User login
The Official Newspaper of the American Association for Thoracic Surgery
Docs Could Face More Cuts in Debt Deal
Legislation to raise the debt ceiling and cut the deficit, signed by the president Aug. 2, leaves physicians in limbo regarding their Medicare payments next year and in the future.
The biggest question is whether the 29.5% cut to Medicare physician fees scheduled for Jan. 1, 2012, will go into effect. This massive payment cut is called for under the Sustainable Growth Rate (SGR) formula used to set Medicare payments to physicians.
Physicians’ groups, led by the American Medical Association, lobbied Congress to include a permanent fix to the SGR in the deficit reduction package. They argued that while fixing the SGR carries a $300 billion price tag, getting the job done now would save the government money down the road. Instead, lawmakers left the SGR out of the package completely.
The new law of the land, the Budget Control Act of 2011, puts into place about $1 trillion in spending cuts over the next decade from the discretionary side of the federal budget. While these immediate cuts do not directly affect physicians, they do impact graduate medical education: Medical students who take out subsidized graduate student loans on or after July 1, 2012, will have to start paying the interest on those loans earlier.
The next round of budget cuts will be determined by the Joint Select Committee on Deficit Reduction, also known as the super committee. The 12-member panel iswill be comprised of legislators from both parties and both houses of Congress.
Sen. Patty Murray (D.-Wash Rep. Dave Camp (R.-Mich.), chairman of the House Ways and Means Committee, Rep. Fred Upton (R.-Mich.), chairman of the House Energy and Commerce Committee, Rep. James E. Clyburn (D.-S.C.), the third-ranking member of the House Democratic leadership, Rep. Xavier Becerra (D.-Calif.), a member of the House Ways and Means Committee, and Rep. Chris Van Hollen (D.-Md.), also a member of the House Ways and Means Committee. The appointments were made by party leaders in the House and Senate.
Party leaders have named the first nine members of the joint committee. Senate Majority Leader Harry Reid (D.-Nev.) appointed«http://democrats.senate.gov/2011/08/09/reid-announces-appointments-to-joint-select-committee-on-deficit-reduction/» Sen. Patty Murray (D.-Wash.)« http://murray.senate.gov/public/», who serves on both the Senate budget and appropriations committees, to co-chair the Joint Select Committee on Deficit Reduction. Her appointment immediately drew criticism from Republicans, who said she is too focused on politics because of her role as chairwoman of the Democratic Senatorial Campaign Committee. Sen. Reid also tapped Sen. Max Baucus (D.-Mont.)« http://baucus.senate.gov/», chairman of the Senate Finance Committee and an architect of the Affordable Care Act, and Sen. John Kerry (D.-Mass.)« http://kerry.senate.gov/», who was the 2004 Democratic presidential nominee, to serve on the joint committee.
Before the joint committee can forward its recommendations to the full Congress, those recommendations must be approved by a majority vote.
"There’s a lot of concern that the committee will be deadlocked," said Edwin Park, vice president for health policy at the Center on Budget and Policy Priorities.
The law requires the joint committee to draft legislation cutting another $1.2 trillion to $1.5 trillion in federal spending over 10 years. The committee has broad authority to consider spending cuts, taxes, and other changes across both discretionary and mandatory government programs. Funding for Affordable Care Act programs is also on the table.
The joint committee must vote on recommendations by Nov. 23, and lawmakers must vote on the joint committee’s bill by Dec. 23.
To keep the legislation from getting bogged down in the Senate, the Budget Control Act requires that the joint committee’s bill be given a fast-track, up-or-down vote requiring a simple majority to pass each chamber.
Should the joint committee’s bill fail, or if the committee deadlocks, the Budget Control Act calls for automatic cuts across the federal government totaling $1.2 trillion over 10 years.
Those cuts would include up to a 2% reduction in Medicare physician payments beginning in 2013. Under a worst-case scenario, physicians could face not only the 29.5% SGR cut in January 2012, but another 2% annual fee cut starting the following year.
The hope for physicians is that the 29.5% cut mandated by the SGR is simply so large that it would be unthinkable for members of Congress to let it go into effect. Many physicians think that Congress will do something to avert the massive SGR cut, even if it’s a temporary fix.
For example, Dr. Jonathan Leffert, chairman of the legislative and regulatory committee for the American Association of Clinical Endocrinologists, said: "Medicare patients not being able to see their physicians is pretty toxic for both Democrats and Republicans."
Legislation to raise the debt ceiling and cut the deficit, signed by the president Aug. 2, leaves physicians in limbo regarding their Medicare payments next year and in the future.
The biggest question is whether the 29.5% cut to Medicare physician fees scheduled for Jan. 1, 2012, will go into effect. This massive payment cut is called for under the Sustainable Growth Rate (SGR) formula used to set Medicare payments to physicians.
Physicians’ groups, led by the American Medical Association, lobbied Congress to include a permanent fix to the SGR in the deficit reduction package. They argued that while fixing the SGR carries a $300 billion price tag, getting the job done now would save the government money down the road. Instead, lawmakers left the SGR out of the package completely.
The new law of the land, the Budget Control Act of 2011, puts into place about $1 trillion in spending cuts over the next decade from the discretionary side of the federal budget. While these immediate cuts do not directly affect physicians, they do impact graduate medical education: Medical students who take out subsidized graduate student loans on or after July 1, 2012, will have to start paying the interest on those loans earlier.
The next round of budget cuts will be determined by the Joint Select Committee on Deficit Reduction, also known as the super committee. The 12-member panel iswill be comprised of legislators from both parties and both houses of Congress.
Sen. Patty Murray (D.-Wash Rep. Dave Camp (R.-Mich.), chairman of the House Ways and Means Committee, Rep. Fred Upton (R.-Mich.), chairman of the House Energy and Commerce Committee, Rep. James E. Clyburn (D.-S.C.), the third-ranking member of the House Democratic leadership, Rep. Xavier Becerra (D.-Calif.), a member of the House Ways and Means Committee, and Rep. Chris Van Hollen (D.-Md.), also a member of the House Ways and Means Committee. The appointments were made by party leaders in the House and Senate.
Party leaders have named the first nine members of the joint committee. Senate Majority Leader Harry Reid (D.-Nev.) appointed«http://democrats.senate.gov/2011/08/09/reid-announces-appointments-to-joint-select-committee-on-deficit-reduction/» Sen. Patty Murray (D.-Wash.)« http://murray.senate.gov/public/», who serves on both the Senate budget and appropriations committees, to co-chair the Joint Select Committee on Deficit Reduction. Her appointment immediately drew criticism from Republicans, who said she is too focused on politics because of her role as chairwoman of the Democratic Senatorial Campaign Committee. Sen. Reid also tapped Sen. Max Baucus (D.-Mont.)« http://baucus.senate.gov/», chairman of the Senate Finance Committee and an architect of the Affordable Care Act, and Sen. John Kerry (D.-Mass.)« http://kerry.senate.gov/», who was the 2004 Democratic presidential nominee, to serve on the joint committee.
Before the joint committee can forward its recommendations to the full Congress, those recommendations must be approved by a majority vote.
"There’s a lot of concern that the committee will be deadlocked," said Edwin Park, vice president for health policy at the Center on Budget and Policy Priorities.
The law requires the joint committee to draft legislation cutting another $1.2 trillion to $1.5 trillion in federal spending over 10 years. The committee has broad authority to consider spending cuts, taxes, and other changes across both discretionary and mandatory government programs. Funding for Affordable Care Act programs is also on the table.
The joint committee must vote on recommendations by Nov. 23, and lawmakers must vote on the joint committee’s bill by Dec. 23.
To keep the legislation from getting bogged down in the Senate, the Budget Control Act requires that the joint committee’s bill be given a fast-track, up-or-down vote requiring a simple majority to pass each chamber.
Should the joint committee’s bill fail, or if the committee deadlocks, the Budget Control Act calls for automatic cuts across the federal government totaling $1.2 trillion over 10 years.
Those cuts would include up to a 2% reduction in Medicare physician payments beginning in 2013. Under a worst-case scenario, physicians could face not only the 29.5% SGR cut in January 2012, but another 2% annual fee cut starting the following year.
The hope for physicians is that the 29.5% cut mandated by the SGR is simply so large that it would be unthinkable for members of Congress to let it go into effect. Many physicians think that Congress will do something to avert the massive SGR cut, even if it’s a temporary fix.
For example, Dr. Jonathan Leffert, chairman of the legislative and regulatory committee for the American Association of Clinical Endocrinologists, said: "Medicare patients not being able to see their physicians is pretty toxic for both Democrats and Republicans."
Legislation to raise the debt ceiling and cut the deficit, signed by the president Aug. 2, leaves physicians in limbo regarding their Medicare payments next year and in the future.
The biggest question is whether the 29.5% cut to Medicare physician fees scheduled for Jan. 1, 2012, will go into effect. This massive payment cut is called for under the Sustainable Growth Rate (SGR) formula used to set Medicare payments to physicians.
Physicians’ groups, led by the American Medical Association, lobbied Congress to include a permanent fix to the SGR in the deficit reduction package. They argued that while fixing the SGR carries a $300 billion price tag, getting the job done now would save the government money down the road. Instead, lawmakers left the SGR out of the package completely.
