User login
A Closer Look at Characteristics of High-Performing HM Groups
Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH

Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH
Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH
Supreme Court: Self-funded insurer does not have to share data
A self-funded insurer does not have to share health data with a state’s all-payer database, according to a March 1 U.S. Supreme Court decision that could affect information-sharing reforms nationwide.
In a 6-2 opinion, the majority justices ruled that the Employee Retirement Income Security Act (ERISA) protects plaintiff Liberty Mutual from having to provide claims and member data to the Vermont Green Mountain Care Board. ERISA, which includes its own reporting, disclosure, and record-keeping provisions, has an express clause that invalidates Vermont’s reporting statute as applied to ERISA plans, Associate Justice Anthony Kennedy wrote in the opinion.

“The state statute imposes duties that are inconsistent with the central design of ERISA, which is to provide a single uniform national scheme for the administration of ERISA plans without interference from laws of the several states even when those laws, to a large extent, impose parallel requirements,” Justice Kennedy wrote.
Associate Justice Ruth Bader-Ginsburg and Associate Justice Sonia Sotomayor dissented with the majority, insisting that Vermont’s database does not infringe on ERISA’s control to regulate self-funded plans. Seventeen other states have enacted similar database systems, which aim to “serve compelling interests,” Justice Ginsburg wrote, such as identifying effective reforms, driving down health care costs, evaluating utility of treatment options, and detecting discrimination in care provision.
“I would hold that Vermont’s effort to track health care services provided to its residents and the cost of those services does not impermissibly intrude on ERISA’s dominion over employee benefit plans,” Justice Ginsburg wrote in her dissent.
The case of Gobeille v. Liberty Mutual Insurance Company stems from a Vermont law that requires all health providers in the state to provide detailed data about their services for the development of an all-payer database. Liberty Mutual argued the law imposed a burden on the self-funded plan because it enforces sharing requirements on top of reporting and disclosure obligations already necessary for the federal Department of Labor. Vermont Green Mountain Care Board Chair Al Gobeille argued the insurer’s purported burdens are trivial because the insurer’s claims administrator already prepares the data required to the state for its non-ERISA operations in Vermont. The 2nd U.S. Circuit Court of Appeals sided with Liberty Mutual.
Liberty Mutual was “pleased,” with the Supreme Court ruling, spokesman John Cusolito said in an interview. He declined to comment further. Mr. Gobeille had not returned a request for comment at press time.
Medical associations expressed disappointment at the ruling.
“It is unfortunate that Vermont’s efforts to increase transparency of health insurance information has been thwarted. The U.S. Supreme Court determined today that a highly complex and confusing federal law can be used to keep the insurance payment process cloaked in mystery,” Dr. Steven J. Stack, president of the American Medical Association said in a statement. “The ruling stands in the way of reform efforts in Vermont and at least 18 other states aimed at providing important information to patients, health professionals and policymakers about health care options, outcomes and costs.”
The American Hospital Association concurred. “Self-insured plans cover a large, growing, and distinctive portion of the population,” AHA spokeswoman Marie Watteau said in a statement. “It is essential that they be included in all-payer databases if those databases are to realize their potential, and if America’s hospitals are to realize their goal of improving community health and controlling costs while providing the high-quality care for which they are known.”
Other medical associations previously weighed in on the case. In a friend-of-the-court brief to the U.S. Supreme Court, the AMA and the Vermont Medical Society said the Gobeille case presents a prime opportunity for the Supreme Court to reexamine ERISA and alleviate confusion between traditional state regulation of health care and exclusive federal regulation of employee benefit plans.
Seventeen states and the District of Columbia issued a joint brief in support of Vermont. A handful of insurers, including the Blue Cross and Blue Shield Association penned briefs in support of Liberty Mutual.
On Twitter @legal_med
A self-funded insurer does not have to share health data with a state’s all-payer database, according to a March 1 U.S. Supreme Court decision that could affect information-sharing reforms nationwide.
In a 6-2 opinion, the majority justices ruled that the Employee Retirement Income Security Act (ERISA) protects plaintiff Liberty Mutual from having to provide claims and member data to the Vermont Green Mountain Care Board. ERISA, which includes its own reporting, disclosure, and record-keeping provisions, has an express clause that invalidates Vermont’s reporting statute as applied to ERISA plans, Associate Justice Anthony Kennedy wrote in the opinion.
“The state statute imposes duties that are inconsistent with the central design of ERISA, which is to provide a single uniform national scheme for the administration of ERISA plans without interference from laws of the several states even when those laws, to a large extent, impose parallel requirements,” Justice Kennedy wrote.
Associate Justice Ruth Bader-Ginsburg and Associate Justice Sonia Sotomayor dissented with the majority, insisting that Vermont’s database does not infringe on ERISA’s control to regulate self-funded plans. Seventeen other states have enacted similar database systems, which aim to “serve compelling interests,” Justice Ginsburg wrote, such as identifying effective reforms, driving down health care costs, evaluating utility of treatment options, and detecting discrimination in care provision.
“I would hold that Vermont’s effort to track health care services provided to its residents and the cost of those services does not impermissibly intrude on ERISA’s dominion over employee benefit plans,” Justice Ginsburg wrote in her dissent.
The case of Gobeille v. Liberty Mutual Insurance Company stems from a Vermont law that requires all health providers in the state to provide detailed data about their services for the development of an all-payer database. Liberty Mutual argued the law imposed a burden on the self-funded plan because it enforces sharing requirements on top of reporting and disclosure obligations already necessary for the federal Department of Labor. Vermont Green Mountain Care Board Chair Al Gobeille argued the insurer’s purported burdens are trivial because the insurer’s claims administrator already prepares the data required to the state for its non-ERISA operations in Vermont. The 2nd U.S. Circuit Court of Appeals sided with Liberty Mutual.
Liberty Mutual was “pleased,” with the Supreme Court ruling, spokesman John Cusolito said in an interview. He declined to comment further. Mr. Gobeille had not returned a request for comment at press time.
Medical associations expressed disappointment at the ruling.
“It is unfortunate that Vermont’s efforts to increase transparency of health insurance information has been thwarted. The U.S. Supreme Court determined today that a highly complex and confusing federal law can be used to keep the insurance payment process cloaked in mystery,” Dr. Steven J. Stack, president of the American Medical Association said in a statement. “The ruling stands in the way of reform efforts in Vermont and at least 18 other states aimed at providing important information to patients, health professionals and policymakers about health care options, outcomes and costs.”
The American Hospital Association concurred. “Self-insured plans cover a large, growing, and distinctive portion of the population,” AHA spokeswoman Marie Watteau said in a statement. “It is essential that they be included in all-payer databases if those databases are to realize their potential, and if America’s hospitals are to realize their goal of improving community health and controlling costs while providing the high-quality care for which they are known.”
Other medical associations previously weighed in on the case. In a friend-of-the-court brief to the U.S. Supreme Court, the AMA and the Vermont Medical Society said the Gobeille case presents a prime opportunity for the Supreme Court to reexamine ERISA and alleviate confusion between traditional state regulation of health care and exclusive federal regulation of employee benefit plans.
Seventeen states and the District of Columbia issued a joint brief in support of Vermont. A handful of insurers, including the Blue Cross and Blue Shield Association penned briefs in support of Liberty Mutual.
On Twitter @legal_med
A self-funded insurer does not have to share health data with a state’s all-payer database, according to a March 1 U.S. Supreme Court decision that could affect information-sharing reforms nationwide.
In a 6-2 opinion, the majority justices ruled that the Employee Retirement Income Security Act (ERISA) protects plaintiff Liberty Mutual from having to provide claims and member data to the Vermont Green Mountain Care Board. ERISA, which includes its own reporting, disclosure, and record-keeping provisions, has an express clause that invalidates Vermont’s reporting statute as applied to ERISA plans, Associate Justice Anthony Kennedy wrote in the opinion.
“The state statute imposes duties that are inconsistent with the central design of ERISA, which is to provide a single uniform national scheme for the administration of ERISA plans without interference from laws of the several states even when those laws, to a large extent, impose parallel requirements,” Justice Kennedy wrote.
Associate Justice Ruth Bader-Ginsburg and Associate Justice Sonia Sotomayor dissented with the majority, insisting that Vermont’s database does not infringe on ERISA’s control to regulate self-funded plans. Seventeen other states have enacted similar database systems, which aim to “serve compelling interests,” Justice Ginsburg wrote, such as identifying effective reforms, driving down health care costs, evaluating utility of treatment options, and detecting discrimination in care provision.
“I would hold that Vermont’s effort to track health care services provided to its residents and the cost of those services does not impermissibly intrude on ERISA’s dominion over employee benefit plans,” Justice Ginsburg wrote in her dissent.
The case of Gobeille v. Liberty Mutual Insurance Company stems from a Vermont law that requires all health providers in the state to provide detailed data about their services for the development of an all-payer database. Liberty Mutual argued the law imposed a burden on the self-funded plan because it enforces sharing requirements on top of reporting and disclosure obligations already necessary for the federal Department of Labor. Vermont Green Mountain Care Board Chair Al Gobeille argued the insurer’s purported burdens are trivial because the insurer’s claims administrator already prepares the data required to the state for its non-ERISA operations in Vermont. The 2nd U.S. Circuit Court of Appeals sided with Liberty Mutual.
Liberty Mutual was “pleased,” with the Supreme Court ruling, spokesman John Cusolito said in an interview. He declined to comment further. Mr. Gobeille had not returned a request for comment at press time.
Medical associations expressed disappointment at the ruling.
“It is unfortunate that Vermont’s efforts to increase transparency of health insurance information has been thwarted. The U.S. Supreme Court determined today that a highly complex and confusing federal law can be used to keep the insurance payment process cloaked in mystery,” Dr. Steven J. Stack, president of the American Medical Association said in a statement. “The ruling stands in the way of reform efforts in Vermont and at least 18 other states aimed at providing important information to patients, health professionals and policymakers about health care options, outcomes and costs.”
The American Hospital Association concurred. “Self-insured plans cover a large, growing, and distinctive portion of the population,” AHA spokeswoman Marie Watteau said in a statement. “It is essential that they be included in all-payer databases if those databases are to realize their potential, and if America’s hospitals are to realize their goal of improving community health and controlling costs while providing the high-quality care for which they are known.”
Other medical associations previously weighed in on the case. In a friend-of-the-court brief to the U.S. Supreme Court, the AMA and the Vermont Medical Society said the Gobeille case presents a prime opportunity for the Supreme Court to reexamine ERISA and alleviate confusion between traditional state regulation of health care and exclusive federal regulation of employee benefit plans.
Seventeen states and the District of Columbia issued a joint brief in support of Vermont. A handful of insurers, including the Blue Cross and Blue Shield Association penned briefs in support of Liberty Mutual.
On Twitter @legal_med

