User login
Society of Hospital Medicine Debuts New Educational Tracks, Pre-Courses at HM14
SHM’s annual meeting offers something new each year. For HM14, a timely new track dubbed “Bending the Cost Curve” will focus on hospitalists’ role in improving cost effectiveness for the healthcare system as a whole.
“The value equation has always been something that’s near and dear to us,” says HM14 course director Daniel Brotman, MD, SFHM. “What’s different now is that cost shifting to the outpatient setting is something that is now being recognized as a potential unintended consequence of rushing through hospitalizations. And as we’re moving into the accountable-care world, making sure that the cost shifting does not occur…is really important.
“That means that hospitalists need to own the care transition.”

–Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course
The debut offerings don’t stop there. Three new pre-courses are on this year’s agenda: “Cardiology: What Hospitalists Need to Know as Front-Line Providers,” “Efficient High-Value Evidence-Based Medicine for the Practicing Hospitalist,” and “NP/PA Playbook for Hospital Medicine.”
“As a pre-course director, I think the educational aspect is what sets the tone for the whole meeting,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course, “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform. “People come looking to improve their clinical skills and their hospitalist groups.”
Pre-courses are critical to the meeting’s educational offerings. In that vein, HM14 is keeping pace with generational reform in care delivery and payment methodologies.
“The educational component—particularly the practice management track—is increasingly important in this era of rapid change,” Flores adds. “I don’t think any hospitalist anywhere in the country can afford to put his or her head in the sand and pretend it’s business as usual.”
To that end, another new feature at HM14 is a panel discussion titled, “Obamacare Is Here: What Does It Mean for You and Your Hospital?” The participants are a who’s who of the specialty’s thought leaders: Centers for Medicare & Medicaid Services chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM; executive director and CEO of the Medical University of South Carolina and former SHM president Patrick Cawley, MD, MHM, FACP; veteran healthcare executive Patrick Courneya, MD; and American Enterprise Institute resident fellow Scott Gottlieb, MD.
“The SHM annual meeting is pretty much the only place a hospitalist can go to learn about these changes,” Flores says, “and how to cope with them from a hospitalist’s perspective.”
Richard Quinn is a freelance writer in New Jersey.
SHM’s annual meeting offers something new each year. For HM14, a timely new track dubbed “Bending the Cost Curve” will focus on hospitalists’ role in improving cost effectiveness for the healthcare system as a whole.
“The value equation has always been something that’s near and dear to us,” says HM14 course director Daniel Brotman, MD, SFHM. “What’s different now is that cost shifting to the outpatient setting is something that is now being recognized as a potential unintended consequence of rushing through hospitalizations. And as we’re moving into the accountable-care world, making sure that the cost shifting does not occur…is really important.
“That means that hospitalists need to own the care transition.”
–Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course
The debut offerings don’t stop there. Three new pre-courses are on this year’s agenda: “Cardiology: What Hospitalists Need to Know as Front-Line Providers,” “Efficient High-Value Evidence-Based Medicine for the Practicing Hospitalist,” and “NP/PA Playbook for Hospital Medicine.”
“As a pre-course director, I think the educational aspect is what sets the tone for the whole meeting,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course, “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform. “People come looking to improve their clinical skills and their hospitalist groups.”
Pre-courses are critical to the meeting’s educational offerings. In that vein, HM14 is keeping pace with generational reform in care delivery and payment methodologies.
“The educational component—particularly the practice management track—is increasingly important in this era of rapid change,” Flores adds. “I don’t think any hospitalist anywhere in the country can afford to put his or her head in the sand and pretend it’s business as usual.”
To that end, another new feature at HM14 is a panel discussion titled, “Obamacare Is Here: What Does It Mean for You and Your Hospital?” The participants are a who’s who of the specialty’s thought leaders: Centers for Medicare & Medicaid Services chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM; executive director and CEO of the Medical University of South Carolina and former SHM president Patrick Cawley, MD, MHM, FACP; veteran healthcare executive Patrick Courneya, MD; and American Enterprise Institute resident fellow Scott Gottlieb, MD.
“The SHM annual meeting is pretty much the only place a hospitalist can go to learn about these changes,” Flores says, “and how to cope with them from a hospitalist’s perspective.”
Richard Quinn is a freelance writer in New Jersey.
SHM’s annual meeting offers something new each year. For HM14, a timely new track dubbed “Bending the Cost Curve” will focus on hospitalists’ role in improving cost effectiveness for the healthcare system as a whole.
“The value equation has always been something that’s near and dear to us,” says HM14 course director Daniel Brotman, MD, SFHM. “What’s different now is that cost shifting to the outpatient setting is something that is now being recognized as a potential unintended consequence of rushing through hospitalizations. And as we’re moving into the accountable-care world, making sure that the cost shifting does not occur…is really important.
“That means that hospitalists need to own the care transition.”
–Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course
The debut offerings don’t stop there. Three new pre-courses are on this year’s agenda: “Cardiology: What Hospitalists Need to Know as Front-Line Providers,” “Efficient High-Value Evidence-Based Medicine for the Practicing Hospitalist,” and “NP/PA Playbook for Hospital Medicine.”
“As a pre-course director, I think the educational aspect is what sets the tone for the whole meeting,” says Leslie Flores, MHA, a partner in Nelson Flores Hospital Medicine Consultants, a member of SHM’s Practice Analysis Committee, and co-director for the practice management pre-course, “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform. “People come looking to improve their clinical skills and their hospitalist groups.”
Pre-courses are critical to the meeting’s educational offerings. In that vein, HM14 is keeping pace with generational reform in care delivery and payment methodologies.
“The educational component—particularly the practice management track—is increasingly important in this era of rapid change,” Flores adds. “I don’t think any hospitalist anywhere in the country can afford to put his or her head in the sand and pretend it’s business as usual.”
To that end, another new feature at HM14 is a panel discussion titled, “Obamacare Is Here: What Does It Mean for You and Your Hospital?” The participants are a who’s who of the specialty’s thought leaders: Centers for Medicare & Medicaid Services chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM; executive director and CEO of the Medical University of South Carolina and former SHM president Patrick Cawley, MD, MHM, FACP; veteran healthcare executive Patrick Courneya, MD; and American Enterprise Institute resident fellow Scott Gottlieb, MD.
“The SHM annual meeting is pretty much the only place a hospitalist can go to learn about these changes,” Flores says, “and how to cope with them from a hospitalist’s perspective.”
Richard Quinn is a freelance writer in New Jersey.
Who gets sued when heart disease is missed?
Primary care physicians are sued more often than physicians from any other specialty for failing to diagnose coronary heart disease in women.
An analysis by medical liability insurer The Doctors Company found primary care doctors are the defendants in half of such lawsuits, compared with cardiologists in 22% of suits and emergency physicians in 17%. Hospitalists and orthopedists each were sued in 6% of cardiac disease–related legal claims.
The findings are "not surprising," said Dr. George P. Rodgers, cochair of the American College of Cardiology (ACC) Board of Trustees’ work group on medical professional liability insurance.
"Primary care physicians encounter many more problems and many more patients," Dr. Rodgers said. "They’re the front line. They’re the gateway to further evaluation or not."

The Doctors Company examined 41 malpractice claims involving alleged injuries and deaths from cardiac disease in women between 2007 and 2013. The majority of plaintiffs alleged misdiagnosis, followed by problems with medical treatment.
In 83% of cases, inadequate patient assessment was identified as a factor in patients’ injuries. Failure or delay to obtain a consult or referral was a contributing factor in 28% of cases, and documentation problems contributed to 22% of cases.
In more than 80% of suits, patients experienced serious or fatal outcomes.
"The problem is that when we deal with heart disease, the stakes are high," Dr. Rodgers said. "If you miss the diagnosis, it could be a disastrous result."
"Because [women] are more difficult to diagnose, one would suspect that physicians who have less experience and maybe less training are more likely to make errors," according to Dr. Sandeep Mangalmurti, a Chicago cardiologist and attorney.
In some cases, patients have a hand in a delayed or missed cardiac disease diagnosis. The Doctors Company analysis found women patients contributed to their injuries in 11% of cases, while men contributed in 20% of cases. Patient factors centered on noncompliance with treatment plans, medications, and follow-up appointments.
One way to reduce legal risks is to ensure medical information is properly communicated between physicians within the care spectrum, said Dr. Mangalmurti, a member of the ACC Board of Trustees’ work group on medical professional liability insurance. "That’s as important as the actual diagnosis."
In many cases, "the problem isn’t that the doctor made a mistake in practicing medicine, but that the information gets lost in translation," he added.
Obtain a sufficient amount of history from the patient, no matter how specific or nonspecific symptoms may be, advised Robin Diamond, senior vice president of patient safety and risk management for The Doctors Company.
Strong documentation is also key, Ms. Diamond said. Making note of all patient interactions and event timelines can help defend against a potential lawsuit later.
"When a suit is filed, it’s really important that the documentation is present to show that the office took the right steps to make sure the patient was seen quickly," she said.
During medical discussions, Dr. Rodgers recommends that physicians engage not only with the patient, but with family members. In many cases, a patient may disagree with a doctor’s orders, but then does not share the doctor’s recommendations with the family, Dr. Rodgers said. When a poor outcome or death results, the family may blame the physician, which can lead to a lawsuit.
"If there’s one single thing you can do [to reduce liability], it’s that we have to have really good communication with the patient and the family, even when things are going badly," he said. "The patient and the family need to know that you care and that you’re trying everything you can."
Primary care physicians are sued more often than physicians from any other specialty for failing to diagnose coronary heart disease in women.
An analysis by medical liability insurer The Doctors Company found primary care doctors are the defendants in half of such lawsuits, compared with cardiologists in 22% of suits and emergency physicians in 17%. Hospitalists and orthopedists each were sued in 6% of cardiac disease–related legal claims.
The findings are "not surprising," said Dr. George P. Rodgers, cochair of the American College of Cardiology (ACC) Board of Trustees’ work group on medical professional liability insurance.
"Primary care physicians encounter many more problems and many more patients," Dr. Rodgers said. "They’re the front line. They’re the gateway to further evaluation or not."
The Doctors Company examined 41 malpractice claims involving alleged injuries and deaths from cardiac disease in women between 2007 and 2013. The majority of plaintiffs alleged misdiagnosis, followed by problems with medical treatment.
In 83% of cases, inadequate patient assessment was identified as a factor in patients’ injuries. Failure or delay to obtain a consult or referral was a contributing factor in 28% of cases, and documentation problems contributed to 22% of cases.
In more than 80% of suits, patients experienced serious or fatal outcomes.
"The problem is that when we deal with heart disease, the stakes are high," Dr. Rodgers said. "If you miss the diagnosis, it could be a disastrous result."
"Because [women] are more difficult to diagnose, one would suspect that physicians who have less experience and maybe less training are more likely to make errors," according to Dr. Sandeep Mangalmurti, a Chicago cardiologist and attorney.
In some cases, patients have a hand in a delayed or missed cardiac disease diagnosis. The Doctors Company analysis found women patients contributed to their injuries in 11% of cases, while men contributed in 20% of cases. Patient factors centered on noncompliance with treatment plans, medications, and follow-up appointments.
One way to reduce legal risks is to ensure medical information is properly communicated between physicians within the care spectrum, said Dr. Mangalmurti, a member of the ACC Board of Trustees’ work group on medical professional liability insurance. "That’s as important as the actual diagnosis."
In many cases, "the problem isn’t that the doctor made a mistake in practicing medicine, but that the information gets lost in translation," he added.
Obtain a sufficient amount of history from the patient, no matter how specific or nonspecific symptoms may be, advised Robin Diamond, senior vice president of patient safety and risk management for The Doctors Company.
Strong documentation is also key, Ms. Diamond said. Making note of all patient interactions and event timelines can help defend against a potential lawsuit later.
"When a suit is filed, it’s really important that the documentation is present to show that the office took the right steps to make sure the patient was seen quickly," she said.
During medical discussions, Dr. Rodgers recommends that physicians engage not only with the patient, but with family members. In many cases, a patient may disagree with a doctor’s orders, but then does not share the doctor’s recommendations with the family, Dr. Rodgers said. When a poor outcome or death results, the family may blame the physician, which can lead to a lawsuit.
"If there’s one single thing you can do [to reduce liability], it’s that we have to have really good communication with the patient and the family, even when things are going badly," he said. "The patient and the family need to know that you care and that you’re trying everything you can."
Primary care physicians are sued more often than physicians from any other specialty for failing to diagnose coronary heart disease in women.
An analysis by medical liability insurer The Doctors Company found primary care doctors are the defendants in half of such lawsuits, compared with cardiologists in 22% of suits and emergency physicians in 17%. Hospitalists and orthopedists each were sued in 6% of cardiac disease–related legal claims.
The findings are "not surprising," said Dr. George P. Rodgers, cochair of the American College of Cardiology (ACC) Board of Trustees’ work group on medical professional liability insurance.
"Primary care physicians encounter many more problems and many more patients," Dr. Rodgers said. "They’re the front line. They’re the gateway to further evaluation or not."
The Doctors Company examined 41 malpractice claims involving alleged injuries and deaths from cardiac disease in women between 2007 and 2013. The majority of plaintiffs alleged misdiagnosis, followed by problems with medical treatment.
In 83% of cases, inadequate patient assessment was identified as a factor in patients’ injuries. Failure or delay to obtain a consult or referral was a contributing factor in 28% of cases, and documentation problems contributed to 22% of cases.
In more than 80% of suits, patients experienced serious or fatal outcomes.
"The problem is that when we deal with heart disease, the stakes are high," Dr. Rodgers said. "If you miss the diagnosis, it could be a disastrous result."
"Because [women] are more difficult to diagnose, one would suspect that physicians who have less experience and maybe less training are more likely to make errors," according to Dr. Sandeep Mangalmurti, a Chicago cardiologist and attorney.
In some cases, patients have a hand in a delayed or missed cardiac disease diagnosis. The Doctors Company analysis found women patients contributed to their injuries in 11% of cases, while men contributed in 20% of cases. Patient factors centered on noncompliance with treatment plans, medications, and follow-up appointments.
One way to reduce legal risks is to ensure medical information is properly communicated between physicians within the care spectrum, said Dr. Mangalmurti, a member of the ACC Board of Trustees’ work group on medical professional liability insurance. "That’s as important as the actual diagnosis."
In many cases, "the problem isn’t that the doctor made a mistake in practicing medicine, but that the information gets lost in translation," he added.
Obtain a sufficient amount of history from the patient, no matter how specific or nonspecific symptoms may be, advised Robin Diamond, senior vice president of patient safety and risk management for The Doctors Company.
Strong documentation is also key, Ms. Diamond said. Making note of all patient interactions and event timelines can help defend against a potential lawsuit later.
"When a suit is filed, it’s really important that the documentation is present to show that the office took the right steps to make sure the patient was seen quickly," she said.
During medical discussions, Dr. Rodgers recommends that physicians engage not only with the patient, but with family members. In many cases, a patient may disagree with a doctor’s orders, but then does not share the doctor’s recommendations with the family, Dr. Rodgers said. When a poor outcome or death results, the family may blame the physician, which can lead to a lawsuit.
"If there’s one single thing you can do [to reduce liability], it’s that we have to have really good communication with the patient and the family, even when things are going badly," he said. "The patient and the family need to know that you care and that you’re trying everything you can."

