User login
Surgeons appeal for change to emergency response protocols
WASHINGTON – A first step to limiting loss of life in mass shooting events is to train law enforcement officers to manage hemorrhaging and ultimately to extend that training to all citizens, a collaborative panel of medical, military, and law enforcement leaders has concluded.
Communities must insist that hemostatic control become a core law-enforcement skill. Rapid hemostatic control has now been shown in several analyses to be critical to the survival of mass-shooting victims, panel members said at the annual clinical congress of the American College of Surgeons.

"Tourniquets don’t belong on an ambulance. They belong in a policeman’s pocket," said Dr. Norman E. McSwain, a panel member and medical director of PreHospital Trauma Life Support, New Orleans.
"If you give these [law-enforcement] officers the training and the equipment, they will absolutely utilize it and you will see an immediate return on your investment. They will make you proud," added Dr. Alexander Eastman, another panel member who also is interim chief of trauma at Parkland Memorial Hospital in Dallas and a lieutenant on the Dallas Police Department SWAT team.
The recommendation discussed by panelists at the meeting is just one from a collaborative committee that included, among others, high-level representatives from the Department of Defense (DOD), the Federal Bureau of Investigation (FBI), and the Federal Emergency Management Agency (FEMA).
According to Dr. Lenworth M. Jacobs, trauma director and chief academic officer for Hartford (Conn.) Hospital, the committee grew out of the "profound effect" he experienced in reviewing the autopsies of the 26 Sandy Hook Elementary School shooting victims in Newtown. The number of dead was over three times greater than the number of injured victims in that attack and the medical examiner on the case asked Dr. Jacobs to help determine why the survival rate was so low.
Dr. Jacobs, a regent with the American College of Surgeons (ACS), approached the ACS Board of Regents about an initiative to develop community responses to mass shootings, because he felt "something good had to come out of" that tragic event. In response, the board tasked Dr. Jacobs and Dr. Michael Rotondo, who chairs the ACS committee on trauma, with forming a consortium of leaders to help communities better prepare for the worst in an era when civilians have access to military-grade weaponry and explosive devices.
The committee met in Hartford in April 2013 and drafted the Hartford Consensus, based on the group’s shared belief that community leaders should approach mass-casualty events like the combat situations they closely resemble. "We need to shift the paradigm and draw from the military to improve survivability in the field," said Dr. David Stuart Wade, chief medical officer for the FBI.
The committee turned to the DOD’s protocols for Tactical Combat Casualty Care. Predicated on a tightly integrated response to an attack, including the "buddy system" of attending to a fellow soldier’s wounds, the protocols were found to have helped reduce the incidence of preventable deaths from extremity hemorrhage to just 2.6% over the course of a decade (J. Trauma Acute Care Surg. 2012;73:S431-7).
In a subsequent interview, Dr. McSwain cited another study (J. Emerg. Med. 2011;41:590-7) that influenced the committee, showing that greater survival rates in 499 soldiers wounded in battle were associated with the prehospital application of tourniquets (89% vs. 78% hospital), particularly when applied before the onset of shock (96% vs. 4% after).
The group also created the THREAT response model for civilian agencies, taking the three current discrete stages of mass casualty–event response in America – threat suppression, medical assessment, and transport – and overlapping them so that definitive care starts immediately to minimize casualties. THREAT stands for Threat suppression, Hemorrhage control, Rapid Evacuation, Assess patient, Transport to trauma center.
Referring to how law enforcement, emergency medical personnel, and other municipal agencies currently are segmented, with each agency acting according to its own objectives, command structures, and vocabularies, Dr. Eastman said that the THREAT model "is 100% a new paradigm" that can make all municipal disaster responses, regardless of the nature of the tragedy, more efficient. "The Hartford Consensus is designed to make these groups, that previously might not have worked well together, become more integrated than ever," he said.
The committee met again in July to draft the Hartford Consensus II, a call to action for local communities across the country to adapt the THREAT model to their current mass casualty–event response plans or to develop a TREAT-based plan if they don’t have one already. "Failing to plan is planning to fail," Dr. Rotondo said during the panel presentation, of which he was the comoderator. "Think the unthinkable and begin to think how you would respond," he said, advising the audience to "practice what you’ve planned. Go deep into your resources."
The Hartford Consensus II also recommends that tourniquets and other medical equipment be prepositioned in appropriate public locations, similar to how automatic external defibrillators are, and that the public be taught how to use them.
In response to questions about training the public, including school teachers, how to protect themselves and others from an active shooter, Dr. Jacobs responded that the best thing to do is to "run, hide, fight." He stated that the time necessary to hide was typically only 15 minutes before the situation is under control.
"I can tell you that a military-grade bullet, shot at point-blank range into anybody, but especially little people, is devastating," Dr. Jacobs said. The weapon used in the Sandy Hook shooting was a military-style semiautomatic Bushmaster .223 rifle. "While you don’t really want to take on an AK-47 or a Bushmaster," Dr. Jacobs said that if it were necessary to confront the shooter, "be as aggressive as possible."
Surgeons can play a part in ensuring the Hartford Consensus is adopted nationally, said Dr. Wade, by becoming "energized" and meeting with their respective local authorities to discuss ways to protect their communities.
"Be a good citizen," Dr. Rotondo told the audience, suggesting they communicate with other hospitals in their hometowns and develop strong relationships with their local leaders to help prepare for such a disaster. He also mentioned that the ACS committee on trauma is available to the surgical community to help activate change.
The committee’s next step, said Dr. Jacobs, is to work with the entertainment industry to start incorporating the THREAT model into movies and television shows so that a measured response to the type of violence that has become a fact of American life can be modeled for the citizenry.
WASHINGTON – A first step to limiting loss of life in mass shooting events is to train law enforcement officers to manage hemorrhaging and ultimately to extend that training to all citizens, a collaborative panel of medical, military, and law enforcement leaders has concluded.
Communities must insist that hemostatic control become a core law-enforcement skill. Rapid hemostatic control has now been shown in several analyses to be critical to the survival of mass-shooting victims, panel members said at the annual clinical congress of the American College of Surgeons.
"Tourniquets don’t belong on an ambulance. They belong in a policeman’s pocket," said Dr. Norman E. McSwain, a panel member and medical director of PreHospital Trauma Life Support, New Orleans.
"If you give these [law-enforcement] officers the training and the equipment, they will absolutely utilize it and you will see an immediate return on your investment. They will make you proud," added Dr. Alexander Eastman, another panel member who also is interim chief of trauma at Parkland Memorial Hospital in Dallas and a lieutenant on the Dallas Police Department SWAT team.
The recommendation discussed by panelists at the meeting is just one from a collaborative committee that included, among others, high-level representatives from the Department of Defense (DOD), the Federal Bureau of Investigation (FBI), and the Federal Emergency Management Agency (FEMA).
According to Dr. Lenworth M. Jacobs, trauma director and chief academic officer for Hartford (Conn.) Hospital, the committee grew out of the "profound effect" he experienced in reviewing the autopsies of the 26 Sandy Hook Elementary School shooting victims in Newtown. The number of dead was over three times greater than the number of injured victims in that attack and the medical examiner on the case asked Dr. Jacobs to help determine why the survival rate was so low.
