User login
Concomitant laparoscopic and vaginal excision of duplicated collecting system

An 80-year-old female developed a painful purulent nodule a day after gardening
. There are more than 100 species of dematiaceous fungi that can cause phaeohyphomycosis, including Alternaria, Exophiala, Phialophora, Wangiella, Bipolaris, Curvularia, and Exserohilum.1,2 The causative fungi are found in plants and soil, so they are commonly seen after activities such as gardening or walking barefoot. Trauma, such as a splinter, typically incites the infection. Infections can present with superficial, cutaneous and subcutaneous involvement.

Sporotrichosis, also called Rose gardener’s disease, is a mycosis caused by Sporothrix schenckii. A typical presentation is when a gardener gets pricked by a rose thorn. Classically, a pustule will develop at the site of inoculation, with additional lesions forming along the path of lymphatic drainage (called a “sporotrichoid” pattern) weeks later. Atypical mycobacterial infections, mainly Mycobacterium marinum, may also present in this way. Histopathology and tissue cultures help to differentiate the two.

An incision and drainage with pathology was performed in the office. Upon opening the nodule, a large wood splinter was extracted. Both the foreign body and a punch biopsy of skin were sent in for examination. Pathology revealed polarizable foreign material in association with suppurative inflammation and dematiaceous fungi. PAS (Periodic-acid Schiff) and GMS (Grocott methenamine silver) stain highlighted fungal forms. Cultures were negative.
Local disease may be treated with excision alone. Oral antifungals, such as itraconazole, fluconazole, or ketoconazole may be used, although may require long treatment courses for months. Amphotericin B and flucytosine may be required in systemic cases. Almost all cases of disseminated disease occur in immunocompromised patients. Our patient’s hand resolved after removal of the causative thorn.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Kradin R. Diagnostic Pathology of Infectious Disease, 1st edition (Saunders, Feb. 2, 2010).
2. Bolognia J et al. Dermatology (St. Louis: Mosby/Elsevier, 2008).
. There are more than 100 species of dematiaceous fungi that can cause phaeohyphomycosis, including Alternaria, Exophiala, Phialophora, Wangiella, Bipolaris, Curvularia, and Exserohilum.1,2 The causative fungi are found in plants and soil, so they are commonly seen after activities such as gardening or walking barefoot. Trauma, such as a splinter, typically incites the infection. Infections can present with superficial, cutaneous and subcutaneous involvement.
Sporotrichosis, also called Rose gardener’s disease, is a mycosis caused by Sporothrix schenckii. A typical presentation is when a gardener gets pricked by a rose thorn. Classically, a pustule will develop at the site of inoculation, with additional lesions forming along the path of lymphatic drainage (called a “sporotrichoid” pattern) weeks later. Atypical mycobacterial infections, mainly Mycobacterium marinum, may also present in this way. Histopathology and tissue cultures help to differentiate the two.
An incision and drainage with pathology was performed in the office. Upon opening the nodule, a large wood splinter was extracted. Both the foreign body and a punch biopsy of skin were sent in for examination. Pathology revealed polarizable foreign material in association with suppurative inflammation and dematiaceous fungi. PAS (Periodic-acid Schiff) and GMS (Grocott methenamine silver) stain highlighted fungal forms. Cultures were negative.
Local disease may be treated with excision alone. Oral antifungals, such as itraconazole, fluconazole, or ketoconazole may be used, although may require long treatment courses for months. Amphotericin B and flucytosine may be required in systemic cases. Almost all cases of disseminated disease occur in immunocompromised patients. Our patient’s hand resolved after removal of the causative thorn.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Kradin R. Diagnostic Pathology of Infectious Disease, 1st edition (Saunders, Feb. 2, 2010).
2. Bolognia J et al. Dermatology (St. Louis: Mosby/Elsevier, 2008).
. There are more than 100 species of dematiaceous fungi that can cause phaeohyphomycosis, including Alternaria, Exophiala, Phialophora, Wangiella, Bipolaris, Curvularia, and Exserohilum.1,2 The causative fungi are found in plants and soil, so they are commonly seen after activities such as gardening or walking barefoot. Trauma, such as a splinter, typically incites the infection. Infections can present with superficial, cutaneous and subcutaneous involvement.
