User login
The Use of Immuno-Oncology Treatments in the VA (FULL)
The following is a lightly edited transcript of a teleconference discussion recorded in April 2018.
Suman Kambhampati, MD. Immuno-oncology is a paradigm-shifting treatment approach. It is an easy-to-understand term for both providers and for patients. The underlying principle is that the body’s own immune system is used or stimulated to fight cancer, and there are drugs that clearly have shown huge promise for this, not only in oncology, but also for other diseases. Time will tell whether that really pans out or not, but to begin with, the emphasis has been inoncology, and therefore, the term immunooncology is fitting.
Dr. Kaster. It was encouraging at first, especially when ipilimumab came out, to see the effects on patients with melanoma. Then the KEYNOTE-024 trial came out, and we were able to jump in anduse monoclonal antibodies directed against programmed death 1 (PD-1) in the first line, which is when things got exciting.1 We have a smaller populationin Boise, so PD-1s in lung cancer have had the biggest impact on our patients so far.
Ellen Nason, RN, MSN. Patients are open to immunotherapies.They’re excited about it. And as the other panelists have said, you can start broadly, as the body fights the cancer on its own, to providing more specific details as a patient wants more information. Immuno-oncology is definitely accepted by patients, and they’re very excited about it, especially with all the news about new therapies.
Dr. Kambhampati. For the Department of Veteran Affairs (VA) population, lung cancer has seen significant impact, and now it’s translating into other diseases through more research, trials, and better understanding about how these drugs are used and work. 
The paradigm is shifting toward offering these drugs not only in metastatic cancers, but also in the surgically resectable tumors. The 2018 American Association for Cancer Research (AACR) meeting, just concluded. At the meeting several abstracts reported instances where immunooncology drugs are being introduced in the early phases of lung cancer and showing outstanding results. It’s very much possible that we’re going to see less use of traditional chemotherapy in the near future.
Ms. Nason. I primarily work with solid tumors,and the majority of the population I work with have lung cancer. So we’re excited about some of the results that we’ve seen and the lower toxicity involved. Recently, we’ve begun using durvalumab with patients with stage III disease. We have about 5 people now that are using it as a maintenance or consolidative treatment vs just using it for patients with stage IV disease. Hopefully, we’ll see some of the same results describedin the paper published on it.2
Dr. Kaster. Yes, we are incorporating these new changes into care as they're coming out. As Ms. Nason mentioned, we're already using immunotherapies in earlier settings, and we are seeing as much research that could be translated into care soon, like combining immunotherapies
in first-line settings, as we see in the Checkmate-227 study with nivolumab and ipilimumab.3,4 The landscape is going to change dramatically in the next couple of years.
Accessing Testing For First-Line Treatments
Dr. Lynch. There has been an ongoing discussionin the literature on accessing appropriate testing—delays in testing can result in patients who are not able to access the best targeted drugs on a first-line basis. The drug companiesand the VA have become highly sensitized to ensuring that veterans are accessing the appropriate testing. We are expanding the capability of VA labs to do that testing.
Ms. Nason. I want to put in a plug for the VA Precision Oncology Program (POP). It’s about 2 years into its existence, and Neil Spector, MD, is the director. The POP pays for sequencing the tumor samples.
A new sequencing contract will go into effect October 2018 and will include sequencing for hematologic malignancies in addition to the current testing of solid tumors. Patients from New York who have been unable to receive testing through the current vendors used by POP, will be included in the new contract. It is important to note that POP is working closely with the National Pharmacy Benefit Management Service (PBM) to develop a policy for approving off-label use of US Food and Drug Administration-approved targeted therapies based on sequenced data collected on patients tested through POP.
In addition, the leadership of POP is working to leverage the molecular testing results conducted through POP to improve veterans' access to clinical trials, both inside and outside the VA. Within the VA people can access information at tinyurl.com/precisiononcology. There is no reason why any eligible patient with cancer in the VA health care system should not have their tumor tissue sequenced through POP, particularly once the new contract goes into effect.
Dr. Lynch. Fortunately, the cost of next-generation sequencing has come down so much that most VA contracted reference laboratories offer next-generation sequencing, including LabCorp (Burlington,NC), Quest Diagnostics (Secaucus, NJ), Fulgent (Temple City, CA), and academic partners such as Oregon Health Sciences University and University of Washington.
Ms. Nason. At the Durham VAMC, sometimes a lack of tissue has been a barrier, but we now have the ability to send blood (liquid biopsy) for next-generation sequencing. Hopefully that will open up options for veterans with inadequate tissue. Importantly, all VA facilities can request liquid biopsiesthrough POP.
Dr. Lynch. That’s an important point. There have been huge advances in liquid biopsy testing.The VA Salt Lake City Health Care System (VASLCHCS) was in talks with Genomic Health (Redwood City, CA) to do a study as part of clinical operations to look at the concordance between the liquid biopsy testing and the precision oncology data. But Genomic Health eventually abandoned its liquid biopsy testing. Currently, the VA is only reimbursing or encouraging liquid biopsy if the tissue is not available or if the veteran has too high a level of comorbidities to undergo tissue biopsy. The main point for the discussion today is that access to testing is a key component of access to all of these advanced drugs.
Dr. Kambhampati. The precision medicine piece will be a game changer—no question about that. Liquid biopsy is very timely. Many patients have difficulty getting rebiopsied, so liquid biopsy is definitely a big, big step forward.
Still, there has not been consistency across the VA as there should be. Perhaps there are a few select centers, including our site in Kansas City, where access to precision medicine is readily available and liquid biopsies are available. We use the PlasmaSELECT test from Personal Genome Diagnostics (Baltimore, MD). We have just added Foundation Medicine (Cambridge, MA) also in hematology. Access to mutational profilingis absolutely a must for precision medicine.
All that being said, the unique issue with immuno-oncology is that it pretty much transcends the mutational profile and perhaps has leveled the playing field, irrespective of the tumor mutation profile or burden. In some solid tumors these immuno-oncology drugs have been shown to work across tumor types and across different mutation types. And there is a hint now in the recent data presented at AACR and in the New England Journalof Medicine showing that the tumor mutational burden is a predictor of pathologic response to at least PD-1 blockade in the resectable stages of lung cancer.1,3 To me, that’s a very important piece of data because that’s something that can be tested and can have a prognostic impact in immuno-oncology, particularly in the early stages of lung cancer and is further proof of the broad value of immunotherapics in targeting tumors irrespective of the precise tumor targets.
Dr. Kaster. Yes, it’s nice to see other options like tumor mutational burden and Lung Immune Prognostic Index being studied.5 It would be nice if we could rely a little more on these, and not PD-L1, which as we all know is a variable and an unreliable target.
Dr. Kambhampati. I agree.
Rural Challenges In A Veterans Population
Dr. Lynch. Providing high-quality cancer care to rural veterans care can be a challenge but it is a VA priority. The VA National Genomic Medicine Services offers better access for rural veterans to germline genetic testing than any other healthcare system in the country. In terms of access to somatic testing and next-generation sequencing, we are working toward providing the same level of cancer care as patients would receive at National Cancer Institute (NCI) cancer centers. The VA oncology leadership has done teleconsults and virtual tumor boards, but for some rural VAMCs, fellowsare leading the clinical care. As we expand use of oral agents for oncology treatment, it will be easier to ensure that rural veterans receive the same standard of care for POP that veterans being cared for at VASLCHCS, Kansas City VAMC, or Durham VAMC get.
Dr. Kambhampati. The Kansas City VAMC in its catchment area includes underserved areas, such as Topeka and Leavenworth, Kansas. What we’ve been able to do here is something that’s unique—Kansas City VAMC is the only standalone VA in the country to be recognized as a primary SWOG (Southwestern Oncology Group) institution, which provides access to many trials, such as the Lung-MAP trial and others. And that has allowed us to use the full expanse of precision medicine without financial barriers. The research has helped us improve the standard of
care for patients across VISN 15.
Dr. Lynch. In precision oncology, the chief of pathology is an important figure in access to advanced care. I’ve worked with Sharad Mathur,MD, of the Kansas City VAMC on many clinical trials. He’s on the Kansas City VAMC Institutional Review Board and the cancer committee and is tuned in to veterans’ access to precision oncology. Kansas City was ordering Foundation One for select patients that met the criteria probably sooner than any other VA and participated in NCI Cooperative Group clinical trials. It is a great example of how veterans are getting access to
the same level of care as are patients who gettreated at NCI partners.
Comorbidities
Dr. Kambhampati. I don’t treat a lot of patients with lung cancer, but I find it easier to use these immuno-oncology drugs than platinums and etoposide. I consider them absolutely nasty chemotherapy drugs now in this era of immuno-oncology and targeted therapy.
Dr. Lynch. The VA is very important in translational lung cancer research and clinical care. It used to be thought that African American patients don’t get epidermal growth factor receptor mutations. And that’s because not enough African American patients with lung cancer were included in the NCI-based clinical trial.There are7,000 veterans who get lung cancer each year, and 20% to 25% of those are African Americans. Prevalence of various mutations and the pharmacogenetics of some of these drugs differ by patient ancestry. Including veterans with lung
cancer in precision oncology clinical trials and clinical care is not just a priority for the VA but a priority for NCI and internationally. I can’t emphasize this enough—veterans with lung cancer should be included in these studies and should be getting the same level of care that our partners are getting at NCI cancer centers. In the VA we’re positioned to do this because of our nationalelectronic health record (EHR) and becauseof our ability to identify patients with specific variants and enroll them in clinical trials.
Ms. Nason. One of the barriers that I find withsome of the patients that I have treated is getting them to a trial. If the trial isn’t available locally, specifically there are socioeconomic and distance issues that are hard to overcome.
Dr. Kaster. For smaller medical centers, getting patients to clinical trials can be difficult. The Boise VAMC is putting together a proposal now to justify hiring a research pharmacist in order to get trials atour site. The goal is to offer trial participation to our patients who otherwise might not be able to participate while offsetting some of the costs of immunotherapy. We are trying to make what could be a negative into a positive.
Measuring Success
Dr. Kambhampati. Unfortunately, we do not have any calculators to incorporate the quality of lives saved to the society. I know there are clearmetrics in transplant and in hematology, but unfortunately, there are no established metrics in solid tumor treatment that allow us to predict the cost savings to the health care system or to society or the benefit to the society. I don’t use any such predictive models or metrics in my decision making. These decisions are made based on existing evidence, and the existing evidence overwhelmingly supports use of immuno-oncology in certain types of solid tumors and in a select group of hematologic malignancies.
Dr. Kaster. This is where you can get more bang for your buck with an oncology pharmacist these days. A pharmacist can make a minor dosing change that will allow the same benefit for the patient, but could equal tens of thousands of dollars in cost-benefit for the VA. They can also be the second set of eyes when adjudicating a nonformulary request to ensure that a patient will benefit.
Dr. Lynch. Inappropriate prescribing is far more expensive than appropriate treatment. And the care for veterans whose long-term health outcomes could be improved by the new immunotherapies. It’s cheaper for veterans to be healthy and live longer than it is to take care of them in
their last 6 weeks of life. Unfortunately, there are not a lot of studies that have demonstrated that empirically, but I think it’s important to do those studies.
Role of Pharmacists
Dr. Lynch. I was at a meeting recently talking about how to improve veteran access to clinical trials. Francesca Cunningham, PharmD, director of the VA Center for Medication Safety of the VA Pharmacy Benefit Management Service (PBM) described the commitment that pharmacy has in taking a leadership role in the integration of precision medicine. Linking veterans’ tumor mutation status and pharmacogenetic variants to pharmacy databases is the best way to ensure treatment is informed by genetics. We have to be realistic about what we’re asking community oncologists to do. With the onset of precision oncology, 10 cancers have become really 100 cancers. In the prior model of care, it was the oncologist, maybe in collaboration with a pathologist, but it was mostly oncologists who determined care.
And in the evolution of precision oncology, Ithink that it’s become an interdisciplinary adventure. Pharmacy is going to play an increasinglyimportant role in precision medicine around all of the molecular alterations, even immuno-oncology regardless of molecular status in which the VA has an advantage. We’re not talking about some community pharmacist. We’re talking about a national health care system where there’s a national EHR, where there’s national PBM systems. So my thoughts on this aspect is that it’s an intricate multidisciplinary team who can ensure that veteran sget the best care possible: the best most cost-effective care possible.
Dr. Kaster. As an oncology pharmacist, I have to second that.
Ms. Nason. As Dr. Kaster said earlier, having a dedicated oncology pharmacist is tremendouslybeneficial. The oncology/hematology pharmacists are following the patients closely and notice when dose adjustments need to be made, optimizing the drug benefit and providing additional safety. Not to mention the cost benefit that can be realized with appropriate adjustment and the expertise they bring to managing possible interactionsand pharmacodynamics.
Dr. Kambhampati. To brag about the Kansas City VAMC program, we have published in Federal Practitioner our best practices showing the collaboration between a pharmacist and providers.6 And we have used several examples of cost savings, which have basically helped us build the research program, and several examples of dual monitoring oral chemotherapy monitoring. And we have created these templates within the EHR that allow everyone to get a quick snapshot of where things are, what needs to be done, and what needs to be monitored.
Now, we are taking it a step further to determine when to stop chemotherapy or when to stop treatments. For example, for chronic myeloid leukemia (CML), there are good data onstopping tyrosine kinase inhibitors.7 And that alone, if implemented across the VA, could bring
in huge cost savings, which perhaps could be put into investments in immuno-oncology or other efforts. We have several examples here that we have published, and we continue to increaseand strengthen our collaboration withour oncology pharmacist. We are very lucky and privileged to have a dedicated oncology pharmacistfor clinics and for research.
Dr. Lynch. The example of CML is perfect, because precision oncology has increased the complexity of care substantially. The VA is wellpositioned to be a leader in this area when care becomes this complex because of its ability to measure access to testing, to translate the results
of testing to pharmacy, to have pharmacists take the lead on prescribing, to have pathologists take the lead on molecular alterations, and to have oncologists take the lead on delivering the cancer care to the patients.
With hematologic malignancies, adherence in the early stages can result in patients getting offcare sooner, which is cost savings. But that requires access to testing, monitoring that testing, and working in partnership with pharmacy. This is a great story about how the VA is positioned to lead in this area of care.
Dr. Kaster. I would like to put a plug in for advanced practice providers and the use of nurse practitioners (NPs) and physician assistants (PAs).The VA is well positioned because it often has established interdisciplinary teams with these providers, pharmacy, nursing, and often social work, to coordinate the care and manage symptoms outside of oncologist visits.
Dr. Lynch. In the NCI cancer center model, once the patient has become stable, the ongoing careis designated to the NP or PA. Then as soon as there’s a change and it requires reevaluation, the oncologist becomes involved again. That pointabout the oncology treatment team is totally in line
with some of the previous comments.
Areas For Further Investigation
Dr. Kaster. There are so many nuances that we’re finding out all of the time about immunotherapies. A recent study brought up the role of antibiotics in the 30 or possibly 60 days prior to immunotherapy.3 How does that change treatment? Which patients are more likely to benefit from immunotherapies, and which are susceptible to “hyperprogression”? How do we integrate palliative care discussions into the carenow that patients are feeling better on treatment and may be less likely to want to discuss palliative care?
Ms. Nason. I absolutely agree with that, especially keeping palliative care integrated within our services. Our focus is now a little different, in thatwe have more optimistic outcomes in mind, butthere still are symptoms and issues where our colleaguesin palliative care are invaluable.
Dr. Lynch. I third that motion. What I would really like to see come out of this discussion is how veterans are getting access to leading oncology care. We just published an analysis of Medicare data and access to EGFR testing. The result of that analysis showed that testing in the VA was consistent with testing in Medicare.
For palliative care, I think the VA does a better job. And it’s just so discouraging as VA employees and as clinicians treating veterans to see publicationsthat suggest that veterans are getting a lower quality of care and that they would be better if care was privatized or outsourced. It’s just fundamentally not the case.
In CML, we see it. We’ve analyzed the data, in that there’s a far lower number of patients with CML who are included in the registry because patients who are diagnosed outside the VA are incorporated in other cancer registries.8 But as soon as their copays increase for access to targeted drugs, they immediately activate their VA benefits so that theycan get their drugs at the VA. For hematologic malignancies that are diagnosed outside the VA and are captured in other cancer registries, as soon as the drugs become expensive, they start getting their care in the VA. I don’t think there’s beena lot of empirical research that’s shown this, but we have the data to illustrate this trend. I hope thatthere are more publications that show that veterans with cancer are getting really good care inside the VA in the existing VA health care system.
Ms. Nason. It is disheartening to see negativepublicity, knowing that I work with colleagues who are strongly committed to providing up-to-date and relevant oncology care.
Dr. Lynch. As we record this conversation, I am in Rotterdam, Netherlands, in a meeting about genomewide testing. In hematologic malignancies, prostate cancer, and breast cancer, it’s a huge issue. And that is the other area that MVP (Million Veteran Program) is leading the way with the MVP biorepository data. Frankly, there’s no other biorepository that has this many patients, that has so many African Americans, and that has such rich EHR data. So inthat other area, the VA is doing really well.
