User login
Renal dosing of non–vitamin K antagonist oral anticoagulants in atrial fibrillation is important in preventing thrombotic and bleeding complications
Clinical question: Does renal underdosing and overdosing of non–vitamin K antagonist oral anticoagulants (NOACs) impact the risk of thrombotic and bleeding complications?
Background: All of the NOACs have at least partial renal clearance, but compliance with Food and Drug Administration–labeled renal dosing recommendations is inconsistent. This study examines the risk of adverse thrombotic and bleeding events in patients with improper anticoagulant dosing.
Study design: Retrospective cohort study.
Setting: United States (OptumLabs data warehouse, a database of over 100 million patients hospitalized in the United States in the last 20 years).
Synopsis: With use of data from the OptumLabs data warehouse of privately insured and Medicare Advantage enrollees, 14,865 patients with nonvalvular atrial fibrillation who were started on NOACs (apixaban, dabigatran, or rivaroxaban) were identified. Creatinine values within the year before treatment were used to calculate an estimated glomerular filtration rate (eGFR).
Of patients qualifying for renal dose reduction, 43% received the standard dosing (overdose). Of patients not qualifying for renal dose reduction, 13% received a reduced dose (underdose). The overdosed group had a higher rate of bleeding events, compared with controls (hazard ratio, 2.19; 95% CI, 1.07-4.46). The underdosed group had a higher rate of stroke (HR, 4.87; 95% CI, 1.30-18.26).
Bottom line: Excessive dosing of NOACs in patients with renal insufficiency is common and is associated with bleeding.Citation: Yao X, Shah ND, Sangaralingham LR, Gersh BJ, and Noseworthy PA. Non–vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. JACC. 2017;69(23):2779-90.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does renal underdosing and overdosing of non–vitamin K antagonist oral anticoagulants (NOACs) impact the risk of thrombotic and bleeding complications?
Background: All of the NOACs have at least partial renal clearance, but compliance with Food and Drug Administration–labeled renal dosing recommendations is inconsistent. This study examines the risk of adverse thrombotic and bleeding events in patients with improper anticoagulant dosing.
Study design: Retrospective cohort study.
Setting: United States (OptumLabs data warehouse, a database of over 100 million patients hospitalized in the United States in the last 20 years).
Synopsis: With use of data from the OptumLabs data warehouse of privately insured and Medicare Advantage enrollees, 14,865 patients with nonvalvular atrial fibrillation who were started on NOACs (apixaban, dabigatran, or rivaroxaban) were identified. Creatinine values within the year before treatment were used to calculate an estimated glomerular filtration rate (eGFR).
Of patients qualifying for renal dose reduction, 43% received the standard dosing (overdose). Of patients not qualifying for renal dose reduction, 13% received a reduced dose (underdose). The overdosed group had a higher rate of bleeding events, compared with controls (hazard ratio, 2.19; 95% CI, 1.07-4.46). The underdosed group had a higher rate of stroke (HR, 4.87; 95% CI, 1.30-18.26).
Bottom line: Excessive dosing of NOACs in patients with renal insufficiency is common and is associated with bleeding.Citation: Yao X, Shah ND, Sangaralingham LR, Gersh BJ, and Noseworthy PA. Non–vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. JACC. 2017;69(23):2779-90.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does renal underdosing and overdosing of non–vitamin K antagonist oral anticoagulants (NOACs) impact the risk of thrombotic and bleeding complications?
Background: All of the NOACs have at least partial renal clearance, but compliance with Food and Drug Administration–labeled renal dosing recommendations is inconsistent. This study examines the risk of adverse thrombotic and bleeding events in patients with improper anticoagulant dosing.
Study design: Retrospective cohort study.
Setting: United States (OptumLabs data warehouse, a database of over 100 million patients hospitalized in the United States in the last 20 years).
Synopsis: With use of data from the OptumLabs data warehouse of privately insured and Medicare Advantage enrollees, 14,865 patients with nonvalvular atrial fibrillation who were started on NOACs (apixaban, dabigatran, or rivaroxaban) were identified. Creatinine values within the year before treatment were used to calculate an estimated glomerular filtration rate (eGFR).
Of patients qualifying for renal dose reduction, 43% received the standard dosing (overdose). Of patients not qualifying for renal dose reduction, 13% received a reduced dose (underdose). The overdosed group had a higher rate of bleeding events, compared with controls (hazard ratio, 2.19; 95% CI, 1.07-4.46). The underdosed group had a higher rate of stroke (HR, 4.87; 95% CI, 1.30-18.26).
