction with overlying melanoma in situ, most commonly lentigo maligna melanoma.1 Histologically, desmoplastic melanomas are characterized by malignant spindle cells within a densely fibrotic stroma (Figure 1). Adjacent lymphoid aggregates and perineural involvement are common features,2 while pigment and atypical mitoses can be infrequent. Desmoplastic melanoma can be classified as mixed or pure based on the degree of desmoplasia and cellularity. Within mixed desmoplastic melanomas, there are areas that have histologic features of conventional melanomas while others demonstrate more typical desmoplastic characteristics. Pure desmoplastic melanoma has a higher degree of desmoplasia and fewer tumor cells than the mixed type.1 The pure subtype tends to be less aggressive and is less likely to metastasize to the lymph nodes.1 In the absence of an in situ component (Figure 2), desmoplastic melanoma may be indistinguishable from other spindle cell tumors on routine hematoxylin and eosin staining; thus, immunohistochemical staining generally is required. The most reliable stains in confirming a diagnosis of desmoplastic melanoma are S100 and SOX10 (SRY-related HMG-box 10)(Figure 3)(eTable).3
Atypical fibroxathoma typically presents as a nodule in the head and neck region or other sun-exposed areas in elderly individuals and is more commonly seen in men than in women.4 Histologically, atypical fibroxanthomas are composed of pleomorphic spindle, epithelioid, and multinucleated giant cells with numerous and atypical mitoses (Figure 4).5 Atypical fibroxanthoma is considered a diagnosis of exclusion; therefore, other dermal spindle cell tumors need to be ruled out before diagnosis can be made. Atypical fibroxanthomas generally stain negative for cytokeratin, S100, SOX10, and desmin, but in some cases there is positive focal staining for smooth muscle actin.4 Multiple immunohistochemical markers, including CD10, have shown reactivity in atypical fibroxanthomas,4 but none of these markers has a high specificity for this tumor; thus, it remains a diagnosis of exclusion.
Cutaneous angiosarcomas are aggressive tumors associated with a high mortality rate despite appropriate treatment with surgical resection and postoperative radiation treatment. They typically present as ecchymotic macules or nodules on the face or scalp of elderly patients.6,7 Ionizing radiation and chronic lymphedema are risk factors for cutaneous angiosarcoma.6 Histologically, well-differentiated cutaneous angiosarcomas are composed of irregular, anastomosing vascular channels that dissect through the dermis (Figure 5).6,7 Less well-differentiated tumors may contain spindle cells and lack obvious vascular structures; thus immunohistochemistry is essential for making the correct diagnosis in these cases. Cutaneous angiosarcomas typically stain positive for ERG (ETS-related gene) protein, CD31, CD34, and factor VIII.6,8 Unfortunately these tumors may also occasionally stain with cytokeratin, which may lead to the erroneous diagnosis of a carcinoma.6
|
|
| |
| Figure 4. Pleomorphic spindle, epithelioid, and multinucleate giant cells with atypical mitoses filling the dermis in atypical fibroxanthoma (H&E, original magnification ×200). | Figure 5. Anastamosing vascular channels dissecting through collagen bundles and consuming the epidermis in cutaneous angiosarcoma (H&E, original magnification ×100). |
Cutaneous leiomyosarcoma is a smooth muscle neoplasm that arises from arrector pili muscles, genital smooth muscles, or vascular smooth muscles. It typically presents as a single plaque or nodule on the arms and legs of individuals older than 50 years of age.9 Cutaneous leiomyosarcomas can be classified as either dermal, in which at least 90% of the tumor is confined to the dermis, or subcutaneous; this distinction is important because the latter type has a higher rate of metastasis and a poorer prognosis.9 Because of this tumor’s smooth muscle derivation, well-differentiated tumors may retain features of typical smooth muscle cells, including cigar-shaped nuclei with adjacent glycogen vacuoles (Figure 6). If fascicle formation is observed, this may be an additional clue to the diagnosis. In poorly differentiated tumors, immunohistochemistry is invaluable. Leiomyosarcoma often stains positive for smooth muscle actin, muscle specific actin, h-caldesmon, desmin, and calponin.9-11
Spindle cell squamous cell carcinomas often present as ulcerated nodules on sun-exposed skin or on sites of prior ionizing radiation.2,12 Like desmoplastic melanoma, spindle cell squamous cell carcinomas are characterized by spindle cells in the dermis. Helpful diagnostic clues may include evidence of squamous differentiation, including keratin pearls or overlying actinic keratosis (Figure 7). However, actinic keratosis is common on sun-damaged skin and cannot be used to definitively confirm this diagnosis. There also may be areas of the tumor with more typical epithelioid cells that are easily identified as squamous cell carcinoma.2 Spindle cell squamous cell carcinoma stains positive for high–molecular weight cytokeratin antibodies and p63,2 which can help to differentiate it from the other spindle cell tumors in the differential.
|
|
| |
| Figure 6. Spindle cells of leiomyosarcoma with cigar-shaped nuclei and adjacent glycogen vacuoles (H&E, original magnification ×600). | Figure 7. Spindle cell squamous cell carcinoma with overlying epidermal atypia that blends with the underlying dermal spindle cells (H&E, original magnification ×100). |
1. Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
2. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
3. Elston DM, Ferringer TC, Ko C, et al. Dermatopathology: Requisites in Dermatology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2014.
4. Luzar B, Calonje E. Morphological and immunohistochemical characteristics of atypical fibroxanthoma with a special emphasis on potential diagnostic pitfalls: a review. J Cutan Pathol. 2010;37:301-309.
5. Iorizzo LJ III, Brown MD. Atypical fibroxanthoma: a review of the literature. Dermatol Surg. 2011;37:146-157.
6. Luca DR. Angiosarcoma, radiation-associated angiosarcoma, and atypical vascular lesion. Arch Pathol Lab Med. 2009;133:1804-1809.
7. Mendenhall WM, Mendenhall CM, Werning JW, et al. Cutaneous angiosarcoma. Am J Oncol. 2006;29:524-528.
8. Thum C, Husain EA, Mulholland K, et al. Atypical fibroxanthoma with pseudoangiomatous features: a histological and immunohistochemical mimic of cutaneous angiosarcoma. Ann Diagn Pathol. 2013;17:502-507.
9. Bolognia JL, Jorizzo JL, Shaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
10. Hall BJ, Grossmann AH, Webber NP, et al. Atypical intradermal smooth muscle neoplasms (formerly cutaneous leiomyosarcomas): case series, immunohistochemical profile and review of the literature. Appl Immunohistochem Mol Morphol. 2013;21:132-138.
11. Perez-Montiel MD, Plaza JA, Dominguez-Malagon H, et al. Differential expression of smooth muscle myosin, smooth muscle actin, h-caldesmon, and calponin in the diagnosis of myofibroblastic and smooth muscle lesions of skin and soft tissue. Am J Dermatopathol. 2006;28:105-111.
12. Cassarino DS, DeRienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification. part one. J Cutan Pathol. 2006;33:191-205.
1. Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
2. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
3. Elston DM, Ferringer TC, Ko C, et al. Dermatopathology: Requisites in Dermatology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2014.
4. Luzar B, Calonje E. Morphological and immunohistochemical characteristics of atypical fibroxanthoma with a special emphasis on potential diagnostic pitfalls: a review. J Cutan Pathol. 2010;37:301-309.
5. Iorizzo LJ III, Brown MD. Atypical fibroxanthoma: a review of the literature. Dermatol Surg. 2011;37:146-157.
6. Luca DR. Angiosarcoma, radiation-associated angiosarcoma, and atypical vascular lesion. Arch Pathol Lab Med. 2009;133:1804-1809.
7. Mendenhall WM, Mendenhall CM, Werning JW, et al. Cutaneous angiosarcoma. Am J Oncol. 2006;29:524-528.
8. Thum C, Husain EA, Mulholland K, et al. Atypical fibroxanthoma with pseudoangiomatous features: a histological and immunohistochemical mimic of cutaneous angiosarcoma. Ann Diagn Pathol. 2013;17:502-507.
9. Bolognia JL, Jorizzo JL, Shaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Elsevier; 2012.
10. Hall BJ, Grossmann AH, Webber NP, et al. Atypical intradermal smooth muscle neoplasms (formerly cutaneous leiomyosarcomas): case series, immunohistochemical profile and review of the literature. Appl Immunohistochem Mol Morphol. 2013;21:132-138.
11. Perez-Montiel MD, Plaza JA, Dominguez-Malagon H, et al. Differential expression of smooth muscle myosin, smooth muscle actin, h-caldesmon, and calponin in the diagnosis of myofibroblastic and smooth muscle lesions of skin and soft tissue. Am J Dermatopathol. 2006;28:105-111.
12. Cassarino DS, DeRienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification. part one. J Cutan Pathol. 2006;33:191-205.

Successive gene mutations causing melanoma progression identified
Several successive genetic alterations have been identified that underlie the progression of melanoma from benign nevus to invasive malignancy, with different melanoma subtypes showing distinct evolutionary trajectories, according to a report published online Nov. 12 in the New England Journal of Medicine.
This discovery can serve as the basis for formulating refined criteria for diagnosing melanoma and predicting its clinical course. It also “revealed an intermediate category of melanocytic neoplasia, characterized by the presence of more than one pathogenic genetic alteration – a finding that helps to resolve the decades-long controversy about dysplastic nevi,” wrote A. Hunter Shain, Ph.D., of the departments of dermatology and pathology and the Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, and his associates.
Many of the pathogenic mutations in melanoma have already been catalogued, but the order in which they occur has never been defined before. “An individual tumor cannot be readily studied as it progresses from benign to malignant,” the investigators explained.
They approached the problem by comparing tissue samples from individual melanomas and melanoma precursor lesions across a spectrum of pathologic levels in different patients. They analyzed 37 melanocytic neoplasms archived at UCSF, St.John’s Hospital in London, and University Hospital Zurich, microdissecting 150 distinct areas of these samples for genetic sequencing. Eight dermatopathologists independently categorized the samples histologically as probably benign, intermediate but probably benign, intermediate but probably malignant, or malignant melanoma.
The investigators discovered “a more or less consistent pattern of genetic changes.” In every case, a single mutation was identified as the putative initiating oncogene. These were always mutations already known to activate the MAPK signaling pathway, usually in the BRAF or NRAS genes.
More advanced lesions harbored a broader spectrum of additional mutations that contributed to progression. Often these mutations affected the TERT promoter region, the CDKN2A gene and similar genes encoding particular protein subunits, or the tumor-suppressor ARID1A gene. A total of 77% of the areas examined in these intermediate tumors and melanomas in situ harbored TERT promoter mutations, which indicates that these mutations occur “at an unexpectedly early stage of the neoplastic progression,” Dr. Shain and his associates said (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMoa1502583).
Only invasive melanomas were characterized by loss of both copies of the CDKN2A gene. Similarly, mutations in the SWI/SNF chromatin remodeling genes emerged primarily at the invasive stage. And losses in the PTEN and TP53 genes occurred exclusively in the thickest invasive melanomas, implying that these mutations occur late in the process of tumor progression. In addition, melanocytic neoplasms transitioned from linear to branched evolution only at later stages of progression, they said.
The investigators noted that “the existence of a category of lesions residing between clearly benign and clearly malignant states has long been proposed, but has remained controversial.” This study demonstrates that these intermediate neoplasms not only exist, but also carry discrete genetic alterations. “Detailed follow-up studies will be necessary to specifically delineate their histopathological characteristics and determine whether genetic or morphologic features can be identified that determine the risk of their progression to melanoma,” they added.
This study was supported by the National Institutes of Health and the Gerson and Barbara Bass Bakar Distinguished Professorship in Cancer Research. Dr. Shain reported having no relevant financial disclosures; one of his associates reported receiving grant support and personal fees from Novartis, Bristol-Myers Squibb, Roche, GlaxoSmithKline, Merck Sharp & Dohme, and Amgen.
Clinical observations and genetic studies like the one by Dr. Shain and his associates have illuminated cancer pathogenesis to a degree that was unimaginable just a short time ago, offering unprecedented opportunities for improved prevention and treatment.
