User login
Cancer treatment delays are deadly: 5- and 10-year data
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
Scant risk for SARS-CoV-2 from hospital air
Everywhere they look within hospitals, researchers find RNA from SARS-CoV-2 in the air. But viable viruses typically are found only close to patients, according to a review of published studies.
The finding supports recommendations to use surgical masks in most parts of the hospital, reserving respirators (such as N95 or FFP2) for aerosol-generating procedures on patients’ respiratory tracts, said Gabriel Birgand, PhD, an infectious disease researcher at Imperial College London.
“When the virus is spreading a lot in the community, it’s probably more likely for you to be contaminated in your friends’ areas or in your building than in your work area, where you are well equipped and compliant with all the measures,” he said in an interview. “So it’s pretty good news.”
The systematic review by Dr. Birgand and colleagues was published in JAMA Network Open.
Recommended precautions to protect health care workers from SARS-CoV-2 infections remain controversial. Most authorities believe droplets are the primary route of transmission, which would mean surgical masks may be sufficient protection. But some research has suggested transmission by aerosols as well, making N95 respirators seem necessary. There is even disagreement about the definitions of the words “aerosol” and “droplet.”
To better understand where traces of the virus can be found in the air in hospitals, Dr. Birgand and colleagues analyzed all the studies they could find on the subject in English.
They identified 24 articles with original data. All of the studies used reverse transcription–polymerase chain reaction (PCR) tests to identify SARS-CoV-2 RNA. In five studies, attempts were also made to culture viable viruses. Three studies assessed the particle size relative to RNA concentration or viral titer.
Of 893 air samples across the 24 studies, 52.7% were taken from areas close to patients, 26.5% were taken in clinical areas, 13.7% in staff areas, 4.7% in public areas, and 2.4% in toilets or bathrooms.
Among those studies that quantified RNA, the median interquartile range of concentrations varied from 1.0 x 103 copies/m3 in clinical areas to 9.7 x 103 copies/m3 in toilets or bathrooms.
One study found an RNA concentration of 2.0 x 103 copies for particle sizes >4 mcm and 1.3 x 103 copies/m3 for particle sizes ≤4 mcm, both in patients’ rooms.
Three studies included viral cultures; of those, two resulted in positive cultures, both in a non-ICU setting. In one study, 3 of 39 samples were positive, and in the other, 4 of 4 were positive. Viral cultures in toilets, clinical areas, staff areas, and public areas were negative.
One of these studies assessed viral concentration and found that the median interquartile range was 4.8 tissue culture infectious dose (TCID50)/m3 for particles <1 mcm, 4.27 TCID50/m3 for particles 1-4 mcm, and 1.82 TCID50/m3 for particles >4 mcm.
Although viable viruses weren’t found in staff areas, the presence of viral RNA in places such as dining rooms and meeting rooms raises a concern, Dr. Birgand said.
“All of these staff areas are probably playing an important role in contamination,” he said. “It’s pretty easy to see when you are dining, you are not wearing a face mask, and it’s associated with a strong risk when there is a strong dissemination of the virus in the community.”
Studies on contact tracing among health care workers have also identified meeting rooms and dining rooms as the second most common source of infection after community contact, he said.
In general, the findings of the review correspond to epidemiologic studies, said Angela Rasmussen, PhD, a virologist with the Georgetown University Center for Global Health Science and Security, Washington, who was not involved in the review. “Absent aerosol-generating procedures, health care workers are largely not getting infected when they take droplet precautions.”
One reason may be that patients shed the most infectious viruses a couple of days before and after symptoms begin. By the time they’re hospitalized, they’re less likely to be contagious but may continue to shed viral RNA.
“We don’t really know the basis for the persistence of RNA being produced long after people have been infected and have recovered from the acute infection,” she said, “but it has been observed quite frequently.”
Although the virus cannot remain viable for very long in the air, remnants may still be detected in the form of RNA, Dr. Rasmussen said. In addition, hospitals often do a good job of ventilation.
She pointed out that it can be difficult to cultivate viruses in air samples because of contaminants such as bacteria and fungi. “That’s one of the limitations of a study like this. You’re not really sure if it’s because there’s no viable virus there or because you just aren’t able to collect samples that would allow you to determine that.”
Dr. Birgand and colleagues acknowledged other limitations. The studies they reviewed used different approaches to sampling. Different procedures may have been underway in the rooms being sampled, and factors such as temperature and humidity could have affected the results. In addition, the studies used different cycle thresholds for PCR positivity.
A version of this article first appeared on Medscape.com.
Everywhere they look within hospitals, researchers find RNA from SARS-CoV-2 in the air. But viable viruses typically are found only close to patients, according to a review of published studies.
The finding supports recommendations to use surgical masks in most parts of the hospital, reserving respirators (such as N95 or FFP2) for aerosol-generating procedures on patients’ respiratory tracts, said Gabriel Birgand, PhD, an infectious disease researcher at Imperial College London.
“When the virus is spreading a lot in the community, it’s probably more likely for you to be contaminated in your friends’ areas or in your building than in your work area, where you are well equipped and compliant with all the measures,” he said in an interview. “So it’s pretty good news.”
The systematic review by Dr. Birgand and colleagues was published in JAMA Network Open.
Recommended precautions to protect health care workers from SARS-CoV-2 infections remain controversial. Most authorities believe droplets are the primary route of transmission, which would mean surgical masks may be sufficient protection. But some research has suggested transmission by aerosols as well, making N95 respirators seem necessary. There is even disagreement about the definitions of the words “aerosol” and “droplet.”
To better understand where traces of the virus can be found in the air in hospitals, Dr. Birgand and colleagues analyzed all the studies they could find on the subject in English.
They identified 24 articles with original data. All of the studies used reverse transcription–polymerase chain reaction (PCR) tests to identify SARS-CoV-2 RNA. In five studies, attempts were also made to culture viable viruses. Three studies assessed the particle size relative to RNA concentration or viral titer.
Of 893 air samples across the 24 studies, 52.7% were taken from areas close to patients, 26.5% were taken in clinical areas, 13.7% in staff areas, 4.7% in public areas, and 2.4% in toilets or bathrooms.
Among those studies that quantified RNA, the median interquartile range of concentrations varied from 1.0 x 103 copies/m3 in clinical areas to 9.7 x 103 copies/m3 in toilets or bathrooms.
One study found an RNA concentration of 2.0 x 103 copies for particle sizes >4 mcm and 1.3 x 103 copies/m3 for particle sizes ≤4 mcm, both in patients’ rooms.
Three studies included viral cultures; of those, two resulted in positive cultures, both in a non-ICU setting. In one study, 3 of 39 samples were positive, and in the other, 4 of 4 were positive. Viral cultures in toilets, clinical areas, staff areas, and public areas were negative.
One of these studies assessed viral concentration and found that the median interquartile range was 4.8 tissue culture infectious dose (TCID50)/m3 for particles <1 mcm, 4.27 TCID50/m3 for particles 1-4 mcm, and 1.82 TCID50/m3 for particles >4 mcm.
Although viable viruses weren’t found in staff areas, the presence of viral RNA in places such as dining rooms and meeting rooms raises a concern, Dr. Birgand said.
“All of these staff areas are probably playing an important role in contamination,” he said. “It’s pretty easy to see when you are dining, you are not wearing a face mask, and it’s associated with a strong risk when there is a strong dissemination of the virus in the community.”
Studies on contact tracing among health care workers have also identified meeting rooms and dining rooms as the second most common source of infection after community contact, he said.
In general, the findings of the review correspond to epidemiologic studies, said Angela Rasmussen, PhD, a virologist with the Georgetown University Center for Global Health Science and Security, Washington, who was not involved in the review. “Absent aerosol-generating procedures, health care workers are largely not getting infected when they take droplet precautions.”
One reason may be that patients shed the most infectious viruses a couple of days before and after symptoms begin. By the time they’re hospitalized, they’re less likely to be contagious but may continue to shed viral RNA.
“We don’t really know the basis for the persistence of RNA being produced long after people have been infected and have recovered from the acute infection,” she said, “but it has been observed quite frequently.”
Although the virus cannot remain viable for very long in the air, remnants may still be detected in the form of RNA, Dr. Rasmussen said. In addition, hospitals often do a good job of ventilation.
She pointed out that it can be difficult to cultivate viruses in air samples because of contaminants such as bacteria and fungi. “That’s one of the limitations of a study like this. You’re not really sure if it’s because there’s no viable virus there or because you just aren’t able to collect samples that would allow you to determine that.”
Dr. Birgand and colleagues acknowledged other limitations. The studies they reviewed used different approaches to sampling. Different procedures may have been underway in the rooms being sampled, and factors such as temperature and humidity could have affected the results. In addition, the studies used different cycle thresholds for PCR positivity.
A version of this article first appeared on Medscape.com.
Everywhere they look within hospitals, researchers find RNA from SARS-CoV-2 in the air. But viable viruses typically are found only close to patients, according to a review of published studies.
The finding supports recommendations to use surgical masks in most parts of the hospital, reserving respirators (such as N95 or FFP2) for aerosol-generating procedures on patients’ respiratory tracts, said Gabriel Birgand, PhD, an infectious disease researcher at Imperial College London.
“When the virus is spreading a lot in the community, it’s probably more likely for you to be contaminated in your friends’ areas or in your building than in your work area, where you are well equipped and compliant with all the measures,” he said in an interview. “So it’s pretty good news.”
The systematic review by Dr. Birgand and colleagues was published in JAMA Network Open.
Recommended precautions to protect health care workers from SARS-CoV-2 infections remain controversial. Most authorities believe droplets are the primary route of transmission, which would mean surgical masks may be sufficient protection. But some research has suggested transmission by aerosols as well, making N95 respirators seem necessary. There is even disagreement about the definitions of the words “aerosol” and “droplet.”
To better understand where traces of the virus can be found in the air in hospitals, Dr. Birgand and colleagues analyzed all the studies they could find on the subject in English.
They identified 24 articles with original data. All of the studies used reverse transcription–polymerase chain reaction (PCR) tests to identify SARS-CoV-2 RNA. In five studies, attempts were also made to culture viable viruses. Three studies assessed the particle size relative to RNA concentration or viral titer.
Of 893 air samples across the 24 studies, 52.7% were taken from areas close to patients, 26.5% were taken in clinical areas, 13.7% in staff areas, 4.7% in public areas, and 2.4% in toilets or bathrooms.
Among those studies that quantified RNA, the median interquartile range of concentrations varied from 1.0 x 103 copies/m3 in clinical areas to 9.7 x 103 copies/m3 in toilets or bathrooms.
One study found an RNA concentration of 2.0 x 103 copies for particle sizes >4 mcm and 1.3 x 103 copies/m3 for particle sizes ≤4 mcm, both in patients’ rooms.
Three studies included viral cultures; of those, two resulted in positive cultures, both in a non-ICU setting. In one study, 3 of 39 samples were positive, and in the other, 4 of 4 were positive. Viral cultures in toilets, clinical areas, staff areas, and public areas were negative.
One of these studies assessed viral concentration and found that the median interquartile range was 4.8 tissue culture infectious dose (TCID50)/m3 for particles <1 mcm, 4.27 TCID50/m3 for particles 1-4 mcm, and 1.82 TCID50/m3 for particles >4 mcm.
Although viable viruses weren’t found in staff areas, the presence of viral RNA in places such as dining rooms and meeting rooms raises a concern, Dr. Birgand said.