Bottom line: Excessive dosing of NOACs in patients with renal insufficiency is common and is associated with bleeding.Citation: Yao X, Shah ND, Sangaralingham LR, Gersh BJ, and Noseworthy PA. Non–vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. JACC. 2017;69(23):2779-90.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
CABG and PCI with drug-eluting stents for left main coronary disease have superior outcomes to medical therapy alone
Clinical question: Does coronary artery bypass grafting (CABG) have superior mortality outcomes to percutaneous coronary intervention (PCI) for left main coronary disease, and how do these interventions compare with medical therapy alone?
Background: Optimal therapy for left main coronary disease is a highly researched topic with CABG having been standard therapy of choice for several decades. However, most studies have not included data comparing CABG to newer drug-eluting stent (DES) generations and no studies have directly compared PCI with DES to medical therapy alone (MTA).
Study design: Meta-analysis.
Setting: Largely European acute care hospitals as well as some VA hospitals.
Synopsis: With PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a review of PubMed and Cochrane databases was conducted, yielding eight RCTs, including a total of 4,850 patients. Six of the RCTs compared CABG with DES, while two compared CABG with MTA. Network meta-analysis was used to compare DES with MTA. At 5 years there were no differences in all-cause mortality between CABG and DES groups (RR, 0.94; 95% CI, 0.68-1.32), though both groups had lower mortality than MTA (RR, 0.21; 95% CI, 0.09-0.47 for CABG vs. MTA and RR, 0.20; 95% CI, 0.08-0.46 for DES vs MTA).
PCI did have higher risk of revascularization at 5 years (RR, 1.68; 95% CI, 1.36-2.08) and lower risk of stroke at 1 year (RR, 0.21; 95% CI, 0.07-0.63), compared with CABG, suggesting younger patients might prefer CABG to avoid revascularization, and older patients may prefer PCI to avoid postprocedural morbidity.
Bottom line: For patients with left main disease, CABG and PCI with DES appear equally effective with regards to prevention of all-cause mortality and both are superior to MTA.
Citation: Shah R, Morsy MS, Weiman DS, and Vetrovec GW. Meta-analysis comparing coronary artery bypass grafting to drug-eluting stents. Am J Cardiol. 2017;120:63-8.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does coronary artery bypass grafting (CABG) have superior mortality outcomes to percutaneous coronary intervention (PCI) for left main coronary disease, and how do these interventions compare with medical therapy alone?
Background: Optimal therapy for left main coronary disease is a highly researched topic with CABG having been standard therapy of choice for several decades. However, most studies have not included data comparing CABG to newer drug-eluting stent (DES) generations and no studies have directly compared PCI with DES to medical therapy alone (MTA).
Study design: Meta-analysis.
Setting: Largely European acute care hospitals as well as some VA hospitals.
Synopsis: With PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a review of PubMed and Cochrane databases was conducted, yielding eight RCTs, including a total of 4,850 patients. Six of the RCTs compared CABG with DES, while two compared CABG with MTA. Network meta-analysis was used to compare DES with MTA. At 5 years there were no differences in all-cause mortality between CABG and DES groups (RR, 0.94; 95% CI, 0.68-1.32), though both groups had lower mortality than MTA (RR, 0.21; 95% CI, 0.09-0.47 for CABG vs. MTA and RR, 0.20; 95% CI, 0.08-0.46 for DES vs MTA).
PCI did have higher risk of revascularization at 5 years (RR, 1.68; 95% CI, 1.36-2.08) and lower risk of stroke at 1 year (RR, 0.21; 95% CI, 0.07-0.63), compared with CABG, suggesting younger patients might prefer CABG to avoid revascularization, and older patients may prefer PCI to avoid postprocedural morbidity.
Bottom line: For patients with left main disease, CABG and PCI with DES appear equally effective with regards to prevention of all-cause mortality and both are superior to MTA.
Citation: Shah R, Morsy MS, Weiman DS, and Vetrovec GW. Meta-analysis comparing coronary artery bypass grafting to drug-eluting stents. Am J Cardiol. 2017;120:63-8.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does coronary artery bypass grafting (CABG) have superior mortality outcomes to percutaneous coronary intervention (PCI) for left main coronary disease, and how do these interventions compare with medical therapy alone?
Background: Optimal therapy for left main coronary disease is a highly researched topic with CABG having been standard therapy of choice for several decades. However, most studies have not included data comparing CABG to newer drug-eluting stent (DES) generations and no studies have directly compared PCI with DES to medical therapy alone (MTA).
Study design: Meta-analysis.
Setting: Largely European acute care hospitals as well as some VA hospitals.
