User login
TBI and growth hormone
In response to “Traumatic brain injury: Pharmacotherapy options for cognitive deficits” (Med/Psych Update, Current Psychiatry, February 2011, p. 21-37), traumatic brain injury (TBI) has been recognized as a risk factor for cognitive impairment, but TBI also has been shown to be a risk factor for hypopituitarism, presenting most frequently with growth hormone deficiency (GHD). GHD is associated not only with changes in body composition but also with impaired quality of life, cognitive dysfunctions, and psychiatric sequelae, usually classified as “depression.”
In a case study we evaluated the impact of GH therapy on the mental status of TBI patients.1 Psychiatric and cognitive functions were tested in 6 GHD patients at baseline (minimum 3 years after TBI) and reassessed after 6 months of GH therapy and 12 months after discontinuing GH therapy. Psychiatric and cognitive examinations included semi-structured interviews and 3 instruments: Symptom Checklist-90-Revised, Zung Depression Inventory, and a standard composite neuropsychological battery.
Our results showed that 6 months of GH therapy in GHD TBI patients improved cognitive abilities (particularly verbal and nonverbal memory) and significantly improved psychiatric functioning. Depression severity decreased, as did intensity of interpersonal sensitivity, hostility, paranoid ideation, anxiety, and psychoticism. Somatization, obsessive-compulsive symptoms, and phobic anxiety decreased in all but 1 patient. In 3 GHD patients who stopped GH therapy for 12 months, we observed worsening verbal and nonverbal memory, interpersonal sensitivity, anxiety, and paranoid ideation. Thus, GHD might be associated with affective and cognitive symptoms in TBI patients and GH replacement therapy could be beneficial. Screening for pituitary dysfunction in TBI patients is strongly recommended, particularly in presence of cognitive and affective symptoms.
Nadja Maric, MD, PhD
Associate Professor
Head of Department for Research and Early
Interventions in Psychiatry
Clinic for Psychiatry, Clinical Centre of Serbia
University of Belgrade School of Medicine
Belgrade, Serbia
1. Maric N, Doknic M, Pavlovic D, et al. Psychiatric and neuropsychological changes in growth hormone-deficient patients after traumatic brain injury in response to growth hormone therapy. J Endocrinol Invest. 2010;33(11):770-775
In response to “Traumatic brain injury: Pharmacotherapy options for cognitive deficits” (Med/Psych Update, Current Psychiatry, February 2011, p. 21-37), traumatic brain injury (TBI) has been recognized as a risk factor for cognitive impairment, but TBI also has been shown to be a risk factor for hypopituitarism, presenting most frequently with growth hormone deficiency (GHD). GHD is associated not only with changes in body composition but also with impaired quality of life, cognitive dysfunctions, and psychiatric sequelae, usually classified as “depression.”
In a case study we evaluated the impact of GH therapy on the mental status of TBI patients.1 Psychiatric and cognitive functions were tested in 6 GHD patients at baseline (minimum 3 years after TBI) and reassessed after 6 months of GH therapy and 12 months after discontinuing GH therapy. Psychiatric and cognitive examinations included semi-structured interviews and 3 instruments: Symptom Checklist-90-Revised, Zung Depression Inventory, and a standard composite neuropsychological battery.
Our results showed that 6 months of GH therapy in GHD TBI patients improved cognitive abilities (particularly verbal and nonverbal memory) and significantly improved psychiatric functioning. Depression severity decreased, as did intensity of interpersonal sensitivity, hostility, paranoid ideation, anxiety, and psychoticism. Somatization, obsessive-compulsive symptoms, and phobic anxiety decreased in all but 1 patient. In 3 GHD patients who stopped GH therapy for 12 months, we observed worsening verbal and nonverbal memory, interpersonal sensitivity, anxiety, and paranoid ideation. Thus, GHD might be associated with affective and cognitive symptoms in TBI patients and GH replacement therapy could be beneficial. Screening for pituitary dysfunction in TBI patients is strongly recommended, particularly in presence of cognitive and affective symptoms.
Nadja Maric, MD, PhD
Associate Professor
Head of Department for Research and Early
Interventions in Psychiatry
Clinic for Psychiatry, Clinical Centre of Serbia
University of Belgrade School of Medicine
Belgrade, Serbia
In response to “Traumatic brain injury: Pharmacotherapy options for cognitive deficits” (Med/Psych Update, Current Psychiatry, February 2011, p. 21-37), traumatic brain injury (TBI) has been recognized as a risk factor for cognitive impairment, but TBI also has been shown to be a risk factor for hypopituitarism, presenting most frequently with growth hormone deficiency (GHD). GHD is associated not only with changes in body composition but also with impaired quality of life, cognitive dysfunctions, and psychiatric sequelae, usually classified as “depression.”
In a case study we evaluated the impact of GH therapy on the mental status of TBI patients.1 Psychiatric and cognitive functions were tested in 6 GHD patients at baseline (minimum 3 years after TBI) and reassessed after 6 months of GH therapy and 12 months after discontinuing GH therapy. Psychiatric and cognitive examinations included semi-structured interviews and 3 instruments: Symptom Checklist-90-Revised, Zung Depression Inventory, and a standard composite neuropsychological battery.
Our results showed that 6 months of GH therapy in GHD TBI patients improved cognitive abilities (particularly verbal and nonverbal memory) and significantly improved psychiatric functioning. Depression severity decreased, as did intensity of interpersonal sensitivity, hostility, paranoid ideation, anxiety, and psychoticism. Somatization, obsessive-compulsive symptoms, and phobic anxiety decreased in all but 1 patient. In 3 GHD patients who stopped GH therapy for 12 months, we observed worsening verbal and nonverbal memory, interpersonal sensitivity, anxiety, and paranoid ideation. Thus, GHD might be associated with affective and cognitive symptoms in TBI patients and GH replacement therapy could be beneficial. Screening for pituitary dysfunction in TBI patients is strongly recommended, particularly in presence of cognitive and affective symptoms.
Nadja Maric, MD, PhD
Associate Professor
Head of Department for Research and Early
Interventions in Psychiatry
Clinic for Psychiatry, Clinical Centre of Serbia
University of Belgrade School of Medicine
Belgrade, Serbia
1. Maric N, Doknic M, Pavlovic D, et al. Psychiatric and neuropsychological changes in growth hormone-deficient patients after traumatic brain injury in response to growth hormone therapy. J Endocrinol Invest. 2010;33(11):770-775
1. Maric N, Doknic M, Pavlovic D, et al. Psychiatric and neuropsychological changes in growth hormone-deficient patients after traumatic brain injury in response to growth hormone therapy. J Endocrinol Invest. 2010;33(11):770-775
Help patients SLEEP without medication
Some of patients’ most common complaints involve sleep: too little, too late, never enough. Although sleep disruptions often are related to the psychiatric disorder for which the person seeks treatment, cognitive and behavioral factors play significant roles.1 Unfortunately, quite often patients expect to be given “something” to foster sleep.
Before writing a prescription, be prepared to evaluate sleep disturbances and educate patients about sleep and how it can be facilitated without medication. The mnemonic SLEEP can help you readily access a basic set of nonpharmacologic aids to assess and treat uncomplicated sleep disturbances.
Schedule. Ask patients about their sleep-wake schedule. Is their pattern routine and regular, or unpredictable? Are they “in synch” with the sleep/activity patterns of those with whom they live, or is their schedule “off track” and disrupted by household noise and activities? Consistency is key to normalizing sleep.
Limit. Sensible limits on caffeinated beverages need to be addressed. Strongly encourage patients to limit nicotine and alcohol in-take. Assess the amount as well as timing of their use of these substances. Remind your patient that alcohol and smoking have a direct impact on sleep initiation and can disrupt sleep because of nocturnal withdrawal.
Eliminate. Removing noxious environmental stimuli is critical. Ask patients about the level of nighttime noise, excessive light, and ventilation and temperature of their sleeping area (cooler is better). Eliminate factors that create a “hostile” sleep environment.
Exercise. Regular exercise performed during the day (but not immediately before going to bed) may be an effective antidote to the psychic stress and physical tension that often contribute to insomnia.2 A several-times-per-week routine of brisk walking, riding a bicycle, swimming, or yoga can reduce sleep-onset latency and improve sleep maintenance. An exercise routine can enhance a patient’s overall health and knock out a daytime sleep habit.
Psychotherapy. Cognitive-behavioral therapy for insomnia has demonstrated efficacy in treating sleep disorders.3 Learning how to “catch, check, and change” distorted and negative cognitions regarding sleep onset can be a valuable tool for persons who are motivated to alter their thoughts and behaviors that contribute to sleep complaints, and may simultaneously improve associated anxiety and/or depression.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep. 2006;9:1398-1414.
2. Passos GS, Povares D, Santana MG, et al. Effect of acute physical exercise on patients with chronic primary insomnia. J Clin Sleep Med. 2010;6:270-275.
3. Edinger JD, Olsen MK, Stechuchak KM, et al. Cognitive behavioral therapy for patients with primary insomnia or insomnia associated predominantly with mixed psychiatric disorders: a randomized clinical trial. Sleep. 2009;32:499-510.
Some of patients’ most common complaints involve sleep: too little, too late, never enough. Although sleep disruptions often are related to the psychiatric disorder for which the person seeks treatment, cognitive and behavioral factors play significant roles.1 Unfortunately, quite often patients expect to be given “something” to foster sleep.
Before writing a prescription, be prepared to evaluate sleep disturbances and educate patients about sleep and how it can be facilitated without medication. The mnemonic SLEEP can help you readily access a basic set of nonpharmacologic aids to assess and treat uncomplicated sleep disturbances.
Schedule. Ask patients about their sleep-wake schedule. Is their pattern routine and regular, or unpredictable? Are they “in synch” with the sleep/activity patterns of those with whom they live, or is their schedule “off track” and disrupted by household noise and activities? Consistency is key to normalizing sleep.
Limit. Sensible limits on caffeinated beverages need to be addressed. Strongly encourage patients to limit nicotine and alcohol in-take. Assess the amount as well as timing of their use of these substances. Remind your patient that alcohol and smoking have a direct impact on sleep initiation and can disrupt sleep because of nocturnal withdrawal.
Eliminate. Removing noxious environmental stimuli is critical. Ask patients about the level of nighttime noise, excessive light, and ventilation and temperature of their sleeping area (cooler is better). Eliminate factors that create a “hostile” sleep environment.
Exercise. Regular exercise performed during the day (but not immediately before going to bed) may be an effective antidote to the psychic stress and physical tension that often contribute to insomnia.2 A several-times-per-week routine of brisk walking, riding a bicycle, swimming, or yoga can reduce sleep-onset latency and improve sleep maintenance. An exercise routine can enhance a patient’s overall health and knock out a daytime sleep habit.
Psychotherapy. Cognitive-behavioral therapy for insomnia has demonstrated efficacy in treating sleep disorders.3 Learning how to “catch, check, and change” distorted and negative cognitions regarding sleep onset can be a valuable tool for persons who are motivated to alter their thoughts and behaviors that contribute to sleep complaints, and may simultaneously improve associated anxiety and/or depression.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Some of patients’ most common complaints involve sleep: too little, too late, never enough. Although sleep disruptions often are related to the psychiatric disorder for which the person seeks treatment, cognitive and behavioral factors play significant roles.1 Unfortunately, quite often patients expect to be given “something” to foster sleep.
Before writing a prescription, be prepared to evaluate sleep disturbances and educate patients about sleep and how it can be facilitated without medication. The mnemonic SLEEP can help you readily access a basic set of nonpharmacologic aids to assess and treat uncomplicated sleep disturbances.
Schedule. Ask patients about their sleep-wake schedule. Is their pattern routine and regular, or unpredictable? Are they “in synch” with the sleep/activity patterns of those with whom they live, or is their schedule “off track” and disrupted by household noise and activities? Consistency is key to normalizing sleep.
Limit. Sensible limits on caffeinated beverages need to be addressed. Strongly encourage patients to limit nicotine and alcohol in-take. Assess the amount as well as timing of their use of these substances. Remind your patient that alcohol and smoking have a direct impact on sleep initiation and can disrupt sleep because of nocturnal withdrawal.
Eliminate. Removing noxious environmental stimuli is critical. Ask patients about the level of nighttime noise, excessive light, and ventilation and temperature of their sleeping area (cooler is better). Eliminate factors that create a “hostile” sleep environment.
Exercise. Regular exercise performed during the day (but not immediately before going to bed) may be an effective antidote to the psychic stress and physical tension that often contribute to insomnia.2 A several-times-per-week routine of brisk walking, riding a bicycle, swimming, or yoga can reduce sleep-onset latency and improve sleep maintenance. An exercise routine can enhance a patient’s overall health and knock out a daytime sleep habit.
Psychotherapy. Cognitive-behavioral therapy for insomnia has demonstrated efficacy in treating sleep disorders.3 Learning how to “catch, check, and change” distorted and negative cognitions regarding sleep onset can be a valuable tool for persons who are motivated to alter their thoughts and behaviors that contribute to sleep complaints, and may simultaneously improve associated anxiety and/or depression.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep. 2006;9:1398-1414.
2. Passos GS, Povares D, Santana MG, et al. Effect of acute physical exercise on patients with chronic primary insomnia. J Clin Sleep Med. 2010;6:270-275.
3. Edinger JD, Olsen MK, Stechuchak KM, et al. Cognitive behavioral therapy for patients with primary insomnia or insomnia associated predominantly with mixed psychiatric disorders: a randomized clinical trial. Sleep. 2009;32:499-510.
1. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep. 2006;9:1398-1414.
2. Passos GS, Povares D, Santana MG, et al. Effect of acute physical exercise on patients with chronic primary insomnia. J Clin Sleep Med. 2010;6:270-275.
3. Edinger JD, Olsen MK, Stechuchak KM, et al. Cognitive behavioral therapy for patients with primary insomnia or insomnia associated predominantly with mixed psychiatric disorders: a randomized clinical trial. Sleep. 2009;32:499-510.
Topical diclofenac for sprains? These doctors say No
“An alternative to oral NSAIDs for acute musculoskeletal injuries,” (PURLs, J Fam Pract. 2011;60:147-148) promotes an unreasonable conclusion. The Cochrane review on which it is based found a 50% response rate to topical diclofenac for ankle sprains, compared with a 25% response to placebo. (A response was defined as ≥50% reduction in pain.) The authors of the Cochrane review seem to think this is adequate, and the authors of this PURL apparently agree.
First, they overstate the benefit. If we consider that 1 in 4 patients respond to placebo, we find that only 1 in 4 patients actually have what the authors describe as an adequate response to topical diclofenac. That still means that half the patients I see for ankle sprain could be calling at 11:00 PM to complain about inadequate pain relief.
Second, the Cochrane reviewers did not use an active control group with oral NSAIDs, leaving us to guess whether oral NSAIDs are equally effective, worse, or better than topical agents. The great majority of people I treat for ankle sprains obtain adequate pain relief with oral therapy. Studies have compared topical and oral NSAIDs, but the authors make no mention of these comparisons.
I trust and rely on the Cochrane reviews, but they are not the word of God. This review did not provide useful information. The space would have been better devoted to a topic I can put into practice.
Dean M. Center, MD
Bozeman, MT
I find it difficult to believe that these ivory tower researchers used topical diclofenac as their base. I’ve used topical agents for acute musculoskeletal pain for 40 years, costing one-tenth (or less) of the price of diclofenac. Only a few patients have complained of skin reactions. For more severe cases, capsaicin is a good choice; otherwise, a methyl salicylate product is very effective, at a concentration of 30% or more. Both are available as generics and do not require a prescription.
Robert Migliorino, DO
Lake Preston, SD
The authors respond:
We appreciate the issues raised by the letter writers. Dr. Center notes that there are few head-to-head trials with other therapy options, such as oral NSAIDs or acetaminophen. We agree. This Cochrane review demonstrates another possible option for pain relief for patients who cannot tolerate oral NSAIDs or prefer not to take them. The body of literature comparing topical to oral NSAIDs is small, but we could not find any high-quality evidence to suggest that oral NSAIDs are more effective.
Dr. Center also questions the clinical utility of a medication that must be given to 4 patients in order for 1 to have a 50% reduction in pain (number needed to treat [NNT]=4). The NNT for topical NSAIDs is about the same.1 For acute musculoskeletal injuries, 1 patient in 4 will respond to placebo, 1 in 4 will respond to active topical or oral therapy, and 2 in 4 will fail treatment. Whether these response rates are acceptable is an individual clinical decision to be made with the patient. We believe they are acceptable to most patients.
We thank Dr. Migliorino for bringing to light other topical pain medications. Diclofenac is the only topical NSAID available in the United States, which is why we chose to highlight it. The Cochrane review did not include salicylates because they are no longer classified as topical NSAIDS, and capsaicin was not included as it is not an NSAID. Both may very well offer pain relief.
The purpose of PURLs (Priority Updates from the Research Literature) is to identify and disseminate evidence that should change the practice of family medicine. We believe that this Cochrane review demonstrates that topical NSAIDs are effective options for acute musculoskeletal injuries and that many primary care physicians would be unfamiliar with this option.
Nina V. Rogers, MD
Kate Rowland, MD
Chicago
Reference
1. Paolini J, Orchard J. The use of therapeutic medications for soft-tissue injuries in sports medicine. Med J Australia. 2005;183:384-388.
“An alternative to oral NSAIDs for acute musculoskeletal injuries,” (PURLs, J Fam Pract. 2011;60:147-148) promotes an unreasonable conclusion. The Cochrane review on which it is based found a 50% response rate to topical diclofenac for ankle sprains, compared with a 25% response to placebo. (A response was defined as ≥50% reduction in pain.) The authors of the Cochrane review seem to think this is adequate, and the authors of this PURL apparently agree.
First, they overstate the benefit. If we consider that 1 in 4 patients respond to placebo, we find that only 1 in 4 patients actually have what the authors describe as an adequate response to topical diclofenac. That still means that half the patients I see for ankle sprain could be calling at 11:00 PM to complain about inadequate pain relief.
Second, the Cochrane reviewers did not use an active control group with oral NSAIDs, leaving us to guess whether oral NSAIDs are equally effective, worse, or better than topical agents. The great majority of people I treat for ankle sprains obtain adequate pain relief with oral therapy. Studies have compared topical and oral NSAIDs, but the authors make no mention of these comparisons.
I trust and rely on the Cochrane reviews, but they are not the word of God. This review did not provide useful information. The space would have been better devoted to a topic I can put into practice.
Dean M. Center, MD
Bozeman, MT
I find it difficult to believe that these ivory tower researchers used topical diclofenac as their base. I’ve used topical agents for acute musculoskeletal pain for 40 years, costing one-tenth (or less) of the price of diclofenac. Only a few patients have complained of skin reactions. For more severe cases, capsaicin is a good choice; otherwise, a methyl salicylate product is very effective, at a concentration of 30% or more. Both are available as generics and do not require a prescription.
Robert Migliorino, DO
Lake Preston, SD
The authors respond:
We appreciate the issues raised by the letter writers. Dr. Center notes that there are few head-to-head trials with other therapy options, such as oral NSAIDs or acetaminophen. We agree. This Cochrane review demonstrates another possible option for pain relief for patients who cannot tolerate oral NSAIDs or prefer not to take them. The body of literature comparing topical to oral NSAIDs is small, but we could not find any high-quality evidence to suggest that oral NSAIDs are more effective.
Dr. Center also questions the clinical utility of a medication that must be given to 4 patients in order for 1 to have a 50% reduction in pain (number needed to treat [NNT]=4). The NNT for topical NSAIDs is about the same.1 For acute musculoskeletal injuries, 1 patient in 4 will respond to placebo, 1 in 4 will respond to active topical or oral therapy, and 2 in 4 will fail treatment. Whether these response rates are acceptable is an individual clinical decision to be made with the patient. We believe they are acceptable to most patients.
We thank Dr. Migliorino for bringing to light other topical pain medications. Diclofenac is the only topical NSAID available in the United States, which is why we chose to highlight it. The Cochrane review did not include salicylates because they are no longer classified as topical NSAIDS, and capsaicin was not included as it is not an NSAID. Both may very well offer pain relief.
The purpose of PURLs (Priority Updates from the Research Literature) is to identify and disseminate evidence that should change the practice of family medicine. We believe that this Cochrane review demonstrates that topical NSAIDs are effective options for acute musculoskeletal injuries and that many primary care physicians would be unfamiliar with this option.
Nina V. Rogers, MD
Kate Rowland, MD
Chicago
“An alternative to oral NSAIDs for acute musculoskeletal injuries,” (PURLs, J Fam Pract. 2011;60:147-148) promotes an unreasonable conclusion. The Cochrane review on which it is based found a 50% response rate to topical diclofenac for ankle sprains, compared with a 25% response to placebo. (A response was defined as ≥50% reduction in pain.) The authors of the Cochrane review seem to think this is adequate, and the authors of this PURL apparently agree.
First, they overstate the benefit. If we consider that 1 in 4 patients respond to placebo, we find that only 1 in 4 patients actually have what the authors describe as an adequate response to topical diclofenac. That still means that half the patients I see for ankle sprain could be calling at 11:00 PM to complain about inadequate pain relief.
Second, the Cochrane reviewers did not use an active control group with oral NSAIDs, leaving us to guess whether oral NSAIDs are equally effective, worse, or better than topical agents. The great majority of people I treat for ankle sprains obtain adequate pain relief with oral therapy. Studies have compared topical and oral NSAIDs, but the authors make no mention of these comparisons.
I trust and rely on the Cochrane reviews, but they are not the word of God. This review did not provide useful information. The space would have been better devoted to a topic I can put into practice.
Dean M. Center, MD
Bozeman, MT
I find it difficult to believe that these ivory tower researchers used topical diclofenac as their base. I’ve used topical agents for acute musculoskeletal pain for 40 years, costing one-tenth (or less) of the price of diclofenac. Only a few patients have complained of skin reactions. For more severe cases, capsaicin is a good choice; otherwise, a methyl salicylate product is very effective, at a concentration of 30% or more. Both are available as generics and do not require a prescription.
Robert Migliorino, DO
Lake Preston, SD
The authors respond:
We appreciate the issues raised by the letter writers. Dr. Center notes that there are few head-to-head trials with other therapy options, such as oral NSAIDs or acetaminophen. We agree. This Cochrane review demonstrates another possible option for pain relief for patients who cannot tolerate oral NSAIDs or prefer not to take them. The body of literature comparing topical to oral NSAIDs is small, but we could not find any high-quality evidence to suggest that oral NSAIDs are more effective.
Dr. Center also questions the clinical utility of a medication that must be given to 4 patients in order for 1 to have a 50% reduction in pain (number needed to treat [NNT]=4). The NNT for topical NSAIDs is about the same.1 For acute musculoskeletal injuries, 1 patient in 4 will respond to placebo, 1 in 4 will respond to active topical or oral therapy, and 2 in 4 will fail treatment. Whether these response rates are acceptable is an individual clinical decision to be made with the patient. We believe they are acceptable to most patients.