Dr. Jacobs, a regent with the American College of Surgeons (ACS), approached the ACS Board of Regents about an initiative to develop community responses to mass shootings, because he felt "something good had to come out of" that tragic event. In response, the board tasked Dr. Jacobs and Dr. Michael Rotondo, who chairs the ACS committee on trauma, with forming a consortium of leaders to help communities better prepare for the worst in an era when civilians have access to military-grade weaponry and explosive devices.
The committee met in Hartford in April 2013 and drafted the Hartford Consensus, based on the group’s shared belief that community leaders should approach mass-casualty events like the combat situations they closely resemble. "We need to shift the paradigm and draw from the military to improve survivability in the field," said Dr. David Stuart Wade, chief medical officer for the FBI.
The committee turned to the DOD’s protocols for Tactical Combat Casualty Care. Predicated on a tightly integrated response to an attack, including the "buddy system" of attending to a fellow soldier’s wounds, the protocols were found to have helped reduce the incidence of preventable deaths from extremity hemorrhage to just 2.6% over the course of a decade (J. Trauma Acute Care Surg. 2012;73:S431-7).
In a subsequent interview, Dr. McSwain cited another study (J. Emerg. Med. 2011;41:590-7) that influenced the committee, showing that greater survival rates in 499 soldiers wounded in battle were associated with the prehospital application of tourniquets (89% vs. 78% hospital), particularly when applied before the onset of shock (96% vs. 4% after).
The group also created the THREAT response model for civilian agencies, taking the three current discrete stages of mass casualty–event response in America – threat suppression, medical assessment, and transport – and overlapping them so that definitive care starts immediately to minimize casualties. THREAT stands for Threat suppression, Hemorrhage control, Rapid Evacuation, Assess patient, Transport to trauma center.
Referring to how law enforcement, emergency medical personnel, and other municipal agencies currently are segmented, with each agency acting according to its own objectives, command structures, and vocabularies, Dr. Eastman said that the THREAT model "is 100% a new paradigm" that can make all municipal disaster responses, regardless of the nature of the tragedy, more efficient. "The Hartford Consensus is designed to make these groups, that previously might not have worked well together, become more integrated than ever," he said.
The committee met again in July to draft the Hartford Consensus II, a call to action for local communities across the country to adapt the THREAT model to their current mass casualty–event response plans or to develop a TREAT-based plan if they don’t have one already. "Failing to plan is planning to fail," Dr. Rotondo said during the panel presentation, of which he was the comoderator. "Think the unthinkable and begin to think how you would respond," he said, advising the audience to "practice what you’ve planned. Go deep into your resources."
The Hartford Consensus II also recommends that tourniquets and other medical equipment be prepositioned in appropriate public locations, similar to how automatic external defibrillators are, and that the public be taught how to use them.
In response to questions about training the public, including school teachers, how to protect themselves and others from an active shooter, Dr. Jacobs responded that the best thing to do is to "run, hide, fight." He stated that the time necessary to hide was typically only 15 minutes before the situation is under control.
"I can tell you that a military-grade bullet, shot at point-blank range into anybody, but especially little people, is devastating," Dr. Jacobs said. The weapon used in the Sandy Hook shooting was a military-style semiautomatic Bushmaster .223 rifle. "While you don’t really want to take on an AK-47 or a Bushmaster," Dr. Jacobs said that if it were necessary to confront the shooter, "be as aggressive as possible."
Surgeons can play a part in ensuring the Hartford Consensus is adopted nationally, said Dr. Wade, by becoming "energized" and meeting with their respective local authorities to discuss ways to protect their communities.
"Be a good citizen," Dr. Rotondo told the audience, suggesting they communicate with other hospitals in their hometowns and develop strong relationships with their local leaders to help prepare for such a disaster. He also mentioned that the ACS committee on trauma is available to the surgical community to help activate change.
The committee’s next step, said Dr. Jacobs, is to work with the entertainment industry to start incorporating the THREAT model into movies and television shows so that a measured response to the type of violence that has become a fact of American life can be modeled for the citizenry.
WASHINGTON – A first step to limiting loss of life in mass shooting events is to train law enforcement officers to manage hemorrhaging and ultimately to extend that training to all citizens, a collaborative panel of medical, military, and law enforcement leaders has concluded.
Communities must insist that hemostatic control become a core law-enforcement skill. Rapid hemostatic control has now been shown in several analyses to be critical to the survival of mass-shooting victims, panel members said at the annual clinical congress of the American College of Surgeons.
"Tourniquets don’t belong on an ambulance. They belong in a policeman’s pocket," said Dr. Norman E. McSwain, a panel member and medical director of PreHospital Trauma Life Support, New Orleans.
"If you give these [law-enforcement] officers the training and the equipment, they will absolutely utilize it and you will see an immediate return on your investment. They will make you proud," added Dr. Alexander Eastman, another panel member who also is interim chief of trauma at Parkland Memorial Hospital in Dallas and a lieutenant on the Dallas Police Department SWAT team.
The recommendation discussed by panelists at the meeting is just one from a collaborative committee that included, among others, high-level representatives from the Department of Defense (DOD), the Federal Bureau of Investigation (FBI), and the Federal Emergency Management Agency (FEMA).
According to Dr. Lenworth M. Jacobs, trauma director and chief academic officer for Hartford (Conn.) Hospital, the committee grew out of the "profound effect" he experienced in reviewing the autopsies of the 26 Sandy Hook Elementary School shooting victims in Newtown. The number of dead was over three times greater than the number of injured victims in that attack and the medical examiner on the case asked Dr. Jacobs to help determine why the survival rate was so low.
Dr. Jacobs, a regent with the American College of Surgeons (ACS), approached the ACS Board of Regents about an initiative to develop community responses to mass shootings, because he felt "something good had to come out of" that tragic event. In response, the board tasked Dr. Jacobs and Dr. Michael Rotondo, who chairs the ACS committee on trauma, with forming a consortium of leaders to help communities better prepare for the worst in an era when civilians have access to military-grade weaponry and explosive devices.
The committee met in Hartford in April 2013 and drafted the Hartford Consensus, based on the group’s shared belief that community leaders should approach mass-casualty events like the combat situations they closely resemble. "We need to shift the paradigm and draw from the military to improve survivability in the field," said Dr. David Stuart Wade, chief medical officer for the FBI.
The committee turned to the DOD’s protocols for Tactical Combat Casualty Care. Predicated on a tightly integrated response to an attack, including the "buddy system" of attending to a fellow soldier’s wounds, the protocols were found to have helped reduce the incidence of preventable deaths from extremity hemorrhage to just 2.6% over the course of a decade (J. Trauma Acute Care Surg. 2012;73:S431-7).
In a subsequent interview, Dr. McSwain cited another study (J. Emerg. Med. 2011;41:590-7) that influenced the committee, showing that greater survival rates in 499 soldiers wounded in battle were associated with the prehospital application of tourniquets (89% vs. 78% hospital), particularly when applied before the onset of shock (96% vs. 4% after).