1. Reck M, Rodríguez-Abreu D, Robinson AG, et al; KEYNOTE-024 Investigators. Pembrolizumab vs chemotherapy for PD-L1-positive non-small cell lung cancer. N Engl J Med. 2016;375(19):1823-1833.
2. Antonia SJ, Villegas A, Daniel D, et al; PACIFIC Investigators. Durvalumab after chemoradiotherapy in stage III non–smallcell lung cancer. N Engl J Med. 2017;377(20):1919-1929.
3. Hellmann MD, Ciuleanu T-E, Pluzansk A, et al. Nivolumab plus ipilimumab in Lung Cancer with a high tumor mutational burden. N Engl J Med. 2018 April 16. [Epub ahead of print.]
4. Motzer RJ, Tannir NM, McDermott DF, et al; CheckMate214 Investigators. Nivolumab plus ipilimumab versus sunitinibin advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277-1290.
5. Derosa L, Hellmann MD, Spaziano M, et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small cell
lung cancer. Ann Oncol. 2018 March 30. [Epub ahead of print.]
6. Heinrichs A, Dessars B, El Housni H, et al. Identification of chronic myeloid leukemia patients treated with imatinib who are potentially eligible for treatment discontinuation by assessingreal-life molecular responses on the international scale in a EUTOS-certified lab. Leuk Res. 2018;67:27-31.
7. Keefe S, Kambhampati S, Powers B. An electronic chemotherapy ordering process and template. Fed Pract. 2015;32(suppl 1):21S-25S.
8. Lynch JA, Berse B, Rabb M, et al. Underutilization and disparities in access to EGFR testing among Medicare patients with lung cancer from 2010 - 2013. BMC Cancer. 2018;18(1):306.
The following is a lightly edited transcript of a teleconference discussion recorded in April 2018.
Suman Kambhampati, MD. Immuno-oncology is a paradigm-shifting treatment approach. It is an easy-to-understand term for both providers and for patients. The underlying principle is that the body’s own immune system is used or stimulated to fight cancer, and there are drugs that clearly have shown huge promise for this, not only in oncology, but also for other diseases. Time will tell whether that really pans out or not, but to begin with, the emphasis has been inoncology, and therefore, the term immunooncology is fitting.
Dr. Kaster. It was encouraging at first, especially when ipilimumab came out, to see the effects on patients with melanoma. Then the KEYNOTE-024 trial came out, and we were able to jump in anduse monoclonal antibodies directed against programmed death 1 (PD-1) in the first line, which is when things got exciting.1 We have a smaller populationin Boise, so PD-1s in lung cancer have had the biggest impact on our patients so far.
Ellen Nason, RN, MSN. Patients are open to immunotherapies.They’re excited about it. And as the other panelists have said, you can start broadly, as the body fights the cancer on its own, to providing more specific details as a patient wants more information. Immuno-oncology is definitely accepted by patients, and they’re very excited about it, especially with all the news about new therapies.
Dr. Kambhampati. For the Department of Veteran Affairs (VA) population, lung cancer has seen significant impact, and now it’s translating into other diseases through more research, trials, and better understanding about how these drugs are used and work.
The paradigm is shifting toward offering these drugs not only in metastatic cancers, but also in the surgically resectable tumors. The 2018 American Association for Cancer Research (AACR) meeting, just concluded. At the meeting several abstracts reported instances where immunooncology drugs are being introduced in the early phases of lung cancer and showing outstanding results. It’s very much possible that we’re going to see less use of traditional chemotherapy in the near future.
Ms. Nason. I primarily work with solid tumors,and the majority of the population I work with have lung cancer. So we’re excited about some of the results that we’ve seen and the lower toxicity involved. Recently, we’ve begun using durvalumab with patients with stage III disease. We have about 5 people now that are using it as a maintenance or consolidative treatment vs just using it for patients with stage IV disease. Hopefully, we’ll see some of the same results describedin the paper published on it.2
Dr. Kaster. Yes, we are incorporating these new changes into care as they're coming out. As Ms. Nason mentioned, we're already using immunotherapies in earlier settings, and we are seeing as much research that could be translated into care soon, like combining immunotherapies
in first-line settings, as we see in the Checkmate-227 study with nivolumab and ipilimumab.3,4 The landscape is going to change dramatically in the next couple of years.
Accessing Testing For First-Line Treatments
Dr. Lynch. There has been an ongoing discussionin the literature on accessing appropriate testing—delays in testing can result in patients who are not able to access the best targeted drugs on a first-line basis. The drug companiesand the VA have become highly sensitized to ensuring that veterans are accessing the appropriate testing. We are expanding the capability of VA labs to do that testing.
Ms. Nason. I want to put in a plug for the VA Precision Oncology Program (POP). It’s about 2 years into its existence, and Neil Spector, MD, is the director. The POP pays for sequencing the tumor samples.
A new sequencing contract will go into effect October 2018 and will include sequencing for hematologic malignancies in addition to the current testing of solid tumors. Patients from New York who have been unable to receive testing through the current vendors used by POP, will be included in the new contract. It is important to note that POP is working closely with the National Pharmacy Benefit Management Service (PBM) to develop a policy for approving off-label use of US Food and Drug Administration-approved targeted therapies based on sequenced data collected on patients tested through POP.
In addition, the leadership of POP is working to leverage the molecular testing results conducted through POP to improve veterans' access to clinical trials, both inside and outside the VA. Within the VA people can access information at tinyurl.com/precisiononcology. There is no reason why any eligible patient with cancer in the VA health care system should not have their tumor tissue sequenced through POP, particularly once the new contract goes into effect.
Dr. Lynch. Fortunately, the cost of next-generation sequencing has come down so much that most VA contracted reference laboratories offer next-generation sequencing, including LabCorp (Burlington,NC), Quest Diagnostics (Secaucus, NJ), Fulgent (Temple City, CA), and academic partners such as Oregon Health Sciences University and University of Washington.
Ms. Nason. At the Durham VAMC, sometimes a lack of tissue has been a barrier, but we now have the ability to send blood (liquid biopsy) for next-generation sequencing. Hopefully that will open up options for veterans with inadequate tissue. Importantly, all VA facilities can request liquid biopsiesthrough POP.
Dr. Lynch. That’s an important point. There have been huge advances in liquid biopsy testing.The VA Salt Lake City Health Care System (VASLCHCS) was in talks with Genomic Health (Redwood City, CA) to do a study as part of clinical operations to look at the concordance between the liquid biopsy testing and the precision oncology data. But Genomic Health eventually abandoned its liquid biopsy testing. Currently, the VA is only reimbursing or encouraging liquid biopsy if the tissue is not available or if the veteran has too high a level of comorbidities to undergo tissue biopsy. The main point for the discussion today is that access to testing is a key component of access to all of these advanced drugs.
Dr. Kambhampati. The precision medicine piece will be a game changer—no question about that. Liquid biopsy is very timely. Many patients have difficulty getting rebiopsied, so liquid biopsy is definitely a big, big step forward.
Still, there has not been consistency across the VA as there should be. Perhaps there are a few select centers, including our site in Kansas City, where access to precision medicine is readily available and liquid biopsies are available. We use the PlasmaSELECT test from Personal Genome Diagnostics (Baltimore, MD). We have just added Foundation Medicine (Cambridge, MA) also in hematology. Access to mutational profilingis absolutely a must for precision medicine.
All that being said, the unique issue with immuno-oncology is that it pretty much transcends the mutational profile and perhaps has leveled the playing field, irrespective of the tumor mutation profile or burden. In some solid tumors these immuno-oncology drugs have been shown to work across tumor types and across different mutation types. And there is a hint now in the recent data presented at AACR and in the New England Journalof Medicine showing that the tumor mutational burden is a predictor of pathologic response to at least PD-1 blockade in the resectable stages of lung cancer.1,3 To me, that’s a very important piece of data because that’s something that can be tested and can have a prognostic impact in immuno-oncology, particularly in the early stages of lung cancer and is further proof of the broad value of immunotherapics in targeting tumors irrespective of the precise tumor targets.
Dr. Kaster. Yes, it’s nice to see other options like tumor mutational burden and Lung Immune Prognostic Index being studied.5 It would be nice if we could rely a little more on these, and not PD-L1, which as we all know is a variable and an unreliable target.
Dr. Kambhampati. I agree.
Rural Challenges In A Veterans Population
Dr. Lynch. Providing high-quality cancer care to rural veterans care can be a challenge but it is a VA priority. The VA National Genomic Medicine Services offers better access for rural veterans to germline genetic testing than any other healthcare system in the country. In terms of access to somatic testing and next-generation sequencing, we are working toward providing the same level of cancer care as patients would receive at National Cancer Institute (NCI) cancer centers. The VA oncology leadership has done teleconsults and virtual tumor boards, but for some rural VAMCs, fellowsare leading the clinical care. As we expand use of oral agents for oncology treatment, it will be easier to ensure that rural veterans receive the same standard of care for POP that veterans being cared for at VASLCHCS, Kansas City VAMC, or Durham VAMC get.
Dr. Kambhampati. The Kansas City VAMC in its catchment area includes underserved areas, such as Topeka and Leavenworth, Kansas. What we’ve been able to do here is something that’s unique—Kansas City VAMC is the only standalone VA in the country to be recognized as a primary SWOG (Southwestern Oncology Group) institution, which provides access to many trials, such as the Lung-MAP trial and others. And that has allowed us to use the full expanse of precision medicine without financial barriers. The research has helped us improve the standard of
care for patients across VISN 15.
Dr. Lynch. In precision oncology, the chief of pathology is an important figure in access to advanced care. I’ve worked with Sharad Mathur,MD, of the Kansas City VAMC on many clinical trials. He’s on the Kansas City VAMC Institutional Review Board and the cancer committee and is tuned in to veterans’ access to precision oncology. Kansas City was ordering Foundation One for select patients that met the criteria probably sooner than any other VA and participated in NCI Cooperative Group clinical trials. It is a great example of how veterans are getting access to
the same level of care as are patients who gettreated at NCI partners.
Comorbidities
Dr. Kambhampati. I don’t treat a lot of patients with lung cancer, but I find it easier to use these immuno-oncology drugs than platinums and etoposide. I consider them absolutely nasty chemotherapy drugs now in this era of immuno-oncology and targeted therapy.
Dr. Lynch. The VA is very important in translational lung cancer research and clinical care. It used to be thought that African American patients don’t get epidermal growth factor receptor mutations. And that’s because not enough African American patients with lung cancer were included in the NCI-based clinical trial.There are7,000 veterans who get lung cancer each year, and 20% to 25% of those are African Americans. Prevalence of various mutations and the pharmacogenetics of some of these drugs differ by patient ancestry. Including veterans with lung
cancer in precision oncology clinical trials and clinical care is not just a priority for the VA but a priority for NCI and internationally. I can’t emphasize this enough—veterans with lung cancer should be included in these studies and should be getting the same level of care that our partners are getting at NCI cancer centers. In the VA we’re positioned to do this because of our nationalelectronic health record (EHR) and becauseof our ability to identify patients with specific variants and enroll them in clinical trials.
Ms. Nason. One of the barriers that I find withsome of the patients that I have treated is getting them to a trial. If the trial isn’t available locally, specifically there are socioeconomic and distance issues that are hard to overcome.
Dr. Kaster. For smaller medical centers, getting patients to clinical trials can be difficult. The Boise VAMC is putting together a proposal now to justify hiring a research pharmacist in order to get trials atour site. The goal is to offer trial participation to our patients who otherwise might not be able to participate while offsetting some of the costs of immunotherapy. We are trying to make what could be a negative into a positive.
Measuring Success
Dr. Kambhampati. Unfortunately, we do not have any calculators to incorporate the quality of lives saved to the society. I know there are clearmetrics in transplant and in hematology, but unfortunately, there are no established metrics in solid tumor treatment that allow us to predict the cost savings to the health care system or to society or the benefit to the society. I don’t use any such predictive models or metrics in my decision making. These decisions are made based on existing evidence, and the existing evidence overwhelmingly supports use of immuno-oncology in certain types of solid tumors and in a select group of hematologic malignancies.
Dr. Kaster. This is where you can get more bang for your buck with an oncology pharmacist these days. A pharmacist can make a minor dosing change that will allow the same benefit for the patient, but could equal tens of thousands of dollars in cost-benefit for the VA. They can also be the second set of eyes when adjudicating a nonformulary request to ensure that a patient will benefit.
Dr. Lynch. Inappropriate prescribing is far more expensive than appropriate treatment. And the care for veterans whose long-term health outcomes could be improved by the new immunotherapies. It’s cheaper for veterans to be healthy and live longer than it is to take care of them in
their last 6 weeks of life. Unfortunately, there are not a lot of studies that have demonstrated that empirically, but I think it’s important to do those studies.
Role of Pharmacists
Dr. Lynch. I was at a meeting recently talking about how to improve veteran access to clinical trials. Francesca Cunningham, PharmD, director of the VA Center for Medication Safety of the VA Pharmacy Benefit Management Service (PBM) described the commitment that pharmacy has in taking a leadership role in the integration of precision medicine. Linking veterans’ tumor mutation status and pharmacogenetic variants to pharmacy databases is the best way to ensure treatment is informed by genetics. We have to be realistic about what we’re asking community oncologists to do. With the onset of precision oncology, 10 cancers have become really 100 cancers. In the prior model of care, it was the oncologist, maybe in collaboration with a pathologist, but it was mostly oncologists who determined care.
And in the evolution of precision oncology, Ithink that it’s become an interdisciplinary adventure. Pharmacy is going to play an increasinglyimportant role in precision medicine around all of the molecular alterations, even immuno-oncology regardless of molecular status in which the VA has an advantage. We’re not talking about some community pharmacist. We’re talking about a national health care system where there’s a national EHR, where there’s national PBM systems. So my thoughts on this aspect is that it’s an intricate multidisciplinary team who can ensure that veteran sget the best care possible: the best most cost-effective care possible.
Dr. Kaster. As an oncology pharmacist, I have to second that.
Ms. Nason. As Dr. Kaster said earlier, having a dedicated oncology pharmacist is tremendouslybeneficial. The oncology/hematology pharmacists are following the patients closely and notice when dose adjustments need to be made, optimizing the drug benefit and providing additional safety. Not to mention the cost benefit that can be realized with appropriate adjustment and the expertise they bring to managing possible interactionsand pharmacodynamics.
Dr. Kambhampati. To brag about the Kansas City VAMC program, we have published in Federal Practitioner our best practices showing the collaboration between a pharmacist and providers.6 And we have used several examples of cost savings, which have basically helped us build the research program, and several examples of dual monitoring oral chemotherapy monitoring. And we have created these templates within the EHR that allow everyone to get a quick snapshot of where things are, what needs to be done, and what needs to be monitored.
Now, we are taking it a step further to determine when to stop chemotherapy or when to stop treatments. For example, for chronic myeloid leukemia (CML), there are good data onstopping tyrosine kinase inhibitors.7 And that alone, if implemented across the VA, could bring
in huge cost savings, which perhaps could be put into investments in immuno-oncology or other efforts. We have several examples here that we have published, and we continue to increaseand strengthen our collaboration withour oncology pharmacist. We are very lucky and privileged to have a dedicated oncology pharmacistfor clinics and for research.
Dr. Lynch. The example of CML is perfect, because precision oncology has increased the complexity of care substantially. The VA is wellpositioned to be a leader in this area when care becomes this complex because of its ability to measure access to testing, to translate the results
of testing to pharmacy, to have pharmacists take the lead on prescribing, to have pathologists take the lead on molecular alterations, and to have oncologists take the lead on delivering the cancer care to the patients.
With hematologic malignancies, adherence in the early stages can result in patients getting offcare sooner, which is cost savings. But that requires access to testing, monitoring that testing, and working in partnership with pharmacy. This is a great story about how the VA is positioned to lead in this area of care.
Dr. Kaster. I would like to put a plug in for advanced practice providers and the use of nurse practitioners (NPs) and physician assistants (PAs).The VA is well positioned because it often has established interdisciplinary teams with these providers, pharmacy, nursing, and often social work, to coordinate the care and manage symptoms outside of oncologist visits.
Dr. Lynch. In the NCI cancer center model, once the patient has become stable, the ongoing careis designated to the NP or PA. Then as soon as there’s a change and it requires reevaluation, the oncologist becomes involved again. That pointabout the oncology treatment team is totally in line
with some of the previous comments.
Areas For Further Investigation
Dr. Kaster. There are so many nuances that we’re finding out all of the time about immunotherapies. A recent study brought up the role of antibiotics in the 30 or possibly 60 days prior to immunotherapy.3 How does that change treatment? Which patients are more likely to benefit from immunotherapies, and which are susceptible to “hyperprogression”? How do we integrate palliative care discussions into the carenow that patients are feeling better on treatment and may be less likely to want to discuss palliative care?
Ms. Nason. I absolutely agree with that, especially keeping palliative care integrated within our services. Our focus is now a little different, in thatwe have more optimistic outcomes in mind, butthere still are symptoms and issues where our colleaguesin palliative care are invaluable.
Dr. Lynch. I third that motion. What I would really like to see come out of this discussion is how veterans are getting access to leading oncology care. We just published an analysis of Medicare data and access to EGFR testing. The result of that analysis showed that testing in the VA was consistent with testing in Medicare.
