User login
Genentech Resubmits T-DM1 to FDA
Two years after the Food and Drug Administration refused to review T-DM1 for accelerated approval, Roche/Genentech Inc. has resubmitted the application with a statistically significant overall survival advantage in hand – FDA’s gold standard for oncology approvals.
The company announced Aug. 27 that it had submitted a biologics license application (BLA) to the FDA for the antibody drug conjugate trastuzumab emtansine, a combination of the monoclonal antibody trastuzumab (Herceptin) with the potent cytotoxic agent DM1, connected by a stable linker based on technology licensed from ImmunoGen Inc.
Genentech expects to submit a marketing authorization application to the European Medicines Agency soon.
[Editor’s note: Genentech has clarified that the updated overall survival analysis was not included in the initial BLA resubmission. It will be provided to FDA during its review of the application.]
The company also announced further results from the EMILIA study, showing T-DM1 had a statistically significant overall survival benefit in HER2-positive metastatic breast cancer, compared with GlaxoSmithKline Inc.’s lapatinib (Tykerb) in combination with capecitabine (Xeloda). Roche did not release actual figures, which will be presented at an upcoming medical meeting.

At the American Society for Clinical Oncology meeting in June, EMILIA authors showed a 3.2-month median progression-free survival benefit. Lead investigator Dr. Kimberly Blackwell, professor of medicine and assistant professor of radiation oncology at Duke Cancer Institute, Duke University, Durham, N.C., also said at the time there was a trend toward an overall survival improvement.
Analysts were not surprised at the news, given the progression-free survival advantage. J.P. Morgan said in an Aug. 27 note that its forecasts already expected a survival benefit in many treatment settings and that while markets reacted favorably to the news, ImmunoGen "already gets credit for this highly promising product."
Priority Review Expected
The positive data also should allow for a quick FDA approval. Priority review would mean action by late February 2013, but J.P. Morgan’s Cory Kasimov indicated that approval could come earlier. The FDA has approved several drugs ahead of the user fee deadline over the past year.
That would be a welcome change for T-DM1 after the FDA refused to file Genentech’s accelerated approval application for the product in 2010. Indeed, the company made the refuse-to-file announcement exactly 2 years before announcing the overall survival benefit – Aug. 27, 2010.
That application was based on the results of one single-arm phase II trial in 110 patients. Tumors shrank in one-third of women with advanced HER2-positive breast cancer, who had received on average seven prior medicines, but the FDA said the filing did not meet the standards for accelerated approval because the company had not exhausted all available treatment options for metastatic breast cancer in the study population.
Roche plans to launch T-DM1 next year as a second-line therapy, although physicians are expected to use it as a first-line therapy, company officials said during an analyst briefing at ASCO in June.
T-DM1 is expected to eventually replace trastuzumab as the standard of care and as the cornerstone of Roche’s breast cancer portfolio. An early 2013 approval will give Roche time to establish the product before the introduction of trastuzumab biosimilars, expected in Europe in 2014 and in the United States in 2019.
The company is already studying T-DM1 in combination with pertuzumab (Perjeta), which could potentially eliminate the need for chemotherapy. Pertuzumab was approved in June for use with trastuzumab and chemotherapy in previously untreated HER2-positive metastatic breast cancer that has recurred after adjuvant or neoadjuvant therapy.
Roche also is expected to be among the first to test a new accelerated approval draft guidance using pathologic complete response to support accelerated approval in neoadjuvant breast cancer. It announced plans for a study testing T-DM1 and pertuzumab just after the draft guidance was released.
The company will face concerns about pricing, especially with the combination of the two targeted agents. But at an ASCO briefing, Roche COO Pascal Soriot pointed out that there will be safety advantages. "There will be a lot of savings for the systems and we need to price that in how we price T-DM1," he said.
Editor’s note: This story appears courtesy of "The Pink Sheet," a weekly Elsevier publication covering pharmaceutical business and policy issues. To learn more, contract customer care at 800-332-2181 or sign up for a free trial.
* This story was updated on 8/28/12 per clarification from Genentech.
Two years after the Food and Drug Administration refused to review T-DM1 for accelerated approval, Roche/Genentech Inc. has resubmitted the application with a statistically significant overall survival advantage in hand – FDA’s gold standard for oncology approvals.
The company announced Aug. 27 that it had submitted a biologics license application (BLA) to the FDA for the antibody drug conjugate trastuzumab emtansine, a combination of the monoclonal antibody trastuzumab (Herceptin) with the potent cytotoxic agent DM1, connected by a stable linker based on technology licensed from ImmunoGen Inc.
Genentech expects to submit a marketing authorization application to the European Medicines Agency soon.
[Editor’s note: Genentech has clarified that the updated overall survival analysis was not included in the initial BLA resubmission. It will be provided to FDA during its review of the application.]
The company also announced further results from the EMILIA study, showing T-DM1 had a statistically significant overall survival benefit in HER2-positive metastatic breast cancer, compared with GlaxoSmithKline Inc.’s lapatinib (Tykerb) in combination with capecitabine (Xeloda). Roche did not release actual figures, which will be presented at an upcoming medical meeting.
At the American Society for Clinical Oncology meeting in June, EMILIA authors showed a 3.2-month median progression-free survival benefit. Lead investigator Dr. Kimberly Blackwell, professor of medicine and assistant professor of radiation oncology at Duke Cancer Institute, Duke University, Durham, N.C., also said at the time there was a trend toward an overall survival improvement.
Analysts were not surprised at the news, given the progression-free survival advantage. J.P. Morgan said in an Aug. 27 note that its forecasts already expected a survival benefit in many treatment settings and that while markets reacted favorably to the news, ImmunoGen "already gets credit for this highly promising product."
Priority Review Expected
The positive data also should allow for a quick FDA approval. Priority review would mean action by late February 2013, but J.P. Morgan’s Cory Kasimov indicated that approval could come earlier. The FDA has approved several drugs ahead of the user fee deadline over the past year.
That would be a welcome change for T-DM1 after the FDA refused to file Genentech’s accelerated approval application for the product in 2010. Indeed, the company made the refuse-to-file announcement exactly 2 years before announcing the overall survival benefit – Aug. 27, 2010.
That application was based on the results of one single-arm phase II trial in 110 patients. Tumors shrank in one-third of women with advanced HER2-positive breast cancer, who had received on average seven prior medicines, but the FDA said the filing did not meet the standards for accelerated approval because the company had not exhausted all available treatment options for metastatic breast cancer in the study population.
Roche plans to launch T-DM1 next year as a second-line therapy, although physicians are expected to use it as a first-line therapy, company officials said during an analyst briefing at ASCO in June.
T-DM1 is expected to eventually replace trastuzumab as the standard of care and as the cornerstone of Roche’s breast cancer portfolio. An early 2013 approval will give Roche time to establish the product before the introduction of trastuzumab biosimilars, expected in Europe in 2014 and in the United States in 2019.
The company is already studying T-DM1 in combination with pertuzumab (Perjeta), which could potentially eliminate the need for chemotherapy. Pertuzumab was approved in June for use with trastuzumab and chemotherapy in previously untreated HER2-positive metastatic breast cancer that has recurred after adjuvant or neoadjuvant therapy.
Roche also is expected to be among the first to test a new accelerated approval draft guidance using pathologic complete response to support accelerated approval in neoadjuvant breast cancer. It announced plans for a study testing T-DM1 and pertuzumab just after the draft guidance was released.
The company will face concerns about pricing, especially with the combination of the two targeted agents. But at an ASCO briefing, Roche COO Pascal Soriot pointed out that there will be safety advantages. "There will be a lot of savings for the systems and we need to price that in how we price T-DM1," he said.
Editor’s note: This story appears courtesy of "The Pink Sheet," a weekly Elsevier publication covering pharmaceutical business and policy issues. To learn more, contract customer care at 800-332-2181 or sign up for a free trial.
* This story was updated on 8/28/12 per clarification from Genentech.
Two years after the Food and Drug Administration refused to review T-DM1 for accelerated approval, Roche/Genentech Inc. has resubmitted the application with a statistically significant overall survival advantage in hand – FDA’s gold standard for oncology approvals.
The company announced Aug. 27 that it had submitted a biologics license application (BLA) to the FDA for the antibody drug conjugate trastuzumab emtansine, a combination of the monoclonal antibody trastuzumab (Herceptin) with the potent cytotoxic agent DM1, connected by a stable linker based on technology licensed from ImmunoGen Inc.
Genentech expects to submit a marketing authorization application to the European Medicines Agency soon.
[Editor’s note: Genentech has clarified that the updated overall survival analysis was not included in the initial BLA resubmission. It will be provided to FDA during its review of the application.]
The company also announced further results from the EMILIA study, showing T-DM1 had a statistically significant overall survival benefit in HER2-positive metastatic breast cancer, compared with GlaxoSmithKline Inc.’s lapatinib (Tykerb) in combination with capecitabine (Xeloda). Roche did not release actual figures, which will be presented at an upcoming medical meeting.
At the American Society for Clinical Oncology meeting in June, EMILIA authors showed a 3.2-month median progression-free survival benefit. Lead investigator Dr. Kimberly Blackwell, professor of medicine and assistant professor of radiation oncology at Duke Cancer Institute, Duke University, Durham, N.C., also said at the time there was a trend toward an overall survival improvement.
Analysts were not surprised at the news, given the progression-free survival advantage. J.P. Morgan said in an Aug. 27 note that its forecasts already expected a survival benefit in many treatment settings and that while markets reacted favorably to the news, ImmunoGen "already gets credit for this highly promising product."
Priority Review Expected
The positive data also should allow for a quick FDA approval. Priority review would mean action by late February 2013, but J.P. Morgan’s Cory Kasimov indicated that approval could come earlier. The FDA has approved several drugs ahead of the user fee deadline over the past year.
That would be a welcome change for T-DM1 after the FDA refused to file Genentech’s accelerated approval application for the product in 2010. Indeed, the company made the refuse-to-file announcement exactly 2 years before announcing the overall survival benefit – Aug. 27, 2010.
That application was based on the results of one single-arm phase II trial in 110 patients. Tumors shrank in one-third of women with advanced HER2-positive breast cancer, who had received on average seven prior medicines, but the FDA said the filing did not meet the standards for accelerated approval because the company had not exhausted all available treatment options for metastatic breast cancer in the study population.
Roche plans to launch T-DM1 next year as a second-line therapy, although physicians are expected to use it as a first-line therapy, company officials said during an analyst briefing at ASCO in June.
T-DM1 is expected to eventually replace trastuzumab as the standard of care and as the cornerstone of Roche’s breast cancer portfolio. An early 2013 approval will give Roche time to establish the product before the introduction of trastuzumab biosimilars, expected in Europe in 2014 and in the United States in 2019.
The company is already studying T-DM1 in combination with pertuzumab (Perjeta), which could potentially eliminate the need for chemotherapy. Pertuzumab was approved in June for use with trastuzumab and chemotherapy in previously untreated HER2-positive metastatic breast cancer that has recurred after adjuvant or neoadjuvant therapy.
Roche also is expected to be among the first to test a new accelerated approval draft guidance using pathologic complete response to support accelerated approval in neoadjuvant breast cancer. It announced plans for a study testing T-DM1 and pertuzumab just after the draft guidance was released.
The company will face concerns about pricing, especially with the combination of the two targeted agents. But at an ASCO briefing, Roche COO Pascal Soriot pointed out that there will be safety advantages. "There will be a lot of savings for the systems and we need to price that in how we price T-DM1," he said.
Editor’s note: This story appears courtesy of "The Pink Sheet," a weekly Elsevier publication covering pharmaceutical business and policy issues. To learn more, contract customer care at 800-332-2181 or sign up for a free trial.
* This story was updated on 8/28/12 per clarification from Genentech.

Acetyl-l-Carnitine Yields Mixed Results for Chemo-Induced Neuropathy
CHICAGO – The impact of acetyl-l-carnitine on chemotherapy-induced peripheral neuropathy may depend largely on the clinical context and patient population, a pair of phase III trials suggests.
Acetyl-l-carnitine (ALC), a natural substance marketed over the counter as a dietary supplement, is popular among cancer patients as a result of preclinical and early-phase data in chemotherapy-related neuropathy and also a study in patients with diabetes-related peripheral neuropathy.
But in a trial among 409 U.S. women receiving adjuvant chemotherapy for breast cancer, those who took ALC not only had no decrease in the development of peripheral neuropathy symptoms relative to peers who were given a placebo, but actually had an increase. And they had a higher rate of serious neuropathy, too.
In contrast, in a trial among more than 200 Chinese patients with various cancers who had peripheral neuropathy from previous chemotherapy, those who took ALC were more likely than those who took a placebo to have an improvement of at least one grade in their neuropathy. They also were more likely to have improvements in fatigue and strength.
Taken together, the two trials, which were reported in a poster discussion session at the annual meeting of the American Society of Clinical Oncology, provide yet another cautionary lesson on the complexity of combining conventional and complementary therapies.
"The use of ALC for prevention is not recommended, and I would say, based on [these results], should be cautioned against. It will be interesting to see the carnitine data and to understand, as much as possible, why the trial was negative," commented Debra L. Barton, Ph.D., of the Mayo Clinic in Rochester, Minn., who was invited to discuss the research. "Further studies are needed to really understand if ALC should be used to treat peripheral neuropathy."
ALC for Prevention of Peripheral Neuropathy

In the first trial, Southwest Oncology Group (SWOG) protocol S0715, investigators led by Dr. Dawn L. Hershman randomized women receiving adjuvant taxane chemotherapy for early breast cancer evenly to either oral ALC 1,000 mg three times daily or matching placebo, for 24 weeks.
Compared with their counterparts in the placebo group, women in the ALC group were more likely to have a greater than 5-point adjusted decrease on the neurotoxicity subscale of the Functional Assessment of Cancer Therapy–Taxane (FACT-NTX) instrument at 12 weeks (odds ratio, 1.48; P = .08) and also at 24 weeks (38% vs. 28%; OR, 1.57; P = .05).
This magnitude of worsening is clinically meaningful, maintained Dr. Hershman of Columbia University in New York, "so this is not like a lot of studies where you find a statistically significant difference that’s not clinically meaningful."
In addition, the incidence of grade 3/4 neurotoxicity was 3.8% with ALC, much higher than the 0.5% seen with placebo.
Patients in the ALC group also had scores on the FACT trial outcome index subscale (FACT-TOI), an overall measure of function, that were on average 3.5 points lower (worse) than those among their placebo counterparts (P = .03). There were no significant differences between groups in terms of fatigue and other toxicities.
The investigators have collected biosamples and will be assessing potential biological correlates with peripheral neuropathy outcomes, according to Dr. Hershman.
"We are looking at DNA, oxidative stress, and carnitine levels to better understand the mechanisms of chemotherapy-induced peripheral neuropathy to begin with, because there is not a whole lot known in terms of mechanism," she said. "If we can figure out what makes people worse, then we will maybe be able to figure out how to make people better from a more mechanistic standpoint, because there are very few drugs to treat chemotherapy-induced peripheral neuropathy."