Allegations: Current Trends in Medical Malpractice, Part 1
We’re lost, but we’re making good time.
-Yogi Berra
As Yogi Berra alludes, it is very easy to get caught up “in the flow” and continue to move along at a good pace, even when one does not know where he or she is ultimately headed. Similarly, in terms of medical malpractice, everyone seems to have an opinion on what should be done to improve the climate of medical malpractice for both providers and patients. Yet, there are many differences in opinions on how to solve these issues, and the “cure” for what “ails” in the system are many—with an undetermined endpoint.
Tort reform is often conjured as the communal fix; yet each state in the Union has its own medical malpractice tort laws, which begs the question of how an issue with so many different facets can be resolved. Additionally, the risk alone of medical malpractice continues to be an important area of concern to emergency physicians (EPs), not only because of the looming threat of malpractice litigation—both real and perceived—but also because of its influence on practice patterns, resource utilization, and patient care in the ED.1,2
Physician Perception
Over the course of a career, an EP faces at least one claim, further perpetuating a common physician perception that the occurrence of a suit is not a condition of “if” but rather of “when.”3 This anxiety and fear among physicians in general are further provoked by the many headlines highlighting massive jury verdicts that dominate the news cycle.4
In addition, the EP’s work and practice are increasingly affected by the impositions of multiple nationally reported quality metrics, institutional throughput goals, and process-improvement efforts. Each of these in turn has the effect of increasing the pace of care and can challenge one’s real-time ability to recognize the dangers of inherent biases, to appreciate and act upon subtle clinical clues, and to rescue patient-experience misadventures. Accordingly, medical malpractice is a frequent topic of discussion for policy proposals among physicians and legislators.
Defensive Medicine and Tort Reform
As spending on health care in the United States topped $3 trillion, or 17.5% of the US gross domestic product in 2014, strategies for cost-containment have become a primary concern across all sectors of the health-care industry.5,6 With defensive medicine proposed by some as a substantial driver of health-care costs, many physicians have focused on tort reform as an avenue to curb defensive testing. This has resulted in substantial policy shifts in a number of jurisdictions.7,8 Some of the policy changes that have taken place over the past few decades have included state-imposed caps on medical malpractice awards and noneconomic damages, caps on attorney fees, and shortened statutes of limitations that require more timely filing of malpractice suits.
Defining Malpractice and Imposing Caps
In 2003, Texas changed its definition of the medical malpractice standard to “willful and wanton negligence”; in Georgia (2005) and South Carolina (2005) the definition was changed to “gross negligence.” Both of these revised definitions are essentially synonymous in a legal sense and are intended to protect physicians working in a high-risk, limited-information, high-intensity environment (eg, the ED) by raising the plaintiff’s responsibility to prove that the defendant physician was aware of the likelihood of serious injury but proceeded with “conscious indifference.”9
It seems, however, that such efforts have been not been entirely effective in reigning in costs of care, decreasing insurance costs, and limiting defensive medicine, particularly in the ED.9 A study by Paik et al10 on the effect of caps on malpractice claims and payouts found that in states with caps, both claims and payouts were effectively reduced, with a large impact on payout per physician and a drop in claims for those cases with larger payouts. While stricter caps had larger effects, the authors did not examine the impact of caps on “defensive medicine.”10 Furthermore, many physicians, health systems, and patient advocacy groups have been exploring and implementing alternative models of claim resolution outside of the legal process.11
Alternative Compensation Models
In the state legislatures of Georgia and Florida, alternative patient-compensation models are currently under proposal. Both models are designed to eliminate the current medical tort system and replace it with an administrative system to compensate patients for medical errors that have caused them harm.12 These proposals are similar to the existing Birth-Related Neurological Injury Compensation Programs (BRNICP) in effect in both Florida and Virginia. The BRNICP in each of these states serves as an administrative system to provide monetary compensation to patients who have clearly suffered only birth-related medical injuries, thus keeping this type of liability out of the court system.
Program Structure
Compensation programs such as the BRNICP in Florida and Virginia would replace traditional tort law. In this system, physicians would pay annually into a compensation fund (as do the physicians in Virginia and Florida), with amounts prorated to liability risk based on practice specialty. A patient harmed by a claimed medical injury that was allegedly caused by the proximate treatment rendered, would apply to the patient compensation system via a designated patient advocate. The advocate would initiate the claim process on behalf of the patient, after which the claim would be reviewed by a panel of medical experts in the appropriate field. If the panel finds the injury was preventable or avoidable, the case would then proceed to a compensation committee to render payment to the injured individual.
This compensation model not only eliminates the need for legal counsel for the patient, but also the need for medical malpractice liability insurance and defense counsel for the physician. Unlike traditional tort law, this alternate process encourages a system of transparency that supports appropriate disclosure of medical error rather than delaying late discovery of error and increased angst both for the patient and the physician.
Potential Benefits
One would anticipate that an alternate compensation model such as the BRNCIP that eliminates the fear of a lawsuit (ie, if patients no longer sued physicians for medical malpractice) would have a significant impact on defensive medicine and its associated costs. A study conducted by Emory University concluded that as much as $7 billion in the state of Georgia could be saved each year if such a program was enacted.13 In addition to the financial benefits, the care of all patients would improve through increased efficiency and better appropriation of finite resources. Moreover, patients harmed in a medical mishap would have a more direct, expedited, and less expensive mechanism of compensation compared to traditional tort systems.
The alternate compensation model would also benefit patients by negating the need for legal counsel. In the current tort system, many cases go unaddressed either because the patient does not have the means to hire counsel or the case seems too inconsequential for a lawyer to accept it. The compensation system would improve access for patients with valid claims, from egregious high impact errors to the lower impact errors, which are still significant.
There are also public health benefits to the alternate compensation model, including advances in patient safety as a result of the transparency of medical error and addressing medical mishaps in a timelier manner, providing an opportunity to improve knowledge and system gaps closer to real-time events. No longer would a patient have to forge an adversarial offensive on a physician. The panel of experts, who becomes the peer of the physician, can fairly assess the conditions of the case and bring forth an impartial recommendation to either reimburse or not reimburse the patient.
By eliminating the punitive nature of tort law upon the physician, and because this system compensates through a state-based compensation program, there is no indelible report made naming the physician to the National Practitioner Data Bank. Further, if a provider is identified as a significant risk to the public, the panel of medical experts can report that physician to the state licensing board immediately, which would prove more effective and efficient than the traditional method of data collection and referral currently in place in most states.
Challenges
Challenges to these bills include resistance from those who may be adversely affected by such legislation—mainly medical malpractice trial lawyers (both plaintiff and defendant) and medical malpractice insurance companies.
Conclusion
In consideration of innovative solutions to medical malpractice reform, the efforts in the states of Georgia and Florida clearly think outside the box. Neither of these proposed solutions is currently operational, but certainly if they become state statutes, they will create a very interesting environment to observe while the effects of such systems play out. The operations of the birth-related injury funds have been successful in states that have already implemented such programs. In the meantime, pending such changes in policy and legislation, EPs can mitigate malpractice risk by maintaining board certification and specialty training requirements, and by employing the following:
Follow the basic principles for every patient. Vital signs are vital for a reason, and all abnormal data must be accounted for;
Maintain open communication with patients—a paramount component in reducing the risk of a malpractice allegation;
Ensure that all members of the care team engender an environment that is focused on patient safety, including open communication with nursing staff and technical support;
Be aware of inherent biases in medical decision-making, which helps to maintain mindfulness in the routine practice of emergency medicine (EM);
Make sure departmental policies and procedures are designed to identify and address all late resulting laboratory results, radiology reading discrepancies and culture results in a timely and uniform manner; and
Provide clear and concise at-home care instructions to patients—prior to discharge—and in a manner the patient can understand.
Part 2 will discuss each of these recommendations in detail and will consider recent trends in medical malpractice as they relate to EM, explore areas of risk, and discuss strategies to reduce medical malpractice risk in the ED.
- Charles SC. Coping with a medical malpractice suit. West J Med. 2001;174(1): 55-58.
- Katz DA, Williams GC, Brown RL, et al. Emergency physicians’ fear of malpractice in evaluating patient with possible acute cardiac ischemia. Ann Emerg Med. 2005;46(6): 525-533.
- Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011; 365(7):629-636.
- Moran B. $6.41 million verdict in Temple malpractice lawsuit. Philadelphia Inquirer. 2012, June 2. http://articles.philly.com/2012-06-02/news/31960243_1_million-verdict-malpractice-massive-heart-attack. Accessed March 1, 2016.
- Martin AB, Hartman M, Benson J, Catlin A; National Health Expenditure Accounts Team. National health spending in 2014: faster growth driven by coverage expansion and prescription drug spending. Health Aff (Millwood). 2015;35(1):150-160.
- Emanuel E, Tanden N, Altman S, et al. A systemic approach to containing health care spending. N Engl J Med. 2012;367(10):949-954.
- Jost TS. Health care reform requires law reform. Health Aff (Millwood). 2009; 28(5): w761-w769.
- Roslund G. The medical malpractice rundown: a state-by-state report card. Emerg Phys Monthly. 2014;July 21. Available at http://epmonthly.com/article/the-medical-malpractice-rundown-a-state-by-state-report-card/. Accessed March 1, 2016.
- Waxman DA, Greenberg MD, Ridgely MS, Kellermann AL, Heaton P. The effect of malpractice reform on emergency department care. N Engl J Med. 2014;371(16):1518-1525.
- Paik M, Black BS, Hyma DA. The receding tide of medical malpractice litigation part 2: effect of damage caps. J Empirical Leg Stud. 2013;10(4):639-669.
- Stamm JA, Korzick KA, Beech K, Wood KE. Medical malpractice: reform for today’s patients and clinicians. Am J Med. 2016;129(1):20-25.
- Segal J. Finally: an end to malpractice litigation? Medscape. Available at http://www.medscape.com/viewarticle/840337_1. March 5,2015. Accessed March 1, 2016.
- Shinkman R. Patient compensation system could replace malpractice torts. Fierce Health Finance Web site. November 9, 2014. Available at http://www.fiercehealthfinance.com/story/patient-compensation-system-could-replace-malpractice-torts/2014-11-09. Accessed March 1, 2016.
