User login
Team engagement and motivation critical to QI success
Thomas McIlraith, MD, SFHM, CLHM, never imagined he would be leading hospitalists and launching quality improvement (QI) initiatives, but only one year out of residency, he was doing just that.
In 2000, Dr. McIlraith had spent a year working as a hospitalist at South Sacramento (Calif.) Kaiser Permanente when he was tapped for the QI program director role.
“Obviously I didn’t have a lot of preparation,” he said of that first job as director. “All of a sudden I found myself in charge of 15 hospitalists, … and I really didn’t know what I was getting myself into.”
But a passion for quality improvement – for striving to always find ways to do better – put Dr. McIlraith on that path and kept him on it through two terms as chair of the hospital medicine department of Mercy Medical Group in Sacramento, where he was hired in 2004. He completed his second term in June 2016 (the department quintupled in size during his tenure), and then chose to return to the ranks as a hospitalist focusing on patient care – and on spending time with his kids before they finished high school.
But quality improvement is in his blood, and he can see himself returning to it someday, Dr. McIlraith said.
“For me it was never about rising up in the ranks of leadership. It was really about making the world I exist in better,” he said.
In recounting some of the lessons he learned over the last 17 years, Dr. McIlraith recalled his first and all-time favorite quality initiative: Central Coordination. It was a concept he implemented around 2002 at Kaiser Permanante that fundamentally changed the way patients were admitted from the emergency department.
The previous system had separate admitting and rounding physicians, which lead to too many patient hand-offs, increased risk of mistakes, poor efficiency, and low patient satisfaction, he said.
“We actually took the job of distributing patients out of physicians’ hands altogether,” Dr. McIlraith explained.
Under Central Coordination, patient assignments were coordinated by a clerical staffer who distributed them evenly among a team of six doctors.
“The most amazing thing was that after this was implemented we went back and looked at ER responsiveness, and our ability to respond to the needs of the ER improved dramatically,” he said. “That wasn’t even an outcome I intended to impact, or look at, but the data were unequivocal. It ended up being really enduring and substantial on many fronts.”
Mercy Medical Group still uses Central Coordination systemwide, and the results of Dr. McIlraith’s initiative were eventually published.
“At the same time, due to my lack of experience in 2002, I definitely made some mistakes,” he said of the undertaking. Among them was failing to recognize just how resistant people can be to change. “I thought [the plan] was so brilliant that everyone would see that and get in line behind me,” he said. “Then I had a rude awakening that not everyone sees things the same way I do. I was completely taken aback by the resistance.”
Even though the existing system left a lot to be desired, the doctors were comfortable with it, Dr. McIlraith explained, stressing that implementing change requires the buy-in of team members.
If he could do it over again, he would follow the eight-step “Road Map for Change” as outlined by Jeffrey Glasheen, MD, SFHM, during the Society of Hospital Medicine’s Leadership Academy, Dr. McIlraith said.
Dr. Glasheen’s road map emphasizes team engagement and motivation, as well as the importance of creating a “burning platform” (the imperative for change).
“You need to be systematic about it to get people to change behaviors,” Dr. McIlraith said, noting that behavioral change is one of the greatest challenges and one of the leading causes of failure to attain the “holy grail” of quality improvement: sustained results.
In fact, the main reason for the enduring success of Central Coordination was that it took the focus off of behavioral change and put it on the process. “We took the behavior aspect out of the equation and put form over function,” Dr. McIlraith said.
One recent quality improvement initiative involved increasing the percentage of discharge orders delivered before 11 a.m. Dr. McIlraith put the lessons he learned to work by creating an “excellence team” that met regularly to identify key problems and to create “SMART (Specific, Measurable, Attainable, Relevant, and Timely) goals,” which are necessary for success.
Because the team not only bought into the plan to meet the target but also helped create the plan, it wasn’t necessary to force behavioral change, Dr. McIlraith said. Instead the team lead the initiative, set the targets and goals, and ended up surpassing the initial goal of reaching 30% of discharge orders in by 11 a.m. (in fact, they hit 40%).
Dr. McIlraith’s advice for QI success is to know the problem you are trying to solve so that you can tell if the solution you implement is having the desired impact and also to measure the impact of that solution using the SMART goals.
For those who hope to follow a quality improvement career path to leadership, he strongly recommends the Society of Hospital Medicine’s Leadership Academies, which are excellent resources for mentorship, networking, and leadership training through SHM.
Ultimately, Dr. McIlraith stressed the importance of mentoring team members for development as future QI leaders. If mentoring relationships are successful, then when the time comes for a QI veteran to “step back” to focus more on family or take a different career path, there will be others who can step in and keep the quality momentum going.
Thomas McIlraith, MD, SFHM, CLHM, never imagined he would be leading hospitalists and launching quality improvement (QI) initiatives, but only one year out of residency, he was doing just that.
In 2000, Dr. McIlraith had spent a year working as a hospitalist at South Sacramento (Calif.) Kaiser Permanente when he was tapped for the QI program director role.
“Obviously I didn’t have a lot of preparation,” he said of that first job as director. “All of a sudden I found myself in charge of 15 hospitalists, … and I really didn’t know what I was getting myself into.”
But a passion for quality improvement – for striving to always find ways to do better – put Dr. McIlraith on that path and kept him on it through two terms as chair of the hospital medicine department of Mercy Medical Group in Sacramento, where he was hired in 2004. He completed his second term in June 2016 (the department quintupled in size during his tenure), and then chose to return to the ranks as a hospitalist focusing on patient care – and on spending time with his kids before they finished high school.
But quality improvement is in his blood, and he can see himself returning to it someday, Dr. McIlraith said.
“For me it was never about rising up in the ranks of leadership. It was really about making the world I exist in better,” he said.
In recounting some of the lessons he learned over the last 17 years, Dr. McIlraith recalled his first and all-time favorite quality initiative: Central Coordination. It was a concept he implemented around 2002 at Kaiser Permanante that fundamentally changed the way patients were admitted from the emergency department.
The previous system had separate admitting and rounding physicians, which lead to too many patient hand-offs, increased risk of mistakes, poor efficiency, and low patient satisfaction, he said.
“We actually took the job of distributing patients out of physicians’ hands altogether,” Dr. McIlraith explained.
Under Central Coordination, patient assignments were coordinated by a clerical staffer who distributed them evenly among a team of six doctors.
“The most amazing thing was that after this was implemented we went back and looked at ER responsiveness, and our ability to respond to the needs of the ER improved dramatically,” he said. “That wasn’t even an outcome I intended to impact, or look at, but the data were unequivocal. It ended up being really enduring and substantial on many fronts.”
Mercy Medical Group still uses Central Coordination systemwide, and the results of Dr. McIlraith’s initiative were eventually published.
“At the same time, due to my lack of experience in 2002, I definitely made some mistakes,” he said of the undertaking. Among them was failing to recognize just how resistant people can be to change. “I thought [the plan] was so brilliant that everyone would see that and get in line behind me,” he said. “Then I had a rude awakening that not everyone sees things the same way I do. I was completely taken aback by the resistance.”
Even though the existing system left a lot to be desired, the doctors were comfortable with it, Dr. McIlraith explained, stressing that implementing change requires the buy-in of team members.
If he could do it over again, he would follow the eight-step “Road Map for Change” as outlined by Jeffrey Glasheen, MD, SFHM, during the Society of Hospital Medicine’s Leadership Academy, Dr. McIlraith said.
Dr. Glasheen’s road map emphasizes team engagement and motivation, as well as the importance of creating a “burning platform” (the imperative for change).
“You need to be systematic about it to get people to change behaviors,” Dr. McIlraith said, noting that behavioral change is one of the greatest challenges and one of the leading causes of failure to attain the “holy grail” of quality improvement: sustained results.
In fact, the main reason for the enduring success of Central Coordination was that it took the focus off of behavioral change and put it on the process. “We took the behavior aspect out of the equation and put form over function,” Dr. McIlraith said.
One recent quality improvement initiative involved increasing the percentage of discharge orders delivered before 11 a.m. Dr. McIlraith put the lessons he learned to work by creating an “excellence team” that met regularly to identify key problems and to create “SMART (Specific, Measurable, Attainable, Relevant, and Timely) goals,” which are necessary for success.
Because the team not only bought into the plan to meet the target but also helped create the plan, it wasn’t necessary to force behavioral change, Dr. McIlraith said. Instead the team lead the initiative, set the targets and goals, and ended up surpassing the initial goal of reaching 30% of discharge orders in by 11 a.m. (in fact, they hit 40%).
Dr. McIlraith’s advice for QI success is to know the problem you are trying to solve so that you can tell if the solution you implement is having the desired impact and also to measure the impact of that solution using the SMART goals.
For those who hope to follow a quality improvement career path to leadership, he strongly recommends the Society of Hospital Medicine’s Leadership Academies, which are excellent resources for mentorship, networking, and leadership training through SHM.
Ultimately, Dr. McIlraith stressed the importance of mentoring team members for development as future QI leaders. If mentoring relationships are successful, then when the time comes for a QI veteran to “step back” to focus more on family or take a different career path, there will be others who can step in and keep the quality momentum going.
Thomas McIlraith, MD, SFHM, CLHM, never imagined he would be leading hospitalists and launching quality improvement (QI) initiatives, but only one year out of residency, he was doing just that.
In 2000, Dr. McIlraith had spent a year working as a hospitalist at South Sacramento (Calif.) Kaiser Permanente when he was tapped for the QI program director role.
“Obviously I didn’t have a lot of preparation,” he said of that first job as director. “All of a sudden I found myself in charge of 15 hospitalists, … and I really didn’t know what I was getting myself into.”
But a passion for quality improvement – for striving to always find ways to do better – put Dr. McIlraith on that path and kept him on it through two terms as chair of the hospital medicine department of Mercy Medical Group in Sacramento, where he was hired in 2004. He completed his second term in June 2016 (the department quintupled in size during his tenure), and then chose to return to the ranks as a hospitalist focusing on patient care – and on spending time with his kids before they finished high school.
But quality improvement is in his blood, and he can see himself returning to it someday, Dr. McIlraith said.
“For me it was never about rising up in the ranks of leadership. It was really about making the world I exist in better,” he said.
In recounting some of the lessons he learned over the last 17 years, Dr. McIlraith recalled his first and all-time favorite quality initiative: Central Coordination. It was a concept he implemented around 2002 at Kaiser Permanante that fundamentally changed the way patients were admitted from the emergency department.
The previous system had separate admitting and rounding physicians, which lead to too many patient hand-offs, increased risk of mistakes, poor efficiency, and low patient satisfaction, he said.
“We actually took the job of distributing patients out of physicians’ hands altogether,” Dr. McIlraith explained.
Under Central Coordination, patient assignments were coordinated by a clerical staffer who distributed them evenly among a team of six doctors.
“The most amazing thing was that after this was implemented we went back and looked at ER responsiveness, and our ability to respond to the needs of the ER improved dramatically,” he said. “That wasn’t even an outcome I intended to impact, or look at, but the data were unequivocal. It ended up being really enduring and substantial on many fronts.”
Mercy Medical Group still uses Central Coordination systemwide, and the results of Dr. McIlraith’s initiative were eventually published.
“At the same time, due to my lack of experience in 2002, I definitely made some mistakes,” he said of the undertaking. Among them was failing to recognize just how resistant people can be to change. “I thought [the plan] was so brilliant that everyone would see that and get in line behind me,” he said. “Then I had a rude awakening that not everyone sees things the same way I do. I was completely taken aback by the resistance.”
Even though the existing system left a lot to be desired, the doctors were comfortable with it, Dr. McIlraith explained, stressing that implementing change requires the buy-in of team members.
If he could do it over again, he would follow the eight-step “Road Map for Change” as outlined by Jeffrey Glasheen, MD, SFHM, during the Society of Hospital Medicine’s Leadership Academy, Dr. McIlraith said.
Dr. Glasheen’s road map emphasizes team engagement and motivation, as well as the importance of creating a “burning platform” (the imperative for change).
“You need to be systematic about it to get people to change behaviors,” Dr. McIlraith said, noting that behavioral change is one of the greatest challenges and one of the leading causes of failure to attain the “holy grail” of quality improvement: sustained results.
In fact, the main reason for the enduring success of Central Coordination was that it took the focus off of behavioral change and put it on the process. “We took the behavior aspect out of the equation and put form over function,” Dr. McIlraith said.
One recent quality improvement initiative involved increasing the percentage of discharge orders delivered before 11 a.m. Dr. McIlraith put the lessons he learned to work by creating an “excellence team” that met regularly to identify key problems and to create “SMART (Specific, Measurable, Attainable, Relevant, and Timely) goals,” which are necessary for success.
Because the team not only bought into the plan to meet the target but also helped create the plan, it wasn’t necessary to force behavioral change, Dr. McIlraith said. Instead the team lead the initiative, set the targets and goals, and ended up surpassing the initial goal of reaching 30% of discharge orders in by 11 a.m. (in fact, they hit 40%).
Dr. McIlraith’s advice for QI success is to know the problem you are trying to solve so that you can tell if the solution you implement is having the desired impact and also to measure the impact of that solution using the SMART goals.
For those who hope to follow a quality improvement career path to leadership, he strongly recommends the Society of Hospital Medicine’s Leadership Academies, which are excellent resources for mentorship, networking, and leadership training through SHM.
Ultimately, Dr. McIlraith stressed the importance of mentoring team members for development as future QI leaders. If mentoring relationships are successful, then when the time comes for a QI veteran to “step back” to focus more on family or take a different career path, there will be others who can step in and keep the quality momentum going.
Migraine May Be an Important Risk Factor for Cardiovascular Diseases
Migraine is associated with increased risk of myocardial infarction, ischemic stroke, hemorrhagic stroke, venous thromboembolism, and atrial fibrillation or atrial flutter, according to a study published online ahead of print January 31 in BMJ. The results suggest that “migraine should be considered a potent and persistent risk factor for most cardiovascular diseases in both men and women,” the researchers said.
Prior studies have found that migraine is associated with ischemic stroke and ischemic heart disease, especially among women and patients with migraine with aura. Convincing epidemiologic evidence of an association between migraine and other cardiovascular events has been lacking, however, said Kasper Adelborg, MD, PhD, of the Department of Clinical Epidemiology at Aarhus University Hospital in Denmark, and colleagues.

To study cardiovascular morbidity associated with migraine, Dr. Adelborg and colleagues conducted a nationwide, population-based cohort study. The study included patients from all Danish hospitals and hospital outpatient clinics between 1995 and 2013. The researchers used Cox regression analysis to assess comorbidity-adjusted hazard ratios of cardiovascular outcomes.
Their analysis included 51,032 patients with migraine and 510,320 people from the general population matched on age, sex, and calendar year. Median age at migraine diagnosis was 35, and 71% of the participants were women.
Incidence per 1,000 People
Patients with incident migraine had greater absolute risk of most cardiovascular outcomes, compared with the general population, across most follow-up periods. After 19 years of follow-up, the cumulative incidences per 1,000 people were greater among migraineurs, compared with the general population, for myocardial infarction (25 vs 17), ischemic stroke (45 vs 25), hemorrhagic stroke (11 vs 6), peripheral artery disease (13 vs 11), venous thromboembolism (27 vs 18), atrial fibrillation or atrial flutter (47 vs 34), and heart failure (19 vs 18).
Migraine was associated with myocardial infarction (adjusted hazard ratio [HR], 1.49), ischemic stroke (adjusted HR, 2.26), and hemorrhagic stroke (adjusted HR, 1.94), as well as venous thromboembolism (adjusted HR, 1.59) and atrial fibrillation or atrial flutter (adjusted HR, 1.25). Migraine was not meaningfully associated with peripheral artery disease or heart failure. “The associations, particularly for stroke outcomes, were stronger during the short term (0–1 years) after diagnosis than the long term (up to 19 years),” the researchers said. In addition, associations were stronger in migraine with aura than in migraine without aura, and in women than in men. In a subcohort of patients with additional data, the associations persisted after additional adjustments for BMI and smoking.
The absolute risk of cardiovascular outcomes was low, which was expected, given the young age of the study population, the researchers noted. Although the investigators adjusted for a range of potential confounders, other unknown or residual confounding (eg, by physical activity) is possible.
Multifactorial mechanisms may explain the observed increased risk of cardiovascular disease in migraine, and different mechanisms may be involved in specific cardiovascular outcomes. Migraine and cardiovascular diseases may share genetic, inflammatory, vascular, endothelial, electrical or depolarizing, or coagulable factors, the researchers said. In addition, migraineurs often use NSAIDs, which are associated with increased risk of cardiovascular events. It is also possible that immobilization due to migraine attacks may increase the risk of venous thromboembolism.
Reducing Risk
“Although the magnitude of the increased cardiovascular risk associated with migraine was fairly small at the individual level, it translates into a substantial increase in risk at the population level, because migraine is a common disease,” Dr. Adelborg and colleagues said. Migraine increasingly is recognized as an important cardiovascular risk factor to consider in clinical practice, and the recently developed QRISK3 algorithm, which predicts 10-year risk of cardiovascular disease in men and women ages 25 to 84, is the first cardiovascular risk-stratification tool to incorporate migraine.
“Ultimately, it will be important to determine whether prevention strategies in patients with migraine can reduce the burden of cardiovascular disease in patients with this common disorder,” the researchers said. “Current migraine guidelines do not recommend use of aspirin and clopidogrel in the prophylaxis of migraine, but clinicians should consider whether patients at particularly high risk of cardiovascular diseases would benefit from anticoagulant treatment.”
The present study and prior research provide “plenty of evidence that migraine should be taken seriously as a strong cardiovascular risk marker,” and data indicate that migraine is associated with “a measurable risk of cardiovascular death,” said Tobias Kurth, MD, Professor of Public Health and Epidemiology and Director of the Institute of Public Health at the Charité-Universitätsmedizin Berlin
Suggested Reading
Adelborg K, Szépligeti SK, Holland-Bill L, et al. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ. 2018 Jan 31 [Epub ahead of print].
Kurth T, Rohmann JL, Shapiro RE. Migraine and risk of cardiovascular disease. BMJ. 2018 Jan 31 [Epub ahead of print].
Migraine is associated with increased risk of myocardial infarction, ischemic stroke, hemorrhagic stroke, venous thromboembolism, and atrial fibrillation or atrial flutter, according to a study published online ahead of print January 31 in BMJ. The results suggest that “migraine should be considered a potent and persistent risk factor for most cardiovascular diseases in both men and women,” the researchers said.
Prior studies have found that migraine is associated with ischemic stroke and ischemic heart disease, especially among women and patients with migraine with aura. Convincing epidemiologic evidence of an association between migraine and other cardiovascular events has been lacking, however, said Kasper Adelborg, MD, PhD, of the Department of Clinical Epidemiology at Aarhus University Hospital in Denmark, and colleagues.
To study cardiovascular morbidity associated with migraine, Dr. Adelborg and colleagues conducted a nationwide, population-based cohort study. The study included patients from all Danish hospitals and hospital outpatient clinics between 1995 and 2013. The researchers used Cox regression analysis to assess comorbidity-adjusted hazard ratios of cardiovascular outcomes.
Their analysis included 51,032 patients with migraine and 510,320 people from the general population matched on age, sex, and calendar year. Median age at migraine diagnosis was 35, and 71% of the participants were women.
Incidence per 1,000 People
Patients with incident migraine had greater absolute risk of most cardiovascular outcomes, compared with the general population, across most follow-up periods. After 19 years of follow-up, the cumulative incidences per 1,000 people were greater among migraineurs, compared with the general population, for myocardial infarction (25 vs 17), ischemic stroke (45 vs 25), hemorrhagic stroke (11 vs 6), peripheral artery disease (13 vs 11), venous thromboembolism (27 vs 18), atrial fibrillation or atrial flutter (47 vs 34), and heart failure (19 vs 18).
Migraine was associated with myocardial infarction (adjusted hazard ratio [HR], 1.49), ischemic stroke (adjusted HR, 2.26), and hemorrhagic stroke (adjusted HR, 1.94), as well as venous thromboembolism (adjusted HR, 1.59) and atrial fibrillation or atrial flutter (adjusted HR, 1.25). Migraine was not meaningfully associated with peripheral artery disease or heart failure. “The associations, particularly for stroke outcomes, were stronger during the short term (0–1 years) after diagnosis than the long term (up to 19 years),” the researchers said. In addition, associations were stronger in migraine with aura than in migraine without aura, and in women than in men. In a subcohort of patients with additional data, the associations persisted after additional adjustments for BMI and smoking.
The absolute risk of cardiovascular outcomes was low, which was expected, given the young age of the study population, the researchers noted. Although the investigators adjusted for a range of potential confounders, other unknown or residual confounding (eg, by physical activity) is possible.
Multifactorial mechanisms may explain the observed increased risk of cardiovascular disease in migraine, and different mechanisms may be involved in specific cardiovascular outcomes. Migraine and cardiovascular diseases may share genetic, inflammatory, vascular, endothelial, electrical or depolarizing, or coagulable factors, the researchers said. In addition, migraineurs often use NSAIDs, which are associated with increased risk of cardiovascular events. It is also possible that immobilization due to migraine attacks may increase the risk of venous thromboembolism.
Reducing Risk
“Although the magnitude of the increased cardiovascular risk associated with migraine was fairly small at the individual level, it translates into a substantial increase in risk at the population level, because migraine is a common disease,” Dr. Adelborg and colleagues said. Migraine increasingly is recognized as an important cardiovascular risk factor to consider in clinical practice, and the recently developed QRISK3 algorithm, which predicts 10-year risk of cardiovascular disease in men and women ages 25 to 84, is the first cardiovascular risk-stratification tool to incorporate migraine.
“Ultimately, it will be important to determine whether prevention strategies in patients with migraine can reduce the burden of cardiovascular disease in patients with this common disorder,” the researchers said. “Current migraine guidelines do not recommend use of aspirin and clopidogrel in the prophylaxis of migraine, but clinicians should consider whether patients at particularly high risk of cardiovascular diseases would benefit from anticoagulant treatment.”
The present study and prior research provide “plenty of evidence that migraine should be taken seriously as a strong cardiovascular risk marker,” and data indicate that migraine is associated with “a measurable risk of cardiovascular death,” said Tobias Kurth, MD, Professor of Public Health and Epidemiology and Director of the Institute of Public Health at the Charité-Universitätsmedizin Berlin
Suggested Reading
Adelborg K, Szépligeti SK, Holland-Bill L, et al. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ. 2018 Jan 31 [Epub ahead of print].
Kurth T, Rohmann JL, Shapiro RE. Migraine and risk of cardiovascular disease. BMJ. 2018 Jan 31 [Epub ahead of print].
Migraine is associated with increased risk of myocardial infarction, ischemic stroke, hemorrhagic stroke, venous thromboembolism, and atrial fibrillation or atrial flutter, according to a study published online ahead of print January 31 in BMJ. The results suggest that “migraine should be considered a potent and persistent risk factor for most cardiovascular diseases in both men and women,” the researchers said.
