User login
Clinical Care Pathway for Cellulitis Can Help Reduce Antibiotic Use, Cost
Clinical question: How would an evidence-based clinical pathway for cellulitis affect process metrics, patient outcomes, and clinical cost?
Background: Cellulitis is a common hospital problem, but its evaluation and treatment vary widely. Specifically, broad-spectrum antibiotics and imaging studies are overutilized when compared to recommended guidelines. A standardized clinical pathway is proposed as a possible solution.
Study design: Retrospective, observational, pre-/post-intervention study.
Setting: University of Utah Health Sciences Center, Salt Lake City.
Synopsis: A multidisciplinary team created a guideline-based care pathway for cellulitis and enrolled 677 adult patients for retrospective analysis during a two-year period. The study showed an overall 59% decrease in the odds of ordering broad-spectrum antibiotics, 23% decrease in pharmacy cost, 44% decrease in laboratory cost, and 13% decrease in overall facility cost, pre-/post-intervention. It also demonstrated no adverse effect on length of stay or 30-day readmission rates.
Given the retrospective, single-center nature of this study, as well as some baseline characteristic differences between enrolled patients, careful conclusions regarding external validity on diverse patient populations must be considered; however, the history of clinical care pathways supports many of the study’s findings. The results make a compelling case for hospitalist groups to implement similar cellulitis pathways and research their effectiveness.
Bottom line: Clinical care pathways for cellulitis provide an opportunity to improve antibiotic stewardship and lower hospital costs without compromising quality of care.
Citation: Yarbrough PM, Kukhareva PV, Spivak ES, Hopkins C, Kawamoto K. Evidence-based care pathway for cellulitis improves process, clinical, and cost outcomes [published online ahead of print July 28, 2015]. J Hosp Med. doi: 10.1002/jhm.2433.
Clinical question: How would an evidence-based clinical pathway for cellulitis affect process metrics, patient outcomes, and clinical cost?
Background: Cellulitis is a common hospital problem, but its evaluation and treatment vary widely. Specifically, broad-spectrum antibiotics and imaging studies are overutilized when compared to recommended guidelines. A standardized clinical pathway is proposed as a possible solution.
Study design: Retrospective, observational, pre-/post-intervention study.
Setting: University of Utah Health Sciences Center, Salt Lake City.
Synopsis: A multidisciplinary team created a guideline-based care pathway for cellulitis and enrolled 677 adult patients for retrospective analysis during a two-year period. The study showed an overall 59% decrease in the odds of ordering broad-spectrum antibiotics, 23% decrease in pharmacy cost, 44% decrease in laboratory cost, and 13% decrease in overall facility cost, pre-/post-intervention. It also demonstrated no adverse effect on length of stay or 30-day readmission rates.
Given the retrospective, single-center nature of this study, as well as some baseline characteristic differences between enrolled patients, careful conclusions regarding external validity on diverse patient populations must be considered; however, the history of clinical care pathways supports many of the study’s findings. The results make a compelling case for hospitalist groups to implement similar cellulitis pathways and research their effectiveness.
Bottom line: Clinical care pathways for cellulitis provide an opportunity to improve antibiotic stewardship and lower hospital costs without compromising quality of care.
Citation: Yarbrough PM, Kukhareva PV, Spivak ES, Hopkins C, Kawamoto K. Evidence-based care pathway for cellulitis improves process, clinical, and cost outcomes [published online ahead of print July 28, 2015]. J Hosp Med. doi: 10.1002/jhm.2433.
Clinical question: How would an evidence-based clinical pathway for cellulitis affect process metrics, patient outcomes, and clinical cost?
Background: Cellulitis is a common hospital problem, but its evaluation and treatment vary widely. Specifically, broad-spectrum antibiotics and imaging studies are overutilized when compared to recommended guidelines. A standardized clinical pathway is proposed as a possible solution.
Study design: Retrospective, observational, pre-/post-intervention study.
Setting: University of Utah Health Sciences Center, Salt Lake City.
Synopsis: A multidisciplinary team created a guideline-based care pathway for cellulitis and enrolled 677 adult patients for retrospective analysis during a two-year period. The study showed an overall 59% decrease in the odds of ordering broad-spectrum antibiotics, 23% decrease in pharmacy cost, 44% decrease in laboratory cost, and 13% decrease in overall facility cost, pre-/post-intervention. It also demonstrated no adverse effect on length of stay or 30-day readmission rates.
Given the retrospective, single-center nature of this study, as well as some baseline characteristic differences between enrolled patients, careful conclusions regarding external validity on diverse patient populations must be considered; however, the history of clinical care pathways supports many of the study’s findings. The results make a compelling case for hospitalist groups to implement similar cellulitis pathways and research their effectiveness.
Bottom line: Clinical care pathways for cellulitis provide an opportunity to improve antibiotic stewardship and lower hospital costs without compromising quality of care.
Citation: Yarbrough PM, Kukhareva PV, Spivak ES, Hopkins C, Kawamoto K. Evidence-based care pathway for cellulitis improves process, clinical, and cost outcomes [published online ahead of print July 28, 2015]. J Hosp Med. doi: 10.1002/jhm.2433.
Practice Administrator Elected Vice President of SHM Maryland Chapter
When you ask Tiffani Panek, division administrator for the division of hospital medicine at Johns Hopkins Bayview Medical Center (BMC) in Baltimore, Md., about her thoughts on the future of hospital medicine, her passion and enthusiasm are immediately apparent. After earning SHM’s Certificate of Leadership in Hospital Medicine, Panek was elected vice president of SHM’s Maryland chapter. She is the only practice administrator currently in chapter leadership.
Her motto? “I’m a hospitalist who happens not to be a clinician.”
The Hospitalist recently spoke with Panek about the future of the HM movement and the roles nonphysician staff play in advancing hospital medicine.
Question: Tell us about your role as division administrator for BMC’s division of hospital medicine.
Answer: As part of the executive leadership team, I serve as the administrative counterpart to site director Flora Kisuule, MD, MPH. I am also the program coordinator for the Academic Hospitalist Fellowship Program and partner with Dr. Kisuule and SHM board member and senior physician advisor Eric Howell, MD, SFHM, on the program’s growing international work to train academic hospitalists and future leaders of hospitalist programs.
Q: What led you to join SHM and get involved in the Practice Administrators Committee?
A: I had never heard of hospital medicine before I started with [my] division, and I really wanted to learn all I could. I was fortunate enough that Dr. Howell was a part of SHM very early, and as my director, he encouraged me to get involved. In the beginning, it was really about educating myself, but after a few years, when I was immersed and truly in love with hospital medicine, I wanted to get more involved and be a part of the change and innovation that SHM and hospital medicine represent. The movement touches so many people in such a direct way. We are in the trenches, taking care of people when they are at their most vulnerable.

Q: How were you able to take what you learned from SHM Leadership Academy and apply it to your professional life and new chapter leader position?
A: I should make a cross-stitch of one of my favorite takeaways: “They won’t care what you know until they know that you care!” The personality and communication lessons have not only helped me develop my own communication skills, but they have helped me become a better supervisor and mentor. I often return to my notes about leading through adversity when faced with challenges at our own facility. I want to bring all of that to the table as the new Maryland chapter vice president, to help us improve the diversity of the chapter and ultimately the hospital medicine movement.
Q: Moving forward, how do you see your role in SHM—and SHM as an organization— impacting positive change for hospitalized patients and the hospitalists who serve them?
A: As an active member, I am excited to leverage SHM, the Practice Administrators Committee, the local chapter, and other meetings to unite talented people working in hospital medicine and work towards the same mission: improving care of hospitalized patients. In addition to bringing our subspecialty colleagues into the fold, we also must improve our inclusivity of nurse practitioners, physician assistants, pharmacists, nurses, and, of course, our administrators. Every single person should feel invested and valued. The diversity of hospital medicine, and of SHM, sets our specialty apart from many others, and we are much stronger for it. There are no healthcare professionals better situated to improve the quality and cost of care than hospitalists.
Brett Radler is SHM’s communications coordinator.
When you ask Tiffani Panek, division administrator for the division of hospital medicine at Johns Hopkins Bayview Medical Center (BMC) in Baltimore, Md., about her thoughts on the future of hospital medicine, her passion and enthusiasm are immediately apparent. After earning SHM’s Certificate of Leadership in Hospital Medicine, Panek was elected vice president of SHM’s Maryland chapter. She is the only practice administrator currently in chapter leadership.
Her motto? “I’m a hospitalist who happens not to be a clinician.”
The Hospitalist recently spoke with Panek about the future of the HM movement and the roles nonphysician staff play in advancing hospital medicine.
Question: Tell us about your role as division administrator for BMC’s division of hospital medicine.
Answer: As part of the executive leadership team, I serve as the administrative counterpart to site director Flora Kisuule, MD, MPH. I am also the program coordinator for the Academic Hospitalist Fellowship Program and partner with Dr. Kisuule and SHM board member and senior physician advisor Eric Howell, MD, SFHM, on the program’s growing international work to train academic hospitalists and future leaders of hospitalist programs.
Q: What led you to join SHM and get involved in the Practice Administrators Committee?
A: I had never heard of hospital medicine before I started with [my] division, and I really wanted to learn all I could. I was fortunate enough that Dr. Howell was a part of SHM very early, and as my director, he encouraged me to get involved. In the beginning, it was really about educating myself, but after a few years, when I was immersed and truly in love with hospital medicine, I wanted to get more involved and be a part of the change and innovation that SHM and hospital medicine represent. The movement touches so many people in such a direct way. We are in the trenches, taking care of people when they are at their most vulnerable.
