User login
The Official Newspaper of the American Association for Thoracic Surgery
AATS: Spare the aortic valve when possible during aortic root replacements
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.

The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.
The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.
The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Your patients will do better with aortic valve–sparing procedures.
Major finding: Aortic valve–sparing procedures are associated with improved long-term freedom from cardiac death (95% at 15 years) when compared with Bentall procedures with biologic valves (93% freedom from cardiac death at 15 years) or mechanical valves (90% freedom at 15 years).
Data source: Review of 1,187 aortic root replacements at the University of Toronto.
Disclosures: The lead investigator has no disclosures.

AATS: No postpneumonectomy survival benefit in adding radiation to chemotherapy for NSCLC
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.

Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.
Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.
Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Limit neoadjuvant treatment to chemotherapy for non–small cell lung cancer patients.
Major finding: About half of patients were alive 5 years after pneumonectomies for lung cancer, whether they had neoadjuvant chemotherapy or chemoradiation.
Data source: Retrospective study of 140 pneumonectomy patients.
Disclosures: Dr. Gebitekin had no disclosures.

With SGR repeal, Medicare refocuses on value
It’s value over volume for Medicare now that the Medicare Access and CHIP Reauthorization Act of 2015 is law.
“This shift in what the country faces in a disease burden really aligns and is helped and facilitated by this updating Medicare to this new disease environment,” Dr. James Madara, CEO of the American Medical Association, said April 15, the day after the Senate passed H.R. 2, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA).
“There are a lot of evolving issues to take care of in this migration toward models of payment delivery that work positively toward impacting quality of care,” Dr. Madara said. “Any time a complex bill as helpful as this one is passed, there are implementation problems that sometimes arise, so one of the areas that we will be strongly attentive to at the AMA is keeping our finger on the pulse of the implementation and working with the federal government to make sure that this tracks in a correct way.”
President Obama signed the bill into law on April 16.
The new law repeals the Medicare Sustainable Growth Rate formula, negating the 21% physician fee cut that was to go into effect April 1. In its place, the law provides a 0.5% pay increase yearly for 5 years as the Medicare program makes the transition away from fee-for-service and to value-based payment.
To help get to a point of value over volume, the bill consolidates existing quality programs – including those regarding the meaningful use of electronic health records – into a single value-based performance program.
“We studied that, along with some of the other physician organizations and our House of Delegates, and the conclusion was that this was not just an improvement, but a significant improvement, over the current set of measurements,” Dr. Madara said.
The new law also incentivizes physicians to use alternate payment models that focus on care coordination and preventive care with a 5% payment bonus. It pushes for more transparency of Medicare data for physicians, providers, and patients.
MACRA also includes funding to help smaller practices participate in alternative payment models or the streamlined quality measurement program, as well as funding to help in the development of quality measures.
“The provisions that allow for continued funding of the quality measurement enterprise in H.R. 2 are a key building block of this important transition and will also facilitate work to continue advancing measurement science,” the National Quality Forum said in a statement. “Ultimately, these efforts will not only help people get better healthcare, but also will reduce costs that strain patients, purchasers, and the system overall.”
Other important provisions in the new law include the reauthorization of several key programs. CHIP (the Children’s Health Insurance Program), the Community Health Center program, the National Health Service Corps, and the Teaching Health Centers program were all reauthorized for 2 years; they had been scheduled to expire later this year. Additionally, the law continues a partial delay of the Medicare two-midnights ruleuntil Sept. 30.
Physicians also cheered provisions of the new law that allay malpractice concerns. The law specifies that the development, recognition, or implementation of any federal health care guideline or standard does not establish a duty of care in medical malpractice claims.
The provision helps distinguish government quality guidelines and payment rules from medical liability standards, according to Brian K. Atchinson, president and CEO of PIAA, a national trade association for medical malpractice liability insurers.
“None of these rules or guidelines were created with the intent to establish a legal standard for negligence, and so it makes sense for Congress to clarify that fact,” Mr. Atchinson said in an interview. “The standard of care provision in the SGR fix bill does just that, and nothing more. It does not shift the playing field to either plaintiffs or defendants. Instead, it ensures that these federal rules are not misused for purposes for which they were never intended.”
H.R. 2 ran into some trouble in the Senate because it does not have a dedicated funding mechanism to cover its full cost. The Congressional Budget Office estimated that enactment of the law will increase the deficit by $141 billion over 10 years. The CBO’s score also found that the legislation would save money, compared with the price of continued patches.
A total of $73 billion of the $214 billion cost of package is offset through spending reductions and revenue increases included in the bill, the CBO found. These include income-related premium adjustments for Medicare Parts B and D, Medigap reforms, an increase of levy authority on payments to Medicare providers with delinquent tax debt, adjustments to inpatient hospital payment rates, a delay of Medicaid Disproportionate Share Hospital changes until 2018, and a 1% market basket update for postacute care providers.
Enactment of the law also looked a bit shaky when the Office of the Actuary for the Centers for Medicare & Medicaid Services released a report April 9 that suggested physicians would see future payment cuts under the law.
“Physician payment rates under H.R. 2 would be lower than scheduled under the current SGR formula by 2048 and would continue to worsen thereafter,” according to the report. “Absent a change in the method or level of update by subsequent legislation, we expect access to Medicare-participating physicians to become a significant issue in the long term under H.R. 2.”
However, the AMA’s Dr. Madara said that he was not concerned about the projections because the report assumes no changes in coming years. “One does not make linear trajectories over a periods of decades or more and assume that that’s where we are going to end up because that assumption is that nothing happens in the interim and, as we all know, that’s just simply not the way life works,” he said.
AMA President Robert Wah noted that the report “fails to take into account the long-range impact such a drastic payment cut [due to the SGR] would have on quality and access for Medicare beneficiaries, or the many options H.R. 2 will make available to physicians for avoiding onerous penalties under current law and the significant positive updates that high performers can earn.”
The American College of Physicians applauded the Senate action.
“We all witnessed something quite extraordinary and historic today when the Senate followed the House in passing comprehensive legislation to repeal Medicare’s Sustainable Growth Rate formula (H.R. 2) and transition us to a new value-based system,” ACP President David Flemming said in a statement.
American Society of Clinical Oncology President Peter Paul Yu said in a statement that “Medicare beneficiaries and their physicians can breathe easier knowing they will no longer face the perennial threat of payment cuts that risk disruption of care and cause anxiety among patients. ... [ASCO] looks forward to working with policymakers to ensure that this new law is effectively implemented and paves the way to new payment models that foster high-quality, value-based health care for all Americans with cancer.”
Similarly, the American Society for Radiation Oncology praised the effort. “Permanently repealing the SGR and replacing it with a stabilized reimbursement plan focused on quality will strengthen Medicare and allow us to enhance cancer care for the more than one million patients treated with radiation therapy each year,” Dr. Bruce G. Haffty, chair of ASTRO’s board of directors, said in a statement.
American College of Cardiology President Kim Allan Williams Sr., in a statement applauding the actions of the Senate, noted that the members “accomplished a major feat by passing legislation that ends a cycle of delays and patches in the law, which created uncertainty for Medicare patients and clinicians for more than an decade.”
The American College of Surgeons lauded the Senate action.
“The reforms set in place by Tuesday’s historic Senate passage of H.R. 2 offers peace of mind to America’s seniors, whose access to medical care through the Medicare program has been threatened for more than 10 years,” Dr. David B. Hoyt, executive director of the American College of Surgeons, said in a statement. “The College is committed to working with policymakers to further develop policies authorized in the legislation that stress quality of care for Medicare beneficiaries.”
The American Psychiatric Association praised the work of the Senate to pass the bill. “The Senate passage of the SGR reform bill is a major step toward a reliable and rational payment system for Medicare beneficiaries and their physicians,” APA President Paul Summergrad said in a statement. “It is long overdue.”
“It is time for a health care system in America that is focused on delivery of quality care, rather than quantity of care,” Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists, said in a statement. “By strengthening the ability of providers to focus on prevention, this bill will help to ensure that more Americans are able to stay healthy, avoiding serious illnesses and their related costs.”
The American College of Emergency Physicians called the move away from the SGR and toward a value-based system “essential to emergency departments. Elderly patients are more likely to need emergency care than any other age group, and the fastest growing segment of the U.S. population is people over 85 years of age. It represents a significant accomplishment for all the emergency physicians who actively made their voices heard in Congress.”
It’s value over volume for Medicare now that the Medicare Access and CHIP Reauthorization Act of 2015 is law.
“This shift in what the country faces in a disease burden really aligns and is helped and facilitated by this updating Medicare to this new disease environment,” Dr. James Madara, CEO of the American Medical Association, said April 15, the day after the Senate passed H.R. 2, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA).
“There are a lot of evolving issues to take care of in this migration toward models of payment delivery that work positively toward impacting quality of care,” Dr. Madara said. “Any time a complex bill as helpful as this one is passed, there are implementation problems that sometimes arise, so one of the areas that we will be strongly attentive to at the AMA is keeping our finger on the pulse of the implementation and working with the federal government to make sure that this tracks in a correct way.”
President Obama signed the bill into law on April 16.
The new law repeals the Medicare Sustainable Growth Rate formula, negating the 21% physician fee cut that was to go into effect April 1. In its place, the law provides a 0.5% pay increase yearly for 5 years as the Medicare program makes the transition away from fee-for-service and to value-based payment.
To help get to a point of value over volume, the bill consolidates existing quality programs – including those regarding the meaningful use of electronic health records – into a single value-based performance program.
“We studied that, along with some of the other physician organizations and our House of Delegates, and the conclusion was that this was not just an improvement, but a significant improvement, over the current set of measurements,” Dr. Madara said.
The new law also incentivizes physicians to use alternate payment models that focus on care coordination and preventive care with a 5% payment bonus. It pushes for more transparency of Medicare data for physicians, providers, and patients.
MACRA also includes funding to help smaller practices participate in alternative payment models or the streamlined quality measurement program, as well as funding to help in the development of quality measures.
“The provisions that allow for continued funding of the quality measurement enterprise in H.R. 2 are a key building block of this important transition and will also facilitate work to continue advancing measurement science,” the National Quality Forum said in a statement. “Ultimately, these efforts will not only help people get better healthcare, but also will reduce costs that strain patients, purchasers, and the system overall.”
Other important provisions in the new law include the reauthorization of several key programs. CHIP (the Children’s Health Insurance Program), the Community Health Center program, the National Health Service Corps, and the Teaching Health Centers program were all reauthorized for 2 years; they had been scheduled to expire later this year. Additionally, the law continues a partial delay of the Medicare two-midnights ruleuntil Sept. 30.
Physicians also cheered provisions of the new law that allay malpractice concerns. The law specifies that the development, recognition, or implementation of any federal health care guideline or standard does not establish a duty of care in medical malpractice claims.
