User login
Comment on "Fractional CO2 Laser Skin Resurfacing for the Treatment of Sun-Damaged Skin and Actinic Keratoses" [letter]
Neurotoxin Treatment: It Ain't What It Used to Be [editorial]
The Vitamin D Debate
Recent media reports suggest that sun exposure is the best source of vitamin D. One study even reports that one minimal erythema dose of sunlight is equivalent to ingesting approximately 20,000 IU of vitamin D2.
The skin produces approximately 10,000 IU of vitamin D in response to 20-30 minutes of sun exposure in the summer – that’s more than 50 times the U.S. government’s daily recommendation, according to the Vitamin D Council, a nonprofit group whose mission is to promote the health benefits of vitamin D (N. Engl. J. Med. 2007;357:266-81).
The American Academy of Dermatology, however, does not recommend getting vitamin D from sun exposure, indoor tanning, or any source that emits ultraviolet radiation. We know that the maximum production of vitamin D occurs after brief exposure to UV radiation; however, the exact amount of time depends on location, time of day, time of year, and skin type.
For a fair-skinned person in the Northeast, that time is 2-5 minutes at noon during the month of June. However, each variable can alter the amount of vitamin D produced. Any additional vitamin D produced by the body is not stored for future use.
Alternatively, the AAD promotes getting vitamin D from the diet, rather than from sun exposure. The Academy also suggests that dietary sources of vitamin D neither prematurely age the skin nor increase risk of developing skin cancer or actinic keratoses. Sources rich in vitamin D include fortified milk, fortified cereal, salmon, mackerel, and cod liver oil. In addition, vitamin D supplements are well tolerated, safe, and effective. In addition, vitamin D is absorbed with calcium, which must be obtained from dietary sources — not the sun. Thus, a healthy diet rich in both calcium and vitamin D is the best way to ensure appropriate levels of both agents without any of the dangers of UV exposure.
The darker the skin and the farther from the equator an individual is, the greater one’s chances of developing a vitamin D deficiency if the diet is inadequate. African Americans, in particular, have lower vitamin D levels overall, compared with age-matched whites. Dr. Michael Holick from Boston University, who is the nation’s leading vitamin D researcher, said he believes that this exaggerated vitamin D deficiency is the reason there is a gap in the health of white vs. black Americans (J. Invest. Dermatol. 2010;130:546-53).
He believes that lower vitamin D levels are why African Americans develop more prostate, breast, and colon cancers. He believes this might also be the reason why the ethnic group may get more aggressive forms of those cancers (N. Engl. J. Med. 2007;357:266-81).
However, there is no good proof in any well-controlled studies to suggest this. None of the studies reflect reduced access to health care, barriers to healthful living, and differences in income and education. In contrast, some recent studies also indicate that the regulation of vitamin D production is independent of skin color (J. Invest. Dermatol. 2010;130:546-53).
Most vitamin D supplements that are available without a prescription contain cholecalciferol (vitamin D3), which is more potent than ergocalciferol vitamin D2 (J. Clin. Endocrinol. Metab. 2004;89:5387-91; Am. J. Clin. Nutr. 2006;84:694-7; and Am. J. Clin. Nutr. 68:854-8).
Multivitamin supplements generally provide 400 IU (10 mcg) of vitamin D. Single ingredient vitamin D supplements may provide between 400 IUs and 2,000 IUs of vitamin D. Calcium supplements can also provide vitamin D.
The National Academy of Sciences Institute of Medicine (IOM) guidelines for vitamin D are a standard reference for advising patients on proper minimal intake levels.
The Department of Agriculture’s Dietary Guidelines recommend those at risk for vitamin D insufficiency to receive supplementation with a total daily dose of 1,000 IUs vitamin D.
In addition, the AAD recommends supplementation with 200 IUs vitamin D from birth to age 50 years for those who are not at increased risk for vitamin D insufficiency. However, the American Academy of Pediatrics recommends supplementation with 400 IU vitamin D/day for children younger than 18 years of age, including infants.
Because vitamin D can be toxic in high doses, the USDA’s Food and Nutrition Board has set an upper limit for safety for vitamin D intake of 2,000 IUs/day for individuals older than 12 months of age and 1,000 IUs/ day for infants.
There is no real answer to the vitamin D debate at this time. Whether the differences in vitamin D levels are because of skin color or diet are still controversial.
We know that ultraviolet radiation can have harmful effects on the skin and that adequate intake can be achieved by diet or oral supplements. So why is there a debate on how much sun one needs to achieve a so-called “normal” vitamin D level? The answer is none. Everyone, regardless of skin color, should take a daily vitamin D supplement (J. Nutr. 2006;136:1126-9; Am. J. Clin. Nutr. 2004;80:1763S-6S).
Recent media reports suggest that sun exposure is the best source of vitamin D. One study even reports that one minimal erythema dose of sunlight is equivalent to ingesting approximately 20,000 IU of vitamin D2.
The skin produces approximately 10,000 IU of vitamin D in response to 20-30 minutes of sun exposure in the summer – that’s more than 50 times the U.S. government’s daily recommendation, according to the Vitamin D Council, a nonprofit group whose mission is to promote the health benefits of vitamin D (N. Engl. J. Med. 2007;357:266-81).
The American Academy of Dermatology, however, does not recommend getting vitamin D from sun exposure, indoor tanning, or any source that emits ultraviolet radiation. We know that the maximum production of vitamin D occurs after brief exposure to UV radiation; however, the exact amount of time depends on location, time of day, time of year, and skin type.
For a fair-skinned person in the Northeast, that time is 2-5 minutes at noon during the month of June. However, each variable can alter the amount of vitamin D produced. Any additional vitamin D produced by the body is not stored for future use.
Alternatively, the AAD promotes getting vitamin D from the diet, rather than from sun exposure. The Academy also suggests that dietary sources of vitamin D neither prematurely age the skin nor increase risk of developing skin cancer or actinic keratoses. Sources rich in vitamin D include fortified milk, fortified cereal, salmon, mackerel, and cod liver oil. In addition, vitamin D supplements are well tolerated, safe, and effective. In addition, vitamin D is absorbed with calcium, which must be obtained from dietary sources — not the sun. Thus, a healthy diet rich in both calcium and vitamin D is the best way to ensure appropriate levels of both agents without any of the dangers of UV exposure.
The darker the skin and the farther from the equator an individual is, the greater one’s chances of developing a vitamin D deficiency if the diet is inadequate. African Americans, in particular, have lower vitamin D levels overall, compared with age-matched whites. Dr. Michael Holick from Boston University, who is the nation’s leading vitamin D researcher, said he believes that this exaggerated vitamin D deficiency is the reason there is a gap in the health of white vs. black Americans (J. Invest. Dermatol. 2010;130:546-53).
He believes that lower vitamin D levels are why African Americans develop more prostate, breast, and colon cancers. He believes this might also be the reason why the ethnic group may get more aggressive forms of those cancers (N. Engl. J. Med. 2007;357:266-81).
However, there is no good proof in any well-controlled studies to suggest this. None of the studies reflect reduced access to health care, barriers to healthful living, and differences in income and education. In contrast, some recent studies also indicate that the regulation of vitamin D production is independent of skin color (J. Invest. Dermatol. 2010;130:546-53).
Most vitamin D supplements that are available without a prescription contain cholecalciferol (vitamin D3), which is more potent than ergocalciferol vitamin D2 (J. Clin. Endocrinol. Metab. 2004;89:5387-91; Am. J. Clin. Nutr. 2006;84:694-7; and Am. J. Clin. Nutr. 68:854-8).
Multivitamin supplements generally provide 400 IU (10 mcg) of vitamin D. Single ingredient vitamin D supplements may provide between 400 IUs and 2,000 IUs of vitamin D. Calcium supplements can also provide vitamin D.
The National Academy of Sciences Institute of Medicine (IOM) guidelines for vitamin D are a standard reference for advising patients on proper minimal intake levels.
The Department of Agriculture’s Dietary Guidelines recommend those at risk for vitamin D insufficiency to receive supplementation with a total daily dose of 1,000 IUs vitamin D.
In addition, the AAD recommends supplementation with 200 IUs vitamin D from birth to age 50 years for those who are not at increased risk for vitamin D insufficiency. However, the American Academy of Pediatrics recommends supplementation with 400 IU vitamin D/day for children younger than 18 years of age, including infants.
Because vitamin D can be toxic in high doses, the USDA’s Food and Nutrition Board has set an upper limit for safety for vitamin D intake of 2,000 IUs/day for individuals older than 12 months of age and 1,000 IUs/ day for infants.
There is no real answer to the vitamin D debate at this time. Whether the differences in vitamin D levels are because of skin color or diet are still controversial.
We know that ultraviolet radiation can have harmful effects on the skin and that adequate intake can be achieved by diet or oral supplements. So why is there a debate on how much sun one needs to achieve a so-called “normal” vitamin D level? The answer is none. Everyone, regardless of skin color, should take a daily vitamin D supplement (J. Nutr. 2006;136:1126-9; Am. J. Clin. Nutr. 2004;80:1763S-6S).
Recent media reports suggest that sun exposure is the best source of vitamin D. One study even reports that one minimal erythema dose of sunlight is equivalent to ingesting approximately 20,000 IU of vitamin D2.
The skin produces approximately 10,000 IU of vitamin D in response to 20-30 minutes of sun exposure in the summer – that’s more than 50 times the U.S. government’s daily recommendation, according to the Vitamin D Council, a nonprofit group whose mission is to promote the health benefits of vitamin D (N. Engl. J. Med. 2007;357:266-81).
