User login
Daratumumab and Darbepoetin for Refractory Warm Autoimmune Hemolytic Anemia: A Novel Duo for a Tough Case
Background
Warm autoimmune hemolytic anemia (wAIHA) is traditionally treated with immunosuppresimmunosuppression, and management of refractory disease is often a challenge. The anti-CD38 antibody daratumumab is emerging as a promising treatment for refractory wAIHA, as it targets autoantibody-producing plasma cells. Here, we present the first reported case of daratumumab used in conjunction with an erythropoiesisstimulating agent (ESA) to salvage refractory wAIHA in a patient with AIDS and bone marrow suppression.
Case Presentation
A middle aged man with HIV (undetectable viral load on antiretroviral treatment but CD4 persistently < 200, requiring chronic antimicrobial prophylaxis) was diagnosed with classic wAIHA in late 2021. The disease initially responded to corticosteroids, but relapsed repeatedly and eventually required IVIG, rituximab, danazol, and three immunosuppressive agents, none of which induced remission. Hemolysis worsened by fall 2024, with hemoglobin 5-6 g/dL despite high-dose corticosteroids and IVIG. Bone marrow biopsy was unrevealing, and he underwent splenectomy. However, recovery was complicated by cutaneous nocardiosis, iron overload, liver injury, and continued hemolysis. Eventually, reticulocytosis also ceased, and hemoglobin declined to 4-5 g/dL. Due to failure of standard therapies and to minimize further immunosuppression, weekly daratumumab injections were initiated, with weekly darbepoetin injections added to aid in compensatory hematopoiesis. With this combination, hemolysis indices improved, reticulocytosis picked up, and hemoglobin increased to 8-9 g/dL. However, the patient continued to struggle with infections, and he succumbed to drug-resistant bacterial sepsis in spring 2025.
Discussion
The patient had very complicated chronic and acute comorbidities, and some simplification was required in order to provide this summary. However, we hope this case adds to the literature on daratumumab as an effective new agent in refractory wAIHA, and also present a novel duo of therapies for patients who may struggle with bone marrow suppression in addition to autoimmune hemolysis. To our knowledge, this is the first reported case of the combination used in this manner.
Conclusions
Daratumumab is an effective and less immunosuppressive alternative for the treatment of heavily pretreated refractory wAIHA. Its combined use with ESA in patients with inadequate reticulocytosis should be studied further to clarify the efficacy and safety in this setting.
Background
Warm autoimmune hemolytic anemia (wAIHA) is traditionally treated with immunosuppresimmunosuppression, and management of refractory disease is often a challenge. The anti-CD38 antibody daratumumab is emerging as a promising treatment for refractory wAIHA, as it targets autoantibody-producing plasma cells. Here, we present the first reported case of daratumumab used in conjunction with an erythropoiesisstimulating agent (ESA) to salvage refractory wAIHA in a patient with AIDS and bone marrow suppression.
Case Presentation
A middle aged man with HIV (undetectable viral load on antiretroviral treatment but CD4 persistently < 200, requiring chronic antimicrobial prophylaxis) was diagnosed with classic wAIHA in late 2021. The disease initially responded to corticosteroids, but relapsed repeatedly and eventually required IVIG, rituximab, danazol, and three immunosuppressive agents, none of which induced remission. Hemolysis worsened by fall 2024, with hemoglobin 5-6 g/dL despite high-dose corticosteroids and IVIG. Bone marrow biopsy was unrevealing, and he underwent splenectomy. However, recovery was complicated by cutaneous nocardiosis, iron overload, liver injury, and continued hemolysis. Eventually, reticulocytosis also ceased, and hemoglobin declined to 4-5 g/dL. Due to failure of standard therapies and to minimize further immunosuppression, weekly daratumumab injections were initiated, with weekly darbepoetin injections added to aid in compensatory hematopoiesis. With this combination, hemolysis indices improved, reticulocytosis picked up, and hemoglobin increased to 8-9 g/dL. However, the patient continued to struggle with infections, and he succumbed to drug-resistant bacterial sepsis in spring 2025.
Discussion
The patient had very complicated chronic and acute comorbidities, and some simplification was required in order to provide this summary. However, we hope this case adds to the literature on daratumumab as an effective new agent in refractory wAIHA, and also present a novel duo of therapies for patients who may struggle with bone marrow suppression in addition to autoimmune hemolysis. To our knowledge, this is the first reported case of the combination used in this manner.
Conclusions
Daratumumab is an effective and less immunosuppressive alternative for the treatment of heavily pretreated refractory wAIHA. Its combined use with ESA in patients with inadequate reticulocytosis should be studied further to clarify the efficacy and safety in this setting.
Background
Warm autoimmune hemolytic anemia (wAIHA) is traditionally treated with immunosuppresimmunosuppression, and management of refractory disease is often a challenge. The anti-CD38 antibody daratumumab is emerging as a promising treatment for refractory wAIHA, as it targets autoantibody-producing plasma cells. Here, we present the first reported case of daratumumab used in conjunction with an erythropoiesisstimulating agent (ESA) to salvage refractory wAIHA in a patient with AIDS and bone marrow suppression.
Case Presentation
A middle aged man with HIV (undetectable viral load on antiretroviral treatment but CD4 persistently < 200, requiring chronic antimicrobial prophylaxis) was diagnosed with classic wAIHA in late 2021. The disease initially responded to corticosteroids, but relapsed repeatedly and eventually required IVIG, rituximab, danazol, and three immunosuppressive agents, none of which induced remission. Hemolysis worsened by fall 2024, with hemoglobin 5-6 g/dL despite high-dose corticosteroids and IVIG. Bone marrow biopsy was unrevealing, and he underwent splenectomy. However, recovery was complicated by cutaneous nocardiosis, iron overload, liver injury, and continued hemolysis. Eventually, reticulocytosis also ceased, and hemoglobin declined to 4-5 g/dL. Due to failure of standard therapies and to minimize further immunosuppression, weekly daratumumab injections were initiated, with weekly darbepoetin injections added to aid in compensatory hematopoiesis. With this combination, hemolysis indices improved, reticulocytosis picked up, and hemoglobin increased to 8-9 g/dL. However, the patient continued to struggle with infections, and he succumbed to drug-resistant bacterial sepsis in spring 2025.
Discussion
The patient had very complicated chronic and acute comorbidities, and some simplification was required in order to provide this summary. However, we hope this case adds to the literature on daratumumab as an effective new agent in refractory wAIHA, and also present a novel duo of therapies for patients who may struggle with bone marrow suppression in addition to autoimmune hemolysis. To our knowledge, this is the first reported case of the combination used in this manner.
Conclusions
Daratumumab is an effective and less immunosuppressive alternative for the treatment of heavily pretreated refractory wAIHA. Its combined use with ESA in patients with inadequate reticulocytosis should be studied further to clarify the efficacy and safety in this setting.
From Screening to Support: Enhancing Cancer Care Through eScreener Technology
Background
Addressing cancer-related distress is a critical component of comprehensive oncology care. In alignment with the National Comprehensive Cancer Network (NCCN) guidelines, which advocate for routine distress screening as a standard of care, our institution aimed to enhance a previously underutilized paper-based screening process by implementing a more efficient and accessible solution.
Objective
To improve screening rates and streamline the identification of psychosocial needs of Veterans who have cancer.
Population
This initiative was conducted in an outpatient Hematology/Oncology clinic at a Midwest Federal Healthcare Center.
Methods
The Plan-Do-Study-Act (PDSA) quality improvement model was used to guide the implementation of the electronic screener. The eScreener was integrated into routine clinical workflow and staff received training to facilitate implementation. Veterans self-identified their needs through the screener, which included a range of practical, family/social, physical, religious or emotional concerns. Clinical staff then review the responses, assessed the identified needs, and entered appropriate referrals into the electronic health record. A dedicated certified nursing assistant (CNA) was incorporated into the workflow to support implementation efforts. As part of their role, the CNA was tasked with ensuring that all Veterans completed the distress screener either electronically or on paper during their visit
Results
Between January 2025 and March 2025, a total of 180 distress screens were completed using the newly implement method. During the same period in the previous year, only 60 screens were completed, representing a 200% increase. The new process enabled timely referrals based on identified needs, resulting in 39 referrals to physicians, 32 to psychologists, 10 to social work, 7 to dieticians, 6 to nurses, and 1 to pastoral care. These outcomes reflect a significant improvement in both accessibility and patient engagement.
Conclusions
The implementation of an electronic cancer distress screener, along with a dedicated staff member resulted in a substantial increase in screening completion rates and multidisciplinary referrals. These preliminary finds suggest that digital tools can significantly enhance psychosocial assessment, improve coordination, and support the delivery of timely, patient-centered oncology care.
Background
Addressing cancer-related distress is a critical component of comprehensive oncology care. In alignment with the National Comprehensive Cancer Network (NCCN) guidelines, which advocate for routine distress screening as a standard of care, our institution aimed to enhance a previously underutilized paper-based screening process by implementing a more efficient and accessible solution.
Objective
To improve screening rates and streamline the identification of psychosocial needs of Veterans who have cancer.
Population
This initiative was conducted in an outpatient Hematology/Oncology clinic at a Midwest Federal Healthcare Center.
Methods
The Plan-Do-Study-Act (PDSA) quality improvement model was used to guide the implementation of the electronic screener. The eScreener was integrated into routine clinical workflow and staff received training to facilitate implementation. Veterans self-identified their needs through the screener, which included a range of practical, family/social, physical, religious or emotional concerns. Clinical staff then review the responses, assessed the identified needs, and entered appropriate referrals into the electronic health record. A dedicated certified nursing assistant (CNA) was incorporated into the workflow to support implementation efforts. As part of their role, the CNA was tasked with ensuring that all Veterans completed the distress screener either electronically or on paper during their visit
Results
Between January 2025 and March 2025, a total of 180 distress screens were completed using the newly implement method. During the same period in the previous year, only 60 screens were completed, representing a 200% increase. The new process enabled timely referrals based on identified needs, resulting in 39 referrals to physicians, 32 to psychologists, 10 to social work, 7 to dieticians, 6 to nurses, and 1 to pastoral care. These outcomes reflect a significant improvement in both accessibility and patient engagement.
Conclusions
The implementation of an electronic cancer distress screener, along with a dedicated staff member resulted in a substantial increase in screening completion rates and multidisciplinary referrals. These preliminary finds suggest that digital tools can significantly enhance psychosocial assessment, improve coordination, and support the delivery of timely, patient-centered oncology care.
Background
Addressing cancer-related distress is a critical component of comprehensive oncology care. In alignment with the National Comprehensive Cancer Network (NCCN) guidelines, which advocate for routine distress screening as a standard of care, our institution aimed to enhance a previously underutilized paper-based screening process by implementing a more efficient and accessible solution.
