User login
A new day for discharges?
“Decrease readmissions, and decrease them stat!” This mantra, or some, perhaps more subtle version thereof, is echoed over and over at hospitals across the country, and for good reason. Not only do readmissions have the potential to cost hospital systems millions of dollars through Medicare payment reductions, they also signal a more important, though less vocalized concern. If our patients keep returning to the hospital, are we really providing them with 100% of the resources they need?
On the surface, it may seem like there is little we can do for that two-pack-per-day smoker with end-stage chronic obstructive pulmonary disease who keeps getting readmitted with an exacerbation. And, while in reality, we may never get him to stop smoking and start taking his mediations as prescribed, perhaps we can help decrease the frequency of readmissions from three to four per year to two to three. While seemingly small, this decrease is actually quite dramatic, correlating to a 25%-50% reduction in the use of hospital services, not to mention the profound impact that fewer days spent in the hospital will have on his quality of life.

It is remarkable how much change occurs in the health care system over time. One year a drug may be touted as a huge breakthrough in treatment, and the next it may be taken off the market because of previously unrecognized, potentially fatal side effects. And just as the field of medicine is ever changing, so are all the fields that support it.
For example, the Agency for Healthcare Research and Qualify (AHRQ) has developed the Re-Engineered Discharge (RED) tool kit, which has been highly successful in reducing hospital readmissions. Originally developed by a group of AHRQ-funded researchers in Boston, RED provides evidence-based tools that help hospitals re-engineer their discharge process. One success story – within 3 months of implementing RED, the Valley Baptist Medical Center in Harlingen, Tex., decreased readmissions from 26% to 15%.
The RED model focuses on comprehensive discharge planning, educating patients about their discharge, and postdischarge follow-up care. It uses dedicated discharge advocates to help patients reconcile their medications and schedule much-needed follow-up appointments.
Other models exist as well. For instance, some hospitals have a palliative care team that focuses not only on keeping patients comfortable while in the hospital, but also on helping them access community services after discharge and make necessary appointments, geared at optimizing their health and ultimately decreasing the need for excessive hospitalizations.
As every health care dollar spent will be scrutinized more and more over time, innovative programs to help us rethink our long-established routines will likely play a major role in catapulting us from where we are to where we want to be.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
“Decrease readmissions, and decrease them stat!” This mantra, or some, perhaps more subtle version thereof, is echoed over and over at hospitals across the country, and for good reason. Not only do readmissions have the potential to cost hospital systems millions of dollars through Medicare payment reductions, they also signal a more important, though less vocalized concern. If our patients keep returning to the hospital, are we really providing them with 100% of the resources they need?
On the surface, it may seem like there is little we can do for that two-pack-per-day smoker with end-stage chronic obstructive pulmonary disease who keeps getting readmitted with an exacerbation. And, while in reality, we may never get him to stop smoking and start taking his mediations as prescribed, perhaps we can help decrease the frequency of readmissions from three to four per year to two to three. While seemingly small, this decrease is actually quite dramatic, correlating to a 25%-50% reduction in the use of hospital services, not to mention the profound impact that fewer days spent in the hospital will have on his quality of life.
It is remarkable how much change occurs in the health care system over time. One year a drug may be touted as a huge breakthrough in treatment, and the next it may be taken off the market because of previously unrecognized, potentially fatal side effects. And just as the field of medicine is ever changing, so are all the fields that support it.
For example, the Agency for Healthcare Research and Qualify (AHRQ) has developed the Re-Engineered Discharge (RED) tool kit, which has been highly successful in reducing hospital readmissions. Originally developed by a group of AHRQ-funded researchers in Boston, RED provides evidence-based tools that help hospitals re-engineer their discharge process. One success story – within 3 months of implementing RED, the Valley Baptist Medical Center in Harlingen, Tex., decreased readmissions from 26% to 15%.
The RED model focuses on comprehensive discharge planning, educating patients about their discharge, and postdischarge follow-up care. It uses dedicated discharge advocates to help patients reconcile their medications and schedule much-needed follow-up appointments.
Other models exist as well. For instance, some hospitals have a palliative care team that focuses not only on keeping patients comfortable while in the hospital, but also on helping them access community services after discharge and make necessary appointments, geared at optimizing their health and ultimately decreasing the need for excessive hospitalizations.
As every health care dollar spent will be scrutinized more and more over time, innovative programs to help us rethink our long-established routines will likely play a major role in catapulting us from where we are to where we want to be.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
“Decrease readmissions, and decrease them stat!” This mantra, or some, perhaps more subtle version thereof, is echoed over and over at hospitals across the country, and for good reason. Not only do readmissions have the potential to cost hospital systems millions of dollars through Medicare payment reductions, they also signal a more important, though less vocalized concern. If our patients keep returning to the hospital, are we really providing them with 100% of the resources they need?
On the surface, it may seem like there is little we can do for that two-pack-per-day smoker with end-stage chronic obstructive pulmonary disease who keeps getting readmitted with an exacerbation. And, while in reality, we may never get him to stop smoking and start taking his mediations as prescribed, perhaps we can help decrease the frequency of readmissions from three to four per year to two to three. While seemingly small, this decrease is actually quite dramatic, correlating to a 25%-50% reduction in the use of hospital services, not to mention the profound impact that fewer days spent in the hospital will have on his quality of life.
It is remarkable how much change occurs in the health care system over time. One year a drug may be touted as a huge breakthrough in treatment, and the next it may be taken off the market because of previously unrecognized, potentially fatal side effects. And just as the field of medicine is ever changing, so are all the fields that support it.
For example, the Agency for Healthcare Research and Qualify (AHRQ) has developed the Re-Engineered Discharge (RED) tool kit, which has been highly successful in reducing hospital readmissions. Originally developed by a group of AHRQ-funded researchers in Boston, RED provides evidence-based tools that help hospitals re-engineer their discharge process. One success story – within 3 months of implementing RED, the Valley Baptist Medical Center in Harlingen, Tex., decreased readmissions from 26% to 15%.
The RED model focuses on comprehensive discharge planning, educating patients about their discharge, and postdischarge follow-up care. It uses dedicated discharge advocates to help patients reconcile their medications and schedule much-needed follow-up appointments.
Other models exist as well. For instance, some hospitals have a palliative care team that focuses not only on keeping patients comfortable while in the hospital, but also on helping them access community services after discharge and make necessary appointments, geared at optimizing their health and ultimately decreasing the need for excessive hospitalizations.
As every health care dollar spent will be scrutinized more and more over time, innovative programs to help us rethink our long-established routines will likely play a major role in catapulting us from where we are to where we want to be.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.

An Update on Acute Care Surgery, Part 2
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD

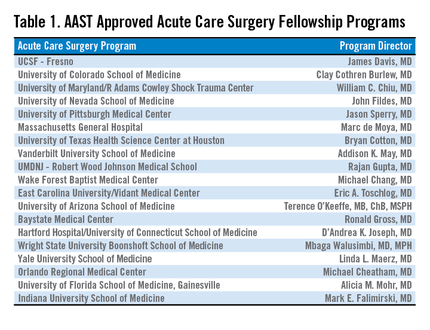
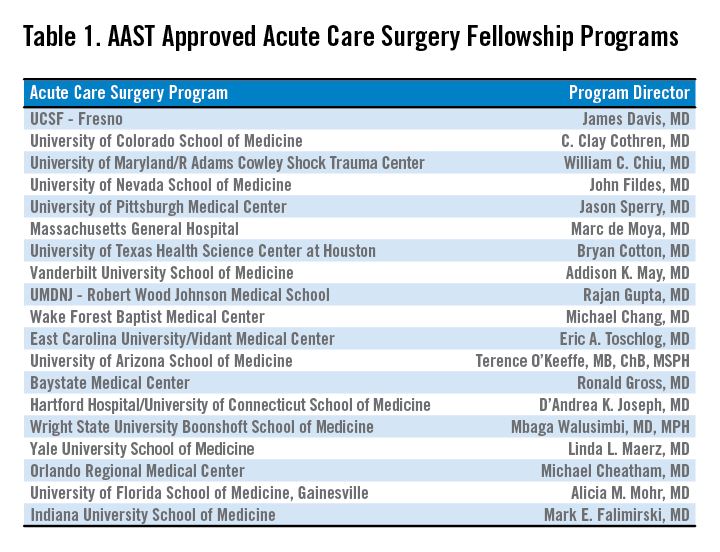
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
In Response to "Online Entry-Level Education: The Jury Is Still Out!"
Dear Dr. Danielsen,
Thank you for addressing this latest controversy in PA/NP issues in the June 2015 Clinician Reviews. I appreciate your candor and your objectiveness in presenting this "hot topic."
I am a currently retired Certified Family Nurse Practitioner after more than 20 years in practice; I graduated from my RN program 40 years ago this month! During my career, I was a clinical instructor in an RN program, as well as a hospital nurse for most of my first two decades of nursing.
After obtaining my MSN/NP education, I preceptored NP students in a master’s prepared program for 20 years. The difference in students who were enrolled in the accelerated programs and those who were in traditional RN to BSN to MSN/NP programs were astonishing to me. They had little to no experience in how to relate to patients or how to take a history, and they certainly were not comfortable with patients.
Another concern is the growing number of "for profit" private schools now offering NP/PA programs, where enrollment seems to be at the price of well-qualified students. Those who cannot meet the requirements of a traditional university setting are now flooding these programs. Just look at the pass rates on exams and the attrition rates along with the high cost they charge.
I am concerned about the move toward e-learning programs. Anybody can memorize pathophysiology, statistics, and biochemistry, but not everyone can learn how to interact with patients and develop critical-thinking and problem-solving skills without direct supervision and experience.
Adequate clinical experience is imperative, and I suggest an internship for NPs and PAs fresh out of school. If we are going to advance our respect in the medical world with our physician colleagues, and continue to provide excellent care in this new era of medicine, then we need to make sure we do not jeopardize the hard work we have all done to bring the current high standards to PA and NP programs.
Janet Evans Emery, RN, MSN, CFNP
Irvine, California
Dear Dr. Danielsen,
Thank you for addressing this latest controversy in PA/NP issues in the June 2015 Clinician Reviews. I appreciate your candor and your objectiveness in presenting this "hot topic."
