User login
Extending Therapy for Breast Cancer
For more presentations from the 9th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO), click here: AVAHO Meeting Presentations
For more presentations from the 9th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO), click here: AVAHO Meeting Presentations
For more presentations from the 9th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO), click here: AVAHO Meeting Presentations

New Breast Cancer Research Group Aims To Improve Veteran Survival Rates
Over 200,000 new cases of breast cancer are diagnosed in the U.S. annually, according to the National Cancer Institute. Dr. Anita Aggarwal, an oncologist at the Washington, DC VAMC, recently completed an extensive study to compare male and female breast cancer in VA patients. The study found that males with breast cancer had higher stage and grade at presentation and higher mortality compared with females. But, when adjusted for age, stage, and grade, males had better survival rates.
Federal Practitioner talked with Dr. Aggarwal about the new breast cancer research group she is currently developing at the Washington, DC VAMC. Dr. Aggarwal’s hope is to help doctors in the federal health system to identify etiology, biology, and improve treatment of both male and female patients with breast cancer.
Federal Practitioner: What is a breast cancer research group, and why do you think one needs to be created at the VA?
Anita Aggarwal, MD: I would like to build a breast cancer research group with the help of all oncologists and health professionals who take care of patients with breast cancer at all VAMCs nationwide. From my retrospective comparison study, breast cancer in our veterans seems to be different than in the general population. The goal of this research group will be to build a data bank with all the pertinent information as well as tissue gene profiling. This will help us to diagnose them early and treat accordingly in a timely fashion.
FP: As more women join the military, do you think breast cancer treatment at the VA will change?
AA: As the number of female veterans increases, I suspect we will see an increase in the number of female patients with breast cancer. As reported by the 2012 Women’s Task Force, women are now the fastest growing cohort within the veteran community. In 2011, there were about 1.8 million women veterans, which is about 8% of the 22.2 million vets in the VA system. That is expected to increase to 2 million in 2020, at which time women will make up to 10.7% of the total vet population. To accommodate these changing needs, the VHA made women’s health programs a priority in 2007, including a recommendation to improve access to screening, mammograms, and related breast care services. The treatment of breast cancer is becoming more personalized with the advent of new, targeted therapies. The treatment will change if we can identify different biological targets in veterans with breast cancer.
FP: Do you think all veterans, male and female, are more susceptible to breast cancer than is the general population?
AA: In general, incidence of breast cancer is decreasing but, as per the Walter Reed General Hospital and USA Today, breast cancer is one of the most common cancers in our veterans. Not only is the number of women with breast cancer increasing, but so too is the number of male veterans with breast cancer. In general, breast cancer in males is rare, < 1% of all breast cancer cases. Our retrospective data from 1995 to 2012 had more than 6,000 patients with breast cancer; out of that, 1,100 were males with breast cancer.
FP: What do you think needs to be changed about how breast cancer is approached in veterans?
AA: I don’t have an answer to that, but if we can build a breast cancer research group, we may be able to answer some of these questions. Collection of the data prospectively on all of breast cancer at all VA facilities will help us to understand etiology, risk factors, and biology by molecular profiling. In turn, this will help health professionals to give personalized treatment to veterans.
Email: anita.aggarwal@va.gov
Read more about Dr. Aggarwal’s breast cancer initiative: http://www.research.va.gov/currents/spring2014/spring2014-45.cfm
Over 200,000 new cases of breast cancer are diagnosed in the U.S. annually, according to the National Cancer Institute. Dr. Anita Aggarwal, an oncologist at the Washington, DC VAMC, recently completed an extensive study to compare male and female breast cancer in VA patients. The study found that males with breast cancer had higher stage and grade at presentation and higher mortality compared with females. But, when adjusted for age, stage, and grade, males had better survival rates.
Federal Practitioner talked with Dr. Aggarwal about the new breast cancer research group she is currently developing at the Washington, DC VAMC. Dr. Aggarwal’s hope is to help doctors in the federal health system to identify etiology, biology, and improve treatment of both male and female patients with breast cancer.
Federal Practitioner: What is a breast cancer research group, and why do you think one needs to be created at the VA?
Anita Aggarwal, MD: I would like to build a breast cancer research group with the help of all oncologists and health professionals who take care of patients with breast cancer at all VAMCs nationwide. From my retrospective comparison study, breast cancer in our veterans seems to be different than in the general population. The goal of this research group will be to build a data bank with all the pertinent information as well as tissue gene profiling. This will help us to diagnose them early and treat accordingly in a timely fashion.
FP: As more women join the military, do you think breast cancer treatment at the VA will change?
AA: As the number of female veterans increases, I suspect we will see an increase in the number of female patients with breast cancer. As reported by the 2012 Women’s Task Force, women are now the fastest growing cohort within the veteran community. In 2011, there were about 1.8 million women veterans, which is about 8% of the 22.2 million vets in the VA system. That is expected to increase to 2 million in 2020, at which time women will make up to 10.7% of the total vet population. To accommodate these changing needs, the VHA made women’s health programs a priority in 2007, including a recommendation to improve access to screening, mammograms, and related breast care services. The treatment of breast cancer is becoming more personalized with the advent of new, targeted therapies. The treatment will change if we can identify different biological targets in veterans with breast cancer.
FP: Do you think all veterans, male and female, are more susceptible to breast cancer than is the general population?
AA: In general, incidence of breast cancer is decreasing but, as per the Walter Reed General Hospital and USA Today, breast cancer is one of the most common cancers in our veterans. Not only is the number of women with breast cancer increasing, but so too is the number of male veterans with breast cancer. In general, breast cancer in males is rare, < 1% of all breast cancer cases. Our retrospective data from 1995 to 2012 had more than 6,000 patients with breast cancer; out of that, 1,100 were males with breast cancer.
FP: What do you think needs to be changed about how breast cancer is approached in veterans?
AA: I don’t have an answer to that, but if we can build a breast cancer research group, we may be able to answer some of these questions. Collection of the data prospectively on all of breast cancer at all VA facilities will help us to understand etiology, risk factors, and biology by molecular profiling. In turn, this will help health professionals to give personalized treatment to veterans.
Email: anita.aggarwal@va.gov
Read more about Dr. Aggarwal’s breast cancer initiative: http://www.research.va.gov/currents/spring2014/spring2014-45.cfm
Over 200,000 new cases of breast cancer are diagnosed in the U.S. annually, according to the National Cancer Institute. Dr. Anita Aggarwal, an oncologist at the Washington, DC VAMC, recently completed an extensive study to compare male and female breast cancer in VA patients. The study found that males with breast cancer had higher stage and grade at presentation and higher mortality compared with females. But, when adjusted for age, stage, and grade, males had better survival rates.
Federal Practitioner talked with Dr. Aggarwal about the new breast cancer research group she is currently developing at the Washington, DC VAMC. Dr. Aggarwal’s hope is to help doctors in the federal health system to identify etiology, biology, and improve treatment of both male and female patients with breast cancer.
Federal Practitioner: What is a breast cancer research group, and why do you think one needs to be created at the VA?
Anita Aggarwal, MD: I would like to build a breast cancer research group with the help of all oncologists and health professionals who take care of patients with breast cancer at all VAMCs nationwide. From my retrospective comparison study, breast cancer in our veterans seems to be different than in the general population. The goal of this research group will be to build a data bank with all the pertinent information as well as tissue gene profiling. This will help us to diagnose them early and treat accordingly in a timely fashion.
FP: As more women join the military, do you think breast cancer treatment at the VA will change?
AA: As the number of female veterans increases, I suspect we will see an increase in the number of female patients with breast cancer. As reported by the 2012 Women’s Task Force, women are now the fastest growing cohort within the veteran community. In 2011, there were about 1.8 million women veterans, which is about 8% of the 22.2 million vets in the VA system. That is expected to increase to 2 million in 2020, at which time women will make up to 10.7% of the total vet population. To accommodate these changing needs, the VHA made women’s health programs a priority in 2007, including a recommendation to improve access to screening, mammograms, and related breast care services. The treatment of breast cancer is becoming more personalized with the advent of new, targeted therapies. The treatment will change if we can identify different biological targets in veterans with breast cancer.
FP: Do you think all veterans, male and female, are more susceptible to breast cancer than is the general population?
AA: In general, incidence of breast cancer is decreasing but, as per the Walter Reed General Hospital and USA Today, breast cancer is one of the most common cancers in our veterans. Not only is the number of women with breast cancer increasing, but so too is the number of male veterans with breast cancer. In general, breast cancer in males is rare, < 1% of all breast cancer cases. Our retrospective data from 1995 to 2012 had more than 6,000 patients with breast cancer; out of that, 1,100 were males with breast cancer.