Objective
To improve screening rates and streamline the identification of psychosocial needs of Veterans who have cancer.
Population
This initiative was conducted in an outpatient Hematology/Oncology clinic at a Midwest Federal Healthcare Center.
Methods
The Plan-Do-Study-Act (PDSA) quality improvement model was used to guide the implementation of the electronic screener. The eScreener was integrated into routine clinical workflow and staff received training to facilitate implementation. Veterans self-identified their needs through the screener, which included a range of practical, family/social, physical, religious or emotional concerns. Clinical staff then review the responses, assessed the identified needs, and entered appropriate referrals into the electronic health record. A dedicated certified nursing assistant (CNA) was incorporated into the workflow to support implementation efforts. As part of their role, the CNA was tasked with ensuring that all Veterans completed the distress screener either electronically or on paper during their visit
Results
Between January 2025 and March 2025, a total of 180 distress screens were completed using the newly implement method. During the same period in the previous year, only 60 screens were completed, representing a 200% increase. The new process enabled timely referrals based on identified needs, resulting in 39 referrals to physicians, 32 to psychologists, 10 to social work, 7 to dieticians, 6 to nurses, and 1 to pastoral care. These outcomes reflect a significant improvement in both accessibility and patient engagement.
Conclusions
The implementation of an electronic cancer distress screener, along with a dedicated staff member resulted in a substantial increase in screening completion rates and multidisciplinary referrals. These preliminary finds suggest that digital tools can significantly enhance psychosocial assessment, improve coordination, and support the delivery of timely, patient-centered oncology care.
Case Presentation: First Ever VA "Bloodless" Autologous Stem Cell Transplant Was a Success
Background
Autologous stem cell transplant (ASCT) is an important part of the treatment paradigm for patients with multiple myeloma (MM) and remains the standard of care for newly diagnosed patients. Blood product transfusion support in the form of platelets and packed red blood cells (pRBCs) is part of the standard of practice as supportive measures during the severely pancytopenic period. Some MM patients, such as those of Jehovah’s Witness (JW) faith, may have religious beliefs or preferences that preclude acceptance of such blood products. Some transplant centers have developed protocols to allow safe “bloodless” ASCT that allows these patients to receive this important treatment while adhering to their beliefs or preferences.
Case Presentation
A 61-year-old veteran of JW faith with newly diagnosed IgG Kappa Multiple Myeloma was referred to the Tennessee Valley Healthcare System (TVHS) Stem Cell Transplant program for consideration of “bloodless” ASCT. With the assistance and expertise of the academic affiliate, Vanderbilt University Medical Center’s established bloodless ASCT protocol, this same protocol was established at TVHS to optimize the patient’s care pretransplant (use of erythropoiesis stimulating agents, intravenous iron, B12 supplementation) as well as post-transplant (use of antifibrinolytics, close inpatient monitoring). Both Ethics and Legal consultation was obtained, and guidance was provided to create a life sustaining treatment (LST) note in the veteran’s electronic health record that captured the veteran’s blood product preference. Once all protocols and guidance were in place, the TVHS SCT/CT program proceeded to treat the veteran with a myeloablative melphalan ASCT. The patient tolerated the procedure exceptionally well with minimal complications. He achieved full engraftment on day +14 after ASCT as expected and was discharged from the inpatient setting. He was monitored in the outpatient setting until day +30 without further complications.
Conclusions
The TVHS SCT/CT performed the first ever bloodless autologous stem cell transplant within the VA. This pioneering effort to establish such protocols to provide care to all veterans whatever their personal or religious preferences is a testament to commitment of VA to provide care for all veterans and the willingness to innovate to do so.
Background
Autologous stem cell transplant (ASCT) is an important part of the treatment paradigm for patients with multiple myeloma (MM) and remains the standard of care for newly diagnosed patients. Blood product transfusion support in the form of platelets and packed red blood cells (pRBCs) is part of the standard of practice as supportive measures during the severely pancytopenic period. Some MM patients, such as those of Jehovah’s Witness (JW) faith, may have religious beliefs or preferences that preclude acceptance of such blood products. Some transplant centers have developed protocols to allow safe “bloodless” ASCT that allows these patients to receive this important treatment while adhering to their beliefs or preferences.
Case Presentation
A 61-year-old veteran of JW faith with newly diagnosed IgG Kappa Multiple Myeloma was referred to the Tennessee Valley Healthcare System (TVHS) Stem Cell Transplant program for consideration of “bloodless” ASCT. With the assistance and expertise of the academic affiliate, Vanderbilt University Medical Center’s established bloodless ASCT protocol, this same protocol was established at TVHS to optimize the patient’s care pretransplant (use of erythropoiesis stimulating agents, intravenous iron, B12 supplementation) as well as post-transplant (use of antifibrinolytics, close inpatient monitoring). Both Ethics and Legal consultation was obtained, and guidance was provided to create a life sustaining treatment (LST) note in the veteran’s electronic health record that captured the veteran’s blood product preference. Once all protocols and guidance were in place, the TVHS SCT/CT program proceeded to treat the veteran with a myeloablative melphalan ASCT. The patient tolerated the procedure exceptionally well with minimal complications. He achieved full engraftment on day +14 after ASCT as expected and was discharged from the inpatient setting. He was monitored in the outpatient setting until day +30 without further complications.
Conclusions
The TVHS SCT/CT performed the first ever bloodless autologous stem cell transplant within the VA. This pioneering effort to establish such protocols to provide care to all veterans whatever their personal or religious preferences is a testament to commitment of VA to provide care for all veterans and the willingness to innovate to do so.
Background
Autologous stem cell transplant (ASCT) is an important part of the treatment paradigm for patients with multiple myeloma (MM) and remains the standard of care for newly diagnosed patients. Blood product transfusion support in the form of platelets and packed red blood cells (pRBCs) is part of the standard of practice as supportive measures during the severely pancytopenic period. Some MM patients, such as those of Jehovah’s Witness (JW) faith, may have religious beliefs or preferences that preclude acceptance of such blood products. Some transplant centers have developed protocols to allow safe “bloodless” ASCT that allows these patients to receive this important treatment while adhering to their beliefs or preferences.
Case Presentation
A 61-year-old veteran of JW faith with newly diagnosed IgG Kappa Multiple Myeloma was referred to the Tennessee Valley Healthcare System (TVHS) Stem Cell Transplant program for consideration of “bloodless” ASCT. With the assistance and expertise of the academic affiliate, Vanderbilt University Medical Center’s established bloodless ASCT protocol, this same protocol was established at TVHS to optimize the patient’s care pretransplant (use of erythropoiesis stimulating agents, intravenous iron, B12 supplementation) as well as post-transplant (use of antifibrinolytics, close inpatient monitoring). Both Ethics and Legal consultation was obtained, and guidance was provided to create a life sustaining treatment (LST) note in the veteran’s electronic health record that captured the veteran’s blood product preference. Once all protocols and guidance were in place, the TVHS SCT/CT program proceeded to treat the veteran with a myeloablative melphalan ASCT. The patient tolerated the procedure exceptionally well with minimal complications. He achieved full engraftment on day +14 after ASCT as expected and was discharged from the inpatient setting. He was monitored in the outpatient setting until day +30 without further complications.
Conclusions
The TVHS SCT/CT performed the first ever bloodless autologous stem cell transplant within the VA. This pioneering effort to establish such protocols to provide care to all veterans whatever their personal or religious preferences is a testament to commitment of VA to provide care for all veterans and the willingness to innovate to do so.
Agent Orange Exposure and Genetic Factors Independently Raise Risk for Multiple Lymphoma Types
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Digital Mindfulness Program May Reduce Anxiety in Patients With Chronic Obstructive Pulmonary Disease
TOPLINE:
An 8-week smartphone-based mindfulness program using audio-guided meditation reduced anxiety and improved emotional well-being in patients with chronic obstructive pulmonary disease (COPD), also providing relief from stress, anxiety, and dyspnea following each session.
METHODOLOGY:
- A considerable proportion of patients with COPD experience clinically significant anxiety and depressive symptoms; psychological interventions that are easy to implement as add-on treatments can alleviate these symptoms.
- In this pilot study, 30 patients (mean age, 62.68 y; 60.5% women) with COPD and subclinical symptoms of anxiety or depression were enrolled and allocated to an 8-week self-administered digital mindfulness-based intervention (n = 14) or the waitlist control (n = 16).
- Patients in the intervention group had an introductory face-to-face session, followed by daily smartphone audio-guided meditation adapted for patients with COPD. The waitlist group received the same intervention after the study period ended.
- The primary endpoints were the feasibility of the intervention and its effects on anxiety and depression symptoms at baseline, 4 weeks, and 8 weeks.
TAKEAWAY:
- Patients in the intervention group practiced mindfulness on 81.38% of the 56 intervention days.
- After 8 weeks, the intervention group showed a significant reduction in anxiety (P = .010) compared with the waitlist group; however, no significant improvement was observed for depression.
- Similarly, significant improvements were reported for emotional functioning (P = .004), but no significant reductions in perceived stress and hair cortisol levels were observed after 8 weeks.
- Significant reductions were reported for momentary subjective stress (P < .001), anxiety (P = .022), and dyspnea (P < .001) immediately after meditation sessions.
IN PRACTICE:
“The investigated self-administered digital MBI [mindfulness-based intervention], including brief 10- to 15-minute meditations, was feasible and holds potential as low-threshold add-on treatment to alleviate anxiety after 8 weeks and reduce momentary subjective stress, anxiety, and dyspnea in everyday life,” the study authors wrote.
SOURCE:
This study was led by Hannah Tschenett, Department of Clinical and Health Psychology, Faculty of Psychology, University of Vienna, Vienna, Austria, and was published online in Respiratory Research.
LIMITATIONS:
This study had several limitations including a small sample size, lack of a true control group, and potential selection bias due to recruitment from centers with patients already interested in mindfulness, which may have inflated adherence. Additionally, generalizability to all patients with COPD was limited, as many were either ineligible or declined to participate.
DISCLOSURES:
This study was funded by the Scientific Medical Fund of the City of Vienna and the Karl Landsteiner Institute (KLI) for Lung Research and Pulmonary Oncology. The KLI received funding from AstraZeneca, Boehringer Ingelheim, Chiesi, Linde plc, Menarini Pharma, Novartis, and Vivisol Austria. Three authors reported being employees of KLI or receiving lecture fees from some of these pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An 8-week smartphone-based mindfulness program using audio-guided meditation reduced anxiety and improved emotional well-being in patients with chronic obstructive pulmonary disease (COPD), also providing relief from stress, anxiety, and dyspnea following each session.