Q: How were you able to take what you learned from SHM Leadership Academy and apply it to your professional life and new chapter leader position?
A: I should make a cross-stitch of one of my favorite takeaways: “They won’t care what you know until they know that you care!” The personality and communication lessons have not only helped me develop my own communication skills, but they have helped me become a better supervisor and mentor. I often return to my notes about leading through adversity when faced with challenges at our own facility. I want to bring all of that to the table as the new Maryland chapter vice president, to help us improve the diversity of the chapter and ultimately the hospital medicine movement.
Q: Moving forward, how do you see your role in SHM—and SHM as an organization— impacting positive change for hospitalized patients and the hospitalists who serve them?
A: As an active member, I am excited to leverage SHM, the Practice Administrators Committee, the local chapter, and other meetings to unite talented people working in hospital medicine and work towards the same mission: improving care of hospitalized patients. In addition to bringing our subspecialty colleagues into the fold, we also must improve our inclusivity of nurse practitioners, physician assistants, pharmacists, nurses, and, of course, our administrators. Every single person should feel invested and valued. The diversity of hospital medicine, and of SHM, sets our specialty apart from many others, and we are much stronger for it. There are no healthcare professionals better situated to improve the quality and cost of care than hospitalists.
Brett Radler is SHM’s communications coordinator.
When you ask Tiffani Panek, division administrator for the division of hospital medicine at Johns Hopkins Bayview Medical Center (BMC) in Baltimore, Md., about her thoughts on the future of hospital medicine, her passion and enthusiasm are immediately apparent. After earning SHM’s Certificate of Leadership in Hospital Medicine, Panek was elected vice president of SHM’s Maryland chapter. She is the only practice administrator currently in chapter leadership.
Her motto? “I’m a hospitalist who happens not to be a clinician.”
The Hospitalist recently spoke with Panek about the future of the HM movement and the roles nonphysician staff play in advancing hospital medicine.
Question: Tell us about your role as division administrator for BMC’s division of hospital medicine.
Answer: As part of the executive leadership team, I serve as the administrative counterpart to site director Flora Kisuule, MD, MPH. I am also the program coordinator for the Academic Hospitalist Fellowship Program and partner with Dr. Kisuule and SHM board member and senior physician advisor Eric Howell, MD, SFHM, on the program’s growing international work to train academic hospitalists and future leaders of hospitalist programs.
Q: What led you to join SHM and get involved in the Practice Administrators Committee?
A: I had never heard of hospital medicine before I started with [my] division, and I really wanted to learn all I could. I was fortunate enough that Dr. Howell was a part of SHM very early, and as my director, he encouraged me to get involved. In the beginning, it was really about educating myself, but after a few years, when I was immersed and truly in love with hospital medicine, I wanted to get more involved and be a part of the change and innovation that SHM and hospital medicine represent. The movement touches so many people in such a direct way. We are in the trenches, taking care of people when they are at their most vulnerable.
Q: How were you able to take what you learned from SHM Leadership Academy and apply it to your professional life and new chapter leader position?
A: I should make a cross-stitch of one of my favorite takeaways: “They won’t care what you know until they know that you care!” The personality and communication lessons have not only helped me develop my own communication skills, but they have helped me become a better supervisor and mentor. I often return to my notes about leading through adversity when faced with challenges at our own facility. I want to bring all of that to the table as the new Maryland chapter vice president, to help us improve the diversity of the chapter and ultimately the hospital medicine movement.
Q: Moving forward, how do you see your role in SHM—and SHM as an organization— impacting positive change for hospitalized patients and the hospitalists who serve them?
A: As an active member, I am excited to leverage SHM, the Practice Administrators Committee, the local chapter, and other meetings to unite talented people working in hospital medicine and work towards the same mission: improving care of hospitalized patients. In addition to bringing our subspecialty colleagues into the fold, we also must improve our inclusivity of nurse practitioners, physician assistants, pharmacists, nurses, and, of course, our administrators. Every single person should feel invested and valued. The diversity of hospital medicine, and of SHM, sets our specialty apart from many others, and we are much stronger for it. There are no healthcare professionals better situated to improve the quality and cost of care than hospitalists.
Brett Radler is SHM’s communications coordinator.
Revolutionizing Quality Improvement in Hospital Medicine
As the senior physician advisor to SHM’s Center for Hospital Innovation and Improvement, Eric Howell, MD, SFHM, bridges the gap between clinical expertise and project support and development. The Hospitalist recently had a conversation with Dr. Howell, a past president of SHM, to learn more about his role and how the Center for Hospital Innovation and Improvement is revolutionizing quality improvement (QI) in hospital medicine.
Question: What is your role as the senior physician advisor to The Center for Hospital Innovation and Improvement?
Answer: I see my role as the intersection of a Venn diagram; one circle involves my clinical know-how, and the other includes the proposals brought to the Center for Hospital Innovation and Improvement by hospitalists and healthcare professionals. Where those two circles intersect is where I am able to use my experience from the front line of patient care to validate potential projects.
In addition to project assessment, I monitor the pulse of healthcare professionals and hospital leadership to ensure we are meeting their needs, including our efforts of convening a recent summit, where hospitalist clinicians … weighed in on how our team could help them improve. I plan to share this feedback in an upcoming feature, centered on emerging topics in hospital medicine, including care transitions, high-risk medications, advance care planning, and others.
Q: Given your clinical experience and involvement with SHM, how would you say hospitalists are positioned to improve quality, safety, and patient outcomes?

appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections.
—Dr. Howell
A: We possess the necessary ingredients to develop a recipe for success in QI from both a clinical and an operational perspective. Hospital medicine is still a young, innovative field that is extremely open to change. Anyone who knows QI knows that it is all about effectively managing and responding to change. Hospitalists also are aware of how to operate in a highly matrixed environment and to collaborate as part of an interdisciplinary team, which are invaluable assets to implementing QI initiatives successfully and proactively monitoring their impact.
Q: What are the biggest assets the Center for Hospital Innovation and Improvement can offer hospitalists in their mission to improve patient care?
A: Our team has resources to help hospitalists improve their skills at whatever stage they are in their careers. If you are just beginning or trying to learn new things independently, you can explore the web-based materials and resource rooms. They are publicly accessible resources that can assist in informing quality improvement efforts in the hospital. For those looking to expand their skills in a more hands-on way, we offer a mentored implementation program, where hospitalists can receive guidance from expert mentors in a number of different clinical areas.
Q: How can the Center for Hospital Innovation and Improvement help hospitalists address emerging challenges in hospital medicine?
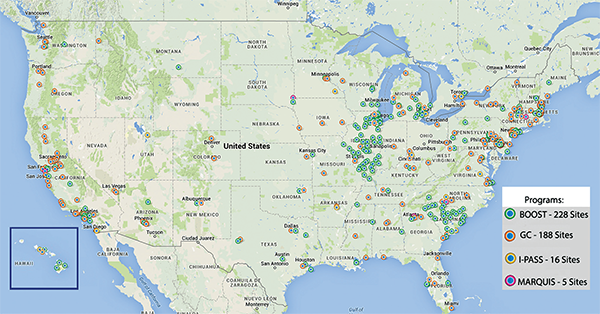
A: You cannot talk about the Center for Hospital Innovation and Improvement without mentioning signature mentored implementation programs like Project BOOST, focused on effective care transitions, and glycemic control—they are juggernauts for SHM’s portfolio because of their proven track records and sustainable frameworks for driving positive change. These two alone have already been implemented at over 400 facilities, with more inquiries each day.
With support from The Milbank Foundation, The Hastings Center and SHM have joined forces and will create new skills-based training resources and a QI framework to improve end-of-life care in the hospital. Our goal is to equip hospital clinicians with the requisite tools to provide adequate palliative care, especially given the policy landscape related to advance care planning discussions.
As antibiotic resistance emerges as a global issue, antibiotic stewardship has continued to be a high priority for hospitalists. After attending the related White House forum earlier this year, SHM committed to cultivating initiatives that emphasize appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections. SHM looks forward to making noteworthy contributions to this initiative, promoting awareness and behavior change through the “Fight the Resistance” campaign.
Q: What is one major takeaway about The Center for Hospital Innovation and Improvement hospitalists should know?
A: The Center for Hospital Innovation and Improvement is not an exclusive club—rather, it is like an open farmers’ market. Anyone with any amount of expertise can get resources through collaboration and partnership. Whether it is residents trying to improve the house staff or professors at major academic centers looking for research partners, The Center for Hospital Innovation and Improvement will welcome you to collaborate and link you to valuable resources.
Brett Radler is SHM’s communications coordinator.
As the senior physician advisor to SHM’s Center for Hospital Innovation and Improvement, Eric Howell, MD, SFHM, bridges the gap between clinical expertise and project support and development. The Hospitalist recently had a conversation with Dr. Howell, a past president of SHM, to learn more about his role and how the Center for Hospital Innovation and Improvement is revolutionizing quality improvement (QI) in hospital medicine.
Question: What is your role as the senior physician advisor to The Center for Hospital Innovation and Improvement?
Answer: I see my role as the intersection of a Venn diagram; one circle involves my clinical know-how, and the other includes the proposals brought to the Center for Hospital Innovation and Improvement by hospitalists and healthcare professionals. Where those two circles intersect is where I am able to use my experience from the front line of patient care to validate potential projects.