FP: What do you think needs to be changed about how breast cancer is approached in veterans?
AA: I don’t have an answer to that, but if we can build a breast cancer research group, we may be able to answer some of these questions. Collection of the data prospectively on all of breast cancer at all VA facilities will help us to understand etiology, risk factors, and biology by molecular profiling. In turn, this will help health professionals to give personalized treatment to veterans.
Email: anita.aggarwal@va.gov
Read more about Dr. Aggarwal’s breast cancer initiative: http://www.research.va.gov/currents/spring2014/spring2014-45.cfm

Hormone therapy for menopausal vasomotor symptoms
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1). 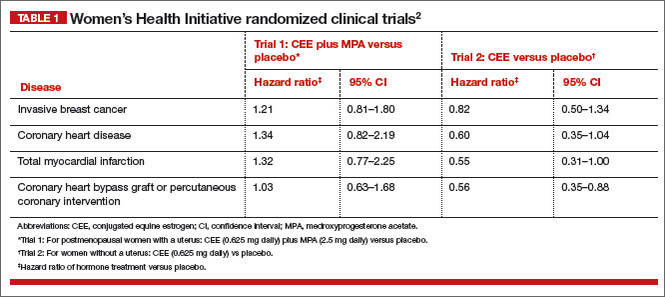
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women. 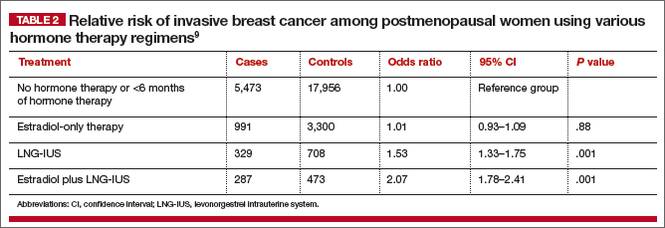
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.

Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1).
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women.
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1).
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women.
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.

Less frequent zoledronic acid an option in metastatic breast cancer
CHICAGO – Women with breast cancer and bone metastases previously treated with bisphosphonates can safely reduce the frequency of their zoledronic acid infusions, according to results from the phase III OPTIMIZE-2 study.
At a median follow-up of 11.9 months, the skeletal-related event (SRE) rate, the study’s primary endpoint, was 23.2% with zoledronic acid (Zometa) every 12 weeks and 22% with zoledronic acid every 4 weeks (P = .724).
The upper limit of the 95% confidence interval for the SRE rate difference was 9.8%, which is below the predefined noninferiority margin of 10%, Dr. Gabriel N. Hortobagyi reported at the annual meeting of the American Society of Clinical Oncology.

Zoledronic acid, a third-generation bisphosphonate, is used to reduce the risk of SREs such as bone fractures and spinal cord compression in patients with bone metastases from solid tumors, and is approved to be administered every 3-4 weeks by intravenous infusion.
It has safety concerns similar to other bisphosphonates such as atypical fractures, chronic kidney impairment, and osteonecrosis of the jaw, and therefore, less frequent dosing could have distinct advantages, Dr. Hortobagyi, professor of medicine at the University of Texas M.D. Anderson Cancer Center, Houston, said during a press briefing highlighting the study.
Dr. Patricia Ganz, professor of medicine at the University of California, Los Angeles, told reporters that for women living with advanced breast cancer and bone metastases, the late-breaking abstract results mean they can spend more time with family and friends and less time in their doctor’s office, with less toxicity and less cost.
"Sometimes we have to add things, but sometimes we have to take away to add value to patients’ care," she said.
The noninferiority, double-blind OPTIMIZE-2 trial enrolled 412 patients with breast cancer and bone metastases and randomly assigned 403 patients to 4 mg intravenous zoledronic acid every 4 weeks or every 12 weeks for 1 year. All participants had received at least nine doses of zoledronic acid or pamidronate prior to study entry. Their average age was 59 years.
The mean skeletal morbidity rate was 0.46 with monthly zoledronic acid and 0.50 with quarterly treatment (P = .854), Dr. Hortobagyi said.
Times to first on-study SRE were also similar in the two arms (Hazard ratio, 1.06; P = .792).
The safety profile was similar in both arms, although there were more kidney-related adverse events in the monthly arm than in the quarterly arm (9.6% vs. 7.9%), he said.
Women dosed monthly had more grade 3/4 adverse events (47.5% vs. 42.6%) and were more likely to stop treatment due to these events (11.6% vs. 8.9%).
Two patients treated monthly developed osteonecrosis of the jaw, whereas none did with quarterly treatment.
Bone marker profiles were similar between arms, Dr. Hortobagyi said. Serum bone-specific alkaline phosphatase was not significantly different at any time point and urinary N-telopeptide/creatinine was significantly different at week 36 only.
Because of study limitations, such as its relatively modest size, and statistical concerns, the inferiority claim should be interpreted with caution, he said. The protocol was revised during the course of the trial including a placebo arm that was dropped because of poor accrual. The sample size was also reduced from 705 to 412 patients based on new data that became available from the ZOOM trial.
As previously reported, ZOOM also demonstrated no difference in skeletal morbidity rate, its primary endpoint, between zoledronic acid dosed quarterly or monthly in women with metastatic breast cancer and bone metastases.
Novartis sponsored the trial. Dr. Hortobagyi disclosed serving as a consultant to Antigen Express, Novartis, and Pfizer, and research funds to his institution from Novartis.
CHICAGO – Women with breast cancer and bone metastases previously treated with bisphosphonates can safely reduce the frequency of their zoledronic acid infusions, according to results from the phase III OPTIMIZE-2 study.
At a median follow-up of 11.9 months, the skeletal-related event (SRE) rate, the study’s primary endpoint, was 23.2% with zoledronic acid (Zometa) every 12 weeks and 22% with zoledronic acid every 4 weeks (P = .724).
The upper limit of the 95% confidence interval for the SRE rate difference was 9.8%, which is below the predefined noninferiority margin of 10%, Dr. Gabriel N. Hortobagyi reported at the annual meeting of the American Society of Clinical Oncology.
Zoledronic acid, a third-generation bisphosphonate, is used to reduce the risk of SREs such as bone fractures and spinal cord compression in patients with bone metastases from solid tumors, and is approved to be administered every 3-4 weeks by intravenous infusion.
It has safety concerns similar to other bisphosphonates such as atypical fractures, chronic kidney impairment, and osteonecrosis of the jaw, and therefore, less frequent dosing could have distinct advantages, Dr. Hortobagyi, professor of medicine at the University of Texas M.D. Anderson Cancer Center, Houston, said during a press briefing highlighting the study.
Dr. Patricia Ganz, professor of medicine at the University of California, Los Angeles, told reporters that for women living with advanced breast cancer and bone metastases, the late-breaking abstract results mean they can spend more time with family and friends and less time in their doctor’s office, with less toxicity and less cost.
"Sometimes we have to add things, but sometimes we have to take away to add value to patients’ care," she said.
The noninferiority, double-blind OPTIMIZE-2 trial enrolled 412 patients with breast cancer and bone metastases and randomly assigned 403 patients to 4 mg intravenous zoledronic acid every 4 weeks or every 12 weeks for 1 year. All participants had received at least nine doses of zoledronic acid or pamidronate prior to study entry. Their average age was 59 years.
The mean skeletal morbidity rate was 0.46 with monthly zoledronic acid and 0.50 with quarterly treatment (P = .854), Dr. Hortobagyi said.
Times to first on-study SRE were also similar in the two arms (Hazard ratio, 1.06; P = .792).
The safety profile was similar in both arms, although there were more kidney-related adverse events in the monthly arm than in the quarterly arm (9.6% vs. 7.9%), he said.
Women dosed monthly had more grade 3/4 adverse events (47.5% vs. 42.6%) and were more likely to stop treatment due to these events (11.6% vs. 8.9%).
Two patients treated monthly developed osteonecrosis of the jaw, whereas none did with quarterly treatment.
Bone marker profiles were similar between arms, Dr. Hortobagyi said. Serum bone-specific alkaline phosphatase was not significantly different at any time point and urinary N-telopeptide/creatinine was significantly different at week 36 only.
Because of study limitations, such as its relatively modest size, and statistical concerns, the inferiority claim should be interpreted with caution, he said. The protocol was revised during the course of the trial including a placebo arm that was dropped because of poor accrual. The sample size was also reduced from 705 to 412 patients based on new data that became available from the ZOOM trial.