The group also created the THREAT response model for civilian agencies, taking the three current discrete stages of mass casualty–event response in America – threat suppression, medical assessment, and transport – and overlapping them so that definitive care starts immediately to minimize casualties. THREAT stands for Threat suppression, Hemorrhage control, Rapid Evacuation, Assess patient, Transport to trauma center.
Referring to how law enforcement, emergency medical personnel, and other municipal agencies currently are segmented, with each agency acting according to its own objectives, command structures, and vocabularies, Dr. Eastman said that the THREAT model "is 100% a new paradigm" that can make all municipal disaster responses, regardless of the nature of the tragedy, more efficient. "The Hartford Consensus is designed to make these groups, that previously might not have worked well together, become more integrated than ever," he said.
The committee met again in July to draft the Hartford Consensus II, a call to action for local communities across the country to adapt the THREAT model to their current mass casualty–event response plans or to develop a TREAT-based plan if they don’t have one already. "Failing to plan is planning to fail," Dr. Rotondo said during the panel presentation, of which he was the comoderator. "Think the unthinkable and begin to think how you would respond," he said, advising the audience to "practice what you’ve planned. Go deep into your resources."
The Hartford Consensus II also recommends that tourniquets and other medical equipment be prepositioned in appropriate public locations, similar to how automatic external defibrillators are, and that the public be taught how to use them.
In response to questions about training the public, including school teachers, how to protect themselves and others from an active shooter, Dr. Jacobs responded that the best thing to do is to "run, hide, fight." He stated that the time necessary to hide was typically only 15 minutes before the situation is under control.
"I can tell you that a military-grade bullet, shot at point-blank range into anybody, but especially little people, is devastating," Dr. Jacobs said. The weapon used in the Sandy Hook shooting was a military-style semiautomatic Bushmaster .223 rifle. "While you don’t really want to take on an AK-47 or a Bushmaster," Dr. Jacobs said that if it were necessary to confront the shooter, "be as aggressive as possible."
Surgeons can play a part in ensuring the Hartford Consensus is adopted nationally, said Dr. Wade, by becoming "energized" and meeting with their respective local authorities to discuss ways to protect their communities.
"Be a good citizen," Dr. Rotondo told the audience, suggesting they communicate with other hospitals in their hometowns and develop strong relationships with their local leaders to help prepare for such a disaster. He also mentioned that the ACS committee on trauma is available to the surgical community to help activate change.
The committee’s next step, said Dr. Jacobs, is to work with the entertainment industry to start incorporating the THREAT model into movies and television shows so that a measured response to the type of violence that has become a fact of American life can be modeled for the citizenry.
AT THE ACS CLINICAL CONGRESS
Major finding: The primary cause of death for mass casualty events is hemorrhaging.
Data source: The Hartford Consensus, published in the American College of Surgeons Bulletin.
Disclosures: The Joint Committee to Create a National Policy to Enhance Survivability from Mass-Casualty Shooting Events sponsored this study. The doctors did not disclose any other relevant disclosures.
ACA exchanges limp along after 2 weeks
The online health insurance marketplaces that are the centerpiece of the Affordable Care Act are off to a rocky start.
In the first 2 weeks of operation, consumers complained about problems using the federally run website – healthcare.gov. They reported trouble getting on the website as well as creating the accounts needed to enroll in health plans.

Health and Human Services (HHS) department officials have acknowledged what they call "glitches" in the system, but said they are working on improving the website as quickly as possible, often through overnight maintenance sessions.
"We have greatly reduced, and even eliminated, wait times at the registration stage, and more people are actively shopping and comparing plans," HHS spokeswoman Joanne Peters said.
The agency is also offering other options for signing up for insurance. Consumers can use the HHS call center (1-800-318-2596) to apply for and enroll over the phone. They can also use the website’s Find Local Help feature to find someone who will work with them in person.
HHS officials cite heavy demand as the major reason for the website’s poor performance. In the first 10 days of operation, the site had 14.6 million unique visitors, according to the agency.
But some technology experts said the problem may go deeper. Now GOP lawmakers in the House and the Senate are launching investigations into how the website was designed and tested, and what problems the administration detected in the months leading up to the Oct. 1 launch.
Rep. Michael Burgess (R-Tex.), who serves on the House Energy and Commerce Committee, said HHS officials need to come to Congress and explain what is happening with the federally run exchanges.
"Members of the administration need to come to the Energy and Commerce Committee and start telling us the truth about this information architecture," Rep. Burgess said. "Taxpayers have spent money – a lot of money – to build these sites. If they’ve been sold a pig in a poke, they need to know."
But while the federally run exchanges have been under fire, the state-run health exchanges have, for the most part, been running more smoothly.
Access Health Connecticut, for example, reported that it had more than 126,000 visitors to its website and has processed almost 2,000 applications. In California, about a million people visited the state’s exchange site in the first 5 days. California consumers submitted 40,000 applications. About 16,000 of those were completed, according to the state.
Officials in Kentucky reported that its exchange site, called Kynect, had 4 million page views in the first 10 days and about 9,000 enrollees. And in Washington state, nearly 10,000 residents had enrolled in either health plans or Medicaid coverage through the state’s exchange.
Currently, there are no data on how many Americans have purchased health insurance through the federally run exchanges. While HHS has released information on traffic to the healthcare.gov site, it will not release enrollment data until November. After that, the administration plans to provide monthly reports.
Individuals have until Dec. 15 to apply for coverage that begins on Jan. 1, 2014. But consumers can continue to enroll in plans through the end of March 2014.
Alicia Ault contributed to this report.
The online health insurance marketplaces that are the centerpiece of the Affordable Care Act are off to a rocky start.
In the first 2 weeks of operation, consumers complained about problems using the federally run website – healthcare.gov. They reported trouble getting on the website as well as creating the accounts needed to enroll in health plans.
Health and Human Services (HHS) department officials have acknowledged what they call "glitches" in the system, but said they are working on improving the website as quickly as possible, often through overnight maintenance sessions.
"We have greatly reduced, and even eliminated, wait times at the registration stage, and more people are actively shopping and comparing plans," HHS spokeswoman Joanne Peters said.
The agency is also offering other options for signing up for insurance. Consumers can use the HHS call center (1-800-318-2596) to apply for and enroll over the phone. They can also use the website’s Find Local Help feature to find someone who will work with them in person.
HHS officials cite heavy demand as the major reason for the website’s poor performance. In the first 10 days of operation, the site had 14.6 million unique visitors, according to the agency.
But some technology experts said the problem may go deeper. Now GOP lawmakers in the House and the Senate are launching investigations into how the website was designed and tested, and what problems the administration detected in the months leading up to the Oct. 1 launch.
Rep. Michael Burgess (R-Tex.), who serves on the House Energy and Commerce Committee, said HHS officials need to come to Congress and explain what is happening with the federally run exchanges.
"Members of the administration need to come to the Energy and Commerce Committee and start telling us the truth about this information architecture," Rep. Burgess said. "Taxpayers have spent money – a lot of money – to build these sites. If they’ve been sold a pig in a poke, they need to know."
But while the federally run exchanges have been under fire, the state-run health exchanges have, for the most part, been running more smoothly.
Access Health Connecticut, for example, reported that it had more than 126,000 visitors to its website and has processed almost 2,000 applications. In California, about a million people visited the state’s exchange site in the first 5 days. California consumers submitted 40,000 applications. About 16,000 of those were completed, according to the state.