I am a currently retired Certified Family Nurse Practitioner after more than 20 years in practice; I graduated from my RN program 40 years ago this month! During my career, I was a clinical instructor in an RN program, as well as a hospital nurse for most of my first two decades of nursing.
After obtaining my MSN/NP education, I preceptored NP students in a master’s prepared program for 20 years. The difference in students who were enrolled in the accelerated programs and those who were in traditional RN to BSN to MSN/NP programs were astonishing to me. They had little to no experience in how to relate to patients or how to take a history, and they certainly were not comfortable with patients.
Another concern is the growing number of "for profit" private schools now offering NP/PA programs, where enrollment seems to be at the price of well-qualified students. Those who cannot meet the requirements of a traditional university setting are now flooding these programs. Just look at the pass rates on exams and the attrition rates along with the high cost they charge.
I am concerned about the move toward e-learning programs. Anybody can memorize pathophysiology, statistics, and biochemistry, but not everyone can learn how to interact with patients and develop critical-thinking and problem-solving skills without direct supervision and experience.
Adequate clinical experience is imperative, and I suggest an internship for NPs and PAs fresh out of school. If we are going to advance our respect in the medical world with our physician colleagues, and continue to provide excellent care in this new era of medicine, then we need to make sure we do not jeopardize the hard work we have all done to bring the current high standards to PA and NP programs.
Janet Evans Emery, RN, MSN, CFNP
Irvine, California
Dear Dr. Danielsen,
Thank you for addressing this latest controversy in PA/NP issues in the June 2015 Clinician Reviews. I appreciate your candor and your objectiveness in presenting this "hot topic."
I am a currently retired Certified Family Nurse Practitioner after more than 20 years in practice; I graduated from my RN program 40 years ago this month! During my career, I was a clinical instructor in an RN program, as well as a hospital nurse for most of my first two decades of nursing.
After obtaining my MSN/NP education, I preceptored NP students in a master’s prepared program for 20 years. The difference in students who were enrolled in the accelerated programs and those who were in traditional RN to BSN to MSN/NP programs were astonishing to me. They had little to no experience in how to relate to patients or how to take a history, and they certainly were not comfortable with patients.
Another concern is the growing number of "for profit" private schools now offering NP/PA programs, where enrollment seems to be at the price of well-qualified students. Those who cannot meet the requirements of a traditional university setting are now flooding these programs. Just look at the pass rates on exams and the attrition rates along with the high cost they charge.
I am concerned about the move toward e-learning programs. Anybody can memorize pathophysiology, statistics, and biochemistry, but not everyone can learn how to interact with patients and develop critical-thinking and problem-solving skills without direct supervision and experience.
Adequate clinical experience is imperative, and I suggest an internship for NPs and PAs fresh out of school. If we are going to advance our respect in the medical world with our physician colleagues, and continue to provide excellent care in this new era of medicine, then we need to make sure we do not jeopardize the hard work we have all done to bring the current high standards to PA and NP programs.
Janet Evans Emery, RN, MSN, CFNP
Irvine, California
Lessons from Charleston
Reverend Clementa Pinckney was 24 when I met him. He had just been elected to the General Assembly in South Carolina from the county adjacent to mine. He was imposing – tall with dark ebony skin, intelligent and in command of the room. This guy, I thought, was going to be the first African-American governor of South Carolina. He had a likability and charisma about him that made him stand out.
As one of my colleagues said, he was one of the good ones. I met then–State Representative Pinckney because I had been lobbying for child health issues, in particular for a gun safety bill. It seems ironic that, almost 20 years later, State Senator Pinckney himself would die from gun violence.
This was the mid 1990’s, and although we never got our gun bill passed, the resulting furor, both here in South Carolina and elsewhere, led to a significant drop in childhood gun mortality that persists to this day. But we still have a long way to go. Somewhere between 30 and 40 young people under the age of 21 die in just South Carolina every year. When are we going to take the steps we know will help reduce even further the ongoing tragedy of too many children dying from bullets?
Two days after the massacre in Charleston, I ran into a colleague. He looked distressed. He told me he had been the alleged murderer’s pediatrician some years ago. Without my prompting he began to think out loud as to whether he could have done something then that would have made a difference. But do we have the systems and procedures in place to identify and help troubled kids? We in pediatrics see them. And we do a lot for them. But so many slip through our fingers. What else can we do as a profession to help identify troubled youth and get them services before it is too late?
Racism is an ugly fact in most societies. I truly believe we have made progress in South Carolina confronting intolerance, but we still have a long way to go. There are significant disparities in health outcomes that are racially linked. I know that I, like most of you, have my own prejudices. The first step is recognizing them. Pediatricians in South Carolina almost universally come in contact with those who are victims of racism, and we need to carefully consider how we overcome our own preconceived notions to provide care to everyone.
I have lost a friend in Clementa Pinckney, but his death causes me to wonder about our own individual and collective responsibility, and what our response should be.
Dr. Rushton is clinical professor of pediatrics at the University of South Carolina, Columbia, and medical director of the Quality Through Technology and Innovation in Pediatrics (QTIP) network. He has practiced pediatrics in Beaufort, S.C., for 32 years.
Reverend Clementa Pinckney was 24 when I met him. He had just been elected to the General Assembly in South Carolina from the county adjacent to mine. He was imposing – tall with dark ebony skin, intelligent and in command of the room. This guy, I thought, was going to be the first African-American governor of South Carolina. He had a likability and charisma about him that made him stand out.
As one of my colleagues said, he was one of the good ones. I met then–State Representative Pinckney because I had been lobbying for child health issues, in particular for a gun safety bill. It seems ironic that, almost 20 years later, State Senator Pinckney himself would die from gun violence.
This was the mid 1990’s, and although we never got our gun bill passed, the resulting furor, both here in South Carolina and elsewhere, led to a significant drop in childhood gun mortality that persists to this day. But we still have a long way to go. Somewhere between 30 and 40 young people under the age of 21 die in just South Carolina every year. When are we going to take the steps we know will help reduce even further the ongoing tragedy of too many children dying from bullets?
Two days after the massacre in Charleston, I ran into a colleague. He looked distressed. He told me he had been the alleged murderer’s pediatrician some years ago. Without my prompting he began to think out loud as to whether he could have done something then that would have made a difference. But do we have the systems and procedures in place to identify and help troubled kids? We in pediatrics see them. And we do a lot for them. But so many slip through our fingers. What else can we do as a profession to help identify troubled youth and get them services before it is too late?
Racism is an ugly fact in most societies. I truly believe we have made progress in South Carolina confronting intolerance, but we still have a long way to go. There are significant disparities in health outcomes that are racially linked. I know that I, like most of you, have my own prejudices. The first step is recognizing them. Pediatricians in South Carolina almost universally come in contact with those who are victims of racism, and we need to carefully consider how we overcome our own preconceived notions to provide care to everyone.
I have lost a friend in Clementa Pinckney, but his death causes me to wonder about our own individual and collective responsibility, and what our response should be.
Dr. Rushton is clinical professor of pediatrics at the University of South Carolina, Columbia, and medical director of the Quality Through Technology and Innovation in Pediatrics (QTIP) network. He has practiced pediatrics in Beaufort, S.C., for 32 years.
Reverend Clementa Pinckney was 24 when I met him. He had just been elected to the General Assembly in South Carolina from the county adjacent to mine. He was imposing – tall with dark ebony skin, intelligent and in command of the room. This guy, I thought, was going to be the first African-American governor of South Carolina. He had a likability and charisma about him that made him stand out.
As one of my colleagues said, he was one of the good ones. I met then–State Representative Pinckney because I had been lobbying for child health issues, in particular for a gun safety bill. It seems ironic that, almost 20 years later, State Senator Pinckney himself would die from gun violence.
This was the mid 1990’s, and although we never got our gun bill passed, the resulting furor, both here in South Carolina and elsewhere, led to a significant drop in childhood gun mortality that persists to this day. But we still have a long way to go. Somewhere between 30 and 40 young people under the age of 21 die in just South Carolina every year. When are we going to take the steps we know will help reduce even further the ongoing tragedy of too many children dying from bullets?
Two days after the massacre in Charleston, I ran into a colleague. He looked distressed. He told me he had been the alleged murderer’s pediatrician some years ago. Without my prompting he began to think out loud as to whether he could have done something then that would have made a difference. But do we have the systems and procedures in place to identify and help troubled kids? We in pediatrics see them. And we do a lot for them. But so many slip through our fingers. What else can we do as a profession to help identify troubled youth and get them services before it is too late?
Racism is an ugly fact in most societies. I truly believe we have made progress in South Carolina confronting intolerance, but we still have a long way to go. There are significant disparities in health outcomes that are racially linked. I know that I, like most of you, have my own prejudices. The first step is recognizing them. Pediatricians in South Carolina almost universally come in contact with those who are victims of racism, and we need to carefully consider how we overcome our own preconceived notions to provide care to everyone.
I have lost a friend in Clementa Pinckney, but his death causes me to wonder about our own individual and collective responsibility, and what our response should be.
Dr. Rushton is clinical professor of pediatrics at the University of South Carolina, Columbia, and medical director of the Quality Through Technology and Innovation in Pediatrics (QTIP) network. He has practiced pediatrics in Beaufort, S.C., for 32 years.

From the Editor: Knights of the Rectangular Table
In my past editorials I have made it abundantly clear that I believe that vascular surgeons, like the Knights of the Round Table in the Arthurian legend, follow a chivalrous code of honor that guides us in placing a patient’s well-being ahead of financial reward. We ride out, catheter and knife at the ready, to defeat the malevolent atherosclerotic enemy. Yet I am now chagrined to acknowledge that we, too, have knights who have forsaken their code of chivalry – vascular surgeons who value the attainment of wealth or prestige as their raison d’être.
Our cadre of ethical doctors far outnumbers the avaricious few. But I am increasingly aware of board certified vascular surgeons offering or carrying out egregious or unnecessary interventions.

The following are but a few illustrations of this behavior:
• A website suggesting all men older than 40 years have a self-paid screening for AAA.
• An 80-year-old woman with recurrent swelling of her right leg being told that she needed an emergency ablation of her saphenous vein.
• An obese 50-year-old with no abdominal symptoms and a patent SMA having a stent placed in his celiac artery.
• A 20-year-old who had her saphenous vein ablated because she had a few spiders on her thigh.
• I encountered a patient after a vascular surgeon had inserted an endograft in an 85-year-old male with a 4.5-cm AAA.