Synopsis: With PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a review of PubMed and Cochrane databases was conducted, yielding eight RCTs, including a total of 4,850 patients. Six of the RCTs compared CABG with DES, while two compared CABG with MTA. Network meta-analysis was used to compare DES with MTA. At 5 years there were no differences in all-cause mortality between CABG and DES groups (RR, 0.94; 95% CI, 0.68-1.32), though both groups had lower mortality than MTA (RR, 0.21; 95% CI, 0.09-0.47 for CABG vs. MTA and RR, 0.20; 95% CI, 0.08-0.46 for DES vs MTA).
PCI did have higher risk of revascularization at 5 years (RR, 1.68; 95% CI, 1.36-2.08) and lower risk of stroke at 1 year (RR, 0.21; 95% CI, 0.07-0.63), compared with CABG, suggesting younger patients might prefer CABG to avoid revascularization, and older patients may prefer PCI to avoid postprocedural morbidity.
Bottom line: For patients with left main disease, CABG and PCI with DES appear equally effective with regards to prevention of all-cause mortality and both are superior to MTA.
Citation: Shah R, Morsy MS, Weiman DS, and Vetrovec GW. Meta-analysis comparing coronary artery bypass grafting to drug-eluting stents. Am J Cardiol. 2017;120:63-8.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Antiplatelet therapy can be continued through surgery without increased risk of reintervention for bleeding
Clinical question: Does continuing antiplatelet therapy through noncardiac surgery increase the risk of postoperative blood transfusion or surgical reintervention for bleeding?
Background: Many prior studies have analyzed the risks and benefits of holding versus continuing antiplatelet therapy in the perioperative setting, but heterogeneity in outcome reporting has limited the ability to compare and contrast studies.
Study design: Meta-analysis.
Setting: Both domestic and international studies were included in the meta-analysis.
Synopsis: With a MEDLINE search, 37 studies with over 30,000 patients total were identified and included in the meta-analysis. Studies compared outcomes of transfusion and surgical reintervention for bleeding in patients receiving noncardiac surgery. Patients were either on no antiplatelet therapy, single therapy, or dual-antiplatelet therapy (DAPT). Relative risk of transfusion escalated in proportion to the amount of antiplatelet therapy; there was a 14% increased risk (95% confidence interval, 1.03-1.26) with aspirin over control and a 33% (95% CI, 1.15-1.55) increased risk with DAPT over control.
Risk of surgical reintervention for bleeding, however, was not increased above control whether on aspirin (relative risk, 0.96; 95% CI, 0.76-1.22), clopidogrel (RR, 1.84; 95% CI, 0.87-3.87), or DAPT (RR, 1.51; (95% CI, 0.92-2.49).
Bottom line: In noncardiac surgery, continuing aspirin or DAPT perioperatively increases the need for transfusion, but not the need for surgical reintervention for bleeding.
Citation: Columbo JA, Lambour AJ, Sundling RA, et. al. A meta-analysis of the impact of aspirin, clopidogrel, and dual-antiplatelet therapy on bleeding complications in noncardiac surgery. Ann Surg. 2017;20(20):1-9.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does continuing antiplatelet therapy through noncardiac surgery increase the risk of postoperative blood transfusion or surgical reintervention for bleeding?
Background: Many prior studies have analyzed the risks and benefits of holding versus continuing antiplatelet therapy in the perioperative setting, but heterogeneity in outcome reporting has limited the ability to compare and contrast studies.
Study design: Meta-analysis.
Setting: Both domestic and international studies were included in the meta-analysis.
Synopsis: With a MEDLINE search, 37 studies with over 30,000 patients total were identified and included in the meta-analysis. Studies compared outcomes of transfusion and surgical reintervention for bleeding in patients receiving noncardiac surgery. Patients were either on no antiplatelet therapy, single therapy, or dual-antiplatelet therapy (DAPT). Relative risk of transfusion escalated in proportion to the amount of antiplatelet therapy; there was a 14% increased risk (95% confidence interval, 1.03-1.26) with aspirin over control and a 33% (95% CI, 1.15-1.55) increased risk with DAPT over control.
Risk of surgical reintervention for bleeding, however, was not increased above control whether on aspirin (relative risk, 0.96; 95% CI, 0.76-1.22), clopidogrel (RR, 1.84; 95% CI, 0.87-3.87), or DAPT (RR, 1.51; (95% CI, 0.92-2.49).
Bottom line: In noncardiac surgery, continuing aspirin or DAPT perioperatively increases the need for transfusion, but not the need for surgical reintervention for bleeding.
Citation: Columbo JA, Lambour AJ, Sundling RA, et. al. A meta-analysis of the impact of aspirin, clopidogrel, and dual-antiplatelet therapy on bleeding complications in noncardiac surgery. Ann Surg. 2017;20(20):1-9.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: Does continuing antiplatelet therapy through noncardiac surgery increase the risk of postoperative blood transfusion or surgical reintervention for bleeding?