For palliative care, I think the VA does a better job. And it’s just so discouraging as VA employees and as clinicians treating veterans to see publicationsthat suggest that veterans are getting a lower quality of care and that they would be better if care was privatized or outsourced. It’s just fundamentally not the case.
In CML, we see it. We’ve analyzed the data, in that there’s a far lower number of patients with CML who are included in the registry because patients who are diagnosed outside the VA are incorporated in other cancer registries.8 But as soon as their copays increase for access to targeted drugs, they immediately activate their VA benefits so that theycan get their drugs at the VA. For hematologic malignancies that are diagnosed outside the VA and are captured in other cancer registries, as soon as the drugs become expensive, they start getting their care in the VA. I don’t think there’s beena lot of empirical research that’s shown this, but we have the data to illustrate this trend. I hope thatthere are more publications that show that veterans with cancer are getting really good care inside the VA in the existing VA health care system.
Ms. Nason. It is disheartening to see negativepublicity, knowing that I work with colleagues who are strongly committed to providing up-to-date and relevant oncology care.
Dr. Lynch. As we record this conversation, I am in Rotterdam, Netherlands, in a meeting about genomewide testing. In hematologic malignancies, prostate cancer, and breast cancer, it’s a huge issue. And that is the other area that MVP (Million Veteran Program) is leading the way with the MVP biorepository data. Frankly, there’s no other biorepository that has this many patients, that has so many African Americans, and that has such rich EHR data. So inthat other area, the VA is doing really well.
The following is a lightly edited transcript of a teleconference discussion recorded in April 2018.
Suman Kambhampati, MD. Immuno-oncology is a paradigm-shifting treatment approach. It is an easy-to-understand term for both providers and for patients. The underlying principle is that the body’s own immune system is used or stimulated to fight cancer, and there are drugs that clearly have shown huge promise for this, not only in oncology, but also for other diseases. Time will tell whether that really pans out or not, but to begin with, the emphasis has been inoncology, and therefore, the term immunooncology is fitting.
Dr. Kaster. It was encouraging at first, especially when ipilimumab came out, to see the effects on patients with melanoma. Then the KEYNOTE-024 trial came out, and we were able to jump in anduse monoclonal antibodies directed against programmed death 1 (PD-1) in the first line, which is when things got exciting.1 We have a smaller populationin Boise, so PD-1s in lung cancer have had the biggest impact on our patients so far.
Ellen Nason, RN, MSN. Patients are open to immunotherapies.They’re excited about it. And as the other panelists have said, you can start broadly, as the body fights the cancer on its own, to providing more specific details as a patient wants more information. Immuno-oncology is definitely accepted by patients, and they’re very excited about it, especially with all the news about new therapies.
Dr. Kambhampati. For the Department of Veteran Affairs (VA) population, lung cancer has seen significant impact, and now it’s translating into other diseases through more research, trials, and better understanding about how these drugs are used and work.
The paradigm is shifting toward offering these drugs not only in metastatic cancers, but also in the surgically resectable tumors. The 2018 American Association for Cancer Research (AACR) meeting, just concluded. At the meeting several abstracts reported instances where immunooncology drugs are being introduced in the early phases of lung cancer and showing outstanding results. It’s very much possible that we’re going to see less use of traditional chemotherapy in the near future.
Ms. Nason. I primarily work with solid tumors,and the majority of the population I work with have lung cancer. So we’re excited about some of the results that we’ve seen and the lower toxicity involved. Recently, we’ve begun using durvalumab with patients with stage III disease. We have about 5 people now that are using it as a maintenance or consolidative treatment vs just using it for patients with stage IV disease. Hopefully, we’ll see some of the same results describedin the paper published on it.2
Dr. Kaster. Yes, we are incorporating these new changes into care as they're coming out. As Ms. Nason mentioned, we're already using immunotherapies in earlier settings, and we are seeing as much research that could be translated into care soon, like combining immunotherapies
in first-line settings, as we see in the Checkmate-227 study with nivolumab and ipilimumab.3,4 The landscape is going to change dramatically in the next couple of years.
Accessing Testing For First-Line Treatments
Dr. Lynch. There has been an ongoing discussionin the literature on accessing appropriate testing—delays in testing can result in patients who are not able to access the best targeted drugs on a first-line basis. The drug companiesand the VA have become highly sensitized to ensuring that veterans are accessing the appropriate testing. We are expanding the capability of VA labs to do that testing.
Ms. Nason. I want to put in a plug for the VA Precision Oncology Program (POP). It’s about 2 years into its existence, and Neil Spector, MD, is the director. The POP pays for sequencing the tumor samples.
A new sequencing contract will go into effect October 2018 and will include sequencing for hematologic malignancies in addition to the current testing of solid tumors. Patients from New York who have been unable to receive testing through the current vendors used by POP, will be included in the new contract. It is important to note that POP is working closely with the National Pharmacy Benefit Management Service (PBM) to develop a policy for approving off-label use of US Food and Drug Administration-approved targeted therapies based on sequenced data collected on patients tested through POP.
In addition, the leadership of POP is working to leverage the molecular testing results conducted through POP to improve veterans' access to clinical trials, both inside and outside the VA. Within the VA people can access information at tinyurl.com/precisiononcology. There is no reason why any eligible patient with cancer in the VA health care system should not have their tumor tissue sequenced through POP, particularly once the new contract goes into effect.
Dr. Lynch. Fortunately, the cost of next-generation sequencing has come down so much that most VA contracted reference laboratories offer next-generation sequencing, including LabCorp (Burlington,NC), Quest Diagnostics (Secaucus, NJ), Fulgent (Temple City, CA), and academic partners such as Oregon Health Sciences University and University of Washington.
Ms. Nason. At the Durham VAMC, sometimes a lack of tissue has been a barrier, but we now have the ability to send blood (liquid biopsy) for next-generation sequencing. Hopefully that will open up options for veterans with inadequate tissue. Importantly, all VA facilities can request liquid biopsiesthrough POP.
Dr. Lynch. That’s an important point. There have been huge advances in liquid biopsy testing.The VA Salt Lake City Health Care System (VASLCHCS) was in talks with Genomic Health (Redwood City, CA) to do a study as part of clinical operations to look at the concordance between the liquid biopsy testing and the precision oncology data. But Genomic Health eventually abandoned its liquid biopsy testing. Currently, the VA is only reimbursing or encouraging liquid biopsy if the tissue is not available or if the veteran has too high a level of comorbidities to undergo tissue biopsy. The main point for the discussion today is that access to testing is a key component of access to all of these advanced drugs.
Dr. Kambhampati. The precision medicine piece will be a game changer—no question about that. Liquid biopsy is very timely. Many patients have difficulty getting rebiopsied, so liquid biopsy is definitely a big, big step forward.
Still, there has not been consistency across the VA as there should be. Perhaps there are a few select centers, including our site in Kansas City, where access to precision medicine is readily available and liquid biopsies are available. We use the PlasmaSELECT test from Personal Genome Diagnostics (Baltimore, MD). We have just added Foundation Medicine (Cambridge, MA) also in hematology. Access to mutational profilingis absolutely a must for precision medicine.
All that being said, the unique issue with immuno-oncology is that it pretty much transcends the mutational profile and perhaps has leveled the playing field, irrespective of the tumor mutation profile or burden. In some solid tumors these immuno-oncology drugs have been shown to work across tumor types and across different mutation types. And there is a hint now in the recent data presented at AACR and in the New England Journalof Medicine showing that the tumor mutational burden is a predictor of pathologic response to at least PD-1 blockade in the resectable stages of lung cancer.1,3 To me, that’s a very important piece of data because that’s something that can be tested and can have a prognostic impact in immuno-oncology, particularly in the early stages of lung cancer and is further proof of the broad value of immunotherapics in targeting tumors irrespective of the precise tumor targets.
Dr. Kaster. Yes, it’s nice to see other options like tumor mutational burden and Lung Immune Prognostic Index being studied.5 It would be nice if we could rely a little more on these, and not PD-L1, which as we all know is a variable and an unreliable target.
Dr. Kambhampati. I agree.
Rural Challenges In A Veterans Population
Dr. Lynch. Providing high-quality cancer care to rural veterans care can be a challenge but it is a VA priority. The VA National Genomic Medicine Services offers better access for rural veterans to germline genetic testing than any other healthcare system in the country. In terms of access to somatic testing and next-generation sequencing, we are working toward providing the same level of cancer care as patients would receive at National Cancer Institute (NCI) cancer centers. The VA oncology leadership has done teleconsults and virtual tumor boards, but for some rural VAMCs, fellowsare leading the clinical care. As we expand use of oral agents for oncology treatment, it will be easier to ensure that rural veterans receive the same standard of care for POP that veterans being cared for at VASLCHCS, Kansas City VAMC, or Durham VAMC get.
Dr. Kambhampati. The Kansas City VAMC in its catchment area includes underserved areas, such as Topeka and Leavenworth, Kansas. What we’ve been able to do here is something that’s unique—Kansas City VAMC is the only standalone VA in the country to be recognized as a primary SWOG (Southwestern Oncology Group) institution, which provides access to many trials, such as the Lung-MAP trial and others. And that has allowed us to use the full expanse of precision medicine without financial barriers. The research has helped us improve the standard of
care for patients across VISN 15.
Dr. Lynch. In precision oncology, the chief of pathology is an important figure in access to advanced care. I’ve worked with Sharad Mathur,MD, of the Kansas City VAMC on many clinical trials. He’s on the Kansas City VAMC Institutional Review Board and the cancer committee and is tuned in to veterans’ access to precision oncology. Kansas City was ordering Foundation One for select patients that met the criteria probably sooner than any other VA and participated in NCI Cooperative Group clinical trials. It is a great example of how veterans are getting access to
the same level of care as are patients who gettreated at NCI partners.
Comorbidities
Dr. Kambhampati. I don’t treat a lot of patients with lung cancer, but I find it easier to use these immuno-oncology drugs than platinums and etoposide. I consider them absolutely nasty chemotherapy drugs now in this era of immuno-oncology and targeted therapy.
Dr. Lynch. The VA is very important in translational lung cancer research and clinical care. It used to be thought that African American patients don’t get epidermal growth factor receptor mutations. And that’s because not enough African American patients with lung cancer were included in the NCI-based clinical trial.There are7,000 veterans who get lung cancer each year, and 20% to 25% of those are African Americans. Prevalence of various mutations and the pharmacogenetics of some of these drugs differ by patient ancestry. Including veterans with lung
cancer in precision oncology clinical trials and clinical care is not just a priority for the VA but a priority for NCI and internationally. I can’t emphasize this enough—veterans with lung cancer should be included in these studies and should be getting the same level of care that our partners are getting at NCI cancer centers. In the VA we’re positioned to do this because of our nationalelectronic health record (EHR) and becauseof our ability to identify patients with specific variants and enroll them in clinical trials.
Ms. Nason. One of the barriers that I find withsome of the patients that I have treated is getting them to a trial. If the trial isn’t available locally, specifically there are socioeconomic and distance issues that are hard to overcome.
Dr. Kaster. For smaller medical centers, getting patients to clinical trials can be difficult. The Boise VAMC is putting together a proposal now to justify hiring a research pharmacist in order to get trials atour site. The goal is to offer trial participation to our patients who otherwise might not be able to participate while offsetting some of the costs of immunotherapy. We are trying to make what could be a negative into a positive.
Measuring Success
Dr. Kambhampati. Unfortunately, we do not have any calculators to incorporate the quality of lives saved to the society. I know there are clearmetrics in transplant and in hematology, but unfortunately, there are no established metrics in solid tumor treatment that allow us to predict the cost savings to the health care system or to society or the benefit to the society. I don’t use any such predictive models or metrics in my decision making. These decisions are made based on existing evidence, and the existing evidence overwhelmingly supports use of immuno-oncology in certain types of solid tumors and in a select group of hematologic malignancies.
Dr. Kaster. This is where you can get more bang for your buck with an oncology pharmacist these days. A pharmacist can make a minor dosing change that will allow the same benefit for the patient, but could equal tens of thousands of dollars in cost-benefit for the VA. They can also be the second set of eyes when adjudicating a nonformulary request to ensure that a patient will benefit.
Dr. Lynch. Inappropriate prescribing is far more expensive than appropriate treatment. And the care for veterans whose long-term health outcomes could be improved by the new immunotherapies. It’s cheaper for veterans to be healthy and live longer than it is to take care of them in
their last 6 weeks of life. Unfortunately, there are not a lot of studies that have demonstrated that empirically, but I think it’s important to do those studies.
Role of Pharmacists
Dr. Lynch. I was at a meeting recently talking about how to improve veteran access to clinical trials. Francesca Cunningham, PharmD, director of the VA Center for Medication Safety of the VA Pharmacy Benefit Management Service (PBM) described the commitment that pharmacy has in taking a leadership role in the integration of precision medicine. Linking veterans’ tumor mutation status and pharmacogenetic variants to pharmacy databases is the best way to ensure treatment is informed by genetics. We have to be realistic about what we’re asking community oncologists to do. With the onset of precision oncology, 10 cancers have become really 100 cancers. In the prior model of care, it was the oncologist, maybe in collaboration with a pathologist, but it was mostly oncologists who determined care.
And in the evolution of precision oncology, Ithink that it’s become an interdisciplinary adventure. Pharmacy is going to play an increasinglyimportant role in precision medicine around all of the molecular alterations, even immuno-oncology regardless of molecular status in which the VA has an advantage. We’re not talking about some community pharmacist. We’re talking about a national health care system where there’s a national EHR, where there’s national PBM systems. So my thoughts on this aspect is that it’s an intricate multidisciplinary team who can ensure that veteran sget the best care possible: the best most cost-effective care possible.
Dr. Kaster. As an oncology pharmacist, I have to second that.
Ms. Nason. As Dr. Kaster said earlier, having a dedicated oncology pharmacist is tremendouslybeneficial. The oncology/hematology pharmacists are following the patients closely and notice when dose adjustments need to be made, optimizing the drug benefit and providing additional safety. Not to mention the cost benefit that can be realized with appropriate adjustment and the expertise they bring to managing possible interactionsand pharmacodynamics.
Dr. Kambhampati. To brag about the Kansas City VAMC program, we have published in Federal Practitioner our best practices showing the collaboration between a pharmacist and providers.6 And we have used several examples of cost savings, which have basically helped us build the research program, and several examples of dual monitoring oral chemotherapy monitoring. And we have created these templates within the EHR that allow everyone to get a quick snapshot of where things are, what needs to be done, and what needs to be monitored.
Now, we are taking it a step further to determine when to stop chemotherapy or when to stop treatments. For example, for chronic myeloid leukemia (CML), there are good data onstopping tyrosine kinase inhibitors.7 And that alone, if implemented across the VA, could bring
in huge cost savings, which perhaps could be put into investments in immuno-oncology or other efforts. We have several examples here that we have published, and we continue to increaseand strengthen our collaboration withour oncology pharmacist. We are very lucky and privileged to have a dedicated oncology pharmacistfor clinics and for research.
Dr. Lynch. The example of CML is perfect, because precision oncology has increased the complexity of care substantially. The VA is wellpositioned to be a leader in this area when care becomes this complex because of its ability to measure access to testing, to translate the results
of testing to pharmacy, to have pharmacists take the lead on prescribing, to have pathologists take the lead on molecular alterations, and to have oncologists take the lead on delivering the cancer care to the patients.
With hematologic malignancies, adherence in the early stages can result in patients getting offcare sooner, which is cost savings. But that requires access to testing, monitoring that testing, and working in partnership with pharmacy. This is a great story about how the VA is positioned to lead in this area of care.
Dr. Kaster. I would like to put a plug in for advanced practice providers and the use of nurse practitioners (NPs) and physician assistants (PAs).The VA is well positioned because it often has established interdisciplinary teams with these providers, pharmacy, nursing, and often social work, to coordinate the care and manage symptoms outside of oncologist visits.
Dr. Lynch. In the NCI cancer center model, once the patient has become stable, the ongoing careis designated to the NP or PA. Then as soon as there’s a change and it requires reevaluation, the oncologist becomes involved again. That pointabout the oncology treatment team is totally in line
with some of the previous comments.
Areas For Further Investigation
Dr. Kaster. There are so many nuances that we’re finding out all of the time about immunotherapies. A recent study brought up the role of antibiotics in the 30 or possibly 60 days prior to immunotherapy.3 How does that change treatment? Which patients are more likely to benefit from immunotherapies, and which are susceptible to “hyperprogression”? How do we integrate palliative care discussions into the carenow that patients are feeling better on treatment and may be less likely to want to discuss palliative care?
Ms. Nason. I absolutely agree with that, especially keeping palliative care integrated within our services. Our focus is now a little different, in thatwe have more optimistic outcomes in mind, butthere still are symptoms and issues where our colleaguesin palliative care are invaluable.
Dr. Lynch. I third that motion. What I would really like to see come out of this discussion is how veterans are getting access to leading oncology care. We just published an analysis of Medicare data and access to EGFR testing. The result of that analysis showed that testing in the VA was consistent with testing in Medicare.
