User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Medication in heart failure: Pro tips on therapy with the ‘four pillars of survival’
On the medication front, there are now “four pillars of survival” in the setting of heart failure with reduced ejection fraction (EF), a cardiologist told hospitalists recently at SHM Converge, the annual conference of the Society of Hospital Medicine.
The quartet of drugs are beta blockers, angiotensin receptor–neprilysin inhibitors, mineralocorticoid receptor antagonists, and the newest addition – sodium-glucose cotransporter 2 inhibitors.
“If we use all four of these medications, the absolute risk reduction [in mortality] is 25% over a 2-year period,” said cardiologist Celeste T. Williams, MD, of Henry Ford Hospital, Detroit. “So it is very important that we use these medications,” she said.
But managing the medications, she said, can be challenging. Dr. Williams offered these tips about the use of medication in heart failure.
Beta blockers are crucial players
“Beta blockers save lives,” Dr. Williams said, “but there’s always a debate about how much we should titrate beta blockers.”
How can you determine the proper titration? Focus on heart rates, she recommended. “We know that higher heart rates in heart failure patients are associated with worse outcomes. There was subgroup analysis in the BEAUTIFUL study that looked at 5,300 patients with EF less than 40% who had CAD [coronary artery disease]. They found that patients with heart rates greater than 70 had a 34% increased risk of cardiovascular death and a 53% increased risk of heart failure hospitalization compared to heart rates less than 70.”
Focus on getting your patient’s heart rate lower than 70 while maintaining their blood pressure, she said.
“Another question we have is, ‘When these patients come into hospitals, what should we do with the beta blocker? Should we continue it? Should we stop it?’ If you can, you always want to continue the beta blocker or the ACE [angiotensin-converting enzyme] inhibitor, because studies have shown us that the likelihood for patients to be on these medications 90 days later is dismal,” she said. “But you also need to look at the patient. If the patient is in cardiogenic shock, their beta blocker should be stopped.”
Consider multiple factors when titrating various medications
“In the hospital, we always will look at hemodynamic compromise in the patient. Is the patient in cardiogenic shock?” Dr. Williams said. “We also must think about compliance concerns. Are the patients even taking their medication? And if they are taking their medications, are they tolerating standard medical therapy? Are they hypotensive? Are they only able to tolerate minimal meds? Have you seen that their creatine continues to rise? Or are they having poor diuresis with the rise in diuretics?”
All these questions are useful, she said, as you determine whether you should titrate medication yourself or refer the patient to an advanced heart failure specialist.
Understand when to stick with guideline-directed medical therapy
Dr. Williams said another question often arises: “If your patient’s EF recovers, should you stop guideline-directed medical therapy [GDMT]?” She highlighted a TRED-HF study that evaluated patients who had recovered from dilated, nonischemic cardiomyopathy and were receiving GDMT. “They withdrew GDMT for half of the patients and looked at their echoes 6 months later. They found that 40% of the patients relapsed. Their EFs went below 40% again. Stopping medications is not the best idea for most of these patients.”
However, she said, there are scenarios in which GDMT may be withdrawn, such as for patients with tachycardia-induced cardiomyopathies whose EF recovers after ablation, those whose EF recovers after alcoholic cardiomyopathy, and those who receive valve replacements. “We need to remember that a lot of the patients who develop stage C heart failure have risk factors. Even though their heart failure has recovered, they have risks that need to be treated, and you can use the same medications that you use for heart failure to control their risk. Therefore, you would not get into trouble by withdrawing their medications.”
She added: “If you’re unable to titrate GDMT because the blood pressure is too soft, the creatine continues to rise, or the patient just has a lot of heart failure symptoms, this is indicative that the patient is sicker than they may appear.” At this point, defer to a heart failure specialist, she said.
Consider ivabradine as an add-on when appropriate
In some cases, a heart rate of less than 70 bpm will not be achieved even with GDMT and maximum tolerated doses, Dr. Williams said. “If they’re in sinus, you can add on a medication called ivabradine, which was studied in the SHIFT study. This looked at patients with EF of less than 35% who had class 2-3 heart failure in sinus rhythm. They had to have a hospitalization within the last 12 months. The patients were randomized to either ivabradine or placebo. The primary outcome was [cardiovascular] death or heart failure hospitalization. They found that patients who had ivabradine had a decrease in heart failure hospitalization.”
The lesson, she said, is that “ivabradine is a great medication to add on to patients who are still tachycardic in sinus when you cannot titrate up the beta blocker.”
Dr. Williams reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On the medication front, there are now “four pillars of survival” in the setting of heart failure with reduced ejection fraction (EF), a cardiologist told hospitalists recently at SHM Converge, the annual conference of the Society of Hospital Medicine.
The quartet of drugs are beta blockers, angiotensin receptor–neprilysin inhibitors, mineralocorticoid receptor antagonists, and the newest addition – sodium-glucose cotransporter 2 inhibitors.
“If we use all four of these medications, the absolute risk reduction [in mortality] is 25% over a 2-year period,” said cardiologist Celeste T. Williams, MD, of Henry Ford Hospital, Detroit. “So it is very important that we use these medications,” she said.
But managing the medications, she said, can be challenging. Dr. Williams offered these tips about the use of medication in heart failure.
Beta blockers are crucial players
“Beta blockers save lives,” Dr. Williams said, “but there’s always a debate about how much we should titrate beta blockers.”
How can you determine the proper titration? Focus on heart rates, she recommended. “We know that higher heart rates in heart failure patients are associated with worse outcomes. There was subgroup analysis in the BEAUTIFUL study that looked at 5,300 patients with EF less than 40% who had CAD [coronary artery disease]. They found that patients with heart rates greater than 70 had a 34% increased risk of cardiovascular death and a 53% increased risk of heart failure hospitalization compared to heart rates less than 70.”
