User login
SGR Reform, ICD-10 Implementation Delays Frustrate Hospitalists, Physicians
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”

The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Hospital employment or physician-led ACO?
Primary care physicians around the country are facing the largest decision of their lives: Do I stay independent and maybe form an accountable care organization with other independent physicians, or do I become an employee of a hospital or health system?
As accountable care is taking hold, new data may alter historic thinking on this "bet-the-practice" question.
Tired of being overworked, undersatisfied, and overwhelmed with growing regulatory requirements, many primary care physicians have sought the security and strength of hospital employment. They say the pressures to invest in technology, billing, coding, and continued reimbursement pressures are just too great.
Yet, the majority of these physicians miss their days of self-employed autonomy, are on average less productive, and worry that the clocks on their compensation guarantees are ticking down.
Most of the moves by your colleagues, and perhaps you, to hospital employment have been defensive. It was just no longer feasible to stay afloat in the current fee-for-service system. You cannot work any harder, faster, or cheaper. You can no longer spend satisfactory time with your patients.
On the other hand, some of you may have joined a hospital or health system to be proactive and gain a solid platform to prepare for the new value-based payment era.
You may have envisioned being integrated with a critical mass of like-minded physicians and facilities, aided by advanced population management tools and a strong balance sheet, and all linked together on the hospital’s health information technology platform. You read that primary care should be in a leadership position and financially incentivized in any accountable care organization – including a hospital’s. Independent physicians could theoretically form ACOs, too, but lack the up-front capital, know-how, and any spare intellectual bandwidth to do so.
So, from a strategic perspective, becoming employed with other physicians by a health system seemed the way to go.
The pace has quickened of health care’s movement away from fee for service or "pay for volume" to payment for better outcomes at lower overall costs, or "pay for value." The factors that applied to the decision to become employed in the fee-for-service era may be yielding to those in the accountable care era sooner than anticipated.
Independent physician-led ACOs appear to be adapting better than hospitals to this change. Although much better prepared fiscally, hospitals are conflicted, or at least hesitant, to make this switch, because much of the savings comes from avoidable admissions and readmissions. On the other hand, emerging data and experience are showing that physician-led ACOs can be very successful.
There are some very integrated and successful hospital-led ACOs or other value-delivery hospital/physician models. In fact, I believe that if the hospital is willing to right-size and truly commit to value, it can be the most successful model.
However, many physicians signed volume-only physician work relative value unit (wRVU) compensation formulas in their hospital employment agreements, with no incentive payments for value. They have not been involved as partners, much less leaders, in any ACO planning. Even though the fee-for-service days are waning and strains are showing for many hospitals that are not adapting, for many employed physicians, the pace of preparedness for the accountable care era has been disappointing.
New data show that while most of the early ACOs in the Medicare Shared Savings Program were hospital led, there are now more physician-led ACOs than any other. At the same time, early results of some modest primary care–only ACOs have been exciting. The rural primary care physician ACO previously reported on in this column, Rio Grande Valley Health Alliance in McAllen, Tex., is preliminarily looking at 90th-percentile quality results and more than $500,000 in (unofficial) savings per physician in their first year under the Medicare Shared Savings Program.
In fact, in a May 14, 2014, article in JAMA, its authors stated: "Even though most adult primary care physicians may not realize it, they each can be seen as a chief executive officer (CEO) in charge of approximately $10 million in annual revenue" (JAMA 2014;311:1855-6). They noted that primary care receives only 5% of that spending, but can control much of the average of $5,000 in annual spending of their 2,000 or so patients. The independent physician-led Palm Beach ACO is cited as an example, with $22 million in savings their first year. The authors recommend physician-led ACOs as the best way to leverage that "CEO" power.
These new success lessons are being learned and need to be shared. Primary care physicians need to understand that the risk of change is now much less than the risk of maintaining the status quo. You need transparency regarding the realities of all your choices, including hospital employment and physician ACOs.
As readers of this column know, I heartily endorse the trend recognized in the JAMA article: "[A]n increasing number of primary care physicians see physician-led ACOs as a powerful opportunity to retain their autonomy and make a positive difference for their patient – as well as their practices’ bottom lines."
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
Primary care physicians around the country are facing the largest decision of their lives: Do I stay independent and maybe form an accountable care organization with other independent physicians, or do I become an employee of a hospital or health system?
As accountable care is taking hold, new data may alter historic thinking on this "bet-the-practice" question.
Tired of being overworked, undersatisfied, and overwhelmed with growing regulatory requirements, many primary care physicians have sought the security and strength of hospital employment. They say the pressures to invest in technology, billing, coding, and continued reimbursement pressures are just too great.
Yet, the majority of these physicians miss their days of self-employed autonomy, are on average less productive, and worry that the clocks on their compensation guarantees are ticking down.
Most of the moves by your colleagues, and perhaps you, to hospital employment have been defensive. It was just no longer feasible to stay afloat in the current fee-for-service system. You cannot work any harder, faster, or cheaper. You can no longer spend satisfactory time with your patients.
On the other hand, some of you may have joined a hospital or health system to be proactive and gain a solid platform to prepare for the new value-based payment era.
You may have envisioned being integrated with a critical mass of like-minded physicians and facilities, aided by advanced population management tools and a strong balance sheet, and all linked together on the hospital’s health information technology platform. You read that primary care should be in a leadership position and financially incentivized in any accountable care organization – including a hospital’s. Independent physicians could theoretically form ACOs, too, but lack the up-front capital, know-how, and any spare intellectual bandwidth to do so.
So, from a strategic perspective, becoming employed with other physicians by a health system seemed the way to go.
The pace has quickened of health care’s movement away from fee for service or "pay for volume" to payment for better outcomes at lower overall costs, or "pay for value." The factors that applied to the decision to become employed in the fee-for-service era may be yielding to those in the accountable care era sooner than anticipated.
Independent physician-led ACOs appear to be adapting better than hospitals to this change. Although much better prepared fiscally, hospitals are conflicted, or at least hesitant, to make this switch, because much of the savings comes from avoidable admissions and readmissions. On the other hand, emerging data and experience are showing that physician-led ACOs can be very successful.
There are some very integrated and successful hospital-led ACOs or other value-delivery hospital/physician models. In fact, I believe that if the hospital is willing to right-size and truly commit to value, it can be the most successful model.
However, many physicians signed volume-only physician work relative value unit (wRVU) compensation formulas in their hospital employment agreements, with no incentive payments for value. They have not been involved as partners, much less leaders, in any ACO planning. Even though the fee-for-service days are waning and strains are showing for many hospitals that are not adapting, for many employed physicians, the pace of preparedness for the accountable care era has been disappointing.
New data show that while most of the early ACOs in the Medicare Shared Savings Program were hospital led, there are now more physician-led ACOs than any other. At the same time, early results of some modest primary care–only ACOs have been exciting. The rural primary care physician ACO previously reported on in this column, Rio Grande Valley Health Alliance in McAllen, Tex., is preliminarily looking at 90th-percentile quality results and more than $500,000 in (unofficial) savings per physician in their first year under the Medicare Shared Savings Program.
In fact, in a May 14, 2014, article in JAMA, its authors stated: "Even though most adult primary care physicians may not realize it, they each can be seen as a chief executive officer (CEO) in charge of approximately $10 million in annual revenue" (JAMA 2014;311:1855-6). They noted that primary care receives only 5% of that spending, but can control much of the average of $5,000 in annual spending of their 2,000 or so patients. The independent physician-led Palm Beach ACO is cited as an example, with $22 million in savings their first year. The authors recommend physician-led ACOs as the best way to leverage that "CEO" power.
These new success lessons are being learned and need to be shared. Primary care physicians need to understand that the risk of change is now much less than the risk of maintaining the status quo. You need transparency regarding the realities of all your choices, including hospital employment and physician ACOs.
As readers of this column know, I heartily endorse the trend recognized in the JAMA article: "[A]n increasing number of primary care physicians see physician-led ACOs as a powerful opportunity to retain their autonomy and make a positive difference for their patient – as well as their practices’ bottom lines."
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
Primary care physicians around the country are facing the largest decision of their lives: Do I stay independent and maybe form an accountable care organization with other independent physicians, or do I become an employee of a hospital or health system?
As accountable care is taking hold, new data may alter historic thinking on this "bet-the-practice" question.
Tired of being overworked, undersatisfied, and overwhelmed with growing regulatory requirements, many primary care physicians have sought the security and strength of hospital employment. They say the pressures to invest in technology, billing, coding, and continued reimbursement pressures are just too great.
Yet, the majority of these physicians miss their days of self-employed autonomy, are on average less productive, and worry that the clocks on their compensation guarantees are ticking down.
Most of the moves by your colleagues, and perhaps you, to hospital employment have been defensive. It was just no longer feasible to stay afloat in the current fee-for-service system. You cannot work any harder, faster, or cheaper. You can no longer spend satisfactory time with your patients.
On the other hand, some of you may have joined a hospital or health system to be proactive and gain a solid platform to prepare for the new value-based payment era.
You may have envisioned being integrated with a critical mass of like-minded physicians and facilities, aided by advanced population management tools and a strong balance sheet, and all linked together on the hospital’s health information technology platform. You read that primary care should be in a leadership position and financially incentivized in any accountable care organization – including a hospital’s. Independent physicians could theoretically form ACOs, too, but lack the up-front capital, know-how, and any spare intellectual bandwidth to do so.
So, from a strategic perspective, becoming employed with other physicians by a health system seemed the way to go.
The pace has quickened of health care’s movement away from fee for service or "pay for volume" to payment for better outcomes at lower overall costs, or "pay for value." The factors that applied to the decision to become employed in the fee-for-service era may be yielding to those in the accountable care era sooner than anticipated.
Independent physician-led ACOs appear to be adapting better than hospitals to this change. Although much better prepared fiscally, hospitals are conflicted, or at least hesitant, to make this switch, because much of the savings comes from avoidable admissions and readmissions. On the other hand, emerging data and experience are showing that physician-led ACOs can be very successful.
There are some very integrated and successful hospital-led ACOs or other value-delivery hospital/physician models. In fact, I believe that if the hospital is willing to right-size and truly commit to value, it can be the most successful model.
However, many physicians signed volume-only physician work relative value unit (wRVU) compensation formulas in their hospital employment agreements, with no incentive payments for value. They have not been involved as partners, much less leaders, in any ACO planning. Even though the fee-for-service days are waning and strains are showing for many hospitals that are not adapting, for many employed physicians, the pace of preparedness for the accountable care era has been disappointing.
New data show that while most of the early ACOs in the Medicare Shared Savings Program were hospital led, there are now more physician-led ACOs than any other. At the same time, early results of some modest primary care–only ACOs have been exciting. The rural primary care physician ACO previously reported on in this column, Rio Grande Valley Health Alliance in McAllen, Tex., is preliminarily looking at 90th-percentile quality results and more than $500,000 in (unofficial) savings per physician in their first year under the Medicare Shared Savings Program.
In fact, in a May 14, 2014, article in JAMA, its authors stated: "Even though most adult primary care physicians may not realize it, they each can be seen as a chief executive officer (CEO) in charge of approximately $10 million in annual revenue" (JAMA 2014;311:1855-6). They noted that primary care receives only 5% of that spending, but can control much of the average of $5,000 in annual spending of their 2,000 or so patients. The independent physician-led Palm Beach ACO is cited as an example, with $22 million in savings their first year. The authors recommend physician-led ACOs as the best way to leverage that "CEO" power.
These new success lessons are being learned and need to be shared. Primary care physicians need to understand that the risk of change is now much less than the risk of maintaining the status quo. You need transparency regarding the realities of all your choices, including hospital employment and physician ACOs.
As readers of this column know, I heartily endorse the trend recognized in the JAMA article: "[A]n increasing number of primary care physicians see physician-led ACOs as a powerful opportunity to retain their autonomy and make a positive difference for their patient – as well as their practices’ bottom lines."
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.

23-year-old woman being treated for opioid dependence, unexpected weight gain
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
Can yoga reduce symptoms of anxiety and depression?
Yes, yoga can reduce symptoms of anxiety and depression (strength of recommendation [SOR]: B, systematic reviews of randomized controlled trials [RCTs] with significant heterogeneity). Across multiple RCTs using varied yoga interventions and diverse study populations, yoga typically improves overall symptom scores for anxiety and depression by about 40%, both by itself and as an adjunctive treatment. It produces no reported harmful side effects.
EVIDENCE SUMMARY
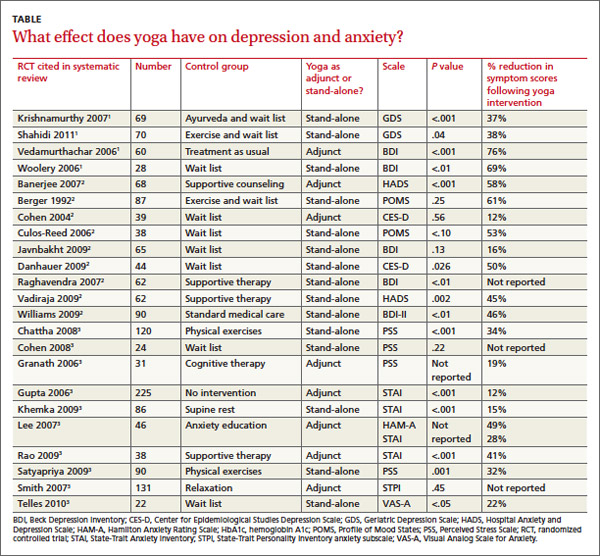
Across 3 systematic reviews of yoga for depression, anxiety, and stress, yoga produced overall reductions of symptoms between 12% and 76%, with an average of 39% net reduction in symptom scores across measures (TABLE).1-3 The RCTs included in the systematic reviews were too heterogeneous to allow quantitative analyses of effect sizes.
Yoga found to significantly reduce depression symptoms
Two 2012 systematic reviews of yoga for depression evaluated 13 RCTs with a total of 782 participants, ages 18 to 80 years with mild to moderate depression. In the 12 RCTs that reported gender, 82% of participants were female; in 6 RCTs a total of 313 patients had cancer.1,2
The RCTs compared yoga to wait-list controls, counseling, education, exercise, or usual care. They evaluated yoga both as a stand-alone intervention and an adjunct to usual care. Yoga sessions varied from 1 hour weekly to 90 minutes daily over 2 to 24 weeks and included physical postures, relaxation, and breathing techniques.
Eight moderate- to high-quality RCTs with a total of 483 participants reported statistically significant reductions in depression symptoms in the yoga groups compared with control groups. In 3 RCTs, yoga was equivalent to wait-list controls; 2 RCTs showed results equivalent to exercise and superior to wait-list controls.
Yoga alleviates anxiety and stress without adverse effects
A 2012 systematic review of yoga for stress and anxiety evaluated 10 RCTs with a total of 813 heterogeneous participants, ages 18 to 76 years, including pregnant women, breast cancer patients, flood survivors, healthy volunteers, patients with chronic illnesses, perimenopausal women, adults with metabolic syndrome, and people working in finance, all with a range of anxiety and stress symptoms.3 The RCTs compared yoga, as an adjunctive or stand-alone treatment, with wait-list controls, relaxation, therapy, anxiety education, rest, or exercise. Yoga regimens varied from a single 20-minute session to 16 weeks of daily 1-hour sessions, with most regimens lasting 6 to 10 weeks.
Of the 10 RCTs reviewed, 7 moderate- to high-quality studies with a total of 627 participants found statistically significant reductions in anxiety and stress in yoga groups compared with control groups. Of the remaining 3 studies, 1 found yoga equivalent to cognitive therapy; 1 found a nonsignificant benefit for yoga compared with wait-list controls; and 1 found no improvement with either yoga or relaxation.
Study limitations included a range of symptom severity, variable type and length of yoga, lack of participant blinding, wait-list rather than active-treatment controls, and a lack of consistent long-term follow-up data. The RCTs didn’t report any adverse effects of yoga, and yoga is considered safe when taught by a competent instructor.3,4
RECOMMENDATIONS
The Institute for Clinical Systems Improvement and the Canadian Network for Mood and Anxiety Treatments recommend yoga as an effective adjunctive treatment to decrease the severity of depression symptoms.5,6
The Veterans Health Administration and the US Department of Defense recommend yoga as a potential adjunctive treatment to manage the hyperarousal symptoms of post-traumatic stress disorder (PTSD).7
The Work Loss Data Institute recommends yoga as an intervention for workers compensation conditions including occupational stress, major depressive disorder, PTSD, and other mental disorders.8
1. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2012;3:117.
2. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
3. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
4. Brown RP, Gerbarg PL. Sudarshan Kriya Yogic breathing in the treatment of stress, anxiety, and depression. Part II—clinical applications and guidelines. J Altern Complement Med. 2005;11:711-717.
5. Mitchell J, Trangle M, Degnan B, et al. Institute for Clinical Systems Improvement. Adult depression primary care. Available at: https://www.icsi.org/_asset/fnhdm3/Depr-Interactive0512b.pdf. Updated September 2013. Accessed March 6, 2014.
6. Ravindran AV, Lam RW, Filteau MJ, et al; Canadian Network for Mood and Anxiety Treatments (CANMAT). Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. V. Complementary and alternative medicine treatments. J Affect Disord. 2009;117(suppl 1):S54-S64.
7. US Department of Veterans Affairs. VA/DoD clinical practice guideline for management of post-traumatic stress disorder and acute stress reaction. US Department of Veterans Affairs Web site. Available at: http://www.healthquality.va.gov/ptsd/. Accessed March 6, 2014.
8. Agency for Healthcare Research and Quality. Mental illness & stress. Agency for Healthcare Research and Quality Web site. Available at: http://www.guideline.gov/content.aspx?id=47588. Updated May 2011. Accessed June 17, 2014
Yes, yoga can reduce symptoms of anxiety and depression (strength of recommendation [SOR]: B, systematic reviews of randomized controlled trials [RCTs] with significant heterogeneity). Across multiple RCTs using varied yoga interventions and diverse study populations, yoga typically improves overall symptom scores for anxiety and depression by about 40%, both by itself and as an adjunctive treatment. It produces no reported harmful side effects.
EVIDENCE SUMMARY
Across 3 systematic reviews of yoga for depression, anxiety, and stress, yoga produced overall reductions of symptoms between 12% and 76%, with an average of 39% net reduction in symptom scores across measures (TABLE).1-3 The RCTs included in the systematic reviews were too heterogeneous to allow quantitative analyses of effect sizes.
Yoga found to significantly reduce depression symptoms
Two 2012 systematic reviews of yoga for depression evaluated 13 RCTs with a total of 782 participants, ages 18 to 80 years with mild to moderate depression. In the 12 RCTs that reported gender, 82% of participants were female; in 6 RCTs a total of 313 patients had cancer.1,2
The RCTs compared yoga to wait-list controls, counseling, education, exercise, or usual care. They evaluated yoga both as a stand-alone intervention and an adjunct to usual care. Yoga sessions varied from 1 hour weekly to 90 minutes daily over 2 to 24 weeks and included physical postures, relaxation, and breathing techniques.