For palliative care, I think the VA does a better job. And it’s just so discouraging as VA employees and as clinicians treating veterans to see publicationsthat suggest that veterans are getting a lower quality of care and that they would be better if care was privatized or outsourced. It’s just fundamentally not the case.
In CML, we see it. We’ve analyzed the data, in that there’s a far lower number of patients with CML who are included in the registry because patients who are diagnosed outside the VA are incorporated in other cancer registries.8 But as soon as their copays increase for access to targeted drugs, they immediately activate their VA benefits so that theycan get their drugs at the VA. For hematologic malignancies that are diagnosed outside the VA and are captured in other cancer registries, as soon as the drugs become expensive, they start getting their care in the VA. I don’t think there’s beena lot of empirical research that’s shown this, but we have the data to illustrate this trend. I hope thatthere are more publications that show that veterans with cancer are getting really good care inside the VA in the existing VA health care system.
Ms. Nason. It is disheartening to see negativepublicity, knowing that I work with colleagues who are strongly committed to providing up-to-date and relevant oncology care.
Dr. Lynch. As we record this conversation, I am in Rotterdam, Netherlands, in a meeting about genomewide testing. In hematologic malignancies, prostate cancer, and breast cancer, it’s a huge issue. And that is the other area that MVP (Million Veteran Program) is leading the way with the MVP biorepository data. Frankly, there’s no other biorepository that has this many patients, that has so many African Americans, and that has such rich EHR data. So inthat other area, the VA is doing really well.
1. Reck M, Rodríguez-Abreu D, Robinson AG, et al; KEYNOTE-024 Investigators. Pembrolizumab vs chemotherapy for PD-L1-positive non-small cell lung cancer. N Engl J Med. 2016;375(19):1823-1833.
2. Antonia SJ, Villegas A, Daniel D, et al; PACIFIC Investigators. Durvalumab after chemoradiotherapy in stage III non–smallcell lung cancer. N Engl J Med. 2017;377(20):1919-1929.
3. Hellmann MD, Ciuleanu T-E, Pluzansk A, et al. Nivolumab plus ipilimumab in Lung Cancer with a high tumor mutational burden. N Engl J Med. 2018 April 16. [Epub ahead of print.]
4. Motzer RJ, Tannir NM, McDermott DF, et al; CheckMate214 Investigators. Nivolumab plus ipilimumab versus sunitinibin advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277-1290.
5. Derosa L, Hellmann MD, Spaziano M, et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small cell
lung cancer. Ann Oncol. 2018 March 30. [Epub ahead of print.]
6. Heinrichs A, Dessars B, El Housni H, et al. Identification of chronic myeloid leukemia patients treated with imatinib who are potentially eligible for treatment discontinuation by assessingreal-life molecular responses on the international scale in a EUTOS-certified lab. Leuk Res. 2018;67:27-31.
7. Keefe S, Kambhampati S, Powers B. An electronic chemotherapy ordering process and template. Fed Pract. 2015;32(suppl 1):21S-25S.
8. Lynch JA, Berse B, Rabb M, et al. Underutilization and disparities in access to EGFR testing among Medicare patients with lung cancer from 2010 - 2013. BMC Cancer. 2018;18(1):306.
1. Reck M, Rodríguez-Abreu D, Robinson AG, et al; KEYNOTE-024 Investigators. Pembrolizumab vs chemotherapy for PD-L1-positive non-small cell lung cancer. N Engl J Med. 2016;375(19):1823-1833.
2. Antonia SJ, Villegas A, Daniel D, et al; PACIFIC Investigators. Durvalumab after chemoradiotherapy in stage III non–smallcell lung cancer. N Engl J Med. 2017;377(20):1919-1929.
3. Hellmann MD, Ciuleanu T-E, Pluzansk A, et al. Nivolumab plus ipilimumab in Lung Cancer with a high tumor mutational burden. N Engl J Med. 2018 April 16. [Epub ahead of print.]
4. Motzer RJ, Tannir NM, McDermott DF, et al; CheckMate214 Investigators. Nivolumab plus ipilimumab versus sunitinibin advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277-1290.
5. Derosa L, Hellmann MD, Spaziano M, et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small cell
lung cancer. Ann Oncol. 2018 March 30. [Epub ahead of print.]
6. Heinrichs A, Dessars B, El Housni H, et al. Identification of chronic myeloid leukemia patients treated with imatinib who are potentially eligible for treatment discontinuation by assessingreal-life molecular responses on the international scale in a EUTOS-certified lab. Leuk Res. 2018;67:27-31.
7. Keefe S, Kambhampati S, Powers B. An electronic chemotherapy ordering process and template. Fed Pract. 2015;32(suppl 1):21S-25S.
8. Lynch JA, Berse B, Rabb M, et al. Underutilization and disparities in access to EGFR testing among Medicare patients with lung cancer from 2010 - 2013. BMC Cancer. 2018;18(1):306.
Lifetime cost of tobacco use tops $1.9 million per smoker
according to the personal financial website WalletHub.
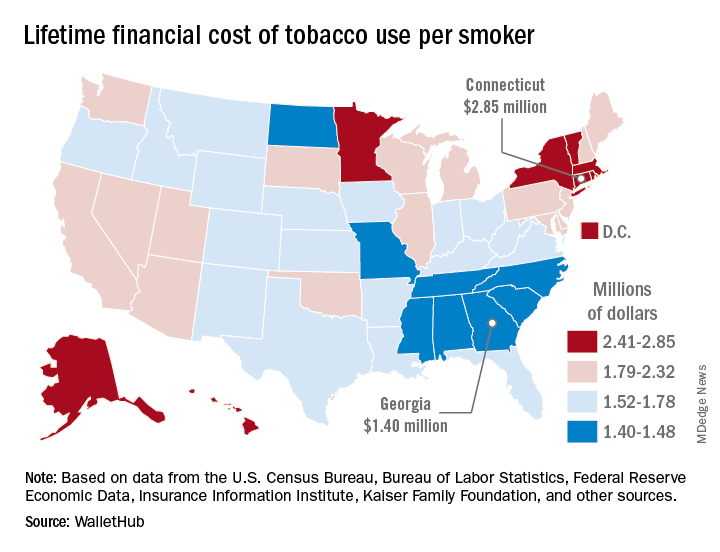
Economic and societal losses related to 37.8 million U.S. tobacco users – including out-of-pocket spending for cigarettes, health care expenses, and lost income – top $300 billion annually, but those costs vary considerably by state, WalletHub said in a recent report.
The state with the highest lifetime cost per smoker is Connecticut, with an estimated total of $2.85 million. That works out to just under $56,000 a year for 51 years because lifetime use was defined as one pack a day starting at age 18 years and continuing until age 69 years. New York has the second-highest lifetime cost, which also rounds off to $2.85 million, followed by the District of Columbia ($2.81 million), Massachusetts ($2.76 million), and Rhode Island ($2.68 million), WalletHub said.
Georgia has the lowest lifetime cost of any state – $1.40 million per smoker – followed by Missouri at $1.41 million, North Carolina at $1.42 million, Mississippi at $1.43 million, and South Carolina at $1.44 million, according to the report.
WalletHub’s formula for total lifetime cost has five components: out-of-pocket cost (one pack of cigarettes per day for 51 years), financial opportunity cost (defined as “the amount of return a person would have earned by instead investing that money in the stock market”), health care cost (spending on treatment for smoking-related health complications), income loss (an average 8% decrease caused by absenteeism and lost productivity), and other costs (loss of a homeowner’s insurance credit and costs of secondhand exposure).
The analysis was based on data from the U.S. Census Bureau, Bureau of Labor Statistics, Centers for Disease Control and Prevention, Insurance Information Institute, Campaign for Tobacco-Free Kids, NYsmokefree.com, Federal Reserve Economic Data, Kaiser Family Foundation, and the Independent Insurance Agents & Brokers of America.
according to the personal financial website WalletHub.
Economic and societal losses related to 37.8 million U.S. tobacco users – including out-of-pocket spending for cigarettes, health care expenses, and lost income – top $300 billion annually, but those costs vary considerably by state, WalletHub said in a recent report.
The state with the highest lifetime cost per smoker is Connecticut, with an estimated total of $2.85 million. That works out to just under $56,000 a year for 51 years because lifetime use was defined as one pack a day starting at age 18 years and continuing until age 69 years. New York has the second-highest lifetime cost, which also rounds off to $2.85 million, followed by the District of Columbia ($2.81 million), Massachusetts ($2.76 million), and Rhode Island ($2.68 million), WalletHub said.
Georgia has the lowest lifetime cost of any state – $1.40 million per smoker – followed by Missouri at $1.41 million, North Carolina at $1.42 million, Mississippi at $1.43 million, and South Carolina at $1.44 million, according to the report.
WalletHub’s formula for total lifetime cost has five components: out-of-pocket cost (one pack of cigarettes per day for 51 years), financial opportunity cost (defined as “the amount of return a person would have earned by instead investing that money in the stock market”), health care cost (spending on treatment for smoking-related health complications), income loss (an average 8% decrease caused by absenteeism and lost productivity), and other costs (loss of a homeowner’s insurance credit and costs of secondhand exposure).
The analysis was based on data from the U.S. Census Bureau, Bureau of Labor Statistics, Centers for Disease Control and Prevention, Insurance Information Institute, Campaign for Tobacco-Free Kids, NYsmokefree.com, Federal Reserve Economic Data, Kaiser Family Foundation, and the Independent Insurance Agents & Brokers of America.
according to the personal financial website WalletHub.
Economic and societal losses related to 37.8 million U.S. tobacco users – including out-of-pocket spending for cigarettes, health care expenses, and lost income – top $300 billion annually, but those costs vary considerably by state, WalletHub said in a recent report.
The state with the highest lifetime cost per smoker is Connecticut, with an estimated total of $2.85 million. That works out to just under $56,000 a year for 51 years because lifetime use was defined as one pack a day starting at age 18 years and continuing until age 69 years. New York has the second-highest lifetime cost, which also rounds off to $2.85 million, followed by the District of Columbia ($2.81 million), Massachusetts ($2.76 million), and Rhode Island ($2.68 million), WalletHub said.
Georgia has the lowest lifetime cost of any state – $1.40 million per smoker – followed by Missouri at $1.41 million, North Carolina at $1.42 million, Mississippi at $1.43 million, and South Carolina at $1.44 million, according to the report.
WalletHub’s formula for total lifetime cost has five components: out-of-pocket cost (one pack of cigarettes per day for 51 years), financial opportunity cost (defined as “the amount of return a person would have earned by instead investing that money in the stock market”), health care cost (spending on treatment for smoking-related health complications), income loss (an average 8% decrease caused by absenteeism and lost productivity), and other costs (loss of a homeowner’s insurance credit and costs of secondhand exposure).
The analysis was based on data from the U.S. Census Bureau, Bureau of Labor Statistics, Centers for Disease Control and Prevention, Insurance Information Institute, Campaign for Tobacco-Free Kids, NYsmokefree.com, Federal Reserve Economic Data, Kaiser Family Foundation, and the Independent Insurance Agents & Brokers of America.
The personal cancer vaccine NEO-PV-01 shows promise in metastatic cancers
WASHINGTON – according to findings from the ongoing phase 1b NT-001study of patients with metastatic melanoma, smoking-associated non–small cell lung cancer (NSCLC), and bladder cancer.

No vaccine-related serious adverse events occurred in 34 patients in a per-protocol set who were treated with the regimen, Siwen Hu-Lieskovan, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We found that NEO-PV-01 in combination with nivolumab was very safe; we did not see any grade 3 to grade 4 toxicity associated with the combination,” said Dr. Hu-Lieskovan, a medical oncologist at the University of California, Los Angeles.
Most adverse events that occurred were mild and related to the local injection, she noted.
Although safety was the primary endpoint of the study, Dr. Hu-Lieskovan and her colleagues also looked at immune responses and treatment efficacy, however, with respect to translational data her presentation addressed only the findings in the melanoma and lung cancer patients.
All patients exhibited an immune response to the vaccine, with 56% of the epitopes generating CD4- and/or CD8-positive T cell responses.
“These immune responses were very durable and still could be detected 52 weeks into the treatment,” she said. Additionally, epitope spreading – increased immune response targeting nonvaccine epitopes (which is indirect evidence of vaccine-induced tumor toxicity) – was observed in 8 of 10 patients tested.
The study subjects, including 16 adults with melanoma, 11 with NSCLC, and 7 with bladder cancer, were treated with nivolumab every 2 weeks for 12 weeks prior to vaccination (while their personalized vaccine was being developed). NEO-PV-01 – which included up to 20 unique peptides plus the immunostimulant poly-ICLC – was then administered subcutaneously in five priming doses followed by two booster doses over the next 12 weeks. Of note, very few patients had programmed cell death protein 1 expression of 50% or greater, including only 13.3%, 28.6%, and 0% of the melanoma, NSCLC, and bladder cancer patients, respectively, and tumor mutation burden was consistent with published reports, she said.
As for efficacy, 11 of 16 melanoma patients (68.6%) had either a partial response (8 pre vaccination and an additional 3 post vaccination) or stable disease. One (6.3%) had a postvaccination complete response, Dr. Hu-Lieskovan said.
“[This is] much better than the historical data,” she noted, adding that 12 patients (75%) are still on the study and continuing treatment with response duration of at least 39.7 weeks.
Of the 11 NSCLC patients, 5 (45.5%) had a partial response (3 pre vaccination and 2 post vaccination), and none had a complete response. Seven (63.6%) remained on the study and were continuing treatment, and response duration was at least 30.6 weeks.
An exploratory analysis of tumor responses after vaccination showed that the majority of melanoma patients and half of the lung cancer patients had further tumor shrinkage after vaccination, and some patients were converted to responders. Most – including some with stable or progressive disease – stayed on treatment, she said.
The findings demonstrate that NEO-PV-01 is very well tolerated and associated with post vaccine responses observed after week 24.
“We saw evidence of vaccination-induced immune response specific to the injected vaccine, as well as epitope spreading, and the T cells induced by these neoantigens can traffic into the tumor and they seem to be functional,” she concluded.
Dr. Hu-Lieskovan reported receiving consulting fees and/or research support from Amgen, BMS, Genmab, Merck, and Vaccinex. She is the UCLA site principal investigator for the NT-001 study and has conducted contracted research for Astellas, F Star, Genentech, Nektar Therapeutics, Neon Therapeutics, Pfizer, Plexxikon, and Xencor.
SOURCE: Hu-Lieskovan S et al. SITC 2018, Abstract 07.
WASHINGTON – according to findings from the ongoing phase 1b NT-001study of patients with metastatic melanoma, smoking-associated non–small cell lung cancer (NSCLC), and bladder cancer.
No vaccine-related serious adverse events occurred in 34 patients in a per-protocol set who were treated with the regimen, Siwen Hu-Lieskovan, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We found that NEO-PV-01 in combination with nivolumab was very safe; we did not see any grade 3 to grade 4 toxicity associated with the combination,” said Dr. Hu-Lieskovan, a medical oncologist at the University of California, Los Angeles.
Most adverse events that occurred were mild and related to the local injection, she noted.
Although safety was the primary endpoint of the study, Dr. Hu-Lieskovan and her colleagues also looked at immune responses and treatment efficacy, however, with respect to translational data her presentation addressed only the findings in the melanoma and lung cancer patients.
All patients exhibited an immune response to the vaccine, with 56% of the epitopes generating CD4- and/or CD8-positive T cell responses.
“These immune responses were very durable and still could be detected 52 weeks into the treatment,” she said. Additionally, epitope spreading – increased immune response targeting nonvaccine epitopes (which is indirect evidence of vaccine-induced tumor toxicity) – was observed in 8 of 10 patients tested.
The study subjects, including 16 adults with melanoma, 11 with NSCLC, and 7 with bladder cancer, were treated with nivolumab every 2 weeks for 12 weeks prior to vaccination (while their personalized vaccine was being developed). NEO-PV-01 – which included up to 20 unique peptides plus the immunostimulant poly-ICLC – was then administered subcutaneously in five priming doses followed by two booster doses over the next 12 weeks. Of note, very few patients had programmed cell death protein 1 expression of 50% or greater, including only 13.3%, 28.6%, and 0% of the melanoma, NSCLC, and bladder cancer patients, respectively, and tumor mutation burden was consistent with published reports, she said.
As for efficacy, 11 of 16 melanoma patients (68.6%) had either a partial response (8 pre vaccination and an additional 3 post vaccination) or stable disease. One (6.3%) had a postvaccination complete response, Dr. Hu-Lieskovan said.
“[This is] much better than the historical data,” she noted, adding that 12 patients (75%) are still on the study and continuing treatment with response duration of at least 39.7 weeks.
Of the 11 NSCLC patients, 5 (45.5%) had a partial response (3 pre vaccination and 2 post vaccination), and none had a complete response. Seven (63.6%) remained on the study and were continuing treatment, and response duration was at least 30.6 weeks.
An exploratory analysis of tumor responses after vaccination showed that the majority of melanoma patients and half of the lung cancer patients had further tumor shrinkage after vaccination, and some patients were converted to responders. Most – including some with stable or progressive disease – stayed on treatment, she said.
The findings demonstrate that NEO-PV-01 is very well tolerated and associated with post vaccine responses observed after week 24.