We thank Dr. Migliorino for bringing to light other topical pain medications. Diclofenac is the only topical NSAID available in the United States, which is why we chose to highlight it. The Cochrane review did not include salicylates because they are no longer classified as topical NSAIDS, and capsaicin was not included as it is not an NSAID. Both may very well offer pain relief.
The purpose of PURLs (Priority Updates from the Research Literature) is to identify and disseminate evidence that should change the practice of family medicine. We believe that this Cochrane review demonstrates that topical NSAIDs are effective options for acute musculoskeletal injuries and that many primary care physicians would be unfamiliar with this option.
Nina V. Rogers, MD
Kate Rowland, MD
Chicago
Reference
1. Paolini J, Orchard J. The use of therapeutic medications for soft-tissue injuries in sports medicine. Med J Australia. 2005;183:384-388.
Reference
1. Paolini J, Orchard J. The use of therapeutic medications for soft-tissue injuries in sports medicine. Med J Australia. 2005;183:384-388.
Forget the mental status test—and learn to listen
My wife was diagnosed with Alzheimer’s disease (AD) at age 63. Unfortunately, her AD went misdiagnosed for several years while I repeatedly tried to convince her doctors that she was experiencing dementia. For 3 years, doctors administered the Mini-Mental State Exam (MMSE) and other cognitive tests, but she consistently did very well (on one occasion scoring 29 out of a possible 30 on the same day that she couldn’t remember our granddaughters’ names). An MRI of her brain showed no definitive signs of AD. Thus, she was treated for stress, anxiety, and depression, although I told both our primary care physician (PCP) and a neurologist that her symptoms couldn’t possibly be due to any of these conditions.
I documented my wife’s behaviors in weekly logs and brought copies to each visit, but invariably my notes went unread or were quickly dismissed. When I told the PCP I thought the medications prescribed by the neurologist weren’t working because she was declining further, he deferred to the specialist, who advised us to “stay the course.” Finally, I convinced my wife to see a psychiatrist affiliated with a major medical center who requested copies of my logs even before our first visit.
At that visit, the psychiatrist interviewed us at length, reviewed previous tests, and administered his own cognitive, physical, and neurological tests. He then ordered a new battery of tests and referred us to his facility’s AD center, where my wife finally received a diagnosis of early-onset Alzheimer’s.
Doctors can improve their chance of accurate diagnosis simply by listening to the spouse or significant other. One recent study found that the AD8, an 8-question, 2-minute screening test given to a close friend or family member, was superior to conventional testing in its ability to detect signs of early dementia.1
Although doctors can’t identify the cause of AD or offer hope for a cure, early diagnosis is important. The sooner the patient starts taking medication designed to help slow the degenerative progression, the more effective the drugs may be.
So please, doctors, if a family member or loved one reports worrisome symptoms of possible dementia, listen carefully. The observations of someone close to the patient just may be more accurate than any screening test you could give.
Allan Vann
Commack, NY
Reference
1. Galvin JE, Fagan AM, Holtzman DM, et al. Relationship of dementia screening tests with biomarkers of Alzheimer’s disease. Brain. 2010;133:3290-3300.
My wife was diagnosed with Alzheimer’s disease (AD) at age 63. Unfortunately, her AD went misdiagnosed for several years while I repeatedly tried to convince her doctors that she was experiencing dementia. For 3 years, doctors administered the Mini-Mental State Exam (MMSE) and other cognitive tests, but she consistently did very well (on one occasion scoring 29 out of a possible 30 on the same day that she couldn’t remember our granddaughters’ names). An MRI of her brain showed no definitive signs of AD. Thus, she was treated for stress, anxiety, and depression, although I told both our primary care physician (PCP) and a neurologist that her symptoms couldn’t possibly be due to any of these conditions.
I documented my wife’s behaviors in weekly logs and brought copies to each visit, but invariably my notes went unread or were quickly dismissed. When I told the PCP I thought the medications prescribed by the neurologist weren’t working because she was declining further, he deferred to the specialist, who advised us to “stay the course.” Finally, I convinced my wife to see a psychiatrist affiliated with a major medical center who requested copies of my logs even before our first visit.
At that visit, the psychiatrist interviewed us at length, reviewed previous tests, and administered his own cognitive, physical, and neurological tests. He then ordered a new battery of tests and referred us to his facility’s AD center, where my wife finally received a diagnosis of early-onset Alzheimer’s.
Doctors can improve their chance of accurate diagnosis simply by listening to the spouse or significant other. One recent study found that the AD8, an 8-question, 2-minute screening test given to a close friend or family member, was superior to conventional testing in its ability to detect signs of early dementia.1
Although doctors can’t identify the cause of AD or offer hope for a cure, early diagnosis is important. The sooner the patient starts taking medication designed to help slow the degenerative progression, the more effective the drugs may be.
So please, doctors, if a family member or loved one reports worrisome symptoms of possible dementia, listen carefully. The observations of someone close to the patient just may be more accurate than any screening test you could give.
Allan Vann
Commack, NY
My wife was diagnosed with Alzheimer’s disease (AD) at age 63. Unfortunately, her AD went misdiagnosed for several years while I repeatedly tried to convince her doctors that she was experiencing dementia. For 3 years, doctors administered the Mini-Mental State Exam (MMSE) and other cognitive tests, but she consistently did very well (on one occasion scoring 29 out of a possible 30 on the same day that she couldn’t remember our granddaughters’ names). An MRI of her brain showed no definitive signs of AD. Thus, she was treated for stress, anxiety, and depression, although I told both our primary care physician (PCP) and a neurologist that her symptoms couldn’t possibly be due to any of these conditions.
I documented my wife’s behaviors in weekly logs and brought copies to each visit, but invariably my notes went unread or were quickly dismissed. When I told the PCP I thought the medications prescribed by the neurologist weren’t working because she was declining further, he deferred to the specialist, who advised us to “stay the course.” Finally, I convinced my wife to see a psychiatrist affiliated with a major medical center who requested copies of my logs even before our first visit.
At that visit, the psychiatrist interviewed us at length, reviewed previous tests, and administered his own cognitive, physical, and neurological tests. He then ordered a new battery of tests and referred us to his facility’s AD center, where my wife finally received a diagnosis of early-onset Alzheimer’s.
Doctors can improve their chance of accurate diagnosis simply by listening to the spouse or significant other. One recent study found that the AD8, an 8-question, 2-minute screening test given to a close friend or family member, was superior to conventional testing in its ability to detect signs of early dementia.1
Although doctors can’t identify the cause of AD or offer hope for a cure, early diagnosis is important. The sooner the patient starts taking medication designed to help slow the degenerative progression, the more effective the drugs may be.
So please, doctors, if a family member or loved one reports worrisome symptoms of possible dementia, listen carefully. The observations of someone close to the patient just may be more accurate than any screening test you could give.
Allan Vann
Commack, NY
Reference
1. Galvin JE, Fagan AM, Holtzman DM, et al. Relationship of dementia screening tests with biomarkers of Alzheimer’s disease. Brain. 2010;133:3290-3300.
Reference
1. Galvin JE, Fagan AM, Holtzman DM, et al. Relationship of dementia screening tests with biomarkers of Alzheimer’s disease. Brain. 2010;133:3290-3300.
Rotavirus infection: Optimal treatment and prevention
• Patients with rotavirus infection require oral, enteral, or intravenous fluids to treat dehydration. A
• Give the first dose of rotavirus (RV) vaccine between the ages of 6 weeks and 14 weeks 6 days; give subsequent doses at 4- to 10-week intervals, completing by 8 months. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Rotavirus is the most common cause of severe gastroenteritis in infants and children younger than 5 years of age, and it accounts for approximately 5% of childhood deaths worldwide.1 In the United States, rotavirus causes numerous cases of dehydrating diarrhea and vomiting, and is responsible for direct and indirect healthcare costs of approximately $1 billion per year. Infection during childhood is almost universal.2
Improved personal hygiene and community sanitation have steadily reduced the prevalence of bacterial and parasitic disease. But these measures have had little effect on the spread of rotavirus and its potential complications of severe dehydration, hospitalization, and even death.1 Importantly, we now have the means to vaccinate against rotavirus infection and dramatically reduce the incidence of disease. In this article, I describe the available vaccines and the vaccination recommendations endorsed by the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP). I also review supportive treatment for rotavirus infection, which entails both do’s and don’ts.
Who is at risk of rotavirus disease?
For most term neonates, rotavirus disease is mild, perhaps because of partial protection from maternal antibodies.3 However, premature infants lacking full maternal antibody protection often suffer from more serious gastroenteritis. The most severe infections usually strike children between the ages of 4 months, when maternally derived antibody protection wanes, and 23 months, when dehydration risk lessens.4-6
The virus spreads from person to person via the fecal–oral route.6,7 Thirty percent to 50% of family members of an infected child may also become infected, but disease in older children and adults is usually subclinical or mild.6 Outbreaks of rotavirus are common in childcare centers and in children’s hospitals.7,8
How the disease presents
Rotavirus gastroenteritis peaks during the winter. With mild cases, a watery diarrhea will last a few days. In severe cases, onset is usually abrupt with fever, abdominal pain, and vomiting, which can precede diarrhea. A third of patients have a temperature higher than 102°F (38.9°C).6 There is a risk of dehydration, shock, and even, occasionally, infant death.9
Typically, the incubation period is 1 to 4 days, and the infection lasts 3 to 7 days. However, damage to the brush border of the intestinal villi can produce persistent disaccharide malabsorption, resulting in prolonged diarrhea even after resolution of infection.10,11 Stools generally do not contain blood or leukocytes. Ultrasound examination during rotavirus infections has shown thickening of the distal ileum and lymphadenopathy, which may predispose to intussusception.12 Other problems possibly linked to wild-type rotavirus infection are Kawasaki disease and sudden infant death syndrome. Recurrent rotavirus infection with one of the many different serotypes is common during childhood.
More than 25 different assays can detect rotavirus in stool, but the most reliable method is direct electron microscopy. A suitable clinically available alternative is enzyme immunoassay testing of stool samples. In mild cases, testing to detect rotavirus is not necessary. But for bloody, severe, or persistent diarrhea, stool testing for rotavirus and other entities is warranted.
Supportive treatment: Do’s and don’ts
No specific antiviral treatment is available for rotavirus infection. That said, the do’s and don’ts that follow will help guide your care.
DO administer oral, enteral, or intravenous (IV) fluids to prevent or correct dehydration. Oral rehydration therapy is the standard treatment for dehydration in anyone with acute gastroenteritis, including that caused by rotavirus. The recommended World Health Organization (WHO) oral rehydration solution contains sodium, chloride, and electrolytes (TABLE 1).13 Rice-based oral rehydration solution is an easily metabolized carbohydrate formulation that helps repair damaged tissues and enhances electrolyte absorption.9 WHO has endorsed guidelines that base fluid replacement on the patient’s age and weight, and that recommend oral zinc intake (10 mg/d for 10-14 days up to age 6 months; 20 mg/d for 10-14 days for older children) for all episodes of diarrhea (http://hetv.org/pdf/diarrhoea-guidelines.pdf). Oral glucose electrolyte solutions containing less sodium and chloride are also effective treatments.
DO recommend frequent small doses of oral rehydration solution, even if the patient is vomiting.14 Rehydration volumes are suggested in TABLE 1. Alternatively, give 10 to 20 mL/kg for each diarrheal episode, and 2 mL/kg for each bout of emesis. Feeding frequent small volumes (30 mL every 5-10 minutes) reduces the risk of emesis.
Although oral rehydration solutions are contraindicated for infants and young children with depressed consciousness, vomiting is not a contraindication to oral intake. About half of the oral intake stays in the stomach, even after vomiting. A single dose of ondansetron may safely reduce vomiting.15
Patients with mainly diarrhea can take fluids or feed at will. With children who refuse to drink, oral rehydration solutions can be administered via nasogastric tube at approximately 5 mL/min to limit vomiting and maintain hydration.14 In dehydrated infants and toddlers with collapsed veins, nasogastric intubation has been shown to be less traumatic than repetitive attempts at placing IV catheters.
DO encourage nursing mothers to con tinue breastfeeding during rehydration treatments. If a mother is bottle feeding, keep this in mind: Rotavirus can cause temporary lactase deficiency for some non-breastfeeding infants; lactose-free formulas may help.
DON’T assume that parents know how to provide proper supplementation. Tell them to avoid fluids containing mostly sugar that lack significant electrolyte supplementation (eg, cola) unless no other fluid alternative is available. Advise caregivers to avoid juices and other liquids high in complex or simple sugars because the osmotic load may worsen diarrhea.14
DON’T give antidiarrheal agents for acute treatment in infants and young children. Such treatment has resulted in death.14
TABLE 1
Prevent or correct dehydration using the WHO-recommended oral rehydration salts solution13
| With this formulation… | …rehydrate per these specifications… | …at this rate | ||
|---|---|---|---|---|
| Component (mmol/L) | Age | Weight (kg) | mL solution/4 h | |
| Sodium (75); chloride (65); glucose (75); potassium (20); citrate (10) | ≤4 mo 4-12 mo 12 mo-2 y 2-5 y | <6 6 to <10 10 to <12 12 to 19 | 200-400 400-700 700-900 900-1400 | |
| WHO, World Health Organization. | ||||
KEEP IN MIND
Hospitalization may be needed to replace fluids via IV or interosseous supplementation. For the severely dehydrated child, 20 mL/kg isotonic fluid can be administered as a rapid bolus.14 It may be necessary to repeat a rapid fluid infusion of 10 to 20 mL/kg every 20 to 30 minutes. For less severely ill infants who require IV rehydration, standard references such as the Harriet Lane Handbook16 provide excellent guidance.
Probiotics may help. Consider probiotics with Lactobacillus or Bifida bacterium to reduce the severity of diarrhea in infants and children who are mildly to moderately ill.17,18 Their usefulness in the severely ill patient has not been demonstrated.
Available vaccines and clinical recommendations
In February 2006, the US Food and Drug Administration (FDA) licensed a 3-dose, oral pentavalent rotavirus vaccine (RV5, RotaTeq) for use among infants. The vaccine contains live reassortant rotaviruses19—4 human rotavirus G outer-surface proteins and 1 human P attachment protein reassorted into a bovine rotavirus not infectious to humans.
In February 2008, the FDA approved a 2-dose, oral monovalent rotavirus vaccine (RV1, Rotarix), an attenuated live human rotavirus containing 1 G protein and 1 P protein. Both vaccines have proven to be clinically effective in rotavirus prevention trials, but effectiveness may depend on which rotavirus serotypes circulate each season.
ACIP, AAP, and AAFP recommend that all infants be routinely vaccinated with either RV5 or RV1.6,20–22 Vaccination should be complete by the time infants reach the age of 8 months (TABLE 2). Guidelines for vaccination emphasize the following points:
Timing. According to the ACIP, the first dose of either vaccine must be administered between the ages of 6 weeks and 14 weeks 6 days (the RV5 manufacturer [Merck] states a maximum age of 12 weeks). Give subsequent doses at 4- to 10-week intervals, as long as all doses are administered by 8 months of age. The RV1 manufacturer (GlaxoSmithKline) suggests completing the second (final) dose of its vaccine by age 24 weeks.
If an infant 15 weeks of age or older accidentally receives a first dose of RV vaccine, the series should be continued, as long as the last dose can be given by 8 months of age. Either vaccine can be administered concurrently with all other vaccines.
Contraindications. The only absolute contraindications to RV5 administration are a demonstrated hypersensitivity to any component of the vaccine and severe combined immunodeficiency disease (SCID). Contraindications to RV1 vaccine are vaccine component hypersensitivity, SCID, latex-induced allergy (anaphylaxis), and uncorrected malformation of the gastrointestinal (GI) tract that might predispose to intussusception.
Precautions. Precautions for vaccines include other forms of primary or secondary immunocompromised or immunodeficiency states, including cancer and acute or chronic GI disorders such as ongoing gastroenteritis or intussusception. Infants with transient mild illness with or without low-grade fever and infants who are breastfeeding can receive either vaccine. RV5 is shed in 9% of recipients and RV1 in 26% of recipients after Dose 1, but transmission of vaccine virus is not known to occur. Likewise, reversion of vaccine virus to more virulent pathogens is not known to occur. A household member with an immuno-compromised condition does not preclude giving either RV vaccine to an infant. The risk of transmitting vaccine virus is much smaller than the risk of acquiring infectious wild-type rotavirus.
Regurgitation of a vaccine dose is uncommon. When it does occur, the RV5 vaccine should not be repeated; some of the vaccine dose is retained and the safety of the additional vaccine from a second dose is unknown. Readministration of a dose of RV1 is not recommended, although not contraindicated.
TABLE 2
Recommended rotavirus live virus vaccine dosing6
| Patient age (mo) | RV5 (RotaTeq) | RV1 (Rotarix) |
|---|---|---|
| 2 | 2 mL | 1 mL |
| 4 | 2 mL | 1 mL* |
| 6 | 2 mlL* | — |
| *The final dose of either vaccine must be given by no later than 8 months of age. | ||
Vaccine efficacy
The safety and efficacy of live rotavirus vaccines were demonstrated in large studies that enrolled 71,725 children in RV5 vaccine trials23 and 24,163 children in RV1 vaccine trials.21 The pivotal RV5 study included a nested substudy to evaluate efficacy against any G1–G4 rotavirus gastroenteritis.
RV5 (RotaTeq) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV5 vaccine effectively prevented severe rotavirus infection in 98% of cases, and reduced hospitalization by 95%, emergency department visits by 94%, physician office visits by 86%, and all rotavirus cases by 74% for infants who received all 3 doses of vaccine according to protocol.23 Hospitalization for any-cause gastroenteritis was reduced by 63%. Second-season data showed persistence of antibody protection. All 3 doses of vaccine are required for maximum protection.23
Both preterm and term infants received their first dose of vaccine between 6 and 12 weeks of life. For preterm infants who are experiencing medical difficulties, the first dose of vaccine may be delayed until the patient is stable, if it can be given before 15 weeks of age.
RV1 (Rotarix) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV1 vaccine was 85% (Latin America) to 96% (Europe) effective in preventing severe rotavirus infection. It reduced hospitalization due to rotavirus by 85% (Latin America) to 100% (Europe), and all rotavirus cases by 87% (Europe) for infants who received both doses of the vaccine according to protocol. For the second season, the vaccine reduced severe rotavirus disease by 70% to 96%, and any rotavirus disease by 73% to 89%, showing persistence of antibody protection.6
Adverse events
With both vaccines, common side effects include irritability, flatulence, fever, vomiting, diarrhea, cough, runny nose, and loss of appetite. The RV5 vaccine has been shown not to increase the risk of intussusception compared with placebo.24,25 The RV1 vaccine should not be used in children with an uncorrected bowel malformation, due to unproven increased risk of intussusception. Risk of death from complications after administration of either vaccine did not differ from that among children receiving placebo.
Postmarketing surveillance of vaccination outcomes
Even though rotavirus vaccine coverage with RV5 RotaTeq in the 2007-2008 and 2008-2009 seasons was far less than that with other childhood immunizations, the number of rotavirus infections dropped by >60% in both 2008 and 2009.26 The number of stool tests for rotavirus and the percentage of positive results also dropped dramatically.
Additionally, the rotavirus peak incidence was delayed 2 to 4 months until April 2008 and March 2009.26 Incidence was reduced in all age groups, suggesting the possibility of herd immunity despite a low vaccine coverage rate (estimates are 57% for ≥1 dose) that would not be expected to provide herd immunity.27 Hospitalizations in the United States for rotavirus gastroenteritis dropped by as much as 85%,28 markedly reducing costs for gastroenteritis.
In a 2010 report from an emergency department in Houston, a complete RV5 vaccine series conferred 82% protection against acute gastroenteritis, 96% against severe rotavirus disease requiring IV rehydration, and 100% against hospitalization.29 For more on the vaccine, see the report by Yen et al.30
Reports of the effectiveness of Rotarix in postmarketing surveillance are limited, but the vaccine does seem to provide broad coverage.31
As of April 11, 2011, RV5 costs $59.76/$69.59 per dose in the public/private sectors, respectively (3-dose series: $179.28/$208.77); RV1 costs $89.25/$102.50 per dose (2-dose series: $178.50/$205). routine vaccination costs about $138 per case averted and $3024 per serious case averted. neither vaccine contains thimerosal. Both vaccines are available in 10-dose packs.
Source: Centers for Disease Control and Prevention. CDC vaccine price list. Prices last reviewed/updated: April 8, 2011. Available at: http://www.cdc.gov/vaccines/programs/vfc/cdc-vac-price-list.htm. Accessed April 11, 2011.
Incorporating rotavirus vaccine into a family medicine practice
Given inadequately reimbursed costs including the cost of stocking RV vaccine (see “Costs of RV vaccines” above), family physicians who treat relatively few infants must determine whether offering RV vaccine fits within their practices.
For family physicians who do treat infants, offering RV vaccination makes sense. These oral vaccines are highly effective, safe, and easy to administer, and will prevent a great deal of worry and calls regarding infants who have a fever or diarrhea or are vomiting. Due to the costs of stocking all vaccines, private practitioners are wise to purchase vaccine loss insurance. Many insurance agencies provide a rider on office insurance policies to cover vaccine supplies.
CORRESPONDENCE
Donald B. Middleton, MD, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; middletondb@upmc.edu
1. Parashar UD, Gibson CJ, Bresee JS, et al. Rotavirus and severe childhood diarrhea. Emerg Infect Dis. 2006;12:304-306.
2. Malek MA, Curns AT, Holman RC, et al. Diarrhea- and rotavirus-associated hospitalizations among children less than 5 years of age: United States, 1997 and 2000. Pediatrics. 2006;117:1887-1892.
3. Xu J, Dennehy P, Keyserling H, et al. Serum antibody responses in children with rotavirus diarrhea can serve as proxy for protection. Clin Diagn Lab Immunol. 2005;12:273-279.
4. World Health Organization. Rotavirus vaccines. Wkly Epidemiol Rec. 2007;82:285-295.
5. Ward RL, Bernstein DI, Staat MA. Rotaviruses. In: Feigin RD, Cherry JD, eds. Textbook of Pediatric Infectious Disease. Vol 2, 6th ed. New York, NY: Saunders; 2009:2245-2270.
6. Centers for Disease Control and Prevention. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2009;58(RR-2):1-25.
7. Butz AM, Fosarelli P, Dick J, et al. Prevalence of rotavirus on high-risk fomites in day-care facilities. Pediatrics. 1993;92:202-205.
8. Fischer TK, Bresee JS, Glass RI. Rotavirus vaccines and the prevention of hospital-acquired diarrhea in children. Vaccine. 2004;22(suppl):S49-S54.