It now appears that most cancers evolve in three broad phases. In the breakthrough phase, a cell acquires a mutation in a specific so-called driver gene and begins to proliferate abnormally. A lesion may or may not be detected at this phase, becoming apparent only after many cell divisions occur over many years. In the expansion phase, a spectrum of new driver-gene mutations arises and enables the cell to thrive in its local environment despite low levels of growth factors, nutrients, and oxygen. This constitutes the abnormal proliferation and disordered cellular architecture characteristic of benign tumors. In the invasive phase, subsequent mutations prompt cells to become malignant, invading normal tissues and growing in otherwise hostile environments. The more invasive-phase cells that are present, the more likely that one of them will succeed in moving to another organ and grow into a clinically important lesion there (metastasizing).
The clinical implications of this process are threefold. First, therapies for advanced cancer will work only if all of the patient’s metastatic lesions harbor a mutation targeted by those therapies. Second, it may be more effective to treat cancers on the basis of their genetic alterations rather than the cell type in which they arose. And third, the progeny of a cell that initiates the breakthrough phase can take decades to progress through the other phases and begin to metastasize because mutations are uncommon, even in tumors. This gives us a large window of time to derail the pathogenetic process.
Dr. Bert Vogelstein and Kenneth W. Kinzler, Ph.D., are with the Ludwig Center and the Howard Hughes Medical Institute at Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore. Dr. Vogelstein and Dr. Kinzler both reported receiving personal fees and other support from Personal Genome Diagnostics, PapGene, Sysmex Ionostics, and Morphotek. They made these remarks in a Perspective essay accompanying Dr. Shain’s report (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMp1508811).
Clinical observations and genetic studies like the one by Dr. Shain and his associates have illuminated cancer pathogenesis to a degree that was unimaginable just a short time ago, offering unprecedented opportunities for improved prevention and treatment.
It now appears that most cancers evolve in three broad phases. In the breakthrough phase, a cell acquires a mutation in a specific so-called driver gene and begins to proliferate abnormally. A lesion may or may not be detected at this phase, becoming apparent only after many cell divisions occur over many years. In the expansion phase, a spectrum of new driver-gene mutations arises and enables the cell to thrive in its local environment despite low levels of growth factors, nutrients, and oxygen. This constitutes the abnormal proliferation and disordered cellular architecture characteristic of benign tumors. In the invasive phase, subsequent mutations prompt cells to become malignant, invading normal tissues and growing in otherwise hostile environments. The more invasive-phase cells that are present, the more likely that one of them will succeed in moving to another organ and grow into a clinically important lesion there (metastasizing).
The clinical implications of this process are threefold. First, therapies for advanced cancer will work only if all of the patient’s metastatic lesions harbor a mutation targeted by those therapies. Second, it may be more effective to treat cancers on the basis of their genetic alterations rather than the cell type in which they arose. And third, the progeny of a cell that initiates the breakthrough phase can take decades to progress through the other phases and begin to metastasize because mutations are uncommon, even in tumors. This gives us a large window of time to derail the pathogenetic process.
Dr. Bert Vogelstein and Kenneth W. Kinzler, Ph.D., are with the Ludwig Center and the Howard Hughes Medical Institute at Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore. Dr. Vogelstein and Dr. Kinzler both reported receiving personal fees and other support from Personal Genome Diagnostics, PapGene, Sysmex Ionostics, and Morphotek. They made these remarks in a Perspective essay accompanying Dr. Shain’s report (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMp1508811).
Clinical observations and genetic studies like the one by Dr. Shain and his associates have illuminated cancer pathogenesis to a degree that was unimaginable just a short time ago, offering unprecedented opportunities for improved prevention and treatment.
It now appears that most cancers evolve in three broad phases. In the breakthrough phase, a cell acquires a mutation in a specific so-called driver gene and begins to proliferate abnormally. A lesion may or may not be detected at this phase, becoming apparent only after many cell divisions occur over many years. In the expansion phase, a spectrum of new driver-gene mutations arises and enables the cell to thrive in its local environment despite low levels of growth factors, nutrients, and oxygen. This constitutes the abnormal proliferation and disordered cellular architecture characteristic of benign tumors. In the invasive phase, subsequent mutations prompt cells to become malignant, invading normal tissues and growing in otherwise hostile environments. The more invasive-phase cells that are present, the more likely that one of them will succeed in moving to another organ and grow into a clinically important lesion there (metastasizing).
The clinical implications of this process are threefold. First, therapies for advanced cancer will work only if all of the patient’s metastatic lesions harbor a mutation targeted by those therapies. Second, it may be more effective to treat cancers on the basis of their genetic alterations rather than the cell type in which they arose. And third, the progeny of a cell that initiates the breakthrough phase can take decades to progress through the other phases and begin to metastasize because mutations are uncommon, even in tumors. This gives us a large window of time to derail the pathogenetic process.
Dr. Bert Vogelstein and Kenneth W. Kinzler, Ph.D., are with the Ludwig Center and the Howard Hughes Medical Institute at Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medical Institutions, Baltimore. Dr. Vogelstein and Dr. Kinzler both reported receiving personal fees and other support from Personal Genome Diagnostics, PapGene, Sysmex Ionostics, and Morphotek. They made these remarks in a Perspective essay accompanying Dr. Shain’s report (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMp1508811).
Several successive genetic alterations have been identified that underlie the progression of melanoma from benign nevus to invasive malignancy, with different melanoma subtypes showing distinct evolutionary trajectories, according to a report published online Nov. 12 in the New England Journal of Medicine.
This discovery can serve as the basis for formulating refined criteria for diagnosing melanoma and predicting its clinical course. It also “revealed an intermediate category of melanocytic neoplasia, characterized by the presence of more than one pathogenic genetic alteration – a finding that helps to resolve the decades-long controversy about dysplastic nevi,” wrote A. Hunter Shain, Ph.D., of the departments of dermatology and pathology and the Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, and his associates.
Many of the pathogenic mutations in melanoma have already been catalogued, but the order in which they occur has never been defined before. “An individual tumor cannot be readily studied as it progresses from benign to malignant,” the investigators explained.
They approached the problem by comparing tissue samples from individual melanomas and melanoma precursor lesions across a spectrum of pathologic levels in different patients. They analyzed 37 melanocytic neoplasms archived at UCSF, St.John’s Hospital in London, and University Hospital Zurich, microdissecting 150 distinct areas of these samples for genetic sequencing. Eight dermatopathologists independently categorized the samples histologically as probably benign, intermediate but probably benign, intermediate but probably malignant, or malignant melanoma.
The investigators discovered “a more or less consistent pattern of genetic changes.” In every case, a single mutation was identified as the putative initiating oncogene. These were always mutations already known to activate the MAPK signaling pathway, usually in the BRAF or NRAS genes.
More advanced lesions harbored a broader spectrum of additional mutations that contributed to progression. Often these mutations affected the TERT promoter region, the CDKN2A gene and similar genes encoding particular protein subunits, or the tumor-suppressor ARID1A gene. A total of 77% of the areas examined in these intermediate tumors and melanomas in situ harbored TERT promoter mutations, which indicates that these mutations occur “at an unexpectedly early stage of the neoplastic progression,” Dr. Shain and his associates said (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMoa1502583).
Only invasive melanomas were characterized by loss of both copies of the CDKN2A gene. Similarly, mutations in the SWI/SNF chromatin remodeling genes emerged primarily at the invasive stage. And losses in the PTEN and TP53 genes occurred exclusively in the thickest invasive melanomas, implying that these mutations occur late in the process of tumor progression. In addition, melanocytic neoplasms transitioned from linear to branched evolution only at later stages of progression, they said.
The investigators noted that “the existence of a category of lesions residing between clearly benign and clearly malignant states has long been proposed, but has remained controversial.” This study demonstrates that these intermediate neoplasms not only exist, but also carry discrete genetic alterations. “Detailed follow-up studies will be necessary to specifically delineate their histopathological characteristics and determine whether genetic or morphologic features can be identified that determine the risk of their progression to melanoma,” they added.
This study was supported by the National Institutes of Health and the Gerson and Barbara Bass Bakar Distinguished Professorship in Cancer Research. Dr. Shain reported having no relevant financial disclosures; one of his associates reported receiving grant support and personal fees from Novartis, Bristol-Myers Squibb, Roche, GlaxoSmithKline, Merck Sharp & Dohme, and Amgen.
Several successive genetic alterations have been identified that underlie the progression of melanoma from benign nevus to invasive malignancy, with different melanoma subtypes showing distinct evolutionary trajectories, according to a report published online Nov. 12 in the New England Journal of Medicine.
This discovery can serve as the basis for formulating refined criteria for diagnosing melanoma and predicting its clinical course. It also “revealed an intermediate category of melanocytic neoplasia, characterized by the presence of more than one pathogenic genetic alteration – a finding that helps to resolve the decades-long controversy about dysplastic nevi,” wrote A. Hunter Shain, Ph.D., of the departments of dermatology and pathology and the Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, and his associates.
Many of the pathogenic mutations in melanoma have already been catalogued, but the order in which they occur has never been defined before. “An individual tumor cannot be readily studied as it progresses from benign to malignant,” the investigators explained.
They approached the problem by comparing tissue samples from individual melanomas and melanoma precursor lesions across a spectrum of pathologic levels in different patients. They analyzed 37 melanocytic neoplasms archived at UCSF, St.John’s Hospital in London, and University Hospital Zurich, microdissecting 150 distinct areas of these samples for genetic sequencing. Eight dermatopathologists independently categorized the samples histologically as probably benign, intermediate but probably benign, intermediate but probably malignant, or malignant melanoma.
The investigators discovered “a more or less consistent pattern of genetic changes.” In every case, a single mutation was identified as the putative initiating oncogene. These were always mutations already known to activate the MAPK signaling pathway, usually in the BRAF or NRAS genes.
More advanced lesions harbored a broader spectrum of additional mutations that contributed to progression. Often these mutations affected the TERT promoter region, the CDKN2A gene and similar genes encoding particular protein subunits, or the tumor-suppressor ARID1A gene. A total of 77% of the areas examined in these intermediate tumors and melanomas in situ harbored TERT promoter mutations, which indicates that these mutations occur “at an unexpectedly early stage of the neoplastic progression,” Dr. Shain and his associates said (N Engl J Med. 2015 Nov 12. doi: 10.1056/NEJMoa1502583).
Only invasive melanomas were characterized by loss of both copies of the CDKN2A gene. Similarly, mutations in the SWI/SNF chromatin remodeling genes emerged primarily at the invasive stage. And losses in the PTEN and TP53 genes occurred exclusively in the thickest invasive melanomas, implying that these mutations occur late in the process of tumor progression. In addition, melanocytic neoplasms transitioned from linear to branched evolution only at later stages of progression, they said.
The investigators noted that “the existence of a category of lesions residing between clearly benign and clearly malignant states has long been proposed, but has remained controversial.” This study demonstrates that these intermediate neoplasms not only exist, but also carry discrete genetic alterations. “Detailed follow-up studies will be necessary to specifically delineate their histopathological characteristics and determine whether genetic or morphologic features can be identified that determine the risk of their progression to melanoma,” they added.
This study was supported by the National Institutes of Health and the Gerson and Barbara Bass Bakar Distinguished Professorship in Cancer Research. Dr. Shain reported having no relevant financial disclosures; one of his associates reported receiving grant support and personal fees from Novartis, Bristol-Myers Squibb, Roche, GlaxoSmithKline, Merck Sharp & Dohme, and Amgen.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Several successive genetic alterations have been identified that underlie the progression of melanoma from benign nevus to invasive malignancy.
Major finding: Every melanocytic neoplasia in this series originated with a single genetic mutation, progressed as a wide spectrum of other specific mutations emerged, and progressed further only in the presence of yet other specific mutations.
Data source: Genetic sequencing of 293 cancer-relevant genes in 150 areas of samples from 37 primary melanomas and their adjacent precursor lesions.
