User login
Moderate drinking shows more benefit for older vs. younger adults
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.

“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.
“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
The health risks and benefits of moderate alcohol consumption are complex and remain a hot topic of debate. The data suggest that small amounts of alcohol may reduce the risk of certain health outcomes over time, but increase the risk of others, wrote Dana Bryazka, MS, a researcher at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, and colleagues, in a paper published in the Lancet.
“The amount of alcohol that minimizes health loss is likely to depend on the distribution of underlying causes of disease burden in a given population. Since this distribution varies widely by geography, age, sex, and time, the level of alcohol consumption associated with the lowest risk to health would depend on the age structure and disease composition of that population,” the researchers wrote.
“We estimate that 1.78 million people worldwide died due to alcohol use in 2020,” Ms. Bryazka said in an interview. “It is important that alcohol consumption guidelines and policies are updated to minimize this harm, particularly in the populations at greatest risk,” she said.
“Existing alcohol consumption guidelines frequently vary by sex, with higher consumption thresholds set for males compared to females. Interestingly, with the currently available data we do not see evidence that risk of alcohol use varies by sex,” she noted.
Methods and results
In the study, the researchers conducted a systematic analysis of burden-weighted dose-response relative risk curves across 22 health outcomes. They used disease rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 for the years 1990-2020 for 21 regions, including 204 countries and territories. The data were analyzed by 5-year age group, sex, and year for individuals aged 15-95 years and older. The researchers estimated the theoretical minimum risk exposure level (TMREL) and nondrinker equivalent (NDE), meaning the amount of alcohol at which the health risk equals that of a nondrinker.
One standard drink was defined as 10 g of pure alcohol, equivalent to a small glass of red wine (100 mL or 3.4 fluid ounces) at 13% alcohol by volume, a can or bottle of beer (375 mL or 12 fluid ounces) at 3.5% alcohol by volume, or a shot of whiskey or other spirits (30 mL or 1.0 fluid ounces) at 40% alcohol by volume.
Overall, the TMREL was low regardless of age, sex, time, or geography, and varied from 0 to 1.87 standard drinks per day. However, it was lowest for males aged 15-39 years (0.136 drinks per day) and only slightly higher for females aged 15-39 (0.273), representing 1-2 tenths of a standard drink.
For adults aged 40 and older without any underlying health conditions, drinking a small amount of alcohol may provide some benefits, such as reducing the risk of ischemic heart disease, stroke, and diabetes, the researchers noted. In general, for individuals aged 40-64 years, TMRELs ranged from about half a standard drink per day (0.527 drinks for males and 0.562 standard drinks per day for females) to almost two standard drinks (1.69 standard drinks per day for males and 1.82 for females). For those older than 65 years, the TMRELs represented just over 3 standard drinks per day (3.19 for males and 3.51 for females). For individuals aged 40 years and older, the distribution of disease burden varied by region, but was J-shaped across all regions, the researchers noted.
The researchers also found that those individuals consuming harmful amounts of alcohol were most likely to be aged 15-39 (59.1%) and male (76.9%).
The study findings were limited by several factors including the observational design and lack of data on drinking patterns, such as binge drinking, the researchers noted. Other limitations include the lack of data reflecting patterns of alcohol consumption during the COVID-19 pandemic, and exclusion of outcomes often associated with alcohol use, such as depression, anxiety, and dementia, that might reduce estimates of TMREL and NDE.
However, the results add to the ongoing discussion of the relationship between moderate alcohol consumption and health, the researchers said.
“The findings of this study support the development of tailored guidelines and recommendations on alcohol consumption by age and across regions and highlight that existing low consumption thresholds are too high for younger populations in all regions,” they concluded.
Consider individual factors when counseling patients
The takeaway message for primary care is that alcohol consumed in moderation can reduce the risk of ischemic heart disease, stroke, and diabetes, Ms. Bryazka noted. “However, it also increases the risk of many cancers, intentional and unintentional injuries, and infectious diseases like tuberculosis,” she said. “Of these health outcomes, young people are most likely to experience injuries, and as a result, we find that there are significant health risks associated with consuming alcohol for young people. Among older individuals, the relative proportions of these outcomes vary by geography, and so do the risks associated with consuming alcohol,” she explained.
“Importantly, our analysis was conducted at the population level; when evaluating risk at the individual level, it is also important to consider other factors such as the presence of comorbidities and interactions between alcohol and medications,” she emphasized.
Health and alcohol interaction is complicated
“These findings seemingly contradict a previous [Global Burden of Diseases, Injuries, and Risk Factors Study] estimate published in The Lancet, which emphasized that any alcohol use, regardless of amount, leads to health loss across populations,” wrote Robyn Burton, PhD, and Nick Sheron, MD, both of King’s College, London, in an accompanying comment.
However, the novel methods of weighting relative risk curves according to levels of underlying disease drive the difference in results, along with disaggregated estimates by age, sex, and region, they said.
“Across most geographical regions in this latest analysis, injuries accounted for most alcohol-related harm in younger age groups. This led to a minimum risk level of zero, or very close to zero, among individuals aged 15-39 years across all geographical regions,” which is lower than the level for older adults because of the shift in alcohol-related disease burden towards cardiovascular disease and cancers, they said. “This highlights the need to consider existing rates of disease in a population when trying to determine the total harm posed by alcohol,” the commentators wrote.
In an additional commentary, Tony Rao, MD, a visiting clinical research fellow in psychiatry at King’s College, London, noted that “the elephant in the room with this study is the interpretation of risk based on outcomes for cardiovascular disease – particularly in older people. We know that any purported health benefits from alcohol on the heart and circulation are balanced out by the increased risk from other conditions such as cancer, liver disease, and mental disorders such as depression and dementia,” Dr. Rao said. “If we are to simply draw the conclusion that older people should continue or start drinking small amounts because it protects against diseases affecting heart and circulation – which still remains controversial – other lifestyle changes or the use of drugs targeted at individual cardiovascular disorders seem like a less harmful way of improving health and wellbeing.”
Data can guide clinical practice
No previous study has examined the effect of the theoretical minimum risk of alcohol consumption by geography, age, sex, and time in the context of background disease rates, said Noel Deep, MD, in an interview.
“This study enabled the researchers to quantify the proportion of the population that consumed alcohol in amounts that exceeded the thresholds by location, age, sex, and year, and this can serve as a guide in our efforts to target the control of alcohol intake by individuals,” said Dr. Deep, a general internist in private practice in Antigo, Wisc. He also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The first take-home message for clinicians is that even low levels of alcohol consumption can have deleterious effects on the health of patients, and patients should be advised accordingly based on the prevalence of diseases in that community and geographic area, Dr. Deep said. “Secondly, clinicians should also consider the risk of alcohol consumption on all forms of health impacts in a given population rather than just focusing on alcohol-related health conditions,” he added.
“This study provides us with the data to tailor our efforts in educating the clinicians and the public about the relationship between alcohol consumption and disease outcomes based on the observed disease rates in each population,” Dr. Deep explained. “The data should provide another reason for physicians to advise their younger patients, especially the younger males, to avoid or minimize alcohol use,” he said. The data also can help clinicians formulate public health messaging and community education to reduce harmful alcohol use, he added.
As for additional research, Dr. Deep said he would like to see data on the difference in the health-related effects of alcohol in binge-drinkers vs. those who regularly consume alcohol on a daily basis. “It would probably also be helpful to figure out what type of alcohol is being studied and the quality of the alcohol,” he said.
The study was supported by the Bill and Melinda Gates Foundation. Ms. Bryazka and colleagues had no financial conflicts to disclose. Dr. Burton disclosed serving as a consultant to the World Health Organization European Office for the Prevention and Control of Noncommunicable Diseases. Dr. Sheron had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose, but serves on the Editorial Advisory Board of Internal Medicine News.
The study was supported by the Bill and Melinda Gates Foundation.
FROM THE LANCET
Fertility doctors, IVF families, post Roe: ‘We’re anxious’
Married for nearly 5 years, Jessica King, 34, and her wife, Sarah, agreed on some things right from the start. “We always knew kids were in the equation,” Jessica says.
Now, Jessica is nearly 20 weeks pregnant, thanks to in vitro fertilization, or IVF. They did “reciprocal” IVF, with Sarah’s egg mixed with donor sperm and the embryo transferred into Jessica. “We’re excited – and terrified,” Jessica says.
But that terror goes beyond the typical concerns of excess weight gain and long labors. They live in Missouri, one of 13 states with so-called trigger laws that went into effect after the Supreme Court overturned Roe v. Wade and the constitutional right to abortion, giving states the power to regulate it. States with trigger laws either banned abortion immediately or within a specified time frame after the ruling. In all, 26 states are expected to have abortion restrictions.
Missouri now allows abortion only for medical emergencies. If her upcoming ultrasound shows serious issues, Jessica says they could easily travel to another state and pay for an abortion. She realizes not everyone can.
However, the concern about trigger laws goes well beyond abortion. Many experts worry about the “spill-over” effects the abortion laws – both the existing ones and future proposals – may have on fertility care and treatments.
‘Personhood’ laws drive the concern
“The current trigger laws on the books are not impacting people’s access to IVF,” says Barbara Collura, president and CEO of RESOLVE, an advocacy group for those with fertility issues. “What we are concerned about is they will come back and make them stronger.”
The chief concern for reproductive rights advocates is so-called “personhood” legislation. According to the Guttmacher Institute, at least six bills about personhood have been introduced in five states, including Iowa, Oklahoma, South Carolina, Vermont, and West Virginia. One of the two Oklahoma bills has gone the farthest, passed by one chamber.
Since the Guttmacher report, Ohio introduced its own personhood legislation July 11, recognizing the personhood of an unborn person from conception.
Personhood legislation defines a fertilized egg or embryo as a legal human entity, says Sean Tipton, chief policy and advocacy officer for the Washington-based American Society of Reproductive Medicine, a nonprofit advocacy group.
“If the legal status of fertilized eggs or early embryos is codified, in vitro fertilization procedures may become legally risky for patients, physicians and staff,” Mr. Tipton wrote in late June in Contemporary OB/GYN Journal. The American Society for Reproductive Medicine has posted a report on state abortion trigger laws and their potential implications for reproductive medicine. Of the 13 with trigger laws in effect, the report found concern about the potential effect on IVF only with Utah’s.
‘Safe’ states?
Even in states without trigger laws or personhood bills, IVF patients say they are anxious about how the Supreme Court ruling may ultimately affect care. Thanks to IVF, Shelly Battista and her husband Robert are expecting twins in December, little sisters to their daughter Emilia, who is 2½.
They live in Illinois, where abortion is legal. “Even though we are safe now, I think the overturning of Roe has made it clear to all of us that none of our freedoms are safe, especially reproductive rights,” Ms. Shelly says.
About one in eight U.S. couples are infertile, according to RESOLVE, In 2019, 2% of all babies born in the United States, or about 78,000 infants, were conceived with the use of assisted reproductive technologies, according to the Centers for Disease Control and Prevention. The most common assisted reproductive technology is IVF, in which the sperm fertilizes the egg outside the body and an embryo is then transferred. The standard of practice is to transfer a single embryo, freezing others for future use.
Trigger state doctors weigh in
Some fertility doctors in those “trigger” states are keeping a close eye on proposed legislation and talking to legislators for interpretation of current and proposed laws.
Eli Reshef, MD, a reproductive endocrinologist and fertility specialist at Bennett Fertility Institute in Oklahoma City, notes that his state has “the strictest abortion law in the land.” The law prohibits all abortions with few exceptions, such as the removal of an ectopic pregnancy (when a fertilized egg implants outside the uterus, such as in the fallopian tubes).
While IVF will not be affected for now, he worries that the Oklahoma law allows a private citizen to sue a health care provider that they feel is performing abortion. The Oklahoma law leaves interpretation of abortion up to the general public, who may be unfamiliar with the language of the law, House Bill 4327.
Dean Moutos, MD, a reproductive endocrinologist and medical director of Arkansas Fertility and Gynecology in Little Rock, says his state’s current trigger law should not affect IVF. “When you read the bill, it says abortion means to terminate the pregnancy of a woman.” Still, he says, “we are concerned about what might happen in the future” and the possibility that some legislators may interpret that differently.
A minority approach
John David Gordon, MD, a reproductive endocrinologist and medical director of Southeastern Fertility Center for Fertility and Reproductive Surgery in Knoxville, Tenn., is also in a trigger state. However, it’s not likely any personhood laws would affect his practice.
That’s because his center, which he acknowledges is clearly in the minority, only performs natural-cycle IVF, which usually results in a single egg, or “mini-stim IVF,” which usually results in three to eight eggs in order to limit the number that may be potentially fertilized. Often, he says, patients choose to freeze unfertilized eggs (alone) to avoid creating an excessive number of embryos. He has a “no discard” program, with any viable embryos frozen or transferred. Abandoned embryos are donated to others.
“This may work for young women,” says Marcelle Cedars, MD, director of reproductive endocrinology at the University of California, San Francisco, and president of the American Society of Reproductive Medicine. However, she says, it will be very inefficient for older patients, since they have a higher percentage of abnormal eggs.
Overall, that approach will also drive up costs, especially for older women, Dr. Cedars says. An average cycle of IVF costs $12,400, and most Americans’ insurance plans don’t cover IVF, according to Mr. Tipton.
Top concerns for IVF
“Personhood” legislation has the potential to upend many common IVF practices, experts say.
Of greatest concern to fertility practices are potential restrictions on the freezing or discarding of embryos, Dr. Cedars says. “This could have a critical impact on practicing the safest, most evidence-based medicine,” she says.