We’re lost, but we’re making good time.
-Yogi Berra
As Yogi Berra alludes, it is very easy to get caught up “in the flow” and continue to move along at a good pace, even when one does not know where he or she is ultimately headed. Similarly, in terms of medical malpractice, everyone seems to have an opinion on what should be done to improve the climate of medical malpractice for both providers and patients. Yet, there are many differences in opinions on how to solve these issues, and the “cure” for what “ails” in the system are many—with an undetermined endpoint.
Tort reform is often conjured as the communal fix; yet each state in the Union has its own medical malpractice tort laws, which begs the question of how an issue with so many different facets can be resolved. Additionally, the risk alone of medical malpractice continues to be an important area of concern to emergency physicians (EPs), not only because of the looming threat of malpractice litigation—both real and perceived—but also because of its influence on practice patterns, resource utilization, and patient care in the ED.1,2
Physician Perception
Over the course of a career, an EP faces at least one claim, further perpetuating a common physician perception that the occurrence of a suit is not a condition of “if” but rather of “when.”3 This anxiety and fear among physicians in general are further provoked by the many headlines highlighting massive jury verdicts that dominate the news cycle.4
In addition, the EP’s work and practice are increasingly affected by the impositions of multiple nationally reported quality metrics, institutional throughput goals, and process-improvement efforts. Each of these in turn has the effect of increasing the pace of care and can challenge one’s real-time ability to recognize the dangers of inherent biases, to appreciate and act upon subtle clinical clues, and to rescue patient-experience misadventures. Accordingly, medical malpractice is a frequent topic of discussion for policy proposals among physicians and legislators.
Defensive Medicine and Tort Reform
As spending on health care in the United States topped $3 trillion, or 17.5% of the US gross domestic product in 2014, strategies for cost-containment have become a primary concern across all sectors of the health-care industry.5,6 With defensive medicine proposed by some as a substantial driver of health-care costs, many physicians have focused on tort reform as an avenue to curb defensive testing. This has resulted in substantial policy shifts in a number of jurisdictions.7,8 Some of the policy changes that have taken place over the past few decades have included state-imposed caps on medical malpractice awards and noneconomic damages, caps on attorney fees, and shortened statutes of limitations that require more timely filing of malpractice suits.
Defining Malpractice and Imposing Caps
In 2003, Texas changed its definition of the medical malpractice standard to “willful and wanton negligence”; in Georgia (2005) and South Carolina (2005) the definition was changed to “gross negligence.” Both of these revised definitions are essentially synonymous in a legal sense and are intended to protect physicians working in a high-risk, limited-information, high-intensity environment (eg, the ED) by raising the plaintiff’s responsibility to prove that the defendant physician was aware of the likelihood of serious injury but proceeded with “conscious indifference.”9
It seems, however, that such efforts have been not been entirely effective in reigning in costs of care, decreasing insurance costs, and limiting defensive medicine, particularly in the ED.9 A study by Paik et al10 on the effect of caps on malpractice claims and payouts found that in states with caps, both claims and payouts were effectively reduced, with a large impact on payout per physician and a drop in claims for those cases with larger payouts. While stricter caps had larger effects, the authors did not examine the impact of caps on “defensive medicine.”10 Furthermore, many physicians, health systems, and patient advocacy groups have been exploring and implementing alternative models of claim resolution outside of the legal process.11
Alternative Compensation Models
In the state legislatures of Georgia and Florida, alternative patient-compensation models are currently under proposal. Both models are designed to eliminate the current medical tort system and replace it with an administrative system to compensate patients for medical errors that have caused them harm.12 These proposals are similar to the existing Birth-Related Neurological Injury Compensation Programs (BRNICP) in effect in both Florida and Virginia. The BRNICP in each of these states serves as an administrative system to provide monetary compensation to patients who have clearly suffered only birth-related medical injuries, thus keeping this type of liability out of the court system.
Program Structure
Compensation programs such as the BRNICP in Florida and Virginia would replace traditional tort law. In this system, physicians would pay annually into a compensation fund (as do the physicians in Virginia and Florida), with amounts prorated to liability risk based on practice specialty. A patient harmed by a claimed medical injury that was allegedly caused by the proximate treatment rendered, would apply to the patient compensation system via a designated patient advocate. The advocate would initiate the claim process on behalf of the patient, after which the claim would be reviewed by a panel of medical experts in the appropriate field. If the panel finds the injury was preventable or avoidable, the case would then proceed to a compensation committee to render payment to the injured individual.
This compensation model not only eliminates the need for legal counsel for the patient, but also the need for medical malpractice liability insurance and defense counsel for the physician. Unlike traditional tort law, this alternate process encourages a system of transparency that supports appropriate disclosure of medical error rather than delaying late discovery of error and increased angst both for the patient and the physician.
Potential Benefits
One would anticipate that an alternate compensation model such as the BRNCIP that eliminates the fear of a lawsuit (ie, if patients no longer sued physicians for medical malpractice) would have a significant impact on defensive medicine and its associated costs. A study conducted by Emory University concluded that as much as $7 billion in the state of Georgia could be saved each year if such a program was enacted.13 In addition to the financial benefits, the care of all patients would improve through increased efficiency and better appropriation of finite resources. Moreover, patients harmed in a medical mishap would have a more direct, expedited, and less expensive mechanism of compensation compared to traditional tort systems.
The alternate compensation model would also benefit patients by negating the need for legal counsel. In the current tort system, many cases go unaddressed either because the patient does not have the means to hire counsel or the case seems too inconsequential for a lawyer to accept it. The compensation system would improve access for patients with valid claims, from egregious high impact errors to the lower impact errors, which are still significant.
There are also public health benefits to the alternate compensation model, including advances in patient safety as a result of the transparency of medical error and addressing medical mishaps in a timelier manner, providing an opportunity to improve knowledge and system gaps closer to real-time events. No longer would a patient have to forge an adversarial offensive on a physician. The panel of experts, who becomes the peer of the physician, can fairly assess the conditions of the case and bring forth an impartial recommendation to either reimburse or not reimburse the patient.
By eliminating the punitive nature of tort law upon the physician, and because this system compensates through a state-based compensation program, there is no indelible report made naming the physician to the National Practitioner Data Bank. Further, if a provider is identified as a significant risk to the public, the panel of medical experts can report that physician to the state licensing board immediately, which would prove more effective and efficient than the traditional method of data collection and referral currently in place in most states.
Challenges
Challenges to these bills include resistance from those who may be adversely affected by such legislation—mainly medical malpractice trial lawyers (both plaintiff and defendant) and medical malpractice insurance companies.
Conclusion
In consideration of innovative solutions to medical malpractice reform, the efforts in the states of Georgia and Florida clearly think outside the box. Neither of these proposed solutions is currently operational, but certainly if they become state statutes, they will create a very interesting environment to observe while the effects of such systems play out. The operations of the birth-related injury funds have been successful in states that have already implemented such programs. In the meantime, pending such changes in policy and legislation, EPs can mitigate malpractice risk by maintaining board certification and specialty training requirements, and by employing the following:
Follow the basic principles for every patient. Vital signs are vital for a reason, and all abnormal data must be accounted for;
Maintain open communication with patients—a paramount component in reducing the risk of a malpractice allegation;
Ensure that all members of the care team engender an environment that is focused on patient safety, including open communication with nursing staff and technical support;
Be aware of inherent biases in medical decision-making, which helps to maintain mindfulness in the routine practice of emergency medicine (EM);
Make sure departmental policies and procedures are designed to identify and address all late resulting laboratory results, radiology reading discrepancies and culture results in a timely and uniform manner; and
Provide clear and concise at-home care instructions to patients—prior to discharge—and in a manner the patient can understand.
Part 2 will discuss each of these recommendations in detail and will consider recent trends in medical malpractice as they relate to EM, explore areas of risk, and discuss strategies to reduce medical malpractice risk in the ED.
We’re lost, but we’re making good time.
-Yogi Berra
As Yogi Berra alludes, it is very easy to get caught up “in the flow” and continue to move along at a good pace, even when one does not know where he or she is ultimately headed. Similarly, in terms of medical malpractice, everyone seems to have an opinion on what should be done to improve the climate of medical malpractice for both providers and patients. Yet, there are many differences in opinions on how to solve these issues, and the “cure” for what “ails” in the system are many—with an undetermined endpoint.
Tort reform is often conjured as the communal fix; yet each state in the Union has its own medical malpractice tort laws, which begs the question of how an issue with so many different facets can be resolved. Additionally, the risk alone of medical malpractice continues to be an important area of concern to emergency physicians (EPs), not only because of the looming threat of malpractice litigation—both real and perceived—but also because of its influence on practice patterns, resource utilization, and patient care in the ED.1,2
Physician Perception
Over the course of a career, an EP faces at least one claim, further perpetuating a common physician perception that the occurrence of a suit is not a condition of “if” but rather of “when.”3 This anxiety and fear among physicians in general are further provoked by the many headlines highlighting massive jury verdicts that dominate the news cycle.4
In addition, the EP’s work and practice are increasingly affected by the impositions of multiple nationally reported quality metrics, institutional throughput goals, and process-improvement efforts. Each of these in turn has the effect of increasing the pace of care and can challenge one’s real-time ability to recognize the dangers of inherent biases, to appreciate and act upon subtle clinical clues, and to rescue patient-experience misadventures. Accordingly, medical malpractice is a frequent topic of discussion for policy proposals among physicians and legislators.
Defensive Medicine and Tort Reform