The provision helps distinguish government quality guidelines and payment rules from medical liability standards, according to Brian K. Atchinson, president and CEO of PIAA, a national trade association for medical malpractice liability insurers.
“None of these rules or guidelines were created with the intent to establish a legal standard for negligence, and so it makes sense for Congress to clarify that fact,” Mr. Atchinson said in an interview. “The standard of care provision in the SGR fix bill does just that, and nothing more. It does not shift the playing field to either plaintiffs or defendants. Instead, it ensures that these federal rules are not misused for purposes for which they were never intended.”
H.R. 2 ran into some trouble in the Senate because it does not have a dedicated funding mechanism to cover its full cost. The Congressional Budget Office estimated that enactment of the law will increase the deficit by $141 billion over 10 years. The CBO’s score also found that the legislation would save money, compared with the price of continued patches.
A total of $73 billion of the $214 billion cost of package is offset through spending reductions and revenue increases included in the bill, the CBO found. These include income-related premium adjustments for Medicare Parts B and D, Medigap reforms, an increase of levy authority on payments to Medicare providers with delinquent tax debt, adjustments to inpatient hospital payment rates, a delay of Medicaid Disproportionate Share Hospital changes until 2018, and a 1% market basket update for postacute care providers.
Enactment of the law also looked a bit shaky when the Office of the Actuary for the Centers for Medicare & Medicaid Services released a report April 9 that suggested physicians would see future payment cuts under the law.
“Physician payment rates under H.R. 2 would be lower than scheduled under the current SGR formula by 2048 and would continue to worsen thereafter,” according to the report. “Absent a change in the method or level of update by subsequent legislation, we expect access to Medicare-participating physicians to become a significant issue in the long term under H.R. 2.”
However, the AMA’s Dr. Madara said that he was not concerned about the projections because the report assumes no changes in coming years. “One does not make linear trajectories over a periods of decades or more and assume that that’s where we are going to end up because that assumption is that nothing happens in the interim and, as we all know, that’s just simply not the way life works,” he said.
AMA President Robert Wah noted that the report “fails to take into account the long-range impact such a drastic payment cut [due to the SGR] would have on quality and access for Medicare beneficiaries, or the many options H.R. 2 will make available to physicians for avoiding onerous penalties under current law and the significant positive updates that high performers can earn.”
The American College of Physicians applauded the Senate action.
“We all witnessed something quite extraordinary and historic today when the Senate followed the House in passing comprehensive legislation to repeal Medicare’s Sustainable Growth Rate formula (H.R. 2) and transition us to a new value-based system,” ACP President David Flemming said in a statement.
American Society of Clinical Oncology President Peter Paul Yu said in a statement that “Medicare beneficiaries and their physicians can breathe easier knowing they will no longer face the perennial threat of payment cuts that risk disruption of care and cause anxiety among patients. ... [ASCO] looks forward to working with policymakers to ensure that this new law is effectively implemented and paves the way to new payment models that foster high-quality, value-based health care for all Americans with cancer.”
Similarly, the American Society for Radiation Oncology praised the effort. “Permanently repealing the SGR and replacing it with a stabilized reimbursement plan focused on quality will strengthen Medicare and allow us to enhance cancer care for the more than one million patients treated with radiation therapy each year,” Dr. Bruce G. Haffty, chair of ASTRO’s board of directors, said in a statement.
American College of Cardiology President Kim Allan Williams Sr., in a statement applauding the actions of the Senate, noted that the members “accomplished a major feat by passing legislation that ends a cycle of delays and patches in the law, which created uncertainty for Medicare patients and clinicians for more than an decade.”
The American College of Surgeons lauded the Senate action.
“The reforms set in place by Tuesday’s historic Senate passage of H.R. 2 offers peace of mind to America’s seniors, whose access to medical care through the Medicare program has been threatened for more than 10 years,” Dr. David B. Hoyt, executive director of the American College of Surgeons, said in a statement. “The College is committed to working with policymakers to further develop policies authorized in the legislation that stress quality of care for Medicare beneficiaries.”
The American Psychiatric Association praised the work of the Senate to pass the bill. “The Senate passage of the SGR reform bill is a major step toward a reliable and rational payment system for Medicare beneficiaries and their physicians,” APA President Paul Summergrad said in a statement. “It is long overdue.”
“It is time for a health care system in America that is focused on delivery of quality care, rather than quantity of care,” Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists, said in a statement. “By strengthening the ability of providers to focus on prevention, this bill will help to ensure that more Americans are able to stay healthy, avoiding serious illnesses and their related costs.”
The American College of Emergency Physicians called the move away from the SGR and toward a value-based system “essential to emergency departments. Elderly patients are more likely to need emergency care than any other age group, and the fastest growing segment of the U.S. population is people over 85 years of age. It represents a significant accomplishment for all the emergency physicians who actively made their voices heard in Congress.”
It’s value over volume for Medicare now that the Medicare Access and CHIP Reauthorization Act of 2015 is law.
“This shift in what the country faces in a disease burden really aligns and is helped and facilitated by this updating Medicare to this new disease environment,” Dr. James Madara, CEO of the American Medical Association, said April 15, the day after the Senate passed H.R. 2, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA).
“There are a lot of evolving issues to take care of in this migration toward models of payment delivery that work positively toward impacting quality of care,” Dr. Madara said. “Any time a complex bill as helpful as this one is passed, there are implementation problems that sometimes arise, so one of the areas that we will be strongly attentive to at the AMA is keeping our finger on the pulse of the implementation and working with the federal government to make sure that this tracks in a correct way.”
President Obama signed the bill into law on April 16.
The new law repeals the Medicare Sustainable Growth Rate formula, negating the 21% physician fee cut that was to go into effect April 1. In its place, the law provides a 0.5% pay increase yearly for 5 years as the Medicare program makes the transition away from fee-for-service and to value-based payment.
To help get to a point of value over volume, the bill consolidates existing quality programs – including those regarding the meaningful use of electronic health records – into a single value-based performance program.
“We studied that, along with some of the other physician organizations and our House of Delegates, and the conclusion was that this was not just an improvement, but a significant improvement, over the current set of measurements,” Dr. Madara said.
The new law also incentivizes physicians to use alternate payment models that focus on care coordination and preventive care with a 5% payment bonus. It pushes for more transparency of Medicare data for physicians, providers, and patients.
MACRA also includes funding to help smaller practices participate in alternative payment models or the streamlined quality measurement program, as well as funding to help in the development of quality measures.
“The provisions that allow for continued funding of the quality measurement enterprise in H.R. 2 are a key building block of this important transition and will also facilitate work to continue advancing measurement science,” the National Quality Forum said in a statement. “Ultimately, these efforts will not only help people get better healthcare, but also will reduce costs that strain patients, purchasers, and the system overall.”
Other important provisions in the new law include the reauthorization of several key programs. CHIP (the Children’s Health Insurance Program), the Community Health Center program, the National Health Service Corps, and the Teaching Health Centers program were all reauthorized for 2 years; they had been scheduled to expire later this year. Additionally, the law continues a partial delay of the Medicare two-midnights ruleuntil Sept. 30.
Physicians also cheered provisions of the new law that allay malpractice concerns. The law specifies that the development, recognition, or implementation of any federal health care guideline or standard does not establish a duty of care in medical malpractice claims.
The provision helps distinguish government quality guidelines and payment rules from medical liability standards, according to Brian K. Atchinson, president and CEO of PIAA, a national trade association for medical malpractice liability insurers.
“None of these rules or guidelines were created with the intent to establish a legal standard for negligence, and so it makes sense for Congress to clarify that fact,” Mr. Atchinson said in an interview. “The standard of care provision in the SGR fix bill does just that, and nothing more. It does not shift the playing field to either plaintiffs or defendants. Instead, it ensures that these federal rules are not misused for purposes for which they were never intended.”
H.R. 2 ran into some trouble in the Senate because it does not have a dedicated funding mechanism to cover its full cost. The Congressional Budget Office estimated that enactment of the law will increase the deficit by $141 billion over 10 years. The CBO’s score also found that the legislation would save money, compared with the price of continued patches.
A total of $73 billion of the $214 billion cost of package is offset through spending reductions and revenue increases included in the bill, the CBO found. These include income-related premium adjustments for Medicare Parts B and D, Medigap reforms, an increase of levy authority on payments to Medicare providers with delinquent tax debt, adjustments to inpatient hospital payment rates, a delay of Medicaid Disproportionate Share Hospital changes until 2018, and a 1% market basket update for postacute care providers.
Enactment of the law also looked a bit shaky when the Office of the Actuary for the Centers for Medicare & Medicaid Services released a report April 9 that suggested physicians would see future payment cuts under the law.
“Physician payment rates under H.R. 2 would be lower than scheduled under the current SGR formula by 2048 and would continue to worsen thereafter,” according to the report. “Absent a change in the method or level of update by subsequent legislation, we expect access to Medicare-participating physicians to become a significant issue in the long term under H.R. 2.”
However, the AMA’s Dr. Madara said that he was not concerned about the projections because the report assumes no changes in coming years. “One does not make linear trajectories over a periods of decades or more and assume that that’s where we are going to end up because that assumption is that nothing happens in the interim and, as we all know, that’s just simply not the way life works,” he said.
AMA President Robert Wah noted that the report “fails to take into account the long-range impact such a drastic payment cut [due to the SGR] would have on quality and access for Medicare beneficiaries, or the many options H.R. 2 will make available to physicians for avoiding onerous penalties under current law and the significant positive updates that high performers can earn.”
The American College of Physicians applauded the Senate action.
“We all witnessed something quite extraordinary and historic today when the Senate followed the House in passing comprehensive legislation to repeal Medicare’s Sustainable Growth Rate formula (H.R. 2) and transition us to a new value-based system,” ACP President David Flemming said in a statement.
American Society of Clinical Oncology President Peter Paul Yu said in a statement that “Medicare beneficiaries and their physicians can breathe easier knowing they will no longer face the perennial threat of payment cuts that risk disruption of care and cause anxiety among patients. ... [ASCO] looks forward to working with policymakers to ensure that this new law is effectively implemented and paves the way to new payment models that foster high-quality, value-based health care for all Americans with cancer.”
Similarly, the American Society for Radiation Oncology praised the effort. “Permanently repealing the SGR and replacing it with a stabilized reimbursement plan focused on quality will strengthen Medicare and allow us to enhance cancer care for the more than one million patients treated with radiation therapy each year,” Dr. Bruce G. Haffty, chair of ASTRO’s board of directors, said in a statement.
American College of Cardiology President Kim Allan Williams Sr., in a statement applauding the actions of the Senate, noted that the members “accomplished a major feat by passing legislation that ends a cycle of delays and patches in the law, which created uncertainty for Medicare patients and clinicians for more than an decade.”
The American College of Surgeons lauded the Senate action.