Focus on getting your patient’s heart rate lower than 70 while maintaining their blood pressure, she said.
“Another question we have is, ‘When these patients come into hospitals, what should we do with the beta blocker? Should we continue it? Should we stop it?’ If you can, you always want to continue the beta blocker or the ACE [angiotensin-converting enzyme] inhibitor, because studies have shown us that the likelihood for patients to be on these medications 90 days later is dismal,” she said. “But you also need to look at the patient. If the patient is in cardiogenic shock, their beta blocker should be stopped.”
Consider multiple factors when titrating various medications
“In the hospital, we always will look at hemodynamic compromise in the patient. Is the patient in cardiogenic shock?” Dr. Williams said. “We also must think about compliance concerns. Are the patients even taking their medication? And if they are taking their medications, are they tolerating standard medical therapy? Are they hypotensive? Are they only able to tolerate minimal meds? Have you seen that their creatine continues to rise? Or are they having poor diuresis with the rise in diuretics?”
All these questions are useful, she said, as you determine whether you should titrate medication yourself or refer the patient to an advanced heart failure specialist.
Understand when to stick with guideline-directed medical therapy
Dr. Williams said another question often arises: “If your patient’s EF recovers, should you stop guideline-directed medical therapy [GDMT]?” She highlighted a TRED-HF study that evaluated patients who had recovered from dilated, nonischemic cardiomyopathy and were receiving GDMT. “They withdrew GDMT for half of the patients and looked at their echoes 6 months later. They found that 40% of the patients relapsed. Their EFs went below 40% again. Stopping medications is not the best idea for most of these patients.”
However, she said, there are scenarios in which GDMT may be withdrawn, such as for patients with tachycardia-induced cardiomyopathies whose EF recovers after ablation, those whose EF recovers after alcoholic cardiomyopathy, and those who receive valve replacements. “We need to remember that a lot of the patients who develop stage C heart failure have risk factors. Even though their heart failure has recovered, they have risks that need to be treated, and you can use the same medications that you use for heart failure to control their risk. Therefore, you would not get into trouble by withdrawing their medications.”
She added: “If you’re unable to titrate GDMT because the blood pressure is too soft, the creatine continues to rise, or the patient just has a lot of heart failure symptoms, this is indicative that the patient is sicker than they may appear.” At this point, defer to a heart failure specialist, she said.
Consider ivabradine as an add-on when appropriate
In some cases, a heart rate of less than 70 bpm will not be achieved even with GDMT and maximum tolerated doses, Dr. Williams said. “If they’re in sinus, you can add on a medication called ivabradine, which was studied in the SHIFT study. This looked at patients with EF of less than 35% who had class 2-3 heart failure in sinus rhythm. They had to have a hospitalization within the last 12 months. The patients were randomized to either ivabradine or placebo. The primary outcome was [cardiovascular] death or heart failure hospitalization. They found that patients who had ivabradine had a decrease in heart failure hospitalization.”
The lesson, she said, is that “ivabradine is a great medication to add on to patients who are still tachycardic in sinus when you cannot titrate up the beta blocker.”
Dr. Williams reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On the medication front, there are now “four pillars of survival” in the setting of heart failure with reduced ejection fraction (EF), a cardiologist told hospitalists recently at SHM Converge, the annual conference of the Society of Hospital Medicine.
The quartet of drugs are beta blockers, angiotensin receptor–neprilysin inhibitors, mineralocorticoid receptor antagonists, and the newest addition – sodium-glucose cotransporter 2 inhibitors.
“If we use all four of these medications, the absolute risk reduction [in mortality] is 25% over a 2-year period,” said cardiologist Celeste T. Williams, MD, of Henry Ford Hospital, Detroit. “So it is very important that we use these medications,” she said.
But managing the medications, she said, can be challenging. Dr. Williams offered these tips about the use of medication in heart failure.
Beta blockers are crucial players
“Beta blockers save lives,” Dr. Williams said, “but there’s always a debate about how much we should titrate beta blockers.”
How can you determine the proper titration? Focus on heart rates, she recommended. “We know that higher heart rates in heart failure patients are associated with worse outcomes. There was subgroup analysis in the BEAUTIFUL study that looked at 5,300 patients with EF less than 40% who had CAD [coronary artery disease]. They found that patients with heart rates greater than 70 had a 34% increased risk of cardiovascular death and a 53% increased risk of heart failure hospitalization compared to heart rates less than 70.”
Focus on getting your patient’s heart rate lower than 70 while maintaining their blood pressure, she said.
“Another question we have is, ‘When these patients come into hospitals, what should we do with the beta blocker? Should we continue it? Should we stop it?’ If you can, you always want to continue the beta blocker or the ACE [angiotensin-converting enzyme] inhibitor, because studies have shown us that the likelihood for patients to be on these medications 90 days later is dismal,” she said. “But you also need to look at the patient. If the patient is in cardiogenic shock, their beta blocker should be stopped.”
Consider multiple factors when titrating various medications
“In the hospital, we always will look at hemodynamic compromise in the patient. Is the patient in cardiogenic shock?” Dr. Williams said. “We also must think about compliance concerns. Are the patients even taking their medication? And if they are taking their medications, are they tolerating standard medical therapy? Are they hypotensive? Are they only able to tolerate minimal meds? Have you seen that their creatine continues to rise? Or are they having poor diuresis with the rise in diuretics?”
All these questions are useful, she said, as you determine whether you should titrate medication yourself or refer the patient to an advanced heart failure specialist.
