User login
Healthcare.gov woes keep 1 million out of insurance marketplace
The technical problems that plagued healthcare.gov throughout October and November could lead to 1 million fewer Americans signing up for health insurance in 2014, according to a report from the Congressional Budget Office.
The CBO previously estimated that 7 million individuals would enroll in health plans through the Affordable Care Act’s (ACA’s) insurance exchanges this year. But a report released Feb. 4 says it’s more likely that 6 million Americans will sign up during the open enrollment period that ends on March 31.

Currently, more than 3 million people have enrolled in health plans through the state- and federally run exchanges, according to the Centers for Medicare & Medicaid Services. But CBO officials said that they expect many people to sign up toward the end of the open enrollment period, especially if they are purchasing a plan primarily to avoid a tax penalty for being uninsured.
"Thus, it is possible that the number of enrollees will reach the 7 million originally projected for 2014, just as it is possible that the number will fall short of the current estimate of 6 million," the report notes.
The CBO predicts that enrollment through the exchanges will reach 22 million by 2016 as people become more familiar with the new insurance options and federal subsidies.
Healthcare.gov’s technical problems likely also depressed enrollment through Medicaid and the Children’s Health Insurance Program (CHIP) this year. The CBO now estimates that 8 million individuals, not the 9 million initially projected, will enroll in Medicaid and CHIP in 2014.
Employment also could take a hit under the ACA, according to the CBO.
Between 2017 and 2024, there could be about a 1.5% to 2% drop in the total number of hours worked in the United States, mostly among low-wage earners as they choose to cut their hours and income to maintain eligibility for federal health insurance subsidies.
On the employer side, the CBO predicts that businesses could cut back on hiring to stay below the 50-worker threshold that requires them to either offer health insurance or pay a penalty. But the CBO also expects that over time, the penalty will have little effect on the hiring of workers because businesses will pass it on to their employees in the form of reduced wages.
Overall, the CBO estimates that the ACA will reduce aggregate compensation by about 1% over the 2017-2024 period, up from a 2010 estimate of 0.5%.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The technical problems that plagued healthcare.gov throughout October and November could lead to 1 million fewer Americans signing up for health insurance in 2014, according to a report from the Congressional Budget Office.
The CBO previously estimated that 7 million individuals would enroll in health plans through the Affordable Care Act’s (ACA’s) insurance exchanges this year. But a report released Feb. 4 says it’s more likely that 6 million Americans will sign up during the open enrollment period that ends on March 31.
Currently, more than 3 million people have enrolled in health plans through the state- and federally run exchanges, according to the Centers for Medicare & Medicaid Services. But CBO officials said that they expect many people to sign up toward the end of the open enrollment period, especially if they are purchasing a plan primarily to avoid a tax penalty for being uninsured.
"Thus, it is possible that the number of enrollees will reach the 7 million originally projected for 2014, just as it is possible that the number will fall short of the current estimate of 6 million," the report notes.
The CBO predicts that enrollment through the exchanges will reach 22 million by 2016 as people become more familiar with the new insurance options and federal subsidies.
Healthcare.gov’s technical problems likely also depressed enrollment through Medicaid and the Children’s Health Insurance Program (CHIP) this year. The CBO now estimates that 8 million individuals, not the 9 million initially projected, will enroll in Medicaid and CHIP in 2014.
Employment also could take a hit under the ACA, according to the CBO.
Between 2017 and 2024, there could be about a 1.5% to 2% drop in the total number of hours worked in the United States, mostly among low-wage earners as they choose to cut their hours and income to maintain eligibility for federal health insurance subsidies.
On the employer side, the CBO predicts that businesses could cut back on hiring to stay below the 50-worker threshold that requires them to either offer health insurance or pay a penalty. But the CBO also expects that over time, the penalty will have little effect on the hiring of workers because businesses will pass it on to their employees in the form of reduced wages.
Overall, the CBO estimates that the ACA will reduce aggregate compensation by about 1% over the 2017-2024 period, up from a 2010 estimate of 0.5%.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The technical problems that plagued healthcare.gov throughout October and November could lead to 1 million fewer Americans signing up for health insurance in 2014, according to a report from the Congressional Budget Office.