“The reforms set in place by Tuesday’s historic Senate passage of H.R. 2 offers peace of mind to America’s seniors, whose access to medical care through the Medicare program has been threatened for more than 10 years,” Dr. David B. Hoyt, executive director of the American College of Surgeons, said in a statement. “The College is committed to working with policymakers to further develop policies authorized in the legislation that stress quality of care for Medicare beneficiaries.”
The American Psychiatric Association praised the work of the Senate to pass the bill. “The Senate passage of the SGR reform bill is a major step toward a reliable and rational payment system for Medicare beneficiaries and their physicians,” APA President Paul Summergrad said in a statement. “It is long overdue.”
“It is time for a health care system in America that is focused on delivery of quality care, rather than quantity of care,” Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists, said in a statement. “By strengthening the ability of providers to focus on prevention, this bill will help to ensure that more Americans are able to stay healthy, avoiding serious illnesses and their related costs.”
The American College of Emergency Physicians called the move away from the SGR and toward a value-based system “essential to emergency departments. Elderly patients are more likely to need emergency care than any other age group, and the fastest growing segment of the U.S. population is people over 85 years of age. It represents a significant accomplishment for all the emergency physicians who actively made their voices heard in Congress.”
EuroPCR: CT-derived FFR promising in evaluating chest pain
PARIS – Noninvasive measurement of computed tomography–derived fractional flow reserve is a potential game changer in the management of patients with stable chest pain.
In a 200-patient proof-of-concept study known as FFR-CT RIPCORD, in which three experienced interventional cardiologists initially devised management plans based on coronary anatomy as defined by the results of CT angiography alone, subsequent knowledge of CT-derived fractional flow reserve (FFR-CT) caused them to change their management strategies in fully 36% of cases, Dr. Nick Curzen reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

“If this novel proof-of-concept result can be confirmed in large-scale trials, this suggests that noninvasive FFR-CT can be used as a clinically relevant tool that mimics the well-described ability of invasive FFR to refine management decisions for patients with chest pain that are made by invasive coronary angiography alone. This would indeed have important implications for routine clinical practice. FFR-CT may have potential as a noninvasive default method for simultaneous assessment of coronary anatomy and physiology in angina patients in order to define their management, which would completely change the way we look after them,” observed Dr. Curzen, professor of interventional cardiology at the University of Southampton (England).
EuroPCR codirector Dr. Williams Wijns was favorably impressed by the FFR-CT RIPCORD findings.
“This, I find just stunning. It’s really far reaching. This is a complete change in paradigm. Many patients that today undergo invasive angiography won’t even be sent to the cath lab. The invasive center becomes only for treatment,” commented Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
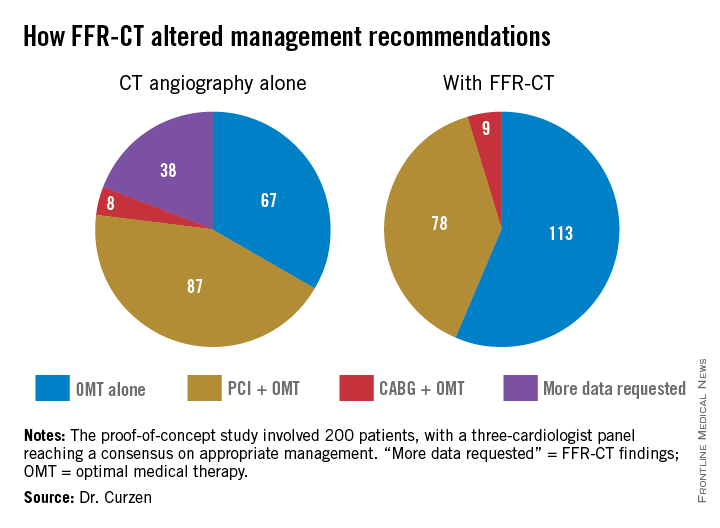
In FFR-CT RIPCORD, the cardiologists received information about a patient’s history and nonvasive CT angiography findings and were asked to reach consensus in selecting one of four management options: optimal medical therapy (OMT) alone, PCI plus OMT, CABG surgery and OMT, or ‘more information needed’ in the form of FFR findings, which identify those coronary lesions that are actually causing ischemia. Instead of receiving the results of conventional invasive FFR obtained using a pressure wire, however, the cardiologists were provided with the noninvasive FFR-CT findings in all 200 cases.
The resultant changes in management were substantial. Thirty percent of the patients initially slated for PCI were reallocated to OMT alone because no ischemic lesions were present. Twelve percent of patients assigned to OMT-only got reassigned to coronary revascularization. Moreover, in 18% of the PCI group, FFR-CT data led to a change in the vessel or vessels targeted for intervention.
“What particularly impressed me were two of those figures: that one-third of PCI patients are redirected to medical therapy, and – even more impressive to me – is the 18% of PCI patients who had a change in their target vessel. That’s a problem we often have in patients with multivessel disease and intermediate lesions: Sometimes we think, for example, the target is the LAD when in fact it’s another vessel,” commented Dr. Jean Fajadet, codirector of the interventional cardiovascular group at the Clinique Pasteur in Toulouse, France.
Dr. Curzen said the exciting thing about FFR-CT is that it could provide in one fell swoop a standardized way of obtaining both the anatomic and physiologic data necessary for informed clinical decision making, and without exposing patients needlessly to the risks of contrast and radiation exposure entailed in invasive coronary angiography.
“When we assess people with stable angina, if you have a room full of invasive cardiologists, we all do it differently at the moment. It’s crazy. A lot of us will do noninvasive tests like stress echo or MRI or some kind of exercise test, and then refer them for an invasive angiogram where we’ll also do an FFR. Some people will go straight for an angiogram. It’s a real mess. The thing I love about FFR-CT is it would be so slick for patients and their families: You see them in a chest pain clinic or your office and you put them in for this test. They don’t have to waste their time coming back several times for different tests. It’s a really beautiful concept,” Dr. Curzen continued.
Right now the turnaround time on FFR-CT is about 12 hours. The dataset has to be sent off to a supercomputer for a complex modeling analysis before the results come back.
“Of course, if this ever becomes clinically proven, I’m sure the turnaround time would become very quick,” according to the cardiologist.
A cost-effectiveness analysis of FFR-CT versus current standard care is ongoing and the results aren’t yet available. However, Dr. Curzen observed, “The cost to the patient is a very important issue: Who would want to have this done invasively if you have a test that proves you don’t need to have an invasive procedure?”
The FFR-CT RIPCORD study was sponsored by Heartflow. Dr. Curzen reported receiving research support from Heartflow, Boston Scientific, Haemonetics, and Medtronic.
PARIS – Noninvasive measurement of computed tomography–derived fractional flow reserve is a potential game changer in the management of patients with stable chest pain.
In a 200-patient proof-of-concept study known as FFR-CT RIPCORD, in which three experienced interventional cardiologists initially devised management plans based on coronary anatomy as defined by the results of CT angiography alone, subsequent knowledge of CT-derived fractional flow reserve (FFR-CT) caused them to change their management strategies in fully 36% of cases, Dr. Nick Curzen reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“If this novel proof-of-concept result can be confirmed in large-scale trials, this suggests that noninvasive FFR-CT can be used as a clinically relevant tool that mimics the well-described ability of invasive FFR to refine management decisions for patients with chest pain that are made by invasive coronary angiography alone. This would indeed have important implications for routine clinical practice. FFR-CT may have potential as a noninvasive default method for simultaneous assessment of coronary anatomy and physiology in angina patients in order to define their management, which would completely change the way we look after them,” observed Dr. Curzen, professor of interventional cardiology at the University of Southampton (England).
EuroPCR codirector Dr. Williams Wijns was favorably impressed by the FFR-CT RIPCORD findings.
“This, I find just stunning. It’s really far reaching. This is a complete change in paradigm. Many patients that today undergo invasive angiography won’t even be sent to the cath lab. The invasive center becomes only for treatment,” commented Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
In FFR-CT RIPCORD, the cardiologists received information about a patient’s history and nonvasive CT angiography findings and were asked to reach consensus in selecting one of four management options: optimal medical therapy (OMT) alone, PCI plus OMT, CABG surgery and OMT, or ‘more information needed’ in the form of FFR findings, which identify those coronary lesions that are actually causing ischemia. Instead of receiving the results of conventional invasive FFR obtained using a pressure wire, however, the cardiologists were provided with the noninvasive FFR-CT findings in all 200 cases.
The resultant changes in management were substantial. Thirty percent of the patients initially slated for PCI were reallocated to OMT alone because no ischemic lesions were present. Twelve percent of patients assigned to OMT-only got reassigned to coronary revascularization. Moreover, in 18% of the PCI group, FFR-CT data led to a change in the vessel or vessels targeted for intervention.
“What particularly impressed me were two of those figures: that one-third of PCI patients are redirected to medical therapy, and – even more impressive to me – is the 18% of PCI patients who had a change in their target vessel. That’s a problem we often have in patients with multivessel disease and intermediate lesions: Sometimes we think, for example, the target is the LAD when in fact it’s another vessel,” commented Dr. Jean Fajadet, codirector of the interventional cardiovascular group at the Clinique Pasteur in Toulouse, France.
Dr. Curzen said the exciting thing about FFR-CT is that it could provide in one fell swoop a standardized way of obtaining both the anatomic and physiologic data necessary for informed clinical decision making, and without exposing patients needlessly to the risks of contrast and radiation exposure entailed in invasive coronary angiography.
“When we assess people with stable angina, if you have a room full of invasive cardiologists, we all do it differently at the moment. It’s crazy. A lot of us will do noninvasive tests like stress echo or MRI or some kind of exercise test, and then refer them for an invasive angiogram where we’ll also do an FFR. Some people will go straight for an angiogram. It’s a real mess. The thing I love about FFR-CT is it would be so slick for patients and their families: You see them in a chest pain clinic or your office and you put them in for this test. They don’t have to waste their time coming back several times for different tests. It’s a really beautiful concept,” Dr. Curzen continued.
Right now the turnaround time on FFR-CT is about 12 hours. The dataset has to be sent off to a supercomputer for a complex modeling analysis before the results come back.
“Of course, if this ever becomes clinically proven, I’m sure the turnaround time would become very quick,” according to the cardiologist.
A cost-effectiveness analysis of FFR-CT versus current standard care is ongoing and the results aren’t yet available. However, Dr. Curzen observed, “The cost to the patient is a very important issue: Who would want to have this done invasively if you have a test that proves you don’t need to have an invasive procedure?”
The FFR-CT RIPCORD study was sponsored by Heartflow. Dr. Curzen reported receiving research support from Heartflow, Boston Scientific, Haemonetics, and Medtronic.
PARIS – Noninvasive measurement of computed tomography–derived fractional flow reserve is a potential game changer in the management of patients with stable chest pain.
