User login
In the Lit: Research You Need to Know
Clinical question: Do hospitals caring for a higher volume of patients with congestive heart failure (CHF) provide better, more efficient care for those patients?
Background: For some surgical and cardiovascular procedures, higher procedure volumes have been associated with better outcomes and lower costs. It is unclear whether this association also exists for common medical conditions, such as CHF.
Study design: Retrospective cohort study.
Setting: National sample of Medicare fee-for-service patients 65 years or older.
Synopsis: National Medicare claims data for more than 1 million discharges from 4,095 hospitals were used to examine the relationship between hospital case volume and quality of care, outcomes, and cost for patients with CHF. Quality of care was defined using the Hospital Quality Alliance (HQA) data on four clinical process measures for CHF from 2007. Hospitals were grouped based on their number of CHF discharges during two years: low volume (25-200), medium volume (201-400), and high volume (>400). Risk adjustment was performed.
Hospitals in the low-volume group had lower performance on the process measures (80.2%) than did medium-volume (87.0%) or high-volume (89.1%) hospitals (P<0.001). Thirty-day mortality was highest in low-volume hospitals (10.2%), when compared to medium-volume (9.3%) and high-volume (8.6%) hospitals (P<0.001). Hospital costs were higher at high-volume hospitals ($8,300) than at medium-volume ($7,700) and low-volume ($7,300) hospitals (P<0.001). Readmission rates were not statistically different between hospital groups.
The relationship between volume and outcomes in the study was not linear, and the incremental benefits seen were small beyond the volume of patients seen at medium-volume hospitals.
Bottom line: Hospitals with higher volumes of CHF patients have better CHF process-of-care measures and lower 30-day CHF mortality but also higher CHF costs.
Citation: Joynt KE, Orav EJ, Jha AK. The association between hospital volume and processes, outcomes, and costs of care for congestive heart failure. Ann Intern Med. 2011;154(2):94-102.
For more physician reviews of HM-related research, visit our website.
Clinical question: Do hospitals caring for a higher volume of patients with congestive heart failure (CHF) provide better, more efficient care for those patients?
Background: For some surgical and cardiovascular procedures, higher procedure volumes have been associated with better outcomes and lower costs. It is unclear whether this association also exists for common medical conditions, such as CHF.
Study design: Retrospective cohort study.
Setting: National sample of Medicare fee-for-service patients 65 years or older.
Synopsis: National Medicare claims data for more than 1 million discharges from 4,095 hospitals were used to examine the relationship between hospital case volume and quality of care, outcomes, and cost for patients with CHF. Quality of care was defined using the Hospital Quality Alliance (HQA) data on four clinical process measures for CHF from 2007. Hospitals were grouped based on their number of CHF discharges during two years: low volume (25-200), medium volume (201-400), and high volume (>400). Risk adjustment was performed.
Hospitals in the low-volume group had lower performance on the process measures (80.2%) than did medium-volume (87.0%) or high-volume (89.1%) hospitals (P<0.001). Thirty-day mortality was highest in low-volume hospitals (10.2%), when compared to medium-volume (9.3%) and high-volume (8.6%) hospitals (P<0.001). Hospital costs were higher at high-volume hospitals ($8,300) than at medium-volume ($7,700) and low-volume ($7,300) hospitals (P<0.001). Readmission rates were not statistically different between hospital groups.
The relationship between volume and outcomes in the study was not linear, and the incremental benefits seen were small beyond the volume of patients seen at medium-volume hospitals.
Bottom line: Hospitals with higher volumes of CHF patients have better CHF process-of-care measures and lower 30-day CHF mortality but also higher CHF costs.
Citation: Joynt KE, Orav EJ, Jha AK. The association between hospital volume and processes, outcomes, and costs of care for congestive heart failure. Ann Intern Med. 2011;154(2):94-102.
For more physician reviews of HM-related research, visit our website.
Clinical question: Do hospitals caring for a higher volume of patients with congestive heart failure (CHF) provide better, more efficient care for those patients?
Background: For some surgical and cardiovascular procedures, higher procedure volumes have been associated with better outcomes and lower costs. It is unclear whether this association also exists for common medical conditions, such as CHF.
Study design: Retrospective cohort study.
Setting: National sample of Medicare fee-for-service patients 65 years or older.
Synopsis: National Medicare claims data for more than 1 million discharges from 4,095 hospitals were used to examine the relationship between hospital case volume and quality of care, outcomes, and cost for patients with CHF. Quality of care was defined using the Hospital Quality Alliance (HQA) data on four clinical process measures for CHF from 2007. Hospitals were grouped based on their number of CHF discharges during two years: low volume (25-200), medium volume (201-400), and high volume (>400). Risk adjustment was performed.
Hospitals in the low-volume group had lower performance on the process measures (80.2%) than did medium-volume (87.0%) or high-volume (89.1%) hospitals (P<0.001). Thirty-day mortality was highest in low-volume hospitals (10.2%), when compared to medium-volume (9.3%) and high-volume (8.6%) hospitals (P<0.001). Hospital costs were higher at high-volume hospitals ($8,300) than at medium-volume ($7,700) and low-volume ($7,300) hospitals (P<0.001). Readmission rates were not statistically different between hospital groups.
The relationship between volume and outcomes in the study was not linear, and the incremental benefits seen were small beyond the volume of patients seen at medium-volume hospitals.
Bottom line: Hospitals with higher volumes of CHF patients have better CHF process-of-care measures and lower 30-day CHF mortality but also higher CHF costs.
Citation: Joynt KE, Orav EJ, Jha AK. The association between hospital volume and processes, outcomes, and costs of care for congestive heart failure. Ann Intern Med. 2011;154(2):94-102.
For more physician reviews of HM-related research, visit our website.