Disclosures: This study was supported by the National Institutes of Health and the Gerson and Barbara Bass Bakar Distinguished Professorship in Cancer Research. Dr. Shain reported having no relevant financial disclosures; one of his associates reported receiving grant support and personal fees from Novartis, Bristol-Myers Squibb, Roche, GlaxoSmithKline, Merck Sharp & Dohme, and Amgen.

Cobimetinib approved as add-on to vemurafenib for advanced melanoma
The Food and Drug Administration has approved the once-daily oral MEK inhibitor cobimetinib in combination with vemurafenib to treat patients with advanced melanoma whose tumors express the BRAF V600E or V600K mutation.
“Today’s approval provides a new targeted treatment that, when added to vemurafenib, demonstrates greater benefit than vemurafenib alone in patients with BRAF mutation–positive melanoma,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, in a press release announcing the approval.
In a pivotal clinical trial, treatment-naive individuals with unresectable, locally advanced or metastatic melanoma whose tumors were positive for BRAF V600E or V600K mutations were randomized to receive the BRAF inhibitor vemurafenib plus placebo (n = 248) or to receive vemurafenib with cobimetinib (n = 247). At the time of data cut-off in May, 2014, median progression-free survival (PFS) was significantly longer for the cobimetinib group (9.9 vs. 6.2 months, hazard ratio, 0.51; P less than .001); PFS was the primary outcome measure.
Of the secondary outcome measures, objective response was seen in two of three patients on cobimetinib, compared with fewer than half of the placebo arm patients (68% vs. 45%; P less than .001). Another secondary outcome measure, overall survival, could not be calculated because too few events had occurred at the end of data collection.
More grade 3 or higher adverse events occurred for patients in the cobimetinib arm than the placebo arm (65% vs. 59%), but the difference was not statistically significant. Patients taking cobimetinib were no more likely than those taking placebo to discontinue taking the study drug.
Side effects most commonly associated with the combination of vemurafenib and cobimetinib included diarrhea, photosensitivity, nausea, fever, and vomiting.
Individuals taking both a BRAF inhibitor and a MEK inhibitor were less likely to develop nonmelanoma secondary skin cancers, a complication that affects about 25% of those taking vemurafenib alone.
Vemurafenib blocks BRAF, part of a molecular signaling pathway implicated in melanoma tumor cell growth and division. Cobimetinib can help delay tumor resistance to vemurafenib by targeting MEK, a gene in the same signaling pathway.
The senior investigator of the pivotal clinical trial, Dr. Antoni Ribas, said in a press release, “Today’s approval is a significant advance in the treatment of metastatic melanoma.
“For patients with a BRAF-mutated melanoma, the combination has higher activity to shrink their tumors, and with less side effects than the drugs on their own,” said Dr. Ribas, a researcher at the University of California, Los Angeles, Jonsson Comprehensive Cancer Center.
The FDA reviewed cobimetinib under its priority review program and gave the drug an orphan drug designation.
Cobimetinib (Cotellic) and vemurafinib (Zelboraf) are both marketed by Genentech.
On Twitter @karioakes
This article was updated November 16, 2015.
The Food and Drug Administration has approved the once-daily oral MEK inhibitor cobimetinib in combination with vemurafenib to treat patients with advanced melanoma whose tumors express the BRAF V600E or V600K mutation.
“Today’s approval provides a new targeted treatment that, when added to vemurafenib, demonstrates greater benefit than vemurafenib alone in patients with BRAF mutation–positive melanoma,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, in a press release announcing the approval.
In a pivotal clinical trial, treatment-naive individuals with unresectable, locally advanced or metastatic melanoma whose tumors were positive for BRAF V600E or V600K mutations were randomized to receive the BRAF inhibitor vemurafenib plus placebo (n = 248) or to receive vemurafenib with cobimetinib (n = 247). At the time of data cut-off in May, 2014, median progression-free survival (PFS) was significantly longer for the cobimetinib group (9.9 vs. 6.2 months, hazard ratio, 0.51; P less than .001); PFS was the primary outcome measure.
Of the secondary outcome measures, objective response was seen in two of three patients on cobimetinib, compared with fewer than half of the placebo arm patients (68% vs. 45%; P less than .001). Another secondary outcome measure, overall survival, could not be calculated because too few events had occurred at the end of data collection.
More grade 3 or higher adverse events occurred for patients in the cobimetinib arm than the placebo arm (65% vs. 59%), but the difference was not statistically significant. Patients taking cobimetinib were no more likely than those taking placebo to discontinue taking the study drug.
Side effects most commonly associated with the combination of vemurafenib and cobimetinib included diarrhea, photosensitivity, nausea, fever, and vomiting.
Individuals taking both a BRAF inhibitor and a MEK inhibitor were less likely to develop nonmelanoma secondary skin cancers, a complication that affects about 25% of those taking vemurafenib alone.
Vemurafenib blocks BRAF, part of a molecular signaling pathway implicated in melanoma tumor cell growth and division. Cobimetinib can help delay tumor resistance to vemurafenib by targeting MEK, a gene in the same signaling pathway.
The senior investigator of the pivotal clinical trial, Dr. Antoni Ribas, said in a press release, “Today’s approval is a significant advance in the treatment of metastatic melanoma.
“For patients with a BRAF-mutated melanoma, the combination has higher activity to shrink their tumors, and with less side effects than the drugs on their own,” said Dr. Ribas, a researcher at the University of California, Los Angeles, Jonsson Comprehensive Cancer Center.
The FDA reviewed cobimetinib under its priority review program and gave the drug an orphan drug designation.
Cobimetinib (Cotellic) and vemurafinib (Zelboraf) are both marketed by Genentech.
On Twitter @karioakes
This article was updated November 16, 2015.
The Food and Drug Administration has approved the once-daily oral MEK inhibitor cobimetinib in combination with vemurafenib to treat patients with advanced melanoma whose tumors express the BRAF V600E or V600K mutation.
“Today’s approval provides a new targeted treatment that, when added to vemurafenib, demonstrates greater benefit than vemurafenib alone in patients with BRAF mutation–positive melanoma,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, in a press release announcing the approval.
In a pivotal clinical trial, treatment-naive individuals with unresectable, locally advanced or metastatic melanoma whose tumors were positive for BRAF V600E or V600K mutations were randomized to receive the BRAF inhibitor vemurafenib plus placebo (n = 248) or to receive vemurafenib with cobimetinib (n = 247). At the time of data cut-off in May, 2014, median progression-free survival (PFS) was significantly longer for the cobimetinib group (9.9 vs. 6.2 months, hazard ratio, 0.51; P less than .001); PFS was the primary outcome measure.
Of the secondary outcome measures, objective response was seen in two of three patients on cobimetinib, compared with fewer than half of the placebo arm patients (68% vs. 45%; P less than .001). Another secondary outcome measure, overall survival, could not be calculated because too few events had occurred at the end of data collection.
More grade 3 or higher adverse events occurred for patients in the cobimetinib arm than the placebo arm (65% vs. 59%), but the difference was not statistically significant. Patients taking cobimetinib were no more likely than those taking placebo to discontinue taking the study drug.
Side effects most commonly associated with the combination of vemurafenib and cobimetinib included diarrhea, photosensitivity, nausea, fever, and vomiting.
Individuals taking both a BRAF inhibitor and a MEK inhibitor were less likely to develop nonmelanoma secondary skin cancers, a complication that affects about 25% of those taking vemurafenib alone.
Vemurafenib blocks BRAF, part of a molecular signaling pathway implicated in melanoma tumor cell growth and division. Cobimetinib can help delay tumor resistance to vemurafenib by targeting MEK, a gene in the same signaling pathway.
The senior investigator of the pivotal clinical trial, Dr. Antoni Ribas, said in a press release, “Today’s approval is a significant advance in the treatment of metastatic melanoma.
“For patients with a BRAF-mutated melanoma, the combination has higher activity to shrink their tumors, and with less side effects than the drugs on their own,” said Dr. Ribas, a researcher at the University of California, Los Angeles, Jonsson Comprehensive Cancer Center.
The FDA reviewed cobimetinib under its priority review program and gave the drug an orphan drug designation.
Cobimetinib (Cotellic) and vemurafinib (Zelboraf) are both marketed by Genentech.
On Twitter @karioakes
This article was updated November 16, 2015.
Lenalidomide plus rituximab achieves 87% response rate
First-line combination biologic therapy with lenalidomide plus rituximab produced an 87% overall response rate in stage 3-4 mantle cell lymphoma, in an industry-sponsored, phase II clinical trial reported online Nov. 5 in the New England Journal of Medicine.
Mantle cell lymphoma is generally incurable, and patients have a median survival of 4-5 years. Initial therapy is usually very intensive, involving high-dose chemotherapy and hematopoietic cell transplantation. Since the malignancy primarily affects older adults who aren’t suitable candidates for intensive regimens, treatment “remains a clinical challenge,” said Dr. Jia Ruan of the Meyer Cancer Center and the division of biostatistics and epidemiology, Weill Cornell Medical College and New York-Presbyterian Hospital, New York, and her associates.
Reasoning that biologic therapy might offer effective disease control with fewer and less intense adverse effects, the investigators performed the open-label, single-group trial over a 3-year period. They treated 38 patients whose mean age was 65 years (range, 42-86 years), most of whom were at intermediate or high risk for imminent progression. These participants received a 12-cycle induction phase of lenalidomide plus rituximab, followed by a maintenance phase until disease progressed, unacceptable adverse effects developed, or patients withdrew from the study. The median follow-up was 30 months (range, 10-42 months).
The primary endpoint – overall response rate – was 87% in the intention-to-treat population, and the complete response rate was 61%. The number of complete responses increased over time with continuing treatment: the median time to a partial response was 3 months, and the median time to a complete response was 11 months. Two-year progression-free survival was 85%, and 2-year overall survival was 97%, the investigators said (New Engl. J. Med. 2015 Nov 5. doi: 10.1056/NEJMoa1505237).
Only eight patients showed progression of mantle cell lymphoma while taking lenalidomide plus rituximab, two of whom died from their disease. The other six patients responded to second-line therapy and remain alive, indicating that this first-line combination biologic therapy doesn’t compromise outcomes after subsequent treatments, Dr. Ruan and her associates said.
Almost as important as these favorable survival results were the findings concerning adverse effects. Scores on several quality-of-life measures either remained stable or improved throughout the induction and maintenance phases of treatment. As expected, grade 3 or 4 hematologic adverse effects included neutropenia (50% of patients), thrombocytopenia (13%), and anemia (11%), all of which resolved; grade 3 or 4 nonhematologic adverse effects included rash (29%), tumor flare (11%), serum sickness (8%), and fatigue (8%), all of which also resolved. All the serious infections that developed during the maintenance phase of treatment, which included pneumonia, cholangitis, and West Nile viral encephalitis, also resolved with antibiotics and supportive care.
Secondary cancers that developed during follow-up included two squamous cell skin cancers, one basal cell skin cancer, two cases of melanoma in situ, one Merkel cell carcinoma, and one pancreatic cancer.
“Our data show that a lower-intensity approach for initial therapy than that usually used in the case of patients with this cancer can be highly active, with durable responses observed in most patients,” Dr. Ruan and her associates said.
This study was supported by Celgene, maker of lenalidomide, and a Weill Cornell Medical College Clinical Translational Science Center grant. Dr. Ruan reported ties to Celgene, and her associates reported ties to numerous industry sources.
First-line combination biologic therapy with lenalidomide plus rituximab produced an 87% overall response rate in stage 3-4 mantle cell lymphoma, in an industry-sponsored, phase II clinical trial reported online Nov. 5 in the New England Journal of Medicine.
Mantle cell lymphoma is generally incurable, and patients have a median survival of 4-5 years. Initial therapy is usually very intensive, involving high-dose chemotherapy and hematopoietic cell transplantation. Since the malignancy primarily affects older adults who aren’t suitable candidates for intensive regimens, treatment “remains a clinical challenge,” said Dr. Jia Ruan of the Meyer Cancer Center and the division of biostatistics and epidemiology, Weill Cornell Medical College and New York-Presbyterian Hospital, New York, and her associates.