9. Kapikian AZ, Hoshino Y, Chanock RM. Rotaviruses. In: Knipe DM, Howley PM, Griffin DE, et al, eds. Fields Virology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2001: 1787-1825.
10. Lorrot M, Vasseur M. How do the rotavirus NSP4 and bacterial enterotoxins lead differently to diarrhea? Virol J. 2007;4:31.-
11. Ramig RF. Pathogenesis of intestinal and systemic rotavirus infection. J Virol. 2004;78:10213-10220.
12. Robinson CG, Hernanz-Schulman M, Zhu Y, et al. Evaluation of anatomic changes in young children with natural rotavirus infection: is intussusception biologically plausible? J Infect Dis. 2004;189:1382-1387.
13. World Health Organization. Oral Rehydration Salts: Production of the New ORS. Geneva, Switzerland: WHO Document Production Services; 2006. Available at: http://whqlibdoc.who.int/hq/2006/WHO_FCH_CAH_06.1.pdf. Accessed April 11, 2011.
14. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1-16.
15. DeCamp LR, Byerley JS, Doshi N, et al. Use of antiemetic agents in acute gastroenteritis: a systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2008;162:858-865.
16. The Johns Hopkins Hospital, Custer JW, Rau RE. Harriet Lane Handbook: A Manual for Pediatric House Officers. 18th ed. St. Louis, Mo: Mosby/Elsevier; 2008.
17. Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ. 2007;335:340.-
18. Van Niel CW, Feudtner C, Garrison MM, et al. Lactobacillus therapy for acute infectious diarrhea in children: a meta- analysis. Pediatrics. 2002;109:678-684.
19. Heaton PM, Goveia MG, Miller JM, et al. Development of a pentavalent rotavirus vaccine against prevalent serotypes of rotavirus gastroenteritis. J Infect Dis. 2005;192(suppl 1):S17-S21.
20. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years — United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(5):1-4.
21. American Academy of Pediatrics (AAP) Committee on Infectious Diseases. Prevention of rotavirus disease: updated guidelines for use of rotavirus vaccine. Pediatrics. 2009;123:1412-1420.
22. Temte JL. Practice guidelines. ACIP releases 2009 child and adolescent immunization schedules. Am Fam Physician. 2009;79:56.-Available at: http://www.aafp.org/afp/2009/0101/p56.html. Accessed January 4, 2010.
23. Vesikari T, Matson DO, Dennehy P, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354:23-33.
24. Centers for Disease Control and Prevention. Intussusception among recipients of rotavirus vaccine: United States, 1998– 1999. MMWR Morb Mortal Wkly Rep. 1999;48:577-581.
25. Centers for Disease Control and Prevention. Postmarketing monitoring of intussusception after RotaTeq vaccine: United States. February 1, 2006–February 15, 2007. MMWR Morb Mortal Wkly Rep. 2007;56:218-222.
26. Centers for Disease Control and Prevention. Reduction in rotavirus after vaccine introduction — United States, 2000-2009. MMWR Morb Mortal Wkly Rep. 2009;58:1146-1149.
27. Clark HF, Lawley D, Mallette LA, et al. Decline in cases of rotavirus gastroenteritis presenting to The Children’s Hospital of Philadelphia after introduction of a pentavalent rotavirus vaccine. Clin Vaccine Immunol. 2009;16:382-386.
28. Chang HG, Smith P, Tserenpuntsag B, et al. Reduction in New York hospitalizations for diarrhea and rotavirus. Presented at: 43rd National Immunization Conference; March 30-April 2, 2009; Dallas, Tex. Abstract 41. Available at: http://cdc.confex.com/cdc/nic2009/webprogram/Paper18073.html. Accessed April 15, 2011.
29. Boom JA, Tate JE, Sahni LC, et al. Effectiveness of pentavalent rotavirus vaccine in a large urban population in the United States. Pediatrics. 2010;125:e199-e207.
30. Yen C, Tate JE, Wenk JD, et al. Diarrhea-associated hospitalizations among US children over 2 rotavirus seasons after vaccine introduction. Pediatrics. 2011;127:e9-e15.
31. Correia JB, Patel MM, Nakagomi O, et al. Effectiveness of monovalent rotavirus vaccine (Rotarix) against severe diarrhea caused by serotypically unrelated G2P[4] strains in Brazil. J Infect Dis. 2010;201:363-369.
• Patients with rotavirus infection require oral, enteral, or intravenous fluids to treat dehydration. A
• Give the first dose of rotavirus (RV) vaccine between the ages of 6 weeks and 14 weeks 6 days; give subsequent doses at 4- to 10-week intervals, completing by 8 months. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Rotavirus is the most common cause of severe gastroenteritis in infants and children younger than 5 years of age, and it accounts for approximately 5% of childhood deaths worldwide.1 In the United States, rotavirus causes numerous cases of dehydrating diarrhea and vomiting, and is responsible for direct and indirect healthcare costs of approximately $1 billion per year. Infection during childhood is almost universal.2
Improved personal hygiene and community sanitation have steadily reduced the prevalence of bacterial and parasitic disease. But these measures have had little effect on the spread of rotavirus and its potential complications of severe dehydration, hospitalization, and even death.1 Importantly, we now have the means to vaccinate against rotavirus infection and dramatically reduce the incidence of disease. In this article, I describe the available vaccines and the vaccination recommendations endorsed by the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP). I also review supportive treatment for rotavirus infection, which entails both do’s and don’ts.
Who is at risk of rotavirus disease?
For most term neonates, rotavirus disease is mild, perhaps because of partial protection from maternal antibodies.3 However, premature infants lacking full maternal antibody protection often suffer from more serious gastroenteritis. The most severe infections usually strike children between the ages of 4 months, when maternally derived antibody protection wanes, and 23 months, when dehydration risk lessens.4-6
The virus spreads from person to person via the fecal–oral route.6,7 Thirty percent to 50% of family members of an infected child may also become infected, but disease in older children and adults is usually subclinical or mild.6 Outbreaks of rotavirus are common in childcare centers and in children’s hospitals.7,8
How the disease presents
Rotavirus gastroenteritis peaks during the winter. With mild cases, a watery diarrhea will last a few days. In severe cases, onset is usually abrupt with fever, abdominal pain, and vomiting, which can precede diarrhea. A third of patients have a temperature higher than 102°F (38.9°C).6 There is a risk of dehydration, shock, and even, occasionally, infant death.9
Typically, the incubation period is 1 to 4 days, and the infection lasts 3 to 7 days. However, damage to the brush border of the intestinal villi can produce persistent disaccharide malabsorption, resulting in prolonged diarrhea even after resolution of infection.10,11 Stools generally do not contain blood or leukocytes. Ultrasound examination during rotavirus infections has shown thickening of the distal ileum and lymphadenopathy, which may predispose to intussusception.12 Other problems possibly linked to wild-type rotavirus infection are Kawasaki disease and sudden infant death syndrome. Recurrent rotavirus infection with one of the many different serotypes is common during childhood.
More than 25 different assays can detect rotavirus in stool, but the most reliable method is direct electron microscopy. A suitable clinically available alternative is enzyme immunoassay testing of stool samples. In mild cases, testing to detect rotavirus is not necessary. But for bloody, severe, or persistent diarrhea, stool testing for rotavirus and other entities is warranted.
Supportive treatment: Do’s and don’ts
No specific antiviral treatment is available for rotavirus infection. That said, the do’s and don’ts that follow will help guide your care.
DO administer oral, enteral, or intravenous (IV) fluids to prevent or correct dehydration. Oral rehydration therapy is the standard treatment for dehydration in anyone with acute gastroenteritis, including that caused by rotavirus. The recommended World Health Organization (WHO) oral rehydration solution contains sodium, chloride, and electrolytes (TABLE 1).13 Rice-based oral rehydration solution is an easily metabolized carbohydrate formulation that helps repair damaged tissues and enhances electrolyte absorption.9 WHO has endorsed guidelines that base fluid replacement on the patient’s age and weight, and that recommend oral zinc intake (10 mg/d for 10-14 days up to age 6 months; 20 mg/d for 10-14 days for older children) for all episodes of diarrhea (http://hetv.org/pdf/diarrhoea-guidelines.pdf). Oral glucose electrolyte solutions containing less sodium and chloride are also effective treatments.
DO recommend frequent small doses of oral rehydration solution, even if the patient is vomiting.14 Rehydration volumes are suggested in TABLE 1. Alternatively, give 10 to 20 mL/kg for each diarrheal episode, and 2 mL/kg for each bout of emesis. Feeding frequent small volumes (30 mL every 5-10 minutes) reduces the risk of emesis.
Although oral rehydration solutions are contraindicated for infants and young children with depressed consciousness, vomiting is not a contraindication to oral intake. About half of the oral intake stays in the stomach, even after vomiting. A single dose of ondansetron may safely reduce vomiting.15
Patients with mainly diarrhea can take fluids or feed at will. With children who refuse to drink, oral rehydration solutions can be administered via nasogastric tube at approximately 5 mL/min to limit vomiting and maintain hydration.14 In dehydrated infants and toddlers with collapsed veins, nasogastric intubation has been shown to be less traumatic than repetitive attempts at placing IV catheters.
DO encourage nursing mothers to con tinue breastfeeding during rehydration treatments. If a mother is bottle feeding, keep this in mind: Rotavirus can cause temporary lactase deficiency for some non-breastfeeding infants; lactose-free formulas may help.
DON’T assume that parents know how to provide proper supplementation. Tell them to avoid fluids containing mostly sugar that lack significant electrolyte supplementation (eg, cola) unless no other fluid alternative is available. Advise caregivers to avoid juices and other liquids high in complex or simple sugars because the osmotic load may worsen diarrhea.14
DON’T give antidiarrheal agents for acute treatment in infants and young children. Such treatment has resulted in death.14
TABLE 1
Prevent or correct dehydration using the WHO-recommended oral rehydration salts solution13
| With this formulation… | …rehydrate per these specifications… | …at this rate | ||
|---|---|---|---|---|
| Component (mmol/L) | Age | Weight (kg) | mL solution/4 h | |
| Sodium (75); chloride (65); glucose (75); potassium (20); citrate (10) | ≤4 mo 4-12 mo 12 mo-2 y 2-5 y | <6 6 to <10 10 to <12 12 to 19 | 200-400 400-700 700-900 900-1400 | |
| WHO, World Health Organization. | ||||
KEEP IN MIND
Hospitalization may be needed to replace fluids via IV or interosseous supplementation. For the severely dehydrated child, 20 mL/kg isotonic fluid can be administered as a rapid bolus.14 It may be necessary to repeat a rapid fluid infusion of 10 to 20 mL/kg every 20 to 30 minutes. For less severely ill infants who require IV rehydration, standard references such as the Harriet Lane Handbook16 provide excellent guidance.
Probiotics may help. Consider probiotics with Lactobacillus or Bifida bacterium to reduce the severity of diarrhea in infants and children who are mildly to moderately ill.17,18 Their usefulness in the severely ill patient has not been demonstrated.
Available vaccines and clinical recommendations
In February 2006, the US Food and Drug Administration (FDA) licensed a 3-dose, oral pentavalent rotavirus vaccine (RV5, RotaTeq) for use among infants. The vaccine contains live reassortant rotaviruses19—4 human rotavirus G outer-surface proteins and 1 human P attachment protein reassorted into a bovine rotavirus not infectious to humans.
In February 2008, the FDA approved a 2-dose, oral monovalent rotavirus vaccine (RV1, Rotarix), an attenuated live human rotavirus containing 1 G protein and 1 P protein. Both vaccines have proven to be clinically effective in rotavirus prevention trials, but effectiveness may depend on which rotavirus serotypes circulate each season.
ACIP, AAP, and AAFP recommend that all infants be routinely vaccinated with either RV5 or RV1.6,20–22 Vaccination should be complete by the time infants reach the age of 8 months (TABLE 2). Guidelines for vaccination emphasize the following points:
Timing. According to the ACIP, the first dose of either vaccine must be administered between the ages of 6 weeks and 14 weeks 6 days (the RV5 manufacturer [Merck] states a maximum age of 12 weeks). Give subsequent doses at 4- to 10-week intervals, as long as all doses are administered by 8 months of age. The RV1 manufacturer (GlaxoSmithKline) suggests completing the second (final) dose of its vaccine by age 24 weeks.
If an infant 15 weeks of age or older accidentally receives a first dose of RV vaccine, the series should be continued, as long as the last dose can be given by 8 months of age. Either vaccine can be administered concurrently with all other vaccines.
Contraindications. The only absolute contraindications to RV5 administration are a demonstrated hypersensitivity to any component of the vaccine and severe combined immunodeficiency disease (SCID). Contraindications to RV1 vaccine are vaccine component hypersensitivity, SCID, latex-induced allergy (anaphylaxis), and uncorrected malformation of the gastrointestinal (GI) tract that might predispose to intussusception.
Precautions. Precautions for vaccines include other forms of primary or secondary immunocompromised or immunodeficiency states, including cancer and acute or chronic GI disorders such as ongoing gastroenteritis or intussusception. Infants with transient mild illness with or without low-grade fever and infants who are breastfeeding can receive either vaccine. RV5 is shed in 9% of recipients and RV1 in 26% of recipients after Dose 1, but transmission of vaccine virus is not known to occur. Likewise, reversion of vaccine virus to more virulent pathogens is not known to occur. A household member with an immuno-compromised condition does not preclude giving either RV vaccine to an infant. The risk of transmitting vaccine virus is much smaller than the risk of acquiring infectious wild-type rotavirus.
Regurgitation of a vaccine dose is uncommon. When it does occur, the RV5 vaccine should not be repeated; some of the vaccine dose is retained and the safety of the additional vaccine from a second dose is unknown. Readministration of a dose of RV1 is not recommended, although not contraindicated.
TABLE 2
Recommended rotavirus live virus vaccine dosing6
| Patient age (mo) | RV5 (RotaTeq) | RV1 (Rotarix) |
|---|---|---|
| 2 | 2 mL | 1 mL |
| 4 | 2 mL | 1 mL* |
| 6 | 2 mlL* | — |
| *The final dose of either vaccine must be given by no later than 8 months of age. | ||
Vaccine efficacy
The safety and efficacy of live rotavirus vaccines were demonstrated in large studies that enrolled 71,725 children in RV5 vaccine trials23 and 24,163 children in RV1 vaccine trials.21 The pivotal RV5 study included a nested substudy to evaluate efficacy against any G1–G4 rotavirus gastroenteritis.
RV5 (RotaTeq) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV5 vaccine effectively prevented severe rotavirus infection in 98% of cases, and reduced hospitalization by 95%, emergency department visits by 94%, physician office visits by 86%, and all rotavirus cases by 74% for infants who received all 3 doses of vaccine according to protocol.23 Hospitalization for any-cause gastroenteritis was reduced by 63%. Second-season data showed persistence of antibody protection. All 3 doses of vaccine are required for maximum protection.23
Both preterm and term infants received their first dose of vaccine between 6 and 12 weeks of life. For preterm infants who are experiencing medical difficulties, the first dose of vaccine may be delayed until the patient is stable, if it can be given before 15 weeks of age.
RV1 (Rotarix) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV1 vaccine was 85% (Latin America) to 96% (Europe) effective in preventing severe rotavirus infection. It reduced hospitalization due to rotavirus by 85% (Latin America) to 100% (Europe), and all rotavirus cases by 87% (Europe) for infants who received both doses of the vaccine according to protocol. For the second season, the vaccine reduced severe rotavirus disease by 70% to 96%, and any rotavirus disease by 73% to 89%, showing persistence of antibody protection.6
Adverse events
With both vaccines, common side effects include irritability, flatulence, fever, vomiting, diarrhea, cough, runny nose, and loss of appetite. The RV5 vaccine has been shown not to increase the risk of intussusception compared with placebo.24,25 The RV1 vaccine should not be used in children with an uncorrected bowel malformation, due to unproven increased risk of intussusception. Risk of death from complications after administration of either vaccine did not differ from that among children receiving placebo.
Postmarketing surveillance of vaccination outcomes
Even though rotavirus vaccine coverage with RV5 RotaTeq in the 2007-2008 and 2008-2009 seasons was far less than that with other childhood immunizations, the number of rotavirus infections dropped by >60% in both 2008 and 2009.26 The number of stool tests for rotavirus and the percentage of positive results also dropped dramatically.
Additionally, the rotavirus peak incidence was delayed 2 to 4 months until April 2008 and March 2009.26 Incidence was reduced in all age groups, suggesting the possibility of herd immunity despite a low vaccine coverage rate (estimates are 57% for ≥1 dose) that would not be expected to provide herd immunity.27 Hospitalizations in the United States for rotavirus gastroenteritis dropped by as much as 85%,28 markedly reducing costs for gastroenteritis.
In a 2010 report from an emergency department in Houston, a complete RV5 vaccine series conferred 82% protection against acute gastroenteritis, 96% against severe rotavirus disease requiring IV rehydration, and 100% against hospitalization.29 For more on the vaccine, see the report by Yen et al.30
Reports of the effectiveness of Rotarix in postmarketing surveillance are limited, but the vaccine does seem to provide broad coverage.31
As of April 11, 2011, RV5 costs $59.76/$69.59 per dose in the public/private sectors, respectively (3-dose series: $179.28/$208.77); RV1 costs $89.25/$102.50 per dose (2-dose series: $178.50/$205). routine vaccination costs about $138 per case averted and $3024 per serious case averted. neither vaccine contains thimerosal. Both vaccines are available in 10-dose packs.
Source: Centers for Disease Control and Prevention. CDC vaccine price list. Prices last reviewed/updated: April 8, 2011. Available at: http://www.cdc.gov/vaccines/programs/vfc/cdc-vac-price-list.htm. Accessed April 11, 2011.
Incorporating rotavirus vaccine into a family medicine practice
Given inadequately reimbursed costs including the cost of stocking RV vaccine (see “Costs of RV vaccines” above), family physicians who treat relatively few infants must determine whether offering RV vaccine fits within their practices.
For family physicians who do treat infants, offering RV vaccination makes sense. These oral vaccines are highly effective, safe, and easy to administer, and will prevent a great deal of worry and calls regarding infants who have a fever or diarrhea or are vomiting. Due to the costs of stocking all vaccines, private practitioners are wise to purchase vaccine loss insurance. Many insurance agencies provide a rider on office insurance policies to cover vaccine supplies.
CORRESPONDENCE
Donald B. Middleton, MD, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; middletondb@upmc.edu
• Patients with rotavirus infection require oral, enteral, or intravenous fluids to treat dehydration. A
• Give the first dose of rotavirus (RV) vaccine between the ages of 6 weeks and 14 weeks 6 days; give subsequent doses at 4- to 10-week intervals, completing by 8 months. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Rotavirus is the most common cause of severe gastroenteritis in infants and children younger than 5 years of age, and it accounts for approximately 5% of childhood deaths worldwide.1 In the United States, rotavirus causes numerous cases of dehydrating diarrhea and vomiting, and is responsible for direct and indirect healthcare costs of approximately $1 billion per year. Infection during childhood is almost universal.2
Improved personal hygiene and community sanitation have steadily reduced the prevalence of bacterial and parasitic disease. But these measures have had little effect on the spread of rotavirus and its potential complications of severe dehydration, hospitalization, and even death.1 Importantly, we now have the means to vaccinate against rotavirus infection and dramatically reduce the incidence of disease. In this article, I describe the available vaccines and the vaccination recommendations endorsed by the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP). I also review supportive treatment for rotavirus infection, which entails both do’s and don’ts.
Who is at risk of rotavirus disease?
For most term neonates, rotavirus disease is mild, perhaps because of partial protection from maternal antibodies.3 However, premature infants lacking full maternal antibody protection often suffer from more serious gastroenteritis. The most severe infections usually strike children between the ages of 4 months, when maternally derived antibody protection wanes, and 23 months, when dehydration risk lessens.4-6
The virus spreads from person to person via the fecal–oral route.6,7 Thirty percent to 50% of family members of an infected child may also become infected, but disease in older children and adults is usually subclinical or mild.6 Outbreaks of rotavirus are common in childcare centers and in children’s hospitals.7,8
How the disease presents
Rotavirus gastroenteritis peaks during the winter. With mild cases, a watery diarrhea will last a few days. In severe cases, onset is usually abrupt with fever, abdominal pain, and vomiting, which can precede diarrhea. A third of patients have a temperature higher than 102°F (38.9°C).6 There is a risk of dehydration, shock, and even, occasionally, infant death.9
Typically, the incubation period is 1 to 4 days, and the infection lasts 3 to 7 days. However, damage to the brush border of the intestinal villi can produce persistent disaccharide malabsorption, resulting in prolonged diarrhea even after resolution of infection.10,11 Stools generally do not contain blood or leukocytes. Ultrasound examination during rotavirus infections has shown thickening of the distal ileum and lymphadenopathy, which may predispose to intussusception.12 Other problems possibly linked to wild-type rotavirus infection are Kawasaki disease and sudden infant death syndrome. Recurrent rotavirus infection with one of the many different serotypes is common during childhood.
More than 25 different assays can detect rotavirus in stool, but the most reliable method is direct electron microscopy. A suitable clinically available alternative is enzyme immunoassay testing of stool samples. In mild cases, testing to detect rotavirus is not necessary. But for bloody, severe, or persistent diarrhea, stool testing for rotavirus and other entities is warranted.
Supportive treatment: Do’s and don’ts
No specific antiviral treatment is available for rotavirus infection. That said, the do’s and don’ts that follow will help guide your care.
DO administer oral, enteral, or intravenous (IV) fluids to prevent or correct dehydration. Oral rehydration therapy is the standard treatment for dehydration in anyone with acute gastroenteritis, including that caused by rotavirus. The recommended World Health Organization (WHO) oral rehydration solution contains sodium, chloride, and electrolytes (TABLE 1).13 Rice-based oral rehydration solution is an easily metabolized carbohydrate formulation that helps repair damaged tissues and enhances electrolyte absorption.9 WHO has endorsed guidelines that base fluid replacement on the patient’s age and weight, and that recommend oral zinc intake (10 mg/d for 10-14 days up to age 6 months; 20 mg/d for 10-14 days for older children) for all episodes of diarrhea (http://hetv.org/pdf/diarrhoea-guidelines.pdf). Oral glucose electrolyte solutions containing less sodium and chloride are also effective treatments.
DO recommend frequent small doses of oral rehydration solution, even if the patient is vomiting.14 Rehydration volumes are suggested in TABLE 1. Alternatively, give 10 to 20 mL/kg for each diarrheal episode, and 2 mL/kg for each bout of emesis. Feeding frequent small volumes (30 mL every 5-10 minutes) reduces the risk of emesis.