EBUS Equals Mediastinoscopy for NSCLC Staging
PHILADELPHIA – Endobronchial ultrasound–guided biopsy of mediastinal lymph nodes in patients with operable non–small cell lung cancer worked as effectively for staging as did the standard approach – mediastinoscopy – in the first head-to-head comparison of the two methods.
"Our results showed that EBUS-TBNA [endobronchial ultrasound–guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.

Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non–small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006–August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUSTBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant. During mediastinoscopy, surgeons successfully biopsied an average of 4 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient. Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
The surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I’m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
PHILADELPHIA – Endobronchial ultrasound–guided biopsy of mediastinal lymph nodes in patients with operable non–small cell lung cancer worked as effectively for staging as did the standard approach – mediastinoscopy – in the first head-to-head comparison of the two methods.
"Our results showed that EBUS-TBNA [endobronchial ultrasound–guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.
Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non–small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006–August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUSTBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant. During mediastinoscopy, surgeons successfully biopsied an average of 4 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient. Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
The surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I’m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
PHILADELPHIA – Endobronchial ultrasound–guided biopsy of mediastinal lymph nodes in patients with operable non–small cell lung cancer worked as effectively for staging as did the standard approach – mediastinoscopy – in the first head-to-head comparison of the two methods.
"Our results showed that EBUS-TBNA [endobronchial ultrasound–guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.
Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non–small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006–August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUSTBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant. During mediastinoscopy, surgeons successfully biopsied an average of 4 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient. Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
The surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I’m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
FROM THE AMERICAN ASSOCIATION FOR THORACIC SURGERY ANNUAL MEETING
Major Finding: EBUS-TBNA proved similar to mediastinoscopy for lymph node staging of patients with operable NSCLC. EBUS-TBNA had a sensitivity of 81%, a negative predictive value of 91%, and 93% accuracy, compared with comparable values of 79%, 90%, and 93%, respectively, for mediastinoscopy when surgeons performed the two methods sequentially in each patient.
Data Source: A single-center study that included 153 patients who were staged by one of seven participating surgeons.
Disclosures: The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
CABG Outcomes Support More Liberal Blood Glucose Range
PHILADELPHIA – A blood glucose target of 121-180 mg/dL for patients following isolated coronary bypass surgery was as clinically effective as was a stricter glucose target and was easier to maintain in a randomized study with 189 patients.
Based on these results, the cardiac surgery program that ran the study switched its blood glucose range for postoperative patients from 90-120 mg/dL to the more liberal range of 121-180 mg/dL, Dr. Shalin P. Desai said at the annual meeting of the American Association for Thoracic Surgery.
"We believe that maintaining patients at a blood glucose level less than 180 mg/dL is safe and effective, and therefore should be considered for patients undergoing coronary artery bypass grafting surgery," said Dr. Desai, a cardiac surgeon at Inova Heart and Vascular Institute in Falls Church, Va.
"We know that a glucose level of less than 180 mg/dL is good, but does it need to be so strict that it’s almost normoglycemic, or can it be more liberal when we know the glucose levels will rise with the stress of surgery and illness? A range of 121-180 mg/dL is probably sufficient," Dr. Desai said in an interview. At that level, "we used less insulin, fewer finger sticks, and fewer resources" than when the target range aims for lower blood glucose levels, he said.
Dr. Desai and his associates enrolled patients undergoing first-time, isolated CABG who had diabetes or required insulin treatment following surgery based on having three consecutive blood glucose readings of at least 150 mg/dL, or one reading of at least 200 mg/dL. The researchers used a bedside, computerized device that regularly assessed blood glucose levels and adjusted the insulin infusion accordingly. The patients averaged 62 years of age, and about 43% had diabetes.
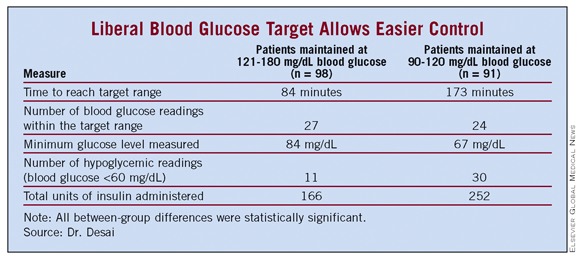
Among the 98 patients maintained on the 121-180 mg/dL regimen, the average time needed to reach the target blood glucose range was 84 minutes – significantly shorter than the average 173 minutes needed for the 91 patients on the strict regimen.
Patients maintained on the liberal target also fared significantly better in their average number of readings within their target range, minimum glucose level, number of hypoglycemic readings, and total insulin dose received (see table).
Assessment of clinical outcomes – renal failure, atrial fibrillation, pneumonia, deep sternal wound infections, prolonged ventilation, prolonged hospitalization, and operative mortality – showed that the liberal range was not inferior to the strict range for preventing these complications in the primary, intention-to-treat analysis. In the as-treated and per-protocol analyses, the liberal-range patients had outcomes that were noninferior to those of the strict control patients for all parameters except for atrial fibrillation. The liberal-range patients showed a small excess of atrial fibrillations in these two additional analyses.
Future studies should look at the same issue in patients undergoing other types of cardiac surgery, such as valve repair or replacement, or a maze procedure, he said.
Dr. Desai said that he had no relevant financial disclosures.
My associates and I recently reported similar results from a randomized study of 82 patients with diabetes who underwent coronary artery bypass grafting surgery. We also compared a target blood glucose range of 90-120 mg/dL with a range of 121-180 mg/dL. Like the current study, we found no difference in the 30-day rates of death, myocardial infarction, neurologic complications, deep sternal wound infections, or atrial fibrillation incidence. The patients maintained with more aggressive glucose control had a higher rate of hypoglycemic events, but this did not result in increased neurologic complications.
