User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
MS and COVID: Docs switched DMTs but maybe didn’t need to
These are the messages of a pair of new studies that examine the impact of the pandemic on the treatment of MS.
One report finds that 80% of specialists surveyed in the summer of 2020 said the pandemic may have changed how they prescribe disease-modifying therapies (DMTs). However, the other report finds no evidence that choice of DMT affects risk of COVID-19 infection. Both studies were presented at the 2021 Annual Meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
For the survey, researchers led by neurologist Elizabeth H. Morrison-Banks, MD, of the University of California, Riverside, sent questions to 188 clinicians who serve on regional National Multiple Sclerosis Society Healthcare Provider Councils. A total of 86 people responded: 45 physicians, 18 rehabilitation therapists, 7 psychologists, 8 advanced practice clinicians, 4 social workers, 2 nurses, a pharmacist, and a researcher.
The results, which were published earlier in 2021 in Multiple Sclerosis and Related Disorders, revealed that the survey participants were prescribing certain DMTs more often: beta-interferons (prescribed more by 28.6% of prescribers), natalizumab (23.8%), and glatiramer acetate (21.4%). Those prescribed less included alemtuzumab (64.2% prescribed it less), cladribine (52.4%), and B cell–depleting agents including ocrelizumab and rituximab (50%). Some specialists suspended drugs entirely (21.4% for alemtuzumab, 16.7% for B cell–depleting agents) or extending dosing intervals (38.1% for natalizumab, 11.9% for fingolimod and siponimod).
“We suspect that some of the lower-efficacy therapies were prescribed more often because these therapies were much less immunosuppressive, and because they did not require in-person visits that would increase risk of viral exposure from infusion center staff, or from other infusion patients,” Dr. Morrison-Banks said in an interview. “We also suspect that some of our survey respondents may have increased the dosing intervals for higher-efficacy therapies such as B cell–modulating agents – or even avoided these therapies altogether – because they were concerned that immunosuppressive agents might trigger severe complications from COVID-19.”
As she noted, “in retrospect, at least some of the concerns expressed in our survey may not have been entirely warranted, but then again, we all knew even less then about COVID-19.”
Indeed, researchers led by neurologist Tyler E. Smith, MD, of New York University Langone Multiple Sclerosis Care Center are reporting that they couldn’t find any link between the following DMTs and higher rates of COVID-19 at the New York City center: rituximab, ocrelizumab, fumerate (dimethyl fumarate, monomethyl fumarate, diroximel fumarate), sphingosine-1-phosphate modulators (fingolimod, siponimod), and natalizumab.
The researchers tracked 1,439 patients with MS who were taking the DMTs from March 2020 to March 2021. Of those, 16.0% were infected with COVID-19 (75% lab confirmed), 6.5% were hospitalized, and 0.9% died.
“We did not find an association between the choice of disease-modifying therapy and developing COVID-19 infection, nor having increased disease severity,” Dr. Smith said in an interview. “We are still analyzing data and hope to publish an updated analysis, but at this point, we don’t have conclusive evidence that DMTs, including anti-CD20 agents, need to be changed to lower the risk of COVID-19.”
Instead, he said, “at this point, we feel our energies should be spent on educating our patients on importance of vaccines and boosters. I don’t think it is necessary to switch DMTs because of COVID-19 concerns. However, this should be reviewed on a case-by-case basis.”
No funding is reported for the survey study, and the authors reported various disclosures. The DMT study was funded by an investigator-initiated grant from the Consortium of Multiple Sclerosis Centers, and the authors reported various disclosures.
These are the messages of a pair of new studies that examine the impact of the pandemic on the treatment of MS.
One report finds that 80% of specialists surveyed in the summer of 2020 said the pandemic may have changed how they prescribe disease-modifying therapies (DMTs). However, the other report finds no evidence that choice of DMT affects risk of COVID-19 infection. Both studies were presented at the 2021 Annual Meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
For the survey, researchers led by neurologist Elizabeth H. Morrison-Banks, MD, of the University of California, Riverside, sent questions to 188 clinicians who serve on regional National Multiple Sclerosis Society Healthcare Provider Councils. A total of 86 people responded: 45 physicians, 18 rehabilitation therapists, 7 psychologists, 8 advanced practice clinicians, 4 social workers, 2 nurses, a pharmacist, and a researcher.
The results, which were published earlier in 2021 in Multiple Sclerosis and Related Disorders, revealed that the survey participants were prescribing certain DMTs more often: beta-interferons (prescribed more by 28.6% of prescribers), natalizumab (23.8%), and glatiramer acetate (21.4%). Those prescribed less included alemtuzumab (64.2% prescribed it less), cladribine (52.4%), and B cell–depleting agents including ocrelizumab and rituximab (50%). Some specialists suspended drugs entirely (21.4% for alemtuzumab, 16.7% for B cell–depleting agents) or extending dosing intervals (38.1% for natalizumab, 11.9% for fingolimod and siponimod).
“We suspect that some of the lower-efficacy therapies were prescribed more often because these therapies were much less immunosuppressive, and because they did not require in-person visits that would increase risk of viral exposure from infusion center staff, or from other infusion patients,” Dr. Morrison-Banks said in an interview. “We also suspect that some of our survey respondents may have increased the dosing intervals for higher-efficacy therapies such as B cell–modulating agents – or even avoided these therapies altogether – because they were concerned that immunosuppressive agents might trigger severe complications from COVID-19.”
As she noted, “in retrospect, at least some of the concerns expressed in our survey may not have been entirely warranted, but then again, we all knew even less then about COVID-19.”
Indeed, researchers led by neurologist Tyler E. Smith, MD, of New York University Langone Multiple Sclerosis Care Center are reporting that they couldn’t find any link between the following DMTs and higher rates of COVID-19 at the New York City center: rituximab, ocrelizumab, fumerate (dimethyl fumarate, monomethyl fumarate, diroximel fumarate), sphingosine-1-phosphate modulators (fingolimod, siponimod), and natalizumab.
The researchers tracked 1,439 patients with MS who were taking the DMTs from March 2020 to March 2021. Of those, 16.0% were infected with COVID-19 (75% lab confirmed), 6.5% were hospitalized, and 0.9% died.
“We did not find an association between the choice of disease-modifying therapy and developing COVID-19 infection, nor having increased disease severity,” Dr. Smith said in an interview. “We are still analyzing data and hope to publish an updated analysis, but at this point, we don’t have conclusive evidence that DMTs, including anti-CD20 agents, need to be changed to lower the risk of COVID-19.”
Instead, he said, “at this point, we feel our energies should be spent on educating our patients on importance of vaccines and boosters. I don’t think it is necessary to switch DMTs because of COVID-19 concerns. However, this should be reviewed on a case-by-case basis.”
No funding is reported for the survey study, and the authors reported various disclosures. The DMT study was funded by an investigator-initiated grant from the Consortium of Multiple Sclerosis Centers, and the authors reported various disclosures.
These are the messages of a pair of new studies that examine the impact of the pandemic on the treatment of MS.
One report finds that 80% of specialists surveyed in the summer of 2020 said the pandemic may have changed how they prescribe disease-modifying therapies (DMTs). However, the other report finds no evidence that choice of DMT affects risk of COVID-19 infection. Both studies were presented at the 2021 Annual Meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
For the survey, researchers led by neurologist Elizabeth H. Morrison-Banks, MD, of the University of California, Riverside, sent questions to 188 clinicians who serve on regional National Multiple Sclerosis Society Healthcare Provider Councils. A total of 86 people responded: 45 physicians, 18 rehabilitation therapists, 7 psychologists, 8 advanced practice clinicians, 4 social workers, 2 nurses, a pharmacist, and a researcher.
The results, which were published earlier in 2021 in Multiple Sclerosis and Related Disorders, revealed that the survey participants were prescribing certain DMTs more often: beta-interferons (prescribed more by 28.6% of prescribers), natalizumab (23.8%), and glatiramer acetate (21.4%). Those prescribed less included alemtuzumab (64.2% prescribed it less), cladribine (52.4%), and B cell–depleting agents including ocrelizumab and rituximab (50%). Some specialists suspended drugs entirely (21.4% for alemtuzumab, 16.7% for B cell–depleting agents) or extending dosing intervals (38.1% for natalizumab, 11.9% for fingolimod and siponimod).
“We suspect that some of the lower-efficacy therapies were prescribed more often because these therapies were much less immunosuppressive, and because they did not require in-person visits that would increase risk of viral exposure from infusion center staff, or from other infusion patients,” Dr. Morrison-Banks said in an interview. “We also suspect that some of our survey respondents may have increased the dosing intervals for higher-efficacy therapies such as B cell–modulating agents – or even avoided these therapies altogether – because they were concerned that immunosuppressive agents might trigger severe complications from COVID-19.”
As she noted, “in retrospect, at least some of the concerns expressed in our survey may not have been entirely warranted, but then again, we all knew even less then about COVID-19.”
Indeed, researchers led by neurologist Tyler E. Smith, MD, of New York University Langone Multiple Sclerosis Care Center are reporting that they couldn’t find any link between the following DMTs and higher rates of COVID-19 at the New York City center: rituximab, ocrelizumab, fumerate (dimethyl fumarate, monomethyl fumarate, diroximel fumarate), sphingosine-1-phosphate modulators (fingolimod, siponimod), and natalizumab.
The researchers tracked 1,439 patients with MS who were taking the DMTs from March 2020 to March 2021. Of those, 16.0% were infected with COVID-19 (75% lab confirmed), 6.5% were hospitalized, and 0.9% died.
“We did not find an association between the choice of disease-modifying therapy and developing COVID-19 infection, nor having increased disease severity,” Dr. Smith said in an interview. “We are still analyzing data and hope to publish an updated analysis, but at this point, we don’t have conclusive evidence that DMTs, including anti-CD20 agents, need to be changed to lower the risk of COVID-19.”
Instead, he said, “at this point, we feel our energies should be spent on educating our patients on importance of vaccines and boosters. I don’t think it is necessary to switch DMTs because of COVID-19 concerns. However, this should be reviewed on a case-by-case basis.”
No funding is reported for the survey study, and the authors reported various disclosures. The DMT study was funded by an investigator-initiated grant from the Consortium of Multiple Sclerosis Centers, and the authors reported various disclosures.
FROM CMSC 2021
Vonoprazan beats PPIs in H. pylori eradication
LAS VEGAS – In the treatment of Helicobacter pylori infection, combination therapies using the oral potassium-competitive acid blocker vonoprazan were superior to standard proton pump inhibitor (PPI)–based triple therapy, producing higher eradication rates, according to combined data from a U.S. and a European phase 3 randomized, controlled trial.
Vonoprazan has been submitted to the Food and Drug Administration for approval with a Fast Track designation in combination with amoxicillin and clarithromycin (triple therapy) or amoxicillin alone (dual therapy) for treating H. pylori infection. It has already been approved in Japan for the treatment of gastric and duodenal ulcers, reflux esophagitis, secondary prevention of low-dose aspirin– or nonsteroidal anti-inflammatory drug–induced gastric mucosal damage, and for first and second-line H. pylori eradication therapy.
Study details
The study included 1,046 treatment-naive patients who had dyspepsia, a recent or new diagnosis of a nonbleeding peptic ulcer, a history of a peptic ulcer, or long-term stable use of an NSAID. Patients were randomized to PPI-based triple therapy (lansoprazole, amoxicillin, clarithromycin), vonoprazan triple therapy (plus amoxicillin, clarithromycin), or vonoprazan dual therapy (amoxicillin). The treatment period was 14 days, followed by 13C urea breath test (UBT) 4 weeks after treatment.
The researchers conducted several analyses, including: Modified intention-to-treat analyses, which included all enrollees; per protocol analyses, which included patients who took at least 75% of each study medication and underwent 13C UBT in the expected time frame; and a safety population of all patients who took at least one study drug.
Among patients with H. pylori strains that were not resistant to clarithromycin, the PPI-based triple-therapy group had an eradication rate of 78.8%, compared with 84.7% in the vonoprazan triple-therapy group (P < .0001), and 78.5% in the vonoprazan dual-therapy group (P = .0037). In the per protocol analysis, PPI-based triple therapy eradicated H. pylori 82.1% of the time, compared with 90.4% in the vonoprazan triple-therapy group (P < .0001) and 81.2% in the vonoprazan dual-therapy group (P = .0077). Both vonoprazan treatment groups were noninferior to PPI-based triple therapy.
A prespecified exploratory analysis found that vonoprazan triple therapy outperformed PPI-based triple therapy in the modified intention-to-treat population (P = .0408) and the per protocol population (P = .0059).
Among patients with clarithromycin-resistant strains of H. pylori, in the modified intention-to-treat population, 31.9% achieved eradication with PPI triple therapy, compared with 65.8% in the vonoprazan triple-therapy group, and 69.6% in the vonoprazan dual-therapy group. In the per protocol population, the numbers were 29.0% versus 67.2% and 79.5%, respectively (P < .0001 for both versus PPI triple therapy).
Among all patients, in the modified intention-to-treat population, 68.5% achieved eradication with PPI triple therapy, 80.8% with vonoprazan triple therapy (P =. 0001), and 77.2% with vonoprazan dual therapy (P = .0063)*. In the per protocol population, the numbers were 70.0%, 85.7% (P < .0001), and 81.1% (P = .0013), respectively.
Safety outcomes were similar among the three groups, with treatment-emergent adverse events occurring in 34.5% of the PPI triple-therapy group (1.2% discontinued), 34.1% of the vonoprazan triple-therapy group (2.3% discontinued), and 29.9% in the vonoprazan dual-therapy group (0.9% discontinued).
Fighting against resistance
The efficacy of PPI-based clarithromycin-based triple therapy has fallen below 80% in the United States and Europe over the past few decades, largely because of antibiotic resistance, said William Chey, MD, during a presentation of the results at the annual meeting of the American College of Gastroenterology. Dr. Chey is a professor of medicine and director of the GI physiology laboratory at Michigan Medicine.
Vonoprazan is more stable in acid than are PPIs, and produces greater and more durable acid reduction, according to Dr. Chey. That’s important for two reasons: One is that some antibiotics are acid-labile, and so may have their efficacy directly impacted in a more acidic environment. The other factor is that most antibiotics work better on bacteria that are actively replicating, and H. pylori reproduces better in a more neutral environment. “So, you increase the replication, you increase the bioavailability of the antibiotics. And therefore, hopefully, that underlies why we see it working better in the patients with [antibiotic] resistance,” Dr. Chey said in an interview.
It remains to be seen whether or not the drug will receive FDA approval, but he pointed to other regimens like bismuth quadruple therapy and rifabutin-based triple therapy that are already available. “If I had the choice, I would never use a PPI-based triple therapy again. People should not be doing that,” said Dr. Chey.
“More successful H. pylori eradication regimens are certainly needed, and these results are particularly relevant and interesting given the increasing failure of initial treatment regimens,” said Kimberly Harer, MD, who moderated the session. She noted that the secondary analysis of patients with clarithromycin-resistant infections was particularly relevant. “The superiority analysis indicating vonoprazan triple therapy resulted in increased H. pylori eradication compared to lanzoprazole triple therapy was especially interesting,” said Dr. Harer, who is a clinical lecturer at University of Michigan Health, Ann Arbor.
One downside to the study is that it didn’t compare vonoprazan combinations to quadruple therapy of a PPI, bismuth, tetracycline, and a nitroimidazole, said Joseph Jennings, MD, who was asked to comment on the study. Other treatment approaches include sequential antibiotics and other combinations. Dr. Jennings also highlighted the findings that the vonoprazan regimens were superior against clarithromycin-resistant strains. “The more different regimens we can add to the armamentarium, the better chance we have because the resistant patterns fluctuate all throughout the world,” said Dr. Jennings, who is an assistant professor of medicine at Georgetown University and director of the center for GI bleeding at MedStar Georgetown University Hospital, both in Washington.
He also pointed out that physicians can face a conundrum when patients fail multiple lines of therapy and have testing done that shows high levels of resistance. Some have allergies that prevent them from turning to other antibiotics. “That’s a market where lots of doctors struggle. Something like this would be a nice add-on,” said Dr. Jennings.
The study was funded by Phathom Pharmaceuticals.** Dr. Chey has consulted and/or received research support from Abbvie, Alfasigma, Allakos, Alnylam, Bayer, Bioamerica, Cosmo, Intrinsic Medicine, Ironwood, Modify Health, My GI Health, My Nutrition Health, Nestle, Phathom Pharmaceuticals, QOL Medical, Redhill, Salix/Valeant, Takeda, Urovant, and Vibrant. Dr. Harer and Dr. Jennings have no relevant financial disclosures.
*Correction, 10/29/21: An earlier version of this article misstated the percentage of patients in the modified intention-to-treat population who achieved eradication with vonoprazan triple therapy.
