User login
The Official Newspaper of the American Association for Thoracic Surgery
Early endoscopic follow-up nets dysplasia in 9.5% of Barrett’s
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.

Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.
Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.
Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
AT DDW 2014
Key clinical point: Early endoscopic follow-up catches 9.5% of dysplasia missed on initial exam, but is not universally recommended by medical societies.
Major finding: Index endoscopy missed 1.9% of high-grade dysplasia or esophageal cancer and 7.6% of low-grade dysplasia.
Data source: A retrospective study in 181 patients with Barrett’s esophagus.
Disclosures: Dr. Visrodia and his coauthors reported no financial disclosures.

Training for minimally invasive cardiac surgery
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.

While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.
While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.
While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.

Attorneys: Doctors' first steps after lawsuit filing vital
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more beneficial resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.

|
| Dr. James A. L. Mathers, Jr. |
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.
|
|
| Dr. James A. L. Mathers, Jr. |
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.
|
|
| Dr. James A. L. Mathers, Jr. |
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more beneficial resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more beneficial resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.

TAVR beat surgery in high-risk aortic stenosis patients
WASHINGTON - A first in transcatheter aortic valve replacement trials, the CoreValve prosthesis was superior to surgical valve replacement in patients with severe aortic stenosis at increased surgical risk, showing a significantly lower risk of mortality 1 year later.
In the U.S. CoreValve High Risk Study, a prospective randomized controlled study of almost 800 patients, the rate of all-cause mortality at 1 year, the primary endpoint, was 14.2% among those in the transcatheter aortic valve replacement (TAVR) group, compared with 19.1% among those in the surgery group, a statistically significant difference that represented a 26% survival benefit at 1 year for the CoreValve, Dr. David H. Adams reported at the annual meeting of the American College of Cardiology.
This is the first prospective, randomized study to show superiority for transcatheter valve therapy over surgery, and "there's no study or trial that I'm aware of that's suggested that TAVR patients would have a superior survival outcome," Dr. Adams of Mount Sinai Medical Center, New York, said in an interview. Based on these results, he said he expects that TAVR "will increasingly become the alternative of choice for patients" at this level of risk.
The study was the high-risk arm of the U.S. CoreValve pivotal trial. The CoreValve self-expanding prosthesis was approved in January 2014 by the Food and Drug Administration for use in extreme risk patients, based on the results of the extreme risk cohort of patients. The data from the study in the high-risk trial are being reviewed at the FDA, according to the manufacturer, Medtronic.
The study compared the safety and effectiveness of TAVR with the CoreValve device to surgical valve replacement in 795 patients at 45 U.S. centers. The patients had severe aortic stenosis, had New York Heart Association class II heart failure or higher, and were judged to have at least a 15% risk of death within 30 days after surgery and less than a 50% risk of death or irreversible complications within 30 days after surgery. Their mean age was about age 83 years, almost half were females, most had class NYHA class III HF, and cardiac risk factors included coronary artery disease (in about two-thirds), previous coronary artery bypass surgery (about 30%), a previous MI (about 25%), and almost all had heart failure.
At 1 year, a composite of major adverse cardiovascular and cerebrovascular events (death from any cause, MI, any stroke, or reintervention), a secondary endpoint, was significantly lower among those on TAVR (20.4%) vs. the surgical group (27.3%). The rate of any stroke at 30 days was 4.9% in TAVR patients and 6.2% in the surgical group; and at 1 year, those rates were 8.8% and 12.6%, respectively; neither difference was statistically significant. Major vascular complications and permanent pacemaker implantations were significantly higher in the TAVR group (22.3% at 1 year, vs. 11.3% in the surgical group). In the TAVR group, there were five cases of cardiac perforation; there were no perforations in the surgical group.
Patients are being followed through 5 years. The 2-year mortality data are encouraging, with continued separation of the all-cause mortality curves, although the numbers are still small, Dr. Adams said.
More patients in the trial refused surgical valve replacement after randomization and the mortality rate within 30 days after surgery was 4.5%, which was lower than the rate specified for inclusion in the study, which was 15% or higher, so the patients may have been at a lower risk than planned, he said.
During the discussion, the inevitable comparisons to the results of the Placement of Aortic Transcatheter Valves A (PARTNER A) study were raised. In PARTNER A, which compared the safety and effectiveness of the balloon-expandable SAPIEN Transcatheter Heart Valve to aortic valve replacement surgery in high-risk patients with severe symptomatic aortic stenosis, found no difference in mortality between the two arms and an increase in cerebrovascular events in the TAVR arm.
Dr. Adams said that different characteristics of the device in the two trials are possible explanations as to why the TAVR results were superior to surgery in the CoreValve study, and not in PARTNER A. "The size of the catheter as well as perhaps the self-expanding nature of the device both could help explain that," he said.
While patient risk was assessed differently in the studies, and the Society of Thoracic Surgeons scores of the patients were different, "we're confident these were patients at increased risk for surgery," he added.
The study was published simultaneously in the New England Journal of Medicine on March 29 (2014 March 29 [doi:10.1056/NEJMoa1400590]).
The study is funded by the CoreValve manufacturer, Medtronic. Dr. Adams disclosed receiving grant support from Medtronic during the conduct of the study and other support from Medtronic and Edwards Lifesciences outside the submitted work.
WASHINGTON - A first in transcatheter aortic valve replacement trials, the CoreValve prosthesis was superior to surgical valve replacement in patients with severe aortic stenosis at increased surgical risk, showing a significantly lower risk of mortality 1 year later.
In the U.S. CoreValve High Risk Study, a prospective randomized controlled study of almost 800 patients, the rate of all-cause mortality at 1 year, the primary endpoint, was 14.2% among those in the transcatheter aortic valve replacement (TAVR) group, compared with 19.1% among those in the surgery group, a statistically significant difference that represented a 26% survival benefit at 1 year for the CoreValve, Dr. David H. Adams reported at the annual meeting of the American College of Cardiology.
This is the first prospective, randomized study to show superiority for transcatheter valve therapy over surgery, and "there's no study or trial that I'm aware of that's suggested that TAVR patients would have a superior survival outcome," Dr. Adams of Mount Sinai Medical Center, New York, said in an interview. Based on these results, he said he expects that TAVR "will increasingly become the alternative of choice for patients" at this level of risk.
The study was the high-risk arm of the U.S. CoreValve pivotal trial. The CoreValve self-expanding prosthesis was approved in January 2014 by the Food and Drug Administration for use in extreme risk patients, based on the results of the extreme risk cohort of patients. The data from the study in the high-risk trial are being reviewed at the FDA, according to the manufacturer, Medtronic.
The study compared the safety and effectiveness of TAVR with the CoreValve device to surgical valve replacement in 795 patients at 45 U.S. centers. The patients had severe aortic stenosis, had New York Heart Association class II heart failure or higher, and were judged to have at least a 15% risk of death within 30 days after surgery and less than a 50% risk of death or irreversible complications within 30 days after surgery. Their mean age was about age 83 years, almost half were females, most had class NYHA class III HF, and cardiac risk factors included coronary artery disease (in about two-thirds), previous coronary artery bypass surgery (about 30%), a previous MI (about 25%), and almost all had heart failure.
