User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Patients trying to lose weight overestimate their diet quality
Only 28% of the participants had good agreement – defined as a difference of 6 points or less – between their perceived diet quality and its actual quality based on Healthy Eating Index–2015 (HEI) scores at the end of the 12-month intervention.
Even fewer – only 13% – had good agreement with their perceived and actual improvement in diet quality.
Jessica Cheng, PhD, Harvard School of Public Health, Boston, presented the findings in an oral session at the American Heart Association scientific sessions.
The study suggests that “patients can benefit from concrete advice on aspects of their diet that could most benefit by being changed,” Dr. Cheng said in an interview.
“But once they know what to change, they may need additional advice on how to make and sustain those changes. Providers may direct their patients to resources such as dietitians, medically tailored meals, MyPlate, healthy recipes, etc.,” she advised.
“The findings are not surprising given that dietary recalls are subject to recall bias and depend on the person’s baseline nutrition knowledge or literacy,” Deepika Laddu, PhD, who was not involved with this research, said in an interview.
Misperception of diet intake is common in individuals with overweight or obesity, and one 90-minute session with a dietitian is not enough, according to Dr. Laddu, assistant professor at the University of Illinois at Chicago.
“The Dietary Guidelines for Americans does a really nice job at presenting all of the options,” she said. However, “understanding what a healthy diet pattern is, or how to adopt it, is confusing, due to a lot of ‘noise’, that is, the mixed messaging and unproven health claims, which add to inadequacies in health or nutrition literacy.”
“It is important to recognize that changing dietary practices is behaviorally challenging and complex,” she emphasized.
People who are interested in making dietary changes need to have ongoing conversations with a qualified health care professional, which most often starts with their primary care clinician.
“Given the well-known time constraints during a typical clinical visit, beyond that initial conversation, it is absolutely critical that patients be referred to qualified healthcare professionals such as a registered dietitian, nurse practitioner, health coach/educator or diabetes educator, etc, for ongoing support.”
These providers can assess the patient’s initial diet, perceptions of a healthy diet, and diet goals, and address any gaps in health literacy, to enable the patient to develop long-lasting, realistic, and healthy eating behaviors.
Perceived vs. actual diet quality
Healthy eating is essential for heart and general health and longevity, but it is unclear if people who make lifestyle (diet and physical activity) changes to lose weight have an accurate perception of diet quality.
The researchers analyzed data from the SMARTER trial of 502 adults aged 35-58 living in the greater Pittsburgh area who were trying to lose weight.
Participants received a 90-minute weight loss counseling session addressing behavioral strategies and establishing dietary and physical activity goals. They all received instructions on how to monitor their diet, physical activity, and weight daily, using a smartphone app, a wristband tracker (Fitbit Charge 2), and a smart wireless scale. Half of the participants also received real-time personalized feedback on those behaviors, up to three times a day, via the study app.
The participants replied to two 24-hour dietary recall questionnaires at study entry and two questionnaires at 12 months.
Researchers analyzed data from the 116 participants who provided information about diet quality. At 1 year, they were asked to rate their diet quality, but also rate their diet quality 12 months earlier at baseline, on a scale of 0-100, where 100 is best.
The average weight loss at 12 months was similar in the groups with and without feedback from the app (roughly 3.2% of baseline weight), so the two study arms were combined. The participants had a mean age of 52 years; 80% were women and 87% were White. They had an average body mass index of 33 kg/m2.
Based on the information from the food recall questionnaires, the researchers calculated the patients’ HEI scores at the start and end of the study. The HEI score is a measure of how well a person’s diet adheres to the 2015-2020 Dietary Guidelines for Americans. It is based on an adequate consumption of nine types of foods – total fruits, whole fruits, total vegetables, greens and beans, total protein foods, seafood, and plant proteins (up to 5 points each), and whole grains, dairy, and fatty acids (up to 10 points each) – and reduced consumption of four dietary components – refined grains, sodium, added sugars, and saturated fats (up to 10 points each).
The healthiest diet has an HEI score of 100, and the Healthy People 2020 goal was an HEI score of 74, Dr. Cheng noted.
At 12 months, on average, the participants rated their diet quality at 70.5 points, whereas the researchers calculated that their average HEI score was only 56.
Participants thought they had improved their diet quality by about 20 points, Dr. Cheng reported. “However, the HEI would suggest they’ve improved it by 1.5 points, which is not a lot out of 100.”
“Future studies should examine the effects of helping people close the gap between their perceptions and objective diet quality measurements,” Dr. Cheng said in a press release from the AHA.
The study was funded by the National Heart, Lung, and Blood Institute, a division of the National Institutes of Health. Dr. Cheng and Dr. Laddu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Only 28% of the participants had good agreement – defined as a difference of 6 points or less – between their perceived diet quality and its actual quality based on Healthy Eating Index–2015 (HEI) scores at the end of the 12-month intervention.
Even fewer – only 13% – had good agreement with their perceived and actual improvement in diet quality.
Jessica Cheng, PhD, Harvard School of Public Health, Boston, presented the findings in an oral session at the American Heart Association scientific sessions.
The study suggests that “patients can benefit from concrete advice on aspects of their diet that could most benefit by being changed,” Dr. Cheng said in an interview.
“But once they know what to change, they may need additional advice on how to make and sustain those changes. Providers may direct their patients to resources such as dietitians, medically tailored meals, MyPlate, healthy recipes, etc.,” she advised.
“The findings are not surprising given that dietary recalls are subject to recall bias and depend on the person’s baseline nutrition knowledge or literacy,” Deepika Laddu, PhD, who was not involved with this research, said in an interview.
Misperception of diet intake is common in individuals with overweight or obesity, and one 90-minute session with a dietitian is not enough, according to Dr. Laddu, assistant professor at the University of Illinois at Chicago.
“The Dietary Guidelines for Americans does a really nice job at presenting all of the options,” she said. However, “understanding what a healthy diet pattern is, or how to adopt it, is confusing, due to a lot of ‘noise’, that is, the mixed messaging and unproven health claims, which add to inadequacies in health or nutrition literacy.”
“It is important to recognize that changing dietary practices is behaviorally challenging and complex,” she emphasized.
People who are interested in making dietary changes need to have ongoing conversations with a qualified health care professional, which most often starts with their primary care clinician.
“Given the well-known time constraints during a typical clinical visit, beyond that initial conversation, it is absolutely critical that patients be referred to qualified healthcare professionals such as a registered dietitian, nurse practitioner, health coach/educator or diabetes educator, etc, for ongoing support.”
These providers can assess the patient’s initial diet, perceptions of a healthy diet, and diet goals, and address any gaps in health literacy, to enable the patient to develop long-lasting, realistic, and healthy eating behaviors.
Perceived vs. actual diet quality
Healthy eating is essential for heart and general health and longevity, but it is unclear if people who make lifestyle (diet and physical activity) changes to lose weight have an accurate perception of diet quality.
The researchers analyzed data from the SMARTER trial of 502 adults aged 35-58 living in the greater Pittsburgh area who were trying to lose weight.
Participants received a 90-minute weight loss counseling session addressing behavioral strategies and establishing dietary and physical activity goals. They all received instructions on how to monitor their diet, physical activity, and weight daily, using a smartphone app, a wristband tracker (Fitbit Charge 2), and a smart wireless scale. Half of the participants also received real-time personalized feedback on those behaviors, up to three times a day, via the study app.
The participants replied to two 24-hour dietary recall questionnaires at study entry and two questionnaires at 12 months.
Researchers analyzed data from the 116 participants who provided information about diet quality. At 1 year, they were asked to rate their diet quality, but also rate their diet quality 12 months earlier at baseline, on a scale of 0-100, where 100 is best.
The average weight loss at 12 months was similar in the groups with and without feedback from the app (roughly 3.2% of baseline weight), so the two study arms were combined. The participants had a mean age of 52 years; 80% were women and 87% were White. They had an average body mass index of 33 kg/m2.
Based on the information from the food recall questionnaires, the researchers calculated the patients’ HEI scores at the start and end of the study. The HEI score is a measure of how well a person’s diet adheres to the 2015-2020 Dietary Guidelines for Americans. It is based on an adequate consumption of nine types of foods – total fruits, whole fruits, total vegetables, greens and beans, total protein foods, seafood, and plant proteins (up to 5 points each), and whole grains, dairy, and fatty acids (up to 10 points each) – and reduced consumption of four dietary components – refined grains, sodium, added sugars, and saturated fats (up to 10 points each).
The healthiest diet has an HEI score of 100, and the Healthy People 2020 goal was an HEI score of 74, Dr. Cheng noted.
At 12 months, on average, the participants rated their diet quality at 70.5 points, whereas the researchers calculated that their average HEI score was only 56.
Participants thought they had improved their diet quality by about 20 points, Dr. Cheng reported. “However, the HEI would suggest they’ve improved it by 1.5 points, which is not a lot out of 100.”
“Future studies should examine the effects of helping people close the gap between their perceptions and objective diet quality measurements,” Dr. Cheng said in a press release from the AHA.
The study was funded by the National Heart, Lung, and Blood Institute, a division of the National Institutes of Health. Dr. Cheng and Dr. Laddu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Only 28% of the participants had good agreement – defined as a difference of 6 points or less – between their perceived diet quality and its actual quality based on Healthy Eating Index–2015 (HEI) scores at the end of the 12-month intervention.
Even fewer – only 13% – had good agreement with their perceived and actual improvement in diet quality.
Jessica Cheng, PhD, Harvard School of Public Health, Boston, presented the findings in an oral session at the American Heart Association scientific sessions.
The study suggests that “patients can benefit from concrete advice on aspects of their diet that could most benefit by being changed,” Dr. Cheng said in an interview.
“But once they know what to change, they may need additional advice on how to make and sustain those changes. Providers may direct their patients to resources such as dietitians, medically tailored meals, MyPlate, healthy recipes, etc.,” she advised.
“The findings are not surprising given that dietary recalls are subject to recall bias and depend on the person’s baseline nutrition knowledge or literacy,” Deepika Laddu, PhD, who was not involved with this research, said in an interview.
Misperception of diet intake is common in individuals with overweight or obesity, and one 90-minute session with a dietitian is not enough, according to Dr. Laddu, assistant professor at the University of Illinois at Chicago.
“The Dietary Guidelines for Americans does a really nice job at presenting all of the options,” she said. However, “understanding what a healthy diet pattern is, or how to adopt it, is confusing, due to a lot of ‘noise’, that is, the mixed messaging and unproven health claims, which add to inadequacies in health or nutrition literacy.”
“It is important to recognize that changing dietary practices is behaviorally challenging and complex,” she emphasized.
People who are interested in making dietary changes need to have ongoing conversations with a qualified health care professional, which most often starts with their primary care clinician.
“Given the well-known time constraints during a typical clinical visit, beyond that initial conversation, it is absolutely critical that patients be referred to qualified healthcare professionals such as a registered dietitian, nurse practitioner, health coach/educator or diabetes educator, etc, for ongoing support.”
These providers can assess the patient’s initial diet, perceptions of a healthy diet, and diet goals, and address any gaps in health literacy, to enable the patient to develop long-lasting, realistic, and healthy eating behaviors.
Perceived vs. actual diet quality
Healthy eating is essential for heart and general health and longevity, but it is unclear if people who make lifestyle (diet and physical activity) changes to lose weight have an accurate perception of diet quality.
The researchers analyzed data from the SMARTER trial of 502 adults aged 35-58 living in the greater Pittsburgh area who were trying to lose weight.
Participants received a 90-minute weight loss counseling session addressing behavioral strategies and establishing dietary and physical activity goals. They all received instructions on how to monitor their diet, physical activity, and weight daily, using a smartphone app, a wristband tracker (Fitbit Charge 2), and a smart wireless scale. Half of the participants also received real-time personalized feedback on those behaviors, up to three times a day, via the study app.
The participants replied to two 24-hour dietary recall questionnaires at study entry and two questionnaires at 12 months.
Researchers analyzed data from the 116 participants who provided information about diet quality. At 1 year, they were asked to rate their diet quality, but also rate their diet quality 12 months earlier at baseline, on a scale of 0-100, where 100 is best.
The average weight loss at 12 months was similar in the groups with and without feedback from the app (roughly 3.2% of baseline weight), so the two study arms were combined. The participants had a mean age of 52 years; 80% were women and 87% were White. They had an average body mass index of 33 kg/m2.
