User login
Handoff intervention cuts medical errors in hospitalized children
An intervention to improve communication and provide more structure to patient "handoffs" among residents dramatically reduced medical errors and preventable adverse events in hospitalized children, according to a report published online Dec. 3 in JAMA.
In a single-center study comparing patient handoffs during the 3-month period before the intervention was implemented against the 3-month period afterward, the rate of medical errors dropped by 46%, from 33.8/100 admissions to 18.3/100. Preventable adverse events similarly decreased, from 3.3/100 admissions to 1.5/100, said Dr. Amy J. Starmer of Boston Children’s Hospital and Harvard Medical School, Boston, and her associates.
"Given the increasing frequency of handoffs in hospitals following resident work-hour reductions and the high frequency with which miscommunications lead to serious medical errors," widespread use of such handoff interventions could have a substantial impact on patient health, they noted.

The investigators performed the before-and-after comparison on two inpatient pediatric units within the same hospital, which included 1,255 children requiring general, subspecialty, and complex-care services during the study period. A total of 42 first-year and third-year residents cared for these patients and participated in the intervention.
Before the intervention, patient handoffs had no standardized structure and involved the use of a printed document that included basic patient information but was not integrated into the electronic health record system.
For the intervention, the residents attended a 2-hour training session in which they discussed best practices for verbal and written handoffs. Handoff procedures were structured to occur on a team basis rather than individually, in a dedicated physical space that was private and quiet, and which were periodically overseen by a chief resident or attending physician.
One of the pediatric units also began using a computerized rather than printed handoff document that was integrated into the electronic health record system and included much more detailed, and regularly updated, patient information.
Overall, 350 medical errors and adverse events were tabulated during the study period, including 77% related to medications, 8.3% related to medical procedures, 4.3% related to diagnostic tests, 3.4% related to other therapies, and 3.7% related to falls.
In particular, the rate of errors that could have had important clinical consequences dropped from 7.3/100 to 3.3/100 admissions, and the rate of errors that could have had such consequences but were prevented decreased from 15/100 to 8.3/100 admissions.
As expected, the rate of nonpreventable errors remained constant (JAMA 2013 Dec. 3 [doi:10.1001/jama.2013.281961]).
Forty of the written handoff documents were reviewed for the presence of 14 important items of patient information. After the intervention, the number of key data omissions was significantly reduced.
"Written handoffs were more comprehensive after the interventions, and verbal handoffs were more likely to occur in a quiet, private location," Dr. Starmer and her associates said.
This study was supported by the Controlled Risk Insurance Company Risk Management Foundation, Boston Children’s Hospital Program for Patient Safety and Quality Research, the Agency for Healthcare Research and Quality, the Child Health Corporation of America, and the National Institutes of Health. No financial conflicts of interest were reported.
Although this study had numerous strengths, its results should be considered preliminary until they can be replicated; further study is still needed to confirm the findings, better characterize and refine the key elements of the handoff intervention, and establish whether the benefits are sustained beyond 3 months, said Dr. Leora I. Horwitz.
Meanwhile, other methods of improving safety at patient handoffs should be considered. "There is now promising work in automatically aggregating data to characterize patients’ clinical condition, identify early deterioration, or prospectively identify patients who have not yet received standard of care, potentially enabling clinicians to convert the existing static handoff process to a real-time dynamic reassessment of clinical condition and patient care," she said.
Dr. Leora I. Horwitz is in the department of internal medicine at Yale University and at the Center for Outcomes Research and Evaluation at Yale–New Haven (Conn.) Hospital. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Starmer’s report (JAMA 2013;310:2255-6).
Although this study had numerous strengths, its results should be considered preliminary until they can be replicated; further study is still needed to confirm the findings, better characterize and refine the key elements of the handoff intervention, and establish whether the benefits are sustained beyond 3 months, said Dr. Leora I. Horwitz.
Meanwhile, other methods of improving safety at patient handoffs should be considered. "There is now promising work in automatically aggregating data to characterize patients’ clinical condition, identify early deterioration, or prospectively identify patients who have not yet received standard of care, potentially enabling clinicians to convert the existing static handoff process to a real-time dynamic reassessment of clinical condition and patient care," she said.
Dr. Leora I. Horwitz is in the department of internal medicine at Yale University and at the Center for Outcomes Research and Evaluation at Yale–New Haven (Conn.) Hospital. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Starmer’s report (JAMA 2013;310:2255-6).
Although this study had numerous strengths, its results should be considered preliminary until they can be replicated; further study is still needed to confirm the findings, better characterize and refine the key elements of the handoff intervention, and establish whether the benefits are sustained beyond 3 months, said Dr. Leora I. Horwitz.
Meanwhile, other methods of improving safety at patient handoffs should be considered. "There is now promising work in automatically aggregating data to characterize patients’ clinical condition, identify early deterioration, or prospectively identify patients who have not yet received standard of care, potentially enabling clinicians to convert the existing static handoff process to a real-time dynamic reassessment of clinical condition and patient care," she said.
Dr. Leora I. Horwitz is in the department of internal medicine at Yale University and at the Center for Outcomes Research and Evaluation at Yale–New Haven (Conn.) Hospital. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Starmer’s report (JAMA 2013;310:2255-6).
An intervention to improve communication and provide more structure to patient "handoffs" among residents dramatically reduced medical errors and preventable adverse events in hospitalized children, according to a report published online Dec. 3 in JAMA.
In a single-center study comparing patient handoffs during the 3-month period before the intervention was implemented against the 3-month period afterward, the rate of medical errors dropped by 46%, from 33.8/100 admissions to 18.3/100. Preventable adverse events similarly decreased, from 3.3/100 admissions to 1.5/100, said Dr. Amy J. Starmer of Boston Children’s Hospital and Harvard Medical School, Boston, and her associates.
"Given the increasing frequency of handoffs in hospitals following resident work-hour reductions and the high frequency with which miscommunications lead to serious medical errors," widespread use of such handoff interventions could have a substantial impact on patient health, they noted.
The investigators performed the before-and-after comparison on two inpatient pediatric units within the same hospital, which included 1,255 children requiring general, subspecialty, and complex-care services during the study period. A total of 42 first-year and third-year residents cared for these patients and participated in the intervention.
Before the intervention, patient handoffs had no standardized structure and involved the use of a printed document that included basic patient information but was not integrated into the electronic health record system.
For the intervention, the residents attended a 2-hour training session in which they discussed best practices for verbal and written handoffs. Handoff procedures were structured to occur on a team basis rather than individually, in a dedicated physical space that was private and quiet, and which were periodically overseen by a chief resident or attending physician.
One of the pediatric units also began using a computerized rather than printed handoff document that was integrated into the electronic health record system and included much more detailed, and regularly updated, patient information.
Overall, 350 medical errors and adverse events were tabulated during the study period, including 77% related to medications, 8.3% related to medical procedures, 4.3% related to diagnostic tests, 3.4% related to other therapies, and 3.7% related to falls.
In particular, the rate of errors that could have had important clinical consequences dropped from 7.3/100 to 3.3/100 admissions, and the rate of errors that could have had such consequences but were prevented decreased from 15/100 to 8.3/100 admissions.
As expected, the rate of nonpreventable errors remained constant (JAMA 2013 Dec. 3 [doi:10.1001/jama.2013.281961]).
Forty of the written handoff documents were reviewed for the presence of 14 important items of patient information. After the intervention, the number of key data omissions was significantly reduced.
"Written handoffs were more comprehensive after the interventions, and verbal handoffs were more likely to occur in a quiet, private location," Dr. Starmer and her associates said.
This study was supported by the Controlled Risk Insurance Company Risk Management Foundation, Boston Children’s Hospital Program for Patient Safety and Quality Research, the Agency for Healthcare Research and Quality, the Child Health Corporation of America, and the National Institutes of Health. No financial conflicts of interest were reported.
An intervention to improve communication and provide more structure to patient "handoffs" among residents dramatically reduced medical errors and preventable adverse events in hospitalized children, according to a report published online Dec. 3 in JAMA.
In a single-center study comparing patient handoffs during the 3-month period before the intervention was implemented against the 3-month period afterward, the rate of medical errors dropped by 46%, from 33.8/100 admissions to 18.3/100. Preventable adverse events similarly decreased, from 3.3/100 admissions to 1.5/100, said Dr. Amy J. Starmer of Boston Children’s Hospital and Harvard Medical School, Boston, and her associates.
"Given the increasing frequency of handoffs in hospitals following resident work-hour reductions and the high frequency with which miscommunications lead to serious medical errors," widespread use of such handoff interventions could have a substantial impact on patient health, they noted.