“All of these staff areas are probably playing an important role in contamination,” he said. “It’s pretty easy to see when you are dining, you are not wearing a face mask, and it’s associated with a strong risk when there is a strong dissemination of the virus in the community.”
Studies on contact tracing among health care workers have also identified meeting rooms and dining rooms as the second most common source of infection after community contact, he said.
In general, the findings of the review correspond to epidemiologic studies, said Angela Rasmussen, PhD, a virologist with the Georgetown University Center for Global Health Science and Security, Washington, who was not involved in the review. “Absent aerosol-generating procedures, health care workers are largely not getting infected when they take droplet precautions.”
One reason may be that patients shed the most infectious viruses a couple of days before and after symptoms begin. By the time they’re hospitalized, they’re less likely to be contagious but may continue to shed viral RNA.
“We don’t really know the basis for the persistence of RNA being produced long after people have been infected and have recovered from the acute infection,” she said, “but it has been observed quite frequently.”
Although the virus cannot remain viable for very long in the air, remnants may still be detected in the form of RNA, Dr. Rasmussen said. In addition, hospitals often do a good job of ventilation.
She pointed out that it can be difficult to cultivate viruses in air samples because of contaminants such as bacteria and fungi. “That’s one of the limitations of a study like this. You’re not really sure if it’s because there’s no viable virus there or because you just aren’t able to collect samples that would allow you to determine that.”
Dr. Birgand and colleagues acknowledged other limitations. The studies they reviewed used different approaches to sampling. Different procedures may have been underway in the rooms being sampled, and factors such as temperature and humidity could have affected the results. In addition, the studies used different cycle thresholds for PCR positivity.
A version of this article first appeared on Medscape.com.
New resilience center targets traumatized health care workers
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.

“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.

But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.

“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.

“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
COVID-19 case fatality doubled in heart transplant patients
Heart transplant recipients infected with SARS-CoV-2 are about twice as likely to die from COVID-19 and should be immediately referred to a transplant center for care, according to transplant experts from Northern Italy.
In a COVID Rapid Report published Dec. 9 in JACC Heart Failure, a group led by Tomaso Bottio, MD, PhD, from the University of Padua, Italy, presented findings on 47 heart transplant recipients who tested positive for SARS-Cov-2 between Feb. 21 and June 30.
The investigators found a case fatality rate of 29.7%, compared with 15.4% in the general population. Prevalence of infection was also much higher at 18 cases (vs. 7) per 1,000 population.
“In our opinion, prompt referral to a heart transplant center is crucial for immunosuppressive therapy optimization and cardiologic follow-up,” Dr. Bottio said in an interview.
Beyond the need for careful adjustment of immunosuppression, graft function should be assessed to “avoid acute rejection or decompensation,” he added.
Dr. Bottio and colleagues tracked COVID-19 cases from among the 2,676 heart transplant recipients alive before the onset of the pandemic at seven heart transplant centers in Northern Italy.
Of the 47 recipients who contracted SARS-CoV-2, 38 required hospitalization while 9 remained at home and 14 died. Mean length of stay in hospital was 17.8 days, much longer in survivors than nonsurvivors (23.2 days vs. 8.5 days; P < .001).
Nonsurvivors were significantly older than survivors (72 vs. 58 years; P = .002). Nonsurvivors were also more likely to present with diabetes (P = .04), extra-cardiac arteriopathy (P = .04), previous percutaneous coronary intervention (P = .04), more allograft vasculopathy (P = .04), and more symptoms of heart failure (P = .02).
Although the authors said the high case fatality rate was, unfortunately, expected, they did not expect so many patients to do well at home.
“What most surprised us was the proportion of a- or pauci-symptomatic heart transplanted patients who did well being treated at home without any therapy modifications,” Dr. Bottio shared. They were also surprised to see there were no cases of graft failure caused by infection-related myocarditis.
These findings from Northern Italy are not dissimilar from the 25% case fatality rate seen in a cohort of heart transplant recipients who caught COVID-19 in New York City early in the pandemic.
In another study, this time looking at a wider group of solid organ transplant recipients with SARS-CoV-2 infection at two centers during the first 3 weeks of the outbreak in New York City, 16 of 90 patients (18%) died.
Treatment recommendations?
Recognizing that there is no randomized trial data informing the treatment of this vulnerable patient population, Dr. Bottio and colleagues suggested that, based on their experience, no change in immunosuppression is needed in those who are “pauci-symptomatic” (mildly symptomatic).
“On the other hand, in hospitalized patients a partial reduction in immunosuppressive therapy avoiding full discontinuation and risk of graft rejection seems to be a common strategy in facing the viral infection,” he said. “In addition, the introduction of corticosteroids could help to suspend the onset of the inflammatory cascade responsible for severe forms of the disease.”
Antibiotic prophylaxis appears to be “fundamental,” he added, particularly in hospitalized patients, but “the role of specific antiviral therapies is still not fully understood in our population.”
Since July 1, they’ve seen an additional six patients with a positive test for SARS-CoV-2. Five were asymptomatic and quarantined at home without changing their immunosuppressive therapy. One patient was hospitalized for pneumonia and had immunosuppressive therapy reduced.
Dr. Bottio and the study coauthors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Heart transplant recipients infected with SARS-CoV-2 are about twice as likely to die from COVID-19 and should be immediately referred to a transplant center for care, according to transplant experts from Northern Italy.
In a COVID Rapid Report published Dec. 9 in JACC Heart Failure, a group led by Tomaso Bottio, MD, PhD, from the University of Padua, Italy, presented findings on 47 heart transplant recipients who tested positive for SARS-Cov-2 between Feb. 21 and June 30.
The investigators found a case fatality rate of 29.7%, compared with 15.4% in the general population. Prevalence of infection was also much higher at 18 cases (vs. 7) per 1,000 population.
“In our opinion, prompt referral to a heart transplant center is crucial for immunosuppressive therapy optimization and cardiologic follow-up,” Dr. Bottio said in an interview.
Beyond the need for careful adjustment of immunosuppression, graft function should be assessed to “avoid acute rejection or decompensation,” he added.
Dr. Bottio and colleagues tracked COVID-19 cases from among the 2,676 heart transplant recipients alive before the onset of the pandemic at seven heart transplant centers in Northern Italy.
Of the 47 recipients who contracted SARS-CoV-2, 38 required hospitalization while 9 remained at home and 14 died. Mean length of stay in hospital was 17.8 days, much longer in survivors than nonsurvivors (23.2 days vs. 8.5 days; P < .001).
Nonsurvivors were significantly older than survivors (72 vs. 58 years; P = .002). Nonsurvivors were also more likely to present with diabetes (P = .04), extra-cardiac arteriopathy (P = .04), previous percutaneous coronary intervention (P = .04), more allograft vasculopathy (P = .04), and more symptoms of heart failure (P = .02).
Although the authors said the high case fatality rate was, unfortunately, expected, they did not expect so many patients to do well at home.
“What most surprised us was the proportion of a- or pauci-symptomatic heart transplanted patients who did well being treated at home without any therapy modifications,” Dr. Bottio shared. They were also surprised to see there were no cases of graft failure caused by infection-related myocarditis.
These findings from Northern Italy are not dissimilar from the 25% case fatality rate seen in a cohort of heart transplant recipients who caught COVID-19 in New York City early in the pandemic.
In another study, this time looking at a wider group of solid organ transplant recipients with SARS-CoV-2 infection at two centers during the first 3 weeks of the outbreak in New York City, 16 of 90 patients (18%) died.
Treatment recommendations?
Recognizing that there is no randomized trial data informing the treatment of this vulnerable patient population, Dr. Bottio and colleagues suggested that, based on their experience, no change in immunosuppression is needed in those who are “pauci-symptomatic” (mildly symptomatic).
“On the other hand, in hospitalized patients a partial reduction in immunosuppressive therapy avoiding full discontinuation and risk of graft rejection seems to be a common strategy in facing the viral infection,” he said. “In addition, the introduction of corticosteroids could help to suspend the onset of the inflammatory cascade responsible for severe forms of the disease.”
Antibiotic prophylaxis appears to be “fundamental,” he added, particularly in hospitalized patients, but “the role of specific antiviral therapies is still not fully understood in our population.”
Since July 1, they’ve seen an additional six patients with a positive test for SARS-CoV-2. Five were asymptomatic and quarantined at home without changing their immunosuppressive therapy. One patient was hospitalized for pneumonia and had immunosuppressive therapy reduced.
Dr. Bottio and the study coauthors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Heart transplant recipients infected with SARS-CoV-2 are about twice as likely to die from COVID-19 and should be immediately referred to a transplant center for care, according to transplant experts from Northern Italy.
In a COVID Rapid Report published Dec. 9 in JACC Heart Failure, a group led by Tomaso Bottio, MD, PhD, from the University of Padua, Italy, presented findings on 47 heart transplant recipients who tested positive for SARS-Cov-2 between Feb. 21 and June 30.
The investigators found a case fatality rate of 29.7%, compared with 15.4% in the general population. Prevalence of infection was also much higher at 18 cases (vs. 7) per 1,000 population.
“In our opinion, prompt referral to a heart transplant center is crucial for immunosuppressive therapy optimization and cardiologic follow-up,” Dr. Bottio said in an interview.
Beyond the need for careful adjustment of immunosuppression, graft function should be assessed to “avoid acute rejection or decompensation,” he added.
Dr. Bottio and colleagues tracked COVID-19 cases from among the 2,676 heart transplant recipients alive before the onset of the pandemic at seven heart transplant centers in Northern Italy.
Of the 47 recipients who contracted SARS-CoV-2, 38 required hospitalization while 9 remained at home and 14 died. Mean length of stay in hospital was 17.8 days, much longer in survivors than nonsurvivors (23.2 days vs. 8.5 days; P < .001).
Nonsurvivors were significantly older than survivors (72 vs. 58 years; P = .002). Nonsurvivors were also more likely to present with diabetes (P = .04), extra-cardiac arteriopathy (P = .04), previous percutaneous coronary intervention (P = .04), more allograft vasculopathy (P = .04), and more symptoms of heart failure (P = .02).
Although the authors said the high case fatality rate was, unfortunately, expected, they did not expect so many patients to do well at home.
“What most surprised us was the proportion of a- or pauci-symptomatic heart transplanted patients who did well being treated at home without any therapy modifications,” Dr. Bottio shared. They were also surprised to see there were no cases of graft failure caused by infection-related myocarditis.
These findings from Northern Italy are not dissimilar from the 25% case fatality rate seen in a cohort of heart transplant recipients who caught COVID-19 in New York City early in the pandemic.
In another study, this time looking at a wider group of solid organ transplant recipients with SARS-CoV-2 infection at two centers during the first 3 weeks of the outbreak in New York City, 16 of 90 patients (18%) died.
Treatment recommendations?
Recognizing that there is no randomized trial data informing the treatment of this vulnerable patient population, Dr. Bottio and colleagues suggested that, based on their experience, no change in immunosuppression is needed in those who are “pauci-symptomatic” (mildly symptomatic).
“On the other hand, in hospitalized patients a partial reduction in immunosuppressive therapy avoiding full discontinuation and risk of graft rejection seems to be a common strategy in facing the viral infection,” he said. “In addition, the introduction of corticosteroids could help to suspend the onset of the inflammatory cascade responsible for severe forms of the disease.”
Antibiotic prophylaxis appears to be “fundamental,” he added, particularly in hospitalized patients, but “the role of specific antiviral therapies is still not fully understood in our population.”