METHODOLOGY:
- A considerable proportion of patients with COPD experience clinically significant anxiety and depressive symptoms; psychological interventions that are easy to implement as add-on treatments can alleviate these symptoms.
- In this pilot study, 30 patients (mean age, 62.68 y; 60.5% women) with COPD and subclinical symptoms of anxiety or depression were enrolled and allocated to an 8-week self-administered digital mindfulness-based intervention (n = 14) or the waitlist control (n = 16).
- Patients in the intervention group had an introductory face-to-face session, followed by daily smartphone audio-guided meditation adapted for patients with COPD. The waitlist group received the same intervention after the study period ended.
- The primary endpoints were the feasibility of the intervention and its effects on anxiety and depression symptoms at baseline, 4 weeks, and 8 weeks.
TAKEAWAY:
- Patients in the intervention group practiced mindfulness on 81.38% of the 56 intervention days.
- After 8 weeks, the intervention group showed a significant reduction in anxiety (P = .010) compared with the waitlist group; however, no significant improvement was observed for depression.
- Similarly, significant improvements were reported for emotional functioning (P = .004), but no significant reductions in perceived stress and hair cortisol levels were observed after 8 weeks.
- Significant reductions were reported for momentary subjective stress (P < .001), anxiety (P = .022), and dyspnea (P < .001) immediately after meditation sessions.
IN PRACTICE:
“The investigated self-administered digital MBI [mindfulness-based intervention], including brief 10- to 15-minute meditations, was feasible and holds potential as low-threshold add-on treatment to alleviate anxiety after 8 weeks and reduce momentary subjective stress, anxiety, and dyspnea in everyday life,” the study authors wrote.
SOURCE:
This study was led by Hannah Tschenett, Department of Clinical and Health Psychology, Faculty of Psychology, University of Vienna, Vienna, Austria, and was published online in Respiratory Research.
LIMITATIONS:
This study had several limitations including a small sample size, lack of a true control group, and potential selection bias due to recruitment from centers with patients already interested in mindfulness, which may have inflated adherence. Additionally, generalizability to all patients with COPD was limited, as many were either ineligible or declined to participate.
DISCLOSURES:
This study was funded by the Scientific Medical Fund of the City of Vienna and the Karl Landsteiner Institute (KLI) for Lung Research and Pulmonary Oncology. The KLI received funding from AstraZeneca, Boehringer Ingelheim, Chiesi, Linde plc, Menarini Pharma, Novartis, and Vivisol Austria. Three authors reported being employees of KLI or receiving lecture fees from some of these pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An 8-week smartphone-based mindfulness program using audio-guided meditation reduced anxiety and improved emotional well-being in patients with chronic obstructive pulmonary disease (COPD), also providing relief from stress, anxiety, and dyspnea following each session.
METHODOLOGY:
- A considerable proportion of patients with COPD experience clinically significant anxiety and depressive symptoms; psychological interventions that are easy to implement as add-on treatments can alleviate these symptoms.
- In this pilot study, 30 patients (mean age, 62.68 y; 60.5% women) with COPD and subclinical symptoms of anxiety or depression were enrolled and allocated to an 8-week self-administered digital mindfulness-based intervention (n = 14) or the waitlist control (n = 16).
- Patients in the intervention group had an introductory face-to-face session, followed by daily smartphone audio-guided meditation adapted for patients with COPD. The waitlist group received the same intervention after the study period ended.
- The primary endpoints were the feasibility of the intervention and its effects on anxiety and depression symptoms at baseline, 4 weeks, and 8 weeks.
TAKEAWAY:
- Patients in the intervention group practiced mindfulness on 81.38% of the 56 intervention days.
- After 8 weeks, the intervention group showed a significant reduction in anxiety (P = .010) compared with the waitlist group; however, no significant improvement was observed for depression.
- Similarly, significant improvements were reported for emotional functioning (P = .004), but no significant reductions in perceived stress and hair cortisol levels were observed after 8 weeks.
- Significant reductions were reported for momentary subjective stress (P < .001), anxiety (P = .022), and dyspnea (P < .001) immediately after meditation sessions.
IN PRACTICE:
“The investigated self-administered digital MBI [mindfulness-based intervention], including brief 10- to 15-minute meditations, was feasible and holds potential as low-threshold add-on treatment to alleviate anxiety after 8 weeks and reduce momentary subjective stress, anxiety, and dyspnea in everyday life,” the study authors wrote.
SOURCE:
This study was led by Hannah Tschenett, Department of Clinical and Health Psychology, Faculty of Psychology, University of Vienna, Vienna, Austria, and was published online in Respiratory Research.
LIMITATIONS:
This study had several limitations including a small sample size, lack of a true control group, and potential selection bias due to recruitment from centers with patients already interested in mindfulness, which may have inflated adherence. Additionally, generalizability to all patients with COPD was limited, as many were either ineligible or declined to participate.
DISCLOSURES:
This study was funded by the Scientific Medical Fund of the City of Vienna and the Karl Landsteiner Institute (KLI) for Lung Research and Pulmonary Oncology. The KLI received funding from AstraZeneca, Boehringer Ingelheim, Chiesi, Linde plc, Menarini Pharma, Novartis, and Vivisol Austria. Three authors reported being employees of KLI or receiving lecture fees from some of these pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Are Your Patients With COPD Inhaling Eucalyptus Oil? Know the Risks
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Single Antiplatelet After TAVR Lowers Risk
Patients who received a single antiplatelet drug therapy — usually aspirin — after transcatheter aortic valve replacement (TAVR) had about half the risk of dying in the subsequent 6 months compared with patients who received dual antiplatelet drug therapy. The findings were similar in men and women and in patients with and without coronary artery disease.
“This is one of the first demonstrations in real-world data that single antiplatelet therapy is not only associated with a lower risk of bleeding but also lower mortality,” said lead author Francesco Pelliccia, MD, PhD, a cardiologist at Sapienza University in Rome, Italy. Mortality rates for those who received dual antiplatelet therapy increased steadily during the 6 months after the procedure, he reported at the Society for Cardiovascular Angiography and Interventions (SCAI) 2025 Scientific Sessions in Washington, DC.
Ischemic and major bleeding events were dramatically reduced in those receiving a single drug, according to a real-world study of 5514 patients undergoing TAVR at 20 centers. The centers participate in the Transfusion Requirements in Transcatheter Aortic Valve Implantation (TRITAVI) registry.
In the 6 months after the procedure, 2.4% of the 3197 patients who received a single antiplatelet drug died of any cause, as did 5.4% of 2317 patients who received two antiplatelet drugs (hazard ratio [HR], 1.65). Dual therapy was associated with a higher risk for death in both men (HR, 2.08) and women (HR, 1.53). Risk for death was also higher in patients with coronary artery disease (HR, 1.83) and without coronary artery disease (HR, 1.52). All results were statistically significant.
Balancing Risks and Benefits
The popularity of TAVR, which was introduced in 2002, has grown to the point that, in 2019, it surpassed the use of surgical aortic valve replacement. But the procedure is associated with an increased risk for both thrombosis and bleeding. Antiplatelet therapy with aspirin and clopidogrel helps prevent thrombosis but can increase the risk of bleeding. This has led to a debate about the best balance for antiplatelet therapy after TAVR with either single therapy — usually with aspirin — or dual therapy with both aspirin and clopidogrel.
A series of studies have addressed this problem. Dual therapy did not show any benefits over single therapy in terms of major adverse cardiac and cerebrovascular events in a 2011 small randomized study. A 2014 small randomized study also showed no benefit for morbidity or mortality from dual therapy. A larger 2017 randomized trial showed that single therapy reduced the risk for major or life-threatening events but did not increase the risk for myocardial infarction or stroke.
Bleeding and bleeding plus thromboembolic events were significantly lower with aspirin than with aspirin plus clopidogrel after a year’s follow-up in the 2020 POPular TAVI trial. Findings from three of these trials were pooled in a 2018 meta-analysis, which showed that dual therapy increased the risk for major adverse events after TAVR and did not prevent ischemic events any more than single therapy.
Based on this evidence, many centers changed their practice. And current European guidelines recommend a single antiplatelet drug for patients undergoing TAVR who do not have additional indications for oral anticoagulation therapy.
By the Numbers
Randomized trials are generally considered the best evidence for medical questions such as this one. “But randomized trials often do not reflect real-world reality. We have to look at what really happens,” Pelliccia said.
Retrospective data from registries can also provide large numbers of patients; in this case, TRITAVI provided data on thousands of patients rather than the hundreds examined in combined randomized trials.
“The results, for the first time, provide clinicians more information on how to treat their patients who are at high risk for bleeding and provide evidence that single antiplatelet therapy should be considered the standard of care in all patients undergoing TAVR,” Pelliccia said.
A version of this article first appeared on Medscape.com.
Patients who received a single antiplatelet drug therapy — usually aspirin — after transcatheter aortic valve replacement (TAVR) had about half the risk of dying in the subsequent 6 months compared with patients who received dual antiplatelet drug therapy. The findings were similar in men and women and in patients with and without coronary artery disease.
“This is one of the first demonstrations in real-world data that single antiplatelet therapy is not only associated with a lower risk of bleeding but also lower mortality,” said lead author Francesco Pelliccia, MD, PhD, a cardiologist at Sapienza University in Rome, Italy. Mortality rates for those who received dual antiplatelet therapy increased steadily during the 6 months after the procedure, he reported at the Society for Cardiovascular Angiography and Interventions (SCAI) 2025 Scientific Sessions in Washington, DC.
Ischemic and major bleeding events were dramatically reduced in those receiving a single drug, according to a real-world study of 5514 patients undergoing TAVR at 20 centers. The centers participate in the Transfusion Requirements in Transcatheter Aortic Valve Implantation (TRITAVI) registry.
In the 6 months after the procedure, 2.4% of the 3197 patients who received a single antiplatelet drug died of any cause, as did 5.4% of 2317 patients who received two antiplatelet drugs (hazard ratio [HR], 1.65). Dual therapy was associated with a higher risk for death in both men (HR, 2.08) and women (HR, 1.53). Risk for death was also higher in patients with coronary artery disease (HR, 1.83) and without coronary artery disease (HR, 1.52). All results were statistically significant.
Balancing Risks and Benefits
The popularity of TAVR, which was introduced in 2002, has grown to the point that, in 2019, it surpassed the use of surgical aortic valve replacement. But the procedure is associated with an increased risk for both thrombosis and bleeding. Antiplatelet therapy with aspirin and clopidogrel helps prevent thrombosis but can increase the risk of bleeding. This has led to a debate about the best balance for antiplatelet therapy after TAVR with either single therapy — usually with aspirin — or dual therapy with both aspirin and clopidogrel.