Officials in Kentucky reported that its exchange site, called Kynect, had 4 million page views in the first 10 days and about 9,000 enrollees. And in Washington state, nearly 10,000 residents had enrolled in either health plans or Medicaid coverage through the state’s exchange.
Currently, there are no data on how many Americans have purchased health insurance through the federally run exchanges. While HHS has released information on traffic to the healthcare.gov site, it will not release enrollment data until November. After that, the administration plans to provide monthly reports.
Individuals have until Dec. 15 to apply for coverage that begins on Jan. 1, 2014. But consumers can continue to enroll in plans through the end of March 2014.
Alicia Ault contributed to this report.
The online health insurance marketplaces that are the centerpiece of the Affordable Care Act are off to a rocky start.
In the first 2 weeks of operation, consumers complained about problems using the federally run website – healthcare.gov. They reported trouble getting on the website as well as creating the accounts needed to enroll in health plans.
Health and Human Services (HHS) department officials have acknowledged what they call "glitches" in the system, but said they are working on improving the website as quickly as possible, often through overnight maintenance sessions.
"We have greatly reduced, and even eliminated, wait times at the registration stage, and more people are actively shopping and comparing plans," HHS spokeswoman Joanne Peters said.
The agency is also offering other options for signing up for insurance. Consumers can use the HHS call center (1-800-318-2596) to apply for and enroll over the phone. They can also use the website’s Find Local Help feature to find someone who will work with them in person.
HHS officials cite heavy demand as the major reason for the website’s poor performance. In the first 10 days of operation, the site had 14.6 million unique visitors, according to the agency.
But some technology experts said the problem may go deeper. Now GOP lawmakers in the House and the Senate are launching investigations into how the website was designed and tested, and what problems the administration detected in the months leading up to the Oct. 1 launch.
Rep. Michael Burgess (R-Tex.), who serves on the House Energy and Commerce Committee, said HHS officials need to come to Congress and explain what is happening with the federally run exchanges.
"Members of the administration need to come to the Energy and Commerce Committee and start telling us the truth about this information architecture," Rep. Burgess said. "Taxpayers have spent money – a lot of money – to build these sites. If they’ve been sold a pig in a poke, they need to know."
But while the federally run exchanges have been under fire, the state-run health exchanges have, for the most part, been running more smoothly.
Access Health Connecticut, for example, reported that it had more than 126,000 visitors to its website and has processed almost 2,000 applications. In California, about a million people visited the state’s exchange site in the first 5 days. California consumers submitted 40,000 applications. About 16,000 of those were completed, according to the state.
Officials in Kentucky reported that its exchange site, called Kynect, had 4 million page views in the first 10 days and about 9,000 enrollees. And in Washington state, nearly 10,000 residents had enrolled in either health plans or Medicaid coverage through the state’s exchange.
Currently, there are no data on how many Americans have purchased health insurance through the federally run exchanges. While HHS has released information on traffic to the healthcare.gov site, it will not release enrollment data until November. After that, the administration plans to provide monthly reports.
Individuals have until Dec. 15 to apply for coverage that begins on Jan. 1, 2014. But consumers can continue to enroll in plans through the end of March 2014.
Alicia Ault contributed to this report.

CMS two-midnight rule begins, but audits are on hold
The Centers for Medicare and Medicaid Services has delayed through December enforcement of its new two-midnight rule, which went into effect Oct. 1. The rule change is an attempt to clarify admission and medical review criteria for inpatient services, while also addressing the growing trend of patients being held in observation for lengthy periods of time.
The new policy states that when a patient’s stay in the hospital surpasses two midnights, the patient is presumed to be an inpatient. Services for patients staying fewer than two midnights are presumed to be provided in the outpatient setting.

Reactions to the policy from providers have been mixed. Hospitals have fiercely opposed the change, which included across-the-board cuts to inpatient Medicare reimbursements.
"The two-midnight rule makes it pretty transparent," said Dr. Evan Pollack, an internist who practices near Philadelphia and is cochair of the American College of Physicians health and public policy committee in Pennsylvania. "I think this brings the decision making back to the treating physician. If you’re not planning to send the patient home the next day, it’s still your decision to admit him."
The policy also takes aim at shorter inpatient hospital stays and could save the Medicare program money, Dr. Pollack said.
At one hospital, data have shown more patients would lose inpatient status than gain it under the new policy, said Dr. Ann Sheehy, who heads the hospital medicine division at the University of Wisconsin in Madison. Dr. Sheehy and her colleagues recently studied observation – which is technically an outpatient service – as well as inpatient stays, at the University of Wisconsin Hospital from July 2010 through December 2011, and determined how many patients would have been affected by the two-midnight rule. They concluded that the hospital would have lost $14.6 million in reimbursements during that period because many more short hospital stays would have been converted to observation stays, for which payments are significantly less than for inpatient services.
The study counters a CMS projection finding the policy will cost the Medicare program $220 million. The agency has offset the amount by reducing hospital payments elsewhere by 0.2%.
Although the data showed the University of Wisconsin Hospital losing Medicare pay, Dr. Sheehy said that the policy change may cost Medicare ultimately. Physician and patient behavior patterns could change as more become aware of the two-midnight benchmark.
"There will be longer stays that are more expensive," Dr. Sheehy said. "Patients will know about the rule and want to stay for another midnight in order to avoid cost-sharing fees. Some will end up staying two midnights because [providers] fear being audited."
Many patients will fall into a "gray area" when spending 26-47 hours in the hospital, she added. Whether some patients cross the two-midnight threshold will depend on the time of day they arrive at the hospital. Patients arriving at 11 p.m., for example, will have shorter stays before reaching two midnights than will others presenting in the morning.
"When rules look like that, it opens the process up to manipulation," Dr. Sheehy said. "Everyone will look at it and ask, ‘How can we get to two midnights?’"
For now, the CMS has instructed Medicare Administrative Contractors and Recovery Audit Contractors to not target hospital inpatient status during reviews for claims with dates of service between Oct. 1 and Dec. 31, according to an agency frequently asked questions page. But the CMS will allow contractors to audit 10-25 cases per hospital during that time for educational purposes.
"We feel it’s giving them a running start," Dr. Sheehy said. Recovery Audit Contractors "will know which hospitals are having problems and go after them in January."
The rule also has faced opposition from Congress. In September, a bipartisan group of more than 100 House members sent a letter to CMS Administrator Marilyn Tavenner urging a 6-month delay to the rule. Patients may face higher out-of-pocket costs while hospitals also have not had enough time to educate providers about the rule.
"We are concerned that hospitals in our districts could be undercompensated for providing medically necessary services that do not meet the new criteria spelled out by the CMS and face administrative challenges in complying with new requirements," the letter stated.
This story was updated 10/15/2013.
The Centers for Medicare and Medicaid Services has delayed through December enforcement of its new two-midnight rule, which went into effect Oct. 1. The rule change is an attempt to clarify admission and medical review criteria for inpatient services, while also addressing the growing trend of patients being held in observation for lengthy periods of time.
