User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
csDMARDs could add to TNF inhibitors’ benefits in SpA
Better retention and remission rates with tumor necrosis factor inhibitors (TNFi) have been observed in patients with spondyloarthritis (SpA) who were also treated with a conventional synthetic disease-modifying antirheumatic drug (csDMARD) rather than monotherapy.
Data from the EuroSpA Research Collaboration have shown that 82% of patients who received TNFi and csDMARD cotherapy were still taking their TNFi at 1 year versus 79% of those who were taking the biologic alone (P < .001).
Combination therapy led to remission in 21.8%, compared with TNFi monotherapy at 19.5% (P < .0001), with rates of remission according to Ankylosing Spondylitis Disease Activity Score <1.3 (23.7% vs. 21.8%, P = .011) and Bath Ankylosing Spondylitis Disease Activity Index <2 (5.9% vs. 7.7%, P < .0001) also favoring the cotherapy group.
“We did see a considerable heterogeneity across the countries in this study, both in the use of csDMARD therapy and in the TNF [inhibitor] retention,” Michael J. Nissen, MBBS, FRACP, MD, a rheumatologist at the University of Geneva, said in an oral abstract presentation at the 12th International Congress on Spondyloarthritides.
“Overall, the 1-year TNFi retention was better with cotherapy, particularly in countries in the Scandinavian region and Switzerland,” Dr. Nissen observed.
“The csDMARD cotherapy significantly improved remission; we could perhaps argue whether these small differences are clinically meaningful, but they were highly significant in the study.”
Why look at csDMARD and TNFi cotherapy?
European guidelines suggest that csDMARDs are not that useful for treating people with SpA, stating that they should not be used in axial disease and used only as monotherapy in those with peripheral disease.
“Nevertheless, these medications are often used, which begs us to ask the question why is that the case?” Dr. Nissen said.
As previous work by Dr. Nissen and others had suggested that there might be a benefit of combining a csDMARD and a TNFi, the aim was to build upon this and see if looking at a very large patient population might be able to provide some clear answers.
The analysis included data from 13 European registries and more than 24,000 patients who had started their first TNFi between 2006 and 2017. The mean age of the study population was 42.5 years, and 58% were male, with an average disease duration of 5.9 years. Nearly one-third of patients were receiving comedication with a csDMARD, although this ranged from 13.5% to 71.2% depending on the country.
The most frequently used TNFi were adalimumab (31% of patients overall), etanercept (24%), and infliximab (25%), and the most-used csDMARDs were methotrexate (56%) and sulfasalazine (45%).
The effectiveness of treatment in achieving clinical remission was examined according to the TNFi used and for the use of csDMARDs.
“We found that sulfasalazine and methotrexate were similarly effective in terms of improving outcomes in addition to a TNF inhibitor,” Dr. Nissen said. For example, the adjusted odds ratios for using sulfasalazine or methotrexate with infliximab were a respective 1.32 and 1.37, and the aORs for uses these specific csDMARDs with etanercept were 1.38 and 1.35.
The researchers reported finding significantly higher aORs if both sulfasalazine and methotrexate were used with a TNFi (1.67 for any TNFi, 1.95 for infliximab, 1.45 foretanercept, and 1.85 for adalimumab).
This perhaps suggests “there’s some role for combining csDMARDs to have an even greater effect,” Dr. Nissen put forward.
A ‘very provocative conclusion’
That’s “a very provocative conclusion” commented Robert Landewé, MD, PhD, of Amsterdam University Medical Center who chaired the sessions. “You can see it by the [number] of people that want to ask questions.”

Désirée van der Heijde, MD, PhD, of Leiden (the Netherlands) University Medical Center, commented these data were “timely as we are updating the ASAS/EULAR [Assessment of SpondyloArthritis international Society/European Alliance of Associations for Rheumatology] recommendations at the moment.” She queried, however, if the differences were clinically significant.
“I think if you have a database of 24,000 patients, highly, statistically significant doesn’t tell me a lot. So, I want to look at the clinical meaning of the differences. So, if you have a 2% difference in retention rate, is that worth prescribing comedication?” Dr. van der Heijde said.
“I think you’re absolutely right,” Dr. Nissen responded. “We’re obviously going to find highly significant differences with such a big patient group.” While the small statistical differences seen may not look very clinically relevant at face value, they could provide some guidance for clinical decision making.
“It may alter our approach if that patient is already on a csDMARD and has peripheral disease; perhaps there’s tendency to then to keep that csDMARD rather than then stopping it and switching to a biologic agent,” Dr. Nissen argued. It’s a topic that has been debated for some time, he added, and further study is needed, but “I think it helps give a little bit more clarity to the idea.”

Another point of discussion was the proportion of patients who had “pure axial disease.” More patients in the comedication group had peripheral disease, Dr. van der Heijde pointed out, “that’s also where we expect to see the differences.”
Further research is needed, but there doesn’t seem to be any impact in terms of the effect on retention, Dr. Nissen said, “but it’s a little bit harder to interpret for efficacy.”
Confounding by indication was another issued raised, which “is very difficult to control for in this type of study,” Dr. Nissen said.
“The hope is that you have a big enough population” so this doesn’t matter, but as is the nature there were lots of missing data that would have been useful to have and adjust for, such as psoriasis and smoking status. There was also no adjustment for the number of patient visits, as it’s very different from registry to registry.
Dr. Nissen disclosed grant/research support from AbbVie and Novartis. He also acknowledged acting as a consultant or speaker for AbbVie, Celgene, Janssen, Eli Lilly, Novartis, and Pfizer.
Better retention and remission rates with tumor necrosis factor inhibitors (TNFi) have been observed in patients with spondyloarthritis (SpA) who were also treated with a conventional synthetic disease-modifying antirheumatic drug (csDMARD) rather than monotherapy.
Data from the EuroSpA Research Collaboration have shown that 82% of patients who received TNFi and csDMARD cotherapy were still taking their TNFi at 1 year versus 79% of those who were taking the biologic alone (P < .001).
Combination therapy led to remission in 21.8%, compared with TNFi monotherapy at 19.5% (P < .0001), with rates of remission according to Ankylosing Spondylitis Disease Activity Score <1.3 (23.7% vs. 21.8%, P = .011) and Bath Ankylosing Spondylitis Disease Activity Index <2 (5.9% vs. 7.7%, P < .0001) also favoring the cotherapy group.
“We did see a considerable heterogeneity across the countries in this study, both in the use of csDMARD therapy and in the TNF [inhibitor] retention,” Michael J. Nissen, MBBS, FRACP, MD, a rheumatologist at the University of Geneva, said in an oral abstract presentation at the 12th International Congress on Spondyloarthritides.
“Overall, the 1-year TNFi retention was better with cotherapy, particularly in countries in the Scandinavian region and Switzerland,” Dr. Nissen observed.
“The csDMARD cotherapy significantly improved remission; we could perhaps argue whether these small differences are clinically meaningful, but they were highly significant in the study.”
Why look at csDMARD and TNFi cotherapy?
European guidelines suggest that csDMARDs are not that useful for treating people with SpA, stating that they should not be used in axial disease and used only as monotherapy in those with peripheral disease.
“Nevertheless, these medications are often used, which begs us to ask the question why is that the case?” Dr. Nissen said.
As previous work by Dr. Nissen and others had suggested that there might be a benefit of combining a csDMARD and a TNFi, the aim was to build upon this and see if looking at a very large patient population might be able to provide some clear answers.
The analysis included data from 13 European registries and more than 24,000 patients who had started their first TNFi between 2006 and 2017. The mean age of the study population was 42.5 years, and 58% were male, with an average disease duration of 5.9 years. Nearly one-third of patients were receiving comedication with a csDMARD, although this ranged from 13.5% to 71.2% depending on the country.
The most frequently used TNFi were adalimumab (31% of patients overall), etanercept (24%), and infliximab (25%), and the most-used csDMARDs were methotrexate (56%) and sulfasalazine (45%).
The effectiveness of treatment in achieving clinical remission was examined according to the TNFi used and for the use of csDMARDs.
“We found that sulfasalazine and methotrexate were similarly effective in terms of improving outcomes in addition to a TNF inhibitor,” Dr. Nissen said. For example, the adjusted odds ratios for using sulfasalazine or methotrexate with infliximab were a respective 1.32 and 1.37, and the aORs for uses these specific csDMARDs with etanercept were 1.38 and 1.35.
The researchers reported finding significantly higher aORs if both sulfasalazine and methotrexate were used with a TNFi (1.67 for any TNFi, 1.95 for infliximab, 1.45 foretanercept, and 1.85 for adalimumab).
This perhaps suggests “there’s some role for combining csDMARDs to have an even greater effect,” Dr. Nissen put forward.
A ‘very provocative conclusion’
That’s “a very provocative conclusion” commented Robert Landewé, MD, PhD, of Amsterdam University Medical Center who chaired the sessions. “You can see it by the [number] of people that want to ask questions.”
Désirée van der Heijde, MD, PhD, of Leiden (the Netherlands) University Medical Center, commented these data were “timely as we are updating the ASAS/EULAR [Assessment of SpondyloArthritis international Society/European Alliance of Associations for Rheumatology] recommendations at the moment.” She queried, however, if the differences were clinically significant.
“I think if you have a database of 24,000 patients, highly, statistically significant doesn’t tell me a lot. So, I want to look at the clinical meaning of the differences. So, if you have a 2% difference in retention rate, is that worth prescribing comedication?” Dr. van der Heijde said.
“I think you’re absolutely right,” Dr. Nissen responded. “We’re obviously going to find highly significant differences with such a big patient group.” While the small statistical differences seen may not look very clinically relevant at face value, they could provide some guidance for clinical decision making.
“It may alter our approach if that patient is already on a csDMARD and has peripheral disease; perhaps there’s tendency to then to keep that csDMARD rather than then stopping it and switching to a biologic agent,” Dr. Nissen argued. It’s a topic that has been debated for some time, he added, and further study is needed, but “I think it helps give a little bit more clarity to the idea.”
Another point of discussion was the proportion of patients who had “pure axial disease.” More patients in the comedication group had peripheral disease, Dr. van der Heijde pointed out, “that’s also where we expect to see the differences.”
Further research is needed, but there doesn’t seem to be any impact in terms of the effect on retention, Dr. Nissen said, “but it’s a little bit harder to interpret for efficacy.”
Confounding by indication was another issued raised, which “is very difficult to control for in this type of study,” Dr. Nissen said.
“The hope is that you have a big enough population” so this doesn’t matter, but as is the nature there were lots of missing data that would have been useful to have and adjust for, such as psoriasis and smoking status. There was also no adjustment for the number of patient visits, as it’s very different from registry to registry.
Dr. Nissen disclosed grant/research support from AbbVie and Novartis. He also acknowledged acting as a consultant or speaker for AbbVie, Celgene, Janssen, Eli Lilly, Novartis, and Pfizer.
Better retention and remission rates with tumor necrosis factor inhibitors (TNFi) have been observed in patients with spondyloarthritis (SpA) who were also treated with a conventional synthetic disease-modifying antirheumatic drug (csDMARD) rather than monotherapy.
Data from the EuroSpA Research Collaboration have shown that 82% of patients who received TNFi and csDMARD cotherapy were still taking their TNFi at 1 year versus 79% of those who were taking the biologic alone (P < .001).
Combination therapy led to remission in 21.8%, compared with TNFi monotherapy at 19.5% (P < .0001), with rates of remission according to Ankylosing Spondylitis Disease Activity Score <1.3 (23.7% vs. 21.8%, P = .011) and Bath Ankylosing Spondylitis Disease Activity Index <2 (5.9% vs. 7.7%, P < .0001) also favoring the cotherapy group.
“We did see a considerable heterogeneity across the countries in this study, both in the use of csDMARD therapy and in the TNF [inhibitor] retention,” Michael J. Nissen, MBBS, FRACP, MD, a rheumatologist at the University of Geneva, said in an oral abstract presentation at the 12th International Congress on Spondyloarthritides.
“Overall, the 1-year TNFi retention was better with cotherapy, particularly in countries in the Scandinavian region and Switzerland,” Dr. Nissen observed.
“The csDMARD cotherapy significantly improved remission; we could perhaps argue whether these small differences are clinically meaningful, but they were highly significant in the study.”
Why look at csDMARD and TNFi cotherapy?
European guidelines suggest that csDMARDs are not that useful for treating people with SpA, stating that they should not be used in axial disease and used only as monotherapy in those with peripheral disease.
“Nevertheless, these medications are often used, which begs us to ask the question why is that the case?” Dr. Nissen said.
As previous work by Dr. Nissen and others had suggested that there might be a benefit of combining a csDMARD and a TNFi, the aim was to build upon this and see if looking at a very large patient population might be able to provide some clear answers.
The analysis included data from 13 European registries and more than 24,000 patients who had started their first TNFi between 2006 and 2017. The mean age of the study population was 42.5 years, and 58% were male, with an average disease duration of 5.9 years. Nearly one-third of patients were receiving comedication with a csDMARD, although this ranged from 13.5% to 71.2% depending on the country.
The most frequently used TNFi were adalimumab (31% of patients overall), etanercept (24%), and infliximab (25%), and the most-used csDMARDs were methotrexate (56%) and sulfasalazine (45%).
The effectiveness of treatment in achieving clinical remission was examined according to the TNFi used and for the use of csDMARDs.
“We found that sulfasalazine and methotrexate were similarly effective in terms of improving outcomes in addition to a TNF inhibitor,” Dr. Nissen said. For example, the adjusted odds ratios for using sulfasalazine or methotrexate with infliximab were a respective 1.32 and 1.37, and the aORs for uses these specific csDMARDs with etanercept were 1.38 and 1.35.
The researchers reported finding significantly higher aORs if both sulfasalazine and methotrexate were used with a TNFi (1.67 for any TNFi, 1.95 for infliximab, 1.45 foretanercept, and 1.85 for adalimumab).
This perhaps suggests “there’s some role for combining csDMARDs to have an even greater effect,” Dr. Nissen put forward.
A ‘very provocative conclusion’
That’s “a very provocative conclusion” commented Robert Landewé, MD, PhD, of Amsterdam University Medical Center who chaired the sessions. “You can see it by the [number] of people that want to ask questions.”
Désirée van der Heijde, MD, PhD, of Leiden (the Netherlands) University Medical Center, commented these data were “timely as we are updating the ASAS/EULAR [Assessment of SpondyloArthritis international Society/European Alliance of Associations for Rheumatology] recommendations at the moment.” She queried, however, if the differences were clinically significant.
“I think if you have a database of 24,000 patients, highly, statistically significant doesn’t tell me a lot. So, I want to look at the clinical meaning of the differences. So, if you have a 2% difference in retention rate, is that worth prescribing comedication?” Dr. van der Heijde said.
“I think you’re absolutely right,” Dr. Nissen responded. “We’re obviously going to find highly significant differences with such a big patient group.” While the small statistical differences seen may not look very clinically relevant at face value, they could provide some guidance for clinical decision making.
“It may alter our approach if that patient is already on a csDMARD and has peripheral disease; perhaps there’s tendency to then to keep that csDMARD rather than then stopping it and switching to a biologic agent,” Dr. Nissen argued. It’s a topic that has been debated for some time, he added, and further study is needed, but “I think it helps give a little bit more clarity to the idea.”
Another point of discussion was the proportion of patients who had “pure axial disease.” More patients in the comedication group had peripheral disease, Dr. van der Heijde pointed out, “that’s also where we expect to see the differences.”
Further research is needed, but there doesn’t seem to be any impact in terms of the effect on retention, Dr. Nissen said, “but it’s a little bit harder to interpret for efficacy.”
Confounding by indication was another issued raised, which “is very difficult to control for in this type of study,” Dr. Nissen said.
“The hope is that you have a big enough population” so this doesn’t matter, but as is the nature there were lots of missing data that would have been useful to have and adjust for, such as psoriasis and smoking status. There was also no adjustment for the number of patient visits, as it’s very different from registry to registry.
Dr. Nissen disclosed grant/research support from AbbVie and Novartis. He also acknowledged acting as a consultant or speaker for AbbVie, Celgene, Janssen, Eli Lilly, Novartis, and Pfizer.
FROM THE 2021 SPA CONGRESS
POSEIDON: Two ICIs plus chemo up survival in mNSCLC
The study involved over 1,000 patients with stage IV NSCLC. Participants were randomly assigned to receive either two ICIs (tremelimumab and durvalumab [Imfinzi]) plus chemotherapy, or one immunotherapy (durvalumab) plus chemotherapy, or chemotherapy alone.
Adding durvalumab to chemotherapy significantly improved PFS by 26% but did not significantly improve OS, the researchers reported. However, adding both tremelimumab and durvalumab significantly increased both PFS (by 28%) and OS (by 23%). Median OS was 14.0 months versus 11.7 months for chemotherapy.
The results were presented on Sept. 9 at a presidential symposium of the World Conference on Lung Cancer 2021.
The two immunotherapies act at different immune checkpoints – tremelimumab acts at CTLA-4, and durvalumab acts at programmed death–1/PD–ligand 1 (PD-L1). Both drugs are from AstraZeneca, which sponsored the POSEIDON trial.
With no new safety signals identified, the triple therapy combination “represents a potential new frontline treatment option for metastatic non–small cell lung cancer,” said lead researcher Melissa L. Johnson, MD, from the Sarah Cannon Research Institute, Nashville, Tenn.
Reacting to the new results in a discussion of the paper, Julie R. Brahmer, MD, from Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medicine, Baltimore, said that, with so many first-line treatment choices now available for advanced NSCLC, she feels like “a kid in the candy store.”
POSEIDON may give her “another choice,” but she pointed out that there are some aspects of the study to consider.
The study required patients to undergo four cycles of chemotherapy along with immunotherapy, “which certainly is standard in many of our practices.”
However, only two cycles of chemotherapy were given in the CheckMate 9LA trial, in which nivolumab (Opdivo) and ipilimumab (Yervoy) were added to chemotherapy for the treatment of stage IV NSCLC. This combination of immunotherapies, which block CTLA-4 and PD-1, is similar to the combination that was studied in the current trial, and it is already approved for use in some patients with lung cancer.
“Also key to point out,” said Dr. Brahmer, is that, in the POSEIDON trial, “there was a trend toward more poor prognostic factors in the chemotherapy arm, where these patients had more liver or central nervous system metastases.”
Despite these differences, the survival outcomes were similar in the two trials, and in both trials, the tails of the curves indicate that “we need to see long-term data” to determine whether the benefit is ongoing.
Which patients for which combos?
Considering all the data from key trials in advanced NSCLC, Dr. Brahmer said that she believes that, for patients with high PD-L1 expression, treatment with a single immunotherapy directed against PD-1 or PD-L1 “is appropriate” and that she didn’t see that adding a CTLA-4 inhibitor to the PD-L1 inhibitor and chemotherapy would give any advantage.
“But for PD-L1–negative disease, I do think CTLA-4 antibodies seem to provide a benefit, specifically seen in the CheckMate studies,” particularly for patients with squamous disease, although she noted that in POSEIDON, histology and PD-L1 status have not been analyzed.
Dr. Brahmer concluded that, although the triple therapy improved survival outcomes in the current study, several key questions remain.
These include determining what CTLA-4 inhibition adds to PD-L1 blockade and asking whether the “slightly increased toxicity” is “worth the slightly increased long-term duration of response” and improved survival outcomes.
Furthermore, it needs to be determined “which populations truly need” the combined approach; “to get to this, we need to find the biomarker for CTLA-4 benefit,” Dr. Brahmer said.
She also noted “a practical question: Is there room in the clinic for another CTLA-4 antibody in addition to the nivolumab/ipilimumab combinations?”
This last point was appreciated on social media. Jill Feldman, a lung cancer patient and advocate, described it on Twitter as a “great question.”
She said that, for her, “options equal hope,” but that it is “critical” to give the “best treatment first. ... So as a patient, I would ask: How do I know/you know which treatment would be best for me?”
With “so many options in the first-line setting,” subsets of patients who may benefit from quadruplet therapy versus monotherapy need to be defined, commented Charu Aggarwal, MD, MPH, Leslye M. Heisler Associate Professor for Lung Cancer Excellence, Penn Medicine, Philadelphia. He added that “PD-L1 may be one biomarker, but we need more.”
More details of the POSEIDON trial
In the POSEIDON trial, investigators had the choice of different chemotherapy regimens: platinum/gemcitabine for patients with squamous disease, platinum/pemetrexed for patients with nonsquamous disease, and nab-paclitaxel/carboplatin for patients with disease of either histology, Dr. Johnson reported.
It is noteworthy that the majority of patients were from Eastern Europe and Asia, “and the proportion of squamous patients enrolled was higher than is typically seen in mixed histology lung cancer studies,” she added.
The patients were stratified by PD-L1 expression at a cutoff of 50%, disease stage, and tumor histology.