Sporotrichosis, also called Rose gardener’s disease, is a mycosis caused by Sporothrix schenckii. A typical presentation is when a gardener gets pricked by a rose thorn. Classically, a pustule will develop at the site of inoculation, with additional lesions forming along the path of lymphatic drainage (called a “sporotrichoid” pattern) weeks later. Atypical mycobacterial infections, mainly Mycobacterium marinum, may also present in this way. Histopathology and tissue cultures help to differentiate the two.
An incision and drainage with pathology was performed in the office. Upon opening the nodule, a large wood splinter was extracted. Both the foreign body and a punch biopsy of skin were sent in for examination. Pathology revealed polarizable foreign material in association with suppurative inflammation and dematiaceous fungi. PAS (Periodic-acid Schiff) and GMS (Grocott methenamine silver) stain highlighted fungal forms. Cultures were negative.
Local disease may be treated with excision alone. Oral antifungals, such as itraconazole, fluconazole, or ketoconazole may be used, although may require long treatment courses for months. Amphotericin B and flucytosine may be required in systemic cases. Almost all cases of disseminated disease occur in immunocompromised patients. Our patient’s hand resolved after removal of the causative thorn.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Kradin R. Diagnostic Pathology of Infectious Disease, 1st edition (Saunders, Feb. 2, 2010).
2. Bolognia J et al. Dermatology (St. Louis: Mosby/Elsevier, 2008).

Outreach Finds Veterans Unaware of Service Connection
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
Duty to Assist: Assisting Veterans with Exposures to Hazardous Materials
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
One in three children fall short of sleep recommendations
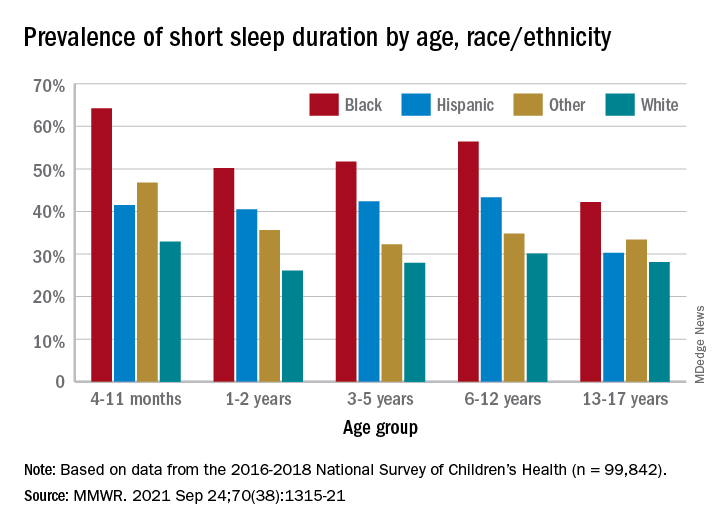
Just over one-third of children in the United States get less sleep than recommended, with higher rates occurring among several racial/ethnic and socioeconomic groups, according to a report from the Centers for Disease Control and Prevention.
, Anne G. Wheaton, PhD, and Angelika H. Claussen, PhD, said in the Morbidity and Mortality Weekly Report.
Unlike previous reports, this analysis showed that adolescents were less likely than infants to have short sleep duration, 31.2% vs. 40.3%. These latest data are based on the 2016-2018 editions of the National Survey of Children’s Health, and the “difference might be explained by NSCH’s reliance on parent report rather than self-report with Youth Risk Behavior Surveys,” they suggested.
Black children had the highest prevalence of any group included in the study, as parents reported that 50.8% of all ages were not getting the recommended amount of sleep, compared with 39.1% among Hispanics, 34.6% for other races, and 28.8% for Whites. The figure for Black infants was 64.2%, almost double the prevalence for White infants (32.9%), said Dr. Wheaton and Dr. Claussen of the CDC.
Short sleep duration also was more common in children from lower-income families and among those with less educated parents. Geography had an effect as well, with prevalence “highest in the Southeast, similar to geographic variation in adequate sleep observed for adults,” they noted.
