User login
FDA Clears First Test to ID Bacteria Associated with Bloodstream Infections
Last month, the Food and Drug Administration cleared a test designed to quickly identify a dozen types of bacteria that can lead to bloodstream infections.
The Verigene GP Blood Culture Nucleic Acid Test, developed by molecular diagnostic firm Nanosphere Inc. of Northbrook, Ill., can identify Staphylococcus (including methicillin-resistant S. aureus, or MRSA), Streptococcus, Enterococcus (including vancomycin-resistant enterococci), and Listeria.
"The current standard of treatment is to provide broad-spectrum antibiotics, including some last-line therapies, such as vancomycin, in order to get coverage for everything," says Mike McGarrity, a Nanosphere executive. "With antibiotic stewardship programs in the majority of hospitals, there is an understanding of the overuse of these last-line therapies and the development of resistance."
Currently, blood cultures can take two to four days to identify certain types of bacteria and determine whether any present are resistant to certain therapies. Once a blood culture is positive, the Nanosphere test can identify bacteria and antimicrobial resistance genes in roughly two and half hours. In a pitch that McGarrity believes will resonate with HM groups, he positions the product as a cost-saver that can reduce length of stay (LOS) for hospitalized patients, as physicians don’t have to wait two days for test results. Quicker identification can also lead to lower mortality rates, he says.
McGarrity, who says Nanosphere will submit an application to the FDA this year for a similar rapid-results test for Clostridium difficile and a broad enteric panel, adds that the test is $75 per use. With LOS reduction and cost savings for targeted de-escalated therapies, he says, there is clear value in the test.
"This gets the attention of stakeholders," he says.
Last month, the Food and Drug Administration cleared a test designed to quickly identify a dozen types of bacteria that can lead to bloodstream infections.
The Verigene GP Blood Culture Nucleic Acid Test, developed by molecular diagnostic firm Nanosphere Inc. of Northbrook, Ill., can identify Staphylococcus (including methicillin-resistant S. aureus, or MRSA), Streptococcus, Enterococcus (including vancomycin-resistant enterococci), and Listeria.
"The current standard of treatment is to provide broad-spectrum antibiotics, including some last-line therapies, such as vancomycin, in order to get coverage for everything," says Mike McGarrity, a Nanosphere executive. "With antibiotic stewardship programs in the majority of hospitals, there is an understanding of the overuse of these last-line therapies and the development of resistance."
Currently, blood cultures can take two to four days to identify certain types of bacteria and determine whether any present are resistant to certain therapies. Once a blood culture is positive, the Nanosphere test can identify bacteria and antimicrobial resistance genes in roughly two and half hours. In a pitch that McGarrity believes will resonate with HM groups, he positions the product as a cost-saver that can reduce length of stay (LOS) for hospitalized patients, as physicians don’t have to wait two days for test results. Quicker identification can also lead to lower mortality rates, he says.
McGarrity, who says Nanosphere will submit an application to the FDA this year for a similar rapid-results test for Clostridium difficile and a broad enteric panel, adds that the test is $75 per use. With LOS reduction and cost savings for targeted de-escalated therapies, he says, there is clear value in the test.
"This gets the attention of stakeholders," he says.
Last month, the Food and Drug Administration cleared a test designed to quickly identify a dozen types of bacteria that can lead to bloodstream infections.
The Verigene GP Blood Culture Nucleic Acid Test, developed by molecular diagnostic firm Nanosphere Inc. of Northbrook, Ill., can identify Staphylococcus (including methicillin-resistant S. aureus, or MRSA), Streptococcus, Enterococcus (including vancomycin-resistant enterococci), and Listeria.
"The current standard of treatment is to provide broad-spectrum antibiotics, including some last-line therapies, such as vancomycin, in order to get coverage for everything," says Mike McGarrity, a Nanosphere executive. "With antibiotic stewardship programs in the majority of hospitals, there is an understanding of the overuse of these last-line therapies and the development of resistance."
Currently, blood cultures can take two to four days to identify certain types of bacteria and determine whether any present are resistant to certain therapies. Once a blood culture is positive, the Nanosphere test can identify bacteria and antimicrobial resistance genes in roughly two and half hours. In a pitch that McGarrity believes will resonate with HM groups, he positions the product as a cost-saver that can reduce length of stay (LOS) for hospitalized patients, as physicians don’t have to wait two days for test results. Quicker identification can also lead to lower mortality rates, he says.
McGarrity, who says Nanosphere will submit an application to the FDA this year for a similar rapid-results test for Clostridium difficile and a broad enteric panel, adds that the test is $75 per use. With LOS reduction and cost savings for targeted de-escalated therapies, he says, there is clear value in the test.
"This gets the attention of stakeholders," he says.
Tech Takes Off: Videoconferences in medical settings is more acceptable and affordable, but hurdles remain
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Hospitalists Should Prepare for the Patient-Centered Medical Home
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.

—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.
—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.
—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
Guidelines for Pneumonia Call for Decreased Use of Broad-Spectrum Antibiotics

Clinical question: What is the impact of a clinical practice guideline for hospitalized children with community-acquired pneumonia (CAP) on antibiotic selection?
Background: CAP is one of the most common reasons for hospitalizations in children. Broad-spectrum antibiotics frequently are prescribed for presumed bacterial pneumonia in children. Recent guidelines for CAP in children have emphasized that ampicillin is an appropriate empiric inpatient treatment option.
Study design: Retrospective review.
Setting: Tertiary referral children’s hospital.
Synopsis: Patients older than two months old with acute, uncomplicated CAP and without significant secondary illness were identified in the 12-month periods preceding and following the implementation of a clinical practice guideline (CPG) that recommended empiric treatment with ampicillin upon admission, and amoxicillin upon discharge.
A total of 1,033 patients were identified, 530 pre-CPG and 503 post-CPG, and the groups were similar. After the CPG, there was a significant increase in empiric ampicillin use (13% to 63%) and concomitant decrease in ceftriaxone use (72% to 21%). Rates of outpatient narrow-spectrum antibiotic prescribing increased as well, and the rate of treatment failure was similar between the groups.
Complex regression analysis was used to analyze the impact of a concomitant antibiotic stewardship program (ASP), implemented three months prior to the initiation of the CPG and demonstrating a separate and additive effect of both initiatives. Thus, changes in antibiotic prescribing were multifactorial over this time period.
The outcomes remain impressive in the context of two increasingly popular QI efforts—CPGs and ASPs. This study represents a meaningful contribution toward demonstration of outcomes-based quality improvement (QI).
Bottom line: In the context of a CPG, antibiotic spectrum may be safely narrowed in pediatric CAP.