“We saw evidence of vaccination-induced immune response specific to the injected vaccine, as well as epitope spreading, and the T cells induced by these neoantigens can traffic into the tumor and they seem to be functional,” she concluded.
Dr. Hu-Lieskovan reported receiving consulting fees and/or research support from Amgen, BMS, Genmab, Merck, and Vaccinex. She is the UCLA site principal investigator for the NT-001 study and has conducted contracted research for Astellas, F Star, Genentech, Nektar Therapeutics, Neon Therapeutics, Pfizer, Plexxikon, and Xencor.
SOURCE: Hu-Lieskovan S et al. SITC 2018, Abstract 07.
WASHINGTON – according to findings from the ongoing phase 1b NT-001study of patients with metastatic melanoma, smoking-associated non–small cell lung cancer (NSCLC), and bladder cancer.
No vaccine-related serious adverse events occurred in 34 patients in a per-protocol set who were treated with the regimen, Siwen Hu-Lieskovan, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We found that NEO-PV-01 in combination with nivolumab was very safe; we did not see any grade 3 to grade 4 toxicity associated with the combination,” said Dr. Hu-Lieskovan, a medical oncologist at the University of California, Los Angeles.
Most adverse events that occurred were mild and related to the local injection, she noted.
Although safety was the primary endpoint of the study, Dr. Hu-Lieskovan and her colleagues also looked at immune responses and treatment efficacy, however, with respect to translational data her presentation addressed only the findings in the melanoma and lung cancer patients.
All patients exhibited an immune response to the vaccine, with 56% of the epitopes generating CD4- and/or CD8-positive T cell responses.
“These immune responses were very durable and still could be detected 52 weeks into the treatment,” she said. Additionally, epitope spreading – increased immune response targeting nonvaccine epitopes (which is indirect evidence of vaccine-induced tumor toxicity) – was observed in 8 of 10 patients tested.
The study subjects, including 16 adults with melanoma, 11 with NSCLC, and 7 with bladder cancer, were treated with nivolumab every 2 weeks for 12 weeks prior to vaccination (while their personalized vaccine was being developed). NEO-PV-01 – which included up to 20 unique peptides plus the immunostimulant poly-ICLC – was then administered subcutaneously in five priming doses followed by two booster doses over the next 12 weeks. Of note, very few patients had programmed cell death protein 1 expression of 50% or greater, including only 13.3%, 28.6%, and 0% of the melanoma, NSCLC, and bladder cancer patients, respectively, and tumor mutation burden was consistent with published reports, she said.
As for efficacy, 11 of 16 melanoma patients (68.6%) had either a partial response (8 pre vaccination and an additional 3 post vaccination) or stable disease. One (6.3%) had a postvaccination complete response, Dr. Hu-Lieskovan said.
“[This is] much better than the historical data,” she noted, adding that 12 patients (75%) are still on the study and continuing treatment with response duration of at least 39.7 weeks.
Of the 11 NSCLC patients, 5 (45.5%) had a partial response (3 pre vaccination and 2 post vaccination), and none had a complete response. Seven (63.6%) remained on the study and were continuing treatment, and response duration was at least 30.6 weeks.
An exploratory analysis of tumor responses after vaccination showed that the majority of melanoma patients and half of the lung cancer patients had further tumor shrinkage after vaccination, and some patients were converted to responders. Most – including some with stable or progressive disease – stayed on treatment, she said.
The findings demonstrate that NEO-PV-01 is very well tolerated and associated with post vaccine responses observed after week 24.
“We saw evidence of vaccination-induced immune response specific to the injected vaccine, as well as epitope spreading, and the T cells induced by these neoantigens can traffic into the tumor and they seem to be functional,” she concluded.
Dr. Hu-Lieskovan reported receiving consulting fees and/or research support from Amgen, BMS, Genmab, Merck, and Vaccinex. She is the UCLA site principal investigator for the NT-001 study and has conducted contracted research for Astellas, F Star, Genentech, Nektar Therapeutics, Neon Therapeutics, Pfizer, Plexxikon, and Xencor.
SOURCE: Hu-Lieskovan S et al. SITC 2018, Abstract 07.
REPORTING FROM SITC 2018
Key clinical point: The NEO-PV-01 personalized cancer vaccine shows good tolerability and safety and appears to have clinical efficacy.
Major finding: There were no vaccine-related serious adverse events, and all patients exhibited an immune response to the vaccine, with 56% of the epitopes generating CD4- and/or CD8-positive T-cell responses.
Study details: A study of the NEO-PV-01 personalized cancer vaccine in 34 patients.
Disclosures: Dr. Hu-Lieskovan reported receiving consulting fees and/or research support from Amgen, BMS, Genmab, Merck, and Vaccinex. She is the UCLA site principal investigator for the NT-001 study and has conducted contracted research for Astellas, F Star, Genentech, Nektar Therapeutics, Neon Therapeutics, Pfizer, Plexxikon, and Xencor.
Source: Hu-Lieskovan S et al. SITC 2018, Abstract 07.
HBV, HCV, HIV testing of new cancer patients advised
Oncologists should consider testing all patients with newly diagnosed cancers for infection with the hepatitis B and C viruses, a multicenter team has recommended.
A prospective study of hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV infections among 3,051 patients with newly diagnosed cancers showed that 6.5% of patients tested positive for previous HBV and 0.6% had chronic HBV infection. In addition, 2.4% of patients were positive for HCV, and 1.1% for HIV infections, reported Scott D. Ramsey, MD, PhD, from the Fred Hutchinson Cancer Research Center in Seattle, and colleagues.
“Many patients had no known risk factors for infection, suggesting that current risk-based models for screening may be insufficient. Thus, we believe our results warrant consideration of universal testing of patients with newly diagnosed cancer for HBV and HCV infection, particularly if such an approach is shown to be cost effective,” they wrote in JAMA Oncology.
The investigators noted that patients with undiagnosed hepatitis and/or HIV infections could transmit them to unsuspecting caregivers, adding that “with effective treatments available, not screening for these viruses misses an opportunity to reduce future morbidity associated with these infections and to avoid viral reactivation during treatment, with resulting morbidity and mortality.”
To estimate the prevalence of the infections in patients with newly diagnosed cancers, investigators looked at a cohort of 3,051 patients with a cancer diagnosis made within the previous 120 days at nine academic medical centers and nine community oncology centers representing a total of 41 cancer clinics affiliated with the SWOG Cancer Research Network (formerly the Southwest Oncology Group).
The median patient age was 60.6 years. Female patients constitute 60.4% of the sample; 18.1% were black, and 18.3% were of Hispanic heritage.
Of 3,050 patients for whom HBV testing results were available, 6.5% (197) were positive for previous HBV infection, compared with an estimated U.S. population prevalence of 4.7%. In addition, 0.6% (19 patients) were found to have chronic HBV, compared with an estimated 0.3% US population prevalence.
HCV infections were detected in 2.4% (71 of 2990 patients), compared with an estimated population prevalence of 1.3%, and HIV infections were detected in 1.1%, compared with a background estimated population prevalence of 0.3%.
In all, 32 patients were diagnosed with viral infections by testing performed for the study, including 8 patients with chronic HBV, 22 with HCV, and 2 with HIV.
Additionally, the authors found that 4 patients with chronic HBV, 23 with HCV, and 7 with HIV had no identifiable risk factors.
The highest prevalence of infections occurred among patients with liver cancer, nonliver and noncolorectal cancers of the gastrointestinal tract, head and neck cancers, lung cancers, and prostate cancer. A finding of viral positivity changed the treatment plan in only 8% of all infected patients, however.
“Given that most HIV-infected patients in our study knew their viral status, the yield of universal HIV testing among patients with newly diagnosed cancer may likely be low. Although age-directed screening is recommended for HIV and HCV, uptake rates in primary care are variable and low overall,” Dr. Ramsey and his colleagues wrote.
The study was supported by grants from the National Cancer Institute. Dr. Ramsey and several co-authors reported receiving NCI grants, and multiple co-authors reported grants and/or consulting fees from various companies.
SOURCE: Ramsey SD et al. JAMA Oncol. 2019 Jan 17. doi: 10.1001/jamaoncol.2018.6437.
Oncologists should consider testing all patients with newly diagnosed cancers for infection with the hepatitis B and C viruses, a multicenter team has recommended.
A prospective study of hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV infections among 3,051 patients with newly diagnosed cancers showed that 6.5% of patients tested positive for previous HBV and 0.6% had chronic HBV infection. In addition, 2.4% of patients were positive for HCV, and 1.1% for HIV infections, reported Scott D. Ramsey, MD, PhD, from the Fred Hutchinson Cancer Research Center in Seattle, and colleagues.
“Many patients had no known risk factors for infection, suggesting that current risk-based models for screening may be insufficient. Thus, we believe our results warrant consideration of universal testing of patients with newly diagnosed cancer for HBV and HCV infection, particularly if such an approach is shown to be cost effective,” they wrote in JAMA Oncology.
The investigators noted that patients with undiagnosed hepatitis and/or HIV infections could transmit them to unsuspecting caregivers, adding that “with effective treatments available, not screening for these viruses misses an opportunity to reduce future morbidity associated with these infections and to avoid viral reactivation during treatment, with resulting morbidity and mortality.”
To estimate the prevalence of the infections in patients with newly diagnosed cancers, investigators looked at a cohort of 3,051 patients with a cancer diagnosis made within the previous 120 days at nine academic medical centers and nine community oncology centers representing a total of 41 cancer clinics affiliated with the SWOG Cancer Research Network (formerly the Southwest Oncology Group).
The median patient age was 60.6 years. Female patients constitute 60.4% of the sample; 18.1% were black, and 18.3% were of Hispanic heritage.
Of 3,050 patients for whom HBV testing results were available, 6.5% (197) were positive for previous HBV infection, compared with an estimated U.S. population prevalence of 4.7%. In addition, 0.6% (19 patients) were found to have chronic HBV, compared with an estimated 0.3% US population prevalence.
HCV infections were detected in 2.4% (71 of 2990 patients), compared with an estimated population prevalence of 1.3%, and HIV infections were detected in 1.1%, compared with a background estimated population prevalence of 0.3%.
In all, 32 patients were diagnosed with viral infections by testing performed for the study, including 8 patients with chronic HBV, 22 with HCV, and 2 with HIV.
Additionally, the authors found that 4 patients with chronic HBV, 23 with HCV, and 7 with HIV had no identifiable risk factors.
The highest prevalence of infections occurred among patients with liver cancer, nonliver and noncolorectal cancers of the gastrointestinal tract, head and neck cancers, lung cancers, and prostate cancer. A finding of viral positivity changed the treatment plan in only 8% of all infected patients, however.
“Given that most HIV-infected patients in our study knew their viral status, the yield of universal HIV testing among patients with newly diagnosed cancer may likely be low. Although age-directed screening is recommended for HIV and HCV, uptake rates in primary care are variable and low overall,” Dr. Ramsey and his colleagues wrote.
The study was supported by grants from the National Cancer Institute. Dr. Ramsey and several co-authors reported receiving NCI grants, and multiple co-authors reported grants and/or consulting fees from various companies.
SOURCE: Ramsey SD et al. JAMA Oncol. 2019 Jan 17. doi: 10.1001/jamaoncol.2018.6437.
Oncologists should consider testing all patients with newly diagnosed cancers for infection with the hepatitis B and C viruses, a multicenter team has recommended.
A prospective study of hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV infections among 3,051 patients with newly diagnosed cancers showed that 6.5% of patients tested positive for previous HBV and 0.6% had chronic HBV infection. In addition, 2.4% of patients were positive for HCV, and 1.1% for HIV infections, reported Scott D. Ramsey, MD, PhD, from the Fred Hutchinson Cancer Research Center in Seattle, and colleagues.
“Many patients had no known risk factors for infection, suggesting that current risk-based models for screening may be insufficient. Thus, we believe our results warrant consideration of universal testing of patients with newly diagnosed cancer for HBV and HCV infection, particularly if such an approach is shown to be cost effective,” they wrote in JAMA Oncology.
The investigators noted that patients with undiagnosed hepatitis and/or HIV infections could transmit them to unsuspecting caregivers, adding that “with effective treatments available, not screening for these viruses misses an opportunity to reduce future morbidity associated with these infections and to avoid viral reactivation during treatment, with resulting morbidity and mortality.”
To estimate the prevalence of the infections in patients with newly diagnosed cancers, investigators looked at a cohort of 3,051 patients with a cancer diagnosis made within the previous 120 days at nine academic medical centers and nine community oncology centers representing a total of 41 cancer clinics affiliated with the SWOG Cancer Research Network (formerly the Southwest Oncology Group).
The median patient age was 60.6 years. Female patients constitute 60.4% of the sample; 18.1% were black, and 18.3% were of Hispanic heritage.
Of 3,050 patients for whom HBV testing results were available, 6.5% (197) were positive for previous HBV infection, compared with an estimated U.S. population prevalence of 4.7%. In addition, 0.6% (19 patients) were found to have chronic HBV, compared with an estimated 0.3% US population prevalence.
HCV infections were detected in 2.4% (71 of 2990 patients), compared with an estimated population prevalence of 1.3%, and HIV infections were detected in 1.1%, compared with a background estimated population prevalence of 0.3%.
In all, 32 patients were diagnosed with viral infections by testing performed for the study, including 8 patients with chronic HBV, 22 with HCV, and 2 with HIV.
Additionally, the authors found that 4 patients with chronic HBV, 23 with HCV, and 7 with HIV had no identifiable risk factors.
The highest prevalence of infections occurred among patients with liver cancer, nonliver and noncolorectal cancers of the gastrointestinal tract, head and neck cancers, lung cancers, and prostate cancer. A finding of viral positivity changed the treatment plan in only 8% of all infected patients, however.
“Given that most HIV-infected patients in our study knew their viral status, the yield of universal HIV testing among patients with newly diagnosed cancer may likely be low. Although age-directed screening is recommended for HIV and HCV, uptake rates in primary care are variable and low overall,” Dr. Ramsey and his colleagues wrote.
The study was supported by grants from the National Cancer Institute. Dr. Ramsey and several co-authors reported receiving NCI grants, and multiple co-authors reported grants and/or consulting fees from various companies.
SOURCE: Ramsey SD et al. JAMA Oncol. 2019 Jan 17. doi: 10.1001/jamaoncol.2018.6437.
FROM JAMA ONCOLOGY
Key clinical point: Patients with newly diagnosed cancers should be screened for viral infections that may pose a transmission risk or could be reactivated by cancer therapies.
Major finding: Infection rates of HBV, HCV, and HIV in patients with newly diagnosed cancers were 6.5%, 2.4%, and 1.1%, respectively.
Study details: Prospective study of viral infections in 3,051 patients with a diagnosis of cancer within the previous 120 days.
Disclosures: The study was supported by grants from the National Cancer Institute. Dr. Ramsey and several coauthors reported receiving NCI grants, and multiple coauthors reported grants and/or consulting fees from various companies.
Source: Ramsey SD et al. JAMA Oncology. 2019 Jan 17. doi: 10.1001/jamaoncol.2018.6437.
Self-reporting extends lung cancer survival
Patients with nonprogressive, metastatic lung cancer who report symptoms through a weekly, web-based monitoring system may survive longer than those who undergo standard imaging surveillance, according to a recent French study.
Self-reporting may notify care providers about adverse effects or recurrence earlier than imaging, suggested lead author, Fabrice Denis, MD, PhD, of Institut Inter-régional de Cancérologie Jean Bernard in Le Mans, France, and his colleagues. Findings were published in a letter in JAMA.
In 2017, a similar, single-center study showed that web-based symptom reporting could improve survival in patients undergoing chemotherapy. The lead investigator on that trial was Ethan Basch, MD, who coauthored the present publication.
The current, prospective study involved 121 patients treated at five centers in France between June 2014 and December 2017. Eligibility required a diagnosis of nonprogressive, metastatic lung cancer, including stage III or IV non–small cell or small cell disease. Patients were treated with antiangiogenic therapy, chemotherapy, immunotherapy, or tyrosine kinase inhibitors.
Patients in the control group had standard follow-up with imaging every 3-6 months. In contrast, the patient-reported outcomes (PRO) group completed a weekly online survey of 13 common symptoms between follow-up visits. If patients reported symptoms that matched with predefined criteria for severity or worsening, then the treating oncologist was notified.
When an 18-month interim analysis showed significant survival advantage in the PRO group, recruitment was stopped, and control patients were moved to the PRO group. After 2 years of follow-up, 40 patients (66.7%) in the control group had died, compared with 29 patients (47.5%) in the PRO group. Before censoring for crossover, median overall survival (OS) was 22.5 months in the PRO group, compared with 14.9 months in the control group (P = .03). Censoring for crossover widened the gap between groups by more than a month (22.5 vs. 13.5 months; P = .005).
“A potential mechanism of action is that symptoms suggesting adverse events or recurrence were detected earlier,” the investigators concluded.
The study was funded by SIVAN Innovation. Investigators reported financial affiliations with AstraZeneca, SIVAN Innovation, Ipsen, Roche, the National Cancer institute, Lilly, and others.
SOURCE: Denis F et al. JAMA. 2019 Jan 22;321(3):306-7.
