User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
COVID-19 vaccine hesitancy still weighs heavy for some rheumatic disease patients
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.

The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.

The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.

Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.
The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.
The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.
Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.
The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.
The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.
Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
FROM THE GRAPPA 2021 ANNUAL MEETING
Medicare rules for CPAP penalize low-income patients for nonadherence
Report from the CHEST Health Policy and Advocacy Committee (HPAC) Conference
The relationship between adherence and benefit for those prescribed continuous positive airway pressure (CPAP) devices is clear. However, a Medicare-reimbursement rule that demands adherence blind to circumstances appears to be denying access to many low-income patients, according to an analysis delivered at the annual CHEST Health Policy and Advocacy Committee (HPAC) conference sponsored by the American College of Chest Physicians.
Over the past several years, adherence to CPAP has improved substantially following a series of studies that demonstrated the device must be used at least 4 hours per night to achieve improved outcomes. Medicare defines adherence as using the device more than 4 hours per night for 70% of nights (21 nights) during a consecutive 30-day period any time in the first 3 months of initial usage.
However, the studies that show improved adherence show a lag among those in the lowest income quartile, according to Sairam Parthasarathy, MD, FCCP, of the Center for Sleep and Circadian Sciences at the University of Arizona, Tucson.
When patients are followed for a year after being prescribed CPAP, the lag for the low-income patients is not seen immediately. Rather, adherence studies show a steady climb in adherence in all income groups initially, but “right at 90 days, there is a marked change,” according to Dr. Parthasarathy.
This change happens to coincide with Medicare policy that denies reimbursement for CPAP after 90 days if patients are not using CPAP at least 4 hours per night, which is the threshold associated with benefit.
The correlation between this policy and income disparity is “observational” rather than proven, but Dr. Parthasarathy is confident it is valid. He believes it is a prime example of a health inequity driven by poorly conceived policy.
“The 90-day rule needs to go,” he said, calling the choice of threshold “man-made.”
“This is the only disease condition for which a therapy is withheld if it is not used according to some magical threshold,” he said. “I cannot think of a more draconian policy.”
In an effort to illustrate the problem, he likened this policy to withholding insulin in a diabetes patient judged nonadherent because of a persistently elevated Hb1Ac.
At 90 days, adherence rates remain at a relatively early point in their upwards trajectory in all income groups. One year later, adherence rates are more than twice as high in the highest income relative to the lowest quartile and approaching twofold greater in quartiles 2 and 3.
“It takes time to get used to these devices,” Dr. Parthasarathy explained. Given studies demonstrating that “more is better” with CPAP, whether measured by sleep scales or quality of life, Dr. Parthasarathy advocates strategies to improve adherence, but he questioned an approach that penalizes low-income patients for a definition of nonadherence at an arbitrary point in time. He suggested it is just one example of health policies that ultimately penalize individuals with lower incomes.
“There are millions of dollars spent every year on understanding the genetics of disease, but the biggest influence on how long you live is the ZIP code of where you live,” said Dr. Parthasarathy, referring to zip codes as a surrogate for socioeconomic status.
This is not to imply, however, that genetics are irrelevant, Dr. Parthasarathy said. He pointed to data linking genetic traits that determine melanin levels and circadian rhythms. He noted one genotype associated with later bedtimes that is more commonly found in African Americans and Hispanics. This has relevance to a variety of sleep disorders and other health conditions, but it might serve as a fundamental disadvantage for children with this genotype, Dr. Parthasarathy maintained. He cited a study conducted at his center that found Hispanic children sleep on average 30 minutes less than white children (Sleep Med. 2016;18:61-66). The reason was simple. Hispanic children went to bed 30 minutes later but rose at the same time.
The later bedtimes and reduced sleep could potentially be one obstacle among many, such as the need for lower income patients to hold several jobs, that prevent these patients from becoming accustomed to CPAP at the same speed as wealthier patients, according to Dr. Parthasarathy.
The current Medicare policy that withholds CPAP on the basis of a single definition of nonadherence appears to lead directly to an inequity in treatment of sleep apnea, Dr. Parthasarathy maintained. Dr. Parthasarathy, who was a coauthor of a recently published paper on addressing disparities in sleep health (Chest. 2021;159:1232-40), described this issue as part of a larger problem of the failure to deliver health care that is sensitive to the cultural and racial differences underlying these inequities.
Kathleen Sarmiento, MD, FCCP, Director, VISN 21 Sleep Clinical Resource Hub for the San Francisco VA Health Care System, agreed. Dr. Sarmiento, a member of the CHEST Health Policy and Advocacy Committee and the moderator of the session in which Dr. Parthasarathy presented his data, said, “This type of issue is exactly what our Committee [HPAC] would like to address.”
The association between the 90-day Medicare rule for CPAP reimbursement and reduced access to this therapy among patients of lower economic status is compelling, she indicated. Within the goal of advocacy for health policies that will reduce inequities, Dr. Sarmiento explained that the committee is attempting to identify and reverse the source of these types of disparity.
“Specific rules or regulations are actionable targets to effect broader change in health care access and health care delivery,” said Dr. Sarmiento, alluding to the mission of HPAC.
Dr. Parthasarathy and Dr. Sarmiento report no relevant conflicts of interest.
Report from the CHEST Health Policy and Advocacy Committee (HPAC) Conference
Report from the CHEST Health Policy and Advocacy Committee (HPAC) Conference
The relationship between adherence and benefit for those prescribed continuous positive airway pressure (CPAP) devices is clear. However, a Medicare-reimbursement rule that demands adherence blind to circumstances appears to be denying access to many low-income patients, according to an analysis delivered at the annual CHEST Health Policy and Advocacy Committee (HPAC) conference sponsored by the American College of Chest Physicians.
Over the past several years, adherence to CPAP has improved substantially following a series of studies that demonstrated the device must be used at least 4 hours per night to achieve improved outcomes. Medicare defines adherence as using the device more than 4 hours per night for 70% of nights (21 nights) during a consecutive 30-day period any time in the first 3 months of initial usage.
However, the studies that show improved adherence show a lag among those in the lowest income quartile, according to Sairam Parthasarathy, MD, FCCP, of the Center for Sleep and Circadian Sciences at the University of Arizona, Tucson.
When patients are followed for a year after being prescribed CPAP, the lag for the low-income patients is not seen immediately. Rather, adherence studies show a steady climb in adherence in all income groups initially, but “right at 90 days, there is a marked change,” according to Dr. Parthasarathy.
This change happens to coincide with Medicare policy that denies reimbursement for CPAP after 90 days if patients are not using CPAP at least 4 hours per night, which is the threshold associated with benefit.
The correlation between this policy and income disparity is “observational” rather than proven, but Dr. Parthasarathy is confident it is valid. He believes it is a prime example of a health inequity driven by poorly conceived policy.
“The 90-day rule needs to go,” he said, calling the choice of threshold “man-made.”
“This is the only disease condition for which a therapy is withheld if it is not used according to some magical threshold,” he said. “I cannot think of a more draconian policy.”
In an effort to illustrate the problem, he likened this policy to withholding insulin in a diabetes patient judged nonadherent because of a persistently elevated Hb1Ac.
At 90 days, adherence rates remain at a relatively early point in their upwards trajectory in all income groups. One year later, adherence rates are more than twice as high in the highest income relative to the lowest quartile and approaching twofold greater in quartiles 2 and 3.
“It takes time to get used to these devices,” Dr. Parthasarathy explained. Given studies demonstrating that “more is better” with CPAP, whether measured by sleep scales or quality of life, Dr. Parthasarathy advocates strategies to improve adherence, but he questioned an approach that penalizes low-income patients for a definition of nonadherence at an arbitrary point in time. He suggested it is just one example of health policies that ultimately penalize individuals with lower incomes.
“There are millions of dollars spent every year on understanding the genetics of disease, but the biggest influence on how long you live is the ZIP code of where you live,” said Dr. Parthasarathy, referring to zip codes as a surrogate for socioeconomic status.
This is not to imply, however, that genetics are irrelevant, Dr. Parthasarathy said. He pointed to data linking genetic traits that determine melanin levels and circadian rhythms. He noted one genotype associated with later bedtimes that is more commonly found in African Americans and Hispanics. This has relevance to a variety of sleep disorders and other health conditions, but it might serve as a fundamental disadvantage for children with this genotype, Dr. Parthasarathy maintained. He cited a study conducted at his center that found Hispanic children sleep on average 30 minutes less than white children (Sleep Med. 2016;18:61-66). The reason was simple. Hispanic children went to bed 30 minutes later but rose at the same time.
The later bedtimes and reduced sleep could potentially be one obstacle among many, such as the need for lower income patients to hold several jobs, that prevent these patients from becoming accustomed to CPAP at the same speed as wealthier patients, according to Dr. Parthasarathy.
The current Medicare policy that withholds CPAP on the basis of a single definition of nonadherence appears to lead directly to an inequity in treatment of sleep apnea, Dr. Parthasarathy maintained. Dr. Parthasarathy, who was a coauthor of a recently published paper on addressing disparities in sleep health (Chest. 2021;159:1232-40), described this issue as part of a larger problem of the failure to deliver health care that is sensitive to the cultural and racial differences underlying these inequities.
Kathleen Sarmiento, MD, FCCP, Director, VISN 21 Sleep Clinical Resource Hub for the San Francisco VA Health Care System, agreed. Dr. Sarmiento, a member of the CHEST Health Policy and Advocacy Committee and the moderator of the session in which Dr. Parthasarathy presented his data, said, “This type of issue is exactly what our Committee [HPAC] would like to address.”
The association between the 90-day Medicare rule for CPAP reimbursement and reduced access to this therapy among patients of lower economic status is compelling, she indicated. Within the goal of advocacy for health policies that will reduce inequities, Dr. Sarmiento explained that the committee is attempting to identify and reverse the source of these types of disparity.
“Specific rules or regulations are actionable targets to effect broader change in health care access and health care delivery,” said Dr. Sarmiento, alluding to the mission of HPAC.
Dr. Parthasarathy and Dr. Sarmiento report no relevant conflicts of interest.
The relationship between adherence and benefit for those prescribed continuous positive airway pressure (CPAP) devices is clear. However, a Medicare-reimbursement rule that demands adherence blind to circumstances appears to be denying access to many low-income patients, according to an analysis delivered at the annual CHEST Health Policy and Advocacy Committee (HPAC) conference sponsored by the American College of Chest Physicians.
Over the past several years, adherence to CPAP has improved substantially following a series of studies that demonstrated the device must be used at least 4 hours per night to achieve improved outcomes. Medicare defines adherence as using the device more than 4 hours per night for 70% of nights (21 nights) during a consecutive 30-day period any time in the first 3 months of initial usage.
However, the studies that show improved adherence show a lag among those in the lowest income quartile, according to Sairam Parthasarathy, MD, FCCP, of the Center for Sleep and Circadian Sciences at the University of Arizona, Tucson.
When patients are followed for a year after being prescribed CPAP, the lag for the low-income patients is not seen immediately. Rather, adherence studies show a steady climb in adherence in all income groups initially, but “right at 90 days, there is a marked change,” according to Dr. Parthasarathy.
This change happens to coincide with Medicare policy that denies reimbursement for CPAP after 90 days if patients are not using CPAP at least 4 hours per night, which is the threshold associated with benefit.
The correlation between this policy and income disparity is “observational” rather than proven, but Dr. Parthasarathy is confident it is valid. He believes it is a prime example of a health inequity driven by poorly conceived policy.
“The 90-day rule needs to go,” he said, calling the choice of threshold “man-made.”
“This is the only disease condition for which a therapy is withheld if it is not used according to some magical threshold,” he said. “I cannot think of a more draconian policy.”
In an effort to illustrate the problem, he likened this policy to withholding insulin in a diabetes patient judged nonadherent because of a persistently elevated Hb1Ac.
At 90 days, adherence rates remain at a relatively early point in their upwards trajectory in all income groups. One year later, adherence rates are more than twice as high in the highest income relative to the lowest quartile and approaching twofold greater in quartiles 2 and 3.
“It takes time to get used to these devices,” Dr. Parthasarathy explained. Given studies demonstrating that “more is better” with CPAP, whether measured by sleep scales or quality of life, Dr. Parthasarathy advocates strategies to improve adherence, but he questioned an approach that penalizes low-income patients for a definition of nonadherence at an arbitrary point in time. He suggested it is just one example of health policies that ultimately penalize individuals with lower incomes.
“There are millions of dollars spent every year on understanding the genetics of disease, but the biggest influence on how long you live is the ZIP code of where you live,” said Dr. Parthasarathy, referring to zip codes as a surrogate for socioeconomic status.
This is not to imply, however, that genetics are irrelevant, Dr. Parthasarathy said. He pointed to data linking genetic traits that determine melanin levels and circadian rhythms. He noted one genotype associated with later bedtimes that is more commonly found in African Americans and Hispanics. This has relevance to a variety of sleep disorders and other health conditions, but it might serve as a fundamental disadvantage for children with this genotype, Dr. Parthasarathy maintained. He cited a study conducted at his center that found Hispanic children sleep on average 30 minutes less than white children (Sleep Med. 2016;18:61-66). The reason was simple. Hispanic children went to bed 30 minutes later but rose at the same time.
The later bedtimes and reduced sleep could potentially be one obstacle among many, such as the need for lower income patients to hold several jobs, that prevent these patients from becoming accustomed to CPAP at the same speed as wealthier patients, according to Dr. Parthasarathy.
The current Medicare policy that withholds CPAP on the basis of a single definition of nonadherence appears to lead directly to an inequity in treatment of sleep apnea, Dr. Parthasarathy maintained. Dr. Parthasarathy, who was a coauthor of a recently published paper on addressing disparities in sleep health (Chest. 2021;159:1232-40), described this issue as part of a larger problem of the failure to deliver health care that is sensitive to the cultural and racial differences underlying these inequities.
Kathleen Sarmiento, MD, FCCP, Director, VISN 21 Sleep Clinical Resource Hub for the San Francisco VA Health Care System, agreed. Dr. Sarmiento, a member of the CHEST Health Policy and Advocacy Committee and the moderator of the session in which Dr. Parthasarathy presented his data, said, “This type of issue is exactly what our Committee [HPAC] would like to address.”
The association between the 90-day Medicare rule for CPAP reimbursement and reduced access to this therapy among patients of lower economic status is compelling, she indicated. Within the goal of advocacy for health policies that will reduce inequities, Dr. Sarmiento explained that the committee is attempting to identify and reverse the source of these types of disparity.
“Specific rules or regulations are actionable targets to effect broader change in health care access and health care delivery,” said Dr. Sarmiento, alluding to the mission of HPAC.
Dr. Parthasarathy and Dr. Sarmiento report no relevant conflicts of interest.
Twice-a-year lenacapavir shows viral suppression in drug-resistant HIV at 26 weeks
With regulatory approval, lenacapavir could become the only HIV-1 treatment option given every 6 months.
“These data support the use of lenacapavir in patients with multidrug-resistant viruses, and according to its long half-life of two subcutaneous injections per year, [it] could help reduce pill burden,” first author Jean-Michel Molina, MD, PhD, professor of infectious diseases and head of the infectious diseases department at the Saint-Louis and Lariboisière Hospitals, Paris, said in an interview.