Since July 1, they’ve seen an additional six patients with a positive test for SARS-CoV-2. Five were asymptomatic and quarantined at home without changing their immunosuppressive therapy. One patient was hospitalized for pneumonia and had immunosuppressive therapy reduced.
Dr. Bottio and the study coauthors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 mortality rates declined, but vary by hospital
Mortality rates for inpatients with COVID-19 dropped significantly during the first 6 months of the pandemic, but outcomes depend on the hospital where patients receive care, new data show.
“[T]he characteristic that is most associated with poor or worsening hospital outcomes is high or increasing community case rates,” write David A. Asch, MD, MBA, executive director of the Center for Health Care Innovation at the University of Pennsylvania in Philadelphia, and colleagues.
The relationship between COVID-19 mortality rates and local disease prevalence suggests that “hospitals do worse when they are burdened with cases and is consistent with imperatives to flatten the curve,” the authors continue. “As case rates of COVID-19 increase across the nation, hospital mortality outcomes may worsen.”
The researchers published their study online December 22 in JAMA Internal Medicine.
The quick and substantial improvement in survival “is a tribute in part to new science — for example, the science that revealed the benefits of dexamethasone,” Asch told Medscape Medical News. “But it’s also a tribute to the doctors and nurses in the hospitals who developed experience. It’s a cliché to refer to them as heroes, but that is what they are. The science and the heroic experience continues on, and so I’m optimistic that we’ll see even more improvement over time.”
However, the data also indicate that “with lots of disease in the community, hospitals may have a harder time keeping patients alive,” Asch said. “And of course the reason this is bad news is that community level case rates are rising all over, and in some cases at rapid rates. With that rise, we might be giving back some of our past gains in survival — just as the vaccine is beginning to be distributed.”
Examining mortality trends
The researchers analyzed administrative claims data from a large national health insurer. They included data from 38,517 adults who were admitted with COVID-19 to 955 US hospitals between January 1 and June 30 of this year. The investigators estimated hospitals’ risk-standardized rate of 30-day in-hospital mortality or referral to hospice, adjusted for patient-level characteristics.
Overall, 3179 patients (8.25%) died, and 1433 patients (3.7%) were referred to hospice. Risk-standardized mortality or hospice referral rates for individual hospitals ranged from 5.7% to 24.7%. The average rate was 9.1% in the best-performing quintile, compared with 15.7% in the worst-performing quintile.
In a subset of 398 hospitals that had at least 10 patients admitted for COVID-19 during early (January 1 through April 30) and later periods (between May 1 and June 30), rates in all but one hospital improved, and 94% improved by at least 25%. The average risk-standardized event rate declined from 16.6% to 9.3%.
“That rate of relative improvement is striking and encouraging, but perhaps not surprising,” Asch and coauthors write. “Early efforts at treating patients with COVID-19 were based on experience with previously known causes of severe respiratory illness. Later efforts could draw on experiences specific to SARS-CoV-2 infection.”
For instance, doctors tried different inpatient management approaches, such as early vs late assisted ventilation, differences in oxygen flow, prone or supine positioning, and anticoagulation. “Those efforts varied in how systematically they were evaluated, but our results suggest that valuable experience was gained,” the authors note.
In addition, variation between hospitals could reflect differences in quality or different admission thresholds, they continue.
The study provides “a reason for optimism that our healthcare system has improved in our ability to care for persons with COVID-19,” write Leon Boudourakis, MD, MHS, and Amit Uppal, MD, in a related commentary. Boudourakis and Uppal are both affiliated with NYC Health + Hospitals in New York City and with SUNY Downstate and New York University School of Medicine, respectively.
Similar improvements in mortality rates have been reported in the United Kingdom and in a New York City hospital system, the editorialists note. The lower mortality rates may represent clinical, healthcare system, and epidemiologic trends.
“Since the first wave of serious COVID-19 cases, physicians have learned a great deal about the best ways to treat this serious infection,” they say. “Steroids may decrease mortality in patients with respiratory failure. Remdesivir may shorten hospitalizations of patients with serious illness. Anticoagulation and prone positioning may help certain patients. Using noninvasive ventilation and high-flow oxygen therapy may spare subsets of patients from the harms of intubation, such as ventilator-induced lung injury.»
Overwhelmed hospitals
“Hospitals do not perform as well when they are overwhelmed,” which may be a reason for the correlation between community prevalence and mortality rates, Boudourakis and Uppal suggested. “In particular, patients with a precarious respiratory status require expert, meticulous therapy to avoid intubation; those who undergo intubation or have kidney failure require nuanced and timely expert care with ventilatory adjustments and kidney replacement therapy, which are difficult to perform optimally when hospital capacity is strained.”
Although the death rate has fallen to about 9% for hospitalized patients, “9% is still high,” Asch said.
“Our results show that hospitals can’t do it on their own,” Asch said. “They need all of us to keep the community spread of the disease down. The right answer now is the right answer since the beginning of the pandemic: Keep your distance, wash your hands, and wear a mask.”
Asch, Boudourakis, and Uppal have disclosed no relevant financial relationships. A study coauthor reported personal fees and grants from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
Mortality rates for inpatients with COVID-19 dropped significantly during the first 6 months of the pandemic, but outcomes depend on the hospital where patients receive care, new data show.
“[T]he characteristic that is most associated with poor or worsening hospital outcomes is high or increasing community case rates,” write David A. Asch, MD, MBA, executive director of the Center for Health Care Innovation at the University of Pennsylvania in Philadelphia, and colleagues.
The relationship between COVID-19 mortality rates and local disease prevalence suggests that “hospitals do worse when they are burdened with cases and is consistent with imperatives to flatten the curve,” the authors continue. “As case rates of COVID-19 increase across the nation, hospital mortality outcomes may worsen.”
The researchers published their study online December 22 in JAMA Internal Medicine.
The quick and substantial improvement in survival “is a tribute in part to new science — for example, the science that revealed the benefits of dexamethasone,” Asch told Medscape Medical News. “But it’s also a tribute to the doctors and nurses in the hospitals who developed experience. It’s a cliché to refer to them as heroes, but that is what they are. The science and the heroic experience continues on, and so I’m optimistic that we’ll see even more improvement over time.”
However, the data also indicate that “with lots of disease in the community, hospitals may have a harder time keeping patients alive,” Asch said. “And of course the reason this is bad news is that community level case rates are rising all over, and in some cases at rapid rates. With that rise, we might be giving back some of our past gains in survival — just as the vaccine is beginning to be distributed.”
Examining mortality trends
The researchers analyzed administrative claims data from a large national health insurer. They included data from 38,517 adults who were admitted with COVID-19 to 955 US hospitals between January 1 and June 30 of this year. The investigators estimated hospitals’ risk-standardized rate of 30-day in-hospital mortality or referral to hospice, adjusted for patient-level characteristics.
Overall, 3179 patients (8.25%) died, and 1433 patients (3.7%) were referred to hospice. Risk-standardized mortality or hospice referral rates for individual hospitals ranged from 5.7% to 24.7%. The average rate was 9.1% in the best-performing quintile, compared with 15.7% in the worst-performing quintile.
In a subset of 398 hospitals that had at least 10 patients admitted for COVID-19 during early (January 1 through April 30) and later periods (between May 1 and June 30), rates in all but one hospital improved, and 94% improved by at least 25%. The average risk-standardized event rate declined from 16.6% to 9.3%.
“That rate of relative improvement is striking and encouraging, but perhaps not surprising,” Asch and coauthors write. “Early efforts at treating patients with COVID-19 were based on experience with previously known causes of severe respiratory illness. Later efforts could draw on experiences specific to SARS-CoV-2 infection.”
For instance, doctors tried different inpatient management approaches, such as early vs late assisted ventilation, differences in oxygen flow, prone or supine positioning, and anticoagulation. “Those efforts varied in how systematically they were evaluated, but our results suggest that valuable experience was gained,” the authors note.
In addition, variation between hospitals could reflect differences in quality or different admission thresholds, they continue.
The study provides “a reason for optimism that our healthcare system has improved in our ability to care for persons with COVID-19,” write Leon Boudourakis, MD, MHS, and Amit Uppal, MD, in a related commentary. Boudourakis and Uppal are both affiliated with NYC Health + Hospitals in New York City and with SUNY Downstate and New York University School of Medicine, respectively.
Similar improvements in mortality rates have been reported in the United Kingdom and in a New York City hospital system, the editorialists note. The lower mortality rates may represent clinical, healthcare system, and epidemiologic trends.
“Since the first wave of serious COVID-19 cases, physicians have learned a great deal about the best ways to treat this serious infection,” they say. “Steroids may decrease mortality in patients with respiratory failure. Remdesivir may shorten hospitalizations of patients with serious illness. Anticoagulation and prone positioning may help certain patients. Using noninvasive ventilation and high-flow oxygen therapy may spare subsets of patients from the harms of intubation, such as ventilator-induced lung injury.»
Overwhelmed hospitals
“Hospitals do not perform as well when they are overwhelmed,” which may be a reason for the correlation between community prevalence and mortality rates, Boudourakis and Uppal suggested. “In particular, patients with a precarious respiratory status require expert, meticulous therapy to avoid intubation; those who undergo intubation or have kidney failure require nuanced and timely expert care with ventilatory adjustments and kidney replacement therapy, which are difficult to perform optimally when hospital capacity is strained.”
Although the death rate has fallen to about 9% for hospitalized patients, “9% is still high,” Asch said.
“Our results show that hospitals can’t do it on their own,” Asch said. “They need all of us to keep the community spread of the disease down. The right answer now is the right answer since the beginning of the pandemic: Keep your distance, wash your hands, and wear a mask.”
Asch, Boudourakis, and Uppal have disclosed no relevant financial relationships. A study coauthor reported personal fees and grants from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
Mortality rates for inpatients with COVID-19 dropped significantly during the first 6 months of the pandemic, but outcomes depend on the hospital where patients receive care, new data show.
“[T]he characteristic that is most associated with poor or worsening hospital outcomes is high or increasing community case rates,” write David A. Asch, MD, MBA, executive director of the Center for Health Care Innovation at the University of Pennsylvania in Philadelphia, and colleagues.
The relationship between COVID-19 mortality rates and local disease prevalence suggests that “hospitals do worse when they are burdened with cases and is consistent with imperatives to flatten the curve,” the authors continue. “As case rates of COVID-19 increase across the nation, hospital mortality outcomes may worsen.”
The researchers published their study online December 22 in JAMA Internal Medicine.
The quick and substantial improvement in survival “is a tribute in part to new science — for example, the science that revealed the benefits of dexamethasone,” Asch told Medscape Medical News. “But it’s also a tribute to the doctors and nurses in the hospitals who developed experience. It’s a cliché to refer to them as heroes, but that is what they are. The science and the heroic experience continues on, and so I’m optimistic that we’ll see even more improvement over time.”
However, the data also indicate that “with lots of disease in the community, hospitals may have a harder time keeping patients alive,” Asch said. “And of course the reason this is bad news is that community level case rates are rising all over, and in some cases at rapid rates. With that rise, we might be giving back some of our past gains in survival — just as the vaccine is beginning to be distributed.”
Examining mortality trends
The researchers analyzed administrative claims data from a large national health insurer. They included data from 38,517 adults who were admitted with COVID-19 to 955 US hospitals between January 1 and June 30 of this year. The investigators estimated hospitals’ risk-standardized rate of 30-day in-hospital mortality or referral to hospice, adjusted for patient-level characteristics.