The American Academy of Dermatology, however, does not recommend getting vitamin D from sun exposure, indoor tanning, or any source that emits ultraviolet radiation. We know that the maximum production of vitamin D occurs after brief exposure to UV radiation; however, the exact amount of time depends on location, time of day, time of year, and skin type.
For a fair-skinned person in the Northeast, that time is 2-5 minutes at noon during the month of June. However, each variable can alter the amount of vitamin D produced. Any additional vitamin D produced by the body is not stored for future use.
Alternatively, the AAD promotes getting vitamin D from the diet, rather than from sun exposure. The Academy also suggests that dietary sources of vitamin D neither prematurely age the skin nor increase risk of developing skin cancer or actinic keratoses. Sources rich in vitamin D include fortified milk, fortified cereal, salmon, mackerel, and cod liver oil. In addition, vitamin D supplements are well tolerated, safe, and effective. In addition, vitamin D is absorbed with calcium, which must be obtained from dietary sources — not the sun. Thus, a healthy diet rich in both calcium and vitamin D is the best way to ensure appropriate levels of both agents without any of the dangers of UV exposure.
The darker the skin and the farther from the equator an individual is, the greater one’s chances of developing a vitamin D deficiency if the diet is inadequate. African Americans, in particular, have lower vitamin D levels overall, compared with age-matched whites. Dr. Michael Holick from Boston University, who is the nation’s leading vitamin D researcher, said he believes that this exaggerated vitamin D deficiency is the reason there is a gap in the health of white vs. black Americans (J. Invest. Dermatol. 2010;130:546-53).
He believes that lower vitamin D levels are why African Americans develop more prostate, breast, and colon cancers. He believes this might also be the reason why the ethnic group may get more aggressive forms of those cancers (N. Engl. J. Med. 2007;357:266-81).
However, there is no good proof in any well-controlled studies to suggest this. None of the studies reflect reduced access to health care, barriers to healthful living, and differences in income and education. In contrast, some recent studies also indicate that the regulation of vitamin D production is independent of skin color (J. Invest. Dermatol. 2010;130:546-53).
Most vitamin D supplements that are available without a prescription contain cholecalciferol (vitamin D3), which is more potent than ergocalciferol vitamin D2 (J. Clin. Endocrinol. Metab. 2004;89:5387-91; Am. J. Clin. Nutr. 2006;84:694-7; and Am. J. Clin. Nutr. 68:854-8).
Multivitamin supplements generally provide 400 IU (10 mcg) of vitamin D. Single ingredient vitamin D supplements may provide between 400 IUs and 2,000 IUs of vitamin D. Calcium supplements can also provide vitamin D.
The National Academy of Sciences Institute of Medicine (IOM) guidelines for vitamin D are a standard reference for advising patients on proper minimal intake levels.
The Department of Agriculture’s Dietary Guidelines recommend those at risk for vitamin D insufficiency to receive supplementation with a total daily dose of 1,000 IUs vitamin D.
In addition, the AAD recommends supplementation with 200 IUs vitamin D from birth to age 50 years for those who are not at increased risk for vitamin D insufficiency. However, the American Academy of Pediatrics recommends supplementation with 400 IU vitamin D/day for children younger than 18 years of age, including infants.
Because vitamin D can be toxic in high doses, the USDA’s Food and Nutrition Board has set an upper limit for safety for vitamin D intake of 2,000 IUs/day for individuals older than 12 months of age and 1,000 IUs/ day for infants.
There is no real answer to the vitamin D debate at this time. Whether the differences in vitamin D levels are because of skin color or diet are still controversial.
We know that ultraviolet radiation can have harmful effects on the skin and that adequate intake can be achieved by diet or oral supplements. So why is there a debate on how much sun one needs to achieve a so-called “normal” vitamin D level? The answer is none. Everyone, regardless of skin color, should take a daily vitamin D supplement (J. Nutr. 2006;136:1126-9; Am. J. Clin. Nutr. 2004;80:1763S-6S).
Expert: Apologize, but Don't Admit Guilt When Things Go Wrong
MONTEREY, CALIF. - When things go horribly wrong for patients, physicians must ask themselves some delicate questions in the art of management.
Should I apologize? How do I deal with the patient? Am I legally obligated to tell the patient what I know about what happened? How do I deal with myself?

Medical negligence may be a factor in some cases, but bad results can happen even when there is no breach of duty, Dr. Clifford Warren Lober noted at the American Society for Mohs Surgery meeting. Especially in cosmetic procedures, the problem may be unmet expectations.
The best thing to do is to anticipate the possibility of a bad outcome to be in the best position to deal with it. Be prepared by maintaining appropriate training and experience. Comply with office surgery rules and develop a good rapport with colleagues. Give the patient a realistic description of expected results. Obtain informed consent from patients and dismiss selected patients if necessary to stay out of trouble, he suggested.
Should the physician apologize when there's a bad outcome? "It depends," said Dr. Lober, a dermatologist in Kissimmee, Fla., who is also an attorney.
Make an effort to show concern, compassion, and empathy. Patients are more likely to sue doctors they perceive as callous or unconcerned but "do not readily sue doctors they like," he said. Some states prohibit expressions of regret, sympathy, or benevolence from being entered into evidence, so apologizing won't necessarily help if a subsequent suit goes to trial. Plus, physicians should ask themselves how effective they are at communicating, because some may come across as arrogant instead of sympathetic.
An apology may deflate the patient's anger and make negotiations possible instead of a lawsuit. Patients may expect an apology--many claim they would not have sued if only the doctor had apologized, Dr. Lober said. Apologizing may be the ethically correct thing to do, help put closure on the problem for both patient and physician, and decrease physician feelings of guilt or distance from the patient.
On the other hand, an apology may be misconstrued as legal weakness and encourage a lawsuit. It could be entered into evidence as an admission of guilt in some states, and malpractice insurers may consider it a breach of contract, so physicians should consult their attorney and malpractice insurer before apologizing.
A physician who chooses to apologize should do it soon after the injury and should be the one who apologizes instead of delegating it to a nurse, attorney, or someone else, Dr. Lober stressed. Sincere expressions of sympathy or remorse are okay, but a physician should never admit guilt, he added.
Seven states--California, Florida, Nevada, New Jersey, Oregon, Pennsylvania, and Vermont--require physicians to notify patients of adverse incidents that seriously harm the patient but specify that this cannot be introduced as evidence or construed as an acknowledgment of liability.
When things go horribly wrong for a patient, the physician may experience anger, self-doubt, or depression. Discuss the situation with your attorney, Dr. Lober advised, but be careful about discussing the circumstances with colleagues, a spouse, or others. Consider psychological counseling if the emotional response is strong or persistent, he added.
Dr. Lober stressed that his comments were for educational purposes only, and he advised physicians to seek legal counsel if an adverse situation arose.n
Dr. Lober reported having no pertinent conflicts of interest.
MONTEREY, CALIF. - When things go horribly wrong for patients, physicians must ask themselves some delicate questions in the art of management.
Should I apologize? How do I deal with the patient? Am I legally obligated to tell the patient what I know about what happened? How do I deal with myself?
Medical negligence may be a factor in some cases, but bad results can happen even when there is no breach of duty, Dr. Clifford Warren Lober noted at the American Society for Mohs Surgery meeting. Especially in cosmetic procedures, the problem may be unmet expectations.
The best thing to do is to anticipate the possibility of a bad outcome to be in the best position to deal with it. Be prepared by maintaining appropriate training and experience. Comply with office surgery rules and develop a good rapport with colleagues. Give the patient a realistic description of expected results. Obtain informed consent from patients and dismiss selected patients if necessary to stay out of trouble, he suggested.
Should the physician apologize when there's a bad outcome? "It depends," said Dr. Lober, a dermatologist in Kissimmee, Fla., who is also an attorney.
Make an effort to show concern, compassion, and empathy. Patients are more likely to sue doctors they perceive as callous or unconcerned but "do not readily sue doctors they like," he said. Some states prohibit expressions of regret, sympathy, or benevolence from being entered into evidence, so apologizing won't necessarily help if a subsequent suit goes to trial. Plus, physicians should ask themselves how effective they are at communicating, because some may come across as arrogant instead of sympathetic.
An apology may deflate the patient's anger and make negotiations possible instead of a lawsuit. Patients may expect an apology--many claim they would not have sued if only the doctor had apologized, Dr. Lober said. Apologizing may be the ethically correct thing to do, help put closure on the problem for both patient and physician, and decrease physician feelings of guilt or distance from the patient.
On the other hand, an apology may be misconstrued as legal weakness and encourage a lawsuit. It could be entered into evidence as an admission of guilt in some states, and malpractice insurers may consider it a breach of contract, so physicians should consult their attorney and malpractice insurer before apologizing.
A physician who chooses to apologize should do it soon after the injury and should be the one who apologizes instead of delegating it to a nurse, attorney, or someone else, Dr. Lober stressed. Sincere expressions of sympathy or remorse are okay, but a physician should never admit guilt, he added.
Seven states--California, Florida, Nevada, New Jersey, Oregon, Pennsylvania, and Vermont--require physicians to notify patients of adverse incidents that seriously harm the patient but specify that this cannot be introduced as evidence or construed as an acknowledgment of liability.
When things go horribly wrong for a patient, the physician may experience anger, self-doubt, or depression. Discuss the situation with your attorney, Dr. Lober advised, but be careful about discussing the circumstances with colleagues, a spouse, or others. Consider psychological counseling if the emotional response is strong or persistent, he added.