Presenting the updated findings from the phase 2/3 CAPELLA trial at the virtual annual meeting of the International AIDS Society conference, Dr. Molina underscored the need for longer-term treatments.
“These patients with multidrug resistances are usually those who have not been fully adherent to their regimen,” he said. “Being able to provide the drug, given every 6 months subcutaneously, provides an ideal treatment for overcoming resistance and lack of adherence.”
The study showed that, after 26 weeks, 81% of heavily treatment-experienced people with HIV in a randomized cohort who were treated with a subcutaneous injection of lenacapavir (927 mg) combined with an optimized background antiretroviral regimen achieved sustained virologic suppression, with an undetectable viral load (<50 copies/mL).
In addition, the lenacapavir-treated patients had a clinically meaningful mean increase in CD4 counts of 81 cells/mcL over the 26 weeks.
The drug was well tolerated, with no drug-related serious adverse events or adverse events leading to discontinuation. The most common adverse events were injection-site reactions, which occurred in 56% of participants, with most being mild or moderate.
Importantly, four participants developed emergent resistances to lenacapavir. One was suppressed with a change in the background regimen and two others were suppressed without a change in regimen.
“We know that these mutations affect viral fitness,” Dr. Molina said in an interview. “We need more studies to assess the real impact of these mutations.”
Dr. Molina noted that a phase 2 study is already underway to evaluate how a pairing of lenacapavir with fellow investigational long-acting drug islatravir (Merck) could offset the risk of developing resistances.
Asked by an audience member whether a two-drug regimen with something like islatravir is likely to successfully prevent resistances, Dr. Molina responded that “it’s too early to know what’s going to happen with [combinations], but these first results are really encouraging when you see the very high rate of being fully suppressed after 26 weeks. The efficacy that we’ve seen after [a previous 2-week analysis] is long lasting.”
Lenacapavir targets multiple viral stages
Unlike other antiviral drugs that target just a single stage of viral replication, lenacapavir takes aim at multiple steps in the viral life cycle, including capsid-mediated uptake of HIV-1 proviral DNA, virus assembly and release, and capsid core formation, Dr. Molina explained.
The CAPELLA trial included participants at research centers in North America, Europe, and Asia, with a median age of 52 years; 25% were female, 38% were Black, and their mean HIV-1 RNA (viral load) was 4.17 log copies/mL.
Overall, 72 patients were divided into two cohorts of 36 patients each, including a randomized and nonrandomized cohort. Dr. Molina primarily reported results from the randomized group.
In that group, patients received either a lead-in of oral lenacapavir (600 mg on day 1 and 2 and 300 mg on day 8) or placebo, in combination with patients’ current failing drug regimens in both groups.
At day 15, all participants were switched to the investigator-selected, optimized background treatment regimen, tailored according to patients’ drug-resistance profiles, and those in the lenacapavir group received the subcutaneous injection of lenacapavir; those in the placebo group were switched to the oral lead-in, followed by subcutaneous lenacapavir every 6 months.
Combined data that included six patients from the nonrandomized cohort showed that 79% of patients had a viral load of less than 50 copies/mL at week 26. The 81% viral suppression rate represented the randomized group (29 of 36).
International AIDS Society cochair Hendrik Streeck, MD, director of the Institute of Virology and Institute for HIV Research at the University Bonn (Germany), said a twice-a-year drug could possibly have profound benefits with a reduction in daily pill burden.
“What makes this an interesting drug is that it is long acting, so one can imagine it has the potential to treat individuals such as those who are not very adherent to the antiretroviral therapy, or who can’t easily access treatment, for example in resource-limited settings,” he said in an interview. “The option to treat patients for the next months in advance could be a very important next step.”
Further data from CALIBRATE
Additional data on lenacapavir from the phase 2 CALIBRATE study, presented in a separate session, further showed the drug, given orally or subcutaneously in combination with oral daily emtricitabine/tenofovir alafenamide, resulted in high rates of viral suppression among 94% of 157 treatment-naive patients after 28 weeks.
Commenting on the research, session moderator Alexandra Calmy, MD, PhD, of the HIV/AIDS unit and LIPO & Metabolism group, infectious diseases division, Geneva University Hospitals, noted the study offered “interesting data indeed” – with some caveats: “Why position a new drug class in naive patients [when] we already have good options, available for a large range of various populations?”
Dr. Calmy noted that, in general, lenacapavir “would certainly be an added value with an adapted 6-monthly companion drug.”
But she raised another key issue: “When will we have data on pregnancy that would allow lenacapavir to really be a game changer worldwide?”
The study was funded by Gilead Sciences. Dr. Molina reported receiving research funding from Gilead and being on advisory boards for Gilead, Merck, ViiV, and Janssen. Dr. Calmy and Dr. Streeck reported no relevant financial relationships.
With regulatory approval, lenacapavir could become the only HIV-1 treatment option given every 6 months.
“These data support the use of lenacapavir in patients with multidrug-resistant viruses, and according to its long half-life of two subcutaneous injections per year, [it] could help reduce pill burden,” first author Jean-Michel Molina, MD, PhD, professor of infectious diseases and head of the infectious diseases department at the Saint-Louis and Lariboisière Hospitals, Paris, said in an interview.
Presenting the updated findings from the phase 2/3 CAPELLA trial at the virtual annual meeting of the International AIDS Society conference, Dr. Molina underscored the need for longer-term treatments.
“These patients with multidrug resistances are usually those who have not been fully adherent to their regimen,” he said. “Being able to provide the drug, given every 6 months subcutaneously, provides an ideal treatment for overcoming resistance and lack of adherence.”
The study showed that, after 26 weeks, 81% of heavily treatment-experienced people with HIV in a randomized cohort who were treated with a subcutaneous injection of lenacapavir (927 mg) combined with an optimized background antiretroviral regimen achieved sustained virologic suppression, with an undetectable viral load (<50 copies/mL).
In addition, the lenacapavir-treated patients had a clinically meaningful mean increase in CD4 counts of 81 cells/mcL over the 26 weeks.
The drug was well tolerated, with no drug-related serious adverse events or adverse events leading to discontinuation. The most common adverse events were injection-site reactions, which occurred in 56% of participants, with most being mild or moderate.
Importantly, four participants developed emergent resistances to lenacapavir. One was suppressed with a change in the background regimen and two others were suppressed without a change in regimen.
“We know that these mutations affect viral fitness,” Dr. Molina said in an interview. “We need more studies to assess the real impact of these mutations.”
Dr. Molina noted that a phase 2 study is already underway to evaluate how a pairing of lenacapavir with fellow investigational long-acting drug islatravir (Merck) could offset the risk of developing resistances.
Asked by an audience member whether a two-drug regimen with something like islatravir is likely to successfully prevent resistances, Dr. Molina responded that “it’s too early to know what’s going to happen with [combinations], but these first results are really encouraging when you see the very high rate of being fully suppressed after 26 weeks. The efficacy that we’ve seen after [a previous 2-week analysis] is long lasting.”
Lenacapavir targets multiple viral stages
Unlike other antiviral drugs that target just a single stage of viral replication, lenacapavir takes aim at multiple steps in the viral life cycle, including capsid-mediated uptake of HIV-1 proviral DNA, virus assembly and release, and capsid core formation, Dr. Molina explained.
The CAPELLA trial included participants at research centers in North America, Europe, and Asia, with a median age of 52 years; 25% were female, 38% were Black, and their mean HIV-1 RNA (viral load) was 4.17 log copies/mL.
Overall, 72 patients were divided into two cohorts of 36 patients each, including a randomized and nonrandomized cohort. Dr. Molina primarily reported results from the randomized group.
In that group, patients received either a lead-in of oral lenacapavir (600 mg on day 1 and 2 and 300 mg on day 8) or placebo, in combination with patients’ current failing drug regimens in both groups.
At day 15, all participants were switched to the investigator-selected, optimized background treatment regimen, tailored according to patients’ drug-resistance profiles, and those in the lenacapavir group received the subcutaneous injection of lenacapavir; those in the placebo group were switched to the oral lead-in, followed by subcutaneous lenacapavir every 6 months.
Combined data that included six patients from the nonrandomized cohort showed that 79% of patients had a viral load of less than 50 copies/mL at week 26. The 81% viral suppression rate represented the randomized group (29 of 36).
International AIDS Society cochair Hendrik Streeck, MD, director of the Institute of Virology and Institute for HIV Research at the University Bonn (Germany), said a twice-a-year drug could possibly have profound benefits with a reduction in daily pill burden.
“What makes this an interesting drug is that it is long acting, so one can imagine it has the potential to treat individuals such as those who are not very adherent to the antiretroviral therapy, or who can’t easily access treatment, for example in resource-limited settings,” he said in an interview. “The option to treat patients for the next months in advance could be a very important next step.”
Further data from CALIBRATE
Additional data on lenacapavir from the phase 2 CALIBRATE study, presented in a separate session, further showed the drug, given orally or subcutaneously in combination with oral daily emtricitabine/tenofovir alafenamide, resulted in high rates of viral suppression among 94% of 157 treatment-naive patients after 28 weeks.
Commenting on the research, session moderator Alexandra Calmy, MD, PhD, of the HIV/AIDS unit and LIPO & Metabolism group, infectious diseases division, Geneva University Hospitals, noted the study offered “interesting data indeed” – with some caveats: “Why position a new drug class in naive patients [when] we already have good options, available for a large range of various populations?”
Dr. Calmy noted that, in general, lenacapavir “would certainly be an added value with an adapted 6-monthly companion drug.”
But she raised another key issue: “When will we have data on pregnancy that would allow lenacapavir to really be a game changer worldwide?”
The study was funded by Gilead Sciences. Dr. Molina reported receiving research funding from Gilead and being on advisory boards for Gilead, Merck, ViiV, and Janssen. Dr. Calmy and Dr. Streeck reported no relevant financial relationships.
With regulatory approval, lenacapavir could become the only HIV-1 treatment option given every 6 months.
“These data support the use of lenacapavir in patients with multidrug-resistant viruses, and according to its long half-life of two subcutaneous injections per year, [it] could help reduce pill burden,” first author Jean-Michel Molina, MD, PhD, professor of infectious diseases and head of the infectious diseases department at the Saint-Louis and Lariboisière Hospitals, Paris, said in an interview.
Presenting the updated findings from the phase 2/3 CAPELLA trial at the virtual annual meeting of the International AIDS Society conference, Dr. Molina underscored the need for longer-term treatments.
“These patients with multidrug resistances are usually those who have not been fully adherent to their regimen,” he said. “Being able to provide the drug, given every 6 months subcutaneously, provides an ideal treatment for overcoming resistance and lack of adherence.”
The study showed that, after 26 weeks, 81% of heavily treatment-experienced people with HIV in a randomized cohort who were treated with a subcutaneous injection of lenacapavir (927 mg) combined with an optimized background antiretroviral regimen achieved sustained virologic suppression, with an undetectable viral load (<50 copies/mL).
In addition, the lenacapavir-treated patients had a clinically meaningful mean increase in CD4 counts of 81 cells/mcL over the 26 weeks.
The drug was well tolerated, with no drug-related serious adverse events or adverse events leading to discontinuation. The most common adverse events were injection-site reactions, which occurred in 56% of participants, with most being mild or moderate.
Importantly, four participants developed emergent resistances to lenacapavir. One was suppressed with a change in the background regimen and two others were suppressed without a change in regimen.
“We know that these mutations affect viral fitness,” Dr. Molina said in an interview. “We need more studies to assess the real impact of these mutations.”
Dr. Molina noted that a phase 2 study is already underway to evaluate how a pairing of lenacapavir with fellow investigational long-acting drug islatravir (Merck) could offset the risk of developing resistances.
Asked by an audience member whether a two-drug regimen with something like islatravir is likely to successfully prevent resistances, Dr. Molina responded that “it’s too early to know what’s going to happen with [combinations], but these first results are really encouraging when you see the very high rate of being fully suppressed after 26 weeks. The efficacy that we’ve seen after [a previous 2-week analysis] is long lasting.”
Lenacapavir targets multiple viral stages
Unlike other antiviral drugs that target just a single stage of viral replication, lenacapavir takes aim at multiple steps in the viral life cycle, including capsid-mediated uptake of HIV-1 proviral DNA, virus assembly and release, and capsid core formation, Dr. Molina explained.
The CAPELLA trial included participants at research centers in North America, Europe, and Asia, with a median age of 52 years; 25% were female, 38% were Black, and their mean HIV-1 RNA (viral load) was 4.17 log copies/mL.
Overall, 72 patients were divided into two cohorts of 36 patients each, including a randomized and nonrandomized cohort. Dr. Molina primarily reported results from the randomized group.
In that group, patients received either a lead-in of oral lenacapavir (600 mg on day 1 and 2 and 300 mg on day 8) or placebo, in combination with patients’ current failing drug regimens in both groups.
At day 15, all participants were switched to the investigator-selected, optimized background treatment regimen, tailored according to patients’ drug-resistance profiles, and those in the lenacapavir group received the subcutaneous injection of lenacapavir; those in the placebo group were switched to the oral lead-in, followed by subcutaneous lenacapavir every 6 months.
Combined data that included six patients from the nonrandomized cohort showed that 79% of patients had a viral load of less than 50 copies/mL at week 26. The 81% viral suppression rate represented the randomized group (29 of 36).
International AIDS Society cochair Hendrik Streeck, MD, director of the Institute of Virology and Institute for HIV Research at the University Bonn (Germany), said a twice-a-year drug could possibly have profound benefits with a reduction in daily pill burden.
“What makes this an interesting drug is that it is long acting, so one can imagine it has the potential to treat individuals such as those who are not very adherent to the antiretroviral therapy, or who can’t easily access treatment, for example in resource-limited settings,” he said in an interview. “The option to treat patients for the next months in advance could be a very important next step.”
Further data from CALIBRATE
Additional data on lenacapavir from the phase 2 CALIBRATE study, presented in a separate session, further showed the drug, given orally or subcutaneously in combination with oral daily emtricitabine/tenofovir alafenamide, resulted in high rates of viral suppression among 94% of 157 treatment-naive patients after 28 weeks.
Commenting on the research, session moderator Alexandra Calmy, MD, PhD, of the HIV/AIDS unit and LIPO & Metabolism group, infectious diseases division, Geneva University Hospitals, noted the study offered “interesting data indeed” – with some caveats: “Why position a new drug class in naive patients [when] we already have good options, available for a large range of various populations?”
Dr. Calmy noted that, in general, lenacapavir “would certainly be an added value with an adapted 6-monthly companion drug.”
But she raised another key issue: “When will we have data on pregnancy that would allow lenacapavir to really be a game changer worldwide?”
The study was funded by Gilead Sciences. Dr. Molina reported receiving research funding from Gilead and being on advisory boards for Gilead, Merck, ViiV, and Janssen. Dr. Calmy and Dr. Streeck reported no relevant financial relationships.
FROM IAS 2021
HIV: Could another two-drug regimen be on the horizon?