Previous research has shown that “sleep disparity was associated with various social determinants of health (e.g., poverty, food insecurity, and perceived racism), which can increase chronic and acute stress and result in environmental and psychological factors that negatively affect sleep duration and can compound long-term health risks,” the investigators wrote.
Short sleep duration by age group was defined as less the following amounts: Twelve hours for infants (4-11 months), 11 hours for children aged 1-2 years, 10 hours for children aged 3-5 years, 9 hours for children aged 6-12, and 8 hours for adolescents (13-17 years), they explained. Responses for the survey’s sleep-duration question totaled 99,842 for the 3 years included.
Just over one-third of children in the United States get less sleep than recommended, with higher rates occurring among several racial/ethnic and socioeconomic groups, according to a report from the Centers for Disease Control and Prevention.
, Anne G. Wheaton, PhD, and Angelika H. Claussen, PhD, said in the Morbidity and Mortality Weekly Report.
Unlike previous reports, this analysis showed that adolescents were less likely than infants to have short sleep duration, 31.2% vs. 40.3%. These latest data are based on the 2016-2018 editions of the National Survey of Children’s Health, and the “difference might be explained by NSCH’s reliance on parent report rather than self-report with Youth Risk Behavior Surveys,” they suggested.
Black children had the highest prevalence of any group included in the study, as parents reported that 50.8% of all ages were not getting the recommended amount of sleep, compared with 39.1% among Hispanics, 34.6% for other races, and 28.8% for Whites. The figure for Black infants was 64.2%, almost double the prevalence for White infants (32.9%), said Dr. Wheaton and Dr. Claussen of the CDC.
Short sleep duration also was more common in children from lower-income families and among those with less educated parents. Geography had an effect as well, with prevalence “highest in the Southeast, similar to geographic variation in adequate sleep observed for adults,” they noted.
Previous research has shown that “sleep disparity was associated with various social determinants of health (e.g., poverty, food insecurity, and perceived racism), which can increase chronic and acute stress and result in environmental and psychological factors that negatively affect sleep duration and can compound long-term health risks,” the investigators wrote.
Short sleep duration by age group was defined as less the following amounts: Twelve hours for infants (4-11 months), 11 hours for children aged 1-2 years, 10 hours for children aged 3-5 years, 9 hours for children aged 6-12, and 8 hours for adolescents (13-17 years), they explained. Responses for the survey’s sleep-duration question totaled 99,842 for the 3 years included.
Just over one-third of children in the United States get less sleep than recommended, with higher rates occurring among several racial/ethnic and socioeconomic groups, according to a report from the Centers for Disease Control and Prevention.
, Anne G. Wheaton, PhD, and Angelika H. Claussen, PhD, said in the Morbidity and Mortality Weekly Report.
Unlike previous reports, this analysis showed that adolescents were less likely than infants to have short sleep duration, 31.2% vs. 40.3%. These latest data are based on the 2016-2018 editions of the National Survey of Children’s Health, and the “difference might be explained by NSCH’s reliance on parent report rather than self-report with Youth Risk Behavior Surveys,” they suggested.
Black children had the highest prevalence of any group included in the study, as parents reported that 50.8% of all ages were not getting the recommended amount of sleep, compared with 39.1% among Hispanics, 34.6% for other races, and 28.8% for Whites. The figure for Black infants was 64.2%, almost double the prevalence for White infants (32.9%), said Dr. Wheaton and Dr. Claussen of the CDC.
Short sleep duration also was more common in children from lower-income families and among those with less educated parents. Geography had an effect as well, with prevalence “highest in the Southeast, similar to geographic variation in adequate sleep observed for adults,” they noted.
Previous research has shown that “sleep disparity was associated with various social determinants of health (e.g., poverty, food insecurity, and perceived racism), which can increase chronic and acute stress and result in environmental and psychological factors that negatively affect sleep duration and can compound long-term health risks,” the investigators wrote.
Short sleep duration by age group was defined as less the following amounts: Twelve hours for infants (4-11 months), 11 hours for children aged 1-2 years, 10 hours for children aged 3-5 years, 9 hours for children aged 6-12, and 8 hours for adolescents (13-17 years), they explained. Responses for the survey’s sleep-duration question totaled 99,842 for the 3 years included.