Most children born in the United States as a result of IVF procedures are born from frozen embryos, according to the Society for Assisted Reproductive Technology, an organization for reproductive specialists.
“The practice of IVF really requires that we generate more embryos than will be used in a given [IVF] cycle,” agrees Kara Goldman, MD, associate professor of obstetrics and gynecology and medical director of the fertility preservation program at Northwestern University, Chicago. She performed the embryo transfer for the Battistas.
In nature, she says, it’s known that only a small number of eggs will be competent to generate a baby. “We see the same thing in IVF.” In a single cycle, 20 eggs may be retrieved, but many fewer typically reach successful fertilization and are able to be implanted.
When patients have completed their family, unused embryos are donated to research, donated for adoption, or destroyed. If embryo destruction is outlawed, Dr. Goldman says, it will have serious ramifications for the practice of IVF.
And if personhood legislation prohibits destroying any embryos, others wonder: Would a lab technician who accidentally dropped and destroyed an embryo be subject to charges? If laws prohibit destruction of embryos, others wonder if will families be forced to pay the embryo storage fees, generally $500-$1,000 a year, in perpetuity.
If an embryo is declared a person, it could also affect a practice called preimplantation genetic testing, or PGT. In PGT, cells are retrieved from an embryo and checked for genetic disorders such as sickle cell anemia and cystic fibrosis, with some parents choosing to discard embryos that are found to be affected.
Some potential parents choose this testing because they know they are carriers for genetic diseases that are serious and even incompatible with life, says Art Caplan, PhD, head of the division of medical ethics at New York University. They may choose to discard embryos that show evidence of the diseases.
Also under fire could be “selective reduction,” reducing multiple fetuses to a single or twin, to reduce risks to babies and mother.
Dr. Caplan predicts if states have many restrictions, some providers will adopt the attitude that “if no one reports, it did not happen.” And those prospective parents with the means, he says, will go to court and fight restrictions. “When they do it, they are saying, ‘You say you are pro-life; I’m trying to have a child. What are you doing getting in my way?’”
IVF families: Tough decisions, emotional times
The Battistas, of Illinois, have had an especially rough road. Shelly was diagnosed with a fast-growing breast cancer in 2020, when Emilia was just an infant. Warned that the chemotherapy she needed would suppress her ovaries, Shelly underwent egg retrieval before starting the cancer treatment.
She opted to have a double mastectomy and her ovaries removed after learning she carried the BRCA1 genetic mutation, boosting the risk of both breast and ovarian cancer.
Once she was cancer-free, she was cleared to start IVF. The first two embryo transfers failed. The third transfer, of a single embryo, was successful. But it split, a rare occurrence, producing two embryos. “It was a big shock, but in the best way,” she says about learning they were having twins. “Now we are over the moon.”
Five frozen embryos remain. At the start, the Battistas decided to discard unused embryos. She and Robert are discussing what to do next. If they decide they are done building their family after the twins’ birth, she wonders, “do we need to discard our [other] embryos before that becomes something that isn’t eligible [possible] for us any longer?” She doesn’t want to be rushed into that decision, however, especially with her medical history.
Jessica King and Sarah have 20 more embryos.
The couple had decided to donate unused embryos for research, when the time comes, and for different reasons. Her wife’s decision is based on her belief in science, while Jessica cites her faith. “As a Jew, it is part of our faith, that we should be doing everything we can to advance humanity,” she says.
In the midst of all the uncertainty, Jessica says, only half-jokingly, that she is tempted to claim the frozen embryos as dependents. “If you are truly going to claim these are precious human lives, you should be giving me all the benefits from having children,” she says.
Shelly knows that having one daughter, with two more on the way, affects her thinking about the court’s ruling. “My overall wish would be that Roe v. Wade is reinstated, and my daughters have the same rights and options that I have … or I did have until my current 36 years of life.”
A version of this article first appeared on WebMD.com.
Married for nearly 5 years, Jessica King, 34, and her wife, Sarah, agreed on some things right from the start. “We always knew kids were in the equation,” Jessica says.
Now, Jessica is nearly 20 weeks pregnant, thanks to in vitro fertilization, or IVF. They did “reciprocal” IVF, with Sarah’s egg mixed with donor sperm and the embryo transferred into Jessica. “We’re excited – and terrified,” Jessica says.
But that terror goes beyond the typical concerns of excess weight gain and long labors. They live in Missouri, one of 13 states with so-called trigger laws that went into effect after the Supreme Court overturned Roe v. Wade and the constitutional right to abortion, giving states the power to regulate it. States with trigger laws either banned abortion immediately or within a specified time frame after the ruling. In all, 26 states are expected to have abortion restrictions.
Missouri now allows abortion only for medical emergencies. If her upcoming ultrasound shows serious issues, Jessica says they could easily travel to another state and pay for an abortion. She realizes not everyone can.
However, the concern about trigger laws goes well beyond abortion. Many experts worry about the “spill-over” effects the abortion laws – both the existing ones and future proposals – may have on fertility care and treatments.
‘Personhood’ laws drive the concern
“The current trigger laws on the books are not impacting people’s access to IVF,” says Barbara Collura, president and CEO of RESOLVE, an advocacy group for those with fertility issues. “What we are concerned about is they will come back and make them stronger.”
The chief concern for reproductive rights advocates is so-called “personhood” legislation. According to the Guttmacher Institute, at least six bills about personhood have been introduced in five states, including Iowa, Oklahoma, South Carolina, Vermont, and West Virginia. One of the two Oklahoma bills has gone the farthest, passed by one chamber.
Since the Guttmacher report, Ohio introduced its own personhood legislation July 11, recognizing the personhood of an unborn person from conception.
Personhood legislation defines a fertilized egg or embryo as a legal human entity, says Sean Tipton, chief policy and advocacy officer for the Washington-based American Society of Reproductive Medicine, a nonprofit advocacy group.
“If the legal status of fertilized eggs or early embryos is codified, in vitro fertilization procedures may become legally risky for patients, physicians and staff,” Mr. Tipton wrote in late June in Contemporary OB/GYN Journal. The American Society for Reproductive Medicine has posted a report on state abortion trigger laws and their potential implications for reproductive medicine. Of the 13 with trigger laws in effect, the report found concern about the potential effect on IVF only with Utah’s.
‘Safe’ states?
Even in states without trigger laws or personhood bills, IVF patients say they are anxious about how the Supreme Court ruling may ultimately affect care. Thanks to IVF, Shelly Battista and her husband Robert are expecting twins in December, little sisters to their daughter Emilia, who is 2½.
They live in Illinois, where abortion is legal. “Even though we are safe now, I think the overturning of Roe has made it clear to all of us that none of our freedoms are safe, especially reproductive rights,” Ms. Shelly says.
About one in eight U.S. couples are infertile, according to RESOLVE, In 2019, 2% of all babies born in the United States, or about 78,000 infants, were conceived with the use of assisted reproductive technologies, according to the Centers for Disease Control and Prevention. The most common assisted reproductive technology is IVF, in which the sperm fertilizes the egg outside the body and an embryo is then transferred. The standard of practice is to transfer a single embryo, freezing others for future use.
Trigger state doctors weigh in
Some fertility doctors in those “trigger” states are keeping a close eye on proposed legislation and talking to legislators for interpretation of current and proposed laws.
Eli Reshef, MD, a reproductive endocrinologist and fertility specialist at Bennett Fertility Institute in Oklahoma City, notes that his state has “the strictest abortion law in the land.” The law prohibits all abortions with few exceptions, such as the removal of an ectopic pregnancy (when a fertilized egg implants outside the uterus, such as in the fallopian tubes).
While IVF will not be affected for now, he worries that the Oklahoma law allows a private citizen to sue a health care provider that they feel is performing abortion. The Oklahoma law leaves interpretation of abortion up to the general public, who may be unfamiliar with the language of the law, House Bill 4327.
Dean Moutos, MD, a reproductive endocrinologist and medical director of Arkansas Fertility and Gynecology in Little Rock, says his state’s current trigger law should not affect IVF. “When you read the bill, it says abortion means to terminate the pregnancy of a woman.” Still, he says, “we are concerned about what might happen in the future” and the possibility that some legislators may interpret that differently.
A minority approach
John David Gordon, MD, a reproductive endocrinologist and medical director of Southeastern Fertility Center for Fertility and Reproductive Surgery in Knoxville, Tenn., is also in a trigger state. However, it’s not likely any personhood laws would affect his practice.
That’s because his center, which he acknowledges is clearly in the minority, only performs natural-cycle IVF, which usually results in a single egg, or “mini-stim IVF,” which usually results in three to eight eggs in order to limit the number that may be potentially fertilized. Often, he says, patients choose to freeze unfertilized eggs (alone) to avoid creating an excessive number of embryos. He has a “no discard” program, with any viable embryos frozen or transferred. Abandoned embryos are donated to others.
“This may work for young women,” says Marcelle Cedars, MD, director of reproductive endocrinology at the University of California, San Francisco, and president of the American Society of Reproductive Medicine. However, she says, it will be very inefficient for older patients, since they have a higher percentage of abnormal eggs.
Overall, that approach will also drive up costs, especially for older women, Dr. Cedars says. An average cycle of IVF costs $12,400, and most Americans’ insurance plans don’t cover IVF, according to Mr. Tipton.
Top concerns for IVF
“Personhood” legislation has the potential to upend many common IVF practices, experts say.
Of greatest concern to fertility practices are potential restrictions on the freezing or discarding of embryos, Dr. Cedars says. “This could have a critical impact on practicing the safest, most evidence-based medicine,” she says.
Most children born in the United States as a result of IVF procedures are born from frozen embryos, according to the Society for Assisted Reproductive Technology, an organization for reproductive specialists.
“The practice of IVF really requires that we generate more embryos than will be used in a given [IVF] cycle,” agrees Kara Goldman, MD, associate professor of obstetrics and gynecology and medical director of the fertility preservation program at Northwestern University, Chicago. She performed the embryo transfer for the Battistas.
In nature, she says, it’s known that only a small number of eggs will be competent to generate a baby. “We see the same thing in IVF.” In a single cycle, 20 eggs may be retrieved, but many fewer typically reach successful fertilization and are able to be implanted.
When patients have completed their family, unused embryos are donated to research, donated for adoption, or destroyed. If embryo destruction is outlawed, Dr. Goldman says, it will have serious ramifications for the practice of IVF.
And if personhood legislation prohibits destroying any embryos, others wonder: Would a lab technician who accidentally dropped and destroyed an embryo be subject to charges? If laws prohibit destruction of embryos, others wonder if will families be forced to pay the embryo storage fees, generally $500-$1,000 a year, in perpetuity.
If an embryo is declared a person, it could also affect a practice called preimplantation genetic testing, or PGT. In PGT, cells are retrieved from an embryo and checked for genetic disorders such as sickle cell anemia and cystic fibrosis, with some parents choosing to discard embryos that are found to be affected.
Some potential parents choose this testing because they know they are carriers for genetic diseases that are serious and even incompatible with life, says Art Caplan, PhD, head of the division of medical ethics at New York University. They may choose to discard embryos that show evidence of the diseases.
Also under fire could be “selective reduction,” reducing multiple fetuses to a single or twin, to reduce risks to babies and mother.
Dr. Caplan predicts if states have many restrictions, some providers will adopt the attitude that “if no one reports, it did not happen.” And those prospective parents with the means, he says, will go to court and fight restrictions. “When they do it, they are saying, ‘You say you are pro-life; I’m trying to have a child. What are you doing getting in my way?’”
IVF families: Tough decisions, emotional times
The Battistas, of Illinois, have had an especially rough road. Shelly was diagnosed with a fast-growing breast cancer in 2020, when Emilia was just an infant. Warned that the chemotherapy she needed would suppress her ovaries, Shelly underwent egg retrieval before starting the cancer treatment.
She opted to have a double mastectomy and her ovaries removed after learning she carried the BRCA1 genetic mutation, boosting the risk of both breast and ovarian cancer.
Once she was cancer-free, she was cleared to start IVF. The first two embryo transfers failed. The third transfer, of a single embryo, was successful. But it split, a rare occurrence, producing two embryos. “It was a big shock, but in the best way,” she says about learning they were having twins. “Now we are over the moon.”
Five frozen embryos remain. At the start, the Battistas decided to discard unused embryos. She and Robert are discussing what to do next. If they decide they are done building their family after the twins’ birth, she wonders, “do we need to discard our [other] embryos before that becomes something that isn’t eligible [possible] for us any longer?” She doesn’t want to be rushed into that decision, however, especially with her medical history.
Jessica King and Sarah have 20 more embryos.
The couple had decided to donate unused embryos for research, when the time comes, and for different reasons. Her wife’s decision is based on her belief in science, while Jessica cites her faith. “As a Jew, it is part of our faith, that we should be doing everything we can to advance humanity,” she says.
In the midst of all the uncertainty, Jessica says, only half-jokingly, that she is tempted to claim the frozen embryos as dependents. “If you are truly going to claim these are precious human lives, you should be giving me all the benefits from having children,” she says.
Shelly knows that having one daughter, with two more on the way, affects her thinking about the court’s ruling. “My overall wish would be that Roe v. Wade is reinstated, and my daughters have the same rights and options that I have … or I did have until my current 36 years of life.”
A version of this article first appeared on WebMD.com.
Married for nearly 5 years, Jessica King, 34, and her wife, Sarah, agreed on some things right from the start. “We always knew kids were in the equation,” Jessica says.
