User login
Genetic analysis links PCSK9 inhibition and CV mortality
, but not all-cause mortality, in a large cohort of individuals.

“We tested the hypothesis that genetically low LDL cholesterol due to PCSK9 [proprotein convertase subtilisin/kexin type 9] variation is causally associated with low cardiovascular and all-cause mortality in a general population of Northern European ancestry,” wrote Marianne Benn, MD, DMSc, and colleagues. The findings were published in the Journal of the American College of Cardiology.
The researchers conducted a large-scale genetic analysis of 109,566 persons from the Copenhagen City Heart Study and Copenhagen General Population Study. In addition, the team included a validation cohort of 431,043 individuals from the UK Biobank.
The median duration of follow-up was 10 years (0-42 years), and the median age at study entry was 57 years.
Study participants were genotyped for several PCSK9 variants and a weighted allele score based the effects of LDL cholesterol, individual allele frequency, and number of variant alleles was calculated for each subject.
Weighted scores were categorized into five stepwise noncontinuous score ranges, with lower levels of LDL cholesterol linked to higher allele scores.
After analysis, the researchers found that a growing number of PCSK9 alleles were associated with lower levels of LDL cholesterol up to 0.61 mmol/L (P for trend less than .001) and reduced CV mortality (P = .001), but not with reduced all-cause mortality (P = .11).
“Our genetic data did not show a reduction in risk of all-cause mortality, and only showed a reduction in risk of all-cause mortality in statin trials and not in the PCSK9-inhibitor trials meta-analyzed,” the researchers wrote. “This may be explained by the low frequency of cardiovascular disease in the 2 populations studied,” they explained.
One key limitation was the homogeneous makeup of the study population. Dr. Benn and colleagues acknowledged this could limit the generalizability of the results.
“Long-term LDL cholesterol treatment (e.g., with PCSK9 inhibitors), may translate into reductions in cardiovascular mortality,” they concluded.
The study was supported by the Danish Council for Independent Research, Medical Sciences, Johan Boserup, and the Lise Boserup’s Fund. The authors reported no conflicts of interest.
SOURCE: Benn M et al. JACC. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.517
One question that remains from the current study is whether prolonged inhibition of PCSK9 in patients with increased LDL cholesterol levels will reduce cardiovascular mortality in the context of primary and secondary prevention.
The recent development of PCSK9 inhibitors was heavily influenced by genetic analyses showing that person-specific variants in the PCSK9 gene could lower LDL levels and reduce rates of coronary heart disease. Because of the rarity of these gene variants, their impact on mortality on a large-scale basis remains unclear.
Although numerous clinical trials have shown that PCSK9 inhibition can reduce CVD-related events in both chronic and high-risk patients, no study has clearly shown an effect on cardiovascular death. However, the relationship between lipid levels and clinical outcomes is difficult to assess owing to the presence of confounding factors. Certain types of genetic analysis may help eliminate these challenges by analyzing large populations over extended periods of time.
The genetic analysis by Dr. Benn and colleagues showed an association between long-term exposure to lower levels of LDL cholesterol, by means of functional variants in the PCSK9 gene, and reduced cardiovascular mortality. These findings, alongside other studies, provide further support for the relationship between PCSK9 inhibition and prevention of cardiovascular mortality.
Gregory G. Schwartz, MD, PhD , and Matthew R.G. Taylor, MD, PhD , are with the University of Colorado in Aurora. Dr. Schwartz reported having financial affiliations with Resverlogix, Roche, Sanofi, and The Medicines Company. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.518 ).
One question that remains from the current study is whether prolonged inhibition of PCSK9 in patients with increased LDL cholesterol levels will reduce cardiovascular mortality in the context of primary and secondary prevention.
The recent development of PCSK9 inhibitors was heavily influenced by genetic analyses showing that person-specific variants in the PCSK9 gene could lower LDL levels and reduce rates of coronary heart disease. Because of the rarity of these gene variants, their impact on mortality on a large-scale basis remains unclear.
Although numerous clinical trials have shown that PCSK9 inhibition can reduce CVD-related events in both chronic and high-risk patients, no study has clearly shown an effect on cardiovascular death. However, the relationship between lipid levels and clinical outcomes is difficult to assess owing to the presence of confounding factors. Certain types of genetic analysis may help eliminate these challenges by analyzing large populations over extended periods of time.
The genetic analysis by Dr. Benn and colleagues showed an association between long-term exposure to lower levels of LDL cholesterol, by means of functional variants in the PCSK9 gene, and reduced cardiovascular mortality. These findings, alongside other studies, provide further support for the relationship between PCSK9 inhibition and prevention of cardiovascular mortality.
Gregory G. Schwartz, MD, PhD , and Matthew R.G. Taylor, MD, PhD , are with the University of Colorado in Aurora. Dr. Schwartz reported having financial affiliations with Resverlogix, Roche, Sanofi, and The Medicines Company. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.518 ).
One question that remains from the current study is whether prolonged inhibition of PCSK9 in patients with increased LDL cholesterol levels will reduce cardiovascular mortality in the context of primary and secondary prevention.
The recent development of PCSK9 inhibitors was heavily influenced by genetic analyses showing that person-specific variants in the PCSK9 gene could lower LDL levels and reduce rates of coronary heart disease. Because of the rarity of these gene variants, their impact on mortality on a large-scale basis remains unclear.
Although numerous clinical trials have shown that PCSK9 inhibition can reduce CVD-related events in both chronic and high-risk patients, no study has clearly shown an effect on cardiovascular death. However, the relationship between lipid levels and clinical outcomes is difficult to assess owing to the presence of confounding factors. Certain types of genetic analysis may help eliminate these challenges by analyzing large populations over extended periods of time.
The genetic analysis by Dr. Benn and colleagues showed an association between long-term exposure to lower levels of LDL cholesterol, by means of functional variants in the PCSK9 gene, and reduced cardiovascular mortality. These findings, alongside other studies, provide further support for the relationship between PCSK9 inhibition and prevention of cardiovascular mortality.
Gregory G. Schwartz, MD, PhD , and Matthew R.G. Taylor, MD, PhD , are with the University of Colorado in Aurora. Dr. Schwartz reported having financial affiliations with Resverlogix, Roche, Sanofi, and The Medicines Company. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.518 ).
, but not all-cause mortality, in a large cohort of individuals.
“We tested the hypothesis that genetically low LDL cholesterol due to PCSK9 [proprotein convertase subtilisin/kexin type 9] variation is causally associated with low cardiovascular and all-cause mortality in a general population of Northern European ancestry,” wrote Marianne Benn, MD, DMSc, and colleagues. The findings were published in the Journal of the American College of Cardiology.
The researchers conducted a large-scale genetic analysis of 109,566 persons from the Copenhagen City Heart Study and Copenhagen General Population Study. In addition, the team included a validation cohort of 431,043 individuals from the UK Biobank.
The median duration of follow-up was 10 years (0-42 years), and the median age at study entry was 57 years.
Study participants were genotyped for several PCSK9 variants and a weighted allele score based the effects of LDL cholesterol, individual allele frequency, and number of variant alleles was calculated for each subject.
Weighted scores were categorized into five stepwise noncontinuous score ranges, with lower levels of LDL cholesterol linked to higher allele scores.
After analysis, the researchers found that a growing number of PCSK9 alleles were associated with lower levels of LDL cholesterol up to 0.61 mmol/L (P for trend less than .001) and reduced CV mortality (P = .001), but not with reduced all-cause mortality (P = .11).
“Our genetic data did not show a reduction in risk of all-cause mortality, and only showed a reduction in risk of all-cause mortality in statin trials and not in the PCSK9-inhibitor trials meta-analyzed,” the researchers wrote. “This may be explained by the low frequency of cardiovascular disease in the 2 populations studied,” they explained.
One key limitation was the homogeneous makeup of the study population. Dr. Benn and colleagues acknowledged this could limit the generalizability of the results.
“Long-term LDL cholesterol treatment (e.g., with PCSK9 inhibitors), may translate into reductions in cardiovascular mortality,” they concluded.
The study was supported by the Danish Council for Independent Research, Medical Sciences, Johan Boserup, and the Lise Boserup’s Fund. The authors reported no conflicts of interest.
SOURCE: Benn M et al. JACC. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.517
, but not all-cause mortality, in a large cohort of individuals.
“We tested the hypothesis that genetically low LDL cholesterol due to PCSK9 [proprotein convertase subtilisin/kexin type 9] variation is causally associated with low cardiovascular and all-cause mortality in a general population of Northern European ancestry,” wrote Marianne Benn, MD, DMSc, and colleagues. The findings were published in the Journal of the American College of Cardiology.
The researchers conducted a large-scale genetic analysis of 109,566 persons from the Copenhagen City Heart Study and Copenhagen General Population Study. In addition, the team included a validation cohort of 431,043 individuals from the UK Biobank.
The median duration of follow-up was 10 years (0-42 years), and the median age at study entry was 57 years.
Study participants were genotyped for several PCSK9 variants and a weighted allele score based the effects of LDL cholesterol, individual allele frequency, and number of variant alleles was calculated for each subject.
Weighted scores were categorized into five stepwise noncontinuous score ranges, with lower levels of LDL cholesterol linked to higher allele scores.
After analysis, the researchers found that a growing number of PCSK9 alleles were associated with lower levels of LDL cholesterol up to 0.61 mmol/L (P for trend less than .001) and reduced CV mortality (P = .001), but not with reduced all-cause mortality (P = .11).
“Our genetic data did not show a reduction in risk of all-cause mortality, and only showed a reduction in risk of all-cause mortality in statin trials and not in the PCSK9-inhibitor trials meta-analyzed,” the researchers wrote. “This may be explained by the low frequency of cardiovascular disease in the 2 populations studied,” they explained.
One key limitation was the homogeneous makeup of the study population. Dr. Benn and colleagues acknowledged this could limit the generalizability of the results.
“Long-term LDL cholesterol treatment (e.g., with PCSK9 inhibitors), may translate into reductions in cardiovascular mortality,” they concluded.
The study was supported by the Danish Council for Independent Research, Medical Sciences, Johan Boserup, and the Lise Boserup’s Fund. The authors reported no conflicts of interest.
SOURCE: Benn M et al. JACC. 2019 Jun 17. doi: 10.1016/j.jacc.2019.03.517
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Cardiovascular events in U.S. RA patients fall to non-RA level
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
REPORTING FROM EULAR 2019 CONGRESS

Having unmet social needs ups cardiovascular risk
WASHINGTON – according to a study.