As previously reported, ZOOM also demonstrated no difference in skeletal morbidity rate, its primary endpoint, between zoledronic acid dosed quarterly or monthly in women with metastatic breast cancer and bone metastases.
Novartis sponsored the trial. Dr. Hortobagyi disclosed serving as a consultant to Antigen Express, Novartis, and Pfizer, and research funds to his institution from Novartis.
CHICAGO – Women with breast cancer and bone metastases previously treated with bisphosphonates can safely reduce the frequency of their zoledronic acid infusions, according to results from the phase III OPTIMIZE-2 study.
At a median follow-up of 11.9 months, the skeletal-related event (SRE) rate, the study’s primary endpoint, was 23.2% with zoledronic acid (Zometa) every 12 weeks and 22% with zoledronic acid every 4 weeks (P = .724).
The upper limit of the 95% confidence interval for the SRE rate difference was 9.8%, which is below the predefined noninferiority margin of 10%, Dr. Gabriel N. Hortobagyi reported at the annual meeting of the American Society of Clinical Oncology.
Zoledronic acid, a third-generation bisphosphonate, is used to reduce the risk of SREs such as bone fractures and spinal cord compression in patients with bone metastases from solid tumors, and is approved to be administered every 3-4 weeks by intravenous infusion.
It has safety concerns similar to other bisphosphonates such as atypical fractures, chronic kidney impairment, and osteonecrosis of the jaw, and therefore, less frequent dosing could have distinct advantages, Dr. Hortobagyi, professor of medicine at the University of Texas M.D. Anderson Cancer Center, Houston, said during a press briefing highlighting the study.
Dr. Patricia Ganz, professor of medicine at the University of California, Los Angeles, told reporters that for women living with advanced breast cancer and bone metastases, the late-breaking abstract results mean they can spend more time with family and friends and less time in their doctor’s office, with less toxicity and less cost.
"Sometimes we have to add things, but sometimes we have to take away to add value to patients’ care," she said.
The noninferiority, double-blind OPTIMIZE-2 trial enrolled 412 patients with breast cancer and bone metastases and randomly assigned 403 patients to 4 mg intravenous zoledronic acid every 4 weeks or every 12 weeks for 1 year. All participants had received at least nine doses of zoledronic acid or pamidronate prior to study entry. Their average age was 59 years.
The mean skeletal morbidity rate was 0.46 with monthly zoledronic acid and 0.50 with quarterly treatment (P = .854), Dr. Hortobagyi said.
Times to first on-study SRE were also similar in the two arms (Hazard ratio, 1.06; P = .792).
The safety profile was similar in both arms, although there were more kidney-related adverse events in the monthly arm than in the quarterly arm (9.6% vs. 7.9%), he said.
Women dosed monthly had more grade 3/4 adverse events (47.5% vs. 42.6%) and were more likely to stop treatment due to these events (11.6% vs. 8.9%).
Two patients treated monthly developed osteonecrosis of the jaw, whereas none did with quarterly treatment.
Bone marker profiles were similar between arms, Dr. Hortobagyi said. Serum bone-specific alkaline phosphatase was not significantly different at any time point and urinary N-telopeptide/creatinine was significantly different at week 36 only.
Because of study limitations, such as its relatively modest size, and statistical concerns, the inferiority claim should be interpreted with caution, he said. The protocol was revised during the course of the trial including a placebo arm that was dropped because of poor accrual. The sample size was also reduced from 705 to 412 patients based on new data that became available from the ZOOM trial.
As previously reported, ZOOM also demonstrated no difference in skeletal morbidity rate, its primary endpoint, between zoledronic acid dosed quarterly or monthly in women with metastatic breast cancer and bone metastases.
Novartis sponsored the trial. Dr. Hortobagyi disclosed serving as a consultant to Antigen Express, Novartis, and Pfizer, and research funds to his institution from Novartis.
AT THE ASCO ANNUAL MEETING 2014
Major finding: The skeletal-related event rate was 23.2% with zoledronic acid every 12 weeks and 22% with zoledronic acid every 4 weeks (P = .724).
Data source: A phase III, double-blind study in 412 women with bone metastases from breast cancer.
Key clinical point: Women with breast cancer and bone metastases can receive bisphosphonates less often without compromising care.
Disclosures: Novartis sponsored the trial. Dr. Hortobagyi disclosed serving as a consultant to Antigen Express, Novartis, and Pfizer, and research funds to his institution from Novartis.

TEXT/SOFT provide practice-changing results for premenopausal breast cancer
CHICAGO – Adjuvant exemestane is more effective at preventing recurrence than tamoxifen is when either is given with ovarian function suppression in premenopausal women with hormone-sensitive breast cancers, according to a joint analysis of the phase III TEXT and SOFT trials.
"Exemestane plus OFS [ovarian function suppression] significantly improves disease-free survival, breast cancer free–interval, and distant recurrence free–interval and is a new treatment option for premenopausal women with hormone receptor-positive early breast cancer," lead study author Dr. Olivia Pagani said during a plenary session at the annual meeting of the American Society of Clinical Oncology.

The results were consistent in TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial), and in women who did and did not receive chemotherapy, said Dr. Pagani, clinical director of the breast unit at the Oncology Institute of Southern Switzerland, Bellinzona.
Among the 43% of women who did not receive chemotherapy, 97.6% of these women in TEXT and 97.5% in SOFT who received the aromatase inhibitor exemestane (Aromasin) remained free from breast cancer at 5 years.
On average, these women had lower-risk features such as older age and smaller tumors, however, 21% of them in TEXT and 8% in SOFT had node-positive disease, she observed. After 5.7 years median follow-up, there were very few distant recurrences in this subgroup, only 1% in the exemestane group.
"These results suggest that some premenopausal women have an excellent prognosis with highly effective endocrine therapy without chemotherapy," Dr. Pagani said.
Invited discussant Dr. Nancy E. Davidson, director of the University of Pittsburgh Cancer Institute, said, "We should remember the power of endocrine therapy in properly selected patients of all ages. Not every premenopausal patient needs chemotherapy."
Dr. Davidson said the results show that the combination of ovarian suppression and an aromatase inhibitor (AI) is "an evidence-based approach and may provide support to use the combination in women who cannot take tamoxifen or perhaps in those at very high risk, especially if they don’t take chemotherapy."
She went on to say, however, that "For now, I’m waiting for the results of SOFT to finalize my approach."
Currently, the standard adjuvant endocrine therapy for premenopausal women is 5 years of tamoxifen, while aromatase inhibitors are primarily used in postmenopausal women, where they have been shown to improve outcomes over tamoxifen.
Physicians in some countries, typically outside the United States, however, recommend adding OFS to tamoxifen in high-risk younger women, but the benefit of this strategy is uncertain. SOFT included a third treatment arm of tamoxifen alone to address the role of OFS for women receiving tamoxifen, but those results are not expected until late 2014.
Study details
The joint analysis, simultaneously published online in the New England Journal of Medicine, included 4,690 premenopausal women with early hormone-sensitive breast cancer, who were randomly assigned to exemestane 25 mg daily or tamoxifen 20 mg daily for 5 years (2014 [doi:10.1056/NEJMoa1404037]).
Randomization occurred within 12 weeks of surgery for all women in TEXT and women in SOFT who did not receive chemotherapy. Women in SOFT who received prior (neo)adjuvant chemotherapy were randomized within 8 months of chemotherapy completion when premenopausal status was demonstrated.
OFS in both trials was achieved through monthly injections of the gonadotropin-releasing hormone agonist triptorelin pamoate (Trelstar Depot), bilateral oophorectomy, or ovarian radiation.
Routine use of bisphosphonates was not permitted, but adjuvant trastuzumab was allowed, if indicated.
Overall, 42% of women were lymph node–positive, 36% had tumors larger than 2 cm, and 12% had human epidermal growth factor receptor 2–positive breast cancer. Their median age was 43 years.
Outcomes
At 5 years, exemestane plus OFS significantly improved the primary endpoint of disease-free survival from 87.3% with tamoxifen plus OFS to 91.1% (hazard ratio, 0.72; P = .0002), Dr. Pagani said.
No striking heterogeneity of treatment effect was observed in prospectively planned subgroup analyses including the cohorts defined by trial, chemotherapy stratum, and node status.
"The relative and absolute differences at 5 years compare favorably with those reported in the practice-changing BIG 1-98 and ATAC [Arimidex, Tamoxifen, Alone or in Combination] trials of aromatase inhibitors vs. tamoxifen in postmenopausal women," she said.
