User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Think Gender, Chronic Bronchitis in COPD
KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.

KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.
KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Adult Phenotypes No Help in Severe Pediatric Asthma
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).

Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).
Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).
Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Alternative to CPAP Arises for Uncomplicated Sleep Apnea
PHOENIX – For uncomplicated, moderate to severe obstructive sleep apnea, autoadjusting positive airway pressure is as effective as continuous positive airway pressure titrated in a sleep laboratory, according to Dr. Neil Freedman, a sleep medicine specialist and pulmonologist in Bannockburn, Ill.
Randomized controlled trials comparing lab-titrated continuous positive airway pressure (CPAP) to autoadjusting positive airway pressure (APAP) in unattended settings have shown similar compliance, apnea-hypopnea index (AHI), and daytime sleepiness improvements (Sleep 2010;33:267-71).

That raises the possibility of sending uncomplicated obstructive sleep apnea patients home with APAP machines to see how they do, instead of to a sleep lab. With insurance companies, among others, interested in that option, "in the near future patients who need CPAP – if they have uncomplicated sleep apnea – are going to get an unattended APAP trial whether they’re going to be treated long-term with it or they are going to be pushed to CPAP. It’s not inappropriate, as long as you know what you’re doing," Dr. Freedman said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
APAP machines don’t provide continuous pressure, but instead detect and respond to changes in upper airway flow or resistance patterns; the idea is to use the minimal effective pressure needed to maintain airway patency, which can change for various reasons, even body position.
Initially, machines are typically set to a minimum pressure of 4 cm H2O and a maximum pressure of 20 cm H2O. Dr. Freedman starts on the higher side with obese patients and those with worse symptoms, and also includes heated humidification and a gradual ramp-up to therapeutic pressures at the start of sleep.
"The overwhelming majority" of patients are going to need pressure of 8 to 12 cm H2O. If patients need more than 14 cm H2O, "there’s probably something else going on," he said.
Despite APAP’s effectiveness, that there are several unresolved issues, he cautioned.
First, the machines use different technologies and algorithms to treat events, so data from one APAP study is specific to the device used in that trial, and cannot be generalized to other machines. It’s important for clinicians to know their device and its weaknesses, but "provider knowledge, patient education, and early follow-up are more important than the type of device used." If patients still complain about snoring, being sleepy during the day, or other issues despite treatment, "look for problems. When in doubt, send them back to the lab," Dr. Freedman said.
Some machines can have trouble distinguishing true obstructive apneic events and central sleep apnea – apneic episodes despite an open airway – and misestimate the apnea-hypopnea index.
Patients may come in with a high AHI and events marked that "should be obstructive events" but that didn’t get better with increased pressure, which suggests central apnea. "If you inappropriately increase the pressure, you may actually make things worse for the patient," he noted. Excessive mask leaking can artificially inflate the AHI as well, so it’s important to use the mask or breathing apparatus recommended for a given machine. A proper fit also helps ensure the machines accurately capture snoring data, a measure of mask vibration, Dr. Freedman said.
Most APAP machines are flow based, which means they rely on the absence of flow back at the machine to detect events. A different approach, the forced oscillation technique (FOT), also is available to differentiate obstructive events from central apneic events. FOT reads changes in patterns of resistance; an absence of flow, despite low resistance, likely indicates a central event.
Dr. Freedman said he had no relevant disclosures.
PHOENIX – For uncomplicated, moderate to severe obstructive sleep apnea, autoadjusting positive airway pressure is as effective as continuous positive airway pressure titrated in a sleep laboratory, according to Dr. Neil Freedman, a sleep medicine specialist and pulmonologist in Bannockburn, Ill.
Randomized controlled trials comparing lab-titrated continuous positive airway pressure (CPAP) to autoadjusting positive airway pressure (APAP) in unattended settings have shown similar compliance, apnea-hypopnea index (AHI), and daytime sleepiness improvements (Sleep 2010;33:267-71).
That raises the possibility of sending uncomplicated obstructive sleep apnea patients home with APAP machines to see how they do, instead of to a sleep lab. With insurance companies, among others, interested in that option, "in the near future patients who need CPAP – if they have uncomplicated sleep apnea – are going to get an unattended APAP trial whether they’re going to be treated long-term with it or they are going to be pushed to CPAP. It’s not inappropriate, as long as you know what you’re doing," Dr. Freedman said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
APAP machines don’t provide continuous pressure, but instead detect and respond to changes in upper airway flow or resistance patterns; the idea is to use the minimal effective pressure needed to maintain airway patency, which can change for various reasons, even body position.
Initially, machines are typically set to a minimum pressure of 4 cm H2O and a maximum pressure of 20 cm H2O. Dr. Freedman starts on the higher side with obese patients and those with worse symptoms, and also includes heated humidification and a gradual ramp-up to therapeutic pressures at the start of sleep.
"The overwhelming majority" of patients are going to need pressure of 8 to 12 cm H2O. If patients need more than 14 cm H2O, "there’s probably something else going on," he said.
Despite APAP’s effectiveness, that there are several unresolved issues, he cautioned.
First, the machines use different technologies and algorithms to treat events, so data from one APAP study is specific to the device used in that trial, and cannot be generalized to other machines. It’s important for clinicians to know their device and its weaknesses, but "provider knowledge, patient education, and early follow-up are more important than the type of device used." If patients still complain about snoring, being sleepy during the day, or other issues despite treatment, "look for problems. When in doubt, send them back to the lab," Dr. Freedman said.
Some machines can have trouble distinguishing true obstructive apneic events and central sleep apnea – apneic episodes despite an open airway – and misestimate the apnea-hypopnea index.
Patients may come in with a high AHI and events marked that "should be obstructive events" but that didn’t get better with increased pressure, which suggests central apnea. "If you inappropriately increase the pressure, you may actually make things worse for the patient," he noted. Excessive mask leaking can artificially inflate the AHI as well, so it’s important to use the mask or breathing apparatus recommended for a given machine. A proper fit also helps ensure the machines accurately capture snoring data, a measure of mask vibration, Dr. Freedman said.
Most APAP machines are flow based, which means they rely on the absence of flow back at the machine to detect events. A different approach, the forced oscillation technique (FOT), also is available to differentiate obstructive events from central apneic events. FOT reads changes in patterns of resistance; an absence of flow, despite low resistance, likely indicates a central event.
Dr. Freedman said he had no relevant disclosures.
PHOENIX – For uncomplicated, moderate to severe obstructive sleep apnea, autoadjusting positive airway pressure is as effective as continuous positive airway pressure titrated in a sleep laboratory, according to Dr. Neil Freedman, a sleep medicine specialist and pulmonologist in Bannockburn, Ill.
Randomized controlled trials comparing lab-titrated continuous positive airway pressure (CPAP) to autoadjusting positive airway pressure (APAP) in unattended settings have shown similar compliance, apnea-hypopnea index (AHI), and daytime sleepiness improvements (Sleep 2010;33:267-71).
That raises the possibility of sending uncomplicated obstructive sleep apnea patients home with APAP machines to see how they do, instead of to a sleep lab. With insurance companies, among others, interested in that option, "in the near future patients who need CPAP – if they have uncomplicated sleep apnea – are going to get an unattended APAP trial whether they’re going to be treated long-term with it or they are going to be pushed to CPAP. It’s not inappropriate, as long as you know what you’re doing," Dr. Freedman said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
APAP machines don’t provide continuous pressure, but instead detect and respond to changes in upper airway flow or resistance patterns; the idea is to use the minimal effective pressure needed to maintain airway patency, which can change for various reasons, even body position.
Initially, machines are typically set to a minimum pressure of 4 cm H2O and a maximum pressure of 20 cm H2O. Dr. Freedman starts on the higher side with obese patients and those with worse symptoms, and also includes heated humidification and a gradual ramp-up to therapeutic pressures at the start of sleep.
"The overwhelming majority" of patients are going to need pressure of 8 to 12 cm H2O. If patients need more than 14 cm H2O, "there’s probably something else going on," he said.
Despite APAP’s effectiveness, that there are several unresolved issues, he cautioned.
First, the machines use different technologies and algorithms to treat events, so data from one APAP study is specific to the device used in that trial, and cannot be generalized to other machines. It’s important for clinicians to know their device and its weaknesses, but "provider knowledge, patient education, and early follow-up are more important than the type of device used." If patients still complain about snoring, being sleepy during the day, or other issues despite treatment, "look for problems. When in doubt, send them back to the lab," Dr. Freedman said.
Some machines can have trouble distinguishing true obstructive apneic events and central sleep apnea – apneic episodes despite an open airway – and misestimate the apnea-hypopnea index.
Patients may come in with a high AHI and events marked that "should be obstructive events" but that didn’t get better with increased pressure, which suggests central apnea. "If you inappropriately increase the pressure, you may actually make things worse for the patient," he noted. Excessive mask leaking can artificially inflate the AHI as well, so it’s important to use the mask or breathing apparatus recommended for a given machine. A proper fit also helps ensure the machines accurately capture snoring data, a measure of mask vibration, Dr. Freedman said.
Most APAP machines are flow based, which means they rely on the absence of flow back at the machine to detect events. A different approach, the forced oscillation technique (FOT), also is available to differentiate obstructive events from central apneic events. FOT reads changes in patterns of resistance; an absence of flow, despite low resistance, likely indicates a central event.