At 1 year, a composite of major adverse cardiovascular and cerebrovascular events (death from any cause, MI, any stroke, or reintervention), a secondary endpoint, was significantly lower among those on TAVR (20.4%) vs. the surgical group (27.3%). The rate of any stroke at 30 days was 4.9% in TAVR patients and 6.2% in the surgical group; and at 1 year, those rates were 8.8% and 12.6%, respectively; neither difference was statistically significant. Major vascular complications and permanent pacemaker implantations were significantly higher in the TAVR group (22.3% at 1 year, vs. 11.3% in the surgical group). In the TAVR group, there were five cases of cardiac perforation; there were no perforations in the surgical group.
Patients are being followed through 5 years. The 2-year mortality data are encouraging, with continued separation of the all-cause mortality curves, although the numbers are still small, Dr. Adams said.
More patients in the trial refused surgical valve replacement after randomization and the mortality rate within 30 days after surgery was 4.5%, which was lower than the rate specified for inclusion in the study, which was 15% or higher, so the patients may have been at a lower risk than planned, he said.
During the discussion, the inevitable comparisons to the results of the Placement of Aortic Transcatheter Valves A (PARTNER A) study were raised. In PARTNER A, which compared the safety and effectiveness of the balloon-expandable SAPIEN Transcatheter Heart Valve to aortic valve replacement surgery in high-risk patients with severe symptomatic aortic stenosis, found no difference in mortality between the two arms and an increase in cerebrovascular events in the TAVR arm.
Dr. Adams said that different characteristics of the device in the two trials are possible explanations as to why the TAVR results were superior to surgery in the CoreValve study, and not in PARTNER A. "The size of the catheter as well as perhaps the self-expanding nature of the device both could help explain that," he said.
While patient risk was assessed differently in the studies, and the Society of Thoracic Surgeons scores of the patients were different, "we're confident these were patients at increased risk for surgery," he added.
The study was published simultaneously in the New England Journal of Medicine on March 29 (2014 March 29 [doi:10.1056/NEJMoa1400590]).
The study is funded by the CoreValve manufacturer, Medtronic. Dr. Adams disclosed receiving grant support from Medtronic during the conduct of the study and other support from Medtronic and Edwards Lifesciences outside the submitted work.
WASHINGTON - A first in transcatheter aortic valve replacement trials, the CoreValve prosthesis was superior to surgical valve replacement in patients with severe aortic stenosis at increased surgical risk, showing a significantly lower risk of mortality 1 year later.
In the U.S. CoreValve High Risk Study, a prospective randomized controlled study of almost 800 patients, the rate of all-cause mortality at 1 year, the primary endpoint, was 14.2% among those in the transcatheter aortic valve replacement (TAVR) group, compared with 19.1% among those in the surgery group, a statistically significant difference that represented a 26% survival benefit at 1 year for the CoreValve, Dr. David H. Adams reported at the annual meeting of the American College of Cardiology.
This is the first prospective, randomized study to show superiority for transcatheter valve therapy over surgery, and "there's no study or trial that I'm aware of that's suggested that TAVR patients would have a superior survival outcome," Dr. Adams of Mount Sinai Medical Center, New York, said in an interview. Based on these results, he said he expects that TAVR "will increasingly become the alternative of choice for patients" at this level of risk.
The study was the high-risk arm of the U.S. CoreValve pivotal trial. The CoreValve self-expanding prosthesis was approved in January 2014 by the Food and Drug Administration for use in extreme risk patients, based on the results of the extreme risk cohort of patients. The data from the study in the high-risk trial are being reviewed at the FDA, according to the manufacturer, Medtronic.
The study compared the safety and effectiveness of TAVR with the CoreValve device to surgical valve replacement in 795 patients at 45 U.S. centers. The patients had severe aortic stenosis, had New York Heart Association class II heart failure or higher, and were judged to have at least a 15% risk of death within 30 days after surgery and less than a 50% risk of death or irreversible complications within 30 days after surgery. Their mean age was about age 83 years, almost half were females, most had class NYHA class III HF, and cardiac risk factors included coronary artery disease (in about two-thirds), previous coronary artery bypass surgery (about 30%), a previous MI (about 25%), and almost all had heart failure.
At 1 year, a composite of major adverse cardiovascular and cerebrovascular events (death from any cause, MI, any stroke, or reintervention), a secondary endpoint, was significantly lower among those on TAVR (20.4%) vs. the surgical group (27.3%). The rate of any stroke at 30 days was 4.9% in TAVR patients and 6.2% in the surgical group; and at 1 year, those rates were 8.8% and 12.6%, respectively; neither difference was statistically significant. Major vascular complications and permanent pacemaker implantations were significantly higher in the TAVR group (22.3% at 1 year, vs. 11.3% in the surgical group). In the TAVR group, there were five cases of cardiac perforation; there were no perforations in the surgical group.
Patients are being followed through 5 years. The 2-year mortality data are encouraging, with continued separation of the all-cause mortality curves, although the numbers are still small, Dr. Adams said.
More patients in the trial refused surgical valve replacement after randomization and the mortality rate within 30 days after surgery was 4.5%, which was lower than the rate specified for inclusion in the study, which was 15% or higher, so the patients may have been at a lower risk than planned, he said.
During the discussion, the inevitable comparisons to the results of the Placement of Aortic Transcatheter Valves A (PARTNER A) study were raised. In PARTNER A, which compared the safety and effectiveness of the balloon-expandable SAPIEN Transcatheter Heart Valve to aortic valve replacement surgery in high-risk patients with severe symptomatic aortic stenosis, found no difference in mortality between the two arms and an increase in cerebrovascular events in the TAVR arm.
Dr. Adams said that different characteristics of the device in the two trials are possible explanations as to why the TAVR results were superior to surgery in the CoreValve study, and not in PARTNER A. "The size of the catheter as well as perhaps the self-expanding nature of the device both could help explain that," he said.
While patient risk was assessed differently in the studies, and the Society of Thoracic Surgeons scores of the patients were different, "we're confident these were patients at increased risk for surgery," he added.
The study was published simultaneously in the New England Journal of Medicine on March 29 (2014 March 29 [doi:10.1056/NEJMoa1400590]).
The study is funded by the CoreValve manufacturer, Medtronic. Dr. Adams disclosed receiving grant support from Medtronic during the conduct of the study and other support from Medtronic and Edwards Lifesciences outside the submitted work.
Major finding: All-cause mortality was 14.2% among high-risk patients with severe aortic stenosis 1 year after TAVR with a self-expanding aortic valve bioprosthesis, vs. 19.1% among those who had surgical aortic valve replacement, a highly statistically significant difference.
Data source: The multicenter prospective U.S. study compared survival at 1 year in 795 patients at high risk for surgery who were randomized to TAVR with the CoreValve device or surgical aortic valve replacement.
Disclosures: The study is funded by the CoreValve manufacturer, Medtronic. Dr. Adams disclosed receiving grant support from Medtronic during the conduct of the study and other support from Medtronic and Edwards Lifesciences outside the study.
Various findings guide approach to indeterminate nodules
SAN DIEGO - About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We're encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.

Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it's important to differentiate - early, accurately, and noninvasively - benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we're wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It's not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going - integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.
SAN DIEGO - About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We're encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.
Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it's important to differentiate - early, accurately, and noninvasively - benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we're wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It's not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going - integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.
SAN DIEGO - About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We're encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.
Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it's important to differentiate - early, accurately, and noninvasively - benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we're wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It's not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going - integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.

Sleeve gastrectomy often worsens GERD
Laparoscopic sleeve gastrectomy not only fails to improve gastroesophageal reflux disease in most patients who undergo the weight-loss procedure, it actually worsens GERD symptoms in many of them and induces GERD in 9%, a study showed.
In addition, patients with preexisting GERD who undergo laparoscopic sleeve gastrectomy (LSG) have high rates of surgical complications; revision surgery; failure to achieve weight loss; and failure to resolve weight-related comorbidities such as diabetes, obstructive sleep apnea, and hypertension. In contrast, patients who undergo gastric bypass show significant improvement in all of these outcomes, said Dr. Cecily E. DuPree and her associates in the department of surgery, Madigan Army Medical Center, Fort Lewis, Wash.

Based on the findings from their study of a national database including 4,832 patients who had laparoscopic sleeve gastrectomy (LSG) and 33,867 who had gastric bypass (GB), "we believe that all patients should be evaluated for the presence and severity of GERD and counseled regarding the relative efficacy of LSG vs. GB or other bariatric operations before surgery. Although there is no definitive evidence to support the listing of GERD as an absolute contraindication to LSG, the available data suggest that the presence of preexisting severe GERD or esophageal dysmotility may be considered a relative contraindication," they said.
They noted that until now, the sleeve procedure's effect on GERD was unknown. Small, single-center series "have raised significant concerns," but no large study has examined the issue. So she and her associates used data from a large, nationwide database (the Bariatric Outcomes Longitudinal Database) to track the resolution, persistence, or development of GERD in 4,832 patients who underwent laparoscopic sleeve gastrectomy in 2007-2010, comparing their outcomes with those of 33,867 patients who underwent gastric bypass during the same period and served as controls.
The prevalence of GERD was 49.7% in the study population, and that of severe GERD was 25.7%, confirming that GERD is very common in candidates for bariatric surgery.
The prevalence of GERD was 44.5% among patients undergoing the sleeve procedure. "This highlights the concern that there is a large population at risk of adverse outcomes after LSG if the procedure is associated with anatomical or physiologic changes that increase the risk of postoperative GERD," the investigators noted.
Most LSG patients (84.1%) had persistent GERD symptoms after the procedure; only 15.9% reported resolution of symptoms. An additional 9.0% of LSG patients reported postoperative worsening of symptoms. And 8.6% of patients who didn't have GERD before undergoing sleeve gastrectomy developed GERD afterward.
In contrast, most patients who underwent gastric bypass showed complete resolution (62.8%) or stabilization (17.6%) of GERD symptoms. Only 2.2% reported worsening GERD symptoms, and none developed de novo symptoms.
Among the LSG patients, the complication rate was significantly higher in those with preexisting GERD (15.1%) or preexisting severe GERD (16.3%) than in those without GERD (10.6%). "There was also a small but statistically significant increase in the need for revisional surgery between LSG patients with and without preoperative GERD symptoms (0.6% vs. 0.3%)" (JAMA Surg. 2014 [doi:10.1001/jamasurg.2013.4323]).
In contrast, the presence of GERD had no effect on complications in the control group. Similarly, the rate of failure to lose weight was higher in LSG patients with preoperative GERD and in LSG patients with severe preoperative GERD than in those without GERD. Again, the presence of GERD had no such effect on weight loss in the gastric bypass patients.
In addition, the percentage of patients who showed resolution of comorbidities was significantly decreased among patients with preoperative GERD who underwent LSG, compared with all other groups.
"These data raise significant concerns about the effect of LSG on the obesity-related comorbidity of GERD and suggest that most patients with preexisting GERD will have either no improvement or possibly worsening of their symptoms after LSG," Dr. DuPree and her associates said.
Modifying surgical technique so that sleeve size and volume are attended to, narrowing of the gastric body or pylorus is avoided, and hiatal hernias are assiduously identified and repaired may reduce the risk of post-LSG GERD, the investigators said.
Laparoscopic sleeve gastrectomy not only fails to improve gastroesophageal reflux disease in most patients who undergo the weight-loss procedure, it actually worsens GERD symptoms in many of them and induces GERD in 9%, a study showed.
In addition, patients with preexisting GERD who undergo laparoscopic sleeve gastrectomy (LSG) have high rates of surgical complications; revision surgery; failure to achieve weight loss; and failure to resolve weight-related comorbidities such as diabetes, obstructive sleep apnea, and hypertension. In contrast, patients who undergo gastric bypass show significant improvement in all of these outcomes, said Dr. Cecily E. DuPree and her associates in the department of surgery, Madigan Army Medical Center, Fort Lewis, Wash.
Based on the findings from their study of a national database including 4,832 patients who had laparoscopic sleeve gastrectomy (LSG) and 33,867 who had gastric bypass (GB), "we believe that all patients should be evaluated for the presence and severity of GERD and counseled regarding the relative efficacy of LSG vs. GB or other bariatric operations before surgery. Although there is no definitive evidence to support the listing of GERD as an absolute contraindication to LSG, the available data suggest that the presence of preexisting severe GERD or esophageal dysmotility may be considered a relative contraindication," they said.