The CBO previously estimated that 7 million individuals would enroll in health plans through the Affordable Care Act’s (ACA’s) insurance exchanges this year. But a report released Feb. 4 says it’s more likely that 6 million Americans will sign up during the open enrollment period that ends on March 31.
Currently, more than 3 million people have enrolled in health plans through the state- and federally run exchanges, according to the Centers for Medicare & Medicaid Services. But CBO officials said that they expect many people to sign up toward the end of the open enrollment period, especially if they are purchasing a plan primarily to avoid a tax penalty for being uninsured.
"Thus, it is possible that the number of enrollees will reach the 7 million originally projected for 2014, just as it is possible that the number will fall short of the current estimate of 6 million," the report notes.
The CBO predicts that enrollment through the exchanges will reach 22 million by 2016 as people become more familiar with the new insurance options and federal subsidies.
Healthcare.gov’s technical problems likely also depressed enrollment through Medicaid and the Children’s Health Insurance Program (CHIP) this year. The CBO now estimates that 8 million individuals, not the 9 million initially projected, will enroll in Medicaid and CHIP in 2014.
Employment also could take a hit under the ACA, according to the CBO.
Between 2017 and 2024, there could be about a 1.5% to 2% drop in the total number of hours worked in the United States, mostly among low-wage earners as they choose to cut their hours and income to maintain eligibility for federal health insurance subsidies.
On the employer side, the CBO predicts that businesses could cut back on hiring to stay below the 50-worker threshold that requires them to either offer health insurance or pay a penalty. But the CBO also expects that over time, the penalty will have little effect on the hiring of workers because businesses will pass it on to their employees in the form of reduced wages.
Overall, the CBO estimates that the ACA will reduce aggregate compensation by about 1% over the 2017-2024 period, up from a 2010 estimate of 0.5%.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Whither IPAB? Cost-cutting board is idle, but not gone
January came and went with nary a whisper from the once feared but now nearly forgotten Independent Payment Advisory Board.
Enacted as part of the Affordable Care Act and originally slated to have made its first cost-cutting recommendations by now, the IPAB has no members and has never met. For 2 years in a row, Congress and the President have stripped most of the board’s funding from the federal budget.
Under the ACA, the IPAB is charged with looking at 5-year Medicare spending trends and recommending cuts for the following year if per capita spending exceeds a set target.
The IPAB’s recommendations in any given year automatically take effect if Congress does not pass legislation to achieve the savings by Aug. 15. The board cannot recommend rationing care, increasing revenues, changing benefits, modifying eligibility, increasing cost-sharing, or changing the percentage of the premium that beneficiaries pay or the subsidies they receive under Medicare Part D.
Last year, the Medicare chief actuary determined spending would stay below the 2015 target, so the IPAB did not need to act. Further, the Congressional Budget Office has estimated that continuing slow growth in health care costs could mean that the board may not be called into play for another decade.
Physician organizations remain interested in either repealing the board or revising its scope and composition.
The American Medical Association objects to the IPAB on principle. In Feb. 2012, AMA Executive Vice President and CEO James L. Madara wrote to congressional leaders in support of a House bill to repeal the IPAB, noting that the IPAB "puts important health care payment and policy decisions in the hands of an independent body that has far too little accountability."
For the American Academy of Family Physicians, the IPAB "just isn’t a high priority right now," Dr. Reid Blackwelder, AAFP president, said in an interview.
The AAFP is more focused on replacing the Medicare Sustainable Growth Rate formula. Should the IPAB’s work get under way, the AAFP would go back to trying to get its recommendations reconsidered, Dr. Blackwelder said.
In fact, the AAFP isn’t completely opposed to the IPAB. "We like the concept, however, we really oppose the way the IPAB was set up," Dr. Blackwelder said.
The AAFP supports several changes to the IPAB, including:
• Addition of a primary care physician and a consumer representative to the board.
• A public comment period after IPAB recommendations are sent to Congress.
• Increased focus on quality improvement.
• Inclusion of all health care sectors – not just physician fees – in the board’s immediate mandate.
While the American College of Physicians supports the general concept of an independent panel to help evaluate Medicare fiscal soundness, it wants primary care representation and equal responsibility for meeting targets among all providers.

Bob Doherty, senior vice president of governmental affairs and public policy at the ACP, said that he does not expect any movement from the IPAB in the near future.