The new law of the land, the Budget Control Act of 2011, puts into place about $1 trillion in spending cuts over the next decade from the discretionary side of the federal budget. While these immediate cuts do not directly affect physicians, they do impact graduate medical education: Medical students who take out subsidized graduate student loans on or after July 1, 2012, will have to start paying the interest on those loans earlier.
The next round of budget cuts will be determined by the Joint Select Committee on Deficit Reduction, also known as the super committee. The 12-member panel iswill be comprised of legislators from both parties and both houses of Congress.
Sen. Patty Murray (D.-Wash Rep. Dave Camp (R.-Mich.), chairman of the House Ways and Means Committee, Rep. Fred Upton (R.-Mich.), chairman of the House Energy and Commerce Committee, Rep. James E. Clyburn (D.-S.C.), the third-ranking member of the House Democratic leadership, Rep. Xavier Becerra (D.-Calif.), a member of the House Ways and Means Committee, and Rep. Chris Van Hollen (D.-Md.), also a member of the House Ways and Means Committee. The appointments were made by party leaders in the House and Senate.
Party leaders have named the first nine members of the joint committee. Senate Majority Leader Harry Reid (D.-Nev.) appointed«http://democrats.senate.gov/2011/08/09/reid-announces-appointments-to-joint-select-committee-on-deficit-reduction/» Sen. Patty Murray (D.-Wash.)« http://murray.senate.gov/public/», who serves on both the Senate budget and appropriations committees, to co-chair the Joint Select Committee on Deficit Reduction. Her appointment immediately drew criticism from Republicans, who said she is too focused on politics because of her role as chairwoman of the Democratic Senatorial Campaign Committee. Sen. Reid also tapped Sen. Max Baucus (D.-Mont.)« http://baucus.senate.gov/», chairman of the Senate Finance Committee and an architect of the Affordable Care Act, and Sen. John Kerry (D.-Mass.)« http://kerry.senate.gov/», who was the 2004 Democratic presidential nominee, to serve on the joint committee.
Before the joint committee can forward its recommendations to the full Congress, those recommendations must be approved by a majority vote.
"There’s a lot of concern that the committee will be deadlocked," said Edwin Park, vice president for health policy at the Center on Budget and Policy Priorities.
The law requires the joint committee to draft legislation cutting another $1.2 trillion to $1.5 trillion in federal spending over 10 years. The committee has broad authority to consider spending cuts, taxes, and other changes across both discretionary and mandatory government programs. Funding for Affordable Care Act programs is also on the table.
The joint committee must vote on recommendations by Nov. 23, and lawmakers must vote on the joint committee’s bill by Dec. 23.
To keep the legislation from getting bogged down in the Senate, the Budget Control Act requires that the joint committee’s bill be given a fast-track, up-or-down vote requiring a simple majority to pass each chamber.
Should the joint committee’s bill fail, or if the committee deadlocks, the Budget Control Act calls for automatic cuts across the federal government totaling $1.2 trillion over 10 years.
Those cuts would include up to a 2% reduction in Medicare physician payments beginning in 2013. Under a worst-case scenario, physicians could face not only the 29.5% SGR cut in January 2012, but another 2% annual fee cut starting the following year.
The hope for physicians is that the 29.5% cut mandated by the SGR is simply so large that it would be unthinkable for members of Congress to let it go into effect. Many physicians think that Congress will do something to avert the massive SGR cut, even if it’s a temporary fix.
For example, Dr. Jonathan Leffert, chairman of the legislative and regulatory committee for the American Association of Clinical Endocrinologists, said: "Medicare patients not being able to see their physicians is pretty toxic for both Democrats and Republicans."
New Data Largely Discount 'July Phenomenon'
"Don’t have surgery in July!" This is the folk wisdom regarding the purported "July Phenomenon" – the perception that it is more dangerous to have an operation in July than at any other time of year. July heralds the onslaught of new interns; July also means that current residents are given additional duties and responsibility. "Why risk an operation in a month when trainee inexperience must surely dilute the quality of patient care?" is the intuitive assumption.
A recent study reported in ‘Surgery’, however, showed that this concern is unfounded.
Multivariate analysis indicated that only 1 out of the 10 most common surgical procedures (lower extremity artery bypass grafting) showed a significant increase in mortality concurrent with the so-called July Phenomenon (odds ratio, 1.34; P = .034).
The researchers also found that there was no significant increase in serious adverse events (SAE) for any of the procedures (Surgery 2011;150:332-8).
The previous medical literature shows no consensus on the subject. The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) suggested that greater rates of postsurgical problems were related to that time of year (Ann. Surg. 2007;246:456-62).
In contrast, studies in obstetrics and neurology showed that no July Phenomenon existed, as did surgical studies in specialties including trauma, pediatric neurosurgery, and cardiac surgery, according to Dr. Bryan A. Ehlert and colleagues at East Carolina University, Greenville, N.C.
To investigate the issue in a broader surgical context, Dr. Ehlert and his colleagues studied the ACS-NSQIP database records of 89,473 patients who had the 10 most common inpatient operative procedures in 2005-2007.
They compared 26,287 patients who had surgery in the July 1–Sept. 30 quarter (called the "first academic quarter," or FAQ) with a control population of 63,186 patients who had equivalent surgery during the rest of the year (Oct. 1–June 30).
They assessed the following 10 procedures: appendectomy, (lower extremity) artery bypass graft, initial reducible ventral hernia repair, laparoscopic appendectomy, laparoscopic cholecystectomy, laparoscopic gastric bypass, partial colectomy, rechanneling of artery, repair of bowel opening, and small-bowel resection.
The two populations showed no significant differences in a wide variety of demographic characteristics including age (average, about 54 years); sex (about 45% male); and presence of coronary artery disease, renal disease, peripheral vascular disease (PVD/PAD), and diabetes. Slight but significant differences were found only in the presence of hypertension (50.0% in the FAQ group vs. 48.4% in controls, respectively) and history of smoking (24.0% vs. 23.4%).
Especially important to the study, there was no significant difference in resident participation in patient care (72.7% vs. 73.0%) or the highest resident level in postgraduate year (2.6 years each).
"Although July might seem intuitively to be a precarious time to undergo an operation due to the influx of new interns and increased responsibilities of rising residents, our findings for the most part discount the presence of a ‘July Phenomenon’ in surgical patients," the authors stated.
Discrepancies between the previous ACS-NSQIP report and their findings were attributed to the much larger sample size in the current study (183 centers vs. 18).
They postulated that the lower extremity bypass graft FAQ group showed greater mortality than did the control group because the vascular subsets had a significantly greater modified Charlson comorbidity index, compared with the nonvascular subsets in the FAQ population (CCI, 3.72 vs. 1.56; P less than .001).
"New surgery interns may not be as adept at recognizing the needs of these patients who are often sicker. As a result, these patient populations may benefit from more senior residents and attending physician involvement as new interns learn how to manage patients with complex cardiovascular disease," they suggested.
A weakness of the study reported by the authors is the crude estimate of patient outcomes, which focuses only on morbidity and mortality and does not include data on duration of stay, medication errors, or cost-effectiveness – all of which could possibly be affected by new interns.
For example, they noted that new interns may be more likely to order more unnecessary laboratory tests, or they may fail to remove invasive devices or monitoring devices that are no longer needed, which may in turn lead to increased infections.
In addition, they also stated that interns may have more difficulties when confronted with rarer operations than the 10 most common procedures that were evaluated.
The researchers disclosed no conflicts that the journal deemed relevant to report.
"Don’t have surgery in July!" This is the folk wisdom regarding the purported "July Phenomenon" – the perception that it is more dangerous to have an operation in July than at any other time of year. July heralds the onslaught of new interns; July also means that current residents are given additional duties and responsibility. "Why risk an operation in a month when trainee inexperience must surely dilute the quality of patient care?" is the intuitive assumption.
A recent study reported in ‘Surgery’, however, showed that this concern is unfounded.
Multivariate analysis indicated that only 1 out of the 10 most common surgical procedures (lower extremity artery bypass grafting) showed a significant increase in mortality concurrent with the so-called July Phenomenon (odds ratio, 1.34; P = .034).
The researchers also found that there was no significant increase in serious adverse events (SAE) for any of the procedures (Surgery 2011;150:332-8).
The previous medical literature shows no consensus on the subject. The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) suggested that greater rates of postsurgical problems were related to that time of year (Ann. Surg. 2007;246:456-62).
In contrast, studies in obstetrics and neurology showed that no July Phenomenon existed, as did surgical studies in specialties including trauma, pediatric neurosurgery, and cardiac surgery, according to Dr. Bryan A. Ehlert and colleagues at East Carolina University, Greenville, N.C.
To investigate the issue in a broader surgical context, Dr. Ehlert and his colleagues studied the ACS-NSQIP database records of 89,473 patients who had the 10 most common inpatient operative procedures in 2005-2007.
They compared 26,287 patients who had surgery in the July 1–Sept. 30 quarter (called the "first academic quarter," or FAQ) with a control population of 63,186 patients who had equivalent surgery during the rest of the year (Oct. 1–June 30).