An obvious concern from the trial’s findings is that ALC may somehow potentiate the neurotoxic effects of taxanes. "Based on these data, physicians should be telling patients not to take ALC during adjuvant chemotherapy," Dr. Hershman concluded. "You need to talk to patients. We know from the literature that overwhelmingly large number of patients take supplements during chemotherapy and afterward, many of which have not been tested. It’s important to get that history from patients."
Dr. Barton, the discussant, praised the trial’s rigorous methodology and proposed that there may have been several reasons for the lack of ALC benefit in preventing neuropathy, despite compelling earlier data.
Previous prevention research was done in animals and thus may not translate to humans, she said. And a positive trial for treatment in humans used intravenous administration, which may result in different bioavailability. Finally, "ALC capsules needed to be taken three times a day, and they are rather large, and these patients were, after all, on chemotherapy. They were likely nauseated [and] dyspeptic, and taking what some might call a horse pill three times a day could not have been an easy task. The study did use pill diaries, but we know those aren’t a perfect tool for adherence."
"The great thing is that the study collected blood and they are able to look at carnitine levels," Dr. Barton said. "So if carnitine is up in the group that got acetyl-carnitine and not in the group that got placebo, well, I think that pretty much confirms that this just didn’t work."
ALC for Treatment of Peripheral Neuropathy
In the second trial, protocol ZHAOKE-2007L03540, investigators led by Dr. Yuanjue Sun of the Sixth Affiliated Hospital of Shanghai (China) Jiao Tong University, enrolled 239 patients who had cancer of various types and stages, had completed chemotherapy, and had had at least grade 2 peripheral neuropathy for up to 6 months.
They were randomly assigned to receive either oral ALC at a dose of 3 g/day or matching placebo, for 8 weeks, with outcomes assessed at clinic visits or by telephone.
Analyses showed that compared with their counterparts in the placebo group, patients in the ALC group were more likely to have had an improvement of at least one grade in their neuropathy, both at 8 weeks (51% vs. 24%; P less than .001) and at 12 weeks (58% vs. 40%; P less than .001).
In terms of secondary outcomes, the ALC group was also more likely to have had an improvement in cancer-related fatigue (31% vs. 20%; P = .048), physical strength (29% vs. 13%; P = .02), and electrophysiology in peripheral nerves (75% vs. 58%; P = .02).
The two groups had statistically indistinguishable rates of adverse events (20% vs. 15%) and adverse reactions (6% vs. 5%). The most common events were gastrointestinal ones and skin allergies.
"This is the first time to confirm that ALC has a positive effect to cure chemotherapy-induced peripheral neuropathy in the Chinese population," Dr. Sun commented through a translator.
"I think the very important thing for this trial is, it is a different kind of patient population. Before this, most clinical trials were performed in [whites] or maybe Americans. This is an only-Asian [population]," he noted, and it is possible that there are genetic differences in how ALC is metabolized.
Dr. Barton, the discussant, took a cautionary view, saying that "there are some things to consider before going out and telling patients to consider acetyl-carnitine for their peripheral neuropathy."
It was unclear from the results reported whether the two treatment groups were well balanced and what criteria were used to define improvement for the secondary outcomes, she noted. Additionally, "outcome measures were all provider graded, [and there were] no self-report measures, so it is difficult to understand the impact of treatment on symptoms, particularly from the patient perspective," she noted.
Dr. Hershman, Dr. Sun, and Dr. Barton disclosed no relevant conflicts of interest; the ZHAOKE-2007L03540 trial was sponsored by Lee’s Pharmaceutical Limited.
CHICAGO – The impact of acetyl-l-carnitine on chemotherapy-induced peripheral neuropathy may depend largely on the clinical context and patient population, a pair of phase III trials suggests.
Acetyl-l-carnitine (ALC), a natural substance marketed over the counter as a dietary supplement, is popular among cancer patients as a result of preclinical and early-phase data in chemotherapy-related neuropathy and also a study in patients with diabetes-related peripheral neuropathy.
But in a trial among 409 U.S. women receiving adjuvant chemotherapy for breast cancer, those who took ALC not only had no decrease in the development of peripheral neuropathy symptoms relative to peers who were given a placebo, but actually had an increase. And they had a higher rate of serious neuropathy, too.
In contrast, in a trial among more than 200 Chinese patients with various cancers who had peripheral neuropathy from previous chemotherapy, those who took ALC were more likely than those who took a placebo to have an improvement of at least one grade in their neuropathy. They also were more likely to have improvements in fatigue and strength.
Taken together, the two trials, which were reported in a poster discussion session at the annual meeting of the American Society of Clinical Oncology, provide yet another cautionary lesson on the complexity of combining conventional and complementary therapies.
"The use of ALC for prevention is not recommended, and I would say, based on [these results], should be cautioned against. It will be interesting to see the carnitine data and to understand, as much as possible, why the trial was negative," commented Debra L. Barton, Ph.D., of the Mayo Clinic in Rochester, Minn., who was invited to discuss the research. "Further studies are needed to really understand if ALC should be used to treat peripheral neuropathy."
ALC for Prevention of Peripheral Neuropathy
In the first trial, Southwest Oncology Group (SWOG) protocol S0715, investigators led by Dr. Dawn L. Hershman randomized women receiving adjuvant taxane chemotherapy for early breast cancer evenly to either oral ALC 1,000 mg three times daily or matching placebo, for 24 weeks.
Compared with their counterparts in the placebo group, women in the ALC group were more likely to have a greater than 5-point adjusted decrease on the neurotoxicity subscale of the Functional Assessment of Cancer Therapy–Taxane (FACT-NTX) instrument at 12 weeks (odds ratio, 1.48; P = .08) and also at 24 weeks (38% vs. 28%; OR, 1.57; P = .05).
This magnitude of worsening is clinically meaningful, maintained Dr. Hershman of Columbia University in New York, "so this is not like a lot of studies where you find a statistically significant difference that’s not clinically meaningful."
In addition, the incidence of grade 3/4 neurotoxicity was 3.8% with ALC, much higher than the 0.5% seen with placebo.
Patients in the ALC group also had scores on the FACT trial outcome index subscale (FACT-TOI), an overall measure of function, that were on average 3.5 points lower (worse) than those among their placebo counterparts (P = .03). There were no significant differences between groups in terms of fatigue and other toxicities.
The investigators have collected biosamples and will be assessing potential biological correlates with peripheral neuropathy outcomes, according to Dr. Hershman.
"We are looking at DNA, oxidative stress, and carnitine levels to better understand the mechanisms of chemotherapy-induced peripheral neuropathy to begin with, because there is not a whole lot known in terms of mechanism," she said. "If we can figure out what makes people worse, then we will maybe be able to figure out how to make people better from a more mechanistic standpoint, because there are very few drugs to treat chemotherapy-induced peripheral neuropathy."
An obvious concern from the trial’s findings is that ALC may somehow potentiate the neurotoxic effects of taxanes. "Based on these data, physicians should be telling patients not to take ALC during adjuvant chemotherapy," Dr. Hershman concluded. "You need to talk to patients. We know from the literature that overwhelmingly large number of patients take supplements during chemotherapy and afterward, many of which have not been tested. It’s important to get that history from patients."
Dr. Barton, the discussant, praised the trial’s rigorous methodology and proposed that there may have been several reasons for the lack of ALC benefit in preventing neuropathy, despite compelling earlier data.
Previous prevention research was done in animals and thus may not translate to humans, she said. And a positive trial for treatment in humans used intravenous administration, which may result in different bioavailability. Finally, "ALC capsules needed to be taken three times a day, and they are rather large, and these patients were, after all, on chemotherapy. They were likely nauseated [and] dyspeptic, and taking what some might call a horse pill three times a day could not have been an easy task. The study did use pill diaries, but we know those aren’t a perfect tool for adherence."
"The great thing is that the study collected blood and they are able to look at carnitine levels," Dr. Barton said. "So if carnitine is up in the group that got acetyl-carnitine and not in the group that got placebo, well, I think that pretty much confirms that this just didn’t work."
ALC for Treatment of Peripheral Neuropathy
In the second trial, protocol ZHAOKE-2007L03540, investigators led by Dr. Yuanjue Sun of the Sixth Affiliated Hospital of Shanghai (China) Jiao Tong University, enrolled 239 patients who had cancer of various types and stages, had completed chemotherapy, and had had at least grade 2 peripheral neuropathy for up to 6 months.
They were randomly assigned to receive either oral ALC at a dose of 3 g/day or matching placebo, for 8 weeks, with outcomes assessed at clinic visits or by telephone.
Analyses showed that compared with their counterparts in the placebo group, patients in the ALC group were more likely to have had an improvement of at least one grade in their neuropathy, both at 8 weeks (51% vs. 24%; P less than .001) and at 12 weeks (58% vs. 40%; P less than .001).
In terms of secondary outcomes, the ALC group was also more likely to have had an improvement in cancer-related fatigue (31% vs. 20%; P = .048), physical strength (29% vs. 13%; P = .02), and electrophysiology in peripheral nerves (75% vs. 58%; P = .02).
The two groups had statistically indistinguishable rates of adverse events (20% vs. 15%) and adverse reactions (6% vs. 5%). The most common events were gastrointestinal ones and skin allergies.
"This is the first time to confirm that ALC has a positive effect to cure chemotherapy-induced peripheral neuropathy in the Chinese population," Dr. Sun commented through a translator.
"I think the very important thing for this trial is, it is a different kind of patient population. Before this, most clinical trials were performed in [whites] or maybe Americans. This is an only-Asian [population]," he noted, and it is possible that there are genetic differences in how ALC is metabolized.
Dr. Barton, the discussant, took a cautionary view, saying that "there are some things to consider before going out and telling patients to consider acetyl-carnitine for their peripheral neuropathy."
It was unclear from the results reported whether the two treatment groups were well balanced and what criteria were used to define improvement for the secondary outcomes, she noted. Additionally, "outcome measures were all provider graded, [and there were] no self-report measures, so it is difficult to understand the impact of treatment on symptoms, particularly from the patient perspective," she noted.
Dr. Hershman, Dr. Sun, and Dr. Barton disclosed no relevant conflicts of interest; the ZHAOKE-2007L03540 trial was sponsored by Lee’s Pharmaceutical Limited.
CHICAGO – The impact of acetyl-l-carnitine on chemotherapy-induced peripheral neuropathy may depend largely on the clinical context and patient population, a pair of phase III trials suggests.
Acetyl-l-carnitine (ALC), a natural substance marketed over the counter as a dietary supplement, is popular among cancer patients as a result of preclinical and early-phase data in chemotherapy-related neuropathy and also a study in patients with diabetes-related peripheral neuropathy.
But in a trial among 409 U.S. women receiving adjuvant chemotherapy for breast cancer, those who took ALC not only had no decrease in the development of peripheral neuropathy symptoms relative to peers who were given a placebo, but actually had an increase. And they had a higher rate of serious neuropathy, too.
In contrast, in a trial among more than 200 Chinese patients with various cancers who had peripheral neuropathy from previous chemotherapy, those who took ALC were more likely than those who took a placebo to have an improvement of at least one grade in their neuropathy. They also were more likely to have improvements in fatigue and strength.
Taken together, the two trials, which were reported in a poster discussion session at the annual meeting of the American Society of Clinical Oncology, provide yet another cautionary lesson on the complexity of combining conventional and complementary therapies.
"The use of ALC for prevention is not recommended, and I would say, based on [these results], should be cautioned against. It will be interesting to see the carnitine data and to understand, as much as possible, why the trial was negative," commented Debra L. Barton, Ph.D., of the Mayo Clinic in Rochester, Minn., who was invited to discuss the research. "Further studies are needed to really understand if ALC should be used to treat peripheral neuropathy."
ALC for Prevention of Peripheral Neuropathy
In the first trial, Southwest Oncology Group (SWOG) protocol S0715, investigators led by Dr. Dawn L. Hershman randomized women receiving adjuvant taxane chemotherapy for early breast cancer evenly to either oral ALC 1,000 mg three times daily or matching placebo, for 24 weeks.
Compared with their counterparts in the placebo group, women in the ALC group were more likely to have a greater than 5-point adjusted decrease on the neurotoxicity subscale of the Functional Assessment of Cancer Therapy–Taxane (FACT-NTX) instrument at 12 weeks (odds ratio, 1.48; P = .08) and also at 24 weeks (38% vs. 28%; OR, 1.57; P = .05).
This magnitude of worsening is clinically meaningful, maintained Dr. Hershman of Columbia University in New York, "so this is not like a lot of studies where you find a statistically significant difference that’s not clinically meaningful."
In addition, the incidence of grade 3/4 neurotoxicity was 3.8% with ALC, much higher than the 0.5% seen with placebo.
Patients in the ALC group also had scores on the FACT trial outcome index subscale (FACT-TOI), an overall measure of function, that were on average 3.5 points lower (worse) than those among their placebo counterparts (P = .03). There were no significant differences between groups in terms of fatigue and other toxicities.
The investigators have collected biosamples and will be assessing potential biological correlates with peripheral neuropathy outcomes, according to Dr. Hershman.
"We are looking at DNA, oxidative stress, and carnitine levels to better understand the mechanisms of chemotherapy-induced peripheral neuropathy to begin with, because there is not a whole lot known in terms of mechanism," she said. "If we can figure out what makes people worse, then we will maybe be able to figure out how to make people better from a more mechanistic standpoint, because there are very few drugs to treat chemotherapy-induced peripheral neuropathy."
An obvious concern from the trial’s findings is that ALC may somehow potentiate the neurotoxic effects of taxanes. "Based on these data, physicians should be telling patients not to take ALC during adjuvant chemotherapy," Dr. Hershman concluded. "You need to talk to patients. We know from the literature that overwhelmingly large number of patients take supplements during chemotherapy and afterward, many of which have not been tested. It’s important to get that history from patients."
Dr. Barton, the discussant, praised the trial’s rigorous methodology and proposed that there may have been several reasons for the lack of ALC benefit in preventing neuropathy, despite compelling earlier data.
Previous prevention research was done in animals and thus may not translate to humans, she said. And a positive trial for treatment in humans used intravenous administration, which may result in different bioavailability. Finally, "ALC capsules needed to be taken three times a day, and they are rather large, and these patients were, after all, on chemotherapy. They were likely nauseated [and] dyspeptic, and taking what some might call a horse pill three times a day could not have been an easy task. The study did use pill diaries, but we know those aren’t a perfect tool for adherence."
"The great thing is that the study collected blood and they are able to look at carnitine levels," Dr. Barton said. "So if carnitine is up in the group that got acetyl-carnitine and not in the group that got placebo, well, I think that pretty much confirms that this just didn’t work."
ALC for Treatment of Peripheral Neuropathy
In the second trial, protocol ZHAOKE-2007L03540, investigators led by Dr. Yuanjue Sun of the Sixth Affiliated Hospital of Shanghai (China) Jiao Tong University, enrolled 239 patients who had cancer of various types and stages, had completed chemotherapy, and had had at least grade 2 peripheral neuropathy for up to 6 months.
They were randomly assigned to receive either oral ALC at a dose of 3 g/day or matching placebo, for 8 weeks, with outcomes assessed at clinic visits or by telephone.
Analyses showed that compared with their counterparts in the placebo group, patients in the ALC group were more likely to have had an improvement of at least one grade in their neuropathy, both at 8 weeks (51% vs. 24%; P less than .001) and at 12 weeks (58% vs. 40%; P less than .001).
