User login
Understanding cultural barriers in hepatitis B virus infection
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
KEY POINTS
- Some Asian Americans have limited proficiency in English and are isolated linguistically, limiting their ability to communicate with health care providers.
- Asian Americans may view Western medicine with suspicion, causing delays in seeking care and making it difficult to successfully manage chronic HBV infection.
- Sensitivity to cultural attitudes may enhance communication and the likelihood that immigrant patients will accept health care providers’ recommendations; cultural sensitivity training may be helpful.
Hepatitis B treatment: Current best practices, avoiding resistance
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
Nucleoside analogues
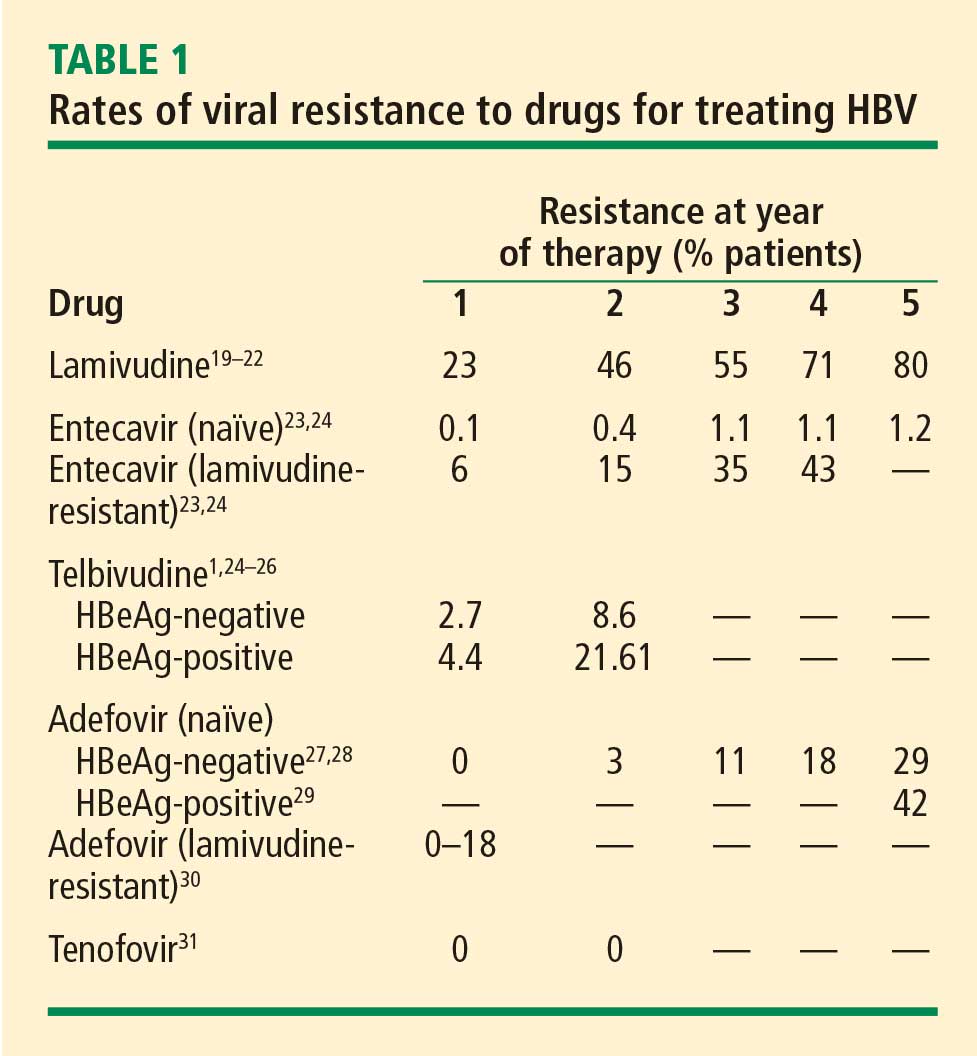
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
Managing resistance
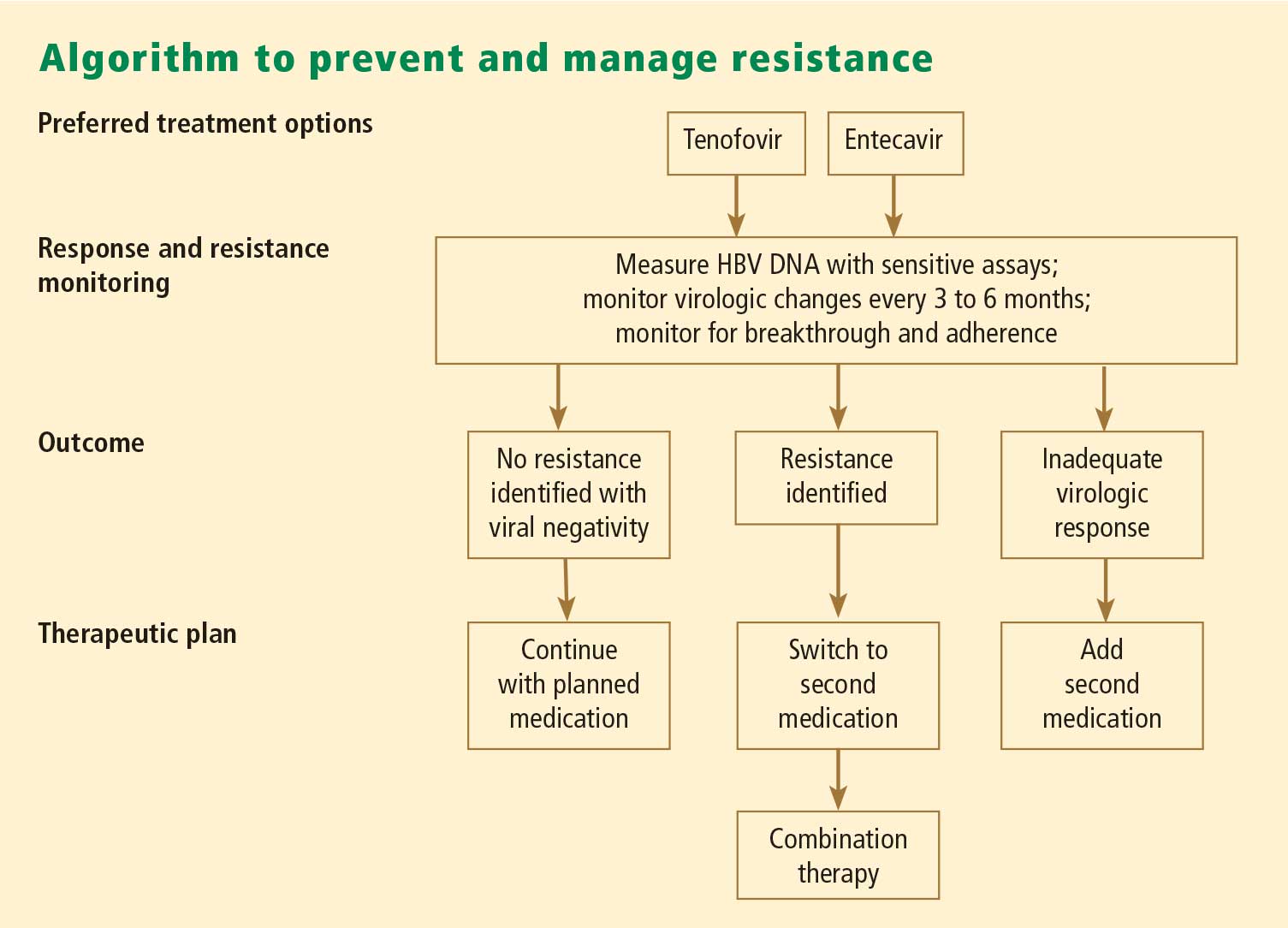
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
Nucleoside analogues
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
Managing resistance
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
Nucleoside analogues
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
Managing resistance
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
KEY POINTS
- Consider treatment for chronic HBV infection for all patients who are positive for HBV DNA, as viral load levels as low as 300 copies/mL confer a risk for hepatocellular carcinoma.
- The goal of therapy is an undetectable level of HBV DNA; initiate therapy with the most potent agent to limit the possibility of resistance.
- Preventing resistance to therapy is crucial for successful treatment of chronic HBV infection.
Monotherapy vs multiple-drug therapy: The experts debate
Monotherapy for treatment-naïve patients
By Robert G. Gish, MD
Powerful antiviral medicines with activity against hepatitis B virus (HBV) have long-term records of potency and safety, supporting the case for monotherapy in treatment-naïve patients. Combination therapy has a limited role in the management of HBV infection; if the approach to treatment is rational from the start, then combination therapy can be reserved for cases of treatment failure or resistance.
THE CASE FOR MONOTHERAPY
Three arguments that favor monotherapy with potent medications are cost, low risk of resistance, and unproven benefit of combination therapy.
Cost
The cost of dual-medication therapy is nearly double that of single-drug therapy, while the benefit is unknown in treatment-naïve patients. My choices for first-line therapy are tenofovir or entecavir, highly potent nucleoside/nucleotide analogues that can cost up to $5,500 and $8,000, respectively, per year of treatment.1 The two in combination would cost nearly $14,000 per year, and benefits have not been proven in the treatment-naïve population.
Low risk of resistance
Potent medications have low rates of resistance, in the range of 1% over 2 to 5 years.2–4 If one starts therapy with the highly potent entecavir, discussions about switching or adding on therapy would be superfluous because of the low rates of resistance and failure associated with entecavir monotherapy. At 5 years, the cumulative rate of entecavir resistance in patients with positive HBV DNA at baseline is 1.2%.5 Tenofovir also produces potent inhibition of HBV DNA and is associated with low rates of resistance,6 although follow-up data with tenofovir extend only to 2 years. Starting therapy with the less potent adefovir, followed by the development of resistance, decreases the probability that tenofovir will achieve HBV DNA suppression during treatment.7 The main driver of resistance is nonadherence with therapy, not treatment failure.
Resistance to pegylated interferon has not been encountered. The therapy is limited in duration (24 to 48 weeks), with durable suppression of HBV DNA and high rates of seroconversion from hepatitis B e antigen (HBeAg)-positive to HBeAg-negative status. Parameters for the use of pegylated interferon as first-line therapy have been established, and include patients with genotype A or B who are young, have HBV DNA levels less than 107 copies/mL, have serum alanine aminotransferase (ALT) levels two to three times the upper limit of normal, and lack significant comorbidities.3,4
Unproven benefit of combination therapy
Perhaps the most convincing argument against combination therapy is that numerous studies of combinations have failed to demonstrate a benefit compared with monotherapy in treatment-naïve patients:
- Interferon in combination with lamivudine has not been shown to be significantly more effective than lamivudine monotherapy.8,9 Further, because of limited information on the safety of interferon in combination with nucleoside or nucleotide analogues, use of the combination is not recommended.4 Neuropathy has been reported with the combination of interferon and telbivudine,4 leading to the release of a warning about its use.10
- A 1-year trial by Lai et al failed to show an improvement in virologic and biochemical responses with the combination of telbivudine and lamivudine compared with telbivudine alone.11
- In patients with lamivudine-resistant chronic HBV infection, adefovir reduced serum HBV DNA levels by 4 weeks whether or not lamivudine therapy was ongoing.12
- Although more patients taking a combination of adefovir and the nucleoside reverse transcriptase inhibitor emtricitabine had normalization of ALT and suppression of HBV DNA to less than 300 copies compared with adefovir monotherapy, rates of HBeAg seroconversion were comparable in the two arms.13
- A recent study that compared tenofovir monotherapy with tenofovir and emtricitabine in combination showed comparable effectiveness for both regimens; the authors concluded that further study is necessary before either choice can be recommended as superior to the other.14
RESISTANCE: IDENTIFY EARLY, ADD ON
To minimize the likelihood of resistance and its impact, HBV DNA levels should be monitored every 3 months; at the first sign of a virologic breakthrough, therapy should be added or switched. Resistance to lamivudine is apparent early; models of treatment response indicate that resistance to lamivudine is likely if HBV DNA does not become undetectable by week 4.
In cases of lamivudine failure, adding adefovir early, when the viral load is less than 107 copies/mL, increases the probability of a virologic response.15 In the situation of lamivudine failure, I prefer adding on to switching to reduce the risk of resistance—a practice supported by the study just cited.15 In lamivudine-resistant patients, adefovir monotherapy was associated with virologic breakthrough and resistance to adefovir in 21% of patients, whereas no patient experienced virologic breakthrough or resistance when adefovir was added to lamivudine.
Successful management involves choosing the best medication up front and educating patients about the importance of taking their medication as instructed. For example, entecavir should be taken without food to maximize its bioavailability. With tenofovir, the risk of renal toxicity is low (1%),16 and can be reduced even further with a pretreatment assessment of the patient.
Multiple-drug therapy is the wave of the future
By Pierre M. Gholam, MD
A concise rationale for multiple-drug therapy is that resistance to monotherapy will occur eventually, with serious consequences in some patients and grave public health implications over the long term. Data from France and Australia indicate that multidrug-resistant HBV is a reality in individual cases. Resistance may be less likely when combinations are used, although little evidence exists at present to support this contention.
COMBINATION THERAPY IS COMMON SENSE
Much of the evidence supporting combination therapy for HBV is common sense:
- Most patients with HBV infection require treatment indefinitely, and duration of therapy that is not finite will inevitably lead to resistance.
- Your first shot is your best shot. Once resistance develops, treatment response will eventually decline.
- Sometimes the stakes are too high to risk breakthroughs. In particular, in patients who have cirrhosis and in those awaiting or following liver transplant, flares and recurrences can have disastrous consequences.
Treatment duration and resistance
As Dr. Gish demonstrated, tenofovir and entecavir are highly potent drugs that suppress viral loads effectively and have high genetic barriers to resistance. On an intent-to-treat basis, HBV DNA levels below the threshold level of detection are achieved at impressive rates with tenofovir and entecavir at 2 years in patients who are either HBeAg negative or positive.5,6,17 When the analyses are limited to patients who actually received the drugs, suppression of HBV DNA to undetectable levels exceeds 90%. Resistance to tenofovir is 0% at 2 years,3 and resistance to entecavir is 1.2% at 5 years.5
Although such data appear to favor monotherapy, most HBV-infected patients who commit to treatment will be treated indefinitely; this applies to patients who are HBeAg negative, who constitute most HBV-infected individuals in the United States and worldwide, or HBeAg positive. There are no established end points for treatment termination in HBeAg-negative patients. The only treatment termination end point that is deemed acceptable in HBeAg-positive patients is a period 6 to 12 months after the loss of HBeAg and the development of antibody to HBeAg, or e antigen seroconversion. Even after many years of treatment that includes the first-line agents tenofovir and entecavir, the likelihood of achieving this end point is fairly low.2,5,18
Adherence is also a consideration. Studies of patients with hypertension, heart disease, and other chronic diseases have shown that strict adherence to therapy over decades is unlikely. The same adherence pattern probably applies to the treatment of chronic HBV infection.
Antiviral drugs used in the treatment of chronic HBV infection are associated with certain resistance mutations that confer additional risk of developing resistance to a subsequent drug. Furthermore, with indefinite duration of therapy, it is realistic to expect that resistance will develop.
Other factors play roles in the development of resistance:
- Mutant viruses. We do not fully understand the potential problem of transmission of mutant viruses. This phenomenon is becoming apparent in endemic areas where treatment-naïve patients harbor mutant viruses acquired through sexual contact with HBV-infected patients who have been treated and in whom the virus has subsequently mutated.
- Barriers to resistance. The genetic barrier to resistance for a single drug will eventually be overcome. It may take longer than it took for adefovir, which is associated with a 30% rate of resistance at 5 years.3 It may take a much longer time for entecavir or tenofovir, but resistance is a biological certainty and we need to contend with it. With human immunodeficiency virus (HIV) infection, we are able to genotype for mutations and tailor treatment accordingly. This strategy is not currently recommended for HBV infection, partly because it is expensive and not routinely available.
- Misuse of therapy. Finally, wider use of antiviral agents for the treatment of HBV may lead to wider misuse, and therefore more resistance. Realistically, not every practitioner will start therapy with entecavir or tenofovir; many of the less potent agents have associated rates of resistance, and these in turn may confer an additional risk of resistance if tenofovir or entecavir is eventually used.
Declining response
Colonno et al19 studied the likelihood of entecavir resistance developing in patients with existing lamivudine resistance. The likelihood of resistance to entecavir at 3 years was 1.2% among patients who had never been exposed to lamivudine. Among patients in whom lamivudine resistance had developed and who were subsequently started on entecavir, resistance to entecavir was 32% at 3 years.19 Resistance has consequences; 25% of lamivudine-resistant patients develop viral breakthrough.
Dr. Gish and I agree that the addition of adefovir to lamivudine is better than switching to adefovir monotherapy in the case of lamivudine failure. Compared with switching, the adefovir-lamivudine combination leads to a lower incidence of virologic breakthrough, a lower likelihood of adefovir resistance over time, a greater probability of achieving undetectable levels of HBV DNA (< 35 copies/mL), and a lower cumulative rate of resistance.20 The superiority of combination therapy in achieving undetectable levels of HBV DNA confers a lower risk of developing resistance over time; by year 4, the likelihood of adefovir resistance is only 4% among lamivudine-resistant patients treated with the combination of adefovir and lamivudine.20
In a study of nucleoside analogue–experienced patients who did not achieve viral suppression, response to tenofovir, defined as HBV DNA less than 400 copies/mL at month 12, was 85% overall and only 30% in adefovir-resistant patients.7 These data demonstrate that, if not starting with combination therapy, it is preferable to initiate treatment with a potent drug that is highly successful at HBV DNA suppression. A second monotherapy will be less successful than the initial attempt.
Consequences of resistance
The consequences of resistance in patients with cirrhosis are significant, prompting strong consideration of combination therapy as a potential means to avoid resistance.
One consequence is a well-documented potential for decompensation in the setting of new-onset resistance as a result of flares. Another is post-transplantation recurrence of HBV, leading to poor outcomes. These risks converge in the patient who is awaiting liver transplantation, in whom combination therapy seems to make the most sense to prevent the development of a flare and a recurrence of HBV infection after transplantation.
WHO SHOULD RECEIVE MULTIPLE-DRUG THERAPY?
The American Association for the Study of Liver Diseases recommends combination therapy as the preferred rescue therapy for primary failure of a first-line agent, citing the possibility of resistance with switching in some circumstances and the superiority of adding on as opposed to switching.2 No data clearly support de novo multiple-drug therapy. Although a number of studies have failed to show an advantage of combination therapy over monotherapy, they were of relatively short duration and focused primarily on viral suppression rather than the occurrence of resistance over time. Long-term studies are needed to determine whether combination therapy is an option de novo.
De novo multiple-drug therapy might be reasonable if a patient is at high risk for resistance—for example, for patients with extraordinarily high levels of HBV DNA or in whom resistance can lead to dire consequences, such as patients with cirrhosis or pretransplant patients.
The HIV pandemic serves as a paradigm for combination therapy. Many agents used to treat HBV infection also have anti-HIV effects; their use as monotherapy should be avoided in order to prevent the development of HIV drug resistance. HIV regimens that include only one HBV antiviral agent with a low genetic barrier to resistance (eg, lamivudine) should also be avoided in order to minimize the risk of HBV drug resistance.
I agree with Dr. Gish that cost and potential toxicity, especially renal toxicity, may limit the widespread use of combination therapies.
Discussion
William D. Carey, MD: I hear more agreement than not between the debaters. Are there any comments from the panel?
Morris Sherman, MD, PhD: I’ll comment on the guidelines for the treatment of HBV infection. Tong et al21 recently examined whether a group of HBV-infected patients who developed cirrhosis and hepatoma would have qualified for treatment under four current sets of guidelines. A startlingly large proportion of patients who developed adverse consequences from their liver disease would not have met the criteria for treatment under any of these major guidelines. As many as one-fourth of patients with chronic HBV infection die as a consequence of their liver disease, and in order to prevent these deaths up to one-half of the patients have to be treated. In the long run, overtreatment may be preferable to undertreatment to reduce the incidence of hepatitis-related deaths. My point is that the treatment guidelines probably exclude many patients who should be treated.
The factors I consider important in my decision to treat are a high viral load, which is indicative of active viral replication, and evidence of liver injury. Patients who have a high viral load and no liver injury won’t experience complications. What do I consider evidence of liver injury? Prolonged elevation of ALT is suggestive, although not necessarily as high as 200 or 300 U/L; it could be in the range of 50 to 80 U/L if fibrosis is significant, which I define as stage 2 or greater on the biopsy. If a high viral load and evidence of significant liver injury are present, I treat the patient regardless of the precise level of the viral load or the ALT.
Dr. Carey: Can you clarify your position? Some of our earlier discussion emphasized the importance of treating when the viral load is high, regardless of other factors. A high viral load by itself may be associated with increased risk of cirrhosis or hepatocellular carcinoma without cirrhosis, so why would a biopsy make a difference?
Dr. Sherman: We can’t predict which younger HBeAg-positive patients with a very high viral load are going to run into trouble down the road. Many will seroconvert spontaneously and never have problems thereafter. In contrast, a patient in his 40s with a high viral load, even if HBeAg positive, and without major fibrosis should be considered for therapy. I tell my patients and the physicians who refer them that once I’m finished with the evaluation, it’s not good-bye. They have to be followed for life because things change.
Tram T. Tran, MD: In the paper by Tong et al,21 all of the patients who subsequently had poor outcomes had low platelet counts. I therefore recommend considering the entire picture in the decision to treat. If physicians followed the treatment guidelines strictly, they would not have treated those patients, but had they noticed thrombocytopenia they would have considered the possibility of advanced fibrosis and considered screening or a biopsy.
- Wong JB. Costs of antiviral therapy of chronic hepatitis B. Paper presented at: Management of Hepatitis B: 2006. National Institutes of Health Workshop. April 6–8, 2006; Bethesda, MD.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Tenney DJ, Pokomowski KA, Rose RE, et al. Entecavir at five years shows long-term maintenance of high genetic barrier to hepatitis B virus resistance [abstract OL-107]. Hepatol Int 2008; 2:S76–S77.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Schalm SW, Heathcote J, Cianciara J, et al. Lamivudine and alpha interferon combination treatment of patients with chronic hepatitis B infection: a randomized trial. Gut 2000; 46:562–568.
- Chan HL-Y, Leung NW-Y, Hui AY, et al. A randomized, controlled trial of combination therapy for chronic hepatitis B: comparing pegylated interferon-a2b and lamivudine with lamivudine alone. Ann Intern Med 2005; 142:240–250.
- Novartis Pharmaceuticals Canada Inc. Risk of peripheral neuropathy in patients treated with telbivudine (SEBIVO®) in combination with interferon. Health Canada Web site. http://www.hc-sc.gc.ca/dhp-mps/alt_formats/hpfb-dgpsa/pdf/medeff/sebivo_pc-cp-eng.pdf. March 12, 2008. Accessed March 12, 2009.
- Lai C-L, Leung N, Teo E-K, et al. A 1-year trial of telbivudine, lamivudine, and the combination in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology 2005; 129:528–536.
- Peters MG, Hann HW, Martin P, et al. Adefovir dipivoxil alone or in combination with lamivudine in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology 2004; 126:91–101.
- Hui C-K, Zhang H-Y, Bowden S, et al. 96 weeks combination of adefovir dipivoxil plus emtricitabine vs. adefovir dipivoxil monotherapy in the treatment of chronic hepatitis B. J Hepatol 2008; 48:714–720.
- Berg T, Moller B, Trinh H, et al. Tenofovir disoproxil fumarate (TDF) versus emtricitabine plus TDF for treatment of chronic hepatitis B (CHB) in subjects with persistent viral replication receiving adefovir dipivoxil (ADV). Paper presented at: 43rd Annual Meeting of the European Association for the Study of the Liver; April 23–27, 2008; Milan, Italy.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
- Szczech LA. Tenofovir nephrotoxicity: focusing research questions and putting them into clinical context. J Infect Dis 2008; 197:7–9.
- Shouval D, Lai C-L, Chang T-T, et al. Three years of entecavir (ETV) retreatment of HBeAg(–) ETV patients who previously discontinued treatment: results from study ETV-901. Poster presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Poster 927.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose RE, Pokornowski K, Baldick CJ, Klesczewski K, Tenney D. Assessment at three years shows high barrier to resistance is maintained in entecavir-treated nucleoside naïve patients while resistance emergence increases over time in lamivudine refractory patients [AASLD abstract 110]. Hepatology 2006; 44(suppl 1):229A–230A.
- Lampertico P, Viganò M, Manenti E, Iavarone M, Sablon E, Colombo M. Low resistance to adefovir combined with lamivudine: a 3-year study of 145 lamivudine-resistant hepatitis B patients. Gastroenterology 2007; 133:1445–1451.
- Tong MJ, Hsien C, Hsu L, Sun HE, Blatt LM. Treatment recommendations for chronic hepatitis B: an evaluation of current guidelines based on a natural history study in the United States. Hepatology 2008; 48:1070–1078.
Monotherapy for treatment-naïve patients
By Robert G. Gish, MD
Powerful antiviral medicines with activity against hepatitis B virus (HBV) have long-term records of potency and safety, supporting the case for monotherapy in treatment-naïve patients. Combination therapy has a limited role in the management of HBV infection; if the approach to treatment is rational from the start, then combination therapy can be reserved for cases of treatment failure or resistance.
THE CASE FOR MONOTHERAPY
Three arguments that favor monotherapy with potent medications are cost, low risk of resistance, and unproven benefit of combination therapy.
Cost
The cost of dual-medication therapy is nearly double that of single-drug therapy, while the benefit is unknown in treatment-naïve patients. My choices for first-line therapy are tenofovir or entecavir, highly potent nucleoside/nucleotide analogues that can cost up to $5,500 and $8,000, respectively, per year of treatment.1 The two in combination would cost nearly $14,000 per year, and benefits have not been proven in the treatment-naïve population.