In a 200-patient proof-of-concept study known as FFR-CT RIPCORD, in which three experienced interventional cardiologists initially devised management plans based on coronary anatomy as defined by the results of CT angiography alone, subsequent knowledge of CT-derived fractional flow reserve (FFR-CT) caused them to change their management strategies in fully 36% of cases, Dr. Nick Curzen reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“If this novel proof-of-concept result can be confirmed in large-scale trials, this suggests that noninvasive FFR-CT can be used as a clinically relevant tool that mimics the well-described ability of invasive FFR to refine management decisions for patients with chest pain that are made by invasive coronary angiography alone. This would indeed have important implications for routine clinical practice. FFR-CT may have potential as a noninvasive default method for simultaneous assessment of coronary anatomy and physiology in angina patients in order to define their management, which would completely change the way we look after them,” observed Dr. Curzen, professor of interventional cardiology at the University of Southampton (England).
EuroPCR codirector Dr. Williams Wijns was favorably impressed by the FFR-CT RIPCORD findings.
“This, I find just stunning. It’s really far reaching. This is a complete change in paradigm. Many patients that today undergo invasive angiography won’t even be sent to the cath lab. The invasive center becomes only for treatment,” commented Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
In FFR-CT RIPCORD, the cardiologists received information about a patient’s history and nonvasive CT angiography findings and were asked to reach consensus in selecting one of four management options: optimal medical therapy (OMT) alone, PCI plus OMT, CABG surgery and OMT, or ‘more information needed’ in the form of FFR findings, which identify those coronary lesions that are actually causing ischemia. Instead of receiving the results of conventional invasive FFR obtained using a pressure wire, however, the cardiologists were provided with the noninvasive FFR-CT findings in all 200 cases.
The resultant changes in management were substantial. Thirty percent of the patients initially slated for PCI were reallocated to OMT alone because no ischemic lesions were present. Twelve percent of patients assigned to OMT-only got reassigned to coronary revascularization. Moreover, in 18% of the PCI group, FFR-CT data led to a change in the vessel or vessels targeted for intervention.
“What particularly impressed me were two of those figures: that one-third of PCI patients are redirected to medical therapy, and – even more impressive to me – is the 18% of PCI patients who had a change in their target vessel. That’s a problem we often have in patients with multivessel disease and intermediate lesions: Sometimes we think, for example, the target is the LAD when in fact it’s another vessel,” commented Dr. Jean Fajadet, codirector of the interventional cardiovascular group at the Clinique Pasteur in Toulouse, France.
Dr. Curzen said the exciting thing about FFR-CT is that it could provide in one fell swoop a standardized way of obtaining both the anatomic and physiologic data necessary for informed clinical decision making, and without exposing patients needlessly to the risks of contrast and radiation exposure entailed in invasive coronary angiography.
“When we assess people with stable angina, if you have a room full of invasive cardiologists, we all do it differently at the moment. It’s crazy. A lot of us will do noninvasive tests like stress echo or MRI or some kind of exercise test, and then refer them for an invasive angiogram where we’ll also do an FFR. Some people will go straight for an angiogram. It’s a real mess. The thing I love about FFR-CT is it would be so slick for patients and their families: You see them in a chest pain clinic or your office and you put them in for this test. They don’t have to waste their time coming back several times for different tests. It’s a really beautiful concept,” Dr. Curzen continued.
Right now the turnaround time on FFR-CT is about 12 hours. The dataset has to be sent off to a supercomputer for a complex modeling analysis before the results come back.
“Of course, if this ever becomes clinically proven, I’m sure the turnaround time would become very quick,” according to the cardiologist.
A cost-effectiveness analysis of FFR-CT versus current standard care is ongoing and the results aren’t yet available. However, Dr. Curzen observed, “The cost to the patient is a very important issue: Who would want to have this done invasively if you have a test that proves you don’t need to have an invasive procedure?”
The FFR-CT RIPCORD study was sponsored by Heartflow. Dr. Curzen reported receiving research support from Heartflow, Boston Scientific, Haemonetics, and Medtronic.
AT EUROPCR
Key clinical point: Clinically decisive anatomic and physiologic data regarding the coronary arteries of patients with stable angina can be obtained noninvasively with a single test: CT-derived fractional flow reserve.
Major finding: Noninvasive FFR-CT findings resulted in a change in management strategy for 36% of patients with stable angina whose initial treatment plan was based on CT angiography alone.
Data source: A proof-of-concept study involving 200 patients with stable angina and a panel of three experienced interventional cardiologists making consensus decisions regarding their appropriate management.
Disclosures: The FFR-CT RIPCORD study was sponsored by Heartflow. The presenter reported having received research support from the company.
Distractions in the OR increase surgeons’ stress
Distractions in the operating room are associated with increased mental strain, stress, and poor teamwork, according to findings of a cross-sectional, prospective observational study of 90 general surgery cases.
Ana Wheelock of the department of surgery and cancer, Imperial College, London, and her associates stated that previous studies have described a variety of distractions in the OR, but have failed to explore the impact of this factor on surgeons, anesthesiologists, and nurses (Ann. Surg. 2015;261:1079-84).
There is evidence to suggest that distractions such as noise and non–case-related conversation in the OR are linked to a higher rate of errors and adverse events, but the chain of events leading to these errors has been understudied (World J. Surg. 2008;32:1643-50; Qual. Saf. Health Care 2007;16:135-9).

For this study, to capture the variety of events and resulting impacts on the work process in the OR, two trained researchers – one surgeon and one behavioral scientist – observed each case. To prevent a Hawthorne effect, the researchers were present in the OR before the study began to acclimatize staff to their presence.
The case sample yielded 69 hours and 40 minutes of real-time observation. Both open and laparoscopic procedures were represented, and cases included appendectomy, inguinal hernia repair, thyroidectomy, varicose vein surgery, and mastectomy. Mean operative time for the cases was 46 minutes, and American Society of Anesthesiologists (ASA) classification of the cases ranged from I to IV. Data were collected from 85 staff (23 surgeons, 28 anesthesiologists, and 34 nurses).
The study focused on three factors with implications for performance: workload, stress, and teamwork. Workload was measured with the validated NASA-Task Load Index tool, widely used in aviation and other high-risk occupations. Six aspects of workload (mental, physical, and temporal demands; frustration; effort; and performance) were measured via interview in each team member after each procedure. Stress level was scored with the State Trait Anxiety Inventory (STAI) in the same way. Teamwork factors were reported with a validated Observational Teamwork Assessment for Surgery (OTAS) tool.
The findings show that distractions were ubiquitous: Fewer than 2% of cases occurred with zero distractions. The most prevalent distraction involved staff entering the OR (81% of which were deemed unnecessary), followed by case-irrelevant conversation, and equipment failures or absences.
The observers noted a wide variety of disruptions: cell phones ringing, missing equipment, malfunctioning lights, requests by an administrator for a few minutes of the surgeon’s time during the operation, overlapping and nonrelevant conversations among nurses about misplaced files and lunch, and external staff entering and leaving the OR. Distractions occurred in 98% of the operations observed and coincided with normal noise of OR machines, dropped instruments, and distant paging. The mean number of intraoperative distractions was 11 per case.

How did these distractions affect surgeons? Teamwork scores (communication, coordination, leadership, and monitoring) were correlated negatively (r = –0.46) with distractions, case-irrelevant conversation initiated by fellow surgeons in particular. Equipment failures also had a negative impact on these teamwork elements for surgeons (r = –0.41). Workload and stress scores for surgeons showed a negative correlation between these factors and the amount of conversation initiated by other surgeons (r = –0.31 and –0.26, respectively). Acoustic distractions from cell phones, monitors, equipment, and dropped instruments were positively associated with higher stress levels among surgeons (r = 0.30).
Fewer distractions were observed, however, in longer cases and also in cases with a higher degree of patient morbidity.
The study is limited by the case mix of relatively short procedures and low patient ASAs. Only global scores were obtained, which did not allow a more detailed analysis of different stages of procedures. In addition, surgical outcomes were not assessed. The researchers noted, however, that “although there were no associations between external distractions and our outcome measures [ASA classification], the sheer number of unnecessary external visitors to the ORs that we observed should be a cause for concern, as high personnel flow through ORs has been significantly associated with hospital acquired infections” (Clin. Infect. Dis. 1991;13:S800-4).
The takeaway from this study, according to the researchers, is that many of these distractions that have a negative impact on workload, stress, and teamwork function are preventable. “Although some distractions may be inevitable, others, particularly during tasks that require undivided attention, should be proactively limited as they can induce human error and have negative consequences on patient safety ... a clearer understanding of the interaction between the team and the OR environment is imperative if we are to truly recognize and mitigate all factors that impact upon team performance and error.”
The (U.K.) National Institute for Health Research funded the study. The authors have no disclosures.
Distractions in the operating room are associated with increased mental strain, stress, and poor teamwork, according to findings of a cross-sectional, prospective observational study of 90 general surgery cases.
Ana Wheelock of the department of surgery and cancer, Imperial College, London, and her associates stated that previous studies have described a variety of distractions in the OR, but have failed to explore the impact of this factor on surgeons, anesthesiologists, and nurses (Ann. Surg. 2015;261:1079-84).
There is evidence to suggest that distractions such as noise and non–case-related conversation in the OR are linked to a higher rate of errors and adverse events, but the chain of events leading to these errors has been understudied (World J. Surg. 2008;32:1643-50; Qual. Saf. Health Care 2007;16:135-9).
For this study, to capture the variety of events and resulting impacts on the work process in the OR, two trained researchers – one surgeon and one behavioral scientist – observed each case. To prevent a Hawthorne effect, the researchers were present in the OR before the study began to acclimatize staff to their presence.
The case sample yielded 69 hours and 40 minutes of real-time observation. Both open and laparoscopic procedures were represented, and cases included appendectomy, inguinal hernia repair, thyroidectomy, varicose vein surgery, and mastectomy. Mean operative time for the cases was 46 minutes, and American Society of Anesthesiologists (ASA) classification of the cases ranged from I to IV. Data were collected from 85 staff (23 surgeons, 28 anesthesiologists, and 34 nurses).
The study focused on three factors with implications for performance: workload, stress, and teamwork. Workload was measured with the validated NASA-Task Load Index tool, widely used in aviation and other high-risk occupations. Six aspects of workload (mental, physical, and temporal demands; frustration; effort; and performance) were measured via interview in each team member after each procedure. Stress level was scored with the State Trait Anxiety Inventory (STAI) in the same way. Teamwork factors were reported with a validated Observational Teamwork Assessment for Surgery (OTAS) tool.
The findings show that distractions were ubiquitous: Fewer than 2% of cases occurred with zero distractions. The most prevalent distraction involved staff entering the OR (81% of which were deemed unnecessary), followed by case-irrelevant conversation, and equipment failures or absences.