Why did tighter glycemic control not produce better outcomes? One possible explanation is that cardiac surgery patients often receive good treatment with cardioprotective drugs, including aspirin, statins, beta-blockers, and angiotensin-converting enzyme inhibitors. Also, the more liberal regimens still produce good glucose control. In our study, the average blood glucose level in the more liberal group was 135 mg/dL.
Tight glucose control may provide long-term benefits that have not yet been identified in these studies. For example, it may improve long-term graft patency and reduce long-term ischemic events. In our studies, we see that more aggressive glucose control results in lower levels of free fatty acids, a marker of inflammation.
Moderate glycemic control produces a significant reduction in morbidity and mortality in cardiac surgery patients that may be hard to improve upon with more aggressive control. I agree that the optimal glucose range following cardiac surgery appears to be 120-180 mg/dL. While the exact level for optimal control remains unknown, the importance of perioperative glycemic control by continuous insulin infusion is now well established.
Dr. Harold L. Lazar is a thoracic surgeon at Boston Medical Center. He said that he has received research support from Eli Lilly to study the effects of glycemic control during cardiac surgery.
My associates and I recently reported similar results from a randomized study of 82 patients with diabetes who underwent coronary artery bypass grafting surgery. We also compared a target blood glucose range of 90-120 mg/dL with a range of 121-180 mg/dL. Like the current study, we found no difference in the 30-day rates of death, myocardial infarction, neurologic complications, deep sternal wound infections, or atrial fibrillation incidence. The patients maintained with more aggressive glucose control had a higher rate of hypoglycemic events, but this did not result in increased neurologic complications.
Why did tighter glycemic control not produce better outcomes? One possible explanation is that cardiac surgery patients often receive good treatment with cardioprotective drugs, including aspirin, statins, beta-blockers, and angiotensin-converting enzyme inhibitors. Also, the more liberal regimens still produce good glucose control. In our study, the average blood glucose level in the more liberal group was 135 mg/dL.
Tight glucose control may provide long-term benefits that have not yet been identified in these studies. For example, it may improve long-term graft patency and reduce long-term ischemic events. In our studies, we see that more aggressive glucose control results in lower levels of free fatty acids, a marker of inflammation.
Moderate glycemic control produces a significant reduction in morbidity and mortality in cardiac surgery patients that may be hard to improve upon with more aggressive control. I agree that the optimal glucose range following cardiac surgery appears to be 120-180 mg/dL. While the exact level for optimal control remains unknown, the importance of perioperative glycemic control by continuous insulin infusion is now well established.
Dr. Harold L. Lazar is a thoracic surgeon at Boston Medical Center. He said that he has received research support from Eli Lilly to study the effects of glycemic control during cardiac surgery.
My associates and I recently reported similar results from a randomized study of 82 patients with diabetes who underwent coronary artery bypass grafting surgery. We also compared a target blood glucose range of 90-120 mg/dL with a range of 121-180 mg/dL. Like the current study, we found no difference in the 30-day rates of death, myocardial infarction, neurologic complications, deep sternal wound infections, or atrial fibrillation incidence. The patients maintained with more aggressive glucose control had a higher rate of hypoglycemic events, but this did not result in increased neurologic complications.
Why did tighter glycemic control not produce better outcomes? One possible explanation is that cardiac surgery patients often receive good treatment with cardioprotective drugs, including aspirin, statins, beta-blockers, and angiotensin-converting enzyme inhibitors. Also, the more liberal regimens still produce good glucose control. In our study, the average blood glucose level in the more liberal group was 135 mg/dL.
Tight glucose control may provide long-term benefits that have not yet been identified in these studies. For example, it may improve long-term graft patency and reduce long-term ischemic events. In our studies, we see that more aggressive glucose control results in lower levels of free fatty acids, a marker of inflammation.
Moderate glycemic control produces a significant reduction in morbidity and mortality in cardiac surgery patients that may be hard to improve upon with more aggressive control. I agree that the optimal glucose range following cardiac surgery appears to be 120-180 mg/dL. While the exact level for optimal control remains unknown, the importance of perioperative glycemic control by continuous insulin infusion is now well established.
Dr. Harold L. Lazar is a thoracic surgeon at Boston Medical Center. He said that he has received research support from Eli Lilly to study the effects of glycemic control during cardiac surgery.
PHILADELPHIA – A blood glucose target of 121-180 mg/dL for patients following isolated coronary bypass surgery was as clinically effective as was a stricter glucose target and was easier to maintain in a randomized study with 189 patients.
Based on these results, the cardiac surgery program that ran the study switched its blood glucose range for postoperative patients from 90-120 mg/dL to the more liberal range of 121-180 mg/dL, Dr. Shalin P. Desai said at the annual meeting of the American Association for Thoracic Surgery.
"We believe that maintaining patients at a blood glucose level less than 180 mg/dL is safe and effective, and therefore should be considered for patients undergoing coronary artery bypass grafting surgery," said Dr. Desai, a cardiac surgeon at Inova Heart and Vascular Institute in Falls Church, Va.
"We know that a glucose level of less than 180 mg/dL is good, but does it need to be so strict that it’s almost normoglycemic, or can it be more liberal when we know the glucose levels will rise with the stress of surgery and illness? A range of 121-180 mg/dL is probably sufficient," Dr. Desai said in an interview. At that level, "we used less insulin, fewer finger sticks, and fewer resources" than when the target range aims for lower blood glucose levels, he said.
Dr. Desai and his associates enrolled patients undergoing first-time, isolated CABG who had diabetes or required insulin treatment following surgery based on having three consecutive blood glucose readings of at least 150 mg/dL, or one reading of at least 200 mg/dL. The researchers used a bedside, computerized device that regularly assessed blood glucose levels and adjusted the insulin infusion accordingly. The patients averaged 62 years of age, and about 43% had diabetes.