**Correction, 10/29/21: An earlier version of this article misstated the name of Phathom Pharmaceuticals.
LAS VEGAS – In the treatment of Helicobacter pylori infection, combination therapies using the oral potassium-competitive acid blocker vonoprazan were superior to standard proton pump inhibitor (PPI)–based triple therapy, producing higher eradication rates, according to combined data from a U.S. and a European phase 3 randomized, controlled trial.
Vonoprazan has been submitted to the Food and Drug Administration for approval with a Fast Track designation in combination with amoxicillin and clarithromycin (triple therapy) or amoxicillin alone (dual therapy) for treating H. pylori infection. It has already been approved in Japan for the treatment of gastric and duodenal ulcers, reflux esophagitis, secondary prevention of low-dose aspirin– or nonsteroidal anti-inflammatory drug–induced gastric mucosal damage, and for first and second-line H. pylori eradication therapy.
Study details
The study included 1,046 treatment-naive patients who had dyspepsia, a recent or new diagnosis of a nonbleeding peptic ulcer, a history of a peptic ulcer, or long-term stable use of an NSAID. Patients were randomized to PPI-based triple therapy (lansoprazole, amoxicillin, clarithromycin), vonoprazan triple therapy (plus amoxicillin, clarithromycin), or vonoprazan dual therapy (amoxicillin). The treatment period was 14 days, followed by 13C urea breath test (UBT) 4 weeks after treatment.
The researchers conducted several analyses, including: Modified intention-to-treat analyses, which included all enrollees; per protocol analyses, which included patients who took at least 75% of each study medication and underwent 13C UBT in the expected time frame; and a safety population of all patients who took at least one study drug.
Among patients with H. pylori strains that were not resistant to clarithromycin, the PPI-based triple-therapy group had an eradication rate of 78.8%, compared with 84.7% in the vonoprazan triple-therapy group (P < .0001), and 78.5% in the vonoprazan dual-therapy group (P = .0037). In the per protocol analysis, PPI-based triple therapy eradicated H. pylori 82.1% of the time, compared with 90.4% in the vonoprazan triple-therapy group (P < .0001) and 81.2% in the vonoprazan dual-therapy group (P = .0077). Both vonoprazan treatment groups were noninferior to PPI-based triple therapy.
A prespecified exploratory analysis found that vonoprazan triple therapy outperformed PPI-based triple therapy in the modified intention-to-treat population (P = .0408) and the per protocol population (P = .0059).
Among patients with clarithromycin-resistant strains of H. pylori, in the modified intention-to-treat population, 31.9% achieved eradication with PPI triple therapy, compared with 65.8% in the vonoprazan triple-therapy group, and 69.6% in the vonoprazan dual-therapy group. In the per protocol population, the numbers were 29.0% versus 67.2% and 79.5%, respectively (P < .0001 for both versus PPI triple therapy).
Among all patients, in the modified intention-to-treat population, 68.5% achieved eradication with PPI triple therapy, 80.8% with vonoprazan triple therapy (P =. 0001), and 77.2% with vonoprazan dual therapy (P = .0063)*. In the per protocol population, the numbers were 70.0%, 85.7% (P < .0001), and 81.1% (P = .0013), respectively.
Safety outcomes were similar among the three groups, with treatment-emergent adverse events occurring in 34.5% of the PPI triple-therapy group (1.2% discontinued), 34.1% of the vonoprazan triple-therapy group (2.3% discontinued), and 29.9% in the vonoprazan dual-therapy group (0.9% discontinued).
Fighting against resistance
The efficacy of PPI-based clarithromycin-based triple therapy has fallen below 80% in the United States and Europe over the past few decades, largely because of antibiotic resistance, said William Chey, MD, during a presentation of the results at the annual meeting of the American College of Gastroenterology. Dr. Chey is a professor of medicine and director of the GI physiology laboratory at Michigan Medicine.
Vonoprazan is more stable in acid than are PPIs, and produces greater and more durable acid reduction, according to Dr. Chey. That’s important for two reasons: One is that some antibiotics are acid-labile, and so may have their efficacy directly impacted in a more acidic environment. The other factor is that most antibiotics work better on bacteria that are actively replicating, and H. pylori reproduces better in a more neutral environment. “So, you increase the replication, you increase the bioavailability of the antibiotics. And therefore, hopefully, that underlies why we see it working better in the patients with [antibiotic] resistance,” Dr. Chey said in an interview.
It remains to be seen whether or not the drug will receive FDA approval, but he pointed to other regimens like bismuth quadruple therapy and rifabutin-based triple therapy that are already available. “If I had the choice, I would never use a PPI-based triple therapy again. People should not be doing that,” said Dr. Chey.
“More successful H. pylori eradication regimens are certainly needed, and these results are particularly relevant and interesting given the increasing failure of initial treatment regimens,” said Kimberly Harer, MD, who moderated the session. She noted that the secondary analysis of patients with clarithromycin-resistant infections was particularly relevant. “The superiority analysis indicating vonoprazan triple therapy resulted in increased H. pylori eradication compared to lanzoprazole triple therapy was especially interesting,” said Dr. Harer, who is a clinical lecturer at University of Michigan Health, Ann Arbor.
One downside to the study is that it didn’t compare vonoprazan combinations to quadruple therapy of a PPI, bismuth, tetracycline, and a nitroimidazole, said Joseph Jennings, MD, who was asked to comment on the study. Other treatment approaches include sequential antibiotics and other combinations. Dr. Jennings also highlighted the findings that the vonoprazan regimens were superior against clarithromycin-resistant strains. “The more different regimens we can add to the armamentarium, the better chance we have because the resistant patterns fluctuate all throughout the world,” said Dr. Jennings, who is an assistant professor of medicine at Georgetown University and director of the center for GI bleeding at MedStar Georgetown University Hospital, both in Washington.
He also pointed out that physicians can face a conundrum when patients fail multiple lines of therapy and have testing done that shows high levels of resistance. Some have allergies that prevent them from turning to other antibiotics. “That’s a market where lots of doctors struggle. Something like this would be a nice add-on,” said Dr. Jennings.
The study was funded by Phathom Pharmaceuticals.** Dr. Chey has consulted and/or received research support from Abbvie, Alfasigma, Allakos, Alnylam, Bayer, Bioamerica, Cosmo, Intrinsic Medicine, Ironwood, Modify Health, My GI Health, My Nutrition Health, Nestle, Phathom Pharmaceuticals, QOL Medical, Redhill, Salix/Valeant, Takeda, Urovant, and Vibrant. Dr. Harer and Dr. Jennings have no relevant financial disclosures.
*Correction, 10/29/21: An earlier version of this article misstated the percentage of patients in the modified intention-to-treat population who achieved eradication with vonoprazan triple therapy.
**Correction, 10/29/21: An earlier version of this article misstated the name of Phathom Pharmaceuticals.
LAS VEGAS – In the treatment of Helicobacter pylori infection, combination therapies using the oral potassium-competitive acid blocker vonoprazan were superior to standard proton pump inhibitor (PPI)–based triple therapy, producing higher eradication rates, according to combined data from a U.S. and a European phase 3 randomized, controlled trial.
Vonoprazan has been submitted to the Food and Drug Administration for approval with a Fast Track designation in combination with amoxicillin and clarithromycin (triple therapy) or amoxicillin alone (dual therapy) for treating H. pylori infection. It has already been approved in Japan for the treatment of gastric and duodenal ulcers, reflux esophagitis, secondary prevention of low-dose aspirin– or nonsteroidal anti-inflammatory drug–induced gastric mucosal damage, and for first and second-line H. pylori eradication therapy.
Study details
The study included 1,046 treatment-naive patients who had dyspepsia, a recent or new diagnosis of a nonbleeding peptic ulcer, a history of a peptic ulcer, or long-term stable use of an NSAID. Patients were randomized to PPI-based triple therapy (lansoprazole, amoxicillin, clarithromycin), vonoprazan triple therapy (plus amoxicillin, clarithromycin), or vonoprazan dual therapy (amoxicillin). The treatment period was 14 days, followed by 13C urea breath test (UBT) 4 weeks after treatment.
The researchers conducted several analyses, including: Modified intention-to-treat analyses, which included all enrollees; per protocol analyses, which included patients who took at least 75% of each study medication and underwent 13C UBT in the expected time frame; and a safety population of all patients who took at least one study drug.
Among patients with H. pylori strains that were not resistant to clarithromycin, the PPI-based triple-therapy group had an eradication rate of 78.8%, compared with 84.7% in the vonoprazan triple-therapy group (P < .0001), and 78.5% in the vonoprazan dual-therapy group (P = .0037). In the per protocol analysis, PPI-based triple therapy eradicated H. pylori 82.1% of the time, compared with 90.4% in the vonoprazan triple-therapy group (P < .0001) and 81.2% in the vonoprazan dual-therapy group (P = .0077). Both vonoprazan treatment groups were noninferior to PPI-based triple therapy.
A prespecified exploratory analysis found that vonoprazan triple therapy outperformed PPI-based triple therapy in the modified intention-to-treat population (P = .0408) and the per protocol population (P = .0059).
Among patients with clarithromycin-resistant strains of H. pylori, in the modified intention-to-treat population, 31.9% achieved eradication with PPI triple therapy, compared with 65.8% in the vonoprazan triple-therapy group, and 69.6% in the vonoprazan dual-therapy group. In the per protocol population, the numbers were 29.0% versus 67.2% and 79.5%, respectively (P < .0001 for both versus PPI triple therapy).
Among all patients, in the modified intention-to-treat population, 68.5% achieved eradication with PPI triple therapy, 80.8% with vonoprazan triple therapy (P =. 0001), and 77.2% with vonoprazan dual therapy (P = .0063)*. In the per protocol population, the numbers were 70.0%, 85.7% (P < .0001), and 81.1% (P = .0013), respectively.
Safety outcomes were similar among the three groups, with treatment-emergent adverse events occurring in 34.5% of the PPI triple-therapy group (1.2% discontinued), 34.1% of the vonoprazan triple-therapy group (2.3% discontinued), and 29.9% in the vonoprazan dual-therapy group (0.9% discontinued).
Fighting against resistance
The efficacy of PPI-based clarithromycin-based triple therapy has fallen below 80% in the United States and Europe over the past few decades, largely because of antibiotic resistance, said William Chey, MD, during a presentation of the results at the annual meeting of the American College of Gastroenterology. Dr. Chey is a professor of medicine and director of the GI physiology laboratory at Michigan Medicine.
Vonoprazan is more stable in acid than are PPIs, and produces greater and more durable acid reduction, according to Dr. Chey. That’s important for two reasons: One is that some antibiotics are acid-labile, and so may have their efficacy directly impacted in a more acidic environment. The other factor is that most antibiotics work better on bacteria that are actively replicating, and H. pylori reproduces better in a more neutral environment. “So, you increase the replication, you increase the bioavailability of the antibiotics. And therefore, hopefully, that underlies why we see it working better in the patients with [antibiotic] resistance,” Dr. Chey said in an interview.
It remains to be seen whether or not the drug will receive FDA approval, but he pointed to other regimens like bismuth quadruple therapy and rifabutin-based triple therapy that are already available. “If I had the choice, I would never use a PPI-based triple therapy again. People should not be doing that,” said Dr. Chey.
“More successful H. pylori eradication regimens are certainly needed, and these results are particularly relevant and interesting given the increasing failure of initial treatment regimens,” said Kimberly Harer, MD, who moderated the session. She noted that the secondary analysis of patients with clarithromycin-resistant infections was particularly relevant. “The superiority analysis indicating vonoprazan triple therapy resulted in increased H. pylori eradication compared to lanzoprazole triple therapy was especially interesting,” said Dr. Harer, who is a clinical lecturer at University of Michigan Health, Ann Arbor.
One downside to the study is that it didn’t compare vonoprazan combinations to quadruple therapy of a PPI, bismuth, tetracycline, and a nitroimidazole, said Joseph Jennings, MD, who was asked to comment on the study. Other treatment approaches include sequential antibiotics and other combinations. Dr. Jennings also highlighted the findings that the vonoprazan regimens were superior against clarithromycin-resistant strains. “The more different regimens we can add to the armamentarium, the better chance we have because the resistant patterns fluctuate all throughout the world,” said Dr. Jennings, who is an assistant professor of medicine at Georgetown University and director of the center for GI bleeding at MedStar Georgetown University Hospital, both in Washington.
He also pointed out that physicians can face a conundrum when patients fail multiple lines of therapy and have testing done that shows high levels of resistance. Some have allergies that prevent them from turning to other antibiotics. “That’s a market where lots of doctors struggle. Something like this would be a nice add-on,” said Dr. Jennings.
The study was funded by Phathom Pharmaceuticals.** Dr. Chey has consulted and/or received research support from Abbvie, Alfasigma, Allakos, Alnylam, Bayer, Bioamerica, Cosmo, Intrinsic Medicine, Ironwood, Modify Health, My GI Health, My Nutrition Health, Nestle, Phathom Pharmaceuticals, QOL Medical, Redhill, Salix/Valeant, Takeda, Urovant, and Vibrant. Dr. Harer and Dr. Jennings have no relevant financial disclosures.
*Correction, 10/29/21: An earlier version of this article misstated the percentage of patients in the modified intention-to-treat population who achieved eradication with vonoprazan triple therapy.
**Correction, 10/29/21: An earlier version of this article misstated the name of Phathom Pharmaceuticals.
AT ACG 2021
Balloon-enhanced colonoscopy finds more adenomas
LAS VEGAS – The G-EYE colonoscope facilitates detection of adenomas more so than does the Endocuff Vision, researchers say.
In the first head-to-head comparison of two mechanical enhancement colonoscopy devices, “the G-EYE demonstrated a meaningful increase in adenoma detection rate [ADR] over Endocuff, particularly for advanced adenomas,” said Seth Gross, MD, a professor of medicine at New York University.
Previous studies have shown that mechanical enhancements are more effective than optical enhancements, Dr. Gross said. “To take it a step further, when you look at mechanical devices, especially these two, in past studies, the G-EYE has been sort of the leader in adenoma detection,” he told this news organization.
But until now, no studies had compared them head to head, said Dr. Gross, who presented the finding here at the American College of Gastroenterology (ACG) 2021 Annual Scientific Meeting.
The two devices work differently. The Endocuff Vision fits onto the colonoscope tip. During withdrawal, it expands radially, and its arms flatten the folds within the colon. The G-EYE balloon is deflated at insertion, then is inflated at the cecum, smoothing the colon wall while centering the colonoscopic view.
To compare the two, Dr. Gross and colleagues randomly assigned 363 patients to undergo colonoscopy with G-EYE and 364 patients to undergo colonoscopy with Endocuff Vision. The two groups were similar in demographics.
Withdrawal times were >6 minutes in both groups. The researchers detected adenomas in a higher percentage of patients with the G-EYE than with the Endocuff Vision. The same was true for advanced adenomas.
When using the G-EYE, the researchers also found more adenomas per patient, more sessile serrated adenomas per patient, more large adenomas per patient, and more right colon adenomas per patient.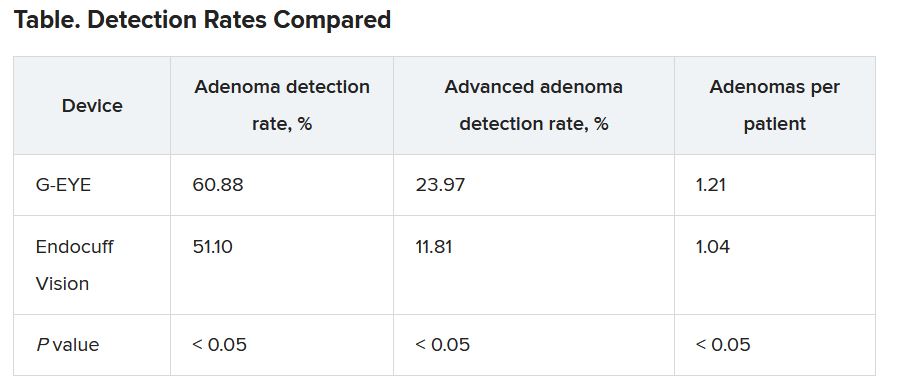
The benchmark for ADR is only 25%, Dr. Gross said, suggesting that both devices are a worthwhile improvement over standard colonoscopes. “It supports the past literature that a mechanical enhancement is something that should be considered during colonoscopy,” he said.
Costs differ as well. The G-EYE requires a permanent modification to the bending rubber of the colonoscope, so the cost is up front. The Endocuff Vision utilizes a single-use cap that is placed on the tip, so costs are spread over time.
The G-EYE gained U.S. Food and Drug Administration clearance in May 2020. In 2016, the Endocuff (an earlier version of the Endocuff Vision) became the first mechanical device the use of which the FDA acknowledged improved ADRs.
