User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Mega vitamin D harms bone in women, not men, without osteoporosis
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
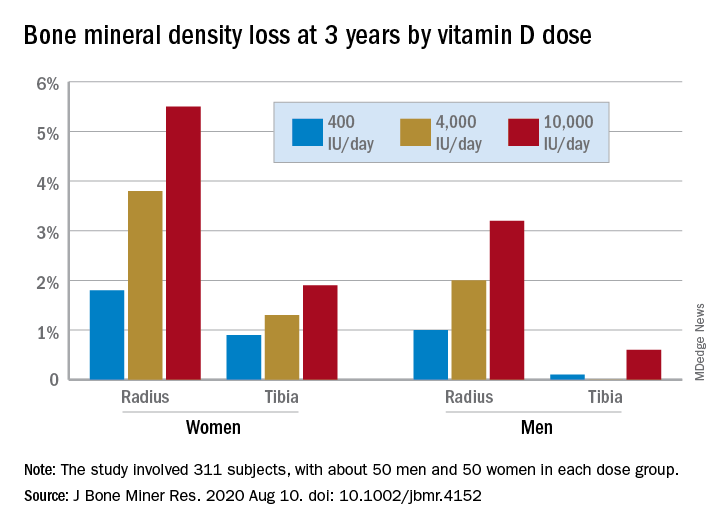
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.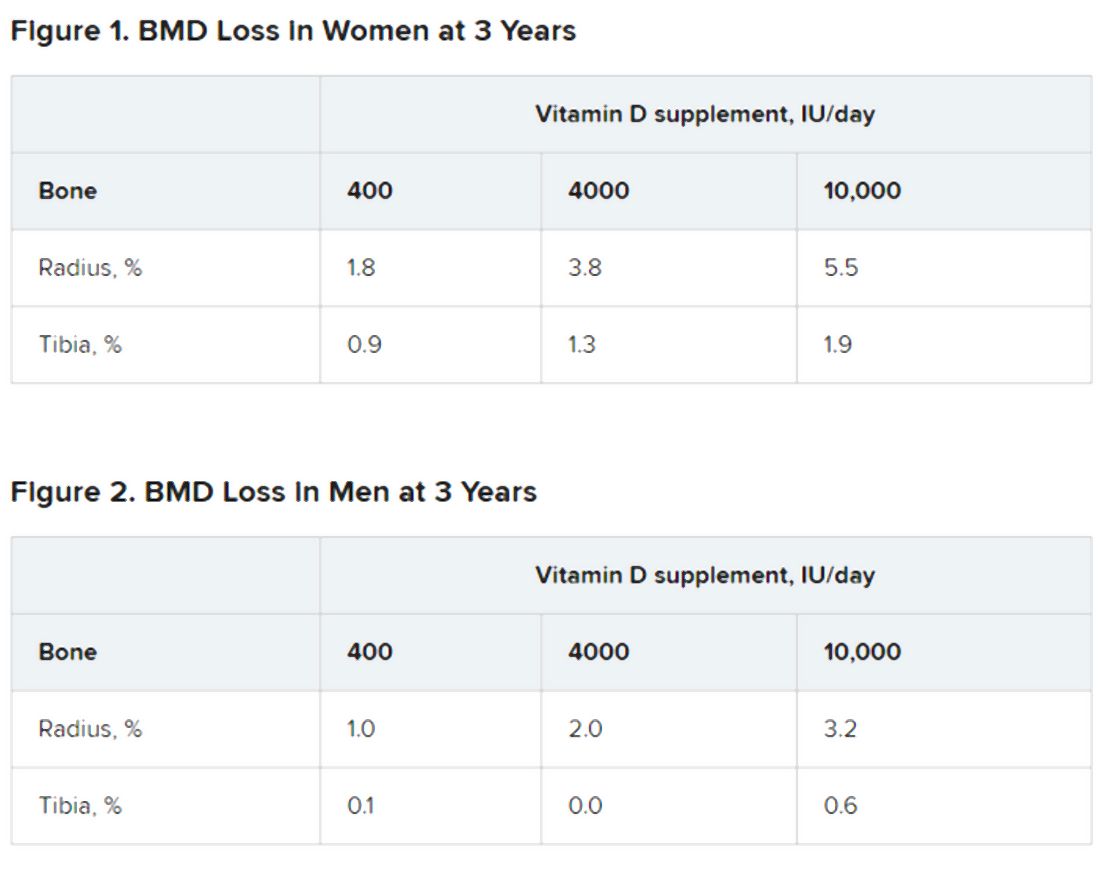
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
The earlier the better for colchicine post-MI: COLCOT
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
Masitinib impresses in nonactive progressive MS
“This is the first time that we have seen significant activity in slowing disability in a population of nonactive primary progressive and secondary progressive MS,” lead investigator, Patrick Vermersch, MD, commented. “There are no drugs available for these patients, which make up the vast majority of progressive MS patients, so these results are impressive. They are definitely a big deal.”
Dr. Vermersch, who is professor of neurology at the University of Lille, France, presented the study at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
“Masitinib – a first-in-class tyrosine kinase inhibitor targeting the innate immune system via inhibition of mast cell and microglia/macrophage activity – may provide a new treatment option for primary progressive and nonactive secondary progressive MS,” he concluded.
This study, known as AB07002, demonstrated a sustained and significant benefit for masitinib at a dose of 4.5 mg/kg per day in Expanded Disability Status Scale (EDSS) score change over 2 years versus placebo, with a 37% reduction in 3-month confirmed disability progression. This change “is relevant from a medical standpoint,” Dr. Vermersch reported.
However, a second dosing schedule, in which the drug was titrated up to 6 mg/kg per day, did not show significant benefit. Dr. Vermersch said this was because of an unexpected improvement in EDSS score in the placebo group.
In the 4.5-mg/kg group, the benefit was demonstrated across a broad population, with no difference with regard to age, duration of disease, or baseline disability. The benefits were similar in both primary and secondary MS phenotypes and were present irrespective of baseline active inflammation status.
Masitinib showed a safety profile “suitable for long-term administration in this population,” Dr. Vermersch said. “Masitinib addresses the huge unmet need in progressive MS,” he said. “The drugs currently used in MS target B cells and T cells. They are immunomodulating drugs and are used for relapsing/remitting MS. But in progressive forms of the disease, there is a strong involvement of innate immunity, so to be effective we need drugs that target this part of the immune system.”
Innate immunity is a major part of the immune system in primates; it is related to the immune cells inside tissues and the CNS and is separate from adaptive peripheral immunity, he explained.
Masitinib is a novel drug for MS in that it inhibits tyrosine kinase and blocks the activity of immune cells involved in the innate immune system – mainly microglia and mast cells. “Both of these types of cells are very involved in progressive MS. Masitinib has no action against T or B cells. It is a small molecule and penetrates the CNS,” Dr. Vermersch noted.
“This has opened up a whole new area of opportunity to develop treatments for progressive MS,” he added.
“We showed a positive significant result in slowing disability in patients with nonactive progressive MS,” he said. “The term ‘nonactive’ is important. Some other drugs [ocrelizumab and siponimod] have shown some modest activity in slowing progressive forms of MS, but this is driven by patients with some degree of inflammatory activity at baseline. Our study excluded such patients.”
The trial tested two different dosing schedules independently, each with its own placebo group. There were two subsets, each with 300 patients. The first subset was randomly assigned in a 2:1 ratio to daily masitinib at 4.5 mg/kg orally or placebo. The second subset was randomly assigned in a 2:1 ratio to daily masitinib titrated to 6 mg/kg or placebo.
The inclusion criteria were patients with primary progressive or secondary progressive MS without relapse (as measured by EDSS progression) within the previous 2 years. “No patients were enrolled who had superimposed relapses during the previous 2 years,” Dr. Vermersch stressed.
Baseline EDSS score was 5.0, and patients had an average disease duration of 15 years. Mean age was 50 years.
The primary endpoint was change from baseline in absolute EDSS value, which was measured every 12 weeks throughout the study, averaged over the 2-year study period (mean change in EDSS score).
Results in the 4.5-mg/kg group showed a mean increase in EDSS score in the masitinib recipients of 0.001 versus 0.098 in the placebo group, giving a mean difference of –0.097 for masitinib (P = 0.025). The results were similar in patients with primary or secondary progressive MS. Sensitivity analysis based on ordinal EDSS change showed a significant 39% increased probability of having more improvements in EDSS or fewer worsening EDSS scores with masitinib (odds ratio, 0.61; P = 0.044). Other results showed that masitinib reduced the risk for first disability progression by 42% (hazard ratio, 0.58; P = 0.034) and the risk for confirmed (3-month) disability progression by 37% (hazard ratio, 0.63; P = 0.15).
Masitinib also showed a 98% reduction in the risk of reaching an EDSS score of 7, corresponding to disability severe enough that the patient is restricted to a wheelchair (hazard ratio, 0.02; P = 0.009). No patients in the masitinib group reached the endpoint of confirmed (3-month) EDSS score of 7, compared with four patients in the placebo group.
In terms of safety in the 4.5-mg/kg group, the most common adverse events were rash (1,5%) gastrointestinal (GI) disturbances (1%), neutropenia (1%), and edema (1%). “We had a couple of patients with skin reactions and neutropenia, but all adverse events were mild to moderate and very manageable,” Dr. Vermersch commented.
He showed just one slide on the subset who were titrated up 6 mg/kg. “Numerically the change in EDSS was comparable in the 6-mg/kg–titrated group as it was in the 4.5-mg/kg group; however, the placebo arm of the 6-mg/kg subset unusually showed an improvement relative to baseline after 96 weeks. The placebo group of the 4.5-mg/kg cohort was consistent with the literature and expected worsening in EDSS score over 96 weeks,” Dr. Vermersch reported.
No new safety signal was observed in the 6-mg/kg cohort. Only the 4.5-mg/kg cohort will be pursued in further trials in MS.
Dr. Vermersch noted that masitinib is also being investigated in other indications and “there are thousands of patient-years of experience which show reassuring safety data.”
“There is some GI disturbances and skin reactions, but a very small percentage of patients discontinue treatment. If the drug is titrated slowly there are fewer adverse effects,” he said. “We will do that in the next study.”
A second confirmatory study is now being planned. The trial will enroll around 700 patients and is expected to recruit quickly because there is such a big unmet need, Dr. Vermersch added.
Commenting on the findings, ACTRIMS president Jeffrey Cohen, MD, of the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, Ohio, said this is “an interesting study from several perspectives.”
“Masitinib is a new drug for MS with a completely novel mechanism of action targeting the innate immune system”, he said. “The study had several innovative features in that it combined primary and secondary progressive MS patients and measured disability in a different way to what we are used to.”
“It did show a slowing of disability, which is great news as we do not have any drugs for these patients at the moment, so this is a very hopeful result,” Dr. Cohen said.
The study was supported by AB Science. Dr. Vermersch reports sitting on advisory boards for Biogen, Sanofi-Genzyme, Teva, Roche, Novartis, Celgene, and Merck KGaA.
A version of this article originally appeared on Medscape.com.
“This is the first time that we have seen significant activity in slowing disability in a population of nonactive primary progressive and secondary progressive MS,” lead investigator, Patrick Vermersch, MD, commented. “There are no drugs available for these patients, which make up the vast majority of progressive MS patients, so these results are impressive. They are definitely a big deal.”
Dr. Vermersch, who is professor of neurology at the University of Lille, France, presented the study at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
“Masitinib – a first-in-class tyrosine kinase inhibitor targeting the innate immune system via inhibition of mast cell and microglia/macrophage activity – may provide a new treatment option for primary progressive and nonactive secondary progressive MS,” he concluded.
This study, known as AB07002, demonstrated a sustained and significant benefit for masitinib at a dose of 4.5 mg/kg per day in Expanded Disability Status Scale (EDSS) score change over 2 years versus placebo, with a 37% reduction in 3-month confirmed disability progression. This change “is relevant from a medical standpoint,” Dr. Vermersch reported.
However, a second dosing schedule, in which the drug was titrated up to 6 mg/kg per day, did not show significant benefit. Dr. Vermersch said this was because of an unexpected improvement in EDSS score in the placebo group.
In the 4.5-mg/kg group, the benefit was demonstrated across a broad population, with no difference with regard to age, duration of disease, or baseline disability. The benefits were similar in both primary and secondary MS phenotypes and were present irrespective of baseline active inflammation status.
Masitinib showed a safety profile “suitable for long-term administration in this population,” Dr. Vermersch said. “Masitinib addresses the huge unmet need in progressive MS,” he said. “The drugs currently used in MS target B cells and T cells. They are immunomodulating drugs and are used for relapsing/remitting MS. But in progressive forms of the disease, there is a strong involvement of innate immunity, so to be effective we need drugs that target this part of the immune system.”
Innate immunity is a major part of the immune system in primates; it is related to the immune cells inside tissues and the CNS and is separate from adaptive peripheral immunity, he explained.
Masitinib is a novel drug for MS in that it inhibits tyrosine kinase and blocks the activity of immune cells involved in the innate immune system – mainly microglia and mast cells. “Both of these types of cells are very involved in progressive MS. Masitinib has no action against T or B cells. It is a small molecule and penetrates the CNS,” Dr. Vermersch noted.