FROM MMWR
RA: Treatment escalation to biologics vs. csDMARD more effective in clinical remission
Key clinical point: In patients with rheumatoid arthritis (RA) in clinical remission, treat-to-target-based treatment escalations to biologics were more effective than escalation to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in improving magnetic resonance imaging (MRI) inflammation, physical function, and clinical disease activity.
Major finding: Escalation to first biologic vs. csDMARD escalation effectively reduced MRI osteitis (difference between least squares means [∆LSM] 1.8; 95% CI 1.0-2.6), Health Assessment Questionnaire score (∆LSM 0.08; 95% CI 0.03-0.1), MRI combined inflammation (∆LSM 2.5; 95% CI 0.9-4.1), and Simplified Disease Activity Index scores (∆LSM 2.7; 95% CI 1.9-3.5).
Study details: This study evaluated the impact of treatment intensification with csDMARDs and biologics in 100 patients with established RA in clinical remission from the IMAGINE-RA trial, who were randomly assigned to MRI treat-to-target strategy.
Disclosures: This research was funded by AbbVie. Some of the authors reported receiving grants and personal fees from various sources including AbbVie.
Source: Møller-Bisgaard S et al. Scand J Rheumatol. 2021 Sep 2. doi: 10.1080/03009742.2021.1935312.
Key clinical point: In patients with rheumatoid arthritis (RA) in clinical remission, treat-to-target-based treatment escalations to biologics were more effective than escalation to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in improving magnetic resonance imaging (MRI) inflammation, physical function, and clinical disease activity.
Major finding: Escalation to first biologic vs. csDMARD escalation effectively reduced MRI osteitis (difference between least squares means [∆LSM] 1.8; 95% CI 1.0-2.6), Health Assessment Questionnaire score (∆LSM 0.08; 95% CI 0.03-0.1), MRI combined inflammation (∆LSM 2.5; 95% CI 0.9-4.1), and Simplified Disease Activity Index scores (∆LSM 2.7; 95% CI 1.9-3.5).
Study details: This study evaluated the impact of treatment intensification with csDMARDs and biologics in 100 patients with established RA in clinical remission from the IMAGINE-RA trial, who were randomly assigned to MRI treat-to-target strategy.
Disclosures: This research was funded by AbbVie. Some of the authors reported receiving grants and personal fees from various sources including AbbVie.
Source: Møller-Bisgaard S et al. Scand J Rheumatol. 2021 Sep 2. doi: 10.1080/03009742.2021.1935312.
Key clinical point: In patients with rheumatoid arthritis (RA) in clinical remission, treat-to-target-based treatment escalations to biologics were more effective than escalation to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in improving magnetic resonance imaging (MRI) inflammation, physical function, and clinical disease activity.
Major finding: Escalation to first biologic vs. csDMARD escalation effectively reduced MRI osteitis (difference between least squares means [∆LSM] 1.8; 95% CI 1.0-2.6), Health Assessment Questionnaire score (∆LSM 0.08; 95% CI 0.03-0.1), MRI combined inflammation (∆LSM 2.5; 95% CI 0.9-4.1), and Simplified Disease Activity Index scores (∆LSM 2.7; 95% CI 1.9-3.5).
Study details: This study evaluated the impact of treatment intensification with csDMARDs and biologics in 100 patients with established RA in clinical remission from the IMAGINE-RA trial, who were randomly assigned to MRI treat-to-target strategy.
Disclosures: This research was funded by AbbVie. Some of the authors reported receiving grants and personal fees from various sources including AbbVie.
Source: Møller-Bisgaard S et al. Scand J Rheumatol. 2021 Sep 2. doi: 10.1080/03009742.2021.1935312.
Abatacept beneficial in csDMARD-refractory RA
Key clinical point: Abatacept appeared to be more efficacious and safer than adding or switching to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in patients with rheumatoid arthritis (RA) of any age who were refractory to csDMARDs.
