Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Author and Disclosure Information
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Author and Disclosure Information
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
References
Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
References
Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4
References
Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4
For understanding the evolution in child neurology over the past 30 years, it would make sense to start with the science, particularly genetics, that have led to treatments and even cures for numerous inherited diseases over that time. When John Bodensteiner, MD, a pillar in the field of child neurology, was asked, he started with something different.
Parent advocacy accelerates advances in rare pediatric diseases
For the progress in many of the rare diseases seen by child neurologists in the last few decades, Dr. Bodensteiner first acknowledged parent support. “The concept was simple initially. For so many of these relatively rare diseases, like the Rett and Sturge-Weber syndromes, parents were learning of them for the first time. The support groups helped parents understand they were not alone. But it then evolved,” recalled Dr. Bodensteiner, who has been a professor of pediatrics and neurology at numerous institutions, most recently the Mayo Clinic in Rochester, Minn.
Many of these support groups first formed, or at least gained momentum, in the 1990s. “As the support groups grew, the members expanded their role to support research, in addition to supporting each other. They ended up volunteering their own data, providing more information about the epidemiology and disease course. They offered tissue samples for experimental studies. They enrolled their children in trials. And they raised funds,” Dr. Bodensteiner explained.
The impact of this advocacy has been enormous, according to Dr. Bodensteiner. As an expert in neuromuscular diseases, he worked directly with several of these groups.
Dr. John Bodensteiner
Although the growth in parent advocacy took place in parallel with major advances in genetics that were driving new insights into disease pathophysiology, Dr. Bodensteiner characterized parent advocates as important partners in accelerating the transition of new information to clinical utility. He suggested that there is little doubt about the importance of their role in moving the science forward by drawing attention to rare disorders that had few, if any, treatment options at the time the advocacy groups were formed.
Since the 1990s, the list of childhood neurologic diseases for which there has been meaningful progress is long. Dr. Bodensteiner selected several examples. For Rett syndrome, key molecular mechanisms have now been isolated, providing meaningful targets that show potential for treatment. For spinal muscular atrophy (SMA), therapies have become available, one of which involves gene replacement that appears to provide cure if initiated early in life. For tuberous sclerosis complex (TSC), gene targets are showing strong promise for controlling seizures and other TSC manifestations.
It has also to be acknowledged that much of the ongoing expansion in knowledge taking place across diseases in pediatric neurology would have taken place with or without parent support. Dr. Bodensteiner singled out seizure disorders only as an illustration. “In the various forms of epilepsy, we now understand mechanisms in much greater detail than we did even a decade ago, let alone 30 years ago,” Dr. Bodensteiner said. In the context of the seizure medicines once widely employed on an empirical basis, “we now often have a clearer picture of why one drug works and not another.”
Growing pains: Child neurology evolves from a subspecialty to a specialty
Until about 10 years ago, child neurology was a subspecialty, variably placed within the departments of pediatrics or neurology based on institution. The decision to elevate child neurology to its own specialty solved some issues but created others, according to Dr. Bodensteiner.
“The initial problem was there was no immediate funding mechanism of residency slots and training,” Dr. Bodensteiner explained. The issue was particularly acute at smaller centers that had been able to support a subspecialty within another department but struggled with a new autonomous unit.
So far, the training requirements for specializing in child neurology remain largely unchanged. Clinical training requires 2 years of straight pediatrics, 1 year of adult neurology, 1 year of basic neurological science,” and 1 year of child neurology, but Dr. Bodensteiner said it might be time to reconsider. He pointed out that neurologists in general and child neurologists specifically are becoming increasingly focused in one area of expertise, such as epilepsy, neuromuscular diseases, and neurodevelopmental delay.
“It can be argued that a few months spent in a dementia clinic during training might not be the best use of time for a child neurologist working in congenital neurological diseases,” he said.
One consequence of the increasing degree of specialization in neurology overall, not just child neurology, has been the changes in recertification, according to Dr. Bodensteiner. Following a model used in other specialties, recertification in child neurology was initially based on an every-10-year examination. Ultimately, this was recognized as inconsistent with the target of keeping clinicians up to date.
“In general, I think that a lot of people waited for 9.5 years before cramming for an examination that was not necessarily relevant to the area in which they were working,” Dr. Bodensteiner said.
The revised process, carried out on an every-3-year cycle, involves board-guided review of the medical literature in 10 topic areas. Child neurologists can elect an article in any of the topic areas, but to complete their recertification process they must read articles in eight of these areas. Dr. Bodensteiner said that this approach has been more popular and is presumably more useful for staying abreast of developments.
The radical increase in specialization in child neurology, like neurology in general, has been a necessary consequence of an avalanche of new information as advances in the field accelerate, but Dr. Bodensteiner cautioned that it is important for those working in these specialized areas to collaborate with others outside of their field of expertise.
“We cannot recognize what we do not know,” Dr. Bodensteiner said. If subspecialization within neurology is critical to stay current with rapid advances in very different diseases, then it also means that clinicians at every level, including within the field of child neurology, need to know when to collaborate or refer to ensure early diagnosis in challenging cases.
“Epileptologists have been trying for years to make it widely known that patients resistant to standard medications deserve referral, but I think this is increasingly true across domains,” Dr. Bodensteiner said. Neurology and child neurology are not alone, but the window of opportunity for effective intervention in children with a progressive disease might be particularly limited.
“The point is that this is more of a risk than it was 20 years ago,” said Dr. Bodensteiner, referring to the growth in new therapies. He cited data suggesting that a causative gene mutation can be identified in about 60% of rare diseases, which is a relatively new phenomenon. Of advances to improve outcomes, faster triage is becoming one of the most important in this increasingly specialized world.
With the growth in knowledge, “there is really no way to be an expert across all diseases in child neurology,” Dr. Bodensteiner said. “As physicians become increasingly insulated in their areas of expertise, I think there needs to be a greater emphasis on communication and collaboration.”
To some degree, this type of specialization has always existed, but Dr. Bodensteiner said the intensification of this trend is among the ways the field has most evolved over the past few decades. In inherited diseases that affect early child development, working together for a prompt diagnosis has assumed a new level of urgency.
For understanding the evolution in child neurology over the past 30 years, it would make sense to start with the science, particularly genetics, that have led to treatments and even cures for numerous inherited diseases over that time. When John Bodensteiner, MD, a pillar in the field of child neurology, was asked, he started with something different.
Parent advocacy accelerates advances in rare pediatric diseases
For the progress in many of the rare diseases seen by child neurologists in the last few decades, Dr. Bodensteiner first acknowledged parent support. “The concept was simple initially. For so many of these relatively rare diseases, like the Rett and Sturge-Weber syndromes, parents were learning of them for the first time. The support groups helped parents understand they were not alone. But it then evolved,” recalled Dr. Bodensteiner, who has been a professor of pediatrics and neurology at numerous institutions, most recently the Mayo Clinic in Rochester, Minn.
Many of these support groups first formed, or at least gained momentum, in the 1990s. “As the support groups grew, the members expanded their role to support research, in addition to supporting each other. They ended up volunteering their own data, providing more information about the epidemiology and disease course. They offered tissue samples for experimental studies. They enrolled their children in trials. And they raised funds,” Dr. Bodensteiner explained.
The impact of this advocacy has been enormous, according to Dr. Bodensteiner. As an expert in neuromuscular diseases, he worked directly with several of these groups.
Dr. John Bodensteiner
Although the growth in parent advocacy took place in parallel with major advances in genetics that were driving new insights into disease pathophysiology, Dr. Bodensteiner characterized parent advocates as important partners in accelerating the transition of new information to clinical utility. He suggested that there is little doubt about the importance of their role in moving the science forward by drawing attention to rare disorders that had few, if any, treatment options at the time the advocacy groups were formed.
Since the 1990s, the list of childhood neurologic diseases for which there has been meaningful progress is long. Dr. Bodensteiner selected several examples. For Rett syndrome, key molecular mechanisms have now been isolated, providing meaningful targets that show potential for treatment. For spinal muscular atrophy (SMA), therapies have become available, one of which involves gene replacement that appears to provide cure if initiated early in life. For tuberous sclerosis complex (TSC), gene targets are showing strong promise for controlling seizures and other TSC manifestations.
It has also to be acknowledged that much of the ongoing expansion in knowledge taking place across diseases in pediatric neurology would have taken place with or without parent support. Dr. Bodensteiner singled out seizure disorders only as an illustration. “In the various forms of epilepsy, we now understand mechanisms in much greater detail than we did even a decade ago, let alone 30 years ago,” Dr. Bodensteiner said. In the context of the seizure medicines once widely employed on an empirical basis, “we now often have a clearer picture of why one drug works and not another.”
Growing pains: Child neurology evolves from a subspecialty to a specialty
Until about 10 years ago, child neurology was a subspecialty, variably placed within the departments of pediatrics or neurology based on institution. The decision to elevate child neurology to its own specialty solved some issues but created others, according to Dr. Bodensteiner.
“The initial problem was there was no immediate funding mechanism of residency slots and training,” Dr. Bodensteiner explained. The issue was particularly acute at smaller centers that had been able to support a subspecialty within another department but struggled with a new autonomous unit.
So far, the training requirements for specializing in child neurology remain largely unchanged. Clinical training requires 2 years of straight pediatrics, 1 year of adult neurology, 1 year of basic neurological science,” and 1 year of child neurology, but Dr. Bodensteiner said it might be time to reconsider. He pointed out that neurologists in general and child neurologists specifically are becoming increasingly focused in one area of expertise, such as epilepsy, neuromuscular diseases, and neurodevelopmental delay.
“It can be argued that a few months spent in a dementia clinic during training might not be the best use of time for a child neurologist working in congenital neurological diseases,” he said.
One consequence of the increasing degree of specialization in neurology overall, not just child neurology, has been the changes in recertification, according to Dr. Bodensteiner. Following a model used in other specialties, recertification in child neurology was initially based on an every-10-year examination. Ultimately, this was recognized as inconsistent with the target of keeping clinicians up to date.
“In general, I think that a lot of people waited for 9.5 years before cramming for an examination that was not necessarily relevant to the area in which they were working,” Dr. Bodensteiner said.
The revised process, carried out on an every-3-year cycle, involves board-guided review of the medical literature in 10 topic areas. Child neurologists can elect an article in any of the topic areas, but to complete their recertification process they must read articles in eight of these areas. Dr. Bodensteiner said that this approach has been more popular and is presumably more useful for staying abreast of developments.
The radical increase in specialization in child neurology, like neurology in general, has been a necessary consequence of an avalanche of new information as advances in the field accelerate, but Dr. Bodensteiner cautioned that it is important for those working in these specialized areas to collaborate with others outside of their field of expertise.
“We cannot recognize what we do not know,” Dr. Bodensteiner said. If subspecialization within neurology is critical to stay current with rapid advances in very different diseases, then it also means that clinicians at every level, including within the field of child neurology, need to know when to collaborate or refer to ensure early diagnosis in challenging cases.
“Epileptologists have been trying for years to make it widely known that patients resistant to standard medications deserve referral, but I think this is increasingly true across domains,” Dr. Bodensteiner said. Neurology and child neurology are not alone, but the window of opportunity for effective intervention in children with a progressive disease might be particularly limited.
“The point is that this is more of a risk than it was 20 years ago,” said Dr. Bodensteiner, referring to the growth in new therapies. He cited data suggesting that a causative gene mutation can be identified in about 60% of rare diseases, which is a relatively new phenomenon. Of advances to improve outcomes, faster triage is becoming one of the most important in this increasingly specialized world.
With the growth in knowledge, “there is really no way to be an expert across all diseases in child neurology,” Dr. Bodensteiner said. “As physicians become increasingly insulated in their areas of expertise, I think there needs to be a greater emphasis on communication and collaboration.”
To some degree, this type of specialization has always existed, but Dr. Bodensteiner said the intensification of this trend is among the ways the field has most evolved over the past few decades. In inherited diseases that affect early child development, working together for a prompt diagnosis has assumed a new level of urgency.
For understanding the evolution in child neurology over the past 30 years, it would make sense to start with the science, particularly genetics, that have led to treatments and even cures for numerous inherited diseases over that time. When John Bodensteiner, MD, a pillar in the field of child neurology, was asked, he started with something different.
Parent advocacy accelerates advances in rare pediatric diseases
For the progress in many of the rare diseases seen by child neurologists in the last few decades, Dr. Bodensteiner first acknowledged parent support. “The concept was simple initially. For so many of these relatively rare diseases, like the Rett and Sturge-Weber syndromes, parents were learning of them for the first time. The support groups helped parents understand they were not alone. But it then evolved,” recalled Dr. Bodensteiner, who has been a professor of pediatrics and neurology at numerous institutions, most recently the Mayo Clinic in Rochester, Minn.
Many of these support groups first formed, or at least gained momentum, in the 1990s. “As the support groups grew, the members expanded their role to support research, in addition to supporting each other. They ended up volunteering their own data, providing more information about the epidemiology and disease course. They offered tissue samples for experimental studies. They enrolled their children in trials. And they raised funds,” Dr. Bodensteiner explained.
The impact of this advocacy has been enormous, according to Dr. Bodensteiner. As an expert in neuromuscular diseases, he worked directly with several of these groups.
Dr. John Bodensteiner
Although the growth in parent advocacy took place in parallel with major advances in genetics that were driving new insights into disease pathophysiology, Dr. Bodensteiner characterized parent advocates as important partners in accelerating the transition of new information to clinical utility. He suggested that there is little doubt about the importance of their role in moving the science forward by drawing attention to rare disorders that had few, if any, treatment options at the time the advocacy groups were formed.
Since the 1990s, the list of childhood neurologic diseases for which there has been meaningful progress is long. Dr. Bodensteiner selected several examples. For Rett syndrome, key molecular mechanisms have now been isolated, providing meaningful targets that show potential for treatment. For spinal muscular atrophy (SMA), therapies have become available, one of which involves gene replacement that appears to provide cure if initiated early in life. For tuberous sclerosis complex (TSC), gene targets are showing strong promise for controlling seizures and other TSC manifestations.
It has also to be acknowledged that much of the ongoing expansion in knowledge taking place across diseases in pediatric neurology would have taken place with or without parent support. Dr. Bodensteiner singled out seizure disorders only as an illustration. “In the various forms of epilepsy, we now understand mechanisms in much greater detail than we did even a decade ago, let alone 30 years ago,” Dr. Bodensteiner said. In the context of the seizure medicines once widely employed on an empirical basis, “we now often have a clearer picture of why one drug works and not another.”