Dr. Freedman said he had no relevant disclosures.
FROM A MEETING ON SLEEP MEDICINE SPONSORED BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Pertussis Immunization Recommended for Adults 65 and Older
ATLANTA – The tetanus-diphtheria-acellular pertussis vaccine should be given to adults aged 65 years and older, according to recommendations from the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
The recommendation, backed by a 14-1 vote among ACIP members, is expected to go into effect when the CDC publishes the guidance, along with other guidance related to use of the adolescent/adult formulation of the tetanus-diphtheria-acellular pertussis vaccine (Tdap).
Of the two currently licensed Tdap vaccines, only GlaxoSmithKline’s Boostrix is approved for adults aged 65 and older. Efficacy data for the other one, Sanofi-Pasteur’s Adacel, had been submitted to the Food and Drug Administration but did not meet immunogenicity end points, the FDA’s representative, Dr. Wellington Sun, told the committee.
The ACIP recommendation will express a preference for use of Boostrix in the 65+ age group but is expected to state that Adacel is acceptable and preferable to delay of vaccination if Boostrix is not available. There were differences of opinion among committee members about whether to express a preference or not, and the exact language for the recommendation was still to be worked out at the time of the vote.
Current recommendations call for a single dose of Tdap for adults aged 19-64 years. Previously, the vaccine had only been recommended for adults 65 and older who were in close contact with an infant less than 12 months of age. With the current vote, ACIP also recommended elimination of the "decennial" interval that had previously been applied to the tetanus-diphtheria vaccine, so that a single dose of Tdap can be given to any adult who has not previously received it, regardless of interval since the last Td, said Dr. Jennifer L. Liang who explained the ACIP Pertussis Vaccines Working Groups’ deliberations.

Liaisons from the American College of Physicians (ACP) and the American Academy of Family Physicians (AAFP) said they supported the vote. "I think the important thing that we did today was in essence make a universal use recommendation for Tdap in adults. Before, it was full of provisos that clinicians couldn’t remember, sort of like the flu [vaccine] story. We’ve made it easy for clinicians by saying every adult deserves a dose of Tdap," ACP liaison Gregory A. Poland said in an interview.
However, "There are unknowns yet. We don’t know the duration of efficacy or the exact level of efficacy, particularly in older adults. Those are data needs that we have," noted Dr. Poland, the Mary Lowell Leary Professor of Medicine and Infectious Diseases at the Mayo Clinic, Rochester, Minn.
According to AAFP liaison Dr. Jamie Loehr, owner of Cayuga Family Medicine, Ithaca, N.Y., "The [AAFP] will review this, and most likely support it as it has in the past. On a practical level, it will be much easier for family physicians to have a blanket immunization recommendation rather than having to pick and chose."
Surveillance data suggest that the incidence of pertussis overall among adults older than 65 in the U.S. ranges from 2.5/100,000 in those aged 65-69 years to 0.8/100,000 in those aged 85 years and older. However, reported rates for adults are believed to be greatly underestimated since adults often don’t exhibit the typical paroxysms, inspiratory whoop, and post-tussive vomiting seen in infants with pertussis. Indeed, data from Australian surveillance and from published studies on varying age groups, some including adults beyond age 65 years, suggest that the incidence actually ranges from 66 to 507 cases/100,000 population, the CDC’s Dr. Anna Acosta told the ACIP.

Girishanthy Krishnarajah of GlaxoSmithKline presented a cost-effectiveness analysis of a one-time Boostrix vaccination among a cohort of U.S. residents aged 65 and older, in which the cost per case averted ranged from $416 to $10,413, depending on the pertussis incidence level. The cost per quality-adjusted life year (QALY) ranged from $13,260 to $332,218, also depending on incidence. When the pertussis incidence in people aged 65 years and older exceeded 110/100,000, the incremental cost-effectiveness ratio falls below $50,000/QALY, the generally accepted cost-effectiveness threshold, she said.
A CDC cost-effectiveness analysis produced similar results, according to Dr. Acosta.
Data suggest that safety and tolerability of Tdap in older adults is similar to that of the Td vaccine. While there are no efficacy data available specifically in the 65+ age group, data suggest that "older adults mount an immune response, likely to provide protection," the CDC’s Dr. Liang said.
Several ACIP members expressed concern that efficacy data were not available, but voted in favor of the recommendation regardless. Dr. Jeffrey Duchin was the sole committee member who cast a vote against the recommendation. "I would have liked to have seen more data on efficacy in the older population. It was assumed in the models. I would like to see more studies," Dr. Duchin, a professor of medicine at the University of Washington in Seattle, said in an interview.
As CDC employees, Dr. Acosta and Dr. Liang had no disclosures. Dr. Loehr and Dr. Duchin stated that they have no disclosures. Dr. Poland consults with companies on novel vaccines, but currently has no relationships with either GlaxoSmithKline or Sanofi-Pasteur.
ATLANTA – The tetanus-diphtheria-acellular pertussis vaccine should be given to adults aged 65 years and older, according to recommendations from the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
The recommendation, backed by a 14-1 vote among ACIP members, is expected to go into effect when the CDC publishes the guidance, along with other guidance related to use of the adolescent/adult formulation of the tetanus-diphtheria-acellular pertussis vaccine (Tdap).
Of the two currently licensed Tdap vaccines, only GlaxoSmithKline’s Boostrix is approved for adults aged 65 and older. Efficacy data for the other one, Sanofi-Pasteur’s Adacel, had been submitted to the Food and Drug Administration but did not meet immunogenicity end points, the FDA’s representative, Dr. Wellington Sun, told the committee.
The ACIP recommendation will express a preference for use of Boostrix in the 65+ age group but is expected to state that Adacel is acceptable and preferable to delay of vaccination if Boostrix is not available. There were differences of opinion among committee members about whether to express a preference or not, and the exact language for the recommendation was still to be worked out at the time of the vote.
Current recommendations call for a single dose of Tdap for adults aged 19-64 years. Previously, the vaccine had only been recommended for adults 65 and older who were in close contact with an infant less than 12 months of age. With the current vote, ACIP also recommended elimination of the "decennial" interval that had previously been applied to the tetanus-diphtheria vaccine, so that a single dose of Tdap can be given to any adult who has not previously received it, regardless of interval since the last Td, said Dr. Jennifer L. Liang who explained the ACIP Pertussis Vaccines Working Groups’ deliberations.
Liaisons from the American College of Physicians (ACP) and the American Academy of Family Physicians (AAFP) said they supported the vote. "I think the important thing that we did today was in essence make a universal use recommendation for Tdap in adults. Before, it was full of provisos that clinicians couldn’t remember, sort of like the flu [vaccine] story. We’ve made it easy for clinicians by saying every adult deserves a dose of Tdap," ACP liaison Gregory A. Poland said in an interview.
However, "There are unknowns yet. We don’t know the duration of efficacy or the exact level of efficacy, particularly in older adults. Those are data needs that we have," noted Dr. Poland, the Mary Lowell Leary Professor of Medicine and Infectious Diseases at the Mayo Clinic, Rochester, Minn.
According to AAFP liaison Dr. Jamie Loehr, owner of Cayuga Family Medicine, Ithaca, N.Y., "The [AAFP] will review this, and most likely support it as it has in the past. On a practical level, it will be much easier for family physicians to have a blanket immunization recommendation rather than having to pick and chose."
Surveillance data suggest that the incidence of pertussis overall among adults older than 65 in the U.S. ranges from 2.5/100,000 in those aged 65-69 years to 0.8/100,000 in those aged 85 years and older. However, reported rates for adults are believed to be greatly underestimated since adults often don’t exhibit the typical paroxysms, inspiratory whoop, and post-tussive vomiting seen in infants with pertussis. Indeed, data from Australian surveillance and from published studies on varying age groups, some including adults beyond age 65 years, suggest that the incidence actually ranges from 66 to 507 cases/100,000 population, the CDC’s Dr. Anna Acosta told the ACIP.
Girishanthy Krishnarajah of GlaxoSmithKline presented a cost-effectiveness analysis of a one-time Boostrix vaccination among a cohort of U.S. residents aged 65 and older, in which the cost per case averted ranged from $416 to $10,413, depending on the pertussis incidence level. The cost per quality-adjusted life year (QALY) ranged from $13,260 to $332,218, also depending on incidence. When the pertussis incidence in people aged 65 years and older exceeded 110/100,000, the incremental cost-effectiveness ratio falls below $50,000/QALY, the generally accepted cost-effectiveness threshold, she said.
A CDC cost-effectiveness analysis produced similar results, according to Dr. Acosta.
Data suggest that safety and tolerability of Tdap in older adults is similar to that of the Td vaccine. While there are no efficacy data available specifically in the 65+ age group, data suggest that "older adults mount an immune response, likely to provide protection," the CDC’s Dr. Liang said.
Several ACIP members expressed concern that efficacy data were not available, but voted in favor of the recommendation regardless. Dr. Jeffrey Duchin was the sole committee member who cast a vote against the recommendation. "I would have liked to have seen more data on efficacy in the older population. It was assumed in the models. I would like to see more studies," Dr. Duchin, a professor of medicine at the University of Washington in Seattle, said in an interview.
As CDC employees, Dr. Acosta and Dr. Liang had no disclosures. Dr. Loehr and Dr. Duchin stated that they have no disclosures. Dr. Poland consults with companies on novel vaccines, but currently has no relationships with either GlaxoSmithKline or Sanofi-Pasteur.