"The administration has made no effort to start the appointment process, which inevitably would run into Republican resistance to recommending appointees and Republican resistance in the Senate to their confirmation," he said. Mr. Doherty noted that many Democrats don’t support the IPAB, either.
That makes the IPAB "a fight that the administration and Democrats don’t need to take on now," Mr. Doherty said.
Paul N. Van de Water, a senior fellow at the Center on Budget and Policy Priorities in Washington, predicted that while action from the IPAB is unlikely in 2014, the board eventually will be called to action.
And, Mr. Van de Water said that he thought that physicians should take a more favorable view of the IPAB. "It allows for the application of expert human judgment about how a cost growth problem should be dealt with," he said.
"It’s not an SGR, an automatic formula that you are stuck with."
On Twitter @aliciaault
January came and went with nary a whisper from the once feared but now nearly forgotten Independent Payment Advisory Board.
Enacted as part of the Affordable Care Act and originally slated to have made its first cost-cutting recommendations by now, the IPAB has no members and has never met. For 2 years in a row, Congress and the President have stripped most of the board’s funding from the federal budget.
Under the ACA, the IPAB is charged with looking at 5-year Medicare spending trends and recommending cuts for the following year if per capita spending exceeds a set target.
The IPAB’s recommendations in any given year automatically take effect if Congress does not pass legislation to achieve the savings by Aug. 15. The board cannot recommend rationing care, increasing revenues, changing benefits, modifying eligibility, increasing cost-sharing, or changing the percentage of the premium that beneficiaries pay or the subsidies they receive under Medicare Part D.
Last year, the Medicare chief actuary determined spending would stay below the 2015 target, so the IPAB did not need to act. Further, the Congressional Budget Office has estimated that continuing slow growth in health care costs could mean that the board may not be called into play for another decade.
Physician organizations remain interested in either repealing the board or revising its scope and composition.
The American Medical Association objects to the IPAB on principle. In Feb. 2012, AMA Executive Vice President and CEO James L. Madara wrote to congressional leaders in support of a House bill to repeal the IPAB, noting that the IPAB "puts important health care payment and policy decisions in the hands of an independent body that has far too little accountability."
For the American Academy of Family Physicians, the IPAB "just isn’t a high priority right now," Dr. Reid Blackwelder, AAFP president, said in an interview.
The AAFP is more focused on replacing the Medicare Sustainable Growth Rate formula. Should the IPAB’s work get under way, the AAFP would go back to trying to get its recommendations reconsidered, Dr. Blackwelder said.
In fact, the AAFP isn’t completely opposed to the IPAB. "We like the concept, however, we really oppose the way the IPAB was set up," Dr. Blackwelder said.
The AAFP supports several changes to the IPAB, including:
• Addition of a primary care physician and a consumer representative to the board.
• A public comment period after IPAB recommendations are sent to Congress.
• Increased focus on quality improvement.
• Inclusion of all health care sectors – not just physician fees – in the board’s immediate mandate.
While the American College of Physicians supports the general concept of an independent panel to help evaluate Medicare fiscal soundness, it wants primary care representation and equal responsibility for meeting targets among all providers.
Bob Doherty, senior vice president of governmental affairs and public policy at the ACP, said that he does not expect any movement from the IPAB in the near future.
"The administration has made no effort to start the appointment process, which inevitably would run into Republican resistance to recommending appointees and Republican resistance in the Senate to their confirmation," he said. Mr. Doherty noted that many Democrats don’t support the IPAB, either.
That makes the IPAB "a fight that the administration and Democrats don’t need to take on now," Mr. Doherty said.
Paul N. Van de Water, a senior fellow at the Center on Budget and Policy Priorities in Washington, predicted that while action from the IPAB is unlikely in 2014, the board eventually will be called to action.
And, Mr. Van de Water said that he thought that physicians should take a more favorable view of the IPAB. "It allows for the application of expert human judgment about how a cost growth problem should be dealt with," he said.
"It’s not an SGR, an automatic formula that you are stuck with."
On Twitter @aliciaault
January came and went with nary a whisper from the once feared but now nearly forgotten Independent Payment Advisory Board.