In terms of secondary outcomes, the ALC group was also more likely to have had an improvement in cancer-related fatigue (31% vs. 20%; P = .048), physical strength (29% vs. 13%; P = .02), and electrophysiology in peripheral nerves (75% vs. 58%; P = .02).
The two groups had statistically indistinguishable rates of adverse events (20% vs. 15%) and adverse reactions (6% vs. 5%). The most common events were gastrointestinal ones and skin allergies.
"This is the first time to confirm that ALC has a positive effect to cure chemotherapy-induced peripheral neuropathy in the Chinese population," Dr. Sun commented through a translator.
"I think the very important thing for this trial is, it is a different kind of patient population. Before this, most clinical trials were performed in [whites] or maybe Americans. This is an only-Asian [population]," he noted, and it is possible that there are genetic differences in how ALC is metabolized.
Dr. Barton, the discussant, took a cautionary view, saying that "there are some things to consider before going out and telling patients to consider acetyl-carnitine for their peripheral neuropathy."
It was unclear from the results reported whether the two treatment groups were well balanced and what criteria were used to define improvement for the secondary outcomes, she noted. Additionally, "outcome measures were all provider graded, [and there were] no self-report measures, so it is difficult to understand the impact of treatment on symptoms, particularly from the patient perspective," she noted.
Dr. Hershman, Dr. Sun, and Dr. Barton disclosed no relevant conflicts of interest; the ZHAOKE-2007L03540 trial was sponsored by Lee’s Pharmaceutical Limited.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Patients taking ALC for prevention were more likely to have a greater than 5-point worsening of FACT-NTX score (38% vs. 28%), whereas patients taking ALC for treatment were more likely to have an improvement of at least one grade in neuropathy (51% vs. 24%).
Data Source: Investigators presented separate, randomized, placebo-controlled phase III trials among 410 women receiving adjuvant taxane chemotherapy for breast cancer and 239 patients with cancer and chemotherapy-induced peripheral neuropathy.
Disclosures: Dr. Hershman, Dr. Sun, and Dr. Barton disclosed no relevant conflicts of interest; the ZHAOKE-2007L03540 trial was sponsored by Lee’s Pharmaceutical Limited.

Breast Cancer Chemoprevention: Hit It Harder
ESTES PARK, COLO. – Primary care physicians appear to have dropped the ball when it comes to primary chemoprevention of breast cancer, studies suggest.
Chemoprevention is enormously underutilized. An estimated 2 million American premenopausal women are candidates for primary chemoprevention of breast cancer with tamoxifen, an agent shown to reduce their risk by 50%. Yet only 4% of them are on this safe and generally well-tolerated estrogen receptor antagonist, Dr. Jennifer R. Diamond said at an update in internal medicine sponsored by the University of Colorado at Denver.

Moreover, when she informally polled her audience at the outset of her talk, 93% indicated via electronic clicker that they were not comfortable with chemoprevention for breast cancer and didn’t commonly use it in appropriately selected patients in their practice.
"The most common side effect I see with tamoxifen for primary chemoprevention is hot flashes. But many young women will do fine. They don’t have any problems. And the opportunity to reduce the risk of breast cancer by 50% in these young women makes this an option I think you really need to be offering to young women" who are at increased risk for breast cancer, said Dr. Diamond, a medical oncologist at the university.
Nearly 230,000 American women will receive a new diagnosis of breast cancer in 2012. More than 39,000 women will die this year from the malignancy.
Secondary chemoprevention is most effective for women who have been diagnosed with lobular carcinoma in situ. The recommendation to embark on secondary chemoprevention usually comes from the patient’s medical oncologist.
In contrast, most candidates for primary chemoprevention have never seen a medical oncologist. Thus, primary chemoprevention falls within the bailiwick of primary care physicians. The latest guidelines from the National Comprehensive Cancer Network identify appropriate candidates for primary chemoprevention as women who have a first-degree relative with breast or ovarian cancer; a history of thoracic irradiation; mutations predisposing to breast cancer; or a 5-year risk of breast cancer of at least 1.7% according to the breast cancer risk assessment tool (the Gail model).
A 5-year risk of 1.7% or greater is not a high bar. It equates on the Gail model to being 65 years old without additional risk factors. "You’ll find that many of your patients are candidates," Dr. Diamond predicted.
Two options are available for primary chemoprevention; the determining factor as to which is best in a given high-risk individual is menopausal status. Premenopausal women can benefit from 5 years of oral tamoxifen at 20 mg/day. In postmenopausal women, however, exemestane (Aromasin), an aromatase inhibitor, is the safer, better choice, even though the drug’s use in chemoprevention is, for now, off label, she continued.
The oft-cited figure of a 50% reduction in breast cancer risk conferred by tamoxifen comes from the landmark randomized, placebo-controlled NSABP (National Surgical Adjuvant Breast and Bowel Project) P-1 trial (J. Natl. Cancer Inst. 1998;90:1371-88). The protective effect continued after treatment ended. The number needed to treat at 20 mg/day for 5 years in order to prevent one additional case of breast cancer was calculated at 95 in 5 years and 56 in 10 years. Women younger than age 50 years experienced no excess risk of serious adverse events.
"The risks of venous thromboembolism and endometrial cancer are what we all worry about with tamoxifen, but they’re actually incredibly uncommon" in women younger than age 50, she said. "I don’t recommend that you use tamoxifen in your postmenopausal women; that’s where you get into trouble with endometrial cancer and thromboembolic events. I believe that you can safely use tamoxifen in premenopausal women without a significantly increased risk of thromboembolic events. I equate the risk to that of birth control pills."
Raloxifene joins tamoxifen as the only other proved drug with Food and Drug Administration approval for primary breast cancer chemoprevention. The NSABP STAR (Study of Tamoxifen and Raloxifene) trial showed that the two medications are equivalent for prevention of invasive breast cancer, but that raloxifene is less effective in preventing ductal carcinoma in situ (JAMA 2006;295:2727-41). For this reason, Dr. Diamond and her colleagues don’t use it.
For postmenopausal women who are candidates for primary chemoprevention, Dr. Diamond said that she turns to exemestane on the basis of the National Cancer Institute of Canada CTG MAP-3 trial, which showed a 65% reduction in the annual incidence of breast cancer with 5 years of the aromatase inhibitor, compared with placebo. (N. Engl. J. Med. 2011;364:2381-91).
The number needed to treat with exemestane at 25 mg/day for 5 years in order to prevent one invasive breast cancer was 94 in 3 years and 26 in 5 years.
"I would argue that this is a really low NNT, and a lot of patients in your practice probably would fall into the category of qualifying for the MAP-3 study," Dr. Diamond said.
There were no serious risks associated with exemestane in MAP-3. Hot flashes and other menopausal symptoms were more common than with placebo, yet reassuringly there was no difference between the exemestane and control groups on quality of life measures.
Bone mineral density decreased over time in the exemestane group; however, patients on the aromatase inhibitor had no increased risk of fractures. Dr. Diamond advised monitoring bone density in exemestane-treated women, and if it drops significantly, consider prescribing denosumab as a subcutaneous injection once every 6 months. Denosumab is already FDA approved to increase bone mass in patients on adjuvant aromatase inhibitor therapy for breast cancer.
Dr. Diamond reported having no financial conflicts.
ESTES PARK, COLO. – Primary care physicians appear to have dropped the ball when it comes to primary chemoprevention of breast cancer, studies suggest.
Chemoprevention is enormously underutilized. An estimated 2 million American premenopausal women are candidates for primary chemoprevention of breast cancer with tamoxifen, an agent shown to reduce their risk by 50%. Yet only 4% of them are on this safe and generally well-tolerated estrogen receptor antagonist, Dr. Jennifer R. Diamond said at an update in internal medicine sponsored by the University of Colorado at Denver.
Moreover, when she informally polled her audience at the outset of her talk, 93% indicated via electronic clicker that they were not comfortable with chemoprevention for breast cancer and didn’t commonly use it in appropriately selected patients in their practice.
"The most common side effect I see with tamoxifen for primary chemoprevention is hot flashes. But many young women will do fine. They don’t have any problems. And the opportunity to reduce the risk of breast cancer by 50% in these young women makes this an option I think you really need to be offering to young women" who are at increased risk for breast cancer, said Dr. Diamond, a medical oncologist at the university.
Nearly 230,000 American women will receive a new diagnosis of breast cancer in 2012. More than 39,000 women will die this year from the malignancy.
Secondary chemoprevention is most effective for women who have been diagnosed with lobular carcinoma in situ. The recommendation to embark on secondary chemoprevention usually comes from the patient’s medical oncologist.
In contrast, most candidates for primary chemoprevention have never seen a medical oncologist. Thus, primary chemoprevention falls within the bailiwick of primary care physicians. The latest guidelines from the National Comprehensive Cancer Network identify appropriate candidates for primary chemoprevention as women who have a first-degree relative with breast or ovarian cancer; a history of thoracic irradiation; mutations predisposing to breast cancer; or a 5-year risk of breast cancer of at least 1.7% according to the breast cancer risk assessment tool (the Gail model).
A 5-year risk of 1.7% or greater is not a high bar. It equates on the Gail model to being 65 years old without additional risk factors. "You’ll find that many of your patients are candidates," Dr. Diamond predicted.
Two options are available for primary chemoprevention; the determining factor as to which is best in a given high-risk individual is menopausal status. Premenopausal women can benefit from 5 years of oral tamoxifen at 20 mg/day. In postmenopausal women, however, exemestane (Aromasin), an aromatase inhibitor, is the safer, better choice, even though the drug’s use in chemoprevention is, for now, off label, she continued.
The oft-cited figure of a 50% reduction in breast cancer risk conferred by tamoxifen comes from the landmark randomized, placebo-controlled NSABP (National Surgical Adjuvant Breast and Bowel Project) P-1 trial (J. Natl. Cancer Inst. 1998;90:1371-88). The protective effect continued after treatment ended. The number needed to treat at 20 mg/day for 5 years in order to prevent one additional case of breast cancer was calculated at 95 in 5 years and 56 in 10 years. Women younger than age 50 years experienced no excess risk of serious adverse events.
"The risks of venous thromboembolism and endometrial cancer are what we all worry about with tamoxifen, but they’re actually incredibly uncommon" in women younger than age 50, she said. "I don’t recommend that you use tamoxifen in your postmenopausal women; that’s where you get into trouble with endometrial cancer and thromboembolic events. I believe that you can safely use tamoxifen in premenopausal women without a significantly increased risk of thromboembolic events. I equate the risk to that of birth control pills."
Raloxifene joins tamoxifen as the only other proved drug with Food and Drug Administration approval for primary breast cancer chemoprevention. The NSABP STAR (Study of Tamoxifen and Raloxifene) trial showed that the two medications are equivalent for prevention of invasive breast cancer, but that raloxifene is less effective in preventing ductal carcinoma in situ (JAMA 2006;295:2727-41). For this reason, Dr. Diamond and her colleagues don’t use it.
For postmenopausal women who are candidates for primary chemoprevention, Dr. Diamond said that she turns to exemestane on the basis of the National Cancer Institute of Canada CTG MAP-3 trial, which showed a 65% reduction in the annual incidence of breast cancer with 5 years of the aromatase inhibitor, compared with placebo. (N. Engl. J. Med. 2011;364:2381-91).
The number needed to treat with exemestane at 25 mg/day for 5 years in order to prevent one invasive breast cancer was 94 in 3 years and 26 in 5 years.
"I would argue that this is a really low NNT, and a lot of patients in your practice probably would fall into the category of qualifying for the MAP-3 study," Dr. Diamond said.
There were no serious risks associated with exemestane in MAP-3. Hot flashes and other menopausal symptoms were more common than with placebo, yet reassuringly there was no difference between the exemestane and control groups on quality of life measures.
Bone mineral density decreased over time in the exemestane group; however, patients on the aromatase inhibitor had no increased risk of fractures. Dr. Diamond advised monitoring bone density in exemestane-treated women, and if it drops significantly, consider prescribing denosumab as a subcutaneous injection once every 6 months. Denosumab is already FDA approved to increase bone mass in patients on adjuvant aromatase inhibitor therapy for breast cancer.
Dr. Diamond reported having no financial conflicts.
ESTES PARK, COLO. – Primary care physicians appear to have dropped the ball when it comes to primary chemoprevention of breast cancer, studies suggest.
Chemoprevention is enormously underutilized. An estimated 2 million American premenopausal women are candidates for primary chemoprevention of breast cancer with tamoxifen, an agent shown to reduce their risk by 50%. Yet only 4% of them are on this safe and generally well-tolerated estrogen receptor antagonist, Dr. Jennifer R. Diamond said at an update in internal medicine sponsored by the University of Colorado at Denver.
Moreover, when she informally polled her audience at the outset of her talk, 93% indicated via electronic clicker that they were not comfortable with chemoprevention for breast cancer and didn’t commonly use it in appropriately selected patients in their practice.
"The most common side effect I see with tamoxifen for primary chemoprevention is hot flashes. But many young women will do fine. They don’t have any problems. And the opportunity to reduce the risk of breast cancer by 50% in these young women makes this an option I think you really need to be offering to young women" who are at increased risk for breast cancer, said Dr. Diamond, a medical oncologist at the university.
Nearly 230,000 American women will receive a new diagnosis of breast cancer in 2012. More than 39,000 women will die this year from the malignancy.
Secondary chemoprevention is most effective for women who have been diagnosed with lobular carcinoma in situ. The recommendation to embark on secondary chemoprevention usually comes from the patient’s medical oncologist.
In contrast, most candidates for primary chemoprevention have never seen a medical oncologist. Thus, primary chemoprevention falls within the bailiwick of primary care physicians. The latest guidelines from the National Comprehensive Cancer Network identify appropriate candidates for primary chemoprevention as women who have a first-degree relative with breast or ovarian cancer; a history of thoracic irradiation; mutations predisposing to breast cancer; or a 5-year risk of breast cancer of at least 1.7% according to the breast cancer risk assessment tool (the Gail model).
A 5-year risk of 1.7% or greater is not a high bar. It equates on the Gail model to being 65 years old without additional risk factors. "You’ll find that many of your patients are candidates," Dr. Diamond predicted.
Two options are available for primary chemoprevention; the determining factor as to which is best in a given high-risk individual is menopausal status. Premenopausal women can benefit from 5 years of oral tamoxifen at 20 mg/day. In postmenopausal women, however, exemestane (Aromasin), an aromatase inhibitor, is the safer, better choice, even though the drug’s use in chemoprevention is, for now, off label, she continued.
The oft-cited figure of a 50% reduction in breast cancer risk conferred by tamoxifen comes from the landmark randomized, placebo-controlled NSABP (National Surgical Adjuvant Breast and Bowel Project) P-1 trial (J. Natl. Cancer Inst. 1998;90:1371-88). The protective effect continued after treatment ended. The number needed to treat at 20 mg/day for 5 years in order to prevent one additional case of breast cancer was calculated at 95 in 5 years and 56 in 10 years. Women younger than age 50 years experienced no excess risk of serious adverse events.