Based on the information from the food recall questionnaires, the researchers calculated the patients’ HEI scores at the start and end of the study. The HEI score is a measure of how well a person’s diet adheres to the 2015-2020 Dietary Guidelines for Americans. It is based on an adequate consumption of nine types of foods – total fruits, whole fruits, total vegetables, greens and beans, total protein foods, seafood, and plant proteins (up to 5 points each), and whole grains, dairy, and fatty acids (up to 10 points each) – and reduced consumption of four dietary components – refined grains, sodium, added sugars, and saturated fats (up to 10 points each).
The healthiest diet has an HEI score of 100, and the Healthy People 2020 goal was an HEI score of 74, Dr. Cheng noted.
At 12 months, on average, the participants rated their diet quality at 70.5 points, whereas the researchers calculated that their average HEI score was only 56.
Participants thought they had improved their diet quality by about 20 points, Dr. Cheng reported. “However, the HEI would suggest they’ve improved it by 1.5 points, which is not a lot out of 100.”
“Future studies should examine the effects of helping people close the gap between their perceptions and objective diet quality measurements,” Dr. Cheng said in a press release from the AHA.
The study was funded by the National Heart, Lung, and Blood Institute, a division of the National Institutes of Health. Dr. Cheng and Dr. Laddu reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AHA 2022
HIV: Treating ‘symptom clusters’ could help improve QOL
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Poor NAFLD outcomes with increased VCTE-measured liver stiffness
according to new findings presented at the annual meeting of the American Association for the Study of Liver Diseases.
Although previous retrospective studies have suggested that increased liver stiffness, as measured by VCTE (FibroScan), is associated with increases in liver-related events, there is a paucity of prospective data, reported Samer Gawrieh, MD, from Indiana University, Carmel and Indianapolis. VCTE is a noninvasive measure of cirrhosis progression.
In their prospective cohort study of patients representing the entire spectrum of NAFLD, the progression to LSM-defined cirrhosis was independently associated with the risk for a composite clinical outcome of death, decompensation, hepatocellular carcinoma, or a Model for End Stage Liver Disease (MELD) score of greater than 15, he said.
Their findings show that “progression to LSM-defined cirrhosis by VCTE is strongly associated with poor clinical outcomes,” Dr. Gawrieh said.
Study findings
Investigators looked at prospective data on 894 patients with biopsy-proven NAFLD in the Nonalcoholic Steatohepatitis (NASH) Clinical Research Network database. The sample included patients with a minimum of two LSM readings taken from 2014 through 2022.
They defined LSM-defined cirrhosis as reaching LSM of greater than 14.9 kPa (90% specificity cutoff) among patients without cirrhosis on the baseline VCTE (a 90% sensitivity cutoff of LSM less than 12.1 kPa).
They also performed a histology-based subanalysis, including data only from those patients who had LSM within 6 months of a liver biopsy.
The median patient age was 60 years, 37% were male, and 80.9% were White and 11.5% were Hispanic/Latino. The median body mass index (BMI) was 32.
Out of all the patients, 119 (13.3%) had progression to LSM-defined cirrhosis.
At a median follow-up of 3.69 years for the 775 patients without LSM progression, 79 (10.2%) had one or more of the events in the composite clinical outcome.
In contrast, after a median 5.48 years of follow-up, 31 of the 119 patients with progression (26.1%) had one or more of the composite events (P < .0001).
The median rates of progression to LSM-defined cirrhosis in the overall cohort were 2% at 1 year, 11% at 3 years, and 16% at 5 years.
Researchers found a correlation between progression to LSM-defined cirrhosis and baseline histological fibrosis stage on biopsy, with a rate of 7% among those with no baseline fibrosis, 9% each for patients with stage I A-C or stage II fibrosis, 24% of those with baseline bridging fibrosis, and 25% of those with baseline cirrhosis.
A comparison of the time to a composite clinical outcome event between patients with progression to LSM-defined cirrhosis and those without progression showed that LSM-defined progression was associated with near doubling in risk, with a hazard ratio of 1.84 (P = .0039).
In a multivariate Cox regression analysis controlling for age, sex, race, BMI, diabetes status, and baseline LSM, only LSM-defined progression (HR, 1.93; P < .01) and age (HR, 1.03; P < .01) were significant predictors.
Dr. Gawrieh noted that while age was a statistically significant factor, it was only weakly associated.
“These data suggest that development of cirrhosis LSM criteria is a promising surrogate for clinical outcomes in patients with NAFLD,” Dr. Gawrieh concluded.
Progression definition questioned
Following the presentation, Nezam Afdhal, MD, chief of the division of gastroenterology, hepatology, and nutrition at Beth Israel Deaconess Hospital in Boston, questioned how 25% of patients who had biopsy-proven cirrhosis could progress to LSM-defined cirrhosis.
Dr. Gawrieh said that, according to inclusion criteria, the patients could not have LSM-defined cirrhosis with the sensitivity cutoff of 12.1 kPa, and that of the 10 patients with baseline cirrhosis in the cohort, all had LSM of less than 12.1 kPa. However, he admitted that because those 10 patients were technically not progressors to cirrhosis, they should have been removed from the analysis for clinical outcomes.
Mark Hartman, MD, a clinical researcher at Eli Lilly and Company in Indianapolis, said the study is valuable but noted that those patients who progressed tended to have higher LSM at baseline as well as a higher [fibrosis-4 score].
Dr. Gawrieh added that the investigators are exploring variables that might explain progression to cirrhosis among patients without high baseline liver stiffness, such as alcohol use or drug-induced liver injury.
The study was supported by the National Institutes of Health and the NASH Clinical Research Network institutions. Dr. Gawrieh disclosed research grants from NIH, Zydus, Viking, and Sonic Incytes, and consulting for TransMedics and Pfizer. Dr. Afdhal and Dr. Hartman reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new findings presented at the annual meeting of the American Association for the Study of Liver Diseases.
Although previous retrospective studies have suggested that increased liver stiffness, as measured by VCTE (FibroScan), is associated with increases in liver-related events, there is a paucity of prospective data, reported Samer Gawrieh, MD, from Indiana University, Carmel and Indianapolis. VCTE is a noninvasive measure of cirrhosis progression.
In their prospective cohort study of patients representing the entire spectrum of NAFLD, the progression to LSM-defined cirrhosis was independently associated with the risk for a composite clinical outcome of death, decompensation, hepatocellular carcinoma, or a Model for End Stage Liver Disease (MELD) score of greater than 15, he said.
Their findings show that “progression to LSM-defined cirrhosis by VCTE is strongly associated with poor clinical outcomes,” Dr. Gawrieh said.
Study findings
Investigators looked at prospective data on 894 patients with biopsy-proven NAFLD in the Nonalcoholic Steatohepatitis (NASH) Clinical Research Network database. The sample included patients with a minimum of two LSM readings taken from 2014 through 2022.
They defined LSM-defined cirrhosis as reaching LSM of greater than 14.9 kPa (90% specificity cutoff) among patients without cirrhosis on the baseline VCTE (a 90% sensitivity cutoff of LSM less than 12.1 kPa).
They also performed a histology-based subanalysis, including data only from those patients who had LSM within 6 months of a liver biopsy.
The median patient age was 60 years, 37% were male, and 80.9% were White and 11.5% were Hispanic/Latino. The median body mass index (BMI) was 32.
Out of all the patients, 119 (13.3%) had progression to LSM-defined cirrhosis.
At a median follow-up of 3.69 years for the 775 patients without LSM progression, 79 (10.2%) had one or more of the events in the composite clinical outcome.
In contrast, after a median 5.48 years of follow-up, 31 of the 119 patients with progression (26.1%) had one or more of the composite events (P < .0001).
The median rates of progression to LSM-defined cirrhosis in the overall cohort were 2% at 1 year, 11% at 3 years, and 16% at 5 years.
Researchers found a correlation between progression to LSM-defined cirrhosis and baseline histological fibrosis stage on biopsy, with a rate of 7% among those with no baseline fibrosis, 9% each for patients with stage I A-C or stage II fibrosis, 24% of those with baseline bridging fibrosis, and 25% of those with baseline cirrhosis.
A comparison of the time to a composite clinical outcome event between patients with progression to LSM-defined cirrhosis and those without progression showed that LSM-defined progression was associated with near doubling in risk, with a hazard ratio of 1.84 (P = .0039).
In a multivariate Cox regression analysis controlling for age, sex, race, BMI, diabetes status, and baseline LSM, only LSM-defined progression (HR, 1.93; P < .01) and age (HR, 1.03; P < .01) were significant predictors.
Dr. Gawrieh noted that while age was a statistically significant factor, it was only weakly associated.
“These data suggest that development of cirrhosis LSM criteria is a promising surrogate for clinical outcomes in patients with NAFLD,” Dr. Gawrieh concluded.
Progression definition questioned
Following the presentation, Nezam Afdhal, MD, chief of the division of gastroenterology, hepatology, and nutrition at Beth Israel Deaconess Hospital in Boston, questioned how 25% of patients who had biopsy-proven cirrhosis could progress to LSM-defined cirrhosis.
Dr. Gawrieh said that, according to inclusion criteria, the patients could not have LSM-defined cirrhosis with the sensitivity cutoff of 12.1 kPa, and that of the 10 patients with baseline cirrhosis in the cohort, all had LSM of less than 12.1 kPa. However, he admitted that because those 10 patients were technically not progressors to cirrhosis, they should have been removed from the analysis for clinical outcomes.
Mark Hartman, MD, a clinical researcher at Eli Lilly and Company in Indianapolis, said the study is valuable but noted that those patients who progressed tended to have higher LSM at baseline as well as a higher [fibrosis-4 score].
Dr. Gawrieh added that the investigators are exploring variables that might explain progression to cirrhosis among patients without high baseline liver stiffness, such as alcohol use or drug-induced liver injury.
The study was supported by the National Institutes of Health and the NASH Clinical Research Network institutions. Dr. Gawrieh disclosed research grants from NIH, Zydus, Viking, and Sonic Incytes, and consulting for TransMedics and Pfizer. Dr. Afdhal and Dr. Hartman reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new findings presented at the annual meeting of the American Association for the Study of Liver Diseases.
Although previous retrospective studies have suggested that increased liver stiffness, as measured by VCTE (FibroScan), is associated with increases in liver-related events, there is a paucity of prospective data, reported Samer Gawrieh, MD, from Indiana University, Carmel and Indianapolis. VCTE is a noninvasive measure of cirrhosis progression.
In their prospective cohort study of patients representing the entire spectrum of NAFLD, the progression to LSM-defined cirrhosis was independently associated with the risk for a composite clinical outcome of death, decompensation, hepatocellular carcinoma, or a Model for End Stage Liver Disease (MELD) score of greater than 15, he said.
Their findings show that “progression to LSM-defined cirrhosis by VCTE is strongly associated with poor clinical outcomes,” Dr. Gawrieh said.
Study findings
Investigators looked at prospective data on 894 patients with biopsy-proven NAFLD in the Nonalcoholic Steatohepatitis (NASH) Clinical Research Network database. The sample included patients with a minimum of two LSM readings taken from 2014 through 2022.
They defined LSM-defined cirrhosis as reaching LSM of greater than 14.9 kPa (90% specificity cutoff) among patients without cirrhosis on the baseline VCTE (a 90% sensitivity cutoff of LSM less than 12.1 kPa).
They also performed a histology-based subanalysis, including data only from those patients who had LSM within 6 months of a liver biopsy.
The median patient age was 60 years, 37% were male, and 80.9% were White and 11.5% were Hispanic/Latino. The median body mass index (BMI) was 32.
Out of all the patients, 119 (13.3%) had progression to LSM-defined cirrhosis.
At a median follow-up of 3.69 years for the 775 patients without LSM progression, 79 (10.2%) had one or more of the events in the composite clinical outcome.
In contrast, after a median 5.48 years of follow-up, 31 of the 119 patients with progression (26.1%) had one or more of the composite events (P < .0001).
The median rates of progression to LSM-defined cirrhosis in the overall cohort were 2% at 1 year, 11% at 3 years, and 16% at 5 years.
Researchers found a correlation between progression to LSM-defined cirrhosis and baseline histological fibrosis stage on biopsy, with a rate of 7% among those with no baseline fibrosis, 9% each for patients with stage I A-C or stage II fibrosis, 24% of those with baseline bridging fibrosis, and 25% of those with baseline cirrhosis.
A comparison of the time to a composite clinical outcome event between patients with progression to LSM-defined cirrhosis and those without progression showed that LSM-defined progression was associated with near doubling in risk, with a hazard ratio of 1.84 (P = .0039).