• Another vascular surgeon performs yearly carotid arteriography to evaluate the possible progression of asymptomatic stenoses.
• Yet another vascular surgeon carried out a carotid endarterectomy for a 60% asymptomatic stenosis in a patient with end-stage lung cancer.
If you find your skin crawling as you read these examples, you are not the perpetrators. If you are blushing, you may be. If you don’t see the problems with these cases you are naive, very poorly educated, or simply greedy. Regardless, these examples shame us all because they bring discredit to a specialty long dedicated to appropriate care. Vascular surgeons are not only our patients’ treating physicians but also their ombudspersons. How is our specialty to be taken seriously when our own members deviate so dramatically from accepted practice guidelines?
The advent of endovascular treatments may explain some of these unnecessary procedures. Endovascular procedures, in general, are much easier to perform than open surgery. Frequently, resultant complications may not be as devastating, so surgeons may be more inclined to intervene earlier in the disease process. Also, it is more cost effective for a vascular surgeon to perform a quick SFA angioplasty and stent rather than a time-consuming and undercompensated femoropopliteal vein bypass. This is especially so if it is performed in the surgeon‘s outpatient facility.
Endovascular technologies also have the cache of being novel and state-of-the-art. Therefore, it is tempting for surgeons to promote their reputation by preferentially performing these ‘advanced’ procedures. New trainees may be especially seduced by the novelty of these techniques, but their lack of clinical experience may result in overutilization.
Clearly, the answer is not that we should perform surgery for surgery’s sake. If a patient has a valid reason for an endovascular procedure, so be it. But if an open procedure is the better option, we must not shy away from it for fear of being regarded as old fashioned.
The increasing adoption of endovascular therapies may not only explain unnecessary procedures but also why vascular surgeons are involved in an identity crisis. As endovascular procedures replace open surgeries, new graduates and even older surgeons may begin to feel uncomfortable performing complex surgeries. As a result, vascular surgeons are now so endo-oriented that we hardly operate. Further, it appears as if our vascular training programs are producing interventional radiologists or cardiologists and not vascular surgeons. If all we offer are endovascular therapies, we will not be able to delineate ourselves from other physicians. We need to reassure our patients and referring doctors that we are still the only specialty that can perform all methods of treatment for our patients, be it medications, surgery, balloons, stents, or whatever. Equally important is that we assure them that the therapeutic modality that we select will be the most appropriate and will not be driven by extraneous factors. Accordingly, we must reign in our wayward colleagues or face unacceptable repercussions.
University institutions have Morbidity and Mortality conferences to evaluate staff surgeons’ performance. Credentials committees have the ability to withdraw privileges for persistent inappropriate indications. Outpatient centers need to establish similar panels so that peer pressure can ensure appropriate treatment. The goal should be remedial education and not punishment. We need to make these “Dark Knights” aware of how their actions have a negative effect on the rest of us. Because, if left unchecked, castigation in the media and government action will punish all vascular surgeons and our legendary contributions to the management of vascular disease will fade from memory, just like Arthur and his knightly court.
Dr. Samson is a physician in the practice of Samson, Showalter, Lepore, and Nair, and clinical professor of surgery, Florida State University.
In my past editorials I have made it abundantly clear that I believe that vascular surgeons, like the Knights of the Round Table in the Arthurian legend, follow a chivalrous code of honor that guides us in placing a patient’s well-being ahead of financial reward. We ride out, catheter and knife at the ready, to defeat the malevolent atherosclerotic enemy. Yet I am now chagrined to acknowledge that we, too, have knights who have forsaken their code of chivalry – vascular surgeons who value the attainment of wealth or prestige as their raison d’être.
Our cadre of ethical doctors far outnumbers the avaricious few. But I am increasingly aware of board certified vascular surgeons offering or carrying out egregious or unnecessary interventions.
The following are but a few illustrations of this behavior:
• A website suggesting all men older than 40 years have a self-paid screening for AAA.
• An 80-year-old woman with recurrent swelling of her right leg being told that she needed an emergency ablation of her saphenous vein.
• An obese 50-year-old with no abdominal symptoms and a patent SMA having a stent placed in his celiac artery.
• A 20-year-old who had her saphenous vein ablated because she had a few spiders on her thigh.
• I encountered a patient after a vascular surgeon had inserted an endograft in an 85-year-old male with a 4.5-cm AAA.
• Another vascular surgeon performs yearly carotid arteriography to evaluate the possible progression of asymptomatic stenoses.
• Yet another vascular surgeon carried out a carotid endarterectomy for a 60% asymptomatic stenosis in a patient with end-stage lung cancer.
If you find your skin crawling as you read these examples, you are not the perpetrators. If you are blushing, you may be. If you don’t see the problems with these cases you are naive, very poorly educated, or simply greedy. Regardless, these examples shame us all because they bring discredit to a specialty long dedicated to appropriate care. Vascular surgeons are not only our patients’ treating physicians but also their ombudspersons. How is our specialty to be taken seriously when our own members deviate so dramatically from accepted practice guidelines?
The advent of endovascular treatments may explain some of these unnecessary procedures. Endovascular procedures, in general, are much easier to perform than open surgery. Frequently, resultant complications may not be as devastating, so surgeons may be more inclined to intervene earlier in the disease process. Also, it is more cost effective for a vascular surgeon to perform a quick SFA angioplasty and stent rather than a time-consuming and undercompensated femoropopliteal vein bypass. This is especially so if it is performed in the surgeon‘s outpatient facility.
Endovascular technologies also have the cache of being novel and state-of-the-art. Therefore, it is tempting for surgeons to promote their reputation by preferentially performing these ‘advanced’ procedures. New trainees may be especially seduced by the novelty of these techniques, but their lack of clinical experience may result in overutilization.
Clearly, the answer is not that we should perform surgery for surgery’s sake. If a patient has a valid reason for an endovascular procedure, so be it. But if an open procedure is the better option, we must not shy away from it for fear of being regarded as old fashioned.
The increasing adoption of endovascular therapies may not only explain unnecessary procedures but also why vascular surgeons are involved in an identity crisis. As endovascular procedures replace open surgeries, new graduates and even older surgeons may begin to feel uncomfortable performing complex surgeries. As a result, vascular surgeons are now so endo-oriented that we hardly operate. Further, it appears as if our vascular training programs are producing interventional radiologists or cardiologists and not vascular surgeons. If all we offer are endovascular therapies, we will not be able to delineate ourselves from other physicians. We need to reassure our patients and referring doctors that we are still the only specialty that can perform all methods of treatment for our patients, be it medications, surgery, balloons, stents, or whatever. Equally important is that we assure them that the therapeutic modality that we select will be the most appropriate and will not be driven by extraneous factors. Accordingly, we must reign in our wayward colleagues or face unacceptable repercussions.
University institutions have Morbidity and Mortality conferences to evaluate staff surgeons’ performance. Credentials committees have the ability to withdraw privileges for persistent inappropriate indications. Outpatient centers need to establish similar panels so that peer pressure can ensure appropriate treatment. The goal should be remedial education and not punishment. We need to make these “Dark Knights” aware of how their actions have a negative effect on the rest of us. Because, if left unchecked, castigation in the media and government action will punish all vascular surgeons and our legendary contributions to the management of vascular disease will fade from memory, just like Arthur and his knightly court.
Dr. Samson is a physician in the practice of Samson, Showalter, Lepore, and Nair, and clinical professor of surgery, Florida State University.
In my past editorials I have made it abundantly clear that I believe that vascular surgeons, like the Knights of the Round Table in the Arthurian legend, follow a chivalrous code of honor that guides us in placing a patient’s well-being ahead of financial reward. We ride out, catheter and knife at the ready, to defeat the malevolent atherosclerotic enemy. Yet I am now chagrined to acknowledge that we, too, have knights who have forsaken their code of chivalry – vascular surgeons who value the attainment of wealth or prestige as their raison d’être.
Our cadre of ethical doctors far outnumbers the avaricious few. But I am increasingly aware of board certified vascular surgeons offering or carrying out egregious or unnecessary interventions.
The following are but a few illustrations of this behavior:
• A website suggesting all men older than 40 years have a self-paid screening for AAA.
• An 80-year-old woman with recurrent swelling of her right leg being told that she needed an emergency ablation of her saphenous vein.
• An obese 50-year-old with no abdominal symptoms and a patent SMA having a stent placed in his celiac artery.
• A 20-year-old who had her saphenous vein ablated because she had a few spiders on her thigh.
• I encountered a patient after a vascular surgeon had inserted an endograft in an 85-year-old male with a 4.5-cm AAA.
• Another vascular surgeon performs yearly carotid arteriography to evaluate the possible progression of asymptomatic stenoses.
• Yet another vascular surgeon carried out a carotid endarterectomy for a 60% asymptomatic stenosis in a patient with end-stage lung cancer.
If you find your skin crawling as you read these examples, you are not the perpetrators. If you are blushing, you may be. If you don’t see the problems with these cases you are naive, very poorly educated, or simply greedy. Regardless, these examples shame us all because they bring discredit to a specialty long dedicated to appropriate care. Vascular surgeons are not only our patients’ treating physicians but also their ombudspersons. How is our specialty to be taken seriously when our own members deviate so dramatically from accepted practice guidelines?
The advent of endovascular treatments may explain some of these unnecessary procedures. Endovascular procedures, in general, are much easier to perform than open surgery. Frequently, resultant complications may not be as devastating, so surgeons may be more inclined to intervene earlier in the disease process. Also, it is more cost effective for a vascular surgeon to perform a quick SFA angioplasty and stent rather than a time-consuming and undercompensated femoropopliteal vein bypass. This is especially so if it is performed in the surgeon‘s outpatient facility.
Endovascular technologies also have the cache of being novel and state-of-the-art. Therefore, it is tempting for surgeons to promote their reputation by preferentially performing these ‘advanced’ procedures. New trainees may be especially seduced by the novelty of these techniques, but their lack of clinical experience may result in overutilization.
Clearly, the answer is not that we should perform surgery for surgery’s sake. If a patient has a valid reason for an endovascular procedure, so be it. But if an open procedure is the better option, we must not shy away from it for fear of being regarded as old fashioned.