Growing pains: Child neurology evolves from a subspecialty to a specialty
Until about 10 years ago, child neurology was a subspecialty, variably placed within the departments of pediatrics or neurology based on institution. The decision to elevate child neurology to its own specialty solved some issues but created others, according to Dr. Bodensteiner.
“The initial problem was there was no immediate funding mechanism of residency slots and training,” Dr. Bodensteiner explained. The issue was particularly acute at smaller centers that had been able to support a subspecialty within another department but struggled with a new autonomous unit.
So far, the training requirements for specializing in child neurology remain largely unchanged. Clinical training requires 2 years of straight pediatrics, 1 year of adult neurology, 1 year of basic neurological science,” and 1 year of child neurology, but Dr. Bodensteiner said it might be time to reconsider. He pointed out that neurologists in general and child neurologists specifically are becoming increasingly focused in one area of expertise, such as epilepsy, neuromuscular diseases, and neurodevelopmental delay.
“It can be argued that a few months spent in a dementia clinic during training might not be the best use of time for a child neurologist working in congenital neurological diseases,” he said.
One consequence of the increasing degree of specialization in neurology overall, not just child neurology, has been the changes in recertification, according to Dr. Bodensteiner. Following a model used in other specialties, recertification in child neurology was initially based on an every-10-year examination. Ultimately, this was recognized as inconsistent with the target of keeping clinicians up to date.
“In general, I think that a lot of people waited for 9.5 years before cramming for an examination that was not necessarily relevant to the area in which they were working,” Dr. Bodensteiner said.
The revised process, carried out on an every-3-year cycle, involves board-guided review of the medical literature in 10 topic areas. Child neurologists can elect an article in any of the topic areas, but to complete their recertification process they must read articles in eight of these areas. Dr. Bodensteiner said that this approach has been more popular and is presumably more useful for staying abreast of developments.
The radical increase in specialization in child neurology, like neurology in general, has been a necessary consequence of an avalanche of new information as advances in the field accelerate, but Dr. Bodensteiner cautioned that it is important for those working in these specialized areas to collaborate with others outside of their field of expertise.
“We cannot recognize what we do not know,” Dr. Bodensteiner said. If subspecialization within neurology is critical to stay current with rapid advances in very different diseases, then it also means that clinicians at every level, including within the field of child neurology, need to know when to collaborate or refer to ensure early diagnosis in challenging cases.
“Epileptologists have been trying for years to make it widely known that patients resistant to standard medications deserve referral, but I think this is increasingly true across domains,” Dr. Bodensteiner said. Neurology and child neurology are not alone, but the window of opportunity for effective intervention in children with a progressive disease might be particularly limited.
“The point is that this is more of a risk than it was 20 years ago,” said Dr. Bodensteiner, referring to the growth in new therapies. He cited data suggesting that a causative gene mutation can be identified in about 60% of rare diseases, which is a relatively new phenomenon. Of advances to improve outcomes, faster triage is becoming one of the most important in this increasingly specialized world.
With the growth in knowledge, “there is really no way to be an expert across all diseases in child neurology,” Dr. Bodensteiner said. “As physicians become increasingly insulated in their areas of expertise, I think there needs to be a greater emphasis on communication and collaboration.”
To some degree, this type of specialization has always existed, but Dr. Bodensteiner said the intensification of this trend is among the ways the field has most evolved over the past few decades. In inherited diseases that affect early child development, working together for a prompt diagnosis has assumed a new level of urgency.
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097/AOG.0000000000005102.
EXPERT COMMENTARY
Stillbirth is defined as intrauterine demise at or beyond 20 weeks’ gestation. Pregestational DM and GDM significantly increase the risk of stillbirth. Both fetal growth restriction and macrosomia are common complications of pregnancies affected by diabetes, and they further increase the risk of stillbirth. While maternal variables such as glycemic control and medication requirement are currently used to assess the risks of expectant management and inform delivery timing, abnormal fetal growth is not.
Investigators sought to evaluate the stillbirth rates per week of expectant management during the late third trimester stratified by birth weight (as a surrogate for fetal growth) in pregnancies complicated by PG-DM or GDM.
Details of the study
McElwee and colleagues used the US National Vital Statistics System to identify nonanomalous singleton pregnancies complicated by PG-DM or GDM from 2014 to 2017.1 Pregnancies were stratified by birth weight and categorized as being LGA (birth weight > 90th percentile for gestational age), SGA (birth weight < 10th percentile for gestational age), or AGA. Stillbirths were identified from 34 0/7 through 39 6/7 weeks of gestation, and conditional stillbirth rates per 10,000 pregnancies were calculated for each week of gestation.
Results. Among 834,631 pregnancies complicated by PG-DM (13.1%) or GDM (86.9%), there were 3,033 stillbirths, of which 61% were in pregnancies with PG-DM. Stillbirth rates increased with advancing gestational age for both PG-DM and GDM regardless of birth weight. In pregnancies with PG-DM, fetuses that were LGA or SGA had a higher relative risk of stillbirth compared with their AGA counterparts at each gestational age. This stillbirth risk was highest in pregnancies with PG-DM that were LGA. At 39 weeks, the stillbirth rate in this population was 96.9/10,000 ongoing pregnancies and was 5 times higher than pregnancies with PG-DM that were AGA. When the GDM-related AGA group was selected as the referent (as the lowest-risk comparison group), pregnancies with PG-DM that were LGA had a 21-times higher relative risk of stillbirth at 37 and 38 weeks of gestation.
Study strengths and limitations
Decisions on the optimal timing of delivery seek to strike a balance between the increased neonatal morbidity with delivery before 39 weeks’ gestation and the increased risk of stillbirth with expectant management. In pregnancies complicated by diabetes, current guidelines from the American College of Obstetricians and Gynecologists recommend consideration of maternal variables, such as medication requirement, glycemic control, and vascular sequelae, to inform decisions on delivery timing, as these factors have been postulated to influence the risk of stillbirth with pregnancy prolongation.2 These recommendations are based largely on expert opinion and retrospective data.
The question of how fetal growth abnormalities factor into this complicated decision making is also an area of low-quality evidence despite studies that demonstrate that both SGA and LGA fetuses in pregnancies complicated by diabetes are at increased risk of stillbirth.3
The large population-based study design by McElwee and colleagues allowed the investigators to examine a rare event (stillbirth) with multiple stratification levels and sufficient statistical power and to contribute to this literature.
Significant limitations, however, must be considered before generalizing these results. The data were restricted to variables available on birth and death certificates, and more granular information—such as the type of DM, level of glycemic control, frequency of antenatal testing, and stillbirth work-up—could not be assessed. Ultrasonographic estimations of fetal weight also were not included. Birth weight data were used as a proxy, although we know that these variables do not always correlate well given the limited accuracy of ultrasonography in assessing projected birth weight, particularly later in pregnancy. The authors also did not control for highly prevalent variables (for example, hypertension, obesity) that are likely associated with abnormal fetal growth and stillbirth in these populations. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The present study demonstrates that both SGA and LGA are significant risk factors for stillbirth in pregnancies with either PG-DM or GDM in the late preterm and early term periods, and this risk should be considered when making decisions on appropriate timing of delivery. The conditional stillbirth rate was highest in pregnancies with PG-DM with LGA fetuses, and this risk increased with each week of expectant management. This population may benefit the most from critical assessment of the risk of stillbirth with ongoing pregnancy. Notably, the quality of evidence is not sufficient to universally alter delivery timing guidelines in this population. We recommend individual assessment of each clinical scenario when making these decisions.
NIGEL MADDEN, MD; MICHELLE A. KOMINIAREK, MD, MS
References
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097 /AOG.0000000000005102
Nigel Madden, MD, is a Maternal-Fetal Medicine Fellow at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Michelle A. Kominiarek, MD, MS, is an Associate Professor of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, at Northwestern University Feinberg School of Medicine, Chicago.
The authors report no financial relationships relevant to this article.
Nigel Madden, MD, is a Maternal-Fetal Medicine Fellow at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Michelle A. Kominiarek, MD, MS, is an Associate Professor of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, at Northwestern University Feinberg School of Medicine, Chicago.
The authors report no financial relationships relevant to this article.
Author and Disclosure Information
Nigel Madden, MD, is a Maternal-Fetal Medicine Fellow at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Michelle A. Kominiarek, MD, MS, is an Associate Professor of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, at Northwestern University Feinberg School of Medicine, Chicago.
The authors report no financial relationships relevant to this article.
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097/AOG.0000000000005102.
EXPERT COMMENTARY
Stillbirth is defined as intrauterine demise at or beyond 20 weeks’ gestation. Pregestational DM and GDM significantly increase the risk of stillbirth. Both fetal growth restriction and macrosomia are common complications of pregnancies affected by diabetes, and they further increase the risk of stillbirth. While maternal variables such as glycemic control and medication requirement are currently used to assess the risks of expectant management and inform delivery timing, abnormal fetal growth is not.
Investigators sought to evaluate the stillbirth rates per week of expectant management during the late third trimester stratified by birth weight (as a surrogate for fetal growth) in pregnancies complicated by PG-DM or GDM.
Details of the study
McElwee and colleagues used the US National Vital Statistics System to identify nonanomalous singleton pregnancies complicated by PG-DM or GDM from 2014 to 2017.1 Pregnancies were stratified by birth weight and categorized as being LGA (birth weight > 90th percentile for gestational age), SGA (birth weight < 10th percentile for gestational age), or AGA. Stillbirths were identified from 34 0/7 through 39 6/7 weeks of gestation, and conditional stillbirth rates per 10,000 pregnancies were calculated for each week of gestation.
Results. Among 834,631 pregnancies complicated by PG-DM (13.1%) or GDM (86.9%), there were 3,033 stillbirths, of which 61% were in pregnancies with PG-DM. Stillbirth rates increased with advancing gestational age for both PG-DM and GDM regardless of birth weight. In pregnancies with PG-DM, fetuses that were LGA or SGA had a higher relative risk of stillbirth compared with their AGA counterparts at each gestational age. This stillbirth risk was highest in pregnancies with PG-DM that were LGA. At 39 weeks, the stillbirth rate in this population was 96.9/10,000 ongoing pregnancies and was 5 times higher than pregnancies with PG-DM that were AGA. When the GDM-related AGA group was selected as the referent (as the lowest-risk comparison group), pregnancies with PG-DM that were LGA had a 21-times higher relative risk of stillbirth at 37 and 38 weeks of gestation.
Study strengths and limitations
Decisions on the optimal timing of delivery seek to strike a balance between the increased neonatal morbidity with delivery before 39 weeks’ gestation and the increased risk of stillbirth with expectant management. In pregnancies complicated by diabetes, current guidelines from the American College of Obstetricians and Gynecologists recommend consideration of maternal variables, such as medication requirement, glycemic control, and vascular sequelae, to inform decisions on delivery timing, as these factors have been postulated to influence the risk of stillbirth with pregnancy prolongation.2 These recommendations are based largely on expert opinion and retrospective data.
The question of how fetal growth abnormalities factor into this complicated decision making is also an area of low-quality evidence despite studies that demonstrate that both SGA and LGA fetuses in pregnancies complicated by diabetes are at increased risk of stillbirth.3
The large population-based study design by McElwee and colleagues allowed the investigators to examine a rare event (stillbirth) with multiple stratification levels and sufficient statistical power and to contribute to this literature.
Significant limitations, however, must be considered before generalizing these results. The data were restricted to variables available on birth and death certificates, and more granular information—such as the type of DM, level of glycemic control, frequency of antenatal testing, and stillbirth work-up—could not be assessed. Ultrasonographic estimations of fetal weight also were not included. Birth weight data were used as a proxy, although we know that these variables do not always correlate well given the limited accuracy of ultrasonography in assessing projected birth weight, particularly later in pregnancy. The authors also did not control for highly prevalent variables (for example, hypertension, obesity) that are likely associated with abnormal fetal growth and stillbirth in these populations. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The present study demonstrates that both SGA and LGA are significant risk factors for stillbirth in pregnancies with either PG-DM or GDM in the late preterm and early term periods, and this risk should be considered when making decisions on appropriate timing of delivery. The conditional stillbirth rate was highest in pregnancies with PG-DM with LGA fetuses, and this risk increased with each week of expectant management. This population may benefit the most from critical assessment of the risk of stillbirth with ongoing pregnancy. Notably, the quality of evidence is not sufficient to universally alter delivery timing guidelines in this population. We recommend individual assessment of each clinical scenario when making these decisions.
NIGEL MADDEN, MD; MICHELLE A. KOMINIAREK, MD, MS
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097/AOG.0000000000005102.
EXPERT COMMENTARY
Stillbirth is defined as intrauterine demise at or beyond 20 weeks’ gestation. Pregestational DM and GDM significantly increase the risk of stillbirth. Both fetal growth restriction and macrosomia are common complications of pregnancies affected by diabetes, and they further increase the risk of stillbirth. While maternal variables such as glycemic control and medication requirement are currently used to assess the risks of expectant management and inform delivery timing, abnormal fetal growth is not.
Investigators sought to evaluate the stillbirth rates per week of expectant management during the late third trimester stratified by birth weight (as a surrogate for fetal growth) in pregnancies complicated by PG-DM or GDM.
Details of the study
McElwee and colleagues used the US National Vital Statistics System to identify nonanomalous singleton pregnancies complicated by PG-DM or GDM from 2014 to 2017.1 Pregnancies were stratified by birth weight and categorized as being LGA (birth weight > 90th percentile for gestational age), SGA (birth weight < 10th percentile for gestational age), or AGA. Stillbirths were identified from 34 0/7 through 39 6/7 weeks of gestation, and conditional stillbirth rates per 10,000 pregnancies were calculated for each week of gestation.
Results. Among 834,631 pregnancies complicated by PG-DM (13.1%) or GDM (86.9%), there were 3,033 stillbirths, of which 61% were in pregnancies with PG-DM. Stillbirth rates increased with advancing gestational age for both PG-DM and GDM regardless of birth weight. In pregnancies with PG-DM, fetuses that were LGA or SGA had a higher relative risk of stillbirth compared with their AGA counterparts at each gestational age. This stillbirth risk was highest in pregnancies with PG-DM that were LGA. At 39 weeks, the stillbirth rate in this population was 96.9/10,000 ongoing pregnancies and was 5 times higher than pregnancies with PG-DM that were AGA. When the GDM-related AGA group was selected as the referent (as the lowest-risk comparison group), pregnancies with PG-DM that were LGA had a 21-times higher relative risk of stillbirth at 37 and 38 weeks of gestation.