Overall, 3179 patients (8.25%) died, and 1433 patients (3.7%) were referred to hospice. Risk-standardized mortality or hospice referral rates for individual hospitals ranged from 5.7% to 24.7%. The average rate was 9.1% in the best-performing quintile, compared with 15.7% in the worst-performing quintile.
In a subset of 398 hospitals that had at least 10 patients admitted for COVID-19 during early (January 1 through April 30) and later periods (between May 1 and June 30), rates in all but one hospital improved, and 94% improved by at least 25%. The average risk-standardized event rate declined from 16.6% to 9.3%.
“That rate of relative improvement is striking and encouraging, but perhaps not surprising,” Asch and coauthors write. “Early efforts at treating patients with COVID-19 were based on experience with previously known causes of severe respiratory illness. Later efforts could draw on experiences specific to SARS-CoV-2 infection.”
For instance, doctors tried different inpatient management approaches, such as early vs late assisted ventilation, differences in oxygen flow, prone or supine positioning, and anticoagulation. “Those efforts varied in how systematically they were evaluated, but our results suggest that valuable experience was gained,” the authors note.
In addition, variation between hospitals could reflect differences in quality or different admission thresholds, they continue.
The study provides “a reason for optimism that our healthcare system has improved in our ability to care for persons with COVID-19,” write Leon Boudourakis, MD, MHS, and Amit Uppal, MD, in a related commentary. Boudourakis and Uppal are both affiliated with NYC Health + Hospitals in New York City and with SUNY Downstate and New York University School of Medicine, respectively.
Similar improvements in mortality rates have been reported in the United Kingdom and in a New York City hospital system, the editorialists note. The lower mortality rates may represent clinical, healthcare system, and epidemiologic trends.
“Since the first wave of serious COVID-19 cases, physicians have learned a great deal about the best ways to treat this serious infection,” they say. “Steroids may decrease mortality in patients with respiratory failure. Remdesivir may shorten hospitalizations of patients with serious illness. Anticoagulation and prone positioning may help certain patients. Using noninvasive ventilation and high-flow oxygen therapy may spare subsets of patients from the harms of intubation, such as ventilator-induced lung injury.»
Overwhelmed hospitals
“Hospitals do not perform as well when they are overwhelmed,” which may be a reason for the correlation between community prevalence and mortality rates, Boudourakis and Uppal suggested. “In particular, patients with a precarious respiratory status require expert, meticulous therapy to avoid intubation; those who undergo intubation or have kidney failure require nuanced and timely expert care with ventilatory adjustments and kidney replacement therapy, which are difficult to perform optimally when hospital capacity is strained.”
Although the death rate has fallen to about 9% for hospitalized patients, “9% is still high,” Asch said.
“Our results show that hospitals can’t do it on their own,” Asch said. “They need all of us to keep the community spread of the disease down. The right answer now is the right answer since the beginning of the pandemic: Keep your distance, wash your hands, and wear a mask.”
Asch, Boudourakis, and Uppal have disclosed no relevant financial relationships. A study coauthor reported personal fees and grants from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
After COVID-19 infection, antibodies highly protective for months, prospective study shows
results of the first prospective study of the subject revealed.

The main message for health care workers is, “if you’ve had COVID, at least in the short term, you are unlikely to get it again,” David Eyre, DPhil, senior author, associate professor at the Big Data Institute and infectious diseases clinician at the University of Oxford (England), said in an interview.
Dr. Eyre and colleagues assessed for the presence of two antibodies to SARS-CoV-2 among 12,541 health care workers in the United Kingdom, including about 10% who had a history of polymerase chain reaction (PCR)–confirmed infection. Of those, 223 who did not have antibodies tested positive on PCR for the virus during 31 weeks of follow-up; two participants who did not have antibodies at baseline tested positive.
The study was published online Dec. 23 in The New England Journal of Medicine.
“It’s great news because there have been so many questions regarding whether or not you can be protected against reinfection, and this health care worker study is really an elegant way to address that question,” Mark Slifka, PhD, said in an interview when asked to comment on the findings.
Although “there are millions of people in the U.S. who have been infected with COVID, we don’t know how common reinfection is,” said Dr. Slifka, a researcher at the Oregon National Primate Research Center and professor at Oregon Health & Science University, Portland.
The likelihood of a subsequent positive PCR test result was 1.09 per 10,000 days at risk among those without antibodies, compared with 0.13 per 10,000 days among those with anti-spike antibodies.
The investigators also assessed for the presence of anti–nucleocapsid IgG antibody titers. They found a significant trend for increasing PCR-positive test results with increasing antibody levels. As with the anti-spike antibody findings, 226 of 11,543 health care providers who did not have anti–nucleocapsid IgG antibodies subsequently tested positive on PCR; by contrast, two of 1,172 participants who did not have antibodies tested positive. Adjusted for age, sex, and calendar time, this finding translates to a 0.11 incidence rate ratio (0.13 per 10,000 days at risk; 95% confidence interval, 0.03-0.45; P = .002).
“This is a study a number of us have been trying to do,” said Christopher L. King, MD, PhD, professor of pathology and associate professor of medicine at Case Western Reserve University, Cleveland.
“To really follow a group like this longitudinally like they’ve done, with a large population, and to see such a big difference – it really confirms our suspicion that those who do become infected and develop an antibody response are significantly protected from reinfection.
“What’s great about this study is it’s nearly a 10-fold reduction in risk if you’ve recovered from COVID and have antibodies,” said Dr. King, who was not involved with the research. “That’s what a lot of us have been wanting to know.”
Unanswered questions remain
“How long this immunity lasts, we don’t know,” Dr. King said. He predicted that antibody protection could last a year to a year and a half. The duration of protection could vary. “We know some people lose their antibodies pretty quickly, and other people don’t,” he said.
Dr. Slifka said the suggestion of “a substantially reduced risk for at least 6 months ... is great news, and the timing couldn’t be better, because we’re rolling out the vaccines.”
Not all antibody responses are alike. For example, data indicate that antibody levels following immunization with the Pfizer/BioNTech or Moderna vaccines are higher on average than those of people who’ve had a natural infection, Dr. King said. He added that initial data on the AstraZeneca COVID-19 vaccine in development showed lower antibody levels compared with natural immunity.
The Centers for Disease Control and Prevention recommends immunization for those with a history of infection. “People who have gotten sick with COVID-19 may still benefit from getting vaccinated,” the CDC notes on its Facts About COVID-19 Vaccines website. “Due to the severe health risks associated with COVID-19 and the fact that re-infection with COVID-19 is possible, people may be advised to get a COVID-19 vaccine even if they have been sick with COVID-19 before,” the CDC stated.
The agency also notes that people appear to become susceptible to reinfection approximately 90 days after onset of infection. However, the new evidence from the UK study that persons have up to 6 months of immune protection might lead to a modification of recommendations, especially at a time when vaccine supplies are limited, Dr. Slifka said.
Another unanswered question is why the two study participants with antibodies subsequently tested positive for reinfection. “There are a lot of things that could have made these people more susceptible,” Dr. King said. For example, they could have been heavily exposed to SARS-CoV-2 or been immunocompromised for another reason.
Furthermore, the immune response involves more than antibody levels, Dr. King noted. Research in rhesus monkeys suggests that T cells play a role, but not as prominent a part as antibodies. “What I think is protecting us from infection is primarily the antibodies, although the T cells are probably important. Once you get infected, the T cells are probably playing a more important role in terms of whether you get very sick or not,” he said.
Multiplication + addition = more protected?
The 90% natural immunity protection in the study approaches the 95% efficacy associated with the Pfizer and Moderna vaccines, Dr. Slifka noted. Even without immunization, this could mean a portion of the U.S. population is already protected against future infection.
Furthermore, the CDC estimates that there are about 7.7 cases of COVID-19 for every case reported.
As of Sept. 30, the CDC reported that there were 6,891,764 confirmed cases. The agency estimated that overall, approximately 53 million people in the United States have been infected. More recent numbers from Johns Hopkins University’s Coronavirus Resource Center indicate that there were 18.2 million cases in the United States as of Dec. 22. If that tally is multiplied by 7.7, the total number protected could approach 140 million, Dr. Slifka said.
“That could really be a boost in terms of knocking this pandemic down in the next couple of months,” Dr. Slifka said.
“Now, if we were to modify the current recommendations and briefly defer vaccination of people with confirmed cases of COVID-19 until later on, we could start reaching herd immunity pretty quickly,” he added.
Real-life implications
“There is no such thing as 100% protection, even from the infection itself. So when you’re dealing with someone with possible exposure to COVID-19, you still need to follow the proper precautions,” Dr. Slifka said.
Nonetheless, he said, “This is great news for those on the front lines who are wondering whether or not they would have any protection if they had COVID-19 before. And the answer is yes – there is a very good chance they will have protection, based on this quite large study.”
One limitation of the study is that the population consisted predominantly of healthy adult health care workers aged 65 years or younger. “Further studies are needed to assess postinfection immunity in other populations, including children, older adults, and persons with coexisting conditions, including immunosuppression,” the researchers noted.
Dr. Eyre plans to continue following the health care workers in the study, some of whom have been vaccinated for COVID-19. This ongoing research will allow him and coinvestigators to “confirm the protection offered by vaccination and investigate how postvaccine antibody responses vary by whether you have had COVID-19 before or not. We also want to understand more about how long postinfection immunity lasts.”
Dr. Eyre has received grants as a Robinson Foundation Fellow and NIHR Oxford BRC senior fellow during the conduct of the study. Dr. Slifka and Dr. King report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results of the first prospective study of the subject revealed.
The main message for health care workers is, “if you’ve had COVID, at least in the short term, you are unlikely to get it again,” David Eyre, DPhil, senior author, associate professor at the Big Data Institute and infectious diseases clinician at the University of Oxford (England), said in an interview.
Dr. Eyre and colleagues assessed for the presence of two antibodies to SARS-CoV-2 among 12,541 health care workers in the United Kingdom, including about 10% who had a history of polymerase chain reaction (PCR)–confirmed infection. Of those, 223 who did not have antibodies tested positive on PCR for the virus during 31 weeks of follow-up; two participants who did not have antibodies at baseline tested positive.
The study was published online Dec. 23 in The New England Journal of Medicine.
“It’s great news because there have been so many questions regarding whether or not you can be protected against reinfection, and this health care worker study is really an elegant way to address that question,” Mark Slifka, PhD, said in an interview when asked to comment on the findings.
Although “there are millions of people in the U.S. who have been infected with COVID, we don’t know how common reinfection is,” said Dr. Slifka, a researcher at the Oregon National Primate Research Center and professor at Oregon Health & Science University, Portland.
The likelihood of a subsequent positive PCR test result was 1.09 per 10,000 days at risk among those without antibodies, compared with 0.13 per 10,000 days among those with anti-spike antibodies.
The investigators also assessed for the presence of anti–nucleocapsid IgG antibody titers. They found a significant trend for increasing PCR-positive test results with increasing antibody levels. As with the anti-spike antibody findings, 226 of 11,543 health care providers who did not have anti–nucleocapsid IgG antibodies subsequently tested positive on PCR; by contrast, two of 1,172 participants who did not have antibodies tested positive. Adjusted for age, sex, and calendar time, this finding translates to a 0.11 incidence rate ratio (0.13 per 10,000 days at risk; 95% confidence interval, 0.03-0.45; P = .002).
