User login
The Official Newspaper of the American Association for Thoracic Surgery
Perspectives on the New Curriculum
The Training Program Experience
By Mara B. Antonoff, M.D., Resident Medical Editor
The new thoracic surgery curriculum has arrived. Debuting this past summer, the curriculum resulted as a joint endeavor of several key organizations heavily vested in thoracic surgical education, with the aim of providing a web-based, multimedia repository of educational materials, accompanied by a formal structure and schedule of weekly topic coverage. Conceptually, the new curriculum has much to offer, with immense theoretical benefits to both the teacher and the student. But what about in practice? Now several months after its launch, the materials provided via the Moodle site and WebBrain have been accessed by the majority of training programs in this country.
How are these tools being utilized by the various programs, and what feedback do they have based on their experiences? The goal of this article will be to explore the various usage patterns of several institutions and their strategies for implementing the materials and integrating them with on-the-ground educational activities. Both the strengths and drawbacks from a programmatic standpoint will be addressed. As you read this article, perhaps you will be motivated to take another look at the curriculum, with new ideas as to how it might best suit your program’s needs.

At Oregon Health and Science University (OHSU), the new curriculum was officially introduced to the trainees and faculty members in a very formal and organized manner, heavily employing the provided instructional videos to become quickly oriented to the new system ("How-To: Utilizing the Thoracic Surgery Brain WebBrain," by Dr. Craig Baker; "How-To: Navigating Moodle," by Dr. Ara Vaporciyan; and "Overview of Teaching Cardiothoracic Surgery" – all available from the Moodle site, http:// jctse.mrooms.net, under Resources on the right hand column). OHSU Program Coordinator Jill Rose reports that she also received helpful information about accessing the curriculum when she attended the "Educate the Educators" course in June, sponsored by the Joint Council on Thoracic Surgery Education (JCTSE). Ms. Rose states, "Faculty and learners enthusiastically adopted this new curriculum and immediately put it to use at least twice a week." When the weekly emails come out, the relevant articles and videos are sent to the trainees and faculty members in the form of a reminder email, including links to the online videos and all related PDF’s as attachments. The residents and fellows then engage in formal curriculum review sessions with faculty, students, and mid-level practitioners – covering the cardiac topics on Monday mornings and thoracic topics on Friday mornings.
At Loma Linda University Health, the residents meet with a faculty moderator on a weekly basis to cover the materials related to the weekly Thoracic Surgery Curriculum topics. The style of presentation is left to the discretion of the attending surgeon, with the majority of the didactic sessions following an oral-board, case-based scenario format. Rather than directly accessing the Moodle pages and WebBrain site, the majority of the faculty and trainees have found that they prefer to have the materials provided to them as hard copies. Consequently, these materials are downloaded and distributed by the program coordinator on a weekly basis.
As with any new educational program, there may be a need for adjustments in initial plans and utilization based on early experiences. For the first few months following release of the curriculum, the Loma Linda group aimed to cover two topics per week – cardiac on Monday mornings and thoracic on Thursday mornings. However, with a tremendous amount of material available for each topic, they ultimately decided to transition to a single weekly session.
While the Loma Linda program has attempted to adhere to the schedule according to the weekly curriculum emails, other programs have chosen to utilize the available materials within the framework of alternative curricular schedules. Rose Haselden, the program coordinator at the Medical University of South Carolina (MUSC), explains that they created their own timeline for covering the materials, based on their specific needs and objectives.
Dr. John Ikonomidis, program director at MUSC, recalls being quick to adopt the new thoracic surgery curriculum. He states, "We were very impressed with its scope and current referencing. When it became available, we went through its entire corpus and divided it into sections which could be covered in 30 minutes. Then we developed a schedule where two topics (one adult or pediatric cardiac and one thoracic) would be covered in our weekly one-hour didactic sessions." Dr. Ikonomidis continues, "The residents are expected to read the material beforehand and faculty are assigned to quiz the residents during the session." In this way, the MUSC program has found a way to use the full breadth of materials, but tailoring the exact learning objectives for their trainees.
While some programs have taken to re-organizing the materials and producing hard copies of the resources for the residents, others have chosen to use the curriculum in its native structure, as a freestanding means of educational supplementation. At Washington University in St. Louis, the trainees are taught how to access the materials and encouraged to both follow the weekly thoracic surgery curriculum emails for independent reading and to utilize the immense resources available for investigating topics relevant to specific cases, conferences, and research interests. Dr. Marc Moon, program director at Washington University, explains that "we have not utilized the materials in any formal, assigned manner; rather, we choose to use the curriculum as a resource for independent study, encouraging our residents to access the multimedia materials both for at-home study and point-of-care reference." Dr. Moon expresses gratitude for the new curriculum, reporting that the faculty members "are grateful that our trainees are able to access these curricular materials through the WebBrain and Moodle, as they serve as an outstanding educational supplement to a high volume operative experience." Dr. Moon further emphasizes, "We find that the new curriculum functions as an excellent adjunct to our clinical teaching."
There are a number of proposed strengths to the new curriculum – its breadth, its ease of access, its correlation with the educational objectives of the American Board of Thoracic Surgery. But what are the benefits being identified from the level of the training program? Dr. Paul Schipper, program director at OHSU, expresses appreciation for the greater volume of material accessible by the trainees, as compared with the older curriculum previously sponsored by the Thoracic Surgery Directors Association (TSDA). States Dr. Schipper, "We’ve been using the TSDA emailed curriculum for several years. With the release of WebBrain, we’ve switched over and been very pleased. Residents are accessing the material and digging deeper into it than previously. In our teaching sessions, we are spending more time on applying the material and less time on explaining it, and I think this is good." Appreciation for the breadth and depth of the material was also noted by Dr. Moon, who identifies the program’s strengths as its ease of access, its large volume, and its applicability to a wide range of educational needs.
Despite the generally laudatory praise, there have been a few issues identified by the training programs that could benefit from some improvement.
Certainly, this is not surprising, as with any educational program, practice and feedback are necessary to optimize the execution for the users. Further, with a resource collection of such enormity, minor tweaks will likely continue in the background at all times in order to ensure ongoing quality-control.
In considering further revision, Dr. Wallen raises some concerns regarding format. He states that "all the moving around on the links makes people crazy," and, for this reason, at Loma Linda, all of the materials are distributed from the WebBrain to the faculty and trainees by the program coordinator. "Otherwise, we would have a revolt," Dr. Jason Wallen explains, This distaste for accessing the materials via the WebBrain is not shared by all users, but it provides feedback, suggesting that changes could be made to optimize formatting to increase ease of use.
Certainly, the leaders in the TSDA, JCTSE, and Thoracic Surgery Residents Association (TSRA) who contributed to the development of the new curriculum are eager for this kind of feedback, welcoming all users to provide constructive criticism. Dr. Ara Vaporciyan, program director at the University of Texas MD Anderson Cancer Center, co-chair of the TSDA/JCTSE Curriculum Committee, and one of the 4 section editors for the curriculum itself, has been a key player in the development of the new curriculum.
States Dr. Vaporciyan, "I never expected this to be perfect on the first try and this is exactly the feedback we need. If we can start an honest conversation about the flaws in the system we can better allocate resources to fixing the most pervasive issues."
Despite the challenges that have been identified, Dr. Wallen remains positive about the curriculum, stating, "We are excited to have an electronic curriculum that our residents can access from anywhere that includes readings and multimedia content. We anticipate that following the curriculum will enhance our residents’ performance on future inservice exams and pave the path to certification."
Dr. Ikonomidis shares Dr. Wallen’s enthusiasm, summarizing that his "residents are constantly engaged and we believe that their learning efficiency has increased." Notes Dr. Schipper, "I am hopeful that this system will stay current and realize and appreciate the effort this has and will take to do so."
Certainly, the new curriculum has already been heavily utilized and appreciated by a number of training programs. While there will always be minor adjustments to be made, the innovators behind the Thoracic Surgery WebBrain and Moodle site are receptive to feedback and clearly dedicated to its ongoing growth.
Perhaps this article has encouraged those of you that aren’t using the curriculum regularly to incorporate it into your institution’s educational structure. For those of you already heavily engaged, perhaps you’ve been inspired to try some new strategies of implementation. Moreover, for all users of the system – trainees, educators, and coordinators – regardless of your program’s current level of use, the take-home message from the creators of the curriculum is that you are encouraged to provide feedback to allow evolution and improvement of the program.
The Trainee Experience
By Sanford M. Zeigler, M.D., Resident Medical Editor
Dr. Antonoff has detailed how different programs have chosen to implement the new curriculum. Of course, in order for the curriculum to work in any setting, people have to actually sit down, access the material, and learn from it. The modules need to be easily accessible, logically organized, and appropriate for the audience for which they are intended. To that end, the folks behind the new curriculum worked diligently to organize all the material into the WebBrain format, which attempts to organize the content by the logic of the human brain, using mind maps, and Moodle, which compartmentalizes the readings into individual curricular assignments that are served up on each resident’s personal Moodle page.

The overall architecture of the WebBrain is very organic; the "Brain" is split into four main branches, comprised of Foundations of Surgery, Cardiovascular, Thoracic, and Congenital headings. From these, the subject matter continues to divide and subdivide again until you reach a terminal branch, where the reader can open a number of different sources, both primary and secondary, on a given subject. The brains’ power lies in the connections that can be made across these fluid boundaries. An example can be seen with one reference that discusses MRI imaging of pericardial disease and cardiac masses. When this is selected, the thought leads the reader back to both the pericardial disease heading and the cardiac tumors heading. The subject selection feature allows the reader to wander throughout the entire WebBrain in a free-flowing but logical manner. Connections across different subjects are, at this point, still rarely utilized. The cross-referencing feature could be a boon for more junior integrated residents and general surgery residents if more of the basic concepts section were connected to cardiac and thoracic subjects, and could allow more self-directed reading to residents that find the time to do so. The WebBrain has some basic search functionality embedded in it that could be used to help understand specific clinical scenarios as they are encountered. Layered upon all of the subject matter are tags, which correspond to the weekly curricular readings. If trainees search for the tag "CV08," for example, they will be directed to each source with that tag, bringing the weekly source matter right to the front. Thus, the WebBrain can be used as a guide for casual reading, as a reference for a particular question or clinical scenario encountered in practice, and also as the source for material covered in didactic session.
The Moodle interface is the gateway to the WebBrain. While it may sound easier to deliver the contents of the WebBrain to each resident rather than go through Moodle, this interface serves two functions. In order to license the content for the curriculum, publishers of many of the textbooks require tight security to prevent unauthorized duplication of the materials. Moodle, by requiring a unique login to access the single WebBrain, provides that security and also allows the WebBrain to be modified in the Cloud, rather than at the level of the end-user. Moodle also provides other testing and tracking tools that have not been completely rolled out. Over the coming months, its full architecture will be used to incorporate quizzes, collaborative message boards, and personal tracking to help residents and their program directors ensure that the material is being covered adequately.
Nearly every resident and faculty member I asked about the new curriculum agreed that the update in content and delivery was badly needed. As an intern in an integrated cardiothoracic surgery program, I remember feeling very jealous of my general surgery colleagues’ access to the SCORE portal, which gave them an easily navigable curriculum accessible from anywhere, with instruction in everything from basic science and physiology to advanced surgical diagnosis and technique. The rollout of the Moodle interface and Web Brain content is the first step to a similar, comprehensive compendium of the necessary knowledge to master cardiac and thoracic surgery.
Response to the rollout has been generally positive from the residents. Most residents agree that the content provides a great sample of landmark papers, lecture videos, book chapters, and consensus statements. A fellow Stanford resident, George Dimeling, wrote: "I like the weekly focus and the topic organization. The content is good, but tough to access." The articles and chapters are often more up to date than printed textbooks, and, once the reader accesses the Brain, are instantly viewable with no further log ins or downloads.
Of course, for a busy resident, it may not always be possible to cover a long book chapter quickly, and the primary literature sometimes fails to cover an entire topic. Justin Schaffer, another Stanford resident, offered this thought: "There’s either a short paper or a 40-page book chapter – there is no solid review of the subject matter. They need something like the Doty lecture series and the TSRA publications to get you warmed up if you don’t have all that time." In fact, the WebBrain incorporates many chapters of the TSRA Cardiothoracic Review book, and the TSRA Clinical Scenarios were added to Moodle on Dec. 12.
One of the more common complaints had little to do with the content but more to do with delivery. At my own institution, most of our hospital computers run an outdated copy of Internet Explorer and have restricted access to update or install a new browser. The out-of-date or restricted software packages that are pervasive in institutional machines nullify many of the advantages of the WebBrain/Moodle format, as the majority of computers at Stanford Hospital cannot access the WebBrain. Furthermore, the WebBrain interface can be laggy and slow even with compatible software.
Others have complained that it is not always easy to find the readings, especially if a program does not follow one of the standardized curricula included with the rollout. First, one must find which content they are responsible for via departmental website or reference to the curricula. Next, the resident logs into the Moodle room, and the proper WebBrain course is launched, then each article for the week is selected and downloaded. Only after that can the content be read, saved, or printed. Using the tag function is helpful, but each time a tagged article is selected, the resident is taken away from the search and to the specific content area, away from the other material assigned for the week. Though it isn’t very difficult to navigate back to the search, all of the steps above make it a bit more of a process to access the material than is convenient for a resident trying to fit in readings between cases or while waiting to round. The new software is a definite improvement, yet still has not reached its full potential.
As Dr. Antonoff pointed out, one residency program has easily overcome this obstacle by consolidating and emailing the appropriate material every week. While the Moodle portion of the curriculum still sees limited functionality, this is probably the best solution to all of the problems. If the articles are in your mailbox, they are accessible anywhere, without the bother of logging in and navigating the Brain.
I discussed this with Dr. Jim Fann, who has been very involved in developing the curriculum, and he explained that direct delivery of the content to each resident had been part of the original goal. As mentioned before, however, publishers require that the delivery of the material is secure from unauthorized duplication. Within the context of an individual institution, those issues are less confining. While individual programs work to integrate the material into their own traditions, it may be worthwhile to designate a resident or office staff member to be in charge of distributing the week’s reading. One little-recognized feature of Moodle is the ability to upload calendars. Perhaps this area could be used by each program to keep the curricular and departmental calendars adjacent to the WebBrain link for easier access.
The recent changes in cardiothoracic surgical education have been myriad, and the rollout of the new curriculum is one of the most pervasive and visible signs of that change. The new curriculum has been designed and updated to reflect not only updates in medical knowledge and consensus, but also changes in the demographic of the cardiothoracic surgery resident and new paradigms in surgical education. The content and delivery systems, while not perfect, remain an ever improving work in progress, which aims to bring cardiothoracic surgical education into the collaborative, cloud based learning era while broadening its reach to both green cardiothoracic surgery interns and traditional fellows with a full general surgery residency behind them. All things considered, the rollout has been very successful, and as more functionality is added and bugs are worked out, things can only improve.
The Training Program Experience
By Mara B. Antonoff, M.D., Resident Medical Editor
The new thoracic surgery curriculum has arrived. Debuting this past summer, the curriculum resulted as a joint endeavor of several key organizations heavily vested in thoracic surgical education, with the aim of providing a web-based, multimedia repository of educational materials, accompanied by a formal structure and schedule of weekly topic coverage. Conceptually, the new curriculum has much to offer, with immense theoretical benefits to both the teacher and the student. But what about in practice? Now several months after its launch, the materials provided via the Moodle site and WebBrain have been accessed by the majority of training programs in this country.
How are these tools being utilized by the various programs, and what feedback do they have based on their experiences? The goal of this article will be to explore the various usage patterns of several institutions and their strategies for implementing the materials and integrating them with on-the-ground educational activities. Both the strengths and drawbacks from a programmatic standpoint will be addressed. As you read this article, perhaps you will be motivated to take another look at the curriculum, with new ideas as to how it might best suit your program’s needs.