At 5 years, 92.8% of women assigned to receive exemestane plus ovarian suppression were free from breast cancer vs. 88.8% of those given tamoxifen plus ovarian suppression (HR, 0.66; P less than .0001).
The rate of freedom from distant recurrence at 5 years was also superior in the exemestane group (93.8% vs. 92%; HR, 0.78; P = .02). In all, 60% of first events involved distant sites.
These benefits, however, have yet to translate into a significant overall survival benefit at 5 years for exemestane plus ovarian suppression, compared with tamoxifen plus ovarian suppression (95.9% vs. 96.9%; HR, 1.14; P = .37), said Dr. Pagani, who added that conclusions about long-term survival are premature at this early follow-up.
Where do we go from here?
ASCO immediate past-president Dr. Clifford Hudis said in a press briefing that the joint analysis provides long-awaited and actionable information on how best to treat premenopausal women with hormone-sensitive breast cancer who appear cured after surgery, but that data from the tamoxifen-alone arm in SOFT are needed to change practice for those unconvinced about the need for ovarian suppression.
Dr. Davidson said she’s left pondering how the results will be integrated into practice. Will clinicians use 10 years of tamoxifen, as supported by the ATLAS and aTTOM trials, or will they use an extended adjuvant approach of 5 years of tamoxifen followed by a switch to 5 years of AI for women who become postmenopausal during their tamoxifen, as supported by the MA 17 trial? It’s also possible some will follow the lead set by TEXT/SOFT and use 5 years of ovarian suppression and AI.
"If the benefits of OFS with AI hold up, we may want to revisit the role of oophorectomy in selected patients, who want to avoid injections and have a permanent menopause," she added. "We will need to make sure we maximize bisphosphonates for bone health, but I’m not prepared to use bisphosphonates as a routine form of adjuvant therapy in these women just yet."
Finally, Dr. Davidson said long-term follow-up of TEXT/SOFT is vital for both benefit and toxicity. Though overall compliance was good, she noted earlier in her talk that 16% of women on exemestane plus OFS prematurely stopped therapy vs. 11% on tamoxifen plus OFS. "Financial toxicity" is also an issue, with the wholesale acquisition cost at her institution for 1 year of exemestane 25 mg daily at $7,344 vs. $1,369 for tamoxifen, she said.
Dr. Pagani stressed during the press briefing that the results do not mean all premenopausal women should be given an AI plus ovarian suppression, but that the decision should be individualized with input from the physician and patient.
The research was supported in part by Pfizer, Ipsen, the International Breast Cancer Study Group, and the National Cancer Institute (NCI). Dr. Pagani reported research funding from Ipsen and Pfizer. Dr. Davidson reported research funding from the Breast Cancer Research Foundation and National Institutes of Health (NIH).
CHICAGO – Adjuvant exemestane is more effective at preventing recurrence than tamoxifen is when either is given with ovarian function suppression in premenopausal women with hormone-sensitive breast cancers, according to a joint analysis of the phase III TEXT and SOFT trials.
"Exemestane plus OFS [ovarian function suppression] significantly improves disease-free survival, breast cancer free–interval, and distant recurrence free–interval and is a new treatment option for premenopausal women with hormone receptor-positive early breast cancer," lead study author Dr. Olivia Pagani said during a plenary session at the annual meeting of the American Society of Clinical Oncology.
The results were consistent in TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial), and in women who did and did not receive chemotherapy, said Dr. Pagani, clinical director of the breast unit at the Oncology Institute of Southern Switzerland, Bellinzona.
Among the 43% of women who did not receive chemotherapy, 97.6% of these women in TEXT and 97.5% in SOFT who received the aromatase inhibitor exemestane (Aromasin) remained free from breast cancer at 5 years.
On average, these women had lower-risk features such as older age and smaller tumors, however, 21% of them in TEXT and 8% in SOFT had node-positive disease, she observed. After 5.7 years median follow-up, there were very few distant recurrences in this subgroup, only 1% in the exemestane group.
"These results suggest that some premenopausal women have an excellent prognosis with highly effective endocrine therapy without chemotherapy," Dr. Pagani said.
Invited discussant Dr. Nancy E. Davidson, director of the University of Pittsburgh Cancer Institute, said, "We should remember the power of endocrine therapy in properly selected patients of all ages. Not every premenopausal patient needs chemotherapy."
Dr. Davidson said the results show that the combination of ovarian suppression and an aromatase inhibitor (AI) is "an evidence-based approach and may provide support to use the combination in women who cannot take tamoxifen or perhaps in those at very high risk, especially if they don’t take chemotherapy."
She went on to say, however, that "For now, I’m waiting for the results of SOFT to finalize my approach."
Currently, the standard adjuvant endocrine therapy for premenopausal women is 5 years of tamoxifen, while aromatase inhibitors are primarily used in postmenopausal women, where they have been shown to improve outcomes over tamoxifen.
Physicians in some countries, typically outside the United States, however, recommend adding OFS to tamoxifen in high-risk younger women, but the benefit of this strategy is uncertain. SOFT included a third treatment arm of tamoxifen alone to address the role of OFS for women receiving tamoxifen, but those results are not expected until late 2014.
Study details
The joint analysis, simultaneously published online in the New England Journal of Medicine, included 4,690 premenopausal women with early hormone-sensitive breast cancer, who were randomly assigned to exemestane 25 mg daily or tamoxifen 20 mg daily for 5 years (2014 [doi:10.1056/NEJMoa1404037]).
Randomization occurred within 12 weeks of surgery for all women in TEXT and women in SOFT who did not receive chemotherapy. Women in SOFT who received prior (neo)adjuvant chemotherapy were randomized within 8 months of chemotherapy completion when premenopausal status was demonstrated.
OFS in both trials was achieved through monthly injections of the gonadotropin-releasing hormone agonist triptorelin pamoate (Trelstar Depot), bilateral oophorectomy, or ovarian radiation.
Routine use of bisphosphonates was not permitted, but adjuvant trastuzumab was allowed, if indicated.
Overall, 42% of women were lymph node–positive, 36% had tumors larger than 2 cm, and 12% had human epidermal growth factor receptor 2–positive breast cancer. Their median age was 43 years.
Outcomes
At 5 years, exemestane plus OFS significantly improved the primary endpoint of disease-free survival from 87.3% with tamoxifen plus OFS to 91.1% (hazard ratio, 0.72; P = .0002), Dr. Pagani said.
No striking heterogeneity of treatment effect was observed in prospectively planned subgroup analyses including the cohorts defined by trial, chemotherapy stratum, and node status.
"The relative and absolute differences at 5 years compare favorably with those reported in the practice-changing BIG 1-98 and ATAC [Arimidex, Tamoxifen, Alone or in Combination] trials of aromatase inhibitors vs. tamoxifen in postmenopausal women," she said.
At 5 years, 92.8% of women assigned to receive exemestane plus ovarian suppression were free from breast cancer vs. 88.8% of those given tamoxifen plus ovarian suppression (HR, 0.66; P less than .0001).
The rate of freedom from distant recurrence at 5 years was also superior in the exemestane group (93.8% vs. 92%; HR, 0.78; P = .02). In all, 60% of first events involved distant sites.
These benefits, however, have yet to translate into a significant overall survival benefit at 5 years for exemestane plus ovarian suppression, compared with tamoxifen plus ovarian suppression (95.9% vs. 96.9%; HR, 1.14; P = .37), said Dr. Pagani, who added that conclusions about long-term survival are premature at this early follow-up.
Where do we go from here?
ASCO immediate past-president Dr. Clifford Hudis said in a press briefing that the joint analysis provides long-awaited and actionable information on how best to treat premenopausal women with hormone-sensitive breast cancer who appear cured after surgery, but that data from the tamoxifen-alone arm in SOFT are needed to change practice for those unconvinced about the need for ovarian suppression.
Dr. Davidson said she’s left pondering how the results will be integrated into practice. Will clinicians use 10 years of tamoxifen, as supported by the ATLAS and aTTOM trials, or will they use an extended adjuvant approach of 5 years of tamoxifen followed by a switch to 5 years of AI for women who become postmenopausal during their tamoxifen, as supported by the MA 17 trial? It’s also possible some will follow the lead set by TEXT/SOFT and use 5 years of ovarian suppression and AI.