Although oral rehydration solutions are contraindicated for infants and young children with depressed consciousness, vomiting is not a contraindication to oral intake. About half of the oral intake stays in the stomach, even after vomiting. A single dose of ondansetron may safely reduce vomiting.15
Patients with mainly diarrhea can take fluids or feed at will. With children who refuse to drink, oral rehydration solutions can be administered via nasogastric tube at approximately 5 mL/min to limit vomiting and maintain hydration.14 In dehydrated infants and toddlers with collapsed veins, nasogastric intubation has been shown to be less traumatic than repetitive attempts at placing IV catheters.
DO encourage nursing mothers to con tinue breastfeeding during rehydration treatments. If a mother is bottle feeding, keep this in mind: Rotavirus can cause temporary lactase deficiency for some non-breastfeeding infants; lactose-free formulas may help.
DON’T assume that parents know how to provide proper supplementation. Tell them to avoid fluids containing mostly sugar that lack significant electrolyte supplementation (eg, cola) unless no other fluid alternative is available. Advise caregivers to avoid juices and other liquids high in complex or simple sugars because the osmotic load may worsen diarrhea.14
DON’T give antidiarrheal agents for acute treatment in infants and young children. Such treatment has resulted in death.14
TABLE 1
Prevent or correct dehydration using the WHO-recommended oral rehydration salts solution13
| With this formulation… | …rehydrate per these specifications… | …at this rate | ||
|---|---|---|---|---|
| Component (mmol/L) | Age | Weight (kg) | mL solution/4 h | |
| Sodium (75); chloride (65); glucose (75); potassium (20); citrate (10) | ≤4 mo 4-12 mo 12 mo-2 y 2-5 y | <6 6 to <10 10 to <12 12 to 19 | 200-400 400-700 700-900 900-1400 | |
| WHO, World Health Organization. | ||||
KEEP IN MIND
Hospitalization may be needed to replace fluids via IV or interosseous supplementation. For the severely dehydrated child, 20 mL/kg isotonic fluid can be administered as a rapid bolus.14 It may be necessary to repeat a rapid fluid infusion of 10 to 20 mL/kg every 20 to 30 minutes. For less severely ill infants who require IV rehydration, standard references such as the Harriet Lane Handbook16 provide excellent guidance.
Probiotics may help. Consider probiotics with Lactobacillus or Bifida bacterium to reduce the severity of diarrhea in infants and children who are mildly to moderately ill.17,18 Their usefulness in the severely ill patient has not been demonstrated.
Available vaccines and clinical recommendations
In February 2006, the US Food and Drug Administration (FDA) licensed a 3-dose, oral pentavalent rotavirus vaccine (RV5, RotaTeq) for use among infants. The vaccine contains live reassortant rotaviruses19—4 human rotavirus G outer-surface proteins and 1 human P attachment protein reassorted into a bovine rotavirus not infectious to humans.
In February 2008, the FDA approved a 2-dose, oral monovalent rotavirus vaccine (RV1, Rotarix), an attenuated live human rotavirus containing 1 G protein and 1 P protein. Both vaccines have proven to be clinically effective in rotavirus prevention trials, but effectiveness may depend on which rotavirus serotypes circulate each season.
ACIP, AAP, and AAFP recommend that all infants be routinely vaccinated with either RV5 or RV1.6,20–22 Vaccination should be complete by the time infants reach the age of 8 months (TABLE 2). Guidelines for vaccination emphasize the following points:
Timing. According to the ACIP, the first dose of either vaccine must be administered between the ages of 6 weeks and 14 weeks 6 days (the RV5 manufacturer [Merck] states a maximum age of 12 weeks). Give subsequent doses at 4- to 10-week intervals, as long as all doses are administered by 8 months of age. The RV1 manufacturer (GlaxoSmithKline) suggests completing the second (final) dose of its vaccine by age 24 weeks.
If an infant 15 weeks of age or older accidentally receives a first dose of RV vaccine, the series should be continued, as long as the last dose can be given by 8 months of age. Either vaccine can be administered concurrently with all other vaccines.
Contraindications. The only absolute contraindications to RV5 administration are a demonstrated hypersensitivity to any component of the vaccine and severe combined immunodeficiency disease (SCID). Contraindications to RV1 vaccine are vaccine component hypersensitivity, SCID, latex-induced allergy (anaphylaxis), and uncorrected malformation of the gastrointestinal (GI) tract that might predispose to intussusception.
Precautions. Precautions for vaccines include other forms of primary or secondary immunocompromised or immunodeficiency states, including cancer and acute or chronic GI disorders such as ongoing gastroenteritis or intussusception. Infants with transient mild illness with or without low-grade fever and infants who are breastfeeding can receive either vaccine. RV5 is shed in 9% of recipients and RV1 in 26% of recipients after Dose 1, but transmission of vaccine virus is not known to occur. Likewise, reversion of vaccine virus to more virulent pathogens is not known to occur. A household member with an immuno-compromised condition does not preclude giving either RV vaccine to an infant. The risk of transmitting vaccine virus is much smaller than the risk of acquiring infectious wild-type rotavirus.
Regurgitation of a vaccine dose is uncommon. When it does occur, the RV5 vaccine should not be repeated; some of the vaccine dose is retained and the safety of the additional vaccine from a second dose is unknown. Readministration of a dose of RV1 is not recommended, although not contraindicated.
TABLE 2
Recommended rotavirus live virus vaccine dosing6
| Patient age (mo) | RV5 (RotaTeq) | RV1 (Rotarix) |
|---|---|---|
| 2 | 2 mL | 1 mL |
| 4 | 2 mL | 1 mL* |
| 6 | 2 mlL* | — |
| *The final dose of either vaccine must be given by no later than 8 months of age. | ||
Vaccine efficacy
The safety and efficacy of live rotavirus vaccines were demonstrated in large studies that enrolled 71,725 children in RV5 vaccine trials23 and 24,163 children in RV1 vaccine trials.21 The pivotal RV5 study included a nested substudy to evaluate efficacy against any G1–G4 rotavirus gastroenteritis.
RV5 (RotaTeq) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV5 vaccine effectively prevented severe rotavirus infection in 98% of cases, and reduced hospitalization by 95%, emergency department visits by 94%, physician office visits by 86%, and all rotavirus cases by 74% for infants who received all 3 doses of vaccine according to protocol.23 Hospitalization for any-cause gastroenteritis was reduced by 63%. Second-season data showed persistence of antibody protection. All 3 doses of vaccine are required for maximum protection.23
Both preterm and term infants received their first dose of vaccine between 6 and 12 weeks of life. For preterm infants who are experiencing medical difficulties, the first dose of vaccine may be delayed until the patient is stable, if it can be given before 15 weeks of age.
RV1 (Rotarix) vaccine. In double-blind, placebo-controlled clinical trials, for the first rotavirus season, live RV1 vaccine was 85% (Latin America) to 96% (Europe) effective in preventing severe rotavirus infection. It reduced hospitalization due to rotavirus by 85% (Latin America) to 100% (Europe), and all rotavirus cases by 87% (Europe) for infants who received both doses of the vaccine according to protocol. For the second season, the vaccine reduced severe rotavirus disease by 70% to 96%, and any rotavirus disease by 73% to 89%, showing persistence of antibody protection.6
Adverse events
With both vaccines, common side effects include irritability, flatulence, fever, vomiting, diarrhea, cough, runny nose, and loss of appetite. The RV5 vaccine has been shown not to increase the risk of intussusception compared with placebo.24,25 The RV1 vaccine should not be used in children with an uncorrected bowel malformation, due to unproven increased risk of intussusception. Risk of death from complications after administration of either vaccine did not differ from that among children receiving placebo.
Postmarketing surveillance of vaccination outcomes
Even though rotavirus vaccine coverage with RV5 RotaTeq in the 2007-2008 and 2008-2009 seasons was far less than that with other childhood immunizations, the number of rotavirus infections dropped by >60% in both 2008 and 2009.26 The number of stool tests for rotavirus and the percentage of positive results also dropped dramatically.
Additionally, the rotavirus peak incidence was delayed 2 to 4 months until April 2008 and March 2009.26 Incidence was reduced in all age groups, suggesting the possibility of herd immunity despite a low vaccine coverage rate (estimates are 57% for ≥1 dose) that would not be expected to provide herd immunity.27 Hospitalizations in the United States for rotavirus gastroenteritis dropped by as much as 85%,28 markedly reducing costs for gastroenteritis.
In a 2010 report from an emergency department in Houston, a complete RV5 vaccine series conferred 82% protection against acute gastroenteritis, 96% against severe rotavirus disease requiring IV rehydration, and 100% against hospitalization.29 For more on the vaccine, see the report by Yen et al.30
Reports of the effectiveness of Rotarix in postmarketing surveillance are limited, but the vaccine does seem to provide broad coverage.31
As of April 11, 2011, RV5 costs $59.76/$69.59 per dose in the public/private sectors, respectively (3-dose series: $179.28/$208.77); RV1 costs $89.25/$102.50 per dose (2-dose series: $178.50/$205). routine vaccination costs about $138 per case averted and $3024 per serious case averted. neither vaccine contains thimerosal. Both vaccines are available in 10-dose packs.
Source: Centers for Disease Control and Prevention. CDC vaccine price list. Prices last reviewed/updated: April 8, 2011. Available at: http://www.cdc.gov/vaccines/programs/vfc/cdc-vac-price-list.htm. Accessed April 11, 2011.
Incorporating rotavirus vaccine into a family medicine practice
Given inadequately reimbursed costs including the cost of stocking RV vaccine (see “Costs of RV vaccines” above), family physicians who treat relatively few infants must determine whether offering RV vaccine fits within their practices.
For family physicians who do treat infants, offering RV vaccination makes sense. These oral vaccines are highly effective, safe, and easy to administer, and will prevent a great deal of worry and calls regarding infants who have a fever or diarrhea or are vomiting. Due to the costs of stocking all vaccines, private practitioners are wise to purchase vaccine loss insurance. Many insurance agencies provide a rider on office insurance policies to cover vaccine supplies.
CORRESPONDENCE
Donald B. Middleton, MD, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; middletondb@upmc.edu
1. Parashar UD, Gibson CJ, Bresee JS, et al. Rotavirus and severe childhood diarrhea. Emerg Infect Dis. 2006;12:304-306.
2. Malek MA, Curns AT, Holman RC, et al. Diarrhea- and rotavirus-associated hospitalizations among children less than 5 years of age: United States, 1997 and 2000. Pediatrics. 2006;117:1887-1892.
3. Xu J, Dennehy P, Keyserling H, et al. Serum antibody responses in children with rotavirus diarrhea can serve as proxy for protection. Clin Diagn Lab Immunol. 2005;12:273-279.
4. World Health Organization. Rotavirus vaccines. Wkly Epidemiol Rec. 2007;82:285-295.
5. Ward RL, Bernstein DI, Staat MA. Rotaviruses. In: Feigin RD, Cherry JD, eds. Textbook of Pediatric Infectious Disease. Vol 2, 6th ed. New York, NY: Saunders; 2009:2245-2270.
6. Centers for Disease Control and Prevention. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2009;58(RR-2):1-25.
7. Butz AM, Fosarelli P, Dick J, et al. Prevalence of rotavirus on high-risk fomites in day-care facilities. Pediatrics. 1993;92:202-205.
8. Fischer TK, Bresee JS, Glass RI. Rotavirus vaccines and the prevention of hospital-acquired diarrhea in children. Vaccine. 2004;22(suppl):S49-S54.
9. Kapikian AZ, Hoshino Y, Chanock RM. Rotaviruses. In: Knipe DM, Howley PM, Griffin DE, et al, eds. Fields Virology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2001: 1787-1825.
10. Lorrot M, Vasseur M. How do the rotavirus NSP4 and bacterial enterotoxins lead differently to diarrhea? Virol J. 2007;4:31.-
11. Ramig RF. Pathogenesis of intestinal and systemic rotavirus infection. J Virol. 2004;78:10213-10220.
12. Robinson CG, Hernanz-Schulman M, Zhu Y, et al. Evaluation of anatomic changes in young children with natural rotavirus infection: is intussusception biologically plausible? J Infect Dis. 2004;189:1382-1387.
13. World Health Organization. Oral Rehydration Salts: Production of the New ORS. Geneva, Switzerland: WHO Document Production Services; 2006. Available at: http://whqlibdoc.who.int/hq/2006/WHO_FCH_CAH_06.1.pdf. Accessed April 11, 2011.
14. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1-16.
15. DeCamp LR, Byerley JS, Doshi N, et al. Use of antiemetic agents in acute gastroenteritis: a systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2008;162:858-865.
16. The Johns Hopkins Hospital, Custer JW, Rau RE. Harriet Lane Handbook: A Manual for Pediatric House Officers. 18th ed. St. Louis, Mo: Mosby/Elsevier; 2008.
17. Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ. 2007;335:340.-
18. Van Niel CW, Feudtner C, Garrison MM, et al. Lactobacillus therapy for acute infectious diarrhea in children: a meta- analysis. Pediatrics. 2002;109:678-684.
19. Heaton PM, Goveia MG, Miller JM, et al. Development of a pentavalent rotavirus vaccine against prevalent serotypes of rotavirus gastroenteritis. J Infect Dis. 2005;192(suppl 1):S17-S21.
20. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years — United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(5):1-4.
21. American Academy of Pediatrics (AAP) Committee on Infectious Diseases. Prevention of rotavirus disease: updated guidelines for use of rotavirus vaccine. Pediatrics. 2009;123:1412-1420.
22. Temte JL. Practice guidelines. ACIP releases 2009 child and adolescent immunization schedules. Am Fam Physician. 2009;79:56.-Available at: http://www.aafp.org/afp/2009/0101/p56.html. Accessed January 4, 2010.
23. Vesikari T, Matson DO, Dennehy P, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354:23-33.
24. Centers for Disease Control and Prevention. Intussusception among recipients of rotavirus vaccine: United States, 1998– 1999. MMWR Morb Mortal Wkly Rep. 1999;48:577-581.
25. Centers for Disease Control and Prevention. Postmarketing monitoring of intussusception after RotaTeq vaccine: United States. February 1, 2006–February 15, 2007. MMWR Morb Mortal Wkly Rep. 2007;56:218-222.
26. Centers for Disease Control and Prevention. Reduction in rotavirus after vaccine introduction — United States, 2000-2009. MMWR Morb Mortal Wkly Rep. 2009;58:1146-1149.
27. Clark HF, Lawley D, Mallette LA, et al. Decline in cases of rotavirus gastroenteritis presenting to The Children’s Hospital of Philadelphia after introduction of a pentavalent rotavirus vaccine. Clin Vaccine Immunol. 2009;16:382-386.
28. Chang HG, Smith P, Tserenpuntsag B, et al. Reduction in New York hospitalizations for diarrhea and rotavirus. Presented at: 43rd National Immunization Conference; March 30-April 2, 2009; Dallas, Tex. Abstract 41. Available at: http://cdc.confex.com/cdc/nic2009/webprogram/Paper18073.html. Accessed April 15, 2011.
29. Boom JA, Tate JE, Sahni LC, et al. Effectiveness of pentavalent rotavirus vaccine in a large urban population in the United States. Pediatrics. 2010;125:e199-e207.
30. Yen C, Tate JE, Wenk JD, et al. Diarrhea-associated hospitalizations among US children over 2 rotavirus seasons after vaccine introduction. Pediatrics. 2011;127:e9-e15.
31. Correia JB, Patel MM, Nakagomi O, et al. Effectiveness of monovalent rotavirus vaccine (Rotarix) against severe diarrhea caused by serotypically unrelated G2P[4] strains in Brazil. J Infect Dis. 2010;201:363-369.
1. Parashar UD, Gibson CJ, Bresee JS, et al. Rotavirus and severe childhood diarrhea. Emerg Infect Dis. 2006;12:304-306.
2. Malek MA, Curns AT, Holman RC, et al. Diarrhea- and rotavirus-associated hospitalizations among children less than 5 years of age: United States, 1997 and 2000. Pediatrics. 2006;117:1887-1892.
3. Xu J, Dennehy P, Keyserling H, et al. Serum antibody responses in children with rotavirus diarrhea can serve as proxy for protection. Clin Diagn Lab Immunol. 2005;12:273-279.
4. World Health Organization. Rotavirus vaccines. Wkly Epidemiol Rec. 2007;82:285-295.
5. Ward RL, Bernstein DI, Staat MA. Rotaviruses. In: Feigin RD, Cherry JD, eds. Textbook of Pediatric Infectious Disease. Vol 2, 6th ed. New York, NY: Saunders; 2009:2245-2270.
6. Centers for Disease Control and Prevention. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2009;58(RR-2):1-25.
7. Butz AM, Fosarelli P, Dick J, et al. Prevalence of rotavirus on high-risk fomites in day-care facilities. Pediatrics. 1993;92:202-205.
8. Fischer TK, Bresee JS, Glass RI. Rotavirus vaccines and the prevention of hospital-acquired diarrhea in children. Vaccine. 2004;22(suppl):S49-S54.
9. Kapikian AZ, Hoshino Y, Chanock RM. Rotaviruses. In: Knipe DM, Howley PM, Griffin DE, et al, eds. Fields Virology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2001: 1787-1825.
10. Lorrot M, Vasseur M. How do the rotavirus NSP4 and bacterial enterotoxins lead differently to diarrhea? Virol J. 2007;4:31.-
11. Ramig RF. Pathogenesis of intestinal and systemic rotavirus infection. J Virol. 2004;78:10213-10220.
12. Robinson CG, Hernanz-Schulman M, Zhu Y, et al. Evaluation of anatomic changes in young children with natural rotavirus infection: is intussusception biologically plausible? J Infect Dis. 2004;189:1382-1387.
13. World Health Organization. Oral Rehydration Salts: Production of the New ORS. Geneva, Switzerland: WHO Document Production Services; 2006. Available at: http://whqlibdoc.who.int/hq/2006/WHO_FCH_CAH_06.1.pdf. Accessed April 11, 2011.
14. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1-16.
15. DeCamp LR, Byerley JS, Doshi N, et al. Use of antiemetic agents in acute gastroenteritis: a systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2008;162:858-865.
16. The Johns Hopkins Hospital, Custer JW, Rau RE. Harriet Lane Handbook: A Manual for Pediatric House Officers. 18th ed. St. Louis, Mo: Mosby/Elsevier; 2008.
17. Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ. 2007;335:340.-
18. Van Niel CW, Feudtner C, Garrison MM, et al. Lactobacillus therapy for acute infectious diarrhea in children: a meta- analysis. Pediatrics. 2002;109:678-684.
19. Heaton PM, Goveia MG, Miller JM, et al. Development of a pentavalent rotavirus vaccine against prevalent serotypes of rotavirus gastroenteritis. J Infect Dis. 2005;192(suppl 1):S17-S21.
20. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years — United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(5):1-4.
21. American Academy of Pediatrics (AAP) Committee on Infectious Diseases. Prevention of rotavirus disease: updated guidelines for use of rotavirus vaccine. Pediatrics. 2009;123:1412-1420.
22. Temte JL. Practice guidelines. ACIP releases 2009 child and adolescent immunization schedules. Am Fam Physician. 2009;79:56.-Available at: http://www.aafp.org/afp/2009/0101/p56.html. Accessed January 4, 2010.
23. Vesikari T, Matson DO, Dennehy P, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354:23-33.
24. Centers for Disease Control and Prevention. Intussusception among recipients of rotavirus vaccine: United States, 1998– 1999. MMWR Morb Mortal Wkly Rep. 1999;48:577-581.
25. Centers for Disease Control and Prevention. Postmarketing monitoring of intussusception after RotaTeq vaccine: United States. February 1, 2006–February 15, 2007. MMWR Morb Mortal Wkly Rep. 2007;56:218-222.
26. Centers for Disease Control and Prevention. Reduction in rotavirus after vaccine introduction — United States, 2000-2009. MMWR Morb Mortal Wkly Rep. 2009;58:1146-1149.
27. Clark HF, Lawley D, Mallette LA, et al. Decline in cases of rotavirus gastroenteritis presenting to The Children’s Hospital of Philadelphia after introduction of a pentavalent rotavirus vaccine. Clin Vaccine Immunol. 2009;16:382-386.
28. Chang HG, Smith P, Tserenpuntsag B, et al. Reduction in New York hospitalizations for diarrhea and rotavirus. Presented at: 43rd National Immunization Conference; March 30-April 2, 2009; Dallas, Tex. Abstract 41. Available at: http://cdc.confex.com/cdc/nic2009/webprogram/Paper18073.html. Accessed April 15, 2011.
29. Boom JA, Tate JE, Sahni LC, et al. Effectiveness of pentavalent rotavirus vaccine in a large urban population in the United States. Pediatrics. 2010;125:e199-e207.
30. Yen C, Tate JE, Wenk JD, et al. Diarrhea-associated hospitalizations among US children over 2 rotavirus seasons after vaccine introduction. Pediatrics. 2011;127:e9-e15.
31. Correia JB, Patel MM, Nakagomi O, et al. Effectiveness of monovalent rotavirus vaccine (Rotarix) against severe diarrhea caused by serotypically unrelated G2P[4] strains in Brazil. J Infect Dis. 2010;201:363-369.
Failure to monitor INR leads to severe bleeding, disability ... Rash and hives not taken seriously enough ... More
Failure to monitor INR leads to severe bleeding, disability
A MAN WITH A HISTORY OF DEEP VEIN THROMBOSIS was taking warfarin 10 mg every even day and 7.5 mg every odd day. His physician changed the warfarin dosage while the patient was taking ciprofloxacin, then resumed the original regimen once the patient finished taking the antibiotic.
No new prescriptions were written to confirm the change nor, the patient claimed, was a proper explanation of the new regimen provided. His international normalized ratio (INR) wasn’t checked after the dosage change.
After 2 weeks on the new warfarin dosage, the patient went to the emergency department (ED) complaining of groin pain and a change in urine color. Urinalysis found red blood cells too numerous to count. Although the patient told the ED staff he was taking warfarin, they didn’t check his INR. He was given a diagnosis of urinary tract infection (UTI) and discharged.
Three days later, the patient returned to the ED because of increased bleeding from his Foley catheter. Once again his INR wasn’t checked and he was discharged with a UTI diagnosis and a prescription for antibiotics. Two days afterwards, he was taken back to the hospital bleeding from all orifices. His INR was 75.
The patient spent a month in the hospital, most of it in the intensive care unit, followed by 3 months in a rehabilitation facility before returning home. He remained confined to a hospital bed.
PLAINTIFF’S CLAIM The physician and hospital were negligent for failing to instruct the patient regarding the change in warfarin dosage and neglecting to check his INR.
THE DEFENSE No information about the defense is available.
VERDICT $700,000 Maryland settlement.
COMMENT The management of anticoagulation has numerous pitfalls for the unwary. Careful monitoring can save lives—and lawsuits.