Overall, 1,013 patients were enrolled. The three treatment arms were relatively well balanced in terms of baseline characteristics.
Dr. Johnson noted that there were “a few minor imbalances” in the durvalumab plus tremelimumab arm, with “fewer females, fewer Asians, and fewer never-smokers relative to the other two arms.”
The primary endpoint analysis after a median follow-up of 10.3 months demonstrated that PFS was significantly improved with durvalumab plus chemotherapy over chemotherapy alone, at a median of 5.5 months versus 4.8 months (hazard ratio, 0.74; P = .00093).
Although OS improved numerically with the addition of durvalumab to chemotherapy, it did not reach significance (13.3 months vs. 11.7 months with chemotherapy alone; HR, 0.86; P = .07581).
The positive PFS benefit with durvalumab plus chemotherapy triggered a secondary endpoint analysis, which showed that adding tremelimumab to durvalumab plus chemotherapy improved both survival outcomes.
Median PFS with the triple combination therapy was 6.2 months, significantly longer than the 4.8 months seen with chemotherapy alone (HR, 0.72; P = .00031).
At 12 months, 26.6% of patients who underwent treatment with durvalumab plus tremelimumab plus chemotherapy had not experienced disease progression, compared with 13.1% in the chemotherapy-alone arm.
OS was also significantly improved, at 14.0 months among patients in the triple therapy arm versus 11.7 in the chemotherapy-alone arm (HR, 0.77; P = .00304).
The results also showed that at 24 months, 32.9% of triple therapy patients were still alive versus 22.1% in the chemotherapy-alone arm.
Analysis indicated that “most subgroups favored the addition of immunotherapy to chemotherapy.” There was a “trend toward improved survival for all patients treated with durvalumab plus tremelimumab plus chemotherapy,” Dr. Johnson said.
This was seen “in particular for the nonsquamous patients” and for those with tumor PD-L1 expression of less than 1%, he added.
It is notable that for a large proportion of combination-therapy patients, response had continued at 12 months. This was the case for 38.9% of those who underwent treatment with durvalumab plus chemotherapy and for 49.7% of those given triple therapy versus 21.4% in the chemotherapy-alone arm.
As was seen across the whole cohort, among patients with nonsquamous disease, PFS and OS improved with the addition of immunotherapy. Of those patients with nonsquamous disease, 95.5% received pemetrexed plus platinum chemotherapy.
However, among patients with squamous tumors, of whom 88.3% received gemcitabine plus platinum chemotherapy, PFS and OS were “poor ... across all treatment arms,” Dr. Johnson reported, “with little separation of the curves.”
She highlighted the fact that the proportion of patients who experienced grade 3/4 adverse events, whether of any cause or treatment related, was only slightly higher in the two immunotherapy arms, indicating that “most events were driven by the chemotherapy.”
The rates of treatment discontinuation and adverse events leading to death were also similar across the three treatment arms, albeit they were slightly higher with the addition of immunotherapy.
Dr. Johnson also noted that, although there were more immune-mediated adverse events with durvalumab plus tremelimumab plus chemotherapy, compared with durvalumab plus chemotherapy, the “majority were grade 1/2 and were manageable.”
The most common immune-mediated events in the two immunotherapy arms were hypothyroid and hepatic events, pneumonitis, dermatitis, and rash.
The study was sponsored by AstraZeneca. Dr. Johnson reported numerous relationships with pharmaceutical companies. Dr. Brahmer reported relationships with Amgen, AstratZeneca, BMA, Genentech/Roche, Eli Lilly, Eisai, GlaxoSmithKline, Janssen, Merck, RAPT Therapeutics, Regeneron, Revolution Medicine, and Sanofi.
A version of this article first appeared on Medscape.com.
The study involved over 1,000 patients with stage IV NSCLC. Participants were randomly assigned to receive either two ICIs (tremelimumab and durvalumab [Imfinzi]) plus chemotherapy, or one immunotherapy (durvalumab) plus chemotherapy, or chemotherapy alone.
Adding durvalumab to chemotherapy significantly improved PFS by 26% but did not significantly improve OS, the researchers reported. However, adding both tremelimumab and durvalumab significantly increased both PFS (by 28%) and OS (by 23%). Median OS was 14.0 months versus 11.7 months for chemotherapy.
The results were presented on Sept. 9 at a presidential symposium of the World Conference on Lung Cancer 2021.
The two immunotherapies act at different immune checkpoints – tremelimumab acts at CTLA-4, and durvalumab acts at programmed death–1/PD–ligand 1 (PD-L1). Both drugs are from AstraZeneca, which sponsored the POSEIDON trial.
With no new safety signals identified, the triple therapy combination “represents a potential new frontline treatment option for metastatic non–small cell lung cancer,” said lead researcher Melissa L. Johnson, MD, from the Sarah Cannon Research Institute, Nashville, Tenn.
Reacting to the new results in a discussion of the paper, Julie R. Brahmer, MD, from Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medicine, Baltimore, said that, with so many first-line treatment choices now available for advanced NSCLC, she feels like “a kid in the candy store.”
POSEIDON may give her “another choice,” but she pointed out that there are some aspects of the study to consider.
The study required patients to undergo four cycles of chemotherapy along with immunotherapy, “which certainly is standard in many of our practices.”
However, only two cycles of chemotherapy were given in the CheckMate 9LA trial, in which nivolumab (Opdivo) and ipilimumab (Yervoy) were added to chemotherapy for the treatment of stage IV NSCLC. This combination of immunotherapies, which block CTLA-4 and PD-1, is similar to the combination that was studied in the current trial, and it is already approved for use in some patients with lung cancer.
“Also key to point out,” said Dr. Brahmer, is that, in the POSEIDON trial, “there was a trend toward more poor prognostic factors in the chemotherapy arm, where these patients had more liver or central nervous system metastases.”
Despite these differences, the survival outcomes were similar in the two trials, and in both trials, the tails of the curves indicate that “we need to see long-term data” to determine whether the benefit is ongoing.
Which patients for which combos?
Considering all the data from key trials in advanced NSCLC, Dr. Brahmer said that she believes that, for patients with high PD-L1 expression, treatment with a single immunotherapy directed against PD-1 or PD-L1 “is appropriate” and that she didn’t see that adding a CTLA-4 inhibitor to the PD-L1 inhibitor and chemotherapy would give any advantage.
“But for PD-L1–negative disease, I do think CTLA-4 antibodies seem to provide a benefit, specifically seen in the CheckMate studies,” particularly for patients with squamous disease, although she noted that in POSEIDON, histology and PD-L1 status have not been analyzed.
Dr. Brahmer concluded that, although the triple therapy improved survival outcomes in the current study, several key questions remain.
These include determining what CTLA-4 inhibition adds to PD-L1 blockade and asking whether the “slightly increased toxicity” is “worth the slightly increased long-term duration of response” and improved survival outcomes.
Furthermore, it needs to be determined “which populations truly need” the combined approach; “to get to this, we need to find the biomarker for CTLA-4 benefit,” Dr. Brahmer said.
She also noted “a practical question: Is there room in the clinic for another CTLA-4 antibody in addition to the nivolumab/ipilimumab combinations?”
This last point was appreciated on social media. Jill Feldman, a lung cancer patient and advocate, described it on Twitter as a “great question.”
She said that, for her, “options equal hope,” but that it is “critical” to give the “best treatment first. ... So as a patient, I would ask: How do I know/you know which treatment would be best for me?”
With “so many options in the first-line setting,” subsets of patients who may benefit from quadruplet therapy versus monotherapy need to be defined, commented Charu Aggarwal, MD, MPH, Leslye M. Heisler Associate Professor for Lung Cancer Excellence, Penn Medicine, Philadelphia. He added that “PD-L1 may be one biomarker, but we need more.”
More details of the POSEIDON trial
In the POSEIDON trial, investigators had the choice of different chemotherapy regimens: platinum/gemcitabine for patients with squamous disease, platinum/pemetrexed for patients with nonsquamous disease, and nab-paclitaxel/carboplatin for patients with disease of either histology, Dr. Johnson reported.
It is noteworthy that the majority of patients were from Eastern Europe and Asia, “and the proportion of squamous patients enrolled was higher than is typically seen in mixed histology lung cancer studies,” she added.
The patients were stratified by PD-L1 expression at a cutoff of 50%, disease stage, and tumor histology.
Overall, 1,013 patients were enrolled. The three treatment arms were relatively well balanced in terms of baseline characteristics.
Dr. Johnson noted that there were “a few minor imbalances” in the durvalumab plus tremelimumab arm, with “fewer females, fewer Asians, and fewer never-smokers relative to the other two arms.”
The primary endpoint analysis after a median follow-up of 10.3 months demonstrated that PFS was significantly improved with durvalumab plus chemotherapy over chemotherapy alone, at a median of 5.5 months versus 4.8 months (hazard ratio, 0.74; P = .00093).
Although OS improved numerically with the addition of durvalumab to chemotherapy, it did not reach significance (13.3 months vs. 11.7 months with chemotherapy alone; HR, 0.86; P = .07581).
The positive PFS benefit with durvalumab plus chemotherapy triggered a secondary endpoint analysis, which showed that adding tremelimumab to durvalumab plus chemotherapy improved both survival outcomes.
Median PFS with the triple combination therapy was 6.2 months, significantly longer than the 4.8 months seen with chemotherapy alone (HR, 0.72; P = .00031).
At 12 months, 26.6% of patients who underwent treatment with durvalumab plus tremelimumab plus chemotherapy had not experienced disease progression, compared with 13.1% in the chemotherapy-alone arm.
OS was also significantly improved, at 14.0 months among patients in the triple therapy arm versus 11.7 in the chemotherapy-alone arm (HR, 0.77; P = .00304).
The results also showed that at 24 months, 32.9% of triple therapy patients were still alive versus 22.1% in the chemotherapy-alone arm.
Analysis indicated that “most subgroups favored the addition of immunotherapy to chemotherapy.” There was a “trend toward improved survival for all patients treated with durvalumab plus tremelimumab plus chemotherapy,” Dr. Johnson said.
This was seen “in particular for the nonsquamous patients” and for those with tumor PD-L1 expression of less than 1%, he added.
It is notable that for a large proportion of combination-therapy patients, response had continued at 12 months. This was the case for 38.9% of those who underwent treatment with durvalumab plus chemotherapy and for 49.7% of those given triple therapy versus 21.4% in the chemotherapy-alone arm.
As was seen across the whole cohort, among patients with nonsquamous disease, PFS and OS improved with the addition of immunotherapy. Of those patients with nonsquamous disease, 95.5% received pemetrexed plus platinum chemotherapy.
However, among patients with squamous tumors, of whom 88.3% received gemcitabine plus platinum chemotherapy, PFS and OS were “poor ... across all treatment arms,” Dr. Johnson reported, “with little separation of the curves.”
She highlighted the fact that the proportion of patients who experienced grade 3/4 adverse events, whether of any cause or treatment related, was only slightly higher in the two immunotherapy arms, indicating that “most events were driven by the chemotherapy.”
The rates of treatment discontinuation and adverse events leading to death were also similar across the three treatment arms, albeit they were slightly higher with the addition of immunotherapy.
Dr. Johnson also noted that, although there were more immune-mediated adverse events with durvalumab plus tremelimumab plus chemotherapy, compared with durvalumab plus chemotherapy, the “majority were grade 1/2 and were manageable.”
The most common immune-mediated events in the two immunotherapy arms were hypothyroid and hepatic events, pneumonitis, dermatitis, and rash.
The study was sponsored by AstraZeneca. Dr. Johnson reported numerous relationships with pharmaceutical companies. Dr. Brahmer reported relationships with Amgen, AstratZeneca, BMA, Genentech/Roche, Eli Lilly, Eisai, GlaxoSmithKline, Janssen, Merck, RAPT Therapeutics, Regeneron, Revolution Medicine, and Sanofi.
A version of this article first appeared on Medscape.com.
The study involved over 1,000 patients with stage IV NSCLC. Participants were randomly assigned to receive either two ICIs (tremelimumab and durvalumab [Imfinzi]) plus chemotherapy, or one immunotherapy (durvalumab) plus chemotherapy, or chemotherapy alone.
Adding durvalumab to chemotherapy significantly improved PFS by 26% but did not significantly improve OS, the researchers reported. However, adding both tremelimumab and durvalumab significantly increased both PFS (by 28%) and OS (by 23%). Median OS was 14.0 months versus 11.7 months for chemotherapy.
The results were presented on Sept. 9 at a presidential symposium of the World Conference on Lung Cancer 2021.
The two immunotherapies act at different immune checkpoints – tremelimumab acts at CTLA-4, and durvalumab acts at programmed death–1/PD–ligand 1 (PD-L1). Both drugs are from AstraZeneca, which sponsored the POSEIDON trial.
With no new safety signals identified, the triple therapy combination “represents a potential new frontline treatment option for metastatic non–small cell lung cancer,” said lead researcher Melissa L. Johnson, MD, from the Sarah Cannon Research Institute, Nashville, Tenn.
Reacting to the new results in a discussion of the paper, Julie R. Brahmer, MD, from Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins Medicine, Baltimore, said that, with so many first-line treatment choices now available for advanced NSCLC, she feels like “a kid in the candy store.”
POSEIDON may give her “another choice,” but she pointed out that there are some aspects of the study to consider.
The study required patients to undergo four cycles of chemotherapy along with immunotherapy, “which certainly is standard in many of our practices.”
However, only two cycles of chemotherapy were given in the CheckMate 9LA trial, in which nivolumab (Opdivo) and ipilimumab (Yervoy) were added to chemotherapy for the treatment of stage IV NSCLC. This combination of immunotherapies, which block CTLA-4 and PD-1, is similar to the combination that was studied in the current trial, and it is already approved for use in some patients with lung cancer.
“Also key to point out,” said Dr. Brahmer, is that, in the POSEIDON trial, “there was a trend toward more poor prognostic factors in the chemotherapy arm, where these patients had more liver or central nervous system metastases.”
Despite these differences, the survival outcomes were similar in the two trials, and in both trials, the tails of the curves indicate that “we need to see long-term data” to determine whether the benefit is ongoing.
Which patients for which combos?
Considering all the data from key trials in advanced NSCLC, Dr. Brahmer said that she believes that, for patients with high PD-L1 expression, treatment with a single immunotherapy directed against PD-1 or PD-L1 “is appropriate” and that she didn’t see that adding a CTLA-4 inhibitor to the PD-L1 inhibitor and chemotherapy would give any advantage.
“But for PD-L1–negative disease, I do think CTLA-4 antibodies seem to provide a benefit, specifically seen in the CheckMate studies,” particularly for patients with squamous disease, although she noted that in POSEIDON, histology and PD-L1 status have not been analyzed.
Dr. Brahmer concluded that, although the triple therapy improved survival outcomes in the current study, several key questions remain.
These include determining what CTLA-4 inhibition adds to PD-L1 blockade and asking whether the “slightly increased toxicity” is “worth the slightly increased long-term duration of response” and improved survival outcomes.
Furthermore, it needs to be determined “which populations truly need” the combined approach; “to get to this, we need to find the biomarker for CTLA-4 benefit,” Dr. Brahmer said.
She also noted “a practical question: Is there room in the clinic for another CTLA-4 antibody in addition to the nivolumab/ipilimumab combinations?”
This last point was appreciated on social media. Jill Feldman, a lung cancer patient and advocate, described it on Twitter as a “great question.”
She said that, for her, “options equal hope,” but that it is “critical” to give the “best treatment first. ... So as a patient, I would ask: How do I know/you know which treatment would be best for me?”
With “so many options in the first-line setting,” subsets of patients who may benefit from quadruplet therapy versus monotherapy need to be defined, commented Charu Aggarwal, MD, MPH, Leslye M. Heisler Associate Professor for Lung Cancer Excellence, Penn Medicine, Philadelphia. He added that “PD-L1 may be one biomarker, but we need more.”
More details of the POSEIDON trial
In the POSEIDON trial, investigators had the choice of different chemotherapy regimens: platinum/gemcitabine for patients with squamous disease, platinum/pemetrexed for patients with nonsquamous disease, and nab-paclitaxel/carboplatin for patients with disease of either histology, Dr. Johnson reported.
It is noteworthy that the majority of patients were from Eastern Europe and Asia, “and the proportion of squamous patients enrolled was higher than is typically seen in mixed histology lung cancer studies,” she added.
The patients were stratified by PD-L1 expression at a cutoff of 50%, disease stage, and tumor histology.
Overall, 1,013 patients were enrolled. The three treatment arms were relatively well balanced in terms of baseline characteristics.
Dr. Johnson noted that there were “a few minor imbalances” in the durvalumab plus tremelimumab arm, with “fewer females, fewer Asians, and fewer never-smokers relative to the other two arms.”
The primary endpoint analysis after a median follow-up of 10.3 months demonstrated that PFS was significantly improved with durvalumab plus chemotherapy over chemotherapy alone, at a median of 5.5 months versus 4.8 months (hazard ratio, 0.74; P = .00093).
Although OS improved numerically with the addition of durvalumab to chemotherapy, it did not reach significance (13.3 months vs. 11.7 months with chemotherapy alone; HR, 0.86; P = .07581).
The positive PFS benefit with durvalumab plus chemotherapy triggered a secondary endpoint analysis, which showed that adding tremelimumab to durvalumab plus chemotherapy improved both survival outcomes.
Median PFS with the triple combination therapy was 6.2 months, significantly longer than the 4.8 months seen with chemotherapy alone (HR, 0.72; P = .00031).
At 12 months, 26.6% of patients who underwent treatment with durvalumab plus tremelimumab plus chemotherapy had not experienced disease progression, compared with 13.1% in the chemotherapy-alone arm.
OS was also significantly improved, at 14.0 months among patients in the triple therapy arm versus 11.7 in the chemotherapy-alone arm (HR, 0.77; P = .00304).
The results also showed that at 24 months, 32.9% of triple therapy patients were still alive versus 22.1% in the chemotherapy-alone arm.
Analysis indicated that “most subgroups favored the addition of immunotherapy to chemotherapy.” There was a “trend toward improved survival for all patients treated with durvalumab plus tremelimumab plus chemotherapy,” Dr. Johnson said.
This was seen “in particular for the nonsquamous patients” and for those with tumor PD-L1 expression of less than 1%, he added.
It is notable that for a large proportion of combination-therapy patients, response had continued at 12 months. This was the case for 38.9% of those who underwent treatment with durvalumab plus chemotherapy and for 49.7% of those given triple therapy versus 21.4% in the chemotherapy-alone arm.
As was seen across the whole cohort, among patients with nonsquamous disease, PFS and OS improved with the addition of immunotherapy. Of those patients with nonsquamous disease, 95.5% received pemetrexed plus platinum chemotherapy.
However, among patients with squamous tumors, of whom 88.3% received gemcitabine plus platinum chemotherapy, PFS and OS were “poor ... across all treatment arms,” Dr. Johnson reported, “with little separation of the curves.”
She highlighted the fact that the proportion of patients who experienced grade 3/4 adverse events, whether of any cause or treatment related, was only slightly higher in the two immunotherapy arms, indicating that “most events were driven by the chemotherapy.”
The rates of treatment discontinuation and adverse events leading to death were also similar across the three treatment arms, albeit they were slightly higher with the addition of immunotherapy.
Dr. Johnson also noted that, although there were more immune-mediated adverse events with durvalumab plus tremelimumab plus chemotherapy, compared with durvalumab plus chemotherapy, the “majority were grade 1/2 and were manageable.”
The most common immune-mediated events in the two immunotherapy arms were hypothyroid and hepatic events, pneumonitis, dermatitis, and rash.
The study was sponsored by AstraZeneca. Dr. Johnson reported numerous relationships with pharmaceutical companies. Dr. Brahmer reported relationships with Amgen, AstratZeneca, BMA, Genentech/Roche, Eli Lilly, Eisai, GlaxoSmithKline, Janssen, Merck, RAPT Therapeutics, Regeneron, Revolution Medicine, and Sanofi.
A version of this article first appeared on Medscape.com.
Combo treatment for NSCLC with brain metastases extends survival by two years for some
The trial is noteworthy because to date, few patients with nonsquamous NSCLC and untreated asymptomatic brain metastases (or those treated with corticosteroids), were ever included in clinical trials that examine the efficacy and safety of chemotherapy and immunotherapy together as first-line treatment, said Ernest Nadal, MD, PhD, of the University of Barcelona Catalan Institute of Oncology at L’Hospitalet de Llobregat. He and his colleagues presented their findings at the meeting, which was organized by the International Association for the Study of Lung Cancer (IASLC).
With only 40 patients, the clinical trial was small, but the safety profile of atezolizumab combined with carboplatin and pemetrexed was favorable in patients with untreated brain metastases and those receiving corticosteroids (dexamethasone of 4 mg once a day or less).