“This has opened up a whole new area of opportunity to develop treatments for progressive MS,” he added.
“We showed a positive significant result in slowing disability in patients with nonactive progressive MS,” he said. “The term ‘nonactive’ is important. Some other drugs [ocrelizumab and siponimod] have shown some modest activity in slowing progressive forms of MS, but this is driven by patients with some degree of inflammatory activity at baseline. Our study excluded such patients.”
The trial tested two different dosing schedules independently, each with its own placebo group. There were two subsets, each with 300 patients. The first subset was randomly assigned in a 2:1 ratio to daily masitinib at 4.5 mg/kg orally or placebo. The second subset was randomly assigned in a 2:1 ratio to daily masitinib titrated to 6 mg/kg or placebo.
The inclusion criteria were patients with primary progressive or secondary progressive MS without relapse (as measured by EDSS progression) within the previous 2 years. “No patients were enrolled who had superimposed relapses during the previous 2 years,” Dr. Vermersch stressed.
Baseline EDSS score was 5.0, and patients had an average disease duration of 15 years. Mean age was 50 years.
The primary endpoint was change from baseline in absolute EDSS value, which was measured every 12 weeks throughout the study, averaged over the 2-year study period (mean change in EDSS score).
Results in the 4.5-mg/kg group showed a mean increase in EDSS score in the masitinib recipients of 0.001 versus 0.098 in the placebo group, giving a mean difference of –0.097 for masitinib (P = 0.025). The results were similar in patients with primary or secondary progressive MS. Sensitivity analysis based on ordinal EDSS change showed a significant 39% increased probability of having more improvements in EDSS or fewer worsening EDSS scores with masitinib (odds ratio, 0.61; P = 0.044). Other results showed that masitinib reduced the risk for first disability progression by 42% (hazard ratio, 0.58; P = 0.034) and the risk for confirmed (3-month) disability progression by 37% (hazard ratio, 0.63; P = 0.15).
Masitinib also showed a 98% reduction in the risk of reaching an EDSS score of 7, corresponding to disability severe enough that the patient is restricted to a wheelchair (hazard ratio, 0.02; P = 0.009). No patients in the masitinib group reached the endpoint of confirmed (3-month) EDSS score of 7, compared with four patients in the placebo group.
In terms of safety in the 4.5-mg/kg group, the most common adverse events were rash (1,5%) gastrointestinal (GI) disturbances (1%), neutropenia (1%), and edema (1%). “We had a couple of patients with skin reactions and neutropenia, but all adverse events were mild to moderate and very manageable,” Dr. Vermersch commented.
He showed just one slide on the subset who were titrated up 6 mg/kg. “Numerically the change in EDSS was comparable in the 6-mg/kg–titrated group as it was in the 4.5-mg/kg group; however, the placebo arm of the 6-mg/kg subset unusually showed an improvement relative to baseline after 96 weeks. The placebo group of the 4.5-mg/kg cohort was consistent with the literature and expected worsening in EDSS score over 96 weeks,” Dr. Vermersch reported.
No new safety signal was observed in the 6-mg/kg cohort. Only the 4.5-mg/kg cohort will be pursued in further trials in MS.
Dr. Vermersch noted that masitinib is also being investigated in other indications and “there are thousands of patient-years of experience which show reassuring safety data.”
“There is some GI disturbances and skin reactions, but a very small percentage of patients discontinue treatment. If the drug is titrated slowly there are fewer adverse effects,” he said. “We will do that in the next study.”
A second confirmatory study is now being planned. The trial will enroll around 700 patients and is expected to recruit quickly because there is such a big unmet need, Dr. Vermersch added.
Commenting on the findings, ACTRIMS president Jeffrey Cohen, MD, of the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, Ohio, said this is “an interesting study from several perspectives.”
“Masitinib is a new drug for MS with a completely novel mechanism of action targeting the innate immune system”, he said. “The study had several innovative features in that it combined primary and secondary progressive MS patients and measured disability in a different way to what we are used to.”
“It did show a slowing of disability, which is great news as we do not have any drugs for these patients at the moment, so this is a very hopeful result,” Dr. Cohen said.
The study was supported by AB Science. Dr. Vermersch reports sitting on advisory boards for Biogen, Sanofi-Genzyme, Teva, Roche, Novartis, Celgene, and Merck KGaA.
A version of this article originally appeared on Medscape.com.
“This is the first time that we have seen significant activity in slowing disability in a population of nonactive primary progressive and secondary progressive MS,” lead investigator, Patrick Vermersch, MD, commented. “There are no drugs available for these patients, which make up the vast majority of progressive MS patients, so these results are impressive. They are definitely a big deal.”
Dr. Vermersch, who is professor of neurology at the University of Lille, France, presented the study at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
“Masitinib – a first-in-class tyrosine kinase inhibitor targeting the innate immune system via inhibition of mast cell and microglia/macrophage activity – may provide a new treatment option for primary progressive and nonactive secondary progressive MS,” he concluded.
This study, known as AB07002, demonstrated a sustained and significant benefit for masitinib at a dose of 4.5 mg/kg per day in Expanded Disability Status Scale (EDSS) score change over 2 years versus placebo, with a 37% reduction in 3-month confirmed disability progression. This change “is relevant from a medical standpoint,” Dr. Vermersch reported.
However, a second dosing schedule, in which the drug was titrated up to 6 mg/kg per day, did not show significant benefit. Dr. Vermersch said this was because of an unexpected improvement in EDSS score in the placebo group.
In the 4.5-mg/kg group, the benefit was demonstrated across a broad population, with no difference with regard to age, duration of disease, or baseline disability. The benefits were similar in both primary and secondary MS phenotypes and were present irrespective of baseline active inflammation status.
Masitinib showed a safety profile “suitable for long-term administration in this population,” Dr. Vermersch said. “Masitinib addresses the huge unmet need in progressive MS,” he said. “The drugs currently used in MS target B cells and T cells. They are immunomodulating drugs and are used for relapsing/remitting MS. But in progressive forms of the disease, there is a strong involvement of innate immunity, so to be effective we need drugs that target this part of the immune system.”
Innate immunity is a major part of the immune system in primates; it is related to the immune cells inside tissues and the CNS and is separate from adaptive peripheral immunity, he explained.
Masitinib is a novel drug for MS in that it inhibits tyrosine kinase and blocks the activity of immune cells involved in the innate immune system – mainly microglia and mast cells. “Both of these types of cells are very involved in progressive MS. Masitinib has no action against T or B cells. It is a small molecule and penetrates the CNS,” Dr. Vermersch noted.
“This has opened up a whole new area of opportunity to develop treatments for progressive MS,” he added.
“We showed a positive significant result in slowing disability in patients with nonactive progressive MS,” he said. “The term ‘nonactive’ is important. Some other drugs [ocrelizumab and siponimod] have shown some modest activity in slowing progressive forms of MS, but this is driven by patients with some degree of inflammatory activity at baseline. Our study excluded such patients.”
The trial tested two different dosing schedules independently, each with its own placebo group. There were two subsets, each with 300 patients. The first subset was randomly assigned in a 2:1 ratio to daily masitinib at 4.5 mg/kg orally or placebo. The second subset was randomly assigned in a 2:1 ratio to daily masitinib titrated to 6 mg/kg or placebo.
The inclusion criteria were patients with primary progressive or secondary progressive MS without relapse (as measured by EDSS progression) within the previous 2 years. “No patients were enrolled who had superimposed relapses during the previous 2 years,” Dr. Vermersch stressed.
Baseline EDSS score was 5.0, and patients had an average disease duration of 15 years. Mean age was 50 years.
The primary endpoint was change from baseline in absolute EDSS value, which was measured every 12 weeks throughout the study, averaged over the 2-year study period (mean change in EDSS score).
Results in the 4.5-mg/kg group showed a mean increase in EDSS score in the masitinib recipients of 0.001 versus 0.098 in the placebo group, giving a mean difference of –0.097 for masitinib (P = 0.025). The results were similar in patients with primary or secondary progressive MS. Sensitivity analysis based on ordinal EDSS change showed a significant 39% increased probability of having more improvements in EDSS or fewer worsening EDSS scores with masitinib (odds ratio, 0.61; P = 0.044). Other results showed that masitinib reduced the risk for first disability progression by 42% (hazard ratio, 0.58; P = 0.034) and the risk for confirmed (3-month) disability progression by 37% (hazard ratio, 0.63; P = 0.15).
Masitinib also showed a 98% reduction in the risk of reaching an EDSS score of 7, corresponding to disability severe enough that the patient is restricted to a wheelchair (hazard ratio, 0.02; P = 0.009). No patients in the masitinib group reached the endpoint of confirmed (3-month) EDSS score of 7, compared with four patients in the placebo group.
In terms of safety in the 4.5-mg/kg group, the most common adverse events were rash (1,5%) gastrointestinal (GI) disturbances (1%), neutropenia (1%), and edema (1%). “We had a couple of patients with skin reactions and neutropenia, but all adverse events were mild to moderate and very manageable,” Dr. Vermersch commented.
He showed just one slide on the subset who were titrated up 6 mg/kg. “Numerically the change in EDSS was comparable in the 6-mg/kg–titrated group as it was in the 4.5-mg/kg group; however, the placebo arm of the 6-mg/kg subset unusually showed an improvement relative to baseline after 96 weeks. The placebo group of the 4.5-mg/kg cohort was consistent with the literature and expected worsening in EDSS score over 96 weeks,” Dr. Vermersch reported.
No new safety signal was observed in the 6-mg/kg cohort. Only the 4.5-mg/kg cohort will be pursued in further trials in MS.
Dr. Vermersch noted that masitinib is also being investigated in other indications and “there are thousands of patient-years of experience which show reassuring safety data.”
“There is some GI disturbances and skin reactions, but a very small percentage of patients discontinue treatment. If the drug is titrated slowly there are fewer adverse effects,” he said. “We will do that in the next study.”
A second confirmatory study is now being planned. The trial will enroll around 700 patients and is expected to recruit quickly because there is such a big unmet need, Dr. Vermersch added.
Commenting on the findings, ACTRIMS president Jeffrey Cohen, MD, of the Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, Ohio, said this is “an interesting study from several perspectives.”
“Masitinib is a new drug for MS with a completely novel mechanism of action targeting the innate immune system”, he said. “The study had several innovative features in that it combined primary and secondary progressive MS patients and measured disability in a different way to what we are used to.”
“It did show a slowing of disability, which is great news as we do not have any drugs for these patients at the moment, so this is a very hopeful result,” Dr. Cohen said.
The study was supported by AB Science. Dr. Vermersch reports sitting on advisory boards for Biogen, Sanofi-Genzyme, Teva, Roche, Novartis, Celgene, and Merck KGaA.
A version of this article originally appeared on Medscape.com.
From MSVirtual2020
Multiple sclerosis prodrome holds promise of earlier diagnosis
“It is time that the prodromal phase of multiple sclerosis [MS] is formally recognized.” That was the conclusion of Helen Tremlett, PhD, delivering the opening plenary session lecture at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
There is a myriad of prodromal features but none that are specific to MS,” Dr. Tremlett said.
“These findings show that in future there could be an earlier window of opportunity to identify and manage MS,” she suggested.
In an interview, Dr. Tremlett, who is professor and Canada Research Chair in Neuroepidemiology and Multiple Sclerosis at the University of British Columbia, Vancouver, explained that for MS a prodrome is a relatively new concept. “Right up until the year 2000, MS leaders were specifically saying that a prodrome did not exist,” she said. “But things have changed. Studies started emerging in the last decade suggestive of a prodrome, and I think we can now say there is definitely proof that a prodrome does exist. If you ask MS patients, the vast majority of them will say they had an increase in health issues in the years before diagnosis.”
In her plenary talk, Dr. Tremlett summarized the available evidence showing that, in the years before the first demyelinating event, patients are more likely to be have multiple health issues and an increase in hospitalizations and physician visits.
In a 2018 study, her group analyzed data from four Canadian provinces, including 14,000 patients with MS and 75,000 matched controls, and found a 75% increase in the rate of hospitalization, a 88% higher rate of physician service use, and a 49% increase in prescription numbers in the 5 years before the first demyelinating event in the patients with MS, compared with controls.
This included a 50% increase in mental health visits to physicians and increased rates of fibromyalgia, pain, headache, migraine, sleep disturbances, urology, and dermatology referrals, as well as irritable bowel syndrome. In addition, there were fewer pregnancies and increased prescriptions for contraception in the female patients later diagnosed with MS.
“There is a huge range of nonspecific symptoms in the 5 years before MS diagnosis, and some of these are really intriguing and unanticipated,” Dr. Tremlett said. “We are not surprised by the findings that fatigue, mental health issues, and bladder and bowel symptoms are increased, but the finding that there are more visits to a dermatologist and an increase in prescriptions for skin conditions was completely unexpected.”
The researchers found that dermatology referrals increased in patients who went on to develop relapsing remitting but not primary progressive forms of MS, which correlates with the established knowledge that the relapsing form has an inflammatory component not seen in progressive MS.