Understand when to stick with guideline-directed medical therapy
Dr. Williams said another question often arises: “If your patient’s EF recovers, should you stop guideline-directed medical therapy [GDMT]?” She highlighted a TRED-HF study that evaluated patients who had recovered from dilated, nonischemic cardiomyopathy and were receiving GDMT. “They withdrew GDMT for half of the patients and looked at their echoes 6 months later. They found that 40% of the patients relapsed. Their EFs went below 40% again. Stopping medications is not the best idea for most of these patients.”
However, she said, there are scenarios in which GDMT may be withdrawn, such as for patients with tachycardia-induced cardiomyopathies whose EF recovers after ablation, those whose EF recovers after alcoholic cardiomyopathy, and those who receive valve replacements. “We need to remember that a lot of the patients who develop stage C heart failure have risk factors. Even though their heart failure has recovered, they have risks that need to be treated, and you can use the same medications that you use for heart failure to control their risk. Therefore, you would not get into trouble by withdrawing their medications.”
She added: “If you’re unable to titrate GDMT because the blood pressure is too soft, the creatine continues to rise, or the patient just has a lot of heart failure symptoms, this is indicative that the patient is sicker than they may appear.” At this point, defer to a heart failure specialist, she said.
Consider ivabradine as an add-on when appropriate
In some cases, a heart rate of less than 70 bpm will not be achieved even with GDMT and maximum tolerated doses, Dr. Williams said. “If they’re in sinus, you can add on a medication called ivabradine, which was studied in the SHIFT study. This looked at patients with EF of less than 35% who had class 2-3 heart failure in sinus rhythm. They had to have a hospitalization within the last 12 months. The patients were randomized to either ivabradine or placebo. The primary outcome was [cardiovascular] death or heart failure hospitalization. They found that patients who had ivabradine had a decrease in heart failure hospitalization.”
The lesson, she said, is that “ivabradine is a great medication to add on to patients who are still tachycardic in sinus when you cannot titrate up the beta blocker.”
Dr. Williams reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Once-weekly oral antipsychotic for schizophrenia on the horizon
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.

The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.
The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel, ultra–long-acting oral formulation of the antipsychotic risperidone (Risperdal) only needs to be taken once weekly and appears to be safe and effective, results of a new phase 2 study suggest.
The new formulation, LYN-005 (Lyndra Therapeutics), quickly reached therapeutic levels in patients, provided sustained exposure to risperidone active moiety over 7 days, and reduced peak drug exposure.
“This novel formulation has the potential to improve treatment adherence and quality of life in patients with schizophrenia or schizoaffective disorder,” study investigator David Walling, PhD, chief clinical officer for the Collaborative NeuroScience Network, Long Beach, Calif., said in an interview.
The findings were presented at the 2021 American Society of Clinical Psychopharmacology annual meeting.
Adherence is key
About 50% of patients don’t take medications as prescribed, creating a significant relapse risk, Dr. Walling noted.
“Here we have the possibility of having a once-weekly oral medication, which means patients don’t have to struggle with the issue of taking the medication daily. Right now, all we have on the market for long-acting medications for schizophrenia are injectables, where the patient has to go get a shot every month or every 2 weeks in order to have the medication in their system for a longer period of time,” he added.
The study included 32 clinically stable patients with a primary diagnosis of schizophrenia or schizoaffective disorder.
Patients received immediate-release (IR) risperidone at 2 mg or 4 mg, based on their current antipsychotic dose, for 13 days.
They were then randomly assigned 3:1 to receive either IR risperidone-matched placebo and LYN-005 at 14 mg or 28 mg risperidone (12 patients per group), or to LYN-005 matched placebo and IR risperidone, 2 mg or 4 mg, (4 patients per group) for 3 weeks.
LYN-05 was administered once weekly for a total of three doses. IR risperidone was administered once daily.
The study’s primary endpoints were pharmacokinetics after LYN-005 and IR risperidone and the incidence of adverse events.
Following LYN-005 administration, systemic exposure to risperidone active moiety (risperidone and 9-hydroxyrisperidone combined) increased with the increasing dose. Peak concentration occurred within the first 3 days of dosing and peak exposures from LYN-005 were lower than with IR risperidone.
“Steady state was achieved around day 15. It didn’t take 3 weeks of dosing for patients to achieve steady state. We achieved that around day 15,” Dr. Walling said.
LYN-005 was well tolerated in the 85% of study participants who received all three doses.
Adverse events occurred in 18 (75%) patients who received LYN-005. Of these, 10 were with the 14-mg dose, and 8 with the 28-mg dose.
The most common AEs were gastrointestinal, which occurred in 13 (54%) patients receiving LYN-005, with a higher incidence in the 28-mg group than in the 14 mg group.
Additionally, nine patients had abdominal pain, discomfort, or tenderness, and five patients (21%) had nausea.
Overall, the incidence of adverse events was higher for LYN-005, compared with IR risperidone, but they were judged to be mild and transitory, with fewer AEs reported with subsequent LYN-005 dosing. After the first dose, 58% of patients reported an AE; this dropped to 18% after the third dose.
An important development
Commenting on the findings, Ira D. Glick, MD, professor emeritus, Stanford (Calif.) University, said: “The major problem with schizophrenia is getting adherence.”
“The better the adherence, the better the outcome, the worst the adherence, the worse the outcome, so being able to take a preparation less often is a very important advance in the field,” said Dr. Glick, who was not involved in the research
Long-acting preparations for chronic mental illness represent a significant advance, he said.
“The future of the treatment of schizophrenia is long-acting injectables. That is the trend,” Dr. Glick explained. “The oral once-a-week preparation may be useful in a group of patients who are phobic about needles, but with the injections, you can be sure that the patient has received their medication. With the oral, there is more of a chance to be noncompliant.