“Although there have been great medical interventions and our technology keeps improving, we can’t prevent the burden of cardiovascular disease. It’s the social factors that are playing this role,” said Ana Palacio, MD, MPH, of the University of Miami during her presentation of the study findings at the annual meeting of the Society of General Internal Medicine.
“We need to address issues at the patient’s home, such as food, isolation, and transportation, to help them prevent cardiovascular risk,” she added.
The study was designed to determine how patient-reported social determinants of health (SDH) had an effect on the Framingham risk score (FRS). Researchers also wanted to assess the relationship between the SDH score and individual risk factors for cardiovascular health, including blood pressure, hemoglobin A1c, LDL cholesterol, body mass index, tobacco use, and physical activity.
Results showed that several SDH factors significantly increase the FRS score, including being born outside of the United States, living alone, having a high social isolation score, and having a low geocoded-based median household income (P less than .01). The calculated SDH score ranged from 0 to 59.
Higher SDH scores were associated with high FRS scores in the areas of poor blood pressure and diabetes control. Additionally, those who had financial strain, poor health literacy, stress, lack of education, and a low median household income were more likely to have a sedentary lifestyle. Black or Hispanic patients who were born outside the United States and had low median household income were at a higher risk of obesity.
The retrospective cohort study originally involved 11,113 primary care patients who received care at the University of Miami Health System between Sept. 16, 2016 and Sept. 10, 2017 and answered an SDH survey. Of this group, 2,876 patients completed the electronic health record data to compile a score. This population had a mean age of 53.8 years and was 61% female; 38% were Hispanic and 9% were black. The mean household income was $53,677 and 87% reported speaking English.
The study examined a total of 11 self-reported and census-based SDH factors. The self-reported factors were race/ethnicity, education, financial strain, stress, tobacco use and physical activity, social isolation, years living in the United States, health literacy, and delayed care. The remaining factors were based on an area deprivation index and census-driven median household income.
“The most surprising finding was how much weight the social factors have in adding to the Framingham risk score, in taking a patient from a medium score to a higher score because of their social environment,” said Dr. Palacio.
The study was funded by the Precision Medicine and Health Disparities Collaborative and was supported by the National Institute on Minority Health and Health Disparities and National Human Genome Research Institute of the National Institutes of Health.
WASHINGTON – according to a study.
“Although there have been great medical interventions and our technology keeps improving, we can’t prevent the burden of cardiovascular disease. It’s the social factors that are playing this role,” said Ana Palacio, MD, MPH, of the University of Miami during her presentation of the study findings at the annual meeting of the Society of General Internal Medicine.
“We need to address issues at the patient’s home, such as food, isolation, and transportation, to help them prevent cardiovascular risk,” she added.
The study was designed to determine how patient-reported social determinants of health (SDH) had an effect on the Framingham risk score (FRS). Researchers also wanted to assess the relationship between the SDH score and individual risk factors for cardiovascular health, including blood pressure, hemoglobin A1c, LDL cholesterol, body mass index, tobacco use, and physical activity.
Results showed that several SDH factors significantly increase the FRS score, including being born outside of the United States, living alone, having a high social isolation score, and having a low geocoded-based median household income (P less than .01). The calculated SDH score ranged from 0 to 59.
Higher SDH scores were associated with high FRS scores in the areas of poor blood pressure and diabetes control. Additionally, those who had financial strain, poor health literacy, stress, lack of education, and a low median household income were more likely to have a sedentary lifestyle. Black or Hispanic patients who were born outside the United States and had low median household income were at a higher risk of obesity.
The retrospective cohort study originally involved 11,113 primary care patients who received care at the University of Miami Health System between Sept. 16, 2016 and Sept. 10, 2017 and answered an SDH survey. Of this group, 2,876 patients completed the electronic health record data to compile a score. This population had a mean age of 53.8 years and was 61% female; 38% were Hispanic and 9% were black. The mean household income was $53,677 and 87% reported speaking English.
The study examined a total of 11 self-reported and census-based SDH factors. The self-reported factors were race/ethnicity, education, financial strain, stress, tobacco use and physical activity, social isolation, years living in the United States, health literacy, and delayed care. The remaining factors were based on an area deprivation index and census-driven median household income.
“The most surprising finding was how much weight the social factors have in adding to the Framingham risk score, in taking a patient from a medium score to a higher score because of their social environment,” said Dr. Palacio.
The study was funded by the Precision Medicine and Health Disparities Collaborative and was supported by the National Institute on Minority Health and Health Disparities and National Human Genome Research Institute of the National Institutes of Health.
WASHINGTON – according to a study.
“Although there have been great medical interventions and our technology keeps improving, we can’t prevent the burden of cardiovascular disease. It’s the social factors that are playing this role,” said Ana Palacio, MD, MPH, of the University of Miami during her presentation of the study findings at the annual meeting of the Society of General Internal Medicine.
“We need to address issues at the patient’s home, such as food, isolation, and transportation, to help them prevent cardiovascular risk,” she added.
The study was designed to determine how patient-reported social determinants of health (SDH) had an effect on the Framingham risk score (FRS). Researchers also wanted to assess the relationship between the SDH score and individual risk factors for cardiovascular health, including blood pressure, hemoglobin A1c, LDL cholesterol, body mass index, tobacco use, and physical activity.
Results showed that several SDH factors significantly increase the FRS score, including being born outside of the United States, living alone, having a high social isolation score, and having a low geocoded-based median household income (P less than .01). The calculated SDH score ranged from 0 to 59.
Higher SDH scores were associated with high FRS scores in the areas of poor blood pressure and diabetes control. Additionally, those who had financial strain, poor health literacy, stress, lack of education, and a low median household income were more likely to have a sedentary lifestyle. Black or Hispanic patients who were born outside the United States and had low median household income were at a higher risk of obesity.
The retrospective cohort study originally involved 11,113 primary care patients who received care at the University of Miami Health System between Sept. 16, 2016 and Sept. 10, 2017 and answered an SDH survey. Of this group, 2,876 patients completed the electronic health record data to compile a score. This population had a mean age of 53.8 years and was 61% female; 38% were Hispanic and 9% were black. The mean household income was $53,677 and 87% reported speaking English.
The study examined a total of 11 self-reported and census-based SDH factors. The self-reported factors were race/ethnicity, education, financial strain, stress, tobacco use and physical activity, social isolation, years living in the United States, health literacy, and delayed care. The remaining factors were based on an area deprivation index and census-driven median household income.
“The most surprising finding was how much weight the social factors have in adding to the Framingham risk score, in taking a patient from a medium score to a higher score because of their social environment,” said Dr. Palacio.
The study was funded by the Precision Medicine and Health Disparities Collaborative and was supported by the National Institute on Minority Health and Health Disparities and National Human Genome Research Institute of the National Institutes of Health.
REPORTING FROM SGIM 2019
Medicaid expansion associated with lower cardiovascular mortality
Counties in states that expanded Medicaid coverage under the Affordable Care Act have experienced a significantly smaller increase in cardiovascular mortality rates among middle-aged adults, compared with counties in states that did not expand coverage, according to findings from a new study.
In expansion-state counties, the change in cardiovascular mortality was stable between the pre-expansion (2010-2013) and postexpansion (2014-2016) periods, at 146.5-146.4 deaths per 100,000 residents per year, compared with mortality rates in nonexpansion counties during the same periods (176.3-180.9 deaths per 100,000), Sameed Ahmed M. Khatana, MD, and colleagues wrote in JAMA Cardiology.
“After accounting for demographic, clinical, and economic differences, counties in expansion states had 4.3 fewer deaths per 100,000 residents per year from cardiovascular causes after Medicaid expansion than if they had followed the same trends as counties in nonexpansion states,” Dr. Khatana, of the University of Pennsylvania, Philadelphia, and colleagues wrote..
That translated into 2,039 fewer total deaths per year in residents aged between 45 and 64 years from cardiovascular causes after Medicaid expansion, the authors noted.
In all, 29 states, plus Washington, D.C., were included in the expansion group, and 19 states were in the nonexpansion (control) group. During the study period, from 2010 to 2016, the number of expansion counties ranged between 912 and 931, and for the nonexpansion counties, between 985 and 1,029. About half of the residents in each group were women. The percentage of black residents was lower in expansion states, but the percentage of Hispanic residents did not differ. Compared with nonexpansion counties, expansion counties also had a lower prevalence of diabetes (8.5% vs. 9.7% in the nonexpansion counties), obesity (26.2% vs. 29.1%), and smoking (17.1 vs. 18.9%); a lower mean percentage of poor residents (14.4% vs 16.6%; all with P less than .001); and a higher median household income.
Expansion counties also fared better when it came to health insurance coverage. In 2010, 14.6% of their residents had no coverage, compared with 19.5% of residents in nonexpansion counties. During the study period, the decrease in the percentage of middle-aged residents without health coverage was larger in expansion than in nonexpansion counties (7.3% vs. 5.6%, respectively), as was the decrease in low-income residents without coverage (19.8% vs. 13.5%).
However, the authors cautioned that, given the observational nature of the study, they were “not able to make a causal association between expansion of Medicaid eligibility and differences in the cardiovascular mortality rates between the two groups of counties. It is possible that there were other unmeasured time varying factors that can explain the observed association.”
Despite that limitation of the study, which observed adults in all income categories and was not limited to low-income residents, the researchers noted that, given the association between Medicaid expansion and cardiovascular mortality rates, as well as the “high burden of cardiovascular risk factors among individuals without insurance and those with lower socioeconomic status,” policy makers might consider the results in future discussions about changes to eligibility for and expansion of Medicaid.
Dr. Khatana is supported by a grant from the National Institutes of Health. Two authors reported relationships with drug companies outside of the reported study; the rest of the authors had no disclosures to report.
SOURCE: Khatana SAM et al. JAMA Cardiol. 2019 Jun 5. doi: 10.1001/jamacardio.2019.1651.
Counties in states that expanded Medicaid coverage under the Affordable Care Act have experienced a significantly smaller increase in cardiovascular mortality rates among middle-aged adults, compared with counties in states that did not expand coverage, according to findings from a new study.
In expansion-state counties, the change in cardiovascular mortality was stable between the pre-expansion (2010-2013) and postexpansion (2014-2016) periods, at 146.5-146.4 deaths per 100,000 residents per year, compared with mortality rates in nonexpansion counties during the same periods (176.3-180.9 deaths per 100,000), Sameed Ahmed M. Khatana, MD, and colleagues wrote in JAMA Cardiology.