In a large U.K. population study of 10,000 patients with MS and 39,000 matched controls sourced from primary care doctors’ records, there was an increase in gastrointestinal and urinary issues, pain, anxiety and depression, insomnia, and fatigue in the 10 years before the first diagnosis of MS or clinically isolated syndrome (CIS) in patients later diagnosed with those conditions, compared with controls, Dr. Tremlett reported.
Other data have suggested that sex and age may affect the prodrome. In a study published this year, anemia was increased in the year before the first demyelinating event and pain was increased for 5 years beforehand. But anemia was more common in male patients later diagnosed with MS/CIS (odds ratio compared with controls, 2.4) than in female patients (OR compared with controls, 1.2).
The increase in pain seemed to be greater with age, with ORs of 1.8 for those younger than 30 years, 2.1 for those age 30-49 years, and 2.4 for those older than 50 years compared with controls.
A Norwegian military study in men that included 900 patients with MS and 19,000 matched controls found that cognitive performance was reduced in the 2 years before MS symptoms developed and up to 20 years before symptoms in those who developed primary progressive MS. “This suggests that primary progressive MS could start decades before the first apparent symptoms become obvious,” Dr. Tremlett commented.
A study in pediatric MS found that the mothers of the patients had higher use of health care (rate ratio, 1.16) and mental health (rate ratio, 1.33) services in the 5 years before their children had their first demyelinating event.
A study in Bavaria, Germany, including 10,000 patients with MS and 73,000 controls, concluded that “many physician visits before MS diagnosis were, in hindsight, likely a demyelinating event,” with the implication that this is evidence of missed opportunity for earlier diagnosis, Dr. Tremlett noted.
In a 2019 study, psychiatric symptoms were more common before MS diagnosis across various different immune-mediated disease (MS, rheumatoid arthritis, inflammatory bowel disease), with an incidence rate ratio of 1.6. The rate was even increased 10 years before diagnosis (incidence rate ratio, 1.5).
“This is evidence for shared prodromal features across immune diseases, but there isn’t a single feature specific to MS,” Dr. Tremlett said. She also referred to evidence that the blood biomarker of neuronal damage, neurofilament light chain (NfL), is raised several years before MS diagnosis. In a U.S. military study that examined serum repository samples, NfL was increased for 6 years before disease onset in 30 patients with MS, compared with 30 matched controls.
What are the implications?
Dr. Tremlett said the immediate impact of these observations about the prodrome is focused on research, particularly investigation of risk factors for MS. “If we want to know what causes MS, we have to be very careful that we are not detecting prodromal symptoms and mistaking that for a causal MS risk factor. We need to make sure we look further back than just the last few years when looking for risk factors.”
She gave the example of the observation that women in the years before MS diagnosis are less likely to have a pregnancy and more likely to fill a prescription for contraception. “This has led to the idea that avoiding pregnancy and using contraceptives increases the risk of MS, but I interpret it as these women know that something odd is going on and make the lifestyle decision not to become pregnant.”
She believes the longer-term impact of the prodrome is going to require much thought. “There is no such diagnosis of prodromal MS at the moment, but there could be in future. But the idea that we can use this information to detect MS earlier is going to require collaboration from many international stakeholders and MS organizations. We can’t automatically suspect MS in people who have these symptoms because they are so nonspecific. I think to request an MRI in patients experiencing headaches/fatigue/bowel issues is jumping the gun at the present moment as these symptoms are very common.”
On the idea of measuring NfL in patients with some of these symptoms, she believes that may be a possibility in the future but much more data are required.“We do have some evidence suggesting that the NfL blood biomarker is raised before MS diagnosis, and this was from a very well-designed study, but it was small so I think it is too early to start looking at this in clinical practice,” she said. “But it does justify doing this as part of a research study. We definitely need more data on this. We must be cautious as NfL is not specific for MS – many other conditions are also associated with raised levels, but it is certainly an interesting marker if used carefully.”
Following in the footsteps of Parkinson disease
She suggested that the way forward will be to package up these symptoms with information on biomarkers, such as NfL and imaging information, to enhance the ability to identify prodromal MS. “We could create a risk score and when a certain level of confidence is reached that this could be prodromal MS, then these patients could be enrolled in an intervention research study.”
Dr. Tremlett pointed out that, in the Parkinson disease field, a set of validated criteria for a prodrome have already been identified. “This is not used in clinical practice yet, but it is being used to identify patients for enrollment into clinical trials. I’m hoping that MS will follow in their footsteps.”
Commenting on the presentation, ACTRIMS president, Jeffrey Cohen, MD, Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, said: “There is no doubt that the MS disease process begins prior to the first attack (in the case of relapsing MS) or the onset of overt disability progression (in the case of primary progressive MS).”
He explained that this is demonstrated by the presence of old lesions on MRI in most patients at the time of presentation, the existence of so-called radiologically isolated syndrome (patients without symptoms of MS who undergo MRI for another reason and are found to have lesions suggesting of MS, many of whom go on to develop MS at a later date), and the occurrence of a variety of symptoms 5-10 years before presentation to a neurologist.
“Those symptoms are ones that are common in MS, though not specific for MS,” Dr. Cohen noted. “The main implication is that the timeline for MS needs to be moved earlier – for diagnosis, categorization of disease course, prognostic studies, and treatment. The issue is that the symptoms of the prodrome are rather nonspecific and most people with those symptoms do not have MS.”
New incoming president of ECTRIMS, Maria Pia Amato, MD, professor of neurology at the University of Florence (Italy), added: “The million-dollar question is when does progression really begin? This plenary talk tells us the disease is there years and years before it manifests itself with first demyelinating event. This opens up an immense opportunity for research and to open the window to the possibility of earlier diagnosis and treatment.”
Dr. Tremlett reports an investment in Precision NanoSystems.
A version of this article originally appeared on Medscape.com.
“It is time that the prodromal phase of multiple sclerosis [MS] is formally recognized.” That was the conclusion of Helen Tremlett, PhD, delivering the opening plenary session lecture at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
There is a myriad of prodromal features but none that are specific to MS,” Dr. Tremlett said.
“These findings show that in future there could be an earlier window of opportunity to identify and manage MS,” she suggested.
In an interview, Dr. Tremlett, who is professor and Canada Research Chair in Neuroepidemiology and Multiple Sclerosis at the University of British Columbia, Vancouver, explained that for MS a prodrome is a relatively new concept. “Right up until the year 2000, MS leaders were specifically saying that a prodrome did not exist,” she said. “But things have changed. Studies started emerging in the last decade suggestive of a prodrome, and I think we can now say there is definitely proof that a prodrome does exist. If you ask MS patients, the vast majority of them will say they had an increase in health issues in the years before diagnosis.”
In her plenary talk, Dr. Tremlett summarized the available evidence showing that, in the years before the first demyelinating event, patients are more likely to be have multiple health issues and an increase in hospitalizations and physician visits.
In a 2018 study, her group analyzed data from four Canadian provinces, including 14,000 patients with MS and 75,000 matched controls, and found a 75% increase in the rate of hospitalization, a 88% higher rate of physician service use, and a 49% increase in prescription numbers in the 5 years before the first demyelinating event in the patients with MS, compared with controls.
This included a 50% increase in mental health visits to physicians and increased rates of fibromyalgia, pain, headache, migraine, sleep disturbances, urology, and dermatology referrals, as well as irritable bowel syndrome. In addition, there were fewer pregnancies and increased prescriptions for contraception in the female patients later diagnosed with MS.
“There is a huge range of nonspecific symptoms in the 5 years before MS diagnosis, and some of these are really intriguing and unanticipated,” Dr. Tremlett said. “We are not surprised by the findings that fatigue, mental health issues, and bladder and bowel symptoms are increased, but the finding that there are more visits to a dermatologist and an increase in prescriptions for skin conditions was completely unexpected.”
The researchers found that dermatology referrals increased in patients who went on to develop relapsing remitting but not primary progressive forms of MS, which correlates with the established knowledge that the relapsing form has an inflammatory component not seen in progressive MS.
In a large U.K. population study of 10,000 patients with MS and 39,000 matched controls sourced from primary care doctors’ records, there was an increase in gastrointestinal and urinary issues, pain, anxiety and depression, insomnia, and fatigue in the 10 years before the first diagnosis of MS or clinically isolated syndrome (CIS) in patients later diagnosed with those conditions, compared with controls, Dr. Tremlett reported.
Other data have suggested that sex and age may affect the prodrome. In a study published this year, anemia was increased in the year before the first demyelinating event and pain was increased for 5 years beforehand. But anemia was more common in male patients later diagnosed with MS/CIS (odds ratio compared with controls, 2.4) than in female patients (OR compared with controls, 1.2).
The increase in pain seemed to be greater with age, with ORs of 1.8 for those younger than 30 years, 2.1 for those age 30-49 years, and 2.4 for those older than 50 years compared with controls.
A Norwegian military study in men that included 900 patients with MS and 19,000 matched controls found that cognitive performance was reduced in the 2 years before MS symptoms developed and up to 20 years before symptoms in those who developed primary progressive MS. “This suggests that primary progressive MS could start decades before the first apparent symptoms become obvious,” Dr. Tremlett commented.
A study in pediatric MS found that the mothers of the patients had higher use of health care (rate ratio, 1.16) and mental health (rate ratio, 1.33) services in the 5 years before their children had their first demyelinating event.
A study in Bavaria, Germany, including 10,000 patients with MS and 73,000 controls, concluded that “many physician visits before MS diagnosis were, in hindsight, likely a demyelinating event,” with the implication that this is evidence of missed opportunity for earlier diagnosis, Dr. Tremlett noted.
In a 2019 study, psychiatric symptoms were more common before MS diagnosis across various different immune-mediated disease (MS, rheumatoid arthritis, inflammatory bowel disease), with an incidence rate ratio of 1.6. The rate was even increased 10 years before diagnosis (incidence rate ratio, 1.5).
“This is evidence for shared prodromal features across immune diseases, but there isn’t a single feature specific to MS,” Dr. Tremlett said. She also referred to evidence that the blood biomarker of neuronal damage, neurofilament light chain (NfL), is raised several years before MS diagnosis. In a U.S. military study that examined serum repository samples, NfL was increased for 6 years before disease onset in 30 patients with MS, compared with 30 matched controls.
What are the implications?
Dr. Tremlett said the immediate impact of these observations about the prodrome is focused on research, particularly investigation of risk factors for MS. “If we want to know what causes MS, we have to be very careful that we are not detecting prodromal symptoms and mistaking that for a causal MS risk factor. We need to make sure we look further back than just the last few years when looking for risk factors.”
She gave the example of the observation that women in the years before MS diagnosis are less likely to have a pregnancy and more likely to fill a prescription for contraception. “This has led to the idea that avoiding pregnancy and using contraceptives increases the risk of MS, but I interpret it as these women know that something odd is going on and make the lifestyle decision not to become pregnant.”
She believes the longer-term impact of the prodrome is going to require much thought. “There is no such diagnosis of prodromal MS at the moment, but there could be in future. But the idea that we can use this information to detect MS earlier is going to require collaboration from many international stakeholders and MS organizations. We can’t automatically suspect MS in people who have these symptoms because they are so nonspecific. I think to request an MRI in patients experiencing headaches/fatigue/bowel issues is jumping the gun at the present moment as these symptoms are very common.”
On the idea of measuring NfL in patients with some of these symptoms, she believes that may be a possibility in the future but much more data are required.“We do have some evidence suggesting that the NfL blood biomarker is raised before MS diagnosis, and this was from a very well-designed study, but it was small so I think it is too early to start looking at this in clinical practice,” she said. “But it does justify doing this as part of a research study. We definitely need more data on this. We must be cautious as NfL is not specific for MS – many other conditions are also associated with raised levels, but it is certainly an interesting marker if used carefully.”
Following in the footsteps of Parkinson disease
She suggested that the way forward will be to package up these symptoms with information on biomarkers, such as NfL and imaging information, to enhance the ability to identify prodromal MS. “We could create a risk score and when a certain level of confidence is reached that this could be prodromal MS, then these patients could be enrolled in an intervention research study.”
Dr. Tremlett pointed out that, in the Parkinson disease field, a set of validated criteria for a prodrome have already been identified. “This is not used in clinical practice yet, but it is being used to identify patients for enrollment into clinical trials. I’m hoping that MS will follow in their footsteps.”
Commenting on the presentation, ACTRIMS president, Jeffrey Cohen, MD, Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, said: “There is no doubt that the MS disease process begins prior to the first attack (in the case of relapsing MS) or the onset of overt disability progression (in the case of primary progressive MS).”
He explained that this is demonstrated by the presence of old lesions on MRI in most patients at the time of presentation, the existence of so-called radiologically isolated syndrome (patients without symptoms of MS who undergo MRI for another reason and are found to have lesions suggesting of MS, many of whom go on to develop MS at a later date), and the occurrence of a variety of symptoms 5-10 years before presentation to a neurologist.
