User login
Long-term antibiotic use may heighten stroke, CHD risk
, according to a study in the European Heart Journal.
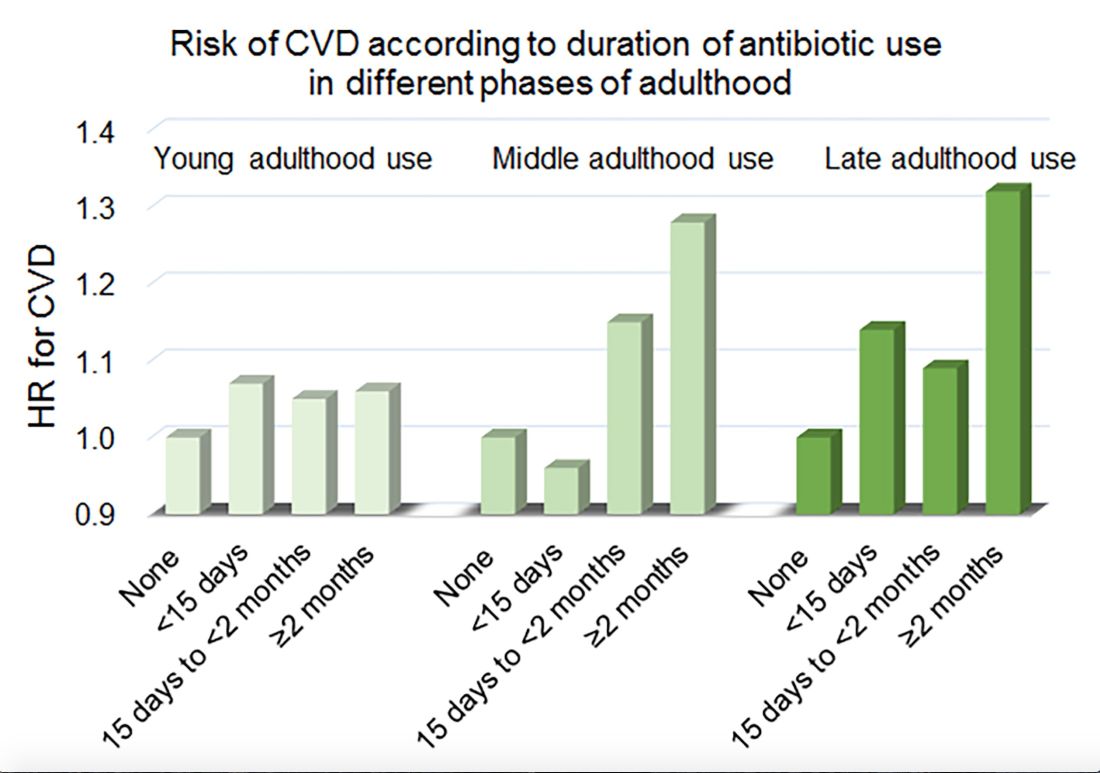
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
, according to a study in the European Heart Journal.
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
, according to a study in the European Heart Journal.
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
FROM THE EUROPEAN HEART JOURNAL
Key clinical point: Among middle-aged and older women, 2 or more months’ exposure to antibiotics is associated with an increased risk of coronary heart disease or stroke.
Major finding: Long-term antibiotic use in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Study details: An analysis of data from nearly 36,500 women in the Nurses’ Health Study.
Disclosures: The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
Source: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
Alirocumab gains indication to reduce cardiovascular risks
Alirocumab has received an updated indication from the Food and Drug Administration for reducing the overall risk of major adverse cardiovascular events in patients with a recent acute coronary event.
![]()
Alirocumab is designed to inhibit the binding of PCSK9 (proprotein convertase subtilisin/kexin type 9) to LDL receptors, thereby lowering LDL cholesterol, according to manufacturer Regeneron, which is developing alirocumab in partnership with Sanofi.
The drug was previously approved in the United States as an adjunct treatment along with diet and maximally tolerated statin therapy to help lower LDL cholesterol in adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease.
The approval of the supplemental Biologics License Application was supported by data from the ODYSSEY Outcomes trial in which 18,924 patients who had an acute coronary syndrome were randomized to alirocumab or placebo plus background high-intensity statin therapy starting at a median of 2.6 months after the event. Over 3 years’ follow-up, a composite endpoint outcome including death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or unstable angina occurred in 9.5% of alirocumab patients and 11.1% of placebo patients.
In the study, patients received subcutaneous dose of 75 mg of alirocumab every 2 weeks, which was adjusted to achieve an LDL cholesterol level of 25-50 mg/dL. The most significant benefits occurred among patients with a baseline LDL cholesterol of 100 mg/dL or higher who were taking high-intensity statins, which supports the role of LDL cholesterol reduction in improving outcomes for coronary syndrome patients, according to study investigators.
Alirocumab is given as a subcutaneous injection. The most common side effects include pain and tenderness at the injection site, and redness, itching, or swelling; some patients have reported symptoms of a common cold or flu.
More details of the ODYSSEY Outcomes trial were presented at the annual meeting of the American College of Cardiology.
Alirocumab has received an updated indication from the Food and Drug Administration for reducing the overall risk of major adverse cardiovascular events in patients with a recent acute coronary event.
![]()
Alirocumab is designed to inhibit the binding of PCSK9 (proprotein convertase subtilisin/kexin type 9) to LDL receptors, thereby lowering LDL cholesterol, according to manufacturer Regeneron, which is developing alirocumab in partnership with Sanofi.
The drug was previously approved in the United States as an adjunct treatment along with diet and maximally tolerated statin therapy to help lower LDL cholesterol in adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease.
The approval of the supplemental Biologics License Application was supported by data from the ODYSSEY Outcomes trial in which 18,924 patients who had an acute coronary syndrome were randomized to alirocumab or placebo plus background high-intensity statin therapy starting at a median of 2.6 months after the event. Over 3 years’ follow-up, a composite endpoint outcome including death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or unstable angina occurred in 9.5% of alirocumab patients and 11.1% of placebo patients.
In the study, patients received subcutaneous dose of 75 mg of alirocumab every 2 weeks, which was adjusted to achieve an LDL cholesterol level of 25-50 mg/dL. The most significant benefits occurred among patients with a baseline LDL cholesterol of 100 mg/dL or higher who were taking high-intensity statins, which supports the role of LDL cholesterol reduction in improving outcomes for coronary syndrome patients, according to study investigators.
Alirocumab is given as a subcutaneous injection. The most common side effects include pain and tenderness at the injection site, and redness, itching, or swelling; some patients have reported symptoms of a common cold or flu.
More details of the ODYSSEY Outcomes trial were presented at the annual meeting of the American College of Cardiology.
Alirocumab has received an updated indication from the Food and Drug Administration for reducing the overall risk of major adverse cardiovascular events in patients with a recent acute coronary event.
![]()
Alirocumab is designed to inhibit the binding of PCSK9 (proprotein convertase subtilisin/kexin type 9) to LDL receptors, thereby lowering LDL cholesterol, according to manufacturer Regeneron, which is developing alirocumab in partnership with Sanofi.
The drug was previously approved in the United States as an adjunct treatment along with diet and maximally tolerated statin therapy to help lower LDL cholesterol in adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease.
The approval of the supplemental Biologics License Application was supported by data from the ODYSSEY Outcomes trial in which 18,924 patients who had an acute coronary syndrome were randomized to alirocumab or placebo plus background high-intensity statin therapy starting at a median of 2.6 months after the event. Over 3 years’ follow-up, a composite endpoint outcome including death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or unstable angina occurred in 9.5% of alirocumab patients and 11.1% of placebo patients.
In the study, patients received subcutaneous dose of 75 mg of alirocumab every 2 weeks, which was adjusted to achieve an LDL cholesterol level of 25-50 mg/dL. The most significant benefits occurred among patients with a baseline LDL cholesterol of 100 mg/dL or higher who were taking high-intensity statins, which supports the role of LDL cholesterol reduction in improving outcomes for coronary syndrome patients, according to study investigators.
Alirocumab is given as a subcutaneous injection. The most common side effects include pain and tenderness at the injection site, and redness, itching, or swelling; some patients have reported symptoms of a common cold or flu.
More details of the ODYSSEY Outcomes trial were presented at the annual meeting of the American College of Cardiology.
Noninvasive FFRCT called ADVANCE in chest pain assessment
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.

In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.

Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.
Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.
Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
REPORTING FROM ACC 19
Cardiac PET/CT can guide CAD therapy
NEW ORLEANS – A PET/CT-derived myocardial ischemic burden in excess of 10% defines a subset of patients with symptomatic CAD who derive significantly greater benefit from an invasive management strategy than a noninvasive one, Kent G. Meredith, MD, reported at the annual meeting of the American College of Cardiology.

Conversely, patients with an ischemia burden of 10% or less have a lower major adverse event rate if they undergo noninvasive treatment.
“We see that cardiac PET/CT-derived ischemic burden provides a convenient and useful tool for predicting clinical outcomes of invasive and noninvasive treatment strategies,”said Dr. Meredith, a cardiologist at Intermountain Medical Center in Murray, Utah.
He presented a retrospective single-center study of 5,528 consecutive patients with symptomatic CAD referred for PET/CT at Intermountain. As a condition for study inclusion, they needed to survive for at least 90 days after imaging, have no elevation of troponin, and have no prior history of CAD.
This was a study of real-world clinical practice featuring standardized institutional protocols. Dr. Meredith explained that the 10% ischemic burden threshold used by cardiologists at Intermountain to help determine an individual’s optimal treatment strategy is based upon “a very important study” in which investigators at Cedars-Sinai Medical Center in Los Angeles showed 16 years ago, in nearly 11,000 consecutive patients, that revascularization had a survival benefit over medical therapy alone at an ischemic burden in excess of 10% as measured by stress myocardial perfusion single photon emission CT (Circulation. 2003 Jun 17;107[23]:2900-7).
Dr. Meredith and his coinvestigators carried out their study to make sure this ischemic burden cutoff is still valid today in view of the considerable changes in imaging technology and optimal medical therapy in the intervening years.
Among the study population, 203 patients had a PET/CT-derived ischemic burden greater than 10% using a well-established scoring system (J Nucl Cardiol. 2006 Nov;13[6]:e157-71), while 5,325 had a lesser ischemic burden. Fifty-six percent of patients with an ischemic burden above the 10% threshold underwent coronary revascularization, 26% had coronary angiography without revascularization, and 18% were managed by optimal medical therapy alone.
The group with an ischemic burden of 10% or less was managed very differently: One percent had revascularization, 3% had angiography without revascularization, and 96% were managed medically.
The higher a patient’s baseline ischemic burden, the higher the major adverse cardiovascular event (MACE) rate during 1-4 years of follow-up. The composite MACE rate, comprising death, hospitalization for acute MI, or late revascularization after 90 days, was 3.9% in patients with an ischemic burden of 10% of less, compared with 8.9% in those above the 10% threshold.
In a multivariate analysis adjusted for demographics, hyperlipidemia, heart failure, and diabetes, patients with an ischemic burden greater than 10% had a 4.6-fold greater risk of MACE if managed medically than if they underwent revascularization. And among those with an ischemic burden of 10% or less, the adjusted risk of MACE was increased 2.8-fold if they received revascularization instead of medical management.
Dr. Meredith reported having no financial conflicts regarding his study, conducted free of commercial sponsorship.
NEW ORLEANS – A PET/CT-derived myocardial ischemic burden in excess of 10% defines a subset of patients with symptomatic CAD who derive significantly greater benefit from an invasive management strategy than a noninvasive one, Kent G. Meredith, MD, reported at the annual meeting of the American College of Cardiology.
Conversely, patients with an ischemia burden of 10% or less have a lower major adverse event rate if they undergo noninvasive treatment.
“We see that cardiac PET/CT-derived ischemic burden provides a convenient and useful tool for predicting clinical outcomes of invasive and noninvasive treatment strategies,”said Dr. Meredith, a cardiologist at Intermountain Medical Center in Murray, Utah.