As spending on health care in the United States topped $3 trillion, or 17.5% of the US gross domestic product in 2014, strategies for cost-containment have become a primary concern across all sectors of the health-care industry.5,6 With defensive medicine proposed by some as a substantial driver of health-care costs, many physicians have focused on tort reform as an avenue to curb defensive testing. This has resulted in substantial policy shifts in a number of jurisdictions.7,8 Some of the policy changes that have taken place over the past few decades have included state-imposed caps on medical malpractice awards and noneconomic damages, caps on attorney fees, and shortened statutes of limitations that require more timely filing of malpractice suits.
Defining Malpractice and Imposing Caps
In 2003, Texas changed its definition of the medical malpractice standard to “willful and wanton negligence”; in Georgia (2005) and South Carolina (2005) the definition was changed to “gross negligence.” Both of these revised definitions are essentially synonymous in a legal sense and are intended to protect physicians working in a high-risk, limited-information, high-intensity environment (eg, the ED) by raising the plaintiff’s responsibility to prove that the defendant physician was aware of the likelihood of serious injury but proceeded with “conscious indifference.”9
It seems, however, that such efforts have been not been entirely effective in reigning in costs of care, decreasing insurance costs, and limiting defensive medicine, particularly in the ED.9 A study by Paik et al10 on the effect of caps on malpractice claims and payouts found that in states with caps, both claims and payouts were effectively reduced, with a large impact on payout per physician and a drop in claims for those cases with larger payouts. While stricter caps had larger effects, the authors did not examine the impact of caps on “defensive medicine.”10 Furthermore, many physicians, health systems, and patient advocacy groups have been exploring and implementing alternative models of claim resolution outside of the legal process.11
Alternative Compensation Models
In the state legislatures of Georgia and Florida, alternative patient-compensation models are currently under proposal. Both models are designed to eliminate the current medical tort system and replace it with an administrative system to compensate patients for medical errors that have caused them harm.12 These proposals are similar to the existing Birth-Related Neurological Injury Compensation Programs (BRNICP) in effect in both Florida and Virginia. The BRNICP in each of these states serves as an administrative system to provide monetary compensation to patients who have clearly suffered only birth-related medical injuries, thus keeping this type of liability out of the court system.
Program Structure
Compensation programs such as the BRNICP in Florida and Virginia would replace traditional tort law. In this system, physicians would pay annually into a compensation fund (as do the physicians in Virginia and Florida), with amounts prorated to liability risk based on practice specialty. A patient harmed by a claimed medical injury that was allegedly caused by the proximate treatment rendered, would apply to the patient compensation system via a designated patient advocate. The advocate would initiate the claim process on behalf of the patient, after which the claim would be reviewed by a panel of medical experts in the appropriate field. If the panel finds the injury was preventable or avoidable, the case would then proceed to a compensation committee to render payment to the injured individual.
This compensation model not only eliminates the need for legal counsel for the patient, but also the need for medical malpractice liability insurance and defense counsel for the physician. Unlike traditional tort law, this alternate process encourages a system of transparency that supports appropriate disclosure of medical error rather than delaying late discovery of error and increased angst both for the patient and the physician.
Potential Benefits
One would anticipate that an alternate compensation model such as the BRNCIP that eliminates the fear of a lawsuit (ie, if patients no longer sued physicians for medical malpractice) would have a significant impact on defensive medicine and its associated costs. A study conducted by Emory University concluded that as much as $7 billion in the state of Georgia could be saved each year if such a program was enacted.13 In addition to the financial benefits, the care of all patients would improve through increased efficiency and better appropriation of finite resources. Moreover, patients harmed in a medical mishap would have a more direct, expedited, and less expensive mechanism of compensation compared to traditional tort systems.
The alternate compensation model would also benefit patients by negating the need for legal counsel. In the current tort system, many cases go unaddressed either because the patient does not have the means to hire counsel or the case seems too inconsequential for a lawyer to accept it. The compensation system would improve access for patients with valid claims, from egregious high impact errors to the lower impact errors, which are still significant.
There are also public health benefits to the alternate compensation model, including advances in patient safety as a result of the transparency of medical error and addressing medical mishaps in a timelier manner, providing an opportunity to improve knowledge and system gaps closer to real-time events. No longer would a patient have to forge an adversarial offensive on a physician. The panel of experts, who becomes the peer of the physician, can fairly assess the conditions of the case and bring forth an impartial recommendation to either reimburse or not reimburse the patient.
By eliminating the punitive nature of tort law upon the physician, and because this system compensates through a state-based compensation program, there is no indelible report made naming the physician to the National Practitioner Data Bank. Further, if a provider is identified as a significant risk to the public, the panel of medical experts can report that physician to the state licensing board immediately, which would prove more effective and efficient than the traditional method of data collection and referral currently in place in most states.
Challenges
Challenges to these bills include resistance from those who may be adversely affected by such legislation—mainly medical malpractice trial lawyers (both plaintiff and defendant) and medical malpractice insurance companies.
Conclusion
In consideration of innovative solutions to medical malpractice reform, the efforts in the states of Georgia and Florida clearly think outside the box. Neither of these proposed solutions is currently operational, but certainly if they become state statutes, they will create a very interesting environment to observe while the effects of such systems play out. The operations of the birth-related injury funds have been successful in states that have already implemented such programs. In the meantime, pending such changes in policy and legislation, EPs can mitigate malpractice risk by maintaining board certification and specialty training requirements, and by employing the following:
Follow the basic principles for every patient. Vital signs are vital for a reason, and all abnormal data must be accounted for;
Maintain open communication with patients—a paramount component in reducing the risk of a malpractice allegation;
Ensure that all members of the care team engender an environment that is focused on patient safety, including open communication with nursing staff and technical support;
Be aware of inherent biases in medical decision-making, which helps to maintain mindfulness in the routine practice of emergency medicine (EM);
Make sure departmental policies and procedures are designed to identify and address all late resulting laboratory results, radiology reading discrepancies and culture results in a timely and uniform manner; and
Provide clear and concise at-home care instructions to patients—prior to discharge—and in a manner the patient can understand.
Part 2 will discuss each of these recommendations in detail and will consider recent trends in medical malpractice as they relate to EM, explore areas of risk, and discuss strategies to reduce medical malpractice risk in the ED.
- Charles SC. Coping with a medical malpractice suit. West J Med. 2001;174(1): 55-58.
- Katz DA, Williams GC, Brown RL, et al. Emergency physicians’ fear of malpractice in evaluating patient with possible acute cardiac ischemia. Ann Emerg Med. 2005;46(6): 525-533.
- Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011; 365(7):629-636.
- Moran B. $6.41 million verdict in Temple malpractice lawsuit. Philadelphia Inquirer. 2012, June 2. http://articles.philly.com/2012-06-02/news/31960243_1_million-verdict-malpractice-massive-heart-attack. Accessed March 1, 2016.
- Martin AB, Hartman M, Benson J, Catlin A; National Health Expenditure Accounts Team. National health spending in 2014: faster growth driven by coverage expansion and prescription drug spending. Health Aff (Millwood). 2015;35(1):150-160.
- Emanuel E, Tanden N, Altman S, et al. A systemic approach to containing health care spending. N Engl J Med. 2012;367(10):949-954.
- Jost TS. Health care reform requires law reform. Health Aff (Millwood). 2009; 28(5): w761-w769.
- Roslund G. The medical malpractice rundown: a state-by-state report card. Emerg Phys Monthly. 2014;July 21. Available at http://epmonthly.com/article/the-medical-malpractice-rundown-a-state-by-state-report-card/. Accessed March 1, 2016.
- Waxman DA, Greenberg MD, Ridgely MS, Kellermann AL, Heaton P. The effect of malpractice reform on emergency department care. N Engl J Med. 2014;371(16):1518-1525.
- Paik M, Black BS, Hyma DA. The receding tide of medical malpractice litigation part 2: effect of damage caps. J Empirical Leg Stud. 2013;10(4):639-669.
- Stamm JA, Korzick KA, Beech K, Wood KE. Medical malpractice: reform for today’s patients and clinicians. Am J Med. 2016;129(1):20-25.
- Segal J. Finally: an end to malpractice litigation? Medscape. Available at http://www.medscape.com/viewarticle/840337_1. March 5,2015. Accessed March 1, 2016.
- Shinkman R. Patient compensation system could replace malpractice torts. Fierce Health Finance Web site. November 9, 2014. Available at http://www.fiercehealthfinance.com/story/patient-compensation-system-could-replace-malpractice-torts/2014-11-09. Accessed March 1, 2016.
- Charles SC. Coping with a medical malpractice suit. West J Med. 2001;174(1): 55-58.
- Katz DA, Williams GC, Brown RL, et al. Emergency physicians’ fear of malpractice in evaluating patient with possible acute cardiac ischemia. Ann Emerg Med. 2005;46(6): 525-533.
- Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011; 365(7):629-636.
- Moran B. $6.41 million verdict in Temple malpractice lawsuit. Philadelphia Inquirer. 2012, June 2. http://articles.philly.com/2012-06-02/news/31960243_1_million-verdict-malpractice-massive-heart-attack. Accessed March 1, 2016.
- Martin AB, Hartman M, Benson J, Catlin A; National Health Expenditure Accounts Team. National health spending in 2014: faster growth driven by coverage expansion and prescription drug spending. Health Aff (Millwood). 2015;35(1):150-160.
- Emanuel E, Tanden N, Altman S, et al. A systemic approach to containing health care spending. N Engl J Med. 2012;367(10):949-954.
- Jost TS. Health care reform requires law reform. Health Aff (Millwood). 2009; 28(5): w761-w769.
- Roslund G. The medical malpractice rundown: a state-by-state report card. Emerg Phys Monthly. 2014;July 21. Available at http://epmonthly.com/article/the-medical-malpractice-rundown-a-state-by-state-report-card/. Accessed March 1, 2016.
- Waxman DA, Greenberg MD, Ridgely MS, Kellermann AL, Heaton P. The effect of malpractice reform on emergency department care. N Engl J Med. 2014;371(16):1518-1525.
- Paik M, Black BS, Hyma DA. The receding tide of medical malpractice litigation part 2: effect of damage caps. J Empirical Leg Stud. 2013;10(4):639-669.
- Stamm JA, Korzick KA, Beech K, Wood KE. Medical malpractice: reform for today’s patients and clinicians. Am J Med. 2016;129(1):20-25.
- Segal J. Finally: an end to malpractice litigation? Medscape. Available at http://www.medscape.com/viewarticle/840337_1. March 5,2015. Accessed March 1, 2016.
- Shinkman R. Patient compensation system could replace malpractice torts. Fierce Health Finance Web site. November 9, 2014. Available at http://www.fiercehealthfinance.com/story/patient-compensation-system-could-replace-malpractice-torts/2014-11-09. Accessed March 1, 2016.