Reasoning that biologic therapy might offer effective disease control with fewer and less intense adverse effects, the investigators performed the open-label, single-group trial over a 3-year period. They treated 38 patients whose mean age was 65 years (range, 42-86 years), most of whom were at intermediate or high risk for imminent progression. These participants received a 12-cycle induction phase of lenalidomide plus rituximab, followed by a maintenance phase until disease progressed, unacceptable adverse effects developed, or patients withdrew from the study. The median follow-up was 30 months (range, 10-42 months).
The primary endpoint – overall response rate – was 87% in the intention-to-treat population, and the complete response rate was 61%. The number of complete responses increased over time with continuing treatment: the median time to a partial response was 3 months, and the median time to a complete response was 11 months. Two-year progression-free survival was 85%, and 2-year overall survival was 97%, the investigators said (New Engl. J. Med. 2015 Nov 5. doi: 10.1056/NEJMoa1505237).
Only eight patients showed progression of mantle cell lymphoma while taking lenalidomide plus rituximab, two of whom died from their disease. The other six patients responded to second-line therapy and remain alive, indicating that this first-line combination biologic therapy doesn’t compromise outcomes after subsequent treatments, Dr. Ruan and her associates said.
Almost as important as these favorable survival results were the findings concerning adverse effects. Scores on several quality-of-life measures either remained stable or improved throughout the induction and maintenance phases of treatment. As expected, grade 3 or 4 hematologic adverse effects included neutropenia (50% of patients), thrombocytopenia (13%), and anemia (11%), all of which resolved; grade 3 or 4 nonhematologic adverse effects included rash (29%), tumor flare (11%), serum sickness (8%), and fatigue (8%), all of which also resolved. All the serious infections that developed during the maintenance phase of treatment, which included pneumonia, cholangitis, and West Nile viral encephalitis, also resolved with antibiotics and supportive care.
Secondary cancers that developed during follow-up included two squamous cell skin cancers, one basal cell skin cancer, two cases of melanoma in situ, one Merkel cell carcinoma, and one pancreatic cancer.
“Our data show that a lower-intensity approach for initial therapy than that usually used in the case of patients with this cancer can be highly active, with durable responses observed in most patients,” Dr. Ruan and her associates said.
This study was supported by Celgene, maker of lenalidomide, and a Weill Cornell Medical College Clinical Translational Science Center grant. Dr. Ruan reported ties to Celgene, and her associates reported ties to numerous industry sources.
First-line combination biologic therapy with lenalidomide plus rituximab produced an 87% overall response rate in stage 3-4 mantle cell lymphoma, in an industry-sponsored, phase II clinical trial reported online Nov. 5 in the New England Journal of Medicine.
Mantle cell lymphoma is generally incurable, and patients have a median survival of 4-5 years. Initial therapy is usually very intensive, involving high-dose chemotherapy and hematopoietic cell transplantation. Since the malignancy primarily affects older adults who aren’t suitable candidates for intensive regimens, treatment “remains a clinical challenge,” said Dr. Jia Ruan of the Meyer Cancer Center and the division of biostatistics and epidemiology, Weill Cornell Medical College and New York-Presbyterian Hospital, New York, and her associates.
Reasoning that biologic therapy might offer effective disease control with fewer and less intense adverse effects, the investigators performed the open-label, single-group trial over a 3-year period. They treated 38 patients whose mean age was 65 years (range, 42-86 years), most of whom were at intermediate or high risk for imminent progression. These participants received a 12-cycle induction phase of lenalidomide plus rituximab, followed by a maintenance phase until disease progressed, unacceptable adverse effects developed, or patients withdrew from the study. The median follow-up was 30 months (range, 10-42 months).
The primary endpoint – overall response rate – was 87% in the intention-to-treat population, and the complete response rate was 61%. The number of complete responses increased over time with continuing treatment: the median time to a partial response was 3 months, and the median time to a complete response was 11 months. Two-year progression-free survival was 85%, and 2-year overall survival was 97%, the investigators said (New Engl. J. Med. 2015 Nov 5. doi: 10.1056/NEJMoa1505237).
Only eight patients showed progression of mantle cell lymphoma while taking lenalidomide plus rituximab, two of whom died from their disease. The other six patients responded to second-line therapy and remain alive, indicating that this first-line combination biologic therapy doesn’t compromise outcomes after subsequent treatments, Dr. Ruan and her associates said.
Almost as important as these favorable survival results were the findings concerning adverse effects. Scores on several quality-of-life measures either remained stable or improved throughout the induction and maintenance phases of treatment. As expected, grade 3 or 4 hematologic adverse effects included neutropenia (50% of patients), thrombocytopenia (13%), and anemia (11%), all of which resolved; grade 3 or 4 nonhematologic adverse effects included rash (29%), tumor flare (11%), serum sickness (8%), and fatigue (8%), all of which also resolved. All the serious infections that developed during the maintenance phase of treatment, which included pneumonia, cholangitis, and West Nile viral encephalitis, also resolved with antibiotics and supportive care.
Secondary cancers that developed during follow-up included two squamous cell skin cancers, one basal cell skin cancer, two cases of melanoma in situ, one Merkel cell carcinoma, and one pancreatic cancer.
“Our data show that a lower-intensity approach for initial therapy than that usually used in the case of patients with this cancer can be highly active, with durable responses observed in most patients,” Dr. Ruan and her associates said.
This study was supported by Celgene, maker of lenalidomide, and a Weill Cornell Medical College Clinical Translational Science Center grant. Dr. Ruan reported ties to Celgene, and her associates reported ties to numerous industry sources.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: First-line combination biologic therapy with lenalidomide plus rituximab produced an 87% overall response rate in stage 3 or 4 mantle cell lymphoma.
Major finding: The primary endpoint – overall response rate – was 87%, and the complete response rate was 61%.
Data source: A multicenter, industry-sponsored, open-label, phase II study involving 38 patients with mantle cell lymphoma followed for a median of 30 months.
Disclosures: This study was supported by Celgene, maker of lenalidomide, and a Weill Cornell Medical College Clinical Translational Science Center grant. Dr. Ruan reported ties to Celgene, and her associates reported ties to numerous industry sources.
Higher risk of basal cell carcinoma linked to menopausal hormone therapy
Late age of natural menopause and use of menopausal hormone therapy were associated with significantly increased risk of basal cell carcinoma (BCC), according to results of a large, nationwide cohort study.
Women who experienced menopause at age 55 years or later, compared with age 50-54 years, had higher BCC risk (hazard ratio, 1.50; 95% confidence interval, 1.04-2.17; P for trend = .017). Among all women, those who had used menopausal hormone therapy had a higher risk (HR, 1.16; 95% confidence interval, 1.03-1.30) (J Clin Oncol. 2015 Nov 2. doi: 10.1200/JCO.2015.62.0625).

The findings are consistent with the hypothesis that exposure to endogenous and exogenous estrogens is photocarcinogenic, according to Dr. Elizabeth Cahoon, research fellow in the Radiation Epidemiology Branch of the National Cancer Institute, Bethesda, Md., and colleagues. Women with the highest observed BCC risk were those who experienced natural menopause and used menopausal hormone therapy for 10 or more years (HR, 1.97; 95% CI, 1.35-2.87; P for trend less than .001).
“In contrast to surgical menopause, which is associated with an immediate and dramatic drop in estrogen levels, women undergoing natural menopause may be exposed to a nontrivial amount of total and unopposed estrogen during the menopausal transition,” they wrote. “In this group, the combination of endogenous and exogenous estrogens may have increased the cumulative estrogen exposure (and, thus, the cumulative phototoxic effects).
The prospective study included 46,100 female, white participants of the US Radiologic Technologists Study, an occupational cohort composed of radiologic technologists. All participants were cancer free at baseline, and 4% had an incident BCC during the approximately 10-year follow-up.
Results showed no association between oral contraceptives and BCC, which may be due a to lower susceptibility in young adults to photosensitizing medications or to the lower doses typical of oral contraceptives. The ethinyl estradiol level in oral contraceptives typically ranges from 20 to 50 mcg, compared with a typical equine estrogen dose in menopausal therapy of 625 mcg.
Most reproductive factors evaluated, including age at menarche, number of live births, and age at first birth, showed no association with BCC.
Dr. Cahoon and coauthors reported having no disclosures.
Late age of natural menopause and use of menopausal hormone therapy were associated with significantly increased risk of basal cell carcinoma (BCC), according to results of a large, nationwide cohort study.
Women who experienced menopause at age 55 years or later, compared with age 50-54 years, had higher BCC risk (hazard ratio, 1.50; 95% confidence interval, 1.04-2.17; P for trend = .017). Among all women, those who had used menopausal hormone therapy had a higher risk (HR, 1.16; 95% confidence interval, 1.03-1.30) (J Clin Oncol. 2015 Nov 2. doi: 10.1200/JCO.2015.62.0625).
The findings are consistent with the hypothesis that exposure to endogenous and exogenous estrogens is photocarcinogenic, according to Dr. Elizabeth Cahoon, research fellow in the Radiation Epidemiology Branch of the National Cancer Institute, Bethesda, Md., and colleagues. Women with the highest observed BCC risk were those who experienced natural menopause and used menopausal hormone therapy for 10 or more years (HR, 1.97; 95% CI, 1.35-2.87; P for trend less than .001).
“In contrast to surgical menopause, which is associated with an immediate and dramatic drop in estrogen levels, women undergoing natural menopause may be exposed to a nontrivial amount of total and unopposed estrogen during the menopausal transition,” they wrote. “In this group, the combination of endogenous and exogenous estrogens may have increased the cumulative estrogen exposure (and, thus, the cumulative phototoxic effects).
The prospective study included 46,100 female, white participants of the US Radiologic Technologists Study, an occupational cohort composed of radiologic technologists. All participants were cancer free at baseline, and 4% had an incident BCC during the approximately 10-year follow-up.
Results showed no association between oral contraceptives and BCC, which may be due a to lower susceptibility in young adults to photosensitizing medications or to the lower doses typical of oral contraceptives. The ethinyl estradiol level in oral contraceptives typically ranges from 20 to 50 mcg, compared with a typical equine estrogen dose in menopausal therapy of 625 mcg.
Most reproductive factors evaluated, including age at menarche, number of live births, and age at first birth, showed no association with BCC.
Dr. Cahoon and coauthors reported having no disclosures.
Late age of natural menopause and use of menopausal hormone therapy were associated with significantly increased risk of basal cell carcinoma (BCC), according to results of a large, nationwide cohort study.
Women who experienced menopause at age 55 years or later, compared with age 50-54 years, had higher BCC risk (hazard ratio, 1.50; 95% confidence interval, 1.04-2.17; P for trend = .017). Among all women, those who had used menopausal hormone therapy had a higher risk (HR, 1.16; 95% confidence interval, 1.03-1.30) (J Clin Oncol. 2015 Nov 2. doi: 10.1200/JCO.2015.62.0625).
The findings are consistent with the hypothesis that exposure to endogenous and exogenous estrogens is photocarcinogenic, according to Dr. Elizabeth Cahoon, research fellow in the Radiation Epidemiology Branch of the National Cancer Institute, Bethesda, Md., and colleagues. Women with the highest observed BCC risk were those who experienced natural menopause and used menopausal hormone therapy for 10 or more years (HR, 1.97; 95% CI, 1.35-2.87; P for trend less than .001).
“In contrast to surgical menopause, which is associated with an immediate and dramatic drop in estrogen levels, women undergoing natural menopause may be exposed to a nontrivial amount of total and unopposed estrogen during the menopausal transition,” they wrote. “In this group, the combination of endogenous and exogenous estrogens may have increased the cumulative estrogen exposure (and, thus, the cumulative phototoxic effects).
The prospective study included 46,100 female, white participants of the US Radiologic Technologists Study, an occupational cohort composed of radiologic technologists. All participants were cancer free at baseline, and 4% had an incident BCC during the approximately 10-year follow-up.
Results showed no association between oral contraceptives and BCC, which may be due a to lower susceptibility in young adults to photosensitizing medications or to the lower doses typical of oral contraceptives. The ethinyl estradiol level in oral contraceptives typically ranges from 20 to 50 mcg, compared with a typical equine estrogen dose in menopausal therapy of 625 mcg.