Headache was the most common adverse event (AE) people experienced in 72 weeks of taking the once-daily investigational two-drug HIV treatment islatravir (ISL; Merck) plus doravirine (DOR; Merck), and those AEs were short-lived and mild, according to a safety analysis presented at the International AIDS Society (IAS) Conference 2021.
That finding, combined with other data showing few changes in metabolic markers, is potentially good news for people living with HIV, inasmuch as two-drug regimens generally have fewer side effects than traditional three- or four-drug regimens, said Jean-Michel Molina, MD, PhD, of Sant-Louis and Lariboisière Hospitals, Paris, who previously presented efficacy data on the combination at the HIV Glasgow 2020 Virtual Conference.
“At this point, it’s encouraging,” Dr. Molina told this news organization. “Safety is good, efficacy seems good. But the data are limited, and it’s too early to tell.”
If it makes it to the clinic, IS/DOR would be the fourth two-drug regimen approved for HIV treatment, following the U.S. Food and Drug Administration approval of dolutegravir/lamivudine (Dovato), dolutegravir/rilpivirine (Juluca), and the monthly injectable cabotegravir long-acting/rilpivirine long-acting (Cabenuva).
DOR, a non-nucleoside reverse transcriptase inhibitor (NNRTI), is currently approved and is part of the three-drug single-pill regimen Delstrigo (doravirine/lamivudine/tenofovir disoproxil fumarate, DOR/3TC/TDF, Merck). ISL is still under development for treatment and prevention. Dr. Molina had previously presented data showing that 81.1% of people living with HIV maintained undetectable viral loads (defined as <50 copies/mL) compared to 80.6% of people who continued treatment with DOR/3TC/TDF. Data on ISL/DOR versus DOR/3TC/TDF for people new to HIV treatment were published May 14 in The Lancet HIV.
The ISL/DOR trial was designed to assess the safety of three doses of ISL with 100 mg of DOR – 0.25 mg, 0.75 mg, and 2.25 mg – as a daily treatment. The investigators randomly assigned 29, 30, and 31 participants, respectively, to each of the dual-therapy arms and 31 people to the DOR/3TC/TDF arm after a 24-week lead-in course of DOR/3TC/TDF. At week 60, everyone in the two-drug arms received 0.75 mg of ISL with DOR.
At HIV Glasgow, Dr. Molina didn’t present details about the safety profile of the two-drug combination. Douglas Cunningham, DO, a primary care provider at Pueblo Family Physicians, Phoenix, presented such data at IAS 2021. What he showed was that over the first 96 weeks of the trial, there were a total of 118 AEs among the 90 participants in the ISL plus DOR arms and 42 among the 31 participants in the three-drug regimen arm, but there were only seven drug-related AEs for people in the ISL plus DOR arm, and all of those occurred during the first 48 weeks. There were none from weeks 48 to 96.
In total, there were no drug-related serious AEs for ISL/DOR; there was one in the DOR/3TC/TDF arm. The most common AE was headache, which occurred in a total of 10 participants in the ISL/DOR arms. There were nine cases of vitamin D deficiency, eight cases of nausea, seven cases of arthralgia, diarrhea, sinus pain, and vomiting, and six cases each of anxiety and rash. Four people experienced pain in their extremities.
In the three-drug combination arm, side effects were far fewer – just 18 occurred in at least 10% of participants. The most common AE among people on the three-drug combination was diarrhea, which occurred in six participants. Nausea occurred in three; vomiting and headache in two; and there was one instance each of vitamin D deficiency, arthralgia, sinus pain, rash, and pain in extremities.
“The majority of these events were mild, transient, and not related to study drug,” Dr. Cunningham said.
Three ISL/DOR participants experienced an increase in fasting triglyceride level of >500-1,000 mg/dL, and six patients experienced grade 4 changes in creatine kinase level of ≥20 IU/L. Dr. Cunningham said that all but one of the cases of an increase in creatinine level were the result of physical exertion by the participants, and all of those changes were found to have resolved at future visits. The bottom line is that the two-drug combination was safe.
“In the islatravir and doravirine arm, there were no serious drug related serious AEs and no discontinuations due to drug-related AEs from week 48 to week 96,” said Dr. Cunningham. “Islatravir in combination with doravirine was generally well tolerated through week 96 with few drug-related AEs.”
Still, the value of this combination is unclear for Laura Waters, MD, consulting physician in HIV and sexual health at Central and Northwest London NHS Trust. She pointed out that the data are preliminary and that islatravir hasn’t yet been shown to lessen the chances of development of treatment-resistant mutations – a big deal for two-drug regimens, inasmuch as early attempts at using only two drugs resulted in incomplete suppression of the virus and resistance. Merck is planning a study of the combination in heavily pretreated individuals.
Merck presented data at IAS on another NNRTI, the investigational MK-8507, in combination with islatravir. MK-8507 has the potential to be used weekly instead of daily. Dr. Waters said she suspects that this trial is just a proof of concept of islatravir in combination with an NNRTI. Merck has signed an agreement with Gilead Sciences to co-develop islatravir with long-acting lenacapravir. Additionally, the two-drug combination of dolutegravir and lamivudine has been very successful.
“I’d be surprised if they developed islatravir/doravirine as a usable combo,” she said. “It’s just too soon to say. My personal view is that people are a bit too overoptimistic about it.”
The study was funded by Merck. Dr. Molina has received grants from Gilead Sciences, Merck, ViiV Healthcare, and Sanofi. Dr. Waters has received speaker or advisory fees during the past 2 years from Gilead Sciences, ViiV Healthcare, Merck, Janssen, Theratech, Sipla, and Mylan.
A version of this article first appeared on Medscape.com.
Headache was the most common adverse event (AE) people experienced in 72 weeks of taking the once-daily investigational two-drug HIV treatment islatravir (ISL; Merck) plus doravirine (DOR; Merck), and those AEs were short-lived and mild, according to a safety analysis presented at the International AIDS Society (IAS) Conference 2021.
That finding, combined with other data showing few changes in metabolic markers, is potentially good news for people living with HIV, inasmuch as two-drug regimens generally have fewer side effects than traditional three- or four-drug regimens, said Jean-Michel Molina, MD, PhD, of Sant-Louis and Lariboisière Hospitals, Paris, who previously presented efficacy data on the combination at the HIV Glasgow 2020 Virtual Conference.
“At this point, it’s encouraging,” Dr. Molina told this news organization. “Safety is good, efficacy seems good. But the data are limited, and it’s too early to tell.”
If it makes it to the clinic, IS/DOR would be the fourth two-drug regimen approved for HIV treatment, following the U.S. Food and Drug Administration approval of dolutegravir/lamivudine (Dovato), dolutegravir/rilpivirine (Juluca), and the monthly injectable cabotegravir long-acting/rilpivirine long-acting (Cabenuva).
DOR, a non-nucleoside reverse transcriptase inhibitor (NNRTI), is currently approved and is part of the three-drug single-pill regimen Delstrigo (doravirine/lamivudine/tenofovir disoproxil fumarate, DOR/3TC/TDF, Merck). ISL is still under development for treatment and prevention. Dr. Molina had previously presented data showing that 81.1% of people living with HIV maintained undetectable viral loads (defined as <50 copies/mL) compared to 80.6% of people who continued treatment with DOR/3TC/TDF. Data on ISL/DOR versus DOR/3TC/TDF for people new to HIV treatment were published May 14 in The Lancet HIV.
The ISL/DOR trial was designed to assess the safety of three doses of ISL with 100 mg of DOR – 0.25 mg, 0.75 mg, and 2.25 mg – as a daily treatment. The investigators randomly assigned 29, 30, and 31 participants, respectively, to each of the dual-therapy arms and 31 people to the DOR/3TC/TDF arm after a 24-week lead-in course of DOR/3TC/TDF. At week 60, everyone in the two-drug arms received 0.75 mg of ISL with DOR.
At HIV Glasgow, Dr. Molina didn’t present details about the safety profile of the two-drug combination. Douglas Cunningham, DO, a primary care provider at Pueblo Family Physicians, Phoenix, presented such data at IAS 2021. What he showed was that over the first 96 weeks of the trial, there were a total of 118 AEs among the 90 participants in the ISL plus DOR arms and 42 among the 31 participants in the three-drug regimen arm, but there were only seven drug-related AEs for people in the ISL plus DOR arm, and all of those occurred during the first 48 weeks. There were none from weeks 48 to 96.
In total, there were no drug-related serious AEs for ISL/DOR; there was one in the DOR/3TC/TDF arm. The most common AE was headache, which occurred in a total of 10 participants in the ISL/DOR arms. There were nine cases of vitamin D deficiency, eight cases of nausea, seven cases of arthralgia, diarrhea, sinus pain, and vomiting, and six cases each of anxiety and rash. Four people experienced pain in their extremities.
In the three-drug combination arm, side effects were far fewer – just 18 occurred in at least 10% of participants. The most common AE among people on the three-drug combination was diarrhea, which occurred in six participants. Nausea occurred in three; vomiting and headache in two; and there was one instance each of vitamin D deficiency, arthralgia, sinus pain, rash, and pain in extremities.
“The majority of these events were mild, transient, and not related to study drug,” Dr. Cunningham said.
Three ISL/DOR participants experienced an increase in fasting triglyceride level of >500-1,000 mg/dL, and six patients experienced grade 4 changes in creatine kinase level of ≥20 IU/L. Dr. Cunningham said that all but one of the cases of an increase in creatinine level were the result of physical exertion by the participants, and all of those changes were found to have resolved at future visits. The bottom line is that the two-drug combination was safe.
“In the islatravir and doravirine arm, there were no serious drug related serious AEs and no discontinuations due to drug-related AEs from week 48 to week 96,” said Dr. Cunningham. “Islatravir in combination with doravirine was generally well tolerated through week 96 with few drug-related AEs.”
Still, the value of this combination is unclear for Laura Waters, MD, consulting physician in HIV and sexual health at Central and Northwest London NHS Trust. She pointed out that the data are preliminary and that islatravir hasn’t yet been shown to lessen the chances of development of treatment-resistant mutations – a big deal for two-drug regimens, inasmuch as early attempts at using only two drugs resulted in incomplete suppression of the virus and resistance. Merck is planning a study of the combination in heavily pretreated individuals.
Merck presented data at IAS on another NNRTI, the investigational MK-8507, in combination with islatravir. MK-8507 has the potential to be used weekly instead of daily. Dr. Waters said she suspects that this trial is just a proof of concept of islatravir in combination with an NNRTI. Merck has signed an agreement with Gilead Sciences to co-develop islatravir with long-acting lenacapravir. Additionally, the two-drug combination of dolutegravir and lamivudine has been very successful.
“I’d be surprised if they developed islatravir/doravirine as a usable combo,” she said. “It’s just too soon to say. My personal view is that people are a bit too overoptimistic about it.”
The study was funded by Merck. Dr. Molina has received grants from Gilead Sciences, Merck, ViiV Healthcare, and Sanofi. Dr. Waters has received speaker or advisory fees during the past 2 years from Gilead Sciences, ViiV Healthcare, Merck, Janssen, Theratech, Sipla, and Mylan.
A version of this article first appeared on Medscape.com.
Headache was the most common adverse event (AE) people experienced in 72 weeks of taking the once-daily investigational two-drug HIV treatment islatravir (ISL; Merck) plus doravirine (DOR; Merck), and those AEs were short-lived and mild, according to a safety analysis presented at the International AIDS Society (IAS) Conference 2021.
That finding, combined with other data showing few changes in metabolic markers, is potentially good news for people living with HIV, inasmuch as two-drug regimens generally have fewer side effects than traditional three- or four-drug regimens, said Jean-Michel Molina, MD, PhD, of Sant-Louis and Lariboisière Hospitals, Paris, who previously presented efficacy data on the combination at the HIV Glasgow 2020 Virtual Conference.
“At this point, it’s encouraging,” Dr. Molina told this news organization. “Safety is good, efficacy seems good. But the data are limited, and it’s too early to tell.”
If it makes it to the clinic, IS/DOR would be the fourth two-drug regimen approved for HIV treatment, following the U.S. Food and Drug Administration approval of dolutegravir/lamivudine (Dovato), dolutegravir/rilpivirine (Juluca), and the monthly injectable cabotegravir long-acting/rilpivirine long-acting (Cabenuva).
DOR, a non-nucleoside reverse transcriptase inhibitor (NNRTI), is currently approved and is part of the three-drug single-pill regimen Delstrigo (doravirine/lamivudine/tenofovir disoproxil fumarate, DOR/3TC/TDF, Merck). ISL is still under development for treatment and prevention. Dr. Molina had previously presented data showing that 81.1% of people living with HIV maintained undetectable viral loads (defined as <50 copies/mL) compared to 80.6% of people who continued treatment with DOR/3TC/TDF. Data on ISL/DOR versus DOR/3TC/TDF for people new to HIV treatment were published May 14 in The Lancet HIV.
The ISL/DOR trial was designed to assess the safety of three doses of ISL with 100 mg of DOR – 0.25 mg, 0.75 mg, and 2.25 mg – as a daily treatment. The investigators randomly assigned 29, 30, and 31 participants, respectively, to each of the dual-therapy arms and 31 people to the DOR/3TC/TDF arm after a 24-week lead-in course of DOR/3TC/TDF. At week 60, everyone in the two-drug arms received 0.75 mg of ISL with DOR.
At HIV Glasgow, Dr. Molina didn’t present details about the safety profile of the two-drug combination. Douglas Cunningham, DO, a primary care provider at Pueblo Family Physicians, Phoenix, presented such data at IAS 2021. What he showed was that over the first 96 weeks of the trial, there were a total of 118 AEs among the 90 participants in the ISL plus DOR arms and 42 among the 31 participants in the three-drug regimen arm, but there were only seven drug-related AEs for people in the ISL plus DOR arm, and all of those occurred during the first 48 weeks. There were none from weeks 48 to 96.
In total, there were no drug-related serious AEs for ISL/DOR; there was one in the DOR/3TC/TDF arm. The most common AE was headache, which occurred in a total of 10 participants in the ISL/DOR arms. There were nine cases of vitamin D deficiency, eight cases of nausea, seven cases of arthralgia, diarrhea, sinus pain, and vomiting, and six cases each of anxiety and rash. Four people experienced pain in their extremities.
In the three-drug combination arm, side effects were far fewer – just 18 occurred in at least 10% of participants. The most common AE among people on the three-drug combination was diarrhea, which occurred in six participants. Nausea occurred in three; vomiting and headache in two; and there was one instance each of vitamin D deficiency, arthralgia, sinus pain, rash, and pain in extremities.
“The majority of these events were mild, transient, and not related to study drug,” Dr. Cunningham said.
Three ISL/DOR participants experienced an increase in fasting triglyceride level of >500-1,000 mg/dL, and six patients experienced grade 4 changes in creatine kinase level of ≥20 IU/L. Dr. Cunningham said that all but one of the cases of an increase in creatinine level were the result of physical exertion by the participants, and all of those changes were found to have resolved at future visits. The bottom line is that the two-drug combination was safe.