The increasing adoption of endovascular therapies may not only explain unnecessary procedures but also why vascular surgeons are involved in an identity crisis. As endovascular procedures replace open surgeries, new graduates and even older surgeons may begin to feel uncomfortable performing complex surgeries. As a result, vascular surgeons are now so endo-oriented that we hardly operate. Further, it appears as if our vascular training programs are producing interventional radiologists or cardiologists and not vascular surgeons. If all we offer are endovascular therapies, we will not be able to delineate ourselves from other physicians. We need to reassure our patients and referring doctors that we are still the only specialty that can perform all methods of treatment for our patients, be it medications, surgery, balloons, stents, or whatever. Equally important is that we assure them that the therapeutic modality that we select will be the most appropriate and will not be driven by extraneous factors. Accordingly, we must reign in our wayward colleagues or face unacceptable repercussions.
University institutions have Morbidity and Mortality conferences to evaluate staff surgeons’ performance. Credentials committees have the ability to withdraw privileges for persistent inappropriate indications. Outpatient centers need to establish similar panels so that peer pressure can ensure appropriate treatment. The goal should be remedial education and not punishment. We need to make these “Dark Knights” aware of how their actions have a negative effect on the rest of us. Because, if left unchecked, castigation in the media and government action will punish all vascular surgeons and our legendary contributions to the management of vascular disease will fade from memory, just like Arthur and his knightly court.
Dr. Samson is a physician in the practice of Samson, Showalter, Lepore, and Nair, and clinical professor of surgery, Florida State University.

Auto accidents in sleepy medical trainees
Question: Driving home after a demanding 24 hours on call, the sleepy and fatigued first-year medical resident momentarily dozed off at the wheel, ran a stop sign, and struck an oncoming car, injuring its driver. In a lawsuit by the injured victim, which of the following answers is best?
A. The residency program is definitely liable, being in violation of Accreditation Council for Graduate Medical Education rules on consecutive work hours.
B. The resident is solely liable, because he’s the one who owed the duty of due care.
C. The hospital may be a named codefendant, because it knew or should have known that sleep deprivation can impair a person’s driving ability.
D. A and C are correct.
E. Only B and C are correct.
Answer: E. Residency training programs face many potential liabilities, such as those arising from disciplinary actions, employer-employee disputes, sexual harassment, and so on. But one issue deserving attention is auto accidents in overfatigued trainees. The incidence of falling asleep at the wheel is very high – in some surveys, close to 50% – and accidents are more likely to occur in the immediate post-call period.
The two main research papers documenting a relationship between extended work duty and auto accidents are from Laura K. Barger, Ph.D., and Dr. Colin P. West.
In the Barger study, the authors conducted a nationwide Web-based survey of 2,737 interns (N. Engl. J. Med. 2005;352:125-34). They found that an extended work shift (greater than 24 hours) was 2.3 times as likely for a motor vehicle crash, and 5.9 times for a near-miss accident. The researchers calculated that every extended shift in the month increased the crash risk by 9.1% and near-miss risk by 16.2%.
In the West study, the authors performed a prospective, 5-year longitudinal study of a cohort of 340 first-year Mayo Clinic residents in internal medicine (Mayo Clin. Proc. 2012;87:1138-44). In self-generated quarterly filings, 11.3% reported a motor vehicle crash and 43.3% a near-miss accident. Sleepiness (as well as other variables such as depression, burnout, diminished quality of life, and fatigue) significantly increased the odds of a motor vehicle incident in the subsequent 3-month period. Each 1-point increase in fatigue or Epworth Sleepiness Scale score was associated with a 52% and 12% respective increase in a motor vehicle crash.
The Accreditation Council for Graduate Medical Education (ACGME) has formulated rules, which have undergone recent changes, regarding consecutive work-duty hours. Its latest edict in June 2014 can be found on its website and stipulates that “Duty periods of PGY-1 residents must not exceed 16 hours in duration,” and “Duty periods of PGY-2 residents and above may be scheduled to a maximum of 24 hours of continuous duty in the hospital.”
Furthermore, programs must encourage residents to use alertness management strategies in the context of patient care responsibilities. Strategic napping, especially after 16 hours of continuous duty and between the hours of 10:00 p.m. and 8:00 a.m., was a strong suggestion.
In a 2005 lawsuit naming Chicago’s Rush Presbyterian-St. Luke’s Medical Center as a defendant, an Illinois court faced the issue of whether a hospital owed a duty to a plaintiff injured by an off-duty resident doctor allegedly suffering from sleep deprivation as a result of a hospital’s policy on working hours (Brewster v. Rush Presbyterian-St. Luke’s Medical Center (836 N.E.2d 635 (Il. App. 2005)). The doctor was an intern who had worked 34 hours of a 36-hour work shift, and fell asleep behind the wheel of her car, striking and seriously injuring the driver of an oncoming car.
In its decision, the court noted the plaintiff’s argument that it was reasonably foreseeable and likely that drivers who were sleep deprived would cause traffic accidents resulting in injuries. For public policy reasons, the plaintiff also maintained that such injuries could be prevented if hospitals either changed work schedules of their residents or provided them with additional rest periods.
However, the court held that there was no liability imputed to health care providers for injuries to nonpatient third parties absent the existence of a “special relationship” between the parties.
Thus, training programs or hospitals may or may not be found liable in future such cases or in other jurisdictions – but the new, stricter ACGME rules suggest that they will, at a minimum, be a named defendant.
Note that in some jurisdictions, injured nonpatient third parties have successfully sued doctors for failing to warn their patients that certain medications can adversely affect their driving ability, and for failing to warn about medical conditions, e.g., syncope, that can adversely impact driving.
Court decisions in analogous factual circumstances have sometimes favored the accident victim.
In Robertson v. LeMaster (301 S.E.2d 563 (W. Va. 1983)), the West Virginia Supreme Court of Appeals noted that the defendant’s employer, Norfolk & Western Railway Company, “could have reasonably foreseen that its exhausted employee, who had been required to work 27 hours without rest, would pose a risk of harm to other motorists.”
In Faverty v. McDonald’s Restaurants of Oregon (892 P.2d 703 (Ore. Ct. App.1995)), an Oregon appeals court held that the defendant corporation (McDonald’s Restaurants of Oregon) knew or should have known that its employee was a hazard to himself and others when he drove home from the workplace after working multiple shifts in a 24-hour period.
On the other hand, in Barclay v. Briscoe (47 A.3d 560 (Md. 2012)), a longshoreman employed by Ports America Baltimore fell asleep at the wheel while traveling home after working a 22-hour shift and caused a head-on collision resulting in catastrophic injuries. Ports America Baltimore contended that it could not be held primarily liable, because it owed no duty to the public to ensure that an employee was fit to drive his personal vehicle home. The trial court agreed, and the Maryland Court of Appeals affirmed.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: Driving home after a demanding 24 hours on call, the sleepy and fatigued first-year medical resident momentarily dozed off at the wheel, ran a stop sign, and struck an oncoming car, injuring its driver. In a lawsuit by the injured victim, which of the following answers is best?
A. The residency program is definitely liable, being in violation of Accreditation Council for Graduate Medical Education rules on consecutive work hours.
B. The resident is solely liable, because he’s the one who owed the duty of due care.
C. The hospital may be a named codefendant, because it knew or should have known that sleep deprivation can impair a person’s driving ability.
D. A and C are correct.
E. Only B and C are correct.
Answer: E. Residency training programs face many potential liabilities, such as those arising from disciplinary actions, employer-employee disputes, sexual harassment, and so on. But one issue deserving attention is auto accidents in overfatigued trainees. The incidence of falling asleep at the wheel is very high – in some surveys, close to 50% – and accidents are more likely to occur in the immediate post-call period.
The two main research papers documenting a relationship between extended work duty and auto accidents are from Laura K. Barger, Ph.D., and Dr. Colin P. West.
In the Barger study, the authors conducted a nationwide Web-based survey of 2,737 interns (N. Engl. J. Med. 2005;352:125-34). They found that an extended work shift (greater than 24 hours) was 2.3 times as likely for a motor vehicle crash, and 5.9 times for a near-miss accident. The researchers calculated that every extended shift in the month increased the crash risk by 9.1% and near-miss risk by 16.2%.
In the West study, the authors performed a prospective, 5-year longitudinal study of a cohort of 340 first-year Mayo Clinic residents in internal medicine (Mayo Clin. Proc. 2012;87:1138-44). In self-generated quarterly filings, 11.3% reported a motor vehicle crash and 43.3% a near-miss accident. Sleepiness (as well as other variables such as depression, burnout, diminished quality of life, and fatigue) significantly increased the odds of a motor vehicle incident in the subsequent 3-month period. Each 1-point increase in fatigue or Epworth Sleepiness Scale score was associated with a 52% and 12% respective increase in a motor vehicle crash.
The Accreditation Council for Graduate Medical Education (ACGME) has formulated rules, which have undergone recent changes, regarding consecutive work-duty hours. Its latest edict in June 2014 can be found on its website and stipulates that “Duty periods of PGY-1 residents must not exceed 16 hours in duration,” and “Duty periods of PGY-2 residents and above may be scheduled to a maximum of 24 hours of continuous duty in the hospital.”
Furthermore, programs must encourage residents to use alertness management strategies in the context of patient care responsibilities. Strategic napping, especially after 16 hours of continuous duty and between the hours of 10:00 p.m. and 8:00 a.m., was a strong suggestion.
In a 2005 lawsuit naming Chicago’s Rush Presbyterian-St. Luke’s Medical Center as a defendant, an Illinois court faced the issue of whether a hospital owed a duty to a plaintiff injured by an off-duty resident doctor allegedly suffering from sleep deprivation as a result of a hospital’s policy on working hours (Brewster v. Rush Presbyterian-St. Luke’s Medical Center (836 N.E.2d 635 (Il. App. 2005)). The doctor was an intern who had worked 34 hours of a 36-hour work shift, and fell asleep behind the wheel of her car, striking and seriously injuring the driver of an oncoming car.
In its decision, the court noted the plaintiff’s argument that it was reasonably foreseeable and likely that drivers who were sleep deprived would cause traffic accidents resulting in injuries. For public policy reasons, the plaintiff also maintained that such injuries could be prevented if hospitals either changed work schedules of their residents or provided them with additional rest periods.
However, the court held that there was no liability imputed to health care providers for injuries to nonpatient third parties absent the existence of a “special relationship” between the parties.