They assessed the following 10 procedures: appendectomy, (lower extremity) artery bypass graft, initial reducible ventral hernia repair, laparoscopic appendectomy, laparoscopic cholecystectomy, laparoscopic gastric bypass, partial colectomy, rechanneling of artery, repair of bowel opening, and small-bowel resection.
The two populations showed no significant differences in a wide variety of demographic characteristics including age (average, about 54 years); sex (about 45% male); and presence of coronary artery disease, renal disease, peripheral vascular disease (PVD/PAD), and diabetes. Slight but significant differences were found only in the presence of hypertension (50.0% in the FAQ group vs. 48.4% in controls, respectively) and history of smoking (24.0% vs. 23.4%).
Especially important to the study, there was no significant difference in resident participation in patient care (72.7% vs. 73.0%) or the highest resident level in postgraduate year (2.6 years each).
"Although July might seem intuitively to be a precarious time to undergo an operation due to the influx of new interns and increased responsibilities of rising residents, our findings for the most part discount the presence of a ‘July Phenomenon’ in surgical patients," the authors stated.
Discrepancies between the previous ACS-NSQIP report and their findings were attributed to the much larger sample size in the current study (183 centers vs. 18).
They postulated that the lower extremity bypass graft FAQ group showed greater mortality than did the control group because the vascular subsets had a significantly greater modified Charlson comorbidity index, compared with the nonvascular subsets in the FAQ population (CCI, 3.72 vs. 1.56; P less than .001).
"New surgery interns may not be as adept at recognizing the needs of these patients who are often sicker. As a result, these patient populations may benefit from more senior residents and attending physician involvement as new interns learn how to manage patients with complex cardiovascular disease," they suggested.
A weakness of the study reported by the authors is the crude estimate of patient outcomes, which focuses only on morbidity and mortality and does not include data on duration of stay, medication errors, or cost-effectiveness – all of which could possibly be affected by new interns.
For example, they noted that new interns may be more likely to order more unnecessary laboratory tests, or they may fail to remove invasive devices or monitoring devices that are no longer needed, which may in turn lead to increased infections.
In addition, they also stated that interns may have more difficulties when confronted with rarer operations than the 10 most common procedures that were evaluated.
The researchers disclosed no conflicts that the journal deemed relevant to report.
"Don’t have surgery in July!" This is the folk wisdom regarding the purported "July Phenomenon" – the perception that it is more dangerous to have an operation in July than at any other time of year. July heralds the onslaught of new interns; July also means that current residents are given additional duties and responsibility. "Why risk an operation in a month when trainee inexperience must surely dilute the quality of patient care?" is the intuitive assumption.
A recent study reported in ‘Surgery’, however, showed that this concern is unfounded.
Multivariate analysis indicated that only 1 out of the 10 most common surgical procedures (lower extremity artery bypass grafting) showed a significant increase in mortality concurrent with the so-called July Phenomenon (odds ratio, 1.34; P = .034).
The researchers also found that there was no significant increase in serious adverse events (SAE) for any of the procedures (Surgery 2011;150:332-8).
The previous medical literature shows no consensus on the subject. The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) suggested that greater rates of postsurgical problems were related to that time of year (Ann. Surg. 2007;246:456-62).
In contrast, studies in obstetrics and neurology showed that no July Phenomenon existed, as did surgical studies in specialties including trauma, pediatric neurosurgery, and cardiac surgery, according to Dr. Bryan A. Ehlert and colleagues at East Carolina University, Greenville, N.C.
To investigate the issue in a broader surgical context, Dr. Ehlert and his colleagues studied the ACS-NSQIP database records of 89,473 patients who had the 10 most common inpatient operative procedures in 2005-2007.
They compared 26,287 patients who had surgery in the July 1–Sept. 30 quarter (called the "first academic quarter," or FAQ) with a control population of 63,186 patients who had equivalent surgery during the rest of the year (Oct. 1–June 30).
They assessed the following 10 procedures: appendectomy, (lower extremity) artery bypass graft, initial reducible ventral hernia repair, laparoscopic appendectomy, laparoscopic cholecystectomy, laparoscopic gastric bypass, partial colectomy, rechanneling of artery, repair of bowel opening, and small-bowel resection.
The two populations showed no significant differences in a wide variety of demographic characteristics including age (average, about 54 years); sex (about 45% male); and presence of coronary artery disease, renal disease, peripheral vascular disease (PVD/PAD), and diabetes. Slight but significant differences were found only in the presence of hypertension (50.0% in the FAQ group vs. 48.4% in controls, respectively) and history of smoking (24.0% vs. 23.4%).
Especially important to the study, there was no significant difference in resident participation in patient care (72.7% vs. 73.0%) or the highest resident level in postgraduate year (2.6 years each).
"Although July might seem intuitively to be a precarious time to undergo an operation due to the influx of new interns and increased responsibilities of rising residents, our findings for the most part discount the presence of a ‘July Phenomenon’ in surgical patients," the authors stated.
Discrepancies between the previous ACS-NSQIP report and their findings were attributed to the much larger sample size in the current study (183 centers vs. 18).
They postulated that the lower extremity bypass graft FAQ group showed greater mortality than did the control group because the vascular subsets had a significantly greater modified Charlson comorbidity index, compared with the nonvascular subsets in the FAQ population (CCI, 3.72 vs. 1.56; P less than .001).
"New surgery interns may not be as adept at recognizing the needs of these patients who are often sicker. As a result, these patient populations may benefit from more senior residents and attending physician involvement as new interns learn how to manage patients with complex cardiovascular disease," they suggested.
A weakness of the study reported by the authors is the crude estimate of patient outcomes, which focuses only on morbidity and mortality and does not include data on duration of stay, medication errors, or cost-effectiveness – all of which could possibly be affected by new interns.
For example, they noted that new interns may be more likely to order more unnecessary laboratory tests, or they may fail to remove invasive devices or monitoring devices that are no longer needed, which may in turn lead to increased infections.
In addition, they also stated that interns may have more difficulties when confronted with rarer operations than the 10 most common procedures that were evaluated.
The researchers disclosed no conflicts that the journal deemed relevant to report.
Major Finding: Mortality was significantly increased (though less than 1%) in only 1 of the 10 most common operations – lower artery bypass grafting – at the beginning of the academic year as compared with any other quarter.
Data Source: A database analysis of 89,473 patients undergoing the 10 most common inpatient operative procedures from 2005 to 2007.
Disclosures: The authors had no disclosures deemed relevant to report by the journal.
Paraesophageal Hernia Repair Boosts Lung Function
COLORADO SPRINGS – Improvements in pulmonary function tests and subjective complaints of breathlessness appear to be underappreciated benefits of the surgical repair of giant paraesophageal hernias.
Symptom assessment of these patients has generally focused on reflux and dysphagia, but these hernias also have adverse impacts on pulmonary function. Repair most benefits patients who are older, have bigger hernias, and worse baseline pulmonary function, said Dr. Philip W. Carrott Jr., of Virginia Mason Medical Center, Seattle.
"Patients with giant paraesophageal hernia and coexistent dyspnea or positional breathlessness should be reviewed by an experienced surgeon for elective repair, even when pulmonary comorbidities exist," Dr. Carrott concluded at the annual meeting of the Western Thoracic Surgical Association.
He based this advice on a single-center, retrospective, cohort study involving 120 patients who had pulmonary function tests preoperatively and again at a median of 106 days after surgery.
The overall group averaged 10% increases over baseline (P less than .001) in forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), vital capacity, and volume-adjusted mid-expiratory flow (IsoFEF25-75), as well as a 2.9% increase in the diffusing capacity of the lung (DLCO).
The larger a patient’s hernia as expressed by percent intrathoracic stomach (ITS) on preoperative contrast studies, the greater the improvement in pulmonary function tests after surgery. Hernia size was the strongest predictor of improvement. For example, forced vital capacity improved by an average of 4.7%, compared with reference values in patients with the smallest hernias as expressed in a percent ITS of less than 50%, as compared with a 6.0% gain in patients with a preop 50%-74% ITS, a 9.1% improvement in those with 75%-99% ITS, and a 14.9% gain in FVC in patients with 100% ITS.
The postoperative improvement in lung function increased with each decade of patient age.
Patients with the worst preoperative lung function tended to have the biggest hernias – and the greatest objective and subjective improvements after surgery. For example, 36% of subjects had a reduced baseline FEV1 not more than 75% of the reference value. Their vital capacity improved by 0.45 L, as compared with 0.23 L in patients without a reduced baseline FEV1. And their DLCO improved by 1.23 mL CO/min/mm Hg, compared with just 0.23 in patients whose baseline FEV1 was more than 75% of the reference value.
Of 63 patients who reported preoperative dyspnea, 47 (75%) noted subjective improvement in their respiratory function after hernia repair. Intriguingly, so did 30 of 57 patients (53%) not complaining of dyspnea at baseline.
Dr. Carrott and his fellow researchers postulate that restoring efficient diaphragmatic function is just part of the explanation. "The stomach probably has a paradoxical motion during respiration, such that the abdominal positive pressure is pushing against the negative effect of the lungs and chest wall," he said.