Study strengths and limitations
Decisions on the optimal timing of delivery seek to strike a balance between the increased neonatal morbidity with delivery before 39 weeks’ gestation and the increased risk of stillbirth with expectant management. In pregnancies complicated by diabetes, current guidelines from the American College of Obstetricians and Gynecologists recommend consideration of maternal variables, such as medication requirement, glycemic control, and vascular sequelae, to inform decisions on delivery timing, as these factors have been postulated to influence the risk of stillbirth with pregnancy prolongation.2 These recommendations are based largely on expert opinion and retrospective data.
The question of how fetal growth abnormalities factor into this complicated decision making is also an area of low-quality evidence despite studies that demonstrate that both SGA and LGA fetuses in pregnancies complicated by diabetes are at increased risk of stillbirth.3
The large population-based study design by McElwee and colleagues allowed the investigators to examine a rare event (stillbirth) with multiple stratification levels and sufficient statistical power and to contribute to this literature.
Significant limitations, however, must be considered before generalizing these results. The data were restricted to variables available on birth and death certificates, and more granular information—such as the type of DM, level of glycemic control, frequency of antenatal testing, and stillbirth work-up—could not be assessed. Ultrasonographic estimations of fetal weight also were not included. Birth weight data were used as a proxy, although we know that these variables do not always correlate well given the limited accuracy of ultrasonography in assessing projected birth weight, particularly later in pregnancy. The authors also did not control for highly prevalent variables (for example, hypertension, obesity) that are likely associated with abnormal fetal growth and stillbirth in these populations. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The present study demonstrates that both SGA and LGA are significant risk factors for stillbirth in pregnancies with either PG-DM or GDM in the late preterm and early term periods, and this risk should be considered when making decisions on appropriate timing of delivery. The conditional stillbirth rate was highest in pregnancies with PG-DM with LGA fetuses, and this risk increased with each week of expectant management. This population may benefit the most from critical assessment of the risk of stillbirth with ongoing pregnancy. Notably, the quality of evidence is not sufficient to universally alter delivery timing guidelines in this population. We recommend individual assessment of each clinical scenario when making these decisions.
NIGEL MADDEN, MD; MICHELLE A. KOMINIAREK, MD, MS
References
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097 /AOG.0000000000005102
Starikov R, Dudley D, Reddy UM. Stillbirth in the pregnancy complicated by diabetes. Curr Diab Rep. 2015;15:11. doi:10.1007/s11892-015-0580-y
References
McElwee ER, Oliver EA, McFarling K, et al. Risk of stillbirth in pregnancies complicated by diabetes, stratified by fetal growth. Obstet Gynecol. 2023;141:801-809. doi:10.1097 /AOG.0000000000005102
Hartwig TJ, Ambye L, Gruhn JR, et al. Cell-free fetal DNA for genetic evaluation in Copenhagen Pregnancy Loss Study (COPL): a prospective cohort study. Lancet. 2023;401:762-771. https://doi.org/10.1016/S0140-6736(22)02610-1.
Expert Commentary
A devastating outcome for women, pregnancy loss is directly proportional to maternal age, estimated to occur in approximately 15% of clinically recognized pregnancies and 30% of preclinical pregnancies.1 Approximately 80% of pregnancy losses occur in the first trimester.2 The frequency of clinically recognized early pregnancy loss for women aged 20–30 years is 9% to 17%, and these rates increase sharply, from 20% at age 35 years to 40% at age 40 years, and 80% at age 45 years. Recurrent pregnancy loss (RPL), defined as the spontaneous loss of 2 or more clinically recognized pregnancies, affects less than 5% of women.3 Genetic testing using chromosomal microarray analysis (CMA) has identified aneuploidy in about 55% of cases of miscarriage.4
Following ASRM guidelines for the evaluation of RPL, which consists of analyzing parental chromosomal abnormalities, congenital and acquired uterine anomalies, endocrine imbalances, and autoimmune factors (including antiphospholipid syndrome), no explainable cause is determined in 50% of cases.3 Recently, it has been shown that more than 90% of patients with RPL will have a probable or definitive cause identified when CMA testing on miscarriage tissue with the ASRM evaluation guidelines.5
Details of the study
In this prospective cohort study from Denmark, the authors analyzed maternal serum for cell-free fetal DNA (cffDNA) to determine the ploidy status of the pregnancy loss. One thousand women older than age 18 were included (those who demonstrated an ultrasound-confirmed intrauterine pregnancy loss prior to 22 weeks’ gestation). Maternal blood was obtained while pregnancy tissue was in situ or within 24 hours of passage of products of conception (POC), then analyzed by genome-wide sequencing of cffDNA.
For the first 333 recruited women (validation phase), direct sequencing of the POC was performed for sensitivity and specificity. Following the elimination of inconclusive samples, 302 of the 333 cases demonstrated a sensitivity of 85% and specificity of 93%. In the subsequent evaluation of 667 women, researchers analyzed maternal serum from the gestational age of fetuses ranging from 35 days to 149 days.
Results.In total, nearly 90% of cases yielded conclusive results, with 50% euploid, 46% aneuploid, and 4% multiple aneuploidies. Earlier gestational ages (less than 7 weeks) had a no-call rate (ie, inconclusive) of approximately 50% (only based on 16 patients), with results typically obtained in maternal serum following passage of POC; in pregnancies at gestational ages past 7 weeks, the no-call rate was about 10%. In general, the longer the time after the pregnancy tissue passed, the higher likelihood of a no-call result.
Applying the technology of single-nucleotide polymorphism (SNP)-based CMA can improve identification of fetal and/or maternal sources as causes of pregnancy loss with accuracy, but it does require collection of POC. Of note, samples were deficient in this study, the authors cite, in one-third of the cases. Given this limitation of collection, the authors argue for use of the noninvasive method of cffDNA, obtained from maternal serum.
Study strengths and weaknesses
Several weaknesses of this study are highlighted. Of the validation cohort, one-third of pregnancy tissue could not be analyzed due to insufficient collection. Only 73% of cases allowed for DNA isolation from fetal tissue or chorionic villi; in 27% of cases samples were labeled “unknown tissue.” In those cases classified as unknown, 70% were further determined to be maternal. When all female and monosomy cases were excluded in an effort to assuredly reduce the risk of contamination with maternal DNA, sensitivity of the cffDNA testing process declined to 78%. Another limitation was the required short window for maternal blood sampling (within 24 hours) and its impact on the no-call rate.
The authors note an association with later-life morbidity in patients with a history of pregnancy loss and RPL (including cardiovascular disease, type 2 diabetes, and mental health disorders), thereby arguing for cffDNA-based testing versus no causal testing; however, no treatment has been proven to be effective at reducing pregnancy loss. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The best management course for unexplained RPL is uncertain. Despite its use for a euploid miscarriage or parental chromosomal structural rearrangement, in vitro fertilization with preimplantation genetic testing remains an unproven modality.6,7 Given that approximately 70% of human conceptions never achieve viability, and 50% fail spontaneously before being detected,8 the authors’ findings demonstrate peripheral maternal blood can provide a reasonably high sensitivity and specificity for fetal ploidy status when compared with direct sequencing of pregnancy tissue. As fetal aneuploidy offers a higher percentage of subsequent successful pregnancy outcomes, cffDNA may offer reassurance, or direct further testing, following a pregnancy loss. As an application of their results, evaluation may be deferred for an aneuploid miscarriage.
—MARK P. TROLICE, MD, MBA
References
Brown S. Miscarriage and its associations. Semin Reprod Med. 2008;26:391-400. doi: 10.1055/s-0028-1087105.
Wang X, Chen C , Wang L, et al. Conception, early pregnancy loss, and time to clinical pregnancy: a population-based prospective study. Fertil Steril. 2003;79:577-584.
Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril. 2012;98: 1103-1111.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/tacg.s320778.
Popescu F, Jaslow FC, Kutteh WH. Recurrent pregnancy loss evaluation combined with 24-chromosome microarray of miscarriage tissue provides a probable or definite cause of pregnancy loss in over 90% of patients. Hum Reprod. 2018;33:579-587. https://doi.org/10.1093/humrep/dey021.
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. https://doi.org/10.1093/humrep/deab194.
Iews M, Tan J, Taskin O, et al. Does preimplantation genetic diagnosis improve reproductive outcome in couples with recurrent pregnancy loss owing to structural chromosomal rearrangement? A systematic review. Reproductive Bio Medicine Online. 2018;36:677-685. https://doi.org/10.1016 /j.rbmo.2018.03.005.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/TACG.S320778.
Hartwig TJ, Ambye L, Gruhn JR, et al. Cell-free fetal DNA for genetic evaluation in Copenhagen Pregnancy Loss Study (COPL): a prospective cohort study. Lancet. 2023;401:762-771. https://doi.org/10.1016/S0140-6736(22)02610-1.
Expert Commentary
A devastating outcome for women, pregnancy loss is directly proportional to maternal age, estimated to occur in approximately 15% of clinically recognized pregnancies and 30% of preclinical pregnancies.1 Approximately 80% of pregnancy losses occur in the first trimester.2 The frequency of clinically recognized early pregnancy loss for women aged 20–30 years is 9% to 17%, and these rates increase sharply, from 20% at age 35 years to 40% at age 40 years, and 80% at age 45 years. Recurrent pregnancy loss (RPL), defined as the spontaneous loss of 2 or more clinically recognized pregnancies, affects less than 5% of women.3 Genetic testing using chromosomal microarray analysis (CMA) has identified aneuploidy in about 55% of cases of miscarriage.4
Following ASRM guidelines for the evaluation of RPL, which consists of analyzing parental chromosomal abnormalities, congenital and acquired uterine anomalies, endocrine imbalances, and autoimmune factors (including antiphospholipid syndrome), no explainable cause is determined in 50% of cases.3 Recently, it has been shown that more than 90% of patients with RPL will have a probable or definitive cause identified when CMA testing on miscarriage tissue with the ASRM evaluation guidelines.5
Details of the study
In this prospective cohort study from Denmark, the authors analyzed maternal serum for cell-free fetal DNA (cffDNA) to determine the ploidy status of the pregnancy loss. One thousand women older than age 18 were included (those who demonstrated an ultrasound-confirmed intrauterine pregnancy loss prior to 22 weeks’ gestation). Maternal blood was obtained while pregnancy tissue was in situ or within 24 hours of passage of products of conception (POC), then analyzed by genome-wide sequencing of cffDNA.
For the first 333 recruited women (validation phase), direct sequencing of the POC was performed for sensitivity and specificity. Following the elimination of inconclusive samples, 302 of the 333 cases demonstrated a sensitivity of 85% and specificity of 93%. In the subsequent evaluation of 667 women, researchers analyzed maternal serum from the gestational age of fetuses ranging from 35 days to 149 days.
Results.In total, nearly 90% of cases yielded conclusive results, with 50% euploid, 46% aneuploid, and 4% multiple aneuploidies. Earlier gestational ages (less than 7 weeks) had a no-call rate (ie, inconclusive) of approximately 50% (only based on 16 patients), with results typically obtained in maternal serum following passage of POC; in pregnancies at gestational ages past 7 weeks, the no-call rate was about 10%. In general, the longer the time after the pregnancy tissue passed, the higher likelihood of a no-call result.
Applying the technology of single-nucleotide polymorphism (SNP)-based CMA can improve identification of fetal and/or maternal sources as causes of pregnancy loss with accuracy, but it does require collection of POC. Of note, samples were deficient in this study, the authors cite, in one-third of the cases. Given this limitation of collection, the authors argue for use of the noninvasive method of cffDNA, obtained from maternal serum.
Study strengths and weaknesses
Several weaknesses of this study are highlighted. Of the validation cohort, one-third of pregnancy tissue could not be analyzed due to insufficient collection. Only 73% of cases allowed for DNA isolation from fetal tissue or chorionic villi; in 27% of cases samples were labeled “unknown tissue.” In those cases classified as unknown, 70% were further determined to be maternal. When all female and monosomy cases were excluded in an effort to assuredly reduce the risk of contamination with maternal DNA, sensitivity of the cffDNA testing process declined to 78%. Another limitation was the required short window for maternal blood sampling (within 24 hours) and its impact on the no-call rate.
The authors note an association with later-life morbidity in patients with a history of pregnancy loss and RPL (including cardiovascular disease, type 2 diabetes, and mental health disorders), thereby arguing for cffDNA-based testing versus no causal testing; however, no treatment has been proven to be effective at reducing pregnancy loss. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The best management course for unexplained RPL is uncertain. Despite its use for a euploid miscarriage or parental chromosomal structural rearrangement, in vitro fertilization with preimplantation genetic testing remains an unproven modality.6,7 Given that approximately 70% of human conceptions never achieve viability, and 50% fail spontaneously before being detected,8 the authors’ findings demonstrate peripheral maternal blood can provide a reasonably high sensitivity and specificity for fetal ploidy status when compared with direct sequencing of pregnancy tissue. As fetal aneuploidy offers a higher percentage of subsequent successful pregnancy outcomes, cffDNA may offer reassurance, or direct further testing, following a pregnancy loss. As an application of their results, evaluation may be deferred for an aneuploid miscarriage.
—MARK P. TROLICE, MD, MBA
Hartwig TJ, Ambye L, Gruhn JR, et al. Cell-free fetal DNA for genetic evaluation in Copenhagen Pregnancy Loss Study (COPL): a prospective cohort study. Lancet. 2023;401:762-771. https://doi.org/10.1016/S0140-6736(22)02610-1.