Citation: Newman RE, Hedican EB, Herigon JC, Williams DD, Williams AR, Newland JG. Impact of a guideline on management of children hospitalized with community-acquired pneumonia. Pediatrics. 2012;129(3):e597-604.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the impact of a clinical practice guideline for hospitalized children with community-acquired pneumonia (CAP) on antibiotic selection?
Background: CAP is one of the most common reasons for hospitalizations in children. Broad-spectrum antibiotics frequently are prescribed for presumed bacterial pneumonia in children. Recent guidelines for CAP in children have emphasized that ampicillin is an appropriate empiric inpatient treatment option.
Study design: Retrospective review.
Setting: Tertiary referral children’s hospital.
Synopsis: Patients older than two months old with acute, uncomplicated CAP and without significant secondary illness were identified in the 12-month periods preceding and following the implementation of a clinical practice guideline (CPG) that recommended empiric treatment with ampicillin upon admission, and amoxicillin upon discharge.
A total of 1,033 patients were identified, 530 pre-CPG and 503 post-CPG, and the groups were similar. After the CPG, there was a significant increase in empiric ampicillin use (13% to 63%) and concomitant decrease in ceftriaxone use (72% to 21%). Rates of outpatient narrow-spectrum antibiotic prescribing increased as well, and the rate of treatment failure was similar between the groups.
Complex regression analysis was used to analyze the impact of a concomitant antibiotic stewardship program (ASP), implemented three months prior to the initiation of the CPG and demonstrating a separate and additive effect of both initiatives. Thus, changes in antibiotic prescribing were multifactorial over this time period.
The outcomes remain impressive in the context of two increasingly popular QI efforts—CPGs and ASPs. This study represents a meaningful contribution toward demonstration of outcomes-based quality improvement (QI).
Bottom line: In the context of a CPG, antibiotic spectrum may be safely narrowed in pediatric CAP.
Citation: Newman RE, Hedican EB, Herigon JC, Williams DD, Williams AR, Newland JG. Impact of a guideline on management of children hospitalized with community-acquired pneumonia. Pediatrics. 2012;129(3):e597-604.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the impact of a clinical practice guideline for hospitalized children with community-acquired pneumonia (CAP) on antibiotic selection?
Background: CAP is one of the most common reasons for hospitalizations in children. Broad-spectrum antibiotics frequently are prescribed for presumed bacterial pneumonia in children. Recent guidelines for CAP in children have emphasized that ampicillin is an appropriate empiric inpatient treatment option.
Study design: Retrospective review.
Setting: Tertiary referral children’s hospital.
Synopsis: Patients older than two months old with acute, uncomplicated CAP and without significant secondary illness were identified in the 12-month periods preceding and following the implementation of a clinical practice guideline (CPG) that recommended empiric treatment with ampicillin upon admission, and amoxicillin upon discharge.
A total of 1,033 patients were identified, 530 pre-CPG and 503 post-CPG, and the groups were similar. After the CPG, there was a significant increase in empiric ampicillin use (13% to 63%) and concomitant decrease in ceftriaxone use (72% to 21%). Rates of outpatient narrow-spectrum antibiotic prescribing increased as well, and the rate of treatment failure was similar between the groups.
Complex regression analysis was used to analyze the impact of a concomitant antibiotic stewardship program (ASP), implemented three months prior to the initiation of the CPG and demonstrating a separate and additive effect of both initiatives. Thus, changes in antibiotic prescribing were multifactorial over this time period.
The outcomes remain impressive in the context of two increasingly popular QI efforts—CPGs and ASPs. This study represents a meaningful contribution toward demonstration of outcomes-based quality improvement (QI).
Bottom line: In the context of a CPG, antibiotic spectrum may be safely narrowed in pediatric CAP.
Citation: Newman RE, Hedican EB, Herigon JC, Williams DD, Williams AR, Newland JG. Impact of a guideline on management of children hospitalized with community-acquired pneumonia. Pediatrics. 2012;129(3):e597-604.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Guidelines for Management of Atrial Fibrillation
Background
Atrial fibrillation (AF) is a common condition, affecting more than 2 million Americans.1 Hospital admissions due to AF have increased 66% in the past two decades. Hospitalization accounts for 52% of the cost of AF management, and the mortality rate of patients with this arrhythmia is twice that of patients in sinus rhythm.1
AF management decisions include choices for rate control, rhythm control, and prevention of thromboembolism. The benefits of a rhythm-control versus a rate-control strategy continue to be evaluated, along with consideration regarding an appropriate heart-rate goal. The modifiable risk factor of stroke in atrial fibrillation also continues to be a target for intervention as atrial fibrillation accounts for one-sixth of all strokes.
Guideline Update
The American College of Cardiology Foundation and American Heart Association (ACC/AHA), in conjunction with the European Society of Cardiology, released practice guidelines on the management of patients with atrial fibrillation in 2006. The ACCF/AHA, writing with the Heart Rhythm Society, released focused updates in early 2011 to be incorporated into the previous guidelines, given new data from major clinical trials and the FDA approval of new medications with indications for AF treatment.2,3
The new recommendations address components of all three major management decisions for AF: rate control, rhythm control, and prevention of thromboembolism.
When managing AF with a rate-control strategy, new guidelines no longer recommend the goal of a resting heart rate of <80 bpm or <115 bpm with activity. This is based on data from the RACE II trial that show no difference in meaningful outcomes with a more aggressive heart-rate goal. Achieving a resting heart rate of 110 bpm was deemed a reasonable approach, as long as the patient has stable ventricular function and acceptable symptoms.
The new drug dronedarone has been introduced in the algorithm for maintenance of sinus rhythm strategy, based on the DIONYSOS, ATHENA, and ANDROMEDA studies. The new algorithm excluded the use of dronedarone in patients with left ventricular hypertrophy, decompensated heart failure, or Class IV heart failure because it was shown to increase mortality in these groups. The guidelines also recommend that it should also be used with caution in patients with bradycardia, prolonged QT interval, increased creatinine, and in patients on agents that moderate CYP3A4 function.
The risks of interventions to decrease thromboembolism against bleeding risk continue to be evaluated in specified patient populations. Although dabigatran did not have FDA approval prior to submission of the 2011 updated guidelines, the 2011 “focused update” incorporated the results of the RE-LY trial. Publication of RE-LY resulted in a Class 1 recommendation for dabigatran as a useful alternative to warfarin in patients with nonvalvular AF without severe renal failure or advanced liver disease.3 However, there is no specific antidote, and dabigatran use is associated with higher rates of dyspepsia and a nonsignificant increase in rates of myocardial infarction. In patients for whom oral anticoagulation with warfarin is considered unsuitable, aspirin with clopidogrel may be considered, although warfarin therapy continues to be a superior therapy to this dual antiplatelet regimen based on the ACTIVE-W and ACTIVE-A studies.2
Established Guideline Analysis
Apart from the listed updates, the management of AF has not changed considerably in the past decade. Rate control continues to be the recommended strategy for older patients along with appropriate symptom control, particularly if they have hypertension or heart disease. Rhythm control is a frequent strategy in AF management, but several studies have not found any difference in quality of life, development or progression of heart failure, or stroke rates in patients for whom a rhythm-control strategy was chosen.
