User login
Found a Peanut: Dealing With Airway Obstructions in Kids
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
FROM A MEETING SPONSORED BY THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Evidence Suggests Pregnancies Can Survive Maternal Cancer Treatment
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.

"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
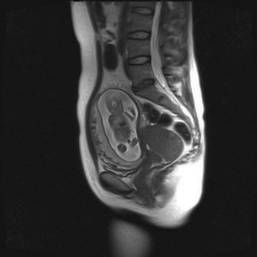
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.

Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience

Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.
"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.
Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience
Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.
"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.
Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience
Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Consider Chemotherapy after Induction Failure for Childhood Leukemia
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: 10-year survival ranged from 4% to 73% in children and adolescents with ALL who failed remission-induction therapy, depending on a wide variety of biological and clinical characteristics.
Data Source: The retrospective observational analysis of data pooled from 14 cooperative study groups in Europe, North America, and Asia, comprised 44,017 children with newly diagnosed ALL enrolled in clinical trials from 1985 through 2000 and followed for a mean of 8 years.
Disclosures: Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
ONLINE EXCLUSIVE: SHM President, NQF CEO Discuss SHM's Earning National Quality Award
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
ONLINE EXCLUSIVE: Listen to new physician editor Danielle Scheurer's vision for The Hospitalist
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
ONLINE EXCLUSIVE: How the School of Medicine at Stanford University Is Addressing Female Physicians and Leadership
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.

—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
ONLINE EXCLUSIVE: Listen to a Hospitalist and Career Expert Discuss What It Takes to Be a Leader
Geriatric Patients Show Greater Cognitive Decline after Hospitalization
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Pudendal Neuralgia
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.

Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
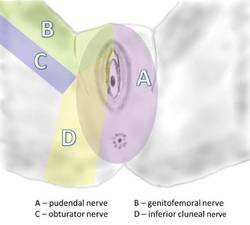
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
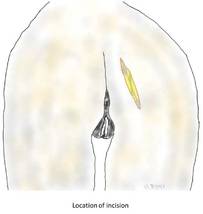
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
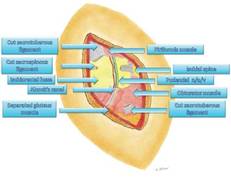
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.
Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.
Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.