They noted that until now, the sleeve procedure's effect on GERD was unknown. Small, single-center series "have raised significant concerns," but no large study has examined the issue. So she and her associates used data from a large, nationwide database (the Bariatric Outcomes Longitudinal Database) to track the resolution, persistence, or development of GERD in 4,832 patients who underwent laparoscopic sleeve gastrectomy in 2007-2010, comparing their outcomes with those of 33,867 patients who underwent gastric bypass during the same period and served as controls.
The prevalence of GERD was 49.7% in the study population, and that of severe GERD was 25.7%, confirming that GERD is very common in candidates for bariatric surgery.
The prevalence of GERD was 44.5% among patients undergoing the sleeve procedure. "This highlights the concern that there is a large population at risk of adverse outcomes after LSG if the procedure is associated with anatomical or physiologic changes that increase the risk of postoperative GERD," the investigators noted.
Most LSG patients (84.1%) had persistent GERD symptoms after the procedure; only 15.9% reported resolution of symptoms. An additional 9.0% of LSG patients reported postoperative worsening of symptoms. And 8.6% of patients who didn't have GERD before undergoing sleeve gastrectomy developed GERD afterward.
In contrast, most patients who underwent gastric bypass showed complete resolution (62.8%) or stabilization (17.6%) of GERD symptoms. Only 2.2% reported worsening GERD symptoms, and none developed de novo symptoms.
Among the LSG patients, the complication rate was significantly higher in those with preexisting GERD (15.1%) or preexisting severe GERD (16.3%) than in those without GERD (10.6%). "There was also a small but statistically significant increase in the need for revisional surgery between LSG patients with and without preoperative GERD symptoms (0.6% vs. 0.3%)" (JAMA Surg. 2014 [doi:10.1001/jamasurg.2013.4323]).
In contrast, the presence of GERD had no effect on complications in the control group. Similarly, the rate of failure to lose weight was higher in LSG patients with preoperative GERD and in LSG patients with severe preoperative GERD than in those without GERD. Again, the presence of GERD had no such effect on weight loss in the gastric bypass patients.
In addition, the percentage of patients who showed resolution of comorbidities was significantly decreased among patients with preoperative GERD who underwent LSG, compared with all other groups.
"These data raise significant concerns about the effect of LSG on the obesity-related comorbidity of GERD and suggest that most patients with preexisting GERD will have either no improvement or possibly worsening of their symptoms after LSG," Dr. DuPree and her associates said.
Modifying surgical technique so that sleeve size and volume are attended to, narrowing of the gastric body or pylorus is avoided, and hiatal hernias are assiduously identified and repaired may reduce the risk of post-LSG GERD, the investigators said.
Laparoscopic sleeve gastrectomy not only fails to improve gastroesophageal reflux disease in most patients who undergo the weight-loss procedure, it actually worsens GERD symptoms in many of them and induces GERD in 9%, a study showed.
In addition, patients with preexisting GERD who undergo laparoscopic sleeve gastrectomy (LSG) have high rates of surgical complications; revision surgery; failure to achieve weight loss; and failure to resolve weight-related comorbidities such as diabetes, obstructive sleep apnea, and hypertension. In contrast, patients who undergo gastric bypass show significant improvement in all of these outcomes, said Dr. Cecily E. DuPree and her associates in the department of surgery, Madigan Army Medical Center, Fort Lewis, Wash.
Based on the findings from their study of a national database including 4,832 patients who had laparoscopic sleeve gastrectomy (LSG) and 33,867 who had gastric bypass (GB), "we believe that all patients should be evaluated for the presence and severity of GERD and counseled regarding the relative efficacy of LSG vs. GB or other bariatric operations before surgery. Although there is no definitive evidence to support the listing of GERD as an absolute contraindication to LSG, the available data suggest that the presence of preexisting severe GERD or esophageal dysmotility may be considered a relative contraindication," they said.
They noted that until now, the sleeve procedure's effect on GERD was unknown. Small, single-center series "have raised significant concerns," but no large study has examined the issue. So she and her associates used data from a large, nationwide database (the Bariatric Outcomes Longitudinal Database) to track the resolution, persistence, or development of GERD in 4,832 patients who underwent laparoscopic sleeve gastrectomy in 2007-2010, comparing their outcomes with those of 33,867 patients who underwent gastric bypass during the same period and served as controls.
The prevalence of GERD was 49.7% in the study population, and that of severe GERD was 25.7%, confirming that GERD is very common in candidates for bariatric surgery.
The prevalence of GERD was 44.5% among patients undergoing the sleeve procedure. "This highlights the concern that there is a large population at risk of adverse outcomes after LSG if the procedure is associated with anatomical or physiologic changes that increase the risk of postoperative GERD," the investigators noted.
Most LSG patients (84.1%) had persistent GERD symptoms after the procedure; only 15.9% reported resolution of symptoms. An additional 9.0% of LSG patients reported postoperative worsening of symptoms. And 8.6% of patients who didn't have GERD before undergoing sleeve gastrectomy developed GERD afterward.
In contrast, most patients who underwent gastric bypass showed complete resolution (62.8%) or stabilization (17.6%) of GERD symptoms. Only 2.2% reported worsening GERD symptoms, and none developed de novo symptoms.
Among the LSG patients, the complication rate was significantly higher in those with preexisting GERD (15.1%) or preexisting severe GERD (16.3%) than in those without GERD (10.6%). "There was also a small but statistically significant increase in the need for revisional surgery between LSG patients with and without preoperative GERD symptoms (0.6% vs. 0.3%)" (JAMA Surg. 2014 [doi:10.1001/jamasurg.2013.4323]).
In contrast, the presence of GERD had no effect on complications in the control group. Similarly, the rate of failure to lose weight was higher in LSG patients with preoperative GERD and in LSG patients with severe preoperative GERD than in those without GERD. Again, the presence of GERD had no such effect on weight loss in the gastric bypass patients.
In addition, the percentage of patients who showed resolution of comorbidities was significantly decreased among patients with preoperative GERD who underwent LSG, compared with all other groups.
"These data raise significant concerns about the effect of LSG on the obesity-related comorbidity of GERD and suggest that most patients with preexisting GERD will have either no improvement or possibly worsening of their symptoms after LSG," Dr. DuPree and her associates said.
Modifying surgical technique so that sleeve size and volume are attended to, narrowing of the gastric body or pylorus is avoided, and hiatal hernias are assiduously identified and repaired may reduce the risk of post-LSG GERD, the investigators said.