Study participants averaged 74 years of age, with a median of four preoperative symptoms. The most common were heartburn in 59%, early satiety in 54%, dyspnea in 52%, dysphagia in 47%, chest pain in 40%, and regurgitation in 39%.
Major comorbidities included pulmonary disease in 29% of subjects, heart disease in 35%, and obesity in 39%. An open Hill repair with no hiatal reinforcement was performed in 99% of patients, and 97% of the operations were elective.
Despite the substantial prevalence of comorbid conditions, there was no operative mortality. The mean length of stay was 4 days. One-third had complications, including six cases of arrhythmia, four instances of nausea delaying discharge, three cases of pneumonia, and two cases each of ileus, wound infection, or delirium.
Discussant Dr. Sean C. Grondin observed that paraesophageal hernia is a relatively common disease in the practice of most thoracic surgeons. And although the study provides some support for the notion that surgical repair may improve pulmonary function, its retrospective nature and only moderate size render it less than fully convincing.
"I think it still falls a little short just yet of providing conclusive evidence. At this time I would caution surgeons from telling patients that they’ll get a definitive improvement in their dyspnea after paraesophageal hernia repair, although it’s certainly a possibility," said Dr. Grondin of the University of Calgary (Alta).
Dr. Ross M. Bremner of St. Joseph’s Hospital and Medical Center, Phoenix, commented that: "I’ve long been telling my patients who have their entire stomach in the chest that they’re likely to get some improvement in their pulmonary function from repair. Now at least I have some data to show them they can get at least 10%-15% improvement."
Dr. Carrott reported that he had no disclosures.
COLORADO SPRINGS – Improvements in pulmonary function tests and subjective complaints of breathlessness appear to be underappreciated benefits of the surgical repair of giant paraesophageal hernias.
Symptom assessment of these patients has generally focused on reflux and dysphagia, but these hernias also have adverse impacts on pulmonary function. Repair most benefits patients who are older, have bigger hernias, and worse baseline pulmonary function, said Dr. Philip W. Carrott Jr., of Virginia Mason Medical Center, Seattle.
"Patients with giant paraesophageal hernia and coexistent dyspnea or positional breathlessness should be reviewed by an experienced surgeon for elective repair, even when pulmonary comorbidities exist," Dr. Carrott concluded at the annual meeting of the Western Thoracic Surgical Association.
He based this advice on a single-center, retrospective, cohort study involving 120 patients who had pulmonary function tests preoperatively and again at a median of 106 days after surgery.
The overall group averaged 10% increases over baseline (P less than .001) in forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), vital capacity, and volume-adjusted mid-expiratory flow (IsoFEF25-75), as well as a 2.9% increase in the diffusing capacity of the lung (DLCO).
The larger a patient’s hernia as expressed by percent intrathoracic stomach (ITS) on preoperative contrast studies, the greater the improvement in pulmonary function tests after surgery. Hernia size was the strongest predictor of improvement. For example, forced vital capacity improved by an average of 4.7%, compared with reference values in patients with the smallest hernias as expressed in a percent ITS of less than 50%, as compared with a 6.0% gain in patients with a preop 50%-74% ITS, a 9.1% improvement in those with 75%-99% ITS, and a 14.9% gain in FVC in patients with 100% ITS.
The postoperative improvement in lung function increased with each decade of patient age.
Patients with the worst preoperative lung function tended to have the biggest hernias – and the greatest objective and subjective improvements after surgery. For example, 36% of subjects had a reduced baseline FEV1 not more than 75% of the reference value. Their vital capacity improved by 0.45 L, as compared with 0.23 L in patients without a reduced baseline FEV1. And their DLCO improved by 1.23 mL CO/min/mm Hg, compared with just 0.23 in patients whose baseline FEV1 was more than 75% of the reference value.
Of 63 patients who reported preoperative dyspnea, 47 (75%) noted subjective improvement in their respiratory function after hernia repair. Intriguingly, so did 30 of 57 patients (53%) not complaining of dyspnea at baseline.
Dr. Carrott and his fellow researchers postulate that restoring efficient diaphragmatic function is just part of the explanation. "The stomach probably has a paradoxical motion during respiration, such that the abdominal positive pressure is pushing against the negative effect of the lungs and chest wall," he said.
Study participants averaged 74 years of age, with a median of four preoperative symptoms. The most common were heartburn in 59%, early satiety in 54%, dyspnea in 52%, dysphagia in 47%, chest pain in 40%, and regurgitation in 39%.
Major comorbidities included pulmonary disease in 29% of subjects, heart disease in 35%, and obesity in 39%. An open Hill repair with no hiatal reinforcement was performed in 99% of patients, and 97% of the operations were elective.
Despite the substantial prevalence of comorbid conditions, there was no operative mortality. The mean length of stay was 4 days. One-third had complications, including six cases of arrhythmia, four instances of nausea delaying discharge, three cases of pneumonia, and two cases each of ileus, wound infection, or delirium.
Discussant Dr. Sean C. Grondin observed that paraesophageal hernia is a relatively common disease in the practice of most thoracic surgeons. And although the study provides some support for the notion that surgical repair may improve pulmonary function, its retrospective nature and only moderate size render it less than fully convincing.
"I think it still falls a little short just yet of providing conclusive evidence. At this time I would caution surgeons from telling patients that they’ll get a definitive improvement in their dyspnea after paraesophageal hernia repair, although it’s certainly a possibility," said Dr. Grondin of the University of Calgary (Alta).
Dr. Ross M. Bremner of St. Joseph’s Hospital and Medical Center, Phoenix, commented that: "I’ve long been telling my patients who have their entire stomach in the chest that they’re likely to get some improvement in their pulmonary function from repair. Now at least I have some data to show them they can get at least 10%-15% improvement."
Dr. Carrott reported that he had no disclosures.
COLORADO SPRINGS – Improvements in pulmonary function tests and subjective complaints of breathlessness appear to be underappreciated benefits of the surgical repair of giant paraesophageal hernias.
Symptom assessment of these patients has generally focused on reflux and dysphagia, but these hernias also have adverse impacts on pulmonary function. Repair most benefits patients who are older, have bigger hernias, and worse baseline pulmonary function, said Dr. Philip W. Carrott Jr., of Virginia Mason Medical Center, Seattle.
"Patients with giant paraesophageal hernia and coexistent dyspnea or positional breathlessness should be reviewed by an experienced surgeon for elective repair, even when pulmonary comorbidities exist," Dr. Carrott concluded at the annual meeting of the Western Thoracic Surgical Association.
He based this advice on a single-center, retrospective, cohort study involving 120 patients who had pulmonary function tests preoperatively and again at a median of 106 days after surgery.
The overall group averaged 10% increases over baseline (P less than .001) in forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), vital capacity, and volume-adjusted mid-expiratory flow (IsoFEF25-75), as well as a 2.9% increase in the diffusing capacity of the lung (DLCO).
The larger a patient’s hernia as expressed by percent intrathoracic stomach (ITS) on preoperative contrast studies, the greater the improvement in pulmonary function tests after surgery. Hernia size was the strongest predictor of improvement. For example, forced vital capacity improved by an average of 4.7%, compared with reference values in patients with the smallest hernias as expressed in a percent ITS of less than 50%, as compared with a 6.0% gain in patients with a preop 50%-74% ITS, a 9.1% improvement in those with 75%-99% ITS, and a 14.9% gain in FVC in patients with 100% ITS.
The postoperative improvement in lung function increased with each decade of patient age.
Patients with the worst preoperative lung function tended to have the biggest hernias – and the greatest objective and subjective improvements after surgery. For example, 36% of subjects had a reduced baseline FEV1 not more than 75% of the reference value. Their vital capacity improved by 0.45 L, as compared with 0.23 L in patients without a reduced baseline FEV1. And their DLCO improved by 1.23 mL CO/min/mm Hg, compared with just 0.23 in patients whose baseline FEV1 was more than 75% of the reference value.
Of 63 patients who reported preoperative dyspnea, 47 (75%) noted subjective improvement in their respiratory function after hernia repair. Intriguingly, so did 30 of 57 patients (53%) not complaining of dyspnea at baseline.
Dr. Carrott and his fellow researchers postulate that restoring efficient diaphragmatic function is just part of the explanation. "The stomach probably has a paradoxical motion during respiration, such that the abdominal positive pressure is pushing against the negative effect of the lungs and chest wall," he said.
Study participants averaged 74 years of age, with a median of four preoperative symptoms. The most common were heartburn in 59%, early satiety in 54%, dyspnea in 52%, dysphagia in 47%, chest pain in 40%, and regurgitation in 39%.
Major comorbidities included pulmonary disease in 29% of subjects, heart disease in 35%, and obesity in 39%. An open Hill repair with no hiatal reinforcement was performed in 99% of patients, and 97% of the operations were elective.
Despite the substantial prevalence of comorbid conditions, there was no operative mortality. The mean length of stay was 4 days. One-third had complications, including six cases of arrhythmia, four instances of nausea delaying discharge, three cases of pneumonia, and two cases each of ileus, wound infection, or delirium.