He presented a retrospective single-center study of 5,528 consecutive patients with symptomatic CAD referred for PET/CT at Intermountain. As a condition for study inclusion, they needed to survive for at least 90 days after imaging, have no elevation of troponin, and have no prior history of CAD.
This was a study of real-world clinical practice featuring standardized institutional protocols. Dr. Meredith explained that the 10% ischemic burden threshold used by cardiologists at Intermountain to help determine an individual’s optimal treatment strategy is based upon “a very important study” in which investigators at Cedars-Sinai Medical Center in Los Angeles showed 16 years ago, in nearly 11,000 consecutive patients, that revascularization had a survival benefit over medical therapy alone at an ischemic burden in excess of 10% as measured by stress myocardial perfusion single photon emission CT (Circulation. 2003 Jun 17;107[23]:2900-7).
Dr. Meredith and his coinvestigators carried out their study to make sure this ischemic burden cutoff is still valid today in view of the considerable changes in imaging technology and optimal medical therapy in the intervening years.
Among the study population, 203 patients had a PET/CT-derived ischemic burden greater than 10% using a well-established scoring system (J Nucl Cardiol. 2006 Nov;13[6]:e157-71), while 5,325 had a lesser ischemic burden. Fifty-six percent of patients with an ischemic burden above the 10% threshold underwent coronary revascularization, 26% had coronary angiography without revascularization, and 18% were managed by optimal medical therapy alone.
The group with an ischemic burden of 10% or less was managed very differently: One percent had revascularization, 3% had angiography without revascularization, and 96% were managed medically.
The higher a patient’s baseline ischemic burden, the higher the major adverse cardiovascular event (MACE) rate during 1-4 years of follow-up. The composite MACE rate, comprising death, hospitalization for acute MI, or late revascularization after 90 days, was 3.9% in patients with an ischemic burden of 10% of less, compared with 8.9% in those above the 10% threshold.
In a multivariate analysis adjusted for demographics, hyperlipidemia, heart failure, and diabetes, patients with an ischemic burden greater than 10% had a 4.6-fold greater risk of MACE if managed medically than if they underwent revascularization. And among those with an ischemic burden of 10% or less, the adjusted risk of MACE was increased 2.8-fold if they received revascularization instead of medical management.
Dr. Meredith reported having no financial conflicts regarding his study, conducted free of commercial sponsorship.
NEW ORLEANS – A PET/CT-derived myocardial ischemic burden in excess of 10% defines a subset of patients with symptomatic CAD who derive significantly greater benefit from an invasive management strategy than a noninvasive one, Kent G. Meredith, MD, reported at the annual meeting of the American College of Cardiology.
Conversely, patients with an ischemia burden of 10% or less have a lower major adverse event rate if they undergo noninvasive treatment.
“We see that cardiac PET/CT-derived ischemic burden provides a convenient and useful tool for predicting clinical outcomes of invasive and noninvasive treatment strategies,”said Dr. Meredith, a cardiologist at Intermountain Medical Center in Murray, Utah.
He presented a retrospective single-center study of 5,528 consecutive patients with symptomatic CAD referred for PET/CT at Intermountain. As a condition for study inclusion, they needed to survive for at least 90 days after imaging, have no elevation of troponin, and have no prior history of CAD.
This was a study of real-world clinical practice featuring standardized institutional protocols. Dr. Meredith explained that the 10% ischemic burden threshold used by cardiologists at Intermountain to help determine an individual’s optimal treatment strategy is based upon “a very important study” in which investigators at Cedars-Sinai Medical Center in Los Angeles showed 16 years ago, in nearly 11,000 consecutive patients, that revascularization had a survival benefit over medical therapy alone at an ischemic burden in excess of 10% as measured by stress myocardial perfusion single photon emission CT (Circulation. 2003 Jun 17;107[23]:2900-7).
Dr. Meredith and his coinvestigators carried out their study to make sure this ischemic burden cutoff is still valid today in view of the considerable changes in imaging technology and optimal medical therapy in the intervening years.
Among the study population, 203 patients had a PET/CT-derived ischemic burden greater than 10% using a well-established scoring system (J Nucl Cardiol. 2006 Nov;13[6]:e157-71), while 5,325 had a lesser ischemic burden. Fifty-six percent of patients with an ischemic burden above the 10% threshold underwent coronary revascularization, 26% had coronary angiography without revascularization, and 18% were managed by optimal medical therapy alone.
The group with an ischemic burden of 10% or less was managed very differently: One percent had revascularization, 3% had angiography without revascularization, and 96% were managed medically.
The higher a patient’s baseline ischemic burden, the higher the major adverse cardiovascular event (MACE) rate during 1-4 years of follow-up. The composite MACE rate, comprising death, hospitalization for acute MI, or late revascularization after 90 days, was 3.9% in patients with an ischemic burden of 10% of less, compared with 8.9% in those above the 10% threshold.
In a multivariate analysis adjusted for demographics, hyperlipidemia, heart failure, and diabetes, patients with an ischemic burden greater than 10% had a 4.6-fold greater risk of MACE if managed medically than if they underwent revascularization. And among those with an ischemic burden of 10% or less, the adjusted risk of MACE was increased 2.8-fold if they received revascularization instead of medical management.
Dr. Meredith reported having no financial conflicts regarding his study, conducted free of commercial sponsorship.
REPORTING FROM ACC 19
Poor response to statins hikes risk of cardiovascular events
About half of patients taking statins for hyperlipidemia don’t adequately respond, leaving them at a 22% increased risk of cardiovascular disease, compared with optimal responders. 
Over 6 years, there were about 2,000 more cardiovascular events among those who failed to experience the national treatment target of at least a 40% reduction in LDL cholesterol, according to Stephen F. Weng, MD, and his colleagues. The report is in Heart.
Physicians’ choice of initial statin weighed heavily in the outcomes. Patients who ended up with an optimal response were more likely to get a more potent statin right off, while those with a poorer response were more likely to get a less-potent statin.
“This study provides ‘real world evidence’ that 50% of patients started on statins do not derive the intended therapeutic benefit from them, significantly increasing their risk of future cardiovascular disease,” wrote Dr. Weng of the University of Nottingham, England, and his colleagues. “These findings contribute to the debate on the effectiveness of statin therapy and highlight the need for personalized medicine in lipid management for patients.”
The study comprised 165,411 primary care patients who had hypercholesterolemia but were free of cardiovascular disease at baseline. Statins were prescribed with the goal of at least a 40% reduction in baseline LDL within 24 months of the start of therapy.
Patients had a mean age of 62 years, with a mean baseline LDL of 4.1 mmol/L (158 mg/dL). About 49% were women.
The primary endpoints were the number of patients who did not achieve the 40% or higher reduction in baseline LDL and the between-group risk differences in cardiovascular events (coronary heart disease, stroke or transient ischemic attack, peripheral vascular disease, cardiovascular death).
After 24 months, 51.2% of patients experienced a suboptimal LDL response, with a mean reduction of 2.1 mmol/L (81 mg/dL) compared with 3.1 mmol/L (120 mg/dL). Compared with optimal responders, these patients were significantly more likely to have received a low-potency statin (29% vs. 18%).
Incident cardiovascular events occurred in 14% of the overall group (coronary artery disease, 8%; stroke/TIA, 3%; peripheral vascular disease 1.9%; cardiovascular death, 1%). All of these outcomes were significantly more common among suboptimal responders than optimal responders.
During a mean of 6 years of follow-up, there were 22,798 cardiovascular disease events overall, with significantly more occurring in suboptimal than optimal responders (12,142 vs. 10,656). This translated to a cardiovascular disease rate of 22.6 and 19.7 per 1,000 person-years, respectively.
In a multivariate analysis controlling for age and baseline LDL level, suboptimal responders were 22% more likely to have a cardiovascular disease incident than were optimal responders.
Among suboptimal responders, every unit decrease of 1 mmol/L (39 mg/dL) conferred a significant 6% risk reduction in cardiovascular disease (odds ratio, 0.94).
The benefit was not universal, the authors pointed out. “In this group, the decreased risk remained significant for only stroke/TIA and was not significant for other constituent cardiovascular disease outcomes. However, in patients with an optimal response, an even greater protective effect of LDL reduction and future cardiovascular disease was seen [13%; OR, 0.87],” and this reduction was significant for all of the individual outcomes.
“The study also highlights the benefit of reducing LDL to optimal values, which would lead to better cardiovascular disease outcomes for patients currently on statins,” the authors concluded.
None of the authors had any relevant financial disclosures.
SOURCE: Weng S. et al. Heart 2019 Apr. doi: 10.1136/heartjnl-2018-314253.
Guidelines always look good on paper, but they’re only as good as their implementation, Márcio S. Bittencourt, MD, wrote in an accompanying editorial.
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) guideline pinned effective statin therapy as a lowering of LDL cholesterol by at least 40%. This target aligns well with data accumulated in randomized controlled studies, but it doesn’t benefit patients unless it can be put into practice.
“An important step after a guideline publication is the assessment of its uptake among health practitioners and patients in the real world, as well as of the impact of its adherence on clinical outcomes. These analyses may not only verify its appropriateness, providing feedback for continuous improvement of recommendations, but also identify targets to optimize delivery of health to the society.”
To understand suboptimal statin response, we must understand the many possible reasons behind it – on the part of both physicians and patients.
Physicians may prefer to prescribe low-potency statins for several reasons, including unawareness of guideline recommendations, doubtfulness of better outcomes with higher potent statins or when a lower LDL is attained, and fear of adverse reactions or drug interactions, Dr. Bittencourt noted. “Moreover, doctors may be reluctant to up-titrate drugs when the treatment goals are not achieved, the so-called therapeutic inertia.”
In this study, for example, optimal responders were more likely to initially receive moderately potent statins. Suboptimal responders, on the other hand, were more likely to receive low-potency statins.
“This probably explains why baseline LDL was higher in optimal responders, indicating that higher LDL motivates the physician to be more aggressive upfront.”
Patients bring their own issues to the treatment table.
“Although an inter-individual response to statins may occur according to the genetic background, most cases where LDL response is less than expected are probably due to lack of adherence or persistence to the treatment. ... Of note, poor adherence to lipid-lowering therapy, together with low-intensity therapy, as opposed to high-intensity treatment, is associated with higher cardiovascular risk.”
Effective implementation of guidelines “has been a challenge for a long time. Both physicians and patients should be targets for approaches aiming at improving adherence to guidelines.”
For clinicians, these could include continuing medical education and simplified treatment algorithms. Patients, too, would benefit from some teaching.
“Patients and society should be educated on the scientific evidence documenting the benefits of lipid-lowering therapy, and antistatin propaganda based on pseudoscience should be strongly disavowed and demystified by health authorities.”
Dr. Bittencourt is an internist at the University Hospital San Paolo, Brazil.
Guidelines always look good on paper, but they’re only as good as their implementation, Márcio S. Bittencourt, MD, wrote in an accompanying editorial.
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) guideline pinned effective statin therapy as a lowering of LDL cholesterol by at least 40%. This target aligns well with data accumulated in randomized controlled studies, but it doesn’t benefit patients unless it can be put into practice.
“An important step after a guideline publication is the assessment of its uptake among health practitioners and patients in the real world, as well as of the impact of its adherence on clinical outcomes. These analyses may not only verify its appropriateness, providing feedback for continuous improvement of recommendations, but also identify targets to optimize delivery of health to the society.”
To understand suboptimal statin response, we must understand the many possible reasons behind it – on the part of both physicians and patients.
Physicians may prefer to prescribe low-potency statins for several reasons, including unawareness of guideline recommendations, doubtfulness of better outcomes with higher potent statins or when a lower LDL is attained, and fear of adverse reactions or drug interactions, Dr. Bittencourt noted. “Moreover, doctors may be reluctant to up-titrate drugs when the treatment goals are not achieved, the so-called therapeutic inertia.”
