User login
Cardiologists’ incomes bounce back from pandemic: Survey
The financial struggles created by the pandemic have eased somewhat, but physicians are still facing an array of challenges, including increased workloads and longer hours. All in all, however, things seem to be looking up.
More than 13,000 physicians in more than 29 specialties shared information about their incomes and other aspects of their careers in a survey conducted by Medscape. The responses showed a trend back to something like normal after the initial blow of the COVID-19 pandemic.
As the profession began to recover from the pandemic, cardiologists reported that their incomes increased in 2021, reaching an average of $490,000 for the year, up from $459,000 the previous year. This was in keeping with physicians in other specialties. “Compensation for most physicians is trending back up, as demands for physicians accelerates,” said James Taylor, group president and chief operating officer of AMN Healthcare’s Physician & Leadership Solutions Division. “The market for physicians has done a complete 180 over just 7 or 8 months.” And though inflation is on everyone’s mind these days, rising salaries have helped physicians keep up with rising prices.
Despite the increase in income (and the accompanying increased workload), nearly 30% of cardiologists have taken on extra work, most of that being medical work, but a few did report unrelated side hustles. This may be due not to a shortfall in income, but rather to a desire to pad the coffers for the future. Lauren Podnos, a financial planner with Wealth Care, a firm that specializes in working with physicians and other health care professionals, points out that many physicians like to build wealth as quickly as possible as a hedge against possible burnout later on. “With physicians,” she said, “we work to get to the point where they have the freedom to do whatever they want – cut back and work part-time or transition into another career – so if they do burn out, they have other options.”
Though physician pay rose overall, not all cardiologists enjoyed a boost in income. However, those who did lose ground did not always lay the blame on COVID-19: General pay cuts were mentioned, for example. For physicians overall, a gender pay gap still remains, with men averaging $373,000 per year, in contrast to women who make $282,000. With more women moving into higher-paying specialties, the gap has narrowed somewhat in recent years, and industry leaders are making efforts to accelerate that trend. “A great many of the specialty organizations have efforts underway not just to increase the number of women in specialties but also to address gender pay gaps and bias in evaluations during residency and fellowship,” said Ron Holder, chief operating officer of the Medical Group Management Association (MGMA).
Incentive bonuses helped bump up income as well. Overall, 57% of physicians receive some kind of incentive bonus; the average for cardiologists was $85,000 last year, up from $71,000 the prior year. While such bonuses can certainly help the bottom line, they’re not always an unmitigated good. A 2021 study found that incentive programs can cause people to prioritize time spent at work and with work colleagues at the expense of family and personal relationships, a potentially troubling finding with so many physicians struggling with depression and burnout. “There’s been a lot of previous evidence showing that the more time we spend with our loved ones the happier we are,” said Julia Hur, PhD, assistant professor of management and organizations at New York University’s Stern School of Business, and lead author of the study. “The core argument of this study is about attention, and performance incentives create an attentional fixation on money,” she said, “causing people to spend more time with work colleagues and people who are helpful to their careers. And that takes away from time for family and friends.”
Still rewarding
Getting paid well is one thing; feeling that you’re being paid well is another. Only 57% of cardiologists who responded to the survey said they felt they were fairly compensated for their work. This puts them at roughly the middle of the pack of specialties. Contrast that with physicians in public health and preventive medicine who topped the charts on this one, with 72% of these doctors feeling that they were being paid fairly for their work.
However, cardiology did rank at the top of specialties whose members said they would choose medicine if they had a chance to do it again, though that number was down from the previous year (81% in 2021 versus 86% in 2020). Of cardiologists surveyed, 88% would choose cardiology if they got a do-over.
Cardiologists spend an average of 16.4 hours each week on paperwork and administration. That’s only slightly higher than the average for all specialties, about 15.5 hours a week. Despite billing hassles and low reimbursement rates, 80% of cardiologists polled say they plan to continue taking new and existing Medicare and Medicaid patients. Though 17% said they could or would drop low-paying insurers, 83% said they could not do that for business, ethical, or other reasons.
Despite its many headaches, medicine is still a rewarding profession. The most rewarding aspects cited by cardiologists were relationships with patients (34%), being good at their work (23%), and knowing they’re making the world a better place (21%). Though this is mostly in line with previous surveys, in recent years physicians have increasingly cited making the world a better place as a key motivation and reward.
The most challenging part of the job? This will not come as a surprise: Having so many rules and regulations. This was the reason given by 26% of respondents. But a close second – at 21% – was having to work long hours. One positive development is that cardiologists are making peace with their EHR systems. Only 10% said this was the most challenging part of the job (the same percentage that cited dealing with difficult patients as most challenging).
The financial struggles created by the pandemic have eased somewhat, but physicians are still facing an array of challenges, including increased workloads and longer hours. All in all, however, things seem to be looking up.
More than 13,000 physicians in more than 29 specialties shared information about their incomes and other aspects of their careers in a survey conducted by Medscape. The responses showed a trend back to something like normal after the initial blow of the COVID-19 pandemic.
As the profession began to recover from the pandemic, cardiologists reported that their incomes increased in 2021, reaching an average of $490,000 for the year, up from $459,000 the previous year. This was in keeping with physicians in other specialties. “Compensation for most physicians is trending back up, as demands for physicians accelerates,” said James Taylor, group president and chief operating officer of AMN Healthcare’s Physician & Leadership Solutions Division. “The market for physicians has done a complete 180 over just 7 or 8 months.” And though inflation is on everyone’s mind these days, rising salaries have helped physicians keep up with rising prices.
Despite the increase in income (and the accompanying increased workload), nearly 30% of cardiologists have taken on extra work, most of that being medical work, but a few did report unrelated side hustles. This may be due not to a shortfall in income, but rather to a desire to pad the coffers for the future. Lauren Podnos, a financial planner with Wealth Care, a firm that specializes in working with physicians and other health care professionals, points out that many physicians like to build wealth as quickly as possible as a hedge against possible burnout later on. “With physicians,” she said, “we work to get to the point where they have the freedom to do whatever they want – cut back and work part-time or transition into another career – so if they do burn out, they have other options.”
Though physician pay rose overall, not all cardiologists enjoyed a boost in income. However, those who did lose ground did not always lay the blame on COVID-19: General pay cuts were mentioned, for example. For physicians overall, a gender pay gap still remains, with men averaging $373,000 per year, in contrast to women who make $282,000. With more women moving into higher-paying specialties, the gap has narrowed somewhat in recent years, and industry leaders are making efforts to accelerate that trend. “A great many of the specialty organizations have efforts underway not just to increase the number of women in specialties but also to address gender pay gaps and bias in evaluations during residency and fellowship,” said Ron Holder, chief operating officer of the Medical Group Management Association (MGMA).
Incentive bonuses helped bump up income as well. Overall, 57% of physicians receive some kind of incentive bonus; the average for cardiologists was $85,000 last year, up from $71,000 the prior year. While such bonuses can certainly help the bottom line, they’re not always an unmitigated good. A 2021 study found that incentive programs can cause people to prioritize time spent at work and with work colleagues at the expense of family and personal relationships, a potentially troubling finding with so many physicians struggling with depression and burnout. “There’s been a lot of previous evidence showing that the more time we spend with our loved ones the happier we are,” said Julia Hur, PhD, assistant professor of management and organizations at New York University’s Stern School of Business, and lead author of the study. “The core argument of this study is about attention, and performance incentives create an attentional fixation on money,” she said, “causing people to spend more time with work colleagues and people who are helpful to their careers. And that takes away from time for family and friends.”
Still rewarding
Getting paid well is one thing; feeling that you’re being paid well is another. Only 57% of cardiologists who responded to the survey said they felt they were fairly compensated for their work. This puts them at roughly the middle of the pack of specialties. Contrast that with physicians in public health and preventive medicine who topped the charts on this one, with 72% of these doctors feeling that they were being paid fairly for their work.
However, cardiology did rank at the top of specialties whose members said they would choose medicine if they had a chance to do it again, though that number was down from the previous year (81% in 2021 versus 86% in 2020). Of cardiologists surveyed, 88% would choose cardiology if they got a do-over.
Cardiologists spend an average of 16.4 hours each week on paperwork and administration. That’s only slightly higher than the average for all specialties, about 15.5 hours a week. Despite billing hassles and low reimbursement rates, 80% of cardiologists polled say they plan to continue taking new and existing Medicare and Medicaid patients. Though 17% said they could or would drop low-paying insurers, 83% said they could not do that for business, ethical, or other reasons.
Despite its many headaches, medicine is still a rewarding profession. The most rewarding aspects cited by cardiologists were relationships with patients (34%), being good at their work (23%), and knowing they’re making the world a better place (21%). Though this is mostly in line with previous surveys, in recent years physicians have increasingly cited making the world a better place as a key motivation and reward.
The most challenging part of the job? This will not come as a surprise: Having so many rules and regulations. This was the reason given by 26% of respondents. But a close second – at 21% – was having to work long hours. One positive development is that cardiologists are making peace with their EHR systems. Only 10% said this was the most challenging part of the job (the same percentage that cited dealing with difficult patients as most challenging).
The financial struggles created by the pandemic have eased somewhat, but physicians are still facing an array of challenges, including increased workloads and longer hours. All in all, however, things seem to be looking up.
More than 13,000 physicians in more than 29 specialties shared information about their incomes and other aspects of their careers in a survey conducted by Medscape. The responses showed a trend back to something like normal after the initial blow of the COVID-19 pandemic.
As the profession began to recover from the pandemic, cardiologists reported that their incomes increased in 2021, reaching an average of $490,000 for the year, up from $459,000 the previous year. This was in keeping with physicians in other specialties. “Compensation for most physicians is trending back up, as demands for physicians accelerates,” said James Taylor, group president and chief operating officer of AMN Healthcare’s Physician & Leadership Solutions Division. “The market for physicians has done a complete 180 over just 7 or 8 months.” And though inflation is on everyone’s mind these days, rising salaries have helped physicians keep up with rising prices.
Despite the increase in income (and the accompanying increased workload), nearly 30% of cardiologists have taken on extra work, most of that being medical work, but a few did report unrelated side hustles. This may be due not to a shortfall in income, but rather to a desire to pad the coffers for the future. Lauren Podnos, a financial planner with Wealth Care, a firm that specializes in working with physicians and other health care professionals, points out that many physicians like to build wealth as quickly as possible as a hedge against possible burnout later on. “With physicians,” she said, “we work to get to the point where they have the freedom to do whatever they want – cut back and work part-time or transition into another career – so if they do burn out, they have other options.”
Though physician pay rose overall, not all cardiologists enjoyed a boost in income. However, those who did lose ground did not always lay the blame on COVID-19: General pay cuts were mentioned, for example. For physicians overall, a gender pay gap still remains, with men averaging $373,000 per year, in contrast to women who make $282,000. With more women moving into higher-paying specialties, the gap has narrowed somewhat in recent years, and industry leaders are making efforts to accelerate that trend. “A great many of the specialty organizations have efforts underway not just to increase the number of women in specialties but also to address gender pay gaps and bias in evaluations during residency and fellowship,” said Ron Holder, chief operating officer of the Medical Group Management Association (MGMA).
Incentive bonuses helped bump up income as well. Overall, 57% of physicians receive some kind of incentive bonus; the average for cardiologists was $85,000 last year, up from $71,000 the prior year. While such bonuses can certainly help the bottom line, they’re not always an unmitigated good. A 2021 study found that incentive programs can cause people to prioritize time spent at work and with work colleagues at the expense of family and personal relationships, a potentially troubling finding with so many physicians struggling with depression and burnout. “There’s been a lot of previous evidence showing that the more time we spend with our loved ones the happier we are,” said Julia Hur, PhD, assistant professor of management and organizations at New York University’s Stern School of Business, and lead author of the study. “The core argument of this study is about attention, and performance incentives create an attentional fixation on money,” she said, “causing people to spend more time with work colleagues and people who are helpful to their careers. And that takes away from time for family and friends.”
Still rewarding
Getting paid well is one thing; feeling that you’re being paid well is another. Only 57% of cardiologists who responded to the survey said they felt they were fairly compensated for their work. This puts them at roughly the middle of the pack of specialties. Contrast that with physicians in public health and preventive medicine who topped the charts on this one, with 72% of these doctors feeling that they were being paid fairly for their work.
However, cardiology did rank at the top of specialties whose members said they would choose medicine if they had a chance to do it again, though that number was down from the previous year (81% in 2021 versus 86% in 2020). Of cardiologists surveyed, 88% would choose cardiology if they got a do-over.
Cardiologists spend an average of 16.4 hours each week on paperwork and administration. That’s only slightly higher than the average for all specialties, about 15.5 hours a week. Despite billing hassles and low reimbursement rates, 80% of cardiologists polled say they plan to continue taking new and existing Medicare and Medicaid patients. Though 17% said they could or would drop low-paying insurers, 83% said they could not do that for business, ethical, or other reasons.
Despite its many headaches, medicine is still a rewarding profession. The most rewarding aspects cited by cardiologists were relationships with patients (34%), being good at their work (23%), and knowing they’re making the world a better place (21%). Though this is mostly in line with previous surveys, in recent years physicians have increasingly cited making the world a better place as a key motivation and reward.
The most challenging part of the job? This will not come as a surprise: Having so many rules and regulations. This was the reason given by 26% of respondents. But a close second – at 21% – was having to work long hours. One positive development is that cardiologists are making peace with their EHR systems. Only 10% said this was the most challenging part of the job (the same percentage that cited dealing with difficult patients as most challenging).
In some states, voters will get to decide the future of abortion rights
As states grapple with the future of abortion in the United States, Michigan, California, and Vermont could become the first states to let voters decide whether the right to abortion should be written into the state constitution.
In Michigan, a proposed constitutional amendment would override a 90-year-old state law that makes abortion a felony even in cases of rape or incest. The U.S. Supreme Court’s overturning of Roe v. Wade could revive that abortion ban – and has galvanized abortion-rights advocates to secure new protections.
Some of the momentum is coming from activists getting involved for the first time.
“I wanted to do something, but I had no political experience or really any experience in activism,” said Amanda Mazur, who lives in rural northwestern Michigan. “But I thought, ‘Maybe I can volunteer and just offer something tangible to the movement.’”
Michigan organizers like Ms. Mazur submitted more than 750,000 signatures – a record number, they said – to state election officials in hopes of having the amendment appear on the November ballot.
If just over half those signatures are validated, Michigan voters will decide whether to amend the state’s constitution to guarantee broad individual rights to “reproductive freedom” that would cover abortion, contraception, and fertility treatments. It would also prevent the state from regulating abortions later in pregnancy if the patient’s “physical or mental health” is at risk.
The ballot initiative has the backing of medical groups like the American College of Obstetricians and Gynecologists, while conservative groups have called it radical and dangerous, claiming it would “allow late-term abortions for practically any reason.”
In California, the push to expand abortion access starts from a very different vantage point: The right to abortion is protected in state statute. And voters will be asked whether they want to enshrine it in the constitution. Proposition 1, which will be on the ballot in November, would prohibit the state from interfering with Californians’ reproductive health decisions, including those related to abortion or contraception.
“I want to know for sure that that right is protected,” state Sen. Toni Atkins (D-Calif.), the Democratic leader in the Senate and lead author of the amendment, said at a legislative hearing in June. “We are protecting ourselves from future courts and future politicians.”
The amendment is one strategy that several California lawmakers are pursuing to protect abortion access in the state. Gov. Gavin Newsom, a Democrat, has signed legislation to eliminate out-of-pocket expenses for abortion for most Californians and to protect California providers that offer abortion services from lawsuits in other states. The recent state budget deal also includes $200 million for reproductive and abortion care.
Earlier in July, Vermont Gov. Phil Scott, a Republican, announced that Proposal 5 will be on the November ballot. He said in a statement: “In Vermont, we solidified the right to choose in law, and now Vermonters have the opportunity to further protect that right in our constitution.”
For Ms. Mazur, the desire to “do something” started in 2017, when she and her husband gave their daughter, then 2 years old, some happy news: She was going to be a big sister. The family was thrilled.
But then doctors told Ms. Mazur something was wrong.
“I found out halfway through the pregnancy that the baby my husband and I hoped for suffered from a rare and life-limiting genetic condition,” Ms. Mazur said. “We ultimately made the compassionate choice to end the pregnancy for my well-being, and for the well-being of our family, and the life of what we thought would be our child.”
Devastated, Ms. Mazur turned to a national online support group and met people having similar experiences. But many group members said they were having a tough time finding a way to terminate their pregnancies.
“It really broke my heart that you’re going through this already devastating experience but have to travel far away from your home across the country ... [and] advocate for yourself like crazy just to get care that you have decided with your doctor is best for you,” Ms. Mazur said.
At the time, abortion rights in Michigan seemed pretty stable, but Ms. Mazur’s political awakening found an outlet this year.
Reproductive Freedom for All, a petition group backed by the American Civil Liberties Union of Michigan and Planned Parenthood Advocates of Michigan, was gathering signatures for the constitutional amendment to enshrine abortion protections in state law. The effort took on new urgency in May after a draft of the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization was leaked and then published.
“Folks realized that this big, scary thing that they did not think would happen might actually happen,” said Jessica Ayoub, a field organizer with the ACLU of Michigan.
Some Michiganders were registering to vote just to be eligible to sign the petition. Jaynie Hoerauf, a 62-year-old attorney in Farwell, drove 40 miles to attend a rally where she knew she could sign it.
“A bunch of us were so ticked off [about Roe being overturned], and we were talking about it. And I was like, ‘I’m just going to go on and find where I can sign the stupid petition,’” Ms. Hoerauf said.
Activists on both sides of the abortion-rights debate expect to spend millions of dollars. They predict that donations will pour in from outside Michigan and that voters in other states will be watching.
“This is just the start of our fight,” Ms. Ayoub said. “We know that it is a long road to November.”
KHN correspondent Rachel Bluth contributed to this report. This story is part of a partnership that includes Michigan Radio, NPR, and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
As states grapple with the future of abortion in the United States, Michigan, California, and Vermont could become the first states to let voters decide whether the right to abortion should be written into the state constitution.
In Michigan, a proposed constitutional amendment would override a 90-year-old state law that makes abortion a felony even in cases of rape or incest. The U.S. Supreme Court’s overturning of Roe v. Wade could revive that abortion ban – and has galvanized abortion-rights advocates to secure new protections.
Some of the momentum is coming from activists getting involved for the first time.
“I wanted to do something, but I had no political experience or really any experience in activism,” said Amanda Mazur, who lives in rural northwestern Michigan. “But I thought, ‘Maybe I can volunteer and just offer something tangible to the movement.’”
Michigan organizers like Ms. Mazur submitted more than 750,000 signatures – a record number, they said – to state election officials in hopes of having the amendment appear on the November ballot.
If just over half those signatures are validated, Michigan voters will decide whether to amend the state’s constitution to guarantee broad individual rights to “reproductive freedom” that would cover abortion, contraception, and fertility treatments. It would also prevent the state from regulating abortions later in pregnancy if the patient’s “physical or mental health” is at risk.
The ballot initiative has the backing of medical groups like the American College of Obstetricians and Gynecologists, while conservative groups have called it radical and dangerous, claiming it would “allow late-term abortions for practically any reason.”
In California, the push to expand abortion access starts from a very different vantage point: The right to abortion is protected in state statute. And voters will be asked whether they want to enshrine it in the constitution. Proposition 1, which will be on the ballot in November, would prohibit the state from interfering with Californians’ reproductive health decisions, including those related to abortion or contraception.
“I want to know for sure that that right is protected,” state Sen. Toni Atkins (D-Calif.), the Democratic leader in the Senate and lead author of the amendment, said at a legislative hearing in June. “We are protecting ourselves from future courts and future politicians.”
The amendment is one strategy that several California lawmakers are pursuing to protect abortion access in the state. Gov. Gavin Newsom, a Democrat, has signed legislation to eliminate out-of-pocket expenses for abortion for most Californians and to protect California providers that offer abortion services from lawsuits in other states. The recent state budget deal also includes $200 million for reproductive and abortion care.
Earlier in July, Vermont Gov. Phil Scott, a Republican, announced that Proposal 5 will be on the November ballot. He said in a statement: “In Vermont, we solidified the right to choose in law, and now Vermonters have the opportunity to further protect that right in our constitution.”
For Ms. Mazur, the desire to “do something” started in 2017, when she and her husband gave their daughter, then 2 years old, some happy news: She was going to be a big sister. The family was thrilled.
But then doctors told Ms. Mazur something was wrong.
“I found out halfway through the pregnancy that the baby my husband and I hoped for suffered from a rare and life-limiting genetic condition,” Ms. Mazur said. “We ultimately made the compassionate choice to end the pregnancy for my well-being, and for the well-being of our family, and the life of what we thought would be our child.”
Devastated, Ms. Mazur turned to a national online support group and met people having similar experiences. But many group members said they were having a tough time finding a way to terminate their pregnancies.
“It really broke my heart that you’re going through this already devastating experience but have to travel far away from your home across the country ... [and] advocate for yourself like crazy just to get care that you have decided with your doctor is best for you,” Ms. Mazur said.
At the time, abortion rights in Michigan seemed pretty stable, but Ms. Mazur’s political awakening found an outlet this year.
Reproductive Freedom for All, a petition group backed by the American Civil Liberties Union of Michigan and Planned Parenthood Advocates of Michigan, was gathering signatures for the constitutional amendment to enshrine abortion protections in state law. The effort took on new urgency in May after a draft of the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization was leaked and then published.
“Folks realized that this big, scary thing that they did not think would happen might actually happen,” said Jessica Ayoub, a field organizer with the ACLU of Michigan.
Some Michiganders were registering to vote just to be eligible to sign the petition. Jaynie Hoerauf, a 62-year-old attorney in Farwell, drove 40 miles to attend a rally where she knew she could sign it.
“A bunch of us were so ticked off [about Roe being overturned], and we were talking about it. And I was like, ‘I’m just going to go on and find where I can sign the stupid petition,’” Ms. Hoerauf said.
Activists on both sides of the abortion-rights debate expect to spend millions of dollars. They predict that donations will pour in from outside Michigan and that voters in other states will be watching.
“This is just the start of our fight,” Ms. Ayoub said. “We know that it is a long road to November.”
KHN correspondent Rachel Bluth contributed to this report. This story is part of a partnership that includes Michigan Radio, NPR, and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
As states grapple with the future of abortion in the United States, Michigan, California, and Vermont could become the first states to let voters decide whether the right to abortion should be written into the state constitution.
In Michigan, a proposed constitutional amendment would override a 90-year-old state law that makes abortion a felony even in cases of rape or incest. The U.S. Supreme Court’s overturning of Roe v. Wade could revive that abortion ban – and has galvanized abortion-rights advocates to secure new protections.
Some of the momentum is coming from activists getting involved for the first time.
“I wanted to do something, but I had no political experience or really any experience in activism,” said Amanda Mazur, who lives in rural northwestern Michigan. “But I thought, ‘Maybe I can volunteer and just offer something tangible to the movement.’”