Among the 98 patients maintained on the 121-180 mg/dL regimen, the average time needed to reach the target blood glucose range was 84 minutes – significantly shorter than the average 173 minutes needed for the 91 patients on the strict regimen.
Patients maintained on the liberal target also fared significantly better in their average number of readings within their target range, minimum glucose level, number of hypoglycemic readings, and total insulin dose received (see table).
Assessment of clinical outcomes – renal failure, atrial fibrillation, pneumonia, deep sternal wound infections, prolonged ventilation, prolonged hospitalization, and operative mortality – showed that the liberal range was not inferior to the strict range for preventing these complications in the primary, intention-to-treat analysis. In the as-treated and per-protocol analyses, the liberal-range patients had outcomes that were noninferior to those of the strict control patients for all parameters except for atrial fibrillation. The liberal-range patients showed a small excess of atrial fibrillations in these two additional analyses.
Future studies should look at the same issue in patients undergoing other types of cardiac surgery, such as valve repair or replacement, or a maze procedure, he said.
Dr. Desai said that he had no relevant financial disclosures.
PHILADELPHIA – A blood glucose target of 121-180 mg/dL for patients following isolated coronary bypass surgery was as clinically effective as was a stricter glucose target and was easier to maintain in a randomized study with 189 patients.
Based on these results, the cardiac surgery program that ran the study switched its blood glucose range for postoperative patients from 90-120 mg/dL to the more liberal range of 121-180 mg/dL, Dr. Shalin P. Desai said at the annual meeting of the American Association for Thoracic Surgery.
"We believe that maintaining patients at a blood glucose level less than 180 mg/dL is safe and effective, and therefore should be considered for patients undergoing coronary artery bypass grafting surgery," said Dr. Desai, a cardiac surgeon at Inova Heart and Vascular Institute in Falls Church, Va.
"We know that a glucose level of less than 180 mg/dL is good, but does it need to be so strict that it’s almost normoglycemic, or can it be more liberal when we know the glucose levels will rise with the stress of surgery and illness? A range of 121-180 mg/dL is probably sufficient," Dr. Desai said in an interview. At that level, "we used less insulin, fewer finger sticks, and fewer resources" than when the target range aims for lower blood glucose levels, he said.
Dr. Desai and his associates enrolled patients undergoing first-time, isolated CABG who had diabetes or required insulin treatment following surgery based on having three consecutive blood glucose readings of at least 150 mg/dL, or one reading of at least 200 mg/dL. The researchers used a bedside, computerized device that regularly assessed blood glucose levels and adjusted the insulin infusion accordingly. The patients averaged 62 years of age, and about 43% had diabetes.
Among the 98 patients maintained on the 121-180 mg/dL regimen, the average time needed to reach the target blood glucose range was 84 minutes – significantly shorter than the average 173 minutes needed for the 91 patients on the strict regimen.
Patients maintained on the liberal target also fared significantly better in their average number of readings within their target range, minimum glucose level, number of hypoglycemic readings, and total insulin dose received (see table).
Assessment of clinical outcomes – renal failure, atrial fibrillation, pneumonia, deep sternal wound infections, prolonged ventilation, prolonged hospitalization, and operative mortality – showed that the liberal range was not inferior to the strict range for preventing these complications in the primary, intention-to-treat analysis. In the as-treated and per-protocol analyses, the liberal-range patients had outcomes that were noninferior to those of the strict control patients for all parameters except for atrial fibrillation. The liberal-range patients showed a small excess of atrial fibrillations in these two additional analyses.
Future studies should look at the same issue in patients undergoing other types of cardiac surgery, such as valve repair or replacement, or a maze procedure, he said.
Dr. Desai said that he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THORACIC SURGERY
Major Finding: A postoperative blood glucose target range of 121-180 mg/dL led to similar clinical outcomes and proved more practical than did a target range of 90-120 mg/dL in patients undergoing first-time, isolated coronary artery bypass grafting surgery.
Data Source: Single-center, randomized trial with 189 patients.
Disclosures: Dr. Desai said he had no relevant financial disclosures.
Pemetrexed Continuation Maintenance Slows NSCLC Progression
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Pemetrexed maintenance therapy plus best supportive care after pemetrexed/cisplatin induction reduced the risk of progression by 38% (log rank P = .00006, HR = 0.62).
Data Source: Phase III study in 939 patients with advanced nonsquamous non–small cell lung cancer.
Disclosures: Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
Pemetrexed Continuation Maintenance Slows NSCLC Progression
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
CHICAGO – Pemetrexed maintenance therapy following pemetrexed plus cisplatin induction reduced the risk of progression by 38% in patients with advanced nonsquamous non–small cell lung cancer in the phase III PARAMOUNT trial.
The study’s primary end point of investigator-assessed progression-free survival was 4.1 months for pemetrexed (Alimta) plus best supportive care and 2.8 months for placebo plus best supportive care (log rank P = .00006; unadjusted hazard ratio, 0.62).
Independent review, completed in 88% of patients, confirmed the robustness of the primary end point, revealing a progression-free survival of 3.9 months for pemetrexed vs. 2.6 months for placebo (log rank P = .0002; HR, 0.64), lead author Dr. Luis Paz-Ares said at the annual meeting of the American Society of Clinical Oncology.
Overall survival data were not mature enough at the time of the analysis, with just 16 deaths.
"The magnitude of the benefit shown on progression-free survival, a 38% decrease in the risk of progression, is in favor of saying this is an effective treatment for patients with advanced nonsquamous non–small cell lung cancer," he said.