A series of studies have addressed this problem. Dual therapy did not show any benefits over single therapy in terms of major adverse cardiac and cerebrovascular events in a 2011 small randomized study. A 2014 small randomized study also showed no benefit for morbidity or mortality from dual therapy. A larger 2017 randomized trial showed that single therapy reduced the risk for major or life-threatening events but did not increase the risk for myocardial infarction or stroke.
Bleeding and bleeding plus thromboembolic events were significantly lower with aspirin than with aspirin plus clopidogrel after a year’s follow-up in the 2020 POPular TAVI trial. Findings from three of these trials were pooled in a 2018 meta-analysis, which showed that dual therapy increased the risk for major adverse events after TAVR and did not prevent ischemic events any more than single therapy.
Based on this evidence, many centers changed their practice. And current European guidelines recommend a single antiplatelet drug for patients undergoing TAVR who do not have additional indications for oral anticoagulation therapy.
By the Numbers
Randomized trials are generally considered the best evidence for medical questions such as this one. “But randomized trials often do not reflect real-world reality. We have to look at what really happens,” Pelliccia said.
Retrospective data from registries can also provide large numbers of patients; in this case, TRITAVI provided data on thousands of patients rather than the hundreds examined in combined randomized trials.
“The results, for the first time, provide clinicians more information on how to treat their patients who are at high risk for bleeding and provide evidence that single antiplatelet therapy should be considered the standard of care in all patients undergoing TAVR,” Pelliccia said.
A version of this article first appeared on Medscape.com.
Patients who received a single antiplatelet drug therapy — usually aspirin — after transcatheter aortic valve replacement (TAVR) had about half the risk of dying in the subsequent 6 months compared with patients who received dual antiplatelet drug therapy. The findings were similar in men and women and in patients with and without coronary artery disease.
“This is one of the first demonstrations in real-world data that single antiplatelet therapy is not only associated with a lower risk of bleeding but also lower mortality,” said lead author Francesco Pelliccia, MD, PhD, a cardiologist at Sapienza University in Rome, Italy. Mortality rates for those who received dual antiplatelet therapy increased steadily during the 6 months after the procedure, he reported at the Society for Cardiovascular Angiography and Interventions (SCAI) 2025 Scientific Sessions in Washington, DC.
Ischemic and major bleeding events were dramatically reduced in those receiving a single drug, according to a real-world study of 5514 patients undergoing TAVR at 20 centers. The centers participate in the Transfusion Requirements in Transcatheter Aortic Valve Implantation (TRITAVI) registry.
In the 6 months after the procedure, 2.4% of the 3197 patients who received a single antiplatelet drug died of any cause, as did 5.4% of 2317 patients who received two antiplatelet drugs (hazard ratio [HR], 1.65). Dual therapy was associated with a higher risk for death in both men (HR, 2.08) and women (HR, 1.53). Risk for death was also higher in patients with coronary artery disease (HR, 1.83) and without coronary artery disease (HR, 1.52). All results were statistically significant.
Balancing Risks and Benefits
The popularity of TAVR, which was introduced in 2002, has grown to the point that, in 2019, it surpassed the use of surgical aortic valve replacement. But the procedure is associated with an increased risk for both thrombosis and bleeding. Antiplatelet therapy with aspirin and clopidogrel helps prevent thrombosis but can increase the risk of bleeding. This has led to a debate about the best balance for antiplatelet therapy after TAVR with either single therapy — usually with aspirin — or dual therapy with both aspirin and clopidogrel.
A series of studies have addressed this problem. Dual therapy did not show any benefits over single therapy in terms of major adverse cardiac and cerebrovascular events in a 2011 small randomized study. A 2014 small randomized study also showed no benefit for morbidity or mortality from dual therapy. A larger 2017 randomized trial showed that single therapy reduced the risk for major or life-threatening events but did not increase the risk for myocardial infarction or stroke.
Bleeding and bleeding plus thromboembolic events were significantly lower with aspirin than with aspirin plus clopidogrel after a year’s follow-up in the 2020 POPular TAVI trial. Findings from three of these trials were pooled in a 2018 meta-analysis, which showed that dual therapy increased the risk for major adverse events after TAVR and did not prevent ischemic events any more than single therapy.
Based on this evidence, many centers changed their practice. And current European guidelines recommend a single antiplatelet drug for patients undergoing TAVR who do not have additional indications for oral anticoagulation therapy.
By the Numbers
Randomized trials are generally considered the best evidence for medical questions such as this one. “But randomized trials often do not reflect real-world reality. We have to look at what really happens,” Pelliccia said.
Retrospective data from registries can also provide large numbers of patients; in this case, TRITAVI provided data on thousands of patients rather than the hundreds examined in combined randomized trials.
“The results, for the first time, provide clinicians more information on how to treat their patients who are at high risk for bleeding and provide evidence that single antiplatelet therapy should be considered the standard of care in all patients undergoing TAVR,” Pelliccia said.
A version of this article first appeared on Medscape.com.
FROM SCAI 2025
Advances in Blood Cancer Care for Veterans
Advances in Blood Cancer Care for Veterans
Click to view more from Cancer Data Trends 2025.
- Li W, ed. The 5th Edition of the World Health Organization Classification of
Hematolymphoid Tumors. In: Leukemia [Internet]. Brisbane (AU): Exon Publications;
October 16, 2022. https://www.ncbi.nlm.nih.gov/books/NBK586208/ - Graf SA, Samples LS, Keating TM, Garcia JM. Clinical research in older adults with
hematologic malignancies: Opportunities for alignment in the Veterans Affairs. Semin
Oncol. 2020;47(1):94-101. doi:10.1053/j.seminoncol.2020.02.010. - Tiu A, McKinnell Z, Liu S, et al. Risk of myeloproliferative neoplasms among
U.S. Veterans from Korean, Vietnam, and Persian Gulf War eras. Am J Hematol.
2024;99(10):1969-1978. doi:10.1002/ajh.27438 - Ma H, Wan JY, Cortessis VK, Gupta P, Cozen W. Survival in Agent Orange
exposed and unexposed Vietnam-era veterans who were diagnosed with
lymphoid malignancies. Blood Adv. 2024;8(4):1037-1041. doi:10.1182/
bloodadvances.2023011999 - Friedman DR, Rodgers TD, Kovalick C, Yellapragada S, Szumita L, Weiss ES. Veterans
with blood cancers: Clinical trial navigation and the challenge of rurality. J Rural
Health. 2024;40(1):114-120. doi:10.1111/jrh.12773 - Parikh DA, Rodgers TD, Passero VA, et al. Teleoncology in the Veterans Health
Administration: Models of Care and the Veteran Experience. Am Soc Clin Oncol Educ
Book. 2024;44(3):e100042. doi:10.1200/EDBK_100042 - Pulumati A, Pulumati A, Dwarakanath BS, Verma A, Papineni RVL. Technological
advancements in cancer diagnostics: Improvements and limitations. Cancer Rep
(Hoboken). 2023;6(2):e1764. doi:10.1002/cnr2.1764
Click to view more from Cancer Data Trends 2025.
Click to view more from Cancer Data Trends 2025.
- Li W, ed. The 5th Edition of the World Health Organization Classification of
Hematolymphoid Tumors. In: Leukemia [Internet]. Brisbane (AU): Exon Publications;
October 16, 2022. https://www.ncbi.nlm.nih.gov/books/NBK586208/ - Graf SA, Samples LS, Keating TM, Garcia JM. Clinical research in older adults with
hematologic malignancies: Opportunities for alignment in the Veterans Affairs. Semin
Oncol. 2020;47(1):94-101. doi:10.1053/j.seminoncol.2020.02.010. - Tiu A, McKinnell Z, Liu S, et al. Risk of myeloproliferative neoplasms among
U.S. Veterans from Korean, Vietnam, and Persian Gulf War eras. Am J Hematol.
2024;99(10):1969-1978. doi:10.1002/ajh.27438 - Ma H, Wan JY, Cortessis VK, Gupta P, Cozen W. Survival in Agent Orange
exposed and unexposed Vietnam-era veterans who were diagnosed with
lymphoid malignancies. Blood Adv. 2024;8(4):1037-1041. doi:10.1182/
bloodadvances.2023011999 - Friedman DR, Rodgers TD, Kovalick C, Yellapragada S, Szumita L, Weiss ES. Veterans
with blood cancers: Clinical trial navigation and the challenge of rurality. J Rural
Health. 2024;40(1):114-120. doi:10.1111/jrh.12773 - Parikh DA, Rodgers TD, Passero VA, et al. Teleoncology in the Veterans Health
Administration: Models of Care and the Veteran Experience. Am Soc Clin Oncol Educ
Book. 2024;44(3):e100042. doi:10.1200/EDBK_100042 - Pulumati A, Pulumati A, Dwarakanath BS, Verma A, Papineni RVL. Technological
advancements in cancer diagnostics: Improvements and limitations. Cancer Rep
(Hoboken). 2023;6(2):e1764. doi:10.1002/cnr2.1764
- Li W, ed. The 5th Edition of the World Health Organization Classification of
Hematolymphoid Tumors. In: Leukemia [Internet]. Brisbane (AU): Exon Publications;
October 16, 2022. https://www.ncbi.nlm.nih.gov/books/NBK586208/ - Graf SA, Samples LS, Keating TM, Garcia JM. Clinical research in older adults with
hematologic malignancies: Opportunities for alignment in the Veterans Affairs. Semin
Oncol. 2020;47(1):94-101. doi:10.1053/j.seminoncol.2020.02.010. - Tiu A, McKinnell Z, Liu S, et al. Risk of myeloproliferative neoplasms among
U.S. Veterans from Korean, Vietnam, and Persian Gulf War eras. Am J Hematol.