At Oregon Health and Science University (OHSU), the new curriculum was officially introduced to the trainees and faculty members in a very formal and organized manner, heavily employing the provided instructional videos to become quickly oriented to the new system ("How-To: Utilizing the Thoracic Surgery Brain WebBrain," by Dr. Craig Baker; "How-To: Navigating Moodle," by Dr. Ara Vaporciyan; and "Overview of Teaching Cardiothoracic Surgery" – all available from the Moodle site, http:// jctse.mrooms.net, under Resources on the right hand column). OHSU Program Coordinator Jill Rose reports that she also received helpful information about accessing the curriculum when she attended the "Educate the Educators" course in June, sponsored by the Joint Council on Thoracic Surgery Education (JCTSE). Ms. Rose states, "Faculty and learners enthusiastically adopted this new curriculum and immediately put it to use at least twice a week." When the weekly emails come out, the relevant articles and videos are sent to the trainees and faculty members in the form of a reminder email, including links to the online videos and all related PDF’s as attachments. The residents and fellows then engage in formal curriculum review sessions with faculty, students, and mid-level practitioners – covering the cardiac topics on Monday mornings and thoracic topics on Friday mornings.
At Loma Linda University Health, the residents meet with a faculty moderator on a weekly basis to cover the materials related to the weekly Thoracic Surgery Curriculum topics. The style of presentation is left to the discretion of the attending surgeon, with the majority of the didactic sessions following an oral-board, case-based scenario format. Rather than directly accessing the Moodle pages and WebBrain site, the majority of the faculty and trainees have found that they prefer to have the materials provided to them as hard copies. Consequently, these materials are downloaded and distributed by the program coordinator on a weekly basis.
As with any new educational program, there may be a need for adjustments in initial plans and utilization based on early experiences. For the first few months following release of the curriculum, the Loma Linda group aimed to cover two topics per week – cardiac on Monday mornings and thoracic on Thursday mornings. However, with a tremendous amount of material available for each topic, they ultimately decided to transition to a single weekly session.
While the Loma Linda program has attempted to adhere to the schedule according to the weekly curriculum emails, other programs have chosen to utilize the available materials within the framework of alternative curricular schedules. Rose Haselden, the program coordinator at the Medical University of South Carolina (MUSC), explains that they created their own timeline for covering the materials, based on their specific needs and objectives.
Dr. John Ikonomidis, program director at MUSC, recalls being quick to adopt the new thoracic surgery curriculum. He states, "We were very impressed with its scope and current referencing. When it became available, we went through its entire corpus and divided it into sections which could be covered in 30 minutes. Then we developed a schedule where two topics (one adult or pediatric cardiac and one thoracic) would be covered in our weekly one-hour didactic sessions." Dr. Ikonomidis continues, "The residents are expected to read the material beforehand and faculty are assigned to quiz the residents during the session." In this way, the MUSC program has found a way to use the full breadth of materials, but tailoring the exact learning objectives for their trainees.
While some programs have taken to re-organizing the materials and producing hard copies of the resources for the residents, others have chosen to use the curriculum in its native structure, as a freestanding means of educational supplementation. At Washington University in St. Louis, the trainees are taught how to access the materials and encouraged to both follow the weekly thoracic surgery curriculum emails for independent reading and to utilize the immense resources available for investigating topics relevant to specific cases, conferences, and research interests. Dr. Marc Moon, program director at Washington University, explains that "we have not utilized the materials in any formal, assigned manner; rather, we choose to use the curriculum as a resource for independent study, encouraging our residents to access the multimedia materials both for at-home study and point-of-care reference." Dr. Moon expresses gratitude for the new curriculum, reporting that the faculty members "are grateful that our trainees are able to access these curricular materials through the WebBrain and Moodle, as they serve as an outstanding educational supplement to a high volume operative experience." Dr. Moon further emphasizes, "We find that the new curriculum functions as an excellent adjunct to our clinical teaching."
There are a number of proposed strengths to the new curriculum – its breadth, its ease of access, its correlation with the educational objectives of the American Board of Thoracic Surgery. But what are the benefits being identified from the level of the training program? Dr. Paul Schipper, program director at OHSU, expresses appreciation for the greater volume of material accessible by the trainees, as compared with the older curriculum previously sponsored by the Thoracic Surgery Directors Association (TSDA). States Dr. Schipper, "We’ve been using the TSDA emailed curriculum for several years. With the release of WebBrain, we’ve switched over and been very pleased. Residents are accessing the material and digging deeper into it than previously. In our teaching sessions, we are spending more time on applying the material and less time on explaining it, and I think this is good." Appreciation for the breadth and depth of the material was also noted by Dr. Moon, who identifies the program’s strengths as its ease of access, its large volume, and its applicability to a wide range of educational needs.
Despite the generally laudatory praise, there have been a few issues identified by the training programs that could benefit from some improvement.
Certainly, this is not surprising, as with any educational program, practice and feedback are necessary to optimize the execution for the users. Further, with a resource collection of such enormity, minor tweaks will likely continue in the background at all times in order to ensure ongoing quality-control.
In considering further revision, Dr. Wallen raises some concerns regarding format. He states that "all the moving around on the links makes people crazy," and, for this reason, at Loma Linda, all of the materials are distributed from the WebBrain to the faculty and trainees by the program coordinator. "Otherwise, we would have a revolt," Dr. Jason Wallen explains, This distaste for accessing the materials via the WebBrain is not shared by all users, but it provides feedback, suggesting that changes could be made to optimize formatting to increase ease of use.
Certainly, the leaders in the TSDA, JCTSE, and Thoracic Surgery Residents Association (TSRA) who contributed to the development of the new curriculum are eager for this kind of feedback, welcoming all users to provide constructive criticism. Dr. Ara Vaporciyan, program director at the University of Texas MD Anderson Cancer Center, co-chair of the TSDA/JCTSE Curriculum Committee, and one of the 4 section editors for the curriculum itself, has been a key player in the development of the new curriculum.
States Dr. Vaporciyan, "I never expected this to be perfect on the first try and this is exactly the feedback we need. If we can start an honest conversation about the flaws in the system we can better allocate resources to fixing the most pervasive issues."
Despite the challenges that have been identified, Dr. Wallen remains positive about the curriculum, stating, "We are excited to have an electronic curriculum that our residents can access from anywhere that includes readings and multimedia content. We anticipate that following the curriculum will enhance our residents’ performance on future inservice exams and pave the path to certification."
Dr. Ikonomidis shares Dr. Wallen’s enthusiasm, summarizing that his "residents are constantly engaged and we believe that their learning efficiency has increased." Notes Dr. Schipper, "I am hopeful that this system will stay current and realize and appreciate the effort this has and will take to do so."
Certainly, the new curriculum has already been heavily utilized and appreciated by a number of training programs. While there will always be minor adjustments to be made, the innovators behind the Thoracic Surgery WebBrain and Moodle site are receptive to feedback and clearly dedicated to its ongoing growth.
Perhaps this article has encouraged those of you that aren’t using the curriculum regularly to incorporate it into your institution’s educational structure. For those of you already heavily engaged, perhaps you’ve been inspired to try some new strategies of implementation. Moreover, for all users of the system – trainees, educators, and coordinators – regardless of your program’s current level of use, the take-home message from the creators of the curriculum is that you are encouraged to provide feedback to allow evolution and improvement of the program.
The Trainee Experience
By Sanford M. Zeigler, M.D., Resident Medical Editor
Dr. Antonoff has detailed how different programs have chosen to implement the new curriculum. Of course, in order for the curriculum to work in any setting, people have to actually sit down, access the material, and learn from it. The modules need to be easily accessible, logically organized, and appropriate for the audience for which they are intended. To that end, the folks behind the new curriculum worked diligently to organize all the material into the WebBrain format, which attempts to organize the content by the logic of the human brain, using mind maps, and Moodle, which compartmentalizes the readings into individual curricular assignments that are served up on each resident’s personal Moodle page.
The overall architecture of the WebBrain is very organic; the "Brain" is split into four main branches, comprised of Foundations of Surgery, Cardiovascular, Thoracic, and Congenital headings. From these, the subject matter continues to divide and subdivide again until you reach a terminal branch, where the reader can open a number of different sources, both primary and secondary, on a given subject. The brains’ power lies in the connections that can be made across these fluid boundaries. An example can be seen with one reference that discusses MRI imaging of pericardial disease and cardiac masses. When this is selected, the thought leads the reader back to both the pericardial disease heading and the cardiac tumors heading. The subject selection feature allows the reader to wander throughout the entire WebBrain in a free-flowing but logical manner. Connections across different subjects are, at this point, still rarely utilized. The cross-referencing feature could be a boon for more junior integrated residents and general surgery residents if more of the basic concepts section were connected to cardiac and thoracic subjects, and could allow more self-directed reading to residents that find the time to do so. The WebBrain has some basic search functionality embedded in it that could be used to help understand specific clinical scenarios as they are encountered. Layered upon all of the subject matter are tags, which correspond to the weekly curricular readings. If trainees search for the tag "CV08," for example, they will be directed to each source with that tag, bringing the weekly source matter right to the front. Thus, the WebBrain can be used as a guide for casual reading, as a reference for a particular question or clinical scenario encountered in practice, and also as the source for material covered in didactic session.
The Moodle interface is the gateway to the WebBrain. While it may sound easier to deliver the contents of the WebBrain to each resident rather than go through Moodle, this interface serves two functions. In order to license the content for the curriculum, publishers of many of the textbooks require tight security to prevent unauthorized duplication of the materials. Moodle, by requiring a unique login to access the single WebBrain, provides that security and also allows the WebBrain to be modified in the Cloud, rather than at the level of the end-user. Moodle also provides other testing and tracking tools that have not been completely rolled out. Over the coming months, its full architecture will be used to incorporate quizzes, collaborative message boards, and personal tracking to help residents and their program directors ensure that the material is being covered adequately.
Nearly every resident and faculty member I asked about the new curriculum agreed that the update in content and delivery was badly needed. As an intern in an integrated cardiothoracic surgery program, I remember feeling very jealous of my general surgery colleagues’ access to the SCORE portal, which gave them an easily navigable curriculum accessible from anywhere, with instruction in everything from basic science and physiology to advanced surgical diagnosis and technique. The rollout of the Moodle interface and Web Brain content is the first step to a similar, comprehensive compendium of the necessary knowledge to master cardiac and thoracic surgery.
Response to the rollout has been generally positive from the residents. Most residents agree that the content provides a great sample of landmark papers, lecture videos, book chapters, and consensus statements. A fellow Stanford resident, George Dimeling, wrote: "I like the weekly focus and the topic organization. The content is good, but tough to access." The articles and chapters are often more up to date than printed textbooks, and, once the reader accesses the Brain, are instantly viewable with no further log ins or downloads.
Of course, for a busy resident, it may not always be possible to cover a long book chapter quickly, and the primary literature sometimes fails to cover an entire topic. Justin Schaffer, another Stanford resident, offered this thought: "There’s either a short paper or a 40-page book chapter – there is no solid review of the subject matter. They need something like the Doty lecture series and the TSRA publications to get you warmed up if you don’t have all that time." In fact, the WebBrain incorporates many chapters of the TSRA Cardiothoracic Review book, and the TSRA Clinical Scenarios were added to Moodle on Dec. 12.
One of the more common complaints had little to do with the content but more to do with delivery. At my own institution, most of our hospital computers run an outdated copy of Internet Explorer and have restricted access to update or install a new browser. The out-of-date or restricted software packages that are pervasive in institutional machines nullify many of the advantages of the WebBrain/Moodle format, as the majority of computers at Stanford Hospital cannot access the WebBrain. Furthermore, the WebBrain interface can be laggy and slow even with compatible software.
Others have complained that it is not always easy to find the readings, especially if a program does not follow one of the standardized curricula included with the rollout. First, one must find which content they are responsible for via departmental website or reference to the curricula. Next, the resident logs into the Moodle room, and the proper WebBrain course is launched, then each article for the week is selected and downloaded. Only after that can the content be read, saved, or printed. Using the tag function is helpful, but each time a tagged article is selected, the resident is taken away from the search and to the specific content area, away from the other material assigned for the week. Though it isn’t very difficult to navigate back to the search, all of the steps above make it a bit more of a process to access the material than is convenient for a resident trying to fit in readings between cases or while waiting to round. The new software is a definite improvement, yet still has not reached its full potential.
As Dr. Antonoff pointed out, one residency program has easily overcome this obstacle by consolidating and emailing the appropriate material every week. While the Moodle portion of the curriculum still sees limited functionality, this is probably the best solution to all of the problems. If the articles are in your mailbox, they are accessible anywhere, without the bother of logging in and navigating the Brain.
I discussed this with Dr. Jim Fann, who has been very involved in developing the curriculum, and he explained that direct delivery of the content to each resident had been part of the original goal. As mentioned before, however, publishers require that the delivery of the material is secure from unauthorized duplication. Within the context of an individual institution, those issues are less confining. While individual programs work to integrate the material into their own traditions, it may be worthwhile to designate a resident or office staff member to be in charge of distributing the week’s reading. One little-recognized feature of Moodle is the ability to upload calendars. Perhaps this area could be used by each program to keep the curricular and departmental calendars adjacent to the WebBrain link for easier access.
The recent changes in cardiothoracic surgical education have been myriad, and the rollout of the new curriculum is one of the most pervasive and visible signs of that change. The new curriculum has been designed and updated to reflect not only updates in medical knowledge and consensus, but also changes in the demographic of the cardiothoracic surgery resident and new paradigms in surgical education. The content and delivery systems, while not perfect, remain an ever improving work in progress, which aims to bring cardiothoracic surgical education into the collaborative, cloud based learning era while broadening its reach to both green cardiothoracic surgery interns and traditional fellows with a full general surgery residency behind them. All things considered, the rollout has been very successful, and as more functionality is added and bugs are worked out, things can only improve.
The Training Program Experience
By Mara B. Antonoff, M.D., Resident Medical Editor
The new thoracic surgery curriculum has arrived. Debuting this past summer, the curriculum resulted as a joint endeavor of several key organizations heavily vested in thoracic surgical education, with the aim of providing a web-based, multimedia repository of educational materials, accompanied by a formal structure and schedule of weekly topic coverage. Conceptually, the new curriculum has much to offer, with immense theoretical benefits to both the teacher and the student. But what about in practice? Now several months after its launch, the materials provided via the Moodle site and WebBrain have been accessed by the majority of training programs in this country.
How are these tools being utilized by the various programs, and what feedback do they have based on their experiences? The goal of this article will be to explore the various usage patterns of several institutions and their strategies for implementing the materials and integrating them with on-the-ground educational activities. Both the strengths and drawbacks from a programmatic standpoint will be addressed. As you read this article, perhaps you will be motivated to take another look at the curriculum, with new ideas as to how it might best suit your program’s needs.
At Oregon Health and Science University (OHSU), the new curriculum was officially introduced to the trainees and faculty members in a very formal and organized manner, heavily employing the provided instructional videos to become quickly oriented to the new system ("How-To: Utilizing the Thoracic Surgery Brain WebBrain," by Dr. Craig Baker; "How-To: Navigating Moodle," by Dr. Ara Vaporciyan; and "Overview of Teaching Cardiothoracic Surgery" – all available from the Moodle site, http:// jctse.mrooms.net, under Resources on the right hand column). OHSU Program Coordinator Jill Rose reports that she also received helpful information about accessing the curriculum when she attended the "Educate the Educators" course in June, sponsored by the Joint Council on Thoracic Surgery Education (JCTSE). Ms. Rose states, "Faculty and learners enthusiastically adopted this new curriculum and immediately put it to use at least twice a week." When the weekly emails come out, the relevant articles and videos are sent to the trainees and faculty members in the form of a reminder email, including links to the online videos and all related PDF’s as attachments. The residents and fellows then engage in formal curriculum review sessions with faculty, students, and mid-level practitioners – covering the cardiac topics on Monday mornings and thoracic topics on Friday mornings.
At Loma Linda University Health, the residents meet with a faculty moderator on a weekly basis to cover the materials related to the weekly Thoracic Surgery Curriculum topics. The style of presentation is left to the discretion of the attending surgeon, with the majority of the didactic sessions following an oral-board, case-based scenario format. Rather than directly accessing the Moodle pages and WebBrain site, the majority of the faculty and trainees have found that they prefer to have the materials provided to them as hard copies. Consequently, these materials are downloaded and distributed by the program coordinator on a weekly basis.