Eight moderate- to high-quality RCTs with a total of 483 participants reported statistically significant reductions in depression symptoms in the yoga groups compared with control groups. In 3 RCTs, yoga was equivalent to wait-list controls; 2 RCTs showed results equivalent to exercise and superior to wait-list controls.
Yoga alleviates anxiety and stress without adverse effects
A 2012 systematic review of yoga for stress and anxiety evaluated 10 RCTs with a total of 813 heterogeneous participants, ages 18 to 76 years, including pregnant women, breast cancer patients, flood survivors, healthy volunteers, patients with chronic illnesses, perimenopausal women, adults with metabolic syndrome, and people working in finance, all with a range of anxiety and stress symptoms.3 The RCTs compared yoga, as an adjunctive or stand-alone treatment, with wait-list controls, relaxation, therapy, anxiety education, rest, or exercise. Yoga regimens varied from a single 20-minute session to 16 weeks of daily 1-hour sessions, with most regimens lasting 6 to 10 weeks.
Of the 10 RCTs reviewed, 7 moderate- to high-quality studies with a total of 627 participants found statistically significant reductions in anxiety and stress in yoga groups compared with control groups. Of the remaining 3 studies, 1 found yoga equivalent to cognitive therapy; 1 found a nonsignificant benefit for yoga compared with wait-list controls; and 1 found no improvement with either yoga or relaxation.
Study limitations included a range of symptom severity, variable type and length of yoga, lack of participant blinding, wait-list rather than active-treatment controls, and a lack of consistent long-term follow-up data. The RCTs didn’t report any adverse effects of yoga, and yoga is considered safe when taught by a competent instructor.3,4
RECOMMENDATIONS
The Institute for Clinical Systems Improvement and the Canadian Network for Mood and Anxiety Treatments recommend yoga as an effective adjunctive treatment to decrease the severity of depression symptoms.5,6
The Veterans Health Administration and the US Department of Defense recommend yoga as a potential adjunctive treatment to manage the hyperarousal symptoms of post-traumatic stress disorder (PTSD).7
The Work Loss Data Institute recommends yoga as an intervention for workers compensation conditions including occupational stress, major depressive disorder, PTSD, and other mental disorders.8
Yes, yoga can reduce symptoms of anxiety and depression (strength of recommendation [SOR]: B, systematic reviews of randomized controlled trials [RCTs] with significant heterogeneity). Across multiple RCTs using varied yoga interventions and diverse study populations, yoga typically improves overall symptom scores for anxiety and depression by about 40%, both by itself and as an adjunctive treatment. It produces no reported harmful side effects.
EVIDENCE SUMMARY
Across 3 systematic reviews of yoga for depression, anxiety, and stress, yoga produced overall reductions of symptoms between 12% and 76%, with an average of 39% net reduction in symptom scores across measures (TABLE).1-3 The RCTs included in the systematic reviews were too heterogeneous to allow quantitative analyses of effect sizes.
Yoga found to significantly reduce depression symptoms
Two 2012 systematic reviews of yoga for depression evaluated 13 RCTs with a total of 782 participants, ages 18 to 80 years with mild to moderate depression. In the 12 RCTs that reported gender, 82% of participants were female; in 6 RCTs a total of 313 patients had cancer.1,2
The RCTs compared yoga to wait-list controls, counseling, education, exercise, or usual care. They evaluated yoga both as a stand-alone intervention and an adjunct to usual care. Yoga sessions varied from 1 hour weekly to 90 minutes daily over 2 to 24 weeks and included physical postures, relaxation, and breathing techniques.
Eight moderate- to high-quality RCTs with a total of 483 participants reported statistically significant reductions in depression symptoms in the yoga groups compared with control groups. In 3 RCTs, yoga was equivalent to wait-list controls; 2 RCTs showed results equivalent to exercise and superior to wait-list controls.
Yoga alleviates anxiety and stress without adverse effects
A 2012 systematic review of yoga for stress and anxiety evaluated 10 RCTs with a total of 813 heterogeneous participants, ages 18 to 76 years, including pregnant women, breast cancer patients, flood survivors, healthy volunteers, patients with chronic illnesses, perimenopausal women, adults with metabolic syndrome, and people working in finance, all with a range of anxiety and stress symptoms.3 The RCTs compared yoga, as an adjunctive or stand-alone treatment, with wait-list controls, relaxation, therapy, anxiety education, rest, or exercise. Yoga regimens varied from a single 20-minute session to 16 weeks of daily 1-hour sessions, with most regimens lasting 6 to 10 weeks.
Of the 10 RCTs reviewed, 7 moderate- to high-quality studies with a total of 627 participants found statistically significant reductions in anxiety and stress in yoga groups compared with control groups. Of the remaining 3 studies, 1 found yoga equivalent to cognitive therapy; 1 found a nonsignificant benefit for yoga compared with wait-list controls; and 1 found no improvement with either yoga or relaxation.
Study limitations included a range of symptom severity, variable type and length of yoga, lack of participant blinding, wait-list rather than active-treatment controls, and a lack of consistent long-term follow-up data. The RCTs didn’t report any adverse effects of yoga, and yoga is considered safe when taught by a competent instructor.3,4
RECOMMENDATIONS
The Institute for Clinical Systems Improvement and the Canadian Network for Mood and Anxiety Treatments recommend yoga as an effective adjunctive treatment to decrease the severity of depression symptoms.5,6
The Veterans Health Administration and the US Department of Defense recommend yoga as a potential adjunctive treatment to manage the hyperarousal symptoms of post-traumatic stress disorder (PTSD).7
The Work Loss Data Institute recommends yoga as an intervention for workers compensation conditions including occupational stress, major depressive disorder, PTSD, and other mental disorders.8
1. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2012;3:117.
2. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
3. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
4. Brown RP, Gerbarg PL. Sudarshan Kriya Yogic breathing in the treatment of stress, anxiety, and depression. Part II—clinical applications and guidelines. J Altern Complement Med. 2005;11:711-717.
5. Mitchell J, Trangle M, Degnan B, et al. Institute for Clinical Systems Improvement. Adult depression primary care. Available at: https://www.icsi.org/_asset/fnhdm3/Depr-Interactive0512b.pdf. Updated September 2013. Accessed March 6, 2014.
6. Ravindran AV, Lam RW, Filteau MJ, et al; Canadian Network for Mood and Anxiety Treatments (CANMAT). Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. V. Complementary and alternative medicine treatments. J Affect Disord. 2009;117(suppl 1):S54-S64.
7. US Department of Veterans Affairs. VA/DoD clinical practice guideline for management of post-traumatic stress disorder and acute stress reaction. US Department of Veterans Affairs Web site. Available at: http://www.healthquality.va.gov/ptsd/. Accessed March 6, 2014.
8. Agency for Healthcare Research and Quality. Mental illness & stress. Agency for Healthcare Research and Quality Web site. Available at: http://www.guideline.gov/content.aspx?id=47588. Updated May 2011. Accessed June 17, 2014
1. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2012;3:117.
2. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
3. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
4. Brown RP, Gerbarg PL. Sudarshan Kriya Yogic breathing in the treatment of stress, anxiety, and depression. Part II—clinical applications and guidelines. J Altern Complement Med. 2005;11:711-717.
5. Mitchell J, Trangle M, Degnan B, et al. Institute for Clinical Systems Improvement. Adult depression primary care. Available at: https://www.icsi.org/_asset/fnhdm3/Depr-Interactive0512b.pdf. Updated September 2013. Accessed March 6, 2014.
6. Ravindran AV, Lam RW, Filteau MJ, et al; Canadian Network for Mood and Anxiety Treatments (CANMAT). Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. V. Complementary and alternative medicine treatments. J Affect Disord. 2009;117(suppl 1):S54-S64.
7. US Department of Veterans Affairs. VA/DoD clinical practice guideline for management of post-traumatic stress disorder and acute stress reaction. US Department of Veterans Affairs Web site. Available at: http://www.healthquality.va.gov/ptsd/. Accessed March 6, 2014.
8. Agency for Healthcare Research and Quality. Mental illness & stress. Agency for Healthcare Research and Quality Web site. Available at: http://www.guideline.gov/content.aspx?id=47588. Updated May 2011. Accessed June 17, 2014
Evidence-based answers from the Family Physicians Inquiries Network
Health Risks Associated with Tattoos and Body Piercing
From the West Virginia University School of Medicine, Morgantown, WV.
Abstract
- Objective: To review the health risks associated with tattoos and body piercing.
- Methods: Review of the literature.
- Results: Tattooing and piercing have become increasingly popular practices in the United States. There are important physical and behavioral risks associated with these forms of body modification. The most common complications from tattooing include skin infections and allergic reactions. Minor complications such as infection and bleeding occur frequently with piercings, but major complications have also been reported. Tattoos and piercings appear to be a marker for risk-taking behavior.
- Conclusion: Clinicians should understand the potential complications of these procedures and be able to counsel patients on how to reduce their health risks.
Tattoos and piercings are ancient practices of body modification that have gained widespread acceptance in modern society, particularly among young adults. Tattoos involve the insertion of colored pigment into the dermal layer of the skin with the goal of creating a permanent marking. They are commonly applied using an electrically powered handheld tattoo machine that moves a needle up and down to inject ink through the epidermis and deposit a drop of ink into the dermis [1]. The cells of the dermis are more stable compared with those of the epidermis, so the ink will mostly stay in place for a person’s lifetime [2].
Body piercing is defined as the insertion of a needle or specially designed piercing gun to create a fistula-like opening into either cartilage or skin for the introduction of decorative ornaments [3]. These ornaments can include jewelry, plastic or wood plugs, beads, or pearls. Body piercing has been part of ritualistic or cultural practices for centuries but is rapidly becoming a worldwide mainstream fashion trend, especially among young women aged 17 to 25 years [4]. Ear piercing has become so well accepted that most studies of body piercing do not include earlobe piercing [5].
There are important physical and behavioral risks associated with body modification. In this paper, we review the epidemiology, potential complications, and behavioral factors associated with tattoos and piercings.
Epidemiology
Tattoos are increasingly popular, with a 2012 Harris poll indicating that 1 in 5 adults has at least 1 tattoo [6], up from 14% in 2008 [7]. In the 2012 poll, adults aged 30 to 39 are most likely to have a tattoo (38%) compared to both those younger (30% of those 25–29 and 22% of those 18–24) and older (27% of those 40–49, 11% of those 50–64 and just 5% of those 65 and older). Women are slightly more likely than men, for the first time since this question was first asked, to have a tattoo (23% versus 19% in men). Current US body piercing rates are approximately 36% [3]. Body piercing is more popular among women than in men [8]. Among adolescents, body piercing is performed considerably earlier than tattooing [9]. The head area is the favored location for piercing, while the most common location for a tattoo is the limb [10].
Associated Health Risks
Tattoos
The most common complications that result from tattooing are skin infections and allergic reactions to the tattoo ink. Extensive skin puncturing can result in bleeding and prolonged leaking of serosanguinous fluid. Pyodermal infections can include temporary inflammation at the site of needle puncture, superficial infections such as impetigo and ecthyma, and deeper infections such as cellulitis, erysipelas, and furunculosis [11]. Unsterile equipment and needles can transmit infectious diseases such as hepatitis [2]. Human immunodeficiency virus is theoretically transmissible this way, but no cases of HIV infection caused by tattooing have been documented [12].
Skin reactions to tattooing include aseptic inflammation and acquired sensitivity to tattoo ink, especially red ink, but also to chromium in green ink, cadmium in yellow ink, and cobalt in blue ink [13]. The reaction can manifest as either allergic contact dermatitis or photo-allergic dermatitis. Cutaneous conditions that localize in tattooed areas include vaccinia, verruca vulgaris, herpes simplex, herpes zoster, psoriasis, lichen planus, keratosis follicularis (Darier disease), chronic discoid lupus erythematosus, and keratoacanthoma. Other possible but less common conditions include keloid, sarcoidal granuloma, erythema multiforme, localized scleroderma, and lymphadenopathy [12].
A recent outbreak of nontuburculous nycobacterial infection was linked to contaminated tattoo inks [14]. Contamination can occur during the manufacturing process due to use of contaminated ingredients or when inks are diluted with nonsterile water by tattoo artists [15]. Investigations of 22 cases of tattoo-associated NTM skin infections in 4 states that occurred during 2011–2012 found that ink was contaminated with NTM before use [16]. M. chelonae, one of several disease-causing NTM species, can cause lung disease, joint infection, eye problems and other organ infections. These infections can be difficult to diagnose and can require treatment lasting 6 months or more [15].
Tattoo laws and regulations vary by state. The inks and ink colorings (pigments) used for tattoos are subject to regulation by the US Food and Drug Administration as cosmetics and color additives. However, the FDA has not traditionally enforced its authority over tattoo inks. The FDA encourages reporting of tattoo-associated complications to its MedWatch program (www.fda.gov/Safety/MedWatch/).
Malignancies reported to develop within tattoos include squamous cell carcinoma, basal cell carcinoma, malignant melanoma, leiomyosarcoma, and dermatofibrosarcoma protuberans [17,18]. These malignancies may be coincidental, but carcinogenicity of the tattoo is as yet unknown. Another concern is that a malignancy within a tattoo is more difficult to identify on skin examination [11,17].
Rarely, tattoos or permanent makeup might cause swelling or burning in the affected areas during magnetic resonance imaging (MRI) exams. The metallic ferric acid pigments used in tattoos can conduct heat on the skin during MRI, resulting in traumatic burns [19]. This has also been reported to occur with tattoos with nonferrous pigments. In some cases, tattoo pigments can interfere with the quality of the image, such as when a person with permanent eyeliner has an MRI of the eye [19].
Patients may self-administer tattoos using sewing needles, forks, paper clips, or pens, and colorants may include charcoal, soot, mascara, or ink. The use of unprofessional tattooists and piercers, who often have limited knowledge of health and hygiene precautions, is more likely to lead to complications [10].
Piercings
While most body piercings are not problematic, the potential for localized infections as well as associated systemic disease is present as long as the piercing site remains open [20]. Bacterial skin infections at or near the site are the most commonly reported complication of body piercings, with causative organisms primarily consisting of Staphylococcus, group A beta-hemolytic Streptococcus, and Pseudomonas [21]. Contributing to the health risks of piercing is the reluctance of patients to seek qualified medical intervention when initial site irritation, pain, or oozing occurs [21].
Systemic infections have been reported. More than 25 infective endocarditis cases in the past decade have come from tongue, navel, earlobe, lower lip, and nipple piercings [21]. Infective endocarditis should be considered in individuals with a new piercing (ie, up to 4 months), with or without a history of congenital heart disease, who present with unexplained fever, night chills, weakness, myalgia, arthralgia, lethargy, or malaise [22]. General complications include allergic contact dermatitis (eg, from nickel or latex), bleeding, scarring and keloid formation, nerve damage, and interference with medical procedures such as intubation and blood/organ donation [20].
Oral piercings may lead to difficulty speaking and eating, excessive salivation, and dental problems. Oral and nasal piercings may be aspirated or become embedded, requiring surgical removal. Tongue piercing, usually performed without anesthesia, may cause damage to teeth and gums, including dental fractures [23] and changes in chewing and speech. Because of the tongue’s vascular nature, prolonged bleeding can result if vessels are punctured during the piercing procedure. In addition, the technique for inserting tongue jewelry may abrade or fracture anterior dentition, and digital manipulation of the jewelry can significantly increase the potential for infection [24]. In fact, complications arising from oral piercing are so numerous—and in some cases life-threatening—that the American Dental Association has issued a formal statement opposing the practice [24].