In this study, for example, optimal responders were more likely to initially receive moderately potent statins. Suboptimal responders, on the other hand, were more likely to receive low-potency statins.
“This probably explains why baseline LDL was higher in optimal responders, indicating that higher LDL motivates the physician to be more aggressive upfront.”
Patients bring their own issues to the treatment table.
“Although an inter-individual response to statins may occur according to the genetic background, most cases where LDL response is less than expected are probably due to lack of adherence or persistence to the treatment. ... Of note, poor adherence to lipid-lowering therapy, together with low-intensity therapy, as opposed to high-intensity treatment, is associated with higher cardiovascular risk.”
Effective implementation of guidelines “has been a challenge for a long time. Both physicians and patients should be targets for approaches aiming at improving adherence to guidelines.”
For clinicians, these could include continuing medical education and simplified treatment algorithms. Patients, too, would benefit from some teaching.
“Patients and society should be educated on the scientific evidence documenting the benefits of lipid-lowering therapy, and antistatin propaganda based on pseudoscience should be strongly disavowed and demystified by health authorities.”
Dr. Bittencourt is an internist at the University Hospital San Paolo, Brazil.
Guidelines always look good on paper, but they’re only as good as their implementation, Márcio S. Bittencourt, MD, wrote in an accompanying editorial.
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) guideline pinned effective statin therapy as a lowering of LDL cholesterol by at least 40%. This target aligns well with data accumulated in randomized controlled studies, but it doesn’t benefit patients unless it can be put into practice.
“An important step after a guideline publication is the assessment of its uptake among health practitioners and patients in the real world, as well as of the impact of its adherence on clinical outcomes. These analyses may not only verify its appropriateness, providing feedback for continuous improvement of recommendations, but also identify targets to optimize delivery of health to the society.”
To understand suboptimal statin response, we must understand the many possible reasons behind it – on the part of both physicians and patients.
Physicians may prefer to prescribe low-potency statins for several reasons, including unawareness of guideline recommendations, doubtfulness of better outcomes with higher potent statins or when a lower LDL is attained, and fear of adverse reactions or drug interactions, Dr. Bittencourt noted. “Moreover, doctors may be reluctant to up-titrate drugs when the treatment goals are not achieved, the so-called therapeutic inertia.”
In this study, for example, optimal responders were more likely to initially receive moderately potent statins. Suboptimal responders, on the other hand, were more likely to receive low-potency statins.
“This probably explains why baseline LDL was higher in optimal responders, indicating that higher LDL motivates the physician to be more aggressive upfront.”
Patients bring their own issues to the treatment table.
“Although an inter-individual response to statins may occur according to the genetic background, most cases where LDL response is less than expected are probably due to lack of adherence or persistence to the treatment. ... Of note, poor adherence to lipid-lowering therapy, together with low-intensity therapy, as opposed to high-intensity treatment, is associated with higher cardiovascular risk.”
Effective implementation of guidelines “has been a challenge for a long time. Both physicians and patients should be targets for approaches aiming at improving adherence to guidelines.”
For clinicians, these could include continuing medical education and simplified treatment algorithms. Patients, too, would benefit from some teaching.
“Patients and society should be educated on the scientific evidence documenting the benefits of lipid-lowering therapy, and antistatin propaganda based on pseudoscience should be strongly disavowed and demystified by health authorities.”
Dr. Bittencourt is an internist at the University Hospital San Paolo, Brazil.
About half of patients taking statins for hyperlipidemia don’t adequately respond, leaving them at a 22% increased risk of cardiovascular disease, compared with optimal responders.
Over 6 years, there were about 2,000 more cardiovascular events among those who failed to experience the national treatment target of at least a 40% reduction in LDL cholesterol, according to Stephen F. Weng, MD, and his colleagues. The report is in Heart.
Physicians’ choice of initial statin weighed heavily in the outcomes. Patients who ended up with an optimal response were more likely to get a more potent statin right off, while those with a poorer response were more likely to get a less-potent statin.
“This study provides ‘real world evidence’ that 50% of patients started on statins do not derive the intended therapeutic benefit from them, significantly increasing their risk of future cardiovascular disease,” wrote Dr. Weng of the University of Nottingham, England, and his colleagues. “These findings contribute to the debate on the effectiveness of statin therapy and highlight the need for personalized medicine in lipid management for patients.”
The study comprised 165,411 primary care patients who had hypercholesterolemia but were free of cardiovascular disease at baseline. Statins were prescribed with the goal of at least a 40% reduction in baseline LDL within 24 months of the start of therapy.
Patients had a mean age of 62 years, with a mean baseline LDL of 4.1 mmol/L (158 mg/dL). About 49% were women.
The primary endpoints were the number of patients who did not achieve the 40% or higher reduction in baseline LDL and the between-group risk differences in cardiovascular events (coronary heart disease, stroke or transient ischemic attack, peripheral vascular disease, cardiovascular death).
After 24 months, 51.2% of patients experienced a suboptimal LDL response, with a mean reduction of 2.1 mmol/L (81 mg/dL) compared with 3.1 mmol/L (120 mg/dL). Compared with optimal responders, these patients were significantly more likely to have received a low-potency statin (29% vs. 18%).
Incident cardiovascular events occurred in 14% of the overall group (coronary artery disease, 8%; stroke/TIA, 3%; peripheral vascular disease 1.9%; cardiovascular death, 1%). All of these outcomes were significantly more common among suboptimal responders than optimal responders.
During a mean of 6 years of follow-up, there were 22,798 cardiovascular disease events overall, with significantly more occurring in suboptimal than optimal responders (12,142 vs. 10,656). This translated to a cardiovascular disease rate of 22.6 and 19.7 per 1,000 person-years, respectively.
In a multivariate analysis controlling for age and baseline LDL level, suboptimal responders were 22% more likely to have a cardiovascular disease incident than were optimal responders.
Among suboptimal responders, every unit decrease of 1 mmol/L (39 mg/dL) conferred a significant 6% risk reduction in cardiovascular disease (odds ratio, 0.94).
The benefit was not universal, the authors pointed out. “In this group, the decreased risk remained significant for only stroke/TIA and was not significant for other constituent cardiovascular disease outcomes. However, in patients with an optimal response, an even greater protective effect of LDL reduction and future cardiovascular disease was seen [13%; OR, 0.87],” and this reduction was significant for all of the individual outcomes.
“The study also highlights the benefit of reducing LDL to optimal values, which would lead to better cardiovascular disease outcomes for patients currently on statins,” the authors concluded.
None of the authors had any relevant financial disclosures.
SOURCE: Weng S. et al. Heart 2019 Apr. doi: 10.1136/heartjnl-2018-314253.
About half of patients taking statins for hyperlipidemia don’t adequately respond, leaving them at a 22% increased risk of cardiovascular disease, compared with optimal responders.
Over 6 years, there were about 2,000 more cardiovascular events among those who failed to experience the national treatment target of at least a 40% reduction in LDL cholesterol, according to Stephen F. Weng, MD, and his colleagues. The report is in Heart.
Physicians’ choice of initial statin weighed heavily in the outcomes. Patients who ended up with an optimal response were more likely to get a more potent statin right off, while those with a poorer response were more likely to get a less-potent statin.
“This study provides ‘real world evidence’ that 50% of patients started on statins do not derive the intended therapeutic benefit from them, significantly increasing their risk of future cardiovascular disease,” wrote Dr. Weng of the University of Nottingham, England, and his colleagues. “These findings contribute to the debate on the effectiveness of statin therapy and highlight the need for personalized medicine in lipid management for patients.”
The study comprised 165,411 primary care patients who had hypercholesterolemia but were free of cardiovascular disease at baseline. Statins were prescribed with the goal of at least a 40% reduction in baseline LDL within 24 months of the start of therapy.
Patients had a mean age of 62 years, with a mean baseline LDL of 4.1 mmol/L (158 mg/dL). About 49% were women.
The primary endpoints were the number of patients who did not achieve the 40% or higher reduction in baseline LDL and the between-group risk differences in cardiovascular events (coronary heart disease, stroke or transient ischemic attack, peripheral vascular disease, cardiovascular death).
After 24 months, 51.2% of patients experienced a suboptimal LDL response, with a mean reduction of 2.1 mmol/L (81 mg/dL) compared with 3.1 mmol/L (120 mg/dL). Compared with optimal responders, these patients were significantly more likely to have received a low-potency statin (29% vs. 18%).
Incident cardiovascular events occurred in 14% of the overall group (coronary artery disease, 8%; stroke/TIA, 3%; peripheral vascular disease 1.9%; cardiovascular death, 1%). All of these outcomes were significantly more common among suboptimal responders than optimal responders.
During a mean of 6 years of follow-up, there were 22,798 cardiovascular disease events overall, with significantly more occurring in suboptimal than optimal responders (12,142 vs. 10,656). This translated to a cardiovascular disease rate of 22.6 and 19.7 per 1,000 person-years, respectively.
In a multivariate analysis controlling for age and baseline LDL level, suboptimal responders were 22% more likely to have a cardiovascular disease incident than were optimal responders.
Among suboptimal responders, every unit decrease of 1 mmol/L (39 mg/dL) conferred a significant 6% risk reduction in cardiovascular disease (odds ratio, 0.94).
The benefit was not universal, the authors pointed out. “In this group, the decreased risk remained significant for only stroke/TIA and was not significant for other constituent cardiovascular disease outcomes. However, in patients with an optimal response, an even greater protective effect of LDL reduction and future cardiovascular disease was seen [13%; OR, 0.87],” and this reduction was significant for all of the individual outcomes.
“The study also highlights the benefit of reducing LDL to optimal values, which would lead to better cardiovascular disease outcomes for patients currently on statins,” the authors concluded.
None of the authors had any relevant financial disclosures.
SOURCE: Weng S. et al. Heart 2019 Apr. doi: 10.1136/heartjnl-2018-314253.
FROM HEART

Atorvastatin appears to lower cardiovascular risk in RA patients
Atorvastatin proved safe and potentially effective in preventing cardiovascular events in RA patients, according to the prematurely terminated TRACE RA trial.
“TRACE RA suggests that atorvastatin 40 mg daily is safe for the primary prevention of [CV events] in patients with RA and appears to confer a similar degree of risk reduction in these patients as in other populations,” wrote George D. Kitas, MD, of the Dudley (England) Group NHS Foundation Trust. The study was published in Arthritis & Rheumatology.
TRACE RA was a multicenter, double-blind, randomized trial that compared atorvastatin with placebo in preventing CV events by reducing LDL cholesterol. Its 3,002 patients with RA were randomized to receive either atorvastatin (1,504) or placebo (1,498). The goal was to follow the participants for 5 years. However, because of an unexpectedly low event rate, the trial was terminated early, resulting in a mean follow-up of 2.5 years.
At the end of the trial, those in the atorvastatin group had 0.77 mmol/L lower LDL cholesterol levels, compared with the placebo group (P less than .0001). Of the patients who received atorvastatin, 24 (1.6%) had a cardiac event versus 36 (2.4%) for placebo (hazard ratio, 0.66; 95% confidence interval, 0.39-1.11; P = .115). The estimated CV event risk reduction per 1 mmol/L reduction in LDL cholesterol was 42% (95% CI, –14% to 70%).
The coauthors acknowledged the study’s limitations, including the fact that it was terminated early because of a lower-than-expected CV event rate. This led to their results not being deemed statistically significant. They noted several reasons why this might have occurred – among them TRACE RA purposely excluding patients with the highest CV event risk – but also recognized that “the low event rate shows that there is a sizeable population of RA patients who have a relatively low CVD risk.”
“This does not support prescribing statins to all RA patients,” they added. “Instead, the decision to prescribe should be based on assessment of the individual RA patient’s risk using, at present, the relevant national or international recommendations and risk assessment tools.”
The study was funded by Arthritis Research UK and the British Heart Foundation. The coauthors report numerous potential conflicts of interest, including receiving honoraria for lectures and advisory boards participation, grant support, and consulting fees from various pharmaceutical companies.
