User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
ARDS Outcome Linked to Oxygenation at 48 Hours
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
FROM THE ANNUAL CONGRESS OF THE SOCIETY OF CRITICAL CARE MEDICINE
Major Finding: The mortality of patients with ARDS who failed to reach a threshold P/F ratio of at least 100 within 48 hours of initiation of high-frequency oscillatory ventilation was 75%, compared with a mortality of 24.3% among similar patients who achieved the ratio.
Data Source: A retrospective study comparing mortality in 58 surgical ICU patients with ARDS who received at least 48 hours of high-frequency oscillatory ventilation.
Disclosures: Dr. Tarras disclosed having no relevant conflicts of interest.
Anticipate Mycobacterial Lung Disease in Anti-TNF Users
SNOWMASS, COLO. – Rheumatoid arthritis patients on tumor necrosis factor inhibitors are at markedly increased risk for both tuberculosis and nontuberculous mycobacterial lung disease, as highlighted in data not yet published from Kaiser Permanente of Northern California that was discussed by investigator Dr. Kevin L. Winthrop at the symposium.
The crude incidence rate of nontuberculous mycobacterial disease in this 3.1-million-member health plan during the study years of 2000-2008 was 4.1 cases/100,000 person-years. The risk rose with age such that among plan members aged 50 years or older the rate was 11.8 cases/100,000 person-years. Plan members with rheumatoid arthritis (RA) who’d never been on a tumor necrosis factor (TNF) inhibitor had a moderately higher rate of 19.2 cases/100,000 person-years, probably because of their use of prednisone. But among 8,418 RA patients on TNF inhibitor therapy, the incidence of nontuberculous mycobacterial pulmonary disease shot up to 112 cases/100,000 person-years.

The tuberculosis incidence followed a similar pattern: 2.8 cases/100,000 person-years among the general Kaiser membership, 5.2 in those aged 50 years or older, 8.7 in RA patients never exposed to a TNF inhibitor, jumping to 56 cases/100,000 person-years among RA patients on an anti-TNF biologic, according to Dr. Winthrop.
In light of these data, physicians need to be on the lookout for nontuberculous mycobacterial pulmonary disease arising in RA patients using a TNF inhibitor.
"You will have patients with this. It’s best to diagnose them early, if possible, and get them off their biologic and also limit or discontinue prednisone," said Dr. Winthrop, an infectious diseases specialist at Oregon Health and Science University, Portland.
It’s his clinical impression, as well as that of other physicians participating in the Infectious Diseases Society of America’s Emerging Infections Network, that people who develop nontuberculous mycobacterial lung disease while on a TNF inhibitor tend to experience more rapid progression of their lung disease, he said at the meeting.
He and his coinvestigators at Kaiser also examined the pulmonary disease rates associated with individual TNF inhibitors. The nontuberculous mycobacterial lung disease rate in patients on etanercept was 35 cases/100,000 person-years of exposure, significantly less than the 116 cases/100,000 person-years with infliximab or 122 with adalimumab.
Similarly, the tuberculosis rate was lowest with etanercept at 17 cases/100,000 person-years as compared to 83 with infliximab and 61 with adalimumab.
The Kaiser experience confirms a 2010 report from the British Society for Rheumatology biologic registry that provided the first solid epidemiologic data showing that TNF inhibitors carry an increased tuberculosis risk. In the U.K. study, etanercept use was associated with a tuberculosis incidence of 39 cases per 100,000 person-years, significantly lower than the 136 cases per 100,000 person-years with infliximab or 144 with adalimumab. In contrast, the tuberculosis rate among more than 3,200 RA patients on a conventional disease-modifying anti-rheumatic drug was zero. The background tuberculosis incidence in the United Kingdom during that time period was about 12 cases/100,000 person-years (Ann. Rheum. Dis. 2010;69:522-8).