A previous trial (Lancet 2009;374:1432-40) showed that switching patients to pemetrexed maintenance improved the time free of cancer, but until now, it was unclear whether patients initially treated with pemetrexed would benefit from maintenance.
"This trial answers that," Dr. Mark Kris, chief of thoracic oncology at Memorial Sloan-Kettering Cancer Center in New York, told reporters in a press briefing at the meeting. "I think it’s very important in that it’s an example of how we can achieve an incremental benefit in our patients by the optimal use of drugs that are already available."
Pemetrexed (Eli Lilly) is approved in combination with cisplatin as first-line therapy for advanced nonsquamous non–small cell lung cancer (NSCLC) and in the second line as maintenance therapy in patients initially treated with chemotherapy.
Standard treatment for nonsquamous NSCLC is to continue bevacizumab until disease progression, but on the basis of these results, clinicians will likely give bevacizumab with pemetrexed, Dr. Kris said in an interview.
"The guidelines don’t say that because they didn’t have any data, but this will be the data that I’m pretty confident will change the guidelines," said Dr. Kris, who also is the William and Joy Ruane Chair in Thoracic Oncology at Sloan-Kettering.
During the formal presentation of the data, invited discussant Dr. Martin Edelman, director of solid tumor oncology at the University of Maryland Greenebaum Cancer Center in Baltimore, described the use of maintenance therapy as a contentious issue. He noted that many questions remain regarding maintenance trials, including the value of progression-free survival as an end point, how and when control patients are crossed over to active treatment, and whether the RECIST criteria should be used to determine progression.
Dr. Edelman described progression-free survival as an arbitrary end point subject to testing interval and considerable bias. To the credit of the PARAMOUNT investigators, he pointed out that there was use of independent review for this end point, but he said it still does not answer the question of overall survival.
"If one is supposed to change practice based on progression-free survival, we really need to know if particularly small differences are really beneficial," Dr. Edelman said. "That is where quality of life analysis can help us."
The PARAMOUNT investigators assessed health-related quality of life using the EuroQol-5D at baseline, day 1 of each cycle of induction or maintenance therapy, and at the 30-day postdiscontinuation visit. Compliance at all time points during the maintenance phase was more than 80%, but no statistical differences in the EQ-5D index score or its visual analog scale were observed between treatment arms, said Dr. Paz-Ares of the Hospital Universitario Virgen del Rocío, Seville, Spain.
A total of 939 patients were enrolled in the trial. They received pemetrexed 500 mg/m2 on day 1 of a 21-day cycle plus cisplatin 75 mg/m2 induction. In all, 539 patients whose disease had not progressed and had a performance status of 0-2 were then randomized to pemetrexed maintenance 500 mg/m2 on day 1 of a 21-day cycle plus best supportive care or placebo plus best supportive care until disease progression.
Dr. Paz-Ares said pemetrexed had a well-tolerated safety profile, similar to that seen in the previous pemetrexed switch maintenance trial. The pemetrexed and placebo groups had similar drug-related deaths (0.6% for both), drug-related serious adverse events (9% vs. 3%, respectively), and discontinuations due to adverse events (5.3% vs. 3.3%). Patients in the pemetrexed arm had significantly more grade 3/4 adverse fatigue (4.2% vs. 0.6%), anemia (4.5% vs. 0.6%), and neutropenia (3.6% vs. 0%). There was one on-study death with pemetrexed (pneumonia) and placebo (not otherwise specified), and one death within 30 days with pemetrexed (endocarditis), Dr. Paz-Ares reported.
"While overall very reasonable, this still comes at a cost in terms of significant toxicity, not to mention the cost of additional treatment," Dr. Edelman observed. "We really need a cost-effectiveness analysis in this era to follow strategies of frequent visits and scanning with early institution of second-line therapy versus the maintenance approach."
Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Pemetrexed maintenance therapy plus best supportive care after pemetrexed/cisplatin induction reduced the risk of progression by 38% (log rank P = .00006, HR = 0.62).
Data Source: Phase III study in 939 patients with advanced nonsquamous non–small cell lung cancer.
Disclosures: Eli Lilly funded the study. Dr. Paz-Ares disclosed no relevant relationships. Several coauthors reported relationships with industry, including employment, stock ownership, honoraria, and consultancy with Lilly, which markets pemetrexed.
Crizotinib Continues to Produce High Response in ALK+ NSCLC
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: In an ongoing phase I trial, the overall response rate to crizotinib was 61%, and the median duration of response was 48 weeks.
Data Source: Clinical trial data from ALK-positive cohort of the second phase of a dose-finding trial.
Disclosures: The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
Crizotinib Continues to Produce High Response in ALK+ NSCLC
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
CHICAGO – Nearly two-thirds of patients with non–small cell lung cancer who were positive for the anaplastic lymphoma kinase responded to the experimental agent crizotinib. The responses were "rapid, dramatic, and durable," investigators reported at the annual meeting of the American Society of Clinical Oncology.
In an ongoing phase I trial, the overall response to crizotinub was 61%, and the median duration of response was 48 weeks. Median progression-free survival was 10 months, reported Dr. D. Ross Camidge, associate clinical director of the thoracic oncology program, University of Colorado, Aurora.
The study and its results are "truly brilliant," commented Dr. Nasser H. Hanna, associate professor of medicine at Indiana University in Indianapolis. Dr. Hanna was the invited discussant.
He added, however, that "most lung cancer is not driven by one or two gene mutations, so ultimately our future success depends upon combining targeted agents in these more complex tumors."
Activation of the anaplastic lymphoma kinase (ALK), primarily through gene rearrangements, is thought to be a primary oncogenic trigger in several different human cancers, including about 3-5% of non-small cell lung cancers (NSCLC).