“This is a study a number of us have been trying to do,” said Christopher L. King, MD, PhD, professor of pathology and associate professor of medicine at Case Western Reserve University, Cleveland.
“To really follow a group like this longitudinally like they’ve done, with a large population, and to see such a big difference – it really confirms our suspicion that those who do become infected and develop an antibody response are significantly protected from reinfection.
“What’s great about this study is it’s nearly a 10-fold reduction in risk if you’ve recovered from COVID and have antibodies,” said Dr. King, who was not involved with the research. “That’s what a lot of us have been wanting to know.”
Unanswered questions remain
“How long this immunity lasts, we don’t know,” Dr. King said. He predicted that antibody protection could last a year to a year and a half. The duration of protection could vary. “We know some people lose their antibodies pretty quickly, and other people don’t,” he said.
Dr. Slifka said the suggestion of “a substantially reduced risk for at least 6 months ... is great news, and the timing couldn’t be better, because we’re rolling out the vaccines.”
Not all antibody responses are alike. For example, data indicate that antibody levels following immunization with the Pfizer/BioNTech or Moderna vaccines are higher on average than those of people who’ve had a natural infection, Dr. King said. He added that initial data on the AstraZeneca COVID-19 vaccine in development showed lower antibody levels compared with natural immunity.
The Centers for Disease Control and Prevention recommends immunization for those with a history of infection. “People who have gotten sick with COVID-19 may still benefit from getting vaccinated,” the CDC notes on its Facts About COVID-19 Vaccines website. “Due to the severe health risks associated with COVID-19 and the fact that re-infection with COVID-19 is possible, people may be advised to get a COVID-19 vaccine even if they have been sick with COVID-19 before,” the CDC stated.
The agency also notes that people appear to become susceptible to reinfection approximately 90 days after onset of infection. However, the new evidence from the UK study that persons have up to 6 months of immune protection might lead to a modification of recommendations, especially at a time when vaccine supplies are limited, Dr. Slifka said.
Another unanswered question is why the two study participants with antibodies subsequently tested positive for reinfection. “There are a lot of things that could have made these people more susceptible,” Dr. King said. For example, they could have been heavily exposed to SARS-CoV-2 or been immunocompromised for another reason.
Furthermore, the immune response involves more than antibody levels, Dr. King noted. Research in rhesus monkeys suggests that T cells play a role, but not as prominent a part as antibodies. “What I think is protecting us from infection is primarily the antibodies, although the T cells are probably important. Once you get infected, the T cells are probably playing a more important role in terms of whether you get very sick or not,” he said.
Multiplication + addition = more protected?
The 90% natural immunity protection in the study approaches the 95% efficacy associated with the Pfizer and Moderna vaccines, Dr. Slifka noted. Even without immunization, this could mean a portion of the U.S. population is already protected against future infection.
Furthermore, the CDC estimates that there are about 7.7 cases of COVID-19 for every case reported.
As of Sept. 30, the CDC reported that there were 6,891,764 confirmed cases. The agency estimated that overall, approximately 53 million people in the United States have been infected. More recent numbers from Johns Hopkins University’s Coronavirus Resource Center indicate that there were 18.2 million cases in the United States as of Dec. 22. If that tally is multiplied by 7.7, the total number protected could approach 140 million, Dr. Slifka said.
“That could really be a boost in terms of knocking this pandemic down in the next couple of months,” Dr. Slifka said.
“Now, if we were to modify the current recommendations and briefly defer vaccination of people with confirmed cases of COVID-19 until later on, we could start reaching herd immunity pretty quickly,” he added.
Real-life implications
“There is no such thing as 100% protection, even from the infection itself. So when you’re dealing with someone with possible exposure to COVID-19, you still need to follow the proper precautions,” Dr. Slifka said.
Nonetheless, he said, “This is great news for those on the front lines who are wondering whether or not they would have any protection if they had COVID-19 before. And the answer is yes – there is a very good chance they will have protection, based on this quite large study.”
One limitation of the study is that the population consisted predominantly of healthy adult health care workers aged 65 years or younger. “Further studies are needed to assess postinfection immunity in other populations, including children, older adults, and persons with coexisting conditions, including immunosuppression,” the researchers noted.
Dr. Eyre plans to continue following the health care workers in the study, some of whom have been vaccinated for COVID-19. This ongoing research will allow him and coinvestigators to “confirm the protection offered by vaccination and investigate how postvaccine antibody responses vary by whether you have had COVID-19 before or not. We also want to understand more about how long postinfection immunity lasts.”
Dr. Eyre has received grants as a Robinson Foundation Fellow and NIHR Oxford BRC senior fellow during the conduct of the study. Dr. Slifka and Dr. King report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results of the first prospective study of the subject revealed.
The main message for health care workers is, “if you’ve had COVID, at least in the short term, you are unlikely to get it again,” David Eyre, DPhil, senior author, associate professor at the Big Data Institute and infectious diseases clinician at the University of Oxford (England), said in an interview.
Dr. Eyre and colleagues assessed for the presence of two antibodies to SARS-CoV-2 among 12,541 health care workers in the United Kingdom, including about 10% who had a history of polymerase chain reaction (PCR)–confirmed infection. Of those, 223 who did not have antibodies tested positive on PCR for the virus during 31 weeks of follow-up; two participants who did not have antibodies at baseline tested positive.
The study was published online Dec. 23 in The New England Journal of Medicine.
“It’s great news because there have been so many questions regarding whether or not you can be protected against reinfection, and this health care worker study is really an elegant way to address that question,” Mark Slifka, PhD, said in an interview when asked to comment on the findings.
Although “there are millions of people in the U.S. who have been infected with COVID, we don’t know how common reinfection is,” said Dr. Slifka, a researcher at the Oregon National Primate Research Center and professor at Oregon Health & Science University, Portland.
The likelihood of a subsequent positive PCR test result was 1.09 per 10,000 days at risk among those without antibodies, compared with 0.13 per 10,000 days among those with anti-spike antibodies.
The investigators also assessed for the presence of anti–nucleocapsid IgG antibody titers. They found a significant trend for increasing PCR-positive test results with increasing antibody levels. As with the anti-spike antibody findings, 226 of 11,543 health care providers who did not have anti–nucleocapsid IgG antibodies subsequently tested positive on PCR; by contrast, two of 1,172 participants who did not have antibodies tested positive. Adjusted for age, sex, and calendar time, this finding translates to a 0.11 incidence rate ratio (0.13 per 10,000 days at risk; 95% confidence interval, 0.03-0.45; P = .002).
“This is a study a number of us have been trying to do,” said Christopher L. King, MD, PhD, professor of pathology and associate professor of medicine at Case Western Reserve University, Cleveland.
“To really follow a group like this longitudinally like they’ve done, with a large population, and to see such a big difference – it really confirms our suspicion that those who do become infected and develop an antibody response are significantly protected from reinfection.
“What’s great about this study is it’s nearly a 10-fold reduction in risk if you’ve recovered from COVID and have antibodies,” said Dr. King, who was not involved with the research. “That’s what a lot of us have been wanting to know.”
Unanswered questions remain
“How long this immunity lasts, we don’t know,” Dr. King said. He predicted that antibody protection could last a year to a year and a half. The duration of protection could vary. “We know some people lose their antibodies pretty quickly, and other people don’t,” he said.
Dr. Slifka said the suggestion of “a substantially reduced risk for at least 6 months ... is great news, and the timing couldn’t be better, because we’re rolling out the vaccines.”
Not all antibody responses are alike. For example, data indicate that antibody levels following immunization with the Pfizer/BioNTech or Moderna vaccines are higher on average than those of people who’ve had a natural infection, Dr. King said. He added that initial data on the AstraZeneca COVID-19 vaccine in development showed lower antibody levels compared with natural immunity.
The Centers for Disease Control and Prevention recommends immunization for those with a history of infection. “People who have gotten sick with COVID-19 may still benefit from getting vaccinated,” the CDC notes on its Facts About COVID-19 Vaccines website. “Due to the severe health risks associated with COVID-19 and the fact that re-infection with COVID-19 is possible, people may be advised to get a COVID-19 vaccine even if they have been sick with COVID-19 before,” the CDC stated.
The agency also notes that people appear to become susceptible to reinfection approximately 90 days after onset of infection. However, the new evidence from the UK study that persons have up to 6 months of immune protection might lead to a modification of recommendations, especially at a time when vaccine supplies are limited, Dr. Slifka said.
Another unanswered question is why the two study participants with antibodies subsequently tested positive for reinfection. “There are a lot of things that could have made these people more susceptible,” Dr. King said. For example, they could have been heavily exposed to SARS-CoV-2 or been immunocompromised for another reason.
Furthermore, the immune response involves more than antibody levels, Dr. King noted. Research in rhesus monkeys suggests that T cells play a role, but not as prominent a part as antibodies. “What I think is protecting us from infection is primarily the antibodies, although the T cells are probably important. Once you get infected, the T cells are probably playing a more important role in terms of whether you get very sick or not,” he said.
Multiplication + addition = more protected?
The 90% natural immunity protection in the study approaches the 95% efficacy associated with the Pfizer and Moderna vaccines, Dr. Slifka noted. Even without immunization, this could mean a portion of the U.S. population is already protected against future infection.
Furthermore, the CDC estimates that there are about 7.7 cases of COVID-19 for every case reported.
As of Sept. 30, the CDC reported that there were 6,891,764 confirmed cases. The agency estimated that overall, approximately 53 million people in the United States have been infected. More recent numbers from Johns Hopkins University’s Coronavirus Resource Center indicate that there were 18.2 million cases in the United States as of Dec. 22. If that tally is multiplied by 7.7, the total number protected could approach 140 million, Dr. Slifka said.
“That could really be a boost in terms of knocking this pandemic down in the next couple of months,” Dr. Slifka said.
“Now, if we were to modify the current recommendations and briefly defer vaccination of people with confirmed cases of COVID-19 until later on, we could start reaching herd immunity pretty quickly,” he added.
Real-life implications
“There is no such thing as 100% protection, even from the infection itself. So when you’re dealing with someone with possible exposure to COVID-19, you still need to follow the proper precautions,” Dr. Slifka said.
Nonetheless, he said, “This is great news for those on the front lines who are wondering whether or not they would have any protection if they had COVID-19 before. And the answer is yes – there is a very good chance they will have protection, based on this quite large study.”
One limitation of the study is that the population consisted predominantly of healthy adult health care workers aged 65 years or younger. “Further studies are needed to assess postinfection immunity in other populations, including children, older adults, and persons with coexisting conditions, including immunosuppression,” the researchers noted.
Dr. Eyre plans to continue following the health care workers in the study, some of whom have been vaccinated for COVID-19. This ongoing research will allow him and coinvestigators to “confirm the protection offered by vaccination and investigate how postvaccine antibody responses vary by whether you have had COVID-19 before or not. We also want to understand more about how long postinfection immunity lasts.”
Dr. Eyre has received grants as a Robinson Foundation Fellow and NIHR Oxford BRC senior fellow during the conduct of the study. Dr. Slifka and Dr. King report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hospital volumes start to fall again, even as COVID-19 soars
Hospital volumes, which had largely recovered in September after crashing last spring, are dropping again, according to new data from Strata Decision Technologies, a Chicago-based analytics firm.