ATLANTA – The tetanus-diphtheria-acellular pertussis vaccine should be given to adults aged 65 years and older, according to recommendations from the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
The recommendation, backed by a 14-1 vote among ACIP members, is expected to go into effect when the CDC publishes the guidance, along with other guidance related to use of the adolescent/adult formulation of the tetanus-diphtheria-acellular pertussis vaccine (Tdap).
Of the two currently licensed Tdap vaccines, only GlaxoSmithKline’s Boostrix is approved for adults aged 65 and older. Efficacy data for the other one, Sanofi-Pasteur’s Adacel, had been submitted to the Food and Drug Administration but did not meet immunogenicity end points, the FDA’s representative, Dr. Wellington Sun, told the committee.
The ACIP recommendation will express a preference for use of Boostrix in the 65+ age group but is expected to state that Adacel is acceptable and preferable to delay of vaccination if Boostrix is not available. There were differences of opinion among committee members about whether to express a preference or not, and the exact language for the recommendation was still to be worked out at the time of the vote.
Current recommendations call for a single dose of Tdap for adults aged 19-64 years. Previously, the vaccine had only been recommended for adults 65 and older who were in close contact with an infant less than 12 months of age. With the current vote, ACIP also recommended elimination of the "decennial" interval that had previously been applied to the tetanus-diphtheria vaccine, so that a single dose of Tdap can be given to any adult who has not previously received it, regardless of interval since the last Td, said Dr. Jennifer L. Liang who explained the ACIP Pertussis Vaccines Working Groups’ deliberations.
Liaisons from the American College of Physicians (ACP) and the American Academy of Family Physicians (AAFP) said they supported the vote. "I think the important thing that we did today was in essence make a universal use recommendation for Tdap in adults. Before, it was full of provisos that clinicians couldn’t remember, sort of like the flu [vaccine] story. We’ve made it easy for clinicians by saying every adult deserves a dose of Tdap," ACP liaison Gregory A. Poland said in an interview.
However, "There are unknowns yet. We don’t know the duration of efficacy or the exact level of efficacy, particularly in older adults. Those are data needs that we have," noted Dr. Poland, the Mary Lowell Leary Professor of Medicine and Infectious Diseases at the Mayo Clinic, Rochester, Minn.
According to AAFP liaison Dr. Jamie Loehr, owner of Cayuga Family Medicine, Ithaca, N.Y., "The [AAFP] will review this, and most likely support it as it has in the past. On a practical level, it will be much easier for family physicians to have a blanket immunization recommendation rather than having to pick and chose."
Surveillance data suggest that the incidence of pertussis overall among adults older than 65 in the U.S. ranges from 2.5/100,000 in those aged 65-69 years to 0.8/100,000 in those aged 85 years and older. However, reported rates for adults are believed to be greatly underestimated since adults often don’t exhibit the typical paroxysms, inspiratory whoop, and post-tussive vomiting seen in infants with pertussis. Indeed, data from Australian surveillance and from published studies on varying age groups, some including adults beyond age 65 years, suggest that the incidence actually ranges from 66 to 507 cases/100,000 population, the CDC’s Dr. Anna Acosta told the ACIP.
Girishanthy Krishnarajah of GlaxoSmithKline presented a cost-effectiveness analysis of a one-time Boostrix vaccination among a cohort of U.S. residents aged 65 and older, in which the cost per case averted ranged from $416 to $10,413, depending on the pertussis incidence level. The cost per quality-adjusted life year (QALY) ranged from $13,260 to $332,218, also depending on incidence. When the pertussis incidence in people aged 65 years and older exceeded 110/100,000, the incremental cost-effectiveness ratio falls below $50,000/QALY, the generally accepted cost-effectiveness threshold, she said.
A CDC cost-effectiveness analysis produced similar results, according to Dr. Acosta.
Data suggest that safety and tolerability of Tdap in older adults is similar to that of the Td vaccine. While there are no efficacy data available specifically in the 65+ age group, data suggest that "older adults mount an immune response, likely to provide protection," the CDC’s Dr. Liang said.
Several ACIP members expressed concern that efficacy data were not available, but voted in favor of the recommendation regardless. Dr. Jeffrey Duchin was the sole committee member who cast a vote against the recommendation. "I would have liked to have seen more data on efficacy in the older population. It was assumed in the models. I would like to see more studies," Dr. Duchin, a professor of medicine at the University of Washington in Seattle, said in an interview.
As CDC employees, Dr. Acosta and Dr. Liang had no disclosures. Dr. Loehr and Dr. Duchin stated that they have no disclosures. Dr. Poland consults with companies on novel vaccines, but currently has no relationships with either GlaxoSmithKline or Sanofi-Pasteur.
FDA Questions CV Events Seen in COPD Drug Trials
Persistent cardiovascular events across the clinical trials for aclidinium bromide may not represent a definite safety signal, according to the Food and Drug Administration, but there is enough concern that an advisory committee will be asked for input on its significance.
The drug’s maker, Forest Laboratories Inc., wants approval of aclidinium bromide for long-term maintenance treatment of bronchospasm from chronic obstructive pulmonary disease, including chronic bronchitis and emphysema. It comes as a dry powder and is dispersed through an inhaler from Almirall SA.
When the FDA’s Pulmonary-Allergy Drugs Advisory Committee considers the product on Feb. 23, the agency wants the panel to discuss the overall safety profile, given the size of the safety database and duration of exposure. The committee also will vote on whether safety has been adequately assessed for the proposed indication.
FDA reviewers identified 10 cardiovascular deaths among patients in aclidinium clinical trials who were treated with the desired 400-mcg dose.
Four of those deaths were caused by cardiac arrest and one was from acute cardiac failure, while only one case of myocardial infarction was reported in patients receiving a 200-mcg dose of aclidinium bromide. None was reported among those receiving placebo. A cardiovascular cause could not be ruled out in two placebo cases, according to FDA documents.
The clinical reviewer said that the significance of the findings is uncertain, but called it "striking" that all the CV deaths in the long-term safety trial were in the 400 mcg–dose group.
Still, the agency said that the incidence rate in the group is lower than would generally be expected in a "real world" COPD population.
"It is difficult to dismiss the apparent imbalance in cardiovascular death between the treatment groups, while at the same time, impossible to conclude that the data represent a true safety signal," the clinical briefing documents conclude.
The size of the safety database was concerning to the FDA. Across all Forest’s trials, 1,471 patients with COPD were exposed to the 400-mcg dose with a mean duration of 211 days, including 733 patients exposed for 182 days or more and 329 exposed for 1 year.
The agency said the size was consistent with international guidelines but was "relatively small compared to the size of programs for other COPD products."
Long-term data combined with additional exposure data suggest that the CV death was possibly dose dependent, the agency said.
"Whether these results represent a spurious finding or a potential safety signal is difficult to discern and may warrant further investigation," the FDA stated.
FDA said the issue is particularly important given the possibility of increased mortality that has been identified with other inhaled anticholinergic agents.
Last year, the FDA ordered large studies of four long-acting beta agonists (LABAs) to assess their safety when used with inhaled corticosteroids versus inhaled corticosteroids alone. It was an outgrowth of a reanalysis of trial data that found LABA use can be associated with severe asthma symptoms, hospitalization, and death.
The FDA said that the reanalysis could be interpreted in different ways and decided new studies were needed.
If the committee decides aclidinium bromide’s safety has not been assessed adequately, it will be asked what other data should be obtained.
Efficacy Data Not Questioned
FDA reviewers did not have any doubts about whether aclidinium bromide’s efficacy had been demonstrated in the three trials that were submitted. The agency said a statistically significant effect compared with placebo was found for the 400-mcg dose, as well as a smaller significant effect for a 200-mcg dose, after 12 weeks of treatment.
The effect from the 400-mcg dose also seemed to persist at week 24 in one of the trials. Subgroup analyses showed effects similar to the overall population, according to FDA briefing documents.
Secondary endpoints such as peak forced expiratory volume in 1 second and rescue medication usage patterns also supported efficacy.
The committee will discuss aclidinium bromide’s efficacy, including its bronchodilatory effect, and vote on whether the efficacy data provide substantial evidence of a clinically meaningful benefit for the 400-mcg dose, which would be given twice daily.
The final voting question asks whether the efficacy and safety data provide substantial evidence for approval.
Forest has proposed the trade name Tudorza Pressair for the pending product.
This coverage is provided courtesy of "The Pink Sheet." Elsevier Global Medical News and "The Pink Sheet" are published by Elsevier.
Persistent cardiovascular events across the clinical trials for aclidinium bromide may not represent a definite safety signal, according to the Food and Drug Administration, but there is enough concern that an advisory committee will be asked for input on its significance.
The drug’s maker, Forest Laboratories Inc., wants approval of aclidinium bromide for long-term maintenance treatment of bronchospasm from chronic obstructive pulmonary disease, including chronic bronchitis and emphysema. It comes as a dry powder and is dispersed through an inhaler from Almirall SA.
When the FDA’s Pulmonary-Allergy Drugs Advisory Committee considers the product on Feb. 23, the agency wants the panel to discuss the overall safety profile, given the size of the safety database and duration of exposure. The committee also will vote on whether safety has been adequately assessed for the proposed indication.
FDA reviewers identified 10 cardiovascular deaths among patients in aclidinium clinical trials who were treated with the desired 400-mcg dose.