Enacted as part of the Affordable Care Act and originally slated to have made its first cost-cutting recommendations by now, the IPAB has no members and has never met. For 2 years in a row, Congress and the President have stripped most of the board’s funding from the federal budget.
Under the ACA, the IPAB is charged with looking at 5-year Medicare spending trends and recommending cuts for the following year if per capita spending exceeds a set target.
The IPAB’s recommendations in any given year automatically take effect if Congress does not pass legislation to achieve the savings by Aug. 15. The board cannot recommend rationing care, increasing revenues, changing benefits, modifying eligibility, increasing cost-sharing, or changing the percentage of the premium that beneficiaries pay or the subsidies they receive under Medicare Part D.
Last year, the Medicare chief actuary determined spending would stay below the 2015 target, so the IPAB did not need to act. Further, the Congressional Budget Office has estimated that continuing slow growth in health care costs could mean that the board may not be called into play for another decade.
Physician organizations remain interested in either repealing the board or revising its scope and composition.
The American Medical Association objects to the IPAB on principle. In Feb. 2012, AMA Executive Vice President and CEO James L. Madara wrote to congressional leaders in support of a House bill to repeal the IPAB, noting that the IPAB "puts important health care payment and policy decisions in the hands of an independent body that has far too little accountability."
For the American Academy of Family Physicians, the IPAB "just isn’t a high priority right now," Dr. Reid Blackwelder, AAFP president, said in an interview.
The AAFP is more focused on replacing the Medicare Sustainable Growth Rate formula. Should the IPAB’s work get under way, the AAFP would go back to trying to get its recommendations reconsidered, Dr. Blackwelder said.
In fact, the AAFP isn’t completely opposed to the IPAB. "We like the concept, however, we really oppose the way the IPAB was set up," Dr. Blackwelder said.
The AAFP supports several changes to the IPAB, including:
• Addition of a primary care physician and a consumer representative to the board.
• A public comment period after IPAB recommendations are sent to Congress.
• Increased focus on quality improvement.
• Inclusion of all health care sectors – not just physician fees – in the board’s immediate mandate.
While the American College of Physicians supports the general concept of an independent panel to help evaluate Medicare fiscal soundness, it wants primary care representation and equal responsibility for meeting targets among all providers.
Bob Doherty, senior vice president of governmental affairs and public policy at the ACP, said that he does not expect any movement from the IPAB in the near future.
"The administration has made no effort to start the appointment process, which inevitably would run into Republican resistance to recommending appointees and Republican resistance in the Senate to their confirmation," he said. Mr. Doherty noted that many Democrats don’t support the IPAB, either.
That makes the IPAB "a fight that the administration and Democrats don’t need to take on now," Mr. Doherty said.
Paul N. Van de Water, a senior fellow at the Center on Budget and Policy Priorities in Washington, predicted that while action from the IPAB is unlikely in 2014, the board eventually will be called to action.
And, Mr. Van de Water said that he thought that physicians should take a more favorable view of the IPAB. "It allows for the application of expert human judgment about how a cost growth problem should be dealt with," he said.
"It’s not an SGR, an automatic formula that you are stuck with."
On Twitter @aliciaault
Likelihood for Readmission of Hospitalized Medicare Patients with Multiple Chronic Conditions Up 600%
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
Shift from Productivity to Value-Based Compensation Gains Momentum
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
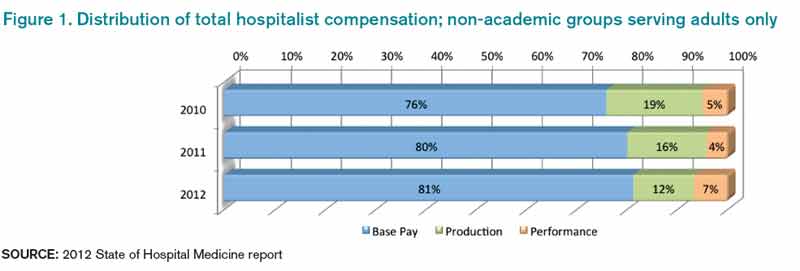
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.