Dr. Gross said that it would be interesting to see whether the mechanical devices and artificial intelligence enhancements could complement each other so as to yield even higher detection rates.
Session moderator Brooks Cash, MD, a professor of medicine at the University of Texas Health Science Center, Houston, said the difference in detection rates made an impressive case for the G-EYE.
“I wouldn’t say I’m convinced,” Dr. Cash said in an interview. “I’d like to see more data. But I think that the plurality of the evidence that they presented and the size of the study were certainly compelling.”
He added that he’d like to see evidence that adding the balloon to a colonoscope doesn’t complicate the cleaning of the device.
Dr. Gross has a financial relationship with Olympus, the maker of the Endocuff Vision. Dr. Cash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
LAS VEGAS – The G-EYE colonoscope facilitates detection of adenomas more so than does the Endocuff Vision, researchers say.
In the first head-to-head comparison of two mechanical enhancement colonoscopy devices, “the G-EYE demonstrated a meaningful increase in adenoma detection rate [ADR] over Endocuff, particularly for advanced adenomas,” said Seth Gross, MD, a professor of medicine at New York University.
Previous studies have shown that mechanical enhancements are more effective than optical enhancements, Dr. Gross said. “To take it a step further, when you look at mechanical devices, especially these two, in past studies, the G-EYE has been sort of the leader in adenoma detection,” he told this news organization.
But until now, no studies had compared them head to head, said Dr. Gross, who presented the finding here at the American College of Gastroenterology (ACG) 2021 Annual Scientific Meeting.
The two devices work differently. The Endocuff Vision fits onto the colonoscope tip. During withdrawal, it expands radially, and its arms flatten the folds within the colon. The G-EYE balloon is deflated at insertion, then is inflated at the cecum, smoothing the colon wall while centering the colonoscopic view.
To compare the two, Dr. Gross and colleagues randomly assigned 363 patients to undergo colonoscopy with G-EYE and 364 patients to undergo colonoscopy with Endocuff Vision. The two groups were similar in demographics.
Withdrawal times were >6 minutes in both groups. The researchers detected adenomas in a higher percentage of patients with the G-EYE than with the Endocuff Vision. The same was true for advanced adenomas.
When using the G-EYE, the researchers also found more adenomas per patient, more sessile serrated adenomas per patient, more large adenomas per patient, and more right colon adenomas per patient.
The benchmark for ADR is only 25%, Dr. Gross said, suggesting that both devices are a worthwhile improvement over standard colonoscopes. “It supports the past literature that a mechanical enhancement is something that should be considered during colonoscopy,” he said.
Costs differ as well. The G-EYE requires a permanent modification to the bending rubber of the colonoscope, so the cost is up front. The Endocuff Vision utilizes a single-use cap that is placed on the tip, so costs are spread over time.
The G-EYE gained U.S. Food and Drug Administration clearance in May 2020. In 2016, the Endocuff (an earlier version of the Endocuff Vision) became the first mechanical device the use of which the FDA acknowledged improved ADRs.
Dr. Gross said that it would be interesting to see whether the mechanical devices and artificial intelligence enhancements could complement each other so as to yield even higher detection rates.
Session moderator Brooks Cash, MD, a professor of medicine at the University of Texas Health Science Center, Houston, said the difference in detection rates made an impressive case for the G-EYE.
“I wouldn’t say I’m convinced,” Dr. Cash said in an interview. “I’d like to see more data. But I think that the plurality of the evidence that they presented and the size of the study were certainly compelling.”
He added that he’d like to see evidence that adding the balloon to a colonoscope doesn’t complicate the cleaning of the device.
Dr. Gross has a financial relationship with Olympus, the maker of the Endocuff Vision. Dr. Cash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
LAS VEGAS – The G-EYE colonoscope facilitates detection of adenomas more so than does the Endocuff Vision, researchers say.
In the first head-to-head comparison of two mechanical enhancement colonoscopy devices, “the G-EYE demonstrated a meaningful increase in adenoma detection rate [ADR] over Endocuff, particularly for advanced adenomas,” said Seth Gross, MD, a professor of medicine at New York University.
Previous studies have shown that mechanical enhancements are more effective than optical enhancements, Dr. Gross said. “To take it a step further, when you look at mechanical devices, especially these two, in past studies, the G-EYE has been sort of the leader in adenoma detection,” he told this news organization.
But until now, no studies had compared them head to head, said Dr. Gross, who presented the finding here at the American College of Gastroenterology (ACG) 2021 Annual Scientific Meeting.
The two devices work differently. The Endocuff Vision fits onto the colonoscope tip. During withdrawal, it expands radially, and its arms flatten the folds within the colon. The G-EYE balloon is deflated at insertion, then is inflated at the cecum, smoothing the colon wall while centering the colonoscopic view.
To compare the two, Dr. Gross and colleagues randomly assigned 363 patients to undergo colonoscopy with G-EYE and 364 patients to undergo colonoscopy with Endocuff Vision. The two groups were similar in demographics.
Withdrawal times were >6 minutes in both groups. The researchers detected adenomas in a higher percentage of patients with the G-EYE than with the Endocuff Vision. The same was true for advanced adenomas.
When using the G-EYE, the researchers also found more adenomas per patient, more sessile serrated adenomas per patient, more large adenomas per patient, and more right colon adenomas per patient.
The benchmark for ADR is only 25%, Dr. Gross said, suggesting that both devices are a worthwhile improvement over standard colonoscopes. “It supports the past literature that a mechanical enhancement is something that should be considered during colonoscopy,” he said.
Costs differ as well. The G-EYE requires a permanent modification to the bending rubber of the colonoscope, so the cost is up front. The Endocuff Vision utilizes a single-use cap that is placed on the tip, so costs are spread over time.
The G-EYE gained U.S. Food and Drug Administration clearance in May 2020. In 2016, the Endocuff (an earlier version of the Endocuff Vision) became the first mechanical device the use of which the FDA acknowledged improved ADRs.
Dr. Gross said that it would be interesting to see whether the mechanical devices and artificial intelligence enhancements could complement each other so as to yield even higher detection rates.
Session moderator Brooks Cash, MD, a professor of medicine at the University of Texas Health Science Center, Houston, said the difference in detection rates made an impressive case for the G-EYE.
“I wouldn’t say I’m convinced,” Dr. Cash said in an interview. “I’d like to see more data. But I think that the plurality of the evidence that they presented and the size of the study were certainly compelling.”
He added that he’d like to see evidence that adding the balloon to a colonoscope doesn’t complicate the cleaning of the device.
Dr. Gross has a financial relationship with Olympus, the maker of the Endocuff Vision. Dr. Cash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ACG 2021
Warn patients about illicit drugs doctored with fentanyl
Fentanyl is now threatening overdoses in patients exposed to essentially any of the full array of recreational drugs – not just opioids – that are being sold illicitly, according to an overview of the problem presented at the virtual Psychopharmacology Update presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.

“Fentanyl can now be found in cocaine and methamphetamine. At this point, there is really no way to predict what is in a [street] drug,” Edwin A. Salsitz, MD, said at the meeting, sponsored by Medscape Live. He is associate clinical professor of medicine who works in the division of chemical dependency at Mount Sinai Beth Israel Medical Center in New York.
As proof of the frequency with which fentanyl is now being used as an additive, most patients with a drug use disorder, regardless of their drug of choice, are testing positive for fentanyl at Dr. Salsitz’s center. Many of those with positive fentanyl tests are unaware that their drugs had been doctored with this agent.
Relative to drugs sold as an opioid, such as heroin or oxycodone, the fentanyl dose in nonopioid drugs is typically more modest, but Dr. Salsitz pointed out that those expecting cocaine or methamphetamine often “have no heroin tolerance, so they are more vulnerable” to the adverse effects of fentanyl, including an overdose.
Although opioid tolerance might improve the chances for surviving a fentanyl overdose, the toxicology of fentanyl is not the same as other opioids. Death from heroin is typically a result of respiratory depression, but the onset is relatively slow, providing a greater opportunity to administer a reversal agent, such as naloxone.
Fentanyl not only produces respiratory depression but skeletal muscle rigidity. The rapid onset of “wooden chest syndrome” can occur within minutes, making the opportunity for intervention much smaller, Dr. Salsitz said.
To illustrate the phenomenon, Dr. Salsitz recounted a case.
After an argument with his mother, a 26-year-old male with a long history of intravenous drug use went to his bedroom. His mother, responding to the sound of a loud thud, rushed to the bedroom to find her son on the floor with a needle still in his arm. Resuscitation efforts by the mother and by the emergency responders, who arrived quickly, failed.
“The speed of his death made it clear that it was fentanyl related, and the postmortem toxicology confirmed that the exposure involved both heroin and fentanyl,” Dr. Salsitz said.
After the first wave of deaths in the opioid epidemic, which was attributed to inappropriate use of prescription opioids, the second wave was driven by heroin. In that wave, patients who became addicted to prescription opioids but were having more difficulty gaining access to them, turned to far cheaper and readily available street heroin. The third wave, driven by fentanyl, began several years ago when sellers of heroin began adding this synthetic opioid, which is relatively cheap, to intensify the high.
It is not expected to end quickly. The fentanyl added to heroin was never a prescription version. Rather, Dr. Salsitz said, it is synthesized in laboratories in China, Mexico, and the United States. It is relatively easy to produce and compact, which makes it easy to transport.
Exacerbating the risks that fentanyl poses when added to street drugs, even more potent versions, such as carfentanil, are also being added to cocaine, methamphetamines, and other nonopioid illicit drugs. When compared on a per-milligram basis, fentanyl is about 100 times more potent than heroin, but carfentanil is about 100 times more potent than fentanyl, according to Dr. Salsitz.
When the third wave of deaths in the opioid epidemic began around 2013, prescriptions of fentanyl, like many other opioid-type therapies were declining. The “perfect storm” that initiated the opioid epidemic was a product of intense focus on pain control and a misperception that prescription opioids posed a low risk of abuse potential, Dr. Salsitz said. By the time fentanyl was driving opioid deaths, the risks of opioids were widely appreciated and their use for prescription analgesia was declining.
Citing several cases, Dr. Salsitz noted that only 20 years after clinicians were being successfully sued for not offering enough analgesia, they were now going to jail for prescribing these drugs too liberally.
According to Dr. Salsitz, While psychiatrists might not have a role in this issue, Dr. Salsitz did see a role for these specialists in protecting patients from the adverse consequences of using illicit drugs doctored with fentanyl.
Noting that individuals with psychiatric disorders are more likely than the general population to self-medicate with drugs purchased illegally, Dr. Salsitz encouraged psychiatrists “to get involved” in asking about drug use and counseling patients on the risks of fentanyl substitution or additives.
“The message is that no one knows what are in these drugs, anymore,” he said.
In addition to making patients aware that many street drugs are now contaminated with fentanyl, Dr. Salsitz provided some safety tips. He suggested instructing patients to take a low dose of any newly acquired drug to gauge its effect, to avoid taking drugs alone, and to avoid mixing drugs. He also recommended using rapid fentanyl test strips in order to detect fentanyl contamination.
Even for the many psychiatrists who do not feel comfortable managing addiction, Dr. Salsitz recommended a proactive approach to address the current threat.
Test strips as an intervention
The seriousness of fentanyl contamination of illicit drugs, including cocaine and methamphetamine, was corroborated by two investigators at the School of Public Health and the Albert Einstein Medical School of Brown University, Providence, R.I. Brandon D.L. Marshall, PhD, associate professor of epidemiology in the School of Public Health, called fentanyl-contaminated cannabis “extremely rare,” but he said that it is being found in counterfeit prescription pills as well as in crystal methamphetamine and in both crack and powder cocaine.
He also advocated the use of fentanyl test strips.
“Test strips are an efficient, inexpensive, and effective way to determine whether fentanyl or related analogs are present in illicit drugs,” he said, noting that he is involved in a trial designed to determine whether fentanyl test strips can reduce the risk of fatal and nonfatal overdoses.
In a pilot study conducted in Baltimore, 69% of the 103 participants engaged in harm reduction behavior after using a fentanyl test strip and receiving a positive result (Addict Behav. 2020;110:106529). It is notable that 86% of the participants had a least one positive result when using the strips. More than half were surprised by the result.
One of the findings from this study was “that the lasting benefit of fentanyl test strip distribution is the opportunity to engage in discussions around safety and relationship building with historically underserved communities,” said the lead author, Ju Nyeong Park, PhD, assistant professor of medicine and epidemiology at Brown University. She moved to Brown after performing this work at Johns Hopkins University, Baltimore.
Dr. Park noted that “many patients in the community already know that they are using drugs containing fentanyl,” but for those who are concerned and wish to avoid contaminated drugs, fentanyl test strips “are a quick screening tool.” However, while the strips are helpful, she cautioned that they cannot be considered a definitive tool for detecting harm in illicit drugs.
“There may also be other chemicals present in tested drugs that confer risk,” she said.
Medscape Live and this news organization are owned by the same parent company. Dr. Salsitz, Dr. Marshall, and Dr. Park reported no potential conflicts of interest.
Fentanyl is now threatening overdoses in patients exposed to essentially any of the full array of recreational drugs – not just opioids – that are being sold illicitly, according to an overview of the problem presented at the virtual Psychopharmacology Update presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“Fentanyl can now be found in cocaine and methamphetamine. At this point, there is really no way to predict what is in a [street] drug,” Edwin A. Salsitz, MD, said at the meeting, sponsored by Medscape Live. He is associate clinical professor of medicine who works in the division of chemical dependency at Mount Sinai Beth Israel Medical Center in New York.
As proof of the frequency with which fentanyl is now being used as an additive, most patients with a drug use disorder, regardless of their drug of choice, are testing positive for fentanyl at Dr. Salsitz’s center. Many of those with positive fentanyl tests are unaware that their drugs had been doctored with this agent.
Relative to drugs sold as an opioid, such as heroin or oxycodone, the fentanyl dose in nonopioid drugs is typically more modest, but Dr. Salsitz pointed out that those expecting cocaine or methamphetamine often “have no heroin tolerance, so they are more vulnerable” to the adverse effects of fentanyl, including an overdose.
Although opioid tolerance might improve the chances for surviving a fentanyl overdose, the toxicology of fentanyl is not the same as other opioids. Death from heroin is typically a result of respiratory depression, but the onset is relatively slow, providing a greater opportunity to administer a reversal agent, such as naloxone.
Fentanyl not only produces respiratory depression but skeletal muscle rigidity. The rapid onset of “wooden chest syndrome” can occur within minutes, making the opportunity for intervention much smaller, Dr. Salsitz said.
To illustrate the phenomenon, Dr. Salsitz recounted a case.
After an argument with his mother, a 26-year-old male with a long history of intravenous drug use went to his bedroom. His mother, responding to the sound of a loud thud, rushed to the bedroom to find her son on the floor with a needle still in his arm. Resuscitation efforts by the mother and by the emergency responders, who arrived quickly, failed.
“The speed of his death made it clear that it was fentanyl related, and the postmortem toxicology confirmed that the exposure involved both heroin and fentanyl,” Dr. Salsitz said.
After the first wave of deaths in the opioid epidemic, which was attributed to inappropriate use of prescription opioids, the second wave was driven by heroin. In that wave, patients who became addicted to prescription opioids but were having more difficulty gaining access to them, turned to far cheaper and readily available street heroin. The third wave, driven by fentanyl, began several years ago when sellers of heroin began adding this synthetic opioid, which is relatively cheap, to intensify the high.
It is not expected to end quickly. The fentanyl added to heroin was never a prescription version. Rather, Dr. Salsitz said, it is synthesized in laboratories in China, Mexico, and the United States. It is relatively easy to produce and compact, which makes it easy to transport.
Exacerbating the risks that fentanyl poses when added to street drugs, even more potent versions, such as carfentanil, are also being added to cocaine, methamphetamines, and other nonopioid illicit drugs. When compared on a per-milligram basis, fentanyl is about 100 times more potent than heroin, but carfentanil is about 100 times more potent than fentanyl, according to Dr. Salsitz.
When the third wave of deaths in the opioid epidemic began around 2013, prescriptions of fentanyl, like many other opioid-type therapies were declining. The “perfect storm” that initiated the opioid epidemic was a product of intense focus on pain control and a misperception that prescription opioids posed a low risk of abuse potential, Dr. Salsitz said. By the time fentanyl was driving opioid deaths, the risks of opioids were widely appreciated and their use for prescription analgesia was declining.
Citing several cases, Dr. Salsitz noted that only 20 years after clinicians were being successfully sued for not offering enough analgesia, they were now going to jail for prescribing these drugs too liberally.