The investigators performed the before-and-after comparison on two inpatient pediatric units within the same hospital, which included 1,255 children requiring general, subspecialty, and complex-care services during the study period. A total of 42 first-year and third-year residents cared for these patients and participated in the intervention.
Before the intervention, patient handoffs had no standardized structure and involved the use of a printed document that included basic patient information but was not integrated into the electronic health record system.
For the intervention, the residents attended a 2-hour training session in which they discussed best practices for verbal and written handoffs. Handoff procedures were structured to occur on a team basis rather than individually, in a dedicated physical space that was private and quiet, and which were periodically overseen by a chief resident or attending physician.
One of the pediatric units also began using a computerized rather than printed handoff document that was integrated into the electronic health record system and included much more detailed, and regularly updated, patient information.
Overall, 350 medical errors and adverse events were tabulated during the study period, including 77% related to medications, 8.3% related to medical procedures, 4.3% related to diagnostic tests, 3.4% related to other therapies, and 3.7% related to falls.
In particular, the rate of errors that could have had important clinical consequences dropped from 7.3/100 to 3.3/100 admissions, and the rate of errors that could have had such consequences but were prevented decreased from 15/100 to 8.3/100 admissions.
As expected, the rate of nonpreventable errors remained constant (JAMA 2013 Dec. 3 [doi:10.1001/jama.2013.281961]).
Forty of the written handoff documents were reviewed for the presence of 14 important items of patient information. After the intervention, the number of key data omissions was significantly reduced.
"Written handoffs were more comprehensive after the interventions, and verbal handoffs were more likely to occur in a quiet, private location," Dr. Starmer and her associates said.
This study was supported by the Controlled Risk Insurance Company Risk Management Foundation, Boston Children’s Hospital Program for Patient Safety and Quality Research, the Agency for Healthcare Research and Quality, the Child Health Corporation of America, and the National Institutes of Health. No financial conflicts of interest were reported.
FROM JAMA
Major finding: The rate of medical errors decreased from 33.8/100 to 18.3/100 admissions after the handoff intervention was implemented, and the rate of preventable adverse events decreased from 3.3/100 to 1.5/100 admissions.
Data source: A prospective intervention study comparing medical errors during the 3 months before and after implementation of an intervention to standardize patient handoffs between resident physicians.
Disclosures: This study was supported by the Controlled Risk Insurance Company Risk Management Foundation, Boston Children’s Hospital Program for Patient Safety and Quality Research, the Agency for Healthcare Research and Quality, the Child Health Corporation of America, and the National Institutes of Health. No financial conflicts of interest were reported.

Medicaid enrollment up 15% in October due to ACA
Medicaid applications were up more than 15% in October in states that are expanding their Medicaid programs under the Affordable Care Act.
The preliminary data, released by the Health and Human Services department Dec. 3, shows that while Americans have been slow to enroll in private health plans through the online exchanges, many low-income individuals are getting access to insurance coverage through the Medicaid program.
As of October, 23 states and the District of Columbia had expanded their Medicaid programs to include individuals with incomes up to 133% of the federal poverty level. That coverage will begin on Jan. 1, 2014. Two more states – Ohio and Michigan – recently announced plans to expand their programs but have not yet begun enrollment.
During October, the number of applications to Medicaid programs and the Children’s Health Insurance Program (CHIP) were up 15.5% overall in states expanding their eligibility, compared with the average monthly number of applications received from July through September. The figures include both individuals who are newly eligible under the ACA and those who were eligible previously. Comparatively, states that opted not to expand their Medicaid programs saw an increase in applications of 4.1%.
Across all states, more than 2.4 million applications were submitted to state Medicaid and CHIP agencies during October. More than 1.4 million individuals were deemed eligible for the programs.
The figures released by the HHS provide a partial picture of Medicaid enrollment under the ACA. Individuals also are applying to the program through the online insurance exchanges. From Oct. 1 to Nov. 2, 396,261 were determined to be eligible for Medicaid or CHIP after applying for insurance through either a state-based exchange or healthcare.gov, according to the HHS.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
Medicaid applications were up more than 15% in October in states that are expanding their Medicaid programs under the Affordable Care Act.
The preliminary data, released by the Health and Human Services department Dec. 3, shows that while Americans have been slow to enroll in private health plans through the online exchanges, many low-income individuals are getting access to insurance coverage through the Medicaid program.
As of October, 23 states and the District of Columbia had expanded their Medicaid programs to include individuals with incomes up to 133% of the federal poverty level. That coverage will begin on Jan. 1, 2014. Two more states – Ohio and Michigan – recently announced plans to expand their programs but have not yet begun enrollment.
During October, the number of applications to Medicaid programs and the Children’s Health Insurance Program (CHIP) were up 15.5% overall in states expanding their eligibility, compared with the average monthly number of applications received from July through September. The figures include both individuals who are newly eligible under the ACA and those who were eligible previously. Comparatively, states that opted not to expand their Medicaid programs saw an increase in applications of 4.1%.
Across all states, more than 2.4 million applications were submitted to state Medicaid and CHIP agencies during October. More than 1.4 million individuals were deemed eligible for the programs.
The figures released by the HHS provide a partial picture of Medicaid enrollment under the ACA. Individuals also are applying to the program through the online insurance exchanges. From Oct. 1 to Nov. 2, 396,261 were determined to be eligible for Medicaid or CHIP after applying for insurance through either a state-based exchange or healthcare.gov, according to the HHS.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
Medicaid applications were up more than 15% in October in states that are expanding their Medicaid programs under the Affordable Care Act.
The preliminary data, released by the Health and Human Services department Dec. 3, shows that while Americans have been slow to enroll in private health plans through the online exchanges, many low-income individuals are getting access to insurance coverage through the Medicaid program.
As of October, 23 states and the District of Columbia had expanded their Medicaid programs to include individuals with incomes up to 133% of the federal poverty level. That coverage will begin on Jan. 1, 2014. Two more states – Ohio and Michigan – recently announced plans to expand their programs but have not yet begun enrollment.
During October, the number of applications to Medicaid programs and the Children’s Health Insurance Program (CHIP) were up 15.5% overall in states expanding their eligibility, compared with the average monthly number of applications received from July through September. The figures include both individuals who are newly eligible under the ACA and those who were eligible previously. Comparatively, states that opted not to expand their Medicaid programs saw an increase in applications of 4.1%.
Across all states, more than 2.4 million applications were submitted to state Medicaid and CHIP agencies during October. More than 1.4 million individuals were deemed eligible for the programs.
The figures released by the HHS provide a partial picture of Medicaid enrollment under the ACA. Individuals also are applying to the program through the online insurance exchanges. From Oct. 1 to Nov. 2, 396,261 were determined to be eligible for Medicaid or CHIP after applying for insurance through either a state-based exchange or healthcare.gov, according to the HHS.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
Physician networks, formularies now viewable on healthcare.gov
Visitors to healthcare.gov now can view physician networks, deductibles, copayments, and formularies as "window shoppers" before they sign up for a health insurance plan – information that both doctors and patients have been seeking.
The new functionality was announced Dec. 2 by the Centers for Medicare and Medicaid Services.
At a Nov. 26 White House meeting on Affordable Care Act concerns, representatives of several physician organizations voiced concern that patients could not see whether their physician or preferred hospital was in a plan’s network during the shopping process, according to Bob Doherty, senior vice president for governmental affairs and public policy for the American College of Physicians.

Mr. Doherty, who attended the White House meeting, said that physician groups also told administration officials that patients and physicians needed information on formularies. Pharmaceuticals – at least one medication from each therapeutic class – must be covered by health exchange plans as an essential health benefit.
"But that doesn’t mean necessarily that your own particular drugs are on that plan’s formulary," Mr. Doherty said. The physician groups argued that more transparency was needed.
The same is true for provider networks. "From a consumer point of view, you may decide that if you can get a plan with lower premium and a deductible you can afford, you may choose to forgo your doctor or hospital," Mr. Doherty said. "That’s okay as long as you make an informed choice," he said, adding that without the ability to see networks, it was impossible to make such a choice.
Now, the networks are visible, but the question is whether the lists are up-to-date, he said. Physician groups also want "more transparency from the insurance industry, disclosing decisions on why they include or don’t include doctors in their networks and why they delist" physicians, Mr. Doherty said.
Physicians are getting help from Rep. Darrell Issa (R-Calif.), chairman of the House Oversight and Government Reform Committee. Rep. Issa sent a letter to 15 insurance companies on Nov. 29, asking for documents "related to the reevaluation of provider networks and payment rates, as well as communications with the administration about potential changes to health plans limiting or changing health care access," according to a statement.