In a multivariate Cox regression analysis controlling for age, sex, race, BMI, diabetes status, and baseline LSM, only LSM-defined progression (HR, 1.93; P < .01) and age (HR, 1.03; P < .01) were significant predictors.
Dr. Gawrieh noted that while age was a statistically significant factor, it was only weakly associated.
“These data suggest that development of cirrhosis LSM criteria is a promising surrogate for clinical outcomes in patients with NAFLD,” Dr. Gawrieh concluded.
Progression definition questioned
Following the presentation, Nezam Afdhal, MD, chief of the division of gastroenterology, hepatology, and nutrition at Beth Israel Deaconess Hospital in Boston, questioned how 25% of patients who had biopsy-proven cirrhosis could progress to LSM-defined cirrhosis.
Dr. Gawrieh said that, according to inclusion criteria, the patients could not have LSM-defined cirrhosis with the sensitivity cutoff of 12.1 kPa, and that of the 10 patients with baseline cirrhosis in the cohort, all had LSM of less than 12.1 kPa. However, he admitted that because those 10 patients were technically not progressors to cirrhosis, they should have been removed from the analysis for clinical outcomes.
Mark Hartman, MD, a clinical researcher at Eli Lilly and Company in Indianapolis, said the study is valuable but noted that those patients who progressed tended to have higher LSM at baseline as well as a higher [fibrosis-4 score].
Dr. Gawrieh added that the investigators are exploring variables that might explain progression to cirrhosis among patients without high baseline liver stiffness, such as alcohol use or drug-induced liver injury.
The study was supported by the National Institutes of Health and the NASH Clinical Research Network institutions. Dr. Gawrieh disclosed research grants from NIH, Zydus, Viking, and Sonic Incytes, and consulting for TransMedics and Pfizer. Dr. Afdhal and Dr. Hartman reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LIVER MEETING
IRONMAN galvanizes case for IV iron repletion in heart failure
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.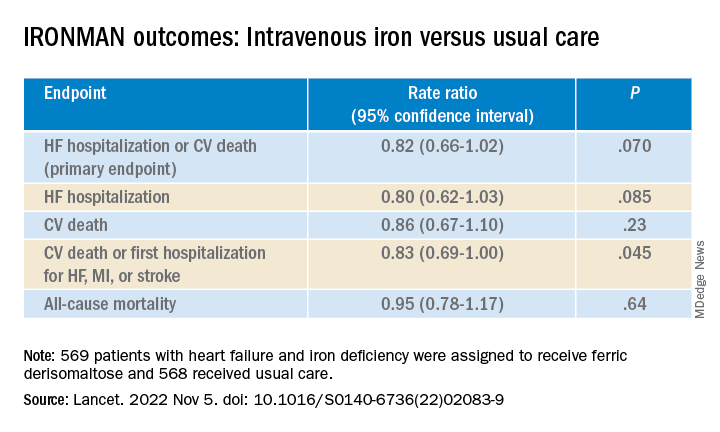
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
AT AHA 2022
Laser pioneer reflects on the future of robots in dermatology
In the opinion of R. Rox Anderson, MD, it’s only a matter of time before true robots make further inroads in dermatology.
“We humans just can’t do everything perfectly,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “We have limited speed and special accuracy and are not good at repetitive tasks. We can’t see in the UV or infrared, and we’re qualitative, not quantitative. ... We’re good at high-level visual assessment.”

During a presentation at the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center, he distinguished between robotics and true robots. A prime example of robotics in medicine is the Da Vinci Surgical System in which a human user “is controlling every movement of this device with capabilities that humans don’t have, such as fine movement and high magnification of imaging,” said Dr. Anderson, who conceived and developed many of the nonscarring laser treatments now widely used in dermatology. “In the military, we have drone aircraft. The pilot is perhaps thousands of miles away; it’s still run by a human being in every way.”
By contrast, true robots are devices in which a human being programs the rules for action but the action itself is not exactly predictable. Artificial intelligence enables robots to perform certain tasks. “If you look at an Amazon warehouse, there’s barely anyone there; robots are packing and unpacking the shelves,” Dr. Anderson said.
Currently, he said, one true robot exists in dermatology: the Food and Drug Administration–cleared ARTAS Robotic Hair Restoration System, which precisely dissects follicular units from the donor area and eliminates the potential for human error. The device “extracts single follicular units from the occipital scalp and makes them available to the surgeon to do an artistic human job of implanting them in the frontal scalp,” Dr. Anderson said.
He predicts that a Mohs surgery robot with image-guided laser ablation would “launch a sea change in the whole field of surgical oncology, and I believe we are in a good position to do it. Everything for this is now sitting on the shelf and it’s unbelievable to me that a company hasn’t accomplished it yet.”
He would also like to see a true laser robot for surgery of tumors that would enable clinicians to download an app for their existing laser instead of having to buy a new device. Currently, “it takes about a half second to make a good optical coherence tomography image of basal cell carcinoma,” he said. “That image could be used for real-time robotic human control of, say, a laser to extirpate the tumor.”
Dr. Anderson’s “wish list” of applications for treatment with a robotic fractional laser includes those that target the sweat glands, sebaceous glands, nerves, inflammatory cells, white hair, blood vessels, lymphatics, hair, tumors, nevi, cysts, and surface contour. “It might be possible to have one software-programmable laser robot for many different applications in dermatology,” he added.
Dr. Anderson reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
In the opinion of R. Rox Anderson, MD, it’s only a matter of time before true robots make further inroads in dermatology.
“We humans just can’t do everything perfectly,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “We have limited speed and special accuracy and are not good at repetitive tasks. We can’t see in the UV or infrared, and we’re qualitative, not quantitative. ... We’re good at high-level visual assessment.”
During a presentation at the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center, he distinguished between robotics and true robots. A prime example of robotics in medicine is the Da Vinci Surgical System in which a human user “is controlling every movement of this device with capabilities that humans don’t have, such as fine movement and high magnification of imaging,” said Dr. Anderson, who conceived and developed many of the nonscarring laser treatments now widely used in dermatology. “In the military, we have drone aircraft. The pilot is perhaps thousands of miles away; it’s still run by a human being in every way.”
By contrast, true robots are devices in which a human being programs the rules for action but the action itself is not exactly predictable. Artificial intelligence enables robots to perform certain tasks. “If you look at an Amazon warehouse, there’s barely anyone there; robots are packing and unpacking the shelves,” Dr. Anderson said.
Currently, he said, one true robot exists in dermatology: the Food and Drug Administration–cleared ARTAS Robotic Hair Restoration System, which precisely dissects follicular units from the donor area and eliminates the potential for human error. The device “extracts single follicular units from the occipital scalp and makes them available to the surgeon to do an artistic human job of implanting them in the frontal scalp,” Dr. Anderson said.
He predicts that a Mohs surgery robot with image-guided laser ablation would “launch a sea change in the whole field of surgical oncology, and I believe we are in a good position to do it. Everything for this is now sitting on the shelf and it’s unbelievable to me that a company hasn’t accomplished it yet.”
He would also like to see a true laser robot for surgery of tumors that would enable clinicians to download an app for their existing laser instead of having to buy a new device. Currently, “it takes about a half second to make a good optical coherence tomography image of basal cell carcinoma,” he said. “That image could be used for real-time robotic human control of, say, a laser to extirpate the tumor.”
Dr. Anderson’s “wish list” of applications for treatment with a robotic fractional laser includes those that target the sweat glands, sebaceous glands, nerves, inflammatory cells, white hair, blood vessels, lymphatics, hair, tumors, nevi, cysts, and surface contour. “It might be possible to have one software-programmable laser robot for many different applications in dermatology,” he added.
Dr. Anderson reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
In the opinion of R. Rox Anderson, MD, it’s only a matter of time before true robots make further inroads in dermatology.
“We humans just can’t do everything perfectly,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “We have limited speed and special accuracy and are not good at repetitive tasks. We can’t see in the UV or infrared, and we’re qualitative, not quantitative. ... We’re good at high-level visual assessment.”
During a presentation at the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center, he distinguished between robotics and true robots. A prime example of robotics in medicine is the Da Vinci Surgical System in which a human user “is controlling every movement of this device with capabilities that humans don’t have, such as fine movement and high magnification of imaging,” said Dr. Anderson, who conceived and developed many of the nonscarring laser treatments now widely used in dermatology. “In the military, we have drone aircraft. The pilot is perhaps thousands of miles away; it’s still run by a human being in every way.”
By contrast, true robots are devices in which a human being programs the rules for action but the action itself is not exactly predictable. Artificial intelligence enables robots to perform certain tasks. “If you look at an Amazon warehouse, there’s barely anyone there; robots are packing and unpacking the shelves,” Dr. Anderson said.
Currently, he said, one true robot exists in dermatology: the Food and Drug Administration–cleared ARTAS Robotic Hair Restoration System, which precisely dissects follicular units from the donor area and eliminates the potential for human error. The device “extracts single follicular units from the occipital scalp and makes them available to the surgeon to do an artistic human job of implanting them in the frontal scalp,” Dr. Anderson said.
He predicts that a Mohs surgery robot with image-guided laser ablation would “launch a sea change in the whole field of surgical oncology, and I believe we are in a good position to do it. Everything for this is now sitting on the shelf and it’s unbelievable to me that a company hasn’t accomplished it yet.”
He would also like to see a true laser robot for surgery of tumors that would enable clinicians to download an app for their existing laser instead of having to buy a new device. Currently, “it takes about a half second to make a good optical coherence tomography image of basal cell carcinoma,” he said. “That image could be used for real-time robotic human control of, say, a laser to extirpate the tumor.”
Dr. Anderson’s “wish list” of applications for treatment with a robotic fractional laser includes those that target the sweat glands, sebaceous glands, nerves, inflammatory cells, white hair, blood vessels, lymphatics, hair, tumors, nevi, cysts, and surface contour. “It might be possible to have one software-programmable laser robot for many different applications in dermatology,” he added.
Dr. Anderson reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
Intensive gout treatment meets urate goal, lowers tophi burden
PHILADELPHIA – Patients with gout who underwent an intensive treat-to-target regimen of monthly up-titration of urate-lowering therapy (ULT) to reach a target serum urate level were significantly more likely to reach that goal at 1 year than were patients who received conventional gout management in a randomized, controlled trial.
These results came from the TICOG (Tight Control of Gout) trial, one of a handful of recent trials to test a treat-to-target strategy with ULT in the management of gout. Beyond the primary outcome of reaching target serum urate level of < 5 mg/dL (< 300 micromol/L), the results also showed that the tight-control strategy significantly lowered urate to a greater extent than conventional management, reduced tophus size in the first metatarsophalangeal (MTP) joint, and improved gray scale synovitis on ultrasound significantly more than with conventional management, Sarah Black, MBBS, a rheumatology trainee at Musgrave Park Hospital, Belfast, Northern Ireland, reported at the American College of Rheumatology annual meeting.
“Based on these outcomes, we question whether gout is best managed in primary or secondary care. We think there is an argument for establishing specialist gout clinics with more time to focus on patient education to help improve outcomes. These clinics could be led by allied health care professionals, such as specialist nurses and pharmacists,” Dr. Black said at the meeting.
Gout management guidelines issued by the British Society for Rheumatology in 2017 call for a target serum urate level of < 5 mg/dL, whereas the ACR’s 2020 guideline for the management of gout endorses a treat-to-target management strategy that aims for a serum urate level of < 6 mg/dL.
The single-center, nonblinded trial recruited 110 patients aged 18-85 years over a 3-year period to take ULT with allopurinol as first-line therapy starting at 100 mg/day. Everyone received the same advice regarding ULT up-titration, lifestyle changes, and gout education at baseline. The second-line agent for ULT was febuxostat (Uloric) 80 mg daily, with uricosuric drugs as third-line agents. All patients received colchicine or NSAID prophylaxis for gout flares for the first 6 months, depending on their comorbidities.
The trial excluded patients who had been treated with ULT within the past 6 months or had experienced prior hypersensitivity to ULT, severe renal impairment (creatinine clearance < 30 mL/min as measured by estimated glomerular filtration rate), significant liver impairment, or any other significant medical disease affecting life expectancy shorter than 1 year.
Conventional management consisted of urate level review at 0, 6, and 12 months with up-titration at each visit and primary care management of ULT between reviews until the target serum urate level was reached. In the tight-control group, monthly up-titrations occurred at the Musgrave Park Hospital at visits with the study team that were led by a rheumatologist and a specialist pharmacist.