At a median follow-up of 17.3 months, median intracranial and systemic progression-free survival – the co-primary study endpoints, along with safety – were 6.9 months and 8.9 months in 40 patients treated with the immune checkpoint inhibitor and chemotherapy combination, and the 18-month progression-free survival rates were 10.4% and 24.9%, respectively, Dr. Nadal said.
Secondary study endpoints included response rate and overall survival rate. The overall response rate was 40% at 12 weeks; 19 patients (47.5%) had stable disease in the central nervous system, and 19 (47.5%) had a systemic response. The median overall survival was 13.6 months, and 2-year overall survival was 32%.
“The 12-week progression-free survival rate was 60%, [which was] above the expected rate of 50%, and the grade 2-4 toxicity rate was 27.5%, [which was] below the threshold of 35%,” Dr. Nadal said.
Four patients achieved complete response in the brain, and four patients had discordance between systemic and central nervous system response: two with progressive disease in the body and stable disease in the brain, and two with progressive disease in the brain and stable disease in the body.
Study subjects were chemotherapy-naive patients with stage IV non-squamous NSCLC without estimated glomerular filtration rate (EGFR) or anaplastic lymphoma kinase (ALK) genetic alterations and with untreated brain metastases. They were enrolled from 11 clinical sites and treated with carboplatin (5 AUCs) and pemetrexed (500 mg/m2) plus atezolizumab (1,200 mg) every 3 weeks for four to six cycles, followed by maintenance with pemetrexed plus atezolizumab for 2 years or until disease progression or unacceptable toxicity.
Grade 3 treatment-related adverse events occurring in at least 5% of patients were anemia (eight patients), back pain (four patients), thrombocytopenia (two patients) and dyspnea, pneumonitis, and elevated alanine transaminase (one patient each). Grade 4 treatment-related adverse events occurred in three patients and included thrombocytopenia, neutropenia, and hallucinations.
“Brain metastases are the most frequent cancer-related neurological complication and have a major impact on the neurocognitive function, quality of life, and the patient’s prognosis,” Dr. Nadal said, adding that local therapy could add toxicity and delay systemic treatment.
The progression-free survival findings in this study are similar to those reported in the KEYNOTE-189 clinical trial in patients with brain metastases, which showed improved outcomes with pembrolizumab plus chemotherapy in patients with previously untreated metastatic nonsquamous NSCLC, Dr. Nadal said.
The safety profile was also favorable – even in the 17 patients receiving corticosteroids at baseline.
“This combination can result in clinical benefit in terms of overall survival in this population “Correlative studies with brain imaging and blood samples are currently ongoing,” he said.
Charu Aggarwal, MD, MPH, an oncologist with Penn Medicine who specializes in lung cancer, said the findings help address how patients with untreated, asymptomatic brain metastases should be treated.
Taken together with findings from other prospective and retrospective trials in this population, the outcomes demonstrate that “in patients with asymptomatic brain metastases, upfront immunochemotherapy is associated with intracranial response rates,” she said. Patients with asymptomatic brain metastases can be safely treated with chemoimmunotherapy, but “proper patient selection is going to be key.”
Unanswered questions from this study include the size of brain metastases at trial enrollment, whether programmed death-ligand 1 status matters, and whether there is an optimal dose of steroids that should be mandated for inclusion into trials, Dr. Aggarwal added, noting that several trials enrolling patients with lung cancer are seeking to answer these questions.
Dr. Nadal reported receiving research support, speaker bureau fees, and/or honoraria from multiple pharmaceutical companies. Dr. Aggarwal reported serving on an advisory board for multiple pharmaceutical companies. She also reported clinical trial funding to her institution from multiple companies.
The trial is noteworthy because to date, few patients with nonsquamous NSCLC and untreated asymptomatic brain metastases (or those treated with corticosteroids), were ever included in clinical trials that examine the efficacy and safety of chemotherapy and immunotherapy together as first-line treatment, said Ernest Nadal, MD, PhD, of the University of Barcelona Catalan Institute of Oncology at L’Hospitalet de Llobregat. He and his colleagues presented their findings at the meeting, which was organized by the International Association for the Study of Lung Cancer (IASLC).
With only 40 patients, the clinical trial was small, but the safety profile of atezolizumab combined with carboplatin and pemetrexed was favorable in patients with untreated brain metastases and those receiving corticosteroids (dexamethasone of 4 mg once a day or less).
At a median follow-up of 17.3 months, median intracranial and systemic progression-free survival – the co-primary study endpoints, along with safety – were 6.9 months and 8.9 months in 40 patients treated with the immune checkpoint inhibitor and chemotherapy combination, and the 18-month progression-free survival rates were 10.4% and 24.9%, respectively, Dr. Nadal said.
Secondary study endpoints included response rate and overall survival rate. The overall response rate was 40% at 12 weeks; 19 patients (47.5%) had stable disease in the central nervous system, and 19 (47.5%) had a systemic response. The median overall survival was 13.6 months, and 2-year overall survival was 32%.
“The 12-week progression-free survival rate was 60%, [which was] above the expected rate of 50%, and the grade 2-4 toxicity rate was 27.5%, [which was] below the threshold of 35%,” Dr. Nadal said.
Four patients achieved complete response in the brain, and four patients had discordance between systemic and central nervous system response: two with progressive disease in the body and stable disease in the brain, and two with progressive disease in the brain and stable disease in the body.
Study subjects were chemotherapy-naive patients with stage IV non-squamous NSCLC without estimated glomerular filtration rate (EGFR) or anaplastic lymphoma kinase (ALK) genetic alterations and with untreated brain metastases. They were enrolled from 11 clinical sites and treated with carboplatin (5 AUCs) and pemetrexed (500 mg/m2) plus atezolizumab (1,200 mg) every 3 weeks for four to six cycles, followed by maintenance with pemetrexed plus atezolizumab for 2 years or until disease progression or unacceptable toxicity.
Grade 3 treatment-related adverse events occurring in at least 5% of patients were anemia (eight patients), back pain (four patients), thrombocytopenia (two patients) and dyspnea, pneumonitis, and elevated alanine transaminase (one patient each). Grade 4 treatment-related adverse events occurred in three patients and included thrombocytopenia, neutropenia, and hallucinations.
“Brain metastases are the most frequent cancer-related neurological complication and have a major impact on the neurocognitive function, quality of life, and the patient’s prognosis,” Dr. Nadal said, adding that local therapy could add toxicity and delay systemic treatment.
The progression-free survival findings in this study are similar to those reported in the KEYNOTE-189 clinical trial in patients with brain metastases, which showed improved outcomes with pembrolizumab plus chemotherapy in patients with previously untreated metastatic nonsquamous NSCLC, Dr. Nadal said.
The safety profile was also favorable – even in the 17 patients receiving corticosteroids at baseline.
“This combination can result in clinical benefit in terms of overall survival in this population “Correlative studies with brain imaging and blood samples are currently ongoing,” he said.
Charu Aggarwal, MD, MPH, an oncologist with Penn Medicine who specializes in lung cancer, said the findings help address how patients with untreated, asymptomatic brain metastases should be treated.
Taken together with findings from other prospective and retrospective trials in this population, the outcomes demonstrate that “in patients with asymptomatic brain metastases, upfront immunochemotherapy is associated with intracranial response rates,” she said. Patients with asymptomatic brain metastases can be safely treated with chemoimmunotherapy, but “proper patient selection is going to be key.”
Unanswered questions from this study include the size of brain metastases at trial enrollment, whether programmed death-ligand 1 status matters, and whether there is an optimal dose of steroids that should be mandated for inclusion into trials, Dr. Aggarwal added, noting that several trials enrolling patients with lung cancer are seeking to answer these questions.
Dr. Nadal reported receiving research support, speaker bureau fees, and/or honoraria from multiple pharmaceutical companies. Dr. Aggarwal reported serving on an advisory board for multiple pharmaceutical companies. She also reported clinical trial funding to her institution from multiple companies.
The trial is noteworthy because to date, few patients with nonsquamous NSCLC and untreated asymptomatic brain metastases (or those treated with corticosteroids), were ever included in clinical trials that examine the efficacy and safety of chemotherapy and immunotherapy together as first-line treatment, said Ernest Nadal, MD, PhD, of the University of Barcelona Catalan Institute of Oncology at L’Hospitalet de Llobregat. He and his colleagues presented their findings at the meeting, which was organized by the International Association for the Study of Lung Cancer (IASLC).
With only 40 patients, the clinical trial was small, but the safety profile of atezolizumab combined with carboplatin and pemetrexed was favorable in patients with untreated brain metastases and those receiving corticosteroids (dexamethasone of 4 mg once a day or less).
At a median follow-up of 17.3 months, median intracranial and systemic progression-free survival – the co-primary study endpoints, along with safety – were 6.9 months and 8.9 months in 40 patients treated with the immune checkpoint inhibitor and chemotherapy combination, and the 18-month progression-free survival rates were 10.4% and 24.9%, respectively, Dr. Nadal said.
Secondary study endpoints included response rate and overall survival rate. The overall response rate was 40% at 12 weeks; 19 patients (47.5%) had stable disease in the central nervous system, and 19 (47.5%) had a systemic response. The median overall survival was 13.6 months, and 2-year overall survival was 32%.
“The 12-week progression-free survival rate was 60%, [which was] above the expected rate of 50%, and the grade 2-4 toxicity rate was 27.5%, [which was] below the threshold of 35%,” Dr. Nadal said.
Four patients achieved complete response in the brain, and four patients had discordance between systemic and central nervous system response: two with progressive disease in the body and stable disease in the brain, and two with progressive disease in the brain and stable disease in the body.
Study subjects were chemotherapy-naive patients with stage IV non-squamous NSCLC without estimated glomerular filtration rate (EGFR) or anaplastic lymphoma kinase (ALK) genetic alterations and with untreated brain metastases. They were enrolled from 11 clinical sites and treated with carboplatin (5 AUCs) and pemetrexed (500 mg/m2) plus atezolizumab (1,200 mg) every 3 weeks for four to six cycles, followed by maintenance with pemetrexed plus atezolizumab for 2 years or until disease progression or unacceptable toxicity.
Grade 3 treatment-related adverse events occurring in at least 5% of patients were anemia (eight patients), back pain (four patients), thrombocytopenia (two patients) and dyspnea, pneumonitis, and elevated alanine transaminase (one patient each). Grade 4 treatment-related adverse events occurred in three patients and included thrombocytopenia, neutropenia, and hallucinations.
“Brain metastases are the most frequent cancer-related neurological complication and have a major impact on the neurocognitive function, quality of life, and the patient’s prognosis,” Dr. Nadal said, adding that local therapy could add toxicity and delay systemic treatment.
The progression-free survival findings in this study are similar to those reported in the KEYNOTE-189 clinical trial in patients with brain metastases, which showed improved outcomes with pembrolizumab plus chemotherapy in patients with previously untreated metastatic nonsquamous NSCLC, Dr. Nadal said.
The safety profile was also favorable – even in the 17 patients receiving corticosteroids at baseline.
“This combination can result in clinical benefit in terms of overall survival in this population “Correlative studies with brain imaging and blood samples are currently ongoing,” he said.
Charu Aggarwal, MD, MPH, an oncologist with Penn Medicine who specializes in lung cancer, said the findings help address how patients with untreated, asymptomatic brain metastases should be treated.
Taken together with findings from other prospective and retrospective trials in this population, the outcomes demonstrate that “in patients with asymptomatic brain metastases, upfront immunochemotherapy is associated with intracranial response rates,” she said. Patients with asymptomatic brain metastases can be safely treated with chemoimmunotherapy, but “proper patient selection is going to be key.”
Unanswered questions from this study include the size of brain metastases at trial enrollment, whether programmed death-ligand 1 status matters, and whether there is an optimal dose of steroids that should be mandated for inclusion into trials, Dr. Aggarwal added, noting that several trials enrolling patients with lung cancer are seeking to answer these questions.
Dr. Nadal reported receiving research support, speaker bureau fees, and/or honoraria from multiple pharmaceutical companies. Dr. Aggarwal reported serving on an advisory board for multiple pharmaceutical companies. She also reported clinical trial funding to her institution from multiple companies.
REPORTING FROM WCLC 2021
COVID is especially dangerous for mesothelioma
according to Susana Cedres, MD, PhD, a thoracic medical oncologist at Vall d’Hebron University Hospital, Barcelona.
At the annual World Conference on Lung Cancer, she reported on her institution’s experience during the first year of the pandemic before widespread vaccine rollouts.
Among 38 malignant pleural mesothelioma (MPM) patients, seven (18%) patients were diagnosed with COVID-19 and of these, three patients were asymptomatic, four (57%) died of complications including bilateral pneumonia within a median of less than half a month after diagnosis, and a fifth patient died from MPM progression.
The findings confirm the particular risk of COVID in MPM. According to researchers reporting in Scientific Reports, mesothelioma was the only cancer linked to significantly worse outcomes. Other risks included tuberculosis, drug use, hepatitis, HIV/AIDS, cardiomyopathy, and diabetes.
However, the Barcelona report only has seven patients, and it’s one of only a few to address the specifics of COVID in MPM.
“There really is a need for more inclusion of MPM patients in international [COVID] registries” to better characterize the course of infection and improve outcomes, said study discussant Francoise Galateau-Salle, MD, PhD, a mesothelioma expert at the Cancer Center Leon Berard in Lyon, France.
Among the seven positive cases in Barcelona, almost all had comorbidities, with the most common being cardiovascular disease in four patients (57%). Only two patients (29%) were on oncologic treatment at the time they were diagnosed, and the median age at diagnosis was 62 years. Four cases were in men, three in women. MPM stage was not reported.
WCLC 2021 was organized by the International Association for the Study of Lung Cancer.
No funding source was reported. Dr. Cedres is an adviser and/or reported travel expenses from a number of companies, including Merck, Pfizer, and Bristol-Myers Squibb. Dr. Galateau-Salle had no disclosures.
according to Susana Cedres, MD, PhD, a thoracic medical oncologist at Vall d’Hebron University Hospital, Barcelona.
At the annual World Conference on Lung Cancer, she reported on her institution’s experience during the first year of the pandemic before widespread vaccine rollouts.
Among 38 malignant pleural mesothelioma (MPM) patients, seven (18%) patients were diagnosed with COVID-19 and of these, three patients were asymptomatic, four (57%) died of complications including bilateral pneumonia within a median of less than half a month after diagnosis, and a fifth patient died from MPM progression.
The findings confirm the particular risk of COVID in MPM. According to researchers reporting in Scientific Reports, mesothelioma was the only cancer linked to significantly worse outcomes. Other risks included tuberculosis, drug use, hepatitis, HIV/AIDS, cardiomyopathy, and diabetes.
However, the Barcelona report only has seven patients, and it’s one of only a few to address the specifics of COVID in MPM.
“There really is a need for more inclusion of MPM patients in international [COVID] registries” to better characterize the course of infection and improve outcomes, said study discussant Francoise Galateau-Salle, MD, PhD, a mesothelioma expert at the Cancer Center Leon Berard in Lyon, France.
Among the seven positive cases in Barcelona, almost all had comorbidities, with the most common being cardiovascular disease in four patients (57%). Only two patients (29%) were on oncologic treatment at the time they were diagnosed, and the median age at diagnosis was 62 years. Four cases were in men, three in women. MPM stage was not reported.
WCLC 2021 was organized by the International Association for the Study of Lung Cancer.
No funding source was reported. Dr. Cedres is an adviser and/or reported travel expenses from a number of companies, including Merck, Pfizer, and Bristol-Myers Squibb. Dr. Galateau-Salle had no disclosures.
according to Susana Cedres, MD, PhD, a thoracic medical oncologist at Vall d’Hebron University Hospital, Barcelona.
At the annual World Conference on Lung Cancer, she reported on her institution’s experience during the first year of the pandemic before widespread vaccine rollouts.
Among 38 malignant pleural mesothelioma (MPM) patients, seven (18%) patients were diagnosed with COVID-19 and of these, three patients were asymptomatic, four (57%) died of complications including bilateral pneumonia within a median of less than half a month after diagnosis, and a fifth patient died from MPM progression.
The findings confirm the particular risk of COVID in MPM. According to researchers reporting in Scientific Reports, mesothelioma was the only cancer linked to significantly worse outcomes. Other risks included tuberculosis, drug use, hepatitis, HIV/AIDS, cardiomyopathy, and diabetes.
However, the Barcelona report only has seven patients, and it’s one of only a few to address the specifics of COVID in MPM.
“There really is a need for more inclusion of MPM patients in international [COVID] registries” to better characterize the course of infection and improve outcomes, said study discussant Francoise Galateau-Salle, MD, PhD, a mesothelioma expert at the Cancer Center Leon Berard in Lyon, France.
Among the seven positive cases in Barcelona, almost all had comorbidities, with the most common being cardiovascular disease in four patients (57%). Only two patients (29%) were on oncologic treatment at the time they were diagnosed, and the median age at diagnosis was 62 years. Four cases were in men, three in women. MPM stage was not reported.
WCLC 2021 was organized by the International Association for the Study of Lung Cancer.
No funding source was reported. Dr. Cedres is an adviser and/or reported travel expenses from a number of companies, including Merck, Pfizer, and Bristol-Myers Squibb. Dr. Galateau-Salle had no disclosures.
FROM WCLC 2021
PRESERVED-HF: Dapagliflozin improves physical limitations in patients with HFpEF
The SGLT2 inhibitor dapagliflozin scored a clear win in a randomized, controlled trial with more than 300 U.S. patients with heart failure with preserved ejection fraction (HFpEF), showing a significant and clinically meaningful benefit for the primary endpoint, a KCCQ measure of symptoms and physical limitations, after 12 weeks of treatment.

These results in the PRESERVED-HF study follow closely on the heals of the initial report from the EMPEROR-Preserved trial that showed a benefit from a different sodium-glucose cotransporter 2 (SGLT2) inhibitor, empagliflozin (Jardiance) in nearly 6,000 randomized patients for the primary endpoint of preventing cardiovascular death or hospitalizations for heart failure.
In PRESERVED-HF, patients with HFpEF who received a standard, once-daily dose of dapagliflozin (Farxiga) had an average 5.8-point improvement in their condition as measured by the Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CS), the study’s primary endpoint.
This is “the first study to demonstrate that an SGLT2 inhibitor dapagliflozin significantly improves symptoms, physical limitations, and 6-minute walking distance in patients with HFpEF,” Mikhail N. Kosiborod, MD, reported at the annual scientific meeting of the Heart Failure Society of America. The secondary endpoint of 6-minute walking distance “has been very difficult to improve in many previous studies of other treatments” tested in patients with HFpEF, noted Dr. Kosiborod, a cardiologist and codirector of the Cardiometabolic Center of Excellence at Saint Luke’s Mid-America Heart Institute.
The results are “highly complementary” to the findings from large outcome trials, such as the findings from EMPEROR-Preserved, he said, and collectively the recent findings from these studies of SGLT2 inhibitors in patients with HFpEF identify drugs in this class as a “new treatment option” for patients with a disorder that until now had no treatment with unequivocally proven efficacy and safety.
‘Impressive and unprecedented’ findings
The findings are “really impressive and unprecedented,” said Milton Packer, MD, a cardiologist at Baylor University Medical Center in Dallas who was not involved in the study. “This is the largest KCCQ benefit ever seen in either patients with HFpEF or in patients with heart failure with reduced ejection fraction,” said Dr. Packer, one of the investigators who led the EMPEROR-Preserved trial.

PRESERVED-HF randomized 324 patients diagnosed with heart failure and with a left ventricular ejection fraction of 45% or higher at any of 26 U.S. centers, with 304 patients completing the planned final analysis after 12 weeks on treatment. Patients could be in New York Heart Association (NYHA) functional class II-IV, they had to have a baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) level of at least 225 pg/mL (or higher if they also had atrial fibrillation), and they required at least one of three markers of established heart failure: recent hospitalization for heart failure or an urgent outpatient visit that required treatment with an IV diuretic, elevated filling pressure measured by left or right catheterization, or structural heart disease detected by echocardiography.
The average age of the enrolled patients was 70 years, and they had been diagnosed with heart failure for about 3 years; 57% were women, 30% were African American, and their median body mass index was 35 kg/m2. Roughly 42% had NYHA class III or IV disease, 56% had type 2 diabetes, their median estimated glomerular filtration rate was about 55 mL/min per 1.73m2, their median KCCQ-CS score at baseline was about 62, and their average 6-minute walk distance was 244 m.
These and other features of the enrolled population define a distinctly U.S. patient population, stressed Dr. Kosiborod, professor of medicine at the University of Missouri–Kansas City.