Michigan organizers like Ms. Mazur submitted more than 750,000 signatures – a record number, they said – to state election officials in hopes of having the amendment appear on the November ballot.
If just over half those signatures are validated, Michigan voters will decide whether to amend the state’s constitution to guarantee broad individual rights to “reproductive freedom” that would cover abortion, contraception, and fertility treatments. It would also prevent the state from regulating abortions later in pregnancy if the patient’s “physical or mental health” is at risk.
The ballot initiative has the backing of medical groups like the American College of Obstetricians and Gynecologists, while conservative groups have called it radical and dangerous, claiming it would “allow late-term abortions for practically any reason.”
In California, the push to expand abortion access starts from a very different vantage point: The right to abortion is protected in state statute. And voters will be asked whether they want to enshrine it in the constitution. Proposition 1, which will be on the ballot in November, would prohibit the state from interfering with Californians’ reproductive health decisions, including those related to abortion or contraception.
“I want to know for sure that that right is protected,” state Sen. Toni Atkins (D-Calif.), the Democratic leader in the Senate and lead author of the amendment, said at a legislative hearing in June. “We are protecting ourselves from future courts and future politicians.”
The amendment is one strategy that several California lawmakers are pursuing to protect abortion access in the state. Gov. Gavin Newsom, a Democrat, has signed legislation to eliminate out-of-pocket expenses for abortion for most Californians and to protect California providers that offer abortion services from lawsuits in other states. The recent state budget deal also includes $200 million for reproductive and abortion care.
Earlier in July, Vermont Gov. Phil Scott, a Republican, announced that Proposal 5 will be on the November ballot. He said in a statement: “In Vermont, we solidified the right to choose in law, and now Vermonters have the opportunity to further protect that right in our constitution.”
For Ms. Mazur, the desire to “do something” started in 2017, when she and her husband gave their daughter, then 2 years old, some happy news: She was going to be a big sister. The family was thrilled.
But then doctors told Ms. Mazur something was wrong.
“I found out halfway through the pregnancy that the baby my husband and I hoped for suffered from a rare and life-limiting genetic condition,” Ms. Mazur said. “We ultimately made the compassionate choice to end the pregnancy for my well-being, and for the well-being of our family, and the life of what we thought would be our child.”
Devastated, Ms. Mazur turned to a national online support group and met people having similar experiences. But many group members said they were having a tough time finding a way to terminate their pregnancies.
“It really broke my heart that you’re going through this already devastating experience but have to travel far away from your home across the country ... [and] advocate for yourself like crazy just to get care that you have decided with your doctor is best for you,” Ms. Mazur said.
At the time, abortion rights in Michigan seemed pretty stable, but Ms. Mazur’s political awakening found an outlet this year.
Reproductive Freedom for All, a petition group backed by the American Civil Liberties Union of Michigan and Planned Parenthood Advocates of Michigan, was gathering signatures for the constitutional amendment to enshrine abortion protections in state law. The effort took on new urgency in May after a draft of the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization was leaked and then published.
“Folks realized that this big, scary thing that they did not think would happen might actually happen,” said Jessica Ayoub, a field organizer with the ACLU of Michigan.
Some Michiganders were registering to vote just to be eligible to sign the petition. Jaynie Hoerauf, a 62-year-old attorney in Farwell, drove 40 miles to attend a rally where she knew she could sign it.
“A bunch of us were so ticked off [about Roe being overturned], and we were talking about it. And I was like, ‘I’m just going to go on and find where I can sign the stupid petition,’” Ms. Hoerauf said.
Activists on both sides of the abortion-rights debate expect to spend millions of dollars. They predict that donations will pour in from outside Michigan and that voters in other states will be watching.
“This is just the start of our fight,” Ms. Ayoub said. “We know that it is a long road to November.”
KHN correspondent Rachel Bluth contributed to this report. This story is part of a partnership that includes Michigan Radio, NPR, and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Children and COVID: Does latest rise in new cases point toward stabilization?
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.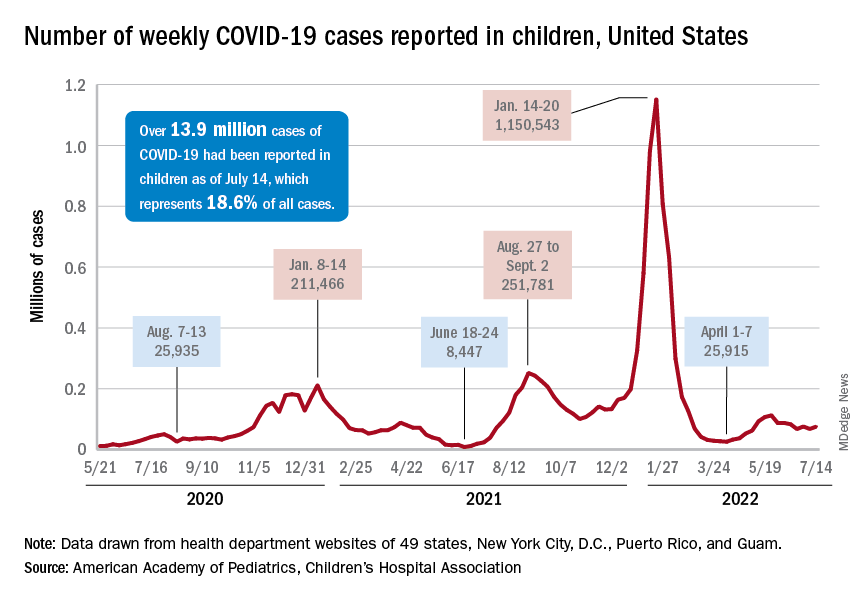
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.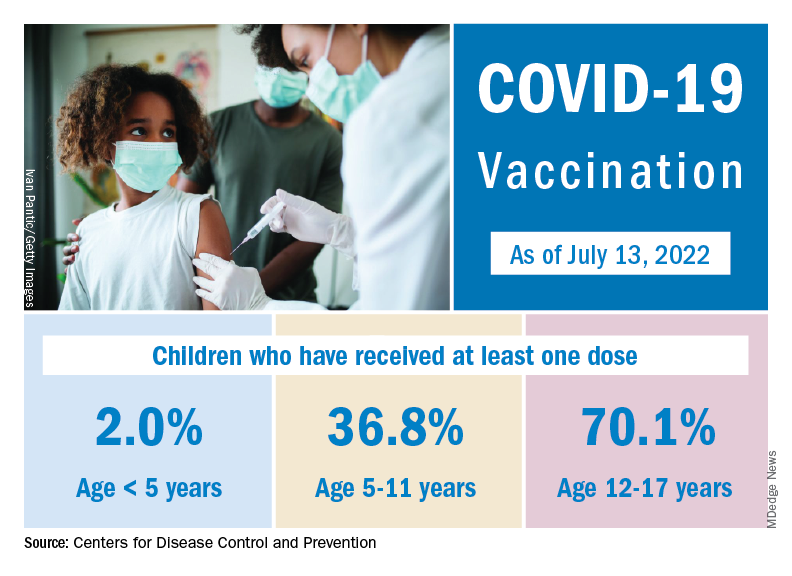
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.
Mark Cuban’s discounted pharmacy offers imatinib at a fraction of the cost
, including several drugs used in oncology.
One of the drugs offering the biggest savings is generic imatinib (originator product Gleevec), which is used for chronic myelogenous leukemia (CML), certain acute lymphocytic leukemia (ALL) and certain types of gastrointestinal stromal tumors (GIST).
Imatinib has a list retail price of $2,502.
At the Mark Cuban pharmacy, it is available for $14.40, which offers a saving of $2,488.
The online pharmacy, known as the Mark Cuban Cost Plus Drug Company (MCCPDC), began operating in January. It is selling more than 100 generic prescription drugs at the cost of ingredients and manufacturing plus 15% margin, $3 pharmacy dispensing fee, and $5 shipping fee.
“We will do whatever it takes to get affordable pharmaceuticals to patients,” said Alex Oshmyansky, MD, PhD, founder and CEO of MCCPDC, in a company statement. “The markup on potentially lifesaving drugs that people depend on is a problem that can’t be ignored. It is imperative that we take action and help expand access to these medications for those who need them most.”
The company is a registered pharmaceutical wholesaler, and as such, can “bypass middlemen and outrageous markups,” the company notes in a press release. They have partnered with the digital health care company Truepill, which built and powers the pharmacy’s website.
At its launch, the pharmacy offered 109 generic medications. So far, the generics offered for oncology include generic anastrozole, letrozole, raloxifene, and tamoxifen for use in breast cancer, as well as the chemotherapy methotrexate and generic imatinib, as mentioned above. All of the drugs sold through the MCCPDC have prices much lower than in the standard marketplace. Becker’s Hospital Review recently published a list of the 50 drugs with the biggest savings at Cuban’s pharmacy.
At the top of the list was albendazole, an anthelmintic that retails for $6,565. In contrast, the MCCPDC price is $453, which translates to a savings of more than $6,000 for a 30-count supply.
The second-largest savings was for imatinib.
For the other cancer drugs, the savings were less substantial, reflecting their much lower retail price, but savings still ranged between $66 and $200 per product.
Overall, 14 of the top 50 discounted drugs are slated to save consumers more than $500 for a 30-count supply when purchased from MCCPDC.
Medicare could save billions
Medicare would save billions if it used this online pharmacy, say researchers from Harvard University, who recently published a study in Annals of Internal Medicine giving some estimates.
The team analyzed 89 generic drugs listed at MCCPDC and found that Medicare Part D could have saved more than $3 billion in 2020 if they had purchased them at these prices. For example, aripiprazole, a commonly used psychiatric medication, was purchased for more than $2 per pill, while the same generic formulation of the drug is sold by Cuban’s company for $0.24 per pill. Overall, just with this one drug, Medicare could have saved $233 million in 2020.
“We found that Medicare spent $9.6 billion on 89 generic drugs in 2020,” commented lead author Hussain S. Lalani, MD, MPH in a tweet. “It could have saved up to $3.6 billion on 77 of the 89 drugs if it purchased them at the largest quantity sold by Mark Cuban’s Cost Plus Drug Company. The other 12 drugs ($1.5B) did not offer savings.”
Dr. Lalani pointed out that the price transparency provided by MCCPDC is “helping us to understand the cost of many generic drugs and highlights inefficiencies in the supply chain for generic drugs.”
In standard practice, there are “multiple actors” involved in distributing the drug from the pharmaceutical manufacturer to the patient, he explained. “Mark Cuban’s company does not accept health insurance, buys from the manufacturer, and sells it directly to consumers online!”
He added that innovation and policy reform are needed. “We know that many drug prices are outrageous, and the supply chain is also expensive & NOT working right,” he tweeted. “We need a system that delivers innovative, affordable, and accessible medicines for all Americans.”
Commenting on Dr. Lalani’s Twitter thread, Eric Topol, MD, Medscape’s editor-in-chief, said that “the many billions the U.S. could save each year by MCCPDC is remarkable.”
Dr. Topol also noted that the savings estimated in the Annals of Internal Medicine paper were based on fewer than 100 generic drugs that are currently available, but he said that “there will be >1,000 more offered in the next year.”
No insurance, no PBMs
Prior to launching the online pharmacy, Mr. Cuban established a pharmacy benefit manager (PBM) operation to serve companies providing prescription coverage in their employee benefit plans. According to a press release, MCCPDC has pledged to be “radically transparent” in its own negotiations as a PBM, revealing the true costs it pays for drugs and eliminating spread pricing and misaligned rebate incentives. MCCPDC anticipates that its PBM could save companies millions of dollars with no changes to its benefits, as it will eliminate the traditional PBM model.
However, the online pharmacy is a cash-only venture, because MCCPDC refuses to pay third-party PBMs in order to be allowed to process insurance claims. But the model allows patients to immediately purchase medications at a cost that is often less than what they might pay when having to deal with deductible and copay requirements.
In the future, MCCPDC plans to start manufacturing medications. The company is currently building a state-of-the-art pharmaceutical facility in Dallas, at which it plans to produce its own high-quality medicines at the lowest possible prices.
A version of this article first appeared on Medscape.com.
, including several drugs used in oncology.
One of the drugs offering the biggest savings is generic imatinib (originator product Gleevec), which is used for chronic myelogenous leukemia (CML), certain acute lymphocytic leukemia (ALL) and certain types of gastrointestinal stromal tumors (GIST).
Imatinib has a list retail price of $2,502.
At the Mark Cuban pharmacy, it is available for $14.40, which offers a saving of $2,488.
The online pharmacy, known as the Mark Cuban Cost Plus Drug Company (MCCPDC), began operating in January. It is selling more than 100 generic prescription drugs at the cost of ingredients and manufacturing plus 15% margin, $3 pharmacy dispensing fee, and $5 shipping fee.
“We will do whatever it takes to get affordable pharmaceuticals to patients,” said Alex Oshmyansky, MD, PhD, founder and CEO of MCCPDC, in a company statement. “The markup on potentially lifesaving drugs that people depend on is a problem that can’t be ignored. It is imperative that we take action and help expand access to these medications for those who need them most.”
The company is a registered pharmaceutical wholesaler, and as such, can “bypass middlemen and outrageous markups,” the company notes in a press release. They have partnered with the digital health care company Truepill, which built and powers the pharmacy’s website.
At its launch, the pharmacy offered 109 generic medications. So far, the generics offered for oncology include generic anastrozole, letrozole, raloxifene, and tamoxifen for use in breast cancer, as well as the chemotherapy methotrexate and generic imatinib, as mentioned above. All of the drugs sold through the MCCPDC have prices much lower than in the standard marketplace. Becker’s Hospital Review recently published a list of the 50 drugs with the biggest savings at Cuban’s pharmacy.
At the top of the list was albendazole, an anthelmintic that retails for $6,565. In contrast, the MCCPDC price is $453, which translates to a savings of more than $6,000 for a 30-count supply.
The second-largest savings was for imatinib.
For the other cancer drugs, the savings were less substantial, reflecting their much lower retail price, but savings still ranged between $66 and $200 per product.
Overall, 14 of the top 50 discounted drugs are slated to save consumers more than $500 for a 30-count supply when purchased from MCCPDC.
Medicare could save billions
Medicare would save billions if it used this online pharmacy, say researchers from Harvard University, who recently published a study in Annals of Internal Medicine giving some estimates.
The team analyzed 89 generic drugs listed at MCCPDC and found that Medicare Part D could have saved more than $3 billion in 2020 if they had purchased them at these prices. For example, aripiprazole, a commonly used psychiatric medication, was purchased for more than $2 per pill, while the same generic formulation of the drug is sold by Cuban’s company for $0.24 per pill. Overall, just with this one drug, Medicare could have saved $233 million in 2020.
“We found that Medicare spent $9.6 billion on 89 generic drugs in 2020,” commented lead author Hussain S. Lalani, MD, MPH in a tweet. “It could have saved up to $3.6 billion on 77 of the 89 drugs if it purchased them at the largest quantity sold by Mark Cuban’s Cost Plus Drug Company. The other 12 drugs ($1.5B) did not offer savings.”
Dr. Lalani pointed out that the price transparency provided by MCCPDC is “helping us to understand the cost of many generic drugs and highlights inefficiencies in the supply chain for generic drugs.”
In standard practice, there are “multiple actors” involved in distributing the drug from the pharmaceutical manufacturer to the patient, he explained. “Mark Cuban’s company does not accept health insurance, buys from the manufacturer, and sells it directly to consumers online!”
He added that innovation and policy reform are needed. “We know that many drug prices are outrageous, and the supply chain is also expensive & NOT working right,” he tweeted. “We need a system that delivers innovative, affordable, and accessible medicines for all Americans.”
Commenting on Dr. Lalani’s Twitter thread, Eric Topol, MD, Medscape’s editor-in-chief, said that “the many billions the U.S. could save each year by MCCPDC is remarkable.”
Dr. Topol also noted that the savings estimated in the Annals of Internal Medicine paper were based on fewer than 100 generic drugs that are currently available, but he said that “there will be >1,000 more offered in the next year.”
No insurance, no PBMs
Prior to launching the online pharmacy, Mr. Cuban established a pharmacy benefit manager (PBM) operation to serve companies providing prescription coverage in their employee benefit plans. According to a press release, MCCPDC has pledged to be “radically transparent” in its own negotiations as a PBM, revealing the true costs it pays for drugs and eliminating spread pricing and misaligned rebate incentives. MCCPDC anticipates that its PBM could save companies millions of dollars with no changes to its benefits, as it will eliminate the traditional PBM model.
However, the online pharmacy is a cash-only venture, because MCCPDC refuses to pay third-party PBMs in order to be allowed to process insurance claims. But the model allows patients to immediately purchase medications at a cost that is often less than what they might pay when having to deal with deductible and copay requirements.
In the future, MCCPDC plans to start manufacturing medications. The company is currently building a state-of-the-art pharmaceutical facility in Dallas, at which it plans to produce its own high-quality medicines at the lowest possible prices.
A version of this article first appeared on Medscape.com.
, including several drugs used in oncology.
One of the drugs offering the biggest savings is generic imatinib (originator product Gleevec), which is used for chronic myelogenous leukemia (CML), certain acute lymphocytic leukemia (ALL) and certain types of gastrointestinal stromal tumors (GIST).
Imatinib has a list retail price of $2,502.
At the Mark Cuban pharmacy, it is available for $14.40, which offers a saving of $2,488.
The online pharmacy, known as the Mark Cuban Cost Plus Drug Company (MCCPDC), began operating in January. It is selling more than 100 generic prescription drugs at the cost of ingredients and manufacturing plus 15% margin, $3 pharmacy dispensing fee, and $5 shipping fee.
“We will do whatever it takes to get affordable pharmaceuticals to patients,” said Alex Oshmyansky, MD, PhD, founder and CEO of MCCPDC, in a company statement. “The markup on potentially lifesaving drugs that people depend on is a problem that can’t be ignored. It is imperative that we take action and help expand access to these medications for those who need them most.”
The company is a registered pharmaceutical wholesaler, and as such, can “bypass middlemen and outrageous markups,” the company notes in a press release. They have partnered with the digital health care company Truepill, which built and powers the pharmacy’s website.
At its launch, the pharmacy offered 109 generic medications. So far, the generics offered for oncology include generic anastrozole, letrozole, raloxifene, and tamoxifen for use in breast cancer, as well as the chemotherapy methotrexate and generic imatinib, as mentioned above. All of the drugs sold through the MCCPDC have prices much lower than in the standard marketplace. Becker’s Hospital Review recently published a list of the 50 drugs with the biggest savings at Cuban’s pharmacy.
At the top of the list was albendazole, an anthelmintic that retails for $6,565. In contrast, the MCCPDC price is $453, which translates to a savings of more than $6,000 for a 30-count supply.
The second-largest savings was for imatinib.
For the other cancer drugs, the savings were less substantial, reflecting their much lower retail price, but savings still ranged between $66 and $200 per product.
Overall, 14 of the top 50 discounted drugs are slated to save consumers more than $500 for a 30-count supply when purchased from MCCPDC.
Medicare could save billions
Medicare would save billions if it used this online pharmacy, say researchers from Harvard University, who recently published a study in Annals of Internal Medicine giving some estimates.
The team analyzed 89 generic drugs listed at MCCPDC and found that Medicare Part D could have saved more than $3 billion in 2020 if they had purchased them at these prices. For example, aripiprazole, a commonly used psychiatric medication, was purchased for more than $2 per pill, while the same generic formulation of the drug is sold by Cuban’s company for $0.24 per pill. Overall, just with this one drug, Medicare could have saved $233 million in 2020.
“We found that Medicare spent $9.6 billion on 89 generic drugs in 2020,” commented lead author Hussain S. Lalani, MD, MPH in a tweet. “It could have saved up to $3.6 billion on 77 of the 89 drugs if it purchased them at the largest quantity sold by Mark Cuban’s Cost Plus Drug Company. The other 12 drugs ($1.5B) did not offer savings.”
Dr. Lalani pointed out that the price transparency provided by MCCPDC is “helping us to understand the cost of many generic drugs and highlights inefficiencies in the supply chain for generic drugs.”
In standard practice, there are “multiple actors” involved in distributing the drug from the pharmaceutical manufacturer to the patient, he explained. “Mark Cuban’s company does not accept health insurance, buys from the manufacturer, and sells it directly to consumers online!”
He added that innovation and policy reform are needed. “We know that many drug prices are outrageous, and the supply chain is also expensive & NOT working right,” he tweeted. “We need a system that delivers innovative, affordable, and accessible medicines for all Americans.”
Commenting on Dr. Lalani’s Twitter thread, Eric Topol, MD, Medscape’s editor-in-chief, said that “the many billions the U.S. could save each year by MCCPDC is remarkable.”
Dr. Topol also noted that the savings estimated in the Annals of Internal Medicine paper were based on fewer than 100 generic drugs that are currently available, but he said that “there will be >1,000 more offered in the next year.”
No insurance, no PBMs
Prior to launching the online pharmacy, Mr. Cuban established a pharmacy benefit manager (PBM) operation to serve companies providing prescription coverage in their employee benefit plans. According to a press release, MCCPDC has pledged to be “radically transparent” in its own negotiations as a PBM, revealing the true costs it pays for drugs and eliminating spread pricing and misaligned rebate incentives. MCCPDC anticipates that its PBM could save companies millions of dollars with no changes to its benefits, as it will eliminate the traditional PBM model.
However, the online pharmacy is a cash-only venture, because MCCPDC refuses to pay third-party PBMs in order to be allowed to process insurance claims. But the model allows patients to immediately purchase medications at a cost that is often less than what they might pay when having to deal with deductible and copay requirements.
In the future, MCCPDC plans to start manufacturing medications. The company is currently building a state-of-the-art pharmaceutical facility in Dallas, at which it plans to produce its own high-quality medicines at the lowest possible prices.
A version of this article first appeared on Medscape.com.
Methotrexate’s impact on COVID-19 vaccination: New insights made
Patients who take methotrexate for a variety of immune-mediated inflammatory diseases and pause taking the drug following receipt of a COVID-19 vaccine dose did not have a higher risk of disease flare and had higher antireceptor binding domain (anti-RBD) antibody titers and increased immunogenicity when compared with continuing the drug, three recent studies suggest.
In one study, British researchers examined the effects of a 2-week break in methotrexate therapy on anti-RBD titers following receipt of a third COVID-19 vaccine dose. In their paper published in The Lancet: Respiratory Medicine, they reported results from a randomized, open-label, superiority trial that suggested pausing the drug improved immunogenicity, compared with no break.
In two trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2022 Congress, a team from India set out to determine whether holding methotrexate after receiving both doses of a COVID-19 vaccine, or holding it only after the second dose, was safe and effective. They found that pausing methotrexate only following the second dose contributed to a lower flare risk, and that patients had higher anti-RBD titers when holding methotrexate for 2 weeks following each dose.