For the 2 weeks that ended Nov. 28, inpatient admissions were 6.2% below what they’d been on Nov. 14 and 2.1% below what they’d been on Oct. 28. Compared with the same intervals in 2019, admissions were off 4.4% for the 14-day period and 3.7% for the 30-day period.
Although those aren’t large percentages, Strata’s report, based on data from about 275 client hospitals, notes that what kept the volumes up was the increasing number of COVID-19 cases. If COVID-19 cases are not considered, admissions would have been down “double digits,” said Steve Lefar, executive director of StrataDataScience, a division of Strata Decision Technologies, in an interview with this news organization.
“Hip and knee replacements, cardiac procedures, and other procedures are significantly down year over year. Infectious disease cases, in contrast, have skyrocketed,” Mr. Lefar said. “Many things went way down that hadn’t fully recovered. It’s COVID-19 that really brought the volume back up.”
Observation and emergency department visits also dropped from already low levels. For the 2 weeks that ended Nov. 28, observation visits were off 8.4%; for the previous month, 10.1%. Compared with 2019, they were down 22.3% and 18.6%, respectively.
ED visits fell 3.7% for the 2-week period, 0.6% for the month. They dropped 21% and 18.7%, respectively, compared with those periods from the previous year.
What these data reflect, Mr. Lefar said, is that people have avoided EDs and are staying away from them more than ever because of COVID-19 fears. This behavior could be problematic for people who have concerning symptoms, such as chest pains, that should be evaluated by an ED physician, he noted.
Daily outpatient visits were down 18.4% for the 14-day period and 9.3% for the 30-day period. But, compared with 2019, ambulatory visits increased 5.8% for the 2-week period and 4.7% for the previous month.
Long-term trends
The outpatient visit data should be viewed in the context of the overall trend since the pandemic began. Strata broke down service lines for the period between March 20 and Nov. 7. The analysis shows that evaluation and management (E/M) encounters, the largest outpatient visit category, fell 58% during this period, compared with the same interval in 2019. Visits for diabetes, hypertension, and minor acute infections and injuries were also way down.
Mr. Lefar observed that the E/M visit category was only for in-person visits, which many patients have ditched in favor of telehealth encounters. At the same time, he noted, “people are going in less for chronic disease visits. So there’s an interplay between less in-person visits, more telehealth, and maybe people going to other sites that aren’t on the hospital campus. But people are going less [to outpatient clinics].”
In the year-to-year comparison, volume was down substantially in other service lines, including cancer (–9.2%), cardiology (–20%), dermatology (–31%), endocrine (–18.8%), ENT (–42.5%), gastroenterology (–24.3%), nephrology (–15%), obstetrics (–15.6%), orthopedics (–28.2%), and general surgery (–22.2%). Major procedures decreased by 21.8%.
In contrast, the infectious disease category jumped 86% over 2019, and “other infectious and parasitic diseases” – i.e., COVID-19 – soared 222%.
There was a much bigger crash in admissions, observation visits, and ED visits last spring than in November, the report shows. “What happened nationally last spring is that everyone shut down,” Mr. Lefar explained. “All the electives were canceled. Even cancer surgery was shut down, along with many other procedures. That’s what drove that crash. But the provider community quickly learned that this is going to be a long haul, and we’re going to have to reopen. We’re going to do it safely, but we’re going to make sure people get the necessary care. We can’t put off cancer care or colonoscopies and other screenings that save lives.”
System starts to break down
The current wave of COVID-19, however, is beginning to change the definition of necessary care, he said. “Hospitals are reaching the breaking point between staff exhaustion and hospital capacity reaching its limit. In Texas, hospitals are starting to shut down certain essential non-COVID care. They’re turning away some nonurgent cases – the electives that were starting to come back.”
How about nonurgent COVID cases? Mr. Lefar said there’s evidence that some of those patients are also being diverted. “Some experts speculate that the turn-away rate of people with confirmed COVID is starting to go up, and hospitals are sending them home with oxygen or an oxygen meter and saying, ‘If it gets worse, come back.’ They just don’t have the critical care capacity – and that should scare the heck out of everybody.”
Strata doesn’t yet have the data to confirm this, he said, “but it appears that some people are being sent home. This may be partly because providers are better at telling which patients are acute, and there are better things they can send them home with. It’s not necessarily worse care, but we don’t know. But we’re definitely seeing a higher send-home rate of patients showing up with COVID.”
Hospital profit margins are cratering again, because the COVID-19 cases aren’t generating nearly as much profit as the lucrative procedures that, in many cases, have been put off, Mr. Lefar said. “Even though CMS is paying 20% more for verified COVID-19 patients, we know that the costs on these patients are much higher than expected, so they’re not making much money on these cases.”
For about a third of hospitals, margins are currently negative, he said. That is about the same percentage as in September. In April, 60% of health systems were losing money, he added. “The CARES Act saved some of them,” he noted.
A version of this article first appeared on Medscape.com.
Hospital volumes, which had largely recovered in September after crashing last spring, are dropping again, according to new data from Strata Decision Technologies, a Chicago-based analytics firm.
For the 2 weeks that ended Nov. 28, inpatient admissions were 6.2% below what they’d been on Nov. 14 and 2.1% below what they’d been on Oct. 28. Compared with the same intervals in 2019, admissions were off 4.4% for the 14-day period and 3.7% for the 30-day period.
Although those aren’t large percentages, Strata’s report, based on data from about 275 client hospitals, notes that what kept the volumes up was the increasing number of COVID-19 cases. If COVID-19 cases are not considered, admissions would have been down “double digits,” said Steve Lefar, executive director of StrataDataScience, a division of Strata Decision Technologies, in an interview with this news organization.
“Hip and knee replacements, cardiac procedures, and other procedures are significantly down year over year. Infectious disease cases, in contrast, have skyrocketed,” Mr. Lefar said. “Many things went way down that hadn’t fully recovered. It’s COVID-19 that really brought the volume back up.”
Observation and emergency department visits also dropped from already low levels. For the 2 weeks that ended Nov. 28, observation visits were off 8.4%; for the previous month, 10.1%. Compared with 2019, they were down 22.3% and 18.6%, respectively.
ED visits fell 3.7% for the 2-week period, 0.6% for the month. They dropped 21% and 18.7%, respectively, compared with those periods from the previous year.
What these data reflect, Mr. Lefar said, is that people have avoided EDs and are staying away from them more than ever because of COVID-19 fears. This behavior could be problematic for people who have concerning symptoms, such as chest pains, that should be evaluated by an ED physician, he noted.
Daily outpatient visits were down 18.4% for the 14-day period and 9.3% for the 30-day period. But, compared with 2019, ambulatory visits increased 5.8% for the 2-week period and 4.7% for the previous month.
Long-term trends
The outpatient visit data should be viewed in the context of the overall trend since the pandemic began. Strata broke down service lines for the period between March 20 and Nov. 7. The analysis shows that evaluation and management (E/M) encounters, the largest outpatient visit category, fell 58% during this period, compared with the same interval in 2019. Visits for diabetes, hypertension, and minor acute infections and injuries were also way down.
Mr. Lefar observed that the E/M visit category was only for in-person visits, which many patients have ditched in favor of telehealth encounters. At the same time, he noted, “people are going in less for chronic disease visits. So there’s an interplay between less in-person visits, more telehealth, and maybe people going to other sites that aren’t on the hospital campus. But people are going less [to outpatient clinics].”
In the year-to-year comparison, volume was down substantially in other service lines, including cancer (–9.2%), cardiology (–20%), dermatology (–31%), endocrine (–18.8%), ENT (–42.5%), gastroenterology (–24.3%), nephrology (–15%), obstetrics (–15.6%), orthopedics (–28.2%), and general surgery (–22.2%). Major procedures decreased by 21.8%.
In contrast, the infectious disease category jumped 86% over 2019, and “other infectious and parasitic diseases” – i.e., COVID-19 – soared 222%.
There was a much bigger crash in admissions, observation visits, and ED visits last spring than in November, the report shows. “What happened nationally last spring is that everyone shut down,” Mr. Lefar explained. “All the electives were canceled. Even cancer surgery was shut down, along with many other procedures. That’s what drove that crash. But the provider community quickly learned that this is going to be a long haul, and we’re going to have to reopen. We’re going to do it safely, but we’re going to make sure people get the necessary care. We can’t put off cancer care or colonoscopies and other screenings that save lives.”
System starts to break down
The current wave of COVID-19, however, is beginning to change the definition of necessary care, he said. “Hospitals are reaching the breaking point between staff exhaustion and hospital capacity reaching its limit. In Texas, hospitals are starting to shut down certain essential non-COVID care. They’re turning away some nonurgent cases – the electives that were starting to come back.”
How about nonurgent COVID cases? Mr. Lefar said there’s evidence that some of those patients are also being diverted. “Some experts speculate that the turn-away rate of people with confirmed COVID is starting to go up, and hospitals are sending them home with oxygen or an oxygen meter and saying, ‘If it gets worse, come back.’ They just don’t have the critical care capacity – and that should scare the heck out of everybody.”
Strata doesn’t yet have the data to confirm this, he said, “but it appears that some people are being sent home. This may be partly because providers are better at telling which patients are acute, and there are better things they can send them home with. It’s not necessarily worse care, but we don’t know. But we’re definitely seeing a higher send-home rate of patients showing up with COVID.”
Hospital profit margins are cratering again, because the COVID-19 cases aren’t generating nearly as much profit as the lucrative procedures that, in many cases, have been put off, Mr. Lefar said. “Even though CMS is paying 20% more for verified COVID-19 patients, we know that the costs on these patients are much higher than expected, so they’re not making much money on these cases.”
For about a third of hospitals, margins are currently negative, he said. That is about the same percentage as in September. In April, 60% of health systems were losing money, he added. “The CARES Act saved some of them,” he noted.
A version of this article first appeared on Medscape.com.
Hospital volumes, which had largely recovered in September after crashing last spring, are dropping again, according to new data from Strata Decision Technologies, a Chicago-based analytics firm.
For the 2 weeks that ended Nov. 28, inpatient admissions were 6.2% below what they’d been on Nov. 14 and 2.1% below what they’d been on Oct. 28. Compared with the same intervals in 2019, admissions were off 4.4% for the 14-day period and 3.7% for the 30-day period.
Although those aren’t large percentages, Strata’s report, based on data from about 275 client hospitals, notes that what kept the volumes up was the increasing number of COVID-19 cases. If COVID-19 cases are not considered, admissions would have been down “double digits,” said Steve Lefar, executive director of StrataDataScience, a division of Strata Decision Technologies, in an interview with this news organization.
“Hip and knee replacements, cardiac procedures, and other procedures are significantly down year over year. Infectious disease cases, in contrast, have skyrocketed,” Mr. Lefar said. “Many things went way down that hadn’t fully recovered. It’s COVID-19 that really brought the volume back up.”
Observation and emergency department visits also dropped from already low levels. For the 2 weeks that ended Nov. 28, observation visits were off 8.4%; for the previous month, 10.1%. Compared with 2019, they were down 22.3% and 18.6%, respectively.
ED visits fell 3.7% for the 2-week period, 0.6% for the month. They dropped 21% and 18.7%, respectively, compared with those periods from the previous year.
What these data reflect, Mr. Lefar said, is that people have avoided EDs and are staying away from them more than ever because of COVID-19 fears. This behavior could be problematic for people who have concerning symptoms, such as chest pains, that should be evaluated by an ED physician, he noted.