At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
What Physicians Should Know About Buying into Hospitalist Practice
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Basic Principles for Pediatric Hospital Medicine Published
Basic Principles for Pediatric Hospital Medicine Published A recent policy statement from the American Academy of Pediatrics (AAP), published online in Pediatrics, urges recognition of the expanded roles and responsibilities of pediatric hospitalists and offers basic principles for pediatric hospital medicine (PHM) programs, including focusing on the unique culture of each program within its parent institution and the importance of coordinated, patient-centered care.4
The article outlines settings available for PHM programs, optimal processes for care transitions, and the need for leadership and goal setting.
“It is implicit in all the aforementioned recommendations that the overarching goal is always to provide the best possible care for children and protect the safety of children in the hospital setting,” the authors note.
AAP’s Section on Hospital Medicine supports a policy of voluntary referrals to pediatric hospital medicine programs.
Basic Principles for Pediatric Hospital Medicine Published A recent policy statement from the American Academy of Pediatrics (AAP), published online in Pediatrics, urges recognition of the expanded roles and responsibilities of pediatric hospitalists and offers basic principles for pediatric hospital medicine (PHM) programs, including focusing on the unique culture of each program within its parent institution and the importance of coordinated, patient-centered care.4
The article outlines settings available for PHM programs, optimal processes for care transitions, and the need for leadership and goal setting.
“It is implicit in all the aforementioned recommendations that the overarching goal is always to provide the best possible care for children and protect the safety of children in the hospital setting,” the authors note.
AAP’s Section on Hospital Medicine supports a policy of voluntary referrals to pediatric hospital medicine programs.
Basic Principles for Pediatric Hospital Medicine Published A recent policy statement from the American Academy of Pediatrics (AAP), published online in Pediatrics, urges recognition of the expanded roles and responsibilities of pediatric hospitalists and offers basic principles for pediatric hospital medicine (PHM) programs, including focusing on the unique culture of each program within its parent institution and the importance of coordinated, patient-centered care.4
The article outlines settings available for PHM programs, optimal processes for care transitions, and the need for leadership and goal setting.
“It is implicit in all the aforementioned recommendations that the overarching goal is always to provide the best possible care for children and protect the safety of children in the hospital setting,” the authors note.
AAP’s Section on Hospital Medicine supports a policy of voluntary referrals to pediatric hospital medicine programs.
Study Suggests Medical Trainees Need Better Manners
Study Suggests Medical Trainees Need More Manners
Researchers at Johns Hopkins Hospital and the University of Maryland Medical Center, both in Baltimore, identified an overall lack of “common courtesy” shown by internal medicine trainees in their interactions with patients.3 Such behavior can lead to lower patient satisfaction and worse medical outcomes, note the authors of the study, which included hospitalist Leonard Feldman, MD, FACP, FAAP, SFHM, an assistant professor of medicine at Hopkins.
The study, published in the November issue of the Journal of Hospital Medicine, followed 29 interns on rounds for three weeks and looked for five key strategies of etiquette-based communication. Researchers found that while the interns asked open-ended questions 75% of the time, they explained their role to the patient only 37% of the time and sat down to talk eye to eye during an encounter only 9% of the time.
The interns performed all five recommended behaviors only 4% of the time.
“These are things that matter to patients and are relatively easy to do,” Dr. Feldman said in a prepared statement. “They’re not being done to the extent they should be.”
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Rizk D, Calabrese R, Page C, Bookbinder M, Flores S, Portenoy R. A unique hospitalist/pain management collaboration to improve pain outcomes [abstract]. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104310. Accessed November 29, 2013.
- American Society for Parenteral and Enteral Nutrition. A.S.P.E.N. supports major medical device changes for improved patient safety. Available at: http://www.nutritioncare.org/Press_Room/Press_Releases/A_S_P_E_N__Supports_Major_Medical_Device_Changes_for_Improved_Patient_Safety/. Accessed November 29, 2013.
- Block LB, Hutzler L, Habicht R, Wu AW, et al. Do internal medicine interns practice etiquette-based communication? A critical look at the inpatient encounter. J Hosp Med. 2013;8(11):631-634.
- Mirkinson LJ, Section on Hospital Medicine. Guiding principles for pediatric hospital medicine programs. Pediatrics. 2013;132(4):782-786.