Low risk of resistance
Potent medications have low rates of resistance, in the range of 1% over 2 to 5 years.2–4 If one starts therapy with the highly potent entecavir, discussions about switching or adding on therapy would be superfluous because of the low rates of resistance and failure associated with entecavir monotherapy. At 5 years, the cumulative rate of entecavir resistance in patients with positive HBV DNA at baseline is 1.2%.5 Tenofovir also produces potent inhibition of HBV DNA and is associated with low rates of resistance,6 although follow-up data with tenofovir extend only to 2 years. Starting therapy with the less potent adefovir, followed by the development of resistance, decreases the probability that tenofovir will achieve HBV DNA suppression during treatment.7 The main driver of resistance is nonadherence with therapy, not treatment failure.
Resistance to pegylated interferon has not been encountered. The therapy is limited in duration (24 to 48 weeks), with durable suppression of HBV DNA and high rates of seroconversion from hepatitis B e antigen (HBeAg)-positive to HBeAg-negative status. Parameters for the use of pegylated interferon as first-line therapy have been established, and include patients with genotype A or B who are young, have HBV DNA levels less than 107 copies/mL, have serum alanine aminotransferase (ALT) levels two to three times the upper limit of normal, and lack significant comorbidities.3,4
Unproven benefit of combination therapy
Perhaps the most convincing argument against combination therapy is that numerous studies of combinations have failed to demonstrate a benefit compared with monotherapy in treatment-naïve patients:
- Interferon in combination with lamivudine has not been shown to be significantly more effective than lamivudine monotherapy.8,9 Further, because of limited information on the safety of interferon in combination with nucleoside or nucleotide analogues, use of the combination is not recommended.4 Neuropathy has been reported with the combination of interferon and telbivudine,4 leading to the release of a warning about its use.10
- A 1-year trial by Lai et al failed to show an improvement in virologic and biochemical responses with the combination of telbivudine and lamivudine compared with telbivudine alone.11
- In patients with lamivudine-resistant chronic HBV infection, adefovir reduced serum HBV DNA levels by 4 weeks whether or not lamivudine therapy was ongoing.12
- Although more patients taking a combination of adefovir and the nucleoside reverse transcriptase inhibitor emtricitabine had normalization of ALT and suppression of HBV DNA to less than 300 copies compared with adefovir monotherapy, rates of HBeAg seroconversion were comparable in the two arms.13
- A recent study that compared tenofovir monotherapy with tenofovir and emtricitabine in combination showed comparable effectiveness for both regimens; the authors concluded that further study is necessary before either choice can be recommended as superior to the other.14
RESISTANCE: IDENTIFY EARLY, ADD ON
To minimize the likelihood of resistance and its impact, HBV DNA levels should be monitored every 3 months; at the first sign of a virologic breakthrough, therapy should be added or switched. Resistance to lamivudine is apparent early; models of treatment response indicate that resistance to lamivudine is likely if HBV DNA does not become undetectable by week 4.
In cases of lamivudine failure, adding adefovir early, when the viral load is less than 107 copies/mL, increases the probability of a virologic response.15 In the situation of lamivudine failure, I prefer adding on to switching to reduce the risk of resistance—a practice supported by the study just cited.15 In lamivudine-resistant patients, adefovir monotherapy was associated with virologic breakthrough and resistance to adefovir in 21% of patients, whereas no patient experienced virologic breakthrough or resistance when adefovir was added to lamivudine.
Successful management involves choosing the best medication up front and educating patients about the importance of taking their medication as instructed. For example, entecavir should be taken without food to maximize its bioavailability. With tenofovir, the risk of renal toxicity is low (1%),16 and can be reduced even further with a pretreatment assessment of the patient.
Multiple-drug therapy is the wave of the future
By Pierre M. Gholam, MD
A concise rationale for multiple-drug therapy is that resistance to monotherapy will occur eventually, with serious consequences in some patients and grave public health implications over the long term. Data from France and Australia indicate that multidrug-resistant HBV is a reality in individual cases. Resistance may be less likely when combinations are used, although little evidence exists at present to support this contention.
COMBINATION THERAPY IS COMMON SENSE
Much of the evidence supporting combination therapy for HBV is common sense:
- Most patients with HBV infection require treatment indefinitely, and duration of therapy that is not finite will inevitably lead to resistance.
- Your first shot is your best shot. Once resistance develops, treatment response will eventually decline.
- Sometimes the stakes are too high to risk breakthroughs. In particular, in patients who have cirrhosis and in those awaiting or following liver transplant, flares and recurrences can have disastrous consequences.
Treatment duration and resistance
As Dr. Gish demonstrated, tenofovir and entecavir are highly potent drugs that suppress viral loads effectively and have high genetic barriers to resistance. On an intent-to-treat basis, HBV DNA levels below the threshold level of detection are achieved at impressive rates with tenofovir and entecavir at 2 years in patients who are either HBeAg negative or positive.5,6,17 When the analyses are limited to patients who actually received the drugs, suppression of HBV DNA to undetectable levels exceeds 90%. Resistance to tenofovir is 0% at 2 years,3 and resistance to entecavir is 1.2% at 5 years.5
Although such data appear to favor monotherapy, most HBV-infected patients who commit to treatment will be treated indefinitely; this applies to patients who are HBeAg negative, who constitute most HBV-infected individuals in the United States and worldwide, or HBeAg positive. There are no established end points for treatment termination in HBeAg-negative patients. The only treatment termination end point that is deemed acceptable in HBeAg-positive patients is a period 6 to 12 months after the loss of HBeAg and the development of antibody to HBeAg, or e antigen seroconversion. Even after many years of treatment that includes the first-line agents tenofovir and entecavir, the likelihood of achieving this end point is fairly low.2,5,18
Adherence is also a consideration. Studies of patients with hypertension, heart disease, and other chronic diseases have shown that strict adherence to therapy over decades is unlikely. The same adherence pattern probably applies to the treatment of chronic HBV infection.
Antiviral drugs used in the treatment of chronic HBV infection are associated with certain resistance mutations that confer additional risk of developing resistance to a subsequent drug. Furthermore, with indefinite duration of therapy, it is realistic to expect that resistance will develop.
Other factors play roles in the development of resistance:
- Mutant viruses. We do not fully understand the potential problem of transmission of mutant viruses. This phenomenon is becoming apparent in endemic areas where treatment-naïve patients harbor mutant viruses acquired through sexual contact with HBV-infected patients who have been treated and in whom the virus has subsequently mutated.
- Barriers to resistance. The genetic barrier to resistance for a single drug will eventually be overcome. It may take longer than it took for adefovir, which is associated with a 30% rate of resistance at 5 years.3 It may take a much longer time for entecavir or tenofovir, but resistance is a biological certainty and we need to contend with it. With human immunodeficiency virus (HIV) infection, we are able to genotype for mutations and tailor treatment accordingly. This strategy is not currently recommended for HBV infection, partly because it is expensive and not routinely available.
- Misuse of therapy. Finally, wider use of antiviral agents for the treatment of HBV may lead to wider misuse, and therefore more resistance. Realistically, not every practitioner will start therapy with entecavir or tenofovir; many of the less potent agents have associated rates of resistance, and these in turn may confer an additional risk of resistance if tenofovir or entecavir is eventually used.
Declining response
Colonno et al19 studied the likelihood of entecavir resistance developing in patients with existing lamivudine resistance. The likelihood of resistance to entecavir at 3 years was 1.2% among patients who had never been exposed to lamivudine. Among patients in whom lamivudine resistance had developed and who were subsequently started on entecavir, resistance to entecavir was 32% at 3 years.19 Resistance has consequences; 25% of lamivudine-resistant patients develop viral breakthrough.
Dr. Gish and I agree that the addition of adefovir to lamivudine is better than switching to adefovir monotherapy in the case of lamivudine failure. Compared with switching, the adefovir-lamivudine combination leads to a lower incidence of virologic breakthrough, a lower likelihood of adefovir resistance over time, a greater probability of achieving undetectable levels of HBV DNA (< 35 copies/mL), and a lower cumulative rate of resistance.20 The superiority of combination therapy in achieving undetectable levels of HBV DNA confers a lower risk of developing resistance over time; by year 4, the likelihood of adefovir resistance is only 4% among lamivudine-resistant patients treated with the combination of adefovir and lamivudine.20
In a study of nucleoside analogue–experienced patients who did not achieve viral suppression, response to tenofovir, defined as HBV DNA less than 400 copies/mL at month 12, was 85% overall and only 30% in adefovir-resistant patients.7 These data demonstrate that, if not starting with combination therapy, it is preferable to initiate treatment with a potent drug that is highly successful at HBV DNA suppression. A second monotherapy will be less successful than the initial attempt.
Consequences of resistance
The consequences of resistance in patients with cirrhosis are significant, prompting strong consideration of combination therapy as a potential means to avoid resistance.
One consequence is a well-documented potential for decompensation in the setting of new-onset resistance as a result of flares. Another is post-transplantation recurrence of HBV, leading to poor outcomes. These risks converge in the patient who is awaiting liver transplantation, in whom combination therapy seems to make the most sense to prevent the development of a flare and a recurrence of HBV infection after transplantation.
WHO SHOULD RECEIVE MULTIPLE-DRUG THERAPY?
The American Association for the Study of Liver Diseases recommends combination therapy as the preferred rescue therapy for primary failure of a first-line agent, citing the possibility of resistance with switching in some circumstances and the superiority of adding on as opposed to switching.2 No data clearly support de novo multiple-drug therapy. Although a number of studies have failed to show an advantage of combination therapy over monotherapy, they were of relatively short duration and focused primarily on viral suppression rather than the occurrence of resistance over time. Long-term studies are needed to determine whether combination therapy is an option de novo.
De novo multiple-drug therapy might be reasonable if a patient is at high risk for resistance—for example, for patients with extraordinarily high levels of HBV DNA or in whom resistance can lead to dire consequences, such as patients with cirrhosis or pretransplant patients.
The HIV pandemic serves as a paradigm for combination therapy. Many agents used to treat HBV infection also have anti-HIV effects; their use as monotherapy should be avoided in order to prevent the development of HIV drug resistance. HIV regimens that include only one HBV antiviral agent with a low genetic barrier to resistance (eg, lamivudine) should also be avoided in order to minimize the risk of HBV drug resistance.
I agree with Dr. Gish that cost and potential toxicity, especially renal toxicity, may limit the widespread use of combination therapies.
Discussion
William D. Carey, MD: I hear more agreement than not between the debaters. Are there any comments from the panel?
Morris Sherman, MD, PhD: I’ll comment on the guidelines for the treatment of HBV infection. Tong et al21 recently examined whether a group of HBV-infected patients who developed cirrhosis and hepatoma would have qualified for treatment under four current sets of guidelines. A startlingly large proportion of patients who developed adverse consequences from their liver disease would not have met the criteria for treatment under any of these major guidelines. As many as one-fourth of patients with chronic HBV infection die as a consequence of their liver disease, and in order to prevent these deaths up to one-half of the patients have to be treated. In the long run, overtreatment may be preferable to undertreatment to reduce the incidence of hepatitis-related deaths. My point is that the treatment guidelines probably exclude many patients who should be treated.
The factors I consider important in my decision to treat are a high viral load, which is indicative of active viral replication, and evidence of liver injury. Patients who have a high viral load and no liver injury won’t experience complications. What do I consider evidence of liver injury? Prolonged elevation of ALT is suggestive, although not necessarily as high as 200 or 300 U/L; it could be in the range of 50 to 80 U/L if fibrosis is significant, which I define as stage 2 or greater on the biopsy. If a high viral load and evidence of significant liver injury are present, I treat the patient regardless of the precise level of the viral load or the ALT.
Dr. Carey: Can you clarify your position? Some of our earlier discussion emphasized the importance of treating when the viral load is high, regardless of other factors. A high viral load by itself may be associated with increased risk of cirrhosis or hepatocellular carcinoma without cirrhosis, so why would a biopsy make a difference?
Dr. Sherman: We can’t predict which younger HBeAg-positive patients with a very high viral load are going to run into trouble down the road. Many will seroconvert spontaneously and never have problems thereafter. In contrast, a patient in his 40s with a high viral load, even if HBeAg positive, and without major fibrosis should be considered for therapy. I tell my patients and the physicians who refer them that once I’m finished with the evaluation, it’s not good-bye. They have to be followed for life because things change.
Tram T. Tran, MD: In the paper by Tong et al,21 all of the patients who subsequently had poor outcomes had low platelet counts. I therefore recommend considering the entire picture in the decision to treat. If physicians followed the treatment guidelines strictly, they would not have treated those patients, but had they noticed thrombocytopenia they would have considered the possibility of advanced fibrosis and considered screening or a biopsy.
Monotherapy for treatment-naïve patients
By Robert G. Gish, MD
Powerful antiviral medicines with activity against hepatitis B virus (HBV) have long-term records of potency and safety, supporting the case for monotherapy in treatment-naïve patients. Combination therapy has a limited role in the management of HBV infection; if the approach to treatment is rational from the start, then combination therapy can be reserved for cases of treatment failure or resistance.
THE CASE FOR MONOTHERAPY
Three arguments that favor monotherapy with potent medications are cost, low risk of resistance, and unproven benefit of combination therapy.
Cost
The cost of dual-medication therapy is nearly double that of single-drug therapy, while the benefit is unknown in treatment-naïve patients. My choices for first-line therapy are tenofovir or entecavir, highly potent nucleoside/nucleotide analogues that can cost up to $5,500 and $8,000, respectively, per year of treatment.1 The two in combination would cost nearly $14,000 per year, and benefits have not been proven in the treatment-naïve population.
Low risk of resistance
Potent medications have low rates of resistance, in the range of 1% over 2 to 5 years.2–4 If one starts therapy with the highly potent entecavir, discussions about switching or adding on therapy would be superfluous because of the low rates of resistance and failure associated with entecavir monotherapy. At 5 years, the cumulative rate of entecavir resistance in patients with positive HBV DNA at baseline is 1.2%.5 Tenofovir also produces potent inhibition of HBV DNA and is associated with low rates of resistance,6 although follow-up data with tenofovir extend only to 2 years. Starting therapy with the less potent adefovir, followed by the development of resistance, decreases the probability that tenofovir will achieve HBV DNA suppression during treatment.7 The main driver of resistance is nonadherence with therapy, not treatment failure.
Resistance to pegylated interferon has not been encountered. The therapy is limited in duration (24 to 48 weeks), with durable suppression of HBV DNA and high rates of seroconversion from hepatitis B e antigen (HBeAg)-positive to HBeAg-negative status. Parameters for the use of pegylated interferon as first-line therapy have been established, and include patients with genotype A or B who are young, have HBV DNA levels less than 107 copies/mL, have serum alanine aminotransferase (ALT) levels two to three times the upper limit of normal, and lack significant comorbidities.3,4
Unproven benefit of combination therapy
Perhaps the most convincing argument against combination therapy is that numerous studies of combinations have failed to demonstrate a benefit compared with monotherapy in treatment-naïve patients:
- Interferon in combination with lamivudine has not been shown to be significantly more effective than lamivudine monotherapy.8,9 Further, because of limited information on the safety of interferon in combination with nucleoside or nucleotide analogues, use of the combination is not recommended.4 Neuropathy has been reported with the combination of interferon and telbivudine,4 leading to the release of a warning about its use.10
- A 1-year trial by Lai et al failed to show an improvement in virologic and biochemical responses with the combination of telbivudine and lamivudine compared with telbivudine alone.11
- In patients with lamivudine-resistant chronic HBV infection, adefovir reduced serum HBV DNA levels by 4 weeks whether or not lamivudine therapy was ongoing.12
- Although more patients taking a combination of adefovir and the nucleoside reverse transcriptase inhibitor emtricitabine had normalization of ALT and suppression of HBV DNA to less than 300 copies compared with adefovir monotherapy, rates of HBeAg seroconversion were comparable in the two arms.13
- A recent study that compared tenofovir monotherapy with tenofovir and emtricitabine in combination showed comparable effectiveness for both regimens; the authors concluded that further study is necessary before either choice can be recommended as superior to the other.14
RESISTANCE: IDENTIFY EARLY, ADD ON
To minimize the likelihood of resistance and its impact, HBV DNA levels should be monitored every 3 months; at the first sign of a virologic breakthrough, therapy should be added or switched. Resistance to lamivudine is apparent early; models of treatment response indicate that resistance to lamivudine is likely if HBV DNA does not become undetectable by week 4.
In cases of lamivudine failure, adding adefovir early, when the viral load is less than 107 copies/mL, increases the probability of a virologic response.15 In the situation of lamivudine failure, I prefer adding on to switching to reduce the risk of resistance—a practice supported by the study just cited.15 In lamivudine-resistant patients, adefovir monotherapy was associated with virologic breakthrough and resistance to adefovir in 21% of patients, whereas no patient experienced virologic breakthrough or resistance when adefovir was added to lamivudine.
Successful management involves choosing the best medication up front and educating patients about the importance of taking their medication as instructed. For example, entecavir should be taken without food to maximize its bioavailability. With tenofovir, the risk of renal toxicity is low (1%),16 and can be reduced even further with a pretreatment assessment of the patient.
Multiple-drug therapy is the wave of the future
By Pierre M. Gholam, MD
A concise rationale for multiple-drug therapy is that resistance to monotherapy will occur eventually, with serious consequences in some patients and grave public health implications over the long term. Data from France and Australia indicate that multidrug-resistant HBV is a reality in individual cases. Resistance may be less likely when combinations are used, although little evidence exists at present to support this contention.
COMBINATION THERAPY IS COMMON SENSE
Much of the evidence supporting combination therapy for HBV is common sense:
- Most patients with HBV infection require treatment indefinitely, and duration of therapy that is not finite will inevitably lead to resistance.
- Your first shot is your best shot. Once resistance develops, treatment response will eventually decline.
- Sometimes the stakes are too high to risk breakthroughs. In particular, in patients who have cirrhosis and in those awaiting or following liver transplant, flares and recurrences can have disastrous consequences.
Treatment duration and resistance
As Dr. Gish demonstrated, tenofovir and entecavir are highly potent drugs that suppress viral loads effectively and have high genetic barriers to resistance. On an intent-to-treat basis, HBV DNA levels below the threshold level of detection are achieved at impressive rates with tenofovir and entecavir at 2 years in patients who are either HBeAg negative or positive.5,6,17 When the analyses are limited to patients who actually received the drugs, suppression of HBV DNA to undetectable levels exceeds 90%. Resistance to tenofovir is 0% at 2 years,3 and resistance to entecavir is 1.2% at 5 years.5
Although such data appear to favor monotherapy, most HBV-infected patients who commit to treatment will be treated indefinitely; this applies to patients who are HBeAg negative, who constitute most HBV-infected individuals in the United States and worldwide, or HBeAg positive. There are no established end points for treatment termination in HBeAg-negative patients. The only treatment termination end point that is deemed acceptable in HBeAg-positive patients is a period 6 to 12 months after the loss of HBeAg and the development of antibody to HBeAg, or e antigen seroconversion. Even after many years of treatment that includes the first-line agents tenofovir and entecavir, the likelihood of achieving this end point is fairly low.2,5,18
Adherence is also a consideration. Studies of patients with hypertension, heart disease, and other chronic diseases have shown that strict adherence to therapy over decades is unlikely. The same adherence pattern probably applies to the treatment of chronic HBV infection.
Antiviral drugs used in the treatment of chronic HBV infection are associated with certain resistance mutations that confer additional risk of developing resistance to a subsequent drug. Furthermore, with indefinite duration of therapy, it is realistic to expect that resistance will develop.
Other factors play roles in the development of resistance:
- Mutant viruses. We do not fully understand the potential problem of transmission of mutant viruses. This phenomenon is becoming apparent in endemic areas where treatment-naïve patients harbor mutant viruses acquired through sexual contact with HBV-infected patients who have been treated and in whom the virus has subsequently mutated.
- Barriers to resistance. The genetic barrier to resistance for a single drug will eventually be overcome. It may take longer than it took for adefovir, which is associated with a 30% rate of resistance at 5 years.3 It may take a much longer time for entecavir or tenofovir, but resistance is a biological certainty and we need to contend with it. With human immunodeficiency virus (HIV) infection, we are able to genotype for mutations and tailor treatment accordingly. This strategy is not currently recommended for HBV infection, partly because it is expensive and not routinely available.
- Misuse of therapy. Finally, wider use of antiviral agents for the treatment of HBV may lead to wider misuse, and therefore more resistance. Realistically, not every practitioner will start therapy with entecavir or tenofovir; many of the less potent agents have associated rates of resistance, and these in turn may confer an additional risk of resistance if tenofovir or entecavir is eventually used.
Declining response
Colonno et al19 studied the likelihood of entecavir resistance developing in patients with existing lamivudine resistance. The likelihood of resistance to entecavir at 3 years was 1.2% among patients who had never been exposed to lamivudine. Among patients in whom lamivudine resistance had developed and who were subsequently started on entecavir, resistance to entecavir was 32% at 3 years.19 Resistance has consequences; 25% of lamivudine-resistant patients develop viral breakthrough.
Dr. Gish and I agree that the addition of adefovir to lamivudine is better than switching to adefovir monotherapy in the case of lamivudine failure. Compared with switching, the adefovir-lamivudine combination leads to a lower incidence of virologic breakthrough, a lower likelihood of adefovir resistance over time, a greater probability of achieving undetectable levels of HBV DNA (< 35 copies/mL), and a lower cumulative rate of resistance.20 The superiority of combination therapy in achieving undetectable levels of HBV DNA confers a lower risk of developing resistance over time; by year 4, the likelihood of adefovir resistance is only 4% among lamivudine-resistant patients treated with the combination of adefovir and lamivudine.20
In a study of nucleoside analogue–experienced patients who did not achieve viral suppression, response to tenofovir, defined as HBV DNA less than 400 copies/mL at month 12, was 85% overall and only 30% in adefovir-resistant patients.7 These data demonstrate that, if not starting with combination therapy, it is preferable to initiate treatment with a potent drug that is highly successful at HBV DNA suppression. A second monotherapy will be less successful than the initial attempt.
Consequences of resistance
The consequences of resistance in patients with cirrhosis are significant, prompting strong consideration of combination therapy as a potential means to avoid resistance.
One consequence is a well-documented potential for decompensation in the setting of new-onset resistance as a result of flares. Another is post-transplantation recurrence of HBV, leading to poor outcomes. These risks converge in the patient who is awaiting liver transplantation, in whom combination therapy seems to make the most sense to prevent the development of a flare and a recurrence of HBV infection after transplantation.
WHO SHOULD RECEIVE MULTIPLE-DRUG THERAPY?
The American Association for the Study of Liver Diseases recommends combination therapy as the preferred rescue therapy for primary failure of a first-line agent, citing the possibility of resistance with switching in some circumstances and the superiority of adding on as opposed to switching.2 No data clearly support de novo multiple-drug therapy. Although a number of studies have failed to show an advantage of combination therapy over monotherapy, they were of relatively short duration and focused primarily on viral suppression rather than the occurrence of resistance over time. Long-term studies are needed to determine whether combination therapy is an option de novo.
De novo multiple-drug therapy might be reasonable if a patient is at high risk for resistance—for example, for patients with extraordinarily high levels of HBV DNA or in whom resistance can lead to dire consequences, such as patients with cirrhosis or pretransplant patients.
The HIV pandemic serves as a paradigm for combination therapy. Many agents used to treat HBV infection also have anti-HIV effects; their use as monotherapy should be avoided in order to prevent the development of HIV drug resistance. HIV regimens that include only one HBV antiviral agent with a low genetic barrier to resistance (eg, lamivudine) should also be avoided in order to minimize the risk of HBV drug resistance.
I agree with Dr. Gish that cost and potential toxicity, especially renal toxicity, may limit the widespread use of combination therapies.
Discussion
William D. Carey, MD: I hear more agreement than not between the debaters. Are there any comments from the panel?
Morris Sherman, MD, PhD: I’ll comment on the guidelines for the treatment of HBV infection. Tong et al21 recently examined whether a group of HBV-infected patients who developed cirrhosis and hepatoma would have qualified for treatment under four current sets of guidelines. A startlingly large proportion of patients who developed adverse consequences from their liver disease would not have met the criteria for treatment under any of these major guidelines. As many as one-fourth of patients with chronic HBV infection die as a consequence of their liver disease, and in order to prevent these deaths up to one-half of the patients have to be treated. In the long run, overtreatment may be preferable to undertreatment to reduce the incidence of hepatitis-related deaths. My point is that the treatment guidelines probably exclude many patients who should be treated.
The factors I consider important in my decision to treat are a high viral load, which is indicative of active viral replication, and evidence of liver injury. Patients who have a high viral load and no liver injury won’t experience complications. What do I consider evidence of liver injury? Prolonged elevation of ALT is suggestive, although not necessarily as high as 200 or 300 U/L; it could be in the range of 50 to 80 U/L if fibrosis is significant, which I define as stage 2 or greater on the biopsy. If a high viral load and evidence of significant liver injury are present, I treat the patient regardless of the precise level of the viral load or the ALT.
Dr. Carey: Can you clarify your position? Some of our earlier discussion emphasized the importance of treating when the viral load is high, regardless of other factors. A high viral load by itself may be associated with increased risk of cirrhosis or hepatocellular carcinoma without cirrhosis, so why would a biopsy make a difference?
Dr. Sherman: We can’t predict which younger HBeAg-positive patients with a very high viral load are going to run into trouble down the road. Many will seroconvert spontaneously and never have problems thereafter. In contrast, a patient in his 40s with a high viral load, even if HBeAg positive, and without major fibrosis should be considered for therapy. I tell my patients and the physicians who refer them that once I’m finished with the evaluation, it’s not good-bye. They have to be followed for life because things change.