Prior studies have found that migraine is associated with ischemic stroke and ischemic heart disease, especially among women and patients with migraine with aura. Convincing epidemiologic evidence of an association between migraine and other cardiovascular events has been lacking, however, said Kasper Adelborg, MD, PhD, of the Department of Clinical Epidemiology at Aarhus University Hospital in Denmark, and colleagues.
To study cardiovascular morbidity associated with migraine, Dr. Adelborg and colleagues conducted a nationwide, population-based cohort study. The study included patients from all Danish hospitals and hospital outpatient clinics between 1995 and 2013. The researchers used Cox regression analysis to assess comorbidity-adjusted hazard ratios of cardiovascular outcomes.
Their analysis included 51,032 patients with migraine and 510,320 people from the general population matched on age, sex, and calendar year. Median age at migraine diagnosis was 35, and 71% of the participants were women.
Incidence per 1,000 People
Patients with incident migraine had greater absolute risk of most cardiovascular outcomes, compared with the general population, across most follow-up periods. After 19 years of follow-up, the cumulative incidences per 1,000 people were greater among migraineurs, compared with the general population, for myocardial infarction (25 vs 17), ischemic stroke (45 vs 25), hemorrhagic stroke (11 vs 6), peripheral artery disease (13 vs 11), venous thromboembolism (27 vs 18), atrial fibrillation or atrial flutter (47 vs 34), and heart failure (19 vs 18).
Migraine was associated with myocardial infarction (adjusted hazard ratio [HR], 1.49), ischemic stroke (adjusted HR, 2.26), and hemorrhagic stroke (adjusted HR, 1.94), as well as venous thromboembolism (adjusted HR, 1.59) and atrial fibrillation or atrial flutter (adjusted HR, 1.25). Migraine was not meaningfully associated with peripheral artery disease or heart failure. “The associations, particularly for stroke outcomes, were stronger during the short term (0–1 years) after diagnosis than the long term (up to 19 years),” the researchers said. In addition, associations were stronger in migraine with aura than in migraine without aura, and in women than in men. In a subcohort of patients with additional data, the associations persisted after additional adjustments for BMI and smoking.
The absolute risk of cardiovascular outcomes was low, which was expected, given the young age of the study population, the researchers noted. Although the investigators adjusted for a range of potential confounders, other unknown or residual confounding (eg, by physical activity) is possible.
Multifactorial mechanisms may explain the observed increased risk of cardiovascular disease in migraine, and different mechanisms may be involved in specific cardiovascular outcomes. Migraine and cardiovascular diseases may share genetic, inflammatory, vascular, endothelial, electrical or depolarizing, or coagulable factors, the researchers said. In addition, migraineurs often use NSAIDs, which are associated with increased risk of cardiovascular events. It is also possible that immobilization due to migraine attacks may increase the risk of venous thromboembolism.
Reducing Risk
“Although the magnitude of the increased cardiovascular risk associated with migraine was fairly small at the individual level, it translates into a substantial increase in risk at the population level, because migraine is a common disease,” Dr. Adelborg and colleagues said. Migraine increasingly is recognized as an important cardiovascular risk factor to consider in clinical practice, and the recently developed QRISK3 algorithm, which predicts 10-year risk of cardiovascular disease in men and women ages 25 to 84, is the first cardiovascular risk-stratification tool to incorporate migraine.
“Ultimately, it will be important to determine whether prevention strategies in patients with migraine can reduce the burden of cardiovascular disease in patients with this common disorder,” the researchers said. “Current migraine guidelines do not recommend use of aspirin and clopidogrel in the prophylaxis of migraine, but clinicians should consider whether patients at particularly high risk of cardiovascular diseases would benefit from anticoagulant treatment.”
The present study and prior research provide “plenty of evidence that migraine should be taken seriously as a strong cardiovascular risk marker,” and data indicate that migraine is associated with “a measurable risk of cardiovascular death,” said Tobias Kurth, MD, Professor of Public Health and Epidemiology and Director of the Institute of Public Health at the Charité-Universitätsmedizin Berlin
Suggested Reading
Adelborg K, Szépligeti SK, Holland-Bill L, et al. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ. 2018 Jan 31 [Epub ahead of print].
Kurth T, Rohmann JL, Shapiro RE. Migraine and risk of cardiovascular disease. BMJ. 2018 Jan 31 [Epub ahead of print].

Conference News Roundup—Association of Academic Physiatrists
Electrical Stimulation Device Improves Motor Function
A person with a spinal cord injury can improve his or her ability to grip and move household objects by using an electrical stimulation device controlled by his or her thoughts, according to researchers. The study suggests that this new technology could one day enhance quality of life among people with disabilities and allow them to live more independently.
People with tetraplegia lose upper-limb strength and dexterity, which has a severe impact on their independence and quality of life. New technology that connects a person’s brain to an implanted functional electrical stimulation orthotics device on the hands could restore manual dexterity and grip strength, thus allowing him or her to perform simple daily tasks like holding a toothbrush without help.
“Individuals with cervical spinal cord injury identify recovery of the use of their hands as the single most impactful way that neurotechnology could change their lives,” said Marcie Bockbrader, MD, PhD, Assistant Professor of Physical Medicine and Rehabilitation at the Ohio State University Wexner Medical Center in Columbus. “Giving a person back [his or her] hands reduces dependence on others. It makes it possible to do the little things—like cutting food or opening a door—that are so essential to being able to take care of oneself.”
To test how well this thought-controlled brain–computer interface system works in real life to improve hand strength and dexterity, Dr. Bockbrader and her research team surgically implanted one of these devices into the hand of a 26-year-old man with C5-level, nonspastic tetraplegia following a spinal cord injury. He practiced using the device three times per week for four hours each session for more than 1,000 days. The research team administered standardized tests of upper-limb motor ability and functional participation to see how well the system improved his grip strength, quickness, and other basic skills.
Using this device improved the man’s upper-limb motor ability dramatically, according to several standardized tests. He improved his ability to grip and manipulate basic objects, and showed that he could perform ordinary tasks with his hands at the speed and dexterity levels of healthy individuals. He could move objects of different sizes and weights. With practice, he improved his ability to manipulate smaller household objects like a toothbrush or hairbrush. He also demonstrated that he could imagine different hand positions to proportionally adjust and control different hand movements.
“Our study demonstrated that patients with tetraplegia might be able to restore some of their skilled hand function with an implanted device that allows them to control movements with their own thoughts,” said Dr. Bockbrader. “Although this technology must be refined and tested before it can go from the laboratory to the public, it may one day offer people with disabilities a way to live and work more independently, and enable them to perform daily tasks.”
Concussion Recovery Varies Among Children
Not all children follow the same path to concussion recovery, nor do they have the same predictors for returning to normal activity, investigators reported. Their study also suggests that younger children should be considered separately from high-school students.
“Concussions are common among children, yet the literature is limited with regard to understanding trajectory of recovery after concussion, particularly in children with non-sports-related injuries and for younger children,” said Kaitlyn Chin, a second-year medical student at University of New England College of Osteopathic Medicine in Biddeford, Maine. “We were particularly interested in understanding how activity levels during recovery from concussion influence time to full recovery, to be able to identify modifiable factors to help guide concussion care. Previous studies have noted differences in the amount of time it takes children to recover from a concussion, and our team recently initiated a study to see if we can identify predictors associated with the amount of time between injury and when a child is medically cleared to return to activities which place the child at risk for reinjury.”
Ms. Chin’s team at Kennedy Krieger Institute in Baltimore reviewed the medical records of 178 children who were treated for concussions at an academically affiliated, rehabilitation-based clinic. The children had been medically cleared to return to play between September 2015 and February 2017. The children included in the study ranged in age from 6 to 17. A slight majority was younger than 14. Each child’s first visit to the clinic was within 60 days of his or her concussion.
The researchers reviewed each child’s record, noting when they had been approved to return to play. Then they looked at several other factors for each child, including sex, cause of the concussion (ie, sports or non-sports-related), number of symptoms, school attendance, and exercise status at the initial visit to the clinic. Finally, they considered these factors when the children were placed into two categories—children under 14 and children over 14—to examine potential differences related to age.
Ms. Chin’s team found that the number of symptoms affected how quickly all children were cleared to return to play. Fewer symptoms were associated with a faster return to play. For older children, male sex and higher level of exercise during recovery were associated with a faster return to play. For younger children, higher levels of exercise and school participation (eg, attending class and completing homework and tests) were associated with faster return to play.
Overall, this study shows that elementary and middle-school-aged children should be considered separately from high-school-aged students when considering risk factors for prolonged recovery from a concussion. Furthermore, Ms. Chin’s team found that school participation and exercise were not harmful and did not prolong recovery.
“Our study adds to the literature supporting that return to cognitive and safe physical activities while a child is still recovering from concussion does not prolong time to recovery,” said Ms. Chin. “Every child is different, and recovery is different for each concussion. [Therefore], a concussion recovery plan should be tailored for each child, and parents should seek help from the child’s pediatrician or other medical professionals for guiding care after a concussion.”
Medicine May Not Affect Concussion Recovery
Medications commonly prescribed to reduce symptoms of concussion may not affect recovery, said investigators. Sports medicine physicians commonly treat patients with concussion, so researchers in Utah investigated how some widely prescribed treatments might affect patients’ recovery.
“We really do not have much other than rest and gentle exercise to combat symptoms of concussion,” said Venessa Lee, MD, a physical medicine and rehabilitation resident at University of Utah Health in Salt Lake City. “Medications are commonly prescribed to help with symptoms, but there is little evidence that they help more than just time and rest.”
Although FDA has not approved any medication to treat concussion, physicians may prescribe medications like gabapentin or tricyclic antidepressants (TCAs) to help reduce symptoms during recovery. To examine whether these drugs benefit patients, Dr. Lee and her research team looked at 277 patients who had been diagnosed with concussion at a local academic sports medicine practice. At each of their visits to the clinic during recovery, patients reported their postconcussion symptoms. The research team used a score sheet to measure their symptoms, and they tracked scores of patients who had more than one visit to the clinic for as long as one year.
Patients were separated into three groups for the study: those not prescribed any medication, those prescribed gabapentin, and those prescribed one of two TCAs, amitriptyline or nortriptyline. Based on self-reported information, investigators gave each patient a score for two factors of postconcussion recovery: headaches and a combination of 22 symptoms, including headaches. Each score was on a scale of 0 to 6.
After they adjusted scores for gender and age, Dr. Lee’s team found that headache and combined symptoms scores decreased significantly within days after the first clinic visit for all three groups of patients—those who had taken no medications, those who had been prescribed gabapentin, and those who had been prescribed a TCA. Patients who had been prescribed any of the medications had significantly higher scores for headaches and overall postconcussion symptoms to begin with, but no one type of medication had any better or worse effect over the duration of the study.
“Patients’ symptoms improve with time after a concussion,” said Dr. Lee. “When we looked at [patients who received] gabapentin and TCAs, their symptoms improved over time as well, but similar to those that did not receive a medication.”
Based on this study, neither gabapentin nor TCAs appear to provide any additional benefit for postconcussion recovery. With this information, patients may be able to avoid taking unnecessary medications as they recover from concussions. Patients should speak with a physician about their symptoms after a concussion, said Dr. Lee.
“Though the two medications we studied did not show a profound improvement in our analysis, this was a retrospective study … which has many drawbacks and limitations. We need to do more research to really find the best method for improving postconcussive symptoms.”
Ballet Helps Children with Musculoskeletal and Neurologic Conditions
Adaptive ballet classes provide functional improvement and social interactions for children with musculoskeletal and neurologic conditions, according to researchers. This type of arts-based adaptive therapy is a promising expansion to successful adaptive sports therapies, said the investigators.
“While great strides have been made in adaptive sports, there are still relatively few opportunities in the arts for people with disabilities,” said Sarah Stauder, MD, a physician at the Medical College of Wisconsin in Milwaukee. “Because of this [scarcity], we wanted to evaluate the effect of adaptive ballet on the physical, emotional, social, and academic function of children with physical impairments. The program is a collaboration between a children’s hospital and a metropolitan ballet company that brings together professional dancers, pediatric doctors, physical and occupational therapists, and children with physical disabilities for a series of dance classes.”
The goal of the study was to see whether a weekly, 45-mintute ballet class with 15 minutes of ballet education over five consecutive weeks would improve the children’s balance, physical functions, social skills, and overall quality of life. Eighteen children (17 girls) from ages 5 to 14, took part in the class. Assessments of each child were performed before and after the series of classes using the Pediatric Quality of Life Inventory, the PEDI-CAT survey, and the Pediatric Balance Scale. Finally, a questionnaire was used to assess each child’s success in achieving individual goals set for the class.
At the end of the five weeks, 94% of participants reached their individual goals for the ballet program. PEDI-CAT scores improved after completion of the program, and the program was most beneficial to participants who had lower functioning and quality of life at the beginning of the program. Finally, the researchers noticed an average improvement in balance among the participants.
“Adaptive programs like the one studied here give children the opportunity to participate in activities they otherwise would have no way to do,” said Dr. Stauder. “More specifically, these dance classes instilled a sense of pride and confidence in the children while improving their physical functioning and quality of life. Our study should open the door to more arts-based therapy for children. It is an effective and enjoyable way for patients to get the therapy they need. When kids are active in an activity that interests them, they naturally make greater strides, and we were able to see this in their day-to-day function.”
Genetic Risk Score Predicts TBI Outcomes
A genetic risk score could help predict a patient’s quality of life after a traumatic brain injury (TBI), said researchers. One day, physicians could have a simple method to forecast a patient’s recovery and personalize therapy to maximize quality of life.
“Gene pathways can influence all of our biologic functions and risk for many health outcomes,” said Mark Linsenmeyer, MD, a resident physician at the University of Pittsburgh Medical Center. “Each person has a unique inherited genetic code. By studying one gene pathway in a large group of people with the same disease or health problem, we hope to unlock clues to why some people have different outcomes than others. This knowledge may be used to help physicians make the best treatment choice for each person.”
Dr. Linsenmeyer and colleagues set out to investigate how genes that affect the brain’s dopamine pathways could predict recovery in people with moderate-to-severe TBI. The team recruited 94 adults with TBI from a level-1 trauma center. They focused on the following five genes in the dopamine pathways: COMT rs4680, VMAT2 rs363226, DRD2 rs6279, ANKK1 Taq1a, and MAOA VNTR. They defined which risk genotypes were associated with lower average scores on surveys filled out by patients with TBI to describe their overall quality of life at six and 12 months after their injuries.
The researchers analyzed how individual variants of each of these five genes could affect patients’ quality of life, and then generated a weighted gene risk score as a measure to reflect cumulative risk represented by all genotypes included in the score. Based on available literature about dopamine pathway genetics, they predicted that their gene risk score calculation tool should be specific to a patient’s sex.
Before they calculated gene risk scores, the research team noticed that only COMT could significantly predict quality of life for a subset of patients six months after their injuries. After generating sex-specific gene risk scores, they found that variants of all five genes on the dopamine pathway could meaningfully contribute to a gene risk score that was highly predictive of quality of life after six months for patients of both sexes with TBI, and also predictive of quality of life after one year for women.
Electrical Stimulation Device Improves Motor Function
A person with a spinal cord injury can improve his or her ability to grip and move household objects by using an electrical stimulation device controlled by his or her thoughts, according to researchers. The study suggests that this new technology could one day enhance quality of life among people with disabilities and allow them to live more independently.
People with tetraplegia lose upper-limb strength and dexterity, which has a severe impact on their independence and quality of life. New technology that connects a person’s brain to an implanted functional electrical stimulation orthotics device on the hands could restore manual dexterity and grip strength, thus allowing him or her to perform simple daily tasks like holding a toothbrush without help.
“Individuals with cervical spinal cord injury identify recovery of the use of their hands as the single most impactful way that neurotechnology could change their lives,” said Marcie Bockbrader, MD, PhD, Assistant Professor of Physical Medicine and Rehabilitation at the Ohio State University Wexner Medical Center in Columbus. “Giving a person back [his or her] hands reduces dependence on others. It makes it possible to do the little things—like cutting food or opening a door—that are so essential to being able to take care of oneself.”
To test how well this thought-controlled brain–computer interface system works in real life to improve hand strength and dexterity, Dr. Bockbrader and her research team surgically implanted one of these devices into the hand of a 26-year-old man with C5-level, nonspastic tetraplegia following a spinal cord injury. He practiced using the device three times per week for four hours each session for more than 1,000 days. The research team administered standardized tests of upper-limb motor ability and functional participation to see how well the system improved his grip strength, quickness, and other basic skills.
Using this device improved the man’s upper-limb motor ability dramatically, according to several standardized tests. He improved his ability to grip and manipulate basic objects, and showed that he could perform ordinary tasks with his hands at the speed and dexterity levels of healthy individuals. He could move objects of different sizes and weights. With practice, he improved his ability to manipulate smaller household objects like a toothbrush or hairbrush. He also demonstrated that he could imagine different hand positions to proportionally adjust and control different hand movements.
“Our study demonstrated that patients with tetraplegia might be able to restore some of their skilled hand function with an implanted device that allows them to control movements with their own thoughts,” said Dr. Bockbrader. “Although this technology must be refined and tested before it can go from the laboratory to the public, it may one day offer people with disabilities a way to live and work more independently, and enable them to perform daily tasks.”
Concussion Recovery Varies Among Children
Not all children follow the same path to concussion recovery, nor do they have the same predictors for returning to normal activity, investigators reported. Their study also suggests that younger children should be considered separately from high-school students.
“Concussions are common among children, yet the literature is limited with regard to understanding trajectory of recovery after concussion, particularly in children with non-sports-related injuries and for younger children,” said Kaitlyn Chin, a second-year medical student at University of New England College of Osteopathic Medicine in Biddeford, Maine. “We were particularly interested in understanding how activity levels during recovery from concussion influence time to full recovery, to be able to identify modifiable factors to help guide concussion care. Previous studies have noted differences in the amount of time it takes children to recover from a concussion, and our team recently initiated a study to see if we can identify predictors associated with the amount of time between injury and when a child is medically cleared to return to activities which place the child at risk for reinjury.”
Ms. Chin’s team at Kennedy Krieger Institute in Baltimore reviewed the medical records of 178 children who were treated for concussions at an academically affiliated, rehabilitation-based clinic. The children had been medically cleared to return to play between September 2015 and February 2017. The children included in the study ranged in age from 6 to 17. A slight majority was younger than 14. Each child’s first visit to the clinic was within 60 days of his or her concussion.
The researchers reviewed each child’s record, noting when they had been approved to return to play. Then they looked at several other factors for each child, including sex, cause of the concussion (ie, sports or non-sports-related), number of symptoms, school attendance, and exercise status at the initial visit to the clinic. Finally, they considered these factors when the children were placed into two categories—children under 14 and children over 14—to examine potential differences related to age.
Ms. Chin’s team found that the number of symptoms affected how quickly all children were cleared to return to play. Fewer symptoms were associated with a faster return to play. For older children, male sex and higher level of exercise during recovery were associated with a faster return to play. For younger children, higher levels of exercise and school participation (eg, attending class and completing homework and tests) were associated with faster return to play.
Overall, this study shows that elementary and middle-school-aged children should be considered separately from high-school-aged students when considering risk factors for prolonged recovery from a concussion. Furthermore, Ms. Chin’s team found that school participation and exercise were not harmful and did not prolong recovery.
“Our study adds to the literature supporting that return to cognitive and safe physical activities while a child is still recovering from concussion does not prolong time to recovery,” said Ms. Chin. “Every child is different, and recovery is different for each concussion. [Therefore], a concussion recovery plan should be tailored for each child, and parents should seek help from the child’s pediatrician or other medical professionals for guiding care after a concussion.”
Medicine May Not Affect Concussion Recovery
Medications commonly prescribed to reduce symptoms of concussion may not affect recovery, said investigators. Sports medicine physicians commonly treat patients with concussion, so researchers in Utah investigated how some widely prescribed treatments might affect patients’ recovery.
“We really do not have much other than rest and gentle exercise to combat symptoms of concussion,” said Venessa Lee, MD, a physical medicine and rehabilitation resident at University of Utah Health in Salt Lake City. “Medications are commonly prescribed to help with symptoms, but there is little evidence that they help more than just time and rest.”
Although FDA has not approved any medication to treat concussion, physicians may prescribe medications like gabapentin or tricyclic antidepressants (TCAs) to help reduce symptoms during recovery. To examine whether these drugs benefit patients, Dr. Lee and her research team looked at 277 patients who had been diagnosed with concussion at a local academic sports medicine practice. At each of their visits to the clinic during recovery, patients reported their postconcussion symptoms. The research team used a score sheet to measure their symptoms, and they tracked scores of patients who had more than one visit to the clinic for as long as one year.
Patients were separated into three groups for the study: those not prescribed any medication, those prescribed gabapentin, and those prescribed one of two TCAs, amitriptyline or nortriptyline. Based on self-reported information, investigators gave each patient a score for two factors of postconcussion recovery: headaches and a combination of 22 symptoms, including headaches. Each score was on a scale of 0 to 6.
After they adjusted scores for gender and age, Dr. Lee’s team found that headache and combined symptoms scores decreased significantly within days after the first clinic visit for all three groups of patients—those who had taken no medications, those who had been prescribed gabapentin, and those who had been prescribed a TCA. Patients who had been prescribed any of the medications had significantly higher scores for headaches and overall postconcussion symptoms to begin with, but no one type of medication had any better or worse effect over the duration of the study.
“Patients’ symptoms improve with time after a concussion,” said Dr. Lee. “When we looked at [patients who received] gabapentin and TCAs, their symptoms improved over time as well, but similar to those that did not receive a medication.”
Based on this study, neither gabapentin nor TCAs appear to provide any additional benefit for postconcussion recovery. With this information, patients may be able to avoid taking unnecessary medications as they recover from concussions. Patients should speak with a physician about their symptoms after a concussion, said Dr. Lee.
“Though the two medications we studied did not show a profound improvement in our analysis, this was a retrospective study … which has many drawbacks and limitations. We need to do more research to really find the best method for improving postconcussive symptoms.”
Ballet Helps Children with Musculoskeletal and Neurologic Conditions
Adaptive ballet classes provide functional improvement and social interactions for children with musculoskeletal and neurologic conditions, according to researchers. This type of arts-based adaptive therapy is a promising expansion to successful adaptive sports therapies, said the investigators.
“While great strides have been made in adaptive sports, there are still relatively few opportunities in the arts for people with disabilities,” said Sarah Stauder, MD, a physician at the Medical College of Wisconsin in Milwaukee. “Because of this [scarcity], we wanted to evaluate the effect of adaptive ballet on the physical, emotional, social, and academic function of children with physical impairments. The program is a collaboration between a children’s hospital and a metropolitan ballet company that brings together professional dancers, pediatric doctors, physical and occupational therapists, and children with physical disabilities for a series of dance classes.”