Crizotinib is a potent and selective oral inhibitor of ALK. Interim results of the agent in ALK-positive NSCLC in a study of 82 patients treated for an average of 6.4 months were reported at the 2010 ASCO annual meeting and in the New England Journal of Medicine (N. Engl. J. Med. 2010; 363:1693-1703). Those data showed an overall response rate of 57% (47 of 82 patients, with 46 confirmed partial responses and 1 confirmed complete response). Additionally, 27 patients (33%) had stable disease.
In the current report, a continuation of the same study with 119 patients, Dr. Camidge reported data on 116 evaluable patients with a median duration of follow-up of 11 months. The median age was 51 years (range 21-79), and the sample was split evenly between men and women. In all, 72% of patients had never smoked. Nearly all of the cancers (97%) were adenocarcinomas.
The median time to response was 8 weeks, although some patients displayed measurable responses in as little as 2 weeks. The disease control rate was 79% at 8 weeks, and 67% at 16 weeks.
Patients 65 and older did slightly better, with a 69% objective response rate (ORR), compared with 60% for those under 65. Patients with no prior systemic therapies fared best, with an 80% ORR, compared with 60% for patients with metastatic disease who had received one prior systemic therapy, and 58% for those who had received at least two lines of therapy. Patients of Asian origin had an 82% ORR, compared with 52% of non-Asians; the difference could be due to pharmacogenomic differences in drug exposure, but the numbers are small and this effect needs to be explored further, Dr. Camidge said.
Median overall survival has not yet been reached. There have been 23 deaths (19%) and 2 patients lost to follow-up, leaving 94 patients (79%) for the overall survival analysis. No treatment-related study deaths have been reported.
Patients with documented disease progression could continue to receive crizotinib if, in the opinion of the investigators, they would derive a clinical benefit. A total of 40 patients (34%) experienced disease progression according to Response Evaluation Criteria in Solid Tumors (RECIST) at the time of the data cutoff (Oct. 29, 2010). Sixteen of these patients continued to receive crizotinib for more than 2 weeks.
Nearly all patients (96%) reported a treatment-related adverse event. Most of the events were grade 1 or 2, although 19 patients (16%) had grade 3 or 4 events. The most common adverse events were visual effects, nausea, diarrhea, vomiting, edema (both localized and peripheral), and constipation.
The results of the trial and another study (PROFILE 1005) have prompted investigators to seek accelerated approval for the drug in patients with ALK-positive NSCLC.
"Preclinical evidence suggests that ALK inhibitors are more effective than chemotherapy in ALK-positive disease, and retrospective clinical data supports this hypothesis. But ultimately, we have to wait for a definitive answer in a phase III trial which has just been completed comparing an ALK inhibitor vs. chemotherapy in this group of patients," Dr. Hanna noted.
The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: In an ongoing phase I trial, the overall response rate to crizotinib was 61%, and the median duration of response was 48 weeks.
Data Source: Clinical trial data from ALK-positive cohort of the second phase of a dose-finding trial.
Disclosures: The study was funded by Pfizer. Dr. Camidge and several of his coauthors have served in an advisory role and received research funding and honoraria from the company. Dr. Hanna had no relevant disclosures.
Higher Methotrexate Dose Fends Off Pediatric Leukemia Recurrence
CHICAGO — A new chemotherapy regimen that starts children and young adults on 50 times the standard dose of methotrexate for high-risk B-precursor acute lymphoblastic leukemia leads to significantly fewer recurrences five years after treatment without an increase in toxicity.
A randomized phase III trial comparing the high-dose regimen to standard therapy was halted in January 2011 after an interim analysis found the 5-year event-free survival rate reached 82% with the new regimen vs. 75% with the old (P = .0006).

Pediatric oncologists began using the new high-dose regimen as standard practice "as soon as we stopped the protocol," Dr. Eric C. Larsen, principal investigator of the study, said at a press briefing June 3, on the opening day of the annual meeting of the American Society of Clinical Oncology. He will present the results June 5 in a plenary session featuring the most important research at the meeting.
Acute lymphoblastic leukemia (ALL) is the most common leukemia in children. Children with high-risk ALL have a high white blood count at diagnosis and/or are 10 years or more of age.
Although pediatric ALL has a high cure rate and the standard regimen had reduced relapses in the bone marrow over time, investigators were concerned that relapses in the central nervous system had not declined as much. Therefore, they sought a regimen with the potential for greater penetration of tumor cells in the central nervous system.
When the study was conceived 10 years ago, the investigators did not have a new drug or targeted therapy, however, said Dr. Larsen, director of the Maine Children’s Cancer Program and the division of pediatric hematology/oncology at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. Therefore, "rather than trying something brand new," they decided to try to optimize treatment with a drug that "had been around for awhile."
One of the earliest chemotherapy drugs, methotrexate promotes cancer cell death by preventing leukemia cells from using folate, an essential vitamin. Its use dates to 1947 when Dr. Sidney Farber induced the first remissions in children with ALL by giving them an early form of methotrexate called aminopterin. It is an essential component of treatment for pediatric ALL, but the optimal regimen was not resolved.
Dr. Richard Schilsky, a professor of medicine and chief of the section of hematology-oncology at the University of Chicago Pritzker School of Medicine, suggested oncologists treating adults have much to learn from how the investigators focused on an existing therapy. "The pediatric oncologists have recognized that to get optimal results in treating cancer you have to optimize the way cancer treatment is given," said Dr. Schilsky, a former ASCO president and moderator of the press briefing.
The Children’s Oncology Group AALL0232 trial started in 2004 and enrolled 3,154 newly diagnosed patients ages 1 to 30. Most pediatric ALL trials do not enroll patients older than 21 years of age, Dr. Larsen said in an interview, but current thinking suggests that young adult patients may do better on pediatric protocols.