"I’m convinced that the monoclonal antibody TNF inhibitors [infliximab and adalimumab] cause more tuberculosis than [does] etanercept. I’m not convinced I know why," Dr. Winthrop admitted.
Numerous potential mechanisms have been floated to explain this differential effect. The two he finds most plausible are that etanercept is less able to penetrate tuberculosis granulomas than are the monoclonal antibody TNF inhibitors, as shown in a mouse model, and the possibility – as yet unproven – that etanercept might also cause less downregulation of CD8 cells producing the antimicrobial peptides perforin and granulysin, which are directed against Mycobacterium tuberculosis.
Dr. Winthrop said the epidemiology of nontuberculous mycobacterial pulmonary disease is changing. Decades ago, it was viewed as a disease of elderly men. As the incidence has climbed during the past 2 decades, however, the disease has come to be recognized as mainly one of postmenopausal women, typically with no history of underlying lung disease or smoking. The phenotype is one of an elderly woman who is tall, slender, and underweight, often with mitral valve prolapse, scoliosis, or pectus defects.
In a large study conducted at four geographically diverse large health plans, the annual prevalence of nontuberculous mycobacterial lung disease among persons age 60 years or older rose from 19.6 cases/100,000 in 1994-1996 to 26.7 cases/100,000 person-years in 2004-2006, a rate two- to threefold greater than the prevalence of tuberculosis at those sites during 2004-2006 (Am. J. Respir. Crit. Care Med. 2010;182:970-6).
Nontuberculous mycobacteria are ubiquitous in tap water and soil. Unlike tuberculosis, which is spread from person to person by coughing, nontuberculous mycobacterial infections are acquired directly from the environment.
Dr. Winthrop said he is reluctant to recommend resuming biologic therapy after a RA patient has been treated for nontuberculous mycobacterial lung disease or coccidioidomycosis.
Dr. Winthrop reported having received consultant fees from Abbott, Amgen, and Pfizer as well as research funding from Pfizer.
SNOWMASS, COLO. – Rheumatoid arthritis patients on tumor necrosis factor inhibitors are at markedly increased risk for both tuberculosis and nontuberculous mycobacterial lung disease, as highlighted in data not yet published from Kaiser Permanente of Northern California that was discussed by investigator Dr. Kevin L. Winthrop at the symposium.
The crude incidence rate of nontuberculous mycobacterial disease in this 3.1-million-member health plan during the study years of 2000-2008 was 4.1 cases/100,000 person-years. The risk rose with age such that among plan members aged 50 years or older the rate was 11.8 cases/100,000 person-years. Plan members with rheumatoid arthritis (RA) who’d never been on a tumor necrosis factor (TNF) inhibitor had a moderately higher rate of 19.2 cases/100,000 person-years, probably because of their use of prednisone. But among 8,418 RA patients on TNF inhibitor therapy, the incidence of nontuberculous mycobacterial pulmonary disease shot up to 112 cases/100,000 person-years.
The tuberculosis incidence followed a similar pattern: 2.8 cases/100,000 person-years among the general Kaiser membership, 5.2 in those aged 50 years or older, 8.7 in RA patients never exposed to a TNF inhibitor, jumping to 56 cases/100,000 person-years among RA patients on an anti-TNF biologic, according to Dr. Winthrop.
In light of these data, physicians need to be on the lookout for nontuberculous mycobacterial pulmonary disease arising in RA patients using a TNF inhibitor.
"You will have patients with this. It’s best to diagnose them early, if possible, and get them off their biologic and also limit or discontinue prednisone," said Dr. Winthrop, an infectious diseases specialist at Oregon Health and Science University, Portland.
It’s his clinical impression, as well as that of other physicians participating in the Infectious Diseases Society of America’s Emerging Infections Network, that people who develop nontuberculous mycobacterial lung disease while on a TNF inhibitor tend to experience more rapid progression of their lung disease, he said at the meeting.