The goal of the study was to see whether a weekly, 45-mintute ballet class with 15 minutes of ballet education over five consecutive weeks would improve the children’s balance, physical functions, social skills, and overall quality of life. Eighteen children (17 girls) from ages 5 to 14, took part in the class. Assessments of each child were performed before and after the series of classes using the Pediatric Quality of Life Inventory, the PEDI-CAT survey, and the Pediatric Balance Scale. Finally, a questionnaire was used to assess each child’s success in achieving individual goals set for the class.
At the end of the five weeks, 94% of participants reached their individual goals for the ballet program. PEDI-CAT scores improved after completion of the program, and the program was most beneficial to participants who had lower functioning and quality of life at the beginning of the program. Finally, the researchers noticed an average improvement in balance among the participants.
“Adaptive programs like the one studied here give children the opportunity to participate in activities they otherwise would have no way to do,” said Dr. Stauder. “More specifically, these dance classes instilled a sense of pride and confidence in the children while improving their physical functioning and quality of life. Our study should open the door to more arts-based therapy for children. It is an effective and enjoyable way for patients to get the therapy they need. When kids are active in an activity that interests them, they naturally make greater strides, and we were able to see this in their day-to-day function.”
Genetic Risk Score Predicts TBI Outcomes
A genetic risk score could help predict a patient’s quality of life after a traumatic brain injury (TBI), said researchers. One day, physicians could have a simple method to forecast a patient’s recovery and personalize therapy to maximize quality of life.
“Gene pathways can influence all of our biologic functions and risk for many health outcomes,” said Mark Linsenmeyer, MD, a resident physician at the University of Pittsburgh Medical Center. “Each person has a unique inherited genetic code. By studying one gene pathway in a large group of people with the same disease or health problem, we hope to unlock clues to why some people have different outcomes than others. This knowledge may be used to help physicians make the best treatment choice for each person.”
Dr. Linsenmeyer and colleagues set out to investigate how genes that affect the brain’s dopamine pathways could predict recovery in people with moderate-to-severe TBI. The team recruited 94 adults with TBI from a level-1 trauma center. They focused on the following five genes in the dopamine pathways: COMT rs4680, VMAT2 rs363226, DRD2 rs6279, ANKK1 Taq1a, and MAOA VNTR. They defined which risk genotypes were associated with lower average scores on surveys filled out by patients with TBI to describe their overall quality of life at six and 12 months after their injuries.
The researchers analyzed how individual variants of each of these five genes could affect patients’ quality of life, and then generated a weighted gene risk score as a measure to reflect cumulative risk represented by all genotypes included in the score. Based on available literature about dopamine pathway genetics, they predicted that their gene risk score calculation tool should be specific to a patient’s sex.
Before they calculated gene risk scores, the research team noticed that only COMT could significantly predict quality of life for a subset of patients six months after their injuries. After generating sex-specific gene risk scores, they found that variants of all five genes on the dopamine pathway could meaningfully contribute to a gene risk score that was highly predictive of quality of life after six months for patients of both sexes with TBI, and also predictive of quality of life after one year for women.
Electrical Stimulation Device Improves Motor Function
A person with a spinal cord injury can improve his or her ability to grip and move household objects by using an electrical stimulation device controlled by his or her thoughts, according to researchers. The study suggests that this new technology could one day enhance quality of life among people with disabilities and allow them to live more independently.
People with tetraplegia lose upper-limb strength and dexterity, which has a severe impact on their independence and quality of life. New technology that connects a person’s brain to an implanted functional electrical stimulation orthotics device on the hands could restore manual dexterity and grip strength, thus allowing him or her to perform simple daily tasks like holding a toothbrush without help.
“Individuals with cervical spinal cord injury identify recovery of the use of their hands as the single most impactful way that neurotechnology could change their lives,” said Marcie Bockbrader, MD, PhD, Assistant Professor of Physical Medicine and Rehabilitation at the Ohio State University Wexner Medical Center in Columbus. “Giving a person back [his or her] hands reduces dependence on others. It makes it possible to do the little things—like cutting food or opening a door—that are so essential to being able to take care of oneself.”
To test how well this thought-controlled brain–computer interface system works in real life to improve hand strength and dexterity, Dr. Bockbrader and her research team surgically implanted one of these devices into the hand of a 26-year-old man with C5-level, nonspastic tetraplegia following a spinal cord injury. He practiced using the device three times per week for four hours each session for more than 1,000 days. The research team administered standardized tests of upper-limb motor ability and functional participation to see how well the system improved his grip strength, quickness, and other basic skills.
Using this device improved the man’s upper-limb motor ability dramatically, according to several standardized tests. He improved his ability to grip and manipulate basic objects, and showed that he could perform ordinary tasks with his hands at the speed and dexterity levels of healthy individuals. He could move objects of different sizes and weights. With practice, he improved his ability to manipulate smaller household objects like a toothbrush or hairbrush. He also demonstrated that he could imagine different hand positions to proportionally adjust and control different hand movements.
“Our study demonstrated that patients with tetraplegia might be able to restore some of their skilled hand function with an implanted device that allows them to control movements with their own thoughts,” said Dr. Bockbrader. “Although this technology must be refined and tested before it can go from the laboratory to the public, it may one day offer people with disabilities a way to live and work more independently, and enable them to perform daily tasks.”
Concussion Recovery Varies Among Children
Not all children follow the same path to concussion recovery, nor do they have the same predictors for returning to normal activity, investigators reported. Their study also suggests that younger children should be considered separately from high-school students.
“Concussions are common among children, yet the literature is limited with regard to understanding trajectory of recovery after concussion, particularly in children with non-sports-related injuries and for younger children,” said Kaitlyn Chin, a second-year medical student at University of New England College of Osteopathic Medicine in Biddeford, Maine. “We were particularly interested in understanding how activity levels during recovery from concussion influence time to full recovery, to be able to identify modifiable factors to help guide concussion care. Previous studies have noted differences in the amount of time it takes children to recover from a concussion, and our team recently initiated a study to see if we can identify predictors associated with the amount of time between injury and when a child is medically cleared to return to activities which place the child at risk for reinjury.”
Ms. Chin’s team at Kennedy Krieger Institute in Baltimore reviewed the medical records of 178 children who were treated for concussions at an academically affiliated, rehabilitation-based clinic. The children had been medically cleared to return to play between September 2015 and February 2017. The children included in the study ranged in age from 6 to 17. A slight majority was younger than 14. Each child’s first visit to the clinic was within 60 days of his or her concussion.
The researchers reviewed each child’s record, noting when they had been approved to return to play. Then they looked at several other factors for each child, including sex, cause of the concussion (ie, sports or non-sports-related), number of symptoms, school attendance, and exercise status at the initial visit to the clinic. Finally, they considered these factors when the children were placed into two categories—children under 14 and children over 14—to examine potential differences related to age.
Ms. Chin’s team found that the number of symptoms affected how quickly all children were cleared to return to play. Fewer symptoms were associated with a faster return to play. For older children, male sex and higher level of exercise during recovery were associated with a faster return to play. For younger children, higher levels of exercise and school participation (eg, attending class and completing homework and tests) were associated with faster return to play.
Overall, this study shows that elementary and middle-school-aged children should be considered separately from high-school-aged students when considering risk factors for prolonged recovery from a concussion. Furthermore, Ms. Chin’s team found that school participation and exercise were not harmful and did not prolong recovery.
“Our study adds to the literature supporting that return to cognitive and safe physical activities while a child is still recovering from concussion does not prolong time to recovery,” said Ms. Chin. “Every child is different, and recovery is different for each concussion. [Therefore], a concussion recovery plan should be tailored for each child, and parents should seek help from the child’s pediatrician or other medical professionals for guiding care after a concussion.”
Medicine May Not Affect Concussion Recovery
Medications commonly prescribed to reduce symptoms of concussion may not affect recovery, said investigators. Sports medicine physicians commonly treat patients with concussion, so researchers in Utah investigated how some widely prescribed treatments might affect patients’ recovery.
“We really do not have much other than rest and gentle exercise to combat symptoms of concussion,” said Venessa Lee, MD, a physical medicine and rehabilitation resident at University of Utah Health in Salt Lake City. “Medications are commonly prescribed to help with symptoms, but there is little evidence that they help more than just time and rest.”
Although FDA has not approved any medication to treat concussion, physicians may prescribe medications like gabapentin or tricyclic antidepressants (TCAs) to help reduce symptoms during recovery. To examine whether these drugs benefit patients, Dr. Lee and her research team looked at 277 patients who had been diagnosed with concussion at a local academic sports medicine practice. At each of their visits to the clinic during recovery, patients reported their postconcussion symptoms. The research team used a score sheet to measure their symptoms, and they tracked scores of patients who had more than one visit to the clinic for as long as one year.
Patients were separated into three groups for the study: those not prescribed any medication, those prescribed gabapentin, and those prescribed one of two TCAs, amitriptyline or nortriptyline. Based on self-reported information, investigators gave each patient a score for two factors of postconcussion recovery: headaches and a combination of 22 symptoms, including headaches. Each score was on a scale of 0 to 6.
After they adjusted scores for gender and age, Dr. Lee’s team found that headache and combined symptoms scores decreased significantly within days after the first clinic visit for all three groups of patients—those who had taken no medications, those who had been prescribed gabapentin, and those who had been prescribed a TCA. Patients who had been prescribed any of the medications had significantly higher scores for headaches and overall postconcussion symptoms to begin with, but no one type of medication had any better or worse effect over the duration of the study.
“Patients’ symptoms improve with time after a concussion,” said Dr. Lee. “When we looked at [patients who received] gabapentin and TCAs, their symptoms improved over time as well, but similar to those that did not receive a medication.”
Based on this study, neither gabapentin nor TCAs appear to provide any additional benefit for postconcussion recovery. With this information, patients may be able to avoid taking unnecessary medications as they recover from concussions. Patients should speak with a physician about their symptoms after a concussion, said Dr. Lee.
“Though the two medications we studied did not show a profound improvement in our analysis, this was a retrospective study … which has many drawbacks and limitations. We need to do more research to really find the best method for improving postconcussive symptoms.”
Ballet Helps Children with Musculoskeletal and Neurologic Conditions
Adaptive ballet classes provide functional improvement and social interactions for children with musculoskeletal and neurologic conditions, according to researchers. This type of arts-based adaptive therapy is a promising expansion to successful adaptive sports therapies, said the investigators.
“While great strides have been made in adaptive sports, there are still relatively few opportunities in the arts for people with disabilities,” said Sarah Stauder, MD, a physician at the Medical College of Wisconsin in Milwaukee. “Because of this [scarcity], we wanted to evaluate the effect of adaptive ballet on the physical, emotional, social, and academic function of children with physical impairments. The program is a collaboration between a children’s hospital and a metropolitan ballet company that brings together professional dancers, pediatric doctors, physical and occupational therapists, and children with physical disabilities for a series of dance classes.”
The goal of the study was to see whether a weekly, 45-mintute ballet class with 15 minutes of ballet education over five consecutive weeks would improve the children’s balance, physical functions, social skills, and overall quality of life. Eighteen children (17 girls) from ages 5 to 14, took part in the class. Assessments of each child were performed before and after the series of classes using the Pediatric Quality of Life Inventory, the PEDI-CAT survey, and the Pediatric Balance Scale. Finally, a questionnaire was used to assess each child’s success in achieving individual goals set for the class.
At the end of the five weeks, 94% of participants reached their individual goals for the ballet program. PEDI-CAT scores improved after completion of the program, and the program was most beneficial to participants who had lower functioning and quality of life at the beginning of the program. Finally, the researchers noticed an average improvement in balance among the participants.
“Adaptive programs like the one studied here give children the opportunity to participate in activities they otherwise would have no way to do,” said Dr. Stauder. “More specifically, these dance classes instilled a sense of pride and confidence in the children while improving their physical functioning and quality of life. Our study should open the door to more arts-based therapy for children. It is an effective and enjoyable way for patients to get the therapy they need. When kids are active in an activity that interests them, they naturally make greater strides, and we were able to see this in their day-to-day function.”
Genetic Risk Score Predicts TBI Outcomes
A genetic risk score could help predict a patient’s quality of life after a traumatic brain injury (TBI), said researchers. One day, physicians could have a simple method to forecast a patient’s recovery and personalize therapy to maximize quality of life.
“Gene pathways can influence all of our biologic functions and risk for many health outcomes,” said Mark Linsenmeyer, MD, a resident physician at the University of Pittsburgh Medical Center. “Each person has a unique inherited genetic code. By studying one gene pathway in a large group of people with the same disease or health problem, we hope to unlock clues to why some people have different outcomes than others. This knowledge may be used to help physicians make the best treatment choice for each person.”
Dr. Linsenmeyer and colleagues set out to investigate how genes that affect the brain’s dopamine pathways could predict recovery in people with moderate-to-severe TBI. The team recruited 94 adults with TBI from a level-1 trauma center. They focused on the following five genes in the dopamine pathways: COMT rs4680, VMAT2 rs363226, DRD2 rs6279, ANKK1 Taq1a, and MAOA VNTR. They defined which risk genotypes were associated with lower average scores on surveys filled out by patients with TBI to describe their overall quality of life at six and 12 months after their injuries.
The researchers analyzed how individual variants of each of these five genes could affect patients’ quality of life, and then generated a weighted gene risk score as a measure to reflect cumulative risk represented by all genotypes included in the score. Based on available literature about dopamine pathway genetics, they predicted that their gene risk score calculation tool should be specific to a patient’s sex.
Before they calculated gene risk scores, the research team noticed that only COMT could significantly predict quality of life for a subset of patients six months after their injuries. After generating sex-specific gene risk scores, they found that variants of all five genes on the dopamine pathway could meaningfully contribute to a gene risk score that was highly predictive of quality of life after six months for patients of both sexes with TBI, and also predictive of quality of life after one year for women.

Advances Broaden Treatment Options for Parkinson’s Disease Motor Symptoms
NAPLES, FL—Although levodopa remains the standard treatment for managing motor symptoms in patients with Parkinson’s disease, many new options are available, and others are in the pipeline. These options include novel modes of carbidopa–levodopa delivery, new adjunctive medications, and innovations in deep brain stimulation (DBS) therapy.

“The explosion of different therapies for Parkinson’s disease is quite exciting,” said Stanley P. Fisher, MD, at the 45thAnnual Meeting of the Southern Clinical Neurological Society. “However, the key is to address individualized management considerations, such as age, cognitive/psychiatric profile, and caregiver status.” Dr. Fisher is Codirector of Saint Luke’s Marion Bloch Neuroscience Institute and Associate Professor of Neurology at the University of Missouri in Kansas City.
Clinical factors to consider include fluctuations in symptom control as the disease progresses—specifically, wearing off (ie, re-emergence of symptoms prior to the next scheduled levodopa dose), on and off time (ie, unpredictable periods of good or poor symptom control), delayed on response (ie, dose takes longer to improve symptoms than previously), dose failure, and levodopa-induced dyskinesia, Dr. Fisher noted. Risk factors for developing dyskinesia include increasing doses of levodopa beyond 400 mg, female gender, low body weight, and earlier age of Parkinson’s disease onset, independent of how many years a patient has been taking levodopa.
Levodopa Preparations
“Levodopa has been used to treat Parkinson’s disease since the early ’70s, and its efficacy is well established,” Dr. Fisher said. “There has been an attempt over the years to create a perfect long-lasting levodopa.” In 1988, the FDA approved Sinemet, an immediate-release combination carbidopa–levodopa oral treatment. Carbidopa prevents the breakdown of levodopa before it crosses the blood–brain barrier, allowing lower doses of levodopa to be used. Sinemet CR (controlled release) has an unpredictable time of onset, Dr. Fisher said. “It should not be used during the day. But it may be helpful to prescribe this drug for use at night, when the time of onset is not critical.”
Parcopa, a carbidopa–levodopa preparation in the form of orally disintegrating tablets, was approved in 2004. “Clinically, it is not much different from Sinemet,” Dr. Fisher said. “However, it is expensive and should be used strictly by people who have difficulty swallowing.”
Duopa, which was approved in 2015, is a carbidopa–levodopa enteral solution delivered by a programmable pump via a transgastric jejunal tube. “It is an intestinal gel that is delivered continuously for at least 16 hours a day,” Dr. Fisher said. “The treatment effect tends to wear off at night, so if the patient does not have a caregiver to help them with the early morning akinesia, using this drug may be quite difficult.”
Rytary is a carbidopa–levodopa extended-release capsule approved in 2015. “The capsules have different beads that allow immediate, intermediate, and long-term release of levodopa, with a half-life of about five hours,” Dr. Fisher said. “Issues related to delayed on and lack of peak-dose effect have limited its widespread use. In addition, the dosing conversion from Sinemet is not intuitive.”
Phase III study results are anticipated for the experimental drug ND0612, a novel liquid carbidopa–levodopa formulation for subcutaneous administration via a pump patch. In a randomized double-blind placebo-controlled parallel group study, investigators are assessing a high dose and a low dose of ND0612 as adjunctive treatment to oral levodopa. Previous research had shown greater bioavailability of the drug with subcutaneous versus oral administration. One study found significantly reduced off time with treatment, with 42% of patients having no off time, Dr. Fisher said.
An inhaled levodopa, CVT-301 (Inbrija), has been submitted to the FDA. The treatment’s novel inhalation system “requires the patient to have intact pulmonary function and certain manual skills. It also requires that oral carbidopa be taken separately,” Dr. Fisher added.
Adjunctive Therapy
“When we started using dopamine agonists and other levodopa-sparing therapies in 1999, it changed the way we treat Parkinson’s disease,” Dr. Fisher said. “Generally, these agents are not as effective as levodopa and potentially have more adverse effects. However, there are some patients with tremor-dominant disease who may respond to dopamine agonists better than to levodopa. Also, for younger patients on 300 mg of levodopa who are not well controlled, prescribing additional dopamine agonists may be the way to go.”
Approved by the FDA in 2004, subcutaneous apomorphine (a non-ergoline dopamine agonist) is delivered via injector pen. Another mode of apomorphine delivery—infusion via injection pump—has been available in Europe for more than 25 years and is being assessed for use in the US. Studies have found that apomorphine infusion may significantly reduce off time and increase on time. The most common adverse effect was skin nodules at the infusion site. In addition, sublingual apomorphine has been studied in a phase III trial and may be available soon, Dr. Fisher said.
Safinamide (Xydago) is a monoamine oxidase type B inhibitor approved in March 2017 indicated for patients who experience off episodes. “While I do not see any dramatic benefit of using this drug, it has two-year data to show that it is safe and effective,” Dr. Fisher noted.
Immediate-release amantadine, an N-methyl-D-aspartate antagonist, has been used to treat Parkinson’s disease since 2003. However, its treatment effect is not well sustained, and multiple doses of the drug throughout the day are not well tolerated, Dr. Fisher said. Extended-release amantadine (Gocovri), approved in August 2017, confers a significant reduction in the Unified Parkinson’s Disease Rating Scale score when given at night. Adverse effects include dizziness, edema, and orthostatic hypotension. “Hallucination is particularly a problem in patients older than 65,” Dr. Fisher said. “The good news is that 57% of hallucination problems resolve within two weeks as patients adjust to the medication. So, it may be worth giving it a try.”
Deep Brain Stimulation
Approved in 2002, the implantable Activa DBS system by Medtronic is indicated for idiopathic Parkinson’s disease of at least four years’ duration in patients who have disabling motor symptoms despite being on an optimized medication regimen but continue, even if briefly, to respond to levodopa, Dr. Fisher said. Used as adjunctive therapy, it provides bilateral stimulation of the internal globus pallidus or the subthalamic nucleus. In one study, patients had significant improvements in on and off time after six months of surgery.
Similar benefits were found for the St. Jude Medical Infinity DBS system, which was approved by the FDA in 2015. The system includes directional lead technology designed to allow physicians to precisely steer current towards the desired structural areas, thereby maximizing symptom management and potentially reducing adverse effects.
The newest DBS system on the market is the Vercise system by Boston Scientific. “This is the only platform that allows independent current delivery to each of the 16 electrodes on the implanted leads,” Dr. Fisher said. “The rechargeable system has a battery life of more than 15 years.” Although the technology has been available in Europe for the last five years, the Vercise system was approved for use in the US in December 2017. Its approval was based on the results of the INTREPID study, the first multicenter, prospective, double-blind, randomized sham-controlled study of DBS for Parkinson’s disease in the US.
“The technology is truly amazing,” Dr. Fisher said. “How the systemperforms in clinical practice remains to be seen.”
—Adriene Marshall
Suggested Reading
Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229-237.
Fahn S, Oakes D, Shoulson I, et al. Levodopa and the progression of Parkinson’s disease. N Engl J Med. 2004;351(24):2498-2508.
Hely MA, Morris JG, Reid WG, Trafficante R. Sydney Multicenter Study of Parkinson’s disease: non-L-dopa-responsive problems dominate at 15 years. Mov Disord. 2005;20(2):190-199.
Pahwa R, Tanner CM, Hauser RA, et al. ADS-5102 (Amantadine) extended-release capsules for levodopa-induced dyskinesia in Parkinson disease (EASE LID Study): a randomized clinical trial. JAMA Neurol. 2017;74(8):941-949.
Schuepbach WM, Rau J, Knudsen K, et al. Neurostimulation for Parkinson’s disease with early motor complications. N Engl J Med. 2013;368(7):610-622.
NAPLES, FL—Although levodopa remains the standard treatment for managing motor symptoms in patients with Parkinson’s disease, many new options are available, and others are in the pipeline. These options include novel modes of carbidopa–levodopa delivery, new adjunctive medications, and innovations in deep brain stimulation (DBS) therapy.
“The explosion of different therapies for Parkinson’s disease is quite exciting,” said Stanley P. Fisher, MD, at the 45thAnnual Meeting of the Southern Clinical Neurological Society. “However, the key is to address individualized management considerations, such as age, cognitive/psychiatric profile, and caregiver status.” Dr. Fisher is Codirector of Saint Luke’s Marion Bloch Neuroscience Institute and Associate Professor of Neurology at the University of Missouri in Kansas City.
Clinical factors to consider include fluctuations in symptom control as the disease progresses—specifically, wearing off (ie, re-emergence of symptoms prior to the next scheduled levodopa dose), on and off time (ie, unpredictable periods of good or poor symptom control), delayed on response (ie, dose takes longer to improve symptoms than previously), dose failure, and levodopa-induced dyskinesia, Dr. Fisher noted. Risk factors for developing dyskinesia include increasing doses of levodopa beyond 400 mg, female gender, low body weight, and earlier age of Parkinson’s disease onset, independent of how many years a patient has been taking levodopa.