SOURCE: Kitas GD et al. Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40892.
Although it did not accomplish exactly what it set out to do, the TRACE RA study is a firm step in the right direction, according to Katherine P. Liao, MD, and Daniel H. Solomon, MD, of Brigham and Women’s Hospital in Boston.
To illustrate their point, Dr. Liao and Dr. Solomon presented a hypothetical RA patient called TR. She is firmly “average,” especially among the population represented in this study. Though she doesn’t seem like a glaring candidate for a statin, we can rightfully assume that – because of RA and a C-reactive protein above 2 mg/dL – her cardiovascular risk is higher than a member of the general population. The next step is determining if a statin will benefit such a patient, something relatively unexplored thus far.
Despite its abrupt termination, the coauthors “laud the investigators of TRACE RA, as this is the first trial among RA patients that was designed to study hard CVD endpoints.” At the very least, the study reinforced that statins are not associated with side effects when paired with typical RA treatments. In the future, Dr. Liao and Dr. Solomon suggested a focus on “better methods for identifying the appropriate patient population in RA to target for CV risk reduction strategies.”
These comments are adapted from an accompanying editorial (Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40891). Dr. Solomon reported receiving salary support through research contracts from AbbVie, Amgen, Corrona, Genentech, Janssen, and Pfizer.
Although it did not accomplish exactly what it set out to do, the TRACE RA study is a firm step in the right direction, according to Katherine P. Liao, MD, and Daniel H. Solomon, MD, of Brigham and Women’s Hospital in Boston.
To illustrate their point, Dr. Liao and Dr. Solomon presented a hypothetical RA patient called TR. She is firmly “average,” especially among the population represented in this study. Though she doesn’t seem like a glaring candidate for a statin, we can rightfully assume that – because of RA and a C-reactive protein above 2 mg/dL – her cardiovascular risk is higher than a member of the general population. The next step is determining if a statin will benefit such a patient, something relatively unexplored thus far.
Despite its abrupt termination, the coauthors “laud the investigators of TRACE RA, as this is the first trial among RA patients that was designed to study hard CVD endpoints.” At the very least, the study reinforced that statins are not associated with side effects when paired with typical RA treatments. In the future, Dr. Liao and Dr. Solomon suggested a focus on “better methods for identifying the appropriate patient population in RA to target for CV risk reduction strategies.”
These comments are adapted from an accompanying editorial (Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40891). Dr. Solomon reported receiving salary support through research contracts from AbbVie, Amgen, Corrona, Genentech, Janssen, and Pfizer.
Although it did not accomplish exactly what it set out to do, the TRACE RA study is a firm step in the right direction, according to Katherine P. Liao, MD, and Daniel H. Solomon, MD, of Brigham and Women’s Hospital in Boston.
To illustrate their point, Dr. Liao and Dr. Solomon presented a hypothetical RA patient called TR. She is firmly “average,” especially among the population represented in this study. Though she doesn’t seem like a glaring candidate for a statin, we can rightfully assume that – because of RA and a C-reactive protein above 2 mg/dL – her cardiovascular risk is higher than a member of the general population. The next step is determining if a statin will benefit such a patient, something relatively unexplored thus far.
Despite its abrupt termination, the coauthors “laud the investigators of TRACE RA, as this is the first trial among RA patients that was designed to study hard CVD endpoints.” At the very least, the study reinforced that statins are not associated with side effects when paired with typical RA treatments. In the future, Dr. Liao and Dr. Solomon suggested a focus on “better methods for identifying the appropriate patient population in RA to target for CV risk reduction strategies.”
These comments are adapted from an accompanying editorial (Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40891). Dr. Solomon reported receiving salary support through research contracts from AbbVie, Amgen, Corrona, Genentech, Janssen, and Pfizer.
Atorvastatin proved safe and potentially effective in preventing cardiovascular events in RA patients, according to the prematurely terminated TRACE RA trial.
“TRACE RA suggests that atorvastatin 40 mg daily is safe for the primary prevention of [CV events] in patients with RA and appears to confer a similar degree of risk reduction in these patients as in other populations,” wrote George D. Kitas, MD, of the Dudley (England) Group NHS Foundation Trust. The study was published in Arthritis & Rheumatology.
TRACE RA was a multicenter, double-blind, randomized trial that compared atorvastatin with placebo in preventing CV events by reducing LDL cholesterol. Its 3,002 patients with RA were randomized to receive either atorvastatin (1,504) or placebo (1,498). The goal was to follow the participants for 5 years. However, because of an unexpectedly low event rate, the trial was terminated early, resulting in a mean follow-up of 2.5 years.
At the end of the trial, those in the atorvastatin group had 0.77 mmol/L lower LDL cholesterol levels, compared with the placebo group (P less than .0001). Of the patients who received atorvastatin, 24 (1.6%) had a cardiac event versus 36 (2.4%) for placebo (hazard ratio, 0.66; 95% confidence interval, 0.39-1.11; P = .115). The estimated CV event risk reduction per 1 mmol/L reduction in LDL cholesterol was 42% (95% CI, –14% to 70%).
The coauthors acknowledged the study’s limitations, including the fact that it was terminated early because of a lower-than-expected CV event rate. This led to their results not being deemed statistically significant. They noted several reasons why this might have occurred – among them TRACE RA purposely excluding patients with the highest CV event risk – but also recognized that “the low event rate shows that there is a sizeable population of RA patients who have a relatively low CVD risk.”
“This does not support prescribing statins to all RA patients,” they added. “Instead, the decision to prescribe should be based on assessment of the individual RA patient’s risk using, at present, the relevant national or international recommendations and risk assessment tools.”
The study was funded by Arthritis Research UK and the British Heart Foundation. The coauthors report numerous potential conflicts of interest, including receiving honoraria for lectures and advisory boards participation, grant support, and consulting fees from various pharmaceutical companies.
SOURCE: Kitas GD et al. Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40892.
Atorvastatin proved safe and potentially effective in preventing cardiovascular events in RA patients, according to the prematurely terminated TRACE RA trial.
“TRACE RA suggests that atorvastatin 40 mg daily is safe for the primary prevention of [CV events] in patients with RA and appears to confer a similar degree of risk reduction in these patients as in other populations,” wrote George D. Kitas, MD, of the Dudley (England) Group NHS Foundation Trust. The study was published in Arthritis & Rheumatology.
TRACE RA was a multicenter, double-blind, randomized trial that compared atorvastatin with placebo in preventing CV events by reducing LDL cholesterol. Its 3,002 patients with RA were randomized to receive either atorvastatin (1,504) or placebo (1,498). The goal was to follow the participants for 5 years. However, because of an unexpectedly low event rate, the trial was terminated early, resulting in a mean follow-up of 2.5 years.
At the end of the trial, those in the atorvastatin group had 0.77 mmol/L lower LDL cholesterol levels, compared with the placebo group (P less than .0001). Of the patients who received atorvastatin, 24 (1.6%) had a cardiac event versus 36 (2.4%) for placebo (hazard ratio, 0.66; 95% confidence interval, 0.39-1.11; P = .115). The estimated CV event risk reduction per 1 mmol/L reduction in LDL cholesterol was 42% (95% CI, –14% to 70%).
The coauthors acknowledged the study’s limitations, including the fact that it was terminated early because of a lower-than-expected CV event rate. This led to their results not being deemed statistically significant. They noted several reasons why this might have occurred – among them TRACE RA purposely excluding patients with the highest CV event risk – but also recognized that “the low event rate shows that there is a sizeable population of RA patients who have a relatively low CVD risk.”
“This does not support prescribing statins to all RA patients,” they added. “Instead, the decision to prescribe should be based on assessment of the individual RA patient’s risk using, at present, the relevant national or international recommendations and risk assessment tools.”
The study was funded by Arthritis Research UK and the British Heart Foundation. The coauthors report numerous potential conflicts of interest, including receiving honoraria for lectures and advisory boards participation, grant support, and consulting fees from various pharmaceutical companies.
SOURCE: Kitas GD et al. Arthritis Rheumatol. 2019 Apr 15. doi: 10.1002/art.40892.
FROM ARTHRITIS & RHEUMATOLOGY
Studies link TMAO to microbiome, reveal new heart disease target
MIAMI – Researchers are one step closer to developing “drugs for bugs” – agents that target the gut microbiome to prevent and treat cardiometabolic diseases, Stanley L. Hazen, MD, PhD, said at the 2019 Gut Microbiota for Health World Summit.

“Each person experiences a meal differently through the filter of their gut microbiome, which helps explain individual differences in susceptibility to disease,” said Dr. Hazen of Cleveland Clinic. “In the future, our medicine cabinets will have drugs in them that not only affect us, but also target the microbial enzymes that affect levels of metabolites like TMAO.”
Trimethylamine N-oxide (TMAO) is produced by gut bacteria. High levels (in one study, approximately 6.2 micromolar) significantly increase the risk of major adverse cardiovascular events even after controlling for traditional demographic and clinical risk factors. Studies indicate that TMAO alters cholesterol and bile acid metabolism, upregulates inflammatory pathways, and promotes foam cell formation, all of which worsen atherosclerosis. In addition, TMAO increases clotting risk by enhancing platelet reactivity.
“Reducing the amount of animal products in one’s diet helps reduce TMAO levels,” said Dr. Hazen. Certain fish – mainly those found in deep, cold water, such as cod – are high in TMAO. However, a bigger culprit in the United States is red meat, which contains two major TMAO precursors – choline and carnitine. In a recent study, Dr. Hazen and his associates gave 113 healthy volunteers three isocaloric diets in random order based on red meat, white meat, or plant-based protein. After 4 weeks, eating the daily equivalent of 8 ounces of steak or two quarter-pound beef patties nearly tripled plasma TMAO levels (P less than .05) from baseline. The white meat and vegetarian diets showed no such effect.
Crucially, the effect of red meat was reversible – TMAO levels fell significantly within 4 weeks after participants stopped consuming red meat. Eating red meat low in saturated fat did not prevent TMAO levels from rising, Dr. Hazen noted at the meeting at the meeting sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility.
In a second study, Dr. Hazen and his associates identified a two-step process by which gut bacteria metabolize carnitine to TMAO. The second step was greatly enhanced in individuals who eat red meat, suggesting a possible therapeutic target. In a third study, they found that high TMAO levels in mice fell significantly with a single oral dose of a second-generation inhibitor of trimethylamine lyase, the enzyme used by gut bacteria to convert choline to TMAO. The inhibitory effect was irreversible, did not reduce the viability of commensal microorganisms, and significantly lowered platelet hyperreactivity and clot formation.
Such results are exciting, but “drugs for bugs” will exhibit varying effects depending on which gut species are present at baseline, Dr. Hazen explained. Investigators will need to understand and account for these differences before therapies for the microbiome can enter the clinic. For now, a blood test for TMAO is available and can help clinicians tailor their suggestions on what to eat.
Dr. Hazen disclosed a consulting relationship with Proctor & Gamble, royalties for patents from Proctor & Gamble, Cleveland Heart Lab, and Quest Diagnostics, and research support from AstraZeneca, Pfizer, Roche Diagnostics, and Proctor & Gamble.
MIAMI – Researchers are one step closer to developing “drugs for bugs” – agents that target the gut microbiome to prevent and treat cardiometabolic diseases, Stanley L. Hazen, MD, PhD, said at the 2019 Gut Microbiota for Health World Summit.
“Each person experiences a meal differently through the filter of their gut microbiome, which helps explain individual differences in susceptibility to disease,” said Dr. Hazen of Cleveland Clinic. “In the future, our medicine cabinets will have drugs in them that not only affect us, but also target the microbial enzymes that affect levels of metabolites like TMAO.”