Most reproductive factors evaluated, including age at menarche, number of live births, and age at first birth, showed no association with BCC.
Dr. Cahoon and coauthors reported having no disclosures.
Key clinical point: Risk of basal cell carcinoma was higher in women with late age of natural menopause and in women who used menopausal hormone therapy.
Major finding: Women who experienced menopause at a late age (55 years or older vs. 50-54 years) had higher BCC risk (HR, 1.50; 95% CI, 1.04-2.17; P for trend = .017), as did women who had ever used menopausal hormone therapy (HR, 1.16; 95% CI, 1.03-1.30).
Data source: The prospective cohort included 46,100 female, white participants of the US Radiologic Technologists Study who were cancer free at baseline; 4% had an incident BCC during the approximately 10-year follow-up.
Disclosures: Dr. Cahoon and coauthors reported having no disclosures.

ASTRO: Combined radioimmunotherapy proves promising in metastatic melanoma
SAN ANTONIO – The combination of the checkpoint inhibitor ipilimumab with palliative doses of radiation therapy was not associated with any unexpected toxicities, and half of the patients with metastatic melanoma who were treated showed a promising clinical response in a phase II study.
The trial included 22 patients with stage IV disease aged a median of 62 years, of whom 11 (50%) responded to the immunotherapy.

So far 3 (14%) of the 11 patients who responded have achieved a complete response (CR) at a median 55 weeks’ follow-up, and 3 (14%) had a partial response at a median 40 weeks’ follow-up, reported the lead study investigator, Dr. Susan Hiniker of Stanford University, during a press briefing at the annual meeting of the American Society for Radiation Oncology. The remaining five (23%) patients who responded had stable disease at a median 39 weeks’ follow-up.
The trial is one of the first prospective studies to report on the combined use of radiation with systemic immunotherapy in this patient population, she observed, noting that the idea behind the combination was that radiation might enhance the immunogenicity of tumors, that may then in turn make systemic immunotherapy more potent.
“Multiple trials have shown that there is still a minority of patients who respond to ipilimumab, with response rates of approximately 15%”, Dr. Hiniker said.
“As such, new methods of potentiating ipilimumab-induced responses are needed,” she added. “Local irradiation can modulate the local tumor environment such as to promote immune responses in a number of ways,” and other preliminary data have suggested that it may be able to increase overall response rates to ipilimumab.
Patients were recruited for the trial if they had stage IV melanoma and were aged between 18 and 65 years. Treatment consisted of palliative radiation delivered to one or two metastatic sites and at least one nonmetastatic site within 5 days of initial immunotherapy treatment with ipilimumab at a dose of 3 mg/kg every 3 weeks for a total of four treatment cycles. The dose and fractionation schedule was at the discretion of the treating physician.
Tumors were assessed for response using Response Evaluation Criteria in Solid Tumors (RECIST) and Immune Response Criteria (IRC) at baseline, 2-4 weeks after the last dose of ipilimumab was given, and then every 3 months thereafter until disease progression.
This being a phase II trial, the primary objective was to look at the safety of the approach; no additional or unexpected toxicities were seen.
“We saw approximately a 14% rate of grade 3-4 toxicity, which is really on par with what has been reported for ipilimumab monotherapy – on the order of 20%,” Dr. Hiniker said in an interview. “But that being said, we don’t believe that radiation itself caused any additional toxicity.”
One of the patients did have a perforated colon, she acknowledged, and for this reason future research may look at the combination of radiation therapy with the PD-1 (programmed T-cell death) inhibitors.
“I think right now everyone is so excited about the PD-1 inhibitors, and think that they’re safer,” Dr. Hiniker suggested. “It’s hard to give someone ipilimumab alone as the first line at this point; although many patients may not experience toxicity, [in] the ones that do, it can be severe.”
Dr. Hiniker also reported that IRC (independent review committee) analysis results suggested that several proinflammatory cytokines were elevated in some patients who responded to treatment. Higher levels of interleukin 2 at baseline, and at two time points during the study, for example, were associated with better response rates than lower levels. The findings also suggested that there might be a relationship between an increased number of elevated CD8-positive T cells and response.
“I think that we will find biomarkers, but we are not there yet, and it would need to be confirmed in a longer, larger study,” Dr. Hiniker said.
From a practical perspective, if a patient is already being treated with ipilimumab, and a physician is considering radiotherapy, then these results suggest that there will be no additional toxicity, she suggested.
“This combination approach does appear to be promising,” she said. “So for a subset of carefully selected patients – and the problem is we don’t totally know how to select them yet – this can be extremely promising.”
Dr. Hiniker had no disclosures to report.
SAN ANTONIO – The combination of the checkpoint inhibitor ipilimumab with palliative doses of radiation therapy was not associated with any unexpected toxicities, and half of the patients with metastatic melanoma who were treated showed a promising clinical response in a phase II study.
The trial included 22 patients with stage IV disease aged a median of 62 years, of whom 11 (50%) responded to the immunotherapy.
So far 3 (14%) of the 11 patients who responded have achieved a complete response (CR) at a median 55 weeks’ follow-up, and 3 (14%) had a partial response at a median 40 weeks’ follow-up, reported the lead study investigator, Dr. Susan Hiniker of Stanford University, during a press briefing at the annual meeting of the American Society for Radiation Oncology. The remaining five (23%) patients who responded had stable disease at a median 39 weeks’ follow-up.
The trial is one of the first prospective studies to report on the combined use of radiation with systemic immunotherapy in this patient population, she observed, noting that the idea behind the combination was that radiation might enhance the immunogenicity of tumors, that may then in turn make systemic immunotherapy more potent.
“Multiple trials have shown that there is still a minority of patients who respond to ipilimumab, with response rates of approximately 15%”, Dr. Hiniker said.
“As such, new methods of potentiating ipilimumab-induced responses are needed,” she added. “Local irradiation can modulate the local tumor environment such as to promote immune responses in a number of ways,” and other preliminary data have suggested that it may be able to increase overall response rates to ipilimumab.
Patients were recruited for the trial if they had stage IV melanoma and were aged between 18 and 65 years. Treatment consisted of palliative radiation delivered to one or two metastatic sites and at least one nonmetastatic site within 5 days of initial immunotherapy treatment with ipilimumab at a dose of 3 mg/kg every 3 weeks for a total of four treatment cycles. The dose and fractionation schedule was at the discretion of the treating physician.
Tumors were assessed for response using Response Evaluation Criteria in Solid Tumors (RECIST) and Immune Response Criteria (IRC) at baseline, 2-4 weeks after the last dose of ipilimumab was given, and then every 3 months thereafter until disease progression.
This being a phase II trial, the primary objective was to look at the safety of the approach; no additional or unexpected toxicities were seen.
“We saw approximately a 14% rate of grade 3-4 toxicity, which is really on par with what has been reported for ipilimumab monotherapy – on the order of 20%,” Dr. Hiniker said in an interview. “But that being said, we don’t believe that radiation itself caused any additional toxicity.”
One of the patients did have a perforated colon, she acknowledged, and for this reason future research may look at the combination of radiation therapy with the PD-1 (programmed T-cell death) inhibitors.
“I think right now everyone is so excited about the PD-1 inhibitors, and think that they’re safer,” Dr. Hiniker suggested. “It’s hard to give someone ipilimumab alone as the first line at this point; although many patients may not experience toxicity, [in] the ones that do, it can be severe.”
Dr. Hiniker also reported that IRC (independent review committee) analysis results suggested that several proinflammatory cytokines were elevated in some patients who responded to treatment. Higher levels of interleukin 2 at baseline, and at two time points during the study, for example, were associated with better response rates than lower levels. The findings also suggested that there might be a relationship between an increased number of elevated CD8-positive T cells and response.
“I think that we will find biomarkers, but we are not there yet, and it would need to be confirmed in a longer, larger study,” Dr. Hiniker said.
From a practical perspective, if a patient is already being treated with ipilimumab, and a physician is considering radiotherapy, then these results suggest that there will be no additional toxicity, she suggested.
“This combination approach does appear to be promising,” she said. “So for a subset of carefully selected patients – and the problem is we don’t totally know how to select them yet – this can be extremely promising.”
Dr. Hiniker had no disclosures to report.
SAN ANTONIO – The combination of the checkpoint inhibitor ipilimumab with palliative doses of radiation therapy was not associated with any unexpected toxicities, and half of the patients with metastatic melanoma who were treated showed a promising clinical response in a phase II study.
The trial included 22 patients with stage IV disease aged a median of 62 years, of whom 11 (50%) responded to the immunotherapy.
So far 3 (14%) of the 11 patients who responded have achieved a complete response (CR) at a median 55 weeks’ follow-up, and 3 (14%) had a partial response at a median 40 weeks’ follow-up, reported the lead study investigator, Dr. Susan Hiniker of Stanford University, during a press briefing at the annual meeting of the American Society for Radiation Oncology. The remaining five (23%) patients who responded had stable disease at a median 39 weeks’ follow-up.
The trial is one of the first prospective studies to report on the combined use of radiation with systemic immunotherapy in this patient population, she observed, noting that the idea behind the combination was that radiation might enhance the immunogenicity of tumors, that may then in turn make systemic immunotherapy more potent.
“Multiple trials have shown that there is still a minority of patients who respond to ipilimumab, with response rates of approximately 15%”, Dr. Hiniker said.
“As such, new methods of potentiating ipilimumab-induced responses are needed,” she added. “Local irradiation can modulate the local tumor environment such as to promote immune responses in a number of ways,” and other preliminary data have suggested that it may be able to increase overall response rates to ipilimumab.
Patients were recruited for the trial if they had stage IV melanoma and were aged between 18 and 65 years. Treatment consisted of palliative radiation delivered to one or two metastatic sites and at least one nonmetastatic site within 5 days of initial immunotherapy treatment with ipilimumab at a dose of 3 mg/kg every 3 weeks for a total of four treatment cycles. The dose and fractionation schedule was at the discretion of the treating physician.
Tumors were assessed for response using Response Evaluation Criteria in Solid Tumors (RECIST) and Immune Response Criteria (IRC) at baseline, 2-4 weeks after the last dose of ipilimumab was given, and then every 3 months thereafter until disease progression.
This being a phase II trial, the primary objective was to look at the safety of the approach; no additional or unexpected toxicities were seen.
“We saw approximately a 14% rate of grade 3-4 toxicity, which is really on par with what has been reported for ipilimumab monotherapy – on the order of 20%,” Dr. Hiniker said in an interview. “But that being said, we don’t believe that radiation itself caused any additional toxicity.”
One of the patients did have a perforated colon, she acknowledged, and for this reason future research may look at the combination of radiation therapy with the PD-1 (programmed T-cell death) inhibitors.
“I think right now everyone is so excited about the PD-1 inhibitors, and think that they’re safer,” Dr. Hiniker suggested. “It’s hard to give someone ipilimumab alone as the first line at this point; although many patients may not experience toxicity, [in] the ones that do, it can be severe.”
Dr. Hiniker also reported that IRC (independent review committee) analysis results suggested that several proinflammatory cytokines were elevated in some patients who responded to treatment. Higher levels of interleukin 2 at baseline, and at two time points during the study, for example, were associated with better response rates than lower levels. The findings also suggested that there might be a relationship between an increased number of elevated CD8-positive T cells and response.
“I think that we will find biomarkers, but we are not there yet, and it would need to be confirmed in a longer, larger study,” Dr. Hiniker said.
From a practical perspective, if a patient is already being treated with ipilimumab, and a physician is considering radiotherapy, then these results suggest that there will be no additional toxicity, she suggested.
“This combination approach does appear to be promising,” she said. “So for a subset of carefully selected patients – and the problem is we don’t totally know how to select them yet – this can be extremely promising.”
Dr. Hiniker had no disclosures to report.
AT THE ASTRO ANNUAL MEETING
Key clinical point: Some patients with metastatic melanoma may benefit from combined use of novel immunotherapies and radiation treatment.
Major finding: No additional toxicity was seen and 50% of patients had a complete or partial response to the treatment regimen of combined radioimmunotherapy.
Data source: Prospective phase II clinical trial of 22 patients with melanoma treated with ipilimumab and palliative radiation therapy.