Now, Jessica is nearly 20 weeks pregnant, thanks to in vitro fertilization, or IVF. They did “reciprocal” IVF, with Sarah’s egg mixed with donor sperm and the embryo transferred into Jessica. “We’re excited – and terrified,” Jessica says.
But that terror goes beyond the typical concerns of excess weight gain and long labors. They live in Missouri, one of 13 states with so-called trigger laws that went into effect after the Supreme Court overturned Roe v. Wade and the constitutional right to abortion, giving states the power to regulate it. States with trigger laws either banned abortion immediately or within a specified time frame after the ruling. In all, 26 states are expected to have abortion restrictions.
Missouri now allows abortion only for medical emergencies. If her upcoming ultrasound shows serious issues, Jessica says they could easily travel to another state and pay for an abortion. She realizes not everyone can.
However, the concern about trigger laws goes well beyond abortion. Many experts worry about the “spill-over” effects the abortion laws – both the existing ones and future proposals – may have on fertility care and treatments.
‘Personhood’ laws drive the concern
“The current trigger laws on the books are not impacting people’s access to IVF,” says Barbara Collura, president and CEO of RESOLVE, an advocacy group for those with fertility issues. “What we are concerned about is they will come back and make them stronger.”
The chief concern for reproductive rights advocates is so-called “personhood” legislation. According to the Guttmacher Institute, at least six bills about personhood have been introduced in five states, including Iowa, Oklahoma, South Carolina, Vermont, and West Virginia. One of the two Oklahoma bills has gone the farthest, passed by one chamber.
Since the Guttmacher report, Ohio introduced its own personhood legislation July 11, recognizing the personhood of an unborn person from conception.
Personhood legislation defines a fertilized egg or embryo as a legal human entity, says Sean Tipton, chief policy and advocacy officer for the Washington-based American Society of Reproductive Medicine, a nonprofit advocacy group.
“If the legal status of fertilized eggs or early embryos is codified, in vitro fertilization procedures may become legally risky for patients, physicians and staff,” Mr. Tipton wrote in late June in Contemporary OB/GYN Journal. The American Society for Reproductive Medicine has posted a report on state abortion trigger laws and their potential implications for reproductive medicine. Of the 13 with trigger laws in effect, the report found concern about the potential effect on IVF only with Utah’s.
‘Safe’ states?
Even in states without trigger laws or personhood bills, IVF patients say they are anxious about how the Supreme Court ruling may ultimately affect care. Thanks to IVF, Shelly Battista and her husband Robert are expecting twins in December, little sisters to their daughter Emilia, who is 2½.
They live in Illinois, where abortion is legal. “Even though we are safe now, I think the overturning of Roe has made it clear to all of us that none of our freedoms are safe, especially reproductive rights,” Ms. Shelly says.
About one in eight U.S. couples are infertile, according to RESOLVE, In 2019, 2% of all babies born in the United States, or about 78,000 infants, were conceived with the use of assisted reproductive technologies, according to the Centers for Disease Control and Prevention. The most common assisted reproductive technology is IVF, in which the sperm fertilizes the egg outside the body and an embryo is then transferred. The standard of practice is to transfer a single embryo, freezing others for future use.
Trigger state doctors weigh in
Some fertility doctors in those “trigger” states are keeping a close eye on proposed legislation and talking to legislators for interpretation of current and proposed laws.
Eli Reshef, MD, a reproductive endocrinologist and fertility specialist at Bennett Fertility Institute in Oklahoma City, notes that his state has “the strictest abortion law in the land.” The law prohibits all abortions with few exceptions, such as the removal of an ectopic pregnancy (when a fertilized egg implants outside the uterus, such as in the fallopian tubes).
While IVF will not be affected for now, he worries that the Oklahoma law allows a private citizen to sue a health care provider that they feel is performing abortion. The Oklahoma law leaves interpretation of abortion up to the general public, who may be unfamiliar with the language of the law, House Bill 4327.
Dean Moutos, MD, a reproductive endocrinologist and medical director of Arkansas Fertility and Gynecology in Little Rock, says his state’s current trigger law should not affect IVF. “When you read the bill, it says abortion means to terminate the pregnancy of a woman.” Still, he says, “we are concerned about what might happen in the future” and the possibility that some legislators may interpret that differently.
A minority approach
John David Gordon, MD, a reproductive endocrinologist and medical director of Southeastern Fertility Center for Fertility and Reproductive Surgery in Knoxville, Tenn., is also in a trigger state. However, it’s not likely any personhood laws would affect his practice.
That’s because his center, which he acknowledges is clearly in the minority, only performs natural-cycle IVF, which usually results in a single egg, or “mini-stim IVF,” which usually results in three to eight eggs in order to limit the number that may be potentially fertilized. Often, he says, patients choose to freeze unfertilized eggs (alone) to avoid creating an excessive number of embryos. He has a “no discard” program, with any viable embryos frozen or transferred. Abandoned embryos are donated to others.
“This may work for young women,” says Marcelle Cedars, MD, director of reproductive endocrinology at the University of California, San Francisco, and president of the American Society of Reproductive Medicine. However, she says, it will be very inefficient for older patients, since they have a higher percentage of abnormal eggs.
Overall, that approach will also drive up costs, especially for older women, Dr. Cedars says. An average cycle of IVF costs $12,400, and most Americans’ insurance plans don’t cover IVF, according to Mr. Tipton.
Top concerns for IVF
“Personhood” legislation has the potential to upend many common IVF practices, experts say.
Of greatest concern to fertility practices are potential restrictions on the freezing or discarding of embryos, Dr. Cedars says. “This could have a critical impact on practicing the safest, most evidence-based medicine,” she says.
Most children born in the United States as a result of IVF procedures are born from frozen embryos, according to the Society for Assisted Reproductive Technology, an organization for reproductive specialists.
“The practice of IVF really requires that we generate more embryos than will be used in a given [IVF] cycle,” agrees Kara Goldman, MD, associate professor of obstetrics and gynecology and medical director of the fertility preservation program at Northwestern University, Chicago. She performed the embryo transfer for the Battistas.
In nature, she says, it’s known that only a small number of eggs will be competent to generate a baby. “We see the same thing in IVF.” In a single cycle, 20 eggs may be retrieved, but many fewer typically reach successful fertilization and are able to be implanted.
When patients have completed their family, unused embryos are donated to research, donated for adoption, or destroyed. If embryo destruction is outlawed, Dr. Goldman says, it will have serious ramifications for the practice of IVF.
And if personhood legislation prohibits destroying any embryos, others wonder: Would a lab technician who accidentally dropped and destroyed an embryo be subject to charges? If laws prohibit destruction of embryos, others wonder if will families be forced to pay the embryo storage fees, generally $500-$1,000 a year, in perpetuity.
If an embryo is declared a person, it could also affect a practice called preimplantation genetic testing, or PGT. In PGT, cells are retrieved from an embryo and checked for genetic disorders such as sickle cell anemia and cystic fibrosis, with some parents choosing to discard embryos that are found to be affected.
Some potential parents choose this testing because they know they are carriers for genetic diseases that are serious and even incompatible with life, says Art Caplan, PhD, head of the division of medical ethics at New York University. They may choose to discard embryos that show evidence of the diseases.
Also under fire could be “selective reduction,” reducing multiple fetuses to a single or twin, to reduce risks to babies and mother.
Dr. Caplan predicts if states have many restrictions, some providers will adopt the attitude that “if no one reports, it did not happen.” And those prospective parents with the means, he says, will go to court and fight restrictions. “When they do it, they are saying, ‘You say you are pro-life; I’m trying to have a child. What are you doing getting in my way?’”
IVF families: Tough decisions, emotional times
The Battistas, of Illinois, have had an especially rough road. Shelly was diagnosed with a fast-growing breast cancer in 2020, when Emilia was just an infant. Warned that the chemotherapy she needed would suppress her ovaries, Shelly underwent egg retrieval before starting the cancer treatment.
She opted to have a double mastectomy and her ovaries removed after learning she carried the BRCA1 genetic mutation, boosting the risk of both breast and ovarian cancer.
Once she was cancer-free, she was cleared to start IVF. The first two embryo transfers failed. The third transfer, of a single embryo, was successful. But it split, a rare occurrence, producing two embryos. “It was a big shock, but in the best way,” she says about learning they were having twins. “Now we are over the moon.”
Five frozen embryos remain. At the start, the Battistas decided to discard unused embryos. She and Robert are discussing what to do next. If they decide they are done building their family after the twins’ birth, she wonders, “do we need to discard our [other] embryos before that becomes something that isn’t eligible [possible] for us any longer?” She doesn’t want to be rushed into that decision, however, especially with her medical history.
Jessica King and Sarah have 20 more embryos.
The couple had decided to donate unused embryos for research, when the time comes, and for different reasons. Her wife’s decision is based on her belief in science, while Jessica cites her faith. “As a Jew, it is part of our faith, that we should be doing everything we can to advance humanity,” she says.
In the midst of all the uncertainty, Jessica says, only half-jokingly, that she is tempted to claim the frozen embryos as dependents. “If you are truly going to claim these are precious human lives, you should be giving me all the benefits from having children,” she says.
Shelly knows that having one daughter, with two more on the way, affects her thinking about the court’s ruling. “My overall wish would be that Roe v. Wade is reinstated, and my daughters have the same rights and options that I have … or I did have until my current 36 years of life.”
A version of this article first appeared on WebMD.com.
Feds warn pharmacists: Don’t refuse to provide abortion pills
The Department of Health & Human Services listed several conditions that are commonly treated with drugs that can induce abortion, warning that withholding the pills could violate civil rights laws and could be considered discrimination based on sex or disability.
“We are committed to ensuring that everyone can access health care, free of discrimination,” Xavier Becerra, the U.S. health and human services secretary, said in a statement. “This includes access to prescription medications for reproductive health and other types of care.”
On July 11, Mr. Becerra issued other guidance to remind hospitals that federal law requires doctors to provide stabilizing treatment for patients with emergency medical conditions, which could include an abortion for those who arrive at emergency departments with a life-threatening issue.
Both actions by the Biden administration assert that federal laws override state laws that have banned or restricted abortion access since the Supreme Court overturned Roe v. Wade, according to The New York Times.
The guidance focuses on Section 1557 of the Affordable Care Act and related federal regulations, which state that recipients of federal financial assistance – including pharmacies that get Medicare and Medicaid payments – can’t discriminate based on race, color, national origin, sex, age, and disability. The guidance highlights that pregnancy discrimination includes discrimination based on current pregnancy, past pregnancy, potential or intended pregnancy, and medical conditions related to pregnancy or childbirth.
Three drugs in particular – mifepristone, misoprostol, and methotrexate – are often prescribed for other medical conditions but can also induce abortions in certain cases. Methotrexate, for example, is used for cancer and autoimmune disorders, such as rheumatoid arthritis.
Mifepristone is often used for patients with Cushing’s syndrome, while misoprostol is often prescribed for ulcers. When used in combination, the two drugs are authorized by the Food and Drug Administration to terminate a pregnancy during the first 10 weeks and after a miscarriage.
Since Roe was overturned, women have posted on social media that they were denied the drugs for their medical conditions due to being of “childbearing age.”
“These are very legitimate issues in terms of people being concerned about having access to the basic medications that they have been receiving for years, just because those medications have the capacity to end a pregnancy,” Alina Salganicoff, PhD, the director of women’s health policy at the Kaiser Family Foundation, told the Times.
“It doesn’t sound like [pharmacies] are blocking this for men,” she said.
The Biden administration’s guidance will likely be challenged in court, the newspaper reported. The update is cautiously written and doesn’t directly say that pharmacies must provide the drugs for the purpose of medication abortion.
In the meantime, pharmacists could feel stuck in the middle. Pharmacists who “believe they are acting in good faith in accordance with their state’s laws on abortion shouldn’t be left without a clear pathway forward,” the National Community Pharmacists Association said in a statement on July 13.
The association, which represents about 19,400 independent pharmacies across the United States, said pharmacies are regulated by states, and most states haven’t advised pharmacists on how to dispense the drugs in question.
“States have provided very little clarity on how pharmacists should proceed in light of conflicting state and federal laws and regulations,” B. Douglas Hoey, the association’s CEO, said in the statement.
“It is highly unfair for state and federal governments to threaten aggressive action against pharmacists who are just trying to serve their patients within new legal boundaries that are still taking shape,” he said.
A version of this article first appeared on WebMD.com.
The Department of Health & Human Services listed several conditions that are commonly treated with drugs that can induce abortion, warning that withholding the pills could violate civil rights laws and could be considered discrimination based on sex or disability.
“We are committed to ensuring that everyone can access health care, free of discrimination,” Xavier Becerra, the U.S. health and human services secretary, said in a statement. “This includes access to prescription medications for reproductive health and other types of care.”
On July 11, Mr. Becerra issued other guidance to remind hospitals that federal law requires doctors to provide stabilizing treatment for patients with emergency medical conditions, which could include an abortion for those who arrive at emergency departments with a life-threatening issue.
Both actions by the Biden administration assert that federal laws override state laws that have banned or restricted abortion access since the Supreme Court overturned Roe v. Wade, according to The New York Times.
The guidance focuses on Section 1557 of the Affordable Care Act and related federal regulations, which state that recipients of federal financial assistance – including pharmacies that get Medicare and Medicaid payments – can’t discriminate based on race, color, national origin, sex, age, and disability. The guidance highlights that pregnancy discrimination includes discrimination based on current pregnancy, past pregnancy, potential or intended pregnancy, and medical conditions related to pregnancy or childbirth.