Tram T. Tran, MD: In the paper by Tong et al,21 all of the patients who subsequently had poor outcomes had low platelet counts. I therefore recommend considering the entire picture in the decision to treat. If physicians followed the treatment guidelines strictly, they would not have treated those patients, but had they noticed thrombocytopenia they would have considered the possibility of advanced fibrosis and considered screening or a biopsy.
- Wong JB. Costs of antiviral therapy of chronic hepatitis B. Paper presented at: Management of Hepatitis B: 2006. National Institutes of Health Workshop. April 6–8, 2006; Bethesda, MD.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Tenney DJ, Pokomowski KA, Rose RE, et al. Entecavir at five years shows long-term maintenance of high genetic barrier to hepatitis B virus resistance [abstract OL-107]. Hepatol Int 2008; 2:S76–S77.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Schalm SW, Heathcote J, Cianciara J, et al. Lamivudine and alpha interferon combination treatment of patients with chronic hepatitis B infection: a randomized trial. Gut 2000; 46:562–568.
- Chan HL-Y, Leung NW-Y, Hui AY, et al. A randomized, controlled trial of combination therapy for chronic hepatitis B: comparing pegylated interferon-a2b and lamivudine with lamivudine alone. Ann Intern Med 2005; 142:240–250.
- Novartis Pharmaceuticals Canada Inc. Risk of peripheral neuropathy in patients treated with telbivudine (SEBIVO®) in combination with interferon. Health Canada Web site. http://www.hc-sc.gc.ca/dhp-mps/alt_formats/hpfb-dgpsa/pdf/medeff/sebivo_pc-cp-eng.pdf. March 12, 2008. Accessed March 12, 2009.
- Lai C-L, Leung N, Teo E-K, et al. A 1-year trial of telbivudine, lamivudine, and the combination in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology 2005; 129:528–536.
- Peters MG, Hann HW, Martin P, et al. Adefovir dipivoxil alone or in combination with lamivudine in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology 2004; 126:91–101.
- Hui C-K, Zhang H-Y, Bowden S, et al. 96 weeks combination of adefovir dipivoxil plus emtricitabine vs. adefovir dipivoxil monotherapy in the treatment of chronic hepatitis B. J Hepatol 2008; 48:714–720.
- Berg T, Moller B, Trinh H, et al. Tenofovir disoproxil fumarate (TDF) versus emtricitabine plus TDF for treatment of chronic hepatitis B (CHB) in subjects with persistent viral replication receiving adefovir dipivoxil (ADV). Paper presented at: 43rd Annual Meeting of the European Association for the Study of the Liver; April 23–27, 2008; Milan, Italy.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
- Szczech LA. Tenofovir nephrotoxicity: focusing research questions and putting them into clinical context. J Infect Dis 2008; 197:7–9.
- Shouval D, Lai C-L, Chang T-T, et al. Three years of entecavir (ETV) retreatment of HBeAg(–) ETV patients who previously discontinued treatment: results from study ETV-901. Poster presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Poster 927.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose RE, Pokornowski K, Baldick CJ, Klesczewski K, Tenney D. Assessment at three years shows high barrier to resistance is maintained in entecavir-treated nucleoside naïve patients while resistance emergence increases over time in lamivudine refractory patients [AASLD abstract 110]. Hepatology 2006; 44(suppl 1):229A–230A.
- Lampertico P, Viganò M, Manenti E, Iavarone M, Sablon E, Colombo M. Low resistance to adefovir combined with lamivudine: a 3-year study of 145 lamivudine-resistant hepatitis B patients. Gastroenterology 2007; 133:1445–1451.
- Tong MJ, Hsien C, Hsu L, Sun HE, Blatt LM. Treatment recommendations for chronic hepatitis B: an evaluation of current guidelines based on a natural history study in the United States. Hepatology 2008; 48:1070–1078.
- Wong JB. Costs of antiviral therapy of chronic hepatitis B. Paper presented at: Management of Hepatitis B: 2006. National Institutes of Health Workshop. April 6–8, 2006; Bethesda, MD.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Tenney DJ, Pokomowski KA, Rose RE, et al. Entecavir at five years shows long-term maintenance of high genetic barrier to hepatitis B virus resistance [abstract OL-107]. Hepatol Int 2008; 2:S76–S77.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Schalm SW, Heathcote J, Cianciara J, et al. Lamivudine and alpha interferon combination treatment of patients with chronic hepatitis B infection: a randomized trial. Gut 2000; 46:562–568.
- Chan HL-Y, Leung NW-Y, Hui AY, et al. A randomized, controlled trial of combination therapy for chronic hepatitis B: comparing pegylated interferon-a2b and lamivudine with lamivudine alone. Ann Intern Med 2005; 142:240–250.
- Novartis Pharmaceuticals Canada Inc. Risk of peripheral neuropathy in patients treated with telbivudine (SEBIVO®) in combination with interferon. Health Canada Web site. http://www.hc-sc.gc.ca/dhp-mps/alt_formats/hpfb-dgpsa/pdf/medeff/sebivo_pc-cp-eng.pdf. March 12, 2008. Accessed March 12, 2009.
- Lai C-L, Leung N, Teo E-K, et al. A 1-year trial of telbivudine, lamivudine, and the combination in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology 2005; 129:528–536.
- Peters MG, Hann HW, Martin P, et al. Adefovir dipivoxil alone or in combination with lamivudine in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology 2004; 126:91–101.
- Hui C-K, Zhang H-Y, Bowden S, et al. 96 weeks combination of adefovir dipivoxil plus emtricitabine vs. adefovir dipivoxil monotherapy in the treatment of chronic hepatitis B. J Hepatol 2008; 48:714–720.
- Berg T, Moller B, Trinh H, et al. Tenofovir disoproxil fumarate (TDF) versus emtricitabine plus TDF for treatment of chronic hepatitis B (CHB) in subjects with persistent viral replication receiving adefovir dipivoxil (ADV). Paper presented at: 43rd Annual Meeting of the European Association for the Study of the Liver; April 23–27, 2008; Milan, Italy.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
- Szczech LA. Tenofovir nephrotoxicity: focusing research questions and putting them into clinical context. J Infect Dis 2008; 197:7–9.
- Shouval D, Lai C-L, Chang T-T, et al. Three years of entecavir (ETV) retreatment of HBeAg(–) ETV patients who previously discontinued treatment: results from study ETV-901. Poster presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Poster 927.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose RE, Pokornowski K, Baldick CJ, Klesczewski K, Tenney D. Assessment at three years shows high barrier to resistance is maintained in entecavir-treated nucleoside naïve patients while resistance emergence increases over time in lamivudine refractory patients [AASLD abstract 110]. Hepatology 2006; 44(suppl 1):229A–230A.
- Lampertico P, Viganò M, Manenti E, Iavarone M, Sablon E, Colombo M. Low resistance to adefovir combined with lamivudine: a 3-year study of 145 lamivudine-resistant hepatitis B patients. Gastroenterology 2007; 133:1445–1451.
- Tong MJ, Hsien C, Hsu L, Sun HE, Blatt LM. Treatment recommendations for chronic hepatitis B: an evaluation of current guidelines based on a natural history study in the United States. Hepatology 2008; 48:1070–1078.
Management of hepatitis B in pregnancy: Weighing the options
The management of hepatitis B virus (HBV) infection in pregnancy is complex. Because infection with HBV in infancy often leads to chronic disease, prevention of perinatal, or vertical, transmission is a worthy goal; yet, prophylactic therapy during pregnancy is not well studied. This article explores the consequences of HBV infection during pregnancy, the specific risks imposed by high viral load, the evidence to support preemptive antiviral therapy, and the timing of therapy during pregnancy.
PERINATAL TRANSMISSION
Perinatal transmission is the most common mode of HBV transmission worldwide; however, the maternal screening programs and universal vaccination in newborns with active and passive immunoprophylaxis have dramatically reduced HBV transmission rates. According to recent data from the US Centers for Disease Control and Prevention, prenatal screening for hepatitis B surface antigen (HBsAg) in the United States is nearly universal; 97% of pregnant women undergo screening before delivery.1 Further, among infants at risk of acquiring HBV infection, 92% complete the three-dose vaccination series by the time they are 3 years old. There is some nationwide variation, however, in the appropriate administration of immunoprophylaxis to infants exposed perinatally, ranging from 78% in Louisiana to 99.8% in one California health maintenance organization.2
Perinatal transmission of HBV infection has declined steadily in the United States over the past 2 decades, consistent with the successful implementation of universal screening of pregnant women and vaccination policies.3 Outside the United States, however, many high-prevalence countries lack vaccination coverage and perinatal transmission is common. In 87 countries with a prevalence of HBV infection that exceeds 8%, the infant vaccine coverage was only 36%.4
Risk of chronic infection
The risk of progression to chronic HBV infection is inversely proportional to the age at which the infection was acquired. Without immunoprophylaxis, up to 90% of infants born to hepatitis B e antigen (HBeAg)-positive mothers become HBV carriers. In comparison, 20% to 30% of children infected between age 1 year and 5 years, and fewer than 5% of immunocompetent adults, become HBV carriers.5–7
If the mother is positive for both HBsAg and HBeAg and her baby does not receive immunoprophylaxis, the risk of the baby developing chronic HBV infection by age 6 months is 70% to 90%.8–10 Of those exposed in early childhood, 28.8% are HBsAg positive by age 4 years.5 These data underscore the need for early vaccination.
In a study of 402 HBsAg-positive pregnant women in China, Xu et al11 found that 3.7% of their newborn infants were HBsAg positive within 24 hours of birth. Of the women who were HBeAg positive, the intrauterine infection rate was 9.8%. Analysis of placental tissue for HBsAg, hepatitis B core antigen (HBcAg), and viral load (HBV DNA) uncovered an overall placental infection rate of 44.6%.
Transplacental transmission of HBV has been observed in multiple studies, especially when mothers are positive for HBsAg and HBeAg and have high viral loads. Among mothers positive for HBeAg, Burk et al12 found an odds ratio of 147 for a persistently infected infant when the maternal HBV DNA level was at least 1.4 ng/mL compared with less than .005 ng/mL. Among the HBeAg-negative mothers, the odds ratio for a persistently infected infant was 19.2 with high versus low maternal HBV DNA levels.
Importance of maternal viremia
Despite successful screening and vaccination programs, high maternal HBV DNA correlates in some studies with perinatal transmission. Wiseman et al13 studied 298 chronically HBV-infected women and their infants, who were tested for HBV at age 9 months. Interim analysis showed a transmission rate of 8.5% for infants born to mothers with virus levels greater than 8 log10 copies/mL. These data suggest that perinatal transmission may still be occurring despite the use of effective active and passive immunoprophylaxis. Additional studies are needed to assess the potential risk reduction associated with treatment of high maternal viremia during pregnancy.
Maternal HBV DNA positivity was associated with a high rate of intrauterine transmission of HBV in a program in India in which 11,524 woman were screened for HBV infection.14 Babies of the 133 women found to be positive at the time of birth were screened for HBsAg, HBeAg, and HBV DNA in serum and cord blood. Of 127 deliveries in which the mothers were positive for HBV DNA, 66% of infants had HBV DNA in their cord blood and 41% had serum markers that were positive at birth. Maternal HBV DNA greater than 1.5 X 105 copies/mL was significantly associated with intrauterine transmission (P = .025), whereas mode of delivery and maternal HBeAg status were not. This study adds to the concern that in some cases, the vaccine and hepatitis B immune globulin (HBIg) given at the time of birth may not prevent infection in those born already infected and further supports the need to assess the treatment of pregnant women with high viral titers.
TREATMENT DURING PREGNANCY
The use of active and passive immunoprophylaxis to reduce the risk of perinatal transmission of HBV is well accepted in clinical practice. HBIg given at the time of birth in combination with three doses of the recombinant hepatitis B vaccine given over the first 6 months of life has been up to 95% effective in preventing perinatal transmission. As noted above, however, the risk of perinatal transmission of HBV increases as the mother’s viral load increases. In one series of mothers with high viral loads, this risk was as high as 28%.15
It stands to reason that if the mother’s viral load can be reduced at the time of birth, the risk of perinatal transmission could also be reduced (see “Case: Minimizing risk in a 29-year-old woman”). In fact, lamivudine treatment of highly viremic HBsAg-positive women during the final months of pregnancy appears safe and may effectively reduce the risk of perinatal transmission of HBV, even in the setting of HBV vaccination plus HBIg.
Evidence for third-trimester treatment
van Zonneveld et al15 studied eight HBeAg-positive women with HBV DNA levels of 1.2 X 109 copies/mL or greater who were treated with 150 mg/day of lamivudine after the 34th week of pregnancy, and compared the rates of perinatal transmission between them and 24 matched historical controls who did not receive treatment. All children received standard immunoprophylaxis at birth and were followed for 12 months. In five of the eight treated mothers, viral load declined to less than 1.2 X 108 copies/mL. Of the eight infants born to treated mothers, four were HBsAg positive at birth, but only one remained positive at 1 year. This 12.5% rate of perinatal transmission was substantially lower than the 28% rate observed among the controls. No adverse events occurred with lamivudine in this study.
In a multicenter, randomized, double-blind, placebo-controlled study in China and the Philippines, Xu et al16 assessed outcomes among 114 HBsAg-positive pregnant women who had high viral loads (HBV DNA > 1,000 mEq/mL). The women were randomized to placebo or treatment with lamivudine starting at 32 weeks of gestation and continuing until 4 weeks postpartum. All of the infants received standard vaccine plus HBIg.
The mothers treated with lamivudine were more likely (98%) to have a reduction in their viral loads to less than 1,000 mEq/mL than the controls (31%). This reduction in viral load translated to improved outcomes for the infants of mothers receiving lamivudine. At 1 year, 18% of infants born to mothers treated with lamivudine were HBsAg positive compared with 39% of infants born to mothers randomized to placebo (P = .014). The rate of HBV DNA positivity at 1 year was reduced by more than half among the infants born to actively treated mothers compared with those who received placebo (20% vs 46%, respectively; P = .003). There was no difference in the rate of adverse events between the treatment and control groups in either the mothers or the infants.
The Xu study suggests that the use of lamivudine in the third trimester in mothers with high viral loads may effectively reduce the risk of perinatal transmission beyond what can be achieved with active and passive immunoprophylaxis. As this study has been presented in abstract form only, we await the final analysis of these data. This therapy appears to be relatively safe for both mother and infant, although the optimal timing and duration of therapy is still unclear.
Treatment options during pregnancy
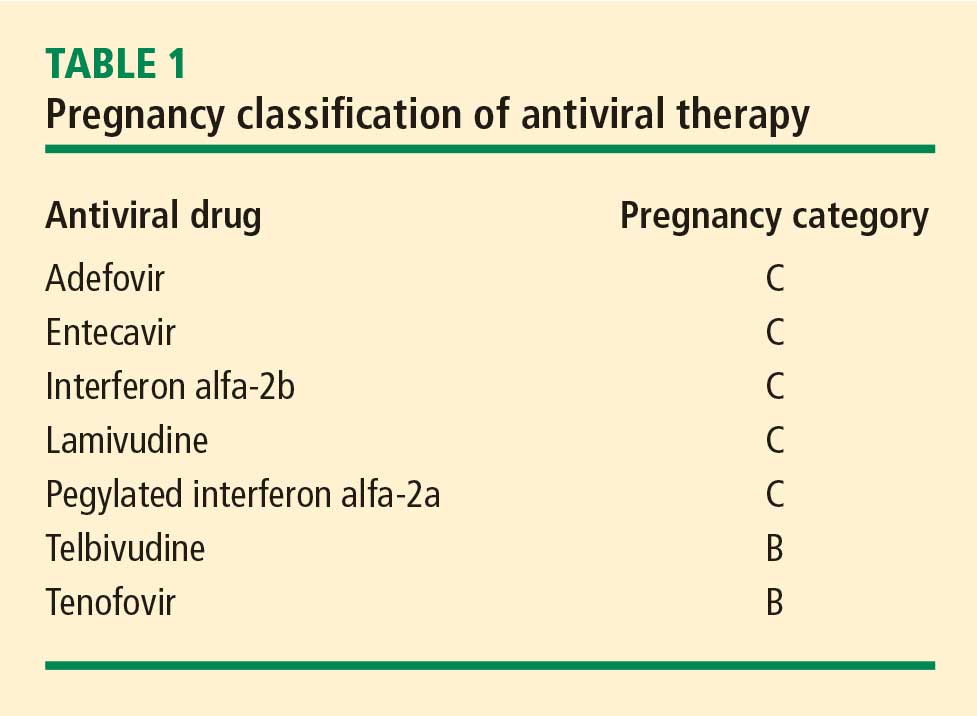
Most human experience with antiviral drug therapy in pregnancy has been with lamivudine. More than 4,600 women have been exposed to the drug during their second or third trimesters.17 Even though lamivudine is classified as FDA pregnancy risk category C, it is associated with a risk of birth defects (2.2% to 2.4%) that is no higher than the baseline birth defect rate.17
Of the two agents classified as FDA pregnancy risk category B, only tenofovir received this classification based on data collected in human exposure. The experience with tenofovir in pregnant women consists of 606 women in their first trimester and 336 in their second trimester.17 The rate of birth defects associated with tenofovir ranges from 1.5% (second-trimester use) to 2.3% (first-trimester use), which is similar to the background rate.17 Telbivudine received its pregnancy risk category B rating based on animal studies; there are few human pregnancy registry data.
Nonpegylated interferon alfa-2b has been shown to have abortifacient effects in rhesus monkeys at 15 and 30 million IU/kg (estimated human equivalent of 5 and 10 million IU/kg, based on body surface area adjustment for a 60-kg adult). Peginterferon alfa-2b should therefore be assumed to also have abortifacient potential, as there are no adequate and well-controlled studies in pregnant women. Peginterferon alfa-2b is to be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. It is recommended for use in fertile women only when they are using effective contraception during the treatment period. Pegylated interferon alfa-2a is approved for treatment of chronic HBV infection, but is not recommended for use during pregnancy.
MANAGEMENT STRATEGY
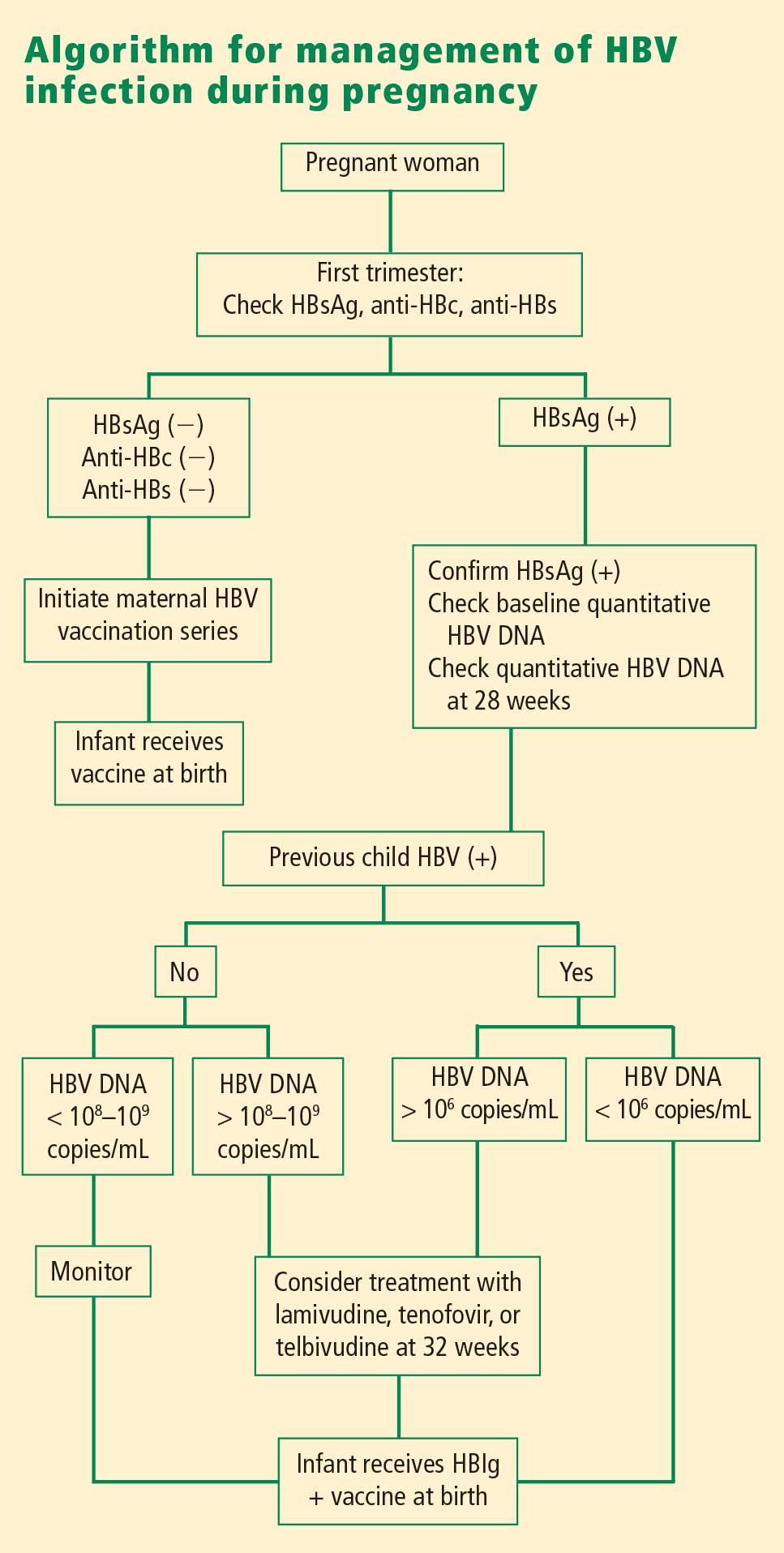
If the mother is HBsAg positive in the first trimester, history of perinatal transmission and an assessment of viral load at week 28 guide further management decisions. All children of HBsAg-positive mothers receive HBIg in addition to vaccination at birth.
Women with high viral loads can be considered for treatment with antiviral therapy, but a comprehensive discussion of risks and benefits needs to take place before opting for treatment as the data are too limited at this time to advocate therapy. One strategy for therapy is the use of lamivudine, tenofovir, or telbivudine starting at 32 weeks of pregnancy; the HBV DNA level that warrants treatment depends on the presence or absence of a history of perinatal transmission. If a previous child was HBV positive, concerns about the risk of perinatal transmission may be higher, so the threshold for treatment may be lower (HBV DNA > 106 copies/mL) than if the previous child were not positive for HBV. If the previous child was not HBV positive, treatment might be considered with HBV DNA levels greater than 108 copies/mL.
SUMMARY
Although a case can be made for treatment of HBV infection during pregnancy, the risks and benefits must be weighed carefully. The benefits of treatment appear to be most pronounced in cases with high maternal viremia; in such instances, treatment should be considered and discussed with the patient at the start of the third trimester. Viable treatment choices are limited to lamivudine, tenofovir, and telbivudine. Of these, lamivudine and tenofovir appear to be the therapeutic options with reasonable human exposure and safety data in pregnancy.
DISCUSSION
William D. Carey, MD: Referring to your case patient, assume that you treat her with tenofovir and her viral load declines. She delivers her baby and then undergoes a thorough workup, including a liver biopsy, that shows no particular liver damage. What would you do?
Tram T. Tran, MD: There are two separate issues: treating the baby and treating the mother. When you’re treating a mother in her third trimester, your goal is to prevent perinatal transmission of HBV. Once the baby is delivered, treated with HBIg, and vaccinated, then your attention turns to the mother. You can then decide based on treatment guidelines and your clinical judgment whether you want to treat the mom.
The period immediately after birth is a time of treatment uncertainty in mothers who choose to breastfeed, because the nucleoside analogues are likely passed in breast milk to some unknown degree, and it’s probably unwise to expose the child this way. In a mother who chooses to breastfeed, I would stop the medication after the delivery, by which time the baby will have received HBIg and the vaccine. When treatment is stopped, you have to think about the potential for a flare; although clinically significant flares are uncommon, the mother should be monitored after stopping treatment. After she stops breastfeeding, you can decide whether to treat her.
Robert G. Gish, MD: What are the effects of tenofovir on bone? Do you talk to your patients about it, and is it an issue during pregnancy or after the baby is delivered?
Dr. Tran: Some data show a decrease in bone mineral density with tenofovir in the human immunodeficiency virus patient population. I definitely talk to my patients about all the potential risks associated with these medicines as, naturally, pregnant women will be very sensitive to any possible risk to their unborn child. Lamivudine probably has the safest profile in pregnancy, given its large body of human experience; however, it is now classified as an FDA pregnancy risk category C drug, whereas tenofovir is classified as category B. This may make a difference to some clinicians.
- Schrag SJ, Arnold KE, Mohle-Boetani JC, et al. Prenatal screening for infectious diseases and opportunities for prevention. Obstet Gynecol 2003; 102:753–760.
- Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev 2006; 28:112–125.
- Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep 2006; 55(RR-16):1–33.
- Centers for Disease Control and Prevention (CDC). Implementation of newborn hepatitis B vaccination—worldwide, 2006. MMWR Morb Mortal Wkly Rep 2008; 57:1249–1252.
- McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1985; 151:599–603.
- Tassopoulos NC, Papaevangelou GJ, Sjogren MH, Roumeliotou-Karayannis A, Gerin JL, Purcell RH. Natural history of acute hepatitis B surface antigen-positive hepatitis in Greek adults. Gastroenterology 1987; 92:1844–1850.
- Chang MH. Natural history of hepatitis B virus infection in children. J Gastroenterol Hepatol 2000; 15(suppl):E16–E19.
- Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol 1977; 105:94–98.
- Wong VC, Ip HM, Reesink HW, et al. Prevention of the HBsAg carrier state in newborn infants of mothers who are chronic carriers of HBsAg and HBeAg by administration of hepatitis-B vaccine and hepatitis-B immunoglobulin: double-blind randomised placebo-controlled study. Lancet 1984; 1(8383):921–926.
- Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. e antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976; 294:746–749.
- Xu DZ, Yan YP, Choi BC, et al. Risk factors and mechanism of transplacental transmission of hepatitis B virus: a case-control study. J Med Virol 2002; 67:20–26.
- Burk RD, Hwang LY, Ho GY, Shafritz DA, Beasley RP. Outcome of perinatal hepatitis B virus exposure is dependent on maternal virus load. J Infect Dis 1994; 170:1418–1423.
- Wiseman E, Fraser MA, Holden S, et al. Perinatal transmission of hepatitis B virus: viral load and HBeAg status are significant risk factors. Presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Abstract 827.
- Pande C, Kumar A, Patra S, Trivedi SS, Dutta AK, Sarin SK. High maternal hepatitis B virus DNA levels but not HBeAg positivity predicts perinatal transmission of hepatitis B to the newborn. Presented at: Digestive Disease Week; May 17–22, 2008; San Diego, CA. Abstract 252.
- van Zonneveld M, van Nunen AB, Niesters HG, de Man RA, Schalm SW, Janssen HL. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Hepat 2003; 10:294–297.
- Xu W-M, Cui Y-T, Wang L, et al. Efficacy and safety of lamivudine in late pregnancy for the prevention of mother-child transmission of hepatitis B: a multicentre, randomised, double-blind, placebo-controlled study [AASLD abstract 246]. Hepatology 2004; 40:272A.
- Antiretroviral Pregnancy Registry Steering Committee. Antiretroviral pregnancy registry international interim report for 1 January 1989 through 31 July 2008. Wilmington, NC: Registry Coordinating Center; 2008. Antiretroviral Pregnancy Registry Web site. http://www.apregistry.com/forms/interim_report.pdf. Accessed December 17, 2008.
- Tran TT, Keeffe EB. Management of the pregnant hepatitis B patient. Current Hepatitis Reports 2008; 7:12–17.
The management of hepatitis B virus (HBV) infection in pregnancy is complex. Because infection with HBV in infancy often leads to chronic disease, prevention of perinatal, or vertical, transmission is a worthy goal; yet, prophylactic therapy during pregnancy is not well studied. This article explores the consequences of HBV infection during pregnancy, the specific risks imposed by high viral load, the evidence to support preemptive antiviral therapy, and the timing of therapy during pregnancy.
PERINATAL TRANSMISSION
Perinatal transmission is the most common mode of HBV transmission worldwide; however, the maternal screening programs and universal vaccination in newborns with active and passive immunoprophylaxis have dramatically reduced HBV transmission rates. According to recent data from the US Centers for Disease Control and Prevention, prenatal screening for hepatitis B surface antigen (HBsAg) in the United States is nearly universal; 97% of pregnant women undergo screening before delivery.1 Further, among infants at risk of acquiring HBV infection, 92% complete the three-dose vaccination series by the time they are 3 years old. There is some nationwide variation, however, in the appropriate administration of immunoprophylaxis to infants exposed perinatally, ranging from 78% in Louisiana to 99.8% in one California health maintenance organization.2
Perinatal transmission of HBV infection has declined steadily in the United States over the past 2 decades, consistent with the successful implementation of universal screening of pregnant women and vaccination policies.3 Outside the United States, however, many high-prevalence countries lack vaccination coverage and perinatal transmission is common. In 87 countries with a prevalence of HBV infection that exceeds 8%, the infant vaccine coverage was only 36%.4
Risk of chronic infection
The risk of progression to chronic HBV infection is inversely proportional to the age at which the infection was acquired. Without immunoprophylaxis, up to 90% of infants born to hepatitis B e antigen (HBeAg)-positive mothers become HBV carriers. In comparison, 20% to 30% of children infected between age 1 year and 5 years, and fewer than 5% of immunocompetent adults, become HBV carriers.5–7
If the mother is positive for both HBsAg and HBeAg and her baby does not receive immunoprophylaxis, the risk of the baby developing chronic HBV infection by age 6 months is 70% to 90%.8–10 Of those exposed in early childhood, 28.8% are HBsAg positive by age 4 years.5 These data underscore the need for early vaccination.
In a study of 402 HBsAg-positive pregnant women in China, Xu et al11 found that 3.7% of their newborn infants were HBsAg positive within 24 hours of birth. Of the women who were HBeAg positive, the intrauterine infection rate was 9.8%. Analysis of placental tissue for HBsAg, hepatitis B core antigen (HBcAg), and viral load (HBV DNA) uncovered an overall placental infection rate of 44.6%.
Transplacental transmission of HBV has been observed in multiple studies, especially when mothers are positive for HBsAg and HBeAg and have high viral loads. Among mothers positive for HBeAg, Burk et al12 found an odds ratio of 147 for a persistently infected infant when the maternal HBV DNA level was at least 1.4 ng/mL compared with less than .005 ng/mL. Among the HBeAg-negative mothers, the odds ratio for a persistently infected infant was 19.2 with high versus low maternal HBV DNA levels.
Importance of maternal viremia
Despite successful screening and vaccination programs, high maternal HBV DNA correlates in some studies with perinatal transmission. Wiseman et al13 studied 298 chronically HBV-infected women and their infants, who were tested for HBV at age 9 months. Interim analysis showed a transmission rate of 8.5% for infants born to mothers with virus levels greater than 8 log10 copies/mL. These data suggest that perinatal transmission may still be occurring despite the use of effective active and passive immunoprophylaxis. Additional studies are needed to assess the potential risk reduction associated with treatment of high maternal viremia during pregnancy.
Maternal HBV DNA positivity was associated with a high rate of intrauterine transmission of HBV in a program in India in which 11,524 woman were screened for HBV infection.14 Babies of the 133 women found to be positive at the time of birth were screened for HBsAg, HBeAg, and HBV DNA in serum and cord blood. Of 127 deliveries in which the mothers were positive for HBV DNA, 66% of infants had HBV DNA in their cord blood and 41% had serum markers that were positive at birth. Maternal HBV DNA greater than 1.5 X 105 copies/mL was significantly associated with intrauterine transmission (P = .025), whereas mode of delivery and maternal HBeAg status were not. This study adds to the concern that in some cases, the vaccine and hepatitis B immune globulin (HBIg) given at the time of birth may not prevent infection in those born already infected and further supports the need to assess the treatment of pregnant women with high viral titers.
TREATMENT DURING PREGNANCY
The use of active and passive immunoprophylaxis to reduce the risk of perinatal transmission of HBV is well accepted in clinical practice. HBIg given at the time of birth in combination with three doses of the recombinant hepatitis B vaccine given over the first 6 months of life has been up to 95% effective in preventing perinatal transmission. As noted above, however, the risk of perinatal transmission of HBV increases as the mother’s viral load increases. In one series of mothers with high viral loads, this risk was as high as 28%.15
It stands to reason that if the mother’s viral load can be reduced at the time of birth, the risk of perinatal transmission could also be reduced (see “Case: Minimizing risk in a 29-year-old woman”). In fact, lamivudine treatment of highly viremic HBsAg-positive women during the final months of pregnancy appears safe and may effectively reduce the risk of perinatal transmission of HBV, even in the setting of HBV vaccination plus HBIg.
Evidence for third-trimester treatment
van Zonneveld et al15 studied eight HBeAg-positive women with HBV DNA levels of 1.2 X 109 copies/mL or greater who were treated with 150 mg/day of lamivudine after the 34th week of pregnancy, and compared the rates of perinatal transmission between them and 24 matched historical controls who did not receive treatment. All children received standard immunoprophylaxis at birth and were followed for 12 months. In five of the eight treated mothers, viral load declined to less than 1.2 X 108 copies/mL. Of the eight infants born to treated mothers, four were HBsAg positive at birth, but only one remained positive at 1 year. This 12.5% rate of perinatal transmission was substantially lower than the 28% rate observed among the controls. No adverse events occurred with lamivudine in this study.
In a multicenter, randomized, double-blind, placebo-controlled study in China and the Philippines, Xu et al16 assessed outcomes among 114 HBsAg-positive pregnant women who had high viral loads (HBV DNA > 1,000 mEq/mL). The women were randomized to placebo or treatment with lamivudine starting at 32 weeks of gestation and continuing until 4 weeks postpartum. All of the infants received standard vaccine plus HBIg.
The mothers treated with lamivudine were more likely (98%) to have a reduction in their viral loads to less than 1,000 mEq/mL than the controls (31%). This reduction in viral load translated to improved outcomes for the infants of mothers receiving lamivudine. At 1 year, 18% of infants born to mothers treated with lamivudine were HBsAg positive compared with 39% of infants born to mothers randomized to placebo (P = .014). The rate of HBV DNA positivity at 1 year was reduced by more than half among the infants born to actively treated mothers compared with those who received placebo (20% vs 46%, respectively; P = .003). There was no difference in the rate of adverse events between the treatment and control groups in either the mothers or the infants.
The Xu study suggests that the use of lamivudine in the third trimester in mothers with high viral loads may effectively reduce the risk of perinatal transmission beyond what can be achieved with active and passive immunoprophylaxis. As this study has been presented in abstract form only, we await the final analysis of these data. This therapy appears to be relatively safe for both mother and infant, although the optimal timing and duration of therapy is still unclear.
Treatment options during pregnancy
Most human experience with antiviral drug therapy in pregnancy has been with lamivudine. More than 4,600 women have been exposed to the drug during their second or third trimesters.17 Even though lamivudine is classified as FDA pregnancy risk category C, it is associated with a risk of birth defects (2.2% to 2.4%) that is no higher than the baseline birth defect rate.17
Of the two agents classified as FDA pregnancy risk category B, only tenofovir received this classification based on data collected in human exposure. The experience with tenofovir in pregnant women consists of 606 women in their first trimester and 336 in their second trimester.17 The rate of birth defects associated with tenofovir ranges from 1.5% (second-trimester use) to 2.3% (first-trimester use), which is similar to the background rate.17 Telbivudine received its pregnancy risk category B rating based on animal studies; there are few human pregnancy registry data.
Nonpegylated interferon alfa-2b has been shown to have abortifacient effects in rhesus monkeys at 15 and 30 million IU/kg (estimated human equivalent of 5 and 10 million IU/kg, based on body surface area adjustment for a 60-kg adult). Peginterferon alfa-2b should therefore be assumed to also have abortifacient potential, as there are no adequate and well-controlled studies in pregnant women. Peginterferon alfa-2b is to be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. It is recommended for use in fertile women only when they are using effective contraception during the treatment period. Pegylated interferon alfa-2a is approved for treatment of chronic HBV infection, but is not recommended for use during pregnancy.
MANAGEMENT STRATEGY
If the mother is HBsAg positive in the first trimester, history of perinatal transmission and an assessment of viral load at week 28 guide further management decisions. All children of HBsAg-positive mothers receive HBIg in addition to vaccination at birth.
Women with high viral loads can be considered for treatment with antiviral therapy, but a comprehensive discussion of risks and benefits needs to take place before opting for treatment as the data are too limited at this time to advocate therapy. One strategy for therapy is the use of lamivudine, tenofovir, or telbivudine starting at 32 weeks of pregnancy; the HBV DNA level that warrants treatment depends on the presence or absence of a history of perinatal transmission. If a previous child was HBV positive, concerns about the risk of perinatal transmission may be higher, so the threshold for treatment may be lower (HBV DNA > 106 copies/mL) than if the previous child were not positive for HBV. If the previous child was not HBV positive, treatment might be considered with HBV DNA levels greater than 108 copies/mL.
SUMMARY
Although a case can be made for treatment of HBV infection during pregnancy, the risks and benefits must be weighed carefully. The benefits of treatment appear to be most pronounced in cases with high maternal viremia; in such instances, treatment should be considered and discussed with the patient at the start of the third trimester. Viable treatment choices are limited to lamivudine, tenofovir, and telbivudine. Of these, lamivudine and tenofovir appear to be the therapeutic options with reasonable human exposure and safety data in pregnancy.
DISCUSSION
William D. Carey, MD: Referring to your case patient, assume that you treat her with tenofovir and her viral load declines. She delivers her baby and then undergoes a thorough workup, including a liver biopsy, that shows no particular liver damage. What would you do?
Tram T. Tran, MD: There are two separate issues: treating the baby and treating the mother. When you’re treating a mother in her third trimester, your goal is to prevent perinatal transmission of HBV. Once the baby is delivered, treated with HBIg, and vaccinated, then your attention turns to the mother. You can then decide based on treatment guidelines and your clinical judgment whether you want to treat the mom.
The period immediately after birth is a time of treatment uncertainty in mothers who choose to breastfeed, because the nucleoside analogues are likely passed in breast milk to some unknown degree, and it’s probably unwise to expose the child this way. In a mother who chooses to breastfeed, I would stop the medication after the delivery, by which time the baby will have received HBIg and the vaccine. When treatment is stopped, you have to think about the potential for a flare; although clinically significant flares are uncommon, the mother should be monitored after stopping treatment. After she stops breastfeeding, you can decide whether to treat her.
Robert G. Gish, MD: What are the effects of tenofovir on bone? Do you talk to your patients about it, and is it an issue during pregnancy or after the baby is delivered?
Dr. Tran: Some data show a decrease in bone mineral density with tenofovir in the human immunodeficiency virus patient population. I definitely talk to my patients about all the potential risks associated with these medicines as, naturally, pregnant women will be very sensitive to any possible risk to their unborn child. Lamivudine probably has the safest profile in pregnancy, given its large body of human experience; however, it is now classified as an FDA pregnancy risk category C drug, whereas tenofovir is classified as category B. This may make a difference to some clinicians.
The management of hepatitis B virus (HBV) infection in pregnancy is complex. Because infection with HBV in infancy often leads to chronic disease, prevention of perinatal, or vertical, transmission is a worthy goal; yet, prophylactic therapy during pregnancy is not well studied. This article explores the consequences of HBV infection during pregnancy, the specific risks imposed by high viral load, the evidence to support preemptive antiviral therapy, and the timing of therapy during pregnancy.
PERINATAL TRANSMISSION
Perinatal transmission is the most common mode of HBV transmission worldwide; however, the maternal screening programs and universal vaccination in newborns with active and passive immunoprophylaxis have dramatically reduced HBV transmission rates. According to recent data from the US Centers for Disease Control and Prevention, prenatal screening for hepatitis B surface antigen (HBsAg) in the United States is nearly universal; 97% of pregnant women undergo screening before delivery.1 Further, among infants at risk of acquiring HBV infection, 92% complete the three-dose vaccination series by the time they are 3 years old. There is some nationwide variation, however, in the appropriate administration of immunoprophylaxis to infants exposed perinatally, ranging from 78% in Louisiana to 99.8% in one California health maintenance organization.2
Perinatal transmission of HBV infection has declined steadily in the United States over the past 2 decades, consistent with the successful implementation of universal screening of pregnant women and vaccination policies.3 Outside the United States, however, many high-prevalence countries lack vaccination coverage and perinatal transmission is common. In 87 countries with a prevalence of HBV infection that exceeds 8%, the infant vaccine coverage was only 36%.4
Risk of chronic infection
The risk of progression to chronic HBV infection is inversely proportional to the age at which the infection was acquired. Without immunoprophylaxis, up to 90% of infants born to hepatitis B e antigen (HBeAg)-positive mothers become HBV carriers. In comparison, 20% to 30% of children infected between age 1 year and 5 years, and fewer than 5% of immunocompetent adults, become HBV carriers.5–7
If the mother is positive for both HBsAg and HBeAg and her baby does not receive immunoprophylaxis, the risk of the baby developing chronic HBV infection by age 6 months is 70% to 90%.8–10 Of those exposed in early childhood, 28.8% are HBsAg positive by age 4 years.5 These data underscore the need for early vaccination.
In a study of 402 HBsAg-positive pregnant women in China, Xu et al11 found that 3.7% of their newborn infants were HBsAg positive within 24 hours of birth. Of the women who were HBeAg positive, the intrauterine infection rate was 9.8%. Analysis of placental tissue for HBsAg, hepatitis B core antigen (HBcAg), and viral load (HBV DNA) uncovered an overall placental infection rate of 44.6%.
Transplacental transmission of HBV has been observed in multiple studies, especially when mothers are positive for HBsAg and HBeAg and have high viral loads. Among mothers positive for HBeAg, Burk et al12 found an odds ratio of 147 for a persistently infected infant when the maternal HBV DNA level was at least 1.4 ng/mL compared with less than .005 ng/mL. Among the HBeAg-negative mothers, the odds ratio for a persistently infected infant was 19.2 with high versus low maternal HBV DNA levels.
Importance of maternal viremia
Despite successful screening and vaccination programs, high maternal HBV DNA correlates in some studies with perinatal transmission. Wiseman et al13 studied 298 chronically HBV-infected women and their infants, who were tested for HBV at age 9 months. Interim analysis showed a transmission rate of 8.5% for infants born to mothers with virus levels greater than 8 log10 copies/mL. These data suggest that perinatal transmission may still be occurring despite the use of effective active and passive immunoprophylaxis. Additional studies are needed to assess the potential risk reduction associated with treatment of high maternal viremia during pregnancy.
Maternal HBV DNA positivity was associated with a high rate of intrauterine transmission of HBV in a program in India in which 11,524 woman were screened for HBV infection.14 Babies of the 133 women found to be positive at the time of birth were screened for HBsAg, HBeAg, and HBV DNA in serum and cord blood. Of 127 deliveries in which the mothers were positive for HBV DNA, 66% of infants had HBV DNA in their cord blood and 41% had serum markers that were positive at birth. Maternal HBV DNA greater than 1.5 X 105 copies/mL was significantly associated with intrauterine transmission (P = .025), whereas mode of delivery and maternal HBeAg status were not. This study adds to the concern that in some cases, the vaccine and hepatitis B immune globulin (HBIg) given at the time of birth may not prevent infection in those born already infected and further supports the need to assess the treatment of pregnant women with high viral titers.
TREATMENT DURING PREGNANCY
The use of active and passive immunoprophylaxis to reduce the risk of perinatal transmission of HBV is well accepted in clinical practice. HBIg given at the time of birth in combination with three doses of the recombinant hepatitis B vaccine given over the first 6 months of life has been up to 95% effective in preventing perinatal transmission. As noted above, however, the risk of perinatal transmission of HBV increases as the mother’s viral load increases. In one series of mothers with high viral loads, this risk was as high as 28%.15
It stands to reason that if the mother’s viral load can be reduced at the time of birth, the risk of perinatal transmission could also be reduced (see “Case: Minimizing risk in a 29-year-old woman”). In fact, lamivudine treatment of highly viremic HBsAg-positive women during the final months of pregnancy appears safe and may effectively reduce the risk of perinatal transmission of HBV, even in the setting of HBV vaccination plus HBIg.
Evidence for third-trimester treatment
van Zonneveld et al15 studied eight HBeAg-positive women with HBV DNA levels of 1.2 X 109 copies/mL or greater who were treated with 150 mg/day of lamivudine after the 34th week of pregnancy, and compared the rates of perinatal transmission between them and 24 matched historical controls who did not receive treatment. All children received standard immunoprophylaxis at birth and were followed for 12 months. In five of the eight treated mothers, viral load declined to less than 1.2 X 108 copies/mL. Of the eight infants born to treated mothers, four were HBsAg positive at birth, but only one remained positive at 1 year. This 12.5% rate of perinatal transmission was substantially lower than the 28% rate observed among the controls. No adverse events occurred with lamivudine in this study.
In a multicenter, randomized, double-blind, placebo-controlled study in China and the Philippines, Xu et al16 assessed outcomes among 114 HBsAg-positive pregnant women who had high viral loads (HBV DNA > 1,000 mEq/mL). The women were randomized to placebo or treatment with lamivudine starting at 32 weeks of gestation and continuing until 4 weeks postpartum. All of the infants received standard vaccine plus HBIg.
The mothers treated with lamivudine were more likely (98%) to have a reduction in their viral loads to less than 1,000 mEq/mL than the controls (31%). This reduction in viral load translated to improved outcomes for the infants of mothers receiving lamivudine. At 1 year, 18% of infants born to mothers treated with lamivudine were HBsAg positive compared with 39% of infants born to mothers randomized to placebo (P = .014). The rate of HBV DNA positivity at 1 year was reduced by more than half among the infants born to actively treated mothers compared with those who received placebo (20% vs 46%, respectively; P = .003). There was no difference in the rate of adverse events between the treatment and control groups in either the mothers or the infants.
The Xu study suggests that the use of lamivudine in the third trimester in mothers with high viral loads may effectively reduce the risk of perinatal transmission beyond what can be achieved with active and passive immunoprophylaxis. As this study has been presented in abstract form only, we await the final analysis of these data. This therapy appears to be relatively safe for both mother and infant, although the optimal timing and duration of therapy is still unclear.
Treatment options during pregnancy
Most human experience with antiviral drug therapy in pregnancy has been with lamivudine. More than 4,600 women have been exposed to the drug during their second or third trimesters.17 Even though lamivudine is classified as FDA pregnancy risk category C, it is associated with a risk of birth defects (2.2% to 2.4%) that is no higher than the baseline birth defect rate.17
Of the two agents classified as FDA pregnancy risk category B, only tenofovir received this classification based on data collected in human exposure. The experience with tenofovir in pregnant women consists of 606 women in their first trimester and 336 in their second trimester.17 The rate of birth defects associated with tenofovir ranges from 1.5% (second-trimester use) to 2.3% (first-trimester use), which is similar to the background rate.17 Telbivudine received its pregnancy risk category B rating based on animal studies; there are few human pregnancy registry data.
Nonpegylated interferon alfa-2b has been shown to have abortifacient effects in rhesus monkeys at 15 and 30 million IU/kg (estimated human equivalent of 5 and 10 million IU/kg, based on body surface area adjustment for a 60-kg adult). Peginterferon alfa-2b should therefore be assumed to also have abortifacient potential, as there are no adequate and well-controlled studies in pregnant women. Peginterferon alfa-2b is to be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. It is recommended for use in fertile women only when they are using effective contraception during the treatment period. Pegylated interferon alfa-2a is approved for treatment of chronic HBV infection, but is not recommended for use during pregnancy.
MANAGEMENT STRATEGY
If the mother is HBsAg positive in the first trimester, history of perinatal transmission and an assessment of viral load at week 28 guide further management decisions. All children of HBsAg-positive mothers receive HBIg in addition to vaccination at birth.
Women with high viral loads can be considered for treatment with antiviral therapy, but a comprehensive discussion of risks and benefits needs to take place before opting for treatment as the data are too limited at this time to advocate therapy. One strategy for therapy is the use of lamivudine, tenofovir, or telbivudine starting at 32 weeks of pregnancy; the HBV DNA level that warrants treatment depends on the presence or absence of a history of perinatal transmission. If a previous child was HBV positive, concerns about the risk of perinatal transmission may be higher, so the threshold for treatment may be lower (HBV DNA > 106 copies/mL) than if the previous child were not positive for HBV. If the previous child was not HBV positive, treatment might be considered with HBV DNA levels greater than 108 copies/mL.
SUMMARY
Although a case can be made for treatment of HBV infection during pregnancy, the risks and benefits must be weighed carefully. The benefits of treatment appear to be most pronounced in cases with high maternal viremia; in such instances, treatment should be considered and discussed with the patient at the start of the third trimester. Viable treatment choices are limited to lamivudine, tenofovir, and telbivudine. Of these, lamivudine and tenofovir appear to be the therapeutic options with reasonable human exposure and safety data in pregnancy.
DISCUSSION
William D. Carey, MD: Referring to your case patient, assume that you treat her with tenofovir and her viral load declines. She delivers her baby and then undergoes a thorough workup, including a liver biopsy, that shows no particular liver damage. What would you do?
Tram T. Tran, MD: There are two separate issues: treating the baby and treating the mother. When you’re treating a mother in her third trimester, your goal is to prevent perinatal transmission of HBV. Once the baby is delivered, treated with HBIg, and vaccinated, then your attention turns to the mother. You can then decide based on treatment guidelines and your clinical judgment whether you want to treat the mom.
The period immediately after birth is a time of treatment uncertainty in mothers who choose to breastfeed, because the nucleoside analogues are likely passed in breast milk to some unknown degree, and it’s probably unwise to expose the child this way. In a mother who chooses to breastfeed, I would stop the medication after the delivery, by which time the baby will have received HBIg and the vaccine. When treatment is stopped, you have to think about the potential for a flare; although clinically significant flares are uncommon, the mother should be monitored after stopping treatment. After she stops breastfeeding, you can decide whether to treat her.
Robert G. Gish, MD: What are the effects of tenofovir on bone? Do you talk to your patients about it, and is it an issue during pregnancy or after the baby is delivered?
Dr. Tran: Some data show a decrease in bone mineral density with tenofovir in the human immunodeficiency virus patient population. I definitely talk to my patients about all the potential risks associated with these medicines as, naturally, pregnant women will be very sensitive to any possible risk to their unborn child. Lamivudine probably has the safest profile in pregnancy, given its large body of human experience; however, it is now classified as an FDA pregnancy risk category C drug, whereas tenofovir is classified as category B. This may make a difference to some clinicians.
- Schrag SJ, Arnold KE, Mohle-Boetani JC, et al. Prenatal screening for infectious diseases and opportunities for prevention. Obstet Gynecol 2003; 102:753–760.
- Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev 2006; 28:112–125.
- Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep 2006; 55(RR-16):1–33.
- Centers for Disease Control and Prevention (CDC). Implementation of newborn hepatitis B vaccination—worldwide, 2006. MMWR Morb Mortal Wkly Rep 2008; 57:1249–1252.
- McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1985; 151:599–603.
- Tassopoulos NC, Papaevangelou GJ, Sjogren MH, Roumeliotou-Karayannis A, Gerin JL, Purcell RH. Natural history of acute hepatitis B surface antigen-positive hepatitis in Greek adults. Gastroenterology 1987; 92:1844–1850.