In addition to project assessment, I monitor the pulse of healthcare professionals and hospital leadership to ensure we are meeting their needs, including our efforts of convening a recent summit, where hospitalist clinicians … weighed in on how our team could help them improve. I plan to share this feedback in an upcoming feature, centered on emerging topics in hospital medicine, including care transitions, high-risk medications, advance care planning, and others.
Q: Given your clinical experience and involvement with SHM, how would you say hospitalists are positioned to improve quality, safety, and patient outcomes?
appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections.
—Dr. Howell
A: We possess the necessary ingredients to develop a recipe for success in QI from both a clinical and an operational perspective. Hospital medicine is still a young, innovative field that is extremely open to change. Anyone who knows QI knows that it is all about effectively managing and responding to change. Hospitalists also are aware of how to operate in a highly matrixed environment and to collaborate as part of an interdisciplinary team, which are invaluable assets to implementing QI initiatives successfully and proactively monitoring their impact.
Q: What are the biggest assets the Center for Hospital Innovation and Improvement can offer hospitalists in their mission to improve patient care?
A: Our team has resources to help hospitalists improve their skills at whatever stage they are in their careers. If you are just beginning or trying to learn new things independently, you can explore the web-based materials and resource rooms. They are publicly accessible resources that can assist in informing quality improvement efforts in the hospital. For those looking to expand their skills in a more hands-on way, we offer a mentored implementation program, where hospitalists can receive guidance from expert mentors in a number of different clinical areas.
Q: How can the Center for Hospital Innovation and Improvement help hospitalists address emerging challenges in hospital medicine?
A: You cannot talk about the Center for Hospital Innovation and Improvement without mentioning signature mentored implementation programs like Project BOOST, focused on effective care transitions, and glycemic control—they are juggernauts for SHM’s portfolio because of their proven track records and sustainable frameworks for driving positive change. These two alone have already been implemented at over 400 facilities, with more inquiries each day.
With support from The Milbank Foundation, The Hastings Center and SHM have joined forces and will create new skills-based training resources and a QI framework to improve end-of-life care in the hospital. Our goal is to equip hospital clinicians with the requisite tools to provide adequate palliative care, especially given the policy landscape related to advance care planning discussions.
As antibiotic resistance emerges as a global issue, antibiotic stewardship has continued to be a high priority for hospitalists. After attending the related White House forum earlier this year, SHM committed to cultivating initiatives that emphasize appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections. SHM looks forward to making noteworthy contributions to this initiative, promoting awareness and behavior change through the “Fight the Resistance” campaign.
Q: What is one major takeaway about The Center for Hospital Innovation and Improvement hospitalists should know?
A: The Center for Hospital Innovation and Improvement is not an exclusive club—rather, it is like an open farmers’ market. Anyone with any amount of expertise can get resources through collaboration and partnership. Whether it is residents trying to improve the house staff or professors at major academic centers looking for research partners, The Center for Hospital Innovation and Improvement will welcome you to collaborate and link you to valuable resources.
Brett Radler is SHM’s communications coordinator.
As the senior physician advisor to SHM’s Center for Hospital Innovation and Improvement, Eric Howell, MD, SFHM, bridges the gap between clinical expertise and project support and development. The Hospitalist recently had a conversation with Dr. Howell, a past president of SHM, to learn more about his role and how the Center for Hospital Innovation and Improvement is revolutionizing quality improvement (QI) in hospital medicine.
Question: What is your role as the senior physician advisor to The Center for Hospital Innovation and Improvement?
Answer: I see my role as the intersection of a Venn diagram; one circle involves my clinical know-how, and the other includes the proposals brought to the Center for Hospital Innovation and Improvement by hospitalists and healthcare professionals. Where those two circles intersect is where I am able to use my experience from the front line of patient care to validate potential projects.
In addition to project assessment, I monitor the pulse of healthcare professionals and hospital leadership to ensure we are meeting their needs, including our efforts of convening a recent summit, where hospitalist clinicians … weighed in on how our team could help them improve. I plan to share this feedback in an upcoming feature, centered on emerging topics in hospital medicine, including care transitions, high-risk medications, advance care planning, and others.
Q: Given your clinical experience and involvement with SHM, how would you say hospitalists are positioned to improve quality, safety, and patient outcomes?
appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections.
—Dr. Howell
A: We possess the necessary ingredients to develop a recipe for success in QI from both a clinical and an operational perspective. Hospital medicine is still a young, innovative field that is extremely open to change. Anyone who knows QI knows that it is all about effectively managing and responding to change. Hospitalists also are aware of how to operate in a highly matrixed environment and to collaborate as part of an interdisciplinary team, which are invaluable assets to implementing QI initiatives successfully and proactively monitoring their impact.
Q: What are the biggest assets the Center for Hospital Innovation and Improvement can offer hospitalists in their mission to improve patient care?
A: Our team has resources to help hospitalists improve their skills at whatever stage they are in their careers. If you are just beginning or trying to learn new things independently, you can explore the web-based materials and resource rooms. They are publicly accessible resources that can assist in informing quality improvement efforts in the hospital. For those looking to expand their skills in a more hands-on way, we offer a mentored implementation program, where hospitalists can receive guidance from expert mentors in a number of different clinical areas.
Q: How can the Center for Hospital Innovation and Improvement help hospitalists address emerging challenges in hospital medicine?
A: You cannot talk about the Center for Hospital Innovation and Improvement without mentioning signature mentored implementation programs like Project BOOST, focused on effective care transitions, and glycemic control—they are juggernauts for SHM’s portfolio because of their proven track records and sustainable frameworks for driving positive change. These two alone have already been implemented at over 400 facilities, with more inquiries each day.
With support from The Milbank Foundation, The Hastings Center and SHM have joined forces and will create new skills-based training resources and a QI framework to improve end-of-life care in the hospital. Our goal is to equip hospital clinicians with the requisite tools to provide adequate palliative care, especially given the policy landscape related to advance care planning discussions.
As antibiotic resistance emerges as a global issue, antibiotic stewardship has continued to be a high priority for hospitalists. After attending the related White House forum earlier this year, SHM committed to cultivating initiatives that emphasize appropriate prescribing practices, which will aid in slowing the emergence of antibiotic-resistant bacteria and prevent the spread of resistant infections. SHM looks forward to making noteworthy contributions to this initiative, promoting awareness and behavior change through the “Fight the Resistance” campaign.
Q: What is one major takeaway about The Center for Hospital Innovation and Improvement hospitalists should know?
A: The Center for Hospital Innovation and Improvement is not an exclusive club—rather, it is like an open farmers’ market. Anyone with any amount of expertise can get resources through collaboration and partnership. Whether it is residents trying to improve the house staff or professors at major academic centers looking for research partners, The Center for Hospital Innovation and Improvement will welcome you to collaborate and link you to valuable resources.
Brett Radler is SHM’s communications coordinator.
Risk Adjusting Readmissions: Coming Soon?
Nearly three-quarters of hospitals will be receiving penalties from the Centers for Medicare and Medicaid Services (CMS) in 2016 for excess readmissions, having failed to prevent enough patients from returning to the hospital 30 days post-discharge. With so many hospitals impacted by penalties, it is understandable that the underlying methodology of the Hospital Readmissions Reduction Program (HRRP) is coming under intense scrutiny.
Research published in JAMA Internal Medicine in September hit upon many of the myriad factors—often outside of the hospital or providers’ control—that influence whether a patient is readmitted to the hospital. This information adds weight to criticism of the measures included in the HRRP and asserts the need to refine or reform the measures to better account for readmissions preventable through the interventions of the healthcare system. The behavior these measures are meant to curb, including poor quality care, inadequate access to follow-up or medications, and gaps in transitions of care, are not identifiable within broad-based, all-cause readmission measures. Instead, hospitals are being penalized for all readmissions, a majority of which may be attributable to community or patient-related factors, such as sociodemographic or housing status, among other variables.
A growing consensus on two fronts asserts that these measures, as currently structured, might not be appropriate for use in pay-for-performance programs. Measure developers, bolstered by a recent decision by the National Quality Forum to institute a trial run of risk adjusting measures for sociodemographic status, are exploring the impact of using different available variables to enhance risk adjusting their measures. Measures for readmissions are at the front of the line of these efforts. Although it is only in the beginning stages, this work could change the foundation of all quality measures used in pay-for-performance programs.
In Congress, legislation has been introduced in both the House of Representatives and the Senate aiming to refine the HRRP through additional risk adjustments. The Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015 (H.R. 1343 and S. 688), introduced by Rep. Jim Renacci (R-Ohio) and Sen. Joe Manchin (D-W.V.), would create immediate relief for hospitals by implementing risk adjustment for dual-eligible patients and the socioeconomic status of the hospital’s patients. At the same time, when reports that are currently in progress about risk adjustment in readmission measures and the use of a 30-day window for categorizing readmissions are completed, CMS would be required to incorporate their findings into the risk adjustment in the HRRP in the future.
SHM is supporting both of these pathways toward improving risk adjustment in readmissions measures. By engaging in the measure process and advocating for the passage of legislation to refine risk adjustment, SHM has taken a stand. The goal of reducing preventable readmissions is too important to use imprecise metrics that seem to penalize the hospitals serving the nation’s neediest patients.
As hospitalists on the front line, you can join SHM in advocating for these common sense, and necessary, changes to the HRRP.
Visit SHM’s Legislative Action Center to send a message to Congress in support of the Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015.