"If the benefits of OFS with AI hold up, we may want to revisit the role of oophorectomy in selected patients, who want to avoid injections and have a permanent menopause," she added. "We will need to make sure we maximize bisphosphonates for bone health, but I’m not prepared to use bisphosphonates as a routine form of adjuvant therapy in these women just yet."
Finally, Dr. Davidson said long-term follow-up of TEXT/SOFT is vital for both benefit and toxicity. Though overall compliance was good, she noted earlier in her talk that 16% of women on exemestane plus OFS prematurely stopped therapy vs. 11% on tamoxifen plus OFS. "Financial toxicity" is also an issue, with the wholesale acquisition cost at her institution for 1 year of exemestane 25 mg daily at $7,344 vs. $1,369 for tamoxifen, she said.
Dr. Pagani stressed during the press briefing that the results do not mean all premenopausal women should be given an AI plus ovarian suppression, but that the decision should be individualized with input from the physician and patient.
The research was supported in part by Pfizer, Ipsen, the International Breast Cancer Study Group, and the National Cancer Institute (NCI). Dr. Pagani reported research funding from Ipsen and Pfizer. Dr. Davidson reported research funding from the Breast Cancer Research Foundation and National Institutes of Health (NIH).
CHICAGO – Adjuvant exemestane is more effective at preventing recurrence than tamoxifen is when either is given with ovarian function suppression in premenopausal women with hormone-sensitive breast cancers, according to a joint analysis of the phase III TEXT and SOFT trials.
"Exemestane plus OFS [ovarian function suppression] significantly improves disease-free survival, breast cancer free–interval, and distant recurrence free–interval and is a new treatment option for premenopausal women with hormone receptor-positive early breast cancer," lead study author Dr. Olivia Pagani said during a plenary session at the annual meeting of the American Society of Clinical Oncology.
The results were consistent in TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial), and in women who did and did not receive chemotherapy, said Dr. Pagani, clinical director of the breast unit at the Oncology Institute of Southern Switzerland, Bellinzona.
Among the 43% of women who did not receive chemotherapy, 97.6% of these women in TEXT and 97.5% in SOFT who received the aromatase inhibitor exemestane (Aromasin) remained free from breast cancer at 5 years.
On average, these women had lower-risk features such as older age and smaller tumors, however, 21% of them in TEXT and 8% in SOFT had node-positive disease, she observed. After 5.7 years median follow-up, there were very few distant recurrences in this subgroup, only 1% in the exemestane group.
"These results suggest that some premenopausal women have an excellent prognosis with highly effective endocrine therapy without chemotherapy," Dr. Pagani said.
Invited discussant Dr. Nancy E. Davidson, director of the University of Pittsburgh Cancer Institute, said, "We should remember the power of endocrine therapy in properly selected patients of all ages. Not every premenopausal patient needs chemotherapy."
Dr. Davidson said the results show that the combination of ovarian suppression and an aromatase inhibitor (AI) is "an evidence-based approach and may provide support to use the combination in women who cannot take tamoxifen or perhaps in those at very high risk, especially if they don’t take chemotherapy."
She went on to say, however, that "For now, I’m waiting for the results of SOFT to finalize my approach."
Currently, the standard adjuvant endocrine therapy for premenopausal women is 5 years of tamoxifen, while aromatase inhibitors are primarily used in postmenopausal women, where they have been shown to improve outcomes over tamoxifen.
Physicians in some countries, typically outside the United States, however, recommend adding OFS to tamoxifen in high-risk younger women, but the benefit of this strategy is uncertain. SOFT included a third treatment arm of tamoxifen alone to address the role of OFS for women receiving tamoxifen, but those results are not expected until late 2014.
Study details
The joint analysis, simultaneously published online in the New England Journal of Medicine, included 4,690 premenopausal women with early hormone-sensitive breast cancer, who were randomly assigned to exemestane 25 mg daily or tamoxifen 20 mg daily for 5 years (2014 [doi:10.1056/NEJMoa1404037]).
Randomization occurred within 12 weeks of surgery for all women in TEXT and women in SOFT who did not receive chemotherapy. Women in SOFT who received prior (neo)adjuvant chemotherapy were randomized within 8 months of chemotherapy completion when premenopausal status was demonstrated.
OFS in both trials was achieved through monthly injections of the gonadotropin-releasing hormone agonist triptorelin pamoate (Trelstar Depot), bilateral oophorectomy, or ovarian radiation.
Routine use of bisphosphonates was not permitted, but adjuvant trastuzumab was allowed, if indicated.
Overall, 42% of women were lymph node–positive, 36% had tumors larger than 2 cm, and 12% had human epidermal growth factor receptor 2–positive breast cancer. Their median age was 43 years.
Outcomes
At 5 years, exemestane plus OFS significantly improved the primary endpoint of disease-free survival from 87.3% with tamoxifen plus OFS to 91.1% (hazard ratio, 0.72; P = .0002), Dr. Pagani said.
No striking heterogeneity of treatment effect was observed in prospectively planned subgroup analyses including the cohorts defined by trial, chemotherapy stratum, and node status.
"The relative and absolute differences at 5 years compare favorably with those reported in the practice-changing BIG 1-98 and ATAC [Arimidex, Tamoxifen, Alone or in Combination] trials of aromatase inhibitors vs. tamoxifen in postmenopausal women," she said.
At 5 years, 92.8% of women assigned to receive exemestane plus ovarian suppression were free from breast cancer vs. 88.8% of those given tamoxifen plus ovarian suppression (HR, 0.66; P less than .0001).
The rate of freedom from distant recurrence at 5 years was also superior in the exemestane group (93.8% vs. 92%; HR, 0.78; P = .02). In all, 60% of first events involved distant sites.
These benefits, however, have yet to translate into a significant overall survival benefit at 5 years for exemestane plus ovarian suppression, compared with tamoxifen plus ovarian suppression (95.9% vs. 96.9%; HR, 1.14; P = .37), said Dr. Pagani, who added that conclusions about long-term survival are premature at this early follow-up.
Where do we go from here?
ASCO immediate past-president Dr. Clifford Hudis said in a press briefing that the joint analysis provides long-awaited and actionable information on how best to treat premenopausal women with hormone-sensitive breast cancer who appear cured after surgery, but that data from the tamoxifen-alone arm in SOFT are needed to change practice for those unconvinced about the need for ovarian suppression.
Dr. Davidson said she’s left pondering how the results will be integrated into practice. Will clinicians use 10 years of tamoxifen, as supported by the ATLAS and aTTOM trials, or will they use an extended adjuvant approach of 5 years of tamoxifen followed by a switch to 5 years of AI for women who become postmenopausal during their tamoxifen, as supported by the MA 17 trial? It’s also possible some will follow the lead set by TEXT/SOFT and use 5 years of ovarian suppression and AI.
"If the benefits of OFS with AI hold up, we may want to revisit the role of oophorectomy in selected patients, who want to avoid injections and have a permanent menopause," she added. "We will need to make sure we maximize bisphosphonates for bone health, but I’m not prepared to use bisphosphonates as a routine form of adjuvant therapy in these women just yet."
Finally, Dr. Davidson said long-term follow-up of TEXT/SOFT is vital for both benefit and toxicity. Though overall compliance was good, she noted earlier in her talk that 16% of women on exemestane plus OFS prematurely stopped therapy vs. 11% on tamoxifen plus OFS. "Financial toxicity" is also an issue, with the wholesale acquisition cost at her institution for 1 year of exemestane 25 mg daily at $7,344 vs. $1,369 for tamoxifen, she said.
Dr. Pagani stressed during the press briefing that the results do not mean all premenopausal women should be given an AI plus ovarian suppression, but that the decision should be individualized with input from the physician and patient.
The research was supported in part by Pfizer, Ipsen, the International Breast Cancer Study Group, and the National Cancer Institute (NCI). Dr. Pagani reported research funding from Ipsen and Pfizer. Dr. Davidson reported research funding from the Breast Cancer Research Foundation and National Institutes of Health (NIH).
AT THE ASCO ANNUAL MEETING 2014
Key clinical point: Exemestane plus OFS is a new treatment option in the setting of premenopausal hormone-sensitive early breast cancer.
Major finding: Exemestane plus OFS significantly improved disease-free survival from 87.3% with tamoxifen plus OFS to 91.1% (HR, 0.72; P = .0002).
Data source: Joint analysis of two phase III studies in 4,690 premenopausal women with hormone receptor-positive, early breast cancer.
Disclosures: The research was supported in part by Pfizer, Ipsen, the International Breast Cancer Study Group, and the NCI. Dr. Pagani reported research funding from Ipsen and Pfizer. Dr. Davidson reported research funding from the Breast Cancer Research Foundation and the NIH.