A total of 48 patients in the conventional arm and 47 in the tight-control arm completed the trial. At baseline, monosodium urate crystals were detected in joint aspirates in 56% of patients receiving tight control and in 58.5% of those receiving conventional management. The mean serum urate level was 490 micromol/L (8.24 mg/dL) for tight-control patients and 470 micromol/L (7.9 mg/dL) for conventionally managed patients.
By 1 year, 89.4% of patients in the tight-control group had achieved the target urate level, compared with 39.6% in the conventional-management group (P < .001). At 6 months, serum urate had declined by 37.6% with tight control vs. 18% with conventional management. By the end of the trial, the median allopurinol dose was 400 mg with tight control (range, 200-900 mg) and 200 mg with conventional management (range, 0-400 mg). A total of 89% of patients were taking allopurinol at the end of the trial.
As expected, tight control led to more flares per month on average (0.35 vs. 0.13) in the 79 patients for whom complete data on flare frequency were available.
On blinded ultrasound evaluations, the median diameter of the first MTP tophus declined significantly more with tight control than with conventional management (–4.65 mm vs. –0.30 mm; P = .003). Gray scale synovitis in the knee improved in 63% of patients undergoing tight control, compared with 14% of conventionally managed patients (P = .043). The researchers observed no difference in resolution of the double-contour sign or in the number of erosions between the groups, although the 1-year time frame may not have been long enough to see resolution and improvement, Dr. Black said.
Dr. Black said that a follow-up study is planned with the same patient cohort at 3 years.
When asked about the feasibility of monthly ULT titration visits for gout management, audience member Tuhina Neogi, MD, professor of epidemiology at Boston University and chief of rheumatology at Boston Medical Center, told this news organization, “We don’t have a lot of data to guide us in that regard, and I also think it depends on what the increment of the dose titration is, but we generally do recognize that therapeutic inertia is bad – keeping someone on a dose for a long time. For me, I don’t think monthly is unreasonable if you have good prophylaxis [against acute flares].”
Dr. Neogi also noted that such monthly assessments don’t have to take place at a hospital. “I think there are many different practice models in which it could be implemented [that are not physician-driven].”
The study had no outside funding. Dr. Black has disclosed no relevant financial relationships. Dr. Neogi has received consulting fees from a variety of pharmaceutical companies, including Alnylam, Regeneron, Eli Lilly, EMD Serono, Novartis, Pfizer, and GlaxoSmithKline.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – Patients with gout who underwent an intensive treat-to-target regimen of monthly up-titration of urate-lowering therapy (ULT) to reach a target serum urate level were significantly more likely to reach that goal at 1 year than were patients who received conventional gout management in a randomized, controlled trial.
These results came from the TICOG (Tight Control of Gout) trial, one of a handful of recent trials to test a treat-to-target strategy with ULT in the management of gout. Beyond the primary outcome of reaching target serum urate level of < 5 mg/dL (< 300 micromol/L), the results also showed that the tight-control strategy significantly lowered urate to a greater extent than conventional management, reduced tophus size in the first metatarsophalangeal (MTP) joint, and improved gray scale synovitis on ultrasound significantly more than with conventional management, Sarah Black, MBBS, a rheumatology trainee at Musgrave Park Hospital, Belfast, Northern Ireland, reported at the American College of Rheumatology annual meeting.
“Based on these outcomes, we question whether gout is best managed in primary or secondary care. We think there is an argument for establishing specialist gout clinics with more time to focus on patient education to help improve outcomes. These clinics could be led by allied health care professionals, such as specialist nurses and pharmacists,” Dr. Black said at the meeting.
Gout management guidelines issued by the British Society for Rheumatology in 2017 call for a target serum urate level of < 5 mg/dL, whereas the ACR’s 2020 guideline for the management of gout endorses a treat-to-target management strategy that aims for a serum urate level of < 6 mg/dL.
The single-center, nonblinded trial recruited 110 patients aged 18-85 years over a 3-year period to take ULT with allopurinol as first-line therapy starting at 100 mg/day. Everyone received the same advice regarding ULT up-titration, lifestyle changes, and gout education at baseline. The second-line agent for ULT was febuxostat (Uloric) 80 mg daily, with uricosuric drugs as third-line agents. All patients received colchicine or NSAID prophylaxis for gout flares for the first 6 months, depending on their comorbidities.
The trial excluded patients who had been treated with ULT within the past 6 months or had experienced prior hypersensitivity to ULT, severe renal impairment (creatinine clearance < 30 mL/min as measured by estimated glomerular filtration rate), significant liver impairment, or any other significant medical disease affecting life expectancy shorter than 1 year.
Conventional management consisted of urate level review at 0, 6, and 12 months with up-titration at each visit and primary care management of ULT between reviews until the target serum urate level was reached. In the tight-control group, monthly up-titrations occurred at the Musgrave Park Hospital at visits with the study team that were led by a rheumatologist and a specialist pharmacist.
A total of 48 patients in the conventional arm and 47 in the tight-control arm completed the trial. At baseline, monosodium urate crystals were detected in joint aspirates in 56% of patients receiving tight control and in 58.5% of those receiving conventional management. The mean serum urate level was 490 micromol/L (8.24 mg/dL) for tight-control patients and 470 micromol/L (7.9 mg/dL) for conventionally managed patients.
By 1 year, 89.4% of patients in the tight-control group had achieved the target urate level, compared with 39.6% in the conventional-management group (P < .001). At 6 months, serum urate had declined by 37.6% with tight control vs. 18% with conventional management. By the end of the trial, the median allopurinol dose was 400 mg with tight control (range, 200-900 mg) and 200 mg with conventional management (range, 0-400 mg). A total of 89% of patients were taking allopurinol at the end of the trial.
As expected, tight control led to more flares per month on average (0.35 vs. 0.13) in the 79 patients for whom complete data on flare frequency were available.
On blinded ultrasound evaluations, the median diameter of the first MTP tophus declined significantly more with tight control than with conventional management (–4.65 mm vs. –0.30 mm; P = .003). Gray scale synovitis in the knee improved in 63% of patients undergoing tight control, compared with 14% of conventionally managed patients (P = .043). The researchers observed no difference in resolution of the double-contour sign or in the number of erosions between the groups, although the 1-year time frame may not have been long enough to see resolution and improvement, Dr. Black said.
Dr. Black said that a follow-up study is planned with the same patient cohort at 3 years.
When asked about the feasibility of monthly ULT titration visits for gout management, audience member Tuhina Neogi, MD, professor of epidemiology at Boston University and chief of rheumatology at Boston Medical Center, told this news organization, “We don’t have a lot of data to guide us in that regard, and I also think it depends on what the increment of the dose titration is, but we generally do recognize that therapeutic inertia is bad – keeping someone on a dose for a long time. For me, I don’t think monthly is unreasonable if you have good prophylaxis [against acute flares].”
Dr. Neogi also noted that such monthly assessments don’t have to take place at a hospital. “I think there are many different practice models in which it could be implemented [that are not physician-driven].”
The study had no outside funding. Dr. Black has disclosed no relevant financial relationships. Dr. Neogi has received consulting fees from a variety of pharmaceutical companies, including Alnylam, Regeneron, Eli Lilly, EMD Serono, Novartis, Pfizer, and GlaxoSmithKline.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – Patients with gout who underwent an intensive treat-to-target regimen of monthly up-titration of urate-lowering therapy (ULT) to reach a target serum urate level were significantly more likely to reach that goal at 1 year than were patients who received conventional gout management in a randomized, controlled trial.
These results came from the TICOG (Tight Control of Gout) trial, one of a handful of recent trials to test a treat-to-target strategy with ULT in the management of gout. Beyond the primary outcome of reaching target serum urate level of < 5 mg/dL (< 300 micromol/L), the results also showed that the tight-control strategy significantly lowered urate to a greater extent than conventional management, reduced tophus size in the first metatarsophalangeal (MTP) joint, and improved gray scale synovitis on ultrasound significantly more than with conventional management, Sarah Black, MBBS, a rheumatology trainee at Musgrave Park Hospital, Belfast, Northern Ireland, reported at the American College of Rheumatology annual meeting.
“Based on these outcomes, we question whether gout is best managed in primary or secondary care. We think there is an argument for establishing specialist gout clinics with more time to focus on patient education to help improve outcomes. These clinics could be led by allied health care professionals, such as specialist nurses and pharmacists,” Dr. Black said at the meeting.
Gout management guidelines issued by the British Society for Rheumatology in 2017 call for a target serum urate level of < 5 mg/dL, whereas the ACR’s 2020 guideline for the management of gout endorses a treat-to-target management strategy that aims for a serum urate level of < 6 mg/dL.
The single-center, nonblinded trial recruited 110 patients aged 18-85 years over a 3-year period to take ULT with allopurinol as first-line therapy starting at 100 mg/day. Everyone received the same advice regarding ULT up-titration, lifestyle changes, and gout education at baseline. The second-line agent for ULT was febuxostat (Uloric) 80 mg daily, with uricosuric drugs as third-line agents. All patients received colchicine or NSAID prophylaxis for gout flares for the first 6 months, depending on their comorbidities.
The trial excluded patients who had been treated with ULT within the past 6 months or had experienced prior hypersensitivity to ULT, severe renal impairment (creatinine clearance < 30 mL/min as measured by estimated glomerular filtration rate), significant liver impairment, or any other significant medical disease affecting life expectancy shorter than 1 year.
Conventional management consisted of urate level review at 0, 6, and 12 months with up-titration at each visit and primary care management of ULT between reviews until the target serum urate level was reached. In the tight-control group, monthly up-titrations occurred at the Musgrave Park Hospital at visits with the study team that were led by a rheumatologist and a specialist pharmacist.
A total of 48 patients in the conventional arm and 47 in the tight-control arm completed the trial. At baseline, monosodium urate crystals were detected in joint aspirates in 56% of patients receiving tight control and in 58.5% of those receiving conventional management. The mean serum urate level was 490 micromol/L (8.24 mg/dL) for tight-control patients and 470 micromol/L (7.9 mg/dL) for conventionally managed patients.
By 1 year, 89.4% of patients in the tight-control group had achieved the target urate level, compared with 39.6% in the conventional-management group (P < .001). At 6 months, serum urate had declined by 37.6% with tight control vs. 18% with conventional management. By the end of the trial, the median allopurinol dose was 400 mg with tight control (range, 200-900 mg) and 200 mg with conventional management (range, 0-400 mg). A total of 89% of patients were taking allopurinol at the end of the trial.
As expected, tight control led to more flares per month on average (0.35 vs. 0.13) in the 79 patients for whom complete data on flare frequency were available.
On blinded ultrasound evaluations, the median diameter of the first MTP tophus declined significantly more with tight control than with conventional management (–4.65 mm vs. –0.30 mm; P = .003). Gray scale synovitis in the knee improved in 63% of patients undergoing tight control, compared with 14% of conventionally managed patients (P = .043). The researchers observed no difference in resolution of the double-contour sign or in the number of erosions between the groups, although the 1-year time frame may not have been long enough to see resolution and improvement, Dr. Black said.
Dr. Black said that a follow-up study is planned with the same patient cohort at 3 years.
When asked about the feasibility of monthly ULT titration visits for gout management, audience member Tuhina Neogi, MD, professor of epidemiology at Boston University and chief of rheumatology at Boston Medical Center, told this news organization, “We don’t have a lot of data to guide us in that regard, and I also think it depends on what the increment of the dose titration is, but we generally do recognize that therapeutic inertia is bad – keeping someone on a dose for a long time. For me, I don’t think monthly is unreasonable if you have good prophylaxis [against acute flares].”
Dr. Neogi also noted that such monthly assessments don’t have to take place at a hospital. “I think there are many different practice models in which it could be implemented [that are not physician-driven].”
The study had no outside funding. Dr. Black has disclosed no relevant financial relationships. Dr. Neogi has received consulting fees from a variety of pharmaceutical companies, including Alnylam, Regeneron, Eli Lilly, EMD Serono, Novartis, Pfizer, and GlaxoSmithKline.
A version of this article first appeared on Medscape.com.
AT ACR 2022
ACR and EULAR roll out updated antiphospholipid syndrome criteria
Draft document widens scope of signs, symptoms
PHILADELPHIA – A draft update of criteria for classifying antiphospholipid syndrome (APS) incorporates a much broader spectrum of disease signs and symptoms, such as kidney disease and more variables for pregnancy, and meets a higher level of specificity than the existing Sapporo criteria, although at the expense of lower sensitivity.