“That said, having an effective, longer-acting oral for those who refuse injections is helpful. to ensure adherence to treatment. We know treatment works, we know it is going to save lives, and that’s what this ultra–long-acting formulation is promoting.”
Dr. Glick has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
ASCO 2021: Breast cancer sessions not to miss
This transcript has been edited for clarity.

Hello. It’s Dr. Kathy Miller from Indiana University.
I have to admit that time has snuck up on me this year. It is already time for the American Society of Clinical Oncology Annual Meeting.
I found it hard to keep track of time this year with the pandemic. Many of the things that help mark the passage of time haven’t happened, have happened at different times of the year than is typical, or have happened in different ways that just haven’t had the same impact in my brain.
Just recently, I was taking a look through the breast cancer program at ASCO and there is a special clinical science symposium that I want to make sure you know about and tune into. It’s the sort of session that might not otherwise reach you.
This has been a year of incredible turmoil and critical thinking about issues of race, ethnicity, justice, and how we can make sure that the medical care we’re providing is inclusive and equitable. How we can make sure we are giving the best outcome to all of our patients.
This special clinical science symposium this year includes several presentations that will delve into how genetically determined ancestry and socially determined race might impact the outcome of our patients. This is a tangled web that is difficult to unpack and separate, but there are clear distinctions here: The genes we inherit do affect how we metabolize drugs, what side effects we might have from drugs, and what drugs might be the best choices for us.
Our socially determined race affects how the world interacts with us. Those biases, be they conscious or unconscious, can affect where we live, where we go to school, how people treat us, what opportunities we have, and how the medical system treats us. They’re related, but they’re not the same. Tune into that clinical science symposium to begin thinking about those differences and how we can make sure we give our patients the best care.
There are other high-profile presentations that you’re going to want to see as well, looking at how we can optimize therapy in patients with HER2-positive disease and beginning to think about who might not need chemotherapy to have an excellent outcome in early-stage disease.
Also, we will be thinking about those patients with triple-negative disease who have residual disease after neoadjuvant chemotherapy. We were all caught off guard with the results of the CREATE-X trial, quite frankly, several years ago.
This year we will hear the results of a postneoadjuvant trial coordinated by the Eastern Cooperative Oncology Group comparing platinum therapy with capecitabine. Tune in to think more about whether capecitabine really should be the standard of care in this population.
As always, I’m interested in your thoughts before or after ASCO. What stood out for you this year in breast cancer? Drop us a comment and let us know about these sessions and what else you found worthwhile.
Dr. Miller is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. Her career has combined both laboratory and clinical research in breast cancer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Dr. Kathy Miller from Indiana University.
I have to admit that time has snuck up on me this year. It is already time for the American Society of Clinical Oncology Annual Meeting.
I found it hard to keep track of time this year with the pandemic. Many of the things that help mark the passage of time haven’t happened, have happened at different times of the year than is typical, or have happened in different ways that just haven’t had the same impact in my brain.
Just recently, I was taking a look through the breast cancer program at ASCO and there is a special clinical science symposium that I want to make sure you know about and tune into. It’s the sort of session that might not otherwise reach you.
This has been a year of incredible turmoil and critical thinking about issues of race, ethnicity, justice, and how we can make sure that the medical care we’re providing is inclusive and equitable. How we can make sure we are giving the best outcome to all of our patients.
This special clinical science symposium this year includes several presentations that will delve into how genetically determined ancestry and socially determined race might impact the outcome of our patients. This is a tangled web that is difficult to unpack and separate, but there are clear distinctions here: The genes we inherit do affect how we metabolize drugs, what side effects we might have from drugs, and what drugs might be the best choices for us.
Our socially determined race affects how the world interacts with us. Those biases, be they conscious or unconscious, can affect where we live, where we go to school, how people treat us, what opportunities we have, and how the medical system treats us. They’re related, but they’re not the same. Tune into that clinical science symposium to begin thinking about those differences and how we can make sure we give our patients the best care.
There are other high-profile presentations that you’re going to want to see as well, looking at how we can optimize therapy in patients with HER2-positive disease and beginning to think about who might not need chemotherapy to have an excellent outcome in early-stage disease.
Also, we will be thinking about those patients with triple-negative disease who have residual disease after neoadjuvant chemotherapy. We were all caught off guard with the results of the CREATE-X trial, quite frankly, several years ago.
This year we will hear the results of a postneoadjuvant trial coordinated by the Eastern Cooperative Oncology Group comparing platinum therapy with capecitabine. Tune in to think more about whether capecitabine really should be the standard of care in this population.
As always, I’m interested in your thoughts before or after ASCO. What stood out for you this year in breast cancer? Drop us a comment and let us know about these sessions and what else you found worthwhile.
Dr. Miller is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. Her career has combined both laboratory and clinical research in breast cancer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Dr. Kathy Miller from Indiana University.
I have to admit that time has snuck up on me this year. It is already time for the American Society of Clinical Oncology Annual Meeting.
I found it hard to keep track of time this year with the pandemic. Many of the things that help mark the passage of time haven’t happened, have happened at different times of the year than is typical, or have happened in different ways that just haven’t had the same impact in my brain.
Just recently, I was taking a look through the breast cancer program at ASCO and there is a special clinical science symposium that I want to make sure you know about and tune into. It’s the sort of session that might not otherwise reach you.
This has been a year of incredible turmoil and critical thinking about issues of race, ethnicity, justice, and how we can make sure that the medical care we’re providing is inclusive and equitable. How we can make sure we are giving the best outcome to all of our patients.