Study Suggests Medical Trainees Need More Manners
Researchers at Johns Hopkins Hospital and the University of Maryland Medical Center, both in Baltimore, identified an overall lack of “common courtesy” shown by internal medicine trainees in their interactions with patients.3 Such behavior can lead to lower patient satisfaction and worse medical outcomes, note the authors of the study, which included hospitalist Leonard Feldman, MD, FACP, FAAP, SFHM, an assistant professor of medicine at Hopkins.
The study, published in the November issue of the Journal of Hospital Medicine, followed 29 interns on rounds for three weeks and looked for five key strategies of etiquette-based communication. Researchers found that while the interns asked open-ended questions 75% of the time, they explained their role to the patient only 37% of the time and sat down to talk eye to eye during an encounter only 9% of the time.
The interns performed all five recommended behaviors only 4% of the time.
“These are things that matter to patients and are relatively easy to do,” Dr. Feldman said in a prepared statement. “They’re not being done to the extent they should be.”
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Rizk D, Calabrese R, Page C, Bookbinder M, Flores S, Portenoy R. A unique hospitalist/pain management collaboration to improve pain outcomes [abstract]. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104310. Accessed November 29, 2013.
- American Society for Parenteral and Enteral Nutrition. A.S.P.E.N. supports major medical device changes for improved patient safety. Available at: http://www.nutritioncare.org/Press_Room/Press_Releases/A_S_P_E_N__Supports_Major_Medical_Device_Changes_for_Improved_Patient_Safety/. Accessed November 29, 2013.
- Block LB, Hutzler L, Habicht R, Wu AW, et al. Do internal medicine interns practice etiquette-based communication? A critical look at the inpatient encounter. J Hosp Med. 2013;8(11):631-634.
- Mirkinson LJ, Section on Hospital Medicine. Guiding principles for pediatric hospital medicine programs. Pediatrics. 2013;132(4):782-786.
Study Suggests Medical Trainees Need More Manners
Researchers at Johns Hopkins Hospital and the University of Maryland Medical Center, both in Baltimore, identified an overall lack of “common courtesy” shown by internal medicine trainees in their interactions with patients.3 Such behavior can lead to lower patient satisfaction and worse medical outcomes, note the authors of the study, which included hospitalist Leonard Feldman, MD, FACP, FAAP, SFHM, an assistant professor of medicine at Hopkins.
The study, published in the November issue of the Journal of Hospital Medicine, followed 29 interns on rounds for three weeks and looked for five key strategies of etiquette-based communication. Researchers found that while the interns asked open-ended questions 75% of the time, they explained their role to the patient only 37% of the time and sat down to talk eye to eye during an encounter only 9% of the time.
The interns performed all five recommended behaviors only 4% of the time.
“These are things that matter to patients and are relatively easy to do,” Dr. Feldman said in a prepared statement. “They’re not being done to the extent they should be.”
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Rizk D, Calabrese R, Page C, Bookbinder M, Flores S, Portenoy R. A unique hospitalist/pain management collaboration to improve pain outcomes [abstract]. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104310. Accessed November 29, 2013.
- American Society for Parenteral and Enteral Nutrition. A.S.P.E.N. supports major medical device changes for improved patient safety. Available at: http://www.nutritioncare.org/Press_Room/Press_Releases/A_S_P_E_N__Supports_Major_Medical_Device_Changes_for_Improved_Patient_Safety/. Accessed November 29, 2013.
- Block LB, Hutzler L, Habicht R, Wu AW, et al. Do internal medicine interns practice etiquette-based communication? A critical look at the inpatient encounter. J Hosp Med. 2013;8(11):631-634.
- Mirkinson LJ, Section on Hospital Medicine. Guiding principles for pediatric hospital medicine programs. Pediatrics. 2013;132(4):782-786.
Hospitalist-Pain Expert Collaboration Educates Providers, Boosts Patient Satisfaction
A collaboration between hospitalists and the pain department at Beth Israel Medical Center in New York City is helping hospitalists address moderate to severe pain and complicating factors in their patients.
“The idea was to impart knowledge from a small group of experts to the hospitalists who manage pain in the majority of hospitalized patients,” says Dahlia Rizk, DO, chief of hospital medicine at Beth Israel and lead author on a poster that described the program and was presented at HM13 in Washington, D.C.1
Dr. Rizk first approached Russell Portenoy, MD, internationally recognized chair of the Department of Pain Management and Palliative Care at Beth Israel, to draw upon his specialized knowledge. Grant funding supported protected time for two hospitalist champions and a nurse practitioner; they reviewed charts on participating units and conducted focus groups with hospitalists to identify barriers to effective pain management. Barriers were compiled into a 56-item menu and shaped the curriculum for weekly training sessions presented by the pain service.