Disclosures: Dr. Hiniker had no disclosures to report.

Ipilimumab approved as adjuvant treatment for resected metastatic melanoma
Ipilimumab is now approved as an adjuvant treatment for patients who have undergone a complete resection of metastatic cutaneous melanoma.
The approval is based on data from a large study showing that ipilimumab, marketed as Yervoy by Bristol-Myers Squibb, improved recurrence-free survival, compared with placebo.

“Today’s approval of Yervoy extends its use to patients who are at high risk of developing recurrence of melanoma after surgery,” Dr. Richard Pazdur, director of the office of hematology and oncology products in Food and Drug Administration’s Center for Drug Evaluation and Research, said in the FDA statement announcing the approval on Oct. 28. “This new use of the drug in earlier stages of the disease builds on our understanding of the immune system’s interaction with cancer.”
Ipilimumab, a monoclonal antibody that blocks cytotoxic T-lymphocyte antigen 4 (CTLA-4), was initially approved in 2011 for the treatment of unresectable or metastatic melanoma.
The new indication is for the adjuvant treatment of patients “with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy.”
In the study of 951 patients, with resected Stage IIIA, IIIB, and IIIC cutaneous melanoma, the median recurrence-free survival was 26 months in the ipilimumab group vs. 17 months in the placebo group; 3-year recurrence-free survival was 46.5% vs. 34.8% (Lancet Oncol. 2015; 16[5]:522-30). The data on overall survival have not yet been analyzed.
The recommended dose and schedule for ipilimumab for adjuvant treatment is 10 mg/kg administered intravenously over 90 minutes every 3 weeks for four doses, followed by 10 mg/kg every 12 weeks for up to 3 years. Doses are omitted, not delayed, if toxicity occurs.
In the study, 52% of those treated with ipilimumab had to discontinue the drug because of adverse reactions. In addition, 41% experienced grade 3-5 immune mediated adverse reactions, including enterocolitis (16%), hepatitis (11%), endocrinopathy (8%), dermatitis (4%), and neuropathy (1.7%).
There were five treatment-related deaths in the study, from immune-mediated adverse reactions, which were enterocolitis (three), Guillain-Barré syndrome (one) and myocarditis (one).The prescribing information includes a boxed warning about the risk of immune-mediated adverse reactions.
In a statement, FDA officials cautioned physicians to carefully monitor patients taking the drug for signs of enterocolitis, dermatitis, neuropathy, and endocrinopathy. Liver function, adrenocorticotropic hormone level, and thyroid function should be measured at baseline and before each dose.
Among the most common reactions were rash, pruritus, diarrhea, nausea, colitis, vomiting, weight loss, fatigue, pyrexia, headache, decreased appetite, and insomnia.
CTLA-4 “may play a role in slowing down or turning off the body’s immune system, and affects its ability to fight off cancerous cells. Yervoy may work by allowing the body’s immune system to recognize, target and attack cells in melanoma tumors,” according to the FDA statement.
Serious adverse events associated with ipilimumab should be reported to the FDA’s MedWatch program or at 800-332-1088.
Ipilimumab is now approved as an adjuvant treatment for patients who have undergone a complete resection of metastatic cutaneous melanoma.
The approval is based on data from a large study showing that ipilimumab, marketed as Yervoy by Bristol-Myers Squibb, improved recurrence-free survival, compared with placebo.
“Today’s approval of Yervoy extends its use to patients who are at high risk of developing recurrence of melanoma after surgery,” Dr. Richard Pazdur, director of the office of hematology and oncology products in Food and Drug Administration’s Center for Drug Evaluation and Research, said in the FDA statement announcing the approval on Oct. 28. “This new use of the drug in earlier stages of the disease builds on our understanding of the immune system’s interaction with cancer.”
Ipilimumab, a monoclonal antibody that blocks cytotoxic T-lymphocyte antigen 4 (CTLA-4), was initially approved in 2011 for the treatment of unresectable or metastatic melanoma.
The new indication is for the adjuvant treatment of patients “with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy.”
In the study of 951 patients, with resected Stage IIIA, IIIB, and IIIC cutaneous melanoma, the median recurrence-free survival was 26 months in the ipilimumab group vs. 17 months in the placebo group; 3-year recurrence-free survival was 46.5% vs. 34.8% (Lancet Oncol. 2015; 16[5]:522-30). The data on overall survival have not yet been analyzed.
The recommended dose and schedule for ipilimumab for adjuvant treatment is 10 mg/kg administered intravenously over 90 minutes every 3 weeks for four doses, followed by 10 mg/kg every 12 weeks for up to 3 years. Doses are omitted, not delayed, if toxicity occurs.
In the study, 52% of those treated with ipilimumab had to discontinue the drug because of adverse reactions. In addition, 41% experienced grade 3-5 immune mediated adverse reactions, including enterocolitis (16%), hepatitis (11%), endocrinopathy (8%), dermatitis (4%), and neuropathy (1.7%).
There were five treatment-related deaths in the study, from immune-mediated adverse reactions, which were enterocolitis (three), Guillain-Barré syndrome (one) and myocarditis (one).The prescribing information includes a boxed warning about the risk of immune-mediated adverse reactions.
In a statement, FDA officials cautioned physicians to carefully monitor patients taking the drug for signs of enterocolitis, dermatitis, neuropathy, and endocrinopathy. Liver function, adrenocorticotropic hormone level, and thyroid function should be measured at baseline and before each dose.
Among the most common reactions were rash, pruritus, diarrhea, nausea, colitis, vomiting, weight loss, fatigue, pyrexia, headache, decreased appetite, and insomnia.
CTLA-4 “may play a role in slowing down or turning off the body’s immune system, and affects its ability to fight off cancerous cells. Yervoy may work by allowing the body’s immune system to recognize, target and attack cells in melanoma tumors,” according to the FDA statement.
Serious adverse events associated with ipilimumab should be reported to the FDA’s MedWatch program or at 800-332-1088.
Ipilimumab is now approved as an adjuvant treatment for patients who have undergone a complete resection of metastatic cutaneous melanoma.
The approval is based on data from a large study showing that ipilimumab, marketed as Yervoy by Bristol-Myers Squibb, improved recurrence-free survival, compared with placebo.
“Today’s approval of Yervoy extends its use to patients who are at high risk of developing recurrence of melanoma after surgery,” Dr. Richard Pazdur, director of the office of hematology and oncology products in Food and Drug Administration’s Center for Drug Evaluation and Research, said in the FDA statement announcing the approval on Oct. 28. “This new use of the drug in earlier stages of the disease builds on our understanding of the immune system’s interaction with cancer.”
Ipilimumab, a monoclonal antibody that blocks cytotoxic T-lymphocyte antigen 4 (CTLA-4), was initially approved in 2011 for the treatment of unresectable or metastatic melanoma.
The new indication is for the adjuvant treatment of patients “with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy.”
In the study of 951 patients, with resected Stage IIIA, IIIB, and IIIC cutaneous melanoma, the median recurrence-free survival was 26 months in the ipilimumab group vs. 17 months in the placebo group; 3-year recurrence-free survival was 46.5% vs. 34.8% (Lancet Oncol. 2015; 16[5]:522-30). The data on overall survival have not yet been analyzed.
The recommended dose and schedule for ipilimumab for adjuvant treatment is 10 mg/kg administered intravenously over 90 minutes every 3 weeks for four doses, followed by 10 mg/kg every 12 weeks for up to 3 years. Doses are omitted, not delayed, if toxicity occurs.
In the study, 52% of those treated with ipilimumab had to discontinue the drug because of adverse reactions. In addition, 41% experienced grade 3-5 immune mediated adverse reactions, including enterocolitis (16%), hepatitis (11%), endocrinopathy (8%), dermatitis (4%), and neuropathy (1.7%).
There were five treatment-related deaths in the study, from immune-mediated adverse reactions, which were enterocolitis (three), Guillain-Barré syndrome (one) and myocarditis (one).The prescribing information includes a boxed warning about the risk of immune-mediated adverse reactions.
In a statement, FDA officials cautioned physicians to carefully monitor patients taking the drug for signs of enterocolitis, dermatitis, neuropathy, and endocrinopathy. Liver function, adrenocorticotropic hormone level, and thyroid function should be measured at baseline and before each dose.
Among the most common reactions were rash, pruritus, diarrhea, nausea, colitis, vomiting, weight loss, fatigue, pyrexia, headache, decreased appetite, and insomnia.
CTLA-4 “may play a role in slowing down or turning off the body’s immune system, and affects its ability to fight off cancerous cells. Yervoy may work by allowing the body’s immune system to recognize, target and attack cells in melanoma tumors,” according to the FDA statement.
Serious adverse events associated with ipilimumab should be reported to the FDA’s MedWatch program or at 800-332-1088.

Biopsy-site photography an easy winner on all counts
CHICAGO – Biopsy-site photography appears to reduce the risk of potential wrong-site surgery and can easily be incorporated into dermatology practice, according to Dr. Jeremy Etzkorn.
When Dr. Etzkorn took on this quality improvement initiative on his own, only 5 of 239 routine biopsy-site photographs evaluated were inadequate. The biopsy site was not clearly marked in two photos with multiple suspicious lesions, and anatomic landmarks were absent in three.
“Almost 98% of the time, the photograph was adequate, which just shows it doesn’t require much training or time to get images of the skin,” the Mohs surgeon said at the annual meeting of the American Society for Dermatologic Surgery.
Biopsy-site photos were taken primarily by medical assistants, as well as nurses, who received minimal, informal training on digital photography and were guided to take at least one photograph with anatomic landmarks present.

Dr. Etzkorn of the University of Pennsylvania Health System, Philadelphia, conducted a prospective, observational cohort study of 329 patients/tumors referred for Mohs micrographic surgery or standard excision to the dermatologic surgery unit at Penn Dermatology. Patients were asked to identify their biopsy site, indicate whether they remembered a photo being taken, and quantify on a 10-point scale their level of confidence that the originally biopsied site was treated on the day of surgery.
Dr. Etzkorn identified the biopsy site before consulting the medical record for a biopsy-site photograph. If the photo was absent and he and the patient agreed on the biopsy site, they proceeded to surgery. If there was any disagreement, surgery was postponed and the referring physician consulted.
Overall, 239 patients (73%) had biopsy-site photographs, and 90 patients (27%), referred to the practice before photography was implemented, did not.
In 12.5% of cases, the patient misidentified the biopsy site, and in 6.7% of cases the physician did, which is similar to what has been reported in the literature, Dr. Etzkorn said.
Biopsy-site photography prevented wrong-site surgery in 3 of the 239 cases (1.25%) where these photographs were available. “Without the photo I would normally have done surgery on that site because the patient was confident it was the right site; I was confident it was the right site,” he said.
Importantly, all three lesions were biopsied, and all were squamous cell carcinoma in situ. So while it was the wrong site, the surgery would not have been inappropriate, Dr. Etzkorn noted.
Surgery was postponed to consult the referring physician in 3% of cases (10/329).
Complete patient confidence (10 of 10 points) that the correct site was treated was achieved in 95% of cases, with most of the remaining patients at 9 of 10 points, he said.
Risk factors for patient biopsy-site misidentification were the inability to see the site without a mirror (odds ratio, 3.95; P = .002) and time between the biopsy and surgery (OR, 2.19; P = .028). Prior studies have also shown that difficult-to-visualize sites are associated with biopsy-site misidentification, he noted.
For Dr. Etzkorn, the risk of biopsy-site misidentification quadrupled if there were multiple simultaneous biopsies from different locations (OR, 4.39; P = .003) and tripled with longer time, defined as longer than a 6-week delay vs. a delay of less than 6 weeks between biopsy and surgery (OR, 3.68; P = .007).
A biopsy-site photograph significantly increased the odds that a patient was completely confident the correct site was treated (OR, 5.48; P = .001), as did the use of Mohs surgery vs. excision (OR, 4.87; P = .017).
Once again, time between the biopsy and surgery was a significant risk factor for postponing surgery (OR, 3.52; P = .035), whereas the presence of a biopsy-site photograph cut that risk by almost 13-fold (OR, 12.5: P less than .001), Dr. Etzkorn reported.