Expert Commentary
A devastating outcome for women, pregnancy loss is directly proportional to maternal age, estimated to occur in approximately 15% of clinically recognized pregnancies and 30% of preclinical pregnancies.1 Approximately 80% of pregnancy losses occur in the first trimester.2 The frequency of clinically recognized early pregnancy loss for women aged 20–30 years is 9% to 17%, and these rates increase sharply, from 20% at age 35 years to 40% at age 40 years, and 80% at age 45 years. Recurrent pregnancy loss (RPL), defined as the spontaneous loss of 2 or more clinically recognized pregnancies, affects less than 5% of women.3 Genetic testing using chromosomal microarray analysis (CMA) has identified aneuploidy in about 55% of cases of miscarriage.4
Following ASRM guidelines for the evaluation of RPL, which consists of analyzing parental chromosomal abnormalities, congenital and acquired uterine anomalies, endocrine imbalances, and autoimmune factors (including antiphospholipid syndrome), no explainable cause is determined in 50% of cases.3 Recently, it has been shown that more than 90% of patients with RPL will have a probable or definitive cause identified when CMA testing on miscarriage tissue with the ASRM evaluation guidelines.5
Details of the study
In this prospective cohort study from Denmark, the authors analyzed maternal serum for cell-free fetal DNA (cffDNA) to determine the ploidy status of the pregnancy loss. One thousand women older than age 18 were included (those who demonstrated an ultrasound-confirmed intrauterine pregnancy loss prior to 22 weeks’ gestation). Maternal blood was obtained while pregnancy tissue was in situ or within 24 hours of passage of products of conception (POC), then analyzed by genome-wide sequencing of cffDNA.
For the first 333 recruited women (validation phase), direct sequencing of the POC was performed for sensitivity and specificity. Following the elimination of inconclusive samples, 302 of the 333 cases demonstrated a sensitivity of 85% and specificity of 93%. In the subsequent evaluation of 667 women, researchers analyzed maternal serum from the gestational age of fetuses ranging from 35 days to 149 days.
Results.In total, nearly 90% of cases yielded conclusive results, with 50% euploid, 46% aneuploid, and 4% multiple aneuploidies. Earlier gestational ages (less than 7 weeks) had a no-call rate (ie, inconclusive) of approximately 50% (only based on 16 patients), with results typically obtained in maternal serum following passage of POC; in pregnancies at gestational ages past 7 weeks, the no-call rate was about 10%. In general, the longer the time after the pregnancy tissue passed, the higher likelihood of a no-call result.
Applying the technology of single-nucleotide polymorphism (SNP)-based CMA can improve identification of fetal and/or maternal sources as causes of pregnancy loss with accuracy, but it does require collection of POC. Of note, samples were deficient in this study, the authors cite, in one-third of the cases. Given this limitation of collection, the authors argue for use of the noninvasive method of cffDNA, obtained from maternal serum.
Study strengths and weaknesses
Several weaknesses of this study are highlighted. Of the validation cohort, one-third of pregnancy tissue could not be analyzed due to insufficient collection. Only 73% of cases allowed for DNA isolation from fetal tissue or chorionic villi; in 27% of cases samples were labeled “unknown tissue.” In those cases classified as unknown, 70% were further determined to be maternal. When all female and monosomy cases were excluded in an effort to assuredly reduce the risk of contamination with maternal DNA, sensitivity of the cffDNA testing process declined to 78%. Another limitation was the required short window for maternal blood sampling (within 24 hours) and its impact on the no-call rate.
The authors note an association with later-life morbidity in patients with a history of pregnancy loss and RPL (including cardiovascular disease, type 2 diabetes, and mental health disorders), thereby arguing for cffDNA-based testing versus no causal testing; however, no treatment has been proven to be effective at reducing pregnancy loss. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The best management course for unexplained RPL is uncertain. Despite its use for a euploid miscarriage or parental chromosomal structural rearrangement, in vitro fertilization with preimplantation genetic testing remains an unproven modality.6,7 Given that approximately 70% of human conceptions never achieve viability, and 50% fail spontaneously before being detected,8 the authors’ findings demonstrate peripheral maternal blood can provide a reasonably high sensitivity and specificity for fetal ploidy status when compared with direct sequencing of pregnancy tissue. As fetal aneuploidy offers a higher percentage of subsequent successful pregnancy outcomes, cffDNA may offer reassurance, or direct further testing, following a pregnancy loss. As an application of their results, evaluation may be deferred for an aneuploid miscarriage.
—MARK P. TROLICE, MD, MBA
References
Brown S. Miscarriage and its associations. Semin Reprod Med. 2008;26:391-400. doi: 10.1055/s-0028-1087105.
Wang X, Chen C , Wang L, et al. Conception, early pregnancy loss, and time to clinical pregnancy: a population-based prospective study. Fertil Steril. 2003;79:577-584.
Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril. 2012;98: 1103-1111.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/tacg.s320778.
Popescu F, Jaslow FC, Kutteh WH. Recurrent pregnancy loss evaluation combined with 24-chromosome microarray of miscarriage tissue provides a probable or definite cause of pregnancy loss in over 90% of patients. Hum Reprod. 2018;33:579-587. https://doi.org/10.1093/humrep/dey021.
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. https://doi.org/10.1093/humrep/deab194.
Iews M, Tan J, Taskin O, et al. Does preimplantation genetic diagnosis improve reproductive outcome in couples with recurrent pregnancy loss owing to structural chromosomal rearrangement? A systematic review. Reproductive Bio Medicine Online. 2018;36:677-685. https://doi.org/10.1016 /j.rbmo.2018.03.005.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/TACG.S320778.
References
Brown S. Miscarriage and its associations. Semin Reprod Med. 2008;26:391-400. doi: 10.1055/s-0028-1087105.
Wang X, Chen C , Wang L, et al. Conception, early pregnancy loss, and time to clinical pregnancy: a population-based prospective study. Fertil Steril. 2003;79:577-584.
Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril. 2012;98: 1103-1111.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/tacg.s320778.
Popescu F, Jaslow FC, Kutteh WH. Recurrent pregnancy loss evaluation combined with 24-chromosome microarray of miscarriage tissue provides a probable or definite cause of pregnancy loss in over 90% of patients. Hum Reprod. 2018;33:579-587. https://doi.org/10.1093/humrep/dey021.
Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. https://doi.org/10.1093/humrep/deab194.
Iews M, Tan J, Taskin O, et al. Does preimplantation genetic diagnosis improve reproductive outcome in couples with recurrent pregnancy loss owing to structural chromosomal rearrangement? A systematic review. Reproductive Bio Medicine Online. 2018;36:677-685. https://doi.org/10.1016 /j.rbmo.2018.03.005.
Papas RS, Kutteh WH. Genetic testing for aneuploidy in patients who have had multiple miscarriages: a review of current literature. Appl Clin Genet. 2021;14:321-329. https://doi.org/10.2147/TACG.S320778.
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
EXPERT COMMENTARY
Maternal mortality rates in the United States were embarrassingly high and rising compared with other high-income countries prior to the onset of the COVID-19 pandemic. Recently, Thoma and Declercq aimed to assess the impact of COVID-19 on pregnancy-related deaths within 42 days of childbirth as well as out to 12 months postpartum.1
During the pandemic, many issues may have affected maternity care and birthing experiences, including changes in prenatal care, restrictions that prevented support people from attending labor, and staffing shortages related to hospital overcrowding with personnel assignments away from labor and delivery. The study by Thoma and Declercq looked at maternal mortality from prior to the onset of the pandemic through changes in the health care environment, availability of vaccines, and emergence of more highly contagious and potentially more lethal viral variants.1 All data were stratified by race, ethnicity, and locale. Death rates were compared between urban, metropolitan regions; suburban, mid-size regions; and rural locations.
Details of the study
Data were collected from the Centers for Disease Control and Prevention’s (CDC) publicly available WONDER database from 2019 to 2021. Because the absolute number of deaths within the American Indian/Alaska Native community was relatively small during that timeframe, data from 2018 also were accessed in order to verify reliability. The authors used the CDC’s definition of pregnancy-related death as “a death while pregnant or within 1 year of the end of pregnancy from any cause related to or aggravated by the pregnancy.”2 International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify maternal deaths. The multiple causes of death file was queried to match maternal deaths with COVID-19 as a contributory cause.
Patterns of maternal deaths were compared with overall COVID-19 cases and COVID-19 death rates for reproductive-age women (ages 15 to 44) by quarters beginning in quarter 1 of 2019. Quarters through the first quarter of 2020 were prepandemic, then quarterly statistics were analyzed from the second quarter of 2020 through the end of 2021 to assess the impact of COVID-19 on early and late maternal mortality.
Findings. Overall maternal mortality rose by 26% from the beginning of 2020 to the second quarter, remained stable through mid-2021, then increased dramatically in the second half of 2021. Maternal mortality unrelated to COVID-19 remained fairly consistent at prior levels, whereas the COVID-19 associateddeaths mirrored the pattern of mortality among reproductive-age nonpregnant women attributed to COVID-19. In addition, the disparities in health outcomes observed in the population at large related to COVID-19 were similar among pregnant people.
American Indian/Alaska Native populations had the largest increase in mortality—more than doubling between early 2020 and the end of 2021. Black people experienced the largest absolute increase in mortality (up to 97.7/100,000 births) while Hispanic birthing people had the highest relative increase (from 19.3 to 29.8/100,000 births). While there were increases in maternal mortality among White and Asian birthing people, these variances were much smaller than for Black, Hispanic, and American Indian/Alaska Native populations.
When comparing mortality stratified by residence areas, early pandemic deaths were higher among birthing people in large urban areas (a 33% increase in 2020); however, later in the pandemic the rates increased substantially in medium-small metropolitan areas (39%) and rural areas (21%).
Study strengths and limitations
The administrative data used to inform this study is a relatively reliable dataset, although errors in both coding for COVID-19 as a contributory cause of maternal death and appropriate ascertainment of race and ethnicity may have occurred. Administrative data can highlight the trends in maternal mortality but cannot identify the root causes of these deaths. We are left with many questions regarding the contribution of staffing, support in labor, changes in prenatal care, and instability in food, housing, and comorbid medical conditions to this devastating rise in maternal mortality. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The COVID-19 pandemic resulted in increased maternal mortality overall but in disproportionate increases in maternal mortality in American Indian/Alaska Native, Black, and Hispanic birthing people. The sharpest rise in mortality occurred with the onset of the Delta variant—and after several COVID-19 vaccines were available, which were not tested in or recommended early in 2021 for pregnant people. Vulnerable populations were at highest risk for death associated with COVID-19 during pregnancy. Perhaps this can inform responses to future pandemics and prompt inclusion of pregnant people early in the development of vaccines and prevention strategies.
BARBARA LEVY, MD
References
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
Centers for Disease Control and Prevention. Pregnancy mortality surveillance system. Accessed April 17, 2023. https://www.cdc.gov/reproductivehealth/maternal -mortality/pregnancy-mortality-surveillance-system.htm
Barbara Levy, MD, is Clinical Professor, Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC; Voluntary Clinical Professor, Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Barbara Levy, MD, is Clinical Professor, Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC; Voluntary Clinical Professor, Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Author and Disclosure Information
Barbara Levy, MD, is Clinical Professor, Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC; Voluntary Clinical Professor, Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
EXPERT COMMENTARY
Maternal mortality rates in the United States were embarrassingly high and rising compared with other high-income countries prior to the onset of the COVID-19 pandemic. Recently, Thoma and Declercq aimed to assess the impact of COVID-19 on pregnancy-related deaths within 42 days of childbirth as well as out to 12 months postpartum.1
During the pandemic, many issues may have affected maternity care and birthing experiences, including changes in prenatal care, restrictions that prevented support people from attending labor, and staffing shortages related to hospital overcrowding with personnel assignments away from labor and delivery. The study by Thoma and Declercq looked at maternal mortality from prior to the onset of the pandemic through changes in the health care environment, availability of vaccines, and emergence of more highly contagious and potentially more lethal viral variants.1 All data were stratified by race, ethnicity, and locale. Death rates were compared between urban, metropolitan regions; suburban, mid-size regions; and rural locations.
Details of the study
Data were collected from the Centers for Disease Control and Prevention’s (CDC) publicly available WONDER database from 2019 to 2021. Because the absolute number of deaths within the American Indian/Alaska Native community was relatively small during that timeframe, data from 2018 also were accessed in order to verify reliability. The authors used the CDC’s definition of pregnancy-related death as “a death while pregnant or within 1 year of the end of pregnancy from any cause related to or aggravated by the pregnancy.”2 International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify maternal deaths. The multiple causes of death file was queried to match maternal deaths with COVID-19 as a contributory cause.
Patterns of maternal deaths were compared with overall COVID-19 cases and COVID-19 death rates for reproductive-age women (ages 15 to 44) by quarters beginning in quarter 1 of 2019. Quarters through the first quarter of 2020 were prepandemic, then quarterly statistics were analyzed from the second quarter of 2020 through the end of 2021 to assess the impact of COVID-19 on early and late maternal mortality.
Findings. Overall maternal mortality rose by 26% from the beginning of 2020 to the second quarter, remained stable through mid-2021, then increased dramatically in the second half of 2021. Maternal mortality unrelated to COVID-19 remained fairly consistent at prior levels, whereas the COVID-19 associateddeaths mirrored the pattern of mortality among reproductive-age nonpregnant women attributed to COVID-19. In addition, the disparities in health outcomes observed in the population at large related to COVID-19 were similar among pregnant people.
American Indian/Alaska Native populations had the largest increase in mortality—more than doubling between early 2020 and the end of 2021. Black people experienced the largest absolute increase in mortality (up to 97.7/100,000 births) while Hispanic birthing people had the highest relative increase (from 19.3 to 29.8/100,000 births). While there were increases in maternal mortality among White and Asian birthing people, these variances were much smaller than for Black, Hispanic, and American Indian/Alaska Native populations.
When comparing mortality stratified by residence areas, early pandemic deaths were higher among birthing people in large urban areas (a 33% increase in 2020); however, later in the pandemic the rates increased substantially in medium-small metropolitan areas (39%) and rural areas (21%).
Study strengths and limitations
The administrative data used to inform this study is a relatively reliable dataset, although errors in both coding for COVID-19 as a contributory cause of maternal death and appropriate ascertainment of race and ethnicity may have occurred. Administrative data can highlight the trends in maternal mortality but cannot identify the root causes of these deaths. We are left with many questions regarding the contribution of staffing, support in labor, changes in prenatal care, and instability in food, housing, and comorbid medical conditions to this devastating rise in maternal mortality. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The COVID-19 pandemic resulted in increased maternal mortality overall but in disproportionate increases in maternal mortality in American Indian/Alaska Native, Black, and Hispanic birthing people. The sharpest rise in mortality occurred with the onset of the Delta variant—and after several COVID-19 vaccines were available, which were not tested in or recommended early in 2021 for pregnant people. Vulnerable populations were at highest risk for death associated with COVID-19 during pregnancy. Perhaps this can inform responses to future pandemics and prompt inclusion of pregnant people early in the development of vaccines and prevention strategies.