"The risks of venous thromboembolism and endometrial cancer are what we all worry about with tamoxifen, but they’re actually incredibly uncommon" in women younger than age 50, she said. "I don’t recommend that you use tamoxifen in your postmenopausal women; that’s where you get into trouble with endometrial cancer and thromboembolic events. I believe that you can safely use tamoxifen in premenopausal women without a significantly increased risk of thromboembolic events. I equate the risk to that of birth control pills."
Raloxifene joins tamoxifen as the only other proved drug with Food and Drug Administration approval for primary breast cancer chemoprevention. The NSABP STAR (Study of Tamoxifen and Raloxifene) trial showed that the two medications are equivalent for prevention of invasive breast cancer, but that raloxifene is less effective in preventing ductal carcinoma in situ (JAMA 2006;295:2727-41). For this reason, Dr. Diamond and her colleagues don’t use it.
For postmenopausal women who are candidates for primary chemoprevention, Dr. Diamond said that she turns to exemestane on the basis of the National Cancer Institute of Canada CTG MAP-3 trial, which showed a 65% reduction in the annual incidence of breast cancer with 5 years of the aromatase inhibitor, compared with placebo. (N. Engl. J. Med. 2011;364:2381-91).
The number needed to treat with exemestane at 25 mg/day for 5 years in order to prevent one invasive breast cancer was 94 in 3 years and 26 in 5 years.
"I would argue that this is a really low NNT, and a lot of patients in your practice probably would fall into the category of qualifying for the MAP-3 study," Dr. Diamond said.
There were no serious risks associated with exemestane in MAP-3. Hot flashes and other menopausal symptoms were more common than with placebo, yet reassuringly there was no difference between the exemestane and control groups on quality of life measures.
Bone mineral density decreased over time in the exemestane group; however, patients on the aromatase inhibitor had no increased risk of fractures. Dr. Diamond advised monitoring bone density in exemestane-treated women, and if it drops significantly, consider prescribing denosumab as a subcutaneous injection once every 6 months. Denosumab is already FDA approved to increase bone mass in patients on adjuvant aromatase inhibitor therapy for breast cancer.
Dr. Diamond reported having no financial conflicts.
EXPERT ANALYSIS FROM AN UPDATE IN INTERNAL MEDICINE SPONSORED BY THE UNIVERSITY OF COLORADO

Dense Breasts Don't Increase Risk of Breast Cancer Death
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
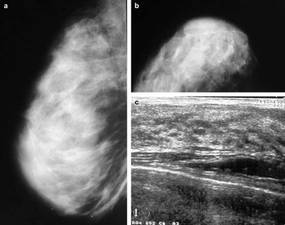
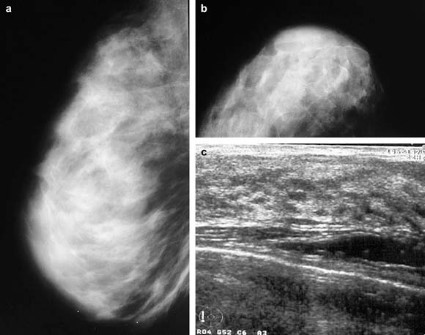
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Prior Thoracic Radiotherapy Warrants Annual Breast MRI
ESTES PARK, COLO. – Primary care physicians are uniquely positioned to help their younger adult female patients who have a history of thoracic radiation therapy for lymphoma by arranging for them to begin undergoing annual screening breast MRI, Dr. Jennifer R. Diamond said.
"That mantle cell radiation includes the upper inner quadrants of both breasts; those patients are at extremely high risk for developing breast cancer," explained Dr. Diamond, a medical oncologist at the University of Colorado, Aurora. "Many times, they’re no longer being followed by their oncologist, and it’s up to their primary care physician to pull the trigger and order the test."

Many patients likely wouldn’t know that they should do breast cancer screening at such an early age, she added, because breast cancer wasn’t an anticipated outcome back when they had their radiotherapy.
National Comprehensive Cancer Network guidelines call for annual breast MRI and mammography along with clinical breast exams every 6-12 months, beginning 8-10 years after thoracic radiotherapy or at age 25 years, whichever occurs later. Dr. Diamond typically has patients stagger the two imaging modalities 6 months apart.
Both annual breast MRI and mammography are necessary. Screening MRI is far more sensitive than mammography alone in high-risk women, and it leads to cancer diagnosis at an earlier stage. However, MRI can miss ductal carcinoma in situ that would be evident as abnormal calcifications on screening mammography, she continued.
Annual breast MRI, in addition to mammography, is also indicated for women at high breast cancer risk as defined by a lifetime estimated risk in excess of 20%, or because they possess a BRCA 1 or 2 mutation, according to the NCCN. Dr. Diamond recommended BRCAPRO as a very useful tool for estimating the lifetime risk of breast cancer in women with no previous breast cancer.
In response to an audience question, she said she’s had no problem in getting insurers to pay for annual breast MRI to supplement annual mammography, so long as she clearly documents in her note that the patient has a greater than 20% lifetime estimated risk of breast cancer.
"They won’t cover it even a week earlier than annually, though," Dr. Diamond added.
She is a big fan of breast tomosynthesis, also known as three-dimensional mammography. The Food and Drug Administration–licensed technology produces a 3-D view of the breast tissue in addition to the standard two-dimensional images, all obtained in one compression with only about 2 seconds of additional compression time. Studies have shown that this tool substantially reduces patient recall rates for nondefinitive mammograms, Dr. Diamond said.
"It allows the mammographer to scroll through the breast, looking up and down sort of like with a CT scan, but without the same radiation exposure," she explained. "It’s a really great new technology, and I think most mammography centers will increasingly turn to it."
Dr. Diamond reported having no financial conflicts.
ESTES PARK, COLO. – Primary care physicians are uniquely positioned to help their younger adult female patients who have a history of thoracic radiation therapy for lymphoma by arranging for them to begin undergoing annual screening breast MRI, Dr. Jennifer R. Diamond said.
"That mantle cell radiation includes the upper inner quadrants of both breasts; those patients are at extremely high risk for developing breast cancer," explained Dr. Diamond, a medical oncologist at the University of Colorado, Aurora. "Many times, they’re no longer being followed by their oncologist, and it’s up to their primary care physician to pull the trigger and order the test."
Many patients likely wouldn’t know that they should do breast cancer screening at such an early age, she added, because breast cancer wasn’t an anticipated outcome back when they had their radiotherapy.
National Comprehensive Cancer Network guidelines call for annual breast MRI and mammography along with clinical breast exams every 6-12 months, beginning 8-10 years after thoracic radiotherapy or at age 25 years, whichever occurs later. Dr. Diamond typically has patients stagger the two imaging modalities 6 months apart.
Both annual breast MRI and mammography are necessary. Screening MRI is far more sensitive than mammography alone in high-risk women, and it leads to cancer diagnosis at an earlier stage. However, MRI can miss ductal carcinoma in situ that would be evident as abnormal calcifications on screening mammography, she continued.
Annual breast MRI, in addition to mammography, is also indicated for women at high breast cancer risk as defined by a lifetime estimated risk in excess of 20%, or because they possess a BRCA 1 or 2 mutation, according to the NCCN. Dr. Diamond recommended BRCAPRO as a very useful tool for estimating the lifetime risk of breast cancer in women with no previous breast cancer.
In response to an audience question, she said she’s had no problem in getting insurers to pay for annual breast MRI to supplement annual mammography, so long as she clearly documents in her note that the patient has a greater than 20% lifetime estimated risk of breast cancer.
"They won’t cover it even a week earlier than annually, though," Dr. Diamond added.
She is a big fan of breast tomosynthesis, also known as three-dimensional mammography. The Food and Drug Administration–licensed technology produces a 3-D view of the breast tissue in addition to the standard two-dimensional images, all obtained in one compression with only about 2 seconds of additional compression time. Studies have shown that this tool substantially reduces patient recall rates for nondefinitive mammograms, Dr. Diamond said.
"It allows the mammographer to scroll through the breast, looking up and down sort of like with a CT scan, but without the same radiation exposure," she explained. "It’s a really great new technology, and I think most mammography centers will increasingly turn to it."
Dr. Diamond reported having no financial conflicts.
ESTES PARK, COLO. – Primary care physicians are uniquely positioned to help their younger adult female patients who have a history of thoracic radiation therapy for lymphoma by arranging for them to begin undergoing annual screening breast MRI, Dr. Jennifer R. Diamond said.
"That mantle cell radiation includes the upper inner quadrants of both breasts; those patients are at extremely high risk for developing breast cancer," explained Dr. Diamond, a medical oncologist at the University of Colorado, Aurora. "Many times, they’re no longer being followed by their oncologist, and it’s up to their primary care physician to pull the trigger and order the test."
Many patients likely wouldn’t know that they should do breast cancer screening at such an early age, she added, because breast cancer wasn’t an anticipated outcome back when they had their radiotherapy.
National Comprehensive Cancer Network guidelines call for annual breast MRI and mammography along with clinical breast exams every 6-12 months, beginning 8-10 years after thoracic radiotherapy or at age 25 years, whichever occurs later. Dr. Diamond typically has patients stagger the two imaging modalities 6 months apart.
Both annual breast MRI and mammography are necessary. Screening MRI is far more sensitive than mammography alone in high-risk women, and it leads to cancer diagnosis at an earlier stage. However, MRI can miss ductal carcinoma in situ that would be evident as abnormal calcifications on screening mammography, she continued.
Annual breast MRI, in addition to mammography, is also indicated for women at high breast cancer risk as defined by a lifetime estimated risk in excess of 20%, or because they possess a BRCA 1 or 2 mutation, according to the NCCN. Dr. Diamond recommended BRCAPRO as a very useful tool for estimating the lifetime risk of breast cancer in women with no previous breast cancer.
In response to an audience question, she said she’s had no problem in getting insurers to pay for annual breast MRI to supplement annual mammography, so long as she clearly documents in her note that the patient has a greater than 20% lifetime estimated risk of breast cancer.
"They won’t cover it even a week earlier than annually, though," Dr. Diamond added.
She is a big fan of breast tomosynthesis, also known as three-dimensional mammography. The Food and Drug Administration–licensed technology produces a 3-D view of the breast tissue in addition to the standard two-dimensional images, all obtained in one compression with only about 2 seconds of additional compression time. Studies have shown that this tool substantially reduces patient recall rates for nondefinitive mammograms, Dr. Diamond said.
"It allows the mammographer to scroll through the breast, looking up and down sort of like with a CT scan, but without the same radiation exposure," she explained. "It’s a really great new technology, and I think most mammography centers will increasingly turn to it."
Dr. Diamond reported having no financial conflicts.
EXPERT ANALYSIS FROM AN UPDATE IN INTERNAL MEDICINE SPONSORED BY THE UNIVERSITY OF COLORADO

Experimental Drug Improves Muscle Strength in Cancer
HOUSTON – An experimental drug significantly improved physical function in men with cancer-related muscle wasting, compared with placebo – and more so in the men with low testosterone levels – in a secondary analysis of a randomized, double-blind, phase II clinical trial.
In all, 60% of the 93 men for whom baseline testosterone levels were available had hypogonadism when the patients were randomized to treatment with daily placebo or 1 mg or 3 mg of enobosarm for 16 weeks. Before treatment, the eugonadal males showed significantly better physical function, as measured by stair-climb power, compared with the hypogonadal patients (174 W vs. 147 W). Lower testosterone levels correlated with lower physical function.
Enobosarm significantly improved physical function (a secondary end point in the trial) with an average 17% increase in stair-climb power in hypogonadal men, and a 12% increase in power in eugonadal men, compared with baseline, Dr. Adrian Dobs and her associates reported at the annual meeting of the Endocrine Society.
Among men on placebo, stair-climb power increased by about 10% in hypogonadal men and by roughly 1% in eugonadal men, compared with baseline, but the changes were not statistically significant, said Dr. Dobs, professor of medicine and oncology at Johns Hopkins University, Baltimore.
Adverse events included fatigue in 21% of both treatment groups, anemia in 19% of those on enobosarm and 15% in those on placebo, nausea in 18% on enobosarm and 14% on placebo, diarrhea in 16% on enobosarm and 14% on placebo, vomiting in 12% of each treatment group, weight decrease in 12% on enobosarm and 10% on placebo, and constipation in 14% on enobosarm and 4% on placebo.
The investigators defined hypogonadism as a testosterone level below 300 ng/dL.
Enobosarm is a nonsteroidal SARM (selective androgen receptor modulator) that produces anabolic effects in bone and muscle without causing the prostate effects in men or hair growth in women that is seen with steroids.
The analysis used data from a larger trial in 159 people with cancer (65% of whom were men) who had lost at least 2% (and an average of 8%) of their weight in the previous 6 months. The men were older than 45 years of age, the women were postmenopausal, and each had a body mass index less than 35 mg/kg2.
The multicenter study as a whole met its primary end point of increasing lean body mass (muscle) and its secondary end point of improving physical function, Dr. Dobs said in an interview. Those results were reported on the website of the company that is developing the drug, GTx Inc., and at previous medical meetings, according to an interview in the Los Angeles Times.
Dr. Dobs did not report results for lean body mass in the current analysis based on gonadal status.
Cancer diagnoses included colorectal cancer, non–small cell lung cancer, non-Hodgkin’s lymphoma, chronic lymphocytic leukemia, and breast cancer. Patients participated in the study prior to or between courses of chemotherapy. Rates of hypogonadism were similar for each type of cancer. Patients with hypogonadism were less likely to complete the study than were eugonadal men.
Patients with cancer develop cachexia (muscle wasting) because of reduced anabolic activity, increased catabolic activity, or both, accounting for a progressive catabolic state. Up to 50% of patients with lung cancer show severe cachexia at the time of diagnosis, and the muscle wasting increases throughout the course of the malignancy, Dr. Dobs said.
Two phase III clinical trials are underway to study effects of 3 mg/day of enobosarm for the prevention and treatment of muscle wasting in patients with non–small cell lung cancer.
GTx Inc., the company that is developing enobosarm, funded the current study. Dr. Dobs reported having no other financial disclosures.
HOUSTON – An experimental drug significantly improved physical function in men with cancer-related muscle wasting, compared with placebo – and more so in the men with low testosterone levels – in a secondary analysis of a randomized, double-blind, phase II clinical trial.
In all, 60% of the 93 men for whom baseline testosterone levels were available had hypogonadism when the patients were randomized to treatment with daily placebo or 1 mg or 3 mg of enobosarm for 16 weeks. Before treatment, the eugonadal males showed significantly better physical function, as measured by stair-climb power, compared with the hypogonadal patients (174 W vs. 147 W). Lower testosterone levels correlated with lower physical function.
Enobosarm significantly improved physical function (a secondary end point in the trial) with an average 17% increase in stair-climb power in hypogonadal men, and a 12% increase in power in eugonadal men, compared with baseline, Dr. Adrian Dobs and her associates reported at the annual meeting of the Endocrine Society.
Among men on placebo, stair-climb power increased by about 10% in hypogonadal men and by roughly 1% in eugonadal men, compared with baseline, but the changes were not statistically significant, said Dr. Dobs, professor of medicine and oncology at Johns Hopkins University, Baltimore.