Thus, training programs or hospitals may or may not be found liable in future such cases or in other jurisdictions – but the new, stricter ACGME rules suggest that they will, at a minimum, be a named defendant.
Note that in some jurisdictions, injured nonpatient third parties have successfully sued doctors for failing to warn their patients that certain medications can adversely affect their driving ability, and for failing to warn about medical conditions, e.g., syncope, that can adversely impact driving.
Court decisions in analogous factual circumstances have sometimes favored the accident victim.
In Robertson v. LeMaster (301 S.E.2d 563 (W. Va. 1983)), the West Virginia Supreme Court of Appeals noted that the defendant’s employer, Norfolk & Western Railway Company, “could have reasonably foreseen that its exhausted employee, who had been required to work 27 hours without rest, would pose a risk of harm to other motorists.”
In Faverty v. McDonald’s Restaurants of Oregon (892 P.2d 703 (Ore. Ct. App.1995)), an Oregon appeals court held that the defendant corporation (McDonald’s Restaurants of Oregon) knew or should have known that its employee was a hazard to himself and others when he drove home from the workplace after working multiple shifts in a 24-hour period.
On the other hand, in Barclay v. Briscoe (47 A.3d 560 (Md. 2012)), a longshoreman employed by Ports America Baltimore fell asleep at the wheel while traveling home after working a 22-hour shift and caused a head-on collision resulting in catastrophic injuries. Ports America Baltimore contended that it could not be held primarily liable, because it owed no duty to the public to ensure that an employee was fit to drive his personal vehicle home. The trial court agreed, and the Maryland Court of Appeals affirmed.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: Driving home after a demanding 24 hours on call, the sleepy and fatigued first-year medical resident momentarily dozed off at the wheel, ran a stop sign, and struck an oncoming car, injuring its driver. In a lawsuit by the injured victim, which of the following answers is best?
A. The residency program is definitely liable, being in violation of Accreditation Council for Graduate Medical Education rules on consecutive work hours.
B. The resident is solely liable, because he’s the one who owed the duty of due care.
C. The hospital may be a named codefendant, because it knew or should have known that sleep deprivation can impair a person’s driving ability.
D. A and C are correct.
E. Only B and C are correct.
Answer: E. Residency training programs face many potential liabilities, such as those arising from disciplinary actions, employer-employee disputes, sexual harassment, and so on. But one issue deserving attention is auto accidents in overfatigued trainees. The incidence of falling asleep at the wheel is very high – in some surveys, close to 50% – and accidents are more likely to occur in the immediate post-call period.
The two main research papers documenting a relationship between extended work duty and auto accidents are from Laura K. Barger, Ph.D., and Dr. Colin P. West.
In the Barger study, the authors conducted a nationwide Web-based survey of 2,737 interns (N. Engl. J. Med. 2005;352:125-34). They found that an extended work shift (greater than 24 hours) was 2.3 times as likely for a motor vehicle crash, and 5.9 times for a near-miss accident. The researchers calculated that every extended shift in the month increased the crash risk by 9.1% and near-miss risk by 16.2%.
In the West study, the authors performed a prospective, 5-year longitudinal study of a cohort of 340 first-year Mayo Clinic residents in internal medicine (Mayo Clin. Proc. 2012;87:1138-44). In self-generated quarterly filings, 11.3% reported a motor vehicle crash and 43.3% a near-miss accident. Sleepiness (as well as other variables such as depression, burnout, diminished quality of life, and fatigue) significantly increased the odds of a motor vehicle incident in the subsequent 3-month period. Each 1-point increase in fatigue or Epworth Sleepiness Scale score was associated with a 52% and 12% respective increase in a motor vehicle crash.
The Accreditation Council for Graduate Medical Education (ACGME) has formulated rules, which have undergone recent changes, regarding consecutive work-duty hours. Its latest edict in June 2014 can be found on its website and stipulates that “Duty periods of PGY-1 residents must not exceed 16 hours in duration,” and “Duty periods of PGY-2 residents and above may be scheduled to a maximum of 24 hours of continuous duty in the hospital.”
Furthermore, programs must encourage residents to use alertness management strategies in the context of patient care responsibilities. Strategic napping, especially after 16 hours of continuous duty and between the hours of 10:00 p.m. and 8:00 a.m., was a strong suggestion.
In a 2005 lawsuit naming Chicago’s Rush Presbyterian-St. Luke’s Medical Center as a defendant, an Illinois court faced the issue of whether a hospital owed a duty to a plaintiff injured by an off-duty resident doctor allegedly suffering from sleep deprivation as a result of a hospital’s policy on working hours (Brewster v. Rush Presbyterian-St. Luke’s Medical Center (836 N.E.2d 635 (Il. App. 2005)). The doctor was an intern who had worked 34 hours of a 36-hour work shift, and fell asleep behind the wheel of her car, striking and seriously injuring the driver of an oncoming car.
In its decision, the court noted the plaintiff’s argument that it was reasonably foreseeable and likely that drivers who were sleep deprived would cause traffic accidents resulting in injuries. For public policy reasons, the plaintiff also maintained that such injuries could be prevented if hospitals either changed work schedules of their residents or provided them with additional rest periods.
However, the court held that there was no liability imputed to health care providers for injuries to nonpatient third parties absent the existence of a “special relationship” between the parties.
Thus, training programs or hospitals may or may not be found liable in future such cases or in other jurisdictions – but the new, stricter ACGME rules suggest that they will, at a minimum, be a named defendant.
Note that in some jurisdictions, injured nonpatient third parties have successfully sued doctors for failing to warn their patients that certain medications can adversely affect their driving ability, and for failing to warn about medical conditions, e.g., syncope, that can adversely impact driving.
Court decisions in analogous factual circumstances have sometimes favored the accident victim.
In Robertson v. LeMaster (301 S.E.2d 563 (W. Va. 1983)), the West Virginia Supreme Court of Appeals noted that the defendant’s employer, Norfolk & Western Railway Company, “could have reasonably foreseen that its exhausted employee, who had been required to work 27 hours without rest, would pose a risk of harm to other motorists.”
In Faverty v. McDonald’s Restaurants of Oregon (892 P.2d 703 (Ore. Ct. App.1995)), an Oregon appeals court held that the defendant corporation (McDonald’s Restaurants of Oregon) knew or should have known that its employee was a hazard to himself and others when he drove home from the workplace after working multiple shifts in a 24-hour period.
On the other hand, in Barclay v. Briscoe (47 A.3d 560 (Md. 2012)), a longshoreman employed by Ports America Baltimore fell asleep at the wheel while traveling home after working a 22-hour shift and caused a head-on collision resulting in catastrophic injuries. Ports America Baltimore contended that it could not be held primarily liable, because it owed no duty to the public to ensure that an employee was fit to drive his personal vehicle home. The trial court agreed, and the Maryland Court of Appeals affirmed.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.

Short on activity
One of the perks that comes with being a grandparent is that you may get the chance to watch your grandchildren practice, play, and perform in a variety of organized activities. If you are retired and are fortunate enough to live in the same town, the opportunities are limitless and change with the season.
Each event is a kaleidoscope of interpersonal and developmental tableaux. First, of course, you are interested to see how your grandchild is doing. Are her skills improving? How do they compare with her peers’? Is she having fun? But then, what is the goal of the activity? Are the coaches/instructors/organizers doing a good job of reaching that goal?
Last week, I was watching my 8-year-old grandson play the last baseball game of his career (“Grampy, baseball is boring. I’m only playing lacrosse next spring.”) Between innings, I thumbed through the June 2015 Pediatrics. I encountered an article that confirmed my suspicions about some of the organized youth activities I had been watching for the last decade, “Physical Activity in Youth Dance Classes” (Pediatrics 2015;135:1067-73). Using accelerometers, researchers from San Diego State University recorded the activity of more than 250 girls, both children and adolescents, in 21 dance studios, both private and community based.
They discovered that the young dancers were, on average, engaged in moderate to vigorous activity 17.2 minutes (plus or minus 8.9 minutes), which amounted to about 36% of the usual class session. Only 8% of the children and 6% of the adolescents met the Centers for Disease Control and Prevention 30-minute guideline for after-school physical activity during dance.
I’ve watched a fair share of dance classes, and these findings come as no surprise. Typically, there is a lot of sitting around cross-legged in a circle, “listening” to “instruction.” There is even more lining up and waiting, and, then of course, adjusting the line, and an abundance of relining up, followed by a 6-second burst of activity. There is considerable poking and/or hugging fellow line mates, that I suspect wouldn’t have budged an accelerometer.
Unfortunately, this degree of inactivity is not unique to little girls’ dance classes. I have observed the same phenomenon during soccer, baseball, lacrosse, and swim classes – in which the ratio of inactivity to activity often exceeds 4:1. Although it may be slightly more prevalent when the instructors are parent/volunteers, professional physical educators also are guilty of injecting too little physical activity into the activities they are managing. Remember gym class. How much time was spent having your attendance taken, being instructed on how to do the activity, and then standing in line waiting your turn?
There are simple solutions, but they require thinking outside the box. Why have two lines of participants? Wouldn’t six lines mean three times as many children would be active at one time? For example, it has taken a while for soccer and hockey programs to catch on, but now both have games on smaller surfaces with less than the usual number of team members, in hopes that more children will be involved and active. Most great coaches have a knack for creating drills that keep the maximum number of participants active, foster the necessary skills, and at the same time are fun for the participants. The bottom line is that most children, particularly the younger ones, learn by imitating, not by being lectured to. They learn even more quickly if they have older children from which to model their behavior.
You could ask, “What’s the big deal?” Am I just venting the frustrations of an efficiency-obsessed former athlete? Does every minute of a child’s organized activity need to be packed with physical activity? No, not if children were allowed more opportunities for free play at other times during the day. No, not if parents were more diligent in restricting screen time. But if parents are going to count on dance classes and organized sports as physically active time for their children, they need to look more carefully at how that time is being used. An hour of dance class or soccer practice may be better than an hour in front of the tube, but it may fall far short of what the child needs.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.”
One of the perks that comes with being a grandparent is that you may get the chance to watch your grandchildren practice, play, and perform in a variety of organized activities. If you are retired and are fortunate enough to live in the same town, the opportunities are limitless and change with the season.