“Those symptoms are ones that are common in MS, though not specific for MS,” Dr. Cohen noted. “The main implication is that the timeline for MS needs to be moved earlier – for diagnosis, categorization of disease course, prognostic studies, and treatment. The issue is that the symptoms of the prodrome are rather nonspecific and most people with those symptoms do not have MS.”
New incoming president of ECTRIMS, Maria Pia Amato, MD, professor of neurology at the University of Florence (Italy), added: “The million-dollar question is when does progression really begin? This plenary talk tells us the disease is there years and years before it manifests itself with first demyelinating event. This opens up an immense opportunity for research and to open the window to the possibility of earlier diagnosis and treatment.”
Dr. Tremlett reports an investment in Precision NanoSystems.
A version of this article originally appeared on Medscape.com.
“It is time that the prodromal phase of multiple sclerosis [MS] is formally recognized.” That was the conclusion of Helen Tremlett, PhD, delivering the opening plenary session lecture at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
There is a myriad of prodromal features but none that are specific to MS,” Dr. Tremlett said.
“These findings show that in future there could be an earlier window of opportunity to identify and manage MS,” she suggested.
In an interview, Dr. Tremlett, who is professor and Canada Research Chair in Neuroepidemiology and Multiple Sclerosis at the University of British Columbia, Vancouver, explained that for MS a prodrome is a relatively new concept. “Right up until the year 2000, MS leaders were specifically saying that a prodrome did not exist,” she said. “But things have changed. Studies started emerging in the last decade suggestive of a prodrome, and I think we can now say there is definitely proof that a prodrome does exist. If you ask MS patients, the vast majority of them will say they had an increase in health issues in the years before diagnosis.”
In her plenary talk, Dr. Tremlett summarized the available evidence showing that, in the years before the first demyelinating event, patients are more likely to be have multiple health issues and an increase in hospitalizations and physician visits.
In a 2018 study, her group analyzed data from four Canadian provinces, including 14,000 patients with MS and 75,000 matched controls, and found a 75% increase in the rate of hospitalization, a 88% higher rate of physician service use, and a 49% increase in prescription numbers in the 5 years before the first demyelinating event in the patients with MS, compared with controls.
This included a 50% increase in mental health visits to physicians and increased rates of fibromyalgia, pain, headache, migraine, sleep disturbances, urology, and dermatology referrals, as well as irritable bowel syndrome. In addition, there were fewer pregnancies and increased prescriptions for contraception in the female patients later diagnosed with MS.
“There is a huge range of nonspecific symptoms in the 5 years before MS diagnosis, and some of these are really intriguing and unanticipated,” Dr. Tremlett said. “We are not surprised by the findings that fatigue, mental health issues, and bladder and bowel symptoms are increased, but the finding that there are more visits to a dermatologist and an increase in prescriptions for skin conditions was completely unexpected.”
The researchers found that dermatology referrals increased in patients who went on to develop relapsing remitting but not primary progressive forms of MS, which correlates with the established knowledge that the relapsing form has an inflammatory component not seen in progressive MS.
In a large U.K. population study of 10,000 patients with MS and 39,000 matched controls sourced from primary care doctors’ records, there was an increase in gastrointestinal and urinary issues, pain, anxiety and depression, insomnia, and fatigue in the 10 years before the first diagnosis of MS or clinically isolated syndrome (CIS) in patients later diagnosed with those conditions, compared with controls, Dr. Tremlett reported.
Other data have suggested that sex and age may affect the prodrome. In a study published this year, anemia was increased in the year before the first demyelinating event and pain was increased for 5 years beforehand. But anemia was more common in male patients later diagnosed with MS/CIS (odds ratio compared with controls, 2.4) than in female patients (OR compared with controls, 1.2).
The increase in pain seemed to be greater with age, with ORs of 1.8 for those younger than 30 years, 2.1 for those age 30-49 years, and 2.4 for those older than 50 years compared with controls.
A Norwegian military study in men that included 900 patients with MS and 19,000 matched controls found that cognitive performance was reduced in the 2 years before MS symptoms developed and up to 20 years before symptoms in those who developed primary progressive MS. “This suggests that primary progressive MS could start decades before the first apparent symptoms become obvious,” Dr. Tremlett commented.
A study in pediatric MS found that the mothers of the patients had higher use of health care (rate ratio, 1.16) and mental health (rate ratio, 1.33) services in the 5 years before their children had their first demyelinating event.
A study in Bavaria, Germany, including 10,000 patients with MS and 73,000 controls, concluded that “many physician visits before MS diagnosis were, in hindsight, likely a demyelinating event,” with the implication that this is evidence of missed opportunity for earlier diagnosis, Dr. Tremlett noted.
In a 2019 study, psychiatric symptoms were more common before MS diagnosis across various different immune-mediated disease (MS, rheumatoid arthritis, inflammatory bowel disease), with an incidence rate ratio of 1.6. The rate was even increased 10 years before diagnosis (incidence rate ratio, 1.5).
“This is evidence for shared prodromal features across immune diseases, but there isn’t a single feature specific to MS,” Dr. Tremlett said. She also referred to evidence that the blood biomarker of neuronal damage, neurofilament light chain (NfL), is raised several years before MS diagnosis. In a U.S. military study that examined serum repository samples, NfL was increased for 6 years before disease onset in 30 patients with MS, compared with 30 matched controls.
What are the implications?
Dr. Tremlett said the immediate impact of these observations about the prodrome is focused on research, particularly investigation of risk factors for MS. “If we want to know what causes MS, we have to be very careful that we are not detecting prodromal symptoms and mistaking that for a causal MS risk factor. We need to make sure we look further back than just the last few years when looking for risk factors.”
She gave the example of the observation that women in the years before MS diagnosis are less likely to have a pregnancy and more likely to fill a prescription for contraception. “This has led to the idea that avoiding pregnancy and using contraceptives increases the risk of MS, but I interpret it as these women know that something odd is going on and make the lifestyle decision not to become pregnant.”
She believes the longer-term impact of the prodrome is going to require much thought. “There is no such diagnosis of prodromal MS at the moment, but there could be in future. But the idea that we can use this information to detect MS earlier is going to require collaboration from many international stakeholders and MS organizations. We can’t automatically suspect MS in people who have these symptoms because they are so nonspecific. I think to request an MRI in patients experiencing headaches/fatigue/bowel issues is jumping the gun at the present moment as these symptoms are very common.”
On the idea of measuring NfL in patients with some of these symptoms, she believes that may be a possibility in the future but much more data are required.“We do have some evidence suggesting that the NfL blood biomarker is raised before MS diagnosis, and this was from a very well-designed study, but it was small so I think it is too early to start looking at this in clinical practice,” she said. “But it does justify doing this as part of a research study. We definitely need more data on this. We must be cautious as NfL is not specific for MS – many other conditions are also associated with raised levels, but it is certainly an interesting marker if used carefully.”
Following in the footsteps of Parkinson disease
She suggested that the way forward will be to package up these symptoms with information on biomarkers, such as NfL and imaging information, to enhance the ability to identify prodromal MS. “We could create a risk score and when a certain level of confidence is reached that this could be prodromal MS, then these patients could be enrolled in an intervention research study.”
Dr. Tremlett pointed out that, in the Parkinson disease field, a set of validated criteria for a prodrome have already been identified. “This is not used in clinical practice yet, but it is being used to identify patients for enrollment into clinical trials. I’m hoping that MS will follow in their footsteps.”
Commenting on the presentation, ACTRIMS president, Jeffrey Cohen, MD, Mellen Center for Multiple Sclerosis Treatment and Research at the Cleveland Clinic, said: “There is no doubt that the MS disease process begins prior to the first attack (in the case of relapsing MS) or the onset of overt disability progression (in the case of primary progressive MS).”
He explained that this is demonstrated by the presence of old lesions on MRI in most patients at the time of presentation, the existence of so-called radiologically isolated syndrome (patients without symptoms of MS who undergo MRI for another reason and are found to have lesions suggesting of MS, many of whom go on to develop MS at a later date), and the occurrence of a variety of symptoms 5-10 years before presentation to a neurologist.
“Those symptoms are ones that are common in MS, though not specific for MS,” Dr. Cohen noted. “The main implication is that the timeline for MS needs to be moved earlier – for diagnosis, categorization of disease course, prognostic studies, and treatment. The issue is that the symptoms of the prodrome are rather nonspecific and most people with those symptoms do not have MS.”
New incoming president of ECTRIMS, Maria Pia Amato, MD, professor of neurology at the University of Florence (Italy), added: “The million-dollar question is when does progression really begin? This plenary talk tells us the disease is there years and years before it manifests itself with first demyelinating event. This opens up an immense opportunity for research and to open the window to the possibility of earlier diagnosis and treatment.”
Dr. Tremlett reports an investment in Precision NanoSystems.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020
Sleep EEG may predict later antidepressant response
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.

This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.

“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.
“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.
“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
FROM ECNP 2020
High plasma GFAP level predicts disability accumulation in secondary progressive MS
according to investigators. The biomarker appears to have a stronger correlation with disability in people with nonactive disease, compared with those with active disease. These data were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.

Astroglial injury and activation is one of the characteristic features of progressive MS. Following such injury, GFAP is released into the cerebrospinal fluid and blood.
“It may be that GFAP plays an especially important role in patients without focal inflammatory activity and is more associated with insidious progression,” said Jens Kuhle, MD, PhD, head of the MS center at University Hospital Basel (Switzerland). “This [finding] needs to be investigated further within the same cohort, but also [within] additional well-characterized other cohorts.”
Dr. Kuhle and colleagues examined GFAP as a prognostic biomarker of disability worsening by analyzing data for patients with active or nonactive secondary progressive MS who participated in the phase 3 EXPAND study, which compared siponimod with placebo. In this post hoc analysis, the investigators quantified baseline GFAP in plasma samples using single-molecule array technology. They categorized GFAP as high or low according to the gender-stratified 80th percentile.
Dr. Kuhle’s group assessed the effect of GFAP on time to an Expanded Disability Status Scale score of 7 (i.e., restriction to wheelchair) using a Cox regression model adjusted for age, gender, disease duration, treatment, relapses in the 24 months prior to study start, and baseline EDSS. In addition, they performed subgroup analyses in patients with active secondary progressive MS and those with nonactive secondary progressive MS. They defined active disease as having relapses at 24 or fewer months before study entry or gadolinium-enhancing T1 lesions at baseline. Participants without these characteristics were classified as having nonactive disease. The investigators also stratified the results by gender.
Correlation was strongest in nonactive disease
The current analysis included samples for 1,405 of the 1,651 patients who had been randomly assigned to treatment in the EXPAND study. The median GFAP level was 119.6 pg/mL among men and 141.4 pg/mL among women.
The risk of reaching an EDSS score of 7 was higher in patients with a high baseline GFAP level. Of 281 (12.1%) participants with a high baseline GFAP level, 34 reached this endpoint, compared with 54 of 1,117 (4.8%) participants with a low baseline GFAP level. For patients with a high GFAP level at baseline, the hazard ratio of this outcome was 1.96.
Subgroup analyses indicated that the increased risk of reaching an EDSS score of 7 was seen mainly in women. Of 169 women (13.6%) with high baseline GFAP level, 23 reached this endpoint, compared with 34 of 673 women (5.1%) without a high baseline GFAP level (HR, 2.22). Among men, the difference was not significant. Of 112 men (9.8%) with a high baseline GFAP level, 11 reached an EDSS score of 7, compared with 20 of 444 men (4.5%) without a high baseline GFAP level (HR, 1.45). The reason for this sex difference is unknown, said Dr. Kuhle. “A next important step is to ensure this [finding] is not influenced by other hidden factors.”
Dr. Kuhle and colleagues also found that the increase in risk of reaching an EDSS score of 7 was mainly observed in patients with nonactive secondary progressive MS. Among 133 such patients with a high baseline GFAP level, 14 (10.5%) reached this endpoint, compared with 22 of 570 patients (3.9%) without a high baseline GFAP level (HR, 3.40). The difference among patients with active secondary progressive MS was not significant (20 of 144 patients [13.9%] with high baseline GFAP level, compared with 30 of 521 patients [5.8%] without a high baseline GFAP level; HR, 1.58). Dr. Kuhle and colleagues found similar trends in the associations between baseline GFAP levels and time to 6-month confirmed disability progression, but these trends were less pronounced.
“The measurement of plasma or blood neurofilament light chain [NfL] is certainly closer to a potential clinical application than [the measurement of] GFAP,” Dr. Kuhle admitted. “However, highly sensitive platforms open the field to the fascinating possibility of finding meaningful biomarkers in the blood compartment in MS.” This development should be developed further. It is necessary to validate the significance of GFAP measures in individual patients and describe them with greater precision before they can be applied clinically. It also is necessary to create normative data and explore for the impact of other variables like age and comorbidities, he added.
“We are currently analyzing the EXPAND data further to see which characteristics at baseline and at end of study are driving plasma GFAP concentrations,” said Dr. Kuhle. “We also need to investigate whether progression events are captured accurately by GFAP in plasma. It will also be important to combine the GFAP data with NfL measures that are already available in this cohort.”