Four of those deaths were caused by cardiac arrest and one was from acute cardiac failure, while only one case of myocardial infarction was reported in patients receiving a 200-mcg dose of aclidinium bromide. None was reported among those receiving placebo. A cardiovascular cause could not be ruled out in two placebo cases, according to FDA documents.
The clinical reviewer said that the significance of the findings is uncertain, but called it "striking" that all the CV deaths in the long-term safety trial were in the 400 mcg–dose group.
Still, the agency said that the incidence rate in the group is lower than would generally be expected in a "real world" COPD population.
"It is difficult to dismiss the apparent imbalance in cardiovascular death between the treatment groups, while at the same time, impossible to conclude that the data represent a true safety signal," the clinical briefing documents conclude.
The size of the safety database was concerning to the FDA. Across all Forest’s trials, 1,471 patients with COPD were exposed to the 400-mcg dose with a mean duration of 211 days, including 733 patients exposed for 182 days or more and 329 exposed for 1 year.
The agency said the size was consistent with international guidelines but was "relatively small compared to the size of programs for other COPD products."
Long-term data combined with additional exposure data suggest that the CV death was possibly dose dependent, the agency said.
"Whether these results represent a spurious finding or a potential safety signal is difficult to discern and may warrant further investigation," the FDA stated.
FDA said the issue is particularly important given the possibility of increased mortality that has been identified with other inhaled anticholinergic agents.
Last year, the FDA ordered large studies of four long-acting beta agonists (LABAs) to assess their safety when used with inhaled corticosteroids versus inhaled corticosteroids alone. It was an outgrowth of a reanalysis of trial data that found LABA use can be associated with severe asthma symptoms, hospitalization, and death.
The FDA said that the reanalysis could be interpreted in different ways and decided new studies were needed.
If the committee decides aclidinium bromide’s safety has not been assessed adequately, it will be asked what other data should be obtained.
Efficacy Data Not Questioned
FDA reviewers did not have any doubts about whether aclidinium bromide’s efficacy had been demonstrated in the three trials that were submitted. The agency said a statistically significant effect compared with placebo was found for the 400-mcg dose, as well as a smaller significant effect for a 200-mcg dose, after 12 weeks of treatment.
The effect from the 400-mcg dose also seemed to persist at week 24 in one of the trials. Subgroup analyses showed effects similar to the overall population, according to FDA briefing documents.
Secondary endpoints such as peak forced expiratory volume in 1 second and rescue medication usage patterns also supported efficacy.
The committee will discuss aclidinium bromide’s efficacy, including its bronchodilatory effect, and vote on whether the efficacy data provide substantial evidence of a clinically meaningful benefit for the 400-mcg dose, which would be given twice daily.
The final voting question asks whether the efficacy and safety data provide substantial evidence for approval.
Forest has proposed the trade name Tudorza Pressair for the pending product.
This coverage is provided courtesy of "The Pink Sheet." Elsevier Global Medical News and "The Pink Sheet" are published by Elsevier.
Persistent cardiovascular events across the clinical trials for aclidinium bromide may not represent a definite safety signal, according to the Food and Drug Administration, but there is enough concern that an advisory committee will be asked for input on its significance.
The drug’s maker, Forest Laboratories Inc., wants approval of aclidinium bromide for long-term maintenance treatment of bronchospasm from chronic obstructive pulmonary disease, including chronic bronchitis and emphysema. It comes as a dry powder and is dispersed through an inhaler from Almirall SA.
When the FDA’s Pulmonary-Allergy Drugs Advisory Committee considers the product on Feb. 23, the agency wants the panel to discuss the overall safety profile, given the size of the safety database and duration of exposure. The committee also will vote on whether safety has been adequately assessed for the proposed indication.
FDA reviewers identified 10 cardiovascular deaths among patients in aclidinium clinical trials who were treated with the desired 400-mcg dose.
Four of those deaths were caused by cardiac arrest and one was from acute cardiac failure, while only one case of myocardial infarction was reported in patients receiving a 200-mcg dose of aclidinium bromide. None was reported among those receiving placebo. A cardiovascular cause could not be ruled out in two placebo cases, according to FDA documents.
The clinical reviewer said that the significance of the findings is uncertain, but called it "striking" that all the CV deaths in the long-term safety trial were in the 400 mcg–dose group.
Still, the agency said that the incidence rate in the group is lower than would generally be expected in a "real world" COPD population.
"It is difficult to dismiss the apparent imbalance in cardiovascular death between the treatment groups, while at the same time, impossible to conclude that the data represent a true safety signal," the clinical briefing documents conclude.
The size of the safety database was concerning to the FDA. Across all Forest’s trials, 1,471 patients with COPD were exposed to the 400-mcg dose with a mean duration of 211 days, including 733 patients exposed for 182 days or more and 329 exposed for 1 year.
The agency said the size was consistent with international guidelines but was "relatively small compared to the size of programs for other COPD products."
Long-term data combined with additional exposure data suggest that the CV death was possibly dose dependent, the agency said.
"Whether these results represent a spurious finding or a potential safety signal is difficult to discern and may warrant further investigation," the FDA stated.
FDA said the issue is particularly important given the possibility of increased mortality that has been identified with other inhaled anticholinergic agents.
Last year, the FDA ordered large studies of four long-acting beta agonists (LABAs) to assess their safety when used with inhaled corticosteroids versus inhaled corticosteroids alone. It was an outgrowth of a reanalysis of trial data that found LABA use can be associated with severe asthma symptoms, hospitalization, and death.
The FDA said that the reanalysis could be interpreted in different ways and decided new studies were needed.
If the committee decides aclidinium bromide’s safety has not been assessed adequately, it will be asked what other data should be obtained.
Efficacy Data Not Questioned
FDA reviewers did not have any doubts about whether aclidinium bromide’s efficacy had been demonstrated in the three trials that were submitted. The agency said a statistically significant effect compared with placebo was found for the 400-mcg dose, as well as a smaller significant effect for a 200-mcg dose, after 12 weeks of treatment.
The effect from the 400-mcg dose also seemed to persist at week 24 in one of the trials. Subgroup analyses showed effects similar to the overall population, according to FDA briefing documents.
Secondary endpoints such as peak forced expiratory volume in 1 second and rescue medication usage patterns also supported efficacy.
The committee will discuss aclidinium bromide’s efficacy, including its bronchodilatory effect, and vote on whether the efficacy data provide substantial evidence of a clinically meaningful benefit for the 400-mcg dose, which would be given twice daily.
The final voting question asks whether the efficacy and safety data provide substantial evidence for approval.
Forest has proposed the trade name Tudorza Pressair for the pending product.
This coverage is provided courtesy of "The Pink Sheet." Elsevier Global Medical News and "The Pink Sheet" are published by Elsevier.
PCV13 Works Best Against Pneumococcal Disease in Adults
The pneumococcal conjugate vaccine, PCV13, may be better in adults than the pneumococcal polysaccharide vaccine, PPSV23, at reducing disease burden because of its potential effectiveness against nonbacteremic pneumococcal pneumonia, according to a report in the Feb. 22/29 issue of JAMA.
PPSV23 covers 23 serotypes while PCV13 covers only 13. However, PPSV23 doesn’t appear to consistently prevent nonbacteremic pneumococcal pneumonia, while PCV13 is more likely to do so, based on preliminary experience.

Because nonbacteremic pneumococcal pneumonia is much more common than invasive pneumococcal disease and is responsible for much more morbidity and mortality, PCV13, despite its narrower serotype coverage, should prevent more pneumococcal disease, reported Dr. Kenneth J. Smith of the section of decision sciences and clinical systems management, University of Pittsburgh, and his associates.
The question of which pneumococcal vaccine to use in adults came to the fore when the Food and Drug Administration recently approved the use of PCV13 in patients aged 50 years and older. Dr. Smith and his colleagues used decision statistical modeling techniques to estimate the cost effectiveness of six different possible pneumococcal vaccine strategies in identical hypothetical cohorts of adults aged 50 and older who were tracked as they aged.
The six strategies were no vaccination, the present U.S. Advisory Committee on Immunization Practices recommendation to vaccinate all adults with PPSV23 at age 65, substituting PCV13 for PPSV23 and vaccinating according to the ACIP recommendations, vaccinating with PCV13 at age 50 and with PPSV23 at age 65, vaccinating with PCV13 at ages 50 and 65 years, and vaccinating with PCV13 at ages 50 and 65, then with PPSV23 at age 75.
The models took into consideration the potential effects of herd immunity, different levels of patient risk of contracting pneumococcal disease, different levels of vaccine effectiveness based on patient age and comorbidity, and three different outcomes after pneumococcal infection: death, disability, or recovery.
"Our analysis favors vaccinating adults with PCV13 instead of PPSV23," chiefly because experts expect that PCV13 will be more effective against nonbacteremic pneumococcal pneumonia than PPSV23 appears to be, the researchers said.
Moreover, the data "suggest that PCV13 administered either as a substitute for PPSV23 [according to] current recommendations or [given] routinely at ages 50 and 65 years might reduce pneumococcal disease burden in an economically reasonable fashion," Dr. Smith and his colleagues wrote (JAMA 2012;307:804-12).