“After accounting for demographic, clinical, and economic differences, counties in expansion states had 4.3 fewer deaths per 100,000 residents per year from cardiovascular causes after Medicaid expansion than if they had followed the same trends as counties in nonexpansion states,” Dr. Khatana, of the University of Pennsylvania, Philadelphia, and colleagues wrote..
That translated into 2,039 fewer total deaths per year in residents aged between 45 and 64 years from cardiovascular causes after Medicaid expansion, the authors noted.
In all, 29 states, plus Washington, D.C., were included in the expansion group, and 19 states were in the nonexpansion (control) group. During the study period, from 2010 to 2016, the number of expansion counties ranged between 912 and 931, and for the nonexpansion counties, between 985 and 1,029. About half of the residents in each group were women. The percentage of black residents was lower in expansion states, but the percentage of Hispanic residents did not differ. Compared with nonexpansion counties, expansion counties also had a lower prevalence of diabetes (8.5% vs. 9.7% in the nonexpansion counties), obesity (26.2% vs. 29.1%), and smoking (17.1 vs. 18.9%); a lower mean percentage of poor residents (14.4% vs 16.6%; all with P less than .001); and a higher median household income.
Expansion counties also fared better when it came to health insurance coverage. In 2010, 14.6% of their residents had no coverage, compared with 19.5% of residents in nonexpansion counties. During the study period, the decrease in the percentage of middle-aged residents without health coverage was larger in expansion than in nonexpansion counties (7.3% vs. 5.6%, respectively), as was the decrease in low-income residents without coverage (19.8% vs. 13.5%).
However, the authors cautioned that, given the observational nature of the study, they were “not able to make a causal association between expansion of Medicaid eligibility and differences in the cardiovascular mortality rates between the two groups of counties. It is possible that there were other unmeasured time varying factors that can explain the observed association.”
Despite that limitation of the study, which observed adults in all income categories and was not limited to low-income residents, the researchers noted that, given the association between Medicaid expansion and cardiovascular mortality rates, as well as the “high burden of cardiovascular risk factors among individuals without insurance and those with lower socioeconomic status,” policy makers might consider the results in future discussions about changes to eligibility for and expansion of Medicaid.
Dr. Khatana is supported by a grant from the National Institutes of Health. Two authors reported relationships with drug companies outside of the reported study; the rest of the authors had no disclosures to report.
SOURCE: Khatana SAM et al. JAMA Cardiol. 2019 Jun 5. doi: 10.1001/jamacardio.2019.1651.
Counties in states that expanded Medicaid coverage under the Affordable Care Act have experienced a significantly smaller increase in cardiovascular mortality rates among middle-aged adults, compared with counties in states that did not expand coverage, according to findings from a new study.
In expansion-state counties, the change in cardiovascular mortality was stable between the pre-expansion (2010-2013) and postexpansion (2014-2016) periods, at 146.5-146.4 deaths per 100,000 residents per year, compared with mortality rates in nonexpansion counties during the same periods (176.3-180.9 deaths per 100,000), Sameed Ahmed M. Khatana, MD, and colleagues wrote in JAMA Cardiology.
“After accounting for demographic, clinical, and economic differences, counties in expansion states had 4.3 fewer deaths per 100,000 residents per year from cardiovascular causes after Medicaid expansion than if they had followed the same trends as counties in nonexpansion states,” Dr. Khatana, of the University of Pennsylvania, Philadelphia, and colleagues wrote..
That translated into 2,039 fewer total deaths per year in residents aged between 45 and 64 years from cardiovascular causes after Medicaid expansion, the authors noted.
In all, 29 states, plus Washington, D.C., were included in the expansion group, and 19 states were in the nonexpansion (control) group. During the study period, from 2010 to 2016, the number of expansion counties ranged between 912 and 931, and for the nonexpansion counties, between 985 and 1,029. About half of the residents in each group were women. The percentage of black residents was lower in expansion states, but the percentage of Hispanic residents did not differ. Compared with nonexpansion counties, expansion counties also had a lower prevalence of diabetes (8.5% vs. 9.7% in the nonexpansion counties), obesity (26.2% vs. 29.1%), and smoking (17.1 vs. 18.9%); a lower mean percentage of poor residents (14.4% vs 16.6%; all with P less than .001); and a higher median household income.
Expansion counties also fared better when it came to health insurance coverage. In 2010, 14.6% of their residents had no coverage, compared with 19.5% of residents in nonexpansion counties. During the study period, the decrease in the percentage of middle-aged residents without health coverage was larger in expansion than in nonexpansion counties (7.3% vs. 5.6%, respectively), as was the decrease in low-income residents without coverage (19.8% vs. 13.5%).
However, the authors cautioned that, given the observational nature of the study, they were “not able to make a causal association between expansion of Medicaid eligibility and differences in the cardiovascular mortality rates between the two groups of counties. It is possible that there were other unmeasured time varying factors that can explain the observed association.”
Despite that limitation of the study, which observed adults in all income categories and was not limited to low-income residents, the researchers noted that, given the association between Medicaid expansion and cardiovascular mortality rates, as well as the “high burden of cardiovascular risk factors among individuals without insurance and those with lower socioeconomic status,” policy makers might consider the results in future discussions about changes to eligibility for and expansion of Medicaid.
Dr. Khatana is supported by a grant from the National Institutes of Health. Two authors reported relationships with drug companies outside of the reported study; the rest of the authors had no disclosures to report.
SOURCE: Khatana SAM et al. JAMA Cardiol. 2019 Jun 5. doi: 10.1001/jamacardio.2019.1651.
FROM JAMA CARDIOLOGY
Key clinical point:
Major finding: Counties in expansion states had 4.3 fewer deaths from cardiovascular causes per 100,000 residents per year after Medicaid expansion, compared with counties in nonexpansion states.
Study details: In this longitudinal, observational study from 2010 to 2016, researchers used a difference-in-difference approach with county-level data for adults from 48 states (excluding Massachusetts and Wisconsin) and Washington, D.C., who were aged between 45 and 64 years. The county-level data were obtained from the Centers for Disease Control and Prevention’s Online Data for Epidemiologic Research mortality database.
Disclosures: Dr. Khatana is supported by a grant from the National Institutes of Health. Two authors reported relationships with drug companies outside of the reported study; the rest of the authors had no disclosures to report.
Source: Khatana SAM et al. JAMA Cardiol. 2019 Jun 5. doi: 10.1001/jamacardio.2019.1651.
Carotid ultrasound may aid cardiovascular risk stratification of patients with psoriatic disease
according to findings from a retrospective study.
When added to the Framingham risk score, the measurement significantly improved its predictive ability, Curtis Sobchak, MD, and colleagues wrote in Arthritis & Rheumatology.
The findings indicate that carotid ultrasound could be a useful addition to cardiovascular risk stratification among these patients.
“Traditional algorithms do not consider other factors that may contribute to increased cardiovascular risk in rheumatic disease patients and tend to underestimate cardiovascular risk,” wrote Dr. Sobchak of the University of Toronto and coauthors.
“The advantage of ultrasound over other modalities for vascular imaging includes lack of radiation, low cost of the examination, and its widespread use in rheumatology for joint evaluation. Thus, this assessment could potentially be performed ‘at the bedside’ during consultation to provide immediate valuable information to complement clinical data from history, physical examination, and laboratory data,” they added.
The study retrospectively examined a prospective, observational cohort of 559 patients with psoriasis alone or psoriasis and psoriatic arthritis enrolled in the University of Toronto Psoriatic Disease Program. The investigators evaluated five ultrasound measures of atherosclerosis, including total plaque area (TPA), mean carotid intima-media thickness (cIMT), maximal cIMT, plaque category, and TPA category. Then they analyzed the risk relationship with major cardiovascular events (CVEs) classified as myocardial infarction, unstable angina, ischemic stroke, revascularization procedures, or cardiovascular-related death. Minor CVEs included stable angina, exacerbation of congestive heart failure, and transient ischemic attack over a mean follow-up close to 4 years.
The mean baseline TPA was 0.18 cm2 and mean cIMT was 639 mcm. Most patients had plaques, including 27.0% with unilateral and 31.5% with bilateral plaques.
The rate of a first CVE during the study period was 1.11 per 100 patient-years, and the rate of a first major CVE was 0.91 per 100 patient-years. The risk of each was significantly related to a higher baseline burden of atherosclerosis.
A multivariate analysis determined that increased TPA at baseline increased the risk of an event by nearly 200% (hazard ratio, 2.85). Mean cIMT was not an independent predictor in the final analysis, “suggesting that TPA is a stronger predictor for CVE than cIMT,” the authors wrote.
Finally, they examined the predictive value of atherosclerosis alone, as well as combined with the Framingham risk score. The 5-year model indicated that the bivariate model was slightly more accurate than the Framingham score alone (area under the curve, 0.84 vs. 0.81), although this was not a significant difference. The predictive value of the Framingham risk score plus maximal cIMT, mean cIMT, or TPA all significantly improved when they were calculated using only high-risk patients (those above the treatment threshold for dyslipidemia).
“To the best of our knowledge this is the first study to assess the utility of various measures of carotid atherosclerosis to predict CVE in patients with psoriasis and PsA [psoriatic arthritis]. ... Combining vascular imaging data with clinical and laboratory measures of traditional cardiovascular risk factors could improve accuracy of cardiovascular risk stratification in patients with psoriatic disease and facilitate earlier initiation of appropriate treatment to reduce CVE in this population,” the investigators wrote.
The study was supported in part by a Young Investigator Operating Grant from the Arthritis Society. Dr. Sobchak had no financial disclosures.
SOURCE: Sobchak C et al. Arthritis Rheumatol. 2019 Jun 5. doi: 10.1002/art.40925.
according to findings from a retrospective study.
When added to the Framingham risk score, the measurement significantly improved its predictive ability, Curtis Sobchak, MD, and colleagues wrote in Arthritis & Rheumatology.
The findings indicate that carotid ultrasound could be a useful addition to cardiovascular risk stratification among these patients.
“Traditional algorithms do not consider other factors that may contribute to increased cardiovascular risk in rheumatic disease patients and tend to underestimate cardiovascular risk,” wrote Dr. Sobchak of the University of Toronto and coauthors.