2024;99(10):1969-1978. doi:10.1002/ajh.27438 - Ma H, Wan JY, Cortessis VK, Gupta P, Cozen W. Survival in Agent Orange
exposed and unexposed Vietnam-era veterans who were diagnosed with
lymphoid malignancies. Blood Adv. 2024;8(4):1037-1041. doi:10.1182/
bloodadvances.2023011999 - Friedman DR, Rodgers TD, Kovalick C, Yellapragada S, Szumita L, Weiss ES. Veterans
with blood cancers: Clinical trial navigation and the challenge of rurality. J Rural
Health. 2024;40(1):114-120. doi:10.1111/jrh.12773 - Parikh DA, Rodgers TD, Passero VA, et al. Teleoncology in the Veterans Health
Administration: Models of Care and the Veteran Experience. Am Soc Clin Oncol Educ
Book. 2024;44(3):e100042. doi:10.1200/EDBK_100042 - Pulumati A, Pulumati A, Dwarakanath BS, Verma A, Papineni RVL. Technological
advancements in cancer diagnostics: Improvements and limitations. Cancer Rep
(Hoboken). 2023;6(2):e1764. doi:10.1002/cnr2.1764
Advances in Blood Cancer Care for Veterans
Advances in Blood Cancer Care for Veterans
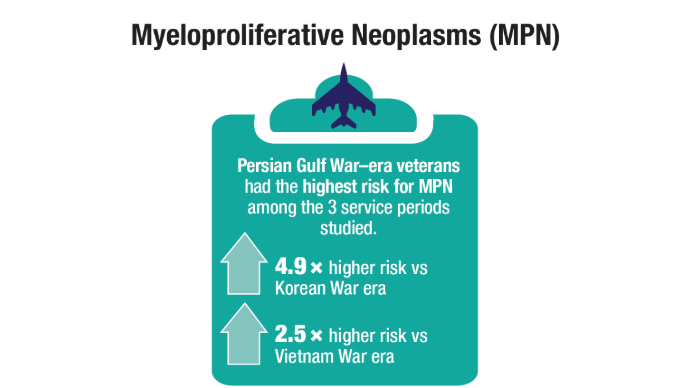
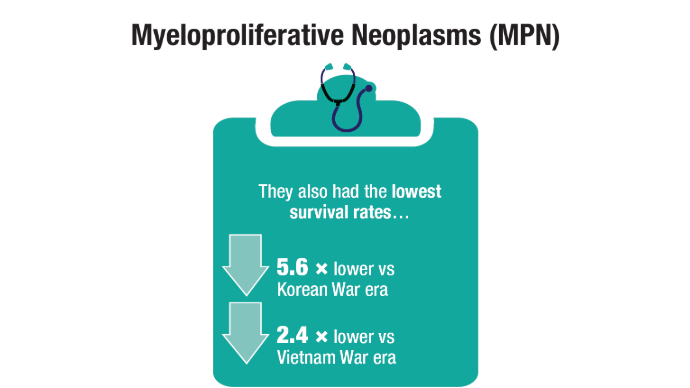
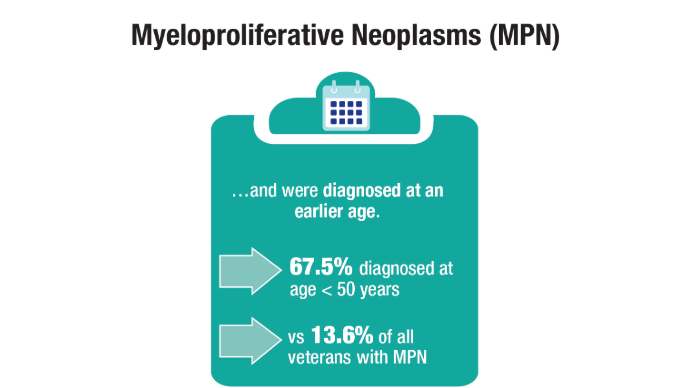
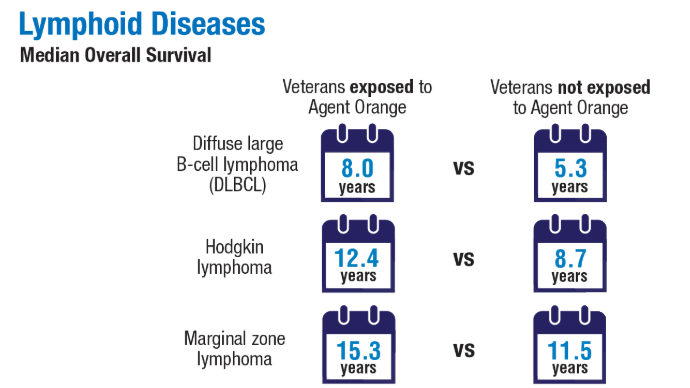
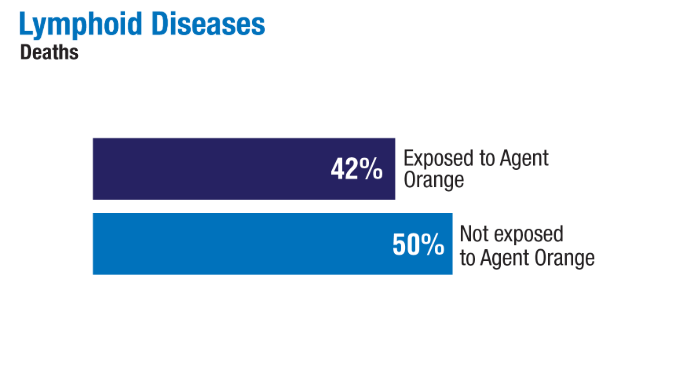
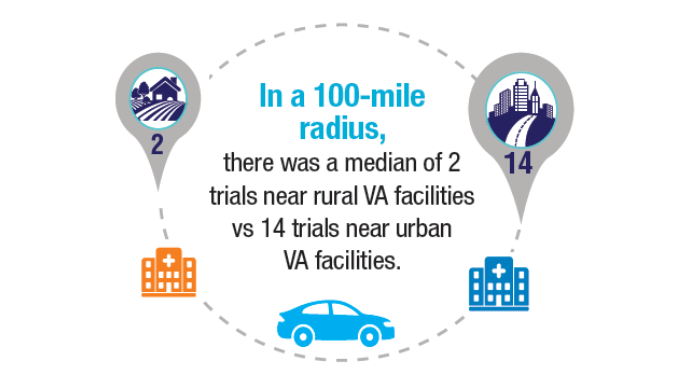
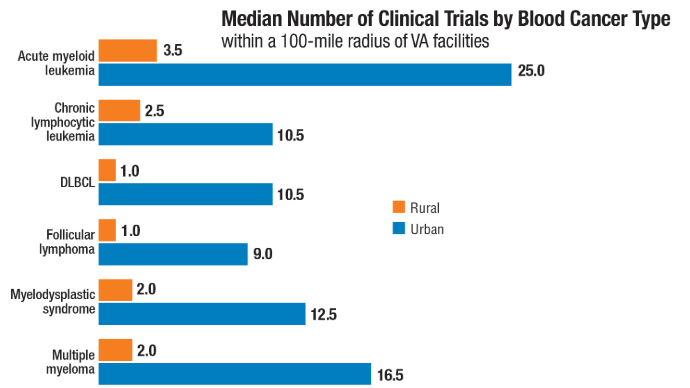
What Hematologists Should Know About Cutaneous Porphyria and Hemochromatosis
One patient, a 39-year-old woman, went to a dermatologist seeking care for fluid-filled blisters over the backs of her hands and arms. Another patient, a 56-year-old man, sought care from his general practitioner owing to fatigue.
Their presentations were quite different, but the two patients shared one thing in common: iron overload. Both ended up in the care of hematologists who diagnosed their conditions as porphyria cutanea tarda (PCT) and hemochromatosis, respectively.
A pair of hematologists discussed the treatment of these disorders at the American Society of Hematology (ASH) 2024 Annual Meeting and in reports in Hematology: American Society of Hematology Education Program. Here’s a look at the guidance they provided.
Porphyria Cutanea Tarda: Skin Trouble
Testing revealed that the female patient had a highly elevated porphyrin levels: Her urine uroporphyrin was 3959 nmol/L (normal, < 30 nmol/L) and plasma uroporphyrin was 2.0 µg/dL (normal, < 1.0 µg/dL). Her serum ferritin level was also high, at 420 ng/mL (normal, < 200 ng/mL).
Rebecca Karp Leaf, MD, of Massachusetts General Hospital and Harvard Medical School, diagnosed her with PCT, a disorder of heme biosynthesis that often presents with skin manifestations.
As co-founder and co-director of the Boston hospital’s Porphyria Center, Karp Leaf is a leading expert in PCT, a rare disease that affects 5-10 people per 100,000. In addition to speaking at the ASH meeting in December, she described PCT in a December 2024 article in Hematology: American Society of Hematology Education Program.
PCT is caused by inhibition of an enzyme in heme biosynthesis and leads to accumulation of porphyrins in the liver and plasma, Karp Leaf said. Through a complex process, excess of iron leads to inhibition of the enzyme, which leads to a buildup of toxic porphyrins, she said. The condition causes painless, blistering lesions on sun-exposed skin, scarring, skin fragility, dark urine, and liver disease.
PCT most commonly occurs in middle age after the age of 40 and affects men more than women. “It’s the only porphyria that can occur absent a genetic variant,” she said, and 75% of cases have no genetic component.
Options for Treatment Include Antivirals and Phlebotomy
Risk factors for PCT include alcohol use, smoking, exogenous estrogen, hepatitis, and HIV mutations.
In regard to treatment, “modification of risk factors can be variably helpful: alcohol and smoking cessation, stopping exogenous estrogen, sun-protective clothing, and steroid-containing creams for lesions,” Karp Leaf said. “Most patients typically require further therapy to reduce liver porphyrins.”
Urine and plasma tests can help with diagnosis, she said. In patients with hepatitis C (HCV), “direct-acting antivirals can actually lead to resolution of PCT without any other therapy. We suspect that with effective antiviral treatment for HCV, the incidence of PCT will really go down.”
Therapeutic phlebotomy — blood removal — is another option. “It’s one of my favorite therapies because you don’t have to give somebody a drug. You can just take out iron,” Karp Leaf said. “Typically, we’ll start with venesection of 450 ccs of whole blood every 2 weeks, We target a ferritin level of 20 [ng/mL] but permit it up to 50 [ng/mL], or a little bit higher.”
The treatment leads to resolution of blisters in about 2-3 months, she said, and normalization of porphyrins by 13 months. Patients typically require about 6-8 treatments, she said.
Another option is iron chelation, iron removal via medicine, “but it’s expensive, has side effects, and is really not recommended if other treatments are available,” she said.
Hydroxychloroquine Can Be Helpful Too
Low-dose hydroxychloroquine can also be effective at 100 mg twice a week, “much lower than what we use in autoimmune disease,” Karp Leaf said. “We suspect that it’s taken up by the hepatic lysosomes and causes release of porphyrins. It causes clinical remission in about 6 months.”
However, higher doses can lead to liver injury, and the drug’s use is limited in end-stage kidney disease since porphyrins are excreted in the urine. These patients are especially difficult to treat, she said.
In the case of the 39-year-old patient, Karp Leaf recommended that the woman reduce her alcohol intake and begin using a copper intrauterine device for contraception instead of a combined oral contraceptive pill, which allowed her to undergo phlebotomy.
“She needed about eight sessions of therapeutic phlebotomy to achieve a ferritin of 30 [ng/mL], and her lesions resolved in 6 months,” Karp Leaf said. “Her plasma porphyrins resolved by 12 months. Her liver biochemistries were a bit elevated, and they subsequently normalized.”
Karp Leaf said she sees the patient about once a year.