“Biopsy-site photography is associated with increased patient confidence that the correct site is treated, decreases in surgical postponement, and the ability to identify wrong-site surgery and prevent it,” he concluded.
Dr. Etzkorn and his coauthor reported having no relevant financial disclosures.
CHICAGO – Biopsy-site photography appears to reduce the risk of potential wrong-site surgery and can easily be incorporated into dermatology practice, according to Dr. Jeremy Etzkorn.
When Dr. Etzkorn took on this quality improvement initiative on his own, only 5 of 239 routine biopsy-site photographs evaluated were inadequate. The biopsy site was not clearly marked in two photos with multiple suspicious lesions, and anatomic landmarks were absent in three.
“Almost 98% of the time, the photograph was adequate, which just shows it doesn’t require much training or time to get images of the skin,” the Mohs surgeon said at the annual meeting of the American Society for Dermatologic Surgery.
Biopsy-site photos were taken primarily by medical assistants, as well as nurses, who received minimal, informal training on digital photography and were guided to take at least one photograph with anatomic landmarks present.
Dr. Etzkorn of the University of Pennsylvania Health System, Philadelphia, conducted a prospective, observational cohort study of 329 patients/tumors referred for Mohs micrographic surgery or standard excision to the dermatologic surgery unit at Penn Dermatology. Patients were asked to identify their biopsy site, indicate whether they remembered a photo being taken, and quantify on a 10-point scale their level of confidence that the originally biopsied site was treated on the day of surgery.
Dr. Etzkorn identified the biopsy site before consulting the medical record for a biopsy-site photograph. If the photo was absent and he and the patient agreed on the biopsy site, they proceeded to surgery. If there was any disagreement, surgery was postponed and the referring physician consulted.
Overall, 239 patients (73%) had biopsy-site photographs, and 90 patients (27%), referred to the practice before photography was implemented, did not.
In 12.5% of cases, the patient misidentified the biopsy site, and in 6.7% of cases the physician did, which is similar to what has been reported in the literature, Dr. Etzkorn said.
Biopsy-site photography prevented wrong-site surgery in 3 of the 239 cases (1.25%) where these photographs were available. “Without the photo I would normally have done surgery on that site because the patient was confident it was the right site; I was confident it was the right site,” he said.
Importantly, all three lesions were biopsied, and all were squamous cell carcinoma in situ. So while it was the wrong site, the surgery would not have been inappropriate, Dr. Etzkorn noted.
Surgery was postponed to consult the referring physician in 3% of cases (10/329).
Complete patient confidence (10 of 10 points) that the correct site was treated was achieved in 95% of cases, with most of the remaining patients at 9 of 10 points, he said.
Risk factors for patient biopsy-site misidentification were the inability to see the site without a mirror (odds ratio, 3.95; P = .002) and time between the biopsy and surgery (OR, 2.19; P = .028). Prior studies have also shown that difficult-to-visualize sites are associated with biopsy-site misidentification, he noted.
For Dr. Etzkorn, the risk of biopsy-site misidentification quadrupled if there were multiple simultaneous biopsies from different locations (OR, 4.39; P = .003) and tripled with longer time, defined as longer than a 6-week delay vs. a delay of less than 6 weeks between biopsy and surgery (OR, 3.68; P = .007).
A biopsy-site photograph significantly increased the odds that a patient was completely confident the correct site was treated (OR, 5.48; P = .001), as did the use of Mohs surgery vs. excision (OR, 4.87; P = .017).
Once again, time between the biopsy and surgery was a significant risk factor for postponing surgery (OR, 3.52; P = .035), whereas the presence of a biopsy-site photograph cut that risk by almost 13-fold (OR, 12.5: P less than .001), Dr. Etzkorn reported.
“Biopsy-site photography is associated with increased patient confidence that the correct site is treated, decreases in surgical postponement, and the ability to identify wrong-site surgery and prevent it,” he concluded.
Dr. Etzkorn and his coauthor reported having no relevant financial disclosures.
CHICAGO – Biopsy-site photography appears to reduce the risk of potential wrong-site surgery and can easily be incorporated into dermatology practice, according to Dr. Jeremy Etzkorn.
When Dr. Etzkorn took on this quality improvement initiative on his own, only 5 of 239 routine biopsy-site photographs evaluated were inadequate. The biopsy site was not clearly marked in two photos with multiple suspicious lesions, and anatomic landmarks were absent in three.
“Almost 98% of the time, the photograph was adequate, which just shows it doesn’t require much training or time to get images of the skin,” the Mohs surgeon said at the annual meeting of the American Society for Dermatologic Surgery.
Biopsy-site photos were taken primarily by medical assistants, as well as nurses, who received minimal, informal training on digital photography and were guided to take at least one photograph with anatomic landmarks present.
Dr. Etzkorn of the University of Pennsylvania Health System, Philadelphia, conducted a prospective, observational cohort study of 329 patients/tumors referred for Mohs micrographic surgery or standard excision to the dermatologic surgery unit at Penn Dermatology. Patients were asked to identify their biopsy site, indicate whether they remembered a photo being taken, and quantify on a 10-point scale their level of confidence that the originally biopsied site was treated on the day of surgery.
Dr. Etzkorn identified the biopsy site before consulting the medical record for a biopsy-site photograph. If the photo was absent and he and the patient agreed on the biopsy site, they proceeded to surgery. If there was any disagreement, surgery was postponed and the referring physician consulted.
Overall, 239 patients (73%) had biopsy-site photographs, and 90 patients (27%), referred to the practice before photography was implemented, did not.
In 12.5% of cases, the patient misidentified the biopsy site, and in 6.7% of cases the physician did, which is similar to what has been reported in the literature, Dr. Etzkorn said.
Biopsy-site photography prevented wrong-site surgery in 3 of the 239 cases (1.25%) where these photographs were available. “Without the photo I would normally have done surgery on that site because the patient was confident it was the right site; I was confident it was the right site,” he said.
Importantly, all three lesions were biopsied, and all were squamous cell carcinoma in situ. So while it was the wrong site, the surgery would not have been inappropriate, Dr. Etzkorn noted.
Surgery was postponed to consult the referring physician in 3% of cases (10/329).
Complete patient confidence (10 of 10 points) that the correct site was treated was achieved in 95% of cases, with most of the remaining patients at 9 of 10 points, he said.
Risk factors for patient biopsy-site misidentification were the inability to see the site without a mirror (odds ratio, 3.95; P = .002) and time between the biopsy and surgery (OR, 2.19; P = .028). Prior studies have also shown that difficult-to-visualize sites are associated with biopsy-site misidentification, he noted.
For Dr. Etzkorn, the risk of biopsy-site misidentification quadrupled if there were multiple simultaneous biopsies from different locations (OR, 4.39; P = .003) and tripled with longer time, defined as longer than a 6-week delay vs. a delay of less than 6 weeks between biopsy and surgery (OR, 3.68; P = .007).
A biopsy-site photograph significantly increased the odds that a patient was completely confident the correct site was treated (OR, 5.48; P = .001), as did the use of Mohs surgery vs. excision (OR, 4.87; P = .017).
Once again, time between the biopsy and surgery was a significant risk factor for postponing surgery (OR, 3.52; P = .035), whereas the presence of a biopsy-site photograph cut that risk by almost 13-fold (OR, 12.5: P less than .001), Dr. Etzkorn reported.
“Biopsy-site photography is associated with increased patient confidence that the correct site is treated, decreases in surgical postponement, and the ability to identify wrong-site surgery and prevent it,” he concluded.
Dr. Etzkorn and his coauthor reported having no relevant financial disclosures.
AT THE ASDS ANNUAL MEETING
Key clinical point: Biopsy-site photography reduces surgical delays, identifies potential wrong-site surgery, and increases patient confidence.
Major finding: Having biopsy-site photos can help prevent wrong-site surgery.
Data source: A prospective, observational cohort study of 329 patients referred for Mohs surgery or standard excision.
Disclosures: Dr. Etzkorn and his coauthor reported having no relevant financial disclosures.

FDA approves T-VEC for metastatic melanoma
The Food and Drug Administration has approved talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, for the local treatment of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that has recurred after initial surgery, the manufacturer Amgen announced today.
The approval officially makes T-VEC (Imlygic) the first virus-based cancer treatment ever approved, as it is derived from the herpes simplex virus. The FDA’s approval comes just months after an FDA advisory panel voiced their support for T-VEC’s approval in a 22-1 vote, based on a phase III study published in the Journal of Clinical Oncology (2015;33 [25]2780-8).

The study looked at 436 individuals with either stage IIIB/C or stage IV (with limited visceral disease burden considered unresectable) and found that patients treated with T-VEC had a significantly higher overall response rate (26.4%) and complete response rate (10.8%) than did those who were treated with subcutaneous granulocyte macrophage colony-stimulating factor (GM-CSF) (5.7% and 0.7%, respectively).
The durable response rate was also significantly higher among T-VEC–treated patients (16.3%) than among those on GM-CSF (2.1%). T-VEC patients also experienced a median overall survival time of 23.3 months, compared with 18.9 months for those on GM-CSF. In the study, cellulitis was noted in about 2% of patients on T-VEC. Fifty-four percent of T-VEC patients who responded to the treatment initially had disease progression before response began.
“The evidence of local and systemic immune responses with T-VEC supports combinations with other immunotherapies as a rational approach. A phase 1b/2 study of T-VEC and ipilimumab is evaluating the safety and efficacy of this combination,” wrote the investigators of the phase III study, which was led by Dr. Robert Andtbacka of the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
T-VEC was also scrutinized in five other studies, all of which reported that the most common adverse events related to the drug were fatigue, chills, and pyrexia and flulike symptoms; severity of these symptoms ranged from mild to moderate.
The manufacturer intends to make the therapy available to patients almost immediately and anticipates its cost to average $65,000, according to a statement.
The Food and Drug Administration has approved talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, for the local treatment of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that has recurred after initial surgery, the manufacturer Amgen announced today.
The approval officially makes T-VEC (Imlygic) the first virus-based cancer treatment ever approved, as it is derived from the herpes simplex virus. The FDA’s approval comes just months after an FDA advisory panel voiced their support for T-VEC’s approval in a 22-1 vote, based on a phase III study published in the Journal of Clinical Oncology (2015;33 [25]2780-8).
The study looked at 436 individuals with either stage IIIB/C or stage IV (with limited visceral disease burden considered unresectable) and found that patients treated with T-VEC had a significantly higher overall response rate (26.4%) and complete response rate (10.8%) than did those who were treated with subcutaneous granulocyte macrophage colony-stimulating factor (GM-CSF) (5.7% and 0.7%, respectively).
The durable response rate was also significantly higher among T-VEC–treated patients (16.3%) than among those on GM-CSF (2.1%). T-VEC patients also experienced a median overall survival time of 23.3 months, compared with 18.9 months for those on GM-CSF. In the study, cellulitis was noted in about 2% of patients on T-VEC. Fifty-four percent of T-VEC patients who responded to the treatment initially had disease progression before response began.
“The evidence of local and systemic immune responses with T-VEC supports combinations with other immunotherapies as a rational approach. A phase 1b/2 study of T-VEC and ipilimumab is evaluating the safety and efficacy of this combination,” wrote the investigators of the phase III study, which was led by Dr. Robert Andtbacka of the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
T-VEC was also scrutinized in five other studies, all of which reported that the most common adverse events related to the drug were fatigue, chills, and pyrexia and flulike symptoms; severity of these symptoms ranged from mild to moderate.
The manufacturer intends to make the therapy available to patients almost immediately and anticipates its cost to average $65,000, according to a statement.
The Food and Drug Administration has approved talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, for the local treatment of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that has recurred after initial surgery, the manufacturer Amgen announced today.
The approval officially makes T-VEC (Imlygic) the first virus-based cancer treatment ever approved, as it is derived from the herpes simplex virus. The FDA’s approval comes just months after an FDA advisory panel voiced their support for T-VEC’s approval in a 22-1 vote, based on a phase III study published in the Journal of Clinical Oncology (2015;33 [25]2780-8).