Adverse events included fatigue in 21% of both treatment groups, anemia in 19% of those on enobosarm and 15% in those on placebo, nausea in 18% on enobosarm and 14% on placebo, diarrhea in 16% on enobosarm and 14% on placebo, vomiting in 12% of each treatment group, weight decrease in 12% on enobosarm and 10% on placebo, and constipation in 14% on enobosarm and 4% on placebo.
The investigators defined hypogonadism as a testosterone level below 300 ng/dL.
Enobosarm is a nonsteroidal SARM (selective androgen receptor modulator) that produces anabolic effects in bone and muscle without causing the prostate effects in men or hair growth in women that is seen with steroids.
The analysis used data from a larger trial in 159 people with cancer (65% of whom were men) who had lost at least 2% (and an average of 8%) of their weight in the previous 6 months. The men were older than 45 years of age, the women were postmenopausal, and each had a body mass index less than 35 mg/kg2.
The multicenter study as a whole met its primary end point of increasing lean body mass (muscle) and its secondary end point of improving physical function, Dr. Dobs said in an interview. Those results were reported on the website of the company that is developing the drug, GTx Inc., and at previous medical meetings, according to an interview in the Los Angeles Times.
Dr. Dobs did not report results for lean body mass in the current analysis based on gonadal status.
Cancer diagnoses included colorectal cancer, non–small cell lung cancer, non-Hodgkin’s lymphoma, chronic lymphocytic leukemia, and breast cancer. Patients participated in the study prior to or between courses of chemotherapy. Rates of hypogonadism were similar for each type of cancer. Patients with hypogonadism were less likely to complete the study than were eugonadal men.
Patients with cancer develop cachexia (muscle wasting) because of reduced anabolic activity, increased catabolic activity, or both, accounting for a progressive catabolic state. Up to 50% of patients with lung cancer show severe cachexia at the time of diagnosis, and the muscle wasting increases throughout the course of the malignancy, Dr. Dobs said.
Two phase III clinical trials are underway to study effects of 3 mg/day of enobosarm for the prevention and treatment of muscle wasting in patients with non–small cell lung cancer.
GTx Inc., the company that is developing enobosarm, funded the current study. Dr. Dobs reported having no other financial disclosures.
HOUSTON – An experimental drug significantly improved physical function in men with cancer-related muscle wasting, compared with placebo – and more so in the men with low testosterone levels – in a secondary analysis of a randomized, double-blind, phase II clinical trial.
In all, 60% of the 93 men for whom baseline testosterone levels were available had hypogonadism when the patients were randomized to treatment with daily placebo or 1 mg or 3 mg of enobosarm for 16 weeks. Before treatment, the eugonadal males showed significantly better physical function, as measured by stair-climb power, compared with the hypogonadal patients (174 W vs. 147 W). Lower testosterone levels correlated with lower physical function.
Enobosarm significantly improved physical function (a secondary end point in the trial) with an average 17% increase in stair-climb power in hypogonadal men, and a 12% increase in power in eugonadal men, compared with baseline, Dr. Adrian Dobs and her associates reported at the annual meeting of the Endocrine Society.
Among men on placebo, stair-climb power increased by about 10% in hypogonadal men and by roughly 1% in eugonadal men, compared with baseline, but the changes were not statistically significant, said Dr. Dobs, professor of medicine and oncology at Johns Hopkins University, Baltimore.
Adverse events included fatigue in 21% of both treatment groups, anemia in 19% of those on enobosarm and 15% in those on placebo, nausea in 18% on enobosarm and 14% on placebo, diarrhea in 16% on enobosarm and 14% on placebo, vomiting in 12% of each treatment group, weight decrease in 12% on enobosarm and 10% on placebo, and constipation in 14% on enobosarm and 4% on placebo.
The investigators defined hypogonadism as a testosterone level below 300 ng/dL.
Enobosarm is a nonsteroidal SARM (selective androgen receptor modulator) that produces anabolic effects in bone and muscle without causing the prostate effects in men or hair growth in women that is seen with steroids.
The analysis used data from a larger trial in 159 people with cancer (65% of whom were men) who had lost at least 2% (and an average of 8%) of their weight in the previous 6 months. The men were older than 45 years of age, the women were postmenopausal, and each had a body mass index less than 35 mg/kg2.
The multicenter study as a whole met its primary end point of increasing lean body mass (muscle) and its secondary end point of improving physical function, Dr. Dobs said in an interview. Those results were reported on the website of the company that is developing the drug, GTx Inc., and at previous medical meetings, according to an interview in the Los Angeles Times.
Dr. Dobs did not report results for lean body mass in the current analysis based on gonadal status.
Cancer diagnoses included colorectal cancer, non–small cell lung cancer, non-Hodgkin’s lymphoma, chronic lymphocytic leukemia, and breast cancer. Patients participated in the study prior to or between courses of chemotherapy. Rates of hypogonadism were similar for each type of cancer. Patients with hypogonadism were less likely to complete the study than were eugonadal men.
Patients with cancer develop cachexia (muscle wasting) because of reduced anabolic activity, increased catabolic activity, or both, accounting for a progressive catabolic state. Up to 50% of patients with lung cancer show severe cachexia at the time of diagnosis, and the muscle wasting increases throughout the course of the malignancy, Dr. Dobs said.
Two phase III clinical trials are underway to study effects of 3 mg/day of enobosarm for the prevention and treatment of muscle wasting in patients with non–small cell lung cancer.
GTx Inc., the company that is developing enobosarm, funded the current study. Dr. Dobs reported having no other financial disclosures.
AT THE ANNUAL MEETING OF THE ENDOCRINE SOCIETY
Major Finding: The experimental drug enobosarm significantly improved physical function on a stair-climb test by 17% in hypogonadal men with cancer and by 12% in eugonadal men with cancer, compared with nonsignificant improvements in men on placebo.
Data Source: Data are from an analysis of data on a secondary end point (physical function) in 93 men from a randomized, double-blind, multicenter trial in 159 cancer patients.
Disclosures: GTx, the company that is developing enobosarm, funded the study. Dr. Dobs reported having no other financial disclosures.

Ovarian Cortex Autografts in Cancer Survivors Yield Live Births
SANTA BARBARA, CALIF. – Ovarian cortex orthotransplantation has resulted in the live births of at least 21 babies to cancer survivors in Europe, where the technique was pioneered and is being refined, Dr. Antonio Pellicer reported at a meeting on in vitro fertilization and embryo transfer.
Unlike the freezing of oocytes or embryos to preserve potential fertility, which requires ovarian stimulation, the ovarian cortex can be harvested from a cancer patient without delay, permitting immediate initiation of chemotherapy and/or radiation therapy. The tissue is cryopreserved until the patient is in remission.
If cancer treatment results in premature ovarian failure and the patient wishes to become pregnant, her autologous ovarian cortex can then be reintroduced.

Ovarian function generally resumes within 3-4 months, said Dr. Pellicer, professor of obstetrics and gynecology and dean of the medical school at the University of Valencia (Spain). Follicle stimulating hormone rates do not reach normal levels, but are sufficient in many cases for resumption of menses and pregnancy, either naturally or through assisted reproductive techniques.
The technique is currently believed to be safe for breast cancer patients and those with Hodgkin’s and non-Hodgkin’s lymphoma, based on histologic and immunologic evaluations of harvested ovarian tissue, Dr. Pellicer said at the meeting, which was sponsored by the University of California, Los Angeles.
It is considered unsafe for patients with leukemia, as metastatic cells might well circulate through the bloodstream to the ovaries. Because of its highly metastatic potential, Ewing’s sarcoma is also considered a contraindication for the procedure, according to Dr. Pellicer.
The technique offers hope, potentially, for prepubertal girls and adolescents with other types of cancer, as well as adult cancer patients, although much remains unknown about the viability and usefulness of the treatment, explained Dr. Pellicer.
At the Valencia Program of Fertility Preservation, more than 600 cancer patients from across Spain have undergone removal of the ovarian cortex around the time of diagnosis, said Dr. Pellicer.
He reported on results in 583 of those patients who were treated since 2005, 55% of whom had been diagnosed with breast cancer.
Regular menses and fertility were restored in some patients who received ovarian autografts, said Dr. Pellicer. In all, 16 pregnancies and 3 live births have occurred, some following in vitro fertilization and some following natural conception.
Those results, along with published studies from programs in France, Germany, Denmark, Belgium, and other countries, indicate that at least 21 and perhaps 23 or more live births have resulted from the technique.
The problem, as Dr. Pellicer sees it, is a lack of cohesive follow-up or evidence that would put those births into perspective.
"We don’t know the number of failed attempts," he said. "There are no registries. There are no real data. Are we doing something which is really helpful? Or are the unsuccessful cases more [typical] than the successful cases?"
"This is a concern to me," he said.
Responding to a question from an audience member, Dr. Pellicer acknowledged that the removal of one ovarian cortex prior to cancer treatment might diminish fertility potential rather than enhance it, because some cancer patients conceive naturally following remission.
Dr. Pellicer reported that he had no relevant financial relationships to disclose.
SANTA BARBARA, CALIF. – Ovarian cortex orthotransplantation has resulted in the live births of at least 21 babies to cancer survivors in Europe, where the technique was pioneered and is being refined, Dr. Antonio Pellicer reported at a meeting on in vitro fertilization and embryo transfer.
Unlike the freezing of oocytes or embryos to preserve potential fertility, which requires ovarian stimulation, the ovarian cortex can be harvested from a cancer patient without delay, permitting immediate initiation of chemotherapy and/or radiation therapy. The tissue is cryopreserved until the patient is in remission.
If cancer treatment results in premature ovarian failure and the patient wishes to become pregnant, her autologous ovarian cortex can then be reintroduced.
Ovarian function generally resumes within 3-4 months, said Dr. Pellicer, professor of obstetrics and gynecology and dean of the medical school at the University of Valencia (Spain). Follicle stimulating hormone rates do not reach normal levels, but are sufficient in many cases for resumption of menses and pregnancy, either naturally or through assisted reproductive techniques.
The technique is currently believed to be safe for breast cancer patients and those with Hodgkin’s and non-Hodgkin’s lymphoma, based on histologic and immunologic evaluations of harvested ovarian tissue, Dr. Pellicer said at the meeting, which was sponsored by the University of California, Los Angeles.
It is considered unsafe for patients with leukemia, as metastatic cells might well circulate through the bloodstream to the ovaries. Because of its highly metastatic potential, Ewing’s sarcoma is also considered a contraindication for the procedure, according to Dr. Pellicer.
The technique offers hope, potentially, for prepubertal girls and adolescents with other types of cancer, as well as adult cancer patients, although much remains unknown about the viability and usefulness of the treatment, explained Dr. Pellicer.
At the Valencia Program of Fertility Preservation, more than 600 cancer patients from across Spain have undergone removal of the ovarian cortex around the time of diagnosis, said Dr. Pellicer.
He reported on results in 583 of those patients who were treated since 2005, 55% of whom had been diagnosed with breast cancer.
Regular menses and fertility were restored in some patients who received ovarian autografts, said Dr. Pellicer. In all, 16 pregnancies and 3 live births have occurred, some following in vitro fertilization and some following natural conception.
Those results, along with published studies from programs in France, Germany, Denmark, Belgium, and other countries, indicate that at least 21 and perhaps 23 or more live births have resulted from the technique.
The problem, as Dr. Pellicer sees it, is a lack of cohesive follow-up or evidence that would put those births into perspective.
"We don’t know the number of failed attempts," he said. "There are no registries. There are no real data. Are we doing something which is really helpful? Or are the unsuccessful cases more [typical] than the successful cases?"
"This is a concern to me," he said.
Responding to a question from an audience member, Dr. Pellicer acknowledged that the removal of one ovarian cortex prior to cancer treatment might diminish fertility potential rather than enhance it, because some cancer patients conceive naturally following remission.
Dr. Pellicer reported that he had no relevant financial relationships to disclose.
SANTA BARBARA, CALIF. – Ovarian cortex orthotransplantation has resulted in the live births of at least 21 babies to cancer survivors in Europe, where the technique was pioneered and is being refined, Dr. Antonio Pellicer reported at a meeting on in vitro fertilization and embryo transfer.
Unlike the freezing of oocytes or embryos to preserve potential fertility, which requires ovarian stimulation, the ovarian cortex can be harvested from a cancer patient without delay, permitting immediate initiation of chemotherapy and/or radiation therapy. The tissue is cryopreserved until the patient is in remission.
If cancer treatment results in premature ovarian failure and the patient wishes to become pregnant, her autologous ovarian cortex can then be reintroduced.
Ovarian function generally resumes within 3-4 months, said Dr. Pellicer, professor of obstetrics and gynecology and dean of the medical school at the University of Valencia (Spain). Follicle stimulating hormone rates do not reach normal levels, but are sufficient in many cases for resumption of menses and pregnancy, either naturally or through assisted reproductive techniques.
The technique is currently believed to be safe for breast cancer patients and those with Hodgkin’s and non-Hodgkin’s lymphoma, based on histologic and immunologic evaluations of harvested ovarian tissue, Dr. Pellicer said at the meeting, which was sponsored by the University of California, Los Angeles.
It is considered unsafe for patients with leukemia, as metastatic cells might well circulate through the bloodstream to the ovaries. Because of its highly metastatic potential, Ewing’s sarcoma is also considered a contraindication for the procedure, according to Dr. Pellicer.
The technique offers hope, potentially, for prepubertal girls and adolescents with other types of cancer, as well as adult cancer patients, although much remains unknown about the viability and usefulness of the treatment, explained Dr. Pellicer.
At the Valencia Program of Fertility Preservation, more than 600 cancer patients from across Spain have undergone removal of the ovarian cortex around the time of diagnosis, said Dr. Pellicer.
He reported on results in 583 of those patients who were treated since 2005, 55% of whom had been diagnosed with breast cancer.
Regular menses and fertility were restored in some patients who received ovarian autografts, said Dr. Pellicer. In all, 16 pregnancies and 3 live births have occurred, some following in vitro fertilization and some following natural conception.
Those results, along with published studies from programs in France, Germany, Denmark, Belgium, and other countries, indicate that at least 21 and perhaps 23 or more live births have resulted from the technique.
The problem, as Dr. Pellicer sees it, is a lack of cohesive follow-up or evidence that would put those births into perspective.
"We don’t know the number of failed attempts," he said. "There are no registries. There are no real data. Are we doing something which is really helpful? Or are the unsuccessful cases more [typical] than the successful cases?"
"This is a concern to me," he said.
Responding to a question from an audience member, Dr. Pellicer acknowledged that the removal of one ovarian cortex prior to cancer treatment might diminish fertility potential rather than enhance it, because some cancer patients conceive naturally following remission.
Dr. Pellicer reported that he had no relevant financial relationships to disclose.
AT A MEETING ON IN VITRO FERTILIZATION AND EMBRYO TRANSFER
Major Finding: Sixteen pregnancies and three live births have occurred, some following in vitro fertilization and some following natural conception.
Data Source: This was a study of 583 patients who received ovarian autografts since 2005, 55% of whom had been diagnosed with breast cancer.
Disclosures: Dr. Pellicer reported that he had no relevant financial relationships to disclose.

Breast Cancer During Pregnancy Can Be Treated as in Nonpregnant Women
It appears that breast cancer diagnosed during pregnancy can be treated much the same as breast cancer diagnosed in nonpregnant women without substantially raising the risks to mother or child, according to a study published online August 16 in the Lancet Oncology .