Dr. Portenoy and the project team also established a metric for “high sustained pain,” patients reporting three or more days of three or more episodes of moderate to severe pain, according to the hospital’s standardized pain assessment scale. The information was captured in a computerized, tablet-based “Live View” tool that shows all of the patients on a unit and their incidences of high sustained pain over a week. The tool is used for rounding on patients and identifying those needing an immediate interdisciplinary focus.
Project results, Dr. Rizk reported, include improvements in high sustained pain scores on six of seven participating units and average reductions in the number of identified barriers to pain. Hospitalists reported increased comfort with adjusting pain therapies, while patient satisfaction scores with pain management also increased.
“Not everyone has access to an expert like Dr. Portenoy, but we’ve now done the root cause analysis and barriers list,” Dr. Rizk says. “I also think this approach could be applied more widely to other problem areas. We plan to try something similar with geriatrics.”
For more information about the collaborative and its pain problem list, contact Dr. Rizk at DRizk@chpnet.org.
A collaboration between hospitalists and the pain department at Beth Israel Medical Center in New York City is helping hospitalists address moderate to severe pain and complicating factors in their patients.
“The idea was to impart knowledge from a small group of experts to the hospitalists who manage pain in the majority of hospitalized patients,” says Dahlia Rizk, DO, chief of hospital medicine at Beth Israel and lead author on a poster that described the program and was presented at HM13 in Washington, D.C.1
Dr. Rizk first approached Russell Portenoy, MD, internationally recognized chair of the Department of Pain Management and Palliative Care at Beth Israel, to draw upon his specialized knowledge. Grant funding supported protected time for two hospitalist champions and a nurse practitioner; they reviewed charts on participating units and conducted focus groups with hospitalists to identify barriers to effective pain management. Barriers were compiled into a 56-item menu and shaped the curriculum for weekly training sessions presented by the pain service.
Dr. Portenoy and the project team also established a metric for “high sustained pain,” patients reporting three or more days of three or more episodes of moderate to severe pain, according to the hospital’s standardized pain assessment scale. The information was captured in a computerized, tablet-based “Live View” tool that shows all of the patients on a unit and their incidences of high sustained pain over a week. The tool is used for rounding on patients and identifying those needing an immediate interdisciplinary focus.
Project results, Dr. Rizk reported, include improvements in high sustained pain scores on six of seven participating units and average reductions in the number of identified barriers to pain. Hospitalists reported increased comfort with adjusting pain therapies, while patient satisfaction scores with pain management also increased.
“Not everyone has access to an expert like Dr. Portenoy, but we’ve now done the root cause analysis and barriers list,” Dr. Rizk says. “I also think this approach could be applied more widely to other problem areas. We plan to try something similar with geriatrics.”
For more information about the collaborative and its pain problem list, contact Dr. Rizk at DRizk@chpnet.org.
A collaboration between hospitalists and the pain department at Beth Israel Medical Center in New York City is helping hospitalists address moderate to severe pain and complicating factors in their patients.
“The idea was to impart knowledge from a small group of experts to the hospitalists who manage pain in the majority of hospitalized patients,” says Dahlia Rizk, DO, chief of hospital medicine at Beth Israel and lead author on a poster that described the program and was presented at HM13 in Washington, D.C.1
Dr. Rizk first approached Russell Portenoy, MD, internationally recognized chair of the Department of Pain Management and Palliative Care at Beth Israel, to draw upon his specialized knowledge. Grant funding supported protected time for two hospitalist champions and a nurse practitioner; they reviewed charts on participating units and conducted focus groups with hospitalists to identify barriers to effective pain management. Barriers were compiled into a 56-item menu and shaped the curriculum for weekly training sessions presented by the pain service.
Dr. Portenoy and the project team also established a metric for “high sustained pain,” patients reporting three or more days of three or more episodes of moderate to severe pain, according to the hospital’s standardized pain assessment scale. The information was captured in a computerized, tablet-based “Live View” tool that shows all of the patients on a unit and their incidences of high sustained pain over a week. The tool is used for rounding on patients and identifying those needing an immediate interdisciplinary focus.