According to Dr. Salsitz, While psychiatrists might not have a role in this issue, Dr. Salsitz did see a role for these specialists in protecting patients from the adverse consequences of using illicit drugs doctored with fentanyl.
Noting that individuals with psychiatric disorders are more likely than the general population to self-medicate with drugs purchased illegally, Dr. Salsitz encouraged psychiatrists “to get involved” in asking about drug use and counseling patients on the risks of fentanyl substitution or additives.
“The message is that no one knows what are in these drugs, anymore,” he said.
In addition to making patients aware that many street drugs are now contaminated with fentanyl, Dr. Salsitz provided some safety tips. He suggested instructing patients to take a low dose of any newly acquired drug to gauge its effect, to avoid taking drugs alone, and to avoid mixing drugs. He also recommended using rapid fentanyl test strips in order to detect fentanyl contamination.
Even for the many psychiatrists who do not feel comfortable managing addiction, Dr. Salsitz recommended a proactive approach to address the current threat.
Test strips as an intervention
The seriousness of fentanyl contamination of illicit drugs, including cocaine and methamphetamine, was corroborated by two investigators at the School of Public Health and the Albert Einstein Medical School of Brown University, Providence, R.I. Brandon D.L. Marshall, PhD, associate professor of epidemiology in the School of Public Health, called fentanyl-contaminated cannabis “extremely rare,” but he said that it is being found in counterfeit prescription pills as well as in crystal methamphetamine and in both crack and powder cocaine.
He also advocated the use of fentanyl test strips.
“Test strips are an efficient, inexpensive, and effective way to determine whether fentanyl or related analogs are present in illicit drugs,” he said, noting that he is involved in a trial designed to determine whether fentanyl test strips can reduce the risk of fatal and nonfatal overdoses.
In a pilot study conducted in Baltimore, 69% of the 103 participants engaged in harm reduction behavior after using a fentanyl test strip and receiving a positive result (Addict Behav. 2020;110:106529). It is notable that 86% of the participants had a least one positive result when using the strips. More than half were surprised by the result.
One of the findings from this study was “that the lasting benefit of fentanyl test strip distribution is the opportunity to engage in discussions around safety and relationship building with historically underserved communities,” said the lead author, Ju Nyeong Park, PhD, assistant professor of medicine and epidemiology at Brown University. She moved to Brown after performing this work at Johns Hopkins University, Baltimore.
Dr. Park noted that “many patients in the community already know that they are using drugs containing fentanyl,” but for those who are concerned and wish to avoid contaminated drugs, fentanyl test strips “are a quick screening tool.” However, while the strips are helpful, she cautioned that they cannot be considered a definitive tool for detecting harm in illicit drugs.
“There may also be other chemicals present in tested drugs that confer risk,” she said.
Medscape Live and this news organization are owned by the same parent company. Dr. Salsitz, Dr. Marshall, and Dr. Park reported no potential conflicts of interest.
Fentanyl is now threatening overdoses in patients exposed to essentially any of the full array of recreational drugs – not just opioids – that are being sold illicitly, according to an overview of the problem presented at the virtual Psychopharmacology Update presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“Fentanyl can now be found in cocaine and methamphetamine. At this point, there is really no way to predict what is in a [street] drug,” Edwin A. Salsitz, MD, said at the meeting, sponsored by Medscape Live. He is associate clinical professor of medicine who works in the division of chemical dependency at Mount Sinai Beth Israel Medical Center in New York.
As proof of the frequency with which fentanyl is now being used as an additive, most patients with a drug use disorder, regardless of their drug of choice, are testing positive for fentanyl at Dr. Salsitz’s center. Many of those with positive fentanyl tests are unaware that their drugs had been doctored with this agent.
Relative to drugs sold as an opioid, such as heroin or oxycodone, the fentanyl dose in nonopioid drugs is typically more modest, but Dr. Salsitz pointed out that those expecting cocaine or methamphetamine often “have no heroin tolerance, so they are more vulnerable” to the adverse effects of fentanyl, including an overdose.
Although opioid tolerance might improve the chances for surviving a fentanyl overdose, the toxicology of fentanyl is not the same as other opioids. Death from heroin is typically a result of respiratory depression, but the onset is relatively slow, providing a greater opportunity to administer a reversal agent, such as naloxone.
Fentanyl not only produces respiratory depression but skeletal muscle rigidity. The rapid onset of “wooden chest syndrome” can occur within minutes, making the opportunity for intervention much smaller, Dr. Salsitz said.
To illustrate the phenomenon, Dr. Salsitz recounted a case.
After an argument with his mother, a 26-year-old male with a long history of intravenous drug use went to his bedroom. His mother, responding to the sound of a loud thud, rushed to the bedroom to find her son on the floor with a needle still in his arm. Resuscitation efforts by the mother and by the emergency responders, who arrived quickly, failed.
“The speed of his death made it clear that it was fentanyl related, and the postmortem toxicology confirmed that the exposure involved both heroin and fentanyl,” Dr. Salsitz said.
After the first wave of deaths in the opioid epidemic, which was attributed to inappropriate use of prescription opioids, the second wave was driven by heroin. In that wave, patients who became addicted to prescription opioids but were having more difficulty gaining access to them, turned to far cheaper and readily available street heroin. The third wave, driven by fentanyl, began several years ago when sellers of heroin began adding this synthetic opioid, which is relatively cheap, to intensify the high.
It is not expected to end quickly. The fentanyl added to heroin was never a prescription version. Rather, Dr. Salsitz said, it is synthesized in laboratories in China, Mexico, and the United States. It is relatively easy to produce and compact, which makes it easy to transport.
Exacerbating the risks that fentanyl poses when added to street drugs, even more potent versions, such as carfentanil, are also being added to cocaine, methamphetamines, and other nonopioid illicit drugs. When compared on a per-milligram basis, fentanyl is about 100 times more potent than heroin, but carfentanil is about 100 times more potent than fentanyl, according to Dr. Salsitz.
When the third wave of deaths in the opioid epidemic began around 2013, prescriptions of fentanyl, like many other opioid-type therapies were declining. The “perfect storm” that initiated the opioid epidemic was a product of intense focus on pain control and a misperception that prescription opioids posed a low risk of abuse potential, Dr. Salsitz said. By the time fentanyl was driving opioid deaths, the risks of opioids were widely appreciated and their use for prescription analgesia was declining.
Citing several cases, Dr. Salsitz noted that only 20 years after clinicians were being successfully sued for not offering enough analgesia, they were now going to jail for prescribing these drugs too liberally.
According to Dr. Salsitz, While psychiatrists might not have a role in this issue, Dr. Salsitz did see a role for these specialists in protecting patients from the adverse consequences of using illicit drugs doctored with fentanyl.
Noting that individuals with psychiatric disorders are more likely than the general population to self-medicate with drugs purchased illegally, Dr. Salsitz encouraged psychiatrists “to get involved” in asking about drug use and counseling patients on the risks of fentanyl substitution or additives.
“The message is that no one knows what are in these drugs, anymore,” he said.
In addition to making patients aware that many street drugs are now contaminated with fentanyl, Dr. Salsitz provided some safety tips. He suggested instructing patients to take a low dose of any newly acquired drug to gauge its effect, to avoid taking drugs alone, and to avoid mixing drugs. He also recommended using rapid fentanyl test strips in order to detect fentanyl contamination.
Even for the many psychiatrists who do not feel comfortable managing addiction, Dr. Salsitz recommended a proactive approach to address the current threat.
Test strips as an intervention
The seriousness of fentanyl contamination of illicit drugs, including cocaine and methamphetamine, was corroborated by two investigators at the School of Public Health and the Albert Einstein Medical School of Brown University, Providence, R.I. Brandon D.L. Marshall, PhD, associate professor of epidemiology in the School of Public Health, called fentanyl-contaminated cannabis “extremely rare,” but he said that it is being found in counterfeit prescription pills as well as in crystal methamphetamine and in both crack and powder cocaine.
He also advocated the use of fentanyl test strips.
“Test strips are an efficient, inexpensive, and effective way to determine whether fentanyl or related analogs are present in illicit drugs,” he said, noting that he is involved in a trial designed to determine whether fentanyl test strips can reduce the risk of fatal and nonfatal overdoses.
In a pilot study conducted in Baltimore, 69% of the 103 participants engaged in harm reduction behavior after using a fentanyl test strip and receiving a positive result (Addict Behav. 2020;110:106529). It is notable that 86% of the participants had a least one positive result when using the strips. More than half were surprised by the result.
One of the findings from this study was “that the lasting benefit of fentanyl test strip distribution is the opportunity to engage in discussions around safety and relationship building with historically underserved communities,” said the lead author, Ju Nyeong Park, PhD, assistant professor of medicine and epidemiology at Brown University. She moved to Brown after performing this work at Johns Hopkins University, Baltimore.
Dr. Park noted that “many patients in the community already know that they are using drugs containing fentanyl,” but for those who are concerned and wish to avoid contaminated drugs, fentanyl test strips “are a quick screening tool.” However, while the strips are helpful, she cautioned that they cannot be considered a definitive tool for detecting harm in illicit drugs.
“There may also be other chemicals present in tested drugs that confer risk,” she said.
Medscape Live and this news organization are owned by the same parent company. Dr. Salsitz, Dr. Marshall, and Dr. Park reported no potential conflicts of interest.
FROM PSYCHOPHARMACOLOGY UPDATE
One of the keys to success on social media? Entertain and educate the public
Social media isn’t everyone’s cup of tea, but

“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
Social media isn’t everyone’s cup of tea, but
“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
Social media isn’t everyone’s cup of tea, but
“I admit that I’m somewhat obsessed with it. I kind of blame it on my work as a dermatologist, that I’m trying to grow my social media as well. It’s interesting to me, fascinating, and I want to understand it more. I think that’s the mindset you need to approach it with.”
Perhaps no other public figure in dermatology has enjoyed success in social media more than Dr. Lee, a board-certified dermatologist who practices in Upland, Calif. In the fall of 2014, she started using Instagram to provide followers a glimpse into her life as a dermatologist, everything from Mohs surgery and Botox to keloid removals and ear lobe repair surgeries. From this she formed her alter ego, “Dr. Pimple Popper,” and became a YouTube sensation, building 7.1 million subscribers over the course of a few years, amounting to 4.5 billion lifetime views. She also grew 12 million followers on TikTok, 4.4 million followers on Instagram, 3 million on Facebook, and more than 139,000 on Twitter. About 80% of her followers are women who range between 18 and 40 years of age.
During the meeting she offered five social media marketing tips for busy clinicians:
You have to ‘play’ to ‘win.’ Active participation in social media is required to develop followers. “You cannot delegate this content,” Dr. Lee said. “You can hire people to help you or leave the task to a social media-savvy medical assistant in your office, but the content should be your responsibility ultimately, because you are the physician,” she added. Not everyone chooses to participate in social media, but it’s also something not to shy away from out of intimidation. “There is some talent associated with it, but it takes a lot of persistence as well,” she said.
Patients come first. Protect them at all costs. Dr. Lee rarely posts the faces of patients she cares for unless they grant consent in advance. “I try to show the work that I do and the beauty of dermatology,” she said during the meeting, which was named “Laser & Aesthetic Skin Therapy: What’s the Truth?” and was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. She added that taking part in social media can help you improve communication skills by engaging with followers who like, share, or respond to the material posted. “When you look back at your posts objectively, you learn about yourself and how you relate to your patients,” she said. “It helps to hone my bedside manner and my skills as a dermatologist.”
Show that you are human. Many dermatologists and other “skin influencers” have established their presence on the Internet and may be direct competitors for patients, but that doesn’t mean you can’t establish your own identity. One way to stand out is by posting content related to your authentic self, such as a photo or video that shows you engaged in a hobby, dining at a favorite restaurant, or visiting a beloved vacation spot. “Your followers don’t want a robot, someone who thinks they’re amazing and can do everything,” said Dr. Lee, who stars in her own TV reality show on TLC. “Show that you have a funny side. You want them to fall in love with you and see a little bit of your world, whatever it might be. Charm the socks off of them.”
Entertain first, educate a close second. The main way you’re going to get people to follow and watch you is to provide some entertainment, “not at the expense of a patient or your practice, though,” she said. “Then you’re going to educate people. We dermatologists have something to teach the world because we are experts on skin, hair, and nails. You want to impart this knowledge in a way that captivates people.” It’s like the sense of accomplishment that comes from learning something new after reading a book or watching a movie, she explained. “You feel good about it, and you can take that knowledge with you somewhere else. I love it when kids come up to me and tell me they know what a lipoma is, what a cyst is, and what psoriasis is because they’ve seen my show, or because they follow me on social media. It’s wonderful because I can see that I’ve educated them.”
Be kind and don’t activate the trolls. Dr. Lee allows positivity and kindness to rule the day on her social media content. “This is what I try to relay to followers, but I also do not engage with the negativity,” she said. “Every now and then, there will be someone who tries to insult what you do or who insults you personally. If you engage with them, it almost invites them to do it more. It almost gives them the ability to fight with you. Try to stay above that; just put out goodness and kindness.”
Several years ago, YouTube and Instagram temporarily shut down Dr. Lee’s accounts because she posted graphic images of skin lesions and procedures – a practice that wasn’t so commonplace at the time. “Don’t just post a graphic image just to be graphic,” she advised. “Make sure it has an educational message associated with it. That will help to validate your content. Posting a warning sign that some images may be graphic could help, too.”
Dr. Lee reported having no relevant financial disclosures.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
Radiation underused as ‘bridge’ to transplant in liver cancer
CHICAGO –It is greatly underutilized compared to other liver-directed therapies, according to new findings.
“This highlights a real-world gap in the treatment armamentarium for hepatocellular carcinoma [HCC],” said Nima Nabavizadeh, MD, associate professor of radiation oncology and residency program director at the Oregon Health and Science University, Portland.
He was speaking at the annual meeting of the American Society for Radiation Oncology.
These new data suggest there is reluctance within transplant programs to utilize radiotherapy as a bridging therapy prior to liver transplant, said Hyun Kim, MD, chief, GI service, department of radiation oncology, Washington University and the Alvin J. Siteman Cancer Center, St. Louis.
“This is despite 10-year-old data from Princess Margaret and Toronto General Hospital showing that external-beam radiation is a safe and feasible bridging therapy,” he said. “More modern data from the same institutions indicate that patients bridged with stereotactic body radiotherapy ablative radiation doses delivered with high conformality have similar survival as patients bridged with radiofrequency ablation.”
Dr. Kim also noted that even after transplant, rates of intrahepatic recurrence can be as high as 10%. Approximately 60% of patients experience recurrence of any type within 3 years.
“Nonablative local therapies leave viable disease, which may permit metastatic progression while the patient awaits transplant,” he said in an interview. This new analysis highlights the need for well-designed clinical trials with modern endpoints to evaluate which bridging therapy is most beneficial for the patient, he added.
In this current “era of radiomics, deep learning, and liquid biopsies, we have unprecedented tools and responsibility to ensure that our practice continues to improve in a data-centric fashion and not remain paused in the paradigm of a previous era,” Dr. Kim said.
A leading cause of death worldwide
HCC is a leading cause of cancer death worldwide, and the incidence is rising within the United States. Transplant is often the best option for long-term survival for patients with localized HCC and advanced cirrhosis, Dr. Nabavizadeh told the meeting.
Because patients often have to wait months to over a year for a transplant, many patients receive liver-directed bridging therapy to prevent tumor growth or spread and to maintain their eligibility for transplant, he explained.
These bridging therapies include thermal ablation procedures, transarterial chemoembolization (TACE), and Y-90 radioembolization, as well as EBRT.
To investigate how these therapies were being used, Dr. Nabavizadeh and colleagues conducted a retrospective study in which they analyzed data from the United Network for Organ Sharing, a nonprofit organization that manages the only national liver transplant waiting list in the United States.
They identified patients on the transplant list who had applied for Model of End-Stage Liver Disease (MELD) exceptions so as to be prioritized on the waiting list.
A total of 18,447 HCC patients submitted MELD exception applications during the study period (October 2013 to June 2020). More than half of these patients (n = 11,171; 60.6%) received a transplant. After submitting the exception application, the median time for receiving a transplant was 7 months.
Of the total group, 15,759 patients (85.4%) received liver-directed therapy while waiting for the transplant, but only 658 patients (3.6% of the overall cohort) received EBRT, either alone or in combination with another therapy.
“The majority of patients received chemoembolization, and ERBT represents a very small percentage,” Dr. Nabavizadeh said.
During the study period, the use of transarterial chemoembolization decreased. It has largely been replaced by thermal ablation and Y-90 radioembolization. The analysis also showed that the use of EBRT had increased over the past several years, but its utilization still remained well below that of the other therapies.