The observers noted a wide variety of disruptions: cell phones ringing, missing equipment, malfunctioning lights, requests by an administrator for a few minutes of the surgeon’s time during the operation, overlapping and nonrelevant conversations among nurses about misplaced files and lunch, and external staff entering and leaving the OR. Distractions occurred in 98% of the operations observed and coincided with normal noise of OR machines, dropped instruments, and distant paging. The mean number of intraoperative distractions was 11 per case.
How did these distractions affect surgeons? Teamwork scores (communication, coordination, leadership, and monitoring) were correlated negatively (r = –0.46) with distractions, case-irrelevant conversation initiated by fellow surgeons in particular. Equipment failures also had a negative impact on these teamwork elements for surgeons (r = –0.41). Workload and stress scores for surgeons showed a negative correlation between these factors and the amount of conversation initiated by other surgeons (r = –0.31 and –0.26, respectively). Acoustic distractions from cell phones, monitors, equipment, and dropped instruments were positively associated with higher stress levels among surgeons (r = 0.30).
Fewer distractions were observed, however, in longer cases and also in cases with a higher degree of patient morbidity.
The study is limited by the case mix of relatively short procedures and low patient ASAs. Only global scores were obtained, which did not allow a more detailed analysis of different stages of procedures. In addition, surgical outcomes were not assessed. The researchers noted, however, that “although there were no associations between external distractions and our outcome measures [ASA classification], the sheer number of unnecessary external visitors to the ORs that we observed should be a cause for concern, as high personnel flow through ORs has been significantly associated with hospital acquired infections” (Clin. Infect. Dis. 1991;13:S800-4).
The takeaway from this study, according to the researchers, is that many of these distractions that have a negative impact on workload, stress, and teamwork function are preventable. “Although some distractions may be inevitable, others, particularly during tasks that require undivided attention, should be proactively limited as they can induce human error and have negative consequences on patient safety ... a clearer understanding of the interaction between the team and the OR environment is imperative if we are to truly recognize and mitigate all factors that impact upon team performance and error.”
The (U.K.) National Institute for Health Research funded the study. The authors have no disclosures.
Distractions in the operating room are associated with increased mental strain, stress, and poor teamwork, according to findings of a cross-sectional, prospective observational study of 90 general surgery cases.
Ana Wheelock of the department of surgery and cancer, Imperial College, London, and her associates stated that previous studies have described a variety of distractions in the OR, but have failed to explore the impact of this factor on surgeons, anesthesiologists, and nurses (Ann. Surg. 2015;261:1079-84).
There is evidence to suggest that distractions such as noise and non–case-related conversation in the OR are linked to a higher rate of errors and adverse events, but the chain of events leading to these errors has been understudied (World J. Surg. 2008;32:1643-50; Qual. Saf. Health Care 2007;16:135-9).
For this study, to capture the variety of events and resulting impacts on the work process in the OR, two trained researchers – one surgeon and one behavioral scientist – observed each case. To prevent a Hawthorne effect, the researchers were present in the OR before the study began to acclimatize staff to their presence.
The case sample yielded 69 hours and 40 minutes of real-time observation. Both open and laparoscopic procedures were represented, and cases included appendectomy, inguinal hernia repair, thyroidectomy, varicose vein surgery, and mastectomy. Mean operative time for the cases was 46 minutes, and American Society of Anesthesiologists (ASA) classification of the cases ranged from I to IV. Data were collected from 85 staff (23 surgeons, 28 anesthesiologists, and 34 nurses).
The study focused on three factors with implications for performance: workload, stress, and teamwork. Workload was measured with the validated NASA-Task Load Index tool, widely used in aviation and other high-risk occupations. Six aspects of workload (mental, physical, and temporal demands; frustration; effort; and performance) were measured via interview in each team member after each procedure. Stress level was scored with the State Trait Anxiety Inventory (STAI) in the same way. Teamwork factors were reported with a validated Observational Teamwork Assessment for Surgery (OTAS) tool.
The findings show that distractions were ubiquitous: Fewer than 2% of cases occurred with zero distractions. The most prevalent distraction involved staff entering the OR (81% of which were deemed unnecessary), followed by case-irrelevant conversation, and equipment failures or absences.
The observers noted a wide variety of disruptions: cell phones ringing, missing equipment, malfunctioning lights, requests by an administrator for a few minutes of the surgeon’s time during the operation, overlapping and nonrelevant conversations among nurses about misplaced files and lunch, and external staff entering and leaving the OR. Distractions occurred in 98% of the operations observed and coincided with normal noise of OR machines, dropped instruments, and distant paging. The mean number of intraoperative distractions was 11 per case.
How did these distractions affect surgeons? Teamwork scores (communication, coordination, leadership, and monitoring) were correlated negatively (r = –0.46) with distractions, case-irrelevant conversation initiated by fellow surgeons in particular. Equipment failures also had a negative impact on these teamwork elements for surgeons (r = –0.41). Workload and stress scores for surgeons showed a negative correlation between these factors and the amount of conversation initiated by other surgeons (r = –0.31 and –0.26, respectively). Acoustic distractions from cell phones, monitors, equipment, and dropped instruments were positively associated with higher stress levels among surgeons (r = 0.30).
Fewer distractions were observed, however, in longer cases and also in cases with a higher degree of patient morbidity.
The study is limited by the case mix of relatively short procedures and low patient ASAs. Only global scores were obtained, which did not allow a more detailed analysis of different stages of procedures. In addition, surgical outcomes were not assessed. The researchers noted, however, that “although there were no associations between external distractions and our outcome measures [ASA classification], the sheer number of unnecessary external visitors to the ORs that we observed should be a cause for concern, as high personnel flow through ORs has been significantly associated with hospital acquired infections” (Clin. Infect. Dis. 1991;13:S800-4).
The takeaway from this study, according to the researchers, is that many of these distractions that have a negative impact on workload, stress, and teamwork function are preventable. “Although some distractions may be inevitable, others, particularly during tasks that require undivided attention, should be proactively limited as they can induce human error and have negative consequences on patient safety ... a clearer understanding of the interaction between the team and the OR environment is imperative if we are to truly recognize and mitigate all factors that impact upon team performance and error.”
The (U.K.) National Institute for Health Research funded the study. The authors have no disclosures.
Key clinical point: Distractions during surgical operations were negatively correlated to stress, workload, and teamwork function scores among surgeons, anesthesiologists, and nurses.
Major finding: Surgeons’ teamwork, workload, and stress scores were negatively associated with case-irrelevant, surgeon-initiated conversation in the OR.
Data source: A cross-sectional, prospective observational study of 90 general surgery cases and 85 staff members.
Disclosures: The National Institute for Health Research funded the study. The authors have no disclosures.
Stricter DVT prophylaxis guidelines needed for cardiac and vascular surgery
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
FROM ANNALS OF VASCULAR SURGERY
Key clinical point: Intraoperative anticoagulation alone does not prevent DVT in patients undergoing vascular and cardiac surgery.
Major finding: The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery.
Data source: Retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database.
Disclosures: The authors did not report any financial disclosures.
ATS: Nintedanib found effective for IPF up to 76 weeks
DENVER – The use of nintedanib 150 mg twice daily has been shown to slow disease progression in patients with idiopathic pulmonary fibrosis up to 76 weeks of treatment, with an acceptable safety and tolerability profile, according to results from a novel study.
Marketed by Boehringer Ingelheim, nintedanib (Ofev)was approved by the FDA in October of 2014 for the treatment of idiopathic pulmonary fibrosis. Data from period 1 of the dose-finding, phase II TOMORROW trial (N. Engl. J. Med. 2011;365:1079–87) and the two replicate Phase III INPULSIS trials (N. Engl. J. Med. 2014;370:2071-82) demonstrated the efficacy and safety of nintedanib 150 mg twice daily over 52 weeks in patients with IPF. After completing period 1 of the TOMORROW trial, study participants had the option to continue treatment in a further blinded treatment phase (period 2).
“Clinicians are always interested in the long-term efficacy and safety of a new drug in patients suffering from a chronic, progressive disease like IPF,” lead study author Dr. Luca Richeldi said in an interview in advance of an international conference of the American Thoracic Society. “These data from period 2 of the TOMORROW trial are the first data to be generated on long-term treatment with nintedanib, i.e., beyond 52 weeks.” In period 2, patients treated with nintedanib in period 1 continued their dose, while placebo-treated patients were switched to nintedanib 50 mg once daily. The researchers evaluated change in forced vital capacity (FVC), acute exacerbations, mortality and adverse events in the nintedanib 150 mg twice daily group vs. the comparator group (placebo/nintedanib 50 mg once daily).

Of the 428 patients treated in period 1, 316 patients completed period 1 and 286 patients continued treatment in period 2. Of these 286 patients, 48 continued to receive nintedanib 150 mg twice daily and 54 were switched from placebo to nintedanib 50 mg once daily (comparator group), said Dr. Richeldi, professor of respiratory medicine and chair of interstitial lung disease at the University of Southampton (United Kingdom).
Dr. Richeldi reported results from a mean exposure of 14.2 months for the nintedanib 150 mg twice daily group and 16.8 months for the comparator group. Across periods 1 and 2, the researchers observed that the mean change in forced vital capacity (FVC) was consistently lower in the nintedanib 150 mg twice daily group, compared with the comparator group, such that by week 76 the absolute change in the percentage of predicted FVC was -3.1% vs. -6.3%, respectively. In addition, the incidence of acute exacerbations at week 76 was lower in the nintedanib 150 mg twice daily group, compared with the comparator group (3.2 vs. 13.4 per 100 patient-years).
A total of 14 patients (16.3%) died in the nintedanib 150 mg twice daily group, compared with 19 patients (21.8%) in the comparator group. However, the proportion of patients with at least one adverse event across period 1 and 2 was similar between both groups (97.6% vs. 96.5%, respectively), as was the proportion of patients with at least one serious adverse event (30.6% vs. 35.3%).
“It was not a surprise to see that the effect of nintedanib 150 mg twice daily on slowing disease progression (as shown by a reduced decline in FVC) was maintained up to week 76,” Dr. Richeldi said. “In addition, we expected that no relevant changes in the safety and tolerability of nintedanib would be observed in period 2 compared with period 1. We were impressed to see that over 90% of patients who completed the first 52 weeks of treatment in the TOMORROW trial (period 1) chose to continue to receive treatment in period 2.”
One limitation of the study was its small sample size, he said, “with FVC data only being available for 80 patients treated with nintedanib twice daily or comparator at week 76. Data from the open-label extension of the INPULSIS trials, INPULSIS-ON, will provide additional data on the long-term efficacy and safety of nintedanib 150 mg twice daily in patients with IPF.”
The study was supported by Boehringer Ingelheim. Dr. Richeldi disclosed that he has received consultation and speaker’s fees from the company. He was also a member of the steering committee for the TOMORROW trial.