Three drugs in particular – mifepristone, misoprostol, and methotrexate – are often prescribed for other medical conditions but can also induce abortions in certain cases. Methotrexate, for example, is used for cancer and autoimmune disorders, such as rheumatoid arthritis.
Mifepristone is often used for patients with Cushing’s syndrome, while misoprostol is often prescribed for ulcers. When used in combination, the two drugs are authorized by the Food and Drug Administration to terminate a pregnancy during the first 10 weeks and after a miscarriage.
Since Roe was overturned, women have posted on social media that they were denied the drugs for their medical conditions due to being of “childbearing age.”
“These are very legitimate issues in terms of people being concerned about having access to the basic medications that they have been receiving for years, just because those medications have the capacity to end a pregnancy,” Alina Salganicoff, PhD, the director of women’s health policy at the Kaiser Family Foundation, told the Times.
“It doesn’t sound like [pharmacies] are blocking this for men,” she said.
The Biden administration’s guidance will likely be challenged in court, the newspaper reported. The update is cautiously written and doesn’t directly say that pharmacies must provide the drugs for the purpose of medication abortion.
In the meantime, pharmacists could feel stuck in the middle. Pharmacists who “believe they are acting in good faith in accordance with their state’s laws on abortion shouldn’t be left without a clear pathway forward,” the National Community Pharmacists Association said in a statement on July 13.
The association, which represents about 19,400 independent pharmacies across the United States, said pharmacies are regulated by states, and most states haven’t advised pharmacists on how to dispense the drugs in question.
“States have provided very little clarity on how pharmacists should proceed in light of conflicting state and federal laws and regulations,” B. Douglas Hoey, the association’s CEO, said in the statement.
“It is highly unfair for state and federal governments to threaten aggressive action against pharmacists who are just trying to serve their patients within new legal boundaries that are still taking shape,” he said.
A version of this article first appeared on WebMD.com.
The Department of Health & Human Services listed several conditions that are commonly treated with drugs that can induce abortion, warning that withholding the pills could violate civil rights laws and could be considered discrimination based on sex or disability.
“We are committed to ensuring that everyone can access health care, free of discrimination,” Xavier Becerra, the U.S. health and human services secretary, said in a statement. “This includes access to prescription medications for reproductive health and other types of care.”
On July 11, Mr. Becerra issued other guidance to remind hospitals that federal law requires doctors to provide stabilizing treatment for patients with emergency medical conditions, which could include an abortion for those who arrive at emergency departments with a life-threatening issue.
Both actions by the Biden administration assert that federal laws override state laws that have banned or restricted abortion access since the Supreme Court overturned Roe v. Wade, according to The New York Times.
The guidance focuses on Section 1557 of the Affordable Care Act and related federal regulations, which state that recipients of federal financial assistance – including pharmacies that get Medicare and Medicaid payments – can’t discriminate based on race, color, national origin, sex, age, and disability. The guidance highlights that pregnancy discrimination includes discrimination based on current pregnancy, past pregnancy, potential or intended pregnancy, and medical conditions related to pregnancy or childbirth.
Three drugs in particular – mifepristone, misoprostol, and methotrexate – are often prescribed for other medical conditions but can also induce abortions in certain cases. Methotrexate, for example, is used for cancer and autoimmune disorders, such as rheumatoid arthritis.
Mifepristone is often used for patients with Cushing’s syndrome, while misoprostol is often prescribed for ulcers. When used in combination, the two drugs are authorized by the Food and Drug Administration to terminate a pregnancy during the first 10 weeks and after a miscarriage.
Since Roe was overturned, women have posted on social media that they were denied the drugs for their medical conditions due to being of “childbearing age.”
“These are very legitimate issues in terms of people being concerned about having access to the basic medications that they have been receiving for years, just because those medications have the capacity to end a pregnancy,” Alina Salganicoff, PhD, the director of women’s health policy at the Kaiser Family Foundation, told the Times.
“It doesn’t sound like [pharmacies] are blocking this for men,” she said.
The Biden administration’s guidance will likely be challenged in court, the newspaper reported. The update is cautiously written and doesn’t directly say that pharmacies must provide the drugs for the purpose of medication abortion.
In the meantime, pharmacists could feel stuck in the middle. Pharmacists who “believe they are acting in good faith in accordance with their state’s laws on abortion shouldn’t be left without a clear pathway forward,” the National Community Pharmacists Association said in a statement on July 13.
The association, which represents about 19,400 independent pharmacies across the United States, said pharmacies are regulated by states, and most states haven’t advised pharmacists on how to dispense the drugs in question.
“States have provided very little clarity on how pharmacists should proceed in light of conflicting state and federal laws and regulations,” B. Douglas Hoey, the association’s CEO, said in the statement.
“It is highly unfair for state and federal governments to threaten aggressive action against pharmacists who are just trying to serve their patients within new legal boundaries that are still taking shape,” he said.
A version of this article first appeared on WebMD.com.
Shift schedule today could worsen that stroke tomorrow
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.

In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.

A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”

KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.

Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.
In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.
A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”
KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.
Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.
In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.
A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”
KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.
Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Hospital-acquired pneumonia is killing patients, yet there is a simple way to stop it
Four years ago, when Dr. Karen Giuliano went to a Boston hospital for hip replacement surgery, she was given a pale-pink bucket of toiletries issued to patients in many hospitals. Inside were tissues, bar soap, deodorant, toothpaste, and, without a doubt, the worst toothbrush she’d ever seen.
“I couldn’t believe it. I got a toothbrush with no bristles,” she said. “It must have not gone through the bristle machine. It was just a stick.”
To most patients, a useless hospital toothbrush would be a mild inconvenience. But to Dr. Giuliano, a nursing professor at the University of Massachusetts, Amherst, it was a reminder of a pervasive “blind spot” in U.S. hospitals: the stunning consequences of unbrushed teeth.
Hospital patients not getting their teeth brushed, or not brushing their teeth themselves, is believed to be a leading cause of hundreds of thousands of cases of pneumonia a year in patients who have not been put on a ventilator. Pneumonia is among the most common infections that occur in health care facilities, and a majority of cases are nonventilator hospital-acquired pneumonia, or NVHAP, which kills up to 30% of those infected, Dr. Giuliano and other experts said.
But unlike many infections that strike within hospitals, the federal government doesn’t require hospitals to report cases of NVHAP. As a result, few hospitals understand the origin of the illness, track its occurrence, or actively work to prevent it, the experts said.
, according to a growing body of peer-reviewed research papers. Instead, many hospitals often skip teeth brushing to prioritize other tasks and provide only cheap, ineffective toothbrushes, often unaware of the consequences, said Dr. Dian Baker, a Sacramento (Calif.) State nursing professor who has spent more than a decade studying NVHAP.
“I’ll tell you that today the vast majority of the tens of thousands of nurses in hospitals have no idea that pneumonia comes from germs in the mouth,” Dr. Baker said.
Pneumonia occurs when germs trigger an infection in the lungs. Although NVHAP accounts for most of the cases that occur in hospitals, it historically has not received the same attention as pneumonia tied to ventilators, which is easier to identify and study because it occurs among a narrow subset of patients.
NVHAP, a risk for virtually all hospital patients, is often caused by bacteria from the mouth that gathers in the scummy biofilm on unbrushed teeth and is aspirated into the lungs. Patients face a higher risk if they lie flat or remain immobile for long periods, so NVHAP can also be prevented by elevating their heads and getting them out of bed more often.
According to the National Organization for NV-HAP Prevention, which was founded in 2020, this pneumonia infects about 1 in every 100 hospital patients and kills 15%-30% of them. For those who survive, the illness often extends their hospital stay by up to 15 days and makes it much more likely they will be readmitted within a month or transferred to an intensive care unit.
John McCleary, 83, of Millinocket, Maine, contracted a likely case of NVHAP in 2008 after he fractured his ankle in a fall and spent 12 days in rehabilitation at a hospital, said his daughter, Kathy Day, a retired nurse and advocate with the Patient Safety Action Network.
Mr. McCleary recovered from the fracture but not from pneumonia. Two days after he returned home, the infection in his lungs caused him to be rushed back to the hospital, where he went into sepsis and spent weeks in treatment before moving to an isolation unit in a nursing home.
He died weeks later, emaciated, largely deaf, unable to eat, and often “too weak to get water through a straw,” his daughter said. After contracting pneumonia, he never walked again.
“It was an astounding assault on his body, from him being here visiting me the week before his fall, to his death just a few months later,” Ms. Day said. “And the whole thing was avoidable.”
While experts describe NVHAP as a largely ignored threat, that appears to be changing.
Last year, a group of researchers – including Dr. Giuliano and Dr. Baker, plus officials from the Centers for Disease Control and Prevention, the Veterans Health Administration, and the Joint Commission – published a “call-to-action” research paper hoping to launch “a national health care conversation about NVHAP prevention.”
The Joint Commission, a nonprofit organization whose accreditation can make or break hospitals, is considering broadening the infection control standards to include more ailments, including NVHAP, said Sylvia Garcia-Houchins, its director of infection prevention and control.
Separately, ECRI, a nonprofit focused on health care safety, this year pinpointed NVHAP as one of its top patient safety concerns.
James Davis, an ECRI infection expert, said the prevalence of NVHAP, while already alarming, is likely “underestimated” and probably worsened as hospitals swelled with patients during the coronavirus pandemic.
“We only know what’s reported,” Mr. Davis said. “Could this be the tip of the iceberg? I would say, in my opinion, probably.”
To better measure the condition, some researchers call for a standardized surveillance definition of NVHAP, which could in time open the door for the federal government to mandate reporting of cases or incentivize prevention. With increasing urgency, researchers are pushing for hospitals not to wait for the federal government to act against NVHAP.
Dr. Baker said she has spoken with hundreds of hospitals about how to prevent NVHAP, but thousands more have yet to take up the cause.
“We are not asking for some big, $300,000 piece of equipment,” Dr. Baker said. “The two things that show the best evidence of preventing this harm are things that should be happening in standard care anyway – brushing teeth and getting patients mobilized.”
That evidence comes from a smattering of studies that show those two strategies can lead to sharp reductions in infection rates.
In California, a study at 21 Kaiser Permanente hospitals used a reprioritization of oral care and getting patients out of bed to reduce rates of hospital-acquired pneumonia by around 70%. At Sutter Medical Center in Sacramento, better oral care reduced NVHAP cases by a yearly average of 35%.
At Orlando Regional Medical Center in Florida, a medical unit and a surgical unit where patients received enhanced oral care reduced NVHAP rates by 85% and 56%, respectively, when compared with similar units that received normal care. A similar study is underway at two hospitals in Illinois.
And the most compelling results come from a veterans’ hospital in Salem, Va., where a 2016 oral care pilot program reduced rates of NVHAP by 92% – saving an estimated 13 lives in just 19 months. The program, the HAPPEN Initiative, has been expanded across the Veterans Health Administration, and experts say it could serve as a model for all U.S. hospitals.
Dr. Michelle Lucatorto, a nursing official who leads HAPPEN, said the program trains nurses to most effectively brush patients’ teeth and educates patients and families on the link between oral care and preventing NVHAP. While teeth brushing may not seem to require training, Dr. Lucatorto made comparisons to how the coronavirus revealed many Americans were doing a lackluster job of another routine hygienic practice: washing their hands.
“Sometimes we are searching for the most complicated intervention,” she said. “We are always looking for that new bypass surgery, or some new technical equipment. And sometimes I think we fail to look at the simple things we can do in our practice to save people’s lives.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Four years ago, when Dr. Karen Giuliano went to a Boston hospital for hip replacement surgery, she was given a pale-pink bucket of toiletries issued to patients in many hospitals. Inside were tissues, bar soap, deodorant, toothpaste, and, without a doubt, the worst toothbrush she’d ever seen.
“I couldn’t believe it. I got a toothbrush with no bristles,” she said. “It must have not gone through the bristle machine. It was just a stick.”
To most patients, a useless hospital toothbrush would be a mild inconvenience. But to Dr. Giuliano, a nursing professor at the University of Massachusetts, Amherst, it was a reminder of a pervasive “blind spot” in U.S. hospitals: the stunning consequences of unbrushed teeth.
Hospital patients not getting their teeth brushed, or not brushing their teeth themselves, is believed to be a leading cause of hundreds of thousands of cases of pneumonia a year in patients who have not been put on a ventilator. Pneumonia is among the most common infections that occur in health care facilities, and a majority of cases are nonventilator hospital-acquired pneumonia, or NVHAP, which kills up to 30% of those infected, Dr. Giuliano and other experts said.
But unlike many infections that strike within hospitals, the federal government doesn’t require hospitals to report cases of NVHAP. As a result, few hospitals understand the origin of the illness, track its occurrence, or actively work to prevent it, the experts said.
, according to a growing body of peer-reviewed research papers. Instead, many hospitals often skip teeth brushing to prioritize other tasks and provide only cheap, ineffective toothbrushes, often unaware of the consequences, said Dr. Dian Baker, a Sacramento (Calif.) State nursing professor who has spent more than a decade studying NVHAP.
“I’ll tell you that today the vast majority of the tens of thousands of nurses in hospitals have no idea that pneumonia comes from germs in the mouth,” Dr. Baker said.
Pneumonia occurs when germs trigger an infection in the lungs. Although NVHAP accounts for most of the cases that occur in hospitals, it historically has not received the same attention as pneumonia tied to ventilators, which is easier to identify and study because it occurs among a narrow subset of patients.