Hemochromatosis: It’s (Probably) a Family Affair
In an adjoining presentation at ASH and in a December 2024 article in Hematology: American Society of Hematology Education Program, hematologist Domenico Girelli, MD, PhD, with the University of Verona, Italy, told colleagues about the 56-year-old male patient with fatigue. He also had a mildly enlarged liver, hyperferritinemia (890 µg/L vs normal value < 300 µg/L) and a mildly increased alanine aminotransferase level (46 U/L vs normal value < 40 U/L).
The patient was diagnosed with hemochromatosis, a genetic disorder caused by mutations that leads to increased transferrin saturation, Girelli said.
“By definition, hemochromatosis is characterized by the absence of signs of a primary red blood cell disorder — different from other disorders like transfusion iron overload or iron-loading anemias,” he said.
It’s also important to consider other possible causes of hyperferritinemia, because most cases of the symptom aren’t related to iron overload, he said. “A careful clinical history and a few laboratory parameters including transferrin saturation are generally sufficient for the differential diagnosis.”
As Girelli noted, “hemochromatosis can have a wide clinical spectrum ranging from mild to severe forms, which are strongly influenced by the co-presence of risk factors like alcohol [use], blood transfusion, and genetic factors captured by polygenic risk score.”
In Many Cases, Hemochromatosis Can Be Successfully Treated
According to Girelli, it’s important to understand the disease stage, because this information can predict the probability of advanced liver fibrosis, which can be a sign of a worse prognosis.
“The strongest clinical predictors of advanced liver fibrosis are ferritin higher than 1000 [µg/L] and the presence of arthropathy [joint disease],” he said. “If both are absent and the patient is asymptomatic, there is no need for further investigation. If both are present, further investigation — including cardiac MRI and full endocrine profile — are indicated. Liver biopsy may be indicated only in uncertain cases.”
Fortunately, “most patients are diagnosed in preclinical or early stage, and their prognosis is excellent, with a normal life expectancy,” he said
Phlebotomy remains the standard of care for hemochromatosis in uncomplicated cases. “It is safe, cheap, well-tolerated, and significantly reduces mortality and morbidity, especially when it is started before the development of cirrhosis,” he said.
Family Members Should Be Tested for Genetic Traits
It’s important to advise patients prior to phlebotomy to avoid undercooked seafood and wound contact with sea water because of the risk for sepsis due to the pathogen Vibrio vulnificus, Girelli said.
And it’s a good idea to test family members to see if they share a genetic risk for hemochromatosis, he said. The 56-year-old patient’s brother turned out to also have genetic risk, and his iron levels were very high. He had recently been diagnosed with seronegative arthritis that could be classified as secondary to hemochromatosis.
For management, Girelli said, patients should minimize or avoid alcohol consumption, eat a healthy diet, and avoid vitamin C and iron supplements even in multivitamin compounds. Patients should be encouraged to exercise and maintain an ideal weight.
The 56-year-old patient fared well, reaching a ferritin target of 50 mg/mL after multiple phlebotomy procedures that removed nearly 5 g of iron.
The patient tolerated the treatment and his fatigue resolved, Girelli said. “The maintenance treatment consisted of 3 phlebotomies per year. The patient remained asymptomatic and was eventually enrolled as a regular blood donor.”
Karp Leaf disclosed relationships with Alnylam, Recordati, and Disc Medicine. She is a member of the Porphyrias Consortium, part of the Rare Diseases Clinical Research Network, funded by the National Institutes of Health and led by the National Center for Advancing Translational Sciences (NCATS). The consortium is funded by NCATS and the National Institute of Diabetes and Digestive and Kidney Diseases. Girelli had no disclosures.
A version of this article first appeared on Medscape.com.
One patient, a 39-year-old woman, went to a dermatologist seeking care for fluid-filled blisters over the backs of her hands and arms. Another patient, a 56-year-old man, sought care from his general practitioner owing to fatigue.
Their presentations were quite different, but the two patients shared one thing in common: iron overload. Both ended up in the care of hematologists who diagnosed their conditions as porphyria cutanea tarda (PCT) and hemochromatosis, respectively.
A pair of hematologists discussed the treatment of these disorders at the American Society of Hematology (ASH) 2024 Annual Meeting and in reports in Hematology: American Society of Hematology Education Program. Here’s a look at the guidance they provided.
Porphyria Cutanea Tarda: Skin Trouble
Testing revealed that the female patient had a highly elevated porphyrin levels: Her urine uroporphyrin was 3959 nmol/L (normal, < 30 nmol/L) and plasma uroporphyrin was 2.0 µg/dL (normal, < 1.0 µg/dL). Her serum ferritin level was also high, at 420 ng/mL (normal, < 200 ng/mL).
Rebecca Karp Leaf, MD, of Massachusetts General Hospital and Harvard Medical School, diagnosed her with PCT, a disorder of heme biosynthesis that often presents with skin manifestations.
As co-founder and co-director of the Boston hospital’s Porphyria Center, Karp Leaf is a leading expert in PCT, a rare disease that affects 5-10 people per 100,000. In addition to speaking at the ASH meeting in December, she described PCT in a December 2024 article in Hematology: American Society of Hematology Education Program.
PCT is caused by inhibition of an enzyme in heme biosynthesis and leads to accumulation of porphyrins in the liver and plasma, Karp Leaf said. Through a complex process, excess of iron leads to inhibition of the enzyme, which leads to a buildup of toxic porphyrins, she said. The condition causes painless, blistering lesions on sun-exposed skin, scarring, skin fragility, dark urine, and liver disease.
PCT most commonly occurs in middle age after the age of 40 and affects men more than women. “It’s the only porphyria that can occur absent a genetic variant,” she said, and 75% of cases have no genetic component.
Options for Treatment Include Antivirals and Phlebotomy
Risk factors for PCT include alcohol use, smoking, exogenous estrogen, hepatitis, and HIV mutations.
In regard to treatment, “modification of risk factors can be variably helpful: alcohol and smoking cessation, stopping exogenous estrogen, sun-protective clothing, and steroid-containing creams for lesions,” Karp Leaf said. “Most patients typically require further therapy to reduce liver porphyrins.”
Urine and plasma tests can help with diagnosis, she said. In patients with hepatitis C (HCV), “direct-acting antivirals can actually lead to resolution of PCT without any other therapy. We suspect that with effective antiviral treatment for HCV, the incidence of PCT will really go down.”
Therapeutic phlebotomy — blood removal — is another option. “It’s one of my favorite therapies because you don’t have to give somebody a drug. You can just take out iron,” Karp Leaf said. “Typically, we’ll start with venesection of 450 ccs of whole blood every 2 weeks, We target a ferritin level of 20 [ng/mL] but permit it up to 50 [ng/mL], or a little bit higher.”
The treatment leads to resolution of blisters in about 2-3 months, she said, and normalization of porphyrins by 13 months. Patients typically require about 6-8 treatments, she said.
Another option is iron chelation, iron removal via medicine, “but it’s expensive, has side effects, and is really not recommended if other treatments are available,” she said.
Hydroxychloroquine Can Be Helpful Too
Low-dose hydroxychloroquine can also be effective at 100 mg twice a week, “much lower than what we use in autoimmune disease,” Karp Leaf said. “We suspect that it’s taken up by the hepatic lysosomes and causes release of porphyrins. It causes clinical remission in about 6 months.”
However, higher doses can lead to liver injury, and the drug’s use is limited in end-stage kidney disease since porphyrins are excreted in the urine. These patients are especially difficult to treat, she said.
In the case of the 39-year-old patient, Karp Leaf recommended that the woman reduce her alcohol intake and begin using a copper intrauterine device for contraception instead of a combined oral contraceptive pill, which allowed her to undergo phlebotomy.
“She needed about eight sessions of therapeutic phlebotomy to achieve a ferritin of 30 [ng/mL], and her lesions resolved in 6 months,” Karp Leaf said. “Her plasma porphyrins resolved by 12 months. Her liver biochemistries were a bit elevated, and they subsequently normalized.”
Karp Leaf said she sees the patient about once a year.
Hemochromatosis: It’s (Probably) a Family Affair
In an adjoining presentation at ASH and in a December 2024 article in Hematology: American Society of Hematology Education Program, hematologist Domenico Girelli, MD, PhD, with the University of Verona, Italy, told colleagues about the 56-year-old male patient with fatigue. He also had a mildly enlarged liver, hyperferritinemia (890 µg/L vs normal value < 300 µg/L) and a mildly increased alanine aminotransferase level (46 U/L vs normal value < 40 U/L).
The patient was diagnosed with hemochromatosis, a genetic disorder caused by mutations that leads to increased transferrin saturation, Girelli said.
“By definition, hemochromatosis is characterized by the absence of signs of a primary red blood cell disorder — different from other disorders like transfusion iron overload or iron-loading anemias,” he said.
It’s also important to consider other possible causes of hyperferritinemia, because most cases of the symptom aren’t related to iron overload, he said. “A careful clinical history and a few laboratory parameters including transferrin saturation are generally sufficient for the differential diagnosis.”
As Girelli noted, “hemochromatosis can have a wide clinical spectrum ranging from mild to severe forms, which are strongly influenced by the co-presence of risk factors like alcohol [use], blood transfusion, and genetic factors captured by polygenic risk score.”
In Many Cases, Hemochromatosis Can Be Successfully Treated
According to Girelli, it’s important to understand the disease stage, because this information can predict the probability of advanced liver fibrosis, which can be a sign of a worse prognosis.
“The strongest clinical predictors of advanced liver fibrosis are ferritin higher than 1000 [µg/L] and the presence of arthropathy [joint disease],” he said. “If both are absent and the patient is asymptomatic, there is no need for further investigation. If both are present, further investigation — including cardiac MRI and full endocrine profile — are indicated. Liver biopsy may be indicated only in uncertain cases.”
Fortunately, “most patients are diagnosed in preclinical or early stage, and their prognosis is excellent, with a normal life expectancy,” he said
Phlebotomy remains the standard of care for hemochromatosis in uncomplicated cases. “It is safe, cheap, well-tolerated, and significantly reduces mortality and morbidity, especially when it is started before the development of cirrhosis,” he said.
Family Members Should Be Tested for Genetic Traits
It’s important to advise patients prior to phlebotomy to avoid undercooked seafood and wound contact with sea water because of the risk for sepsis due to the pathogen Vibrio vulnificus, Girelli said.
And it’s a good idea to test family members to see if they share a genetic risk for hemochromatosis, he said. The 56-year-old patient’s brother turned out to also have genetic risk, and his iron levels were very high. He had recently been diagnosed with seronegative arthritis that could be classified as secondary to hemochromatosis.