Major finding: At 24 weeks, European League Against Rheumatism good or moderate response was achieved by a significantly higher proportion of older patients aged 65 years or above (odds ratio [OR] 7.770; P < .0001) and younger patients (OR 4.089; P = .005) receiving abatacept vs. csDMARDs. Few serious adverse events were reported.
Study details: This was a prospective, multicenter study involving 202 bio-naive, csDMARD-refractory patients with RA. The patients were categorized into older (n=67) and younger (n=47) patients receiving abatacept and older (n=48) and younger (n=40) patients receiving csDMARDs.
Disclosures: This study was supported by Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd. The authors including the lead author reported receiving grants and personal/consultancy/speakers’ fees from various sources including Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd.
Source: Muraoka S et al. Rheumatol Ther. 2021 Aug 26. doi: 10.1007/s40744-021-00356-2.
Key clinical point: Abatacept appeared to be more efficacious and safer than adding or switching to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in patients with rheumatoid arthritis (RA) of any age who were refractory to csDMARDs.
Major finding: At 24 weeks, European League Against Rheumatism good or moderate response was achieved by a significantly higher proportion of older patients aged 65 years or above (odds ratio [OR] 7.770; P < .0001) and younger patients (OR 4.089; P = .005) receiving abatacept vs. csDMARDs. Few serious adverse events were reported.
Study details: This was a prospective, multicenter study involving 202 bio-naive, csDMARD-refractory patients with RA. The patients were categorized into older (n=67) and younger (n=47) patients receiving abatacept and older (n=48) and younger (n=40) patients receiving csDMARDs.
Disclosures: This study was supported by Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd. The authors including the lead author reported receiving grants and personal/consultancy/speakers’ fees from various sources including Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd.
Source: Muraoka S et al. Rheumatol Ther. 2021 Aug 26. doi: 10.1007/s40744-021-00356-2.
Key clinical point: Abatacept appeared to be more efficacious and safer than adding or switching to conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in patients with rheumatoid arthritis (RA) of any age who were refractory to csDMARDs.
Major finding: At 24 weeks, European League Against Rheumatism good or moderate response was achieved by a significantly higher proportion of older patients aged 65 years or above (odds ratio [OR] 7.770; P < .0001) and younger patients (OR 4.089; P = .005) receiving abatacept vs. csDMARDs. Few serious adverse events were reported.
Study details: This was a prospective, multicenter study involving 202 bio-naive, csDMARD-refractory patients with RA. The patients were categorized into older (n=67) and younger (n=47) patients receiving abatacept and older (n=48) and younger (n=40) patients receiving csDMARDs.
Disclosures: This study was supported by Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd. The authors including the lead author reported receiving grants and personal/consultancy/speakers’ fees from various sources including Bristol Myers Squibb K.K. and Ono Pharmaceutical Co., Ltd.
Source: Muraoka S et al. Rheumatol Ther. 2021 Aug 26. doi: 10.1007/s40744-021-00356-2.
Bronchiectasis is a common extra-articular feature of RA
Key clinical point: The incidence of rheumatoid arthritis-related bronchiectasis (RA-BR) was almost 20%, suggesting that bronchiectasis is a common extra-articular feature of rheumatoid arthritis (RA).
Major finding: The pooled overall prevalence of RA-BR was 18.7% (95% CI 13.7%-24.3%) in the random effects meta-analysis and 22.6% (95% CI 16.8%-29.0%) in studies that used high-resolution chest computed tomography imaging.
Study details: Findings are from a systematic review and meta-analysis of 41 studies that reported on RA-BR prevalence, risk factors, or both.
Disclosures: The study did not receive any external funding. Dr. Sparks, Dr. Doyle, and Dr. Shadick reported receiving research support and consultancy fees from various sources.
Source: Martin LW et al. Semin Arthritis Rheum. 2021 Aug 20. doi: 10.1016/j.semarthrit.2021.08.005.
Key clinical point: The incidence of rheumatoid arthritis-related bronchiectasis (RA-BR) was almost 20%, suggesting that bronchiectasis is a common extra-articular feature of rheumatoid arthritis (RA).
Major finding: The pooled overall prevalence of RA-BR was 18.7% (95% CI 13.7%-24.3%) in the random effects meta-analysis and 22.6% (95% CI 16.8%-29.0%) in studies that used high-resolution chest computed tomography imaging.