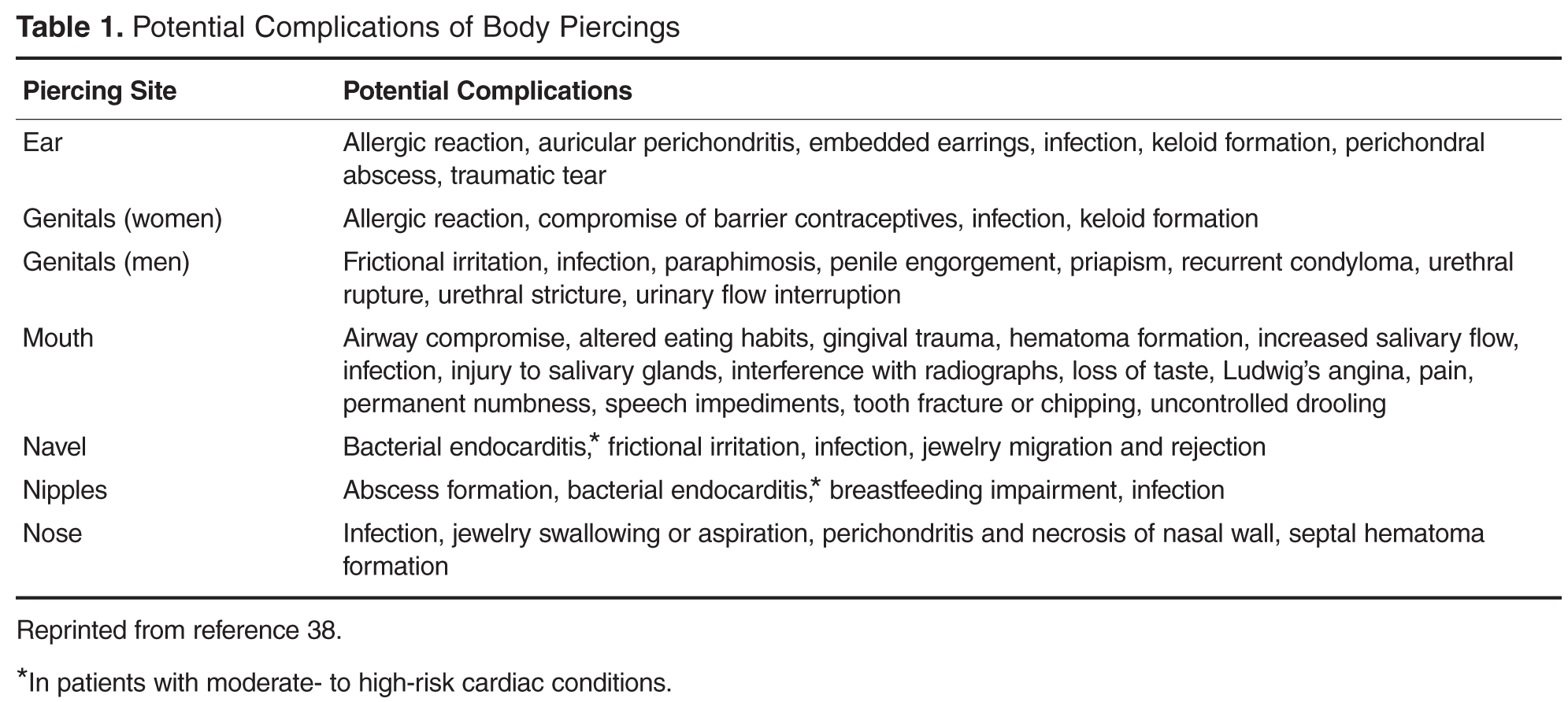
Behavioral Risk
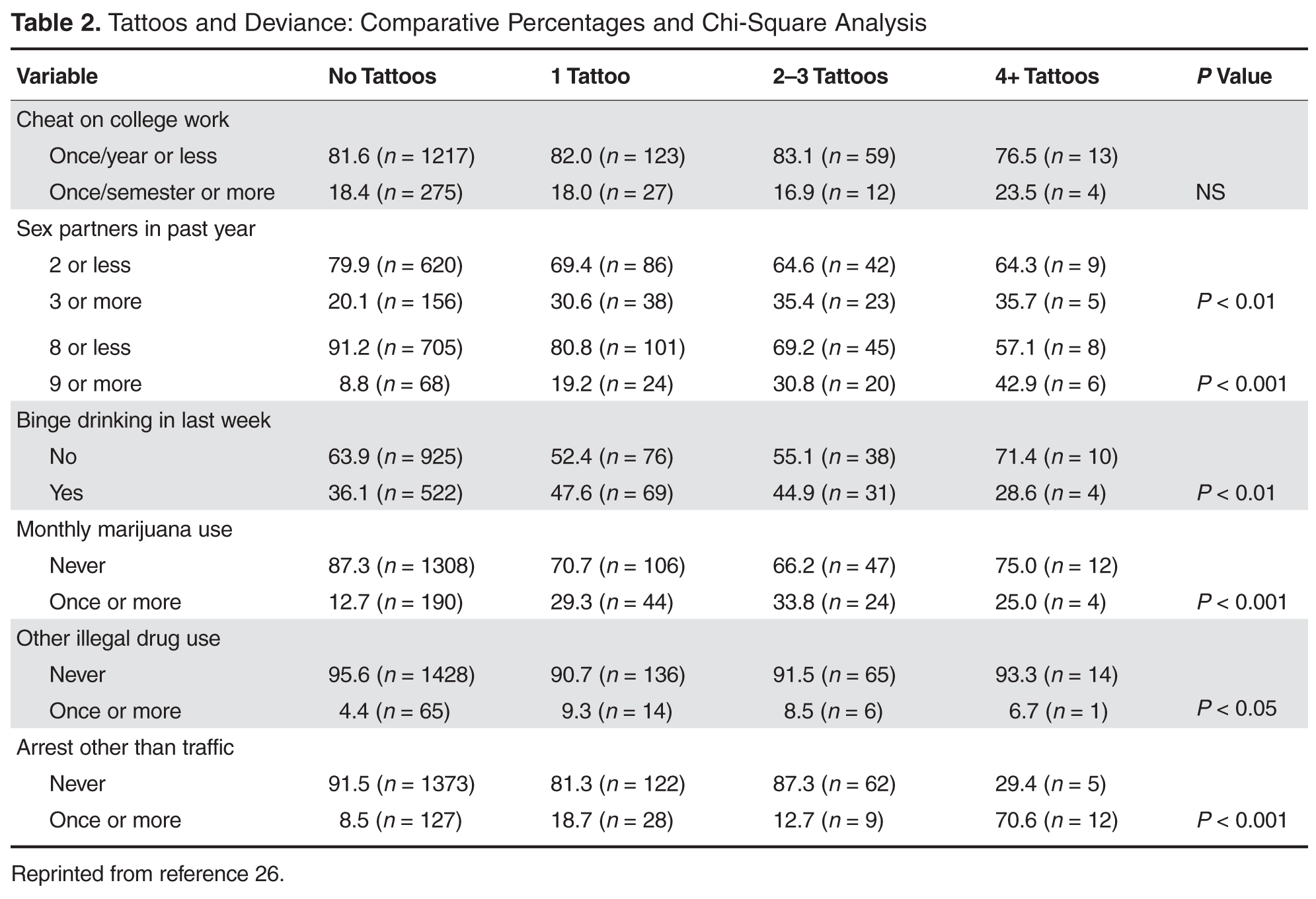
Several studies have found that those with body modifications engaged in earlier or more frequent sexual activity and had a greater number of sexual partners [26–28]. A study by Deschesnes and colleagues [29] reported that certain “externalized” risk behaviors were more commonly associated with tattooed and pierced youth than with their unmodified counterparts, including the use of drugs, gang affiliation, school truancy, and problem gambling. Other studies of high school youth have found that tattooing was significantly and independently associated with other high-risk behaviors, including sexual intercourse, binge drinking, smoking, marijuana use, gang membership, truancy, and school failure [30]. However, a survey of college students found that, compared to individuals with no body art, individuals with 1 tattoo and less than 4 piercings had no greater likelihood to engage in high-risk behaviors [31].
Conversely, some researchers have attempted to show a positive association for body modification. In a study of women with eating disorders, the authors suggested that body piercing could be seen as reflecting a positive attitude towards the body, an expression of self-care [32]. In addition, people with piercings are more likely to give attention to their physical appearance and are less likely to be overweight than people without piercings [33].
Stirn and Hinz [34] concluded that most people who partake in body modification clearly do not do it because they have any psychological problems. However, for a few, modifications may be utilized as a convenient means to either realize psychopathological inclinations, such as self-injury, or to overcome psychological traumas. The prevalence of self-injury is unknown, though it is believed to be a growing problem. While self-injury is believed to be a low-lethality behavior, teens who hurt themselves are at increased risk for suicide related to their underlying anxiety or depression. Moreover, self-harmers report that they often had their skin tattooed or body pierced to help overcome a negative experience, or simply to experience physical pain. Another clue that self-harm and piercing/tattooing might in some cases be linked derives from the fact that many of the self-harmers said they had ceased cutting themselves after obtaining their first piercing or tattoo [35]. The increasing incidence makes deliberate self-harm a problem that all health care providers dealing with adolescents are likely to encounter.
Given the link between body modification and “externalized risk behaviors” in young people, tattooing and body piercing may serve as clinical markers for health care professionals, potentially identifying those who may be involved in activities that hinder their health and development [29]. For example, closer examination of teens who wear long sleeves or clothing inappropriate for weather could reveal cuts, burns, carvings, or bruises that are self-inflicted.
Patients are more likely to discuss the issue of body art if the clinician does not speak or act judgmentally [1]. Practitioners who are concerned that their tattooed patient might be self-injuring or engaging in other risky behaviors should invite a discussion with the patient, perhaps using general terms, such as “Sometimes people may get involved in self-injury and don’t know where to turn for help. I will try to help you if you are ever worried about that.” As always, if the clinician suspects a patient is engaged in self-harming activities, an immediate referral should be made for mental health evaluation and any necessary intervention.
Preventatively, clinicians should provide targeted and repeated education to transmit the message of effective decision-making and evaluation of risks to children in the early elementary grades, since some students start to obtain body art as early as fifth grade.
Regret and Removal
Over time, many individuals regret getting tattoos and wish to have them removed [35]. In some cases, delayed complications, like the development of allergic, hypersensitivity, or granulomatous reactions, require tattoo removal. On average, tattoo regret occurs 14 years after tattooing and by the age of 40 years.
Removal is more painful and laborious than the tattooing itself, and complete removal, with no scarring, is often not possible. The American Society for Dermatologic Surgery reports that in 2011, its doctors performed nearly 100,000 tattoo removal procedures, up from the 86,000 performed in 2010 [36]. Pulsed lasers have been used to remove tattoos for more than 20 years. With this procedure, pulses of high-intensity laser energy pass through the epidermis and are selectively absorbed by the tattoo pigment. The laser breaks the pigment into smaller particles, which may be metabolized or excreted by the body, or transported to and stored in lymph nodes or other tissues [37].
Other removal techniques include dermabrasion and surgical excision. Do-it-yourself tattoo removal ointments and creams can be purchased online, but they have not been approved by the FDA and there is no clinical evidence that they work. Furthermore, tattoo removal ointments and creams may cause unexpected reactions, such as rashes, burning, scarring, or changes in skin pigmentation [37].
Clinician’s Role
Body art provides a window into an individual’s uniqueness, and acknowledging body modifications can help build trust and develop the physician/patient relationship. The health professional armed with knowledge about body modifications can forge more functional relationships, obtain critical historical information, and provide better treatment and referral for this population [5].
Having a clinician who is a trusted, nonjudgmental source of information and intervention for patients who choose body art will reduce the health risk of complications associated with tattooing and piercing [1]. Unfortunately, only 14% of the population identify health care professionals as a common resource for information on body modification. Instead, young adults endorsed friends (82%), body piercing shops (61%), and tattoo shops (51%) as their top information sources. Clinicians should help patients make informed decisions about body art and counsel them about the importance of universal precautions [35].
Corresponding author: Susannah Grimm Poe, EdD, 176 Gilboa Rd., Fairmont, WV 26554, spoe@hsc.wvu.edu.
Financial disclosures: None.
1. Schmidt R, Armstrong M. Tattooing in adolescents and adults. Up to Date 2013. Available at www.uptodate.com.
2. US Food and Drug Administration. Tattoos and permanent makeup. 2009. Available at www.fda.gov/Cosmetics/ProductandIngredientSafety/ProductInformation/ucm108530.htm.
3. Armstrong ML, Koch JR, Saunders JC, et al. The hole picture: risks, decision making, purpose, regulations, and the future of body piercing. Clin Dermatol 2007;25:398-406.
4. Schorzman CM, Gold MA, Downs JS, Murray PJ. Body art: attitudes and practices regarding body piercing among urban undergraduates. J Am Osteopath Assoc 2007;107:432-8.
5. Urdang, M, Mallek, J, Mallon, W. Tattoos and piercings: a review for the emergency physician. West J Emerg Med 2011;12:393–8.
6. Braverman S. One in five US adults now has a tattoo. New York: Harris Interactive; 2012.
7. Corso RA. Nationwide Harris poll. New York: Harris Interactive; 2008.
8. Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol 2006;55:413–21.
9. Antoszewski B, Sitek A, Fijałkowska M, et al. Tattooing and body piercing--what motivates you to do it? Int J Soc Psychiatry. 2010;56:471–9.
10. Quaranta A, Napoli C, Fasano F, et al. Body piercing and tattoos: a survey on young adults’ knowledge of the risks and practices in body art. BMC Public Health 2011;11:774.
11. Glassy C, Glassy M, Aldasoiuqi A. Tattooing: medical uses and problems. Clev Clin J Med 2012;79:761–70.
12. Sperry K. Tattoos and tattooing. Part II: gross pathology, histopathology, medical complications, and applications. Am J Forensic Med Pathol 1992;13:7–17.
13. Kaur RR, Kirby W, Maibach H. Cutaneous allergic reactions to tattoo ink. J Cosmet Dermatol 2009; 8:295–300.
14. Kennedy BS, Bedard B, Younge M, et al. Outbreak of Mycobacterium chelonae infection associated with tattoo ink. N Engl J Med 2012;367:1020–4.
15. CDC. The hidden dangers of getting inked. Available at http://blogs.cdc.gov/publichealthmatters/2012/08/the-hidden-dangers-of-getting-inked.
16. LeBlanc PM, Hollinger KA, Klontz KC. Tattoo ink-related infections—awareness, diagnosis, reporting, and prevention. N Engl J Med 2012;367:985–7.
17. Shinohara MM, Nguyen J, Gardner J, Rosenbach M, Elenitsas R. The histopathologic spectrum of decorative tattoo complications. J Cutan Pathol 2012;39:1110–8.
18. Reddy KK, Hanke CW, Tierney EP. Malignancy arising within cutaneous tattoos: case of dermatofibrosarcoma protuberans and review of literature. J Drugs Dermatol 2011;10:837–42.
19. Tope WD, Shellock FG. Magnetic resonance imaging and permanent cosmetics (tattoos): survey of complications and adverse events. J Magn Reson Imaging 2002;15:180–4.
20. Holbrook, J, Minocha J, Laumann A. Body piercing: complications and prevention of health risks. Am J Clin Dermatol 2012;13:1–17.
21. Hogan L, Armstrong ML. Body piercing: more than skin deep. Skin therapy letter. Available at www.skintherapyletter.com/2009/14.7/2.html.
22. Raja SG, Shad SK, Dreyfus GD. Body piercing: a rare cause of mitral valve endocarditis. J Heart Valve Dis 2004;13:854.
23. Botchway C, Kuc I. Tongue piercing and associated tooth fracture. J Can Dent Assoc 1998;64:803–5.
24. American Dental Association. Statement on intraoral/perioral piercing and tongue splitting. 2012. Available at www.ada.org/prof/resources/positions/statements/piercing.asp.
25. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205–15.
26. Koch R, Roberts AE, Armstrong ML, Owen DC. Body art, deviance, and American college students. Soc Sci J 2010;47:151–61.
27. Gueguen N. Tattoos, piercings, and sexual activity. Social Behav Personality 2012;40:1543–7.
28. Skegg K, Nada-Raja S, Paul C, et al. Body piercing, personality, and sexual behavior. Arch Sex Behav 2007; 36:47–54.
29. Deschesnes M, Fines P, Demers S. Are tattooing and body piercing indicators of risk-taking behaviours among high school students? J Adolesc 2006; 29:379–93.
30. Roberts TA, Ryan SA. Tattooing and high-risk behavior in adolescents. Pediatrics 2002;110:1058–63.
31. Owen DC, Armstrong ML, Koch JR, Roberts AE. College students with body art: well-being or high-risk behavior? J Psychosoc Nurs Ment Health Serv 2013;51:20–8.
32. Claes L, Vandereycken W, Vertommen H. Self-care versus self-harm: piercing, tattooing, and self-injuring in eating disorders. Eur Eat Disord Rev 2004;13:11–18.
33. Hicinbothem J, Gonsalves S, Lester D. Body modification and suicidal behavior. Death Stud 2006; 30:351–63.
34. Stirn A, Hinz A. Tattoos, body piercings, and self-injury: Is there a connection? Psychotherapy Res 2008;18:326–33.
35. Burris K, Kim K. Tattoo removal. Clin Dermatol 2007;25:388–92.
36. American Society for Dermatologic Surgery. Unwanted tattoos. Available at www.asds.net/tattooremovalinformation.aspx.
37. US Food and Drug Administration. Inked and regretful: removing tattoos. 2013. Available at www.fda.gov/ForConsumers/ucm336842.htm.
38. Meltzer DI. Complications of body piercing. Am Fam Physician 2005;72:2029–34.
From the West Virginia University School of Medicine, Morgantown, WV.
Abstract
- Objective: To review the health risks associated with tattoos and body piercing.
- Methods: Review of the literature.
- Results: Tattooing and piercing have become increasingly popular practices in the United States. There are important physical and behavioral risks associated with these forms of body modification. The most common complications from tattooing include skin infections and allergic reactions. Minor complications such as infection and bleeding occur frequently with piercings, but major complications have also been reported. Tattoos and piercings appear to be a marker for risk-taking behavior.
- Conclusion: Clinicians should understand the potential complications of these procedures and be able to counsel patients on how to reduce their health risks.
Tattoos and piercings are ancient practices of body modification that have gained widespread acceptance in modern society, particularly among young adults. Tattoos involve the insertion of colored pigment into the dermal layer of the skin with the goal of creating a permanent marking. They are commonly applied using an electrically powered handheld tattoo machine that moves a needle up and down to inject ink through the epidermis and deposit a drop of ink into the dermis [1]. The cells of the dermis are more stable compared with those of the epidermis, so the ink will mostly stay in place for a person’s lifetime [2].
Body piercing is defined as the insertion of a needle or specially designed piercing gun to create a fistula-like opening into either cartilage or skin for the introduction of decorative ornaments [3]. These ornaments can include jewelry, plastic or wood plugs, beads, or pearls. Body piercing has been part of ritualistic or cultural practices for centuries but is rapidly becoming a worldwide mainstream fashion trend, especially among young women aged 17 to 25 years [4]. Ear piercing has become so well accepted that most studies of body piercing do not include earlobe piercing [5].
There are important physical and behavioral risks associated with body modification. In this paper, we review the epidemiology, potential complications, and behavioral factors associated with tattoos and piercings.
Epidemiology
Tattoos are increasingly popular, with a 2012 Harris poll indicating that 1 in 5 adults has at least 1 tattoo [6], up from 14% in 2008 [7]. In the 2012 poll, adults aged 30 to 39 are most likely to have a tattoo (38%) compared to both those younger (30% of those 25–29 and 22% of those 18–24) and older (27% of those 40–49, 11% of those 50–64 and just 5% of those 65 and older). Women are slightly more likely than men, for the first time since this question was first asked, to have a tattoo (23% versus 19% in men). Current US body piercing rates are approximately 36% [3]. Body piercing is more popular among women than in men [8]. Among adolescents, body piercing is performed considerably earlier than tattooing [9]. The head area is the favored location for piercing, while the most common location for a tattoo is the limb [10].
Associated Health Risks
Tattoos
The most common complications that result from tattooing are skin infections and allergic reactions to the tattoo ink. Extensive skin puncturing can result in bleeding and prolonged leaking of serosanguinous fluid. Pyodermal infections can include temporary inflammation at the site of needle puncture, superficial infections such as impetigo and ecthyma, and deeper infections such as cellulitis, erysipelas, and furunculosis [11]. Unsterile equipment and needles can transmit infectious diseases such as hepatitis [2]. Human immunodeficiency virus is theoretically transmissible this way, but no cases of HIV infection caused by tattooing have been documented [12].
Skin reactions to tattooing include aseptic inflammation and acquired sensitivity to tattoo ink, especially red ink, but also to chromium in green ink, cadmium in yellow ink, and cobalt in blue ink [13]. The reaction can manifest as either allergic contact dermatitis or photo-allergic dermatitis. Cutaneous conditions that localize in tattooed areas include vaccinia, verruca vulgaris, herpes simplex, herpes zoster, psoriasis, lichen planus, keratosis follicularis (Darier disease), chronic discoid lupus erythematosus, and keratoacanthoma. Other possible but less common conditions include keloid, sarcoidal granuloma, erythema multiforme, localized scleroderma, and lymphadenopathy [12].
A recent outbreak of nontuburculous nycobacterial infection was linked to contaminated tattoo inks [14]. Contamination can occur during the manufacturing process due to use of contaminated ingredients or when inks are diluted with nonsterile water by tattoo artists [15]. Investigations of 22 cases of tattoo-associated NTM skin infections in 4 states that occurred during 2011–2012 found that ink was contaminated with NTM before use [16]. M. chelonae, one of several disease-causing NTM species, can cause lung disease, joint infection, eye problems and other organ infections. These infections can be difficult to diagnose and can require treatment lasting 6 months or more [15].