Levodopa Preparations
“Levodopa has been used to treat Parkinson’s disease since the early ’70s, and its efficacy is well established,” Dr. Fisher said. “There has been an attempt over the years to create a perfect long-lasting levodopa.” In 1988, the FDA approved Sinemet, an immediate-release combination carbidopa–levodopa oral treatment. Carbidopa prevents the breakdown of levodopa before it crosses the blood–brain barrier, allowing lower doses of levodopa to be used. Sinemet CR (controlled release) has an unpredictable time of onset, Dr. Fisher said. “It should not be used during the day. But it may be helpful to prescribe this drug for use at night, when the time of onset is not critical.”
Parcopa, a carbidopa–levodopa preparation in the form of orally disintegrating tablets, was approved in 2004. “Clinically, it is not much different from Sinemet,” Dr. Fisher said. “However, it is expensive and should be used strictly by people who have difficulty swallowing.”
Duopa, which was approved in 2015, is a carbidopa–levodopa enteral solution delivered by a programmable pump via a transgastric jejunal tube. “It is an intestinal gel that is delivered continuously for at least 16 hours a day,” Dr. Fisher said. “The treatment effect tends to wear off at night, so if the patient does not have a caregiver to help them with the early morning akinesia, using this drug may be quite difficult.”
Rytary is a carbidopa–levodopa extended-release capsule approved in 2015. “The capsules have different beads that allow immediate, intermediate, and long-term release of levodopa, with a half-life of about five hours,” Dr. Fisher said. “Issues related to delayed on and lack of peak-dose effect have limited its widespread use. In addition, the dosing conversion from Sinemet is not intuitive.”
Phase III study results are anticipated for the experimental drug ND0612, a novel liquid carbidopa–levodopa formulation for subcutaneous administration via a pump patch. In a randomized double-blind placebo-controlled parallel group study, investigators are assessing a high dose and a low dose of ND0612 as adjunctive treatment to oral levodopa. Previous research had shown greater bioavailability of the drug with subcutaneous versus oral administration. One study found significantly reduced off time with treatment, with 42% of patients having no off time, Dr. Fisher said.
An inhaled levodopa, CVT-301 (Inbrija), has been submitted to the FDA. The treatment’s novel inhalation system “requires the patient to have intact pulmonary function and certain manual skills. It also requires that oral carbidopa be taken separately,” Dr. Fisher added.
Adjunctive Therapy
“When we started using dopamine agonists and other levodopa-sparing therapies in 1999, it changed the way we treat Parkinson’s disease,” Dr. Fisher said. “Generally, these agents are not as effective as levodopa and potentially have more adverse effects. However, there are some patients with tremor-dominant disease who may respond to dopamine agonists better than to levodopa. Also, for younger patients on 300 mg of levodopa who are not well controlled, prescribing additional dopamine agonists may be the way to go.”
Approved by the FDA in 2004, subcutaneous apomorphine (a non-ergoline dopamine agonist) is delivered via injector pen. Another mode of apomorphine delivery—infusion via injection pump—has been available in Europe for more than 25 years and is being assessed for use in the US. Studies have found that apomorphine infusion may significantly reduce off time and increase on time. The most common adverse effect was skin nodules at the infusion site. In addition, sublingual apomorphine has been studied in a phase III trial and may be available soon, Dr. Fisher said.
Safinamide (Xydago) is a monoamine oxidase type B inhibitor approved in March 2017 indicated for patients who experience off episodes. “While I do not see any dramatic benefit of using this drug, it has two-year data to show that it is safe and effective,” Dr. Fisher noted.
Immediate-release amantadine, an N-methyl-D-aspartate antagonist, has been used to treat Parkinson’s disease since 2003. However, its treatment effect is not well sustained, and multiple doses of the drug throughout the day are not well tolerated, Dr. Fisher said. Extended-release amantadine (Gocovri), approved in August 2017, confers a significant reduction in the Unified Parkinson’s Disease Rating Scale score when given at night. Adverse effects include dizziness, edema, and orthostatic hypotension. “Hallucination is particularly a problem in patients older than 65,” Dr. Fisher said. “The good news is that 57% of hallucination problems resolve within two weeks as patients adjust to the medication. So, it may be worth giving it a try.”
Deep Brain Stimulation
Approved in 2002, the implantable Activa DBS system by Medtronic is indicated for idiopathic Parkinson’s disease of at least four years’ duration in patients who have disabling motor symptoms despite being on an optimized medication regimen but continue, even if briefly, to respond to levodopa, Dr. Fisher said. Used as adjunctive therapy, it provides bilateral stimulation of the internal globus pallidus or the subthalamic nucleus. In one study, patients had significant improvements in on and off time after six months of surgery.
Similar benefits were found for the St. Jude Medical Infinity DBS system, which was approved by the FDA in 2015. The system includes directional lead technology designed to allow physicians to precisely steer current towards the desired structural areas, thereby maximizing symptom management and potentially reducing adverse effects.
The newest DBS system on the market is the Vercise system by Boston Scientific. “This is the only platform that allows independent current delivery to each of the 16 electrodes on the implanted leads,” Dr. Fisher said. “The rechargeable system has a battery life of more than 15 years.” Although the technology has been available in Europe for the last five years, the Vercise system was approved for use in the US in December 2017. Its approval was based on the results of the INTREPID study, the first multicenter, prospective, double-blind, randomized sham-controlled study of DBS for Parkinson’s disease in the US.
“The technology is truly amazing,” Dr. Fisher said. “How the systemperforms in clinical practice remains to be seen.”
—Adriene Marshall
Suggested Reading
Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229-237.
Fahn S, Oakes D, Shoulson I, et al. Levodopa and the progression of Parkinson’s disease. N Engl J Med. 2004;351(24):2498-2508.
Hely MA, Morris JG, Reid WG, Trafficante R. Sydney Multicenter Study of Parkinson’s disease: non-L-dopa-responsive problems dominate at 15 years. Mov Disord. 2005;20(2):190-199.
Pahwa R, Tanner CM, Hauser RA, et al. ADS-5102 (Amantadine) extended-release capsules for levodopa-induced dyskinesia in Parkinson disease (EASE LID Study): a randomized clinical trial. JAMA Neurol. 2017;74(8):941-949.
Schuepbach WM, Rau J, Knudsen K, et al. Neurostimulation for Parkinson’s disease with early motor complications. N Engl J Med. 2013;368(7):610-622.
NAPLES, FL—Although levodopa remains the standard treatment for managing motor symptoms in patients with Parkinson’s disease, many new options are available, and others are in the pipeline. These options include novel modes of carbidopa–levodopa delivery, new adjunctive medications, and innovations in deep brain stimulation (DBS) therapy.
“The explosion of different therapies for Parkinson’s disease is quite exciting,” said Stanley P. Fisher, MD, at the 45thAnnual Meeting of the Southern Clinical Neurological Society. “However, the key is to address individualized management considerations, such as age, cognitive/psychiatric profile, and caregiver status.” Dr. Fisher is Codirector of Saint Luke’s Marion Bloch Neuroscience Institute and Associate Professor of Neurology at the University of Missouri in Kansas City.
Clinical factors to consider include fluctuations in symptom control as the disease progresses—specifically, wearing off (ie, re-emergence of symptoms prior to the next scheduled levodopa dose), on and off time (ie, unpredictable periods of good or poor symptom control), delayed on response (ie, dose takes longer to improve symptoms than previously), dose failure, and levodopa-induced dyskinesia, Dr. Fisher noted. Risk factors for developing dyskinesia include increasing doses of levodopa beyond 400 mg, female gender, low body weight, and earlier age of Parkinson’s disease onset, independent of how many years a patient has been taking levodopa.
Levodopa Preparations
“Levodopa has been used to treat Parkinson’s disease since the early ’70s, and its efficacy is well established,” Dr. Fisher said. “There has been an attempt over the years to create a perfect long-lasting levodopa.” In 1988, the FDA approved Sinemet, an immediate-release combination carbidopa–levodopa oral treatment. Carbidopa prevents the breakdown of levodopa before it crosses the blood–brain barrier, allowing lower doses of levodopa to be used. Sinemet CR (controlled release) has an unpredictable time of onset, Dr. Fisher said. “It should not be used during the day. But it may be helpful to prescribe this drug for use at night, when the time of onset is not critical.”
Parcopa, a carbidopa–levodopa preparation in the form of orally disintegrating tablets, was approved in 2004. “Clinically, it is not much different from Sinemet,” Dr. Fisher said. “However, it is expensive and should be used strictly by people who have difficulty swallowing.”
Duopa, which was approved in 2015, is a carbidopa–levodopa enteral solution delivered by a programmable pump via a transgastric jejunal tube. “It is an intestinal gel that is delivered continuously for at least 16 hours a day,” Dr. Fisher said. “The treatment effect tends to wear off at night, so if the patient does not have a caregiver to help them with the early morning akinesia, using this drug may be quite difficult.”
Rytary is a carbidopa–levodopa extended-release capsule approved in 2015. “The capsules have different beads that allow immediate, intermediate, and long-term release of levodopa, with a half-life of about five hours,” Dr. Fisher said. “Issues related to delayed on and lack of peak-dose effect have limited its widespread use. In addition, the dosing conversion from Sinemet is not intuitive.”
Phase III study results are anticipated for the experimental drug ND0612, a novel liquid carbidopa–levodopa formulation for subcutaneous administration via a pump patch. In a randomized double-blind placebo-controlled parallel group study, investigators are assessing a high dose and a low dose of ND0612 as adjunctive treatment to oral levodopa. Previous research had shown greater bioavailability of the drug with subcutaneous versus oral administration. One study found significantly reduced off time with treatment, with 42% of patients having no off time, Dr. Fisher said.
An inhaled levodopa, CVT-301 (Inbrija), has been submitted to the FDA. The treatment’s novel inhalation system “requires the patient to have intact pulmonary function and certain manual skills. It also requires that oral carbidopa be taken separately,” Dr. Fisher added.
Adjunctive Therapy
“When we started using dopamine agonists and other levodopa-sparing therapies in 1999, it changed the way we treat Parkinson’s disease,” Dr. Fisher said. “Generally, these agents are not as effective as levodopa and potentially have more adverse effects. However, there are some patients with tremor-dominant disease who may respond to dopamine agonists better than to levodopa. Also, for younger patients on 300 mg of levodopa who are not well controlled, prescribing additional dopamine agonists may be the way to go.”
Approved by the FDA in 2004, subcutaneous apomorphine (a non-ergoline dopamine agonist) is delivered via injector pen. Another mode of apomorphine delivery—infusion via injection pump—has been available in Europe for more than 25 years and is being assessed for use in the US. Studies have found that apomorphine infusion may significantly reduce off time and increase on time. The most common adverse effect was skin nodules at the infusion site. In addition, sublingual apomorphine has been studied in a phase III trial and may be available soon, Dr. Fisher said.
Safinamide (Xydago) is a monoamine oxidase type B inhibitor approved in March 2017 indicated for patients who experience off episodes. “While I do not see any dramatic benefit of using this drug, it has two-year data to show that it is safe and effective,” Dr. Fisher noted.
Immediate-release amantadine, an N-methyl-D-aspartate antagonist, has been used to treat Parkinson’s disease since 2003. However, its treatment effect is not well sustained, and multiple doses of the drug throughout the day are not well tolerated, Dr. Fisher said. Extended-release amantadine (Gocovri), approved in August 2017, confers a significant reduction in the Unified Parkinson’s Disease Rating Scale score when given at night. Adverse effects include dizziness, edema, and orthostatic hypotension. “Hallucination is particularly a problem in patients older than 65,” Dr. Fisher said. “The good news is that 57% of hallucination problems resolve within two weeks as patients adjust to the medication. So, it may be worth giving it a try.”
Deep Brain Stimulation
Approved in 2002, the implantable Activa DBS system by Medtronic is indicated for idiopathic Parkinson’s disease of at least four years’ duration in patients who have disabling motor symptoms despite being on an optimized medication regimen but continue, even if briefly, to respond to levodopa, Dr. Fisher said. Used as adjunctive therapy, it provides bilateral stimulation of the internal globus pallidus or the subthalamic nucleus. In one study, patients had significant improvements in on and off time after six months of surgery.
Similar benefits were found for the St. Jude Medical Infinity DBS system, which was approved by the FDA in 2015. The system includes directional lead technology designed to allow physicians to precisely steer current towards the desired structural areas, thereby maximizing symptom management and potentially reducing adverse effects.
The newest DBS system on the market is the Vercise system by Boston Scientific. “This is the only platform that allows independent current delivery to each of the 16 electrodes on the implanted leads,” Dr. Fisher said. “The rechargeable system has a battery life of more than 15 years.” Although the technology has been available in Europe for the last five years, the Vercise system was approved for use in the US in December 2017. Its approval was based on the results of the INTREPID study, the first multicenter, prospective, double-blind, randomized sham-controlled study of DBS for Parkinson’s disease in the US.
“The technology is truly amazing,” Dr. Fisher said. “How the systemperforms in clinical practice remains to be seen.”
—Adriene Marshall
Suggested Reading
Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229-237.
Fahn S, Oakes D, Shoulson I, et al. Levodopa and the progression of Parkinson’s disease. N Engl J Med. 2004;351(24):2498-2508.
Hely MA, Morris JG, Reid WG, Trafficante R. Sydney Multicenter Study of Parkinson’s disease: non-L-dopa-responsive problems dominate at 15 years. Mov Disord. 2005;20(2):190-199.
Pahwa R, Tanner CM, Hauser RA, et al. ADS-5102 (Amantadine) extended-release capsules for levodopa-induced dyskinesia in Parkinson disease (EASE LID Study): a randomized clinical trial. JAMA Neurol. 2017;74(8):941-949.
Schuepbach WM, Rau J, Knudsen K, et al. Neurostimulation for Parkinson’s disease with early motor complications. N Engl J Med. 2013;368(7):610-622.

How Are Newer DMTs Used in Pediatric MS?
SAN DIEGO—Newer oral and IV disease-modifying therapies (DMTs) for multiple sclerosis (MS) increasingly are used in children, according to data presented at the ACTRIMS 2018 Forum. These DMTs often are second-line therapies, but some patients receive them as first-line treatment.
“Newer DMTs … are being started more often over time at clinics participating in the US Network of Pediatric MS Centers,” said Kristen M. Krysko, MD, Clinical Fellow at the University of California, San Francisco School of Medicine, and colleagues.

The short-term side effect profile of newer DMTs in children is similar to that in adults. The study may have underestimated side effects, however, and long-term safety data are lacking, the researchers noted.
Treatment Challenges
About 5% of patients with MS develop symptoms before age 18. “Treatment of pediatric MS is challenging, given high relapse rates and the lack of safety and efficacy data for DMTs in children,” Dr. Krysko and colleagues said. “Conventionally, first-line treatments for pediatric MS include interferon beta and glatiramer acetate, but these agents may be poorly tolerated, since they are given by injection, and may not adequately control the disease. Those with breakthrough events require escalation to more potent agents, which are increasingly used off-label in pediatric MS despite limited data about safety or efficacy in children.”
To characterize the use and safety of newer DMTs in children with MS and clinically isolated syndrome (CIS), Dr. Krysko and colleagues conducted a retrospective cohort study of prospectively collected data at 12 clinics participating in the US Network of Pediatric MS Centers as of August 2017.
The researchers examined patterns of newer DMT use and newer DMT side effects. They classified DMTs as injectable (ie, glatiramer acetate and beta-interferons), oral (ie, dimethyl fumarate, fingolimod, and teriflunomide), or IV (ie, natalizumab, rituximab, alemtuzumab, and ocrelizumab). The researchers considered dimethyl fumarate, fingolimod, teriflunomide, natalizumab, rituximab, ocrelizumab, alemtuzumab, and daclizumab to be newer therapies.
The cohort included more than 1,000 patients with MS or CIS. In all, 618 patients had received a DMT before age 18 (587 patients with a diagnosis of MS at last follow-up and 31 patients with a diagnosis of CIS at last follow-up). About 66% were female, and patients’ mean age at MS onset was approximately 13.
The Use of Oral and IV DMTs
From 2008 to 2017, use of newer oral and IV DMTs increased overall and as first-line therapy in patients younger than 12 and in patients 12 or older. Of the 618 patients who received a DMT before age 18, 259 (42%) received a newer DMT, and 104 (17%) received a newer DMT as a first-line therapy.
Newer DMTs used in patients before age 18 included natalizumab in 101 patients, dimethyl fumarate in 100 patients, rituximab in 57 patients, fingolimod in 37 patients, daclizumab in five patients, and teriflunomide in three patients. Newer DMTs used as first-line therapy in patients before age 18 included dimethyl fumarate in 36 patients, natalizumab in 30 patients, rituximab in 22 patients, fingolimod in 14 patients, and teriflunomide in two patients.
Patients were exposed to dimethyl fumarate for 149 person-years, natalizumab for 140 person-years, rituximab for 75 person-years, fingolimod for 55 person-years, daclizumab for 10 person-years, and teriflunomide for one person-year.
Randomized controlled trials of the efficacy of DMTs in children with MS are ongoing. Future studies may explore predictors of newer DMT use in children with MS, the researchers said.
—Jake Remaly
SAN DIEGO—Newer oral and IV disease-modifying therapies (DMTs) for multiple sclerosis (MS) increasingly are used in children, according to data presented at the ACTRIMS 2018 Forum. These DMTs often are second-line therapies, but some patients receive them as first-line treatment.
“Newer DMTs … are being started more often over time at clinics participating in the US Network of Pediatric MS Centers,” said Kristen M. Krysko, MD, Clinical Fellow at the University of California, San Francisco School of Medicine, and colleagues.
The short-term side effect profile of newer DMTs in children is similar to that in adults. The study may have underestimated side effects, however, and long-term safety data are lacking, the researchers noted.
Treatment Challenges
About 5% of patients with MS develop symptoms before age 18. “Treatment of pediatric MS is challenging, given high relapse rates and the lack of safety and efficacy data for DMTs in children,” Dr. Krysko and colleagues said. “Conventionally, first-line treatments for pediatric MS include interferon beta and glatiramer acetate, but these agents may be poorly tolerated, since they are given by injection, and may not adequately control the disease. Those with breakthrough events require escalation to more potent agents, which are increasingly used off-label in pediatric MS despite limited data about safety or efficacy in children.”
To characterize the use and safety of newer DMTs in children with MS and clinically isolated syndrome (CIS), Dr. Krysko and colleagues conducted a retrospective cohort study of prospectively collected data at 12 clinics participating in the US Network of Pediatric MS Centers as of August 2017.
The researchers examined patterns of newer DMT use and newer DMT side effects. They classified DMTs as injectable (ie, glatiramer acetate and beta-interferons), oral (ie, dimethyl fumarate, fingolimod, and teriflunomide), or IV (ie, natalizumab, rituximab, alemtuzumab, and ocrelizumab). The researchers considered dimethyl fumarate, fingolimod, teriflunomide, natalizumab, rituximab, ocrelizumab, alemtuzumab, and daclizumab to be newer therapies.
The cohort included more than 1,000 patients with MS or CIS. In all, 618 patients had received a DMT before age 18 (587 patients with a diagnosis of MS at last follow-up and 31 patients with a diagnosis of CIS at last follow-up). About 66% were female, and patients’ mean age at MS onset was approximately 13.
The Use of Oral and IV DMTs
From 2008 to 2017, use of newer oral and IV DMTs increased overall and as first-line therapy in patients younger than 12 and in patients 12 or older. Of the 618 patients who received a DMT before age 18, 259 (42%) received a newer DMT, and 104 (17%) received a newer DMT as a first-line therapy.
Newer DMTs used in patients before age 18 included natalizumab in 101 patients, dimethyl fumarate in 100 patients, rituximab in 57 patients, fingolimod in 37 patients, daclizumab in five patients, and teriflunomide in three patients. Newer DMTs used as first-line therapy in patients before age 18 included dimethyl fumarate in 36 patients, natalizumab in 30 patients, rituximab in 22 patients, fingolimod in 14 patients, and teriflunomide in two patients.
Patients were exposed to dimethyl fumarate for 149 person-years, natalizumab for 140 person-years, rituximab for 75 person-years, fingolimod for 55 person-years, daclizumab for 10 person-years, and teriflunomide for one person-year.
Randomized controlled trials of the efficacy of DMTs in children with MS are ongoing. Future studies may explore predictors of newer DMT use in children with MS, the researchers said.
—Jake Remaly
SAN DIEGO—Newer oral and IV disease-modifying therapies (DMTs) for multiple sclerosis (MS) increasingly are used in children, according to data presented at the ACTRIMS 2018 Forum. These DMTs often are second-line therapies, but some patients receive them as first-line treatment.
“Newer DMTs … are being started more often over time at clinics participating in the US Network of Pediatric MS Centers,” said Kristen M. Krysko, MD, Clinical Fellow at the University of California, San Francisco School of Medicine, and colleagues.
The short-term side effect profile of newer DMTs in children is similar to that in adults. The study may have underestimated side effects, however, and long-term safety data are lacking, the researchers noted.
Treatment Challenges
About 5% of patients with MS develop symptoms before age 18. “Treatment of pediatric MS is challenging, given high relapse rates and the lack of safety and efficacy data for DMTs in children,” Dr. Krysko and colleagues said. “Conventionally, first-line treatments for pediatric MS include interferon beta and glatiramer acetate, but these agents may be poorly tolerated, since they are given by injection, and may not adequately control the disease. Those with breakthrough events require escalation to more potent agents, which are increasingly used off-label in pediatric MS despite limited data about safety or efficacy in children.”
To characterize the use and safety of newer DMTs in children with MS and clinically isolated syndrome (CIS), Dr. Krysko and colleagues conducted a retrospective cohort study of prospectively collected data at 12 clinics participating in the US Network of Pediatric MS Centers as of August 2017.
The researchers examined patterns of newer DMT use and newer DMT side effects. They classified DMTs as injectable (ie, glatiramer acetate and beta-interferons), oral (ie, dimethyl fumarate, fingolimod, and teriflunomide), or IV (ie, natalizumab, rituximab, alemtuzumab, and ocrelizumab). The researchers considered dimethyl fumarate, fingolimod, teriflunomide, natalizumab, rituximab, ocrelizumab, alemtuzumab, and daclizumab to be newer therapies.
The cohort included more than 1,000 patients with MS or CIS. In all, 618 patients had received a DMT before age 18 (587 patients with a diagnosis of MS at last follow-up and 31 patients with a diagnosis of CIS at last follow-up). About 66% were female, and patients’ mean age at MS onset was approximately 13.
The Use of Oral and IV DMTs
From 2008 to 2017, use of newer oral and IV DMTs increased overall and as first-line therapy in patients younger than 12 and in patients 12 or older. Of the 618 patients who received a DMT before age 18, 259 (42%) received a newer DMT, and 104 (17%) received a newer DMT as a first-line therapy.