Study details: Findings are from a systematic review and meta-analysis of 41 studies that reported on RA-BR prevalence, risk factors, or both.
Disclosures: The study did not receive any external funding. Dr. Sparks, Dr. Doyle, and Dr. Shadick reported receiving research support and consultancy fees from various sources.
Source: Martin LW et al. Semin Arthritis Rheum. 2021 Aug 20. doi: 10.1016/j.semarthrit.2021.08.005.
Key clinical point: The incidence of rheumatoid arthritis-related bronchiectasis (RA-BR) was almost 20%, suggesting that bronchiectasis is a common extra-articular feature of rheumatoid arthritis (RA).
Major finding: The pooled overall prevalence of RA-BR was 18.7% (95% CI 13.7%-24.3%) in the random effects meta-analysis and 22.6% (95% CI 16.8%-29.0%) in studies that used high-resolution chest computed tomography imaging.
Study details: Findings are from a systematic review and meta-analysis of 41 studies that reported on RA-BR prevalence, risk factors, or both.
Disclosures: The study did not receive any external funding. Dr. Sparks, Dr. Doyle, and Dr. Shadick reported receiving research support and consultancy fees from various sources.
Source: Martin LW et al. Semin Arthritis Rheum. 2021 Aug 20. doi: 10.1016/j.semarthrit.2021.08.005.
Early disease remission reduces fatigue risk in RA
Key clinical point: Disease activity is associated with fatigue in early rheumatoid arthritis (RA), and patients who achieve early remission are at lower risk for experiencing fatigue.
Major finding: Patients who achieved remission at 6 months had a lower chance of experiencing fatigue at 24 months (Disease Activity Score 44 remission, odds ratio [OR] 0.31; P < .001). Fewer swollen joints (OR 0.92; P = .006), lower power Doppler ultrasound score (OR 0.95; P = .027), and a higher patient global assessment score (OR 1.03; P < .001) raised the likelihood of clinically relevant fatigue at 24 months.
Study details: The findings come from the analysis of 205 individuals from the ARCTIC trial. Patients were randomly assigned to a treat-to-target approach with and without musculoskeletal ultrasonography during clinical examinations and treatment decisions.
Disclosures: This work was supported by the DAM Foundation. Some of the authors declared receiving personal fees, personal honoraria, consultancy honorariums/fees, and serving on the data safety monitoring board or advisory board of various sources.
Source: Holton K et al. Ann Rheum Dis. 2021 Aug 13. doi: 10.1136/annrheumdis-2021-220750.
Key clinical point: Disease activity is associated with fatigue in early rheumatoid arthritis (RA), and patients who achieve early remission are at lower risk for experiencing fatigue.
Major finding: Patients who achieved remission at 6 months had a lower chance of experiencing fatigue at 24 months (Disease Activity Score 44 remission, odds ratio [OR] 0.31; P < .001). Fewer swollen joints (OR 0.92; P = .006), lower power Doppler ultrasound score (OR 0.95; P = .027), and a higher patient global assessment score (OR 1.03; P < .001) raised the likelihood of clinically relevant fatigue at 24 months.
Study details: The findings come from the analysis of 205 individuals from the ARCTIC trial. Patients were randomly assigned to a treat-to-target approach with and without musculoskeletal ultrasonography during clinical examinations and treatment decisions.
Disclosures: This work was supported by the DAM Foundation. Some of the authors declared receiving personal fees, personal honoraria, consultancy honorariums/fees, and serving on the data safety monitoring board or advisory board of various sources.
Source: Holton K et al. Ann Rheum Dis. 2021 Aug 13. doi: 10.1136/annrheumdis-2021-220750.
Key clinical point: Disease activity is associated with fatigue in early rheumatoid arthritis (RA), and patients who achieve early remission are at lower risk for experiencing fatigue.
Major finding: Patients who achieved remission at 6 months had a lower chance of experiencing fatigue at 24 months (Disease Activity Score 44 remission, odds ratio [OR] 0.31; P < .001). Fewer swollen joints (OR 0.92; P = .006), lower power Doppler ultrasound score (OR 0.95; P = .027), and a higher patient global assessment score (OR 1.03; P < .001) raised the likelihood of clinically relevant fatigue at 24 months.