Tattoo laws and regulations vary by state. The inks and ink colorings (pigments) used for tattoos are subject to regulation by the US Food and Drug Administration as cosmetics and color additives. However, the FDA has not traditionally enforced its authority over tattoo inks. The FDA encourages reporting of tattoo-associated complications to its MedWatch program (www.fda.gov/Safety/MedWatch/).
Malignancies reported to develop within tattoos include squamous cell carcinoma, basal cell carcinoma, malignant melanoma, leiomyosarcoma, and dermatofibrosarcoma protuberans [17,18]. These malignancies may be coincidental, but carcinogenicity of the tattoo is as yet unknown. Another concern is that a malignancy within a tattoo is more difficult to identify on skin examination [11,17].
Rarely, tattoos or permanent makeup might cause swelling or burning in the affected areas during magnetic resonance imaging (MRI) exams. The metallic ferric acid pigments used in tattoos can conduct heat on the skin during MRI, resulting in traumatic burns [19]. This has also been reported to occur with tattoos with nonferrous pigments. In some cases, tattoo pigments can interfere with the quality of the image, such as when a person with permanent eyeliner has an MRI of the eye [19].
Patients may self-administer tattoos using sewing needles, forks, paper clips, or pens, and colorants may include charcoal, soot, mascara, or ink. The use of unprofessional tattooists and piercers, who often have limited knowledge of health and hygiene precautions, is more likely to lead to complications [10].
Piercings
While most body piercings are not problematic, the potential for localized infections as well as associated systemic disease is present as long as the piercing site remains open [20]. Bacterial skin infections at or near the site are the most commonly reported complication of body piercings, with causative organisms primarily consisting of Staphylococcus, group A beta-hemolytic Streptococcus, and Pseudomonas [21]. Contributing to the health risks of piercing is the reluctance of patients to seek qualified medical intervention when initial site irritation, pain, or oozing occurs [21].
Systemic infections have been reported. More than 25 infective endocarditis cases in the past decade have come from tongue, navel, earlobe, lower lip, and nipple piercings [21]. Infective endocarditis should be considered in individuals with a new piercing (ie, up to 4 months), with or without a history of congenital heart disease, who present with unexplained fever, night chills, weakness, myalgia, arthralgia, lethargy, or malaise [22]. General complications include allergic contact dermatitis (eg, from nickel or latex), bleeding, scarring and keloid formation, nerve damage, and interference with medical procedures such as intubation and blood/organ donation [20].
Oral piercings may lead to difficulty speaking and eating, excessive salivation, and dental problems. Oral and nasal piercings may be aspirated or become embedded, requiring surgical removal. Tongue piercing, usually performed without anesthesia, may cause damage to teeth and gums, including dental fractures [23] and changes in chewing and speech. Because of the tongue’s vascular nature, prolonged bleeding can result if vessels are punctured during the piercing procedure. In addition, the technique for inserting tongue jewelry may abrade or fracture anterior dentition, and digital manipulation of the jewelry can significantly increase the potential for infection [24]. In fact, complications arising from oral piercing are so numerous—and in some cases life-threatening—that the American Dental Association has issued a formal statement opposing the practice [24].
Behavioral Risk
Several studies have found that those with body modifications engaged in earlier or more frequent sexual activity and had a greater number of sexual partners [26–28]. A study by Deschesnes and colleagues [29] reported that certain “externalized” risk behaviors were more commonly associated with tattooed and pierced youth than with their unmodified counterparts, including the use of drugs, gang affiliation, school truancy, and problem gambling. Other studies of high school youth have found that tattooing was significantly and independently associated with other high-risk behaviors, including sexual intercourse, binge drinking, smoking, marijuana use, gang membership, truancy, and school failure [30]. However, a survey of college students found that, compared to individuals with no body art, individuals with 1 tattoo and less than 4 piercings had no greater likelihood to engage in high-risk behaviors [31].
Conversely, some researchers have attempted to show a positive association for body modification. In a study of women with eating disorders, the authors suggested that body piercing could be seen as reflecting a positive attitude towards the body, an expression of self-care [32]. In addition, people with piercings are more likely to give attention to their physical appearance and are less likely to be overweight than people without piercings [33].
Stirn and Hinz [34] concluded that most people who partake in body modification clearly do not do it because they have any psychological problems. However, for a few, modifications may be utilized as a convenient means to either realize psychopathological inclinations, such as self-injury, or to overcome psychological traumas. The prevalence of self-injury is unknown, though it is believed to be a growing problem. While self-injury is believed to be a low-lethality behavior, teens who hurt themselves are at increased risk for suicide related to their underlying anxiety or depression. Moreover, self-harmers report that they often had their skin tattooed or body pierced to help overcome a negative experience, or simply to experience physical pain. Another clue that self-harm and piercing/tattooing might in some cases be linked derives from the fact that many of the self-harmers said they had ceased cutting themselves after obtaining their first piercing or tattoo [35]. The increasing incidence makes deliberate self-harm a problem that all health care providers dealing with adolescents are likely to encounter.
Given the link between body modification and “externalized risk behaviors” in young people, tattooing and body piercing may serve as clinical markers for health care professionals, potentially identifying those who may be involved in activities that hinder their health and development [29]. For example, closer examination of teens who wear long sleeves or clothing inappropriate for weather could reveal cuts, burns, carvings, or bruises that are self-inflicted.
Patients are more likely to discuss the issue of body art if the clinician does not speak or act judgmentally [1]. Practitioners who are concerned that their tattooed patient might be self-injuring or engaging in other risky behaviors should invite a discussion with the patient, perhaps using general terms, such as “Sometimes people may get involved in self-injury and don’t know where to turn for help. I will try to help you if you are ever worried about that.” As always, if the clinician suspects a patient is engaged in self-harming activities, an immediate referral should be made for mental health evaluation and any necessary intervention.
Preventatively, clinicians should provide targeted and repeated education to transmit the message of effective decision-making and evaluation of risks to children in the early elementary grades, since some students start to obtain body art as early as fifth grade.
Regret and Removal
Over time, many individuals regret getting tattoos and wish to have them removed [35]. In some cases, delayed complications, like the development of allergic, hypersensitivity, or granulomatous reactions, require tattoo removal. On average, tattoo regret occurs 14 years after tattooing and by the age of 40 years.
Removal is more painful and laborious than the tattooing itself, and complete removal, with no scarring, is often not possible. The American Society for Dermatologic Surgery reports that in 2011, its doctors performed nearly 100,000 tattoo removal procedures, up from the 86,000 performed in 2010 [36]. Pulsed lasers have been used to remove tattoos for more than 20 years. With this procedure, pulses of high-intensity laser energy pass through the epidermis and are selectively absorbed by the tattoo pigment. The laser breaks the pigment into smaller particles, which may be metabolized or excreted by the body, or transported to and stored in lymph nodes or other tissues [37].
Other removal techniques include dermabrasion and surgical excision. Do-it-yourself tattoo removal ointments and creams can be purchased online, but they have not been approved by the FDA and there is no clinical evidence that they work. Furthermore, tattoo removal ointments and creams may cause unexpected reactions, such as rashes, burning, scarring, or changes in skin pigmentation [37].
Clinician’s Role
Body art provides a window into an individual’s uniqueness, and acknowledging body modifications can help build trust and develop the physician/patient relationship. The health professional armed with knowledge about body modifications can forge more functional relationships, obtain critical historical information, and provide better treatment and referral for this population [5].
Having a clinician who is a trusted, nonjudgmental source of information and intervention for patients who choose body art will reduce the health risk of complications associated with tattooing and piercing [1]. Unfortunately, only 14% of the population identify health care professionals as a common resource for information on body modification. Instead, young adults endorsed friends (82%), body piercing shops (61%), and tattoo shops (51%) as their top information sources. Clinicians should help patients make informed decisions about body art and counsel them about the importance of universal precautions [35].
Corresponding author: Susannah Grimm Poe, EdD, 176 Gilboa Rd., Fairmont, WV 26554, spoe@hsc.wvu.edu.
Financial disclosures: None.
From the West Virginia University School of Medicine, Morgantown, WV.
Abstract
- Objective: To review the health risks associated with tattoos and body piercing.
- Methods: Review of the literature.
- Results: Tattooing and piercing have become increasingly popular practices in the United States. There are important physical and behavioral risks associated with these forms of body modification. The most common complications from tattooing include skin infections and allergic reactions. Minor complications such as infection and bleeding occur frequently with piercings, but major complications have also been reported. Tattoos and piercings appear to be a marker for risk-taking behavior.
- Conclusion: Clinicians should understand the potential complications of these procedures and be able to counsel patients on how to reduce their health risks.
Tattoos and piercings are ancient practices of body modification that have gained widespread acceptance in modern society, particularly among young adults. Tattoos involve the insertion of colored pigment into the dermal layer of the skin with the goal of creating a permanent marking. They are commonly applied using an electrically powered handheld tattoo machine that moves a needle up and down to inject ink through the epidermis and deposit a drop of ink into the dermis [1]. The cells of the dermis are more stable compared with those of the epidermis, so the ink will mostly stay in place for a person’s lifetime [2].
Body piercing is defined as the insertion of a needle or specially designed piercing gun to create a fistula-like opening into either cartilage or skin for the introduction of decorative ornaments [3]. These ornaments can include jewelry, plastic or wood plugs, beads, or pearls. Body piercing has been part of ritualistic or cultural practices for centuries but is rapidly becoming a worldwide mainstream fashion trend, especially among young women aged 17 to 25 years [4]. Ear piercing has become so well accepted that most studies of body piercing do not include earlobe piercing [5].
There are important physical and behavioral risks associated with body modification. In this paper, we review the epidemiology, potential complications, and behavioral factors associated with tattoos and piercings.
Epidemiology
Tattoos are increasingly popular, with a 2012 Harris poll indicating that 1 in 5 adults has at least 1 tattoo [6], up from 14% in 2008 [7]. In the 2012 poll, adults aged 30 to 39 are most likely to have a tattoo (38%) compared to both those younger (30% of those 25–29 and 22% of those 18–24) and older (27% of those 40–49, 11% of those 50–64 and just 5% of those 65 and older). Women are slightly more likely than men, for the first time since this question was first asked, to have a tattoo (23% versus 19% in men). Current US body piercing rates are approximately 36% [3]. Body piercing is more popular among women than in men [8]. Among adolescents, body piercing is performed considerably earlier than tattooing [9]. The head area is the favored location for piercing, while the most common location for a tattoo is the limb [10].
Associated Health Risks
Tattoos
The most common complications that result from tattooing are skin infections and allergic reactions to the tattoo ink. Extensive skin puncturing can result in bleeding and prolonged leaking of serosanguinous fluid. Pyodermal infections can include temporary inflammation at the site of needle puncture, superficial infections such as impetigo and ecthyma, and deeper infections such as cellulitis, erysipelas, and furunculosis [11]. Unsterile equipment and needles can transmit infectious diseases such as hepatitis [2]. Human immunodeficiency virus is theoretically transmissible this way, but no cases of HIV infection caused by tattooing have been documented [12].
Skin reactions to tattooing include aseptic inflammation and acquired sensitivity to tattoo ink, especially red ink, but also to chromium in green ink, cadmium in yellow ink, and cobalt in blue ink [13]. The reaction can manifest as either allergic contact dermatitis or photo-allergic dermatitis. Cutaneous conditions that localize in tattooed areas include vaccinia, verruca vulgaris, herpes simplex, herpes zoster, psoriasis, lichen planus, keratosis follicularis (Darier disease), chronic discoid lupus erythematosus, and keratoacanthoma. Other possible but less common conditions include keloid, sarcoidal granuloma, erythema multiforme, localized scleroderma, and lymphadenopathy [12].
A recent outbreak of nontuburculous nycobacterial infection was linked to contaminated tattoo inks [14]. Contamination can occur during the manufacturing process due to use of contaminated ingredients or when inks are diluted with nonsterile water by tattoo artists [15]. Investigations of 22 cases of tattoo-associated NTM skin infections in 4 states that occurred during 2011–2012 found that ink was contaminated with NTM before use [16]. M. chelonae, one of several disease-causing NTM species, can cause lung disease, joint infection, eye problems and other organ infections. These infections can be difficult to diagnose and can require treatment lasting 6 months or more [15].
Tattoo laws and regulations vary by state. The inks and ink colorings (pigments) used for tattoos are subject to regulation by the US Food and Drug Administration as cosmetics and color additives. However, the FDA has not traditionally enforced its authority over tattoo inks. The FDA encourages reporting of tattoo-associated complications to its MedWatch program (www.fda.gov/Safety/MedWatch/).
Malignancies reported to develop within tattoos include squamous cell carcinoma, basal cell carcinoma, malignant melanoma, leiomyosarcoma, and dermatofibrosarcoma protuberans [17,18]. These malignancies may be coincidental, but carcinogenicity of the tattoo is as yet unknown. Another concern is that a malignancy within a tattoo is more difficult to identify on skin examination [11,17].
Rarely, tattoos or permanent makeup might cause swelling or burning in the affected areas during magnetic resonance imaging (MRI) exams. The metallic ferric acid pigments used in tattoos can conduct heat on the skin during MRI, resulting in traumatic burns [19]. This has also been reported to occur with tattoos with nonferrous pigments. In some cases, tattoo pigments can interfere with the quality of the image, such as when a person with permanent eyeliner has an MRI of the eye [19].
Patients may self-administer tattoos using sewing needles, forks, paper clips, or pens, and colorants may include charcoal, soot, mascara, or ink. The use of unprofessional tattooists and piercers, who often have limited knowledge of health and hygiene precautions, is more likely to lead to complications [10].
Piercings
While most body piercings are not problematic, the potential for localized infections as well as associated systemic disease is present as long as the piercing site remains open [20]. Bacterial skin infections at or near the site are the most commonly reported complication of body piercings, with causative organisms primarily consisting of Staphylococcus, group A beta-hemolytic Streptococcus, and Pseudomonas [21]. Contributing to the health risks of piercing is the reluctance of patients to seek qualified medical intervention when initial site irritation, pain, or oozing occurs [21].
Systemic infections have been reported. More than 25 infective endocarditis cases in the past decade have come from tongue, navel, earlobe, lower lip, and nipple piercings [21]. Infective endocarditis should be considered in individuals with a new piercing (ie, up to 4 months), with or without a history of congenital heart disease, who present with unexplained fever, night chills, weakness, myalgia, arthralgia, lethargy, or malaise [22]. General complications include allergic contact dermatitis (eg, from nickel or latex), bleeding, scarring and keloid formation, nerve damage, and interference with medical procedures such as intubation and blood/organ donation [20].
Oral piercings may lead to difficulty speaking and eating, excessive salivation, and dental problems. Oral and nasal piercings may be aspirated or become embedded, requiring surgical removal. Tongue piercing, usually performed without anesthesia, may cause damage to teeth and gums, including dental fractures [23] and changes in chewing and speech. Because of the tongue’s vascular nature, prolonged bleeding can result if vessels are punctured during the piercing procedure. In addition, the technique for inserting tongue jewelry may abrade or fracture anterior dentition, and digital manipulation of the jewelry can significantly increase the potential for infection [24]. In fact, complications arising from oral piercing are so numerous—and in some cases life-threatening—that the American Dental Association has issued a formal statement opposing the practice [24].
Behavioral Risk
Several studies have found that those with body modifications engaged in earlier or more frequent sexual activity and had a greater number of sexual partners [26–28]. A study by Deschesnes and colleagues [29] reported that certain “externalized” risk behaviors were more commonly associated with tattooed and pierced youth than with their unmodified counterparts, including the use of drugs, gang affiliation, school truancy, and problem gambling. Other studies of high school youth have found that tattooing was significantly and independently associated with other high-risk behaviors, including sexual intercourse, binge drinking, smoking, marijuana use, gang membership, truancy, and school failure [30]. However, a survey of college students found that, compared to individuals with no body art, individuals with 1 tattoo and less than 4 piercings had no greater likelihood to engage in high-risk behaviors [31].
Conversely, some researchers have attempted to show a positive association for body modification. In a study of women with eating disorders, the authors suggested that body piercing could be seen as reflecting a positive attitude towards the body, an expression of self-care [32]. In addition, people with piercings are more likely to give attention to their physical appearance and are less likely to be overweight than people without piercings [33].
Stirn and Hinz [34] concluded that most people who partake in body modification clearly do not do it because they have any psychological problems. However, for a few, modifications may be utilized as a convenient means to either realize psychopathological inclinations, such as self-injury, or to overcome psychological traumas. The prevalence of self-injury is unknown, though it is believed to be a growing problem. While self-injury is believed to be a low-lethality behavior, teens who hurt themselves are at increased risk for suicide related to their underlying anxiety or depression. Moreover, self-harmers report that they often had their skin tattooed or body pierced to help overcome a negative experience, or simply to experience physical pain. Another clue that self-harm and piercing/tattooing might in some cases be linked derives from the fact that many of the self-harmers said they had ceased cutting themselves after obtaining their first piercing or tattoo [35]. The increasing incidence makes deliberate self-harm a problem that all health care providers dealing with adolescents are likely to encounter.
Given the link between body modification and “externalized risk behaviors” in young people, tattooing and body piercing may serve as clinical markers for health care professionals, potentially identifying those who may be involved in activities that hinder their health and development [29]. For example, closer examination of teens who wear long sleeves or clothing inappropriate for weather could reveal cuts, burns, carvings, or bruises that are self-inflicted.
Patients are more likely to discuss the issue of body art if the clinician does not speak or act judgmentally [1]. Practitioners who are concerned that their tattooed patient might be self-injuring or engaging in other risky behaviors should invite a discussion with the patient, perhaps using general terms, such as “Sometimes people may get involved in self-injury and don’t know where to turn for help. I will try to help you if you are ever worried about that.” As always, if the clinician suspects a patient is engaged in self-harming activities, an immediate referral should be made for mental health evaluation and any necessary intervention.
Preventatively, clinicians should provide targeted and repeated education to transmit the message of effective decision-making and evaluation of risks to children in the early elementary grades, since some students start to obtain body art as early as fifth grade.
Regret and Removal
Over time, many individuals regret getting tattoos and wish to have them removed [35]. In some cases, delayed complications, like the development of allergic, hypersensitivity, or granulomatous reactions, require tattoo removal. On average, tattoo regret occurs 14 years after tattooing and by the age of 40 years.
Removal is more painful and laborious than the tattooing itself, and complete removal, with no scarring, is often not possible. The American Society for Dermatologic Surgery reports that in 2011, its doctors performed nearly 100,000 tattoo removal procedures, up from the 86,000 performed in 2010 [36]. Pulsed lasers have been used to remove tattoos for more than 20 years. With this procedure, pulses of high-intensity laser energy pass through the epidermis and are selectively absorbed by the tattoo pigment. The laser breaks the pigment into smaller particles, which may be metabolized or excreted by the body, or transported to and stored in lymph nodes or other tissues [37].