Trimethylamine N-oxide (TMAO) is produced by gut bacteria. High levels (in one study, approximately 6.2 micromolar) significantly increase the risk of major adverse cardiovascular events even after controlling for traditional demographic and clinical risk factors. Studies indicate that TMAO alters cholesterol and bile acid metabolism, upregulates inflammatory pathways, and promotes foam cell formation, all of which worsen atherosclerosis. In addition, TMAO increases clotting risk by enhancing platelet reactivity.
“Reducing the amount of animal products in one’s diet helps reduce TMAO levels,” said Dr. Hazen. Certain fish – mainly those found in deep, cold water, such as cod – are high in TMAO. However, a bigger culprit in the United States is red meat, which contains two major TMAO precursors – choline and carnitine. In a recent study, Dr. Hazen and his associates gave 113 healthy volunteers three isocaloric diets in random order based on red meat, white meat, or plant-based protein. After 4 weeks, eating the daily equivalent of 8 ounces of steak or two quarter-pound beef patties nearly tripled plasma TMAO levels (P less than .05) from baseline. The white meat and vegetarian diets showed no such effect.
Crucially, the effect of red meat was reversible – TMAO levels fell significantly within 4 weeks after participants stopped consuming red meat. Eating red meat low in saturated fat did not prevent TMAO levels from rising, Dr. Hazen noted at the meeting at the meeting sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility.
In a second study, Dr. Hazen and his associates identified a two-step process by which gut bacteria metabolize carnitine to TMAO. The second step was greatly enhanced in individuals who eat red meat, suggesting a possible therapeutic target. In a third study, they found that high TMAO levels in mice fell significantly with a single oral dose of a second-generation inhibitor of trimethylamine lyase, the enzyme used by gut bacteria to convert choline to TMAO. The inhibitory effect was irreversible, did not reduce the viability of commensal microorganisms, and significantly lowered platelet hyperreactivity and clot formation.
Such results are exciting, but “drugs for bugs” will exhibit varying effects depending on which gut species are present at baseline, Dr. Hazen explained. Investigators will need to understand and account for these differences before therapies for the microbiome can enter the clinic. For now, a blood test for TMAO is available and can help clinicians tailor their suggestions on what to eat.
Dr. Hazen disclosed a consulting relationship with Proctor & Gamble, royalties for patents from Proctor & Gamble, Cleveland Heart Lab, and Quest Diagnostics, and research support from AstraZeneca, Pfizer, Roche Diagnostics, and Proctor & Gamble.
MIAMI – Researchers are one step closer to developing “drugs for bugs” – agents that target the gut microbiome to prevent and treat cardiometabolic diseases, Stanley L. Hazen, MD, PhD, said at the 2019 Gut Microbiota for Health World Summit.
“Each person experiences a meal differently through the filter of their gut microbiome, which helps explain individual differences in susceptibility to disease,” said Dr. Hazen of Cleveland Clinic. “In the future, our medicine cabinets will have drugs in them that not only affect us, but also target the microbial enzymes that affect levels of metabolites like TMAO.”
Trimethylamine N-oxide (TMAO) is produced by gut bacteria. High levels (in one study, approximately 6.2 micromolar) significantly increase the risk of major adverse cardiovascular events even after controlling for traditional demographic and clinical risk factors. Studies indicate that TMAO alters cholesterol and bile acid metabolism, upregulates inflammatory pathways, and promotes foam cell formation, all of which worsen atherosclerosis. In addition, TMAO increases clotting risk by enhancing platelet reactivity.
“Reducing the amount of animal products in one’s diet helps reduce TMAO levels,” said Dr. Hazen. Certain fish – mainly those found in deep, cold water, such as cod – are high in TMAO. However, a bigger culprit in the United States is red meat, which contains two major TMAO precursors – choline and carnitine. In a recent study, Dr. Hazen and his associates gave 113 healthy volunteers three isocaloric diets in random order based on red meat, white meat, or plant-based protein. After 4 weeks, eating the daily equivalent of 8 ounces of steak or two quarter-pound beef patties nearly tripled plasma TMAO levels (P less than .05) from baseline. The white meat and vegetarian diets showed no such effect.
Crucially, the effect of red meat was reversible – TMAO levels fell significantly within 4 weeks after participants stopped consuming red meat. Eating red meat low in saturated fat did not prevent TMAO levels from rising, Dr. Hazen noted at the meeting at the meeting sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility.
In a second study, Dr. Hazen and his associates identified a two-step process by which gut bacteria metabolize carnitine to TMAO. The second step was greatly enhanced in individuals who eat red meat, suggesting a possible therapeutic target. In a third study, they found that high TMAO levels in mice fell significantly with a single oral dose of a second-generation inhibitor of trimethylamine lyase, the enzyme used by gut bacteria to convert choline to TMAO. The inhibitory effect was irreversible, did not reduce the viability of commensal microorganisms, and significantly lowered platelet hyperreactivity and clot formation.
Such results are exciting, but “drugs for bugs” will exhibit varying effects depending on which gut species are present at baseline, Dr. Hazen explained. Investigators will need to understand and account for these differences before therapies for the microbiome can enter the clinic. For now, a blood test for TMAO is available and can help clinicians tailor their suggestions on what to eat.
Dr. Hazen disclosed a consulting relationship with Proctor & Gamble, royalties for patents from Proctor & Gamble, Cleveland Heart Lab, and Quest Diagnostics, and research support from AstraZeneca, Pfizer, Roche Diagnostics, and Proctor & Gamble.
REPORTING FROM GMFH 2019

CAC score over 1,000 carries higher risks
, based on data from a large retrospective study presented by Allison W. Peng at the annual meeting of the American College of Cardiology.
“Our data argues for consideration of CAC 1000 (or more) as a distinct group with CVD mortality greater than that of contemporary secondary prevention trials ... We showed that those with CAC 1000 (or more) have both a higher area and density of calcification, a more dispersed pattern of calcification in their coronary artery tree (the majority with 4-vessel disease), with a markedly more diffuse distribution of extra-coronary calcification compared to the other CAC groups,” Ms. Peng and her colleagues wrote in the study, which was published online in the Journal of the American College of Cardiology.
Future guidelines should address these patients as a distinct risk group that might gain the most benefit from targeted, aggressive preventive therapy, the researchers said.
Current guidelines identify individuals with CAC scores over 400 as the highest risk group. With a mean follow-up time of 12.3 years, the results from 66,636 asymptomatic individuals in the CAC consortium study, which included over 2,800 patients with CAC (Agatston) scores of 1,000 or more, indicate patients with CAC scores of 1000 or more have nearly a 2-fold higher risk of CVD mortality compared to those with CAC scores of 400-999. While the mortality risk levels off slightly in those with scores exceeding 1000, all-cause and cause-specific mortality risk still increases with no apparent upper CAC threshold.
Patients with a CAC score of at least 1000 were 66.3 years old, on average; 86.3% were male, 52.4% had 4-vessel CAC, and they had a larger total CAC area.
Compared to patients with CAC scores of 400-999, those with a CAC score of 1000 or more had a greater risk of cardiovascular disease (HR, 1.71; 95% CI, 1.41-2.08), coronary heart disease (HR, 1.84; 95% CI, 1.43-2.36), cancer (HR, 1.36; 95% CI, 1.07-1.73), and all-cause mortality (HR, 1.51; 95% CI, 1.33-1.70).
Those with CAC scores of 400-999 had a 2.1, 3.6, 2.7, and 9.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively. But those with CAC scores of 1000 of more had a 5.1, 8.0, 4.6, and 18.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively.
The leading cause of death was CVD; 36.5% in the CAC 400-999 group and 42.6% in the CAC 1000 or more group. CHD mortality, as a subset of CVD mortality, constituted 21.1% of deaths in the CAC 400-999 group and 27.1% of deaths in the CAC 1000 or more group.
“Future randomized controlled trials of aggressive preventative therapies, for example PCSK9-inhibitors and anti-inflammatory drugs, in patients with CAC ≥ 1000, may prove helpful to evaluate the benefits of such treatment in this unique group,” the authors wrote. They also urged updating current guidelines to reflect best practices for these patients.
The study was funded by The National Institutes of Health. The authors have no relevant financial disclosures.
SOURCE: Peng A et al. Journal of the American College of Cardiology.
, based on data from a large retrospective study presented by Allison W. Peng at the annual meeting of the American College of Cardiology.
“Our data argues for consideration of CAC 1000 (or more) as a distinct group with CVD mortality greater than that of contemporary secondary prevention trials ... We showed that those with CAC 1000 (or more) have both a higher area and density of calcification, a more dispersed pattern of calcification in their coronary artery tree (the majority with 4-vessel disease), with a markedly more diffuse distribution of extra-coronary calcification compared to the other CAC groups,” Ms. Peng and her colleagues wrote in the study, which was published online in the Journal of the American College of Cardiology.
Future guidelines should address these patients as a distinct risk group that might gain the most benefit from targeted, aggressive preventive therapy, the researchers said.
Current guidelines identify individuals with CAC scores over 400 as the highest risk group. With a mean follow-up time of 12.3 years, the results from 66,636 asymptomatic individuals in the CAC consortium study, which included over 2,800 patients with CAC (Agatston) scores of 1,000 or more, indicate patients with CAC scores of 1000 or more have nearly a 2-fold higher risk of CVD mortality compared to those with CAC scores of 400-999. While the mortality risk levels off slightly in those with scores exceeding 1000, all-cause and cause-specific mortality risk still increases with no apparent upper CAC threshold.
Patients with a CAC score of at least 1000 were 66.3 years old, on average; 86.3% were male, 52.4% had 4-vessel CAC, and they had a larger total CAC area.
Compared to patients with CAC scores of 400-999, those with a CAC score of 1000 or more had a greater risk of cardiovascular disease (HR, 1.71; 95% CI, 1.41-2.08), coronary heart disease (HR, 1.84; 95% CI, 1.43-2.36), cancer (HR, 1.36; 95% CI, 1.07-1.73), and all-cause mortality (HR, 1.51; 95% CI, 1.33-1.70).
Those with CAC scores of 400-999 had a 2.1, 3.6, 2.7, and 9.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively. But those with CAC scores of 1000 of more had a 5.1, 8.0, 4.6, and 18.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively.
The leading cause of death was CVD; 36.5% in the CAC 400-999 group and 42.6% in the CAC 1000 or more group. CHD mortality, as a subset of CVD mortality, constituted 21.1% of deaths in the CAC 400-999 group and 27.1% of deaths in the CAC 1000 or more group.
“Future randomized controlled trials of aggressive preventative therapies, for example PCSK9-inhibitors and anti-inflammatory drugs, in patients with CAC ≥ 1000, may prove helpful to evaluate the benefits of such treatment in this unique group,” the authors wrote. They also urged updating current guidelines to reflect best practices for these patients.
The study was funded by The National Institutes of Health. The authors have no relevant financial disclosures.
SOURCE: Peng A et al. Journal of the American College of Cardiology.
, based on data from a large retrospective study presented by Allison W. Peng at the annual meeting of the American College of Cardiology.
“Our data argues for consideration of CAC 1000 (or more) as a distinct group with CVD mortality greater than that of contemporary secondary prevention trials ... We showed that those with CAC 1000 (or more) have both a higher area and density of calcification, a more dispersed pattern of calcification in their coronary artery tree (the majority with 4-vessel disease), with a markedly more diffuse distribution of extra-coronary calcification compared to the other CAC groups,” Ms. Peng and her colleagues wrote in the study, which was published online in the Journal of the American College of Cardiology.
Future guidelines should address these patients as a distinct risk group that might gain the most benefit from targeted, aggressive preventive therapy, the researchers said.
Current guidelines identify individuals with CAC scores over 400 as the highest risk group. With a mean follow-up time of 12.3 years, the results from 66,636 asymptomatic individuals in the CAC consortium study, which included over 2,800 patients with CAC (Agatston) scores of 1,000 or more, indicate patients with CAC scores of 1000 or more have nearly a 2-fold higher risk of CVD mortality compared to those with CAC scores of 400-999. While the mortality risk levels off slightly in those with scores exceeding 1000, all-cause and cause-specific mortality risk still increases with no apparent upper CAC threshold.