"Even among the individuals fortunate enough to keep their plans, many Americans are finding that access to their preferred doctor(s) is being abruptly terminated," wrote Rep. Issa, adding, "Some health insurers have acknowledged that they are slashing provider payment rates for plans offered on Obamacare exchanges."
The letter requested a response from the insurers by Dec. 13.
aault@frontlinemedcom.com
On Twitter @aliciaault
Visitors to healthcare.gov now can view physician networks, deductibles, copayments, and formularies as "window shoppers" before they sign up for a health insurance plan – information that both doctors and patients have been seeking.
The new functionality was announced Dec. 2 by the Centers for Medicare and Medicaid Services.
At a Nov. 26 White House meeting on Affordable Care Act concerns, representatives of several physician organizations voiced concern that patients could not see whether their physician or preferred hospital was in a plan’s network during the shopping process, according to Bob Doherty, senior vice president for governmental affairs and public policy for the American College of Physicians.
Mr. Doherty, who attended the White House meeting, said that physician groups also told administration officials that patients and physicians needed information on formularies. Pharmaceuticals – at least one medication from each therapeutic class – must be covered by health exchange plans as an essential health benefit.
"But that doesn’t mean necessarily that your own particular drugs are on that plan’s formulary," Mr. Doherty said. The physician groups argued that more transparency was needed.
The same is true for provider networks. "From a consumer point of view, you may decide that if you can get a plan with lower premium and a deductible you can afford, you may choose to forgo your doctor or hospital," Mr. Doherty said. "That’s okay as long as you make an informed choice," he said, adding that without the ability to see networks, it was impossible to make such a choice.
Now, the networks are visible, but the question is whether the lists are up-to-date, he said. Physician groups also want "more transparency from the insurance industry, disclosing decisions on why they include or don’t include doctors in their networks and why they delist" physicians, Mr. Doherty said.
Physicians are getting help from Rep. Darrell Issa (R-Calif.), chairman of the House Oversight and Government Reform Committee. Rep. Issa sent a letter to 15 insurance companies on Nov. 29, asking for documents "related to the reevaluation of provider networks and payment rates, as well as communications with the administration about potential changes to health plans limiting or changing health care access," according to a statement.
"Even among the individuals fortunate enough to keep their plans, many Americans are finding that access to their preferred doctor(s) is being abruptly terminated," wrote Rep. Issa, adding, "Some health insurers have acknowledged that they are slashing provider payment rates for plans offered on Obamacare exchanges."
The letter requested a response from the insurers by Dec. 13.
aault@frontlinemedcom.com
On Twitter @aliciaault
Visitors to healthcare.gov now can view physician networks, deductibles, copayments, and formularies as "window shoppers" before they sign up for a health insurance plan – information that both doctors and patients have been seeking.
The new functionality was announced Dec. 2 by the Centers for Medicare and Medicaid Services.
At a Nov. 26 White House meeting on Affordable Care Act concerns, representatives of several physician organizations voiced concern that patients could not see whether their physician or preferred hospital was in a plan’s network during the shopping process, according to Bob Doherty, senior vice president for governmental affairs and public policy for the American College of Physicians.
Mr. Doherty, who attended the White House meeting, said that physician groups also told administration officials that patients and physicians needed information on formularies. Pharmaceuticals – at least one medication from each therapeutic class – must be covered by health exchange plans as an essential health benefit.
"But that doesn’t mean necessarily that your own particular drugs are on that plan’s formulary," Mr. Doherty said. The physician groups argued that more transparency was needed.
The same is true for provider networks. "From a consumer point of view, you may decide that if you can get a plan with lower premium and a deductible you can afford, you may choose to forgo your doctor or hospital," Mr. Doherty said. "That’s okay as long as you make an informed choice," he said, adding that without the ability to see networks, it was impossible to make such a choice.
Now, the networks are visible, but the question is whether the lists are up-to-date, he said. Physician groups also want "more transparency from the insurance industry, disclosing decisions on why they include or don’t include doctors in their networks and why they delist" physicians, Mr. Doherty said.
Physicians are getting help from Rep. Darrell Issa (R-Calif.), chairman of the House Oversight and Government Reform Committee. Rep. Issa sent a letter to 15 insurance companies on Nov. 29, asking for documents "related to the reevaluation of provider networks and payment rates, as well as communications with the administration about potential changes to health plans limiting or changing health care access," according to a statement.
"Even among the individuals fortunate enough to keep their plans, many Americans are finding that access to their preferred doctor(s) is being abruptly terminated," wrote Rep. Issa, adding, "Some health insurers have acknowledged that they are slashing provider payment rates for plans offered on Obamacare exchanges."
The letter requested a response from the insurers by Dec. 13.
aault@frontlinemedcom.com
On Twitter @aliciaault

Medicare finalizes plan for non-face-to-face payments
Starting in 2015, primary care physicians will get paid for some of the chronic care management work they do outside of office visits.
As part of the 2014 Medicare physician fee schedule final rule, officials at the Centers for Medicare and Medicaid Services (CMS) finalized plans to begin paying physicians separately for services such as development and revision of a care plan, communication with other treating providers, review of lab results, and adjustment of medications.
The agency established a new G-code that physicians can use to bill for non-face-to-face care management services for Medicare patients with two or more significant chronic conditions. The code, which will apply to 20 minutes or more of chronic care management services during a 30-day period, takes effect on Jan. 1, 2015.
Physicians who wish to use the new code will have to meet a series of requirements laid out by the CMS, including providing 24-7 access, coordination with home- and community-based service providers, and patient access to the practice through secure messaging or patient portals.
The new codes are part of a recent move by Medicare officials to emphasize primary care and to pay for services that happen outside of the traditional office visit. In 2012, the CMS established codes for transitional care management services for patients moving from a hospital or skilled nursing facility to home. Those codes, which took effect this year, included payment for some non-face-to-face activities.
The news was greeted as a step in the right direction by the American Academy of Family Physicians.
"Elderly and disabled patients have complex, multiple, and chronic health conditions that require the whole-person medical attention available only through primary care physicians," Dr. Reid Blackwelder, AAFP president, said in a statement. "Placing appropriate value on the primary care services these patients require and establishing codes for chronic care management are important steps in meeting their needs."
The final fee schedule rule also provides a new estimate for how deep the Sustainable Growth Rate (SGR) formula cut will be in 2014. The across-the-board cut, which will take effect on Jan. 1 unless Congress takes action to avert it, will be 20.1%, down from an earlier estimate of 24.4%.
The somewhat smaller cut was not seen as good news by physician groups, which are increasingly fed up with the SGR formula.
The American Medical Association urged Congress to act quickly, not on a temporary patch, but on a permanent repeal of the SGR formula.
"The clock is ticking," Dr. Ardis Dee Hoven, AMA president, said in a statement. "At stake are innovations that would make Medicare more cost effective for current and future generations of seniors. These innovations are not possible if physicians are worried about drastic cuts to Medicare rates that have remained almost flat since 2001, while the cost of caring for patients has gone up by 25 percent."
The 2014 fee schedule also continues to phase in the Physician Value-Based Payment Modifier program. The program links Medicare payments to performance on cost and quality of care. The first payment adjustments will come in January 2015 for practices of 100 or more providers. In January 2016, the program will extend to groups with 10 or more eligible professionals. The CMS estimates that nearly 60% of physicians will be paid under the value-based payment modifier program in 2016. The remainder of physicians will be included in the program starting in January 2017.
But the CMS urged physicians to plan ahead. While payments won’t be affected until those dates, the performance measurement will occur earlier. For instance, for small group practices that will enter the program in 2017, the performance year is 2015. Physicians in small practices should use 2014 as a "practice year" and report to the Physician Quality Reporting System (PQRS) program so that they will be ready in 2015, according to the CMS.
The fee schedule will be published in the Federal Register on Dec. 10. The deadline for public comments on the rule is Jan. 27, 2014.
Starting in 2015, primary care physicians will get paid for some of the chronic care management work they do outside of office visits.
As part of the 2014 Medicare physician fee schedule final rule, officials at the Centers for Medicare and Medicaid Services (CMS) finalized plans to begin paying physicians separately for services such as development and revision of a care plan, communication with other treating providers, review of lab results, and adjustment of medications.
The agency established a new G-code that physicians can use to bill for non-face-to-face care management services for Medicare patients with two or more significant chronic conditions. The code, which will apply to 20 minutes or more of chronic care management services during a 30-day period, takes effect on Jan. 1, 2015.
Physicians who wish to use the new code will have to meet a series of requirements laid out by the CMS, including providing 24-7 access, coordination with home- and community-based service providers, and patient access to the practice through secure messaging or patient portals.