Testing now is critical to ICD-10 readiness
Still not prepared for the switch over to ICD-10? Experts say there’s still time to catch up before the Oct. 1 compliance date.
In an ideal world, physicians, their coders, and office staff would have already fully assessed the cost of transitioning to ICD-10, would have undergone training about how to improve clinical documentation and appropriate use of the new diagnosis codes, and would have internally tested their upgraded software. That would leave more than half a year to complete external testing with health plans to ensure that they get paid in October.

The reality? Few are on track to meet those milestones on time.
"Everybody is behind, not just practices," said Robert Tennant, senior policy adviser at the Medical Group Management Association (MGMA). For a practice to be ready for ICD-10, the "key trading partners have to be ready and our surveys are indicating that they are not," he said.
Those partners include practice management software vendors, electronic health record (EHR) vendors, clearinghouses, and private and public payers.
So does that mean another ICD-10 delay is likely? The Centers for Medicare and Medicaid Services says no.
Part of the reason may be that health plans, which are investing money in upgrading their own systems, are pushing the agency to move forward on time. They are signaling to the government that they don’t want another delay, Mr. Tennant said.
The MGMA is advising its members to prepare for an Oct. 1 launch of ICD-10. But Mr. Tennant said he’s not entirely convinced that the CMS will stick to the date if much of the health care industry is unprepared to make the switch.
"Claims have to be paid," he said. "The system cannot grind to a halt because practices that aren’t paid can’t see patients."
Start with training
Assuming that most physician offices have assessed which parts of their practice management and EHR systems need to be upgraded, and have determined the cost for upgrades and training, it’s time to get familiar with the new diagnosis coding system.

Coders and billers will need the most training on the new coding methodology, but doctors still need to get familiar with the level of documentation that’s need for their most frequently used codes. In general, the new system calls for great specificity, though it’s not an absolute rule.
For instance, the classification for asthma has changed from ICD-9 to ICD-10. Physicians will need to provide more specific documentation about the severity level (moderately persistent, severely persistent, etc.) for their coders to select the appropriate ICD-10 code, according to Kathryn DeVault, a coding expert at the American Health Information Management Association (AHIMA).
"The good news is that as different as ICD-10 and ICD-9 are, they are similar," Ms. DeVault said. "If there’s a familiarity or comfort level working with ICD-9, it’s a natural transition to ICD-10."
While there are some significant changes, especially related to orthopedic codes, for many subspecialties the differences will be minimal, she said.
Ms. DeVault recommended having the practice manager or lead coder identify the top 20 diagnosis codes for every physician in the practice and build some education around those frequently used codes.
She cautioned doctors not to skimp on the time and money needed to thoroughly train themselves and their staffs. "The key here is to do it right and do it right the first time," she said.
Check the books
Physicians and their staff also need to evaluate their current cash flow and revenue cycle, including the age of account balances, billing lag time, and other issues that may result in delayed or denied claims, said Asia Blunt, practice management strategist at the American Academy of Family Physicians. Correct those problems now, she said, then reevaluate between April and August.