Additionally, these patients still require anticoagulation, and the side effects of anti-arrhythmic drugs might offset the benefits of sinus rhythm. Therefore, rate control is an appropriate strategy. The stroke rate and side-effect risks with anti-arrhythmics are considerably lower in younger patients or those with paroxysmal lone AF, and so a rhythm-control strategy in these groups is reasonable.
Stroke rate in AF increases with known high-risk factors (prior thromboembolism or rheumatic mitral stenosis) and moderate-risk factors (heart failure, hypertension, age over 75, and diabetes). Less validated risk factors include female gender, age 65-74, thyrotoxicosis, and the presence of coronary artery disease.
There are well-defined recommendations for how to anticoagulate specific subgroups that pose clinical challenges not directly addressed in studies, but the guidelines do assist with:
- Patients who have a stroke with a therapeutic INR: Rather than adding antiplatelet agents, INR goal can be raised to 3-3.5;
- Patients >75 years old who are at a high risk for bleeding: A target INR of 2.0 (target range 1.6-2.5) seems reasonable;1 and
- Patients with stable coronary artery disease and AF: Warfarin anticoagulation alone should provide satisfactory antithrombotic prophylaxis against cerebrovascular and coronary atheroembolic events.1
Decisions involving perioperative management of anticoagulation in patients with AF frequently arise. Per the guidelines, in patients with nonvalvular AF, anticoagulation can be stopped for up to one week without bridging for surgical or diagnostic procedures, but bridging should be considered in high-risk patients.
HM Takeaways
Hospitalists are likely to manage AF, whether alone or in conjunction with cardiology consultation. These new comprehensive guidelines deal with rate control, rhythm control, and prevention of thromboembolism. Hospitalists should take particular interest in the guidelines regarding lenient rate control, dronedarone for rhythm control, and dabigatran as a new alternative for anticoagulation in appropriate populations.
Drs. Farrell and Carbo are hospitalists at Beth Israel Deaconess Medical Center in Boston.
References
- Fuster V, Rydén LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011;57(11):e101-98.
- Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Heart Rhythm. 2011;8(1):157-76.
- Wann LS, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2011;57(11):1330-7.
Background
Atrial fibrillation (AF) is a common condition, affecting more than 2 million Americans.1 Hospital admissions due to AF have increased 66% in the past two decades. Hospitalization accounts for 52% of the cost of AF management, and the mortality rate of patients with this arrhythmia is twice that of patients in sinus rhythm.1
AF management decisions include choices for rate control, rhythm control, and prevention of thromboembolism. The benefits of a rhythm-control versus a rate-control strategy continue to be evaluated, along with consideration regarding an appropriate heart-rate goal. The modifiable risk factor of stroke in atrial fibrillation also continues to be a target for intervention as atrial fibrillation accounts for one-sixth of all strokes.
Guideline Update
The American College of Cardiology Foundation and American Heart Association (ACC/AHA), in conjunction with the European Society of Cardiology, released practice guidelines on the management of patients with atrial fibrillation in 2006. The ACCF/AHA, writing with the Heart Rhythm Society, released focused updates in early 2011 to be incorporated into the previous guidelines, given new data from major clinical trials and the FDA approval of new medications with indications for AF treatment.2,3
The new recommendations address components of all three major management decisions for AF: rate control, rhythm control, and prevention of thromboembolism.
When managing AF with a rate-control strategy, new guidelines no longer recommend the goal of a resting heart rate of <80 bpm or <115 bpm with activity. This is based on data from the RACE II trial that show no difference in meaningful outcomes with a more aggressive heart-rate goal. Achieving a resting heart rate of 110 bpm was deemed a reasonable approach, as long as the patient has stable ventricular function and acceptable symptoms.
The new drug dronedarone has been introduced in the algorithm for maintenance of sinus rhythm strategy, based on the DIONYSOS, ATHENA, and ANDROMEDA studies. The new algorithm excluded the use of dronedarone in patients with left ventricular hypertrophy, decompensated heart failure, or Class IV heart failure because it was shown to increase mortality in these groups. The guidelines also recommend that it should also be used with caution in patients with bradycardia, prolonged QT interval, increased creatinine, and in patients on agents that moderate CYP3A4 function.
The risks of interventions to decrease thromboembolism against bleeding risk continue to be evaluated in specified patient populations. Although dabigatran did not have FDA approval prior to submission of the 2011 updated guidelines, the 2011 “focused update” incorporated the results of the RE-LY trial. Publication of RE-LY resulted in a Class 1 recommendation for dabigatran as a useful alternative to warfarin in patients with nonvalvular AF without severe renal failure or advanced liver disease.3 However, there is no specific antidote, and dabigatran use is associated with higher rates of dyspepsia and a nonsignificant increase in rates of myocardial infarction. In patients for whom oral anticoagulation with warfarin is considered unsuitable, aspirin with clopidogrel may be considered, although warfarin therapy continues to be a superior therapy to this dual antiplatelet regimen based on the ACTIVE-W and ACTIVE-A studies.2
Established Guideline Analysis
Apart from the listed updates, the management of AF has not changed considerably in the past decade. Rate control continues to be the recommended strategy for older patients along with appropriate symptom control, particularly if they have hypertension or heart disease. Rhythm control is a frequent strategy in AF management, but several studies have not found any difference in quality of life, development or progression of heart failure, or stroke rates in patients for whom a rhythm-control strategy was chosen.
Additionally, these patients still require anticoagulation, and the side effects of anti-arrhythmic drugs might offset the benefits of sinus rhythm. Therefore, rate control is an appropriate strategy. The stroke rate and side-effect risks with anti-arrhythmics are considerably lower in younger patients or those with paroxysmal lone AF, and so a rhythm-control strategy in these groups is reasonable.
Stroke rate in AF increases with known high-risk factors (prior thromboembolism or rheumatic mitral stenosis) and moderate-risk factors (heart failure, hypertension, age over 75, and diabetes). Less validated risk factors include female gender, age 65-74, thyrotoxicosis, and the presence of coronary artery disease.