Joshua Lapps is SHM’s government relations manager.
Nearly three-quarters of hospitals will be receiving penalties from the Centers for Medicare and Medicaid Services (CMS) in 2016 for excess readmissions, having failed to prevent enough patients from returning to the hospital 30 days post-discharge. With so many hospitals impacted by penalties, it is understandable that the underlying methodology of the Hospital Readmissions Reduction Program (HRRP) is coming under intense scrutiny.
Research published in JAMA Internal Medicine in September hit upon many of the myriad factors—often outside of the hospital or providers’ control—that influence whether a patient is readmitted to the hospital. This information adds weight to criticism of the measures included in the HRRP and asserts the need to refine or reform the measures to better account for readmissions preventable through the interventions of the healthcare system. The behavior these measures are meant to curb, including poor quality care, inadequate access to follow-up or medications, and gaps in transitions of care, are not identifiable within broad-based, all-cause readmission measures. Instead, hospitals are being penalized for all readmissions, a majority of which may be attributable to community or patient-related factors, such as sociodemographic or housing status, among other variables.
A growing consensus on two fronts asserts that these measures, as currently structured, might not be appropriate for use in pay-for-performance programs. Measure developers, bolstered by a recent decision by the National Quality Forum to institute a trial run of risk adjusting measures for sociodemographic status, are exploring the impact of using different available variables to enhance risk adjusting their measures. Measures for readmissions are at the front of the line of these efforts. Although it is only in the beginning stages, this work could change the foundation of all quality measures used in pay-for-performance programs.
In Congress, legislation has been introduced in both the House of Representatives and the Senate aiming to refine the HRRP through additional risk adjustments. The Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015 (H.R. 1343 and S. 688), introduced by Rep. Jim Renacci (R-Ohio) and Sen. Joe Manchin (D-W.V.), would create immediate relief for hospitals by implementing risk adjustment for dual-eligible patients and the socioeconomic status of the hospital’s patients. At the same time, when reports that are currently in progress about risk adjustment in readmission measures and the use of a 30-day window for categorizing readmissions are completed, CMS would be required to incorporate their findings into the risk adjustment in the HRRP in the future.
SHM is supporting both of these pathways toward improving risk adjustment in readmissions measures. By engaging in the measure process and advocating for the passage of legislation to refine risk adjustment, SHM has taken a stand. The goal of reducing preventable readmissions is too important to use imprecise metrics that seem to penalize the hospitals serving the nation’s neediest patients.
As hospitalists on the front line, you can join SHM in advocating for these common sense, and necessary, changes to the HRRP.
Visit SHM’s Legislative Action Center to send a message to Congress in support of the Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015.
Joshua Lapps is SHM’s government relations manager.
Nearly three-quarters of hospitals will be receiving penalties from the Centers for Medicare and Medicaid Services (CMS) in 2016 for excess readmissions, having failed to prevent enough patients from returning to the hospital 30 days post-discharge. With so many hospitals impacted by penalties, it is understandable that the underlying methodology of the Hospital Readmissions Reduction Program (HRRP) is coming under intense scrutiny.
Research published in JAMA Internal Medicine in September hit upon many of the myriad factors—often outside of the hospital or providers’ control—that influence whether a patient is readmitted to the hospital. This information adds weight to criticism of the measures included in the HRRP and asserts the need to refine or reform the measures to better account for readmissions preventable through the interventions of the healthcare system. The behavior these measures are meant to curb, including poor quality care, inadequate access to follow-up or medications, and gaps in transitions of care, are not identifiable within broad-based, all-cause readmission measures. Instead, hospitals are being penalized for all readmissions, a majority of which may be attributable to community or patient-related factors, such as sociodemographic or housing status, among other variables.
A growing consensus on two fronts asserts that these measures, as currently structured, might not be appropriate for use in pay-for-performance programs. Measure developers, bolstered by a recent decision by the National Quality Forum to institute a trial run of risk adjusting measures for sociodemographic status, are exploring the impact of using different available variables to enhance risk adjusting their measures. Measures for readmissions are at the front of the line of these efforts. Although it is only in the beginning stages, this work could change the foundation of all quality measures used in pay-for-performance programs.
In Congress, legislation has been introduced in both the House of Representatives and the Senate aiming to refine the HRRP through additional risk adjustments. The Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015 (H.R. 1343 and S. 688), introduced by Rep. Jim Renacci (R-Ohio) and Sen. Joe Manchin (D-W.V.), would create immediate relief for hospitals by implementing risk adjustment for dual-eligible patients and the socioeconomic status of the hospital’s patients. At the same time, when reports that are currently in progress about risk adjustment in readmission measures and the use of a 30-day window for categorizing readmissions are completed, CMS would be required to incorporate their findings into the risk adjustment in the HRRP in the future.
SHM is supporting both of these pathways toward improving risk adjustment in readmissions measures. By engaging in the measure process and advocating for the passage of legislation to refine risk adjustment, SHM has taken a stand. The goal of reducing preventable readmissions is too important to use imprecise metrics that seem to penalize the hospitals serving the nation’s neediest patients.
As hospitalists on the front line, you can join SHM in advocating for these common sense, and necessary, changes to the HRRP.
Visit SHM’s Legislative Action Center to send a message to Congress in support of the Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015.
Joshua Lapps is SHM’s government relations manager.
Which Hospitalist Should Bill for Inpatient Stays with Multiple Providers?

During a facility stay, a patient could be attended to by more than one hospitalist. For example, perhaps one hospitalist is the admitting physician, but the patient has a three-day stay and may be seen by three different hospitalists. Are there any guidelines as to which physician should be billed on the facility claim? Thank you for any remarks, suggestions, or references.
—Anonymous
Dr. Hospitalist responds:
Most of us can definitely relate to the concerns you have about properly billing during the patient’s hospital stay. By facility claim, I’m assuming you mean the physician’s bill for services rendered to a hospitalized patient. After querying the Centers for Medicare and Medicaid (CMS) website and discussing the question with several of our coding and billing gurus, as far as I can tell, there are no specific guidelines pertaining to which physician in a multiphysician group should bill. CMS guidelines are clear that you should only bill for the services you provide. CMS is very specific about allowing only one physician of the same specialty billing per day (reference the CMS Manual, Chapter 12, 30.6.9-Payment for Inpatient Hospital Visits).
In our very large group, we bill daily for the individual inpatient services we provide. That way, when the bill goes out, the clinician author is responsible for its validity and can support the level of care as documented.
Billing and coding is such an arduous process, I can’t imagine attempting it without an electronic interface. Most hospitalist groups have some form of electronic billing software that has integrated checks and balances to catch the common mistakes. Improper billing done by anyone in the group can expose the entire group to an audit. With ICD-10 now upon us, this becomes ever more important.
Good luck!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
During a facility stay, a patient could be attended to by more than one hospitalist. For example, perhaps one hospitalist is the admitting physician, but the patient has a three-day stay and may be seen by three different hospitalists. Are there any guidelines as to which physician should be billed on the facility claim? Thank you for any remarks, suggestions, or references.
—Anonymous
Dr. Hospitalist responds:
Most of us can definitely relate to the concerns you have about properly billing during the patient’s hospital stay. By facility claim, I’m assuming you mean the physician’s bill for services rendered to a hospitalized patient. After querying the Centers for Medicare and Medicaid (CMS) website and discussing the question with several of our coding and billing gurus, as far as I can tell, there are no specific guidelines pertaining to which physician in a multiphysician group should bill. CMS guidelines are clear that you should only bill for the services you provide. CMS is very specific about allowing only one physician of the same specialty billing per day (reference the CMS Manual, Chapter 12, 30.6.9-Payment for Inpatient Hospital Visits).
In our very large group, we bill daily for the individual inpatient services we provide. That way, when the bill goes out, the clinician author is responsible for its validity and can support the level of care as documented.
Billing and coding is such an arduous process, I can’t imagine attempting it without an electronic interface. Most hospitalist groups have some form of electronic billing software that has integrated checks and balances to catch the common mistakes. Improper billing done by anyone in the group can expose the entire group to an audit. With ICD-10 now upon us, this becomes ever more important.
Good luck!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
During a facility stay, a patient could be attended to by more than one hospitalist. For example, perhaps one hospitalist is the admitting physician, but the patient has a three-day stay and may be seen by three different hospitalists. Are there any guidelines as to which physician should be billed on the facility claim? Thank you for any remarks, suggestions, or references.
—Anonymous
Dr. Hospitalist responds:
Most of us can definitely relate to the concerns you have about properly billing during the patient’s hospital stay. By facility claim, I’m assuming you mean the physician’s bill for services rendered to a hospitalized patient. After querying the Centers for Medicare and Medicaid (CMS) website and discussing the question with several of our coding and billing gurus, as far as I can tell, there are no specific guidelines pertaining to which physician in a multiphysician group should bill. CMS guidelines are clear that you should only bill for the services you provide. CMS is very specific about allowing only one physician of the same specialty billing per day (reference the CMS Manual, Chapter 12, 30.6.9-Payment for Inpatient Hospital Visits).
In our very large group, we bill daily for the individual inpatient services we provide. That way, when the bill goes out, the clinician author is responsible for its validity and can support the level of care as documented.
Billing and coding is such an arduous process, I can’t imagine attempting it without an electronic interface. Most hospitalist groups have some form of electronic billing software that has integrated checks and balances to catch the common mistakes. Improper billing done by anyone in the group can expose the entire group to an audit. With ICD-10 now upon us, this becomes ever more important.