Experts at the AAFP are recommending that physicians put aside a cash reserve, if possible, to cover expenses during the first 3 months of the transition in case large numbers of claims are denied. (See below for more tips on planning for the worst.)
Testing with vendors, payers
Internal and external testing is also key. Before Oct. 1, practices should have completed end-to-end testing of their upgraded systems, ensuring that everything works smoothly from the time they code a claim to when they receive payment from the health insurer.
Practices can begin internal testing as soon as they have upgraded their software. But external testing will depend on when clearinghouses and health plans are ready.
The CMS will provide the first testing opportunity March 3-7. The agency will hold a national ICD-10 testing week allowing practices and clearinghouses to submit claims using the new coding system. Practices will receive an acknowledgement that the claims were either accepted or rejected by the system. Practices must register in advance through their local Medicare Administrative Contractor (MAC) website to test. Find your local MAC here.
But this type of front-end testing is only a first step, Mr. Tennant said. Front-end testing determines whether the claim contains an ICD-10 code and if it is in the right place and the right format. But practices will need to conduct further testing with payers to determine if the code they used is appropriate and whether they will get paid.
For instance, when submitting a claim for a sprained ankle under ICD-10, the coder might specify right or left ankle, or leave it as unspecified. Depending on the health insurer’s policy around the code, the insurer could pay the claim, reject it, or hold or "pend" it while seeking additional information. The complicating factor, Mr. Tennant said, is that each health insurer has different coding policies and those policies have yet to be released for ICD-10.
"It’s very frustrating for everybody," Mr. Tennant said.
To minimize the impact, Mr. Tennant recommended identifying the payers responsible for the majority of your claims. Keep in contact with them about the release of their payment policies and testing schedules, he said.
"Be aggressive in your outreach to those plans," he said.
Contingency plans
Just in case a worst-case scenario develops, Mr. Tennant offered the advice on ICD-10 contingency plans:
• Research back-up options for practice management systems and clearinghouses. If the vendors aren’t providing a clear answer on when they will be ready to offer upgrades and testing, start researching alternatives. Ask colleagues if they have vendors that are prepared for the transition.
• Don’t rely on one coder. Train more than one staff member on how to use the new coding system. That way, if the chief coder leaves 3 weeks before the compliance date, someone else can step in.
• Limit vacations around the Oct. 1 compliance date. This is not a time to operate short staffed.
• Don’t wait around for health plans to start ICD-10 testing. Start with context testing. Take a subset of high-dollar, high-volume ICD-9 claims that have already been paid by the health plan and practice coding them in ICD-10. Similarly, begin to code claims in parallel in both ICD-9 and ICD-10 and move them through your internal workflow. In both of these testing approaches, check if the documentation provided is sufficient to identify the best ICD-10 code. If not, it’s time for more training.
• Ensure you have enough cash to operate in case claims are rejected or delayed. Setting aside cash reserves is a good move. Consider postponing major capital investments for a few months before and after Oct. 1. Obtaining a line of credit to cover a few months of operating expenses is another option.
• Submit as many of claims as possible with ICD-9 codes before Oct. 1.
Free ICD-10 resources
• ICD-10 guide with checklists and timelines (CMS).
• Sample letter to gauge vendors’ ICD-10 readiness (AHIMA).
• Cost calculator and ICD-10 timeline (AAFP).
• Twelve step transition plan, white papers, and practice tool (AMA)
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Still not prepared for the switch over to ICD-10? Experts say there’s still time to catch up before the Oct. 1 compliance date.
In an ideal world, physicians, their coders, and office staff would have already fully assessed the cost of transitioning to ICD-10, would have undergone training about how to improve clinical documentation and appropriate use of the new diagnosis codes, and would have internally tested their upgraded software. That would leave more than half a year to complete external testing with health plans to ensure that they get paid in October.
The reality? Few are on track to meet those milestones on time.
"Everybody is behind, not just practices," said Robert Tennant, senior policy adviser at the Medical Group Management Association (MGMA). For a practice to be ready for ICD-10, the "key trading partners have to be ready and our surveys are indicating that they are not," he said.
Those partners include practice management software vendors, electronic health record (EHR) vendors, clearinghouses, and private and public payers.
So does that mean another ICD-10 delay is likely? The Centers for Medicare and Medicaid Services says no.
Part of the reason may be that health plans, which are investing money in upgrading their own systems, are pushing the agency to move forward on time. They are signaling to the government that they don’t want another delay, Mr. Tennant said.
The MGMA is advising its members to prepare for an Oct. 1 launch of ICD-10. But Mr. Tennant said he’s not entirely convinced that the CMS will stick to the date if much of the health care industry is unprepared to make the switch.
"Claims have to be paid," he said. "The system cannot grind to a halt because practices that aren’t paid can’t see patients."
Start with training
Assuming that most physician offices have assessed which parts of their practice management and EHR systems need to be upgraded, and have determined the cost for upgrades and training, it’s time to get familiar with the new diagnosis coding system.
Coders and billers will need the most training on the new coding methodology, but doctors still need to get familiar with the level of documentation that’s need for their most frequently used codes. In general, the new system calls for great specificity, though it’s not an absolute rule.
For instance, the classification for asthma has changed from ICD-9 to ICD-10. Physicians will need to provide more specific documentation about the severity level (moderately persistent, severely persistent, etc.) for their coders to select the appropriate ICD-10 code, according to Kathryn DeVault, a coding expert at the American Health Information Management Association (AHIMA).
"The good news is that as different as ICD-10 and ICD-9 are, they are similar," Ms. DeVault said. "If there’s a familiarity or comfort level working with ICD-9, it’s a natural transition to ICD-10."
While there are some significant changes, especially related to orthopedic codes, for many subspecialties the differences will be minimal, she said.
Ms. DeVault recommended having the practice manager or lead coder identify the top 20 diagnosis codes for every physician in the practice and build some education around those frequently used codes.
She cautioned doctors not to skimp on the time and money needed to thoroughly train themselves and their staffs. "The key here is to do it right and do it right the first time," she said.
Check the books
Physicians and their staff also need to evaluate their current cash flow and revenue cycle, including the age of account balances, billing lag time, and other issues that may result in delayed or denied claims, said Asia Blunt, practice management strategist at the American Academy of Family Physicians. Correct those problems now, she said, then reevaluate between April and August.
Experts at the AAFP are recommending that physicians put aside a cash reserve, if possible, to cover expenses during the first 3 months of the transition in case large numbers of claims are denied. (See below for more tips on planning for the worst.)
Testing with vendors, payers
Internal and external testing is also key. Before Oct. 1, practices should have completed end-to-end testing of their upgraded systems, ensuring that everything works smoothly from the time they code a claim to when they receive payment from the health insurer.
Practices can begin internal testing as soon as they have upgraded their software. But external testing will depend on when clearinghouses and health plans are ready.
The CMS will provide the first testing opportunity March 3-7. The agency will hold a national ICD-10 testing week allowing practices and clearinghouses to submit claims using the new coding system. Practices will receive an acknowledgement that the claims were either accepted or rejected by the system. Practices must register in advance through their local Medicare Administrative Contractor (MAC) website to test. Find your local MAC here.
But this type of front-end testing is only a first step, Mr. Tennant said. Front-end testing determines whether the claim contains an ICD-10 code and if it is in the right place and the right format. But practices will need to conduct further testing with payers to determine if the code they used is appropriate and whether they will get paid.
For instance, when submitting a claim for a sprained ankle under ICD-10, the coder might specify right or left ankle, or leave it as unspecified. Depending on the health insurer’s policy around the code, the insurer could pay the claim, reject it, or hold or "pend" it while seeking additional information. The complicating factor, Mr. Tennant said, is that each health insurer has different coding policies and those policies have yet to be released for ICD-10.
"It’s very frustrating for everybody," Mr. Tennant said.
To minimize the impact, Mr. Tennant recommended identifying the payers responsible for the majority of your claims. Keep in contact with them about the release of their payment policies and testing schedules, he said.
"Be aggressive in your outreach to those plans," he said.
Contingency plans
Just in case a worst-case scenario develops, Mr. Tennant offered the advice on ICD-10 contingency plans:
• Research back-up options for practice management systems and clearinghouses. If the vendors aren’t providing a clear answer on when they will be ready to offer upgrades and testing, start researching alternatives. Ask colleagues if they have vendors that are prepared for the transition.
• Don’t rely on one coder. Train more than one staff member on how to use the new coding system. That way, if the chief coder leaves 3 weeks before the compliance date, someone else can step in.
• Limit vacations around the Oct. 1 compliance date. This is not a time to operate short staffed.
• Don’t wait around for health plans to start ICD-10 testing. Start with context testing. Take a subset of high-dollar, high-volume ICD-9 claims that have already been paid by the health plan and practice coding them in ICD-10. Similarly, begin to code claims in parallel in both ICD-9 and ICD-10 and move them through your internal workflow. In both of these testing approaches, check if the documentation provided is sufficient to identify the best ICD-10 code. If not, it’s time for more training.
• Ensure you have enough cash to operate in case claims are rejected or delayed. Setting aside cash reserves is a good move. Consider postponing major capital investments for a few months before and after Oct. 1. Obtaining a line of credit to cover a few months of operating expenses is another option.
• Submit as many of claims as possible with ICD-9 codes before Oct. 1.
Free ICD-10 resources
• ICD-10 guide with checklists and timelines (CMS).
• Sample letter to gauge vendors’ ICD-10 readiness (AHIMA).
• Cost calculator and ICD-10 timeline (AAFP).
• Twelve step transition plan, white papers, and practice tool (AMA)
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Still not prepared for the switch over to ICD-10? Experts say there’s still time to catch up before the Oct. 1 compliance date.
In an ideal world, physicians, their coders, and office staff would have already fully assessed the cost of transitioning to ICD-10, would have undergone training about how to improve clinical documentation and appropriate use of the new diagnosis codes, and would have internally tested their upgraded software. That would leave more than half a year to complete external testing with health plans to ensure that they get paid in October.
The reality? Few are on track to meet those milestones on time.
"Everybody is behind, not just practices," said Robert Tennant, senior policy adviser at the Medical Group Management Association (MGMA). For a practice to be ready for ICD-10, the "key trading partners have to be ready and our surveys are indicating that they are not," he said.
Those partners include practice management software vendors, electronic health record (EHR) vendors, clearinghouses, and private and public payers.
So does that mean another ICD-10 delay is likely? The Centers for Medicare and Medicaid Services says no.
Part of the reason may be that health plans, which are investing money in upgrading their own systems, are pushing the agency to move forward on time. They are signaling to the government that they don’t want another delay, Mr. Tennant said.
The MGMA is advising its members to prepare for an Oct. 1 launch of ICD-10. But Mr. Tennant said he’s not entirely convinced that the CMS will stick to the date if much of the health care industry is unprepared to make the switch.
"Claims have to be paid," he said. "The system cannot grind to a halt because practices that aren’t paid can’t see patients."
Start with training
Assuming that most physician offices have assessed which parts of their practice management and EHR systems need to be upgraded, and have determined the cost for upgrades and training, it’s time to get familiar with the new diagnosis coding system.
Coders and billers will need the most training on the new coding methodology, but doctors still need to get familiar with the level of documentation that’s need for their most frequently used codes. In general, the new system calls for great specificity, though it’s not an absolute rule.
For instance, the classification for asthma has changed from ICD-9 to ICD-10. Physicians will need to provide more specific documentation about the severity level (moderately persistent, severely persistent, etc.) for their coders to select the appropriate ICD-10 code, according to Kathryn DeVault, a coding expert at the American Health Information Management Association (AHIMA).
"The good news is that as different as ICD-10 and ICD-9 are, they are similar," Ms. DeVault said. "If there’s a familiarity or comfort level working with ICD-9, it’s a natural transition to ICD-10."
While there are some significant changes, especially related to orthopedic codes, for many subspecialties the differences will be minimal, she said.
Ms. DeVault recommended having the practice manager or lead coder identify the top 20 diagnosis codes for every physician in the practice and build some education around those frequently used codes.
She cautioned doctors not to skimp on the time and money needed to thoroughly train themselves and their staffs. "The key here is to do it right and do it right the first time," she said.
Check the books
Physicians and their staff also need to evaluate their current cash flow and revenue cycle, including the age of account balances, billing lag time, and other issues that may result in delayed or denied claims, said Asia Blunt, practice management strategist at the American Academy of Family Physicians. Correct those problems now, she said, then reevaluate between April and August.
Experts at the AAFP are recommending that physicians put aside a cash reserve, if possible, to cover expenses during the first 3 months of the transition in case large numbers of claims are denied. (See below for more tips on planning for the worst.)
Testing with vendors, payers
Internal and external testing is also key. Before Oct. 1, practices should have completed end-to-end testing of their upgraded systems, ensuring that everything works smoothly from the time they code a claim to when they receive payment from the health insurer.
Practices can begin internal testing as soon as they have upgraded their software. But external testing will depend on when clearinghouses and health plans are ready.
The CMS will provide the first testing opportunity March 3-7. The agency will hold a national ICD-10 testing week allowing practices and clearinghouses to submit claims using the new coding system. Practices will receive an acknowledgement that the claims were either accepted or rejected by the system. Practices must register in advance through their local Medicare Administrative Contractor (MAC) website to test. Find your local MAC here.
But this type of front-end testing is only a first step, Mr. Tennant said. Front-end testing determines whether the claim contains an ICD-10 code and if it is in the right place and the right format. But practices will need to conduct further testing with payers to determine if the code they used is appropriate and whether they will get paid.
For instance, when submitting a claim for a sprained ankle under ICD-10, the coder might specify right or left ankle, or leave it as unspecified. Depending on the health insurer’s policy around the code, the insurer could pay the claim, reject it, or hold or "pend" it while seeking additional information. The complicating factor, Mr. Tennant said, is that each health insurer has different coding policies and those policies have yet to be released for ICD-10.
"It’s very frustrating for everybody," Mr. Tennant said.
To minimize the impact, Mr. Tennant recommended identifying the payers responsible for the majority of your claims. Keep in contact with them about the release of their payment policies and testing schedules, he said.
"Be aggressive in your outreach to those plans," he said.
Contingency plans
Just in case a worst-case scenario develops, Mr. Tennant offered the advice on ICD-10 contingency plans:
• Research back-up options for practice management systems and clearinghouses. If the vendors aren’t providing a clear answer on when they will be ready to offer upgrades and testing, start researching alternatives. Ask colleagues if they have vendors that are prepared for the transition.
• Don’t rely on one coder. Train more than one staff member on how to use the new coding system. That way, if the chief coder leaves 3 weeks before the compliance date, someone else can step in.
• Limit vacations around the Oct. 1 compliance date. This is not a time to operate short staffed.
• Don’t wait around for health plans to start ICD-10 testing. Start with context testing. Take a subset of high-dollar, high-volume ICD-9 claims that have already been paid by the health plan and practice coding them in ICD-10. Similarly, begin to code claims in parallel in both ICD-9 and ICD-10 and move them through your internal workflow. In both of these testing approaches, check if the documentation provided is sufficient to identify the best ICD-10 code. If not, it’s time for more training.
• Ensure you have enough cash to operate in case claims are rejected or delayed. Setting aside cash reserves is a good move. Consider postponing major capital investments for a few months before and after Oct. 1. Obtaining a line of credit to cover a few months of operating expenses is another option.
• Submit as many of claims as possible with ICD-9 codes before Oct. 1.
Free ICD-10 resources
• ICD-10 guide with checklists and timelines (CMS).
• Sample letter to gauge vendors’ ICD-10 readiness (AHIMA).
• Cost calculator and ICD-10 timeline (AAFP).
• Twelve step transition plan, white papers, and practice tool (AMA)
mschneider@frontlinemedcom.com
On Twitter @maryellenny

SGR fix could cost as much as $150 billion
Current proposals to repeal the Medicare Sustainable Growth Rate formula and replace it with a new payment system could cost anywhere from $121 billion to $150 billion over the next decade, according to new estimates from the Congressional Budget Office.
Legislation (H.R. 2810) approved by the House Ways and Means Committee in December is the least expensive option. It would cost about $121 billion over 10 years, according to the CBO projection. That bill includes 2 years of 0.5% pay updates for physicians and begins to partially tie payment to performance.
A more expensive option (S. 1871), approved by the Senate Finance Committee in December, would cost $150.4 billion through 2023, the CBO estimated. The Senate version would freeze physician payments for the next decade, but would allow physicians to earn more by participating in alternative payment models or another incentive program that measures quality of care and resource use.