There are well-defined recommendations for how to anticoagulate specific subgroups that pose clinical challenges not directly addressed in studies, but the guidelines do assist with:
- Patients who have a stroke with a therapeutic INR: Rather than adding antiplatelet agents, INR goal can be raised to 3-3.5;
- Patients >75 years old who are at a high risk for bleeding: A target INR of 2.0 (target range 1.6-2.5) seems reasonable;1 and
- Patients with stable coronary artery disease and AF: Warfarin anticoagulation alone should provide satisfactory antithrombotic prophylaxis against cerebrovascular and coronary atheroembolic events.1
Decisions involving perioperative management of anticoagulation in patients with AF frequently arise. Per the guidelines, in patients with nonvalvular AF, anticoagulation can be stopped for up to one week without bridging for surgical or diagnostic procedures, but bridging should be considered in high-risk patients.
HM Takeaways
Hospitalists are likely to manage AF, whether alone or in conjunction with cardiology consultation. These new comprehensive guidelines deal with rate control, rhythm control, and prevention of thromboembolism. Hospitalists should take particular interest in the guidelines regarding lenient rate control, dronedarone for rhythm control, and dabigatran as a new alternative for anticoagulation in appropriate populations.
Drs. Farrell and Carbo are hospitalists at Beth Israel Deaconess Medical Center in Boston.
References
- Fuster V, Rydén LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011;57(11):e101-98.
- Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Heart Rhythm. 2011;8(1):157-76.
- Wann LS, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2011;57(11):1330-7.
Background
Atrial fibrillation (AF) is a common condition, affecting more than 2 million Americans.1 Hospital admissions due to AF have increased 66% in the past two decades. Hospitalization accounts for 52% of the cost of AF management, and the mortality rate of patients with this arrhythmia is twice that of patients in sinus rhythm.1
AF management decisions include choices for rate control, rhythm control, and prevention of thromboembolism. The benefits of a rhythm-control versus a rate-control strategy continue to be evaluated, along with consideration regarding an appropriate heart-rate goal. The modifiable risk factor of stroke in atrial fibrillation also continues to be a target for intervention as atrial fibrillation accounts for one-sixth of all strokes.
Guideline Update
The American College of Cardiology Foundation and American Heart Association (ACC/AHA), in conjunction with the European Society of Cardiology, released practice guidelines on the management of patients with atrial fibrillation in 2006. The ACCF/AHA, writing with the Heart Rhythm Society, released focused updates in early 2011 to be incorporated into the previous guidelines, given new data from major clinical trials and the FDA approval of new medications with indications for AF treatment.2,3
The new recommendations address components of all three major management decisions for AF: rate control, rhythm control, and prevention of thromboembolism.
When managing AF with a rate-control strategy, new guidelines no longer recommend the goal of a resting heart rate of <80 bpm or <115 bpm with activity. This is based on data from the RACE II trial that show no difference in meaningful outcomes with a more aggressive heart-rate goal. Achieving a resting heart rate of 110 bpm was deemed a reasonable approach, as long as the patient has stable ventricular function and acceptable symptoms.
The new drug dronedarone has been introduced in the algorithm for maintenance of sinus rhythm strategy, based on the DIONYSOS, ATHENA, and ANDROMEDA studies. The new algorithm excluded the use of dronedarone in patients with left ventricular hypertrophy, decompensated heart failure, or Class IV heart failure because it was shown to increase mortality in these groups. The guidelines also recommend that it should also be used with caution in patients with bradycardia, prolonged QT interval, increased creatinine, and in patients on agents that moderate CYP3A4 function.
The risks of interventions to decrease thromboembolism against bleeding risk continue to be evaluated in specified patient populations. Although dabigatran did not have FDA approval prior to submission of the 2011 updated guidelines, the 2011 “focused update” incorporated the results of the RE-LY trial. Publication of RE-LY resulted in a Class 1 recommendation for dabigatran as a useful alternative to warfarin in patients with nonvalvular AF without severe renal failure or advanced liver disease.3 However, there is no specific antidote, and dabigatran use is associated with higher rates of dyspepsia and a nonsignificant increase in rates of myocardial infarction. In patients for whom oral anticoagulation with warfarin is considered unsuitable, aspirin with clopidogrel may be considered, although warfarin therapy continues to be a superior therapy to this dual antiplatelet regimen based on the ACTIVE-W and ACTIVE-A studies.2
Established Guideline Analysis
Apart from the listed updates, the management of AF has not changed considerably in the past decade. Rate control continues to be the recommended strategy for older patients along with appropriate symptom control, particularly if they have hypertension or heart disease. Rhythm control is a frequent strategy in AF management, but several studies have not found any difference in quality of life, development or progression of heart failure, or stroke rates in patients for whom a rhythm-control strategy was chosen.
Additionally, these patients still require anticoagulation, and the side effects of anti-arrhythmic drugs might offset the benefits of sinus rhythm. Therefore, rate control is an appropriate strategy. The stroke rate and side-effect risks with anti-arrhythmics are considerably lower in younger patients or those with paroxysmal lone AF, and so a rhythm-control strategy in these groups is reasonable.
Stroke rate in AF increases with known high-risk factors (prior thromboembolism or rheumatic mitral stenosis) and moderate-risk factors (heart failure, hypertension, age over 75, and diabetes). Less validated risk factors include female gender, age 65-74, thyrotoxicosis, and the presence of coronary artery disease.
There are well-defined recommendations for how to anticoagulate specific subgroups that pose clinical challenges not directly addressed in studies, but the guidelines do assist with:
- Patients who have a stroke with a therapeutic INR: Rather than adding antiplatelet agents, INR goal can be raised to 3-3.5;
- Patients >75 years old who are at a high risk for bleeding: A target INR of 2.0 (target range 1.6-2.5) seems reasonable;1 and
- Patients with stable coronary artery disease and AF: Warfarin anticoagulation alone should provide satisfactory antithrombotic prophylaxis against cerebrovascular and coronary atheroembolic events.1
Decisions involving perioperative management of anticoagulation in patients with AF frequently arise. Per the guidelines, in patients with nonvalvular AF, anticoagulation can be stopped for up to one week without bridging for surgical or diagnostic procedures, but bridging should be considered in high-risk patients.
HM Takeaways
Hospitalists are likely to manage AF, whether alone or in conjunction with cardiology consultation. These new comprehensive guidelines deal with rate control, rhythm control, and prevention of thromboembolism. Hospitalists should take particular interest in the guidelines regarding lenient rate control, dronedarone for rhythm control, and dabigatran as a new alternative for anticoagulation in appropriate populations.
Drs. Farrell and Carbo are hospitalists at Beth Israel Deaconess Medical Center in Boston.
References
- Fuster V, Rydén LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011;57(11):e101-98.
- Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Heart Rhythm. 2011;8(1):157-76.
- Wann LS, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2011;57(11):1330-7.