Good luck!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
Eliminations Hospitalist Groups Should Consider

Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.

Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.
Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.
Medicare’s Readmission Reduction Program Cuts $420M to U.S. Hospitals This Year
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
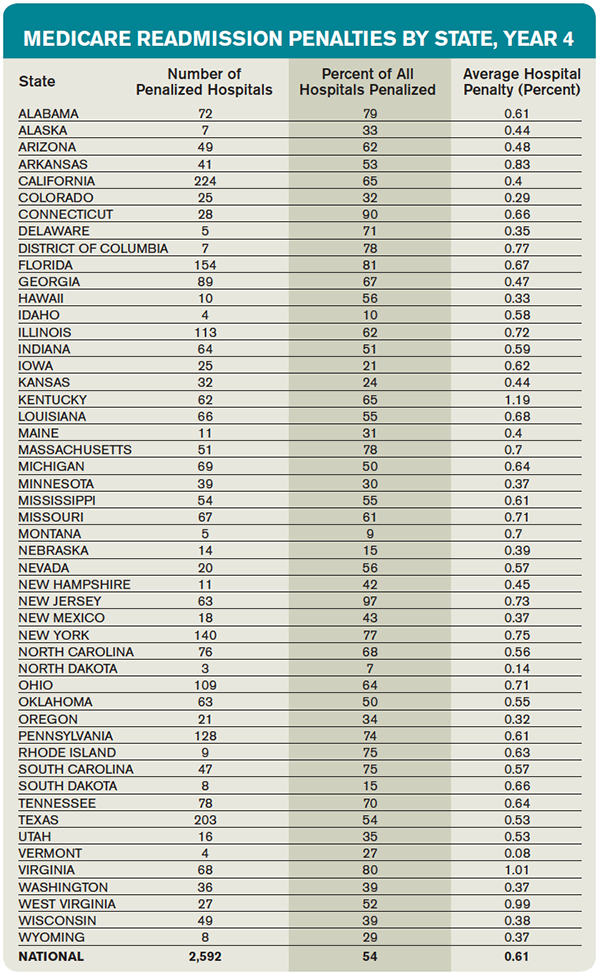
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.

References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
SHM Holding Roundtable for Hospitalist Practice Administrators
Are you a hospitalist practice administrator in a new role? SHM can help—and the upcoming roundtable discussion presented by Glenn Appelbaum, CHE, CPA, and Heather Fordyce, BS, on December 9 can help you find the resources to enable you to manage your practice effectively and efficiently. For details and to pre-register, visit the “Practice Administrators”.
Are you a hospitalist practice administrator in a new role? SHM can help—and the upcoming roundtable discussion presented by Glenn Appelbaum, CHE, CPA, and Heather Fordyce, BS, on December 9 can help you find the resources to enable you to manage your practice effectively and efficiently. For details and to pre-register, visit the “Practice Administrators”.
Are you a hospitalist practice administrator in a new role? SHM can help—and the upcoming roundtable discussion presented by Glenn Appelbaum, CHE, CPA, and Heather Fordyce, BS, on December 9 can help you find the resources to enable you to manage your practice effectively and efficiently. For details and to pre-register, visit the “Practice Administrators”.
Antimicrobial Stewardship Resources Often Lacking in Hospitalists' Routines
The best antibiotic stewardship programs weave improvements into the routines of hospitalists. But at the end of the day, developing and overseeing these important programs does require some level of time and money. And setting aside that time and money has been the exception rather than the rule.
According to early results from an SHM survey, nine of 123 hospitalists said that they are compensated for work on antimicrobial stewardship programs at their hospitals. That’s a mere 7%. Only 10 out of 122 respondents said they have “protected time” for work on an antimicrobial stewardship program. That’s about 8%. And it’s possible that the survey results are actually skewed somewhat, receiving responses from more proactive centers. One hundred fifteen out of 178 respondents, or 65%, said that they have an antimicrobial stewardship program at their centers.
Arjun Srinivasan, the CDC’s associate director for healthcare-associated infection prevention programs, says he has found that typically about half of U.S. hospitals have such programs. Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Johns Hopkins Bayview Medical Center in Baltimore, says change can be a slow process, but he expects initiatives like SHM’s new antibiotic stewardship campaign to help tip the scales toward more resources and more change. It’s a matter of “making the case that, No. 1, this is a problem and, No. 2, there are solutions out there and, No. 3, these solutions are cost effective, as well as improving quality.” Demonstrating the effects on cost and outcomes, he says, is “likely the tipping point [where] we will see real change.”

“If we don’t change, we’re going to run out of antibiotics,” says Dr. Howell, who is also senior physician advisor to SHM’s Center for Hospital Innovation and Improvement. “People are sort of really panic-stricken. And that fear is helping to motivate them to drive change, too.”
Jonathan Zenilman, MD, chief of the division of infectious diseases at Bayview, says that his team worked with a non-Hopkins hospital in Delaware and found they saved about $80,000 a year just by eliminating the use of ertapenem for pre-operative prophylaxis for abdominal surgery. Numbers like that, he says, show that the case for savings can be made to hospital administration. Then again, it’s often easier to make the case before a program is started—and harder to keep it going after that first year.
“Between the second and the third year, you’re not going to generate much savings, if anything,” he says. If a new administrator is in place, it can be a challenge to get them to realize that costs will go back up once a program is dismantled.
“They look at this as an additional business model,” Dr. Zenilman explains. “They’ll say, ‘Where does my revenue offset the costs?’ And sometimes they just don’t get the value proposition…It needs to be pitched as a value proposition and not as a revenue proposition.”
The culture change toward value in the U.S. is helping, though, he says. “Now the business case is easier,” he says, “because there’s clearly this regulatory push towards doing it.” TH
The best antibiotic stewardship programs weave improvements into the routines of hospitalists. But at the end of the day, developing and overseeing these important programs does require some level of time and money. And setting aside that time and money has been the exception rather than the rule.
According to early results from an SHM survey, nine of 123 hospitalists said that they are compensated for work on antimicrobial stewardship programs at their hospitals. That’s a mere 7%. Only 10 out of 122 respondents said they have “protected time” for work on an antimicrobial stewardship program. That’s about 8%. And it’s possible that the survey results are actually skewed somewhat, receiving responses from more proactive centers. One hundred fifteen out of 178 respondents, or 65%, said that they have an antimicrobial stewardship program at their centers.
Arjun Srinivasan, the CDC’s associate director for healthcare-associated infection prevention programs, says he has found that typically about half of U.S. hospitals have such programs. Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Johns Hopkins Bayview Medical Center in Baltimore, says change can be a slow process, but he expects initiatives like SHM’s new antibiotic stewardship campaign to help tip the scales toward more resources and more change. It’s a matter of “making the case that, No. 1, this is a problem and, No. 2, there are solutions out there and, No. 3, these solutions are cost effective, as well as improving quality.” Demonstrating the effects on cost and outcomes, he says, is “likely the tipping point [where] we will see real change.”
“If we don’t change, we’re going to run out of antibiotics,” says Dr. Howell, who is also senior physician advisor to SHM’s Center for Hospital Innovation and Improvement. “People are sort of really panic-stricken. And that fear is helping to motivate them to drive change, too.”
Jonathan Zenilman, MD, chief of the division of infectious diseases at Bayview, says that his team worked with a non-Hopkins hospital in Delaware and found they saved about $80,000 a year just by eliminating the use of ertapenem for pre-operative prophylaxis for abdominal surgery. Numbers like that, he says, show that the case for savings can be made to hospital administration. Then again, it’s often easier to make the case before a program is started—and harder to keep it going after that first year.
“Between the second and the third year, you’re not going to generate much savings, if anything,” he says. If a new administrator is in place, it can be a challenge to get them to realize that costs will go back up once a program is dismantled.
“They look at this as an additional business model,” Dr. Zenilman explains. “They’ll say, ‘Where does my revenue offset the costs?’ And sometimes they just don’t get the value proposition…It needs to be pitched as a value proposition and not as a revenue proposition.”
The culture change toward value in the U.S. is helping, though, he says. “Now the business case is easier,” he says, “because there’s clearly this regulatory push towards doing it.” TH
The best antibiotic stewardship programs weave improvements into the routines of hospitalists. But at the end of the day, developing and overseeing these important programs does require some level of time and money. And setting aside that time and money has been the exception rather than the rule.
According to early results from an SHM survey, nine of 123 hospitalists said that they are compensated for work on antimicrobial stewardship programs at their hospitals. That’s a mere 7%. Only 10 out of 122 respondents said they have “protected time” for work on an antimicrobial stewardship program. That’s about 8%. And it’s possible that the survey results are actually skewed somewhat, receiving responses from more proactive centers. One hundred fifteen out of 178 respondents, or 65%, said that they have an antimicrobial stewardship program at their centers.
Arjun Srinivasan, the CDC’s associate director for healthcare-associated infection prevention programs, says he has found that typically about half of U.S. hospitals have such programs. Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Johns Hopkins Bayview Medical Center in Baltimore, says change can be a slow process, but he expects initiatives like SHM’s new antibiotic stewardship campaign to help tip the scales toward more resources and more change. It’s a matter of “making the case that, No. 1, this is a problem and, No. 2, there are solutions out there and, No. 3, these solutions are cost effective, as well as improving quality.” Demonstrating the effects on cost and outcomes, he says, is “likely the tipping point [where] we will see real change.”