The additional cost for this bill comes from extending some Medicare and Medicaid programs; the physician payment portion alone would cost about $111.5 billion over 10 years, CBO predicted.
The price tag will have a big impact on whether Congress can pass an SGR repeal bill this year. The Medicare fee cut for 2014 – which was to kick in Jan. 1 – was replaced by a 0.5% physician pay increase through March 31. But the cut will take effect on April 1 if Congress does not enact either another temporary SGR fix or a permanent repeal of the formula.
While there has been widespread bipartisan support for SGR repeal, there has yet to be any serious discussion of how lawmakers would pay for the fix. Physician groups, which have been deeply involved in the policy discussions surrounding SGR repeal, have also remained silent on how to pay for it.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Current proposals to repeal the Medicare Sustainable Growth Rate formula and replace it with a new payment system could cost anywhere from $121 billion to $150 billion over the next decade, according to new estimates from the Congressional Budget Office.
Legislation (H.R. 2810) approved by the House Ways and Means Committee in December is the least expensive option. It would cost about $121 billion over 10 years, according to the CBO projection. That bill includes 2 years of 0.5% pay updates for physicians and begins to partially tie payment to performance.
A more expensive option (S. 1871), approved by the Senate Finance Committee in December, would cost $150.4 billion through 2023, the CBO estimated. The Senate version would freeze physician payments for the next decade, but would allow physicians to earn more by participating in alternative payment models or another incentive program that measures quality of care and resource use.
The additional cost for this bill comes from extending some Medicare and Medicaid programs; the physician payment portion alone would cost about $111.5 billion over 10 years, CBO predicted.
The price tag will have a big impact on whether Congress can pass an SGR repeal bill this year. The Medicare fee cut for 2014 – which was to kick in Jan. 1 – was replaced by a 0.5% physician pay increase through March 31. But the cut will take effect on April 1 if Congress does not enact either another temporary SGR fix or a permanent repeal of the formula.
While there has been widespread bipartisan support for SGR repeal, there has yet to be any serious discussion of how lawmakers would pay for the fix. Physician groups, which have been deeply involved in the policy discussions surrounding SGR repeal, have also remained silent on how to pay for it.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Current proposals to repeal the Medicare Sustainable Growth Rate formula and replace it with a new payment system could cost anywhere from $121 billion to $150 billion over the next decade, according to new estimates from the Congressional Budget Office.
Legislation (H.R. 2810) approved by the House Ways and Means Committee in December is the least expensive option. It would cost about $121 billion over 10 years, according to the CBO projection. That bill includes 2 years of 0.5% pay updates for physicians and begins to partially tie payment to performance.
A more expensive option (S. 1871), approved by the Senate Finance Committee in December, would cost $150.4 billion through 2023, the CBO estimated. The Senate version would freeze physician payments for the next decade, but would allow physicians to earn more by participating in alternative payment models or another incentive program that measures quality of care and resource use.
The additional cost for this bill comes from extending some Medicare and Medicaid programs; the physician payment portion alone would cost about $111.5 billion over 10 years, CBO predicted.
The price tag will have a big impact on whether Congress can pass an SGR repeal bill this year. The Medicare fee cut for 2014 – which was to kick in Jan. 1 – was replaced by a 0.5% physician pay increase through March 31. But the cut will take effect on April 1 if Congress does not enact either another temporary SGR fix or a permanent repeal of the formula.
While there has been widespread bipartisan support for SGR repeal, there has yet to be any serious discussion of how lawmakers would pay for the fix. Physician groups, which have been deeply involved in the policy discussions surrounding SGR repeal, have also remained silent on how to pay for it.
mschneider@frontlinemedcom.com
On Twitter @maryellenny

Joint Commission targets patient flow in 2014
The Joint Commission is continuing its focus on reducing emergency department boarding with the introduction of additional standards aimed at improving the flow of patients throughout the hospital.
In performance standards that went into effect on Jan. 1, the Joint Commission is requiring its accredited hospitals to measure and set goals for "mitigating and managing" the boarding of patients who come through the emergency department. And the organization recommends that hospitals try to limit boarding to no more than 4 hours after the decision to admit or transfer has been made, though the 4-hour time frame is a guideline and hospitals won’t be scored on whether they can meet it.

The Joint Commission is also requiring hospitals to do more to curb the boarding of patients with mental health or substance abuse emergencies in particular. In a new standard that took effect on Jan. 1, hospital leaders are required to reach out to behavioral health care providers in the community whenever they encounter patients at risk for boarding due to a behavioral health emergency.
The new standards come a year after hospitals were asked to make reducing boarding in the ED, a hospital-wide mission by setting specific goals on ensuring the availability of patient beds and maintaining proper throughput in laboratories, operating rooms, inpatient units, telemetry, radiology, and the postanesthesia-care unit. Also in 2013, hospitals were asked to create a safe, monitored location to board behavioral health patients awaiting treatment.
The standards are mostly good news for emergency physicians, said Dr. Frederick C. Blum, a past president of the American College of Emergency Physicians and an attending physician in the department of emergency medicine at West Virginia University in Morgantown, because they pull the hospital leadership into the issues of ED boarding in general and how to handle boarding of behavioral health patients.
"Previously, the hospitals have not given this issue as much attention," he said. "This at least makes them partners with us to try solve this problem of ED boarding."
But even with the whole hospital behind the problem, it will remain a challenge, Dr. Blum said. One complicating factor is the Affordable Care Act. No one knows for sure how the ACA will change the volume of patients coming to the ED, Dr. Blum said, and hospitals still have to deal with persistent problems such as the shortage of hospital beds.
For hospitalists, the increased focus on patient flow could bring some major changes, according to Dr. David Yu, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M.
Currently, hospitalist groups are structured financially for maximum productivity not patient flow. And, as a result, efficiently discharging patients and freeing up hospital beds isn’t a top priority for hospitalists, he said.
"It’s going to be a paradigm shift," Dr. Yu said.
To get hospitalists and other specialists in the hospital focused on improving patient flow, hospital leaders will need to switch up the financial incentives and set a hospital-wide budget that makes patient flow a priority, Dr. Yu said.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Joint Commission is continuing its focus on reducing emergency department boarding with the introduction of additional standards aimed at improving the flow of patients throughout the hospital.
In performance standards that went into effect on Jan. 1, the Joint Commission is requiring its accredited hospitals to measure and set goals for "mitigating and managing" the boarding of patients who come through the emergency department. And the organization recommends that hospitals try to limit boarding to no more than 4 hours after the decision to admit or transfer has been made, though the 4-hour time frame is a guideline and hospitals won’t be scored on whether they can meet it.
The Joint Commission is also requiring hospitals to do more to curb the boarding of patients with mental health or substance abuse emergencies in particular. In a new standard that took effect on Jan. 1, hospital leaders are required to reach out to behavioral health care providers in the community whenever they encounter patients at risk for boarding due to a behavioral health emergency.
The new standards come a year after hospitals were asked to make reducing boarding in the ED, a hospital-wide mission by setting specific goals on ensuring the availability of patient beds and maintaining proper throughput in laboratories, operating rooms, inpatient units, telemetry, radiology, and the postanesthesia-care unit. Also in 2013, hospitals were asked to create a safe, monitored location to board behavioral health patients awaiting treatment.
The standards are mostly good news for emergency physicians, said Dr. Frederick C. Blum, a past president of the American College of Emergency Physicians and an attending physician in the department of emergency medicine at West Virginia University in Morgantown, because they pull the hospital leadership into the issues of ED boarding in general and how to handle boarding of behavioral health patients.
"Previously, the hospitals have not given this issue as much attention," he said. "This at least makes them partners with us to try solve this problem of ED boarding."
But even with the whole hospital behind the problem, it will remain a challenge, Dr. Blum said. One complicating factor is the Affordable Care Act. No one knows for sure how the ACA will change the volume of patients coming to the ED, Dr. Blum said, and hospitals still have to deal with persistent problems such as the shortage of hospital beds.
For hospitalists, the increased focus on patient flow could bring some major changes, according to Dr. David Yu, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M.
Currently, hospitalist groups are structured financially for maximum productivity not patient flow. And, as a result, efficiently discharging patients and freeing up hospital beds isn’t a top priority for hospitalists, he said.
"It’s going to be a paradigm shift," Dr. Yu said.
To get hospitalists and other specialists in the hospital focused on improving patient flow, hospital leaders will need to switch up the financial incentives and set a hospital-wide budget that makes patient flow a priority, Dr. Yu said.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Joint Commission is continuing its focus on reducing emergency department boarding with the introduction of additional standards aimed at improving the flow of patients throughout the hospital.
In performance standards that went into effect on Jan. 1, the Joint Commission is requiring its accredited hospitals to measure and set goals for "mitigating and managing" the boarding of patients who come through the emergency department. And the organization recommends that hospitals try to limit boarding to no more than 4 hours after the decision to admit or transfer has been made, though the 4-hour time frame is a guideline and hospitals won’t be scored on whether they can meet it.
The Joint Commission is also requiring hospitals to do more to curb the boarding of patients with mental health or substance abuse emergencies in particular. In a new standard that took effect on Jan. 1, hospital leaders are required to reach out to behavioral health care providers in the community whenever they encounter patients at risk for boarding due to a behavioral health emergency.
The new standards come a year after hospitals were asked to make reducing boarding in the ED, a hospital-wide mission by setting specific goals on ensuring the availability of patient beds and maintaining proper throughput in laboratories, operating rooms, inpatient units, telemetry, radiology, and the postanesthesia-care unit. Also in 2013, hospitals were asked to create a safe, monitored location to board behavioral health patients awaiting treatment.
The standards are mostly good news for emergency physicians, said Dr. Frederick C. Blum, a past president of the American College of Emergency Physicians and an attending physician in the department of emergency medicine at West Virginia University in Morgantown, because they pull the hospital leadership into the issues of ED boarding in general and how to handle boarding of behavioral health patients.
"Previously, the hospitals have not given this issue as much attention," he said. "This at least makes them partners with us to try solve this problem of ED boarding."
But even with the whole hospital behind the problem, it will remain a challenge, Dr. Blum said. One complicating factor is the Affordable Care Act. No one knows for sure how the ACA will change the volume of patients coming to the ED, Dr. Blum said, and hospitals still have to deal with persistent problems such as the shortage of hospital beds.
For hospitalists, the increased focus on patient flow could bring some major changes, according to Dr. David Yu, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M.
Currently, hospitalist groups are structured financially for maximum productivity not patient flow. And, as a result, efficiently discharging patients and freeing up hospital beds isn’t a top priority for hospitalists, he said.
"It’s going to be a paradigm shift," Dr. Yu said.
To get hospitalists and other specialists in the hospital focused on improving patient flow, hospital leaders will need to switch up the financial incentives and set a hospital-wide budget that makes patient flow a priority, Dr. Yu said.
mschneider@frontlinemedcom.com
On Twitter @maryellenny