“The patients we enrolled are the patients we see in U.S. clinical practice,” he said in an interview. Importantly, the patient profile of a median BMI of 35 kg/m2, a median KCCQ-CS score of 62 – “quite low,” noted Dr. Kosiborod – and having more than 40% of patients in NYHA functional class III defines a study population with a substantially greater burden of obesity, symptoms, and functional impairment compared with those enrolled in prior trials involving patients with HFpEF such as EMPEROR-Preserved.
Results complement findings from larger trials
PRESERVED-HF was an investigator-initiated study designed to inform clinical practice, not as a pivotal trial like EMPEROR-Preserved, which aims to gather evidence to support a new indication for regulatory approval. (On Sept. 9, 2021, the Food and Drug Administration granted empagliflozin “breakthrough therapy” status for treating HFpEF based on the EMPEROR-Preserved results, which will fast-track the agency’s decision on this indication.)
Dr. Kosiborod noted that he and his associates designed PRESERVED-HF with adequate patient numbers to power a statistically valid assessment of effect on KCCQ-CS score. While the new findings will not by themselves lead to a new indication for dapagliflozin to treat patients with HFpEF, they will potentially complement the pending results of another trial, DELIVER, by showing efficacy and safety in a uniquely U.S. patient population. DELIVER is a pivotal, global trial of dapagliflozin in more than 6,000 patients with HFpEF that’s on track to report findings in 2022.
Dr. Kosiborod also stressed that dapagliflozin has U.S.-approved indications for treating patients with type 2 diabetes, and for patients with chronic kidney disease, and that a majority of patients enrolled in PRESERVED-HF had one or both of these conditions. That makes the new findings especially compelling for patients with either type 2 diabetes or chronic kidney disease and HFpEF who are not already receiving an SGLT2 inhibitor.
Other findings that he reported showed a range of benefits consistent with the primary endpoint, including the KCCQ overall summary score, which also showed a significant 4.5-point average increase over placebo after 12 weeks. Analysis by the percentage of patients achieving at least a 5-point improvement in the KCCQ clinical summary score (the threshold for a clinically meaningful improvement) showed that about 45% of patients treated with dapagliflozin reached this mark compared with roughly 35% of patients in the placebo arm, indicating a number needed to treat of nine to have one additional patient achieve this threshold after 12 weeks. Average improvement in 6-minute walk distance was about 20 m with dapagliflozin compared with placebo.
No heterogeneity of effect by baseline ejection fraction.
Subgroup analyses showed no heterogeneity of response across 12 different ways of subdividing the study population, including age, sex, race, diabetes status, and BMI. The median left ventricular ejection fraction among enrolled patients was 60%, and the findings showed identical KCCQ improvements among patients with ejection fractions less than the median and those with an ejection fraction above the median.
This last finding was especially relevant because the EMPEROR-Preserved results showed a possible signal of heterogeneity by ejection fraction and an attenuated effect among patients with HFpEF and an ejection fraction above the 60%-65% range, although the certainty of this finding is currently controversial.
The impact of empagliflozin on KCCQ clinical summary score in EMPEROR-Preserved showed an average incremental improvement of 1.32 points compared with placebo, a significant difference, but more modest than the increment from dapagliflozin treatment seen in PRESERVED-HF. Dr. Kosiborod hypothesized that this difference might be mostly because of the different patient populations enrolled in the two studies.
Dr. Kosiborod noted that a report on the PRESERVED-HF results will soon appear in Nature Medicine.
PRESERVED-HF was funded by AstraZeneca, which markets dapagliflozin (Farxiga), but the trials’ design and conduct were independent of this funding source. Dr. Kosiborod has been a consultant to AstraZeneca and numerous other companies, and he has received research funding from AstraZeneca and Boehringer Ingelheim. Dr. Packer has had financial relationships with AstraZeneca and numerous other companies.
The SGLT2 inhibitor dapagliflozin scored a clear win in a randomized, controlled trial with more than 300 U.S. patients with heart failure with preserved ejection fraction (HFpEF), showing a significant and clinically meaningful benefit for the primary endpoint, a KCCQ measure of symptoms and physical limitations, after 12 weeks of treatment.
These results in the PRESERVED-HF study follow closely on the heals of the initial report from the EMPEROR-Preserved trial that showed a benefit from a different sodium-glucose cotransporter 2 (SGLT2) inhibitor, empagliflozin (Jardiance) in nearly 6,000 randomized patients for the primary endpoint of preventing cardiovascular death or hospitalizations for heart failure.
In PRESERVED-HF, patients with HFpEF who received a standard, once-daily dose of dapagliflozin (Farxiga) had an average 5.8-point improvement in their condition as measured by the Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CS), the study’s primary endpoint.
This is “the first study to demonstrate that an SGLT2 inhibitor dapagliflozin significantly improves symptoms, physical limitations, and 6-minute walking distance in patients with HFpEF,” Mikhail N. Kosiborod, MD, reported at the annual scientific meeting of the Heart Failure Society of America. The secondary endpoint of 6-minute walking distance “has been very difficult to improve in many previous studies of other treatments” tested in patients with HFpEF, noted Dr. Kosiborod, a cardiologist and codirector of the Cardiometabolic Center of Excellence at Saint Luke’s Mid-America Heart Institute.
The results are “highly complementary” to the findings from large outcome trials, such as the findings from EMPEROR-Preserved, he said, and collectively the recent findings from these studies of SGLT2 inhibitors in patients with HFpEF identify drugs in this class as a “new treatment option” for patients with a disorder that until now had no treatment with unequivocally proven efficacy and safety.
‘Impressive and unprecedented’ findings
The findings are “really impressive and unprecedented,” said Milton Packer, MD, a cardiologist at Baylor University Medical Center in Dallas who was not involved in the study. “This is the largest KCCQ benefit ever seen in either patients with HFpEF or in patients with heart failure with reduced ejection fraction,” said Dr. Packer, one of the investigators who led the EMPEROR-Preserved trial.
PRESERVED-HF randomized 324 patients diagnosed with heart failure and with a left ventricular ejection fraction of 45% or higher at any of 26 U.S. centers, with 304 patients completing the planned final analysis after 12 weeks on treatment. Patients could be in New York Heart Association (NYHA) functional class II-IV, they had to have a baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) level of at least 225 pg/mL (or higher if they also had atrial fibrillation), and they required at least one of three markers of established heart failure: recent hospitalization for heart failure or an urgent outpatient visit that required treatment with an IV diuretic, elevated filling pressure measured by left or right catheterization, or structural heart disease detected by echocardiography.
The average age of the enrolled patients was 70 years, and they had been diagnosed with heart failure for about 3 years; 57% were women, 30% were African American, and their median body mass index was 35 kg/m2. Roughly 42% had NYHA class III or IV disease, 56% had type 2 diabetes, their median estimated glomerular filtration rate was about 55 mL/min per 1.73m2, their median KCCQ-CS score at baseline was about 62, and their average 6-minute walk distance was 244 m.
These and other features of the enrolled population define a distinctly U.S. patient population, stressed Dr. Kosiborod, professor of medicine at the University of Missouri–Kansas City.
“The patients we enrolled are the patients we see in U.S. clinical practice,” he said in an interview. Importantly, the patient profile of a median BMI of 35 kg/m2, a median KCCQ-CS score of 62 – “quite low,” noted Dr. Kosiborod – and having more than 40% of patients in NYHA functional class III defines a study population with a substantially greater burden of obesity, symptoms, and functional impairment compared with those enrolled in prior trials involving patients with HFpEF such as EMPEROR-Preserved.
Results complement findings from larger trials
PRESERVED-HF was an investigator-initiated study designed to inform clinical practice, not as a pivotal trial like EMPEROR-Preserved, which aims to gather evidence to support a new indication for regulatory approval. (On Sept. 9, 2021, the Food and Drug Administration granted empagliflozin “breakthrough therapy” status for treating HFpEF based on the EMPEROR-Preserved results, which will fast-track the agency’s decision on this indication.)
Dr. Kosiborod noted that he and his associates designed PRESERVED-HF with adequate patient numbers to power a statistically valid assessment of effect on KCCQ-CS score. While the new findings will not by themselves lead to a new indication for dapagliflozin to treat patients with HFpEF, they will potentially complement the pending results of another trial, DELIVER, by showing efficacy and safety in a uniquely U.S. patient population. DELIVER is a pivotal, global trial of dapagliflozin in more than 6,000 patients with HFpEF that’s on track to report findings in 2022.
Dr. Kosiborod also stressed that dapagliflozin has U.S.-approved indications for treating patients with type 2 diabetes, and for patients with chronic kidney disease, and that a majority of patients enrolled in PRESERVED-HF had one or both of these conditions. That makes the new findings especially compelling for patients with either type 2 diabetes or chronic kidney disease and HFpEF who are not already receiving an SGLT2 inhibitor.
Other findings that he reported showed a range of benefits consistent with the primary endpoint, including the KCCQ overall summary score, which also showed a significant 4.5-point average increase over placebo after 12 weeks. Analysis by the percentage of patients achieving at least a 5-point improvement in the KCCQ clinical summary score (the threshold for a clinically meaningful improvement) showed that about 45% of patients treated with dapagliflozin reached this mark compared with roughly 35% of patients in the placebo arm, indicating a number needed to treat of nine to have one additional patient achieve this threshold after 12 weeks. Average improvement in 6-minute walk distance was about 20 m with dapagliflozin compared with placebo.
No heterogeneity of effect by baseline ejection fraction.
Subgroup analyses showed no heterogeneity of response across 12 different ways of subdividing the study population, including age, sex, race, diabetes status, and BMI. The median left ventricular ejection fraction among enrolled patients was 60%, and the findings showed identical KCCQ improvements among patients with ejection fractions less than the median and those with an ejection fraction above the median.
This last finding was especially relevant because the EMPEROR-Preserved results showed a possible signal of heterogeneity by ejection fraction and an attenuated effect among patients with HFpEF and an ejection fraction above the 60%-65% range, although the certainty of this finding is currently controversial.
The impact of empagliflozin on KCCQ clinical summary score in EMPEROR-Preserved showed an average incremental improvement of 1.32 points compared with placebo, a significant difference, but more modest than the increment from dapagliflozin treatment seen in PRESERVED-HF. Dr. Kosiborod hypothesized that this difference might be mostly because of the different patient populations enrolled in the two studies.
Dr. Kosiborod noted that a report on the PRESERVED-HF results will soon appear in Nature Medicine.
PRESERVED-HF was funded by AstraZeneca, which markets dapagliflozin (Farxiga), but the trials’ design and conduct were independent of this funding source. Dr. Kosiborod has been a consultant to AstraZeneca and numerous other companies, and he has received research funding from AstraZeneca and Boehringer Ingelheim. Dr. Packer has had financial relationships with AstraZeneca and numerous other companies.
The SGLT2 inhibitor dapagliflozin scored a clear win in a randomized, controlled trial with more than 300 U.S. patients with heart failure with preserved ejection fraction (HFpEF), showing a significant and clinically meaningful benefit for the primary endpoint, a KCCQ measure of symptoms and physical limitations, after 12 weeks of treatment.
These results in the PRESERVED-HF study follow closely on the heals of the initial report from the EMPEROR-Preserved trial that showed a benefit from a different sodium-glucose cotransporter 2 (SGLT2) inhibitor, empagliflozin (Jardiance) in nearly 6,000 randomized patients for the primary endpoint of preventing cardiovascular death or hospitalizations for heart failure.
In PRESERVED-HF, patients with HFpEF who received a standard, once-daily dose of dapagliflozin (Farxiga) had an average 5.8-point improvement in their condition as measured by the Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CS), the study’s primary endpoint.
This is “the first study to demonstrate that an SGLT2 inhibitor dapagliflozin significantly improves symptoms, physical limitations, and 6-minute walking distance in patients with HFpEF,” Mikhail N. Kosiborod, MD, reported at the annual scientific meeting of the Heart Failure Society of America. The secondary endpoint of 6-minute walking distance “has been very difficult to improve in many previous studies of other treatments” tested in patients with HFpEF, noted Dr. Kosiborod, a cardiologist and codirector of the Cardiometabolic Center of Excellence at Saint Luke’s Mid-America Heart Institute.
The results are “highly complementary” to the findings from large outcome trials, such as the findings from EMPEROR-Preserved, he said, and collectively the recent findings from these studies of SGLT2 inhibitors in patients with HFpEF identify drugs in this class as a “new treatment option” for patients with a disorder that until now had no treatment with unequivocally proven efficacy and safety.
‘Impressive and unprecedented’ findings
The findings are “really impressive and unprecedented,” said Milton Packer, MD, a cardiologist at Baylor University Medical Center in Dallas who was not involved in the study. “This is the largest KCCQ benefit ever seen in either patients with HFpEF or in patients with heart failure with reduced ejection fraction,” said Dr. Packer, one of the investigators who led the EMPEROR-Preserved trial.
PRESERVED-HF randomized 324 patients diagnosed with heart failure and with a left ventricular ejection fraction of 45% or higher at any of 26 U.S. centers, with 304 patients completing the planned final analysis after 12 weeks on treatment. Patients could be in New York Heart Association (NYHA) functional class II-IV, they had to have a baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) level of at least 225 pg/mL (or higher if they also had atrial fibrillation), and they required at least one of three markers of established heart failure: recent hospitalization for heart failure or an urgent outpatient visit that required treatment with an IV diuretic, elevated filling pressure measured by left or right catheterization, or structural heart disease detected by echocardiography.
The average age of the enrolled patients was 70 years, and they had been diagnosed with heart failure for about 3 years; 57% were women, 30% were African American, and their median body mass index was 35 kg/m2. Roughly 42% had NYHA class III or IV disease, 56% had type 2 diabetes, their median estimated glomerular filtration rate was about 55 mL/min per 1.73m2, their median KCCQ-CS score at baseline was about 62, and their average 6-minute walk distance was 244 m.
These and other features of the enrolled population define a distinctly U.S. patient population, stressed Dr. Kosiborod, professor of medicine at the University of Missouri–Kansas City.
“The patients we enrolled are the patients we see in U.S. clinical practice,” he said in an interview. Importantly, the patient profile of a median BMI of 35 kg/m2, a median KCCQ-CS score of 62 – “quite low,” noted Dr. Kosiborod – and having more than 40% of patients in NYHA functional class III defines a study population with a substantially greater burden of obesity, symptoms, and functional impairment compared with those enrolled in prior trials involving patients with HFpEF such as EMPEROR-Preserved.
Results complement findings from larger trials
PRESERVED-HF was an investigator-initiated study designed to inform clinical practice, not as a pivotal trial like EMPEROR-Preserved, which aims to gather evidence to support a new indication for regulatory approval. (On Sept. 9, 2021, the Food and Drug Administration granted empagliflozin “breakthrough therapy” status for treating HFpEF based on the EMPEROR-Preserved results, which will fast-track the agency’s decision on this indication.)
Dr. Kosiborod noted that he and his associates designed PRESERVED-HF with adequate patient numbers to power a statistically valid assessment of effect on KCCQ-CS score. While the new findings will not by themselves lead to a new indication for dapagliflozin to treat patients with HFpEF, they will potentially complement the pending results of another trial, DELIVER, by showing efficacy and safety in a uniquely U.S. patient population. DELIVER is a pivotal, global trial of dapagliflozin in more than 6,000 patients with HFpEF that’s on track to report findings in 2022.
Dr. Kosiborod also stressed that dapagliflozin has U.S.-approved indications for treating patients with type 2 diabetes, and for patients with chronic kidney disease, and that a majority of patients enrolled in PRESERVED-HF had one or both of these conditions. That makes the new findings especially compelling for patients with either type 2 diabetes or chronic kidney disease and HFpEF who are not already receiving an SGLT2 inhibitor.
Other findings that he reported showed a range of benefits consistent with the primary endpoint, including the KCCQ overall summary score, which also showed a significant 4.5-point average increase over placebo after 12 weeks. Analysis by the percentage of patients achieving at least a 5-point improvement in the KCCQ clinical summary score (the threshold for a clinically meaningful improvement) showed that about 45% of patients treated with dapagliflozin reached this mark compared with roughly 35% of patients in the placebo arm, indicating a number needed to treat of nine to have one additional patient achieve this threshold after 12 weeks. Average improvement in 6-minute walk distance was about 20 m with dapagliflozin compared with placebo.
No heterogeneity of effect by baseline ejection fraction.
Subgroup analyses showed no heterogeneity of response across 12 different ways of subdividing the study population, including age, sex, race, diabetes status, and BMI. The median left ventricular ejection fraction among enrolled patients was 60%, and the findings showed identical KCCQ improvements among patients with ejection fractions less than the median and those with an ejection fraction above the median.
This last finding was especially relevant because the EMPEROR-Preserved results showed a possible signal of heterogeneity by ejection fraction and an attenuated effect among patients with HFpEF and an ejection fraction above the 60%-65% range, although the certainty of this finding is currently controversial.
The impact of empagliflozin on KCCQ clinical summary score in EMPEROR-Preserved showed an average incremental improvement of 1.32 points compared with placebo, a significant difference, but more modest than the increment from dapagliflozin treatment seen in PRESERVED-HF. Dr. Kosiborod hypothesized that this difference might be mostly because of the different patient populations enrolled in the two studies.
Dr. Kosiborod noted that a report on the PRESERVED-HF results will soon appear in Nature Medicine.
PRESERVED-HF was funded by AstraZeneca, which markets dapagliflozin (Farxiga), but the trials’ design and conduct were independent of this funding source. Dr. Kosiborod has been a consultant to AstraZeneca and numerous other companies, and he has received research funding from AstraZeneca and Boehringer Ingelheim. Dr. Packer has had financial relationships with AstraZeneca and numerous other companies.
FROM HFSA 2021
Obese children with asthma are resistant to ICS
Obese or overweight children with asthma could be using inhaled corticosteroids (ICS) to no avail, combined results from observational studies suggest.

Using Mendelian randomization, a method for reducing bias in observational studies, investigators from the University of Amsterdam Medical Center performed an analysis of data from four cross-sectional studies and one cohort study on a total of 1,511 children with asthma.
They showed that every 1-unit increase in the body mass index (BMI) z score was associated with a more than twofold higher odds ratio for exacerbation, reported Cristina Longo, PhD, a former postdoctoral fellow at AMC, and assistant professor of medicine at the University of Montreal.
“In this large, multicenter Mendelian randomization study, our findings support current evidence that children with higher BMI status respond inadequately to inhaled corticosteroids, and that this association is likely not explained by measured confounding or reverse causation,” she said in an oral abstract presentation during the European Respiratory Society International Congress.
Unmeasured confounding
The obese-asthma phenotype in children is characterized by reduced lung function, high symptom expression, poor response to ICS, and high health care utilization.
“While most observational studies suggest that weight status is associated with asthma exacerbations, despite using inhaled corticosteroids, it’s unclear whether these associations may be due to unmeasured confounding or reverse causation, which captures the idea that perhaps obesity is a consequence rather than a cause of uncontrolled severe asthma,” she said.
Traditional observational studies of the obesity-asthma link rely on comparing data on asthma in a target population and comparing nonobese patients with obese patients. The problem with this method, Dr. Longo contended, is that the exposure assignment – weight status – is not random, and could lead to bias from potential imbalance of confounders, leading to unintentionally biased results.
In contrast, Mendelian randomization uses genetic data to approximate random assignment of exposures, using a risk score for BMI based on genetic susceptibility. The score is based on the accumulation of genetic variants (single-nucleotide polymorphisms, or SNPs) that predispose individuals to obesity, with higher numbers of variants results in a higher risk score.
The scores are then used to determine the comparison groups for evaluating the obesity-asthma association.
Alphabet soup
Dr. Longo and colleagues analyzed data on a total 1,511 children enrolled in four observational studies (PACMAN, PAGES, HPR, CLARA) and one cohort study (ALSPAC).
They included children with an asthma diagnosis who used ICS and had available information on both BMI and genetics.
The Mendelian randomization analysis was based on a weighted allele score based on 97 SNPs predictive of BMI based on large-scale genomewide association studies. The exposure for the analysis was age- and sex-adjusted BMI z scores based on World Health Organization growth charts for children.
They found that using the Mendelian randomization approach, for each standard deviation increase in BMI, the OR for any parent-reported asthma exacerbations, including urgent care visits or use of oral corticosteroids, was 2.31 (95% confidence interval, 1.26-4.25).
In contrast, if the traditional observational model had been used, the OR would be a nonsignificant 1.10 (95% CI, 0.99-1.22).
“Treatment guidelines recommend steroids for children with asthma who have a higher-than-normal BMI,” Dr. Longo said in a statement. “Our research group felt that the one-size fits-all approach to treating children with asthma with inhaled steroids as their first-line treatment, particularly those with excess weight, warrants revision. At the very least, research identifying potential alternative treatments should be encouraged and prioritized, especially since 30% of children with asthma are also obese. With the childhood obesity epidemic rising, we expect this percentage to increase meaning this problem of poor control will be seen more frequently in routine clinical practice.”