Discussant Dr. Sean C. Grondin observed that paraesophageal hernia is a relatively common disease in the practice of most thoracic surgeons. And although the study provides some support for the notion that surgical repair may improve pulmonary function, its retrospective nature and only moderate size render it less than fully convincing.
"I think it still falls a little short just yet of providing conclusive evidence. At this time I would caution surgeons from telling patients that they’ll get a definitive improvement in their dyspnea after paraesophageal hernia repair, although it’s certainly a possibility," said Dr. Grondin of the University of Calgary (Alta).
Dr. Ross M. Bremner of St. Joseph’s Hospital and Medical Center, Phoenix, commented that: "I’ve long been telling my patients who have their entire stomach in the chest that they’re likely to get some improvement in their pulmonary function from repair. Now at least I have some data to show them they can get at least 10%-15% improvement."
Dr. Carrott reported that he had no disclosures.
Major Finding: Forced vital capacity improved by an average of 4.7%, compared with reference values in patients with the smallest paraesophageal hernias, those with a preoperative intrathoracic stomach (ITS) of less than 50%. FVC improved 6.0% in patients with a 50%-74% ITS, 9.1% in those with 75%-99% ITS, and 15% in patients with 100% ITS.
Data Source: A single-center, retrospective, cohort study involving 120 patients who underwent repair of paraesophageal hernia and had pulmonary function measured preoperatively and again a median of 106 days post-surgery.
Disclosures: No financial conflicts of interest.
HHS Plans Revamp of Human Research Rules
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.

"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.
"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.
"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
Joint Commission Steps Up Efforts to Reduce Wrong-Site Surgery
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
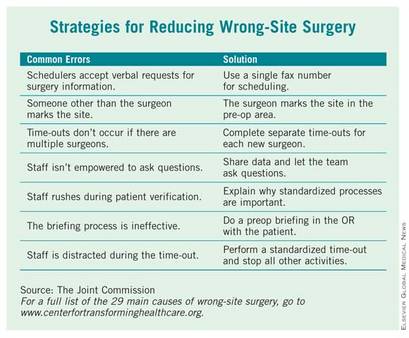
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
CMS Proposes 30% Pay Cut for 2012
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1. The 29.5% pay cut is scheduled to take effect Jan. 1, 2012, unless Congress once again intervenes.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
"We need a permanent SGR fix to solve this problem once and for all. That’s why the president’s budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix," Dr. Berwick said.
"We are pleased that there is support from the administration and bipartisan members of Congress for permanent reform of this broken system, but agreement is not enough – action is needed," said Dr. Peter W. Carmel, president of the American Medical Association, in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. That review has not yet begun, but revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula, said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units. Additional changes will also be made because of the implementation of some recommendations of the American Medical Association/Specialty Society Resource Based Relative Value Scale Update Committee (RUC).
The CMS said in a statement that it is proposing to continue efforts to identify what it calls "potentially misvalued codes." As part of those efforts, the agency will look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
CMS estimates that the additional changes included in the proposed fee schedule will result in a 0% total payment change for general surgery services. Whereas general surgery still will be subject to the 29.5% Medicare payment reduction if Congress fails to act, this update also means that, unlike some other specialties, general surgery will not be subject to any further payment reductions in 2012.
CMS wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound. The agency said the reduction would affect about 100 types of services. Reducing that component by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session would result in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
Also included in the rule are proposals that would update a number of physician incentive programs, including the Physician Quality Reporting System, the e-Prescribing Incentive Program, and the Electronic Health Records Incentive Program. Additionally, it calls for expanding the multiple procedure payment reduction policy and for using quality and cost measures to establish a new physician value-based payment modifier.
The American College of Surgeons (ACS) continues to work with CMS on all of the programs addressed in the current proposed rule. Ten surgical organizations, including the ACS, recently sent a letter to U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius and CMS Administrator Berwick expressing concern regarding CMS’s action in the last Medicare Physician Fee Schedule. The organizations identified CMS’s departure from past practice in which it has traditionally accepted more than 90% of the RUC’s recommendations. The letter noted that CMS accepted only 71% of the 2010 RUC recommendations.
Citing the need to accurately reflect the work associated with a variety of physician services, the surgical organizations asked CMS to adopt the work values that were developed by the RUC. The organizations also stated that CMS’s decision regarding the valuation of work for physician services "must be made using a transparent, consistent process, and must be based on credible data."
A final rule is expected by Nov. 1.
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1. The 29.5% pay cut is scheduled to take effect Jan. 1, 2012, unless Congress once again intervenes.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
"We need a permanent SGR fix to solve this problem once and for all. That’s why the president’s budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix," Dr. Berwick said.
"We are pleased that there is support from the administration and bipartisan members of Congress for permanent reform of this broken system, but agreement is not enough – action is needed," said Dr. Peter W. Carmel, president of the American Medical Association, in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. That review has not yet begun, but revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula, said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units. Additional changes will also be made because of the implementation of some recommendations of the American Medical Association/Specialty Society Resource Based Relative Value Scale Update Committee (RUC).
The CMS said in a statement that it is proposing to continue efforts to identify what it calls "potentially misvalued codes." As part of those efforts, the agency will look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
CMS estimates that the additional changes included in the proposed fee schedule will result in a 0% total payment change for general surgery services. Whereas general surgery still will be subject to the 29.5% Medicare payment reduction if Congress fails to act, this update also means that, unlike some other specialties, general surgery will not be subject to any further payment reductions in 2012.
CMS wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound. The agency said the reduction would affect about 100 types of services. Reducing that component by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session would result in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
Also included in the rule are proposals that would update a number of physician incentive programs, including the Physician Quality Reporting System, the e-Prescribing Incentive Program, and the Electronic Health Records Incentive Program. Additionally, it calls for expanding the multiple procedure payment reduction policy and for using quality and cost measures to establish a new physician value-based payment modifier.
The American College of Surgeons (ACS) continues to work with CMS on all of the programs addressed in the current proposed rule. Ten surgical organizations, including the ACS, recently sent a letter to U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius and CMS Administrator Berwick expressing concern regarding CMS’s action in the last Medicare Physician Fee Schedule. The organizations identified CMS’s departure from past practice in which it has traditionally accepted more than 90% of the RUC’s recommendations. The letter noted that CMS accepted only 71% of the 2010 RUC recommendations.
Citing the need to accurately reflect the work associated with a variety of physician services, the surgical organizations asked CMS to adopt the work values that were developed by the RUC. The organizations also stated that CMS’s decision regarding the valuation of work for physician services "must be made using a transparent, consistent process, and must be based on credible data."
A final rule is expected by Nov. 1.
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1. The 29.5% pay cut is scheduled to take effect Jan. 1, 2012, unless Congress once again intervenes.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
"We need a permanent SGR fix to solve this problem once and for all. That’s why the president’s budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix," Dr. Berwick said.
"We are pleased that there is support from the administration and bipartisan members of Congress for permanent reform of this broken system, but agreement is not enough – action is needed," said Dr. Peter W. Carmel, president of the American Medical Association, in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. That review has not yet begun, but revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula, said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units. Additional changes will also be made because of the implementation of some recommendations of the American Medical Association/Specialty Society Resource Based Relative Value Scale Update Committee (RUC).
The CMS said in a statement that it is proposing to continue efforts to identify what it calls "potentially misvalued codes." As part of those efforts, the agency will look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
CMS estimates that the additional changes included in the proposed fee schedule will result in a 0% total payment change for general surgery services. Whereas general surgery still will be subject to the 29.5% Medicare payment reduction if Congress fails to act, this update also means that, unlike some other specialties, general surgery will not be subject to any further payment reductions in 2012.
CMS wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound. The agency said the reduction would affect about 100 types of services. Reducing that component by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session would result in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
Also included in the rule are proposals that would update a number of physician incentive programs, including the Physician Quality Reporting System, the e-Prescribing Incentive Program, and the Electronic Health Records Incentive Program. Additionally, it calls for expanding the multiple procedure payment reduction policy and for using quality and cost measures to establish a new physician value-based payment modifier.
The American College of Surgeons (ACS) continues to work with CMS on all of the programs addressed in the current proposed rule. Ten surgical organizations, including the ACS, recently sent a letter to U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius and CMS Administrator Berwick expressing concern regarding CMS’s action in the last Medicare Physician Fee Schedule. The organizations identified CMS’s departure from past practice in which it has traditionally accepted more than 90% of the RUC’s recommendations. The letter noted that CMS accepted only 71% of the 2010 RUC recommendations.
Citing the need to accurately reflect the work associated with a variety of physician services, the surgical organizations asked CMS to adopt the work values that were developed by the RUC. The organizations also stated that CMS’s decision regarding the valuation of work for physician services "must be made using a transparent, consistent process, and must be based on credible data."
A final rule is expected by Nov. 1.
CABG, PCI Trends Suggest Many Not Treated Optimally
The rate of coronary artery bypass grafting performed in U.S. hospitals declined by approximately one-third between 2001 and 2008, according to an analysis of the Agency for Healthcare Research and Quality database.
During the same period, the rate of percutaneous coronary interventions (PCIs) showed a far more modest decrease.