Feds: Major EHR companies will remove interoperability roadblocks
LAS VEGAS – Health care data interoperability should get a huge boost under a public-private effort announced Feb. 29 by U.S. Department of Health and Human Services Secretary Sylvia Burwell.
The nation’s top five health care systems and companies, which provide the electronic health record systems that cover more than 90% of U.S. hospital patients, have agreed to principles designed to improve patient access to health data and eliminate the practice of data blocking.
They also have agreed to adopt federally recognized, national interoperability standards, Ms. Burwell announced at the annual meeting of the Healthcare Information and Management Systems Society.
“Technology is not just one leg of our strategy to build a better health care system for our nation – it supports the entire effort,” Ms. Burwell said. “We are working to unlock health care data and information so that providers are better informed and patients and families can access their health care information, making them empowered, active participants in their own care.”

In a show of support, medical specialty societies including the American Academy of Family Physicians, the American College of Physicians, the American Society of Clinical Oncology, and the American Medical Association also signed on to the commitment.
“We have made tremendous progress to bring health care into the 21st century,” Ms. Burwell said. “In 6 short years, we have tripled the adoption of electronic health records. Today, three-quarters of physicians are using them. And nearly every hospital uses EHRs, meaning that there is now a digital care footprint for almost everyone in this country.”
To unlock all those data and make them useful to health care providers and patients, the health IT companies and health care systems have agreed to the following steps:
• Implement application programming interface (API) technology so that smartphone and tablet apps can be created, facilitating patient use and transfer of their health care data.
• Work so providers can share patient health care data with patients and other providers whenever permitted by law, while not blocking such sharing either intentionally or unintentionally.
• Use the federally recognized Fast Healthcare Interoperability Resources (FHIR) data standard.
This commitment is a “major step forward” to help patients “not just in one episode, but over the long term,” explained Dr. Karen DeSalvo, National Coordinator for Health Information Technology. The agreement means the health care system is “on the threshold of a truly historic opportunity to transform quality of care,” she added.
Federal officials have a timeline for progress toward these goals by 2018, Dr. DeSalvo noted. But “the private sector wants to pull that forward and be leaders with us,” she said. “So, our expectation is that the calls and the commitments and the associated actions that these developers have declared will be seeing some changes by the fall.”
To highlight health information technology’s promise, Ms. Burwell shared a story about electronic health records’ use to find children affected by lead pollution in the water supplies of Flint, Mich.
Alerted to the problem by a friend, pediatrician Mona Hanna-Attisha of Hurley Medical Center in Flint tried to determine whether pipe corrosion might leach dangerous levels of lead into the water supply, Ms. Burwell said.
“She knew the danger lead posed and began what she called a ‘crusade’ to find out if it was affecting children,” Ms. Burwell explained. Dr. Hanna-Attisha mined Hurley’s medical records to “compare blood test results from more than 700 children in the area and map home addresses for geographic variations.
“She quickly discovered that the percentage of children in Flint with lead poisoning had doubled, and even tripled, in some neighborhoods,” Burwell said.
If those results had still been on paper, “it would have taken forever to get these results,” she said.
“Dr. Hanna-Attisha’s story shows us the power of putting health care data to work,” Ms. Burwell noted. “It allows us to see the connections in our communities and helps us put patients in the center of their care.”
Dr. David Classen, chief information officer of the patient safety organization Pascal Metrics and an author of a 2011 Institute of Medicine report on health IT and patient safety, applauded the announcement and the commitment from major EHR vendors and hospital systems have signed on.
“That was one of the things [the IOM expert panel] envisioned – a public-private partnership that would really help this. That’s close to optimal in my view.”
But “the devil’s in the details,” said Dr. Classen, associate professor of medicine at the University of Utah. “When it comes to sharing safety information, it’s not just removal of the gag clauses, it’s also the confidentiality clauses, and the intellectual property protections. Those things too can inhibit sharing of safety information. The challenge here is that [EHR vendors] worry that if they’re so interoperable, they convert their proprietary technology into something that could virtually be open source...and everyone can look at it. Those are legitimate concerns.”
Another concern is agreeing on a common alphabet. “Without that, this is not going to work,” he said. “All these vendor products grew up in silos, without standards imposed on them. So naturally, they’re going to have a Tower of Babel, which means most of them aren’t going to be speaking the same language.”
LAS VEGAS – Health care data interoperability should get a huge boost under a public-private effort announced Feb. 29 by U.S. Department of Health and Human Services Secretary Sylvia Burwell.
The nation’s top five health care systems and companies, which provide the electronic health record systems that cover more than 90% of U.S. hospital patients, have agreed to principles designed to improve patient access to health data and eliminate the practice of data blocking.
They also have agreed to adopt federally recognized, national interoperability standards, Ms. Burwell announced at the annual meeting of the Healthcare Information and Management Systems Society.
“Technology is not just one leg of our strategy to build a better health care system for our nation – it supports the entire effort,” Ms. Burwell said. “We are working to unlock health care data and information so that providers are better informed and patients and families can access their health care information, making them empowered, active participants in their own care.”
In a show of support, medical specialty societies including the American Academy of Family Physicians, the American College of Physicians, the American Society of Clinical Oncology, and the American Medical Association also signed on to the commitment.
“We have made tremendous progress to bring health care into the 21st century,” Ms. Burwell said. “In 6 short years, we have tripled the adoption of electronic health records. Today, three-quarters of physicians are using them. And nearly every hospital uses EHRs, meaning that there is now a digital care footprint for almost everyone in this country.”
To unlock all those data and make them useful to health care providers and patients, the health IT companies and health care systems have agreed to the following steps:
• Implement application programming interface (API) technology so that smartphone and tablet apps can be created, facilitating patient use and transfer of their health care data.
• Work so providers can share patient health care data with patients and other providers whenever permitted by law, while not blocking such sharing either intentionally or unintentionally.
• Use the federally recognized Fast Healthcare Interoperability Resources (FHIR) data standard.
This commitment is a “major step forward” to help patients “not just in one episode, but over the long term,” explained Dr. Karen DeSalvo, National Coordinator for Health Information Technology. The agreement means the health care system is “on the threshold of a truly historic opportunity to transform quality of care,” she added.
Federal officials have a timeline for progress toward these goals by 2018, Dr. DeSalvo noted. But “the private sector wants to pull that forward and be leaders with us,” she said. “So, our expectation is that the calls and the commitments and the associated actions that these developers have declared will be seeing some changes by the fall.”
To highlight health information technology’s promise, Ms. Burwell shared a story about electronic health records’ use to find children affected by lead pollution in the water supplies of Flint, Mich.
Alerted to the problem by a friend, pediatrician Mona Hanna-Attisha of Hurley Medical Center in Flint tried to determine whether pipe corrosion might leach dangerous levels of lead into the water supply, Ms. Burwell said.
“She knew the danger lead posed and began what she called a ‘crusade’ to find out if it was affecting children,” Ms. Burwell explained. Dr. Hanna-Attisha mined Hurley’s medical records to “compare blood test results from more than 700 children in the area and map home addresses for geographic variations.
“She quickly discovered that the percentage of children in Flint with lead poisoning had doubled, and even tripled, in some neighborhoods,” Burwell said.
If those results had still been on paper, “it would have taken forever to get these results,” she said.
“Dr. Hanna-Attisha’s story shows us the power of putting health care data to work,” Ms. Burwell noted. “It allows us to see the connections in our communities and helps us put patients in the center of their care.”
Dr. David Classen, chief information officer of the patient safety organization Pascal Metrics and an author of a 2011 Institute of Medicine report on health IT and patient safety, applauded the announcement and the commitment from major EHR vendors and hospital systems have signed on.
“That was one of the things [the IOM expert panel] envisioned – a public-private partnership that would really help this. That’s close to optimal in my view.”
But “the devil’s in the details,” said Dr. Classen, associate professor of medicine at the University of Utah. “When it comes to sharing safety information, it’s not just removal of the gag clauses, it’s also the confidentiality clauses, and the intellectual property protections. Those things too can inhibit sharing of safety information. The challenge here is that [EHR vendors] worry that if they’re so interoperable, they convert their proprietary technology into something that could virtually be open source...and everyone can look at it. Those are legitimate concerns.”
Another concern is agreeing on a common alphabet. “Without that, this is not going to work,” he said. “All these vendor products grew up in silos, without standards imposed on them. So naturally, they’re going to have a Tower of Babel, which means most of them aren’t going to be speaking the same language.”
LAS VEGAS – Health care data interoperability should get a huge boost under a public-private effort announced Feb. 29 by U.S. Department of Health and Human Services Secretary Sylvia Burwell.
The nation’s top five health care systems and companies, which provide the electronic health record systems that cover more than 90% of U.S. hospital patients, have agreed to principles designed to improve patient access to health data and eliminate the practice of data blocking.
They also have agreed to adopt federally recognized, national interoperability standards, Ms. Burwell announced at the annual meeting of the Healthcare Information and Management Systems Society.
“Technology is not just one leg of our strategy to build a better health care system for our nation – it supports the entire effort,” Ms. Burwell said. “We are working to unlock health care data and information so that providers are better informed and patients and families can access their health care information, making them empowered, active participants in their own care.”
In a show of support, medical specialty societies including the American Academy of Family Physicians, the American College of Physicians, the American Society of Clinical Oncology, and the American Medical Association also signed on to the commitment.
“We have made tremendous progress to bring health care into the 21st century,” Ms. Burwell said. “In 6 short years, we have tripled the adoption of electronic health records. Today, three-quarters of physicians are using them. And nearly every hospital uses EHRs, meaning that there is now a digital care footprint for almost everyone in this country.”
To unlock all those data and make them useful to health care providers and patients, the health IT companies and health care systems have agreed to the following steps:
• Implement application programming interface (API) technology so that smartphone and tablet apps can be created, facilitating patient use and transfer of their health care data.
• Work so providers can share patient health care data with patients and other providers whenever permitted by law, while not blocking such sharing either intentionally or unintentionally.
• Use the federally recognized Fast Healthcare Interoperability Resources (FHIR) data standard.
This commitment is a “major step forward” to help patients “not just in one episode, but over the long term,” explained Dr. Karen DeSalvo, National Coordinator for Health Information Technology. The agreement means the health care system is “on the threshold of a truly historic opportunity to transform quality of care,” she added.
Federal officials have a timeline for progress toward these goals by 2018, Dr. DeSalvo noted. But “the private sector wants to pull that forward and be leaders with us,” she said. “So, our expectation is that the calls and the commitments and the associated actions that these developers have declared will be seeing some changes by the fall.”
To highlight health information technology’s promise, Ms. Burwell shared a story about electronic health records’ use to find children affected by lead pollution in the water supplies of Flint, Mich.
Alerted to the problem by a friend, pediatrician Mona Hanna-Attisha of Hurley Medical Center in Flint tried to determine whether pipe corrosion might leach dangerous levels of lead into the water supply, Ms. Burwell said.
“She knew the danger lead posed and began what she called a ‘crusade’ to find out if it was affecting children,” Ms. Burwell explained. Dr. Hanna-Attisha mined Hurley’s medical records to “compare blood test results from more than 700 children in the area and map home addresses for geographic variations.
“She quickly discovered that the percentage of children in Flint with lead poisoning had doubled, and even tripled, in some neighborhoods,” Burwell said.
If those results had still been on paper, “it would have taken forever to get these results,” she said.
“Dr. Hanna-Attisha’s story shows us the power of putting health care data to work,” Ms. Burwell noted. “It allows us to see the connections in our communities and helps us put patients in the center of their care.”
Dr. David Classen, chief information officer of the patient safety organization Pascal Metrics and an author of a 2011 Institute of Medicine report on health IT and patient safety, applauded the announcement and the commitment from major EHR vendors and hospital systems have signed on.
“That was one of the things [the IOM expert panel] envisioned – a public-private partnership that would really help this. That’s close to optimal in my view.”
But “the devil’s in the details,” said Dr. Classen, associate professor of medicine at the University of Utah. “When it comes to sharing safety information, it’s not just removal of the gag clauses, it’s also the confidentiality clauses, and the intellectual property protections. Those things too can inhibit sharing of safety information. The challenge here is that [EHR vendors] worry that if they’re so interoperable, they convert their proprietary technology into something that could virtually be open source...and everyone can look at it. Those are legitimate concerns.”
Another concern is agreeing on a common alphabet. “Without that, this is not going to work,” he said. “All these vendor products grew up in silos, without standards imposed on them. So naturally, they’re going to have a Tower of Babel, which means most of them aren’t going to be speaking the same language.”
AT HIMSS16