Dr. Lober stressed that his comments were for educational purposes only, and he advised physicians to seek legal counsel if an adverse situation arose.n
Dr. Lober reported having no pertinent conflicts of interest.
MONTEREY, CALIF. - When things go horribly wrong for patients, physicians must ask themselves some delicate questions in the art of management.
Should I apologize? How do I deal with the patient? Am I legally obligated to tell the patient what I know about what happened? How do I deal with myself?
Medical negligence may be a factor in some cases, but bad results can happen even when there is no breach of duty, Dr. Clifford Warren Lober noted at the American Society for Mohs Surgery meeting. Especially in cosmetic procedures, the problem may be unmet expectations.
The best thing to do is to anticipate the possibility of a bad outcome to be in the best position to deal with it. Be prepared by maintaining appropriate training and experience. Comply with office surgery rules and develop a good rapport with colleagues. Give the patient a realistic description of expected results. Obtain informed consent from patients and dismiss selected patients if necessary to stay out of trouble, he suggested.
Should the physician apologize when there's a bad outcome? "It depends," said Dr. Lober, a dermatologist in Kissimmee, Fla., who is also an attorney.
Make an effort to show concern, compassion, and empathy. Patients are more likely to sue doctors they perceive as callous or unconcerned but "do not readily sue doctors they like," he said. Some states prohibit expressions of regret, sympathy, or benevolence from being entered into evidence, so apologizing won't necessarily help if a subsequent suit goes to trial. Plus, physicians should ask themselves how effective they are at communicating, because some may come across as arrogant instead of sympathetic.
An apology may deflate the patient's anger and make negotiations possible instead of a lawsuit. Patients may expect an apology--many claim they would not have sued if only the doctor had apologized, Dr. Lober said. Apologizing may be the ethically correct thing to do, help put closure on the problem for both patient and physician, and decrease physician feelings of guilt or distance from the patient.
On the other hand, an apology may be misconstrued as legal weakness and encourage a lawsuit. It could be entered into evidence as an admission of guilt in some states, and malpractice insurers may consider it a breach of contract, so physicians should consult their attorney and malpractice insurer before apologizing.
A physician who chooses to apologize should do it soon after the injury and should be the one who apologizes instead of delegating it to a nurse, attorney, or someone else, Dr. Lober stressed. Sincere expressions of sympathy or remorse are okay, but a physician should never admit guilt, he added.
Seven states--California, Florida, Nevada, New Jersey, Oregon, Pennsylvania, and Vermont--require physicians to notify patients of adverse incidents that seriously harm the patient but specify that this cannot be introduced as evidence or construed as an acknowledgment of liability.
When things go horribly wrong for a patient, the physician may experience anger, self-doubt, or depression. Discuss the situation with your attorney, Dr. Lober advised, but be careful about discussing the circumstances with colleagues, a spouse, or others. Consider psychological counseling if the emotional response is strong or persistent, he added.
Dr. Lober stressed that his comments were for educational purposes only, and he advised physicians to seek legal counsel if an adverse situation arose.n
Dr. Lober reported having no pertinent conflicts of interest.
Mohs Infection Rates Equal With Sterile Versus Clean Gloves
NEW YORK - Clean, nonsterile gloves are just as effective in preventing infection in Mohs surgery as their more expensive sterile counterparts.
These findings from two studies add to a growing body of data that support the use of clean technique and could translate into significant cost savings for Mohs surgeons - up to several thousand dollars a year, by one estimate.
In the first study presented at the annual meeting of the American College of Mohs Surgery, researchers led by Dr. Heather D. Rogers of the University of Washington, Seattle, sought to evaluate the rate of surgical site infection (SSI) in Mohs surgery patients using clean surgical technique versus sterile technique for "all steps of MMS [Mohs micrographic surgery], including wound reconstruction, in the absence of prophylactic antibiotics."
The researchers evaluated 1,000 patients undergoing MMS using clean technique, which included the use of clean (vs. sterile) gloves, clean (vs. sterile) towels, and a "single pack" of sterile instruments for the entire wound reconstruction.
Infection was classified according to the Centers for Disease Control and Prevention parameters: A site was considered infected if it expressed purulent discharge, if it displayed edema or erythema, and if the patient complained of pain or tenderness at the site.
"There were 11 infections in 1,000 patients with 1,204 tumors," said Dr. Rogers, for an infection rate of 0.91%. Three of the infections were complications of hematomas.
"Our SSI rate of 0.91% is extremely low," she said, "underscoring the overall safety of MMS and its performance in the outpatient setting without the use of antibiotic prophylaxis or sterile technique."
The second study was presented by Dr. Yang Xia of the division of Mohs surgery at the Scripps Clinic, La Jolla, Calif. Dr. Xia conducted a prospective, subject-blinded pilot study of 60 patients at the clinic to assess the difference in infection rate between clean, nonsterile gloves and sterile gloves for the repair of surgical defects in MMS.
"Clean gloves were used for all patients in the tumor removal phase," said Dr. Xia.
After tumors were removed, patients were randomized to repair with either clean or sterile gloves. A total of 30 patients were enrolled in each arm. Sterile paper and trays were used during all repairs. The mean age of the clean group was 69 years (26 men); the mean age of the sterile group was 74 years (28 men). Patients were excluded from the study if they were taking antibiotics at the time of the procedure or if they had any serious comorbidities, such as HIV.
After surgery, patients were followed up for 5-21 days, and the wounds were assessed by a nurse or assistant who was not affiliated with the study.
In the clean group, there was one SSI, in a 67-year-old man who cultured positive for methicillin-susceptible Staphylococcus aureus (MSSA). He was prescribed cephalexin.
In the sterile group, there were two SSIs: one case of MSSA, which was treated with cephalexin and resolved, and one case of methicillin-resistant Staphylococcus aureus (MRSA), which resolved with administration of Septra (trimethoprim and sulfamethoxazole) twice a day for 14 days.
Given the equally low rates of infection in the two study arms, the potential cost-savings of switching from sterile to clean gloves for these procedures could be tremendous, Dr. Xia said. One online search put the cost of a box of 100 clean gloves at $4-$9, although Dr. Xia gave a figure of $4-$29 for a box of 150 gloves. In contrast, a box of 100 sterile surgical gloves costs $74-$250, according to Dr. Xia. (A separate online search found a box of 100 sterile gloves available for $45-$275.)
Depending on the annual volume of a surgeon's cases, switching from sterile to clean gloves could save $6,000 to $20,000 a year, Dr. Xia estimated.
Dr. Rogers and Dr. Xia said they had no disclosures to make in relation to their presentations.
NEW YORK - Clean, nonsterile gloves are just as effective in preventing infection in Mohs surgery as their more expensive sterile counterparts.
These findings from two studies add to a growing body of data that support the use of clean technique and could translate into significant cost savings for Mohs surgeons - up to several thousand dollars a year, by one estimate.
In the first study presented at the annual meeting of the American College of Mohs Surgery, researchers led by Dr. Heather D. Rogers of the University of Washington, Seattle, sought to evaluate the rate of surgical site infection (SSI) in Mohs surgery patients using clean surgical technique versus sterile technique for "all steps of MMS [Mohs micrographic surgery], including wound reconstruction, in the absence of prophylactic antibiotics."
The researchers evaluated 1,000 patients undergoing MMS using clean technique, which included the use of clean (vs. sterile) gloves, clean (vs. sterile) towels, and a "single pack" of sterile instruments for the entire wound reconstruction.
Infection was classified according to the Centers for Disease Control and Prevention parameters: A site was considered infected if it expressed purulent discharge, if it displayed edema or erythema, and if the patient complained of pain or tenderness at the site.
"There were 11 infections in 1,000 patients with 1,204 tumors," said Dr. Rogers, for an infection rate of 0.91%. Three of the infections were complications of hematomas.
"Our SSI rate of 0.91% is extremely low," she said, "underscoring the overall safety of MMS and its performance in the outpatient setting without the use of antibiotic prophylaxis or sterile technique."
The second study was presented by Dr. Yang Xia of the division of Mohs surgery at the Scripps Clinic, La Jolla, Calif. Dr. Xia conducted a prospective, subject-blinded pilot study of 60 patients at the clinic to assess the difference in infection rate between clean, nonsterile gloves and sterile gloves for the repair of surgical defects in MMS.
"Clean gloves were used for all patients in the tumor removal phase," said Dr. Xia.
After tumors were removed, patients were randomized to repair with either clean or sterile gloves. A total of 30 patients were enrolled in each arm. Sterile paper and trays were used during all repairs. The mean age of the clean group was 69 years (26 men); the mean age of the sterile group was 74 years (28 men). Patients were excluded from the study if they were taking antibiotics at the time of the procedure or if they had any serious comorbidities, such as HIV.
After surgery, patients were followed up for 5-21 days, and the wounds were assessed by a nurse or assistant who was not affiliated with the study.
In the clean group, there was one SSI, in a 67-year-old man who cultured positive for methicillin-susceptible Staphylococcus aureus (MSSA). He was prescribed cephalexin.
In the sterile group, there were two SSIs: one case of MSSA, which was treated with cephalexin and resolved, and one case of methicillin-resistant Staphylococcus aureus (MRSA), which resolved with administration of Septra (trimethoprim and sulfamethoxazole) twice a day for 14 days.