“In the islatravir and doravirine arm, there were no serious drug related serious AEs and no discontinuations due to drug-related AEs from week 48 to week 96,” said Dr. Cunningham. “Islatravir in combination with doravirine was generally well tolerated through week 96 with few drug-related AEs.”
Still, the value of this combination is unclear for Laura Waters, MD, consulting physician in HIV and sexual health at Central and Northwest London NHS Trust. She pointed out that the data are preliminary and that islatravir hasn’t yet been shown to lessen the chances of development of treatment-resistant mutations – a big deal for two-drug regimens, inasmuch as early attempts at using only two drugs resulted in incomplete suppression of the virus and resistance. Merck is planning a study of the combination in heavily pretreated individuals.
Merck presented data at IAS on another NNRTI, the investigational MK-8507, in combination with islatravir. MK-8507 has the potential to be used weekly instead of daily. Dr. Waters said she suspects that this trial is just a proof of concept of islatravir in combination with an NNRTI. Merck has signed an agreement with Gilead Sciences to co-develop islatravir with long-acting lenacapravir. Additionally, the two-drug combination of dolutegravir and lamivudine has been very successful.
“I’d be surprised if they developed islatravir/doravirine as a usable combo,” she said. “It’s just too soon to say. My personal view is that people are a bit too overoptimistic about it.”
The study was funded by Merck. Dr. Molina has received grants from Gilead Sciences, Merck, ViiV Healthcare, and Sanofi. Dr. Waters has received speaker or advisory fees during the past 2 years from Gilead Sciences, ViiV Healthcare, Merck, Janssen, Theratech, Sipla, and Mylan.
A version of this article first appeared on Medscape.com.
HIV increases risk for severe COVID-19
according to a report from the World Health Organization on COVID-19 outcomes among people living with HIV. The study primarily included people from South Africa but also some data from other parts of the world, including the United States.
However, the report, presented at the 11th IAS Conference on HIV Science (IAS 2021), couldn’t answer some crucial questions clinicians have been wondering about since the COVID-19 pandemic began. For example, was the increase in COVID risk a result of the presence of HIV or because of the immune compromise caused by untreated HIV?
The report didn’t include data on viral load or CD counts, both used to evaluate the health of a person’s immune system. On effective treatment, people living with HIV have a lifespan close to their HIV-negative peers. And effective treatment causes undetectable viral loads which, when maintained for 6 months or more, eliminates transmission of HIV to sexual partners.
What’s clear is that in people with HIV, as in people without HIV, older people, men, and people with diabetes, hypertension, or obesity had the worst outcomes and were most likely to die from COVID-19.
For David Malebranche, MD, MPH, an internal medicine doctor who provides primary care for people in Atlanta, and who was not involved in the study, the WHO study didn’t add anything new. He already recommends the COVID-19 vaccine for all of his patients, HIV-positive or not.
“We don’t have any information from this about the T-cell counts [or] the rates of viral suppression, which I think is tremendously important,” he told this news organization. “To bypass that and not include that in any of the discussion puts the results in a questionable place for me.”
The results come from the WHO Clinical Platform, which culls data from WHO member country surveillance as well as manual case reports from all over the world. By April 29, data on 268,412 people hospitalized with COVID-19 from 37 countries were reported to the platform. Of those, 22,640 people are from the U.S.
A total of 15,522 participants worldwide were living with HIV, 664 in the United States. All U.S. cases were reported from the New York City Health and Hospitals system, Henry Ford Hospital in Detroit, and BronxCare Health System in New York City. Almost all of the remaining participants lived in South Africa – 14,682 of the 15,522, or 94.5%.
Of the 15,522 people living with HIV in the overall group, 37.1% of participants were male, and their median age was 45 years. More than 1 in 3 (36.2%) were admitted with severe or critical COVID-19, and nearly one quarter – 23.1% – with a known outcome died. More than half had one or more chronic conditions, including those that themselves are associated with worse COVID-19 outcomes, such as hypertension (in 33.2% of the participants), diabetes (22.7%), and BMIs above 30 (16.9%). In addition, 8.9% were smokers, 6.6% had chronic pulmonary disease, and 4.3% had chronic heart disease.
After adjusting for those chronic conditions, age, and sex, people living with HIV had a 6% higher rate of severe or critical COVID-19 illness. When investigators adjusted the analysis additionally to differentiate outcomes based on not just the presence of comorbid conditions but the number of them a person had, that increased risk rose to 13%. HIV itself is a comorbid condition, though it wasn’t counted as one in this adjusted analysis.
It didn’t matter whether researchers looked at risk for severe outcomes or deaths after removing the significant co-occurring conditions or if they looked at number of chronic illnesses (aside from HIV), said Silvia Bertagnolio, MD, medical officer at the World Health Organization and co-author of the analysis.
“Both models show almost identical [adjusted odds ratios], meaning that HIV was independently significantly associated with severe/critical presentation,” she told this news organization.
As for death, the analysis showed that, overall, people living with HIV were 30% more likely to die of COVID-19 compared with those not living with HIV. And while this held true even when they adjusted the data for comorbidities, people with HIV were more likely to die if they were over age 65 (risk increased by 82%), male (risk increased by 21%), had diabetes (risk increased by 50%), or had hypertension (risk increased by 26%).
When they broke down the data by WHO region – Africa, Europe, the Americas – investigators found that the increased risk for death held true in Africa. But there were not enough data from the other regions to model mortality risk. What’s more, when they broke the data down by country and excluded South Africa, they found that the elevated risk for death in people living with HIV did not reach statistical significance. Dr. Bertagnolio said she suspects that the small sample sizes from other regions made it impossible to detect a difference, but one could still be present.
One thing conspicuously absent from the analysis was information on viral load, CD4 T-cell count, progression of HIV to AIDS, and whether individuals were in HIV care. The first three factors were not reported in the platform, and the fourth was available for 60% of participants but was not included in the analysis. Dr. Bertagnolio pointed out that, for those 60% of participants, 91.8% were on antiretroviral treatment (ART).
“The majority of patients come from South Africa, and we know that in South Africa, over 90% of people receiving ART are virologically suppressed,” she told this news organization. “So we could speculate that this effect persists despite the use of ART, in a population likely to be virally suppressed, although we cannot assess this with certainty through the data set we had.”
A much smaller study of 749 people living with HIV and diagnosed with SARS-CoV-2, also presented at the conference, found that detectable HIV viral load was significantly associated with a slightly higher risk of severe outcomes (P < .039), but CD4 counts less than 200 cells/mm3 was not (P = .15).
And although both Dr. Bertagnolio and conference organizers presented this data as proof that HIV increases the risk for poor COVID-19 outcomes, Dr. Malebranche isn’t so sure. He estimates that only about half his patients have received the COVID-19 vaccine. But this study is unlikely to make him forcefully recommend a COVID-19 vaccination with young, otherwise healthy, and undetectable people in his care who express particular concern about long-term effects of the vaccine. He also manages a lot of people with HIV who have undetectable viral loads and CD4 counts of up to 1,200 but are older, with diabetes, obesity, and high blood pressure. Those are the people he will target with stronger messages regarding the vaccine.
“The young patients who are healthy, virally suppressed, and doing well may very much argue with me, ‘I’m not going to push it,’ but I will bring it up on the next visit,” he said. The analysis “just helps reinforce in me that I need to have these conversations and be a little bit more persuasive to my older patients with comorbid conditions.”
Dr. Bertagnolio has disclosed no relevant financial relationships. Dr. Malebranche serves on the pre-exposure prophylaxis (PrEP) speakers bureau for Gilead Sciences and has consulted and advised for ViiV Healthcare. This study was funded by the World Health Organization.
A version of this article first appeared on Medscape.com.
according to a report from the World Health Organization on COVID-19 outcomes among people living with HIV. The study primarily included people from South Africa but also some data from other parts of the world, including the United States.
However, the report, presented at the 11th IAS Conference on HIV Science (IAS 2021), couldn’t answer some crucial questions clinicians have been wondering about since the COVID-19 pandemic began. For example, was the increase in COVID risk a result of the presence of HIV or because of the immune compromise caused by untreated HIV?
The report didn’t include data on viral load or CD counts, both used to evaluate the health of a person’s immune system. On effective treatment, people living with HIV have a lifespan close to their HIV-negative peers. And effective treatment causes undetectable viral loads which, when maintained for 6 months or more, eliminates transmission of HIV to sexual partners.
What’s clear is that in people with HIV, as in people without HIV, older people, men, and people with diabetes, hypertension, or obesity had the worst outcomes and were most likely to die from COVID-19.
For David Malebranche, MD, MPH, an internal medicine doctor who provides primary care for people in Atlanta, and who was not involved in the study, the WHO study didn’t add anything new. He already recommends the COVID-19 vaccine for all of his patients, HIV-positive or not.
“We don’t have any information from this about the T-cell counts [or] the rates of viral suppression, which I think is tremendously important,” he told this news organization. “To bypass that and not include that in any of the discussion puts the results in a questionable place for me.”
The results come from the WHO Clinical Platform, which culls data from WHO member country surveillance as well as manual case reports from all over the world. By April 29, data on 268,412 people hospitalized with COVID-19 from 37 countries were reported to the platform. Of those, 22,640 people are from the U.S.
A total of 15,522 participants worldwide were living with HIV, 664 in the United States. All U.S. cases were reported from the New York City Health and Hospitals system, Henry Ford Hospital in Detroit, and BronxCare Health System in New York City. Almost all of the remaining participants lived in South Africa – 14,682 of the 15,522, or 94.5%.
Of the 15,522 people living with HIV in the overall group, 37.1% of participants were male, and their median age was 45 years. More than 1 in 3 (36.2%) were admitted with severe or critical COVID-19, and nearly one quarter – 23.1% – with a known outcome died. More than half had one or more chronic conditions, including those that themselves are associated with worse COVID-19 outcomes, such as hypertension (in 33.2% of the participants), diabetes (22.7%), and BMIs above 30 (16.9%). In addition, 8.9% were smokers, 6.6% had chronic pulmonary disease, and 4.3% had chronic heart disease.
After adjusting for those chronic conditions, age, and sex, people living with HIV had a 6% higher rate of severe or critical COVID-19 illness. When investigators adjusted the analysis additionally to differentiate outcomes based on not just the presence of comorbid conditions but the number of them a person had, that increased risk rose to 13%. HIV itself is a comorbid condition, though it wasn’t counted as one in this adjusted analysis.
It didn’t matter whether researchers looked at risk for severe outcomes or deaths after removing the significant co-occurring conditions or if they looked at number of chronic illnesses (aside from HIV), said Silvia Bertagnolio, MD, medical officer at the World Health Organization and co-author of the analysis.
“Both models show almost identical [adjusted odds ratios], meaning that HIV was independently significantly associated with severe/critical presentation,” she told this news organization.
As for death, the analysis showed that, overall, people living with HIV were 30% more likely to die of COVID-19 compared with those not living with HIV. And while this held true even when they adjusted the data for comorbidities, people with HIV were more likely to die if they were over age 65 (risk increased by 82%), male (risk increased by 21%), had diabetes (risk increased by 50%), or had hypertension (risk increased by 26%).
When they broke down the data by WHO region – Africa, Europe, the Americas – investigators found that the increased risk for death held true in Africa. But there were not enough data from the other regions to model mortality risk. What’s more, when they broke the data down by country and excluded South Africa, they found that the elevated risk for death in people living with HIV did not reach statistical significance. Dr. Bertagnolio said she suspects that the small sample sizes from other regions made it impossible to detect a difference, but one could still be present.
One thing conspicuously absent from the analysis was information on viral load, CD4 T-cell count, progression of HIV to AIDS, and whether individuals were in HIV care. The first three factors were not reported in the platform, and the fourth was available for 60% of participants but was not included in the analysis. Dr. Bertagnolio pointed out that, for those 60% of participants, 91.8% were on antiretroviral treatment (ART).
“The majority of patients come from South Africa, and we know that in South Africa, over 90% of people receiving ART are virologically suppressed,” she told this news organization. “So we could speculate that this effect persists despite the use of ART, in a population likely to be virally suppressed, although we cannot assess this with certainty through the data set we had.”
A much smaller study of 749 people living with HIV and diagnosed with SARS-CoV-2, also presented at the conference, found that detectable HIV viral load was significantly associated with a slightly higher risk of severe outcomes (P < .039), but CD4 counts less than 200 cells/mm3 was not (P = .15).
And although both Dr. Bertagnolio and conference organizers presented this data as proof that HIV increases the risk for poor COVID-19 outcomes, Dr. Malebranche isn’t so sure. He estimates that only about half his patients have received the COVID-19 vaccine. But this study is unlikely to make him forcefully recommend a COVID-19 vaccination with young, otherwise healthy, and undetectable people in his care who express particular concern about long-term effects of the vaccine. He also manages a lot of people with HIV who have undetectable viral loads and CD4 counts of up to 1,200 but are older, with diabetes, obesity, and high blood pressure. Those are the people he will target with stronger messages regarding the vaccine.
“The young patients who are healthy, virally suppressed, and doing well may very much argue with me, ‘I’m not going to push it,’ but I will bring it up on the next visit,” he said. The analysis “just helps reinforce in me that I need to have these conversations and be a little bit more persuasive to my older patients with comorbid conditions.”
Dr. Bertagnolio has disclosed no relevant financial relationships. Dr. Malebranche serves on the pre-exposure prophylaxis (PrEP) speakers bureau for Gilead Sciences and has consulted and advised for ViiV Healthcare. This study was funded by the World Health Organization.
A version of this article first appeared on Medscape.com.
according to a report from the World Health Organization on COVID-19 outcomes among people living with HIV. The study primarily included people from South Africa but also some data from other parts of the world, including the United States.
However, the report, presented at the 11th IAS Conference on HIV Science (IAS 2021), couldn’t answer some crucial questions clinicians have been wondering about since the COVID-19 pandemic began. For example, was the increase in COVID risk a result of the presence of HIV or because of the immune compromise caused by untreated HIV?
The report didn’t include data on viral load or CD counts, both used to evaluate the health of a person’s immune system. On effective treatment, people living with HIV have a lifespan close to their HIV-negative peers. And effective treatment causes undetectable viral loads which, when maintained for 6 months or more, eliminates transmission of HIV to sexual partners.
What’s clear is that in people with HIV, as in people without HIV, older people, men, and people with diabetes, hypertension, or obesity had the worst outcomes and were most likely to die from COVID-19.
For David Malebranche, MD, MPH, an internal medicine doctor who provides primary care for people in Atlanta, and who was not involved in the study, the WHO study didn’t add anything new. He already recommends the COVID-19 vaccine for all of his patients, HIV-positive or not.
“We don’t have any information from this about the T-cell counts [or] the rates of viral suppression, which I think is tremendously important,” he told this news organization. “To bypass that and not include that in any of the discussion puts the results in a questionable place for me.”
The results come from the WHO Clinical Platform, which culls data from WHO member country surveillance as well as manual case reports from all over the world. By April 29, data on 268,412 people hospitalized with COVID-19 from 37 countries were reported to the platform. Of those, 22,640 people are from the U.S.