Other removal techniques include dermabrasion and surgical excision. Do-it-yourself tattoo removal ointments and creams can be purchased online, but they have not been approved by the FDA and there is no clinical evidence that they work. Furthermore, tattoo removal ointments and creams may cause unexpected reactions, such as rashes, burning, scarring, or changes in skin pigmentation [37].
Clinician’s Role
Body art provides a window into an individual’s uniqueness, and acknowledging body modifications can help build trust and develop the physician/patient relationship. The health professional armed with knowledge about body modifications can forge more functional relationships, obtain critical historical information, and provide better treatment and referral for this population [5].
Having a clinician who is a trusted, nonjudgmental source of information and intervention for patients who choose body art will reduce the health risk of complications associated with tattooing and piercing [1]. Unfortunately, only 14% of the population identify health care professionals as a common resource for information on body modification. Instead, young adults endorsed friends (82%), body piercing shops (61%), and tattoo shops (51%) as their top information sources. Clinicians should help patients make informed decisions about body art and counsel them about the importance of universal precautions [35].
Corresponding author: Susannah Grimm Poe, EdD, 176 Gilboa Rd., Fairmont, WV 26554, spoe@hsc.wvu.edu.
Financial disclosures: None.
1. Schmidt R, Armstrong M. Tattooing in adolescents and adults. Up to Date 2013. Available at www.uptodate.com.
2. US Food and Drug Administration. Tattoos and permanent makeup. 2009. Available at www.fda.gov/Cosmetics/ProductandIngredientSafety/ProductInformation/ucm108530.htm.
3. Armstrong ML, Koch JR, Saunders JC, et al. The hole picture: risks, decision making, purpose, regulations, and the future of body piercing. Clin Dermatol 2007;25:398-406.
4. Schorzman CM, Gold MA, Downs JS, Murray PJ. Body art: attitudes and practices regarding body piercing among urban undergraduates. J Am Osteopath Assoc 2007;107:432-8.
5. Urdang, M, Mallek, J, Mallon, W. Tattoos and piercings: a review for the emergency physician. West J Emerg Med 2011;12:393–8.
6. Braverman S. One in five US adults now has a tattoo. New York: Harris Interactive; 2012.
7. Corso RA. Nationwide Harris poll. New York: Harris Interactive; 2008.
8. Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol 2006;55:413–21.
9. Antoszewski B, Sitek A, Fijałkowska M, et al. Tattooing and body piercing--what motivates you to do it? Int J Soc Psychiatry. 2010;56:471–9.
10. Quaranta A, Napoli C, Fasano F, et al. Body piercing and tattoos: a survey on young adults’ knowledge of the risks and practices in body art. BMC Public Health 2011;11:774.
11. Glassy C, Glassy M, Aldasoiuqi A. Tattooing: medical uses and problems. Clev Clin J Med 2012;79:761–70.
12. Sperry K. Tattoos and tattooing. Part II: gross pathology, histopathology, medical complications, and applications. Am J Forensic Med Pathol 1992;13:7–17.
13. Kaur RR, Kirby W, Maibach H. Cutaneous allergic reactions to tattoo ink. J Cosmet Dermatol 2009; 8:295–300.
14. Kennedy BS, Bedard B, Younge M, et al. Outbreak of Mycobacterium chelonae infection associated with tattoo ink. N Engl J Med 2012;367:1020–4.
15. CDC. The hidden dangers of getting inked. Available at http://blogs.cdc.gov/publichealthmatters/2012/08/the-hidden-dangers-of-getting-inked.
16. LeBlanc PM, Hollinger KA, Klontz KC. Tattoo ink-related infections—awareness, diagnosis, reporting, and prevention. N Engl J Med 2012;367:985–7.
17. Shinohara MM, Nguyen J, Gardner J, Rosenbach M, Elenitsas R. The histopathologic spectrum of decorative tattoo complications. J Cutan Pathol 2012;39:1110–8.
18. Reddy KK, Hanke CW, Tierney EP. Malignancy arising within cutaneous tattoos: case of dermatofibrosarcoma protuberans and review of literature. J Drugs Dermatol 2011;10:837–42.
19. Tope WD, Shellock FG. Magnetic resonance imaging and permanent cosmetics (tattoos): survey of complications and adverse events. J Magn Reson Imaging 2002;15:180–4.
20. Holbrook, J, Minocha J, Laumann A. Body piercing: complications and prevention of health risks. Am J Clin Dermatol 2012;13:1–17.
21. Hogan L, Armstrong ML. Body piercing: more than skin deep. Skin therapy letter. Available at www.skintherapyletter.com/2009/14.7/2.html.
22. Raja SG, Shad SK, Dreyfus GD. Body piercing: a rare cause of mitral valve endocarditis. J Heart Valve Dis 2004;13:854.
23. Botchway C, Kuc I. Tongue piercing and associated tooth fracture. J Can Dent Assoc 1998;64:803–5.
24. American Dental Association. Statement on intraoral/perioral piercing and tongue splitting. 2012. Available at www.ada.org/prof/resources/positions/statements/piercing.asp.
25. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205–15.
26. Koch R, Roberts AE, Armstrong ML, Owen DC. Body art, deviance, and American college students. Soc Sci J 2010;47:151–61.
27. Gueguen N. Tattoos, piercings, and sexual activity. Social Behav Personality 2012;40:1543–7.
28. Skegg K, Nada-Raja S, Paul C, et al. Body piercing, personality, and sexual behavior. Arch Sex Behav 2007; 36:47–54.
29. Deschesnes M, Fines P, Demers S. Are tattooing and body piercing indicators of risk-taking behaviours among high school students? J Adolesc 2006; 29:379–93.
30. Roberts TA, Ryan SA. Tattooing and high-risk behavior in adolescents. Pediatrics 2002;110:1058–63.
31. Owen DC, Armstrong ML, Koch JR, Roberts AE. College students with body art: well-being or high-risk behavior? J Psychosoc Nurs Ment Health Serv 2013;51:20–8.
32. Claes L, Vandereycken W, Vertommen H. Self-care versus self-harm: piercing, tattooing, and self-injuring in eating disorders. Eur Eat Disord Rev 2004;13:11–18.
33. Hicinbothem J, Gonsalves S, Lester D. Body modification and suicidal behavior. Death Stud 2006; 30:351–63.
34. Stirn A, Hinz A. Tattoos, body piercings, and self-injury: Is there a connection? Psychotherapy Res 2008;18:326–33.
35. Burris K, Kim K. Tattoo removal. Clin Dermatol 2007;25:388–92.
36. American Society for Dermatologic Surgery. Unwanted tattoos. Available at www.asds.net/tattooremovalinformation.aspx.
37. US Food and Drug Administration. Inked and regretful: removing tattoos. 2013. Available at www.fda.gov/ForConsumers/ucm336842.htm.
38. Meltzer DI. Complications of body piercing. Am Fam Physician 2005;72:2029–34.
1. Schmidt R, Armstrong M. Tattooing in adolescents and adults. Up to Date 2013. Available at www.uptodate.com.
2. US Food and Drug Administration. Tattoos and permanent makeup. 2009. Available at www.fda.gov/Cosmetics/ProductandIngredientSafety/ProductInformation/ucm108530.htm.
3. Armstrong ML, Koch JR, Saunders JC, et al. The hole picture: risks, decision making, purpose, regulations, and the future of body piercing. Clin Dermatol 2007;25:398-406.
4. Schorzman CM, Gold MA, Downs JS, Murray PJ. Body art: attitudes and practices regarding body piercing among urban undergraduates. J Am Osteopath Assoc 2007;107:432-8.
5. Urdang, M, Mallek, J, Mallon, W. Tattoos and piercings: a review for the emergency physician. West J Emerg Med 2011;12:393–8.
6. Braverman S. One in five US adults now has a tattoo. New York: Harris Interactive; 2012.
7. Corso RA. Nationwide Harris poll. New York: Harris Interactive; 2008.
8. Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol 2006;55:413–21.
9. Antoszewski B, Sitek A, Fijałkowska M, et al. Tattooing and body piercing--what motivates you to do it? Int J Soc Psychiatry. 2010;56:471–9.
10. Quaranta A, Napoli C, Fasano F, et al. Body piercing and tattoos: a survey on young adults’ knowledge of the risks and practices in body art. BMC Public Health 2011;11:774.
11. Glassy C, Glassy M, Aldasoiuqi A. Tattooing: medical uses and problems. Clev Clin J Med 2012;79:761–70.
12. Sperry K. Tattoos and tattooing. Part II: gross pathology, histopathology, medical complications, and applications. Am J Forensic Med Pathol 1992;13:7–17.
13. Kaur RR, Kirby W, Maibach H. Cutaneous allergic reactions to tattoo ink. J Cosmet Dermatol 2009; 8:295–300.
14. Kennedy BS, Bedard B, Younge M, et al. Outbreak of Mycobacterium chelonae infection associated with tattoo ink. N Engl J Med 2012;367:1020–4.
15. CDC. The hidden dangers of getting inked. Available at http://blogs.cdc.gov/publichealthmatters/2012/08/the-hidden-dangers-of-getting-inked.
16. LeBlanc PM, Hollinger KA, Klontz KC. Tattoo ink-related infections—awareness, diagnosis, reporting, and prevention. N Engl J Med 2012;367:985–7.
17. Shinohara MM, Nguyen J, Gardner J, Rosenbach M, Elenitsas R. The histopathologic spectrum of decorative tattoo complications. J Cutan Pathol 2012;39:1110–8.
18. Reddy KK, Hanke CW, Tierney EP. Malignancy arising within cutaneous tattoos: case of dermatofibrosarcoma protuberans and review of literature. J Drugs Dermatol 2011;10:837–42.
19. Tope WD, Shellock FG. Magnetic resonance imaging and permanent cosmetics (tattoos): survey of complications and adverse events. J Magn Reson Imaging 2002;15:180–4.
20. Holbrook, J, Minocha J, Laumann A. Body piercing: complications and prevention of health risks. Am J Clin Dermatol 2012;13:1–17.
21. Hogan L, Armstrong ML. Body piercing: more than skin deep. Skin therapy letter. Available at www.skintherapyletter.com/2009/14.7/2.html.
22. Raja SG, Shad SK, Dreyfus GD. Body piercing: a rare cause of mitral valve endocarditis. J Heart Valve Dis 2004;13:854.
23. Botchway C, Kuc I. Tongue piercing and associated tooth fracture. J Can Dent Assoc 1998;64:803–5.
24. American Dental Association. Statement on intraoral/perioral piercing and tongue splitting. 2012. Available at www.ada.org/prof/resources/positions/statements/piercing.asp.
25. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205–15.
26. Koch R, Roberts AE, Armstrong ML, Owen DC. Body art, deviance, and American college students. Soc Sci J 2010;47:151–61.
27. Gueguen N. Tattoos, piercings, and sexual activity. Social Behav Personality 2012;40:1543–7.
28. Skegg K, Nada-Raja S, Paul C, et al. Body piercing, personality, and sexual behavior. Arch Sex Behav 2007; 36:47–54.
29. Deschesnes M, Fines P, Demers S. Are tattooing and body piercing indicators of risk-taking behaviours among high school students? J Adolesc 2006; 29:379–93.
30. Roberts TA, Ryan SA. Tattooing and high-risk behavior in adolescents. Pediatrics 2002;110:1058–63.
31. Owen DC, Armstrong ML, Koch JR, Roberts AE. College students with body art: well-being or high-risk behavior? J Psychosoc Nurs Ment Health Serv 2013;51:20–8.
32. Claes L, Vandereycken W, Vertommen H. Self-care versus self-harm: piercing, tattooing, and self-injuring in eating disorders. Eur Eat Disord Rev 2004;13:11–18.
33. Hicinbothem J, Gonsalves S, Lester D. Body modification and suicidal behavior. Death Stud 2006; 30:351–63.
34. Stirn A, Hinz A. Tattoos, body piercings, and self-injury: Is there a connection? Psychotherapy Res 2008;18:326–33.
35. Burris K, Kim K. Tattoo removal. Clin Dermatol 2007;25:388–92.
36. American Society for Dermatologic Surgery. Unwanted tattoos. Available at www.asds.net/tattooremovalinformation.aspx.
37. US Food and Drug Administration. Inked and regretful: removing tattoos. 2013. Available at www.fda.gov/ForConsumers/ucm336842.htm.
38. Meltzer DI. Complications of body piercing. Am Fam Physician 2005;72:2029–34.
Two Home Health Agencies Reduce Readmissions Among Heart Failure Patients Using a Quality Improvement Approach
From Collaborative Healthcare Strategies, Lexington, MA (Dr. Boutwell), and the National Home Health Corporation, Scarsdale, NY.
Abstract
- Objective: To describe a quality improvement initiative implemented by 2 home health care agencies to reduce readmissions.
- Methods: The agencies reviewed their data and identified best practices for reducing acute hospital transfers among their high-risk heart failure patients, focusing on the first 14 days of the care episode. Care intensity was increased during the first 3 days, and an active surveillance approach was used during the first 2 weeks. Training for staff, called “Heart Failure Boot Camp,” was introduced and made part of new employee orientation.
- Results: The 30-day rehospitalization rate was reduced from 31% to 17%.
- Conclusion: A data-driven transitional care model can lead to reductions in 30-day readmissions among high-risk patients receiving home health care.
Hospital readmissions are frequent, costly, and can be a marker of poorly coordinated postdischarge care [1]. Since the passage of the Affordable Care Act in 2010, reducing readmissions has become a national priority, as reflected in the emergence of accountable care organizations, bundled payments, and readmission penalties for hospitals, among other efforts. With the increasing attention on reducing readmissions, home health care agencies are under pressure to identify opportunities to improve performance. Two affiliated home health care agencies in Massachusetts and Connecticut made reducing their all-cause 30-day readmission rate a strategic priority. In this article, we describe their approach.
Setting
New England Home Care (NEHC, Cromwell, CT) is a regional agency that serves 7 of the 8 counties in Connecticut and over 7400 patients annually. Medical Resources Home Health (Newton, MA) is a regional agency that serves 8 of the 12 counties in Massachusetts and 2000 patients annually. These home health agencies are both owned by National Home Health Care Corporation (Scarsdale, NY) but are independently managed, with separate staff and regional market differences.
Data Analysis

Opportunities for Improvement The data analysis highlighted several immediate opportunities for improvement. First, the data showed that the first 3 days of the home health episode are a period of increased risk. Thus, intensification of care—and successful first contacts—during the first 3 days of the home health episode was an important target goal. Similarly, the first 14 days were a period of increased risk, suggesting the potential benefit of home health staff proactively monitoring patients during this time to identify clinical or other needs early in the effort to avert a hospitalization. In addition, while respiratory symptoms were among the top reasons for acute care hospitalization within 30 days of episode initiation, many other diagnoses were also implicated. Nine conditions comprised 80% of coded reasons for hospitalization, suggesting that vigilance around respiratory complaints is important but cannot be the exclusive focus of symptom management in this population.
Approach The agencies started this performance improvement initiative by focusing on one patient subgroup (heart failure patients) served by one of the agencies (NEHC). New approaches were tried, and effective approaches were codified through training, on-the job coaching, and performance feedback to front-line clinicians. This approach facilitated the spread of these changes to the second agency, and subsequently both agencies expanded their focus beyond heart failure to other common diagnoses in the home health population.
Changes to Standard Care Practices Based on identified opportunities for improvement, the agency incorporated modifications to standard care utilizing existing resources and within the construct of a certified Medicare home health episode (Medicare’s required specific services, assessments, and other activities that a home health agency must provide in order to bill for an episode). First, working with managers and front-line clinicians, they focused on establishing successful contact during the first 3 days of an episode of care. Front-line staff reported that some patients did not respond to the first attempt to establish contact, and staff thought that it indicated that the patient did not want home health care. The agency designed a new initial contact protocol to increase the likelihood of a successful first contact with the patient. Second, staff increased the frequency of contact in the first 3 days of the episode, either through home visits or phone calls. Increased contact served to allowed the home health staff to get to know the patient and have more points of reference upon which to identify whether symptoms were developing or changing. In addition, increase initial frequency served to increase the comfort and confidence that the patient and their family had in the agency. Third, in the context of increasing the frequency and effectiveness of contacts in the first 14 days, home care staff were trained to adopt an “active surveillance” approach. This staff development and re-training initiative instructed staff on practices to increase their awareness and recognition of patient needs or changing circumstances, outside the specific problem-defined focus area(s) of the home health episode. Frequent contact in the first 14 days creates an opportunity for home health staff to intervene proactively in the confusion or symptoms that lead patients or their families to call 911. Fourth, home care staff received professional development training specifically focused on heart failure, called “Heart Failure Boot Camp.” This training provided a review and update on the clinical management best practices for home care for heart failure patients. This training was conducted by the agency’s staff clinical educator at each local field office. Once all the agencies’ existing staff were trained, the training materials were included in new employee orientation. Rate of acute care hospitalizations was tracked and reports were provided to each local field office on a quarterly basis. Agency leadership included review of these data with local field office managers in their existing management meetings to reinforce the importance of this initiative for the agency at the highest levels. As the efforts to reduce hospitalizations evolved to include patients with conditions other than heart failure, the agencies developed a readmission risk assessment that included the number of medications ( < 5; 6–10; 11–15; 16–20; or > 20) and number of hospitalizations within the past 12 months. Staff could act upon the risk elements identified to reduce each individual patient’s risk of readmission.
Adding Enhanced Service to Standard Care: The Transitional Care Liaison
ollowing the implementation of the above changes to standard home health care practices, the agencies subsequently deployed full-time transitional care liaisons at local hospitals. This was a new role, requiring newly dedicated resources for the position. The role is modeled upon the Care Transitions Intervention [2],which emphasizes the value of initiating transitional care during the hospitalization. In this new role, the hospital-based home care liaisons establish a relationship with the patient, schedule immediate follow-up, review medications and the plan to obtain new medications, and review the plan of care in the hospital, prior to the transition home. On-site transitional care liaisons greatly facilitate clinical collaboration, allowing the “receiving” provider to request clarifications prior to discharge. On-site relationships also enable formal and informal mutual improvements in the transition process. An unanticipated benefit to this collaboration is that the agencies are able to identify some high-utilizing patients who are served by several area hospitals. Thus the agencies were able to add to the list of highest-risk patients for some hospitals that were otherwise unidentified.
Outcomes
The 30-day rehospitalization rate for NEHC was 31% during the baseline period (9/30/2008 to 6/30/2010). The quarterly variability in readmission rates was high, ranging from 20% to 42% in any given quarter. Following the start of the performance improvement initiative in Quarter 3 of 2010, and through the most recent quarter for which data are available (Quarter 3 2013) the quarterly 30-day readmission rates demonstrated decreased variability (15% to 22%) and the 30-day readmission rate was reduced to 17%—a 45% reduction in rehospitalizations. The agencies’ rehospitalization rates are lower than local benchmarks [1].