This conclusion, from an observational study involving 447 European women included in registries of cancers diagnosed during pregnancy, must still be validated in other studies. But until then, the current evidence indicates that pregnancy outcomes are not significantly different between women who receive breast cancer chemotherapy during the second or third trimesters and those who wait until after delivery to start treatment, said Dr. Sibylle Loibl of the German Breast Group, Neu-Isenburg, Germany, and her associates.
In this study, infants exposed to their mothers’ breast cancer chemotherapy while in utero had slightly lower birth weights and slightly more complications than those not exposed to chemotherapy, but these differences were not clinically significant.
Breast cancer diagnosed during pregnancy is rare, estimated to occur in less than 1% of breast cancers in Europe. But its incidence is increasing in high-income countries due to the trend of women delaying childbirth until they are older, when breast cancer is more prevalent.
The German Breast Group established its Breast Cancer During Pregnancy registry in 2003 and expanded it to include cases in the Netherlands, the United Kingdom, Poland, Italy, and the Czech Republic in 2009. In the same time period, Belgium also established a registry of all cancers diagnosed during pregnancy. Dr. Loibl and her colleagues assessed outcomes in 447 cases from these registries in which women were diagnosed as having early (413 patients) or metastatic (34 patients) breast cancer while pregnant (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70261-9]).
The median gestational age at diagnosis was 24 weeks (range, 5-40 weeks), and the median age of the women was 33 years (range, 22-51 years).
Data on chemotherapy were available for 368 women. Of these, 197 received chemotherapy while pregnant and 171 received it after delivery.
Overall, 1,187 cycles of chemotherapy were given, and 63% of these were given during pregnancy. The women received a median of four cycles (range, one to eight cycles) during pregnancy.
A total of 90% of those treated during pregnancy received an anthracyline; 8% received a combination of cyclophosphamide, methotrexate, and fluorouracil; and 7% received a taxane. None of the women received trastuzumab, endocrine therapy, or radiotherapy during pregnancy.
Women with early breast cancer who opted for chemotherapy during pregnancy tended to have more advanced disease, with more unfavorable tumor stage and nodal status, than did those who chose to begin chemotherapy after delivery. After the data were adjusted to account for this difference, the researchers found no significant difference between the two groups in disease-free or overall survival.
The estimated 3-year disease-free survival was 70.2% in women with early disease who underwent chemotherapy while pregnant and 74.3% in those who waited until after delivery. Similarly, the estimated overall 3-year survival was 84.9% in women with early breast cancer who underwent chemotherapy while pregnant and 87.4% in those who delayed chemotherapy until after delivery.
The estimated 5-year disease-free survival was 61.1% in women who had chemotherapy while pregnant and 64.4% in those who waited, and the estimated 5-year overall survival was 77% and 82.4%, respectively.
Data were available for 373 newborns, of whom 203 had been exposed to chemotherapy in utero and 170 had not.
Birth weight was slightly lower in the exposed than in the nonexposed infants, but this difference was judged to be "clinically irrelevant" because it didn’t affect the health of the babies, Dr. Loibl and her associates said.
Moreover, there were no significant differences between the two groups in major birth defects, infant height, Apgar scores, hemoglobin concentration, leukocyte counts, thrombocyte counts, or alopecia. And there was no significant difference in the proportion of infants discharged with their mothers (34% vs. 41%).
Adverse events occurred more often when chemotherapy was received during pregnancy (15%) than when it was delayed (4%). However, this difference was attributed to the higher rates of preterm labor and premature rupture of the membrane among exposed pregnancies. "Most complications were reported in babies who were delivered prematurely, regardless of exposure to chemotherapy," the investigators said.
The data were not adequate to determine why women who received chemotherapy had a higher rate of preterm delivery. Both physical stress and psychological stress may have played a role, and it is possible that women who received chemotherapy were more prone to infections that may have triggered labor.
In addition, the cytotoxic agents themselves may have hastened labor through some as yet unknown mechanism. However, the rate of preeclampsia was similar between the two groups, so oxidative stress, which is known to be induced by cytoxic agents, was not responsible.
Further study of the data being collected in the registries of cancers diagnosed during pregnancy will likely shed light on these issues. Dr. Loibl and her colleagues are now performing a matched-pair analysis to assess whether the prognosis of breast cancer in nonpregnant women differs from that in pregnant women when the latter are treated according to current guidelines.
This study was supported by BANSS Foundation, University Hospital Frankfurt, the German Breast Group, Research Foundation-Flanders, Clinical Research Fund-UZ Gasthuisberg, and the Belgian Cancer Plan. No financial conflicts of interest were reported.
Future studies should address not just the toxic effects of chemotherapy during pregnancy but also the pharmacokinetics of cytotoxic agents in pregnant women, because the physiologic changes of pregnancy can greatly affect drug disposition, said Dr. Olivier Mir and Dr. Paul Berveiller.
"Whether doses should be increased in this population is uncertain because such increases could result in severe thrombocytopenia, neutropenia, and infection, with potentially devastating consequences for both mother and baby," they noted.
More research also is needed to determine whether the slightly increased fetal risks identified by Dr. Loibl and her colleagues could be minimized with better drug selection and dosing, they added.
Dr. Mir and Dr. Berveiller are in the Cancer Associated With Pregnancy Network, Paris. Dr. Mir is also in the department of medical oncology at Hôpital Cochin at the Université René Descartes, Paris. Dr. Mir reported ties to Roche, Pfizer, and Servier. These remarks were taken from their editorial comment accompanying Dr. Loibl’s report (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70331-5]).
Future studies should address not just the toxic effects of chemotherapy during pregnancy but also the pharmacokinetics of cytotoxic agents in pregnant women, because the physiologic changes of pregnancy can greatly affect drug disposition, said Dr. Olivier Mir and Dr. Paul Berveiller.
"Whether doses should be increased in this population is uncertain because such increases could result in severe thrombocytopenia, neutropenia, and infection, with potentially devastating consequences for both mother and baby," they noted.
More research also is needed to determine whether the slightly increased fetal risks identified by Dr. Loibl and her colleagues could be minimized with better drug selection and dosing, they added.
Dr. Mir and Dr. Berveiller are in the Cancer Associated With Pregnancy Network, Paris. Dr. Mir is also in the department of medical oncology at Hôpital Cochin at the Université René Descartes, Paris. Dr. Mir reported ties to Roche, Pfizer, and Servier. These remarks were taken from their editorial comment accompanying Dr. Loibl’s report (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70331-5]).
Future studies should address not just the toxic effects of chemotherapy during pregnancy but also the pharmacokinetics of cytotoxic agents in pregnant women, because the physiologic changes of pregnancy can greatly affect drug disposition, said Dr. Olivier Mir and Dr. Paul Berveiller.
"Whether doses should be increased in this population is uncertain because such increases could result in severe thrombocytopenia, neutropenia, and infection, with potentially devastating consequences for both mother and baby," they noted.
More research also is needed to determine whether the slightly increased fetal risks identified by Dr. Loibl and her colleagues could be minimized with better drug selection and dosing, they added.
Dr. Mir and Dr. Berveiller are in the Cancer Associated With Pregnancy Network, Paris. Dr. Mir is also in the department of medical oncology at Hôpital Cochin at the Université René Descartes, Paris. Dr. Mir reported ties to Roche, Pfizer, and Servier. These remarks were taken from their editorial comment accompanying Dr. Loibl’s report (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70331-5]).
It appears that breast cancer diagnosed during pregnancy can be treated much the same as breast cancer diagnosed in nonpregnant women without substantially raising the risks to mother or child, according to a study published online August 16 in the Lancet Oncology .
This conclusion, from an observational study involving 447 European women included in registries of cancers diagnosed during pregnancy, must still be validated in other studies. But until then, the current evidence indicates that pregnancy outcomes are not significantly different between women who receive breast cancer chemotherapy during the second or third trimesters and those who wait until after delivery to start treatment, said Dr. Sibylle Loibl of the German Breast Group, Neu-Isenburg, Germany, and her associates.
In this study, infants exposed to their mothers’ breast cancer chemotherapy while in utero had slightly lower birth weights and slightly more complications than those not exposed to chemotherapy, but these differences were not clinically significant.
Breast cancer diagnosed during pregnancy is rare, estimated to occur in less than 1% of breast cancers in Europe. But its incidence is increasing in high-income countries due to the trend of women delaying childbirth until they are older, when breast cancer is more prevalent.
The German Breast Group established its Breast Cancer During Pregnancy registry in 2003 and expanded it to include cases in the Netherlands, the United Kingdom, Poland, Italy, and the Czech Republic in 2009. In the same time period, Belgium also established a registry of all cancers diagnosed during pregnancy. Dr. Loibl and her colleagues assessed outcomes in 447 cases from these registries in which women were diagnosed as having early (413 patients) or metastatic (34 patients) breast cancer while pregnant (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70261-9]).
The median gestational age at diagnosis was 24 weeks (range, 5-40 weeks), and the median age of the women was 33 years (range, 22-51 years).
Data on chemotherapy were available for 368 women. Of these, 197 received chemotherapy while pregnant and 171 received it after delivery.
Overall, 1,187 cycles of chemotherapy were given, and 63% of these were given during pregnancy. The women received a median of four cycles (range, one to eight cycles) during pregnancy.
A total of 90% of those treated during pregnancy received an anthracyline; 8% received a combination of cyclophosphamide, methotrexate, and fluorouracil; and 7% received a taxane. None of the women received trastuzumab, endocrine therapy, or radiotherapy during pregnancy.
Women with early breast cancer who opted for chemotherapy during pregnancy tended to have more advanced disease, with more unfavorable tumor stage and nodal status, than did those who chose to begin chemotherapy after delivery. After the data were adjusted to account for this difference, the researchers found no significant difference between the two groups in disease-free or overall survival.
The estimated 3-year disease-free survival was 70.2% in women with early disease who underwent chemotherapy while pregnant and 74.3% in those who waited until after delivery. Similarly, the estimated overall 3-year survival was 84.9% in women with early breast cancer who underwent chemotherapy while pregnant and 87.4% in those who delayed chemotherapy until after delivery.
The estimated 5-year disease-free survival was 61.1% in women who had chemotherapy while pregnant and 64.4% in those who waited, and the estimated 5-year overall survival was 77% and 82.4%, respectively.
Data were available for 373 newborns, of whom 203 had been exposed to chemotherapy in utero and 170 had not.
Birth weight was slightly lower in the exposed than in the nonexposed infants, but this difference was judged to be "clinically irrelevant" because it didn’t affect the health of the babies, Dr. Loibl and her associates said.
Moreover, there were no significant differences between the two groups in major birth defects, infant height, Apgar scores, hemoglobin concentration, leukocyte counts, thrombocyte counts, or alopecia. And there was no significant difference in the proportion of infants discharged with their mothers (34% vs. 41%).
Adverse events occurred more often when chemotherapy was received during pregnancy (15%) than when it was delayed (4%). However, this difference was attributed to the higher rates of preterm labor and premature rupture of the membrane among exposed pregnancies. "Most complications were reported in babies who were delivered prematurely, regardless of exposure to chemotherapy," the investigators said.
The data were not adequate to determine why women who received chemotherapy had a higher rate of preterm delivery. Both physical stress and psychological stress may have played a role, and it is possible that women who received chemotherapy were more prone to infections that may have triggered labor.
In addition, the cytotoxic agents themselves may have hastened labor through some as yet unknown mechanism. However, the rate of preeclampsia was similar between the two groups, so oxidative stress, which is known to be induced by cytoxic agents, was not responsible.
Further study of the data being collected in the registries of cancers diagnosed during pregnancy will likely shed light on these issues. Dr. Loibl and her colleagues are now performing a matched-pair analysis to assess whether the prognosis of breast cancer in nonpregnant women differs from that in pregnant women when the latter are treated according to current guidelines.
This study was supported by BANSS Foundation, University Hospital Frankfurt, the German Breast Group, Research Foundation-Flanders, Clinical Research Fund-UZ Gasthuisberg, and the Belgian Cancer Plan. No financial conflicts of interest were reported.
It appears that breast cancer diagnosed during pregnancy can be treated much the same as breast cancer diagnosed in nonpregnant women without substantially raising the risks to mother or child, according to a study published online August 16 in the Lancet Oncology .
This conclusion, from an observational study involving 447 European women included in registries of cancers diagnosed during pregnancy, must still be validated in other studies. But until then, the current evidence indicates that pregnancy outcomes are not significantly different between women who receive breast cancer chemotherapy during the second or third trimesters and those who wait until after delivery to start treatment, said Dr. Sibylle Loibl of the German Breast Group, Neu-Isenburg, Germany, and her associates.
In this study, infants exposed to their mothers’ breast cancer chemotherapy while in utero had slightly lower birth weights and slightly more complications than those not exposed to chemotherapy, but these differences were not clinically significant.
Breast cancer diagnosed during pregnancy is rare, estimated to occur in less than 1% of breast cancers in Europe. But its incidence is increasing in high-income countries due to the trend of women delaying childbirth until they are older, when breast cancer is more prevalent.
The German Breast Group established its Breast Cancer During Pregnancy registry in 2003 and expanded it to include cases in the Netherlands, the United Kingdom, Poland, Italy, and the Czech Republic in 2009. In the same time period, Belgium also established a registry of all cancers diagnosed during pregnancy. Dr. Loibl and her colleagues assessed outcomes in 447 cases from these registries in which women were diagnosed as having early (413 patients) or metastatic (34 patients) breast cancer while pregnant (Lancet Oncol. 2012 Aug. 15 [doi:10.1016/S1470-2045(12)70261-9]).
The median gestational age at diagnosis was 24 weeks (range, 5-40 weeks), and the median age of the women was 33 years (range, 22-51 years).
Data on chemotherapy were available for 368 women. Of these, 197 received chemotherapy while pregnant and 171 received it after delivery.
Overall, 1,187 cycles of chemotherapy were given, and 63% of these were given during pregnancy. The women received a median of four cycles (range, one to eight cycles) during pregnancy.
A total of 90% of those treated during pregnancy received an anthracyline; 8% received a combination of cyclophosphamide, methotrexate, and fluorouracil; and 7% received a taxane. None of the women received trastuzumab, endocrine therapy, or radiotherapy during pregnancy.
Women with early breast cancer who opted for chemotherapy during pregnancy tended to have more advanced disease, with more unfavorable tumor stage and nodal status, than did those who chose to begin chemotherapy after delivery. After the data were adjusted to account for this difference, the researchers found no significant difference between the two groups in disease-free or overall survival.
The estimated 3-year disease-free survival was 70.2% in women with early disease who underwent chemotherapy while pregnant and 74.3% in those who waited until after delivery. Similarly, the estimated overall 3-year survival was 84.9% in women with early breast cancer who underwent chemotherapy while pregnant and 87.4% in those who delayed chemotherapy until after delivery.
The estimated 5-year disease-free survival was 61.1% in women who had chemotherapy while pregnant and 64.4% in those who waited, and the estimated 5-year overall survival was 77% and 82.4%, respectively.
Data were available for 373 newborns, of whom 203 had been exposed to chemotherapy in utero and 170 had not.