“If we don’t change, we’re going to run out of antibiotics,” says Dr. Howell, who is also senior physician advisor to SHM’s Center for Hospital Innovation and Improvement. “People are sort of really panic-stricken. And that fear is helping to motivate them to drive change, too.”
Jonathan Zenilman, MD, chief of the division of infectious diseases at Bayview, says that his team worked with a non-Hopkins hospital in Delaware and found they saved about $80,000 a year just by eliminating the use of ertapenem for pre-operative prophylaxis for abdominal surgery. Numbers like that, he says, show that the case for savings can be made to hospital administration. Then again, it’s often easier to make the case before a program is started—and harder to keep it going after that first year.
“Between the second and the third year, you’re not going to generate much savings, if anything,” he says. If a new administrator is in place, it can be a challenge to get them to realize that costs will go back up once a program is dismantled.
“They look at this as an additional business model,” Dr. Zenilman explains. “They’ll say, ‘Where does my revenue offset the costs?’ And sometimes they just don’t get the value proposition…It needs to be pitched as a value proposition and not as a revenue proposition.”
The culture change toward value in the U.S. is helping, though, he says. “Now the business case is easier,” he says, “because there’s clearly this regulatory push towards doing it.” TH
Society of Hospital Medicine Launches Antimicrobial Stewardship Campaign
In 2006, infectious disease specialists and pharmacists at Johns Hopkins Bayview Medical Center in Baltimore took a look at the pharmacy budget and were jarred by the numbers.
“The proportion of the pharmacy budget that was antimicrobials was much larger than we would expect,” says Jonathan Zenilman, MD, chief of infectious diseases at Bayview.
The pharmacy and ID teams implemented antibiotic stewardship tools, including medication reassessments after two or three days and quicker conversion to oral drugs when appropriate. They also did something that was fairly new at the time: A hospitalist was incorporated into the team. The tactic was employed out of need—the ID department was stretched too thin—but it made perfect sense, Dr. Zenilman says. Most of the patients seen by hospitalists have bread-and-butter conditions that comprise a lot of the center’s antibiotic use.
“Patients on a typical hospital medicine series are not on advanced antifungals and complicated antibiotic regimens,” he says.
The arrangement worked: The center achieved a more than 50% reduction in the main target drug, Zosyn, and a hospitalist is still typically part of the antibiotic stewardship team.
That might have been a new concept then, but fast forward a decade: ID and public health experts are increasingly seeing hospitalists as central to the effort to limit antibiotic overuse and stall the development of drug resistance in antimicrobial organisms.
Now, SHM is about to launch a campaign to get more hospitalists to see themselves as central to that effort. SHM will formally kick off the “Fight the Resistance” campaign on November 9. It’s an awareness and behavior change campaign that builds on SHM’s participation in a White House forum on antibiotic resistance that was held in June.

“We wanted to not only enhance awareness among hospitalists about what appropriate antimicrobial prescribing is, but also to change behaviors and ultimately change culture to facilitate appropriate antibiotic use,” says Jenna Goldstein, director of SHM’s Center for Hospital Innovation and Improvement (CHII), who is leading the initiative along with Mobola Owolabi, SHM project manager.
Behavior Change
The society will provide educational inserts hospitalists can use at their hospitals, as well as downloadable posters that will help raise awareness on appropriate antibiotic use. The campaign will be highlighted in SHM’s online and social media presence.
Hospitalists will be asked to make behavior changes in their antibiotic-related practices that will promote better stewardship, such as taking an antibiotic “timeout” during which usage is revisited and changed or discontinued if antibiotic use is not appropriate.
“We’re specifically asking hospitalists to engage in behavior changes and we plan to assess outcomes and results after implementation,” Goldstein says. “Our ultimate goal, although we realize this is a much longer-term goal and certainly more arduous to measure, is to change the culture in the hospital related to prescribing, so that hospitalists are prescribing only when appropriate, only when there’s an indicated infection, and according to the evidence base for prescribing antimicrobials for their patients.”

Future plans will include developing a mentored implementation program in which SHM will provide guidance for hospitalists who want to develop or improve a stewardship program at their hospital. The guidance will be based in part on the CDC’s “Core Elements of Hospital Antibiotic Stewardship Programs,” a kind of guidebook on antibiotic stewardship.1
Read more about antibiotic stewardship resources.
Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Bayview, associate professor of medicine at Johns Hopkins University School of Medicine, and CHII’s senior physician advisor, says it’s time for hospitalists to take on a bigger role.
“Doing ‘just in case’ antibiotics is really not appropriate and should be strongly discouraged, unless the risks are very high for a specific patient,” he says. A past president of SHM, Dr. Howell has long advocated that hospitalists take the time to explain the risk of excessive antibiotic use to their patients, even on a busy day.
“It’s our duty as physicians to make sure our patients get the best care possible, and often that means the physicians themselves have to do the educating,” he says. “I would say that, in general, it doesn’t take that much time. Having a conversation with your patient to educate them about anything—heart failure, diabetes, appropriate antibiotics—must be built into the care that we provide our patients somehow.”
That communication doesn’t necessarily have to be performed by the hospitalist, he notes. The pharmacist, nurse, or written material can relay this information. But somewhere along the line, he says, the antibiotic education must happen.
SHM’s initiative should help, simply because “knowledge is good,” says Dr. Zenilman, the ID expert at Hopkins Bayview. Key to success, he says, will be what happens when hospitalists are taking care of a patient—will they actually be willing to cut their regimens?
“People overuse antibiotics, sometimes not out of education issues, but because they’re anxious,” Dr. Zenilman says. “The more challenging part is getting people to deal with the uncertainty and recognizing intuitively that overuse has enormous complications.”
The literature is now replete with studies showing how antibiotic stewardship measures help curb resistance, eliminate incorrect antibiotic prescribing, lower antibiotic use, and lower costs.
A web-based program was projected to save almost $400,000 a year linked to restricted antibiotic use at Johns Hopkins, according to a 2008 study.2
In Canada, according to a 2007 study, a program including recommendations for alternative drugs and shorter, guideline-based treatment durations helped reduce Clostridium difficile infections by 60% over a two-year period.3
An analysis published in August, using data from the CDC’s National Healthcare Safety Network and Emerging Infections Program, concluded that a nationwide infection control and antibiotic stewardship intervention could, over five years, avoid an estimated 619,000 hospital-acquired infections from carbapenem-resistant Enterobacteriaceae, multidrug-resistant Pseudomonas aeruginosa, invasive methicillin-resistant Staphylococcus aureus (MRSA), or C. diff.4
In spite of the evidence, preliminary results of a recent SHM survey on antibiotic stewardship found very little support, in terms of money and protected time, for hospitalists to be involved in antibiotic stewardship programs.
UM’s Success Story
A kind of microcosm of what is possible can be seen at the University of Michigan. There, Scott Flanders, MD, MHM, clinical professor of internal medicine and past president of SHM, has led an effort, along with the CDC and the Institute for Healthcare Improvement, to look at hospitalist-led interventions for smarter antimicrobial use.
Hospitalists in several programs around the country were asked to focus on a few key improvement strategies that are believed to improve use. For instance, when guidelines give a range of duration of dosing, physicians often lean toward the higher end (when the range is seven to 21 days, the default was typically closer to 21), even when that might not be necessary in a given situation. So, more specific guidelines for common situations were applied.
Hospitalists also worked to improve documentation to make antibiotic use more visible at the point of care: which drug it is, when it was started, what day of therapy it is that day, how many more days are left.
An antibiotic “timeout” at 48 to 72 hours was implemented to determine whether the treatment course should be maintained, changed, or eliminated.
The idea was for hospitalists to track this as part of the usual care process.
“We didn’t want people to create whole new systems to do these things,” says Dr. Flanders, who has consulted with SHM for its stewardship initiative. “We wanted people, for example, to use their multidisciplinary rounds that they were already having to just add one thing to the checklist.”
The process was shown to be workable. All steps of the stewardship protocol were performed 70% of the time after the initiative began, compared with just 20% of the time before it began, Dr. Flanders says. Additionally, about 25% of patients had a “significant and important” change made to their antibiotic treatment following the “timeout.”

“During this timeout, a lot of action happened,” Dr. Flanders says. More study is needed to show exactly how much of a change occurred and whether it led to cost savings, he says, but “I suspect it will.”
Much-Anticipated Partnership
Arjun Srinivasan, MD, associate director for healthcare-associated infection prevention programs at the CDC, says he is eager to continue to work with SHM on its antibiotic stewardship efforts, but he cautions that hospitalists should not try to do too much too quickly in implementing change.
“Success generally comes from starting small, from starting with a focused approach to something that you know is a problem in your facility,” Dr. Srinivasan says. “When you try to delve into everything all at once, you can very quickly get overwhelmed.”
Although smaller centers might have less manpower and face a bigger challenge in leading a stewardship program, it can be done, he says.
“We see some very small hospitals that have fantastic stewardship programs and some very small hospitals that are struggling,” he says. “We know it’s doable across the spectrum of the sizes of hospital.”
Hospitalists, he adds, “are the tip of the spear. They are probably prescribing most of the antibiotics [for inpatients] … and diagnosing most of the infections. So arming them with the information they need, working with them to develop a process that makes prescribing optimal and most efficient is obviously hugely beneficial.
“You’re going to have a tremendous impact by reaching that particular group.”
Tom Collins is a freelance writer in South Florida.
References
- Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. May 7, 2015. Accessed October 6, 2015.