Lessons Learned
The agencies experience with this initiative has led to several lessons learned that may be of interest to other agencies and providers looking to design and implement care models to reduce rehospitalizations.
First, it was essential to supplement our knowledge of best practices from the literature and industry experts with an examination of our own data. In addition to examining rates of rehospitalization, we were able to identify patients at highest risk so we could intensify services early for this group.
Second, the 2 agencies participating in this effort are affiliated but independently managed, with separate staff and regional market differences. We were pleased to learn that a common service delivery model could be successfully implemented in both agencies. This suggests that this structured care delivery improvement approach can be replicated in other organizations and local contexts.
Third, by no means was the staff development and retraining a “one and done” effort; continuous reinforcement of the rationale for the practice change and the protocols for optimizing engagement to reduce rehospitalizations was required.
Finally, the performance improvement initiative started with an initial focus on heart failure patients. Over the course of the Initiative we named the series of practice changes our “Healthy@Home” model of care. As we expanded our focus to all patients at high risk of readmission (as identified by our risk assessment score), we learned that staff thought the Healthy@Home practice changes only applied to heart failure patients. This required re-messaging with the staff and regional supervisors.
Conclusion
As rehospitalizations continue to be a prominent measure of quality, cost, and patient experience and a measure for which hospitals and post-acute and community-based providers are either penalized or rewarded, there is a growing awareness of the many factors outside the walls of the hospital that determine whether a patient will return within a defined period of time. Many home health agencies see this as an opportune moment to highlight the critical role they play in care transitions across settings and over time. In this article, we describe the experience of 2 affiliated regional home health care agencies as they engaged in a structured performance improvement effort to reduce readmissions among their high-risk patients. This effort involving data analysis, identification of locally relevant opportunities for improvement, modifications to standard care utilizing existing resources, adding a new service, and expansion beyond the initial target population to all patients at high risk of readmission. This 3-year effort has resulted in a substantial and sustained reduction in rehospitalization rates.
1. Masspro, Massachusetts’ Quality Improvement Organization. State of the state: readmissions in Massachusetts January 1 2009-September 30 2013. Accessed 14 April 2014 at www.masspro.org/files/tools/12_13_state_of_the_state.pdf.
2. Coleman EA, Parry C, Chalmers S, Min S. The care transitions intervention. Arch Intern Med 2006;166:1822–8.
From Collaborative Healthcare Strategies, Lexington, MA (Dr. Boutwell), and the National Home Health Corporation, Scarsdale, NY.
Abstract
- Objective: To describe a quality improvement initiative implemented by 2 home health care agencies to reduce readmissions.
- Methods: The agencies reviewed their data and identified best practices for reducing acute hospital transfers among their high-risk heart failure patients, focusing on the first 14 days of the care episode. Care intensity was increased during the first 3 days, and an active surveillance approach was used during the first 2 weeks. Training for staff, called “Heart Failure Boot Camp,” was introduced and made part of new employee orientation.
- Results: The 30-day rehospitalization rate was reduced from 31% to 17%.
- Conclusion: A data-driven transitional care model can lead to reductions in 30-day readmissions among high-risk patients receiving home health care.
Hospital readmissions are frequent, costly, and can be a marker of poorly coordinated postdischarge care [1]. Since the passage of the Affordable Care Act in 2010, reducing readmissions has become a national priority, as reflected in the emergence of accountable care organizations, bundled payments, and readmission penalties for hospitals, among other efforts. With the increasing attention on reducing readmissions, home health care agencies are under pressure to identify opportunities to improve performance. Two affiliated home health care agencies in Massachusetts and Connecticut made reducing their all-cause 30-day readmission rate a strategic priority. In this article, we describe their approach.
Setting
New England Home Care (NEHC, Cromwell, CT) is a regional agency that serves 7 of the 8 counties in Connecticut and over 7400 patients annually. Medical Resources Home Health (Newton, MA) is a regional agency that serves 8 of the 12 counties in Massachusetts and 2000 patients annually. These home health agencies are both owned by National Home Health Care Corporation (Scarsdale, NY) but are independently managed, with separate staff and regional market differences.
Data Analysis
Opportunities for Improvement The data analysis highlighted several immediate opportunities for improvement. First, the data showed that the first 3 days of the home health episode are a period of increased risk. Thus, intensification of care—and successful first contacts—during the first 3 days of the home health episode was an important target goal. Similarly, the first 14 days were a period of increased risk, suggesting the potential benefit of home health staff proactively monitoring patients during this time to identify clinical or other needs early in the effort to avert a hospitalization. In addition, while respiratory symptoms were among the top reasons for acute care hospitalization within 30 days of episode initiation, many other diagnoses were also implicated. Nine conditions comprised 80% of coded reasons for hospitalization, suggesting that vigilance around respiratory complaints is important but cannot be the exclusive focus of symptom management in this population.
Approach The agencies started this performance improvement initiative by focusing on one patient subgroup (heart failure patients) served by one of the agencies (NEHC). New approaches were tried, and effective approaches were codified through training, on-the job coaching, and performance feedback to front-line clinicians. This approach facilitated the spread of these changes to the second agency, and subsequently both agencies expanded their focus beyond heart failure to other common diagnoses in the home health population.
Changes to Standard Care Practices Based on identified opportunities for improvement, the agency incorporated modifications to standard care utilizing existing resources and within the construct of a certified Medicare home health episode (Medicare’s required specific services, assessments, and other activities that a home health agency must provide in order to bill for an episode). First, working with managers and front-line clinicians, they focused on establishing successful contact during the first 3 days of an episode of care. Front-line staff reported that some patients did not respond to the first attempt to establish contact, and staff thought that it indicated that the patient did not want home health care. The agency designed a new initial contact protocol to increase the likelihood of a successful first contact with the patient. Second, staff increased the frequency of contact in the first 3 days of the episode, either through home visits or phone calls. Increased contact served to allowed the home health staff to get to know the patient and have more points of reference upon which to identify whether symptoms were developing or changing. In addition, increase initial frequency served to increase the comfort and confidence that the patient and their family had in the agency. Third, in the context of increasing the frequency and effectiveness of contacts in the first 14 days, home care staff were trained to adopt an “active surveillance” approach. This staff development and re-training initiative instructed staff on practices to increase their awareness and recognition of patient needs or changing circumstances, outside the specific problem-defined focus area(s) of the home health episode. Frequent contact in the first 14 days creates an opportunity for home health staff to intervene proactively in the confusion or symptoms that lead patients or their families to call 911. Fourth, home care staff received professional development training specifically focused on heart failure, called “Heart Failure Boot Camp.” This training provided a review and update on the clinical management best practices for home care for heart failure patients. This training was conducted by the agency’s staff clinical educator at each local field office. Once all the agencies’ existing staff were trained, the training materials were included in new employee orientation. Rate of acute care hospitalizations was tracked and reports were provided to each local field office on a quarterly basis. Agency leadership included review of these data with local field office managers in their existing management meetings to reinforce the importance of this initiative for the agency at the highest levels. As the efforts to reduce hospitalizations evolved to include patients with conditions other than heart failure, the agencies developed a readmission risk assessment that included the number of medications ( < 5; 6–10; 11–15; 16–20; or > 20) and number of hospitalizations within the past 12 months. Staff could act upon the risk elements identified to reduce each individual patient’s risk of readmission.
Adding Enhanced Service to Standard Care: The Transitional Care Liaison
ollowing the implementation of the above changes to standard home health care practices, the agencies subsequently deployed full-time transitional care liaisons at local hospitals. This was a new role, requiring newly dedicated resources for the position. The role is modeled upon the Care Transitions Intervention [2],which emphasizes the value of initiating transitional care during the hospitalization. In this new role, the hospital-based home care liaisons establish a relationship with the patient, schedule immediate follow-up, review medications and the plan to obtain new medications, and review the plan of care in the hospital, prior to the transition home. On-site transitional care liaisons greatly facilitate clinical collaboration, allowing the “receiving” provider to request clarifications prior to discharge. On-site relationships also enable formal and informal mutual improvements in the transition process. An unanticipated benefit to this collaboration is that the agencies are able to identify some high-utilizing patients who are served by several area hospitals. Thus the agencies were able to add to the list of highest-risk patients for some hospitals that were otherwise unidentified.
Outcomes
The 30-day rehospitalization rate for NEHC was 31% during the baseline period (9/30/2008 to 6/30/2010). The quarterly variability in readmission rates was high, ranging from 20% to 42% in any given quarter. Following the start of the performance improvement initiative in Quarter 3 of 2010, and through the most recent quarter for which data are available (Quarter 3 2013) the quarterly 30-day readmission rates demonstrated decreased variability (15% to 22%) and the 30-day readmission rate was reduced to 17%—a 45% reduction in rehospitalizations. The agencies’ rehospitalization rates are lower than local benchmarks [1].
Lessons Learned
The agencies experience with this initiative has led to several lessons learned that may be of interest to other agencies and providers looking to design and implement care models to reduce rehospitalizations.
First, it was essential to supplement our knowledge of best practices from the literature and industry experts with an examination of our own data. In addition to examining rates of rehospitalization, we were able to identify patients at highest risk so we could intensify services early for this group.
Second, the 2 agencies participating in this effort are affiliated but independently managed, with separate staff and regional market differences. We were pleased to learn that a common service delivery model could be successfully implemented in both agencies. This suggests that this structured care delivery improvement approach can be replicated in other organizations and local contexts.
Third, by no means was the staff development and retraining a “one and done” effort; continuous reinforcement of the rationale for the practice change and the protocols for optimizing engagement to reduce rehospitalizations was required.
Finally, the performance improvement initiative started with an initial focus on heart failure patients. Over the course of the Initiative we named the series of practice changes our “Healthy@Home” model of care. As we expanded our focus to all patients at high risk of readmission (as identified by our risk assessment score), we learned that staff thought the Healthy@Home practice changes only applied to heart failure patients. This required re-messaging with the staff and regional supervisors.
Conclusion
As rehospitalizations continue to be a prominent measure of quality, cost, and patient experience and a measure for which hospitals and post-acute and community-based providers are either penalized or rewarded, there is a growing awareness of the many factors outside the walls of the hospital that determine whether a patient will return within a defined period of time. Many home health agencies see this as an opportune moment to highlight the critical role they play in care transitions across settings and over time. In this article, we describe the experience of 2 affiliated regional home health care agencies as they engaged in a structured performance improvement effort to reduce readmissions among their high-risk patients. This effort involving data analysis, identification of locally relevant opportunities for improvement, modifications to standard care utilizing existing resources, adding a new service, and expansion beyond the initial target population to all patients at high risk of readmission. This 3-year effort has resulted in a substantial and sustained reduction in rehospitalization rates.
From Collaborative Healthcare Strategies, Lexington, MA (Dr. Boutwell), and the National Home Health Corporation, Scarsdale, NY.
Abstract
- Objective: To describe a quality improvement initiative implemented by 2 home health care agencies to reduce readmissions.
- Methods: The agencies reviewed their data and identified best practices for reducing acute hospital transfers among their high-risk heart failure patients, focusing on the first 14 days of the care episode. Care intensity was increased during the first 3 days, and an active surveillance approach was used during the first 2 weeks. Training for staff, called “Heart Failure Boot Camp,” was introduced and made part of new employee orientation.
- Results: The 30-day rehospitalization rate was reduced from 31% to 17%.
- Conclusion: A data-driven transitional care model can lead to reductions in 30-day readmissions among high-risk patients receiving home health care.
Hospital readmissions are frequent, costly, and can be a marker of poorly coordinated postdischarge care [1]. Since the passage of the Affordable Care Act in 2010, reducing readmissions has become a national priority, as reflected in the emergence of accountable care organizations, bundled payments, and readmission penalties for hospitals, among other efforts. With the increasing attention on reducing readmissions, home health care agencies are under pressure to identify opportunities to improve performance. Two affiliated home health care agencies in Massachusetts and Connecticut made reducing their all-cause 30-day readmission rate a strategic priority. In this article, we describe their approach.
Setting
New England Home Care (NEHC, Cromwell, CT) is a regional agency that serves 7 of the 8 counties in Connecticut and over 7400 patients annually. Medical Resources Home Health (Newton, MA) is a regional agency that serves 8 of the 12 counties in Massachusetts and 2000 patients annually. These home health agencies are both owned by National Home Health Care Corporation (Scarsdale, NY) but are independently managed, with separate staff and regional market differences.
Data Analysis
Opportunities for Improvement The data analysis highlighted several immediate opportunities for improvement. First, the data showed that the first 3 days of the home health episode are a period of increased risk. Thus, intensification of care—and successful first contacts—during the first 3 days of the home health episode was an important target goal. Similarly, the first 14 days were a period of increased risk, suggesting the potential benefit of home health staff proactively monitoring patients during this time to identify clinical or other needs early in the effort to avert a hospitalization. In addition, while respiratory symptoms were among the top reasons for acute care hospitalization within 30 days of episode initiation, many other diagnoses were also implicated. Nine conditions comprised 80% of coded reasons for hospitalization, suggesting that vigilance around respiratory complaints is important but cannot be the exclusive focus of symptom management in this population.
Approach The agencies started this performance improvement initiative by focusing on one patient subgroup (heart failure patients) served by one of the agencies (NEHC). New approaches were tried, and effective approaches were codified through training, on-the job coaching, and performance feedback to front-line clinicians. This approach facilitated the spread of these changes to the second agency, and subsequently both agencies expanded their focus beyond heart failure to other common diagnoses in the home health population.
Changes to Standard Care Practices Based on identified opportunities for improvement, the agency incorporated modifications to standard care utilizing existing resources and within the construct of a certified Medicare home health episode (Medicare’s required specific services, assessments, and other activities that a home health agency must provide in order to bill for an episode). First, working with managers and front-line clinicians, they focused on establishing successful contact during the first 3 days of an episode of care. Front-line staff reported that some patients did not respond to the first attempt to establish contact, and staff thought that it indicated that the patient did not want home health care. The agency designed a new initial contact protocol to increase the likelihood of a successful first contact with the patient. Second, staff increased the frequency of contact in the first 3 days of the episode, either through home visits or phone calls. Increased contact served to allowed the home health staff to get to know the patient and have more points of reference upon which to identify whether symptoms were developing or changing. In addition, increase initial frequency served to increase the comfort and confidence that the patient and their family had in the agency. Third, in the context of increasing the frequency and effectiveness of contacts in the first 14 days, home care staff were trained to adopt an “active surveillance” approach. This staff development and re-training initiative instructed staff on practices to increase their awareness and recognition of patient needs or changing circumstances, outside the specific problem-defined focus area(s) of the home health episode. Frequent contact in the first 14 days creates an opportunity for home health staff to intervene proactively in the confusion or symptoms that lead patients or their families to call 911. Fourth, home care staff received professional development training specifically focused on heart failure, called “Heart Failure Boot Camp.” This training provided a review and update on the clinical management best practices for home care for heart failure patients. This training was conducted by the agency’s staff clinical educator at each local field office. Once all the agencies’ existing staff were trained, the training materials were included in new employee orientation. Rate of acute care hospitalizations was tracked and reports were provided to each local field office on a quarterly basis. Agency leadership included review of these data with local field office managers in their existing management meetings to reinforce the importance of this initiative for the agency at the highest levels. As the efforts to reduce hospitalizations evolved to include patients with conditions other than heart failure, the agencies developed a readmission risk assessment that included the number of medications ( < 5; 6–10; 11–15; 16–20; or > 20) and number of hospitalizations within the past 12 months. Staff could act upon the risk elements identified to reduce each individual patient’s risk of readmission.
Adding Enhanced Service to Standard Care: The Transitional Care Liaison
ollowing the implementation of the above changes to standard home health care practices, the agencies subsequently deployed full-time transitional care liaisons at local hospitals. This was a new role, requiring newly dedicated resources for the position. The role is modeled upon the Care Transitions Intervention [2],which emphasizes the value of initiating transitional care during the hospitalization. In this new role, the hospital-based home care liaisons establish a relationship with the patient, schedule immediate follow-up, review medications and the plan to obtain new medications, and review the plan of care in the hospital, prior to the transition home. On-site transitional care liaisons greatly facilitate clinical collaboration, allowing the “receiving” provider to request clarifications prior to discharge. On-site relationships also enable formal and informal mutual improvements in the transition process. An unanticipated benefit to this collaboration is that the agencies are able to identify some high-utilizing patients who are served by several area hospitals. Thus the agencies were able to add to the list of highest-risk patients for some hospitals that were otherwise unidentified.
Outcomes
The 30-day rehospitalization rate for NEHC was 31% during the baseline period (9/30/2008 to 6/30/2010). The quarterly variability in readmission rates was high, ranging from 20% to 42% in any given quarter. Following the start of the performance improvement initiative in Quarter 3 of 2010, and through the most recent quarter for which data are available (Quarter 3 2013) the quarterly 30-day readmission rates demonstrated decreased variability (15% to 22%) and the 30-day readmission rate was reduced to 17%—a 45% reduction in rehospitalizations. The agencies’ rehospitalization rates are lower than local benchmarks [1].
Lessons Learned
The agencies experience with this initiative has led to several lessons learned that may be of interest to other agencies and providers looking to design and implement care models to reduce rehospitalizations.
First, it was essential to supplement our knowledge of best practices from the literature and industry experts with an examination of our own data. In addition to examining rates of rehospitalization, we were able to identify patients at highest risk so we could intensify services early for this group.
Second, the 2 agencies participating in this effort are affiliated but independently managed, with separate staff and regional market differences. We were pleased to learn that a common service delivery model could be successfully implemented in both agencies. This suggests that this structured care delivery improvement approach can be replicated in other organizations and local contexts.
Third, by no means was the staff development and retraining a “one and done” effort; continuous reinforcement of the rationale for the practice change and the protocols for optimizing engagement to reduce rehospitalizations was required.
Finally, the performance improvement initiative started with an initial focus on heart failure patients. Over the course of the Initiative we named the series of practice changes our “Healthy@Home” model of care. As we expanded our focus to all patients at high risk of readmission (as identified by our risk assessment score), we learned that staff thought the Healthy@Home practice changes only applied to heart failure patients. This required re-messaging with the staff and regional supervisors.
Conclusion
As rehospitalizations continue to be a prominent measure of quality, cost, and patient experience and a measure for which hospitals and post-acute and community-based providers are either penalized or rewarded, there is a growing awareness of the many factors outside the walls of the hospital that determine whether a patient will return within a defined period of time. Many home health agencies see this as an opportune moment to highlight the critical role they play in care transitions across settings and over time. In this article, we describe the experience of 2 affiliated regional home health care agencies as they engaged in a structured performance improvement effort to reduce readmissions among their high-risk patients. This effort involving data analysis, identification of locally relevant opportunities for improvement, modifications to standard care utilizing existing resources, adding a new service, and expansion beyond the initial target population to all patients at high risk of readmission. This 3-year effort has resulted in a substantial and sustained reduction in rehospitalization rates.