Interns Learn Ultrasound-Guided Procedures
Internal medicine (IM) interns at the University of Texas Health Sciences Center in San Antonio are learning how to perform ultrasound-guided procedures (e.g. thoracentesis, paracentesis, lumbar puncture), gaining confidence in procedural skills that they can then take into residency and beyond,
according to an innovation poster presented at HM12.1 The procedure service, which is a monthlong, mandatory rotation for IM interns, had its origins in funds allocated for an additional chief resident position that focused on quality and patient safety and the championing of procedures by one of the program’s directors, says David Schmit, MD, a chief resident and the abstract’s lead author.
Three chief residents, who lead the service, developed and teach its structured curriculum, which includes an instructional video, didactic presentations on indications, contraindications, risks and benefits, practice on a simulator, and instruction in obtaining appropriate consents from patients. Trainees perform each procedure under the chief residents’ supervision and complete competency checklists. Many participants complete the required five supervised procedures while still interns. “We since opened the service to second-year residents” so they can go back and master its curriculum, Dr. Schmit says.
Results in the first seven months of the service included 342 procedures performed by medical trainees, with 100% success for paracentesis and thoracentesis; slightly lower rates were seen for lumbar puncture. The rate of pneumothorax resulting from procedures declined to 4% from 12.5%, and the overall complication rate was 2.6%. Equally important, Dr. Schmit says, were 85 requests for procedures that were not performed because trainees recognized contraindications or safety considerations.
Reference
Internal medicine (IM) interns at the University of Texas Health Sciences Center in San Antonio are learning how to perform ultrasound-guided procedures (e.g. thoracentesis, paracentesis, lumbar puncture), gaining confidence in procedural skills that they can then take into residency and beyond,
according to an innovation poster presented at HM12.1 The procedure service, which is a monthlong, mandatory rotation for IM interns, had its origins in funds allocated for an additional chief resident position that focused on quality and patient safety and the championing of procedures by one of the program’s directors, says David Schmit, MD, a chief resident and the abstract’s lead author.
Three chief residents, who lead the service, developed and teach its structured curriculum, which includes an instructional video, didactic presentations on indications, contraindications, risks and benefits, practice on a simulator, and instruction in obtaining appropriate consents from patients. Trainees perform each procedure under the chief residents’ supervision and complete competency checklists. Many participants complete the required five supervised procedures while still interns. “We since opened the service to second-year residents” so they can go back and master its curriculum, Dr. Schmit says.
Results in the first seven months of the service included 342 procedures performed by medical trainees, with 100% success for paracentesis and thoracentesis; slightly lower rates were seen for lumbar puncture. The rate of pneumothorax resulting from procedures declined to 4% from 12.5%, and the overall complication rate was 2.6%. Equally important, Dr. Schmit says, were 85 requests for procedures that were not performed because trainees recognized contraindications or safety considerations.
Reference
Internal medicine (IM) interns at the University of Texas Health Sciences Center in San Antonio are learning how to perform ultrasound-guided procedures (e.g. thoracentesis, paracentesis, lumbar puncture), gaining confidence in procedural skills that they can then take into residency and beyond,
according to an innovation poster presented at HM12.1 The procedure service, which is a monthlong, mandatory rotation for IM interns, had its origins in funds allocated for an additional chief resident position that focused on quality and patient safety and the championing of procedures by one of the program’s directors, says David Schmit, MD, a chief resident and the abstract’s lead author.
Three chief residents, who lead the service, developed and teach its structured curriculum, which includes an instructional video, didactic presentations on indications, contraindications, risks and benefits, practice on a simulator, and instruction in obtaining appropriate consents from patients. Trainees perform each procedure under the chief residents’ supervision and complete competency checklists. Many participants complete the required five supervised procedures while still interns. “We since opened the service to second-year residents” so they can go back and master its curriculum, Dr. Schmit says.
Results in the first seven months of the service included 342 procedures performed by medical trainees, with 100% success for paracentesis and thoracentesis; slightly lower rates were seen for lumbar puncture. The rate of pneumothorax resulting from procedures declined to 4% from 12.5%, and the overall complication rate was 2.6%. Equally important, Dr. Schmit says, were 85 requests for procedures that were not performed because trainees recognized contraindications or safety considerations.
Reference
Guidelines Urge Transfer of Subarachnoid Hemorrhage Patients
The new “Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage,” published online May 3 in Stroke, call for hospitals treating fewer than 10 aneurysmal subarachnoid hemorrhage (aSAH) cases per year to consider their immediate transfer to facilities that handle at least 35 such cases annually.1 The recommendation is based on research suggesting that 30-day death rates were significantly higher in low-volume facilities (39%) vs. facilities treating more than 35 cases per year (27%), reflecting the latter’s greater access to cerebrovascular surgeons, endovascular specialists, and neuro-intensive-care services.
This type of hemorrhage accounts for 5% of all strokes and affects more than 30,000 Americans annually.
Reference
The new “Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage,” published online May 3 in Stroke, call for hospitals treating fewer than 10 aneurysmal subarachnoid hemorrhage (aSAH) cases per year to consider their immediate transfer to facilities that handle at least 35 such cases annually.1 The recommendation is based on research suggesting that 30-day death rates were significantly higher in low-volume facilities (39%) vs. facilities treating more than 35 cases per year (27%), reflecting the latter’s greater access to cerebrovascular surgeons, endovascular specialists, and neuro-intensive-care services.
This type of hemorrhage accounts for 5% of all strokes and affects more than 30,000 Americans annually.
Reference
The new “Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage,” published online May 3 in Stroke, call for hospitals treating fewer than 10 aneurysmal subarachnoid hemorrhage (aSAH) cases per year to consider their immediate transfer to facilities that handle at least 35 such cases annually.1 The recommendation is based on research suggesting that 30-day death rates were significantly higher in low-volume facilities (39%) vs. facilities treating more than 35 cases per year (27%), reflecting the latter’s greater access to cerebrovascular surgeons, endovascular specialists, and neuro-intensive-care services.
This type of hemorrhage accounts for 5% of all strokes and affects more than 30,000 Americans annually.
Reference
Win Whitcomb: Staying ... and Paying

Take a minute to recall your last credit-card statement. On it, say, is the hotel charge from your last out-of-town CME excursion. Below the total charge you were expecting is a separate line-item charge of $75 for a “recreational fee.” Puzzled, you call the hotel. They inform you that because you used the gym and pool—accessed with your room key—they levied the fee. No signs, alerts, or postings to denote such a policy, you innocently expected inclusive use of the facilities in the price of your visit.
Capture the emotion of that moment. It is likely your heart will race and you will think to yourself, “Get me the manager!”
Out of vigilance for penalties and fraud from recovery audit contractor (RAC) investigations, as well attentiveness to unnecessary readmissions, hospitals increasingly are categorizing Medicare patients under observation, rather than inpatient, status. This is to avoid conflict with regulators. Beneficiaries are in the crosshairs because of this designation change and, much in the same way as with our hotel charge, they also experience sticker shock when they get their bills. It is leading to confusion among providers, and consternation within the Medicare recipient community.