Daily outpatient visits were down 18.4% for the 14-day period and 9.3% for the 30-day period. But, compared with 2019, ambulatory visits increased 5.8% for the 2-week period and 4.7% for the previous month.
Long-term trends
The outpatient visit data should be viewed in the context of the overall trend since the pandemic began. Strata broke down service lines for the period between March 20 and Nov. 7. The analysis shows that evaluation and management (E/M) encounters, the largest outpatient visit category, fell 58% during this period, compared with the same interval in 2019. Visits for diabetes, hypertension, and minor acute infections and injuries were also way down.
Mr. Lefar observed that the E/M visit category was only for in-person visits, which many patients have ditched in favor of telehealth encounters. At the same time, he noted, “people are going in less for chronic disease visits. So there’s an interplay between less in-person visits, more telehealth, and maybe people going to other sites that aren’t on the hospital campus. But people are going less [to outpatient clinics].”
In the year-to-year comparison, volume was down substantially in other service lines, including cancer (–9.2%), cardiology (–20%), dermatology (–31%), endocrine (–18.8%), ENT (–42.5%), gastroenterology (–24.3%), nephrology (–15%), obstetrics (–15.6%), orthopedics (–28.2%), and general surgery (–22.2%). Major procedures decreased by 21.8%.
In contrast, the infectious disease category jumped 86% over 2019, and “other infectious and parasitic diseases” – i.e., COVID-19 – soared 222%.
There was a much bigger crash in admissions, observation visits, and ED visits last spring than in November, the report shows. “What happened nationally last spring is that everyone shut down,” Mr. Lefar explained. “All the electives were canceled. Even cancer surgery was shut down, along with many other procedures. That’s what drove that crash. But the provider community quickly learned that this is going to be a long haul, and we’re going to have to reopen. We’re going to do it safely, but we’re going to make sure people get the necessary care. We can’t put off cancer care or colonoscopies and other screenings that save lives.”
System starts to break down
The current wave of COVID-19, however, is beginning to change the definition of necessary care, he said. “Hospitals are reaching the breaking point between staff exhaustion and hospital capacity reaching its limit. In Texas, hospitals are starting to shut down certain essential non-COVID care. They’re turning away some nonurgent cases – the electives that were starting to come back.”
How about nonurgent COVID cases? Mr. Lefar said there’s evidence that some of those patients are also being diverted. “Some experts speculate that the turn-away rate of people with confirmed COVID is starting to go up, and hospitals are sending them home with oxygen or an oxygen meter and saying, ‘If it gets worse, come back.’ They just don’t have the critical care capacity – and that should scare the heck out of everybody.”
Strata doesn’t yet have the data to confirm this, he said, “but it appears that some people are being sent home. This may be partly because providers are better at telling which patients are acute, and there are better things they can send them home with. It’s not necessarily worse care, but we don’t know. But we’re definitely seeing a higher send-home rate of patients showing up with COVID.”
Hospital profit margins are cratering again, because the COVID-19 cases aren’t generating nearly as much profit as the lucrative procedures that, in many cases, have been put off, Mr. Lefar said. “Even though CMS is paying 20% more for verified COVID-19 patients, we know that the costs on these patients are much higher than expected, so they’re not making much money on these cases.”
For about a third of hospitals, margins are currently negative, he said. That is about the same percentage as in September. In April, 60% of health systems were losing money, he added. “The CARES Act saved some of them,” he noted.
A version of this article first appeared on Medscape.com.
Pregnant women should be offered COVID-19 vaccine, experts agree
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.

Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.
Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.
Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
Moderna’s COVID-19 vaccine deemed ‘highly effective,’ but further studies needed
The Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) evaluated
The panel acknowledged that further studies will be required post issuance of an Emergency Use Authorization (EUA) to collect additional data on the safety and effectiveness of the vaccine. A briefing document released by the FDA on Dec. 17, 2020, summarized interim results and included recommendations from VRBPAC on use of Moderna’s mRNA-1273 COVID-19 vaccine.
“On November 30, 2020, ModernaTX (the Sponsor) submitted an EUA request to FDA for an investigational COVID-19 vaccine (mRNA-1273) intended to prevent COVID-19,” the committee wrote.
The mRNA-1273 vaccine trial
Among 30,351 individuals aged 18 years and older, the efficacy, safety, and immunogenicity of the mRNA-1273 vaccine candidate was evaluated in a randomized, stratified, observer-blind, placebo-controlled phase 3 study. Participants were randomly assigned (1:1) to receive two injections of either 100 mcg of mRNA-1273 (n = 15,181) or saline placebo (n = 15,170) administered intramuscularly on day 1 and day 29.
The primary efficacy endpoint was efficacy of mRNA-1273 against PCR-confirmed COVID-19 with onset at least 14 days following the second dose. The primary safety endpoint was to characterize the safety of the vaccine following one or two doses.
Efficacy
Among 27,817 subjects included in the first interim analysis (data cutoff: Nov. 7, 2020), 5 cases of COVID-19 with onset at least 14 days after the second dose occurred among vaccine recipients and 90 case occurred among placebo recipients, corresponding to 94.5% vaccine efficacy (95% confidence interval, 86.5%-97.8%).
“Subgroup analyses of the primary efficacy endpoint showed similar efficacy point estimates across age groups, genders, racial and ethnic groups, and participants with medical comorbidities associated with high risk of severe COVID-19,” they reported.
Data from the final scheduled analysis of the primary efficacy endpoint (data cutoff: Nov. 21, 2020; median follow-up of >2 months after dose 2), demonstrated 94.1% vaccine efficacy (95% confidence interval, 89.3%-96.8%), corresponding to 11 cases of COVID-19 in the vaccine group and 185 cases in the placebo group.
When stratified by age, the vaccine efficacy was 95.6% (95% CI, 90.6%-97.9%) for individuals 18-64 years of age and 86.4% (95% CI, 61.4%-95.5%) for those 65 years of age or older.
In addition, results from secondary analyses indicated benefit for mRNA-1273 in preventing severe COVID-19 cases, COVID-19 in those with prior SARS-CoV-2 infection, and infection after the first dose, but these data were not conclusive.
Safety
Among 30,350 subjects included in the first interim analysis (data cutoff: Nov. 11, 2020; median follow-up of 7 weeks post second dose), no specific safety concerns were observed that would prevent issuance of an EUA.

Additional safety data (data cutoff: Nov. 25, 2020; median follow-up of 9 weeks post second dose) were provided on Dec. 7, 2020, but did not change the conclusions from the first interim analysis.
The most common vaccine-related adverse reactions were injection site pain (91.6%), fatigue (68.5%), headache (63.0%), muscle pain (59.6%), joint pain (44.8%), and chills (43.4%).
“The frequency of serious adverse events (SAEs) was low (1.0% in the mRNA-1273 arm and 1.0% in the placebo arm), without meaningful imbalances between study arms,” they reported.
Myocardial infarction (0.03%), nephrolithiasis (0.02%), and cholecystitis (0.02%) were the most common SAEs that were numerically greater in the vaccine arm than the placebo arm; however, the small number of cases does not infer a casual relationship.
“The 2-dose vaccination regimen was highly effective in preventing PCR-confirmed COVID-19 occurring at least 14 days after receipt of the second dose,” the committee wrote. “[However], it is critical to continue to gather data about the vaccine even after it is made available under EUA.”
The associated phase 3 study was sponsored by ModernaTX.
SOURCE: FDA Briefing Document: Moderna COVID-19 Vaccine. FDA Vaccines and Related Biological Products Advisory Committee. Published Dec. 17, 2020.
The Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) evaluated
The panel acknowledged that further studies will be required post issuance of an Emergency Use Authorization (EUA) to collect additional data on the safety and effectiveness of the vaccine. A briefing document released by the FDA on Dec. 17, 2020, summarized interim results and included recommendations from VRBPAC on use of Moderna’s mRNA-1273 COVID-19 vaccine.
“On November 30, 2020, ModernaTX (the Sponsor) submitted an EUA request to FDA for an investigational COVID-19 vaccine (mRNA-1273) intended to prevent COVID-19,” the committee wrote.
The mRNA-1273 vaccine trial
Among 30,351 individuals aged 18 years and older, the efficacy, safety, and immunogenicity of the mRNA-1273 vaccine candidate was evaluated in a randomized, stratified, observer-blind, placebo-controlled phase 3 study. Participants were randomly assigned (1:1) to receive two injections of either 100 mcg of mRNA-1273 (n = 15,181) or saline placebo (n = 15,170) administered intramuscularly on day 1 and day 29.
The primary efficacy endpoint was efficacy of mRNA-1273 against PCR-confirmed COVID-19 with onset at least 14 days following the second dose. The primary safety endpoint was to characterize the safety of the vaccine following one or two doses.
Efficacy
Among 27,817 subjects included in the first interim analysis (data cutoff: Nov. 7, 2020), 5 cases of COVID-19 with onset at least 14 days after the second dose occurred among vaccine recipients and 90 case occurred among placebo recipients, corresponding to 94.5% vaccine efficacy (95% confidence interval, 86.5%-97.8%).
“Subgroup analyses of the primary efficacy endpoint showed similar efficacy point estimates across age groups, genders, racial and ethnic groups, and participants with medical comorbidities associated with high risk of severe COVID-19,” they reported.
Data from the final scheduled analysis of the primary efficacy endpoint (data cutoff: Nov. 21, 2020; median follow-up of >2 months after dose 2), demonstrated 94.1% vaccine efficacy (95% confidence interval, 89.3%-96.8%), corresponding to 11 cases of COVID-19 in the vaccine group and 185 cases in the placebo group.
When stratified by age, the vaccine efficacy was 95.6% (95% CI, 90.6%-97.9%) for individuals 18-64 years of age and 86.4% (95% CI, 61.4%-95.5%) for those 65 years of age or older.
In addition, results from secondary analyses indicated benefit for mRNA-1273 in preventing severe COVID-19 cases, COVID-19 in those with prior SARS-CoV-2 infection, and infection after the first dose, but these data were not conclusive.
Safety
Among 30,350 subjects included in the first interim analysis (data cutoff: Nov. 11, 2020; median follow-up of 7 weeks post second dose), no specific safety concerns were observed that would prevent issuance of an EUA.
Additional safety data (data cutoff: Nov. 25, 2020; median follow-up of 9 weeks post second dose) were provided on Dec. 7, 2020, but did not change the conclusions from the first interim analysis.
The most common vaccine-related adverse reactions were injection site pain (91.6%), fatigue (68.5%), headache (63.0%), muscle pain (59.6%), joint pain (44.8%), and chills (43.4%).
“The frequency of serious adverse events (SAEs) was low (1.0% in the mRNA-1273 arm and 1.0% in the placebo arm), without meaningful imbalances between study arms,” they reported.
Myocardial infarction (0.03%), nephrolithiasis (0.02%), and cholecystitis (0.02%) were the most common SAEs that were numerically greater in the vaccine arm than the placebo arm; however, the small number of cases does not infer a casual relationship.
“The 2-dose vaccination regimen was highly effective in preventing PCR-confirmed COVID-19 occurring at least 14 days after receipt of the second dose,” the committee wrote. “[However], it is critical to continue to gather data about the vaccine even after it is made available under EUA.”
The associated phase 3 study was sponsored by ModernaTX.
SOURCE: FDA Briefing Document: Moderna COVID-19 Vaccine. FDA Vaccines and Related Biological Products Advisory Committee. Published Dec. 17, 2020.
The Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) evaluated
The panel acknowledged that further studies will be required post issuance of an Emergency Use Authorization (EUA) to collect additional data on the safety and effectiveness of the vaccine. A briefing document released by the FDA on Dec. 17, 2020, summarized interim results and included recommendations from VRBPAC on use of Moderna’s mRNA-1273 COVID-19 vaccine.
“On November 30, 2020, ModernaTX (the Sponsor) submitted an EUA request to FDA for an investigational COVID-19 vaccine (mRNA-1273) intended to prevent COVID-19,” the committee wrote.
The mRNA-1273 vaccine trial
Among 30,351 individuals aged 18 years and older, the efficacy, safety, and immunogenicity of the mRNA-1273 vaccine candidate was evaluated in a randomized, stratified, observer-blind, placebo-controlled phase 3 study. Participants were randomly assigned (1:1) to receive two injections of either 100 mcg of mRNA-1273 (n = 15,181) or saline placebo (n = 15,170) administered intramuscularly on day 1 and day 29.
The primary efficacy endpoint was efficacy of mRNA-1273 against PCR-confirmed COVID-19 with onset at least 14 days following the second dose. The primary safety endpoint was to characterize the safety of the vaccine following one or two doses.
Efficacy
Among 27,817 subjects included in the first interim analysis (data cutoff: Nov. 7, 2020), 5 cases of COVID-19 with onset at least 14 days after the second dose occurred among vaccine recipients and 90 case occurred among placebo recipients, corresponding to 94.5% vaccine efficacy (95% confidence interval, 86.5%-97.8%).
“Subgroup analyses of the primary efficacy endpoint showed similar efficacy point estimates across age groups, genders, racial and ethnic groups, and participants with medical comorbidities associated with high risk of severe COVID-19,” they reported.
Data from the final scheduled analysis of the primary efficacy endpoint (data cutoff: Nov. 21, 2020; median follow-up of >2 months after dose 2), demonstrated 94.1% vaccine efficacy (95% confidence interval, 89.3%-96.8%), corresponding to 11 cases of COVID-19 in the vaccine group and 185 cases in the placebo group.
When stratified by age, the vaccine efficacy was 95.6% (95% CI, 90.6%-97.9%) for individuals 18-64 years of age and 86.4% (95% CI, 61.4%-95.5%) for those 65 years of age or older.
In addition, results from secondary analyses indicated benefit for mRNA-1273 in preventing severe COVID-19 cases, COVID-19 in those with prior SARS-CoV-2 infection, and infection after the first dose, but these data were not conclusive.
Safety
Among 30,350 subjects included in the first interim analysis (data cutoff: Nov. 11, 2020; median follow-up of 7 weeks post second dose), no specific safety concerns were observed that would prevent issuance of an EUA.
Additional safety data (data cutoff: Nov. 25, 2020; median follow-up of 9 weeks post second dose) were provided on Dec. 7, 2020, but did not change the conclusions from the first interim analysis.
The most common vaccine-related adverse reactions were injection site pain (91.6%), fatigue (68.5%), headache (63.0%), muscle pain (59.6%), joint pain (44.8%), and chills (43.4%).
“The frequency of serious adverse events (SAEs) was low (1.0% in the mRNA-1273 arm and 1.0% in the placebo arm), without meaningful imbalances between study arms,” they reported.
Myocardial infarction (0.03%), nephrolithiasis (0.02%), and cholecystitis (0.02%) were the most common SAEs that were numerically greater in the vaccine arm than the placebo arm; however, the small number of cases does not infer a casual relationship.
“The 2-dose vaccination regimen was highly effective in preventing PCR-confirmed COVID-19 occurring at least 14 days after receipt of the second dose,” the committee wrote. “[However], it is critical to continue to gather data about the vaccine even after it is made available under EUA.”
The associated phase 3 study was sponsored by ModernaTX.
SOURCE: FDA Briefing Document: Moderna COVID-19 Vaccine. FDA Vaccines and Related Biological Products Advisory Committee. Published Dec. 17, 2020.
Key clinical point: The FDA’s Vaccines and Related Biological Products Advisory Committee regarded Moderna’s COVID-19 vaccine as highly effective with a favorable safety profile, based on interim phase 3 results.
Major finding: The two-dose vaccine regimen had a low frequency of serious adverse events (1.0% each in the mRNA-1273 and placebo arms, respectively) and demonstrated 94.1% (95% CI, 89.3%-96.8%) vaccine efficacy.
Study details: A briefing document summarized interim data and recommendations from the FDA’s VRBPAC on Moderna’s mRNA-1273 COVID-19 vaccine.
Disclosures: The associated phase 3 study was sponsored by ModernaTX.
Source: FDA Briefing Document: Moderna COVID-19 Vaccine. FDA Vaccines and Related Biological Products Advisory Committee. Published Dec. 17, 2020.
Child abuse visits to EDs declined in 2020, but not admissions
but the visits in 2020 were significantly more likely to result in hospitalization, based on analysis of a national ED database.
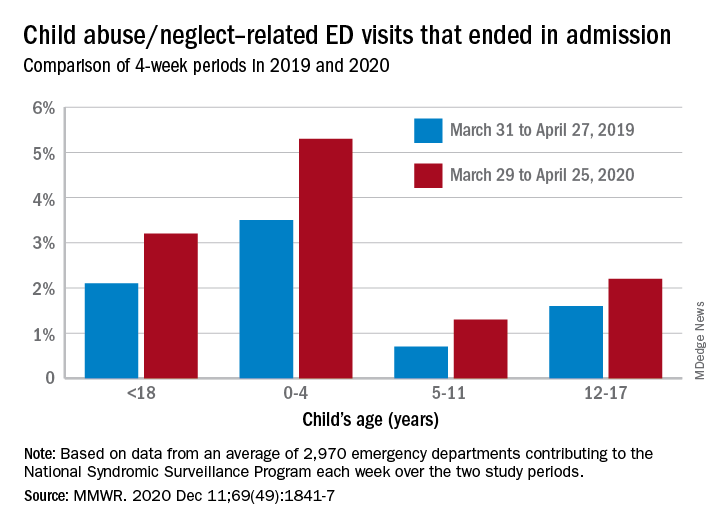
The number of ED visits involving child abuse and neglect was down by 53% during the 4-week period from March 29 to April 25, 2020, compared with the 4 weeks from March 31 to April 27, 2019. The proportion of those ED visits that ended in hospitalizations, however, increased from 2.1% in 2019 to 3.2% in 2020, Elizabeth Swedo, MD, and associates at the Centers for Disease Control and Prevention said in the Morbidity and Mortality Weekly Report.
“ED visits related to suspected or confirmed child abuse and neglect decreased beginning the week of March 15, 2020, coinciding with the declaration of a national emergency related to COVID-19 and implementation of community mitigation measures,” they wrote.
An earlier study involving the same database (the National Syndromic Surveillance Program) showed that, over the two same 4-week periods, the volume of all ED visits in 2020 was down 72% for children aged 10 years and younger and 71% for those aged 11-14 years.
In the current study, however, all age subgroups had significant increases in hospital admissions. The proportion of ED visits related to child abuse and neglect that resulted in hospitalization rose from 3.5% in 2019 to 5.3% in 2020 among ages 0-4 years, 0.7% to 1.3% for ages 5-11 years, and 1.6% to 2.2% for adolescents aged 12-17, Dr. Swedo and associates reported.
The absence of a corresponding drop in hospitalizations may be tied to risk factors related to the pandemic, “such as loss of income, increased stress related to parental child care and schooling responsibilities, and increased substance use and mental health conditions among adults,” the investigators added.
The National Syndromic Surveillance Program receives daily data from 3,310 EDs in 47 states, but the number of facilities meeting the investigators’ criteria averaged 2,970 a week for the 8 weeks of the study period.
SOURCE: Swedo E et al. MMWR. 2020 Dec. 11;69(49):1841-7.
but the visits in 2020 were significantly more likely to result in hospitalization, based on analysis of a national ED database.
The number of ED visits involving child abuse and neglect was down by 53% during the 4-week period from March 29 to April 25, 2020, compared with the 4 weeks from March 31 to April 27, 2019. The proportion of those ED visits that ended in hospitalizations, however, increased from 2.1% in 2019 to 3.2% in 2020, Elizabeth Swedo, MD, and associates at the Centers for Disease Control and Prevention said in the Morbidity and Mortality Weekly Report.
“ED visits related to suspected or confirmed child abuse and neglect decreased beginning the week of March 15, 2020, coinciding with the declaration of a national emergency related to COVID-19 and implementation of community mitigation measures,” they wrote.
An earlier study involving the same database (the National Syndromic Surveillance Program) showed that, over the two same 4-week periods, the volume of all ED visits in 2020 was down 72% for children aged 10 years and younger and 71% for those aged 11-14 years.
In the current study, however, all age subgroups had significant increases in hospital admissions. The proportion of ED visits related to child abuse and neglect that resulted in hospitalization rose from 3.5% in 2019 to 5.3% in 2020 among ages 0-4 years, 0.7% to 1.3% for ages 5-11 years, and 1.6% to 2.2% for adolescents aged 12-17, Dr. Swedo and associates reported.
The absence of a corresponding drop in hospitalizations may be tied to risk factors related to the pandemic, “such as loss of income, increased stress related to parental child care and schooling responsibilities, and increased substance use and mental health conditions among adults,” the investigators added.
The National Syndromic Surveillance Program receives daily data from 3,310 EDs in 47 states, but the number of facilities meeting the investigators’ criteria averaged 2,970 a week for the 8 weeks of the study period.
SOURCE: Swedo E et al. MMWR. 2020 Dec. 11;69(49):1841-7.
but the visits in 2020 were significantly more likely to result in hospitalization, based on analysis of a national ED database.
The number of ED visits involving child abuse and neglect was down by 53% during the 4-week period from March 29 to April 25, 2020, compared with the 4 weeks from March 31 to April 27, 2019. The proportion of those ED visits that ended in hospitalizations, however, increased from 2.1% in 2019 to 3.2% in 2020, Elizabeth Swedo, MD, and associates at the Centers for Disease Control and Prevention said in the Morbidity and Mortality Weekly Report.
“ED visits related to suspected or confirmed child abuse and neglect decreased beginning the week of March 15, 2020, coinciding with the declaration of a national emergency related to COVID-19 and implementation of community mitigation measures,” they wrote.
An earlier study involving the same database (the National Syndromic Surveillance Program) showed that, over the two same 4-week periods, the volume of all ED visits in 2020 was down 72% for children aged 10 years and younger and 71% for those aged 11-14 years.
In the current study, however, all age subgroups had significant increases in hospital admissions. The proportion of ED visits related to child abuse and neglect that resulted in hospitalization rose from 3.5% in 2019 to 5.3% in 2020 among ages 0-4 years, 0.7% to 1.3% for ages 5-11 years, and 1.6% to 2.2% for adolescents aged 12-17, Dr. Swedo and associates reported.
The absence of a corresponding drop in hospitalizations may be tied to risk factors related to the pandemic, “such as loss of income, increased stress related to parental child care and schooling responsibilities, and increased substance use and mental health conditions among adults,” the investigators added.
The National Syndromic Surveillance Program receives daily data from 3,310 EDs in 47 states, but the number of facilities meeting the investigators’ criteria averaged 2,970 a week for the 8 weeks of the study period.
SOURCE: Swedo E et al. MMWR. 2020 Dec. 11;69(49):1841-7.
FROM MMWR