Christopher E. Brightling, PhD, professor of respiratory medicine at the University of Leicester (England), commented that “this is very good and fascinating research with findings that are important and novel.
“It sheds light on the complex interplay between genes, weight, and response to inhaled corticosteroids, underscoring the need to combine drug treatments with lifestyle and diet modifications. Policy makers, health care providers and families need to do much more to tackle the growing obesity epidemic in young people,” he said.
Dr. Brightling was not involved in the study.
The study was supported by the ERS and the European Union’s H2020 research and innovation program. Dr. Longo was a Horizon 2020 Marie-Sklodowska Cure Respire-3 fellow. Dr. Brightling reported no relevant disclosures.
Obese or overweight children with asthma could be using inhaled corticosteroids (ICS) to no avail, combined results from observational studies suggest.
Using Mendelian randomization, a method for reducing bias in observational studies, investigators from the University of Amsterdam Medical Center performed an analysis of data from four cross-sectional studies and one cohort study on a total of 1,511 children with asthma.
They showed that every 1-unit increase in the body mass index (BMI) z score was associated with a more than twofold higher odds ratio for exacerbation, reported Cristina Longo, PhD, a former postdoctoral fellow at AMC, and assistant professor of medicine at the University of Montreal.
“In this large, multicenter Mendelian randomization study, our findings support current evidence that children with higher BMI status respond inadequately to inhaled corticosteroids, and that this association is likely not explained by measured confounding or reverse causation,” she said in an oral abstract presentation during the European Respiratory Society International Congress.
Unmeasured confounding
The obese-asthma phenotype in children is characterized by reduced lung function, high symptom expression, poor response to ICS, and high health care utilization.
“While most observational studies suggest that weight status is associated with asthma exacerbations, despite using inhaled corticosteroids, it’s unclear whether these associations may be due to unmeasured confounding or reverse causation, which captures the idea that perhaps obesity is a consequence rather than a cause of uncontrolled severe asthma,” she said.
Traditional observational studies of the obesity-asthma link rely on comparing data on asthma in a target population and comparing nonobese patients with obese patients. The problem with this method, Dr. Longo contended, is that the exposure assignment – weight status – is not random, and could lead to bias from potential imbalance of confounders, leading to unintentionally biased results.
In contrast, Mendelian randomization uses genetic data to approximate random assignment of exposures, using a risk score for BMI based on genetic susceptibility. The score is based on the accumulation of genetic variants (single-nucleotide polymorphisms, or SNPs) that predispose individuals to obesity, with higher numbers of variants results in a higher risk score.
The scores are then used to determine the comparison groups for evaluating the obesity-asthma association.
Alphabet soup
Dr. Longo and colleagues analyzed data on a total 1,511 children enrolled in four observational studies (PACMAN, PAGES, HPR, CLARA) and one cohort study (ALSPAC).
They included children with an asthma diagnosis who used ICS and had available information on both BMI and genetics.
The Mendelian randomization analysis was based on a weighted allele score based on 97 SNPs predictive of BMI based on large-scale genomewide association studies. The exposure for the analysis was age- and sex-adjusted BMI z scores based on World Health Organization growth charts for children.
They found that using the Mendelian randomization approach, for each standard deviation increase in BMI, the OR for any parent-reported asthma exacerbations, including urgent care visits or use of oral corticosteroids, was 2.31 (95% confidence interval, 1.26-4.25).
In contrast, if the traditional observational model had been used, the OR would be a nonsignificant 1.10 (95% CI, 0.99-1.22).
“Treatment guidelines recommend steroids for children with asthma who have a higher-than-normal BMI,” Dr. Longo said in a statement. “Our research group felt that the one-size fits-all approach to treating children with asthma with inhaled steroids as their first-line treatment, particularly those with excess weight, warrants revision. At the very least, research identifying potential alternative treatments should be encouraged and prioritized, especially since 30% of children with asthma are also obese. With the childhood obesity epidemic rising, we expect this percentage to increase meaning this problem of poor control will be seen more frequently in routine clinical practice.”
Christopher E. Brightling, PhD, professor of respiratory medicine at the University of Leicester (England), commented that “this is very good and fascinating research with findings that are important and novel.
“It sheds light on the complex interplay between genes, weight, and response to inhaled corticosteroids, underscoring the need to combine drug treatments with lifestyle and diet modifications. Policy makers, health care providers and families need to do much more to tackle the growing obesity epidemic in young people,” he said.
Dr. Brightling was not involved in the study.
The study was supported by the ERS and the European Union’s H2020 research and innovation program. Dr. Longo was a Horizon 2020 Marie-Sklodowska Cure Respire-3 fellow. Dr. Brightling reported no relevant disclosures.
Obese or overweight children with asthma could be using inhaled corticosteroids (ICS) to no avail, combined results from observational studies suggest.
Using Mendelian randomization, a method for reducing bias in observational studies, investigators from the University of Amsterdam Medical Center performed an analysis of data from four cross-sectional studies and one cohort study on a total of 1,511 children with asthma.
They showed that every 1-unit increase in the body mass index (BMI) z score was associated with a more than twofold higher odds ratio for exacerbation, reported Cristina Longo, PhD, a former postdoctoral fellow at AMC, and assistant professor of medicine at the University of Montreal.
“In this large, multicenter Mendelian randomization study, our findings support current evidence that children with higher BMI status respond inadequately to inhaled corticosteroids, and that this association is likely not explained by measured confounding or reverse causation,” she said in an oral abstract presentation during the European Respiratory Society International Congress.
Unmeasured confounding
The obese-asthma phenotype in children is characterized by reduced lung function, high symptom expression, poor response to ICS, and high health care utilization.
“While most observational studies suggest that weight status is associated with asthma exacerbations, despite using inhaled corticosteroids, it’s unclear whether these associations may be due to unmeasured confounding or reverse causation, which captures the idea that perhaps obesity is a consequence rather than a cause of uncontrolled severe asthma,” she said.
Traditional observational studies of the obesity-asthma link rely on comparing data on asthma in a target population and comparing nonobese patients with obese patients. The problem with this method, Dr. Longo contended, is that the exposure assignment – weight status – is not random, and could lead to bias from potential imbalance of confounders, leading to unintentionally biased results.
In contrast, Mendelian randomization uses genetic data to approximate random assignment of exposures, using a risk score for BMI based on genetic susceptibility. The score is based on the accumulation of genetic variants (single-nucleotide polymorphisms, or SNPs) that predispose individuals to obesity, with higher numbers of variants results in a higher risk score.
The scores are then used to determine the comparison groups for evaluating the obesity-asthma association.
Alphabet soup
Dr. Longo and colleagues analyzed data on a total 1,511 children enrolled in four observational studies (PACMAN, PAGES, HPR, CLARA) and one cohort study (ALSPAC).
They included children with an asthma diagnosis who used ICS and had available information on both BMI and genetics.
The Mendelian randomization analysis was based on a weighted allele score based on 97 SNPs predictive of BMI based on large-scale genomewide association studies. The exposure for the analysis was age- and sex-adjusted BMI z scores based on World Health Organization growth charts for children.
They found that using the Mendelian randomization approach, for each standard deviation increase in BMI, the OR for any parent-reported asthma exacerbations, including urgent care visits or use of oral corticosteroids, was 2.31 (95% confidence interval, 1.26-4.25).
In contrast, if the traditional observational model had been used, the OR would be a nonsignificant 1.10 (95% CI, 0.99-1.22).
“Treatment guidelines recommend steroids for children with asthma who have a higher-than-normal BMI,” Dr. Longo said in a statement. “Our research group felt that the one-size fits-all approach to treating children with asthma with inhaled steroids as their first-line treatment, particularly those with excess weight, warrants revision. At the very least, research identifying potential alternative treatments should be encouraged and prioritized, especially since 30% of children with asthma are also obese. With the childhood obesity epidemic rising, we expect this percentage to increase meaning this problem of poor control will be seen more frequently in routine clinical practice.”
Christopher E. Brightling, PhD, professor of respiratory medicine at the University of Leicester (England), commented that “this is very good and fascinating research with findings that are important and novel.
“It sheds light on the complex interplay between genes, weight, and response to inhaled corticosteroids, underscoring the need to combine drug treatments with lifestyle and diet modifications. Policy makers, health care providers and families need to do much more to tackle the growing obesity epidemic in young people,” he said.
Dr. Brightling was not involved in the study.
The study was supported by the ERS and the European Union’s H2020 research and innovation program. Dr. Longo was a Horizon 2020 Marie-Sklodowska Cure Respire-3 fellow. Dr. Brightling reported no relevant disclosures.
FROM ERS 2021
Are ESC’s new heart failure guidelines already outdated?
The new guideline on management of heart failure (HF) from the European Society of Cardiology seemed to bear an asterisk or footnote even before its full unveiling in the early hours of ESC Congress 2021.

The document would offer little new in the arena of HF with preserved ejection fraction (HFpEF), so understandably the fast-approaching presentation of a major HFpEF trial – arguably the conference’s marquee event – would feel to some like the elephant in the room.
“I’d like to highlight this unfortunate timing of the guideline, because it’s an hour or 2 before we hear the full story from EMPEROR-Preserved, which I’m sure will change the guidelines,” Faiez Zannad, MD, PhD, University of Lorraine, Vandoeuvre-Les-Nancy, France, said wryly.
Anticipation of the trial’s full presentation was intense as the ESC congress got underway, in part because the top-line and incomplete message from EMPEROR-Preserved had already been released: Patients with HFpEF treated with the sodium-glucose cotransporter 2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Eli Lilly) showed a significant benefit for the primary endpoint of cardiovascular (CV) death or HF hospitalization.
Although empagliflozin is the first medication to achieve that status in a major HFpEF trial, conspicuously absent from the early announcement were the magnitude of “benefit” and any data. Still, the tantalizing top-line results mean that technically, at least, “we have a drug which is effective in reduced and preserved ejection fraction,” Dr. Zannad said.
But the new guideline, published online Aug. 27, 2021, in the European Heart Journal and comprehensively described that day at the congress, was never really expected to consider results from EMPEROR-Reduced. “These new indications do need to go through the regulatory authorities,” such as the European Medicines Agency and the U.S. Food and Drug Administration, observed Carlos Aguiar, MD, Hospital Santa Cruz, Carnaxide, Portugal.
“It does take some time for the whole process to be concluded and, finally, as physicians, being able to implement it in clinical practice,” Dr. Aguiar said as moderator of press briefing prior to the ESC congress.
The ESC guideline’s next iteration or update could well include an SGLT2 inhibitor recommendation that applies beyond the ejection fraction limits of HFrEF. Still, the document summarized that day reflects a number of pivotal concepts with profound treatment implications. Among them are the field’s latest paradigm for medical therapy of HFrEF and the increasingly accepted division of traditional HFpEF into two entities: HF with mildly reduced ejection fraction (HFmrEF); and HFpEF, with its left ventricular ejection fraction (LVEF) threshold raised to 50%.
In fact, HFmrEF in the new document is a drug-therapy indication that barely existed a few years ago but grew in prominence after secondary findings from trials like TOPCAT for spironolactone and PARAGON-HF for sacubitril-valsartan (Entresto, Novartis), an angiotensin-receptor/neprilysin inhibitor (ARNI). Still, the HFmrEF recommendations come with different class and level-of-evidence designations.
Those new guideline features and others in the realm of pharmacologic therapy were summarized by the document’s authors at the 2021 Heart Failure Association of the European Society of Cardiology (ESC-HFA) meeting, and covered at the time by this news organization
The ‘fantastic four’
One of the document’s central recommendations specifies which contemporary drug classes should be initiated, and when, in patients with HFrEF. An ACE inhibitor or ARNI, a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and an SGLT2 inhibitor collectively earned a class I recommendation, “given the importance of these key HFrEF therapies, some of which have been shown to improve outcomes within a month of initiation,” observed Roy S. Gardner, MBChB, MD.
An agent from each of the four classes is to be “commenced and up-titrated as quickly and as safely as possible, whilst using the lowest effective dose of loop diuretic to relieve congestion,” said Dr. Gardner, from Golden Jubilee National Hospital, Clydebank, Scotland, when presenting the full HFrEF portion of the guidelines.
The oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo, Merck), which recently emerged from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization, gained a class IIb recommendation.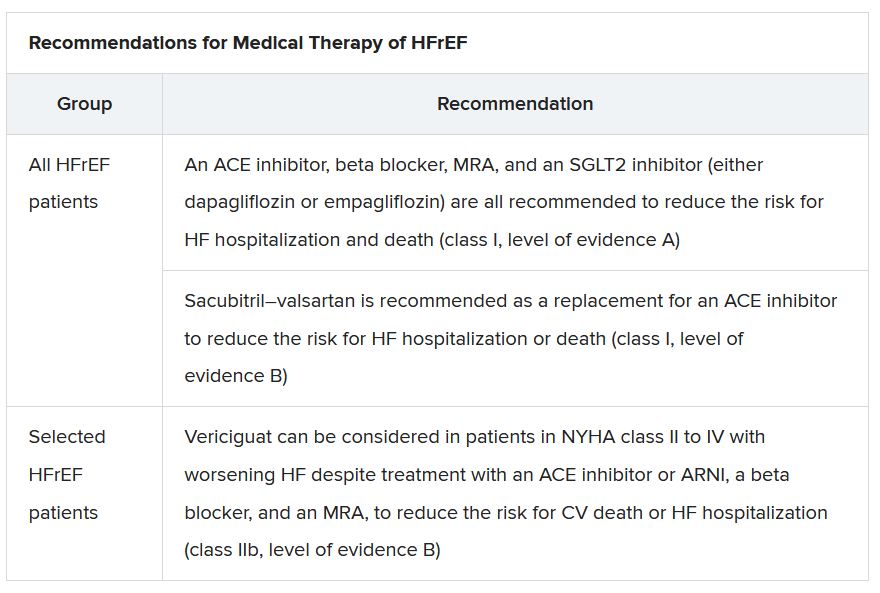
The document’s “simplified algorithm” for managing such patients overall and the advent of SGLT2 inhibitors are new twists in ESC guidelines for HF. But the way the four drug classes are started in patients is key and could take some practitioners time to get used to. There is no prespecified order of initiation.
“We’ve left the door open for clinicians to evaluate the evidence to make sure these four drugs are started, and to tailor how to do it according to the patient,” based on clinical considerations such as blood pressure or renal function, said Theresa A. McDonagh, MD, King’s College London, cochair of the guideline task force.
“The SGLT2 inhibitor trials were done on top of therapy with ACE inhibitors or ARNI, beta-blockers, and MRAs, so some people no doubt will choose to follow a sequenced approach,” Dr. McDonagh said. Other practitioners will consider each patient and attempt to get all four started “as quickly and safely as possible based on the phenotype.”
Importantly, clinicians “should not wait for weeks, months, or years until you have the four drugs in the patient, but you should do this within weeks,” cautioned Johann Bauersachs, MD, Hannover (Germany) Medical School, a discussant for the guideline presentation who is listed as a reviewer on the document.
Although angiotensin-receptor blockers (ARBs) and ACE inhibitors are sometimes thought of as interchangeable, the new guideline does not give them the same weight. “The angiotensin-receptor blocker valsartan is a constituent of the ARNI,” Dr. McDonagh noted. “So, the place of ARBs in heart failure has been downgraded in HFrEF. They are really for those who are intolerant of an ACE inhibitor or an ARNI.”
In practice, ARBs are likely to be used as first-line therapy in some circumstances, observed Dr. Bauersachs. They are “the default option in, unfortunately, many low-income countries that may not afford sacubitril-valsartan. And I know that there are many of them.”
Tweaks to device recommendations
The new document contains several new wrinkles in the recommendations for HF device therapy, which should usually be considered only if still appropriate after at least 3 months of optimal medical therapy, Dr. Gardner said.
For example, use of an implantable cardioverter-defibrillator (ICD) has been demoted from its previous class I recommendation to class II, level of evidence A, in patients with nonischemic cardiomyopathy “in light of the data from the DANISH study,” Dr. Gardner said.
The 2016 DANISH trial was noteworthy for questioning the survival benefits of ICDs in patients with nonischemic cardiomyopathy, whether or not they were also receiving cardiac resynchronization therapy (CRT).
The new document also puts greater emphasis on a range of specific CRT patient-selection criteria. Beyond the conventional recommended standards of an LVEF of 35% or less, QRS of at least 150 ms, and left-bundle-branch block on optimal meds, consideration can be given to CRT if the QRS is only 130 ms or greater. “And where it’s appropriate to do so, an ICD could be an option,” Dr. Gardner said.
It also recommends CRT as a replacement for right ventricular pacing in patients with high-degree atrioventricular block. “And this, for the first time, includes patients with atrial fibrillation,” he said. “The previous indications for CRT were in individuals in sinus rhythm.”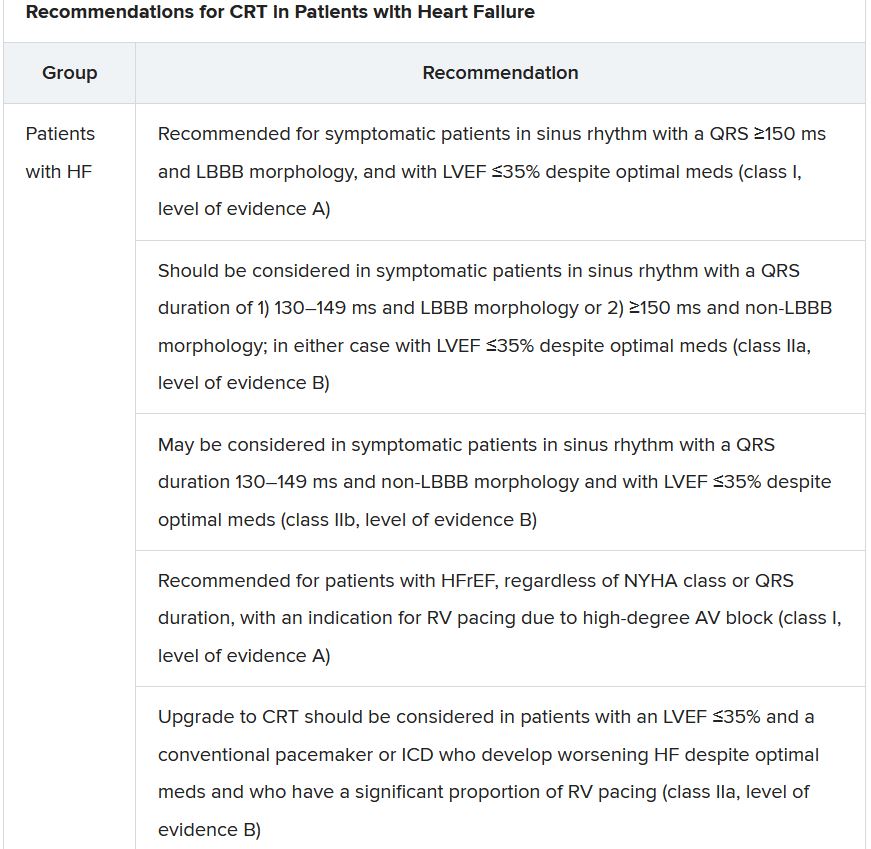
The new document recommends that HF in any patient be classified as HFrEF, defined by an LVEF of ≤40%; HFmrEF, defined by an LVEF of 41%-49%; or HFpEF, defined by an LVEF of at least 50%. “Importantly, for all forms, the presence of the clinical syndrome of heart failure is a prerequisite,” observed Carolyn S.P. Lam, MBBS, PhD, Duke-NUS Graduate Medical School, Singapore, at the presentation.
In a critical update from previous guidelines, the term HF with “mid-range” ejection fraction was replaced by the term specifying “mildly reduced” ejection fraction, Dr. Lam noted. The shift retains the acronym but now reflects growing appreciation that HFmrEF patients can benefit from treatments also used in HFrEF, including ACE inhibitors, ARBs, beta-blockers, MRAs, and sacubitril-valsartan, she said.
Support for that relationship comes largely from post hoc subgroup analyses of trials that featured some patients with LVEF 40%-49%. That includes most HFpEF trials represented in the guideline document, but also EMPEROR-Preserved, which saw gains for the primary outcome across the entire range of LVEF above 40%.