Patients with a CAC score of at least 1000 were 66.3 years old, on average; 86.3% were male, 52.4% had 4-vessel CAC, and they had a larger total CAC area.
Compared to patients with CAC scores of 400-999, those with a CAC score of 1000 or more had a greater risk of cardiovascular disease (HR, 1.71; 95% CI, 1.41-2.08), coronary heart disease (HR, 1.84; 95% CI, 1.43-2.36), cancer (HR, 1.36; 95% CI, 1.07-1.73), and all-cause mortality (HR, 1.51; 95% CI, 1.33-1.70).
Those with CAC scores of 400-999 had a 2.1, 3.6, 2.7, and 9.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively. But those with CAC scores of 1000 of more had a 5.1, 8.0, 4.6, and 18.8 mortality rate per 1000 person-years for CHD, CVD, cancer, and all-cause mortality, respectively.
The leading cause of death was CVD; 36.5% in the CAC 400-999 group and 42.6% in the CAC 1000 or more group. CHD mortality, as a subset of CVD mortality, constituted 21.1% of deaths in the CAC 400-999 group and 27.1% of deaths in the CAC 1000 or more group.
“Future randomized controlled trials of aggressive preventative therapies, for example PCSK9-inhibitors and anti-inflammatory drugs, in patients with CAC ≥ 1000, may prove helpful to evaluate the benefits of such treatment in this unique group,” the authors wrote. They also urged updating current guidelines to reflect best practices for these patients.
The study was funded by The National Institutes of Health. The authors have no relevant financial disclosures.
SOURCE: Peng A et al. Journal of the American College of Cardiology.
FROM ACC 2019
Light physical activity lowers CVD risk in older women
Even light physical activity can significantly reduce the risks of acquiring coronary heart disease specifically and the broad range of cardiovascular diseases in older women, new data suggests.
A paper published in JAMA Network Open reported the outcome of a prospective cohort study in 5,861 women, with a mean age of 78.5 years, who wore accelerometers for 7 days to measure physical activity.
than those in the lowest quartile of activity, who engaged in less than 3.9 hours per day, after adjusting for factors such as comorbidities, lifestyle, and cardiovascular risk.
Similarly, those in the highest quartile had an 18% lower risk of cardiovascular disease than those in the lowest quartile, after adjusting for potential confounders.
Researchers saw a significant dose-dependent decrease in the risk for incident coronary heart disease and cardiovascular disease with increasing light physical activity, such that each 1-hour increment of activity was associated with a 20% decrease in coronary heart disease risk and 10% decrease in cardiovascular disease risk.
Andrea Z. LaCroix, PhD, from the University of California, San Diego, and her coauthors noted that physical activity guidelines for aerobic activity suggest 75 minutes of vigorous physical activity or 150 minutes of moderate activity each day, but only around 25% of U.S. women aged over 75 years are estimated to meet this requirement.
“These guidelines may have discouraged PA [physical activity] when perceived to be unattainable by large segments of the population,” they wrote.
While the majority of active time in older adults is spent doing light physical activity, little is known about the cardiovascular effects of participating in this level of activity. “A major barrier has been that self-reported questionnaires measuring leisure-time PA do not adequately capture light PA that is acquired throughout the day in activities of daily living,” they wrote.
The study also looked at the impact of moderate to vigorous physical activity, finding a significant 46% reduction between the highest to lowest quartiles of activity in coronary heart disease risk and a 31% reduction in cardiovascular disease risk.
Even after adjusting for the use of lipid-lowering medication, antihypertensive medication or healthy eating scores, the results remained unchanged. The researchers also saw no change when women with angina and heart failure at baseline were excluded or when they excluded cardiovascular events that occurred during the first 6 months of follow-up.
The study was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; and the Department of Health & Human Services. Six authors reported receiving funding from the study supporters and other research institutions, and one reported membership on the advisory committee for physical activity guidelines. No other conflicts of interest were reported.
SOURCE: LaCroix AZ et al. JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0419.
Older women do not get enough physical activity, so this finding that light physical activity is associated with improved coronary heart disease and cardiovascular disease outcomes supports the recent scientific report by the 2018 Physical Activity Guidelines Advisory Committee. It is also helpful in extending the evidence about the benefits of physical activity in reducing incident coronary heart disease to older women, as previous studies on this topic showed such benefits in men.
These findings should remind health care professionals, systems, and agencies to promote the 2018 Physical Activity Guidelines for Americans to all patients. Otherwise, the future health and well-being of older women is likely to suffer from the consequences of sedentary behavior and inadequate physical activity.
Gregory W. Heath, DHSc, MPH, is from the department of health and human performance at the University of Tennessee, Chattanooga. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0405). No conflicts of interest were reported.
Older women do not get enough physical activity, so this finding that light physical activity is associated with improved coronary heart disease and cardiovascular disease outcomes supports the recent scientific report by the 2018 Physical Activity Guidelines Advisory Committee. It is also helpful in extending the evidence about the benefits of physical activity in reducing incident coronary heart disease to older women, as previous studies on this topic showed such benefits in men.
These findings should remind health care professionals, systems, and agencies to promote the 2018 Physical Activity Guidelines for Americans to all patients. Otherwise, the future health and well-being of older women is likely to suffer from the consequences of sedentary behavior and inadequate physical activity.
Gregory W. Heath, DHSc, MPH, is from the department of health and human performance at the University of Tennessee, Chattanooga. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0405). No conflicts of interest were reported.
Older women do not get enough physical activity, so this finding that light physical activity is associated with improved coronary heart disease and cardiovascular disease outcomes supports the recent scientific report by the 2018 Physical Activity Guidelines Advisory Committee. It is also helpful in extending the evidence about the benefits of physical activity in reducing incident coronary heart disease to older women, as previous studies on this topic showed such benefits in men.
These findings should remind health care professionals, systems, and agencies to promote the 2018 Physical Activity Guidelines for Americans to all patients. Otherwise, the future health and well-being of older women is likely to suffer from the consequences of sedentary behavior and inadequate physical activity.
Gregory W. Heath, DHSc, MPH, is from the department of health and human performance at the University of Tennessee, Chattanooga. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0405). No conflicts of interest were reported.
Even light physical activity can significantly reduce the risks of acquiring coronary heart disease specifically and the broad range of cardiovascular diseases in older women, new data suggests.
A paper published in JAMA Network Open reported the outcome of a prospective cohort study in 5,861 women, with a mean age of 78.5 years, who wore accelerometers for 7 days to measure physical activity.
than those in the lowest quartile of activity, who engaged in less than 3.9 hours per day, after adjusting for factors such as comorbidities, lifestyle, and cardiovascular risk.
Similarly, those in the highest quartile had an 18% lower risk of cardiovascular disease than those in the lowest quartile, after adjusting for potential confounders.
Researchers saw a significant dose-dependent decrease in the risk for incident coronary heart disease and cardiovascular disease with increasing light physical activity, such that each 1-hour increment of activity was associated with a 20% decrease in coronary heart disease risk and 10% decrease in cardiovascular disease risk.
Andrea Z. LaCroix, PhD, from the University of California, San Diego, and her coauthors noted that physical activity guidelines for aerobic activity suggest 75 minutes of vigorous physical activity or 150 minutes of moderate activity each day, but only around 25% of U.S. women aged over 75 years are estimated to meet this requirement.
“These guidelines may have discouraged PA [physical activity] when perceived to be unattainable by large segments of the population,” they wrote.
While the majority of active time in older adults is spent doing light physical activity, little is known about the cardiovascular effects of participating in this level of activity. “A major barrier has been that self-reported questionnaires measuring leisure-time PA do not adequately capture light PA that is acquired throughout the day in activities of daily living,” they wrote.
The study also looked at the impact of moderate to vigorous physical activity, finding a significant 46% reduction between the highest to lowest quartiles of activity in coronary heart disease risk and a 31% reduction in cardiovascular disease risk.
Even after adjusting for the use of lipid-lowering medication, antihypertensive medication or healthy eating scores, the results remained unchanged. The researchers also saw no change when women with angina and heart failure at baseline were excluded or when they excluded cardiovascular events that occurred during the first 6 months of follow-up.
The study was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; and the Department of Health & Human Services. Six authors reported receiving funding from the study supporters and other research institutions, and one reported membership on the advisory committee for physical activity guidelines. No other conflicts of interest were reported.
SOURCE: LaCroix AZ et al. JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0419.
Even light physical activity can significantly reduce the risks of acquiring coronary heart disease specifically and the broad range of cardiovascular diseases in older women, new data suggests.
A paper published in JAMA Network Open reported the outcome of a prospective cohort study in 5,861 women, with a mean age of 78.5 years, who wore accelerometers for 7 days to measure physical activity.
than those in the lowest quartile of activity, who engaged in less than 3.9 hours per day, after adjusting for factors such as comorbidities, lifestyle, and cardiovascular risk.
Similarly, those in the highest quartile had an 18% lower risk of cardiovascular disease than those in the lowest quartile, after adjusting for potential confounders.
Researchers saw a significant dose-dependent decrease in the risk for incident coronary heart disease and cardiovascular disease with increasing light physical activity, such that each 1-hour increment of activity was associated with a 20% decrease in coronary heart disease risk and 10% decrease in cardiovascular disease risk.
Andrea Z. LaCroix, PhD, from the University of California, San Diego, and her coauthors noted that physical activity guidelines for aerobic activity suggest 75 minutes of vigorous physical activity or 150 minutes of moderate activity each day, but only around 25% of U.S. women aged over 75 years are estimated to meet this requirement.
“These guidelines may have discouraged PA [physical activity] when perceived to be unattainable by large segments of the population,” they wrote.
While the majority of active time in older adults is spent doing light physical activity, little is known about the cardiovascular effects of participating in this level of activity. “A major barrier has been that self-reported questionnaires measuring leisure-time PA do not adequately capture light PA that is acquired throughout the day in activities of daily living,” they wrote.
The study also looked at the impact of moderate to vigorous physical activity, finding a significant 46% reduction between the highest to lowest quartiles of activity in coronary heart disease risk and a 31% reduction in cardiovascular disease risk.
Even after adjusting for the use of lipid-lowering medication, antihypertensive medication or healthy eating scores, the results remained unchanged. The researchers also saw no change when women with angina and heart failure at baseline were excluded or when they excluded cardiovascular events that occurred during the first 6 months of follow-up.
The study was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; and the Department of Health & Human Services. Six authors reported receiving funding from the study supporters and other research institutions, and one reported membership on the advisory committee for physical activity guidelines. No other conflicts of interest were reported.
SOURCE: LaCroix AZ et al. JAMA Netw Open. 2019 Mar 15. doi: 10.1001/jamanetworkopen.2019.0419.
FROM JAMA NETWORK OPEN
Bempedoic acid safely dropped LDL, now seeks FDA approval
Based on its performance, bempedoic acid seems on track for agency approval.
Aside from demonstrating safety, the efficacy goal of the CLEAR Harmony (Evaluation of Long-Term Safety and Tolerability of ETC-1002 in High-Risk Patients With Hyperlipidemia and High CV Risk) trial was to cut LDL cholesterol as an add-on to maximally tolerated statin treatment, as well as discretionary use of other lipid-lowering agents in patients with atherosclerotic cardiovascular disease.
That goal appeared to be met by the CLEAR Harmony results, as well as the results from four other studies that contributed data to the approval application filed for bempedoic acid. A clinical outcomes study is underway with more than 12,000 patients aimed at showing incremental clinical benefit from bempedoic acid on top of approved treatments for lowering LDL cholesterol, but those results are not expected until 2022. Until then, the application’s data focus on the evidence that the new drug safely lowers LDL cholesterol when used on top of existing treatments.