Three members of the core planning group that wrote the update, jointly commissioned by the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR), reviewed the proposed criteria at the annual meeting of the ACR.
If ACR and EULAR adopt the new criteria, it would be an update to the Sapporo classification criteria for APS, which was last updated in 2006. The pending criteria consist of the following eight domains encompassing clinical findings and laboratory test results:
- Macrovascular – venous thromboembolism (VTE) with and without high VTE risk profile.
- Macrovascular – arterial thrombosis with and without a high cardiovascular disease risk profile.
- Microvascular – additional categories for kidney disease, pulmonary embolism, and other conditions for both suspected and established APS.
- Obstetric – expanded definitions to account for the absence or presence of preeclampsia or premature birth with or without fetal death.
- Cardiac valve – accounts for thickening and vegetation.
- Hematologic – includes thrombocytopenia (defined as the lowest platelet count, 20-130 x 109/L).
- Antiphospholipid (aPL) test – coagulation-based functional assay, assigning greater weight to persistent over one-time positive test results.
- aPL test by solid-phase assay – includes anticardiolipin enzyme-linked immunosorbent assay (aCL ELISA), and aCL/anti-beta 2 glycoprotein-I (aCL/anti-beta 2 GPI) tests, with greater weight assigned for moderate-to-high positive results depending on isotype, whether immunoglobulin G or M.
Changes from Sapporo criteria
The existing Sapporo criteria include two clinical categories, vascular thrombosis and pregnancy morbidity; and three laboratory categories, positive lupus anticoagulant, medium or high antibody titers, and high aCL/anti-beta 2 GPI measured by ELISA. All of these are included in the draft criteria under two domains.
“These novel clinical features will help us better stratify patients according to the risk factor profile,” Stéphane Zuily, MD, PhD, a vascular specialist and European co-principal investigator of the planning group, said in explaining the proposed updated domains.
“We well-defined the microvascular domain items further than the aPL nephropathy; we redefined pregnancy morbidities; we added cardiac valve disease and thrombocytopenia; and, through gathering novel laboratory features, we were able to quantify single, double, and triple aPL positivity based on different domains and weights,” said Dr. Zuily, professor of medicine at Lorraine University in Nancy, France.
Also noteworthy is the separation of aCL/anti-beta 2 GPI testing by IgG and IgM isotypes. “And we were also able to identify different thresholds in terms of aPL positivity,” Dr. Zuily said.
Rationale and methodology
Planning group member Medha Barbhaiya, MD, MPH, an attending physician at the Hospital for Special Surgery and assistant professor at Weill Cornell Medicine in New York, explained the rationale for the update. “The existing criteria were drafted in 1999 and updated in 2006 and require one clinical criterion, either vascular thrombosis event or pregnancy morbidity along with antiphospholipid antibodies,” she said.
Those 16-year-old criteria also ignored heterogeneous manifestations such as heart valve disease or thrombocytopenia, failed to stratify thrombotic events as risk factors, and used an outdated definition of pregnancy morbidity related to APS, she said.
“These findings helped to support our rationale for new criteria development, along with the fact that over the last 1 to 2 decades there have been important advancements in the methodology of classification criteria development,” she said. ACR and EULAR both endorsed the new methodology for developing the classification criteria, Dr. Barbhaiya added.
That methodology involved multidisciplinary international panels of experts and data-driven efforts, with the goal of identifying patients with a high likelihood of APS for research purposes. The planning group collected 568 cases from 29 international centers, dividing them into two validation cohorts of 284 cases each.
How classification criteria work
Doruk Erkan, MD, MPH, coprincipal investigator representing the United States on the planning group, an attending physician at the Hospital for Special Surgery in New York, and a professor at Weill Cornell Medicine in New York, explained how the classification system works. “If you have a patient that you are considering for APS classification, the story starts with entry criteria, which are one documented clinical criterion plus a positive aPL [antiphospholipid] test within 3 years of observation of the clinical criteria,” he said.
Once the entry criteria for APS are met, there are the clinical and laboratory domains. Dr. Erkan explained that weighted point values are assigned to individual categories under each domain. For example, in the macrovascular VTE domain, VTE with a high VTE risk profile is worth 1 point, but VTE without a high VTE risk profile is worth 3 points.
“APS classification will be achieved with at least three points from clinical domains and at least three points from the laboratory domains,” he said.
The planning group conducted a sensitivity and specificity analysis of the draft classification system using the two validation cohorts. “Our goal was very high specificity to improve the homogeneity in APS research, and we achieved this in both cohorts with 99% specificity,” Dr. Erkan said. That compares to sensitivity of 91% and 86% of the Sapporo criteria in the validation cohorts.
“Our sensitivity was 83% and 84% capturing a broad spectrum of patients assessed with APS suspicion,” he added, vs. 100% and 99% with the Sapporo criteria.
These criteria are not absolute and are structured to permit future modifications, Dr. Erkan said. “When this work is completed, another chapter will start,” he said. “If a case doesn’t meet APS classification criteria, the case may still be uncertain or equivocal rather than not APS. Uncertain or controversial cases should be studied separately to guide future updates of the new criteria.”
Comment: Why these updates are needed
April Jorge, MD, a rheumatologist at Massachusetts General Hospital in Boston and moderator of the session on the draft APS criteria, explained why these updated criteria are needed. “It’s very important to get the updated criteria because, as the speakers mentioned, the prior Sapporo criteria were limited to just large-vessel venous thrombosis or pregnancy complications, and so that makes it difficult to study the disease in other manifestations, such as kidney manifestations, if they’re not part of the criteria.”

She added, “I think there was a need for clear classification criteria that was thought to be highly specific for the disease so that future studies can be done in this population.”
Dr. Jorge called the 99% specificity described in the analysis “impressive” and “promising.”
Dr. Barbhaiya and Dr. Zuily have no relevant disclosures. Dr. Erkan disclosed relationships with Aurinia, Eli Lilly, Exagen, and GlaxoSmithKline. Dr. Jorge has no relevant disclosures.
Draft document widens scope of signs, symptoms
Draft document widens scope of signs, symptoms
PHILADELPHIA – A draft update of criteria for classifying antiphospholipid syndrome (APS) incorporates a much broader spectrum of disease signs and symptoms, such as kidney disease and more variables for pregnancy, and meets a higher level of specificity than the existing Sapporo criteria, although at the expense of lower sensitivity.
Three members of the core planning group that wrote the update, jointly commissioned by the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR), reviewed the proposed criteria at the annual meeting of the ACR.
If ACR and EULAR adopt the new criteria, it would be an update to the Sapporo classification criteria for APS, which was last updated in 2006. The pending criteria consist of the following eight domains encompassing clinical findings and laboratory test results:
- Macrovascular – venous thromboembolism (VTE) with and without high VTE risk profile.
- Macrovascular – arterial thrombosis with and without a high cardiovascular disease risk profile.
- Microvascular – additional categories for kidney disease, pulmonary embolism, and other conditions for both suspected and established APS.
- Obstetric – expanded definitions to account for the absence or presence of preeclampsia or premature birth with or without fetal death.
- Cardiac valve – accounts for thickening and vegetation.
- Hematologic – includes thrombocytopenia (defined as the lowest platelet count, 20-130 x 109/L).
- Antiphospholipid (aPL) test – coagulation-based functional assay, assigning greater weight to persistent over one-time positive test results.
- aPL test by solid-phase assay – includes anticardiolipin enzyme-linked immunosorbent assay (aCL ELISA), and aCL/anti-beta 2 glycoprotein-I (aCL/anti-beta 2 GPI) tests, with greater weight assigned for moderate-to-high positive results depending on isotype, whether immunoglobulin G or M.
Changes from Sapporo criteria
The existing Sapporo criteria include two clinical categories, vascular thrombosis and pregnancy morbidity; and three laboratory categories, positive lupus anticoagulant, medium or high antibody titers, and high aCL/anti-beta 2 GPI measured by ELISA. All of these are included in the draft criteria under two domains.
“These novel clinical features will help us better stratify patients according to the risk factor profile,” Stéphane Zuily, MD, PhD, a vascular specialist and European co-principal investigator of the planning group, said in explaining the proposed updated domains.
“We well-defined the microvascular domain items further than the aPL nephropathy; we redefined pregnancy morbidities; we added cardiac valve disease and thrombocytopenia; and, through gathering novel laboratory features, we were able to quantify single, double, and triple aPL positivity based on different domains and weights,” said Dr. Zuily, professor of medicine at Lorraine University in Nancy, France.
Also noteworthy is the separation of aCL/anti-beta 2 GPI testing by IgG and IgM isotypes. “And we were also able to identify different thresholds in terms of aPL positivity,” Dr. Zuily said.
Rationale and methodology
Planning group member Medha Barbhaiya, MD, MPH, an attending physician at the Hospital for Special Surgery and assistant professor at Weill Cornell Medicine in New York, explained the rationale for the update. “The existing criteria were drafted in 1999 and updated in 2006 and require one clinical criterion, either vascular thrombosis event or pregnancy morbidity along with antiphospholipid antibodies,” she said.
Those 16-year-old criteria also ignored heterogeneous manifestations such as heart valve disease or thrombocytopenia, failed to stratify thrombotic events as risk factors, and used an outdated definition of pregnancy morbidity related to APS, she said.
“These findings helped to support our rationale for new criteria development, along with the fact that over the last 1 to 2 decades there have been important advancements in the methodology of classification criteria development,” she said. ACR and EULAR both endorsed the new methodology for developing the classification criteria, Dr. Barbhaiya added.
That methodology involved multidisciplinary international panels of experts and data-driven efforts, with the goal of identifying patients with a high likelihood of APS for research purposes. The planning group collected 568 cases from 29 international centers, dividing them into two validation cohorts of 284 cases each.
How classification criteria work
Doruk Erkan, MD, MPH, coprincipal investigator representing the United States on the planning group, an attending physician at the Hospital for Special Surgery in New York, and a professor at Weill Cornell Medicine in New York, explained how the classification system works. “If you have a patient that you are considering for APS classification, the story starts with entry criteria, which are one documented clinical criterion plus a positive aPL [antiphospholipid] test within 3 years of observation of the clinical criteria,” he said.
Once the entry criteria for APS are met, there are the clinical and laboratory domains. Dr. Erkan explained that weighted point values are assigned to individual categories under each domain. For example, in the macrovascular VTE domain, VTE with a high VTE risk profile is worth 1 point, but VTE without a high VTE risk profile is worth 3 points.
“APS classification will be achieved with at least three points from clinical domains and at least three points from the laboratory domains,” he said.
The planning group conducted a sensitivity and specificity analysis of the draft classification system using the two validation cohorts. “Our goal was very high specificity to improve the homogeneity in APS research, and we achieved this in both cohorts with 99% specificity,” Dr. Erkan said. That compares to sensitivity of 91% and 86% of the Sapporo criteria in the validation cohorts.
“Our sensitivity was 83% and 84% capturing a broad spectrum of patients assessed with APS suspicion,” he added, vs. 100% and 99% with the Sapporo criteria.
These criteria are not absolute and are structured to permit future modifications, Dr. Erkan said. “When this work is completed, another chapter will start,” he said. “If a case doesn’t meet APS classification criteria, the case may still be uncertain or equivocal rather than not APS. Uncertain or controversial cases should be studied separately to guide future updates of the new criteria.”
Comment: Why these updates are needed
April Jorge, MD, a rheumatologist at Massachusetts General Hospital in Boston and moderator of the session on the draft APS criteria, explained why these updated criteria are needed. “It’s very important to get the updated criteria because, as the speakers mentioned, the prior Sapporo criteria were limited to just large-vessel venous thrombosis or pregnancy complications, and so that makes it difficult to study the disease in other manifestations, such as kidney manifestations, if they’re not part of the criteria.”
She added, “I think there was a need for clear classification criteria that was thought to be highly specific for the disease so that future studies can be done in this population.”
Dr. Jorge called the 99% specificity described in the analysis “impressive” and “promising.”
Dr. Barbhaiya and Dr. Zuily have no relevant disclosures. Dr. Erkan disclosed relationships with Aurinia, Eli Lilly, Exagen, and GlaxoSmithKline. Dr. Jorge has no relevant disclosures.
PHILADELPHIA – A draft update of criteria for classifying antiphospholipid syndrome (APS) incorporates a much broader spectrum of disease signs and symptoms, such as kidney disease and more variables for pregnancy, and meets a higher level of specificity than the existing Sapporo criteria, although at the expense of lower sensitivity.