Newer DMTs used in patients before age 18 included natalizumab in 101 patients, dimethyl fumarate in 100 patients, rituximab in 57 patients, fingolimod in 37 patients, daclizumab in five patients, and teriflunomide in three patients. Newer DMTs used as first-line therapy in patients before age 18 included dimethyl fumarate in 36 patients, natalizumab in 30 patients, rituximab in 22 patients, fingolimod in 14 patients, and teriflunomide in two patients.
Patients were exposed to dimethyl fumarate for 149 person-years, natalizumab for 140 person-years, rituximab for 75 person-years, fingolimod for 55 person-years, daclizumab for 10 person-years, and teriflunomide for one person-year.
Randomized controlled trials of the efficacy of DMTs in children with MS are ongoing. Future studies may explore predictors of newer DMT use in children with MS, the researchers said.
—Jake Remaly
Overweight and obese individuals face greater cardiovascular morbidity
.
In a report published online Feb. 28 in JAMA Cardiology, researchers presented an analysis of pooled data from 190,672 participants and 3.2 million person-years of follow-up in 10 prospective cohort studies, including the Framingham Heart Study, the Multi-Ethnic Study of Atherosclerosis, and the Atherosclerosis Risk in Communities Study.
Incident cardiovascular events occurred in 37% of overweight middle-aged men and 28% of overweight middle-aged women. In obese middle-aged men and women, those figures were 47% and 39%, respectively, and in the morbidly obese they were 65% and 48%. By comparison, incident cardiovascular events occurred in 32% of middle-aged men of normal BMI, and 22% of women.
Across all the studies, there were 7,136 fatal or nonfatal myocardial infarctions, 3,733 fatal or nonfatal strokes, 4,614 diagnoses of heart failure, and 13,457 cardiovascular disease events during 856,532 person-years of follow-up in middle-aged adults.
After adjustment for age, ethnicity, and smoking status, the competing hazard ratios for experiencing a cardiovascular disease event compared to a noncardiovascular disease death were greater in the higher-BMI categories, and greatest among morbidly obese middle-aged men and women, largely because of a greater proportion of coronary heart disease and heart failure events.
“In addition, greater all-cause mortality in higher-BMI categories occurred at the expense of a greater proportion of deaths from cardiovascular causes in middle-aged men and women who are overweight and obese,” wrote Sadiya S. Khan, MD, MSc, of Northwestern University, Chicago, and her coauthors.
The research suggested that for each increasing unit of BMI in middle-aged men and women, the adjusted competing hazard ratios of incident cardiovascular disease events increased by a significant 5%.
The study found that middle-aged men in the normal and overweight BMI group enjoyed more years free from cardiovascular disease than did obese middle-aged men. In middle-aged women, those who were in the normal BMI range had significantly more years lived free of cardiovascular disease than did overweight or obese women.
The incidence of cardiovascular disease was significantly delayed by an average of 7.5 years in middle-aged men of normal BMI and 7.1 years in middle-aged women of normal BMI, compared with those with morbid obesity.
In terms of longevity, men and women with normal BMI lived on average 5.6 years and 2 years longer, respectively, than did men and women with morbid obesity.
“The results of this study build on prior research from the Cardiovascular Disease Lifetime Risk Pooling Project highlighting marked differences in lifetime risks of CVD and further highlight the importance of consideration of BMI as a risk factor for diminished healthy longevity and greater overall CVD morbidity and mortality,” the authors wrote.
The study was intended to address recent controversy over the health implications of overweight, with some evidence suggesting that overweight individuals have all-cause mortality similar to or lower than that of normal-weight groups.
“While we do observe evidence of the well-described overweight and obesity paradox, in which heavier individuals appear to live longer on average after diagnosis of CVD compared with individuals with normal BMI, our data when following up individuals prior to the onset of CVD indicate that this occurs because of a trend toward earlier onset of disease in individuals who are overweight and obese,” they wrote.
The study did not account for change in BMI over the course of follow-up, nor did it use data on fat distribution or the degree of visceral adiposity, the researchers noted.
“Additional important outcomes of obesity-related morbidity, such as atrial fibrillation, sleep-disordered breathing, and chronic liver disease, were not ascertained routinely in our cohort studies, and we likely underestimated the overall comorbidity burden of excess weight.”
The National Heart, Lung, and Blood Institute supported the study. No conflicts of interest were declared.
SOURCE: Khan SS et al. JAMA Cardiol. 2018 Feb 28. doi: 10.1001/jamacardio.2018.0022.
.
In a report published online Feb. 28 in JAMA Cardiology, researchers presented an analysis of pooled data from 190,672 participants and 3.2 million person-years of follow-up in 10 prospective cohort studies, including the Framingham Heart Study, the Multi-Ethnic Study of Atherosclerosis, and the Atherosclerosis Risk in Communities Study.
Incident cardiovascular events occurred in 37% of overweight middle-aged men and 28% of overweight middle-aged women. In obese middle-aged men and women, those figures were 47% and 39%, respectively, and in the morbidly obese they were 65% and 48%. By comparison, incident cardiovascular events occurred in 32% of middle-aged men of normal BMI, and 22% of women.
Across all the studies, there were 7,136 fatal or nonfatal myocardial infarctions, 3,733 fatal or nonfatal strokes, 4,614 diagnoses of heart failure, and 13,457 cardiovascular disease events during 856,532 person-years of follow-up in middle-aged adults.
After adjustment for age, ethnicity, and smoking status, the competing hazard ratios for experiencing a cardiovascular disease event compared to a noncardiovascular disease death were greater in the higher-BMI categories, and greatest among morbidly obese middle-aged men and women, largely because of a greater proportion of coronary heart disease and heart failure events.
“In addition, greater all-cause mortality in higher-BMI categories occurred at the expense of a greater proportion of deaths from cardiovascular causes in middle-aged men and women who are overweight and obese,” wrote Sadiya S. Khan, MD, MSc, of Northwestern University, Chicago, and her coauthors.
The research suggested that for each increasing unit of BMI in middle-aged men and women, the adjusted competing hazard ratios of incident cardiovascular disease events increased by a significant 5%.
The study found that middle-aged men in the normal and overweight BMI group enjoyed more years free from cardiovascular disease than did obese middle-aged men. In middle-aged women, those who were in the normal BMI range had significantly more years lived free of cardiovascular disease than did overweight or obese women.
The incidence of cardiovascular disease was significantly delayed by an average of 7.5 years in middle-aged men of normal BMI and 7.1 years in middle-aged women of normal BMI, compared with those with morbid obesity.
In terms of longevity, men and women with normal BMI lived on average 5.6 years and 2 years longer, respectively, than did men and women with morbid obesity.
“The results of this study build on prior research from the Cardiovascular Disease Lifetime Risk Pooling Project highlighting marked differences in lifetime risks of CVD and further highlight the importance of consideration of BMI as a risk factor for diminished healthy longevity and greater overall CVD morbidity and mortality,” the authors wrote.
The study was intended to address recent controversy over the health implications of overweight, with some evidence suggesting that overweight individuals have all-cause mortality similar to or lower than that of normal-weight groups.
“While we do observe evidence of the well-described overweight and obesity paradox, in which heavier individuals appear to live longer on average after diagnosis of CVD compared with individuals with normal BMI, our data when following up individuals prior to the onset of CVD indicate that this occurs because of a trend toward earlier onset of disease in individuals who are overweight and obese,” they wrote.
The study did not account for change in BMI over the course of follow-up, nor did it use data on fat distribution or the degree of visceral adiposity, the researchers noted.
“Additional important outcomes of obesity-related morbidity, such as atrial fibrillation, sleep-disordered breathing, and chronic liver disease, were not ascertained routinely in our cohort studies, and we likely underestimated the overall comorbidity burden of excess weight.”
The National Heart, Lung, and Blood Institute supported the study. No conflicts of interest were declared.
SOURCE: Khan SS et al. JAMA Cardiol. 2018 Feb 28. doi: 10.1001/jamacardio.2018.0022.
.
In a report published online Feb. 28 in JAMA Cardiology, researchers presented an analysis of pooled data from 190,672 participants and 3.2 million person-years of follow-up in 10 prospective cohort studies, including the Framingham Heart Study, the Multi-Ethnic Study of Atherosclerosis, and the Atherosclerosis Risk in Communities Study.
Incident cardiovascular events occurred in 37% of overweight middle-aged men and 28% of overweight middle-aged women. In obese middle-aged men and women, those figures were 47% and 39%, respectively, and in the morbidly obese they were 65% and 48%. By comparison, incident cardiovascular events occurred in 32% of middle-aged men of normal BMI, and 22% of women.
Across all the studies, there were 7,136 fatal or nonfatal myocardial infarctions, 3,733 fatal or nonfatal strokes, 4,614 diagnoses of heart failure, and 13,457 cardiovascular disease events during 856,532 person-years of follow-up in middle-aged adults.
After adjustment for age, ethnicity, and smoking status, the competing hazard ratios for experiencing a cardiovascular disease event compared to a noncardiovascular disease death were greater in the higher-BMI categories, and greatest among morbidly obese middle-aged men and women, largely because of a greater proportion of coronary heart disease and heart failure events.
“In addition, greater all-cause mortality in higher-BMI categories occurred at the expense of a greater proportion of deaths from cardiovascular causes in middle-aged men and women who are overweight and obese,” wrote Sadiya S. Khan, MD, MSc, of Northwestern University, Chicago, and her coauthors.
The research suggested that for each increasing unit of BMI in middle-aged men and women, the adjusted competing hazard ratios of incident cardiovascular disease events increased by a significant 5%.
The study found that middle-aged men in the normal and overweight BMI group enjoyed more years free from cardiovascular disease than did obese middle-aged men. In middle-aged women, those who were in the normal BMI range had significantly more years lived free of cardiovascular disease than did overweight or obese women.
The incidence of cardiovascular disease was significantly delayed by an average of 7.5 years in middle-aged men of normal BMI and 7.1 years in middle-aged women of normal BMI, compared with those with morbid obesity.
In terms of longevity, men and women with normal BMI lived on average 5.6 years and 2 years longer, respectively, than did men and women with morbid obesity.
“The results of this study build on prior research from the Cardiovascular Disease Lifetime Risk Pooling Project highlighting marked differences in lifetime risks of CVD and further highlight the importance of consideration of BMI as a risk factor for diminished healthy longevity and greater overall CVD morbidity and mortality,” the authors wrote.
The study was intended to address recent controversy over the health implications of overweight, with some evidence suggesting that overweight individuals have all-cause mortality similar to or lower than that of normal-weight groups.
“While we do observe evidence of the well-described overweight and obesity paradox, in which heavier individuals appear to live longer on average after diagnosis of CVD compared with individuals with normal BMI, our data when following up individuals prior to the onset of CVD indicate that this occurs because of a trend toward earlier onset of disease in individuals who are overweight and obese,” they wrote.
The study did not account for change in BMI over the course of follow-up, nor did it use data on fat distribution or the degree of visceral adiposity, the researchers noted.
“Additional important outcomes of obesity-related morbidity, such as atrial fibrillation, sleep-disordered breathing, and chronic liver disease, were not ascertained routinely in our cohort studies, and we likely underestimated the overall comorbidity burden of excess weight.”
The National Heart, Lung, and Blood Institute supported the study. No conflicts of interest were declared.
SOURCE: Khan SS et al. JAMA Cardiol. 2018 Feb 28. doi: 10.1001/jamacardio.2018.0022.
FROM JAMA CARDIOLOGY
Key clinical point: Obese individuals have shorter life spans and spend significantly more time dealing with the burden of cardiovascular morbidity than do normal-weight individuals.
Major finding: Overweight and obese middle-aged individuals have a significantly higher incidence of cardiovascular events and mortality compared with normal-weight middle-aged individuals.
Data source: Analysis of pooled data from 190,672 participants and 3.2 million person-years of follow-up in 10 prospective cohort studies.
Disclosures: The National Heart, Lung, and Blood Institute supported the study. No conflicts of interest were declared.
Source: Khan SS et al. JAMA Cardiol. 2018 Feb 28. doi: 10.1001/jamacardio.2018.0022
Mexican Americans With Midlife Stroke May Have Worse Outcomes Than Non-Hispanic Whites
LOS ANGELES—Mexican Americans with midlife stroke may have significantly worse 90-day outcomes, compared with non-Hispanic whites, according to a study presented at the International Stroke Conference 2018. Mexican Americans had lower physical quality of life scores and a high prevalence of depression, the authors noted.
“The growing number of midlife stroke survivors will have unique rehabilitation and health care resource needs,” said Lynda D. Lisabeth, PhD, MPH, Professor of Epidemiology at the University of Michigan Medical School in Ann Arbor. “Particular attention to Mexican American midlife stroke survivors is warranted.”

Midlife stroke can result in many years of stroke-related disability, and midlife stroke rates are stable or increasing. The impact of midlife stroke may be worse in Mexican Americans, who have higher stroke rates, earlier strokes, and appear to have worse outcomes, said the researchers. To compare stroke outcomes in Mexican Americans and non-Hispanic whites younger than 65, Dr. Lisabeth and colleagues analyzed data from the population-based Brain Attack Surveillance in Corpus Christi (BASIC) project in South Texas.
The researchers identified patients younger than 65 with incident ischemic stroke between 2008 and 2015. Strokes were identified using active and passive stroke surveillance and validated by a physician blinded to patients’ ethnicity. Investigators conducted in-person interviews with patients or proxies at baseline and at 90 days. The researchers assessed patients’ functional, neurologic, and cognitive outcomes, quality of life, and depression.
Of 925 patients with a first ischemic stroke between the ages of 45 and 64, 508 patients had outcome data (341 Mexican Americans and 167 non-Hispanic whites). At baseline, Mexican Americans had lower levels of education, higher average BMI, and were more likely to have hypertension and diabetes, compared with non-Hispanic whites. Mexican Americans were less likely to smoke than non-Hispanic whites, however.
After adjusting for confounders (eg, age, sex, education, insurance, marital status, stroke severity, stroke treatment, risk factors, prestroke function, cognition, and comorbidity level), Mexican Americans had significantly worse 90-day outcomes than non-Hispanic whites in every domain except depression. Among Mexican Americans, the median functional outcome score (ie, total Activities of Daily Living/Instrumental Activities of Daily Living score, range 1–4, higher scores worse) was 1.9, compared with 1.5 among non-Hispanic whites (adjusted mean difference, 0.26). The median NIH Stroke Scale score (range 0–42, higher scores worse) was 2 among Mexican Americans, compared with 1 among non-Hispanic whites (adjusted mean difference, 26%).
In addition, the median score on the Modified Mini-Mental State Examination (range 0–100, higher scores better) was 90 for Mexican Americans, compared with 94.5 for non-Hispanic whites. Mexican Americans had a lower median total Stroke-Specific Quality of Life score (range 1–5, higher scores better) and lower median scores on the physical and psychosocial Stroke-Specific Quality of Life subscales, compared with non-Hispanic whites (3.3 vs 3.8, 2.5 vs 3.2, and 4.2 vs 4.5, respectively). In addition, a greater percentage of Mexican Americans had depression, compared with non-Hispanic whites (41.1% vs 34.5%), but this difference was not significant, likely due to the smaller sample size for this outcome.
—Erica Tricarico
LOS ANGELES—Mexican Americans with midlife stroke may have significantly worse 90-day outcomes, compared with non-Hispanic whites, according to a study presented at the International Stroke Conference 2018. Mexican Americans had lower physical quality of life scores and a high prevalence of depression, the authors noted.
“The growing number of midlife stroke survivors will have unique rehabilitation and health care resource needs,” said Lynda D. Lisabeth, PhD, MPH, Professor of Epidemiology at the University of Michigan Medical School in Ann Arbor. “Particular attention to Mexican American midlife stroke survivors is warranted.”
Midlife stroke can result in many years of stroke-related disability, and midlife stroke rates are stable or increasing. The impact of midlife stroke may be worse in Mexican Americans, who have higher stroke rates, earlier strokes, and appear to have worse outcomes, said the researchers. To compare stroke outcomes in Mexican Americans and non-Hispanic whites younger than 65, Dr. Lisabeth and colleagues analyzed data from the population-based Brain Attack Surveillance in Corpus Christi (BASIC) project in South Texas.
The researchers identified patients younger than 65 with incident ischemic stroke between 2008 and 2015. Strokes were identified using active and passive stroke surveillance and validated by a physician blinded to patients’ ethnicity. Investigators conducted in-person interviews with patients or proxies at baseline and at 90 days. The researchers assessed patients’ functional, neurologic, and cognitive outcomes, quality of life, and depression.
Of 925 patients with a first ischemic stroke between the ages of 45 and 64, 508 patients had outcome data (341 Mexican Americans and 167 non-Hispanic whites). At baseline, Mexican Americans had lower levels of education, higher average BMI, and were more likely to have hypertension and diabetes, compared with non-Hispanic whites. Mexican Americans were less likely to smoke than non-Hispanic whites, however.
After adjusting for confounders (eg, age, sex, education, insurance, marital status, stroke severity, stroke treatment, risk factors, prestroke function, cognition, and comorbidity level), Mexican Americans had significantly worse 90-day outcomes than non-Hispanic whites in every domain except depression. Among Mexican Americans, the median functional outcome score (ie, total Activities of Daily Living/Instrumental Activities of Daily Living score, range 1–4, higher scores worse) was 1.9, compared with 1.5 among non-Hispanic whites (adjusted mean difference, 0.26). The median NIH Stroke Scale score (range 0–42, higher scores worse) was 2 among Mexican Americans, compared with 1 among non-Hispanic whites (adjusted mean difference, 26%).
In addition, the median score on the Modified Mini-Mental State Examination (range 0–100, higher scores better) was 90 for Mexican Americans, compared with 94.5 for non-Hispanic whites. Mexican Americans had a lower median total Stroke-Specific Quality of Life score (range 1–5, higher scores better) and lower median scores on the physical and psychosocial Stroke-Specific Quality of Life subscales, compared with non-Hispanic whites (3.3 vs 3.8, 2.5 vs 3.2, and 4.2 vs 4.5, respectively). In addition, a greater percentage of Mexican Americans had depression, compared with non-Hispanic whites (41.1% vs 34.5%), but this difference was not significant, likely due to the smaller sample size for this outcome.
—Erica Tricarico
LOS ANGELES—Mexican Americans with midlife stroke may have significantly worse 90-day outcomes, compared with non-Hispanic whites, according to a study presented at the International Stroke Conference 2018. Mexican Americans had lower physical quality of life scores and a high prevalence of depression, the authors noted.
“The growing number of midlife stroke survivors will have unique rehabilitation and health care resource needs,” said Lynda D. Lisabeth, PhD, MPH, Professor of Epidemiology at the University of Michigan Medical School in Ann Arbor. “Particular attention to Mexican American midlife stroke survivors is warranted.”
Midlife stroke can result in many years of stroke-related disability, and midlife stroke rates are stable or increasing. The impact of midlife stroke may be worse in Mexican Americans, who have higher stroke rates, earlier strokes, and appear to have worse outcomes, said the researchers. To compare stroke outcomes in Mexican Americans and non-Hispanic whites younger than 65, Dr. Lisabeth and colleagues analyzed data from the population-based Brain Attack Surveillance in Corpus Christi (BASIC) project in South Texas.
The researchers identified patients younger than 65 with incident ischemic stroke between 2008 and 2015. Strokes were identified using active and passive stroke surveillance and validated by a physician blinded to patients’ ethnicity. Investigators conducted in-person interviews with patients or proxies at baseline and at 90 days. The researchers assessed patients’ functional, neurologic, and cognitive outcomes, quality of life, and depression.
Of 925 patients with a first ischemic stroke between the ages of 45 and 64, 508 patients had outcome data (341 Mexican Americans and 167 non-Hispanic whites). At baseline, Mexican Americans had lower levels of education, higher average BMI, and were more likely to have hypertension and diabetes, compared with non-Hispanic whites. Mexican Americans were less likely to smoke than non-Hispanic whites, however.
After adjusting for confounders (eg, age, sex, education, insurance, marital status, stroke severity, stroke treatment, risk factors, prestroke function, cognition, and comorbidity level), Mexican Americans had significantly worse 90-day outcomes than non-Hispanic whites in every domain except depression. Among Mexican Americans, the median functional outcome score (ie, total Activities of Daily Living/Instrumental Activities of Daily Living score, range 1–4, higher scores worse) was 1.9, compared with 1.5 among non-Hispanic whites (adjusted mean difference, 0.26). The median NIH Stroke Scale score (range 0–42, higher scores worse) was 2 among Mexican Americans, compared with 1 among non-Hispanic whites (adjusted mean difference, 26%).
In addition, the median score on the Modified Mini-Mental State Examination (range 0–100, higher scores better) was 90 for Mexican Americans, compared with 94.5 for non-Hispanic whites. Mexican Americans had a lower median total Stroke-Specific Quality of Life score (range 1–5, higher scores better) and lower median scores on the physical and psychosocial Stroke-Specific Quality of Life subscales, compared with non-Hispanic whites (3.3 vs 3.8, 2.5 vs 3.2, and 4.2 vs 4.5, respectively). In addition, a greater percentage of Mexican Americans had depression, compared with non-Hispanic whites (41.1% vs 34.5%), but this difference was not significant, likely due to the smaller sample size for this outcome.
—Erica Tricarico
What Is the Impact of Poststroke Cognitive Impairment in Patients With Mild Stroke?
LOS ANGELES—Poststroke cognitive impairment is associated with inability to return to work and to drive, according to research presented at the International Stroke Conference 2018. Patients who are able to return to work appear to have higher Montreal Cognitive Assessment (MOCA) scores. In addition, factors such as being older than 65, having a history of stroke and diabetes, being unemployed, and living in a facility may suggest a higher risk of poststroke cognitive impairment, the authors noted.
“Since cognitive impairment can impact life quality, screening, even in mild stroke, could be beneficial,” said Ilavarasy Maran, MD, a resident at the University of Connecticut Health/Hartford Hospital.

Two of the main causes of dependency in stroke survivors are poststroke cognitive impairment and poststroke dementia. Approximately two-thirds of patients with stroke develop cognitive decline. This prevalence is expected to rise because of the aging population, said the researchers.
To evaluate the burden and risk factors associated with cognitive impairment after mild stroke, Dr. Maran and colleagues conducted a retrospective observational cohort study of 56 patients (51 with ischemic stroke, five with hemorrhagic stroke) evaluated between July 2016 and June 2017. Patients completed a questionnaire that elicited demographic information and history, as well as previously known cognitive impairment. Researchers used MOCA to evaluate cognition.
Median age was 61.5, 66.1% of patients were men, 76.8% were Caucasian, and the median discharge NIH Stroke Scale score was 1. Four percent of patients presented to the clinic at fewer than six weeks, 71.4% presented to the clinic at six to 12 weeks, 17.9% presented to the clinic at 12 to 24 weeks, and 7.1% of patients presented to the clinic at more than 24 weeks after discharge for stroke. None of the patients had a previous history of dementia, said the researchers.