Study addresses a clinical need
“There is great need for a reliable, easy-to-measure, and relevant fluid biomarker for use in MS,” said Robert J. Fox, MD, staff neurologist at the Cleveland Clinic’s Mellen Center for MS. Neurofilaments have been a leading candidate among biomarkers, but researchers are exploring other candidates as well. An advantage of the present study is that Dr. Kuhle and colleagues examined a large number of patients with secondary progressive MS who underwent highly structured follow-up over several years, Dr. Fox said.
“What is most interesting is that the predictive capacity was greater in nonrelapsing secondary progressive MS, and so may have advantages over neurofilament in this group of patients,” he added. “Currently, GFAP is a research test and isn’t available for clinical practice.”
Researchers should investigate other ways in which GFAP is related to future disease activity (e.g., in the form of relapses or new MRI lesions) as well as to other measures of disability progression besides restriction to a wheelchair, said Dr. Fox. “Future research needs to examine whether this biomarker is helpful at the individual patient level. Can it guide a patient’s clinician toward treatment recommendations?”
This study was funded by Novartis. Neither Dr. Kuhle nor Dr. Fox had no relevant disclosures to report.
This article was updated 9/14/2020.
according to investigators. The biomarker appears to have a stronger correlation with disability in people with nonactive disease, compared with those with active disease. These data were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Astroglial injury and activation is one of the characteristic features of progressive MS. Following such injury, GFAP is released into the cerebrospinal fluid and blood.
“It may be that GFAP plays an especially important role in patients without focal inflammatory activity and is more associated with insidious progression,” said Jens Kuhle, MD, PhD, head of the MS center at University Hospital Basel (Switzerland). “This [finding] needs to be investigated further within the same cohort, but also [within] additional well-characterized other cohorts.”
Dr. Kuhle and colleagues examined GFAP as a prognostic biomarker of disability worsening by analyzing data for patients with active or nonactive secondary progressive MS who participated in the phase 3 EXPAND study, which compared siponimod with placebo. In this post hoc analysis, the investigators quantified baseline GFAP in plasma samples using single-molecule array technology. They categorized GFAP as high or low according to the gender-stratified 80th percentile.
Dr. Kuhle’s group assessed the effect of GFAP on time to an Expanded Disability Status Scale score of 7 (i.e., restriction to wheelchair) using a Cox regression model adjusted for age, gender, disease duration, treatment, relapses in the 24 months prior to study start, and baseline EDSS. In addition, they performed subgroup analyses in patients with active secondary progressive MS and those with nonactive secondary progressive MS. They defined active disease as having relapses at 24 or fewer months before study entry or gadolinium-enhancing T1 lesions at baseline. Participants without these characteristics were classified as having nonactive disease. The investigators also stratified the results by gender.
Correlation was strongest in nonactive disease
The current analysis included samples for 1,405 of the 1,651 patients who had been randomly assigned to treatment in the EXPAND study. The median GFAP level was 119.6 pg/mL among men and 141.4 pg/mL among women.
The risk of reaching an EDSS score of 7 was higher in patients with a high baseline GFAP level. Of 281 (12.1%) participants with a high baseline GFAP level, 34 reached this endpoint, compared with 54 of 1,117 (4.8%) participants with a low baseline GFAP level. For patients with a high GFAP level at baseline, the hazard ratio of this outcome was 1.96.
Subgroup analyses indicated that the increased risk of reaching an EDSS score of 7 was seen mainly in women. Of 169 women (13.6%) with high baseline GFAP level, 23 reached this endpoint, compared with 34 of 673 women (5.1%) without a high baseline GFAP level (HR, 2.22). Among men, the difference was not significant. Of 112 men (9.8%) with a high baseline GFAP level, 11 reached an EDSS score of 7, compared with 20 of 444 men (4.5%) without a high baseline GFAP level (HR, 1.45). The reason for this sex difference is unknown, said Dr. Kuhle. “A next important step is to ensure this [finding] is not influenced by other hidden factors.”
Dr. Kuhle and colleagues also found that the increase in risk of reaching an EDSS score of 7 was mainly observed in patients with nonactive secondary progressive MS. Among 133 such patients with a high baseline GFAP level, 14 (10.5%) reached this endpoint, compared with 22 of 570 patients (3.9%) without a high baseline GFAP level (HR, 3.40). The difference among patients with active secondary progressive MS was not significant (20 of 144 patients [13.9%] with high baseline GFAP level, compared with 30 of 521 patients [5.8%] without a high baseline GFAP level; HR, 1.58). Dr. Kuhle and colleagues found similar trends in the associations between baseline GFAP levels and time to 6-month confirmed disability progression, but these trends were less pronounced.
“The measurement of plasma or blood neurofilament light chain [NfL] is certainly closer to a potential clinical application than [the measurement of] GFAP,” Dr. Kuhle admitted. “However, highly sensitive platforms open the field to the fascinating possibility of finding meaningful biomarkers in the blood compartment in MS.” This development should be developed further. It is necessary to validate the significance of GFAP measures in individual patients and describe them with greater precision before they can be applied clinically. It also is necessary to create normative data and explore for the impact of other variables like age and comorbidities, he added.
“We are currently analyzing the EXPAND data further to see which characteristics at baseline and at end of study are driving plasma GFAP concentrations,” said Dr. Kuhle. “We also need to investigate whether progression events are captured accurately by GFAP in plasma. It will also be important to combine the GFAP data with NfL measures that are already available in this cohort.”
Study addresses a clinical need
“There is great need for a reliable, easy-to-measure, and relevant fluid biomarker for use in MS,” said Robert J. Fox, MD, staff neurologist at the Cleveland Clinic’s Mellen Center for MS. Neurofilaments have been a leading candidate among biomarkers, but researchers are exploring other candidates as well. An advantage of the present study is that Dr. Kuhle and colleagues examined a large number of patients with secondary progressive MS who underwent highly structured follow-up over several years, Dr. Fox said.
“What is most interesting is that the predictive capacity was greater in nonrelapsing secondary progressive MS, and so may have advantages over neurofilament in this group of patients,” he added. “Currently, GFAP is a research test and isn’t available for clinical practice.”
Researchers should investigate other ways in which GFAP is related to future disease activity (e.g., in the form of relapses or new MRI lesions) as well as to other measures of disability progression besides restriction to a wheelchair, said Dr. Fox. “Future research needs to examine whether this biomarker is helpful at the individual patient level. Can it guide a patient’s clinician toward treatment recommendations?”
This study was funded by Novartis. Neither Dr. Kuhle nor Dr. Fox had no relevant disclosures to report.
This article was updated 9/14/2020.
according to investigators. The biomarker appears to have a stronger correlation with disability in people with nonactive disease, compared with those with active disease. These data were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
Astroglial injury and activation is one of the characteristic features of progressive MS. Following such injury, GFAP is released into the cerebrospinal fluid and blood.
“It may be that GFAP plays an especially important role in patients without focal inflammatory activity and is more associated with insidious progression,” said Jens Kuhle, MD, PhD, head of the MS center at University Hospital Basel (Switzerland). “This [finding] needs to be investigated further within the same cohort, but also [within] additional well-characterized other cohorts.”
Dr. Kuhle and colleagues examined GFAP as a prognostic biomarker of disability worsening by analyzing data for patients with active or nonactive secondary progressive MS who participated in the phase 3 EXPAND study, which compared siponimod with placebo. In this post hoc analysis, the investigators quantified baseline GFAP in plasma samples using single-molecule array technology. They categorized GFAP as high or low according to the gender-stratified 80th percentile.
Dr. Kuhle’s group assessed the effect of GFAP on time to an Expanded Disability Status Scale score of 7 (i.e., restriction to wheelchair) using a Cox regression model adjusted for age, gender, disease duration, treatment, relapses in the 24 months prior to study start, and baseline EDSS. In addition, they performed subgroup analyses in patients with active secondary progressive MS and those with nonactive secondary progressive MS. They defined active disease as having relapses at 24 or fewer months before study entry or gadolinium-enhancing T1 lesions at baseline. Participants without these characteristics were classified as having nonactive disease. The investigators also stratified the results by gender.
Correlation was strongest in nonactive disease
The current analysis included samples for 1,405 of the 1,651 patients who had been randomly assigned to treatment in the EXPAND study. The median GFAP level was 119.6 pg/mL among men and 141.4 pg/mL among women.
The risk of reaching an EDSS score of 7 was higher in patients with a high baseline GFAP level. Of 281 (12.1%) participants with a high baseline GFAP level, 34 reached this endpoint, compared with 54 of 1,117 (4.8%) participants with a low baseline GFAP level. For patients with a high GFAP level at baseline, the hazard ratio of this outcome was 1.96.
Subgroup analyses indicated that the increased risk of reaching an EDSS score of 7 was seen mainly in women. Of 169 women (13.6%) with high baseline GFAP level, 23 reached this endpoint, compared with 34 of 673 women (5.1%) without a high baseline GFAP level (HR, 2.22). Among men, the difference was not significant. Of 112 men (9.8%) with a high baseline GFAP level, 11 reached an EDSS score of 7, compared with 20 of 444 men (4.5%) without a high baseline GFAP level (HR, 1.45). The reason for this sex difference is unknown, said Dr. Kuhle. “A next important step is to ensure this [finding] is not influenced by other hidden factors.”
Dr. Kuhle and colleagues also found that the increase in risk of reaching an EDSS score of 7 was mainly observed in patients with nonactive secondary progressive MS. Among 133 such patients with a high baseline GFAP level, 14 (10.5%) reached this endpoint, compared with 22 of 570 patients (3.9%) without a high baseline GFAP level (HR, 3.40). The difference among patients with active secondary progressive MS was not significant (20 of 144 patients [13.9%] with high baseline GFAP level, compared with 30 of 521 patients [5.8%] without a high baseline GFAP level; HR, 1.58). Dr. Kuhle and colleagues found similar trends in the associations between baseline GFAP levels and time to 6-month confirmed disability progression, but these trends were less pronounced.
“The measurement of plasma or blood neurofilament light chain [NfL] is certainly closer to a potential clinical application than [the measurement of] GFAP,” Dr. Kuhle admitted. “However, highly sensitive platforms open the field to the fascinating possibility of finding meaningful biomarkers in the blood compartment in MS.” This development should be developed further. It is necessary to validate the significance of GFAP measures in individual patients and describe them with greater precision before they can be applied clinically. It also is necessary to create normative data and explore for the impact of other variables like age and comorbidities, he added.
“We are currently analyzing the EXPAND data further to see which characteristics at baseline and at end of study are driving plasma GFAP concentrations,” said Dr. Kuhle. “We also need to investigate whether progression events are captured accurately by GFAP in plasma. It will also be important to combine the GFAP data with NfL measures that are already available in this cohort.”
Study addresses a clinical need
“There is great need for a reliable, easy-to-measure, and relevant fluid biomarker for use in MS,” said Robert J. Fox, MD, staff neurologist at the Cleveland Clinic’s Mellen Center for MS. Neurofilaments have been a leading candidate among biomarkers, but researchers are exploring other candidates as well. An advantage of the present study is that Dr. Kuhle and colleagues examined a large number of patients with secondary progressive MS who underwent highly structured follow-up over several years, Dr. Fox said.
“What is most interesting is that the predictive capacity was greater in nonrelapsing secondary progressive MS, and so may have advantages over neurofilament in this group of patients,” he added. “Currently, GFAP is a research test and isn’t available for clinical practice.”
Researchers should investigate other ways in which GFAP is related to future disease activity (e.g., in the form of relapses or new MRI lesions) as well as to other measures of disability progression besides restriction to a wheelchair, said Dr. Fox. “Future research needs to examine whether this biomarker is helpful at the individual patient level. Can it guide a patient’s clinician toward treatment recommendations?”
This study was funded by Novartis. Neither Dr. Kuhle nor Dr. Fox had no relevant disclosures to report.
This article was updated 9/14/2020.
FROM MSVIRTUAL2020
ISCHEMIA trial revisited: Some MAY benefit from invasive strategy
The landmark ISCHEMIA trial rattled the cardiology world with its message that clinical outcomes weren’t significantly better with a routine initial invasive strategy than with medical therapy alone in patients with stable coronary artery disease and moderate or severe myocardial ischemia on noninvasive testing. But

ISCHEMIA participants in the sweet spot for an initial invasive strategy were the ones with a baseline history of mild to moderate heart failure symptoms and a left ventricular ejection fraction (LVEF) of 35%-45%, Renato Lopes, MD, PhD, reported at the virtual annual congress of the European Society of Cardiology.
“An invasive approach may be beneficial in this subgroup of high-risk patients with moderate to severe ischemia and a history of heart failure and left ventricular dysfunction,” declared Dr. Lopes, professor of medicine at Duke University, Durham, N.C.
He was quick to add, however, that this finding from ISCHEMIA should be considered hypothesis generating in light of the small sample size in the subgroup analysis.
The ISCHEMIA trial randomized 5,179 patients with stable CAD and at least moderate myocardial ischemia on noninvasive testing to a routine invasive or conservative management strategy. At 4 years of follow-up there was no significant between-group difference in cardiovascular outcomes (N Engl J Med. 2020 Apr 9;382[15]:1395-407).