BARBARA LEVY, MD
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
EXPERT COMMENTARY
Maternal mortality rates in the United States were embarrassingly high and rising compared with other high-income countries prior to the onset of the COVID-19 pandemic. Recently, Thoma and Declercq aimed to assess the impact of COVID-19 on pregnancy-related deaths within 42 days of childbirth as well as out to 12 months postpartum.1
During the pandemic, many issues may have affected maternity care and birthing experiences, including changes in prenatal care, restrictions that prevented support people from attending labor, and staffing shortages related to hospital overcrowding with personnel assignments away from labor and delivery. The study by Thoma and Declercq looked at maternal mortality from prior to the onset of the pandemic through changes in the health care environment, availability of vaccines, and emergence of more highly contagious and potentially more lethal viral variants.1 All data were stratified by race, ethnicity, and locale. Death rates were compared between urban, metropolitan regions; suburban, mid-size regions; and rural locations.
Details of the study
Data were collected from the Centers for Disease Control and Prevention’s (CDC) publicly available WONDER database from 2019 to 2021. Because the absolute number of deaths within the American Indian/Alaska Native community was relatively small during that timeframe, data from 2018 also were accessed in order to verify reliability. The authors used the CDC’s definition of pregnancy-related death as “a death while pregnant or within 1 year of the end of pregnancy from any cause related to or aggravated by the pregnancy.”2 International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify maternal deaths. The multiple causes of death file was queried to match maternal deaths with COVID-19 as a contributory cause.
Patterns of maternal deaths were compared with overall COVID-19 cases and COVID-19 death rates for reproductive-age women (ages 15 to 44) by quarters beginning in quarter 1 of 2019. Quarters through the first quarter of 2020 were prepandemic, then quarterly statistics were analyzed from the second quarter of 2020 through the end of 2021 to assess the impact of COVID-19 on early and late maternal mortality.
Findings. Overall maternal mortality rose by 26% from the beginning of 2020 to the second quarter, remained stable through mid-2021, then increased dramatically in the second half of 2021. Maternal mortality unrelated to COVID-19 remained fairly consistent at prior levels, whereas the COVID-19 associateddeaths mirrored the pattern of mortality among reproductive-age nonpregnant women attributed to COVID-19. In addition, the disparities in health outcomes observed in the population at large related to COVID-19 were similar among pregnant people.
American Indian/Alaska Native populations had the largest increase in mortality—more than doubling between early 2020 and the end of 2021. Black people experienced the largest absolute increase in mortality (up to 97.7/100,000 births) while Hispanic birthing people had the highest relative increase (from 19.3 to 29.8/100,000 births). While there were increases in maternal mortality among White and Asian birthing people, these variances were much smaller than for Black, Hispanic, and American Indian/Alaska Native populations.
When comparing mortality stratified by residence areas, early pandemic deaths were higher among birthing people in large urban areas (a 33% increase in 2020); however, later in the pandemic the rates increased substantially in medium-small metropolitan areas (39%) and rural areas (21%).
Study strengths and limitations
The administrative data used to inform this study is a relatively reliable dataset, although errors in both coding for COVID-19 as a contributory cause of maternal death and appropriate ascertainment of race and ethnicity may have occurred. Administrative data can highlight the trends in maternal mortality but cannot identify the root causes of these deaths. We are left with many questions regarding the contribution of staffing, support in labor, changes in prenatal care, and instability in food, housing, and comorbid medical conditions to this devastating rise in maternal mortality. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The COVID-19 pandemic resulted in increased maternal mortality overall but in disproportionate increases in maternal mortality in American Indian/Alaska Native, Black, and Hispanic birthing people. The sharpest rise in mortality occurred with the onset of the Delta variant—and after several COVID-19 vaccines were available, which were not tested in or recommended early in 2021 for pregnant people. Vulnerable populations were at highest risk for death associated with COVID-19 during pregnancy. Perhaps this can inform responses to future pandemics and prompt inclusion of pregnant people early in the development of vaccines and prevention strategies.
BARBARA LEVY, MD
References
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
Centers for Disease Control and Prevention. Pregnancy mortality surveillance system. Accessed April 17, 2023. https://www.cdc.gov/reproductivehealth/maternal -mortality/pregnancy-mortality-surveillance-system.htm
References
Thoma ME, Declercq ER. Changes in pregnancy-related mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the United States. Obstet Gynecol. 2023. doi:10.1097/AOG0000000000005182.
Centers for Disease Control and Prevention. Pregnancy mortality surveillance system. Accessed April 17, 2023. https://www.cdc.gov/reproductivehealth/maternal -mortality/pregnancy-mortality-surveillance-system.htm
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
EXPERT COMMENTARY
Aspirin is, to date, the only proven preventative treatment to reduce the risk of preeclampsia in pregnancy. While aspirin initiation, optimally prior to 16 weeks, generally is accepted, the best timing for discontinuation remains uncertain due to conflicting data on risk of bleeding and different doses used. The American College of Obstetricians and Gynecologists recommends a broad range of patients eligible for low-dose aspirin with continuation through delivery, citing data that support no increase in either maternal or fetal/neonatal complications, including bleeding complications.1 Other guidelines recommend reduction in pregnancy exposure to aspirin with strict guidelines for which patients are considered “high risk” as well as discontinuation at 36 weeks prior to labor onset to reduce the risk of potential bleeding complications.
Recently, Mendoza and colleagues tested the hypothesis that, in patients at high risk for preterm preeclampsia (based on high-risk first-trimester screening followed by a low risk of preeclampsia at 24 to 28 weeks based on a normal sFlt-1:PlGF [soluble fms-like tyrosine kinase-1 to placental growth factor] ratio), discontinuing aspirin is noninferior in preventing preterm preeclampsia compared with continuing aspirin until 36 weeks.2
Details of the study
Mendoza and colleagues conducted a multicenter, open label, randomized, phase 3, noninferiority trial that randomly assigned 968 participants prior to stopping recruitment based on the findings from a planned interim analysis.2
The patient population included women with singleton pregnancies between 24 and 28 weeks who had initiated aspirin 150 mg daily by 16 6/7 weeks due to high-risk first- trimester screening for preterm preeclampsia. Additionally, these patients also had an sFlt-1:PlGR ratio of 38 or less between 24 and 28 weeks’ gestation, which prior studies have demonstrated to exclude the diagnosis of preeclampsia.
Patients were randomly assigned to either discontinue aspirin at 24 to 28 weeks’ gestation (intervention group) or continue aspirin until 36 weeks’ gestation (control group). The primary outcome was delivery due to preeclampsia at less than 37 weeks, with secondary outcomes of preeclampsia at less than 34 weeks, preeclampsia at 37 or more weeks, or other adverse pregnancy outcomes.
Results.For the primary outcome (936 participants’ data analyzed), the incidence of preeclampsia at less than 37 weeks was 1.48% in the intervention group and 1.73% in the control group (absolute difference, -0.25%, which meets study criteria for noninferiority).
No difference occurred in the secondary outcomes of adverse outcomes at less than 34 weeks or at less than 37 weeks. While there was no difference in the incidence of the individual adverse outcomes at 37 or more weeks, the intervention group had a decrease in the incidence of having “any” adverse outcome (-5.04%) as well as a decrease in minor antepartum hemorrhage (nose and/or gum bleeding) (-4.7%).
The authors therefore concluded that aspirin discontinuation at 24 to 28 weeks’ gestation in pregnant patients at high risk for preterm preeclampsia and a normal sFlt-1:PlGF ratio is noninferior to aspirin continuation for prevention of preterm preeclampsia. They also suggested that this discontinuation may reduce the risk of adverse pregnancy outcomes at 37 or more weeks as well as minor bleeding complications.
Study strengths and limitations
The authors cited the novelty of this study at considering using aspirin for the prevention of preterm preeclampsia in a specific patient group for the shortest amount of time needed to achieve this goal. Potential benefits could be decreased bleeding complications, cost, anxiety, and visits.
They also noted the following study limitations: open-label design, a predominantly White patient population, early termination due to the interim analysis, inadequate power for more rare complications, and a query as to the appropriate choice for the threshold for noninferiority. Noninferiority trials have inherent weaknesses as a group that should be considered before major practice changes occur as a result of their findings.
Several other factors in the study limit the generalizability of the authors’ recommendations, especially to patient populations in the United States. For example, the study used an aspirin dose of 150 mg daily, which is almost double the dose recommended in the United States (81 mg). The reasoning for this was that doses higher than 100 mg have been shown to be the most effective for preeclampsia prevention but also may have higher rates of bleeding complications, including placental abruption. The demonstrated increase in complications may not hold at a lower dose.
Additionally, patients in this study were selected for aspirin by a first-trimester algorithm that may not be in general use everywhere (and differs from the US Preventive Services Task Force recommendations for low-dose aspirin use in pregnancy). Finally, although extremely interesting, the use of the sFlt-1:PlFG ratio at 24 to 28 weeks is not in widespread use in the United States and may incur an additional cost not equivalent to the low cost of a daily aspirin.
Essentially, this is an extremely limited study for a very specific population. Before globally discontinuing low-dose aspirin in high-risk patients, the different doses and eligibility criteria should be studied for effect of early discontinuation. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Low-dose aspirin should continue to be used for prevention of preeclampsia in high-risk pregnant patients, optimally starting at 12 to 16 weeks’ gestation and continuing either through 36 weeks or delivery. Further study is needed to determine the optimal timing for earlier discontinuation of aspirin based on dose, risk factors, and other measures of preeclampsia risk as the pregnancy progresses.
JAIMEY M. PAULI, MD
References
ACOG committee opinion no. 743: low-dose aspirin use during pregnancy. Obstet Gynecol. 2018;132:e44-e52. doi:10.1097/AOG.0000000000002708.
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
Jaimey M. Pauli, MD, is Professor, Department of Obstetrics and Gynecology; Chief, Division of Maternal-Fetal Medicine, Pennsylvania State College of Medicine, Milton S. Hershey Medical Center, Hershey, Pennsylvania. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Jaimey M. Pauli, MD, is Professor, Department of Obstetrics and Gynecology; Chief, Division of Maternal-Fetal Medicine, Pennsylvania State College of Medicine, Milton S. Hershey Medical Center, Hershey, Pennsylvania. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Author and Disclosure Information
Jaimey M. Pauli, MD, is Professor, Department of Obstetrics and Gynecology; Chief, Division of Maternal-Fetal Medicine, Pennsylvania State College of Medicine, Milton S. Hershey Medical Center, Hershey, Pennsylvania. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
EXPERT COMMENTARY
Aspirin is, to date, the only proven preventative treatment to reduce the risk of preeclampsia in pregnancy. While aspirin initiation, optimally prior to 16 weeks, generally is accepted, the best timing for discontinuation remains uncertain due to conflicting data on risk of bleeding and different doses used. The American College of Obstetricians and Gynecologists recommends a broad range of patients eligible for low-dose aspirin with continuation through delivery, citing data that support no increase in either maternal or fetal/neonatal complications, including bleeding complications.1 Other guidelines recommend reduction in pregnancy exposure to aspirin with strict guidelines for which patients are considered “high risk” as well as discontinuation at 36 weeks prior to labor onset to reduce the risk of potential bleeding complications.
Recently, Mendoza and colleagues tested the hypothesis that, in patients at high risk for preterm preeclampsia (based on high-risk first-trimester screening followed by a low risk of preeclampsia at 24 to 28 weeks based on a normal sFlt-1:PlGF [soluble fms-like tyrosine kinase-1 to placental growth factor] ratio), discontinuing aspirin is noninferior in preventing preterm preeclampsia compared with continuing aspirin until 36 weeks.2
Details of the study
Mendoza and colleagues conducted a multicenter, open label, randomized, phase 3, noninferiority trial that randomly assigned 968 participants prior to stopping recruitment based on the findings from a planned interim analysis.2
The patient population included women with singleton pregnancies between 24 and 28 weeks who had initiated aspirin 150 mg daily by 16 6/7 weeks due to high-risk first- trimester screening for preterm preeclampsia. Additionally, these patients also had an sFlt-1:PlGR ratio of 38 or less between 24 and 28 weeks’ gestation, which prior studies have demonstrated to exclude the diagnosis of preeclampsia.
Patients were randomly assigned to either discontinue aspirin at 24 to 28 weeks’ gestation (intervention group) or continue aspirin until 36 weeks’ gestation (control group). The primary outcome was delivery due to preeclampsia at less than 37 weeks, with secondary outcomes of preeclampsia at less than 34 weeks, preeclampsia at 37 or more weeks, or other adverse pregnancy outcomes.
Results.For the primary outcome (936 participants’ data analyzed), the incidence of preeclampsia at less than 37 weeks was 1.48% in the intervention group and 1.73% in the control group (absolute difference, -0.25%, which meets study criteria for noninferiority).
No difference occurred in the secondary outcomes of adverse outcomes at less than 34 weeks or at less than 37 weeks. While there was no difference in the incidence of the individual adverse outcomes at 37 or more weeks, the intervention group had a decrease in the incidence of having “any” adverse outcome (-5.04%) as well as a decrease in minor antepartum hemorrhage (nose and/or gum bleeding) (-4.7%).
The authors therefore concluded that aspirin discontinuation at 24 to 28 weeks’ gestation in pregnant patients at high risk for preterm preeclampsia and a normal sFlt-1:PlGF ratio is noninferior to aspirin continuation for prevention of preterm preeclampsia. They also suggested that this discontinuation may reduce the risk of adverse pregnancy outcomes at 37 or more weeks as well as minor bleeding complications.
Study strengths and limitations
The authors cited the novelty of this study at considering using aspirin for the prevention of preterm preeclampsia in a specific patient group for the shortest amount of time needed to achieve this goal. Potential benefits could be decreased bleeding complications, cost, anxiety, and visits.
They also noted the following study limitations: open-label design, a predominantly White patient population, early termination due to the interim analysis, inadequate power for more rare complications, and a query as to the appropriate choice for the threshold for noninferiority. Noninferiority trials have inherent weaknesses as a group that should be considered before major practice changes occur as a result of their findings.