According to their models, substituting PCV13 for PPSV23 would cost $28,900 per quality-adjusted life-year, while staying with PPSV23 would cost $34,000 per quality-adjusted life-year. Even giving PCV13 at age 50 and again at age 65, which would cost $45,100 per quality-adjusted life-year, would still be cost effective, they noted.
However, the study results would not hold true if PCV13’s effectiveness against nonbacteremic pneumococcal pneumonia proves to have been overestimated. If it turns out that PCV13 is not very effective against nonbacteremic pneumococcal pneumonia, then the current PPSV23 recommendations would be superior, the investigators said.
Similarly, the results of this study would not hold true if it turns out that childhood vaccination with PCV13, which has only recently begun, substantially changes herd immunity, reducing disease rates in adults.
This study was supported by the National Institute of Allergy and Infectious Diseases. No relevant financial disclosures were reported among the study’s authors.
“Although the
results of the cost-effectiveness analysis by Smith et al. are robust for most variables
in the model, the findings are vulnerable to estimates of two key parameters
about which there is still considerable uncertainty,” said Dr. Eugene D. Shapiro.
The first unknown is whether
PCV13 will be effective against nonbacteremic pneumococcal pneumonia (NPP). “A
large clinical trial is being conducted ... to try to answer this question, but
because of the difficulty of diagnosing NPP, it is not clear that a definitive
answer will be forthcoming.”
The second key unknown is
how the recent introduction of the PCV13 among children will affect herd
immunity, and thus how it will affect adults’ risks.
“As often happens, policy
makers likely will need to decide whether to recommend a change in the strategy
for immunization of adults in the absence of definitive data on all values that
contribute to analysis of the potential cost effectiveness of a change in
policy.” The analysis by Dr. Smith and his colleagues provides “a reasonable
framework with which to approach this issue. However, if recommendations are
made to switch to PCV13 for adults, the degree to which subsequent decreases in
rates of both invasive pneumococcal infections and NPP among adults are due to
a switch to PCV13 for adults or to the already-implemented administration of PCV13
to children might never be known.”
DR. SHAPIRO is in the departments of pediatrics, epidemiology, and investigative medicine at Yale University, New Haven, Conn. He reported haing no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Smith's report (JAMA 2012;307:847-9).
“Although the
results of the cost-effectiveness analysis by Smith et al. are robust for most variables
in the model, the findings are vulnerable to estimates of two key parameters
about which there is still considerable uncertainty,” said Dr. Eugene D. Shapiro.
The first unknown is whether
PCV13 will be effective against nonbacteremic pneumococcal pneumonia (NPP). “A
large clinical trial is being conducted ... to try to answer this question, but
because of the difficulty of diagnosing NPP, it is not clear that a definitive
answer will be forthcoming.”
The second key unknown is
how the recent introduction of the PCV13 among children will affect herd
immunity, and thus how it will affect adults’ risks.
“As often happens, policy
makers likely will need to decide whether to recommend a change in the strategy
for immunization of adults in the absence of definitive data on all values that
contribute to analysis of the potential cost effectiveness of a change in
policy.” The analysis by Dr. Smith and his colleagues provides “a reasonable
framework with which to approach this issue. However, if recommendations are
made to switch to PCV13 for adults, the degree to which subsequent decreases in
rates of both invasive pneumococcal infections and NPP among adults are due to
a switch to PCV13 for adults or to the already-implemented administration of PCV13
to children might never be known.”
DR. SHAPIRO is in the departments of pediatrics, epidemiology, and investigative medicine at Yale University, New Haven, Conn. He reported haing no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Smith's report (JAMA 2012;307:847-9).
“Although the
results of the cost-effectiveness analysis by Smith et al. are robust for most variables
in the model, the findings are vulnerable to estimates of two key parameters
about which there is still considerable uncertainty,” said Dr. Eugene D. Shapiro.
The first unknown is whether
PCV13 will be effective against nonbacteremic pneumococcal pneumonia (NPP). “A
large clinical trial is being conducted ... to try to answer this question, but
because of the difficulty of diagnosing NPP, it is not clear that a definitive
answer will be forthcoming.”
The second key unknown is
how the recent introduction of the PCV13 among children will affect herd
immunity, and thus how it will affect adults’ risks.
“As often happens, policy
makers likely will need to decide whether to recommend a change in the strategy
for immunization of adults in the absence of definitive data on all values that
contribute to analysis of the potential cost effectiveness of a change in
policy.” The analysis by Dr. Smith and his colleagues provides “a reasonable
framework with which to approach this issue. However, if recommendations are
made to switch to PCV13 for adults, the degree to which subsequent decreases in
rates of both invasive pneumococcal infections and NPP among adults are due to
a switch to PCV13 for adults or to the already-implemented administration of PCV13
to children might never be known.”
DR. SHAPIRO is in the departments of pediatrics, epidemiology, and investigative medicine at Yale University, New Haven, Conn. He reported haing no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Smith's report (JAMA 2012;307:847-9).
The pneumococcal conjugate vaccine, PCV13, may be better in adults than the pneumococcal polysaccharide vaccine, PPSV23, at reducing disease burden because of its potential effectiveness against nonbacteremic pneumococcal pneumonia, according to a report in the Feb. 22/29 issue of JAMA.
PPSV23 covers 23 serotypes while PCV13 covers only 13. However, PPSV23 doesn’t appear to consistently prevent nonbacteremic pneumococcal pneumonia, while PCV13 is more likely to do so, based on preliminary experience.
Because nonbacteremic pneumococcal pneumonia is much more common than invasive pneumococcal disease and is responsible for much more morbidity and mortality, PCV13, despite its narrower serotype coverage, should prevent more pneumococcal disease, reported Dr. Kenneth J. Smith of the section of decision sciences and clinical systems management, University of Pittsburgh, and his associates.
The question of which pneumococcal vaccine to use in adults came to the fore when the Food and Drug Administration recently approved the use of PCV13 in patients aged 50 years and older. Dr. Smith and his colleagues used decision statistical modeling techniques to estimate the cost effectiveness of six different possible pneumococcal vaccine strategies in identical hypothetical cohorts of adults aged 50 and older who were tracked as they aged.
The six strategies were no vaccination, the present U.S. Advisory Committee on Immunization Practices recommendation to vaccinate all adults with PPSV23 at age 65, substituting PCV13 for PPSV23 and vaccinating according to the ACIP recommendations, vaccinating with PCV13 at age 50 and with PPSV23 at age 65, vaccinating with PCV13 at ages 50 and 65 years, and vaccinating with PCV13 at ages 50 and 65, then with PPSV23 at age 75.
The models took into consideration the potential effects of herd immunity, different levels of patient risk of contracting pneumococcal disease, different levels of vaccine effectiveness based on patient age and comorbidity, and three different outcomes after pneumococcal infection: death, disability, or recovery.
"Our analysis favors vaccinating adults with PCV13 instead of PPSV23," chiefly because experts expect that PCV13 will be more effective against nonbacteremic pneumococcal pneumonia than PPSV23 appears to be, the researchers said.
Moreover, the data "suggest that PCV13 administered either as a substitute for PPSV23 [according to] current recommendations or [given] routinely at ages 50 and 65 years might reduce pneumococcal disease burden in an economically reasonable fashion," Dr. Smith and his colleagues wrote (JAMA 2012;307:804-12).
According to their models, substituting PCV13 for PPSV23 would cost $28,900 per quality-adjusted life-year, while staying with PPSV23 would cost $34,000 per quality-adjusted life-year. Even giving PCV13 at age 50 and again at age 65, which would cost $45,100 per quality-adjusted life-year, would still be cost effective, they noted.
However, the study results would not hold true if PCV13’s effectiveness against nonbacteremic pneumococcal pneumonia proves to have been overestimated. If it turns out that PCV13 is not very effective against nonbacteremic pneumococcal pneumonia, then the current PPSV23 recommendations would be superior, the investigators said.
Similarly, the results of this study would not hold true if it turns out that childhood vaccination with PCV13, which has only recently begun, substantially changes herd immunity, reducing disease rates in adults.
This study was supported by the National Institute of Allergy and Infectious Diseases. No relevant financial disclosures were reported among the study’s authors.
The pneumococcal conjugate vaccine, PCV13, may be better in adults than the pneumococcal polysaccharide vaccine, PPSV23, at reducing disease burden because of its potential effectiveness against nonbacteremic pneumococcal pneumonia, according to a report in the Feb. 22/29 issue of JAMA.
PPSV23 covers 23 serotypes while PCV13 covers only 13. However, PPSV23 doesn’t appear to consistently prevent nonbacteremic pneumococcal pneumonia, while PCV13 is more likely to do so, based on preliminary experience.
Because nonbacteremic pneumococcal pneumonia is much more common than invasive pneumococcal disease and is responsible for much more morbidity and mortality, PCV13, despite its narrower serotype coverage, should prevent more pneumococcal disease, reported Dr. Kenneth J. Smith of the section of decision sciences and clinical systems management, University of Pittsburgh, and his associates.
The question of which pneumococcal vaccine to use in adults came to the fore when the Food and Drug Administration recently approved the use of PCV13 in patients aged 50 years and older. Dr. Smith and his colleagues used decision statistical modeling techniques to estimate the cost effectiveness of six different possible pneumococcal vaccine strategies in identical hypothetical cohorts of adults aged 50 and older who were tracked as they aged.