TACE was the most utilized therapy. It was used for 39.6% of patients, followed by thermal ablation (12.8%) and radioembolization (8.7%). Almost a quarter of patients (22.2%) received a combination of non-EBRT therapies.
“We found that EBRT use significantly differed by region,” Dr. Nabavizadeh said. The highest usage (8.7%) was in Great Lakes states. In the Southeast, it was used for 1.7% patients.
No statistical differences were observed in clinicopathologic factors between the patients who received EBRT and those who did not.
Transplant is curative
Transplant is curative both for cancer and underlying cirrhosis, but patients may experience disease progression while waiting for transplant, noted Jessica Karen Wong, MD, assistant professor, department of radiation oncology, Fox Chase Cancer Center, Philadelphia, who was approached for comment.
“Radiation, specifically, stereotactic body radiation therapy, is a safe and effective bridging therapy but was only used in a small minority of eligible patients in this national database,” she said. “Although the use of radiation as bridging therapy is increasing over time, it continues to be underutilized. Increasing the use of radiation provides an opportunity to improve patient care for hepatocellular carcinoma patients awaiting a liver transplant.”
Dr. Nabavizadeh and Dr. Wong have disclosed no relevant financial relationships. Dr. Kim has received research funding and speaker honorarium from Varian and ViewRay.
A version of this article first appeared on Medscape.com.
CHICAGO –It is greatly underutilized compared to other liver-directed therapies, according to new findings.
“This highlights a real-world gap in the treatment armamentarium for hepatocellular carcinoma [HCC],” said Nima Nabavizadeh, MD, associate professor of radiation oncology and residency program director at the Oregon Health and Science University, Portland.
He was speaking at the annual meeting of the American Society for Radiation Oncology.
These new data suggest there is reluctance within transplant programs to utilize radiotherapy as a bridging therapy prior to liver transplant, said Hyun Kim, MD, chief, GI service, department of radiation oncology, Washington University and the Alvin J. Siteman Cancer Center, St. Louis.
“This is despite 10-year-old data from Princess Margaret and Toronto General Hospital showing that external-beam radiation is a safe and feasible bridging therapy,” he said. “More modern data from the same institutions indicate that patients bridged with stereotactic body radiotherapy ablative radiation doses delivered with high conformality have similar survival as patients bridged with radiofrequency ablation.”
Dr. Kim also noted that even after transplant, rates of intrahepatic recurrence can be as high as 10%. Approximately 60% of patients experience recurrence of any type within 3 years.
“Nonablative local therapies leave viable disease, which may permit metastatic progression while the patient awaits transplant,” he said in an interview. This new analysis highlights the need for well-designed clinical trials with modern endpoints to evaluate which bridging therapy is most beneficial for the patient, he added.
In this current “era of radiomics, deep learning, and liquid biopsies, we have unprecedented tools and responsibility to ensure that our practice continues to improve in a data-centric fashion and not remain paused in the paradigm of a previous era,” Dr. Kim said.
A leading cause of death worldwide
HCC is a leading cause of cancer death worldwide, and the incidence is rising within the United States. Transplant is often the best option for long-term survival for patients with localized HCC and advanced cirrhosis, Dr. Nabavizadeh told the meeting.
Because patients often have to wait months to over a year for a transplant, many patients receive liver-directed bridging therapy to prevent tumor growth or spread and to maintain their eligibility for transplant, he explained.
These bridging therapies include thermal ablation procedures, transarterial chemoembolization (TACE), and Y-90 radioembolization, as well as EBRT.
To investigate how these therapies were being used, Dr. Nabavizadeh and colleagues conducted a retrospective study in which they analyzed data from the United Network for Organ Sharing, a nonprofit organization that manages the only national liver transplant waiting list in the United States.
They identified patients on the transplant list who had applied for Model of End-Stage Liver Disease (MELD) exceptions so as to be prioritized on the waiting list.
A total of 18,447 HCC patients submitted MELD exception applications during the study period (October 2013 to June 2020). More than half of these patients (n = 11,171; 60.6%) received a transplant. After submitting the exception application, the median time for receiving a transplant was 7 months.
Of the total group, 15,759 patients (85.4%) received liver-directed therapy while waiting for the transplant, but only 658 patients (3.6% of the overall cohort) received EBRT, either alone or in combination with another therapy.
“The majority of patients received chemoembolization, and ERBT represents a very small percentage,” Dr. Nabavizadeh said.
During the study period, the use of transarterial chemoembolization decreased. It has largely been replaced by thermal ablation and Y-90 radioembolization. The analysis also showed that the use of EBRT had increased over the past several years, but its utilization still remained well below that of the other therapies.
TACE was the most utilized therapy. It was used for 39.6% of patients, followed by thermal ablation (12.8%) and radioembolization (8.7%). Almost a quarter of patients (22.2%) received a combination of non-EBRT therapies.
“We found that EBRT use significantly differed by region,” Dr. Nabavizadeh said. The highest usage (8.7%) was in Great Lakes states. In the Southeast, it was used for 1.7% patients.
No statistical differences were observed in clinicopathologic factors between the patients who received EBRT and those who did not.
Transplant is curative
Transplant is curative both for cancer and underlying cirrhosis, but patients may experience disease progression while waiting for transplant, noted Jessica Karen Wong, MD, assistant professor, department of radiation oncology, Fox Chase Cancer Center, Philadelphia, who was approached for comment.
“Radiation, specifically, stereotactic body radiation therapy, is a safe and effective bridging therapy but was only used in a small minority of eligible patients in this national database,” she said. “Although the use of radiation as bridging therapy is increasing over time, it continues to be underutilized. Increasing the use of radiation provides an opportunity to improve patient care for hepatocellular carcinoma patients awaiting a liver transplant.”
Dr. Nabavizadeh and Dr. Wong have disclosed no relevant financial relationships. Dr. Kim has received research funding and speaker honorarium from Varian and ViewRay.
A version of this article first appeared on Medscape.com.
CHICAGO –It is greatly underutilized compared to other liver-directed therapies, according to new findings.
“This highlights a real-world gap in the treatment armamentarium for hepatocellular carcinoma [HCC],” said Nima Nabavizadeh, MD, associate professor of radiation oncology and residency program director at the Oregon Health and Science University, Portland.
He was speaking at the annual meeting of the American Society for Radiation Oncology.
These new data suggest there is reluctance within transplant programs to utilize radiotherapy as a bridging therapy prior to liver transplant, said Hyun Kim, MD, chief, GI service, department of radiation oncology, Washington University and the Alvin J. Siteman Cancer Center, St. Louis.
“This is despite 10-year-old data from Princess Margaret and Toronto General Hospital showing that external-beam radiation is a safe and feasible bridging therapy,” he said. “More modern data from the same institutions indicate that patients bridged with stereotactic body radiotherapy ablative radiation doses delivered with high conformality have similar survival as patients bridged with radiofrequency ablation.”
Dr. Kim also noted that even after transplant, rates of intrahepatic recurrence can be as high as 10%. Approximately 60% of patients experience recurrence of any type within 3 years.
“Nonablative local therapies leave viable disease, which may permit metastatic progression while the patient awaits transplant,” he said in an interview. This new analysis highlights the need for well-designed clinical trials with modern endpoints to evaluate which bridging therapy is most beneficial for the patient, he added.
In this current “era of radiomics, deep learning, and liquid biopsies, we have unprecedented tools and responsibility to ensure that our practice continues to improve in a data-centric fashion and not remain paused in the paradigm of a previous era,” Dr. Kim said.
A leading cause of death worldwide
HCC is a leading cause of cancer death worldwide, and the incidence is rising within the United States. Transplant is often the best option for long-term survival for patients with localized HCC and advanced cirrhosis, Dr. Nabavizadeh told the meeting.
Because patients often have to wait months to over a year for a transplant, many patients receive liver-directed bridging therapy to prevent tumor growth or spread and to maintain their eligibility for transplant, he explained.
These bridging therapies include thermal ablation procedures, transarterial chemoembolization (TACE), and Y-90 radioembolization, as well as EBRT.
To investigate how these therapies were being used, Dr. Nabavizadeh and colleagues conducted a retrospective study in which they analyzed data from the United Network for Organ Sharing, a nonprofit organization that manages the only national liver transplant waiting list in the United States.
They identified patients on the transplant list who had applied for Model of End-Stage Liver Disease (MELD) exceptions so as to be prioritized on the waiting list.
A total of 18,447 HCC patients submitted MELD exception applications during the study period (October 2013 to June 2020). More than half of these patients (n = 11,171; 60.6%) received a transplant. After submitting the exception application, the median time for receiving a transplant was 7 months.
Of the total group, 15,759 patients (85.4%) received liver-directed therapy while waiting for the transplant, but only 658 patients (3.6% of the overall cohort) received EBRT, either alone or in combination with another therapy.
“The majority of patients received chemoembolization, and ERBT represents a very small percentage,” Dr. Nabavizadeh said.
During the study period, the use of transarterial chemoembolization decreased. It has largely been replaced by thermal ablation and Y-90 radioembolization. The analysis also showed that the use of EBRT had increased over the past several years, but its utilization still remained well below that of the other therapies.
TACE was the most utilized therapy. It was used for 39.6% of patients, followed by thermal ablation (12.8%) and radioembolization (8.7%). Almost a quarter of patients (22.2%) received a combination of non-EBRT therapies.
“We found that EBRT use significantly differed by region,” Dr. Nabavizadeh said. The highest usage (8.7%) was in Great Lakes states. In the Southeast, it was used for 1.7% patients.
No statistical differences were observed in clinicopathologic factors between the patients who received EBRT and those who did not.
Transplant is curative
Transplant is curative both for cancer and underlying cirrhosis, but patients may experience disease progression while waiting for transplant, noted Jessica Karen Wong, MD, assistant professor, department of radiation oncology, Fox Chase Cancer Center, Philadelphia, who was approached for comment.
“Radiation, specifically, stereotactic body radiation therapy, is a safe and effective bridging therapy but was only used in a small minority of eligible patients in this national database,” she said. “Although the use of radiation as bridging therapy is increasing over time, it continues to be underutilized. Increasing the use of radiation provides an opportunity to improve patient care for hepatocellular carcinoma patients awaiting a liver transplant.”
Dr. Nabavizadeh and Dr. Wong have disclosed no relevant financial relationships. Dr. Kim has received research funding and speaker honorarium from Varian and ViewRay.
A version of this article first appeared on Medscape.com.
FROM ASTRO 2021
After POEM, FLIP matches HRM for measuring patient response
LAS VEGAS – Functional lumen imaging probe (FLIP) was equivalent to high-resolution manometry (HRM) in predicting clinical response by Eckardt score 6 months or more after per oral endoscopic myotomy (POEM) for achalasia or esophagogastric junction (EGJ) outlet obstruction (EGJOO).

Measures for clinical response following lower esophageal sphincter myotomy procedures include Eckardt Score, timed barium esophagram, HRM, and FLIP. However, since FLIP is a relatively new technique, there are few clinical data comparing its efficacy versus HRM in patients who have a positive response to POEM measured by the Eckardt score, according to John DeWitt, MD, who presented the research at the annual meeting of the American College of Gastroenterology.
FLIP can be performed during a follow-up endoscopy while a patient is sedated, while HRM requires the patient to be awake. Some patients find the procedure intolerable, and Dr. DeWitt estimates that 10%-20% of patients don’t return for follow-up assessments because of the discomfort.
“[FLIP] is a relatively new technology, the role of which is still being discovered. We have a lot more information on the diagnosis side of things. The role in follow-up, particularly after myotomy, is really not defined well. This is the first study to my knowledge that has evaluated manometry and FLIP head-to-head to compare patient-reported outcomes,” said Dr. DeWitt in an interview. He is a professor of medicine and the director of endoscopic ultrasound at Indiana University Medical Center, in Indianapolis.
Going head-to-head
The researchers conducted a retrospective, single-center study of 265 consecutive patients who underwent POEM for achalasia or EGJOO from 2016 through 2020. A clinical response was defined as an Eckardt score ≤3, EGJ distensibility index (EGJ-DI) higher than 2.8 mm2/mm Hg, maximum integrated relaxation pressure (IRP) <15 mm Hg, or a maximum EGJ diameter greater than 14 mm at any balloon distension.
In all, 126 patients returned for follow-up and completed an upper endoscopy with FLIP, HRM, and Eckardt scores within a 6-12 month period after the POEM procedure.
With respect to HRM, an IRP measurement <15 mm Hg predicted post-POEM Eckardt score with a sensitivity of 86.7% (95% confidence interval, 79.3-92.2) and a specificity of 33.3% (95% CI, 4.3-77.7), with an area under the curve of 0.60 (95% CI, 0.39-0.81). A maximum EJG diameter ≥ 14 mm had a sensitivity of 77.5% (95% CI, 69.0-84.6) and a specificity of 33.3% (95% CI, 4.3-77.7), with an AUC of 0.55 (95% CI, 0.34-0.76).
The performance was similar with FLIP: EGJ-DI > 2.8 mm2/mm Hg at any balloon setting had a sensitivity of 95.0% (95% CI, 89.4-98.1) and a specificity% of 0.0, and an AUC of 0.53 (95% CI, 0.51-0.55). A similar measurement at 40 mL or 50 mL distension had a sensitivity of 93.3% (95% CI, 87.3-97.1) and a specificity of 16.7% (95% CI, 0.4-64.1), with an AUC of 0.55 (95% CI, 0.39-0.72). Receiver operator characteristic analysis showed no significant difference between ability of FLIP and HRM to predict a normal Eckardt score.
If the study is repeated in other patient populations, Dr. DeWitt hopes that it could eliminate manometry altogether in a large majority of patients. “That would be potentially a game changer for bringing patients back to see how well they’re doing,” said Dr. DeWitt.
Not all patients who undergo POEM would be good candidates for FLIP, said Dr. DeWitt. The study was limited to patients with hypertension in the lower esophageal sphincter. Other disorders such as diffuse esophageal spasm, jackhammer esophagus, and type III achalasia would not likely be candidates for FLIP. “Those patients are going to probably still need manometry because if the esophageal body abnormalities are still present, then repeat testing might need to be performed,” said Dr. DeWitt. Still, he estimated about 80% of patients could be eligible for FLIP instead.
Impact on patients
“I think it’s interesting new data,” said Patrick Young, MD, who comoderated the session where the research was presented. He noted that the treatment of achalasia is evolving away from surgery, and the techniques to measure response are evolving along with it. “As we progress in that technology and using that procedure, we need to understand better how to follow those people up. I think adding this new device may help us to understand who’s going to respond well, and who’s not going to respond well. This is an early investigation, so I think we’ll need to do trials, but I think this is a good first step,” said Dr. Young, who is a professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md.

Comoderator Mohammad Yaghoobi, MD, also praised the study, but noted that the cost of FLIP could be a concern. “We want to have a reasonable ratio of the cost versus the effectiveness,” said Dr. Yaghoobi, who is an associate professor of medicine at McMaster University in Hamilton, Ont.
Dr. DeWitt, Dr. Young, and Dr. Yaghoobi had no relevant disclosures.
LAS VEGAS – Functional lumen imaging probe (FLIP) was equivalent to high-resolution manometry (HRM) in predicting clinical response by Eckardt score 6 months or more after per oral endoscopic myotomy (POEM) for achalasia or esophagogastric junction (EGJ) outlet obstruction (EGJOO).
Measures for clinical response following lower esophageal sphincter myotomy procedures include Eckardt Score, timed barium esophagram, HRM, and FLIP. However, since FLIP is a relatively new technique, there are few clinical data comparing its efficacy versus HRM in patients who have a positive response to POEM measured by the Eckardt score, according to John DeWitt, MD, who presented the research at the annual meeting of the American College of Gastroenterology.
FLIP can be performed during a follow-up endoscopy while a patient is sedated, while HRM requires the patient to be awake. Some patients find the procedure intolerable, and Dr. DeWitt estimates that 10%-20% of patients don’t return for follow-up assessments because of the discomfort.
“[FLIP] is a relatively new technology, the role of which is still being discovered. We have a lot more information on the diagnosis side of things. The role in follow-up, particularly after myotomy, is really not defined well. This is the first study to my knowledge that has evaluated manometry and FLIP head-to-head to compare patient-reported outcomes,” said Dr. DeWitt in an interview. He is a professor of medicine and the director of endoscopic ultrasound at Indiana University Medical Center, in Indianapolis.
Going head-to-head
The researchers conducted a retrospective, single-center study of 265 consecutive patients who underwent POEM for achalasia or EGJOO from 2016 through 2020. A clinical response was defined as an Eckardt score ≤3, EGJ distensibility index (EGJ-DI) higher than 2.8 mm2/mm Hg, maximum integrated relaxation pressure (IRP) <15 mm Hg, or a maximum EGJ diameter greater than 14 mm at any balloon distension.