1. Masspro, Massachusetts’ Quality Improvement Organization. State of the state: readmissions in Massachusetts January 1 2009-September 30 2013. Accessed 14 April 2014 at www.masspro.org/files/tools/12_13_state_of_the_state.pdf.
2. Coleman EA, Parry C, Chalmers S, Min S. The care transitions intervention. Arch Intern Med 2006;166:1822–8.
1. Masspro, Massachusetts’ Quality Improvement Organization. State of the state: readmissions in Massachusetts January 1 2009-September 30 2013. Accessed 14 April 2014 at www.masspro.org/files/tools/12_13_state_of_the_state.pdf.
2. Coleman EA, Parry C, Chalmers S, Min S. The care transitions intervention. Arch Intern Med 2006;166:1822–8.
Young girl with lower leg rash
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.

English Ability and Glycemic Control in Latinos with Diabetes
Study Overview
Objective. To determine if there is an association between self-reported English language ability and glycemic control in Latinos with type 2 diabetes.
Design. Descriptive correlational study using data from a larger cross-sectional study.
Setting and participants. 167 adults with diabetes who self-identified as Latino or Hispanic recruited at clinics in the Chicago area from May 2004 to May 2006. The dataset was collected using face-to-face interviews with diabetic patients aged ≥ 18 years. All participants attended clinics affiliated with an academic medical center or physician offices affiliated with a suburban hospital. Patients with type 1 diabetes and those with < 17 points on the Mini-Mental State Examination were excluded. English speaking ability was categorized as speaking English “not at all,” “not well,” “well,” or “very well” based on patient self-report. A multivariable logistic regression model was used to examine the predictive relationship between English language skills and HbA1c levels, with covariates selected if they were significantly correlated with English language ability. The final regression model accounted for age, sex, education, annual income, health insurance status, duration of diabetes, birth in the United States, and years in the United States.
Main outcome measure. HbA1c ≥ 7.0% as captured by chart review.
Main results. Of the 167 patients, 38% reported speaking English very well, 21% reported speaking well, 26% reported speaking not very well, and 14% did not speak English at all. Reflecting immigration-sensitive patterns, patients who spoke English very well were younger and more likely to have graduated high school and have an annual income over $25,000 per year. Comorbidities and complications did not differ by English speaking ability except for diabetic eye disease, which was was more prevalent among those who did not speak English at all (42%, p = 0.04). Whether speaking ability was treated as a continuous or dichotomous variable, HbA1c levels formed a U-shaped curve: those who spoke English very well (odds ratio [OR] 2.32, 95% CI, 1.00–5.41) or not at all (OR 4.11, 95% CI 1.35–12.54) had higher odds of having an elevated HbA1c than those who spoke English well, although this was only statistically significant for those who spoke no English. In adjusted analyses, the U-shaped curve persisted with the highest odds among those who spoke English very well (OR 3.20, 95% CI 1.05–9.79) or not at all (OR 4.95, 95% CI 1.29–18.92).
Conclusion. The relationship between English speaking ability and diabetes management is more complex than previously described. Interventions aimed at improving diabetes outcomes may need to be tailored to specific subgroups within the Latino population.
Commentary
Immigrant health is complex and language is an understudied factor in health transitions of those who migrate for new lives or temporary work. For Latinos, migration abroad was once thought to improve health, but a recent systematic review by Teruya et al [1] suggests that the migration experience has a wide variety of effects on health, many of which can be negative.
The notion that English fluency confers health care benefits is questionable, as the authors state. Those unfamiliar with the acculturation literature might think that English speaking ability is a good marker of acculturation, but recent research on the subject suggests otherwise. Acculturation is a complex phenomenon that cannot be measured or gauged by a single variable [2–5]. Among the many factors influencing acculturation, the migration experience and country of origin will play a major role in acculturation and how it occurs in the arrival country. Health care providers seeking to understand the complexity of acculturation better to improve care for their immigrant patients would benefit from examining the extensive social science literature on the subject. The results of this study suggest that providers should not take for granted someone’s English speaking ability as a marker of acculturation and thus assume that their health outcomes would be equivalent to native born populations.
This study has number of weaknesses. The main concern is that the study did not consider a number of important health service delivery factors. The researchers did not assess for the number of visits the patient had with appropriate interpretation services, whether or not there were language concordant visits between patients and providers (limited English proficiency patients are more likely to form consistent service relationships with language concordant providers [6–10]), or whether the patient had diabetes education classes or individual counseling sessions to facilitate self-management. These service-based factors could potentially explain some of the results seen. The small sample size, age of the data in the study, and failure to distinguish the country of origin of the Latino patients are other weaknesses.
Applications for Clinical Practice
Providers can improve their clinical practice with limited English proficiency Latino patients with diabetes by being more sensitive to the potential effects of language on diabetes outcomes in this population. The results suggest that providers should not assume that a Latino patient’s English language skills mean that they are better at self-managing their diabetes and will have better outcomes. Asking patients about their country of origin and migration experiences may help differentiate the effects of language in concert with other potentially confounding variables that can help elucidate the effects of language on diabetes related outcomes.
—Allison Squires, PhD, RN
1. Teruya SA, Bazargan-Hejazi S. The immigrant and Hispanic paradoxes: a systematic review of their predictions and effects. Hisp J Behav Sci 2013 Sep 5;35:486–509.
2. Rudmin FW. Phenomenology of acculturation: retrospective reports from the Philippines, Japan, Quebec, and Norway. Cult Psychol 2010;16:313–32.
3. Matsunaga M, Hecht ML, Elek E, Ndiaye K. Ethnic identity development and acculturation: a longitudinal analysis of Mexican-heritage youth in the Southwest United States. J Cross Cult Psychol 2010;41:410–27.
4. Siatkowski A. Hispanic acculturation: a concept analysis. J Transcult Nurs 2007;18:316–23.
5. Horevitz E, Organista KC. The Mexican health paradox: expanding the explanatory power of the acculturation construct. Hisp J Behav Sci 2012;35:3–34.
6. Gany F, Leng J, Shapiro E, et al. Patient satisfaction with different interpreting methods: a randomized controlled trial. J Gen Intern Med 2007;22 Suppl 2:312–8.
7. Grover A, Deakyne S, Bajaj L, Roosevelt GE. Comparison of throughput times for limited English proficiency patient visits in the emergency department between different interpreter modalities. J Immigr Minor Health 2012;14:602–7.
8. Ngo-Metzger Q, Sorkin DH, Phillips RS, et al. Providing high-quality care for limited English proficient patients: the importance of language concordance and interpreter use. J Gen Intern Med 2007;22 Suppl 2:324–30.
9. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
10. Arauz Boudreau AD, Fluet CF, Reuland CP, et al. Associations of providers’ language and cultural skills with Latino parents’ perceptions of well-child care. Acad Pediatr 2010;10:172–8.
Study Overview
Objective. To determine if there is an association between self-reported English language ability and glycemic control in Latinos with type 2 diabetes.
Design. Descriptive correlational study using data from a larger cross-sectional study.
Setting and participants. 167 adults with diabetes who self-identified as Latino or Hispanic recruited at clinics in the Chicago area from May 2004 to May 2006. The dataset was collected using face-to-face interviews with diabetic patients aged ≥ 18 years. All participants attended clinics affiliated with an academic medical center or physician offices affiliated with a suburban hospital. Patients with type 1 diabetes and those with < 17 points on the Mini-Mental State Examination were excluded. English speaking ability was categorized as speaking English “not at all,” “not well,” “well,” or “very well” based on patient self-report. A multivariable logistic regression model was used to examine the predictive relationship between English language skills and HbA1c levels, with covariates selected if they were significantly correlated with English language ability. The final regression model accounted for age, sex, education, annual income, health insurance status, duration of diabetes, birth in the United States, and years in the United States.
Main outcome measure. HbA1c ≥ 7.0% as captured by chart review.
Main results. Of the 167 patients, 38% reported speaking English very well, 21% reported speaking well, 26% reported speaking not very well, and 14% did not speak English at all. Reflecting immigration-sensitive patterns, patients who spoke English very well were younger and more likely to have graduated high school and have an annual income over $25,000 per year. Comorbidities and complications did not differ by English speaking ability except for diabetic eye disease, which was was more prevalent among those who did not speak English at all (42%, p = 0.04). Whether speaking ability was treated as a continuous or dichotomous variable, HbA1c levels formed a U-shaped curve: those who spoke English very well (odds ratio [OR] 2.32, 95% CI, 1.00–5.41) or not at all (OR 4.11, 95% CI 1.35–12.54) had higher odds of having an elevated HbA1c than those who spoke English well, although this was only statistically significant for those who spoke no English. In adjusted analyses, the U-shaped curve persisted with the highest odds among those who spoke English very well (OR 3.20, 95% CI 1.05–9.79) or not at all (OR 4.95, 95% CI 1.29–18.92).
Conclusion. The relationship between English speaking ability and diabetes management is more complex than previously described. Interventions aimed at improving diabetes outcomes may need to be tailored to specific subgroups within the Latino population.
Commentary
Immigrant health is complex and language is an understudied factor in health transitions of those who migrate for new lives or temporary work. For Latinos, migration abroad was once thought to improve health, but a recent systematic review by Teruya et al [1] suggests that the migration experience has a wide variety of effects on health, many of which can be negative.
The notion that English fluency confers health care benefits is questionable, as the authors state. Those unfamiliar with the acculturation literature might think that English speaking ability is a good marker of acculturation, but recent research on the subject suggests otherwise. Acculturation is a complex phenomenon that cannot be measured or gauged by a single variable [2–5]. Among the many factors influencing acculturation, the migration experience and country of origin will play a major role in acculturation and how it occurs in the arrival country. Health care providers seeking to understand the complexity of acculturation better to improve care for their immigrant patients would benefit from examining the extensive social science literature on the subject. The results of this study suggest that providers should not take for granted someone’s English speaking ability as a marker of acculturation and thus assume that their health outcomes would be equivalent to native born populations.
This study has number of weaknesses. The main concern is that the study did not consider a number of important health service delivery factors. The researchers did not assess for the number of visits the patient had with appropriate interpretation services, whether or not there were language concordant visits between patients and providers (limited English proficiency patients are more likely to form consistent service relationships with language concordant providers [6–10]), or whether the patient had diabetes education classes or individual counseling sessions to facilitate self-management. These service-based factors could potentially explain some of the results seen. The small sample size, age of the data in the study, and failure to distinguish the country of origin of the Latino patients are other weaknesses.
Applications for Clinical Practice
Providers can improve their clinical practice with limited English proficiency Latino patients with diabetes by being more sensitive to the potential effects of language on diabetes outcomes in this population. The results suggest that providers should not assume that a Latino patient’s English language skills mean that they are better at self-managing their diabetes and will have better outcomes. Asking patients about their country of origin and migration experiences may help differentiate the effects of language in concert with other potentially confounding variables that can help elucidate the effects of language on diabetes related outcomes.
—Allison Squires, PhD, RN
Study Overview
Objective. To determine if there is an association between self-reported English language ability and glycemic control in Latinos with type 2 diabetes.
Design. Descriptive correlational study using data from a larger cross-sectional study.
Setting and participants. 167 adults with diabetes who self-identified as Latino or Hispanic recruited at clinics in the Chicago area from May 2004 to May 2006. The dataset was collected using face-to-face interviews with diabetic patients aged ≥ 18 years. All participants attended clinics affiliated with an academic medical center or physician offices affiliated with a suburban hospital. Patients with type 1 diabetes and those with < 17 points on the Mini-Mental State Examination were excluded. English speaking ability was categorized as speaking English “not at all,” “not well,” “well,” or “very well” based on patient self-report. A multivariable logistic regression model was used to examine the predictive relationship between English language skills and HbA1c levels, with covariates selected if they were significantly correlated with English language ability. The final regression model accounted for age, sex, education, annual income, health insurance status, duration of diabetes, birth in the United States, and years in the United States.
Main outcome measure. HbA1c ≥ 7.0% as captured by chart review.
Main results. Of the 167 patients, 38% reported speaking English very well, 21% reported speaking well, 26% reported speaking not very well, and 14% did not speak English at all. Reflecting immigration-sensitive patterns, patients who spoke English very well were younger and more likely to have graduated high school and have an annual income over $25,000 per year. Comorbidities and complications did not differ by English speaking ability except for diabetic eye disease, which was was more prevalent among those who did not speak English at all (42%, p = 0.04). Whether speaking ability was treated as a continuous or dichotomous variable, HbA1c levels formed a U-shaped curve: those who spoke English very well (odds ratio [OR] 2.32, 95% CI, 1.00–5.41) or not at all (OR 4.11, 95% CI 1.35–12.54) had higher odds of having an elevated HbA1c than those who spoke English well, although this was only statistically significant for those who spoke no English. In adjusted analyses, the U-shaped curve persisted with the highest odds among those who spoke English very well (OR 3.20, 95% CI 1.05–9.79) or not at all (OR 4.95, 95% CI 1.29–18.92).
Conclusion. The relationship between English speaking ability and diabetes management is more complex than previously described. Interventions aimed at improving diabetes outcomes may need to be tailored to specific subgroups within the Latino population.
Commentary
Immigrant health is complex and language is an understudied factor in health transitions of those who migrate for new lives or temporary work. For Latinos, migration abroad was once thought to improve health, but a recent systematic review by Teruya et al [1] suggests that the migration experience has a wide variety of effects on health, many of which can be negative.
The notion that English fluency confers health care benefits is questionable, as the authors state. Those unfamiliar with the acculturation literature might think that English speaking ability is a good marker of acculturation, but recent research on the subject suggests otherwise. Acculturation is a complex phenomenon that cannot be measured or gauged by a single variable [2–5]. Among the many factors influencing acculturation, the migration experience and country of origin will play a major role in acculturation and how it occurs in the arrival country. Health care providers seeking to understand the complexity of acculturation better to improve care for their immigrant patients would benefit from examining the extensive social science literature on the subject. The results of this study suggest that providers should not take for granted someone’s English speaking ability as a marker of acculturation and thus assume that their health outcomes would be equivalent to native born populations.
This study has number of weaknesses. The main concern is that the study did not consider a number of important health service delivery factors. The researchers did not assess for the number of visits the patient had with appropriate interpretation services, whether or not there were language concordant visits between patients and providers (limited English proficiency patients are more likely to form consistent service relationships with language concordant providers [6–10]), or whether the patient had diabetes education classes or individual counseling sessions to facilitate self-management. These service-based factors could potentially explain some of the results seen. The small sample size, age of the data in the study, and failure to distinguish the country of origin of the Latino patients are other weaknesses.
Applications for Clinical Practice
Providers can improve their clinical practice with limited English proficiency Latino patients with diabetes by being more sensitive to the potential effects of language on diabetes outcomes in this population. The results suggest that providers should not assume that a Latino patient’s English language skills mean that they are better at self-managing their diabetes and will have better outcomes. Asking patients about their country of origin and migration experiences may help differentiate the effects of language in concert with other potentially confounding variables that can help elucidate the effects of language on diabetes related outcomes.
—Allison Squires, PhD, RN
1. Teruya SA, Bazargan-Hejazi S. The immigrant and Hispanic paradoxes: a systematic review of their predictions and effects. Hisp J Behav Sci 2013 Sep 5;35:486–509.
2. Rudmin FW. Phenomenology of acculturation: retrospective reports from the Philippines, Japan, Quebec, and Norway. Cult Psychol 2010;16:313–32.
3. Matsunaga M, Hecht ML, Elek E, Ndiaye K. Ethnic identity development and acculturation: a longitudinal analysis of Mexican-heritage youth in the Southwest United States. J Cross Cult Psychol 2010;41:410–27.
4. Siatkowski A. Hispanic acculturation: a concept analysis. J Transcult Nurs 2007;18:316–23.
5. Horevitz E, Organista KC. The Mexican health paradox: expanding the explanatory power of the acculturation construct. Hisp J Behav Sci 2012;35:3–34.
6. Gany F, Leng J, Shapiro E, et al. Patient satisfaction with different interpreting methods: a randomized controlled trial. J Gen Intern Med 2007;22 Suppl 2:312–8.
7. Grover A, Deakyne S, Bajaj L, Roosevelt GE. Comparison of throughput times for limited English proficiency patient visits in the emergency department between different interpreter modalities. J Immigr Minor Health 2012;14:602–7.
8. Ngo-Metzger Q, Sorkin DH, Phillips RS, et al. Providing high-quality care for limited English proficient patients: the importance of language concordance and interpreter use. J Gen Intern Med 2007;22 Suppl 2:324–30.
9. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
10. Arauz Boudreau AD, Fluet CF, Reuland CP, et al. Associations of providers’ language and cultural skills with Latino parents’ perceptions of well-child care. Acad Pediatr 2010;10:172–8.
1. Teruya SA, Bazargan-Hejazi S. The immigrant and Hispanic paradoxes: a systematic review of their predictions and effects. Hisp J Behav Sci 2013 Sep 5;35:486–509.
2. Rudmin FW. Phenomenology of acculturation: retrospective reports from the Philippines, Japan, Quebec, and Norway. Cult Psychol 2010;16:313–32.
3. Matsunaga M, Hecht ML, Elek E, Ndiaye K. Ethnic identity development and acculturation: a longitudinal analysis of Mexican-heritage youth in the Southwest United States. J Cross Cult Psychol 2010;41:410–27.
4. Siatkowski A. Hispanic acculturation: a concept analysis. J Transcult Nurs 2007;18:316–23.
5. Horevitz E, Organista KC. The Mexican health paradox: expanding the explanatory power of the acculturation construct. Hisp J Behav Sci 2012;35:3–34.
6. Gany F, Leng J, Shapiro E, et al. Patient satisfaction with different interpreting methods: a randomized controlled trial. J Gen Intern Med 2007;22 Suppl 2:312–8.
7. Grover A, Deakyne S, Bajaj L, Roosevelt GE. Comparison of throughput times for limited English proficiency patient visits in the emergency department between different interpreter modalities. J Immigr Minor Health 2012;14:602–7.
8. Ngo-Metzger Q, Sorkin DH, Phillips RS, et al. Providing high-quality care for limited English proficient patients: the importance of language concordance and interpreter use. J Gen Intern Med 2007;22 Suppl 2:324–30.
9. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
10. Arauz Boudreau AD, Fluet CF, Reuland CP, et al. Associations of providers’ language and cultural skills with Latino parents’ perceptions of well-child care. Acad Pediatr 2010;10:172–8.
Skip the compression stockings following DVT
Do not recommend elastic compression stockings (ECS) to decrease the incidence of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).1
Strength of recommendation
B: Based on a large, randomized controlled trial
Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
Illustrative case
A 56-year-old man comes to your clinic 3 days after receiving a diagnosis of lower extremity deep vein thrombosis (DVT). He was prescribed warfarin, 5 mg/d, with enoxaparin bridging, 120 mg/d. He has read about post-thrombotic syndrome (PTS) online and is very concerned about this possible side effect. He is asking about using elastic compression stockings (ECS). What should you tell him?