Rash and hives not taken seriously enough
A HISTORY OF 3 SEIZURES in a 7-year-old boy prompted a neurologist to prescribe valproic acid. The neurologist later added lamotrigine because of the child’s behavior problems. After taking both medications for 2 weeks, the child developed a rash, at which point the neurologist discontinued the lamotrigine and started diphenhydramine.
The following day, the child was brought to the ED with an itchy rash and hives on his torso and extremities. An allergic reaction was diagnosed and the child was discharged with instructions to take diphenhydramine along with acetaminophen and ibuprofen as needed. When informed of the ED visit, the neurologist requested a follow-up appointment in 4 weeks.
Two days later, the child was back in the ED because the rash had progressed to include redness and swelling of the face. Once again, he was discharged with a diagnosis of allergic reaction and instructions to take diphenhydramine and acetaminophen.
Two days afterward, the child was taken to a different ED, from which he was airlifted to a tertiary care center and admitted to the intensive care unit for treatment of Stevens-Johnson syndrome. The condition advanced to toxic epidermal necrolysis with sloughing of skin and the lining of the gastrointestinal tract. Several weeks later, the child died.
PLAINTIFF’S CLAIM The neurologist was negligent in prescribing lamotrigine for the behavior problem instead of referring the boy to a child psychologist. The lamotrigine dosage was excessive; the neurologist didn’t respond properly to the report of a rash.
The pharmacist was negligent in failing to contact the neurologist to discuss the excessive dosage. Discharging the child from the ED with a life-threatening drug reaction was unreasonable.
THE DEFENSE The defendants denied that they were negligent or caused the child’s death. They were prepared to present the histories of the parents, whose backgrounds included drug abuse, and state investigations regarding the care of the child.
VERDICT $1.55 million Washington settlement.
COMMENT When prescribing a drug with a potentially serious adverse effect, it’s always prudent to document patient education and follow-up thoroughly. Even though hindsight is 20/20, an “allergic reaction” in a patient on lamotrigine should raise red flags.
Delay in spotting compartment syndrome has permanent consequences
SEVERE NUMBNESS, TINGLING, AND PAIN IN HER LEFT CALF brought a 20-year-old woman to the ED. She couldn’t lift her left foot or bear weight on her left foot or leg. She reported awakening with the symptoms after a New Year’s Eve party the previous evening. After an examination, but no tests, she was discharged with a diagnosis of “floppy foot syndrome” and a prescription for a non-narcotic pain medication.
The young woman went to another ED the next day, complaining of continued pain and swelling in her left calf. She was admitted to the hospital for an orthopedic consultation, which resulted in a diagnosis of compartment syndrome. By that time, the patient had gone into renal failure from rhabdomyolysis caused by tissue breakdown. She underwent a fasciotomy, after which she required hemodialysis (until her kidney function returned) and rehabilitation. Damage to the nerves of her left calf and leg left her with permanent foot drop.
PLAINTIFF’S CLAIM The hospital was negligent in failing to diagnose compartment syndrome when the woman went to the ED. Proper diagnosis and treatment at that time would have prevented the nerve damage and foot drop.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Maryland settlement.
COMMENT Compartment syndrome can be challenging to recognize. Recently I have come across several allegations of malpractice for untimely diagnosis. Remember this important problem when faced with a patient with leg pain.
Multiple errors end in death from pneumonia
A 24-YEAR-OLD MAN WITH CHEST PAIN AND A COUGH went to his physician, who diagnosed chest wall pain and prescribed a narcotic pain reliever. The young man returned the next day complaining of increased chest pain. He said he’d been spitting up blood-stained sputum. He was perspiring and vomited in the doctor’s waiting room. The doctor diagnosed an upper respiratory infection and prescribed a cough syrup containing more narcotics.
Later that day the patient had a radiograph at a hospital. It revealed pneumonia. Shortly afterward, the hospital confirmed by fax with the doctor’s office that the doctor had received the results. The doctor didn’t read the radiograph results for 2 days.
After the doctor read the radiograph report, his office tried to contact the patient but misdialed his phone number, then made no further attempts at contact. The patient’s former wife found him at home unresponsive. He was admitted to the ED, where he died of pneumonia shortly thereafter.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE No information about the defense is available.
VERDICT $1.85 million net verdict in Virginia.
COMMENT A cascade of mistakes (sometimes referred to as the Swiss cheese effect) occurs, and a preventable death results. Are you at risk for such an event? What fail-safe measures do you have in place in your practice?
Failure to monitor INR leads to severe bleeding, disability
A MAN WITH A HISTORY OF DEEP VEIN THROMBOSIS was taking warfarin 10 mg every even day and 7.5 mg every odd day. His physician changed the warfarin dosage while the patient was taking ciprofloxacin, then resumed the original regimen once the patient finished taking the antibiotic.
No new prescriptions were written to confirm the change nor, the patient claimed, was a proper explanation of the new regimen provided. His international normalized ratio (INR) wasn’t checked after the dosage change.
After 2 weeks on the new warfarin dosage, the patient went to the emergency department (ED) complaining of groin pain and a change in urine color. Urinalysis found red blood cells too numerous to count. Although the patient told the ED staff he was taking warfarin, they didn’t check his INR. He was given a diagnosis of urinary tract infection (UTI) and discharged.
Three days later, the patient returned to the ED because of increased bleeding from his Foley catheter. Once again his INR wasn’t checked and he was discharged with a UTI diagnosis and a prescription for antibiotics. Two days afterwards, he was taken back to the hospital bleeding from all orifices. His INR was 75.
The patient spent a month in the hospital, most of it in the intensive care unit, followed by 3 months in a rehabilitation facility before returning home. He remained confined to a hospital bed.
PLAINTIFF’S CLAIM The physician and hospital were negligent for failing to instruct the patient regarding the change in warfarin dosage and neglecting to check his INR.
THE DEFENSE No information about the defense is available.
VERDICT $700,000 Maryland settlement.
COMMENT The management of anticoagulation has numerous pitfalls for the unwary. Careful monitoring can save lives—and lawsuits.
Rash and hives not taken seriously enough
A HISTORY OF 3 SEIZURES in a 7-year-old boy prompted a neurologist to prescribe valproic acid. The neurologist later added lamotrigine because of the child’s behavior problems. After taking both medications for 2 weeks, the child developed a rash, at which point the neurologist discontinued the lamotrigine and started diphenhydramine.
The following day, the child was brought to the ED with an itchy rash and hives on his torso and extremities. An allergic reaction was diagnosed and the child was discharged with instructions to take diphenhydramine along with acetaminophen and ibuprofen as needed. When informed of the ED visit, the neurologist requested a follow-up appointment in 4 weeks.
Two days later, the child was back in the ED because the rash had progressed to include redness and swelling of the face. Once again, he was discharged with a diagnosis of allergic reaction and instructions to take diphenhydramine and acetaminophen.
Two days afterward, the child was taken to a different ED, from which he was airlifted to a tertiary care center and admitted to the intensive care unit for treatment of Stevens-Johnson syndrome. The condition advanced to toxic epidermal necrolysis with sloughing of skin and the lining of the gastrointestinal tract. Several weeks later, the child died.
PLAINTIFF’S CLAIM The neurologist was negligent in prescribing lamotrigine for the behavior problem instead of referring the boy to a child psychologist. The lamotrigine dosage was excessive; the neurologist didn’t respond properly to the report of a rash.
The pharmacist was negligent in failing to contact the neurologist to discuss the excessive dosage. Discharging the child from the ED with a life-threatening drug reaction was unreasonable.
THE DEFENSE The defendants denied that they were negligent or caused the child’s death. They were prepared to present the histories of the parents, whose backgrounds included drug abuse, and state investigations regarding the care of the child.
VERDICT $1.55 million Washington settlement.
COMMENT When prescribing a drug with a potentially serious adverse effect, it’s always prudent to document patient education and follow-up thoroughly. Even though hindsight is 20/20, an “allergic reaction” in a patient on lamotrigine should raise red flags.
Delay in spotting compartment syndrome has permanent consequences
SEVERE NUMBNESS, TINGLING, AND PAIN IN HER LEFT CALF brought a 20-year-old woman to the ED. She couldn’t lift her left foot or bear weight on her left foot or leg. She reported awakening with the symptoms after a New Year’s Eve party the previous evening. After an examination, but no tests, she was discharged with a diagnosis of “floppy foot syndrome” and a prescription for a non-narcotic pain medication.
The young woman went to another ED the next day, complaining of continued pain and swelling in her left calf. She was admitted to the hospital for an orthopedic consultation, which resulted in a diagnosis of compartment syndrome. By that time, the patient had gone into renal failure from rhabdomyolysis caused by tissue breakdown. She underwent a fasciotomy, after which she required hemodialysis (until her kidney function returned) and rehabilitation. Damage to the nerves of her left calf and leg left her with permanent foot drop.
PLAINTIFF’S CLAIM The hospital was negligent in failing to diagnose compartment syndrome when the woman went to the ED. Proper diagnosis and treatment at that time would have prevented the nerve damage and foot drop.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Maryland settlement.
COMMENT Compartment syndrome can be challenging to recognize. Recently I have come across several allegations of malpractice for untimely diagnosis. Remember this important problem when faced with a patient with leg pain.
Multiple errors end in death from pneumonia
A 24-YEAR-OLD MAN WITH CHEST PAIN AND A COUGH went to his physician, who diagnosed chest wall pain and prescribed a narcotic pain reliever. The young man returned the next day complaining of increased chest pain. He said he’d been spitting up blood-stained sputum. He was perspiring and vomited in the doctor’s waiting room. The doctor diagnosed an upper respiratory infection and prescribed a cough syrup containing more narcotics.
Later that day the patient had a radiograph at a hospital. It revealed pneumonia. Shortly afterward, the hospital confirmed by fax with the doctor’s office that the doctor had received the results. The doctor didn’t read the radiograph results for 2 days.
After the doctor read the radiograph report, his office tried to contact the patient but misdialed his phone number, then made no further attempts at contact. The patient’s former wife found him at home unresponsive. He was admitted to the ED, where he died of pneumonia shortly thereafter.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE No information about the defense is available.
VERDICT $1.85 million net verdict in Virginia.
COMMENT A cascade of mistakes (sometimes referred to as the Swiss cheese effect) occurs, and a preventable death results. Are you at risk for such an event? What fail-safe measures do you have in place in your practice?
Failure to monitor INR leads to severe bleeding, disability
A MAN WITH A HISTORY OF DEEP VEIN THROMBOSIS was taking warfarin 10 mg every even day and 7.5 mg every odd day. His physician changed the warfarin dosage while the patient was taking ciprofloxacin, then resumed the original regimen once the patient finished taking the antibiotic.
No new prescriptions were written to confirm the change nor, the patient claimed, was a proper explanation of the new regimen provided. His international normalized ratio (INR) wasn’t checked after the dosage change.
After 2 weeks on the new warfarin dosage, the patient went to the emergency department (ED) complaining of groin pain and a change in urine color. Urinalysis found red blood cells too numerous to count. Although the patient told the ED staff he was taking warfarin, they didn’t check his INR. He was given a diagnosis of urinary tract infection (UTI) and discharged.
Three days later, the patient returned to the ED because of increased bleeding from his Foley catheter. Once again his INR wasn’t checked and he was discharged with a UTI diagnosis and a prescription for antibiotics. Two days afterwards, he was taken back to the hospital bleeding from all orifices. His INR was 75.
The patient spent a month in the hospital, most of it in the intensive care unit, followed by 3 months in a rehabilitation facility before returning home. He remained confined to a hospital bed.
PLAINTIFF’S CLAIM The physician and hospital were negligent for failing to instruct the patient regarding the change in warfarin dosage and neglecting to check his INR.
THE DEFENSE No information about the defense is available.
VERDICT $700,000 Maryland settlement.
COMMENT The management of anticoagulation has numerous pitfalls for the unwary. Careful monitoring can save lives—and lawsuits.
Rash and hives not taken seriously enough
A HISTORY OF 3 SEIZURES in a 7-year-old boy prompted a neurologist to prescribe valproic acid. The neurologist later added lamotrigine because of the child’s behavior problems. After taking both medications for 2 weeks, the child developed a rash, at which point the neurologist discontinued the lamotrigine and started diphenhydramine.
The following day, the child was brought to the ED with an itchy rash and hives on his torso and extremities. An allergic reaction was diagnosed and the child was discharged with instructions to take diphenhydramine along with acetaminophen and ibuprofen as needed. When informed of the ED visit, the neurologist requested a follow-up appointment in 4 weeks.
Two days later, the child was back in the ED because the rash had progressed to include redness and swelling of the face. Once again, he was discharged with a diagnosis of allergic reaction and instructions to take diphenhydramine and acetaminophen.
Two days afterward, the child was taken to a different ED, from which he was airlifted to a tertiary care center and admitted to the intensive care unit for treatment of Stevens-Johnson syndrome. The condition advanced to toxic epidermal necrolysis with sloughing of skin and the lining of the gastrointestinal tract. Several weeks later, the child died.
PLAINTIFF’S CLAIM The neurologist was negligent in prescribing lamotrigine for the behavior problem instead of referring the boy to a child psychologist. The lamotrigine dosage was excessive; the neurologist didn’t respond properly to the report of a rash.
The pharmacist was negligent in failing to contact the neurologist to discuss the excessive dosage. Discharging the child from the ED with a life-threatening drug reaction was unreasonable.
THE DEFENSE The defendants denied that they were negligent or caused the child’s death. They were prepared to present the histories of the parents, whose backgrounds included drug abuse, and state investigations regarding the care of the child.
VERDICT $1.55 million Washington settlement.
COMMENT When prescribing a drug with a potentially serious adverse effect, it’s always prudent to document patient education and follow-up thoroughly. Even though hindsight is 20/20, an “allergic reaction” in a patient on lamotrigine should raise red flags.
Delay in spotting compartment syndrome has permanent consequences
SEVERE NUMBNESS, TINGLING, AND PAIN IN HER LEFT CALF brought a 20-year-old woman to the ED. She couldn’t lift her left foot or bear weight on her left foot or leg. She reported awakening with the symptoms after a New Year’s Eve party the previous evening. After an examination, but no tests, she was discharged with a diagnosis of “floppy foot syndrome” and a prescription for a non-narcotic pain medication.
The young woman went to another ED the next day, complaining of continued pain and swelling in her left calf. She was admitted to the hospital for an orthopedic consultation, which resulted in a diagnosis of compartment syndrome. By that time, the patient had gone into renal failure from rhabdomyolysis caused by tissue breakdown. She underwent a fasciotomy, after which she required hemodialysis (until her kidney function returned) and rehabilitation. Damage to the nerves of her left calf and leg left her with permanent foot drop.
PLAINTIFF’S CLAIM The hospital was negligent in failing to diagnose compartment syndrome when the woman went to the ED. Proper diagnosis and treatment at that time would have prevented the nerve damage and foot drop.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Maryland settlement.
COMMENT Compartment syndrome can be challenging to recognize. Recently I have come across several allegations of malpractice for untimely diagnosis. Remember this important problem when faced with a patient with leg pain.
Multiple errors end in death from pneumonia
A 24-YEAR-OLD MAN WITH CHEST PAIN AND A COUGH went to his physician, who diagnosed chest wall pain and prescribed a narcotic pain reliever. The young man returned the next day complaining of increased chest pain. He said he’d been spitting up blood-stained sputum. He was perspiring and vomited in the doctor’s waiting room. The doctor diagnosed an upper respiratory infection and prescribed a cough syrup containing more narcotics.
Later that day the patient had a radiograph at a hospital. It revealed pneumonia. Shortly afterward, the hospital confirmed by fax with the doctor’s office that the doctor had received the results. The doctor didn’t read the radiograph results for 2 days.
After the doctor read the radiograph report, his office tried to contact the patient but misdialed his phone number, then made no further attempts at contact. The patient’s former wife found him at home unresponsive. He was admitted to the ED, where he died of pneumonia shortly thereafter.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE No information about the defense is available.
VERDICT $1.85 million net verdict in Virginia.
COMMENT A cascade of mistakes (sometimes referred to as the Swiss cheese effect) occurs, and a preventable death results. Are you at risk for such an event? What fail-safe measures do you have in place in your practice?
ACIP immunization update
Keeping up with the ever-changing immunization schedules recommended by the Centers for Disease Control and Prevention (CDC)’s Advisory Committee on Immunization Practices (ACIP) can be difficult. The most recent changes are the interim recommendations from the February 2011 ACIP meeting pertaining to tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine immunization and postexposure prophylaxis (PEP) for health care personnel. Updated schedules for routine immunization of children and adults that incorporate additions and changes made in the preceding year were published by the CDC in February.1,2
ACIP widens the scope of pertussis prevention
The past decade has seen an increase in pertussis cases, including an increase in the number of cases among infants and adolescents (FIGURE). In 2010, California reported 8383 cases, including 10 infant deaths. This was the highest number and rate of cases reported in more than 50 years.3 Other states have also experienced recent increases.
This evolving epidemiology of pertussis has prompted ACIP to recommend a routine single Tdap dose for adolescents between the ages of 11 and 18 years who have completed the recommended DTP/DTaP (diphtheria and tetanus toxoids and pertussis/diphtheria and tetanus toxoids and acellular pertussis) vaccination series and for adults ages 19 to 64 years. ACIP also recommends a single dose for children ages 7 to 10 if they are not fully vaccinated against pertussis and for adults 65 and older who have not previously received Tdap and who are in close contact with infants. The last 2 are off-label recommendations. ACIP has also eliminated any recommended interval between the time of vaccination with tetanus or diphtheriatoxoid (Td) containing vaccine and the administration of Tdap.4
FIGURE
Reported pertussis incidence by age group, 1990-2009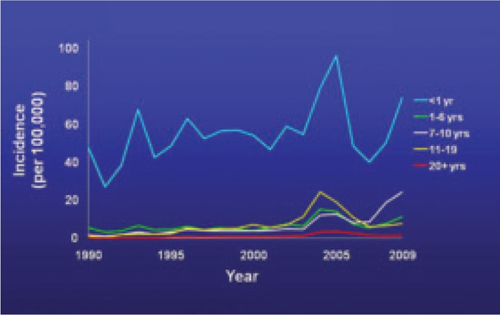
Source: Centers for Disease Control and Prevention. Pertussis (whooping cough): surveillance and reporting. Available at: www.cdc.gov/pertussis/surv-reporting.html. Accessed March 21, 2011.
2 new recommendations for clinician postexposure prophylaxis
Interim recommendations from the most recent ACIP meeting in February 20115 re-emphasize that health care personnel should receive Tdap and recommend that health care facilities take steps to increase adherence, including providing the vaccine at no cost.5
Since health care personnel are at increased risk of exposure to pertussis, ACIP also made 2 recommendations for PEP.
- All health care personnel (vaccinated or not) in close contact with a pertussis patient (as defined in TABLE 1) who are likely to expose patients at high risk for complications from pertussis (infants <1 year of age and those with certain immunodeficiency conditions, chronic lung disease, respiratory insufficiency, or cystic fibrosis) should receive PEP.
- Exposed personnel who do not work with high-risk patients should receive PEP or be monitored daily for 21 days, treated at first signs of infection, and excluded from patient contact for 5 days if symptoms develop. The antimicrobials and doses for treatment and prevention of pertussis have been published in the Morbidity and Mortality Weekly Report.6 Options for PEP include azithromycin, clarithromycin, erythromycin, and trimethoprim-sulfamethoxazole.6
TABLE 1
Definition of close contact with a pertussis patient
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2005.6 |
Coming soon: Complete vaccine recommendations for health care workers
Recent experience with pertussis (and influenza) has highlighted the need for health care personnel to be vaccinated against infectious diseases to protect themselves, their patients, and their families. To that end, ACIP plans to publish a compendium later this year that brings together all recommendations regarding immunizations for health care personnel. When it becomes available, family physicians will be able to refer to this document to ensure that they and their staff are immunized in line with CDC recommendations.
The latest on influenza vaccine, PCV13, MCV4, hepatitis B, and HPV
The most notable additions to the routine schedules ACIP announced during the past year are universal, yearly influenza immunization from the age of 6 months on and the replacement of the 7-valent pneumococcal conjugate vaccine (PCV7) with a 13-valent product (PCV13) for infants and children. Details of these recommendations, including how to transition from PCV7 to PCV13, were published late last year by the CDC and described in another Practice Alert.7-9
In addition, changes were made in the schedules for meningococcal conjugate vaccine. A 2-dose primary series, instead of a single dose, of MCV4 is now recommended for those with compromised immunity. A booster of MCV4 is now recommended at age 16 for those vaccinated at 11 or 12 years, and at age 16 to 18 for those vaccinated at 13 to 15 years.10 The MCV4 recommendations are summarized in TABLE 2.
More schedule details in the footnotes. The new schedules contain a number of clarifications in the footnotes that:1,11
- explain the spacing of the 3-dose primary series for hepatitis B vaccine (HepB) for infants if they do not receive a dose immediately after birth
- clarify the circumstances in which children younger than age 9 need 2 doses of influenza vaccine
- describe the availability of both a quadrivalent human papillomavirus vaccine (HPV4) and a bivalent vaccine (HPV2) to prevent precancerous cervical lesions and cancer
- list the option for using HPV4 for males for the prevention of genital warts.
TABLE 2
Meningococcal conjugate vaccine recommendations by risk group, ACIP 2010
| Risk group | Primary series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at age 11 or 12 years |
|
| HIV-infected individuals ages 11-18 years | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with persistent complement component deficiency such as C5-C9, properdin, or factor D, or functional or anatomic asplenia | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with prolonged increased risk of exposure, such as microbiologists routinely working with Neisseria meningitidis and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose |
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2011.10 | ||
1. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2011. MMWR Morb Mortal Wkly Rep QuickGuide. 2011;60(5):1-4.
2. Centers for Disease Control and Prevention. Recommended adult immunization schedule-United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(4):1-4.
3. Centers for Disease Control and Prevention. Pertussis (whooping cough): outbreaks. Available at: http://www.cdc.gov/pertussis/outbreaks.html. Accessed March 19, 2011.
4. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60(1):13-15.
5. Centers for Disease Control and Prevention. ACIP presentation slides: February 2011 meeting. Available at www.cdc.gov/vaccines/recs/acip/slides-feb11.htm#pertussis. Accessed March 19, 2011.
6. Centers for Disease Control and Prevention. Recommended antimicrobial agents for treatment and postexposure prophylaxis of pertussis: 2005 CDC guidelines. MMWR Recomm Rep. 2005;54(RR-14):1-16.
7. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm Rep. 2010;59(RR-8):1-62.
8. Centers for Disease Control and Prevention. Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59(RR-11):1-18.
9. Campos-Outcalt D. Your guide to the new pneumococcal vaccine for children. J Fam Pract. 2010;59:394-398.
10. Centers for Disease Control and Prevention. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
11. Centers for Disease Control and Prevention. FDA licensure of bivalent human papillomavirus vaccine (HPV2, Cervarix) for use in females and updated HPV vaccination recommendations from the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2010;59:626-629.