A total of 15,522 participants worldwide were living with HIV, 664 in the United States. All U.S. cases were reported from the New York City Health and Hospitals system, Henry Ford Hospital in Detroit, and BronxCare Health System in New York City. Almost all of the remaining participants lived in South Africa – 14,682 of the 15,522, or 94.5%.
Of the 15,522 people living with HIV in the overall group, 37.1% of participants were male, and their median age was 45 years. More than 1 in 3 (36.2%) were admitted with severe or critical COVID-19, and nearly one quarter – 23.1% – with a known outcome died. More than half had one or more chronic conditions, including those that themselves are associated with worse COVID-19 outcomes, such as hypertension (in 33.2% of the participants), diabetes (22.7%), and BMIs above 30 (16.9%). In addition, 8.9% were smokers, 6.6% had chronic pulmonary disease, and 4.3% had chronic heart disease.
After adjusting for those chronic conditions, age, and sex, people living with HIV had a 6% higher rate of severe or critical COVID-19 illness. When investigators adjusted the analysis additionally to differentiate outcomes based on not just the presence of comorbid conditions but the number of them a person had, that increased risk rose to 13%. HIV itself is a comorbid condition, though it wasn’t counted as one in this adjusted analysis.
It didn’t matter whether researchers looked at risk for severe outcomes or deaths after removing the significant co-occurring conditions or if they looked at number of chronic illnesses (aside from HIV), said Silvia Bertagnolio, MD, medical officer at the World Health Organization and co-author of the analysis.
“Both models show almost identical [adjusted odds ratios], meaning that HIV was independently significantly associated with severe/critical presentation,” she told this news organization.
As for death, the analysis showed that, overall, people living with HIV were 30% more likely to die of COVID-19 compared with those not living with HIV. And while this held true even when they adjusted the data for comorbidities, people with HIV were more likely to die if they were over age 65 (risk increased by 82%), male (risk increased by 21%), had diabetes (risk increased by 50%), or had hypertension (risk increased by 26%).
When they broke down the data by WHO region – Africa, Europe, the Americas – investigators found that the increased risk for death held true in Africa. But there were not enough data from the other regions to model mortality risk. What’s more, when they broke the data down by country and excluded South Africa, they found that the elevated risk for death in people living with HIV did not reach statistical significance. Dr. Bertagnolio said she suspects that the small sample sizes from other regions made it impossible to detect a difference, but one could still be present.
One thing conspicuously absent from the analysis was information on viral load, CD4 T-cell count, progression of HIV to AIDS, and whether individuals were in HIV care. The first three factors were not reported in the platform, and the fourth was available for 60% of participants but was not included in the analysis. Dr. Bertagnolio pointed out that, for those 60% of participants, 91.8% were on antiretroviral treatment (ART).
“The majority of patients come from South Africa, and we know that in South Africa, over 90% of people receiving ART are virologically suppressed,” she told this news organization. “So we could speculate that this effect persists despite the use of ART, in a population likely to be virally suppressed, although we cannot assess this with certainty through the data set we had.”
A much smaller study of 749 people living with HIV and diagnosed with SARS-CoV-2, also presented at the conference, found that detectable HIV viral load was significantly associated with a slightly higher risk of severe outcomes (P < .039), but CD4 counts less than 200 cells/mm3 was not (P = .15).
And although both Dr. Bertagnolio and conference organizers presented this data as proof that HIV increases the risk for poor COVID-19 outcomes, Dr. Malebranche isn’t so sure. He estimates that only about half his patients have received the COVID-19 vaccine. But this study is unlikely to make him forcefully recommend a COVID-19 vaccination with young, otherwise healthy, and undetectable people in his care who express particular concern about long-term effects of the vaccine. He also manages a lot of people with HIV who have undetectable viral loads and CD4 counts of up to 1,200 but are older, with diabetes, obesity, and high blood pressure. Those are the people he will target with stronger messages regarding the vaccine.
“The young patients who are healthy, virally suppressed, and doing well may very much argue with me, ‘I’m not going to push it,’ but I will bring it up on the next visit,” he said. The analysis “just helps reinforce in me that I need to have these conversations and be a little bit more persuasive to my older patients with comorbid conditions.”
Dr. Bertagnolio has disclosed no relevant financial relationships. Dr. Malebranche serves on the pre-exposure prophylaxis (PrEP) speakers bureau for Gilead Sciences and has consulted and advised for ViiV Healthcare. This study was funded by the World Health Organization.
A version of this article first appeared on Medscape.com.
Long COVID seen in patients with severe and mild disease
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.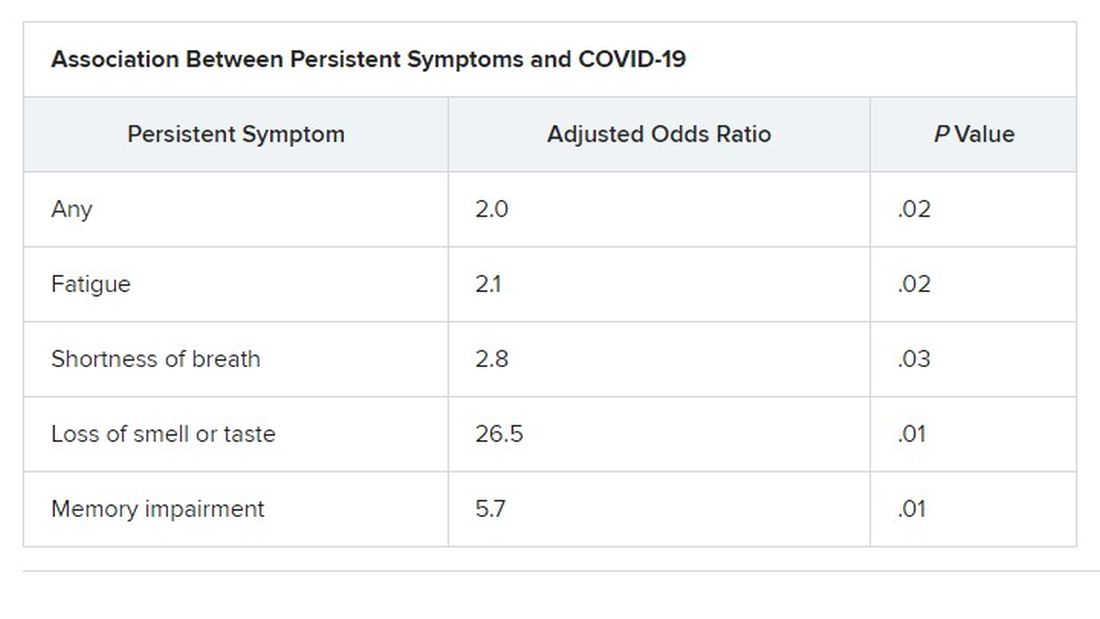
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN CONGRESS OF CLINICAL MICROBIOLOGY & INFECTIOUS DISEASES
Resistant TB: Adjustments to BPaL regimen reduce AEs, not efficacy
Lower doses of linezolid in the BPaL drug regimen (bedaquiline, pretomanid, and linezolid) significantly reduce the adverse events associated with the treatment for patients with highly drug-resistant tuberculosis (TB) without compromising its high efficacy, new research shows.
“The ZeNix trial shows that reduced doses and/or shorter durations of linezolid appear to have high efficacy and improved safety,” said first author Francesca Conradie, MB, BCh, of the clinical HIV research unit, faculty of health sciences, University of Witwatersrand, Johannesburg, South Africa, in presenting the findings at the virtual meeting of the International AIDS Society conference.
As recently reported in the pivotal Nix-TB trial, the BPaL regimen yielded a 90% treatment success rate among people with highly drug-resistant forms of TB.
However, a 6-month regimen that included linezolid 1,200 mg resulted in toxic effects: 81% of patients in the study experienced peripheral neuropathy, and myelosuppression occurred in 48%. These effects often led to dose reductions or treatment interruption.
Adjustments in the dose of linezolid in the new ZeNix trial substantially reduced peripheral neuropathy to 13% and myelosuppression to 7%, with no significant reduction in the treatment response.
Importantly, the results were similar among patients with and those without HIV. This is of note because TB is the leading cause of death among patients with HIV.
“In the ZeNix trial, only 20% of patients were HIV infected, but in the [previous] Nix-TB trial, 30% were infected, so we have experience now in about 70 patients who were infected, and the outcomes were no different,” Dr. Conradie said in an interview.
Experts say the findings represent an important turn in the steep challenge of tackling highly resistant TB.
“In our opinion, these are exciting results that could change treatment guidelines for highly drug-resistant tuberculosis, with real benefits for the patients,” said Hendrik Streeck, MD, International AIDS Society cochair and director of the Institute of Virology and the Institute for HIV Research at the University Bonn (Germany), in a press conference.
Payam Nahid, MD, MPH, director of the Center for Tuberculosis at theUniversity of California, San Francisco, agreed.
“The results of this trial will impact global practices in treating drug-resistant TB as well as the design and conduct of future TB clinical trials,” Dr. Nahid said in an interview.
ZeNix trial
The phase 3 ZeNix trial included 181 patients with highly resistant TB in South Africa, Russia, Georgia, and Moldova. The mean age of the patients was 37 years; 67.4% were men, 63.5% were White, and 19.9% were HIV positive.
All patients were treated for 6 months with bedaquiline 200 mg daily for 8 weeks followed by 100 mg daily for 18 weeks, as well as pretomanid 200 mg daily.
The patients were randomly assigned to receive one of four daily doses of linezolid: 1,200 mg for 6 months (the original dose from the Nix-TB trial; n = 45) or 2 months (n = 46), or 600 mg for 6 or 2 months (45 patients each).
Percentages of patients with HIV were equal among the four groups, at about 20% each.
The primary outcomes – resolution of clinical disease and a negative culture status after 6 months – were observed across all linezolid dose groups. The success rate was 93% for those receiving 1,200 mg for 6 months, 89% for those receiving 1,200 mg for 2 months, 91% for those receiving 600 mg for 6 months, and 84% for those receiving 600 mg for 2 months.
With regard to the key adverse events of peripheral neuropathy and myelosuppression, manifested as anemia, the highest rates were among those who received linezolid 1,200 mg for 6 month, at 38% and 22%, respectively, compared with 24% and 17.4% among those who received 1,200 mg for 2 months, 24% and 2% among those who received 600 mg for 6 months, and 13% and 6.7% among those who received 600 mg for 2 months.
Four cases of optic neuropathy occurred among those who received 1,200 mg for 6 months; all cases resolved.
Patients who received 1,200 mg for 6 months required the highest number of linezolid dose modifications; 51% required changes that included reduction, interruption, or discontinuation, compared with 28% among those who received 1,200 mg for 2 months and 13% each in the other two groups.
On the basis of these results, “my personal opinion is that 600 mg at 6 months [of linezolid] is most likely the best strategy for the treatment of this highly resistant treatment population group,” Dr. Conradie told this news organization.
Findings represent ‘great news’ in addressing concerns
Dr. Nahid further commented that the results are highly encouraging in light of the ongoing concerns about the effects of linezolid in the BPaL regimen.
“This is great news,” he said. “The ZeNix trial addresses a key concern that providers and patients have had regarding the safety and tolerability of taking 6 months of linezolid at 1200 mg/d as part of the BPaL regimen.
“The findings that doses lower and durations shorter than the current 1,200 mg linezolid daily for 6 months will significantly expand the usability of the BPaL regimen worldwide.”
The inclusion of patients with HIV was essential in the trial, he noted.
“There are drug-drug interactions to be considered, among other factors that impact drug exposure,” Dr. Nahid said.
“Inclusion of patients living with HIV in this study means that any modifications to the BPaL regimen considered by the WHO [World Health Organization] and other policy decision makers will include data from this key population,” he said. “Of course, more data are needed on safety, tolerability, and efficacy on BPaL in general, and there are international cohorts and demonstration projects underway that will enhance our understanding of the regimen in HIV and in other special populations.”
The authors, Dr. Streeck, and Dr. Nahid have disclosed no relevant financial relationships.
This article was updated 7/21/21.
Lower doses of linezolid in the BPaL drug regimen (bedaquiline, pretomanid, and linezolid) significantly reduce the adverse events associated with the treatment for patients with highly drug-resistant tuberculosis (TB) without compromising its high efficacy, new research shows.
“The ZeNix trial shows that reduced doses and/or shorter durations of linezolid appear to have high efficacy and improved safety,” said first author Francesca Conradie, MB, BCh, of the clinical HIV research unit, faculty of health sciences, University of Witwatersrand, Johannesburg, South Africa, in presenting the findings at the virtual meeting of the International AIDS Society conference.
As recently reported in the pivotal Nix-TB trial, the BPaL regimen yielded a 90% treatment success rate among people with highly drug-resistant forms of TB.
However, a 6-month regimen that included linezolid 1,200 mg resulted in toxic effects: 81% of patients in the study experienced peripheral neuropathy, and myelosuppression occurred in 48%. These effects often led to dose reductions or treatment interruption.
Adjustments in the dose of linezolid in the new ZeNix trial substantially reduced peripheral neuropathy to 13% and myelosuppression to 7%, with no significant reduction in the treatment response.
Importantly, the results were similar among patients with and those without HIV. This is of note because TB is the leading cause of death among patients with HIV.
“In the ZeNix trial, only 20% of patients were HIV infected, but in the [previous] Nix-TB trial, 30% were infected, so we have experience now in about 70 patients who were infected, and the outcomes were no different,” Dr. Conradie said in an interview.
Experts say the findings represent an important turn in the steep challenge of tackling highly resistant TB.
“In our opinion, these are exciting results that could change treatment guidelines for highly drug-resistant tuberculosis, with real benefits for the patients,” said Hendrik Streeck, MD, International AIDS Society cochair and director of the Institute of Virology and the Institute for HIV Research at the University Bonn (Germany), in a press conference.
Payam Nahid, MD, MPH, director of the Center for Tuberculosis at theUniversity of California, San Francisco, agreed.
“The results of this trial will impact global practices in treating drug-resistant TB as well as the design and conduct of future TB clinical trials,” Dr. Nahid said in an interview.
ZeNix trial
The phase 3 ZeNix trial included 181 patients with highly resistant TB in South Africa, Russia, Georgia, and Moldova. The mean age of the patients was 37 years; 67.4% were men, 63.5% were White, and 19.9% were HIV positive.
All patients were treated for 6 months with bedaquiline 200 mg daily for 8 weeks followed by 100 mg daily for 18 weeks, as well as pretomanid 200 mg daily.
The patients were randomly assigned to receive one of four daily doses of linezolid: 1,200 mg for 6 months (the original dose from the Nix-TB trial; n = 45) or 2 months (n = 46), or 600 mg for 6 or 2 months (45 patients each).
Percentages of patients with HIV were equal among the four groups, at about 20% each.
The primary outcomes – resolution of clinical disease and a negative culture status after 6 months – were observed across all linezolid dose groups. The success rate was 93% for those receiving 1,200 mg for 6 months, 89% for those receiving 1,200 mg for 2 months, 91% for those receiving 600 mg for 6 months, and 84% for those receiving 600 mg for 2 months.