Why is this occurring? The dilemma stems from Medicare payments and the key distinction between inpatient coverage (Part A) and outpatient coverage (Parts B and D). When a patient receives their discharge notification—without an “official” inpatient designation—sometimes staying greater than 24 to 48 hours in the ED or in a specially defined observation unit can mean that beneficiary charges are different. This could result in discrete and sometimes jolting copayments and deductibles for drugs and services.
Worse, if beneficiaries require a skilled nursing facility stay (the “three-day stay” inpatient requirement), Medicare will not pay because they never registered “official” hospital time. Patients and caregivers are not prepared for the unexpected bills, and, consequently, tempers are rising.
The rules for Medicare Advantage enrollees, who make up 25% of the program, differ from conventional Medicare. However, commercial plans often shadow traditional fee-for-service in their policies, and, consequently, no exemplar of success in this realm exits.
Hospitals have increased both the number of their observation stays, as well as their hourly lengths (>48 hours). Because the definition of “observation status” is vague, and even the one- to two-day window is inflating, hospitals and hospitalists are often left to navigate without a compass. Again, fear of fraud and penalties places hospitals—and, indirectly, hospitalists, who often make judgments on admission grade—in a precarious position.
The responsibility of hospitals to notify beneficiaries of their status hinges on this murky determination milieu, which might change in real time during the stay and makes for an unsatisfactory standard. Understandably, CMS is attempting to rectify this quandary, taking into account a hospital’s need to clarify its billing and designation practices as well as beneficiaries’ desire to obtain clear guidance on their responsibilities both during and after a stay.
Hospitalists, of course, want direction on coding and an understanding of the impact their decisions will have on patients and subspecialty colleagues. To that end, Patrick Conway, MD, SFHM, chief medical officer for the Centers for Medicare & Medicaid (CMS), offers some enlightenment on this matter:
Q: Is it tenable to keep the current system in place? However, as a fix, require payors and providers to inform beneficiaries of inpatient versus observation status at time zero in a more rigorous, yet-to-be determined manner?
A: Current regulations only require CMS to inform beneficiaries when they are admitted as an inpatient and not when they are an outpatient receiving observation services. There are important implications for coverage for beneficiaries post-hospital stay, coverage of self-administered drugs, and beneficiary coinsurance from this distinction. As a hospitalist, I think it is best to inform the patient of their status, especially if it has the potential to impact beneficiary liability, including coverage of post-acute care. CMS prepared a pamphlet in 2009, “Are You a Hospital Inpatient or Outpatient? If You Have Medicare, Ask!” to educate beneficiaries on this issue. The pamphlet can found at http://www.medicare.gov/Publications/Pubs/pdf/11435.pdf.
Q: Due to the nature of how hospital care is changing, are admission decisions potentially becoming too conflicted an endeavor for inpatient caregivers?
A: We want admission decisions to be based on clinical considerations. The decision to admit a patient should be based on the clinical judgment of the primary care, emergency medicine, and/or hospital medicine clinician.
Q: Before the U.S. healthcare system matures to a more integrated model with internalized risk, can you envision any near-term code changes that might simplify the difficulties all parties are facing, in a budget-neutral fashion?
A: CMS is currently investigating options to clarify when it is appropriate to admit the patient as an inpatient versus keeping the patient as an outpatient receiving observation services. We understand that this issue is of concern to hospitals, hospitalists, and patients, and we are considering carefully how to simplify the rules in a way that best meets the needs of patients and providers without increasing costs to the system.
I expect we will hear more from Medicare in the near-term on this matter. Stay tuned.
For more about the patient’s perspective on this issue, please see Brad’s blog: www.hospitalmedicine.org/pmblog.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Take a minute to recall your last credit-card statement. On it, say, is the hotel charge from your last out-of-town CME excursion. Below the total charge you were expecting is a separate line-item charge of $75 for a “recreational fee.” Puzzled, you call the hotel. They inform you that because you used the gym and pool—accessed with your room key—they levied the fee. No signs, alerts, or postings to denote such a policy, you innocently expected inclusive use of the facilities in the price of your visit.
Capture the emotion of that moment. It is likely your heart will race and you will think to yourself, “Get me the manager!”
Out of vigilance for penalties and fraud from recovery audit contractor (RAC) investigations, as well attentiveness to unnecessary readmissions, hospitals increasingly are categorizing Medicare patients under observation, rather than inpatient, status. This is to avoid conflict with regulators. Beneficiaries are in the crosshairs because of this designation change and, much in the same way as with our hotel charge, they also experience sticker shock when they get their bills. It is leading to confusion among providers, and consternation within the Medicare recipient community.
Why is this occurring? The dilemma stems from Medicare payments and the key distinction between inpatient coverage (Part A) and outpatient coverage (Parts B and D). When a patient receives their discharge notification—without an “official” inpatient designation—sometimes staying greater than 24 to 48 hours in the ED or in a specially defined observation unit can mean that beneficiary charges are different. This could result in discrete and sometimes jolting copayments and deductibles for drugs and services.
Worse, if beneficiaries require a skilled nursing facility stay (the “three-day stay” inpatient requirement), Medicare will not pay because they never registered “official” hospital time. Patients and caregivers are not prepared for the unexpected bills, and, consequently, tempers are rising.
The rules for Medicare Advantage enrollees, who make up 25% of the program, differ from conventional Medicare. However, commercial plans often shadow traditional fee-for-service in their policies, and, consequently, no exemplar of success in this realm exits.
Hospitals have increased both the number of their observation stays, as well as their hourly lengths (>48 hours). Because the definition of “observation status” is vague, and even the one- to two-day window is inflating, hospitals and hospitalists are often left to navigate without a compass. Again, fear of fraud and penalties places hospitals—and, indirectly, hospitalists, who often make judgments on admission grade—in a precarious position.
The responsibility of hospitals to notify beneficiaries of their status hinges on this murky determination milieu, which might change in real time during the stay and makes for an unsatisfactory standard. Understandably, CMS is attempting to rectify this quandary, taking into account a hospital’s need to clarify its billing and designation practices as well as beneficiaries’ desire to obtain clear guidance on their responsibilities both during and after a stay.
Hospitalists, of course, want direction on coding and an understanding of the impact their decisions will have on patients and subspecialty colleagues. To that end, Patrick Conway, MD, SFHM, chief medical officer for the Centers for Medicare & Medicaid (CMS), offers some enlightenment on this matter:
Q: Is it tenable to keep the current system in place? However, as a fix, require payors and providers to inform beneficiaries of inpatient versus observation status at time zero in a more rigorous, yet-to-be determined manner?