Background: Many prior studies have analyzed the risks and benefits of holding versus continuing antiplatelet therapy in the perioperative setting, but heterogeneity in outcome reporting has limited the ability to compare and contrast studies.
Study design: Meta-analysis.
Setting: Both domestic and international studies were included in the meta-analysis.
Synopsis: With a MEDLINE search, 37 studies with over 30,000 patients total were identified and included in the meta-analysis. Studies compared outcomes of transfusion and surgical reintervention for bleeding in patients receiving noncardiac surgery. Patients were either on no antiplatelet therapy, single therapy, or dual-antiplatelet therapy (DAPT). Relative risk of transfusion escalated in proportion to the amount of antiplatelet therapy; there was a 14% increased risk (95% confidence interval, 1.03-1.26) with aspirin over control and a 33% (95% CI, 1.15-1.55) increased risk with DAPT over control.
Risk of surgical reintervention for bleeding, however, was not increased above control whether on aspirin (relative risk, 0.96; 95% CI, 0.76-1.22), clopidogrel (RR, 1.84; 95% CI, 0.87-3.87), or DAPT (RR, 1.51; (95% CI, 0.92-2.49).
Bottom line: In noncardiac surgery, continuing aspirin or DAPT perioperatively increases the need for transfusion, but not the need for surgical reintervention for bleeding.
Citation: Columbo JA, Lambour AJ, Sundling RA, et. al. A meta-analysis of the impact of aspirin, clopidogrel, and dual-antiplatelet therapy on bleeding complications in noncardiac surgery. Ann Surg. 2017;20(20):1-9.
Dr. Portnoy is hospitalist and instructor of medicine, Icahn School of Medicine of the Mount Sinai Health System.
Public health hazard: Bring your flu to work day
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.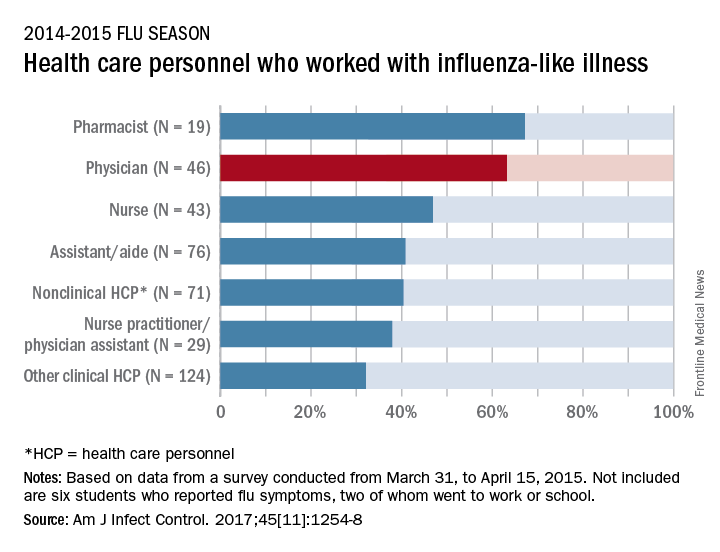
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
FROM THE AMERICAN JOURNAL OF INFECTION CONTROL
Identifying high-value care practices
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
Reference
Sy CD, McDaniel C, Bradford M, et al. The Development and Validation of a High Value Care Rounding Tool Using the Delphi Method [abstract]. J Hosp Med. 2017; 12 (suppl 2). http://www.shmabstracts.com/abstract/the-development-and-validation-of-a-high-value-care-rounding-tool-using-the-delphi-method/. Accessed June 6, 2017.
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
Reference
Sy CD, McDaniel C, Bradford M, et al. The Development and Validation of a High Value Care Rounding Tool Using the Delphi Method [abstract]. J Hosp Med. 2017; 12 (suppl 2). http://www.shmabstracts.com/abstract/the-development-and-validation-of-a-high-value-care-rounding-tool-using-the-delphi-method/. Accessed June 6, 2017.
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
Reference
Sy CD, McDaniel C, Bradford M, et al. The Development and Validation of a High Value Care Rounding Tool Using the Delphi Method [abstract]. J Hosp Med. 2017; 12 (suppl 2). http://www.shmabstracts.com/abstract/the-development-and-validation-of-a-high-value-care-rounding-tool-using-the-delphi-method/. Accessed June 6, 2017.
SHORT TAKES
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores

In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores
In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores
In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
Infections increase risk of idiopathic VTE
Infection and infection sites have been found to be associated with a significant increased risk of venous thromboembolism, according to results of a population-based, matched, case-control analysis of medical records covering the 13-year period 1988-2000.