Pausing methotrexate after booster
The 2-week methotrexate break and booster vaccine dose data in the Vaccine Response On Off Methotrexate (VROOM) trial showed that after a month, the geometric mean antispike 1 (S1)-RBD antibody titer was 10,798 U/mL (95% confidence interval [CI], 8,970-12,997) in the group that continued methotrexate and 22,750 U/mL (95% CI, 19,314-26,796) in the group that suspended methotrexate; the geometric mean ratio was 2.19 (P < .0001; mixed-effects model), reported Abhishek Abhishek, MD, PhD, professor of rheumatology at the University of Nottingham in Nottingham, England, and colleagues.
Prior research showed that stopping methotrexate therapy for 2 weeks following the seasonal influenza vaccine contributed to better vaccine immunity among patients with rheumatoid arthritis, but there was no impact of stopping the drug for up to 4 weeks before vaccination on vaccine-related immunity, the researchers noted.
It is crucial in maximizing long-lasting vaccine protection in people who are possibly susceptible through immune suppression at this point in the COVID-19 vaccination regimen, the study team noted.
“Evidence from this study will be useful for policymakers, national immunization advisory committees, and specialist societies formulating recommendations on the use of methotrexate around the time of COVID-19 vaccination. This evidence will help patients and clinicians make informed choices about the risks and benefits of interrupting methotrexate treatment around the time of COVID-19 vaccination, with implications for the potential to extend such approaches to other therapeutics,” they wrote.
In American College of Rheumatology (ACR) guidance for COVID-19 vaccination, the organization advised against using standard synthetic disease-modifying antirheumatic medicines such as methotrexate “for 1-2 weeks (as disease activity allows) after each COVID-19 vaccine dose,” given the at-risk population and public health concerns, Jeffrey A. Sparks, MD, MMSc, assistant professor of medicine and associate physician at Brigham and Women’s Hospital and Harvard Medical School, Boston, and Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, noted in an accompanying editorial in The Lancet: Respiratory Medicine.
However, when the ACR developed this statement, there was only one trial involving patients with rheumatoid arthritis who paused methotrexate following seasonal influenza vaccination, the editorialists said.

“Although this finding adds to the evidence base to support interruption of methotrexate after vaccination, a shared decision process is needed to weigh the possible benefit of optimizing protection from COVID-19 and the possible risk of underlying disease flare,” they added.

Dr. Abhishek and colleagues assessed 254 patients with immune-mediated inflammatory disease from dermatology and rheumatology clinics across 26 hospitals in the United Kingdom. Participants had been diagnosed with systemic lupus erythematosus, rheumatoid arthritis, atopic dermatitis, polymyalgia rheumatica, axial spondyloarthritis, and psoriasis without or with arthritis. They had also been taking up to 25 mg of methotrexate per week for 3 months or longer and had received two doses of either the Pfizer/BioNTech BNT162b2 vaccine or AstraZeneca/Oxford viral vector vaccine. The booster dose was most often the Pfizer BNT162b2 vaccine (82%). The patients’ mean age was 59 years, with females comprising 61% of the cohort. Participants were randomly assigned 1:1 to either group.
Investigators performing laboratory analysis were masked to cohort assignment, and clinical research staff, data analysts, participants, and researchers were unmasked.
The elevated antibody response of patients who suspended methotrexate was the same across different kinds of immune-mediated inflammatory disease, primary vaccination platform, SARS-CoV-2 infection history, and age.
Notably, no intervention-associated adverse events were reported, the study team noted.
The conclusions that could be drawn from the booster-dose study were limited by the trial’s modest cohort size, the small number of patients in exploratory subgroup analyses, a lack of information about differences in prescription drug behavior, and early termination’s effect on the researchers’ ability to identify differences between subgroups and in secondary outcomes, the authors noted.
Other limitations included a lack of generalizability to patients with active disease who couldn’t stop therapy and were not included in the investigation, and participants were not blinded to what group they were in, the researchers said.
Expert commentary
This current study is consistent with other studies over the last several months showing that methotrexate harms both humoral and cell-mediated COVID-19 responses, noted Kevin Winthrop, MD, MPH, professor of infectious disease and public health at Oregon Health & Science University, Portland, who was not involved in the study. “And so now the new wave of studies are like this one, where they are holding methotrexate experimentally and seeing if it makes a difference,” he said.

“The one shortcoming of this study – and so far, the studies to date – is that no one has looked at whether the experimental hold has resulted in a change in T-cell responses, which ... we are [now] recognizing [the importance of] more and more in long-term protection, particularly in severe disease. Theoretically, holding [methotrexate] might help enhance T-cell responses, but that hasn’t been shown experimentally.”
Dr. Winthrop pointed out that one might get the same benefit from holding methotrexate for 1 week instead of 2 and that there likely is a reduced risk of flare-up from underlying autoimmune disease.
It is still not certain that this benefit extends to other vaccines, Dr. Winthrop noted. “It is probably true for most vaccines that if you hold methotrexate for 1 or 2 weeks, you might see some short-term benefit in responsiveness, but you don’t know that there is any clinical meaningfulness of this. That’s going to take other long-term studies. You don’t know how long this benefit lasts.”
Pausing methotrexate during initial COVID vaccine doses
Patients with either rheumatoid arthritis or psoriatic arthritis had higher anti-RBD antibody titers when methotrexate was stopped after both doses of the AstraZeneca vaccine, or simply after the second dose, than when methotrexate was continued, according to results from two single-center, randomized controlled trials called MIVAC I and II, Anu Sreekanth, MD, of Sree Sudheendra Medical Mission in Kochi, Kerala, India, and colleagues reported at EULAR 2022.

Results from MIVAC I indicated that there was a higher flare rate when methotrexate was stopped after both vaccine doses, but there was no difference in flare rate in MIVAC II when methotrexate was stopped only after the second dose as opposed to stopping it after both doses.
In the MIVAC I trial, 158 unvaccinated patients were randomized 1:1 to a cohort in which methotrexate was held for 2 weeks after both doses and a cohort in which methotrexate was continued despite the vaccine. In MIVAC II, 157 patients continued methotrexate while receiving the first vaccine dose. These patients were subsequently randomized either to continue or to stop methotrexate for 2 weeks following the second dose.
The findings from MIVAC I demonstrated the flare rate was lower in the methotrexate-continue group than in the methotrexate-pause group (8% vs. 25%; P = .005) and that the median anti-RBD titer was significantly higher for the methotrexate-pause group than the methotrexate-continue group (2,484 vs. 1,147; P = .001).
The results from MIVAC II trial indicated that there was no difference in flare rates between the two study groups (7.9% vs. 11.8%; P = .15). Yet, the median anti-RBD titer was significantly higher in the methotrexate-pause cohort than in the methotrexate-continue cohort (2,553 vs. 990; P = .001).
The report suggests there is a flare risk when methotrexate is stopped, Dr. Sreekanth noted. “It appears more logical to hold only after the second dose, as comparable anti-RBD titers are generated” with either approach, Dr. Sreekanth said.
Expert commentary: MIVAC I and II
Inés Colmegna, MD, associate professor at McGill University in Montreal, noted that it was intriguing that the risk of flares in MIVAC II is half of that reported after each of the doses of MIVAC I. “It is also worth emphasizing that despite the reported frequency of flares, the actual disease activity [as measured by the Disease Activity Score in 28 joints] in patients who did or did not withhold methotrexate was similar.

“MIVAC I and II have practical implications as they help to adequately inform patients about the risk and benefit trade of withholding methotrexate post–COVID-19 vaccination,” Dr. Colmegna told this news organization.
“Additional information would help to [further] interpret the findings of these studies, including whether any of the participants were taking any other DMARDs; data on the severity of the flares and functional impact; analysis of factors that predict the risk of flares, such as higher doses of methotrexate; [and change in] disease activity scores pre- and postvaccination,” Dr. Colmegna concluded.
Dr. Abhishek disclosed relationships with Springer, UpTodate, Oxford, Immunotec, AstraZeneca, Inflazome, NGM Biopharmaceuticals, Menarini Pharmaceuticals, and Cadila Pharmaceuticals. Dr. Abhishek is cochair of the ACR/EULAR CPPD Classification Criteria Working Group and the OMERACT CPPD Working Group. Dr. Sparks disclosed relationships with Gilead, Boehringer Ingelheim, Amgen, Bristol-Myers Squibb, and AbbVie, unrelated to this study. Dr. Tedeschi disclosed relationships with ModernaTx and NGM Biopharmaceuticals. Dr. Winthrop disclosed a research grant and serving as a scientific consultant for Pfizer. Dr. Sreekanth and Dr. Colmegna have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who take methotrexate for a variety of immune-mediated inflammatory diseases and pause taking the drug following receipt of a COVID-19 vaccine dose did not have a higher risk of disease flare and had higher antireceptor binding domain (anti-RBD) antibody titers and increased immunogenicity when compared with continuing the drug, three recent studies suggest.
In one study, British researchers examined the effects of a 2-week break in methotrexate therapy on anti-RBD titers following receipt of a third COVID-19 vaccine dose. In their paper published in The Lancet: Respiratory Medicine, they reported results from a randomized, open-label, superiority trial that suggested pausing the drug improved immunogenicity, compared with no break.
In two trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2022 Congress, a team from India set out to determine whether holding methotrexate after receiving both doses of a COVID-19 vaccine, or holding it only after the second dose, was safe and effective. They found that pausing methotrexate only following the second dose contributed to a lower flare risk, and that patients had higher anti-RBD titers when holding methotrexate for 2 weeks following each dose.
Pausing methotrexate after booster
The 2-week methotrexate break and booster vaccine dose data in the Vaccine Response On Off Methotrexate (VROOM) trial showed that after a month, the geometric mean antispike 1 (S1)-RBD antibody titer was 10,798 U/mL (95% confidence interval [CI], 8,970-12,997) in the group that continued methotrexate and 22,750 U/mL (95% CI, 19,314-26,796) in the group that suspended methotrexate; the geometric mean ratio was 2.19 (P < .0001; mixed-effects model), reported Abhishek Abhishek, MD, PhD, professor of rheumatology at the University of Nottingham in Nottingham, England, and colleagues.
Prior research showed that stopping methotrexate therapy for 2 weeks following the seasonal influenza vaccine contributed to better vaccine immunity among patients with rheumatoid arthritis, but there was no impact of stopping the drug for up to 4 weeks before vaccination on vaccine-related immunity, the researchers noted.
It is crucial in maximizing long-lasting vaccine protection in people who are possibly susceptible through immune suppression at this point in the COVID-19 vaccination regimen, the study team noted.
“Evidence from this study will be useful for policymakers, national immunization advisory committees, and specialist societies formulating recommendations on the use of methotrexate around the time of COVID-19 vaccination. This evidence will help patients and clinicians make informed choices about the risks and benefits of interrupting methotrexate treatment around the time of COVID-19 vaccination, with implications for the potential to extend such approaches to other therapeutics,” they wrote.
In American College of Rheumatology (ACR) guidance for COVID-19 vaccination, the organization advised against using standard synthetic disease-modifying antirheumatic medicines such as methotrexate “for 1-2 weeks (as disease activity allows) after each COVID-19 vaccine dose,” given the at-risk population and public health concerns, Jeffrey A. Sparks, MD, MMSc, assistant professor of medicine and associate physician at Brigham and Women’s Hospital and Harvard Medical School, Boston, and Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, noted in an accompanying editorial in The Lancet: Respiratory Medicine.
However, when the ACR developed this statement, there was only one trial involving patients with rheumatoid arthritis who paused methotrexate following seasonal influenza vaccination, the editorialists said.
“Although this finding adds to the evidence base to support interruption of methotrexate after vaccination, a shared decision process is needed to weigh the possible benefit of optimizing protection from COVID-19 and the possible risk of underlying disease flare,” they added.
Dr. Abhishek and colleagues assessed 254 patients with immune-mediated inflammatory disease from dermatology and rheumatology clinics across 26 hospitals in the United Kingdom. Participants had been diagnosed with systemic lupus erythematosus, rheumatoid arthritis, atopic dermatitis, polymyalgia rheumatica, axial spondyloarthritis, and psoriasis without or with arthritis. They had also been taking up to 25 mg of methotrexate per week for 3 months or longer and had received two doses of either the Pfizer/BioNTech BNT162b2 vaccine or AstraZeneca/Oxford viral vector vaccine. The booster dose was most often the Pfizer BNT162b2 vaccine (82%). The patients’ mean age was 59 years, with females comprising 61% of the cohort. Participants were randomly assigned 1:1 to either group.
Investigators performing laboratory analysis were masked to cohort assignment, and clinical research staff, data analysts, participants, and researchers were unmasked.
The elevated antibody response of patients who suspended methotrexate was the same across different kinds of immune-mediated inflammatory disease, primary vaccination platform, SARS-CoV-2 infection history, and age.
Notably, no intervention-associated adverse events were reported, the study team noted.
The conclusions that could be drawn from the booster-dose study were limited by the trial’s modest cohort size, the small number of patients in exploratory subgroup analyses, a lack of information about differences in prescription drug behavior, and early termination’s effect on the researchers’ ability to identify differences between subgroups and in secondary outcomes, the authors noted.
Other limitations included a lack of generalizability to patients with active disease who couldn’t stop therapy and were not included in the investigation, and participants were not blinded to what group they were in, the researchers said.
Expert commentary
This current study is consistent with other studies over the last several months showing that methotrexate harms both humoral and cell-mediated COVID-19 responses, noted Kevin Winthrop, MD, MPH, professor of infectious disease and public health at Oregon Health & Science University, Portland, who was not involved in the study. “And so now the new wave of studies are like this one, where they are holding methotrexate experimentally and seeing if it makes a difference,” he said.
“The one shortcoming of this study – and so far, the studies to date – is that no one has looked at whether the experimental hold has resulted in a change in T-cell responses, which ... we are [now] recognizing [the importance of] more and more in long-term protection, particularly in severe disease. Theoretically, holding [methotrexate] might help enhance T-cell responses, but that hasn’t been shown experimentally.”
Dr. Winthrop pointed out that one might get the same benefit from holding methotrexate for 1 week instead of 2 and that there likely is a reduced risk of flare-up from underlying autoimmune disease.
It is still not certain that this benefit extends to other vaccines, Dr. Winthrop noted. “It is probably true for most vaccines that if you hold methotrexate for 1 or 2 weeks, you might see some short-term benefit in responsiveness, but you don’t know that there is any clinical meaningfulness of this. That’s going to take other long-term studies. You don’t know how long this benefit lasts.”
Pausing methotrexate during initial COVID vaccine doses
Patients with either rheumatoid arthritis or psoriatic arthritis had higher anti-RBD antibody titers when methotrexate was stopped after both doses of the AstraZeneca vaccine, or simply after the second dose, than when methotrexate was continued, according to results from two single-center, randomized controlled trials called MIVAC I and II, Anu Sreekanth, MD, of Sree Sudheendra Medical Mission in Kochi, Kerala, India, and colleagues reported at EULAR 2022.
Results from MIVAC I indicated that there was a higher flare rate when methotrexate was stopped after both vaccine doses, but there was no difference in flare rate in MIVAC II when methotrexate was stopped only after the second dose as opposed to stopping it after both doses.
In the MIVAC I trial, 158 unvaccinated patients were randomized 1:1 to a cohort in which methotrexate was held for 2 weeks after both doses and a cohort in which methotrexate was continued despite the vaccine. In MIVAC II, 157 patients continued methotrexate while receiving the first vaccine dose. These patients were subsequently randomized either to continue or to stop methotrexate for 2 weeks following the second dose.
The findings from MIVAC I demonstrated the flare rate was lower in the methotrexate-continue group than in the methotrexate-pause group (8% vs. 25%; P = .005) and that the median anti-RBD titer was significantly higher for the methotrexate-pause group than the methotrexate-continue group (2,484 vs. 1,147; P = .001).
The results from MIVAC II trial indicated that there was no difference in flare rates between the two study groups (7.9% vs. 11.8%; P = .15). Yet, the median anti-RBD titer was significantly higher in the methotrexate-pause cohort than in the methotrexate-continue cohort (2,553 vs. 990; P = .001).
The report suggests there is a flare risk when methotrexate is stopped, Dr. Sreekanth noted. “It appears more logical to hold only after the second dose, as comparable anti-RBD titers are generated” with either approach, Dr. Sreekanth said.
Expert commentary: MIVAC I and II
Inés Colmegna, MD, associate professor at McGill University in Montreal, noted that it was intriguing that the risk of flares in MIVAC II is half of that reported after each of the doses of MIVAC I. “It is also worth emphasizing that despite the reported frequency of flares, the actual disease activity [as measured by the Disease Activity Score in 28 joints] in patients who did or did not withhold methotrexate was similar.
“MIVAC I and II have practical implications as they help to adequately inform patients about the risk and benefit trade of withholding methotrexate post–COVID-19 vaccination,” Dr. Colmegna told this news organization.
“Additional information would help to [further] interpret the findings of these studies, including whether any of the participants were taking any other DMARDs; data on the severity of the flares and functional impact; analysis of factors that predict the risk of flares, such as higher doses of methotrexate; [and change in] disease activity scores pre- and postvaccination,” Dr. Colmegna concluded.
Dr. Abhishek disclosed relationships with Springer, UpTodate, Oxford, Immunotec, AstraZeneca, Inflazome, NGM Biopharmaceuticals, Menarini Pharmaceuticals, and Cadila Pharmaceuticals. Dr. Abhishek is cochair of the ACR/EULAR CPPD Classification Criteria Working Group and the OMERACT CPPD Working Group. Dr. Sparks disclosed relationships with Gilead, Boehringer Ingelheim, Amgen, Bristol-Myers Squibb, and AbbVie, unrelated to this study. Dr. Tedeschi disclosed relationships with ModernaTx and NGM Biopharmaceuticals. Dr. Winthrop disclosed a research grant and serving as a scientific consultant for Pfizer. Dr. Sreekanth and Dr. Colmegna have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who take methotrexate for a variety of immune-mediated inflammatory diseases and pause taking the drug following receipt of a COVID-19 vaccine dose did not have a higher risk of disease flare and had higher antireceptor binding domain (anti-RBD) antibody titers and increased immunogenicity when compared with continuing the drug, three recent studies suggest.
In one study, British researchers examined the effects of a 2-week break in methotrexate therapy on anti-RBD titers following receipt of a third COVID-19 vaccine dose. In their paper published in The Lancet: Respiratory Medicine, they reported results from a randomized, open-label, superiority trial that suggested pausing the drug improved immunogenicity, compared with no break.
In two trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2022 Congress, a team from India set out to determine whether holding methotrexate after receiving both doses of a COVID-19 vaccine, or holding it only after the second dose, was safe and effective. They found that pausing methotrexate only following the second dose contributed to a lower flare risk, and that patients had higher anti-RBD titers when holding methotrexate for 2 weeks following each dose.
Pausing methotrexate after booster
The 2-week methotrexate break and booster vaccine dose data in the Vaccine Response On Off Methotrexate (VROOM) trial showed that after a month, the geometric mean antispike 1 (S1)-RBD antibody titer was 10,798 U/mL (95% confidence interval [CI], 8,970-12,997) in the group that continued methotrexate and 22,750 U/mL (95% CI, 19,314-26,796) in the group that suspended methotrexate; the geometric mean ratio was 2.19 (P < .0001; mixed-effects model), reported Abhishek Abhishek, MD, PhD, professor of rheumatology at the University of Nottingham in Nottingham, England, and colleagues.
Prior research showed that stopping methotrexate therapy for 2 weeks following the seasonal influenza vaccine contributed to better vaccine immunity among patients with rheumatoid arthritis, but there was no impact of stopping the drug for up to 4 weeks before vaccination on vaccine-related immunity, the researchers noted.
It is crucial in maximizing long-lasting vaccine protection in people who are possibly susceptible through immune suppression at this point in the COVID-19 vaccination regimen, the study team noted.
“Evidence from this study will be useful for policymakers, national immunization advisory committees, and specialist societies formulating recommendations on the use of methotrexate around the time of COVID-19 vaccination. This evidence will help patients and clinicians make informed choices about the risks and benefits of interrupting methotrexate treatment around the time of COVID-19 vaccination, with implications for the potential to extend such approaches to other therapeutics,” they wrote.
In American College of Rheumatology (ACR) guidance for COVID-19 vaccination, the organization advised against using standard synthetic disease-modifying antirheumatic medicines such as methotrexate “for 1-2 weeks (as disease activity allows) after each COVID-19 vaccine dose,” given the at-risk population and public health concerns, Jeffrey A. Sparks, MD, MMSc, assistant professor of medicine and associate physician at Brigham and Women’s Hospital and Harvard Medical School, Boston, and Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, noted in an accompanying editorial in The Lancet: Respiratory Medicine.
However, when the ACR developed this statement, there was only one trial involving patients with rheumatoid arthritis who paused methotrexate following seasonal influenza vaccination, the editorialists said.
“Although this finding adds to the evidence base to support interruption of methotrexate after vaccination, a shared decision process is needed to weigh the possible benefit of optimizing protection from COVID-19 and the possible risk of underlying disease flare,” they added.
Dr. Abhishek and colleagues assessed 254 patients with immune-mediated inflammatory disease from dermatology and rheumatology clinics across 26 hospitals in the United Kingdom. Participants had been diagnosed with systemic lupus erythematosus, rheumatoid arthritis, atopic dermatitis, polymyalgia rheumatica, axial spondyloarthritis, and psoriasis without or with arthritis. They had also been taking up to 25 mg of methotrexate per week for 3 months or longer and had received two doses of either the Pfizer/BioNTech BNT162b2 vaccine or AstraZeneca/Oxford viral vector vaccine. The booster dose was most often the Pfizer BNT162b2 vaccine (82%). The patients’ mean age was 59 years, with females comprising 61% of the cohort. Participants were randomly assigned 1:1 to either group.
Investigators performing laboratory analysis were masked to cohort assignment, and clinical research staff, data analysts, participants, and researchers were unmasked.
The elevated antibody response of patients who suspended methotrexate was the same across different kinds of immune-mediated inflammatory disease, primary vaccination platform, SARS-CoV-2 infection history, and age.
Notably, no intervention-associated adverse events were reported, the study team noted.
The conclusions that could be drawn from the booster-dose study were limited by the trial’s modest cohort size, the small number of patients in exploratory subgroup analyses, a lack of information about differences in prescription drug behavior, and early termination’s effect on the researchers’ ability to identify differences between subgroups and in secondary outcomes, the authors noted.
Other limitations included a lack of generalizability to patients with active disease who couldn’t stop therapy and were not included in the investigation, and participants were not blinded to what group they were in, the researchers said.
Expert commentary
This current study is consistent with other studies over the last several months showing that methotrexate harms both humoral and cell-mediated COVID-19 responses, noted Kevin Winthrop, MD, MPH, professor of infectious disease and public health at Oregon Health & Science University, Portland, who was not involved in the study. “And so now the new wave of studies are like this one, where they are holding methotrexate experimentally and seeing if it makes a difference,” he said.