Study details: The findings come from the analysis of 205 individuals from the ARCTIC trial. Patients were randomly assigned to a treat-to-target approach with and without musculoskeletal ultrasonography during clinical examinations and treatment decisions.
Disclosures: This work was supported by the DAM Foundation. Some of the authors declared receiving personal fees, personal honoraria, consultancy honorariums/fees, and serving on the data safety monitoring board or advisory board of various sources.
Source: Holton K et al. Ann Rheum Dis. 2021 Aug 13. doi: 10.1136/annrheumdis-2021-220750.
No link between recent antibiotic use and RA risk later in life
Key clinical point: Over 6 years of prospective follow-up found no association between recent antibiotic use and subsequent risk for rheumatoid arthritis (RA) later in life.
Major finding: Compared with no antibiotic usage, short-term (adjusted hazard ratio [aHR] 0.88; 95% CI 0.38-1.38) and middle-to-long-term (aHR 1.06; 95% CI 0.42-1.71) antibiotic use was not associated with an increased risk for RA.
Study details: The study included 1,33,125 female participants from Nurses' Health Study (NHS; n=58,757) and NHS II (n=74,368) databases. Based on antibiotic usage, participants were categorized into nonuse, short-term use (1-14 days), and middle-to-long-term use (15 or more days) groups.
Disclosures: This work was supported by the Natural Science Foundation of China, the Guangdong Provincial Key Laboratory of Digestive Cancer Research, the Startup Fund for the 100 Top Talents Program, the Sun Yat-sen University, and the National Institutes of Health. All the authors reported no conflict of interests.
Source: Liu Y et al. Expert Opin Drug Saf. 2021 Aug 25. doi: 10.1080/14740338.2021.1970134.
Key clinical point: Over 6 years of prospective follow-up found no association between recent antibiotic use and subsequent risk for rheumatoid arthritis (RA) later in life.
Major finding: Compared with no antibiotic usage, short-term (adjusted hazard ratio [aHR] 0.88; 95% CI 0.38-1.38) and middle-to-long-term (aHR 1.06; 95% CI 0.42-1.71) antibiotic use was not associated with an increased risk for RA.
Study details: The study included 1,33,125 female participants from Nurses' Health Study (NHS; n=58,757) and NHS II (n=74,368) databases. Based on antibiotic usage, participants were categorized into nonuse, short-term use (1-14 days), and middle-to-long-term use (15 or more days) groups.
Disclosures: This work was supported by the Natural Science Foundation of China, the Guangdong Provincial Key Laboratory of Digestive Cancer Research, the Startup Fund for the 100 Top Talents Program, the Sun Yat-sen University, and the National Institutes of Health. All the authors reported no conflict of interests.
Source: Liu Y et al. Expert Opin Drug Saf. 2021 Aug 25. doi: 10.1080/14740338.2021.1970134.
Key clinical point: Over 6 years of prospective follow-up found no association between recent antibiotic use and subsequent risk for rheumatoid arthritis (RA) later in life.
Major finding: Compared with no antibiotic usage, short-term (adjusted hazard ratio [aHR] 0.88; 95% CI 0.38-1.38) and middle-to-long-term (aHR 1.06; 95% CI 0.42-1.71) antibiotic use was not associated with an increased risk for RA.
Study details: The study included 1,33,125 female participants from Nurses' Health Study (NHS; n=58,757) and NHS II (n=74,368) databases. Based on antibiotic usage, participants were categorized into nonuse, short-term use (1-14 days), and middle-to-long-term use (15 or more days) groups.
Disclosures: This work was supported by the Natural Science Foundation of China, the Guangdong Provincial Key Laboratory of Digestive Cancer Research, the Startup Fund for the 100 Top Talents Program, the Sun Yat-sen University, and the National Institutes of Health. All the authors reported no conflict of interests.
Source: Liu Y et al. Expert Opin Drug Saf. 2021 Aug 25. doi: 10.1080/14740338.2021.1970134.