“The advantage of ultrasound over other modalities for vascular imaging includes lack of radiation, low cost of the examination, and its widespread use in rheumatology for joint evaluation. Thus, this assessment could potentially be performed ‘at the bedside’ during consultation to provide immediate valuable information to complement clinical data from history, physical examination, and laboratory data,” they added.
The study retrospectively examined a prospective, observational cohort of 559 patients with psoriasis alone or psoriasis and psoriatic arthritis enrolled in the University of Toronto Psoriatic Disease Program. The investigators evaluated five ultrasound measures of atherosclerosis, including total plaque area (TPA), mean carotid intima-media thickness (cIMT), maximal cIMT, plaque category, and TPA category. Then they analyzed the risk relationship with major cardiovascular events (CVEs) classified as myocardial infarction, unstable angina, ischemic stroke, revascularization procedures, or cardiovascular-related death. Minor CVEs included stable angina, exacerbation of congestive heart failure, and transient ischemic attack over a mean follow-up close to 4 years.
The mean baseline TPA was 0.18 cm2 and mean cIMT was 639 mcm. Most patients had plaques, including 27.0% with unilateral and 31.5% with bilateral plaques.
The rate of a first CVE during the study period was 1.11 per 100 patient-years, and the rate of a first major CVE was 0.91 per 100 patient-years. The risk of each was significantly related to a higher baseline burden of atherosclerosis.
A multivariate analysis determined that increased TPA at baseline increased the risk of an event by nearly 200% (hazard ratio, 2.85). Mean cIMT was not an independent predictor in the final analysis, “suggesting that TPA is a stronger predictor for CVE than cIMT,” the authors wrote.
Finally, they examined the predictive value of atherosclerosis alone, as well as combined with the Framingham risk score. The 5-year model indicated that the bivariate model was slightly more accurate than the Framingham score alone (area under the curve, 0.84 vs. 0.81), although this was not a significant difference. The predictive value of the Framingham risk score plus maximal cIMT, mean cIMT, or TPA all significantly improved when they were calculated using only high-risk patients (those above the treatment threshold for dyslipidemia).
“To the best of our knowledge this is the first study to assess the utility of various measures of carotid atherosclerosis to predict CVE in patients with psoriasis and PsA [psoriatic arthritis]. ... Combining vascular imaging data with clinical and laboratory measures of traditional cardiovascular risk factors could improve accuracy of cardiovascular risk stratification in patients with psoriatic disease and facilitate earlier initiation of appropriate treatment to reduce CVE in this population,” the investigators wrote.
The study was supported in part by a Young Investigator Operating Grant from the Arthritis Society. Dr. Sobchak had no financial disclosures.
SOURCE: Sobchak C et al. Arthritis Rheumatol. 2019 Jun 5. doi: 10.1002/art.40925.
according to findings from a retrospective study.
When added to the Framingham risk score, the measurement significantly improved its predictive ability, Curtis Sobchak, MD, and colleagues wrote in Arthritis & Rheumatology.
The findings indicate that carotid ultrasound could be a useful addition to cardiovascular risk stratification among these patients.
“Traditional algorithms do not consider other factors that may contribute to increased cardiovascular risk in rheumatic disease patients and tend to underestimate cardiovascular risk,” wrote Dr. Sobchak of the University of Toronto and coauthors.
“The advantage of ultrasound over other modalities for vascular imaging includes lack of radiation, low cost of the examination, and its widespread use in rheumatology for joint evaluation. Thus, this assessment could potentially be performed ‘at the bedside’ during consultation to provide immediate valuable information to complement clinical data from history, physical examination, and laboratory data,” they added.
The study retrospectively examined a prospective, observational cohort of 559 patients with psoriasis alone or psoriasis and psoriatic arthritis enrolled in the University of Toronto Psoriatic Disease Program. The investigators evaluated five ultrasound measures of atherosclerosis, including total plaque area (TPA), mean carotid intima-media thickness (cIMT), maximal cIMT, plaque category, and TPA category. Then they analyzed the risk relationship with major cardiovascular events (CVEs) classified as myocardial infarction, unstable angina, ischemic stroke, revascularization procedures, or cardiovascular-related death. Minor CVEs included stable angina, exacerbation of congestive heart failure, and transient ischemic attack over a mean follow-up close to 4 years.
The mean baseline TPA was 0.18 cm2 and mean cIMT was 639 mcm. Most patients had plaques, including 27.0% with unilateral and 31.5% with bilateral plaques.
The rate of a first CVE during the study period was 1.11 per 100 patient-years, and the rate of a first major CVE was 0.91 per 100 patient-years. The risk of each was significantly related to a higher baseline burden of atherosclerosis.
A multivariate analysis determined that increased TPA at baseline increased the risk of an event by nearly 200% (hazard ratio, 2.85). Mean cIMT was not an independent predictor in the final analysis, “suggesting that TPA is a stronger predictor for CVE than cIMT,” the authors wrote.
Finally, they examined the predictive value of atherosclerosis alone, as well as combined with the Framingham risk score. The 5-year model indicated that the bivariate model was slightly more accurate than the Framingham score alone (area under the curve, 0.84 vs. 0.81), although this was not a significant difference. The predictive value of the Framingham risk score plus maximal cIMT, mean cIMT, or TPA all significantly improved when they were calculated using only high-risk patients (those above the treatment threshold for dyslipidemia).
“To the best of our knowledge this is the first study to assess the utility of various measures of carotid atherosclerosis to predict CVE in patients with psoriasis and PsA [psoriatic arthritis]. ... Combining vascular imaging data with clinical and laboratory measures of traditional cardiovascular risk factors could improve accuracy of cardiovascular risk stratification in patients with psoriatic disease and facilitate earlier initiation of appropriate treatment to reduce CVE in this population,” the investigators wrote.
The study was supported in part by a Young Investigator Operating Grant from the Arthritis Society. Dr. Sobchak had no financial disclosures.
SOURCE: Sobchak C et al. Arthritis Rheumatol. 2019 Jun 5. doi: 10.1002/art.40925.
FROM ARTHRITIS & RHEUMATOLOGY
FDA grants Priority Review to Vascepa for cardiovascular risk reduction
The Food and Drug Administration has granted a Priority Review to the supplemental new drug application for icosapent ethyl (Vascepa).

If approved, Vascepa – which is produced by Amarin – would be the first drug indicated to reduce residual cardiovascular risk in patients with LDL cholesterol managed by statins who still have persistent elevated triglycerides. The drug is now approved for reducing triglyceride levels in patients with baseline values of 500 mg/dL or greater.
The Priority Review is based on results of REDUCE-IT, a landmark cardiovascular outcomes trial whose primary results were presented at the American Heart Association scientific sessions last November and published in the New England Journal of Medicine. Vascepa achieved the primary study endpoint, reducing the relative risk for the first occurrence of a major adverse cardiovascular event significantly, by 25%.
The drug also met the study’s key secondary endpoint, reducing the incidence of a composite of cardiovascular death, nonfatal heart attack, and nonfatal stroke by 26%. Significant adverse events associated with Vascepa in the trial were peripheral edema, constipation, and atrial fibrillation.
Vascepa is currently indicated as an adjunct to diet to reduce triglyceride in adults with severe hypertriglyceridemia, a significantly smaller population than that represented in REDUCE-IT.
“We expect earlier approval of an expanded indication for Vascepa to lead to faster improvements in care for millions of patients with residual cardiovascular risk after statin therapy,” John F. Thero, president and CEO of Amarin, said in the statement.
The FDA is expected to issue a complete response by the end of September. Find the full press release on the Amarin website.
The Food and Drug Administration has granted a Priority Review to the supplemental new drug application for icosapent ethyl (Vascepa).
If approved, Vascepa – which is produced by Amarin – would be the first drug indicated to reduce residual cardiovascular risk in patients with LDL cholesterol managed by statins who still have persistent elevated triglycerides. The drug is now approved for reducing triglyceride levels in patients with baseline values of 500 mg/dL or greater.
The Priority Review is based on results of REDUCE-IT, a landmark cardiovascular outcomes trial whose primary results were presented at the American Heart Association scientific sessions last November and published in the New England Journal of Medicine. Vascepa achieved the primary study endpoint, reducing the relative risk for the first occurrence of a major adverse cardiovascular event significantly, by 25%.
The drug also met the study’s key secondary endpoint, reducing the incidence of a composite of cardiovascular death, nonfatal heart attack, and nonfatal stroke by 26%. Significant adverse events associated with Vascepa in the trial were peripheral edema, constipation, and atrial fibrillation.
Vascepa is currently indicated as an adjunct to diet to reduce triglyceride in adults with severe hypertriglyceridemia, a significantly smaller population than that represented in REDUCE-IT.
“We expect earlier approval of an expanded indication for Vascepa to lead to faster improvements in care for millions of patients with residual cardiovascular risk after statin therapy,” John F. Thero, president and CEO of Amarin, said in the statement.
The FDA is expected to issue a complete response by the end of September. Find the full press release on the Amarin website.
The Food and Drug Administration has granted a Priority Review to the supplemental new drug application for icosapent ethyl (Vascepa).
If approved, Vascepa – which is produced by Amarin – would be the first drug indicated to reduce residual cardiovascular risk in patients with LDL cholesterol managed by statins who still have persistent elevated triglycerides. The drug is now approved for reducing triglyceride levels in patients with baseline values of 500 mg/dL or greater.
The Priority Review is based on results of REDUCE-IT, a landmark cardiovascular outcomes trial whose primary results were presented at the American Heart Association scientific sessions last November and published in the New England Journal of Medicine. Vascepa achieved the primary study endpoint, reducing the relative risk for the first occurrence of a major adverse cardiovascular event significantly, by 25%.
The drug also met the study’s key secondary endpoint, reducing the incidence of a composite of cardiovascular death, nonfatal heart attack, and nonfatal stroke by 26%. Significant adverse events associated with Vascepa in the trial were peripheral edema, constipation, and atrial fibrillation.
Vascepa is currently indicated as an adjunct to diet to reduce triglyceride in adults with severe hypertriglyceridemia, a significantly smaller population than that represented in REDUCE-IT.
“We expect earlier approval of an expanded indication for Vascepa to lead to faster improvements in care for millions of patients with residual cardiovascular risk after statin therapy,” John F. Thero, president and CEO of Amarin, said in the statement.
The FDA is expected to issue a complete response by the end of September. Find the full press release on the Amarin website.