Dr. Kevin P. Cohoon and his colleagues at the Mayo Clinic, Rochester, Minn., developed models using conditional logistic regression analysis to stratify the risk associated with specific infections and infection sites.

Five hundred thirteen (39.4%) cases and 189 (12.7%) controls had an infection within the previous 92 days (odds ratio, 4.5; P less than .0001). Known VTE risk factors and potentially confounding variables were used in the adjusted univariate and multivariate models, as reported in the American Journal of Medicine (2017. doi: 10.1016/j.amjmed.2017.09.015).
Dr. Cohoon and his colleagues reported that univariate analysis showed “most infection sites were strongly associated with venous thromboembolism” and the adjusted multivariate model resulted in 2.4-fold (P less than .0001) higher odds for VTE incidence, compared with uninfected controls.
Adjusted multivariate analysis ranked the odds of VTE according to specific infections. Dr. Cohoon and his colleagues reported that this modeling showed that the “highest magnitude of risk, compared with no infection, was imparted by intra-abdominal infection (OR, 18) followed by oral infection (OR, 12), systematic blood stream infection (OR, 11), lower respiratory infection such as pneumonia (OR, 3.6), and symptomatic urinary tract infection (OR, 2.2).”
The researchers concluded that their findings may allow for further refinement of inpatient VTE risk-prediction models such as the Padua prediction score and “future studies are required to assess the utility of venous thromboembolism prophylaxis among outpatients with high venous thromboembolism risk infections.”
The authors reported that they had no conflicts of interest.
Infection and infection sites have been found to be associated with a significant increased risk of venous thromboembolism, according to results of a population-based, matched, case-control analysis of medical records covering the 13-year period 1988-2000.
Dr. Kevin P. Cohoon and his colleagues at the Mayo Clinic, Rochester, Minn., developed models using conditional logistic regression analysis to stratify the risk associated with specific infections and infection sites.
Five hundred thirteen (39.4%) cases and 189 (12.7%) controls had an infection within the previous 92 days (odds ratio, 4.5; P less than .0001). Known VTE risk factors and potentially confounding variables were used in the adjusted univariate and multivariate models, as reported in the American Journal of Medicine (2017. doi: 10.1016/j.amjmed.2017.09.015).
Dr. Cohoon and his colleagues reported that univariate analysis showed “most infection sites were strongly associated with venous thromboembolism” and the adjusted multivariate model resulted in 2.4-fold (P less than .0001) higher odds for VTE incidence, compared with uninfected controls.
Adjusted multivariate analysis ranked the odds of VTE according to specific infections. Dr. Cohoon and his colleagues reported that this modeling showed that the “highest magnitude of risk, compared with no infection, was imparted by intra-abdominal infection (OR, 18) followed by oral infection (OR, 12), systematic blood stream infection (OR, 11), lower respiratory infection such as pneumonia (OR, 3.6), and symptomatic urinary tract infection (OR, 2.2).”
The researchers concluded that their findings may allow for further refinement of inpatient VTE risk-prediction models such as the Padua prediction score and “future studies are required to assess the utility of venous thromboembolism prophylaxis among outpatients with high venous thromboembolism risk infections.”
The authors reported that they had no conflicts of interest.
Infection and infection sites have been found to be associated with a significant increased risk of venous thromboembolism, according to results of a population-based, matched, case-control analysis of medical records covering the 13-year period 1988-2000.
Dr. Kevin P. Cohoon and his colleagues at the Mayo Clinic, Rochester, Minn., developed models using conditional logistic regression analysis to stratify the risk associated with specific infections and infection sites.
Five hundred thirteen (39.4%) cases and 189 (12.7%) controls had an infection within the previous 92 days (odds ratio, 4.5; P less than .0001). Known VTE risk factors and potentially confounding variables were used in the adjusted univariate and multivariate models, as reported in the American Journal of Medicine (2017. doi: 10.1016/j.amjmed.2017.09.015).
Dr. Cohoon and his colleagues reported that univariate analysis showed “most infection sites were strongly associated with venous thromboembolism” and the adjusted multivariate model resulted in 2.4-fold (P less than .0001) higher odds for VTE incidence, compared with uninfected controls.
Adjusted multivariate analysis ranked the odds of VTE according to specific infections. Dr. Cohoon and his colleagues reported that this modeling showed that the “highest magnitude of risk, compared with no infection, was imparted by intra-abdominal infection (OR, 18) followed by oral infection (OR, 12), systematic blood stream infection (OR, 11), lower respiratory infection such as pneumonia (OR, 3.6), and symptomatic urinary tract infection (OR, 2.2).”