TSRA - Advocates for the CT Surgical Trainee
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
DECAAF: Assess extent of fibrosis before AF ablation
For patients scheduled to undergo AF catheter ablation, estimating the extent of atrial fibrosis using delayed enhancement MRI can help distinguish those likely to respond from patients likely to have recurrent arrhythmia, according to a report published online Feb. 4 in JAMA.
In the prospective, observational DECAAF (Delayed-Enhancement MRI Determinant of Successful Radiofrequency Ablation of Atrial Fibrillation) study, 260 such patients (mean age, 59 years) underwent quantification of left atrial fibrosis via delayed enhancement MRI with gadolinium at 15 medical centers in six countries, before undergoing AF ablation. These centers had varying levels of experience with cardiac imaging and used different ablation procedures, said Dr. Nassir F. Marrouche, director of the comprehensive arrhythmia and research management center, University of Utah, Salt Lake City, and his associates.

Four categories of fibrosis were used: involvement of less than 10% of the atrial wall (stage 1, 49 patients), 10%-19% of the atrial wall (stage 2, 107 patients), 20%-29% of the atrial wall (stage 3, 80 patients), and 30% or more of the atrial wall (stage 4, 24 patients). The estimated percentage of atrial fibrosis strongly correlated with arrhythmia recurrence at 1 year, even after the data were adjusted to account for variables such as patient age and sex; the presence of hypertension, heart failure, mitral valve disease, or diabetes; and the type of AF (paroxysmal vs persistent).
The hazard ratio for recurrent arrhythmia was 1.06 for every 1% increase in the extent of atrial fibrosis (JAMA 2014 Feb. 4 [doi:10.1001/jama.2014.3]).
This is the first multicenter study to demonstrate the feasibility and potential clinical value of quantifying the degree of AF fibrosis using delayed enhancement MRI before performing ablation, offering a noninvasive, effective method for determining which patients are likely to benefit and which should avoid the procedure, Dr. Marrouche and his associates said.
The JAMA report expands on results presented at the annual meeting of the Heart Rhythm Society last year.
The study was funded by the Comprehensive Arrhythmia and Research Management Center at the University of Utah and the George S. and Dolores Dore Eccles Foundation. Dr. Marrouche reported owning stock and being named in two patents licensed to Marrek; his associates reported numerous ties to industry sources.
For patients scheduled to undergo AF catheter ablation, estimating the extent of atrial fibrosis using delayed enhancement MRI can help distinguish those likely to respond from patients likely to have recurrent arrhythmia, according to a report published online Feb. 4 in JAMA.
In the prospective, observational DECAAF (Delayed-Enhancement MRI Determinant of Successful Radiofrequency Ablation of Atrial Fibrillation) study, 260 such patients (mean age, 59 years) underwent quantification of left atrial fibrosis via delayed enhancement MRI with gadolinium at 15 medical centers in six countries, before undergoing AF ablation. These centers had varying levels of experience with cardiac imaging and used different ablation procedures, said Dr. Nassir F. Marrouche, director of the comprehensive arrhythmia and research management center, University of Utah, Salt Lake City, and his associates.
Four categories of fibrosis were used: involvement of less than 10% of the atrial wall (stage 1, 49 patients), 10%-19% of the atrial wall (stage 2, 107 patients), 20%-29% of the atrial wall (stage 3, 80 patients), and 30% or more of the atrial wall (stage 4, 24 patients). The estimated percentage of atrial fibrosis strongly correlated with arrhythmia recurrence at 1 year, even after the data were adjusted to account for variables such as patient age and sex; the presence of hypertension, heart failure, mitral valve disease, or diabetes; and the type of AF (paroxysmal vs persistent).
The hazard ratio for recurrent arrhythmia was 1.06 for every 1% increase in the extent of atrial fibrosis (JAMA 2014 Feb. 4 [doi:10.1001/jama.2014.3]).
This is the first multicenter study to demonstrate the feasibility and potential clinical value of quantifying the degree of AF fibrosis using delayed enhancement MRI before performing ablation, offering a noninvasive, effective method for determining which patients are likely to benefit and which should avoid the procedure, Dr. Marrouche and his associates said.
The JAMA report expands on results presented at the annual meeting of the Heart Rhythm Society last year.
The study was funded by the Comprehensive Arrhythmia and Research Management Center at the University of Utah and the George S. and Dolores Dore Eccles Foundation. Dr. Marrouche reported owning stock and being named in two patents licensed to Marrek; his associates reported numerous ties to industry sources.
For patients scheduled to undergo AF catheter ablation, estimating the extent of atrial fibrosis using delayed enhancement MRI can help distinguish those likely to respond from patients likely to have recurrent arrhythmia, according to a report published online Feb. 4 in JAMA.
In the prospective, observational DECAAF (Delayed-Enhancement MRI Determinant of Successful Radiofrequency Ablation of Atrial Fibrillation) study, 260 such patients (mean age, 59 years) underwent quantification of left atrial fibrosis via delayed enhancement MRI with gadolinium at 15 medical centers in six countries, before undergoing AF ablation. These centers had varying levels of experience with cardiac imaging and used different ablation procedures, said Dr. Nassir F. Marrouche, director of the comprehensive arrhythmia and research management center, University of Utah, Salt Lake City, and his associates.
Four categories of fibrosis were used: involvement of less than 10% of the atrial wall (stage 1, 49 patients), 10%-19% of the atrial wall (stage 2, 107 patients), 20%-29% of the atrial wall (stage 3, 80 patients), and 30% or more of the atrial wall (stage 4, 24 patients). The estimated percentage of atrial fibrosis strongly correlated with arrhythmia recurrence at 1 year, even after the data were adjusted to account for variables such as patient age and sex; the presence of hypertension, heart failure, mitral valve disease, or diabetes; and the type of AF (paroxysmal vs persistent).
The hazard ratio for recurrent arrhythmia was 1.06 for every 1% increase in the extent of atrial fibrosis (JAMA 2014 Feb. 4 [doi:10.1001/jama.2014.3]).
This is the first multicenter study to demonstrate the feasibility and potential clinical value of quantifying the degree of AF fibrosis using delayed enhancement MRI before performing ablation, offering a noninvasive, effective method for determining which patients are likely to benefit and which should avoid the procedure, Dr. Marrouche and his associates said.
The JAMA report expands on results presented at the annual meeting of the Heart Rhythm Society last year.
The study was funded by the Comprehensive Arrhythmia and Research Management Center at the University of Utah and the George S. and Dolores Dore Eccles Foundation. Dr. Marrouche reported owning stock and being named in two patents licensed to Marrek; his associates reported numerous ties to industry sources.

Frailty assessment central to TAVR decision
SNOWMASS, COLO.– Transcatheter aortic valve replacement in nonsurgical candidates with severe symptomatic aortic stenosis carries a hefty price tag of $116,500 per quality-adjusted life-year gained over medical management.
That’s the bottom line in a cost-effectiveness study led by cardiologist Dr. Mark A. Hlatky. The investigators applied data on the costs and benefits of transfemoral transcatheter aortic valve replacement (TAVR) as documented in the landmark PARTNER (Placement of Aortic Transcatheter Valves) trial in their Markov model involving a hypothetical patient cohort. The estimated incremental cost-effectiveness of $116,500 per quality-adjusted life-year gained is well in excess of the $50,000 figure widely accepted by health policy makers as defining a cutoff for cost-effective therapy.