This special clinical science symposium this year includes several presentations that will delve into how genetically determined ancestry and socially determined race might impact the outcome of our patients. This is a tangled web that is difficult to unpack and separate, but there are clear distinctions here: The genes we inherit do affect how we metabolize drugs, what side effects we might have from drugs, and what drugs might be the best choices for us.
Our socially determined race affects how the world interacts with us. Those biases, be they conscious or unconscious, can affect where we live, where we go to school, how people treat us, what opportunities we have, and how the medical system treats us. They’re related, but they’re not the same. Tune into that clinical science symposium to begin thinking about those differences and how we can make sure we give our patients the best care.
There are other high-profile presentations that you’re going to want to see as well, looking at how we can optimize therapy in patients with HER2-positive disease and beginning to think about who might not need chemotherapy to have an excellent outcome in early-stage disease.
Also, we will be thinking about those patients with triple-negative disease who have residual disease after neoadjuvant chemotherapy. We were all caught off guard with the results of the CREATE-X trial, quite frankly, several years ago.
This year we will hear the results of a postneoadjuvant trial coordinated by the Eastern Cooperative Oncology Group comparing platinum therapy with capecitabine. Tune in to think more about whether capecitabine really should be the standard of care in this population.
As always, I’m interested in your thoughts before or after ASCO. What stood out for you this year in breast cancer? Drop us a comment and let us know about these sessions and what else you found worthwhile.
Dr. Miller is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. Her career has combined both laboratory and clinical research in breast cancer.
A version of this article first appeared on Medscape.com.

'Exciting': Olaparib benefit also in early BRCA+ breast cancer
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
Mavacamten boosts quality of life in patients with hypertrophic cardiomyopathy
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.

The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.

EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.
The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.
EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.
The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.
EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
FROM ACC 2021
Nintedanib slows interstitial lung disease in RA patients
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.

“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
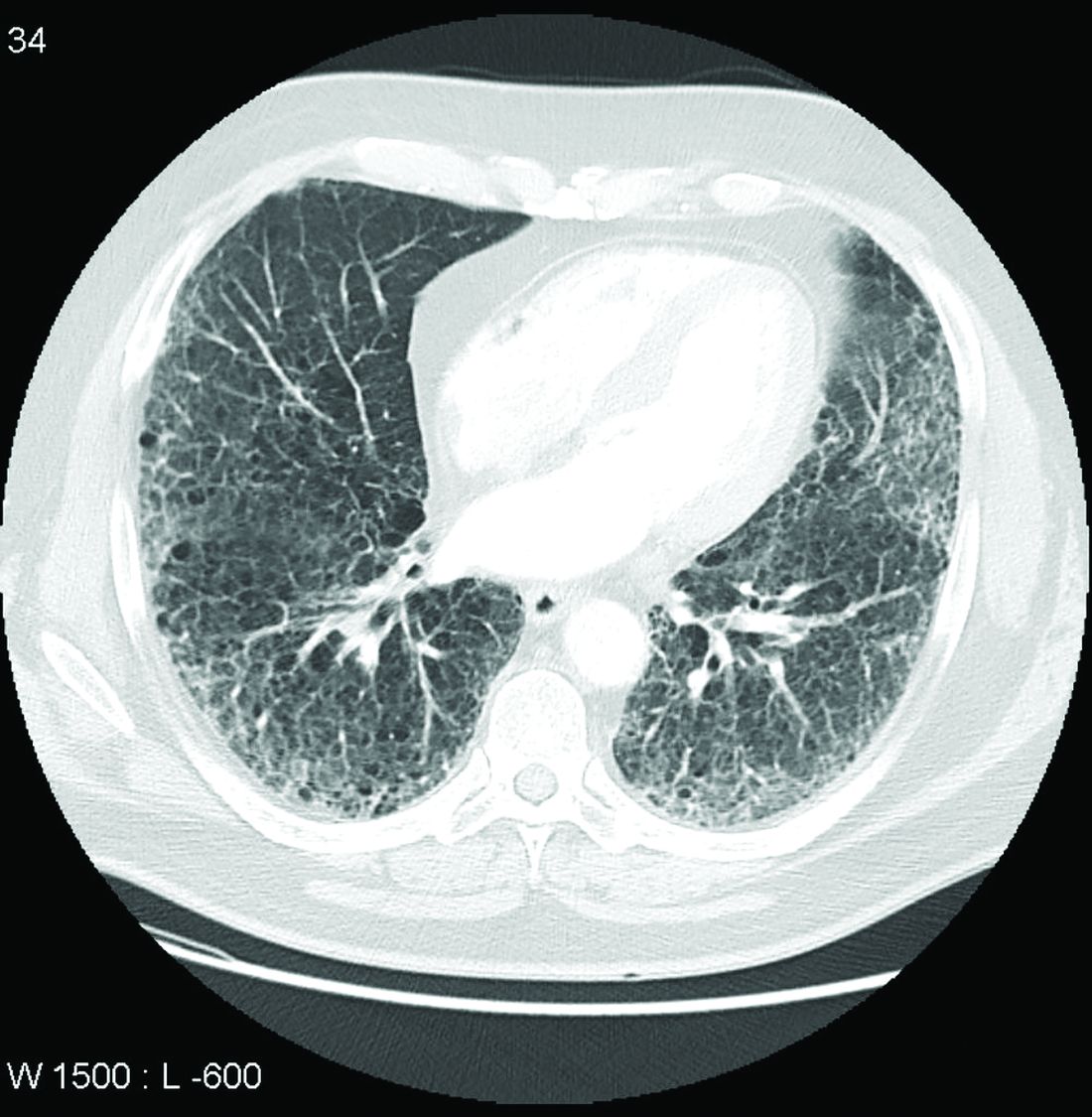
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
FROM THE EULAR 2021 CONGRESS
IL-6 levels predict distant breast cancer recurrence
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
FROM ASCO 2021
NCAA athletes: ECG abnormalities persist after COVID-19
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intersection of trauma and race in pregnancy calls for more study
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
FROM ACOG 2021
BEAT-LUPUS: Belimumab after rituximab delays severe flares
Using belimumab after rituximab to treat patients with systemic lupus erythematosus (SLE) refractory to conventional therapy not only significantly decreased levels of serum IgG anti-dsDNA antibody levels but also prolonged the time before severe flares of disease occurred in the phase 2b BEAT-LUPUS (Belimumab after B cell depletion in SLE) study.