Several other factors in the study limit the generalizability of the authors’ recommendations, especially to patient populations in the United States. For example, the study used an aspirin dose of 150 mg daily, which is almost double the dose recommended in the United States (81 mg). The reasoning for this was that doses higher than 100 mg have been shown to be the most effective for preeclampsia prevention but also may have higher rates of bleeding complications, including placental abruption. The demonstrated increase in complications may not hold at a lower dose.
Additionally, patients in this study were selected for aspirin by a first-trimester algorithm that may not be in general use everywhere (and differs from the US Preventive Services Task Force recommendations for low-dose aspirin use in pregnancy). Finally, although extremely interesting, the use of the sFlt-1:PlFG ratio at 24 to 28 weeks is not in widespread use in the United States and may incur an additional cost not equivalent to the low cost of a daily aspirin.
Essentially, this is an extremely limited study for a very specific population. Before globally discontinuing low-dose aspirin in high-risk patients, the different doses and eligibility criteria should be studied for effect of early discontinuation. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Low-dose aspirin should continue to be used for prevention of preeclampsia in high-risk pregnant patients, optimally starting at 12 to 16 weeks’ gestation and continuing either through 36 weeks or delivery. Further study is needed to determine the optimal timing for earlier discontinuation of aspirin based on dose, risk factors, and other measures of preeclampsia risk as the pregnancy progresses.
JAIMEY M. PAULI, MD
Photo: antoniodiaz/Shutterstock
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
EXPERT COMMENTARY
Aspirin is, to date, the only proven preventative treatment to reduce the risk of preeclampsia in pregnancy. While aspirin initiation, optimally prior to 16 weeks, generally is accepted, the best timing for discontinuation remains uncertain due to conflicting data on risk of bleeding and different doses used. The American College of Obstetricians and Gynecologists recommends a broad range of patients eligible for low-dose aspirin with continuation through delivery, citing data that support no increase in either maternal or fetal/neonatal complications, including bleeding complications.1 Other guidelines recommend reduction in pregnancy exposure to aspirin with strict guidelines for which patients are considered “high risk” as well as discontinuation at 36 weeks prior to labor onset to reduce the risk of potential bleeding complications.
Recently, Mendoza and colleagues tested the hypothesis that, in patients at high risk for preterm preeclampsia (based on high-risk first-trimester screening followed by a low risk of preeclampsia at 24 to 28 weeks based on a normal sFlt-1:PlGF [soluble fms-like tyrosine kinase-1 to placental growth factor] ratio), discontinuing aspirin is noninferior in preventing preterm preeclampsia compared with continuing aspirin until 36 weeks.2
Details of the study
Mendoza and colleagues conducted a multicenter, open label, randomized, phase 3, noninferiority trial that randomly assigned 968 participants prior to stopping recruitment based on the findings from a planned interim analysis.2
The patient population included women with singleton pregnancies between 24 and 28 weeks who had initiated aspirin 150 mg daily by 16 6/7 weeks due to high-risk first- trimester screening for preterm preeclampsia. Additionally, these patients also had an sFlt-1:PlGR ratio of 38 or less between 24 and 28 weeks’ gestation, which prior studies have demonstrated to exclude the diagnosis of preeclampsia.
Patients were randomly assigned to either discontinue aspirin at 24 to 28 weeks’ gestation (intervention group) or continue aspirin until 36 weeks’ gestation (control group). The primary outcome was delivery due to preeclampsia at less than 37 weeks, with secondary outcomes of preeclampsia at less than 34 weeks, preeclampsia at 37 or more weeks, or other adverse pregnancy outcomes.
Results.For the primary outcome (936 participants’ data analyzed), the incidence of preeclampsia at less than 37 weeks was 1.48% in the intervention group and 1.73% in the control group (absolute difference, -0.25%, which meets study criteria for noninferiority).
No difference occurred in the secondary outcomes of adverse outcomes at less than 34 weeks or at less than 37 weeks. While there was no difference in the incidence of the individual adverse outcomes at 37 or more weeks, the intervention group had a decrease in the incidence of having “any” adverse outcome (-5.04%) as well as a decrease in minor antepartum hemorrhage (nose and/or gum bleeding) (-4.7%).
The authors therefore concluded that aspirin discontinuation at 24 to 28 weeks’ gestation in pregnant patients at high risk for preterm preeclampsia and a normal sFlt-1:PlGF ratio is noninferior to aspirin continuation for prevention of preterm preeclampsia. They also suggested that this discontinuation may reduce the risk of adverse pregnancy outcomes at 37 or more weeks as well as minor bleeding complications.
Study strengths and limitations
The authors cited the novelty of this study at considering using aspirin for the prevention of preterm preeclampsia in a specific patient group for the shortest amount of time needed to achieve this goal. Potential benefits could be decreased bleeding complications, cost, anxiety, and visits.
They also noted the following study limitations: open-label design, a predominantly White patient population, early termination due to the interim analysis, inadequate power for more rare complications, and a query as to the appropriate choice for the threshold for noninferiority. Noninferiority trials have inherent weaknesses as a group that should be considered before major practice changes occur as a result of their findings.
Several other factors in the study limit the generalizability of the authors’ recommendations, especially to patient populations in the United States. For example, the study used an aspirin dose of 150 mg daily, which is almost double the dose recommended in the United States (81 mg). The reasoning for this was that doses higher than 100 mg have been shown to be the most effective for preeclampsia prevention but also may have higher rates of bleeding complications, including placental abruption. The demonstrated increase in complications may not hold at a lower dose.
Additionally, patients in this study were selected for aspirin by a first-trimester algorithm that may not be in general use everywhere (and differs from the US Preventive Services Task Force recommendations for low-dose aspirin use in pregnancy). Finally, although extremely interesting, the use of the sFlt-1:PlFG ratio at 24 to 28 weeks is not in widespread use in the United States and may incur an additional cost not equivalent to the low cost of a daily aspirin.
Essentially, this is an extremely limited study for a very specific population. Before globally discontinuing low-dose aspirin in high-risk patients, the different doses and eligibility criteria should be studied for effect of early discontinuation. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Low-dose aspirin should continue to be used for prevention of preeclampsia in high-risk pregnant patients, optimally starting at 12 to 16 weeks’ gestation and continuing either through 36 weeks or delivery. Further study is needed to determine the optimal timing for earlier discontinuation of aspirin based on dose, risk factors, and other measures of preeclampsia risk as the pregnancy progresses.
JAIMEY M. PAULI, MD
References
ACOG committee opinion no. 743: low-dose aspirin use during pregnancy. Obstet Gynecol. 2018;132:e44-e52. doi:10.1097/AOG.0000000000002708.
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
References
ACOG committee opinion no. 743: low-dose aspirin use during pregnancy. Obstet Gynecol. 2018;132:e44-e52. doi:10.1097/AOG.0000000000002708.
Mendoza M, Bonacina E, Garcia-Manau P, et al. Aspirin discontinuation at 24 to 28 weeks’ gestation in pregnancies at high risk of preterm preeclampsia: a randomized clinical trial. JAMA. 2023;329:542-550. doi:10.1001/jama.2023.0691.
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
EXPERT COMMENTARY
Cervical cancer screening guidelines recommend screening cessation at age 65 once specific exit criteria are met. (According to the American Cancer Society, individuals aged >65 years who have no history of cervical intraepithelial neoplasia [CIN] grade 2 or more severe disease within the past 25 years, and who have documented adequate negative prior screening in the prior 10 years, discontinue all cervical cancer screening.)1 We know, however, that about one-fifth of all cervical cancer cases are diagnosed among individuals aged 65 or older, and for Black women that proportion is even higher when data are appropriately adjusted to account for the increased rate of hysterectomy among Black versus White women.2-4
Early-stage cervical cancer is largely a curable disease with very high 5-year overall survival rates. Unfortunately, more than half of all cervical cancer is diagnosed at a more advanced stage, and survival rates are much lower for this population.5
Cervical cancer incidence rates plummeted in the United States after the introduction of the Pap test for cervical cancer screening. However, the percentage of women who are not up to date with cervical cancer screening may now be increasing, from 14% in 2005 to 23% in 2019 according to one study from the US Preventive Services Task Force.6 When looking at cervical cancer screening rates by age, researchers from the Centers for Disease Control and Prevention estimate that the proportion of patients who have not been recently screened goes up as patients get older, with approximately 845,000 American women aged 61 to 65 not adequately screened in 2015 alone.7
Details of the study
Cooley and colleagues sought to better characterize the cohort of women diagnosed with cervical cancer at a later age, specifically the stage at diagnosis and survival.8 They used data from the California Cancer Registry (CCR), a large state-mandated, population-based data repository that is affiliated with the Surveillance, Epidemiology, and End Results (SEER) program.
The researchers identified 12,442 womenin the CCR who were newly diagnosed with cervical cancer from 2009 to 2018, 17.4% of whom were age 65 or older. They looked at cancer stage at diagnosis as it relates to relative survival rate (“the ratio of the observed survival rate among those who have cancer divided by the expected survival rate for people of the same sex, race/ethnicity, and age who do not have cancer”), Charlson comorbidity score, socioeconomic status, health insurance status, urbanicity, and race/ethnicity.
Results.In this study, 71% of women aged 65 or older presented with advanced-stage disease (FIGO [International Federation of Gynecology and Obstetrics] stage II–IV) as compared with only 48% in those aged 21 to 64. Five-year relative survival rates also were lower in the older cohort—23% to 37%, compared with 42% to 52% in the younger patients. In a sensitivity analysis, late-stage disease was associated with older age, increasing medical comorbidities, and nonadenocarcinoma histology.
Interestingly, older women of Hispanic ethnicity were less likely to be diagnosed with late-stage disease when compared with non-Hispanic White women.
Study strengths and limitations
Although this study’s conclusions—that patients with advanced-stage cancer are more likely to do poorly than those with early-stage cancer—may seem obvious to some even without the proven data, it is still important to highlight what a clinician may intuit with data to support that intuition. It is particularly important to emphasize this risk in older women in light of the aging population in the United States, with adults older than age 65 expected to account for more than 20% of the nation’s population by 2030.9
The study by Cooley and colleagues adds value to the existing literature due to its large study population, which included more than 12,000 patients diagnosed with cervical cancer.8 And although its results may not be completely generalizable as the data were gathered from only a California-specific population, the sample was diverse with significant portions of Hispanic and Black patients. This study supports previous data that showed high rates of advanced cervical cancer in women older than age 65, with resultant worse 5-year relative survival in this population of older women specifically.4 ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Cervical cancer is both common and deadly in older women. Although current cervical cancer screening guidelines recommend screening cessation after age 65, remember that this is based on strict exit criteria. Consider screening older women (especially with human papillomavirus [HPV] testing) for cervical cancer if they have risk factors (such as smoking, multiple sexual partners, inconsistent or infrequent screening, history of abnormal Pap or HPV tests), and keep cervical cancer on your differential diagnosis in women who present with postmenopausal bleeding, vaginal discharge, pelvic pain, recurrent urinary tract infections, or other concerning symptoms.
SARAH DILLEY, MD, MPH, AND WARNER HUH, MD
References
Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
Dilley S, Huh W, Blechter B, et al. It’s time to re-evaluate cervical cancer screening after age 65. Gynecol Oncol. 2021;162:200-202. doi:10.1016/j.ygyno.2021.04.027.
Rositch AF, Nowak RG, Gravitt PE. Increased age and racespecific incidence of cervical cancer after correction for hysterectomy prevalence in the United States from 2000 to 2009. Cancer. 2014;120:2032-2038. doi:10.1002/cncr.28548.
Beavis AL, Gravitt PE, Rositch AF. Hysterectomy-corrected cervical cancer mortality rates reveal a larger racial disparity in the United States. Cancer. 2017;123:1044-1050. doi:10.1002 /cncr.30507.
Cancer Stat Facts. National Cancer Institute Surveillance, Epidemiology, and End Results Program. https://seer.cancer .gov/statfacts/html/cervix.html
Suk R, Hong YR, Rajan SS, et al. Assessment of US Preventive Services Task Force guideline-concordant cervical cancer screening rates and reasons for underscreening by age, race and ethnicity, sexual orientation, rurality, and insurance, 2005 to 2019. JAMA Netw Open. 2022;5:e2143582. doi:10.1001 /jamanetworkopen.2021.43582.
White MC, Shoemaker ML, Benard VB. Cervical cancer screening and incidence by age: unmet needs near and after the stopping age for screening. Am J Prev Med. 2017;53:392395. doi:10.1016/j.amepre.2017.02.024.
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
Ortman JM, Velkoff VA, Hogan H. An aging nation: the older population in the United States. May 2014. United States Census Bureau. Accessed April 12, 2023. https://www.census .gov/library/publications/2014/demo/p25-1140.html
Sarah Dilley, MD, MPH, is Assistant Professor, Gynecologic Oncology, Department of Gynecology and Obstetrics, Emory University, Atlanta, Georgia.
Warner Huh, MD, is Professor, Gynecologic Oncology, and Chair, Department of Obstetrics and Gynecology, University of Alabama at Birmingham, Birmingham, Alabama.
The authors report no financial relationships relevant to this article.
Sarah Dilley, MD, MPH, is Assistant Professor, Gynecologic Oncology, Department of Gynecology and Obstetrics, Emory University, Atlanta, Georgia.
Warner Huh, MD, is Professor, Gynecologic Oncology, and Chair, Department of Obstetrics and Gynecology, University of Alabama at Birmingham, Birmingham, Alabama.
The authors report no financial relationships relevant to this article.
Author and Disclosure Information
Sarah Dilley, MD, MPH, is Assistant Professor, Gynecologic Oncology, Department of Gynecology and Obstetrics, Emory University, Atlanta, Georgia.
Warner Huh, MD, is Professor, Gynecologic Oncology, and Chair, Department of Obstetrics and Gynecology, University of Alabama at Birmingham, Birmingham, Alabama.
The authors report no financial relationships relevant to this article.