Cholesterol guideline: Risk assessment gets personal
according to the 2018 update to U.S. guidelines for cholesterol management from the American Heart Association and the American College of Cardiology.
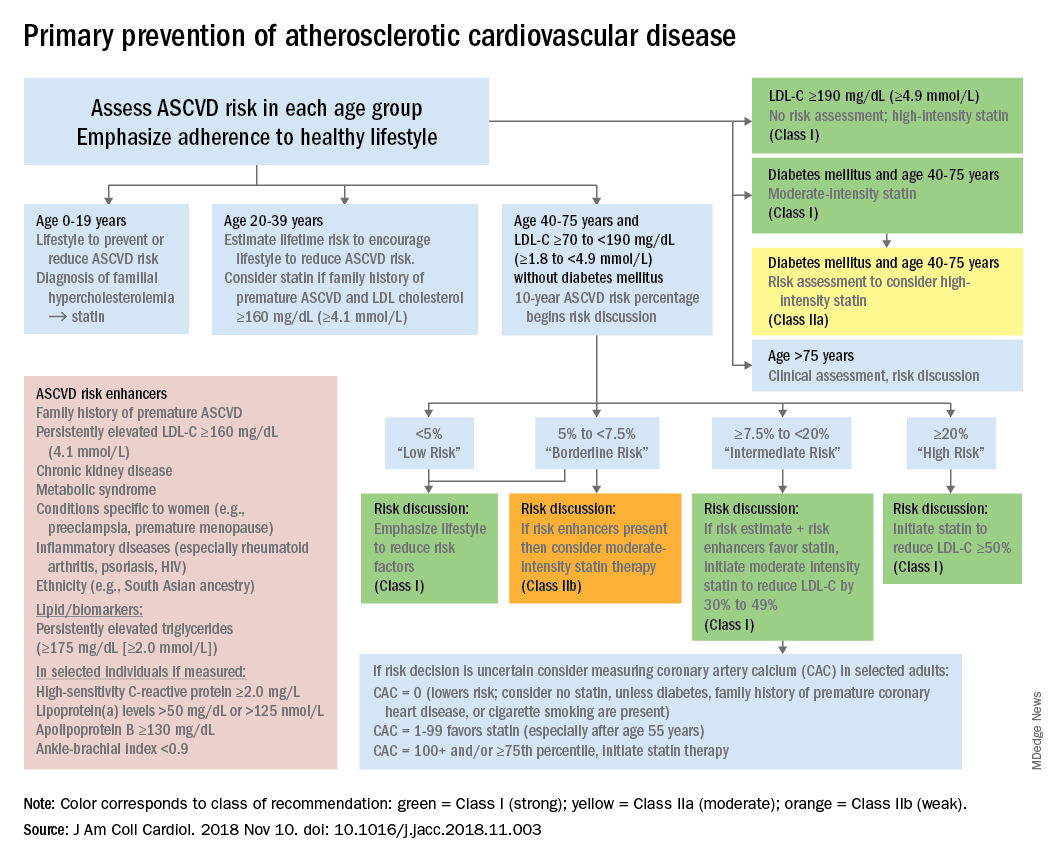
The guideline also emphasizes “careful adherence to lifestyle recommendations at an early age [to] reduce risk factor burden over the lifespan and decrease the need for preventive drug therapies later in life,” Scott M. Grundy, MD, PhD, and Neil J. Stone, MD, said in a synopsis of the document in the Annals of Internal Medicine.
For primary prevention in patients aged 40-75 years, estimation of 10-year ASCVD risk – introduced in the 2013 guidelines – and stratification into one of four categories should set the stage for clinician-patient discussion. A score of less than 5% indicates low risk and should prompt a risk discussion that emphasizes lifestyle recommendations. “Statins are clinically efficacious in the latter three categories, but the higher the risk, the stronger the statin indication,” said Dr. Grundy of the University of Texas, Dallas, and Dr. Stone of Northwestern University, Chicago.
When risk status is uncertain, measurement of coronary artery calcium should be considered in patients aged 40-75 years with LDL cholesterol levels of 70-189 mg/dL who do no not have diabetes, they noted.
The guideline emphasizes secondary prevention with “maximally tolerated doses of statins” and the use of nonstatin drugs such as ezetimibe and PCSK9 inhibitors for patients with very high ASCVD risk – defined as a history of multiple major events or one event and other high-risk conditions, Dr. Grundy and Dr. Stone wrote.
Financial support for the Guideline Writing Committee for the 2018 Cholesterol Guidelines came from the AHA and the ACC. Dr. Grundy and Dr. Stone said that they had no relevant conflicts of interest.
SOURCE: Grundy SM and Stone NJ. Ann Intern Med. 2019 May 28. doi: 10.7326/M19-0365.
according to the 2018 update to U.S. guidelines for cholesterol management from the American Heart Association and the American College of Cardiology.
The guideline also emphasizes “careful adherence to lifestyle recommendations at an early age [to] reduce risk factor burden over the lifespan and decrease the need for preventive drug therapies later in life,” Scott M. Grundy, MD, PhD, and Neil J. Stone, MD, said in a synopsis of the document in the Annals of Internal Medicine.
For primary prevention in patients aged 40-75 years, estimation of 10-year ASCVD risk – introduced in the 2013 guidelines – and stratification into one of four categories should set the stage for clinician-patient discussion. A score of less than 5% indicates low risk and should prompt a risk discussion that emphasizes lifestyle recommendations. “Statins are clinically efficacious in the latter three categories, but the higher the risk, the stronger the statin indication,” said Dr. Grundy of the University of Texas, Dallas, and Dr. Stone of Northwestern University, Chicago.
When risk status is uncertain, measurement of coronary artery calcium should be considered in patients aged 40-75 years with LDL cholesterol levels of 70-189 mg/dL who do no not have diabetes, they noted.
The guideline emphasizes secondary prevention with “maximally tolerated doses of statins” and the use of nonstatin drugs such as ezetimibe and PCSK9 inhibitors for patients with very high ASCVD risk – defined as a history of multiple major events or one event and other high-risk conditions, Dr. Grundy and Dr. Stone wrote.
Financial support for the Guideline Writing Committee for the 2018 Cholesterol Guidelines came from the AHA and the ACC. Dr. Grundy and Dr. Stone said that they had no relevant conflicts of interest.
SOURCE: Grundy SM and Stone NJ. Ann Intern Med. 2019 May 28. doi: 10.7326/M19-0365.
according to the 2018 update to U.S. guidelines for cholesterol management from the American Heart Association and the American College of Cardiology.
The guideline also emphasizes “careful adherence to lifestyle recommendations at an early age [to] reduce risk factor burden over the lifespan and decrease the need for preventive drug therapies later in life,” Scott M. Grundy, MD, PhD, and Neil J. Stone, MD, said in a synopsis of the document in the Annals of Internal Medicine.
For primary prevention in patients aged 40-75 years, estimation of 10-year ASCVD risk – introduced in the 2013 guidelines – and stratification into one of four categories should set the stage for clinician-patient discussion. A score of less than 5% indicates low risk and should prompt a risk discussion that emphasizes lifestyle recommendations. “Statins are clinically efficacious in the latter three categories, but the higher the risk, the stronger the statin indication,” said Dr. Grundy of the University of Texas, Dallas, and Dr. Stone of Northwestern University, Chicago.
When risk status is uncertain, measurement of coronary artery calcium should be considered in patients aged 40-75 years with LDL cholesterol levels of 70-189 mg/dL who do no not have diabetes, they noted.
The guideline emphasizes secondary prevention with “maximally tolerated doses of statins” and the use of nonstatin drugs such as ezetimibe and PCSK9 inhibitors for patients with very high ASCVD risk – defined as a history of multiple major events or one event and other high-risk conditions, Dr. Grundy and Dr. Stone wrote.
Financial support for the Guideline Writing Committee for the 2018 Cholesterol Guidelines came from the AHA and the ACC. Dr. Grundy and Dr. Stone said that they had no relevant conflicts of interest.
SOURCE: Grundy SM and Stone NJ. Ann Intern Med. 2019 May 28. doi: 10.7326/M19-0365.
FROM THE ANNALS OF INTERNAL MEDICINE
Significant increase in low-attenuation coronary plaques found in lupus
SAN FRANCISCO – according to an investigation from Johns Hopkins University, Baltimore.
All of the 102 lupus patients in the coronary artery CT angiography study also had positive plaque remodeling, meaning that at least one low-attenuation plaque was growing into the lumen wall, not the lumen itself, which makes them difficult to detect on standard imaging. Low-attenuation plaques were defined in the study as a plaque larger than 1 mm2 with a radiodensity below 30 Hounsfield units.
Low-attenuation plaques are inherently unstable; they’re fatty, necrotic, and have a high risk of rupturing; their presence in the lumen wall is especially worrisome. In the general population, they sometimes regress, scarring down over time and no longer posing a threat. That didn’t happen in the 30 lupus patients who had follow-up CT angiographies, some 9 years after their first.
The team conducted the study to help understand why cardiovascular disease is so common in lupus, and the leading cause of death. Hopkins investigators have shown previously that statins have no effect on the risk or plaque occurrence and progression, and the cardiovascular risk doesn’t always seem to correlate with disease control. For those and other reasons, the current thinking at Hopkins is that cardiovascular disease in lupus is somehow different than in the general population, said George Stojan, MD, an assistant professor of rheumatology at the school and codirector of the Hopkins Lupus Center.
The goal is “to figure out exactly what to look for when we assess the risk; I don’t think we understand that at this point. We assume patients with lupus behave exactly like patients who don’t have lupus, but they obviously don’t. They do not respond to statins. They have a higher risk no matter what you do for them, even when their disease activity is low, and how much plaque they have over time doesn’t really correlate with disease activity,” he said at an international conference on systemic lupus erythematosus.
“Once we understand” the mechanism, “then we can try to [alter] it. Maybe we can look at new drugs, like the PCSK9 inhibitors which have shown a lot of promise in the general population.” At this point, however, “we don’t really know how to intervene,” Dr. Stojan said.
In the meantime, positive remodeling and low-attenuation, noncalcified plaques (LANCPs) might be something to look for when assessing systemic lupus erythematosus cardiovascular risk. “A simple coronary calcium score, something that all doctors do,” is not enough in lupus, nor is simply checking for lumen obstruction. Also, it’s important not to be misled by an overall reduction in noncalcified plaques. “Low-attenuation, noncalcified plaques don’t [regress] over time in lupus, and they are the ones that lead to cardiovascular events,” he said.