The trial’s primary outcome of serum IgG anti-dsDNA antibody levels showed a decline from a geometric mean of 162 IU/mL at baseline to 69 IU/mL at 24 weeks and 47 IU/mL at 1 year in patients treated with belimumab (Benlysta) after rituximab (Rituxan and biosimilars). These reductions were significantly lower than the values seen in the placebo after rituximab arm (a respective 121 IU/mL, 99 IU/mL, and 103 IU/mL; P < .001).
Just 3 patients who received belimumab versus 10 who received placebo after rituximab experienced a severe BILAG (British Isles Lupus Assessment Group) index A flare by the end of the study at 52 weeks. The hazard ratio (HR) for the flare reduction was 0.27 (P = .03), indicating a 73% reduction.
The use of belimumab rather than a placebo also led to a small reduction in total serum IgG, and significantly suppressed B-cell repopulation (P = .03).
These results need confirming in a larger, phase 3 trial, the trial’s principal investigator, Michael Ehrenstein, PhD, said at the annual European Congress of Rheumatology. They are “clearly encouraging” and “support the hypothesis that BAFF [B-cell–activating factor] can drive flares after rituximab,” he said.
Although B-cell depletion with rituximab is recommended by national and international guidelines to treat some patients with SLE who are refractory to conventional therapy, its use is not licensed.
“Certainly, rituximab is a controversial drug in lupus,” Dr. Ehrenstein, a consultant rheumatologist based at University College London, said in an interview. Although there is real-world evidence from registries and open-label studies suggesting that it is widely used and effective in some patients, the randomized, controlled trials conducted with rituximab about 10 years ago failed to meet their primary endpoints.
“A lot has been written about why that was, but probably the biggest reason was the high dose of steroids in both groups,” Dr. Ehrenstein said. To try to avoid muddying the waters of the BEAT-LUPUS trial findings, the maximum dose of prednisolone allowed to be used as background therapy was 20 mg/day. The trial’s investigators were also encouraged to reduce the baseline steroid dose to at least 50% by the trial’s 6-month halfway point.
“We tried to reflect what was going on in the U.K.,” Dr. Ehrenstein said, noting that the inspiration for the trial was a patient who had received sequential rituximab treatment. Although she got better with each cycle of rituximab, when her disease flared it would be worse than the time before, with increasingly higher anti-dsDNA levels recorded. The reason for this seemed to be because of increasing BAFF levels, and so the hypothesis was that if rituximab was associated with increased BAFF levels, then co-targeting BAFF with belimumab should be able to prevent those flares from happening.
The BEAT-LUPUS trial has been a huge collaborative effort and was conducted across 16 U.K. centers. From initial funding to the data analysis, it has taken 6 years to complete and was made possible by a unique partnership between Versus Arthritis, University College London Hospitals Biomedical Research Center, the National Institute for Health Research UK Musculoskeletal Translational Research Collaboration, and GlaxoSmithKline (GSK). GSK provided belimumab free of charge, as well as additional funding, but had no role in the design of the study and will not have any role going forward.
From an initial 172 patients assessed for eligibility, 52 patients were finally enrolled into the trial and received rituximab as two infusions given 2 weeks apart. Patients were then randomized in a double-blind manner to receive either belimumab (n = 26) or placebo (n = 26) 4-8 weeks after their first dose of rituximab. The intention-to-treat population consisted of 43 patients.
The use of belimumab after rituximab did not increase the risk for infection – serious or otherwise – or adverse effects, Dr. Ehrenstein reported. Serious adverse events were reported in six (23%) patients in each arm, and serious infections were seen in two (8%) of the belimumab- and four (15%) of the placebo-treated patients.
“I think the take-home message is that it seems that belimumab can reduce the number of severe flares that occur after rituximab therapy,” Dr. Ehrenstein said. “It’s promising, but not definitive,” he added. The next step is of course to publish these data and to perform a phase 3 trial.

In the discussion time following the presentation, session moderator Xavier Mariette, MD, PhD, of Bicêtre Hospital, Paris-Saclay University, asked why not give belimumab first before rituximab if using belimumab afterward works?
“Our strategy was driven by the observation that BAFF levels surged after rituximab, and therefore it’s logical to give the belimumab to block that BAFF surge,” he answered.
“Certainly, there are ideas that belimumab releases mature B cells into the circulation and rituximab can target that,” he added. That strategy is under investigation in the BLISS-BELIEVE trial, which should also report by the end of this year. It’s a much larger, phase 3 trial, involving nearly 300 patients and is sponsored by GSK.
“Clearly, this is a combination treatment [but] whether you give one before the other is uncertain,” Dr. Ehrenstein observed.
Another member of the viewing audience asked whether it would have been a fairer comparison if another dose of rituximab had been given to patients at week 24 instead of no treatment. Dr. Ehrenstein noted that it was a “good point” to make, but the investigators mainly wanted to answer whether giving belimumab after rituximab would target BAFF and thereby drop serum anti-dsDNA antibody levels. He said that a full trial of rituximab for patients with SLE, perhaps adding this extra dose, needs to be conducted.