Patients with a baseline LVEF below 35% weren’t eligible for enrollment in ISCHEMIA. That’s because the prior Surgical Treatment for Ischemic Heart Failure Extension Study (STICHES) showed patients with ischemic cardiomyopathy and an LVEF below 35% had a significantly lower cardiovascular death rate with surgical revascularization plus medical therapy than optimal medical therapy alone at 10 years of follow-up (N Engl J Med. 2016 Apr 21;374[16]:1511-20).
But what about the impact of immediate revascularization as compared with medical management alone in patients with milder impairment of LVEF in the 35%-45% range and/or a history of symptomatic heart failure? Theoretically, the improved blood flow to ischemic myocardium obtained via revascularization in such patients might activate hibernating myocardium and reduce ventricular dysfunction, thereby reducing the risk of cardiovascular events. The ISCHEMIA trial provided a unique opportunity to prospectively examine this question in 398 affected study participants, Dr. Lopes explained.
This 398-patient subgroup with a baseline history of heart failure and/or left ventricular dysfunction (HF/LVD) was at higher risk than patients without those features. Indeed, the primary outcome in ISCHEMIA – a composite of cardiovascular death, nonfatal MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest – occurred in 22.7% of the HF/LVD group at 4 years of follow-up, compared with 13.8% of the much larger group without HF/LVD. The HF/LVD group also had significantly higher rates of the secondary composite endpoints of cardiovascular death or MI (19.7% vs. 12.3%) and all-cause mortality or heart failure (15% vs. 6.9%).
The provocative central finding in this new subanalysis was that patients in the HF/LVD subgroup fared significantly better in terms of cardiovascular events if randomized to the initial invasive approach. Indeed, their 4-year rate of the primary outcome was 17.2%, compared with 29.3% with an initial conservative approach. The various secondary outcomes followed suit. In contrast, the primary outcome occurred in 13% of patients without HF/LVD who were randomized to the invasive strategy, not significantly different from the 14.6% rate with conservative management.
Drilling deeper into the data, Dr. Lopes and coinvestigators found that the enhanced event-free survival benefit of an initial invasive strategy was restricted to the 28 patients having both a baseline history of symptomatic heart failure and an LVEF of 35%-45%. There was no significant difference in outcomes with an invasive versus conservative strategy in the 177 patients with a history of heart failure whose LVEF was greater than 50% – that is, patients with heart failure with preserved ejection fraction – nor in the 193 participants with an LVEF of 35%-45% but no history of symptomatic heart failure.
In an interview, Mark H. Drazner, MD, commented, “this is an interesting hypothesis, for sure, that warrants further study to confirm whether it’s valid. And if it is valid, there could be real implications. If this is true, I think there could be a decent number of patients out there that this would have implications for.
“The ISCHEMIA trial was a heroic effort. While there are certainly logistical hurdles involved in anybody doing an ISCHEMIA 2 trial based on this small subgroup analysis, other people could start looking at retrospective datasets and see if they can confirm these findings to build momentum to study this further,” said Dr. Drazner, professor of medicine and chief of clinical cardiology at the University of Texas Southwestern Medical Center, Dallas, as well as an associate editor at Circulation.
Dr. Lopes reported receiving research grants from Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi-Aventis as well as serving as a consultant to a handful of pharmaceutical companies, none relevant to his presentation.
Simultaneous with his presentation at ESC Congress 2020, Dr. Lopes’ study was published online in Circulation.
SOURCE: Lopes R et al. Circulation. 2020 Aug 29. doi: 10.1161/CIRCULATIONAHA.120.050304.
The landmark ISCHEMIA trial rattled the cardiology world with its message that clinical outcomes weren’t significantly better with a routine initial invasive strategy than with medical therapy alone in patients with stable coronary artery disease and moderate or severe myocardial ischemia on noninvasive testing. But
ISCHEMIA participants in the sweet spot for an initial invasive strategy were the ones with a baseline history of mild to moderate heart failure symptoms and a left ventricular ejection fraction (LVEF) of 35%-45%, Renato Lopes, MD, PhD, reported at the virtual annual congress of the European Society of Cardiology.
“An invasive approach may be beneficial in this subgroup of high-risk patients with moderate to severe ischemia and a history of heart failure and left ventricular dysfunction,” declared Dr. Lopes, professor of medicine at Duke University, Durham, N.C.
He was quick to add, however, that this finding from ISCHEMIA should be considered hypothesis generating in light of the small sample size in the subgroup analysis.
The ISCHEMIA trial randomized 5,179 patients with stable CAD and at least moderate myocardial ischemia on noninvasive testing to a routine invasive or conservative management strategy. At 4 years of follow-up there was no significant between-group difference in cardiovascular outcomes (N Engl J Med. 2020 Apr 9;382[15]:1395-407).
Patients with a baseline LVEF below 35% weren’t eligible for enrollment in ISCHEMIA. That’s because the prior Surgical Treatment for Ischemic Heart Failure Extension Study (STICHES) showed patients with ischemic cardiomyopathy and an LVEF below 35% had a significantly lower cardiovascular death rate with surgical revascularization plus medical therapy than optimal medical therapy alone at 10 years of follow-up (N Engl J Med. 2016 Apr 21;374[16]:1511-20).
But what about the impact of immediate revascularization as compared with medical management alone in patients with milder impairment of LVEF in the 35%-45% range and/or a history of symptomatic heart failure? Theoretically, the improved blood flow to ischemic myocardium obtained via revascularization in such patients might activate hibernating myocardium and reduce ventricular dysfunction, thereby reducing the risk of cardiovascular events. The ISCHEMIA trial provided a unique opportunity to prospectively examine this question in 398 affected study participants, Dr. Lopes explained.
This 398-patient subgroup with a baseline history of heart failure and/or left ventricular dysfunction (HF/LVD) was at higher risk than patients without those features. Indeed, the primary outcome in ISCHEMIA – a composite of cardiovascular death, nonfatal MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest – occurred in 22.7% of the HF/LVD group at 4 years of follow-up, compared with 13.8% of the much larger group without HF/LVD. The HF/LVD group also had significantly higher rates of the secondary composite endpoints of cardiovascular death or MI (19.7% vs. 12.3%) and all-cause mortality or heart failure (15% vs. 6.9%).
The provocative central finding in this new subanalysis was that patients in the HF/LVD subgroup fared significantly better in terms of cardiovascular events if randomized to the initial invasive approach. Indeed, their 4-year rate of the primary outcome was 17.2%, compared with 29.3% with an initial conservative approach. The various secondary outcomes followed suit. In contrast, the primary outcome occurred in 13% of patients without HF/LVD who were randomized to the invasive strategy, not significantly different from the 14.6% rate with conservative management.
Drilling deeper into the data, Dr. Lopes and coinvestigators found that the enhanced event-free survival benefit of an initial invasive strategy was restricted to the 28 patients having both a baseline history of symptomatic heart failure and an LVEF of 35%-45%. There was no significant difference in outcomes with an invasive versus conservative strategy in the 177 patients with a history of heart failure whose LVEF was greater than 50% – that is, patients with heart failure with preserved ejection fraction – nor in the 193 participants with an LVEF of 35%-45% but no history of symptomatic heart failure.
In an interview, Mark H. Drazner, MD, commented, “this is an interesting hypothesis, for sure, that warrants further study to confirm whether it’s valid. And if it is valid, there could be real implications. If this is true, I think there could be a decent number of patients out there that this would have implications for.
“The ISCHEMIA trial was a heroic effort. While there are certainly logistical hurdles involved in anybody doing an ISCHEMIA 2 trial based on this small subgroup analysis, other people could start looking at retrospective datasets and see if they can confirm these findings to build momentum to study this further,” said Dr. Drazner, professor of medicine and chief of clinical cardiology at the University of Texas Southwestern Medical Center, Dallas, as well as an associate editor at Circulation.
Dr. Lopes reported receiving research grants from Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi-Aventis as well as serving as a consultant to a handful of pharmaceutical companies, none relevant to his presentation.
Simultaneous with his presentation at ESC Congress 2020, Dr. Lopes’ study was published online in Circulation.
SOURCE: Lopes R et al. Circulation. 2020 Aug 29. doi: 10.1161/CIRCULATIONAHA.120.050304.
The landmark ISCHEMIA trial rattled the cardiology world with its message that clinical outcomes weren’t significantly better with a routine initial invasive strategy than with medical therapy alone in patients with stable coronary artery disease and moderate or severe myocardial ischemia on noninvasive testing. But
ISCHEMIA participants in the sweet spot for an initial invasive strategy were the ones with a baseline history of mild to moderate heart failure symptoms and a left ventricular ejection fraction (LVEF) of 35%-45%, Renato Lopes, MD, PhD, reported at the virtual annual congress of the European Society of Cardiology.
“An invasive approach may be beneficial in this subgroup of high-risk patients with moderate to severe ischemia and a history of heart failure and left ventricular dysfunction,” declared Dr. Lopes, professor of medicine at Duke University, Durham, N.C.
He was quick to add, however, that this finding from ISCHEMIA should be considered hypothesis generating in light of the small sample size in the subgroup analysis.
The ISCHEMIA trial randomized 5,179 patients with stable CAD and at least moderate myocardial ischemia on noninvasive testing to a routine invasive or conservative management strategy. At 4 years of follow-up there was no significant between-group difference in cardiovascular outcomes (N Engl J Med. 2020 Apr 9;382[15]:1395-407).
Patients with a baseline LVEF below 35% weren’t eligible for enrollment in ISCHEMIA. That’s because the prior Surgical Treatment for Ischemic Heart Failure Extension Study (STICHES) showed patients with ischemic cardiomyopathy and an LVEF below 35% had a significantly lower cardiovascular death rate with surgical revascularization plus medical therapy than optimal medical therapy alone at 10 years of follow-up (N Engl J Med. 2016 Apr 21;374[16]:1511-20).
But what about the impact of immediate revascularization as compared with medical management alone in patients with milder impairment of LVEF in the 35%-45% range and/or a history of symptomatic heart failure? Theoretically, the improved blood flow to ischemic myocardium obtained via revascularization in such patients might activate hibernating myocardium and reduce ventricular dysfunction, thereby reducing the risk of cardiovascular events. The ISCHEMIA trial provided a unique opportunity to prospectively examine this question in 398 affected study participants, Dr. Lopes explained.
This 398-patient subgroup with a baseline history of heart failure and/or left ventricular dysfunction (HF/LVD) was at higher risk than patients without those features. Indeed, the primary outcome in ISCHEMIA – a composite of cardiovascular death, nonfatal MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest – occurred in 22.7% of the HF/LVD group at 4 years of follow-up, compared with 13.8% of the much larger group without HF/LVD. The HF/LVD group also had significantly higher rates of the secondary composite endpoints of cardiovascular death or MI (19.7% vs. 12.3%) and all-cause mortality or heart failure (15% vs. 6.9%).
The provocative central finding in this new subanalysis was that patients in the HF/LVD subgroup fared significantly better in terms of cardiovascular events if randomized to the initial invasive approach. Indeed, their 4-year rate of the primary outcome was 17.2%, compared with 29.3% with an initial conservative approach. The various secondary outcomes followed suit. In contrast, the primary outcome occurred in 13% of patients without HF/LVD who were randomized to the invasive strategy, not significantly different from the 14.6% rate with conservative management.
Drilling deeper into the data, Dr. Lopes and coinvestigators found that the enhanced event-free survival benefit of an initial invasive strategy was restricted to the 28 patients having both a baseline history of symptomatic heart failure and an LVEF of 35%-45%. There was no significant difference in outcomes with an invasive versus conservative strategy in the 177 patients with a history of heart failure whose LVEF was greater than 50% – that is, patients with heart failure with preserved ejection fraction – nor in the 193 participants with an LVEF of 35%-45% but no history of symptomatic heart failure.
In an interview, Mark H. Drazner, MD, commented, “this is an interesting hypothesis, for sure, that warrants further study to confirm whether it’s valid. And if it is valid, there could be real implications. If this is true, I think there could be a decent number of patients out there that this would have implications for.
“The ISCHEMIA trial was a heroic effort. While there are certainly logistical hurdles involved in anybody doing an ISCHEMIA 2 trial based on this small subgroup analysis, other people could start looking at retrospective datasets and see if they can confirm these findings to build momentum to study this further,” said Dr. Drazner, professor of medicine and chief of clinical cardiology at the University of Texas Southwestern Medical Center, Dallas, as well as an associate editor at Circulation.
Dr. Lopes reported receiving research grants from Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi-Aventis as well as serving as a consultant to a handful of pharmaceutical companies, none relevant to his presentation.
Simultaneous with his presentation at ESC Congress 2020, Dr. Lopes’ study was published online in Circulation.
SOURCE: Lopes R et al. Circulation. 2020 Aug 29. doi: 10.1161/CIRCULATIONAHA.120.050304.
FROM ESC CONGRESS 2020
No one-size-fits-all approach to tissue-tightening devices
.