In all, 50% of patients had no cognitive impairment, 19.6% had mild impairment, 16.1% had moderate impairment, and 14.3% had dementia. In addition, 50% of patients who had been working previously were able to return to work. This group had higher MOCA scores than did participants who did not return to work. Approximately 19.6% of patients who stopped driving did so due to cognitive impairment. No significant difference in MOCA scores based on the location of the stroke was reported.
Researchers also observed that patients with cognitive impairment had a previous history of hypertension and that history of depression did not appear to influence poststroke cognitive impairment.
—Erica Tricarico
LOS ANGELES—Poststroke cognitive impairment is associated with inability to return to work and to drive, according to research presented at the International Stroke Conference 2018. Patients who are able to return to work appear to have higher Montreal Cognitive Assessment (MOCA) scores. In addition, factors such as being older than 65, having a history of stroke and diabetes, being unemployed, and living in a facility may suggest a higher risk of poststroke cognitive impairment, the authors noted.
“Since cognitive impairment can impact life quality, screening, even in mild stroke, could be beneficial,” said Ilavarasy Maran, MD, a resident at the University of Connecticut Health/Hartford Hospital.
Two of the main causes of dependency in stroke survivors are poststroke cognitive impairment and poststroke dementia. Approximately two-thirds of patients with stroke develop cognitive decline. This prevalence is expected to rise because of the aging population, said the researchers.
To evaluate the burden and risk factors associated with cognitive impairment after mild stroke, Dr. Maran and colleagues conducted a retrospective observational cohort study of 56 patients (51 with ischemic stroke, five with hemorrhagic stroke) evaluated between July 2016 and June 2017. Patients completed a questionnaire that elicited demographic information and history, as well as previously known cognitive impairment. Researchers used MOCA to evaluate cognition.
Median age was 61.5, 66.1% of patients were men, 76.8% were Caucasian, and the median discharge NIH Stroke Scale score was 1. Four percent of patients presented to the clinic at fewer than six weeks, 71.4% presented to the clinic at six to 12 weeks, 17.9% presented to the clinic at 12 to 24 weeks, and 7.1% of patients presented to the clinic at more than 24 weeks after discharge for stroke. None of the patients had a previous history of dementia, said the researchers.
In all, 50% of patients had no cognitive impairment, 19.6% had mild impairment, 16.1% had moderate impairment, and 14.3% had dementia. In addition, 50% of patients who had been working previously were able to return to work. This group had higher MOCA scores than did participants who did not return to work. Approximately 19.6% of patients who stopped driving did so due to cognitive impairment. No significant difference in MOCA scores based on the location of the stroke was reported.
Researchers also observed that patients with cognitive impairment had a previous history of hypertension and that history of depression did not appear to influence poststroke cognitive impairment.
—Erica Tricarico
LOS ANGELES—Poststroke cognitive impairment is associated with inability to return to work and to drive, according to research presented at the International Stroke Conference 2018. Patients who are able to return to work appear to have higher Montreal Cognitive Assessment (MOCA) scores. In addition, factors such as being older than 65, having a history of stroke and diabetes, being unemployed, and living in a facility may suggest a higher risk of poststroke cognitive impairment, the authors noted.
“Since cognitive impairment can impact life quality, screening, even in mild stroke, could be beneficial,” said Ilavarasy Maran, MD, a resident at the University of Connecticut Health/Hartford Hospital.
Two of the main causes of dependency in stroke survivors are poststroke cognitive impairment and poststroke dementia. Approximately two-thirds of patients with stroke develop cognitive decline. This prevalence is expected to rise because of the aging population, said the researchers.
To evaluate the burden and risk factors associated with cognitive impairment after mild stroke, Dr. Maran and colleagues conducted a retrospective observational cohort study of 56 patients (51 with ischemic stroke, five with hemorrhagic stroke) evaluated between July 2016 and June 2017. Patients completed a questionnaire that elicited demographic information and history, as well as previously known cognitive impairment. Researchers used MOCA to evaluate cognition.
Median age was 61.5, 66.1% of patients were men, 76.8% were Caucasian, and the median discharge NIH Stroke Scale score was 1. Four percent of patients presented to the clinic at fewer than six weeks, 71.4% presented to the clinic at six to 12 weeks, 17.9% presented to the clinic at 12 to 24 weeks, and 7.1% of patients presented to the clinic at more than 24 weeks after discharge for stroke. None of the patients had a previous history of dementia, said the researchers.
In all, 50% of patients had no cognitive impairment, 19.6% had mild impairment, 16.1% had moderate impairment, and 14.3% had dementia. In addition, 50% of patients who had been working previously were able to return to work. This group had higher MOCA scores than did participants who did not return to work. Approximately 19.6% of patients who stopped driving did so due to cognitive impairment. No significant difference in MOCA scores based on the location of the stroke was reported.
Researchers also observed that patients with cognitive impairment had a previous history of hypertension and that history of depression did not appear to influence poststroke cognitive impairment.
—Erica Tricarico
EMS Stroke Field Triage Improves Outcomes
LOS ANGELES—An emergency medical services (EMS) protocol to identify large-vessel occlusions and deliver patients to a comprehensive stroke center (CSC) within 30 minutes reduced the time to recanalization, when compared with a protocol that optimized the transfer of such patients from primary stroke centers (PSCs) to CSCs. The study was presented at the International Stroke Conference 2018.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in EMS units will improve outcomes. The controversy arose from concerns that stroke severity scores measured in the field are not always accurate, and that longer travel to a CSC could delay treatment for a patient who does not need thrombectomy.
“A lot of people have done mathematical modeling, but nobody has done the work to change the system so we can see what happens. This is the first study that has shown a real-world example of what it means for patients,” said Ryan McTaggart, MD, Director of Interventional Neuroradiology at Brown University Rhode Island Hospital in Providence.

Instituting a Transfer Protocol
The region where the study was carried out has one CSC and eight PSCs. The large-vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS) and to conduct CT and CT angiography. The PSC was instructed to share the images with the CSC, which decided whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would be delivered to the CSC if it was within 30 minutes of their current location. Patients scoring less than 4 would be brought to the nearest facility. When the field LAMS score was 4 or greater and the nearest CSC was more than 30 minutes away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than the CSC, process outcomes were better with the field triage protocol. “Despite eight additional minutes of transport time, IV t-PA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is two or three, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it is a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was difficult. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It is a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients, but for the economics of the health care system. We are potentially saving patients from disability health care costs,” he said.
Travel Time Increased
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during the following three time periods: before PSC–CSC transfer optimization and before field triage (ie, July 2015 to January 2016), after transfer optimization and with voluntary field triage (ie, January 2016 to January 2017), and when transfer optimization and field triage were mandatory (ie, January 2017 to January 2018).
The patients had an anterior large-vessel occlusion and mild-to-moderate early ischemic change. Outcomes included time from hospital arrival (ie, PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (ie, modified Rankin scale score 0–2) at 90 days, or discharge with an NIH Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any procedural change occurred, 100 after transfer optimization, and 94 after transfer optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to the CSC instead of a PSC was eight minutes.
The time to first use of IV alteplase decreased from 54 minutes before any procedural change to 49 minutes after transfer optimization and to 36 minutes after transfer optimization and field triage. Similar decreases were seen in time to arterial puncture (105 minutes, 101 minutes, and 88 minutes, respectively) and time to recanalization (156 minutes, 132 minutes, and 116 minutes, respectively). These differences did not reach statistical significance.
The clinical outcomes also became more favorable. Approximately 58% of patients had a favorable outcome at 90 days with both protocols in place, compared with 51% with only transfer optimization and 31% before any procedural changes.
The researchers conducted a subanalysis of 150 patients for whom a PSC was closer than the CSC. Of these patients, 94 went to the CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV t-PA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs. The time to arterial puncture was also shorter (98 minutes vs 155 minutes), as was time to recanalization (131 minutes vs 174 minutes).
Patients taken to the CSC were more likely to have a favorable outcome (65% vs 42%).
The study received no external funding. Dr. McTaggart reported no financial disclosures.
—Jim Kling
LOS ANGELES—An emergency medical services (EMS) protocol to identify large-vessel occlusions and deliver patients to a comprehensive stroke center (CSC) within 30 minutes reduced the time to recanalization, when compared with a protocol that optimized the transfer of such patients from primary stroke centers (PSCs) to CSCs. The study was presented at the International Stroke Conference 2018.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in EMS units will improve outcomes. The controversy arose from concerns that stroke severity scores measured in the field are not always accurate, and that longer travel to a CSC could delay treatment for a patient who does not need thrombectomy.
“A lot of people have done mathematical modeling, but nobody has done the work to change the system so we can see what happens. This is the first study that has shown a real-world example of what it means for patients,” said Ryan McTaggart, MD, Director of Interventional Neuroradiology at Brown University Rhode Island Hospital in Providence.
Instituting a Transfer Protocol
The region where the study was carried out has one CSC and eight PSCs. The large-vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS) and to conduct CT and CT angiography. The PSC was instructed to share the images with the CSC, which decided whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would be delivered to the CSC if it was within 30 minutes of their current location. Patients scoring less than 4 would be brought to the nearest facility. When the field LAMS score was 4 or greater and the nearest CSC was more than 30 minutes away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than the CSC, process outcomes were better with the field triage protocol. “Despite eight additional minutes of transport time, IV t-PA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is two or three, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it is a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was difficult. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It is a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients, but for the economics of the health care system. We are potentially saving patients from disability health care costs,” he said.
Travel Time Increased
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during the following three time periods: before PSC–CSC transfer optimization and before field triage (ie, July 2015 to January 2016), after transfer optimization and with voluntary field triage (ie, January 2016 to January 2017), and when transfer optimization and field triage were mandatory (ie, January 2017 to January 2018).
The patients had an anterior large-vessel occlusion and mild-to-moderate early ischemic change. Outcomes included time from hospital arrival (ie, PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (ie, modified Rankin scale score 0–2) at 90 days, or discharge with an NIH Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any procedural change occurred, 100 after transfer optimization, and 94 after transfer optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to the CSC instead of a PSC was eight minutes.
The time to first use of IV alteplase decreased from 54 minutes before any procedural change to 49 minutes after transfer optimization and to 36 minutes after transfer optimization and field triage. Similar decreases were seen in time to arterial puncture (105 minutes, 101 minutes, and 88 minutes, respectively) and time to recanalization (156 minutes, 132 minutes, and 116 minutes, respectively). These differences did not reach statistical significance.
The clinical outcomes also became more favorable. Approximately 58% of patients had a favorable outcome at 90 days with both protocols in place, compared with 51% with only transfer optimization and 31% before any procedural changes.
The researchers conducted a subanalysis of 150 patients for whom a PSC was closer than the CSC. Of these patients, 94 went to the CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV t-PA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs. The time to arterial puncture was also shorter (98 minutes vs 155 minutes), as was time to recanalization (131 minutes vs 174 minutes).
Patients taken to the CSC were more likely to have a favorable outcome (65% vs 42%).
The study received no external funding. Dr. McTaggart reported no financial disclosures.
—Jim Kling
LOS ANGELES—An emergency medical services (EMS) protocol to identify large-vessel occlusions and deliver patients to a comprehensive stroke center (CSC) within 30 minutes reduced the time to recanalization, when compared with a protocol that optimized the transfer of such patients from primary stroke centers (PSCs) to CSCs. The study was presented at the International Stroke Conference 2018.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in EMS units will improve outcomes. The controversy arose from concerns that stroke severity scores measured in the field are not always accurate, and that longer travel to a CSC could delay treatment for a patient who does not need thrombectomy.
“A lot of people have done mathematical modeling, but nobody has done the work to change the system so we can see what happens. This is the first study that has shown a real-world example of what it means for patients,” said Ryan McTaggart, MD, Director of Interventional Neuroradiology at Brown University Rhode Island Hospital in Providence.
Instituting a Transfer Protocol
The region where the study was carried out has one CSC and eight PSCs. The large-vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS) and to conduct CT and CT angiography. The PSC was instructed to share the images with the CSC, which decided whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would be delivered to the CSC if it was within 30 minutes of their current location. Patients scoring less than 4 would be brought to the nearest facility. When the field LAMS score was 4 or greater and the nearest CSC was more than 30 minutes away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than the CSC, process outcomes were better with the field triage protocol. “Despite eight additional minutes of transport time, IV t-PA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is two or three, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it is a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was difficult. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It is a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients, but for the economics of the health care system. We are potentially saving patients from disability health care costs,” he said.
Travel Time Increased
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during the following three time periods: before PSC–CSC transfer optimization and before field triage (ie, July 2015 to January 2016), after transfer optimization and with voluntary field triage (ie, January 2016 to January 2017), and when transfer optimization and field triage were mandatory (ie, January 2017 to January 2018).
The patients had an anterior large-vessel occlusion and mild-to-moderate early ischemic change. Outcomes included time from hospital arrival (ie, PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (ie, modified Rankin scale score 0–2) at 90 days, or discharge with an NIH Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any procedural change occurred, 100 after transfer optimization, and 94 after transfer optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to the CSC instead of a PSC was eight minutes.
The time to first use of IV alteplase decreased from 54 minutes before any procedural change to 49 minutes after transfer optimization and to 36 minutes after transfer optimization and field triage. Similar decreases were seen in time to arterial puncture (105 minutes, 101 minutes, and 88 minutes, respectively) and time to recanalization (156 minutes, 132 minutes, and 116 minutes, respectively). These differences did not reach statistical significance.
The clinical outcomes also became more favorable. Approximately 58% of patients had a favorable outcome at 90 days with both protocols in place, compared with 51% with only transfer optimization and 31% before any procedural changes.
The researchers conducted a subanalysis of 150 patients for whom a PSC was closer than the CSC. Of these patients, 94 went to the CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV t-PA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs. The time to arterial puncture was also shorter (98 minutes vs 155 minutes), as was time to recanalization (131 minutes vs 174 minutes).
Patients taken to the CSC were more likely to have a favorable outcome (65% vs 42%).
The study received no external funding. Dr. McTaggart reported no financial disclosures.
—Jim Kling
Endometriosis: Expert perspectives on medical and surgical management
Endometriosis is one of the more daunting diagnoses that gynecologists treat. In this roundtable discussion, moderated by
First-time evaluation
Arnold P. Advincula, MD: When a patient presents to your practice for the first time and you suspect endometriosis, what considerations tailor your evaluation, and what does that evaluation involve?
Hye-Chun Hur, MD, MPH: The diagnosis is contingent on a patient’s presenting profile. How symptomatic is she? How old is she? What are her reproductive goals? The gold standard for diagnosis is a histologic diagnosis, which is surgical. Depending on the age profile, however, and how close she is to menopause, the patient may be managed medically. Even women in the young reproductive age group may be managed medically if symptoms are responsive to medical treatment.
Douglas N. Brown, MD: I agree. When a patient presents without a laparoscopy, or a tissue diagnosis, but the symptoms are consistent with likely endometriosis (depending on where she is in her reproductive cycle and what her goals are), I think treating with a first-line therapy—hormonal treatments such as progestin-only oral contraceptive pills—is acceptable. I usually conduct a treatment trial period of 3 to 6 months to see if she obtains any symptom relief.
If that first-line treatment fails, generally you can move to a second-line treatment.
I have a discussion in which I either offer a second-line treatment, such as medroxyprogesterone (Depo-Provera) or leuprolide acetate (Lupron Depot), or get a tissue diagnosis, if possible, by performing laparoscopy. If first-line or even second-line therapy fails, you need to consider doing a diagnostic laparoscopy to confirm or deny the diagnosis.
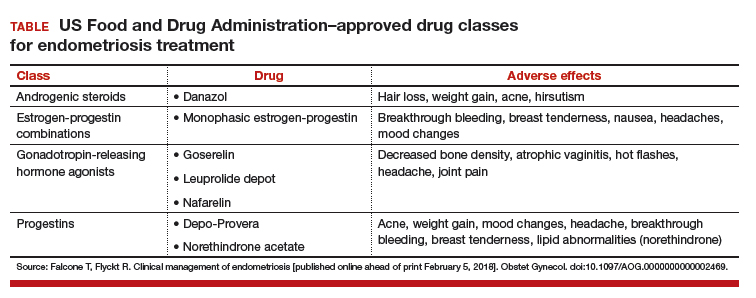
Dr. Advincula: Are there any points in the evaluation of a patient who visits your practice for the first time where you would immediately offer a surgical approach, as opposed to starting with medical management?
Dr. Hur: A large percentage of my patients undergo surgical evaluation, as surgical diagnosis is the gold standard. If you look at the literature, even among surgeons, the accuracy of visual diagnosis is not great.1,2 I target individuals who are either not responsive to medical treatment or who have never tried medical treatment but are trying to conceive, so they are not medical candidates, or individuals who genuinely want a diagnosis for surgical management—sometimes even before first-line medical treatment.
Dr. Brown: Your examination sometimes also dictates your approach. A patient may never have had a laparoscopy or hormone therapy, but if you find uterosacral ligament nodularity, extreme pain on examination, and suspicious findings on ultrasound or otherwise, a diagnostic laparoscopy may be warranted to confirm the diagnosis.
Endometrioma management
Dr. Advincula: Let’s jump ahead. You have decided to proceed with laparoscopy and you encounter an endometrioma. What is your management strategy, particularly in a fertility-desiring patient?
Dr. Hur: Even if a woman has not undergone first-line medical treatment, if she is trying to conceive or presents with infertility, it’s a different balancing act for approaching the patient. When a woman presents, either with an ultrasound finding or an intraoperative finding of an endometrioma, I am a strong advocate of treating symptomatic disease, which means complete cyst excision. Good clinical data suggest that reproductive outcomes are improved for spontaneous pregnancy rates when you excise an endometrioma.3-6
Dr. Advincula: What are the risks of excision of an endometrioma cyst that patients need to know about?
Dr. Brown: Current standard of care is cystectomy, stripping the cyst wall away from the ovarian cortex. There is some concern that the stripping process, depending on how long the endometrioma has been present within the ovary, can cause some destruction to the underlying oocytes and perhaps impact that ovary’s ability to produce viable eggs.
Some studies, from France in particular, have investigated different energy sources, such as plasma energy, that make it possible to remove part of the cyst and then use the plasma energy to vaporize the rest of the cyst wall that may be lying on the cortex. Researchers looked at anti-Müllerian hormone levels, and there does seem to be a difference in terms of how you remove the cyst.7-9 This energy source is not available to everyone; it’s similar to laser but does not have as much penetration. Standard of care is still ovarian stripping.
The conversation with the patient—if she is already infertile and this cyst is a problem—would be that it likely needs to be removed. There is a chance that she may need assisted reproduction; she might not be able to get pregnant on her own due either to the presence of the endometrioma or to the surgical process of removing it and stripping.
Dr. Advincula: How soon after surgery can a patient start to pursue trying to get pregnant?
Dr. Hur: I think there is no time restraint outside of recovery. As long as the patient has a routine postoperative course, she can try to conceive, spontaneously or with assisted reproduction. Some data suggest, however, that ovarian reserve is diminished immediately after surgery.10–12 If you look at the spontaneous clinical pregnancy outcomes, they are comparable 3 to 6 months postsurgery.4,12–14
Dr. Brown: I agree. Time is of the essence with a lot of patients, many of whom present after age 35.
Dr. Hur: It’s also important to highlight that there are 2 presentations with endometrioma: the symptomatic patient and the asymptomatic patient. In the asymptomatic patient, her age, reproductive goals, and the bilaterality (whether it is present on both sides or on one side) of the endometrioma are important in deciding on a patient-centered surgical plan. For someone with a smaller cyst, unilateral presentation, and maybe older age at presentation, it may or may not impact assisted reproductive outcomes.
If the patient is not symptomatic and she is older with bilateral endometriomas less than 4 cm, some data suggest that patient might be better served in a conservative fashion.6,15–17 Then, once she is done with assisted reproduction, we might be more aggressive surgically by treating the finding that would not resolve spontaneously without surgical management. It is important to highlight that endometriomas do not resolve on their own; they require surgical management.
Read about managing endometriosis for the patient not seeking fertility
Endometriosis management for the patient not seeking fertility
Dr. Advincula: Let’s now consider a patient on whom you have performed laparoscopy not only to diagnose and confirm the evidence of endometriosis but also to treat endometriosis, an endometrioma, and potentially deeply infiltrative disease. But this person is not trying to get pregnant. Postoperatively, what is your approach?
Dr. Brown: Suppressive therapy for this patient could be first-line or second-line therapy, such as a Lupron Depot or Depo-Provera. We keep the patient on suppressive therapy (whatever treatments work for her), until she’s ready to get pregnant; then we take her off. Hopefully she gets pregnant. After she delivers, we reinitiate suppressive therapy. I will follow these women throughout their reproductive cycle, and I think having a team of physicians who are all on the same page can help this patient manage her disease through her reproductive years.
Dr. Hur: If a patient presented warranting surgical management once, and she is not menopausal, the likelihood that disease will recur is quite high. Understanding the nature and the pathology of the disease, hormonal suppression would be warranted. Suppression is not just for between pregnancies, it’s until the patient reaches natural menopause. It’s also in the hopes of suppressing the disease so she does not need recurrent surgeries.
We typically do not operate unless patients have recurrence of symptoms that no longer respond to medical therapy. Our hope is to buy them more time closer to the age of natural menopause so that medical repercussions do not result in hysterectomy and ovary removal, which have other nongynecologic manifestations, including negative impact on bone and cardiac health.
Hye-Chun Hur, MD, MPH: I am a strong advocate of excision of endometriosis. I believe that it's essential to excise for 2 very important reasons. One reason is for diagnosis. Accurately diagnosing endometriosis through visualization alone is poor, even among gynecologic surgeons. It is very important to have an accurate diagnosis of endometriosis, since the diagnosis will then dictate the treatment for the rest of a patient's reproductive life.
The second reason that excision is essential is because you just do not know how much disease there is "behind the scenes." When you start to excise, you begin to appreciate the depth of the disease, and often fibrosis or inflammation is present even behind the endometriosis implant that is visualized.
Douglas N. Brown, MD: I approach endometriosis in the same way that an oncologist would approach cancer. I call it cytoreduction--reducing the disease. There is this iceberg phenomenon, where the tip of the iceberg is seen in the water, but you have no idea how deep it actually goes. That is very much deep, infiltrative endometriosis. Performing an ablation on the top does almost nothing for the patient and may actually complicate the situation by causing scar tissue. If a patient has symptoms, I firmly believe that you must resect the disease, whether it is on the peritoneum, bladder, bowel, or near the ureter. Now, these are radical surgeries, and not every patient should have a radical surgery. It is very much based on the patient's pain complaints and issues at that time, but excision of endometriosis really, in my opinion, should be the standard of care.