Key Elements of Critical Care
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.

Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1

Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
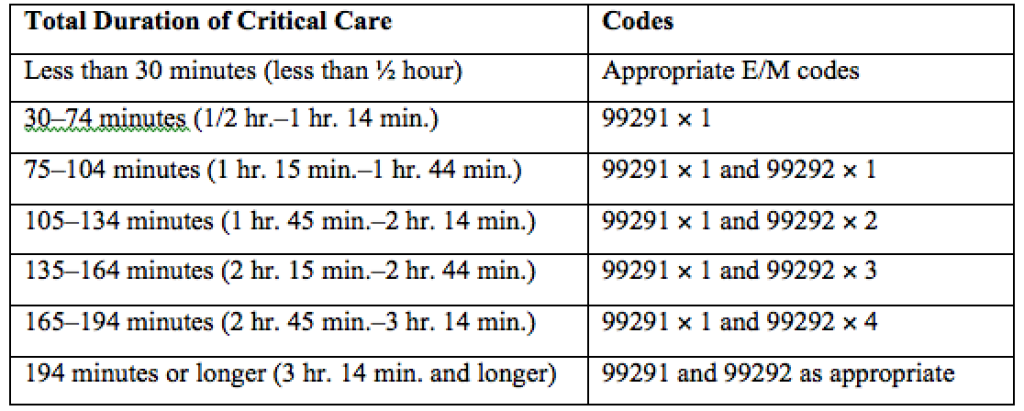
Medicare Grants Billing Code for Hospitalists
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
VIDEO: Beware legal land mines when working with PAs, NPs
AUSTIN, TEX. – As use of mid-level providers grows, legal risks for practices also can rise.
In this video interview at an American Health Lawyers Association conference, attorney Alex T. Krouse discusses common liability dangers that arise when working with physician assistants and nurse practitioners. Mr. Krouse also speaks about frequent billing errors that can happen within provider teams and breaks down the difference between physician supervision and physician collaboration.
On Twitter @legal_med
AUSTIN, TEX. – As use of mid-level providers grows, legal risks for practices also can rise.
In this video interview at an American Health Lawyers Association conference, attorney Alex T. Krouse discusses common liability dangers that arise when working with physician assistants and nurse practitioners. Mr. Krouse also speaks about frequent billing errors that can happen within provider teams and breaks down the difference between physician supervision and physician collaboration.
On Twitter @legal_med
AUSTIN, TEX. – As use of mid-level providers grows, legal risks for practices also can rise.
In this video interview at an American Health Lawyers Association conference, attorney Alex T. Krouse discusses common liability dangers that arise when working with physician assistants and nurse practitioners. Mr. Krouse also speaks about frequent billing errors that can happen within provider teams and breaks down the difference between physician supervision and physician collaboration.
On Twitter @legal_med
EXPERT ANALYSIS FROM THE PHYSICIANS & HOSPITALS LAW INSTITUTE

Marijuana tourists also visiting Colorado EDs
Out-of-state residents appear to be driving the recent increases in marijuana-related emergency department visits in Colorado, Dr. Howard S. Kim and his associates reported online Feb. 24 in the New England Journal of Medicine.
Using statewide data from the Colorado Hospital Association, they found that ED visits related to cannabis by out-of-state residents rose from 78 per 10,000 ED visits in 2012 to 163 per 10,000 in 2014, an increase of 109%. For Colorado residents, cannabis-related ED admissions over that same time period went up 44% – from 70 per 10,000 to 101, said Dr. Kim of Northwestern University, Chicago, and his associates (N Engl J Med. 2016 Feb 24;374[8]:797-8. doi:10.1056/NEJMc1515009).

The investigators also looked at a single urban academic hospital in Aurora, Colo., and found that cannabis-related ED visits there for out-of-state residents went from 85 per 10,000 visits in 2013 to 168 per 10,000 in 2014, compared with respective rates of 106 and 112 for Colorado residents.
“The flattening of the rates of ED visits possibly related to cannabis use among Colorado residents in an urban hospital may represent a learning curve during the period when marijuana was potentially available to Colorado residents for medical use (medical marijuana period) but was largely inaccessible to out-of-state residents,” they suggested.
Out-of-state residents appear to be driving the recent increases in marijuana-related emergency department visits in Colorado, Dr. Howard S. Kim and his associates reported online Feb. 24 in the New England Journal of Medicine.
Using statewide data from the Colorado Hospital Association, they found that ED visits related to cannabis by out-of-state residents rose from 78 per 10,000 ED visits in 2012 to 163 per 10,000 in 2014, an increase of 109%. For Colorado residents, cannabis-related ED admissions over that same time period went up 44% – from 70 per 10,000 to 101, said Dr. Kim of Northwestern University, Chicago, and his associates (N Engl J Med. 2016 Feb 24;374[8]:797-8. doi:10.1056/NEJMc1515009).
The investigators also looked at a single urban academic hospital in Aurora, Colo., and found that cannabis-related ED visits there for out-of-state residents went from 85 per 10,000 visits in 2013 to 168 per 10,000 in 2014, compared with respective rates of 106 and 112 for Colorado residents.
“The flattening of the rates of ED visits possibly related to cannabis use among Colorado residents in an urban hospital may represent a learning curve during the period when marijuana was potentially available to Colorado residents for medical use (medical marijuana period) but was largely inaccessible to out-of-state residents,” they suggested.
Out-of-state residents appear to be driving the recent increases in marijuana-related emergency department visits in Colorado, Dr. Howard S. Kim and his associates reported online Feb. 24 in the New England Journal of Medicine.
Using statewide data from the Colorado Hospital Association, they found that ED visits related to cannabis by out-of-state residents rose from 78 per 10,000 ED visits in 2012 to 163 per 10,000 in 2014, an increase of 109%. For Colorado residents, cannabis-related ED admissions over that same time period went up 44% – from 70 per 10,000 to 101, said Dr. Kim of Northwestern University, Chicago, and his associates (N Engl J Med. 2016 Feb 24;374[8]:797-8. doi:10.1056/NEJMc1515009).
The investigators also looked at a single urban academic hospital in Aurora, Colo., and found that cannabis-related ED visits there for out-of-state residents went from 85 per 10,000 visits in 2013 to 168 per 10,000 in 2014, compared with respective rates of 106 and 112 for Colorado residents.
“The flattening of the rates of ED visits possibly related to cannabis use among Colorado residents in an urban hospital may represent a learning curve during the period when marijuana was potentially available to Colorado residents for medical use (medical marijuana period) but was largely inaccessible to out-of-state residents,” they suggested.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
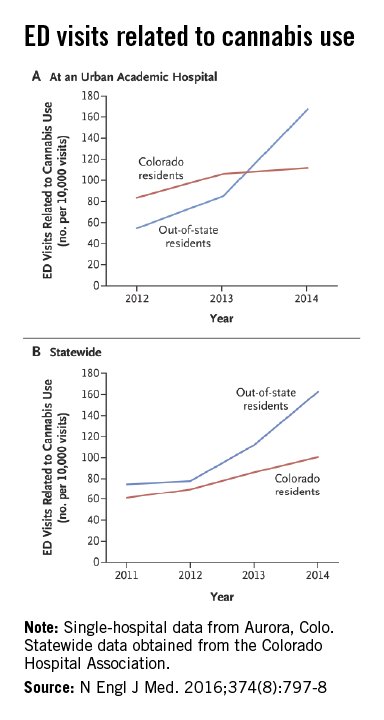
AMA’s Stack ‘cautiously optimistic’ about MACRA implementation
WASHINGTON – Coming regulations to implement the MACRA legislation also could include sweeping reforms to meaningful use and quality reporting programs, said Dr. Steven J. Stack, president of the American Medical Association.
Dr. Stack expressed “cautious optimism” that the regulations would help doctors to return to focusing on treating patients and away from meeting the myriad of regulatory requirements that have piled up in recent years.