- Chang MH. Natural history of hepatitis B virus infection in children. J Gastroenterol Hepatol 2000; 15(suppl):E16–E19.
- Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol 1977; 105:94–98.
- Wong VC, Ip HM, Reesink HW, et al. Prevention of the HBsAg carrier state in newborn infants of mothers who are chronic carriers of HBsAg and HBeAg by administration of hepatitis-B vaccine and hepatitis-B immunoglobulin: double-blind randomised placebo-controlled study. Lancet 1984; 1(8383):921–926.
- Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. e antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976; 294:746–749.
- Xu DZ, Yan YP, Choi BC, et al. Risk factors and mechanism of transplacental transmission of hepatitis B virus: a case-control study. J Med Virol 2002; 67:20–26.
- Burk RD, Hwang LY, Ho GY, Shafritz DA, Beasley RP. Outcome of perinatal hepatitis B virus exposure is dependent on maternal virus load. J Infect Dis 1994; 170:1418–1423.
- Wiseman E, Fraser MA, Holden S, et al. Perinatal transmission of hepatitis B virus: viral load and HBeAg status are significant risk factors. Presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Abstract 827.
- Pande C, Kumar A, Patra S, Trivedi SS, Dutta AK, Sarin SK. High maternal hepatitis B virus DNA levels but not HBeAg positivity predicts perinatal transmission of hepatitis B to the newborn. Presented at: Digestive Disease Week; May 17–22, 2008; San Diego, CA. Abstract 252.
- van Zonneveld M, van Nunen AB, Niesters HG, de Man RA, Schalm SW, Janssen HL. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Hepat 2003; 10:294–297.
- Xu W-M, Cui Y-T, Wang L, et al. Efficacy and safety of lamivudine in late pregnancy for the prevention of mother-child transmission of hepatitis B: a multicentre, randomised, double-blind, placebo-controlled study [AASLD abstract 246]. Hepatology 2004; 40:272A.
- Antiretroviral Pregnancy Registry Steering Committee. Antiretroviral pregnancy registry international interim report for 1 January 1989 through 31 July 2008. Wilmington, NC: Registry Coordinating Center; 2008. Antiretroviral Pregnancy Registry Web site. http://www.apregistry.com/forms/interim_report.pdf. Accessed December 17, 2008.
- Tran TT, Keeffe EB. Management of the pregnant hepatitis B patient. Current Hepatitis Reports 2008; 7:12–17.
- Schrag SJ, Arnold KE, Mohle-Boetani JC, et al. Prenatal screening for infectious diseases and opportunities for prevention. Obstet Gynecol 2003; 102:753–760.
- Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev 2006; 28:112–125.
- Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep 2006; 55(RR-16):1–33.
- Centers for Disease Control and Prevention (CDC). Implementation of newborn hepatitis B vaccination—worldwide, 2006. MMWR Morb Mortal Wkly Rep 2008; 57:1249–1252.
- McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1985; 151:599–603.
- Tassopoulos NC, Papaevangelou GJ, Sjogren MH, Roumeliotou-Karayannis A, Gerin JL, Purcell RH. Natural history of acute hepatitis B surface antigen-positive hepatitis in Greek adults. Gastroenterology 1987; 92:1844–1850.
- Chang MH. Natural history of hepatitis B virus infection in children. J Gastroenterol Hepatol 2000; 15(suppl):E16–E19.
- Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol 1977; 105:94–98.
- Wong VC, Ip HM, Reesink HW, et al. Prevention of the HBsAg carrier state in newborn infants of mothers who are chronic carriers of HBsAg and HBeAg by administration of hepatitis-B vaccine and hepatitis-B immunoglobulin: double-blind randomised placebo-controlled study. Lancet 1984; 1(8383):921–926.
- Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. e antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976; 294:746–749.
- Xu DZ, Yan YP, Choi BC, et al. Risk factors and mechanism of transplacental transmission of hepatitis B virus: a case-control study. J Med Virol 2002; 67:20–26.
- Burk RD, Hwang LY, Ho GY, Shafritz DA, Beasley RP. Outcome of perinatal hepatitis B virus exposure is dependent on maternal virus load. J Infect Dis 1994; 170:1418–1423.
- Wiseman E, Fraser MA, Holden S, et al. Perinatal transmission of hepatitis B virus: viral load and HBeAg status are significant risk factors. Presented at: 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31–November 4, 2008; San Francisco, CA. Abstract 827.
- Pande C, Kumar A, Patra S, Trivedi SS, Dutta AK, Sarin SK. High maternal hepatitis B virus DNA levels but not HBeAg positivity predicts perinatal transmission of hepatitis B to the newborn. Presented at: Digestive Disease Week; May 17–22, 2008; San Diego, CA. Abstract 252.
- van Zonneveld M, van Nunen AB, Niesters HG, de Man RA, Schalm SW, Janssen HL. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Hepat 2003; 10:294–297.
- Xu W-M, Cui Y-T, Wang L, et al. Efficacy and safety of lamivudine in late pregnancy for the prevention of mother-child transmission of hepatitis B: a multicentre, randomised, double-blind, placebo-controlled study [AASLD abstract 246]. Hepatology 2004; 40:272A.
- Antiretroviral Pregnancy Registry Steering Committee. Antiretroviral pregnancy registry international interim report for 1 January 1989 through 31 July 2008. Wilmington, NC: Registry Coordinating Center; 2008. Antiretroviral Pregnancy Registry Web site. http://www.apregistry.com/forms/interim_report.pdf. Accessed December 17, 2008.
- Tran TT, Keeffe EB. Management of the pregnant hepatitis B patient. Current Hepatitis Reports 2008; 7:12–17.
KEY POINTS
- Hepatitis B immune globulin at the time of birth plus three doses of the recombinant hepatitis B vaccine over the first 6 months of life is up to 95% effective in
preventing perinatal transmission. - Despite successful screening and vaccination, perinatal transmission of HBV is still possible if maternal viral load is high.
- Antiviral treatment during the third trimester of pregnancy may reduce perinatal transmission of HBV; the benefit appears most pronounced with high maternal viremia.
Strategies for managing coinfection with hepatitis B virus and HIV
Worldwide, 40 million people are infected with the human immunodeficiency virus (HIV). As many as 4 million of them are coinfected with hepatitis B virus (HBV).1 In North America and Europe, the highest prevalence of HBV/HIV coinfection is in men who have sex with men. Approximately half of HIV-positive men who have sex with men have evidence of prior or active HBV infection, and 5% to 10% have chronic HBV infection. Among those who acquire HIV through injected drug use or through heterosexual transmission, the coinfection rate is much lower.2,3
Coinfection with HBV and HIV follows a different course elsewhere in the world. For example, in Africa and Asia, HBV is usually acquired first through neonatal or childhood infection, with either vertical or horizontal transmission after birth.4,5 In parts of Africa, ritual scarification is likely a major player in the adolescent transmission of HBV. (Ritual scarification is the practice of creating small incisions in the skin of adolescents and rubbing black ash in the wounds to form scars; the cutting instruments are not sterilized between rituals.)
NATURAL HISTORY
In general, HBV tends to be more aggressive in HIV-positive individuals than in monoinfected individuals,2,6 with higher HBV carrier rates, higher levels of HBV viremia, more frequent episodes of activation, and faster progression to cirrhosis.
Hepatocellular carcinoma occurs more often, its onset is earlier, and its course is more aggressive in coinfected individuals than in monoinfected individuals.7,8 Using data from a prospective cohort study, Thio et al9 found that among men coinfected with HIV and HBV, liver-related mortality was almost 19 times greater compared with men infected with HBV only and more than seven times greater compared with those infected with HIV only.
In an observational longitudinal cohort study,10 the risk of death from liver disease in HIV-positive persons was nearly three times greater among those also infected with HBV (P < .0001).
ASSESSING WHEN TO TREAT
The objectives of HBV therapy in individuals coinfected with HIV are similar to those in the population infected with HBV alone. Suppression of viral replication is the major goal. Ideally, the viral load should be reduced to an undetectable level, which will result in normalization of alanine aminotransferase (ALT) level, improved liver histology, reduced risk of progression to cirrhosis and liver failure (although supportive evidence from controlled clinical trials is lacking), and likely reduced incidence of hepatocellular carcinoma.
For those who are hepatitis B e antigen (HBeAg) positive, seroconversion may be a convenient end point for treatment, although for many patients seroconversion is not associated with remission of disease activity or viral replication.
Treatment decisions depend on whether or not the patient requires highly active antiretroviral therapy (HAART) for HIV infection. If HAART is indicated, then HIV agents that have HBV activity are incorporated into the regimen. If the patient does not yet require HAART for HIV but requires treatment for hepatitis B, this is itself an indication for HAART, since monotherapy for HBV is associated with the development of HIV resistance.
Viral load and ALT
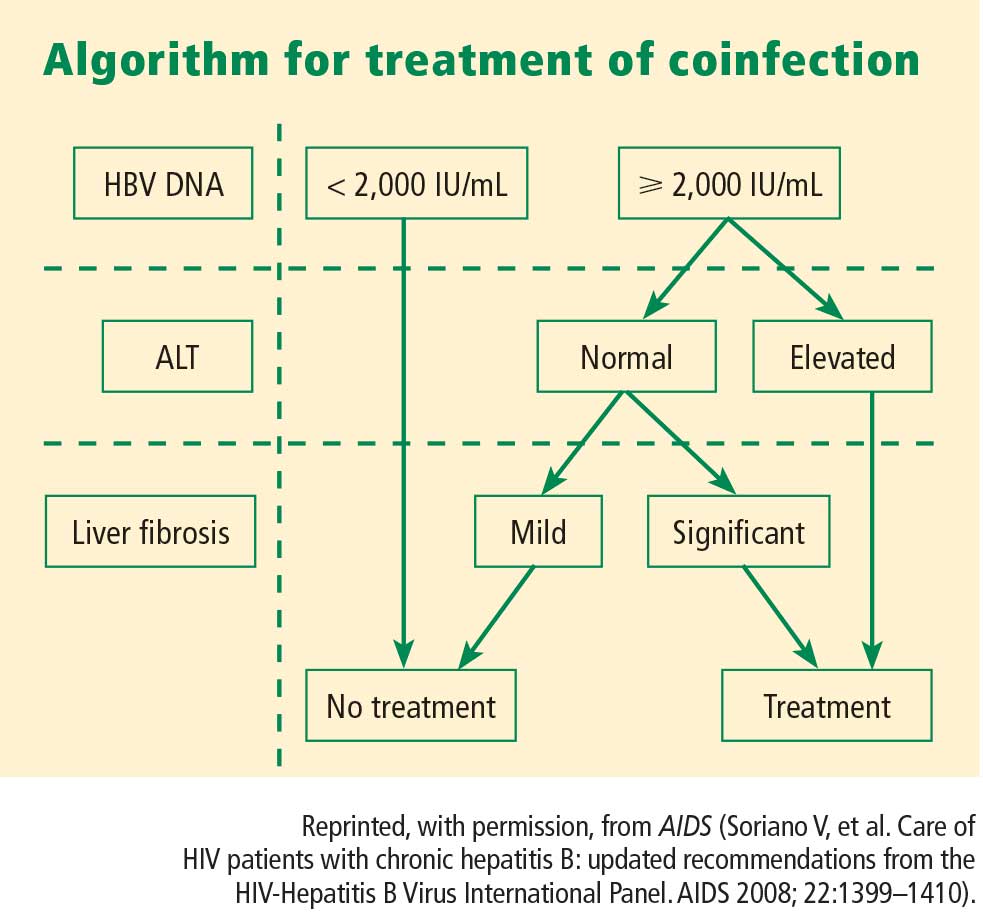
Liver biopsy
If the ALT is normal in the presence of a high HBV DNA level, a liver biopsy is recommended, partly because the ALT level is an inadequate indicator of the severity of liver disease. If significant fibrosis is present, treatment is recommended. No treatment is required if fibrosis is mild, but liver biopsies should be repeated every 3 to 5 years in this group because a hallmark of HBV infection is its variability in time to progression. The extent of fibrosis may influence the choice of therapy.
Often in the coinfected patient, HBV-related liver injury must be distinguished from other forms of liver injury. For instance, some of the drugs used to treat HIV infection can induce nonalcoholic fatty liver disease and lipodystrophy. Because the risk of advanced fibrosis is higher in the coinfected patient than in the patient infected only with HBV, the threshold for biopsy in the coinfected patient should be lower.
At present, noninvasive tools to assess the extent of liver injury have not been validated in chronic HBV infection, unlike in hepatitis C virus infection.
TREATMENT OPTIONS
The potential therapies for HBV in the coinfected patient are the same as those for the patient infected with HBV alone (see “Hepatitis B treatment: Current best practices, avoiding resistance”), with the addition of tenofovir and emtricitabine in combination.
Interferon
Early studies of interferon for the treatment of chronic HBV infection included many patients who were also HIV positive. These early studies revealed a lower rate of HBeAg seroconversion in HIV-positive patients compared with HIV-negative patients. Di Martino et al11 found that approximately half (26 of 50) of HIV-negative patients treated with interferon seroconverted at 6 years, compared with only 4 of 26 interferon-treated patients with chronic HBV who were coinfected with HIV. Based on results such as these, interferon therapy in the HBV/HIV-coinfected patient should be limited to patients who are likely to seroconvert: ie, those who are female and younger than 40 years with high ALT levels, low serum HBV DNA levels, and active liver histology (a subgroup that is more likely to undergo spontaneous seroconversion than other HBV-infected groups).
Standard or pegylated interferon is a treatment option for coinfected patients who do not yet require HAART, especially patients who have high ALT levels, low viral loads, and positive HBeAg status without liver decompensation.12
Nucleoside and nucleotide analogues
The nucleoside and nucleotide analogues used for HBV therapy have different degrees of effectiveness against HIV polymerase, but none can be used as monotherapy because of the risk of inducing HIV resistance. Lamivudine and tenofovir are used as part of the standard cocktail for the treatment of HIV (see “Case: HIV/HBV with resistance to tenofovir”). Entecavir is now recognized as a partial inhibitor of HIV replication. Both lamivudine and entecavir induce the YMDD mutation, an indication of resistance to therapy, in HIV polymerase. Tenofovir also may select for resistance mutations in HIV polymerase.
At dosages used for the treatment of HBV infection, adefovir has weak activity against HIV, and therefore HIV would not be under significant selective pressure to develop resistance mutations. In HIV polymerase, the mutations that confer resistance to adefovir also confer resistance to tenofovir, and therefore use of adefovir may induce tenofovir resistance.
Telbivudine has not been studied in HIV-infected patients, but its resistance profile is similar to that of lamivudine.
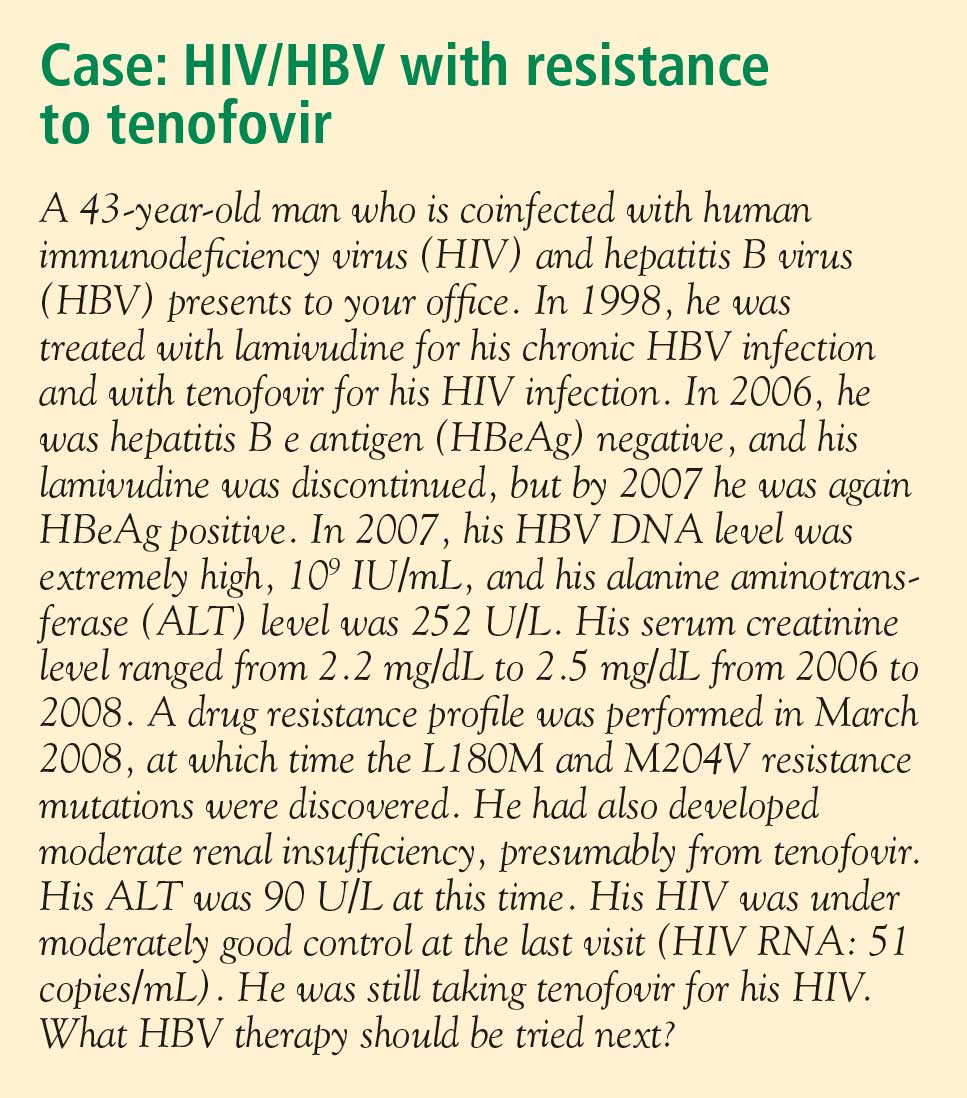
Treating both infections
When both HBV and HIV infections require treatment, HAART is necessary for HIV.12 The treatment strategy for coinfection is to use standard therapy for HIV, selecting two agents that are effective against HBV infection.
The need to avoid antiviral resistance complicates the selection of active agents. Resistance to HIV therapy limits the choices for treatment of HBV infection. The immediate aim of therapy, an undetectable level of HBV DNA, eliminates the use of less potent agents. The best choice for therapy is the most potent agent that can be used, such as tenofovir plus lamivudine or tenofovir plus emtricitabine.
Antiviral resistance
For the coinfected patient who develops resistance to lamivudine, the recommendation is to treat with tenofovir plus entecavir (the preferable choice because of absence of cross-reactivity between the two agents) or tenofovir plus lamivudine or emtricitabine. There is some evidence that lamivudine resistance predisposes to entecavir resistance, but the studies that generated these results were conducted in patients who had very high baseline viral loads13; the effectiveness of entecavir in patients with low baseline viral loads is unknown. Presumably, when entecavir is used in combination with another potent nucleoside analogue in coinfected patients, the sensitivity of HBV will be more durable than when entecavir is used as monotherapy.
Long-term monitoring
Long-term monitoring for the coinfected patient is similar to that for the patient infected with HBV only. HBV DNA levels should be monitored every 3 months for signs of resistance until levels have plateaued or become undetectable. Once the HBV DNA level is stable or undetectable, the monitoring interval can be extended. Ultrasonographic screening for hepatocellular carcinoma should be conducted every 6 months. Patients with cirrhosis should be screened for esophageal varices.
SUMMARY
HBV in the setting of HIV is more aggressive than in a patient infected with HBV only, and treatment must be comparably aggressive and carefully selected. The primary goal of HBV treatment in a coinfected patient is the same as in a patient with HBV infection only: reduction of viral load to undetectable levels. Treatment decisions are based on viral load, ALT level, findings on liver biopsy, the need for HAART, and the drug’s resistance profile. None of the nucleoside or nucleotide analogues can be used as monotherapy in the coinfected patient because of the risk of inducing resistance to HIV therapy. When the patient requires HAART, then the general recommendation is to select a combination of two drugs that have activity against HIV. If resistance develops, the preferred strategy is treatment with tenofovir plus entecavir. Monitoring includes measurement of HBV DNA levels every 3 months and ultrasonographic screening for hepatocellular carcinoma every 6 months.
- Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006; 44(suppl 1):S6–S9.
- Soriano V, Puoti M, Peters M, et al. Care of HIV patients with chronic hepatitis B: updated recommendations from the HIV-Hepatitis B Virus International Panel. AIDS 2008; 22:1399–1410.
- Núñez M, Soriano V. Management of patients co-infected with hepatitis B virus and HIV. Lancet Infect Dis 2005; 5:374–382.
- Modi AA, Feld JJ. Viral hepatitis and HIV in Africa. AIDS Rev 2007; 9:25–39.
- Hoffman CJ, Thio CL. Clinical implications of HIV and hepatitis B coinfection in Asia and Africa. Lancet Infect Dis 2007; 7:402–409.
- Puoti M, Torti C, Bruno R, Filice G, Carosi G. Natural history of chronic hepatitis B in co-infected patients. J Hepatol 2006; 44(suppl 1):S65–S70.
- Puoti M, Bruno R, Soriano V, et al. Hepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation and outcome. AIDS 2004; 18:2285–2293.
- Bräu N, Fox RK, Xiao P, et al. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: a US-Canadian multicenter study. J Hepatol 2007; 47:527–537.
- Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002; 360:1921–1926.
- Mocroft A, Soriano V, Rockstroh J, et al. Is there evidence for an increase in the death rate from liver-related disease in patients with HIV? AIDS 2005; 19:2117–2125.
- Di Martino V, Thevenot T, Colin J-F, et al. Influence of HIV infection on the response to interferon therapy and the long-term outcome of chronic hepatitis B. Gastroenterology 2002; 123:1812–1822.
- Iser DM, Sasadeusz JJ. Current treatment of HIV/hepatitis B virus coinfection. J Gastroenterol Hepatol 2008; 23:699–706.
- Sherman M, Yurdaydin C, Sollano J, et al; AI463026 BEHoLD Study Group. Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B. Gastroenterology 2006; 130:2039–2049.
Worldwide, 40 million people are infected with the human immunodeficiency virus (HIV). As many as 4 million of them are coinfected with hepatitis B virus (HBV).1 In North America and Europe, the highest prevalence of HBV/HIV coinfection is in men who have sex with men. Approximately half of HIV-positive men who have sex with men have evidence of prior or active HBV infection, and 5% to 10% have chronic HBV infection. Among those who acquire HIV through injected drug use or through heterosexual transmission, the coinfection rate is much lower.2,3
Coinfection with HBV and HIV follows a different course elsewhere in the world. For example, in Africa and Asia, HBV is usually acquired first through neonatal or childhood infection, with either vertical or horizontal transmission after birth.4,5 In parts of Africa, ritual scarification is likely a major player in the adolescent transmission of HBV. (Ritual scarification is the practice of creating small incisions in the skin of adolescents and rubbing black ash in the wounds to form scars; the cutting instruments are not sterilized between rituals.)
NATURAL HISTORY
In general, HBV tends to be more aggressive in HIV-positive individuals than in monoinfected individuals,2,6 with higher HBV carrier rates, higher levels of HBV viremia, more frequent episodes of activation, and faster progression to cirrhosis.
Hepatocellular carcinoma occurs more often, its onset is earlier, and its course is more aggressive in coinfected individuals than in monoinfected individuals.7,8 Using data from a prospective cohort study, Thio et al9 found that among men coinfected with HIV and HBV, liver-related mortality was almost 19 times greater compared with men infected with HBV only and more than seven times greater compared with those infected with HIV only.
In an observational longitudinal cohort study,10 the risk of death from liver disease in HIV-positive persons was nearly three times greater among those also infected with HBV (P < .0001).
ASSESSING WHEN TO TREAT
The objectives of HBV therapy in individuals coinfected with HIV are similar to those in the population infected with HBV alone. Suppression of viral replication is the major goal. Ideally, the viral load should be reduced to an undetectable level, which will result in normalization of alanine aminotransferase (ALT) level, improved liver histology, reduced risk of progression to cirrhosis and liver failure (although supportive evidence from controlled clinical trials is lacking), and likely reduced incidence of hepatocellular carcinoma.
For those who are hepatitis B e antigen (HBeAg) positive, seroconversion may be a convenient end point for treatment, although for many patients seroconversion is not associated with remission of disease activity or viral replication.
Treatment decisions depend on whether or not the patient requires highly active antiretroviral therapy (HAART) for HIV infection. If HAART is indicated, then HIV agents that have HBV activity are incorporated into the regimen. If the patient does not yet require HAART for HIV but requires treatment for hepatitis B, this is itself an indication for HAART, since monotherapy for HBV is associated with the development of HIV resistance.
Viral load and ALT
Liver biopsy
If the ALT is normal in the presence of a high HBV DNA level, a liver biopsy is recommended, partly because the ALT level is an inadequate indicator of the severity of liver disease. If significant fibrosis is present, treatment is recommended. No treatment is required if fibrosis is mild, but liver biopsies should be repeated every 3 to 5 years in this group because a hallmark of HBV infection is its variability in time to progression. The extent of fibrosis may influence the choice of therapy.
Often in the coinfected patient, HBV-related liver injury must be distinguished from other forms of liver injury. For instance, some of the drugs used to treat HIV infection can induce nonalcoholic fatty liver disease and lipodystrophy. Because the risk of advanced fibrosis is higher in the coinfected patient than in the patient infected only with HBV, the threshold for biopsy in the coinfected patient should be lower.
At present, noninvasive tools to assess the extent of liver injury have not been validated in chronic HBV infection, unlike in hepatitis C virus infection.
TREATMENT OPTIONS
The potential therapies for HBV in the coinfected patient are the same as those for the patient infected with HBV alone (see “Hepatitis B treatment: Current best practices, avoiding resistance”), with the addition of tenofovir and emtricitabine in combination.