In all, 126 patients returned for follow-up and completed an upper endoscopy with FLIP, HRM, and Eckardt scores within a 6-12 month period after the POEM procedure.
With respect to HRM, an IRP measurement <15 mm Hg predicted post-POEM Eckardt score with a sensitivity of 86.7% (95% confidence interval, 79.3-92.2) and a specificity of 33.3% (95% CI, 4.3-77.7), with an area under the curve of 0.60 (95% CI, 0.39-0.81). A maximum EJG diameter ≥ 14 mm had a sensitivity of 77.5% (95% CI, 69.0-84.6) and a specificity of 33.3% (95% CI, 4.3-77.7), with an AUC of 0.55 (95% CI, 0.34-0.76).
The performance was similar with FLIP: EGJ-DI > 2.8 mm2/mm Hg at any balloon setting had a sensitivity of 95.0% (95% CI, 89.4-98.1) and a specificity% of 0.0, and an AUC of 0.53 (95% CI, 0.51-0.55). A similar measurement at 40 mL or 50 mL distension had a sensitivity of 93.3% (95% CI, 87.3-97.1) and a specificity of 16.7% (95% CI, 0.4-64.1), with an AUC of 0.55 (95% CI, 0.39-0.72). Receiver operator characteristic analysis showed no significant difference between ability of FLIP and HRM to predict a normal Eckardt score.
If the study is repeated in other patient populations, Dr. DeWitt hopes that it could eliminate manometry altogether in a large majority of patients. “That would be potentially a game changer for bringing patients back to see how well they’re doing,” said Dr. DeWitt.
Not all patients who undergo POEM would be good candidates for FLIP, said Dr. DeWitt. The study was limited to patients with hypertension in the lower esophageal sphincter. Other disorders such as diffuse esophageal spasm, jackhammer esophagus, and type III achalasia would not likely be candidates for FLIP. “Those patients are going to probably still need manometry because if the esophageal body abnormalities are still present, then repeat testing might need to be performed,” said Dr. DeWitt. Still, he estimated about 80% of patients could be eligible for FLIP instead.
Impact on patients
“I think it’s interesting new data,” said Patrick Young, MD, who comoderated the session where the research was presented. He noted that the treatment of achalasia is evolving away from surgery, and the techniques to measure response are evolving along with it. “As we progress in that technology and using that procedure, we need to understand better how to follow those people up. I think adding this new device may help us to understand who’s going to respond well, and who’s not going to respond well. This is an early investigation, so I think we’ll need to do trials, but I think this is a good first step,” said Dr. Young, who is a professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md.
Comoderator Mohammad Yaghoobi, MD, also praised the study, but noted that the cost of FLIP could be a concern. “We want to have a reasonable ratio of the cost versus the effectiveness,” said Dr. Yaghoobi, who is an associate professor of medicine at McMaster University in Hamilton, Ont.
Dr. DeWitt, Dr. Young, and Dr. Yaghoobi had no relevant disclosures.
LAS VEGAS – Functional lumen imaging probe (FLIP) was equivalent to high-resolution manometry (HRM) in predicting clinical response by Eckardt score 6 months or more after per oral endoscopic myotomy (POEM) for achalasia or esophagogastric junction (EGJ) outlet obstruction (EGJOO).
Measures for clinical response following lower esophageal sphincter myotomy procedures include Eckardt Score, timed barium esophagram, HRM, and FLIP. However, since FLIP is a relatively new technique, there are few clinical data comparing its efficacy versus HRM in patients who have a positive response to POEM measured by the Eckardt score, according to John DeWitt, MD, who presented the research at the annual meeting of the American College of Gastroenterology.
FLIP can be performed during a follow-up endoscopy while a patient is sedated, while HRM requires the patient to be awake. Some patients find the procedure intolerable, and Dr. DeWitt estimates that 10%-20% of patients don’t return for follow-up assessments because of the discomfort.
“[FLIP] is a relatively new technology, the role of which is still being discovered. We have a lot more information on the diagnosis side of things. The role in follow-up, particularly after myotomy, is really not defined well. This is the first study to my knowledge that has evaluated manometry and FLIP head-to-head to compare patient-reported outcomes,” said Dr. DeWitt in an interview. He is a professor of medicine and the director of endoscopic ultrasound at Indiana University Medical Center, in Indianapolis.
Going head-to-head
The researchers conducted a retrospective, single-center study of 265 consecutive patients who underwent POEM for achalasia or EGJOO from 2016 through 2020. A clinical response was defined as an Eckardt score ≤3, EGJ distensibility index (EGJ-DI) higher than 2.8 mm2/mm Hg, maximum integrated relaxation pressure (IRP) <15 mm Hg, or a maximum EGJ diameter greater than 14 mm at any balloon distension.
In all, 126 patients returned for follow-up and completed an upper endoscopy with FLIP, HRM, and Eckardt scores within a 6-12 month period after the POEM procedure.
With respect to HRM, an IRP measurement <15 mm Hg predicted post-POEM Eckardt score with a sensitivity of 86.7% (95% confidence interval, 79.3-92.2) and a specificity of 33.3% (95% CI, 4.3-77.7), with an area under the curve of 0.60 (95% CI, 0.39-0.81). A maximum EJG diameter ≥ 14 mm had a sensitivity of 77.5% (95% CI, 69.0-84.6) and a specificity of 33.3% (95% CI, 4.3-77.7), with an AUC of 0.55 (95% CI, 0.34-0.76).
The performance was similar with FLIP: EGJ-DI > 2.8 mm2/mm Hg at any balloon setting had a sensitivity of 95.0% (95% CI, 89.4-98.1) and a specificity% of 0.0, and an AUC of 0.53 (95% CI, 0.51-0.55). A similar measurement at 40 mL or 50 mL distension had a sensitivity of 93.3% (95% CI, 87.3-97.1) and a specificity of 16.7% (95% CI, 0.4-64.1), with an AUC of 0.55 (95% CI, 0.39-0.72). Receiver operator characteristic analysis showed no significant difference between ability of FLIP and HRM to predict a normal Eckardt score.
If the study is repeated in other patient populations, Dr. DeWitt hopes that it could eliminate manometry altogether in a large majority of patients. “That would be potentially a game changer for bringing patients back to see how well they’re doing,” said Dr. DeWitt.
Not all patients who undergo POEM would be good candidates for FLIP, said Dr. DeWitt. The study was limited to patients with hypertension in the lower esophageal sphincter. Other disorders such as diffuse esophageal spasm, jackhammer esophagus, and type III achalasia would not likely be candidates for FLIP. “Those patients are going to probably still need manometry because if the esophageal body abnormalities are still present, then repeat testing might need to be performed,” said Dr. DeWitt. Still, he estimated about 80% of patients could be eligible for FLIP instead.
Impact on patients
“I think it’s interesting new data,” said Patrick Young, MD, who comoderated the session where the research was presented. He noted that the treatment of achalasia is evolving away from surgery, and the techniques to measure response are evolving along with it. “As we progress in that technology and using that procedure, we need to understand better how to follow those people up. I think adding this new device may help us to understand who’s going to respond well, and who’s not going to respond well. This is an early investigation, so I think we’ll need to do trials, but I think this is a good first step,” said Dr. Young, who is a professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md.
Comoderator Mohammad Yaghoobi, MD, also praised the study, but noted that the cost of FLIP could be a concern. “We want to have a reasonable ratio of the cost versus the effectiveness,” said Dr. Yaghoobi, who is an associate professor of medicine at McMaster University in Hamilton, Ont.
Dr. DeWitt, Dr. Young, and Dr. Yaghoobi had no relevant disclosures.
AT ACG 2021
Dupilumab shows long-term efficacy in EoE
LAS VEGAS –Data from the 28-week extension of the Liberty EoE TREET phase 3 clinical trial showed that the anti–interleukin-4/IL-13 antibody dupilumab led to long-term improvement in eosinophil count, histology, and patient-reported symptoms of eosinophilic esophagitis (EoE) out to 28 weeks. Dupilumab is Food and Drug Administration approved for the treatment of atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.

Many patients don’t respond to the standard therapies of proton pump inhibitors, steroids, or diet. Some evidence suggests that EoE might be driven by type 2 inflammation, and dupilumab’s effect on the shared receptor of IL-4 and IL-13 directly counters that pathway.
“The current treatments are [proton pump inhibitors], steroids, or diet – a good proportion of patients don’t respond to them. And they’re also not targeted,” Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, said in an interview. Dr. Dellon presented the research at the annual meeting of the American College of Gastroenterology.
“The bottom line is that people who responded up front to dupilumab maintain that response to a year, and the people on placebo gained a similar response as the people who were treated. It looked good. It was histologic, symptomatic, and endoscopic outcomes,” said Dr. Dellon.
Many of the patients in the new study were steroid refractory, making it a difficult population to treat, according to Dr. Dellon. “You can’t compare to the steroid-treated patients, but the 6-month data showed about a 60% response rate histologically, which is right up there with where steroids and diet are for easier to treat patients. So the fact that it’s a harder to treat cohort is pretty impressive from that standpoint,” said Dr. Dellon.
Data from the first 24 weeks was previously reported at UEG Week 2020 and showed that dupilumab outperformed placebo in EoE patients aged 12 years and older, with dupilumab producing better outcomes in peak esophageal intraepithelial eosinophil count and change in Dysphagia Symptom Questionnaire (DSQ) Score at 24 weeks.
At ACG 2021, Dr. Dellon reported on 52-week results, where all patients from both treated and placebo groups received dupilumab after the initial 24-week phase. Dupilumab reduced dysphagia symptoms as measured by the absolute change in DSQ score at 24 weeks (–21.9 vs. –9.6; P < .001). At 52 weeks, the dupilumab group showed a change of –23.4 from the start of the study, and the placebo-to-dupilumab group had a DSQ score change of –21.7. Dupilumab also led to a greater percentage reduction in DSQ score by 24 weeks (69.2% versus 31.7%; P < .001); at 52 weeks, the dupilumab group had a 75.9% reduction and the placebo-to-dupilumab group had a 65.9% reduction (no significant difference).
The dupilumab group had a greater proportion of patients who achieved peak esophageal eosinophil count of 6 eosinophils or less per high power field at 24 weeks (59.5% vs. 5.1%); at 52 weeks, 55.9% had achieved this measure, versus 60.0% of the placebo-to-dupilumab group. At 24 weeks, the dupilumab group had a 71.2% reduction in peak eosinophil count from baseline versus –3.0% in placebo (P < .001). At week 52, the reductions were 88.6% and 83.8%, respectively.
Histology features were improved with dupilumab. At week 24, the absolute change in histology scoring system mean grade score (histologic severity) from initial baseline was greater in the dupilumab group (least squares mean, –0.761 vs. –0.001; P < .001). The improvement continued at week 52 (LS mean, –0.87) and occurred in the placebo-to-dupilumab group (LS mean, –0.87). The dupilumab group had a greater absolute change in mean stage score at 24 weeks (histologic extent, LS mean, –0.753 vs. –0.012; P < .001) and 52 weeks (LS mean, –0.89), while the placebo-to-dupilumab group achieved a similar change at 52 weeks (LS mean, –0.87).
Endoscopic features improved in the dupilumab group as measured by endoscopic reference score at 24 weeks (LS mean, –3.2 versus –0.3; P <.001) and at 52 weeks (LS mean, –4.1). The placebo-to-dupilumab group had a similar outcome at 52 weeks (LS mean, –3.9).
Dupilumab was well tolerated, with the only significant difference in treatment-emergent adverse events being injection-site reactions and injection-site erythema.
“I thought the data was really impressive and compelling,” said Amy Oxentenko, MD, chair of medicine at the Mayo Clinic in Phoenix, who comoderated the session. “It’d be nice to have something like this that is a targeted therapy that clearly shows improvement in not only some of the symptoms and histology, but also having an impact possibly on that fibrotic piece, which I think is really the area of morbidity in these patients long term.”
If approved, dupilumab could improve compliance among patients, who sometimes struggle with taking topical steroids properly, said comoderator David Hass, MD, who is an associate clinical professor at Yale University, New Haven, Conn. He also agreed that the potential for remodeling would be a significant benefit over steroids.
One concern with dupilumab would be any potential for immune suppression. “It’s always something to think about,” Dr. Hass said.
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon has consulted and received research support from numerous pharmaceutical companies. Dr. Oxentenko and Dr. Hass have no relevant financial disclosures.
This article was updated Nov. 4, 2021.
LAS VEGAS –Data from the 28-week extension of the Liberty EoE TREET phase 3 clinical trial showed that the anti–interleukin-4/IL-13 antibody dupilumab led to long-term improvement in eosinophil count, histology, and patient-reported symptoms of eosinophilic esophagitis (EoE) out to 28 weeks. Dupilumab is Food and Drug Administration approved for the treatment of atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.
Many patients don’t respond to the standard therapies of proton pump inhibitors, steroids, or diet. Some evidence suggests that EoE might be driven by type 2 inflammation, and dupilumab’s effect on the shared receptor of IL-4 and IL-13 directly counters that pathway.
“The current treatments are [proton pump inhibitors], steroids, or diet – a good proportion of patients don’t respond to them. And they’re also not targeted,” Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, said in an interview. Dr. Dellon presented the research at the annual meeting of the American College of Gastroenterology.
“The bottom line is that people who responded up front to dupilumab maintain that response to a year, and the people on placebo gained a similar response as the people who were treated. It looked good. It was histologic, symptomatic, and endoscopic outcomes,” said Dr. Dellon.
Many of the patients in the new study were steroid refractory, making it a difficult population to treat, according to Dr. Dellon. “You can’t compare to the steroid-treated patients, but the 6-month data showed about a 60% response rate histologically, which is right up there with where steroids and diet are for easier to treat patients. So the fact that it’s a harder to treat cohort is pretty impressive from that standpoint,” said Dr. Dellon.
Data from the first 24 weeks was previously reported at UEG Week 2020 and showed that dupilumab outperformed placebo in EoE patients aged 12 years and older, with dupilumab producing better outcomes in peak esophageal intraepithelial eosinophil count and change in Dysphagia Symptom Questionnaire (DSQ) Score at 24 weeks.
At ACG 2021, Dr. Dellon reported on 52-week results, where all patients from both treated and placebo groups received dupilumab after the initial 24-week phase. Dupilumab reduced dysphagia symptoms as measured by the absolute change in DSQ score at 24 weeks (–21.9 vs. –9.6; P < .001). At 52 weeks, the dupilumab group showed a change of –23.4 from the start of the study, and the placebo-to-dupilumab group had a DSQ score change of –21.7. Dupilumab also led to a greater percentage reduction in DSQ score by 24 weeks (69.2% versus 31.7%; P < .001); at 52 weeks, the dupilumab group had a 75.9% reduction and the placebo-to-dupilumab group had a 65.9% reduction (no significant difference).
The dupilumab group had a greater proportion of patients who achieved peak esophageal eosinophil count of 6 eosinophils or less per high power field at 24 weeks (59.5% vs. 5.1%); at 52 weeks, 55.9% had achieved this measure, versus 60.0% of the placebo-to-dupilumab group. At 24 weeks, the dupilumab group had a 71.2% reduction in peak eosinophil count from baseline versus –3.0% in placebo (P < .001). At week 52, the reductions were 88.6% and 83.8%, respectively.
Histology features were improved with dupilumab. At week 24, the absolute change in histology scoring system mean grade score (histologic severity) from initial baseline was greater in the dupilumab group (least squares mean, –0.761 vs. –0.001; P < .001). The improvement continued at week 52 (LS mean, –0.87) and occurred in the placebo-to-dupilumab group (LS mean, –0.87). The dupilumab group had a greater absolute change in mean stage score at 24 weeks (histologic extent, LS mean, –0.753 vs. –0.012; P < .001) and 52 weeks (LS mean, –0.89), while the placebo-to-dupilumab group achieved a similar change at 52 weeks (LS mean, –0.87).
Endoscopic features improved in the dupilumab group as measured by endoscopic reference score at 24 weeks (LS mean, –3.2 versus –0.3; P <.001) and at 52 weeks (LS mean, –4.1). The placebo-to-dupilumab group had a similar outcome at 52 weeks (LS mean, –3.9).
Dupilumab was well tolerated, with the only significant difference in treatment-emergent adverse events being injection-site reactions and injection-site erythema.
“I thought the data was really impressive and compelling,” said Amy Oxentenko, MD, chair of medicine at the Mayo Clinic in Phoenix, who comoderated the session. “It’d be nice to have something like this that is a targeted therapy that clearly shows improvement in not only some of the symptoms and histology, but also having an impact possibly on that fibrotic piece, which I think is really the area of morbidity in these patients long term.”