The AMA has been working closely with the Centers for Medicare & Medicaid Services “very candidly and very constructively” and the agency has “demonstrated a willingness to reconsider things,” Dr. Stack said at the AMA National Advocacy Conference.
The regulations to implement MACRA (the Medicare Access and CHIP Reauthorization Act of 2015) “offers CMS an uncommonly robust opportunity to take things like [the Physician Quality Reporting System], meaningful use, value-based purchasing and reconceptualize, now that we have the opportunity under one rulemaking, to say how should all of these really work together,” Dr. Stack said.
Indeed, during a keynote address at the AMA conference, CMS Administrator Andy Slavitt said one of the goals for the agency this year was to simplify things for doctors.
“We must reduce burden and give physicians back more time to spend with patients,” Mr. Slavitt said. “Several years ago, we launched an initiative that is reducing regulatory burden and saving hospitals $3.2 billion over 5 years. But we are barely scratching the surface. We have a strategic effort this year designed to reduce burden and create efficiencies in the physician’s office.”
He hinted that the MACRA regulations would be used to redefine how health IT is utilized, noting the emphasis will be on rewarding outcomes that technology helps achieve, rather than simply incentivizing the use of it; providing more flexibility to meet physician needs; leveling the playing field to allow more competition from vendors; and to address ongoing interoperability issues.
The concern Dr. Stack addressed during the press meeting was the ongoing opioid epidemic, one of the few things he expects to see legislative action on during this presidential election year.
He called for thoughtful, comprehensive solutions to addressing the problem so that it allows patients with a true medical need for chronic pain management to be able to continue to have access to needed prescription pain medications. Arbitrary prescribing caps and other fixes that, on the surface, are simple and easy to implement, should be avoided, he said.
“Those kinds of approaches for this problem could have the really undesired consequences of rather than solving the problem,” Dr. Stack said, adding that they could drive even more people from prescription pills to heroin. That “causes deaths far more rapidly than the other stuff, which takes tens of millions of Americans with legitimate chronic pain who are legitimately suffering and throwing them into horrific life problems without access to care they need.”
As an adjunct to that, Dr. Stack also addressed drug pricing, using naloxone, which is used to help patients experiencing and opioid overdose, as something that has skyrocketed in price.
In looking at 5 years of drug prices in his state of Kentucky, naloxone has gone up from just over $4.50 a pill in 2010 to $38 a pill in 2015.
“If there is one thing that I will be absolutely clear on as a physician in the United States, this is not the time for the pharmaceutical industry to play games in the midst of an epidemic that taking over a quarter-million people’s lives over the documented course of this problem,” Dr. Stack said. “This is the time for the pharmaceutical industry to do its part and make sure that naloxone is as cheap as water from a tap so that patients in need can get the care they need and have this life-saving drug. This is not a profiteering opportunity for anyone.”
WASHINGTON – Coming regulations to implement the MACRA legislation also could include sweeping reforms to meaningful use and quality reporting programs, said Dr. Steven J. Stack, president of the American Medical Association.
Dr. Stack expressed “cautious optimism” that the regulations would help doctors to return to focusing on treating patients and away from meeting the myriad of regulatory requirements that have piled up in recent years.
The AMA has been working closely with the Centers for Medicare & Medicaid Services “very candidly and very constructively” and the agency has “demonstrated a willingness to reconsider things,” Dr. Stack said at the AMA National Advocacy Conference.
The regulations to implement MACRA (the Medicare Access and CHIP Reauthorization Act of 2015) “offers CMS an uncommonly robust opportunity to take things like [the Physician Quality Reporting System], meaningful use, value-based purchasing and reconceptualize, now that we have the opportunity under one rulemaking, to say how should all of these really work together,” Dr. Stack said.
Indeed, during a keynote address at the AMA conference, CMS Administrator Andy Slavitt said one of the goals for the agency this year was to simplify things for doctors.
“We must reduce burden and give physicians back more time to spend with patients,” Mr. Slavitt said. “Several years ago, we launched an initiative that is reducing regulatory burden and saving hospitals $3.2 billion over 5 years. But we are barely scratching the surface. We have a strategic effort this year designed to reduce burden and create efficiencies in the physician’s office.”
He hinted that the MACRA regulations would be used to redefine how health IT is utilized, noting the emphasis will be on rewarding outcomes that technology helps achieve, rather than simply incentivizing the use of it; providing more flexibility to meet physician needs; leveling the playing field to allow more competition from vendors; and to address ongoing interoperability issues.
The concern Dr. Stack addressed during the press meeting was the ongoing opioid epidemic, one of the few things he expects to see legislative action on during this presidential election year.
He called for thoughtful, comprehensive solutions to addressing the problem so that it allows patients with a true medical need for chronic pain management to be able to continue to have access to needed prescription pain medications. Arbitrary prescribing caps and other fixes that, on the surface, are simple and easy to implement, should be avoided, he said.
“Those kinds of approaches for this problem could have the really undesired consequences of rather than solving the problem,” Dr. Stack said, adding that they could drive even more people from prescription pills to heroin. That “causes deaths far more rapidly than the other stuff, which takes tens of millions of Americans with legitimate chronic pain who are legitimately suffering and throwing them into horrific life problems without access to care they need.”
As an adjunct to that, Dr. Stack also addressed drug pricing, using naloxone, which is used to help patients experiencing and opioid overdose, as something that has skyrocketed in price.
In looking at 5 years of drug prices in his state of Kentucky, naloxone has gone up from just over $4.50 a pill in 2010 to $38 a pill in 2015.
“If there is one thing that I will be absolutely clear on as a physician in the United States, this is not the time for the pharmaceutical industry to play games in the midst of an epidemic that taking over a quarter-million people’s lives over the documented course of this problem,” Dr. Stack said. “This is the time for the pharmaceutical industry to do its part and make sure that naloxone is as cheap as water from a tap so that patients in need can get the care they need and have this life-saving drug. This is not a profiteering opportunity for anyone.”
WASHINGTON – Coming regulations to implement the MACRA legislation also could include sweeping reforms to meaningful use and quality reporting programs, said Dr. Steven J. Stack, president of the American Medical Association.
Dr. Stack expressed “cautious optimism” that the regulations would help doctors to return to focusing on treating patients and away from meeting the myriad of regulatory requirements that have piled up in recent years.
The AMA has been working closely with the Centers for Medicare & Medicaid Services “very candidly and very constructively” and the agency has “demonstrated a willingness to reconsider things,” Dr. Stack said at the AMA National Advocacy Conference.
The regulations to implement MACRA (the Medicare Access and CHIP Reauthorization Act of 2015) “offers CMS an uncommonly robust opportunity to take things like [the Physician Quality Reporting System], meaningful use, value-based purchasing and reconceptualize, now that we have the opportunity under one rulemaking, to say how should all of these really work together,” Dr. Stack said.
Indeed, during a keynote address at the AMA conference, CMS Administrator Andy Slavitt said one of the goals for the agency this year was to simplify things for doctors.
“We must reduce burden and give physicians back more time to spend with patients,” Mr. Slavitt said. “Several years ago, we launched an initiative that is reducing regulatory burden and saving hospitals $3.2 billion over 5 years. But we are barely scratching the surface. We have a strategic effort this year designed to reduce burden and create efficiencies in the physician’s office.”
He hinted that the MACRA regulations would be used to redefine how health IT is utilized, noting the emphasis will be on rewarding outcomes that technology helps achieve, rather than simply incentivizing the use of it; providing more flexibility to meet physician needs; leveling the playing field to allow more competition from vendors; and to address ongoing interoperability issues.
The concern Dr. Stack addressed during the press meeting was the ongoing opioid epidemic, one of the few things he expects to see legislative action on during this presidential election year.
He called for thoughtful, comprehensive solutions to addressing the problem so that it allows patients with a true medical need for chronic pain management to be able to continue to have access to needed prescription pain medications. Arbitrary prescribing caps and other fixes that, on the surface, are simple and easy to implement, should be avoided, he said.
“Those kinds of approaches for this problem could have the really undesired consequences of rather than solving the problem,” Dr. Stack said, adding that they could drive even more people from prescription pills to heroin. That “causes deaths far more rapidly than the other stuff, which takes tens of millions of Americans with legitimate chronic pain who are legitimately suffering and throwing them into horrific life problems without access to care they need.”
As an adjunct to that, Dr. Stack also addressed drug pricing, using naloxone, which is used to help patients experiencing and opioid overdose, as something that has skyrocketed in price.
In looking at 5 years of drug prices in his state of Kentucky, naloxone has gone up from just over $4.50 a pill in 2010 to $38 a pill in 2015.
“If there is one thing that I will be absolutely clear on as a physician in the United States, this is not the time for the pharmaceutical industry to play games in the midst of an epidemic that taking over a quarter-million people’s lives over the documented course of this problem,” Dr. Stack said. “This is the time for the pharmaceutical industry to do its part and make sure that naloxone is as cheap as water from a tap so that patients in need can get the care they need and have this life-saving drug. This is not a profiteering opportunity for anyone.”
AT THE AMA NATIONAL ADVOCACY CONFERENCE

Dr. Robert Califf confirmed as FDA commissioner
Dr. Robert M. Califf was confirmed as Commissioner of the Food and Drug Administration by an 89-4 vote of the full Senate on Feb. 24.
Physician associations praised the Senate’s confirmation, calling Dr. Califf a strong voice in the cardiovascular community who will bring valuable perspective to the FDA role.

“Dr. Califf is an acclaimed leader in the cardiovascular community who brings impressive medical knowledge, clinical research experience and leadership capabilities to the FDA,” Dr. Kim Allan Williams Sr., American College of Cardiology president, said in a statement. “He has made important contributions to the field of medicine and has the vision required to lead the FDA in its efforts to promote and protect public health.”
Dr. Califf has served as FDA deputy commissioner for medical products and tobacco since February 2015. He is a former vice chancellor of clinical and translational research and professor of medicine in the division of cardiology at Duke University, Durham, N.C. He served as director of the Duke Translational Medicine Institute and founding director of the Duke Clinical Research Institute. Dr. Califf has led countless landmark clinical trials and is one of the most frequently cited authors in biomedical science, with more than 1,200 publications in the peer-reviewed literature, according to his biography on the FDA website.
The New England Journal of Medicine endorsed Dr. Califf’s nomination in an editorial published online in October 2015. They noted that Dr. Califf’s experience with clinical trials and drug data should be considered advantages to the FDA and would further the agency’s aim to improve drug safety (N Engl J Med. 2016 Jan 14; 374:176-7).
“Califf’s experience, his proven leadership abilities, his record of robust research to guide clinical practice, and his unwavering dedication to improving patient outcomes are unsurpassed qualifications for the post of commissioner of the FDA,” according to the editorial signed by Dr. Jeffrey M. Drazen, editor in chief.
Dr. Califf’s nomination was contested by legislators including Sen. Bernie Sanders (I-Vt.), who opposed Dr. Califf’s ties to the pharmaceutical industry. Dr. Califf is founding director of the Duke Clinical Research Institute, which has conducted extensive clinical trials for the drug industry. Dr. Califf, in the past, disclosed receiving consulting fees from pharmaceutical manufactures.