"Our data imply a sizeable shift in cardiovascular clinical practice patterns away from surgical treatment toward percutaneous, catheter-based interventions," said Andrew J. Epstein, Ph.D., of the Philadelphia Veterans Affairs? Center for Health Equity Research and Promotion and the University of Pennsylvania, and his associates.
Given that coronary artery bypass grafting remains the better choice for patients with previously untreated three-vessel or left main coronary artery disease, according to the results of the SYNTAX trial (N. Engl. J. Med. 2009;360:961-72), it appears that CABG is being underused, the authors wrote.
It seems likely that in recent years, "patients who would have been optimally treated with CABG surgery were instead treated with PCI," they noted.
To assess temporal trends in coronary revascularization procedures, the investigators examined a nationally representative sample of hospitalization claims using an Agency for Healthcare Research and Quality database.
The database includes discharge data from approximately 1,000 nonfederal hospitals in 42 states, which covers 20% of U.S. hospitals and allows accurate estimates for the entire population of hospitalized patients, regardless of payer or insurance status.
Between 2001 and 2008, the total number of coronary revascularizations decreased "modestly," by approximately 15%.
There was a "substantial," statistically significant, 38% decrease in the annual rate of CABG surgery, from 1,742 per million adults in the first year of the study period to 1,081 per million in the final year.
This decline was roughly linear throughout the 8-year study period, suggesting that it "was not triggered by any single event occurring during the past decade, such as the introduction of competing technologies, advances in CABG surgical techniques, publication of clinical trials, or issuance of clinical guidelines."
CABG procedures decreased across all sex, age, racial, and regional subgroups.
In contrast, the PCI rate remained fairly constant, showing a "modest" 4% decrease from 3,827 per million adults per year in the first year of the study to 3,667 in the final year.
"Projected to the entire U.S. population, these rate changes implied that 130,000 fewer CABG surgeries were performed in 2008 compared to 2001," Dr. Epstein and his colleagues noted (JAMA 2011;305:1769-76).
The data did not allow the researchers to distinguish which patients may have been more appropriate candidates for CABG than for PCI, so "it cannot be known with certainty whether physicians were increasingly substituting PCI for CABG surgery during the past decade. ... [But] our findings suggest the possibility that several thousand patients who underwent PCI in 2008 would have undergone CABG surgery had patterns of care not changed markedly," they said.
The preferences of patients were also not discernible from the data, lead investigator Dr. Peter W. Groeneveld said in an interview. "However, if patient preference [for PCI vs. CABG] was the driving factor, there would have to be some reason that PCI was even more preferable to patients in 2008 than it was in 2001.
This scenario seems unlikely since the procedures haven?t changed that much," said Dr. Groeneveld, assistant professor of medicine at the University of Pennsylvania and staff physician at the Philadelphia Veterans Affairs Medical Center.
Another important finding was that during this interval, the number of hospitals providing CABG increased. Combined with the drop in the number of CABG surgeries, this resulted in a 28% decline in the median caseload per hospital, "and a substantial increase in the number of hospitals that provided fewer than 100 CABG surgeries per year."
Whether or not low-volume centers inherently have worse CABG outcomes can be debated, but either way "our findings highlight the increasing role of low-volume hospitals in the provision of CABG surgery," Dr. Epstein and his associates said.
The final trend in coronary revascularizations revealed in these data was the marked surge in PCI procedures using drug-eluting stents soon after two devices were approved by the Food and Drug Administration in 2003.
By mid-2005, 90% of PCI procedures involved drug-eluting stents, reflecting "a high level of clinician enthusiasm" for the devices.
This peak was soon followed by a marked decline after the publication of safety concerns such as late in-stent thrombosis, "as well as increasing clinician awareness of the imperative for ... adherence to long-duration antiplatelet therapy."
By the beginning of 2008, only 61% of PCI procedures involved placement of drug-eluting stents, but that rate increased steadily during that year, which also saw the adoption of second-generation stents that carried lower restenosis rates.
"An important implication of this volatility is that thousands of patients may have received drug-eluting stents during the peak years who would have received bare-metal stents [in later years].
"Whether these patients were appropriately treated ... during these years of ?high enthusiasm? for drug-eluting stents is uncertain," the investigators noted.
This study was supported by the National Heart, Lung, and Blood Institute; the Agency for Healthcare Research and Quality; and the Pennsylvania Department of Health. ☐
The rate of coronary artery bypass grafting performed in U.S. hospitals declined by approximately one-third between 2001 and 2008, according to an analysis of the Agency for Healthcare Research and Quality database.
During the same period, the rate of percutaneous coronary interventions (PCIs) showed a far more modest decrease.
"Our data imply a sizeable shift in cardiovascular clinical practice patterns away from surgical treatment toward percutaneous, catheter-based interventions," said Andrew J. Epstein, Ph.D., of the Philadelphia Veterans Affairs? Center for Health Equity Research and Promotion and the University of Pennsylvania, and his associates.
Given that coronary artery bypass grafting remains the better choice for patients with previously untreated three-vessel or left main coronary artery disease, according to the results of the SYNTAX trial (N. Engl. J. Med. 2009;360:961-72), it appears that CABG is being underused, the authors wrote.
It seems likely that in recent years, "patients who would have been optimally treated with CABG surgery were instead treated with PCI," they noted.
To assess temporal trends in coronary revascularization procedures, the investigators examined a nationally representative sample of hospitalization claims using an Agency for Healthcare Research and Quality database.
The database includes discharge data from approximately 1,000 nonfederal hospitals in 42 states, which covers 20% of U.S. hospitals and allows accurate estimates for the entire population of hospitalized patients, regardless of payer or insurance status.
Between 2001 and 2008, the total number of coronary revascularizations decreased "modestly," by approximately 15%.
There was a "substantial," statistically significant, 38% decrease in the annual rate of CABG surgery, from 1,742 per million adults in the first year of the study period to 1,081 per million in the final year.
This decline was roughly linear throughout the 8-year study period, suggesting that it "was not triggered by any single event occurring during the past decade, such as the introduction of competing technologies, advances in CABG surgical techniques, publication of clinical trials, or issuance of clinical guidelines."
CABG procedures decreased across all sex, age, racial, and regional subgroups.
In contrast, the PCI rate remained fairly constant, showing a "modest" 4% decrease from 3,827 per million adults per year in the first year of the study to 3,667 in the final year.
"Projected to the entire U.S. population, these rate changes implied that 130,000 fewer CABG surgeries were performed in 2008 compared to 2001," Dr. Epstein and his colleagues noted (JAMA 2011;305:1769-76).
The data did not allow the researchers to distinguish which patients may have been more appropriate candidates for CABG than for PCI, so "it cannot be known with certainty whether physicians were increasingly substituting PCI for CABG surgery during the past decade. ... [But] our findings suggest the possibility that several thousand patients who underwent PCI in 2008 would have undergone CABG surgery had patterns of care not changed markedly," they said.
The preferences of patients were also not discernible from the data, lead investigator Dr. Peter W. Groeneveld said in an interview. "However, if patient preference [for PCI vs. CABG] was the driving factor, there would have to be some reason that PCI was even more preferable to patients in 2008 than it was in 2001.
This scenario seems unlikely since the procedures haven?t changed that much," said Dr. Groeneveld, assistant professor of medicine at the University of Pennsylvania and staff physician at the Philadelphia Veterans Affairs Medical Center.
Another important finding was that during this interval, the number of hospitals providing CABG increased. Combined with the drop in the number of CABG surgeries, this resulted in a 28% decline in the median caseload per hospital, "and a substantial increase in the number of hospitals that provided fewer than 100 CABG surgeries per year."
Whether or not low-volume centers inherently have worse CABG outcomes can be debated, but either way "our findings highlight the increasing role of low-volume hospitals in the provision of CABG surgery," Dr. Epstein and his associates said.
The final trend in coronary revascularizations revealed in these data was the marked surge in PCI procedures using drug-eluting stents soon after two devices were approved by the Food and Drug Administration in 2003.
By mid-2005, 90% of PCI procedures involved drug-eluting stents, reflecting "a high level of clinician enthusiasm" for the devices.
This peak was soon followed by a marked decline after the publication of safety concerns such as late in-stent thrombosis, "as well as increasing clinician awareness of the imperative for ... adherence to long-duration antiplatelet therapy."
By the beginning of 2008, only 61% of PCI procedures involved placement of drug-eluting stents, but that rate increased steadily during that year, which also saw the adoption of second-generation stents that carried lower restenosis rates.
"An important implication of this volatility is that thousands of patients may have received drug-eluting stents during the peak years who would have received bare-metal stents [in later years].
"Whether these patients were appropriately treated ... during these years of ?high enthusiasm? for drug-eluting stents is uncertain," the investigators noted.
This study was supported by the National Heart, Lung, and Blood Institute; the Agency for Healthcare Research and Quality; and the Pennsylvania Department of Health. ☐
The rate of coronary artery bypass grafting performed in U.S. hospitals declined by approximately one-third between 2001 and 2008, according to an analysis of the Agency for Healthcare Research and Quality database.