In this cost-effectiveness analysis (Circ. Cardiovasc. Qual. Outcomes 2013;6:419-28), TAVR boosted life expectancy by roughly 11 months, from 2.08 years with medical therapy to 2.93 years. Quality-adjusted life expectancy rose from 1.19 to 1.93 years. TAVR also resulted in 1.4 fewer hospitalizations than with medical management. However, undergoing TAVR rather than medical management raised the lifetime stroke risk from 1% to 11% and increased lifetime health care costs from $83,600 to $169,100, reported the group led by Dr. Hlatky, professor of health research and policy and also professor of medicine at Stanford (Calif.) University.
"This is a fascinating study," Dr. Karen P. Alexander said at the Annual Cardiovascular Conference at Snowmass. "I think the lesson here is that futility from a cost perspective is also something that should be in the discussion" regarding TAVR vs. medical therapy in patients with inoperable aortic stenosis.
She highlighted the Hlatky study in discussing the key role frailty assessment plays in considering TAVR. The study showed that the cost-effectiveness of TAVR is greater in patients with a lower burden of noncardiac disease, which is another way saying "those who are less frail."
This conclusion underscores a statement in the 2012 American College of Cardiology/American Association for Thoracic Surgery/Society for Cardiovascular Angiography and Interventions/Society of Thoracic Surgeons expert consensus document on TAVR paraphrased by Dr. Alexander: Frailty will assume central importance in patient selection for TAVR by virtue of the extensive comorbidities in this population. Existing models do not have predictive variables of interest in high-risk patients. (J. Am. Coll. Cardiol. 2012;59:1200-54).
Dr. Alexander of Duke University in Durham, N.C., said frailty is important when considering TAVR because it has been shown to be associated with increased rates of post-TAVR 30-day morbidity and mortality, prolonged hospital length of stay, and 1-year mortality.
She defined frailty as a multisystem impairment resulting in reduced physiologic reserve and increased vulnerability to stress. Frailty is a physiologic phenotype associated with slow gait, weakness, weight loss, exhaustion, and a low daily activity level.
While the degree of a patient’s frailty is an important consideration in deciding on TAVR vs. medical management, frailty per se is no contraindication to the procedure. Indeed, the prevalence of frailty as defined simply by a baseline 5-meter walk time in excess of 6 seconds was 72% among the 7,710 TAVR patients, mean age 84 years, included in the recent first report of the comprehensive national STS/ACC Transcatheter Valve Therapy Registry (JAMA 2013;310:2069-77). That’s nearly twice the 38% prevalence among community-dwelling 85-year-olds, Dr. Alexander noted, citing data from the Canadian Study of Health and Aging (CMAJ 2011;183:e487-94).
More than 20 different frailty risk scores are now in circulation. Dr. Alexander is particularly enthusiastic about the frailty risk tool developed as part of the ACC’s new Championing Care for the Patient With Aortic Stenosis Initiative. It efficiently assesses five domains of frailty – slowness, weakness, malnutrition, inactivity with loss of independence, and malnutrition – and generates a clinically useful qualitative frailty rating. A patient with a high frailty score may not have sufficient life expectancy to obtain the benefits of TAVR.
With regard to treatment futility, Dr. Alexander observed that it can be defined as either lack of medical efficacy as judged by physicians or as lack of meaningful survival as judged by a patient’s personal values. Yet one in four Americans aged 75 years or older has given little or no thought to their own wishes for end-of-life medical therapy, according to a recent Pew Research Center survey.
The telephone survey, conducted last spring, included a representative sample of 1,994 U.S. adults. While 47% of respondents aged 75 years or older indicated they had given their own wishes for end-of-life medical care a great deal of thought, 25% said they had given the matter "not much or none." Reflection on those personal wishes needs to be part of the physician/patient discussion about TAVR, according to Dr. Alexander.
With regard to general views on end-of-life therapy, 74% of surveyed individuals age 75 and up declared there should be circumstances in which a patient should be allowed to die. Another 22% said medical staff should do everything possible to save a patient’s life under all circumstances.
Dr. Alexander reported serving as a consultant to Gilead and Pozen.
SNOWMASS, COLO.– Transcatheter aortic valve replacement in nonsurgical candidates with severe symptomatic aortic stenosis carries a hefty price tag of $116,500 per quality-adjusted life-year gained over medical management.
That’s the bottom line in a cost-effectiveness study led by cardiologist Dr. Mark A. Hlatky. The investigators applied data on the costs and benefits of transfemoral transcatheter aortic valve replacement (TAVR) as documented in the landmark PARTNER (Placement of Aortic Transcatheter Valves) trial in their Markov model involving a hypothetical patient cohort. The estimated incremental cost-effectiveness of $116,500 per quality-adjusted life-year gained is well in excess of the $50,000 figure widely accepted by health policy makers as defining a cutoff for cost-effective therapy.