The CT angiography findings were compared with findings in 100 healthy controls who had two CT angiograms in a University of California, Los Angeles, cohort. Overall, there was a mean of 458 LANCPs among lupus patients, versus 42 among controls, a more than 900% difference (P less than .001).
Women with lupus aged under 44 years had a mean of 63 LANCPs; none were detected in healthy women under 44 years. Among women aged 45-59 years, there was a mean of 451 LANCPs in the lupus group versus 53 in the control arm. The findings were highly statistically significant, and almost statistically significant for women 60 years or older, 695 lesions among lupus patients versus 22 (P = .0576).
There were only nine men with lupus in the study, but the findings were similar versus male controls.
While mean LANCP volume regressed over time in the control group (mean, –6.90 mm3; P = .0002), a mean regression of –13.56 mm3 in the lupus group was not statistically significant (P = .4570).
Both controls and lupus patients had a positive remodeling index. It progressed in the lupus group over time, and regressed in controls, but the findings were not statistically significant.
“Statins did nothing for the lupus patients. They didn’t affect progress of coronary plaques at all. We still treat patients because theoretically we don’t have anything better, but we know that they don’t really work in this population,” Dr. Stojan said
The work is funded by the National Institutes of Health. Dr. Stojan didn’t report any relevant disclosures.
SOURCE: Stojan G et al. Lupus Sci Med. 2019;6[suppl 1]:A200, Abstract 274.
SAN FRANCISCO – according to an investigation from Johns Hopkins University, Baltimore.
All of the 102 lupus patients in the coronary artery CT angiography study also had positive plaque remodeling, meaning that at least one low-attenuation plaque was growing into the lumen wall, not the lumen itself, which makes them difficult to detect on standard imaging. Low-attenuation plaques were defined in the study as a plaque larger than 1 mm2 with a radiodensity below 30 Hounsfield units.
Low-attenuation plaques are inherently unstable; they’re fatty, necrotic, and have a high risk of rupturing; their presence in the lumen wall is especially worrisome. In the general population, they sometimes regress, scarring down over time and no longer posing a threat. That didn’t happen in the 30 lupus patients who had follow-up CT angiographies, some 9 years after their first.
The team conducted the study to help understand why cardiovascular disease is so common in lupus, and the leading cause of death. Hopkins investigators have shown previously that statins have no effect on the risk or plaque occurrence and progression, and the cardiovascular risk doesn’t always seem to correlate with disease control. For those and other reasons, the current thinking at Hopkins is that cardiovascular disease in lupus is somehow different than in the general population, said George Stojan, MD, an assistant professor of rheumatology at the school and codirector of the Hopkins Lupus Center.
The goal is “to figure out exactly what to look for when we assess the risk; I don’t think we understand that at this point. We assume patients with lupus behave exactly like patients who don’t have lupus, but they obviously don’t. They do not respond to statins. They have a higher risk no matter what you do for them, even when their disease activity is low, and how much plaque they have over time doesn’t really correlate with disease activity,” he said at an international conference on systemic lupus erythematosus.
“Once we understand” the mechanism, “then we can try to [alter] it. Maybe we can look at new drugs, like the PCSK9 inhibitors which have shown a lot of promise in the general population.” At this point, however, “we don’t really know how to intervene,” Dr. Stojan said.
In the meantime, positive remodeling and low-attenuation, noncalcified plaques (LANCPs) might be something to look for when assessing systemic lupus erythematosus cardiovascular risk. “A simple coronary calcium score, something that all doctors do,” is not enough in lupus, nor is simply checking for lumen obstruction. Also, it’s important not to be misled by an overall reduction in noncalcified plaques. “Low-attenuation, noncalcified plaques don’t [regress] over time in lupus, and they are the ones that lead to cardiovascular events,” he said.
The CT angiography findings were compared with findings in 100 healthy controls who had two CT angiograms in a University of California, Los Angeles, cohort. Overall, there was a mean of 458 LANCPs among lupus patients, versus 42 among controls, a more than 900% difference (P less than .001).
Women with lupus aged under 44 years had a mean of 63 LANCPs; none were detected in healthy women under 44 years. Among women aged 45-59 years, there was a mean of 451 LANCPs in the lupus group versus 53 in the control arm. The findings were highly statistically significant, and almost statistically significant for women 60 years or older, 695 lesions among lupus patients versus 22 (P = .0576).
There were only nine men with lupus in the study, but the findings were similar versus male controls.
While mean LANCP volume regressed over time in the control group (mean, –6.90 mm3; P = .0002), a mean regression of –13.56 mm3 in the lupus group was not statistically significant (P = .4570).
Both controls and lupus patients had a positive remodeling index. It progressed in the lupus group over time, and regressed in controls, but the findings were not statistically significant.
“Statins did nothing for the lupus patients. They didn’t affect progress of coronary plaques at all. We still treat patients because theoretically we don’t have anything better, but we know that they don’t really work in this population,” Dr. Stojan said
The work is funded by the National Institutes of Health. Dr. Stojan didn’t report any relevant disclosures.
SOURCE: Stojan G et al. Lupus Sci Med. 2019;6[suppl 1]:A200, Abstract 274.
SAN FRANCISCO – according to an investigation from Johns Hopkins University, Baltimore.
All of the 102 lupus patients in the coronary artery CT angiography study also had positive plaque remodeling, meaning that at least one low-attenuation plaque was growing into the lumen wall, not the lumen itself, which makes them difficult to detect on standard imaging. Low-attenuation plaques were defined in the study as a plaque larger than 1 mm2 with a radiodensity below 30 Hounsfield units.
Low-attenuation plaques are inherently unstable; they’re fatty, necrotic, and have a high risk of rupturing; their presence in the lumen wall is especially worrisome. In the general population, they sometimes regress, scarring down over time and no longer posing a threat. That didn’t happen in the 30 lupus patients who had follow-up CT angiographies, some 9 years after their first.
The team conducted the study to help understand why cardiovascular disease is so common in lupus, and the leading cause of death. Hopkins investigators have shown previously that statins have no effect on the risk or plaque occurrence and progression, and the cardiovascular risk doesn’t always seem to correlate with disease control. For those and other reasons, the current thinking at Hopkins is that cardiovascular disease in lupus is somehow different than in the general population, said George Stojan, MD, an assistant professor of rheumatology at the school and codirector of the Hopkins Lupus Center.
The goal is “to figure out exactly what to look for when we assess the risk; I don’t think we understand that at this point. We assume patients with lupus behave exactly like patients who don’t have lupus, but they obviously don’t. They do not respond to statins. They have a higher risk no matter what you do for them, even when their disease activity is low, and how much plaque they have over time doesn’t really correlate with disease activity,” he said at an international conference on systemic lupus erythematosus.
“Once we understand” the mechanism, “then we can try to [alter] it. Maybe we can look at new drugs, like the PCSK9 inhibitors which have shown a lot of promise in the general population.” At this point, however, “we don’t really know how to intervene,” Dr. Stojan said.
In the meantime, positive remodeling and low-attenuation, noncalcified plaques (LANCPs) might be something to look for when assessing systemic lupus erythematosus cardiovascular risk. “A simple coronary calcium score, something that all doctors do,” is not enough in lupus, nor is simply checking for lumen obstruction. Also, it’s important not to be misled by an overall reduction in noncalcified plaques. “Low-attenuation, noncalcified plaques don’t [regress] over time in lupus, and they are the ones that lead to cardiovascular events,” he said.
The CT angiography findings were compared with findings in 100 healthy controls who had two CT angiograms in a University of California, Los Angeles, cohort. Overall, there was a mean of 458 LANCPs among lupus patients, versus 42 among controls, a more than 900% difference (P less than .001).
Women with lupus aged under 44 years had a mean of 63 LANCPs; none were detected in healthy women under 44 years. Among women aged 45-59 years, there was a mean of 451 LANCPs in the lupus group versus 53 in the control arm. The findings were highly statistically significant, and almost statistically significant for women 60 years or older, 695 lesions among lupus patients versus 22 (P = .0576).
There were only nine men with lupus in the study, but the findings were similar versus male controls.
While mean LANCP volume regressed over time in the control group (mean, –6.90 mm3; P = .0002), a mean regression of –13.56 mm3 in the lupus group was not statistically significant (P = .4570).
Both controls and lupus patients had a positive remodeling index. It progressed in the lupus group over time, and regressed in controls, but the findings were not statistically significant.
“Statins did nothing for the lupus patients. They didn’t affect progress of coronary plaques at all. We still treat patients because theoretically we don’t have anything better, but we know that they don’t really work in this population,” Dr. Stojan said
The work is funded by the National Institutes of Health. Dr. Stojan didn’t report any relevant disclosures.
SOURCE: Stojan G et al. Lupus Sci Med. 2019;6[suppl 1]:A200, Abstract 274.
REPORTING FROM LUPUS 2019
Key clinical point: Positive remodeling and low-attenuation, noncalcified plaques might be something to look for when assessing systemic lupus erythematosus cardiovascular risk.
Major finding: There was a mean of 458 low-attenuation, noncalcified plaques among lupus patients versus 42 among controls, a more than 900% difference (P less than .001)
Study details: Coronary CT angiography in 102 lupus patients and 100 healthy controls
Disclosures: The National Institutes of Health funded the work. The lead investigator didn’t report any relevant disclosures.
Source: Stojan G et al. Lupus Sci Med. 2019;6[suppl 1]:A200, Abstract 274.
WISE sheds light on angina in INOCA
NEW ORLEANS – A higher baseline average coronary peak flow velocity is an independent predictor of angina in women with symptomatic ischemia and nonobstructive coronary artery disease (INOCA), according to a new report from the WISE-CVD study.

WISE-CVD (the Women’s Ischemia Syndrome Evaluation: Coronary Vascular Dysfunction) project is a National Institutes of Health–sponsored series of studies. WISE investigators have previously shown that higher baseline average peak flow velocity (BAPV) is correlated with volumetric flow and is an independent predictor of major adverse cardiovascular events. However, until now the relationship between BAPV and anginal symptoms hadn’t been investigated, Nissi S. Suppogu, MD, observed at the annual meeting of the American College of Cardiology.
She reported on 260 women with angiographically evaluated symptomatic INOCA who participated in WISE-CVD. They were divided into two groups based upon their BAPV: 123 had a BAPV of 22 cm/sec or more, and 137 had a BAPV of less than 22 cm/sec.