During the same period, the rate of percutaneous coronary interventions (PCIs) showed a far more modest decrease.
"Our data imply a sizeable shift in cardiovascular clinical practice patterns away from surgical treatment toward percutaneous, catheter-based interventions," said Andrew J. Epstein, Ph.D., of the Philadelphia Veterans Affairs? Center for Health Equity Research and Promotion and the University of Pennsylvania, and his associates.
Given that coronary artery bypass grafting remains the better choice for patients with previously untreated three-vessel or left main coronary artery disease, according to the results of the SYNTAX trial (N. Engl. J. Med. 2009;360:961-72), it appears that CABG is being underused, the authors wrote.
It seems likely that in recent years, "patients who would have been optimally treated with CABG surgery were instead treated with PCI," they noted.
To assess temporal trends in coronary revascularization procedures, the investigators examined a nationally representative sample of hospitalization claims using an Agency for Healthcare Research and Quality database.
The database includes discharge data from approximately 1,000 nonfederal hospitals in 42 states, which covers 20% of U.S. hospitals and allows accurate estimates for the entire population of hospitalized patients, regardless of payer or insurance status.
Between 2001 and 2008, the total number of coronary revascularizations decreased "modestly," by approximately 15%.
There was a "substantial," statistically significant, 38% decrease in the annual rate of CABG surgery, from 1,742 per million adults in the first year of the study period to 1,081 per million in the final year.
This decline was roughly linear throughout the 8-year study period, suggesting that it "was not triggered by any single event occurring during the past decade, such as the introduction of competing technologies, advances in CABG surgical techniques, publication of clinical trials, or issuance of clinical guidelines."
CABG procedures decreased across all sex, age, racial, and regional subgroups.
In contrast, the PCI rate remained fairly constant, showing a "modest" 4% decrease from 3,827 per million adults per year in the first year of the study to 3,667 in the final year.
"Projected to the entire U.S. population, these rate changes implied that 130,000 fewer CABG surgeries were performed in 2008 compared to 2001," Dr. Epstein and his colleagues noted (JAMA 2011;305:1769-76).
The data did not allow the researchers to distinguish which patients may have been more appropriate candidates for CABG than for PCI, so "it cannot be known with certainty whether physicians were increasingly substituting PCI for CABG surgery during the past decade. ... [But] our findings suggest the possibility that several thousand patients who underwent PCI in 2008 would have undergone CABG surgery had patterns of care not changed markedly," they said.
The preferences of patients were also not discernible from the data, lead investigator Dr. Peter W. Groeneveld said in an interview. "However, if patient preference [for PCI vs. CABG] was the driving factor, there would have to be some reason that PCI was even more preferable to patients in 2008 than it was in 2001.
This scenario seems unlikely since the procedures haven?t changed that much," said Dr. Groeneveld, assistant professor of medicine at the University of Pennsylvania and staff physician at the Philadelphia Veterans Affairs Medical Center.
Another important finding was that during this interval, the number of hospitals providing CABG increased. Combined with the drop in the number of CABG surgeries, this resulted in a 28% decline in the median caseload per hospital, "and a substantial increase in the number of hospitals that provided fewer than 100 CABG surgeries per year."
Whether or not low-volume centers inherently have worse CABG outcomes can be debated, but either way "our findings highlight the increasing role of low-volume hospitals in the provision of CABG surgery," Dr. Epstein and his associates said.
The final trend in coronary revascularizations revealed in these data was the marked surge in PCI procedures using drug-eluting stents soon after two devices were approved by the Food and Drug Administration in 2003.
By mid-2005, 90% of PCI procedures involved drug-eluting stents, reflecting "a high level of clinician enthusiasm" for the devices.
This peak was soon followed by a marked decline after the publication of safety concerns such as late in-stent thrombosis, "as well as increasing clinician awareness of the imperative for ... adherence to long-duration antiplatelet therapy."
By the beginning of 2008, only 61% of PCI procedures involved placement of drug-eluting stents, but that rate increased steadily during that year, which also saw the adoption of second-generation stents that carried lower restenosis rates.
"An important implication of this volatility is that thousands of patients may have received drug-eluting stents during the peak years who would have received bare-metal stents [in later years].
"Whether these patients were appropriately treated ... during these years of ?high enthusiasm? for drug-eluting stents is uncertain," the investigators noted.
This study was supported by the National Heart, Lung, and Blood Institute; the Agency for Healthcare Research and Quality; and the Pennsylvania Department of Health. ☐
Major Finding: The rate of CABG surgeries declined by approximately one-third and that of PCI procedures fell by 4% between 2001 and 2008, while the number of hospitals providing CABG increased by 12% and the number providing PCI rose by 26% during the same period.
Data Source: A nationwide serial cross-sectional study of time trends in coronary revascularization procedures.
Disclosures: This study was supported by the National Heart, Lung, and Blood Institute; the Agency for Healthcare Research and Quality; and the Pennsylvania Department of Health.
Staging: EBUS Equals Mediastinoscopy?
PHILADELPHIA - Endobronchial ultrasound-guided biopsy of mediastinal lymph nodes in patients with operable non-small cell lung cancer worked as effectively for staging as did the standard approach - mediastinoscopy in a head-to-head comparison of the two methods.
"Our results have shown that EBUS-TBNA [endobronchial ultrasound-guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.

Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non?small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006?August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUS-TBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant.
During mediastinoscopy, surgeons successfully biopsied an average of 3.8 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient.
Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
Despite any sampling differences, the surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I?m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
PHILADELPHIA - Endobronchial ultrasound-guided biopsy of mediastinal lymph nodes in patients with operable non-small cell lung cancer worked as effectively for staging as did the standard approach - mediastinoscopy in a head-to-head comparison of the two methods.
"Our results have shown that EBUS-TBNA [endobronchial ultrasound-guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.
Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non?small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006?August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUS-TBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant.
During mediastinoscopy, surgeons successfully biopsied an average of 3.8 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient.
Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
Despite any sampling differences, the surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I?m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
PHILADELPHIA - Endobronchial ultrasound-guided biopsy of mediastinal lymph nodes in patients with operable non-small cell lung cancer worked as effectively for staging as did the standard approach - mediastinoscopy in a head-to-head comparison of the two methods.
"Our results have shown that EBUS-TBNA [endobronchial ultrasound-guided transbronchial needle aspiration], when performed as in this study, can replace mediastinoscopy for accurate staging of the mediastinum in potentially resectable lung cancer," Dr. Kazuhiro Yasufuku said at the annual meeting of the American Association for Thoracic Surgery.
Based on these results, which were obtained in 153 patients treated by any one of seven surgeons working at Toronto General Hospital, Dr. Yasufuku and his colleagues now routinely use EBUS-TBNA as their initial approach for staging patients with inoperable non?small cell lung cancer (NSCLC), who account for about 70% of all NSCLC patients they treat. As long as they can collect adequate cell specimens for cytologic analysis from the lymph node stations they routinely assess, they rely exclusively on EBUS-TBNA for staging, which allows them to avoid mediastinoscopy for most of their patients, Dr. Yasufuku said in an interview.
"We knew that EBUS-TBNA was good, but [until now] we never knew how it compared with the gold standard, mediastinoscopy," he said. The major limiting factor is lymph node size, he noted. Surgeons find it challenging to routinely obtain an adequate cell specimen from nodes smaller than 5 mm in diameter, Dr. Yasufuku said. "The smaller the node, the harder it is to put a needle into it."
The Toronto group uses rapid, onsite cytologic evaluation, which means that a cytologist attends the procedure in the combined surgical and endoscopy suite. In the study, and also in routine practice, "we can make repeated needle passes until we obtain good specimens. The surgeon can learn how to place the needle by getting immediate feedback" on the specimens, he said.
The specimens obtained allow for a tissue diagnosis, and typically provide enough material to assess cells for the presence of epidermal growth factor receptor mutations, he added.
EBUS-TBNA uses local rather than general anesthesia, is less invasive, and has fewer complications compared with mediastinoscopy, said Dr. Yasufuku, a thoracic surgeon and director of the interventional thoracic surgery program at Toronto General and the University of Toronto.
The study enrolled adults with NSCLC who required mediastinoscopy as part of their staging to determine their suitability for lung cancer resection. The study excluded patients who were not fit for definitive surgical resection, because the researchers used the status of the surgically excised lymph nodes as the basis for judging the diagnostic accuracy of both techniques.
During July 2006?August 2010, they enrolled 153 patients with an average age of 69 years. The most common NSCLC histologic subtype was adenocarcinoma (59%), followed by squamous cell carcinoma (25%). Staging by ultrasound imaging identified 57% of the patients with stage I or II disease, and 39% with stage IIIA disease. The remaining 4% had stage IIIB or stage IV disease.
All patients underwent general anesthesia. A surgeon first performed EBUS-TBNA on each patient, followed immediately by mediastinoscopy. All patients then underwent surgical lymph node resection to definitively assess their nodes if EBUS-TBNA, mediastinoscopy, or both did not show signs of metastatic disease.