Interferon
Early studies of interferon for the treatment of chronic HBV infection included many patients who were also HIV positive. These early studies revealed a lower rate of HBeAg seroconversion in HIV-positive patients compared with HIV-negative patients. Di Martino et al11 found that approximately half (26 of 50) of HIV-negative patients treated with interferon seroconverted at 6 years, compared with only 4 of 26 interferon-treated patients with chronic HBV who were coinfected with HIV. Based on results such as these, interferon therapy in the HBV/HIV-coinfected patient should be limited to patients who are likely to seroconvert: ie, those who are female and younger than 40 years with high ALT levels, low serum HBV DNA levels, and active liver histology (a subgroup that is more likely to undergo spontaneous seroconversion than other HBV-infected groups).
Standard or pegylated interferon is a treatment option for coinfected patients who do not yet require HAART, especially patients who have high ALT levels, low viral loads, and positive HBeAg status without liver decompensation.12
Nucleoside and nucleotide analogues
The nucleoside and nucleotide analogues used for HBV therapy have different degrees of effectiveness against HIV polymerase, but none can be used as monotherapy because of the risk of inducing HIV resistance. Lamivudine and tenofovir are used as part of the standard cocktail for the treatment of HIV (see “Case: HIV/HBV with resistance to tenofovir”). Entecavir is now recognized as a partial inhibitor of HIV replication. Both lamivudine and entecavir induce the YMDD mutation, an indication of resistance to therapy, in HIV polymerase. Tenofovir also may select for resistance mutations in HIV polymerase.
At dosages used for the treatment of HBV infection, adefovir has weak activity against HIV, and therefore HIV would not be under significant selective pressure to develop resistance mutations. In HIV polymerase, the mutations that confer resistance to adefovir also confer resistance to tenofovir, and therefore use of adefovir may induce tenofovir resistance.
Telbivudine has not been studied in HIV-infected patients, but its resistance profile is similar to that of lamivudine.
Treating both infections
When both HBV and HIV infections require treatment, HAART is necessary for HIV.12 The treatment strategy for coinfection is to use standard therapy for HIV, selecting two agents that are effective against HBV infection.
The need to avoid antiviral resistance complicates the selection of active agents. Resistance to HIV therapy limits the choices for treatment of HBV infection. The immediate aim of therapy, an undetectable level of HBV DNA, eliminates the use of less potent agents. The best choice for therapy is the most potent agent that can be used, such as tenofovir plus lamivudine or tenofovir plus emtricitabine.
Antiviral resistance
For the coinfected patient who develops resistance to lamivudine, the recommendation is to treat with tenofovir plus entecavir (the preferable choice because of absence of cross-reactivity between the two agents) or tenofovir plus lamivudine or emtricitabine. There is some evidence that lamivudine resistance predisposes to entecavir resistance, but the studies that generated these results were conducted in patients who had very high baseline viral loads13; the effectiveness of entecavir in patients with low baseline viral loads is unknown. Presumably, when entecavir is used in combination with another potent nucleoside analogue in coinfected patients, the sensitivity of HBV will be more durable than when entecavir is used as monotherapy.
Long-term monitoring
Long-term monitoring for the coinfected patient is similar to that for the patient infected with HBV only. HBV DNA levels should be monitored every 3 months for signs of resistance until levels have plateaued or become undetectable. Once the HBV DNA level is stable or undetectable, the monitoring interval can be extended. Ultrasonographic screening for hepatocellular carcinoma should be conducted every 6 months. Patients with cirrhosis should be screened for esophageal varices.
SUMMARY
HBV in the setting of HIV is more aggressive than in a patient infected with HBV only, and treatment must be comparably aggressive and carefully selected. The primary goal of HBV treatment in a coinfected patient is the same as in a patient with HBV infection only: reduction of viral load to undetectable levels. Treatment decisions are based on viral load, ALT level, findings on liver biopsy, the need for HAART, and the drug’s resistance profile. None of the nucleoside or nucleotide analogues can be used as monotherapy in the coinfected patient because of the risk of inducing resistance to HIV therapy. When the patient requires HAART, then the general recommendation is to select a combination of two drugs that have activity against HIV. If resistance develops, the preferred strategy is treatment with tenofovir plus entecavir. Monitoring includes measurement of HBV DNA levels every 3 months and ultrasonographic screening for hepatocellular carcinoma every 6 months.
Worldwide, 40 million people are infected with the human immunodeficiency virus (HIV). As many as 4 million of them are coinfected with hepatitis B virus (HBV).1 In North America and Europe, the highest prevalence of HBV/HIV coinfection is in men who have sex with men. Approximately half of HIV-positive men who have sex with men have evidence of prior or active HBV infection, and 5% to 10% have chronic HBV infection. Among those who acquire HIV through injected drug use or through heterosexual transmission, the coinfection rate is much lower.2,3
Coinfection with HBV and HIV follows a different course elsewhere in the world. For example, in Africa and Asia, HBV is usually acquired first through neonatal or childhood infection, with either vertical or horizontal transmission after birth.4,5 In parts of Africa, ritual scarification is likely a major player in the adolescent transmission of HBV. (Ritual scarification is the practice of creating small incisions in the skin of adolescents and rubbing black ash in the wounds to form scars; the cutting instruments are not sterilized between rituals.)
NATURAL HISTORY
In general, HBV tends to be more aggressive in HIV-positive individuals than in monoinfected individuals,2,6 with higher HBV carrier rates, higher levels of HBV viremia, more frequent episodes of activation, and faster progression to cirrhosis.
Hepatocellular carcinoma occurs more often, its onset is earlier, and its course is more aggressive in coinfected individuals than in monoinfected individuals.7,8 Using data from a prospective cohort study, Thio et al9 found that among men coinfected with HIV and HBV, liver-related mortality was almost 19 times greater compared with men infected with HBV only and more than seven times greater compared with those infected with HIV only.
In an observational longitudinal cohort study,10 the risk of death from liver disease in HIV-positive persons was nearly three times greater among those also infected with HBV (P < .0001).
ASSESSING WHEN TO TREAT
The objectives of HBV therapy in individuals coinfected with HIV are similar to those in the population infected with HBV alone. Suppression of viral replication is the major goal. Ideally, the viral load should be reduced to an undetectable level, which will result in normalization of alanine aminotransferase (ALT) level, improved liver histology, reduced risk of progression to cirrhosis and liver failure (although supportive evidence from controlled clinical trials is lacking), and likely reduced incidence of hepatocellular carcinoma.
For those who are hepatitis B e antigen (HBeAg) positive, seroconversion may be a convenient end point for treatment, although for many patients seroconversion is not associated with remission of disease activity or viral replication.
Treatment decisions depend on whether or not the patient requires highly active antiretroviral therapy (HAART) for HIV infection. If HAART is indicated, then HIV agents that have HBV activity are incorporated into the regimen. If the patient does not yet require HAART for HIV but requires treatment for hepatitis B, this is itself an indication for HAART, since monotherapy for HBV is associated with the development of HIV resistance.
Viral load and ALT
Liver biopsy
If the ALT is normal in the presence of a high HBV DNA level, a liver biopsy is recommended, partly because the ALT level is an inadequate indicator of the severity of liver disease. If significant fibrosis is present, treatment is recommended. No treatment is required if fibrosis is mild, but liver biopsies should be repeated every 3 to 5 years in this group because a hallmark of HBV infection is its variability in time to progression. The extent of fibrosis may influence the choice of therapy.
Often in the coinfected patient, HBV-related liver injury must be distinguished from other forms of liver injury. For instance, some of the drugs used to treat HIV infection can induce nonalcoholic fatty liver disease and lipodystrophy. Because the risk of advanced fibrosis is higher in the coinfected patient than in the patient infected only with HBV, the threshold for biopsy in the coinfected patient should be lower.
At present, noninvasive tools to assess the extent of liver injury have not been validated in chronic HBV infection, unlike in hepatitis C virus infection.
TREATMENT OPTIONS
The potential therapies for HBV in the coinfected patient are the same as those for the patient infected with HBV alone (see “Hepatitis B treatment: Current best practices, avoiding resistance”), with the addition of tenofovir and emtricitabine in combination.
Interferon
Early studies of interferon for the treatment of chronic HBV infection included many patients who were also HIV positive. These early studies revealed a lower rate of HBeAg seroconversion in HIV-positive patients compared with HIV-negative patients. Di Martino et al11 found that approximately half (26 of 50) of HIV-negative patients treated with interferon seroconverted at 6 years, compared with only 4 of 26 interferon-treated patients with chronic HBV who were coinfected with HIV. Based on results such as these, interferon therapy in the HBV/HIV-coinfected patient should be limited to patients who are likely to seroconvert: ie, those who are female and younger than 40 years with high ALT levels, low serum HBV DNA levels, and active liver histology (a subgroup that is more likely to undergo spontaneous seroconversion than other HBV-infected groups).
Standard or pegylated interferon is a treatment option for coinfected patients who do not yet require HAART, especially patients who have high ALT levels, low viral loads, and positive HBeAg status without liver decompensation.12
Nucleoside and nucleotide analogues
The nucleoside and nucleotide analogues used for HBV therapy have different degrees of effectiveness against HIV polymerase, but none can be used as monotherapy because of the risk of inducing HIV resistance. Lamivudine and tenofovir are used as part of the standard cocktail for the treatment of HIV (see “Case: HIV/HBV with resistance to tenofovir”). Entecavir is now recognized as a partial inhibitor of HIV replication. Both lamivudine and entecavir induce the YMDD mutation, an indication of resistance to therapy, in HIV polymerase. Tenofovir also may select for resistance mutations in HIV polymerase.
At dosages used for the treatment of HBV infection, adefovir has weak activity against HIV, and therefore HIV would not be under significant selective pressure to develop resistance mutations. In HIV polymerase, the mutations that confer resistance to adefovir also confer resistance to tenofovir, and therefore use of adefovir may induce tenofovir resistance.
Telbivudine has not been studied in HIV-infected patients, but its resistance profile is similar to that of lamivudine.
Treating both infections
When both HBV and HIV infections require treatment, HAART is necessary for HIV.12 The treatment strategy for coinfection is to use standard therapy for HIV, selecting two agents that are effective against HBV infection.
The need to avoid antiviral resistance complicates the selection of active agents. Resistance to HIV therapy limits the choices for treatment of HBV infection. The immediate aim of therapy, an undetectable level of HBV DNA, eliminates the use of less potent agents. The best choice for therapy is the most potent agent that can be used, such as tenofovir plus lamivudine or tenofovir plus emtricitabine.
Antiviral resistance
For the coinfected patient who develops resistance to lamivudine, the recommendation is to treat with tenofovir plus entecavir (the preferable choice because of absence of cross-reactivity between the two agents) or tenofovir plus lamivudine or emtricitabine. There is some evidence that lamivudine resistance predisposes to entecavir resistance, but the studies that generated these results were conducted in patients who had very high baseline viral loads13; the effectiveness of entecavir in patients with low baseline viral loads is unknown. Presumably, when entecavir is used in combination with another potent nucleoside analogue in coinfected patients, the sensitivity of HBV will be more durable than when entecavir is used as monotherapy.
Long-term monitoring
Long-term monitoring for the coinfected patient is similar to that for the patient infected with HBV only. HBV DNA levels should be monitored every 3 months for signs of resistance until levels have plateaued or become undetectable. Once the HBV DNA level is stable or undetectable, the monitoring interval can be extended. Ultrasonographic screening for hepatocellular carcinoma should be conducted every 6 months. Patients with cirrhosis should be screened for esophageal varices.
SUMMARY
HBV in the setting of HIV is more aggressive than in a patient infected with HBV only, and treatment must be comparably aggressive and carefully selected. The primary goal of HBV treatment in a coinfected patient is the same as in a patient with HBV infection only: reduction of viral load to undetectable levels. Treatment decisions are based on viral load, ALT level, findings on liver biopsy, the need for HAART, and the drug’s resistance profile. None of the nucleoside or nucleotide analogues can be used as monotherapy in the coinfected patient because of the risk of inducing resistance to HIV therapy. When the patient requires HAART, then the general recommendation is to select a combination of two drugs that have activity against HIV. If resistance develops, the preferred strategy is treatment with tenofovir plus entecavir. Monitoring includes measurement of HBV DNA levels every 3 months and ultrasonographic screening for hepatocellular carcinoma every 6 months.
- Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006; 44(suppl 1):S6–S9.
- Soriano V, Puoti M, Peters M, et al. Care of HIV patients with chronic hepatitis B: updated recommendations from the HIV-Hepatitis B Virus International Panel. AIDS 2008; 22:1399–1410.
- Núñez M, Soriano V. Management of patients co-infected with hepatitis B virus and HIV. Lancet Infect Dis 2005; 5:374–382.
- Modi AA, Feld JJ. Viral hepatitis and HIV in Africa. AIDS Rev 2007; 9:25–39.
- Hoffman CJ, Thio CL. Clinical implications of HIV and hepatitis B coinfection in Asia and Africa. Lancet Infect Dis 2007; 7:402–409.
- Puoti M, Torti C, Bruno R, Filice G, Carosi G. Natural history of chronic hepatitis B in co-infected patients. J Hepatol 2006; 44(suppl 1):S65–S70.
- Puoti M, Bruno R, Soriano V, et al. Hepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation and outcome. AIDS 2004; 18:2285–2293.
- Bräu N, Fox RK, Xiao P, et al. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: a US-Canadian multicenter study. J Hepatol 2007; 47:527–537.
- Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002; 360:1921–1926.
- Mocroft A, Soriano V, Rockstroh J, et al. Is there evidence for an increase in the death rate from liver-related disease in patients with HIV? AIDS 2005; 19:2117–2125.
- Di Martino V, Thevenot T, Colin J-F, et al. Influence of HIV infection on the response to interferon therapy and the long-term outcome of chronic hepatitis B. Gastroenterology 2002; 123:1812–1822.
- Iser DM, Sasadeusz JJ. Current treatment of HIV/hepatitis B virus coinfection. J Gastroenterol Hepatol 2008; 23:699–706.
- Sherman M, Yurdaydin C, Sollano J, et al; AI463026 BEHoLD Study Group. Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B. Gastroenterology 2006; 130:2039–2049.
- Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006; 44(suppl 1):S6–S9.
- Soriano V, Puoti M, Peters M, et al. Care of HIV patients with chronic hepatitis B: updated recommendations from the HIV-Hepatitis B Virus International Panel. AIDS 2008; 22:1399–1410.
- Núñez M, Soriano V. Management of patients co-infected with hepatitis B virus and HIV. Lancet Infect Dis 2005; 5:374–382.
- Modi AA, Feld JJ. Viral hepatitis and HIV in Africa. AIDS Rev 2007; 9:25–39.
- Hoffman CJ, Thio CL. Clinical implications of HIV and hepatitis B coinfection in Asia and Africa. Lancet Infect Dis 2007; 7:402–409.
- Puoti M, Torti C, Bruno R, Filice G, Carosi G. Natural history of chronic hepatitis B in co-infected patients. J Hepatol 2006; 44(suppl 1):S65–S70.
- Puoti M, Bruno R, Soriano V, et al. Hepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation and outcome. AIDS 2004; 18:2285–2293.
- Bräu N, Fox RK, Xiao P, et al. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: a US-Canadian multicenter study. J Hepatol 2007; 47:527–537.
- Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002; 360:1921–1926.
- Mocroft A, Soriano V, Rockstroh J, et al. Is there evidence for an increase in the death rate from liver-related disease in patients with HIV? AIDS 2005; 19:2117–2125.
- Di Martino V, Thevenot T, Colin J-F, et al. Influence of HIV infection on the response to interferon therapy and the long-term outcome of chronic hepatitis B. Gastroenterology 2002; 123:1812–1822.
- Iser DM, Sasadeusz JJ. Current treatment of HIV/hepatitis B virus coinfection. J Gastroenterol Hepatol 2008; 23:699–706.
- Sherman M, Yurdaydin C, Sollano J, et al; AI463026 BEHoLD Study Group. Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B. Gastroenterology 2006; 130:2039–2049.
KEY POINTS
- Patients with HBV/HIV coinfection are at relatively high risk of frequent HBV activation, progression to cirrhosis, and death from liver-related causes.
- If the patient does not yet require HAART but requires treatment for HBV, this is itself an indication for HAART, since monotherapy for HBV is associated with development of resistance to HIV therapy.
- Nucleoside and nucleotide analogues should not be used as monotherapy in the HBV/HIV-coinfected patient because of the risk of inducing HIV resistance.
Salary One Part of the Compensation Package
Salary One Part of the Compensation Package
I am a senior medical resident who intends to start a new job as a hospitalist later this year. I have been interviewing and feel fortunate to have several offers of employment. Is there anything I should be looking for in employment contracts?
M. Berkowitz, DO, Manchester, N.H.

Dr. Hospitalist responds:
Congratulations on your graduation, and welcome to the rest of your career. I have worked in HM for more than a decade. You have made a wonderful career choice; there is no better time to be a hospitalist.
Selecting the right job is important. I recognize it’s not easy to determine the best employer for you. All too often, I hear about physicians taking a job because the employer offered the highest salary. Money is important, but it’s not the only variable you should consider when sorting out offers. I have no formal training in human resources or employment law, but I have been hiring physicians for more than a decade, and I believe there are very important elements of compensation in any job offer aside from salary. For example, benefit packages and benefits costs to the employee and employer vary from job to job. Some employee benefits cost the HM group 25% of salary. Compare a job offer with paid benefits to a job offer with a similar salary and no paid benefits. When you do the math, you’ll understand why salary isn’t the only variable you should consider.
Take time to understand retirement plan offerings, including the short- and long-term implications. Some employers offer pension plans; most offer access to 401(k) or 403(b) plans. Some employers match employee contributions, while others do not. Over the long term, match programs offer a huge investment advantage. However, it is important to know the terms of the plan—namely, the vesting period. The vesting period is the number of months or years an individual must be employed to qualify for matching contributions. Ideally, you want a retirement plan that vests immediately.
Another important benefit is malpractice insurance. Do not assume that your employer will provide malpractice insurance at no additional cost to you. Do not assume that all malpractice insurance policies are the same. Most policies provide a monetary amount of coverage for each incident with an annual aggregate limit. For example, a 1/3 policy covers up to $1 million per incident and up to $3 million in annual aggregate. Higher amounts of coverage will offer greater protection against high-dollar verdicts but might make the insured an attractive candidate for litigation in the eyes of some plaintiffs.
Most hospitals require that physicians carry a medical malpractice policy with a minimum amount of coverage before they grant privileges. Some policies, such as occurrence policies, provide coverage for incidents that occur during your period of employment, even if you leave your job.
Claims-made medical malpractice policies typically are less expensive, but they will not provide coverage after you leave an employer unless the policy includes “tail coverage.” If you have a claims-made policy, I urge you to consider purchasing tail coverage. The take-home message is that medical malpractice insurance should be figured into your employment decision.
Also consider whether prospective employers offer signing bonuses; reimbursement for continuing medical education; and health, life, disability, and accidental death and dismemberment insurance coverage for you and your family. I suggest you examine the language of each individual insurance policy to understand what coverage is offered.
Perhaps the most important piece of advice I have for you is to retain the services of a healthcare attorney. Make sure this person is familiar with physician employment agreements in the state where you plan to work. TH
Salary One Part of the Compensation Package
I am a senior medical resident who intends to start a new job as a hospitalist later this year. I have been interviewing and feel fortunate to have several offers of employment. Is there anything I should be looking for in employment contracts?
M. Berkowitz, DO, Manchester, N.H.
Dr. Hospitalist responds:
Congratulations on your graduation, and welcome to the rest of your career. I have worked in HM for more than a decade. You have made a wonderful career choice; there is no better time to be a hospitalist.
Selecting the right job is important. I recognize it’s not easy to determine the best employer for you. All too often, I hear about physicians taking a job because the employer offered the highest salary. Money is important, but it’s not the only variable you should consider when sorting out offers. I have no formal training in human resources or employment law, but I have been hiring physicians for more than a decade, and I believe there are very important elements of compensation in any job offer aside from salary. For example, benefit packages and benefits costs to the employee and employer vary from job to job. Some employee benefits cost the HM group 25% of salary. Compare a job offer with paid benefits to a job offer with a similar salary and no paid benefits. When you do the math, you’ll understand why salary isn’t the only variable you should consider.
Take time to understand retirement plan offerings, including the short- and long-term implications. Some employers offer pension plans; most offer access to 401(k) or 403(b) plans. Some employers match employee contributions, while others do not. Over the long term, match programs offer a huge investment advantage. However, it is important to know the terms of the plan—namely, the vesting period. The vesting period is the number of months or years an individual must be employed to qualify for matching contributions. Ideally, you want a retirement plan that vests immediately.
Another important benefit is malpractice insurance. Do not assume that your employer will provide malpractice insurance at no additional cost to you. Do not assume that all malpractice insurance policies are the same. Most policies provide a monetary amount of coverage for each incident with an annual aggregate limit. For example, a 1/3 policy covers up to $1 million per incident and up to $3 million in annual aggregate. Higher amounts of coverage will offer greater protection against high-dollar verdicts but might make the insured an attractive candidate for litigation in the eyes of some plaintiffs.
Most hospitals require that physicians carry a medical malpractice policy with a minimum amount of coverage before they grant privileges. Some policies, such as occurrence policies, provide coverage for incidents that occur during your period of employment, even if you leave your job.
Claims-made medical malpractice policies typically are less expensive, but they will not provide coverage after you leave an employer unless the policy includes “tail coverage.” If you have a claims-made policy, I urge you to consider purchasing tail coverage. The take-home message is that medical malpractice insurance should be figured into your employment decision.
Also consider whether prospective employers offer signing bonuses; reimbursement for continuing medical education; and health, life, disability, and accidental death and dismemberment insurance coverage for you and your family. I suggest you examine the language of each individual insurance policy to understand what coverage is offered.
Perhaps the most important piece of advice I have for you is to retain the services of a healthcare attorney. Make sure this person is familiar with physician employment agreements in the state where you plan to work. TH
Salary One Part of the Compensation Package
I am a senior medical resident who intends to start a new job as a hospitalist later this year. I have been interviewing and feel fortunate to have several offers of employment. Is there anything I should be looking for in employment contracts?
M. Berkowitz, DO, Manchester, N.H.
Dr. Hospitalist responds:
Congratulations on your graduation, and welcome to the rest of your career. I have worked in HM for more than a decade. You have made a wonderful career choice; there is no better time to be a hospitalist.
Selecting the right job is important. I recognize it’s not easy to determine the best employer for you. All too often, I hear about physicians taking a job because the employer offered the highest salary. Money is important, but it’s not the only variable you should consider when sorting out offers. I have no formal training in human resources or employment law, but I have been hiring physicians for more than a decade, and I believe there are very important elements of compensation in any job offer aside from salary. For example, benefit packages and benefits costs to the employee and employer vary from job to job. Some employee benefits cost the HM group 25% of salary. Compare a job offer with paid benefits to a job offer with a similar salary and no paid benefits. When you do the math, you’ll understand why salary isn’t the only variable you should consider.
Take time to understand retirement plan offerings, including the short- and long-term implications. Some employers offer pension plans; most offer access to 401(k) or 403(b) plans. Some employers match employee contributions, while others do not. Over the long term, match programs offer a huge investment advantage. However, it is important to know the terms of the plan—namely, the vesting period. The vesting period is the number of months or years an individual must be employed to qualify for matching contributions. Ideally, you want a retirement plan that vests immediately.
Another important benefit is malpractice insurance. Do not assume that your employer will provide malpractice insurance at no additional cost to you. Do not assume that all malpractice insurance policies are the same. Most policies provide a monetary amount of coverage for each incident with an annual aggregate limit. For example, a 1/3 policy covers up to $1 million per incident and up to $3 million in annual aggregate. Higher amounts of coverage will offer greater protection against high-dollar verdicts but might make the insured an attractive candidate for litigation in the eyes of some plaintiffs.
Most hospitals require that physicians carry a medical malpractice policy with a minimum amount of coverage before they grant privileges. Some policies, such as occurrence policies, provide coverage for incidents that occur during your period of employment, even if you leave your job.
Claims-made medical malpractice policies typically are less expensive, but they will not provide coverage after you leave an employer unless the policy includes “tail coverage.” If you have a claims-made policy, I urge you to consider purchasing tail coverage. The take-home message is that medical malpractice insurance should be figured into your employment decision.
Also consider whether prospective employers offer signing bonuses; reimbursement for continuing medical education; and health, life, disability, and accidental death and dismemberment insurance coverage for you and your family. I suggest you examine the language of each individual insurance policy to understand what coverage is offered.
Perhaps the most important piece of advice I have for you is to retain the services of a healthcare attorney. Make sure this person is familiar with physician employment agreements in the state where you plan to work. TH
Under Pressure
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
Hospitalist Stephanie Jackson, MD, medical director of patient safety at Sacred Heart Medical Center in Eugene, Ore., was preparing for SHM’s meeting with lawmakers in Washington, D.C., in March. As a member of SHM’s Public Policy Committee, she knew the annual powwow with Congressional leaders would be particularly sensitive this year as the economy continues to crater, healthcare reform hangs in political purgatory, and HM advocates look to insulate the industry from growing pressures.
But while she was prepping to tackle national issues, Dr. Jackson was dealing with serious problems closer to home. Her own hospital administrators were preparing to slash the safety initiatives she was championing, including an ambitious new bar-coding system to reduce medication errors and a long-planned information technology upgrade, from the budget. Hospital executives held emergency financial meetings two weeks running. At the time, Sacred Heart had less than 70 days’ cash on hand, compared with its usual 350-day buffer. In essence, the threat to her HM program had sprouted up so severely and quickly that Dr. Jackson was too busy batting them down to travel 3,000 miles to talk about the issues.