The researchers concluded that their findings may allow for further refinement of inpatient VTE risk-prediction models such as the Padua prediction score and “future studies are required to assess the utility of venous thromboembolism prophylaxis among outpatients with high venous thromboembolism risk infections.”
The authors reported that they had no conflicts of interest.
FROM THE AMERICAN JOURNAL OF MEDICINE
Key clinical point:
Major finding: A significantly greater number of patients with infections developed VTE as compared with uninfected controls (OR, 4.5; P less than .0001).
Data source: Study was a retrospective database analysis of 1,303 VTE patients and 1,494 paired controls.
Disclosures: The authors reported that they had no conflicts of interest.
Developing machines that detect disease
Smells – of skin, breath, or bodily fluids – can, in some cases, reveal the presence of disease. This fact has led researchers to try to build an odor sensor that could make a fast, reliable diagnosis, and now the field may be on the verge of a breakthrough, according to a recent article in the New York Times.
In addition to various efforts in Austria, Switzerland, and Japan, an English manufacturer – Owlstone Medical – has been making headway with an odor analysis technology. It will be part of a National Health Service trial that will test the sensor for diagnosing lung cancer. The company also is conducting a trial using urine samples to detect colon cancer; its program allows changing the software to change what disease you detect.
Meanwhile, an Israeli chemical engineer, Hossam Haick, is using similar technology, with molecular receptors that have an affinity for certain biomarkers of disease found in the breath. Artificial intelligence allows the sensors to improve with each use, and a paper published last year showed that this system could distinguish among 17 different diseases with up to 86% accuracy.
And in the United States, researchers from the Monell Chemical Senses Center and the University of Pennsylvania are working on an odor sensor that detects ovarian cancer in samples of blood plasma. They chose plasma because it is less likely than breath or urine to be affected by other factors such as diet or environmental chemicals.
These technologies could be available to doctors in 3-5 years, experts say.
Reference
Murphy K. One Day, a Machine Will Smell Whether You’re Sick . New York Times. May 1, 2017. Accessed May 29, 2017.
Smells – of skin, breath, or bodily fluids – can, in some cases, reveal the presence of disease. This fact has led researchers to try to build an odor sensor that could make a fast, reliable diagnosis, and now the field may be on the verge of a breakthrough, according to a recent article in the New York Times.
In addition to various efforts in Austria, Switzerland, and Japan, an English manufacturer – Owlstone Medical – has been making headway with an odor analysis technology. It will be part of a National Health Service trial that will test the sensor for diagnosing lung cancer. The company also is conducting a trial using urine samples to detect colon cancer; its program allows changing the software to change what disease you detect.
Meanwhile, an Israeli chemical engineer, Hossam Haick, is using similar technology, with molecular receptors that have an affinity for certain biomarkers of disease found in the breath. Artificial intelligence allows the sensors to improve with each use, and a paper published last year showed that this system could distinguish among 17 different diseases with up to 86% accuracy.
And in the United States, researchers from the Monell Chemical Senses Center and the University of Pennsylvania are working on an odor sensor that detects ovarian cancer in samples of blood plasma. They chose plasma because it is less likely than breath or urine to be affected by other factors such as diet or environmental chemicals.
These technologies could be available to doctors in 3-5 years, experts say.
Reference
Murphy K. One Day, a Machine Will Smell Whether You’re Sick . New York Times. May 1, 2017. Accessed May 29, 2017.
Smells – of skin, breath, or bodily fluids – can, in some cases, reveal the presence of disease. This fact has led researchers to try to build an odor sensor that could make a fast, reliable diagnosis, and now the field may be on the verge of a breakthrough, according to a recent article in the New York Times.
In addition to various efforts in Austria, Switzerland, and Japan, an English manufacturer – Owlstone Medical – has been making headway with an odor analysis technology. It will be part of a National Health Service trial that will test the sensor for diagnosing lung cancer. The company also is conducting a trial using urine samples to detect colon cancer; its program allows changing the software to change what disease you detect.
Meanwhile, an Israeli chemical engineer, Hossam Haick, is using similar technology, with molecular receptors that have an affinity for certain biomarkers of disease found in the breath. Artificial intelligence allows the sensors to improve with each use, and a paper published last year showed that this system could distinguish among 17 different diseases with up to 86% accuracy.
And in the United States, researchers from the Monell Chemical Senses Center and the University of Pennsylvania are working on an odor sensor that detects ovarian cancer in samples of blood plasma. They chose plasma because it is less likely than breath or urine to be affected by other factors such as diet or environmental chemicals.
These technologies could be available to doctors in 3-5 years, experts say.