The new policy states that when a patient’s stay in the hospital surpasses two midnights, the patient is presumed to be an inpatient. Services for patients staying fewer than two midnights are presumed to be provided in the outpatient setting.
Reactions to the policy from providers have been mixed. Hospitals have fiercely opposed the change, which included across-the-board cuts to inpatient Medicare reimbursements.
"The two-midnight rule makes it pretty transparent," said Dr. Evan Pollack, an internist who practices near Philadelphia and is cochair of the American College of Physicians health and public policy committee in Pennsylvania. "I think this brings the decision making back to the treating physician. If you’re not planning to send the patient home the next day, it’s still your decision to admit him."
The policy also takes aim at shorter inpatient hospital stays and could save the Medicare program money, Dr. Pollack said.
At one hospital, data have shown more patients would lose inpatient status than gain it under the new policy, said Dr. Ann Sheehy, who heads the hospital medicine division at the University of Wisconsin in Madison. Dr. Sheehy and her colleagues recently studied observation – which is technically an outpatient service – as well as inpatient stays, at the University of Wisconsin Hospital from July 2010 through December 2011, and determined how many patients would have been affected by the two-midnight rule. They concluded that the hospital would have lost $14.6 million in reimbursements during that period because many more short hospital stays would have been converted to observation stays, for which payments are significantly less than for inpatient services.
The study counters a CMS projection finding the policy will cost the Medicare program $220 million. The agency has offset the amount by reducing hospital payments elsewhere by 0.2%.
Although the data showed the University of Wisconsin Hospital losing Medicare pay, Dr. Sheehy said that the policy change may cost Medicare ultimately. Physician and patient behavior patterns could change as more become aware of the two-midnight benchmark.
"There will be longer stays that are more expensive," Dr. Sheehy said. "Patients will know about the rule and want to stay for another midnight in order to avoid cost-sharing fees. Some will end up staying two midnights because [providers] fear being audited."
Many patients will fall into a "gray area" when spending 26-47 hours in the hospital, she added. Whether some patients cross the two-midnight threshold will depend on the time of day they arrive at the hospital. Patients arriving at 11 p.m., for example, will have shorter stays before reaching two midnights than will others presenting in the morning.
"When rules look like that, it opens the process up to manipulation," Dr. Sheehy said. "Everyone will look at it and ask, ‘How can we get to two midnights?’"
For now, the CMS has instructed Medicare Administrative Contractors and Recovery Audit Contractors to not target hospital inpatient status during reviews for claims with dates of service between Oct. 1 and Dec. 31, according to an agency frequently asked questions page. But the CMS will allow contractors to audit 10-25 cases per hospital during that time for educational purposes.
"We feel it’s giving them a running start," Dr. Sheehy said. Recovery Audit Contractors "will know which hospitals are having problems and go after them in January."
The rule also has faced opposition from Congress. In September, a bipartisan group of more than 100 House members sent a letter to CMS Administrator Marilyn Tavenner urging a 6-month delay to the rule. Patients may face higher out-of-pocket costs while hospitals also have not had enough time to educate providers about the rule.
"We are concerned that hospitals in our districts could be undercompensated for providing medically necessary services that do not meet the new criteria spelled out by the CMS and face administrative challenges in complying with new requirements," the letter stated.
This story was updated 10/15/2013.
The Centers for Medicare and Medicaid Services has delayed through December enforcement of its new two-midnight rule, which went into effect Oct. 1. The rule change is an attempt to clarify admission and medical review criteria for inpatient services, while also addressing the growing trend of patients being held in observation for lengthy periods of time.
The new policy states that when a patient’s stay in the hospital surpasses two midnights, the patient is presumed to be an inpatient. Services for patients staying fewer than two midnights are presumed to be provided in the outpatient setting.
Reactions to the policy from providers have been mixed. Hospitals have fiercely opposed the change, which included across-the-board cuts to inpatient Medicare reimbursements.
"The two-midnight rule makes it pretty transparent," said Dr. Evan Pollack, an internist who practices near Philadelphia and is cochair of the American College of Physicians health and public policy committee in Pennsylvania. "I think this brings the decision making back to the treating physician. If you’re not planning to send the patient home the next day, it’s still your decision to admit him."
The policy also takes aim at shorter inpatient hospital stays and could save the Medicare program money, Dr. Pollack said.
At one hospital, data have shown more patients would lose inpatient status than gain it under the new policy, said Dr. Ann Sheehy, who heads the hospital medicine division at the University of Wisconsin in Madison. Dr. Sheehy and her colleagues recently studied observation – which is technically an outpatient service – as well as inpatient stays, at the University of Wisconsin Hospital from July 2010 through December 2011, and determined how many patients would have been affected by the two-midnight rule. They concluded that the hospital would have lost $14.6 million in reimbursements during that period because many more short hospital stays would have been converted to observation stays, for which payments are significantly less than for inpatient services.
The study counters a CMS projection finding the policy will cost the Medicare program $220 million. The agency has offset the amount by reducing hospital payments elsewhere by 0.2%.
Although the data showed the University of Wisconsin Hospital losing Medicare pay, Dr. Sheehy said that the policy change may cost Medicare ultimately. Physician and patient behavior patterns could change as more become aware of the two-midnight benchmark.
"There will be longer stays that are more expensive," Dr. Sheehy said. "Patients will know about the rule and want to stay for another midnight in order to avoid cost-sharing fees. Some will end up staying two midnights because [providers] fear being audited."
Many patients will fall into a "gray area" when spending 26-47 hours in the hospital, she added. Whether some patients cross the two-midnight threshold will depend on the time of day they arrive at the hospital. Patients arriving at 11 p.m., for example, will have shorter stays before reaching two midnights than will others presenting in the morning.
"When rules look like that, it opens the process up to manipulation," Dr. Sheehy said. "Everyone will look at it and ask, ‘How can we get to two midnights?’"
For now, the CMS has instructed Medicare Administrative Contractors and Recovery Audit Contractors to not target hospital inpatient status during reviews for claims with dates of service between Oct. 1 and Dec. 31, according to an agency frequently asked questions page. But the CMS will allow contractors to audit 10-25 cases per hospital during that time for educational purposes.
"We feel it’s giving them a running start," Dr. Sheehy said. Recovery Audit Contractors "will know which hospitals are having problems and go after them in January."
The rule also has faced opposition from Congress. In September, a bipartisan group of more than 100 House members sent a letter to CMS Administrator Marilyn Tavenner urging a 6-month delay to the rule. Patients may face higher out-of-pocket costs while hospitals also have not had enough time to educate providers about the rule.
"We are concerned that hospitals in our districts could be undercompensated for providing medically necessary services that do not meet the new criteria spelled out by the CMS and face administrative challenges in complying with new requirements," the letter stated.
This story was updated 10/15/2013.

Surgeons call for change in mass casualty response
WASHINGTON – In the aftermath of the Sandy Hook Elementary School shootings, Dr. Lenworth Jacobs, a regent of the American College of Surgeons (ACS) and vice president of academic affairs at Hartford (Conn.) Hospital, was called to examine the autopsies of the victims. What he saw affected him so profoundly that he asked the ACS how surgeons might help communities to respond to such chaotic tragedies and minimize the enormous loss of life that occurs.