Each event is a kaleidoscope of interpersonal and developmental tableaux. First, of course, you are interested to see how your grandchild is doing. Are her skills improving? How do they compare with her peers’? Is she having fun? But then, what is the goal of the activity? Are the coaches/instructors/organizers doing a good job of reaching that goal?
Last week, I was watching my 8-year-old grandson play the last baseball game of his career (“Grampy, baseball is boring. I’m only playing lacrosse next spring.”) Between innings, I thumbed through the June 2015 Pediatrics. I encountered an article that confirmed my suspicions about some of the organized youth activities I had been watching for the last decade, “Physical Activity in Youth Dance Classes” (Pediatrics 2015;135:1067-73). Using accelerometers, researchers from San Diego State University recorded the activity of more than 250 girls, both children and adolescents, in 21 dance studios, both private and community based.
They discovered that the young dancers were, on average, engaged in moderate to vigorous activity 17.2 minutes (plus or minus 8.9 minutes), which amounted to about 36% of the usual class session. Only 8% of the children and 6% of the adolescents met the Centers for Disease Control and Prevention 30-minute guideline for after-school physical activity during dance.
I’ve watched a fair share of dance classes, and these findings come as no surprise. Typically, there is a lot of sitting around cross-legged in a circle, “listening” to “instruction.” There is even more lining up and waiting, and, then of course, adjusting the line, and an abundance of relining up, followed by a 6-second burst of activity. There is considerable poking and/or hugging fellow line mates, that I suspect wouldn’t have budged an accelerometer.
Unfortunately, this degree of inactivity is not unique to little girls’ dance classes. I have observed the same phenomenon during soccer, baseball, lacrosse, and swim classes – in which the ratio of inactivity to activity often exceeds 4:1. Although it may be slightly more prevalent when the instructors are parent/volunteers, professional physical educators also are guilty of injecting too little physical activity into the activities they are managing. Remember gym class. How much time was spent having your attendance taken, being instructed on how to do the activity, and then standing in line waiting your turn?
There are simple solutions, but they require thinking outside the box. Why have two lines of participants? Wouldn’t six lines mean three times as many children would be active at one time? For example, it has taken a while for soccer and hockey programs to catch on, but now both have games on smaller surfaces with less than the usual number of team members, in hopes that more children will be involved and active. Most great coaches have a knack for creating drills that keep the maximum number of participants active, foster the necessary skills, and at the same time are fun for the participants. The bottom line is that most children, particularly the younger ones, learn by imitating, not by being lectured to. They learn even more quickly if they have older children from which to model their behavior.
You could ask, “What’s the big deal?” Am I just venting the frustrations of an efficiency-obsessed former athlete? Does every minute of a child’s organized activity need to be packed with physical activity? No, not if children were allowed more opportunities for free play at other times during the day. No, not if parents were more diligent in restricting screen time. But if parents are going to count on dance classes and organized sports as physically active time for their children, they need to look more carefully at how that time is being used. An hour of dance class or soccer practice may be better than an hour in front of the tube, but it may fall far short of what the child needs.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.”
One of the perks that comes with being a grandparent is that you may get the chance to watch your grandchildren practice, play, and perform in a variety of organized activities. If you are retired and are fortunate enough to live in the same town, the opportunities are limitless and change with the season.
Each event is a kaleidoscope of interpersonal and developmental tableaux. First, of course, you are interested to see how your grandchild is doing. Are her skills improving? How do they compare with her peers’? Is she having fun? But then, what is the goal of the activity? Are the coaches/instructors/organizers doing a good job of reaching that goal?
Last week, I was watching my 8-year-old grandson play the last baseball game of his career (“Grampy, baseball is boring. I’m only playing lacrosse next spring.”) Between innings, I thumbed through the June 2015 Pediatrics. I encountered an article that confirmed my suspicions about some of the organized youth activities I had been watching for the last decade, “Physical Activity in Youth Dance Classes” (Pediatrics 2015;135:1067-73). Using accelerometers, researchers from San Diego State University recorded the activity of more than 250 girls, both children and adolescents, in 21 dance studios, both private and community based.
They discovered that the young dancers were, on average, engaged in moderate to vigorous activity 17.2 minutes (plus or minus 8.9 minutes), which amounted to about 36% of the usual class session. Only 8% of the children and 6% of the adolescents met the Centers for Disease Control and Prevention 30-minute guideline for after-school physical activity during dance.
I’ve watched a fair share of dance classes, and these findings come as no surprise. Typically, there is a lot of sitting around cross-legged in a circle, “listening” to “instruction.” There is even more lining up and waiting, and, then of course, adjusting the line, and an abundance of relining up, followed by a 6-second burst of activity. There is considerable poking and/or hugging fellow line mates, that I suspect wouldn’t have budged an accelerometer.
Unfortunately, this degree of inactivity is not unique to little girls’ dance classes. I have observed the same phenomenon during soccer, baseball, lacrosse, and swim classes – in which the ratio of inactivity to activity often exceeds 4:1. Although it may be slightly more prevalent when the instructors are parent/volunteers, professional physical educators also are guilty of injecting too little physical activity into the activities they are managing. Remember gym class. How much time was spent having your attendance taken, being instructed on how to do the activity, and then standing in line waiting your turn?
There are simple solutions, but they require thinking outside the box. Why have two lines of participants? Wouldn’t six lines mean three times as many children would be active at one time? For example, it has taken a while for soccer and hockey programs to catch on, but now both have games on smaller surfaces with less than the usual number of team members, in hopes that more children will be involved and active. Most great coaches have a knack for creating drills that keep the maximum number of participants active, foster the necessary skills, and at the same time are fun for the participants. The bottom line is that most children, particularly the younger ones, learn by imitating, not by being lectured to. They learn even more quickly if they have older children from which to model their behavior.
You could ask, “What’s the big deal?” Am I just venting the frustrations of an efficiency-obsessed former athlete? Does every minute of a child’s organized activity need to be packed with physical activity? No, not if children were allowed more opportunities for free play at other times during the day. No, not if parents were more diligent in restricting screen time. But if parents are going to count on dance classes and organized sports as physically active time for their children, they need to look more carefully at how that time is being used. An hour of dance class or soccer practice may be better than an hour in front of the tube, but it may fall far short of what the child needs.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.”
Physician suicide needs attention
Recently, there have been several news stories about physicians committing suicide. This is across all levels of the profession, including medical students, residents, and attendings.
Historically, doctors have had a higher rate of suicide than most professions. I’m not sure if that number has crept up recently, or if events are garnering more attention than before. They’re certainly mentioned prominently on various medical blogs.
Why do you see this in medicine? There are probably a number of factors that overlap:
• A high pressure job, where mistakes aren’t allowed (which isn’t humanly possible).
• A culture of litigation, where even minor mistakes are taken to court.
• Declining financial reimbursement, making it harder to support a practice and family, especially when you’re already six figures in debt coming out of medical school.
• Pressure to work longer hours and see far more patients than is possible, which increases the potential for mistakes. This further reduces the amount of family and recreational time available to balance ourselves.
• An increase in “empowered patients” demanding unnecessary tests and treatments because it said so on the Internet.
• A general lack of respect for the profession, to where we’re now “providers” who are vilified for political reasons by insurance companies, consumer groups, and both major parties.
• The need for us not to admit or seek treatment for human vulnerabilities. Our own health (mental and physical) is neglected because we can’t take time off to address it and a fear that doing so may result in us having our licenses penalized.
Any of the above makes life unpleasant, but when you combine them … it can be a perfect storm that tips a person over the edge.
In medicine, seeking help is often seen as a weakness, and even the most rational person under difficult circumstances can snap. None of the physicians who’ve ended their lives started out saying that was how they wanted their medical career to wind up. But when stressors pile up, it may appear to them to be the only way out. In that frame of mind, you think doing something so drastic is better for everyone around you. It isn’t true, but at that point you don’t believe it.
A physician’s suicide, even outside of its effects on their family, is a loss. A physician is a community resource, leaving behind relationships with patients in various stages of work-ups and treatments. There’s always another doctor, but it’s not easy, or immediate, to find someone who’s a good fit for the area.
I don’t know if this is a peculiarly American phenomenon or if my colleagues in Canada, Europe, and elsewhere face similar challenges. If the suicide rate elsewhere is lower, what can we learn from them to make things better here? If it’s the same, what can we do collectively to find an answer? Every country needs doctors and can’t afford to lose them.
Is there an easy solution? Probably not. Too many factors to fix. But it’s a serious problem and needs attention.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, there have been several news stories about physicians committing suicide. This is across all levels of the profession, including medical students, residents, and attendings.
Historically, doctors have had a higher rate of suicide than most professions. I’m not sure if that number has crept up recently, or if events are garnering more attention than before. They’re certainly mentioned prominently on various medical blogs.
Why do you see this in medicine? There are probably a number of factors that overlap:
• A high pressure job, where mistakes aren’t allowed (which isn’t humanly possible).
• A culture of litigation, where even minor mistakes are taken to court.
• Declining financial reimbursement, making it harder to support a practice and family, especially when you’re already six figures in debt coming out of medical school.
• Pressure to work longer hours and see far more patients than is possible, which increases the potential for mistakes. This further reduces the amount of family and recreational time available to balance ourselves.
• An increase in “empowered patients” demanding unnecessary tests and treatments because it said so on the Internet.
• A general lack of respect for the profession, to where we’re now “providers” who are vilified for political reasons by insurance companies, consumer groups, and both major parties.
• The need for us not to admit or seek treatment for human vulnerabilities. Our own health (mental and physical) is neglected because we can’t take time off to address it and a fear that doing so may result in us having our licenses penalized.
Any of the above makes life unpleasant, but when you combine them … it can be a perfect storm that tips a person over the edge.
In medicine, seeking help is often seen as a weakness, and even the most rational person under difficult circumstances can snap. None of the physicians who’ve ended their lives started out saying that was how they wanted their medical career to wind up. But when stressors pile up, it may appear to them to be the only way out. In that frame of mind, you think doing something so drastic is better for everyone around you. It isn’t true, but at that point you don’t believe it.
A physician’s suicide, even outside of its effects on their family, is a loss. A physician is a community resource, leaving behind relationships with patients in various stages of work-ups and treatments. There’s always another doctor, but it’s not easy, or immediate, to find someone who’s a good fit for the area.