NVHAP, a risk for virtually all hospital patients, is often caused by bacteria from the mouth that gathers in the scummy biofilm on unbrushed teeth and is aspirated into the lungs. Patients face a higher risk if they lie flat or remain immobile for long periods, so NVHAP can also be prevented by elevating their heads and getting them out of bed more often.
According to the National Organization for NV-HAP Prevention, which was founded in 2020, this pneumonia infects about 1 in every 100 hospital patients and kills 15%-30% of them. For those who survive, the illness often extends their hospital stay by up to 15 days and makes it much more likely they will be readmitted within a month or transferred to an intensive care unit.
John McCleary, 83, of Millinocket, Maine, contracted a likely case of NVHAP in 2008 after he fractured his ankle in a fall and spent 12 days in rehabilitation at a hospital, said his daughter, Kathy Day, a retired nurse and advocate with the Patient Safety Action Network.
Mr. McCleary recovered from the fracture but not from pneumonia. Two days after he returned home, the infection in his lungs caused him to be rushed back to the hospital, where he went into sepsis and spent weeks in treatment before moving to an isolation unit in a nursing home.
He died weeks later, emaciated, largely deaf, unable to eat, and often “too weak to get water through a straw,” his daughter said. After contracting pneumonia, he never walked again.
“It was an astounding assault on his body, from him being here visiting me the week before his fall, to his death just a few months later,” Ms. Day said. “And the whole thing was avoidable.”
While experts describe NVHAP as a largely ignored threat, that appears to be changing.
Last year, a group of researchers – including Dr. Giuliano and Dr. Baker, plus officials from the Centers for Disease Control and Prevention, the Veterans Health Administration, and the Joint Commission – published a “call-to-action” research paper hoping to launch “a national health care conversation about NVHAP prevention.”
The Joint Commission, a nonprofit organization whose accreditation can make or break hospitals, is considering broadening the infection control standards to include more ailments, including NVHAP, said Sylvia Garcia-Houchins, its director of infection prevention and control.
Separately, ECRI, a nonprofit focused on health care safety, this year pinpointed NVHAP as one of its top patient safety concerns.
James Davis, an ECRI infection expert, said the prevalence of NVHAP, while already alarming, is likely “underestimated” and probably worsened as hospitals swelled with patients during the coronavirus pandemic.
“We only know what’s reported,” Mr. Davis said. “Could this be the tip of the iceberg? I would say, in my opinion, probably.”
To better measure the condition, some researchers call for a standardized surveillance definition of NVHAP, which could in time open the door for the federal government to mandate reporting of cases or incentivize prevention. With increasing urgency, researchers are pushing for hospitals not to wait for the federal government to act against NVHAP.
Dr. Baker said she has spoken with hundreds of hospitals about how to prevent NVHAP, but thousands more have yet to take up the cause.
“We are not asking for some big, $300,000 piece of equipment,” Dr. Baker said. “The two things that show the best evidence of preventing this harm are things that should be happening in standard care anyway – brushing teeth and getting patients mobilized.”
That evidence comes from a smattering of studies that show those two strategies can lead to sharp reductions in infection rates.
In California, a study at 21 Kaiser Permanente hospitals used a reprioritization of oral care and getting patients out of bed to reduce rates of hospital-acquired pneumonia by around 70%. At Sutter Medical Center in Sacramento, better oral care reduced NVHAP cases by a yearly average of 35%.
At Orlando Regional Medical Center in Florida, a medical unit and a surgical unit where patients received enhanced oral care reduced NVHAP rates by 85% and 56%, respectively, when compared with similar units that received normal care. A similar study is underway at two hospitals in Illinois.
And the most compelling results come from a veterans’ hospital in Salem, Va., where a 2016 oral care pilot program reduced rates of NVHAP by 92% – saving an estimated 13 lives in just 19 months. The program, the HAPPEN Initiative, has been expanded across the Veterans Health Administration, and experts say it could serve as a model for all U.S. hospitals.
Dr. Michelle Lucatorto, a nursing official who leads HAPPEN, said the program trains nurses to most effectively brush patients’ teeth and educates patients and families on the link between oral care and preventing NVHAP. While teeth brushing may not seem to require training, Dr. Lucatorto made comparisons to how the coronavirus revealed many Americans were doing a lackluster job of another routine hygienic practice: washing their hands.
“Sometimes we are searching for the most complicated intervention,” she said. “We are always looking for that new bypass surgery, or some new technical equipment. And sometimes I think we fail to look at the simple things we can do in our practice to save people’s lives.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Four years ago, when Dr. Karen Giuliano went to a Boston hospital for hip replacement surgery, she was given a pale-pink bucket of toiletries issued to patients in many hospitals. Inside were tissues, bar soap, deodorant, toothpaste, and, without a doubt, the worst toothbrush she’d ever seen.
“I couldn’t believe it. I got a toothbrush with no bristles,” she said. “It must have not gone through the bristle machine. It was just a stick.”
To most patients, a useless hospital toothbrush would be a mild inconvenience. But to Dr. Giuliano, a nursing professor at the University of Massachusetts, Amherst, it was a reminder of a pervasive “blind spot” in U.S. hospitals: the stunning consequences of unbrushed teeth.
Hospital patients not getting their teeth brushed, or not brushing their teeth themselves, is believed to be a leading cause of hundreds of thousands of cases of pneumonia a year in patients who have not been put on a ventilator. Pneumonia is among the most common infections that occur in health care facilities, and a majority of cases are nonventilator hospital-acquired pneumonia, or NVHAP, which kills up to 30% of those infected, Dr. Giuliano and other experts said.
But unlike many infections that strike within hospitals, the federal government doesn’t require hospitals to report cases of NVHAP. As a result, few hospitals understand the origin of the illness, track its occurrence, or actively work to prevent it, the experts said.
, according to a growing body of peer-reviewed research papers. Instead, many hospitals often skip teeth brushing to prioritize other tasks and provide only cheap, ineffective toothbrushes, often unaware of the consequences, said Dr. Dian Baker, a Sacramento (Calif.) State nursing professor who has spent more than a decade studying NVHAP.
“I’ll tell you that today the vast majority of the tens of thousands of nurses in hospitals have no idea that pneumonia comes from germs in the mouth,” Dr. Baker said.
Pneumonia occurs when germs trigger an infection in the lungs. Although NVHAP accounts for most of the cases that occur in hospitals, it historically has not received the same attention as pneumonia tied to ventilators, which is easier to identify and study because it occurs among a narrow subset of patients.
NVHAP, a risk for virtually all hospital patients, is often caused by bacteria from the mouth that gathers in the scummy biofilm on unbrushed teeth and is aspirated into the lungs. Patients face a higher risk if they lie flat or remain immobile for long periods, so NVHAP can also be prevented by elevating their heads and getting them out of bed more often.
According to the National Organization for NV-HAP Prevention, which was founded in 2020, this pneumonia infects about 1 in every 100 hospital patients and kills 15%-30% of them. For those who survive, the illness often extends their hospital stay by up to 15 days and makes it much more likely they will be readmitted within a month or transferred to an intensive care unit.
John McCleary, 83, of Millinocket, Maine, contracted a likely case of NVHAP in 2008 after he fractured his ankle in a fall and spent 12 days in rehabilitation at a hospital, said his daughter, Kathy Day, a retired nurse and advocate with the Patient Safety Action Network.
Mr. McCleary recovered from the fracture but not from pneumonia. Two days after he returned home, the infection in his lungs caused him to be rushed back to the hospital, where he went into sepsis and spent weeks in treatment before moving to an isolation unit in a nursing home.
He died weeks later, emaciated, largely deaf, unable to eat, and often “too weak to get water through a straw,” his daughter said. After contracting pneumonia, he never walked again.
“It was an astounding assault on his body, from him being here visiting me the week before his fall, to his death just a few months later,” Ms. Day said. “And the whole thing was avoidable.”
While experts describe NVHAP as a largely ignored threat, that appears to be changing.
Last year, a group of researchers – including Dr. Giuliano and Dr. Baker, plus officials from the Centers for Disease Control and Prevention, the Veterans Health Administration, and the Joint Commission – published a “call-to-action” research paper hoping to launch “a national health care conversation about NVHAP prevention.”
The Joint Commission, a nonprofit organization whose accreditation can make or break hospitals, is considering broadening the infection control standards to include more ailments, including NVHAP, said Sylvia Garcia-Houchins, its director of infection prevention and control.
Separately, ECRI, a nonprofit focused on health care safety, this year pinpointed NVHAP as one of its top patient safety concerns.
James Davis, an ECRI infection expert, said the prevalence of NVHAP, while already alarming, is likely “underestimated” and probably worsened as hospitals swelled with patients during the coronavirus pandemic.
“We only know what’s reported,” Mr. Davis said. “Could this be the tip of the iceberg? I would say, in my opinion, probably.”
To better measure the condition, some researchers call for a standardized surveillance definition of NVHAP, which could in time open the door for the federal government to mandate reporting of cases or incentivize prevention. With increasing urgency, researchers are pushing for hospitals not to wait for the federal government to act against NVHAP.
Dr. Baker said she has spoken with hundreds of hospitals about how to prevent NVHAP, but thousands more have yet to take up the cause.
“We are not asking for some big, $300,000 piece of equipment,” Dr. Baker said. “The two things that show the best evidence of preventing this harm are things that should be happening in standard care anyway – brushing teeth and getting patients mobilized.”
That evidence comes from a smattering of studies that show those two strategies can lead to sharp reductions in infection rates.
In California, a study at 21 Kaiser Permanente hospitals used a reprioritization of oral care and getting patients out of bed to reduce rates of hospital-acquired pneumonia by around 70%. At Sutter Medical Center in Sacramento, better oral care reduced NVHAP cases by a yearly average of 35%.
At Orlando Regional Medical Center in Florida, a medical unit and a surgical unit where patients received enhanced oral care reduced NVHAP rates by 85% and 56%, respectively, when compared with similar units that received normal care. A similar study is underway at two hospitals in Illinois.
And the most compelling results come from a veterans’ hospital in Salem, Va., where a 2016 oral care pilot program reduced rates of NVHAP by 92% – saving an estimated 13 lives in just 19 months. The program, the HAPPEN Initiative, has been expanded across the Veterans Health Administration, and experts say it could serve as a model for all U.S. hospitals.
Dr. Michelle Lucatorto, a nursing official who leads HAPPEN, said the program trains nurses to most effectively brush patients’ teeth and educates patients and families on the link between oral care and preventing NVHAP. While teeth brushing may not seem to require training, Dr. Lucatorto made comparisons to how the coronavirus revealed many Americans were doing a lackluster job of another routine hygienic practice: washing their hands.
“Sometimes we are searching for the most complicated intervention,” she said. “We are always looking for that new bypass surgery, or some new technical equipment. And sometimes I think we fail to look at the simple things we can do in our practice to save people’s lives.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Pulse oximeters lead to less oxygen supplementation for people of color
The new research suggests that skin color–related differences in pulse oximeter readings are in fact impacting clinical decision-making, lead author Eric R. Gottlieb, MD, of Brigham and Women’s Hospital and Massachusetts Institute of Technology, both in Boston, and colleagues wrote. This suggests that technology needs to updated to improve health equity, they continued, in their paper published in JAMA Internal Medicine.

“It has been known for decades that these readings are affected by various surface pigmentations, including nail polish and skin melanin, which may affect light absorption and scattering,” the investigators wrote. “This increases the risk of hidden hypoxemia [among patients with darker skin], in which patients have falsely elevated SpO2 readings, usually defined as 92% or greater, with a blood hemoglobin oxygen saturation less than 88%.”
Although published reports on this phenomenon date back to the 1980s, clinical significance has been largely discounted, they said, citing a 2008 paper on the topic, which stated that “oximetry need not have exact accuracy” to determine if a patient needs oxygen supplementation.
‘We’re not providing equal care’
Questioning the validity of this statement, Dr. Gottlieb and colleagues conducted a retrospective cohort study involving 3,069 patients admitted to intensive care at the Beth Israel Deaconess Medical Center in Boston between 2008 and 2019, thereby excluding patients treated during the COVID-19 pandemic. The population consisted of four races/ethnicities: White (87%), Black (7%), Hispanic (4%), and Asian (3%).
Aligning with previous studies, multivariable linear regression analyses showed that Asian, Black, and Hispanic patients had significantly higher SpO2 readings than White patients in relation to hemoglobin oxygen saturation values, suggesting falsely elevated readings.
Further modeling showed that these same patient groups also received lower oxygen delivery rates, which were not explained directly by race/ethnicity, but instead were mediated by the discrepancy between SpO2 and hemoglobin oxygen saturation values. In other words, physicians were responding consistently to pulse oximetry readings, rather than exhibiting a direct racial/ethnic bias in their clinical decision-making.
“We’re not providing equal care,” Dr. Gottlieb said in an interview. “It’s not that the patients are sicker, or have other socioeconomic explanations for why this happens to them. It’s us. It’s our technology. And that’s something that really has to be fixed.”
The investigators offered a cautionary view of corrective algorithms, as these “have exacerbated disparities and are subject to ethical concerns;” for example, with glomerular filtration rate estimations in Black patients.
Dr. Gottlieb also cautioned against action by individual physicians, who may now be inclined to change how they interpret pulse oximeter readings based on a patient’s race or ethnicity.
“I don’t think that we can expect physicians, every time they see a patient, to be second guessing whether the number basically reflects the truth,” he said.
Instead, Dr. Gottlieb suggested that the burden of change rests upon the shoulders of institutions, including hospitals and device manufacturers, both of which “really need to take the responsibility” for making sure that pulse oximeters are “equitable and have similar performance across races.”