Malpractice Counsel
Case 1: Follow-up in Community-Acquired Methicillin- Resistant Staphylococcus Aureus Pharyngitis
A 73-year-old woman presented to the ED complaining of injuries she sustained following a minor fall at home. The patient’s past medical history was remarkable for diabetes mellitus (DM), hypertension, cerebrovascular accident, and a history of chronic pain. During the course of evaluation, the patient mentioned that she had experienced a sore throat. In addition to X-rays, the emergency physician (EP) ordered a rapid strep test (RST). All studies were normal and the patient was discharged home.
Over the next 2 months, the patient received medical treatment from other medical professionals, but not at the previous hospital. Reportedly, she did not complain of a sore throat during this time period. The patient did return to the same ED approximately 2 months later, complaining of cough and difficulty breathing; she died 5 days thereafter. No autopsy was performed.
A lawsuit was filed on behalf of the patient, stating the hospital breached the standard of care by not reporting the finding of MRSA directly to the treating physician, and that this led directly to the patient’s death by MRSA pneumonia. The jury returned a verdict in favor of the plaintiff for $32 million.
Discussion
This case illustrates two simple but important points: managing community-acquired MRSA (CA-MRSA) infections is a growing challenge for physicians; and hospital follow-up systems for positive findings (ie, fractures, blood cultures, etc) need to be consistently reliable.
It is estimated that 30% of healthy people carry S aureus in their anterior nares; colonization rates for the throat are much less studied. In one recent study, 265 throat swabs were collected from patients aged 14 to 65 years old, who complained of pharyngitis in an outpatient setting.1 A total of 165 S aureus isolates (62.3%) were recovered from the 265 swabs. For the S aureus isolates, 38.2% (63) grew CA-MRSA; the remaining 68.1% (102) were methicillin-sensitive S aureus (MSSA). Interestingly, of the 63 MRSA-positive swabs, over half also grew Group A Streptococcus. The natural disease progression of CA-MRSA pharyngitis is still unknown, as is what to do with a positive throat swab for CA-MRSA. While there are a few case reports of bacteremia and Lemmiere syndrome possibly related to CA-MRSA pharyngitis,2,3 more information is clearly needed. For this case, it is not possible to definitively determine the role of the positive throat swab for CAMRSA in the patient’s subsequent death.
The other teaching point in this case is much simpler and well defined. Simply put, patients expect to be informed of positive findings, whether the result is known at the time of their ED visit or sometime afterward. There needs to be a system in place that consistently and reliably provides important information to either the patient’s treating physician or to the patient. The manners in which this information is communicated are myriad and should take into account hospital resources, the role of the EP and nurse, and what works best for your locality. The “who” and “how” of the contact is not important: reliability, timeliness, and consistency need to be the key drivers of the system.
Case 2: Arterial Occlusion
A 61-year-old woman called emergency medical services (EMS) after noticing her feet felt cold to the touch and having difficulty ambulating. The paramedics noted the patient had normal vital signs and normal circulation in her legs, and she was transported to the ED without incident. Upon arrival to the ED, she was triaged as nonurgent and placed in the minor-care area. On nursing assessment, the patient’s feet were found to be cold, but with palpable pulses bilaterally. Her past medical history was significant for hypertension and DM.
The patient was seen by a physician assistant (PA), who found both feet cool to the touch, but with bilateral pulses present. She was administered intravenous morphine for pain and laboratory studies were ordered. At the time, the PA was concerned about arterial occlusion versus deep vein thrombosis (DVT) versus cellulitis. A venous ultrasound examination was ordered and shown to be negative for DVT. A complete blood count was remarkable only for mild leukocytosis. The PA discussed the case with the supervising EP; they agreed on a diagnosis of cellulitis and discharged the patient home with antibiotics and analgesics.
Approximately 12 hours after discharge, the patient presented back to the ED via ambulance. At that time, she was hypotensive and tachypneic, with a thready palpable pulse. On repeat examination, she no longer had pulses present in her feet. An arteriogram found complete occlusion of her arterial circulation at the level of the knees bilaterally, requiring bilateral belowthe- knee amputation.
The patient sued both the emergency medicine physician and the PA for failure to provide her with the necessary care during her initial ED visit, resulting in loss of limbs. The defendants claimed the patient could not prove gross negligence by clear and convincing evidence, as required by state law. Following the ensuing trial, the jury returned a $5 million verdict in favor of the plaintiff.
Discussion
First, it is important to remember that just because a patient has been triaged to a low-acuity area does not mean she or he must have a minor problem. The provider still must maintain a high level of vigilance— regardless of the location of the patient in the ED.
Second, was this patient in atrial fibrillation, which is responsible in approximately 65% of all peripheral emboli? The abrupt onset of this patient’s symptoms is much more compatible with an embolic origin of her symptoms rather than a thrombus (ie, symptoms of claudication).
Lastly, a diagnosis of cellulitis is inconsistent with the physical findings of the PA, as well as those of the triage nurse and paramedics. This patient’s feet were cool to the touch whereas cellulitis presents with erythema and increased warmth. While the presence of pulses was somewhat reassuring, the cool temperature of the feet and complaint of pain were indicators of the need to evaluate for a possible arterial origin of these findings. However, if this were an embolic phenomenon, peripheral arterial ultrasound would have probably been normal, and the outcome unchanged.
Case 3: Failure to Communicate
A 59-year-old man presented to his primary care physician (PCP) for intermittent right-hand weakness and numbness and tingling in his right arm during the previous 24 hours. As the PCP was concerned that the patient might be experiencing a transient ischemic attack (TIA), the patient and his wife were instructed to go directly to the ED of the local hospital. The PCP wrote a note stating that the patient needed “a stroke work up,” gave the note to the patient, and told him to give it to the ED staff.
The patient went directly to the ED and was immediately seen by a “rapid triage nurse.” He gave the note to the nurse and told her of the PCP’s concerns. The nurse documented on the hospital assessment form that the patient was high priority and needed to be seen immediately. She attached the PCP’s note to the front of the form.
The patient was then seen by the traditional triage nurse. After evaluation, she changed the priority from high to low acuity. The triage nurse later stated later that she never saw the PCP’s note, nor did she obtain any history regarding the concerns of the PCP.
The patient was then evaluated by an EP in the low-acuity (or minor-care) area of the ED. The EP later stated that he never saw the note from the PCP, and had not received any information regarding a suspected TIA or stroke. The EP ordered a right wrist X-ray, diagnosed carpel tunnel syndrome, and prescribed an anti-inflammatory medication as well as follow-up with a hand surgeon.
The initial (rapid triage) nurse saw the patient leaving the ED at the time of discharge and thought he had not been in the ED long enough to have undergone a stroke work up. She reviewed his paperwork and saw the patient had not received the indicated work up. The nurse called the patient’s house and left a message on the answering machine notifying him of the need to return to the ED. The patient arrived back to the ED approximately 2 hours later.
On the second ED presentation that day, the patient was evaluated by a different EP. The patient had blood drawn, an electrocardiogram, and a noncontrast computed tomography scan of the brain, the results of which were all normal. The EP concluded the patient required admission to the hospital for additional work up (eg, carotid Doppler ultrasound). The hospitalist was paged, and told the EP he would be there “as soon as possible.” However, after several hours delay, and no hospitalist, the patient became impatient and expressed the desire to go home. The EP urged the patient to follow up with his PCP in the morning to complete the evaluation.
The next day, before seeing his PCP, the patient suffered an ischemic stroke with right-sided hemiparesis. The case went to trial, and the jury found in favor of the plaintiff.
Discussion
Unfortunately, multiple opportunities were lost in obtaining the correct care at the right time for this patient. Lack of communication and poor communication are frequently cited as causes in medical malpractice cases, and this case perfectly illustrates this problem.
First, the PCP should have called the ED and spoken to the EP directly. This would have provided the PCP the opportunity to express his concerns directly to the treating physician. This kind of one-on-one communication between physicians will always be superior to a hand-written note.
Second, it is unclear why the triage nurse changed the initial nurse’s correct assessment. It is also unclear what happened to the PCP’s note—it was never seen again. Clearly there was miscommunication at this point between the triage nurse and the patient. This case further illustrates the importance of good triage. Once a patient is directed down the wrong pathway (ie, to minor care rather than the main treatment area), the situation becomes much more difficult to correct.
Next, the EP in the low-acuity area was probably falsely assured this patient had only a “minor” problem problem, and not something serious. Emergency physicians must be vigilant to the possibility that the patient can have something seriously wrong even if he or she has been triaged to a low-acuity area. A minor sore throat can turn out to be epiglottitis and a viral stomachache can turn out to be appendicitis. These patients deserve the same quality of history, physical examination, and differential diagnosis as any other patient in the ED.
Finally, while we are not responsible for hospitalists or consultants, we do have a responsibility to our patients. We need to ensure that the care they receive is the appropriate care. Possible alternatives to discharging this patient would have been to call another hospitalist for admission or to seek the input of the chief of the medical staff or the on-call hospital administrator. As EPs, we are frequently required to serve as the primary advocate for our patients.
There is the possibility that even if the patient had been admitted to the hospital, the outcome would have been the same. However, since he might have been a candidate for tissue plasminogen activator or interventional radiology if he had suffered the cerebrovascular accident as an inpatient, he lost his best chance for a good outcome.
- Gowrishankar S, Thenmozhi R, Balaji K, Pandian SK. Emergence of methicillin-resistant, vancomycin-intermediate Staphylococcus aureus among patients associated with group A Streptococcal pharyngitis infection in southern India. Infect Genet Evol. 2013;14:383-389.
- Wang LJ, Du XQ, Nyirimigabo E, Shou ST. A case report: concurrent infectious mononucleosis and community-associated methicillinresistant Staphylococcus aureus bacteremia. Am J Emerg Med. 2013. doi:10.1016/j.ajem.2013.10.033
- Kizhner VZ, Samara GJ, Panesar R, Krespi YP. MRSA bacteremia associated with Lemierre syndrome. Otolaryngol Head Neck Surg. 2011;145(suppl 2):P152,P153.
Case 1: Follow-up in Community-Acquired Methicillin- Resistant Staphylococcus Aureus Pharyngitis
A 73-year-old woman presented to the ED complaining of injuries she sustained following a minor fall at home. The patient’s past medical history was remarkable for diabetes mellitus (DM), hypertension, cerebrovascular accident, and a history of chronic pain. During the course of evaluation, the patient mentioned that she had experienced a sore throat. In addition to X-rays, the emergency physician (EP) ordered a rapid strep test (RST). All studies were normal and the patient was discharged home.
Over the next 2 months, the patient received medical treatment from other medical professionals, but not at the previous hospital. Reportedly, she did not complain of a sore throat during this time period. The patient did return to the same ED approximately 2 months later, complaining of cough and difficulty breathing; she died 5 days thereafter. No autopsy was performed.
A lawsuit was filed on behalf of the patient, stating the hospital breached the standard of care by not reporting the finding of MRSA directly to the treating physician, and that this led directly to the patient’s death by MRSA pneumonia. The jury returned a verdict in favor of the plaintiff for $32 million.
Discussion
This case illustrates two simple but important points: managing community-acquired MRSA (CA-MRSA) infections is a growing challenge for physicians; and hospital follow-up systems for positive findings (ie, fractures, blood cultures, etc) need to be consistently reliable.
It is estimated that 30% of healthy people carry S aureus in their anterior nares; colonization rates for the throat are much less studied. In one recent study, 265 throat swabs were collected from patients aged 14 to 65 years old, who complained of pharyngitis in an outpatient setting.1 A total of 165 S aureus isolates (62.3%) were recovered from the 265 swabs. For the S aureus isolates, 38.2% (63) grew CA-MRSA; the remaining 68.1% (102) were methicillin-sensitive S aureus (MSSA). Interestingly, of the 63 MRSA-positive swabs, over half also grew Group A Streptococcus. The natural disease progression of CA-MRSA pharyngitis is still unknown, as is what to do with a positive throat swab for CA-MRSA. While there are a few case reports of bacteremia and Lemmiere syndrome possibly related to CA-MRSA pharyngitis,2,3 more information is clearly needed. For this case, it is not possible to definitively determine the role of the positive throat swab for CAMRSA in the patient’s subsequent death.
The other teaching point in this case is much simpler and well defined. Simply put, patients expect to be informed of positive findings, whether the result is known at the time of their ED visit or sometime afterward. There needs to be a system in place that consistently and reliably provides important information to either the patient’s treating physician or to the patient. The manners in which this information is communicated are myriad and should take into account hospital resources, the role of the EP and nurse, and what works best for your locality. The “who” and “how” of the contact is not important: reliability, timeliness, and consistency need to be the key drivers of the system.
Case 2: Arterial Occlusion
A 61-year-old woman called emergency medical services (EMS) after noticing her feet felt cold to the touch and having difficulty ambulating. The paramedics noted the patient had normal vital signs and normal circulation in her legs, and she was transported to the ED without incident. Upon arrival to the ED, she was triaged as nonurgent and placed in the minor-care area. On nursing assessment, the patient’s feet were found to be cold, but with palpable pulses bilaterally. Her past medical history was significant for hypertension and DM.
The patient was seen by a physician assistant (PA), who found both feet cool to the touch, but with bilateral pulses present. She was administered intravenous morphine for pain and laboratory studies were ordered. At the time, the PA was concerned about arterial occlusion versus deep vein thrombosis (DVT) versus cellulitis. A venous ultrasound examination was ordered and shown to be negative for DVT. A complete blood count was remarkable only for mild leukocytosis. The PA discussed the case with the supervising EP; they agreed on a diagnosis of cellulitis and discharged the patient home with antibiotics and analgesics.
Approximately 12 hours after discharge, the patient presented back to the ED via ambulance. At that time, she was hypotensive and tachypneic, with a thready palpable pulse. On repeat examination, she no longer had pulses present in her feet. An arteriogram found complete occlusion of her arterial circulation at the level of the knees bilaterally, requiring bilateral belowthe- knee amputation.
The patient sued both the emergency medicine physician and the PA for failure to provide her with the necessary care during her initial ED visit, resulting in loss of limbs. The defendants claimed the patient could not prove gross negligence by clear and convincing evidence, as required by state law. Following the ensuing trial, the jury returned a $5 million verdict in favor of the plaintiff.
Discussion
First, it is important to remember that just because a patient has been triaged to a low-acuity area does not mean she or he must have a minor problem. The provider still must maintain a high level of vigilance— regardless of the location of the patient in the ED.
Second, was this patient in atrial fibrillation, which is responsible in approximately 65% of all peripheral emboli? The abrupt onset of this patient’s symptoms is much more compatible with an embolic origin of her symptoms rather than a thrombus (ie, symptoms of claudication).
Lastly, a diagnosis of cellulitis is inconsistent with the physical findings of the PA, as well as those of the triage nurse and paramedics. This patient’s feet were cool to the touch whereas cellulitis presents with erythema and increased warmth. While the presence of pulses was somewhat reassuring, the cool temperature of the feet and complaint of pain were indicators of the need to evaluate for a possible arterial origin of these findings. However, if this were an embolic phenomenon, peripheral arterial ultrasound would have probably been normal, and the outcome unchanged.