Given the equally low rates of infection in the two study arms, the potential cost-savings of switching from sterile to clean gloves for these procedures could be tremendous, Dr. Xia said. One online search put the cost of a box of 100 clean gloves at $4-$9, although Dr. Xia gave a figure of $4-$29 for a box of 150 gloves. In contrast, a box of 100 sterile surgical gloves costs $74-$250, according to Dr. Xia. (A separate online search found a box of 100 sterile gloves available for $45-$275.)
Depending on the annual volume of a surgeon's cases, switching from sterile to clean gloves could save $6,000 to $20,000 a year, Dr. Xia estimated.
Dr. Rogers and Dr. Xia said they had no disclosures to make in relation to their presentations.
NEW YORK - Clean, nonsterile gloves are just as effective in preventing infection in Mohs surgery as their more expensive sterile counterparts.
These findings from two studies add to a growing body of data that support the use of clean technique and could translate into significant cost savings for Mohs surgeons - up to several thousand dollars a year, by one estimate.
In the first study presented at the annual meeting of the American College of Mohs Surgery, researchers led by Dr. Heather D. Rogers of the University of Washington, Seattle, sought to evaluate the rate of surgical site infection (SSI) in Mohs surgery patients using clean surgical technique versus sterile technique for "all steps of MMS [Mohs micrographic surgery], including wound reconstruction, in the absence of prophylactic antibiotics."
The researchers evaluated 1,000 patients undergoing MMS using clean technique, which included the use of clean (vs. sterile) gloves, clean (vs. sterile) towels, and a "single pack" of sterile instruments for the entire wound reconstruction.
Infection was classified according to the Centers for Disease Control and Prevention parameters: A site was considered infected if it expressed purulent discharge, if it displayed edema or erythema, and if the patient complained of pain or tenderness at the site.
"There were 11 infections in 1,000 patients with 1,204 tumors," said Dr. Rogers, for an infection rate of 0.91%. Three of the infections were complications of hematomas.
"Our SSI rate of 0.91% is extremely low," she said, "underscoring the overall safety of MMS and its performance in the outpatient setting without the use of antibiotic prophylaxis or sterile technique."
The second study was presented by Dr. Yang Xia of the division of Mohs surgery at the Scripps Clinic, La Jolla, Calif. Dr. Xia conducted a prospective, subject-blinded pilot study of 60 patients at the clinic to assess the difference in infection rate between clean, nonsterile gloves and sterile gloves for the repair of surgical defects in MMS.
"Clean gloves were used for all patients in the tumor removal phase," said Dr. Xia.
After tumors were removed, patients were randomized to repair with either clean or sterile gloves. A total of 30 patients were enrolled in each arm. Sterile paper and trays were used during all repairs. The mean age of the clean group was 69 years (26 men); the mean age of the sterile group was 74 years (28 men). Patients were excluded from the study if they were taking antibiotics at the time of the procedure or if they had any serious comorbidities, such as HIV.
After surgery, patients were followed up for 5-21 days, and the wounds were assessed by a nurse or assistant who was not affiliated with the study.
In the clean group, there was one SSI, in a 67-year-old man who cultured positive for methicillin-susceptible Staphylococcus aureus (MSSA). He was prescribed cephalexin.
In the sterile group, there were two SSIs: one case of MSSA, which was treated with cephalexin and resolved, and one case of methicillin-resistant Staphylococcus aureus (MRSA), which resolved with administration of Septra (trimethoprim and sulfamethoxazole) twice a day for 14 days.
Given the equally low rates of infection in the two study arms, the potential cost-savings of switching from sterile to clean gloves for these procedures could be tremendous, Dr. Xia said. One online search put the cost of a box of 100 clean gloves at $4-$9, although Dr. Xia gave a figure of $4-$29 for a box of 150 gloves. In contrast, a box of 100 sterile surgical gloves costs $74-$250, according to Dr. Xia. (A separate online search found a box of 100 sterile gloves available for $45-$275.)
Depending on the annual volume of a surgeon's cases, switching from sterile to clean gloves could save $6,000 to $20,000 a year, Dr. Xia estimated.
Dr. Rogers and Dr. Xia said they had no disclosures to make in relation to their presentations.
"Incisionless" Neck Lift System
Dr. Gregory P. Mueller explains how to perform the "incisionless" neck lift, a recently launched advancement in cosmetic surgery.
Dr. Gregory P. Mueller explains how to perform the "incisionless" neck lift, a recently launched advancement in cosmetic surgery.
Dr. Gregory P. Mueller explains how to perform the "incisionless" neck lift, a recently launched advancement in cosmetic surgery.
Techniques Not Equal for Flattening Mohs Specimens
MONTEREY, Calif. — Stainless steel embedding wells may be the best of several mechanisms available to flatten or “conform” tissue specimens for sectioning in Mohs surgery, in one expert’s opinion.
Sectioning of the peripheral/epidermal margin of the lesion is essential for Mohs surgery to ensure complete margin assessment. Most Mohs surgeons require that 90% or more of the epidermis be present to feel that they’re assessing an adequate epidermal margin, Dr. David F. Butler explained at a meeting of the American Society for Mohs Surgery.
Only two mechanisms can flatten multiple tissue specimens at once: the $20,000 CryoHist machine, or the $529 stainless steel embedding wells, said Dr. Butler, chair of dermatology at the Scott and White Hospital and Clinic and professor of medicine at Texas A&M University, both in Temple, Tex.
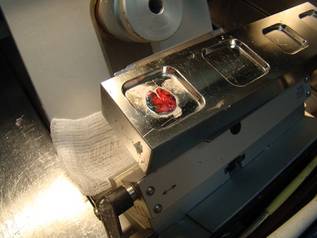
Lower cost, convenience, and quality results make him a fan of the stainless steel embedding wells, which consist of 1-inch steel bars with wells cut out in different sizes and depths. The bars reside within a cryostat, which provides a heat sink for the rapid freezing of the specimen.
The surgeon or other operator places a specimen facedown on the smooth surface of a well and presses down on the peripheral edge of the specimen with a gloved finger. “Like putting your tongue to a cold flagpole in Wisconsin in winter, it sticks,” he said.
Optimal cutting temperature (OCT) compound—a cryopreservation medium—is then applied over the specimen, and a metal chuck with a cross-grid pattern to better hold onto frozen OCT is applied to the OCT. A freezing block that’s been kept cold within the cryostat can be placed over the stem of the chuck to freeze the specimen more quickly.
As Dr. Butler described it, one of the sets includes one freezing bar with a 24-mm well, a 36-mm chuck, and the overchuck freezing block. He described the complete set as three bars with different well sizes, six small chucks, four large chucks, four overchuck freezing blocks, a chuck bin, an elevated embedding block, and angled freezing forceps.
The stainless steel embedding wells are available from Dr. Stephen R. Peters, the pathologist who designed them, Dr. Butler said. Dr. Peters is at Hackensack (N.J.) University Medical Center and can be reached through his Web site or via e-mail.
In using the stainless steel embedding wells for seven consecutive specimens, Dr. Butler found that five of the seven specimens (71%) met the goal of having more than 90% of the epidermis present by the sixth retained section.
He compared the time needed to freeze a specimen and mount the block using several mechanisms. It took 105 seconds with the embedding wells, 56 seconds with the CryoHist, 68 seconds with the Miami Special, and 91 seconds with the Cryocup. Only the embedding wells and CryoHist could freeze and mount multiple specimens at the same time “so the overall process doesn’t take very long,” he said.
The CryoHist is a large machine, plumbed for liquid nitrogen that flattens specimens via a vacuum suction. Compared with embedding wells, its disadvantages include the high cost and the need for greater space, external power and liquid nitrogen, and consumables such as a plastic film that is used in the process, Dr. Butler said.
The Miami Special is a long-handled clamp with flat metal plates at the end on which partially frozen OCT and a chuck are placed. The specimen is placed on the OCT and the clamp is closed and dipped in liquid nitrogen to freeze. “The problem is that it’s very cumbersome and can only do one at a time,” he said.
The Davidson Cryocup is a metal device with a long handle and a cup at one end in which tissue is placed facedown and covered with OCT and a chuck. The cup is lowered into liquid nitrogen to freeze. “It has the same problem as the Miami Special: You can only process one specimen at a time,” he said.
Other mechanisms include the inexpensive cryomold, small plastic trays of different sizes and depths on which specimens are placed facedown and covered with OCT and a chuck before placement in a cryostat. The plastic cryomold is peeled back before sectioning, one specimen at a time.
An older technique employs a heat extractor that resides within some cryostats and remains cold. A chuck is placed on the rack within the cryostat, OCT is applied, and the specimen is placed “deep side up” on the OCT, he said. A cold round bar of the heat extractor is pressed down on the specimen and OCT until frozen.
Dr. Butler said he has no pertinent conflicts of interest.
MONTEREY, Calif. — Stainless steel embedding wells may be the best of several mechanisms available to flatten or “conform” tissue specimens for sectioning in Mohs surgery, in one expert’s opinion.
Sectioning of the peripheral/epidermal margin of the lesion is essential for Mohs surgery to ensure complete margin assessment. Most Mohs surgeons require that 90% or more of the epidermis be present to feel that they’re assessing an adequate epidermal margin, Dr. David F. Butler explained at a meeting of the American Society for Mohs Surgery.
Only two mechanisms can flatten multiple tissue specimens at once: the $20,000 CryoHist machine, or the $529 stainless steel embedding wells, said Dr. Butler, chair of dermatology at the Scott and White Hospital and Clinic and professor of medicine at Texas A&M University, both in Temple, Tex.