For management, Girelli said, patients should minimize or avoid alcohol consumption, eat a healthy diet, and avoid vitamin C and iron supplements even in multivitamin compounds. Patients should be encouraged to exercise and maintain an ideal weight.
The 56-year-old patient fared well, reaching a ferritin target of 50 mg/mL after multiple phlebotomy procedures that removed nearly 5 g of iron.
The patient tolerated the treatment and his fatigue resolved, Girelli said. “The maintenance treatment consisted of 3 phlebotomies per year. The patient remained asymptomatic and was eventually enrolled as a regular blood donor.”
Karp Leaf disclosed relationships with Alnylam, Recordati, and Disc Medicine. She is a member of the Porphyrias Consortium, part of the Rare Diseases Clinical Research Network, funded by the National Institutes of Health and led by the National Center for Advancing Translational Sciences (NCATS). The consortium is funded by NCATS and the National Institute of Diabetes and Digestive and Kidney Diseases. Girelli had no disclosures.
A version of this article first appeared on Medscape.com.
One patient, a 39-year-old woman, went to a dermatologist seeking care for fluid-filled blisters over the backs of her hands and arms. Another patient, a 56-year-old man, sought care from his general practitioner owing to fatigue.
Their presentations were quite different, but the two patients shared one thing in common: iron overload. Both ended up in the care of hematologists who diagnosed their conditions as porphyria cutanea tarda (PCT) and hemochromatosis, respectively.
A pair of hematologists discussed the treatment of these disorders at the American Society of Hematology (ASH) 2024 Annual Meeting and in reports in Hematology: American Society of Hematology Education Program. Here’s a look at the guidance they provided.
Porphyria Cutanea Tarda: Skin Trouble
Testing revealed that the female patient had a highly elevated porphyrin levels: Her urine uroporphyrin was 3959 nmol/L (normal, < 30 nmol/L) and plasma uroporphyrin was 2.0 µg/dL (normal, < 1.0 µg/dL). Her serum ferritin level was also high, at 420 ng/mL (normal, < 200 ng/mL).
Rebecca Karp Leaf, MD, of Massachusetts General Hospital and Harvard Medical School, diagnosed her with PCT, a disorder of heme biosynthesis that often presents with skin manifestations.
As co-founder and co-director of the Boston hospital’s Porphyria Center, Karp Leaf is a leading expert in PCT, a rare disease that affects 5-10 people per 100,000. In addition to speaking at the ASH meeting in December, she described PCT in a December 2024 article in Hematology: American Society of Hematology Education Program.
PCT is caused by inhibition of an enzyme in heme biosynthesis and leads to accumulation of porphyrins in the liver and plasma, Karp Leaf said. Through a complex process, excess of iron leads to inhibition of the enzyme, which leads to a buildup of toxic porphyrins, she said. The condition causes painless, blistering lesions on sun-exposed skin, scarring, skin fragility, dark urine, and liver disease.
PCT most commonly occurs in middle age after the age of 40 and affects men more than women. “It’s the only porphyria that can occur absent a genetic variant,” she said, and 75% of cases have no genetic component.
Options for Treatment Include Antivirals and Phlebotomy
Risk factors for PCT include alcohol use, smoking, exogenous estrogen, hepatitis, and HIV mutations.
In regard to treatment, “modification of risk factors can be variably helpful: alcohol and smoking cessation, stopping exogenous estrogen, sun-protective clothing, and steroid-containing creams for lesions,” Karp Leaf said. “Most patients typically require further therapy to reduce liver porphyrins.”
Urine and plasma tests can help with diagnosis, she said. In patients with hepatitis C (HCV), “direct-acting antivirals can actually lead to resolution of PCT without any other therapy. We suspect that with effective antiviral treatment for HCV, the incidence of PCT will really go down.”
Therapeutic phlebotomy — blood removal — is another option. “It’s one of my favorite therapies because you don’t have to give somebody a drug. You can just take out iron,” Karp Leaf said. “Typically, we’ll start with venesection of 450 ccs of whole blood every 2 weeks, We target a ferritin level of 20 [ng/mL] but permit it up to 50 [ng/mL], or a little bit higher.”
The treatment leads to resolution of blisters in about 2-3 months, she said, and normalization of porphyrins by 13 months. Patients typically require about 6-8 treatments, she said.
Another option is iron chelation, iron removal via medicine, “but it’s expensive, has side effects, and is really not recommended if other treatments are available,” she said.
Hydroxychloroquine Can Be Helpful Too
Low-dose hydroxychloroquine can also be effective at 100 mg twice a week, “much lower than what we use in autoimmune disease,” Karp Leaf said. “We suspect that it’s taken up by the hepatic lysosomes and causes release of porphyrins. It causes clinical remission in about 6 months.”
However, higher doses can lead to liver injury, and the drug’s use is limited in end-stage kidney disease since porphyrins are excreted in the urine. These patients are especially difficult to treat, she said.
In the case of the 39-year-old patient, Karp Leaf recommended that the woman reduce her alcohol intake and begin using a copper intrauterine device for contraception instead of a combined oral contraceptive pill, which allowed her to undergo phlebotomy.
“She needed about eight sessions of therapeutic phlebotomy to achieve a ferritin of 30 [ng/mL], and her lesions resolved in 6 months,” Karp Leaf said. “Her plasma porphyrins resolved by 12 months. Her liver biochemistries were a bit elevated, and they subsequently normalized.”
Karp Leaf said she sees the patient about once a year.
Hemochromatosis: It’s (Probably) a Family Affair
In an adjoining presentation at ASH and in a December 2024 article in Hematology: American Society of Hematology Education Program, hematologist Domenico Girelli, MD, PhD, with the University of Verona, Italy, told colleagues about the 56-year-old male patient with fatigue. He also had a mildly enlarged liver, hyperferritinemia (890 µg/L vs normal value < 300 µg/L) and a mildly increased alanine aminotransferase level (46 U/L vs normal value < 40 U/L).
The patient was diagnosed with hemochromatosis, a genetic disorder caused by mutations that leads to increased transferrin saturation, Girelli said.
“By definition, hemochromatosis is characterized by the absence of signs of a primary red blood cell disorder — different from other disorders like transfusion iron overload or iron-loading anemias,” he said.
It’s also important to consider other possible causes of hyperferritinemia, because most cases of the symptom aren’t related to iron overload, he said. “A careful clinical history and a few laboratory parameters including transferrin saturation are generally sufficient for the differential diagnosis.”
As Girelli noted, “hemochromatosis can have a wide clinical spectrum ranging from mild to severe forms, which are strongly influenced by the co-presence of risk factors like alcohol [use], blood transfusion, and genetic factors captured by polygenic risk score.”
In Many Cases, Hemochromatosis Can Be Successfully Treated
According to Girelli, it’s important to understand the disease stage, because this information can predict the probability of advanced liver fibrosis, which can be a sign of a worse prognosis.
“The strongest clinical predictors of advanced liver fibrosis are ferritin higher than 1000 [µg/L] and the presence of arthropathy [joint disease],” he said. “If both are absent and the patient is asymptomatic, there is no need for further investigation. If both are present, further investigation — including cardiac MRI and full endocrine profile — are indicated. Liver biopsy may be indicated only in uncertain cases.”
Fortunately, “most patients are diagnosed in preclinical or early stage, and their prognosis is excellent, with a normal life expectancy,” he said
Phlebotomy remains the standard of care for hemochromatosis in uncomplicated cases. “It is safe, cheap, well-tolerated, and significantly reduces mortality and morbidity, especially when it is started before the development of cirrhosis,” he said.
Family Members Should Be Tested for Genetic Traits
It’s important to advise patients prior to phlebotomy to avoid undercooked seafood and wound contact with sea water because of the risk for sepsis due to the pathogen Vibrio vulnificus, Girelli said.
And it’s a good idea to test family members to see if they share a genetic risk for hemochromatosis, he said. The 56-year-old patient’s brother turned out to also have genetic risk, and his iron levels were very high. He had recently been diagnosed with seronegative arthritis that could be classified as secondary to hemochromatosis.
For management, Girelli said, patients should minimize or avoid alcohol consumption, eat a healthy diet, and avoid vitamin C and iron supplements even in multivitamin compounds. Patients should be encouraged to exercise and maintain an ideal weight.
The 56-year-old patient fared well, reaching a ferritin target of 50 mg/mL after multiple phlebotomy procedures that removed nearly 5 g of iron.
The patient tolerated the treatment and his fatigue resolved, Girelli said. “The maintenance treatment consisted of 3 phlebotomies per year. The patient remained asymptomatic and was eventually enrolled as a regular blood donor.”
Karp Leaf disclosed relationships with Alnylam, Recordati, and Disc Medicine. She is a member of the Porphyrias Consortium, part of the Rare Diseases Clinical Research Network, funded by the National Institutes of Health and led by the National Center for Advancing Translational Sciences (NCATS). The consortium is funded by NCATS and the National Institute of Diabetes and Digestive and Kidney Diseases. Girelli had no disclosures.
A version of this article first appeared on Medscape.com.
Heavy Menstrual Bleeding: How Hematologists Can Help
Heavy menstrual bleeding is more than an inconvenience in adolescents: It often leads to significant medical complications, in addition to disruptions in quality of life. While measuring the true level of bleeding can be a challenge, hematologists say treatments are helpful and can be as simple — and surprising — as doses of aspirin.
About 90% of adolescents with heavy menstrual bleeding will have low ferritin, and 70% will develop anemia, said benign hematologist Juliana Perez Botero, MD, of the Mayo Clinic in Rochester, Minnesota, in a presentation at the American Society of Hematology (ASH) 2024 Annual Meeting. “This is an issue of big magnitude that has public health implications, but it’s also an issue of gender equality and social justice.”
Measuring Menstruation: What Counts as Heavy Bleeding?
According to hematologist Allison Wheeler, MD, of the University of Washington in Seattle, normal menstrual bleeding is defined as lasting for about 5 days with 30-50 mL of blood loss.
“Historically, heavy menstrual bleeding was defined as bleeding as > 7 days or > 80 mL of blood loss,” Wheeler said. “It’s pretty hard to measure those mL. So a more modern definition is increased menstrual blood loss that interferes with a female’s physical, social, emotional, or material quality of life.”
Measuring blood loss during menstruation isn’t simple. The alkaline hematin method, which measures blood in feminine hygiene products, is the “gold standard, but that’s all I’m going to say about that,” Wheeler said.
An alternative is the Pictorial Blood Loss Assessment Chart, a visual tool that patients can use to estimate blood loss, she said, although there have been questions about its accuracy. In addition, it only covers pads and tampons even though other products are now available.