Risks of excision of endometriosis
Dr. Brown: The risks of disease excision depend on whether a patient has ureteral disease, bladder disease, or bowel disease, suggested through a preoperative or another operative report or imaging. If this is the case, we have a preoperative discussion with the patient about, "To what extent do you want me to go to remove the disease from your pelvis? If I remove it from your peritoneum and your bladder, there is the chance that you'll have to go home with a Foley catheter for a few days. If the bowel is involved, do you want me to try to resect the disease or shave it off the bowel? If we get into a problem, are you okay with me resecting that bowel?" These are the issues that we have to discuss, because there are potential complications, although known.
The role of the LNG-IUD
Dr. Advincula: Something that often comes up is the role of a levonorgestrel-releasing intrauterine device (LNG-IUD) as one therapy option, either preoperatively or postoperatively. What is your perspective?
Dr. Hur: I reserve the LNG-IUD as a second-line therapy for patients, predominantly because it allows direct delivery of the medication to the womb (rather than systemic exposure of the medication). For patients who experience adverse effects due to systemic exposure to first-line treatments, it might be a great option. However, I do not believe that it consistently suppresses the ovaries, which we understand feeds the pathology of the hormonal stimulation, and so typically I will reserve it as a second-line treatment.
Dr. Brown: I utilize the LNG-IUD in a similar fashion. I may have patients who have had a diagnostic laparoscopy somewhere else and were referred to me because they now have known stage 3 or 4 endometriosis without endometriomas. Those patients, if they are going to need suppressive therapy after surgery and are not ready to get pregnant, do very well with the LNG-IUD, and I will place it during surgery under anesthesia. If a patient has endometriomas seen at the time of surgery, we could still place an LNG-IUD at the time of surgery. We may need to add on an additional medication, however, like another oral progesterone. I do have patients that use both an IUD and either combined oral contraceptive pills and/or oral progestins. Those patients usually have complicated cases with very deep infiltrative disease.
Read about managing endometriosis involving the bowel
Managing endometriosis involving the bowel
Dr. Advincula: Patients often are quite concerned when the words “endometriosis” and “bowel” come together. How do you manage disease that involves the bowel?

Dr. Hur: A lot of patients with endometriosis have what I call neighboring disease—it’s not limited just to the pelvis, but it involves the neighboring organs including the bowel and bladder. Patients can present with symptoms related to those adjacent organs. However, not all disease involving the bowel or bladder manifests with symptoms, and patients with symptoms may not have visible disease.
Typically, when a patient presents with symptoms of bowel involvement, where the bowel lumen is narrowed to more than 50% and/or she has functional manifestations (signs of obstruction that result in abnormal bowel function), we have serious conversations about a bowel resection. If she has full-thickness disease without significant bowel dysfunction—other than blood in her stool—sometimes we talk about more conservative treatment because of the long-term manifestations that a bowel resection could have.
Dr. Brown: I agree completely. It is important to have a good relationship with our colorectal surgeons. If I suspect that the patient has narrowing of the lumen of the large bowel or she actually has symptoms such as bloody diarrhea during menstruation—which is suggestive of deep, infiltrative and penetrative disease—I will often order a colonoscopy ahead of time to get confirmed biopsies. Then the patient discussion occurs with our colorectal surgeon, who operates with me jointly if we decide to proceed with a bowel resection. It’s important to have subspecialty colleagues involved in this care, because a low anterior resection is a very big surgery and there can be down-the-stream complications.
The importance of multidisciplinary care
Dr. Advincula: What are your perspectives on a multidisciplinary or interdisciplinary approach to the patient with endometriosis?
Dr. Brown: As I previously mentioned, it is important to develop a good relationship with colorectal surgery/urology. In addition, behavioral therapists may be involved in the care of patients with endometriosis, for a number of reasons. The disease process is fluid. It will change during the patient’s reproductive years, and you need to manage it accordingly based on her symptoms. Sometimes the diagnosis is not made for 5 to 10 years, and that can lead to other issues: depression, fibromyalgia, or irritable bowel syndrome.
The patient may have multiple issues plus endometriosis. I think having specialists such as gastroenterologists and behavioral therapists on board, as well as colorectal and urological surgeons who can perform these complex surgeries, is very beneficial to the patient. That way, she benefits from the team’s focus and is cared for from start to finish.
Dr. Hur: I like to call the abdomen a studio. It does not have separate compartments for each organ system. It’s one big room, and often the neighboring organs are involved, including the bowel and bladder. I think Dr. Brown’s observation—the multidisciplinary approach to a patient’s comprehensive care—is critical. Like any surgery, preoperative planning and preoperative assessment are essential, and these steps should include the patient. The discussion should cover not only the surgical outcomes that the surgeons expect, but also what the patient expects to be improved. For example, for patients with extensive disease and bowel involvement, a bowel resection is not always the right approach because it can have potential long-term sequelae. Balancing the risks associated with surgery with the long-term benefits is an important part of the discussion.
Dr. Advincula: Those are both excellent perspectives. Endometriosis is a very complicated disease state, does require a multidisciplinary approach to management, and there are implications and strategies that involve both the medical approach to management and the surgical approach.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Wykes CB, Clark TJ, Khan KS. Accuracy of laparoscopy in the diagnosis of endometriosis: a systematic quantitative review. BJOG. 2004;111(11):1204–1212.
- Fernando S, Soh PQ, Cooper M, et al. Reliability of visual diagnosis of endometriosis. J Minim Invasive Gynecol. 2013;20(6):783–789.
- Alborzi S, Momtahan M, Parsanezhad ME, Dehbashi S, Zolghadri J, Alborzi S. A prospective, randomized study comparing laparoscopic ovarian cystectomy versus fenestration and coagulation in patients with endometriomas. Fertil Steril. 2004;82(6):1633–1637.
- Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomized clinical trial of two laparoscopic treatments of endometriomas: cystectomy versus drainage and coagulation. Fertil Steril. 1998;70(6):1176–1180.
- Hart RJ, Hickey M, Maouris P, Buckett W, Garry R. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst Rev. 2005;(3):CD004992.
- Dunselman GA, Vermeulen N, Becker C, et al; European Society of Human Reproduction and Embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412.
- Stochino-Loi E, Darwish B, Mircea O, et al. Does preoperative antimüllerian hormone level influence postoperative pregnancy rate in women undergoing surgery for severe endometriosis? Fertil Steril. 2017;107(3):707–713.e3.
- Motte I, Roman H, Clavier B, et al. In vitro fertilization outcomes after ablation of endometriomas using plasma energy: A retrospective case-control study. Gynecol Obstet Fertil. 2016;44(10):541–547.
- Roman H, Bubenheim M, Auber M, Marpeau L, Puscasiu L. Antimullerian hormone level and endometrioma ablation using plasma energy. JSLS. 2014;18(3).
- Saito N, Okuda K, Yuguchi H, Yamashita Y, Terai Y, Ohmichi M. Compared with cystectomy, is ovarian vaporization of endometriotic cysts truly more effective in maintaining ovarian reserve? J Minim Invasive Gynecol. 2014;21(5):804–810.
- Giampaolino P, Bifulco G, Di Spiezio Sardo A, Mercorio A, Bruzzese D, Di Carlo C. Endometrioma size is a relevant factor in selection of the most appropriate surgical technique: a prospective randomized preliminary study. Eur J Obstet Gynecol Reprod Biol. 2015;195:88–93.
- Chang HJ, Han SH, Lee JR, et al. Impact of laparoscopic cystectomy on ovarian reserve: serial changes of serum anti-MTimes New Romanüllerian hormone levels. Fertil Steril. 2010;94(1):343–349.
- Ding Y, Yuan Y, Ding J, Chen Y, Zhang X, Hua K. Comprehensive assessment of the impact of laparoscopic ovarian cystectomy on ovarian reserve. J Minim Invasive Gynecol. 2015;22(7):1252–1259.
- Mircea O, Puscasiu L, Resch B, et al. Fertility outcomes after ablation using plasma energy versus cystectomy in infertile women with ovarian endometrioma: A multicentric comparative study. J Minim Invasive Gynecol. 2016;23(7):1138–1145.
- Ozaki R, Kumakiri J, Tinelli A, Grimbizis GF, Kitade M, Takeda S. Evaluation of factors predicting diminished ovarian reserve before and after laparoscopic cystectomy for ovarian endometriomas: a prospective cohort study. J Ovarian Res. 2016;9(1):37.
- Demirol A, Guven S, Baykal C, Gurgan T. Effect of endometrioma cystectomy on IVF outcome: A prospective randomized study. Reprod Biomed Online. 2006;12(5):639–643.
- Kennedy S, Bergqvist A, Chapron C, et al; ESHRE Special Interest Group for Endometriosis and Endometrium Guideline Development Group. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20(10):2698–2704.
OBG Management Expert Panel

Arnold P. Advincula, MD
Levine Family Professor of Women's Health
Vice-Chair, Department of Obstetrics & Gynecology
Chief of Gynecology, Sloane Hospital for Women
Medical Director, Mary & Michael Jaharis Simulation Center
Columbia University Medical Center
New York-Presbyterian Hospital, New York, New York

Douglas N. Brown, MD
Chief, Minimally Invasive Gynecologic Surgery
Director, Center for Minimally Invasive Gynecologic Surgery
Vincent Department of Obstetrics & Gynecology
Massachusetts General Hospital
Assistant Professor of Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School, Boston, Massachusetts

Hye-Chun Hur, MD, MPH
Director, Division of Minimally Invasive Gynecologic Surgery
Beth Israel Deaconess Medical Center
Assistant Professor, Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School
Dr. Advincula reports being a consultant to AbbVie, Applied Medical, ConMed, CooperSurgical, Intuitive Surgical, and Titan Medical and receiving royalties from CooperSurgical. Dr. Brown reports being a consultant to Medtronic and CooperSurgical. Dr. Hur reports no financial relationships relevant to this article.
OBG Management Expert Panel
Arnold P. Advincula, MD
Levine Family Professor of Women's Health
Vice-Chair, Department of Obstetrics & Gynecology
Chief of Gynecology, Sloane Hospital for Women
Medical Director, Mary & Michael Jaharis Simulation Center
Columbia University Medical Center
New York-Presbyterian Hospital, New York, New York
Douglas N. Brown, MD
Chief, Minimally Invasive Gynecologic Surgery
Director, Center for Minimally Invasive Gynecologic Surgery
Vincent Department of Obstetrics & Gynecology
Massachusetts General Hospital
Assistant Professor of Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School, Boston, Massachusetts
Hye-Chun Hur, MD, MPH
Director, Division of Minimally Invasive Gynecologic Surgery
Beth Israel Deaconess Medical Center
Assistant Professor, Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School
Dr. Advincula reports being a consultant to AbbVie, Applied Medical, ConMed, CooperSurgical, Intuitive Surgical, and Titan Medical and receiving royalties from CooperSurgical. Dr. Brown reports being a consultant to Medtronic and CooperSurgical. Dr. Hur reports no financial relationships relevant to this article.
OBG Management Expert Panel
Arnold P. Advincula, MD
Levine Family Professor of Women's Health
Vice-Chair, Department of Obstetrics & Gynecology
Chief of Gynecology, Sloane Hospital for Women
Medical Director, Mary & Michael Jaharis Simulation Center
Columbia University Medical Center
New York-Presbyterian Hospital, New York, New York
Douglas N. Brown, MD
Chief, Minimally Invasive Gynecologic Surgery
Director, Center for Minimally Invasive Gynecologic Surgery
Vincent Department of Obstetrics & Gynecology
Massachusetts General Hospital
Assistant Professor of Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School, Boston, Massachusetts
Hye-Chun Hur, MD, MPH
Director, Division of Minimally Invasive Gynecologic Surgery
Beth Israel Deaconess Medical Center
Assistant Professor, Obstetrics, Gynecology, and Reproductive Biology
Harvard Medical School
Dr. Advincula reports being a consultant to AbbVie, Applied Medical, ConMed, CooperSurgical, Intuitive Surgical, and Titan Medical and receiving royalties from CooperSurgical. Dr. Brown reports being a consultant to Medtronic and CooperSurgical. Dr. Hur reports no financial relationships relevant to this article.
Endometriosis is one of the more daunting diagnoses that gynecologists treat. In this roundtable discussion, moderated by
First-time evaluation
Arnold P. Advincula, MD: When a patient presents to your practice for the first time and you suspect endometriosis, what considerations tailor your evaluation, and what does that evaluation involve?
Hye-Chun Hur, MD, MPH: The diagnosis is contingent on a patient’s presenting profile. How symptomatic is she? How old is she? What are her reproductive goals? The gold standard for diagnosis is a histologic diagnosis, which is surgical. Depending on the age profile, however, and how close she is to menopause, the patient may be managed medically. Even women in the young reproductive age group may be managed medically if symptoms are responsive to medical treatment.
Douglas N. Brown, MD: I agree. When a patient presents without a laparoscopy, or a tissue diagnosis, but the symptoms are consistent with likely endometriosis (depending on where she is in her reproductive cycle and what her goals are), I think treating with a first-line therapy—hormonal treatments such as progestin-only oral contraceptive pills—is acceptable. I usually conduct a treatment trial period of 3 to 6 months to see if she obtains any symptom relief.
If that first-line treatment fails, generally you can move to a second-line treatment.
I have a discussion in which I either offer a second-line treatment, such as medroxyprogesterone (Depo-Provera) or leuprolide acetate (Lupron Depot), or get a tissue diagnosis, if possible, by performing laparoscopy. If first-line or even second-line therapy fails, you need to consider doing a diagnostic laparoscopy to confirm or deny the diagnosis.
Dr. Advincula: Are there any points in the evaluation of a patient who visits your practice for the first time where you would immediately offer a surgical approach, as opposed to starting with medical management?
Dr. Hur: A large percentage of my patients undergo surgical evaluation, as surgical diagnosis is the gold standard. If you look at the literature, even among surgeons, the accuracy of visual diagnosis is not great.1,2 I target individuals who are either not responsive to medical treatment or who have never tried medical treatment but are trying to conceive, so they are not medical candidates, or individuals who genuinely want a diagnosis for surgical management—sometimes even before first-line medical treatment.
Dr. Brown: Your examination sometimes also dictates your approach. A patient may never have had a laparoscopy or hormone therapy, but if you find uterosacral ligament nodularity, extreme pain on examination, and suspicious findings on ultrasound or otherwise, a diagnostic laparoscopy may be warranted to confirm the diagnosis.
Endometrioma management
Dr. Advincula: Let’s jump ahead. You have decided to proceed with laparoscopy and you encounter an endometrioma. What is your management strategy, particularly in a fertility-desiring patient?
Dr. Hur: Even if a woman has not undergone first-line medical treatment, if she is trying to conceive or presents with infertility, it’s a different balancing act for approaching the patient. When a woman presents, either with an ultrasound finding or an intraoperative finding of an endometrioma, I am a strong advocate of treating symptomatic disease, which means complete cyst excision. Good clinical data suggest that reproductive outcomes are improved for spontaneous pregnancy rates when you excise an endometrioma.3-6
Dr. Advincula: What are the risks of excision of an endometrioma cyst that patients need to know about?
Dr. Brown: Current standard of care is cystectomy, stripping the cyst wall away from the ovarian cortex. There is some concern that the stripping process, depending on how long the endometrioma has been present within the ovary, can cause some destruction to the underlying oocytes and perhaps impact that ovary’s ability to produce viable eggs.
Some studies, from France in particular, have investigated different energy sources, such as plasma energy, that make it possible to remove part of the cyst and then use the plasma energy to vaporize the rest of the cyst wall that may be lying on the cortex. Researchers looked at anti-Müllerian hormone levels, and there does seem to be a difference in terms of how you remove the cyst.7-9 This energy source is not available to everyone; it’s similar to laser but does not have as much penetration. Standard of care is still ovarian stripping.
The conversation with the patient—if she is already infertile and this cyst is a problem—would be that it likely needs to be removed. There is a chance that she may need assisted reproduction; she might not be able to get pregnant on her own due either to the presence of the endometrioma or to the surgical process of removing it and stripping.
Dr. Advincula: How soon after surgery can a patient start to pursue trying to get pregnant?
Dr. Hur: I think there is no time restraint outside of recovery. As long as the patient has a routine postoperative course, she can try to conceive, spontaneously or with assisted reproduction. Some data suggest, however, that ovarian reserve is diminished immediately after surgery.10–12 If you look at the spontaneous clinical pregnancy outcomes, they are comparable 3 to 6 months postsurgery.4,12–14
Dr. Brown: I agree. Time is of the essence with a lot of patients, many of whom present after age 35.
Dr. Hur: It’s also important to highlight that there are 2 presentations with endometrioma: the symptomatic patient and the asymptomatic patient. In the asymptomatic patient, her age, reproductive goals, and the bilaterality (whether it is present on both sides or on one side) of the endometrioma are important in deciding on a patient-centered surgical plan. For someone with a smaller cyst, unilateral presentation, and maybe older age at presentation, it may or may not impact assisted reproductive outcomes.
If the patient is not symptomatic and she is older with bilateral endometriomas less than 4 cm, some data suggest that patient might be better served in a conservative fashion.6,15–17 Then, once she is done with assisted reproduction, we might be more aggressive surgically by treating the finding that would not resolve spontaneously without surgical management. It is important to highlight that endometriomas do not resolve on their own; they require surgical management.
Read about managing endometriosis for the patient not seeking fertility
Endometriosis management for the patient not seeking fertility
Dr. Advincula: Let’s now consider a patient on whom you have performed laparoscopy not only to diagnose and confirm the evidence of endometriosis but also to treat endometriosis, an endometrioma, and potentially deeply infiltrative disease. But this person is not trying to get pregnant. Postoperatively, what is your approach?
Dr. Brown: Suppressive therapy for this patient could be first-line or second-line therapy, such as a Lupron Depot or Depo-Provera. We keep the patient on suppressive therapy (whatever treatments work for her), until she’s ready to get pregnant; then we take her off. Hopefully she gets pregnant. After she delivers, we reinitiate suppressive therapy. I will follow these women throughout their reproductive cycle, and I think having a team of physicians who are all on the same page can help this patient manage her disease through her reproductive years.
Dr. Hur: If a patient presented warranting surgical management once, and she is not menopausal, the likelihood that disease will recur is quite high. Understanding the nature and the pathology of the disease, hormonal suppression would be warranted. Suppression is not just for between pregnancies, it’s until the patient reaches natural menopause. It’s also in the hopes of suppressing the disease so she does not need recurrent surgeries.
We typically do not operate unless patients have recurrence of symptoms that no longer respond to medical therapy. Our hope is to buy them more time closer to the age of natural menopause so that medical repercussions do not result in hysterectomy and ovary removal, which have other nongynecologic manifestations, including negative impact on bone and cardiac health.
Hye-Chun Hur, MD, MPH: I am a strong advocate of excision of endometriosis. I believe that it's essential to excise for 2 very important reasons. One reason is for diagnosis. Accurately diagnosing endometriosis through visualization alone is poor, even among gynecologic surgeons. It is very important to have an accurate diagnosis of endometriosis, since the diagnosis will then dictate the treatment for the rest of a patient's reproductive life.
The second reason that excision is essential is because you just do not know how much disease there is "behind the scenes." When you start to excise, you begin to appreciate the depth of the disease, and often fibrosis or inflammation is present even behind the endometriosis implant that is visualized.
Douglas N. Brown, MD: I approach endometriosis in the same way that an oncologist would approach cancer. I call it cytoreduction--reducing the disease. There is this iceberg phenomenon, where the tip of the iceberg is seen in the water, but you have no idea how deep it actually goes. That is very much deep, infiltrative endometriosis. Performing an ablation on the top does almost nothing for the patient and may actually complicate the situation by causing scar tissue. If a patient has symptoms, I firmly believe that you must resect the disease, whether it is on the peritoneum, bladder, bowel, or near the ureter. Now, these are radical surgeries, and not every patient should have a radical surgery. It is very much based on the patient's pain complaints and issues at that time, but excision of endometriosis really, in my opinion, should be the standard of care.
Risks of excision of endometriosis
Dr. Brown: The risks of disease excision depend on whether a patient has ureteral disease, bladder disease, or bowel disease, suggested through a preoperative or another operative report or imaging. If this is the case, we have a preoperative discussion with the patient about, "To what extent do you want me to go to remove the disease from your pelvis? If I remove it from your peritoneum and your bladder, there is the chance that you'll have to go home with a Foley catheter for a few days. If the bowel is involved, do you want me to try to resect the disease or shave it off the bowel? If we get into a problem, are you okay with me resecting that bowel?" These are the issues that we have to discuss, because there are potential complications, although known.
The role of the LNG-IUD
Dr. Advincula: Something that often comes up is the role of a levonorgestrel-releasing intrauterine device (LNG-IUD) as one therapy option, either preoperatively or postoperatively. What is your perspective?
Dr. Hur: I reserve the LNG-IUD as a second-line therapy for patients, predominantly because it allows direct delivery of the medication to the womb (rather than systemic exposure of the medication). For patients who experience adverse effects due to systemic exposure to first-line treatments, it might be a great option. However, I do not believe that it consistently suppresses the ovaries, which we understand feeds the pathology of the hormonal stimulation, and so typically I will reserve it as a second-line treatment.
Dr. Brown: I utilize the LNG-IUD in a similar fashion. I may have patients who have had a diagnostic laparoscopy somewhere else and were referred to me because they now have known stage 3 or 4 endometriosis without endometriomas. Those patients, if they are going to need suppressive therapy after surgery and are not ready to get pregnant, do very well with the LNG-IUD, and I will place it during surgery under anesthesia. If a patient has endometriomas seen at the time of surgery, we could still place an LNG-IUD at the time of surgery. We may need to add on an additional medication, however, like another oral progesterone. I do have patients that use both an IUD and either combined oral contraceptive pills and/or oral progestins. Those patients usually have complicated cases with very deep infiltrative disease.
Read about managing endometriosis involving the bowel
Managing endometriosis involving the bowel
Dr. Advincula: Patients often are quite concerned when the words “endometriosis” and “bowel” come together. How do you manage disease that involves the bowel?
Dr. Hur: A lot of patients with endometriosis have what I call neighboring disease—it’s not limited just to the pelvis, but it involves the neighboring organs including the bowel and bladder. Patients can present with symptoms related to those adjacent organs. However, not all disease involving the bowel or bladder manifests with symptoms, and patients with symptoms may not have visible disease.
Typically, when a patient presents with symptoms of bowel involvement, where the bowel lumen is narrowed to more than 50% and/or she has functional manifestations (signs of obstruction that result in abnormal bowel function), we have serious conversations about a bowel resection. If she has full-thickness disease without significant bowel dysfunction—other than blood in her stool—sometimes we talk about more conservative treatment because of the long-term manifestations that a bowel resection could have.