As with any new educational program, there may be a need for adjustments in initial plans and utilization based on early experiences. For the first few months following release of the curriculum, the Loma Linda group aimed to cover two topics per week – cardiac on Monday mornings and thoracic on Thursday mornings. However, with a tremendous amount of material available for each topic, they ultimately decided to transition to a single weekly session.
While the Loma Linda program has attempted to adhere to the schedule according to the weekly curriculum emails, other programs have chosen to utilize the available materials within the framework of alternative curricular schedules. Rose Haselden, the program coordinator at the Medical University of South Carolina (MUSC), explains that they created their own timeline for covering the materials, based on their specific needs and objectives.
Dr. John Ikonomidis, program director at MUSC, recalls being quick to adopt the new thoracic surgery curriculum. He states, "We were very impressed with its scope and current referencing. When it became available, we went through its entire corpus and divided it into sections which could be covered in 30 minutes. Then we developed a schedule where two topics (one adult or pediatric cardiac and one thoracic) would be covered in our weekly one-hour didactic sessions." Dr. Ikonomidis continues, "The residents are expected to read the material beforehand and faculty are assigned to quiz the residents during the session." In this way, the MUSC program has found a way to use the full breadth of materials, but tailoring the exact learning objectives for their trainees.
While some programs have taken to re-organizing the materials and producing hard copies of the resources for the residents, others have chosen to use the curriculum in its native structure, as a freestanding means of educational supplementation. At Washington University in St. Louis, the trainees are taught how to access the materials and encouraged to both follow the weekly thoracic surgery curriculum emails for independent reading and to utilize the immense resources available for investigating topics relevant to specific cases, conferences, and research interests. Dr. Marc Moon, program director at Washington University, explains that "we have not utilized the materials in any formal, assigned manner; rather, we choose to use the curriculum as a resource for independent study, encouraging our residents to access the multimedia materials both for at-home study and point-of-care reference." Dr. Moon expresses gratitude for the new curriculum, reporting that the faculty members "are grateful that our trainees are able to access these curricular materials through the WebBrain and Moodle, as they serve as an outstanding educational supplement to a high volume operative experience." Dr. Moon further emphasizes, "We find that the new curriculum functions as an excellent adjunct to our clinical teaching."
There are a number of proposed strengths to the new curriculum – its breadth, its ease of access, its correlation with the educational objectives of the American Board of Thoracic Surgery. But what are the benefits being identified from the level of the training program? Dr. Paul Schipper, program director at OHSU, expresses appreciation for the greater volume of material accessible by the trainees, as compared with the older curriculum previously sponsored by the Thoracic Surgery Directors Association (TSDA). States Dr. Schipper, "We’ve been using the TSDA emailed curriculum for several years. With the release of WebBrain, we’ve switched over and been very pleased. Residents are accessing the material and digging deeper into it than previously. In our teaching sessions, we are spending more time on applying the material and less time on explaining it, and I think this is good." Appreciation for the breadth and depth of the material was also noted by Dr. Moon, who identifies the program’s strengths as its ease of access, its large volume, and its applicability to a wide range of educational needs.
Despite the generally laudatory praise, there have been a few issues identified by the training programs that could benefit from some improvement.
Certainly, this is not surprising, as with any educational program, practice and feedback are necessary to optimize the execution for the users. Further, with a resource collection of such enormity, minor tweaks will likely continue in the background at all times in order to ensure ongoing quality-control.
In considering further revision, Dr. Wallen raises some concerns regarding format. He states that "all the moving around on the links makes people crazy," and, for this reason, at Loma Linda, all of the materials are distributed from the WebBrain to the faculty and trainees by the program coordinator. "Otherwise, we would have a revolt," Dr. Jason Wallen explains, This distaste for accessing the materials via the WebBrain is not shared by all users, but it provides feedback, suggesting that changes could be made to optimize formatting to increase ease of use.
Certainly, the leaders in the TSDA, JCTSE, and Thoracic Surgery Residents Association (TSRA) who contributed to the development of the new curriculum are eager for this kind of feedback, welcoming all users to provide constructive criticism. Dr. Ara Vaporciyan, program director at the University of Texas MD Anderson Cancer Center, co-chair of the TSDA/JCTSE Curriculum Committee, and one of the 4 section editors for the curriculum itself, has been a key player in the development of the new curriculum.
States Dr. Vaporciyan, "I never expected this to be perfect on the first try and this is exactly the feedback we need. If we can start an honest conversation about the flaws in the system we can better allocate resources to fixing the most pervasive issues."
Despite the challenges that have been identified, Dr. Wallen remains positive about the curriculum, stating, "We are excited to have an electronic curriculum that our residents can access from anywhere that includes readings and multimedia content. We anticipate that following the curriculum will enhance our residents’ performance on future inservice exams and pave the path to certification."
Dr. Ikonomidis shares Dr. Wallen’s enthusiasm, summarizing that his "residents are constantly engaged and we believe that their learning efficiency has increased." Notes Dr. Schipper, "I am hopeful that this system will stay current and realize and appreciate the effort this has and will take to do so."
Certainly, the new curriculum has already been heavily utilized and appreciated by a number of training programs. While there will always be minor adjustments to be made, the innovators behind the Thoracic Surgery WebBrain and Moodle site are receptive to feedback and clearly dedicated to its ongoing growth.
Perhaps this article has encouraged those of you that aren’t using the curriculum regularly to incorporate it into your institution’s educational structure. For those of you already heavily engaged, perhaps you’ve been inspired to try some new strategies of implementation. Moreover, for all users of the system – trainees, educators, and coordinators – regardless of your program’s current level of use, the take-home message from the creators of the curriculum is that you are encouraged to provide feedback to allow evolution and improvement of the program.
The Trainee Experience
By Sanford M. Zeigler, M.D., Resident Medical Editor
Dr. Antonoff has detailed how different programs have chosen to implement the new curriculum. Of course, in order for the curriculum to work in any setting, people have to actually sit down, access the material, and learn from it. The modules need to be easily accessible, logically organized, and appropriate for the audience for which they are intended. To that end, the folks behind the new curriculum worked diligently to organize all the material into the WebBrain format, which attempts to organize the content by the logic of the human brain, using mind maps, and Moodle, which compartmentalizes the readings into individual curricular assignments that are served up on each resident’s personal Moodle page.
The overall architecture of the WebBrain is very organic; the "Brain" is split into four main branches, comprised of Foundations of Surgery, Cardiovascular, Thoracic, and Congenital headings. From these, the subject matter continues to divide and subdivide again until you reach a terminal branch, where the reader can open a number of different sources, both primary and secondary, on a given subject. The brains’ power lies in the connections that can be made across these fluid boundaries. An example can be seen with one reference that discusses MRI imaging of pericardial disease and cardiac masses. When this is selected, the thought leads the reader back to both the pericardial disease heading and the cardiac tumors heading. The subject selection feature allows the reader to wander throughout the entire WebBrain in a free-flowing but logical manner. Connections across different subjects are, at this point, still rarely utilized. The cross-referencing feature could be a boon for more junior integrated residents and general surgery residents if more of the basic concepts section were connected to cardiac and thoracic subjects, and could allow more self-directed reading to residents that find the time to do so. The WebBrain has some basic search functionality embedded in it that could be used to help understand specific clinical scenarios as they are encountered. Layered upon all of the subject matter are tags, which correspond to the weekly curricular readings. If trainees search for the tag "CV08," for example, they will be directed to each source with that tag, bringing the weekly source matter right to the front. Thus, the WebBrain can be used as a guide for casual reading, as a reference for a particular question or clinical scenario encountered in practice, and also as the source for material covered in didactic session.
The Moodle interface is the gateway to the WebBrain. While it may sound easier to deliver the contents of the WebBrain to each resident rather than go through Moodle, this interface serves two functions. In order to license the content for the curriculum, publishers of many of the textbooks require tight security to prevent unauthorized duplication of the materials. Moodle, by requiring a unique login to access the single WebBrain, provides that security and also allows the WebBrain to be modified in the Cloud, rather than at the level of the end-user. Moodle also provides other testing and tracking tools that have not been completely rolled out. Over the coming months, its full architecture will be used to incorporate quizzes, collaborative message boards, and personal tracking to help residents and their program directors ensure that the material is being covered adequately.
Nearly every resident and faculty member I asked about the new curriculum agreed that the update in content and delivery was badly needed. As an intern in an integrated cardiothoracic surgery program, I remember feeling very jealous of my general surgery colleagues’ access to the SCORE portal, which gave them an easily navigable curriculum accessible from anywhere, with instruction in everything from basic science and physiology to advanced surgical diagnosis and technique. The rollout of the Moodle interface and Web Brain content is the first step to a similar, comprehensive compendium of the necessary knowledge to master cardiac and thoracic surgery.
Response to the rollout has been generally positive from the residents. Most residents agree that the content provides a great sample of landmark papers, lecture videos, book chapters, and consensus statements. A fellow Stanford resident, George Dimeling, wrote: "I like the weekly focus and the topic organization. The content is good, but tough to access." The articles and chapters are often more up to date than printed textbooks, and, once the reader accesses the Brain, are instantly viewable with no further log ins or downloads.
Of course, for a busy resident, it may not always be possible to cover a long book chapter quickly, and the primary literature sometimes fails to cover an entire topic. Justin Schaffer, another Stanford resident, offered this thought: "There’s either a short paper or a 40-page book chapter – there is no solid review of the subject matter. They need something like the Doty lecture series and the TSRA publications to get you warmed up if you don’t have all that time." In fact, the WebBrain incorporates many chapters of the TSRA Cardiothoracic Review book, and the TSRA Clinical Scenarios were added to Moodle on Dec. 12.
One of the more common complaints had little to do with the content but more to do with delivery. At my own institution, most of our hospital computers run an outdated copy of Internet Explorer and have restricted access to update or install a new browser. The out-of-date or restricted software packages that are pervasive in institutional machines nullify many of the advantages of the WebBrain/Moodle format, as the majority of computers at Stanford Hospital cannot access the WebBrain. Furthermore, the WebBrain interface can be laggy and slow even with compatible software.
Others have complained that it is not always easy to find the readings, especially if a program does not follow one of the standardized curricula included with the rollout. First, one must find which content they are responsible for via departmental website or reference to the curricula. Next, the resident logs into the Moodle room, and the proper WebBrain course is launched, then each article for the week is selected and downloaded. Only after that can the content be read, saved, or printed. Using the tag function is helpful, but each time a tagged article is selected, the resident is taken away from the search and to the specific content area, away from the other material assigned for the week. Though it isn’t very difficult to navigate back to the search, all of the steps above make it a bit more of a process to access the material than is convenient for a resident trying to fit in readings between cases or while waiting to round. The new software is a definite improvement, yet still has not reached its full potential.
As Dr. Antonoff pointed out, one residency program has easily overcome this obstacle by consolidating and emailing the appropriate material every week. While the Moodle portion of the curriculum still sees limited functionality, this is probably the best solution to all of the problems. If the articles are in your mailbox, they are accessible anywhere, without the bother of logging in and navigating the Brain.
I discussed this with Dr. Jim Fann, who has been very involved in developing the curriculum, and he explained that direct delivery of the content to each resident had been part of the original goal. As mentioned before, however, publishers require that the delivery of the material is secure from unauthorized duplication. Within the context of an individual institution, those issues are less confining. While individual programs work to integrate the material into their own traditions, it may be worthwhile to designate a resident or office staff member to be in charge of distributing the week’s reading. One little-recognized feature of Moodle is the ability to upload calendars. Perhaps this area could be used by each program to keep the curricular and departmental calendars adjacent to the WebBrain link for easier access.
The recent changes in cardiothoracic surgical education have been myriad, and the rollout of the new curriculum is one of the most pervasive and visible signs of that change. The new curriculum has been designed and updated to reflect not only updates in medical knowledge and consensus, but also changes in the demographic of the cardiothoracic surgery resident and new paradigms in surgical education. The content and delivery systems, while not perfect, remain an ever improving work in progress, which aims to bring cardiothoracic surgical education into the collaborative, cloud based learning era while broadening its reach to both green cardiothoracic surgery interns and traditional fellows with a full general surgery residency behind them. All things considered, the rollout has been very successful, and as more functionality is added and bugs are worked out, things can only improve.

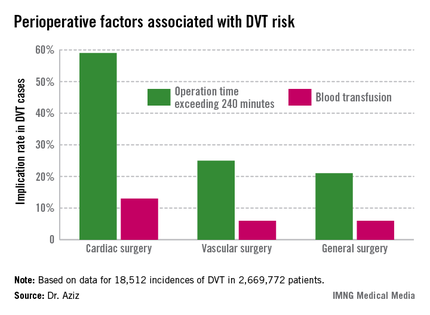
DVT risk higher in cardiac and vascular surgery
WASHINGTON - Cardiac and vascular surgery patients are at higher risk for deep vein thrombosis than are general surgery patients, according to data presented at the annual clinical congress of the American College of Surgeons.
In a retrospective analysis of 2,669,772 patients with a median age of 64 years, 43% of whom were males, in the ACS-National Surgical Quality Improvement Program (NSQIP) during 2005-2009, Dr. Faisal Aziz of Penn State Hershey (Pa.) Heart and Vascular Institute and his colleagues sought to determine the actual rate of deep vein thrombosis (DVT) during revascularization procedures, compared with general surgery.
The researchers sorted patients according to DVT risk factors such as age, gender, body mass index over 40 kg/m2, and whether the surgery was acute. They then assessed intraoperative factors such as total time to completion and the American Society of Anesthesiology score. They then considered the postoperative factors associated with DVT, such as blood transfusions, return to the operating room, deep wound infection, cardiac arrest, and mortality.
There were 18,512 incidences of DVT, equaling 0.69% of all patients studied. Of those, 0.66% occurred during general surgery, 2.08% occurred during cardiac surgery, and 1% occurred during vascular surgery.
"The implications of our study are that, contrary to popular belief, the incidence of postop DVT is actually higher after cardiac surgery and vascular surgery procedures," he said.
The cardiac surgery procedures associated with the highest DVT incidence rate were tricuspid valve replacement (8%), thoracic endovascular aortic repair (5%), thoracic aortic graft replacement (4%), and pericardial window (4%).
In a comparison of cardiac procedures, tricuspid valve replacement vs. aortic valve replacement had a risk ratio of 3.5 (P < .001). In tricuspid valve replacement vs. coronary artery bypass, the former had a risk ratio of 11.24 (P < .001).
Vascular surgeries with the highest DVT incidence rates were peripheral bypass (1%), amputation (trans-metatarsal, 0.75%; below knee, 1%; above the knee, 1%), and ruptured aortic aneurysms (3.5%).
Comparatively, in ruptured endovascular aneurysm repair (EVAR) vs. elective EVAR, the risk ratio was 3.55 (P < .001). In abdominal aortic aneurysm (AAA) repair, ruptured vs. elective surgeries had a risk ratio of 2.37 (P < .001).
Compared with 80% of general surgery patients, 74% of cardiac surgery patients were 70 years or older (relative risk, 1.12; P = .13); 86% of vascular surgery patients were 70 years or older (RR, 1.1; P < .05).
Male gender was an associated risk factor in 49% of general surgery patients, compared with 70% for cardiac patients (RR, 1.4; P < .001) and 51% for vascular patients (RR, 1.1; P < .001).
Intra- and postoperative factors associated with DVT risk included operation times exceeding 240 minutes and previous DVT. Compared with 21% of general surgery patients, operation time was implicated in 59% of cardiac surgery patients (relative risk, 2.72; P < .001) and 25% of vascular surgery patients (RR, 1.14; P <.001). Blood transfusions affected 13% of cardiac surgery patients (RR, 2.3; P < .001), 6% of vascular surgery patients (RR, 1.3; P < .001), and 6% of general surgery patients.
Compared with 24% for general surgery patients, returning to the operating room was implicated in 27% of cardiac patients (RR, 1.4; P = .27) and 32% of vascular surgery patients (RR, 1.3; P < .001).
"Procedures and perioperative factors associated with high risk of postoperative DVT should be identified, and adequate DVT prophylaxis should be ensured for these patients," Dr. Aziz concluded.