With regard to the key adverse events of peripheral neuropathy and myelosuppression, manifested as anemia, the highest rates were among those who received linezolid 1,200 mg for 6 month, at 38% and 22%, respectively, compared with 24% and 17.4% among those who received 1,200 mg for 2 months, 24% and 2% among those who received 600 mg for 6 months, and 13% and 6.7% among those who received 600 mg for 2 months.
Four cases of optic neuropathy occurred among those who received 1,200 mg for 6 months; all cases resolved.
Patients who received 1,200 mg for 6 months required the highest number of linezolid dose modifications; 51% required changes that included reduction, interruption, or discontinuation, compared with 28% among those who received 1,200 mg for 2 months and 13% each in the other two groups.
On the basis of these results, “my personal opinion is that 600 mg at 6 months [of linezolid] is most likely the best strategy for the treatment of this highly resistant treatment population group,” Dr. Conradie told this news organization.
Findings represent ‘great news’ in addressing concerns
Dr. Nahid further commented that the results are highly encouraging in light of the ongoing concerns about the effects of linezolid in the BPaL regimen.
“This is great news,” he said. “The ZeNix trial addresses a key concern that providers and patients have had regarding the safety and tolerability of taking 6 months of linezolid at 1200 mg/d as part of the BPaL regimen.
“The findings that doses lower and durations shorter than the current 1,200 mg linezolid daily for 6 months will significantly expand the usability of the BPaL regimen worldwide.”
The inclusion of patients with HIV was essential in the trial, he noted.
“There are drug-drug interactions to be considered, among other factors that impact drug exposure,” Dr. Nahid said.
“Inclusion of patients living with HIV in this study means that any modifications to the BPaL regimen considered by the WHO [World Health Organization] and other policy decision makers will include data from this key population,” he said. “Of course, more data are needed on safety, tolerability, and efficacy on BPaL in general, and there are international cohorts and demonstration projects underway that will enhance our understanding of the regimen in HIV and in other special populations.”
The authors, Dr. Streeck, and Dr. Nahid have disclosed no relevant financial relationships.
This article was updated 7/21/21.
Lower doses of linezolid in the BPaL drug regimen (bedaquiline, pretomanid, and linezolid) significantly reduce the adverse events associated with the treatment for patients with highly drug-resistant tuberculosis (TB) without compromising its high efficacy, new research shows.
“The ZeNix trial shows that reduced doses and/or shorter durations of linezolid appear to have high efficacy and improved safety,” said first author Francesca Conradie, MB, BCh, of the clinical HIV research unit, faculty of health sciences, University of Witwatersrand, Johannesburg, South Africa, in presenting the findings at the virtual meeting of the International AIDS Society conference.
As recently reported in the pivotal Nix-TB trial, the BPaL regimen yielded a 90% treatment success rate among people with highly drug-resistant forms of TB.
However, a 6-month regimen that included linezolid 1,200 mg resulted in toxic effects: 81% of patients in the study experienced peripheral neuropathy, and myelosuppression occurred in 48%. These effects often led to dose reductions or treatment interruption.
Adjustments in the dose of linezolid in the new ZeNix trial substantially reduced peripheral neuropathy to 13% and myelosuppression to 7%, with no significant reduction in the treatment response.
Importantly, the results were similar among patients with and those without HIV. This is of note because TB is the leading cause of death among patients with HIV.
“In the ZeNix trial, only 20% of patients were HIV infected, but in the [previous] Nix-TB trial, 30% were infected, so we have experience now in about 70 patients who were infected, and the outcomes were no different,” Dr. Conradie said in an interview.
Experts say the findings represent an important turn in the steep challenge of tackling highly resistant TB.
“In our opinion, these are exciting results that could change treatment guidelines for highly drug-resistant tuberculosis, with real benefits for the patients,” said Hendrik Streeck, MD, International AIDS Society cochair and director of the Institute of Virology and the Institute for HIV Research at the University Bonn (Germany), in a press conference.
Payam Nahid, MD, MPH, director of the Center for Tuberculosis at theUniversity of California, San Francisco, agreed.
“The results of this trial will impact global practices in treating drug-resistant TB as well as the design and conduct of future TB clinical trials,” Dr. Nahid said in an interview.
ZeNix trial
The phase 3 ZeNix trial included 181 patients with highly resistant TB in South Africa, Russia, Georgia, and Moldova. The mean age of the patients was 37 years; 67.4% were men, 63.5% were White, and 19.9% were HIV positive.
All patients were treated for 6 months with bedaquiline 200 mg daily for 8 weeks followed by 100 mg daily for 18 weeks, as well as pretomanid 200 mg daily.
The patients were randomly assigned to receive one of four daily doses of linezolid: 1,200 mg for 6 months (the original dose from the Nix-TB trial; n = 45) or 2 months (n = 46), or 600 mg for 6 or 2 months (45 patients each).
Percentages of patients with HIV were equal among the four groups, at about 20% each.
The primary outcomes – resolution of clinical disease and a negative culture status after 6 months – were observed across all linezolid dose groups. The success rate was 93% for those receiving 1,200 mg for 6 months, 89% for those receiving 1,200 mg for 2 months, 91% for those receiving 600 mg for 6 months, and 84% for those receiving 600 mg for 2 months.
With regard to the key adverse events of peripheral neuropathy and myelosuppression, manifested as anemia, the highest rates were among those who received linezolid 1,200 mg for 6 month, at 38% and 22%, respectively, compared with 24% and 17.4% among those who received 1,200 mg for 2 months, 24% and 2% among those who received 600 mg for 6 months, and 13% and 6.7% among those who received 600 mg for 2 months.
Four cases of optic neuropathy occurred among those who received 1,200 mg for 6 months; all cases resolved.
Patients who received 1,200 mg for 6 months required the highest number of linezolid dose modifications; 51% required changes that included reduction, interruption, or discontinuation, compared with 28% among those who received 1,200 mg for 2 months and 13% each in the other two groups.
On the basis of these results, “my personal opinion is that 600 mg at 6 months [of linezolid] is most likely the best strategy for the treatment of this highly resistant treatment population group,” Dr. Conradie told this news organization.
Findings represent ‘great news’ in addressing concerns
Dr. Nahid further commented that the results are highly encouraging in light of the ongoing concerns about the effects of linezolid in the BPaL regimen.
“This is great news,” he said. “The ZeNix trial addresses a key concern that providers and patients have had regarding the safety and tolerability of taking 6 months of linezolid at 1200 mg/d as part of the BPaL regimen.
“The findings that doses lower and durations shorter than the current 1,200 mg linezolid daily for 6 months will significantly expand the usability of the BPaL regimen worldwide.”
The inclusion of patients with HIV was essential in the trial, he noted.
“There are drug-drug interactions to be considered, among other factors that impact drug exposure,” Dr. Nahid said.
“Inclusion of patients living with HIV in this study means that any modifications to the BPaL regimen considered by the WHO [World Health Organization] and other policy decision makers will include data from this key population,” he said. “Of course, more data are needed on safety, tolerability, and efficacy on BPaL in general, and there are international cohorts and demonstration projects underway that will enhance our understanding of the regimen in HIV and in other special populations.”
The authors, Dr. Streeck, and Dr. Nahid have disclosed no relevant financial relationships.
This article was updated 7/21/21.
FROM IAS 2021
Targeted outreach increases Black COVID-19 vaccination rates
Thoughtful, targeted approaches are needed to increase COVID-19 vaccination rates in Black and Latinx communities, which often distrust the health care system and face barriers to vaccine access, new data show.
“Black, Latinx, and Native American individuals represent about a combined 60% of COVID-19 deaths, despite comprising significantly less of the United States population,” said Jacinda C. Abdul-Mutakabbir, PharmD, from Loma Linda (Calif.) University.
“To put this into perspective, Black individuals represent 13.4% of the United States population, while Native Americans represent 1.6%, clearly showing the disproportionate outcomes here,” she explained during her online presentation at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
The vaccine creates an opportunity to change the disproportionate way COVID-19 has affected racial and ethnic communities, said Dr. Abdul-Mutakabbir, but “a long history of mistreatment within the U.S. health care system decreases their trust for the system to use fair practices when delivering these vaccines.”
For people in minority communities, often “the fear of cost associated with health care keeps them from being vaccinated,” she said. “Also, there is a lack of vaccines actually allocated to these communities, or inconsistent computer-based sign-ups that make WiFi mandatory, which in turn has created additional barriers for vaccination access.”
Loma Linda University maintains the largest mass-vaccination site in San Bernardino County, the fourth-largest county in southern California. However, only 3.0% of the people vaccinated there have been Black. And although 8% of the state’s population is Black, only 2.7% of the Black population has been vaccinated.
In contrast, Black Californians have accounted for about 20% of COVID-19 cases in the state, and 20%-30% of COVID-19 deaths.
To promote equitable access to COVID-19 vaccines, Dr. Abdul-Mutakabbir and colleagues developed a “three-tiered approach.” First, they had local Black faith leaders hold summits ahead of the vaccination clinics. Next, at those summits, they had a Black pharmacist educate attendees about the vaccines. And finally, they held a low-barrier community vaccination clinic in a Black community, where the pharmacist oversaw the transport and preparation of the vaccines.
Because access, transportation, and internet are all barriers to vaccination, the clinic used paper-based registration and was held as a pop-up clinic at a local Black church. The team held two clinics for the first Moderna dose, one clinic for the second Moderna dose, and one clinic for the Johnson & Johnson one-dose vaccine.
During the Moderna first-dose clinics, 673 vaccinations were administered, and during the second-dose clinic, 366 were administered. Early data showed a return rate of 87%, but the team has yet to update the final numbers, Dr. Abdul-Mutakabbir reported. During the Johnson & Johnson clinic, 314 vaccinations were administered, nearly half to Black people. After the community vaccination clinics, the mass vaccination site saw a 0.6% increase in vaccinations for Black people.
Dr. Abdul-Mutakabbir’s team also held three community clinics in Latinx communities. During the first-dose Moderna pop-up clinic, 258 vaccinations were administered, and during the second-dose clinic, 253 were, for a 98% return rate. Approximately 92% of those vaccinated were Latinx.
The study findings are not surprising, said Rhea Boyd, MD, director of equity and justice for California Children’s Trust.
“The barriers to vaccination are known and clear,” she said in an interview. “Mobile clinics with paper appointments address a number of those barriers head on, like transportation, internet access, and accessibility. Having Black providers leading the effort and church leaders involved also has been shown to increase confidence in the operations and process.”
Information campaigns can help counter online disinformation. Ultimately, however, “the main barrier to vaccination is access,” Dr. Boyd said. “Address access and rates will increase.”
The health inequities seen in vaccination rates among Black and Latinx people “are a product of structural and systemic racism,” Dr. Abdul-Mutakabbir said. “To create equitable processes, it is essential that we evaluate how we approach each of these different minoritized groups.”
Dr. Abdul-Mutakabbir disclosed no relevant financial relationships. Dr. Boyd codeveloped THE CONVERSATION, a national campaign to bring credible information about the COVID vaccines to Black and Latinx communities in partnership with KFF, BCAC, and Unidos US.
A version of this article first appeared on Medscape.com.
Thoughtful, targeted approaches are needed to increase COVID-19 vaccination rates in Black and Latinx communities, which often distrust the health care system and face barriers to vaccine access, new data show.
“Black, Latinx, and Native American individuals represent about a combined 60% of COVID-19 deaths, despite comprising significantly less of the United States population,” said Jacinda C. Abdul-Mutakabbir, PharmD, from Loma Linda (Calif.) University.
“To put this into perspective, Black individuals represent 13.4% of the United States population, while Native Americans represent 1.6%, clearly showing the disproportionate outcomes here,” she explained during her online presentation at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
The vaccine creates an opportunity to change the disproportionate way COVID-19 has affected racial and ethnic communities, said Dr. Abdul-Mutakabbir, but “a long history of mistreatment within the U.S. health care system decreases their trust for the system to use fair practices when delivering these vaccines.”
For people in minority communities, often “the fear of cost associated with health care keeps them from being vaccinated,” she said. “Also, there is a lack of vaccines actually allocated to these communities, or inconsistent computer-based sign-ups that make WiFi mandatory, which in turn has created additional barriers for vaccination access.”
Loma Linda University maintains the largest mass-vaccination site in San Bernardino County, the fourth-largest county in southern California. However, only 3.0% of the people vaccinated there have been Black. And although 8% of the state’s population is Black, only 2.7% of the Black population has been vaccinated.
In contrast, Black Californians have accounted for about 20% of COVID-19 cases in the state, and 20%-30% of COVID-19 deaths.
To promote equitable access to COVID-19 vaccines, Dr. Abdul-Mutakabbir and colleagues developed a “three-tiered approach.” First, they had local Black faith leaders hold summits ahead of the vaccination clinics. Next, at those summits, they had a Black pharmacist educate attendees about the vaccines. And finally, they held a low-barrier community vaccination clinic in a Black community, where the pharmacist oversaw the transport and preparation of the vaccines.
Because access, transportation, and internet are all barriers to vaccination, the clinic used paper-based registration and was held as a pop-up clinic at a local Black church. The team held two clinics for the first Moderna dose, one clinic for the second Moderna dose, and one clinic for the Johnson & Johnson one-dose vaccine.
During the Moderna first-dose clinics, 673 vaccinations were administered, and during the second-dose clinic, 366 were administered. Early data showed a return rate of 87%, but the team has yet to update the final numbers, Dr. Abdul-Mutakabbir reported. During the Johnson & Johnson clinic, 314 vaccinations were administered, nearly half to Black people. After the community vaccination clinics, the mass vaccination site saw a 0.6% increase in vaccinations for Black people.
Dr. Abdul-Mutakabbir’s team also held three community clinics in Latinx communities. During the first-dose Moderna pop-up clinic, 258 vaccinations were administered, and during the second-dose clinic, 253 were, for a 98% return rate. Approximately 92% of those vaccinated were Latinx.
The study findings are not surprising, said Rhea Boyd, MD, director of equity and justice for California Children’s Trust.
“The barriers to vaccination are known and clear,” she said in an interview. “Mobile clinics with paper appointments address a number of those barriers head on, like transportation, internet access, and accessibility. Having Black providers leading the effort and church leaders involved also has been shown to increase confidence in the operations and process.”
Information campaigns can help counter online disinformation. Ultimately, however, “the main barrier to vaccination is access,” Dr. Boyd said. “Address access and rates will increase.”
The health inequities seen in vaccination rates among Black and Latinx people “are a product of structural and systemic racism,” Dr. Abdul-Mutakabbir said. “To create equitable processes, it is essential that we evaluate how we approach each of these different minoritized groups.”
Dr. Abdul-Mutakabbir disclosed no relevant financial relationships. Dr. Boyd codeveloped THE CONVERSATION, a national campaign to bring credible information about the COVID vaccines to Black and Latinx communities in partnership with KFF, BCAC, and Unidos US.
A version of this article first appeared on Medscape.com.
Thoughtful, targeted approaches are needed to increase COVID-19 vaccination rates in Black and Latinx communities, which often distrust the health care system and face barriers to vaccine access, new data show.