“It’s hard to leave when your organization is not doing well,” she says. “You need to be home. Our whole mission is to provide safe, high-quality, compassionate patient care. When budget cuts are made, it will affect patient care. There’s absolutely no way it can’t.”
It’s the new HM paradigm: a landscape in which hospitalists confront a growing confluence of threats to their livelihood. The pressures are rooted in the economic downturn, as hospitals nationwide face sagging revenues and daily fights to raise capital as investors lower their investment ratings. Questions abound:
- Will more primary-care physicians (PCPs) return to hospitals to supplement their practices, siphoning encounters from HM groups?
- Will an infusion of government money into community health centers draw patients away from hospital stays?
- Will HM’s workforce expansion continue as hospitals close or lose the ability to pay competitive subsidies? Even the Federal Reserve, in its latest Beige Book survey, reported falling patient volumes for elective procedures and an increase in emergency services.
- Will the very real fears of physician overload and burnout—and the possible departure of qualified hospitalists for other specialties or careers—grow as institutions cut ancillary medical staff and put more duties on the HM checklist?
The threats are real, of course, but HM advocates and practitioners say that, for now, they remain just that. HM groups continue to grow, and HM job postings are plenty. To date, hospital administrators have been mostly loathe to lay off the staffers they count on to lower costs through patient safety initiatives, reduced length of stay, and faster throughput. The most optimistic of hospitalists view the threats as opportunities to further establish themselves as thought leaders who can prove their worth through quantifiable metrics. Still, hospitals are increasingly in dire straits, and that means hospitalists could be in the same situation.
“The dilemma is that hospitalists are tied to the hospital as an institution,” says Larry Wellikson, MD, CEO of SHM. “It doesn’t really matter what causes the hospital to have less discretionary capital. … These things play against the hospitalist.”
Beyond Staff Cuts
Dr. Jackson’s case is typical. Her institution—a two-hospital center with 510 combined beds—recently eliminated 70 positions. None were physicians, but several care-management jobs were lost. Add in a local unemployment rate of almost 12%, and it’s no surprise the hospital is buckling under the weight of uncompensated charity care. And even though Sacred Heart lists patient safety initiatives as a top priority, “it always comes up that it can be cut,” Dr. Jackson says.
The bar-coding initiative was put on hold until the end of 2010, despite the hospital’s purchase of a packager that separates medications into individual packets. Dr. Jackson thinks the new technology could cut medication errors by at least 25%. Updates in information technology have been put on hold. And even if President Obama’s stimulus plan supplies money for electronic medical records (EMR), much of that money might not make it to the hospital-floor level for another 12 to 18 months.
Budget cuts aren’t relegated to large-scale initiatives, either. “Positions have been frozen, perks disappearing,” Dr. Jackson says. “At medical staff meetings, food is getting sparse. Educational opportunities that would have been there before, they’re not going to pay for that. My money to go to [HM09] is frozen right now.”
Stay the Course
Greg Maynard, MD, MS, clinical professor of medicine and chief of the division of hospital medicine at the University of California at San Diego Medical Center, also identifies the threats to HM in personal terms. Cutbacks on spending are hard to avoid in tough economic times, he reasons, but the key for hospitalists is to not allow those discussions to affect the interpersonal relationships between HM groups and hospital executives. He also echoes the sentiments of burnout fears and morale issues. In the past year, his 24-member HM group has added primary coverage of the adult oncology unit and adult cystic fibrosis patients, among other responsibilities. It also started night coverage shifts. All the while, Dr. Maynard and his staff have heard UC San Diego is having financial issues, including troubles with its pension investments. Budget discussions are more strained because of the overall economic crisis, which makes professional relationships even more important to maintain, he says.
—Greg Maynard, MD, chief, hospital medicine division, UC San Diego Medical Center
“You have to empathize with the medical center administrators as they struggle,” he adds. “I think there’s a threat of a dialogue. When pressure comes on, debates can become contentious. It’s important to avoid that.”
Dr. Maynard blames some of the current friction between hospitals and hospitalists on HM’s growth—estimated at 28,000 physicians and still growing—and the lagging increases in Medicare, Medicaid, and private insurer reimbursement. A new reimbursement system is at the top of Obama’s agenda for national healthcare reform; however, the economy has slowed the advance of those initiatives. Obama has set aside roughly $20 billion in stimulus funding to encourage EMR programs.
Other plans are likely to gain momentum in coming months, with the expected confirmation of Kansas Gov. Kathleen Sebelius as secretary of the U.S. Department of Health and Human Services.
“You can’t grow and grow, and not grow the amount of money needed,” Dr. Maynard says.
Return of the PCP
Another oft-discussed threat to the HM model is the potential return of primary-care physicians (PCPs) to the hospital. PCPs pulling back to focus on their private outpatient practices helped birth the HM movement. Many of the nation’s uninsured forego primary care and instead seek care in the ED, which often leads to hospital admission and HM care. If PCPs return to the hospital, it could mean a decrease in hospitalist patient census.
The plight of the unemployed, which has ballooned to more than 500,000 per month since December 2008, is another consideration. Will PCPs need to fill an encounter gap when millions of American families lose their employee-funded medical benefits? And what about the billions being set aside to open new community health centers, which theoretically would siphon potential PCP patients—and revenue? Will these centers push PCPs to resume caring for hospitalized patients?
“The only threat to HM is if we had major healthcare reform that included comprehensiveness, that included something to make it worthwhile for the PCPs to take care of their patients in the hospital,” says Robert M. Centor, MD, FACP, associate dean and director of the division of general internal medicine at Huntsville Regional Medical Campus in Alabama. “For more and more family physicians … it doesn’t make financial sense to travel to the hospital.”
Gene “Rusty” Kallenberg, MD, chief of family medicine at UC San Diego’s School of Medicine, points out PCPs can hurt hospitalists without returning to the hospital. More patients treated in primary care means fewer patients whom hospitalists can charge. Should Obama extend healthcare coverage to the estimated 47 million uninsured people in the U.S., patients once treated in the ED and admitted through HM programs likely would seek primary care before heading to the hospital, further limiting billing opportunities for HM groups. The irony, Dr. Kallenberg says, is that what is best for the patient isn’t necessarily best for the industry—HM included—that treats them.
“If you reward PCPs for doing what’s right, then somebody has to pay for it,” he says. “The specialists are going to pay for it. If what happens is epidemiologically fine, that we lower the census … where is the money coming from?”
For the well-positioned HM group, the money will come from the savings it can prove to hospital administrators, says Dr. Centor, a nationally recognized voice in the debate on the value of hospitalists. He and Dr. Wellikson agree that hospitalists should be viewed as even more valuable to a hospital in financial trouble.
“Good hospitalists demonstrate their value with pay-for-performance-type things, with the avoidance of events, getting involved in quality committees,” Dr. Centor says. “A really good hospitalist program is worth its weight in gold and makes the hospital money. If you’re in a hospitalist group that is just churning out patients and isn’t involved in quality and isn’t considered good clinically, then you might be in danger.”
Integration Model
At Boston Medical Center, hospitalists have a more secure place—even in worsening economic times—through a vertical integration program that uses physicians hired through the Department of Family Medicine. The doctors split time between community health centers and hospital inpatient units, and work directly with hospitalists led by Jeffrey Greenwald, MD, HM director and associate professor of medicine at Boston University School of Medicine.
Larry Culpepper, MD, MPH, chairman of family medicine at Boston University School of Medicine and Boston Medical Center, says the vertical integration helps the family medicine physician and hospitalist to find efficiencies. “It has huge advantages,” Dr. Culpepper says. “They’re closely tied to the hospital this way. They’re not out in the community health center getting burned out and drifting away from mainstream medicine. … They see—face to face—the urologist or the cardiologist. They’ve got great communication that helps both ways.”
Collaborative programs are likely to crop up more in the next 12 to 18 months as HM leaders look for creative ways to justify their hospital support. More than 90% of HM groups receive hospital support payments, and the average subsidy is nearly $900,000 per year, according to SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine.” Dr. Wellikson says hospitalists are establishing initiatives to demonstrate their value, but independent experts say more empirical data is needed to quantify that value.
“Many studies report that hospitalist care is associated with shorter lengths of stay and reduced costs,” say the authors of a recent study in the New England Journal of Medicine.1 “However, most studies were single-center, observational studies, and the results of the few available randomized trials have been mixed.”
Dr. Wellikson says recognition of the symbiotic relationship between hospitals and the hospitalists that work there is a major step in and of itself. HM leaders need to recognize and appreciate the litany of current statistics tied to hospitals. He frequently quotes recent hospital data that show 65% of institutions experienced both a drop in elective procedures and an uptick in charity care.
Combine that information with fact that many hospitals saw credit ratings downgraded and investment portfolios trimmed to the tune of $1 billion, and it’s clear hospitalists need to be cognizant of the threats to their livelihood. That means HM and hospitals need to work together, Dr. Wellikson says, to make both businesses financially viable. Thought leaders who take a long-term view, one that aligns HM fortunes with hospitals’ fate, would be in the strongest position moving forward, he says.
“In any cycle in any industry, you have fat times and lean times,” he says. “You have to manage in both times, and this is the first lean time. … Eventually, this recession will pass and the strong hospitals will survive. The better hospitalists will survive, because they’re going to be more valuable to their institution.” TH
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. NEJM. 2009;360(11):1141-1143.
Bright Lights, Big City

It wasn’t that long ago that SHM was pretty excited to see that the word “hospitalist” had been added to the dictionary, but to have hospitalists mentioned on Oprah Winfrey’s television show, on The Today Show, and in the New England Journal of Medicine (NEJM) all in the same week is a watershed moment. It’s further recognition that HM is part of the fabric of this country and an established specialty in America’s healthcare system.
It all started in March, when SHM President Pat Cawley, MD, was quoted in O, The Oprah Magazine, which has a circulation of more than 2 million. Later that month, Oprah had Dennis Quaid on her show to discuss the overdose of anticoagulant his newborn twins were given at a Los Angeles hospital. The conversation quickly turned to patient safety and performance expectations for hospitalized patients. Dr. Mehmet Oz, the resident medical guru for Oprah’s show, created a list of eight essential steps for hospitalized patients to take in order to have the best and safest hospital experience. No. 7 on this list was “Get to know your hospitalist.” It’s the kind of exposure that drives 10,000 to 20,000 people to go online and discover hospitalists.
That same week, The Today Show featured Geno Merli, MD, chief medical officer at Jefferson Medical College in Philadelphia, an SHM member, and our representative to the Coalition to Prevent DVT (www.preventDVT.org). Dr. Merli discussed deep-vein thrombosis (DVT) and pulmonary embolism (PE) prevention, as well as efforts to engage patients and their physicians in this effort. SHM has assumed a leadership role in this 60-group coalition, which is providing DVT awareness to millions of people.
And to top off a banner week, NEJM ran a story and editorial about the rapid growth of HM, based on a study analyzing Medicare data from 1997 to 2006. In “Growth in the Care of Older Patients by Hospitalists in the United States,” by Kuo et al, the main finding was the very rapid growth of HM. The editorial authors noted “the odds that a Medicare patient would be cared for by a hospitalist grew by 29% per year from 1997 through 2006.”
The cherry on the sundae was when other media outlets followed up on the Oprah story, and even more jumped on the NEJM article. Hundreds of media outlets seized the opportunity to tout the growth of HM and our role in patient safety and performance improvement. The reach of these messages, through a national consumer audience and through a prestigious medical journal, should not be underestimated. SHM couldn’t buy that kind of message and deliver it to our patients and their families.
No Slowing Down
It was interesting that I was at SHM’s Leadership Academy in Hawaii when all the stories broke, which made it seem more tangible and brought it home on a personal level as a hospitalist. Just being around 120 current and future HM leaders made me realize that we have the manpower (and womanpower) to continue to create the needed change for our health system.
Hospitalist leaders took a week off from their overwhelming, day-to-day responsibilities to learn how to be more effective leaders. This is the ninth time SHM has brought together more than 100 hospitalist leaders, and every time, we find bright, young—and some not-so-young—hospitalists who thirst for direction to manage their group of hospitalists, to create a team of health professionals, to reshape and fix the hospitals they work in, to move from volume to value, and to do all of the hundreds of other things hospitalist leaders get handed to them every day.
The energy in our specialty will also be felt at HM09. Despite the recession and the recent falloff in attendance at many medical meetings, SHM’s annual meeting—the largest gathering in HM, which will occur in Chicago this month—is having its best registration ever. More than 2,000 stakeholders will come together to network, train to be a better hospitalist, and learn how to effect real change at their hospitals.
As President Obama has mentioned time and again, there are plenty of companies and organizations that continue to produce the products and services that Americans want and need, and even though we are in tough times, those organizations will prevail. Hospitalists clearly are in demand. Even in tough economic times, hospitals, medical staffs, and our patients continue to look to us for answers.
HM is growing exponentially, even when many still know little about hospitalists and what we do. With voices like Oprah, Today, and NEJM highlighting our good work, more light will be shed on our specialty. And I believe we are ready for the scrutiny and the recognition.
Hospitalists earn their keep by taking over a greater share of the management of the acutely ill patient, in working with our primary-care physician, subspecialty, and surgical colleagues, and by being strong team members with our allied health professionals. In many ways, HM remains a work in progress. Although we have accomplished much in a little more than a decade, our best days are still ahead of us.
Just turn on the TV or open a magazine to hear all about it. TH
Dr. Wellikson is CEO of SHM.
It wasn’t that long ago that SHM was pretty excited to see that the word “hospitalist” had been added to the dictionary, but to have hospitalists mentioned on Oprah Winfrey’s television show, on The Today Show, and in the New England Journal of Medicine (NEJM) all in the same week is a watershed moment. It’s further recognition that HM is part of the fabric of this country and an established specialty in America’s healthcare system.
It all started in March, when SHM President Pat Cawley, MD, was quoted in O, The Oprah Magazine, which has a circulation of more than 2 million. Later that month, Oprah had Dennis Quaid on her show to discuss the overdose of anticoagulant his newborn twins were given at a Los Angeles hospital. The conversation quickly turned to patient safety and performance expectations for hospitalized patients. Dr. Mehmet Oz, the resident medical guru for Oprah’s show, created a list of eight essential steps for hospitalized patients to take in order to have the best and safest hospital experience. No. 7 on this list was “Get to know your hospitalist.” It’s the kind of exposure that drives 10,000 to 20,000 people to go online and discover hospitalists.
That same week, The Today Show featured Geno Merli, MD, chief medical officer at Jefferson Medical College in Philadelphia, an SHM member, and our representative to the Coalition to Prevent DVT (www.preventDVT.org). Dr. Merli discussed deep-vein thrombosis (DVT) and pulmonary embolism (PE) prevention, as well as efforts to engage patients and their physicians in this effort. SHM has assumed a leadership role in this 60-group coalition, which is providing DVT awareness to millions of people.
And to top off a banner week, NEJM ran a story and editorial about the rapid growth of HM, based on a study analyzing Medicare data from 1997 to 2006. In “Growth in the Care of Older Patients by Hospitalists in the United States,” by Kuo et al, the main finding was the very rapid growth of HM. The editorial authors noted “the odds that a Medicare patient would be cared for by a hospitalist grew by 29% per year from 1997 through 2006.”
The cherry on the sundae was when other media outlets followed up on the Oprah story, and even more jumped on the NEJM article. Hundreds of media outlets seized the opportunity to tout the growth of HM and our role in patient safety and performance improvement. The reach of these messages, through a national consumer audience and through a prestigious medical journal, should not be underestimated. SHM couldn’t buy that kind of message and deliver it to our patients and their families.
No Slowing Down
It was interesting that I was at SHM’s Leadership Academy in Hawaii when all the stories broke, which made it seem more tangible and brought it home on a personal level as a hospitalist. Just being around 120 current and future HM leaders made me realize that we have the manpower (and womanpower) to continue to create the needed change for our health system.
Hospitalist leaders took a week off from their overwhelming, day-to-day responsibilities to learn how to be more effective leaders. This is the ninth time SHM has brought together more than 100 hospitalist leaders, and every time, we find bright, young—and some not-so-young—hospitalists who thirst for direction to manage their group of hospitalists, to create a team of health professionals, to reshape and fix the hospitals they work in, to move from volume to value, and to do all of the hundreds of other things hospitalist leaders get handed to them every day.
The energy in our specialty will also be felt at HM09. Despite the recession and the recent falloff in attendance at many medical meetings, SHM’s annual meeting—the largest gathering in HM, which will occur in Chicago this month—is having its best registration ever. More than 2,000 stakeholders will come together to network, train to be a better hospitalist, and learn how to effect real change at their hospitals.
As President Obama has mentioned time and again, there are plenty of companies and organizations that continue to produce the products and services that Americans want and need, and even though we are in tough times, those organizations will prevail. Hospitalists clearly are in demand. Even in tough economic times, hospitals, medical staffs, and our patients continue to look to us for answers.
HM is growing exponentially, even when many still know little about hospitalists and what we do. With voices like Oprah, Today, and NEJM highlighting our good work, more light will be shed on our specialty. And I believe we are ready for the scrutiny and the recognition.
Hospitalists earn their keep by taking over a greater share of the management of the acutely ill patient, in working with our primary-care physician, subspecialty, and surgical colleagues, and by being strong team members with our allied health professionals. In many ways, HM remains a work in progress. Although we have accomplished much in a little more than a decade, our best days are still ahead of us.
Just turn on the TV or open a magazine to hear all about it. TH
Dr. Wellikson is CEO of SHM.
It wasn’t that long ago that SHM was pretty excited to see that the word “hospitalist” had been added to the dictionary, but to have hospitalists mentioned on Oprah Winfrey’s television show, on The Today Show, and in the New England Journal of Medicine (NEJM) all in the same week is a watershed moment. It’s further recognition that HM is part of the fabric of this country and an established specialty in America’s healthcare system.
It all started in March, when SHM President Pat Cawley, MD, was quoted in O, The Oprah Magazine, which has a circulation of more than 2 million. Later that month, Oprah had Dennis Quaid on her show to discuss the overdose of anticoagulant his newborn twins were given at a Los Angeles hospital. The conversation quickly turned to patient safety and performance expectations for hospitalized patients. Dr. Mehmet Oz, the resident medical guru for Oprah’s show, created a list of eight essential steps for hospitalized patients to take in order to have the best and safest hospital experience. No. 7 on this list was “Get to know your hospitalist.” It’s the kind of exposure that drives 10,000 to 20,000 people to go online and discover hospitalists.
That same week, The Today Show featured Geno Merli, MD, chief medical officer at Jefferson Medical College in Philadelphia, an SHM member, and our representative to the Coalition to Prevent DVT (www.preventDVT.org). Dr. Merli discussed deep-vein thrombosis (DVT) and pulmonary embolism (PE) prevention, as well as efforts to engage patients and their physicians in this effort. SHM has assumed a leadership role in this 60-group coalition, which is providing DVT awareness to millions of people.
And to top off a banner week, NEJM ran a story and editorial about the rapid growth of HM, based on a study analyzing Medicare data from 1997 to 2006. In “Growth in the Care of Older Patients by Hospitalists in the United States,” by Kuo et al, the main finding was the very rapid growth of HM. The editorial authors noted “the odds that a Medicare patient would be cared for by a hospitalist grew by 29% per year from 1997 through 2006.”
The cherry on the sundae was when other media outlets followed up on the Oprah story, and even more jumped on the NEJM article. Hundreds of media outlets seized the opportunity to tout the growth of HM and our role in patient safety and performance improvement. The reach of these messages, through a national consumer audience and through a prestigious medical journal, should not be underestimated. SHM couldn’t buy that kind of message and deliver it to our patients and their families.
No Slowing Down
It was interesting that I was at SHM’s Leadership Academy in Hawaii when all the stories broke, which made it seem more tangible and brought it home on a personal level as a hospitalist. Just being around 120 current and future HM leaders made me realize that we have the manpower (and womanpower) to continue to create the needed change for our health system.
Hospitalist leaders took a week off from their overwhelming, day-to-day responsibilities to learn how to be more effective leaders. This is the ninth time SHM has brought together more than 100 hospitalist leaders, and every time, we find bright, young—and some not-so-young—hospitalists who thirst for direction to manage their group of hospitalists, to create a team of health professionals, to reshape and fix the hospitals they work in, to move from volume to value, and to do all of the hundreds of other things hospitalist leaders get handed to them every day.
The energy in our specialty will also be felt at HM09. Despite the recession and the recent falloff in attendance at many medical meetings, SHM’s annual meeting—the largest gathering in HM, which will occur in Chicago this month—is having its best registration ever. More than 2,000 stakeholders will come together to network, train to be a better hospitalist, and learn how to effect real change at their hospitals.
As President Obama has mentioned time and again, there are plenty of companies and organizations that continue to produce the products and services that Americans want and need, and even though we are in tough times, those organizations will prevail. Hospitalists clearly are in demand. Even in tough economic times, hospitals, medical staffs, and our patients continue to look to us for answers.
HM is growing exponentially, even when many still know little about hospitalists and what we do. With voices like Oprah, Today, and NEJM highlighting our good work, more light will be shed on our specialty. And I believe we are ready for the scrutiny and the recognition.
Hospitalists earn their keep by taking over a greater share of the management of the acutely ill patient, in working with our primary-care physician, subspecialty, and surgical colleagues, and by being strong team members with our allied health professionals. In many ways, HM remains a work in progress. Although we have accomplished much in a little more than a decade, our best days are still ahead of us.
Just turn on the TV or open a magazine to hear all about it. TH
Dr. Wellikson is CEO of SHM.
The Bigger They Are ...

Editor’s note: This is the first of a two-part series addressing large HM group issues.
In the mid-1990s, when I first became interested in how other hospitalist groups were organized, I started surveying by phone all the groups I could find. It was really unusual to find a group larger than four or five full-time equivalent (FTE) hospitalists. Since then, the size of a typical hospitalist group has grown steadily, and data reported in SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine” shows the median number of FTE physicians in HM groups is 8.0 (mean of 9.75). So in just a few years, our field has grown in such a way that half of all groups in operation now have more than eight physician FTEs. I think most future growth in numbers of hospitalists will be due to individual practices getting larger, rather than new practices starting up.
I work regularly with groups that have more than 20 FTEs, and I have found that large groups tend to have a number of attributes in common.
Separate Daytime Admitter and Rounder Functions
Large groups almost always staff admitter and rounder functions with separate doctors around the clock. That means patients arriving during regular business hours are admitted by a different doctor (the admitter) than the doctor who will provide their care on Day Two and beyond (the rounder).
Although such a system is popular, I suggest every group challenge itself to think about whether it really is the best system. Most groups, regardless of size, have about a quarter to a third of their new admits and consults arrive between 7 a.m. and 5 p.m. If the group did away with a separate admitter during the day and moved all daytime admitters into additional rounder positions, all the daytime admissions could be rotated among all of the daytime doctors, and those patients would typically be seen by the same hospitalist the next day. That would improve hospitalist-patient continuity for the patients who arrive during the day, which might improve the group’s overall efficiency as well as quality and patient satisfaction. Each rounder would become responsible for seeing up to three new consults or admissions during the course of the daytime rounding shift, and the list of new patients to take over each morning—patients admitted by the evening and night admitters—would be smaller.
Of course, one significant benefit of having a separate admitter shift during the day is relieving the rounding doctors of the stress of interrupting rounds for an unpredictable number of new admissions each day. And if the new admissions arrive in the morning, throughput may suffer as it might mean the rounding doctor may see “dischargeable” patients later in the day.
I think there is room for debate about whether it is best for large groups to have a separate admitter during the day, but whatever approach a group chooses, it should acknowledge the costs of that approach and not just assume that it is the only one that is feasible or reasonable.
Who Is Caring for Whom?
The larger the hospitalist group, the more difficulty nurses and other staff have understanding exactly how patients are distributed among the doctors. When one hospitalist rotates “off service” to be replaced by another the next day, or when overnight admissions are “picked up” by a rounding doctor the next morning, it can be difficult for nurses to know which hospitalist is responsible for the patient at a given moment.
All groups, regardless of size, should ensure that the hospitalist who picks up patients from a colleague who has rotated off the day before writes an order in the chart indicating “change attending to Dr. Jones,” or clearly communicates who the new hospitalist is by some other means, such as an electronic medical record or a phone call from a clerk. It isn’t enough that patients are assigned to a particular team—say, the “white team” or the “green team”—for their entire stay. Nurses and other staff need to know which hospitalist is covering that team each day.
One test of how well your system is working is to assess how the nurse answers when a patient or family asks, “Which doctor will be in to see me today?” It isn’t good enough for the nurse to just say, “The green-team doctor will see you, but I don’t know who that is today.” The nurse needs to be able to provide the name of the doctor who will be in. If nurses at your hospital regularly page the wrong hospitalist, or must call around just to figure out who the attending hospitalist is for a particular patient, then you have an opportunity to improve how you communicate this information to the nurse and others.
Even if you have a system in which it is clear to everyone which hospitalist has taken over for one who has rotated off-service, you need to ensure that nurses can easily determine the attending hospitalist for patients admitted the night before. Night-shift staff not knowing which doctor will take over in the morning is an all-too-common problem, and it results in too many staffers not knowing who is caring for the patient from the time the night doctor goes off (e.g., 7 a.m.) until the rounder taking over gets to that patient on rounds. Having evening/night admitters assign attending, or rounder, hospitalists at the time of each admission is a great solution, and I’ll provide ideas about how to do this in next month’s column.
I worry about patient satisfaction if the evening/night admitter can’t tell the patient the name of the hospitalist who will take over in the morning. How can the patient feel that they’re getting personalized care when they’re told, “I don’t know which of my partners will take over your care tomorrow. They all get together and divide up the patients each morning and will assign a doctor to you then”? It’s different if the admitter tells the patient, “I’m on call for our group tonight, but will be home sleeping tomorrow and my colleague, Dr. Clapton, will take over your care in the morning.” I usually go on to say with a wink that the patient is getting an upgrade, because Dr. Clapton is so much smarter and better-looking than me. I’ll understand if the embellishment doesn’t feel right for you, but I think there is value in the admitter, or a hospitalist rotating off-service, taking a minute to say something nice about the hospitalist who will take over next.