To screen or not to screen: lung and breast cancer
Although the incidence of lung cancer in the United States has been falling in recent years because of a decrease in cigarette smoking, the disease is still the third most common cancer, and the leading cause of cancer death. In March 2014, the US Preventive Services Task Force (USPSTF) updated its 2004 recommendations for lung cancer screening by commissioning a systematic evidence review of low-dose computed tomography (CT) by focusing on new evidence from randomized clinical trials published since 2004. In addition, a modeling study provided information about the optimum screening age, screening interval, and the risk-benefit ratio for screening.
Click on the PDF icon at the top of this introduction to read the full article.
Although the incidence of lung cancer in the United States has been falling in recent years because of a decrease in cigarette smoking, the disease is still the third most common cancer, and the leading cause of cancer death. In March 2014, the US Preventive Services Task Force (USPSTF) updated its 2004 recommendations for lung cancer screening by commissioning a systematic evidence review of low-dose computed tomography (CT) by focusing on new evidence from randomized clinical trials published since 2004. In addition, a modeling study provided information about the optimum screening age, screening interval, and the risk-benefit ratio for screening.
Click on the PDF icon at the top of this introduction to read the full article.
Although the incidence of lung cancer in the United States has been falling in recent years because of a decrease in cigarette smoking, the disease is still the third most common cancer, and the leading cause of cancer death. In March 2014, the US Preventive Services Task Force (USPSTF) updated its 2004 recommendations for lung cancer screening by commissioning a systematic evidence review of low-dose computed tomography (CT) by focusing on new evidence from randomized clinical trials published since 2004. In addition, a modeling study provided information about the optimum screening age, screening interval, and the risk-benefit ratio for screening.
Click on the PDF icon at the top of this introduction to read the full article.
Short-term outcomes of the implementation of a computer-based breast cancer risk assessment program during screening mammography
Background Barriers to assessing a patient’s risk for breast cancer include the inadequate documentation of family history, the complexity of risk calculation and model selection, and a lack of awareness of risk on the part of the patient and/or provider. We have established computer-based, real-time assessment of a patient’s risk for breast cancer at the time of having a mammogram.
Objective To facilitate identification of high-risk patients who need genetic counseling and testing and magnetic resonance imaging screening based on the results of the risk assessment.
Methods Since November 23, 2010, all mammogram patients have completed questionnaires using a wireless tablet. On the basis of a real-time calculation for a patient’s risk of BRCA1/BRCA2 mutation (Myriad, Tyrer-Cuzick, BRCAPRO) and lifetime risk of breast cancer (Gail, Claus, Tyrer-Cuzick, BRCAPRO) using Hughes riskApps, patients were categorized as high risk (≥ 10% BRCA mutation or ≥ 20% lifetime breast cancer risk) or average risk and received a risk assessment letter. The risk data was integrated into our mammography information system (PenRad) at the same time. High-risk patients were contacted to facilitate evaluation.
Results As of June 30, 2012, a total of 24,213 unaffected patients completed the risk assessment. There were 2,196 patients (9.1%) identified as high risk: 1,051 (4.3%) had a BRCA mutation risk, 1,570 (6.5%) had lifetime breast cancer risk, and 425 (1.8%) had risk for both. Of the high-risk patients, 416 (18.7%) were evaluated by our APN and/or genetic counselor. Of the 231 who were evaluated by a genetic counselor, 97 had genetic testing and 9 (8.3%) were BRCA positive. Annual MRI screening was recommended to 254 patients.
Conclusions We have successfully implemented breast cancer risk assessment through our screening mammography service. Results suggest that 9.1% of our patients can benefit from risk assessment, 4.3% should consider genetic testing, and 6.5% may benefit from screening MRI. We strive to improve compliance through patient education.
Click on the PDF icon at the top of this introduction to read the full article.
Background Barriers to assessing a patient’s risk for breast cancer include the inadequate documentation of family history, the complexity of risk calculation and model selection, and a lack of awareness of risk on the part of the patient and/or provider. We have established computer-based, real-time assessment of a patient’s risk for breast cancer at the time of having a mammogram.
Objective To facilitate identification of high-risk patients who need genetic counseling and testing and magnetic resonance imaging screening based on the results of the risk assessment.
Methods Since November 23, 2010, all mammogram patients have completed questionnaires using a wireless tablet. On the basis of a real-time calculation for a patient’s risk of BRCA1/BRCA2 mutation (Myriad, Tyrer-Cuzick, BRCAPRO) and lifetime risk of breast cancer (Gail, Claus, Tyrer-Cuzick, BRCAPRO) using Hughes riskApps, patients were categorized as high risk (≥ 10% BRCA mutation or ≥ 20% lifetime breast cancer risk) or average risk and received a risk assessment letter. The risk data was integrated into our mammography information system (PenRad) at the same time. High-risk patients were contacted to facilitate evaluation.
Results As of June 30, 2012, a total of 24,213 unaffected patients completed the risk assessment. There were 2,196 patients (9.1%) identified as high risk: 1,051 (4.3%) had a BRCA mutation risk, 1,570 (6.5%) had lifetime breast cancer risk, and 425 (1.8%) had risk for both. Of the high-risk patients, 416 (18.7%) were evaluated by our APN and/or genetic counselor. Of the 231 who were evaluated by a genetic counselor, 97 had genetic testing and 9 (8.3%) were BRCA positive. Annual MRI screening was recommended to 254 patients.
Conclusions We have successfully implemented breast cancer risk assessment through our screening mammography service. Results suggest that 9.1% of our patients can benefit from risk assessment, 4.3% should consider genetic testing, and 6.5% may benefit from screening MRI. We strive to improve compliance through patient education.
Click on the PDF icon at the top of this introduction to read the full article.
Background Barriers to assessing a patient’s risk for breast cancer include the inadequate documentation of family history, the complexity of risk calculation and model selection, and a lack of awareness of risk on the part of the patient and/or provider. We have established computer-based, real-time assessment of a patient’s risk for breast cancer at the time of having a mammogram.
Objective To facilitate identification of high-risk patients who need genetic counseling and testing and magnetic resonance imaging screening based on the results of the risk assessment.
Methods Since November 23, 2010, all mammogram patients have completed questionnaires using a wireless tablet. On the basis of a real-time calculation for a patient’s risk of BRCA1/BRCA2 mutation (Myriad, Tyrer-Cuzick, BRCAPRO) and lifetime risk of breast cancer (Gail, Claus, Tyrer-Cuzick, BRCAPRO) using Hughes riskApps, patients were categorized as high risk (≥ 10% BRCA mutation or ≥ 20% lifetime breast cancer risk) or average risk and received a risk assessment letter. The risk data was integrated into our mammography information system (PenRad) at the same time. High-risk patients were contacted to facilitate evaluation.
Results As of June 30, 2012, a total of 24,213 unaffected patients completed the risk assessment. There were 2,196 patients (9.1%) identified as high risk: 1,051 (4.3%) had a BRCA mutation risk, 1,570 (6.5%) had lifetime breast cancer risk, and 425 (1.8%) had risk for both. Of the high-risk patients, 416 (18.7%) were evaluated by our APN and/or genetic counselor. Of the 231 who were evaluated by a genetic counselor, 97 had genetic testing and 9 (8.3%) were BRCA positive. Annual MRI screening was recommended to 254 patients.
Conclusions We have successfully implemented breast cancer risk assessment through our screening mammography service. Results suggest that 9.1% of our patients can benefit from risk assessment, 4.3% should consider genetic testing, and 6.5% may benefit from screening MRI. We strive to improve compliance through patient education.
Click on the PDF icon at the top of this introduction to read the full article.
Targeted sessions for targeted therapies at ASCO
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
Adding tomosynthesis improved mammography’s cancer detection
Adding tomosynthesis to screening digital mammography decreases the "recall" rate by 15% while increasing the cancer detection rate by 29%, according to a report published online June 25 in JAMA.
Researchers compared the performance of screening digital mammography alone (281,187 cases) against the performance after tomosynthesis was added to mammography (173,663 cases) at 13 sites in geographically diverse regions across the country. The work was funded primarily by Hologic, maker of the only Food and Drug Administration–approved tomosynthesis equipment at the time of this retrospective study, said Dr. Sarah M. Friedewald of the Caldwell Breast Center, Advocate Lutheran General Hospital, Park Ridge, Ill., and her associates.