Case 3: Failure to Communicate
A 59-year-old man presented to his primary care physician (PCP) for intermittent right-hand weakness and numbness and tingling in his right arm during the previous 24 hours. As the PCP was concerned that the patient might be experiencing a transient ischemic attack (TIA), the patient and his wife were instructed to go directly to the ED of the local hospital. The PCP wrote a note stating that the patient needed “a stroke work up,” gave the note to the patient, and told him to give it to the ED staff.
The patient went directly to the ED and was immediately seen by a “rapid triage nurse.” He gave the note to the nurse and told her of the PCP’s concerns. The nurse documented on the hospital assessment form that the patient was high priority and needed to be seen immediately. She attached the PCP’s note to the front of the form.
The patient was then seen by the traditional triage nurse. After evaluation, she changed the priority from high to low acuity. The triage nurse later stated later that she never saw the PCP’s note, nor did she obtain any history regarding the concerns of the PCP.
The patient was then evaluated by an EP in the low-acuity (or minor-care) area of the ED. The EP later stated that he never saw the note from the PCP, and had not received any information regarding a suspected TIA or stroke. The EP ordered a right wrist X-ray, diagnosed carpel tunnel syndrome, and prescribed an anti-inflammatory medication as well as follow-up with a hand surgeon.
The initial (rapid triage) nurse saw the patient leaving the ED at the time of discharge and thought he had not been in the ED long enough to have undergone a stroke work up. She reviewed his paperwork and saw the patient had not received the indicated work up. The nurse called the patient’s house and left a message on the answering machine notifying him of the need to return to the ED. The patient arrived back to the ED approximately 2 hours later.
On the second ED presentation that day, the patient was evaluated by a different EP. The patient had blood drawn, an electrocardiogram, and a noncontrast computed tomography scan of the brain, the results of which were all normal. The EP concluded the patient required admission to the hospital for additional work up (eg, carotid Doppler ultrasound). The hospitalist was paged, and told the EP he would be there “as soon as possible.” However, after several hours delay, and no hospitalist, the patient became impatient and expressed the desire to go home. The EP urged the patient to follow up with his PCP in the morning to complete the evaluation.
The next day, before seeing his PCP, the patient suffered an ischemic stroke with right-sided hemiparesis. The case went to trial, and the jury found in favor of the plaintiff.
Discussion
Unfortunately, multiple opportunities were lost in obtaining the correct care at the right time for this patient. Lack of communication and poor communication are frequently cited as causes in medical malpractice cases, and this case perfectly illustrates this problem.
First, the PCP should have called the ED and spoken to the EP directly. This would have provided the PCP the opportunity to express his concerns directly to the treating physician. This kind of one-on-one communication between physicians will always be superior to a hand-written note.
Second, it is unclear why the triage nurse changed the initial nurse’s correct assessment. It is also unclear what happened to the PCP’s note—it was never seen again. Clearly there was miscommunication at this point between the triage nurse and the patient. This case further illustrates the importance of good triage. Once a patient is directed down the wrong pathway (ie, to minor care rather than the main treatment area), the situation becomes much more difficult to correct.
Next, the EP in the low-acuity area was probably falsely assured this patient had only a “minor” problem problem, and not something serious. Emergency physicians must be vigilant to the possibility that the patient can have something seriously wrong even if he or she has been triaged to a low-acuity area. A minor sore throat can turn out to be epiglottitis and a viral stomachache can turn out to be appendicitis. These patients deserve the same quality of history, physical examination, and differential diagnosis as any other patient in the ED.
Finally, while we are not responsible for hospitalists or consultants, we do have a responsibility to our patients. We need to ensure that the care they receive is the appropriate care. Possible alternatives to discharging this patient would have been to call another hospitalist for admission or to seek the input of the chief of the medical staff or the on-call hospital administrator. As EPs, we are frequently required to serve as the primary advocate for our patients.
There is the possibility that even if the patient had been admitted to the hospital, the outcome would have been the same. However, since he might have been a candidate for tissue plasminogen activator or interventional radiology if he had suffered the cerebrovascular accident as an inpatient, he lost his best chance for a good outcome.
Case 1: Follow-up in Community-Acquired Methicillin- Resistant Staphylococcus Aureus Pharyngitis
A 73-year-old woman presented to the ED complaining of injuries she sustained following a minor fall at home. The patient’s past medical history was remarkable for diabetes mellitus (DM), hypertension, cerebrovascular accident, and a history of chronic pain. During the course of evaluation, the patient mentioned that she had experienced a sore throat. In addition to X-rays, the emergency physician (EP) ordered a rapid strep test (RST). All studies were normal and the patient was discharged home.
Over the next 2 months, the patient received medical treatment from other medical professionals, but not at the previous hospital. Reportedly, she did not complain of a sore throat during this time period. The patient did return to the same ED approximately 2 months later, complaining of cough and difficulty breathing; she died 5 days thereafter. No autopsy was performed.
A lawsuit was filed on behalf of the patient, stating the hospital breached the standard of care by not reporting the finding of MRSA directly to the treating physician, and that this led directly to the patient’s death by MRSA pneumonia. The jury returned a verdict in favor of the plaintiff for $32 million.
Discussion
This case illustrates two simple but important points: managing community-acquired MRSA (CA-MRSA) infections is a growing challenge for physicians; and hospital follow-up systems for positive findings (ie, fractures, blood cultures, etc) need to be consistently reliable.
It is estimated that 30% of healthy people carry S aureus in their anterior nares; colonization rates for the throat are much less studied. In one recent study, 265 throat swabs were collected from patients aged 14 to 65 years old, who complained of pharyngitis in an outpatient setting.1 A total of 165 S aureus isolates (62.3%) were recovered from the 265 swabs. For the S aureus isolates, 38.2% (63) grew CA-MRSA; the remaining 68.1% (102) were methicillin-sensitive S aureus (MSSA). Interestingly, of the 63 MRSA-positive swabs, over half also grew Group A Streptococcus. The natural disease progression of CA-MRSA pharyngitis is still unknown, as is what to do with a positive throat swab for CA-MRSA. While there are a few case reports of bacteremia and Lemmiere syndrome possibly related to CA-MRSA pharyngitis,2,3 more information is clearly needed. For this case, it is not possible to definitively determine the role of the positive throat swab for CAMRSA in the patient’s subsequent death.
The other teaching point in this case is much simpler and well defined. Simply put, patients expect to be informed of positive findings, whether the result is known at the time of their ED visit or sometime afterward. There needs to be a system in place that consistently and reliably provides important information to either the patient’s treating physician or to the patient. The manners in which this information is communicated are myriad and should take into account hospital resources, the role of the EP and nurse, and what works best for your locality. The “who” and “how” of the contact is not important: reliability, timeliness, and consistency need to be the key drivers of the system.
Case 2: Arterial Occlusion
A 61-year-old woman called emergency medical services (EMS) after noticing her feet felt cold to the touch and having difficulty ambulating. The paramedics noted the patient had normal vital signs and normal circulation in her legs, and she was transported to the ED without incident. Upon arrival to the ED, she was triaged as nonurgent and placed in the minor-care area. On nursing assessment, the patient’s feet were found to be cold, but with palpable pulses bilaterally. Her past medical history was significant for hypertension and DM.
The patient was seen by a physician assistant (PA), who found both feet cool to the touch, but with bilateral pulses present. She was administered intravenous morphine for pain and laboratory studies were ordered. At the time, the PA was concerned about arterial occlusion versus deep vein thrombosis (DVT) versus cellulitis. A venous ultrasound examination was ordered and shown to be negative for DVT. A complete blood count was remarkable only for mild leukocytosis. The PA discussed the case with the supervising EP; they agreed on a diagnosis of cellulitis and discharged the patient home with antibiotics and analgesics.
Approximately 12 hours after discharge, the patient presented back to the ED via ambulance. At that time, she was hypotensive and tachypneic, with a thready palpable pulse. On repeat examination, she no longer had pulses present in her feet. An arteriogram found complete occlusion of her arterial circulation at the level of the knees bilaterally, requiring bilateral belowthe- knee amputation.
The patient sued both the emergency medicine physician and the PA for failure to provide her with the necessary care during her initial ED visit, resulting in loss of limbs. The defendants claimed the patient could not prove gross negligence by clear and convincing evidence, as required by state law. Following the ensuing trial, the jury returned a $5 million verdict in favor of the plaintiff.
Discussion
First, it is important to remember that just because a patient has been triaged to a low-acuity area does not mean she or he must have a minor problem. The provider still must maintain a high level of vigilance— regardless of the location of the patient in the ED.
Second, was this patient in atrial fibrillation, which is responsible in approximately 65% of all peripheral emboli? The abrupt onset of this patient’s symptoms is much more compatible with an embolic origin of her symptoms rather than a thrombus (ie, symptoms of claudication).
Lastly, a diagnosis of cellulitis is inconsistent with the physical findings of the PA, as well as those of the triage nurse and paramedics. This patient’s feet were cool to the touch whereas cellulitis presents with erythema and increased warmth. While the presence of pulses was somewhat reassuring, the cool temperature of the feet and complaint of pain were indicators of the need to evaluate for a possible arterial origin of these findings. However, if this were an embolic phenomenon, peripheral arterial ultrasound would have probably been normal, and the outcome unchanged.
Case 3: Failure to Communicate
A 59-year-old man presented to his primary care physician (PCP) for intermittent right-hand weakness and numbness and tingling in his right arm during the previous 24 hours. As the PCP was concerned that the patient might be experiencing a transient ischemic attack (TIA), the patient and his wife were instructed to go directly to the ED of the local hospital. The PCP wrote a note stating that the patient needed “a stroke work up,” gave the note to the patient, and told him to give it to the ED staff.
The patient went directly to the ED and was immediately seen by a “rapid triage nurse.” He gave the note to the nurse and told her of the PCP’s concerns. The nurse documented on the hospital assessment form that the patient was high priority and needed to be seen immediately. She attached the PCP’s note to the front of the form.
The patient was then seen by the traditional triage nurse. After evaluation, she changed the priority from high to low acuity. The triage nurse later stated later that she never saw the PCP’s note, nor did she obtain any history regarding the concerns of the PCP.
The patient was then evaluated by an EP in the low-acuity (or minor-care) area of the ED. The EP later stated that he never saw the note from the PCP, and had not received any information regarding a suspected TIA or stroke. The EP ordered a right wrist X-ray, diagnosed carpel tunnel syndrome, and prescribed an anti-inflammatory medication as well as follow-up with a hand surgeon.
The initial (rapid triage) nurse saw the patient leaving the ED at the time of discharge and thought he had not been in the ED long enough to have undergone a stroke work up. She reviewed his paperwork and saw the patient had not received the indicated work up. The nurse called the patient’s house and left a message on the answering machine notifying him of the need to return to the ED. The patient arrived back to the ED approximately 2 hours later.
On the second ED presentation that day, the patient was evaluated by a different EP. The patient had blood drawn, an electrocardiogram, and a noncontrast computed tomography scan of the brain, the results of which were all normal. The EP concluded the patient required admission to the hospital for additional work up (eg, carotid Doppler ultrasound). The hospitalist was paged, and told the EP he would be there “as soon as possible.” However, after several hours delay, and no hospitalist, the patient became impatient and expressed the desire to go home. The EP urged the patient to follow up with his PCP in the morning to complete the evaluation.
The next day, before seeing his PCP, the patient suffered an ischemic stroke with right-sided hemiparesis. The case went to trial, and the jury found in favor of the plaintiff.
Discussion
Unfortunately, multiple opportunities were lost in obtaining the correct care at the right time for this patient. Lack of communication and poor communication are frequently cited as causes in medical malpractice cases, and this case perfectly illustrates this problem.
First, the PCP should have called the ED and spoken to the EP directly. This would have provided the PCP the opportunity to express his concerns directly to the treating physician. This kind of one-on-one communication between physicians will always be superior to a hand-written note.
Second, it is unclear why the triage nurse changed the initial nurse’s correct assessment. It is also unclear what happened to the PCP’s note—it was never seen again. Clearly there was miscommunication at this point between the triage nurse and the patient. This case further illustrates the importance of good triage. Once a patient is directed down the wrong pathway (ie, to minor care rather than the main treatment area), the situation becomes much more difficult to correct.
Next, the EP in the low-acuity area was probably falsely assured this patient had only a “minor” problem problem, and not something serious. Emergency physicians must be vigilant to the possibility that the patient can have something seriously wrong even if he or she has been triaged to a low-acuity area. A minor sore throat can turn out to be epiglottitis and a viral stomachache can turn out to be appendicitis. These patients deserve the same quality of history, physical examination, and differential diagnosis as any other patient in the ED.
Finally, while we are not responsible for hospitalists or consultants, we do have a responsibility to our patients. We need to ensure that the care they receive is the appropriate care. Possible alternatives to discharging this patient would have been to call another hospitalist for admission or to seek the input of the chief of the medical staff or the on-call hospital administrator. As EPs, we are frequently required to serve as the primary advocate for our patients.
There is the possibility that even if the patient had been admitted to the hospital, the outcome would have been the same. However, since he might have been a candidate for tissue plasminogen activator or interventional radiology if he had suffered the cerebrovascular accident as an inpatient, he lost his best chance for a good outcome.
- Gowrishankar S, Thenmozhi R, Balaji K, Pandian SK. Emergence of methicillin-resistant, vancomycin-intermediate Staphylococcus aureus among patients associated with group A Streptococcal pharyngitis infection in southern India. Infect Genet Evol. 2013;14:383-389.
- Wang LJ, Du XQ, Nyirimigabo E, Shou ST. A case report: concurrent infectious mononucleosis and community-associated methicillinresistant Staphylococcus aureus bacteremia. Am J Emerg Med. 2013. doi:10.1016/j.ajem.2013.10.033
- Kizhner VZ, Samara GJ, Panesar R, Krespi YP. MRSA bacteremia associated with Lemierre syndrome. Otolaryngol Head Neck Surg. 2011;145(suppl 2):P152,P153.
- Gowrishankar S, Thenmozhi R, Balaji K, Pandian SK. Emergence of methicillin-resistant, vancomycin-intermediate Staphylococcus aureus among patients associated with group A Streptococcal pharyngitis infection in southern India. Infect Genet Evol. 2013;14:383-389.
- Wang LJ, Du XQ, Nyirimigabo E, Shou ST. A case report: concurrent infectious mononucleosis and community-associated methicillinresistant Staphylococcus aureus bacteremia. Am J Emerg Med. 2013. doi:10.1016/j.ajem.2013.10.033
- Kizhner VZ, Samara GJ, Panesar R, Krespi YP. MRSA bacteremia associated with Lemierre syndrome. Otolaryngol Head Neck Surg. 2011;145(suppl 2):P152,P153.
2014 budget reduces spending for ACA, IPAB
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.