On Twitter @dougbrunk
DENVER – The use of nintedanib 150 mg twice daily has been shown to slow disease progression in patients with idiopathic pulmonary fibrosis up to 76 weeks of treatment, with an acceptable safety and tolerability profile, according to results from a novel study.
Marketed by Boehringer Ingelheim, nintedanib (Ofev)was approved by the FDA in October of 2014 for the treatment of idiopathic pulmonary fibrosis. Data from period 1 of the dose-finding, phase II TOMORROW trial (N. Engl. J. Med. 2011;365:1079–87) and the two replicate Phase III INPULSIS trials (N. Engl. J. Med. 2014;370:2071-82) demonstrated the efficacy and safety of nintedanib 150 mg twice daily over 52 weeks in patients with IPF. After completing period 1 of the TOMORROW trial, study participants had the option to continue treatment in a further blinded treatment phase (period 2).
“Clinicians are always interested in the long-term efficacy and safety of a new drug in patients suffering from a chronic, progressive disease like IPF,” lead study author Dr. Luca Richeldi said in an interview in advance of an international conference of the American Thoracic Society. “These data from period 2 of the TOMORROW trial are the first data to be generated on long-term treatment with nintedanib, i.e., beyond 52 weeks.” In period 2, patients treated with nintedanib in period 1 continued their dose, while placebo-treated patients were switched to nintedanib 50 mg once daily. The researchers evaluated change in forced vital capacity (FVC), acute exacerbations, mortality and adverse events in the nintedanib 150 mg twice daily group vs. the comparator group (placebo/nintedanib 50 mg once daily).
Of the 428 patients treated in period 1, 316 patients completed period 1 and 286 patients continued treatment in period 2. Of these 286 patients, 48 continued to receive nintedanib 150 mg twice daily and 54 were switched from placebo to nintedanib 50 mg once daily (comparator group), said Dr. Richeldi, professor of respiratory medicine and chair of interstitial lung disease at the University of Southampton (United Kingdom).
Dr. Richeldi reported results from a mean exposure of 14.2 months for the nintedanib 150 mg twice daily group and 16.8 months for the comparator group. Across periods 1 and 2, the researchers observed that the mean change in forced vital capacity (FVC) was consistently lower in the nintedanib 150 mg twice daily group, compared with the comparator group, such that by week 76 the absolute change in the percentage of predicted FVC was -3.1% vs. -6.3%, respectively. In addition, the incidence of acute exacerbations at week 76 was lower in the nintedanib 150 mg twice daily group, compared with the comparator group (3.2 vs. 13.4 per 100 patient-years).
A total of 14 patients (16.3%) died in the nintedanib 150 mg twice daily group, compared with 19 patients (21.8%) in the comparator group. However, the proportion of patients with at least one adverse event across period 1 and 2 was similar between both groups (97.6% vs. 96.5%, respectively), as was the proportion of patients with at least one serious adverse event (30.6% vs. 35.3%).
“It was not a surprise to see that the effect of nintedanib 150 mg twice daily on slowing disease progression (as shown by a reduced decline in FVC) was maintained up to week 76,” Dr. Richeldi said. “In addition, we expected that no relevant changes in the safety and tolerability of nintedanib would be observed in period 2 compared with period 1. We were impressed to see that over 90% of patients who completed the first 52 weeks of treatment in the TOMORROW trial (period 1) chose to continue to receive treatment in period 2.”
One limitation of the study was its small sample size, he said, “with FVC data only being available for 80 patients treated with nintedanib twice daily or comparator at week 76. Data from the open-label extension of the INPULSIS trials, INPULSIS-ON, will provide additional data on the long-term efficacy and safety of nintedanib 150 mg twice daily in patients with IPF.”
The study was supported by Boehringer Ingelheim. Dr. Richeldi disclosed that he has received consultation and speaker’s fees from the company. He was also a member of the steering committee for the TOMORROW trial.
On Twitter @dougbrunk
DENVER – The use of nintedanib 150 mg twice daily has been shown to slow disease progression in patients with idiopathic pulmonary fibrosis up to 76 weeks of treatment, with an acceptable safety and tolerability profile, according to results from a novel study.
Marketed by Boehringer Ingelheim, nintedanib (Ofev)was approved by the FDA in October of 2014 for the treatment of idiopathic pulmonary fibrosis. Data from period 1 of the dose-finding, phase II TOMORROW trial (N. Engl. J. Med. 2011;365:1079–87) and the two replicate Phase III INPULSIS trials (N. Engl. J. Med. 2014;370:2071-82) demonstrated the efficacy and safety of nintedanib 150 mg twice daily over 52 weeks in patients with IPF. After completing period 1 of the TOMORROW trial, study participants had the option to continue treatment in a further blinded treatment phase (period 2).
“Clinicians are always interested in the long-term efficacy and safety of a new drug in patients suffering from a chronic, progressive disease like IPF,” lead study author Dr. Luca Richeldi said in an interview in advance of an international conference of the American Thoracic Society. “These data from period 2 of the TOMORROW trial are the first data to be generated on long-term treatment with nintedanib, i.e., beyond 52 weeks.” In period 2, patients treated with nintedanib in period 1 continued their dose, while placebo-treated patients were switched to nintedanib 50 mg once daily. The researchers evaluated change in forced vital capacity (FVC), acute exacerbations, mortality and adverse events in the nintedanib 150 mg twice daily group vs. the comparator group (placebo/nintedanib 50 mg once daily).
Of the 428 patients treated in period 1, 316 patients completed period 1 and 286 patients continued treatment in period 2. Of these 286 patients, 48 continued to receive nintedanib 150 mg twice daily and 54 were switched from placebo to nintedanib 50 mg once daily (comparator group), said Dr. Richeldi, professor of respiratory medicine and chair of interstitial lung disease at the University of Southampton (United Kingdom).
Dr. Richeldi reported results from a mean exposure of 14.2 months for the nintedanib 150 mg twice daily group and 16.8 months for the comparator group. Across periods 1 and 2, the researchers observed that the mean change in forced vital capacity (FVC) was consistently lower in the nintedanib 150 mg twice daily group, compared with the comparator group, such that by week 76 the absolute change in the percentage of predicted FVC was -3.1% vs. -6.3%, respectively. In addition, the incidence of acute exacerbations at week 76 was lower in the nintedanib 150 mg twice daily group, compared with the comparator group (3.2 vs. 13.4 per 100 patient-years).
A total of 14 patients (16.3%) died in the nintedanib 150 mg twice daily group, compared with 19 patients (21.8%) in the comparator group. However, the proportion of patients with at least one adverse event across period 1 and 2 was similar between both groups (97.6% vs. 96.5%, respectively), as was the proportion of patients with at least one serious adverse event (30.6% vs. 35.3%).
“It was not a surprise to see that the effect of nintedanib 150 mg twice daily on slowing disease progression (as shown by a reduced decline in FVC) was maintained up to week 76,” Dr. Richeldi said. “In addition, we expected that no relevant changes in the safety and tolerability of nintedanib would be observed in period 2 compared with period 1. We were impressed to see that over 90% of patients who completed the first 52 weeks of treatment in the TOMORROW trial (period 1) chose to continue to receive treatment in period 2.”
One limitation of the study was its small sample size, he said, “with FVC data only being available for 80 patients treated with nintedanib twice daily or comparator at week 76. Data from the open-label extension of the INPULSIS trials, INPULSIS-ON, will provide additional data on the long-term efficacy and safety of nintedanib 150 mg twice daily in patients with IPF.”
The study was supported by Boehringer Ingelheim. Dr. Richeldi disclosed that he has received consultation and speaker’s fees from the company. He was also a member of the steering committee for the TOMORROW trial.
On Twitter @dougbrunk
AT ATS 2015
Key clinical point: The effect of nintedanib on idiopathic pulmonary fibrosis was maintained up to 76 >weeks.
Major finding: The mean change in forced vital capacity (FVC) was consistently lower in the nintedanib 150 mg twice daily group, compared with the comparator group, such that by week 76 the absolute change in the percentage of predicted FVC was -3.1% vs. -6.3%, respectively.
Data source: A study of 102 patients from the TOMORROW trial who continued treatment with nintedanib 150 mg twice daily or nintedanib 50 mg once daily (comparator group) for up to 76 weeks.
Disclosures: The study was supported by Boehringer Ingelheim. Dr. Richeldi disclosed that he has received consultation and speaker’s fees from the company. He was also a member of the steering committee for the TOMORROW trial.

DDW: Barrett’s ‘indefinite for dysplasia’ may be cancer harbinger
WASHINGTON – A diagnosis of Barrett’s esophagus “indefinite for dysplasia” doesn’t mean that the patient is home free; it may, in fact, be an indicator of increased risk for progression to high-grade dysplasia or esophageal adenocarcinoma, investigators suggest.
Among 87 patients who had follow-up endoscopies and biopsies within a year of a diagnosis of Barrett’s indefinite for dysplasia (IND), 7 had progression of disease, including 5 who developed high-grade dysplasia or adenocarcinoma, and 2 who developed low-grade disease.

Of these seven patients, four had disease progression with 6 months of a diagnosis of Barrett’s IND, Dr, Michelle Ma reported at the annual Digestive Disease Week.
“Indefinite for dysplasia is an important diagnostic category that is associated with an increased risk for prevalent dysplasia, particularly within the first 6 months after diagnosis. After 12 months, the risk for progressing to advanced neoplasia is low, and similar to other studies,” said Dr. Ma of the University of Pennsylvania, Philadelphia.
Although there is fairly strong evidence to guide the management of patients with low-grade and high-grade dysplasia, it’s less clear whether Barrett’s IND is risk marker for progression. Dr. Ma said, citing a somewhat fuzzy definition of the term: “Epithelial abnormalities insufficient to diagnose dysplasia, or epithelial abnormalities unclear due to inflammation or sampling.”
Uncertainty about the natural history of IND is reflected in practice guidelines, which either don’t address it, call for repeat endoscopy in 6 months, or call for an expert gastrointestinal pathology review with repeat endoscopy to clarify dysplasia status if the evidence is of low quality, Dr. Ma said.
To determine the rate of, and risk factors for, neoplastic progression of IND, the authors took a retrospective look at patients in their center’s pathology database and Barrett’s esophagus register with a histopathologic diagnosis of IND from 2000 through 2014. They excluded patients with frank dysplasia or carcinoma on diagnosis, and those who did not have follow-up endoscopies.
The investigatoes factored demographic variables into their analysis, including age, gender, body-mass index, smoking history, use of proton-pump inhibitors (PPI), nonsteroidal anti-inflammatory drugs, and family history of Barrett’s or esophageal adenocarcinoma. They also considered endoscopic/pathologic characteristics such as hiatal hernia size, Barrett’s segment length, muscosal nodularity, and multifocal IND.