“The one shortcoming of this study – and so far, the studies to date – is that no one has looked at whether the experimental hold has resulted in a change in T-cell responses, which ... we are [now] recognizing [the importance of] more and more in long-term protection, particularly in severe disease. Theoretically, holding [methotrexate] might help enhance T-cell responses, but that hasn’t been shown experimentally.”
Dr. Winthrop pointed out that one might get the same benefit from holding methotrexate for 1 week instead of 2 and that there likely is a reduced risk of flare-up from underlying autoimmune disease.
It is still not certain that this benefit extends to other vaccines, Dr. Winthrop noted. “It is probably true for most vaccines that if you hold methotrexate for 1 or 2 weeks, you might see some short-term benefit in responsiveness, but you don’t know that there is any clinical meaningfulness of this. That’s going to take other long-term studies. You don’t know how long this benefit lasts.”
Pausing methotrexate during initial COVID vaccine doses
Patients with either rheumatoid arthritis or psoriatic arthritis had higher anti-RBD antibody titers when methotrexate was stopped after both doses of the AstraZeneca vaccine, or simply after the second dose, than when methotrexate was continued, according to results from two single-center, randomized controlled trials called MIVAC I and II, Anu Sreekanth, MD, of Sree Sudheendra Medical Mission in Kochi, Kerala, India, and colleagues reported at EULAR 2022.
Results from MIVAC I indicated that there was a higher flare rate when methotrexate was stopped after both vaccine doses, but there was no difference in flare rate in MIVAC II when methotrexate was stopped only after the second dose as opposed to stopping it after both doses.
In the MIVAC I trial, 158 unvaccinated patients were randomized 1:1 to a cohort in which methotrexate was held for 2 weeks after both doses and a cohort in which methotrexate was continued despite the vaccine. In MIVAC II, 157 patients continued methotrexate while receiving the first vaccine dose. These patients were subsequently randomized either to continue or to stop methotrexate for 2 weeks following the second dose.
The findings from MIVAC I demonstrated the flare rate was lower in the methotrexate-continue group than in the methotrexate-pause group (8% vs. 25%; P = .005) and that the median anti-RBD titer was significantly higher for the methotrexate-pause group than the methotrexate-continue group (2,484 vs. 1,147; P = .001).
The results from MIVAC II trial indicated that there was no difference in flare rates between the two study groups (7.9% vs. 11.8%; P = .15). Yet, the median anti-RBD titer was significantly higher in the methotrexate-pause cohort than in the methotrexate-continue cohort (2,553 vs. 990; P = .001).
The report suggests there is a flare risk when methotrexate is stopped, Dr. Sreekanth noted. “It appears more logical to hold only after the second dose, as comparable anti-RBD titers are generated” with either approach, Dr. Sreekanth said.
Expert commentary: MIVAC I and II
Inés Colmegna, MD, associate professor at McGill University in Montreal, noted that it was intriguing that the risk of flares in MIVAC II is half of that reported after each of the doses of MIVAC I. “It is also worth emphasizing that despite the reported frequency of flares, the actual disease activity [as measured by the Disease Activity Score in 28 joints] in patients who did or did not withhold methotrexate was similar.
“MIVAC I and II have practical implications as they help to adequately inform patients about the risk and benefit trade of withholding methotrexate post–COVID-19 vaccination,” Dr. Colmegna told this news organization.
“Additional information would help to [further] interpret the findings of these studies, including whether any of the participants were taking any other DMARDs; data on the severity of the flares and functional impact; analysis of factors that predict the risk of flares, such as higher doses of methotrexate; [and change in] disease activity scores pre- and postvaccination,” Dr. Colmegna concluded.
Dr. Abhishek disclosed relationships with Springer, UpTodate, Oxford, Immunotec, AstraZeneca, Inflazome, NGM Biopharmaceuticals, Menarini Pharmaceuticals, and Cadila Pharmaceuticals. Dr. Abhishek is cochair of the ACR/EULAR CPPD Classification Criteria Working Group and the OMERACT CPPD Working Group. Dr. Sparks disclosed relationships with Gilead, Boehringer Ingelheim, Amgen, Bristol-Myers Squibb, and AbbVie, unrelated to this study. Dr. Tedeschi disclosed relationships with ModernaTx and NGM Biopharmaceuticals. Dr. Winthrop disclosed a research grant and serving as a scientific consultant for Pfizer. Dr. Sreekanth and Dr. Colmegna have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Her ex-husband is suing a clinic over the abortion she had 4 years ago
A judge allowed the woman’s ex-husband to establish an estate for the embryo, which had been aborted in its seventh week of development. The ex-husband filed a wrongful death lawsuit against the clinic and its doctors in 2020, alleging that physicians failed to obtain proper informed consent from the woman as required by Arizona law.
Across the United States, people have sued for negligence in the death of a fetus or embryo in cases where a pregnant person has been killed in a car crash or a pregnancy was lost because of alleged wrongdoing by a physician. But a court action claiming the wrongful death of an aborted embryo or fetus is a more novel strategy, legal experts said.
The experts said this rare tactic could become more common, as anti-abortion groups have signaled their desire to further limit reproductive rights following the U.S. Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade. The Arizona lawsuit and others that may follow could also be an attempt to discourage and intimidate providers and harass plaintiffs’ former romantic partners, experts said.
Lucinda Finley, a law professor at the University at Buffalo who specializes in tort law and reproductive rights, said the Arizona case is a “harbinger of things to come” and called it “troubling for the future.”
Ms. Finley said she expects state lawmakers and anti-abortion groups to use “unprecedented strategies” to try to prevent people from traveling to obtain abortions or block them from obtaining information on where to seek one.
Perhaps the most extreme example is in Texas, where the Texas Heartbeat Act, signed into law in May 2021 and upheld by the U.S. Supreme Court in December, allows private citizens to sue a person who performs or aids in an abortion.
“It’s much bigger than these wrongful death suits,” Ms. Finley said.
Civia Tamarkin, president of the National Council of Jewish Women Arizona, which advocates for reproductive rights, said the Arizona lawsuit is part of a larger agenda that anti-abortion advocates are working toward.
“It’s a lawsuit that appears to be a trial balloon to see how far the attorney and the plaintiff can push the limits of the law, the limits of reason, the limits of science and medicine,” Ms. Tamarkin said.
In July 2018, the ex-husband, Mario Villegas, accompanied his then-wife to three medical appointments – a consultation, the abortion, and a follow-up. The woman, who ProPublica is not identifying for privacy reasons, said in a deposition in the wrongful death suit that at the time of the procedure the two were already talking about obtaining a divorce, which was finalized later that year.
“We were not happy together at all,” she said.
Mr. Villegas, a former Marine from Globe, Ariz., a mining town east of Phoenix, had been married twice before and has other children. He has since moved out of state.
In a form his then-wife filled out at the clinic, she said she was seeking an abortion because she was not ready to be a parent and her relationship with Mr. Villegas was unstable, according to court records. She also checked a box affirming that “I am comfortable with my decision to terminate this pregnancy.” The woman declined to speak on the record with ProPublica out of fear for her safety.
The following year, in 2019, Mr. Villegas learned about an Alabama man who hadn’t wanted his ex-girlfriend to have an abortion and sued the Alabama Women’s Center for Reproductive Alternatives in Huntsville on behalf of an embryo that was aborted at six weeks.
To sue on behalf of the embryo, the would-be father, Ryan Magers, went to probate court where he asked a judge to appoint him as the personal representative of the estate. In probate court, a judge may appoint someone to represent the estate of a person who has died without a will. That representative then has the authority to distribute the estate’s assets to beneficiaries.
When Mr. Magers filed to open an estate for the embryo, his attorney cited various Alabama court rulings involving pregnant people and a 2018 amendment to the Alabama Constitution recognizing the “sanctity of unborn life and the rights of unborn children.”
A probate judge appointed Mr. Magers representative of the estate, giving him legal standing to sue for damages in the wrongful death claim. The case, believed to be the first instance in which an aborted embryo was given legal rights, made national headlines.
It’s unclear how many states allow an estate to be opened on behalf of an embryo or fetus. Some states, like Arizona, don’t explicitly define what counts as a deceased person in their probate code, leaving it to a judge to decide. In a handful of states, laws define embryos and fetuses as a person at conception, which could allow for an estate, but it’s rare.
An Alabama circuit court judge eventually dismissed Mr. Magers’ wrongful death lawsuit, stating that the claims were “precluded by State and Federal laws.”
Mr. Villegas contacted Mr. Magers’ attorney, Brent Helms, about pursuing a similar action in Arizona and was referred to J. Stanley Martineau, an Arizona attorney who had flown to Alabama to talk to Mr. Helms about Mr. Magers’ case.
In August 2020, Mr. Villegas filed a petition to be appointed personal representative of the estate of “Baby Villegas.” His ex-wife opposed the action and contacted a legal advocacy organization focused on reproductive justice, which helped her obtain a lawyer.
In court filings, Mr. Villegas said he prefers to think of “Baby Villegas” as a girl, although the sex of the embryo was never determined, and his lawyer argued that there isn’t an Arizona case that explicitly defines a deceased person, “so the issue appears to be an open one in Arizona.”
In a 2021 motion arguing for dismissal, the ex-wife’s attorney, Louis Silverman, argued that Arizona’s probate code doesn’t authorize the appointment of a personal representative for an embryo, and that granting Mr. Villegas’ request would violate a woman’s constitutional right to decide whether to carry a pregnancy to term.
“U.S. Supreme Court precedent has long protected the constitutional right of a woman to obtain an abortion, including that the decision whether to do so belongs to the woman alone – even where her partner, spouse, or ex-spouse disagrees with that decision,” Mr. Silverman said last year.
Gila County Superior Court Judge Bryan B. Chambers said in an order denying the motion that his decision allows Mr. Villegas to make the argument that the embryo is a person in a wrongful death lawsuit, but that he has not reached that conclusion at this stage. Mr. Villegas was later appointed the personal representative of the estate.
As states determine what is legal in the wake of Dobbs and legislators propose new abortion laws, anti-abortion groups such as the National Right to Life Committee see civil suits as a way to enforce abortion bans and have released model legislation they hope sympathetic legislators will duplicate in statehouses nationwide.
“In addition to criminal penalties and medical license revocation, civil remedies will be critical to ensure that unborn lives are protected from illegal abortions,” the group wrote in a June 15 letter to its state affiliates that included the model legislation.
James Bopp Jr., general counsel for the committee, said in an interview with ProPublica that such actions will be necessary because some “radical Democrat” prosecutors have signaled they won’t enforce criminal abortion bans. Last month, 90 prosecutors from across the country indicated that they would not prosecute those who seek abortions.
“The civil remedies follow what the criminal law makes unlawful,” he said. “And that’s what we’re doing.”
The National Right to Life Committee’s model legislation, which advocates prohibiting abortion except to prevent the death of the pregnant person, recommends that states permit civil actions against people or entities that violate abortion laws “to prevent future violations.” It also suggests that people who have had or have sought to have an illegal abortion, as well as the expectant father and the parents of a pregnant minor, be allowed to pursue wrongful death actions.
Under the legislation, an action for wrongful death of an “unborn child” would be treated like that of a child who died after being born.
In one regard, Arizona has already implemented a piece of this model legislation as the state’s lawmakers have chipped away at access to abortion and enacted a myriad of regulations on doctors who provide the procedure.
The state’s “informed consent” statute for abortion, first signed into law by then-Gov. Jan Brewer in 2009, mandated an in-person counseling session and a 24-hour waiting period before an abortion. It allows a pregnant person, their husband or a maternal grandparent of a minor to sue if a physician does not properly obtain the pregnant person’s informed consent, and to receive damages for psychological, emotional and physical injuries, statutory damages and attorney fees.
The informed consent laws, which have changed over time, mandate that the patient be told about the “probable anatomical and physiological characteristics” of the embryo or fetus and the “immediate and long-term medical risks” associated with abortion, as well as alternatives to the procedure. Some abortion-rights groups and medical professionals have criticized informed consent processes, arguing the materials can be misleading and personify the embryo or fetus. A 2018 review of numerous studies concluded that having an abortion does not increase a person’s risk of infertility in their next pregnancy, nor is it linked to a higher risk of breast cancer or preterm birth, among other issues.
The wrongful death suit comes at a time of extraordinary confusion over abortion law in Arizona.
Until Roe v. Wade was handed down in 1973, establishing a constitutional right to abortion, a law dating to before statehood had banned the procedure. In March, Gov. Doug Ducey, a Republican who has called Arizona “the most pro-life state in the country,” signed into law a bill outlawing abortions after 15 weeks, and said that law would supersede the pre-statehood ban if Roe were overturned. But now that Roe has been overturned, Arizona Attorney General Mark Brnovich, another Republican, said he intends to enforce the pre-statehood ban, which outlawed abortion except to preserve the life of the person seeking the procedure. On July 14, he filed a motion to lift an injunction on the law, which would make it enforceable.
Adding to the muddle, a U.S. district court judge on July 11 blocked part of a 2021 Arizona law that would classify fertilized eggs, embryos and fetuses as people starting at conception, ruling that the attorney general cannot use the so-called personhood law against abortion providers. Following the Supreme Court decision in Dobbs, eight of the state’s nine abortion providers – all located in three Arizona counties – halted abortion services, but following the emergency injunction some are again offering them.
In the wrongful death claim, Mr. Martineau argued that the woman’s consent was invalidated because the doctors didn’t follow the informed consent statute. Although the woman signed four consent documents, the suit claims that “evidence shows that in her rush to maximize profits,” the clinic’s owner, Dr. Gabrielle Goodrick, “cut corners.” Mr. Martineau alleged that Dr. Goodrick and another doctor didn’t inform the woman of the loss of “maternal-fetal” attachment, about the alternatives to abortion or that if not for the abortion, the embryo would likely have been “delivered to term,” among other violations.
Tom Slutes, Dr. Goodrick’s lawyer, called the lawsuit “ridiculous.”
“They didn’t cut any corners,” he said, adding that the woman “clearly knew what was going to happen and definitely, strongly” wanted the abortion. Regardless of the information the woman received, she wouldn’t have changed her mind, Mr. Slutes said. Mr. Slutes referenced the deposition, where the woman said she “felt completely informed.”
Mr. Martineau said in an interview that Mr. Villegas isn’t motivated by collecting money from the lawsuit.
“He has no desire to harass” his ex-wife, Mr. Martineau said. “All he wants to do is make sure it doesn’t happen to another father.”
In a deposition, Mr. Villegas’ ex-wife said that he was emotionally abusive during their marriage, which lasted nearly 5 years. At first, she said, Mr. Villegas seemed like the “greatest guy I’ve ever met in my life,” taking her to California for a week as a birthday gift. But as the marriage progressed, she said, there were times he wouldn’t allow her to get a job or leave the house unless she was with him.
The woman alleged that Mr. Villegas made fake social media profiles, hacked into her social media accounts and threatened to “blackmail” her if she left him during his failed campaign to be a justice of the peace in Gila County, outside of Phoenix.
Mr. Villegas denied the allegations about his relationship but declined to comment further for this story, Mr. Martineau said.
Carliss Chatman, an associate law professor at Washington and Lee University in Virginia, said certain civil remedies can also be a mechanism for men to continue to abuse their former partners through the court system.
“What happens if the father who is suing on behalf of the fetus is your rapist or your abuser? It’s another way to torture a woman,” Ms. Chatman said.
Ms. Chatman added that these legal actions can be a deterrent for physicians in states where abortion is banned after a certain gestational period, because the threat of civil suits makes it harder for doctors to get insurance.
The lawsuit has added to the stresses on Dr. Goodrick, who has been performing abortions in Arizona since the mid-1990s, and her practice. She said that, since the lawsuit was filed, the annual cost of her medical malpractice insurance has risen from $32,000 to $67,000.
Before providers in Arizona halted abortions following the Supreme Court decision, people would begin lining up outside Dr. Goodrick’s clinic at 6 a.m., sometimes with lawn chairs in hand, like “a concert line,” Dr. Goodrick said.
“Every year there’s something and we never know what it’s going to be,” Dr. Goodrick said recently at her Phoenix clinic. “I’m kind of desensitized to it all.”
Nicole Santa Cruz is a reporter covering issues of inequality in the Southwest.
This story was originally published on ProPublica. ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive their biggest stories as soon as they’re published.
A judge allowed the woman’s ex-husband to establish an estate for the embryo, which had been aborted in its seventh week of development. The ex-husband filed a wrongful death lawsuit against the clinic and its doctors in 2020, alleging that physicians failed to obtain proper informed consent from the woman as required by Arizona law.
Across the United States, people have sued for negligence in the death of a fetus or embryo in cases where a pregnant person has been killed in a car crash or a pregnancy was lost because of alleged wrongdoing by a physician. But a court action claiming the wrongful death of an aborted embryo or fetus is a more novel strategy, legal experts said.
The experts said this rare tactic could become more common, as anti-abortion groups have signaled their desire to further limit reproductive rights following the U.S. Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade. The Arizona lawsuit and others that may follow could also be an attempt to discourage and intimidate providers and harass plaintiffs’ former romantic partners, experts said.
Lucinda Finley, a law professor at the University at Buffalo who specializes in tort law and reproductive rights, said the Arizona case is a “harbinger of things to come” and called it “troubling for the future.”
Ms. Finley said she expects state lawmakers and anti-abortion groups to use “unprecedented strategies” to try to prevent people from traveling to obtain abortions or block them from obtaining information on where to seek one.
Perhaps the most extreme example is in Texas, where the Texas Heartbeat Act, signed into law in May 2021 and upheld by the U.S. Supreme Court in December, allows private citizens to sue a person who performs or aids in an abortion.
“It’s much bigger than these wrongful death suits,” Ms. Finley said.
Civia Tamarkin, president of the National Council of Jewish Women Arizona, which advocates for reproductive rights, said the Arizona lawsuit is part of a larger agenda that anti-abortion advocates are working toward.
“It’s a lawsuit that appears to be a trial balloon to see how far the attorney and the plaintiff can push the limits of the law, the limits of reason, the limits of science and medicine,” Ms. Tamarkin said.
In July 2018, the ex-husband, Mario Villegas, accompanied his then-wife to three medical appointments – a consultation, the abortion, and a follow-up. The woman, who ProPublica is not identifying for privacy reasons, said in a deposition in the wrongful death suit that at the time of the procedure the two were already talking about obtaining a divorce, which was finalized later that year.
“We were not happy together at all,” she said.
Mr. Villegas, a former Marine from Globe, Ariz., a mining town east of Phoenix, had been married twice before and has other children. He has since moved out of state.
In a form his then-wife filled out at the clinic, she said she was seeking an abortion because she was not ready to be a parent and her relationship with Mr. Villegas was unstable, according to court records. She also checked a box affirming that “I am comfortable with my decision to terminate this pregnancy.” The woman declined to speak on the record with ProPublica out of fear for her safety.
The following year, in 2019, Mr. Villegas learned about an Alabama man who hadn’t wanted his ex-girlfriend to have an abortion and sued the Alabama Women’s Center for Reproductive Alternatives in Huntsville on behalf of an embryo that was aborted at six weeks.
To sue on behalf of the embryo, the would-be father, Ryan Magers, went to probate court where he asked a judge to appoint him as the personal representative of the estate. In probate court, a judge may appoint someone to represent the estate of a person who has died without a will. That representative then has the authority to distribute the estate’s assets to beneficiaries.
When Mr. Magers filed to open an estate for the embryo, his attorney cited various Alabama court rulings involving pregnant people and a 2018 amendment to the Alabama Constitution recognizing the “sanctity of unborn life and the rights of unborn children.”
A probate judge appointed Mr. Magers representative of the estate, giving him legal standing to sue for damages in the wrongful death claim. The case, believed to be the first instance in which an aborted embryo was given legal rights, made national headlines.
It’s unclear how many states allow an estate to be opened on behalf of an embryo or fetus. Some states, like Arizona, don’t explicitly define what counts as a deceased person in their probate code, leaving it to a judge to decide. In a handful of states, laws define embryos and fetuses as a person at conception, which could allow for an estate, but it’s rare.
An Alabama circuit court judge eventually dismissed Mr. Magers’ wrongful death lawsuit, stating that the claims were “precluded by State and Federal laws.”
Mr. Villegas contacted Mr. Magers’ attorney, Brent Helms, about pursuing a similar action in Arizona and was referred to J. Stanley Martineau, an Arizona attorney who had flown to Alabama to talk to Mr. Helms about Mr. Magers’ case.
In August 2020, Mr. Villegas filed a petition to be appointed personal representative of the estate of “Baby Villegas.” His ex-wife opposed the action and contacted a legal advocacy organization focused on reproductive justice, which helped her obtain a lawyer.
In court filings, Mr. Villegas said he prefers to think of “Baby Villegas” as a girl, although the sex of the embryo was never determined, and his lawyer argued that there isn’t an Arizona case that explicitly defines a deceased person, “so the issue appears to be an open one in Arizona.”
In a 2021 motion arguing for dismissal, the ex-wife’s attorney, Louis Silverman, argued that Arizona’s probate code doesn’t authorize the appointment of a personal representative for an embryo, and that granting Mr. Villegas’ request would violate a woman’s constitutional right to decide whether to carry a pregnancy to term.
“U.S. Supreme Court precedent has long protected the constitutional right of a woman to obtain an abortion, including that the decision whether to do so belongs to the woman alone – even where her partner, spouse, or ex-spouse disagrees with that decision,” Mr. Silverman said last year.
Gila County Superior Court Judge Bryan B. Chambers said in an order denying the motion that his decision allows Mr. Villegas to make the argument that the embryo is a person in a wrongful death lawsuit, but that he has not reached that conclusion at this stage. Mr. Villegas was later appointed the personal representative of the estate.
As states determine what is legal in the wake of Dobbs and legislators propose new abortion laws, anti-abortion groups such as the National Right to Life Committee see civil suits as a way to enforce abortion bans and have released model legislation they hope sympathetic legislators will duplicate in statehouses nationwide.
“In addition to criminal penalties and medical license revocation, civil remedies will be critical to ensure that unborn lives are protected from illegal abortions,” the group wrote in a June 15 letter to its state affiliates that included the model legislation.
James Bopp Jr., general counsel for the committee, said in an interview with ProPublica that such actions will be necessary because some “radical Democrat” prosecutors have signaled they won’t enforce criminal abortion bans. Last month, 90 prosecutors from across the country indicated that they would not prosecute those who seek abortions.
“The civil remedies follow what the criminal law makes unlawful,” he said. “And that’s what we’re doing.”
The National Right to Life Committee’s model legislation, which advocates prohibiting abortion except to prevent the death of the pregnant person, recommends that states permit civil actions against people or entities that violate abortion laws “to prevent future violations.” It also suggests that people who have had or have sought to have an illegal abortion, as well as the expectant father and the parents of a pregnant minor, be allowed to pursue wrongful death actions.
Under the legislation, an action for wrongful death of an “unborn child” would be treated like that of a child who died after being born.
In one regard, Arizona has already implemented a piece of this model legislation as the state’s lawmakers have chipped away at access to abortion and enacted a myriad of regulations on doctors who provide the procedure.