- Agwu AL, Lee CK, Jain SK. A World Wide Web-based antimicrobial stewardship program improves efficiency, communication, and user satisfaction and reduces cost in a tertiary care pediatric medical center. Clin Infect Dis. 2008 Sep 15;47(6):747-753.
- Valiquette L, Cossette B, Garant MP, Diab H, Pépin J. Impact of a reduction in the use of high-risk antibiotics on the course of an epidemic of Clostridium difficile-associated disease caused by the hypervirulent NAP1/027 strain. Clin Infect Dis. 2007;45 Suppl 2:S112-S121.
- Slayton RB, Toth D, Lee BY, et al. Vital signs: estimated effects of a coordinated approach for action to reduce antibiotic-resistant infections in health care facilities - United States. MMWR Morb Mortal Wkly Rep. 2015;64(30):826-831.
In 2006, infectious disease specialists and pharmacists at Johns Hopkins Bayview Medical Center in Baltimore took a look at the pharmacy budget and were jarred by the numbers.
“The proportion of the pharmacy budget that was antimicrobials was much larger than we would expect,” says Jonathan Zenilman, MD, chief of infectious diseases at Bayview.
The pharmacy and ID teams implemented antibiotic stewardship tools, including medication reassessments after two or three days and quicker conversion to oral drugs when appropriate. They also did something that was fairly new at the time: A hospitalist was incorporated into the team. The tactic was employed out of need—the ID department was stretched too thin—but it made perfect sense, Dr. Zenilman says. Most of the patients seen by hospitalists have bread-and-butter conditions that comprise a lot of the center’s antibiotic use.
“Patients on a typical hospital medicine series are not on advanced antifungals and complicated antibiotic regimens,” he says.
The arrangement worked: The center achieved a more than 50% reduction in the main target drug, Zosyn, and a hospitalist is still typically part of the antibiotic stewardship team.
That might have been a new concept then, but fast forward a decade: ID and public health experts are increasingly seeing hospitalists as central to the effort to limit antibiotic overuse and stall the development of drug resistance in antimicrobial organisms.
Now, SHM is about to launch a campaign to get more hospitalists to see themselves as central to that effort. SHM will formally kick off the “Fight the Resistance” campaign on November 9. It’s an awareness and behavior change campaign that builds on SHM’s participation in a White House forum on antibiotic resistance that was held in June.
“We wanted to not only enhance awareness among hospitalists about what appropriate antimicrobial prescribing is, but also to change behaviors and ultimately change culture to facilitate appropriate antibiotic use,” says Jenna Goldstein, director of SHM’s Center for Hospital Innovation and Improvement (CHII), who is leading the initiative along with Mobola Owolabi, SHM project manager.
Behavior Change
The society will provide educational inserts hospitalists can use at their hospitals, as well as downloadable posters that will help raise awareness on appropriate antibiotic use. The campaign will be highlighted in SHM’s online and social media presence.
Hospitalists will be asked to make behavior changes in their antibiotic-related practices that will promote better stewardship, such as taking an antibiotic “timeout” during which usage is revisited and changed or discontinued if antibiotic use is not appropriate.
“We’re specifically asking hospitalists to engage in behavior changes and we plan to assess outcomes and results after implementation,” Goldstein says. “Our ultimate goal, although we realize this is a much longer-term goal and certainly more arduous to measure, is to change the culture in the hospital related to prescribing, so that hospitalists are prescribing only when appropriate, only when there’s an indicated infection, and according to the evidence base for prescribing antimicrobials for their patients.”
Future plans will include developing a mentored implementation program in which SHM will provide guidance for hospitalists who want to develop or improve a stewardship program at their hospital. The guidance will be based in part on the CDC’s “Core Elements of Hospital Antibiotic Stewardship Programs,” a kind of guidebook on antibiotic stewardship.1
Read more about antibiotic stewardship resources.
Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Bayview, associate professor of medicine at Johns Hopkins University School of Medicine, and CHII’s senior physician advisor, says it’s time for hospitalists to take on a bigger role.
“Doing ‘just in case’ antibiotics is really not appropriate and should be strongly discouraged, unless the risks are very high for a specific patient,” he says. A past president of SHM, Dr. Howell has long advocated that hospitalists take the time to explain the risk of excessive antibiotic use to their patients, even on a busy day.
“It’s our duty as physicians to make sure our patients get the best care possible, and often that means the physicians themselves have to do the educating,” he says. “I would say that, in general, it doesn’t take that much time. Having a conversation with your patient to educate them about anything—heart failure, diabetes, appropriate antibiotics—must be built into the care that we provide our patients somehow.”
That communication doesn’t necessarily have to be performed by the hospitalist, he notes. The pharmacist, nurse, or written material can relay this information. But somewhere along the line, he says, the antibiotic education must happen.
SHM’s initiative should help, simply because “knowledge is good,” says Dr. Zenilman, the ID expert at Hopkins Bayview. Key to success, he says, will be what happens when hospitalists are taking care of a patient—will they actually be willing to cut their regimens?
“People overuse antibiotics, sometimes not out of education issues, but because they’re anxious,” Dr. Zenilman says. “The more challenging part is getting people to deal with the uncertainty and recognizing intuitively that overuse has enormous complications.”
The literature is now replete with studies showing how antibiotic stewardship measures help curb resistance, eliminate incorrect antibiotic prescribing, lower antibiotic use, and lower costs.
A web-based program was projected to save almost $400,000 a year linked to restricted antibiotic use at Johns Hopkins, according to a 2008 study.2
In Canada, according to a 2007 study, a program including recommendations for alternative drugs and shorter, guideline-based treatment durations helped reduce Clostridium difficile infections by 60% over a two-year period.3
An analysis published in August, using data from the CDC’s National Healthcare Safety Network and Emerging Infections Program, concluded that a nationwide infection control and antibiotic stewardship intervention could, over five years, avoid an estimated 619,000 hospital-acquired infections from carbapenem-resistant Enterobacteriaceae, multidrug-resistant Pseudomonas aeruginosa, invasive methicillin-resistant Staphylococcus aureus (MRSA), or C. diff.4
In spite of the evidence, preliminary results of a recent SHM survey on antibiotic stewardship found very little support, in terms of money and protected time, for hospitalists to be involved in antibiotic stewardship programs.
UM’s Success Story
A kind of microcosm of what is possible can be seen at the University of Michigan. There, Scott Flanders, MD, MHM, clinical professor of internal medicine and past president of SHM, has led an effort, along with the CDC and the Institute for Healthcare Improvement, to look at hospitalist-led interventions for smarter antimicrobial use.
Hospitalists in several programs around the country were asked to focus on a few key improvement strategies that are believed to improve use. For instance, when guidelines give a range of duration of dosing, physicians often lean toward the higher end (when the range is seven to 21 days, the default was typically closer to 21), even when that might not be necessary in a given situation. So, more specific guidelines for common situations were applied.
Hospitalists also worked to improve documentation to make antibiotic use more visible at the point of care: which drug it is, when it was started, what day of therapy it is that day, how many more days are left.
An antibiotic “timeout” at 48 to 72 hours was implemented to determine whether the treatment course should be maintained, changed, or eliminated.
The idea was for hospitalists to track this as part of the usual care process.
“We didn’t want people to create whole new systems to do these things,” says Dr. Flanders, who has consulted with SHM for its stewardship initiative. “We wanted people, for example, to use their multidisciplinary rounds that they were already having to just add one thing to the checklist.”
The process was shown to be workable. All steps of the stewardship protocol were performed 70% of the time after the initiative began, compared with just 20% of the time before it began, Dr. Flanders says. Additionally, about 25% of patients had a “significant and important” change made to their antibiotic treatment following the “timeout.”
“During this timeout, a lot of action happened,” Dr. Flanders says. More study is needed to show exactly how much of a change occurred and whether it led to cost savings, he says, but “I suspect it will.”
Much-Anticipated Partnership
Arjun Srinivasan, MD, associate director for healthcare-associated infection prevention programs at the CDC, says he is eager to continue to work with SHM on its antibiotic stewardship efforts, but he cautions that hospitalists should not try to do too much too quickly in implementing change.
“Success generally comes from starting small, from starting with a focused approach to something that you know is a problem in your facility,” Dr. Srinivasan says. “When you try to delve into everything all at once, you can very quickly get overwhelmed.”
Although smaller centers might have less manpower and face a bigger challenge in leading a stewardship program, it can be done, he says.
“We see some very small hospitals that have fantastic stewardship programs and some very small hospitals that are struggling,” he says. “We know it’s doable across the spectrum of the sizes of hospital.”
Hospitalists, he adds, “are the tip of the spear. They are probably prescribing most of the antibiotics [for inpatients] … and diagnosing most of the infections. So arming them with the information they need, working with them to develop a process that makes prescribing optimal and most efficient is obviously hugely beneficial.
“You’re going to have a tremendous impact by reaching that particular group.”
Tom Collins is a freelance writer in South Florida.
References
- Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. May 7, 2015. Accessed October 6, 2015.
- Agwu AL, Lee CK, Jain SK. A World Wide Web-based antimicrobial stewardship program improves efficiency, communication, and user satisfaction and reduces cost in a tertiary care pediatric medical center. Clin Infect Dis. 2008 Sep 15;47(6):747-753.
- Valiquette L, Cossette B, Garant MP, Diab H, Pépin J. Impact of a reduction in the use of high-risk antibiotics on the course of an epidemic of Clostridium difficile-associated disease caused by the hypervirulent NAP1/027 strain. Clin Infect Dis. 2007;45 Suppl 2:S112-S121.