“Bempedoic acid provides an additional therapeutic option to safely lower LDL cholesterol in patients with high risk for atherosclerotic cardiovascular disease already treated with a statin,” Kausik K. Ray, MD, said when he first reported these findings during the annual meeting of the European Society of Cardiology last August in Munich. The same results appeared in a newly released article (N Engl J Med. 2019 Mar 14;380[11]:1022-32).

Maximum recommended statin dosages exist because, for every doubling of the statin dosage, LDL cholesterol levels drop by about another 6%, but adverse events grow more common. Because bempedoic acid and other ATP citrate lyase inhibitors work via the same metabolic pathway as that of statins – HMG CoA reductase inhibitors – “we did not know whether squeezing another 20% of LDL cholesterol lowering would be tolerated. What we have clearly and reassuringly shown is it is well tolerated,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
The CLEAR Harmony results showed in 2,230 randomized patients that treatment with bempedoic acid cut LDL cholesterol levels by an average of 18% more compared with placebo in the intention-to-treat analysis, and by 20% in an on-treatment analysis.
By seeking U.S. marketing approval for bempedoic acid based on LDL-lowering and safety only, but without data on clinical endpoints, the company developing the drug is following a path already established by several other lipid-lowering drug classes.

“Statins, ezetimibe and the PCSK9 inhibitors were all approved based on clinical trial results that showed LDL-cholesterol reductions with what the FDA judged to be acceptable safety, but without results from completed outcomes trials,” Christie M. Ballantyne, MD, a coauthor of the CLEAR Harmony study and professor and chief of cardiology at Baylor College of Medicine in Houston, said in an interview.
Stephen Nicholls, MD, professor of cardiology at Monash University in Melbourne, added in an interview that “the precedent has been to conditionally approve LDL cholesterol–lowering drugs at this stage of development, based on the large body of evidence demonstrating that LDL cholesterol–lowering consistently produces clinical benefit.”

To gain more confidence that treatment with bempedoic acid exerts a benefit to patients prior to availability of clinical-outcome results, the developing company sponsored a genetic and epidemiologic study that looked at the association between naturally occurring mutations that dampen the activity of ATP citrate lyase, an enzyme that metabolically sits just upstream from HMG CoA reductase, the enzyme that statins target. Dr. Nicholls, Dr. Ray, and several other collaborators devised “genetic scores” that took into account variants of the gene that codes for ATP citrate lyase, and a separate score for HMG CoA reductase variants. Each score estimated a person’s activity for each of these enzymes. The researchers then used the scores to classify enzymatic activity in more than 650,000 people in several different databases, including more than 100,000 people with a history of major cardiovascular events.
The results showed that “genetic variants that mimic the effect of ATP citrate lyase inhibitors and statins appeared to lower plasma LDL cholesterol levels by the same mechanism of action. They were associated with nearly identical effects on the risk of cardiovascular disease and cancer per unit decrease in the LDL cholesterol level,” the investigators said in an article published concurrently with the CLEAR Harmony results (N Engl J Med. 2019 March 14;380[11]:1033-42).

This finding “strengthens the likelihood that an outcome trial will show benefits,” Steven E. Nissen, MD, chairman of cardiovascular medicine at the Cleveland Clinic Foundation, and a lead investigator in the bempedoic acid outcomes trial, CLEAR Outcomes, said in an interview.
Dr. Nicholls noted that, on the basis of the genetic study’s results “it would seem very reasonable to extrapolate and expect that bempedoic acid should reduce cardiovascular events.”
The data reported by Dr. Ray and his associates from the CLEAR Harmony trial showed that overall, the adverse-event rates associated with bempedoic acid treatment were similar to the rates seen in patients who received placebo. But Michael V. Holmes, MD, who wrote an editorial that accompanied both reports, highlighted a few differences in the adverse event rates that concerned him. These were a statistically significant higher rate of gout and blood uric acid levels on bempedoic acid treatment compared with controls, a significantly higher rate of discontinuations because of adverse events, and nominally higher rates of death, cardiovascular death, and heart failure hospitalization, said Dr. Holmes, an epidemiologist at the University of Oxford, England.
But Dr. Nissen said that “the safety ‘signals’ involve very small numbers of patients and do not raise major concerns. The increases in gout and uric acid are worth noting, but are less weighty than the disease the drug is intended to treat: major cardiovascular events.”
Dr. Nichols added that “the large cardiovascular outcome trial will provide the opportunity to further study safety and potential side effects. I’m hesitant to overinterpret event data from a relatively small clinical trial that primarily focused on the lipid effects.”
Despite recent success of the PCSK9 inhibitors as an add-on or substitute for statin treatment of elevated LDL cholesterol, the cost of the drugs in this class has made the cardiovascular disease community eager for another alternative to statins.
“The PCSK9 inhibitors are extremely effective, but uptake has been slow due to their cost and formulary restrictions,” said Dr. Ballantyne. “Many high-risk patients continue to have persistently elevated levels of LDL cholesterol.” Bempedoic acid is “a new therapy that can help people who continue to have elevations of LDL cholesterol despite current therapies.”
CLEAR Harmony and the genetic study were sponsored by Esperion, the company developing bempedoic acid. Dr. Ray has been a consultant to several drug companies but had no other financial relationship to Esperion. Dr. Ballantyne and Dr. Nicholls have been consultants to and have received research funding from Esperion and from several other companies. Dr. Nissen is leading an Esperion-sponsored study but has no financial relationships with the company or with other companies.
SOURCEs: N Engl J Med. 2019 Mar 14;380[11]:1022-32 and 1033-42.
The primary endpoint of bempedoic acid’s safety, assessed by means of the incidence of adverse events and changes in safety laboratory variables during the CLEAR Harmony trial, did not differ meaningfully between the bempedoic acid group and the placebo group. However, patients in the bempedoic acid group had an excess risk of adverse events leading to discontinuation of the blinded trial regimen, an excess risk of gout, and higher blood concentrations of uric acid than those in the placebo group.
In further analyses of nonprimary and secondary endpoints, there were additional potentially troubling signals, although the 95% confidence intervals were wide: 0.9% of the patients treated with bempedoic acid died, compared with 0.3% of those in the placebo group; 0.4% and 0.1%, respectively, died from adjudicated cardiovascular disease; and 0.6% and 0.1%, respectively, were hospitalized for heart failure. Although the findings are potentially alarming, the imprecision that is reflected in the 95% confidence intervals renders the relative risk values virtually meaningless, but can these effect estimates be unseen?
The cumulative data from randomized treatment trials and from studies of human genetics say that, for a given reduction in the LDL cholesterol level, drugs that inhibit ATP citrate lyase and do not have off-target effects ought to yield reductions in the risk of cardiovascular disease that are similar to those achieved with statins. However, analysis of endpoints in treatment trials for which there is marginal statistical power is best avoided. Fortunately for bempedoic acid, an ongoing phase 3, cardiovascular outcome trial will provide additional information.
More broadly, the genetic characterization of drug targets is set to revolutionize how we develop medicines.
Michael V. Holmes, MD, is an epidemiologist at the University of Oxford, England. He made these comments in a published editorial (N Engl J Med. 2019 Mar 14;380[11]:1076-9). He had no disclosures.
The primary endpoint of bempedoic acid’s safety, assessed by means of the incidence of adverse events and changes in safety laboratory variables during the CLEAR Harmony trial, did not differ meaningfully between the bempedoic acid group and the placebo group. However, patients in the bempedoic acid group had an excess risk of adverse events leading to discontinuation of the blinded trial regimen, an excess risk of gout, and higher blood concentrations of uric acid than those in the placebo group.
In further analyses of nonprimary and secondary endpoints, there were additional potentially troubling signals, although the 95% confidence intervals were wide: 0.9% of the patients treated with bempedoic acid died, compared with 0.3% of those in the placebo group; 0.4% and 0.1%, respectively, died from adjudicated cardiovascular disease; and 0.6% and 0.1%, respectively, were hospitalized for heart failure. Although the findings are potentially alarming, the imprecision that is reflected in the 95% confidence intervals renders the relative risk values virtually meaningless, but can these effect estimates be unseen?
The cumulative data from randomized treatment trials and from studies of human genetics say that, for a given reduction in the LDL cholesterol level, drugs that inhibit ATP citrate lyase and do not have off-target effects ought to yield reductions in the risk of cardiovascular disease that are similar to those achieved with statins. However, analysis of endpoints in treatment trials for which there is marginal statistical power is best avoided. Fortunately for bempedoic acid, an ongoing phase 3, cardiovascular outcome trial will provide additional information.
More broadly, the genetic characterization of drug targets is set to revolutionize how we develop medicines.
Michael V. Holmes, MD, is an epidemiologist at the University of Oxford, England. He made these comments in a published editorial (N Engl J Med. 2019 Mar 14;380[11]:1076-9). He had no disclosures.
The primary endpoint of bempedoic acid’s safety, assessed by means of the incidence of adverse events and changes in safety laboratory variables during the CLEAR Harmony trial, did not differ meaningfully between the bempedoic acid group and the placebo group. However, patients in the bempedoic acid group had an excess risk of adverse events leading to discontinuation of the blinded trial regimen, an excess risk of gout, and higher blood concentrations of uric acid than those in the placebo group.
In further analyses of nonprimary and secondary endpoints, there were additional potentially troubling signals, although the 95% confidence intervals were wide: 0.9% of the patients treated with bempedoic acid died, compared with 0.3% of those in the placebo group; 0.4% and 0.1%, respectively, died from adjudicated cardiovascular disease; and 0.6% and 0.1%, respectively, were hospitalized for heart failure. Although the findings are potentially alarming, the imprecision that is reflected in the 95% confidence intervals renders the relative risk values virtually meaningless, but can these effect estimates be unseen?
The cumulative data from randomized treatment trials and from studies of human genetics say that, for a given reduction in the LDL cholesterol level, drugs that inhibit ATP citrate lyase and do not have off-target effects ought to yield reductions in the risk of cardiovascular disease that are similar to those achieved with statins. However, analysis of endpoints in treatment trials for which there is marginal statistical power is best avoided. Fortunately for bempedoic acid, an ongoing phase 3, cardiovascular outcome trial will provide additional information.
More broadly, the genetic characterization of drug targets is set to revolutionize how we develop medicines.
Michael V. Holmes, MD, is an epidemiologist at the University of Oxford, England. He made these comments in a published editorial (N Engl J Med. 2019 Mar 14;380[11]:1076-9). He had no disclosures.
Based on its performance, bempedoic acid seems on track for agency approval.
Aside from demonstrating safety, the efficacy goal of the CLEAR Harmony (Evaluation of Long-Term Safety and Tolerability of ETC-1002 in High-Risk Patients With Hyperlipidemia and High CV Risk) trial was to cut LDL cholesterol as an add-on to maximally tolerated statin treatment, as well as discretionary use of other lipid-lowering agents in patients with atherosclerotic cardiovascular disease.
That goal appeared to be met by the CLEAR Harmony results, as well as the results from four other studies that contributed data to the approval application filed for bempedoic acid. A clinical outcomes study is underway with more than 12,000 patients aimed at showing incremental clinical benefit from bempedoic acid on top of approved treatments for lowering LDL cholesterol, but those results are not expected until 2022. Until then, the application’s data focus on the evidence that the new drug safely lowers LDL cholesterol when used on top of existing treatments.
“Bempedoic acid provides an additional therapeutic option to safely lower LDL cholesterol in patients with high risk for atherosclerotic cardiovascular disease already treated with a statin,” Kausik K. Ray, MD, said when he first reported these findings during the annual meeting of the European Society of Cardiology last August in Munich. The same results appeared in a newly released article (N Engl J Med. 2019 Mar 14;380[11]:1022-32).
Maximum recommended statin dosages exist because, for every doubling of the statin dosage, LDL cholesterol levels drop by about another 6%, but adverse events grow more common. Because bempedoic acid and other ATP citrate lyase inhibitors work via the same metabolic pathway as that of statins – HMG CoA reductase inhibitors – “we did not know whether squeezing another 20% of LDL cholesterol lowering would be tolerated. What we have clearly and reassuringly shown is it is well tolerated,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
The CLEAR Harmony results showed in 2,230 randomized patients that treatment with bempedoic acid cut LDL cholesterol levels by an average of 18% more compared with placebo in the intention-to-treat analysis, and by 20% in an on-treatment analysis.