The "recall" rate – the proportion of patients requiring additional imaging based on the results of their screening mammography – declined from 107 per 1,000 screens with digital mammography alone to 91 per 1,000 screens when tomosynthesis was added, a relative reduction of 15%. At the same time, the cancer detection rate rose from 4.2 to 5.4 per 1,000 scans, a relative increase of 29%. After tomosynthesis was introduced, the detection rate of invasive cancers rose from 2.9 to 4.1 per 1,000 scans, while that of ductal carcinoma in situ remained unchanged at 1.4 per 1,000, the investigators said (JAMA 2014 June 25 [doi:10.1001/jama.2014.6095]).
It is important to note that this study did not assess clinical outcomes, so it remains to be seen whether these improvements in screening mammography translate into clinically relevant improvements in breast cancer mortality. In addition, this study was limited in that it was retrospective and nonrandomized, they wrote.
This study was funded by tomosynthesis equipment maker Hologic and the National Cancer Institute. Dr. Friedewald and her associates also reported other ties to Hologic.
Tomosynthesis likely represents an advance over digital mammography for breast cancer screening, but only appropriately powered, prospective, randomized, multicenter clinical trials involving all four currently available tomosynthesis systems will answer this question definitively, said Dr. Etta D. Pisano and Martin J. Yaffe, Ph.D.
Despite the promising results of Friedewald et al., it is still uncertain whether women should specifically ask for tomosynthesis or whether screening centers should convert to tomosynthesis. People who believe screening mammography saves lives without undue false-positive results and overdiagnosis will likely advocate the addition of tomosynthesis; those who question the utility of screening mammography will not likely change their views after seeing these results, Dr. Pisano and Dr. Yaffe said.
Dr. Pisano is at the Medical University of South Carolina, Charleston. Dr. Yaffe is at the Ontario Institute for Cancer Research at the University of Toronto. Dr. Pisano reported ties to FujiFilm, Koning Corp., Siemens, Philips, and NextRay Inc.; Dr. Yaffe reported ties to GE Healthcare and Mammographic Physics Inc. These remarks were taken from their editorial accompanying Dr. Friedewald’s report (JAMA 2014;311:2488-9).
Tomosynthesis likely represents an advance over digital mammography for breast cancer screening, but only appropriately powered, prospective, randomized, multicenter clinical trials involving all four currently available tomosynthesis systems will answer this question definitively, said Dr. Etta D. Pisano and Martin J. Yaffe, Ph.D.
Despite the promising results of Friedewald et al., it is still uncertain whether women should specifically ask for tomosynthesis or whether screening centers should convert to tomosynthesis. People who believe screening mammography saves lives without undue false-positive results and overdiagnosis will likely advocate the addition of tomosynthesis; those who question the utility of screening mammography will not likely change their views after seeing these results, Dr. Pisano and Dr. Yaffe said.
Dr. Pisano is at the Medical University of South Carolina, Charleston. Dr. Yaffe is at the Ontario Institute for Cancer Research at the University of Toronto. Dr. Pisano reported ties to FujiFilm, Koning Corp., Siemens, Philips, and NextRay Inc.; Dr. Yaffe reported ties to GE Healthcare and Mammographic Physics Inc. These remarks were taken from their editorial accompanying Dr. Friedewald’s report (JAMA 2014;311:2488-9).
Tomosynthesis likely represents an advance over digital mammography for breast cancer screening, but only appropriately powered, prospective, randomized, multicenter clinical trials involving all four currently available tomosynthesis systems will answer this question definitively, said Dr. Etta D. Pisano and Martin J. Yaffe, Ph.D.
Despite the promising results of Friedewald et al., it is still uncertain whether women should specifically ask for tomosynthesis or whether screening centers should convert to tomosynthesis. People who believe screening mammography saves lives without undue false-positive results and overdiagnosis will likely advocate the addition of tomosynthesis; those who question the utility of screening mammography will not likely change their views after seeing these results, Dr. Pisano and Dr. Yaffe said.
Dr. Pisano is at the Medical University of South Carolina, Charleston. Dr. Yaffe is at the Ontario Institute for Cancer Research at the University of Toronto. Dr. Pisano reported ties to FujiFilm, Koning Corp., Siemens, Philips, and NextRay Inc.; Dr. Yaffe reported ties to GE Healthcare and Mammographic Physics Inc. These remarks were taken from their editorial accompanying Dr. Friedewald’s report (JAMA 2014;311:2488-9).
Adding tomosynthesis to screening digital mammography decreases the "recall" rate by 15% while increasing the cancer detection rate by 29%, according to a report published online June 25 in JAMA.
Researchers compared the performance of screening digital mammography alone (281,187 cases) against the performance after tomosynthesis was added to mammography (173,663 cases) at 13 sites in geographically diverse regions across the country. The work was funded primarily by Hologic, maker of the only Food and Drug Administration–approved tomosynthesis equipment at the time of this retrospective study, said Dr. Sarah M. Friedewald of the Caldwell Breast Center, Advocate Lutheran General Hospital, Park Ridge, Ill., and her associates.
The "recall" rate – the proportion of patients requiring additional imaging based on the results of their screening mammography – declined from 107 per 1,000 screens with digital mammography alone to 91 per 1,000 screens when tomosynthesis was added, a relative reduction of 15%. At the same time, the cancer detection rate rose from 4.2 to 5.4 per 1,000 scans, a relative increase of 29%. After tomosynthesis was introduced, the detection rate of invasive cancers rose from 2.9 to 4.1 per 1,000 scans, while that of ductal carcinoma in situ remained unchanged at 1.4 per 1,000, the investigators said (JAMA 2014 June 25 [doi:10.1001/jama.2014.6095]).
It is important to note that this study did not assess clinical outcomes, so it remains to be seen whether these improvements in screening mammography translate into clinically relevant improvements in breast cancer mortality. In addition, this study was limited in that it was retrospective and nonrandomized, they wrote.
This study was funded by tomosynthesis equipment maker Hologic and the National Cancer Institute. Dr. Friedewald and her associates also reported other ties to Hologic.
Adding tomosynthesis to screening digital mammography decreases the "recall" rate by 15% while increasing the cancer detection rate by 29%, according to a report published online June 25 in JAMA.
Researchers compared the performance of screening digital mammography alone (281,187 cases) against the performance after tomosynthesis was added to mammography (173,663 cases) at 13 sites in geographically diverse regions across the country. The work was funded primarily by Hologic, maker of the only Food and Drug Administration–approved tomosynthesis equipment at the time of this retrospective study, said Dr. Sarah M. Friedewald of the Caldwell Breast Center, Advocate Lutheran General Hospital, Park Ridge, Ill., and her associates.
The "recall" rate – the proportion of patients requiring additional imaging based on the results of their screening mammography – declined from 107 per 1,000 screens with digital mammography alone to 91 per 1,000 screens when tomosynthesis was added, a relative reduction of 15%. At the same time, the cancer detection rate rose from 4.2 to 5.4 per 1,000 scans, a relative increase of 29%. After tomosynthesis was introduced, the detection rate of invasive cancers rose from 2.9 to 4.1 per 1,000 scans, while that of ductal carcinoma in situ remained unchanged at 1.4 per 1,000, the investigators said (JAMA 2014 June 25 [doi:10.1001/jama.2014.6095]).
It is important to note that this study did not assess clinical outcomes, so it remains to be seen whether these improvements in screening mammography translate into clinically relevant improvements in breast cancer mortality. In addition, this study was limited in that it was retrospective and nonrandomized, they wrote.
This study was funded by tomosynthesis equipment maker Hologic and the National Cancer Institute. Dr. Friedewald and her associates also reported other ties to Hologic.
FROM JAMA
Key clinical point: Tomosynthesis may reduce the need for repeat imaging to detect breast cancer.
Major finding: The "recall" rate declined from 107 per 1,000 screens with digital mammography alone to 91 per 1,000 screens when tomosynthesis was added, a relative reduction of 15%; at the same time, the cancer detection rate rose from 4.2 to 5.4 per 1,000 scans, a relative increase of 29%.
Data source: A retrospective multicenter analysis of screening digital mammography’s performance before (281,187 scans) and after (173,663 scans) the introduction of tomosynthesis to improve its accuracy.
Disclosures: This study was funded by Hologic and the National Cancer Institute. Dr. Friedewald and her associates also reported other ties to Hologic, which makes tomosynthesis equipment.

Combined imaging differentiated benign, cancerous breast tumors
Combined imaging techniques using multiparametric 18fluorodeoxyglucose PET-MRI allow differentiation between benign and malignant breast tumors with a diagnostic accuracy of 96%, according to a report published online June 24 in Clinical Cancer Research.