Lower cost, convenience, and quality results make him a fan of the stainless steel embedding wells, which consist of 1-inch steel bars with wells cut out in different sizes and depths. The bars reside within a cryostat, which provides a heat sink for the rapid freezing of the specimen.
The surgeon or other operator places a specimen facedown on the smooth surface of a well and presses down on the peripheral edge of the specimen with a gloved finger. “Like putting your tongue to a cold flagpole in Wisconsin in winter, it sticks,” he said.
Optimal cutting temperature (OCT) compound—a cryopreservation medium—is then applied over the specimen, and a metal chuck with a cross-grid pattern to better hold onto frozen OCT is applied to the OCT. A freezing block that’s been kept cold within the cryostat can be placed over the stem of the chuck to freeze the specimen more quickly.
As Dr. Butler described it, one of the sets includes one freezing bar with a 24-mm well, a 36-mm chuck, and the overchuck freezing block. He described the complete set as three bars with different well sizes, six small chucks, four large chucks, four overchuck freezing blocks, a chuck bin, an elevated embedding block, and angled freezing forceps.
The stainless steel embedding wells are available from Dr. Stephen R. Peters, the pathologist who designed them, Dr. Butler said. Dr. Peters is at Hackensack (N.J.) University Medical Center and can be reached through his Web site or via e-mail.
In using the stainless steel embedding wells for seven consecutive specimens, Dr. Butler found that five of the seven specimens (71%) met the goal of having more than 90% of the epidermis present by the sixth retained section.
He compared the time needed to freeze a specimen and mount the block using several mechanisms. It took 105 seconds with the embedding wells, 56 seconds with the CryoHist, 68 seconds with the Miami Special, and 91 seconds with the Cryocup. Only the embedding wells and CryoHist could freeze and mount multiple specimens at the same time “so the overall process doesn’t take very long,” he said.
The CryoHist is a large machine, plumbed for liquid nitrogen that flattens specimens via a vacuum suction. Compared with embedding wells, its disadvantages include the high cost and the need for greater space, external power and liquid nitrogen, and consumables such as a plastic film that is used in the process, Dr. Butler said.
The Miami Special is a long-handled clamp with flat metal plates at the end on which partially frozen OCT and a chuck are placed. The specimen is placed on the OCT and the clamp is closed and dipped in liquid nitrogen to freeze. “The problem is that it’s very cumbersome and can only do one at a time,” he said.
The Davidson Cryocup is a metal device with a long handle and a cup at one end in which tissue is placed facedown and covered with OCT and a chuck. The cup is lowered into liquid nitrogen to freeze. “It has the same problem as the Miami Special: You can only process one specimen at a time,” he said.
Other mechanisms include the inexpensive cryomold, small plastic trays of different sizes and depths on which specimens are placed facedown and covered with OCT and a chuck before placement in a cryostat. The plastic cryomold is peeled back before sectioning, one specimen at a time.
An older technique employs a heat extractor that resides within some cryostats and remains cold. A chuck is placed on the rack within the cryostat, OCT is applied, and the specimen is placed “deep side up” on the OCT, he said. A cold round bar of the heat extractor is pressed down on the specimen and OCT until frozen.
Dr. Butler said he has no pertinent conflicts of interest.
MONTEREY, Calif. — Stainless steel embedding wells may be the best of several mechanisms available to flatten or “conform” tissue specimens for sectioning in Mohs surgery, in one expert’s opinion.
Sectioning of the peripheral/epidermal margin of the lesion is essential for Mohs surgery to ensure complete margin assessment. Most Mohs surgeons require that 90% or more of the epidermis be present to feel that they’re assessing an adequate epidermal margin, Dr. David F. Butler explained at a meeting of the American Society for Mohs Surgery.
Only two mechanisms can flatten multiple tissue specimens at once: the $20,000 CryoHist machine, or the $529 stainless steel embedding wells, said Dr. Butler, chair of dermatology at the Scott and White Hospital and Clinic and professor of medicine at Texas A&M University, both in Temple, Tex.
Lower cost, convenience, and quality results make him a fan of the stainless steel embedding wells, which consist of 1-inch steel bars with wells cut out in different sizes and depths. The bars reside within a cryostat, which provides a heat sink for the rapid freezing of the specimen.
The surgeon or other operator places a specimen facedown on the smooth surface of a well and presses down on the peripheral edge of the specimen with a gloved finger. “Like putting your tongue to a cold flagpole in Wisconsin in winter, it sticks,” he said.
Optimal cutting temperature (OCT) compound—a cryopreservation medium—is then applied over the specimen, and a metal chuck with a cross-grid pattern to better hold onto frozen OCT is applied to the OCT. A freezing block that’s been kept cold within the cryostat can be placed over the stem of the chuck to freeze the specimen more quickly.
As Dr. Butler described it, one of the sets includes one freezing bar with a 24-mm well, a 36-mm chuck, and the overchuck freezing block. He described the complete set as three bars with different well sizes, six small chucks, four large chucks, four overchuck freezing blocks, a chuck bin, an elevated embedding block, and angled freezing forceps.
The stainless steel embedding wells are available from Dr. Stephen R. Peters, the pathologist who designed them, Dr. Butler said. Dr. Peters is at Hackensack (N.J.) University Medical Center and can be reached through his Web site or via e-mail.
In using the stainless steel embedding wells for seven consecutive specimens, Dr. Butler found that five of the seven specimens (71%) met the goal of having more than 90% of the epidermis present by the sixth retained section.
He compared the time needed to freeze a specimen and mount the block using several mechanisms. It took 105 seconds with the embedding wells, 56 seconds with the CryoHist, 68 seconds with the Miami Special, and 91 seconds with the Cryocup. Only the embedding wells and CryoHist could freeze and mount multiple specimens at the same time “so the overall process doesn’t take very long,” he said.
The CryoHist is a large machine, plumbed for liquid nitrogen that flattens specimens via a vacuum suction. Compared with embedding wells, its disadvantages include the high cost and the need for greater space, external power and liquid nitrogen, and consumables such as a plastic film that is used in the process, Dr. Butler said.
The Miami Special is a long-handled clamp with flat metal plates at the end on which partially frozen OCT and a chuck are placed. The specimen is placed on the OCT and the clamp is closed and dipped in liquid nitrogen to freeze. “The problem is that it’s very cumbersome and can only do one at a time,” he said.
The Davidson Cryocup is a metal device with a long handle and a cup at one end in which tissue is placed facedown and covered with OCT and a chuck. The cup is lowered into liquid nitrogen to freeze. “It has the same problem as the Miami Special: You can only process one specimen at a time,” he said.
Other mechanisms include the inexpensive cryomold, small plastic trays of different sizes and depths on which specimens are placed facedown and covered with OCT and a chuck before placement in a cryostat. The plastic cryomold is peeled back before sectioning, one specimen at a time.
An older technique employs a heat extractor that resides within some cryostats and remains cold. A chuck is placed on the rack within the cryostat, OCT is applied, and the specimen is placed “deep side up” on the OCT, he said. A cold round bar of the heat extractor is pressed down on the specimen and OCT until frozen.
Dr. Butler said he has no pertinent conflicts of interest.
The Juicy Benefits of Açaí Berry
Native to South America, particularly the Amazon River and its tributaries and estuaries (J. Agric. Food Chem. 2006;54:8,598-603), the açaí palm (Euterpe oleracea Mart.) has become a subject of great interest in recent years, because its fruit is believed by many to boast significant antioxidant capacity.

The juice and pulp of açaí are popular beverage components in juice blends, smoothies, and other drinks in Central and South America. Mainstream attention, including features on popular U.S. television programs, “has increased interest in the United States in the potential and rumored health effects of açaí. This column will briefly review recent findings regarding this increasingly popular antioxidant-rich plant.
Juicy Benefits
In 2008, investigators studied the antioxidant and anti-inflammatory activities of a commercial juice blend (MonaVie Active) containing açaí as the main ingredient. Anthocyanins, the primary active phenolic components in açaí, were found to be the main antioxidants in the juice, particularly cyanidin 3-rutoside, cyanidin 3-diglycoside, and cyanidin 3-glucoside. In vitro, the antioxidants in the blend were shown to protect against oxidative damage. Polymorphonuclear cells exhibited decreased formation of free radicals and lower migration toward certain proinflammatory chemoattractants.
In vivo, a randomized, double-blind, placebo-controlled crossover trial with 12 healthy participants revealed within-subject increases in serum antioxidants 1 hour and 2 hours after consumption of MonaVie Active, and suppression of lipid peroxidation 2 hours after consumption (J. Agric. Food Chem. 2008;56:8,326-33).
In another study, a four-way crossover clinical trial compared açaí pulp and clarified açaí juice, with applesauce and a nonantioxidant drink as controls. Twelve healthy volunteers were dosed at 7 mL/kg of body weight following a washout phase and overnight fast. The investigators noted that plasma antioxidant capacity increased 2.3- and 3.0-fold for açaí juice and pulp, respectively, 2 hours after consumption of the beverage (J. Agric. Food Chem. 2008;56:7,796-802).
Additional recent research on antioxidant beverages has involved açaí. A study using four tests of antioxidant strength evaluated the relative antioxidant capacities of several polyphenol-rich beverages available on the U.S. market. These beverages included açaí juice, apple juice, black cherry juice, blueberry juice, Concord grape juice, cranberry juice, orange juice, pomegranate juice, red wines, and iced tea (black, green, and white). The in vitro antioxidant capacity of açaí juice was found to be in the middle of the pack, more potent than apple juice, cranberry juice, orange juice, and iced tea. The researchers cautioned, however, that in vitro antioxidant strength does not necessarily translate to in vivo biologic activity (J. Agric. Food Chem. 2008;56:1,415-22).