The six strategies were no vaccination, the present U.S. Advisory Committee on Immunization Practices recommendation to vaccinate all adults with PPSV23 at age 65, substituting PCV13 for PPSV23 and vaccinating according to the ACIP recommendations, vaccinating with PCV13 at age 50 and with PPSV23 at age 65, vaccinating with PCV13 at ages 50 and 65 years, and vaccinating with PCV13 at ages 50 and 65, then with PPSV23 at age 75.
The models took into consideration the potential effects of herd immunity, different levels of patient risk of contracting pneumococcal disease, different levels of vaccine effectiveness based on patient age and comorbidity, and three different outcomes after pneumococcal infection: death, disability, or recovery.
"Our analysis favors vaccinating adults with PCV13 instead of PPSV23," chiefly because experts expect that PCV13 will be more effective against nonbacteremic pneumococcal pneumonia than PPSV23 appears to be, the researchers said.
Moreover, the data "suggest that PCV13 administered either as a substitute for PPSV23 [according to] current recommendations or [given] routinely at ages 50 and 65 years might reduce pneumococcal disease burden in an economically reasonable fashion," Dr. Smith and his colleagues wrote (JAMA 2012;307:804-12).
According to their models, substituting PCV13 for PPSV23 would cost $28,900 per quality-adjusted life-year, while staying with PPSV23 would cost $34,000 per quality-adjusted life-year. Even giving PCV13 at age 50 and again at age 65, which would cost $45,100 per quality-adjusted life-year, would still be cost effective, they noted.
However, the study results would not hold true if PCV13’s effectiveness against nonbacteremic pneumococcal pneumonia proves to have been overestimated. If it turns out that PCV13 is not very effective against nonbacteremic pneumococcal pneumonia, then the current PPSV23 recommendations would be superior, the investigators said.
Similarly, the results of this study would not hold true if it turns out that childhood vaccination with PCV13, which has only recently begun, substantially changes herd immunity, reducing disease rates in adults.
This study was supported by the National Institute of Allergy and Infectious Diseases. No relevant financial disclosures were reported among the study’s authors.
FROM JAMA
Major Finding:
Substituting PCV13 for PPSV23 would cost $28,900 per quality-adjusted
life-year, while staying with PPSV23 would cost $34,000 per quality-adjusted
life-year.
Data Source: This
was an analysis of statistical models predicting the effectiveness and costs of
enacting six different vaccination strategies in identical hypothetical cohorts
of adults aged 50 and older.
Disclosures: The
study was supported by the National Institute
of Allergy and Infectious
Diseases. No relevant financial disclosures were reported among the study’s
authors.
Quality of Dyspnea Directs Diagnosis, Management
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.

For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.
For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.
For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Early Strides Made in Personalized Refractory Asthma Care
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."

Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
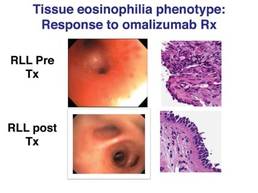
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Major Finding: Six phenotypes have been identified using bronchoscopy and a supraglottic index that can be used to evaluate and direct therapy for refractory asthma.
Data Source: Data were taken from an observational treatment study of 58 patients with difficult to treat, refractory asthma.
Disclosures: Dr. Martin and his coauthors reported no relevant conflicts of interest.
Extended-Release Gabapentin an Option for Augmentation in RLS
PHOENIX – Sometimes, treating restless legs syndrome with dopaminergic agents can make the problem worse.
After months of use, patients might report that they still have symptoms in their calves, and now also in their thighs and arms, and not just at bedtime.
"It’s pretty dreadful when you see it. It happens as soon as they sit down in the evening. It might be much more intense than before," said Dr. Barbara A. Phillips a professor of medicine at the University of Kentucky, Lexington, and medical director of the school’s sleep disorders center.
The phenomena, known as augmentation, probably occurs in "something like 80%" of RLS patients treated with carbidopa-levodopa (Sinemet) nightly, and maybe up to 20% treated with pramipexole (Mirapex) and ropinirole (Requip), she said.
"The bad news is that it’s pretty common. The good news is there’s never been a case report that it didn’t go away when the drug was stopped," said Dr. Phillips, who is also the current president of the Sleep Institute of the American College of Chest Physicians.
Studies on how to manage augmentation are lacking, "but if [patients] are on Sinemet, stop it, and don’t ever use it again. If they’re on pramipexole, you could try switching them to ropinirole. If augmentation happens earlier in the day, you could split the dose and give them an earlier dose. Your strategy really has to be tailored to how the augmentation presents," she said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
Following its recent Food and Drug Administration approval for RLS, patients could also be switched to extended-release gabapentin (Horizant), an anticonvulsant, not a dopamine agonist, "but I can’t point to any science" supporting the move; "What I’m telling you here is opinion," Dr. Phillips said.
Compulsive behaviors – overeating, hair eating, gambling, and spree shopping, for instance – can also be a problem with dopaminergic agents at RLS doses. "If you’re going to use these agents, patients need to be asked ... and warned about such behaviors," she said.
Ropinirole and pramipexole must be titrated to effect; nausea is usually the limiting factor. Dr. Phillips and her colleagues typically start ropinirole patients on 0.5 mg and then titrate up every 3-6 days. In clinical trials, the average dosage was about 2 mg/day. "Sometimes, patients don’t think it’s helping, but often that’s because they’re still on 0.5 mg, which is probably not enough, or they are taking it right at bedtime," instead of 1-2 hours before bed, as required with dopaminergic RLS treatment.
Pramipexole is more potent, "so start at 0.125 mg and titrate up every 3-5 days," Dr. Phillips said. The average dosage in therapeutic trials was 0.25 mg/day, she added.
Ropinirole is hepatically metabolized and might be a good choice for people with renal failure. Pramipexole is renally excreted and might be the way to go for liver failure patients or those on other drugs metabolized by the liver.
Unlike ropinirole and pramipexole, levodopa does not carry an FDA indication for RLS, but is, nonetheless, effective. It can also cause nausea, but doesn’t have to be titrated and can be used as needed, making it a good option for people with infrequent attacks.
"Some people can predict they are going to have RLS if they are going to go out to dinner, have a glass of wine, sit in a small chair in the front row of the opera, and stay up late. But that’s only going to happen four times a year. They may not want to take a drug that has to be titrated and taken every night in order to deal with" an intermittent problem, she said.
Extended-release gabapentin is not associated with compulsive behaviors, but it’s expensive and likely associated with drowsiness at the 600-mg daily RLS dose. "And remember, all anticonvulsants carry various suicide warnings," Dr. Phillips said.
Dr. Phillips disclosed that she has been a speaker or consultant for groups funded by Cephalon, ResMed, and Respironics.
PHOENIX – Sometimes, treating restless legs syndrome with dopaminergic agents can make the problem worse.
After months of use, patients might report that they still have symptoms in their calves, and now also in their thighs and arms, and not just at bedtime.
"It’s pretty dreadful when you see it. It happens as soon as they sit down in the evening. It might be much more intense than before," said Dr. Barbara A. Phillips a professor of medicine at the University of Kentucky, Lexington, and medical director of the school’s sleep disorders center.
The phenomena, known as augmentation, probably occurs in "something like 80%" of RLS patients treated with carbidopa-levodopa (Sinemet) nightly, and maybe up to 20% treated with pramipexole (Mirapex) and ropinirole (Requip), she said.
"The bad news is that it’s pretty common. The good news is there’s never been a case report that it didn’t go away when the drug was stopped," said Dr. Phillips, who is also the current president of the Sleep Institute of the American College of Chest Physicians.
Studies on how to manage augmentation are lacking, "but if [patients] are on Sinemet, stop it, and don’t ever use it again. If they’re on pramipexole, you could try switching them to ropinirole. If augmentation happens earlier in the day, you could split the dose and give them an earlier dose. Your strategy really has to be tailored to how the augmentation presents," she said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
Following its recent Food and Drug Administration approval for RLS, patients could also be switched to extended-release gabapentin (Horizant), an anticonvulsant, not a dopamine agonist, "but I can’t point to any science" supporting the move; "What I’m telling you here is opinion," Dr. Phillips said.
Compulsive behaviors – overeating, hair eating, gambling, and spree shopping, for instance – can also be a problem with dopaminergic agents at RLS doses. "If you’re going to use these agents, patients need to be asked ... and warned about such behaviors," she said.
Ropinirole and pramipexole must be titrated to effect; nausea is usually the limiting factor. Dr. Phillips and her colleagues typically start ropinirole patients on 0.5 mg and then titrate up every 3-6 days. In clinical trials, the average dosage was about 2 mg/day. "Sometimes, patients don’t think it’s helping, but often that’s because they’re still on 0.5 mg, which is probably not enough, or they are taking it right at bedtime," instead of 1-2 hours before bed, as required with dopaminergic RLS treatment.
Pramipexole is more potent, "so start at 0.125 mg and titrate up every 3-5 days," Dr. Phillips said. The average dosage in therapeutic trials was 0.25 mg/day, she added.
Ropinirole is hepatically metabolized and might be a good choice for people with renal failure. Pramipexole is renally excreted and might be the way to go for liver failure patients or those on other drugs metabolized by the liver.
Unlike ropinirole and pramipexole, levodopa does not carry an FDA indication for RLS, but is, nonetheless, effective. It can also cause nausea, but doesn’t have to be titrated and can be used as needed, making it a good option for people with infrequent attacks.