Another option is the Adolescent Menstrual Bleeding Questionnaire. “It captures both how much patients are bleeding and a lot of quality-of-life aspects,” she said.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), Surprisingly, Can Be Effective Treatments
It seems counterintuitive that NSAIDs can be helpful in patients with heavy bleeding. “We don’t think about them because Cox inhibition ends up leading to decreases in thromboxane A2, which is going to increase bleeding,” Wheeler said. However, she said, the drugs also decrease prostaglandin within the endometrium, which can improve menstrual bleeding.
“In a meta-analysis, when NSAIDs were compared to placebo, there was decreased menstrual bleeding,” she said. “It was pretty similar to estrogen-progesterone formulations together. And when compared to antifibrinolytics, there was a little more menstrual bleeding with the NSAID use.”
Wheeler cautioned that “it’s important to optimize NSAID dosage. You really can’t use lower doses, and you can’t use sporadic doses.”
Other Options: Tranexamic Acid, Hormone Management
Tranexamic acid is the most common antifibrinolytic treatment for heavy bleeding, Wheeler said. “This is a lysine analog that’s going to inhibit the conversion from plasminogen to plasmin,” she said. “This is going to strengthen and stabilize blood clots that are already formed.”
Multiple clinical trials have studied the treatment in heavy menstrual bleeding, she said. “There’s no increased risk of venous or arterial thrombosis among participants in these clinical trials, but patients with a history of thrombosis were excluded from the majority of them. So we do need to keep that in mind.”
As for adverse effects, they’re mild and sporadic and include headaches and stomach upset, she said.
Another treatment option is estrogen and progesterone therapy using pill, patch, or vaginal ring, Wheeler said. The treatment leads to a “stable and thin very endometrium,” and typically takes 3-6 months to fully kick in. Studies have suggested the therapy can lead to 35%-80% reduction in menstrual blood loss, she said.
Keep in mind, Wheeler noted, “that there are many contraindications associated with estrogen use. Please take note of this, especially in consideration of discussions with patients shifting over to progesterone-only hormonal therapy” — another option to treat excess bleeding.
In most patients, she added, progesterone-only therapy “is going to result in irregular bleeding when you first start taking it. That irregular bleeding can last from up to 3-6 months. It’s something that’s really important to discuss with patients.”
She also noted that this therapy can be given to patients in forms that do not prevent pregnancy.
Botero had no disclosures. Wheeler reported relationships with Novo Nordisk, Bayer, BioMarin, Bioverativ, CSL Behring, Genentech, HEMA, Octapharma, Pfizer, Sanofi-Aventis, Shire North America, Spark, and Takeda.
A version of this article first appeared on Medscape.com.
Heavy menstrual bleeding is more than an inconvenience in adolescents: It often leads to significant medical complications, in addition to disruptions in quality of life. While measuring the true level of bleeding can be a challenge, hematologists say treatments are helpful and can be as simple — and surprising — as doses of aspirin.
About 90% of adolescents with heavy menstrual bleeding will have low ferritin, and 70% will develop anemia, said benign hematologist Juliana Perez Botero, MD, of the Mayo Clinic in Rochester, Minnesota, in a presentation at the American Society of Hematology (ASH) 2024 Annual Meeting. “This is an issue of big magnitude that has public health implications, but it’s also an issue of gender equality and social justice.”
Measuring Menstruation: What Counts as Heavy Bleeding?
According to hematologist Allison Wheeler, MD, of the University of Washington in Seattle, normal menstrual bleeding is defined as lasting for about 5 days with 30-50 mL of blood loss.
“Historically, heavy menstrual bleeding was defined as bleeding as > 7 days or > 80 mL of blood loss,” Wheeler said. “It’s pretty hard to measure those mL. So a more modern definition is increased menstrual blood loss that interferes with a female’s physical, social, emotional, or material quality of life.”
Measuring blood loss during menstruation isn’t simple. The alkaline hematin method, which measures blood in feminine hygiene products, is the “gold standard, but that’s all I’m going to say about that,” Wheeler said.
An alternative is the Pictorial Blood Loss Assessment Chart, a visual tool that patients can use to estimate blood loss, she said, although there have been questions about its accuracy. In addition, it only covers pads and tampons even though other products are now available.
Another option is the Adolescent Menstrual Bleeding Questionnaire. “It captures both how much patients are bleeding and a lot of quality-of-life aspects,” she said.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), Surprisingly, Can Be Effective Treatments
It seems counterintuitive that NSAIDs can be helpful in patients with heavy bleeding. “We don’t think about them because Cox inhibition ends up leading to decreases in thromboxane A2, which is going to increase bleeding,” Wheeler said. However, she said, the drugs also decrease prostaglandin within the endometrium, which can improve menstrual bleeding.
“In a meta-analysis, when NSAIDs were compared to placebo, there was decreased menstrual bleeding,” she said. “It was pretty similar to estrogen-progesterone formulations together. And when compared to antifibrinolytics, there was a little more menstrual bleeding with the NSAID use.”
Wheeler cautioned that “it’s important to optimize NSAID dosage. You really can’t use lower doses, and you can’t use sporadic doses.”
Other Options: Tranexamic Acid, Hormone Management
Tranexamic acid is the most common antifibrinolytic treatment for heavy bleeding, Wheeler said. “This is a lysine analog that’s going to inhibit the conversion from plasminogen to plasmin,” she said. “This is going to strengthen and stabilize blood clots that are already formed.”
Multiple clinical trials have studied the treatment in heavy menstrual bleeding, she said. “There’s no increased risk of venous or arterial thrombosis among participants in these clinical trials, but patients with a history of thrombosis were excluded from the majority of them. So we do need to keep that in mind.”
As for adverse effects, they’re mild and sporadic and include headaches and stomach upset, she said.
Another treatment option is estrogen and progesterone therapy using pill, patch, or vaginal ring, Wheeler said. The treatment leads to a “stable and thin very endometrium,” and typically takes 3-6 months to fully kick in. Studies have suggested the therapy can lead to 35%-80% reduction in menstrual blood loss, she said.
Keep in mind, Wheeler noted, “that there are many contraindications associated with estrogen use. Please take note of this, especially in consideration of discussions with patients shifting over to progesterone-only hormonal therapy” — another option to treat excess bleeding.
In most patients, she added, progesterone-only therapy “is going to result in irregular bleeding when you first start taking it. That irregular bleeding can last from up to 3-6 months. It’s something that’s really important to discuss with patients.”
She also noted that this therapy can be given to patients in forms that do not prevent pregnancy.
Botero had no disclosures. Wheeler reported relationships with Novo Nordisk, Bayer, BioMarin, Bioverativ, CSL Behring, Genentech, HEMA, Octapharma, Pfizer, Sanofi-Aventis, Shire North America, Spark, and Takeda.
A version of this article first appeared on Medscape.com.
Heavy menstrual bleeding is more than an inconvenience in adolescents: It often leads to significant medical complications, in addition to disruptions in quality of life. While measuring the true level of bleeding can be a challenge, hematologists say treatments are helpful and can be as simple — and surprising — as doses of aspirin.
About 90% of adolescents with heavy menstrual bleeding will have low ferritin, and 70% will develop anemia, said benign hematologist Juliana Perez Botero, MD, of the Mayo Clinic in Rochester, Minnesota, in a presentation at the American Society of Hematology (ASH) 2024 Annual Meeting. “This is an issue of big magnitude that has public health implications, but it’s also an issue of gender equality and social justice.”
Measuring Menstruation: What Counts as Heavy Bleeding?
According to hematologist Allison Wheeler, MD, of the University of Washington in Seattle, normal menstrual bleeding is defined as lasting for about 5 days with 30-50 mL of blood loss.
“Historically, heavy menstrual bleeding was defined as bleeding as > 7 days or > 80 mL of blood loss,” Wheeler said. “It’s pretty hard to measure those mL. So a more modern definition is increased menstrual blood loss that interferes with a female’s physical, social, emotional, or material quality of life.”
Measuring blood loss during menstruation isn’t simple. The alkaline hematin method, which measures blood in feminine hygiene products, is the “gold standard, but that’s all I’m going to say about that,” Wheeler said.
An alternative is the Pictorial Blood Loss Assessment Chart, a visual tool that patients can use to estimate blood loss, she said, although there have been questions about its accuracy. In addition, it only covers pads and tampons even though other products are now available.
Another option is the Adolescent Menstrual Bleeding Questionnaire. “It captures both how much patients are bleeding and a lot of quality-of-life aspects,” she said.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), Surprisingly, Can Be Effective Treatments
It seems counterintuitive that NSAIDs can be helpful in patients with heavy bleeding. “We don’t think about them because Cox inhibition ends up leading to decreases in thromboxane A2, which is going to increase bleeding,” Wheeler said. However, she said, the drugs also decrease prostaglandin within the endometrium, which can improve menstrual bleeding.
“In a meta-analysis, when NSAIDs were compared to placebo, there was decreased menstrual bleeding,” she said. “It was pretty similar to estrogen-progesterone formulations together. And when compared to antifibrinolytics, there was a little more menstrual bleeding with the NSAID use.”
Wheeler cautioned that “it’s important to optimize NSAID dosage. You really can’t use lower doses, and you can’t use sporadic doses.”
Other Options: Tranexamic Acid, Hormone Management
Tranexamic acid is the most common antifibrinolytic treatment for heavy bleeding, Wheeler said. “This is a lysine analog that’s going to inhibit the conversion from plasminogen to plasmin,” she said. “This is going to strengthen and stabilize blood clots that are already formed.”
Multiple clinical trials have studied the treatment in heavy menstrual bleeding, she said. “There’s no increased risk of venous or arterial thrombosis among participants in these clinical trials, but patients with a history of thrombosis were excluded from the majority of them. So we do need to keep that in mind.”
As for adverse effects, they’re mild and sporadic and include headaches and stomach upset, she said.
Another treatment option is estrogen and progesterone therapy using pill, patch, or vaginal ring, Wheeler said. The treatment leads to a “stable and thin very endometrium,” and typically takes 3-6 months to fully kick in. Studies have suggested the therapy can lead to 35%-80% reduction in menstrual blood loss, she said.
Keep in mind, Wheeler noted, “that there are many contraindications associated with estrogen use. Please take note of this, especially in consideration of discussions with patients shifting over to progesterone-only hormonal therapy” — another option to treat excess bleeding.
In most patients, she added, progesterone-only therapy “is going to result in irregular bleeding when you first start taking it. That irregular bleeding can last from up to 3-6 months. It’s something that’s really important to discuss with patients.”
She also noted that this therapy can be given to patients in forms that do not prevent pregnancy.
Botero had no disclosures. Wheeler reported relationships with Novo Nordisk, Bayer, BioMarin, Bioverativ, CSL Behring, Genentech, HEMA, Octapharma, Pfizer, Sanofi-Aventis, Shire North America, Spark, and Takeda.
A version of this article first appeared on Medscape.com.