Reference
Murphy K. One Day, a Machine Will Smell Whether You’re Sick . New York Times. May 1, 2017. Accessed May 29, 2017.
Rates, predictors, and variability of interhospital transfers
Clinical question: What is the national frequency of interhospital transfers, and are there any patient or hospital factors that predict these transfers?
Background: Interhospital patient transfers may be due to the need for a specialized service, but the factors and patterns have not been well studied.
Setting: All acute care hospitals in the United States.
Synopsis: Using data from the 2013 Centers for Medicare & Medicaid Services and the 2013 American Hospital Association, this study showed that 1.5% of the 6.6 million eligible beneficiaries underwent interhospital transfer (IHT). Patient and hospital characteristics that increased the odds of IHT included age 74-85 years, nonblack race, higher comorbidity, lower diagnosis-related group weight, fewer recent hospitalizations, and hospitalization in the Northeast region of the United States. Lower case mix index was associated with increased odds of IHT. Rates of IHT remain variable, after adjusting for patient and hospital characteristics. This study was restricted to the Medicare population so did not represent all populations. IHT from the emergency room was not assessed, and those who were transferred more than once (to another hospital and back) were not included.
Bottom line: A large number of Medicare patients undergo IHT nationally, and the rate varies widely based on patient factors, geography, and other factors unrelated to patient or hospital characteristics.
Citation: Mueller SK, Jie Zheng, Orav EJ, Schnipper JL. Rates, predictors, and variability of interhospital transfers: A national evaluation. J Hosp Med. 2017;6:435-42.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.
Clinical question: What is the national frequency of interhospital transfers, and are there any patient or hospital factors that predict these transfers?
Background: Interhospital patient transfers may be due to the need for a specialized service, but the factors and patterns have not been well studied.
Setting: All acute care hospitals in the United States.
Synopsis: Using data from the 2013 Centers for Medicare & Medicaid Services and the 2013 American Hospital Association, this study showed that 1.5% of the 6.6 million eligible beneficiaries underwent interhospital transfer (IHT). Patient and hospital characteristics that increased the odds of IHT included age 74-85 years, nonblack race, higher comorbidity, lower diagnosis-related group weight, fewer recent hospitalizations, and hospitalization in the Northeast region of the United States. Lower case mix index was associated with increased odds of IHT. Rates of IHT remain variable, after adjusting for patient and hospital characteristics. This study was restricted to the Medicare population so did not represent all populations. IHT from the emergency room was not assessed, and those who were transferred more than once (to another hospital and back) were not included.
Bottom line: A large number of Medicare patients undergo IHT nationally, and the rate varies widely based on patient factors, geography, and other factors unrelated to patient or hospital characteristics.
Citation: Mueller SK, Jie Zheng, Orav EJ, Schnipper JL. Rates, predictors, and variability of interhospital transfers: A national evaluation. J Hosp Med. 2017;6:435-42.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.
Clinical question: What is the national frequency of interhospital transfers, and are there any patient or hospital factors that predict these transfers?
Background: Interhospital patient transfers may be due to the need for a specialized service, but the factors and patterns have not been well studied.
Setting: All acute care hospitals in the United States.
Synopsis: Using data from the 2013 Centers for Medicare & Medicaid Services and the 2013 American Hospital Association, this study showed that 1.5% of the 6.6 million eligible beneficiaries underwent interhospital transfer (IHT). Patient and hospital characteristics that increased the odds of IHT included age 74-85 years, nonblack race, higher comorbidity, lower diagnosis-related group weight, fewer recent hospitalizations, and hospitalization in the Northeast region of the United States. Lower case mix index was associated with increased odds of IHT. Rates of IHT remain variable, after adjusting for patient and hospital characteristics. This study was restricted to the Medicare population so did not represent all populations. IHT from the emergency room was not assessed, and those who were transferred more than once (to another hospital and back) were not included.
Bottom line: A large number of Medicare patients undergo IHT nationally, and the rate varies widely based on patient factors, geography, and other factors unrelated to patient or hospital characteristics.
Citation: Mueller SK, Jie Zheng, Orav EJ, Schnipper JL. Rates, predictors, and variability of interhospital transfers: A national evaluation. J Hosp Med. 2017;6:435-42.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.
Rib fracture diagnosis in the panscan era
Clinical question: Do rib fractures observed on chest CT carry the same morbidity and mortality risk as those observed in chest radiograph?
Background: Traditionally studies have shown that first and second rib fractures on chest radiograph after blunt trauma are associated with substantial morbidity and mortality. With growing frequency of CT imaging in the “panscan” era, it is unknown whether similar rib fractures found on CT carry the same meaning.
Setting: 10 level I trauma centers.