Birth weight was slightly lower in the exposed than in the nonexposed infants, but this difference was judged to be "clinically irrelevant" because it didn’t affect the health of the babies, Dr. Loibl and her associates said.
Moreover, there were no significant differences between the two groups in major birth defects, infant height, Apgar scores, hemoglobin concentration, leukocyte counts, thrombocyte counts, or alopecia. And there was no significant difference in the proportion of infants discharged with their mothers (34% vs. 41%).
Adverse events occurred more often when chemotherapy was received during pregnancy (15%) than when it was delayed (4%). However, this difference was attributed to the higher rates of preterm labor and premature rupture of the membrane among exposed pregnancies. "Most complications were reported in babies who were delivered prematurely, regardless of exposure to chemotherapy," the investigators said.
The data were not adequate to determine why women who received chemotherapy had a higher rate of preterm delivery. Both physical stress and psychological stress may have played a role, and it is possible that women who received chemotherapy were more prone to infections that may have triggered labor.
In addition, the cytotoxic agents themselves may have hastened labor through some as yet unknown mechanism. However, the rate of preeclampsia was similar between the two groups, so oxidative stress, which is known to be induced by cytoxic agents, was not responsible.
Further study of the data being collected in the registries of cancers diagnosed during pregnancy will likely shed light on these issues. Dr. Loibl and her colleagues are now performing a matched-pair analysis to assess whether the prognosis of breast cancer in nonpregnant women differs from that in pregnant women when the latter are treated according to current guidelines.
This study was supported by BANSS Foundation, University Hospital Frankfurt, the German Breast Group, Research Foundation-Flanders, Clinical Research Fund-UZ Gasthuisberg, and the Belgian Cancer Plan. No financial conflicts of interest were reported.
FROM THE LANCET ONCOLOGY
Major Finding: Rates of low birth weight and adverse events were slightly higher when women underwent breast cancer chemotherapy while pregnant than when they delayed chemotherapy until after delivery, but the small differences were deemed clinically irrelevant.
Data Source: An observational study of pregnancy outcomes in European women diagnosed as having breast cancer during pregnancy, of whom 197 received chemotherapy while pregnant and 171 delayed chemotherapy until after delivery.
Disclosures: This study was supported by BANSS Foundation, University Hospital Frankfurt, the German Breast Group, Research Foundation-Flanders, Clinical Research Fund-UZ Gasthuisberg, and the Belgian Cancer Plan. No financial conflicts of interest were reported.
Romidepsin-Decitabine Duo Battles Breast and Kidney Cancers
Two blood cancer drugs, romidepsin and decitabine, may form a partnership that can treat specific types of breast and kidney cancers, based on data from a stem cell study published online in Molecular Cancer Therapeutics.
Each drug is approved by the Food and Drug Administration to treat hematologic cancer, but this study uniquely combined romidepsin (Istodax) and decitabine (Dacogen) to activate a tumor suppressor gene that is inactive in triple-negative breast cancer and clear cell renal cell carcinoma.
Activating the gene known as secreted frizzled-related protein 1 (sFRP1) killed kidney and breast cancer cells in multiple cell lines tested, but only when the drugs were used in tandem (Mol. Cancer Ther. July 23, 2012 [doi:10.1158/1535-7163.MCT-11-0873]).
Ultimately, clinicians may be able to target treatment of triple-negative breast cancer and clear cell renal cell carcinoma by identifying which patients have tumors in which sFRP1 is inactivated, the researchers noted. "We predict that there are a number of drug targetable genes that are re-expressed after combinatorial treatment that possess antitumor activity," they said.
"We now have the basis for a clinical trial aimed at providing effective therapy for two drug-resistant cancers and perhaps many more tumor types in the future," senior author John A. Copland, Ph.D., of the Mayo Clinic in Jacksonville, Florida, added in a statement issued July 31 by the Mayo Clinic.
The researchers had no financial conflicts to disclose. The study was funded in part by grants from several organizations, including the National Cancer Institute; Kidney Cancer Research at Mayo Clinic, Florida; and the Breast Cancer Research Foundation.
Two blood cancer drugs, romidepsin and decitabine, may form a partnership that can treat specific types of breast and kidney cancers, based on data from a stem cell study published online in Molecular Cancer Therapeutics.
Each drug is approved by the Food and Drug Administration to treat hematologic cancer, but this study uniquely combined romidepsin (Istodax) and decitabine (Dacogen) to activate a tumor suppressor gene that is inactive in triple-negative breast cancer and clear cell renal cell carcinoma.
Activating the gene known as secreted frizzled-related protein 1 (sFRP1) killed kidney and breast cancer cells in multiple cell lines tested, but only when the drugs were used in tandem (Mol. Cancer Ther. July 23, 2012 [doi:10.1158/1535-7163.MCT-11-0873]).
Ultimately, clinicians may be able to target treatment of triple-negative breast cancer and clear cell renal cell carcinoma by identifying which patients have tumors in which sFRP1 is inactivated, the researchers noted. "We predict that there are a number of drug targetable genes that are re-expressed after combinatorial treatment that possess antitumor activity," they said.
"We now have the basis for a clinical trial aimed at providing effective therapy for two drug-resistant cancers and perhaps many more tumor types in the future," senior author John A. Copland, Ph.D., of the Mayo Clinic in Jacksonville, Florida, added in a statement issued July 31 by the Mayo Clinic.
The researchers had no financial conflicts to disclose. The study was funded in part by grants from several organizations, including the National Cancer Institute; Kidney Cancer Research at Mayo Clinic, Florida; and the Breast Cancer Research Foundation.
Two blood cancer drugs, romidepsin and decitabine, may form a partnership that can treat specific types of breast and kidney cancers, based on data from a stem cell study published online in Molecular Cancer Therapeutics.
Each drug is approved by the Food and Drug Administration to treat hematologic cancer, but this study uniquely combined romidepsin (Istodax) and decitabine (Dacogen) to activate a tumor suppressor gene that is inactive in triple-negative breast cancer and clear cell renal cell carcinoma.
Activating the gene known as secreted frizzled-related protein 1 (sFRP1) killed kidney and breast cancer cells in multiple cell lines tested, but only when the drugs were used in tandem (Mol. Cancer Ther. July 23, 2012 [doi:10.1158/1535-7163.MCT-11-0873]).
Ultimately, clinicians may be able to target treatment of triple-negative breast cancer and clear cell renal cell carcinoma by identifying which patients have tumors in which sFRP1 is inactivated, the researchers noted. "We predict that there are a number of drug targetable genes that are re-expressed after combinatorial treatment that possess antitumor activity," they said.
"We now have the basis for a clinical trial aimed at providing effective therapy for two drug-resistant cancers and perhaps many more tumor types in the future," senior author John A. Copland, Ph.D., of the Mayo Clinic in Jacksonville, Florida, added in a statement issued July 31 by the Mayo Clinic.
The researchers had no financial conflicts to disclose. The study was funded in part by grants from several organizations, including the National Cancer Institute; Kidney Cancer Research at Mayo Clinic, Florida; and the Breast Cancer Research Foundation.
FROM MOLECULAR CANCER THERAPEUTICS
Faster Injectable Trastuzumab Matches Intravenous in Response Rates
A subcutaneous injectable form of trastuzumab achieved pharmacokinetic and clinical outcomes that equaled those of intravenous infusion for women with HER2-positive breast cancers in a randomized open-label phase III study.
The international HannaH trial found no significant differences in presurgical serum trough levels at any time during the six-cycle neoadjuvant treatment. At the end of the year-long study, 45% of the subcutaneous group and 41% of the intravenous group had a pathological complete response (pCR).
The subcutaneous form of trastuzumab (Herceptin) takes 5 minutes to administer; patients can self-administer the drug at home. The infusion takes 90 minutes and must be done in the clinic.
If clinical results are equivalent, the injection could become an attractive alternative to intravenous treatment, Dr. Gustavo Ismael of the Hospital Amaral Carvalho, Jaú, Brazil, and his coauthors proposed in the Aug. 9 online issue of the Lancet Oncology (2012 [doi.org/10.1016/S1470-2045(12)70329-7]).*
"The shortened duration of administration with subcutaneous trastuzumab ... suggests the potential for substantial time saving for patients, physicians, and nursing staff," the investigators wrote.
Susan Willson, a spokesperson for Genentech, said the company is looking at the HannaH data, as well as that of other studies, to determine whether the subcutaneous form of trastuzumab will be put forth to the Food and Drug Administration.
Earlier this year, Roche, Genetech’s parent company, submitted a line extension application for subcutaneous trastuzumab to the European Medicines Association. The requested indication is the treatment of HER-2-positive breast cancer.
Trastuzumab Given with Neoadjuvant Chemo
The HannaH (enHANced treatment with NeoAdjuvant Herceptin) trial randomized 596 women with HER-2 positive breast cancer to six cycles of neoadjuvant chemotherapy with either the injections or intravenous infusions; both were administered once every 3 weeks.
The injection was a fixed dose of 600 mg trastuzumab with recombinant hyaluronidase PH-20 delivered to the thigh by study nurses. The enzyme temporarily degrades interstitial hyaluronan, expanding the space to accommodate the volume of the injection.
Women in the subcutaneous group did not take a loading dose of the medication. Those in the intravenous group received an 8 mg/kg loading dose followed by a 6 mg/kg maintenance dose. The follow-up period was 24 months or until disease recurrence
The chemotherapy regimen for both groups consisted of four 3-week cycles of docetaxel (Taxotere) followed by four cycles of fluorouracil and cyclophosphamide. After surgery, all patients continued their trastuzumab regimen for 1 year.
Median patient age was 50 years. About 50% were positive for estrogen receptor tumors. More than half had operable cancer; more than a third had locally advanced cancer; and about 6% had inflammatory breast cancer. Median follow-up in both groups was a little more than 1 year.
The pharmacokinetic profile was similar between the two forms of trastuzumab. After the first cycle, the mean trough serum level was similar between the injectable and intravenous forms (32.7 mcg/mL vs. 34.5 mcg/mL). The levels were also similar before the third cycle (45 and 48 mcg/mL). Almost all patients (98%) reached the therapeutic level of more than 20 micrograms/ml by cycle 8.
The mean presurgical trough level of the subcutaneous form was 58 mcg/mL; for the intravenous form, the mean level was 79 mcg/mL.
Similar Efficacy and Toxicity
The efficacy analysis included 523 patients and showed noninferiority of subcutaneous trastuzumab to intravenous trastuzumab. A pathological complete response occurred in 45% of the subcutaneous group and in 41% of the intravenous group in a per-protocol analysis. An intent-to-treat analysis showed similar numbers, with a complete pathological response in 42% of the subcutaneous group an 37% of the intravenous group.
Overall responses rates, including complete and partial responses, were comparable. Event-free and overall survival data were not yet mature, and have yet to be reported.
The rate of adverse events was similar between the subcutaneous and intravenous groups: alopecia (63% each), nausea (49% each), neutropenia (44% subcutaneous vs. 46% intravenous), diarrhea (34% subcutaneous vs. 37% intravenous), asthenia (25% each), and fatigue (23% subcutaneous vs. 26% intravenous).
The same proportion of patients in each group experienced at least one serious adverse event (52%). The most common were neutropenia, leucopenia, and febrile neutropenia.
Four adverse events lead to death – one in the subcutaneous group and three in the intravenous group during neoadjuvant treatment. These included a fatal acute pneumonia in an obese 66-year-old with pulmonary fibrosis in the subcutaneous group. In the intravenous group, the deaths were a myocardial infarction in an obese patient with a history of hypertension; a sudden death in an overweight patient who with hypertension and diabetes; fatal septic shock in a patient who developed febrile neutropenia. The septic shock and cardiac deaths were attributed to the treatment, the investigators said.
The proportion of grade 3 adverse events was similar in both groups, but the relative percentage of those classified as serious adverse events was 7.7% for the intravenous group and 18% for the subcutaneous group. "A similar finding was made for grade 2 adverse events, of which 0.5% was classed as serous ... in the intravenous group versus 1.5% in the subcutaneous group," they wrote. The investigators could not find an explanation for the imbalance in reporting of serious adverse events, but suggested that they may have been more conservative in assessing the subcutaneous arm of the trial.
Two patients in the subcutaneous group had mild congestive heart failure; both were obese with a history of hypertension. Six patients in the intravenous group and seven in the subcutaneous group had a significant decrease in left ventricular ejection fraction.
Antitrastuzumab antibodies developed in 10 patients in the intravenous group and 20 in the subcutaneous group, but these did not affect serum trough levels.
F. Hoffman-LaRoche funded the study Dr. Ismael disclosed that he has received honoraria from the company. His co-investigators also reported several financial relationships, including travels grants, speakers fees, research support, and employment.
Click here to hear Dr. Ismael discuss the trial in a podcast at the Lancet Oncology website.
*Correction, 08/13/12: This sentence was corrected to state that injectable trastuzumab could become an alternative to intravenous treatment. Weekly treatment was not specified.
A rapid, subcutaneous delivery of trastuzumab could come with several big advantages, Dr. Jose Perez-Garcia and Dr. Javier Cortes wrote in an accompanying editorial (Lancet Onc. 2012 Aug. 9 [doi.org/10.1016/S1470-2045(12)70367-4]).
"First, the ability to deliver the drug in about 5 minutes without the need to secure intravenous access makes subcutaneous treatment more convenient," wrote Dr. Perez-Garcia and Dr. Cortes of Vall d’Hebron Institute of Oncology, Barcelona. "Second, in addition to time savings, once the drug can be administered at home, patients will be able to continue their lives with less hospital dependence, which is an important psychological aspect."
The study didn’t address which drug delivery method patients preferred, or how an at-home subcutaneous administration might affect their quality of life. But another randomized study, PrefHer, aims to explore that, they wrote. PrefHer will evaluate patients' preference and healthcare satisfaction with subcutaneous vs. intravenous trastuzumab.
They also noted that the HannaH study could set a precedent for rapid approval of neoadjuvant drugs based on the pathological complete response (pCR) – but that pCR as an end point has not yet been fully vetted. "This approach appears to have at least two major limitations. First, we do not know what improvement in pCR would be necessary to translate into disease-free survival or overall survival benefit. Second, we also do not know what proportion of patients achieving a pCR would be needed to establish noninferiority between two drugs or between two methods of administering the same drug."
Finally, they wrote. "Third, the method of categorizing long-term adverse effects might be insufficient because many adverse events might appear after pCR, so if pCR is enough for regulatory purposes, the consequences of these long-term events might not be taken into account."
Dr. Perez-Garcia is an oncologist in the breast cancer program at Vall d’Hebron Institute of Oncology, Barcelona. He had no financial disclosures. Dr. Cortes, of the same institution, disclosed relationships with Roche and other companies.
A rapid, subcutaneous delivery of trastuzumab could come with several big advantages, Dr. Jose Perez-Garcia and Dr. Javier Cortes wrote in an accompanying editorial (Lancet Onc. 2012 Aug. 9 [doi.org/10.1016/S1470-2045(12)70367-4]).
"First, the ability to deliver the drug in about 5 minutes without the need to secure intravenous access makes subcutaneous treatment more convenient," wrote Dr. Perez-Garcia and Dr. Cortes of Vall d’Hebron Institute of Oncology, Barcelona. "Second, in addition to time savings, once the drug can be administered at home, patients will be able to continue their lives with less hospital dependence, which is an important psychological aspect."