The new codes are part of a recent move by Medicare officials to emphasize primary care and to pay for services that happen outside of the traditional office visit. In 2012, the CMS established codes for transitional care management services for patients moving from a hospital or skilled nursing facility to home. Those codes, which took effect this year, included payment for some non-face-to-face activities.
The news was greeted as a step in the right direction by the American Academy of Family Physicians.
"Elderly and disabled patients have complex, multiple, and chronic health conditions that require the whole-person medical attention available only through primary care physicians," Dr. Reid Blackwelder, AAFP president, said in a statement. "Placing appropriate value on the primary care services these patients require and establishing codes for chronic care management are important steps in meeting their needs."
The final fee schedule rule also provides a new estimate for how deep the Sustainable Growth Rate (SGR) formula cut will be in 2014. The across-the-board cut, which will take effect on Jan. 1 unless Congress takes action to avert it, will be 20.1%, down from an earlier estimate of 24.4%.
The somewhat smaller cut was not seen as good news by physician groups, which are increasingly fed up with the SGR formula.
The American Medical Association urged Congress to act quickly, not on a temporary patch, but on a permanent repeal of the SGR formula.
"The clock is ticking," Dr. Ardis Dee Hoven, AMA president, said in a statement. "At stake are innovations that would make Medicare more cost effective for current and future generations of seniors. These innovations are not possible if physicians are worried about drastic cuts to Medicare rates that have remained almost flat since 2001, while the cost of caring for patients has gone up by 25 percent."
The 2014 fee schedule also continues to phase in the Physician Value-Based Payment Modifier program. The program links Medicare payments to performance on cost and quality of care. The first payment adjustments will come in January 2015 for practices of 100 or more providers. In January 2016, the program will extend to groups with 10 or more eligible professionals. The CMS estimates that nearly 60% of physicians will be paid under the value-based payment modifier program in 2016. The remainder of physicians will be included in the program starting in January 2017.
But the CMS urged physicians to plan ahead. While payments won’t be affected until those dates, the performance measurement will occur earlier. For instance, for small group practices that will enter the program in 2017, the performance year is 2015. Physicians in small practices should use 2014 as a "practice year" and report to the Physician Quality Reporting System (PQRS) program so that they will be ready in 2015, according to the CMS.
The fee schedule will be published in the Federal Register on Dec. 10. The deadline for public comments on the rule is Jan. 27, 2014.
Starting in 2015, primary care physicians will get paid for some of the chronic care management work they do outside of office visits.
As part of the 2014 Medicare physician fee schedule final rule, officials at the Centers for Medicare and Medicaid Services (CMS) finalized plans to begin paying physicians separately for services such as development and revision of a care plan, communication with other treating providers, review of lab results, and adjustment of medications.
The agency established a new G-code that physicians can use to bill for non-face-to-face care management services for Medicare patients with two or more significant chronic conditions. The code, which will apply to 20 minutes or more of chronic care management services during a 30-day period, takes effect on Jan. 1, 2015.
Physicians who wish to use the new code will have to meet a series of requirements laid out by the CMS, including providing 24-7 access, coordination with home- and community-based service providers, and patient access to the practice through secure messaging or patient portals.
The new codes are part of a recent move by Medicare officials to emphasize primary care and to pay for services that happen outside of the traditional office visit. In 2012, the CMS established codes for transitional care management services for patients moving from a hospital or skilled nursing facility to home. Those codes, which took effect this year, included payment for some non-face-to-face activities.
The news was greeted as a step in the right direction by the American Academy of Family Physicians.
"Elderly and disabled patients have complex, multiple, and chronic health conditions that require the whole-person medical attention available only through primary care physicians," Dr. Reid Blackwelder, AAFP president, said in a statement. "Placing appropriate value on the primary care services these patients require and establishing codes for chronic care management are important steps in meeting their needs."
The final fee schedule rule also provides a new estimate for how deep the Sustainable Growth Rate (SGR) formula cut will be in 2014. The across-the-board cut, which will take effect on Jan. 1 unless Congress takes action to avert it, will be 20.1%, down from an earlier estimate of 24.4%.
The somewhat smaller cut was not seen as good news by physician groups, which are increasingly fed up with the SGR formula.
The American Medical Association urged Congress to act quickly, not on a temporary patch, but on a permanent repeal of the SGR formula.
"The clock is ticking," Dr. Ardis Dee Hoven, AMA president, said in a statement. "At stake are innovations that would make Medicare more cost effective for current and future generations of seniors. These innovations are not possible if physicians are worried about drastic cuts to Medicare rates that have remained almost flat since 2001, while the cost of caring for patients has gone up by 25 percent."
The 2014 fee schedule also continues to phase in the Physician Value-Based Payment Modifier program. The program links Medicare payments to performance on cost and quality of care. The first payment adjustments will come in January 2015 for practices of 100 or more providers. In January 2016, the program will extend to groups with 10 or more eligible professionals. The CMS estimates that nearly 60% of physicians will be paid under the value-based payment modifier program in 2016. The remainder of physicians will be included in the program starting in January 2017.
But the CMS urged physicians to plan ahead. While payments won’t be affected until those dates, the performance measurement will occur earlier. For instance, for small group practices that will enter the program in 2017, the performance year is 2015. Physicians in small practices should use 2014 as a "practice year" and report to the Physician Quality Reporting System (PQRS) program so that they will be ready in 2015, according to the CMS.
The fee schedule will be published in the Federal Register on Dec. 10. The deadline for public comments on the rule is Jan. 27, 2014.
Feds make significant progress on HealthCare.gov
The federal insurance website, HealthCare.gov, is now faster and more reliable, but more work still needs to be done, according to an assessment by the Centers for Medicare and Medicaid Services.
About 80% of users are now able to complete the online application and enrollment process, meeting the goal set by the agency to get the website running smoothly for the majority of users by the end of November, Julie Bataille, director of the office of communications at CMS, said at a Dec. 1 press briefing.
CMS officials reported that they have improved the website’s response times, decreased the per-page error rate, and improved system stability and capacity. The improved performance is a "night and day" difference from how the site operated during October, according to Jeff Zients, a consultant brought in to improve the website.
Response time to user requests has been reduced from about 8 seconds in late October to 1 second on Nov. 30, Ms. Bataille reported. Similar reductions have been made to the error rate (percentage of per page system time outs and failures). In early October, the error rate was more than 6%; on Nov. 30, it was less than 1%.
Site stability also has improved, Ms. Bataille said, meaning that HealthCare.gov is "up" more than 90% of the time now – excluding scheduled maintenance – in comparison to 42.9% of the time in early November.
Federal officials said they are hopeful that the site will be able to handle a surge in users in December as the enrollment deadline approaches for consumers who want insurance coverage on Jan. 1. They have increased capacity on the site to about 50,000 simultaneous users and more than 800,000 users per day.
Mr. Zients said that, even with the improvements, the website may not have enough capacity to handle some peak user loads. As a result, CMS has put in place a queuing system that will serve users in order. The system will e-mail those users who could not get through and invite them back to the site when it’s not as busy.
Mr. Zients said that he expects consumers will continue to encounter glitches. However, the issues should be resolved much quicker now that they will have a rapid response team monitoring and responding to problems 24 hours a day.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
The federal insurance website, HealthCare.gov, is now faster and more reliable, but more work still needs to be done, according to an assessment by the Centers for Medicare and Medicaid Services.
About 80% of users are now able to complete the online application and enrollment process, meeting the goal set by the agency to get the website running smoothly for the majority of users by the end of November, Julie Bataille, director of the office of communications at CMS, said at a Dec. 1 press briefing.
CMS officials reported that they have improved the website’s response times, decreased the per-page error rate, and improved system stability and capacity. The improved performance is a "night and day" difference from how the site operated during October, according to Jeff Zients, a consultant brought in to improve the website.
Response time to user requests has been reduced from about 8 seconds in late October to 1 second on Nov. 30, Ms. Bataille reported. Similar reductions have been made to the error rate (percentage of per page system time outs and failures). In early October, the error rate was more than 6%; on Nov. 30, it was less than 1%.
Site stability also has improved, Ms. Bataille said, meaning that HealthCare.gov is "up" more than 90% of the time now – excluding scheduled maintenance – in comparison to 42.9% of the time in early November.
Federal officials said they are hopeful that the site will be able to handle a surge in users in December as the enrollment deadline approaches for consumers who want insurance coverage on Jan. 1. They have increased capacity on the site to about 50,000 simultaneous users and more than 800,000 users per day.
Mr. Zients said that, even with the improvements, the website may not have enough capacity to handle some peak user loads. As a result, CMS has put in place a queuing system that will serve users in order. The system will e-mail those users who could not get through and invite them back to the site when it’s not as busy.