Synopsis: Data from the National Emergency X-Radiography Utilization Study showed that, of the 8,661 patients who suffered blunt trauma and received both chest radiograph and chest CT, 23.9% had rib fractures. Rib fractures were observed in 66.1% of chest CT–only cases. Patients with rib fractures had a higher admission rate (88.7% versus 45.8%) and higher mortality (5.6% versus 2.7%) than patients without rib fractures. Mortality rate and great-vessel injury were higher in those with first or second rib fractures. The mortality of patients with rib fractures observed only on chest CT was not statistically different from those whose fractures were also seen in chest radiograph. The study included patients who were more severely injured and may have been more likely to receive a CT, which may have led to an overestimation of fractures found. The actual causes of admission and death were not reviewed.
Bottom line: CT in trauma-imaging protocol can identify patients with rib fractures well, compared with combined CT with chest radiograph. Rib fractures are associated with higher rates of admission and mortality risk than those without rib fractures. Specifically, first or second rib fractures are found to have greater risk for mortality and great-vessel injury.
Citation: Murphy CE 4th, Raja AS, Baumann BM, et al. Rib fracture diagnosis in the panscan era. Ann Emerg Med. 2017. doi: 10.1016/j.annemergmed.2017.04.011.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.
Clinical question: Do rib fractures observed on chest CT carry the same morbidity and mortality risk as those observed in chest radiograph?
Background: Traditionally studies have shown that first and second rib fractures on chest radiograph after blunt trauma are associated with substantial morbidity and mortality. With growing frequency of CT imaging in the “panscan” era, it is unknown whether similar rib fractures found on CT carry the same meaning.
Setting: 10 level I trauma centers.
Synopsis: Data from the National Emergency X-Radiography Utilization Study showed that, of the 8,661 patients who suffered blunt trauma and received both chest radiograph and chest CT, 23.9% had rib fractures. Rib fractures were observed in 66.1% of chest CT–only cases. Patients with rib fractures had a higher admission rate (88.7% versus 45.8%) and higher mortality (5.6% versus 2.7%) than patients without rib fractures. Mortality rate and great-vessel injury were higher in those with first or second rib fractures. The mortality of patients with rib fractures observed only on chest CT was not statistically different from those whose fractures were also seen in chest radiograph. The study included patients who were more severely injured and may have been more likely to receive a CT, which may have led to an overestimation of fractures found. The actual causes of admission and death were not reviewed.
Bottom line: CT in trauma-imaging protocol can identify patients with rib fractures well, compared with combined CT with chest radiograph. Rib fractures are associated with higher rates of admission and mortality risk than those without rib fractures. Specifically, first or second rib fractures are found to have greater risk for mortality and great-vessel injury.
Citation: Murphy CE 4th, Raja AS, Baumann BM, et al. Rib fracture diagnosis in the panscan era. Ann Emerg Med. 2017. doi: 10.1016/j.annemergmed.2017.04.011.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.
Clinical question: Do rib fractures observed on chest CT carry the same morbidity and mortality risk as those observed in chest radiograph?
Background: Traditionally studies have shown that first and second rib fractures on chest radiograph after blunt trauma are associated with substantial morbidity and mortality. With growing frequency of CT imaging in the “panscan” era, it is unknown whether similar rib fractures found on CT carry the same meaning.
Setting: 10 level I trauma centers.
Synopsis: Data from the National Emergency X-Radiography Utilization Study showed that, of the 8,661 patients who suffered blunt trauma and received both chest radiograph and chest CT, 23.9% had rib fractures. Rib fractures were observed in 66.1% of chest CT–only cases. Patients with rib fractures had a higher admission rate (88.7% versus 45.8%) and higher mortality (5.6% versus 2.7%) than patients without rib fractures. Mortality rate and great-vessel injury were higher in those with first or second rib fractures. The mortality of patients with rib fractures observed only on chest CT was not statistically different from those whose fractures were also seen in chest radiograph. The study included patients who were more severely injured and may have been more likely to receive a CT, which may have led to an overestimation of fractures found. The actual causes of admission and death were not reviewed.
Bottom line: CT in trauma-imaging protocol can identify patients with rib fractures well, compared with combined CT with chest radiograph. Rib fractures are associated with higher rates of admission and mortality risk than those without rib fractures. Specifically, first or second rib fractures are found to have greater risk for mortality and great-vessel injury.
Citation: Murphy CE 4th, Raja AS, Baumann BM, et al. Rib fracture diagnosis in the panscan era. Ann Emerg Med. 2017. doi: 10.1016/j.annemergmed.2017.04.011.
Dr. Xu is assistant professor and hospitalist, Icahn School of Medicine of the Mount Sinai Health System, New York.