The study looked at 436 individuals with either stage IIIB/C or stage IV (with limited visceral disease burden considered unresectable) and found that patients treated with T-VEC had a significantly higher overall response rate (26.4%) and complete response rate (10.8%) than did those who were treated with subcutaneous granulocyte macrophage colony-stimulating factor (GM-CSF) (5.7% and 0.7%, respectively).
The durable response rate was also significantly higher among T-VEC–treated patients (16.3%) than among those on GM-CSF (2.1%). T-VEC patients also experienced a median overall survival time of 23.3 months, compared with 18.9 months for those on GM-CSF. In the study, cellulitis was noted in about 2% of patients on T-VEC. Fifty-four percent of T-VEC patients who responded to the treatment initially had disease progression before response began.
“The evidence of local and systemic immune responses with T-VEC supports combinations with other immunotherapies as a rational approach. A phase 1b/2 study of T-VEC and ipilimumab is evaluating the safety and efficacy of this combination,” wrote the investigators of the phase III study, which was led by Dr. Robert Andtbacka of the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
T-VEC was also scrutinized in five other studies, all of which reported that the most common adverse events related to the drug were fatigue, chills, and pyrexia and flulike symptoms; severity of these symptoms ranged from mild to moderate.
The manufacturer intends to make the therapy available to patients almost immediately and anticipates its cost to average $65,000, according to a statement.
FROM THE FDA

Spitzoid melanoma mortality on par with conventional melanoma
CHICAGO – One in four patients with an invasive spitzoid melanoma died from melanoma within 10 years of diagnosis, according to a large SEER database analysis.
The risk of death due to melanoma increased significantly with tumor thickness, metastatic disease, head and neck lesions, male sex, and older age, Dr. Sultan Mirza reported at the annual meeting of the American Society for Dermatologic Surgery.
Spitzoid tumors represent a group of melanocytic neoplasms composed of distinct epithelioid and/or spindle cells and are important because of their mimicry of malignant melanoma.
Although there is a paucity of data, several smaller studies have suggested spitzoid melanomas are less aggressive and have a lower mortality rate when compared with conventional malignant melanoma, he said.
“Our study found spitzoid melanoma–specific mortality to be quite high and is likely to be more on par with the mortality of the conventional malignant melanoma,” Dr. Mirza of Mayo Clinic, Rochester, Minn., said in an interview.
“Given a lack of broadly accepted and well-defined diagnostic criteria, it is our suspicion that many cases of these tumors go unrecognized or are classified under various other types of neoplastic proliferations at the time of diagnosis. This, therefore, hinders our knowledge of the true prognosis of the spitzoid tumors.”
Using the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) database, the investigators identified 2,025 patients who were diagnosed between 1992 and 2010 with an epithelioid/spindle cell melanoma, epithelial cell melanoma, spindle cell melanoma not otherwise specified, or spindle cell melanoma type A or type B. After excluding patients with missing data including microscopic confirmation of malignancy or cause of death, 1,997 patients remained.
Most were white (96%), male (61%), and had invasive disease (98%). Their average age at diagnosis was 64 years, with 21 patients younger than 18 years of age. Median follow-up was 5.6 years.
Of the 1,997 patients, 773 (39%) were deceased at last follow-up. Of these, 331 (43%) died due to metastatic melanoma, Dr. Mirza said. The median time to death was 1.8 years after diagnosis.
Among the 1,956 patients with invasive disease, melanoma cause-specific survival at years 1, 5, 10, and 15 was 95%, 81%, 76%, and 74%, respectively.
Among 41 patients with in situ spitzoid melanoma, the melanoma cause-specific survival was 100% at years 1, 5, and 10.In survival analyses, a Breslow tumor depth of more than 4 mm carried a five times higher risk of melanoma-specific death than a depth of less than 1 mm (hazard ratio, 5.0; P less than .001), Dr. Mirza said.
The risk of death from melanoma increased dramatically as the stage of melanoma advanced from localized (referent) to regional (HR, 4.3; P = .001) and then to distant (HR, 19.4; P = .001).
A similar pattern was observed as patient age increased from 52 years or younger (referent) to 53-66 years (HR, 1.7; P = .001), 67- 77 years (HR, 1.7; P = .001), and finally to age 78 years and older (HR, 2.6; P = .001).
Men were twice as likely to die from melanoma as women (HR, 1.9; P = .001), he said.
The worst anatomic site for a lesion was on the head and scalp, which carried more than twice the risk of melanoma-specific death as lesions on the face and ears (HR, 2.3; P = .001).Limitations of the study were the lack of fluorescence in situ hybridization data, an inability to review and categorize tumor pathology, and confusing terminology regarding spitzoid tumors in the database, resulting in possible inclusion of other types of melanomas, Dr. Mirza said.
This variance of terminology emphasizes the need for standardized nomenclature and once accomplished, will hopefully provide further clarity regarding types of spitzoid growths, so we can know the true prognosis and treatment, he added.
CHICAGO – One in four patients with an invasive spitzoid melanoma died from melanoma within 10 years of diagnosis, according to a large SEER database analysis.
The risk of death due to melanoma increased significantly with tumor thickness, metastatic disease, head and neck lesions, male sex, and older age, Dr. Sultan Mirza reported at the annual meeting of the American Society for Dermatologic Surgery.
Spitzoid tumors represent a group of melanocytic neoplasms composed of distinct epithelioid and/or spindle cells and are important because of their mimicry of malignant melanoma.
Although there is a paucity of data, several smaller studies have suggested spitzoid melanomas are less aggressive and have a lower mortality rate when compared with conventional malignant melanoma, he said.
“Our study found spitzoid melanoma–specific mortality to be quite high and is likely to be more on par with the mortality of the conventional malignant melanoma,” Dr. Mirza of Mayo Clinic, Rochester, Minn., said in an interview.
“Given a lack of broadly accepted and well-defined diagnostic criteria, it is our suspicion that many cases of these tumors go unrecognized or are classified under various other types of neoplastic proliferations at the time of diagnosis. This, therefore, hinders our knowledge of the true prognosis of the spitzoid tumors.”
Using the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) database, the investigators identified 2,025 patients who were diagnosed between 1992 and 2010 with an epithelioid/spindle cell melanoma, epithelial cell melanoma, spindle cell melanoma not otherwise specified, or spindle cell melanoma type A or type B. After excluding patients with missing data including microscopic confirmation of malignancy or cause of death, 1,997 patients remained.
Most were white (96%), male (61%), and had invasive disease (98%). Their average age at diagnosis was 64 years, with 21 patients younger than 18 years of age. Median follow-up was 5.6 years.
Of the 1,997 patients, 773 (39%) were deceased at last follow-up. Of these, 331 (43%) died due to metastatic melanoma, Dr. Mirza said. The median time to death was 1.8 years after diagnosis.
Among the 1,956 patients with invasive disease, melanoma cause-specific survival at years 1, 5, 10, and 15 was 95%, 81%, 76%, and 74%, respectively.
Among 41 patients with in situ spitzoid melanoma, the melanoma cause-specific survival was 100% at years 1, 5, and 10.In survival analyses, a Breslow tumor depth of more than 4 mm carried a five times higher risk of melanoma-specific death than a depth of less than 1 mm (hazard ratio, 5.0; P less than .001), Dr. Mirza said.
The risk of death from melanoma increased dramatically as the stage of melanoma advanced from localized (referent) to regional (HR, 4.3; P = .001) and then to distant (HR, 19.4; P = .001).
A similar pattern was observed as patient age increased from 52 years or younger (referent) to 53-66 years (HR, 1.7; P = .001), 67- 77 years (HR, 1.7; P = .001), and finally to age 78 years and older (HR, 2.6; P = .001).
Men were twice as likely to die from melanoma as women (HR, 1.9; P = .001), he said.
The worst anatomic site for a lesion was on the head and scalp, which carried more than twice the risk of melanoma-specific death as lesions on the face and ears (HR, 2.3; P = .001).Limitations of the study were the lack of fluorescence in situ hybridization data, an inability to review and categorize tumor pathology, and confusing terminology regarding spitzoid tumors in the database, resulting in possible inclusion of other types of melanomas, Dr. Mirza said.
This variance of terminology emphasizes the need for standardized nomenclature and once accomplished, will hopefully provide further clarity regarding types of spitzoid growths, so we can know the true prognosis and treatment, he added.
CHICAGO – One in four patients with an invasive spitzoid melanoma died from melanoma within 10 years of diagnosis, according to a large SEER database analysis.
The risk of death due to melanoma increased significantly with tumor thickness, metastatic disease, head and neck lesions, male sex, and older age, Dr. Sultan Mirza reported at the annual meeting of the American Society for Dermatologic Surgery.
Spitzoid tumors represent a group of melanocytic neoplasms composed of distinct epithelioid and/or spindle cells and are important because of their mimicry of malignant melanoma.
Although there is a paucity of data, several smaller studies have suggested spitzoid melanomas are less aggressive and have a lower mortality rate when compared with conventional malignant melanoma, he said.
“Our study found spitzoid melanoma–specific mortality to be quite high and is likely to be more on par with the mortality of the conventional malignant melanoma,” Dr. Mirza of Mayo Clinic, Rochester, Minn., said in an interview.
“Given a lack of broadly accepted and well-defined diagnostic criteria, it is our suspicion that many cases of these tumors go unrecognized or are classified under various other types of neoplastic proliferations at the time of diagnosis. This, therefore, hinders our knowledge of the true prognosis of the spitzoid tumors.”
Using the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) database, the investigators identified 2,025 patients who were diagnosed between 1992 and 2010 with an epithelioid/spindle cell melanoma, epithelial cell melanoma, spindle cell melanoma not otherwise specified, or spindle cell melanoma type A or type B. After excluding patients with missing data including microscopic confirmation of malignancy or cause of death, 1,997 patients remained.
Most were white (96%), male (61%), and had invasive disease (98%). Their average age at diagnosis was 64 years, with 21 patients younger than 18 years of age. Median follow-up was 5.6 years.
Of the 1,997 patients, 773 (39%) were deceased at last follow-up. Of these, 331 (43%) died due to metastatic melanoma, Dr. Mirza said. The median time to death was 1.8 years after diagnosis.
Among the 1,956 patients with invasive disease, melanoma cause-specific survival at years 1, 5, 10, and 15 was 95%, 81%, 76%, and 74%, respectively.
Among 41 patients with in situ spitzoid melanoma, the melanoma cause-specific survival was 100% at years 1, 5, and 10.In survival analyses, a Breslow tumor depth of more than 4 mm carried a five times higher risk of melanoma-specific death than a depth of less than 1 mm (hazard ratio, 5.0; P less than .001), Dr. Mirza said.
The risk of death from melanoma increased dramatically as the stage of melanoma advanced from localized (referent) to regional (HR, 4.3; P = .001) and then to distant (HR, 19.4; P = .001).
A similar pattern was observed as patient age increased from 52 years or younger (referent) to 53-66 years (HR, 1.7; P = .001), 67- 77 years (HR, 1.7; P = .001), and finally to age 78 years and older (HR, 2.6; P = .001).
Men were twice as likely to die from melanoma as women (HR, 1.9; P = .001), he said.
The worst anatomic site for a lesion was on the head and scalp, which carried more than twice the risk of melanoma-specific death as lesions on the face and ears (HR, 2.3; P = .001).Limitations of the study were the lack of fluorescence in situ hybridization data, an inability to review and categorize tumor pathology, and confusing terminology regarding spitzoid tumors in the database, resulting in possible inclusion of other types of melanomas, Dr. Mirza said.
This variance of terminology emphasizes the need for standardized nomenclature and once accomplished, will hopefully provide further clarity regarding types of spitzoid growths, so we can know the true prognosis and treatment, he added.
AT THE ASDS ANNUAL MEETING
Key clinical point: One-fourth of patients with invasive spitzoid melanoma died from their disease within 10 years of diagnosis.
Major finding: Melanoma-specific mortality was 24% at 10 years.
Data source: SEER database analysis of 1,997 patients with Spitz cutaneous melanoma.
Disclosures: The authors reported having no financial disclosures.