“Black, Latinx, and Native American individuals represent about a combined 60% of COVID-19 deaths, despite comprising significantly less of the United States population,” said Jacinda C. Abdul-Mutakabbir, PharmD, from Loma Linda (Calif.) University.
“To put this into perspective, Black individuals represent 13.4% of the United States population, while Native Americans represent 1.6%, clearly showing the disproportionate outcomes here,” she explained during her online presentation at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
The vaccine creates an opportunity to change the disproportionate way COVID-19 has affected racial and ethnic communities, said Dr. Abdul-Mutakabbir, but “a long history of mistreatment within the U.S. health care system decreases their trust for the system to use fair practices when delivering these vaccines.”
For people in minority communities, often “the fear of cost associated with health care keeps them from being vaccinated,” she said. “Also, there is a lack of vaccines actually allocated to these communities, or inconsistent computer-based sign-ups that make WiFi mandatory, which in turn has created additional barriers for vaccination access.”
Loma Linda University maintains the largest mass-vaccination site in San Bernardino County, the fourth-largest county in southern California. However, only 3.0% of the people vaccinated there have been Black. And although 8% of the state’s population is Black, only 2.7% of the Black population has been vaccinated.
In contrast, Black Californians have accounted for about 20% of COVID-19 cases in the state, and 20%-30% of COVID-19 deaths.
To promote equitable access to COVID-19 vaccines, Dr. Abdul-Mutakabbir and colleagues developed a “three-tiered approach.” First, they had local Black faith leaders hold summits ahead of the vaccination clinics. Next, at those summits, they had a Black pharmacist educate attendees about the vaccines. And finally, they held a low-barrier community vaccination clinic in a Black community, where the pharmacist oversaw the transport and preparation of the vaccines.
Because access, transportation, and internet are all barriers to vaccination, the clinic used paper-based registration and was held as a pop-up clinic at a local Black church. The team held two clinics for the first Moderna dose, one clinic for the second Moderna dose, and one clinic for the Johnson & Johnson one-dose vaccine.
During the Moderna first-dose clinics, 673 vaccinations were administered, and during the second-dose clinic, 366 were administered. Early data showed a return rate of 87%, but the team has yet to update the final numbers, Dr. Abdul-Mutakabbir reported. During the Johnson & Johnson clinic, 314 vaccinations were administered, nearly half to Black people. After the community vaccination clinics, the mass vaccination site saw a 0.6% increase in vaccinations for Black people.
Dr. Abdul-Mutakabbir’s team also held three community clinics in Latinx communities. During the first-dose Moderna pop-up clinic, 258 vaccinations were administered, and during the second-dose clinic, 253 were, for a 98% return rate. Approximately 92% of those vaccinated were Latinx.
The study findings are not surprising, said Rhea Boyd, MD, director of equity and justice for California Children’s Trust.
“The barriers to vaccination are known and clear,” she said in an interview. “Mobile clinics with paper appointments address a number of those barriers head on, like transportation, internet access, and accessibility. Having Black providers leading the effort and church leaders involved also has been shown to increase confidence in the operations and process.”
Information campaigns can help counter online disinformation. Ultimately, however, “the main barrier to vaccination is access,” Dr. Boyd said. “Address access and rates will increase.”
The health inequities seen in vaccination rates among Black and Latinx people “are a product of structural and systemic racism,” Dr. Abdul-Mutakabbir said. “To create equitable processes, it is essential that we evaluate how we approach each of these different minoritized groups.”
Dr. Abdul-Mutakabbir disclosed no relevant financial relationships. Dr. Boyd codeveloped THE CONVERSATION, a national campaign to bring credible information about the COVID vaccines to Black and Latinx communities in partnership with KFF, BCAC, and Unidos US.
A version of this article first appeared on Medscape.com.
Dupilumab safe, effective in kids 6-11 with moderate-to-severe asthma
Dupilumab (Dupixent, Sanofi and Regeneron) significantly reduced exacerbations compared with placebo in children ages 6-11 years who had moderate-to-severe asthma in a phase 3 trial.
A fully human monoclonal antibody, dupilumab also improved lung function versus placebo by week 12, an improvement that lasted the length of the 52-week trial.
Dupilumab previously had been shown to be safe and effective in adolescents and adults with moderate-to-severe asthma, patients 6 years and older with moderate-to-severe atopic dermatitis, and adults with chronic rhinosinusitis with nasal polyposis, but its safety and effectiveness for moderate-to-severe asthma in the 6-11 years age group was not known.
Results from the randomized, double-blind VOYAGE study conducted across several countries were presented Saturday, July 10, at the European Academy of Allergy and Clinical Immunology (EAACI) Hybrid Congress 2021.
Leonard B. Bacharier, MD, professor of pediatrics, allergy/immunology/pulmonary medicine at Vanderbilt University Medical Center in Nashville, Tennessee, presented the results from the trial, which was funded by Sanofi/Regeneron.
Researchers enrolled 408 children ages 6-11 years with uncontrolled moderate-to-severe asthma. Children on high-dose inhaled corticosteroids (ICS) alone or medium-to-high–dose ICS with a second controller were randomly assigned either to add-on subcutaneous dupilumab 100 mg or 200 mg, based on body weight at study start, or to placebo every 2 weeks for 52 weeks.
Analyses were done in two populations: 350 patients with markers of type 2 inflammation (baseline blood eosinophils ≥150 cells/μl or fractional exhaled nitric oxide [FeNO] ≥20 ppb) and 259 patients with baseline blood eosinophils ≥300 cells/µl.
“The primary endpoint was the annualized rate of severe asthma exacerbations,” Dr. Bacharier said. “The key secondary endpoint was change in percent predicted prebronchodilator FEV1 [forced expiratory volume at 1 second] from baseline to week 12.”
At week 12, the annualized severe asthma exacerbation rate was reduced by 59% (P < .0001) in children with blood eosinophils ≥300 cells/µL and results were similar in those with the type 2 inflammatory phenotype compared with placebo.
Results also indicate a favorable safety profile for dupilumab.
James M. Tracy, DO, an expert with the American College of Allergy, Asthma, and Immunology, told this news organization that adding the dupilumab option for children in the 6-11 age group is “huge.”
Dr. Tracy, who was not involved with the study, said although omalizumab (Xolair, Genentech) is also available for these children, dupilumab stands out because of the range of comorbidities it can treat.
“[Children] don’t have the same rhinosinusitis and polyposis that adults would have, but a lot of them have eczema, and this drug with multiple prongs is incredibly useful and addresses a broad array of allergic conditions,” Dr. Tracy said.
More than 90% of children in the study had at least one concurrent type 2 inflammatory condition, including atopic dermatitis and eosinophilic esophagitis. Dupilumab blocks the shared receptor for interleukin (IL)-4/IL-13, which are key drivers of type 2 inflammation in multiple diseases.
Dr. Tracy said that while dupilumab is not the only drug available to treat children 6-11 years with moderate-to-severe asthma, it is “a significant and unique addition to the armamentarium of the individual practitioner taking care of these very severe asthmatics in the 6-11 age group.”
Dupilumab also led to rapid and sustained improvement in lung function. At 12 weeks, children assigned dupilumab improved their lung function as measured by FEV1 by 5.21% (P = .0009), and that continued through the 52-week study period.
“What we know is the [improved lung function] effect is sustained. What we don’t know is how long you have to keep on the drug for a more permanent effect, which is an issue for all these biologics,” Tracy said.
Dr. Bacharier reported speaker fees and research support from Sanofi/Regeneron. Dr. Tracy has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dupilumab (Dupixent, Sanofi and Regeneron) significantly reduced exacerbations compared with placebo in children ages 6-11 years who had moderate-to-severe asthma in a phase 3 trial.
A fully human monoclonal antibody, dupilumab also improved lung function versus placebo by week 12, an improvement that lasted the length of the 52-week trial.
Dupilumab previously had been shown to be safe and effective in adolescents and adults with moderate-to-severe asthma, patients 6 years and older with moderate-to-severe atopic dermatitis, and adults with chronic rhinosinusitis with nasal polyposis, but its safety and effectiveness for moderate-to-severe asthma in the 6-11 years age group was not known.
Results from the randomized, double-blind VOYAGE study conducted across several countries were presented Saturday, July 10, at the European Academy of Allergy and Clinical Immunology (EAACI) Hybrid Congress 2021.
Leonard B. Bacharier, MD, professor of pediatrics, allergy/immunology/pulmonary medicine at Vanderbilt University Medical Center in Nashville, Tennessee, presented the results from the trial, which was funded by Sanofi/Regeneron.
Researchers enrolled 408 children ages 6-11 years with uncontrolled moderate-to-severe asthma. Children on high-dose inhaled corticosteroids (ICS) alone or medium-to-high–dose ICS with a second controller were randomly assigned either to add-on subcutaneous dupilumab 100 mg or 200 mg, based on body weight at study start, or to placebo every 2 weeks for 52 weeks.
Analyses were done in two populations: 350 patients with markers of type 2 inflammation (baseline blood eosinophils ≥150 cells/μl or fractional exhaled nitric oxide [FeNO] ≥20 ppb) and 259 patients with baseline blood eosinophils ≥300 cells/µl.
“The primary endpoint was the annualized rate of severe asthma exacerbations,” Dr. Bacharier said. “The key secondary endpoint was change in percent predicted prebronchodilator FEV1 [forced expiratory volume at 1 second] from baseline to week 12.”
At week 12, the annualized severe asthma exacerbation rate was reduced by 59% (P < .0001) in children with blood eosinophils ≥300 cells/µL and results were similar in those with the type 2 inflammatory phenotype compared with placebo.
Results also indicate a favorable safety profile for dupilumab.
James M. Tracy, DO, an expert with the American College of Allergy, Asthma, and Immunology, told this news organization that adding the dupilumab option for children in the 6-11 age group is “huge.”
Dr. Tracy, who was not involved with the study, said although omalizumab (Xolair, Genentech) is also available for these children, dupilumab stands out because of the range of comorbidities it can treat.
“[Children] don’t have the same rhinosinusitis and polyposis that adults would have, but a lot of them have eczema, and this drug with multiple prongs is incredibly useful and addresses a broad array of allergic conditions,” Dr. Tracy said.
More than 90% of children in the study had at least one concurrent type 2 inflammatory condition, including atopic dermatitis and eosinophilic esophagitis. Dupilumab blocks the shared receptor for interleukin (IL)-4/IL-13, which are key drivers of type 2 inflammation in multiple diseases.
Dr. Tracy said that while dupilumab is not the only drug available to treat children 6-11 years with moderate-to-severe asthma, it is “a significant and unique addition to the armamentarium of the individual practitioner taking care of these very severe asthmatics in the 6-11 age group.”
Dupilumab also led to rapid and sustained improvement in lung function. At 12 weeks, children assigned dupilumab improved their lung function as measured by FEV1 by 5.21% (P = .0009), and that continued through the 52-week study period.
“What we know is the [improved lung function] effect is sustained. What we don’t know is how long you have to keep on the drug for a more permanent effect, which is an issue for all these biologics,” Tracy said.
Dr. Bacharier reported speaker fees and research support from Sanofi/Regeneron. Dr. Tracy has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dupilumab (Dupixent, Sanofi and Regeneron) significantly reduced exacerbations compared with placebo in children ages 6-11 years who had moderate-to-severe asthma in a phase 3 trial.
A fully human monoclonal antibody, dupilumab also improved lung function versus placebo by week 12, an improvement that lasted the length of the 52-week trial.
Dupilumab previously had been shown to be safe and effective in adolescents and adults with moderate-to-severe asthma, patients 6 years and older with moderate-to-severe atopic dermatitis, and adults with chronic rhinosinusitis with nasal polyposis, but its safety and effectiveness for moderate-to-severe asthma in the 6-11 years age group was not known.
Results from the randomized, double-blind VOYAGE study conducted across several countries were presented Saturday, July 10, at the European Academy of Allergy and Clinical Immunology (EAACI) Hybrid Congress 2021.
Leonard B. Bacharier, MD, professor of pediatrics, allergy/immunology/pulmonary medicine at Vanderbilt University Medical Center in Nashville, Tennessee, presented the results from the trial, which was funded by Sanofi/Regeneron.
Researchers enrolled 408 children ages 6-11 years with uncontrolled moderate-to-severe asthma. Children on high-dose inhaled corticosteroids (ICS) alone or medium-to-high–dose ICS with a second controller were randomly assigned either to add-on subcutaneous dupilumab 100 mg or 200 mg, based on body weight at study start, or to placebo every 2 weeks for 52 weeks.
Analyses were done in two populations: 350 patients with markers of type 2 inflammation (baseline blood eosinophils ≥150 cells/μl or fractional exhaled nitric oxide [FeNO] ≥20 ppb) and 259 patients with baseline blood eosinophils ≥300 cells/µl.
“The primary endpoint was the annualized rate of severe asthma exacerbations,” Dr. Bacharier said. “The key secondary endpoint was change in percent predicted prebronchodilator FEV1 [forced expiratory volume at 1 second] from baseline to week 12.”
At week 12, the annualized severe asthma exacerbation rate was reduced by 59% (P < .0001) in children with blood eosinophils ≥300 cells/µL and results were similar in those with the type 2 inflammatory phenotype compared with placebo.
Results also indicate a favorable safety profile for dupilumab.
James M. Tracy, DO, an expert with the American College of Allergy, Asthma, and Immunology, told this news organization that adding the dupilumab option for children in the 6-11 age group is “huge.”
Dr. Tracy, who was not involved with the study, said although omalizumab (Xolair, Genentech) is also available for these children, dupilumab stands out because of the range of comorbidities it can treat.
“[Children] don’t have the same rhinosinusitis and polyposis that adults would have, but a lot of them have eczema, and this drug with multiple prongs is incredibly useful and addresses a broad array of allergic conditions,” Dr. Tracy said.
More than 90% of children in the study had at least one concurrent type 2 inflammatory condition, including atopic dermatitis and eosinophilic esophagitis. Dupilumab blocks the shared receptor for interleukin (IL)-4/IL-13, which are key drivers of type 2 inflammation in multiple diseases.
Dr. Tracy said that while dupilumab is not the only drug available to treat children 6-11 years with moderate-to-severe asthma, it is “a significant and unique addition to the armamentarium of the individual practitioner taking care of these very severe asthmatics in the 6-11 age group.”
Dupilumab also led to rapid and sustained improvement in lung function. At 12 weeks, children assigned dupilumab improved their lung function as measured by FEV1 by 5.21% (P = .0009), and that continued through the 52-week study period.
“What we know is the [improved lung function] effect is sustained. What we don’t know is how long you have to keep on the drug for a more permanent effect, which is an issue for all these biologics,” Tracy said.
Dr. Bacharier reported speaker fees and research support from Sanofi/Regeneron. Dr. Tracy has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pediatric alopecia areata in the U.S. has increased twofold since 2009, study finds
according to results from the largest study to date on the topic.