The LVEF-based definitions are consistent with a recent HF classification proposal endorsed by the ESC and subspecialty societies in Europe, North America, Japan, India, Australia, New Zealand, and China.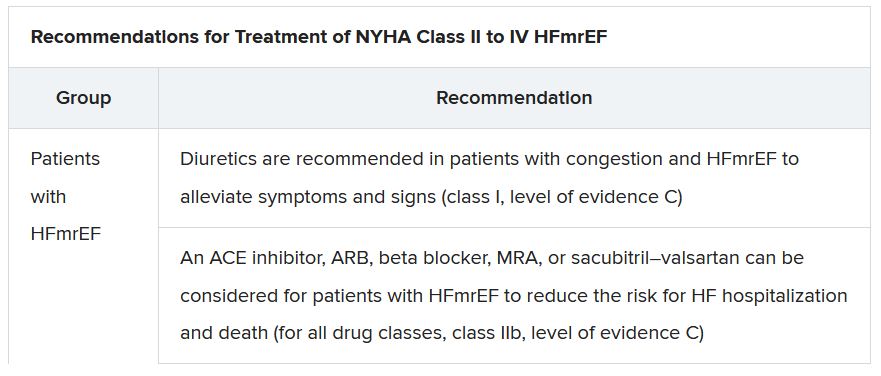
The document doesn’t update recommendations for HFpEF, in which “no treatment has been shown to convincingly reduce mortality or morbidity,” Dr. Lam observed. Still, she noted, the guideline task force “acknowledges that treatment options for HFpEF are being revised even as the guidelines have been published.”
That could be a reference to empagliflozin in EMPEROR-Preserved, but it also refers to the strikingly broad wording of an expanded indication for sacubitril-valsartan in the United States – “to reduce the risk of cardiovascular death and hospitalization for heart failure in adult patients with chronic heart failure” – without specific restrictions on the basis of LVEF. The new indication was announced in early 2021, too late to be considered in the new guidelines.
Whither LVEF-based definitions?
During discussion after the guideline presentation, Dr. Zannad speculated on the future of HF classifications based on ventricular function, given trial evidence in recent years that some agents – notably spironolactone, sacubitril-valsartan, and now, apparently, empagliflozin – might be effective in HFpEF as well as HFrEF.
Will the field continue with “LVEF-centric” distinctions across the range of HF, or transition to “some definition in which drug therapies can be used independently across the full spectrum of ejection fraction?” Dr. Zannad posed.
“I think we need to wait and see what some of these trials with the SGLT2 inhibitors are going to show in heart failure with preserved ejection fraction,” Dr. McDonagh replied. “And I think that will be a step for the next guideline, completely redefining heart failure.”
A version of this article first appeared on Medscape.com.
The new guideline on management of heart failure (HF) from the European Society of Cardiology seemed to bear an asterisk or footnote even before its full unveiling in the early hours of ESC Congress 2021.
The document would offer little new in the arena of HF with preserved ejection fraction (HFpEF), so understandably the fast-approaching presentation of a major HFpEF trial – arguably the conference’s marquee event – would feel to some like the elephant in the room.
“I’d like to highlight this unfortunate timing of the guideline, because it’s an hour or 2 before we hear the full story from EMPEROR-Preserved, which I’m sure will change the guidelines,” Faiez Zannad, MD, PhD, University of Lorraine, Vandoeuvre-Les-Nancy, France, said wryly.
Anticipation of the trial’s full presentation was intense as the ESC congress got underway, in part because the top-line and incomplete message from EMPEROR-Preserved had already been released: Patients with HFpEF treated with the sodium-glucose cotransporter 2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Eli Lilly) showed a significant benefit for the primary endpoint of cardiovascular (CV) death or HF hospitalization.
Although empagliflozin is the first medication to achieve that status in a major HFpEF trial, conspicuously absent from the early announcement were the magnitude of “benefit” and any data. Still, the tantalizing top-line results mean that technically, at least, “we have a drug which is effective in reduced and preserved ejection fraction,” Dr. Zannad said.
But the new guideline, published online Aug. 27, 2021, in the European Heart Journal and comprehensively described that day at the congress, was never really expected to consider results from EMPEROR-Reduced. “These new indications do need to go through the regulatory authorities,” such as the European Medicines Agency and the U.S. Food and Drug Administration, observed Carlos Aguiar, MD, Hospital Santa Cruz, Carnaxide, Portugal.
“It does take some time for the whole process to be concluded and, finally, as physicians, being able to implement it in clinical practice,” Dr. Aguiar said as moderator of press briefing prior to the ESC congress.
The ESC guideline’s next iteration or update could well include an SGLT2 inhibitor recommendation that applies beyond the ejection fraction limits of HFrEF. Still, the document summarized that day reflects a number of pivotal concepts with profound treatment implications. Among them are the field’s latest paradigm for medical therapy of HFrEF and the increasingly accepted division of traditional HFpEF into two entities: HF with mildly reduced ejection fraction (HFmrEF); and HFpEF, with its left ventricular ejection fraction (LVEF) threshold raised to 50%.
In fact, HFmrEF in the new document is a drug-therapy indication that barely existed a few years ago but grew in prominence after secondary findings from trials like TOPCAT for spironolactone and PARAGON-HF for sacubitril-valsartan (Entresto, Novartis), an angiotensin-receptor/neprilysin inhibitor (ARNI). Still, the HFmrEF recommendations come with different class and level-of-evidence designations.
Those new guideline features and others in the realm of pharmacologic therapy were summarized by the document’s authors at the 2021 Heart Failure Association of the European Society of Cardiology (ESC-HFA) meeting, and covered at the time by this news organization
The ‘fantastic four’
One of the document’s central recommendations specifies which contemporary drug classes should be initiated, and when, in patients with HFrEF. An ACE inhibitor or ARNI, a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and an SGLT2 inhibitor collectively earned a class I recommendation, “given the importance of these key HFrEF therapies, some of which have been shown to improve outcomes within a month of initiation,” observed Roy S. Gardner, MBChB, MD.
An agent from each of the four classes is to be “commenced and up-titrated as quickly and as safely as possible, whilst using the lowest effective dose of loop diuretic to relieve congestion,” said Dr. Gardner, from Golden Jubilee National Hospital, Clydebank, Scotland, when presenting the full HFrEF portion of the guidelines.
The oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo, Merck), which recently emerged from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization, gained a class IIb recommendation.
The document’s “simplified algorithm” for managing such patients overall and the advent of SGLT2 inhibitors are new twists in ESC guidelines for HF. But the way the four drug classes are started in patients is key and could take some practitioners time to get used to. There is no prespecified order of initiation.
“We’ve left the door open for clinicians to evaluate the evidence to make sure these four drugs are started, and to tailor how to do it according to the patient,” based on clinical considerations such as blood pressure or renal function, said Theresa A. McDonagh, MD, King’s College London, cochair of the guideline task force.
“The SGLT2 inhibitor trials were done on top of therapy with ACE inhibitors or ARNI, beta-blockers, and MRAs, so some people no doubt will choose to follow a sequenced approach,” Dr. McDonagh said. Other practitioners will consider each patient and attempt to get all four started “as quickly and safely as possible based on the phenotype.”
Importantly, clinicians “should not wait for weeks, months, or years until you have the four drugs in the patient, but you should do this within weeks,” cautioned Johann Bauersachs, MD, Hannover (Germany) Medical School, a discussant for the guideline presentation who is listed as a reviewer on the document.
Although angiotensin-receptor blockers (ARBs) and ACE inhibitors are sometimes thought of as interchangeable, the new guideline does not give them the same weight. “The angiotensin-receptor blocker valsartan is a constituent of the ARNI,” Dr. McDonagh noted. “So, the place of ARBs in heart failure has been downgraded in HFrEF. They are really for those who are intolerant of an ACE inhibitor or an ARNI.”
In practice, ARBs are likely to be used as first-line therapy in some circumstances, observed Dr. Bauersachs. They are “the default option in, unfortunately, many low-income countries that may not afford sacubitril-valsartan. And I know that there are many of them.”
Tweaks to device recommendations
The new document contains several new wrinkles in the recommendations for HF device therapy, which should usually be considered only if still appropriate after at least 3 months of optimal medical therapy, Dr. Gardner said.
For example, use of an implantable cardioverter-defibrillator (ICD) has been demoted from its previous class I recommendation to class II, level of evidence A, in patients with nonischemic cardiomyopathy “in light of the data from the DANISH study,” Dr. Gardner said.
The 2016 DANISH trial was noteworthy for questioning the survival benefits of ICDs in patients with nonischemic cardiomyopathy, whether or not they were also receiving cardiac resynchronization therapy (CRT).
The new document also puts greater emphasis on a range of specific CRT patient-selection criteria. Beyond the conventional recommended standards of an LVEF of 35% or less, QRS of at least 150 ms, and left-bundle-branch block on optimal meds, consideration can be given to CRT if the QRS is only 130 ms or greater. “And where it’s appropriate to do so, an ICD could be an option,” Dr. Gardner said.
It also recommends CRT as a replacement for right ventricular pacing in patients with high-degree atrioventricular block. “And this, for the first time, includes patients with atrial fibrillation,” he said. “The previous indications for CRT were in individuals in sinus rhythm.”
The new document recommends that HF in any patient be classified as HFrEF, defined by an LVEF of ≤40%; HFmrEF, defined by an LVEF of 41%-49%; or HFpEF, defined by an LVEF of at least 50%. “Importantly, for all forms, the presence of the clinical syndrome of heart failure is a prerequisite,” observed Carolyn S.P. Lam, MBBS, PhD, Duke-NUS Graduate Medical School, Singapore, at the presentation.
In a critical update from previous guidelines, the term HF with “mid-range” ejection fraction was replaced by the term specifying “mildly reduced” ejection fraction, Dr. Lam noted. The shift retains the acronym but now reflects growing appreciation that HFmrEF patients can benefit from treatments also used in HFrEF, including ACE inhibitors, ARBs, beta-blockers, MRAs, and sacubitril-valsartan, she said.
Support for that relationship comes largely from post hoc subgroup analyses of trials that featured some patients with LVEF 40%-49%. That includes most HFpEF trials represented in the guideline document, but also EMPEROR-Preserved, which saw gains for the primary outcome across the entire range of LVEF above 40%.
The LVEF-based definitions are consistent with a recent HF classification proposal endorsed by the ESC and subspecialty societies in Europe, North America, Japan, India, Australia, New Zealand, and China.
The document doesn’t update recommendations for HFpEF, in which “no treatment has been shown to convincingly reduce mortality or morbidity,” Dr. Lam observed. Still, she noted, the guideline task force “acknowledges that treatment options for HFpEF are being revised even as the guidelines have been published.”
That could be a reference to empagliflozin in EMPEROR-Preserved, but it also refers to the strikingly broad wording of an expanded indication for sacubitril-valsartan in the United States – “to reduce the risk of cardiovascular death and hospitalization for heart failure in adult patients with chronic heart failure” – without specific restrictions on the basis of LVEF. The new indication was announced in early 2021, too late to be considered in the new guidelines.
Whither LVEF-based definitions?
During discussion after the guideline presentation, Dr. Zannad speculated on the future of HF classifications based on ventricular function, given trial evidence in recent years that some agents – notably spironolactone, sacubitril-valsartan, and now, apparently, empagliflozin – might be effective in HFpEF as well as HFrEF.
Will the field continue with “LVEF-centric” distinctions across the range of HF, or transition to “some definition in which drug therapies can be used independently across the full spectrum of ejection fraction?” Dr. Zannad posed.
“I think we need to wait and see what some of these trials with the SGLT2 inhibitors are going to show in heart failure with preserved ejection fraction,” Dr. McDonagh replied. “And I think that will be a step for the next guideline, completely redefining heart failure.”
A version of this article first appeared on Medscape.com.
The new guideline on management of heart failure (HF) from the European Society of Cardiology seemed to bear an asterisk or footnote even before its full unveiling in the early hours of ESC Congress 2021.
The document would offer little new in the arena of HF with preserved ejection fraction (HFpEF), so understandably the fast-approaching presentation of a major HFpEF trial – arguably the conference’s marquee event – would feel to some like the elephant in the room.
“I’d like to highlight this unfortunate timing of the guideline, because it’s an hour or 2 before we hear the full story from EMPEROR-Preserved, which I’m sure will change the guidelines,” Faiez Zannad, MD, PhD, University of Lorraine, Vandoeuvre-Les-Nancy, France, said wryly.
Anticipation of the trial’s full presentation was intense as the ESC congress got underway, in part because the top-line and incomplete message from EMPEROR-Preserved had already been released: Patients with HFpEF treated with the sodium-glucose cotransporter 2 inhibitor empagliflozin (Jardiance, Boehringer Ingelheim/Eli Lilly) showed a significant benefit for the primary endpoint of cardiovascular (CV) death or HF hospitalization.
Although empagliflozin is the first medication to achieve that status in a major HFpEF trial, conspicuously absent from the early announcement were the magnitude of “benefit” and any data. Still, the tantalizing top-line results mean that technically, at least, “we have a drug which is effective in reduced and preserved ejection fraction,” Dr. Zannad said.
But the new guideline, published online Aug. 27, 2021, in the European Heart Journal and comprehensively described that day at the congress, was never really expected to consider results from EMPEROR-Reduced. “These new indications do need to go through the regulatory authorities,” such as the European Medicines Agency and the U.S. Food and Drug Administration, observed Carlos Aguiar, MD, Hospital Santa Cruz, Carnaxide, Portugal.
“It does take some time for the whole process to be concluded and, finally, as physicians, being able to implement it in clinical practice,” Dr. Aguiar said as moderator of press briefing prior to the ESC congress.
The ESC guideline’s next iteration or update could well include an SGLT2 inhibitor recommendation that applies beyond the ejection fraction limits of HFrEF. Still, the document summarized that day reflects a number of pivotal concepts with profound treatment implications. Among them are the field’s latest paradigm for medical therapy of HFrEF and the increasingly accepted division of traditional HFpEF into two entities: HF with mildly reduced ejection fraction (HFmrEF); and HFpEF, with its left ventricular ejection fraction (LVEF) threshold raised to 50%.
In fact, HFmrEF in the new document is a drug-therapy indication that barely existed a few years ago but grew in prominence after secondary findings from trials like TOPCAT for spironolactone and PARAGON-HF for sacubitril-valsartan (Entresto, Novartis), an angiotensin-receptor/neprilysin inhibitor (ARNI). Still, the HFmrEF recommendations come with different class and level-of-evidence designations.
Those new guideline features and others in the realm of pharmacologic therapy were summarized by the document’s authors at the 2021 Heart Failure Association of the European Society of Cardiology (ESC-HFA) meeting, and covered at the time by this news organization
The ‘fantastic four’
One of the document’s central recommendations specifies which contemporary drug classes should be initiated, and when, in patients with HFrEF. An ACE inhibitor or ARNI, a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and an SGLT2 inhibitor collectively earned a class I recommendation, “given the importance of these key HFrEF therapies, some of which have been shown to improve outcomes within a month of initiation,” observed Roy S. Gardner, MBChB, MD.
An agent from each of the four classes is to be “commenced and up-titrated as quickly and as safely as possible, whilst using the lowest effective dose of loop diuretic to relieve congestion,” said Dr. Gardner, from Golden Jubilee National Hospital, Clydebank, Scotland, when presenting the full HFrEF portion of the guidelines.
The oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo, Merck), which recently emerged from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization, gained a class IIb recommendation.
The document’s “simplified algorithm” for managing such patients overall and the advent of SGLT2 inhibitors are new twists in ESC guidelines for HF. But the way the four drug classes are started in patients is key and could take some practitioners time to get used to. There is no prespecified order of initiation.
“We’ve left the door open for clinicians to evaluate the evidence to make sure these four drugs are started, and to tailor how to do it according to the patient,” based on clinical considerations such as blood pressure or renal function, said Theresa A. McDonagh, MD, King’s College London, cochair of the guideline task force.
“The SGLT2 inhibitor trials were done on top of therapy with ACE inhibitors or ARNI, beta-blockers, and MRAs, so some people no doubt will choose to follow a sequenced approach,” Dr. McDonagh said. Other practitioners will consider each patient and attempt to get all four started “as quickly and safely as possible based on the phenotype.”
Importantly, clinicians “should not wait for weeks, months, or years until you have the four drugs in the patient, but you should do this within weeks,” cautioned Johann Bauersachs, MD, Hannover (Germany) Medical School, a discussant for the guideline presentation who is listed as a reviewer on the document.
Although angiotensin-receptor blockers (ARBs) and ACE inhibitors are sometimes thought of as interchangeable, the new guideline does not give them the same weight. “The angiotensin-receptor blocker valsartan is a constituent of the ARNI,” Dr. McDonagh noted. “So, the place of ARBs in heart failure has been downgraded in HFrEF. They are really for those who are intolerant of an ACE inhibitor or an ARNI.”
In practice, ARBs are likely to be used as first-line therapy in some circumstances, observed Dr. Bauersachs. They are “the default option in, unfortunately, many low-income countries that may not afford sacubitril-valsartan. And I know that there are many of them.”
Tweaks to device recommendations
The new document contains several new wrinkles in the recommendations for HF device therapy, which should usually be considered only if still appropriate after at least 3 months of optimal medical therapy, Dr. Gardner said.
For example, use of an implantable cardioverter-defibrillator (ICD) has been demoted from its previous class I recommendation to class II, level of evidence A, in patients with nonischemic cardiomyopathy “in light of the data from the DANISH study,” Dr. Gardner said.
The 2016 DANISH trial was noteworthy for questioning the survival benefits of ICDs in patients with nonischemic cardiomyopathy, whether or not they were also receiving cardiac resynchronization therapy (CRT).
The new document also puts greater emphasis on a range of specific CRT patient-selection criteria. Beyond the conventional recommended standards of an LVEF of 35% or less, QRS of at least 150 ms, and left-bundle-branch block on optimal meds, consideration can be given to CRT if the QRS is only 130 ms or greater. “And where it’s appropriate to do so, an ICD could be an option,” Dr. Gardner said.
It also recommends CRT as a replacement for right ventricular pacing in patients with high-degree atrioventricular block. “And this, for the first time, includes patients with atrial fibrillation,” he said. “The previous indications for CRT were in individuals in sinus rhythm.”
The new document recommends that HF in any patient be classified as HFrEF, defined by an LVEF of ≤40%; HFmrEF, defined by an LVEF of 41%-49%; or HFpEF, defined by an LVEF of at least 50%. “Importantly, for all forms, the presence of the clinical syndrome of heart failure is a prerequisite,” observed Carolyn S.P. Lam, MBBS, PhD, Duke-NUS Graduate Medical School, Singapore, at the presentation.
In a critical update from previous guidelines, the term HF with “mid-range” ejection fraction was replaced by the term specifying “mildly reduced” ejection fraction, Dr. Lam noted. The shift retains the acronym but now reflects growing appreciation that HFmrEF patients can benefit from treatments also used in HFrEF, including ACE inhibitors, ARBs, beta-blockers, MRAs, and sacubitril-valsartan, she said.
Support for that relationship comes largely from post hoc subgroup analyses of trials that featured some patients with LVEF 40%-49%. That includes most HFpEF trials represented in the guideline document, but also EMPEROR-Preserved, which saw gains for the primary outcome across the entire range of LVEF above 40%.
The LVEF-based definitions are consistent with a recent HF classification proposal endorsed by the ESC and subspecialty societies in Europe, North America, Japan, India, Australia, New Zealand, and China.
The document doesn’t update recommendations for HFpEF, in which “no treatment has been shown to convincingly reduce mortality or morbidity,” Dr. Lam observed. Still, she noted, the guideline task force “acknowledges that treatment options for HFpEF are being revised even as the guidelines have been published.”
That could be a reference to empagliflozin in EMPEROR-Preserved, but it also refers to the strikingly broad wording of an expanded indication for sacubitril-valsartan in the United States – “to reduce the risk of cardiovascular death and hospitalization for heart failure in adult patients with chronic heart failure” – without specific restrictions on the basis of LVEF. The new indication was announced in early 2021, too late to be considered in the new guidelines.
Whither LVEF-based definitions?
During discussion after the guideline presentation, Dr. Zannad speculated on the future of HF classifications based on ventricular function, given trial evidence in recent years that some agents – notably spironolactone, sacubitril-valsartan, and now, apparently, empagliflozin – might be effective in HFpEF as well as HFrEF.
Will the field continue with “LVEF-centric” distinctions across the range of HF, or transition to “some definition in which drug therapies can be used independently across the full spectrum of ejection fraction?” Dr. Zannad posed.
“I think we need to wait and see what some of these trials with the SGLT2 inhibitors are going to show in heart failure with preserved ejection fraction,” Dr. McDonagh replied. “And I think that will be a step for the next guideline, completely redefining heart failure.”
A version of this article first appeared on Medscape.com.
Pandemic strategies to boost trial enrollment should stay
Although enrollment into lung cancer clinical trials fell during the early months of the COVID-19 pandemic, it increased after a number of mitigation strategies were introduced.
These strategies should now be maintained, say experts, in order to improve enrollment and access to trials and to ensure that trials are more pragmatic and streamlined.