The state’s “informed consent” statute for abortion, first signed into law by then-Gov. Jan Brewer in 2009, mandated an in-person counseling session and a 24-hour waiting period before an abortion. It allows a pregnant person, their husband or a maternal grandparent of a minor to sue if a physician does not properly obtain the pregnant person’s informed consent, and to receive damages for psychological, emotional and physical injuries, statutory damages and attorney fees.
The informed consent laws, which have changed over time, mandate that the patient be told about the “probable anatomical and physiological characteristics” of the embryo or fetus and the “immediate and long-term medical risks” associated with abortion, as well as alternatives to the procedure. Some abortion-rights groups and medical professionals have criticized informed consent processes, arguing the materials can be misleading and personify the embryo or fetus. A 2018 review of numerous studies concluded that having an abortion does not increase a person’s risk of infertility in their next pregnancy, nor is it linked to a higher risk of breast cancer or preterm birth, among other issues.
The wrongful death suit comes at a time of extraordinary confusion over abortion law in Arizona.
Until Roe v. Wade was handed down in 1973, establishing a constitutional right to abortion, a law dating to before statehood had banned the procedure. In March, Gov. Doug Ducey, a Republican who has called Arizona “the most pro-life state in the country,” signed into law a bill outlawing abortions after 15 weeks, and said that law would supersede the pre-statehood ban if Roe were overturned. But now that Roe has been overturned, Arizona Attorney General Mark Brnovich, another Republican, said he intends to enforce the pre-statehood ban, which outlawed abortion except to preserve the life of the person seeking the procedure. On July 14, he filed a motion to lift an injunction on the law, which would make it enforceable.
Adding to the muddle, a U.S. district court judge on July 11 blocked part of a 2021 Arizona law that would classify fertilized eggs, embryos and fetuses as people starting at conception, ruling that the attorney general cannot use the so-called personhood law against abortion providers. Following the Supreme Court decision in Dobbs, eight of the state’s nine abortion providers – all located in three Arizona counties – halted abortion services, but following the emergency injunction some are again offering them.
In the wrongful death claim, Mr. Martineau argued that the woman’s consent was invalidated because the doctors didn’t follow the informed consent statute. Although the woman signed four consent documents, the suit claims that “evidence shows that in her rush to maximize profits,” the clinic’s owner, Dr. Gabrielle Goodrick, “cut corners.” Mr. Martineau alleged that Dr. Goodrick and another doctor didn’t inform the woman of the loss of “maternal-fetal” attachment, about the alternatives to abortion or that if not for the abortion, the embryo would likely have been “delivered to term,” among other violations.
Tom Slutes, Dr. Goodrick’s lawyer, called the lawsuit “ridiculous.”
“They didn’t cut any corners,” he said, adding that the woman “clearly knew what was going to happen and definitely, strongly” wanted the abortion. Regardless of the information the woman received, she wouldn’t have changed her mind, Mr. Slutes said. Mr. Slutes referenced the deposition, where the woman said she “felt completely informed.”
Mr. Martineau said in an interview that Mr. Villegas isn’t motivated by collecting money from the lawsuit.
“He has no desire to harass” his ex-wife, Mr. Martineau said. “All he wants to do is make sure it doesn’t happen to another father.”
In a deposition, Mr. Villegas’ ex-wife said that he was emotionally abusive during their marriage, which lasted nearly 5 years. At first, she said, Mr. Villegas seemed like the “greatest guy I’ve ever met in my life,” taking her to California for a week as a birthday gift. But as the marriage progressed, she said, there were times he wouldn’t allow her to get a job or leave the house unless she was with him.
The woman alleged that Mr. Villegas made fake social media profiles, hacked into her social media accounts and threatened to “blackmail” her if she left him during his failed campaign to be a justice of the peace in Gila County, outside of Phoenix.
Mr. Villegas denied the allegations about his relationship but declined to comment further for this story, Mr. Martineau said.
Carliss Chatman, an associate law professor at Washington and Lee University in Virginia, said certain civil remedies can also be a mechanism for men to continue to abuse their former partners through the court system.
“What happens if the father who is suing on behalf of the fetus is your rapist or your abuser? It’s another way to torture a woman,” Ms. Chatman said.
Ms. Chatman added that these legal actions can be a deterrent for physicians in states where abortion is banned after a certain gestational period, because the threat of civil suits makes it harder for doctors to get insurance.
The lawsuit has added to the stresses on Dr. Goodrick, who has been performing abortions in Arizona since the mid-1990s, and her practice. She said that, since the lawsuit was filed, the annual cost of her medical malpractice insurance has risen from $32,000 to $67,000.
Before providers in Arizona halted abortions following the Supreme Court decision, people would begin lining up outside Dr. Goodrick’s clinic at 6 a.m., sometimes with lawn chairs in hand, like “a concert line,” Dr. Goodrick said.
“Every year there’s something and we never know what it’s going to be,” Dr. Goodrick said recently at her Phoenix clinic. “I’m kind of desensitized to it all.”
Nicole Santa Cruz is a reporter covering issues of inequality in the Southwest.
This story was originally published on ProPublica. ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive their biggest stories as soon as they’re published.
A judge allowed the woman’s ex-husband to establish an estate for the embryo, which had been aborted in its seventh week of development. The ex-husband filed a wrongful death lawsuit against the clinic and its doctors in 2020, alleging that physicians failed to obtain proper informed consent from the woman as required by Arizona law.
Across the United States, people have sued for negligence in the death of a fetus or embryo in cases where a pregnant person has been killed in a car crash or a pregnancy was lost because of alleged wrongdoing by a physician. But a court action claiming the wrongful death of an aborted embryo or fetus is a more novel strategy, legal experts said.
The experts said this rare tactic could become more common, as anti-abortion groups have signaled their desire to further limit reproductive rights following the U.S. Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade. The Arizona lawsuit and others that may follow could also be an attempt to discourage and intimidate providers and harass plaintiffs’ former romantic partners, experts said.
Lucinda Finley, a law professor at the University at Buffalo who specializes in tort law and reproductive rights, said the Arizona case is a “harbinger of things to come” and called it “troubling for the future.”
Ms. Finley said she expects state lawmakers and anti-abortion groups to use “unprecedented strategies” to try to prevent people from traveling to obtain abortions or block them from obtaining information on where to seek one.
Perhaps the most extreme example is in Texas, where the Texas Heartbeat Act, signed into law in May 2021 and upheld by the U.S. Supreme Court in December, allows private citizens to sue a person who performs or aids in an abortion.
“It’s much bigger than these wrongful death suits,” Ms. Finley said.
Civia Tamarkin, president of the National Council of Jewish Women Arizona, which advocates for reproductive rights, said the Arizona lawsuit is part of a larger agenda that anti-abortion advocates are working toward.
“It’s a lawsuit that appears to be a trial balloon to see how far the attorney and the plaintiff can push the limits of the law, the limits of reason, the limits of science and medicine,” Ms. Tamarkin said.
In July 2018, the ex-husband, Mario Villegas, accompanied his then-wife to three medical appointments – a consultation, the abortion, and a follow-up. The woman, who ProPublica is not identifying for privacy reasons, said in a deposition in the wrongful death suit that at the time of the procedure the two were already talking about obtaining a divorce, which was finalized later that year.
“We were not happy together at all,” she said.
Mr. Villegas, a former Marine from Globe, Ariz., a mining town east of Phoenix, had been married twice before and has other children. He has since moved out of state.
In a form his then-wife filled out at the clinic, she said she was seeking an abortion because she was not ready to be a parent and her relationship with Mr. Villegas was unstable, according to court records. She also checked a box affirming that “I am comfortable with my decision to terminate this pregnancy.” The woman declined to speak on the record with ProPublica out of fear for her safety.
The following year, in 2019, Mr. Villegas learned about an Alabama man who hadn’t wanted his ex-girlfriend to have an abortion and sued the Alabama Women’s Center for Reproductive Alternatives in Huntsville on behalf of an embryo that was aborted at six weeks.
To sue on behalf of the embryo, the would-be father, Ryan Magers, went to probate court where he asked a judge to appoint him as the personal representative of the estate. In probate court, a judge may appoint someone to represent the estate of a person who has died without a will. That representative then has the authority to distribute the estate’s assets to beneficiaries.
When Mr. Magers filed to open an estate for the embryo, his attorney cited various Alabama court rulings involving pregnant people and a 2018 amendment to the Alabama Constitution recognizing the “sanctity of unborn life and the rights of unborn children.”
A probate judge appointed Mr. Magers representative of the estate, giving him legal standing to sue for damages in the wrongful death claim. The case, believed to be the first instance in which an aborted embryo was given legal rights, made national headlines.
It’s unclear how many states allow an estate to be opened on behalf of an embryo or fetus. Some states, like Arizona, don’t explicitly define what counts as a deceased person in their probate code, leaving it to a judge to decide. In a handful of states, laws define embryos and fetuses as a person at conception, which could allow for an estate, but it’s rare.
An Alabama circuit court judge eventually dismissed Mr. Magers’ wrongful death lawsuit, stating that the claims were “precluded by State and Federal laws.”
Mr. Villegas contacted Mr. Magers’ attorney, Brent Helms, about pursuing a similar action in Arizona and was referred to J. Stanley Martineau, an Arizona attorney who had flown to Alabama to talk to Mr. Helms about Mr. Magers’ case.
In August 2020, Mr. Villegas filed a petition to be appointed personal representative of the estate of “Baby Villegas.” His ex-wife opposed the action and contacted a legal advocacy organization focused on reproductive justice, which helped her obtain a lawyer.
In court filings, Mr. Villegas said he prefers to think of “Baby Villegas” as a girl, although the sex of the embryo was never determined, and his lawyer argued that there isn’t an Arizona case that explicitly defines a deceased person, “so the issue appears to be an open one in Arizona.”
In a 2021 motion arguing for dismissal, the ex-wife’s attorney, Louis Silverman, argued that Arizona’s probate code doesn’t authorize the appointment of a personal representative for an embryo, and that granting Mr. Villegas’ request would violate a woman’s constitutional right to decide whether to carry a pregnancy to term.
“U.S. Supreme Court precedent has long protected the constitutional right of a woman to obtain an abortion, including that the decision whether to do so belongs to the woman alone – even where her partner, spouse, or ex-spouse disagrees with that decision,” Mr. Silverman said last year.
Gila County Superior Court Judge Bryan B. Chambers said in an order denying the motion that his decision allows Mr. Villegas to make the argument that the embryo is a person in a wrongful death lawsuit, but that he has not reached that conclusion at this stage. Mr. Villegas was later appointed the personal representative of the estate.
As states determine what is legal in the wake of Dobbs and legislators propose new abortion laws, anti-abortion groups such as the National Right to Life Committee see civil suits as a way to enforce abortion bans and have released model legislation they hope sympathetic legislators will duplicate in statehouses nationwide.
“In addition to criminal penalties and medical license revocation, civil remedies will be critical to ensure that unborn lives are protected from illegal abortions,” the group wrote in a June 15 letter to its state affiliates that included the model legislation.
James Bopp Jr., general counsel for the committee, said in an interview with ProPublica that such actions will be necessary because some “radical Democrat” prosecutors have signaled they won’t enforce criminal abortion bans. Last month, 90 prosecutors from across the country indicated that they would not prosecute those who seek abortions.
“The civil remedies follow what the criminal law makes unlawful,” he said. “And that’s what we’re doing.”
The National Right to Life Committee’s model legislation, which advocates prohibiting abortion except to prevent the death of the pregnant person, recommends that states permit civil actions against people or entities that violate abortion laws “to prevent future violations.” It also suggests that people who have had or have sought to have an illegal abortion, as well as the expectant father and the parents of a pregnant minor, be allowed to pursue wrongful death actions.
Under the legislation, an action for wrongful death of an “unborn child” would be treated like that of a child who died after being born.
In one regard, Arizona has already implemented a piece of this model legislation as the state’s lawmakers have chipped away at access to abortion and enacted a myriad of regulations on doctors who provide the procedure.
The state’s “informed consent” statute for abortion, first signed into law by then-Gov. Jan Brewer in 2009, mandated an in-person counseling session and a 24-hour waiting period before an abortion. It allows a pregnant person, their husband or a maternal grandparent of a minor to sue if a physician does not properly obtain the pregnant person’s informed consent, and to receive damages for psychological, emotional and physical injuries, statutory damages and attorney fees.
The informed consent laws, which have changed over time, mandate that the patient be told about the “probable anatomical and physiological characteristics” of the embryo or fetus and the “immediate and long-term medical risks” associated with abortion, as well as alternatives to the procedure. Some abortion-rights groups and medical professionals have criticized informed consent processes, arguing the materials can be misleading and personify the embryo or fetus. A 2018 review of numerous studies concluded that having an abortion does not increase a person’s risk of infertility in their next pregnancy, nor is it linked to a higher risk of breast cancer or preterm birth, among other issues.
The wrongful death suit comes at a time of extraordinary confusion over abortion law in Arizona.
Until Roe v. Wade was handed down in 1973, establishing a constitutional right to abortion, a law dating to before statehood had banned the procedure. In March, Gov. Doug Ducey, a Republican who has called Arizona “the most pro-life state in the country,” signed into law a bill outlawing abortions after 15 weeks, and said that law would supersede the pre-statehood ban if Roe were overturned. But now that Roe has been overturned, Arizona Attorney General Mark Brnovich, another Republican, said he intends to enforce the pre-statehood ban, which outlawed abortion except to preserve the life of the person seeking the procedure. On July 14, he filed a motion to lift an injunction on the law, which would make it enforceable.
Adding to the muddle, a U.S. district court judge on July 11 blocked part of a 2021 Arizona law that would classify fertilized eggs, embryos and fetuses as people starting at conception, ruling that the attorney general cannot use the so-called personhood law against abortion providers. Following the Supreme Court decision in Dobbs, eight of the state’s nine abortion providers – all located in three Arizona counties – halted abortion services, but following the emergency injunction some are again offering them.
In the wrongful death claim, Mr. Martineau argued that the woman’s consent was invalidated because the doctors didn’t follow the informed consent statute. Although the woman signed four consent documents, the suit claims that “evidence shows that in her rush to maximize profits,” the clinic’s owner, Dr. Gabrielle Goodrick, “cut corners.” Mr. Martineau alleged that Dr. Goodrick and another doctor didn’t inform the woman of the loss of “maternal-fetal” attachment, about the alternatives to abortion or that if not for the abortion, the embryo would likely have been “delivered to term,” among other violations.
Tom Slutes, Dr. Goodrick’s lawyer, called the lawsuit “ridiculous.”
“They didn’t cut any corners,” he said, adding that the woman “clearly knew what was going to happen and definitely, strongly” wanted the abortion. Regardless of the information the woman received, she wouldn’t have changed her mind, Mr. Slutes said. Mr. Slutes referenced the deposition, where the woman said she “felt completely informed.”
Mr. Martineau said in an interview that Mr. Villegas isn’t motivated by collecting money from the lawsuit.
“He has no desire to harass” his ex-wife, Mr. Martineau said. “All he wants to do is make sure it doesn’t happen to another father.”
In a deposition, Mr. Villegas’ ex-wife said that he was emotionally abusive during their marriage, which lasted nearly 5 years. At first, she said, Mr. Villegas seemed like the “greatest guy I’ve ever met in my life,” taking her to California for a week as a birthday gift. But as the marriage progressed, she said, there were times he wouldn’t allow her to get a job or leave the house unless she was with him.
The woman alleged that Mr. Villegas made fake social media profiles, hacked into her social media accounts and threatened to “blackmail” her if she left him during his failed campaign to be a justice of the peace in Gila County, outside of Phoenix.
Mr. Villegas denied the allegations about his relationship but declined to comment further for this story, Mr. Martineau said.
Carliss Chatman, an associate law professor at Washington and Lee University in Virginia, said certain civil remedies can also be a mechanism for men to continue to abuse their former partners through the court system.
“What happens if the father who is suing on behalf of the fetus is your rapist or your abuser? It’s another way to torture a woman,” Ms. Chatman said.
Ms. Chatman added that these legal actions can be a deterrent for physicians in states where abortion is banned after a certain gestational period, because the threat of civil suits makes it harder for doctors to get insurance.
The lawsuit has added to the stresses on Dr. Goodrick, who has been performing abortions in Arizona since the mid-1990s, and her practice. She said that, since the lawsuit was filed, the annual cost of her medical malpractice insurance has risen from $32,000 to $67,000.
Before providers in Arizona halted abortions following the Supreme Court decision, people would begin lining up outside Dr. Goodrick’s clinic at 6 a.m., sometimes with lawn chairs in hand, like “a concert line,” Dr. Goodrick said.
“Every year there’s something and we never know what it’s going to be,” Dr. Goodrick said recently at her Phoenix clinic. “I’m kind of desensitized to it all.”
Nicole Santa Cruz is a reporter covering issues of inequality in the Southwest.
This story was originally published on ProPublica. ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive their biggest stories as soon as they’re published.
Nurse midwives step up to provide prenatal care after two rural hospitals shutter birthing centers
MUSCATINE, IOWA – Bailee Tordai, who was 33 weeks into her pregnancy, barely made it to the prenatal checkup. Her clunky old Jeep couldn’t complete the 2-mile trip from her house to the University of Iowa’s outreach clinic in her southeastern Iowa hometown. It was a hot June day, and a wiring problem made the Jeep conk out in the street.
A passerby helped Ms.Tordai, 22, push her stricken vehicle off the road and into a parking lot. Then she called her stepdad for a ride to the clinic.
Jaclyn Roman, a nurse-midwife, walked into the exam room. “I heard your car broke down.”
“Yup. You want to buy it? Five bucks!” Ms. Tordai joked.
Her lack of reliable transportation won’t be a laughing matter in August, when her baby is due. She will need to arrange for someone to drive her about 40 miles northwest to the University of Iowa Hospitals and Clinics in Iowa City. She can’t give birth at Muscatine’s hospital because it shuttered its birthing unit in 2020.
Ms. Roman is part of an unusual effort to minimize the harm caused by such closures. She’s one of 11 certified nurse-midwives from the University of Iowa who travel regularly to Muscatine and Washington, another southeastern Iowa town where the local hospital closed its birthing unit. The university’s pilot project, which is supported by a federal grant, doesn’t aim to reopen shuttered birthing units. Instead, the midwife team helps ensure area women receive related services. Last year, it served more than 500 patients in Muscatine and Washington.
Muscatine is one of hundreds of rural areas in the United States where hospitals have dropped birthing services during the past 2 decades, often because they lack obstetricians and other specialized staff members.
Hospital industry leaders say birthing units also tend to lose money, largely because of low payments from Medicaid, the public health insurance program that covers more than 40% of births in the United States and an even greater share in many rural areas.
The loss of labor-and-delivery services hits especially hard for women who lack resources and time to travel for care.
Muscatine, which is on the Mississippi River, has more than 23,000 residents, making it a relatively large town by Iowa standards. But its hospital is one of 41 Iowa facilities that have closed their birthing units since 2000, according to the Iowa Department of Public Health. Most were in rural areas. Just one has reopened, and only 56 Iowa hospitals now have birthing units.
The nurse-midwife team’s work includes crucial prenatal checkups. Most pregnant people are supposed to have a dozen or more such appointments before giving birth. Health care providers use the checkups to track how a pregnancy is progressing and to watch for signs of high blood pressure and other problems that can lead to premature births, stillbirths, or even maternal deaths. The midwives also advise women on how to keep themselves and their babies healthy after birth.
Karen Jefferson, DM, director of midwifery practice for the American College of Nurse-Midwives, said the University of Iowa team’s approach is an innovative way to address needs in rural areas that have lost hospital birthing units. “How wonderful would it be to see a provider in your town, instead of driving 40 miles for your prenatal visits – especially toward the end of pregnancy, when you’re going every week,” said Dr. Jefferson, who lives in rural New York.
Midwives can provide many other types of care for women and for babies. In theory, they could even open rural birthing centers outside of hospitals, Dr. Jefferson said. But they would need to overcome concerns about financing and about the availability of surgeons to do emergency cesarean sections, which she said are rarely needed in low-risk births.
The University of Iowa midwives focus on low-risk pregnancies, referring patients with significant health issues to physician specialists in Iowa City. Often, those specialists can visit with the patients and the midwives via video conference in the small-town clinics.
The loss of a hospital obstetrics unit can make finding local maternity care harder for rural families.
Ms. Tordai can attest that if patients must travel far for prenatal appointments, they’re less likely to get to them all. If she had to go to Iowa City for each of hers, repeatedly taking 3 hours off from her job managing a pizza restaurant would be tough, she said. On that June day her Jeep broke down, she would have canceled her appointment.
Instead, she wound up on an exam table at the Muscatine clinic listening to her baby’s heartbeat on a monitor and watching as Ms. Roman measured her belly.
“Nice job being perfect,” the midwife told her during the checkup.
Ms. Roman asked Ms. Tordai to describe her baby’s movements. “Constant,” she replied with a smile.
Ms. Roman asked whether she planned to breastfeed. Ms. Tordai said she didn’t have much luck with her first daughter, Aspen, now 4.
“Have you thought about a breastfeeding class?” the midwife asked.
“I don’t have time for that,” Ms. Tordai replied. Ms. Roman continued to coax her, noting where a breastfeeding class is available online.
Near the end of the appointment, Ms. Tordai asked Ms. Roman whether she could schedule an induced birth at the University of Iowa hospital. The midwife told her that, in general, letting labor begin on its own is better than artificially starting it.
But there was the matter of unreliable transportation. Ms. Tordai explained that scheduling the birth would help her arrange to have her mother drive her to the hospital in Iowa City. Ms. Roman agreed that transportation is a legitimate reason and arranged for an induced labor on Aug. 10.
The University of Iowa midwife team started offering services in 2020 in a clinic about 2 miles from Trinity Muscatine hospital. The hospital is owned by UnityPoint Health, a large nonprofit hospital system that blamed a lack of available obstetricians for the closure of the Muscatine birthing unit. At the time, UnityPoint leaders said they hoped to reopen the unit if they could recruit new obstetricians to the area.
Kristy Phillipson, a UnityPoint Health spokesperson, told KHN in June that the company has continued to try to recruit physicians, including for the Muscatine hospital. Although it has not reopened the birthing unit, the company regularly sends an obstetrician and other staff members to provide prenatal care and related services, she said.
Most pregnant patients from the area who choose UnityPoint for their care wind up giving birth at the system’s hospital in Bettendorf, a 45-minute drive to the east.
The University of Iowa midwife team has no plans to open its own birthing centers, but it hopes to expand its rural clinic service to other underserved towns. To do so, the university would need to hire more nurse-midwives, which could be a challenge. According to the Iowa Board of Nursing, 120 licensed nurse-midwives live in the state of 3 million people.
The University of Iowa plans to address that by starting the state’s first nurse-midwife training program in 2023. The master’s degree program, which will emphasize rural service, will train registered nurses to become nurse-midwives. It eventually could graduate eight people per year, said Amber Goodrich, a University of Iowa midwife helping lead the effort.