Keeping up with the ever-changing immunization schedules recommended by the Centers for Disease Control and Prevention (CDC)’s Advisory Committee on Immunization Practices (ACIP) can be difficult. The most recent changes are the interim recommendations from the February 2011 ACIP meeting pertaining to tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine immunization and postexposure prophylaxis (PEP) for health care personnel. Updated schedules for routine immunization of children and adults that incorporate additions and changes made in the preceding year were published by the CDC in February.1,2
ACIP widens the scope of pertussis prevention
The past decade has seen an increase in pertussis cases, including an increase in the number of cases among infants and adolescents (FIGURE). In 2010, California reported 8383 cases, including 10 infant deaths. This was the highest number and rate of cases reported in more than 50 years.3 Other states have also experienced recent increases.
This evolving epidemiology of pertussis has prompted ACIP to recommend a routine single Tdap dose for adolescents between the ages of 11 and 18 years who have completed the recommended DTP/DTaP (diphtheria and tetanus toxoids and pertussis/diphtheria and tetanus toxoids and acellular pertussis) vaccination series and for adults ages 19 to 64 years. ACIP also recommends a single dose for children ages 7 to 10 if they are not fully vaccinated against pertussis and for adults 65 and older who have not previously received Tdap and who are in close contact with infants. The last 2 are off-label recommendations. ACIP has also eliminated any recommended interval between the time of vaccination with tetanus or diphtheriatoxoid (Td) containing vaccine and the administration of Tdap.4
FIGURE
Reported pertussis incidence by age group, 1990-2009
Source: Centers for Disease Control and Prevention. Pertussis (whooping cough): surveillance and reporting. Available at: www.cdc.gov/pertussis/surv-reporting.html. Accessed March 21, 2011.
2 new recommendations for clinician postexposure prophylaxis
Interim recommendations from the most recent ACIP meeting in February 20115 re-emphasize that health care personnel should receive Tdap and recommend that health care facilities take steps to increase adherence, including providing the vaccine at no cost.5
Since health care personnel are at increased risk of exposure to pertussis, ACIP also made 2 recommendations for PEP.
- All health care personnel (vaccinated or not) in close contact with a pertussis patient (as defined in TABLE 1) who are likely to expose patients at high risk for complications from pertussis (infants <1 year of age and those with certain immunodeficiency conditions, chronic lung disease, respiratory insufficiency, or cystic fibrosis) should receive PEP.
- Exposed personnel who do not work with high-risk patients should receive PEP or be monitored daily for 21 days, treated at first signs of infection, and excluded from patient contact for 5 days if symptoms develop. The antimicrobials and doses for treatment and prevention of pertussis have been published in the Morbidity and Mortality Weekly Report.6 Options for PEP include azithromycin, clarithromycin, erythromycin, and trimethoprim-sulfamethoxazole.6
TABLE 1
Definition of close contact with a pertussis patient
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2005.6 |
Coming soon: Complete vaccine recommendations for health care workers
Recent experience with pertussis (and influenza) has highlighted the need for health care personnel to be vaccinated against infectious diseases to protect themselves, their patients, and their families. To that end, ACIP plans to publish a compendium later this year that brings together all recommendations regarding immunizations for health care personnel. When it becomes available, family physicians will be able to refer to this document to ensure that they and their staff are immunized in line with CDC recommendations.
The latest on influenza vaccine, PCV13, MCV4, hepatitis B, and HPV
The most notable additions to the routine schedules ACIP announced during the past year are universal, yearly influenza immunization from the age of 6 months on and the replacement of the 7-valent pneumococcal conjugate vaccine (PCV7) with a 13-valent product (PCV13) for infants and children. Details of these recommendations, including how to transition from PCV7 to PCV13, were published late last year by the CDC and described in another Practice Alert.7-9
In addition, changes were made in the schedules for meningococcal conjugate vaccine. A 2-dose primary series, instead of a single dose, of MCV4 is now recommended for those with compromised immunity. A booster of MCV4 is now recommended at age 16 for those vaccinated at 11 or 12 years, and at age 16 to 18 for those vaccinated at 13 to 15 years.10 The MCV4 recommendations are summarized in TABLE 2.
More schedule details in the footnotes. The new schedules contain a number of clarifications in the footnotes that:1,11
- explain the spacing of the 3-dose primary series for hepatitis B vaccine (HepB) for infants if they do not receive a dose immediately after birth
- clarify the circumstances in which children younger than age 9 need 2 doses of influenza vaccine
- describe the availability of both a quadrivalent human papillomavirus vaccine (HPV4) and a bivalent vaccine (HPV2) to prevent precancerous cervical lesions and cancer
- list the option for using HPV4 for males for the prevention of genital warts.
TABLE 2
Meningococcal conjugate vaccine recommendations by risk group, ACIP 2010
| Risk group | Primary series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at age 11 or 12 years |
|
| HIV-infected individuals ages 11-18 years | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with persistent complement component deficiency such as C5-C9, properdin, or factor D, or functional or anatomic asplenia | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with prolonged increased risk of exposure, such as microbiologists routinely working with Neisseria meningitidis and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose |
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2011.10 | ||
Keeping up with the ever-changing immunization schedules recommended by the Centers for Disease Control and Prevention (CDC)’s Advisory Committee on Immunization Practices (ACIP) can be difficult. The most recent changes are the interim recommendations from the February 2011 ACIP meeting pertaining to tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine immunization and postexposure prophylaxis (PEP) for health care personnel. Updated schedules for routine immunization of children and adults that incorporate additions and changes made in the preceding year were published by the CDC in February.1,2
ACIP widens the scope of pertussis prevention
The past decade has seen an increase in pertussis cases, including an increase in the number of cases among infants and adolescents (FIGURE). In 2010, California reported 8383 cases, including 10 infant deaths. This was the highest number and rate of cases reported in more than 50 years.3 Other states have also experienced recent increases.
This evolving epidemiology of pertussis has prompted ACIP to recommend a routine single Tdap dose for adolescents between the ages of 11 and 18 years who have completed the recommended DTP/DTaP (diphtheria and tetanus toxoids and pertussis/diphtheria and tetanus toxoids and acellular pertussis) vaccination series and for adults ages 19 to 64 years. ACIP also recommends a single dose for children ages 7 to 10 if they are not fully vaccinated against pertussis and for adults 65 and older who have not previously received Tdap and who are in close contact with infants. The last 2 are off-label recommendations. ACIP has also eliminated any recommended interval between the time of vaccination with tetanus or diphtheriatoxoid (Td) containing vaccine and the administration of Tdap.4
FIGURE
Reported pertussis incidence by age group, 1990-2009
Source: Centers for Disease Control and Prevention. Pertussis (whooping cough): surveillance and reporting. Available at: www.cdc.gov/pertussis/surv-reporting.html. Accessed March 21, 2011.
2 new recommendations for clinician postexposure prophylaxis
Interim recommendations from the most recent ACIP meeting in February 20115 re-emphasize that health care personnel should receive Tdap and recommend that health care facilities take steps to increase adherence, including providing the vaccine at no cost.5
Since health care personnel are at increased risk of exposure to pertussis, ACIP also made 2 recommendations for PEP.
- All health care personnel (vaccinated or not) in close contact with a pertussis patient (as defined in TABLE 1) who are likely to expose patients at high risk for complications from pertussis (infants <1 year of age and those with certain immunodeficiency conditions, chronic lung disease, respiratory insufficiency, or cystic fibrosis) should receive PEP.
- Exposed personnel who do not work with high-risk patients should receive PEP or be monitored daily for 21 days, treated at first signs of infection, and excluded from patient contact for 5 days if symptoms develop. The antimicrobials and doses for treatment and prevention of pertussis have been published in the Morbidity and Mortality Weekly Report.6 Options for PEP include azithromycin, clarithromycin, erythromycin, and trimethoprim-sulfamethoxazole.6
TABLE 1
Definition of close contact with a pertussis patient
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2005.6 |
Coming soon: Complete vaccine recommendations for health care workers
Recent experience with pertussis (and influenza) has highlighted the need for health care personnel to be vaccinated against infectious diseases to protect themselves, their patients, and their families. To that end, ACIP plans to publish a compendium later this year that brings together all recommendations regarding immunizations for health care personnel. When it becomes available, family physicians will be able to refer to this document to ensure that they and their staff are immunized in line with CDC recommendations.
The latest on influenza vaccine, PCV13, MCV4, hepatitis B, and HPV
The most notable additions to the routine schedules ACIP announced during the past year are universal, yearly influenza immunization from the age of 6 months on and the replacement of the 7-valent pneumococcal conjugate vaccine (PCV7) with a 13-valent product (PCV13) for infants and children. Details of these recommendations, including how to transition from PCV7 to PCV13, were published late last year by the CDC and described in another Practice Alert.7-9
In addition, changes were made in the schedules for meningococcal conjugate vaccine. A 2-dose primary series, instead of a single dose, of MCV4 is now recommended for those with compromised immunity. A booster of MCV4 is now recommended at age 16 for those vaccinated at 11 or 12 years, and at age 16 to 18 for those vaccinated at 13 to 15 years.10 The MCV4 recommendations are summarized in TABLE 2.
More schedule details in the footnotes. The new schedules contain a number of clarifications in the footnotes that:1,11
- explain the spacing of the 3-dose primary series for hepatitis B vaccine (HepB) for infants if they do not receive a dose immediately after birth
- clarify the circumstances in which children younger than age 9 need 2 doses of influenza vaccine
- describe the availability of both a quadrivalent human papillomavirus vaccine (HPV4) and a bivalent vaccine (HPV2) to prevent precancerous cervical lesions and cancer
- list the option for using HPV4 for males for the prevention of genital warts.
TABLE 2
Meningococcal conjugate vaccine recommendations by risk group, ACIP 2010
| Risk group | Primary series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at age 11 or 12 years |
|
| HIV-infected individuals ages 11-18 years | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with persistent complement component deficiency such as C5-C9, properdin, or factor D, or functional or anatomic asplenia | 2 doses, 2 months apart |
|
| Individuals ages 2-55 years with prolonged increased risk of exposure, such as microbiologists routinely working with Neisseria meningitidis and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose |
|
| Source: Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2011.10 | ||
1. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2011. MMWR Morb Mortal Wkly Rep QuickGuide. 2011;60(5):1-4.
2. Centers for Disease Control and Prevention. Recommended adult immunization schedule-United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(4):1-4.
3. Centers for Disease Control and Prevention. Pertussis (whooping cough): outbreaks. Available at: http://www.cdc.gov/pertussis/outbreaks.html. Accessed March 19, 2011.
4. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60(1):13-15.
5. Centers for Disease Control and Prevention. ACIP presentation slides: February 2011 meeting. Available at www.cdc.gov/vaccines/recs/acip/slides-feb11.htm#pertussis. Accessed March 19, 2011.
6. Centers for Disease Control and Prevention. Recommended antimicrobial agents for treatment and postexposure prophylaxis of pertussis: 2005 CDC guidelines. MMWR Recomm Rep. 2005;54(RR-14):1-16.
7. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm Rep. 2010;59(RR-8):1-62.
8. Centers for Disease Control and Prevention. Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59(RR-11):1-18.
9. Campos-Outcalt D. Your guide to the new pneumococcal vaccine for children. J Fam Pract. 2010;59:394-398.
10. Centers for Disease Control and Prevention. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
11. Centers for Disease Control and Prevention. FDA licensure of bivalent human papillomavirus vaccine (HPV2, Cervarix) for use in females and updated HPV vaccination recommendations from the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2010;59:626-629.
1. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2011. MMWR Morb Mortal Wkly Rep QuickGuide. 2011;60(5):1-4.
2. Centers for Disease Control and Prevention. Recommended adult immunization schedule-United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(4):1-4.
3. Centers for Disease Control and Prevention. Pertussis (whooping cough): outbreaks. Available at: http://www.cdc.gov/pertussis/outbreaks.html. Accessed March 19, 2011.
4. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60(1):13-15.
5. Centers for Disease Control and Prevention. ACIP presentation slides: February 2011 meeting. Available at www.cdc.gov/vaccines/recs/acip/slides-feb11.htm#pertussis. Accessed March 19, 2011.
6. Centers for Disease Control and Prevention. Recommended antimicrobial agents for treatment and postexposure prophylaxis of pertussis: 2005 CDC guidelines. MMWR Recomm Rep. 2005;54(RR-14):1-16.
7. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm Rep. 2010;59(RR-8):1-62.
8. Centers for Disease Control and Prevention. Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59(RR-11):1-18.
9. Campos-Outcalt D. Your guide to the new pneumococcal vaccine for children. J Fam Pract. 2010;59:394-398.
10. Centers for Disease Control and Prevention. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
11. Centers for Disease Control and Prevention. FDA licensure of bivalent human papillomavirus vaccine (HPV2, Cervarix) for use in females and updated HPV vaccination recommendations from the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2010;59:626-629.
Returning traveler with painful penile mass
WORRIED THAT HE MIGHT HAVE CONTRACTED CHLAMYDIA, a 27-year-old man visited our clinic for treatment. About 5 days earlier, he’d begun experiencing pain and a burning feeling when he urinated. Three days earlier, a painful lump near the head of his penis developed; the lump was growing.
The patient, who was otherwise healthy, had recently returned from a trip to Vietnam during which he reported having had sex with one female partner. He said, “I thought I was safe. I used a condom.”
On examination, he had a purulent urethral discharge and there was a fluctuant, yellowish-white, tender swelling on the left side of the frenulum (FIGURE). There were no ulcers. There was, however, a single 2-cm lymph node in the right inguinal area that was mobile, nontender, nonfluctuant, and of normal consistency.
FIGURE
Swelling with purulent discharge
In addition to the fluctuant, yellowish white, tender swelling on the left side of the frenulum, the patient had purulent urethral discharge and a single, 2-cm lymph node in the right inguinal area.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tysonitis
The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
Case reports of gonorrheal infection of Tyson’s gland have documented infection with and without symptoms of urethritis.2-4 Diagnosis in this case was confirmed by sending the discharge for nucleic acid amplification testing (NAAT), which was positive for Neisseria gonorrhoeae and negative for Chlamydia trachomatis.
Other diagnostic possibilities. The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.5
How this patient’s attempt at “safe sex” failed
Oropharyngeal gonococcal infection was the route of transmission implicated in this patient’s infection. When specifically asked about his sexual encounter, our patient admitted that while he was diligent about using a condom for intercourse, he did not use a condom when he received oral sex.
The prevalence of pharyngeal involvement is estimated to be 10% to 20% among women and MSM (men who have sex with men) who have genital gonorrheal infection.6 The risk of contracting N gonorrhoeae when receiving oral sex from an infected partner is unknown.
A common disease, a not-so-common complication
Genital infection by N gonorrhoeae remains the second most common notifiable disease in the United States, with 301,174 cases reported in 2009.7 Effective antimicrobial treatment has reduced the occurrence of local complications of gonococcal infection. Nevertheless, complications of gonococcal urethritis like the ones that follow do occur.
Acute epididymitis is the most common complication of urethral gonorrhea. It is characterized by a swollen and inflamed scrotum, localized epididymal pain, fever, and pyuria.8
Penile edema (“bull-headed clap”) is another common complication.8 It may be limited to the meatus or extend to the distal penile shaft and prepuce and may occur in the absence of other inflammatory signs.
Urethral stricture, once thought to be a common complication, is actually relatively rare, occurring in just 0.5% of cases.6 Urethral strictures attributed to gonorrheal urethritis during the pre-antibiotic era may have actually resulted from the caustic treatments administered during that time.
Acute prostatitis with sudden onset of chills, fever, malaise, and warmth and swelling of the prostate can also develop, although it is more commonly caused by gram-negative rods, such as Escherichia coli or Proteus mirabilis.8
Chronic prostatitis, usually caused by recurrent urinary tract infections, has also been documented as a complication of gonorrheal infection.9
Infection of the Cowper’s, or bulbourethral glands, can occur, leading to perineal swelling.10
Periurethral abscess results when an infected Littre’s or Tyson’s gland ruptures and the infection extends into the deeper tissues.11
Seminal vesiculitis has previously been described as an uncommon complication of gonorrheal infection. However, a recent small study showed ultrasonographic evidence of vesiculitis in 46% of patients with urethritis due to gonorrhea or chlamydia.12
Penile sclerosing lymphangitis presents as an acute, firm, cordlike lesion of the coronal sulcus. A quarter of reported cases have been linked to sexually transmitted infections, including gonorrhea.13
NAAT is key to diagnosis
Infection with genitourinary N gonorrhoeae can be detected in various ways, including gram staining of a male urethral specimen, culture, nucleic acid hybridization, and NAAT. NAAT, which we used with our patient, has the advantage of being approved for use with urine specimens from men and women, as well as with endocervical or urethral samples.
Diagnosis of nongenital infection (ie, pharynx, rectum) typically requires culture. Other diagnostic methods are not FDA-approved for use with specimens from nongenital sites and may yield false-positive results due to cross-reactivity with organisms other than N gonorrhoeae.14 Patients tested for gonorrhea should also be tested for other sexually transmitted infections, including chlamydia, syphilis, and human immunodeficiency virus.
Treat patients with ceftriaxone
Treatment for tysonitis is similar to treatment for gonococcal urethritis and centers on the use of appropriate antibiotics.15 Quinolone-resistant N gonorrhoeae is increasingly common; it is estimated that up to 40% of strains in Asia are now quinolone resistant.16 Because of this, the CDC recommends treatment with ceftriaxone and azithromycin.17 As with urethritis, presumptive treatment for chlamydia is warranted. For tysonitis, incision and drainage may also be necessary.18
A good outcome for our patient
This patient was treated with ceftriaxone 250 mg intramuscularly and azithromycin 1 g as a single oral dose. The abscess was incised and drained under local anesthesia, with 2 cc of pus obtained.
Five days after treatment, the patient reported feeling much better. He was told to call the clinic if he didn’t have complete resolution in 2 weeks. He did not report any further problems.
CORRESPONDENCE Andrew Schechtman, MD, San Jose-O’Connor Hospital Family Medicine Residency, 455 O’Connor Drive,#210, San Jose, CA 95128; aschecht@stanford.edu
1. Batistatou A, Panelos J, Zioga A, et al. Ectomic modified sebaceous glands in human penis. Int J Surg Pathol. 2006;14:355-356.
2. Burgess JA. Gonococcal tysonitis without urethritis after prophylactic post-coital urination. Br J Vener Dis. 1971;47:40-41.
3. Bavidge KJ. Letter: gonococcal infection of the penis. Br J Vener Dis. 1976;52:66.-
4. Abdul Gaffoor PM. Gonococcal tysonitis. Postgrad Med J. 1986;62:869-870.
5. Frenkl T, Potts J. Sexually transmitted diseases. In: Wein AJ, Kavoussi LR, Novick AC, et al, eds. Campbell-Walsh Urology. 9th ed. Philadelphia, Pa: Saunders; 2007:371–385.
6. Nelson AL. Gonorrheal infections. In: Nelson AL, Woodward JA, eds. Sexually Transmitted Diseases: A Practical Guide for Primary Care. Totowa, NJ: Humana Press; 2007:153–182.
7. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2009. Available at: www.cdc.gov/std/stats09/surv2009-Complete.pdf. Accessed March 25, 2011.
8. Marrazzo JM, Handsfield HH, Sparling PF. Neisseria gonorrhoeae. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia, Pa: Churchill Livingstone 2009;2753-2770.
9. Adler MW. ABC of sexually transmitted diseases: complications of common genital infections and infections in other sites. Br Med J. 1983;287:1709-1712.
10. Subramanian S. Gonococcal urethritis with bilateral tysonitis and periurethral abscess. Sex Transm Dis. 1981;8:77-78.
11. Komolafe AJ, Cornford PA, Fordham MV, et al. Periurethral abscess complicating male gonococcal urethritis treated by surgical incision and drainage. Int J STD AIDS. 2002;13:857-858.
12. Furuya R, Takahashi S, Furuya S, et al. Is urethritis accompanied by seminal vesiculitis? Int J Urol. 2009;16:628-631.
13. Rosen T, Hwong H. Sclerosing lymphangitis of the penis. J Am Acad Dermatol. 2003;49:916-918.
14. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. Diseases characterized by urethritis and cervicitis. Available at: http://www.cdc.gov/STD/treatment/2006/urethritis-and-cervicitis.htm#uc6. Accessed January 26, 2010.
15. el-Benhawi MO, el-Tonsy MH. Gonococcal urethritis with bilateral tysonitis. Cutis. 1988;41:425-426.
16. Centers for Disease Control and Prevention. Increases in fluoroquinolone-resistant Neisseria gonorrhoeae—Hawaii and California, 2001. MMWR Morb Mortal Wkly Rep. 2002;51:1041-1044.
17. Workowski KA, Berman S. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
18. Fiumara NJ. Gonococcal tysonitis. Br J Vener Dis. 1977;53:145.
WORRIED THAT HE MIGHT HAVE CONTRACTED CHLAMYDIA, a 27-year-old man visited our clinic for treatment. About 5 days earlier, he’d begun experiencing pain and a burning feeling when he urinated. Three days earlier, a painful lump near the head of his penis developed; the lump was growing.
The patient, who was otherwise healthy, had recently returned from a trip to Vietnam during which he reported having had sex with one female partner. He said, “I thought I was safe. I used a condom.”
On examination, he had a purulent urethral discharge and there was a fluctuant, yellowish-white, tender swelling on the left side of the frenulum (FIGURE). There were no ulcers. There was, however, a single 2-cm lymph node in the right inguinal area that was mobile, nontender, nonfluctuant, and of normal consistency.
FIGURE
Swelling with purulent discharge
In addition to the fluctuant, yellowish white, tender swelling on the left side of the frenulum, the patient had purulent urethral discharge and a single, 2-cm lymph node in the right inguinal area.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tysonitis
The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
Case reports of gonorrheal infection of Tyson’s gland have documented infection with and without symptoms of urethritis.2-4 Diagnosis in this case was confirmed by sending the discharge for nucleic acid amplification testing (NAAT), which was positive for Neisseria gonorrhoeae and negative for Chlamydia trachomatis.
Other diagnostic possibilities. The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.5
How this patient’s attempt at “safe sex” failed
Oropharyngeal gonococcal infection was the route of transmission implicated in this patient’s infection. When specifically asked about his sexual encounter, our patient admitted that while he was diligent about using a condom for intercourse, he did not use a condom when he received oral sex.
The prevalence of pharyngeal involvement is estimated to be 10% to 20% among women and MSM (men who have sex with men) who have genital gonorrheal infection.6 The risk of contracting N gonorrhoeae when receiving oral sex from an infected partner is unknown.