He had no disclosures.
WASHINGTON - Cardiac and vascular surgery patients are at higher risk for deep vein thrombosis than are general surgery patients, according to data presented at the annual clinical congress of the American College of Surgeons.
In a retrospective analysis of 2,669,772 patients with a median age of 64 years, 43% of whom were males, in the ACS-National Surgical Quality Improvement Program (NSQIP) during 2005-2009, Dr. Faisal Aziz of Penn State Hershey (Pa.) Heart and Vascular Institute and his colleagues sought to determine the actual rate of deep vein thrombosis (DVT) during revascularization procedures, compared with general surgery.
The researchers sorted patients according to DVT risk factors such as age, gender, body mass index over 40 kg/m2, and whether the surgery was acute. They then assessed intraoperative factors such as total time to completion and the American Society of Anesthesiology score. They then considered the postoperative factors associated with DVT, such as blood transfusions, return to the operating room, deep wound infection, cardiac arrest, and mortality.
There were 18,512 incidences of DVT, equaling 0.69% of all patients studied. Of those, 0.66% occurred during general surgery, 2.08% occurred during cardiac surgery, and 1% occurred during vascular surgery.
"The implications of our study are that, contrary to popular belief, the incidence of postop DVT is actually higher after cardiac surgery and vascular surgery procedures," he said.
The cardiac surgery procedures associated with the highest DVT incidence rate were tricuspid valve replacement (8%), thoracic endovascular aortic repair (5%), thoracic aortic graft replacement (4%), and pericardial window (4%).
In a comparison of cardiac procedures, tricuspid valve replacement vs. aortic valve replacement had a risk ratio of 3.5 (P < .001). In tricuspid valve replacement vs. coronary artery bypass, the former had a risk ratio of 11.24 (P < .001).
Vascular surgeries with the highest DVT incidence rates were peripheral bypass (1%), amputation (trans-metatarsal, 0.75%; below knee, 1%; above the knee, 1%), and ruptured aortic aneurysms (3.5%).
Comparatively, in ruptured endovascular aneurysm repair (EVAR) vs. elective EVAR, the risk ratio was 3.55 (P < .001). In abdominal aortic aneurysm (AAA) repair, ruptured vs. elective surgeries had a risk ratio of 2.37 (P < .001).
Compared with 80% of general surgery patients, 74% of cardiac surgery patients were 70 years or older (relative risk, 1.12; P = .13); 86% of vascular surgery patients were 70 years or older (RR, 1.1; P < .05).
Male gender was an associated risk factor in 49% of general surgery patients, compared with 70% for cardiac patients (RR, 1.4; P < .001) and 51% for vascular patients (RR, 1.1; P < .001).
Intra- and postoperative factors associated with DVT risk included operation times exceeding 240 minutes and previous DVT. Compared with 21% of general surgery patients, operation time was implicated in 59% of cardiac surgery patients (relative risk, 2.72; P < .001) and 25% of vascular surgery patients (RR, 1.14; P <.001). Blood transfusions affected 13% of cardiac surgery patients (RR, 2.3; P < .001), 6% of vascular surgery patients (RR, 1.3; P < .001), and 6% of general surgery patients.
Compared with 24% for general surgery patients, returning to the operating room was implicated in 27% of cardiac patients (RR, 1.4; P = .27) and 32% of vascular surgery patients (RR, 1.3; P < .001).
"Procedures and perioperative factors associated with high risk of postoperative DVT should be identified, and adequate DVT prophylaxis should be ensured for these patients," Dr. Aziz concluded.
He had no disclosures.
WASHINGTON - Cardiac and vascular surgery patients are at higher risk for deep vein thrombosis than are general surgery patients, according to data presented at the annual clinical congress of the American College of Surgeons.
In a retrospective analysis of 2,669,772 patients with a median age of 64 years, 43% of whom were males, in the ACS-National Surgical Quality Improvement Program (NSQIP) during 2005-2009, Dr. Faisal Aziz of Penn State Hershey (Pa.) Heart and Vascular Institute and his colleagues sought to determine the actual rate of deep vein thrombosis (DVT) during revascularization procedures, compared with general surgery.
The researchers sorted patients according to DVT risk factors such as age, gender, body mass index over 40 kg/m2, and whether the surgery was acute. They then assessed intraoperative factors such as total time to completion and the American Society of Anesthesiology score. They then considered the postoperative factors associated with DVT, such as blood transfusions, return to the operating room, deep wound infection, cardiac arrest, and mortality.
There were 18,512 incidences of DVT, equaling 0.69% of all patients studied. Of those, 0.66% occurred during general surgery, 2.08% occurred during cardiac surgery, and 1% occurred during vascular surgery.
"The implications of our study are that, contrary to popular belief, the incidence of postop DVT is actually higher after cardiac surgery and vascular surgery procedures," he said.
The cardiac surgery procedures associated with the highest DVT incidence rate were tricuspid valve replacement (8%), thoracic endovascular aortic repair (5%), thoracic aortic graft replacement (4%), and pericardial window (4%).
In a comparison of cardiac procedures, tricuspid valve replacement vs. aortic valve replacement had a risk ratio of 3.5 (P < .001). In tricuspid valve replacement vs. coronary artery bypass, the former had a risk ratio of 11.24 (P < .001).
Vascular surgeries with the highest DVT incidence rates were peripheral bypass (1%), amputation (trans-metatarsal, 0.75%; below knee, 1%; above the knee, 1%), and ruptured aortic aneurysms (3.5%).
Comparatively, in ruptured endovascular aneurysm repair (EVAR) vs. elective EVAR, the risk ratio was 3.55 (P < .001). In abdominal aortic aneurysm (AAA) repair, ruptured vs. elective surgeries had a risk ratio of 2.37 (P < .001).
Compared with 80% of general surgery patients, 74% of cardiac surgery patients were 70 years or older (relative risk, 1.12; P = .13); 86% of vascular surgery patients were 70 years or older (RR, 1.1; P < .05).
Male gender was an associated risk factor in 49% of general surgery patients, compared with 70% for cardiac patients (RR, 1.4; P < .001) and 51% for vascular patients (RR, 1.1; P < .001).
Intra- and postoperative factors associated with DVT risk included operation times exceeding 240 minutes and previous DVT. Compared with 21% of general surgery patients, operation time was implicated in 59% of cardiac surgery patients (relative risk, 2.72; P < .001) and 25% of vascular surgery patients (RR, 1.14; P <.001). Blood transfusions affected 13% of cardiac surgery patients (RR, 2.3; P < .001), 6% of vascular surgery patients (RR, 1.3; P < .001), and 6% of general surgery patients.
Compared with 24% for general surgery patients, returning to the operating room was implicated in 27% of cardiac patients (RR, 1.4; P = .27) and 32% of vascular surgery patients (RR, 1.3; P < .001).
"Procedures and perioperative factors associated with high risk of postoperative DVT should be identified, and adequate DVT prophylaxis should be ensured for these patients," Dr. Aziz concluded.
He had no disclosures.
Budget, short-term SGR fix signed
Physicians will get a 0.5% raise in Medicare pay on Jan. 1, thanks to a last-minute legislative fix to the Sustainable Growth Rate formula signed into law by President Obama on Dec. 26.
The Pathway for SGR Reform Act of 2013 was attached as an amendment to the Bipartisan Budget Agreement of 2013. The budget deal, brokered by Sen. Patty Murray (D-Wash.) and Rep. Paul Ryan (R-Wis.), passed the House on Dec. 12 and the Senate on Dec. 18. The Congressional Budget Office estimated that the temporary fix would cost $3.3 billion in 2014 and a total of $7.3 billion through 2023. It would be paid for by cutting Medicaid payments for hospital-based charity care and to long-term care hospitals.

The law also extends the 2% sequestration cut to Medicare payments by 2 years, to 2023.
It encourages the CMS to simplify physicians’ administrative burden by more closely coordinating quality measure requirements and giving doctors timely feedback.
The law extends funding for a variety of other health-related federal programs for an additional 3 months, including for Area Agencies on Aging. Finally, the law delays enforcement of the "two-midnight rule" until October 2014. The goal of the rule is to cut down on hospitals using observation status to keep from admitting patients. Hospitals have until Oct. 1, 2014, to adjust to the new policy, which requires admission if a physician thinks a patient will need a stay longer than 48 hours.
Congress was expected to consider a permanent replacement for the SGR when it returned on Jan. 6.
Physicians will get a 0.5% raise in Medicare pay on Jan. 1, thanks to a last-minute legislative fix to the Sustainable Growth Rate formula signed into law by President Obama on Dec. 26.
The Pathway for SGR Reform Act of 2013 was attached as an amendment to the Bipartisan Budget Agreement of 2013. The budget deal, brokered by Sen. Patty Murray (D-Wash.) and Rep. Paul Ryan (R-Wis.), passed the House on Dec. 12 and the Senate on Dec. 18. The Congressional Budget Office estimated that the temporary fix would cost $3.3 billion in 2014 and a total of $7.3 billion through 2023. It would be paid for by cutting Medicaid payments for hospital-based charity care and to long-term care hospitals.
The law also extends the 2% sequestration cut to Medicare payments by 2 years, to 2023.
It encourages the CMS to simplify physicians’ administrative burden by more closely coordinating quality measure requirements and giving doctors timely feedback.
The law extends funding for a variety of other health-related federal programs for an additional 3 months, including for Area Agencies on Aging. Finally, the law delays enforcement of the "two-midnight rule" until October 2014. The goal of the rule is to cut down on hospitals using observation status to keep from admitting patients. Hospitals have until Oct. 1, 2014, to adjust to the new policy, which requires admission if a physician thinks a patient will need a stay longer than 48 hours.
Congress was expected to consider a permanent replacement for the SGR when it returned on Jan. 6.
Physicians will get a 0.5% raise in Medicare pay on Jan. 1, thanks to a last-minute legislative fix to the Sustainable Growth Rate formula signed into law by President Obama on Dec. 26.
The Pathway for SGR Reform Act of 2013 was attached as an amendment to the Bipartisan Budget Agreement of 2013. The budget deal, brokered by Sen. Patty Murray (D-Wash.) and Rep. Paul Ryan (R-Wis.), passed the House on Dec. 12 and the Senate on Dec. 18. The Congressional Budget Office estimated that the temporary fix would cost $3.3 billion in 2014 and a total of $7.3 billion through 2023. It would be paid for by cutting Medicaid payments for hospital-based charity care and to long-term care hospitals.
The law also extends the 2% sequestration cut to Medicare payments by 2 years, to 2023.
It encourages the CMS to simplify physicians’ administrative burden by more closely coordinating quality measure requirements and giving doctors timely feedback.
The law extends funding for a variety of other health-related federal programs for an additional 3 months, including for Area Agencies on Aging. Finally, the law delays enforcement of the "two-midnight rule" until October 2014. The goal of the rule is to cut down on hospitals using observation status to keep from admitting patients. Hospitals have until Oct. 1, 2014, to adjust to the new policy, which requires admission if a physician thinks a patient will need a stay longer than 48 hours.
Congress was expected to consider a permanent replacement for the SGR when it returned on Jan. 6.

Mitral valve repair seen as no better than replacement
Mitral valve repair was no better than chordal-sparing mitral valve replacement in the first randomized clinical trial attempting to settle the controversy over which procedure is superior for treating functional ischemic mitral regurgitation, which was simultaneously reported at the annual scientific sessions of the American Heart Association and online in the New England Journal of Medicine.
In the past few years, the use of mitral valve repair has far exceeded that of mitral valve replacement for this indication, largely on the basis of reports that the repair procedure yields lower operative mortality, improved left ventricular function, and higher long-term survival rates. In particular, a 2011 meta-analysis found a 35% lower relative risk of death in the long term with mitral valve repair, compared with replacement, said Dr. Michael A. Acker and his associates in the Cardiothoracic Surgical Trials Network (CTSN).
But in their multicenter study directly comparing the two procedures in 251 patients with severe functional ischemic mitral regurgitation, there was no significant difference between the surgeries in left ventricular end-systolic volume index at 1 year, nor in mortality at either 1 month or 1 year.
Moreover, study participants who underwent mitral valve repair showed a disturbing excess in the rate of recurrence of mitral regurgitation at 1 year, with a rate that was 30 percentage points higher than that among patients who underwent mitral valve replacement. "This lack of durability in correction of mitral regurgitation is disconcerting, given its reported association with further progression and long-term negative outcomes," said Dr. Acker of the division of cardiovascular surgery, University of Pennsylvania, Philadelphia, and his associates.
Functional ischemic mitral regurgitation, a "high-prevalence" condition affecting an estimated 2-3 million Americans, differs from primary degenerative mitral regurgitation in that the valve leaflets themselves remain normal while the defect occurs in the myocardium. "Ischemic mitral regurgitation is a consequence of adverse left ventricular remodeling after myocardial injury, with enlargement of the left ventricular chamber and mitral annulus, apical and lateral migration of the papillary muscles, leaflet retethering, and reduced closing forces. These processes lead to malcoaptation of the leaflets and variable degrees of mitral regurgitation that can fluctuate dynamically as a function of volume status, afterload, heart rhythm, and residual ischemia," the researchers said.
Current guidelines recommend mitral valve repair or chordal-sparing mitral valve replacement for severe regurgitation unresponsive to medical therapy, but do not specify which procedure is preferred because there is no conclusive evidence demonstrating the superiority of one over the other. "Recently, the field has embraced mitral valve repair over replacement," even without such evidence, Dr. Acker and his colleagues said.
The CTSN performed this study at 22 medical centers to assess the relative benefits of the two surgeries, with 126 patients randomized to undergo mitral valve repair and 125 to undergo replacement that included complete preservation of the subvalvular apparatus.
The primary endpoint was the degree of LV reverse remodeling, as measured by the left ventricular end-systolic volume index (LVESVI) on transthoracic echocardiography, at 1 year. The mean LVESVI was not significantly different between the repair group (54.6 mL per square meter) and the replacement group (60.7 mL per square meter), reflecting decreases of 6.6 mL per square meter and 6.8 mL per square meter, respectively, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1312808]).
The median between group difference in the change in LVESVI score after surgery also was not clinically significant. However, 32.6% of patients who underwent mitral valve repair had a recurrence of regurgitation within 1 year, compared with only 2.3% of those who had mitral valve replacement. Three patients in the repair group required reoperation, compared with none in the replacement group.
There were no significant differences in cumulative mortality, 30-day postoperative mortality, or 1-year mortality between the two groups, and no significant difference in a composite endpoint of major adverse cardiac or cerebrovascular events.
Rates of serious adverse events were similar, and the durations of hospitalization were similar between the two study groups, as were rates of readmission. All measures of quality of life and functional status on two assessment tools were similar.
"Our findings contradict much of the published literature on this topic, which reports several advantages to mitral valve repair over replacement, including lower operative mortality, improved left ventricular function, and higher rates of long-term survival," Dr. Acker and his associates noted.
The evolution of the valve replacement procedure, which now includes chordal sparing, "may account for the improved results we observed, as compared with previous studies, since the retention of the internal architectural support of the left ventricle may preserve contractile efficiency and reduce left ventricular dilatation and dysfunction," they said.
Dr. Acker reported no conflicts.
Mitral valve repair was no better than chordal-sparing mitral valve replacement in the first randomized clinical trial attempting to settle the controversy over which procedure is superior for treating functional ischemic mitral regurgitation, which was simultaneously reported at the annual scientific sessions of the American Heart Association and online in the New England Journal of Medicine.
In the past few years, the use of mitral valve repair has far exceeded that of mitral valve replacement for this indication, largely on the basis of reports that the repair procedure yields lower operative mortality, improved left ventricular function, and higher long-term survival rates. In particular, a 2011 meta-analysis found a 35% lower relative risk of death in the long term with mitral valve repair, compared with replacement, said Dr. Michael A. Acker and his associates in the Cardiothoracic Surgical Trials Network (CTSN).
But in their multicenter study directly comparing the two procedures in 251 patients with severe functional ischemic mitral regurgitation, there was no significant difference between the surgeries in left ventricular end-systolic volume index at 1 year, nor in mortality at either 1 month or 1 year.