The surgeons attempted biopsies at five lymph node stations in each patient: stations 2R, 2L, 4R, 4L, and 7. They successfully biopsied an average of three stations per patient using EBUS-TBNA, with an inadequate specimen obtained on an average of one station per patient. Average lymph node diameter on the short axis was 7 mm, and the procedure averaged a total of 20 minutes per patient. Overall, EBUS-TBNA identified 78 biopsies as malignant.
During mediastinoscopy, surgeons successfully biopsied an average of 3.8 nodes per patient, with inadequate specimens obtained from 10 nodes, an average of fewer than 0.1 inadequate specimen per patient.
Mediastinoscopy retrieved 79 biopsies that were identified as malignant.
Despite any sampling differences, the surgeons reached an identical and correct diagnosis using both modalities in 136 patients (89%). Neither modality produced the correct diagnosis in four patients (3%), which meant that overall EBUS-TBNA and mediastinoscopy agreed 92% of the time. EBUS-TBNA was correct and mediastinoscopy incorrect in seven patients, and mediastinoscopy was correct and EBUS-TBNA incorrect in six patients.
These outcomes meant that EBUS-TBNA had 81% sensitivity, 91% negative predictive value, and 93% diagnostic accuracy. Mediastinoscopy led to 79% sensitivity, 90% negative predictive value, and 93% accuracy. Both methods had a specificity and positive predictive value of 100%, Dr. Yasufuku said.
No complications occurred after EBUS-TBNA, but there were four minor complications following subsequent mediastinoscopy: Two patients had a hematoma, one had a recurrent nerve injury, and one had a wound infection.
"It was a very clean study, showing that in the hands of a trained surgeon in our setting, EBUS-TBNA works very well. We clearly showed that the diagnostic yield is similar, and that patients who require mediastinoscopy as part of their staging can undergo EBUS-TBNA as their initial modality. Depending on what you find, you want to also do mediastinoscopy," he added.
"I?m convinced that [Dr. Yasufuku has] demonstrated equivalent ability to stage the mediastinum with EBUS-TBNA and with mediastinoscopy," commented Dr. Joel D. Cooper, professor of surgery and chief of thoracic surgery at the University of Pennsylvania in Philadelphia.
The study was supported by Olympus Medical Systems, a company that markets an EBUS-TBNA system. Dr. Yasufuku said that he has received research support from Olympus. Dr. Cooper said that he had no relevant disclosures.
Most Stable CAD Goes Right to PCI
Contrary to clinical practice guidelines and simple logic, most patients who have stable coronary artery disease are not given optimal medical therapy before undergoing percutaneous coronary intervention, according to a recent study reported in JAMA.
In March 2007, "the most definitive randomized trial" comparing percutaneous coronary intervention (PCI) to optimal medical therapy, determined that PCI is no more effective than drug treatment at preventing MI or death in stable CAD. But even with this evidence, there was little change in the pattern of stable CAD patients going straight to PCI, said Dr. William B. Borden of Weill Cornell Medical College in New York, and his associates.
Dr. Borden and his colleagues assessed the practice patterns regarding the use of optimal medical therapy before and after PCI using data obtained from the national CathPCI Registry.
The researchers examined a 19-month interval occurring before publication of the trial results of Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) (N. Engl. J. Med. 2007;356:1503-16) and a 24-month period occuring afterward, to determine whether physicians had been inspired to transfer those findings into clinical practice.
The study population comprised 467,211 patients treated at 1,013 U.S. hospitals, which constituted about 28% of the total CathPCI population during the study period.
Optimal medical therapy was defined as being prescribed aspirin, a beta-blocker, and a statin before PCI and being prescribed aspirin or thienopyridine, a beta-blocker, a statin, and an ACE inhibitor or angiotensin receptor blocker after PCI, or having specific contraindications to these medications.
Overall, fewer than half of PCI patients ? 45% ? received optimal medical therapy before undergoing PCI. Current guidelines recommend maximizing medical therapy because that often relieves symptoms, obviating the need for PCI.
The rates of optimal medical therapy increased only slightly after publication of the COURAGE results, from 43% to 45%. This increase "was of little clinical significance," the investigators said (JAMA 2011:305:1882-9).
Dr. Borden disclosed ties to the pharmaceutical Kowa Company.
Contrary to clinical practice guidelines and simple logic, most patients who have stable coronary artery disease are not given optimal medical therapy before undergoing percutaneous coronary intervention, according to a recent study reported in JAMA.
In March 2007, "the most definitive randomized trial" comparing percutaneous coronary intervention (PCI) to optimal medical therapy, determined that PCI is no more effective than drug treatment at preventing MI or death in stable CAD. But even with this evidence, there was little change in the pattern of stable CAD patients going straight to PCI, said Dr. William B. Borden of Weill Cornell Medical College in New York, and his associates.
Dr. Borden and his colleagues assessed the practice patterns regarding the use of optimal medical therapy before and after PCI using data obtained from the national CathPCI Registry.
The researchers examined a 19-month interval occurring before publication of the trial results of Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) (N. Engl. J. Med. 2007;356:1503-16) and a 24-month period occuring afterward, to determine whether physicians had been inspired to transfer those findings into clinical practice.
The study population comprised 467,211 patients treated at 1,013 U.S. hospitals, which constituted about 28% of the total CathPCI population during the study period.
Optimal medical therapy was defined as being prescribed aspirin, a beta-blocker, and a statin before PCI and being prescribed aspirin or thienopyridine, a beta-blocker, a statin, and an ACE inhibitor or angiotensin receptor blocker after PCI, or having specific contraindications to these medications.
Overall, fewer than half of PCI patients ? 45% ? received optimal medical therapy before undergoing PCI. Current guidelines recommend maximizing medical therapy because that often relieves symptoms, obviating the need for PCI.
The rates of optimal medical therapy increased only slightly after publication of the COURAGE results, from 43% to 45%. This increase "was of little clinical significance," the investigators said (JAMA 2011:305:1882-9).
Dr. Borden disclosed ties to the pharmaceutical Kowa Company.
Contrary to clinical practice guidelines and simple logic, most patients who have stable coronary artery disease are not given optimal medical therapy before undergoing percutaneous coronary intervention, according to a recent study reported in JAMA.
In March 2007, "the most definitive randomized trial" comparing percutaneous coronary intervention (PCI) to optimal medical therapy, determined that PCI is no more effective than drug treatment at preventing MI or death in stable CAD. But even with this evidence, there was little change in the pattern of stable CAD patients going straight to PCI, said Dr. William B. Borden of Weill Cornell Medical College in New York, and his associates.
Dr. Borden and his colleagues assessed the practice patterns regarding the use of optimal medical therapy before and after PCI using data obtained from the national CathPCI Registry.
The researchers examined a 19-month interval occurring before publication of the trial results of Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) (N. Engl. J. Med. 2007;356:1503-16) and a 24-month period occuring afterward, to determine whether physicians had been inspired to transfer those findings into clinical practice.
The study population comprised 467,211 patients treated at 1,013 U.S. hospitals, which constituted about 28% of the total CathPCI population during the study period.
Optimal medical therapy was defined as being prescribed aspirin, a beta-blocker, and a statin before PCI and being prescribed aspirin or thienopyridine, a beta-blocker, a statin, and an ACE inhibitor or angiotensin receptor blocker after PCI, or having specific contraindications to these medications.
Overall, fewer than half of PCI patients ? 45% ? received optimal medical therapy before undergoing PCI. Current guidelines recommend maximizing medical therapy because that often relieves symptoms, obviating the need for PCI.
The rates of optimal medical therapy increased only slightly after publication of the COURAGE results, from 43% to 45%. This increase "was of little clinical significance," the investigators said (JAMA 2011:305:1882-9).
Dr. Borden disclosed ties to the pharmaceutical Kowa Company.
CMS Plans to Pay Hospitals for Quality
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) this Spring.
The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare’s Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and to how their performance has improved over time.
The new program is the first step in shifting payments toward quality and away from volume, aacording to Dr. Donald Berwick, a CMS administrator, who spoke during a press conference.
"This is one of those areas where improvement of quality and reduction in cost go hand-in-hand," Dr. Berwick said. "My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care."
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness.
A complete list of the measures is available online at www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html.
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare’s Hospital Compare website.
The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia.
And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing was published in the Federal Register in May and becomes final in July.
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) this Spring.
The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare’s Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and to how their performance has improved over time.
The new program is the first step in shifting payments toward quality and away from volume, aacording to Dr. Donald Berwick, a CMS administrator, who spoke during a press conference.
"This is one of those areas where improvement of quality and reduction in cost go hand-in-hand," Dr. Berwick said. "My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care."
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness.
A complete list of the measures is available online at www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html.
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare’s Hospital Compare website.
The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia.
And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing was published in the Federal Register in May and becomes final in July.
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) this Spring.
The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare’s Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and to how their performance has improved over time.
The new program is the first step in shifting payments toward quality and away from volume, aacording to Dr. Donald Berwick, a CMS administrator, who spoke during a press conference.
"This is one of those areas where improvement of quality and reduction in cost go hand-in-hand," Dr. Berwick said. "My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care."
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness.
A complete list of the measures is available online at www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html.
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare’s Hospital Compare website.
The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia.
And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing was published in the Federal Register in May and becomes final in July.