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
EXPERT COMMENTARY
Cervical cancer screening guidelines recommend screening cessation at age 65 once specific exit criteria are met. (According to the American Cancer Society, individuals aged >65 years who have no history of cervical intraepithelial neoplasia [CIN] grade 2 or more severe disease within the past 25 years, and who have documented adequate negative prior screening in the prior 10 years, discontinue all cervical cancer screening.)1 We know, however, that about one-fifth of all cervical cancer cases are diagnosed among individuals aged 65 or older, and for Black women that proportion is even higher when data are appropriately adjusted to account for the increased rate of hysterectomy among Black versus White women.2-4
Early-stage cervical cancer is largely a curable disease with very high 5-year overall survival rates. Unfortunately, more than half of all cervical cancer is diagnosed at a more advanced stage, and survival rates are much lower for this population.5
Cervical cancer incidence rates plummeted in the United States after the introduction of the Pap test for cervical cancer screening. However, the percentage of women who are not up to date with cervical cancer screening may now be increasing, from 14% in 2005 to 23% in 2019 according to one study from the US Preventive Services Task Force.6 When looking at cervical cancer screening rates by age, researchers from the Centers for Disease Control and Prevention estimate that the proportion of patients who have not been recently screened goes up as patients get older, with approximately 845,000 American women aged 61 to 65 not adequately screened in 2015 alone.7
Details of the study
Cooley and colleagues sought to better characterize the cohort of women diagnosed with cervical cancer at a later age, specifically the stage at diagnosis and survival.8 They used data from the California Cancer Registry (CCR), a large state-mandated, population-based data repository that is affiliated with the Surveillance, Epidemiology, and End Results (SEER) program.
The researchers identified 12,442 womenin the CCR who were newly diagnosed with cervical cancer from 2009 to 2018, 17.4% of whom were age 65 or older. They looked at cancer stage at diagnosis as it relates to relative survival rate (“the ratio of the observed survival rate among those who have cancer divided by the expected survival rate for people of the same sex, race/ethnicity, and age who do not have cancer”), Charlson comorbidity score, socioeconomic status, health insurance status, urbanicity, and race/ethnicity.
Results.In this study, 71% of women aged 65 or older presented with advanced-stage disease (FIGO [International Federation of Gynecology and Obstetrics] stage II–IV) as compared with only 48% in those aged 21 to 64. Five-year relative survival rates also were lower in the older cohort—23% to 37%, compared with 42% to 52% in the younger patients. In a sensitivity analysis, late-stage disease was associated with older age, increasing medical comorbidities, and nonadenocarcinoma histology.
Interestingly, older women of Hispanic ethnicity were less likely to be diagnosed with late-stage disease when compared with non-Hispanic White women.
Study strengths and limitations
Although this study’s conclusions—that patients with advanced-stage cancer are more likely to do poorly than those with early-stage cancer—may seem obvious to some even without the proven data, it is still important to highlight what a clinician may intuit with data to support that intuition. It is particularly important to emphasize this risk in older women in light of the aging population in the United States, with adults older than age 65 expected to account for more than 20% of the nation’s population by 2030.9
The study by Cooley and colleagues adds value to the existing literature due to its large study population, which included more than 12,000 patients diagnosed with cervical cancer.8 And although its results may not be completely generalizable as the data were gathered from only a California-specific population, the sample was diverse with significant portions of Hispanic and Black patients. This study supports previous data that showed high rates of advanced cervical cancer in women older than age 65, with resultant worse 5-year relative survival in this population of older women specifically.4 ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Cervical cancer is both common and deadly in older women. Although current cervical cancer screening guidelines recommend screening cessation after age 65, remember that this is based on strict exit criteria. Consider screening older women (especially with human papillomavirus [HPV] testing) for cervical cancer if they have risk factors (such as smoking, multiple sexual partners, inconsistent or infrequent screening, history of abnormal Pap or HPV tests), and keep cervical cancer on your differential diagnosis in women who present with postmenopausal bleeding, vaginal discharge, pelvic pain, recurrent urinary tract infections, or other concerning symptoms.
SARAH DILLEY, MD, MPH, AND WARNER HUH, MD
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
EXPERT COMMENTARY
Cervical cancer screening guidelines recommend screening cessation at age 65 once specific exit criteria are met. (According to the American Cancer Society, individuals aged >65 years who have no history of cervical intraepithelial neoplasia [CIN] grade 2 or more severe disease within the past 25 years, and who have documented adequate negative prior screening in the prior 10 years, discontinue all cervical cancer screening.)1 We know, however, that about one-fifth of all cervical cancer cases are diagnosed among individuals aged 65 or older, and for Black women that proportion is even higher when data are appropriately adjusted to account for the increased rate of hysterectomy among Black versus White women.2-4
Early-stage cervical cancer is largely a curable disease with very high 5-year overall survival rates. Unfortunately, more than half of all cervical cancer is diagnosed at a more advanced stage, and survival rates are much lower for this population.5
Cervical cancer incidence rates plummeted in the United States after the introduction of the Pap test for cervical cancer screening. However, the percentage of women who are not up to date with cervical cancer screening may now be increasing, from 14% in 2005 to 23% in 2019 according to one study from the US Preventive Services Task Force.6 When looking at cervical cancer screening rates by age, researchers from the Centers for Disease Control and Prevention estimate that the proportion of patients who have not been recently screened goes up as patients get older, with approximately 845,000 American women aged 61 to 65 not adequately screened in 2015 alone.7
Details of the study
Cooley and colleagues sought to better characterize the cohort of women diagnosed with cervical cancer at a later age, specifically the stage at diagnosis and survival.8 They used data from the California Cancer Registry (CCR), a large state-mandated, population-based data repository that is affiliated with the Surveillance, Epidemiology, and End Results (SEER) program.
The researchers identified 12,442 womenin the CCR who were newly diagnosed with cervical cancer from 2009 to 2018, 17.4% of whom were age 65 or older. They looked at cancer stage at diagnosis as it relates to relative survival rate (“the ratio of the observed survival rate among those who have cancer divided by the expected survival rate for people of the same sex, race/ethnicity, and age who do not have cancer”), Charlson comorbidity score, socioeconomic status, health insurance status, urbanicity, and race/ethnicity.
Results.In this study, 71% of women aged 65 or older presented with advanced-stage disease (FIGO [International Federation of Gynecology and Obstetrics] stage II–IV) as compared with only 48% in those aged 21 to 64. Five-year relative survival rates also were lower in the older cohort—23% to 37%, compared with 42% to 52% in the younger patients. In a sensitivity analysis, late-stage disease was associated with older age, increasing medical comorbidities, and nonadenocarcinoma histology.
Interestingly, older women of Hispanic ethnicity were less likely to be diagnosed with late-stage disease when compared with non-Hispanic White women.
Study strengths and limitations
Although this study’s conclusions—that patients with advanced-stage cancer are more likely to do poorly than those with early-stage cancer—may seem obvious to some even without the proven data, it is still important to highlight what a clinician may intuit with data to support that intuition. It is particularly important to emphasize this risk in older women in light of the aging population in the United States, with adults older than age 65 expected to account for more than 20% of the nation’s population by 2030.9
The study by Cooley and colleagues adds value to the existing literature due to its large study population, which included more than 12,000 patients diagnosed with cervical cancer.8 And although its results may not be completely generalizable as the data were gathered from only a California-specific population, the sample was diverse with significant portions of Hispanic and Black patients. This study supports previous data that showed high rates of advanced cervical cancer in women older than age 65, with resultant worse 5-year relative survival in this population of older women specifically.4 ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Cervical cancer is both common and deadly in older women. Although current cervical cancer screening guidelines recommend screening cessation after age 65, remember that this is based on strict exit criteria. Consider screening older women (especially with human papillomavirus [HPV] testing) for cervical cancer if they have risk factors (such as smoking, multiple sexual partners, inconsistent or infrequent screening, history of abnormal Pap or HPV tests), and keep cervical cancer on your differential diagnosis in women who present with postmenopausal bleeding, vaginal discharge, pelvic pain, recurrent urinary tract infections, or other concerning symptoms.
SARAH DILLEY, MD, MPH, AND WARNER HUH, MD
References
Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
Dilley S, Huh W, Blechter B, et al. It’s time to re-evaluate cervical cancer screening after age 65. Gynecol Oncol. 2021;162:200-202. doi:10.1016/j.ygyno.2021.04.027.
Rositch AF, Nowak RG, Gravitt PE. Increased age and racespecific incidence of cervical cancer after correction for hysterectomy prevalence in the United States from 2000 to 2009. Cancer. 2014;120:2032-2038. doi:10.1002/cncr.28548.
Beavis AL, Gravitt PE, Rositch AF. Hysterectomy-corrected cervical cancer mortality rates reveal a larger racial disparity in the United States. Cancer. 2017;123:1044-1050. doi:10.1002 /cncr.30507.
Cancer Stat Facts. National Cancer Institute Surveillance, Epidemiology, and End Results Program. https://seer.cancer .gov/statfacts/html/cervix.html
Suk R, Hong YR, Rajan SS, et al. Assessment of US Preventive Services Task Force guideline-concordant cervical cancer screening rates and reasons for underscreening by age, race and ethnicity, sexual orientation, rurality, and insurance, 2005 to 2019. JAMA Netw Open. 2022;5:e2143582. doi:10.1001 /jamanetworkopen.2021.43582.
White MC, Shoemaker ML, Benard VB. Cervical cancer screening and incidence by age: unmet needs near and after the stopping age for screening. Am J Prev Med. 2017;53:392395. doi:10.1016/j.amepre.2017.02.024.
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
Ortman JM, Velkoff VA, Hogan H. An aging nation: the older population in the United States. May 2014. United States Census Bureau. Accessed April 12, 2023. https://www.census .gov/library/publications/2014/demo/p25-1140.html
References
Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
Dilley S, Huh W, Blechter B, et al. It’s time to re-evaluate cervical cancer screening after age 65. Gynecol Oncol. 2021;162:200-202. doi:10.1016/j.ygyno.2021.04.027.
Rositch AF, Nowak RG, Gravitt PE. Increased age and racespecific incidence of cervical cancer after correction for hysterectomy prevalence in the United States from 2000 to 2009. Cancer. 2014;120:2032-2038. doi:10.1002/cncr.28548.
Beavis AL, Gravitt PE, Rositch AF. Hysterectomy-corrected cervical cancer mortality rates reveal a larger racial disparity in the United States. Cancer. 2017;123:1044-1050. doi:10.1002 /cncr.30507.
Cancer Stat Facts. National Cancer Institute Surveillance, Epidemiology, and End Results Program. https://seer.cancer .gov/statfacts/html/cervix.html
Suk R, Hong YR, Rajan SS, et al. Assessment of US Preventive Services Task Force guideline-concordant cervical cancer screening rates and reasons for underscreening by age, race and ethnicity, sexual orientation, rurality, and insurance, 2005 to 2019. JAMA Netw Open. 2022;5:e2143582. doi:10.1001 /jamanetworkopen.2021.43582.
White MC, Shoemaker ML, Benard VB. Cervical cancer screening and incidence by age: unmet needs near and after the stopping age for screening. Am J Prev Med. 2017;53:392395. doi:10.1016/j.amepre.2017.02.024.
Cooley JJ, Maguire FB, Morris CR, et al. Cervical cancer stage at diagnosis and survival among women ≥65 years in California. Cancer Epidemiol Biomarkers Prev. 2023;32:91-97. doi:10.1158/1055-9965.EPI-22-0793.
Ortman JM, Velkoff VA, Hogan H. An aging nation: the older population in the United States. May 2014. United States Census Bureau. Accessed April 12, 2023. https://www.census .gov/library/publications/2014/demo/p25-1140.html
Although the past 30 years have stirred up a whirlwind of neurological research that has dramatically expanded therapeutic options for patients with epilepsy, historical pioneers in the field might be disappointed at the fact that treatment response has remained stubbornly stagnant. “Plus ça change, plus c’est la même chose,” they might say: The more things change, the more they stay the same. In fact, since 1993, despite an explosion of third-generation drugs, an abundance of new surgical approaches, and a whole new category of treatment in the form of neurostimulation devices, response rates in epilepsy have not budged, with roughly two-thirds of patients achieving seizure freedom and a third still struggling with treatment resistance.
Dr. Jacqueline A. French
But if you widen the lens and look towards the horizon, things are “on the cusp and going like a rocket,” said Jacqueline A. French, MD, professor of neurology in the Comprehensive Epilepsy Center at NYU Langone Health, New York. While treatment response rates may be stuck, adverse effects of those treatments have plummeted, and even treatment-resistant patients dealing with residual seizures live a much freer life with far fewer and less serious episodes.
Simpler times
In the late 1980s, just as Dr. French was finishing her second epilepsy fellowship at Yale, it was “almost laughable that things were so simple,” she recalls. “There were a few major centers that were doing epilepsy surgery … and in the world of medication, there were just five major drugs: phenobarbital, primidone, carbamazepine, phenytoin, and valproate.” That all changed as she was settling in to her first academic position at the University of Pennsylvania, with the “explosive” introduction of felbamate, a new antiseizure drug whose precipitous rise and fall from favor cast a sobering shadow which set the course for future drug development in the field.
“The felbamate story has a lot to do with what came after, but it was a drug that was much more advantageous in regards to a lot of the things that we didn’t like about antiseizure medicines or antiepileptic drugs as we called them at that time,” she said. The older drugs affected the cerebellum, making people sleepy and unable to concentrate. They also came with the risk of serious adverse effects such as hepatic enzyme induction and teratogenicity. Not only was felbamate nonsedating, “it actually was a little bit alerting,” said Dr. French. “People felt so different and so great on it, and it was effective for some seizure types that we didn’t really have good drugs for.” Very quickly, felbamate became a first-line therapy. Within its first year on the market, 150,000 newly diagnosed patients were started on it, “which is unthinkable now,” she said.
Sure enough, it all came crashing down a year later, on Aug. 1, 1994, when the drug was urgently withdrawn by the U.S. Food and Drug Administration after being linked to the development of aplastic anemia. “There was a day that anybody who was there at the time will remember when we all got the news, that everybody had to be taken off the drug,” Dr. French recalled. “We spent the weekend in the chart room, looking chart by chart by chart, for who was on felbamate.”
Until then, Dr. French had been straddling the line between her interests in pharmacologic versus surgical treatments for epilepsy. In fact, during her second epilepsy fellowship, which was dedicated to surgery, she published “Characteristics of medial temporal lobe epilepsy” in Annals of Neurology, one of the most-cited papers of her career. “Epilepsy from the temporal lobe is the biggest and best shot on goal when you’re talking about sending somebody to epilepsy surgery and rendering them completely seizure free,” she said. “Early in my career at the University of Pennsylvania, it was all about identifying those patients. And you know, there is nothing more gratifying than taking somebody whose life has been devastated by frequent seizures, who is injuring themselves and not able to be independent, and doing a surgery, which is very safe, and then all the seizures are gone – which is probably why I was so excited by surgery at the time.”