Moreover, study participants who underwent mitral valve repair showed a disturbing excess in the rate of recurrence of mitral regurgitation at 1 year, with a rate that was 30 percentage points higher than that among patients who underwent mitral valve replacement. "This lack of durability in correction of mitral regurgitation is disconcerting, given its reported association with further progression and long-term negative outcomes," said Dr. Acker of the division of cardiovascular surgery, University of Pennsylvania, Philadelphia, and his associates.
Functional ischemic mitral regurgitation, a "high-prevalence" condition affecting an estimated 2-3 million Americans, differs from primary degenerative mitral regurgitation in that the valve leaflets themselves remain normal while the defect occurs in the myocardium. "Ischemic mitral regurgitation is a consequence of adverse left ventricular remodeling after myocardial injury, with enlargement of the left ventricular chamber and mitral annulus, apical and lateral migration of the papillary muscles, leaflet retethering, and reduced closing forces. These processes lead to malcoaptation of the leaflets and variable degrees of mitral regurgitation that can fluctuate dynamically as a function of volume status, afterload, heart rhythm, and residual ischemia," the researchers said.
Current guidelines recommend mitral valve repair or chordal-sparing mitral valve replacement for severe regurgitation unresponsive to medical therapy, but do not specify which procedure is preferred because there is no conclusive evidence demonstrating the superiority of one over the other. "Recently, the field has embraced mitral valve repair over replacement," even without such evidence, Dr. Acker and his colleagues said.
The CTSN performed this study at 22 medical centers to assess the relative benefits of the two surgeries, with 126 patients randomized to undergo mitral valve repair and 125 to undergo replacement that included complete preservation of the subvalvular apparatus.
The primary endpoint was the degree of LV reverse remodeling, as measured by the left ventricular end-systolic volume index (LVESVI) on transthoracic echocardiography, at 1 year. The mean LVESVI was not significantly different between the repair group (54.6 mL per square meter) and the replacement group (60.7 mL per square meter), reflecting decreases of 6.6 mL per square meter and 6.8 mL per square meter, respectively, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1312808]).
The median between group difference in the change in LVESVI score after surgery also was not clinically significant. However, 32.6% of patients who underwent mitral valve repair had a recurrence of regurgitation within 1 year, compared with only 2.3% of those who had mitral valve replacement. Three patients in the repair group required reoperation, compared with none in the replacement group.
There were no significant differences in cumulative mortality, 30-day postoperative mortality, or 1-year mortality between the two groups, and no significant difference in a composite endpoint of major adverse cardiac or cerebrovascular events.
Rates of serious adverse events were similar, and the durations of hospitalization were similar between the two study groups, as were rates of readmission. All measures of quality of life and functional status on two assessment tools were similar.
"Our findings contradict much of the published literature on this topic, which reports several advantages to mitral valve repair over replacement, including lower operative mortality, improved left ventricular function, and higher rates of long-term survival," Dr. Acker and his associates noted.
The evolution of the valve replacement procedure, which now includes chordal sparing, "may account for the improved results we observed, as compared with previous studies, since the retention of the internal architectural support of the left ventricle may preserve contractile efficiency and reduce left ventricular dilatation and dysfunction," they said.
Dr. Acker reported no conflicts.
Mitral valve repair was no better than chordal-sparing mitral valve replacement in the first randomized clinical trial attempting to settle the controversy over which procedure is superior for treating functional ischemic mitral regurgitation, which was simultaneously reported at the annual scientific sessions of the American Heart Association and online in the New England Journal of Medicine.
In the past few years, the use of mitral valve repair has far exceeded that of mitral valve replacement for this indication, largely on the basis of reports that the repair procedure yields lower operative mortality, improved left ventricular function, and higher long-term survival rates. In particular, a 2011 meta-analysis found a 35% lower relative risk of death in the long term with mitral valve repair, compared with replacement, said Dr. Michael A. Acker and his associates in the Cardiothoracic Surgical Trials Network (CTSN).
But in their multicenter study directly comparing the two procedures in 251 patients with severe functional ischemic mitral regurgitation, there was no significant difference between the surgeries in left ventricular end-systolic volume index at 1 year, nor in mortality at either 1 month or 1 year.
Moreover, study participants who underwent mitral valve repair showed a disturbing excess in the rate of recurrence of mitral regurgitation at 1 year, with a rate that was 30 percentage points higher than that among patients who underwent mitral valve replacement. "This lack of durability in correction of mitral regurgitation is disconcerting, given its reported association with further progression and long-term negative outcomes," said Dr. Acker of the division of cardiovascular surgery, University of Pennsylvania, Philadelphia, and his associates.
Functional ischemic mitral regurgitation, a "high-prevalence" condition affecting an estimated 2-3 million Americans, differs from primary degenerative mitral regurgitation in that the valve leaflets themselves remain normal while the defect occurs in the myocardium. "Ischemic mitral regurgitation is a consequence of adverse left ventricular remodeling after myocardial injury, with enlargement of the left ventricular chamber and mitral annulus, apical and lateral migration of the papillary muscles, leaflet retethering, and reduced closing forces. These processes lead to malcoaptation of the leaflets and variable degrees of mitral regurgitation that can fluctuate dynamically as a function of volume status, afterload, heart rhythm, and residual ischemia," the researchers said.
Current guidelines recommend mitral valve repair or chordal-sparing mitral valve replacement for severe regurgitation unresponsive to medical therapy, but do not specify which procedure is preferred because there is no conclusive evidence demonstrating the superiority of one over the other. "Recently, the field has embraced mitral valve repair over replacement," even without such evidence, Dr. Acker and his colleagues said.
The CTSN performed this study at 22 medical centers to assess the relative benefits of the two surgeries, with 126 patients randomized to undergo mitral valve repair and 125 to undergo replacement that included complete preservation of the subvalvular apparatus.
The primary endpoint was the degree of LV reverse remodeling, as measured by the left ventricular end-systolic volume index (LVESVI) on transthoracic echocardiography, at 1 year. The mean LVESVI was not significantly different between the repair group (54.6 mL per square meter) and the replacement group (60.7 mL per square meter), reflecting decreases of 6.6 mL per square meter and 6.8 mL per square meter, respectively, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1312808]).
The median between group difference in the change in LVESVI score after surgery also was not clinically significant. However, 32.6% of patients who underwent mitral valve repair had a recurrence of regurgitation within 1 year, compared with only 2.3% of those who had mitral valve replacement. Three patients in the repair group required reoperation, compared with none in the replacement group.
There were no significant differences in cumulative mortality, 30-day postoperative mortality, or 1-year mortality between the two groups, and no significant difference in a composite endpoint of major adverse cardiac or cerebrovascular events.
Rates of serious adverse events were similar, and the durations of hospitalization were similar between the two study groups, as were rates of readmission. All measures of quality of life and functional status on two assessment tools were similar.
"Our findings contradict much of the published literature on this topic, which reports several advantages to mitral valve repair over replacement, including lower operative mortality, improved left ventricular function, and higher rates of long-term survival," Dr. Acker and his associates noted.
The evolution of the valve replacement procedure, which now includes chordal sparing, "may account for the improved results we observed, as compared with previous studies, since the retention of the internal architectural support of the left ventricle may preserve contractile efficiency and reduce left ventricular dilatation and dysfunction," they said.
Dr. Acker reported no conflicts.
Major Finding: The primary end point ? the degree of LV reverse remodeling, as measured by the left ventricular end-systolic volume index on transthoracic echocardiography at 1 year ? was not significantly different between the repair group (54.6 mL per square meter) and the replacement group (60.7 mL per square meter).
Data Source: A randomized clinical trial involving 126 patients with severe functional ischemic mitral regurgitation who underwent mitral valve repair and 125 who underwent chordal-sparing mitral valve replacement, and who were followed for 1 year.
Disclosures: This study was funded by the National Heart, Lung, and Blood Institute, the National Institute of Neurological Diseases and Stroke, and the Canadian Institutes of Health Research. Dr. Acker and his associates reported no financial conflicts of interest.
CoreValve Extreme Risk study is promising
SAN FRANCISCO – Trans-catheter aortic valve replacement with the self-expanding CoreValve in patients at extreme surgical risk significantly reduced the rate of death or major stroke at 1 year, from 43% to 26%, in a 487-patient pivotal trial.
The CoreValve Extreme Risk study gathered data from a registry of patients with symptomatic severe aortic stenosis who attempted an iliofemoral implantation procedure with the CoreValve at 40 U.S. sites. Results were compared with an "objective performance goal" derived from two sources: a meta-analysis of five contemporary balloon valvuloplasty series that found a 43% mortality and major stroke rate at 1 year, and the 1-year rate from the PARTNER B trial in inoperable patients (Placement of Aortic Transcatheter Valves, Cohort B), which was 50% but had a lower confidence bound of 43%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The performance-goal comparison was necessary in the current study because randomizing these patients to medical therapy in a control group is no longer an acceptable option in the United States, Dr. Jeffrey J. Popma said at the Transcatheter Cardiovascular Therapeutics annual meeting.
The 1-year all-cause mortality rate was 24%, and the cardiovascular mortality was 18%, reported Dr. Popma, professor of medicine at Harvard Medical School, Boston.
Two percent of patients developed a major stroke within 1 month and 4% did so within 1 year.
Data from a continued access study involving another 830 extreme-risk patients who received the CoreValve through an iliofemoral approach are showing even better results, with a 16% rate of mortality or major stroke at 6 months.

Among secondary endpoints at 1 year in the main study, 7% of patients developed any kind of stroke, 2% had an MI, 2% needed reintervention, 41% had bleeding that met Valve Academic Research Consortium criteria, 8% had major vascular complications, and 27% required implantation of a permanent pacemaker, Dr. Popma reported at the meeting, cosponsored by the American College of Cardiology. Ninety percent of patients improved by at least one New York Heart Association functional class and 60% improved by at least two classes at 1 year of follow-up.
Paravalvular regurgitation of any severity was seen in 53% of patients 1 month after implantation and in 33% at 1 year. Moderate paravalvular leakage (PVL) affected 9% at 1 month and 4% at 1 year, and severe PVL affected 1.6% at 1 month and no patients at 1 year, Dr. Popma said. Among the 11% of patients with moderate PVL at 1 month, 80% of those who survived to 1 year had a reduction in leakage over time.
"We believe that’s why we did not find an association in the study between mild or moderate aortic regurgitation with respect to late-term mortality," though mortality risk was substantially higher with severe regurgitation, he said. One-year mortality rates were 86% with severe PVL and 24% with either moderate or mild PVL, compared with 18% in patients with no PVL.
The improvement in PVL rates over time may be due to use of CT angiography to select appropriate valve sizes for patients and continued expansion of the self-expanding frame over time. "That’s a remarkable finding, and it needs to be confirmed," Dr. Popma said.
The study focused on patients whose severe frailty, comorbidity, or disability put them at extreme risk of at least a 50% chance of death or irreversible morbidity within 30 days had they undergone surgical aortic valve replacement. A second U.S. pivotal trial of the CoreValve is focusing on patients at high (but not extreme) risk.
Most of the sites in the study had no experience with CoreValve before this study, Dr. Michael J. Mack noted at a press briefing. "The results are outstanding, but especially putting it in that light," said Dr. Mack, a member of the steering committee for the PARTNER trial.
Dr. Popma reported financial ties with Medtronic, which sponsored the study and makes CoreValve.
This is a brilliantly executed, rigorously performed study. After doing sham-control studies, as we did, in these extreme-risk patients, it’s difficult to do a randomized trial. I think these investigators did they best that they could. Using a performance goal standard was the right thing to do.

|
| Dr. Martin B. Leon |
I think that the results are good. It’s always difficult to compare study to study. They’re at different points in time, and we learn things over time. The CoreValve device is a lower-profile device, so there were fewer vascular complications, there was less major bleeding. Those things, in fact, can have an impact on 1-year mortality. The overall 1-year mortality was lower than in PARTNER. In PARTNER by intention to treat the mortality rate was 30.7%, and in the CoreValve study it was in the low 20% range. I think that that’s encouraging.
The stroke rates are encouraging. The pacemaker rates are predictable; it’s a by-product of the specific device. The importance of that is debatable, but it’s not really a concern. It was anticipated.
The paravalvular leakage (PVL) rate is interesting. Many studies with CoreValve suggest that either moderate or severe PVL is associated with an increase in late mortality, if not at 1 year later. It’s not a huge sample size; maybe over time with different definitions of PVL we’d begin to see that.
I am surprised by the 30-day to 1-year data that suggest a reduced PVL rate. I can understand how a self-expanding platform might change in the first 30 days; I can’t quite understand how it would change between 1 month and 12 months in a way that PVL would go down.
Martin B. Leon, M.D., is director of the Center for Interventional Vascular Therapy at Columbia University, New York, and served as principal investigator of the PARTNER trial of the competing Sapien valve.
This is a brilliantly executed, rigorously performed study. After doing sham-control studies, as we did, in these extreme-risk patients, it’s difficult to do a randomized trial. I think these investigators did they best that they could. Using a performance goal standard was the right thing to do.
|
|
| Dr. Martin B. Leon |
I think that the results are good. It’s always difficult to compare study to study. They’re at different points in time, and we learn things over time. The CoreValve device is a lower-profile device, so there were fewer vascular complications, there was less major bleeding. Those things, in fact, can have an impact on 1-year mortality. The overall 1-year mortality was lower than in PARTNER. In PARTNER by intention to treat the mortality rate was 30.7%, and in the CoreValve study it was in the low 20% range. I think that that’s encouraging.
The stroke rates are encouraging. The pacemaker rates are predictable; it’s a by-product of the specific device. The importance of that is debatable, but it’s not really a concern. It was anticipated.
The paravalvular leakage (PVL) rate is interesting. Many studies with CoreValve suggest that either moderate or severe PVL is associated with an increase in late mortality, if not at 1 year later. It’s not a huge sample size; maybe over time with different definitions of PVL we’d begin to see that.
I am surprised by the 30-day to 1-year data that suggest a reduced PVL rate. I can understand how a self-expanding platform might change in the first 30 days; I can’t quite understand how it would change between 1 month and 12 months in a way that PVL would go down.
Martin B. Leon, M.D., is director of the Center for Interventional Vascular Therapy at Columbia University, New York, and served as principal investigator of the PARTNER trial of the competing Sapien valve.
This is a brilliantly executed, rigorously performed study. After doing sham-control studies, as we did, in these extreme-risk patients, it’s difficult to do a randomized trial. I think these investigators did they best that they could. Using a performance goal standard was the right thing to do.
|
|
| Dr. Martin B. Leon |
I think that the results are good. It’s always difficult to compare study to study. They’re at different points in time, and we learn things over time. The CoreValve device is a lower-profile device, so there were fewer vascular complications, there was less major bleeding. Those things, in fact, can have an impact on 1-year mortality. The overall 1-year mortality was lower than in PARTNER. In PARTNER by intention to treat the mortality rate was 30.7%, and in the CoreValve study it was in the low 20% range. I think that that’s encouraging.
The stroke rates are encouraging. The pacemaker rates are predictable; it’s a by-product of the specific device. The importance of that is debatable, but it’s not really a concern. It was anticipated.
The paravalvular leakage (PVL) rate is interesting. Many studies with CoreValve suggest that either moderate or severe PVL is associated with an increase in late mortality, if not at 1 year later. It’s not a huge sample size; maybe over time with different definitions of PVL we’d begin to see that.
I am surprised by the 30-day to 1-year data that suggest a reduced PVL rate. I can understand how a self-expanding platform might change in the first 30 days; I can’t quite understand how it would change between 1 month and 12 months in a way that PVL would go down.
Martin B. Leon, M.D., is director of the Center for Interventional Vascular Therapy at Columbia University, New York, and served as principal investigator of the PARTNER trial of the competing Sapien valve.
SAN FRANCISCO – Trans-catheter aortic valve replacement with the self-expanding CoreValve in patients at extreme surgical risk significantly reduced the rate of death or major stroke at 1 year, from 43% to 26%, in a 487-patient pivotal trial.