Patients with nonprogressive, metastatic lung cancer who report symptoms through a weekly, web-based monitoring system may survive longer than those who undergo standard imaging surveillance, according to a recent French study.
Self-reporting may notify care providers about adverse effects or recurrence earlier than imaging, suggested lead author, Fabrice Denis, MD, PhD, of Institut Inter-régional de Cancérologie Jean Bernard in Le Mans, France, and his colleagues. Findings were published in a letter in JAMA.
In 2017, a similar, single-center study showed that web-based symptom reporting could improve survival in patients undergoing chemotherapy. The lead investigator on that trial was Ethan Basch, MD, who coauthored the present publication.
The current, prospective study involved 121 patients treated at five centers in France between June 2014 and December 2017. Eligibility required a diagnosis of nonprogressive, metastatic lung cancer, including stage III or IV non–small cell or small cell disease. Patients were treated with antiangiogenic therapy, chemotherapy, immunotherapy, or tyrosine kinase inhibitors.
Patients in the control group had standard follow-up with imaging every 3-6 months. In contrast, the patient-reported outcomes (PRO) group completed a weekly online survey of 13 common symptoms between follow-up visits. If patients reported symptoms that matched with predefined criteria for severity or worsening, then the treating oncologist was notified.
When an 18-month interim analysis showed significant survival advantage in the PRO group, recruitment was stopped, and control patients were moved to the PRO group. After 2 years of follow-up, 40 patients (66.7%) in the control group had died, compared with 29 patients (47.5%) in the PRO group. Before censoring for crossover, median overall survival (OS) was 22.5 months in the PRO group, compared with 14.9 months in the control group (P = .03). Censoring for crossover widened the gap between groups by more than a month (22.5 vs. 13.5 months; P = .005).
“A potential mechanism of action is that symptoms suggesting adverse events or recurrence were detected earlier,” the investigators concluded.
The study was funded by SIVAN Innovation. Investigators reported financial affiliations with AstraZeneca, SIVAN Innovation, Ipsen, Roche, the National Cancer institute, Lilly, and others.
SOURCE: Denis F et al. JAMA. 2019 Jan 22;321(3):306-7.
Patients with nonprogressive, metastatic lung cancer who report symptoms through a weekly, web-based monitoring system may survive longer than those who undergo standard imaging surveillance, according to a recent French study.
Self-reporting may notify care providers about adverse effects or recurrence earlier than imaging, suggested lead author, Fabrice Denis, MD, PhD, of Institut Inter-régional de Cancérologie Jean Bernard in Le Mans, France, and his colleagues. Findings were published in a letter in JAMA.
In 2017, a similar, single-center study showed that web-based symptom reporting could improve survival in patients undergoing chemotherapy. The lead investigator on that trial was Ethan Basch, MD, who coauthored the present publication.
The current, prospective study involved 121 patients treated at five centers in France between June 2014 and December 2017. Eligibility required a diagnosis of nonprogressive, metastatic lung cancer, including stage III or IV non–small cell or small cell disease. Patients were treated with antiangiogenic therapy, chemotherapy, immunotherapy, or tyrosine kinase inhibitors.
Patients in the control group had standard follow-up with imaging every 3-6 months. In contrast, the patient-reported outcomes (PRO) group completed a weekly online survey of 13 common symptoms between follow-up visits. If patients reported symptoms that matched with predefined criteria for severity or worsening, then the treating oncologist was notified.
When an 18-month interim analysis showed significant survival advantage in the PRO group, recruitment was stopped, and control patients were moved to the PRO group. After 2 years of follow-up, 40 patients (66.7%) in the control group had died, compared with 29 patients (47.5%) in the PRO group. Before censoring for crossover, median overall survival (OS) was 22.5 months in the PRO group, compared with 14.9 months in the control group (P = .03). Censoring for crossover widened the gap between groups by more than a month (22.5 vs. 13.5 months; P = .005).
“A potential mechanism of action is that symptoms suggesting adverse events or recurrence were detected earlier,” the investigators concluded.
The study was funded by SIVAN Innovation. Investigators reported financial affiliations with AstraZeneca, SIVAN Innovation, Ipsen, Roche, the National Cancer institute, Lilly, and others.
SOURCE: Denis F et al. JAMA. 2019 Jan 22;321(3):306-7.
FROM JAMA
Key clinical point: Patients with nonprogressive, metastatic lung cancer who report symptoms through a weekly, web-based monitoring system may survive longer than those who undergo standard imaging surveillance.
Major finding: Median overall survival (OS) of patients in the web-based monitoring group was 22.5 months versus 13.5 months for patients in the standard imaging group (P = .005).
Study details: A prospective study of 121 nonprogressive, metastatic lung cancer patients being treated with antiangiogenic therapy, chemotherapy, immunotherapy, or tyrosine kinase inhibitors.
Disclosures: The study was funded by SIVAN Innovation. Investigators reported financial affiliations with AstraZeneca, SIVAN Innovation, Ipsen, Roche, the National Cancer Institute, Lilly, and others.
Source: Denis F et al. JAMA. 2019 Jan 22;321(3):306-7.
Platinum-etoposide, taxanes best for small cell transformed EGFR-mutant lung cancer
Epidermal growth factor receptor (EGFR)–mutant non–small cell lung tumors transformed to small cell disease an average of 17.8 months after diagnosis, and this shift often involved Rb1, TP53, and PIK3CA mutations, according to the findings of a multicenter retrospective study of 67 patients.
After transformation, platinum-etoposide, paclitaxel, and nab-paclitaxel each yielded clinical response rates of 71%, while patients did not respond to programmed death-1 or programmed death-ligand 1 checkpoint inhibition, reported Nicolas Marcoux, MD, of Massachusetts General Hospital in Boston and his associates. “Indeed, none of the 17 patients [who received a checkpoint inhibitor] even seemed to derive clinical benefit from these therapies, as the longest time to progression was only 9 weeks,” the researchers wrote in the Journal of Clinical Oncology.
Interestingly, docetaxel produced no responses among six treated patients. Transformation often led to central nervous system metastases and patients survived a median of 10.7 months after transformation (95% confidence interval, 8.0-13.7 months).
Repeat biopsies showed that 3%-10% of EGFR-mutant non–small cell lung cancers transformed to small cell lung cancers. However, the subsequent clinical course has not been well characterized. Patients in this study were treated at eight cancer centers, had a history of EGFR-mutant small cell lung cancer, and most (87%) had non–small cell histology at diagnosis and received at least one EGFR tyrosine kinase inhibitor. The other nine patients had de novo small cell lung cancer or mixed histology.
All 59 patients with tissue genotyping at first evidence of small cell lung cancer retained their founder EGFR mutations, Dr. Marcoux and his associates reported. Among 19 patients with a history of EGFR T790M positivity, 15 patients were T790 wild-type at transformation. “Other recurrent mutations included TP53, Rb1, and PIK3CA,” they wrote.
The study supports the first-line use of platinum-etoposide for EGFR-mutant lung cancers that transform to small cell lung cancer, the researchers concluded. “Conversely, these tumors do not respond well to checkpoint inhibitors and the use of these therapies outside of a clinical trial should currently be discouraged.”
Funders included the National Institutes of Health, LungStrong, Targeting a Cure for Lung Cancer, Be a Piece of the Solution, the Susanne E. Coyne Memorial Fund, and a STOP Cancer Carrie Scott Grant. Dr. Marcoux disclosed honoraria from Bristol-Myers Squibb.
SOURCE: Marcoux N et al. J Clin Oncol. 2018 Dec 14. doi: 10.1200/JCO.18.01585.
Epidermal growth factor receptor (EGFR)–mutant non–small cell lung tumors transformed to small cell disease an average of 17.8 months after diagnosis, and this shift often involved Rb1, TP53, and PIK3CA mutations, according to the findings of a multicenter retrospective study of 67 patients.
After transformation, platinum-etoposide, paclitaxel, and nab-paclitaxel each yielded clinical response rates of 71%, while patients did not respond to programmed death-1 or programmed death-ligand 1 checkpoint inhibition, reported Nicolas Marcoux, MD, of Massachusetts General Hospital in Boston and his associates. “Indeed, none of the 17 patients [who received a checkpoint inhibitor] even seemed to derive clinical benefit from these therapies, as the longest time to progression was only 9 weeks,” the researchers wrote in the Journal of Clinical Oncology.
Interestingly, docetaxel produced no responses among six treated patients. Transformation often led to central nervous system metastases and patients survived a median of 10.7 months after transformation (95% confidence interval, 8.0-13.7 months).
Repeat biopsies showed that 3%-10% of EGFR-mutant non–small cell lung cancers transformed to small cell lung cancers. However, the subsequent clinical course has not been well characterized. Patients in this study were treated at eight cancer centers, had a history of EGFR-mutant small cell lung cancer, and most (87%) had non–small cell histology at diagnosis and received at least one EGFR tyrosine kinase inhibitor. The other nine patients had de novo small cell lung cancer or mixed histology.
All 59 patients with tissue genotyping at first evidence of small cell lung cancer retained their founder EGFR mutations, Dr. Marcoux and his associates reported. Among 19 patients with a history of EGFR T790M positivity, 15 patients were T790 wild-type at transformation. “Other recurrent mutations included TP53, Rb1, and PIK3CA,” they wrote.
The study supports the first-line use of platinum-etoposide for EGFR-mutant lung cancers that transform to small cell lung cancer, the researchers concluded. “Conversely, these tumors do not respond well to checkpoint inhibitors and the use of these therapies outside of a clinical trial should currently be discouraged.”
Funders included the National Institutes of Health, LungStrong, Targeting a Cure for Lung Cancer, Be a Piece of the Solution, the Susanne E. Coyne Memorial Fund, and a STOP Cancer Carrie Scott Grant. Dr. Marcoux disclosed honoraria from Bristol-Myers Squibb.
SOURCE: Marcoux N et al. J Clin Oncol. 2018 Dec 14. doi: 10.1200/JCO.18.01585.
Epidermal growth factor receptor (EGFR)–mutant non–small cell lung tumors transformed to small cell disease an average of 17.8 months after diagnosis, and this shift often involved Rb1, TP53, and PIK3CA mutations, according to the findings of a multicenter retrospective study of 67 patients.
After transformation, platinum-etoposide, paclitaxel, and nab-paclitaxel each yielded clinical response rates of 71%, while patients did not respond to programmed death-1 or programmed death-ligand 1 checkpoint inhibition, reported Nicolas Marcoux, MD, of Massachusetts General Hospital in Boston and his associates. “Indeed, none of the 17 patients [who received a checkpoint inhibitor] even seemed to derive clinical benefit from these therapies, as the longest time to progression was only 9 weeks,” the researchers wrote in the Journal of Clinical Oncology.
Interestingly, docetaxel produced no responses among six treated patients. Transformation often led to central nervous system metastases and patients survived a median of 10.7 months after transformation (95% confidence interval, 8.0-13.7 months).
Repeat biopsies showed that 3%-10% of EGFR-mutant non–small cell lung cancers transformed to small cell lung cancers. However, the subsequent clinical course has not been well characterized. Patients in this study were treated at eight cancer centers, had a history of EGFR-mutant small cell lung cancer, and most (87%) had non–small cell histology at diagnosis and received at least one EGFR tyrosine kinase inhibitor. The other nine patients had de novo small cell lung cancer or mixed histology.
All 59 patients with tissue genotyping at first evidence of small cell lung cancer retained their founder EGFR mutations, Dr. Marcoux and his associates reported. Among 19 patients with a history of EGFR T790M positivity, 15 patients were T790 wild-type at transformation. “Other recurrent mutations included TP53, Rb1, and PIK3CA,” they wrote.
The study supports the first-line use of platinum-etoposide for EGFR-mutant lung cancers that transform to small cell lung cancer, the researchers concluded. “Conversely, these tumors do not respond well to checkpoint inhibitors and the use of these therapies outside of a clinical trial should currently be discouraged.”
Funders included the National Institutes of Health, LungStrong, Targeting a Cure for Lung Cancer, Be a Piece of the Solution, the Susanne E. Coyne Memorial Fund, and a STOP Cancer Carrie Scott Grant. Dr. Marcoux disclosed honoraria from Bristol-Myers Squibb.
SOURCE: Marcoux N et al. J Clin Oncol. 2018 Dec 14. doi: 10.1200/JCO.18.01585.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Platinum-etoposide and taxane therapies elicited high response rates after transformation of EGFR-mutant non–small cell lung cancer.
Major finding: Median time to transformation was 17.8 months (95% CI, 14.3-26.2 months). Both platinum-etoposide and taxane therapies produced high response rates (71% each), but patients did not respond to checkpoint inhibitor therapy.
Data source: Multicenter retrospective study of 67 patients with EGFR-mutant small cell lung cancer.
Disclosures: Funders included the National Institutes of Health, LungStrong, Targeting a Cure for Lung Cancer, Be a Piece of the Solution, the Susanne E. Coyne Memorial Fund, and a STOP Cancer Carrie Scott Grant. Dr. Marcoux disclosed honoraria from Bristol-Myers Squibb.
Source: Marcoux N et al. J Clin Oncol. 2018 Dec 14. doi: 10.1200/JCO.18.01585.
Lung screening complications costly, more prevalent than in trial setting
The real-world rate of is substantially higher than in clinical trials, a study suggests.
Those complications related to low-dose computed tomography (LDCT) screening are potentially costly, according to the analysis of commercial and Medicare claims data for nearly 350,000 individuals.
While tentative, these results emphasize the need to discuss the risk of adverse events and their costs as part of the shared decision-making process between physicians and patients, researchers said in a report on their study in JAMA Internal Medicine.
“As the number of individuals seeking lung cancer screening with LDCT increases, so too will the number of individuals undergoing invasive diagnostic procedures as a results of abnormal findings,” said Jinhai Huo, MD, PhD, of the department of health services research, management, and policy at the University of Florida, Gainesville.
The retrospective cohort study included 174,702 individuals who underwent an invasive diagnostic procedure related to lung cancer screening and 169,808 control subjects.
All individuals studied were between 55 and 77 years old, the targeted age range for lung cancer screening specified by the Centers for Medicare & Medicaid Services.
Complication rates were about twice as high as they were in the landmark National Lung Screening Trial (NLST), both for a younger cohort of individuals aged 55-64 years, and an older Medicare age group of individuals aged 65 to 77 years, Dr. Huo and coinvestigators reported.
The estimated rate of complications was 22.0% (95% confidence interval, 21.7%-22.7%) in the younger age group, and even higher in the older age group, at 23.8% (95% CI, 23.0%-24.6%), according to investigators. By contrast, complication rates in the NLST were 9.8% and 8.5% for younger and older age cohorts, respectively.
The cost of managing postprocedural complications was higher than the cost of the diagnostic procedures, investigators said.
Mean costs ranged from $6,320 for minor complications to $56,845 for major complications, they reported.
The most common invasive diagnostic procedure in the study cohort was cytology test or biopsy in 26.1%, followed by bronchoscopy in 25.6%, according to study data. Another 5.4% underwent thoracic surgery.
In a previous Medicare advisory committee meeting, some experts expressed concern that complication rates in settings outside of the NLST would be higher than what was reported in that study, Dr. Huo and coauthors noted in their report.
“Our findings echoed this concern,” they said in a discussion of their results.
Dr. Huo and coauthors reported no conflicts of interest related to the research, which was supported in part by grants or fellowships from the University of Texas MD Anderson Cancer Center, the University of Florida, the National Cancer Institute, and the National Institutes of Health.
SOURCE: Huo J et al. JAMA Intern Med. 2019 Jan 14.
“The conversations that are occurring about lung cancer screening are woefully inadequate and do not discuss harms,” wrote Rita F. Redberg, MD, in an editorial note. Shared decision-making visits were made mandatory prior to lung cancer screening by the Centers for Medicare & Medicaid Services. That decision was made because of an evidence review suggesting a “low likelihood” that benefits of lung cancer screening would exceed harms in the Medicare population, Dr. Redberg wrote. Despite that, most Medicare beneficiaries are not having the required visit for shared decision making before they undergo the CT scan.

“It is likely that patients’ decisions not to undergo low-dose computed tomography for lung cancer screening are driven by the high false-positive rate, high chance of incidental findings, and subsequent need for invasive procedures, and small chance of benefit,” she said in her comment.
Shared decision-making visits are also rarely happening in the privately insured population, as shown in previous research, Dr. Redberg noted.
She reported no conflicts of interest related to her Editor’s Note, which appears in JAMA Internal Medicine (2019 Jan 14).
Dr. Redberg is with the department of medicine, University of California, San Francisco.
“The conversations that are occurring about lung cancer screening are woefully inadequate and do not discuss harms,” wrote Rita F. Redberg, MD, in an editorial note. Shared decision-making visits were made mandatory prior to lung cancer screening by the Centers for Medicare & Medicaid Services. That decision was made because of an evidence review suggesting a “low likelihood” that benefits of lung cancer screening would exceed harms in the Medicare population, Dr. Redberg wrote. Despite that, most Medicare beneficiaries are not having the required visit for shared decision making before they undergo the CT scan.
“It is likely that patients’ decisions not to undergo low-dose computed tomography for lung cancer screening are driven by the high false-positive rate, high chance of incidental findings, and subsequent need for invasive procedures, and small chance of benefit,” she said in her comment.