The resulting Hartford Consensus – a document created by members of the ACS, the FBI, and various law enforcement and military organizations that calls for a new paradigm in emergency response – was presented at the annual clinical congress of the American College of Surgeons.
WASHINGTON – In the aftermath of the Sandy Hook Elementary School shootings, Dr. Lenworth Jacobs, a regent of the American College of Surgeons (ACS) and vice president of academic affairs at Hartford (Conn.) Hospital, was called to examine the autopsies of the victims. What he saw affected him so profoundly that he asked the ACS how surgeons might help communities to respond to such chaotic tragedies and minimize the enormous loss of life that occurs.
The resulting Hartford Consensus – a document created by members of the ACS, the FBI, and various law enforcement and military organizations that calls for a new paradigm in emergency response – was presented at the annual clinical congress of the American College of Surgeons.
WASHINGTON – In the aftermath of the Sandy Hook Elementary School shootings, Dr. Lenworth Jacobs, a regent of the American College of Surgeons (ACS) and vice president of academic affairs at Hartford (Conn.) Hospital, was called to examine the autopsies of the victims. What he saw affected him so profoundly that he asked the ACS how surgeons might help communities to respond to such chaotic tragedies and minimize the enormous loss of life that occurs.
The resulting Hartford Consensus – a document created by members of the ACS, the FBI, and various law enforcement and military organizations that calls for a new paradigm in emergency response – was presented at the annual clinical congress of the American College of Surgeons.
AT THE ACS CLINICAL CONGRESS

What you need to know about health insurance exchanges
As the state and federal health insurance exchanges get up and running, physicians will face questions from patients about eligibility, enrollment, and how the marketplaces work.
The dizzying array of plans, costs, subsidies, and more could easily overwhelm even those who have been closely following the implementation of the Affordable Care Act, which established the exchanges.
Physicians don’t have to go it alone. Several organizations – including the American Medical Association, the American College of Physicians, and the American Academy of Family Physicians – have set up websites to help doctors help their patients through the open enrollment period (Oct. 1, 2013, to March 31, 2014).

"We’re going to give facts, figures, and information to doctors so they have it in their offices, to help them and their staff navigate this period of time," Dr. Ardis Dee Hoven, AMA president, said in an interview.
Dr. Reid Blackwelder, president of the AAFP, agreed that physicians did not have to be the only ones helping patients. Family physicians, in particular, "often feel we’re supposed to have the answer for everything, and that’s not really possible," he said in an interview.
Knowing about the exchanges, whether one agrees with the premise of the ACA or not, is important to patient care, Dr. Blackwelder said. "Even if physicians are not happy with [the law], they need to help patients recognize this is an option available to them to help them with their health care costs."
Dr. Charles Cutler, chairman of the ACP Board of Regents, said, "personally, this is a conversation I want to have with the patient." He said that a physician is most knowledgeable about that patient’s medical needs and can help guide what kind of coverage to choose.
There will be much to navigate. To a large extent, what doctors tell patients about the exchanges will depend on where they practice.
Each state has chosen its own pathway for an exchange as well as whether it will expand Medicaid eligibility, which impacts how, and how many, patients will receive coverage.
Under the ACA, Medicaid coverage is available to all Americans who earn up to 133% of the federal poverty level ($14,856 for an individual and $30,657 for a family of four). Twenty-four states have said they will make Medicaid available at that level or higher, 21 won’t expand, and 5 are uncommitted.
That means a lot of people will make too little to buy coverage on an exchange and too much to get Medicaid. According to a recent study by the Commonwealth Fund, in states that aren’t expanding, about 42% of adults who were uninsured for any time over the past 2 years won’t have access to new coverage.
At press time, 16 states and the District of Columbia had created their own exchanges, 26 states were letting the federal government run the exchange, and 7 states were operating partnership with the feds. In Utah, the state has opened an exchange for small businesses, but the federal government runs the exchange for individuals.
There are a lot of questions about how many patients will enroll through exchanges and how diligently they will stick with the new insurance plans.
*In the first week the exchanges were open, some 8 million people visited the federal exchanges' healthcare.gov website. The Department of Health and Human Services (HHS) was not able to say how many of them had actually applied for insurance coverage. The number of hits and applications on the state exchange sites varied, but in most states, the initial amount of traffic was massive.
Families USA has estimated that as many as 26 million Americans who make between 100% and 400% of the federal poverty level (between $24,000 and $94,000 for a family of four) will be eligible for tax credits to buy insurance.
Although individuals will be required to have health insurance beginning in January, some will choose not to. Those who opt out in 2014 will pay a penalty to the federal government with their 2015 tax return. The penalty will be either 1% of their income or $95, whichever is higher. By 2016, that amount rises to 2.5% of income or $695 per person, with exceptions for low-income individuals.
The government is also cutting enrollees a break on premium payments. As long as they have paid at least one premium, they’ll have a 90-day grace period to pay the next one. If they don’t pay, the insurer can drop the patient from the plan. But, if they’ve received services during that 90-day period, the insurer is not obligated to pay. That doesn't sit well with many physicians.
"It makes no sense at all – the patient is protected but the rest of the system isn’t and that’s not how it’s supposed to work," the AMA’s Dr. Hoven said.
Much remains to be seen with how the exchanges work, including what kind of clout they will have in negotiating with physicians. Many predict that the exchanges will grow as forces to be reckoned with in the insurance market.
Eventually, they will be able to set quality standards, bar plans that don’t meet certain standards, and limit the sale of insurance outside exchanges, according to Henry Aaron of the Brookings Institution and Kevin W. Lucia of Georgetown University (N. Engl. J. Med. doi:10.1056/NEJMp1308032).
Vermont and Washington, D.C., already prohibit sales of individual policies outside their exchanges.
The insurance exchanges also are expected to expand their reach. They will start offering plans to employers with 51 to 100 workers in 2016, and could be adding larger employers in 2017. Over time, "we believe that the exchanges will be seen as a means for promoting a competitive insurance market in which consumers can make rational decisions, and that they will become an instrument that can reshape the health care delivery system," wrote Mr. Aaron and Mr. Lucia.

Exchanges will vary from state to state
*The Commonwealth Fund has mapped it out, with links to each state's exchange website, details on how each exchange is governed, who serves on the board of directors, and whether and when quality data have to be reported.
*Not every insurer in every state is participating. In some states, only one insurer is offering plans. A list of every insurer and all the plans being offered in every state can be found at The Centers for Medicare and Medicaid Services website. There is also information on insurers participating in the federally-run exchanges at www.healthcare.gov.
Each state exchange is using different ways to get patients enrolled. For the most part, physicians are not being asked to get involved personally; however, the department of Health and Human Services has enlisted physician organizations – such as the AMA, the AAFP, the ACP, and the American Academy of Pediatrics – as "Champions for Coverage," to help spread the word.
Plans offered through the exchanges will have to cover a set of essential benefits. All Medicaid plans have to cover those services as well.
Exchange plans can’t deny coverage or charge higher premiums for preexisting conditions, and premiums can’t be different for men and women. Insurers can still charge more as people age, except in Vermont and New York, which prohibit age-rating by state law.