“Alopecia areata is a relatively common cause of nonscarring hair loss in children,” Paige McKenzie said during the annual meeting of the Society for Pediatric Dermatology. “The only two epidemiologic studies that have been performed in children have been based on registry or survey data which is inherently at risk for bias,” she added, referring to studies published in 2017 and 2018. “Additionally, epidemiologic descriptions of alopecia areata in adults are limited and overall estimates have varied from 0.2% to 2%. Current understanding is also largely based on population studies in Olmsted County, Minnesota, an area with mostly White racial demographics, so it’s not representative of the U.S. population as a whole.”
To identify the incidence and prevalence of pediatric AA over time, and across age, race/ethnicity, and sex, Ms. McKenzie and colleagues conducted a retrospective cohort study from 2009 to 2020 using PEDSnet, a network of seven U.S. pediatric health institutions with a database of more than 6.5 million children. “PEDSnet is unique because it uses a common data model to standardize EHR data across different health systems and uses SNOMED [Systematized Nomenclature of Medicine]–Clinical Terms to identify specific patient populations,” said Ms. McKenzie, who was a clinical research fellow in the section of dermatology at the Children’s Hospital of Philadelphia during the 2020-2021 academic year.
She and her coauthors limited their analysis to children younger than age 18 who were assigned a SNOMED code for AA during at least one dermatology physician visit or at least two nondermatology physician visits. They also identified an incidence cohort that was a subset of the study cohort who had at least 12 months of follow-up. “To determine the accuracy of AA patient identification, we also reviewed 100 cases at random from one institution with a threshold of greater than 95% accuracy,” said Ms. McKenzie, who is now a fourth-year medical student at the University of Texas Southwestern Medical Center, Dallas.
Of 5,409,919 children included in the study, 5,801 had AA, for an overall prevalence of 0.11%. The prevalence doubled from 0.04% in 2009 to 0.08% in 2019. “It fell in 2020, which we believe is a result of the COVID-19 pandemic’s effects on health care utilization,” she said. AA prevalence peaked at 9 years of age and was higher among females, compared with males (0.12% vs. 0.09%, respectively). The prevalence was highest among Hispanic children (0.23%), followed by Asian children (0.17%), Black children (0.12%), and White children (0.08%).
The incidence cohort consisted of 2,896,241 children. Of these, 2,398 had AA between 2009-2020, for an overall incidence of 13.6 cases per 100,000 patient-years. The incidence rate of AA by age was normally distributed and peaked at 6 years of age. Rates were 22.8% higher in female patients than in male patients. In addition, incidence rates were highest among Hispanics (31.5/100,000 person-years), followed by Asians (23.1/100,000 person-years), Blacks (17.0/100,000 person-years), and Whites (8.8/100,000).
Logistic regression analysis showed general agreement with the unadjusted incidence data. Males were less likely to be diagnosed with AA, compared with females (adjusted odds ratio, 0.80; P < .001). Analysis across race/ethnicity revealed significantly increased rates among children from minority backgrounds when compared with white children. Hispanic children had the greatest risk of developing AA (aOR, 3.07), followed by Asian children (aOR, 2.02), and Black children (aOR, 1.73) (P < .001 for all associations). Patients with atopic dermatitis, thyroid disease, psoriasis, vitiligo, and trisomy 21 prior to AA diagnosis all had a significantly higher risk of developing AA, compared with those without those diagnoses.
“This is the largest description of pediatric AA to date,” Ms. McKenzie said. “The prevalence has increased steadily, with a twofold increase over the last 10 years, which mirrors other autoimmune disorders. Children who identify as Hispanic, Asian, and Black have significantly higher incidence rates of alopecia areata compared to those who identify as White.”
Moving forward, she added, “efforts should focus on increasing education and awareness of AA in diverse communities and in community pediatricians so that patients can be diagnosed correctly early on. We can also use this data to ensure that representative populations are included in clinical trials for patients with AA.”
Asked to comment on the results Maria Hordinsky, MD, professor and chair of the department of dermatology at the University of Minnesota, Minneapolis, said that the study “is a great contribution to our understanding of the epidemiology of pediatric alopecia areata and also highlights how common alopecia areata is in children.” In an interview, she said that it would be interesting to see if this is a worldwide phenomenon or unique to the United States.
Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study, characterized the work as being “very informative. Looking at a large cohort of pediatric patients with alopecia areata diagnosed by a dermatologist or two or more nondermatologists, the authors found a higher incidence and prevalence in nonwhite children here in the United States. I am worried in fact, the true incidence could be even higher than noted in the searched database because nonwhite children can often come from underserved and undercared for areas.”
The other authors were Christopher B. Forrest, MD, PhD, Mitchell Maltenfort, PhD, and Leslie Castelo-Soccio, MD, PhD, of Children’s Hospital of Philadelphia. Dr. Castelo-Soccio is a consultant for Pfizer; the other authors reported having no financial disclosures. Dr. Hordinsky disclosed receiving grant support for clinical research work on hair diseases from Pfizer, Eli Lilly, Concert Pharmaceuticals, and Target Derm and grant support from the National Alopecia Areata Foundation; and is on an advisory panel for Cassiopea. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
*This story was updated on 7/19/21.
according to results from the largest study to date on the topic.
“Alopecia areata is a relatively common cause of nonscarring hair loss in children,” Paige McKenzie said during the annual meeting of the Society for Pediatric Dermatology. “The only two epidemiologic studies that have been performed in children have been based on registry or survey data which is inherently at risk for bias,” she added, referring to studies published in 2017 and 2018. “Additionally, epidemiologic descriptions of alopecia areata in adults are limited and overall estimates have varied from 0.2% to 2%. Current understanding is also largely based on population studies in Olmsted County, Minnesota, an area with mostly White racial demographics, so it’s not representative of the U.S. population as a whole.”
To identify the incidence and prevalence of pediatric AA over time, and across age, race/ethnicity, and sex, Ms. McKenzie and colleagues conducted a retrospective cohort study from 2009 to 2020 using PEDSnet, a network of seven U.S. pediatric health institutions with a database of more than 6.5 million children. “PEDSnet is unique because it uses a common data model to standardize EHR data across different health systems and uses SNOMED [Systematized Nomenclature of Medicine]–Clinical Terms to identify specific patient populations,” said Ms. McKenzie, who was a clinical research fellow in the section of dermatology at the Children’s Hospital of Philadelphia during the 2020-2021 academic year.
She and her coauthors limited their analysis to children younger than age 18 who were assigned a SNOMED code for AA during at least one dermatology physician visit or at least two nondermatology physician visits. They also identified an incidence cohort that was a subset of the study cohort who had at least 12 months of follow-up. “To determine the accuracy of AA patient identification, we also reviewed 100 cases at random from one institution with a threshold of greater than 95% accuracy,” said Ms. McKenzie, who is now a fourth-year medical student at the University of Texas Southwestern Medical Center, Dallas.
Of 5,409,919 children included in the study, 5,801 had AA, for an overall prevalence of 0.11%. The prevalence doubled from 0.04% in 2009 to 0.08% in 2019. “It fell in 2020, which we believe is a result of the COVID-19 pandemic’s effects on health care utilization,” she said. AA prevalence peaked at 9 years of age and was higher among females, compared with males (0.12% vs. 0.09%, respectively). The prevalence was highest among Hispanic children (0.23%), followed by Asian children (0.17%), Black children (0.12%), and White children (0.08%).
The incidence cohort consisted of 2,896,241 children. Of these, 2,398 had AA between 2009-2020, for an overall incidence of 13.6 cases per 100,000 patient-years. The incidence rate of AA by age was normally distributed and peaked at 6 years of age. Rates were 22.8% higher in female patients than in male patients. In addition, incidence rates were highest among Hispanics (31.5/100,000 person-years), followed by Asians (23.1/100,000 person-years), Blacks (17.0/100,000 person-years), and Whites (8.8/100,000).
Logistic regression analysis showed general agreement with the unadjusted incidence data. Males were less likely to be diagnosed with AA, compared with females (adjusted odds ratio, 0.80; P < .001). Analysis across race/ethnicity revealed significantly increased rates among children from minority backgrounds when compared with white children. Hispanic children had the greatest risk of developing AA (aOR, 3.07), followed by Asian children (aOR, 2.02), and Black children (aOR, 1.73) (P < .001 for all associations). Patients with atopic dermatitis, thyroid disease, psoriasis, vitiligo, and trisomy 21 prior to AA diagnosis all had a significantly higher risk of developing AA, compared with those without those diagnoses.
“This is the largest description of pediatric AA to date,” Ms. McKenzie said. “The prevalence has increased steadily, with a twofold increase over the last 10 years, which mirrors other autoimmune disorders. Children who identify as Hispanic, Asian, and Black have significantly higher incidence rates of alopecia areata compared to those who identify as White.”
Moving forward, she added, “efforts should focus on increasing education and awareness of AA in diverse communities and in community pediatricians so that patients can be diagnosed correctly early on. We can also use this data to ensure that representative populations are included in clinical trials for patients with AA.”
Asked to comment on the results Maria Hordinsky, MD, professor and chair of the department of dermatology at the University of Minnesota, Minneapolis, said that the study “is a great contribution to our understanding of the epidemiology of pediatric alopecia areata and also highlights how common alopecia areata is in children.” In an interview, she said that it would be interesting to see if this is a worldwide phenomenon or unique to the United States.
Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study, characterized the work as being “very informative. Looking at a large cohort of pediatric patients with alopecia areata diagnosed by a dermatologist or two or more nondermatologists, the authors found a higher incidence and prevalence in nonwhite children here in the United States. I am worried in fact, the true incidence could be even higher than noted in the searched database because nonwhite children can often come from underserved and undercared for areas.”
The other authors were Christopher B. Forrest, MD, PhD, Mitchell Maltenfort, PhD, and Leslie Castelo-Soccio, MD, PhD, of Children’s Hospital of Philadelphia. Dr. Castelo-Soccio is a consultant for Pfizer; the other authors reported having no financial disclosures. Dr. Hordinsky disclosed receiving grant support for clinical research work on hair diseases from Pfizer, Eli Lilly, Concert Pharmaceuticals, and Target Derm and grant support from the National Alopecia Areata Foundation; and is on an advisory panel for Cassiopea. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
*This story was updated on 7/19/21.
according to results from the largest study to date on the topic.
“Alopecia areata is a relatively common cause of nonscarring hair loss in children,” Paige McKenzie said during the annual meeting of the Society for Pediatric Dermatology. “The only two epidemiologic studies that have been performed in children have been based on registry or survey data which is inherently at risk for bias,” she added, referring to studies published in 2017 and 2018. “Additionally, epidemiologic descriptions of alopecia areata in adults are limited and overall estimates have varied from 0.2% to 2%. Current understanding is also largely based on population studies in Olmsted County, Minnesota, an area with mostly White racial demographics, so it’s not representative of the U.S. population as a whole.”
To identify the incidence and prevalence of pediatric AA over time, and across age, race/ethnicity, and sex, Ms. McKenzie and colleagues conducted a retrospective cohort study from 2009 to 2020 using PEDSnet, a network of seven U.S. pediatric health institutions with a database of more than 6.5 million children. “PEDSnet is unique because it uses a common data model to standardize EHR data across different health systems and uses SNOMED [Systematized Nomenclature of Medicine]–Clinical Terms to identify specific patient populations,” said Ms. McKenzie, who was a clinical research fellow in the section of dermatology at the Children’s Hospital of Philadelphia during the 2020-2021 academic year.
She and her coauthors limited their analysis to children younger than age 18 who were assigned a SNOMED code for AA during at least one dermatology physician visit or at least two nondermatology physician visits. They also identified an incidence cohort that was a subset of the study cohort who had at least 12 months of follow-up. “To determine the accuracy of AA patient identification, we also reviewed 100 cases at random from one institution with a threshold of greater than 95% accuracy,” said Ms. McKenzie, who is now a fourth-year medical student at the University of Texas Southwestern Medical Center, Dallas.
Of 5,409,919 children included in the study, 5,801 had AA, for an overall prevalence of 0.11%. The prevalence doubled from 0.04% in 2009 to 0.08% in 2019. “It fell in 2020, which we believe is a result of the COVID-19 pandemic’s effects on health care utilization,” she said. AA prevalence peaked at 9 years of age and was higher among females, compared with males (0.12% vs. 0.09%, respectively). The prevalence was highest among Hispanic children (0.23%), followed by Asian children (0.17%), Black children (0.12%), and White children (0.08%).
The incidence cohort consisted of 2,896,241 children. Of these, 2,398 had AA between 2009-2020, for an overall incidence of 13.6 cases per 100,000 patient-years. The incidence rate of AA by age was normally distributed and peaked at 6 years of age. Rates were 22.8% higher in female patients than in male patients. In addition, incidence rates were highest among Hispanics (31.5/100,000 person-years), followed by Asians (23.1/100,000 person-years), Blacks (17.0/100,000 person-years), and Whites (8.8/100,000).
Logistic regression analysis showed general agreement with the unadjusted incidence data. Males were less likely to be diagnosed with AA, compared with females (adjusted odds ratio, 0.80; P < .001). Analysis across race/ethnicity revealed significantly increased rates among children from minority backgrounds when compared with white children. Hispanic children had the greatest risk of developing AA (aOR, 3.07), followed by Asian children (aOR, 2.02), and Black children (aOR, 1.73) (P < .001 for all associations). Patients with atopic dermatitis, thyroid disease, psoriasis, vitiligo, and trisomy 21 prior to AA diagnosis all had a significantly higher risk of developing AA, compared with those without those diagnoses.
“This is the largest description of pediatric AA to date,” Ms. McKenzie said. “The prevalence has increased steadily, with a twofold increase over the last 10 years, which mirrors other autoimmune disorders. Children who identify as Hispanic, Asian, and Black have significantly higher incidence rates of alopecia areata compared to those who identify as White.”
Moving forward, she added, “efforts should focus on increasing education and awareness of AA in diverse communities and in community pediatricians so that patients can be diagnosed correctly early on. We can also use this data to ensure that representative populations are included in clinical trials for patients with AA.”
Asked to comment on the results Maria Hordinsky, MD, professor and chair of the department of dermatology at the University of Minnesota, Minneapolis, said that the study “is a great contribution to our understanding of the epidemiology of pediatric alopecia areata and also highlights how common alopecia areata is in children.” In an interview, she said that it would be interesting to see if this is a worldwide phenomenon or unique to the United States.
Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study, characterized the work as being “very informative. Looking at a large cohort of pediatric patients with alopecia areata diagnosed by a dermatologist or two or more nondermatologists, the authors found a higher incidence and prevalence in nonwhite children here in the United States. I am worried in fact, the true incidence could be even higher than noted in the searched database because nonwhite children can often come from underserved and undercared for areas.”
The other authors were Christopher B. Forrest, MD, PhD, Mitchell Maltenfort, PhD, and Leslie Castelo-Soccio, MD, PhD, of Children’s Hospital of Philadelphia. Dr. Castelo-Soccio is a consultant for Pfizer; the other authors reported having no financial disclosures. Dr. Hordinsky disclosed receiving grant support for clinical research work on hair diseases from Pfizer, Eli Lilly, Concert Pharmaceuticals, and Target Derm and grant support from the National Alopecia Areata Foundation; and is on an advisory panel for Cassiopea. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
*This story was updated on 7/19/21.
FROM SPD 2021