“There are many devices on the market, but their efficacy is not consistent,” Catherine M. DiGiorgio, MS, MD, said during the virtual annual Masters of Aesthetics Symposium. “The key to maximizing patient satisfaction is patient selection and setting realistic expectations.”
She avoids recommending the use of tissue-tightening devices for patients who require surgical correction and for those who find the idea of minimal improvement unacceptable. “These are not the treatments for them,” she said. “I also find that when a patient uses her fingers to pull her face back and says, ‘I want to look like this,’ this is not the right patient for these devices. They can get a good amount of improvement, but efficacy is not consistent.”
Still, patients favor noninvasive or minimally invasive procedures for skin tightening now more than ever before. “They are not willing to undergo surgical treatments, and they want something with low downtime,” she said.
Dr. DiGiorgio, who practices at the Boston Center for Facial Rejuvenation, began a review of tissue-tightening devices on the market by discussing the role of ablative fractional lasers such as the carbon dioxide 10,600-nm laser and the Erbium:YAG 2,940-nm laser, which carry risks and downtime. “I don’t view these lasers as a tissue-tightening devices, but they are included because they can provide a little bit of tightening,” she said.
The ideal candidate is someone with skin type I-II and mild skin laxity. “These lasers are really good at improving rhytides,” she noted. “The patient needs to be able to tolerate the discomfort and manage the healing process. Sometimes you can get blepharoplastylike results with some patients. This can be combined with vascular lasers and pigment-targeting lasers to improve the overall texture and tone of the skin. Many combine this with a face-lift or a blepharoplasty. You should wait at least 6-8 weeks after a face-lift before performing this procedure. Some plastic surgeons do combine this with blepharoplasty in the same visit.”
A less invasive option for skin tightening is the delivery of radiofrequency energy, which disrupts hydrogen bonds of the collagen triple helix. This occurs in temperatures greater than 60° C and results in collagen contraction and tightening and neocollagenesis. There are several devices available including transcutaneous monopolar radiofrequency (Thermage, TempSure), subsurface thermistor–controlled monopolar radiofrequency (ThermiTight), and fractional microneedling radiofrequency (Profound RF, Genius RF, Vivace, and Secret RF). The transcutaneous monopolar radiofrequency device delivers energy uniformly via a treatment tip that has contact cooling and coupling fluid. Collagen is denatured at 65° C and fibroblasts are stimulated to form new collagen. The healing process provides additional tightening.
“These treatments are noninvasive; there’s no downtime, and there’s mild discomfort,” Dr. DiGiorgio commented. “Treatments can be done around the eyes, on the face and body. When treating around the eyes with these devices you want to use a corneal plastic eye shield. Contraindications include having a pacemaker, defibrillator, or other electronic implantable device.”
In her opinion, the ideal patient for this device has mild skin laxity or is younger and seeking to maintain a youthful appearance. “It’s great for mild upper eyelid laxity and for temporary improvement of cellulite appearance,” she said. “The patient should not require surgical intervention and the patient should also agree to undergo multiple treatment sessions. Just one treatment session is not going to cut it.”
Another device in this class of technology is subsurface thermistor–controlled monopolar radiofrequency, “which is basically a probe that’s inserted into the skin, most commonly in the submental area,” Dr. DiGiorgio said. An external infrared camera monitors the epidermal temperature, which should not exceed 45°C. This results in a controlled deep dermal and subdermal delivery of thermal energy. “It requires light tumescent anesthesia, and it can be combined with liposuction,” she said. “Common side effects include erythema, edema, and bruising, and sometimes contour irregularities or nodules.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical correction. “You can combine this with liposuction, but you can achieve good results without it,” she said.
The next device in this class of technology that Dr. DiGiorgio discussed is fractional microneedling radiofrequency. Of several such devices on the market, some have adjustable depths up to 4 mm while others have fixed depths. The energy is adjustable, and the tips can be insulated or noninsulated. “Insulated tips make it safer to perform in darker skin types because the proximal portion of the needle is insulated and the epidermis is spared from damage,” she explained. “Some devices are a bit more painful than others. It does require topical anesthesia; some require local injection anesthesia. Patients have erythema for about 24 hours, and treatments are recommended monthly.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical intervention but who seeks to maintain a youthful appearance. “Patients should understand that multiple treatments will be required to achieve optimal results,” she said. “I find that there is less improvement in older patients. This can be combined with thread lifts, vascular lasers, pigment-targeting lasers, and CO2 lasers.”
The next device for skin tightening that she discussed is microfocused ultrasound (Ultherapy), which delivers millisecond domain pulses at three different depths that are determined by the transducer that you use. It can go as deep as 4.5 mm. “Each pulse delivers a focal zone of coagulation to achieve tissue contraction,” Dr. DiGiorgio said. “There’s an ultrasound-imaging device attached to it to ensure proper skin contact and the delivery of energy at an appropriate depth. Patients can have a little bit of pain and erythema and edema, sometime bruising. Usually there is not much downtime with these treatments.”
A newcomer in this class of technology is SoftWave, an intense ultrasound beam array (IUB), which delivers energy precisely to the middermis at a depth of 1.5 mm. “With each pulse, the hand piece has seven transducers that deliver energy in 3-dimensional cylindrical thermal zones,” Dr. DiGiorgio said. “You get greater than 25% tissue coverage in one treatment, and there is no injury to the epidermis or deeper structures. It has unique vectors that are along the lines of facial wrinkles, so you get tightening along those lines.”
The procedure takes about 30 minutes, there is no downtime, and it causes no pain, she said. Pretreatment, patients receive topical anesthesia. “This device has active skin cooling and has an ultrasound gel,” she added. “It does not have an imaging platform like the microfocused ultrasound does, because the depth is fixed. You get significant wrinkle reduction and decrease in submental fullness with improvement in jawline definition, eyebrow position, fine lines, and texture.” In her opinion, the ideal candidate for this device is a patient in the mid-40s to early 50s with mild to moderate elastosis, fullness, texture irregularities, laxity, rhytids, elastosis, and photoaging.
She reported having no financial disclosures.
.
“There are many devices on the market, but their efficacy is not consistent,” Catherine M. DiGiorgio, MS, MD, said during the virtual annual Masters of Aesthetics Symposium. “The key to maximizing patient satisfaction is patient selection and setting realistic expectations.”
She avoids recommending the use of tissue-tightening devices for patients who require surgical correction and for those who find the idea of minimal improvement unacceptable. “These are not the treatments for them,” she said. “I also find that when a patient uses her fingers to pull her face back and says, ‘I want to look like this,’ this is not the right patient for these devices. They can get a good amount of improvement, but efficacy is not consistent.”
Still, patients favor noninvasive or minimally invasive procedures for skin tightening now more than ever before. “They are not willing to undergo surgical treatments, and they want something with low downtime,” she said.
Dr. DiGiorgio, who practices at the Boston Center for Facial Rejuvenation, began a review of tissue-tightening devices on the market by discussing the role of ablative fractional lasers such as the carbon dioxide 10,600-nm laser and the Erbium:YAG 2,940-nm laser, which carry risks and downtime. “I don’t view these lasers as a tissue-tightening devices, but they are included because they can provide a little bit of tightening,” she said.
The ideal candidate is someone with skin type I-II and mild skin laxity. “These lasers are really good at improving rhytides,” she noted. “The patient needs to be able to tolerate the discomfort and manage the healing process. Sometimes you can get blepharoplastylike results with some patients. This can be combined with vascular lasers and pigment-targeting lasers to improve the overall texture and tone of the skin. Many combine this with a face-lift or a blepharoplasty. You should wait at least 6-8 weeks after a face-lift before performing this procedure. Some plastic surgeons do combine this with blepharoplasty in the same visit.”
A less invasive option for skin tightening is the delivery of radiofrequency energy, which disrupts hydrogen bonds of the collagen triple helix. This occurs in temperatures greater than 60° C and results in collagen contraction and tightening and neocollagenesis. There are several devices available including transcutaneous monopolar radiofrequency (Thermage, TempSure), subsurface thermistor–controlled monopolar radiofrequency (ThermiTight), and fractional microneedling radiofrequency (Profound RF, Genius RF, Vivace, and Secret RF). The transcutaneous monopolar radiofrequency device delivers energy uniformly via a treatment tip that has contact cooling and coupling fluid. Collagen is denatured at 65° C and fibroblasts are stimulated to form new collagen. The healing process provides additional tightening.
“These treatments are noninvasive; there’s no downtime, and there’s mild discomfort,” Dr. DiGiorgio commented. “Treatments can be done around the eyes, on the face and body. When treating around the eyes with these devices you want to use a corneal plastic eye shield. Contraindications include having a pacemaker, defibrillator, or other electronic implantable device.”
In her opinion, the ideal patient for this device has mild skin laxity or is younger and seeking to maintain a youthful appearance. “It’s great for mild upper eyelid laxity and for temporary improvement of cellulite appearance,” she said. “The patient should not require surgical intervention and the patient should also agree to undergo multiple treatment sessions. Just one treatment session is not going to cut it.”
Another device in this class of technology is subsurface thermistor–controlled monopolar radiofrequency, “which is basically a probe that’s inserted into the skin, most commonly in the submental area,” Dr. DiGiorgio said. An external infrared camera monitors the epidermal temperature, which should not exceed 45°C. This results in a controlled deep dermal and subdermal delivery of thermal energy. “It requires light tumescent anesthesia, and it can be combined with liposuction,” she said. “Common side effects include erythema, edema, and bruising, and sometimes contour irregularities or nodules.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical correction. “You can combine this with liposuction, but you can achieve good results without it,” she said.
The next device in this class of technology that Dr. DiGiorgio discussed is fractional microneedling radiofrequency. Of several such devices on the market, some have adjustable depths up to 4 mm while others have fixed depths. The energy is adjustable, and the tips can be insulated or noninsulated. “Insulated tips make it safer to perform in darker skin types because the proximal portion of the needle is insulated and the epidermis is spared from damage,” she explained. “Some devices are a bit more painful than others. It does require topical anesthesia; some require local injection anesthesia. Patients have erythema for about 24 hours, and treatments are recommended monthly.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical intervention but who seeks to maintain a youthful appearance. “Patients should understand that multiple treatments will be required to achieve optimal results,” she said. “I find that there is less improvement in older patients. This can be combined with thread lifts, vascular lasers, pigment-targeting lasers, and CO2 lasers.”
The next device for skin tightening that she discussed is microfocused ultrasound (Ultherapy), which delivers millisecond domain pulses at three different depths that are determined by the transducer that you use. It can go as deep as 4.5 mm. “Each pulse delivers a focal zone of coagulation to achieve tissue contraction,” Dr. DiGiorgio said. “There’s an ultrasound-imaging device attached to it to ensure proper skin contact and the delivery of energy at an appropriate depth. Patients can have a little bit of pain and erythema and edema, sometime bruising. Usually there is not much downtime with these treatments.”
A newcomer in this class of technology is SoftWave, an intense ultrasound beam array (IUB), which delivers energy precisely to the middermis at a depth of 1.5 mm. “With each pulse, the hand piece has seven transducers that deliver energy in 3-dimensional cylindrical thermal zones,” Dr. DiGiorgio said. “You get greater than 25% tissue coverage in one treatment, and there is no injury to the epidermis or deeper structures. It has unique vectors that are along the lines of facial wrinkles, so you get tightening along those lines.”
The procedure takes about 30 minutes, there is no downtime, and it causes no pain, she said. Pretreatment, patients receive topical anesthesia. “This device has active skin cooling and has an ultrasound gel,” she added. “It does not have an imaging platform like the microfocused ultrasound does, because the depth is fixed. You get significant wrinkle reduction and decrease in submental fullness with improvement in jawline definition, eyebrow position, fine lines, and texture.” In her opinion, the ideal candidate for this device is a patient in the mid-40s to early 50s with mild to moderate elastosis, fullness, texture irregularities, laxity, rhytids, elastosis, and photoaging.
She reported having no financial disclosures.
.
“There are many devices on the market, but their efficacy is not consistent,” Catherine M. DiGiorgio, MS, MD, said during the virtual annual Masters of Aesthetics Symposium. “The key to maximizing patient satisfaction is patient selection and setting realistic expectations.”
She avoids recommending the use of tissue-tightening devices for patients who require surgical correction and for those who find the idea of minimal improvement unacceptable. “These are not the treatments for them,” she said. “I also find that when a patient uses her fingers to pull her face back and says, ‘I want to look like this,’ this is not the right patient for these devices. They can get a good amount of improvement, but efficacy is not consistent.”
Still, patients favor noninvasive or minimally invasive procedures for skin tightening now more than ever before. “They are not willing to undergo surgical treatments, and they want something with low downtime,” she said.
Dr. DiGiorgio, who practices at the Boston Center for Facial Rejuvenation, began a review of tissue-tightening devices on the market by discussing the role of ablative fractional lasers such as the carbon dioxide 10,600-nm laser and the Erbium:YAG 2,940-nm laser, which carry risks and downtime. “I don’t view these lasers as a tissue-tightening devices, but they are included because they can provide a little bit of tightening,” she said.