Shared decision-making visits are also rarely happening in the privately insured population, as shown in previous research, Dr. Redberg noted.
She reported no conflicts of interest related to her Editor’s Note, which appears in JAMA Internal Medicine (2019 Jan 14).
Dr. Redberg is with the department of medicine, University of California, San Francisco.
“The conversations that are occurring about lung cancer screening are woefully inadequate and do not discuss harms,” wrote Rita F. Redberg, MD, in an editorial note. Shared decision-making visits were made mandatory prior to lung cancer screening by the Centers for Medicare & Medicaid Services. That decision was made because of an evidence review suggesting a “low likelihood” that benefits of lung cancer screening would exceed harms in the Medicare population, Dr. Redberg wrote. Despite that, most Medicare beneficiaries are not having the required visit for shared decision making before they undergo the CT scan.
“It is likely that patients’ decisions not to undergo low-dose computed tomography for lung cancer screening are driven by the high false-positive rate, high chance of incidental findings, and subsequent need for invasive procedures, and small chance of benefit,” she said in her comment.
Shared decision-making visits are also rarely happening in the privately insured population, as shown in previous research, Dr. Redberg noted.
She reported no conflicts of interest related to her Editor’s Note, which appears in JAMA Internal Medicine (2019 Jan 14).
Dr. Redberg is with the department of medicine, University of California, San Francisco.
The real-world rate of is substantially higher than in clinical trials, a study suggests.
Those complications related to low-dose computed tomography (LDCT) screening are potentially costly, according to the analysis of commercial and Medicare claims data for nearly 350,000 individuals.
While tentative, these results emphasize the need to discuss the risk of adverse events and their costs as part of the shared decision-making process between physicians and patients, researchers said in a report on their study in JAMA Internal Medicine.
“As the number of individuals seeking lung cancer screening with LDCT increases, so too will the number of individuals undergoing invasive diagnostic procedures as a results of abnormal findings,” said Jinhai Huo, MD, PhD, of the department of health services research, management, and policy at the University of Florida, Gainesville.
The retrospective cohort study included 174,702 individuals who underwent an invasive diagnostic procedure related to lung cancer screening and 169,808 control subjects.
All individuals studied were between 55 and 77 years old, the targeted age range for lung cancer screening specified by the Centers for Medicare & Medicaid Services.
Complication rates were about twice as high as they were in the landmark National Lung Screening Trial (NLST), both for a younger cohort of individuals aged 55-64 years, and an older Medicare age group of individuals aged 65 to 77 years, Dr. Huo and coinvestigators reported.
The estimated rate of complications was 22.0% (95% confidence interval, 21.7%-22.7%) in the younger age group, and even higher in the older age group, at 23.8% (95% CI, 23.0%-24.6%), according to investigators. By contrast, complication rates in the NLST were 9.8% and 8.5% for younger and older age cohorts, respectively.
The cost of managing postprocedural complications was higher than the cost of the diagnostic procedures, investigators said.
Mean costs ranged from $6,320 for minor complications to $56,845 for major complications, they reported.
The most common invasive diagnostic procedure in the study cohort was cytology test or biopsy in 26.1%, followed by bronchoscopy in 25.6%, according to study data. Another 5.4% underwent thoracic surgery.
In a previous Medicare advisory committee meeting, some experts expressed concern that complication rates in settings outside of the NLST would be higher than what was reported in that study, Dr. Huo and coauthors noted in their report.
“Our findings echoed this concern,” they said in a discussion of their results.
Dr. Huo and coauthors reported no conflicts of interest related to the research, which was supported in part by grants or fellowships from the University of Texas MD Anderson Cancer Center, the University of Florida, the National Cancer Institute, and the National Institutes of Health.
SOURCE: Huo J et al. JAMA Intern Med. 2019 Jan 14.
The real-world rate of is substantially higher than in clinical trials, a study suggests.
Those complications related to low-dose computed tomography (LDCT) screening are potentially costly, according to the analysis of commercial and Medicare claims data for nearly 350,000 individuals.
While tentative, these results emphasize the need to discuss the risk of adverse events and their costs as part of the shared decision-making process between physicians and patients, researchers said in a report on their study in JAMA Internal Medicine.
“As the number of individuals seeking lung cancer screening with LDCT increases, so too will the number of individuals undergoing invasive diagnostic procedures as a results of abnormal findings,” said Jinhai Huo, MD, PhD, of the department of health services research, management, and policy at the University of Florida, Gainesville.
The retrospective cohort study included 174,702 individuals who underwent an invasive diagnostic procedure related to lung cancer screening and 169,808 control subjects.
All individuals studied were between 55 and 77 years old, the targeted age range for lung cancer screening specified by the Centers for Medicare & Medicaid Services.
Complication rates were about twice as high as they were in the landmark National Lung Screening Trial (NLST), both for a younger cohort of individuals aged 55-64 years, and an older Medicare age group of individuals aged 65 to 77 years, Dr. Huo and coinvestigators reported.
The estimated rate of complications was 22.0% (95% confidence interval, 21.7%-22.7%) in the younger age group, and even higher in the older age group, at 23.8% (95% CI, 23.0%-24.6%), according to investigators. By contrast, complication rates in the NLST were 9.8% and 8.5% for younger and older age cohorts, respectively.
The cost of managing postprocedural complications was higher than the cost of the diagnostic procedures, investigators said.
Mean costs ranged from $6,320 for minor complications to $56,845 for major complications, they reported.
The most common invasive diagnostic procedure in the study cohort was cytology test or biopsy in 26.1%, followed by bronchoscopy in 25.6%, according to study data. Another 5.4% underwent thoracic surgery.
In a previous Medicare advisory committee meeting, some experts expressed concern that complication rates in settings outside of the NLST would be higher than what was reported in that study, Dr. Huo and coauthors noted in their report.
“Our findings echoed this concern,” they said in a discussion of their results.
Dr. Huo and coauthors reported no conflicts of interest related to the research, which was supported in part by grants or fellowships from the University of Texas MD Anderson Cancer Center, the University of Florida, the National Cancer Institute, and the National Institutes of Health.
SOURCE: Huo J et al. JAMA Intern Med. 2019 Jan 14.
FROM JAMA INTERNAL MEDICINE
Key clinical point: The risk of complications following lung cancer screening is higher in a real-world setting as compared with the landmark National Lung Screening Trial (NLST).
Major finding: Estimated complication rates were 22.0%-23.8%, compared with 8.5%-9.8% in the NLST.
Study details: A retrospective cohort study including 174,702 individuals who underwent an invasive diagnostic procedure related to lung cancer screening and 169,808 controls.
Disclosures: Authors reported no conflicts of interest. The research was supported in part by grants or fellowships from the University of Texas MD Anderson Cancer Center, the University of Florida, the National Cancer Institute, and the National Institutes of Health.
Source: Huo J et al. JAMA Intern Med. 2019 Jan 14.
More benefit to chemoradiation in earlier small cell lung cancer
In response to chemoradiation, patients with stage I or II small cell lung cancer (SCLC) have a significantly longer overall survival than do those with stage III disease, according to a post hoc analysis of a randomized trial of chemoradiation in patients with early stages of SCLC.
The fact that overall survival is better in stage I and II than in stage III SCLC isn’t surprising. But the data confirm that stage I and II SCLC responds differently to chemoradiation than does stage III, providing a benchmark for safety and efficacy, according to the study authors.
The phase 3 CONVERT trial, from which the data were drawn, randomized patients with limited-stage SCLC to twice-daily (45 Gy in 30 fractions) or once-daily (66 Gy in 33 fractions) radiation after initiating cisplatin-etoposide chemotherapy (Lancet Oncol. 2017 Aug;18[8]:1116-25). Additional prophylactic cranial irradiation was permitted for those with an indication.
Contrary to the researcher’s hypothesis, once-daily radiation was not more effective for the primary outcome of overall survival in CONVERT, which limited enrollment to patients with local disease but did not stratify outcomes by SCLC stage. The purpose of the new post hoc analysis was to compare outcomes in those early-disease SCLC patients stratified by stage, which the authors noted is now recommended by several guidelines.
Because there were only four patients in CONVERT with stage I SCLC, those with either stage I or II SCLC, totaling 86 patients, were combined and then compared with the 423 with stage III SCLC.
At baseline, there were no significant differences between stage I/II and III groups for median age, smoking history, ECOG performance status, or dyspnea score at baseline. Similar proportions of patients completed the planned therapy.
However, the median survival was twice as long in the stage I/II group, compared with those with stage III SCLC (50 vs. 25 months), producing a hazard ratio for this outcome of 0.60 (P = .001). At 5 years, 49% of the stage I/II patients were alive, compared with 28% of the stage III patients (P = .001).
Other outcomes, such as progression-free survival at 5 years (47% vs. 26%; P = .003) also favored those with earlier-stage disease.
The incidence of adverse events associated with chemoradiation was not significantly different for the two groups, with the exception of acute esophagitis, which was less frequent in patients with earlier stage disease.
“The low incidence of severe toxic effects is a valid rationale to consider future radiotherapy dose intensification trials to improve outcomes” in patients with stage I/II disease, according to study author Ahmed Salem, MB, ChB, of the University of Manchester, England, and his coinvestigators.
The data from the post hoc analysis support guideline recommendations to stage even early and local SCLC when evaluating response to therapy in clinical trials, noted Howard (Jack) West, MD, of Swedish Cancer Institute, Seattle, in an accompanying editorial (JAMA Oncol. 2018 Dec 6. doi: 10.1001/jamaoncol.2018.5187). Dr. West suggested that such staging information might be useful when counseling patients about treatment options.
“These results imply that we may do our patients a disservice by dispensing with clinically relevant staging information that can lead to a more refined assessment of prognosis and optimal treatment,” Dr. West wrote.
SOURCE: Salem A et al. JAMA Oncol. 2018 Dec 6:e185335. doi: 10.1001/jamaoncol.2018.5335.
In response to chemoradiation, patients with stage I or II small cell lung cancer (SCLC) have a significantly longer overall survival than do those with stage III disease, according to a post hoc analysis of a randomized trial of chemoradiation in patients with early stages of SCLC.
The fact that overall survival is better in stage I and II than in stage III SCLC isn’t surprising. But the data confirm that stage I and II SCLC responds differently to chemoradiation than does stage III, providing a benchmark for safety and efficacy, according to the study authors.
The phase 3 CONVERT trial, from which the data were drawn, randomized patients with limited-stage SCLC to twice-daily (45 Gy in 30 fractions) or once-daily (66 Gy in 33 fractions) radiation after initiating cisplatin-etoposide chemotherapy (Lancet Oncol. 2017 Aug;18[8]:1116-25). Additional prophylactic cranial irradiation was permitted for those with an indication.
Contrary to the researcher’s hypothesis, once-daily radiation was not more effective for the primary outcome of overall survival in CONVERT, which limited enrollment to patients with local disease but did not stratify outcomes by SCLC stage. The purpose of the new post hoc analysis was to compare outcomes in those early-disease SCLC patients stratified by stage, which the authors noted is now recommended by several guidelines.
Because there were only four patients in CONVERT with stage I SCLC, those with either stage I or II SCLC, totaling 86 patients, were combined and then compared with the 423 with stage III SCLC.
At baseline, there were no significant differences between stage I/II and III groups for median age, smoking history, ECOG performance status, or dyspnea score at baseline. Similar proportions of patients completed the planned therapy.
However, the median survival was twice as long in the stage I/II group, compared with those with stage III SCLC (50 vs. 25 months), producing a hazard ratio for this outcome of 0.60 (P = .001). At 5 years, 49% of the stage I/II patients were alive, compared with 28% of the stage III patients (P = .001).
Other outcomes, such as progression-free survival at 5 years (47% vs. 26%; P = .003) also favored those with earlier-stage disease.
The incidence of adverse events associated with chemoradiation was not significantly different for the two groups, with the exception of acute esophagitis, which was less frequent in patients with earlier stage disease.
“The low incidence of severe toxic effects is a valid rationale to consider future radiotherapy dose intensification trials to improve outcomes” in patients with stage I/II disease, according to study author Ahmed Salem, MB, ChB, of the University of Manchester, England, and his coinvestigators.
The data from the post hoc analysis support guideline recommendations to stage even early and local SCLC when evaluating response to therapy in clinical trials, noted Howard (Jack) West, MD, of Swedish Cancer Institute, Seattle, in an accompanying editorial (JAMA Oncol. 2018 Dec 6. doi: 10.1001/jamaoncol.2018.5187). Dr. West suggested that such staging information might be useful when counseling patients about treatment options.
“These results imply that we may do our patients a disservice by dispensing with clinically relevant staging information that can lead to a more refined assessment of prognosis and optimal treatment,” Dr. West wrote.
SOURCE: Salem A et al. JAMA Oncol. 2018 Dec 6:e185335. doi: 10.1001/jamaoncol.2018.5335.
In response to chemoradiation, patients with stage I or II small cell lung cancer (SCLC) have a significantly longer overall survival than do those with stage III disease, according to a post hoc analysis of a randomized trial of chemoradiation in patients with early stages of SCLC.
The fact that overall survival is better in stage I and II than in stage III SCLC isn’t surprising. But the data confirm that stage I and II SCLC responds differently to chemoradiation than does stage III, providing a benchmark for safety and efficacy, according to the study authors.
The phase 3 CONVERT trial, from which the data were drawn, randomized patients with limited-stage SCLC to twice-daily (45 Gy in 30 fractions) or once-daily (66 Gy in 33 fractions) radiation after initiating cisplatin-etoposide chemotherapy (Lancet Oncol. 2017 Aug;18[8]:1116-25). Additional prophylactic cranial irradiation was permitted for those with an indication.
Contrary to the researcher’s hypothesis, once-daily radiation was not more effective for the primary outcome of overall survival in CONVERT, which limited enrollment to patients with local disease but did not stratify outcomes by SCLC stage. The purpose of the new post hoc analysis was to compare outcomes in those early-disease SCLC patients stratified by stage, which the authors noted is now recommended by several guidelines.
Because there were only four patients in CONVERT with stage I SCLC, those with either stage I or II SCLC, totaling 86 patients, were combined and then compared with the 423 with stage III SCLC.
At baseline, there were no significant differences between stage I/II and III groups for median age, smoking history, ECOG performance status, or dyspnea score at baseline. Similar proportions of patients completed the planned therapy.
However, the median survival was twice as long in the stage I/II group, compared with those with stage III SCLC (50 vs. 25 months), producing a hazard ratio for this outcome of 0.60 (P = .001). At 5 years, 49% of the stage I/II patients were alive, compared with 28% of the stage III patients (P = .001).
Other outcomes, such as progression-free survival at 5 years (47% vs. 26%; P = .003) also favored those with earlier-stage disease.
The incidence of adverse events associated with chemoradiation was not significantly different for the two groups, with the exception of acute esophagitis, which was less frequent in patients with earlier stage disease.
“The low incidence of severe toxic effects is a valid rationale to consider future radiotherapy dose intensification trials to improve outcomes” in patients with stage I/II disease, according to study author Ahmed Salem, MB, ChB, of the University of Manchester, England, and his coinvestigators.
The data from the post hoc analysis support guideline recommendations to stage even early and local SCLC when evaluating response to therapy in clinical trials, noted Howard (Jack) West, MD, of Swedish Cancer Institute, Seattle, in an accompanying editorial (JAMA Oncol. 2018 Dec 6. doi: 10.1001/jamaoncol.2018.5187). Dr. West suggested that such staging information might be useful when counseling patients about treatment options.
“These results imply that we may do our patients a disservice by dispensing with clinically relevant staging information that can lead to a more refined assessment of prognosis and optimal treatment,” Dr. West wrote.
SOURCE: Salem A et al. JAMA Oncol. 2018 Dec 6:e185335. doi: 10.1001/jamaoncol.2018.5335.
FROM JAMA ONCOLOGY
Key clinical point: Overall survival after chemoradiation is longer in stages I and II versus stage III small cell lung cancer.
Major finding: The hazard ratio for overall survival was 0.60 (P = .001), signifying 40% risk reduction for stage I/II versus stage III SCLC.
Study details: A post hoc secondary analysis of a phase 3 randomized trial.
Disclosures: The authors declared no potential conflicts of interest.
Source: Salem A et al. JAMA Oncol. 2018 Dec 6:e185335. doi: 10.1001/jamaoncol.2018.5335.
Adding veliparib to doublet therapy for NSCLC gives slight boost in PFS
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor veliparib to platinum doublet chemotherapy modestly improved progression-free survival in a randomized, placebo-controlled, phase 2 trial of 128 patients with extensive-stage non–small cell lung cancer.
Improved progression-free survival (PFS) “did not translate into reduction in overall mortality for patients treated with veliparib. However, the improvement in the point estimate of PFS was quite modest at 6.1 months, compared with 5.5 months [in the placebo control arm],” wrote Taofeek K. Owonikoko, MD, PhD, of Emory University, Atlanta, together with his coinvestigators in the Journal of Clinical Oncology.