Those graduates could fill gaps throughout rural areas, where even more hospitals may shutter their birthing units in the coming years.
“This crisis is going nowhere fast,” Ms. Goodrich said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
MUSCATINE, IOWA – Bailee Tordai, who was 33 weeks into her pregnancy, barely made it to the prenatal checkup. Her clunky old Jeep couldn’t complete the 2-mile trip from her house to the University of Iowa’s outreach clinic in her southeastern Iowa hometown. It was a hot June day, and a wiring problem made the Jeep conk out in the street.
A passerby helped Ms.Tordai, 22, push her stricken vehicle off the road and into a parking lot. Then she called her stepdad for a ride to the clinic.
Jaclyn Roman, a nurse-midwife, walked into the exam room. “I heard your car broke down.”
“Yup. You want to buy it? Five bucks!” Ms. Tordai joked.
Her lack of reliable transportation won’t be a laughing matter in August, when her baby is due. She will need to arrange for someone to drive her about 40 miles northwest to the University of Iowa Hospitals and Clinics in Iowa City. She can’t give birth at Muscatine’s hospital because it shuttered its birthing unit in 2020.
Ms. Roman is part of an unusual effort to minimize the harm caused by such closures. She’s one of 11 certified nurse-midwives from the University of Iowa who travel regularly to Muscatine and Washington, another southeastern Iowa town where the local hospital closed its birthing unit. The university’s pilot project, which is supported by a federal grant, doesn’t aim to reopen shuttered birthing units. Instead, the midwife team helps ensure area women receive related services. Last year, it served more than 500 patients in Muscatine and Washington.
Muscatine is one of hundreds of rural areas in the United States where hospitals have dropped birthing services during the past 2 decades, often because they lack obstetricians and other specialized staff members.
Hospital industry leaders say birthing units also tend to lose money, largely because of low payments from Medicaid, the public health insurance program that covers more than 40% of births in the United States and an even greater share in many rural areas.
The loss of labor-and-delivery services hits especially hard for women who lack resources and time to travel for care.
Muscatine, which is on the Mississippi River, has more than 23,000 residents, making it a relatively large town by Iowa standards. But its hospital is one of 41 Iowa facilities that have closed their birthing units since 2000, according to the Iowa Department of Public Health. Most were in rural areas. Just one has reopened, and only 56 Iowa hospitals now have birthing units.
The nurse-midwife team’s work includes crucial prenatal checkups. Most pregnant people are supposed to have a dozen or more such appointments before giving birth. Health care providers use the checkups to track how a pregnancy is progressing and to watch for signs of high blood pressure and other problems that can lead to premature births, stillbirths, or even maternal deaths. The midwives also advise women on how to keep themselves and their babies healthy after birth.
Karen Jefferson, DM, director of midwifery practice for the American College of Nurse-Midwives, said the University of Iowa team’s approach is an innovative way to address needs in rural areas that have lost hospital birthing units. “How wonderful would it be to see a provider in your town, instead of driving 40 miles for your prenatal visits – especially toward the end of pregnancy, when you’re going every week,” said Dr. Jefferson, who lives in rural New York.
Midwives can provide many other types of care for women and for babies. In theory, they could even open rural birthing centers outside of hospitals, Dr. Jefferson said. But they would need to overcome concerns about financing and about the availability of surgeons to do emergency cesarean sections, which she said are rarely needed in low-risk births.
The University of Iowa midwives focus on low-risk pregnancies, referring patients with significant health issues to physician specialists in Iowa City. Often, those specialists can visit with the patients and the midwives via video conference in the small-town clinics.
The loss of a hospital obstetrics unit can make finding local maternity care harder for rural families.
Ms. Tordai can attest that if patients must travel far for prenatal appointments, they’re less likely to get to them all. If she had to go to Iowa City for each of hers, repeatedly taking 3 hours off from her job managing a pizza restaurant would be tough, she said. On that June day her Jeep broke down, she would have canceled her appointment.
Instead, she wound up on an exam table at the Muscatine clinic listening to her baby’s heartbeat on a monitor and watching as Ms. Roman measured her belly.
“Nice job being perfect,” the midwife told her during the checkup.
Ms. Roman asked Ms. Tordai to describe her baby’s movements. “Constant,” she replied with a smile.
Ms. Roman asked whether she planned to breastfeed. Ms. Tordai said she didn’t have much luck with her first daughter, Aspen, now 4.
“Have you thought about a breastfeeding class?” the midwife asked.
“I don’t have time for that,” Ms. Tordai replied. Ms. Roman continued to coax her, noting where a breastfeeding class is available online.
Near the end of the appointment, Ms. Tordai asked Ms. Roman whether she could schedule an induced birth at the University of Iowa hospital. The midwife told her that, in general, letting labor begin on its own is better than artificially starting it.
But there was the matter of unreliable transportation. Ms. Tordai explained that scheduling the birth would help her arrange to have her mother drive her to the hospital in Iowa City. Ms. Roman agreed that transportation is a legitimate reason and arranged for an induced labor on Aug. 10.
The University of Iowa midwife team started offering services in 2020 in a clinic about 2 miles from Trinity Muscatine hospital. The hospital is owned by UnityPoint Health, a large nonprofit hospital system that blamed a lack of available obstetricians for the closure of the Muscatine birthing unit. At the time, UnityPoint leaders said they hoped to reopen the unit if they could recruit new obstetricians to the area.
Kristy Phillipson, a UnityPoint Health spokesperson, told KHN in June that the company has continued to try to recruit physicians, including for the Muscatine hospital. Although it has not reopened the birthing unit, the company regularly sends an obstetrician and other staff members to provide prenatal care and related services, she said.
Most pregnant patients from the area who choose UnityPoint for their care wind up giving birth at the system’s hospital in Bettendorf, a 45-minute drive to the east.
The University of Iowa midwife team has no plans to open its own birthing centers, but it hopes to expand its rural clinic service to other underserved towns. To do so, the university would need to hire more nurse-midwives, which could be a challenge. According to the Iowa Board of Nursing, 120 licensed nurse-midwives live in the state of 3 million people.
The University of Iowa plans to address that by starting the state’s first nurse-midwife training program in 2023. The master’s degree program, which will emphasize rural service, will train registered nurses to become nurse-midwives. It eventually could graduate eight people per year, said Amber Goodrich, a University of Iowa midwife helping lead the effort.
Those graduates could fill gaps throughout rural areas, where even more hospitals may shutter their birthing units in the coming years.
“This crisis is going nowhere fast,” Ms. Goodrich said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
MUSCATINE, IOWA – Bailee Tordai, who was 33 weeks into her pregnancy, barely made it to the prenatal checkup. Her clunky old Jeep couldn’t complete the 2-mile trip from her house to the University of Iowa’s outreach clinic in her southeastern Iowa hometown. It was a hot June day, and a wiring problem made the Jeep conk out in the street.
A passerby helped Ms.Tordai, 22, push her stricken vehicle off the road and into a parking lot. Then she called her stepdad for a ride to the clinic.
Jaclyn Roman, a nurse-midwife, walked into the exam room. “I heard your car broke down.”
“Yup. You want to buy it? Five bucks!” Ms. Tordai joked.
Her lack of reliable transportation won’t be a laughing matter in August, when her baby is due. She will need to arrange for someone to drive her about 40 miles northwest to the University of Iowa Hospitals and Clinics in Iowa City. She can’t give birth at Muscatine’s hospital because it shuttered its birthing unit in 2020.
Ms. Roman is part of an unusual effort to minimize the harm caused by such closures. She’s one of 11 certified nurse-midwives from the University of Iowa who travel regularly to Muscatine and Washington, another southeastern Iowa town where the local hospital closed its birthing unit. The university’s pilot project, which is supported by a federal grant, doesn’t aim to reopen shuttered birthing units. Instead, the midwife team helps ensure area women receive related services. Last year, it served more than 500 patients in Muscatine and Washington.
Muscatine is one of hundreds of rural areas in the United States where hospitals have dropped birthing services during the past 2 decades, often because they lack obstetricians and other specialized staff members.
Hospital industry leaders say birthing units also tend to lose money, largely because of low payments from Medicaid, the public health insurance program that covers more than 40% of births in the United States and an even greater share in many rural areas.
The loss of labor-and-delivery services hits especially hard for women who lack resources and time to travel for care.
Muscatine, which is on the Mississippi River, has more than 23,000 residents, making it a relatively large town by Iowa standards. But its hospital is one of 41 Iowa facilities that have closed their birthing units since 2000, according to the Iowa Department of Public Health. Most were in rural areas. Just one has reopened, and only 56 Iowa hospitals now have birthing units.
The nurse-midwife team’s work includes crucial prenatal checkups. Most pregnant people are supposed to have a dozen or more such appointments before giving birth. Health care providers use the checkups to track how a pregnancy is progressing and to watch for signs of high blood pressure and other problems that can lead to premature births, stillbirths, or even maternal deaths. The midwives also advise women on how to keep themselves and their babies healthy after birth.
Karen Jefferson, DM, director of midwifery practice for the American College of Nurse-Midwives, said the University of Iowa team’s approach is an innovative way to address needs in rural areas that have lost hospital birthing units. “How wonderful would it be to see a provider in your town, instead of driving 40 miles for your prenatal visits – especially toward the end of pregnancy, when you’re going every week,” said Dr. Jefferson, who lives in rural New York.
Midwives can provide many other types of care for women and for babies. In theory, they could even open rural birthing centers outside of hospitals, Dr. Jefferson said. But they would need to overcome concerns about financing and about the availability of surgeons to do emergency cesarean sections, which she said are rarely needed in low-risk births.
The University of Iowa midwives focus on low-risk pregnancies, referring patients with significant health issues to physician specialists in Iowa City. Often, those specialists can visit with the patients and the midwives via video conference in the small-town clinics.
The loss of a hospital obstetrics unit can make finding local maternity care harder for rural families.
Ms. Tordai can attest that if patients must travel far for prenatal appointments, they’re less likely to get to them all. If she had to go to Iowa City for each of hers, repeatedly taking 3 hours off from her job managing a pizza restaurant would be tough, she said. On that June day her Jeep broke down, she would have canceled her appointment.
Instead, she wound up on an exam table at the Muscatine clinic listening to her baby’s heartbeat on a monitor and watching as Ms. Roman measured her belly.
“Nice job being perfect,” the midwife told her during the checkup.
Ms. Roman asked Ms. Tordai to describe her baby’s movements. “Constant,” she replied with a smile.
Ms. Roman asked whether she planned to breastfeed. Ms. Tordai said she didn’t have much luck with her first daughter, Aspen, now 4.
“Have you thought about a breastfeeding class?” the midwife asked.
“I don’t have time for that,” Ms. Tordai replied. Ms. Roman continued to coax her, noting where a breastfeeding class is available online.
Near the end of the appointment, Ms. Tordai asked Ms. Roman whether she could schedule an induced birth at the University of Iowa hospital. The midwife told her that, in general, letting labor begin on its own is better than artificially starting it.
But there was the matter of unreliable transportation. Ms. Tordai explained that scheduling the birth would help her arrange to have her mother drive her to the hospital in Iowa City. Ms. Roman agreed that transportation is a legitimate reason and arranged for an induced labor on Aug. 10.
The University of Iowa midwife team started offering services in 2020 in a clinic about 2 miles from Trinity Muscatine hospital. The hospital is owned by UnityPoint Health, a large nonprofit hospital system that blamed a lack of available obstetricians for the closure of the Muscatine birthing unit. At the time, UnityPoint leaders said they hoped to reopen the unit if they could recruit new obstetricians to the area.
Kristy Phillipson, a UnityPoint Health spokesperson, told KHN in June that the company has continued to try to recruit physicians, including for the Muscatine hospital. Although it has not reopened the birthing unit, the company regularly sends an obstetrician and other staff members to provide prenatal care and related services, she said.
Most pregnant patients from the area who choose UnityPoint for their care wind up giving birth at the system’s hospital in Bettendorf, a 45-minute drive to the east.
The University of Iowa midwife team has no plans to open its own birthing centers, but it hopes to expand its rural clinic service to other underserved towns. To do so, the university would need to hire more nurse-midwives, which could be a challenge. According to the Iowa Board of Nursing, 120 licensed nurse-midwives live in the state of 3 million people.
The University of Iowa plans to address that by starting the state’s first nurse-midwife training program in 2023. The master’s degree program, which will emphasize rural service, will train registered nurses to become nurse-midwives. It eventually could graduate eight people per year, said Amber Goodrich, a University of Iowa midwife helping lead the effort.
Those graduates could fill gaps throughout rural areas, where even more hospitals may shutter their birthing units in the coming years.
“This crisis is going nowhere fast,” Ms. Goodrich said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Red Flag: Suicide risk
How AI is helping prevent suicide in veterans

Medically reviewed by Jennifer Casarella, MD
Dan Miller has parked his Nissan Altima on the side of the road near a field outside Chicago and is holding a gun to his head.
Haunted for years by the compounded trauma of tours of duty in the Middle East and his work as a police officer in Chicago, at that moment, Dr. Miller saw no reason to live. And there were troubles at home with his wife and children, who had grown fearful of his behavior.
“My whole world was falling apart,” he says of that dark night in 2014. “It left a hole I didn’t know how to fill.”
He chose not to pull the trigger after a brochure on the passenger seat of his car gave him an unexpected perspective – and launched him on a path to help others in his situation.
Had Mr. Miller taken his life that night, he would have joined thousands of other veterans who died by suicide. About 17 U.S. veterans lose their lives this way each day, on average, according to the Department of Veterans Affairs. In 2019, the last year for which records are available, 6,261 veterans took their own lives – and the suicide rate for veterans was 52% higher than for nonveterans, the agency’s records show.
The problem has become so severe that
But that wasn’t available when Dan Miller’s life was unraveling.
In the years leading up to his near-suicide, his wife had pushed him to get help. “She said, ‘You’re not the same person you were when you left. The kids are scared of you. The pets are scared of you,” he recalls.
He resisted, even when his wife threatened divorce. Rising through the ranks of the Marines, Mr. Miller had become more emotionally isolated. He feared losing his job and the respect of others if he let anyone know what he was going through.
Finally, he gave the VHA a chance. He went in for an initial consultation in 2010 and didn’t find it helpful. He didn’t like being told what to do. So he stopped. He turned to obsessive exercise and excessive drinking.
That day in 2014, Mr. Miller’s wife told him she was taking the kids out for a playdate. After she left, he was served with divorce papers. Less than an hour later, he was parked in his car with his gun, ready to end his life.
But if it all had happened just a few years later, things might never have gotten to that point.
Scanning for suicide risk
In 2017, the VHA piloted its AI program, called REACH VET, that aims to help prevent veterans from dying by suicide.
Every month, a computer scans the electronic health records of all VHA patients who’ve had a health care visit for any reason in the last 2 years. It checks more than 140 variables and weights them to estimate someone’s overall suicide risk at that moment in time.
To build the risk algorithm, a computer combed through the medical records of 6,360 veterans confirmed to have died by suicide between 2009 and 2011. (The VHA continually updates the list of variables from the health records of VHA patients, including those who have died by suicide since then and others.)
Some variables are things you’d expect:
- A past suicide attempt.
- A diagnosis of depression or other mental illness.
- A diagnosis of a terminal illness.
Others are more surprising. For example, a diagnosis of arthritis or diabetes adds weight.
REACH VET flags the riskiest cases – the top 0.1% – for a mental health or primary care provider to review. They reach out to the patient to tell them how and why their record was flagged, discuss any recommended treatment changes, and ask them to come in for a visit.
“It’s an opportunity to talk about their risk factors, which is designed to lead to a conversation about safety planning,” says clinical psychologist Matthew Miller, PhD, national director of the U.S. Department of Veterans Affairs’ Suicide Prevention Program. He’s not related to Dan Miller.
Making a suicide safety plan
A safety plan is a document that outlines how a person can help prevent their own suicide in a crisis.
The plan may include:
- A list of personal triggers or warning signs.
- What’s helped them in the past.
- Names of people or organizations who can support them.
- Plans to remove means of suicide, such as guns, from their environment.
- Their reasons for living.
In people at risk for suicide, research shows that having a safety plan reduces suicidal thoughts and attempts, lowers rates of depression and hopelessness, and boosts veterans’ engagement with the health care system. It may also help people manage things that trigger their suicidal thoughts.
Getting the call
What if REACH VET had been around when Dan Miller was in crisis – and he’d gotten a call from the VHA?
“It absolutely, positively would have helped because one of the biggest things on that day when I got served was feeling completely alone and that I had no one to turn to,” Mr. Miller says. He’s now a speaker for the Wounded Warrior Project, a nonprofit that serves veterans and active-duty service people.
Vets’ reactions to the unexpected VHA phone call, psychologist Dr. Miller says, “run the gamut from ‘Thank you for contacting me. Let’s talk,’ to ‘What are you talking about? Leave me alone!’ ”
Nothing stops all suicides. But REACH VET is having an impact. In a clinical trial, vets contacted through REACH VET had more doctor visits, were more likely to have a written suicide prevention safety plan, and had fewer hospital admissions for mental health, ER visits, and suicide attempts.

An assist from AI
Even simple outreach can make a big difference. And there’s research to prove it.
One study included 4,730 veterans recently discharged from psychiatric care at the VHA, a group considered at high risk for suicide.
Half of them got 13 caring emails from hospital staff in the weeks after leaving the hospital. The emails mentioned personal things the patient had shared, like a love of hiking, and wished them well. The other veterans got routine follow-up but no emails.
Two years later, those who got the caring emails were less likely to have died by suicide than the other vets. The study was published in 2014 in Contemporary Clinical Trials.
Researchers have done studies like this many times: with handwritten notes from the primary care doctor, postcards from the ER, and so forth. The results never vary: The notes reduce suicide risk.
“If we could use AI to identify people to receive notes or phone calls, it would be a very effective and inexpensive way to guide follow-up care,” says Rebecca Bernert, PhD, director and founder of the Suicide Prevention Research Laboratory at Stanford (Calif.) University.
AI doesn’t replace clinical judgment.
“AI can capture data that we miss due to the limits of our humanity,” psychologist Dr. Miller says. “There’s suicide prevention processes founded on big data and AI, and there are processes founded in clinical intuition and acumen.”
AI is only as good as the data it’s based on. If that data lacks diversity, it may miss things. And variables that apply to veterans may differ in civilians.
Stopping suicidal thoughts
Google is putting AI to work against suicide, too. Its MUM (Multitask Unified Model) technology seeks to understand the intent behind what we google.
MUM powers Google Search. It can often tell the difference between a search for information about suicide for someone writing a research paper on the topic and a search for information on how or where to carry out a suicide.
When Google Search detects that someone in the United States might be in crisis and at risk of suicide, the first search results that person gets are the number for the National Suicide Prevention Lifeline and other resources for people in crisis.
Google Home Assistant works in the same way. When a user makes a query that signals a suicide-related crisis, the gadget serves up resources that offer help.
MUM is working to understand the nuances of crisis language in 75 languages so that Google Search can provide people in crisis with hotlines or other resources in many countries.
“We want to find partners that are accessible to users in terms of hours of operation. We have a strong preference for finding partners that promise confidentiality and privacy to the extent that those are permitted [in that country],” says Anne Merritt, MD, a product manager at Google Search.
Other companies are working on apps that use AI to spot suicide risk in other ways, including voice technology that may notice subtle changes in the voice of someone who’s depressed and may be thinking of suicide. Those are still in development but show promise. Keep in mind that apps do not require government approval, so if you try one, be sure to let your health care provider know.
Changing the channel
Seeing a hotline number on your phone or computer screen can help, Dan Miller says. “If I happened to be online, searching maybe for a bridge to jump off of ... and suddenly that pops up on the screen, it’s like it changes the channel.”
It may not work for everyone, he says, but that search result could interrupt someone’s suicidal train of thought.
That’s crucial, psychologist Dr. Miller says, because most suicide attempts escalate from first thought to potentially fatal action in just 1 hour. That’s how fast it happened for Dan Miller in 2014.
“When you’re able to put time and space between the suicidal thought and the access to the method to act on that thought, you save lives,” Dr. Bernert says.
Making a different choice
An interruption in Mr. Miller’s thinking is what had saved his life.
Holding the gun to his head, Mr. Miller looked over at the passenger seat at a brochure from Wounded Warrior Project, which he had just learned about. Mr. Miller noticed a photo of a man in a wheelchair, a veteran like him, who had no legs. He thought that the man looked worse off than him but hadn’t given up.
Mr. Miller put down his gun and decided to get help.
Recovering from a near suicide attempt, he says, is a journey. It doesn’t happen overnight. Now, 8 years later, Mr. Miller is planning a brief break from the speaker circuit. He plans to spend 2 weeks in an outpatient counseling program for posttraumatic stress disorder and traumatic brain injury.
“Telling my story to strangers – part of it is healing me in a way, but I’m learning that repeating the story over and over again is also keeping me from letting it go. And I’m still healing.”
A version of this article first appeared on WebMD.com.
How AI is helping prevent suicide in veterans
How AI is helping prevent suicide in veterans
Medically reviewed by Jennifer Casarella, MD
Dan Miller has parked his Nissan Altima on the side of the road near a field outside Chicago and is holding a gun to his head.
Haunted for years by the compounded trauma of tours of duty in the Middle East and his work as a police officer in Chicago, at that moment, Dr. Miller saw no reason to live. And there were troubles at home with his wife and children, who had grown fearful of his behavior.
“My whole world was falling apart,” he says of that dark night in 2014. “It left a hole I didn’t know how to fill.”
He chose not to pull the trigger after a brochure on the passenger seat of his car gave him an unexpected perspective – and launched him on a path to help others in his situation.
Had Mr. Miller taken his life that night, he would have joined thousands of other veterans who died by suicide. About 17 U.S. veterans lose their lives this way each day, on average, according to the Department of Veterans Affairs. In 2019, the last year for which records are available, 6,261 veterans took their own lives – and the suicide rate for veterans was 52% higher than for nonveterans, the agency’s records show.
The problem has become so severe that
But that wasn’t available when Dan Miller’s life was unraveling.
In the years leading up to his near-suicide, his wife had pushed him to get help. “She said, ‘You’re not the same person you were when you left. The kids are scared of you. The pets are scared of you,” he recalls.
He resisted, even when his wife threatened divorce. Rising through the ranks of the Marines, Mr. Miller had become more emotionally isolated. He feared losing his job and the respect of others if he let anyone know what he was going through.
Finally, he gave the VHA a chance. He went in for an initial consultation in 2010 and didn’t find it helpful. He didn’t like being told what to do. So he stopped. He turned to obsessive exercise and excessive drinking.
That day in 2014, Mr. Miller’s wife told him she was taking the kids out for a playdate. After she left, he was served with divorce papers. Less than an hour later, he was parked in his car with his gun, ready to end his life.
But if it all had happened just a few years later, things might never have gotten to that point.
Scanning for suicide risk
In 2017, the VHA piloted its AI program, called REACH VET, that aims to help prevent veterans from dying by suicide.