The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.
The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.
The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault

United States earns D+ on support for emergency care
State and federal lawmakers are doing a dismal job of supporting the nation’s emergency departments, creating poor access to emergency care, a volatile medical liability environment, and providing insufficient resources for disaster preparedness, according to a national and state-level report card from the American College of Emergency Physicians.
The organization gave the nation an overall grade of D+ for its policies on emergency care.
The report does not address the quality of care provided directly by emergency physicians and other providers.

The emergency care environment has worsened over the last few years, ACEP found. In 2009, the last time the college issued a report card, the U.S. earned an overall grade of C-. The lower grade this year is due in part to state-level funding cuts for emergency departments.
"This report card is sounding an alarm. Rhetoric and policy for the past several years has focused primarily on preventing emergency visits. Is it any surprise that our national grade has dropped to a D+?" said Dr. Alex Rosenau, president of the American College of Emergency Physicians.
The report card is also a call to action for Congress and the president, Dr. Rosenau said, because the Affordable Care Act is likely to put an even greater strain on struggling emergency departments.
EDs can expect an influx of patients as millions of Americans are insured for the first time, said Dr. Rosenau, senior vice chair of emergency medicine at Lehigh Valley Health Network in Allentown, Pa. Primary care physician shortages – combined with low Medicaid payments – mean that the ED is likely to be the main source of care for many of these newly insured patients, he said.
"More patients are coming," he said. "We want to be ready."

The report card scores the measures related to access to emergency care, quality and patient safety, the medical liability environment, public health and injury prevention, and disaster preparedness. An ACEP task force analyzed data from the Centers for Disease Control and Prevention, the National Highway Traffic Safety Administration, the Centers for Medicare and Medicaid Services, and the American Medical Association.
The nation’s lowest grade was for access to emergency care (D–), which examines the number of emergency physicians, access to treatment centers, financial barriers, and hospital capacity. The poor grade reflects recent hospital closures, coupled with the growing shortage of psychiatric care beds and hospital inpatient beds.
In the area of quality and patient safety, which measures the implementation of triage policies, as well as the use of computerized practitioner order entry, the U.S. received a C.
The United States received a C– in the area of medical liability, which examines state tort reform efforts and the general legal atmosphere for physicians.
The country also got a C for policies related to public health, including traffic safety and drunk driving, immunizations, and injury prevention.
Finally, ACEP awarded a grade of C– for disaster preparedness, which includes funding for state coordination and training not only during natural disasters, but also during terrorist events and health outbreaks.
"I am alarmed by the lack of support for emergency care," said Dr. Jon Mark Hirshon, chair of the report card task force who is with the department of emergency medicine at the University of Maryland, Baltimore. "When you need an emergency department, you need it. We must send a clear message to our state and federal legislators to support this crucial part of the health care system."
The report card also graded state-level support of emergency medicine. The District of Columbia earned the highest overall (B-) and was joined in the top five by Massachusetts, Maine, Nebraska, and Colorado. In contrast, Wyoming ranked last, earned a failing grade overall. The other bottom-ranked states were Arkansas, New Mexico, Montana, and Kentucky.
ACEP officials called the report a "roadmap" for improving emergency care in this country. The college called on Congress to:
• Fund the Workforce Commission, created under the ACA, to investigate health provider shortages.
• Pass legislation to provide limited liability protections for emergency and on-call physicians who perform services mandated by the federal Emergency Medical Treatment & Labor Act (EMTALA).
• Fund ACA pilot programs to design innovative models of regionalized emergency care and trauma systems.
• Fund the Emergency Care Coordination Center at the Health and Human Services department.
• Fund graduate medical education program in emergency care.
• Hold hearings to examine how the ACA is impacting the emergency department safety net.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
State and federal lawmakers are doing a dismal job of supporting the nation’s emergency departments, creating poor access to emergency care, a volatile medical liability environment, and providing insufficient resources for disaster preparedness, according to a national and state-level report card from the American College of Emergency Physicians.
The organization gave the nation an overall grade of D+ for its policies on emergency care.
The report does not address the quality of care provided directly by emergency physicians and other providers.
The emergency care environment has worsened over the last few years, ACEP found. In 2009, the last time the college issued a report card, the U.S. earned an overall grade of C-. The lower grade this year is due in part to state-level funding cuts for emergency departments.
"This report card is sounding an alarm. Rhetoric and policy for the past several years has focused primarily on preventing emergency visits. Is it any surprise that our national grade has dropped to a D+?" said Dr. Alex Rosenau, president of the American College of Emergency Physicians.
The report card is also a call to action for Congress and the president, Dr. Rosenau said, because the Affordable Care Act is likely to put an even greater strain on struggling emergency departments.
EDs can expect an influx of patients as millions of Americans are insured for the first time, said Dr. Rosenau, senior vice chair of emergency medicine at Lehigh Valley Health Network in Allentown, Pa. Primary care physician shortages – combined with low Medicaid payments – mean that the ED is likely to be the main source of care for many of these newly insured patients, he said.
"More patients are coming," he said. "We want to be ready."
The report card scores the measures related to access to emergency care, quality and patient safety, the medical liability environment, public health and injury prevention, and disaster preparedness. An ACEP task force analyzed data from the Centers for Disease Control and Prevention, the National Highway Traffic Safety Administration, the Centers for Medicare and Medicaid Services, and the American Medical Association.
The nation’s lowest grade was for access to emergency care (D–), which examines the number of emergency physicians, access to treatment centers, financial barriers, and hospital capacity. The poor grade reflects recent hospital closures, coupled with the growing shortage of psychiatric care beds and hospital inpatient beds.
In the area of quality and patient safety, which measures the implementation of triage policies, as well as the use of computerized practitioner order entry, the U.S. received a C.
The United States received a C– in the area of medical liability, which examines state tort reform efforts and the general legal atmosphere for physicians.
The country also got a C for policies related to public health, including traffic safety and drunk driving, immunizations, and injury prevention.
Finally, ACEP awarded a grade of C– for disaster preparedness, which includes funding for state coordination and training not only during natural disasters, but also during terrorist events and health outbreaks.
"I am alarmed by the lack of support for emergency care," said Dr. Jon Mark Hirshon, chair of the report card task force who is with the department of emergency medicine at the University of Maryland, Baltimore. "When you need an emergency department, you need it. We must send a clear message to our state and federal legislators to support this crucial part of the health care system."
The report card also graded state-level support of emergency medicine. The District of Columbia earned the highest overall (B-) and was joined in the top five by Massachusetts, Maine, Nebraska, and Colorado. In contrast, Wyoming ranked last, earned a failing grade overall. The other bottom-ranked states were Arkansas, New Mexico, Montana, and Kentucky.
ACEP officials called the report a "roadmap" for improving emergency care in this country. The college called on Congress to:
• Fund the Workforce Commission, created under the ACA, to investigate health provider shortages.
• Pass legislation to provide limited liability protections for emergency and on-call physicians who perform services mandated by the federal Emergency Medical Treatment & Labor Act (EMTALA).
• Fund ACA pilot programs to design innovative models of regionalized emergency care and trauma systems.
• Fund the Emergency Care Coordination Center at the Health and Human Services department.
• Fund graduate medical education program in emergency care.
• Hold hearings to examine how the ACA is impacting the emergency department safety net.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
State and federal lawmakers are doing a dismal job of supporting the nation’s emergency departments, creating poor access to emergency care, a volatile medical liability environment, and providing insufficient resources for disaster preparedness, according to a national and state-level report card from the American College of Emergency Physicians.
The organization gave the nation an overall grade of D+ for its policies on emergency care.
The report does not address the quality of care provided directly by emergency physicians and other providers.
The emergency care environment has worsened over the last few years, ACEP found. In 2009, the last time the college issued a report card, the U.S. earned an overall grade of C-. The lower grade this year is due in part to state-level funding cuts for emergency departments.
"This report card is sounding an alarm. Rhetoric and policy for the past several years has focused primarily on preventing emergency visits. Is it any surprise that our national grade has dropped to a D+?" said Dr. Alex Rosenau, president of the American College of Emergency Physicians.
The report card is also a call to action for Congress and the president, Dr. Rosenau said, because the Affordable Care Act is likely to put an even greater strain on struggling emergency departments.
EDs can expect an influx of patients as millions of Americans are insured for the first time, said Dr. Rosenau, senior vice chair of emergency medicine at Lehigh Valley Health Network in Allentown, Pa. Primary care physician shortages – combined with low Medicaid payments – mean that the ED is likely to be the main source of care for many of these newly insured patients, he said.
"More patients are coming," he said. "We want to be ready."
The report card scores the measures related to access to emergency care, quality and patient safety, the medical liability environment, public health and injury prevention, and disaster preparedness. An ACEP task force analyzed data from the Centers for Disease Control and Prevention, the National Highway Traffic Safety Administration, the Centers for Medicare and Medicaid Services, and the American Medical Association.
The nation’s lowest grade was for access to emergency care (D–), which examines the number of emergency physicians, access to treatment centers, financial barriers, and hospital capacity. The poor grade reflects recent hospital closures, coupled with the growing shortage of psychiatric care beds and hospital inpatient beds.
In the area of quality and patient safety, which measures the implementation of triage policies, as well as the use of computerized practitioner order entry, the U.S. received a C.
The United States received a C– in the area of medical liability, which examines state tort reform efforts and the general legal atmosphere for physicians.
The country also got a C for policies related to public health, including traffic safety and drunk driving, immunizations, and injury prevention.
Finally, ACEP awarded a grade of C– for disaster preparedness, which includes funding for state coordination and training not only during natural disasters, but also during terrorist events and health outbreaks.
"I am alarmed by the lack of support for emergency care," said Dr. Jon Mark Hirshon, chair of the report card task force who is with the department of emergency medicine at the University of Maryland, Baltimore. "When you need an emergency department, you need it. We must send a clear message to our state and federal legislators to support this crucial part of the health care system."
The report card also graded state-level support of emergency medicine. The District of Columbia earned the highest overall (B-) and was joined in the top five by Massachusetts, Maine, Nebraska, and Colorado. In contrast, Wyoming ranked last, earned a failing grade overall. The other bottom-ranked states were Arkansas, New Mexico, Montana, and Kentucky.
ACEP officials called the report a "roadmap" for improving emergency care in this country. The college called on Congress to:
• Fund the Workforce Commission, created under the ACA, to investigate health provider shortages.
• Pass legislation to provide limited liability protections for emergency and on-call physicians who perform services mandated by the federal Emergency Medical Treatment & Labor Act (EMTALA).
• Fund ACA pilot programs to design innovative models of regionalized emergency care and trauma systems.
• Fund the Emergency Care Coordination Center at the Health and Human Services department.
• Fund graduate medical education program in emergency care.
• Hold hearings to examine how the ACA is impacting the emergency department safety net.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY

Hawaii named healthiest state in 2013
Residents of Hawaii are living in America’s healthiest state, according to "America's Health Rankings- 2013 Edition."
Hawaii, which has never finished out of the top six since the rankings began in 1990, reclaimed the top spot it last held in 2008. Vermont, which finished first in each of the previous 4 years, was second in 2013, followed by Minnesota, Massachusetts, and New Hampshire.
The bottom five consisted of West Virginia (46) and four states in the Southeast: Alabama (47), Louisiana (48), Arkansas (49), and Mississippi (50). Mississippi has finished "among the bottom three states since the inception of the rankings in 1990," the report said.
For the 2013 report, each state was ranked using 27 measures that represent various aspects of health, grouped into five categories: behaviors, community and environment, policy, clinical care, and outcomes.
"America’s Health Rankings" is published jointly by the United Health Foundation, the American Public Health Association, and the Partnership for Prevention. The private, not-for-profit United Health Foundation was founded in 1999 by UnitedHealth Group, which operates UnitedHealthcare.

Residents of Hawaii are living in America’s healthiest state, according to "America's Health Rankings- 2013 Edition."
Hawaii, which has never finished out of the top six since the rankings began in 1990, reclaimed the top spot it last held in 2008. Vermont, which finished first in each of the previous 4 years, was second in 2013, followed by Minnesota, Massachusetts, and New Hampshire.
The bottom five consisted of West Virginia (46) and four states in the Southeast: Alabama (47), Louisiana (48), Arkansas (49), and Mississippi (50). Mississippi has finished "among the bottom three states since the inception of the rankings in 1990," the report said.
For the 2013 report, each state was ranked using 27 measures that represent various aspects of health, grouped into five categories: behaviors, community and environment, policy, clinical care, and outcomes.
"America’s Health Rankings" is published jointly by the United Health Foundation, the American Public Health Association, and the Partnership for Prevention. The private, not-for-profit United Health Foundation was founded in 1999 by UnitedHealth Group, which operates UnitedHealthcare.
Residents of Hawaii are living in America’s healthiest state, according to "America's Health Rankings- 2013 Edition."
Hawaii, which has never finished out of the top six since the rankings began in 1990, reclaimed the top spot it last held in 2008. Vermont, which finished first in each of the previous 4 years, was second in 2013, followed by Minnesota, Massachusetts, and New Hampshire.
The bottom five consisted of West Virginia (46) and four states in the Southeast: Alabama (47), Louisiana (48), Arkansas (49), and Mississippi (50). Mississippi has finished "among the bottom three states since the inception of the rankings in 1990," the report said.
For the 2013 report, each state was ranked using 27 measures that represent various aspects of health, grouped into five categories: behaviors, community and environment, policy, clinical care, and outcomes.
"America’s Health Rankings" is published jointly by the United Health Foundation, the American Public Health Association, and the Partnership for Prevention. The private, not-for-profit United Health Foundation was founded in 1999 by UnitedHealth Group, which operates UnitedHealthcare.
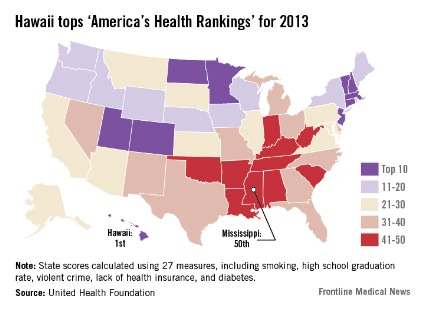
Medicare to start releasing individual physician payment data
Reversing more than 30 years of policy, federal officials announced they would soon begin releasing data on how much Medicare pays to individual physicians.
Officials at the Centers for Medicare and Medicaid Services (CMS) announced Jan. 14 that they would take a "case-by-case" approach to the release of individual physician payment information, weighing the right for privacy against the value to the public in each Freedom of Information Act request they receive.

In addition to fielding individual requests for physician data, the agency plans to generate and publish aggregate data sets on physician services.
The policy change will take effect on March 18.
"As CMS makes a determination about how and when to disclose any information on a physician’s Medicare payment, we intend to consider the importance of protecting physicians’ privacy and ensuring the accuracy of any data released as well as appropriate protections to limit potential misuse of the information," Jonathan Blum, CMS Principal Deputy Administrator, wrote in a blog post on Jan. 14.
Last May, a federal judge cleared the way for this policy shift back by lifting an injunction that had previously barred the agency from making public its database of Medicare physician claims.
The new policy has plenty of benefits, Mr. Blum wrote, including allowing providers to collaborate on better care management, giving consumers more reliable measures of quality and performance, and allowing journalists and researchers to identify Medicare waste, fraud, and abuse.
The change is also part of a broader effort at the CMS to make health care prices more transparent.
Last May, the CMS published the average charges for the 100 most common inpatient services at hospitals around the country. And in June, the agency released average charges for 30 selected outpatient procedures, ranging from echocardiograms to pulmonary tests.
Physicians’ groups have been urging caution as the CMS evaluated the release of physician data. In a Sept. 5 letter signed by the American Medical Association as well as several specialty and state medical societies, physicians said that the CMS must educate the public about the limitations of analyzing Medicare claims data. For example, Medicare claims may not include many factors that influence the cost of medical care, including specialty, location, patient mix, other demographics, and practice costs.
In the letter, the physician organizations urged the CMS to provide access to data to organizations that have experience in handling and analyzing Medicare data. And they called for the opportunity to review and correct their information in a timely manner.
"Medicare data is highly susceptible to misleading conclusions," the letter said. "CMS should undertake a detailed educational program to explain any Medicare data release program and openly address its limitations, including that the data may take into account only a small fraction of a physician’s patient population or may be outdated."
Reversing more than 30 years of policy, federal officials announced they would soon begin releasing data on how much Medicare pays to individual physicians.
Officials at the Centers for Medicare and Medicaid Services (CMS) announced Jan. 14 that they would take a "case-by-case" approach to the release of individual physician payment information, weighing the right for privacy against the value to the public in each Freedom of Information Act request they receive.
In addition to fielding individual requests for physician data, the agency plans to generate and publish aggregate data sets on physician services.
The policy change will take effect on March 18.
"As CMS makes a determination about how and when to disclose any information on a physician’s Medicare payment, we intend to consider the importance of protecting physicians’ privacy and ensuring the accuracy of any data released as well as appropriate protections to limit potential misuse of the information," Jonathan Blum, CMS Principal Deputy Administrator, wrote in a blog post on Jan. 14.
Last May, a federal judge cleared the way for this policy shift back by lifting an injunction that had previously barred the agency from making public its database of Medicare physician claims.
The new policy has plenty of benefits, Mr. Blum wrote, including allowing providers to collaborate on better care management, giving consumers more reliable measures of quality and performance, and allowing journalists and researchers to identify Medicare waste, fraud, and abuse.
The change is also part of a broader effort at the CMS to make health care prices more transparent.
Last May, the CMS published the average charges for the 100 most common inpatient services at hospitals around the country. And in June, the agency released average charges for 30 selected outpatient procedures, ranging from echocardiograms to pulmonary tests.
Physicians’ groups have been urging caution as the CMS evaluated the release of physician data. In a Sept. 5 letter signed by the American Medical Association as well as several specialty and state medical societies, physicians said that the CMS must educate the public about the limitations of analyzing Medicare claims data. For example, Medicare claims may not include many factors that influence the cost of medical care, including specialty, location, patient mix, other demographics, and practice costs.
In the letter, the physician organizations urged the CMS to provide access to data to organizations that have experience in handling and analyzing Medicare data. And they called for the opportunity to review and correct their information in a timely manner.
"Medicare data is highly susceptible to misleading conclusions," the letter said. "CMS should undertake a detailed educational program to explain any Medicare data release program and openly address its limitations, including that the data may take into account only a small fraction of a physician’s patient population or may be outdated."
Reversing more than 30 years of policy, federal officials announced they would soon begin releasing data on how much Medicare pays to individual physicians.
Officials at the Centers for Medicare and Medicaid Services (CMS) announced Jan. 14 that they would take a "case-by-case" approach to the release of individual physician payment information, weighing the right for privacy against the value to the public in each Freedom of Information Act request they receive.
In addition to fielding individual requests for physician data, the agency plans to generate and publish aggregate data sets on physician services.
The policy change will take effect on March 18.
"As CMS makes a determination about how and when to disclose any information on a physician’s Medicare payment, we intend to consider the importance of protecting physicians’ privacy and ensuring the accuracy of any data released as well as appropriate protections to limit potential misuse of the information," Jonathan Blum, CMS Principal Deputy Administrator, wrote in a blog post on Jan. 14.
Last May, a federal judge cleared the way for this policy shift back by lifting an injunction that had previously barred the agency from making public its database of Medicare physician claims.
The new policy has plenty of benefits, Mr. Blum wrote, including allowing providers to collaborate on better care management, giving consumers more reliable measures of quality and performance, and allowing journalists and researchers to identify Medicare waste, fraud, and abuse.
The change is also part of a broader effort at the CMS to make health care prices more transparent.
Last May, the CMS published the average charges for the 100 most common inpatient services at hospitals around the country. And in June, the agency released average charges for 30 selected outpatient procedures, ranging from echocardiograms to pulmonary tests.
Physicians’ groups have been urging caution as the CMS evaluated the release of physician data. In a Sept. 5 letter signed by the American Medical Association as well as several specialty and state medical societies, physicians said that the CMS must educate the public about the limitations of analyzing Medicare claims data. For example, Medicare claims may not include many factors that influence the cost of medical care, including specialty, location, patient mix, other demographics, and practice costs.
In the letter, the physician organizations urged the CMS to provide access to data to organizations that have experience in handling and analyzing Medicare data. And they called for the opportunity to review and correct their information in a timely manner.
"Medicare data is highly susceptible to misleading conclusions," the letter said. "CMS should undertake a detailed educational program to explain any Medicare data release program and openly address its limitations, including that the data may take into account only a small fraction of a physician’s patient population or may be outdated."