At the time of the interim analysis, 2,426 patients had been randomized. About half the population in the interim analysis, 1,217 patients, was treated with a standard Capizzi regimen in which intravenous methotrexate is delivered at a starting dose of 100 mg/m2 and escalated by 50 mg/m2 every 10 days up to a maximum of 5 doses depending on the child’s ability to tolerate the medication. In this regimen methotrexate is followed by a second chemotherapy drug called asparaginase.
The other 1,209 patients were assigned to the high-dose arm, and received 5 g/m2 – that is, 5,000 mg/m2 of methotrexate biweekly in four doses.
Despite concerns that the high-dose regimen would lead to more toxicity, febrile neutropenia occurred less in the experimental arm of the trial: 5.2% vs. 8.2% in the standard arm (P = .005). Leucovorin rescue was available for patients on high-dose methotrexate, which may partially explain the lower incidence of neutropenia in this group. Acute neurotoxicity, osteonecrosis, and other clinically relevant side effects were not significantly different.
Investigators are not sure why the high-dose regimen is less toxic, but side effects with standard therapy may be more the result of the combination of drugs in the Capizzi regimen than of methotrexate itself, Dr. Larsen said.
A substudy is looking at the comparative costs of the two regimens, he added. Methotrexate is inexpensive, but the high-dose regimen requires hospitalization. This needs to be balanced against the cost of hospitalizing and treating with antibiotics the greater proportion of children developing febrile neutropenia, a serious toxicity, on the Capizzi regimen.
A new wrinkle, Dr. Larsen noted, is that the Children’s Oncology Group and the adult Cancer and Leukemia Group B are planning a joint trial comparing adult and children’s regimens for teens and young adults with ALL. It was scheduled to use the Capizzi regimen but needs to be reconsidered.
The National Institutes of Health provided funds for the trial. Two co-authors said they received research funding from Becton-Dickinson.
methotrexate, ASCO, american society of oncology
CHICAGO — A new chemotherapy regimen that starts children and young adults on 50 times the standard dose of methotrexate for high-risk B-precursor acute lymphoblastic leukemia leads to significantly fewer recurrences five years after treatment without an increase in toxicity.
A randomized phase III trial comparing the high-dose regimen to standard therapy was halted in January 2011 after an interim analysis found the 5-year event-free survival rate reached 82% with the new regimen vs. 75% with the old (P = .0006).
Pediatric oncologists began using the new high-dose regimen as standard practice "as soon as we stopped the protocol," Dr. Eric C. Larsen, principal investigator of the study, said at a press briefing June 3, on the opening day of the annual meeting of the American Society of Clinical Oncology. He will present the results June 5 in a plenary session featuring the most important research at the meeting.
Acute lymphoblastic leukemia (ALL) is the most common leukemia in children. Children with high-risk ALL have a high white blood count at diagnosis and/or are 10 years or more of age.
Although pediatric ALL has a high cure rate and the standard regimen had reduced relapses in the bone marrow over time, investigators were concerned that relapses in the central nervous system had not declined as much. Therefore, they sought a regimen with the potential for greater penetration of tumor cells in the central nervous system.
When the study was conceived 10 years ago, the investigators did not have a new drug or targeted therapy, however, said Dr. Larsen, director of the Maine Children’s Cancer Program and the division of pediatric hematology/oncology at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. Therefore, "rather than trying something brand new," they decided to try to optimize treatment with a drug that "had been around for awhile."
One of the earliest chemotherapy drugs, methotrexate promotes cancer cell death by preventing leukemia cells from using folate, an essential vitamin. Its use dates to 1947 when Dr. Sidney Farber induced the first remissions in children with ALL by giving them an early form of methotrexate called aminopterin. It is an essential component of treatment for pediatric ALL, but the optimal regimen was not resolved.
Dr. Richard Schilsky, a professor of medicine and chief of the section of hematology-oncology at the University of Chicago Pritzker School of Medicine, suggested oncologists treating adults have much to learn from how the investigators focused on an existing therapy. "The pediatric oncologists have recognized that to get optimal results in treating cancer you have to optimize the way cancer treatment is given," said Dr. Schilsky, a former ASCO president and moderator of the press briefing.
The Children’s Oncology Group AALL0232 trial started in 2004 and enrolled 3,154 newly diagnosed patients ages 1 to 30. Most pediatric ALL trials do not enroll patients older than 21 years of age, Dr. Larsen said in an interview, but current thinking suggests that young adult patients may do better on pediatric protocols.
At the time of the interim analysis, 2,426 patients had been randomized. About half the population in the interim analysis, 1,217 patients, was treated with a standard Capizzi regimen in which intravenous methotrexate is delivered at a starting dose of 100 mg/m2 and escalated by 50 mg/m2 every 10 days up to a maximum of 5 doses depending on the child’s ability to tolerate the medication. In this regimen methotrexate is followed by a second chemotherapy drug called asparaginase.
The other 1,209 patients were assigned to the high-dose arm, and received 5 g/m2 – that is, 5,000 mg/m2 of methotrexate biweekly in four doses.
Despite concerns that the high-dose regimen would lead to more toxicity, febrile neutropenia occurred less in the experimental arm of the trial: 5.2% vs. 8.2% in the standard arm (P = .005). Leucovorin rescue was available for patients on high-dose methotrexate, which may partially explain the lower incidence of neutropenia in this group. Acute neurotoxicity, osteonecrosis, and other clinically relevant side effects were not significantly different.
Investigators are not sure why the high-dose regimen is less toxic, but side effects with standard therapy may be more the result of the combination of drugs in the Capizzi regimen than of methotrexate itself, Dr. Larsen said.