I don’t know if this is a peculiarly American phenomenon or if my colleagues in Canada, Europe, and elsewhere face similar challenges. If the suicide rate elsewhere is lower, what can we learn from them to make things better here? If it’s the same, what can we do collectively to find an answer? Every country needs doctors and can’t afford to lose them.
Is there an easy solution? Probably not. Too many factors to fix. But it’s a serious problem and needs attention.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, there have been several news stories about physicians committing suicide. This is across all levels of the profession, including medical students, residents, and attendings.
Historically, doctors have had a higher rate of suicide than most professions. I’m not sure if that number has crept up recently, or if events are garnering more attention than before. They’re certainly mentioned prominently on various medical blogs.
Why do you see this in medicine? There are probably a number of factors that overlap:
• A high pressure job, where mistakes aren’t allowed (which isn’t humanly possible).
• A culture of litigation, where even minor mistakes are taken to court.
• Declining financial reimbursement, making it harder to support a practice and family, especially when you’re already six figures in debt coming out of medical school.
• Pressure to work longer hours and see far more patients than is possible, which increases the potential for mistakes. This further reduces the amount of family and recreational time available to balance ourselves.
• An increase in “empowered patients” demanding unnecessary tests and treatments because it said so on the Internet.
• A general lack of respect for the profession, to where we’re now “providers” who are vilified for political reasons by insurance companies, consumer groups, and both major parties.
• The need for us not to admit or seek treatment for human vulnerabilities. Our own health (mental and physical) is neglected because we can’t take time off to address it and a fear that doing so may result in us having our licenses penalized.
Any of the above makes life unpleasant, but when you combine them … it can be a perfect storm that tips a person over the edge.
In medicine, seeking help is often seen as a weakness, and even the most rational person under difficult circumstances can snap. None of the physicians who’ve ended their lives started out saying that was how they wanted their medical career to wind up. But when stressors pile up, it may appear to them to be the only way out. In that frame of mind, you think doing something so drastic is better for everyone around you. It isn’t true, but at that point you don’t believe it.
A physician’s suicide, even outside of its effects on their family, is a loss. A physician is a community resource, leaving behind relationships with patients in various stages of work-ups and treatments. There’s always another doctor, but it’s not easy, or immediate, to find someone who’s a good fit for the area.
I don’t know if this is a peculiarly American phenomenon or if my colleagues in Canada, Europe, and elsewhere face similar challenges. If the suicide rate elsewhere is lower, what can we learn from them to make things better here? If it’s the same, what can we do collectively to find an answer? Every country needs doctors and can’t afford to lose them.
Is there an easy solution? Probably not. Too many factors to fix. But it’s a serious problem and needs attention.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

To FDA: Wait for clinical outcomes data
The recent endorsements by the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee of the new genetically manufactured, subcutaneously administered cholesterol-lowering agents alirocumab (Sanofi-Regeneron) and evolocumab (Pfizer) have sent a jolt through the world of cholesterol therapy. Proposed for the treatment of patients with high-risk cardiovascular disease and homozygous familial hypercholesterolemia (HoFH), the decisions suggest that the committee has developed a severe case of scientific amnesia.
A case can be made for the approval for the very-high-risk and untreatable patients with HoFH, but the decision to treat millions of Americans based on the paucity of clinical data available would be disturbing, if not irresponsible.
It is clear that these proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors provide a powerful therapy for reducing LDL cholesterol, with a reported decrease of about 60% after only 12 or 52 weeks of treatment. Based on four small studies lasting 10-12 weeks and without any clinical outcome data, the committee recommended approving evolocumab for lifetime therapy without anything to support its clinical effectiveness or safety.
Dr. Robert J. Smith, who chaired the advisory committee meeting, faced with approving the drug or delaying a decision until a randomized clinical trial can be completed said, “I am unwilling to subject patients to the wait.” A publication of the American College of Cardiology suggested that these two monoclonal antibody drugs could replace generic statins in 70 million Americans at an estimated cost of $7,000-$12,000 a year. Talk about breaking the bank.
Only recently, we decided that the appropriate statin therapy for cholesterol control should use the dosing from the original clinical trials rather than chasing LDL levels to the lowest level possible. We now have a class of drugs that clearly can lower the cholesterol to a level never seen before, and we are about to discard that therapeutic advice.
We have experience in chasing blood levels with uncertain outcomes. Reducing blood sugar to a very low hemoglobin A1c level led to adverse clinical events and increased mortality in type 2 diabetes. Raising HDL with the cholesterol ester transfer protein (CETP) inhibitor torcetrapib in a study of 15,000 patients in an outcome trial carried out over a number of years led to increased blood pressure and mortality by 58%, which was associated with a 25% decrease in LDL cholesterol and a 72% increase in HDL, both effects presumed to be remarkably beneficial (N. Engl. J. Med. 2007;357:2109-22).
It is quite possible that these new agents can further decrease coronary vascular mortality. A healthy controversy has raged for some time in regard to the “LDL hypothesis,” compared with therapy based upon the clinical trial outcome. The recent IMPROVE-IT report (N. Engl. J. Med. 2015;372:2387-97) provides some data to support the LDL hypothesis. In that study, the addition of 10 mg of ezetimibe to 40 mg of simvastatin in 18,144 patients followed for up to 6 years resulted in a 2% decrease in mortality associated with a 15.8-mg decrease in serum LDL.
Would it not be prudent to have similar data with the new drug on the street? If it is as potent as it appears to be, a trial of much shorter duration might demonstrate its potency and safety before it is offered to 70 million Americans. The FDA has been reluctant to use surrogate endpoints for approving drugs, but its position has not always been consistent. For some time the FDA has, on occasion, approved drugs that can lower cholesterol with limited outcome data as it did with ezetimibe. However, the decision in regard to the PCSK9 inhibitors will have a much larger impact on care than an add-on drug like ezetimibe. Let’s hope that the FDA shows better judgment than its advisory committee.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The recent endorsements by the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee of the new genetically manufactured, subcutaneously administered cholesterol-lowering agents alirocumab (Sanofi-Regeneron) and evolocumab (Pfizer) have sent a jolt through the world of cholesterol therapy. Proposed for the treatment of patients with high-risk cardiovascular disease and homozygous familial hypercholesterolemia (HoFH), the decisions suggest that the committee has developed a severe case of scientific amnesia.
A case can be made for the approval for the very-high-risk and untreatable patients with HoFH, but the decision to treat millions of Americans based on the paucity of clinical data available would be disturbing, if not irresponsible.
It is clear that these proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors provide a powerful therapy for reducing LDL cholesterol, with a reported decrease of about 60% after only 12 or 52 weeks of treatment. Based on four small studies lasting 10-12 weeks and without any clinical outcome data, the committee recommended approving evolocumab for lifetime therapy without anything to support its clinical effectiveness or safety.
Dr. Robert J. Smith, who chaired the advisory committee meeting, faced with approving the drug or delaying a decision until a randomized clinical trial can be completed said, “I am unwilling to subject patients to the wait.” A publication of the American College of Cardiology suggested that these two monoclonal antibody drugs could replace generic statins in 70 million Americans at an estimated cost of $7,000-$12,000 a year. Talk about breaking the bank.
Only recently, we decided that the appropriate statin therapy for cholesterol control should use the dosing from the original clinical trials rather than chasing LDL levels to the lowest level possible. We now have a class of drugs that clearly can lower the cholesterol to a level never seen before, and we are about to discard that therapeutic advice.
We have experience in chasing blood levels with uncertain outcomes. Reducing blood sugar to a very low hemoglobin A1c level led to adverse clinical events and increased mortality in type 2 diabetes. Raising HDL with the cholesterol ester transfer protein (CETP) inhibitor torcetrapib in a study of 15,000 patients in an outcome trial carried out over a number of years led to increased blood pressure and mortality by 58%, which was associated with a 25% decrease in LDL cholesterol and a 72% increase in HDL, both effects presumed to be remarkably beneficial (N. Engl. J. Med. 2007;357:2109-22).
It is quite possible that these new agents can further decrease coronary vascular mortality. A healthy controversy has raged for some time in regard to the “LDL hypothesis,” compared with therapy based upon the clinical trial outcome. The recent IMPROVE-IT report (N. Engl. J. Med. 2015;372:2387-97) provides some data to support the LDL hypothesis. In that study, the addition of 10 mg of ezetimibe to 40 mg of simvastatin in 18,144 patients followed for up to 6 years resulted in a 2% decrease in mortality associated with a 15.8-mg decrease in serum LDL.
Would it not be prudent to have similar data with the new drug on the street? If it is as potent as it appears to be, a trial of much shorter duration might demonstrate its potency and safety before it is offered to 70 million Americans. The FDA has been reluctant to use surrogate endpoints for approving drugs, but its position has not always been consistent. For some time the FDA has, on occasion, approved drugs that can lower cholesterol with limited outcome data as it did with ezetimibe. However, the decision in regard to the PCSK9 inhibitors will have a much larger impact on care than an add-on drug like ezetimibe. Let’s hope that the FDA shows better judgment than its advisory committee.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The recent endorsements by the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee of the new genetically manufactured, subcutaneously administered cholesterol-lowering agents alirocumab (Sanofi-Regeneron) and evolocumab (Pfizer) have sent a jolt through the world of cholesterol therapy. Proposed for the treatment of patients with high-risk cardiovascular disease and homozygous familial hypercholesterolemia (HoFH), the decisions suggest that the committee has developed a severe case of scientific amnesia.
A case can be made for the approval for the very-high-risk and untreatable patients with HoFH, but the decision to treat millions of Americans based on the paucity of clinical data available would be disturbing, if not irresponsible.
It is clear that these proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors provide a powerful therapy for reducing LDL cholesterol, with a reported decrease of about 60% after only 12 or 52 weeks of treatment. Based on four small studies lasting 10-12 weeks and without any clinical outcome data, the committee recommended approving evolocumab for lifetime therapy without anything to support its clinical effectiveness or safety.
Dr. Robert J. Smith, who chaired the advisory committee meeting, faced with approving the drug or delaying a decision until a randomized clinical trial can be completed said, “I am unwilling to subject patients to the wait.” A publication of the American College of Cardiology suggested that these two monoclonal antibody drugs could replace generic statins in 70 million Americans at an estimated cost of $7,000-$12,000 a year. Talk about breaking the bank.