While Dr. Gottlieb said that skin color likely plays the greatest role in measurement discrepancies, he encouraged stakeholders “to think broadly about this, and not just assume that it’s entirely skin color,” noting a small amount of evidence indicating that blood chemistry may also play a role. Still, he predicted that colorimetry – the direct measurement of skin color – will probably be incorporated into pulse oximeters of the future.
Black patients 3X more likely to have hidden hypoxia than White patients
Michael Sjoding, MD, of the University of Michigan, Ann Arbor, was one of the first to raise awareness of skin color–related issues with pulse oximeters during the throes of the COVID-19 pandemic. His study, which involved more than 10,000 patients, showed that Black patients were threefold more likely to have hidden hypoxia than White patients.

The present study shows that such discrepancies are indeed clinically significant, Dr. Sjoding said in an interview. And these data are needed, he added, to bring about change.
“What is being asked is potentially a big deal,” Dr. Sjoding said. “Pulse oximeters are everywhere, and it would be a big undertaking to redesign pulse oximeters and purchase new pulse oximeters. You need a compelling body of evidence to do that. I think it’s there now, clearly. So I’m hopeful that we’re going to finally move forward, towards having devices that we are confident work accurately in everyone.”
Why it has taken so long to gather this evidence, however, is a thornier topic, considering race-related discrepancies in pulse oximeter readings were first documented more than 3 decades ago.
“We sort of rediscovered something that had been known and had been described in the past,” Dr. Sjoding said. He explained how he and many of his colleagues had completed pulmonary fellowships, yet none of them knew of these potential issues with pulse oximeters until they began to observe differences in their own patients during the pandemic.
“I’ll give previous generations of researchers the benefit of the doubt,” Dr. Sjoding said, pointing out that techniques in data gathering and analysis have advanced considerably over the years. “The types of studies that were done before were very different than what we did.”
Yet Dr. Sjoding entertained the possibility that other factors may have been at play.
“I think definitely there’s a social commentary on prioritization of research,” he said.
The study was supported by grants from the National Institutes of Health. The investigators and Dr. Sjoding reported no conflicts of interest.
The new research suggests that skin color–related differences in pulse oximeter readings are in fact impacting clinical decision-making, lead author Eric R. Gottlieb, MD, of Brigham and Women’s Hospital and Massachusetts Institute of Technology, both in Boston, and colleagues wrote. This suggests that technology needs to updated to improve health equity, they continued, in their paper published in JAMA Internal Medicine.
“It has been known for decades that these readings are affected by various surface pigmentations, including nail polish and skin melanin, which may affect light absorption and scattering,” the investigators wrote. “This increases the risk of hidden hypoxemia [among patients with darker skin], in which patients have falsely elevated SpO2 readings, usually defined as 92% or greater, with a blood hemoglobin oxygen saturation less than 88%.”
Although published reports on this phenomenon date back to the 1980s, clinical significance has been largely discounted, they said, citing a 2008 paper on the topic, which stated that “oximetry need not have exact accuracy” to determine if a patient needs oxygen supplementation.
‘We’re not providing equal care’
Questioning the validity of this statement, Dr. Gottlieb and colleagues conducted a retrospective cohort study involving 3,069 patients admitted to intensive care at the Beth Israel Deaconess Medical Center in Boston between 2008 and 2019, thereby excluding patients treated during the COVID-19 pandemic. The population consisted of four races/ethnicities: White (87%), Black (7%), Hispanic (4%), and Asian (3%).
Aligning with previous studies, multivariable linear regression analyses showed that Asian, Black, and Hispanic patients had significantly higher SpO2 readings than White patients in relation to hemoglobin oxygen saturation values, suggesting falsely elevated readings.
Further modeling showed that these same patient groups also received lower oxygen delivery rates, which were not explained directly by race/ethnicity, but instead were mediated by the discrepancy between SpO2 and hemoglobin oxygen saturation values. In other words, physicians were responding consistently to pulse oximetry readings, rather than exhibiting a direct racial/ethnic bias in their clinical decision-making.
“We’re not providing equal care,” Dr. Gottlieb said in an interview. “It’s not that the patients are sicker, or have other socioeconomic explanations for why this happens to them. It’s us. It’s our technology. And that’s something that really has to be fixed.”
The investigators offered a cautionary view of corrective algorithms, as these “have exacerbated disparities and are subject to ethical concerns;” for example, with glomerular filtration rate estimations in Black patients.
Dr. Gottlieb also cautioned against action by individual physicians, who may now be inclined to change how they interpret pulse oximeter readings based on a patient’s race or ethnicity.
“I don’t think that we can expect physicians, every time they see a patient, to be second guessing whether the number basically reflects the truth,” he said.
Instead, Dr. Gottlieb suggested that the burden of change rests upon the shoulders of institutions, including hospitals and device manufacturers, both of which “really need to take the responsibility” for making sure that pulse oximeters are “equitable and have similar performance across races.”
While Dr. Gottlieb said that skin color likely plays the greatest role in measurement discrepancies, he encouraged stakeholders “to think broadly about this, and not just assume that it’s entirely skin color,” noting a small amount of evidence indicating that blood chemistry may also play a role. Still, he predicted that colorimetry – the direct measurement of skin color – will probably be incorporated into pulse oximeters of the future.
Black patients 3X more likely to have hidden hypoxia than White patients
Michael Sjoding, MD, of the University of Michigan, Ann Arbor, was one of the first to raise awareness of skin color–related issues with pulse oximeters during the throes of the COVID-19 pandemic. His study, which involved more than 10,000 patients, showed that Black patients were threefold more likely to have hidden hypoxia than White patients.
The present study shows that such discrepancies are indeed clinically significant, Dr. Sjoding said in an interview. And these data are needed, he added, to bring about change.
“What is being asked is potentially a big deal,” Dr. Sjoding said. “Pulse oximeters are everywhere, and it would be a big undertaking to redesign pulse oximeters and purchase new pulse oximeters. You need a compelling body of evidence to do that. I think it’s there now, clearly. So I’m hopeful that we’re going to finally move forward, towards having devices that we are confident work accurately in everyone.”
Why it has taken so long to gather this evidence, however, is a thornier topic, considering race-related discrepancies in pulse oximeter readings were first documented more than 3 decades ago.
“We sort of rediscovered something that had been known and had been described in the past,” Dr. Sjoding said. He explained how he and many of his colleagues had completed pulmonary fellowships, yet none of them knew of these potential issues with pulse oximeters until they began to observe differences in their own patients during the pandemic.
“I’ll give previous generations of researchers the benefit of the doubt,” Dr. Sjoding said, pointing out that techniques in data gathering and analysis have advanced considerably over the years. “The types of studies that were done before were very different than what we did.”
Yet Dr. Sjoding entertained the possibility that other factors may have been at play.
“I think definitely there’s a social commentary on prioritization of research,” he said.
The study was supported by grants from the National Institutes of Health. The investigators and Dr. Sjoding reported no conflicts of interest.
The new research suggests that skin color–related differences in pulse oximeter readings are in fact impacting clinical decision-making, lead author Eric R. Gottlieb, MD, of Brigham and Women’s Hospital and Massachusetts Institute of Technology, both in Boston, and colleagues wrote. This suggests that technology needs to updated to improve health equity, they continued, in their paper published in JAMA Internal Medicine.
“It has been known for decades that these readings are affected by various surface pigmentations, including nail polish and skin melanin, which may affect light absorption and scattering,” the investigators wrote. “This increases the risk of hidden hypoxemia [among patients with darker skin], in which patients have falsely elevated SpO2 readings, usually defined as 92% or greater, with a blood hemoglobin oxygen saturation less than 88%.”
Although published reports on this phenomenon date back to the 1980s, clinical significance has been largely discounted, they said, citing a 2008 paper on the topic, which stated that “oximetry need not have exact accuracy” to determine if a patient needs oxygen supplementation.
‘We’re not providing equal care’
Questioning the validity of this statement, Dr. Gottlieb and colleagues conducted a retrospective cohort study involving 3,069 patients admitted to intensive care at the Beth Israel Deaconess Medical Center in Boston between 2008 and 2019, thereby excluding patients treated during the COVID-19 pandemic. The population consisted of four races/ethnicities: White (87%), Black (7%), Hispanic (4%), and Asian (3%).
Aligning with previous studies, multivariable linear regression analyses showed that Asian, Black, and Hispanic patients had significantly higher SpO2 readings than White patients in relation to hemoglobin oxygen saturation values, suggesting falsely elevated readings.
Further modeling showed that these same patient groups also received lower oxygen delivery rates, which were not explained directly by race/ethnicity, but instead were mediated by the discrepancy between SpO2 and hemoglobin oxygen saturation values. In other words, physicians were responding consistently to pulse oximetry readings, rather than exhibiting a direct racial/ethnic bias in their clinical decision-making.
“We’re not providing equal care,” Dr. Gottlieb said in an interview. “It’s not that the patients are sicker, or have other socioeconomic explanations for why this happens to them. It’s us. It’s our technology. And that’s something that really has to be fixed.”
The investigators offered a cautionary view of corrective algorithms, as these “have exacerbated disparities and are subject to ethical concerns;” for example, with glomerular filtration rate estimations in Black patients.
Dr. Gottlieb also cautioned against action by individual physicians, who may now be inclined to change how they interpret pulse oximeter readings based on a patient’s race or ethnicity.
“I don’t think that we can expect physicians, every time they see a patient, to be second guessing whether the number basically reflects the truth,” he said.
Instead, Dr. Gottlieb suggested that the burden of change rests upon the shoulders of institutions, including hospitals and device manufacturers, both of which “really need to take the responsibility” for making sure that pulse oximeters are “equitable and have similar performance across races.”
While Dr. Gottlieb said that skin color likely plays the greatest role in measurement discrepancies, he encouraged stakeholders “to think broadly about this, and not just assume that it’s entirely skin color,” noting a small amount of evidence indicating that blood chemistry may also play a role. Still, he predicted that colorimetry – the direct measurement of skin color – will probably be incorporated into pulse oximeters of the future.
Black patients 3X more likely to have hidden hypoxia than White patients
Michael Sjoding, MD, of the University of Michigan, Ann Arbor, was one of the first to raise awareness of skin color–related issues with pulse oximeters during the throes of the COVID-19 pandemic. His study, which involved more than 10,000 patients, showed that Black patients were threefold more likely to have hidden hypoxia than White patients.
The present study shows that such discrepancies are indeed clinically significant, Dr. Sjoding said in an interview. And these data are needed, he added, to bring about change.
“What is being asked is potentially a big deal,” Dr. Sjoding said. “Pulse oximeters are everywhere, and it would be a big undertaking to redesign pulse oximeters and purchase new pulse oximeters. You need a compelling body of evidence to do that. I think it’s there now, clearly. So I’m hopeful that we’re going to finally move forward, towards having devices that we are confident work accurately in everyone.”
Why it has taken so long to gather this evidence, however, is a thornier topic, considering race-related discrepancies in pulse oximeter readings were first documented more than 3 decades ago.
“We sort of rediscovered something that had been known and had been described in the past,” Dr. Sjoding said. He explained how he and many of his colleagues had completed pulmonary fellowships, yet none of them knew of these potential issues with pulse oximeters until they began to observe differences in their own patients during the pandemic.
“I’ll give previous generations of researchers the benefit of the doubt,” Dr. Sjoding said, pointing out that techniques in data gathering and analysis have advanced considerably over the years. “The types of studies that were done before were very different than what we did.”
Yet Dr. Sjoding entertained the possibility that other factors may have been at play.
“I think definitely there’s a social commentary on prioritization of research,” he said.
The study was supported by grants from the National Institutes of Health. The investigators and Dr. Sjoding reported no conflicts of interest.
FROM JAMA INTERNAL MEDICINE
Physicians urged to write indications on drug scripts as methotrexate users face new barriers with SCOTUS decision
.
The Court’s 5-4 decision in Dobbs v. Jackson Women’s Health Organization, which halted abortion procedures across the country, also appears to be affecting certain drug regimens. Reports have emerged that pharmacies are denying access to methotrexate (MTX), a drug often used in patients with arthritis or cancer, as well as psoriasis and other skin diseases. In very high doses, MTX it is used to terminate an ectopic pregnancy after miscarriage. The drug can also lead to birth defects.
“It’s happening all over,” Donald Miller, PharmD, professor of pharmacy practice at North Dakota State University, Fargo, said in an interview. “Pharmacists are reluctant to dispense it, and rheumatologists are reluctant to prescribe it because they’re afraid of going to jail.”
Becky Schwartz, a patient who takes MTX for lupus, recently tweeted that her physician’s office stopped prescribing the drug because it is considered an abortifacient. “I had care that made my disabled life easier, and [the Supreme Court] took that from me,” Ms. Schwartz wrote.
Prior to the Supreme Court’s ruling, physicians were concerned about the impact an overturning of the 1973 law would have on patient access to MTX and other prescription medications with abortifacient properties. Doctors in general are becoming afraid of prescribing anything that’s a teratogen, said Dr. Miller.
MTX is used far more often for autoimmune disease than as an abortifacient, said rheumatologist Kristen Young, MD, clinical assistant professor at the University of Arizona College of Medicine, Phoenix. It’s a slippery slope if states reacting to the Supreme Court ruling start regulating oral abortifacients, she added. Specifically, this will have a significant impact on patients with rheumatic disease.