Women in the high BAPV group had more frequent angina as shown by their average score of 50 on that domain of the Seattle Angina Questionnaire, compared with 60 in the low-BAPV group. The high-BAPV group also had significantly worse angina-related quality of life as reflected in their lower score on that dimension of a related instrument, the Seattle Angina Questionnaire–7.
Further support for the notion that high-BAPV women with INOCA have more severe angina than those with low BAPV comes from the finding that they were significantly more likely to use nitrates (37.6% of them did so, compared with 22.6% of low-BAPV women) and ranolazine, or Ranexa (7.9% versus 1.7%). In addition, the high-BAPV patients had numerically greater usage of other antianginal agents – beta-blockers, calcium channel blockers, and ACE inhibitors or angiotensin receptor blockers – although these differences didn’t reach statistical significance, reported Dr. Suppogu of Cedars-Sinai Medical Center in Los Angeles.
She reported having no financial conflicts regarding her presentation.
NEW ORLEANS – A higher baseline average coronary peak flow velocity is an independent predictor of angina in women with symptomatic ischemia and nonobstructive coronary artery disease (INOCA), according to a new report from the WISE-CVD study.
WISE-CVD (the Women’s Ischemia Syndrome Evaluation: Coronary Vascular Dysfunction) project is a National Institutes of Health–sponsored series of studies. WISE investigators have previously shown that higher baseline average peak flow velocity (BAPV) is correlated with volumetric flow and is an independent predictor of major adverse cardiovascular events. However, until now the relationship between BAPV and anginal symptoms hadn’t been investigated, Nissi S. Suppogu, MD, observed at the annual meeting of the American College of Cardiology.
She reported on 260 women with angiographically evaluated symptomatic INOCA who participated in WISE-CVD. They were divided into two groups based upon their BAPV: 123 had a BAPV of 22 cm/sec or more, and 137 had a BAPV of less than 22 cm/sec.
Women in the high BAPV group had more frequent angina as shown by their average score of 50 on that domain of the Seattle Angina Questionnaire, compared with 60 in the low-BAPV group. The high-BAPV group also had significantly worse angina-related quality of life as reflected in their lower score on that dimension of a related instrument, the Seattle Angina Questionnaire–7.
Further support for the notion that high-BAPV women with INOCA have more severe angina than those with low BAPV comes from the finding that they were significantly more likely to use nitrates (37.6% of them did so, compared with 22.6% of low-BAPV women) and ranolazine, or Ranexa (7.9% versus 1.7%). In addition, the high-BAPV patients had numerically greater usage of other antianginal agents – beta-blockers, calcium channel blockers, and ACE inhibitors or angiotensin receptor blockers – although these differences didn’t reach statistical significance, reported Dr. Suppogu of Cedars-Sinai Medical Center in Los Angeles.
She reported having no financial conflicts regarding her presentation.
NEW ORLEANS – A higher baseline average coronary peak flow velocity is an independent predictor of angina in women with symptomatic ischemia and nonobstructive coronary artery disease (INOCA), according to a new report from the WISE-CVD study.
WISE-CVD (the Women’s Ischemia Syndrome Evaluation: Coronary Vascular Dysfunction) project is a National Institutes of Health–sponsored series of studies. WISE investigators have previously shown that higher baseline average peak flow velocity (BAPV) is correlated with volumetric flow and is an independent predictor of major adverse cardiovascular events. However, until now the relationship between BAPV and anginal symptoms hadn’t been investigated, Nissi S. Suppogu, MD, observed at the annual meeting of the American College of Cardiology.
She reported on 260 women with angiographically evaluated symptomatic INOCA who participated in WISE-CVD. They were divided into two groups based upon their BAPV: 123 had a BAPV of 22 cm/sec or more, and 137 had a BAPV of less than 22 cm/sec.
Women in the high BAPV group had more frequent angina as shown by their average score of 50 on that domain of the Seattle Angina Questionnaire, compared with 60 in the low-BAPV group. The high-BAPV group also had significantly worse angina-related quality of life as reflected in their lower score on that dimension of a related instrument, the Seattle Angina Questionnaire–7.
Further support for the notion that high-BAPV women with INOCA have more severe angina than those with low BAPV comes from the finding that they were significantly more likely to use nitrates (37.6% of them did so, compared with 22.6% of low-BAPV women) and ranolazine, or Ranexa (7.9% versus 1.7%). In addition, the high-BAPV patients had numerically greater usage of other antianginal agents – beta-blockers, calcium channel blockers, and ACE inhibitors or angiotensin receptor blockers – although these differences didn’t reach statistical significance, reported Dr. Suppogu of Cedars-Sinai Medical Center in Los Angeles.
She reported having no financial conflicts regarding her presentation.
REPORTING FROM ACC 19
Weight-loss drug options expand, but beware cardiac risk
LOS ANGELES – Newer medications are much more powerful, but they come with cautions – insurer coverage can be a hurdle, and there are significant gaps in knowledge about their risks for patients with heart disease, Ken Fujioka, MD, told colleagues at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.

Dr. Fujioka, of Scripps Clinic in San Diego, shared some tips with his peers about using medications to reduce weight.
Diabetes drugs help, but may need a boost
Metformin can reduce weight by as much as 3%, Dr. Fujioka said. And there may be another benefit related to long-term weight loss maintenance, he said, citing a 15-year study of overweight or obese patients at high risk for diabetes who either received metformin, underwent an intensive lifestyle intervention, or took a placebo. Of the participants with weight loss of at least 5% after the first year, those originally assigned to receive metformin had the greatest weight loss during years 6-15. Older age, the amount of weight initially lost, and continued used of metformin were predictors of long-term weight loss maintenance, according to the researchers (Ann Intern Med. 2019 Apr 23. doi: 10.7326/M18-1605).
There are other options among diabetes drugs. Sodium-glucose cotransporter 2 (SGLT2) inhibitors – a class of drugs that includes canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance) – have a striking effect on weight loss, Dr. Fujioka said. They can cause 300 calories to be flushed out in the urine each day. But that typically doesn’t translate into weight loss of more than 20 pounds, he said, because the body doesn’t fully adjust to fewer calories.
“The patients begin to eat more,” he said. “They have to take in more calories to make up for [the loss]. They’re not consciously trying to do this. It’s a metabolic adaptation, so 2%-3% [weight loss] is about all you’ll get. You won’t get 10% or 20%.”
To drive up weight loss, Dr. Fujioka recommended adding the glucagonlike peptide–1 [GLP1] receptor diabetes drug exenatide (Byetta; Bydureon) or the appetite suppressant phentermine (Adipex-p; Lomaira) to an SGLT2 inhibitor. Recent studies have shown that the drug combinations have a greater impact on weight loss than when taken separately (Lancet Diabetes Endocrinol. 2016 Dec;4[12]:1004-16; Diabetes Care. 2017 May;40[5]:632-9).
In regard to phentermine, which acts similarly to amphetamine, Dr. Fujioka advised colleagues to be aware that “15 mg or less is really safe, but you drive pulse and heart rate beyond that.”
Consider insurance coverage and other factors
Often, insurers will pay for GLP1-receptor and SGLT2-inhibitor medications in patients with diabetes, even if their hemoglobin A1c is in the healthy range, Dr. Fujioka said, but they’ll balk at paying for specific weight-loss medications, although that can vary by the region of the country. He added that cash discount cards are available for several weight-loss drugs.
Newer weight-loss drugs ...
Dr. Fujioka highlighted a quartet of weight-loss drugs that have been approved in recent years.
- Lorcaserin (Belviq), a selective serotonin 2C receptor agonist, has shown unique benefits in patients with diabetes. A large, multinational, randomized controlled trial found that the drug reduced the risk for incident diabetes, induced remission of hyperglycemia, and reduced the risk of microvascular complications in obese and overweight patients (Lancet. 2018 Nov 24;392[10161]:2269-79).
- Phentermine/topiramate (Qsymia), a combination of an antiseizure medication (topiramate) and an appetite suppressant (phentermine). A 2014 study found that the drug, together with lifestyle modification, effectively promoted weight loss and improved glycemic control in obese or overweight patients with type 2 diabetes (Diabetes Care. 2014 Dec;37[12]:3309-16).
- Naltrexone/bupropion (Contrave), a combination of an addiction drug (naltrexone) and an antidepressant (bupropion). Findings from a 2013 study reported that the drug “in overweight/obese patients with type 2 diabetes induced weight loss... was associated with improvements in glycemic control and select cardiovascular risk factors and was generally well tolerated with a safety profile similar to that in patients without diabetes.” (Diabetes Care. 2013 Dec;36[12]:4022-9).
- Liraglutide, an injectable GLP1 agonist that has been approved for diabetes (Victoza) and weight loss (Saxenda). Dr. Fujioka was coauthor for a study in which the findings suggested that the drug could prevent prediabetes from turning into diabetes. (Lancet. 2017 Apr 8;389[10077]:1399-409).
... but watch out for safety in patients with heart disease
Two of the newer weight-loss drugs are OK to prescribe for diabetic patients with heart disease, Dr. Fujioka said, but two are not, because no cardiac safety trials have been completed for them.
Liraglutide (at a dose of 3.0 mg) is considered safe based on previous data (Diabetes Obes Metab. 2018 Mar;20[3]:734-9), Dr. Fujioka said. Likewise, findings from a trial with lorcaserin in which 12,000 overweight or obese patients with atherosclerotic cardiovascular disease or multiple cardiovascular risk factors received either lorcaserin (10 mg twice daily) or placebo, suggested that lorcaserin helped sustain weight loss without a higher rate of major cardiovascular events compared with placebo (N Engl J Med. 2018 Sep 20;379[12]:1107-17).However, no such cardiac safety trials have been completed for naltrexone/bupropion or phentermine/topiramate, said Dr. Fujioka. As a result, he said he could not recommend either of them for patients with high-risk cardiovascular disease.
Dr. Fujioka disclosed relationships of various types with Novo Nordisk, Eisai, Gelesis, KVK Tech, Amgen, Sunovion, Boehringer Ingelheim, and Janssen Global Services.
LOS ANGELES – Newer medications are much more powerful, but they come with cautions – insurer coverage can be a hurdle, and there are significant gaps in knowledge about their risks for patients with heart disease, Ken Fujioka, MD, told colleagues at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.
Dr. Fujioka, of Scripps Clinic in San Diego, shared some tips with his peers about using medications to reduce weight.