If approved, dupilumab could improve compliance among patients, who sometimes struggle with taking topical steroids properly, said comoderator David Hass, MD, who is an associate clinical professor at Yale University, New Haven, Conn. He also agreed that the potential for remodeling would be a significant benefit over steroids.
One concern with dupilumab would be any potential for immune suppression. “It’s always something to think about,” Dr. Hass said.
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon has consulted and received research support from numerous pharmaceutical companies. Dr. Oxentenko and Dr. Hass have no relevant financial disclosures.
This article was updated Nov. 4, 2021.
LAS VEGAS –Data from the 28-week extension of the Liberty EoE TREET phase 3 clinical trial showed that the anti–interleukin-4/IL-13 antibody dupilumab led to long-term improvement in eosinophil count, histology, and patient-reported symptoms of eosinophilic esophagitis (EoE) out to 28 weeks. Dupilumab is Food and Drug Administration approved for the treatment of atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis.
Many patients don’t respond to the standard therapies of proton pump inhibitors, steroids, or diet. Some evidence suggests that EoE might be driven by type 2 inflammation, and dupilumab’s effect on the shared receptor of IL-4 and IL-13 directly counters that pathway.
“The current treatments are [proton pump inhibitors], steroids, or diet – a good proportion of patients don’t respond to them. And they’re also not targeted,” Evan Dellon, MD, professor of medicine and epidemiology at the University of North Carolina at Chapel Hill, said in an interview. Dr. Dellon presented the research at the annual meeting of the American College of Gastroenterology.
“The bottom line is that people who responded up front to dupilumab maintain that response to a year, and the people on placebo gained a similar response as the people who were treated. It looked good. It was histologic, symptomatic, and endoscopic outcomes,” said Dr. Dellon.
Many of the patients in the new study were steroid refractory, making it a difficult population to treat, according to Dr. Dellon. “You can’t compare to the steroid-treated patients, but the 6-month data showed about a 60% response rate histologically, which is right up there with where steroids and diet are for easier to treat patients. So the fact that it’s a harder to treat cohort is pretty impressive from that standpoint,” said Dr. Dellon.
Data from the first 24 weeks was previously reported at UEG Week 2020 and showed that dupilumab outperformed placebo in EoE patients aged 12 years and older, with dupilumab producing better outcomes in peak esophageal intraepithelial eosinophil count and change in Dysphagia Symptom Questionnaire (DSQ) Score at 24 weeks.
At ACG 2021, Dr. Dellon reported on 52-week results, where all patients from both treated and placebo groups received dupilumab after the initial 24-week phase. Dupilumab reduced dysphagia symptoms as measured by the absolute change in DSQ score at 24 weeks (–21.9 vs. –9.6; P < .001). At 52 weeks, the dupilumab group showed a change of –23.4 from the start of the study, and the placebo-to-dupilumab group had a DSQ score change of –21.7. Dupilumab also led to a greater percentage reduction in DSQ score by 24 weeks (69.2% versus 31.7%; P < .001); at 52 weeks, the dupilumab group had a 75.9% reduction and the placebo-to-dupilumab group had a 65.9% reduction (no significant difference).
The dupilumab group had a greater proportion of patients who achieved peak esophageal eosinophil count of 6 eosinophils or less per high power field at 24 weeks (59.5% vs. 5.1%); at 52 weeks, 55.9% had achieved this measure, versus 60.0% of the placebo-to-dupilumab group. At 24 weeks, the dupilumab group had a 71.2% reduction in peak eosinophil count from baseline versus –3.0% in placebo (P < .001). At week 52, the reductions were 88.6% and 83.8%, respectively.
Histology features were improved with dupilumab. At week 24, the absolute change in histology scoring system mean grade score (histologic severity) from initial baseline was greater in the dupilumab group (least squares mean, –0.761 vs. –0.001; P < .001). The improvement continued at week 52 (LS mean, –0.87) and occurred in the placebo-to-dupilumab group (LS mean, –0.87). The dupilumab group had a greater absolute change in mean stage score at 24 weeks (histologic extent, LS mean, –0.753 vs. –0.012; P < .001) and 52 weeks (LS mean, –0.89), while the placebo-to-dupilumab group achieved a similar change at 52 weeks (LS mean, –0.87).
Endoscopic features improved in the dupilumab group as measured by endoscopic reference score at 24 weeks (LS mean, –3.2 versus –0.3; P <.001) and at 52 weeks (LS mean, –4.1). The placebo-to-dupilumab group had a similar outcome at 52 weeks (LS mean, –3.9).
Dupilumab was well tolerated, with the only significant difference in treatment-emergent adverse events being injection-site reactions and injection-site erythema.
“I thought the data was really impressive and compelling,” said Amy Oxentenko, MD, chair of medicine at the Mayo Clinic in Phoenix, who comoderated the session. “It’d be nice to have something like this that is a targeted therapy that clearly shows improvement in not only some of the symptoms and histology, but also having an impact possibly on that fibrotic piece, which I think is really the area of morbidity in these patients long term.”
If approved, dupilumab could improve compliance among patients, who sometimes struggle with taking topical steroids properly, said comoderator David Hass, MD, who is an associate clinical professor at Yale University, New Haven, Conn. He also agreed that the potential for remodeling would be a significant benefit over steroids.
One concern with dupilumab would be any potential for immune suppression. “It’s always something to think about,” Dr. Hass said.
LIBERTY EoE TREET was funded by Sanofi and Regeneron. Dr. Dellon has consulted and received research support from numerous pharmaceutical companies. Dr. Oxentenko and Dr. Hass have no relevant financial disclosures.
This article was updated Nov. 4, 2021.
AT AGC 2021
Tracking adenomas per colonoscopy shows promise as quality measure
The number of adenomas per colonoscopy (APC) is inversely correlated with postcolonoscopy colorectal cancer (PCCRC), which supports use of APC as a new quality control measure, according to investigators.

Data from 138 endoscopists showed that patients screened by physicians with higher APCs had significantly lower rates of PCCRC, and an APC of 0.6 offered more protection than either an APC of 0.4 or an adenoma detection rate (ADR) of 25%, reported lead author Joseph C. Anderson, MD, of White River Junction VA Medical Center, Hanover, N.H., and colleagues.
“Unfortunately, APC has never been validated as a quality measure by demonstrating a reduction in PCCRC in exams performed by endoscopists with higher rates,” Dr. Anderson said at the annual meeting of the American College of Gastroenterology.
To this end, Dr. Anderson and colleagues reviewed data from the New Hampshire Colonoscopy Registry (NHCR), including 9,023 screening colonoscopies with a follow-up event 6-60 months after the initial exam. Procedures were conducted by 138 endoscopists in New Hampshire, Vermont, Massachusetts, and Maine.
Three quality measures were analyzed for associations with PCCRC: an APC of 0.4, an APC of 0.6, and an ADR of 25%. Hazard ratios were calculated for all PCCRCs, as well as PCCRCs diagnosed at first follow-up event. Rates were reported for two time periods: 6-36 months and 6-60 months.
From 6 to 60 months, 82 cases of PCCRC were diagnosed, among which 50 were diagnosed between 6 and 36 months.
For both periods, all three quality measures were significantly associated with reductions in PCCRC. The higher APC of 0.6, however, offered greater protection, reducing all PCCRCs by 71% and 61% in the shorter and longer period, respectively. In comparison, the lower APC of 0.4 reduced rates by 63% and 53%, while the ADR benchmark reduced rates by 62% and 42%.
These trends were maintained for PCCRCs diagnosed at first follow-up event. An APC of 0.6 was associated with respective reductions of 79% and 65% for the shorter and longer period, compared with 64% and 57% for the lower APC, and 67% and 49% for ADR.
Additional analysis clarified the relationship between APC level and likelihood of developing PCCRC. In terms of absolute risk, patients screened by an endoscopist with an APC greater than 0.6 had a 0.5% chance of developing PCCRC from 6 to 36 months, compared with 0.7% for an APC of 0.4-0.6, and 2.1% for an APC of less than 0.4 (P = .0001). This pattern held through 60 months, during which time an APC greater than 0.6 was associated with an absolute risk of PCCRC of 0.4%, compared with 0.7% for an APC of 0.4-0.6, and 1.6% for an APC less than 0.4 (P = .0001).
“Our novel data support the use of APC as a quality measure by demonstrating a reduction in PCCRC risk in exams performed by endoscopists with higher APCs,” Dr. Anderson concluded, noting that an APC of 0.6 appeared to offer more protection than an APC of 0.4. “I feel that ... APC as a quality measure, now that we’ve validated it, may be accepted because of its ability to differentiate endoscopists on their adenoma detection skills.”
According to Lawrence Hookey, MD, of Queen’s University, Kingston, Ont., “It’s an important study that will probably contribute to where we’re going forward.”
Dr. Lawrence, chair of the division and medical director of the endoscopy units at Kingston General and Hotel Dieu hospitals, said that APC may overcome the main concern with ADR – that endoscopists who find one adenoma may not be motivated to seek out as many as possible.
“The problem with ADR, in general, is that if you find one polyp, and if ADR is the stat you’re living by, then you don’t need to find any other polyps, and that obviously doesn’t do that patient a favor, necessarily,” Dr. Hookey said in an interview. “It does bring them back sooner for surveillance, but it doesn’t help remove the rest of the polyps that they have. And not that someone is going to find one polyp and turn off the light and pull the scope out, but you may not be looking as hard.”
APC mitigates this issue, he explained, because it determines “whether or not you’re truly clearing things out and getting rid of as many [polyps] as possible.”
Dr. Hookey said that APC is “probably the best” quality control measure on the horizon, and he suggested that more work is needed to determine the optimal benchmark figure, which should ideally be investigated through larger studies.
“I just want to see it in bigger groups,” he said.
The investigators and Dr. Hookey reported no conflicts of interest.
The number of adenomas per colonoscopy (APC) is inversely correlated with postcolonoscopy colorectal cancer (PCCRC), which supports use of APC as a new quality control measure, according to investigators.
Data from 138 endoscopists showed that patients screened by physicians with higher APCs had significantly lower rates of PCCRC, and an APC of 0.6 offered more protection than either an APC of 0.4 or an adenoma detection rate (ADR) of 25%, reported lead author Joseph C. Anderson, MD, of White River Junction VA Medical Center, Hanover, N.H., and colleagues.
“Unfortunately, APC has never been validated as a quality measure by demonstrating a reduction in PCCRC in exams performed by endoscopists with higher rates,” Dr. Anderson said at the annual meeting of the American College of Gastroenterology.
To this end, Dr. Anderson and colleagues reviewed data from the New Hampshire Colonoscopy Registry (NHCR), including 9,023 screening colonoscopies with a follow-up event 6-60 months after the initial exam. Procedures were conducted by 138 endoscopists in New Hampshire, Vermont, Massachusetts, and Maine.
Three quality measures were analyzed for associations with PCCRC: an APC of 0.4, an APC of 0.6, and an ADR of 25%. Hazard ratios were calculated for all PCCRCs, as well as PCCRCs diagnosed at first follow-up event. Rates were reported for two time periods: 6-36 months and 6-60 months.
From 6 to 60 months, 82 cases of PCCRC were diagnosed, among which 50 were diagnosed between 6 and 36 months.
For both periods, all three quality measures were significantly associated with reductions in PCCRC. The higher APC of 0.6, however, offered greater protection, reducing all PCCRCs by 71% and 61% in the shorter and longer period, respectively. In comparison, the lower APC of 0.4 reduced rates by 63% and 53%, while the ADR benchmark reduced rates by 62% and 42%.
These trends were maintained for PCCRCs diagnosed at first follow-up event. An APC of 0.6 was associated with respective reductions of 79% and 65% for the shorter and longer period, compared with 64% and 57% for the lower APC, and 67% and 49% for ADR.
Additional analysis clarified the relationship between APC level and likelihood of developing PCCRC. In terms of absolute risk, patients screened by an endoscopist with an APC greater than 0.6 had a 0.5% chance of developing PCCRC from 6 to 36 months, compared with 0.7% for an APC of 0.4-0.6, and 2.1% for an APC of less than 0.4 (P = .0001). This pattern held through 60 months, during which time an APC greater than 0.6 was associated with an absolute risk of PCCRC of 0.4%, compared with 0.7% for an APC of 0.4-0.6, and 1.6% for an APC less than 0.4 (P = .0001).
“Our novel data support the use of APC as a quality measure by demonstrating a reduction in PCCRC risk in exams performed by endoscopists with higher APCs,” Dr. Anderson concluded, noting that an APC of 0.6 appeared to offer more protection than an APC of 0.4. “I feel that ... APC as a quality measure, now that we’ve validated it, may be accepted because of its ability to differentiate endoscopists on their adenoma detection skills.”
According to Lawrence Hookey, MD, of Queen’s University, Kingston, Ont., “It’s an important study that will probably contribute to where we’re going forward.”
Dr. Lawrence, chair of the division and medical director of the endoscopy units at Kingston General and Hotel Dieu hospitals, said that APC may overcome the main concern with ADR – that endoscopists who find one adenoma may not be motivated to seek out as many as possible.
“The problem with ADR, in general, is that if you find one polyp, and if ADR is the stat you’re living by, then you don’t need to find any other polyps, and that obviously doesn’t do that patient a favor, necessarily,” Dr. Hookey said in an interview. “It does bring them back sooner for surveillance, but it doesn’t help remove the rest of the polyps that they have. And not that someone is going to find one polyp and turn off the light and pull the scope out, but you may not be looking as hard.”
APC mitigates this issue, he explained, because it determines “whether or not you’re truly clearing things out and getting rid of as many [polyps] as possible.”
Dr. Hookey said that APC is “probably the best” quality control measure on the horizon, and he suggested that more work is needed to determine the optimal benchmark figure, which should ideally be investigated through larger studies.
“I just want to see it in bigger groups,” he said.
The investigators and Dr. Hookey reported no conflicts of interest.
The number of adenomas per colonoscopy (APC) is inversely correlated with postcolonoscopy colorectal cancer (PCCRC), which supports use of APC as a new quality control measure, according to investigators.
Data from 138 endoscopists showed that patients screened by physicians with higher APCs had significantly lower rates of PCCRC, and an APC of 0.6 offered more protection than either an APC of 0.4 or an adenoma detection rate (ADR) of 25%, reported lead author Joseph C. Anderson, MD, of White River Junction VA Medical Center, Hanover, N.H., and colleagues.
“Unfortunately, APC has never been validated as a quality measure by demonstrating a reduction in PCCRC in exams performed by endoscopists with higher rates,” Dr. Anderson said at the annual meeting of the American College of Gastroenterology.
To this end, Dr. Anderson and colleagues reviewed data from the New Hampshire Colonoscopy Registry (NHCR), including 9,023 screening colonoscopies with a follow-up event 6-60 months after the initial exam. Procedures were conducted by 138 endoscopists in New Hampshire, Vermont, Massachusetts, and Maine.
Three quality measures were analyzed for associations with PCCRC: an APC of 0.4, an APC of 0.6, and an ADR of 25%. Hazard ratios were calculated for all PCCRCs, as well as PCCRCs diagnosed at first follow-up event. Rates were reported for two time periods: 6-36 months and 6-60 months.
From 6 to 60 months, 82 cases of PCCRC were diagnosed, among which 50 were diagnosed between 6 and 36 months.
For both periods, all three quality measures were significantly associated with reductions in PCCRC. The higher APC of 0.6, however, offered greater protection, reducing all PCCRCs by 71% and 61% in the shorter and longer period, respectively. In comparison, the lower APC of 0.4 reduced rates by 63% and 53%, while the ADR benchmark reduced rates by 62% and 42%.
These trends were maintained for PCCRCs diagnosed at first follow-up event. An APC of 0.6 was associated with respective reductions of 79% and 65% for the shorter and longer period, compared with 64% and 57% for the lower APC, and 67% and 49% for ADR.
Additional analysis clarified the relationship between APC level and likelihood of developing PCCRC. In terms of absolute risk, patients screened by an endoscopist with an APC greater than 0.6 had a 0.5% chance of developing PCCRC from 6 to 36 months, compared with 0.7% for an APC of 0.4-0.6, and 2.1% for an APC of less than 0.4 (P = .0001). This pattern held through 60 months, during which time an APC greater than 0.6 was associated with an absolute risk of PCCRC of 0.4%, compared with 0.7% for an APC of 0.4-0.6, and 1.6% for an APC less than 0.4 (P = .0001).
“Our novel data support the use of APC as a quality measure by demonstrating a reduction in PCCRC risk in exams performed by endoscopists with higher APCs,” Dr. Anderson concluded, noting that an APC of 0.6 appeared to offer more protection than an APC of 0.4. “I feel that ... APC as a quality measure, now that we’ve validated it, may be accepted because of its ability to differentiate endoscopists on their adenoma detection skills.”