"Some people can predict they are going to have RLS if they are going to go out to dinner, have a glass of wine, sit in a small chair in the front row of the opera, and stay up late. But that’s only going to happen four times a year. They may not want to take a drug that has to be titrated and taken every night in order to deal with" an intermittent problem, she said.
Extended-release gabapentin is not associated with compulsive behaviors, but it’s expensive and likely associated with drowsiness at the 600-mg daily RLS dose. "And remember, all anticonvulsants carry various suicide warnings," Dr. Phillips said.
Dr. Phillips disclosed that she has been a speaker or consultant for groups funded by Cephalon, ResMed, and Respironics.
PHOENIX – Sometimes, treating restless legs syndrome with dopaminergic agents can make the problem worse.
After months of use, patients might report that they still have symptoms in their calves, and now also in their thighs and arms, and not just at bedtime.
"It’s pretty dreadful when you see it. It happens as soon as they sit down in the evening. It might be much more intense than before," said Dr. Barbara A. Phillips a professor of medicine at the University of Kentucky, Lexington, and medical director of the school’s sleep disorders center.
The phenomena, known as augmentation, probably occurs in "something like 80%" of RLS patients treated with carbidopa-levodopa (Sinemet) nightly, and maybe up to 20% treated with pramipexole (Mirapex) and ropinirole (Requip), she said.
"The bad news is that it’s pretty common. The good news is there’s never been a case report that it didn’t go away when the drug was stopped," said Dr. Phillips, who is also the current president of the Sleep Institute of the American College of Chest Physicians.
Studies on how to manage augmentation are lacking, "but if [patients] are on Sinemet, stop it, and don’t ever use it again. If they’re on pramipexole, you could try switching them to ropinirole. If augmentation happens earlier in the day, you could split the dose and give them an earlier dose. Your strategy really has to be tailored to how the augmentation presents," she said at a meeting on sleep medicine sponsored by the American College of Chest Physicians.
Following its recent Food and Drug Administration approval for RLS, patients could also be switched to extended-release gabapentin (Horizant), an anticonvulsant, not a dopamine agonist, "but I can’t point to any science" supporting the move; "What I’m telling you here is opinion," Dr. Phillips said.
Compulsive behaviors – overeating, hair eating, gambling, and spree shopping, for instance – can also be a problem with dopaminergic agents at RLS doses. "If you’re going to use these agents, patients need to be asked ... and warned about such behaviors," she said.
Ropinirole and pramipexole must be titrated to effect; nausea is usually the limiting factor. Dr. Phillips and her colleagues typically start ropinirole patients on 0.5 mg and then titrate up every 3-6 days. In clinical trials, the average dosage was about 2 mg/day. "Sometimes, patients don’t think it’s helping, but often that’s because they’re still on 0.5 mg, which is probably not enough, or they are taking it right at bedtime," instead of 1-2 hours before bed, as required with dopaminergic RLS treatment.
Pramipexole is more potent, "so start at 0.125 mg and titrate up every 3-5 days," Dr. Phillips said. The average dosage in therapeutic trials was 0.25 mg/day, she added.
Ropinirole is hepatically metabolized and might be a good choice for people with renal failure. Pramipexole is renally excreted and might be the way to go for liver failure patients or those on other drugs metabolized by the liver.
Unlike ropinirole and pramipexole, levodopa does not carry an FDA indication for RLS, but is, nonetheless, effective. It can also cause nausea, but doesn’t have to be titrated and can be used as needed, making it a good option for people with infrequent attacks.
"Some people can predict they are going to have RLS if they are going to go out to dinner, have a glass of wine, sit in a small chair in the front row of the opera, and stay up late. But that’s only going to happen four times a year. They may not want to take a drug that has to be titrated and taken every night in order to deal with" an intermittent problem, she said.
Extended-release gabapentin is not associated with compulsive behaviors, but it’s expensive and likely associated with drowsiness at the 600-mg daily RLS dose. "And remember, all anticonvulsants carry various suicide warnings," Dr. Phillips said.
Dr. Phillips disclosed that she has been a speaker or consultant for groups funded by Cephalon, ResMed, and Respironics.
FROM A MEETING ON SLEEP MEDICINE SPONSORED BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Prophylactic Semuloparin Cuts Rate of VTE in Cancer Patients
Semuloparin, an ultralow-molecular-weight heparin, reduced the incidence of venous thromboembolic events when given prophylactically to patients with a variety of metastatic or locally advanced solid tumors, according to a report in the Feb. 16 issue of the New England Journal of Medicine.
Semuloparin prevented both deep vein thrombosis and pulmonary embolism (PE) without raising the risk of major bleeding in patients undergoing chemotherapy for lung, pancreatic, stomach, colon, rectal, bladder, or ovarian cancer. It did not improve overall survival, however, said Dr. Giancarlo Agnelli of the department of internal medicine at the University of Perugia (Italy) and his associates.

The investigators assessed the safety and efficacy of semuloparin because this patient population has a high incidence of venous thromboembolism (VTE). They conducted the SAVE-ONCO trial (NCT00694382), which was sponsored by semuloparin’s manufacturer, Sanofi-Aventis, at 395 medical centers in 47 countries.
A total of 3,212 patients were randomly assigned to receive daily subcutaneous injections of either semuloparin (1,608 patients) or placebo (1,604 patients), beginning on the first day of chemotherapy and continuing until chemotherapy was stopped or changed to a different regimen. The concomitant use of antiplatelet agents and nonsteroidal anti-inflammatory drugs (NSAIDs) was permitted at the treating physician’s discretion.
The mean duration of treatment was 3.5 months. The reasons for discontinuing treatment were similar between patients receiving semuloparin and those receiving placebo – chiefly adverse events (15.9% and 17.5%, respectively) and the patient’s request to discontinue treatment (18.1% and 17.4%, respectively).
The primary efficacy outcome – a composite end point of any symptomatic deep vein thrombosis in the lower or upper limbs, any nonfatal pulmonary embolism, or death related to VTE – occurred in 1.2% of the semuloparin group, a significantly lower rate than the 3.4% rate in the placebo group.
Semuloparin significantly reduced the incidence of deep vein thrombosis, fatal PE, and nonfatal PE. This benefit was seen across all groups of patients categorized by cancer stage, cancer site, and geographic region, Dr. Agnelli and his colleagues reported (N. Engl. J. Med. 2012;366:601-9).
The treatment benefit also was consistent across numerous baseline risks for VTE, such as personal or family history of VTE; use of a central venous catheter; obesity; age of 75 years or more; presence of chronic respiratory or heart failure; presence of venous insufficiency or varicose veins; and use of hormone therapy.
However, semuloparin did not improve overall survival. Mortality was 43.4% in the semuloparin group and 44.5% in the placebo group.
The overall rate of major and clinically relevant nonmajor bleeding was 2.8% with semuloparin and 2.0% with placebo, a nonsignificant difference. Two fatal bleeding events occurred with semuloparin and four with placebo. "Five episodes of nonfatal bleeding in a critical area or organ were noted, all in the semuloparin group," the researchers said.
Serious adverse events developed in 26.3% of patients taking semuloparin and 25.5% of those taking placebo, a nonsignificant difference. In particular, there were no cases of heparin-induced thrombocytopenia, and the rates of thrombocytopenia were comparable between the semuloparin and placebo groups (7.1% and 7.6%, respectively).
"Current guidelines recommend antithrombotic prophylaxis for patients with cancer who are admitted to the hospital for medical illness (administered for the duration of the hospital stay) and for patients who have undergone surgery for cancer (extended for up to 5 weeks) but not for routine use in ambulatory patients receiving chemotherapy. This study suggests a benefit from antithrombotic prophylaxis with semuloparin in patients receiving chemotherapy for cancer," Dr. Agnelli and his associates said.
This study was supported by Sanofi, manufacturer of semuloparin. Dr. Agnelli and his associates reported ties to numerous industry sources.
The findings by Agnelli et al. indicate that many cancer patients "can probably avert hospitalization for deep vein thrombosis and pulmonary embolism and might live longer, if they accept an increased risk of bleeding and its subsequent treatment," said Dr. Elie A. Aki and Dr. Holger J. Schünemann.
According to the SAVE-ONCO data, if 1,000 cancer patients used a prophylactic dose of ultralow-molecular-weight heparin, "over a period of 12 months death would be averted in approximately 30 patients, venous thromboembolism would be averted in 20, and 1 would have a major bleeding episode," they noted.
Elie A. Akl, M.D., Ph.D., is in the department of medicine, State University of New York at Buffalo, and the departments of clinical epidemiology and biostatistics at McMaster University, Hamilton, Ont. Holger J. Schünemann, M.D., Ph.D., is in the departments of medicine and clinical epidemiology and biostatistics at McMaster University. They reported no relevant financial conflicts of interest. These remarks were taken from their editorial accompanying the report of Dr. Agnelli and his colleagues (N. Engl. J. Med. 2012;366:661-2).
The findings by Agnelli et al. indicate that many cancer patients "can probably avert hospitalization for deep vein thrombosis and pulmonary embolism and might live longer, if they accept an increased risk of bleeding and its subsequent treatment," said Dr. Elie A. Aki and Dr. Holger J. Schünemann.
According to the SAVE-ONCO data, if 1,000 cancer patients used a prophylactic dose of ultralow-molecular-weight heparin, "over a period of 12 months death would be averted in approximately 30 patients, venous thromboembolism would be averted in 20, and 1 would have a major bleeding episode," they noted.