PTS can be a frustrating, debilitating condition. Its clinical features range from minor limb swelling to severe edema and pain, irreversible skin changes, and leg ulcerations.2 It occurs in 25% to 50% of patients after DVT.3 Because current PTS treatments are not very effective, prevention is essential.4,5
Patients are frequently encouraged to wear ECS after DVT to reduce the incidence of PTS by reducing venous hypertension and reflux. These stockings are expensive and uncomfortable. Prior studies suggested that using ECS can cut the incidence of PTS in half.6,7 However, these were small, single-center studies, and they were not placebo-controlled.6,7
STUDY SUMMARY: RCT sets aside a common practice
Kahn et al1 conducted a randomized, placebo-controlled trial of active vs placebo ECS in patients from 24 centers in the United States and Canada who’d had an ultrasound-confirmed proximal DVT (in the popliteal or more proximal deep leg vein) within the previous 14 days. Most patients received standard anticoagulation therapy to treat their DVT (5-10 days of heparin and 3-6 months of warfarin). Patients were excluded if they had received thrombolytics, had arterial claudication, had a life expectancy of <6 months, were unable to put on ECS due to physical disabilities or allergy, or were unable to participate in follow-up visits.
Patients were randomly assigned to wear active (30-40 mm Hg graduated) ECS or identical-looking placebo ECS with <5 mm Hg compression at the ankle for 2 years. Providers, study personnel and statisticians, and patients were all blinded to treatment allocation. Patients were asked to wear the stocking on the affected leg each day from when they woke until they went to bed.
Participants were followed at one, 6, 12, 18, and 24 months. The primary outcome was the cumulative incidence of PTS diagnosed at 6 months or later using Ginsberg’s criteria of ipsilateral pain and swelling of at least 1 month’s duration.8 Secondary outcomes included severity of PTS, presence of leg ulcers, recurrence of venous thromboembolism (VTE), death, adverse events, venous valvular reflux, and quality of life (QOL). Outcomes were measured objectively using a validated scale (the Villalta scale) for PTS severity and the 36-item Short Form Health Survey (SF-36) and the Venous Insufficiency Epidemiological and Economic Study Quality of Life (VEINES-QOL) questionnaire to measure QOL.9-11
There were 409 patients in the ECS group and 394 in the placebo group. Baseline characteristics, including body mass index (BMI), VTE risk factors, and anticoagulation treatment regimens, were similar between groups. The average age was 55.4 years in the study group (standard deviation [SD] ± 15.3 years) and 54.8 years (SD ± 15.8 years) in the place- bo group. Men comprised 62.4% of the active group and 57.9% of the placebo group. Approximately 90% of the participants in both groups were white.
At one month, approximately 95% of participants in both the active and placebo groups used the stockings; at 24 months, a little less than 70% of the participants in both groups continued to use the stockings. The percentage of people who used the stockings for at least 3 days a week was similar across both groups.
The cumulative incidence of PTS during follow-up was 14.2% in the active group vs 12.7% in the placebo group, with a hazard ratio of 1.13 (95% confidence interval [CI], .73-1.76; P=.58). There were no differences in any of the secondary outcomes. Prespecified subgroup analyses found that age, BMI, and severity of DVT had no effect on the outcomes. There was a marginal benefit for ECS for women (P=.047) over men, but this does not likely reflect a true difference because the CIs surrounding the hazard ratios for men and women overlapped and crossed the null value.
WHAT'S NEW: New evidence contradicts previous studies
Two prior studies showed that using 30 to 40 mm Hg ECS decreased the incidence of PTS after proximal DVT.6,7 However, these were smaller, open-label, single-center studies. This study by Kahn et al1 was the first placebo-controlled, randomized, multicenter study that used validated instruments to measure PTS and QOL. It found no benefit in using ECS, thus contradicting the results of the prior studies.
There are currently no guidelines or consensus statements for or against the use of ECS after DVT.
CAVEATS: High nonadherence rates might have affected the results
In both groups, adherence to the assigned intervention diminished throughout the study. Overall, approximately 95% of patients reported wearing their stockings at one month; this dropped to just under 70% by 2 years. Theoretically, this could have affected efficacy outcomes. However, the decrease was similar in both groups and represents what is observed in clinical practice. A prespecified per protocol analysis of patients who wore their ECS more regularly found no benefit.
It is possible that a “placebo effect” could explain the lack of difference between groups. However, the placebo stockings provided virtually no compression, and the 2-year cumulative incidence of PTS in both the treatment and placebo groups was similar to that seen in control groups in prior studies.6,7
Finally, the incidence of PTS in this study was much lower than the 25% to 50% incidence reported in previous studies. Kahn et al1 suggested that this was because they used more stringent and standardized criteria for PTS than was used in previous research.
CHALLENGES TO IMPLEMENTATION: There are no barriers to ending this practice
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
2. Kahn SR, Shrier I, Julian JA, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149:698-707.
3. Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125:1-7.
4. Cohen JM, Akl EA, Kahn SR. Pharmacologic and compression therapies for postthrombotic syndrome: a systematic review of randomized controlled trials. Chest. 2012;141:308-320.
5. Henke PK, Comerota AJ. An update on etiology, prevention, and therapy of postthrombotic syndrome. J Vasc Surg. 2011;53:500- 509.
6. Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
7. Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
8. Ginsberg JS, Hirsh J, Julian J, et al. Prevention and treatment of postphlebitic syndrome: results of a 3-part study. Arch Intern Med. 2001;161:2105-2109.
9. Villalta S, Bagatella P, Piccioli A, et al. Assessment of validity and reproducibility of a clinical scale for the post-thrombotic syndrome. Haemostasis. 1994;24:158a.
10. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31:247-263.
11. Kahn SR, Lamping DL, Ducruet T, et al; VETO Study Investigators. VEINES-QOL/Sym questionnaire was a reliable and valid disease-specific quality of life measure for deep venous thrombosis. J Clin Epidemiol. 2006;59:1049-1056.
Do not recommend elastic compression stockings (ECS) to decrease the incidence of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).1
Strength of recommendation
B: Based on a large, randomized controlled trial
Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
Illustrative case
A 56-year-old man comes to your clinic 3 days after receiving a diagnosis of lower extremity deep vein thrombosis (DVT). He was prescribed warfarin, 5 mg/d, with enoxaparin bridging, 120 mg/d. He has read about post-thrombotic syndrome (PTS) online and is very concerned about this possible side effect. He is asking about using elastic compression stockings (ECS). What should you tell him?
PTS can be a frustrating, debilitating condition. Its clinical features range from minor limb swelling to severe edema and pain, irreversible skin changes, and leg ulcerations.2 It occurs in 25% to 50% of patients after DVT.3 Because current PTS treatments are not very effective, prevention is essential.4,5
Patients are frequently encouraged to wear ECS after DVT to reduce the incidence of PTS by reducing venous hypertension and reflux. These stockings are expensive and uncomfortable. Prior studies suggested that using ECS can cut the incidence of PTS in half.6,7 However, these were small, single-center studies, and they were not placebo-controlled.6,7
STUDY SUMMARY: RCT sets aside a common practice
Kahn et al1 conducted a randomized, placebo-controlled trial of active vs placebo ECS in patients from 24 centers in the United States and Canada who’d had an ultrasound-confirmed proximal DVT (in the popliteal or more proximal deep leg vein) within the previous 14 days. Most patients received standard anticoagulation therapy to treat their DVT (5-10 days of heparin and 3-6 months of warfarin). Patients were excluded if they had received thrombolytics, had arterial claudication, had a life expectancy of <6 months, were unable to put on ECS due to physical disabilities or allergy, or were unable to participate in follow-up visits.
Patients were randomly assigned to wear active (30-40 mm Hg graduated) ECS or identical-looking placebo ECS with <5 mm Hg compression at the ankle for 2 years. Providers, study personnel and statisticians, and patients were all blinded to treatment allocation. Patients were asked to wear the stocking on the affected leg each day from when they woke until they went to bed.
Participants were followed at one, 6, 12, 18, and 24 months. The primary outcome was the cumulative incidence of PTS diagnosed at 6 months or later using Ginsberg’s criteria of ipsilateral pain and swelling of at least 1 month’s duration.8 Secondary outcomes included severity of PTS, presence of leg ulcers, recurrence of venous thromboembolism (VTE), death, adverse events, venous valvular reflux, and quality of life (QOL). Outcomes were measured objectively using a validated scale (the Villalta scale) for PTS severity and the 36-item Short Form Health Survey (SF-36) and the Venous Insufficiency Epidemiological and Economic Study Quality of Life (VEINES-QOL) questionnaire to measure QOL.9-11
There were 409 patients in the ECS group and 394 in the placebo group. Baseline characteristics, including body mass index (BMI), VTE risk factors, and anticoagulation treatment regimens, were similar between groups. The average age was 55.4 years in the study group (standard deviation [SD] ± 15.3 years) and 54.8 years (SD ± 15.8 years) in the place- bo group. Men comprised 62.4% of the active group and 57.9% of the placebo group. Approximately 90% of the participants in both groups were white.
At one month, approximately 95% of participants in both the active and placebo groups used the stockings; at 24 months, a little less than 70% of the participants in both groups continued to use the stockings. The percentage of people who used the stockings for at least 3 days a week was similar across both groups.
The cumulative incidence of PTS during follow-up was 14.2% in the active group vs 12.7% in the placebo group, with a hazard ratio of 1.13 (95% confidence interval [CI], .73-1.76; P=.58). There were no differences in any of the secondary outcomes. Prespecified subgroup analyses found that age, BMI, and severity of DVT had no effect on the outcomes. There was a marginal benefit for ECS for women (P=.047) over men, but this does not likely reflect a true difference because the CIs surrounding the hazard ratios for men and women overlapped and crossed the null value.
WHAT'S NEW: New evidence contradicts previous studies
Two prior studies showed that using 30 to 40 mm Hg ECS decreased the incidence of PTS after proximal DVT.6,7 However, these were smaller, open-label, single-center studies. This study by Kahn et al1 was the first placebo-controlled, randomized, multicenter study that used validated instruments to measure PTS and QOL. It found no benefit in using ECS, thus contradicting the results of the prior studies.
There are currently no guidelines or consensus statements for or against the use of ECS after DVT.
CAVEATS: High nonadherence rates might have affected the results
In both groups, adherence to the assigned intervention diminished throughout the study. Overall, approximately 95% of patients reported wearing their stockings at one month; this dropped to just under 70% by 2 years. Theoretically, this could have affected efficacy outcomes. However, the decrease was similar in both groups and represents what is observed in clinical practice. A prespecified per protocol analysis of patients who wore their ECS more regularly found no benefit.
It is possible that a “placebo effect” could explain the lack of difference between groups. However, the placebo stockings provided virtually no compression, and the 2-year cumulative incidence of PTS in both the treatment and placebo groups was similar to that seen in control groups in prior studies.6,7
Finally, the incidence of PTS in this study was much lower than the 25% to 50% incidence reported in previous studies. Kahn et al1 suggested that this was because they used more stringent and standardized criteria for PTS than was used in previous research.
CHALLENGES TO IMPLEMENTATION: There are no barriers to ending this practice
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Do not recommend elastic compression stockings (ECS) to decrease the incidence of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).1
Strength of recommendation
B: Based on a large, randomized controlled trial
Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
Illustrative case
A 56-year-old man comes to your clinic 3 days after receiving a diagnosis of lower extremity deep vein thrombosis (DVT). He was prescribed warfarin, 5 mg/d, with enoxaparin bridging, 120 mg/d. He has read about post-thrombotic syndrome (PTS) online and is very concerned about this possible side effect. He is asking about using elastic compression stockings (ECS). What should you tell him?
PTS can be a frustrating, debilitating condition. Its clinical features range from minor limb swelling to severe edema and pain, irreversible skin changes, and leg ulcerations.2 It occurs in 25% to 50% of patients after DVT.3 Because current PTS treatments are not very effective, prevention is essential.4,5
Patients are frequently encouraged to wear ECS after DVT to reduce the incidence of PTS by reducing venous hypertension and reflux. These stockings are expensive and uncomfortable. Prior studies suggested that using ECS can cut the incidence of PTS in half.6,7 However, these were small, single-center studies, and they were not placebo-controlled.6,7
STUDY SUMMARY: RCT sets aside a common practice
Kahn et al1 conducted a randomized, placebo-controlled trial of active vs placebo ECS in patients from 24 centers in the United States and Canada who’d had an ultrasound-confirmed proximal DVT (in the popliteal or more proximal deep leg vein) within the previous 14 days. Most patients received standard anticoagulation therapy to treat their DVT (5-10 days of heparin and 3-6 months of warfarin). Patients were excluded if they had received thrombolytics, had arterial claudication, had a life expectancy of <6 months, were unable to put on ECS due to physical disabilities or allergy, or were unable to participate in follow-up visits.
Patients were randomly assigned to wear active (30-40 mm Hg graduated) ECS or identical-looking placebo ECS with <5 mm Hg compression at the ankle for 2 years. Providers, study personnel and statisticians, and patients were all blinded to treatment allocation. Patients were asked to wear the stocking on the affected leg each day from when they woke until they went to bed.
Participants were followed at one, 6, 12, 18, and 24 months. The primary outcome was the cumulative incidence of PTS diagnosed at 6 months or later using Ginsberg’s criteria of ipsilateral pain and swelling of at least 1 month’s duration.8 Secondary outcomes included severity of PTS, presence of leg ulcers, recurrence of venous thromboembolism (VTE), death, adverse events, venous valvular reflux, and quality of life (QOL). Outcomes were measured objectively using a validated scale (the Villalta scale) for PTS severity and the 36-item Short Form Health Survey (SF-36) and the Venous Insufficiency Epidemiological and Economic Study Quality of Life (VEINES-QOL) questionnaire to measure QOL.9-11
There were 409 patients in the ECS group and 394 in the placebo group. Baseline characteristics, including body mass index (BMI), VTE risk factors, and anticoagulation treatment regimens, were similar between groups. The average age was 55.4 years in the study group (standard deviation [SD] ± 15.3 years) and 54.8 years (SD ± 15.8 years) in the place- bo group. Men comprised 62.4% of the active group and 57.9% of the placebo group. Approximately 90% of the participants in both groups were white.
At one month, approximately 95% of participants in both the active and placebo groups used the stockings; at 24 months, a little less than 70% of the participants in both groups continued to use the stockings. The percentage of people who used the stockings for at least 3 days a week was similar across both groups.
The cumulative incidence of PTS during follow-up was 14.2% in the active group vs 12.7% in the placebo group, with a hazard ratio of 1.13 (95% confidence interval [CI], .73-1.76; P=.58). There were no differences in any of the secondary outcomes. Prespecified subgroup analyses found that age, BMI, and severity of DVT had no effect on the outcomes. There was a marginal benefit for ECS for women (P=.047) over men, but this does not likely reflect a true difference because the CIs surrounding the hazard ratios for men and women overlapped and crossed the null value.
WHAT'S NEW: New evidence contradicts previous studies
Two prior studies showed that using 30 to 40 mm Hg ECS decreased the incidence of PTS after proximal DVT.6,7 However, these were smaller, open-label, single-center studies. This study by Kahn et al1 was the first placebo-controlled, randomized, multicenter study that used validated instruments to measure PTS and QOL. It found no benefit in using ECS, thus contradicting the results of the prior studies.
There are currently no guidelines or consensus statements for or against the use of ECS after DVT.
CAVEATS: High nonadherence rates might have affected the results
In both groups, adherence to the assigned intervention diminished throughout the study. Overall, approximately 95% of patients reported wearing their stockings at one month; this dropped to just under 70% by 2 years. Theoretically, this could have affected efficacy outcomes. However, the decrease was similar in both groups and represents what is observed in clinical practice. A prespecified per protocol analysis of patients who wore their ECS more regularly found no benefit.
It is possible that a “placebo effect” could explain the lack of difference between groups. However, the placebo stockings provided virtually no compression, and the 2-year cumulative incidence of PTS in both the treatment and placebo groups was similar to that seen in control groups in prior studies.6,7
Finally, the incidence of PTS in this study was much lower than the 25% to 50% incidence reported in previous studies. Kahn et al1 suggested that this was because they used more stringent and standardized criteria for PTS than was used in previous research.
CHALLENGES TO IMPLEMENTATION: There are no barriers to ending this practice
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
2. Kahn SR, Shrier I, Julian JA, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149:698-707.
3. Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125:1-7.
4. Cohen JM, Akl EA, Kahn SR. Pharmacologic and compression therapies for postthrombotic syndrome: a systematic review of randomized controlled trials. Chest. 2012;141:308-320.
5. Henke PK, Comerota AJ. An update on etiology, prevention, and therapy of postthrombotic syndrome. J Vasc Surg. 2011;53:500- 509.
6. Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
7. Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
8. Ginsberg JS, Hirsh J, Julian J, et al. Prevention and treatment of postphlebitic syndrome: results of a 3-part study. Arch Intern Med. 2001;161:2105-2109.
9. Villalta S, Bagatella P, Piccioli A, et al. Assessment of validity and reproducibility of a clinical scale for the post-thrombotic syndrome. Haemostasis. 1994;24:158a.
10. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31:247-263.
11. Kahn SR, Lamping DL, Ducruet T, et al; VETO Study Investigators. VEINES-QOL/Sym questionnaire was a reliable and valid disease-specific quality of life measure for deep venous thrombosis. J Clin Epidemiol. 2006;59:1049-1056.
1. Kahn SR, Shapiro S, Wells PS, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383:880-888.
2. Kahn SR, Shrier I, Julian JA, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149:698-707.
3. Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125:1-7.
4. Cohen JM, Akl EA, Kahn SR. Pharmacologic and compression therapies for postthrombotic syndrome: a systematic review of randomized controlled trials. Chest. 2012;141:308-320.
5. Henke PK, Comerota AJ. An update on etiology, prevention, and therapy of postthrombotic syndrome. J Vasc Surg. 2011;53:500- 509.
6. Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
7. Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
8. Ginsberg JS, Hirsh J, Julian J, et al. Prevention and treatment of postphlebitic syndrome: results of a 3-part study. Arch Intern Med. 2001;161:2105-2109.
9. Villalta S, Bagatella P, Piccioli A, et al. Assessment of validity and reproducibility of a clinical scale for the post-thrombotic syndrome. Haemostasis. 1994;24:158a.
10. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31:247-263.
11. Kahn SR, Lamping DL, Ducruet T, et al; VETO Study Investigators. VEINES-QOL/Sym questionnaire was a reliable and valid disease-specific quality of life measure for deep venous thrombosis. J Clin Epidemiol. 2006;59:1049-1056.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.