A substudy is looking at the comparative costs of the two regimens, he added. Methotrexate is inexpensive, but the high-dose regimen requires hospitalization. This needs to be balanced against the cost of hospitalizing and treating with antibiotics the greater proportion of children developing febrile neutropenia, a serious toxicity, on the Capizzi regimen.
A new wrinkle, Dr. Larsen noted, is that the Children’s Oncology Group and the adult Cancer and Leukemia Group B are planning a joint trial comparing adult and children’s regimens for teens and young adults with ALL. It was scheduled to use the Capizzi regimen but needs to be reconsidered.
The National Institutes of Health provided funds for the trial. Two co-authors said they received research funding from Becton-Dickinson.
CHICAGO — A new chemotherapy regimen that starts children and young adults on 50 times the standard dose of methotrexate for high-risk B-precursor acute lymphoblastic leukemia leads to significantly fewer recurrences five years after treatment without an increase in toxicity.
A randomized phase III trial comparing the high-dose regimen to standard therapy was halted in January 2011 after an interim analysis found the 5-year event-free survival rate reached 82% with the new regimen vs. 75% with the old (P = .0006).
Pediatric oncologists began using the new high-dose regimen as standard practice "as soon as we stopped the protocol," Dr. Eric C. Larsen, principal investigator of the study, said at a press briefing June 3, on the opening day of the annual meeting of the American Society of Clinical Oncology. He will present the results June 5 in a plenary session featuring the most important research at the meeting.
Acute lymphoblastic leukemia (ALL) is the most common leukemia in children. Children with high-risk ALL have a high white blood count at diagnosis and/or are 10 years or more of age.
Although pediatric ALL has a high cure rate and the standard regimen had reduced relapses in the bone marrow over time, investigators were concerned that relapses in the central nervous system had not declined as much. Therefore, they sought a regimen with the potential for greater penetration of tumor cells in the central nervous system.
When the study was conceived 10 years ago, the investigators did not have a new drug or targeted therapy, however, said Dr. Larsen, director of the Maine Children’s Cancer Program and the division of pediatric hematology/oncology at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. Therefore, "rather than trying something brand new," they decided to try to optimize treatment with a drug that "had been around for awhile."
One of the earliest chemotherapy drugs, methotrexate promotes cancer cell death by preventing leukemia cells from using folate, an essential vitamin. Its use dates to 1947 when Dr. Sidney Farber induced the first remissions in children with ALL by giving them an early form of methotrexate called aminopterin. It is an essential component of treatment for pediatric ALL, but the optimal regimen was not resolved.
Dr. Richard Schilsky, a professor of medicine and chief of the section of hematology-oncology at the University of Chicago Pritzker School of Medicine, suggested oncologists treating adults have much to learn from how the investigators focused on an existing therapy. "The pediatric oncologists have recognized that to get optimal results in treating cancer you have to optimize the way cancer treatment is given," said Dr. Schilsky, a former ASCO president and moderator of the press briefing.
The Children’s Oncology Group AALL0232 trial started in 2004 and enrolled 3,154 newly diagnosed patients ages 1 to 30. Most pediatric ALL trials do not enroll patients older than 21 years of age, Dr. Larsen said in an interview, but current thinking suggests that young adult patients may do better on pediatric protocols.
At the time of the interim analysis, 2,426 patients had been randomized. About half the population in the interim analysis, 1,217 patients, was treated with a standard Capizzi regimen in which intravenous methotrexate is delivered at a starting dose of 100 mg/m2 and escalated by 50 mg/m2 every 10 days up to a maximum of 5 doses depending on the child’s ability to tolerate the medication. In this regimen methotrexate is followed by a second chemotherapy drug called asparaginase.
The other 1,209 patients were assigned to the high-dose arm, and received 5 g/m2 – that is, 5,000 mg/m2 of methotrexate biweekly in four doses.
Despite concerns that the high-dose regimen would lead to more toxicity, febrile neutropenia occurred less in the experimental arm of the trial: 5.2% vs. 8.2% in the standard arm (P = .005). Leucovorin rescue was available for patients on high-dose methotrexate, which may partially explain the lower incidence of neutropenia in this group. Acute neurotoxicity, osteonecrosis, and other clinically relevant side effects were not significantly different.
Investigators are not sure why the high-dose regimen is less toxic, but side effects with standard therapy may be more the result of the combination of drugs in the Capizzi regimen than of methotrexate itself, Dr. Larsen said.
A substudy is looking at the comparative costs of the two regimens, he added. Methotrexate is inexpensive, but the high-dose regimen requires hospitalization. This needs to be balanced against the cost of hospitalizing and treating with antibiotics the greater proportion of children developing febrile neutropenia, a serious toxicity, on the Capizzi regimen.
A new wrinkle, Dr. Larsen noted, is that the Children’s Oncology Group and the adult Cancer and Leukemia Group B are planning a joint trial comparing adult and children’s regimens for teens and young adults with ALL. It was scheduled to use the Capizzi regimen but needs to be reconsidered.
The National Institutes of Health provided funds for the trial. Two co-authors said they received research funding from Becton-Dickinson.
methotrexate, ASCO, american society of oncology
methotrexate, ASCO, american society of oncology
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Event-free survival at 5 years was 82% in the high-dose methotrexate arm and 75% with a standard Capizzi regimen (P=.006).
Data Source: Randomization of 2,426 children and young adults with high-risk ALL.
Disclosures: The National Institutes of Health provided funds for the trial. Two co-authors said they received research funding from Becton-Dickinson.
ONLINE EXCLUSIVE: Listen to Dr. Conway chat about his new role at the Centers for Medicare & Medicaid Services
Click here to listen to Dr. Conway
Click here to listen to Dr. Conway
Click here to listen to Dr. Conway
Patients Unaware of DVT Risk, Survey Shows
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."