The CoreValve Extreme Risk study gathered data from a registry of patients with symptomatic severe aortic stenosis who attempted an iliofemoral implantation procedure with the CoreValve at 40 U.S. sites. Results were compared with an "objective performance goal" derived from two sources: a meta-analysis of five contemporary balloon valvuloplasty series that found a 43% mortality and major stroke rate at 1 year, and the 1-year rate from the PARTNER B trial in inoperable patients (Placement of Aortic Transcatheter Valves, Cohort B), which was 50% but had a lower confidence bound of 43%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The performance-goal comparison was necessary in the current study because randomizing these patients to medical therapy in a control group is no longer an acceptable option in the United States, Dr. Jeffrey J. Popma said at the Transcatheter Cardiovascular Therapeutics annual meeting.
The 1-year all-cause mortality rate was 24%, and the cardiovascular mortality was 18%, reported Dr. Popma, professor of medicine at Harvard Medical School, Boston.
Two percent of patients developed a major stroke within 1 month and 4% did so within 1 year.
Data from a continued access study involving another 830 extreme-risk patients who received the CoreValve through an iliofemoral approach are showing even better results, with a 16% rate of mortality or major stroke at 6 months.
Among secondary endpoints at 1 year in the main study, 7% of patients developed any kind of stroke, 2% had an MI, 2% needed reintervention, 41% had bleeding that met Valve Academic Research Consortium criteria, 8% had major vascular complications, and 27% required implantation of a permanent pacemaker, Dr. Popma reported at the meeting, cosponsored by the American College of Cardiology. Ninety percent of patients improved by at least one New York Heart Association functional class and 60% improved by at least two classes at 1 year of follow-up.
Paravalvular regurgitation of any severity was seen in 53% of patients 1 month after implantation and in 33% at 1 year. Moderate paravalvular leakage (PVL) affected 9% at 1 month and 4% at 1 year, and severe PVL affected 1.6% at 1 month and no patients at 1 year, Dr. Popma said. Among the 11% of patients with moderate PVL at 1 month, 80% of those who survived to 1 year had a reduction in leakage over time.
"We believe that’s why we did not find an association in the study between mild or moderate aortic regurgitation with respect to late-term mortality," though mortality risk was substantially higher with severe regurgitation, he said. One-year mortality rates were 86% with severe PVL and 24% with either moderate or mild PVL, compared with 18% in patients with no PVL.
The improvement in PVL rates over time may be due to use of CT angiography to select appropriate valve sizes for patients and continued expansion of the self-expanding frame over time. "That’s a remarkable finding, and it needs to be confirmed," Dr. Popma said.
The study focused on patients whose severe frailty, comorbidity, or disability put them at extreme risk of at least a 50% chance of death or irreversible morbidity within 30 days had they undergone surgical aortic valve replacement. A second U.S. pivotal trial of the CoreValve is focusing on patients at high (but not extreme) risk.
Most of the sites in the study had no experience with CoreValve before this study, Dr. Michael J. Mack noted at a press briefing. "The results are outstanding, but especially putting it in that light," said Dr. Mack, a member of the steering committee for the PARTNER trial.
Dr. Popma reported financial ties with Medtronic, which sponsored the study and makes CoreValve.
SAN FRANCISCO – Trans-catheter aortic valve replacement with the self-expanding CoreValve in patients at extreme surgical risk significantly reduced the rate of death or major stroke at 1 year, from 43% to 26%, in a 487-patient pivotal trial.
The CoreValve Extreme Risk study gathered data from a registry of patients with symptomatic severe aortic stenosis who attempted an iliofemoral implantation procedure with the CoreValve at 40 U.S. sites. Results were compared with an "objective performance goal" derived from two sources: a meta-analysis of five contemporary balloon valvuloplasty series that found a 43% mortality and major stroke rate at 1 year, and the 1-year rate from the PARTNER B trial in inoperable patients (Placement of Aortic Transcatheter Valves, Cohort B), which was 50% but had a lower confidence bound of 43%.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The performance-goal comparison was necessary in the current study because randomizing these patients to medical therapy in a control group is no longer an acceptable option in the United States, Dr. Jeffrey J. Popma said at the Transcatheter Cardiovascular Therapeutics annual meeting.
The 1-year all-cause mortality rate was 24%, and the cardiovascular mortality was 18%, reported Dr. Popma, professor of medicine at Harvard Medical School, Boston.
Two percent of patients developed a major stroke within 1 month and 4% did so within 1 year.
Data from a continued access study involving another 830 extreme-risk patients who received the CoreValve through an iliofemoral approach are showing even better results, with a 16% rate of mortality or major stroke at 6 months.
Among secondary endpoints at 1 year in the main study, 7% of patients developed any kind of stroke, 2% had an MI, 2% needed reintervention, 41% had bleeding that met Valve Academic Research Consortium criteria, 8% had major vascular complications, and 27% required implantation of a permanent pacemaker, Dr. Popma reported at the meeting, cosponsored by the American College of Cardiology. Ninety percent of patients improved by at least one New York Heart Association functional class and 60% improved by at least two classes at 1 year of follow-up.
Paravalvular regurgitation of any severity was seen in 53% of patients 1 month after implantation and in 33% at 1 year. Moderate paravalvular leakage (PVL) affected 9% at 1 month and 4% at 1 year, and severe PVL affected 1.6% at 1 month and no patients at 1 year, Dr. Popma said. Among the 11% of patients with moderate PVL at 1 month, 80% of those who survived to 1 year had a reduction in leakage over time.
"We believe that’s why we did not find an association in the study between mild or moderate aortic regurgitation with respect to late-term mortality," though mortality risk was substantially higher with severe regurgitation, he said. One-year mortality rates were 86% with severe PVL and 24% with either moderate or mild PVL, compared with 18% in patients with no PVL.
The improvement in PVL rates over time may be due to use of CT angiography to select appropriate valve sizes for patients and continued expansion of the self-expanding frame over time. "That’s a remarkable finding, and it needs to be confirmed," Dr. Popma said.
The study focused on patients whose severe frailty, comorbidity, or disability put them at extreme risk of at least a 50% chance of death or irreversible morbidity within 30 days had they undergone surgical aortic valve replacement. A second U.S. pivotal trial of the CoreValve is focusing on patients at high (but not extreme) risk.
Most of the sites in the study had no experience with CoreValve before this study, Dr. Michael J. Mack noted at a press briefing. "The results are outstanding, but especially putting it in that light," said Dr. Mack, a member of the steering committee for the PARTNER trial.
Dr. Popma reported financial ties with Medtronic, which sponsored the study and makes CoreValve.
Major finding: The rate of all-cause mortality or stroke at 1 year was 26%, compared with an objective performance goal of 43%.
Data source: Study of registry data on 487 patients with symptomatic severe aortic stenosis and attempted CoreValve implantation via iliofemoral access.
Disclosures: Dr. Popma reported financial associations with Medtronic, which sponsored the study and makes CoreValve, and with six other companies.

Ten-year outcomes for ablation in atrial fibrillation impressive
DALLAS - At 10 years after their procedures, the rate of freedom from atrial fibrillation and atrial tachycardia was 87% in 513 patients who underwent pulmonary vein antrum isolation for drug-refractory paroxysmal atrial fibrillation at a single high-volume center in Texas.
After a single radiofrequency ablation procedure, 59% of patients remained arrhythmia free for the full decade and another 28% of the cohort was rendered arrhythmia free after an average of two repeat ablation procedures, Dr. Pasquale Santangeli reported at the American Heart Association scientific sessions.
A particularly striking finding in this series was the low 4% rate of recurrent atrial arrhythmias during years 3-6 of follow-up, and the 5% rate between years 6 and 10. Those late recurrence rates are much lower than those in previous reports from other centers. The likely explanation lies in the fact that electrophysiologists at the Austin center routinely extended their pulmonary vein antrum isolation to the posterior wall and performed empiric isolation of the superior vena cava in all patients. Other centers reporting long-term outcomes generally performed segmental or less extensive antral isolation, observed Dr. Santangeli of the Texas Cardiac Arrhythmia Institute at St. David?s Medical Center in Austin, Tex., and the University of Foggia (Italy).
Follow-up, including Holter monitoring, was performed every 3 months during year 1 and every 6-9 months thereafter. The rate of recurrent atrial arrhythmia was 21% at 1 year and 11% during years 1-3.
All patients with a recurrence were offered a repeat procedure, and 74% of them underwent repeat ablation. Reconnection in the pulmonary vein antrum was found in 31% of patients at the time of their first repeat procedure and in no patients who underwent a second repeat ablation.
Patients with recurrent atrial arrhythmia after two failed procedures underwent a high-dose isoproterenol challenge to identify nonpulmonary vein triggers, which were then targeted for ablation. The predictors of very late recurrence due to nonpulmonary vein triggers were increased left atrial size, obesity, and female gender.
Dr. Santangeli reported having no financial conflicts in connection with this study, which was honored as the top presentation by an early career investigator in the core area of heart rhythm disorders and resuscitation science at the annual meeting.
DALLAS - At 10 years after their procedures, the rate of freedom from atrial fibrillation and atrial tachycardia was 87% in 513 patients who underwent pulmonary vein antrum isolation for drug-refractory paroxysmal atrial fibrillation at a single high-volume center in Texas.
After a single radiofrequency ablation procedure, 59% of patients remained arrhythmia free for the full decade and another 28% of the cohort was rendered arrhythmia free after an average of two repeat ablation procedures, Dr. Pasquale Santangeli reported at the American Heart Association scientific sessions.
A particularly striking finding in this series was the low 4% rate of recurrent atrial arrhythmias during years 3-6 of follow-up, and the 5% rate between years 6 and 10. Those late recurrence rates are much lower than those in previous reports from other centers. The likely explanation lies in the fact that electrophysiologists at the Austin center routinely extended their pulmonary vein antrum isolation to the posterior wall and performed empiric isolation of the superior vena cava in all patients. Other centers reporting long-term outcomes generally performed segmental or less extensive antral isolation, observed Dr. Santangeli of the Texas Cardiac Arrhythmia Institute at St. David?s Medical Center in Austin, Tex., and the University of Foggia (Italy).
Follow-up, including Holter monitoring, was performed every 3 months during year 1 and every 6-9 months thereafter. The rate of recurrent atrial arrhythmia was 21% at 1 year and 11% during years 1-3.
All patients with a recurrence were offered a repeat procedure, and 74% of them underwent repeat ablation. Reconnection in the pulmonary vein antrum was found in 31% of patients at the time of their first repeat procedure and in no patients who underwent a second repeat ablation.
Patients with recurrent atrial arrhythmia after two failed procedures underwent a high-dose isoproterenol challenge to identify nonpulmonary vein triggers, which were then targeted for ablation. The predictors of very late recurrence due to nonpulmonary vein triggers were increased left atrial size, obesity, and female gender.
Dr. Santangeli reported having no financial conflicts in connection with this study, which was honored as the top presentation by an early career investigator in the core area of heart rhythm disorders and resuscitation science at the annual meeting.
DALLAS - At 10 years after their procedures, the rate of freedom from atrial fibrillation and atrial tachycardia was 87% in 513 patients who underwent pulmonary vein antrum isolation for drug-refractory paroxysmal atrial fibrillation at a single high-volume center in Texas.
After a single radiofrequency ablation procedure, 59% of patients remained arrhythmia free for the full decade and another 28% of the cohort was rendered arrhythmia free after an average of two repeat ablation procedures, Dr. Pasquale Santangeli reported at the American Heart Association scientific sessions.
A particularly striking finding in this series was the low 4% rate of recurrent atrial arrhythmias during years 3-6 of follow-up, and the 5% rate between years 6 and 10. Those late recurrence rates are much lower than those in previous reports from other centers. The likely explanation lies in the fact that electrophysiologists at the Austin center routinely extended their pulmonary vein antrum isolation to the posterior wall and performed empiric isolation of the superior vena cava in all patients. Other centers reporting long-term outcomes generally performed segmental or less extensive antral isolation, observed Dr. Santangeli of the Texas Cardiac Arrhythmia Institute at St. David?s Medical Center in Austin, Tex., and the University of Foggia (Italy).
Follow-up, including Holter monitoring, was performed every 3 months during year 1 and every 6-9 months thereafter. The rate of recurrent atrial arrhythmia was 21% at 1 year and 11% during years 1-3.
All patients with a recurrence were offered a repeat procedure, and 74% of them underwent repeat ablation. Reconnection in the pulmonary vein antrum was found in 31% of patients at the time of their first repeat procedure and in no patients who underwent a second repeat ablation.
Patients with recurrent atrial arrhythmia after two failed procedures underwent a high-dose isoproterenol challenge to identify nonpulmonary vein triggers, which were then targeted for ablation. The predictors of very late recurrence due to nonpulmonary vein triggers were increased left atrial size, obesity, and female gender.
Dr. Santangeli reported having no financial conflicts in connection with this study, which was honored as the top presentation by an early career investigator in the core area of heart rhythm disorders and resuscitation science at the annual meeting.
AT THE AHA SCIENTIFIC SESSIONS
Major finding: A decade after 513 patients underwent extensive pulmonary vein antrum isolation for drug-resistant paroxysmal atrial fibrillation, 87% were free of atrial fibrillation/atrial tachycardia, including 59% with single-procedure arrhythmia-free survival.
Data source: A retrospective case series involving 513 patients who underwent pulmonary vein antrum isolation during 2000-2002 at a single high-volume center.
Disclosures: The presenter reported having no financial conflicts.
Transradial PCI seems feasible in women
SAN FRANCISCO – Rates of bleeding or vascular complications in women undergoing percutaneous coronary intervention were 59% lower using radial access, compared with femoral access, a difference that did not reach statistical significance in a randomized study of 1,787 patients.
Bleeding or vascular complications within 72 hours or at hospital discharge were seen in 1.2% of 345 women who had transradial percutaneous coronary intervention (PCI) and 2.9% of 345 women who had transfemoral PCI, Dr. Sunil V. Rao reported at the Trans-catheter Cardiovascular Therapeutics annual meeting.

Although that difference was not statistically significant in this prespecified analysis of patients who actually underwent PCI, the rate of bleeding and vascular complications was significantly lower for the group randomized to radial access in an analysis of the whole cohort, regardless of whether they had PCI or just diagnostic catheterization. Bleeding and vascular complication rates were 0.6% in those randomized to radial access and 1.7% in those randomized to femoral access.
In both the PCI cohort and the total cohort, significantly more women in the radial group needed to cross over to femoral access for PCI compared with the crossover rate in the femoral group. In the PCI cohort, 6.1% of the radial group crossed over, as did 1.7% of the femoral group. In the total cohort, crossover was needed in 6.7% of the radial group and 1.9% of the femoral group, said Dr. Rao of Duke University, Durham, N.C. The main reason for crossover from radial to femoral access was radial artery spasm, in 43% of cases.
The Study of Access Site for Enhancement of PCI for Women (SAFE-PCI) leveraged data from the National Cardiovascular Data Registry’s CathPCI Registry from 60 institutions on adult women undergoing elective or urgent PCI or undergoing diagnostic angiography to evaluate ischemic symptoms with the possibility of PCI. The primary outcome measure was Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding events and vascular complications requiring intervention.
The investigators had planned to randomize 3,000 women to obtain 1,800 who underwent PCI, but a routine review after randomizing 1,120 patients suggested that the trial would be too small to show a difference because of lower-than-expected bleeding rates. Because no harm was noted in either the radial or femoral group, the investigators continued until they had enough patients for a quality-of-life substudy, then prematurely discontinued the trial.
The reduction in bleeding with the radial approach was similar to reductions seen in previous studies, Dr. Rao said at the meeting, cosponsored by the American College of Cardiology. The conversion rate from radial to femoral access was similar to the 7.6% rate reported in a prior trial (Lancet 2011;377:1409-20).
Compared with men, women have an increased risk for bleeding from antithrombotic therapy and from femoral access for PCI. Radial access can decrease bleeding risk, but trans-radial PCI has been less common in women, in part because they have smaller radial arteries.
The current trial’s results suggest that "an initial strategy of radial access is reasonable and may be preferred by some operators for women undergoing cardiac catheterization or PCI, with the recognition that a proportion of patients will require conversion to femoral access," he said.