Sen. Joe Manchin (D-W.Va.) and Sen. Edward Markey (D-Mass.) also opposed the nomination. They, however, said they wished to block Dr. Califf’s nomination because they believe the FDA is failing to adequately regulate opioids entering the U.S. market. Sen. Manchin and Sen. Markey were joined by Sen. Kelly Ayotte (R-N.H.) and Sen. Richard Blumenthal (D-Conn.) in voting against Dr. Califf.
“The FDA is supposed to be our nation’s pharmacist, but right now, it is prescribing dangerous and addictive painkillers without limits, without supervision and without consequence,” Sen. Markey said in a Feb. 22 statement. “We need the leader of the FDA to be a tough cop on the beat, not a rubber stamp approving the latest Big Pharma painkillers that are the cause of this deadly scourge of opioid addiction and overdoses.”
On Feb. 4, Dr. Califf called for a sweeping overhaul of the FDA’s approach to opioid medications, including renewed efforts to improve how opioids are approved, labeled, and prescribed. Under the new plan, the FDA will convene an advisory committee before approving new drug applications for opioids that do not have abuse-deterrent properties and develop changes to immediate-release opioid labeling. The agency also plans to expand access to abuse-deterrent formulations of opioid products and improve the availability of naloxone and medication-assisted treatment options for patients with opioid use disorders.
“Things are getting worse, not better, with the epidemic of opioid misuse, abuse and dependence,” Dr. Califf said in a statement. “It’s time we all took a step back to look at what is working and what we need to change to impact this crisis.”

Just prior to the full Senate vote, Sen. Patty Murray (D-Wash.), ranking member of the Health, Education, Labor, and Pensions Committee, spoke in support of Dr. Califf’s nomination.
“After careful review, I believe Dr. Califf’s experience and expertise will allow him to lead the FDA in a way that puts patients and families first and upholds the highest standards of patient and consumer safety,” Sen. Murray said on the Senate floor. “Dr. Califf has led one of our country’s largest clinical research organizations and has a record of advancing medical breakthroughs on especially difficult-to-treat illnesses.”
Senators opposing Dr. Califf’s nomination attempted to filibuster the body’s consideration and vote on Dr. Califf’s nomination on Feb. 22. Their efforts were voted down 80-6.
On Twitter @legal_med
Dr. Robert M. Califf was confirmed as Commissioner of the Food and Drug Administration by an 89-4 vote of the full Senate on Feb. 24.
Physician associations praised the Senate’s confirmation, calling Dr. Califf a strong voice in the cardiovascular community who will bring valuable perspective to the FDA role.
“Dr. Califf is an acclaimed leader in the cardiovascular community who brings impressive medical knowledge, clinical research experience and leadership capabilities to the FDA,” Dr. Kim Allan Williams Sr., American College of Cardiology president, said in a statement. “He has made important contributions to the field of medicine and has the vision required to lead the FDA in its efforts to promote and protect public health.”
Dr. Califf has served as FDA deputy commissioner for medical products and tobacco since February 2015. He is a former vice chancellor of clinical and translational research and professor of medicine in the division of cardiology at Duke University, Durham, N.C. He served as director of the Duke Translational Medicine Institute and founding director of the Duke Clinical Research Institute. Dr. Califf has led countless landmark clinical trials and is one of the most frequently cited authors in biomedical science, with more than 1,200 publications in the peer-reviewed literature, according to his biography on the FDA website.
The New England Journal of Medicine endorsed Dr. Califf’s nomination in an editorial published online in October 2015. They noted that Dr. Califf’s experience with clinical trials and drug data should be considered advantages to the FDA and would further the agency’s aim to improve drug safety (N Engl J Med. 2016 Jan 14; 374:176-7).
“Califf’s experience, his proven leadership abilities, his record of robust research to guide clinical practice, and his unwavering dedication to improving patient outcomes are unsurpassed qualifications for the post of commissioner of the FDA,” according to the editorial signed by Dr. Jeffrey M. Drazen, editor in chief.
Dr. Califf’s nomination was contested by legislators including Sen. Bernie Sanders (I-Vt.), who opposed Dr. Califf’s ties to the pharmaceutical industry. Dr. Califf is founding director of the Duke Clinical Research Institute, which has conducted extensive clinical trials for the drug industry. Dr. Califf, in the past, disclosed receiving consulting fees from pharmaceutical manufactures.
Sen. Joe Manchin (D-W.Va.) and Sen. Edward Markey (D-Mass.) also opposed the nomination. They, however, said they wished to block Dr. Califf’s nomination because they believe the FDA is failing to adequately regulate opioids entering the U.S. market. Sen. Manchin and Sen. Markey were joined by Sen. Kelly Ayotte (R-N.H.) and Sen. Richard Blumenthal (D-Conn.) in voting against Dr. Califf.
“The FDA is supposed to be our nation’s pharmacist, but right now, it is prescribing dangerous and addictive painkillers without limits, without supervision and without consequence,” Sen. Markey said in a Feb. 22 statement. “We need the leader of the FDA to be a tough cop on the beat, not a rubber stamp approving the latest Big Pharma painkillers that are the cause of this deadly scourge of opioid addiction and overdoses.”
On Feb. 4, Dr. Califf called for a sweeping overhaul of the FDA’s approach to opioid medications, including renewed efforts to improve how opioids are approved, labeled, and prescribed. Under the new plan, the FDA will convene an advisory committee before approving new drug applications for opioids that do not have abuse-deterrent properties and develop changes to immediate-release opioid labeling. The agency also plans to expand access to abuse-deterrent formulations of opioid products and improve the availability of naloxone and medication-assisted treatment options for patients with opioid use disorders.
“Things are getting worse, not better, with the epidemic of opioid misuse, abuse and dependence,” Dr. Califf said in a statement. “It’s time we all took a step back to look at what is working and what we need to change to impact this crisis.”
Just prior to the full Senate vote, Sen. Patty Murray (D-Wash.), ranking member of the Health, Education, Labor, and Pensions Committee, spoke in support of Dr. Califf’s nomination.
“After careful review, I believe Dr. Califf’s experience and expertise will allow him to lead the FDA in a way that puts patients and families first and upholds the highest standards of patient and consumer safety,” Sen. Murray said on the Senate floor. “Dr. Califf has led one of our country’s largest clinical research organizations and has a record of advancing medical breakthroughs on especially difficult-to-treat illnesses.”
Senators opposing Dr. Califf’s nomination attempted to filibuster the body’s consideration and vote on Dr. Califf’s nomination on Feb. 22. Their efforts were voted down 80-6.
On Twitter @legal_med
Dr. Robert M. Califf was confirmed as Commissioner of the Food and Drug Administration by an 89-4 vote of the full Senate on Feb. 24.
Physician associations praised the Senate’s confirmation, calling Dr. Califf a strong voice in the cardiovascular community who will bring valuable perspective to the FDA role.
“Dr. Califf is an acclaimed leader in the cardiovascular community who brings impressive medical knowledge, clinical research experience and leadership capabilities to the FDA,” Dr. Kim Allan Williams Sr., American College of Cardiology president, said in a statement. “He has made important contributions to the field of medicine and has the vision required to lead the FDA in its efforts to promote and protect public health.”
Dr. Califf has served as FDA deputy commissioner for medical products and tobacco since February 2015. He is a former vice chancellor of clinical and translational research and professor of medicine in the division of cardiology at Duke University, Durham, N.C. He served as director of the Duke Translational Medicine Institute and founding director of the Duke Clinical Research Institute. Dr. Califf has led countless landmark clinical trials and is one of the most frequently cited authors in biomedical science, with more than 1,200 publications in the peer-reviewed literature, according to his biography on the FDA website.
The New England Journal of Medicine endorsed Dr. Califf’s nomination in an editorial published online in October 2015. They noted that Dr. Califf’s experience with clinical trials and drug data should be considered advantages to the FDA and would further the agency’s aim to improve drug safety (N Engl J Med. 2016 Jan 14; 374:176-7).
“Califf’s experience, his proven leadership abilities, his record of robust research to guide clinical practice, and his unwavering dedication to improving patient outcomes are unsurpassed qualifications for the post of commissioner of the FDA,” according to the editorial signed by Dr. Jeffrey M. Drazen, editor in chief.
Dr. Califf’s nomination was contested by legislators including Sen. Bernie Sanders (I-Vt.), who opposed Dr. Califf’s ties to the pharmaceutical industry. Dr. Califf is founding director of the Duke Clinical Research Institute, which has conducted extensive clinical trials for the drug industry. Dr. Califf, in the past, disclosed receiving consulting fees from pharmaceutical manufactures.
Sen. Joe Manchin (D-W.Va.) and Sen. Edward Markey (D-Mass.) also opposed the nomination. They, however, said they wished to block Dr. Califf’s nomination because they believe the FDA is failing to adequately regulate opioids entering the U.S. market. Sen. Manchin and Sen. Markey were joined by Sen. Kelly Ayotte (R-N.H.) and Sen. Richard Blumenthal (D-Conn.) in voting against Dr. Califf.
“The FDA is supposed to be our nation’s pharmacist, but right now, it is prescribing dangerous and addictive painkillers without limits, without supervision and without consequence,” Sen. Markey said in a Feb. 22 statement. “We need the leader of the FDA to be a tough cop on the beat, not a rubber stamp approving the latest Big Pharma painkillers that are the cause of this deadly scourge of opioid addiction and overdoses.”
On Feb. 4, Dr. Califf called for a sweeping overhaul of the FDA’s approach to opioid medications, including renewed efforts to improve how opioids are approved, labeled, and prescribed. Under the new plan, the FDA will convene an advisory committee before approving new drug applications for opioids that do not have abuse-deterrent properties and develop changes to immediate-release opioid labeling. The agency also plans to expand access to abuse-deterrent formulations of opioid products and improve the availability of naloxone and medication-assisted treatment options for patients with opioid use disorders.
“Things are getting worse, not better, with the epidemic of opioid misuse, abuse and dependence,” Dr. Califf said in a statement. “It’s time we all took a step back to look at what is working and what we need to change to impact this crisis.”
Just prior to the full Senate vote, Sen. Patty Murray (D-Wash.), ranking member of the Health, Education, Labor, and Pensions Committee, spoke in support of Dr. Califf’s nomination.
“After careful review, I believe Dr. Califf’s experience and expertise will allow him to lead the FDA in a way that puts patients and families first and upholds the highest standards of patient and consumer safety,” Sen. Murray said on the Senate floor. “Dr. Califf has led one of our country’s largest clinical research organizations and has a record of advancing medical breakthroughs on especially difficult-to-treat illnesses.”
Senators opposing Dr. Califf’s nomination attempted to filibuster the body’s consideration and vote on Dr. Califf’s nomination on Feb. 22. Their efforts were voted down 80-6.
On Twitter @legal_med