- Slayton RB, Toth D, Lee BY, et al. Vital signs: estimated effects of a coordinated approach for action to reduce antibiotic-resistant infections in health care facilities - United States. MMWR Morb Mortal Wkly Rep. 2015;64(30):826-831.
In 2006, infectious disease specialists and pharmacists at Johns Hopkins Bayview Medical Center in Baltimore took a look at the pharmacy budget and were jarred by the numbers.
“The proportion of the pharmacy budget that was antimicrobials was much larger than we would expect,” says Jonathan Zenilman, MD, chief of infectious diseases at Bayview.
The pharmacy and ID teams implemented antibiotic stewardship tools, including medication reassessments after two or three days and quicker conversion to oral drugs when appropriate. They also did something that was fairly new at the time: A hospitalist was incorporated into the team. The tactic was employed out of need—the ID department was stretched too thin—but it made perfect sense, Dr. Zenilman says. Most of the patients seen by hospitalists have bread-and-butter conditions that comprise a lot of the center’s antibiotic use.
“Patients on a typical hospital medicine series are not on advanced antifungals and complicated antibiotic regimens,” he says.
The arrangement worked: The center achieved a more than 50% reduction in the main target drug, Zosyn, and a hospitalist is still typically part of the antibiotic stewardship team.
That might have been a new concept then, but fast forward a decade: ID and public health experts are increasingly seeing hospitalists as central to the effort to limit antibiotic overuse and stall the development of drug resistance in antimicrobial organisms.
Now, SHM is about to launch a campaign to get more hospitalists to see themselves as central to that effort. SHM will formally kick off the “Fight the Resistance” campaign on November 9. It’s an awareness and behavior change campaign that builds on SHM’s participation in a White House forum on antibiotic resistance that was held in June.
“We wanted to not only enhance awareness among hospitalists about what appropriate antimicrobial prescribing is, but also to change behaviors and ultimately change culture to facilitate appropriate antibiotic use,” says Jenna Goldstein, director of SHM’s Center for Hospital Innovation and Improvement (CHII), who is leading the initiative along with Mobola Owolabi, SHM project manager.
Behavior Change
The society will provide educational inserts hospitalists can use at their hospitals, as well as downloadable posters that will help raise awareness on appropriate antibiotic use. The campaign will be highlighted in SHM’s online and social media presence.
Hospitalists will be asked to make behavior changes in their antibiotic-related practices that will promote better stewardship, such as taking an antibiotic “timeout” during which usage is revisited and changed or discontinued if antibiotic use is not appropriate.
“We’re specifically asking hospitalists to engage in behavior changes and we plan to assess outcomes and results after implementation,” Goldstein says. “Our ultimate goal, although we realize this is a much longer-term goal and certainly more arduous to measure, is to change the culture in the hospital related to prescribing, so that hospitalists are prescribing only when appropriate, only when there’s an indicated infection, and according to the evidence base for prescribing antimicrobials for their patients.”
Future plans will include developing a mentored implementation program in which SHM will provide guidance for hospitalists who want to develop or improve a stewardship program at their hospital. The guidance will be based in part on the CDC’s “Core Elements of Hospital Antibiotic Stewardship Programs,” a kind of guidebook on antibiotic stewardship.1
Read more about antibiotic stewardship resources.
Eric Howell, MD, SFHM, director of the collaborative inpatient medicine service at Bayview, associate professor of medicine at Johns Hopkins University School of Medicine, and CHII’s senior physician advisor, says it’s time for hospitalists to take on a bigger role.
“Doing ‘just in case’ antibiotics is really not appropriate and should be strongly discouraged, unless the risks are very high for a specific patient,” he says. A past president of SHM, Dr. Howell has long advocated that hospitalists take the time to explain the risk of excessive antibiotic use to their patients, even on a busy day.
“It’s our duty as physicians to make sure our patients get the best care possible, and often that means the physicians themselves have to do the educating,” he says. “I would say that, in general, it doesn’t take that much time. Having a conversation with your patient to educate them about anything—heart failure, diabetes, appropriate antibiotics—must be built into the care that we provide our patients somehow.”
That communication doesn’t necessarily have to be performed by the hospitalist, he notes. The pharmacist, nurse, or written material can relay this information. But somewhere along the line, he says, the antibiotic education must happen.
SHM’s initiative should help, simply because “knowledge is good,” says Dr. Zenilman, the ID expert at Hopkins Bayview. Key to success, he says, will be what happens when hospitalists are taking care of a patient—will they actually be willing to cut their regimens?
“People overuse antibiotics, sometimes not out of education issues, but because they’re anxious,” Dr. Zenilman says. “The more challenging part is getting people to deal with the uncertainty and recognizing intuitively that overuse has enormous complications.”
The literature is now replete with studies showing how antibiotic stewardship measures help curb resistance, eliminate incorrect antibiotic prescribing, lower antibiotic use, and lower costs.
A web-based program was projected to save almost $400,000 a year linked to restricted antibiotic use at Johns Hopkins, according to a 2008 study.2
In Canada, according to a 2007 study, a program including recommendations for alternative drugs and shorter, guideline-based treatment durations helped reduce Clostridium difficile infections by 60% over a two-year period.3
An analysis published in August, using data from the CDC’s National Healthcare Safety Network and Emerging Infections Program, concluded that a nationwide infection control and antibiotic stewardship intervention could, over five years, avoid an estimated 619,000 hospital-acquired infections from carbapenem-resistant Enterobacteriaceae, multidrug-resistant Pseudomonas aeruginosa, invasive methicillin-resistant Staphylococcus aureus (MRSA), or C. diff.4
In spite of the evidence, preliminary results of a recent SHM survey on antibiotic stewardship found very little support, in terms of money and protected time, for hospitalists to be involved in antibiotic stewardship programs.
UM’s Success Story
A kind of microcosm of what is possible can be seen at the University of Michigan. There, Scott Flanders, MD, MHM, clinical professor of internal medicine and past president of SHM, has led an effort, along with the CDC and the Institute for Healthcare Improvement, to look at hospitalist-led interventions for smarter antimicrobial use.
Hospitalists in several programs around the country were asked to focus on a few key improvement strategies that are believed to improve use. For instance, when guidelines give a range of duration of dosing, physicians often lean toward the higher end (when the range is seven to 21 days, the default was typically closer to 21), even when that might not be necessary in a given situation. So, more specific guidelines for common situations were applied.
Hospitalists also worked to improve documentation to make antibiotic use more visible at the point of care: which drug it is, when it was started, what day of therapy it is that day, how many more days are left.
An antibiotic “timeout” at 48 to 72 hours was implemented to determine whether the treatment course should be maintained, changed, or eliminated.
The idea was for hospitalists to track this as part of the usual care process.
“We didn’t want people to create whole new systems to do these things,” says Dr. Flanders, who has consulted with SHM for its stewardship initiative. “We wanted people, for example, to use their multidisciplinary rounds that they were already having to just add one thing to the checklist.”
The process was shown to be workable. All steps of the stewardship protocol were performed 70% of the time after the initiative began, compared with just 20% of the time before it began, Dr. Flanders says. Additionally, about 25% of patients had a “significant and important” change made to their antibiotic treatment following the “timeout.”
“During this timeout, a lot of action happened,” Dr. Flanders says. More study is needed to show exactly how much of a change occurred and whether it led to cost savings, he says, but “I suspect it will.”
Much-Anticipated Partnership
Arjun Srinivasan, MD, associate director for healthcare-associated infection prevention programs at the CDC, says he is eager to continue to work with SHM on its antibiotic stewardship efforts, but he cautions that hospitalists should not try to do too much too quickly in implementing change.
“Success generally comes from starting small, from starting with a focused approach to something that you know is a problem in your facility,” Dr. Srinivasan says. “When you try to delve into everything all at once, you can very quickly get overwhelmed.”
Although smaller centers might have less manpower and face a bigger challenge in leading a stewardship program, it can be done, he says.
“We see some very small hospitals that have fantastic stewardship programs and some very small hospitals that are struggling,” he says. “We know it’s doable across the spectrum of the sizes of hospital.”
Hospitalists, he adds, “are the tip of the spear. They are probably prescribing most of the antibiotics [for inpatients] … and diagnosing most of the infections. So arming them with the information they need, working with them to develop a process that makes prescribing optimal and most efficient is obviously hugely beneficial.
“You’re going to have a tremendous impact by reaching that particular group.”
Tom Collins is a freelance writer in South Florida.
References
- Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. May 7, 2015. Accessed October 6, 2015.
- Agwu AL, Lee CK, Jain SK. A World Wide Web-based antimicrobial stewardship program improves efficiency, communication, and user satisfaction and reduces cost in a tertiary care pediatric medical center. Clin Infect Dis. 2008 Sep 15;47(6):747-753.
- Valiquette L, Cossette B, Garant MP, Diab H, Pépin J. Impact of a reduction in the use of high-risk antibiotics on the course of an epidemic of Clostridium difficile-associated disease caused by the hypervirulent NAP1/027 strain. Clin Infect Dis. 2007;45 Suppl 2:S112-S121.
- Slayton RB, Toth D, Lee BY, et al. Vital signs: estimated effects of a coordinated approach for action to reduce antibiotic-resistant infections in health care facilities - United States. MMWR Morb Mortal Wkly Rep. 2015;64(30):826-831.