Texas pharmacies target two drugs
MTX denials have caught the attention of health care organizations. “Uncertainty in financial and criminal liability for health care professionals in certain state laws and regulations are possibly compromising continuity of care and access [to] medications proven to be safe and effective by the Food and Drug Administration for these indications,” warned the American Pharmacists Association (APhA) in a statement to this news organization.
The APhA said that it was monitoring this situation to assess the effect on patients and pharmacists.
The Arthritis Foundation was made aware of challenges from patients in accessing their MTX prescription for managing their arthritis and shared a statement on the Foundation’s website.
In Texas, pharmacists can refuse to fill scripts for misoprostol and MTX, a combination used for medical abortions. According to the foundation, “Already there are reports that people in Texas who miscarry or take methotrexate for arthritis [are] having trouble getting their prescriptions filled.”
MTX, approved by the FDA in 1985, “is the absolute cornerstone of rheumatoid arthritis. We cannot deny our patients this incredibly valuable drug,” said John Reveille, MD, vice-chair for the department of medicine at the University of Texas McGovern School of Medicine and a member of the Arthritis Foundation expert panel, in an interview.
“While it’s true that methotrexate can be lethal to the fetus, misoprostol is much more likely to cause a spontaneous abortion, and the combination is especially effective,” he said.
“If you look at Cochrane clinical studies, the dose of misoprostol contained in certain combinations with NSAIDs [nonsteroidal anti-inflammatory drugs] can induce spontaneous abortions. It’s surprising that pharmacists are targeting methotrexate, an essential drug in arthritis treatment, when there are medications available that do not have this benefit that can by themselves cause loss of the fetus, such as mifepristone,” added Dr. Reveille.
The Dobbs ruling could also affect the ability of oncologists to provide lifesaving cancer care, according to Jason Westin, MD, an oncologist at the University of Texas MD Anderson Cancer Center in the department of lymphoma and myeloma.
“We have heard of medications with multiple indications, such as methotrexate, not being dispensed by pharmacies due to confusion regarding the intended use and potential consequences for the health care team,” he said in an interview.
Conflicting laws pose challenges for physicians
In North Dakota, inconsistencies in several laws are making it difficult for physicians and pharmacists to make decisions. “Lots of confusion can result when people pass laws against abortion. There’s sometimes no insight into the ramifications of those laws,” said Dr. Miller.
North Dakota approved a trigger law several years ago that makes abortion illegal 30 days after an overturning of Roe. However, another law that regulates abortion conflicts with the trigger law. “Some of the language will need clarification in the next legislative session,” he said.
APhA and other pharmacy associations strongly favor not interfering with the doctor- or pharmacist-patient relationship. The law needs to defer to appropriate care between doctor and patient, said Dr. Miller. State pharmacy associations in North Dakota are working with legislatures to clarify any exceptions in the law, he added.
Arizona lawmakers are trying to reconcile two abortion laws on the books. One, based on an 1864 territorial law, deems abortion illegal. In addition, a newly approved law bans abortions after 15 weeks. The latter will go into effect in September 2022. In both laws, a risk to the mother’s life is the only exception for abortion, said Dr. Young.
Denials aren’t widespread
Not all doctors are seeing MTX denials, but they’re worried about the future. “To date, we have not encountered difficulty in obtaining methotrexate based upon state abortion restrictions but are concerned that this could occur and result in dangerous delays in care,” said Dr. Westin.
Dr. Reveille, who practices rheumatology in Houston, has not yet received any complaints from patients. Things may be different in more rural parts of Texas, where pharmacists could be denying prescriptions based on religious issues, he offered.
It’s a little soon to see what repercussions may result from the Supreme Court ruling and state actions, said Dr. Reveille. “In Texas, we’re a bit ahead of the tidal wave.”
Access problems also haven’t shown up at the university clinic where Dr. Young practices. “In Arizona, it’s unclear if there would be a legal basis to refuse a person methotrexate on the basis that it can be used as an abortifacient,” she said.
Specificity is key in writing Rx scripts
Physicians can make things easier for patients by writing the indication and dose for the drug on the prescription slip. For example, a 10-mg script for MTX is not going to be used for an abortion, said Dr. Miller.
Rheumatologists in Texas have been doing this for some time, even before the Supreme Court ruling, said Fehmida Zahabi, MD, FACR, president of the Society of Texas Association of Rheumatology. For MTX prescriptions in premenopausal women, “patients are told their doctor needs to call the pharmacist. In the small print, we are asked to give a diagnosis to make sure we aren’t using it to terminate pregnancies,” said Dr. Zahabi.
She further noted that if the diagnosis is already indicated on the script, pharmacies generally won’t give patients a hard time.
Patients can also ask their physicians for a letter of medical necessity that confirms a drug’s use for a specific medical condition.
Mail order is another option if a local pharmacy won’t fill a prescription, said Dr. Miller. “This is legal unless a state makes it illegal to send an abortifacient across state lines,” he added.
Many medications used in rheumatic diseases are harmful in pregnancy, and it’s important to routinely discuss pregnancy risk and planning in the rheumatology clinic, said Dr. Young. This should include a thorough discussion and referral for long-acting reversible contraception in most cases, she suggested.
Actions at the federal, state level
President Joe Biden recently signed an executive order prompting federal regulators to protect access to medication abortions, among other steps to safeguard access to reproductive services.
In a statement on Twitter, the American College of Rheumatology (ACR) said that it was “ ... following this issue closely to determine if rheumatology providers and patients are experiencing any widespread difficulty accessing methotrexate or if any initial disruptions are potentially temporary and due to the independent actions of pharmacists trying to figure out what is and isn’t allowed where they practice.”
ACR has assembled a task force of medical and policy experts to determine the best course of action for patients.
The Arthritis Foundation also continues to monitor the situation, encouraging patients to call its hotline, said Steven Schultz, director of state legislative affairs, in an interview.
“We are analyzing how medication abortion could cause confusion on the part of providers or pharmacists dispensing the medication and what this means for specific patients,” said Mr. Schultz. Through a survey, the foundation hopes to get a better idea of what’s going on in the states at a macro level.
This may take some time, as states go through a process of lawsuits, injunctions, or coming into session to do something that may affect access to MTX, said Mr. Schultz.
Being involved in local advocacy is more important than ever, stressed Dr. Young. “Additionally, being plugged into what the ACR and other advocacy groups are doing on the national level is helpful as well to know the status of these medication access issues.”
Rheumatologists have a unique voice in this discussion, she added. “We guide our patients to stability for a safe pregnancy, and even with careful planning, we see patients who become critically ill during pregnancy and require lifesaving treatment, which at times can mean an abortion is necessary.”
Oncologists also advocate for their patients on a regular basis to make sure they have access to the care they need, said Dr. Westin. This situation with Roe is no different, he added. “We will continue to use our unique expertise to advocate for policies that assure access to high-quality, evidence-based care – and to help our patients overcome barriers that may interfere.”
Dr. Reveille participated on an advisory board with Eli Lilly in October 2021.
A version of this article first appeared on Medscape.com.
.
The Court’s 5-4 decision in Dobbs v. Jackson Women’s Health Organization, which halted abortion procedures across the country, also appears to be affecting certain drug regimens. Reports have emerged that pharmacies are denying access to methotrexate (MTX), a drug often used in patients with arthritis or cancer, as well as psoriasis and other skin diseases. In very high doses, MTX it is used to terminate an ectopic pregnancy after miscarriage. The drug can also lead to birth defects.
“It’s happening all over,” Donald Miller, PharmD, professor of pharmacy practice at North Dakota State University, Fargo, said in an interview. “Pharmacists are reluctant to dispense it, and rheumatologists are reluctant to prescribe it because they’re afraid of going to jail.”
Becky Schwartz, a patient who takes MTX for lupus, recently tweeted that her physician’s office stopped prescribing the drug because it is considered an abortifacient. “I had care that made my disabled life easier, and [the Supreme Court] took that from me,” Ms. Schwartz wrote.
Prior to the Supreme Court’s ruling, physicians were concerned about the impact an overturning of the 1973 law would have on patient access to MTX and other prescription medications with abortifacient properties. Doctors in general are becoming afraid of prescribing anything that’s a teratogen, said Dr. Miller.
MTX is used far more often for autoimmune disease than as an abortifacient, said rheumatologist Kristen Young, MD, clinical assistant professor at the University of Arizona College of Medicine, Phoenix. It’s a slippery slope if states reacting to the Supreme Court ruling start regulating oral abortifacients, she added. Specifically, this will have a significant impact on patients with rheumatic disease.
Texas pharmacies target two drugs
MTX denials have caught the attention of health care organizations. “Uncertainty in financial and criminal liability for health care professionals in certain state laws and regulations are possibly compromising continuity of care and access [to] medications proven to be safe and effective by the Food and Drug Administration for these indications,” warned the American Pharmacists Association (APhA) in a statement to this news organization.
The APhA said that it was monitoring this situation to assess the effect on patients and pharmacists.
The Arthritis Foundation was made aware of challenges from patients in accessing their MTX prescription for managing their arthritis and shared a statement on the Foundation’s website.
In Texas, pharmacists can refuse to fill scripts for misoprostol and MTX, a combination used for medical abortions. According to the foundation, “Already there are reports that people in Texas who miscarry or take methotrexate for arthritis [are] having trouble getting their prescriptions filled.”
MTX, approved by the FDA in 1985, “is the absolute cornerstone of rheumatoid arthritis. We cannot deny our patients this incredibly valuable drug,” said John Reveille, MD, vice-chair for the department of medicine at the University of Texas McGovern School of Medicine and a member of the Arthritis Foundation expert panel, in an interview.
“While it’s true that methotrexate can be lethal to the fetus, misoprostol is much more likely to cause a spontaneous abortion, and the combination is especially effective,” he said.
“If you look at Cochrane clinical studies, the dose of misoprostol contained in certain combinations with NSAIDs [nonsteroidal anti-inflammatory drugs] can induce spontaneous abortions. It’s surprising that pharmacists are targeting methotrexate, an essential drug in arthritis treatment, when there are medications available that do not have this benefit that can by themselves cause loss of the fetus, such as mifepristone,” added Dr. Reveille.
The Dobbs ruling could also affect the ability of oncologists to provide lifesaving cancer care, according to Jason Westin, MD, an oncologist at the University of Texas MD Anderson Cancer Center in the department of lymphoma and myeloma.
“We have heard of medications with multiple indications, such as methotrexate, not being dispensed by pharmacies due to confusion regarding the intended use and potential consequences for the health care team,” he said in an interview.
Conflicting laws pose challenges for physicians
In North Dakota, inconsistencies in several laws are making it difficult for physicians and pharmacists to make decisions. “Lots of confusion can result when people pass laws against abortion. There’s sometimes no insight into the ramifications of those laws,” said Dr. Miller.
North Dakota approved a trigger law several years ago that makes abortion illegal 30 days after an overturning of Roe. However, another law that regulates abortion conflicts with the trigger law. “Some of the language will need clarification in the next legislative session,” he said.
APhA and other pharmacy associations strongly favor not interfering with the doctor- or pharmacist-patient relationship. The law needs to defer to appropriate care between doctor and patient, said Dr. Miller. State pharmacy associations in North Dakota are working with legislatures to clarify any exceptions in the law, he added.
Arizona lawmakers are trying to reconcile two abortion laws on the books. One, based on an 1864 territorial law, deems abortion illegal. In addition, a newly approved law bans abortions after 15 weeks. The latter will go into effect in September 2022. In both laws, a risk to the mother’s life is the only exception for abortion, said Dr. Young.
Denials aren’t widespread
Not all doctors are seeing MTX denials, but they’re worried about the future. “To date, we have not encountered difficulty in obtaining methotrexate based upon state abortion restrictions but are concerned that this could occur and result in dangerous delays in care,” said Dr. Westin.
Dr. Reveille, who practices rheumatology in Houston, has not yet received any complaints from patients. Things may be different in more rural parts of Texas, where pharmacists could be denying prescriptions based on religious issues, he offered.
It’s a little soon to see what repercussions may result from the Supreme Court ruling and state actions, said Dr. Reveille. “In Texas, we’re a bit ahead of the tidal wave.”
Access problems also haven’t shown up at the university clinic where Dr. Young practices. “In Arizona, it’s unclear if there would be a legal basis to refuse a person methotrexate on the basis that it can be used as an abortifacient,” she said.
Specificity is key in writing Rx scripts
Physicians can make things easier for patients by writing the indication and dose for the drug on the prescription slip. For example, a 10-mg script for MTX is not going to be used for an abortion, said Dr. Miller.
Rheumatologists in Texas have been doing this for some time, even before the Supreme Court ruling, said Fehmida Zahabi, MD, FACR, president of the Society of Texas Association of Rheumatology. For MTX prescriptions in premenopausal women, “patients are told their doctor needs to call the pharmacist. In the small print, we are asked to give a diagnosis to make sure we aren’t using it to terminate pregnancies,” said Dr. Zahabi.
She further noted that if the diagnosis is already indicated on the script, pharmacies generally won’t give patients a hard time.
Patients can also ask their physicians for a letter of medical necessity that confirms a drug’s use for a specific medical condition.
Mail order is another option if a local pharmacy won’t fill a prescription, said Dr. Miller. “This is legal unless a state makes it illegal to send an abortifacient across state lines,” he added.
Many medications used in rheumatic diseases are harmful in pregnancy, and it’s important to routinely discuss pregnancy risk and planning in the rheumatology clinic, said Dr. Young. This should include a thorough discussion and referral for long-acting reversible contraception in most cases, she suggested.