Every month, a computer scans the electronic health records of all VHA patients who’ve had a health care visit for any reason in the last 2 years. It checks more than 140 variables and weights them to estimate someone’s overall suicide risk at that moment in time.
To build the risk algorithm, a computer combed through the medical records of 6,360 veterans confirmed to have died by suicide between 2009 and 2011. (The VHA continually updates the list of variables from the health records of VHA patients, including those who have died by suicide since then and others.)
Some variables are things you’d expect:
- A past suicide attempt.
- A diagnosis of depression or other mental illness.
- A diagnosis of a terminal illness.
Others are more surprising. For example, a diagnosis of arthritis or diabetes adds weight.
REACH VET flags the riskiest cases – the top 0.1% – for a mental health or primary care provider to review. They reach out to the patient to tell them how and why their record was flagged, discuss any recommended treatment changes, and ask them to come in for a visit.
“It’s an opportunity to talk about their risk factors, which is designed to lead to a conversation about safety planning,” says clinical psychologist Matthew Miller, PhD, national director of the U.S. Department of Veterans Affairs’ Suicide Prevention Program. He’s not related to Dan Miller.
Making a suicide safety plan
A safety plan is a document that outlines how a person can help prevent their own suicide in a crisis.
The plan may include:
- A list of personal triggers or warning signs.
- What’s helped them in the past.
- Names of people or organizations who can support them.
- Plans to remove means of suicide, such as guns, from their environment.
- Their reasons for living.
In people at risk for suicide, research shows that having a safety plan reduces suicidal thoughts and attempts, lowers rates of depression and hopelessness, and boosts veterans’ engagement with the health care system. It may also help people manage things that trigger their suicidal thoughts.
Getting the call
What if REACH VET had been around when Dan Miller was in crisis – and he’d gotten a call from the VHA?
“It absolutely, positively would have helped because one of the biggest things on that day when I got served was feeling completely alone and that I had no one to turn to,” Mr. Miller says. He’s now a speaker for the Wounded Warrior Project, a nonprofit that serves veterans and active-duty service people.
Vets’ reactions to the unexpected VHA phone call, psychologist Dr. Miller says, “run the gamut from ‘Thank you for contacting me. Let’s talk,’ to ‘What are you talking about? Leave me alone!’ ”
Nothing stops all suicides. But REACH VET is having an impact. In a clinical trial, vets contacted through REACH VET had more doctor visits, were more likely to have a written suicide prevention safety plan, and had fewer hospital admissions for mental health, ER visits, and suicide attempts.
An assist from AI
Even simple outreach can make a big difference. And there’s research to prove it.
One study included 4,730 veterans recently discharged from psychiatric care at the VHA, a group considered at high risk for suicide.
Half of them got 13 caring emails from hospital staff in the weeks after leaving the hospital. The emails mentioned personal things the patient had shared, like a love of hiking, and wished them well. The other veterans got routine follow-up but no emails.
Two years later, those who got the caring emails were less likely to have died by suicide than the other vets. The study was published in 2014 in Contemporary Clinical Trials.
Researchers have done studies like this many times: with handwritten notes from the primary care doctor, postcards from the ER, and so forth. The results never vary: The notes reduce suicide risk.
“If we could use AI to identify people to receive notes or phone calls, it would be a very effective and inexpensive way to guide follow-up care,” says Rebecca Bernert, PhD, director and founder of the Suicide Prevention Research Laboratory at Stanford (Calif.) University.
AI doesn’t replace clinical judgment.
“AI can capture data that we miss due to the limits of our humanity,” psychologist Dr. Miller says. “There’s suicide prevention processes founded on big data and AI, and there are processes founded in clinical intuition and acumen.”
AI is only as good as the data it’s based on. If that data lacks diversity, it may miss things. And variables that apply to veterans may differ in civilians.
Stopping suicidal thoughts
Google is putting AI to work against suicide, too. Its MUM (Multitask Unified Model) technology seeks to understand the intent behind what we google.
MUM powers Google Search. It can often tell the difference between a search for information about suicide for someone writing a research paper on the topic and a search for information on how or where to carry out a suicide.
When Google Search detects that someone in the United States might be in crisis and at risk of suicide, the first search results that person gets are the number for the National Suicide Prevention Lifeline and other resources for people in crisis.
Google Home Assistant works in the same way. When a user makes a query that signals a suicide-related crisis, the gadget serves up resources that offer help.
MUM is working to understand the nuances of crisis language in 75 languages so that Google Search can provide people in crisis with hotlines or other resources in many countries.
“We want to find partners that are accessible to users in terms of hours of operation. We have a strong preference for finding partners that promise confidentiality and privacy to the extent that those are permitted [in that country],” says Anne Merritt, MD, a product manager at Google Search.
Other companies are working on apps that use AI to spot suicide risk in other ways, including voice technology that may notice subtle changes in the voice of someone who’s depressed and may be thinking of suicide. Those are still in development but show promise. Keep in mind that apps do not require government approval, so if you try one, be sure to let your health care provider know.
Changing the channel
Seeing a hotline number on your phone or computer screen can help, Dan Miller says. “If I happened to be online, searching maybe for a bridge to jump off of ... and suddenly that pops up on the screen, it’s like it changes the channel.”
It may not work for everyone, he says, but that search result could interrupt someone’s suicidal train of thought.
That’s crucial, psychologist Dr. Miller says, because most suicide attempts escalate from first thought to potentially fatal action in just 1 hour. That’s how fast it happened for Dan Miller in 2014.
“When you’re able to put time and space between the suicidal thought and the access to the method to act on that thought, you save lives,” Dr. Bernert says.
Making a different choice
An interruption in Mr. Miller’s thinking is what had saved his life.
Holding the gun to his head, Mr. Miller looked over at the passenger seat at a brochure from Wounded Warrior Project, which he had just learned about. Mr. Miller noticed a photo of a man in a wheelchair, a veteran like him, who had no legs. He thought that the man looked worse off than him but hadn’t given up.
Mr. Miller put down his gun and decided to get help.
Recovering from a near suicide attempt, he says, is a journey. It doesn’t happen overnight. Now, 8 years later, Mr. Miller is planning a brief break from the speaker circuit. He plans to spend 2 weeks in an outpatient counseling program for posttraumatic stress disorder and traumatic brain injury.
“Telling my story to strangers – part of it is healing me in a way, but I’m learning that repeating the story over and over again is also keeping me from letting it go. And I’m still healing.”
A version of this article first appeared on WebMD.com.
Medically reviewed by Jennifer Casarella, MD
Dan Miller has parked his Nissan Altima on the side of the road near a field outside Chicago and is holding a gun to his head.
Haunted for years by the compounded trauma of tours of duty in the Middle East and his work as a police officer in Chicago, at that moment, Dr. Miller saw no reason to live. And there were troubles at home with his wife and children, who had grown fearful of his behavior.
“My whole world was falling apart,” he says of that dark night in 2014. “It left a hole I didn’t know how to fill.”
He chose not to pull the trigger after a brochure on the passenger seat of his car gave him an unexpected perspective – and launched him on a path to help others in his situation.
Had Mr. Miller taken his life that night, he would have joined thousands of other veterans who died by suicide. About 17 U.S. veterans lose their lives this way each day, on average, according to the Department of Veterans Affairs. In 2019, the last year for which records are available, 6,261 veterans took their own lives – and the suicide rate for veterans was 52% higher than for nonveterans, the agency’s records show.
The problem has become so severe that
But that wasn’t available when Dan Miller’s life was unraveling.
In the years leading up to his near-suicide, his wife had pushed him to get help. “She said, ‘You’re not the same person you were when you left. The kids are scared of you. The pets are scared of you,” he recalls.
He resisted, even when his wife threatened divorce. Rising through the ranks of the Marines, Mr. Miller had become more emotionally isolated. He feared losing his job and the respect of others if he let anyone know what he was going through.
Finally, he gave the VHA a chance. He went in for an initial consultation in 2010 and didn’t find it helpful. He didn’t like being told what to do. So he stopped. He turned to obsessive exercise and excessive drinking.
That day in 2014, Mr. Miller’s wife told him she was taking the kids out for a playdate. After she left, he was served with divorce papers. Less than an hour later, he was parked in his car with his gun, ready to end his life.
But if it all had happened just a few years later, things might never have gotten to that point.
Scanning for suicide risk
In 2017, the VHA piloted its AI program, called REACH VET, that aims to help prevent veterans from dying by suicide.
Every month, a computer scans the electronic health records of all VHA patients who’ve had a health care visit for any reason in the last 2 years. It checks more than 140 variables and weights them to estimate someone’s overall suicide risk at that moment in time.
To build the risk algorithm, a computer combed through the medical records of 6,360 veterans confirmed to have died by suicide between 2009 and 2011. (The VHA continually updates the list of variables from the health records of VHA patients, including those who have died by suicide since then and others.)
Some variables are things you’d expect:
- A past suicide attempt.
- A diagnosis of depression or other mental illness.
- A diagnosis of a terminal illness.
Others are more surprising. For example, a diagnosis of arthritis or diabetes adds weight.
REACH VET flags the riskiest cases – the top 0.1% – for a mental health or primary care provider to review. They reach out to the patient to tell them how and why their record was flagged, discuss any recommended treatment changes, and ask them to come in for a visit.
“It’s an opportunity to talk about their risk factors, which is designed to lead to a conversation about safety planning,” says clinical psychologist Matthew Miller, PhD, national director of the U.S. Department of Veterans Affairs’ Suicide Prevention Program. He’s not related to Dan Miller.
Making a suicide safety plan
A safety plan is a document that outlines how a person can help prevent their own suicide in a crisis.
The plan may include:
- A list of personal triggers or warning signs.
- What’s helped them in the past.
- Names of people or organizations who can support them.
- Plans to remove means of suicide, such as guns, from their environment.
- Their reasons for living.
In people at risk for suicide, research shows that having a safety plan reduces suicidal thoughts and attempts, lowers rates of depression and hopelessness, and boosts veterans’ engagement with the health care system. It may also help people manage things that trigger their suicidal thoughts.
Getting the call
What if REACH VET had been around when Dan Miller was in crisis – and he’d gotten a call from the VHA?
“It absolutely, positively would have helped because one of the biggest things on that day when I got served was feeling completely alone and that I had no one to turn to,” Mr. Miller says. He’s now a speaker for the Wounded Warrior Project, a nonprofit that serves veterans and active-duty service people.
Vets’ reactions to the unexpected VHA phone call, psychologist Dr. Miller says, “run the gamut from ‘Thank you for contacting me. Let’s talk,’ to ‘What are you talking about? Leave me alone!’ ”
Nothing stops all suicides. But REACH VET is having an impact. In a clinical trial, vets contacted through REACH VET had more doctor visits, were more likely to have a written suicide prevention safety plan, and had fewer hospital admissions for mental health, ER visits, and suicide attempts.
An assist from AI
Even simple outreach can make a big difference. And there’s research to prove it.
One study included 4,730 veterans recently discharged from psychiatric care at the VHA, a group considered at high risk for suicide.
Half of them got 13 caring emails from hospital staff in the weeks after leaving the hospital. The emails mentioned personal things the patient had shared, like a love of hiking, and wished them well. The other veterans got routine follow-up but no emails.
Two years later, those who got the caring emails were less likely to have died by suicide than the other vets. The study was published in 2014 in Contemporary Clinical Trials.
Researchers have done studies like this many times: with handwritten notes from the primary care doctor, postcards from the ER, and so forth. The results never vary: The notes reduce suicide risk.
“If we could use AI to identify people to receive notes or phone calls, it would be a very effective and inexpensive way to guide follow-up care,” says Rebecca Bernert, PhD, director and founder of the Suicide Prevention Research Laboratory at Stanford (Calif.) University.
AI doesn’t replace clinical judgment.
“AI can capture data that we miss due to the limits of our humanity,” psychologist Dr. Miller says. “There’s suicide prevention processes founded on big data and AI, and there are processes founded in clinical intuition and acumen.”
AI is only as good as the data it’s based on. If that data lacks diversity, it may miss things. And variables that apply to veterans may differ in civilians.
Stopping suicidal thoughts
Google is putting AI to work against suicide, too. Its MUM (Multitask Unified Model) technology seeks to understand the intent behind what we google.
MUM powers Google Search. It can often tell the difference between a search for information about suicide for someone writing a research paper on the topic and a search for information on how or where to carry out a suicide.
When Google Search detects that someone in the United States might be in crisis and at risk of suicide, the first search results that person gets are the number for the National Suicide Prevention Lifeline and other resources for people in crisis.
Google Home Assistant works in the same way. When a user makes a query that signals a suicide-related crisis, the gadget serves up resources that offer help.
MUM is working to understand the nuances of crisis language in 75 languages so that Google Search can provide people in crisis with hotlines or other resources in many countries.
“We want to find partners that are accessible to users in terms of hours of operation. We have a strong preference for finding partners that promise confidentiality and privacy to the extent that those are permitted [in that country],” says Anne Merritt, MD, a product manager at Google Search.
Other companies are working on apps that use AI to spot suicide risk in other ways, including voice technology that may notice subtle changes in the voice of someone who’s depressed and may be thinking of suicide. Those are still in development but show promise. Keep in mind that apps do not require government approval, so if you try one, be sure to let your health care provider know.
Changing the channel
Seeing a hotline number on your phone or computer screen can help, Dan Miller says. “If I happened to be online, searching maybe for a bridge to jump off of ... and suddenly that pops up on the screen, it’s like it changes the channel.”
It may not work for everyone, he says, but that search result could interrupt someone’s suicidal train of thought.
That’s crucial, psychologist Dr. Miller says, because most suicide attempts escalate from first thought to potentially fatal action in just 1 hour. That’s how fast it happened for Dan Miller in 2014.
“When you’re able to put time and space between the suicidal thought and the access to the method to act on that thought, you save lives,” Dr. Bernert says.
Making a different choice
An interruption in Mr. Miller’s thinking is what had saved his life.
Holding the gun to his head, Mr. Miller looked over at the passenger seat at a brochure from Wounded Warrior Project, which he had just learned about. Mr. Miller noticed a photo of a man in a wheelchair, a veteran like him, who had no legs. He thought that the man looked worse off than him but hadn’t given up.
Mr. Miller put down his gun and decided to get help.
Recovering from a near suicide attempt, he says, is a journey. It doesn’t happen overnight. Now, 8 years later, Mr. Miller is planning a brief break from the speaker circuit. He plans to spend 2 weeks in an outpatient counseling program for posttraumatic stress disorder and traumatic brain injury.
“Telling my story to strangers – part of it is healing me in a way, but I’m learning that repeating the story over and over again is also keeping me from letting it go. And I’m still healing.”
A version of this article first appeared on WebMD.com.
Violent patient throws scalding oil on MD; other patient dangers
Ralph Newman, MD, got a taste of how dangerous medicine could be at age 10, when he witnessed a physician being shot by a patient.
“I was visiting a friend whose father was a psychiatrist,” Dr. Newman recalled. “We were playing in the living room when the doorbell rang. My friend went to the door and opened it. Then I heard a shot. I ran to the front hall and saw my friend’s father slumped at the bottom of the stairs. He had come down the stairs to see who was there. It was a patient armed with a shotgun.”
As a result of the shooting, a large portion of the psychiatrist’s intestines was removed. In spite of this traumatic incident, Dr. Newman went on to become a psychiatrist – who treated many violent prisoners. “I knew it was dangerous,” he said, “but I rationalized that I wouldn’t be attacked because I would be nicer.”
That attitude seemed to work until 2002, when a prisoner threw boiling oil on him. Dr. Newman was working at the Federal Medical Center Butner, a facility for prisoners in North Carolina. “A prisoner I had been treating was denied parole, based on my recommendation,” he said. “From then on, he was looking for a way to exact revenge.”
“One day I was sitting in the nursing station, typing up notes,” Dr. Newman said. “Two new nurses, who were also there, had forgotten to lock the door, and the prisoner noticed that. He heated up some baby oil in a microwave, which was available to prisoners at the time. Then he walked into the office, threw the oil on my back, and came at me with a sharp pencil.”
Dr. Newman said the nurses fled to an adjoining office, locked the door, and wouldn’t let him in. He went into another office and collapsed in exhaustion. He was saved by an inmate who came on the scene, fended off the attacker, and called for help.
“I was taken to the burn unit,” Dr. Newman recalled. “I had second- and third-degree burns on 9% of my body. It was extremely painful. It took me 45 days to recover enough to get back to work.” The two nurses were fired.
Doctors take threats by patients more seriously now
When orthopedic surgeon Preston Phillips, MD, was killed by a patient in Tulsa, Okla., on June 1, Jennifer M. Weiss, MD, recognized the potential danger to physicians.
“The news left me feeling very shaken,” said Dr. Weiss, a pediatric orthopedic surgeon at Southern California Permanente Medical Group, Los Angeles. “Every orthopedic surgeon I talked to about it felt shaken.”
Dr. Weiss said the impact of that event prompted her to take a patient’s abuse more seriously than she might have previously. “Before the killing, my colleagues and I might have swept the incident under the rug, but we reported it to the authorities,” she said.
“What happened was I told a parent of a school-aged child that the child wasn’t ready to go back to sports,” Dr. Weiss says. “This parent was incredibly triggered – screaming and making verbal threats. The parent was standing between me and the door, so I couldn’t get out.”
Coworkers down the hall heard the yelling and helped Dr. Weiss get out of the room. “The parent was escorted out of the building, and the incident was reported to our risk management team,” she said.
Shooters/killers vs. agitated patients
Patients who shoot to kill are very different from agitated patients seen by many doctors on a regular basis – particularly in emergency departments (EDs), psychiatric units, and pain clinics, said Scott Zeller, MD, a psychiatrist who is vice president of Acute Psychiatric Medicine at Vituity, a multistate physician partnership based in Emeryville, California.
“Agitated patients have trouble communicating their needs and can become physically and verbally aggressive,” Dr. Zeller said. He reports that there are 1.7 million such incidents a year in this country, but most of the incidents of verbal aggression can be kept from exploding into physical violence.
Shooters, however, are very hard to stop because they usually plan the action in advance, Dr. Zeller said. He recalled the 2017 murder of Todd Graham, MD, a friend from medical school. Dr. Graham, an orthopedic surgeon in South Bend, Ind., was gunned down by the husband of one of his patients after Dr. Graham declined to prescribe opioids for her.
Playing down the risk of violence
Doctors may play down the risk of violence, even after they have experienced it personally. “Patients can get angry and may make threatening comments,” Dr. Weiss said. “A lot of doctors just brush it off.”
Simple remarks can set off violence-prone patients, as happened to James P. Phillips, MD, director of disaster and operational medicine at George Washington University, Washington. He recalled asking a prisoner who was visiting his hospital to “lower the volume,” and the man exploded. “Even though he was handcuffed to the bed, he heaved an oxygen tank into a window,” Dr. Phillips said. “He said he would be coming back to kill me.”
Sometimes threats or other types of verbal abuse can be as destructive as physical violence. Diann Krywko, MD, an emergency physician at the Medical University of South Carolina (MUSC) Health, Charleston, has had some tough assignments. She worked in EDs in Detroit and Flint, Mich., for a decade before coming to MUSC, where she serves as director of wellness, health, and resilience. One of the incidents that has bothered her the most involved a threat.
It happened when Dr. Krywko denied a patient’s request for narcotics. “She was very angry and said she’d come to my home and cut my children’s heads off,” Dr. Krywko said. “To this day, what she said horrifies me. I still see her smile as she said that.”
Dr. Krywko considered filing for a restraining order against the patient but didn’t because the patient could have learned her address. Dr. Phillips said fear of retaliation is one reason many doctors don’t report threats from patients. “The patient you report knows where you work and may come there to take revenge,” he said. “Also, you may have to continue caring for the person who punched you.”
Online threats also may cause a great deal of angst. Dr. Phillips said he received many online threats when was a medical analyst for CNN in 2020. “Someone sent my address to his Twitter followers, and they shared it with others, so now the whole world knows where I live,” he said. “I had to upgrade security at my home.”
How to deal with volatile patients
Being nice may not always work, but in many cases, it can keep a volatile situation from exploding, according to Dr. Krywko.
“When patients begin to show signs of agitation or are already there, we always try to verbally deescalate the situation, which involves listening,” Dr. Krywko said. “They want someone to hear them out.”
Doctors speak to patients from a position of authority, but Dr. Krywko advises that they should not be too blunt. “Don’t tell patients they’re wrong,” she said. “Even if they may be incorrect, they feel their viewpoint is valid. Encourage a dialogue with words like, ‘Tell me more,’ ” Dr. Krywko said.
Defending yourself
Doctors may have little warning of an impending attack because a patient’s mood can change quickly. This happened several years ago to Jennifer Casaletto, MD, an emergency physician in Charlotte, N.C.
“A man was brought into my ED by ambulance,” she said. “He seemed very calm for a long while, but then he became completely unhinged. A male nurse placed himself between the patient and others and was attacked. He got hurt but was able to continue working.”
Dr. Zeller said health care teams sometimes overreact when patients lash out. “The old-fashioned way to deal with an agitated patient is to call in the cavalry – everyone does a group takedown,” he said. “The patient is put in restraints and heavily sedated. This is not good for anybody. Not only is it likely to injure and traumatize the patient, it can also injure the care team.”
Many hospital EDs have security guards. “I feel safer when a hospital has armed security guards, but they need to be well trained,” Dr. Casaletto said. “Many small hospitals and freestanding EDs do not have security officers at all, or the guards are undertrained or told not to touch anybody.”
In many electronic health record systems, doctors can flag violent patients so future caregivers can be forewarned. However, Dr. Zeller advises against writing about patients’ violence or rudeness in the medical record, because patients can have access to it and might take revenge.
Rising violence from patients
“It feels like it has become much more dangerous to work in the ED,” said Hasan Gokal, MD, an emergency physician working in EDs at the Texas Medical Center. “Just last week, a woman pulled out a gun and fired it in an ED near Houston.”
The statistics back up Dr. Gokal’s assessment. Injuries caused by violent attacks against medical professionals grew by 67% from 2011 to 2018, according to the U.S. Bureau of Labor Statistics. Those levels rose even more during the COVID-19 pandemic – the assault rate in hospitals rose 23% just in 2020.
Dr. Krywko said she had “a patient who said she wanted to hurt the next person who irritated her, and that happened to me. She jumped out of her bed swinging and punching, and I wasn’t ready for it. I yelled for help and the care team came.”
“The rise in violence has to do with a decline in respect for authority,” Dr. Phillips said. “Some people now believe doctors are lying to them about the need for COVID precautions because they are taking money from the vaccine companies. The pandemic has exacerbated violence in every way.”
Dr. Phillips said that a growing lack of resources had led to more anger among patients. “There are fewer nurses and reduced physician coverage,” he said. “That means longer wait times for patients, which increases patients’ frustrations.”
Dr. Weiss said patients have higher expectations. “In sports medicine, the expectations are incredible,” she said. “Parents want their kids to get back to playing as soon as possible.”