Mr. Zients said that he expects consumers will continue to encounter glitches. However, the issues should be resolved much quicker now that they will have a rapid response team monitoring and responding to problems 24 hours a day.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
The federal insurance website, HealthCare.gov, is now faster and more reliable, but more work still needs to be done, according to an assessment by the Centers for Medicare and Medicaid Services.
About 80% of users are now able to complete the online application and enrollment process, meeting the goal set by the agency to get the website running smoothly for the majority of users by the end of November, Julie Bataille, director of the office of communications at CMS, said at a Dec. 1 press briefing.
CMS officials reported that they have improved the website’s response times, decreased the per-page error rate, and improved system stability and capacity. The improved performance is a "night and day" difference from how the site operated during October, according to Jeff Zients, a consultant brought in to improve the website.
Response time to user requests has been reduced from about 8 seconds in late October to 1 second on Nov. 30, Ms. Bataille reported. Similar reductions have been made to the error rate (percentage of per page system time outs and failures). In early October, the error rate was more than 6%; on Nov. 30, it was less than 1%.
Site stability also has improved, Ms. Bataille said, meaning that HealthCare.gov is "up" more than 90% of the time now – excluding scheduled maintenance – in comparison to 42.9% of the time in early November.
Federal officials said they are hopeful that the site will be able to handle a surge in users in December as the enrollment deadline approaches for consumers who want insurance coverage on Jan. 1. They have increased capacity on the site to about 50,000 simultaneous users and more than 800,000 users per day.
Mr. Zients said that, even with the improvements, the website may not have enough capacity to handle some peak user loads. As a result, CMS has put in place a queuing system that will serve users in order. The system will e-mail those users who could not get through and invite them back to the site when it’s not as busy.
Mr. Zients said that he expects consumers will continue to encounter glitches. However, the issues should be resolved much quicker now that they will have a rapid response team monitoring and responding to problems 24 hours a day.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
What To Do When the Hospitalist Group Leader Refuses to See Patients

My hospitalist group, which has nine employees, is hospital-employed in a small Midwest town. We use the traditional seven-on and seven-off rotation and hire locum tenens to fill schedule gaps, as we have a couple of MDs who recently left the group. A few of us are concerned because our “boss,” who controls the schedule, does not put himself in rotation regularly. Instead, he puts locum or part-timers on the schedule, even on weeks when he is available. We all know that the hospital is paying him extra to take care of administrative work, and that it costs more for the hospital to pay part-time/locums. In your experience, is this a common occurrence? Should we be upset? Lastly, should we bring this issue to administration, because many of us think that they are not aware this is happening.
–Mismatched in the Midwest
Dr. Hospitalist responds:
Opinions vary when it comes to the amount of clinical time hospitalist leaders should devote to their groups. As we have become more involved in the administrative aspects of the hospital, there are increasing demands placed on directors. Along with increased administrative demands comes the desire of many of these physician-leaders to remain adept in the practice of hospital medicine. Without a strong clinical connection and familiarity with what the others experience day to day, the group leader risks losing credibility and whatever leverage the title might offer.
Many groups have devised formulas based on the number of members in the group to help them derive a “fair” amount of administrative time to allow the director. For example, for every five full-time equivalents (FTEs) on staff, the director receives 0.1 FTE in admin time; so, for a group of 25 members, the director would get 0.5 admin time. The remainder of time would be clinical, but again, how that clinical time is managed is also highly variable.
This seems like a reasonable formula to me, because those with larger programs will have larger hospitals, more people to manage, and more personalities to deal with. The potential rewards and job satisfaction are also greater. (Another potential scheduling issue: Does the group leader “fall right into” the rotation or only work the services with light census or teaching services in an academic institution?)
Some groups that work the traditional seven-on/seven-off schedule have allowed the hospitalist physician-leader to work Monday through Friday and carry a smaller census (10-12). This allows the leader to be in the hospital during those critical times when most administrative duties are fulfilled, while also allowing for a mechanism to place overflow patients on those high census days—as long as it is a rare occurrence. He or she should also occasionally work all the different shifts (nocturnist, admitter, teams, and so on) to best understand the group’s opportunities for improvement and its challenges.
There are likely as many iterations of how to devise a fair division of time as there are hospitalist groups, but, most importantly, the days of getting someone to volunteer to be a hospitalist director without some form of compensation are long gone. In most programs, the job has become much more complex.
Many believe it is a conflict of interest for the group leader to prepare the schedule. There is too much room for perceived favoritism or mistreatment by the members when the schedule doesn’t work in everyone’s favor (which it never will). There are proprietary programs on the market that allow for easy and reliable scheduling; they also remove the potential for bias. In a group as small as yours, an astute administrative assistant or associate director can be entrusted with the schedule.
With regard to speaking up, you say a “few” in your group are concerned, so I assume more than one but still a small number of your group has expressed some dissatisfaction. There may be other members with similar sentiments, so it is important to have a discussion with all the group members and solicit their opinions. Instead of approaching the administrators with your concerns, I suggest you and your colleagues have an open and candid discussion with your group leader. After the discussion, if you still remain dissatisfied with the director’s level of clinical involvement, you are left with several choices:
- Approach hospital administration and see if they approve of how your director is carrying out his clinical responsibilities. Be prepared for the director to find out.
- Continue to do your job and let this issue rest.
- Start looking for another job. If the situation really bothers you, I favor the latter!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
My hospitalist group, which has nine employees, is hospital-employed in a small Midwest town. We use the traditional seven-on and seven-off rotation and hire locum tenens to fill schedule gaps, as we have a couple of MDs who recently left the group. A few of us are concerned because our “boss,” who controls the schedule, does not put himself in rotation regularly. Instead, he puts locum or part-timers on the schedule, even on weeks when he is available. We all know that the hospital is paying him extra to take care of administrative work, and that it costs more for the hospital to pay part-time/locums. In your experience, is this a common occurrence? Should we be upset? Lastly, should we bring this issue to administration, because many of us think that they are not aware this is happening.
–Mismatched in the Midwest
Dr. Hospitalist responds:
Opinions vary when it comes to the amount of clinical time hospitalist leaders should devote to their groups. As we have become more involved in the administrative aspects of the hospital, there are increasing demands placed on directors. Along with increased administrative demands comes the desire of many of these physician-leaders to remain adept in the practice of hospital medicine. Without a strong clinical connection and familiarity with what the others experience day to day, the group leader risks losing credibility and whatever leverage the title might offer.
Many groups have devised formulas based on the number of members in the group to help them derive a “fair” amount of administrative time to allow the director. For example, for every five full-time equivalents (FTEs) on staff, the director receives 0.1 FTE in admin time; so, for a group of 25 members, the director would get 0.5 admin time. The remainder of time would be clinical, but again, how that clinical time is managed is also highly variable.
This seems like a reasonable formula to me, because those with larger programs will have larger hospitals, more people to manage, and more personalities to deal with. The potential rewards and job satisfaction are also greater. (Another potential scheduling issue: Does the group leader “fall right into” the rotation or only work the services with light census or teaching services in an academic institution?)
Some groups that work the traditional seven-on/seven-off schedule have allowed the hospitalist physician-leader to work Monday through Friday and carry a smaller census (10-12). This allows the leader to be in the hospital during those critical times when most administrative duties are fulfilled, while also allowing for a mechanism to place overflow patients on those high census days—as long as it is a rare occurrence. He or she should also occasionally work all the different shifts (nocturnist, admitter, teams, and so on) to best understand the group’s opportunities for improvement and its challenges.
There are likely as many iterations of how to devise a fair division of time as there are hospitalist groups, but, most importantly, the days of getting someone to volunteer to be a hospitalist director without some form of compensation are long gone. In most programs, the job has become much more complex.
Many believe it is a conflict of interest for the group leader to prepare the schedule. There is too much room for perceived favoritism or mistreatment by the members when the schedule doesn’t work in everyone’s favor (which it never will). There are proprietary programs on the market that allow for easy and reliable scheduling; they also remove the potential for bias. In a group as small as yours, an astute administrative assistant or associate director can be entrusted with the schedule.
With regard to speaking up, you say a “few” in your group are concerned, so I assume more than one but still a small number of your group has expressed some dissatisfaction. There may be other members with similar sentiments, so it is important to have a discussion with all the group members and solicit their opinions. Instead of approaching the administrators with your concerns, I suggest you and your colleagues have an open and candid discussion with your group leader. After the discussion, if you still remain dissatisfied with the director’s level of clinical involvement, you are left with several choices:
- Approach hospital administration and see if they approve of how your director is carrying out his clinical responsibilities. Be prepared for the director to find out.