This in turn permits a "remarkable" reduction in breast biopsies, said Dr. Katja Pinker and her associates at the Medical University of Vienna.

In a single-center feasibility study, the investigators compared the prognostic accuracy of several different combinations of breast imaging in 76 consecutive women aged 25-86 years (mean age, 55.7 years) who were seen during a 3-year period and had suspicious findings on mammography or breast ultrasonography. The lesions ranged in size from 5 mm to 77 mm (median, 29.2 mm); 53 proved to be malignant and 23 were benign.
Only one combination of imaging techniques – multiparametric 18fluorodeoxyglucose (FDG) PET-MRI – achieved an overall diagnostic accuracy of 96%, with a sensitivity of 100% and a specificity of 87% in distinguishing cancers from benign tumors.
Multiparametric FDG PET-MRI includes:
• Dynamic contrast-enhanced MRI, which provides high-resolution anatomic information and depicts increased microvascular density and capillary leaks, which are markers of angiogenesis in malignant tumors.
• Diffusion-weighted imaging that shows cellular diffusivity on a molecular level, which typically is restricted in malignant tissue.
• Three-dimensional proton spectroscopic imaging, which detects elevated levels of the metabolite choline, a marker of increased cell-membrane turnover.
• FDG PET that allows assessment of glucose consumption, which typically is increased in neoplastic processes.
Thus, this combination of imaging techniques simultaneously assesses several processes involved in cancer development: angiogenesis, molecular capabilities, glucose consumption, and metabolite concentration, the investigators said (Clin. Cancer Res. 2014 June 24 [doi: 10.1158/1055-9965.EPI-13-1284]).
Fluorodeoxyglucose, "currently the ‘workhorse’ in clinical PET imaging, has a good sensitivity but limited specificity, as several types of benign breast tumors and conditions can be 18FDG-avid and mimic malignancy," Dr. Pinker and her associates wrote. "However, a multitude of new, targeted radiotracers for visualization of processes involved in cancer evolution are being developed and investigated." These tracers should increase the specificity of this combination of imaging techniques, which will soon make multiparametric PET-MRI an important tool in detecting breast cancer, staging the disease, and monitoring treatment response, they said.
This study was funded by the Austrian Society of Senology, the Austrian National Bank "Jubiläumsfond," and the Medical Scientific Fund of the Mayor of Vienna. Dr. Pinker and her associates reported no financial conflicts of interest.
Combined imaging techniques using multiparametric 18fluorodeoxyglucose PET-MRI allow differentiation between benign and malignant breast tumors with a diagnostic accuracy of 96%, according to a report published online June 24 in Clinical Cancer Research.
This in turn permits a "remarkable" reduction in breast biopsies, said Dr. Katja Pinker and her associates at the Medical University of Vienna.
In a single-center feasibility study, the investigators compared the prognostic accuracy of several different combinations of breast imaging in 76 consecutive women aged 25-86 years (mean age, 55.7 years) who were seen during a 3-year period and had suspicious findings on mammography or breast ultrasonography. The lesions ranged in size from 5 mm to 77 mm (median, 29.2 mm); 53 proved to be malignant and 23 were benign.
Only one combination of imaging techniques – multiparametric 18fluorodeoxyglucose (FDG) PET-MRI – achieved an overall diagnostic accuracy of 96%, with a sensitivity of 100% and a specificity of 87% in distinguishing cancers from benign tumors.
Multiparametric FDG PET-MRI includes:
• Dynamic contrast-enhanced MRI, which provides high-resolution anatomic information and depicts increased microvascular density and capillary leaks, which are markers of angiogenesis in malignant tumors.
• Diffusion-weighted imaging that shows cellular diffusivity on a molecular level, which typically is restricted in malignant tissue.
• Three-dimensional proton spectroscopic imaging, which detects elevated levels of the metabolite choline, a marker of increased cell-membrane turnover.
• FDG PET that allows assessment of glucose consumption, which typically is increased in neoplastic processes.
Thus, this combination of imaging techniques simultaneously assesses several processes involved in cancer development: angiogenesis, molecular capabilities, glucose consumption, and metabolite concentration, the investigators said (Clin. Cancer Res. 2014 June 24 [doi: 10.1158/1055-9965.EPI-13-1284]).
Fluorodeoxyglucose, "currently the ‘workhorse’ in clinical PET imaging, has a good sensitivity but limited specificity, as several types of benign breast tumors and conditions can be 18FDG-avid and mimic malignancy," Dr. Pinker and her associates wrote. "However, a multitude of new, targeted radiotracers for visualization of processes involved in cancer evolution are being developed and investigated." These tracers should increase the specificity of this combination of imaging techniques, which will soon make multiparametric PET-MRI an important tool in detecting breast cancer, staging the disease, and monitoring treatment response, they said.
This study was funded by the Austrian Society of Senology, the Austrian National Bank "Jubiläumsfond," and the Medical Scientific Fund of the Mayor of Vienna. Dr. Pinker and her associates reported no financial conflicts of interest.
Combined imaging techniques using multiparametric 18fluorodeoxyglucose PET-MRI allow differentiation between benign and malignant breast tumors with a diagnostic accuracy of 96%, according to a report published online June 24 in Clinical Cancer Research.
This in turn permits a "remarkable" reduction in breast biopsies, said Dr. Katja Pinker and her associates at the Medical University of Vienna.
In a single-center feasibility study, the investigators compared the prognostic accuracy of several different combinations of breast imaging in 76 consecutive women aged 25-86 years (mean age, 55.7 years) who were seen during a 3-year period and had suspicious findings on mammography or breast ultrasonography. The lesions ranged in size from 5 mm to 77 mm (median, 29.2 mm); 53 proved to be malignant and 23 were benign.
Only one combination of imaging techniques – multiparametric 18fluorodeoxyglucose (FDG) PET-MRI – achieved an overall diagnostic accuracy of 96%, with a sensitivity of 100% and a specificity of 87% in distinguishing cancers from benign tumors.
Multiparametric FDG PET-MRI includes:
• Dynamic contrast-enhanced MRI, which provides high-resolution anatomic information and depicts increased microvascular density and capillary leaks, which are markers of angiogenesis in malignant tumors.
• Diffusion-weighted imaging that shows cellular diffusivity on a molecular level, which typically is restricted in malignant tissue.
• Three-dimensional proton spectroscopic imaging, which detects elevated levels of the metabolite choline, a marker of increased cell-membrane turnover.
• FDG PET that allows assessment of glucose consumption, which typically is increased in neoplastic processes.
Thus, this combination of imaging techniques simultaneously assesses several processes involved in cancer development: angiogenesis, molecular capabilities, glucose consumption, and metabolite concentration, the investigators said (Clin. Cancer Res. 2014 June 24 [doi: 10.1158/1055-9965.EPI-13-1284]).
Fluorodeoxyglucose, "currently the ‘workhorse’ in clinical PET imaging, has a good sensitivity but limited specificity, as several types of benign breast tumors and conditions can be 18FDG-avid and mimic malignancy," Dr. Pinker and her associates wrote. "However, a multitude of new, targeted radiotracers for visualization of processes involved in cancer evolution are being developed and investigated." These tracers should increase the specificity of this combination of imaging techniques, which will soon make multiparametric PET-MRI an important tool in detecting breast cancer, staging the disease, and monitoring treatment response, they said.
This study was funded by the Austrian Society of Senology, the Austrian National Bank "Jubiläumsfond," and the Medical Scientific Fund of the Mayor of Vienna. Dr. Pinker and her associates reported no financial conflicts of interest.
FROM CLINICAL CANCER RESEARCH
Key clinical point: A combination of imaging techniques, which simultaneously assesses several processes involved in cancer development, achieved high diagnostic accuracy in distinguishing breast cancers from benign lesions.
Major finding: Only one combination of imaging techniques – 18fluorodeoxyglucose PET-MRI – achieved an overall diagnostic accuracy of 96%, with a sensitivity of 100% and a specificity of 87% in distinguishing malignancies from benign lesions.
Data source: A prospective, single-center feasibility study involving different combinations of breast imaging techniques to assess the likelihood of malignancy in 76 consecutive women who had suspicious findings on mammography or ultrasonography.
Disclosures: This study was funded by the Austrian Society of Senology, the Austrian National Bank "Jubiläumsfond," and the Medical Scientific Fund of the Mayor of Vienna. Dr. Pinker and her associates reported no financial conflicts of interest.