For a while, in the early 1990s, temporal lobectomy eclipsed many of the other avenues in epilepsy treatment, but it too has given way to a much wider variety of more complex techniques, which may be less curative but more palliative.
More drug options
Meanwhile, the felbamate story had ignited debate in the field about safer drug development – pushing Dr. French into establishing what was then known as the Antiepileptic Drug Trials conference, later renamed the Epilepsy Therapies & Diagnostics Development Symposium – a forum that encouraged safer, but also swifter movement of drugs through the pipeline and onto the market. “After felbamate, came gabapentin, and then came to topiramate and lamotrigine, and very quickly there were many, many, many choices,” she explained. “But once stung, twice shy. Felbamate really gave us a new perspective on which patients we put on the new drugs. Now we have a process of starting them in people with treatment-resistant epilepsy first. The risk-benefit equation is more reasonable because they have lots of risks. And then we work our way back to people with newly diagnosed epilepsy.”
Disease-modifying therapies
Today, the medications used to treat epilepsy are referred to as antiseizure rather than antiepileptic drugs because they simply suppress seizure symptoms and do not address the cause. But the rocket that Dr. French is watching gain speed and momentum is the disease-modifying gene therapies – true antiepileptics that may significantly move the needle on the number and type of patients who can reach seizure freedom. “We spent the last 25 years not even thinking we would ever have antiepileptic therapies, and now in the last 5 years or so, we were pretty sure we will,” she said. “We have gene therapies that can intervene now – none yet that have actually reached approval, these are all currently in trials – but we certainly have high expectations that they will very soon be available.”
Improving patients’ lives
While gene therapy rockets ahead, new device developments are already improving life for patients, even despite ongoing seizures. A drug-delivering pump is still in trials, but could make a big difference to daily medication adherence, and wearable or implantable devices are being developed to track seizures. More accurate tracking has also revealed that many people’s seizures are actually quite predictable, with regular cycles allowing for the possibility of prophylactic medication when increased seizure activity is expected.
Despite 30 years of no change in the proportion of epilepsy patients experiencing treatment resistance, Dr. French said that drugs, devices, and surgeries have improved the lives of all patients – both treatment resistant and treatment sensitive. “The difference between almost seizure free and completely seizure free is a big one because it means you can’t drive, you may have difficulty with your employment, but being able to take a pill every day and feel otherwise completely normal? We’ve come a long way.”
Although the past 30 years have stirred up a whirlwind of neurological research that has dramatically expanded therapeutic options for patients with epilepsy, historical pioneers in the field might be disappointed at the fact that treatment response has remained stubbornly stagnant. “Plus ça change, plus c’est la même chose,” they might say: The more things change, the more they stay the same. In fact, since 1993, despite an explosion of third-generation drugs, an abundance of new surgical approaches, and a whole new category of treatment in the form of neurostimulation devices, response rates in epilepsy have not budged, with roughly two-thirds of patients achieving seizure freedom and a third still struggling with treatment resistance.
Dr. Jacqueline A. French
But if you widen the lens and look towards the horizon, things are “on the cusp and going like a rocket,” said Jacqueline A. French, MD, professor of neurology in the Comprehensive Epilepsy Center at NYU Langone Health, New York. While treatment response rates may be stuck, adverse effects of those treatments have plummeted, and even treatment-resistant patients dealing with residual seizures live a much freer life with far fewer and less serious episodes.
Simpler times
In the late 1980s, just as Dr. French was finishing her second epilepsy fellowship at Yale, it was “almost laughable that things were so simple,” she recalls. “There were a few major centers that were doing epilepsy surgery … and in the world of medication, there were just five major drugs: phenobarbital, primidone, carbamazepine, phenytoin, and valproate.” That all changed as she was settling in to her first academic position at the University of Pennsylvania, with the “explosive” introduction of felbamate, a new antiseizure drug whose precipitous rise and fall from favor cast a sobering shadow which set the course for future drug development in the field.
“The felbamate story has a lot to do with what came after, but it was a drug that was much more advantageous in regards to a lot of the things that we didn’t like about antiseizure medicines or antiepileptic drugs as we called them at that time,” she said. The older drugs affected the cerebellum, making people sleepy and unable to concentrate. They also came with the risk of serious adverse effects such as hepatic enzyme induction and teratogenicity. Not only was felbamate nonsedating, “it actually was a little bit alerting,” said Dr. French. “People felt so different and so great on it, and it was effective for some seizure types that we didn’t really have good drugs for.” Very quickly, felbamate became a first-line therapy. Within its first year on the market, 150,000 newly diagnosed patients were started on it, “which is unthinkable now,” she said.
Sure enough, it all came crashing down a year later, on Aug. 1, 1994, when the drug was urgently withdrawn by the U.S. Food and Drug Administration after being linked to the development of aplastic anemia. “There was a day that anybody who was there at the time will remember when we all got the news, that everybody had to be taken off the drug,” Dr. French recalled. “We spent the weekend in the chart room, looking chart by chart by chart, for who was on felbamate.”
Until then, Dr. French had been straddling the line between her interests in pharmacologic versus surgical treatments for epilepsy. In fact, during her second epilepsy fellowship, which was dedicated to surgery, she published “Characteristics of medial temporal lobe epilepsy” in Annals of Neurology, one of the most-cited papers of her career. “Epilepsy from the temporal lobe is the biggest and best shot on goal when you’re talking about sending somebody to epilepsy surgery and rendering them completely seizure free,” she said. “Early in my career at the University of Pennsylvania, it was all about identifying those patients. And you know, there is nothing more gratifying than taking somebody whose life has been devastated by frequent seizures, who is injuring themselves and not able to be independent, and doing a surgery, which is very safe, and then all the seizures are gone – which is probably why I was so excited by surgery at the time.”
For a while, in the early 1990s, temporal lobectomy eclipsed many of the other avenues in epilepsy treatment, but it too has given way to a much wider variety of more complex techniques, which may be less curative but more palliative.
More drug options
Meanwhile, the felbamate story had ignited debate in the field about safer drug development – pushing Dr. French into establishing what was then known as the Antiepileptic Drug Trials conference, later renamed the Epilepsy Therapies & Diagnostics Development Symposium – a forum that encouraged safer, but also swifter movement of drugs through the pipeline and onto the market. “After felbamate, came gabapentin, and then came to topiramate and lamotrigine, and very quickly there were many, many, many choices,” she explained. “But once stung, twice shy. Felbamate really gave us a new perspective on which patients we put on the new drugs. Now we have a process of starting them in people with treatment-resistant epilepsy first. The risk-benefit equation is more reasonable because they have lots of risks. And then we work our way back to people with newly diagnosed epilepsy.”
Disease-modifying therapies
Today, the medications used to treat epilepsy are referred to as antiseizure rather than antiepileptic drugs because they simply suppress seizure symptoms and do not address the cause. But the rocket that Dr. French is watching gain speed and momentum is the disease-modifying gene therapies – true antiepileptics that may significantly move the needle on the number and type of patients who can reach seizure freedom. “We spent the last 25 years not even thinking we would ever have antiepileptic therapies, and now in the last 5 years or so, we were pretty sure we will,” she said. “We have gene therapies that can intervene now – none yet that have actually reached approval, these are all currently in trials – but we certainly have high expectations that they will very soon be available.”
Improving patients’ lives
While gene therapy rockets ahead, new device developments are already improving life for patients, even despite ongoing seizures. A drug-delivering pump is still in trials, but could make a big difference to daily medication adherence, and wearable or implantable devices are being developed to track seizures. More accurate tracking has also revealed that many people’s seizures are actually quite predictable, with regular cycles allowing for the possibility of prophylactic medication when increased seizure activity is expected.
Despite 30 years of no change in the proportion of epilepsy patients experiencing treatment resistance, Dr. French said that drugs, devices, and surgeries have improved the lives of all patients – both treatment resistant and treatment sensitive. “The difference between almost seizure free and completely seizure free is a big one because it means you can’t drive, you may have difficulty with your employment, but being able to take a pill every day and feel otherwise completely normal? We’ve come a long way.”
Although the past 30 years have stirred up a whirlwind of neurological research that has dramatically expanded therapeutic options for patients with epilepsy, historical pioneers in the field might be disappointed at the fact that treatment response has remained stubbornly stagnant. “Plus ça change, plus c’est la même chose,” they might say: The more things change, the more they stay the same. In fact, since 1993, despite an explosion of third-generation drugs, an abundance of new surgical approaches, and a whole new category of treatment in the form of neurostimulation devices, response rates in epilepsy have not budged, with roughly two-thirds of patients achieving seizure freedom and a third still struggling with treatment resistance.
Dr. Jacqueline A. French
But if you widen the lens and look towards the horizon, things are “on the cusp and going like a rocket,” said Jacqueline A. French, MD, professor of neurology in the Comprehensive Epilepsy Center at NYU Langone Health, New York. While treatment response rates may be stuck, adverse effects of those treatments have plummeted, and even treatment-resistant patients dealing with residual seizures live a much freer life with far fewer and less serious episodes.
Simpler times
In the late 1980s, just as Dr. French was finishing her second epilepsy fellowship at Yale, it was “almost laughable that things were so simple,” she recalls. “There were a few major centers that were doing epilepsy surgery … and in the world of medication, there were just five major drugs: phenobarbital, primidone, carbamazepine, phenytoin, and valproate.” That all changed as she was settling in to her first academic position at the University of Pennsylvania, with the “explosive” introduction of felbamate, a new antiseizure drug whose precipitous rise and fall from favor cast a sobering shadow which set the course for future drug development in the field.
“The felbamate story has a lot to do with what came after, but it was a drug that was much more advantageous in regards to a lot of the things that we didn’t like about antiseizure medicines or antiepileptic drugs as we called them at that time,” she said. The older drugs affected the cerebellum, making people sleepy and unable to concentrate. They also came with the risk of serious adverse effects such as hepatic enzyme induction and teratogenicity. Not only was felbamate nonsedating, “it actually was a little bit alerting,” said Dr. French. “People felt so different and so great on it, and it was effective for some seizure types that we didn’t really have good drugs for.” Very quickly, felbamate became a first-line therapy. Within its first year on the market, 150,000 newly diagnosed patients were started on it, “which is unthinkable now,” she said.
Sure enough, it all came crashing down a year later, on Aug. 1, 1994, when the drug was urgently withdrawn by the U.S. Food and Drug Administration after being linked to the development of aplastic anemia. “There was a day that anybody who was there at the time will remember when we all got the news, that everybody had to be taken off the drug,” Dr. French recalled. “We spent the weekend in the chart room, looking chart by chart by chart, for who was on felbamate.”
Until then, Dr. French had been straddling the line between her interests in pharmacologic versus surgical treatments for epilepsy. In fact, during her second epilepsy fellowship, which was dedicated to surgery, she published “Characteristics of medial temporal lobe epilepsy” in Annals of Neurology, one of the most-cited papers of her career. “Epilepsy from the temporal lobe is the biggest and best shot on goal when you’re talking about sending somebody to epilepsy surgery and rendering them completely seizure free,” she said. “Early in my career at the University of Pennsylvania, it was all about identifying those patients. And you know, there is nothing more gratifying than taking somebody whose life has been devastated by frequent seizures, who is injuring themselves and not able to be independent, and doing a surgery, which is very safe, and then all the seizures are gone – which is probably why I was so excited by surgery at the time.”
For a while, in the early 1990s, temporal lobectomy eclipsed many of the other avenues in epilepsy treatment, but it too has given way to a much wider variety of more complex techniques, which may be less curative but more palliative.
More drug options
Meanwhile, the felbamate story had ignited debate in the field about safer drug development – pushing Dr. French into establishing what was then known as the Antiepileptic Drug Trials conference, later renamed the Epilepsy Therapies & Diagnostics Development Symposium – a forum that encouraged safer, but also swifter movement of drugs through the pipeline and onto the market. “After felbamate, came gabapentin, and then came to topiramate and lamotrigine, and very quickly there were many, many, many choices,” she explained. “But once stung, twice shy. Felbamate really gave us a new perspective on which patients we put on the new drugs. Now we have a process of starting them in people with treatment-resistant epilepsy first. The risk-benefit equation is more reasonable because they have lots of risks. And then we work our way back to people with newly diagnosed epilepsy.”
Disease-modifying therapies
Today, the medications used to treat epilepsy are referred to as antiseizure rather than antiepileptic drugs because they simply suppress seizure symptoms and do not address the cause. But the rocket that Dr. French is watching gain speed and momentum is the disease-modifying gene therapies – true antiepileptics that may significantly move the needle on the number and type of patients who can reach seizure freedom. “We spent the last 25 years not even thinking we would ever have antiepileptic therapies, and now in the last 5 years or so, we were pretty sure we will,” she said. “We have gene therapies that can intervene now – none yet that have actually reached approval, these are all currently in trials – but we certainly have high expectations that they will very soon be available.”
Improving patients’ lives
While gene therapy rockets ahead, new device developments are already improving life for patients, even despite ongoing seizures. A drug-delivering pump is still in trials, but could make a big difference to daily medication adherence, and wearable or implantable devices are being developed to track seizures. More accurate tracking has also revealed that many people’s seizures are actually quite predictable, with regular cycles allowing for the possibility of prophylactic medication when increased seizure activity is expected.
Despite 30 years of no change in the proportion of epilepsy patients experiencing treatment resistance, Dr. French said that drugs, devices, and surgeries have improved the lives of all patients – both treatment resistant and treatment sensitive. “The difference between almost seizure free and completely seizure free is a big one because it means you can’t drive, you may have difficulty with your employment, but being able to take a pill every day and feel otherwise completely normal? We’ve come a long way.”


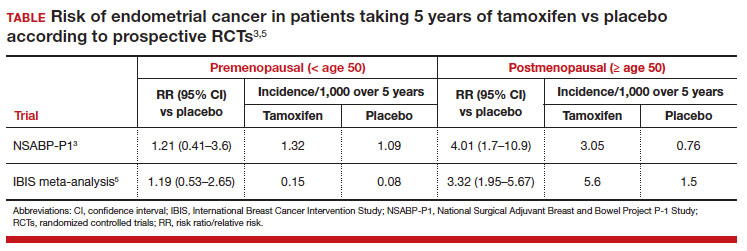

 PHOTO: BETAVERSO/SHUTTERSTOCK
PHOTO: BETAVERSO/SHUTTERSTOCK