Plans will be able to offer five levels of coverage, ranging from the least protective and least expensive to the most protective and most expensive: catastrophic, bronze, silver, gold, and platinum. Not every state requires that every level of coverage be offered.
Premiums will be based on income and age. An individual with an income below $45,960 and a family of four with an income below $94,200 will be eligible for some kind of assistance. Tax credits are given directly to the insurance company so that the enrollee doesn’t have to pay the higher premium up front. Out-of-pocket costs will also be limited, depending on income.
The Kaiser Family Foundation has estimated that older Americans, those between 60-65 years, are likely to benefit the most from subsidies.
On Twitter @aliciaault
*Updated 10/9/13
As the state and federal health insurance exchanges get up and running, physicians will face questions from patients about eligibility, enrollment, and how the marketplaces work.
The dizzying array of plans, costs, subsidies, and more could easily overwhelm even those who have been closely following the implementation of the Affordable Care Act, which established the exchanges.
Physicians don’t have to go it alone. Several organizations – including the American Medical Association, the American College of Physicians, and the American Academy of Family Physicians – have set up websites to help doctors help their patients through the open enrollment period (Oct. 1, 2013, to March 31, 2014).
"We’re going to give facts, figures, and information to doctors so they have it in their offices, to help them and their staff navigate this period of time," Dr. Ardis Dee Hoven, AMA president, said in an interview.
Dr. Reid Blackwelder, president of the AAFP, agreed that physicians did not have to be the only ones helping patients. Family physicians, in particular, "often feel we’re supposed to have the answer for everything, and that’s not really possible," he said in an interview.
Knowing about the exchanges, whether one agrees with the premise of the ACA or not, is important to patient care, Dr. Blackwelder said. "Even if physicians are not happy with [the law], they need to help patients recognize this is an option available to them to help them with their health care costs."
Dr. Charles Cutler, chairman of the ACP Board of Regents, said, "personally, this is a conversation I want to have with the patient." He said that a physician is most knowledgeable about that patient’s medical needs and can help guide what kind of coverage to choose.
There will be much to navigate. To a large extent, what doctors tell patients about the exchanges will depend on where they practice.
Each state has chosen its own pathway for an exchange as well as whether it will expand Medicaid eligibility, which impacts how, and how many, patients will receive coverage.
Under the ACA, Medicaid coverage is available to all Americans who earn up to 133% of the federal poverty level ($14,856 for an individual and $30,657 for a family of four). Twenty-four states have said they will make Medicaid available at that level or higher, 21 won’t expand, and 5 are uncommitted.
That means a lot of people will make too little to buy coverage on an exchange and too much to get Medicaid. According to a recent study by the Commonwealth Fund, in states that aren’t expanding, about 42% of adults who were uninsured for any time over the past 2 years won’t have access to new coverage.
At press time, 16 states and the District of Columbia had created their own exchanges, 26 states were letting the federal government run the exchange, and 7 states were operating partnership with the feds. In Utah, the state has opened an exchange for small businesses, but the federal government runs the exchange for individuals.
There are a lot of questions about how many patients will enroll through exchanges and how diligently they will stick with the new insurance plans.
*In the first week the exchanges were open, some 8 million people visited the federal exchanges' healthcare.gov website. The Department of Health and Human Services (HHS) was not able to say how many of them had actually applied for insurance coverage. The number of hits and applications on the state exchange sites varied, but in most states, the initial amount of traffic was massive.
Families USA has estimated that as many as 26 million Americans who make between 100% and 400% of the federal poverty level (between $24,000 and $94,000 for a family of four) will be eligible for tax credits to buy insurance.
Although individuals will be required to have health insurance beginning in January, some will choose not to. Those who opt out in 2014 will pay a penalty to the federal government with their 2015 tax return. The penalty will be either 1% of their income or $95, whichever is higher. By 2016, that amount rises to 2.5% of income or $695 per person, with exceptions for low-income individuals.
The government is also cutting enrollees a break on premium payments. As long as they have paid at least one premium, they’ll have a 90-day grace period to pay the next one. If they don’t pay, the insurer can drop the patient from the plan. But, if they’ve received services during that 90-day period, the insurer is not obligated to pay. That doesn't sit well with many physicians.
"It makes no sense at all – the patient is protected but the rest of the system isn’t and that’s not how it’s supposed to work," the AMA’s Dr. Hoven said.
Much remains to be seen with how the exchanges work, including what kind of clout they will have in negotiating with physicians. Many predict that the exchanges will grow as forces to be reckoned with in the insurance market.
Eventually, they will be able to set quality standards, bar plans that don’t meet certain standards, and limit the sale of insurance outside exchanges, according to Henry Aaron of the Brookings Institution and Kevin W. Lucia of Georgetown University (N. Engl. J. Med. doi:10.1056/NEJMp1308032).
Vermont and Washington, D.C., already prohibit sales of individual policies outside their exchanges.
The insurance exchanges also are expected to expand their reach. They will start offering plans to employers with 51 to 100 workers in 2016, and could be adding larger employers in 2017. Over time, "we believe that the exchanges will be seen as a means for promoting a competitive insurance market in which consumers can make rational decisions, and that they will become an instrument that can reshape the health care delivery system," wrote Mr. Aaron and Mr. Lucia.
Exchanges will vary from state to state
*The Commonwealth Fund has mapped it out, with links to each state's exchange website, details on how each exchange is governed, who serves on the board of directors, and whether and when quality data have to be reported.
*Not every insurer in every state is participating. In some states, only one insurer is offering plans. A list of every insurer and all the plans being offered in every state can be found at The Centers for Medicare and Medicaid Services website. There is also information on insurers participating in the federally-run exchanges at www.healthcare.gov.
Each state exchange is using different ways to get patients enrolled. For the most part, physicians are not being asked to get involved personally; however, the department of Health and Human Services has enlisted physician organizations – such as the AMA, the AAFP, the ACP, and the American Academy of Pediatrics – as "Champions for Coverage," to help spread the word.
Plans offered through the exchanges will have to cover a set of essential benefits. All Medicaid plans have to cover those services as well.
Exchange plans can’t deny coverage or charge higher premiums for preexisting conditions, and premiums can’t be different for men and women. Insurers can still charge more as people age, except in Vermont and New York, which prohibit age-rating by state law.
Plans will be able to offer five levels of coverage, ranging from the least protective and least expensive to the most protective and most expensive: catastrophic, bronze, silver, gold, and platinum. Not every state requires that every level of coverage be offered.
Premiums will be based on income and age. An individual with an income below $45,960 and a family of four with an income below $94,200 will be eligible for some kind of assistance. Tax credits are given directly to the insurance company so that the enrollee doesn’t have to pay the higher premium up front. Out-of-pocket costs will also be limited, depending on income.
The Kaiser Family Foundation has estimated that older Americans, those between 60-65 years, are likely to benefit the most from subsidies.
On Twitter @aliciaault
*Updated 10/9/13
As the state and federal health insurance exchanges get up and running, physicians will face questions from patients about eligibility, enrollment, and how the marketplaces work.
The dizzying array of plans, costs, subsidies, and more could easily overwhelm even those who have been closely following the implementation of the Affordable Care Act, which established the exchanges.