Next month, I will continue to explore issues that are particularly problematic for larger groups. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a two-part series addressing large HM group issues.
In the mid-1990s, when I first became interested in how other hospitalist groups were organized, I started surveying by phone all the groups I could find. It was really unusual to find a group larger than four or five full-time equivalent (FTE) hospitalists. Since then, the size of a typical hospitalist group has grown steadily, and data reported in SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine” shows the median number of FTE physicians in HM groups is 8.0 (mean of 9.75). So in just a few years, our field has grown in such a way that half of all groups in operation now have more than eight physician FTEs. I think most future growth in numbers of hospitalists will be due to individual practices getting larger, rather than new practices starting up.
I work regularly with groups that have more than 20 FTEs, and I have found that large groups tend to have a number of attributes in common.
Separate Daytime Admitter and Rounder Functions
Large groups almost always staff admitter and rounder functions with separate doctors around the clock. That means patients arriving during regular business hours are admitted by a different doctor (the admitter) than the doctor who will provide their care on Day Two and beyond (the rounder).
Although such a system is popular, I suggest every group challenge itself to think about whether it really is the best system. Most groups, regardless of size, have about a quarter to a third of their new admits and consults arrive between 7 a.m. and 5 p.m. If the group did away with a separate admitter during the day and moved all daytime admitters into additional rounder positions, all the daytime admissions could be rotated among all of the daytime doctors, and those patients would typically be seen by the same hospitalist the next day. That would improve hospitalist-patient continuity for the patients who arrive during the day, which might improve the group’s overall efficiency as well as quality and patient satisfaction. Each rounder would become responsible for seeing up to three new consults or admissions during the course of the daytime rounding shift, and the list of new patients to take over each morning—patients admitted by the evening and night admitters—would be smaller.
Of course, one significant benefit of having a separate admitter shift during the day is relieving the rounding doctors of the stress of interrupting rounds for an unpredictable number of new admissions each day. And if the new admissions arrive in the morning, throughput may suffer as it might mean the rounding doctor may see “dischargeable” patients later in the day.
I think there is room for debate about whether it is best for large groups to have a separate admitter during the day, but whatever approach a group chooses, it should acknowledge the costs of that approach and not just assume that it is the only one that is feasible or reasonable.
Who Is Caring for Whom?
The larger the hospitalist group, the more difficulty nurses and other staff have understanding exactly how patients are distributed among the doctors. When one hospitalist rotates “off service” to be replaced by another the next day, or when overnight admissions are “picked up” by a rounding doctor the next morning, it can be difficult for nurses to know which hospitalist is responsible for the patient at a given moment.
All groups, regardless of size, should ensure that the hospitalist who picks up patients from a colleague who has rotated off the day before writes an order in the chart indicating “change attending to Dr. Jones,” or clearly communicates who the new hospitalist is by some other means, such as an electronic medical record or a phone call from a clerk. It isn’t enough that patients are assigned to a particular team—say, the “white team” or the “green team”—for their entire stay. Nurses and other staff need to know which hospitalist is covering that team each day.
One test of how well your system is working is to assess how the nurse answers when a patient or family asks, “Which doctor will be in to see me today?” It isn’t good enough for the nurse to just say, “The green-team doctor will see you, but I don’t know who that is today.” The nurse needs to be able to provide the name of the doctor who will be in. If nurses at your hospital regularly page the wrong hospitalist, or must call around just to figure out who the attending hospitalist is for a particular patient, then you have an opportunity to improve how you communicate this information to the nurse and others.
Even if you have a system in which it is clear to everyone which hospitalist has taken over for one who has rotated off-service, you need to ensure that nurses can easily determine the attending hospitalist for patients admitted the night before. Night-shift staff not knowing which doctor will take over in the morning is an all-too-common problem, and it results in too many staffers not knowing who is caring for the patient from the time the night doctor goes off (e.g., 7 a.m.) until the rounder taking over gets to that patient on rounds. Having evening/night admitters assign attending, or rounder, hospitalists at the time of each admission is a great solution, and I’ll provide ideas about how to do this in next month’s column.
I worry about patient satisfaction if the evening/night admitter can’t tell the patient the name of the hospitalist who will take over in the morning. How can the patient feel that they’re getting personalized care when they’re told, “I don’t know which of my partners will take over your care tomorrow. They all get together and divide up the patients each morning and will assign a doctor to you then”? It’s different if the admitter tells the patient, “I’m on call for our group tonight, but will be home sleeping tomorrow and my colleague, Dr. Clapton, will take over your care in the morning.” I usually go on to say with a wink that the patient is getting an upgrade, because Dr. Clapton is so much smarter and better-looking than me. I’ll understand if the embellishment doesn’t feel right for you, but I think there is value in the admitter, or a hospitalist rotating off-service, taking a minute to say something nice about the hospitalist who will take over next.
Next month, I will continue to explore issues that are particularly problematic for larger groups. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a two-part series addressing large HM group issues.
In the mid-1990s, when I first became interested in how other hospitalist groups were organized, I started surveying by phone all the groups I could find. It was really unusual to find a group larger than four or five full-time equivalent (FTE) hospitalists. Since then, the size of a typical hospitalist group has grown steadily, and data reported in SHM’s “2007-2008 Bi-Annual Survey on the State of Hospital Medicine” shows the median number of FTE physicians in HM groups is 8.0 (mean of 9.75). So in just a few years, our field has grown in such a way that half of all groups in operation now have more than eight physician FTEs. I think most future growth in numbers of hospitalists will be due to individual practices getting larger, rather than new practices starting up.
I work regularly with groups that have more than 20 FTEs, and I have found that large groups tend to have a number of attributes in common.
Separate Daytime Admitter and Rounder Functions
Large groups almost always staff admitter and rounder functions with separate doctors around the clock. That means patients arriving during regular business hours are admitted by a different doctor (the admitter) than the doctor who will provide their care on Day Two and beyond (the rounder).
Although such a system is popular, I suggest every group challenge itself to think about whether it really is the best system. Most groups, regardless of size, have about a quarter to a third of their new admits and consults arrive between 7 a.m. and 5 p.m. If the group did away with a separate admitter during the day and moved all daytime admitters into additional rounder positions, all the daytime admissions could be rotated among all of the daytime doctors, and those patients would typically be seen by the same hospitalist the next day. That would improve hospitalist-patient continuity for the patients who arrive during the day, which might improve the group’s overall efficiency as well as quality and patient satisfaction. Each rounder would become responsible for seeing up to three new consults or admissions during the course of the daytime rounding shift, and the list of new patients to take over each morning—patients admitted by the evening and night admitters—would be smaller.
Of course, one significant benefit of having a separate admitter shift during the day is relieving the rounding doctors of the stress of interrupting rounds for an unpredictable number of new admissions each day. And if the new admissions arrive in the morning, throughput may suffer as it might mean the rounding doctor may see “dischargeable” patients later in the day.
I think there is room for debate about whether it is best for large groups to have a separate admitter during the day, but whatever approach a group chooses, it should acknowledge the costs of that approach and not just assume that it is the only one that is feasible or reasonable.
Who Is Caring for Whom?
The larger the hospitalist group, the more difficulty nurses and other staff have understanding exactly how patients are distributed among the doctors. When one hospitalist rotates “off service” to be replaced by another the next day, or when overnight admissions are “picked up” by a rounding doctor the next morning, it can be difficult for nurses to know which hospitalist is responsible for the patient at a given moment.
All groups, regardless of size, should ensure that the hospitalist who picks up patients from a colleague who has rotated off the day before writes an order in the chart indicating “change attending to Dr. Jones,” or clearly communicates who the new hospitalist is by some other means, such as an electronic medical record or a phone call from a clerk. It isn’t enough that patients are assigned to a particular team—say, the “white team” or the “green team”—for their entire stay. Nurses and other staff need to know which hospitalist is covering that team each day.
One test of how well your system is working is to assess how the nurse answers when a patient or family asks, “Which doctor will be in to see me today?” It isn’t good enough for the nurse to just say, “The green-team doctor will see you, but I don’t know who that is today.” The nurse needs to be able to provide the name of the doctor who will be in. If nurses at your hospital regularly page the wrong hospitalist, or must call around just to figure out who the attending hospitalist is for a particular patient, then you have an opportunity to improve how you communicate this information to the nurse and others.
Even if you have a system in which it is clear to everyone which hospitalist has taken over for one who has rotated off-service, you need to ensure that nurses can easily determine the attending hospitalist for patients admitted the night before. Night-shift staff not knowing which doctor will take over in the morning is an all-too-common problem, and it results in too many staffers not knowing who is caring for the patient from the time the night doctor goes off (e.g., 7 a.m.) until the rounder taking over gets to that patient on rounds. Having evening/night admitters assign attending, or rounder, hospitalists at the time of each admission is a great solution, and I’ll provide ideas about how to do this in next month’s column.
I worry about patient satisfaction if the evening/night admitter can’t tell the patient the name of the hospitalist who will take over in the morning. How can the patient feel that they’re getting personalized care when they’re told, “I don’t know which of my partners will take over your care tomorrow. They all get together and divide up the patients each morning and will assign a doctor to you then”? It’s different if the admitter tells the patient, “I’m on call for our group tonight, but will be home sleeping tomorrow and my colleague, Dr. Clapton, will take over your care in the morning.” I usually go on to say with a wink that the patient is getting an upgrade, because Dr. Clapton is so much smarter and better-looking than me. I’ll understand if the embellishment doesn’t feel right for you, but I think there is value in the admitter, or a hospitalist rotating off-service, taking a minute to say something nice about the hospitalist who will take over next.
Next month, I will continue to explore issues that are particularly problematic for larger groups. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Read All About It

In the aftermath of the recent shuttering of Colorado’s oldest newspaper, The Rocky Mountain News, a couple of colleagues and I were discussing how unlikely it seemed just a few months ago that this could happen. It wasn’t long until we made the theoretical leap to what it would take for our hospitalist group to go out of business. Of course, this seems highly unlikely, but then again, the closing of a 150-year-old metropolitan newspaper seemed a preposterous proposition.
In the course of this discussion, we conjured myriad internal or external factors that could adversely affect our program. Although this was a tangential, lunchtime discussion, it did reverberate against the tuning fork of a faltering U.S. economy, especially regarding the financial sector and the automotive industry.
With that as a frame, I thought I’d take a dip into Paranoia Pond and look at potential threats to the HM model. Let me start by saying that I believe—deeply—in the hospitalist movement, the strides we’ve made, and the bright path that lies before us. I am not stating that any of these potential perils will put hospitalists out of business. However, the list below includes several risks that, if not properly mitigated, could alter our future course.
Here are 10 potential threats to the HM business model that you should keep an eye on:
1. Failure to Embrace QI
Those who fundamentally improve outcomes will write the future of medicine. Hospitalists are perfectly positioned—and expected—to do this. I believe most hospital CEOs think this is part of the contract: funding for quality. A failure to live up to our end of the bargain puts us at great risk. If your group isn’t able to demonstrate measurable improvements in processes and clinical outcomes, then you are at risk of losing hospital funding. As the economy recedes further and hospital reimbursement is more closely tied to quality, this will quickly move beyond a potential threat to a reality.
2. Lack of New Data to Support the HM Model
A corollary of No. 1 is our ability to show how we work. This burden, by and large, falls to my academic colleagues. After a rash of early studies showed the benefits of the hospitalist model, more recent data has been less convincing. This doesn’t mean we aren’t improving outcomes; rather, it means we aren’t always measuring and proving it. HM must get past the easy-to-measure endpoints, such as length-of-stay reduction and cost savings, to more meaningful endpoints, such as readmission rates, mortality, and clinical improvements. Ultimately, HM depends on robust, published data that clearly illustrate our benefit to hospitals and patients. Anything short of that intensifies the pressure to achieve No. 1.
3. Decreased Admissions
Our mother ship is under fire. Each wound our hospitals suffer is a wound to us. Erosion of hospital margins likely will translate to decreased levels of support. Nearly 40% of hospitals are experiencing a decrease in admissions. Coupled with economy-induced increases in the number of uninsured patients, this looms as a major threat to our future stability.
4. Elective Procedures
Thirty-one percent of hospitals have witnessed a decrease in lucrative, elective procedures. It began with the rise of procedural centers (e.g., surgery, gastroenterology, radiology) and is being exacerbated by the wheezing U.S. economy. Each 1% increase in unemployment results in roughly 2.5 million Americans losing their employer-provided health benefits. That means fewer elective procedures, which directly threatens the profitability of HM groups who depend on co-management revenue.
5. Recruitment
For years, HM has battled a workforce shortage, which has stifled growth and pushed providers to the verge of exhaustion. This problem persists despite offers of lucrative salaries, significant free time, and specialty status. The continuing workforce shortage should serve as a call to arms to improve recruitment into the field. An inability to increase the flow of providers will limit growth and tax the hospitalists we have in place. Ultimately, we will retard our progress toward achieving the improved outcomes articulated in No. 1.
6. Retention
We must address burnout and career satisfaction issues. Although exact numbers are tough to come by, it’s clear that many hospitalists are exhausted and overworked. This should not come as a surprise, considering we are a rapidly growing field constantly tasked with seeing more patients and solving all of a hospital’s problems. However, an inability to keep our current workforce sated and in HM jobs will amplify the workforce shortage.
7. PCPs Return
One interesting theory is that the floundering economy could prompt primary-care physicians (PCPs), whose hospital exodus we backfilled, to return to inpatient care in order to supplement their income. This isn’t likely to happen unless outpatient providers see such a drop in business that they cannot field a large-enough insured panel of patients to make ends meet. The possibility of PCPs seeing insured inpatients and leaving hospitalists with a largely uninsured population would be a game-changer. In the face of a large PCP shortage, however, this seems an unlikely scenario.
8. PCP Payment Reform
It is more likely our primary-care colleagues will get an ever-so-deserved pay raise. This is central to the proposed medical-home model and a key point of many healthcare reform plans. To stay competitive, hospitalists might also see a resultant pay increase. Anything short of this could further strain HM recruitment, as working hospitalists and new grads might migrate back toward primary-care jobs.
9. Bundling
It’s too early to know the effects of the proposed bundling of physician and hospital payments into one fee, which would compensate both hospitals and physicians. On the one hand, it could be a boon, as HM efficiency could be rewarded in ways not currently allowed. On the other hand, if hospitals continue to struggle financially and we are completely dependent upon bundled payments for our revenue, it could be a financial calamity.
10. Healthcare Reform
Without a clear sense of President Obama’s plans for healthcare reform, it’s tough to predict the future. We could try to paint numerous rosy scenarios that derive from a plan that includes a universal payor, improved access, and increased technology. However, it’s possible this reform would hamstring our efforts through reduced reimbursement, increased regulation, and cumbersome federal mandates.
Final Thought
I believe HM is strong and will overcome future threats. But it pays to consider and mitigate the hazards we might confront. Still, after much deliberation, I just cannot conceive of a reasonable scenario that results in a future without hospitalists.
Then again, Henry Ford probably felt the same about cars. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.
In the aftermath of the recent shuttering of Colorado’s oldest newspaper, The Rocky Mountain News, a couple of colleagues and I were discussing how unlikely it seemed just a few months ago that this could happen. It wasn’t long until we made the theoretical leap to what it would take for our hospitalist group to go out of business. Of course, this seems highly unlikely, but then again, the closing of a 150-year-old metropolitan newspaper seemed a preposterous proposition.
In the course of this discussion, we conjured myriad internal or external factors that could adversely affect our program. Although this was a tangential, lunchtime discussion, it did reverberate against the tuning fork of a faltering U.S. economy, especially regarding the financial sector and the automotive industry.
With that as a frame, I thought I’d take a dip into Paranoia Pond and look at potential threats to the HM model. Let me start by saying that I believe—deeply—in the hospitalist movement, the strides we’ve made, and the bright path that lies before us. I am not stating that any of these potential perils will put hospitalists out of business. However, the list below includes several risks that, if not properly mitigated, could alter our future course.
Here are 10 potential threats to the HM business model that you should keep an eye on:
1. Failure to Embrace QI
Those who fundamentally improve outcomes will write the future of medicine. Hospitalists are perfectly positioned—and expected—to do this. I believe most hospital CEOs think this is part of the contract: funding for quality. A failure to live up to our end of the bargain puts us at great risk. If your group isn’t able to demonstrate measurable improvements in processes and clinical outcomes, then you are at risk of losing hospital funding. As the economy recedes further and hospital reimbursement is more closely tied to quality, this will quickly move beyond a potential threat to a reality.
2. Lack of New Data to Support the HM Model
A corollary of No. 1 is our ability to show how we work. This burden, by and large, falls to my academic colleagues. After a rash of early studies showed the benefits of the hospitalist model, more recent data has been less convincing. This doesn’t mean we aren’t improving outcomes; rather, it means we aren’t always measuring and proving it. HM must get past the easy-to-measure endpoints, such as length-of-stay reduction and cost savings, to more meaningful endpoints, such as readmission rates, mortality, and clinical improvements. Ultimately, HM depends on robust, published data that clearly illustrate our benefit to hospitals and patients. Anything short of that intensifies the pressure to achieve No. 1.
3. Decreased Admissions
Our mother ship is under fire. Each wound our hospitals suffer is a wound to us. Erosion of hospital margins likely will translate to decreased levels of support. Nearly 40% of hospitals are experiencing a decrease in admissions. Coupled with economy-induced increases in the number of uninsured patients, this looms as a major threat to our future stability.
4. Elective Procedures
Thirty-one percent of hospitals have witnessed a decrease in lucrative, elective procedures. It began with the rise of procedural centers (e.g., surgery, gastroenterology, radiology) and is being exacerbated by the wheezing U.S. economy. Each 1% increase in unemployment results in roughly 2.5 million Americans losing their employer-provided health benefits. That means fewer elective procedures, which directly threatens the profitability of HM groups who depend on co-management revenue.
5. Recruitment
For years, HM has battled a workforce shortage, which has stifled growth and pushed providers to the verge of exhaustion. This problem persists despite offers of lucrative salaries, significant free time, and specialty status. The continuing workforce shortage should serve as a call to arms to improve recruitment into the field. An inability to increase the flow of providers will limit growth and tax the hospitalists we have in place. Ultimately, we will retard our progress toward achieving the improved outcomes articulated in No. 1.
6. Retention
We must address burnout and career satisfaction issues. Although exact numbers are tough to come by, it’s clear that many hospitalists are exhausted and overworked. This should not come as a surprise, considering we are a rapidly growing field constantly tasked with seeing more patients and solving all of a hospital’s problems. However, an inability to keep our current workforce sated and in HM jobs will amplify the workforce shortage.
7. PCPs Return
One interesting theory is that the floundering economy could prompt primary-care physicians (PCPs), whose hospital exodus we backfilled, to return to inpatient care in order to supplement their income. This isn’t likely to happen unless outpatient providers see such a drop in business that they cannot field a large-enough insured panel of patients to make ends meet. The possibility of PCPs seeing insured inpatients and leaving hospitalists with a largely uninsured population would be a game-changer. In the face of a large PCP shortage, however, this seems an unlikely scenario.
8. PCP Payment Reform
It is more likely our primary-care colleagues will get an ever-so-deserved pay raise. This is central to the proposed medical-home model and a key point of many healthcare reform plans. To stay competitive, hospitalists might also see a resultant pay increase. Anything short of this could further strain HM recruitment, as working hospitalists and new grads might migrate back toward primary-care jobs.
9. Bundling
It’s too early to know the effects of the proposed bundling of physician and hospital payments into one fee, which would compensate both hospitals and physicians. On the one hand, it could be a boon, as HM efficiency could be rewarded in ways not currently allowed. On the other hand, if hospitals continue to struggle financially and we are completely dependent upon bundled payments for our revenue, it could be a financial calamity.
10. Healthcare Reform
Without a clear sense of President Obama’s plans for healthcare reform, it’s tough to predict the future. We could try to paint numerous rosy scenarios that derive from a plan that includes a universal payor, improved access, and increased technology. However, it’s possible this reform would hamstring our efforts through reduced reimbursement, increased regulation, and cumbersome federal mandates.
Final Thought
I believe HM is strong and will overcome future threats. But it pays to consider and mitigate the hazards we might confront. Still, after much deliberation, I just cannot conceive of a reasonable scenario that results in a future without hospitalists.
Then again, Henry Ford probably felt the same about cars. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.
In the aftermath of the recent shuttering of Colorado’s oldest newspaper, The Rocky Mountain News, a couple of colleagues and I were discussing how unlikely it seemed just a few months ago that this could happen. It wasn’t long until we made the theoretical leap to what it would take for our hospitalist group to go out of business. Of course, this seems highly unlikely, but then again, the closing of a 150-year-old metropolitan newspaper seemed a preposterous proposition.
In the course of this discussion, we conjured myriad internal or external factors that could adversely affect our program. Although this was a tangential, lunchtime discussion, it did reverberate against the tuning fork of a faltering U.S. economy, especially regarding the financial sector and the automotive industry.
With that as a frame, I thought I’d take a dip into Paranoia Pond and look at potential threats to the HM model. Let me start by saying that I believe—deeply—in the hospitalist movement, the strides we’ve made, and the bright path that lies before us. I am not stating that any of these potential perils will put hospitalists out of business. However, the list below includes several risks that, if not properly mitigated, could alter our future course.
Here are 10 potential threats to the HM business model that you should keep an eye on:
1. Failure to Embrace QI
Those who fundamentally improve outcomes will write the future of medicine. Hospitalists are perfectly positioned—and expected—to do this. I believe most hospital CEOs think this is part of the contract: funding for quality. A failure to live up to our end of the bargain puts us at great risk. If your group isn’t able to demonstrate measurable improvements in processes and clinical outcomes, then you are at risk of losing hospital funding. As the economy recedes further and hospital reimbursement is more closely tied to quality, this will quickly move beyond a potential threat to a reality.
2. Lack of New Data to Support the HM Model
A corollary of No. 1 is our ability to show how we work. This burden, by and large, falls to my academic colleagues. After a rash of early studies showed the benefits of the hospitalist model, more recent data has been less convincing. This doesn’t mean we aren’t improving outcomes; rather, it means we aren’t always measuring and proving it. HM must get past the easy-to-measure endpoints, such as length-of-stay reduction and cost savings, to more meaningful endpoints, such as readmission rates, mortality, and clinical improvements. Ultimately, HM depends on robust, published data that clearly illustrate our benefit to hospitals and patients. Anything short of that intensifies the pressure to achieve No. 1.
3. Decreased Admissions
Our mother ship is under fire. Each wound our hospitals suffer is a wound to us. Erosion of hospital margins likely will translate to decreased levels of support. Nearly 40% of hospitals are experiencing a decrease in admissions. Coupled with economy-induced increases in the number of uninsured patients, this looms as a major threat to our future stability.
4. Elective Procedures
Thirty-one percent of hospitals have witnessed a decrease in lucrative, elective procedures. It began with the rise of procedural centers (e.g., surgery, gastroenterology, radiology) and is being exacerbated by the wheezing U.S. economy. Each 1% increase in unemployment results in roughly 2.5 million Americans losing their employer-provided health benefits. That means fewer elective procedures, which directly threatens the profitability of HM groups who depend on co-management revenue.
5. Recruitment
For years, HM has battled a workforce shortage, which has stifled growth and pushed providers to the verge of exhaustion. This problem persists despite offers of lucrative salaries, significant free time, and specialty status. The continuing workforce shortage should serve as a call to arms to improve recruitment into the field. An inability to increase the flow of providers will limit growth and tax the hospitalists we have in place. Ultimately, we will retard our progress toward achieving the improved outcomes articulated in No. 1.
6. Retention
We must address burnout and career satisfaction issues. Although exact numbers are tough to come by, it’s clear that many hospitalists are exhausted and overworked. This should not come as a surprise, considering we are a rapidly growing field constantly tasked with seeing more patients and solving all of a hospital’s problems. However, an inability to keep our current workforce sated and in HM jobs will amplify the workforce shortage.
7. PCPs Return
One interesting theory is that the floundering economy could prompt primary-care physicians (PCPs), whose hospital exodus we backfilled, to return to inpatient care in order to supplement their income. This isn’t likely to happen unless outpatient providers see such a drop in business that they cannot field a large-enough insured panel of patients to make ends meet. The possibility of PCPs seeing insured inpatients and leaving hospitalists with a largely uninsured population would be a game-changer. In the face of a large PCP shortage, however, this seems an unlikely scenario.
8. PCP Payment Reform
It is more likely our primary-care colleagues will get an ever-so-deserved pay raise. This is central to the proposed medical-home model and a key point of many healthcare reform plans. To stay competitive, hospitalists might also see a resultant pay increase. Anything short of this could further strain HM recruitment, as working hospitalists and new grads might migrate back toward primary-care jobs.
9. Bundling
It’s too early to know the effects of the proposed bundling of physician and hospital payments into one fee, which would compensate both hospitals and physicians. On the one hand, it could be a boon, as HM efficiency could be rewarded in ways not currently allowed. On the other hand, if hospitals continue to struggle financially and we are completely dependent upon bundled payments for our revenue, it could be a financial calamity.
10. Healthcare Reform
Without a clear sense of President Obama’s plans for healthcare reform, it’s tough to predict the future. We could try to paint numerous rosy scenarios that derive from a plan that includes a universal payor, improved access, and increased technology. However, it’s possible this reform would hamstring our efforts through reduced reimbursement, increased regulation, and cumbersome federal mandates.
Final Thought
I believe HM is strong and will overcome future threats. But it pays to consider and mitigate the hazards we might confront. Still, after much deliberation, I just cannot conceive of a reasonable scenario that results in a future without hospitalists.
Then again, Henry Ford probably felt the same about cars. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.