By seeking U.S. marketing approval for bempedoic acid based on LDL-lowering and safety only, but without data on clinical endpoints, the company developing the drug is following a path already established by several other lipid-lowering drug classes.
“Statins, ezetimibe and the PCSK9 inhibitors were all approved based on clinical trial results that showed LDL-cholesterol reductions with what the FDA judged to be acceptable safety, but without results from completed outcomes trials,” Christie M. Ballantyne, MD, a coauthor of the CLEAR Harmony study and professor and chief of cardiology at Baylor College of Medicine in Houston, said in an interview.
Stephen Nicholls, MD, professor of cardiology at Monash University in Melbourne, added in an interview that “the precedent has been to conditionally approve LDL cholesterol–lowering drugs at this stage of development, based on the large body of evidence demonstrating that LDL cholesterol–lowering consistently produces clinical benefit.”
To gain more confidence that treatment with bempedoic acid exerts a benefit to patients prior to availability of clinical-outcome results, the developing company sponsored a genetic and epidemiologic study that looked at the association between naturally occurring mutations that dampen the activity of ATP citrate lyase, an enzyme that metabolically sits just upstream from HMG CoA reductase, the enzyme that statins target. Dr. Nicholls, Dr. Ray, and several other collaborators devised “genetic scores” that took into account variants of the gene that codes for ATP citrate lyase, and a separate score for HMG CoA reductase variants. Each score estimated a person’s activity for each of these enzymes. The researchers then used the scores to classify enzymatic activity in more than 650,000 people in several different databases, including more than 100,000 people with a history of major cardiovascular events.
The results showed that “genetic variants that mimic the effect of ATP citrate lyase inhibitors and statins appeared to lower plasma LDL cholesterol levels by the same mechanism of action. They were associated with nearly identical effects on the risk of cardiovascular disease and cancer per unit decrease in the LDL cholesterol level,” the investigators said in an article published concurrently with the CLEAR Harmony results (N Engl J Med. 2019 March 14;380[11]:1033-42).
This finding “strengthens the likelihood that an outcome trial will show benefits,” Steven E. Nissen, MD, chairman of cardiovascular medicine at the Cleveland Clinic Foundation, and a lead investigator in the bempedoic acid outcomes trial, CLEAR Outcomes, said in an interview.
Dr. Nicholls noted that, on the basis of the genetic study’s results “it would seem very reasonable to extrapolate and expect that bempedoic acid should reduce cardiovascular events.”
The data reported by Dr. Ray and his associates from the CLEAR Harmony trial showed that overall, the adverse-event rates associated with bempedoic acid treatment were similar to the rates seen in patients who received placebo. But Michael V. Holmes, MD, who wrote an editorial that accompanied both reports, highlighted a few differences in the adverse event rates that concerned him. These were a statistically significant higher rate of gout and blood uric acid levels on bempedoic acid treatment compared with controls, a significantly higher rate of discontinuations because of adverse events, and nominally higher rates of death, cardiovascular death, and heart failure hospitalization, said Dr. Holmes, an epidemiologist at the University of Oxford, England.
But Dr. Nissen said that “the safety ‘signals’ involve very small numbers of patients and do not raise major concerns. The increases in gout and uric acid are worth noting, but are less weighty than the disease the drug is intended to treat: major cardiovascular events.”
Dr. Nichols added that “the large cardiovascular outcome trial will provide the opportunity to further study safety and potential side effects. I’m hesitant to overinterpret event data from a relatively small clinical trial that primarily focused on the lipid effects.”
Despite recent success of the PCSK9 inhibitors as an add-on or substitute for statin treatment of elevated LDL cholesterol, the cost of the drugs in this class has made the cardiovascular disease community eager for another alternative to statins.
“The PCSK9 inhibitors are extremely effective, but uptake has been slow due to their cost and formulary restrictions,” said Dr. Ballantyne. “Many high-risk patients continue to have persistently elevated levels of LDL cholesterol.” Bempedoic acid is “a new therapy that can help people who continue to have elevations of LDL cholesterol despite current therapies.”
CLEAR Harmony and the genetic study were sponsored by Esperion, the company developing bempedoic acid. Dr. Ray has been a consultant to several drug companies but had no other financial relationship to Esperion. Dr. Ballantyne and Dr. Nicholls have been consultants to and have received research funding from Esperion and from several other companies. Dr. Nissen is leading an Esperion-sponsored study but has no financial relationships with the company or with other companies.
SOURCEs: N Engl J Med. 2019 Mar 14;380[11]:1022-32 and 1033-42.
Based on its performance, bempedoic acid seems on track for agency approval.
Aside from demonstrating safety, the efficacy goal of the CLEAR Harmony (Evaluation of Long-Term Safety and Tolerability of ETC-1002 in High-Risk Patients With Hyperlipidemia and High CV Risk) trial was to cut LDL cholesterol as an add-on to maximally tolerated statin treatment, as well as discretionary use of other lipid-lowering agents in patients with atherosclerotic cardiovascular disease.
That goal appeared to be met by the CLEAR Harmony results, as well as the results from four other studies that contributed data to the approval application filed for bempedoic acid. A clinical outcomes study is underway with more than 12,000 patients aimed at showing incremental clinical benefit from bempedoic acid on top of approved treatments for lowering LDL cholesterol, but those results are not expected until 2022. Until then, the application’s data focus on the evidence that the new drug safely lowers LDL cholesterol when used on top of existing treatments.
“Bempedoic acid provides an additional therapeutic option to safely lower LDL cholesterol in patients with high risk for atherosclerotic cardiovascular disease already treated with a statin,” Kausik K. Ray, MD, said when he first reported these findings during the annual meeting of the European Society of Cardiology last August in Munich. The same results appeared in a newly released article (N Engl J Med. 2019 Mar 14;380[11]:1022-32).
Maximum recommended statin dosages exist because, for every doubling of the statin dosage, LDL cholesterol levels drop by about another 6%, but adverse events grow more common. Because bempedoic acid and other ATP citrate lyase inhibitors work via the same metabolic pathway as that of statins – HMG CoA reductase inhibitors – “we did not know whether squeezing another 20% of LDL cholesterol lowering would be tolerated. What we have clearly and reassuringly shown is it is well tolerated,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
The CLEAR Harmony results showed in 2,230 randomized patients that treatment with bempedoic acid cut LDL cholesterol levels by an average of 18% more compared with placebo in the intention-to-treat analysis, and by 20% in an on-treatment analysis.
By seeking U.S. marketing approval for bempedoic acid based on LDL-lowering and safety only, but without data on clinical endpoints, the company developing the drug is following a path already established by several other lipid-lowering drug classes.
“Statins, ezetimibe and the PCSK9 inhibitors were all approved based on clinical trial results that showed LDL-cholesterol reductions with what the FDA judged to be acceptable safety, but without results from completed outcomes trials,” Christie M. Ballantyne, MD, a coauthor of the CLEAR Harmony study and professor and chief of cardiology at Baylor College of Medicine in Houston, said in an interview.
Stephen Nicholls, MD, professor of cardiology at Monash University in Melbourne, added in an interview that “the precedent has been to conditionally approve LDL cholesterol–lowering drugs at this stage of development, based on the large body of evidence demonstrating that LDL cholesterol–lowering consistently produces clinical benefit.”
To gain more confidence that treatment with bempedoic acid exerts a benefit to patients prior to availability of clinical-outcome results, the developing company sponsored a genetic and epidemiologic study that looked at the association between naturally occurring mutations that dampen the activity of ATP citrate lyase, an enzyme that metabolically sits just upstream from HMG CoA reductase, the enzyme that statins target. Dr. Nicholls, Dr. Ray, and several other collaborators devised “genetic scores” that took into account variants of the gene that codes for ATP citrate lyase, and a separate score for HMG CoA reductase variants. Each score estimated a person’s activity for each of these enzymes. The researchers then used the scores to classify enzymatic activity in more than 650,000 people in several different databases, including more than 100,000 people with a history of major cardiovascular events.
The results showed that “genetic variants that mimic the effect of ATP citrate lyase inhibitors and statins appeared to lower plasma LDL cholesterol levels by the same mechanism of action. They were associated with nearly identical effects on the risk of cardiovascular disease and cancer per unit decrease in the LDL cholesterol level,” the investigators said in an article published concurrently with the CLEAR Harmony results (N Engl J Med. 2019 March 14;380[11]:1033-42).
This finding “strengthens the likelihood that an outcome trial will show benefits,” Steven E. Nissen, MD, chairman of cardiovascular medicine at the Cleveland Clinic Foundation, and a lead investigator in the bempedoic acid outcomes trial, CLEAR Outcomes, said in an interview.
Dr. Nicholls noted that, on the basis of the genetic study’s results “it would seem very reasonable to extrapolate and expect that bempedoic acid should reduce cardiovascular events.”
The data reported by Dr. Ray and his associates from the CLEAR Harmony trial showed that overall, the adverse-event rates associated with bempedoic acid treatment were similar to the rates seen in patients who received placebo. But Michael V. Holmes, MD, who wrote an editorial that accompanied both reports, highlighted a few differences in the adverse event rates that concerned him. These were a statistically significant higher rate of gout and blood uric acid levels on bempedoic acid treatment compared with controls, a significantly higher rate of discontinuations because of adverse events, and nominally higher rates of death, cardiovascular death, and heart failure hospitalization, said Dr. Holmes, an epidemiologist at the University of Oxford, England.
But Dr. Nissen said that “the safety ‘signals’ involve very small numbers of patients and do not raise major concerns. The increases in gout and uric acid are worth noting, but are less weighty than the disease the drug is intended to treat: major cardiovascular events.”
Dr. Nichols added that “the large cardiovascular outcome trial will provide the opportunity to further study safety and potential side effects. I’m hesitant to overinterpret event data from a relatively small clinical trial that primarily focused on the lipid effects.”
Despite recent success of the PCSK9 inhibitors as an add-on or substitute for statin treatment of elevated LDL cholesterol, the cost of the drugs in this class has made the cardiovascular disease community eager for another alternative to statins.
“The PCSK9 inhibitors are extremely effective, but uptake has been slow due to their cost and formulary restrictions,” said Dr. Ballantyne. “Many high-risk patients continue to have persistently elevated levels of LDL cholesterol.” Bempedoic acid is “a new therapy that can help people who continue to have elevations of LDL cholesterol despite current therapies.”
CLEAR Harmony and the genetic study were sponsored by Esperion, the company developing bempedoic acid. Dr. Ray has been a consultant to several drug companies but had no other financial relationship to Esperion. Dr. Ballantyne and Dr. Nicholls have been consultants to and have received research funding from Esperion and from several other companies. Dr. Nissen is leading an Esperion-sponsored study but has no financial relationships with the company or with other companies.
SOURCEs: N Engl J Med. 2019 Mar 14;380[11]:1022-32 and 1033-42.
Key clinical point: Bempedoic acid safely lowed LDL cholesterol levels in a pivotal trial.
Major finding: In the intention-to-treat analysis, bempedoic acid cut LDL cholesterol by 18%; by 20% in an on-treatment analysis.
Study details: CLEAR Harmony, a multicenter, randomized trial with 2,230 patients.
Disclosures: CLEAR Harmony and the genetic study were sponsored by Esperion, the company developing bempedoic acid. Dr. Ray has been a consultant to several drug companies but had no other financial relationship to Esperion. Dr. Ballantyne and Dr. Nicholls have been consultants to and have received research funding from Esperion and from several other companies. Dr. Nissen is leading an Esperion-sponsored study but has no financial relationships with the company or with other companies.
Sources: N Engl J Med. 2019 Mar 14;380[11]:1022-32 and 1033-42.