These were the findings from a survey sent to 173 sites of clinical trials in 45 countries around the world. The findings were presented recently at the World Conference on Lung Cancer (WCLC) 2021. The meeting and the survey were organized by the International Association for the Study of Lung Cancer (IASLC).
Responses to the survey revealed that enrollment into lung cancer trials fell by 43% during the early months of the pandemic. Patients stopped attending clinics, and some trials were suspended.
Patients were less willing to visit clinical trial sites, and lockdown restrictions made travel difficult.
Organizers of clinical trials responded by implementing mitigation strategies, such as changing monitoring requirements, increasing use of telehealth, and using local non-study facilities for laboratory and radiology services.
These measures led to an increase in trial enrollment toward the end of 2020, the survey results show.
“The COVID-19 pandemic created many challenges [that led to] reductions in lung cancer clinical trial enrollment,” commented study presenter Matthew P. Smeltzer, PhD, from the Division of Epidemiology, Biostatistics, and Environmental Health, University of Memphis.
The employment of mitigation strategies allowed the removal of “barriers,” and although the pandemic “worsened, trial enrollment began to improve due in part to these strategies,” Dr. Smeltzer said.
Many of these measures were successful and should be maintained, he suggested. Strategies include allowing telehealth visits, performing testing at local laboratories, using local radiology services, mailing experimental agents “where possible,” and allowing flexibility in trial schedules.
This is a “very important” study, commented Marina Garassino, MD, professor of medicine, hematology, and oncology, the University of Chicago Medicine, in her discussion of the abstract.
Irrespective of the pandemic, the regulation and the bureaucracy of clinical trials hinder participation by patients and physicians, she said.
Many of the mitigation strategies highlighted by the survey were similar to recommendations on the conduct of clinical trials published by the American Society of Clinical Oncology during the pandemic. Those recommendations emphasize the use of telehealth and offsite strategies to help with patient monitoring, she noted.
The findings from the survey show that it is possible to conduct more “streamlined and pragmatic trials,” she said.
“More flexible approaches should be approved by the sponsors of clinical trials and global regulatory bodies,” she added.
However, she expressed concern that “with the telehealth visits, we can create some disparities.”
“We have to remember that lung cancer patients are sometimes a very old population, and they are not digitally evolved,” she commented.
Commenting on Twitter, Jennifer C. King, PhD, chief scientific officer at the GO2 Foundation for Lung Cancer, in Washington, D.C., agreed that many of the mitigation strategies identified in the study “are good for patients all of the time, not just during a pandemic.”
Impact on lung cancer clinical trials
The survey, which included 64 questions, was intended to assess the impact of the COVID pandemic on lung cancer clinical trials.
Most of the survey responses came from sites in Europe (37.6%); 21.4% came from Asia, 13.3% came from the United States, and 7.5% came from Canada.
The team found that enrollment into lung cancer trials declined by 43% in 2020 compared to 2019, at an incidence rate ratio of 0.57 (P = .0115).
The largest decreases in enrollment were between April and August 2020, Dr. Smeltzer noted. However, in the last quarter of 2020 (October to December), the differences in enrollment were significantly smaller (P = .0160), despite a marked increase in global COVID-19 cases per month, he added.
The most common challenges faced by clinical trial sites during the pandemic were the following: There were fewer eligible patients (cited by 67% of respondents); compliance protocol was worse (61%); trials were suspended (60%); there was a lack of research staff (48%); and there were institutional closures (39%).
Regarding patient-related challenges, 67% of sites cited less willingness to visit the site. Other challenges included less ability to travel (cited by 60%), reduced access to the trial site (52%), quarantining because of exposure to COVID-19 (40%), and SARS-CoV-2 infection (26%).
Concerns of patients included the following: Fear of SARS-CoV-2 infection, which was cited by 83%; travel restrictions (47%); securing transportation (38%); and access to the laboratory/radiology services (14%).
“Patient willingness to visit the site was a consistent barrier reported across Europe, the U.S., and Canada,” said Dr. Smeltzer, although the effect was smaller in North America, he added.
Regarding mitigation strategies that were employed during the pandemic to combat the challenges and concerns, the team found that the most common measure was the modification of monitoring requirements, used by 44% of sites.
This was followed by the use of telehealth visits (43% sites), the use of laboratories at non-study facilities ( 27%), and alterations to the number of required visits (25%).
Other mitigation strategies included use of mail-order medications, (24%), using radiology services at a non-study site (20%), and altering the trial schedules (19%).
The most effective mitigation strategies were felt to be those that allowed flexibility with respect to location. These measures included use of remote monitoring, remote diagnostics, telehealth visits, and modified symptom monitoring.
Effective strategies that increased flexibility in time were delayed visits, delayed assessments, and changes to the Institutional Review Board.
The study was funded by the IASLC, which received industry support to conduct the project. Dr. Smeltzer reported no relevant financial relationships. Dr. Garassino has relationships with AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Ignyta, Incyte, MedImmune, Mirati, MSD International, Novartis, Pfizer, Regeneron, Roche, Takeda, and Seattle Genetics.
A version of this article first appeared on Medscape.com.
Although enrollment into lung cancer clinical trials fell during the early months of the COVID-19 pandemic, it increased after a number of mitigation strategies were introduced.
These strategies should now be maintained, say experts, in order to improve enrollment and access to trials and to ensure that trials are more pragmatic and streamlined.
These were the findings from a survey sent to 173 sites of clinical trials in 45 countries around the world. The findings were presented recently at the World Conference on Lung Cancer (WCLC) 2021. The meeting and the survey were organized by the International Association for the Study of Lung Cancer (IASLC).
Responses to the survey revealed that enrollment into lung cancer trials fell by 43% during the early months of the pandemic. Patients stopped attending clinics, and some trials were suspended.
Patients were less willing to visit clinical trial sites, and lockdown restrictions made travel difficult.
Organizers of clinical trials responded by implementing mitigation strategies, such as changing monitoring requirements, increasing use of telehealth, and using local non-study facilities for laboratory and radiology services.
These measures led to an increase in trial enrollment toward the end of 2020, the survey results show.
“The COVID-19 pandemic created many challenges [that led to] reductions in lung cancer clinical trial enrollment,” commented study presenter Matthew P. Smeltzer, PhD, from the Division of Epidemiology, Biostatistics, and Environmental Health, University of Memphis.
The employment of mitigation strategies allowed the removal of “barriers,” and although the pandemic “worsened, trial enrollment began to improve due in part to these strategies,” Dr. Smeltzer said.
Many of these measures were successful and should be maintained, he suggested. Strategies include allowing telehealth visits, performing testing at local laboratories, using local radiology services, mailing experimental agents “where possible,” and allowing flexibility in trial schedules.
This is a “very important” study, commented Marina Garassino, MD, professor of medicine, hematology, and oncology, the University of Chicago Medicine, in her discussion of the abstract.
Irrespective of the pandemic, the regulation and the bureaucracy of clinical trials hinder participation by patients and physicians, she said.
Many of the mitigation strategies highlighted by the survey were similar to recommendations on the conduct of clinical trials published by the American Society of Clinical Oncology during the pandemic. Those recommendations emphasize the use of telehealth and offsite strategies to help with patient monitoring, she noted.
The findings from the survey show that it is possible to conduct more “streamlined and pragmatic trials,” she said.
“More flexible approaches should be approved by the sponsors of clinical trials and global regulatory bodies,” she added.
However, she expressed concern that “with the telehealth visits, we can create some disparities.”
“We have to remember that lung cancer patients are sometimes a very old population, and they are not digitally evolved,” she commented.
Commenting on Twitter, Jennifer C. King, PhD, chief scientific officer at the GO2 Foundation for Lung Cancer, in Washington, D.C., agreed that many of the mitigation strategies identified in the study “are good for patients all of the time, not just during a pandemic.”
Impact on lung cancer clinical trials
The survey, which included 64 questions, was intended to assess the impact of the COVID pandemic on lung cancer clinical trials.
Most of the survey responses came from sites in Europe (37.6%); 21.4% came from Asia, 13.3% came from the United States, and 7.5% came from Canada.
The team found that enrollment into lung cancer trials declined by 43% in 2020 compared to 2019, at an incidence rate ratio of 0.57 (P = .0115).
The largest decreases in enrollment were between April and August 2020, Dr. Smeltzer noted. However, in the last quarter of 2020 (October to December), the differences in enrollment were significantly smaller (P = .0160), despite a marked increase in global COVID-19 cases per month, he added.
The most common challenges faced by clinical trial sites during the pandemic were the following: There were fewer eligible patients (cited by 67% of respondents); compliance protocol was worse (61%); trials were suspended (60%); there was a lack of research staff (48%); and there were institutional closures (39%).
Regarding patient-related challenges, 67% of sites cited less willingness to visit the site. Other challenges included less ability to travel (cited by 60%), reduced access to the trial site (52%), quarantining because of exposure to COVID-19 (40%), and SARS-CoV-2 infection (26%).
Concerns of patients included the following: Fear of SARS-CoV-2 infection, which was cited by 83%; travel restrictions (47%); securing transportation (38%); and access to the laboratory/radiology services (14%).
“Patient willingness to visit the site was a consistent barrier reported across Europe, the U.S., and Canada,” said Dr. Smeltzer, although the effect was smaller in North America, he added.
Regarding mitigation strategies that were employed during the pandemic to combat the challenges and concerns, the team found that the most common measure was the modification of monitoring requirements, used by 44% of sites.
This was followed by the use of telehealth visits (43% sites), the use of laboratories at non-study facilities ( 27%), and alterations to the number of required visits (25%).
Other mitigation strategies included use of mail-order medications, (24%), using radiology services at a non-study site (20%), and altering the trial schedules (19%).
The most effective mitigation strategies were felt to be those that allowed flexibility with respect to location. These measures included use of remote monitoring, remote diagnostics, telehealth visits, and modified symptom monitoring.
Effective strategies that increased flexibility in time were delayed visits, delayed assessments, and changes to the Institutional Review Board.
The study was funded by the IASLC, which received industry support to conduct the project. Dr. Smeltzer reported no relevant financial relationships. Dr. Garassino has relationships with AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Ignyta, Incyte, MedImmune, Mirati, MSD International, Novartis, Pfizer, Regeneron, Roche, Takeda, and Seattle Genetics.
A version of this article first appeared on Medscape.com.
Although enrollment into lung cancer clinical trials fell during the early months of the COVID-19 pandemic, it increased after a number of mitigation strategies were introduced.
These strategies should now be maintained, say experts, in order to improve enrollment and access to trials and to ensure that trials are more pragmatic and streamlined.
These were the findings from a survey sent to 173 sites of clinical trials in 45 countries around the world. The findings were presented recently at the World Conference on Lung Cancer (WCLC) 2021. The meeting and the survey were organized by the International Association for the Study of Lung Cancer (IASLC).
Responses to the survey revealed that enrollment into lung cancer trials fell by 43% during the early months of the pandemic. Patients stopped attending clinics, and some trials were suspended.
Patients were less willing to visit clinical trial sites, and lockdown restrictions made travel difficult.
Organizers of clinical trials responded by implementing mitigation strategies, such as changing monitoring requirements, increasing use of telehealth, and using local non-study facilities for laboratory and radiology services.
These measures led to an increase in trial enrollment toward the end of 2020, the survey results show.
“The COVID-19 pandemic created many challenges [that led to] reductions in lung cancer clinical trial enrollment,” commented study presenter Matthew P. Smeltzer, PhD, from the Division of Epidemiology, Biostatistics, and Environmental Health, University of Memphis.
The employment of mitigation strategies allowed the removal of “barriers,” and although the pandemic “worsened, trial enrollment began to improve due in part to these strategies,” Dr. Smeltzer said.
Many of these measures were successful and should be maintained, he suggested. Strategies include allowing telehealth visits, performing testing at local laboratories, using local radiology services, mailing experimental agents “where possible,” and allowing flexibility in trial schedules.
This is a “very important” study, commented Marina Garassino, MD, professor of medicine, hematology, and oncology, the University of Chicago Medicine, in her discussion of the abstract.
Irrespective of the pandemic, the regulation and the bureaucracy of clinical trials hinder participation by patients and physicians, she said.
Many of the mitigation strategies highlighted by the survey were similar to recommendations on the conduct of clinical trials published by the American Society of Clinical Oncology during the pandemic. Those recommendations emphasize the use of telehealth and offsite strategies to help with patient monitoring, she noted.
The findings from the survey show that it is possible to conduct more “streamlined and pragmatic trials,” she said.
“More flexible approaches should be approved by the sponsors of clinical trials and global regulatory bodies,” she added.
However, she expressed concern that “with the telehealth visits, we can create some disparities.”
“We have to remember that lung cancer patients are sometimes a very old population, and they are not digitally evolved,” she commented.
Commenting on Twitter, Jennifer C. King, PhD, chief scientific officer at the GO2 Foundation for Lung Cancer, in Washington, D.C., agreed that many of the mitigation strategies identified in the study “are good for patients all of the time, not just during a pandemic.”
Impact on lung cancer clinical trials
The survey, which included 64 questions, was intended to assess the impact of the COVID pandemic on lung cancer clinical trials.
Most of the survey responses came from sites in Europe (37.6%); 21.4% came from Asia, 13.3% came from the United States, and 7.5% came from Canada.
The team found that enrollment into lung cancer trials declined by 43% in 2020 compared to 2019, at an incidence rate ratio of 0.57 (P = .0115).
The largest decreases in enrollment were between April and August 2020, Dr. Smeltzer noted. However, in the last quarter of 2020 (October to December), the differences in enrollment were significantly smaller (P = .0160), despite a marked increase in global COVID-19 cases per month, he added.
The most common challenges faced by clinical trial sites during the pandemic were the following: There were fewer eligible patients (cited by 67% of respondents); compliance protocol was worse (61%); trials were suspended (60%); there was a lack of research staff (48%); and there were institutional closures (39%).
Regarding patient-related challenges, 67% of sites cited less willingness to visit the site. Other challenges included less ability to travel (cited by 60%), reduced access to the trial site (52%), quarantining because of exposure to COVID-19 (40%), and SARS-CoV-2 infection (26%).
Concerns of patients included the following: Fear of SARS-CoV-2 infection, which was cited by 83%; travel restrictions (47%); securing transportation (38%); and access to the laboratory/radiology services (14%).
“Patient willingness to visit the site was a consistent barrier reported across Europe, the U.S., and Canada,” said Dr. Smeltzer, although the effect was smaller in North America, he added.
Regarding mitigation strategies that were employed during the pandemic to combat the challenges and concerns, the team found that the most common measure was the modification of monitoring requirements, used by 44% of sites.
This was followed by the use of telehealth visits (43% sites), the use of laboratories at non-study facilities ( 27%), and alterations to the number of required visits (25%).
Other mitigation strategies included use of mail-order medications, (24%), using radiology services at a non-study site (20%), and altering the trial schedules (19%).
The most effective mitigation strategies were felt to be those that allowed flexibility with respect to location. These measures included use of remote monitoring, remote diagnostics, telehealth visits, and modified symptom monitoring.
Effective strategies that increased flexibility in time were delayed visits, delayed assessments, and changes to the Institutional Review Board.
The study was funded by the IASLC, which received industry support to conduct the project. Dr. Smeltzer reported no relevant financial relationships. Dr. Garassino has relationships with AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Ignyta, Incyte, MedImmune, Mirati, MSD International, Novartis, Pfizer, Regeneron, Roche, Takeda, and Seattle Genetics.
A version of this article first appeared on Medscape.com.
Air pollution – second leading cause of lung cancer

The new data show that the rate of lung cancer deaths attributable to air pollution varies widely between countries. Serbia, Poland, China, Mongolia, and Turkey are among the worst affected. The analysis shows an association between deaths from lung cancer and the proportion of national energy that is produced from coal.
“Both smoking and air pollution are important causes of lung cancer,” said study presenter Christine D. Berg, MD, former codirector of the National Lung Screening Trial, and “both need to be eliminated to help prevent lung cancer and save lives.
“As lung cancer professionals, we can mitigate the effects of air pollution on causing lung cancer by speaking out for clean energy standards,” she said.
Dr. Berg presented the new analysis on Sept. 9 at the 2021 World Conference on Lung Cancer, which was organized by the International Association for the Study of Lung Cancer.
She welcomed the recent statement issued by the IASLC in support of the International Day of Clean Air for Blue Skies, which took place on Sept. 7. It was a call for action that emphasized the need for further efforts to improve air quality to protect human health.
The findings from the new analysis are “depressing,” commented Joachim G. J. V. Aerts, MD. PhD, department of pulmonary diseases, Erasmus University Medical Center, Rotterdam, the Netherlands.
It is now clear that air pollution has an impact not only on the incidence of lung cancer but also on its outcome, he added.
Indeed, previous research showed that each 10 mcg/m3 increase in particular matter of 2.5 mcg in size was associated with a 15%-27% increase in lung cancer mortality. There was no difference in rates between women and men.
A key question, Dr. Aerts said, is whether reducing air pollution would be beneficial.
Efforts to reduce air pollution over recent decades in the United Kingdom have not led to a reduction in lung cancer deaths. This is because of the increase in life expectancy – individuals have been exposed to pollution for longer, albeit at lower levels, he pointed out.
Because of lockdowns during the COVID pandemic, travel has been greatly reduced. This has resulted in a dramatic reduction in air pollution, “and this led to a decrease in the number of children born with low birth weight,” said Dr. Aerts.
Hopefully, that benefit will also be seen regarding other diseases, he added.
The call to action to reduce air pollution is of the “utmost importance,” he said. He noted that the focus should be on global, national, local, and personal preventive measures.
“It is time to join forces,” he added, “to ‘clean the air.’ ”
Dr. Berg’s presentation was warmly received on social media.
It was “fabulous,” commented Eric H. Bernicker, MD, director of medical thoracic oncology at Houston Methodist Cancer Center.
“Thoracic oncologists need to add air pollution to things they advocate about; we have an important voice here,” he added.
It is “so important to understand that air pollution is a human carcinogen,” commented Ivy Elkins, a lung cancer survivor and advocate and cofounder of the EGFR Resisters Lung Cancer Patient Group. “All you need are lungs to get lung cancer!”
Contribution of air pollution to lung cancer
In her presentation, Dr. Berg emphasized that lung cancer is the leading cause of cancer death worldwide, although the distribution between countries “depends on historical and current smoking patterns and the demographics of the population.”
Overall, data from GLOBOCAN 2018 indicate that annually there are approximately 2.1 million incident cases of lung cancer and almost 1.8 million lung cancer deaths around the globe.
A recent study estimated that, worldwide, 14.1% of all lung cancer deaths, including in never-smokers, are directly linked to air pollution.
Dr. Berg said that this makes it the “second-leading cause of lung cancer” behind smoking.
The figure is somewhat lower for the United States, where around 4.7% of lung cancer deaths each year are directly attributable to pollution. However, with “the wildfires out West, we’re going to be seeing more of a toll from air pollution,” she predicted.
She pointed out that the International Agency for Research on Cancer classifies outdoor air pollution, especially particulate matter, as a human carcinogen on the basis of evidence of an association with lung cancer.
It is thought that direct deposits and local effects of particulate matter lead to oxidative damage and low-grade chronic inflammation. These in turn result in molecular changes that affect DNA and gene transcription and inhibit apoptosis, all of which lead to the development of cancerous lesions, she explained.
Synthesizing various estimates on global burden of disease, Dr. Berg and colleagues calculated that in 2019 the rate of lung cancer deaths attributable to particular matter in people aged 50-69 years was highest in Serbia, at 36.88 attributable deaths per 100,000.
Next was Poland, with a rate of 27.97 per 100,000, followed by China at 24.63 per 100,000, Mongolia at 19.71 per 100,000, and Turkey at 19.2 per 100,000.
The major sources of air pollution in the most affected countries were transportation, indoor cooking, and energy sources, she said.
In Serbia, 70% of energy production was from coal. It was 74% in Poland, 65% in China, 80% in Mongolia, 35% in Turkey, and 19% in the United States.
At the time of the analysis, only 17.3% of U.S. adults were smokers, and the air concentration of particular matter of 2.5 mcm was 9.6% mcg/m3. Both of these rates are far below those seen in more severely affected countries.
“But 40% of our energy now comes from natural gas,” noted Dr. Berg, “which is still a pollutant and a source of methane. It’s a very potent greenhouse gas.”
No funding for the study has been reported. Dr. Berg has relationships with GRAIL and Mercy BioAnalytics. Dr. Aerts has relationships with Amphera, AstraZeneca, Bayer, BIOCAD, Bristol-Myers Squibb, Eli Lilly, and Roche.
A version of this article first appeared on Medscape.com.
The new data show that the rate of lung cancer deaths attributable to air pollution varies widely between countries. Serbia, Poland, China, Mongolia, and Turkey are among the worst affected. The analysis shows an association between deaths from lung cancer and the proportion of national energy that is produced from coal.