A: Current regulations only require CMS to inform beneficiaries when they are admitted as an inpatient and not when they are an outpatient receiving observation services. There are important implications for coverage for beneficiaries post-hospital stay, coverage of self-administered drugs, and beneficiary coinsurance from this distinction. As a hospitalist, I think it is best to inform the patient of their status, especially if it has the potential to impact beneficiary liability, including coverage of post-acute care. CMS prepared a pamphlet in 2009, “Are You a Hospital Inpatient or Outpatient? If You Have Medicare, Ask!” to educate beneficiaries on this issue. The pamphlet can found at http://www.medicare.gov/Publications/Pubs/pdf/11435.pdf.
Q: Due to the nature of how hospital care is changing, are admission decisions potentially becoming too conflicted an endeavor for inpatient caregivers?
A: We want admission decisions to be based on clinical considerations. The decision to admit a patient should be based on the clinical judgment of the primary care, emergency medicine, and/or hospital medicine clinician.
Q: Before the U.S. healthcare system matures to a more integrated model with internalized risk, can you envision any near-term code changes that might simplify the difficulties all parties are facing, in a budget-neutral fashion?
A: CMS is currently investigating options to clarify when it is appropriate to admit the patient as an inpatient versus keeping the patient as an outpatient receiving observation services. We understand that this issue is of concern to hospitals, hospitalists, and patients, and we are considering carefully how to simplify the rules in a way that best meets the needs of patients and providers without increasing costs to the system.
I expect we will hear more from Medicare in the near-term on this matter. Stay tuned.
For more about the patient’s perspective on this issue, please see Brad’s blog: www.hospitalmedicine.org/pmblog.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Take a minute to recall your last credit-card statement. On it, say, is the hotel charge from your last out-of-town CME excursion. Below the total charge you were expecting is a separate line-item charge of $75 for a “recreational fee.” Puzzled, you call the hotel. They inform you that because you used the gym and pool—accessed with your room key—they levied the fee. No signs, alerts, or postings to denote such a policy, you innocently expected inclusive use of the facilities in the price of your visit.
Capture the emotion of that moment. It is likely your heart will race and you will think to yourself, “Get me the manager!”
Out of vigilance for penalties and fraud from recovery audit contractor (RAC) investigations, as well attentiveness to unnecessary readmissions, hospitals increasingly are categorizing Medicare patients under observation, rather than inpatient, status. This is to avoid conflict with regulators. Beneficiaries are in the crosshairs because of this designation change and, much in the same way as with our hotel charge, they also experience sticker shock when they get their bills. It is leading to confusion among providers, and consternation within the Medicare recipient community.
Why is this occurring? The dilemma stems from Medicare payments and the key distinction between inpatient coverage (Part A) and outpatient coverage (Parts B and D). When a patient receives their discharge notification—without an “official” inpatient designation—sometimes staying greater than 24 to 48 hours in the ED or in a specially defined observation unit can mean that beneficiary charges are different. This could result in discrete and sometimes jolting copayments and deductibles for drugs and services.
Worse, if beneficiaries require a skilled nursing facility stay (the “three-day stay” inpatient requirement), Medicare will not pay because they never registered “official” hospital time. Patients and caregivers are not prepared for the unexpected bills, and, consequently, tempers are rising.
The rules for Medicare Advantage enrollees, who make up 25% of the program, differ from conventional Medicare. However, commercial plans often shadow traditional fee-for-service in their policies, and, consequently, no exemplar of success in this realm exits.
Hospitals have increased both the number of their observation stays, as well as their hourly lengths (>48 hours). Because the definition of “observation status” is vague, and even the one- to two-day window is inflating, hospitals and hospitalists are often left to navigate without a compass. Again, fear of fraud and penalties places hospitals—and, indirectly, hospitalists, who often make judgments on admission grade—in a precarious position.
The responsibility of hospitals to notify beneficiaries of their status hinges on this murky determination milieu, which might change in real time during the stay and makes for an unsatisfactory standard. Understandably, CMS is attempting to rectify this quandary, taking into account a hospital’s need to clarify its billing and designation practices as well as beneficiaries’ desire to obtain clear guidance on their responsibilities both during and after a stay.
Hospitalists, of course, want direction on coding and an understanding of the impact their decisions will have on patients and subspecialty colleagues. To that end, Patrick Conway, MD, SFHM, chief medical officer for the Centers for Medicare & Medicaid (CMS), offers some enlightenment on this matter:
Q: Is it tenable to keep the current system in place? However, as a fix, require payors and providers to inform beneficiaries of inpatient versus observation status at time zero in a more rigorous, yet-to-be determined manner?
A: Current regulations only require CMS to inform beneficiaries when they are admitted as an inpatient and not when they are an outpatient receiving observation services. There are important implications for coverage for beneficiaries post-hospital stay, coverage of self-administered drugs, and beneficiary coinsurance from this distinction. As a hospitalist, I think it is best to inform the patient of their status, especially if it has the potential to impact beneficiary liability, including coverage of post-acute care. CMS prepared a pamphlet in 2009, “Are You a Hospital Inpatient or Outpatient? If You Have Medicare, Ask!” to educate beneficiaries on this issue. The pamphlet can found at http://www.medicare.gov/Publications/Pubs/pdf/11435.pdf.
Q: Due to the nature of how hospital care is changing, are admission decisions potentially becoming too conflicted an endeavor for inpatient caregivers?
A: We want admission decisions to be based on clinical considerations. The decision to admit a patient should be based on the clinical judgment of the primary care, emergency medicine, and/or hospital medicine clinician.
Q: Before the U.S. healthcare system matures to a more integrated model with internalized risk, can you envision any near-term code changes that might simplify the difficulties all parties are facing, in a budget-neutral fashion?
A: CMS is currently investigating options to clarify when it is appropriate to admit the patient as an inpatient versus keeping the patient as an outpatient receiving observation services. We understand that this issue is of concern to hospitals, hospitalists, and patients, and we are considering carefully how to simplify the rules in a way that best meets the needs of patients and providers without increasing costs to the system.
I expect we will hear more from Medicare in the near-term on this matter. Stay tuned.
For more about the patient’s perspective on this issue, please see Brad’s blog: www.hospitalmedicine.org/pmblog.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Unit-Based Rounding: A Holy Grail?