Only recently, we decided that the appropriate statin therapy for cholesterol control should use the dosing from the original clinical trials rather than chasing LDL levels to the lowest level possible. We now have a class of drugs that clearly can lower the cholesterol to a level never seen before, and we are about to discard that therapeutic advice.
We have experience in chasing blood levels with uncertain outcomes. Reducing blood sugar to a very low hemoglobin A1c level led to adverse clinical events and increased mortality in type 2 diabetes. Raising HDL with the cholesterol ester transfer protein (CETP) inhibitor torcetrapib in a study of 15,000 patients in an outcome trial carried out over a number of years led to increased blood pressure and mortality by 58%, which was associated with a 25% decrease in LDL cholesterol and a 72% increase in HDL, both effects presumed to be remarkably beneficial (N. Engl. J. Med. 2007;357:2109-22).
It is quite possible that these new agents can further decrease coronary vascular mortality. A healthy controversy has raged for some time in regard to the “LDL hypothesis,” compared with therapy based upon the clinical trial outcome. The recent IMPROVE-IT report (N. Engl. J. Med. 2015;372:2387-97) provides some data to support the LDL hypothesis. In that study, the addition of 10 mg of ezetimibe to 40 mg of simvastatin in 18,144 patients followed for up to 6 years resulted in a 2% decrease in mortality associated with a 15.8-mg decrease in serum LDL.
Would it not be prudent to have similar data with the new drug on the street? If it is as potent as it appears to be, a trial of much shorter duration might demonstrate its potency and safety before it is offered to 70 million Americans. The FDA has been reluctant to use surrogate endpoints for approving drugs, but its position has not always been consistent. For some time the FDA has, on occasion, approved drugs that can lower cholesterol with limited outcome data as it did with ezetimibe. However, the decision in regard to the PCSK9 inhibitors will have a much larger impact on care than an add-on drug like ezetimibe. Let’s hope that the FDA shows better judgment than its advisory committee.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Ego depletion in the clinic
A study published in JAMA Internal Medicine in December 2014 looked at decision fatigue in primary care providers. The researchers focused on antibiotic prescriptions for acute respiratory infections (including those for which antibiotics are never indicated) over a 16-month period covering 21,867 visits to 204 clinicians. They compared the rate of antibiotic prescription at the first, second, third, and fourth hour of clinic, with the premise being that over a period of repeated decision making the quality of the decisions declines (JAMA Intern. Med. 2014;174:2029-31).
If, like me, you think you have unrealistic expectations about physicians being unimpeachable, you might be disappointed to learn that antibiotic prescriptions were significantly higher for the third and fourth hour of clinic. It seems that as the clinic session wore on, physicians opted for the “safer,” “easier” option.

Another paper involving similarly weighty consequences was published in 2011 in Proceedings of the National Academy of Sciences (and cited as one of only six references in the JAMA paper). The researchers looked at parole decisions made by judges in four Israeli prisons. Data from 1,112 judicial rulings involving eight judges showed that “the percentage of favorable rulings drops gradually from ~65% to nearly zero within each decision session and returns abruptly to ~65% after a break” (Proc. Natl. Acad. Sci. U.S.A. 2011;108:6889-92). (Breaks lasted about 30 minutes and involved a meal.) That’s a pretty dramatic rate of change. It is sobering to think of lives being hugely affected by such seemingly irrelevant details. Talk about fate being fickle.
Decision fatigue suggests that when we make repeated decisions over a brief period of time there is an erosion of self-control and we are more likely to choose the “affectively pleasing” option. It has been written about in psychology journals for the past 2 decades, but for practical and ethical reasons, most studies on the subject involve minor decisions, such as what to choose at the grocery store or which items to add to one’s wedding registry. The concept has become quite popular in the fields of behavioral economic and advertising. It is the reason groceries display candy at the cash register.
Decision fatigue is part of a larger theory on our executive functions, proposed by Dr. Roy Baumeister, professor of social psychology at the University of Florida. His central idea is that self-control, volitional acts, responsibility, and self-regulatory efforts “draw upon a common resource and deplete it.” He calls it ego depletion. In one simple but powerful experiment, researchers conducted a study where students were asked to commit either two digits or seven digits to memory. When offered a choice of fruit salad or chocolate cake as compensation for participation in the study, those who had to remember seven digits were far more likely to choose the chocolate cake – certainly the more “affectively pleasing” option. So ego depletion is to blame for my constant kitchen-grazing behavior at the end of a trying clinic day. Apart from affecting my waistline, I’m sure it affects me in ways that I am unaware of, ways that may have an impact not just on patients but on society, too.
The JAMA Internal Medicine article seems to be the first of its kind in the medical literature. To me, it is hugely important because it reminds us of two major truths: that there are often bigger things at stake, and that doctors, being mere mortals, are not exempt from human frailty.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A study published in JAMA Internal Medicine in December 2014 looked at decision fatigue in primary care providers. The researchers focused on antibiotic prescriptions for acute respiratory infections (including those for which antibiotics are never indicated) over a 16-month period covering 21,867 visits to 204 clinicians. They compared the rate of antibiotic prescription at the first, second, third, and fourth hour of clinic, with the premise being that over a period of repeated decision making the quality of the decisions declines (JAMA Intern. Med. 2014;174:2029-31).
If, like me, you think you have unrealistic expectations about physicians being unimpeachable, you might be disappointed to learn that antibiotic prescriptions were significantly higher for the third and fourth hour of clinic. It seems that as the clinic session wore on, physicians opted for the “safer,” “easier” option.
Another paper involving similarly weighty consequences was published in 2011 in Proceedings of the National Academy of Sciences (and cited as one of only six references in the JAMA paper). The researchers looked at parole decisions made by judges in four Israeli prisons. Data from 1,112 judicial rulings involving eight judges showed that “the percentage of favorable rulings drops gradually from ~65% to nearly zero within each decision session and returns abruptly to ~65% after a break” (Proc. Natl. Acad. Sci. U.S.A. 2011;108:6889-92). (Breaks lasted about 30 minutes and involved a meal.) That’s a pretty dramatic rate of change. It is sobering to think of lives being hugely affected by such seemingly irrelevant details. Talk about fate being fickle.
Decision fatigue suggests that when we make repeated decisions over a brief period of time there is an erosion of self-control and we are more likely to choose the “affectively pleasing” option. It has been written about in psychology journals for the past 2 decades, but for practical and ethical reasons, most studies on the subject involve minor decisions, such as what to choose at the grocery store or which items to add to one’s wedding registry. The concept has become quite popular in the fields of behavioral economic and advertising. It is the reason groceries display candy at the cash register.
Decision fatigue is part of a larger theory on our executive functions, proposed by Dr. Roy Baumeister, professor of social psychology at the University of Florida. His central idea is that self-control, volitional acts, responsibility, and self-regulatory efforts “draw upon a common resource and deplete it.” He calls it ego depletion. In one simple but powerful experiment, researchers conducted a study where students were asked to commit either two digits or seven digits to memory. When offered a choice of fruit salad or chocolate cake as compensation for participation in the study, those who had to remember seven digits were far more likely to choose the chocolate cake – certainly the more “affectively pleasing” option. So ego depletion is to blame for my constant kitchen-grazing behavior at the end of a trying clinic day. Apart from affecting my waistline, I’m sure it affects me in ways that I am unaware of, ways that may have an impact not just on patients but on society, too.
The JAMA Internal Medicine article seems to be the first of its kind in the medical literature. To me, it is hugely important because it reminds us of two major truths: that there are often bigger things at stake, and that doctors, being mere mortals, are not exempt from human frailty.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A study published in JAMA Internal Medicine in December 2014 looked at decision fatigue in primary care providers. The researchers focused on antibiotic prescriptions for acute respiratory infections (including those for which antibiotics are never indicated) over a 16-month period covering 21,867 visits to 204 clinicians. They compared the rate of antibiotic prescription at the first, second, third, and fourth hour of clinic, with the premise being that over a period of repeated decision making the quality of the decisions declines (JAMA Intern. Med. 2014;174:2029-31).
If, like me, you think you have unrealistic expectations about physicians being unimpeachable, you might be disappointed to learn that antibiotic prescriptions were significantly higher for the third and fourth hour of clinic. It seems that as the clinic session wore on, physicians opted for the “safer,” “easier” option.
Another paper involving similarly weighty consequences was published in 2011 in Proceedings of the National Academy of Sciences (and cited as one of only six references in the JAMA paper). The researchers looked at parole decisions made by judges in four Israeli prisons. Data from 1,112 judicial rulings involving eight judges showed that “the percentage of favorable rulings drops gradually from ~65% to nearly zero within each decision session and returns abruptly to ~65% after a break” (Proc. Natl. Acad. Sci. U.S.A. 2011;108:6889-92). (Breaks lasted about 30 minutes and involved a meal.) That’s a pretty dramatic rate of change. It is sobering to think of lives being hugely affected by such seemingly irrelevant details. Talk about fate being fickle.
Decision fatigue suggests that when we make repeated decisions over a brief period of time there is an erosion of self-control and we are more likely to choose the “affectively pleasing” option. It has been written about in psychology journals for the past 2 decades, but for practical and ethical reasons, most studies on the subject involve minor decisions, such as what to choose at the grocery store or which items to add to one’s wedding registry. The concept has become quite popular in the fields of behavioral economic and advertising. It is the reason groceries display candy at the cash register.
Decision fatigue is part of a larger theory on our executive functions, proposed by Dr. Roy Baumeister, professor of social psychology at the University of Florida. His central idea is that self-control, volitional acts, responsibility, and self-regulatory efforts “draw upon a common resource and deplete it.” He calls it ego depletion. In one simple but powerful experiment, researchers conducted a study where students were asked to commit either two digits or seven digits to memory. When offered a choice of fruit salad or chocolate cake as compensation for participation in the study, those who had to remember seven digits were far more likely to choose the chocolate cake – certainly the more “affectively pleasing” option. So ego depletion is to blame for my constant kitchen-grazing behavior at the end of a trying clinic day. Apart from affecting my waistline, I’m sure it affects me in ways that I am unaware of, ways that may have an impact not just on patients but on society, too.
The JAMA Internal Medicine article seems to be the first of its kind in the medical literature. To me, it is hugely important because it reminds us of two major truths: that there are often bigger things at stake, and that doctors, being mere mortals, are not exempt from human frailty.
Dr. Chan practices rheumatology in Pawtucket, R.I.