“Both smoking and air pollution are important causes of lung cancer,” said study presenter Christine D. Berg, MD, former codirector of the National Lung Screening Trial, and “both need to be eliminated to help prevent lung cancer and save lives.
“As lung cancer professionals, we can mitigate the effects of air pollution on causing lung cancer by speaking out for clean energy standards,” she said.
Dr. Berg presented the new analysis on Sept. 9 at the 2021 World Conference on Lung Cancer, which was organized by the International Association for the Study of Lung Cancer.
She welcomed the recent statement issued by the IASLC in support of the International Day of Clean Air for Blue Skies, which took place on Sept. 7. It was a call for action that emphasized the need for further efforts to improve air quality to protect human health.
The findings from the new analysis are “depressing,” commented Joachim G. J. V. Aerts, MD. PhD, department of pulmonary diseases, Erasmus University Medical Center, Rotterdam, the Netherlands.
It is now clear that air pollution has an impact not only on the incidence of lung cancer but also on its outcome, he added.
Indeed, previous research showed that each 10 mcg/m3 increase in particular matter of 2.5 mcg in size was associated with a 15%-27% increase in lung cancer mortality. There was no difference in rates between women and men.
A key question, Dr. Aerts said, is whether reducing air pollution would be beneficial.
Efforts to reduce air pollution over recent decades in the United Kingdom have not led to a reduction in lung cancer deaths. This is because of the increase in life expectancy – individuals have been exposed to pollution for longer, albeit at lower levels, he pointed out.
Because of lockdowns during the COVID pandemic, travel has been greatly reduced. This has resulted in a dramatic reduction in air pollution, “and this led to a decrease in the number of children born with low birth weight,” said Dr. Aerts.
Hopefully, that benefit will also be seen regarding other diseases, he added.
The call to action to reduce air pollution is of the “utmost importance,” he said. He noted that the focus should be on global, national, local, and personal preventive measures.
“It is time to join forces,” he added, “to ‘clean the air.’ ”
Dr. Berg’s presentation was warmly received on social media.
It was “fabulous,” commented Eric H. Bernicker, MD, director of medical thoracic oncology at Houston Methodist Cancer Center.
“Thoracic oncologists need to add air pollution to things they advocate about; we have an important voice here,” he added.
It is “so important to understand that air pollution is a human carcinogen,” commented Ivy Elkins, a lung cancer survivor and advocate and cofounder of the EGFR Resisters Lung Cancer Patient Group. “All you need are lungs to get lung cancer!”
Contribution of air pollution to lung cancer
In her presentation, Dr. Berg emphasized that lung cancer is the leading cause of cancer death worldwide, although the distribution between countries “depends on historical and current smoking patterns and the demographics of the population.”
Overall, data from GLOBOCAN 2018 indicate that annually there are approximately 2.1 million incident cases of lung cancer and almost 1.8 million lung cancer deaths around the globe.
A recent study estimated that, worldwide, 14.1% of all lung cancer deaths, including in never-smokers, are directly linked to air pollution.
Dr. Berg said that this makes it the “second-leading cause of lung cancer” behind smoking.
The figure is somewhat lower for the United States, where around 4.7% of lung cancer deaths each year are directly attributable to pollution. However, with “the wildfires out West, we’re going to be seeing more of a toll from air pollution,” she predicted.
She pointed out that the International Agency for Research on Cancer classifies outdoor air pollution, especially particulate matter, as a human carcinogen on the basis of evidence of an association with lung cancer.
It is thought that direct deposits and local effects of particulate matter lead to oxidative damage and low-grade chronic inflammation. These in turn result in molecular changes that affect DNA and gene transcription and inhibit apoptosis, all of which lead to the development of cancerous lesions, she explained.
Synthesizing various estimates on global burden of disease, Dr. Berg and colleagues calculated that in 2019 the rate of lung cancer deaths attributable to particular matter in people aged 50-69 years was highest in Serbia, at 36.88 attributable deaths per 100,000.
Next was Poland, with a rate of 27.97 per 100,000, followed by China at 24.63 per 100,000, Mongolia at 19.71 per 100,000, and Turkey at 19.2 per 100,000.
The major sources of air pollution in the most affected countries were transportation, indoor cooking, and energy sources, she said.
In Serbia, 70% of energy production was from coal. It was 74% in Poland, 65% in China, 80% in Mongolia, 35% in Turkey, and 19% in the United States.
At the time of the analysis, only 17.3% of U.S. adults were smokers, and the air concentration of particular matter of 2.5 mcm was 9.6% mcg/m3. Both of these rates are far below those seen in more severely affected countries.
“But 40% of our energy now comes from natural gas,” noted Dr. Berg, “which is still a pollutant and a source of methane. It’s a very potent greenhouse gas.”
No funding for the study has been reported. Dr. Berg has relationships with GRAIL and Mercy BioAnalytics. Dr. Aerts has relationships with Amphera, AstraZeneca, Bayer, BIOCAD, Bristol-Myers Squibb, Eli Lilly, and Roche.
A version of this article first appeared on Medscape.com.
The new data show that the rate of lung cancer deaths attributable to air pollution varies widely between countries. Serbia, Poland, China, Mongolia, and Turkey are among the worst affected. The analysis shows an association between deaths from lung cancer and the proportion of national energy that is produced from coal.
“Both smoking and air pollution are important causes of lung cancer,” said study presenter Christine D. Berg, MD, former codirector of the National Lung Screening Trial, and “both need to be eliminated to help prevent lung cancer and save lives.
“As lung cancer professionals, we can mitigate the effects of air pollution on causing lung cancer by speaking out for clean energy standards,” she said.
Dr. Berg presented the new analysis on Sept. 9 at the 2021 World Conference on Lung Cancer, which was organized by the International Association for the Study of Lung Cancer.
She welcomed the recent statement issued by the IASLC in support of the International Day of Clean Air for Blue Skies, which took place on Sept. 7. It was a call for action that emphasized the need for further efforts to improve air quality to protect human health.
The findings from the new analysis are “depressing,” commented Joachim G. J. V. Aerts, MD. PhD, department of pulmonary diseases, Erasmus University Medical Center, Rotterdam, the Netherlands.
It is now clear that air pollution has an impact not only on the incidence of lung cancer but also on its outcome, he added.
Indeed, previous research showed that each 10 mcg/m3 increase in particular matter of 2.5 mcg in size was associated with a 15%-27% increase in lung cancer mortality. There was no difference in rates between women and men.
A key question, Dr. Aerts said, is whether reducing air pollution would be beneficial.
Efforts to reduce air pollution over recent decades in the United Kingdom have not led to a reduction in lung cancer deaths. This is because of the increase in life expectancy – individuals have been exposed to pollution for longer, albeit at lower levels, he pointed out.
Because of lockdowns during the COVID pandemic, travel has been greatly reduced. This has resulted in a dramatic reduction in air pollution, “and this led to a decrease in the number of children born with low birth weight,” said Dr. Aerts.
Hopefully, that benefit will also be seen regarding other diseases, he added.
The call to action to reduce air pollution is of the “utmost importance,” he said. He noted that the focus should be on global, national, local, and personal preventive measures.
“It is time to join forces,” he added, “to ‘clean the air.’ ”
Dr. Berg’s presentation was warmly received on social media.
It was “fabulous,” commented Eric H. Bernicker, MD, director of medical thoracic oncology at Houston Methodist Cancer Center.
“Thoracic oncologists need to add air pollution to things they advocate about; we have an important voice here,” he added.
It is “so important to understand that air pollution is a human carcinogen,” commented Ivy Elkins, a lung cancer survivor and advocate and cofounder of the EGFR Resisters Lung Cancer Patient Group. “All you need are lungs to get lung cancer!”
Contribution of air pollution to lung cancer
In her presentation, Dr. Berg emphasized that lung cancer is the leading cause of cancer death worldwide, although the distribution between countries “depends on historical and current smoking patterns and the demographics of the population.”
Overall, data from GLOBOCAN 2018 indicate that annually there are approximately 2.1 million incident cases of lung cancer and almost 1.8 million lung cancer deaths around the globe.
A recent study estimated that, worldwide, 14.1% of all lung cancer deaths, including in never-smokers, are directly linked to air pollution.
Dr. Berg said that this makes it the “second-leading cause of lung cancer” behind smoking.
The figure is somewhat lower for the United States, where around 4.7% of lung cancer deaths each year are directly attributable to pollution. However, with “the wildfires out West, we’re going to be seeing more of a toll from air pollution,” she predicted.
She pointed out that the International Agency for Research on Cancer classifies outdoor air pollution, especially particulate matter, as a human carcinogen on the basis of evidence of an association with lung cancer.
It is thought that direct deposits and local effects of particulate matter lead to oxidative damage and low-grade chronic inflammation. These in turn result in molecular changes that affect DNA and gene transcription and inhibit apoptosis, all of which lead to the development of cancerous lesions, she explained.
Synthesizing various estimates on global burden of disease, Dr. Berg and colleagues calculated that in 2019 the rate of lung cancer deaths attributable to particular matter in people aged 50-69 years was highest in Serbia, at 36.88 attributable deaths per 100,000.
Next was Poland, with a rate of 27.97 per 100,000, followed by China at 24.63 per 100,000, Mongolia at 19.71 per 100,000, and Turkey at 19.2 per 100,000.
The major sources of air pollution in the most affected countries were transportation, indoor cooking, and energy sources, she said.
In Serbia, 70% of energy production was from coal. It was 74% in Poland, 65% in China, 80% in Mongolia, 35% in Turkey, and 19% in the United States.
At the time of the analysis, only 17.3% of U.S. adults were smokers, and the air concentration of particular matter of 2.5 mcm was 9.6% mcg/m3. Both of these rates are far below those seen in more severely affected countries.
“But 40% of our energy now comes from natural gas,” noted Dr. Berg, “which is still a pollutant and a source of methane. It’s a very potent greenhouse gas.”
No funding for the study has been reported. Dr. Berg has relationships with GRAIL and Mercy BioAnalytics. Dr. Aerts has relationships with Amphera, AstraZeneca, Bayer, BIOCAD, Bristol-Myers Squibb, Eli Lilly, and Roche.
A version of this article first appeared on Medscape.com.
Infants breathe better when pregnant moms exercise
Lung function in early infancy may be influenced by the mother’s level of physical activity during pregnancy, results of a study from Sweden suggest.
Low-lung function at 3 months of age, as measured by the ratio of time to peak tidal expiratory flow to expiratory time (tPTEF/tE), was more frequent among children whose mothers were physically inactive during the first half of pregnancy compared with those who exercised either moderately or strenuously, reported Hrefna Katrin Gudmundsdottir, MD, a pediatrician and PhD candidate at the University of Oslo, Norway. The results were based on a prospective observational study of 841 mother-child pairs.
“The potential link between maternal inactivity and low lung function in infancy adds to the importance of advising pregnant women and women of childbearing age on physical activity,” she said in an oral abstract presented during the virtual European Respiratory Society (ERS) International Congress.
Jonathan Grigg, MD, professor of pediatric respiratory and environmental medicine at Queen Mary University of London, who was not involved in the study, commented that it “offers a fascinating hint that increased physical activity of mothers is associated with better lung function in their babies and, therefore, possibly their health in later life. More research is needed to confirm this link, but it is important that women feel supported by their health care providers to be active in a way that is comfortable and accessible to them.”
Impaired lung function in infancy is associated with wheezing and asthma in childhood, and lower lung function later in life, Dr. Gudmundsdottir said. She also noted that impaired lung function begins in utero and is related to fetal and infant size, family history of asthma, and/or maternal smoking.
Physical activity during pregnancy has been demonstrated to reduce the risk of preterm birth and cesarean birth and of children being born either abnormally small or abnormally large for their gestational age, she explained.
To see where physical inactivity in the first half of pregnancy is associated with lower lung function in otherwise healthy 3-month old infants, Dr. Gudmundsdottir and colleagues looked at data on a mother-child cohort from the prospective population-based PreventADALL study, which was designed to study prevention of atopic dermatitis and allergies in children in Norway and Sweden.
A total of 814 infants (49% female) had available measures of tidal flow volume in the awake state at 3 months, as well as mother-reported data on physical activity at 18 weeks of pregnancy.
The investigators categorized the mothers as inactive, with either no or only low-intensity physical activity, “fairly” active, or “very” active based on self reporting.
The average tPTEF/tE value among all infants in the study was 0.391. The average value for 290 infants born to inactive mothers was 0.387, compared with 0.394 for 299 infants born to very active mothers, a difference that was not statistically significant.
Maternal physical activity level was not significantly associated with continuous tPTEF/tE, but the investigators did find that the offspring of inactive mothers were significantly more likely than the children of fairly or very active mothers to have a tPTEF/tE below 0.25 in both univariate analysis (odds ratio, 2.15; P = .011), and in multivariate analysis controlling for maternal age, education, parity, prepregnancy body-mass index, parental atopy, and in-utero exposure to nicotine (OR, 2.18; P = .013).
In univariate but not multivariate analysis, children of inactive mothers were significantly more likely than infants of more active mothers to have tPTEF/tE values below the 50th percentile (OR, 1.35; P = .042).
“We observed a trend that adds to the importance of advising women of childbearing age and pregnant women about physical activity. However, there may be factors that affect both maternal physical activity and lung function in offspring that we have not accounted for and could affect the results, so more research is needed,” Dr. Gudmundsdottir said in a statement.
Dr. Grigg pointed out that “it’s also worth keeping in mind that the single most important thing that mothers can do for their own health and that of their baby is to ensure that they do not smoke or use other tobacco products before, during, and after pregnancy. A smoke-free home has the biggest impact on lung function and health in childhood and later life.”
The study was supported by the University of Oslo. Dr. Gudmundsdottir and Dr. Grigg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lung function in early infancy may be influenced by the mother’s level of physical activity during pregnancy, results of a study from Sweden suggest.
Low-lung function at 3 months of age, as measured by the ratio of time to peak tidal expiratory flow to expiratory time (tPTEF/tE), was more frequent among children whose mothers were physically inactive during the first half of pregnancy compared with those who exercised either moderately or strenuously, reported Hrefna Katrin Gudmundsdottir, MD, a pediatrician and PhD candidate at the University of Oslo, Norway. The results were based on a prospective observational study of 841 mother-child pairs.
“The potential link between maternal inactivity and low lung function in infancy adds to the importance of advising pregnant women and women of childbearing age on physical activity,” she said in an oral abstract presented during the virtual European Respiratory Society (ERS) International Congress.
Jonathan Grigg, MD, professor of pediatric respiratory and environmental medicine at Queen Mary University of London, who was not involved in the study, commented that it “offers a fascinating hint that increased physical activity of mothers is associated with better lung function in their babies and, therefore, possibly their health in later life. More research is needed to confirm this link, but it is important that women feel supported by their health care providers to be active in a way that is comfortable and accessible to them.”
Impaired lung function in infancy is associated with wheezing and asthma in childhood, and lower lung function later in life, Dr. Gudmundsdottir said. She also noted that impaired lung function begins in utero and is related to fetal and infant size, family history of asthma, and/or maternal smoking.
Physical activity during pregnancy has been demonstrated to reduce the risk of preterm birth and cesarean birth and of children being born either abnormally small or abnormally large for their gestational age, she explained.
To see where physical inactivity in the first half of pregnancy is associated with lower lung function in otherwise healthy 3-month old infants, Dr. Gudmundsdottir and colleagues looked at data on a mother-child cohort from the prospective population-based PreventADALL study, which was designed to study prevention of atopic dermatitis and allergies in children in Norway and Sweden.
A total of 814 infants (49% female) had available measures of tidal flow volume in the awake state at 3 months, as well as mother-reported data on physical activity at 18 weeks of pregnancy.
The investigators categorized the mothers as inactive, with either no or only low-intensity physical activity, “fairly” active, or “very” active based on self reporting.
The average tPTEF/tE value among all infants in the study was 0.391. The average value for 290 infants born to inactive mothers was 0.387, compared with 0.394 for 299 infants born to very active mothers, a difference that was not statistically significant.
Maternal physical activity level was not significantly associated with continuous tPTEF/tE, but the investigators did find that the offspring of inactive mothers were significantly more likely than the children of fairly or very active mothers to have a tPTEF/tE below 0.25 in both univariate analysis (odds ratio, 2.15; P = .011), and in multivariate analysis controlling for maternal age, education, parity, prepregnancy body-mass index, parental atopy, and in-utero exposure to nicotine (OR, 2.18; P = .013).
In univariate but not multivariate analysis, children of inactive mothers were significantly more likely than infants of more active mothers to have tPTEF/tE values below the 50th percentile (OR, 1.35; P = .042).
“We observed a trend that adds to the importance of advising women of childbearing age and pregnant women about physical activity. However, there may be factors that affect both maternal physical activity and lung function in offspring that we have not accounted for and could affect the results, so more research is needed,” Dr. Gudmundsdottir said in a statement.
Dr. Grigg pointed out that “it’s also worth keeping in mind that the single most important thing that mothers can do for their own health and that of their baby is to ensure that they do not smoke or use other tobacco products before, during, and after pregnancy. A smoke-free home has the biggest impact on lung function and health in childhood and later life.”
The study was supported by the University of Oslo. Dr. Gudmundsdottir and Dr. Grigg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lung function in early infancy may be influenced by the mother’s level of physical activity during pregnancy, results of a study from Sweden suggest.
Low-lung function at 3 months of age, as measured by the ratio of time to peak tidal expiratory flow to expiratory time (tPTEF/tE), was more frequent among children whose mothers were physically inactive during the first half of pregnancy compared with those who exercised either moderately or strenuously, reported Hrefna Katrin Gudmundsdottir, MD, a pediatrician and PhD candidate at the University of Oslo, Norway. The results were based on a prospective observational study of 841 mother-child pairs.
“The potential link between maternal inactivity and low lung function in infancy adds to the importance of advising pregnant women and women of childbearing age on physical activity,” she said in an oral abstract presented during the virtual European Respiratory Society (ERS) International Congress.
Jonathan Grigg, MD, professor of pediatric respiratory and environmental medicine at Queen Mary University of London, who was not involved in the study, commented that it “offers a fascinating hint that increased physical activity of mothers is associated with better lung function in their babies and, therefore, possibly their health in later life. More research is needed to confirm this link, but it is important that women feel supported by their health care providers to be active in a way that is comfortable and accessible to them.”
Impaired lung function in infancy is associated with wheezing and asthma in childhood, and lower lung function later in life, Dr. Gudmundsdottir said. She also noted that impaired lung function begins in utero and is related to fetal and infant size, family history of asthma, and/or maternal smoking.
Physical activity during pregnancy has been demonstrated to reduce the risk of preterm birth and cesarean birth and of children being born either abnormally small or abnormally large for their gestational age, she explained.
To see where physical inactivity in the first half of pregnancy is associated with lower lung function in otherwise healthy 3-month old infants, Dr. Gudmundsdottir and colleagues looked at data on a mother-child cohort from the prospective population-based PreventADALL study, which was designed to study prevention of atopic dermatitis and allergies in children in Norway and Sweden.
A total of 814 infants (49% female) had available measures of tidal flow volume in the awake state at 3 months, as well as mother-reported data on physical activity at 18 weeks of pregnancy.
The investigators categorized the mothers as inactive, with either no or only low-intensity physical activity, “fairly” active, or “very” active based on self reporting.
The average tPTEF/tE value among all infants in the study was 0.391. The average value for 290 infants born to inactive mothers was 0.387, compared with 0.394 for 299 infants born to very active mothers, a difference that was not statistically significant.
Maternal physical activity level was not significantly associated with continuous tPTEF/tE, but the investigators did find that the offspring of inactive mothers were significantly more likely than the children of fairly or very active mothers to have a tPTEF/tE below 0.25 in both univariate analysis (odds ratio, 2.15; P = .011), and in multivariate analysis controlling for maternal age, education, parity, prepregnancy body-mass index, parental atopy, and in-utero exposure to nicotine (OR, 2.18; P = .013).
In univariate but not multivariate analysis, children of inactive mothers were significantly more likely than infants of more active mothers to have tPTEF/tE values below the 50th percentile (OR, 1.35; P = .042).
“We observed a trend that adds to the importance of advising women of childbearing age and pregnant women about physical activity. However, there may be factors that affect both maternal physical activity and lung function in offspring that we have not accounted for and could affect the results, so more research is needed,” Dr. Gudmundsdottir said in a statement.
Dr. Grigg pointed out that “it’s also worth keeping in mind that the single most important thing that mothers can do for their own health and that of their baby is to ensure that they do not smoke or use other tobacco products before, during, and after pregnancy. A smoke-free home has the biggest impact on lung function and health in childhood and later life.”
The study was supported by the University of Oslo. Dr. Gudmundsdottir and Dr. Grigg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.