The study didn’t address which drug delivery method patients preferred, or how an at-home subcutaneous administration might affect their quality of life. But another randomized study, PrefHer, aims to explore that, they wrote. PrefHer will evaluate patients' preference and healthcare satisfaction with subcutaneous vs. intravenous trastuzumab.
They also noted that the HannaH study could set a precedent for rapid approval of neoadjuvant drugs based on the pathological complete response (pCR) – but that pCR as an end point has not yet been fully vetted. "This approach appears to have at least two major limitations. First, we do not know what improvement in pCR would be necessary to translate into disease-free survival or overall survival benefit. Second, we also do not know what proportion of patients achieving a pCR would be needed to establish noninferiority between two drugs or between two methods of administering the same drug."
Finally, they wrote. "Third, the method of categorizing long-term adverse effects might be insufficient because many adverse events might appear after pCR, so if pCR is enough for regulatory purposes, the consequences of these long-term events might not be taken into account."
Dr. Perez-Garcia is an oncologist in the breast cancer program at Vall d’Hebron Institute of Oncology, Barcelona. He had no financial disclosures. Dr. Cortes, of the same institution, disclosed relationships with Roche and other companies.
A rapid, subcutaneous delivery of trastuzumab could come with several big advantages, Dr. Jose Perez-Garcia and Dr. Javier Cortes wrote in an accompanying editorial (Lancet Onc. 2012 Aug. 9 [doi.org/10.1016/S1470-2045(12)70367-4]).
"First, the ability to deliver the drug in about 5 minutes without the need to secure intravenous access makes subcutaneous treatment more convenient," wrote Dr. Perez-Garcia and Dr. Cortes of Vall d’Hebron Institute of Oncology, Barcelona. "Second, in addition to time savings, once the drug can be administered at home, patients will be able to continue their lives with less hospital dependence, which is an important psychological aspect."
The study didn’t address which drug delivery method patients preferred, or how an at-home subcutaneous administration might affect their quality of life. But another randomized study, PrefHer, aims to explore that, they wrote. PrefHer will evaluate patients' preference and healthcare satisfaction with subcutaneous vs. intravenous trastuzumab.
They also noted that the HannaH study could set a precedent for rapid approval of neoadjuvant drugs based on the pathological complete response (pCR) – but that pCR as an end point has not yet been fully vetted. "This approach appears to have at least two major limitations. First, we do not know what improvement in pCR would be necessary to translate into disease-free survival or overall survival benefit. Second, we also do not know what proportion of patients achieving a pCR would be needed to establish noninferiority between two drugs or between two methods of administering the same drug."
Finally, they wrote. "Third, the method of categorizing long-term adverse effects might be insufficient because many adverse events might appear after pCR, so if pCR is enough for regulatory purposes, the consequences of these long-term events might not be taken into account."
Dr. Perez-Garcia is an oncologist in the breast cancer program at Vall d’Hebron Institute of Oncology, Barcelona. He had no financial disclosures. Dr. Cortes, of the same institution, disclosed relationships with Roche and other companies.
A subcutaneous injectable form of trastuzumab achieved pharmacokinetic and clinical outcomes that equaled those of intravenous infusion for women with HER2-positive breast cancers in a randomized open-label phase III study.
The international HannaH trial found no significant differences in presurgical serum trough levels at any time during the six-cycle neoadjuvant treatment. At the end of the year-long study, 45% of the subcutaneous group and 41% of the intravenous group had a pathological complete response (pCR).
The subcutaneous form of trastuzumab (Herceptin) takes 5 minutes to administer; patients can self-administer the drug at home. The infusion takes 90 minutes and must be done in the clinic.
If clinical results are equivalent, the injection could become an attractive alternative to intravenous treatment, Dr. Gustavo Ismael of the Hospital Amaral Carvalho, Jaú, Brazil, and his coauthors proposed in the Aug. 9 online issue of the Lancet Oncology (2012 [doi.org/10.1016/S1470-2045(12)70329-7]).*
"The shortened duration of administration with subcutaneous trastuzumab ... suggests the potential for substantial time saving for patients, physicians, and nursing staff," the investigators wrote.
Susan Willson, a spokesperson for Genentech, said the company is looking at the HannaH data, as well as that of other studies, to determine whether the subcutaneous form of trastuzumab will be put forth to the Food and Drug Administration.
Earlier this year, Roche, Genetech’s parent company, submitted a line extension application for subcutaneous trastuzumab to the European Medicines Association. The requested indication is the treatment of HER-2-positive breast cancer.
Trastuzumab Given with Neoadjuvant Chemo
The HannaH (enHANced treatment with NeoAdjuvant Herceptin) trial randomized 596 women with HER-2 positive breast cancer to six cycles of neoadjuvant chemotherapy with either the injections or intravenous infusions; both were administered once every 3 weeks.
The injection was a fixed dose of 600 mg trastuzumab with recombinant hyaluronidase PH-20 delivered to the thigh by study nurses. The enzyme temporarily degrades interstitial hyaluronan, expanding the space to accommodate the volume of the injection.
Women in the subcutaneous group did not take a loading dose of the medication. Those in the intravenous group received an 8 mg/kg loading dose followed by a 6 mg/kg maintenance dose. The follow-up period was 24 months or until disease recurrence
The chemotherapy regimen for both groups consisted of four 3-week cycles of docetaxel (Taxotere) followed by four cycles of fluorouracil and cyclophosphamide. After surgery, all patients continued their trastuzumab regimen for 1 year.
Median patient age was 50 years. About 50% were positive for estrogen receptor tumors. More than half had operable cancer; more than a third had locally advanced cancer; and about 6% had inflammatory breast cancer. Median follow-up in both groups was a little more than 1 year.
The pharmacokinetic profile was similar between the two forms of trastuzumab. After the first cycle, the mean trough serum level was similar between the injectable and intravenous forms (32.7 mcg/mL vs. 34.5 mcg/mL). The levels were also similar before the third cycle (45 and 48 mcg/mL). Almost all patients (98%) reached the therapeutic level of more than 20 micrograms/ml by cycle 8.
The mean presurgical trough level of the subcutaneous form was 58 mcg/mL; for the intravenous form, the mean level was 79 mcg/mL.
Similar Efficacy and Toxicity
The efficacy analysis included 523 patients and showed noninferiority of subcutaneous trastuzumab to intravenous trastuzumab. A pathological complete response occurred in 45% of the subcutaneous group and in 41% of the intravenous group in a per-protocol analysis. An intent-to-treat analysis showed similar numbers, with a complete pathological response in 42% of the subcutaneous group an 37% of the intravenous group.
Overall responses rates, including complete and partial responses, were comparable. Event-free and overall survival data were not yet mature, and have yet to be reported.
The rate of adverse events was similar between the subcutaneous and intravenous groups: alopecia (63% each), nausea (49% each), neutropenia (44% subcutaneous vs. 46% intravenous), diarrhea (34% subcutaneous vs. 37% intravenous), asthenia (25% each), and fatigue (23% subcutaneous vs. 26% intravenous).
The same proportion of patients in each group experienced at least one serious adverse event (52%). The most common were neutropenia, leucopenia, and febrile neutropenia.
Four adverse events lead to death – one in the subcutaneous group and three in the intravenous group during neoadjuvant treatment. These included a fatal acute pneumonia in an obese 66-year-old with pulmonary fibrosis in the subcutaneous group. In the intravenous group, the deaths were a myocardial infarction in an obese patient with a history of hypertension; a sudden death in an overweight patient who with hypertension and diabetes; fatal septic shock in a patient who developed febrile neutropenia. The septic shock and cardiac deaths were attributed to the treatment, the investigators said.
The proportion of grade 3 adverse events was similar in both groups, but the relative percentage of those classified as serious adverse events was 7.7% for the intravenous group and 18% for the subcutaneous group. "A similar finding was made for grade 2 adverse events, of which 0.5% was classed as serous ... in the intravenous group versus 1.5% in the subcutaneous group," they wrote. The investigators could not find an explanation for the imbalance in reporting of serious adverse events, but suggested that they may have been more conservative in assessing the subcutaneous arm of the trial.
Two patients in the subcutaneous group had mild congestive heart failure; both were obese with a history of hypertension. Six patients in the intravenous group and seven in the subcutaneous group had a significant decrease in left ventricular ejection fraction.
Antitrastuzumab antibodies developed in 10 patients in the intravenous group and 20 in the subcutaneous group, but these did not affect serum trough levels.
F. Hoffman-LaRoche funded the study Dr. Ismael disclosed that he has received honoraria from the company. His co-investigators also reported several financial relationships, including travels grants, speakers fees, research support, and employment.
Click here to hear Dr. Ismael discuss the trial in a podcast at the Lancet Oncology website.
*Correction, 08/13/12: This sentence was corrected to state that injectable trastuzumab could become an alternative to intravenous treatment. Weekly treatment was not specified.
A subcutaneous injectable form of trastuzumab achieved pharmacokinetic and clinical outcomes that equaled those of intravenous infusion for women with HER2-positive breast cancers in a randomized open-label phase III study.
The international HannaH trial found no significant differences in presurgical serum trough levels at any time during the six-cycle neoadjuvant treatment. At the end of the year-long study, 45% of the subcutaneous group and 41% of the intravenous group had a pathological complete response (pCR).
The subcutaneous form of trastuzumab (Herceptin) takes 5 minutes to administer; patients can self-administer the drug at home. The infusion takes 90 minutes and must be done in the clinic.
If clinical results are equivalent, the injection could become an attractive alternative to intravenous treatment, Dr. Gustavo Ismael of the Hospital Amaral Carvalho, Jaú, Brazil, and his coauthors proposed in the Aug. 9 online issue of the Lancet Oncology (2012 [doi.org/10.1016/S1470-2045(12)70329-7]).*
"The shortened duration of administration with subcutaneous trastuzumab ... suggests the potential for substantial time saving for patients, physicians, and nursing staff," the investigators wrote.
Susan Willson, a spokesperson for Genentech, said the company is looking at the HannaH data, as well as that of other studies, to determine whether the subcutaneous form of trastuzumab will be put forth to the Food and Drug Administration.
Earlier this year, Roche, Genetech’s parent company, submitted a line extension application for subcutaneous trastuzumab to the European Medicines Association. The requested indication is the treatment of HER-2-positive breast cancer.
Trastuzumab Given with Neoadjuvant Chemo
The HannaH (enHANced treatment with NeoAdjuvant Herceptin) trial randomized 596 women with HER-2 positive breast cancer to six cycles of neoadjuvant chemotherapy with either the injections or intravenous infusions; both were administered once every 3 weeks.
The injection was a fixed dose of 600 mg trastuzumab with recombinant hyaluronidase PH-20 delivered to the thigh by study nurses. The enzyme temporarily degrades interstitial hyaluronan, expanding the space to accommodate the volume of the injection.
Women in the subcutaneous group did not take a loading dose of the medication. Those in the intravenous group received an 8 mg/kg loading dose followed by a 6 mg/kg maintenance dose. The follow-up period was 24 months or until disease recurrence
The chemotherapy regimen for both groups consisted of four 3-week cycles of docetaxel (Taxotere) followed by four cycles of fluorouracil and cyclophosphamide. After surgery, all patients continued their trastuzumab regimen for 1 year.
Median patient age was 50 years. About 50% were positive for estrogen receptor tumors. More than half had operable cancer; more than a third had locally advanced cancer; and about 6% had inflammatory breast cancer. Median follow-up in both groups was a little more than 1 year.
The pharmacokinetic profile was similar between the two forms of trastuzumab. After the first cycle, the mean trough serum level was similar between the injectable and intravenous forms (32.7 mcg/mL vs. 34.5 mcg/mL). The levels were also similar before the third cycle (45 and 48 mcg/mL). Almost all patients (98%) reached the therapeutic level of more than 20 micrograms/ml by cycle 8.
The mean presurgical trough level of the subcutaneous form was 58 mcg/mL; for the intravenous form, the mean level was 79 mcg/mL.
Similar Efficacy and Toxicity
The efficacy analysis included 523 patients and showed noninferiority of subcutaneous trastuzumab to intravenous trastuzumab. A pathological complete response occurred in 45% of the subcutaneous group and in 41% of the intravenous group in a per-protocol analysis. An intent-to-treat analysis showed similar numbers, with a complete pathological response in 42% of the subcutaneous group an 37% of the intravenous group.
Overall responses rates, including complete and partial responses, were comparable. Event-free and overall survival data were not yet mature, and have yet to be reported.
The rate of adverse events was similar between the subcutaneous and intravenous groups: alopecia (63% each), nausea (49% each), neutropenia (44% subcutaneous vs. 46% intravenous), diarrhea (34% subcutaneous vs. 37% intravenous), asthenia (25% each), and fatigue (23% subcutaneous vs. 26% intravenous).
The same proportion of patients in each group experienced at least one serious adverse event (52%). The most common were neutropenia, leucopenia, and febrile neutropenia.
Four adverse events lead to death – one in the subcutaneous group and three in the intravenous group during neoadjuvant treatment. These included a fatal acute pneumonia in an obese 66-year-old with pulmonary fibrosis in the subcutaneous group. In the intravenous group, the deaths were a myocardial infarction in an obese patient with a history of hypertension; a sudden death in an overweight patient who with hypertension and diabetes; fatal septic shock in a patient who developed febrile neutropenia. The septic shock and cardiac deaths were attributed to the treatment, the investigators said.
The proportion of grade 3 adverse events was similar in both groups, but the relative percentage of those classified as serious adverse events was 7.7% for the intravenous group and 18% for the subcutaneous group. "A similar finding was made for grade 2 adverse events, of which 0.5% was classed as serous ... in the intravenous group versus 1.5% in the subcutaneous group," they wrote. The investigators could not find an explanation for the imbalance in reporting of serious adverse events, but suggested that they may have been more conservative in assessing the subcutaneous arm of the trial.
Two patients in the subcutaneous group had mild congestive heart failure; both were obese with a history of hypertension. Six patients in the intravenous group and seven in the subcutaneous group had a significant decrease in left ventricular ejection fraction.
Antitrastuzumab antibodies developed in 10 patients in the intravenous group and 20 in the subcutaneous group, but these did not affect serum trough levels.
F. Hoffman-LaRoche funded the study Dr. Ismael disclosed that he has received honoraria from the company. His co-investigators also reported several financial relationships, including travels grants, speakers fees, research support, and employment.
Click here to hear Dr. Ismael discuss the trial in a podcast at the Lancet Oncology website.
*Correction, 08/13/12: This sentence was corrected to state that injectable trastuzumab could become an alternative to intravenous treatment. Weekly treatment was not specified.
FROM LANCET ONCOLOGY
Major Finding: A pathologic complete response occurred in 45% of those who used a subcutaneous injectable trastuzumab and 41% of those who underwent the traditional intravenous treatment.
Data Source: HannaH was an open-label, randomized study of 596 women with HER2-positive breast cancer.
Disclosures: F. Hoffman-LaRoche funded the study Dr. Ismael disclosed that he has received honoraria from the company. His co-investigators also reported financial relationships, including travels grants, speakers’ fees, research support, and employment.