Preclinical studies suggest that veliparib helps potentiate standard chemotherapy of non–small cell lung cancer (NSCLC), but clinical trials have yielded mixed results for PARP inhibition in this cancer. Patients in this study had untreated, extensive-stage NSCLC and an Eastern Cooperative Oncology Group performance status of 0 or 1. They received four 3-week cycles of cisplatin-etoposide (75 mg/m2 intravenously on day 1 and 100 mg/m2 on days 1-3) plus either veliparib (100 mg orally twice per day on days 1-7) or placebo.
Grade 3 or higher lymphopenia and neutropenia were more common in the veliparib arm but did not reduce treatment delivery. After a median follow-up time of 18.5 months, overall response rate was 72% in the veliparib arm versus 66% in the control arm (P =.57). Median overall survival times were 10.3 months and 8.9 months, respectively (hazard ratio, 0.83; P = .17).
The unstratified HR for PFS favored the veliparib-doublet arm but did not reach statistical significance (0.75; P = .06). After stratifying patients by sex and serum lactate dehydrogenase levels, the HR for PFS favored veliparib-doublet chemotherapy (0.63; P = .01). However, veliparib showed a much stronger effect in the subgroup of men with abnormal lactate dehydrogenase levels (adjusted HR, 0.34; P less than .001), which violated the “proportional hazards within strata assumption” on which this model was based, rendering the overall stratified HR uninterpretable, the researchers wrote.
They added that, before pursuing a larger definitive clinical trial, they await results from the ongoing phase 2 M14-361 study, in which patients with extensive-stage NSCLC are receiving platinum doublet therapy with carboplatin-etoposide plus either veliparib or placebo.
Funders included the Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group and the National Cancer Institute. Dr. Owonikoko reported ties to Novartis, Astellas Pharma, Celgene, and several other pharmaceutical companies.
SOURCE: Owonikoko TK et al. J Clin Oncol. 2018 Dec 5. doi: 10.1200/JCO.18.00264.
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor veliparib to platinum doublet chemotherapy modestly improved progression-free survival in a randomized, placebo-controlled, phase 2 trial of 128 patients with extensive-stage non–small cell lung cancer.
Improved progression-free survival (PFS) “did not translate into reduction in overall mortality for patients treated with veliparib. However, the improvement in the point estimate of PFS was quite modest at 6.1 months, compared with 5.5 months [in the placebo control arm],” wrote Taofeek K. Owonikoko, MD, PhD, of Emory University, Atlanta, together with his coinvestigators in the Journal of Clinical Oncology.
Preclinical studies suggest that veliparib helps potentiate standard chemotherapy of non–small cell lung cancer (NSCLC), but clinical trials have yielded mixed results for PARP inhibition in this cancer. Patients in this study had untreated, extensive-stage NSCLC and an Eastern Cooperative Oncology Group performance status of 0 or 1. They received four 3-week cycles of cisplatin-etoposide (75 mg/m2 intravenously on day 1 and 100 mg/m2 on days 1-3) plus either veliparib (100 mg orally twice per day on days 1-7) or placebo.
Grade 3 or higher lymphopenia and neutropenia were more common in the veliparib arm but did not reduce treatment delivery. After a median follow-up time of 18.5 months, overall response rate was 72% in the veliparib arm versus 66% in the control arm (P =.57). Median overall survival times were 10.3 months and 8.9 months, respectively (hazard ratio, 0.83; P = .17).
The unstratified HR for PFS favored the veliparib-doublet arm but did not reach statistical significance (0.75; P = .06). After stratifying patients by sex and serum lactate dehydrogenase levels, the HR for PFS favored veliparib-doublet chemotherapy (0.63; P = .01). However, veliparib showed a much stronger effect in the subgroup of men with abnormal lactate dehydrogenase levels (adjusted HR, 0.34; P less than .001), which violated the “proportional hazards within strata assumption” on which this model was based, rendering the overall stratified HR uninterpretable, the researchers wrote.
They added that, before pursuing a larger definitive clinical trial, they await results from the ongoing phase 2 M14-361 study, in which patients with extensive-stage NSCLC are receiving platinum doublet therapy with carboplatin-etoposide plus either veliparib or placebo.
Funders included the Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group and the National Cancer Institute. Dr. Owonikoko reported ties to Novartis, Astellas Pharma, Celgene, and several other pharmaceutical companies.
SOURCE: Owonikoko TK et al. J Clin Oncol. 2018 Dec 5. doi: 10.1200/JCO.18.00264.
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor veliparib to platinum doublet chemotherapy modestly improved progression-free survival in a randomized, placebo-controlled, phase 2 trial of 128 patients with extensive-stage non–small cell lung cancer.
Improved progression-free survival (PFS) “did not translate into reduction in overall mortality for patients treated with veliparib. However, the improvement in the point estimate of PFS was quite modest at 6.1 months, compared with 5.5 months [in the placebo control arm],” wrote Taofeek K. Owonikoko, MD, PhD, of Emory University, Atlanta, together with his coinvestigators in the Journal of Clinical Oncology.
Preclinical studies suggest that veliparib helps potentiate standard chemotherapy of non–small cell lung cancer (NSCLC), but clinical trials have yielded mixed results for PARP inhibition in this cancer. Patients in this study had untreated, extensive-stage NSCLC and an Eastern Cooperative Oncology Group performance status of 0 or 1. They received four 3-week cycles of cisplatin-etoposide (75 mg/m2 intravenously on day 1 and 100 mg/m2 on days 1-3) plus either veliparib (100 mg orally twice per day on days 1-7) or placebo.
Grade 3 or higher lymphopenia and neutropenia were more common in the veliparib arm but did not reduce treatment delivery. After a median follow-up time of 18.5 months, overall response rate was 72% in the veliparib arm versus 66% in the control arm (P =.57). Median overall survival times were 10.3 months and 8.9 months, respectively (hazard ratio, 0.83; P = .17).
The unstratified HR for PFS favored the veliparib-doublet arm but did not reach statistical significance (0.75; P = .06). After stratifying patients by sex and serum lactate dehydrogenase levels, the HR for PFS favored veliparib-doublet chemotherapy (0.63; P = .01). However, veliparib showed a much stronger effect in the subgroup of men with abnormal lactate dehydrogenase levels (adjusted HR, 0.34; P less than .001), which violated the “proportional hazards within strata assumption” on which this model was based, rendering the overall stratified HR uninterpretable, the researchers wrote.
They added that, before pursuing a larger definitive clinical trial, they await results from the ongoing phase 2 M14-361 study, in which patients with extensive-stage NSCLC are receiving platinum doublet therapy with carboplatin-etoposide plus either veliparib or placebo.
Funders included the Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group and the National Cancer Institute. Dr. Owonikoko reported ties to Novartis, Astellas Pharma, Celgene, and several other pharmaceutical companies.
SOURCE: Owonikoko TK et al. J Clin Oncol. 2018 Dec 5. doi: 10.1200/JCO.18.00264.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Adding veliparib to platinum-based doublet chemotherapy modestly improved progression-free survival in patients with extensive-stage non–small cell lung cancer.
Major finding: After a median follow-up of 18.5 months, median progression-free survival was 6.1 months for veliparib plus cisplatin-etoposide versus 5.5 months for placebo plus cisplatin-etoposide (unstratified hazard ratio, 0.75; P = .06).
Data source: A phase 2, randomized, placebo-controlled trial of 128 adults with untreated, extensive-stage non–small cell lung cancer (ECOG-ACRIN 2511).
Disclosures: Funders included the Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group and the National Cancer Institute. Dr. Owonikoko reported ties to Novartis, Astellas Pharma, Celgene, and several other pharmaceutical companies.
Source: Owonikoko TK et al. J Clin Oncol. 2018 Dec 5. doi: 10.1200/JCO.18.00264.
Pyrotinib shows promise in HER2-mutant non–small cell lung cancer
Pyrotinib, an irreversible pan-HER receptor tyrosine kinase inhibitor, showed promising safety and efficacy in a phase 2 trial of 15 adults with HER2-mutant non–small cell lung cancer and also topped afatinib in in vitro and murine studies, investigators reported.
In the phase 2 trial, objective response rate was 53%, a median overall survival was 12.9 months, and median progression-free survival was 6.4 months, wrote Yan Wang of Tongji University, Shanghai, China, together with associates. Pyrotinib showed superior antitumor activity, compared with afatinib, in a patient-derived organoid (P = .004) and xenograft mouse model (P = .0471), they reported in Annals of Oncology.
About 2% to 3% of patients with non–small cell lung cancer (NSCLC) have HER2 mutations, which most often involve an exon 20 insertion. Because HER2-targeting agents such as afatinib, dacomitinib, neratinib, and trastuzumab have limited activity against these cancers, patients usually receive chemotherapy, even though it is less effective than in lung cancers with ALK or ROS1 rearrangements.
To seek a better treatment option, the researchers created a HER2YVMA insertion patient-derived organoid model and a patient-derived xenograft mouse model, both of which confirmed the superior antitumor activity of pyrotinib, compared with afatinib or T-DM1 (ado-trastuzumab emtansine). For example, tumor burdens in mice fell by an average of 52% with pyrotinib but rose by 25% on afatinib and by 11% on T-DM1.
Accordingly, the researchers conducted a phase 2 trial of oral pyrotinib (400 mg daily) in 15 adults with NSCLC characterized by HER2 mutations in exon 20 or exon 19, the tyrosine kinase domain. Patients had an Eastern Cooperative Oncology Group performance status of 0-2, lacked symptomatic brain metastases, and had progressed on standard therapy.
In all, nine patients (60%) developed adverse events, the most common of which were grade 1 or 2 diarrhea, decreased hemoglobin levels, and hypocalcemia. There were no grade 3 or 4 events. Progression-free survival ranged from 1.7 to 23.4 months and one-third of patients stayed on pyrotinib for more than 1 year. Among two patients with asymptomatic brain metastases, one stopped pyrotinib at 4 weeks because of primary tumor progression but the other achieved stable disease on treatment. Three (23%) patients developed incident brain metastases on pyrotinib. The sole patient who progressed on a prior HER2-targeted therapy (afatinib) responded to pyrotinib.
Taken together, these findings support further study of pyrotinib in patients with NSCLC with HER2 exon 20 mutations, the researchers wrote. They have initiated a multicenter, phase 2 trial, which is currently in progress.
Funders included the National Natural Science Foundation of China, the “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission, the Science and Technology Commission of Shanghai Municipality, the Development Fund for Shanghai Talents, the University of Iowa Start-up Funds, and the American Cancer Society. The investigators reported having no conflicts of interest.
SOURCE: Wang Y et al. Ann Oncol. 2018 Dec 31. doi: 10.1093/annonc/mdy542.
Pyrotinib, an irreversible pan-HER receptor tyrosine kinase inhibitor, showed promising safety and efficacy in a phase 2 trial of 15 adults with HER2-mutant non–small cell lung cancer and also topped afatinib in in vitro and murine studies, investigators reported.
In the phase 2 trial, objective response rate was 53%, a median overall survival was 12.9 months, and median progression-free survival was 6.4 months, wrote Yan Wang of Tongji University, Shanghai, China, together with associates. Pyrotinib showed superior antitumor activity, compared with afatinib, in a patient-derived organoid (P = .004) and xenograft mouse model (P = .0471), they reported in Annals of Oncology.
About 2% to 3% of patients with non–small cell lung cancer (NSCLC) have HER2 mutations, which most often involve an exon 20 insertion. Because HER2-targeting agents such as afatinib, dacomitinib, neratinib, and trastuzumab have limited activity against these cancers, patients usually receive chemotherapy, even though it is less effective than in lung cancers with ALK or ROS1 rearrangements.
To seek a better treatment option, the researchers created a HER2YVMA insertion patient-derived organoid model and a patient-derived xenograft mouse model, both of which confirmed the superior antitumor activity of pyrotinib, compared with afatinib or T-DM1 (ado-trastuzumab emtansine). For example, tumor burdens in mice fell by an average of 52% with pyrotinib but rose by 25% on afatinib and by 11% on T-DM1.
Accordingly, the researchers conducted a phase 2 trial of oral pyrotinib (400 mg daily) in 15 adults with NSCLC characterized by HER2 mutations in exon 20 or exon 19, the tyrosine kinase domain. Patients had an Eastern Cooperative Oncology Group performance status of 0-2, lacked symptomatic brain metastases, and had progressed on standard therapy.
In all, nine patients (60%) developed adverse events, the most common of which were grade 1 or 2 diarrhea, decreased hemoglobin levels, and hypocalcemia. There were no grade 3 or 4 events. Progression-free survival ranged from 1.7 to 23.4 months and one-third of patients stayed on pyrotinib for more than 1 year. Among two patients with asymptomatic brain metastases, one stopped pyrotinib at 4 weeks because of primary tumor progression but the other achieved stable disease on treatment. Three (23%) patients developed incident brain metastases on pyrotinib. The sole patient who progressed on a prior HER2-targeted therapy (afatinib) responded to pyrotinib.
Taken together, these findings support further study of pyrotinib in patients with NSCLC with HER2 exon 20 mutations, the researchers wrote. They have initiated a multicenter, phase 2 trial, which is currently in progress.
Funders included the National Natural Science Foundation of China, the “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission, the Science and Technology Commission of Shanghai Municipality, the Development Fund for Shanghai Talents, the University of Iowa Start-up Funds, and the American Cancer Society. The investigators reported having no conflicts of interest.
SOURCE: Wang Y et al. Ann Oncol. 2018 Dec 31. doi: 10.1093/annonc/mdy542.
Pyrotinib, an irreversible pan-HER receptor tyrosine kinase inhibitor, showed promising safety and efficacy in a phase 2 trial of 15 adults with HER2-mutant non–small cell lung cancer and also topped afatinib in in vitro and murine studies, investigators reported.
In the phase 2 trial, objective response rate was 53%, a median overall survival was 12.9 months, and median progression-free survival was 6.4 months, wrote Yan Wang of Tongji University, Shanghai, China, together with associates. Pyrotinib showed superior antitumor activity, compared with afatinib, in a patient-derived organoid (P = .004) and xenograft mouse model (P = .0471), they reported in Annals of Oncology.
About 2% to 3% of patients with non–small cell lung cancer (NSCLC) have HER2 mutations, which most often involve an exon 20 insertion. Because HER2-targeting agents such as afatinib, dacomitinib, neratinib, and trastuzumab have limited activity against these cancers, patients usually receive chemotherapy, even though it is less effective than in lung cancers with ALK or ROS1 rearrangements.
To seek a better treatment option, the researchers created a HER2YVMA insertion patient-derived organoid model and a patient-derived xenograft mouse model, both of which confirmed the superior antitumor activity of pyrotinib, compared with afatinib or T-DM1 (ado-trastuzumab emtansine). For example, tumor burdens in mice fell by an average of 52% with pyrotinib but rose by 25% on afatinib and by 11% on T-DM1.
Accordingly, the researchers conducted a phase 2 trial of oral pyrotinib (400 mg daily) in 15 adults with NSCLC characterized by HER2 mutations in exon 20 or exon 19, the tyrosine kinase domain. Patients had an Eastern Cooperative Oncology Group performance status of 0-2, lacked symptomatic brain metastases, and had progressed on standard therapy.
In all, nine patients (60%) developed adverse events, the most common of which were grade 1 or 2 diarrhea, decreased hemoglobin levels, and hypocalcemia. There were no grade 3 or 4 events. Progression-free survival ranged from 1.7 to 23.4 months and one-third of patients stayed on pyrotinib for more than 1 year. Among two patients with asymptomatic brain metastases, one stopped pyrotinib at 4 weeks because of primary tumor progression but the other achieved stable disease on treatment. Three (23%) patients developed incident brain metastases on pyrotinib. The sole patient who progressed on a prior HER2-targeted therapy (afatinib) responded to pyrotinib.
Taken together, these findings support further study of pyrotinib in patients with NSCLC with HER2 exon 20 mutations, the researchers wrote. They have initiated a multicenter, phase 2 trial, which is currently in progress.
Funders included the National Natural Science Foundation of China, the “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission, the Science and Technology Commission of Shanghai Municipality, the Development Fund for Shanghai Talents, the University of Iowa Start-up Funds, and the American Cancer Society. The investigators reported having no conflicts of interest.
SOURCE: Wang Y et al. Ann Oncol. 2018 Dec 31. doi: 10.1093/annonc/mdy542.
FROM ANNALS OF ONCOLOGY
Key clinical point: Pyrotinib showed promising antitumor activity in patients with HER2-mutant non–small cell lung cancer.
Major finding: The objective response rate was 53%, median overall survival was 12.9 months, and median progression-free survival was 6.4 months. Pyrotinib showed superior antitumor activity, compared with afatinib in vitro (P = .004) and in a patient-derived xenograft model (P = .0471).
Study details: A phase 2 trial of 15 adults with progressive HER2-mutant non–small cell lung cancer, along with organoid and patient-derived xenograft models.
Disclosures: Funders included the National Natural Science Foundation of China, the “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission, the Science and Technology Commission of Shanghai Municipality, the Development Fund for Shanghai Talents, the University of Iowa Start-up Funds, and the American Cancer Society. The investigators reported having no conflicts of interest.
Source: Wang Y et al. Ann Oncol. 2018 Dec 31. doi: 10.1093/annonc/mdy542.