Three members of the core planning group that wrote the update, jointly commissioned by the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR), reviewed the proposed criteria at the annual meeting of the ACR.
If ACR and EULAR adopt the new criteria, it would be an update to the Sapporo classification criteria for APS, which was last updated in 2006. The pending criteria consist of the following eight domains encompassing clinical findings and laboratory test results:
- Macrovascular – venous thromboembolism (VTE) with and without high VTE risk profile.
- Macrovascular – arterial thrombosis with and without a high cardiovascular disease risk profile.
- Microvascular – additional categories for kidney disease, pulmonary embolism, and other conditions for both suspected and established APS.
- Obstetric – expanded definitions to account for the absence or presence of preeclampsia or premature birth with or without fetal death.
- Cardiac valve – accounts for thickening and vegetation.
- Hematologic – includes thrombocytopenia (defined as the lowest platelet count, 20-130 x 109/L).
- Antiphospholipid (aPL) test – coagulation-based functional assay, assigning greater weight to persistent over one-time positive test results.
- aPL test by solid-phase assay – includes anticardiolipin enzyme-linked immunosorbent assay (aCL ELISA), and aCL/anti-beta 2 glycoprotein-I (aCL/anti-beta 2 GPI) tests, with greater weight assigned for moderate-to-high positive results depending on isotype, whether immunoglobulin G or M.
Changes from Sapporo criteria
The existing Sapporo criteria include two clinical categories, vascular thrombosis and pregnancy morbidity; and three laboratory categories, positive lupus anticoagulant, medium or high antibody titers, and high aCL/anti-beta 2 GPI measured by ELISA. All of these are included in the draft criteria under two domains.
“These novel clinical features will help us better stratify patients according to the risk factor profile,” Stéphane Zuily, MD, PhD, a vascular specialist and European co-principal investigator of the planning group, said in explaining the proposed updated domains.
“We well-defined the microvascular domain items further than the aPL nephropathy; we redefined pregnancy morbidities; we added cardiac valve disease and thrombocytopenia; and, through gathering novel laboratory features, we were able to quantify single, double, and triple aPL positivity based on different domains and weights,” said Dr. Zuily, professor of medicine at Lorraine University in Nancy, France.
Also noteworthy is the separation of aCL/anti-beta 2 GPI testing by IgG and IgM isotypes. “And we were also able to identify different thresholds in terms of aPL positivity,” Dr. Zuily said.
Rationale and methodology
Planning group member Medha Barbhaiya, MD, MPH, an attending physician at the Hospital for Special Surgery and assistant professor at Weill Cornell Medicine in New York, explained the rationale for the update. “The existing criteria were drafted in 1999 and updated in 2006 and require one clinical criterion, either vascular thrombosis event or pregnancy morbidity along with antiphospholipid antibodies,” she said.
Those 16-year-old criteria also ignored heterogeneous manifestations such as heart valve disease or thrombocytopenia, failed to stratify thrombotic events as risk factors, and used an outdated definition of pregnancy morbidity related to APS, she said.
“These findings helped to support our rationale for new criteria development, along with the fact that over the last 1 to 2 decades there have been important advancements in the methodology of classification criteria development,” she said. ACR and EULAR both endorsed the new methodology for developing the classification criteria, Dr. Barbhaiya added.
That methodology involved multidisciplinary international panels of experts and data-driven efforts, with the goal of identifying patients with a high likelihood of APS for research purposes. The planning group collected 568 cases from 29 international centers, dividing them into two validation cohorts of 284 cases each.
How classification criteria work
Doruk Erkan, MD, MPH, coprincipal investigator representing the United States on the planning group, an attending physician at the Hospital for Special Surgery in New York, and a professor at Weill Cornell Medicine in New York, explained how the classification system works. “If you have a patient that you are considering for APS classification, the story starts with entry criteria, which are one documented clinical criterion plus a positive aPL [antiphospholipid] test within 3 years of observation of the clinical criteria,” he said.
Once the entry criteria for APS are met, there are the clinical and laboratory domains. Dr. Erkan explained that weighted point values are assigned to individual categories under each domain. For example, in the macrovascular VTE domain, VTE with a high VTE risk profile is worth 1 point, but VTE without a high VTE risk profile is worth 3 points.
“APS classification will be achieved with at least three points from clinical domains and at least three points from the laboratory domains,” he said.
The planning group conducted a sensitivity and specificity analysis of the draft classification system using the two validation cohorts. “Our goal was very high specificity to improve the homogeneity in APS research, and we achieved this in both cohorts with 99% specificity,” Dr. Erkan said. That compares to sensitivity of 91% and 86% of the Sapporo criteria in the validation cohorts.
“Our sensitivity was 83% and 84% capturing a broad spectrum of patients assessed with APS suspicion,” he added, vs. 100% and 99% with the Sapporo criteria.
These criteria are not absolute and are structured to permit future modifications, Dr. Erkan said. “When this work is completed, another chapter will start,” he said. “If a case doesn’t meet APS classification criteria, the case may still be uncertain or equivocal rather than not APS. Uncertain or controversial cases should be studied separately to guide future updates of the new criteria.”
Comment: Why these updates are needed
April Jorge, MD, a rheumatologist at Massachusetts General Hospital in Boston and moderator of the session on the draft APS criteria, explained why these updated criteria are needed. “It’s very important to get the updated criteria because, as the speakers mentioned, the prior Sapporo criteria were limited to just large-vessel venous thrombosis or pregnancy complications, and so that makes it difficult to study the disease in other manifestations, such as kidney manifestations, if they’re not part of the criteria.”
She added, “I think there was a need for clear classification criteria that was thought to be highly specific for the disease so that future studies can be done in this population.”
Dr. Jorge called the 99% specificity described in the analysis “impressive” and “promising.”
Dr. Barbhaiya and Dr. Zuily have no relevant disclosures. Dr. Erkan disclosed relationships with Aurinia, Eli Lilly, Exagen, and GlaxoSmithKline. Dr. Jorge has no relevant disclosures.
AT ACR 2022
Be aware, mindfulness training can lower systolic BP: MB-BP
CHICAGO – It’s been said that one can observe a lot just by watching. Turning such observation inward, new evidence suggests, might lead to blood pressure (BP) reductions that approach what’s possible from an antihypertensive agent.
Systolic BP fell over 6 months by almost 6 mm Hg, on average, in people with elevated BP who participated in an 8-week mindful awareness program as part of a randomized trial that included a usual-care control group.
The program taught established mindfulness-training techniques aimed at modifying behaviors regarding diet, exercise, and other controllable influences on the success of antihypertensive therapy.
Participants in the program, called Mindfulness-Based Blood Pressure Reduction (MB-BP), also the name of the single-center study, “showed potentially clinically relevant reductions in systolic blood pressure,” said principal investigator Eric B. Loucks, PhD, Brown University, Providence, R.I.
The phase 2 trial has some limitations, he observed, including on generalizability. For example, it entered about 200 mostly White, college-educated adults from one metropolitan area.
But if these findings are replicated in further studies, “preferably by other research groups, in a larger and broader population, and with longer follow-up,” Dr. Loucks said, the MB-BP intervention could become “an appealing approach to help control blood pressure.”
Dr. Loucks made the comments at a press conference prior to his formal presentation of MB-BP Nov. 6 at American Heart Association (AHA) Scientific Sessions 2022, held in Chicago and virtually.
Mindfulness-based interventions for elevated BP have not been widely studied, “so this is exactly what we need: a well-done trial with a control group to show that it actually works,” Amit Khera, MD, not connected with MB-BP, told this news organization.
The trial is “really important for proof of concept, but it had only 200 people. You need a larger one, and you need longer-term data,” agreed Dr. Khera, who directs the preventive cardiology program at the University of Texas Southwestern Medical Center, in Dallas. “Six months is good, but we want to see if it’s durable.”
Rhian M. Touyz, MBBCh, also not part of MB-BP, agreed that the nearly 6 mm Hg mean systolic BP reduction among program participants is clinically relevant. “I think in the context of global risk and reduction of target organ damage and cardiovascular events, it is significant in terms of events at a population level,” Dr. Touyz, McGill University Health Centre, Montreal, told this news organization.
Many patients on antihypertensive therapy that’s falling short resist the addition of another such agent, she observed, and instead might show further BP reduction from mindfulness training. The intervention probably also “would benefit health in general.” Mindfulness-based approaches could therefore be useful additions to treatment protocols for elevated BP, Dr. Touyz said.
How the training works
The MB-BP program used validated mindfulness-based stress-management techniques, adapted to address elevated BP, that included “personalized feedback and education about hypertension risk factors, mindful awareness training of participants’ relationships with hypertension risk factors, and support for behavior change,” Dr. Loucks and colleagues reported.
Participants were trained in mindfulness skills that included “self-awareness and emotion regulation,” Dr. Loucks said, which they then could apply to their “relationships with the things that we know influence blood pressure, like physical activity, diet, antihypertensive medication adherence, or alcohol consumption.”
One goal is to promote greater “attention control,” he said, “so that there’s some self-awareness that arises in terms of how we feel the next day, after a lot of alcohol consumption, for example, or lack of physical activity.” The process can provide insights that inspire patients to modify behaviors and risk factors that elevate BP, Dr. Loucks explained.
Effects on medication use
Systolic BP responses led some program participants to be managed on fewer or reduced dosages of antihypertensive meds, he told this news organization. Physicians seen outside of the trial could adjust their prescriptions, intensifying or pulling back on meds depending on their assessments of the patient. Any prescription changes would be documented by the researchers at the patient’s next class or trial-clinic visit.
The group that did the training, Dr. Loucks said, was 33% less likely to increase and 30% more likely to decrease their use of BP-lowering medications compared with the control group.
Elevated BP is so common and undertreated that “there is a need for every possible level of intervention, starting from the population level to the individual and everything else in between,” nephrologist Janani Rangaswami, MD, George Washington University, Washington, said at the press conference.
Therefore, “this mindfulness-based approach, in addition to standard of care with pharmacotherapy, is a really welcome addition to the hypertension literature,” said Dr. Rangaswami, who directs her center’s cardiorenal program. The systolic BP reduction seen in the intervention group, she agreed, was “clinically important and meaningful.”
Blinded assessments
The trial entered 201 patients with systolic and diastolic BP greater than 120 mm Hg and 80 mm Hg, respectively; 58.7% were women, 81% were White, and 73% were college-educated, Dr. Loucks reported.
The 100 assigned to the “enhanced usual care” control group received educational materials on controlling high BP. They and the 101 who followed the mindfulness-based program were given and trained on a home BP-monitoring device. They were then followed for the primary endpoint of change in systolic BP at 6 months.
Data management and outcomes assessments were conducted by trialists not involved in the training intervention who were blinded to randomization assignment.
In a prespecified unadjusted analysis by intention-to-treat, systolic BP in the intervention group dropped by a mean of 5.9 mm Hg (P < .001) compared with baseline and 4.5 mm Hg (P = .045), compared with the control group.
A post hoc analysis adjusted for sex and baseline BP showed an average 4.3 mm Hg reduction (P = .056) in those following the MB-BP program, compared with controls.
There were no observed significant effects on diastolic BP.
The study offered clues to how engagement in the MB-BP program might promote reductions in systolic BP, Dr. Loucks observed. For example, it may have led to increased activity levels, reduced sodium intake, and other dietary improvements.
Indeed, program participants averaged about 351 minutes less sedentary time (P = .02) and showed a 0.32-point improvement in Dietary Approaches to Stop Hypertension scores (P = .08), compared with the control group, Dr. Loucks reported. Other modifiable risk factors for elevated BP that could have responded to the mindfulness-based training, he proposed, include obesity, alcohol intake, and reaction to stress.
Dr. Loucks reports that he developed the MB-BP training and was a program instructor but did not receive related financial compensation; he had no other disclosures. Dr. Khera, Dr. Touyz, and Dr. Rangaswami had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – It’s been said that one can observe a lot just by watching. Turning such observation inward, new evidence suggests, might lead to blood pressure (BP) reductions that approach what’s possible from an antihypertensive agent.
Systolic BP fell over 6 months by almost 6 mm Hg, on average, in people with elevated BP who participated in an 8-week mindful awareness program as part of a randomized trial that included a usual-care control group.
The program taught established mindfulness-training techniques aimed at modifying behaviors regarding diet, exercise, and other controllable influences on the success of antihypertensive therapy.