In this cost-effectiveness analysis (Circ. Cardiovasc. Qual. Outcomes 2013;6:419-28), TAVR boosted life expectancy by roughly 11 months, from 2.08 years with medical therapy to 2.93 years. Quality-adjusted life expectancy rose from 1.19 to 1.93 years. TAVR also resulted in 1.4 fewer hospitalizations than with medical management. However, undergoing TAVR rather than medical management raised the lifetime stroke risk from 1% to 11% and increased lifetime health care costs from $83,600 to $169,100, reported the group led by Dr. Hlatky, professor of health research and policy and also professor of medicine at Stanford (Calif.) University.
"This is a fascinating study," Dr. Karen P. Alexander said at the Annual Cardiovascular Conference at Snowmass. "I think the lesson here is that futility from a cost perspective is also something that should be in the discussion" regarding TAVR vs. medical therapy in patients with inoperable aortic stenosis.
She highlighted the Hlatky study in discussing the key role frailty assessment plays in considering TAVR. The study showed that the cost-effectiveness of TAVR is greater in patients with a lower burden of noncardiac disease, which is another way saying "those who are less frail."
This conclusion underscores a statement in the 2012 American College of Cardiology/American Association for Thoracic Surgery/Society for Cardiovascular Angiography and Interventions/Society of Thoracic Surgeons expert consensus document on TAVR paraphrased by Dr. Alexander: Frailty will assume central importance in patient selection for TAVR by virtue of the extensive comorbidities in this population. Existing models do not have predictive variables of interest in high-risk patients. (J. Am. Coll. Cardiol. 2012;59:1200-54).
Dr. Alexander of Duke University in Durham, N.C., said frailty is important when considering TAVR because it has been shown to be associated with increased rates of post-TAVR 30-day morbidity and mortality, prolonged hospital length of stay, and 1-year mortality.
She defined frailty as a multisystem impairment resulting in reduced physiologic reserve and increased vulnerability to stress. Frailty is a physiologic phenotype associated with slow gait, weakness, weight loss, exhaustion, and a low daily activity level.
While the degree of a patient’s frailty is an important consideration in deciding on TAVR vs. medical management, frailty per se is no contraindication to the procedure. Indeed, the prevalence of frailty as defined simply by a baseline 5-meter walk time in excess of 6 seconds was 72% among the 7,710 TAVR patients, mean age 84 years, included in the recent first report of the comprehensive national STS/ACC Transcatheter Valve Therapy Registry (JAMA 2013;310:2069-77). That’s nearly twice the 38% prevalence among community-dwelling 85-year-olds, Dr. Alexander noted, citing data from the Canadian Study of Health and Aging (CMAJ 2011;183:e487-94).
More than 20 different frailty risk scores are now in circulation. Dr. Alexander is particularly enthusiastic about the frailty risk tool developed as part of the ACC’s new Championing Care for the Patient With Aortic Stenosis Initiative. It efficiently assesses five domains of frailty – slowness, weakness, malnutrition, inactivity with loss of independence, and malnutrition – and generates a clinically useful qualitative frailty rating. A patient with a high frailty score may not have sufficient life expectancy to obtain the benefits of TAVR.
With regard to treatment futility, Dr. Alexander observed that it can be defined as either lack of medical efficacy as judged by physicians or as lack of meaningful survival as judged by a patient’s personal values. Yet one in four Americans aged 75 years or older has given little or no thought to their own wishes for end-of-life medical therapy, according to a recent Pew Research Center survey.
The telephone survey, conducted last spring, included a representative sample of 1,994 U.S. adults. While 47% of respondents aged 75 years or older indicated they had given their own wishes for end-of-life medical care a great deal of thought, 25% said they had given the matter "not much or none." Reflection on those personal wishes needs to be part of the physician/patient discussion about TAVR, according to Dr. Alexander.
With regard to general views on end-of-life therapy, 74% of surveyed individuals age 75 and up declared there should be circumstances in which a patient should be allowed to die. Another 22% said medical staff should do everything possible to save a patient’s life under all circumstances.
Dr. Alexander reported serving as a consultant to Gilead and Pozen.
SNOWMASS, COLO.– Transcatheter aortic valve replacement in nonsurgical candidates with severe symptomatic aortic stenosis carries a hefty price tag of $116,500 per quality-adjusted life-year gained over medical management.