- Continue to do your job and let this issue rest.
- Start looking for another job. If the situation really bothers you, I favor the latter!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
My hospitalist group, which has nine employees, is hospital-employed in a small Midwest town. We use the traditional seven-on and seven-off rotation and hire locum tenens to fill schedule gaps, as we have a couple of MDs who recently left the group. A few of us are concerned because our “boss,” who controls the schedule, does not put himself in rotation regularly. Instead, he puts locum or part-timers on the schedule, even on weeks when he is available. We all know that the hospital is paying him extra to take care of administrative work, and that it costs more for the hospital to pay part-time/locums. In your experience, is this a common occurrence? Should we be upset? Lastly, should we bring this issue to administration, because many of us think that they are not aware this is happening.
–Mismatched in the Midwest
Dr. Hospitalist responds:
Opinions vary when it comes to the amount of clinical time hospitalist leaders should devote to their groups. As we have become more involved in the administrative aspects of the hospital, there are increasing demands placed on directors. Along with increased administrative demands comes the desire of many of these physician-leaders to remain adept in the practice of hospital medicine. Without a strong clinical connection and familiarity with what the others experience day to day, the group leader risks losing credibility and whatever leverage the title might offer.
Many groups have devised formulas based on the number of members in the group to help them derive a “fair” amount of administrative time to allow the director. For example, for every five full-time equivalents (FTEs) on staff, the director receives 0.1 FTE in admin time; so, for a group of 25 members, the director would get 0.5 admin time. The remainder of time would be clinical, but again, how that clinical time is managed is also highly variable.
This seems like a reasonable formula to me, because those with larger programs will have larger hospitals, more people to manage, and more personalities to deal with. The potential rewards and job satisfaction are also greater. (Another potential scheduling issue: Does the group leader “fall right into” the rotation or only work the services with light census or teaching services in an academic institution?)
Some groups that work the traditional seven-on/seven-off schedule have allowed the hospitalist physician-leader to work Monday through Friday and carry a smaller census (10-12). This allows the leader to be in the hospital during those critical times when most administrative duties are fulfilled, while also allowing for a mechanism to place overflow patients on those high census days—as long as it is a rare occurrence. He or she should also occasionally work all the different shifts (nocturnist, admitter, teams, and so on) to best understand the group’s opportunities for improvement and its challenges.
There are likely as many iterations of how to devise a fair division of time as there are hospitalist groups, but, most importantly, the days of getting someone to volunteer to be a hospitalist director without some form of compensation are long gone. In most programs, the job has become much more complex.
Many believe it is a conflict of interest for the group leader to prepare the schedule. There is too much room for perceived favoritism or mistreatment by the members when the schedule doesn’t work in everyone’s favor (which it never will). There are proprietary programs on the market that allow for easy and reliable scheduling; they also remove the potential for bias. In a group as small as yours, an astute administrative assistant or associate director can be entrusted with the schedule.
With regard to speaking up, you say a “few” in your group are concerned, so I assume more than one but still a small number of your group has expressed some dissatisfaction. There may be other members with similar sentiments, so it is important to have a discussion with all the group members and solicit their opinions. Instead of approaching the administrators with your concerns, I suggest you and your colleagues have an open and candid discussion with your group leader. After the discussion, if you still remain dissatisfied with the director’s level of clinical involvement, you are left with several choices:
- Approach hospital administration and see if they approve of how your director is carrying out his clinical responsibilities. Be prepared for the director to find out.
- Continue to do your job and let this issue rest.
- Start looking for another job. If the situation really bothers you, I favor the latter!
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
Get Ready for Transition to ICD-10 Medical Coding

By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
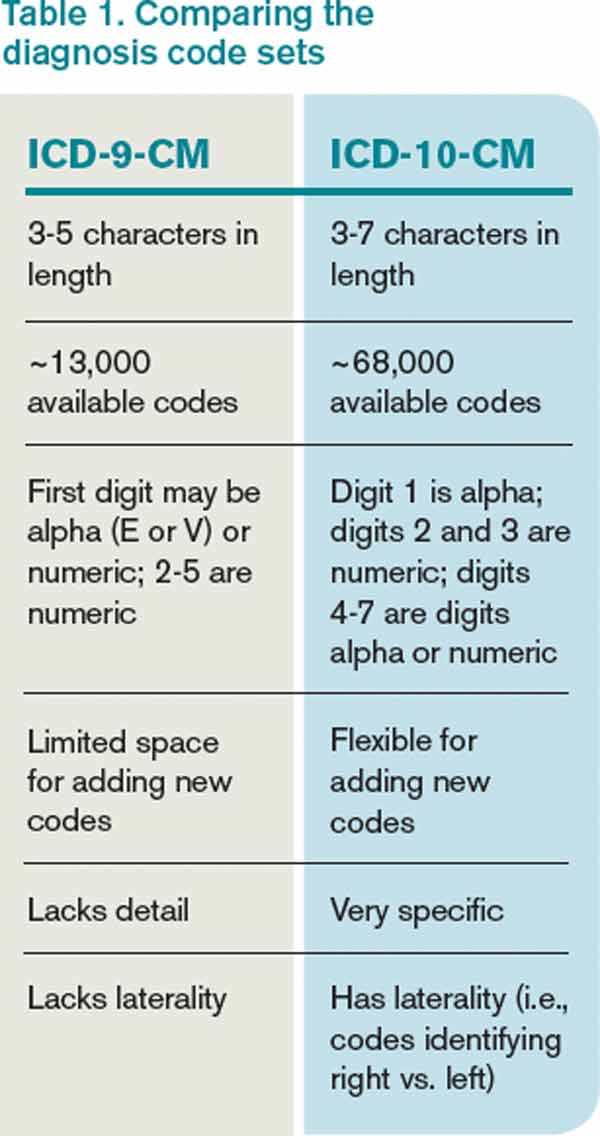
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Large Hospital Systems, Physician Groups Most Likely to Form Accountable Care Organizations
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
Workflow Interruptions Threaten Patient Safety, Hospitalists' Job Satisfaction


When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
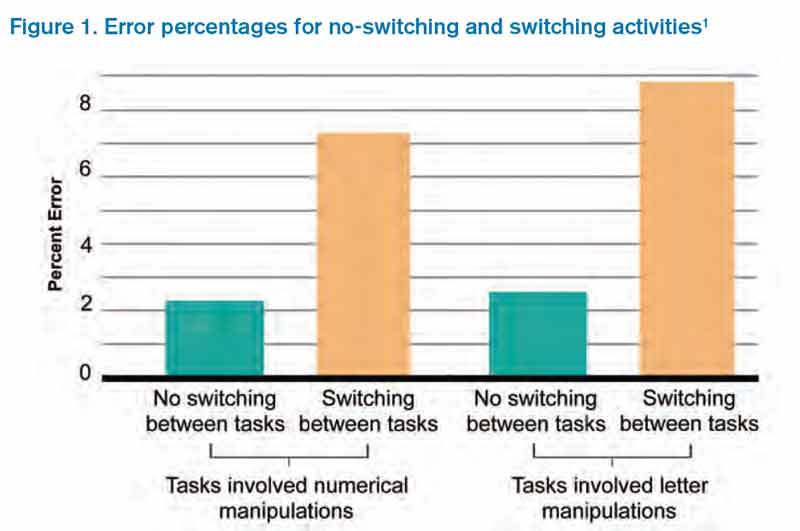
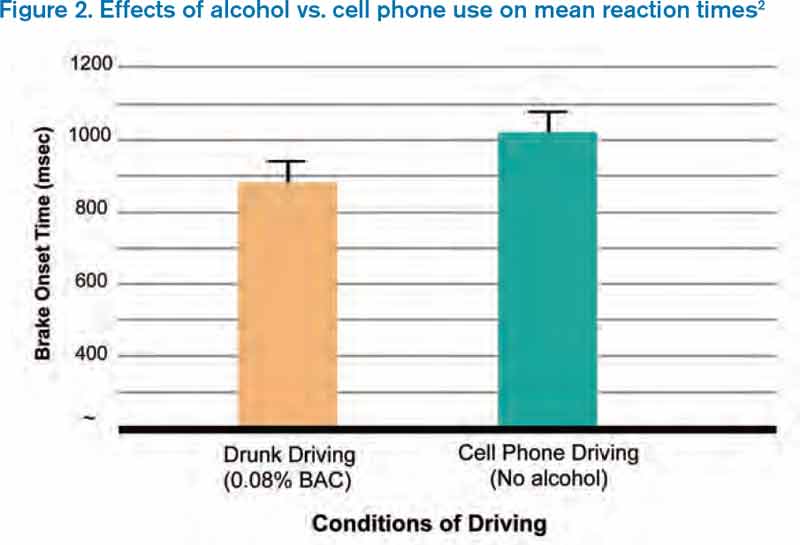
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
Society of Hospital Medicine (SHM) Epitomizes Professional Diversity

I just got back from a trip to SHM headquarters in Philadelphia, and all I can say is “wow.” I was visiting there for a meeting with the staff, many SHM members and committee leaders, and the SHM board of directors. The first day we all went into a big, modern, beautiful room at SHM headquarters—there must have been more than 100 people—and we went around the room and introduced ourselves. The diversity of the staff that support our society, and the diversity of the members there, was truly breathtaking. What I saw was a microcosm of our society and our specialty.