Women preferred the radial approach over femoral access in the study, he added.
The results could be looked at as a glass half empty or half full, Dr. Roxana Mehran said as the discussant of the study at the meeting. She served on the executive committee of the SAFE-PCI trial.
In the eyes of a purist statistician, the results show no significant evidence that radial access prevents bleeding or vascular complications, the primary endpoint, said Dr. Mehran, professor of medicine and director of interventional cardiovascular research at Mount Sinai School of Medicine, New York.
From a clinician’s viewpoint, however, the estimates of benefit from radial access in the overall cohort and the PCI cohort were similar, yielding approximately a 60% reduction in bleeding with radial access, she noted. "The study provides evidence, albeit not conclusive, for greater efficacy with radial access in women," she said.
The crossover rates suggest that for every bleeding event or vascular complication prevented in the radial access group, three patients would cross over. "While there’s a higher crossover from [the] radial to the femoral approach, it’s reasonable and intuitive to begin with the radial approach in women," she said, "especially in those women at high risk for bleeding."
Dr. Rao has been a consultant for the Medicines Co., which helped fund the trial, and for AstraZeneca. Dr. Mehran reported financial associations with these companies and with Abbott Vascular and Daiichi-Sankyo/Eli Lilly & Co., which also funded the trial. Other funders of the study included Terumo Medical, Medtronic, ACIST Medical Systems, and Guerbet. Dr. Mehran also reported financial associations with nine other medical companies.
I don’t think we have the data to say that this is a positive study or that we should change our practice because of these results. It’s an incomplete study, so we really don’t have the data. We need to think about why we didn’t have the anticipated enrollment and why the bleeding rate was lower than expected in the femoral access group. Those are the things that I think led to the futility. But it’s not really a negative trial. We simply don’t know whether radial access will be better in high-risk women undergoing PCI. It’s promising, and it makes all the sense in the world because of the bleeding risk in women.
Dr. Alice K. Jacobs is a professor of medicine and director of the cardiac catheterization laboratory and interventional cardiology at Boston University. She gave these remarks at a press briefing. Dr. Jacobs reported having no relevant financial disclosures.
I don’t think we have the data to say that this is a positive study or that we should change our practice because of these results. It’s an incomplete study, so we really don’t have the data. We need to think about why we didn’t have the anticipated enrollment and why the bleeding rate was lower than expected in the femoral access group. Those are the things that I think led to the futility. But it’s not really a negative trial. We simply don’t know whether radial access will be better in high-risk women undergoing PCI. It’s promising, and it makes all the sense in the world because of the bleeding risk in women.
Dr. Alice K. Jacobs is a professor of medicine and director of the cardiac catheterization laboratory and interventional cardiology at Boston University. She gave these remarks at a press briefing. Dr. Jacobs reported having no relevant financial disclosures.
I don’t think we have the data to say that this is a positive study or that we should change our practice because of these results. It’s an incomplete study, so we really don’t have the data. We need to think about why we didn’t have the anticipated enrollment and why the bleeding rate was lower than expected in the femoral access group. Those are the things that I think led to the futility. But it’s not really a negative trial. We simply don’t know whether radial access will be better in high-risk women undergoing PCI. It’s promising, and it makes all the sense in the world because of the bleeding risk in women.
Dr. Alice K. Jacobs is a professor of medicine and director of the cardiac catheterization laboratory and interventional cardiology at Boston University. She gave these remarks at a press briefing. Dr. Jacobs reported having no relevant financial disclosures.
SAN FRANCISCO – Rates of bleeding or vascular complications in women undergoing percutaneous coronary intervention were 59% lower using radial access, compared with femoral access, a difference that did not reach statistical significance in a randomized study of 1,787 patients.
Bleeding or vascular complications within 72 hours or at hospital discharge were seen in 1.2% of 345 women who had transradial percutaneous coronary intervention (PCI) and 2.9% of 345 women who had transfemoral PCI, Dr. Sunil V. Rao reported at the Trans-catheter Cardiovascular Therapeutics annual meeting.
Although that difference was not statistically significant in this prespecified analysis of patients who actually underwent PCI, the rate of bleeding and vascular complications was significantly lower for the group randomized to radial access in an analysis of the whole cohort, regardless of whether they had PCI or just diagnostic catheterization. Bleeding and vascular complication rates were 0.6% in those randomized to radial access and 1.7% in those randomized to femoral access.
In both the PCI cohort and the total cohort, significantly more women in the radial group needed to cross over to femoral access for PCI compared with the crossover rate in the femoral group. In the PCI cohort, 6.1% of the radial group crossed over, as did 1.7% of the femoral group. In the total cohort, crossover was needed in 6.7% of the radial group and 1.9% of the femoral group, said Dr. Rao of Duke University, Durham, N.C. The main reason for crossover from radial to femoral access was radial artery spasm, in 43% of cases.
The Study of Access Site for Enhancement of PCI for Women (SAFE-PCI) leveraged data from the National Cardiovascular Data Registry’s CathPCI Registry from 60 institutions on adult women undergoing elective or urgent PCI or undergoing diagnostic angiography to evaluate ischemic symptoms with the possibility of PCI. The primary outcome measure was Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding events and vascular complications requiring intervention.
The investigators had planned to randomize 3,000 women to obtain 1,800 who underwent PCI, but a routine review after randomizing 1,120 patients suggested that the trial would be too small to show a difference because of lower-than-expected bleeding rates. Because no harm was noted in either the radial or femoral group, the investigators continued until they had enough patients for a quality-of-life substudy, then prematurely discontinued the trial.
The reduction in bleeding with the radial approach was similar to reductions seen in previous studies, Dr. Rao said at the meeting, cosponsored by the American College of Cardiology. The conversion rate from radial to femoral access was similar to the 7.6% rate reported in a prior trial (Lancet 2011;377:1409-20).
Compared with men, women have an increased risk for bleeding from antithrombotic therapy and from femoral access for PCI. Radial access can decrease bleeding risk, but trans-radial PCI has been less common in women, in part because they have smaller radial arteries.
The current trial’s results suggest that "an initial strategy of radial access is reasonable and may be preferred by some operators for women undergoing cardiac catheterization or PCI, with the recognition that a proportion of patients will require conversion to femoral access," he said.
Women preferred the radial approach over femoral access in the study, he added.
The results could be looked at as a glass half empty or half full, Dr. Roxana Mehran said as the discussant of the study at the meeting. She served on the executive committee of the SAFE-PCI trial.
In the eyes of a purist statistician, the results show no significant evidence that radial access prevents bleeding or vascular complications, the primary endpoint, said Dr. Mehran, professor of medicine and director of interventional cardiovascular research at Mount Sinai School of Medicine, New York.
From a clinician’s viewpoint, however, the estimates of benefit from radial access in the overall cohort and the PCI cohort were similar, yielding approximately a 60% reduction in bleeding with radial access, she noted. "The study provides evidence, albeit not conclusive, for greater efficacy with radial access in women," she said.
The crossover rates suggest that for every bleeding event or vascular complication prevented in the radial access group, three patients would cross over. "While there’s a higher crossover from [the] radial to the femoral approach, it’s reasonable and intuitive to begin with the radial approach in women," she said, "especially in those women at high risk for bleeding."
Dr. Rao has been a consultant for the Medicines Co., which helped fund the trial, and for AstraZeneca. Dr. Mehran reported financial associations with these companies and with Abbott Vascular and Daiichi-Sankyo/Eli Lilly & Co., which also funded the trial. Other funders of the study included Terumo Medical, Medtronic, ACIST Medical Systems, and Guerbet. Dr. Mehran also reported financial associations with nine other medical companies.
SAN FRANCISCO – Rates of bleeding or vascular complications in women undergoing percutaneous coronary intervention were 59% lower using radial access, compared with femoral access, a difference that did not reach statistical significance in a randomized study of 1,787 patients.
Bleeding or vascular complications within 72 hours or at hospital discharge were seen in 1.2% of 345 women who had transradial percutaneous coronary intervention (PCI) and 2.9% of 345 women who had transfemoral PCI, Dr. Sunil V. Rao reported at the Trans-catheter Cardiovascular Therapeutics annual meeting.
Although that difference was not statistically significant in this prespecified analysis of patients who actually underwent PCI, the rate of bleeding and vascular complications was significantly lower for the group randomized to radial access in an analysis of the whole cohort, regardless of whether they had PCI or just diagnostic catheterization. Bleeding and vascular complication rates were 0.6% in those randomized to radial access and 1.7% in those randomized to femoral access.
In both the PCI cohort and the total cohort, significantly more women in the radial group needed to cross over to femoral access for PCI compared with the crossover rate in the femoral group. In the PCI cohort, 6.1% of the radial group crossed over, as did 1.7% of the femoral group. In the total cohort, crossover was needed in 6.7% of the radial group and 1.9% of the femoral group, said Dr. Rao of Duke University, Durham, N.C. The main reason for crossover from radial to femoral access was radial artery spasm, in 43% of cases.
The Study of Access Site for Enhancement of PCI for Women (SAFE-PCI) leveraged data from the National Cardiovascular Data Registry’s CathPCI Registry from 60 institutions on adult women undergoing elective or urgent PCI or undergoing diagnostic angiography to evaluate ischemic symptoms with the possibility of PCI. The primary outcome measure was Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding events and vascular complications requiring intervention.
The investigators had planned to randomize 3,000 women to obtain 1,800 who underwent PCI, but a routine review after randomizing 1,120 patients suggested that the trial would be too small to show a difference because of lower-than-expected bleeding rates. Because no harm was noted in either the radial or femoral group, the investigators continued until they had enough patients for a quality-of-life substudy, then prematurely discontinued the trial.
The reduction in bleeding with the radial approach was similar to reductions seen in previous studies, Dr. Rao said at the meeting, cosponsored by the American College of Cardiology. The conversion rate from radial to femoral access was similar to the 7.6% rate reported in a prior trial (Lancet 2011;377:1409-20).
Compared with men, women have an increased risk for bleeding from antithrombotic therapy and from femoral access for PCI. Radial access can decrease bleeding risk, but trans-radial PCI has been less common in women, in part because they have smaller radial arteries.
The current trial’s results suggest that "an initial strategy of radial access is reasonable and may be preferred by some operators for women undergoing cardiac catheterization or PCI, with the recognition that a proportion of patients will require conversion to femoral access," he said.
Women preferred the radial approach over femoral access in the study, he added.
The results could be looked at as a glass half empty or half full, Dr. Roxana Mehran said as the discussant of the study at the meeting. She served on the executive committee of the SAFE-PCI trial.
In the eyes of a purist statistician, the results show no significant evidence that radial access prevents bleeding or vascular complications, the primary endpoint, said Dr. Mehran, professor of medicine and director of interventional cardiovascular research at Mount Sinai School of Medicine, New York.
From a clinician’s viewpoint, however, the estimates of benefit from radial access in the overall cohort and the PCI cohort were similar, yielding approximately a 60% reduction in bleeding with radial access, she noted. "The study provides evidence, albeit not conclusive, for greater efficacy with radial access in women," she said.
The crossover rates suggest that for every bleeding event or vascular complication prevented in the radial access group, three patients would cross over. "While there’s a higher crossover from [the] radial to the femoral approach, it’s reasonable and intuitive to begin with the radial approach in women," she said, "especially in those women at high risk for bleeding."
Dr. Rao has been a consultant for the Medicines Co., which helped fund the trial, and for AstraZeneca. Dr. Mehran reported financial associations with these companies and with Abbott Vascular and Daiichi-Sankyo/Eli Lilly & Co., which also funded the trial. Other funders of the study included Terumo Medical, Medtronic, ACIST Medical Systems, and Guerbet. Dr. Mehran also reported financial associations with nine other medical companies.
Major finding: Rates of bleeding or vascular complications were 1.2% using radial access and 2.9% using femoral access in the PCI subgroup and 6.7% and 1.9%, respectively, in the entire cohort.
Data source: A randomized study of 1,787 women undergoing definite or possible PCI at 60 institutions.
Disclosures: Dr. Rao has been a consultant for the Medicines Co., which helped fund the trial, and for AstraZeneca. Dr. Mehran reported financial associations with these companies and with Abbott Vascular and Daiichi-Sankyo/Eli Lilly & Co., which also funded the trial. Other funders of the study included Abbott Vascular, Daiichi-Sankyo/Eli Lilly & Co., Terumo Medical, Medtronic, ACIST Medical Systems, and Guerbet. Dr. Mehran also reported financial associations with nine other medical companies.

Bipartisan SGR repeal plan unveiled
The Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.
Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."
The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.
The Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.
Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."
The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.
The Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.
Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."
The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.

VTE rate not an accurate measure of hospital quality
Postoperative venous thromboembolism rates may not be an effective way of measuring hospital quality, according to Dr. Karl Y. Bilimoria and his colleagues.
The investigators calculated patient-level rates of venous thromboembolism as well as rates of imaging for VTE using data from the American Hospital Association and Medicare Compare from 2009 to 2010 from nearly 1 million patients discharged from 2,786 hospitals after a major surgery.

They sought to determine the association between hospital adherence to VTE reduction protocols (Surgical Care Improvement Project for VTE or SCIP-VTE-2) and risk-adjusted rates of VTE as measured by Patient Safety Indicator 12 (PSI-12) from the Agency for Healthcare Research and Quality. They also looked at how overall hospital quality scores correlated with VTE prophylaxis and risk-adjusted VTE scores.
They presented their findigns at the annual clinical congress of the American College of Surgeons and in JAMA [doi:10.1001/jama.2013.280048]).
Hospitals that adhered consistently to VTE reduction protocols paradoxically had higher PSI-12 scores, although not significantly so (P = .03). Hospitals with higher overall quality scores also adhered to VTE reduction protocols at a higher rate (93.3% in the lowest quartile vs. 95.5% in the highest) and had significantly higher risk-adjusted VTE event scores (P less than .001).
"Most important, hospital VTE rates were associated with the intensity of detecting VTE with imaging studies," the investigators said. Mean VTE diagnostic imaging rates ranged from 32/1,000 in the lowest quartile to 167/1,000 in the highest. Hospitals with the lowest imaging rates diagnosed 5.0 VTEs per 1,000 discharges, compared with hospitals with the highest imaging rates diagnosing 13.5 VTEs per 1,000 discharges.
In effect, PSI-12 scores the use of VTE imaging by hospitals instead of the quality of care provided, the investigators said. Further, surveillance bias impedes quality performance improvements; thus, decision making becomes more difficult for "patients seeking to identify a high-quality hospital."
In an accompanying editorial, Dr. Edwin H. Livingston, deputy editor of JAMA, noted that hypervigilance of VTEs might further worsen care in that "the very high compliance rate with VTE prophylaxis might result from many patients receiving treatments from which they are not likely to benefit. This is because current process measures were based on older guidelines that overestimated the benefits of VTE prophylaxis" (JAMA [doi:10.1001/jama.2013.280049]).
For that reason, Dr. Livingston recommended that public reporting of VTEs be "reconsidered or curtailed because few hospitals have sufficient numbers of patients to show statistically significant effects of prophylactic measures on VTE rates."
Measuring outcomes in general and safety events in particular is a complex proposition. This is particularly true when using patient safety indicators (PSIs) and hospital-acquired conditions as outcome metrics to compare performance across organizations.
In addition to the usual challenging nuances such as severity of illness adjustment, these indicators rely on accurate documentation and coding and as the Agency for Healthcare Research and Quality states: PSIs identify "potential in-hospital complications and adverse events following surgeries, procedures, and childbirth."
This is well meaning when an analytic team uses these metrics as part of a comprehensive quality and patient safety program to identify potential internal improvement opportunities. However, there are real limitations when using these metrics as outcomes that are tied to public reporting initiatives, payment incentives, and rankings.
The study in JAMA by Dr. Bilimoria and his colleagues highlights another limitation of some of these metrics – that of surveillance bias. Using PSI-12 (postoperative venous thromboembolism), risk-adjusted VTE rates were shown to correlate positively with intensity of imaging use (surveillance) and inversely with other measures of quality such as structure or process.
Thus, those with the highest VTE rates did everything right, but also looked for events more often.