A common disease, a not-so-common complication
Genital infection by N gonorrhoeae remains the second most common notifiable disease in the United States, with 301,174 cases reported in 2009.7 Effective antimicrobial treatment has reduced the occurrence of local complications of gonococcal infection. Nevertheless, complications of gonococcal urethritis like the ones that follow do occur.
Acute epididymitis is the most common complication of urethral gonorrhea. It is characterized by a swollen and inflamed scrotum, localized epididymal pain, fever, and pyuria.8
Penile edema (“bull-headed clap”) is another common complication.8 It may be limited to the meatus or extend to the distal penile shaft and prepuce and may occur in the absence of other inflammatory signs.
Urethral stricture, once thought to be a common complication, is actually relatively rare, occurring in just 0.5% of cases.6 Urethral strictures attributed to gonorrheal urethritis during the pre-antibiotic era may have actually resulted from the caustic treatments administered during that time.
Acute prostatitis with sudden onset of chills, fever, malaise, and warmth and swelling of the prostate can also develop, although it is more commonly caused by gram-negative rods, such as Escherichia coli or Proteus mirabilis.8
Chronic prostatitis, usually caused by recurrent urinary tract infections, has also been documented as a complication of gonorrheal infection.9
Infection of the Cowper’s, or bulbourethral glands, can occur, leading to perineal swelling.10
Periurethral abscess results when an infected Littre’s or Tyson’s gland ruptures and the infection extends into the deeper tissues.11
Seminal vesiculitis has previously been described as an uncommon complication of gonorrheal infection. However, a recent small study showed ultrasonographic evidence of vesiculitis in 46% of patients with urethritis due to gonorrhea or chlamydia.12
Penile sclerosing lymphangitis presents as an acute, firm, cordlike lesion of the coronal sulcus. A quarter of reported cases have been linked to sexually transmitted infections, including gonorrhea.13
NAAT is key to diagnosis
Infection with genitourinary N gonorrhoeae can be detected in various ways, including gram staining of a male urethral specimen, culture, nucleic acid hybridization, and NAAT. NAAT, which we used with our patient, has the advantage of being approved for use with urine specimens from men and women, as well as with endocervical or urethral samples.
Diagnosis of nongenital infection (ie, pharynx, rectum) typically requires culture. Other diagnostic methods are not FDA-approved for use with specimens from nongenital sites and may yield false-positive results due to cross-reactivity with organisms other than N gonorrhoeae.14 Patients tested for gonorrhea should also be tested for other sexually transmitted infections, including chlamydia, syphilis, and human immunodeficiency virus.
Treat patients with ceftriaxone
Treatment for tysonitis is similar to treatment for gonococcal urethritis and centers on the use of appropriate antibiotics.15 Quinolone-resistant N gonorrhoeae is increasingly common; it is estimated that up to 40% of strains in Asia are now quinolone resistant.16 Because of this, the CDC recommends treatment with ceftriaxone and azithromycin.17 As with urethritis, presumptive treatment for chlamydia is warranted. For tysonitis, incision and drainage may also be necessary.18
A good outcome for our patient
This patient was treated with ceftriaxone 250 mg intramuscularly and azithromycin 1 g as a single oral dose. The abscess was incised and drained under local anesthesia, with 2 cc of pus obtained.
Five days after treatment, the patient reported feeling much better. He was told to call the clinic if he didn’t have complete resolution in 2 weeks. He did not report any further problems.
CORRESPONDENCE Andrew Schechtman, MD, San Jose-O’Connor Hospital Family Medicine Residency, 455 O’Connor Drive,#210, San Jose, CA 95128; aschecht@stanford.edu
WORRIED THAT HE MIGHT HAVE CONTRACTED CHLAMYDIA, a 27-year-old man visited our clinic for treatment. About 5 days earlier, he’d begun experiencing pain and a burning feeling when he urinated. Three days earlier, a painful lump near the head of his penis developed; the lump was growing.
The patient, who was otherwise healthy, had recently returned from a trip to Vietnam during which he reported having had sex with one female partner. He said, “I thought I was safe. I used a condom.”
On examination, he had a purulent urethral discharge and there was a fluctuant, yellowish-white, tender swelling on the left side of the frenulum (FIGURE). There were no ulcers. There was, however, a single 2-cm lymph node in the right inguinal area that was mobile, nontender, nonfluctuant, and of normal consistency.
FIGURE
Swelling with purulent discharge
In addition to the fluctuant, yellowish white, tender swelling on the left side of the frenulum, the patient had purulent urethral discharge and a single, 2-cm lymph node in the right inguinal area.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tysonitis
The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
Case reports of gonorrheal infection of Tyson’s gland have documented infection with and without symptoms of urethritis.2-4 Diagnosis in this case was confirmed by sending the discharge for nucleic acid amplification testing (NAAT), which was positive for Neisseria gonorrhoeae and negative for Chlamydia trachomatis.
Other diagnostic possibilities. The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.5
How this patient’s attempt at “safe sex” failed
Oropharyngeal gonococcal infection was the route of transmission implicated in this patient’s infection. When specifically asked about his sexual encounter, our patient admitted that while he was diligent about using a condom for intercourse, he did not use a condom when he received oral sex.
The prevalence of pharyngeal involvement is estimated to be 10% to 20% among women and MSM (men who have sex with men) who have genital gonorrheal infection.6 The risk of contracting N gonorrhoeae when receiving oral sex from an infected partner is unknown.
A common disease, a not-so-common complication
Genital infection by N gonorrhoeae remains the second most common notifiable disease in the United States, with 301,174 cases reported in 2009.7 Effective antimicrobial treatment has reduced the occurrence of local complications of gonococcal infection. Nevertheless, complications of gonococcal urethritis like the ones that follow do occur.
Acute epididymitis is the most common complication of urethral gonorrhea. It is characterized by a swollen and inflamed scrotum, localized epididymal pain, fever, and pyuria.8
Penile edema (“bull-headed clap”) is another common complication.8 It may be limited to the meatus or extend to the distal penile shaft and prepuce and may occur in the absence of other inflammatory signs.
Urethral stricture, once thought to be a common complication, is actually relatively rare, occurring in just 0.5% of cases.6 Urethral strictures attributed to gonorrheal urethritis during the pre-antibiotic era may have actually resulted from the caustic treatments administered during that time.
Acute prostatitis with sudden onset of chills, fever, malaise, and warmth and swelling of the prostate can also develop, although it is more commonly caused by gram-negative rods, such as Escherichia coli or Proteus mirabilis.8
Chronic prostatitis, usually caused by recurrent urinary tract infections, has also been documented as a complication of gonorrheal infection.9
Infection of the Cowper’s, or bulbourethral glands, can occur, leading to perineal swelling.10
Periurethral abscess results when an infected Littre’s or Tyson’s gland ruptures and the infection extends into the deeper tissues.11
Seminal vesiculitis has previously been described as an uncommon complication of gonorrheal infection. However, a recent small study showed ultrasonographic evidence of vesiculitis in 46% of patients with urethritis due to gonorrhea or chlamydia.12
Penile sclerosing lymphangitis presents as an acute, firm, cordlike lesion of the coronal sulcus. A quarter of reported cases have been linked to sexually transmitted infections, including gonorrhea.13
NAAT is key to diagnosis
Infection with genitourinary N gonorrhoeae can be detected in various ways, including gram staining of a male urethral specimen, culture, nucleic acid hybridization, and NAAT. NAAT, which we used with our patient, has the advantage of being approved for use with urine specimens from men and women, as well as with endocervical or urethral samples.
Diagnosis of nongenital infection (ie, pharynx, rectum) typically requires culture. Other diagnostic methods are not FDA-approved for use with specimens from nongenital sites and may yield false-positive results due to cross-reactivity with organisms other than N gonorrhoeae.14 Patients tested for gonorrhea should also be tested for other sexually transmitted infections, including chlamydia, syphilis, and human immunodeficiency virus.
Treat patients with ceftriaxone
Treatment for tysonitis is similar to treatment for gonococcal urethritis and centers on the use of appropriate antibiotics.15 Quinolone-resistant N gonorrhoeae is increasingly common; it is estimated that up to 40% of strains in Asia are now quinolone resistant.16 Because of this, the CDC recommends treatment with ceftriaxone and azithromycin.17 As with urethritis, presumptive treatment for chlamydia is warranted. For tysonitis, incision and drainage may also be necessary.18
A good outcome for our patient
This patient was treated with ceftriaxone 250 mg intramuscularly and azithromycin 1 g as a single oral dose. The abscess was incised and drained under local anesthesia, with 2 cc of pus obtained.
Five days after treatment, the patient reported feeling much better. He was told to call the clinic if he didn’t have complete resolution in 2 weeks. He did not report any further problems.
CORRESPONDENCE Andrew Schechtman, MD, San Jose-O’Connor Hospital Family Medicine Residency, 455 O’Connor Drive,#210, San Jose, CA 95128; aschecht@stanford.edu
1. Batistatou A, Panelos J, Zioga A, et al. Ectomic modified sebaceous glands in human penis. Int J Surg Pathol. 2006;14:355-356.
2. Burgess JA. Gonococcal tysonitis without urethritis after prophylactic post-coital urination. Br J Vener Dis. 1971;47:40-41.
3. Bavidge KJ. Letter: gonococcal infection of the penis. Br J Vener Dis. 1976;52:66.-
4. Abdul Gaffoor PM. Gonococcal tysonitis. Postgrad Med J. 1986;62:869-870.
5. Frenkl T, Potts J. Sexually transmitted diseases. In: Wein AJ, Kavoussi LR, Novick AC, et al, eds. Campbell-Walsh Urology. 9th ed. Philadelphia, Pa: Saunders; 2007:371–385.
6. Nelson AL. Gonorrheal infections. In: Nelson AL, Woodward JA, eds. Sexually Transmitted Diseases: A Practical Guide for Primary Care. Totowa, NJ: Humana Press; 2007:153–182.
7. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2009. Available at: www.cdc.gov/std/stats09/surv2009-Complete.pdf. Accessed March 25, 2011.
8. Marrazzo JM, Handsfield HH, Sparling PF. Neisseria gonorrhoeae. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia, Pa: Churchill Livingstone 2009;2753-2770.
9. Adler MW. ABC of sexually transmitted diseases: complications of common genital infections and infections in other sites. Br Med J. 1983;287:1709-1712.
10. Subramanian S. Gonococcal urethritis with bilateral tysonitis and periurethral abscess. Sex Transm Dis. 1981;8:77-78.
11. Komolafe AJ, Cornford PA, Fordham MV, et al. Periurethral abscess complicating male gonococcal urethritis treated by surgical incision and drainage. Int J STD AIDS. 2002;13:857-858.
12. Furuya R, Takahashi S, Furuya S, et al. Is urethritis accompanied by seminal vesiculitis? Int J Urol. 2009;16:628-631.
13. Rosen T, Hwong H. Sclerosing lymphangitis of the penis. J Am Acad Dermatol. 2003;49:916-918.
14. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. Diseases characterized by urethritis and cervicitis. Available at: http://www.cdc.gov/STD/treatment/2006/urethritis-and-cervicitis.htm#uc6. Accessed January 26, 2010.
15. el-Benhawi MO, el-Tonsy MH. Gonococcal urethritis with bilateral tysonitis. Cutis. 1988;41:425-426.
16. Centers for Disease Control and Prevention. Increases in fluoroquinolone-resistant Neisseria gonorrhoeae—Hawaii and California, 2001. MMWR Morb Mortal Wkly Rep. 2002;51:1041-1044.
17. Workowski KA, Berman S. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
18. Fiumara NJ. Gonococcal tysonitis. Br J Vener Dis. 1977;53:145.
1. Batistatou A, Panelos J, Zioga A, et al. Ectomic modified sebaceous glands in human penis. Int J Surg Pathol. 2006;14:355-356.
2. Burgess JA. Gonococcal tysonitis without urethritis after prophylactic post-coital urination. Br J Vener Dis. 1971;47:40-41.
3. Bavidge KJ. Letter: gonococcal infection of the penis. Br J Vener Dis. 1976;52:66.-
4. Abdul Gaffoor PM. Gonococcal tysonitis. Postgrad Med J. 1986;62:869-870.
5. Frenkl T, Potts J. Sexually transmitted diseases. In: Wein AJ, Kavoussi LR, Novick AC, et al, eds. Campbell-Walsh Urology. 9th ed. Philadelphia, Pa: Saunders; 2007:371–385.
6. Nelson AL. Gonorrheal infections. In: Nelson AL, Woodward JA, eds. Sexually Transmitted Diseases: A Practical Guide for Primary Care. Totowa, NJ: Humana Press; 2007:153–182.
7. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2009. Available at: www.cdc.gov/std/stats09/surv2009-Complete.pdf. Accessed March 25, 2011.
8. Marrazzo JM, Handsfield HH, Sparling PF. Neisseria gonorrhoeae. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia, Pa: Churchill Livingstone 2009;2753-2770.
9. Adler MW. ABC of sexually transmitted diseases: complications of common genital infections and infections in other sites. Br Med J. 1983;287:1709-1712.
10. Subramanian S. Gonococcal urethritis with bilateral tysonitis and periurethral abscess. Sex Transm Dis. 1981;8:77-78.
11. Komolafe AJ, Cornford PA, Fordham MV, et al. Periurethral abscess complicating male gonococcal urethritis treated by surgical incision and drainage. Int J STD AIDS. 2002;13:857-858.
12. Furuya R, Takahashi S, Furuya S, et al. Is urethritis accompanied by seminal vesiculitis? Int J Urol. 2009;16:628-631.
13. Rosen T, Hwong H. Sclerosing lymphangitis of the penis. J Am Acad Dermatol. 2003;49:916-918.
14. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. Diseases characterized by urethritis and cervicitis. Available at: http://www.cdc.gov/STD/treatment/2006/urethritis-and-cervicitis.htm#uc6. Accessed January 26, 2010.
15. el-Benhawi MO, el-Tonsy MH. Gonococcal urethritis with bilateral tysonitis. Cutis. 1988;41:425-426.
16. Centers for Disease Control and Prevention. Increases in fluoroquinolone-resistant Neisseria gonorrhoeae—Hawaii and California, 2001. MMWR Morb Mortal Wkly Rep. 2002;51:1041-1044.
17. Workowski KA, Berman S. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
18. Fiumara NJ. Gonococcal tysonitis. Br J Vener Dis. 1977;53:145.
How effective—and safe—are systemic steroids for acute low back pain?
SHORT COURSES OF SYSTEMIC STEROIDS ARE LIKELY SAFE, but they are ineffective. A single dose of intramuscular (IM) or intravenous (IV) methylprednisolone doesn’t improve long-term pain scores in patients with low back pain and sciatica and produces conflicting effects on function. Oral prednisone (9-day taper) doesn’t improve pain or function in patients with back pain and sciatica. A single IM dose of methylprednisolone doesn’t improve pain scores or function in patients with back pain without sciatica (strength of recommendation: B, randomized controlled trials [RCTs]).
No trials of corticosteroids for back pain reported an increase in adverse outcomes, but studies were small, and only short-term (1 month) follow-up data are available.
Evidence summary
A double-blind RCT of 82 patients who reported to an emergency department with acute low back pain and sciatica compared the efficacy of a single IM dose of 160 mg methylprednisolone with placebo.1 Sciatica was confirmed with a positive straight leg test. All patients were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score, rated on a 0-to-10 visual analog scale (VAS).
Pain scores dropped in both groups over time. The magnitude of the change was not significantly greater in the steroid group (at 1 week: mean difference=1.1; 95% confidence interval [CI], –0.5 to 2.8; at 1 month: mean difference=1.3; 95% CI, –0.5 to 2.7).
Among secondary outcomes at 1 month, 19% of the methylprednisolone group reported continued functional disability compared with 49% of the placebo group (absolute difference=30%; 95% CI, 9-49; P=.007). Analgesic use in the previous 24 hours was similar for both groups (22% with steroid injection vs 43% with placebo; P=.06). There were no reports of gastrointestinal bleeding, osteonecrosis, infection, or serious hyperglycemia.
The same applies to back pain without sciatica
Another double-blind RCT of 87 patients evaluated IM methylprednisolone for acute low back pain of less than 1 week duration without sciatica.2 Patients received a single IM dose of 160 mg methylprednisolone or placebo. Both groups were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score on a 0-to-10 VAS.
Pain scores dropped in both groups over time, but the reduction wasn’t significantly larger in the steroid group (at 1 week: mean difference=0.6; 95% CI, –0.9 to 2.2; at 1 month: mean difference=0.6; 95% CI, –1.0 to 2.2). At 1 month, neither functional status nor “medication use in the preceding 24 hours” differed between the 2 groups.
The most common adverse effects were upper gastrointestinal complaints, drowsiness, and weakness. Adverse effect rates were comparable for the 2 groups and believed to be caused by the naproxen and oxycodone all patients received.
Relief of sciatica with IV steroids is short-lived
A double-blind RCT evaluated the efficacy of a single IV dose of 500 mg methylprednisolone or placebo for 65 patients with leg sciatica (with or without back pain) associated with imaging-confirmed lumbar disk disease.3 The primary outcome was reduction in sciatic leg pain during the first 3 days after injection as measured on a 100-mm VAS. All patients received standard pain medication and physical therapy.
At day 1, 48% of the methylprednisolone group and 28% of the placebo group showed a decrease on the VAS for sciatic pain of 20 mm or more (P=.04; number needed to treat=5). Pain measurements at 2, 3, 10, and 30 days found no significant difference between the groups, however. Nor did the groups differ significantly in functional status or medication use. The study didn’t assess adverse events.
Oral prednisone relieves back pain with sciatica no better than placebo
A double-blind RCT compared an oral prednisone taper (60 mg, 40 mg, and 20 mg each for 3 days) with placebo for treating 27 patients with acute low back pain and sciatica.4 All patients received nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotics for pain control, directions to engage in activity as tolerated, and a referral for physical therapy. Outcomes were evaluated weekly for 1 month, then monthly for 5 months.
Pain scores, functional ability, and medication use didn’t differ significantly between the 2 groups. Steroid injections were later given to 15% of the oral steroid group and 43% of the control group, but the difference in outcomes wasn’t statistically significant. Investigators didn’t assess adverse events.
Recommendations
The joint guidelines of the American College of Physicians and the American Pain Society recommend acetaminophen and NSAIDs as first-line treatments for back pain and back pain with sciatica.5 The guidelines advise against using systemic corticosteroids because “they have not been shown to be more effective than placebo.”
1. Friedman BW, Esses D, Solorzano C, et al. A randomized placebo-controlled trial of single-dose IM corticosteroid for radicular low back pain. Spine. 2008;33:E624-E629.
2. Friedman BW, Holden L, Esses D, et al. Parenteral corticosteroids for emergency department patients with nonradicular low back pain. J Emerg Med. 2006;31:365-370.
3. Finckh A, Zufferey P, Schurch MA, et al. Short-term efficacy of intravenous pulse glucocorticoids in acute discogenic sciatica: a randomized controlled trial. Spine. 2006;31:377-381.
4. Holve RL, Barkan H. Oral steroids in initial treatment of acute sciatica. J Am Board Fam Med. 2008;21:469-474.
5. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
SHORT COURSES OF SYSTEMIC STEROIDS ARE LIKELY SAFE, but they are ineffective. A single dose of intramuscular (IM) or intravenous (IV) methylprednisolone doesn’t improve long-term pain scores in patients with low back pain and sciatica and produces conflicting effects on function. Oral prednisone (9-day taper) doesn’t improve pain or function in patients with back pain and sciatica. A single IM dose of methylprednisolone doesn’t improve pain scores or function in patients with back pain without sciatica (strength of recommendation: B, randomized controlled trials [RCTs]).
No trials of corticosteroids for back pain reported an increase in adverse outcomes, but studies were small, and only short-term (1 month) follow-up data are available.
Evidence summary
A double-blind RCT of 82 patients who reported to an emergency department with acute low back pain and sciatica compared the efficacy of a single IM dose of 160 mg methylprednisolone with placebo.1 Sciatica was confirmed with a positive straight leg test. All patients were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score, rated on a 0-to-10 visual analog scale (VAS).
Pain scores dropped in both groups over time. The magnitude of the change was not significantly greater in the steroid group (at 1 week: mean difference=1.1; 95% confidence interval [CI], –0.5 to 2.8; at 1 month: mean difference=1.3; 95% CI, –0.5 to 2.7).
Among secondary outcomes at 1 month, 19% of the methylprednisolone group reported continued functional disability compared with 49% of the placebo group (absolute difference=30%; 95% CI, 9-49; P=.007). Analgesic use in the previous 24 hours was similar for both groups (22% with steroid injection vs 43% with placebo; P=.06). There were no reports of gastrointestinal bleeding, osteonecrosis, infection, or serious hyperglycemia.
The same applies to back pain without sciatica
Another double-blind RCT of 87 patients evaluated IM methylprednisolone for acute low back pain of less than 1 week duration without sciatica.2 Patients received a single IM dose of 160 mg methylprednisolone or placebo. Both groups were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score on a 0-to-10 VAS.
Pain scores dropped in both groups over time, but the reduction wasn’t significantly larger in the steroid group (at 1 week: mean difference=0.6; 95% CI, –0.9 to 2.2; at 1 month: mean difference=0.6; 95% CI, –1.0 to 2.2). At 1 month, neither functional status nor “medication use in the preceding 24 hours” differed between the 2 groups.
The most common adverse effects were upper gastrointestinal complaints, drowsiness, and weakness. Adverse effect rates were comparable for the 2 groups and believed to be caused by the naproxen and oxycodone all patients received.
Relief of sciatica with IV steroids is short-lived
A double-blind RCT evaluated the efficacy of a single IV dose of 500 mg methylprednisolone or placebo for 65 patients with leg sciatica (with or without back pain) associated with imaging-confirmed lumbar disk disease.3 The primary outcome was reduction in sciatic leg pain during the first 3 days after injection as measured on a 100-mm VAS. All patients received standard pain medication and physical therapy.
At day 1, 48% of the methylprednisolone group and 28% of the placebo group showed a decrease on the VAS for sciatic pain of 20 mm or more (P=.04; number needed to treat=5). Pain measurements at 2, 3, 10, and 30 days found no significant difference between the groups, however. Nor did the groups differ significantly in functional status or medication use. The study didn’t assess adverse events.
Oral prednisone relieves back pain with sciatica no better than placebo
A double-blind RCT compared an oral prednisone taper (60 mg, 40 mg, and 20 mg each for 3 days) with placebo for treating 27 patients with acute low back pain and sciatica.4 All patients received nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotics for pain control, directions to engage in activity as tolerated, and a referral for physical therapy. Outcomes were evaluated weekly for 1 month, then monthly for 5 months.
Pain scores, functional ability, and medication use didn’t differ significantly between the 2 groups. Steroid injections were later given to 15% of the oral steroid group and 43% of the control group, but the difference in outcomes wasn’t statistically significant. Investigators didn’t assess adverse events.