Anthocyanins
In 2004, investigators studied anthocyanins and other polyphenolic components of açaí in order to identify their contributions to the overall antioxidant profile of the fruit. They also sought to determine the color stability of anthocyanins against hydrogen peroxide at various termperatures. The researchers found that cyanidin 3-glucoside was the prevailing anthocyanin among 16 other polyphenolics in the tropical fruit, and the most influential in terms of its antioxidant capacity. In the presence of hydrogen peroxide, red grape anthocyanins were most stable, with açaí and pigments rich in acylated anthocyanins exhibiting lower color stability in a temperature-dependent fashion. In the presence of ascorbic acid, acylated anthocyanin sources displayed increased color stability. The authors concluded that açaí demonstrated functional characteristics that would be useful in food and nutraceutical products (J. Agric. Food Chem. 2004;52:1539-45).
Subsequently, some of the same researchers studied the effects of açaí polyphenolics on antiproliferation and induction of apoptosis in HL-60 human leukemia cells. They found that the açaí polyphenols indeed lowered leukemia cell proliferation in vitro, and concluded that açaí is a rich source of bioactive polyphenolic compounds (J. Agric. Food Chem. 2006;54:1,222-9).
Fruit Consumption
On the basis of discoveries that açaí fruit exhibits potent antioxidant capacity in vitro, particularly against superoxide and peroxyl radicals, Schauss et al. set out in 2006 to examine the potential health benefits that açaí fruit might impart. They investigated the antioxidant activity of a standardized freeze-dried açaí fruit pulp/skin powder (OptiAcai) in various assays using several sources of free radicals. The researchers found evidence in support of açaí’s antioxidant capacity against superoxide and peroxyl radicals, including strong scavenging of superoxide and the highest antioxidant activity of any food against the peroxyl radical. Mild activity was noted against the peroxynitrite and hydroxyl radicals.
The investigators also performed an assay to assess the inhibition of free radical development in freshly purified human neutrophils, which revealed that the antioxidants in açaí can, at very low doses, penetrate human cells and exhibit oxygen-quenching activity. Finally, the investigators studied the anti-inflammatory and immune bioactivities of açaí components, and observed that the fruit has the potential to inhibit cyclo-oxygenase (COX)-1 and COX-2 (J. Agric. Food Chem. 2006;54:8,604-10).
In a separate study, Schauss et al. analyzed OptiAcai and identified anthocyanins (chiefly cyanidin 3-glucoside and cyanidin 3-rutinoside), proanthocyanidins (mainly polymers), and other flavonoids (i.e., homoorientin, orientin, isovitexin, scoparin, and taxifolin deoxyhexose, along with several unknown ones) as the primary phytochemical constituents. They also found oleic and palmitic acids to be the prevailing fatty acid components. Resveratrol was identified at trace levels, and 19 amino acids were found, comprising 7.59% of the total weight (J. Agric. Food Chem. 2006;54:8,598-603).
Nutritional Components
In a far-ranging study of açaí pulp culled in the Venezuelan Amazon from two harvests of the year 2005, investigators used spectrophotometric methods to determine the content of polyphenols, tannins, and anthocynanins. The study sought to characterize the polyphenolic content and antioxidant capacity of the fruit, along with other qualities, such as fatty acid content. Antioxidant capacity was analyzed through the 2,2-diphenyl-1-picrylhydrazyl method.
The researchers found that açaí has a high content of lipids, particularly oleic acid, as well as large amounts of protein, ash, and total dietary fiber. The antioxidant capacity was 88%. The investigators concluded that açaí confers significant nutritional value and contains antioxidant constituents such as polyphenols, tannins, and anthocyanins that may render the fruit ripe for industrialization (Arch. Latinoam. Nutr. 2007;57:94-8).
Researchers studying the antioxidant capacities of 11 commercial and noncommercial varieties of açaí fruit pulp against three reactive oxygen species found that all purple açaí samples were potent scavengers of peroxyl radicals, good against peroxynitrite, and poor against hydroxyl radicals, compared with recently studied common European fruit and vegetable juices. One white açaí species displayed low antioxidant capacity against all three reactive oxygen species. Anthocyanins were found to account for only about 10% of the overall antioxidant capacities of the fruit. The investigators concluded that as-yet unidentified constituents of the açaí fruit pulp appeared to be responsible for most of its antioxidant activity (Int. J. Food Sci. Nutr. 2005;56:53-64).
Seed Extracts
The same researchers, along with others, later assessed the antioxidant capacity of methanol and ethanol seed extracts from açaí against peroxyl radicals, peroxynitrite, and hydroxyl radicals. They found that the antioxidant activity of the seed extracts was similar to that of the pulp against peroxyl radicals, and was greater against peroxynitrite and hydroxyl radicals. They also determined that procyanidins contribute significantly to the overall antioxidant capacity of açaí, but as-yet unidentified compounds account for the majority of such activity (J. Agric. Food Chem. 2006;54:4,162-7).
In a recent study, Pacheco-Palencia et al. examined the absorption and antiproliferative effects of açaí pulp extracts and a polyphenolic-enriched oil derived from the fruit pulp of the açaí berry. Investigators ascertained the chemical composition, antioxidant activity, and polyphenolic absorption of phytochemical fractions in a Caco-2 monolayer, in addition to their cytotoxicity in a human colon cancer cell line (HT-29 adenocarcinoma cells).
In general, the study added to the relatively slim body of literature on the bioactive properties, chemical composition, and cellular absorption of açaí polyphenolics. The investigators found that polyphenolic mixtures from the açaí pulp and oil significantly inhibited cell proliferation, and that standardized extracts featured a preponderance of hydroxybenzoic acids, monomeric flavan-3-ols, and procyanidin dimers and trimers (J. Agric. Food Chem. 2008;56:3,593-600).
Phenolic Constituents
Later in 2008, Pacheco-Palencia and two of the same researchers identified for the first time the phenolic constituents in crude oil extracts of the açaí berry. Like the berry, the oil was found to contain high concentrations of phenolic acids (i.e., vanillic acid, syringic acid, p-hydroxybenzoic acid, protocatechuic acid, and ferulic acid), (+)-catechin, and several procyanidin oligomers. The researchers evaluated the thermal stability of the oil during short- and long-term storage for lipid oxidation and phenolic retention, in terms of the effects on antioxidant activity. They found that phenolic acids underwent a 16% loss at 20° or 30° C after 10 weeks of storage, and a 33% loss at 40° C. Procyanidin oligomers showed greater degradation: 23% at 20° C, 39% at 30° C, and 74% at 40° C, in both high- and low-phenolic açaí oils. Phenolic and antioxidant capacity decreased less than 10% during short-term (20 minutes) heating at 150° C and 170° C. The investigators concluded that the high phenolic composition of açaí oil renders it a potentially beneficial food and supplement option, as well as a promising cosmetic agent (J. Agric. Food Chem. 2008;56:4,631-6).
Conclusions
Açaí berry is a popular ingredient in beverages in Central and South America, and its popularity is steadily increasing in North America. It is highly touted for its antioxidant potency. The berry is available in oral supplement form and is advertised as a miraculous weight-loss elixir. It is not often found in topical preparations because of its blue color.
While some of the scant research on açaí is compelling and, indeed, suggests significant antioxidant capacity, there is no evidence to support the use of açaí for weight loss. It is important that practitioners deflate the hype surrounding this botanical and indicate to patients that much more research is necessary to determine whether the antioxidant properties of açaí can be appropriately harnessed in topical or oral skin products.
That said, while I strongly recommend disabusing patients of the notion that açaí will help them lose weight, adding a sizable portion or portions of anthocyanin-containing berries, including açaí, in one’s diet is a healthy choice. As always, it’s best to suggest whole foods – real fruit – as opposed to diluted but sugared fruit drinks.
Native to South America, particularly the Amazon River and its tributaries and estuaries (J. Agric. Food Chem. 2006;54:8,598-603), the açaí palm (Euterpe oleracea Mart.) has become a subject of great interest in recent years, because its fruit is believed by many to boast significant antioxidant capacity.
The juice and pulp of açaí are popular beverage components in juice blends, smoothies, and other drinks in Central and South America. Mainstream attention, including features on popular U.S. television programs, “has increased interest in the United States in the potential and rumored health effects of açaí. This column will briefly review recent findings regarding this increasingly popular antioxidant-rich plant.
Juicy Benefits
In 2008, investigators studied the antioxidant and anti-inflammatory activities of a commercial juice blend (MonaVie Active) containing açaí as the main ingredient. Anthocyanins, the primary active phenolic components in açaí, were found to be the main antioxidants in the juice, particularly cyanidin 3-rutoside, cyanidin 3-diglycoside, and cyanidin 3-glucoside. In vitro, the antioxidants in the blend were shown to protect against oxidative damage. Polymorphonuclear cells exhibited decreased formation of free radicals and lower migration toward certain proinflammatory chemoattractants.
In vivo, a randomized, double-blind, placebo-controlled crossover trial with 12 healthy participants revealed within-subject increases in serum antioxidants 1 hour and 2 hours after consumption of MonaVie Active, and suppression of lipid peroxidation 2 hours after consumption (J. Agric. Food Chem. 2008;56:8,326-33).