According to Lawrence Hookey, MD, of Queen’s University, Kingston, Ont., “It’s an important study that will probably contribute to where we’re going forward.”
Dr. Lawrence, chair of the division and medical director of the endoscopy units at Kingston General and Hotel Dieu hospitals, said that APC may overcome the main concern with ADR – that endoscopists who find one adenoma may not be motivated to seek out as many as possible.
“The problem with ADR, in general, is that if you find one polyp, and if ADR is the stat you’re living by, then you don’t need to find any other polyps, and that obviously doesn’t do that patient a favor, necessarily,” Dr. Hookey said in an interview. “It does bring them back sooner for surveillance, but it doesn’t help remove the rest of the polyps that they have. And not that someone is going to find one polyp and turn off the light and pull the scope out, but you may not be looking as hard.”
APC mitigates this issue, he explained, because it determines “whether or not you’re truly clearing things out and getting rid of as many [polyps] as possible.”
Dr. Hookey said that APC is “probably the best” quality control measure on the horizon, and he suggested that more work is needed to determine the optimal benchmark figure, which should ideally be investigated through larger studies.
“I just want to see it in bigger groups,” he said.
The investigators and Dr. Hookey reported no conflicts of interest.
FROM ACG 2021
Immune response detected in most IBD patients after COVID vaccines
Most patients with inflammatory bowel disease (IBD) develop a humoral immune response after completing an mRNA SARS-CoV-2 vaccine series, according to data from almost 800 patients.

Anti–receptor binding domain IgG antibodies specific to SARS-CoV-2 were detectable in 95% of patients, with “generally similar” results across vaccine type, age group, and medication class, apart from corticosteroid users, who had an 86% antibody detection rate, reported lead author Kimberly N. Weaver, MD, of the University of North Carolina at Chapel Hill, and colleagues.
“Patients with IBD on immunosuppressive medications have the potential for attenuated response to the SARS-CoV-2 vaccination,” Dr. Weaver said at the annual meeting of the American College of Gastroenterology.
In support of this possibility, Dr. Weaver cited two recent trials from earlier in 2021: one demonstrated blunted antibody responses in IBD patients taking infliximab, while the other showed that full vaccination was less effective at preventing SARS-CoV-2 infection among patients with IBD than nonimmunosuppressed individuals.
To better characterize antibody responses after receiving an mRNA vaccination series, Dr. Weaver and colleagues launched the PREVENT-COVID trial, including the present dataset of 787 patients with IBD older than 12 years, all of whom provided serum samples 8 weeks after completing an mRNA vaccine series. Patients with positive nucleocapsid antibody (indicating prior infection), and/or those who reported prior COVID-19 infection, were excluded. Most patients were White (95%) and female (73%), with an average age of 48 years. Slightly more patients received the BNT162b2 vaccine than the mRNA-1273 vaccine (58% vs. 42%).
At 8 weeks, 752 out of 787 patients had detectable antibodies (95%). Antibody rates were highest among patients receiving vedolizumab monotherapy (n = 83; 99%) or ustekinumab monotherapy (n = 102; 99%), followed by mercaptopurine, azathioprine, or methotrexate monotherapy (n = 67; 97%); anti–tumor necrosis factor monotherapy (n = 270; 96%); mesalamine, sulfasalazine, or budesonide monotherapy or no medication (n = 143; 95%); and finally anti-TNF/immunosuppressive combination therapy (n = 75; 86%). Median and mean antibody titers were lowest for anti-TNF combination therapy and highest for vedolizumab.
Thirty-five patients taking corticosteroids had an antibody detection rate of 85.7% (95% CI, 70.6-93.7), compared with 95.9% (95% CI, 94.2-97.1) among nonsteroid users. In contrast, antibody detection rates were not significantly affected by age or vaccine type.
“Reassuringly, most IBD medications do not prevent an initial antibody response after SARS-CoV-2 vaccination, and this is unlike other classes of immune suppression such as B-cell depletion therapy,” Dr. Weaver concluded. “Additional data are forthcoming on a larger subset of participants in the PREVENT-COVID study which will allow for analysis of factors associated with humoral immune response and potential optimization of immunization strategies.” She described a dataset of about 500 IBD patients in which booster vaccines overcame poor antibody responses to the initial vaccine series.
‘The data we need’
Serre-yu Wong, MD, PhD, of Icahn School of Medicine at Mount Sinai, New York, agreed that the findings should offer some reassurance to patients with IBD and their care providers.

“At the end of the day we have really nice seroconversion rates for the IBD population,” Dr. Wong said.
In April 2021, Dr. Wong and the ICARUS-IBD Working Group published a similar report of 48 patients with IBD receiving biologic therapies, among whom the seroconversion rate was 100%.
“A lot of the early data, including ours, are on infusion medications, and that’s sort of a practical thing because those were the only patients we could get samples from, but [Dr. Weaver and colleagues] were able to get samples from patients not on medications, on oral medications, and on other injection medications that people can take at home, and these are really the data we need for all of our other IBD patients,” Dr. Wong said.
Dr. Wong highlighted that both trials showed some IBD patients generating “very, very high” titers, many of them above the threshold needed for donating convalescent plasma for COVID-19 treatment; still, exact titer levels needed to protect against SARS-CoV-2 infection remain unclear.
“This is going to require longitudinal studies,” Dr. Wong said. “We can’t answer that perfectly right now. We don’t know the magic level of antibodies. I don’t know if you need a titer of 1:100 or 1:1,000.”
Although postvaccination antibody testing is not recommended by the Centers for Disease Control and Prevention, Dr. Wong said that “many patients” check their titers anyway, leading to anxiety if antibodies are low or undetectable.
“I know that it’s very disconcerting sometimes when you don’t see an antibody response, and this is one of the hardest things to try to explain to patients,” Dr. Wong said. “[It’s necessary] to have a frank discussion about the fact that we don’t know the magic level of antibodies, and that there are also other parts of the immune system that we haven’t tested with antibodies. We haven’t tested the T-cell response, and we do know you can have a T-cell response even if you don’t have a B-cell response.”
Dr. Wong suggested that more work is needed to determine the impact of the IBD disease process on susceptibility to SARS-CoV-2 infection, and the rates of antibody responses for the various other vaccines being used around the world.
The PREVENT-COVID study was supported by the Leona M. and Harry B. Helmsley Charitable Trust. The investigators disclosed additional relationships with AbbVie, Johnson & Johnson, Genentech, and others. Dr. Wong reported no relevant conflicts of interest.
This article was updated Oct. 28, 2021.
Most patients with inflammatory bowel disease (IBD) develop a humoral immune response after completing an mRNA SARS-CoV-2 vaccine series, according to data from almost 800 patients.
Anti–receptor binding domain IgG antibodies specific to SARS-CoV-2 were detectable in 95% of patients, with “generally similar” results across vaccine type, age group, and medication class, apart from corticosteroid users, who had an 86% antibody detection rate, reported lead author Kimberly N. Weaver, MD, of the University of North Carolina at Chapel Hill, and colleagues.
“Patients with IBD on immunosuppressive medications have the potential for attenuated response to the SARS-CoV-2 vaccination,” Dr. Weaver said at the annual meeting of the American College of Gastroenterology.
In support of this possibility, Dr. Weaver cited two recent trials from earlier in 2021: one demonstrated blunted antibody responses in IBD patients taking infliximab, while the other showed that full vaccination was less effective at preventing SARS-CoV-2 infection among patients with IBD than nonimmunosuppressed individuals.
To better characterize antibody responses after receiving an mRNA vaccination series, Dr. Weaver and colleagues launched the PREVENT-COVID trial, including the present dataset of 787 patients with IBD older than 12 years, all of whom provided serum samples 8 weeks after completing an mRNA vaccine series. Patients with positive nucleocapsid antibody (indicating prior infection), and/or those who reported prior COVID-19 infection, were excluded. Most patients were White (95%) and female (73%), with an average age of 48 years. Slightly more patients received the BNT162b2 vaccine than the mRNA-1273 vaccine (58% vs. 42%).
At 8 weeks, 752 out of 787 patients had detectable antibodies (95%). Antibody rates were highest among patients receiving vedolizumab monotherapy (n = 83; 99%) or ustekinumab monotherapy (n = 102; 99%), followed by mercaptopurine, azathioprine, or methotrexate monotherapy (n = 67; 97%); anti–tumor necrosis factor monotherapy (n = 270; 96%); mesalamine, sulfasalazine, or budesonide monotherapy or no medication (n = 143; 95%); and finally anti-TNF/immunosuppressive combination therapy (n = 75; 86%). Median and mean antibody titers were lowest for anti-TNF combination therapy and highest for vedolizumab.
Thirty-five patients taking corticosteroids had an antibody detection rate of 85.7% (95% CI, 70.6-93.7), compared with 95.9% (95% CI, 94.2-97.1) among nonsteroid users. In contrast, antibody detection rates were not significantly affected by age or vaccine type.
“Reassuringly, most IBD medications do not prevent an initial antibody response after SARS-CoV-2 vaccination, and this is unlike other classes of immune suppression such as B-cell depletion therapy,” Dr. Weaver concluded. “Additional data are forthcoming on a larger subset of participants in the PREVENT-COVID study which will allow for analysis of factors associated with humoral immune response and potential optimization of immunization strategies.” She described a dataset of about 500 IBD patients in which booster vaccines overcame poor antibody responses to the initial vaccine series.
‘The data we need’
Serre-yu Wong, MD, PhD, of Icahn School of Medicine at Mount Sinai, New York, agreed that the findings should offer some reassurance to patients with IBD and their care providers.
“At the end of the day we have really nice seroconversion rates for the IBD population,” Dr. Wong said.
In April 2021, Dr. Wong and the ICARUS-IBD Working Group published a similar report of 48 patients with IBD receiving biologic therapies, among whom the seroconversion rate was 100%.
“A lot of the early data, including ours, are on infusion medications, and that’s sort of a practical thing because those were the only patients we could get samples from, but [Dr. Weaver and colleagues] were able to get samples from patients not on medications, on oral medications, and on other injection medications that people can take at home, and these are really the data we need for all of our other IBD patients,” Dr. Wong said.
Dr. Wong highlighted that both trials showed some IBD patients generating “very, very high” titers, many of them above the threshold needed for donating convalescent plasma for COVID-19 treatment; still, exact titer levels needed to protect against SARS-CoV-2 infection remain unclear.
“This is going to require longitudinal studies,” Dr. Wong said. “We can’t answer that perfectly right now. We don’t know the magic level of antibodies. I don’t know if you need a titer of 1:100 or 1:1,000.”
Although postvaccination antibody testing is not recommended by the Centers for Disease Control and Prevention, Dr. Wong said that “many patients” check their titers anyway, leading to anxiety if antibodies are low or undetectable.
“I know that it’s very disconcerting sometimes when you don’t see an antibody response, and this is one of the hardest things to try to explain to patients,” Dr. Wong said. “[It’s necessary] to have a frank discussion about the fact that we don’t know the magic level of antibodies, and that there are also other parts of the immune system that we haven’t tested with antibodies. We haven’t tested the T-cell response, and we do know you can have a T-cell response even if you don’t have a B-cell response.”
Dr. Wong suggested that more work is needed to determine the impact of the IBD disease process on susceptibility to SARS-CoV-2 infection, and the rates of antibody responses for the various other vaccines being used around the world.
The PREVENT-COVID study was supported by the Leona M. and Harry B. Helmsley Charitable Trust. The investigators disclosed additional relationships with AbbVie, Johnson & Johnson, Genentech, and others. Dr. Wong reported no relevant conflicts of interest.
This article was updated Oct. 28, 2021.
Most patients with inflammatory bowel disease (IBD) develop a humoral immune response after completing an mRNA SARS-CoV-2 vaccine series, according to data from almost 800 patients.
Anti–receptor binding domain IgG antibodies specific to SARS-CoV-2 were detectable in 95% of patients, with “generally similar” results across vaccine type, age group, and medication class, apart from corticosteroid users, who had an 86% antibody detection rate, reported lead author Kimberly N. Weaver, MD, of the University of North Carolina at Chapel Hill, and colleagues.
“Patients with IBD on immunosuppressive medications have the potential for attenuated response to the SARS-CoV-2 vaccination,” Dr. Weaver said at the annual meeting of the American College of Gastroenterology.
In support of this possibility, Dr. Weaver cited two recent trials from earlier in 2021: one demonstrated blunted antibody responses in IBD patients taking infliximab, while the other showed that full vaccination was less effective at preventing SARS-CoV-2 infection among patients with IBD than nonimmunosuppressed individuals.
To better characterize antibody responses after receiving an mRNA vaccination series, Dr. Weaver and colleagues launched the PREVENT-COVID trial, including the present dataset of 787 patients with IBD older than 12 years, all of whom provided serum samples 8 weeks after completing an mRNA vaccine series. Patients with positive nucleocapsid antibody (indicating prior infection), and/or those who reported prior COVID-19 infection, were excluded. Most patients were White (95%) and female (73%), with an average age of 48 years. Slightly more patients received the BNT162b2 vaccine than the mRNA-1273 vaccine (58% vs. 42%).
At 8 weeks, 752 out of 787 patients had detectable antibodies (95%). Antibody rates were highest among patients receiving vedolizumab monotherapy (n = 83; 99%) or ustekinumab monotherapy (n = 102; 99%), followed by mercaptopurine, azathioprine, or methotrexate monotherapy (n = 67; 97%); anti–tumor necrosis factor monotherapy (n = 270; 96%); mesalamine, sulfasalazine, or budesonide monotherapy or no medication (n = 143; 95%); and finally anti-TNF/immunosuppressive combination therapy (n = 75; 86%). Median and mean antibody titers were lowest for anti-TNF combination therapy and highest for vedolizumab.
Thirty-five patients taking corticosteroids had an antibody detection rate of 85.7% (95% CI, 70.6-93.7), compared with 95.9% (95% CI, 94.2-97.1) among nonsteroid users. In contrast, antibody detection rates were not significantly affected by age or vaccine type.
“Reassuringly, most IBD medications do not prevent an initial antibody response after SARS-CoV-2 vaccination, and this is unlike other classes of immune suppression such as B-cell depletion therapy,” Dr. Weaver concluded. “Additional data are forthcoming on a larger subset of participants in the PREVENT-COVID study which will allow for analysis of factors associated with humoral immune response and potential optimization of immunization strategies.” She described a dataset of about 500 IBD patients in which booster vaccines overcame poor antibody responses to the initial vaccine series.
‘The data we need’
Serre-yu Wong, MD, PhD, of Icahn School of Medicine at Mount Sinai, New York, agreed that the findings should offer some reassurance to patients with IBD and their care providers.
“At the end of the day we have really nice seroconversion rates for the IBD population,” Dr. Wong said.
In April 2021, Dr. Wong and the ICARUS-IBD Working Group published a similar report of 48 patients with IBD receiving biologic therapies, among whom the seroconversion rate was 100%.
“A lot of the early data, including ours, are on infusion medications, and that’s sort of a practical thing because those were the only patients we could get samples from, but [Dr. Weaver and colleagues] were able to get samples from patients not on medications, on oral medications, and on other injection medications that people can take at home, and these are really the data we need for all of our other IBD patients,” Dr. Wong said.
Dr. Wong highlighted that both trials showed some IBD patients generating “very, very high” titers, many of them above the threshold needed for donating convalescent plasma for COVID-19 treatment; still, exact titer levels needed to protect against SARS-CoV-2 infection remain unclear.
“This is going to require longitudinal studies,” Dr. Wong said. “We can’t answer that perfectly right now. We don’t know the magic level of antibodies. I don’t know if you need a titer of 1:100 or 1:1,000.”
Although postvaccination antibody testing is not recommended by the Centers for Disease Control and Prevention, Dr. Wong said that “many patients” check their titers anyway, leading to anxiety if antibodies are low or undetectable.
“I know that it’s very disconcerting sometimes when you don’t see an antibody response, and this is one of the hardest things to try to explain to patients,” Dr. Wong said. “[It’s necessary] to have a frank discussion about the fact that we don’t know the magic level of antibodies, and that there are also other parts of the immune system that we haven’t tested with antibodies. We haven’t tested the T-cell response, and we do know you can have a T-cell response even if you don’t have a B-cell response.”
Dr. Wong suggested that more work is needed to determine the impact of the IBD disease process on susceptibility to SARS-CoV-2 infection, and the rates of antibody responses for the various other vaccines being used around the world.
The PREVENT-COVID study was supported by the Leona M. and Harry B. Helmsley Charitable Trust. The investigators disclosed additional relationships with AbbVie, Johnson & Johnson, Genentech, and others. Dr. Wong reported no relevant conflicts of interest.
This article was updated Oct. 28, 2021.
AT ACG 2021