Dr. Ehrenstein disclosed receiving research funding and educational grants from GSK and participating in advisory panels for the company.
Using belimumab after rituximab to treat patients with systemic lupus erythematosus (SLE) refractory to conventional therapy not only significantly decreased levels of serum IgG anti-dsDNA antibody levels but also prolonged the time before severe flares of disease occurred in the phase 2b BEAT-LUPUS (Belimumab after B cell depletion in SLE) study.
The trial’s primary outcome of serum IgG anti-dsDNA antibody levels showed a decline from a geometric mean of 162 IU/mL at baseline to 69 IU/mL at 24 weeks and 47 IU/mL at 1 year in patients treated with belimumab (Benlysta) after rituximab (Rituxan and biosimilars). These reductions were significantly lower than the values seen in the placebo after rituximab arm (a respective 121 IU/mL, 99 IU/mL, and 103 IU/mL; P < .001).
Just 3 patients who received belimumab versus 10 who received placebo after rituximab experienced a severe BILAG (British Isles Lupus Assessment Group) index A flare by the end of the study at 52 weeks. The hazard ratio (HR) for the flare reduction was 0.27 (P = .03), indicating a 73% reduction.
The use of belimumab rather than a placebo also led to a small reduction in total serum IgG, and significantly suppressed B-cell repopulation (P = .03).
These results need confirming in a larger, phase 3 trial, the trial’s principal investigator, Michael Ehrenstein, PhD, said at the annual European Congress of Rheumatology. They are “clearly encouraging” and “support the hypothesis that BAFF [B-cell–activating factor] can drive flares after rituximab,” he said.
Although B-cell depletion with rituximab is recommended by national and international guidelines to treat some patients with SLE who are refractory to conventional therapy, its use is not licensed.
“Certainly, rituximab is a controversial drug in lupus,” Dr. Ehrenstein, a consultant rheumatologist based at University College London, said in an interview. Although there is real-world evidence from registries and open-label studies suggesting that it is widely used and effective in some patients, the randomized, controlled trials conducted with rituximab about 10 years ago failed to meet their primary endpoints.
“A lot has been written about why that was, but probably the biggest reason was the high dose of steroids in both groups,” Dr. Ehrenstein said. To try to avoid muddying the waters of the BEAT-LUPUS trial findings, the maximum dose of prednisolone allowed to be used as background therapy was 20 mg/day. The trial’s investigators were also encouraged to reduce the baseline steroid dose to at least 50% by the trial’s 6-month halfway point.
“We tried to reflect what was going on in the U.K.,” Dr. Ehrenstein said, noting that the inspiration for the trial was a patient who had received sequential rituximab treatment. Although she got better with each cycle of rituximab, when her disease flared it would be worse than the time before, with increasingly higher anti-dsDNA levels recorded. The reason for this seemed to be because of increasing BAFF levels, and so the hypothesis was that if rituximab was associated with increased BAFF levels, then co-targeting BAFF with belimumab should be able to prevent those flares from happening.
The BEAT-LUPUS trial has been a huge collaborative effort and was conducted across 16 U.K. centers. From initial funding to the data analysis, it has taken 6 years to complete and was made possible by a unique partnership between Versus Arthritis, University College London Hospitals Biomedical Research Center, the National Institute for Health Research UK Musculoskeletal Translational Research Collaboration, and GlaxoSmithKline (GSK). GSK provided belimumab free of charge, as well as additional funding, but had no role in the design of the study and will not have any role going forward.
From an initial 172 patients assessed for eligibility, 52 patients were finally enrolled into the trial and received rituximab as two infusions given 2 weeks apart. Patients were then randomized in a double-blind manner to receive either belimumab (n = 26) or placebo (n = 26) 4-8 weeks after their first dose of rituximab. The intention-to-treat population consisted of 43 patients.
The use of belimumab after rituximab did not increase the risk for infection – serious or otherwise – or adverse effects, Dr. Ehrenstein reported. Serious adverse events were reported in six (23%) patients in each arm, and serious infections were seen in two (8%) of the belimumab- and four (15%) of the placebo-treated patients.
“I think the take-home message is that it seems that belimumab can reduce the number of severe flares that occur after rituximab therapy,” Dr. Ehrenstein said. “It’s promising, but not definitive,” he added. The next step is of course to publish these data and to perform a phase 3 trial.
In the discussion time following the presentation, session moderator Xavier Mariette, MD, PhD, of Bicêtre Hospital, Paris-Saclay University, asked why not give belimumab first before rituximab if using belimumab afterward works?
“Our strategy was driven by the observation that BAFF levels surged after rituximab, and therefore it’s logical to give the belimumab to block that BAFF surge,” he answered.
“Certainly, there are ideas that belimumab releases mature B cells into the circulation and rituximab can target that,” he added. That strategy is under investigation in the BLISS-BELIEVE trial, which should also report by the end of this year. It’s a much larger, phase 3 trial, involving nearly 300 patients and is sponsored by GSK.
“Clearly, this is a combination treatment [but] whether you give one before the other is uncertain,” Dr. Ehrenstein observed.
Another member of the viewing audience asked whether it would have been a fairer comparison if another dose of rituximab had been given to patients at week 24 instead of no treatment. Dr. Ehrenstein noted that it was a “good point” to make, but the investigators mainly wanted to answer whether giving belimumab after rituximab would target BAFF and thereby drop serum anti-dsDNA antibody levels. He said that a full trial of rituximab for patients with SLE, perhaps adding this extra dose, needs to be conducted.