Recommendations
The joint guidelines of the American College of Physicians and the American Pain Society recommend acetaminophen and NSAIDs as first-line treatments for back pain and back pain with sciatica.5 The guidelines advise against using systemic corticosteroids because “they have not been shown to be more effective than placebo.”
SHORT COURSES OF SYSTEMIC STEROIDS ARE LIKELY SAFE, but they are ineffective. A single dose of intramuscular (IM) or intravenous (IV) methylprednisolone doesn’t improve long-term pain scores in patients with low back pain and sciatica and produces conflicting effects on function. Oral prednisone (9-day taper) doesn’t improve pain or function in patients with back pain and sciatica. A single IM dose of methylprednisolone doesn’t improve pain scores or function in patients with back pain without sciatica (strength of recommendation: B, randomized controlled trials [RCTs]).
No trials of corticosteroids for back pain reported an increase in adverse outcomes, but studies were small, and only short-term (1 month) follow-up data are available.
Evidence summary
A double-blind RCT of 82 patients who reported to an emergency department with acute low back pain and sciatica compared the efficacy of a single IM dose of 160 mg methylprednisolone with placebo.1 Sciatica was confirmed with a positive straight leg test. All patients were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score, rated on a 0-to-10 visual analog scale (VAS).
Pain scores dropped in both groups over time. The magnitude of the change was not significantly greater in the steroid group (at 1 week: mean difference=1.1; 95% confidence interval [CI], –0.5 to 2.8; at 1 month: mean difference=1.3; 95% CI, –0.5 to 2.7).
Among secondary outcomes at 1 month, 19% of the methylprednisolone group reported continued functional disability compared with 49% of the placebo group (absolute difference=30%; 95% CI, 9-49; P=.007). Analgesic use in the previous 24 hours was similar for both groups (22% with steroid injection vs 43% with placebo; P=.06). There were no reports of gastrointestinal bleeding, osteonecrosis, infection, or serious hyperglycemia.
The same applies to back pain without sciatica
Another double-blind RCT of 87 patients evaluated IM methylprednisolone for acute low back pain of less than 1 week duration without sciatica.2 Patients received a single IM dose of 160 mg methylprednisolone or placebo. Both groups were given an instruction sheet and a small supply of naproxen and oxycodone with acetaminophen. The primary outcome was change in pain score on a 0-to-10 VAS.
Pain scores dropped in both groups over time, but the reduction wasn’t significantly larger in the steroid group (at 1 week: mean difference=0.6; 95% CI, –0.9 to 2.2; at 1 month: mean difference=0.6; 95% CI, –1.0 to 2.2). At 1 month, neither functional status nor “medication use in the preceding 24 hours” differed between the 2 groups.
The most common adverse effects were upper gastrointestinal complaints, drowsiness, and weakness. Adverse effect rates were comparable for the 2 groups and believed to be caused by the naproxen and oxycodone all patients received.
Relief of sciatica with IV steroids is short-lived
A double-blind RCT evaluated the efficacy of a single IV dose of 500 mg methylprednisolone or placebo for 65 patients with leg sciatica (with or without back pain) associated with imaging-confirmed lumbar disk disease.3 The primary outcome was reduction in sciatic leg pain during the first 3 days after injection as measured on a 100-mm VAS. All patients received standard pain medication and physical therapy.
At day 1, 48% of the methylprednisolone group and 28% of the placebo group showed a decrease on the VAS for sciatic pain of 20 mm or more (P=.04; number needed to treat=5). Pain measurements at 2, 3, 10, and 30 days found no significant difference between the groups, however. Nor did the groups differ significantly in functional status or medication use. The study didn’t assess adverse events.
Oral prednisone relieves back pain with sciatica no better than placebo
A double-blind RCT compared an oral prednisone taper (60 mg, 40 mg, and 20 mg each for 3 days) with placebo for treating 27 patients with acute low back pain and sciatica.4 All patients received nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotics for pain control, directions to engage in activity as tolerated, and a referral for physical therapy. Outcomes were evaluated weekly for 1 month, then monthly for 5 months.
Pain scores, functional ability, and medication use didn’t differ significantly between the 2 groups. Steroid injections were later given to 15% of the oral steroid group and 43% of the control group, but the difference in outcomes wasn’t statistically significant. Investigators didn’t assess adverse events.
Recommendations
The joint guidelines of the American College of Physicians and the American Pain Society recommend acetaminophen and NSAIDs as first-line treatments for back pain and back pain with sciatica.5 The guidelines advise against using systemic corticosteroids because “they have not been shown to be more effective than placebo.”
1. Friedman BW, Esses D, Solorzano C, et al. A randomized placebo-controlled trial of single-dose IM corticosteroid for radicular low back pain. Spine. 2008;33:E624-E629.
2. Friedman BW, Holden L, Esses D, et al. Parenteral corticosteroids for emergency department patients with nonradicular low back pain. J Emerg Med. 2006;31:365-370.
3. Finckh A, Zufferey P, Schurch MA, et al. Short-term efficacy of intravenous pulse glucocorticoids in acute discogenic sciatica: a randomized controlled trial. Spine. 2006;31:377-381.
4. Holve RL, Barkan H. Oral steroids in initial treatment of acute sciatica. J Am Board Fam Med. 2008;21:469-474.
5. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
1. Friedman BW, Esses D, Solorzano C, et al. A randomized placebo-controlled trial of single-dose IM corticosteroid for radicular low back pain. Spine. 2008;33:E624-E629.
2. Friedman BW, Holden L, Esses D, et al. Parenteral corticosteroids for emergency department patients with nonradicular low back pain. J Emerg Med. 2006;31:365-370.
3. Finckh A, Zufferey P, Schurch MA, et al. Short-term efficacy of intravenous pulse glucocorticoids in acute discogenic sciatica: a randomized controlled trial. Spine. 2006;31:377-381.
4. Holve RL, Barkan H. Oral steroids in initial treatment of acute sciatica. J Am Board Fam Med. 2008;21:469-474.
5. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
Evidence-based answers from the Family Physicians Inquiries Network
What are the adverse effects of prolonged opioid use in patients with chronic pain?
CONSTIPATION, NAUSEA, AND DYSPEPSIA are the most common long-term adverse effects of chronic opioid use (strength of recommendation [SOR]: B, systematic review of low-quality studies). Men may experience depression, fatigue, and sexual dysfunction (SOR: B, 2 observational studies). Prolonged use of opioids also may increase sensitivity to pain (SOR: C, review of case reports and case series). (This review does not address drug seeking or drug escalating.)
Patients on long-term methadone are at risk for cardiac arrhythmias caused by prolonged QT intervals and torsades de pointes (SOR: C, case reports).
Patients taking buprenorphine for opioid dependence may experience acute hepatitis (SOR: C, 1 case report).
Evidence summary
Chronic pain is usually defined as pain persisting longer than 3 months. Evidence of the efficacy of opioids for noncancer pain has led to increased opioid prescribing over the past 20 years and with it, growing concern about adverse effects from long-term use.1
Nausea, constipation, dyspepsia lead side-effects parade
A Cochrane systematic review of 26 studies (25 observational studies and 1 randomized controlled trial [RCT]) of adults who had taken opioids for noncancer pain for at least 6 months assessed the adverse effects of long-term opioid therapy.2 Although the authors couldn’t quantify the incidence of adverse effects because of inconsistent reporting and definition of effects, they stated that the most common complications were nausea, constipation, and dyspepsia. The review found that 22.9% of patients (95% confidence interval [CI], 15.3-32.8) discontinued oral opioids because of adverse effects.
A cross-sectional observational study evaluated self-reported adverse effects in 889 patients who received opioid therapy for noncancer pain lasting at least 3 months.3 Forty percent of patients reported constipation and 18% sexual dysfunction. Patients taking opioids daily experienced more constipation than patients taking the drugs intermittently (39% vs 24%; number needed to harm [NNH]=7; P<.05).
Sexual dysfunction, fatigue, depression aren’t far behind
A case-control study of 20 male cancer survivors with neuropathic pain who took 200 mg of morphine-equivalent daily for a year found that 90% of patients in the opioid group experienced hypogonadism with symptoms of sexual dysfunction, fatigue, and depression, compared with 40% of the 20 controls (NNH=2; 95% CI, 1-5).4
A case-controlled observational study of 54 men with noncancer pain who took opioids for 1 year found that 39 of 45 men who had normal erectile function before opioid therapy reported severe erectile dysfunction while taking the drugs.5 Levels of testosterone and estradiol were significantly lower (P<.0001) in the men taking opioids than the 27 opioid-free controls.
Potentially fatal arrhythmias are a risk for some patients
From 1969 to 2002, 59 cases of QT prolongation or torsades de pointes in methadone users, 5 (8.5%) of them fatal, were reported to the US Food and Drug Administration’s Medwatch Database.6 The mean daily methadone dose was 410 mg (median dose 345 mg, range 29-1680 mg). Length of therapy was not reported. In 44 (75%) of reported cases, patients had other known risks for QT prolongation or torsades de pointes, including female sex, interacting medications, potassium or magnesium abnormalities, and structural heart disease.
Buprenorphine may cause acute hepatitis
No apparent long-term hepatic adverse effects are associated with chronic opioid use. However, a 2004 case series described acute cytolytic hepatitis in 7 patients taking buprenorphine, all with hepatitis C and a history of intravenous drug abuse.7 Acute symptoms resolved quickly in all cases, and only 3 patients required a reduction in buprenorphine dosage.
Prolonged use may increase sensitivity to pain
Case reports and case series have found that prolonged use of opioids causes increased sensitivity to pain in some patients, which is difficult to differentiate from opioid tolerance.8
Recommendations
The American Pain Society (APS) recommends anticipating, identifying, and treating opioid-related adverse effects such as constipation or nausea.1 APS advises against using opioid antagonists to prevent or treat bowel dysfunction, and encourages older patients or patients with an increased risk of developing constipation to start a bowel regimen. Patients with complaints suggesting hypogonadism should be tested for hormonal deficiencies.
The Center for Substance Abuse and Treatment recommends obtaining a cardiac history and an electrocardiogram (EKG) on all patients before starting methadone and repeating the EKG at 30 days and annually thereafter to evaluate for QT prolongation.9 Prescribers should also warn patients of the risk of methadone-induced arrhythmias and be aware of interacting medications that prolong the QT interval or reduce methadone elimination.
1. Chou R, Fanciullo GJ, Adler JA, et al. Clinical guidelines for the use of chronic opioid therapy in chronic non-cancer pain. J Pain. 2009;10:113-130.
2. Noble M, Treadwell JR, Tregear SJ, et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev. 2010;(1):CD006605.-
3. Brown RT, Zuelsdorff M, Fleming M. Adverse effects and cognitive function among primary care patients taking opioids for chronic nonmalignant pain. J Opioid Manag. 2006;2:137-146.
4. Rajagopal A, Vassilopoulou-Sellin R, Palmer JL, et al. Symptomatic hypogonadism in male survivors of cancer with chronic exposure to opioids. Cancer. 2004;100:851-858.
5. Daniell HW. Hypogonadism in men consuming sustained-action oral opioids. J Pain. 2002;3:377-384.
6. Pearson EC, Woosley RL. QT prolongation and torsades de pointes among methadone users: reports to the FDA spontaneous reporting system. Pharmacoepidemiol Drug Saf. 2005;14:747-753.
7. Hervé S, Riachi G, Noblet C, et al. Acute hepatitis due to buprenorphine administration. Eur J Gastroenterol Hepatol. 2004;16:1033-1037.
8. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;20:1943-1953.
9. Krantz MJ, Martin J, Stimmel B, et al. QTc interval screening in methadone treatment. Ann Intern Med. 2009;150:387-395.
CONSTIPATION, NAUSEA, AND DYSPEPSIA are the most common long-term adverse effects of chronic opioid use (strength of recommendation [SOR]: B, systematic review of low-quality studies). Men may experience depression, fatigue, and sexual dysfunction (SOR: B, 2 observational studies). Prolonged use of opioids also may increase sensitivity to pain (SOR: C, review of case reports and case series). (This review does not address drug seeking or drug escalating.)
Patients on long-term methadone are at risk for cardiac arrhythmias caused by prolonged QT intervals and torsades de pointes (SOR: C, case reports).
Patients taking buprenorphine for opioid dependence may experience acute hepatitis (SOR: C, 1 case report).
Evidence summary
Chronic pain is usually defined as pain persisting longer than 3 months. Evidence of the efficacy of opioids for noncancer pain has led to increased opioid prescribing over the past 20 years and with it, growing concern about adverse effects from long-term use.1
Nausea, constipation, dyspepsia lead side-effects parade
A Cochrane systematic review of 26 studies (25 observational studies and 1 randomized controlled trial [RCT]) of adults who had taken opioids for noncancer pain for at least 6 months assessed the adverse effects of long-term opioid therapy.2 Although the authors couldn’t quantify the incidence of adverse effects because of inconsistent reporting and definition of effects, they stated that the most common complications were nausea, constipation, and dyspepsia. The review found that 22.9% of patients (95% confidence interval [CI], 15.3-32.8) discontinued oral opioids because of adverse effects.
A cross-sectional observational study evaluated self-reported adverse effects in 889 patients who received opioid therapy for noncancer pain lasting at least 3 months.3 Forty percent of patients reported constipation and 18% sexual dysfunction. Patients taking opioids daily experienced more constipation than patients taking the drugs intermittently (39% vs 24%; number needed to harm [NNH]=7; P<.05).
Sexual dysfunction, fatigue, depression aren’t far behind
A case-control study of 20 male cancer survivors with neuropathic pain who took 200 mg of morphine-equivalent daily for a year found that 90% of patients in the opioid group experienced hypogonadism with symptoms of sexual dysfunction, fatigue, and depression, compared with 40% of the 20 controls (NNH=2; 95% CI, 1-5).4
A case-controlled observational study of 54 men with noncancer pain who took opioids for 1 year found that 39 of 45 men who had normal erectile function before opioid therapy reported severe erectile dysfunction while taking the drugs.5 Levels of testosterone and estradiol were significantly lower (P<.0001) in the men taking opioids than the 27 opioid-free controls.
Potentially fatal arrhythmias are a risk for some patients
From 1969 to 2002, 59 cases of QT prolongation or torsades de pointes in methadone users, 5 (8.5%) of them fatal, were reported to the US Food and Drug Administration’s Medwatch Database.6 The mean daily methadone dose was 410 mg (median dose 345 mg, range 29-1680 mg). Length of therapy was not reported. In 44 (75%) of reported cases, patients had other known risks for QT prolongation or torsades de pointes, including female sex, interacting medications, potassium or magnesium abnormalities, and structural heart disease.
Buprenorphine may cause acute hepatitis
No apparent long-term hepatic adverse effects are associated with chronic opioid use. However, a 2004 case series described acute cytolytic hepatitis in 7 patients taking buprenorphine, all with hepatitis C and a history of intravenous drug abuse.7 Acute symptoms resolved quickly in all cases, and only 3 patients required a reduction in buprenorphine dosage.
Prolonged use may increase sensitivity to pain
Case reports and case series have found that prolonged use of opioids causes increased sensitivity to pain in some patients, which is difficult to differentiate from opioid tolerance.8
Recommendations
The American Pain Society (APS) recommends anticipating, identifying, and treating opioid-related adverse effects such as constipation or nausea.1 APS advises against using opioid antagonists to prevent or treat bowel dysfunction, and encourages older patients or patients with an increased risk of developing constipation to start a bowel regimen. Patients with complaints suggesting hypogonadism should be tested for hormonal deficiencies.
The Center for Substance Abuse and Treatment recommends obtaining a cardiac history and an electrocardiogram (EKG) on all patients before starting methadone and repeating the EKG at 30 days and annually thereafter to evaluate for QT prolongation.9 Prescribers should also warn patients of the risk of methadone-induced arrhythmias and be aware of interacting medications that prolong the QT interval or reduce methadone elimination.
CONSTIPATION, NAUSEA, AND DYSPEPSIA are the most common long-term adverse effects of chronic opioid use (strength of recommendation [SOR]: B, systematic review of low-quality studies). Men may experience depression, fatigue, and sexual dysfunction (SOR: B, 2 observational studies). Prolonged use of opioids also may increase sensitivity to pain (SOR: C, review of case reports and case series). (This review does not address drug seeking or drug escalating.)
Patients on long-term methadone are at risk for cardiac arrhythmias caused by prolonged QT intervals and torsades de pointes (SOR: C, case reports).
Patients taking buprenorphine for opioid dependence may experience acute hepatitis (SOR: C, 1 case report).
Evidence summary
Chronic pain is usually defined as pain persisting longer than 3 months. Evidence of the efficacy of opioids for noncancer pain has led to increased opioid prescribing over the past 20 years and with it, growing concern about adverse effects from long-term use.1
Nausea, constipation, dyspepsia lead side-effects parade
A Cochrane systematic review of 26 studies (25 observational studies and 1 randomized controlled trial [RCT]) of adults who had taken opioids for noncancer pain for at least 6 months assessed the adverse effects of long-term opioid therapy.2 Although the authors couldn’t quantify the incidence of adverse effects because of inconsistent reporting and definition of effects, they stated that the most common complications were nausea, constipation, and dyspepsia. The review found that 22.9% of patients (95% confidence interval [CI], 15.3-32.8) discontinued oral opioids because of adverse effects.
A cross-sectional observational study evaluated self-reported adverse effects in 889 patients who received opioid therapy for noncancer pain lasting at least 3 months.3 Forty percent of patients reported constipation and 18% sexual dysfunction. Patients taking opioids daily experienced more constipation than patients taking the drugs intermittently (39% vs 24%; number needed to harm [NNH]=7; P<.05).
Sexual dysfunction, fatigue, depression aren’t far behind
A case-control study of 20 male cancer survivors with neuropathic pain who took 200 mg of morphine-equivalent daily for a year found that 90% of patients in the opioid group experienced hypogonadism with symptoms of sexual dysfunction, fatigue, and depression, compared with 40% of the 20 controls (NNH=2; 95% CI, 1-5).4
A case-controlled observational study of 54 men with noncancer pain who took opioids for 1 year found that 39 of 45 men who had normal erectile function before opioid therapy reported severe erectile dysfunction while taking the drugs.5 Levels of testosterone and estradiol were significantly lower (P<.0001) in the men taking opioids than the 27 opioid-free controls.
Potentially fatal arrhythmias are a risk for some patients
From 1969 to 2002, 59 cases of QT prolongation or torsades de pointes in methadone users, 5 (8.5%) of them fatal, were reported to the US Food and Drug Administration’s Medwatch Database.6 The mean daily methadone dose was 410 mg (median dose 345 mg, range 29-1680 mg). Length of therapy was not reported. In 44 (75%) of reported cases, patients had other known risks for QT prolongation or torsades de pointes, including female sex, interacting medications, potassium or magnesium abnormalities, and structural heart disease.
Buprenorphine may cause acute hepatitis
No apparent long-term hepatic adverse effects are associated with chronic opioid use. However, a 2004 case series described acute cytolytic hepatitis in 7 patients taking buprenorphine, all with hepatitis C and a history of intravenous drug abuse.7 Acute symptoms resolved quickly in all cases, and only 3 patients required a reduction in buprenorphine dosage.
Prolonged use may increase sensitivity to pain
Case reports and case series have found that prolonged use of opioids causes increased sensitivity to pain in some patients, which is difficult to differentiate from opioid tolerance.8
Recommendations
The American Pain Society (APS) recommends anticipating, identifying, and treating opioid-related adverse effects such as constipation or nausea.1 APS advises against using opioid antagonists to prevent or treat bowel dysfunction, and encourages older patients or patients with an increased risk of developing constipation to start a bowel regimen. Patients with complaints suggesting hypogonadism should be tested for hormonal deficiencies.
The Center for Substance Abuse and Treatment recommends obtaining a cardiac history and an electrocardiogram (EKG) on all patients before starting methadone and repeating the EKG at 30 days and annually thereafter to evaluate for QT prolongation.9 Prescribers should also warn patients of the risk of methadone-induced arrhythmias and be aware of interacting medications that prolong the QT interval or reduce methadone elimination.
1. Chou R, Fanciullo GJ, Adler JA, et al. Clinical guidelines for the use of chronic opioid therapy in chronic non-cancer pain. J Pain. 2009;10:113-130.
2. Noble M, Treadwell JR, Tregear SJ, et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev. 2010;(1):CD006605.-
3. Brown RT, Zuelsdorff M, Fleming M. Adverse effects and cognitive function among primary care patients taking opioids for chronic nonmalignant pain. J Opioid Manag. 2006;2:137-146.
4. Rajagopal A, Vassilopoulou-Sellin R, Palmer JL, et al. Symptomatic hypogonadism in male survivors of cancer with chronic exposure to opioids. Cancer. 2004;100:851-858.
5. Daniell HW. Hypogonadism in men consuming sustained-action oral opioids. J Pain. 2002;3:377-384.
6. Pearson EC, Woosley RL. QT prolongation and torsades de pointes among methadone users: reports to the FDA spontaneous reporting system. Pharmacoepidemiol Drug Saf. 2005;14:747-753.
7. Hervé S, Riachi G, Noblet C, et al. Acute hepatitis due to buprenorphine administration. Eur J Gastroenterol Hepatol. 2004;16:1033-1037.
8. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;20:1943-1953.
9. Krantz MJ, Martin J, Stimmel B, et al. QTc interval screening in methadone treatment. Ann Intern Med. 2009;150:387-395.
1. Chou R, Fanciullo GJ, Adler JA, et al. Clinical guidelines for the use of chronic opioid therapy in chronic non-cancer pain. J Pain. 2009;10:113-130.
2. Noble M, Treadwell JR, Tregear SJ, et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev. 2010;(1):CD006605.-
3. Brown RT, Zuelsdorff M, Fleming M. Adverse effects and cognitive function among primary care patients taking opioids for chronic nonmalignant pain. J Opioid Manag. 2006;2:137-146.
4. Rajagopal A, Vassilopoulou-Sellin R, Palmer JL, et al. Symptomatic hypogonadism in male survivors of cancer with chronic exposure to opioids. Cancer. 2004;100:851-858.
5. Daniell HW. Hypogonadism in men consuming sustained-action oral opioids. J Pain. 2002;3:377-384.
6. Pearson EC, Woosley RL. QT prolongation and torsades de pointes among methadone users: reports to the FDA spontaneous reporting system. Pharmacoepidemiol Drug Saf. 2005;14:747-753.
7. Hervé S, Riachi G, Noblet C, et al. Acute hepatitis due to buprenorphine administration. Eur J Gastroenterol Hepatol. 2004;16:1033-1037.
8. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;20:1943-1953.
9. Krantz MJ, Martin J, Stimmel B, et al. QTc interval screening in methadone treatment. Ann Intern Med. 2009;150:387-395.
Evidence-based answers from the Family Physicians Inquiries Network