Dr. Brown: I agree completely. It is important to have a good relationship with our colorectal surgeons. If I suspect that the patient has narrowing of the lumen of the large bowel or she actually has symptoms such as bloody diarrhea during menstruation—which is suggestive of deep, infiltrative and penetrative disease—I will often order a colonoscopy ahead of time to get confirmed biopsies. Then the patient discussion occurs with our colorectal surgeon, who operates with me jointly if we decide to proceed with a bowel resection. It’s important to have subspecialty colleagues involved in this care, because a low anterior resection is a very big surgery and there can be down-the-stream complications.
The importance of multidisciplinary care
Dr. Advincula: What are your perspectives on a multidisciplinary or interdisciplinary approach to the patient with endometriosis?
Dr. Brown: As I previously mentioned, it is important to develop a good relationship with colorectal surgery/urology. In addition, behavioral therapists may be involved in the care of patients with endometriosis, for a number of reasons. The disease process is fluid. It will change during the patient’s reproductive years, and you need to manage it accordingly based on her symptoms. Sometimes the diagnosis is not made for 5 to 10 years, and that can lead to other issues: depression, fibromyalgia, or irritable bowel syndrome.
The patient may have multiple issues plus endometriosis. I think having specialists such as gastroenterologists and behavioral therapists on board, as well as colorectal and urological surgeons who can perform these complex surgeries, is very beneficial to the patient. That way, she benefits from the team’s focus and is cared for from start to finish.
Dr. Hur: I like to call the abdomen a studio. It does not have separate compartments for each organ system. It’s one big room, and often the neighboring organs are involved, including the bowel and bladder. I think Dr. Brown’s observation—the multidisciplinary approach to a patient’s comprehensive care—is critical. Like any surgery, preoperative planning and preoperative assessment are essential, and these steps should include the patient. The discussion should cover not only the surgical outcomes that the surgeons expect, but also what the patient expects to be improved. For example, for patients with extensive disease and bowel involvement, a bowel resection is not always the right approach because it can have potential long-term sequelae. Balancing the risks associated with surgery with the long-term benefits is an important part of the discussion.
Dr. Advincula: Those are both excellent perspectives. Endometriosis is a very complicated disease state, does require a multidisciplinary approach to management, and there are implications and strategies that involve both the medical approach to management and the surgical approach.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Endometriosis is one of the more daunting diagnoses that gynecologists treat. In this roundtable discussion, moderated by
First-time evaluation
Arnold P. Advincula, MD: When a patient presents to your practice for the first time and you suspect endometriosis, what considerations tailor your evaluation, and what does that evaluation involve?
Hye-Chun Hur, MD, MPH: The diagnosis is contingent on a patient’s presenting profile. How symptomatic is she? How old is she? What are her reproductive goals? The gold standard for diagnosis is a histologic diagnosis, which is surgical. Depending on the age profile, however, and how close she is to menopause, the patient may be managed medically. Even women in the young reproductive age group may be managed medically if symptoms are responsive to medical treatment.
Douglas N. Brown, MD: I agree. When a patient presents without a laparoscopy, or a tissue diagnosis, but the symptoms are consistent with likely endometriosis (depending on where she is in her reproductive cycle and what her goals are), I think treating with a first-line therapy—hormonal treatments such as progestin-only oral contraceptive pills—is acceptable. I usually conduct a treatment trial period of 3 to 6 months to see if she obtains any symptom relief.
If that first-line treatment fails, generally you can move to a second-line treatment.
I have a discussion in which I either offer a second-line treatment, such as medroxyprogesterone (Depo-Provera) or leuprolide acetate (Lupron Depot), or get a tissue diagnosis, if possible, by performing laparoscopy. If first-line or even second-line therapy fails, you need to consider doing a diagnostic laparoscopy to confirm or deny the diagnosis.
Dr. Advincula: Are there any points in the evaluation of a patient who visits your practice for the first time where you would immediately offer a surgical approach, as opposed to starting with medical management?
Dr. Hur: A large percentage of my patients undergo surgical evaluation, as surgical diagnosis is the gold standard. If you look at the literature, even among surgeons, the accuracy of visual diagnosis is not great.1,2 I target individuals who are either not responsive to medical treatment or who have never tried medical treatment but are trying to conceive, so they are not medical candidates, or individuals who genuinely want a diagnosis for surgical management—sometimes even before first-line medical treatment.
Dr. Brown: Your examination sometimes also dictates your approach. A patient may never have had a laparoscopy or hormone therapy, but if you find uterosacral ligament nodularity, extreme pain on examination, and suspicious findings on ultrasound or otherwise, a diagnostic laparoscopy may be warranted to confirm the diagnosis.
Endometrioma management
Dr. Advincula: Let’s jump ahead. You have decided to proceed with laparoscopy and you encounter an endometrioma. What is your management strategy, particularly in a fertility-desiring patient?
Dr. Hur: Even if a woman has not undergone first-line medical treatment, if she is trying to conceive or presents with infertility, it’s a different balancing act for approaching the patient. When a woman presents, either with an ultrasound finding or an intraoperative finding of an endometrioma, I am a strong advocate of treating symptomatic disease, which means complete cyst excision. Good clinical data suggest that reproductive outcomes are improved for spontaneous pregnancy rates when you excise an endometrioma.3-6
Dr. Advincula: What are the risks of excision of an endometrioma cyst that patients need to know about?
Dr. Brown: Current standard of care is cystectomy, stripping the cyst wall away from the ovarian cortex. There is some concern that the stripping process, depending on how long the endometrioma has been present within the ovary, can cause some destruction to the underlying oocytes and perhaps impact that ovary’s ability to produce viable eggs.
Some studies, from France in particular, have investigated different energy sources, such as plasma energy, that make it possible to remove part of the cyst and then use the plasma energy to vaporize the rest of the cyst wall that may be lying on the cortex. Researchers looked at anti-Müllerian hormone levels, and there does seem to be a difference in terms of how you remove the cyst.7-9 This energy source is not available to everyone; it’s similar to laser but does not have as much penetration. Standard of care is still ovarian stripping.
The conversation with the patient—if she is already infertile and this cyst is a problem—would be that it likely needs to be removed. There is a chance that she may need assisted reproduction; she might not be able to get pregnant on her own due either to the presence of the endometrioma or to the surgical process of removing it and stripping.
Dr. Advincula: How soon after surgery can a patient start to pursue trying to get pregnant?
Dr. Hur: I think there is no time restraint outside of recovery. As long as the patient has a routine postoperative course, she can try to conceive, spontaneously or with assisted reproduction. Some data suggest, however, that ovarian reserve is diminished immediately after surgery.10–12 If you look at the spontaneous clinical pregnancy outcomes, they are comparable 3 to 6 months postsurgery.4,12–14
Dr. Brown: I agree. Time is of the essence with a lot of patients, many of whom present after age 35.
Dr. Hur: It’s also important to highlight that there are 2 presentations with endometrioma: the symptomatic patient and the asymptomatic patient. In the asymptomatic patient, her age, reproductive goals, and the bilaterality (whether it is present on both sides or on one side) of the endometrioma are important in deciding on a patient-centered surgical plan. For someone with a smaller cyst, unilateral presentation, and maybe older age at presentation, it may or may not impact assisted reproductive outcomes.
If the patient is not symptomatic and she is older with bilateral endometriomas less than 4 cm, some data suggest that patient might be better served in a conservative fashion.6,15–17 Then, once she is done with assisted reproduction, we might be more aggressive surgically by treating the finding that would not resolve spontaneously without surgical management. It is important to highlight that endometriomas do not resolve on their own; they require surgical management.
Read about managing endometriosis for the patient not seeking fertility
Endometriosis management for the patient not seeking fertility
Dr. Advincula: Let’s now consider a patient on whom you have performed laparoscopy not only to diagnose and confirm the evidence of endometriosis but also to treat endometriosis, an endometrioma, and potentially deeply infiltrative disease. But this person is not trying to get pregnant. Postoperatively, what is your approach?
Dr. Brown: Suppressive therapy for this patient could be first-line or second-line therapy, such as a Lupron Depot or Depo-Provera. We keep the patient on suppressive therapy (whatever treatments work for her), until she’s ready to get pregnant; then we take her off. Hopefully she gets pregnant. After she delivers, we reinitiate suppressive therapy. I will follow these women throughout their reproductive cycle, and I think having a team of physicians who are all on the same page can help this patient manage her disease through her reproductive years.
Dr. Hur: If a patient presented warranting surgical management once, and she is not menopausal, the likelihood that disease will recur is quite high. Understanding the nature and the pathology of the disease, hormonal suppression would be warranted. Suppression is not just for between pregnancies, it’s until the patient reaches natural menopause. It’s also in the hopes of suppressing the disease so she does not need recurrent surgeries.
We typically do not operate unless patients have recurrence of symptoms that no longer respond to medical therapy. Our hope is to buy them more time closer to the age of natural menopause so that medical repercussions do not result in hysterectomy and ovary removal, which have other nongynecologic manifestations, including negative impact on bone and cardiac health.
Hye-Chun Hur, MD, MPH: I am a strong advocate of excision of endometriosis. I believe that it's essential to excise for 2 very important reasons. One reason is for diagnosis. Accurately diagnosing endometriosis through visualization alone is poor, even among gynecologic surgeons. It is very important to have an accurate diagnosis of endometriosis, since the diagnosis will then dictate the treatment for the rest of a patient's reproductive life.
The second reason that excision is essential is because you just do not know how much disease there is "behind the scenes." When you start to excise, you begin to appreciate the depth of the disease, and often fibrosis or inflammation is present even behind the endometriosis implant that is visualized.
Douglas N. Brown, MD: I approach endometriosis in the same way that an oncologist would approach cancer. I call it cytoreduction--reducing the disease. There is this iceberg phenomenon, where the tip of the iceberg is seen in the water, but you have no idea how deep it actually goes. That is very much deep, infiltrative endometriosis. Performing an ablation on the top does almost nothing for the patient and may actually complicate the situation by causing scar tissue. If a patient has symptoms, I firmly believe that you must resect the disease, whether it is on the peritoneum, bladder, bowel, or near the ureter. Now, these are radical surgeries, and not every patient should have a radical surgery. It is very much based on the patient's pain complaints and issues at that time, but excision of endometriosis really, in my opinion, should be the standard of care.
Risks of excision of endometriosis
Dr. Brown: The risks of disease excision depend on whether a patient has ureteral disease, bladder disease, or bowel disease, suggested through a preoperative or another operative report or imaging. If this is the case, we have a preoperative discussion with the patient about, "To what extent do you want me to go to remove the disease from your pelvis? If I remove it from your peritoneum and your bladder, there is the chance that you'll have to go home with a Foley catheter for a few days. If the bowel is involved, do you want me to try to resect the disease or shave it off the bowel? If we get into a problem, are you okay with me resecting that bowel?" These are the issues that we have to discuss, because there are potential complications, although known.
The role of the LNG-IUD
Dr. Advincula: Something that often comes up is the role of a levonorgestrel-releasing intrauterine device (LNG-IUD) as one therapy option, either preoperatively or postoperatively. What is your perspective?
Dr. Hur: I reserve the LNG-IUD as a second-line therapy for patients, predominantly because it allows direct delivery of the medication to the womb (rather than systemic exposure of the medication). For patients who experience adverse effects due to systemic exposure to first-line treatments, it might be a great option. However, I do not believe that it consistently suppresses the ovaries, which we understand feeds the pathology of the hormonal stimulation, and so typically I will reserve it as a second-line treatment.
Dr. Brown: I utilize the LNG-IUD in a similar fashion. I may have patients who have had a diagnostic laparoscopy somewhere else and were referred to me because they now have known stage 3 or 4 endometriosis without endometriomas. Those patients, if they are going to need suppressive therapy after surgery and are not ready to get pregnant, do very well with the LNG-IUD, and I will place it during surgery under anesthesia. If a patient has endometriomas seen at the time of surgery, we could still place an LNG-IUD at the time of surgery. We may need to add on an additional medication, however, like another oral progesterone. I do have patients that use both an IUD and either combined oral contraceptive pills and/or oral progestins. Those patients usually have complicated cases with very deep infiltrative disease.
Read about managing endometriosis involving the bowel
Managing endometriosis involving the bowel
Dr. Advincula: Patients often are quite concerned when the words “endometriosis” and “bowel” come together. How do you manage disease that involves the bowel?
Dr. Hur: A lot of patients with endometriosis have what I call neighboring disease—it’s not limited just to the pelvis, but it involves the neighboring organs including the bowel and bladder. Patients can present with symptoms related to those adjacent organs. However, not all disease involving the bowel or bladder manifests with symptoms, and patients with symptoms may not have visible disease.
Typically, when a patient presents with symptoms of bowel involvement, where the bowel lumen is narrowed to more than 50% and/or she has functional manifestations (signs of obstruction that result in abnormal bowel function), we have serious conversations about a bowel resection. If she has full-thickness disease without significant bowel dysfunction—other than blood in her stool—sometimes we talk about more conservative treatment because of the long-term manifestations that a bowel resection could have.
Dr. Brown: I agree completely. It is important to have a good relationship with our colorectal surgeons. If I suspect that the patient has narrowing of the lumen of the large bowel or she actually has symptoms such as bloody diarrhea during menstruation—which is suggestive of deep, infiltrative and penetrative disease—I will often order a colonoscopy ahead of time to get confirmed biopsies. Then the patient discussion occurs with our colorectal surgeon, who operates with me jointly if we decide to proceed with a bowel resection. It’s important to have subspecialty colleagues involved in this care, because a low anterior resection is a very big surgery and there can be down-the-stream complications.
The importance of multidisciplinary care
Dr. Advincula: What are your perspectives on a multidisciplinary or interdisciplinary approach to the patient with endometriosis?
Dr. Brown: As I previously mentioned, it is important to develop a good relationship with colorectal surgery/urology. In addition, behavioral therapists may be involved in the care of patients with endometriosis, for a number of reasons. The disease process is fluid. It will change during the patient’s reproductive years, and you need to manage it accordingly based on her symptoms. Sometimes the diagnosis is not made for 5 to 10 years, and that can lead to other issues: depression, fibromyalgia, or irritable bowel syndrome.
The patient may have multiple issues plus endometriosis. I think having specialists such as gastroenterologists and behavioral therapists on board, as well as colorectal and urological surgeons who can perform these complex surgeries, is very beneficial to the patient. That way, she benefits from the team’s focus and is cared for from start to finish.
Dr. Hur: I like to call the abdomen a studio. It does not have separate compartments for each organ system. It’s one big room, and often the neighboring organs are involved, including the bowel and bladder. I think Dr. Brown’s observation—the multidisciplinary approach to a patient’s comprehensive care—is critical. Like any surgery, preoperative planning and preoperative assessment are essential, and these steps should include the patient. The discussion should cover not only the surgical outcomes that the surgeons expect, but also what the patient expects to be improved. For example, for patients with extensive disease and bowel involvement, a bowel resection is not always the right approach because it can have potential long-term sequelae. Balancing the risks associated with surgery with the long-term benefits is an important part of the discussion.
Dr. Advincula: Those are both excellent perspectives. Endometriosis is a very complicated disease state, does require a multidisciplinary approach to management, and there are implications and strategies that involve both the medical approach to management and the surgical approach.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Wykes CB, Clark TJ, Khan KS. Accuracy of laparoscopy in the diagnosis of endometriosis: a systematic quantitative review. BJOG. 2004;111(11):1204–1212.
- Fernando S, Soh PQ, Cooper M, et al. Reliability of visual diagnosis of endometriosis. J Minim Invasive Gynecol. 2013;20(6):783–789.
- Alborzi S, Momtahan M, Parsanezhad ME, Dehbashi S, Zolghadri J, Alborzi S. A prospective, randomized study comparing laparoscopic ovarian cystectomy versus fenestration and coagulation in patients with endometriomas. Fertil Steril. 2004;82(6):1633–1637.
- Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomized clinical trial of two laparoscopic treatments of endometriomas: cystectomy versus drainage and coagulation. Fertil Steril. 1998;70(6):1176–1180.
- Hart RJ, Hickey M, Maouris P, Buckett W, Garry R. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst Rev. 2005;(3):CD004992.
- Dunselman GA, Vermeulen N, Becker C, et al; European Society of Human Reproduction and Embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412.
- Stochino-Loi E, Darwish B, Mircea O, et al. Does preoperative antimüllerian hormone level influence postoperative pregnancy rate in women undergoing surgery for severe endometriosis? Fertil Steril. 2017;107(3):707–713.e3.
- Motte I, Roman H, Clavier B, et al. In vitro fertilization outcomes after ablation of endometriomas using plasma energy: A retrospective case-control study. Gynecol Obstet Fertil. 2016;44(10):541–547.
- Roman H, Bubenheim M, Auber M, Marpeau L, Puscasiu L. Antimullerian hormone level and endometrioma ablation using plasma energy. JSLS. 2014;18(3).
- Saito N, Okuda K, Yuguchi H, Yamashita Y, Terai Y, Ohmichi M. Compared with cystectomy, is ovarian vaporization of endometriotic cysts truly more effective in maintaining ovarian reserve? J Minim Invasive Gynecol. 2014;21(5):804–810.
- Giampaolino P, Bifulco G, Di Spiezio Sardo A, Mercorio A, Bruzzese D, Di Carlo C. Endometrioma size is a relevant factor in selection of the most appropriate surgical technique: a prospective randomized preliminary study. Eur J Obstet Gynecol Reprod Biol. 2015;195:88–93.
- Chang HJ, Han SH, Lee JR, et al. Impact of laparoscopic cystectomy on ovarian reserve: serial changes of serum anti-MTimes New Romanüllerian hormone levels. Fertil Steril. 2010;94(1):343–349.
- Ding Y, Yuan Y, Ding J, Chen Y, Zhang X, Hua K. Comprehensive assessment of the impact of laparoscopic ovarian cystectomy on ovarian reserve. J Minim Invasive Gynecol. 2015;22(7):1252–1259.
- Mircea O, Puscasiu L, Resch B, et al. Fertility outcomes after ablation using plasma energy versus cystectomy in infertile women with ovarian endometrioma: A multicentric comparative study. J Minim Invasive Gynecol. 2016;23(7):1138–1145.
- Ozaki R, Kumakiri J, Tinelli A, Grimbizis GF, Kitade M, Takeda S. Evaluation of factors predicting diminished ovarian reserve before and after laparoscopic cystectomy for ovarian endometriomas: a prospective cohort study. J Ovarian Res. 2016;9(1):37.
- Demirol A, Guven S, Baykal C, Gurgan T. Effect of endometrioma cystectomy on IVF outcome: A prospective randomized study. Reprod Biomed Online. 2006;12(5):639–643.
- Kennedy S, Bergqvist A, Chapron C, et al; ESHRE Special Interest Group for Endometriosis and Endometrium Guideline Development Group. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20(10):2698–2704.
- Wykes CB, Clark TJ, Khan KS. Accuracy of laparoscopy in the diagnosis of endometriosis: a systematic quantitative review. BJOG. 2004;111(11):1204–1212.
- Fernando S, Soh PQ, Cooper M, et al. Reliability of visual diagnosis of endometriosis. J Minim Invasive Gynecol. 2013;20(6):783–789.
- Alborzi S, Momtahan M, Parsanezhad ME, Dehbashi S, Zolghadri J, Alborzi S. A prospective, randomized study comparing laparoscopic ovarian cystectomy versus fenestration and coagulation in patients with endometriomas. Fertil Steril. 2004;82(6):1633–1637.
- Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomized clinical trial of two laparoscopic treatments of endometriomas: cystectomy versus drainage and coagulation. Fertil Steril. 1998;70(6):1176–1180.
- Hart RJ, Hickey M, Maouris P, Buckett W, Garry R. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst Rev. 2005;(3):CD004992.
- Dunselman GA, Vermeulen N, Becker C, et al; European Society of Human Reproduction and Embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412.
- Stochino-Loi E, Darwish B, Mircea O, et al. Does preoperative antimüllerian hormone level influence postoperative pregnancy rate in women undergoing surgery for severe endometriosis? Fertil Steril. 2017;107(3):707–713.e3.
- Motte I, Roman H, Clavier B, et al. In vitro fertilization outcomes after ablation of endometriomas using plasma energy: A retrospective case-control study. Gynecol Obstet Fertil. 2016;44(10):541–547.
- Roman H, Bubenheim M, Auber M, Marpeau L, Puscasiu L. Antimullerian hormone level and endometrioma ablation using plasma energy. JSLS. 2014;18(3).
- Saito N, Okuda K, Yuguchi H, Yamashita Y, Terai Y, Ohmichi M. Compared with cystectomy, is ovarian vaporization of endometriotic cysts truly more effective in maintaining ovarian reserve? J Minim Invasive Gynecol. 2014;21(5):804–810.
- Giampaolino P, Bifulco G, Di Spiezio Sardo A, Mercorio A, Bruzzese D, Di Carlo C. Endometrioma size is a relevant factor in selection of the most appropriate surgical technique: a prospective randomized preliminary study. Eur J Obstet Gynecol Reprod Biol. 2015;195:88–93.
- Chang HJ, Han SH, Lee JR, et al. Impact of laparoscopic cystectomy on ovarian reserve: serial changes of serum anti-MTimes New Romanüllerian hormone levels. Fertil Steril. 2010;94(1):343–349.
- Ding Y, Yuan Y, Ding J, Chen Y, Zhang X, Hua K. Comprehensive assessment of the impact of laparoscopic ovarian cystectomy on ovarian reserve. J Minim Invasive Gynecol. 2015;22(7):1252–1259.
- Mircea O, Puscasiu L, Resch B, et al. Fertility outcomes after ablation using plasma energy versus cystectomy in infertile women with ovarian endometrioma: A multicentric comparative study. J Minim Invasive Gynecol. 2016;23(7):1138–1145.
- Ozaki R, Kumakiri J, Tinelli A, Grimbizis GF, Kitade M, Takeda S. Evaluation of factors predicting diminished ovarian reserve before and after laparoscopic cystectomy for ovarian endometriomas: a prospective cohort study. J Ovarian Res. 2016;9(1):37.
- Demirol A, Guven S, Baykal C, Gurgan T. Effect of endometrioma cystectomy on IVF outcome: A prospective randomized study. Reprod Biomed Online. 2006;12(5):639–643.
- Kennedy S, Bergqvist A, Chapron C, et al; ESHRE Special Interest Group for Endometriosis and Endometrium Guideline Development Group. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20(10):2698–2704.
Take-home points
- Endometriosis management involves fluidity of care. Treatment approaches will change throughout a patient's reproductive life, depending on the patient's presenting symptoms and reproductive goals.
- Inform the patient of the disease process and how it may affect her menstrual pain symptoms and family planning.
- Educate patients so they may effectively participate in the management discussion. Hear the voice of the patient to make a tailored plan of care for each individual.
- Endometriosis can be a complex medical problem. Use a comprehensive multidisciplinary approach when appropriate.
Watch: Video roundtable–Endometriosis: Expert perspectives on medical and surgical management