A total of 106 patients with IND were eligible for the analysis, 87 of whom had follow-up endoscopy and biopsy within a year of diagnosis. As noted before, 7 of these patients had prevalent disease, with prevalence rates of 2.3% for low-grade dysplasia, 4.6% for high-grade dysplasia, and 1.1% for esophageal adenocarcinoma.
To determine the incidence of dysplasia, the authors first excluded the 7 patients with prevealent dysplasia and 33 patients who did not have a surveillance endoscopy in the first year following a diagnosis of IND, leaving 66 patients for analysis. Of this group, 3 developed incident dysplasia or adenocarcinoma, yielding an incidence of 4.5% over a median of 32 months of follow-up.
An analysis of risk factors for prevalent dysplasia showed that none of the variables was significant, although Barrett’s segment length approached statistical significance. Looking at risk factors for incident dysplasia, both smoking status (P = .0207) and segment length (P = .0253) were significant predictors.
A pathologist who was not involved in the study pointed out that a diagnosis of IND can mean many things to many people.
“Indefinite for dysplasia is really not an entity, it’s about 5,000 things that we choose to put into that category. It’s a horribly non-reproducible diagnosis,” commented Dr. Henry D. Appelman, a professor of anatomic pathology at the University of Michigan in Ann Arbor, during a aquestion-and-answer period.
He questioned whether the diagnoses of IND were subject to review at her center.
Dr. Ma noted that Barrett’s specimens at her institution are routinely reviewed by pathologists specializing in Barrett’s, who will also review slides of patients referred to the center from other institutions.
The study was internally funded. The authors reported no conflicts of interest.
WASHINGTON – A diagnosis of Barrett’s esophagus “indefinite for dysplasia” doesn’t mean that the patient is home free; it may, in fact, be an indicator of increased risk for progression to high-grade dysplasia or esophageal adenocarcinoma, investigators suggest.
Among 87 patients who had follow-up endoscopies and biopsies within a year of a diagnosis of Barrett’s indefinite for dysplasia (IND), 7 had progression of disease, including 5 who developed high-grade dysplasia or adenocarcinoma, and 2 who developed low-grade disease.
Of these seven patients, four had disease progression with 6 months of a diagnosis of Barrett’s IND, Dr, Michelle Ma reported at the annual Digestive Disease Week.
“Indefinite for dysplasia is an important diagnostic category that is associated with an increased risk for prevalent dysplasia, particularly within the first 6 months after diagnosis. After 12 months, the risk for progressing to advanced neoplasia is low, and similar to other studies,” said Dr. Ma of the University of Pennsylvania, Philadelphia.
Although there is fairly strong evidence to guide the management of patients with low-grade and high-grade dysplasia, it’s less clear whether Barrett’s IND is risk marker for progression. Dr. Ma said, citing a somewhat fuzzy definition of the term: “Epithelial abnormalities insufficient to diagnose dysplasia, or epithelial abnormalities unclear due to inflammation or sampling.”
Uncertainty about the natural history of IND is reflected in practice guidelines, which either don’t address it, call for repeat endoscopy in 6 months, or call for an expert gastrointestinal pathology review with repeat endoscopy to clarify dysplasia status if the evidence is of low quality, Dr. Ma said.
To determine the rate of, and risk factors for, neoplastic progression of IND, the authors took a retrospective look at patients in their center’s pathology database and Barrett’s esophagus register with a histopathologic diagnosis of IND from 2000 through 2014. They excluded patients with frank dysplasia or carcinoma on diagnosis, and those who did not have follow-up endoscopies.
The investigatoes factored demographic variables into their analysis, including age, gender, body-mass index, smoking history, use of proton-pump inhibitors (PPI), nonsteroidal anti-inflammatory drugs, and family history of Barrett’s or esophageal adenocarcinoma. They also considered endoscopic/pathologic characteristics such as hiatal hernia size, Barrett’s segment length, muscosal nodularity, and multifocal IND.
A total of 106 patients with IND were eligible for the analysis, 87 of whom had follow-up endoscopy and biopsy within a year of diagnosis. As noted before, 7 of these patients had prevalent disease, with prevalence rates of 2.3% for low-grade dysplasia, 4.6% for high-grade dysplasia, and 1.1% for esophageal adenocarcinoma.
To determine the incidence of dysplasia, the authors first excluded the 7 patients with prevealent dysplasia and 33 patients who did not have a surveillance endoscopy in the first year following a diagnosis of IND, leaving 66 patients for analysis. Of this group, 3 developed incident dysplasia or adenocarcinoma, yielding an incidence of 4.5% over a median of 32 months of follow-up.
An analysis of risk factors for prevalent dysplasia showed that none of the variables was significant, although Barrett’s segment length approached statistical significance. Looking at risk factors for incident dysplasia, both smoking status (P = .0207) and segment length (P = .0253) were significant predictors.
A pathologist who was not involved in the study pointed out that a diagnosis of IND can mean many things to many people.
“Indefinite for dysplasia is really not an entity, it’s about 5,000 things that we choose to put into that category. It’s a horribly non-reproducible diagnosis,” commented Dr. Henry D. Appelman, a professor of anatomic pathology at the University of Michigan in Ann Arbor, during a aquestion-and-answer period.
He questioned whether the diagnoses of IND were subject to review at her center.
Dr. Ma noted that Barrett’s specimens at her institution are routinely reviewed by pathologists specializing in Barrett’s, who will also review slides of patients referred to the center from other institutions.
The study was internally funded. The authors reported no conflicts of interest.
WASHINGTON – A diagnosis of Barrett’s esophagus “indefinite for dysplasia” doesn’t mean that the patient is home free; it may, in fact, be an indicator of increased risk for progression to high-grade dysplasia or esophageal adenocarcinoma, investigators suggest.
Among 87 patients who had follow-up endoscopies and biopsies within a year of a diagnosis of Barrett’s indefinite for dysplasia (IND), 7 had progression of disease, including 5 who developed high-grade dysplasia or adenocarcinoma, and 2 who developed low-grade disease.
Of these seven patients, four had disease progression with 6 months of a diagnosis of Barrett’s IND, Dr, Michelle Ma reported at the annual Digestive Disease Week.
“Indefinite for dysplasia is an important diagnostic category that is associated with an increased risk for prevalent dysplasia, particularly within the first 6 months after diagnosis. After 12 months, the risk for progressing to advanced neoplasia is low, and similar to other studies,” said Dr. Ma of the University of Pennsylvania, Philadelphia.
Although there is fairly strong evidence to guide the management of patients with low-grade and high-grade dysplasia, it’s less clear whether Barrett’s IND is risk marker for progression. Dr. Ma said, citing a somewhat fuzzy definition of the term: “Epithelial abnormalities insufficient to diagnose dysplasia, or epithelial abnormalities unclear due to inflammation or sampling.”
Uncertainty about the natural history of IND is reflected in practice guidelines, which either don’t address it, call for repeat endoscopy in 6 months, or call for an expert gastrointestinal pathology review with repeat endoscopy to clarify dysplasia status if the evidence is of low quality, Dr. Ma said.
To determine the rate of, and risk factors for, neoplastic progression of IND, the authors took a retrospective look at patients in their center’s pathology database and Barrett’s esophagus register with a histopathologic diagnosis of IND from 2000 through 2014. They excluded patients with frank dysplasia or carcinoma on diagnosis, and those who did not have follow-up endoscopies.
The investigatoes factored demographic variables into their analysis, including age, gender, body-mass index, smoking history, use of proton-pump inhibitors (PPI), nonsteroidal anti-inflammatory drugs, and family history of Barrett’s or esophageal adenocarcinoma. They also considered endoscopic/pathologic characteristics such as hiatal hernia size, Barrett’s segment length, muscosal nodularity, and multifocal IND.
A total of 106 patients with IND were eligible for the analysis, 87 of whom had follow-up endoscopy and biopsy within a year of diagnosis. As noted before, 7 of these patients had prevalent disease, with prevalence rates of 2.3% for low-grade dysplasia, 4.6% for high-grade dysplasia, and 1.1% for esophageal adenocarcinoma.
To determine the incidence of dysplasia, the authors first excluded the 7 patients with prevealent dysplasia and 33 patients who did not have a surveillance endoscopy in the first year following a diagnosis of IND, leaving 66 patients for analysis. Of this group, 3 developed incident dysplasia or adenocarcinoma, yielding an incidence of 4.5% over a median of 32 months of follow-up.
An analysis of risk factors for prevalent dysplasia showed that none of the variables was significant, although Barrett’s segment length approached statistical significance. Looking at risk factors for incident dysplasia, both smoking status (P = .0207) and segment length (P = .0253) were significant predictors.
A pathologist who was not involved in the study pointed out that a diagnosis of IND can mean many things to many people.
“Indefinite for dysplasia is really not an entity, it’s about 5,000 things that we choose to put into that category. It’s a horribly non-reproducible diagnosis,” commented Dr. Henry D. Appelman, a professor of anatomic pathology at the University of Michigan in Ann Arbor, during a aquestion-and-answer period.
He questioned whether the diagnoses of IND were subject to review at her center.
Dr. Ma noted that Barrett’s specimens at her institution are routinely reviewed by pathologists specializing in Barrett’s, who will also review slides of patients referred to the center from other institutions.
The study was internally funded. The authors reported no conflicts of interest.
AT DDW 2015
Key clinical point: Barrett’s esophagus indefinite for dysplasia may progress to dysplasia or adenocarcinoma within a year of diagnosis.
Major finding: Seven of 87 patients with a diagnosis of Barrett’s indefinite for dysplasia (IND) had disease progression within 1 year.
Data source: Retrospective case series of 87 patients who had follow-up endoscopies and biopsies within a year of a diagnosis of Barrett’s IND.
Disclosures: The study was internally funded. The authors reported no conflicts of interest.

The May issue of Thoracic Surgery News is now available online
Be sure to visit our interactive digital or PDF version of the May issue of Thoracic Surgery News, now available online. This month we feature several more articles from the Journal of Cardiovascular and Thoracic Surgery, an update of the IMPROVE-IT study results, and two articles focusing on TAVR.
And stay tuned next month for the start of our coverage of the Mitral Conclave and the 95th AATS Annual Meeting.
Click to view our May digital edition here.
Be sure to visit our interactive digital or PDF version of the May issue of Thoracic Surgery News, now available online. This month we feature several more articles from the Journal of Cardiovascular and Thoracic Surgery, an update of the IMPROVE-IT study results, and two articles focusing on TAVR.
And stay tuned next month for the start of our coverage of the Mitral Conclave and the 95th AATS Annual Meeting.
Click to view our May digital edition here.
Be sure to visit our interactive digital or PDF version of the May issue of Thoracic Surgery News, now available online. This month we feature several more articles from the Journal of Cardiovascular and Thoracic Surgery, an update of the IMPROVE-IT study results, and two articles focusing on TAVR.