Dr. Ehrenstein disclosed receiving research funding and educational grants from GSK and participating in advisory panels for the company.
Using belimumab after rituximab to treat patients with systemic lupus erythematosus (SLE) refractory to conventional therapy not only significantly decreased levels of serum IgG anti-dsDNA antibody levels but also prolonged the time before severe flares of disease occurred in the phase 2b BEAT-LUPUS (Belimumab after B cell depletion in SLE) study.
The trial’s primary outcome of serum IgG anti-dsDNA antibody levels showed a decline from a geometric mean of 162 IU/mL at baseline to 69 IU/mL at 24 weeks and 47 IU/mL at 1 year in patients treated with belimumab (Benlysta) after rituximab (Rituxan and biosimilars). These reductions were significantly lower than the values seen in the placebo after rituximab arm (a respective 121 IU/mL, 99 IU/mL, and 103 IU/mL; P < .001).
Just 3 patients who received belimumab versus 10 who received placebo after rituximab experienced a severe BILAG (British Isles Lupus Assessment Group) index A flare by the end of the study at 52 weeks. The hazard ratio (HR) for the flare reduction was 0.27 (P = .03), indicating a 73% reduction.
The use of belimumab rather than a placebo also led to a small reduction in total serum IgG, and significantly suppressed B-cell repopulation (P = .03).
These results need confirming in a larger, phase 3 trial, the trial’s principal investigator, Michael Ehrenstein, PhD, said at the annual European Congress of Rheumatology. They are “clearly encouraging” and “support the hypothesis that BAFF [B-cell–activating factor] can drive flares after rituximab,” he said.
Although B-cell depletion with rituximab is recommended by national and international guidelines to treat some patients with SLE who are refractory to conventional therapy, its use is not licensed.
“Certainly, rituximab is a controversial drug in lupus,” Dr. Ehrenstein, a consultant rheumatologist based at University College London, said in an interview. Although there is real-world evidence from registries and open-label studies suggesting that it is widely used and effective in some patients, the randomized, controlled trials conducted with rituximab about 10 years ago failed to meet their primary endpoints.
“A lot has been written about why that was, but probably the biggest reason was the high dose of steroids in both groups,” Dr. Ehrenstein said. To try to avoid muddying the waters of the BEAT-LUPUS trial findings, the maximum dose of prednisolone allowed to be used as background therapy was 20 mg/day. The trial’s investigators were also encouraged to reduce the baseline steroid dose to at least 50% by the trial’s 6-month halfway point.
“We tried to reflect what was going on in the U.K.,” Dr. Ehrenstein said, noting that the inspiration for the trial was a patient who had received sequential rituximab treatment. Although she got better with each cycle of rituximab, when her disease flared it would be worse than the time before, with increasingly higher anti-dsDNA levels recorded. The reason for this seemed to be because of increasing BAFF levels, and so the hypothesis was that if rituximab was associated with increased BAFF levels, then co-targeting BAFF with belimumab should be able to prevent those flares from happening.
The BEAT-LUPUS trial has been a huge collaborative effort and was conducted across 16 U.K. centers. From initial funding to the data analysis, it has taken 6 years to complete and was made possible by a unique partnership between Versus Arthritis, University College London Hospitals Biomedical Research Center, the National Institute for Health Research UK Musculoskeletal Translational Research Collaboration, and GlaxoSmithKline (GSK). GSK provided belimumab free of charge, as well as additional funding, but had no role in the design of the study and will not have any role going forward.
From an initial 172 patients assessed for eligibility, 52 patients were finally enrolled into the trial and received rituximab as two infusions given 2 weeks apart. Patients were then randomized in a double-blind manner to receive either belimumab (n = 26) or placebo (n = 26) 4-8 weeks after their first dose of rituximab. The intention-to-treat population consisted of 43 patients.
The use of belimumab after rituximab did not increase the risk for infection – serious or otherwise – or adverse effects, Dr. Ehrenstein reported. Serious adverse events were reported in six (23%) patients in each arm, and serious infections were seen in two (8%) of the belimumab- and four (15%) of the placebo-treated patients.
“I think the take-home message is that it seems that belimumab can reduce the number of severe flares that occur after rituximab therapy,” Dr. Ehrenstein said. “It’s promising, but not definitive,” he added. The next step is of course to publish these data and to perform a phase 3 trial.
In the discussion time following the presentation, session moderator Xavier Mariette, MD, PhD, of Bicêtre Hospital, Paris-Saclay University, asked why not give belimumab first before rituximab if using belimumab afterward works?
“Our strategy was driven by the observation that BAFF levels surged after rituximab, and therefore it’s logical to give the belimumab to block that BAFF surge,” he answered.
“Certainly, there are ideas that belimumab releases mature B cells into the circulation and rituximab can target that,” he added. That strategy is under investigation in the BLISS-BELIEVE trial, which should also report by the end of this year. It’s a much larger, phase 3 trial, involving nearly 300 patients and is sponsored by GSK.
“Clearly, this is a combination treatment [but] whether you give one before the other is uncertain,” Dr. Ehrenstein observed.
Another member of the viewing audience asked whether it would have been a fairer comparison if another dose of rituximab had been given to patients at week 24 instead of no treatment. Dr. Ehrenstein noted that it was a “good point” to make, but the investigators mainly wanted to answer whether giving belimumab after rituximab would target BAFF and thereby drop serum anti-dsDNA antibody levels. He said that a full trial of rituximab for patients with SLE, perhaps adding this extra dose, needs to be conducted.
Dr. Ehrenstein disclosed receiving research funding and educational grants from GSK and participating in advisory panels for the company.
FROM THE EULAR 2021 CONGRESS