Participants in the program, called Mindfulness-Based Blood Pressure Reduction (MB-BP), also the name of the single-center study, “showed potentially clinically relevant reductions in systolic blood pressure,” said principal investigator Eric B. Loucks, PhD, Brown University, Providence, R.I.
The phase 2 trial has some limitations, he observed, including on generalizability. For example, it entered about 200 mostly White, college-educated adults from one metropolitan area.
But if these findings are replicated in further studies, “preferably by other research groups, in a larger and broader population, and with longer follow-up,” Dr. Loucks said, the MB-BP intervention could become “an appealing approach to help control blood pressure.”
Dr. Loucks made the comments at a press conference prior to his formal presentation of MB-BP Nov. 6 at American Heart Association (AHA) Scientific Sessions 2022, held in Chicago and virtually.
Mindfulness-based interventions for elevated BP have not been widely studied, “so this is exactly what we need: a well-done trial with a control group to show that it actually works,” Amit Khera, MD, not connected with MB-BP, told this news organization.
The trial is “really important for proof of concept, but it had only 200 people. You need a larger one, and you need longer-term data,” agreed Dr. Khera, who directs the preventive cardiology program at the University of Texas Southwestern Medical Center, in Dallas. “Six months is good, but we want to see if it’s durable.”
Rhian M. Touyz, MBBCh, also not part of MB-BP, agreed that the nearly 6 mm Hg mean systolic BP reduction among program participants is clinically relevant. “I think in the context of global risk and reduction of target organ damage and cardiovascular events, it is significant in terms of events at a population level,” Dr. Touyz, McGill University Health Centre, Montreal, told this news organization.
Many patients on antihypertensive therapy that’s falling short resist the addition of another such agent, she observed, and instead might show further BP reduction from mindfulness training. The intervention probably also “would benefit health in general.” Mindfulness-based approaches could therefore be useful additions to treatment protocols for elevated BP, Dr. Touyz said.
How the training works
The MB-BP program used validated mindfulness-based stress-management techniques, adapted to address elevated BP, that included “personalized feedback and education about hypertension risk factors, mindful awareness training of participants’ relationships with hypertension risk factors, and support for behavior change,” Dr. Loucks and colleagues reported.
Participants were trained in mindfulness skills that included “self-awareness and emotion regulation,” Dr. Loucks said, which they then could apply to their “relationships with the things that we know influence blood pressure, like physical activity, diet, antihypertensive medication adherence, or alcohol consumption.”
One goal is to promote greater “attention control,” he said, “so that there’s some self-awareness that arises in terms of how we feel the next day, after a lot of alcohol consumption, for example, or lack of physical activity.” The process can provide insights that inspire patients to modify behaviors and risk factors that elevate BP, Dr. Loucks explained.
Effects on medication use
Systolic BP responses led some program participants to be managed on fewer or reduced dosages of antihypertensive meds, he told this news organization. Physicians seen outside of the trial could adjust their prescriptions, intensifying or pulling back on meds depending on their assessments of the patient. Any prescription changes would be documented by the researchers at the patient’s next class or trial-clinic visit.
The group that did the training, Dr. Loucks said, was 33% less likely to increase and 30% more likely to decrease their use of BP-lowering medications compared with the control group.
Elevated BP is so common and undertreated that “there is a need for every possible level of intervention, starting from the population level to the individual and everything else in between,” nephrologist Janani Rangaswami, MD, George Washington University, Washington, said at the press conference.
Therefore, “this mindfulness-based approach, in addition to standard of care with pharmacotherapy, is a really welcome addition to the hypertension literature,” said Dr. Rangaswami, who directs her center’s cardiorenal program. The systolic BP reduction seen in the intervention group, she agreed, was “clinically important and meaningful.”
Blinded assessments
The trial entered 201 patients with systolic and diastolic BP greater than 120 mm Hg and 80 mm Hg, respectively; 58.7% were women, 81% were White, and 73% were college-educated, Dr. Loucks reported.
The 100 assigned to the “enhanced usual care” control group received educational materials on controlling high BP. They and the 101 who followed the mindfulness-based program were given and trained on a home BP-monitoring device. They were then followed for the primary endpoint of change in systolic BP at 6 months.
Data management and outcomes assessments were conducted by trialists not involved in the training intervention who were blinded to randomization assignment.
In a prespecified unadjusted analysis by intention-to-treat, systolic BP in the intervention group dropped by a mean of 5.9 mm Hg (P < .001) compared with baseline and 4.5 mm Hg (P = .045), compared with the control group.
A post hoc analysis adjusted for sex and baseline BP showed an average 4.3 mm Hg reduction (P = .056) in those following the MB-BP program, compared with controls.
There were no observed significant effects on diastolic BP.
The study offered clues to how engagement in the MB-BP program might promote reductions in systolic BP, Dr. Loucks observed. For example, it may have led to increased activity levels, reduced sodium intake, and other dietary improvements.
Indeed, program participants averaged about 351 minutes less sedentary time (P = .02) and showed a 0.32-point improvement in Dietary Approaches to Stop Hypertension scores (P = .08), compared with the control group, Dr. Loucks reported. Other modifiable risk factors for elevated BP that could have responded to the mindfulness-based training, he proposed, include obesity, alcohol intake, and reaction to stress.
Dr. Loucks reports that he developed the MB-BP training and was a program instructor but did not receive related financial compensation; he had no other disclosures. Dr. Khera, Dr. Touyz, and Dr. Rangaswami had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – It’s been said that one can observe a lot just by watching. Turning such observation inward, new evidence suggests, might lead to blood pressure (BP) reductions that approach what’s possible from an antihypertensive agent.
Systolic BP fell over 6 months by almost 6 mm Hg, on average, in people with elevated BP who participated in an 8-week mindful awareness program as part of a randomized trial that included a usual-care control group.
The program taught established mindfulness-training techniques aimed at modifying behaviors regarding diet, exercise, and other controllable influences on the success of antihypertensive therapy.
Participants in the program, called Mindfulness-Based Blood Pressure Reduction (MB-BP), also the name of the single-center study, “showed potentially clinically relevant reductions in systolic blood pressure,” said principal investigator Eric B. Loucks, PhD, Brown University, Providence, R.I.
The phase 2 trial has some limitations, he observed, including on generalizability. For example, it entered about 200 mostly White, college-educated adults from one metropolitan area.
But if these findings are replicated in further studies, “preferably by other research groups, in a larger and broader population, and with longer follow-up,” Dr. Loucks said, the MB-BP intervention could become “an appealing approach to help control blood pressure.”
Dr. Loucks made the comments at a press conference prior to his formal presentation of MB-BP Nov. 6 at American Heart Association (AHA) Scientific Sessions 2022, held in Chicago and virtually.
Mindfulness-based interventions for elevated BP have not been widely studied, “so this is exactly what we need: a well-done trial with a control group to show that it actually works,” Amit Khera, MD, not connected with MB-BP, told this news organization.
The trial is “really important for proof of concept, but it had only 200 people. You need a larger one, and you need longer-term data,” agreed Dr. Khera, who directs the preventive cardiology program at the University of Texas Southwestern Medical Center, in Dallas. “Six months is good, but we want to see if it’s durable.”
Rhian M. Touyz, MBBCh, also not part of MB-BP, agreed that the nearly 6 mm Hg mean systolic BP reduction among program participants is clinically relevant. “I think in the context of global risk and reduction of target organ damage and cardiovascular events, it is significant in terms of events at a population level,” Dr. Touyz, McGill University Health Centre, Montreal, told this news organization.
Many patients on antihypertensive therapy that’s falling short resist the addition of another such agent, she observed, and instead might show further BP reduction from mindfulness training. The intervention probably also “would benefit health in general.” Mindfulness-based approaches could therefore be useful additions to treatment protocols for elevated BP, Dr. Touyz said.
How the training works
The MB-BP program used validated mindfulness-based stress-management techniques, adapted to address elevated BP, that included “personalized feedback and education about hypertension risk factors, mindful awareness training of participants’ relationships with hypertension risk factors, and support for behavior change,” Dr. Loucks and colleagues reported.
Participants were trained in mindfulness skills that included “self-awareness and emotion regulation,” Dr. Loucks said, which they then could apply to their “relationships with the things that we know influence blood pressure, like physical activity, diet, antihypertensive medication adherence, or alcohol consumption.”
One goal is to promote greater “attention control,” he said, “so that there’s some self-awareness that arises in terms of how we feel the next day, after a lot of alcohol consumption, for example, or lack of physical activity.” The process can provide insights that inspire patients to modify behaviors and risk factors that elevate BP, Dr. Loucks explained.
Effects on medication use
Systolic BP responses led some program participants to be managed on fewer or reduced dosages of antihypertensive meds, he told this news organization. Physicians seen outside of the trial could adjust their prescriptions, intensifying or pulling back on meds depending on their assessments of the patient. Any prescription changes would be documented by the researchers at the patient’s next class or trial-clinic visit.
The group that did the training, Dr. Loucks said, was 33% less likely to increase and 30% more likely to decrease their use of BP-lowering medications compared with the control group.
Elevated BP is so common and undertreated that “there is a need for every possible level of intervention, starting from the population level to the individual and everything else in between,” nephrologist Janani Rangaswami, MD, George Washington University, Washington, said at the press conference.
Therefore, “this mindfulness-based approach, in addition to standard of care with pharmacotherapy, is a really welcome addition to the hypertension literature,” said Dr. Rangaswami, who directs her center’s cardiorenal program. The systolic BP reduction seen in the intervention group, she agreed, was “clinically important and meaningful.”
Blinded assessments
The trial entered 201 patients with systolic and diastolic BP greater than 120 mm Hg and 80 mm Hg, respectively; 58.7% were women, 81% were White, and 73% were college-educated, Dr. Loucks reported.
The 100 assigned to the “enhanced usual care” control group received educational materials on controlling high BP. They and the 101 who followed the mindfulness-based program were given and trained on a home BP-monitoring device. They were then followed for the primary endpoint of change in systolic BP at 6 months.
Data management and outcomes assessments were conducted by trialists not involved in the training intervention who were blinded to randomization assignment.
In a prespecified unadjusted analysis by intention-to-treat, systolic BP in the intervention group dropped by a mean of 5.9 mm Hg (P < .001) compared with baseline and 4.5 mm Hg (P = .045), compared with the control group.
A post hoc analysis adjusted for sex and baseline BP showed an average 4.3 mm Hg reduction (P = .056) in those following the MB-BP program, compared with controls.
There were no observed significant effects on diastolic BP.
The study offered clues to how engagement in the MB-BP program might promote reductions in systolic BP, Dr. Loucks observed. For example, it may have led to increased activity levels, reduced sodium intake, and other dietary improvements.
Indeed, program participants averaged about 351 minutes less sedentary time (P = .02) and showed a 0.32-point improvement in Dietary Approaches to Stop Hypertension scores (P = .08), compared with the control group, Dr. Loucks reported. Other modifiable risk factors for elevated BP that could have responded to the mindfulness-based training, he proposed, include obesity, alcohol intake, and reaction to stress.
Dr. Loucks reports that he developed the MB-BP training and was a program instructor but did not receive related financial compensation; he had no other disclosures. Dr. Khera, Dr. Touyz, and Dr. Rangaswami had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AHA 2022
First classification criteria proposed for chronic osteomyelitis
PHILADELPHIA – An international group of researchers has proposed the first classification criteria for chronic nonbacterial osteomyelitis (CNO) and a severe form of it, chronic recurrent multifocal osteomyelitis (CRMO).
CNO/CRMO most frequently affect children and adolescents and can significantly affect quality of life.

Yongdong (Dan) Zhao, MD, PhD, a pediatric rheumatologist at Seattle Children’s Hospital, Seattle, Washington, and Seza Ozen, MD, MSc, medical faculty head at Hacettepe University in Ankara, Turkey – members of the expert panel for criteria development – explained the proposed criteria, developed over 6 years, at the American College of Rheumatology 2022 Annual Meeting.
They gave examples of the point system that will help researchers correctly classify CNO/CRMO if the criteria are approved by ACR and the European Alliance of Associations for Rheumatology (EULAR).

Melissa S. Oliver, MD, a pediatric rheumatologist at Riley Children’s Hospital and Indiana University, Indianapolis, told this news organization: “This proposal is important because CNO/CRMO has primarily been a diagnosis of exclusion. There are no specific tests or biomarkers for this disease. It can mimic malignancy and infectious osteomyelitis in its presentation, and these must be ruled out thoroughly first.”