And stay tuned next month for the start of our coverage of the Mitral Conclave and the 95th AATS Annual Meeting.
Click to view our May digital edition here.

Ultrasound accurately predicts trauma thoracotomy survival
SAN DIEGO – The few trauma patients who will survive a high-risk thoracotomy procedure for cardiac arrest can be predicted by the presence of cardiac motion as detected by a quick and inexpensive bedside ultrasound, a prospective study conducted at a level I trauma center showed.
Focused assessment with sonography in trauma (FAST) was 100% sensitive and 62% specific in predicting those who would survive or be eligible for organ donation after receiving a resuscitative thoracotomy for traumatic cardiac arrest, said Dr. Kenji Inaba of the department of surgery at the University of Southern California Medical Center in Los Angeles.

Resuscitative thoracotomy, said Dr. Inaba, is a salvage procedure performed after cardiac arrest. It is a “high-risk, resource-intensive procedure, with a low quantitative yield. And yet, patients do survive.” Previous retrospective studies found that of those receiving resuscitative thoracotomy for traumatic arrest, 7.4% survived, with more than 90% of survivors retaining neurologic function; an additional 4.2% of recipients were potentially eligible for organ donation. Thus, a tool to identify potential survivors among those who present in post-traumatic cardiac arrest would help avoid unnecessary use of a procedure with such risks and resource burdens.
FAST, an inexpensive procedure that is standard for other indications in trauma, has been effective in identifying potential survivors in thoracotomy for nontrauma cardiac arrests, Dr. Inaba said at the annual meeting of the American Surgical Association.
The technique “has near-universal availability, can be performed immediately at the bedside without moving the patient, and yields real-time results with no radiation involved,” he said.
For the current prospective study, the specific aim was to examine the ability of FAST to differentiate survivors and potential organ donors from those who would not survive resuscitative thoracotomy among those presenting in traumatic cardiac arrest. Dr. Inaba and his associates examined the predictive value of cardiac motion and the presence of pericardial fluid for survival, as well as the adequacy of the FAST study for each patient.
The single-center study, conducted from 2010 to 2014, enrolled 187 patients (mean age, 31; 84.5% male) presenting in traumatic arrest who received resuscitative thoracotomy in the emergency department and also received a FAST. The scans were performed by emergency medicine residents under direct faculty supervision. Of the 187 patients studied, 6 (3.2%) survived, 3 (1.6%) became organ donors, and 178 (95.2%) died but were not organ donor eligible.
Cardiac motion was detected by FAST in 54 (28.9%) individuals in the total study population; among these were all nine of the survivors and donors, yielding a sensitivity of 100% and a specificity of 73.7% for survival (P < .001). All 16 of the patients with pericardial fluid detected by FAST died, as did all 7 patients in whom the study was deemed inadequate. Put simply, Dr. Inaba said, “no cardiac motion equals no survival.”
If thoracotomies had been performed only on patients in the study group who had cardiac motion on FAST, more than half of the unsuccessful resuscitative thoracotomies would have been avoided, Dr. Inaba noted. The study, he said, has particular application for lower-volume trauma centers, which must carefully weigh the prolonged use of limited resources required in a resuscitative thoracotomy.
Dr. David Spain, chief of trauma and critical care surgery at Stanford (Calif.) University, asked whether the study captured the mechanism of injury. Though the study did not do so, said Dr. Inaba, he and his colleagues realized that a subset of patients who went immediately to the operating room were not included in the study, a potential limitation. This group of patients included those with a penetrating cardiac injury – a possible reason, he said, why no patients among the survivors had a cardiac injury.
The authors reported no relevant financial disclosures.
SAN DIEGO – The few trauma patients who will survive a high-risk thoracotomy procedure for cardiac arrest can be predicted by the presence of cardiac motion as detected by a quick and inexpensive bedside ultrasound, a prospective study conducted at a level I trauma center showed.
Focused assessment with sonography in trauma (FAST) was 100% sensitive and 62% specific in predicting those who would survive or be eligible for organ donation after receiving a resuscitative thoracotomy for traumatic cardiac arrest, said Dr. Kenji Inaba of the department of surgery at the University of Southern California Medical Center in Los Angeles.
Resuscitative thoracotomy, said Dr. Inaba, is a salvage procedure performed after cardiac arrest. It is a “high-risk, resource-intensive procedure, with a low quantitative yield. And yet, patients do survive.” Previous retrospective studies found that of those receiving resuscitative thoracotomy for traumatic arrest, 7.4% survived, with more than 90% of survivors retaining neurologic function; an additional 4.2% of recipients were potentially eligible for organ donation. Thus, a tool to identify potential survivors among those who present in post-traumatic cardiac arrest would help avoid unnecessary use of a procedure with such risks and resource burdens.
FAST, an inexpensive procedure that is standard for other indications in trauma, has been effective in identifying potential survivors in thoracotomy for nontrauma cardiac arrests, Dr. Inaba said at the annual meeting of the American Surgical Association.
The technique “has near-universal availability, can be performed immediately at the bedside without moving the patient, and yields real-time results with no radiation involved,” he said.
For the current prospective study, the specific aim was to examine the ability of FAST to differentiate survivors and potential organ donors from those who would not survive resuscitative thoracotomy among those presenting in traumatic cardiac arrest. Dr. Inaba and his associates examined the predictive value of cardiac motion and the presence of pericardial fluid for survival, as well as the adequacy of the FAST study for each patient.
The single-center study, conducted from 2010 to 2014, enrolled 187 patients (mean age, 31; 84.5% male) presenting in traumatic arrest who received resuscitative thoracotomy in the emergency department and also received a FAST. The scans were performed by emergency medicine residents under direct faculty supervision. Of the 187 patients studied, 6 (3.2%) survived, 3 (1.6%) became organ donors, and 178 (95.2%) died but were not organ donor eligible.
Cardiac motion was detected by FAST in 54 (28.9%) individuals in the total study population; among these were all nine of the survivors and donors, yielding a sensitivity of 100% and a specificity of 73.7% for survival (P < .001). All 16 of the patients with pericardial fluid detected by FAST died, as did all 7 patients in whom the study was deemed inadequate. Put simply, Dr. Inaba said, “no cardiac motion equals no survival.”
If thoracotomies had been performed only on patients in the study group who had cardiac motion on FAST, more than half of the unsuccessful resuscitative thoracotomies would have been avoided, Dr. Inaba noted. The study, he said, has particular application for lower-volume trauma centers, which must carefully weigh the prolonged use of limited resources required in a resuscitative thoracotomy.
Dr. David Spain, chief of trauma and critical care surgery at Stanford (Calif.) University, asked whether the study captured the mechanism of injury. Though the study did not do so, said Dr. Inaba, he and his colleagues realized that a subset of patients who went immediately to the operating room were not included in the study, a potential limitation. This group of patients included those with a penetrating cardiac injury – a possible reason, he said, why no patients among the survivors had a cardiac injury.
The authors reported no relevant financial disclosures.
SAN DIEGO – The few trauma patients who will survive a high-risk thoracotomy procedure for cardiac arrest can be predicted by the presence of cardiac motion as detected by a quick and inexpensive bedside ultrasound, a prospective study conducted at a level I trauma center showed.
Focused assessment with sonography in trauma (FAST) was 100% sensitive and 62% specific in predicting those who would survive or be eligible for organ donation after receiving a resuscitative thoracotomy for traumatic cardiac arrest, said Dr. Kenji Inaba of the department of surgery at the University of Southern California Medical Center in Los Angeles.
Resuscitative thoracotomy, said Dr. Inaba, is a salvage procedure performed after cardiac arrest. It is a “high-risk, resource-intensive procedure, with a low quantitative yield. And yet, patients do survive.” Previous retrospective studies found that of those receiving resuscitative thoracotomy for traumatic arrest, 7.4% survived, with more than 90% of survivors retaining neurologic function; an additional 4.2% of recipients were potentially eligible for organ donation. Thus, a tool to identify potential survivors among those who present in post-traumatic cardiac arrest would help avoid unnecessary use of a procedure with such risks and resource burdens.
FAST, an inexpensive procedure that is standard for other indications in trauma, has been effective in identifying potential survivors in thoracotomy for nontrauma cardiac arrests, Dr. Inaba said at the annual meeting of the American Surgical Association.
The technique “has near-universal availability, can be performed immediately at the bedside without moving the patient, and yields real-time results with no radiation involved,” he said.
For the current prospective study, the specific aim was to examine the ability of FAST to differentiate survivors and potential organ donors from those who would not survive resuscitative thoracotomy among those presenting in traumatic cardiac arrest. Dr. Inaba and his associates examined the predictive value of cardiac motion and the presence of pericardial fluid for survival, as well as the adequacy of the FAST study for each patient.
The single-center study, conducted from 2010 to 2014, enrolled 187 patients (mean age, 31; 84.5% male) presenting in traumatic arrest who received resuscitative thoracotomy in the emergency department and also received a FAST. The scans were performed by emergency medicine residents under direct faculty supervision. Of the 187 patients studied, 6 (3.2%) survived, 3 (1.6%) became organ donors, and 178 (95.2%) died but were not organ donor eligible.
Cardiac motion was detected by FAST in 54 (28.9%) individuals in the total study population; among these were all nine of the survivors and donors, yielding a sensitivity of 100% and a specificity of 73.7% for survival (P < .001). All 16 of the patients with pericardial fluid detected by FAST died, as did all 7 patients in whom the study was deemed inadequate. Put simply, Dr. Inaba said, “no cardiac motion equals no survival.”
If thoracotomies had been performed only on patients in the study group who had cardiac motion on FAST, more than half of the unsuccessful resuscitative thoracotomies would have been avoided, Dr. Inaba noted. The study, he said, has particular application for lower-volume trauma centers, which must carefully weigh the prolonged use of limited resources required in a resuscitative thoracotomy.
Dr. David Spain, chief of trauma and critical care surgery at Stanford (Calif.) University, asked whether the study captured the mechanism of injury. Though the study did not do so, said Dr. Inaba, he and his colleagues realized that a subset of patients who went immediately to the operating room were not included in the study, a potential limitation. This group of patients included those with a penetrating cardiac injury – a possible reason, he said, why no patients among the survivors had a cardiac injury.
The authors reported no relevant financial disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point: Trauma arrest victims who will survive resuscitative thoracotomy can be predicted using focused assessment with sonography in trauma.
Major findings: FAST was 100% sensitive for detecting survivors after resuscitative thoracotomy for traumatic cardiac arrest.
Data source: A prospective series of 187 trauma patients in cardiac arrest undergoing resuscitative thoracotomy from 2010 to 2014 at a level I trauma center.
Disclosures: The authors reported no relevant financial disclosures.