“Hospitals in particular are soft targets for violence,” Dr. Phillips said. “People know you can’t assault a flight attendant, because it’s a federal offense, but there is no such federal offense for violence against health care personnel.”
A version of this article first appeared on Medscape.com.
Ralph Newman, MD, got a taste of how dangerous medicine could be at age 10, when he witnessed a physician being shot by a patient.
“I was visiting a friend whose father was a psychiatrist,” Dr. Newman recalled. “We were playing in the living room when the doorbell rang. My friend went to the door and opened it. Then I heard a shot. I ran to the front hall and saw my friend’s father slumped at the bottom of the stairs. He had come down the stairs to see who was there. It was a patient armed with a shotgun.”
As a result of the shooting, a large portion of the psychiatrist’s intestines was removed. In spite of this traumatic incident, Dr. Newman went on to become a psychiatrist – who treated many violent prisoners. “I knew it was dangerous,” he said, “but I rationalized that I wouldn’t be attacked because I would be nicer.”
That attitude seemed to work until 2002, when a prisoner threw boiling oil on him. Dr. Newman was working at the Federal Medical Center Butner, a facility for prisoners in North Carolina. “A prisoner I had been treating was denied parole, based on my recommendation,” he said. “From then on, he was looking for a way to exact revenge.”
“One day I was sitting in the nursing station, typing up notes,” Dr. Newman said. “Two new nurses, who were also there, had forgotten to lock the door, and the prisoner noticed that. He heated up some baby oil in a microwave, which was available to prisoners at the time. Then he walked into the office, threw the oil on my back, and came at me with a sharp pencil.”
Dr. Newman said the nurses fled to an adjoining office, locked the door, and wouldn’t let him in. He went into another office and collapsed in exhaustion. He was saved by an inmate who came on the scene, fended off the attacker, and called for help.
“I was taken to the burn unit,” Dr. Newman recalled. “I had second- and third-degree burns on 9% of my body. It was extremely painful. It took me 45 days to recover enough to get back to work.” The two nurses were fired.
Doctors take threats by patients more seriously now
When orthopedic surgeon Preston Phillips, MD, was killed by a patient in Tulsa, Okla., on June 1, Jennifer M. Weiss, MD, recognized the potential danger to physicians.
“The news left me feeling very shaken,” said Dr. Weiss, a pediatric orthopedic surgeon at Southern California Permanente Medical Group, Los Angeles. “Every orthopedic surgeon I talked to about it felt shaken.”
Dr. Weiss said the impact of that event prompted her to take a patient’s abuse more seriously than she might have previously. “Before the killing, my colleagues and I might have swept the incident under the rug, but we reported it to the authorities,” she said.
“What happened was I told a parent of a school-aged child that the child wasn’t ready to go back to sports,” Dr. Weiss says. “This parent was incredibly triggered – screaming and making verbal threats. The parent was standing between me and the door, so I couldn’t get out.”
Coworkers down the hall heard the yelling and helped Dr. Weiss get out of the room. “The parent was escorted out of the building, and the incident was reported to our risk management team,” she said.
Shooters/killers vs. agitated patients
Patients who shoot to kill are very different from agitated patients seen by many doctors on a regular basis – particularly in emergency departments (EDs), psychiatric units, and pain clinics, said Scott Zeller, MD, a psychiatrist who is vice president of Acute Psychiatric Medicine at Vituity, a multistate physician partnership based in Emeryville, California.
“Agitated patients have trouble communicating their needs and can become physically and verbally aggressive,” Dr. Zeller said. He reports that there are 1.7 million such incidents a year in this country, but most of the incidents of verbal aggression can be kept from exploding into physical violence.
Shooters, however, are very hard to stop because they usually plan the action in advance, Dr. Zeller said. He recalled the 2017 murder of Todd Graham, MD, a friend from medical school. Dr. Graham, an orthopedic surgeon in South Bend, Ind., was gunned down by the husband of one of his patients after Dr. Graham declined to prescribe opioids for her.
Playing down the risk of violence
Doctors may play down the risk of violence, even after they have experienced it personally. “Patients can get angry and may make threatening comments,” Dr. Weiss said. “A lot of doctors just brush it off.”
Simple remarks can set off violence-prone patients, as happened to James P. Phillips, MD, director of disaster and operational medicine at George Washington University, Washington. He recalled asking a prisoner who was visiting his hospital to “lower the volume,” and the man exploded. “Even though he was handcuffed to the bed, he heaved an oxygen tank into a window,” Dr. Phillips said. “He said he would be coming back to kill me.”
Sometimes threats or other types of verbal abuse can be as destructive as physical violence. Diann Krywko, MD, an emergency physician at the Medical University of South Carolina (MUSC) Health, Charleston, has had some tough assignments. She worked in EDs in Detroit and Flint, Mich., for a decade before coming to MUSC, where she serves as director of wellness, health, and resilience. One of the incidents that has bothered her the most involved a threat.
It happened when Dr. Krywko denied a patient’s request for narcotics. “She was very angry and said she’d come to my home and cut my children’s heads off,” Dr. Krywko said. “To this day, what she said horrifies me. I still see her smile as she said that.”
Dr. Krywko considered filing for a restraining order against the patient but didn’t because the patient could have learned her address. Dr. Phillips said fear of retaliation is one reason many doctors don’t report threats from patients. “The patient you report knows where you work and may come there to take revenge,” he said. “Also, you may have to continue caring for the person who punched you.”
Online threats also may cause a great deal of angst. Dr. Phillips said he received many online threats when was a medical analyst for CNN in 2020. “Someone sent my address to his Twitter followers, and they shared it with others, so now the whole world knows where I live,” he said. “I had to upgrade security at my home.”
How to deal with volatile patients
Being nice may not always work, but in many cases, it can keep a volatile situation from exploding, according to Dr. Krywko.
“When patients begin to show signs of agitation or are already there, we always try to verbally deescalate the situation, which involves listening,” Dr. Krywko said. “They want someone to hear them out.”
Doctors speak to patients from a position of authority, but Dr. Krywko advises that they should not be too blunt. “Don’t tell patients they’re wrong,” she said. “Even if they may be incorrect, they feel their viewpoint is valid. Encourage a dialogue with words like, ‘Tell me more,’ ” Dr. Krywko said.
Defending yourself
Doctors may have little warning of an impending attack because a patient’s mood can change quickly. This happened several years ago to Jennifer Casaletto, MD, an emergency physician in Charlotte, N.C.
“A man was brought into my ED by ambulance,” she said. “He seemed very calm for a long while, but then he became completely unhinged. A male nurse placed himself between the patient and others and was attacked. He got hurt but was able to continue working.”
Dr. Zeller said health care teams sometimes overreact when patients lash out. “The old-fashioned way to deal with an agitated patient is to call in the cavalry – everyone does a group takedown,” he said. “The patient is put in restraints and heavily sedated. This is not good for anybody. Not only is it likely to injure and traumatize the patient, it can also injure the care team.”
Many hospital EDs have security guards. “I feel safer when a hospital has armed security guards, but they need to be well trained,” Dr. Casaletto said. “Many small hospitals and freestanding EDs do not have security officers at all, or the guards are undertrained or told not to touch anybody.”
In many electronic health record systems, doctors can flag violent patients so future caregivers can be forewarned. However, Dr. Zeller advises against writing about patients’ violence or rudeness in the medical record, because patients can have access to it and might take revenge.
Rising violence from patients
“It feels like it has become much more dangerous to work in the ED,” said Hasan Gokal, MD, an emergency physician working in EDs at the Texas Medical Center. “Just last week, a woman pulled out a gun and fired it in an ED near Houston.”
The statistics back up Dr. Gokal’s assessment. Injuries caused by violent attacks against medical professionals grew by 67% from 2011 to 2018, according to the U.S. Bureau of Labor Statistics. Those levels rose even more during the COVID-19 pandemic – the assault rate in hospitals rose 23% just in 2020.
Dr. Krywko said she had “a patient who said she wanted to hurt the next person who irritated her, and that happened to me. She jumped out of her bed swinging and punching, and I wasn’t ready for it. I yelled for help and the care team came.”
“The rise in violence has to do with a decline in respect for authority,” Dr. Phillips said. “Some people now believe doctors are lying to them about the need for COVID precautions because they are taking money from the vaccine companies. The pandemic has exacerbated violence in every way.”
Dr. Phillips said that a growing lack of resources had led to more anger among patients. “There are fewer nurses and reduced physician coverage,” he said. “That means longer wait times for patients, which increases patients’ frustrations.”
Dr. Weiss said patients have higher expectations. “In sports medicine, the expectations are incredible,” she said. “Parents want their kids to get back to playing as soon as possible.”
“Hospitals in particular are soft targets for violence,” Dr. Phillips said. “People know you can’t assault a flight attendant, because it’s a federal offense, but there is no such federal offense for violence against health care personnel.”
A version of this article first appeared on Medscape.com.
Ralph Newman, MD, got a taste of how dangerous medicine could be at age 10, when he witnessed a physician being shot by a patient.
“I was visiting a friend whose father was a psychiatrist,” Dr. Newman recalled. “We were playing in the living room when the doorbell rang. My friend went to the door and opened it. Then I heard a shot. I ran to the front hall and saw my friend’s father slumped at the bottom of the stairs. He had come down the stairs to see who was there. It was a patient armed with a shotgun.”
As a result of the shooting, a large portion of the psychiatrist’s intestines was removed. In spite of this traumatic incident, Dr. Newman went on to become a psychiatrist – who treated many violent prisoners. “I knew it was dangerous,” he said, “but I rationalized that I wouldn’t be attacked because I would be nicer.”
That attitude seemed to work until 2002, when a prisoner threw boiling oil on him. Dr. Newman was working at the Federal Medical Center Butner, a facility for prisoners in North Carolina. “A prisoner I had been treating was denied parole, based on my recommendation,” he said. “From then on, he was looking for a way to exact revenge.”
“One day I was sitting in the nursing station, typing up notes,” Dr. Newman said. “Two new nurses, who were also there, had forgotten to lock the door, and the prisoner noticed that. He heated up some baby oil in a microwave, which was available to prisoners at the time. Then he walked into the office, threw the oil on my back, and came at me with a sharp pencil.”
Dr. Newman said the nurses fled to an adjoining office, locked the door, and wouldn’t let him in. He went into another office and collapsed in exhaustion. He was saved by an inmate who came on the scene, fended off the attacker, and called for help.
“I was taken to the burn unit,” Dr. Newman recalled. “I had second- and third-degree burns on 9% of my body. It was extremely painful. It took me 45 days to recover enough to get back to work.” The two nurses were fired.
Doctors take threats by patients more seriously now
When orthopedic surgeon Preston Phillips, MD, was killed by a patient in Tulsa, Okla., on June 1, Jennifer M. Weiss, MD, recognized the potential danger to physicians.
“The news left me feeling very shaken,” said Dr. Weiss, a pediatric orthopedic surgeon at Southern California Permanente Medical Group, Los Angeles. “Every orthopedic surgeon I talked to about it felt shaken.”
Dr. Weiss said the impact of that event prompted her to take a patient’s abuse more seriously than she might have previously. “Before the killing, my colleagues and I might have swept the incident under the rug, but we reported it to the authorities,” she said.
“What happened was I told a parent of a school-aged child that the child wasn’t ready to go back to sports,” Dr. Weiss says. “This parent was incredibly triggered – screaming and making verbal threats. The parent was standing between me and the door, so I couldn’t get out.”
Coworkers down the hall heard the yelling and helped Dr. Weiss get out of the room. “The parent was escorted out of the building, and the incident was reported to our risk management team,” she said.
Shooters/killers vs. agitated patients
Patients who shoot to kill are very different from agitated patients seen by many doctors on a regular basis – particularly in emergency departments (EDs), psychiatric units, and pain clinics, said Scott Zeller, MD, a psychiatrist who is vice president of Acute Psychiatric Medicine at Vituity, a multistate physician partnership based in Emeryville, California.
“Agitated patients have trouble communicating their needs and can become physically and verbally aggressive,” Dr. Zeller said. He reports that there are 1.7 million such incidents a year in this country, but most of the incidents of verbal aggression can be kept from exploding into physical violence.
Shooters, however, are very hard to stop because they usually plan the action in advance, Dr. Zeller said. He recalled the 2017 murder of Todd Graham, MD, a friend from medical school. Dr. Graham, an orthopedic surgeon in South Bend, Ind., was gunned down by the husband of one of his patients after Dr. Graham declined to prescribe opioids for her.
Playing down the risk of violence
Doctors may play down the risk of violence, even after they have experienced it personally. “Patients can get angry and may make threatening comments,” Dr. Weiss said. “A lot of doctors just brush it off.”
Simple remarks can set off violence-prone patients, as happened to James P. Phillips, MD, director of disaster and operational medicine at George Washington University, Washington. He recalled asking a prisoner who was visiting his hospital to “lower the volume,” and the man exploded. “Even though he was handcuffed to the bed, he heaved an oxygen tank into a window,” Dr. Phillips said. “He said he would be coming back to kill me.”
Sometimes threats or other types of verbal abuse can be as destructive as physical violence. Diann Krywko, MD, an emergency physician at the Medical University of South Carolina (MUSC) Health, Charleston, has had some tough assignments. She worked in EDs in Detroit and Flint, Mich., for a decade before coming to MUSC, where she serves as director of wellness, health, and resilience. One of the incidents that has bothered her the most involved a threat.
It happened when Dr. Krywko denied a patient’s request for narcotics. “She was very angry and said she’d come to my home and cut my children’s heads off,” Dr. Krywko said. “To this day, what she said horrifies me. I still see her smile as she said that.”
Dr. Krywko considered filing for a restraining order against the patient but didn’t because the patient could have learned her address. Dr. Phillips said fear of retaliation is one reason many doctors don’t report threats from patients. “The patient you report knows where you work and may come there to take revenge,” he said. “Also, you may have to continue caring for the person who punched you.”
Online threats also may cause a great deal of angst. Dr. Phillips said he received many online threats when was a medical analyst for CNN in 2020. “Someone sent my address to his Twitter followers, and they shared it with others, so now the whole world knows where I live,” he said. “I had to upgrade security at my home.”
How to deal with volatile patients
Being nice may not always work, but in many cases, it can keep a volatile situation from exploding, according to Dr. Krywko.
“When patients begin to show signs of agitation or are already there, we always try to verbally deescalate the situation, which involves listening,” Dr. Krywko said. “They want someone to hear them out.”
Doctors speak to patients from a position of authority, but Dr. Krywko advises that they should not be too blunt. “Don’t tell patients they’re wrong,” she said. “Even if they may be incorrect, they feel their viewpoint is valid. Encourage a dialogue with words like, ‘Tell me more,’ ” Dr. Krywko said.
Defending yourself
Doctors may have little warning of an impending attack because a patient’s mood can change quickly. This happened several years ago to Jennifer Casaletto, MD, an emergency physician in Charlotte, N.C.
“A man was brought into my ED by ambulance,” she said. “He seemed very calm for a long while, but then he became completely unhinged. A male nurse placed himself between the patient and others and was attacked. He got hurt but was able to continue working.”
Dr. Zeller said health care teams sometimes overreact when patients lash out. “The old-fashioned way to deal with an agitated patient is to call in the cavalry – everyone does a group takedown,” he said. “The patient is put in restraints and heavily sedated. This is not good for anybody. Not only is it likely to injure and traumatize the patient, it can also injure the care team.”
Many hospital EDs have security guards. “I feel safer when a hospital has armed security guards, but they need to be well trained,” Dr. Casaletto said. “Many small hospitals and freestanding EDs do not have security officers at all, or the guards are undertrained or told not to touch anybody.”
In many electronic health record systems, doctors can flag violent patients so future caregivers can be forewarned. However, Dr. Zeller advises against writing about patients’ violence or rudeness in the medical record, because patients can have access to it and might take revenge.
Rising violence from patients
“It feels like it has become much more dangerous to work in the ED,” said Hasan Gokal, MD, an emergency physician working in EDs at the Texas Medical Center. “Just last week, a woman pulled out a gun and fired it in an ED near Houston.”
The statistics back up Dr. Gokal’s assessment. Injuries caused by violent attacks against medical professionals grew by 67% from 2011 to 2018, according to the U.S. Bureau of Labor Statistics. Those levels rose even more during the COVID-19 pandemic – the assault rate in hospitals rose 23% just in 2020.
Dr. Krywko said she had “a patient who said she wanted to hurt the next person who irritated her, and that happened to me. She jumped out of her bed swinging and punching, and I wasn’t ready for it. I yelled for help and the care team came.”
“The rise in violence has to do with a decline in respect for authority,” Dr. Phillips said. “Some people now believe doctors are lying to them about the need for COVID precautions because they are taking money from the vaccine companies. The pandemic has exacerbated violence in every way.”
Dr. Phillips said that a growing lack of resources had led to more anger among patients. “There are fewer nurses and reduced physician coverage,” he said. “That means longer wait times for patients, which increases patients’ frustrations.”
Dr. Weiss said patients have higher expectations. “In sports medicine, the expectations are incredible,” she said. “Parents want their kids to get back to playing as soon as possible.”
“Hospitals in particular are soft targets for violence,” Dr. Phillips said. “People know you can’t assault a flight attendant, because it’s a federal offense, but there is no such federal offense for violence against health care personnel.”
A version of this article first appeared on Medscape.com.
Drug shortages plague hematology, but preparedness helps
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.
Just before he took a call from a reporter asking about the impact of drug shortages in hematology, Bill Greene, PharmD, chief pharmaceutical officer at St. Jude Children’s Research Hospital, had spent an hour on the phone overseeing his institution’s response to a hematology drug shortage. The chemotherapy drug fludarabine, used to treat chronic lymphocytic leukemia, was in short supply.
“There are 5 different manufacturers, but none of them have had drug available over the past 2 weeks,” Dr. Greene said. “We’re trying to chase some emergency supplies to be able to continue treatment for patients who’ve had their treatments initiated and planned.”
Over the past several years, this predicament has become common at hematology clinics across the country. In fact, management of scarce medication resources has become a significant part of Dr. Greene’s workload these days, as critical drugs fail to show up on time or manufacturer supplies run low at his hospital in Memphis.
This shortage of hematology drugs got a new dose of national attention, thanks to a recent episode of CBS News’ “60 Minutes.” Through interviews with physicians and parents of children who suddenly could not get vital medications, the report highlighted the recent shortage of another leukemia drug, vincristine.
“As a cancer mom, we shouldn’t be fighting for our children to get a drug that is needed,” Cyndi Valenta was quoted as saying. She recalled that when the shortage began in 2019, her 13-year-old son, a leukemia patient at Loma Linda (Calif.) University Hospital, felt frightened. Ms. Valenta said she felt a “gut-wrenching feeling of just fear and anger.” They were finally able to get doses of the drug after launching a social media campaign.
Such drug shortages are especially widespread in oncology and hematology, according to a survey of oncology pharmacists at 68 organizations nationwide. Published in the May 2022 issue of Oncology Practice, the study showed that 63% of institutions reported one or more drug shortages every month, with a 34% increase in 2019, compared with 2018. Treatment delays, reduced doses, or alternative regimens were reported by 75% of respondents, the authors wrote.
The pharmacists surveyed between May 2019 and July 2020 were asked about the three most hard-to-get chemotherapy and supportive care agents. Vincristine topped the list, followed by vinblastine, IVIG, leucovorin, and BCG, as well as difficult-to-obtain ropine, erwinia asparaginase, etoposide, and leuprolide. Several of these drugs are used to treat conditions such as lymphoma and leukemia.
Eighty-two percent of respondents reported shortages of decitabine (IV), often used as part of a cocktail with vinblastine and other drugs to treat Hodgkin lymphoma.
The reasons for drug shortages are varied. The CBS News report declared that “pharmaceutical companies have stopped producing many life-saving generic drugs because they make too little profit,” and it suggested that the federal government isn’t doing enough.
But government action actually might be making a difference. According to the FDA, the number of new drug shortages has fallen dramatically from 250 in 2011 to 41 in 2021, and the number of prevented drug shortages rose from nearly 200 to more than 300 over that same period. Still, the number of ongoing drug shortages has risen from around 40 in 2017 to about 80 in 2021.
Reasons for the paucity of certain drugs are often unclear. In a June 12, 2022 post, for example, the American Society of Health-System Pharmacists’ drug shortage database noted that the chemotherapy drug fludarabine was in short supply and provided details about when some of the 5 manufacturers expected to have it available. (This is the shortage that Dr. Greene was trying to manage.) But 4 of the 5 manufacturers “did not provide a reason,” and the fifth blamed manufacturing delays.
“There’s a lot of closely held trade secrets that hinder the ability to share good information,” said Dr. Greene. To make things more complicated, shipping times are often unreliable. “The product doesn’t show up today, we place another order. Sometimes it will show up tomorrow, sometimes it doesn’t,” he said. “If you’re not tracking it carefully, you deplete your own supply.”
Patients’ families have grown used to dealing with drug shortages, and “they’re less quick to blame personnel at our institution.”
How can hematologists cope with this issue? “The best thing in the immediate term is to advocate for their hospital to have a pharmacist dedicated to shortage monitoring and taking proactive steps to obviate shortages,” hematologist/oncologist Andrew Hantel, MD, an instructor at Dana-Farber Cancer Institute, Harvard Medical School, Boston, said in an interview.
“We have ongoing communications with other large cancer centers and the FDA to recognize shortages early and develop plans to make sure we stay ahead of them,” Dr. Hantel said. “Most often this involves assessing supply, use rates, alternative manufacturers, and additional measures the Food and Drug Administration can take (for example, importation), and occasionally working with clinical teams to see if other medications are feasible alternatives.”
If a drug is unavailable, it can also be helpful to discuss alternative approaches. “We did not have any frank shortages of vincristine,” Dr. Hantel said, “but we did focus on conservation measures and considered different ethically appropriate ways to distribute vincristine if there was a point at which we did not have enough for everyone who needed it.”
If a drug is in short supply, options can include delaying treatment, giving an alternative, or providing the rest of the regimen without the scarce drug, he said. In a 2021 report in The Lancet Hematology, Dr. Hantel and his colleagues offered “model solutions for ethical allocation during cancer medicine shortages.”
The authors of the May 2022 drug-shortage report highlighted an alternative regimen in hematology. They noted that manufacturing delays have limited the supply of dacarbazine, used for Hodgkin lymphoma. Due to the current shortages, they wrote, clinicians are considering the use of escalated bleomycin, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, replacing dacarbazine with procarbazine and using the doxorubicin, bleomycin, vinblastine, procarbazine, and prednisone regimen, or replacing dacarbazine with cyclophosphamide.
Dr. Greene emphasized the importance of tracking the news and the drug shortage websites run by the FDA and the American Society of Health-System Pharmacists.
It’s also crucial to have a good relationship with your wholesaler, he added, and to communicate about these problems within your facility. At his hospital, the pharmaceutical staff holds a multi-disciplinary meeting at least weekly to discuss the supply of medications. As he put it, “it’s a challenging environment.”
Dr. Greene and Dr. Hantel reported no relevant disclosures.