However, she noted, this can be challenging and can delay diagnosis and treatment.
The classification criteria are novel, she said, because an international collaborative group used a consensus process involving physicians managing CNO and patients or caregivers of children with CNO.
Findings for and against CNO
Dr. Ozen summarized some examples of findings for and against a CNO/CRMO classification.
Statistically significant findings in favor of CNO/CRMO, she said, include intermittent bone pain; bone pain in upper torso; swelling of upper torso; presence of symmetric lesions; and presence of adaptive immune cell and/or fibrosis in biopsy.
Conversely, findings against CNO/CRMO include fever; signs of infection by labs; signs of cancer by biopsy; specific abnormal x-ray/CT scan; specific abnormal MRI; or pain resolved with antibiotics alone.
Dr. Zhao described a point system with a threshold of 55 points for classification of CNO/CRMO.
He gave actual examples from the registry to demonstrate high and low probability of CNO/CRMO.
Pro-CNO example
The first was a boy, aged 7 years 10 months, who had a year and a half of pain in his back and legs, but no fever. Pain was constant, waxing and waning. He had a personal and family history of psoriasis and was tender to palpation at multiple sites. Labs were normal and bone biopsy and vitamin C tests were not done; imaging findings showed multiple bones were affected. There was no antibiotic treatment.
That patient was scored 81, much higher than the threshold of 55, and would be classified as having CNO.
Non-CNO example
Conversely, the following example of a patient would score 47 – under the threshold – and would not be classified as having CNO.
That patient was an 11-year-old boy who had 2 months of pain in his right thigh with no fever. The pain was constantly waxing and waning. He was tender to palpation at only his right thigh without swelling. Labs were normal. He had no coexisting conditions. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were not measured, and no vitamin C test was performed. Imaging showed one right femur lesion on a PET-CT scan. There was no antibiotic treatment, and a bone biopsy culture showed malignancy but no inflammation or fibrosis.
Dr. Zhao said the mimickers most likely to be misclassified are vitamin C deficiency; hypophosphatasia; benign bone tumor, such as osteogenic osteoma; and a malignancy with normal labs and multifocal pattern of bone lesions.
The classification criteria will be “extremely helpful to diagnose patients with CNO/CRMO earlier,” said Dr. Oliver, who helped develop the criteria.
“The goal is that the proposed classification criteria will be used by all physicians to diagnose suspected CNO patients earlier and refer to a rheumatologist earlier so that appropriate therapies will not be delayed.”
The group will seek ACR and EULAR endorsement, and if granted, work toward widespread implementation. The criteria will allow researchers to have a more homogeneous study population for future clinical trials, Dr. Zhao said.
Dr. Zhao, Dr. Ozen, and Dr. Oliver declared no relevant financial relationships. Dr. Oliver helped develop the proposed guidelines.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – An international group of researchers has proposed the first classification criteria for chronic nonbacterial osteomyelitis (CNO) and a severe form of it, chronic recurrent multifocal osteomyelitis (CRMO).
CNO/CRMO most frequently affect children and adolescents and can significantly affect quality of life.
Yongdong (Dan) Zhao, MD, PhD, a pediatric rheumatologist at Seattle Children’s Hospital, Seattle, Washington, and Seza Ozen, MD, MSc, medical faculty head at Hacettepe University in Ankara, Turkey – members of the expert panel for criteria development – explained the proposed criteria, developed over 6 years, at the American College of Rheumatology 2022 Annual Meeting.
They gave examples of the point system that will help researchers correctly classify CNO/CRMO if the criteria are approved by ACR and the European Alliance of Associations for Rheumatology (EULAR).
Melissa S. Oliver, MD, a pediatric rheumatologist at Riley Children’s Hospital and Indiana University, Indianapolis, told this news organization: “This proposal is important because CNO/CRMO has primarily been a diagnosis of exclusion. There are no specific tests or biomarkers for this disease. It can mimic malignancy and infectious osteomyelitis in its presentation, and these must be ruled out thoroughly first.”
However, she noted, this can be challenging and can delay diagnosis and treatment.
The classification criteria are novel, she said, because an international collaborative group used a consensus process involving physicians managing CNO and patients or caregivers of children with CNO.
Findings for and against CNO
Dr. Ozen summarized some examples of findings for and against a CNO/CRMO classification.
Statistically significant findings in favor of CNO/CRMO, she said, include intermittent bone pain; bone pain in upper torso; swelling of upper torso; presence of symmetric lesions; and presence of adaptive immune cell and/or fibrosis in biopsy.
Conversely, findings against CNO/CRMO include fever; signs of infection by labs; signs of cancer by biopsy; specific abnormal x-ray/CT scan; specific abnormal MRI; or pain resolved with antibiotics alone.
Dr. Zhao described a point system with a threshold of 55 points for classification of CNO/CRMO.
He gave actual examples from the registry to demonstrate high and low probability of CNO/CRMO.
Pro-CNO example
The first was a boy, aged 7 years 10 months, who had a year and a half of pain in his back and legs, but no fever. Pain was constant, waxing and waning. He had a personal and family history of psoriasis and was tender to palpation at multiple sites. Labs were normal and bone biopsy and vitamin C tests were not done; imaging findings showed multiple bones were affected. There was no antibiotic treatment.
That patient was scored 81, much higher than the threshold of 55, and would be classified as having CNO.
Non-CNO example
Conversely, the following example of a patient would score 47 – under the threshold – and would not be classified as having CNO.
That patient was an 11-year-old boy who had 2 months of pain in his right thigh with no fever. The pain was constantly waxing and waning. He was tender to palpation at only his right thigh without swelling. Labs were normal. He had no coexisting conditions. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were not measured, and no vitamin C test was performed. Imaging showed one right femur lesion on a PET-CT scan. There was no antibiotic treatment, and a bone biopsy culture showed malignancy but no inflammation or fibrosis.
Dr. Zhao said the mimickers most likely to be misclassified are vitamin C deficiency; hypophosphatasia; benign bone tumor, such as osteogenic osteoma; and a malignancy with normal labs and multifocal pattern of bone lesions.
The classification criteria will be “extremely helpful to diagnose patients with CNO/CRMO earlier,” said Dr. Oliver, who helped develop the criteria.
“The goal is that the proposed classification criteria will be used by all physicians to diagnose suspected CNO patients earlier and refer to a rheumatologist earlier so that appropriate therapies will not be delayed.”
The group will seek ACR and EULAR endorsement, and if granted, work toward widespread implementation. The criteria will allow researchers to have a more homogeneous study population for future clinical trials, Dr. Zhao said.
Dr. Zhao, Dr. Ozen, and Dr. Oliver declared no relevant financial relationships. Dr. Oliver helped develop the proposed guidelines.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – An international group of researchers has proposed the first classification criteria for chronic nonbacterial osteomyelitis (CNO) and a severe form of it, chronic recurrent multifocal osteomyelitis (CRMO).
CNO/CRMO most frequently affect children and adolescents and can significantly affect quality of life.
Yongdong (Dan) Zhao, MD, PhD, a pediatric rheumatologist at Seattle Children’s Hospital, Seattle, Washington, and Seza Ozen, MD, MSc, medical faculty head at Hacettepe University in Ankara, Turkey – members of the expert panel for criteria development – explained the proposed criteria, developed over 6 years, at the American College of Rheumatology 2022 Annual Meeting.
They gave examples of the point system that will help researchers correctly classify CNO/CRMO if the criteria are approved by ACR and the European Alliance of Associations for Rheumatology (EULAR).
Melissa S. Oliver, MD, a pediatric rheumatologist at Riley Children’s Hospital and Indiana University, Indianapolis, told this news organization: “This proposal is important because CNO/CRMO has primarily been a diagnosis of exclusion. There are no specific tests or biomarkers for this disease. It can mimic malignancy and infectious osteomyelitis in its presentation, and these must be ruled out thoroughly first.”
However, she noted, this can be challenging and can delay diagnosis and treatment.
The classification criteria are novel, she said, because an international collaborative group used a consensus process involving physicians managing CNO and patients or caregivers of children with CNO.
Findings for and against CNO
Dr. Ozen summarized some examples of findings for and against a CNO/CRMO classification.
Statistically significant findings in favor of CNO/CRMO, she said, include intermittent bone pain; bone pain in upper torso; swelling of upper torso; presence of symmetric lesions; and presence of adaptive immune cell and/or fibrosis in biopsy.
Conversely, findings against CNO/CRMO include fever; signs of infection by labs; signs of cancer by biopsy; specific abnormal x-ray/CT scan; specific abnormal MRI; or pain resolved with antibiotics alone.
Dr. Zhao described a point system with a threshold of 55 points for classification of CNO/CRMO.
He gave actual examples from the registry to demonstrate high and low probability of CNO/CRMO.
Pro-CNO example
The first was a boy, aged 7 years 10 months, who had a year and a half of pain in his back and legs, but no fever. Pain was constant, waxing and waning. He had a personal and family history of psoriasis and was tender to palpation at multiple sites. Labs were normal and bone biopsy and vitamin C tests were not done; imaging findings showed multiple bones were affected. There was no antibiotic treatment.
That patient was scored 81, much higher than the threshold of 55, and would be classified as having CNO.
Non-CNO example
Conversely, the following example of a patient would score 47 – under the threshold – and would not be classified as having CNO.
That patient was an 11-year-old boy who had 2 months of pain in his right thigh with no fever. The pain was constantly waxing and waning. He was tender to palpation at only his right thigh without swelling. Labs were normal. He had no coexisting conditions. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were not measured, and no vitamin C test was performed. Imaging showed one right femur lesion on a PET-CT scan. There was no antibiotic treatment, and a bone biopsy culture showed malignancy but no inflammation or fibrosis.
Dr. Zhao said the mimickers most likely to be misclassified are vitamin C deficiency; hypophosphatasia; benign bone tumor, such as osteogenic osteoma; and a malignancy with normal labs and multifocal pattern of bone lesions.
The classification criteria will be “extremely helpful to diagnose patients with CNO/CRMO earlier,” said Dr. Oliver, who helped develop the criteria.
“The goal is that the proposed classification criteria will be used by all physicians to diagnose suspected CNO patients earlier and refer to a rheumatologist earlier so that appropriate therapies will not be delayed.”
The group will seek ACR and EULAR endorsement, and if granted, work toward widespread implementation. The criteria will allow researchers to have a more homogeneous study population for future clinical trials, Dr. Zhao said.
Dr. Zhao, Dr. Ozen, and Dr. Oliver declared no relevant financial relationships. Dr. Oliver helped develop the proposed guidelines.
A version of this article first appeared on Medscape.com.
AT ACR 2022
More weight loss with surgery than new obesity meds: meta-analysis
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.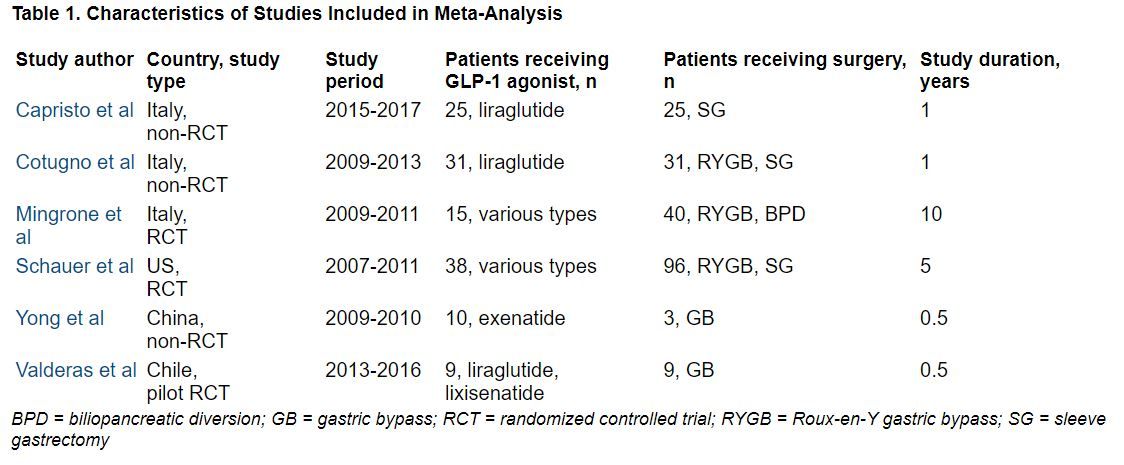
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT OBESITYWEEK®