Diabetes drugs help, but may need a boost
Metformin can reduce weight by as much as 3%, Dr. Fujioka said. And there may be another benefit related to long-term weight loss maintenance, he said, citing a 15-year study of overweight or obese patients at high risk for diabetes who either received metformin, underwent an intensive lifestyle intervention, or took a placebo. Of the participants with weight loss of at least 5% after the first year, those originally assigned to receive metformin had the greatest weight loss during years 6-15. Older age, the amount of weight initially lost, and continued used of metformin were predictors of long-term weight loss maintenance, according to the researchers (Ann Intern Med. 2019 Apr 23. doi: 10.7326/M18-1605).
There are other options among diabetes drugs. Sodium-glucose cotransporter 2 (SGLT2) inhibitors – a class of drugs that includes canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance) – have a striking effect on weight loss, Dr. Fujioka said. They can cause 300 calories to be flushed out in the urine each day. But that typically doesn’t translate into weight loss of more than 20 pounds, he said, because the body doesn’t fully adjust to fewer calories.
“The patients begin to eat more,” he said. “They have to take in more calories to make up for [the loss]. They’re not consciously trying to do this. It’s a metabolic adaptation, so 2%-3% [weight loss] is about all you’ll get. You won’t get 10% or 20%.”
To drive up weight loss, Dr. Fujioka recommended adding the glucagonlike peptide–1 [GLP1] receptor diabetes drug exenatide (Byetta; Bydureon) or the appetite suppressant phentermine (Adipex-p; Lomaira) to an SGLT2 inhibitor. Recent studies have shown that the drug combinations have a greater impact on weight loss than when taken separately (Lancet Diabetes Endocrinol. 2016 Dec;4[12]:1004-16; Diabetes Care. 2017 May;40[5]:632-9).
In regard to phentermine, which acts similarly to amphetamine, Dr. Fujioka advised colleagues to be aware that “15 mg or less is really safe, but you drive pulse and heart rate beyond that.”
Consider insurance coverage and other factors
Often, insurers will pay for GLP1-receptor and SGLT2-inhibitor medications in patients with diabetes, even if their hemoglobin A1c is in the healthy range, Dr. Fujioka said, but they’ll balk at paying for specific weight-loss medications, although that can vary by the region of the country. He added that cash discount cards are available for several weight-loss drugs.
Newer weight-loss drugs ...
Dr. Fujioka highlighted a quartet of weight-loss drugs that have been approved in recent years.
- Lorcaserin (Belviq), a selective serotonin 2C receptor agonist, has shown unique benefits in patients with diabetes. A large, multinational, randomized controlled trial found that the drug reduced the risk for incident diabetes, induced remission of hyperglycemia, and reduced the risk of microvascular complications in obese and overweight patients (Lancet. 2018 Nov 24;392[10161]:2269-79).
- Phentermine/topiramate (Qsymia), a combination of an antiseizure medication (topiramate) and an appetite suppressant (phentermine). A 2014 study found that the drug, together with lifestyle modification, effectively promoted weight loss and improved glycemic control in obese or overweight patients with type 2 diabetes (Diabetes Care. 2014 Dec;37[12]:3309-16).
- Naltrexone/bupropion (Contrave), a combination of an addiction drug (naltrexone) and an antidepressant (bupropion). Findings from a 2013 study reported that the drug “in overweight/obese patients with type 2 diabetes induced weight loss... was associated with improvements in glycemic control and select cardiovascular risk factors and was generally well tolerated with a safety profile similar to that in patients without diabetes.” (Diabetes Care. 2013 Dec;36[12]:4022-9).
- Liraglutide, an injectable GLP1 agonist that has been approved for diabetes (Victoza) and weight loss (Saxenda). Dr. Fujioka was coauthor for a study in which the findings suggested that the drug could prevent prediabetes from turning into diabetes. (Lancet. 2017 Apr 8;389[10077]:1399-409).
... but watch out for safety in patients with heart disease
Two of the newer weight-loss drugs are OK to prescribe for diabetic patients with heart disease, Dr. Fujioka said, but two are not, because no cardiac safety trials have been completed for them.
Liraglutide (at a dose of 3.0 mg) is considered safe based on previous data (Diabetes Obes Metab. 2018 Mar;20[3]:734-9), Dr. Fujioka said. Likewise, findings from a trial with lorcaserin in which 12,000 overweight or obese patients with atherosclerotic cardiovascular disease or multiple cardiovascular risk factors received either lorcaserin (10 mg twice daily) or placebo, suggested that lorcaserin helped sustain weight loss without a higher rate of major cardiovascular events compared with placebo (N Engl J Med. 2018 Sep 20;379[12]:1107-17).However, no such cardiac safety trials have been completed for naltrexone/bupropion or phentermine/topiramate, said Dr. Fujioka. As a result, he said he could not recommend either of them for patients with high-risk cardiovascular disease.
Dr. Fujioka disclosed relationships of various types with Novo Nordisk, Eisai, Gelesis, KVK Tech, Amgen, Sunovion, Boehringer Ingelheim, and Janssen Global Services.
LOS ANGELES – Newer medications are much more powerful, but they come with cautions – insurer coverage can be a hurdle, and there are significant gaps in knowledge about their risks for patients with heart disease, Ken Fujioka, MD, told colleagues at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.
Dr. Fujioka, of Scripps Clinic in San Diego, shared some tips with his peers about using medications to reduce weight.
Diabetes drugs help, but may need a boost
Metformin can reduce weight by as much as 3%, Dr. Fujioka said. And there may be another benefit related to long-term weight loss maintenance, he said, citing a 15-year study of overweight or obese patients at high risk for diabetes who either received metformin, underwent an intensive lifestyle intervention, or took a placebo. Of the participants with weight loss of at least 5% after the first year, those originally assigned to receive metformin had the greatest weight loss during years 6-15. Older age, the amount of weight initially lost, and continued used of metformin were predictors of long-term weight loss maintenance, according to the researchers (Ann Intern Med. 2019 Apr 23. doi: 10.7326/M18-1605).
There are other options among diabetes drugs. Sodium-glucose cotransporter 2 (SGLT2) inhibitors – a class of drugs that includes canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance) – have a striking effect on weight loss, Dr. Fujioka said. They can cause 300 calories to be flushed out in the urine each day. But that typically doesn’t translate into weight loss of more than 20 pounds, he said, because the body doesn’t fully adjust to fewer calories.
“The patients begin to eat more,” he said. “They have to take in more calories to make up for [the loss]. They’re not consciously trying to do this. It’s a metabolic adaptation, so 2%-3% [weight loss] is about all you’ll get. You won’t get 10% or 20%.”
To drive up weight loss, Dr. Fujioka recommended adding the glucagonlike peptide–1 [GLP1] receptor diabetes drug exenatide (Byetta; Bydureon) or the appetite suppressant phentermine (Adipex-p; Lomaira) to an SGLT2 inhibitor. Recent studies have shown that the drug combinations have a greater impact on weight loss than when taken separately (Lancet Diabetes Endocrinol. 2016 Dec;4[12]:1004-16; Diabetes Care. 2017 May;40[5]:632-9).
In regard to phentermine, which acts similarly to amphetamine, Dr. Fujioka advised colleagues to be aware that “15 mg or less is really safe, but you drive pulse and heart rate beyond that.”
Consider insurance coverage and other factors
Often, insurers will pay for GLP1-receptor and SGLT2-inhibitor medications in patients with diabetes, even if their hemoglobin A1c is in the healthy range, Dr. Fujioka said, but they’ll balk at paying for specific weight-loss medications, although that can vary by the region of the country. He added that cash discount cards are available for several weight-loss drugs.
Newer weight-loss drugs ...
Dr. Fujioka highlighted a quartet of weight-loss drugs that have been approved in recent years.
- Lorcaserin (Belviq), a selective serotonin 2C receptor agonist, has shown unique benefits in patients with diabetes. A large, multinational, randomized controlled trial found that the drug reduced the risk for incident diabetes, induced remission of hyperglycemia, and reduced the risk of microvascular complications in obese and overweight patients (Lancet. 2018 Nov 24;392[10161]:2269-79).
- Phentermine/topiramate (Qsymia), a combination of an antiseizure medication (topiramate) and an appetite suppressant (phentermine). A 2014 study found that the drug, together with lifestyle modification, effectively promoted weight loss and improved glycemic control in obese or overweight patients with type 2 diabetes (Diabetes Care. 2014 Dec;37[12]:3309-16).
- Naltrexone/bupropion (Contrave), a combination of an addiction drug (naltrexone) and an antidepressant (bupropion). Findings from a 2013 study reported that the drug “in overweight/obese patients with type 2 diabetes induced weight loss... was associated with improvements in glycemic control and select cardiovascular risk factors and was generally well tolerated with a safety profile similar to that in patients without diabetes.” (Diabetes Care. 2013 Dec;36[12]:4022-9).
- Liraglutide, an injectable GLP1 agonist that has been approved for diabetes (Victoza) and weight loss (Saxenda). Dr. Fujioka was coauthor for a study in which the findings suggested that the drug could prevent prediabetes from turning into diabetes. (Lancet. 2017 Apr 8;389[10077]:1399-409).
... but watch out for safety in patients with heart disease
Two of the newer weight-loss drugs are OK to prescribe for diabetic patients with heart disease, Dr. Fujioka said, but two are not, because no cardiac safety trials have been completed for them.
Liraglutide (at a dose of 3.0 mg) is considered safe based on previous data (Diabetes Obes Metab. 2018 Mar;20[3]:734-9), Dr. Fujioka said. Likewise, findings from a trial with lorcaserin in which 12,000 overweight or obese patients with atherosclerotic cardiovascular disease or multiple cardiovascular risk factors received either lorcaserin (10 mg twice daily) or placebo, suggested that lorcaserin helped sustain weight loss without a higher rate of major cardiovascular events compared with placebo (N Engl J Med. 2018 Sep 20;379[12]:1107-17).However, no such cardiac safety trials have been completed for naltrexone/bupropion or phentermine/topiramate, said Dr. Fujioka. As a result, he said he could not recommend either of them for patients with high-risk cardiovascular disease.
Dr. Fujioka disclosed relationships of various types with Novo Nordisk, Eisai, Gelesis, KVK Tech, Amgen, Sunovion, Boehringer Ingelheim, and Janssen Global Services.
EXPERT ANALYSIS FROM AACE 2019