That’s the bottom line in a cost-effectiveness study led by cardiologist Dr. Mark A. Hlatky. The investigators applied data on the costs and benefits of transfemoral transcatheter aortic valve replacement (TAVR) as documented in the landmark PARTNER (Placement of Aortic Transcatheter Valves) trial in their Markov model involving a hypothetical patient cohort. The estimated incremental cost-effectiveness of $116,500 per quality-adjusted life-year gained is well in excess of the $50,000 figure widely accepted by health policy makers as defining a cutoff for cost-effective therapy.
In this cost-effectiveness analysis (Circ. Cardiovasc. Qual. Outcomes 2013;6:419-28), TAVR boosted life expectancy by roughly 11 months, from 2.08 years with medical therapy to 2.93 years. Quality-adjusted life expectancy rose from 1.19 to 1.93 years. TAVR also resulted in 1.4 fewer hospitalizations than with medical management. However, undergoing TAVR rather than medical management raised the lifetime stroke risk from 1% to 11% and increased lifetime health care costs from $83,600 to $169,100, reported the group led by Dr. Hlatky, professor of health research and policy and also professor of medicine at Stanford (Calif.) University.
"This is a fascinating study," Dr. Karen P. Alexander said at the Annual Cardiovascular Conference at Snowmass. "I think the lesson here is that futility from a cost perspective is also something that should be in the discussion" regarding TAVR vs. medical therapy in patients with inoperable aortic stenosis.
She highlighted the Hlatky study in discussing the key role frailty assessment plays in considering TAVR. The study showed that the cost-effectiveness of TAVR is greater in patients with a lower burden of noncardiac disease, which is another way saying "those who are less frail."
This conclusion underscores a statement in the 2012 American College of Cardiology/American Association for Thoracic Surgery/Society for Cardiovascular Angiography and Interventions/Society of Thoracic Surgeons expert consensus document on TAVR paraphrased by Dr. Alexander: Frailty will assume central importance in patient selection for TAVR by virtue of the extensive comorbidities in this population. Existing models do not have predictive variables of interest in high-risk patients. (J. Am. Coll. Cardiol. 2012;59:1200-54).
Dr. Alexander of Duke University in Durham, N.C., said frailty is important when considering TAVR because it has been shown to be associated with increased rates of post-TAVR 30-day morbidity and mortality, prolonged hospital length of stay, and 1-year mortality.
She defined frailty as a multisystem impairment resulting in reduced physiologic reserve and increased vulnerability to stress. Frailty is a physiologic phenotype associated with slow gait, weakness, weight loss, exhaustion, and a low daily activity level.
While the degree of a patient’s frailty is an important consideration in deciding on TAVR vs. medical management, frailty per se is no contraindication to the procedure. Indeed, the prevalence of frailty as defined simply by a baseline 5-meter walk time in excess of 6 seconds was 72% among the 7,710 TAVR patients, mean age 84 years, included in the recent first report of the comprehensive national STS/ACC Transcatheter Valve Therapy Registry (JAMA 2013;310:2069-77). That’s nearly twice the 38% prevalence among community-dwelling 85-year-olds, Dr. Alexander noted, citing data from the Canadian Study of Health and Aging (CMAJ 2011;183:e487-94).
More than 20 different frailty risk scores are now in circulation. Dr. Alexander is particularly enthusiastic about the frailty risk tool developed as part of the ACC’s new Championing Care for the Patient With Aortic Stenosis Initiative. It efficiently assesses five domains of frailty – slowness, weakness, malnutrition, inactivity with loss of independence, and malnutrition – and generates a clinically useful qualitative frailty rating. A patient with a high frailty score may not have sufficient life expectancy to obtain the benefits of TAVR.
With regard to treatment futility, Dr. Alexander observed that it can be defined as either lack of medical efficacy as judged by physicians or as lack of meaningful survival as judged by a patient’s personal values. Yet one in four Americans aged 75 years or older has given little or no thought to their own wishes for end-of-life medical therapy, according to a recent Pew Research Center survey.
The telephone survey, conducted last spring, included a representative sample of 1,994 U.S. adults. While 47% of respondents aged 75 years or older indicated they had given their own wishes for end-of-life medical care a great deal of thought, 25% said they had given the matter "not much or none." Reflection on those personal wishes needs to be part of the physician/patient discussion about TAVR, according to Dr. Alexander.
With regard to general views on end-of-life therapy, 74% of surveyed individuals age 75 and up declared there should be circumstances in which a patient should be allowed to die. Another 22% said medical staff should do everything possible to save a patient’s life under all circumstances.
Dr. Alexander reported serving as a consultant to Gilead and Pozen.

Commentary: Performing clinical research as a CT trainee
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.

So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
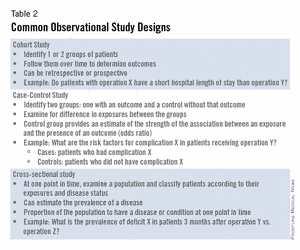
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
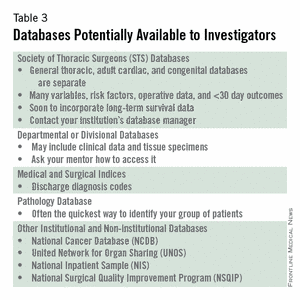
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.