The ideal candidate is someone with skin type I-II and mild skin laxity. “These lasers are really good at improving rhytides,” she noted. “The patient needs to be able to tolerate the discomfort and manage the healing process. Sometimes you can get blepharoplastylike results with some patients. This can be combined with vascular lasers and pigment-targeting lasers to improve the overall texture and tone of the skin. Many combine this with a face-lift or a blepharoplasty. You should wait at least 6-8 weeks after a face-lift before performing this procedure. Some plastic surgeons do combine this with blepharoplasty in the same visit.”
A less invasive option for skin tightening is the delivery of radiofrequency energy, which disrupts hydrogen bonds of the collagen triple helix. This occurs in temperatures greater than 60° C and results in collagen contraction and tightening and neocollagenesis. There are several devices available including transcutaneous monopolar radiofrequency (Thermage, TempSure), subsurface thermistor–controlled monopolar radiofrequency (ThermiTight), and fractional microneedling radiofrequency (Profound RF, Genius RF, Vivace, and Secret RF). The transcutaneous monopolar radiofrequency device delivers energy uniformly via a treatment tip that has contact cooling and coupling fluid. Collagen is denatured at 65° C and fibroblasts are stimulated to form new collagen. The healing process provides additional tightening.
“These treatments are noninvasive; there’s no downtime, and there’s mild discomfort,” Dr. DiGiorgio commented. “Treatments can be done around the eyes, on the face and body. When treating around the eyes with these devices you want to use a corneal plastic eye shield. Contraindications include having a pacemaker, defibrillator, or other electronic implantable device.”
In her opinion, the ideal patient for this device has mild skin laxity or is younger and seeking to maintain a youthful appearance. “It’s great for mild upper eyelid laxity and for temporary improvement of cellulite appearance,” she said. “The patient should not require surgical intervention and the patient should also agree to undergo multiple treatment sessions. Just one treatment session is not going to cut it.”
Another device in this class of technology is subsurface thermistor–controlled monopolar radiofrequency, “which is basically a probe that’s inserted into the skin, most commonly in the submental area,” Dr. DiGiorgio said. An external infrared camera monitors the epidermal temperature, which should not exceed 45°C. This results in a controlled deep dermal and subdermal delivery of thermal energy. “It requires light tumescent anesthesia, and it can be combined with liposuction,” she said. “Common side effects include erythema, edema, and bruising, and sometimes contour irregularities or nodules.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical correction. “You can combine this with liposuction, but you can achieve good results without it,” she said.
The next device in this class of technology that Dr. DiGiorgio discussed is fractional microneedling radiofrequency. Of several such devices on the market, some have adjustable depths up to 4 mm while others have fixed depths. The energy is adjustable, and the tips can be insulated or noninsulated. “Insulated tips make it safer to perform in darker skin types because the proximal portion of the needle is insulated and the epidermis is spared from damage,” she explained. “Some devices are a bit more painful than others. It does require topical anesthesia; some require local injection anesthesia. Patients have erythema for about 24 hours, and treatments are recommended monthly.” In her opinion, the ideal candidate for this device is someone with mild to moderate skin laxity who does not require surgical intervention but who seeks to maintain a youthful appearance. “Patients should understand that multiple treatments will be required to achieve optimal results,” she said. “I find that there is less improvement in older patients. This can be combined with thread lifts, vascular lasers, pigment-targeting lasers, and CO2 lasers.”
The next device for skin tightening that she discussed is microfocused ultrasound (Ultherapy), which delivers millisecond domain pulses at three different depths that are determined by the transducer that you use. It can go as deep as 4.5 mm. “Each pulse delivers a focal zone of coagulation to achieve tissue contraction,” Dr. DiGiorgio said. “There’s an ultrasound-imaging device attached to it to ensure proper skin contact and the delivery of energy at an appropriate depth. Patients can have a little bit of pain and erythema and edema, sometime bruising. Usually there is not much downtime with these treatments.”
A newcomer in this class of technology is SoftWave, an intense ultrasound beam array (IUB), which delivers energy precisely to the middermis at a depth of 1.5 mm. “With each pulse, the hand piece has seven transducers that deliver energy in 3-dimensional cylindrical thermal zones,” Dr. DiGiorgio said. “You get greater than 25% tissue coverage in one treatment, and there is no injury to the epidermis or deeper structures. It has unique vectors that are along the lines of facial wrinkles, so you get tightening along those lines.”
The procedure takes about 30 minutes, there is no downtime, and it causes no pain, she said. Pretreatment, patients receive topical anesthesia. “This device has active skin cooling and has an ultrasound gel,” she added. “It does not have an imaging platform like the microfocused ultrasound does, because the depth is fixed. You get significant wrinkle reduction and decrease in submental fullness with improvement in jawline definition, eyebrow position, fine lines, and texture.” In her opinion, the ideal candidate for this device is a patient in the mid-40s to early 50s with mild to moderate elastosis, fullness, texture irregularities, laxity, rhytids, elastosis, and photoaging.
She reported having no financial disclosures.
REPORTING FROM MOA 2020
App for MS aims to capture elusive signals of progression

At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
At the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020, researchers at the University Hospital and University of Basel in Switzerland, presented data on their dreaMS app. The investigators are validating the app in a nonblinded cohort of 30 people with MS in the early to middle stages of progression and 30 controls without MS.
The application comprises a series of active tests measuring movement, fine motor skills, cognition, and vision, as well as questionnaires to assess quality of life, walking ability, and fatigue in people with Expanded Disability Status Scale (EDSS) scores of 6.5 or lower. A wrist device, used concurrently with the app, passively monitors subjects’ step count, heart rate, and different measures of activity.
If validated, such smartphone-based “digital biomarkers” will provide clinicians and investigators with a steadier flow of information for assessing MS disease progression and informing clinical decision-making. In June, Ludwig Kappos, MD, the app study’s senior researcher, co-authored an analysis of randomized trial data that argued for discarding the standard categories of relapsing and progressive MS in favor of seeing the disease as a continuum, in which progression can and does occur in the absence of relapses.
The digital biomarker work builds on that more unified view of the disease, Dr. Kappos said in an interview.
Outside of disease exacerbations or relapses, “progression can be very difficult to capture, especially in the first stage of the disease because of compensation in the central nervous system,” he said. “Our ability to see these very slight changes during a neurological examination is limited even if we do it very thoroughly. But by having these more frequent assessments we may be able to.”
Smartphone-gleaned biomarkers may have implications for prognosis and for choice of therapy, Dr. Kappos added. “We expect that these digital biomarkers will be even more sensitive and to be able to recognize before severe deficits are evident who is a candidate for a more intensive treatment and who is not.”
At the MSVirtual2020 congress, Dr. Kappos’s colleagues at the university Johannes Lorscheider, MD, and Yvonne Naegelin, MD, presented their feasibility and acceptance study currently underway in 60 volunteers. One of the concerns the investigators have had was whether engaged users would remain with the app. “We have designed the tests as little challenges to help keep people interested—we want to make these tests as appealing as possible,” Dr. Kappos said.
In this study, the reliability of each test is determined by intra-class correlation and median coefficient of variation. Preliminary reliability testing with healthy controls showed intra-class correlation coefficients of greater than 60% for the digital biomarkers and greater than 80% for at least one in every domain.
Once the best tests are selected and the app is fine-tuned, the group intends to embark on larger studies of the digital biomarkers. The next, planned for 2021, will recruit approximately 400 patients from the Swiss MS cohort, whose 1,000-some MS participants are followed with standardized examination and imaging protocols across healthcare centers.
“This is a very well characterized group of patients who are followed continuously with state-of-the-art neurological examinations, high-end MRI, and blood biomarkers,” Dr. Kappos said. “We want to see if we can add value by using digital biomarkers.”
The dreaMS app project is an independent investigator-initiated venture in cooperation with a technological partner. The study was supported by the Swiss Innovation Agency. The University Hospital Basel has received research funding for clinical trials from a number of pharmaceutical manufacturers.
SOURCE: Lorscheider J, et al. MSVirtual2020. Abstract P0069.
FROM MSVirtual2020
Satralizumab reduces risk of severe NMOSD relapse
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.

NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
(NMOSD), according to investigators. The drug also was associated with a lower likelihood of using acute relapse therapy.
These results were presented at the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS–ACTRIMS) 2020, this year known as MSVirtual2020.
NMOSD is characterized by acute relapses that are unpredictable and lead to the accumulation of disability. “Patients with NMOSD often recover poorly from relapses, therefore, the primary goal for disease management is to reduce attack frequency,” said Ingo Kleiter, MD, medical director of Marianne-Strauß-Klinik in Berg, Germany. “In the two phase 3 trials SAkuraSky and SAkuraStar, the IL-6 receptor inhibitor satralizumab was found to significantly reduce the risk of relapses versus placebo.” Satralizumab is a humanized, monoclonal, recycling antibody that targets the interleukin-6 receptor.
Dr. Kleiter and colleagues examined pooled data from the two phase 3 trials of satralizumab to determine the treatment’s effect on relapse severity in patients with NMOSD. Participants in those trials received placebo or 120 mg of satralizumab at weeks 0, 2, 4, and every 4 weeks thereafter.
For their research, the investigators analyzed data from the pooled intention-to-treat population in the double-blind periods of both studies. To evaluate the severity of protocol-defined relapses, they compared patients’ Expanded Disability Status Scale (EDSS) scores at the time of relapse with their scores before the relapse (i.e., their scores at the last scheduled study visit). Using the visual Functional Systems Score (FSS), Dr. Kleiter and colleagues performed a similar analysis on optic neuritis relapses. They categorized a protocol-defined relapse as severe if it entailed a change of two or more points on the EDSS or visual FSS. The investigators conducted Kaplan-Meier analyses to evaluate the time to first severe protocol-defined relapse. They also compared the number of patients receiving acute therapy for any relapse between treatment groups.
Safety profile confirmed
Dr. Kleiter and colleagues included 178 patients in their analyses. A total of 27 of 104 patients (26%) who received satralizumab had a protocol-defined relapse, compared with 34 of 74 patients (46%) who received placebo. The number and proportion of severe protocol-defined relapses were lower in the satralizumab group (5 of 27 events [19%]), compared with the placebo group (12 of 34 events [35%]). In addition, the number and proportion of severe protocol-defined optic neuritis relapses were lower in patients receiving satralizumab (2 of 8 events [25%]), compared with those receiving placebo (5 of 13 events [39%]). Compared with placebo, satralizumab was associated with a 79% reduction in the risk of severe protocol-defined relapse (hazard ratio, 0.21).
A lower proportion of patients receiving satralizumab was prescribed acute relapse therapy (38%), compared with patients receiving placebo (58%). The odds ratio of receiving a prescription of acute relapse therapy was 0.46 among patients receiving satralizumab.
The activity of IL-6 may cause neurologic damage in patients with NMOSD through astrocytic damage, disruption of the blood–brain barrier, and T cell polarization. “It is proposed that through inhibiting IL-6 across these multiple mechanisms, satralizumab reduces the risk and severity of NMOSD attacks,” Dr. Kleiter said.
To date, the rates of infection and serious infection for patients treated with satralizumab in the combined double-blind and open-label extension periods have been consistent with those for patients treated with satralizumab in the double-blind portion. These rates have not increased over time. Satralizumab is administered as a subcutaneous injection every 4 weeks, and treatment can be self-administered at the discretion of the managing physician. “These data provide reassurance to physicians about the overall profile of satralizumab, with respect to efficacy and safety in the longer term,” said Dr. Kleiter.
Does satralizumab differ from other new agents?
The main strength of the study is that sufficient numbers of relapses were available for analysis in the active and control groups, said Achim Berthele, MD, associate professor of neurology at the Technical University of Munich. This allowed the researchers to examine whether satralizumab led to a better outcome after each relapse, which it did. “A weakness is how the severity of relapses was quantified,” said Dr. Berthele. “The EDSS as a measure is not linear, and its functional systems are not clinically equivalent. However, the whole NMOSD community is struggling with this problem.”
The study’s implications for neurologists’ clinical practice are unclear, however. “Although the results presented are encouraging, the data are still too small to say with certainty that satralizumab does indeed improve the outcome of relapses,” said Dr. Berthele. “It is also an open question whether satralizumab differs in this respect from the other new immunotherapeutic agents.”
Investigators must collect further data on the outcome of relapses that occur during treatment with modern immunomodulatory therapy, Dr. Berthele added. Future research could examine whether the new anti-inflammatory immunotherapeutic agents also are suitable drugs for relapse therapy. Another salient question is whether clinical vigilance or relapse therapy in NMOSD has improved in general. “This is what Kleiter and colleagues show as well: The number of severe relapses under placebo was much lower than expected,” said Dr. Berthele.
Chugai/Roche funded the study. Dr. Kleiter has received compensation for consulting, speaking, or serving on advisory boards for Alexion, Biogen, Celgene, Merck, and Roche. Dr. Berthele was not involved in any of the satralizumab trials, but is an investigator and coauthor of the PREVENT trial of eculizumab.
SOURCE: Kleiter I, et al. MSVirtual2020. Abstract FC01.03.
FROM MSVirtual2020