In another study, a four-way crossover clinical trial compared açaí pulp and clarified açaí juice, with applesauce and a nonantioxidant drink as controls. Twelve healthy volunteers were dosed at 7 mL/kg of body weight following a washout phase and overnight fast. The investigators noted that plasma antioxidant capacity increased 2.3- and 3.0-fold for açaí juice and pulp, respectively, 2 hours after consumption of the beverage (J. Agric. Food Chem. 2008;56:7,796-802).
Additional recent research on antioxidant beverages has involved açaí. A study using four tests of antioxidant strength evaluated the relative antioxidant capacities of several polyphenol-rich beverages available on the U.S. market. These beverages included açaí juice, apple juice, black cherry juice, blueberry juice, Concord grape juice, cranberry juice, orange juice, pomegranate juice, red wines, and iced tea (black, green, and white). The in vitro antioxidant capacity of açaí juice was found to be in the middle of the pack, more potent than apple juice, cranberry juice, orange juice, and iced tea. The researchers cautioned, however, that in vitro antioxidant strength does not necessarily translate to in vivo biologic activity (J. Agric. Food Chem. 2008;56:1,415-22).
Anthocyanins
In 2004, investigators studied anthocyanins and other polyphenolic components of açaí in order to identify their contributions to the overall antioxidant profile of the fruit. They also sought to determine the color stability of anthocyanins against hydrogen peroxide at various termperatures. The researchers found that cyanidin 3-glucoside was the prevailing anthocyanin among 16 other polyphenolics in the tropical fruit, and the most influential in terms of its antioxidant capacity. In the presence of hydrogen peroxide, red grape anthocyanins were most stable, with açaí and pigments rich in acylated anthocyanins exhibiting lower color stability in a temperature-dependent fashion. In the presence of ascorbic acid, acylated anthocyanin sources displayed increased color stability. The authors concluded that açaí demonstrated functional characteristics that would be useful in food and nutraceutical products (J. Agric. Food Chem. 2004;52:1539-45).
Subsequently, some of the same researchers studied the effects of açaí polyphenolics on antiproliferation and induction of apoptosis in HL-60 human leukemia cells. They found that the açaí polyphenols indeed lowered leukemia cell proliferation in vitro, and concluded that açaí is a rich source of bioactive polyphenolic compounds (J. Agric. Food Chem. 2006;54:1,222-9).
Fruit Consumption
On the basis of discoveries that açaí fruit exhibits potent antioxidant capacity in vitro, particularly against superoxide and peroxyl radicals, Schauss et al. set out in 2006 to examine the potential health benefits that açaí fruit might impart. They investigated the antioxidant activity of a standardized freeze-dried açaí fruit pulp/skin powder (OptiAcai) in various assays using several sources of free radicals. The researchers found evidence in support of açaí’s antioxidant capacity against superoxide and peroxyl radicals, including strong scavenging of superoxide and the highest antioxidant activity of any food against the peroxyl radical. Mild activity was noted against the peroxynitrite and hydroxyl radicals.
The investigators also performed an assay to assess the inhibition of free radical development in freshly purified human neutrophils, which revealed that the antioxidants in açaí can, at very low doses, penetrate human cells and exhibit oxygen-quenching activity. Finally, the investigators studied the anti-inflammatory and immune bioactivities of açaí components, and observed that the fruit has the potential to inhibit cyclo-oxygenase (COX)-1 and COX-2 (J. Agric. Food Chem. 2006;54:8,604-10).
In a separate study, Schauss et al. analyzed OptiAcai and identified anthocyanins (chiefly cyanidin 3-glucoside and cyanidin 3-rutinoside), proanthocyanidins (mainly polymers), and other flavonoids (i.e., homoorientin, orientin, isovitexin, scoparin, and taxifolin deoxyhexose, along with several unknown ones) as the primary phytochemical constituents. They also found oleic and palmitic acids to be the prevailing fatty acid components. Resveratrol was identified at trace levels, and 19 amino acids were found, comprising 7.59% of the total weight (J. Agric. Food Chem. 2006;54:8,598-603).
Nutritional Components
In a far-ranging study of açaí pulp culled in the Venezuelan Amazon from two harvests of the year 2005, investigators used spectrophotometric methods to determine the content of polyphenols, tannins, and anthocynanins. The study sought to characterize the polyphenolic content and antioxidant capacity of the fruit, along with other qualities, such as fatty acid content. Antioxidant capacity was analyzed through the 2,2-diphenyl-1-picrylhydrazyl method.
The researchers found that açaí has a high content of lipids, particularly oleic acid, as well as large amounts of protein, ash, and total dietary fiber. The antioxidant capacity was 88%. The investigators concluded that açaí confers significant nutritional value and contains antioxidant constituents such as polyphenols, tannins, and anthocyanins that may render the fruit ripe for industrialization (Arch. Latinoam. Nutr. 2007;57:94-8).
Researchers studying the antioxidant capacities of 11 commercial and noncommercial varieties of açaí fruit pulp against three reactive oxygen species found that all purple açaí samples were potent scavengers of peroxyl radicals, good against peroxynitrite, and poor against hydroxyl radicals, compared with recently studied common European fruit and vegetable juices. One white açaí species displayed low antioxidant capacity against all three reactive oxygen species. Anthocyanins were found to account for only about 10% of the overall antioxidant capacities of the fruit. The investigators concluded that as-yet unidentified constituents of the açaí fruit pulp appeared to be responsible for most of its antioxidant activity (Int. J. Food Sci. Nutr. 2005;56:53-64).
Seed Extracts
The same researchers, along with others, later assessed the antioxidant capacity of methanol and ethanol seed extracts from açaí against peroxyl radicals, peroxynitrite, and hydroxyl radicals. They found that the antioxidant activity of the seed extracts was similar to that of the pulp against peroxyl radicals, and was greater against peroxynitrite and hydroxyl radicals. They also determined that procyanidins contribute significantly to the overall antioxidant capacity of açaí, but as-yet unidentified compounds account for the majority of such activity (J. Agric. Food Chem. 2006;54:4,162-7).
In a recent study, Pacheco-Palencia et al. examined the absorption and antiproliferative effects of açaí pulp extracts and a polyphenolic-enriched oil derived from the fruit pulp of the açaí berry. Investigators ascertained the chemical composition, antioxidant activity, and polyphenolic absorption of phytochemical fractions in a Caco-2 monolayer, in addition to their cytotoxicity in a human colon cancer cell line (HT-29 adenocarcinoma cells).
In general, the study added to the relatively slim body of literature on the bioactive properties, chemical composition, and cellular absorption of açaí polyphenolics. The investigators found that polyphenolic mixtures from the açaí pulp and oil significantly inhibited cell proliferation, and that standardized extracts featured a preponderance of hydroxybenzoic acids, monomeric flavan-3-ols, and procyanidin dimers and trimers (J. Agric. Food Chem. 2008;56:3,593-600).
Phenolic Constituents
Later in 2008, Pacheco-Palencia and two of the same researchers identified for the first time the phenolic constituents in crude oil extracts of the açaí berry. Like the berry, the oil was found to contain high concentrations of phenolic acids (i.e., vanillic acid, syringic acid, p-hydroxybenzoic acid, protocatechuic acid, and ferulic acid), (+)-catechin, and several procyanidin oligomers. The researchers evaluated the thermal stability of the oil during short- and long-term storage for lipid oxidation and phenolic retention, in terms of the effects on antioxidant activity. They found that phenolic acids underwent a 16% loss at 20° or 30° C after 10 weeks of storage, and a 33% loss at 40° C. Procyanidin oligomers showed greater degradation: 23% at 20° C, 39% at 30° C, and 74% at 40° C, in both high- and low-phenolic açaí oils. Phenolic and antioxidant capacity decreased less than 10% during short-term (20 minutes) heating at 150° C and 170° C. The investigators concluded that the high phenolic composition of açaí oil renders it a potentially beneficial food and supplement option, as well as a promising cosmetic agent (J. Agric. Food Chem. 2008;56:4,631-6).
Conclusions
Açaí berry is a popular ingredient in beverages in Central and South America, and its popularity is steadily increasing in North America. It is highly touted for its antioxidant potency. The berry is available in oral supplement form and is advertised as a miraculous weight-loss elixir. It is not often found in topical preparations because of its blue color.
While some of the scant research on açaí is compelling and, indeed, suggests significant antioxidant capacity, there is no evidence to support the use of açaí for weight loss. It is important that practitioners deflate the hype surrounding this botanical and indicate to patients that much more research is necessary to determine whether the antioxidant properties of açaí can be appropriately harnessed in topical or oral skin products.
That said, while I strongly recommend disabusing patients of the notion that açaí will help them lose weight, adding a sizable portion or portions of anthocyanin-containing berries, including açaí, in one’s diet is a healthy choice. As always, it’s best to suggest whole foods – real fruit – as opposed to diluted but sugared fruit drinks.
Native to South America, particularly the Amazon River and its tributaries and estuaries (J. Agric. Food Chem. 2006;54:8,598-603), the açaí palm (Euterpe oleracea Mart.) has become a subject of great interest in recent years, because its fruit is believed by many to boast significant antioxidant capacity.
The juice and pulp of açaí are popular beverage components in juice blends, smoothies, and other drinks in Central and South America. Mainstream attention, including features on popular U.S. television programs, “has increased interest in the United States in the potential and rumored health effects of açaí. This column will briefly review recent findings regarding this increasingly popular antioxidant-rich plant.