Looking around the room, it was easy to see some aspects of our diverse organization: both genders and a variety of ethnicities and age groups were well represented. These traditional measures of diversity are critical to a healthy environment, in my opinion, and the data bear out the idea that a diverse workforce can reduce turnover and be more creative and qualified.1,2 Our diversity is not an accident. It is part of a larger, deliberate strategy by SHM to be “the home” for healthcare professionals who provide hospital-based patient care. SHM embraces diversity, whether it’s skin deep or deeply cognitive.
Although we are continually working to enrich the traditional aspects of diversity, we are also very hard at work to make SHM a place of professional diversity.
Open and Inclusive
Over the past several years, SHM has worked hard to be openly inclusive. Many of the committees and sections within the society have been developed specifically to embrace important aspects of hospital medicine that have special or common interests, characteristics, or needs. Examples include the international section, med-peds section, administrators’ committee, and the nurse practitioner and physician assistant committee. These venues allow individuals under a Big Tent to find others with similar interests or training, so that they can address unique aspects of hospital medicine as it relates directly to them. SHM’s virtual world is following our committee and section structure, which has some of the most actively growing HMXchange communities coming from the “administrators” community and the “NP/PA” community.
SHM has put its money where its mouth is, dedicating significant resources for educational programs that will help benefit professionals with a variety of backgrounds. Some are focused on the special needs of our diverse physician population, including the Academic Hospitalist Academy, the Quality and Safety Educators Academy, and the Pediatric Hospital Medicine annual meeting (through a partnership with the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association). Other events are focused specifically on helping our non-physician colleagues, like the boot camp that is presented in collaboration with the American Academy of Physician Assistants and American Association of Nurse Practitioners. The SHM Leadership Academies attract a venerable alphabet soup of professional designations, including many MDs and DOs, of course, but also increasing numbers of PAs and NPs, a growing number of administrators, and now even a few ED and OB docs! Now that’s a Big Tent.
My understanding is that these events are always popular and often sold out.
Maybe the most powerful evidence that our Big Tent philosophy is working is found in the relationships SHM has forged with other hospital-based specialties, like obstetrics, neurology, and surgery. The president of the Society of OB/GYN Hospitalists (societyofobgynhospitalists.com) has attended the SHM annual meeting and at least one of the Leadership Academies. Although “traditional” hospitalists like me may not be able to help in the OR or birthing suite, we have a lot of experience in quality improvement, leadership, and, of course, addressing the needs of a new and growing professional segment. The emergence and growth of these “specialty hospitalists” offers a unique opportunity for traditional hospitalists to partner with our subspecialty colleagues in a new way, so that together we can continue to improve patient care within the hospital across multiple disciplines.
What’s Ahead?
Based on the data I recently saw while at SHM headquarters, the Big Tent philosophy is a measurable success. Membership for NPs, PAs, and administrators is growing, with nearly 200 new members in those categories combined. Incredibly, we have ED physicians joining our organization—albeit, at a number dwarfed by internists—and the relationships with the specialty hospitalists are moving forward in a meaningful way. Looking at committees and committee chairs, there is plenty of ethnic, professional, and gender diversity.
What does all of this focus outside of internal medicine and physician groups mean for us internists? Will we be left behind? Fret not. Physicians make up more than 85% of our 12,000-plus members, with internists outnumbering—by a huge number—all of the other segments of our society combined. There is no Big Tent so large that physicians, or even internists, will ever be in jeopardy. We occupy plenty of space under this Big Tent and still have lots of room to spare for our colleagues. In welcoming others, we all strengthen our own standing, by elevating the entire field.
As a terrific mentor once said, a rising tide floats all boats. And the way to raise the tide of hospital medicine can be through partnerships whose gravity is a strong pull on the hospital medicine tide, as the moon pulls the ocean’s tides.
One area in which our society plans to place more effort in expanding the Big Tent is with trainees. Students and housestaff are one of the smallest groups in our organization, with the smallest growth. Those statistics are cause for concern. The need for future hospitalist growth, both in numbers and skill set, makes attracting this segment of paramount importance, in my view.
Fortunately, SHM is developing a strategy to make our society a valuable home to trainees. I have touched on those strategies previously, including a Physicians in Training Committee, free membership for students, $100 memberships for housestaff, and our “1,000 Challenge” to recruit 1,000 students and housestaff in the coming months.
In Sum
I am a firm believer in professional and personal diversity. I am proud to work in a society that also embraces this philosophy, places real value on it, and works hard to be inclusive. So, the next time you meet an NP, PA, student, or even a hospital-based OB physician, bring them under the SHM Big Tent, and encourage them to join us in making the hospital world a better place. They, we, and our patients will be better off for it.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to ehowell@jhmi.edu.
References
- Egan ME. Global diversity and inclusion: Fostering innovation through a diverse workforce. Forbes Insights. Forbes website. Available at: http://images.forbes.com/forbesinsights/StudyPDFs/Innovation_Through_Diversity.pdf. Accessed October 23, 2013.
- Kerby S, Burns C. The top 10 economic facts of diversity in the workplace. Center for American Progress website. Available at: http://www.americanprogress.org/issues/labor/news/2012/07/12/11900/the-top-10-economic-facts-of-diversity-in-the-workplace. Accessed October 23, 2013.
I just got back from a trip to SHM headquarters in Philadelphia, and all I can say is “wow.” I was visiting there for a meeting with the staff, many SHM members and committee leaders, and the SHM board of directors. The first day we all went into a big, modern, beautiful room at SHM headquarters—there must have been more than 100 people—and we went around the room and introduced ourselves. The diversity of the staff that support our society, and the diversity of the members there, was truly breathtaking. What I saw was a microcosm of our society and our specialty.
Looking around the room, it was easy to see some aspects of our diverse organization: both genders and a variety of ethnicities and age groups were well represented. These traditional measures of diversity are critical to a healthy environment, in my opinion, and the data bear out the idea that a diverse workforce can reduce turnover and be more creative and qualified.1,2 Our diversity is not an accident. It is part of a larger, deliberate strategy by SHM to be “the home” for healthcare professionals who provide hospital-based patient care. SHM embraces diversity, whether it’s skin deep or deeply cognitive.
Although we are continually working to enrich the traditional aspects of diversity, we are also very hard at work to make SHM a place of professional diversity.
Open and Inclusive
Over the past several years, SHM has worked hard to be openly inclusive. Many of the committees and sections within the society have been developed specifically to embrace important aspects of hospital medicine that have special or common interests, characteristics, or needs. Examples include the international section, med-peds section, administrators’ committee, and the nurse practitioner and physician assistant committee. These venues allow individuals under a Big Tent to find others with similar interests or training, so that they can address unique aspects of hospital medicine as it relates directly to them. SHM’s virtual world is following our committee and section structure, which has some of the most actively growing HMXchange communities coming from the “administrators” community and the “NP/PA” community.
SHM has put its money where its mouth is, dedicating significant resources for educational programs that will help benefit professionals with a variety of backgrounds. Some are focused on the special needs of our diverse physician population, including the Academic Hospitalist Academy, the Quality and Safety Educators Academy, and the Pediatric Hospital Medicine annual meeting (through a partnership with the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association). Other events are focused specifically on helping our non-physician colleagues, like the boot camp that is presented in collaboration with the American Academy of Physician Assistants and American Association of Nurse Practitioners. The SHM Leadership Academies attract a venerable alphabet soup of professional designations, including many MDs and DOs, of course, but also increasing numbers of PAs and NPs, a growing number of administrators, and now even a few ED and OB docs! Now that’s a Big Tent.
My understanding is that these events are always popular and often sold out.