This finding complicates the use of PSI-12 as an indicator to compare outcomes across health care systems. However, when used as an internal driver in the context of other local metrics of quality and safety, the original intent of PSI-12 as an indicator of potential hospital complications does not change.
This highlights the importance of health care systems in understanding the strengths and limitations of quality and safety metrics and in developing the analytic capabilities to turn data points into real opportunities to deliver better care, rather than going down the proverbial rabbit hole. Yet, regulatory agencies should also recognize that using imperfect metrics as a part of payment-reform initiatives needs to be done with extreme caution or there will be unintended consequences that do not lead to our collective goal of exceptional value in health care for our patients.
Dr. Robert Pendleton is chief medical quality officer for University of Utah Health Care, Salt Lake City.
Measuring outcomes in general and safety events in particular is a complex proposition. This is particularly true when using patient safety indicators (PSIs) and hospital-acquired conditions as outcome metrics to compare performance across organizations.
In addition to the usual challenging nuances such as severity of illness adjustment, these indicators rely on accurate documentation and coding and as the Agency for Healthcare Research and Quality states: PSIs identify "potential in-hospital complications and adverse events following surgeries, procedures, and childbirth."
This is well meaning when an analytic team uses these metrics as part of a comprehensive quality and patient safety program to identify potential internal improvement opportunities. However, there are real limitations when using these metrics as outcomes that are tied to public reporting initiatives, payment incentives, and rankings.
The study in JAMA by Dr. Bilimoria and his colleagues highlights another limitation of some of these metrics – that of surveillance bias. Using PSI-12 (postoperative venous thromboembolism), risk-adjusted VTE rates were shown to correlate positively with intensity of imaging use (surveillance) and inversely with other measures of quality such as structure or process.
Thus, those with the highest VTE rates did everything right, but also looked for events more often.
This finding complicates the use of PSI-12 as an indicator to compare outcomes across health care systems. However, when used as an internal driver in the context of other local metrics of quality and safety, the original intent of PSI-12 as an indicator of potential hospital complications does not change.
This highlights the importance of health care systems in understanding the strengths and limitations of quality and safety metrics and in developing the analytic capabilities to turn data points into real opportunities to deliver better care, rather than going down the proverbial rabbit hole. Yet, regulatory agencies should also recognize that using imperfect metrics as a part of payment-reform initiatives needs to be done with extreme caution or there will be unintended consequences that do not lead to our collective goal of exceptional value in health care for our patients.
Dr. Robert Pendleton is chief medical quality officer for University of Utah Health Care, Salt Lake City.
Measuring outcomes in general and safety events in particular is a complex proposition. This is particularly true when using patient safety indicators (PSIs) and hospital-acquired conditions as outcome metrics to compare performance across organizations.
In addition to the usual challenging nuances such as severity of illness adjustment, these indicators rely on accurate documentation and coding and as the Agency for Healthcare Research and Quality states: PSIs identify "potential in-hospital complications and adverse events following surgeries, procedures, and childbirth."
This is well meaning when an analytic team uses these metrics as part of a comprehensive quality and patient safety program to identify potential internal improvement opportunities. However, there are real limitations when using these metrics as outcomes that are tied to public reporting initiatives, payment incentives, and rankings.
The study in JAMA by Dr. Bilimoria and his colleagues highlights another limitation of some of these metrics – that of surveillance bias. Using PSI-12 (postoperative venous thromboembolism), risk-adjusted VTE rates were shown to correlate positively with intensity of imaging use (surveillance) and inversely with other measures of quality such as structure or process.
Thus, those with the highest VTE rates did everything right, but also looked for events more often.
This finding complicates the use of PSI-12 as an indicator to compare outcomes across health care systems. However, when used as an internal driver in the context of other local metrics of quality and safety, the original intent of PSI-12 as an indicator of potential hospital complications does not change.
This highlights the importance of health care systems in understanding the strengths and limitations of quality and safety metrics and in developing the analytic capabilities to turn data points into real opportunities to deliver better care, rather than going down the proverbial rabbit hole. Yet, regulatory agencies should also recognize that using imperfect metrics as a part of payment-reform initiatives needs to be done with extreme caution or there will be unintended consequences that do not lead to our collective goal of exceptional value in health care for our patients.
Dr. Robert Pendleton is chief medical quality officer for University of Utah Health Care, Salt Lake City.
Postoperative venous thromboembolism rates may not be an effective way of measuring hospital quality, according to Dr. Karl Y. Bilimoria and his colleagues.
The investigators calculated patient-level rates of venous thromboembolism as well as rates of imaging for VTE using data from the American Hospital Association and Medicare Compare from 2009 to 2010 from nearly 1 million patients discharged from 2,786 hospitals after a major surgery.
They sought to determine the association between hospital adherence to VTE reduction protocols (Surgical Care Improvement Project for VTE or SCIP-VTE-2) and risk-adjusted rates of VTE as measured by Patient Safety Indicator 12 (PSI-12) from the Agency for Healthcare Research and Quality. They also looked at how overall hospital quality scores correlated with VTE prophylaxis and risk-adjusted VTE scores.
They presented their findigns at the annual clinical congress of the American College of Surgeons and in JAMA [doi:10.1001/jama.2013.280048]).
Hospitals that adhered consistently to VTE reduction protocols paradoxically had higher PSI-12 scores, although not significantly so (P = .03). Hospitals with higher overall quality scores also adhered to VTE reduction protocols at a higher rate (93.3% in the lowest quartile vs. 95.5% in the highest) and had significantly higher risk-adjusted VTE event scores (P less than .001).
"Most important, hospital VTE rates were associated with the intensity of detecting VTE with imaging studies," the investigators said. Mean VTE diagnostic imaging rates ranged from 32/1,000 in the lowest quartile to 167/1,000 in the highest. Hospitals with the lowest imaging rates diagnosed 5.0 VTEs per 1,000 discharges, compared with hospitals with the highest imaging rates diagnosing 13.5 VTEs per 1,000 discharges.
In effect, PSI-12 scores the use of VTE imaging by hospitals instead of the quality of care provided, the investigators said. Further, surveillance bias impedes quality performance improvements; thus, decision making becomes more difficult for "patients seeking to identify a high-quality hospital."
In an accompanying editorial, Dr. Edwin H. Livingston, deputy editor of JAMA, noted that hypervigilance of VTEs might further worsen care in that "the very high compliance rate with VTE prophylaxis might result from many patients receiving treatments from which they are not likely to benefit. This is because current process measures were based on older guidelines that overestimated the benefits of VTE prophylaxis" (JAMA [doi:10.1001/jama.2013.280049]).
For that reason, Dr. Livingston recommended that public reporting of VTEs be "reconsidered or curtailed because few hospitals have sufficient numbers of patients to show statistically significant effects of prophylactic measures on VTE rates."
Postoperative venous thromboembolism rates may not be an effective way of measuring hospital quality, according to Dr. Karl Y. Bilimoria and his colleagues.
The investigators calculated patient-level rates of venous thromboembolism as well as rates of imaging for VTE using data from the American Hospital Association and Medicare Compare from 2009 to 2010 from nearly 1 million patients discharged from 2,786 hospitals after a major surgery.
They sought to determine the association between hospital adherence to VTE reduction protocols (Surgical Care Improvement Project for VTE or SCIP-VTE-2) and risk-adjusted rates of VTE as measured by Patient Safety Indicator 12 (PSI-12) from the Agency for Healthcare Research and Quality. They also looked at how overall hospital quality scores correlated with VTE prophylaxis and risk-adjusted VTE scores.
They presented their findigns at the annual clinical congress of the American College of Surgeons and in JAMA [doi:10.1001/jama.2013.280048]).
Hospitals that adhered consistently to VTE reduction protocols paradoxically had higher PSI-12 scores, although not significantly so (P = .03). Hospitals with higher overall quality scores also adhered to VTE reduction protocols at a higher rate (93.3% in the lowest quartile vs. 95.5% in the highest) and had significantly higher risk-adjusted VTE event scores (P less than .001).
"Most important, hospital VTE rates were associated with the intensity of detecting VTE with imaging studies," the investigators said. Mean VTE diagnostic imaging rates ranged from 32/1,000 in the lowest quartile to 167/1,000 in the highest. Hospitals with the lowest imaging rates diagnosed 5.0 VTEs per 1,000 discharges, compared with hospitals with the highest imaging rates diagnosing 13.5 VTEs per 1,000 discharges.
In effect, PSI-12 scores the use of VTE imaging by hospitals instead of the quality of care provided, the investigators said. Further, surveillance bias impedes quality performance improvements; thus, decision making becomes more difficult for "patients seeking to identify a high-quality hospital."
In an accompanying editorial, Dr. Edwin H. Livingston, deputy editor of JAMA, noted that hypervigilance of VTEs might further worsen care in that "the very high compliance rate with VTE prophylaxis might result from many patients receiving treatments from which they are not likely to benefit. This is because current process measures were based on older guidelines that overestimated the benefits of VTE prophylaxis" (JAMA [doi:10.1001/jama.2013.280049]).
For that reason, Dr. Livingston recommended that public reporting of VTEs be "reconsidered or curtailed because few hospitals have sufficient numbers of patients to show statistically significant effects of prophylactic measures on VTE rates."
Major finding: Hospitals that adhered consistently to VTE reduction protocols had higher rates of VTE, although not significantly so (P = .03).
Data source: Study of hospital risk-adjusted VTE prophylaxis adherence rates to postoperative VTE event rates in 2,786 hospitals.
Disclosures: The study was funded by the AHRQ and Northwestern University. Dr. Bilimoria has received honoraria from hospitals, professional societies, and continuing medical education companies for presentation on quality improvement.

How to foil post-CABG aspirin resistance
AMSTERDAM (IMNG) – Giving low-dose aspirin four times per day in the first days after coronary artery bypass graft surgery suppresses serum thromboxane levels far more effectively than does conventional once-daily dosing at 325 mg, according to a randomized trial.
The clinical implication of this finding is that more frequent dosing of aspirin may prevent the serious problem of premature vein graft failure from the development of aspirin resistance in the postoperative period, although at this point this is a hypothesis that requires testing in a future study, Dr. Jeremy S. Paikin said at the annual congress of the European Society of Cardiology.
He reported on 110 on-pump coronary artery bypass graft (CABG) patients randomized on postoperative day 1 to aspirin either at 81 mg four times daily, the standard 325 mg once daily, or to 81 mg once daily.
The primary study endpoint was the serum thromboxane level on the morning of postoperative day 4. The median level was 13.3 ng/mL in the group on aspirin at 81 mg once daily, 3.4 ng/mL with 325 mg once daily, and significantly lower at 1.1 ng/mL in patients on 81 mg four times daily.
"With 81 mg QD [four times daily], there’s almost complete suppression of serum thromboxane throughout the course of the hospital stay," according to Dr. Paikin of McMaster University, Hamilton, Ont.
Aspirin is known to prevent CABG graft failure, but its effectiveness is limited by the not-infrequent development of aspirin hyporesponsiveness in the postoperative period. The underlying mechanism involved in this aspirin resistance was previously unknown; however, in their randomized trial Dr. Paikin and coinvestigators established that the hyporesponsiveness is caused at least in part by increased platelet turnover in the postoperative period. The investigators showed that platelet turnover per day was increased two- to threefold in the week after CABG, compared with presurgical levels, a finding Dr. Paikin termed "quite exciting."
Recognizing that administration of any drug four times daily raises formidable adherence obstacles, he and his coworkers are just about to start a clinical trial looking at twice-daily aspirin dosing post CABG. They’re also interested in drawing a firm evidentiary connection between serum thromboxane levels and risk of premature graft failure.
Dr. Paikin reported having no financial conflicts of interest.
AMSTERDAM (IMNG) – Giving low-dose aspirin four times per day in the first days after coronary artery bypass graft surgery suppresses serum thromboxane levels far more effectively than does conventional once-daily dosing at 325 mg, according to a randomized trial.
The clinical implication of this finding is that more frequent dosing of aspirin may prevent the serious problem of premature vein graft failure from the development of aspirin resistance in the postoperative period, although at this point this is a hypothesis that requires testing in a future study, Dr. Jeremy S. Paikin said at the annual congress of the European Society of Cardiology.
He reported on 110 on-pump coronary artery bypass graft (CABG) patients randomized on postoperative day 1 to aspirin either at 81 mg four times daily, the standard 325 mg once daily, or to 81 mg once daily.
The primary study endpoint was the serum thromboxane level on the morning of postoperative day 4. The median level was 13.3 ng/mL in the group on aspirin at 81 mg once daily, 3.4 ng/mL with 325 mg once daily, and significantly lower at 1.1 ng/mL in patients on 81 mg four times daily.
"With 81 mg QD [four times daily], there’s almost complete suppression of serum thromboxane throughout the course of the hospital stay," according to Dr. Paikin of McMaster University, Hamilton, Ont.
Aspirin is known to prevent CABG graft failure, but its effectiveness is limited by the not-infrequent development of aspirin hyporesponsiveness in the postoperative period. The underlying mechanism involved in this aspirin resistance was previously unknown; however, in their randomized trial Dr. Paikin and coinvestigators established that the hyporesponsiveness is caused at least in part by increased platelet turnover in the postoperative period. The investigators showed that platelet turnover per day was increased two- to threefold in the week after CABG, compared with presurgical levels, a finding Dr. Paikin termed "quite exciting."
Recognizing that administration of any drug four times daily raises formidable adherence obstacles, he and his coworkers are just about to start a clinical trial looking at twice-daily aspirin dosing post CABG. They’re also interested in drawing a firm evidentiary connection between serum thromboxane levels and risk of premature graft failure.
Dr. Paikin reported having no financial conflicts of interest.
AMSTERDAM (IMNG) – Giving low-dose aspirin four times per day in the first days after coronary artery bypass graft surgery suppresses serum thromboxane levels far more effectively than does conventional once-daily dosing at 325 mg, according to a randomized trial.
The clinical implication of this finding is that more frequent dosing of aspirin may prevent the serious problem of premature vein graft failure from the development of aspirin resistance in the postoperative period, although at this point this is a hypothesis that requires testing in a future study, Dr. Jeremy S. Paikin said at the annual congress of the European Society of Cardiology.
He reported on 110 on-pump coronary artery bypass graft (CABG) patients randomized on postoperative day 1 to aspirin either at 81 mg four times daily, the standard 325 mg once daily, or to 81 mg once daily.
The primary study endpoint was the serum thromboxane level on the morning of postoperative day 4. The median level was 13.3 ng/mL in the group on aspirin at 81 mg once daily, 3.4 ng/mL with 325 mg once daily, and significantly lower at 1.1 ng/mL in patients on 81 mg four times daily.
"With 81 mg QD [four times daily], there’s almost complete suppression of serum thromboxane throughout the course of the hospital stay," according to Dr. Paikin of McMaster University, Hamilton, Ont.
Aspirin is known to prevent CABG graft failure, but its effectiveness is limited by the not-infrequent development of aspirin hyporesponsiveness in the postoperative period. The underlying mechanism involved in this aspirin resistance was previously unknown; however, in their randomized trial Dr. Paikin and coinvestigators established that the hyporesponsiveness is caused at least in part by increased platelet turnover in the postoperative period. The investigators showed that platelet turnover per day was increased two- to threefold in the week after CABG, compared with presurgical levels, a finding Dr. Paikin termed "quite exciting."
Recognizing that administration of any drug four times daily raises formidable adherence obstacles, he and his coworkers are just about to start a clinical trial looking at twice-daily aspirin dosing post CABG. They’re also interested in drawing a firm evidentiary connection between serum thromboxane levels and risk of premature graft failure.
Dr. Paikin reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2013
Major finding: The median serum thromboxane level on the morning of post CABG day 4 was 13.3 ng/mL in the group on aspirin at 81 mg once daily, 3.4 ng/mL with 325 mg once daily, and significantly lower at 1.1 ng/mL in patients on 81 mg four times daily.
Data source: A randomized clinical trial in which 110 patients who underwent on-pump CABG surgery were randomized on postoperative day 1 to aspirin at either 81 mg four times daily, 325 mg once daily, or 81 mg once daily.
Disclosures: The study presenter reported having no financial conflicts.