Actions at the federal, state level
President Joe Biden recently signed an executive order prompting federal regulators to protect access to medication abortions, among other steps to safeguard access to reproductive services.
In a statement on Twitter, the American College of Rheumatology (ACR) said that it was “ ... following this issue closely to determine if rheumatology providers and patients are experiencing any widespread difficulty accessing methotrexate or if any initial disruptions are potentially temporary and due to the independent actions of pharmacists trying to figure out what is and isn’t allowed where they practice.”
ACR has assembled a task force of medical and policy experts to determine the best course of action for patients.
The Arthritis Foundation also continues to monitor the situation, encouraging patients to call its hotline, said Steven Schultz, director of state legislative affairs, in an interview.
“We are analyzing how medication abortion could cause confusion on the part of providers or pharmacists dispensing the medication and what this means for specific patients,” said Mr. Schultz. Through a survey, the foundation hopes to get a better idea of what’s going on in the states at a macro level.
This may take some time, as states go through a process of lawsuits, injunctions, or coming into session to do something that may affect access to MTX, said Mr. Schultz.
Being involved in local advocacy is more important than ever, stressed Dr. Young. “Additionally, being plugged into what the ACR and other advocacy groups are doing on the national level is helpful as well to know the status of these medication access issues.”
Rheumatologists have a unique voice in this discussion, she added. “We guide our patients to stability for a safe pregnancy, and even with careful planning, we see patients who become critically ill during pregnancy and require lifesaving treatment, which at times can mean an abortion is necessary.”
Oncologists also advocate for their patients on a regular basis to make sure they have access to the care they need, said Dr. Westin. This situation with Roe is no different, he added. “We will continue to use our unique expertise to advocate for policies that assure access to high-quality, evidence-based care – and to help our patients overcome barriers that may interfere.”
Dr. Reveille participated on an advisory board with Eli Lilly in October 2021.
A version of this article first appeared on Medscape.com.
.
The Court’s 5-4 decision in Dobbs v. Jackson Women’s Health Organization, which halted abortion procedures across the country, also appears to be affecting certain drug regimens. Reports have emerged that pharmacies are denying access to methotrexate (MTX), a drug often used in patients with arthritis or cancer, as well as psoriasis and other skin diseases. In very high doses, MTX it is used to terminate an ectopic pregnancy after miscarriage. The drug can also lead to birth defects.
“It’s happening all over,” Donald Miller, PharmD, professor of pharmacy practice at North Dakota State University, Fargo, said in an interview. “Pharmacists are reluctant to dispense it, and rheumatologists are reluctant to prescribe it because they’re afraid of going to jail.”
Becky Schwartz, a patient who takes MTX for lupus, recently tweeted that her physician’s office stopped prescribing the drug because it is considered an abortifacient. “I had care that made my disabled life easier, and [the Supreme Court] took that from me,” Ms. Schwartz wrote.
Prior to the Supreme Court’s ruling, physicians were concerned about the impact an overturning of the 1973 law would have on patient access to MTX and other prescription medications with abortifacient properties. Doctors in general are becoming afraid of prescribing anything that’s a teratogen, said Dr. Miller.
MTX is used far more often for autoimmune disease than as an abortifacient, said rheumatologist Kristen Young, MD, clinical assistant professor at the University of Arizona College of Medicine, Phoenix. It’s a slippery slope if states reacting to the Supreme Court ruling start regulating oral abortifacients, she added. Specifically, this will have a significant impact on patients with rheumatic disease.
Texas pharmacies target two drugs
MTX denials have caught the attention of health care organizations. “Uncertainty in financial and criminal liability for health care professionals in certain state laws and regulations are possibly compromising continuity of care and access [to] medications proven to be safe and effective by the Food and Drug Administration for these indications,” warned the American Pharmacists Association (APhA) in a statement to this news organization.
The APhA said that it was monitoring this situation to assess the effect on patients and pharmacists.
The Arthritis Foundation was made aware of challenges from patients in accessing their MTX prescription for managing their arthritis and shared a statement on the Foundation’s website.
In Texas, pharmacists can refuse to fill scripts for misoprostol and MTX, a combination used for medical abortions. According to the foundation, “Already there are reports that people in Texas who miscarry or take methotrexate for arthritis [are] having trouble getting their prescriptions filled.”
MTX, approved by the FDA in 1985, “is the absolute cornerstone of rheumatoid arthritis. We cannot deny our patients this incredibly valuable drug,” said John Reveille, MD, vice-chair for the department of medicine at the University of Texas McGovern School of Medicine and a member of the Arthritis Foundation expert panel, in an interview.
“While it’s true that methotrexate can be lethal to the fetus, misoprostol is much more likely to cause a spontaneous abortion, and the combination is especially effective,” he said.
“If you look at Cochrane clinical studies, the dose of misoprostol contained in certain combinations with NSAIDs [nonsteroidal anti-inflammatory drugs] can induce spontaneous abortions. It’s surprising that pharmacists are targeting methotrexate, an essential drug in arthritis treatment, when there are medications available that do not have this benefit that can by themselves cause loss of the fetus, such as mifepristone,” added Dr. Reveille.
The Dobbs ruling could also affect the ability of oncologists to provide lifesaving cancer care, according to Jason Westin, MD, an oncologist at the University of Texas MD Anderson Cancer Center in the department of lymphoma and myeloma.
“We have heard of medications with multiple indications, such as methotrexate, not being dispensed by pharmacies due to confusion regarding the intended use and potential consequences for the health care team,” he said in an interview.
Conflicting laws pose challenges for physicians
In North Dakota, inconsistencies in several laws are making it difficult for physicians and pharmacists to make decisions. “Lots of confusion can result when people pass laws against abortion. There’s sometimes no insight into the ramifications of those laws,” said Dr. Miller.
North Dakota approved a trigger law several years ago that makes abortion illegal 30 days after an overturning of Roe. However, another law that regulates abortion conflicts with the trigger law. “Some of the language will need clarification in the next legislative session,” he said.
APhA and other pharmacy associations strongly favor not interfering with the doctor- or pharmacist-patient relationship. The law needs to defer to appropriate care between doctor and patient, said Dr. Miller. State pharmacy associations in North Dakota are working with legislatures to clarify any exceptions in the law, he added.
Arizona lawmakers are trying to reconcile two abortion laws on the books. One, based on an 1864 territorial law, deems abortion illegal. In addition, a newly approved law bans abortions after 15 weeks. The latter will go into effect in September 2022. In both laws, a risk to the mother’s life is the only exception for abortion, said Dr. Young.
Denials aren’t widespread
Not all doctors are seeing MTX denials, but they’re worried about the future. “To date, we have not encountered difficulty in obtaining methotrexate based upon state abortion restrictions but are concerned that this could occur and result in dangerous delays in care,” said Dr. Westin.
Dr. Reveille, who practices rheumatology in Houston, has not yet received any complaints from patients. Things may be different in more rural parts of Texas, where pharmacists could be denying prescriptions based on religious issues, he offered.
It’s a little soon to see what repercussions may result from the Supreme Court ruling and state actions, said Dr. Reveille. “In Texas, we’re a bit ahead of the tidal wave.”
Access problems also haven’t shown up at the university clinic where Dr. Young practices. “In Arizona, it’s unclear if there would be a legal basis to refuse a person methotrexate on the basis that it can be used as an abortifacient,” she said.
Specificity is key in writing Rx scripts
Physicians can make things easier for patients by writing the indication and dose for the drug on the prescription slip. For example, a 10-mg script for MTX is not going to be used for an abortion, said Dr. Miller.
Rheumatologists in Texas have been doing this for some time, even before the Supreme Court ruling, said Fehmida Zahabi, MD, FACR, president of the Society of Texas Association of Rheumatology. For MTX prescriptions in premenopausal women, “patients are told their doctor needs to call the pharmacist. In the small print, we are asked to give a diagnosis to make sure we aren’t using it to terminate pregnancies,” said Dr. Zahabi.
She further noted that if the diagnosis is already indicated on the script, pharmacies generally won’t give patients a hard time.
Patients can also ask their physicians for a letter of medical necessity that confirms a drug’s use for a specific medical condition.
Mail order is another option if a local pharmacy won’t fill a prescription, said Dr. Miller. “This is legal unless a state makes it illegal to send an abortifacient across state lines,” he added.
Many medications used in rheumatic diseases are harmful in pregnancy, and it’s important to routinely discuss pregnancy risk and planning in the rheumatology clinic, said Dr. Young. This should include a thorough discussion and referral for long-acting reversible contraception in most cases, she suggested.
Actions at the federal, state level
President Joe Biden recently signed an executive order prompting federal regulators to protect access to medication abortions, among other steps to safeguard access to reproductive services.
In a statement on Twitter, the American College of Rheumatology (ACR) said that it was “ ... following this issue closely to determine if rheumatology providers and patients are experiencing any widespread difficulty accessing methotrexate or if any initial disruptions are potentially temporary and due to the independent actions of pharmacists trying to figure out what is and isn’t allowed where they practice.”
ACR has assembled a task force of medical and policy experts to determine the best course of action for patients.
The Arthritis Foundation also continues to monitor the situation, encouraging patients to call its hotline, said Steven Schultz, director of state legislative affairs, in an interview.
“We are analyzing how medication abortion could cause confusion on the part of providers or pharmacists dispensing the medication and what this means for specific patients,” said Mr. Schultz. Through a survey, the foundation hopes to get a better idea of what’s going on in the states at a macro level.
This may take some time, as states go through a process of lawsuits, injunctions, or coming into session to do something that may affect access to MTX, said Mr. Schultz.
Being involved in local advocacy is more important than ever, stressed Dr. Young. “Additionally, being plugged into what the ACR and other advocacy groups are doing on the national level is helpful as well to know the status of these medication access issues.”
Rheumatologists have a unique voice in this discussion, she added. “We guide our patients to stability for a safe pregnancy, and even with careful planning, we see patients who become critically ill during pregnancy and require lifesaving treatment, which at times can mean an abortion is necessary.”
Oncologists also advocate for their patients on a regular basis to make sure they have access to the care they need, said Dr. Westin. This situation with Roe is no different, he added. “We will continue to use our unique expertise to advocate for policies that assure access to high-quality, evidence-based care – and to help our patients overcome barriers that may interfere.”
Dr. Reveille participated on an advisory board with Eli Lilly in October 2021.
A version of this article first appeared on Medscape.com.
Children and COVID: Vaccination a harder sell in the summer
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.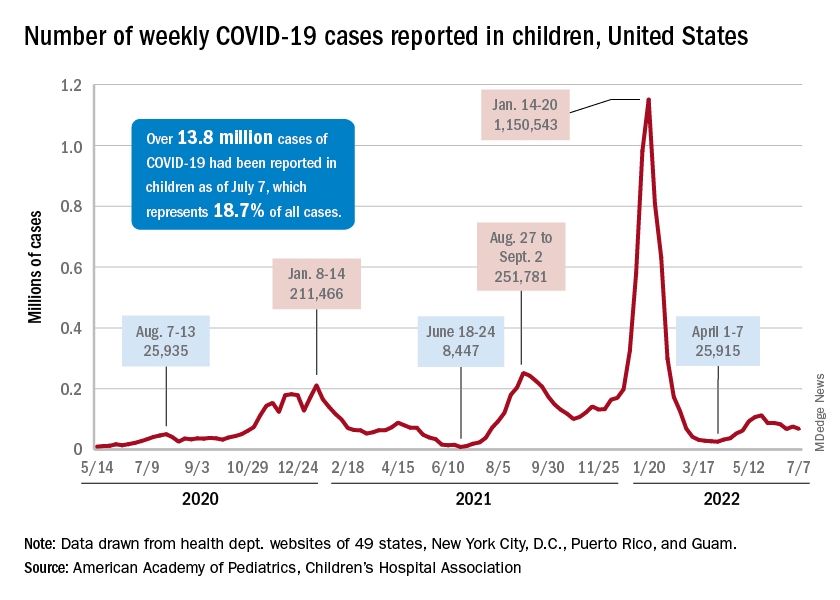
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
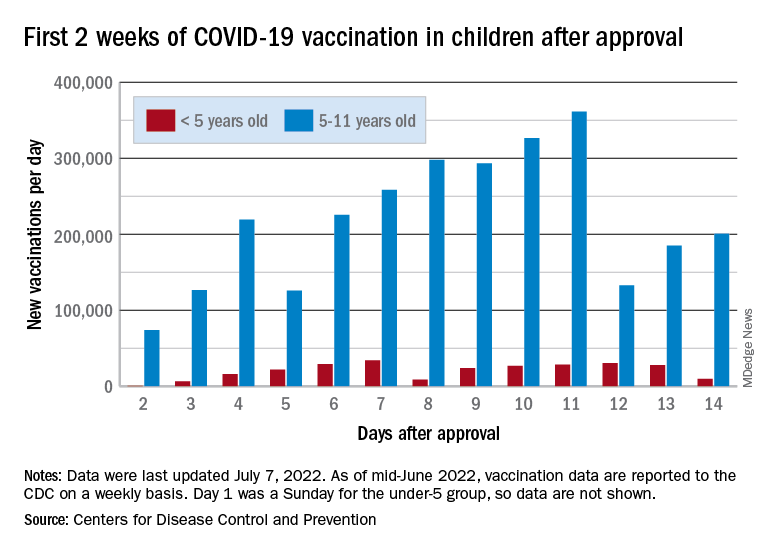
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
Inflation and health care: The prognosis for doctors
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Gender surgeons on TikTok, Instagram: Appropriate or not?
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.