Elie A. Akl, M.D., Ph.D., is in the department of medicine, State University of New York at Buffalo, and the departments of clinical epidemiology and biostatistics at McMaster University, Hamilton, Ont. Holger J. Schünemann, M.D., Ph.D., is in the departments of medicine and clinical epidemiology and biostatistics at McMaster University. They reported no relevant financial conflicts of interest. These remarks were taken from their editorial accompanying the report of Dr. Agnelli and his colleagues (N. Engl. J. Med. 2012;366:661-2).
The findings by Agnelli et al. indicate that many cancer patients "can probably avert hospitalization for deep vein thrombosis and pulmonary embolism and might live longer, if they accept an increased risk of bleeding and its subsequent treatment," said Dr. Elie A. Aki and Dr. Holger J. Schünemann.
According to the SAVE-ONCO data, if 1,000 cancer patients used a prophylactic dose of ultralow-molecular-weight heparin, "over a period of 12 months death would be averted in approximately 30 patients, venous thromboembolism would be averted in 20, and 1 would have a major bleeding episode," they noted.
Elie A. Akl, M.D., Ph.D., is in the department of medicine, State University of New York at Buffalo, and the departments of clinical epidemiology and biostatistics at McMaster University, Hamilton, Ont. Holger J. Schünemann, M.D., Ph.D., is in the departments of medicine and clinical epidemiology and biostatistics at McMaster University. They reported no relevant financial conflicts of interest. These remarks were taken from their editorial accompanying the report of Dr. Agnelli and his colleagues (N. Engl. J. Med. 2012;366:661-2).
Semuloparin, an ultralow-molecular-weight heparin, reduced the incidence of venous thromboembolic events when given prophylactically to patients with a variety of metastatic or locally advanced solid tumors, according to a report in the Feb. 16 issue of the New England Journal of Medicine.
Semuloparin prevented both deep vein thrombosis and pulmonary embolism (PE) without raising the risk of major bleeding in patients undergoing chemotherapy for lung, pancreatic, stomach, colon, rectal, bladder, or ovarian cancer. It did not improve overall survival, however, said Dr. Giancarlo Agnelli of the department of internal medicine at the University of Perugia (Italy) and his associates.
The investigators assessed the safety and efficacy of semuloparin because this patient population has a high incidence of venous thromboembolism (VTE). They conducted the SAVE-ONCO trial (NCT00694382), which was sponsored by semuloparin’s manufacturer, Sanofi-Aventis, at 395 medical centers in 47 countries.
A total of 3,212 patients were randomly assigned to receive daily subcutaneous injections of either semuloparin (1,608 patients) or placebo (1,604 patients), beginning on the first day of chemotherapy and continuing until chemotherapy was stopped or changed to a different regimen. The concomitant use of antiplatelet agents and nonsteroidal anti-inflammatory drugs (NSAIDs) was permitted at the treating physician’s discretion.
The mean duration of treatment was 3.5 months. The reasons for discontinuing treatment were similar between patients receiving semuloparin and those receiving placebo – chiefly adverse events (15.9% and 17.5%, respectively) and the patient’s request to discontinue treatment (18.1% and 17.4%, respectively).
The primary efficacy outcome – a composite end point of any symptomatic deep vein thrombosis in the lower or upper limbs, any nonfatal pulmonary embolism, or death related to VTE – occurred in 1.2% of the semuloparin group, a significantly lower rate than the 3.4% rate in the placebo group.
Semuloparin significantly reduced the incidence of deep vein thrombosis, fatal PE, and nonfatal PE. This benefit was seen across all groups of patients categorized by cancer stage, cancer site, and geographic region, Dr. Agnelli and his colleagues reported (N. Engl. J. Med. 2012;366:601-9).
The treatment benefit also was consistent across numerous baseline risks for VTE, such as personal or family history of VTE; use of a central venous catheter; obesity; age of 75 years or more; presence of chronic respiratory or heart failure; presence of venous insufficiency or varicose veins; and use of hormone therapy.
However, semuloparin did not improve overall survival. Mortality was 43.4% in the semuloparin group and 44.5% in the placebo group.
The overall rate of major and clinically relevant nonmajor bleeding was 2.8% with semuloparin and 2.0% with placebo, a nonsignificant difference. Two fatal bleeding events occurred with semuloparin and four with placebo. "Five episodes of nonfatal bleeding in a critical area or organ were noted, all in the semuloparin group," the researchers said.
Serious adverse events developed in 26.3% of patients taking semuloparin and 25.5% of those taking placebo, a nonsignificant difference. In particular, there were no cases of heparin-induced thrombocytopenia, and the rates of thrombocytopenia were comparable between the semuloparin and placebo groups (7.1% and 7.6%, respectively).
"Current guidelines recommend antithrombotic prophylaxis for patients with cancer who are admitted to the hospital for medical illness (administered for the duration of the hospital stay) and for patients who have undergone surgery for cancer (extended for up to 5 weeks) but not for routine use in ambulatory patients receiving chemotherapy. This study suggests a benefit from antithrombotic prophylaxis with semuloparin in patients receiving chemotherapy for cancer," Dr. Agnelli and his associates said.
This study was supported by Sanofi, manufacturer of semuloparin. Dr. Agnelli and his associates reported ties to numerous industry sources.
Semuloparin, an ultralow-molecular-weight heparin, reduced the incidence of venous thromboembolic events when given prophylactically to patients with a variety of metastatic or locally advanced solid tumors, according to a report in the Feb. 16 issue of the New England Journal of Medicine.
Semuloparin prevented both deep vein thrombosis and pulmonary embolism (PE) without raising the risk of major bleeding in patients undergoing chemotherapy for lung, pancreatic, stomach, colon, rectal, bladder, or ovarian cancer. It did not improve overall survival, however, said Dr. Giancarlo Agnelli of the department of internal medicine at the University of Perugia (Italy) and his associates.
The investigators assessed the safety and efficacy of semuloparin because this patient population has a high incidence of venous thromboembolism (VTE). They conducted the SAVE-ONCO trial (NCT00694382), which was sponsored by semuloparin’s manufacturer, Sanofi-Aventis, at 395 medical centers in 47 countries.
A total of 3,212 patients were randomly assigned to receive daily subcutaneous injections of either semuloparin (1,608 patients) or placebo (1,604 patients), beginning on the first day of chemotherapy and continuing until chemotherapy was stopped or changed to a different regimen. The concomitant use of antiplatelet agents and nonsteroidal anti-inflammatory drugs (NSAIDs) was permitted at the treating physician’s discretion.
The mean duration of treatment was 3.5 months. The reasons for discontinuing treatment were similar between patients receiving semuloparin and those receiving placebo – chiefly adverse events (15.9% and 17.5%, respectively) and the patient’s request to discontinue treatment (18.1% and 17.4%, respectively).
The primary efficacy outcome – a composite end point of any symptomatic deep vein thrombosis in the lower or upper limbs, any nonfatal pulmonary embolism, or death related to VTE – occurred in 1.2% of the semuloparin group, a significantly lower rate than the 3.4% rate in the placebo group.
Semuloparin significantly reduced the incidence of deep vein thrombosis, fatal PE, and nonfatal PE. This benefit was seen across all groups of patients categorized by cancer stage, cancer site, and geographic region, Dr. Agnelli and his colleagues reported (N. Engl. J. Med. 2012;366:601-9).
The treatment benefit also was consistent across numerous baseline risks for VTE, such as personal or family history of VTE; use of a central venous catheter; obesity; age of 75 years or more; presence of chronic respiratory or heart failure; presence of venous insufficiency or varicose veins; and use of hormone therapy.
However, semuloparin did not improve overall survival. Mortality was 43.4% in the semuloparin group and 44.5% in the placebo group.
The overall rate of major and clinically relevant nonmajor bleeding was 2.8% with semuloparin and 2.0% with placebo, a nonsignificant difference. Two fatal bleeding events occurred with semuloparin and four with placebo. "Five episodes of nonfatal bleeding in a critical area or organ were noted, all in the semuloparin group," the researchers said.
Serious adverse events developed in 26.3% of patients taking semuloparin and 25.5% of those taking placebo, a nonsignificant difference. In particular, there were no cases of heparin-induced thrombocytopenia, and the rates of thrombocytopenia were comparable between the semuloparin and placebo groups (7.1% and 7.6%, respectively).
"Current guidelines recommend antithrombotic prophylaxis for patients with cancer who are admitted to the hospital for medical illness (administered for the duration of the hospital stay) and for patients who have undergone surgery for cancer (extended for up to 5 weeks) but not for routine use in ambulatory patients receiving chemotherapy. This study suggests a benefit from antithrombotic prophylaxis with semuloparin in patients receiving chemotherapy for cancer," Dr. Agnelli and his associates said.
This study was supported by Sanofi, manufacturer of semuloparin. Dr. Agnelli and his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: VTE occurred in 1.2% of cancer patients taking semuloparin, which was significantly lower than the 3.4% rate in the placebo group.
Data Source: SAVE-ONCO was a double-blind, international clinical trial comparing 3 months of daily subcutaneous injections of semuloparin against placebo in 3,212 patients who were undergoing a broad range of chemotherapy regimens for a variety of tumors.
Disclosures: This study was supported by Sanofi, manufacturer of semuloparin. Dr. Agnelli and his associates reported ties to numerous industry sources.