Project results, Dr. Rizk reported, include improvements in high sustained pain scores on six of seven participating units and average reductions in the number of identified barriers to pain. Hospitalists reported increased comfort with adjusting pain therapies, while patient satisfaction scores with pain management also increased.
“Not everyone has access to an expert like Dr. Portenoy, but we’ve now done the root cause analysis and barriers list,” Dr. Rizk says. “I also think this approach could be applied more widely to other problem areas. We plan to try something similar with geriatrics.”
For more information about the collaborative and its pain problem list, contact Dr. Rizk at DRizk@chpnet.org.
Society of Hospital Medicine's CODE-H Helps Hospitalists Avoid Coding Issues
Use SHM’s CODE-H Interactive to Avoid Coding Issues
Coding is a part of every hospitalist’s life, but tips from the experts can make that life easier, more efficient, and more compliant. That’s why SHM’s CODE-H program teaches hospitalists and hospitalist group managers and administrators how to stay up to date with the latest in the best
practices of coding and documentation.
On March 20, coding expert Barbara Pierce, CCS-P, ACS-EM, will present an online session on some of the most important coding topics for hospitalists, including:
- Critical care;
- Prolonged services;
- Documentation when working with NPs and PAs;
- Teaching physician rules; and
- Tips to avoid billing issues and potential denials.
This session is the third in a series of seven that cover the full range of coding topics, from developing a compliance plan and internal auditing process to ICD-10, PQRS, and Medicare’s Physician Value-Based Payment Modifier.
CME credits are offered through post-tests following each webinar, and each participant is eligible for up to seven credits throughout the series. Up to 10 individuals in a group can sign up through a single registration.
For more information, visit www.hospitalmedicine.org/codeh.
Use SHM’s CODE-H Interactive to Avoid Coding Issues
Coding is a part of every hospitalist’s life, but tips from the experts can make that life easier, more efficient, and more compliant. That’s why SHM’s CODE-H program teaches hospitalists and hospitalist group managers and administrators how to stay up to date with the latest in the best
practices of coding and documentation.
On March 20, coding expert Barbara Pierce, CCS-P, ACS-EM, will present an online session on some of the most important coding topics for hospitalists, including:
- Critical care;
- Prolonged services;
- Documentation when working with NPs and PAs;
- Teaching physician rules; and
- Tips to avoid billing issues and potential denials.
This session is the third in a series of seven that cover the full range of coding topics, from developing a compliance plan and internal auditing process to ICD-10, PQRS, and Medicare’s Physician Value-Based Payment Modifier.
CME credits are offered through post-tests following each webinar, and each participant is eligible for up to seven credits throughout the series. Up to 10 individuals in a group can sign up through a single registration.
For more information, visit www.hospitalmedicine.org/codeh.
Use SHM’s CODE-H Interactive to Avoid Coding Issues
Coding is a part of every hospitalist’s life, but tips from the experts can make that life easier, more efficient, and more compliant. That’s why SHM’s CODE-H program teaches hospitalists and hospitalist group managers and administrators how to stay up to date with the latest in the best
practices of coding and documentation.
On March 20, coding expert Barbara Pierce, CCS-P, ACS-EM, will present an online session on some of the most important coding topics for hospitalists, including:
- Critical care;
- Prolonged services;
- Documentation when working with NPs and PAs;
- Teaching physician rules; and
- Tips to avoid billing issues and potential denials.
This session is the third in a series of seven that cover the full range of coding topics, from developing a compliance plan and internal auditing process to ICD-10, PQRS, and Medicare’s Physician Value-Based Payment Modifier.
CME credits are offered through post-tests following each webinar, and each participant is eligible for up to seven credits throughout the series. Up to 10 individuals in a group can sign up through a single registration.
For more information, visit www.hospitalmedicine.org/codeh.
Apply Now for Society of Hospital Medicine's Project BOOST
BOOST Makes a Difference

For more info, visit www.hospitalmedicine.org/boost.
BOOST Makes a Difference
For more info, visit www.hospitalmedicine.org/boost.
BOOST Makes a Difference
For more info, visit www.hospitalmedicine.org/boost.