Maybe the most powerful evidence that our Big Tent philosophy is working is found in the relationships SHM has forged with other hospital-based specialties, like obstetrics, neurology, and surgery. The president of the Society of OB/GYN Hospitalists (societyofobgynhospitalists.com) has attended the SHM annual meeting and at least one of the Leadership Academies. Although “traditional” hospitalists like me may not be able to help in the OR or birthing suite, we have a lot of experience in quality improvement, leadership, and, of course, addressing the needs of a new and growing professional segment. The emergence and growth of these “specialty hospitalists” offers a unique opportunity for traditional hospitalists to partner with our subspecialty colleagues in a new way, so that together we can continue to improve patient care within the hospital across multiple disciplines.
What’s Ahead?
Based on the data I recently saw while at SHM headquarters, the Big Tent philosophy is a measurable success. Membership for NPs, PAs, and administrators is growing, with nearly 200 new members in those categories combined. Incredibly, we have ED physicians joining our organization—albeit, at a number dwarfed by internists—and the relationships with the specialty hospitalists are moving forward in a meaningful way. Looking at committees and committee chairs, there is plenty of ethnic, professional, and gender diversity.
What does all of this focus outside of internal medicine and physician groups mean for us internists? Will we be left behind? Fret not. Physicians make up more than 85% of our 12,000-plus members, with internists outnumbering—by a huge number—all of the other segments of our society combined. There is no Big Tent so large that physicians, or even internists, will ever be in jeopardy. We occupy plenty of space under this Big Tent and still have lots of room to spare for our colleagues. In welcoming others, we all strengthen our own standing, by elevating the entire field.
As a terrific mentor once said, a rising tide floats all boats. And the way to raise the tide of hospital medicine can be through partnerships whose gravity is a strong pull on the hospital medicine tide, as the moon pulls the ocean’s tides.
One area in which our society plans to place more effort in expanding the Big Tent is with trainees. Students and housestaff are one of the smallest groups in our organization, with the smallest growth. Those statistics are cause for concern. The need for future hospitalist growth, both in numbers and skill set, makes attracting this segment of paramount importance, in my view.
Fortunately, SHM is developing a strategy to make our society a valuable home to trainees. I have touched on those strategies previously, including a Physicians in Training Committee, free membership for students, $100 memberships for housestaff, and our “1,000 Challenge” to recruit 1,000 students and housestaff in the coming months.
In Sum
I am a firm believer in professional and personal diversity. I am proud to work in a society that also embraces this philosophy, places real value on it, and works hard to be inclusive. So, the next time you meet an NP, PA, student, or even a hospital-based OB physician, bring them under the SHM Big Tent, and encourage them to join us in making the hospital world a better place. They, we, and our patients will be better off for it.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to ehowell@jhmi.edu.
References
- Egan ME. Global diversity and inclusion: Fostering innovation through a diverse workforce. Forbes Insights. Forbes website. Available at: http://images.forbes.com/forbesinsights/StudyPDFs/Innovation_Through_Diversity.pdf. Accessed October 23, 2013.
- Kerby S, Burns C. The top 10 economic facts of diversity in the workplace. Center for American Progress website. Available at: http://www.americanprogress.org/issues/labor/news/2012/07/12/11900/the-top-10-economic-facts-of-diversity-in-the-workplace. Accessed October 23, 2013.
I just got back from a trip to SHM headquarters in Philadelphia, and all I can say is “wow.” I was visiting there for a meeting with the staff, many SHM members and committee leaders, and the SHM board of directors. The first day we all went into a big, modern, beautiful room at SHM headquarters—there must have been more than 100 people—and we went around the room and introduced ourselves. The diversity of the staff that support our society, and the diversity of the members there, was truly breathtaking. What I saw was a microcosm of our society and our specialty.
Looking around the room, it was easy to see some aspects of our diverse organization: both genders and a variety of ethnicities and age groups were well represented. These traditional measures of diversity are critical to a healthy environment, in my opinion, and the data bear out the idea that a diverse workforce can reduce turnover and be more creative and qualified.1,2 Our diversity is not an accident. It is part of a larger, deliberate strategy by SHM to be “the home” for healthcare professionals who provide hospital-based patient care. SHM embraces diversity, whether it’s skin deep or deeply cognitive.
Although we are continually working to enrich the traditional aspects of diversity, we are also very hard at work to make SHM a place of professional diversity.
Open and Inclusive
Over the past several years, SHM has worked hard to be openly inclusive. Many of the committees and sections within the society have been developed specifically to embrace important aspects of hospital medicine that have special or common interests, characteristics, or needs. Examples include the international section, med-peds section, administrators’ committee, and the nurse practitioner and physician assistant committee. These venues allow individuals under a Big Tent to find others with similar interests or training, so that they can address unique aspects of hospital medicine as it relates directly to them. SHM’s virtual world is following our committee and section structure, which has some of the most actively growing HMXchange communities coming from the “administrators” community and the “NP/PA” community.
SHM has put its money where its mouth is, dedicating significant resources for educational programs that will help benefit professionals with a variety of backgrounds. Some are focused on the special needs of our diverse physician population, including the Academic Hospitalist Academy, the Quality and Safety Educators Academy, and the Pediatric Hospital Medicine annual meeting (through a partnership with the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association). Other events are focused specifically on helping our non-physician colleagues, like the boot camp that is presented in collaboration with the American Academy of Physician Assistants and American Association of Nurse Practitioners. The SHM Leadership Academies attract a venerable alphabet soup of professional designations, including many MDs and DOs, of course, but also increasing numbers of PAs and NPs, a growing number of administrators, and now even a few ED and OB docs! Now that’s a Big Tent.
My understanding is that these events are always popular and often sold out.
Maybe the most powerful evidence that our Big Tent philosophy is working is found in the relationships SHM has forged with other hospital-based specialties, like obstetrics, neurology, and surgery. The president of the Society of OB/GYN Hospitalists (societyofobgynhospitalists.com) has attended the SHM annual meeting and at least one of the Leadership Academies. Although “traditional” hospitalists like me may not be able to help in the OR or birthing suite, we have a lot of experience in quality improvement, leadership, and, of course, addressing the needs of a new and growing professional segment. The emergence and growth of these “specialty hospitalists” offers a unique opportunity for traditional hospitalists to partner with our subspecialty colleagues in a new way, so that together we can continue to improve patient care within the hospital across multiple disciplines.
What’s Ahead?
Based on the data I recently saw while at SHM headquarters, the Big Tent philosophy is a measurable success. Membership for NPs, PAs, and administrators is growing, with nearly 200 new members in those categories combined. Incredibly, we have ED physicians joining our organization—albeit, at a number dwarfed by internists—and the relationships with the specialty hospitalists are moving forward in a meaningful way. Looking at committees and committee chairs, there is plenty of ethnic, professional, and gender diversity.
What does all of this focus outside of internal medicine and physician groups mean for us internists? Will we be left behind? Fret not. Physicians make up more than 85% of our 12,000-plus members, with internists outnumbering—by a huge number—all of the other segments of our society combined. There is no Big Tent so large that physicians, or even internists, will ever be in jeopardy. We occupy plenty of space under this Big Tent and still have lots of room to spare for our colleagues. In welcoming others, we all strengthen our own standing, by elevating the entire field.
As a terrific mentor once said, a rising tide floats all boats. And the way to raise the tide of hospital medicine can be through partnerships whose gravity is a strong pull on the hospital medicine tide, as the moon pulls the ocean’s tides.
One area in which our society plans to place more effort in expanding the Big Tent is with trainees. Students and housestaff are one of the smallest groups in our organization, with the smallest growth. Those statistics are cause for concern. The need for future hospitalist growth, both in numbers and skill set, makes attracting this segment of paramount importance, in my view.
Fortunately, SHM is developing a strategy to make our society a valuable home to trainees. I have touched on those strategies previously, including a Physicians in Training Committee, free membership for students, $100 memberships for housestaff, and our “1,000 Challenge” to recruit 1,000 students and housestaff in the coming months.
In Sum
I am a firm believer in professional and personal diversity. I am proud to work in a society that also embraces this philosophy, places real value on it, and works hard to be inclusive. So, the next time you meet an NP, PA, student, or even a hospital-based OB physician, bring them under the SHM Big Tent, and encourage them to join us in making the hospital world a better place. They, we, and our patients will be better off for it.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to ehowell@jhmi.edu.
References
- Egan ME. Global diversity and inclusion: Fostering innovation through a diverse workforce. Forbes Insights. Forbes website. Available at: http://images.forbes.com/forbesinsights/StudyPDFs/Innovation_Through_Diversity.pdf. Accessed October 23, 2013.
- Kerby S, Burns C. The top 10 economic facts of diversity in the workplace. Center for American Progress website. Available at: http://www.americanprogress.org/issues/labor/news/2012/07/12/11900/the-top-10-economic-facts-of-diversity-in-the-workplace. Accessed October 23, 2013.