The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
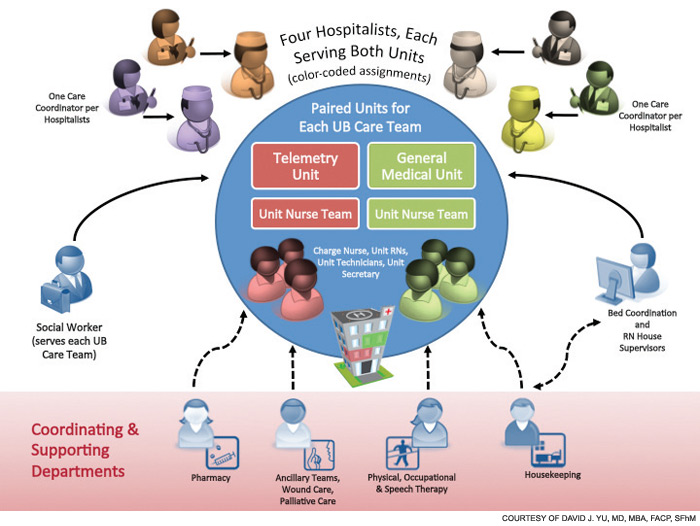
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.

Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The Patient-Centered Medical Home: A Primer
The term “patient-centered medical home” has a nice ring to it, but what does it really mean? And how does it function in the real world? The model is evolving, but here are the main components of the PCMH and how they’ve been implemented in real practice, at least so far:
“PERSONAL” PHYSICIAN: This is the doctor, usually a family or general practice physician, who shepherds patients through the medical system. In practice, this means things like encouraging patient questions about their care, extra efforts to educate patients on their health, and nurses making detailed follow-up calls with patients to make sure they’ve gotten their medications and know how to take them, and communicating any other steps the patient should be taking.
“Whole-person orientation”: The personal physician is responsible for taking care of all of the patient’s medical needs, either himself or by arranging care with specialists. The care ranges from preventive to chronic to end-of-life. In practice, this often means having appointments made with another doctor, if necessary, before the patient leaves the primary-care doctor, or seeing several doctors of different specialties during the same appointment.
Coordinated or integrated care: Care in the PCMH spans all aspects of the healthcare system, from subspecialists to the hospital to the nursing home. In practice, this means the use of electronic registries and health information exchange systems to make sure every health professional has all the information they should have about the patient.
Quality and safety: In practice, it means the development of a care plan that is bolstered by close relationships between patients, doctors, and family members. Plus, a good PCMH will have a more collegial atmosphere, with regular meetings among doctors of varying specialties. Evidence-based medicine is the guide. And feedback from the patient is sought more aggressively. Practices also can undergo a voluntary recognition process by a non-government-related healthcare quality organization, such as the National Committee for Quality Assurance.
Enhanced access: So that patients get the care when they need it, same-day scheduling is often offered. There are expanded hours, and phone and email communication is used more often.
Payment: The payment system in a PCMH encourages better primary care and prevention of illness. Still, most PCMH practices currently use a blend of fee-for-service, a monthly “care coordination” fee, and incentives for quality care.
Source: Adapted from 2007’s Joint Statement on Patient-Centered Medical Home, Agency for Healthcare Research and Quality
The term “patient-centered medical home” has a nice ring to it, but what does it really mean? And how does it function in the real world? The model is evolving, but here are the main components of the PCMH and how they’ve been implemented in real practice, at least so far:
“PERSONAL” PHYSICIAN: This is the doctor, usually a family or general practice physician, who shepherds patients through the medical system. In practice, this means things like encouraging patient questions about their care, extra efforts to educate patients on their health, and nurses making detailed follow-up calls with patients to make sure they’ve gotten their medications and know how to take them, and communicating any other steps the patient should be taking.
“Whole-person orientation”: The personal physician is responsible for taking care of all of the patient’s medical needs, either himself or by arranging care with specialists. The care ranges from preventive to chronic to end-of-life. In practice, this often means having appointments made with another doctor, if necessary, before the patient leaves the primary-care doctor, or seeing several doctors of different specialties during the same appointment.
Coordinated or integrated care: Care in the PCMH spans all aspects of the healthcare system, from subspecialists to the hospital to the nursing home. In practice, this means the use of electronic registries and health information exchange systems to make sure every health professional has all the information they should have about the patient.
Quality and safety: In practice, it means the development of a care plan that is bolstered by close relationships between patients, doctors, and family members. Plus, a good PCMH will have a more collegial atmosphere, with regular meetings among doctors of varying specialties. Evidence-based medicine is the guide. And feedback from the patient is sought more aggressively. Practices also can undergo a voluntary recognition process by a non-government-related healthcare quality organization, such as the National Committee for Quality Assurance.
Enhanced access: So that patients get the care when they need it, same-day scheduling is often offered. There are expanded hours, and phone and email communication is used more often.
Payment: The payment system in a PCMH encourages better primary care and prevention of illness. Still, most PCMH practices currently use a blend of fee-for-service, a monthly “care coordination” fee, and incentives for quality care.
Source: Adapted from 2007’s Joint Statement on Patient-Centered Medical Home, Agency for Healthcare Research and Quality
The term “patient-centered medical home” has a nice ring to it, but what does it really mean? And how does it function in the real world? The model is evolving, but here are the main components of the PCMH and how they’ve been implemented in real practice, at least so far:
“PERSONAL” PHYSICIAN: This is the doctor, usually a family or general practice physician, who shepherds patients through the medical system. In practice, this means things like encouraging patient questions about their care, extra efforts to educate patients on their health, and nurses making detailed follow-up calls with patients to make sure they’ve gotten their medications and know how to take them, and communicating any other steps the patient should be taking.
“Whole-person orientation”: The personal physician is responsible for taking care of all of the patient’s medical needs, either himself or by arranging care with specialists. The care ranges from preventive to chronic to end-of-life. In practice, this often means having appointments made with another doctor, if necessary, before the patient leaves the primary-care doctor, or seeing several doctors of different specialties during the same appointment.
Coordinated or integrated care: Care in the PCMH spans all aspects of the healthcare system, from subspecialists to the hospital to the nursing home. In practice, this means the use of electronic registries and health information exchange systems to make sure every health professional has all the information they should have about the patient.
Quality and safety: In practice, it means the development of a care plan that is bolstered by close relationships between patients, doctors, and family members. Plus, a good PCMH will have a more collegial atmosphere, with regular meetings among doctors of varying specialties. Evidence-based medicine is the guide. And feedback from the patient is sought more aggressively. Practices also can undergo a voluntary recognition process by a non-government-related healthcare quality organization, such as the National Committee for Quality Assurance.
Enhanced access: So that patients get the care when they need it, same-day scheduling is often offered. There are expanded hours, and phone and email communication is used more often.
Payment: The payment system in a PCMH encourages better primary care and prevention of illness. Still, most PCMH practices currently use a blend of fee-for-service, a monthly “care coordination” fee, and incentives for quality care.
Source: Adapted from 2007’s Joint Statement on Patient-Centered Medical Home, Agency for Healthcare Research and Quality