Juicy Benefits
In 2008, investigators studied the antioxidant and anti-inflammatory activities of a commercial juice blend (MonaVie Active) containing açaí as the main ingredient. Anthocyanins, the primary active phenolic components in açaí, were found to be the main antioxidants in the juice, particularly cyanidin 3-rutoside, cyanidin 3-diglycoside, and cyanidin 3-glucoside. In vitro, the antioxidants in the blend were shown to protect against oxidative damage. Polymorphonuclear cells exhibited decreased formation of free radicals and lower migration toward certain proinflammatory chemoattractants.
In vivo, a randomized, double-blind, placebo-controlled crossover trial with 12 healthy participants revealed within-subject increases in serum antioxidants 1 hour and 2 hours after consumption of MonaVie Active, and suppression of lipid peroxidation 2 hours after consumption (J. Agric. Food Chem. 2008;56:8,326-33).
In another study, a four-way crossover clinical trial compared açaí pulp and clarified açaí juice, with applesauce and a nonantioxidant drink as controls. Twelve healthy volunteers were dosed at 7 mL/kg of body weight following a washout phase and overnight fast. The investigators noted that plasma antioxidant capacity increased 2.3- and 3.0-fold for açaí juice and pulp, respectively, 2 hours after consumption of the beverage (J. Agric. Food Chem. 2008;56:7,796-802).
Additional recent research on antioxidant beverages has involved açaí. A study using four tests of antioxidant strength evaluated the relative antioxidant capacities of several polyphenol-rich beverages available on the U.S. market. These beverages included açaí juice, apple juice, black cherry juice, blueberry juice, Concord grape juice, cranberry juice, orange juice, pomegranate juice, red wines, and iced tea (black, green, and white). The in vitro antioxidant capacity of açaí juice was found to be in the middle of the pack, more potent than apple juice, cranberry juice, orange juice, and iced tea. The researchers cautioned, however, that in vitro antioxidant strength does not necessarily translate to in vivo biologic activity (J. Agric. Food Chem. 2008;56:1,415-22).
Anthocyanins
In 2004, investigators studied anthocyanins and other polyphenolic components of açaí in order to identify their contributions to the overall antioxidant profile of the fruit. They also sought to determine the color stability of anthocyanins against hydrogen peroxide at various termperatures. The researchers found that cyanidin 3-glucoside was the prevailing anthocyanin among 16 other polyphenolics in the tropical fruit, and the most influential in terms of its antioxidant capacity. In the presence of hydrogen peroxide, red grape anthocyanins were most stable, with açaí and pigments rich in acylated anthocyanins exhibiting lower color stability in a temperature-dependent fashion. In the presence of ascorbic acid, acylated anthocyanin sources displayed increased color stability. The authors concluded that açaí demonstrated functional characteristics that would be useful in food and nutraceutical products (J. Agric. Food Chem. 2004;52:1539-45).
Subsequently, some of the same researchers studied the effects of açaí polyphenolics on antiproliferation and induction of apoptosis in HL-60 human leukemia cells. They found that the açaí polyphenols indeed lowered leukemia cell proliferation in vitro, and concluded that açaí is a rich source of bioactive polyphenolic compounds (J. Agric. Food Chem. 2006;54:1,222-9).
Fruit Consumption
On the basis of discoveries that açaí fruit exhibits potent antioxidant capacity in vitro, particularly against superoxide and peroxyl radicals, Schauss et al. set out in 2006 to examine the potential health benefits that açaí fruit might impart. They investigated the antioxidant activity of a standardized freeze-dried açaí fruit pulp/skin powder (OptiAcai) in various assays using several sources of free radicals. The researchers found evidence in support of açaí’s antioxidant capacity against superoxide and peroxyl radicals, including strong scavenging of superoxide and the highest antioxidant activity of any food against the peroxyl radical. Mild activity was noted against the peroxynitrite and hydroxyl radicals.
The investigators also performed an assay to assess the inhibition of free radical development in freshly purified human neutrophils, which revealed that the antioxidants in açaí can, at very low doses, penetrate human cells and exhibit oxygen-quenching activity. Finally, the investigators studied the anti-inflammatory and immune bioactivities of açaí components, and observed that the fruit has the potential to inhibit cyclo-oxygenase (COX)-1 and COX-2 (J. Agric. Food Chem. 2006;54:8,604-10).
In a separate study, Schauss et al. analyzed OptiAcai and identified anthocyanins (chiefly cyanidin 3-glucoside and cyanidin 3-rutinoside), proanthocyanidins (mainly polymers), and other flavonoids (i.e., homoorientin, orientin, isovitexin, scoparin, and taxifolin deoxyhexose, along with several unknown ones) as the primary phytochemical constituents. They also found oleic and palmitic acids to be the prevailing fatty acid components. Resveratrol was identified at trace levels, and 19 amino acids were found, comprising 7.59% of the total weight (J. Agric. Food Chem. 2006;54:8,598-603).
Nutritional Components
In a far-ranging study of açaí pulp culled in the Venezuelan Amazon from two harvests of the year 2005, investigators used spectrophotometric methods to determine the content of polyphenols, tannins, and anthocynanins. The study sought to characterize the polyphenolic content and antioxidant capacity of the fruit, along with other qualities, such as fatty acid content. Antioxidant capacity was analyzed through the 2,2-diphenyl-1-picrylhydrazyl method.
The researchers found that açaí has a high content of lipids, particularly oleic acid, as well as large amounts of protein, ash, and total dietary fiber. The antioxidant capacity was 88%. The investigators concluded that açaí confers significant nutritional value and contains antioxidant constituents such as polyphenols, tannins, and anthocyanins that may render the fruit ripe for industrialization (Arch. Latinoam. Nutr. 2007;57:94-8).
Researchers studying the antioxidant capacities of 11 commercial and noncommercial varieties of açaí fruit pulp against three reactive oxygen species found that all purple açaí samples were potent scavengers of peroxyl radicals, good against peroxynitrite, and poor against hydroxyl radicals, compared with recently studied common European fruit and vegetable juices. One white açaí species displayed low antioxidant capacity against all three reactive oxygen species. Anthocyanins were found to account for only about 10% of the overall antioxidant capacities of the fruit. The investigators concluded that as-yet unidentified constituents of the açaí fruit pulp appeared to be responsible for most of its antioxidant activity (Int. J. Food Sci. Nutr. 2005;56:53-64).
Seed Extracts
The same researchers, along with others, later assessed the antioxidant capacity of methanol and ethanol seed extracts from açaí against peroxyl radicals, peroxynitrite, and hydroxyl radicals. They found that the antioxidant activity of the seed extracts was similar to that of the pulp against peroxyl radicals, and was greater against peroxynitrite and hydroxyl radicals. They also determined that procyanidins contribute significantly to the overall antioxidant capacity of açaí, but as-yet unidentified compounds account for the majority of such activity (J. Agric. Food Chem. 2006;54:4,162-7).
In a recent study, Pacheco-Palencia et al. examined the absorption and antiproliferative effects of açaí pulp extracts and a polyphenolic-enriched oil derived from the fruit pulp of the açaí berry. Investigators ascertained the chemical composition, antioxidant activity, and polyphenolic absorption of phytochemical fractions in a Caco-2 monolayer, in addition to their cytotoxicity in a human colon cancer cell line (HT-29 adenocarcinoma cells).
In general, the study added to the relatively slim body of literature on the bioactive properties, chemical composition, and cellular absorption of açaí polyphenolics. The investigators found that polyphenolic mixtures from the açaí pulp and oil significantly inhibited cell proliferation, and that standardized extracts featured a preponderance of hydroxybenzoic acids, monomeric flavan-3-ols, and procyanidin dimers and trimers (J. Agric. Food Chem. 2008;56:3,593-600).
Phenolic Constituents
Later in 2008, Pacheco-Palencia and two of the same researchers identified for the first time the phenolic constituents in crude oil extracts of the açaí berry. Like the berry, the oil was found to contain high concentrations of phenolic acids (i.e., vanillic acid, syringic acid, p-hydroxybenzoic acid, protocatechuic acid, and ferulic acid), (+)-catechin, and several procyanidin oligomers. The researchers evaluated the thermal stability of the oil during short- and long-term storage for lipid oxidation and phenolic retention, in terms of the effects on antioxidant activity. They found that phenolic acids underwent a 16% loss at 20° or 30° C after 10 weeks of storage, and a 33% loss at 40° C. Procyanidin oligomers showed greater degradation: 23% at 20° C, 39% at 30° C, and 74% at 40° C, in both high- and low-phenolic açaí oils. Phenolic and antioxidant capacity decreased less than 10% during short-term (20 minutes) heating at 150° C and 170° C. The investigators concluded that the high phenolic composition of açaí oil renders it a potentially beneficial food and supplement option, as well as a promising cosmetic agent (J. Agric. Food Chem. 2008;56:4,631-6).
Conclusions
Açaí berry is a popular ingredient in beverages in Central and South America, and its popularity is steadily increasing in North America. It is highly touted for its antioxidant potency. The berry is available in oral supplement form and is advertised as a miraculous weight-loss elixir. It is not often found in topical preparations because of its blue color.
While some of the scant research on açaí is compelling and, indeed, suggests significant antioxidant capacity, there is no evidence to support the use of açaí for weight loss. It is important that practitioners deflate the hype surrounding this botanical and indicate to patients that much more research is necessary to determine whether the antioxidant properties of açaí can be appropriately harnessed in topical or oral skin products.
That said, while I strongly recommend disabusing patients of the notion that açaí will help them lose weight, adding a sizable portion or portions of anthocyanin-containing berries, including açaí, in one’s diet is a healthy choice. As always, it’s best to suggest whole foods – real fruit – as opposed to diluted but sugared fruit drinks.