Physicians don’t have to go it alone. Several organizations – including the American Medical Association, the American College of Physicians, and the American Academy of Family Physicians – have set up websites to help doctors help their patients through the open enrollment period (Oct. 1, 2013, to March 31, 2014).
"We’re going to give facts, figures, and information to doctors so they have it in their offices, to help them and their staff navigate this period of time," Dr. Ardis Dee Hoven, AMA president, said in an interview.
Dr. Reid Blackwelder, president of the AAFP, agreed that physicians did not have to be the only ones helping patients. Family physicians, in particular, "often feel we’re supposed to have the answer for everything, and that’s not really possible," he said in an interview.
Knowing about the exchanges, whether one agrees with the premise of the ACA or not, is important to patient care, Dr. Blackwelder said. "Even if physicians are not happy with [the law], they need to help patients recognize this is an option available to them to help them with their health care costs."
Dr. Charles Cutler, chairman of the ACP Board of Regents, said, "personally, this is a conversation I want to have with the patient." He said that a physician is most knowledgeable about that patient’s medical needs and can help guide what kind of coverage to choose.
There will be much to navigate. To a large extent, what doctors tell patients about the exchanges will depend on where they practice.
Each state has chosen its own pathway for an exchange as well as whether it will expand Medicaid eligibility, which impacts how, and how many, patients will receive coverage.
Under the ACA, Medicaid coverage is available to all Americans who earn up to 133% of the federal poverty level ($14,856 for an individual and $30,657 for a family of four). Twenty-four states have said they will make Medicaid available at that level or higher, 21 won’t expand, and 5 are uncommitted.
That means a lot of people will make too little to buy coverage on an exchange and too much to get Medicaid. According to a recent study by the Commonwealth Fund, in states that aren’t expanding, about 42% of adults who were uninsured for any time over the past 2 years won’t have access to new coverage.
At press time, 16 states and the District of Columbia had created their own exchanges, 26 states were letting the federal government run the exchange, and 7 states were operating partnership with the feds. In Utah, the state has opened an exchange for small businesses, but the federal government runs the exchange for individuals.
There are a lot of questions about how many patients will enroll through exchanges and how diligently they will stick with the new insurance plans.
*In the first week the exchanges were open, some 8 million people visited the federal exchanges' healthcare.gov website. The Department of Health and Human Services (HHS) was not able to say how many of them had actually applied for insurance coverage. The number of hits and applications on the state exchange sites varied, but in most states, the initial amount of traffic was massive.
Families USA has estimated that as many as 26 million Americans who make between 100% and 400% of the federal poverty level (between $24,000 and $94,000 for a family of four) will be eligible for tax credits to buy insurance.
Although individuals will be required to have health insurance beginning in January, some will choose not to. Those who opt out in 2014 will pay a penalty to the federal government with their 2015 tax return. The penalty will be either 1% of their income or $95, whichever is higher. By 2016, that amount rises to 2.5% of income or $695 per person, with exceptions for low-income individuals.
The government is also cutting enrollees a break on premium payments. As long as they have paid at least one premium, they’ll have a 90-day grace period to pay the next one. If they don’t pay, the insurer can drop the patient from the plan. But, if they’ve received services during that 90-day period, the insurer is not obligated to pay. That doesn't sit well with many physicians.
"It makes no sense at all – the patient is protected but the rest of the system isn’t and that’s not how it’s supposed to work," the AMA’s Dr. Hoven said.
Much remains to be seen with how the exchanges work, including what kind of clout they will have in negotiating with physicians. Many predict that the exchanges will grow as forces to be reckoned with in the insurance market.
Eventually, they will be able to set quality standards, bar plans that don’t meet certain standards, and limit the sale of insurance outside exchanges, according to Henry Aaron of the Brookings Institution and Kevin W. Lucia of Georgetown University (N. Engl. J. Med. doi:10.1056/NEJMp1308032).
Vermont and Washington, D.C., already prohibit sales of individual policies outside their exchanges.
The insurance exchanges also are expected to expand their reach. They will start offering plans to employers with 51 to 100 workers in 2016, and could be adding larger employers in 2017. Over time, "we believe that the exchanges will be seen as a means for promoting a competitive insurance market in which consumers can make rational decisions, and that they will become an instrument that can reshape the health care delivery system," wrote Mr. Aaron and Mr. Lucia.
Exchanges will vary from state to state
*The Commonwealth Fund has mapped it out, with links to each state's exchange website, details on how each exchange is governed, who serves on the board of directors, and whether and when quality data have to be reported.
*Not every insurer in every state is participating. In some states, only one insurer is offering plans. A list of every insurer and all the plans being offered in every state can be found at The Centers for Medicare and Medicaid Services website. There is also information on insurers participating in the federally-run exchanges at www.healthcare.gov.
Each state exchange is using different ways to get patients enrolled. For the most part, physicians are not being asked to get involved personally; however, the department of Health and Human Services has enlisted physician organizations – such as the AMA, the AAFP, the ACP, and the American Academy of Pediatrics – as "Champions for Coverage," to help spread the word.
Plans offered through the exchanges will have to cover a set of essential benefits. All Medicaid plans have to cover those services as well.
Exchange plans can’t deny coverage or charge higher premiums for preexisting conditions, and premiums can’t be different for men and women. Insurers can still charge more as people age, except in Vermont and New York, which prohibit age-rating by state law.
Plans will be able to offer five levels of coverage, ranging from the least protective and least expensive to the most protective and most expensive: catastrophic, bronze, silver, gold, and platinum. Not every state requires that every level of coverage be offered.
Premiums will be based on income and age. An individual with an income below $45,960 and a family of four with an income below $94,200 will be eligible for some kind of assistance. Tax credits are given directly to the insurance company so that the enrollee doesn’t have to pay the higher premium up front. Out-of-pocket costs will also be limited, depending on income.
The Kaiser Family Foundation has estimated that older Americans, those between 60-65 years, are likely to benefit the most from subsidies.
On Twitter @aliciaault
*Updated 10/9/13
The Why and How Data Mining Is Applicable to Hospital Medicine
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
MGMA Surveys Make Hospitalists' Productivity Hard to Assess


The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
New Rules for Value-Based Purchasing, Readmission Penalties, Admissions


The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
How To Avoid Medicare Denials for Critical-Care Billing

Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
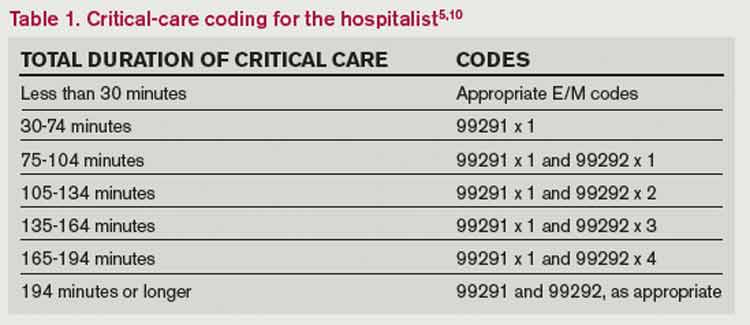
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Feds Extend HIPAA Obligations, Violation Penalties
Key Takeaways for Hospitalist Groups

- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.