He and his coinvestigators at Kaiser also examined the pulmonary disease rates associated with individual TNF inhibitors. The nontuberculous mycobacterial lung disease rate in patients on etanercept was 35 cases/100,000 person-years of exposure, significantly less than the 116 cases/100,000 person-years with infliximab or 122 with adalimumab.
Similarly, the tuberculosis rate was lowest with etanercept at 17 cases/100,000 person-years as compared to 83 with infliximab and 61 with adalimumab.
The Kaiser experience confirms a 2010 report from the British Society for Rheumatology biologic registry that provided the first solid epidemiologic data showing that TNF inhibitors carry an increased tuberculosis risk. In the U.K. study, etanercept use was associated with a tuberculosis incidence of 39 cases per 100,000 person-years, significantly lower than the 136 cases per 100,000 person-years with infliximab or 144 with adalimumab. In contrast, the tuberculosis rate among more than 3,200 RA patients on a conventional disease-modifying anti-rheumatic drug was zero. The background tuberculosis incidence in the United Kingdom during that time period was about 12 cases/100,000 person-years (Ann. Rheum. Dis. 2010;69:522-8).
"I’m convinced that the monoclonal antibody TNF inhibitors [infliximab and adalimumab] cause more tuberculosis than [does] etanercept. I’m not convinced I know why," Dr. Winthrop admitted.
Numerous potential mechanisms have been floated to explain this differential effect. The two he finds most plausible are that etanercept is less able to penetrate tuberculosis granulomas than are the monoclonal antibody TNF inhibitors, as shown in a mouse model, and the possibility – as yet unproven – that etanercept might also cause less downregulation of CD8 cells producing the antimicrobial peptides perforin and granulysin, which are directed against Mycobacterium tuberculosis.
Dr. Winthrop said the epidemiology of nontuberculous mycobacterial pulmonary disease is changing. Decades ago, it was viewed as a disease of elderly men. As the incidence has climbed during the past 2 decades, however, the disease has come to be recognized as mainly one of postmenopausal women, typically with no history of underlying lung disease or smoking. The phenotype is one of an elderly woman who is tall, slender, and underweight, often with mitral valve prolapse, scoliosis, or pectus defects.
In a large study conducted at four geographically diverse large health plans, the annual prevalence of nontuberculous mycobacterial lung disease among persons age 60 years or older rose from 19.6 cases/100,000 in 1994-1996 to 26.7 cases/100,000 person-years in 2004-2006, a rate two- to threefold greater than the prevalence of tuberculosis at those sites during 2004-2006 (Am. J. Respir. Crit. Care Med. 2010;182:970-6).
Nontuberculous mycobacteria are ubiquitous in tap water and soil. Unlike tuberculosis, which is spread from person to person by coughing, nontuberculous mycobacterial infections are acquired directly from the environment.
Dr. Winthrop said he is reluctant to recommend resuming biologic therapy after a RA patient has been treated for nontuberculous mycobacterial lung disease or coccidioidomycosis.
Dr. Winthrop reported having received consultant fees from Abbott, Amgen, and Pfizer as well as research funding from Pfizer.
SNOWMASS, COLO. – Rheumatoid arthritis patients on tumor necrosis factor inhibitors are at markedly increased risk for both tuberculosis and nontuberculous mycobacterial lung disease, as highlighted in data not yet published from Kaiser Permanente of Northern California that was discussed by investigator Dr. Kevin L. Winthrop at the symposium.
The crude incidence rate of nontuberculous mycobacterial disease in this 3.1-million-member health plan during the study years of 2000-2008 was 4.1 cases/100,000 person-years. The risk rose with age such that among plan members aged 50 years or older the rate was 11.8 cases/100,000 person-years. Plan members with rheumatoid arthritis (RA) who’d never been on a tumor necrosis factor (TNF) inhibitor had a moderately higher rate of 19.2 cases/100,000 person-years, probably because of their use of prednisone. But among 8,418 RA patients on TNF inhibitor therapy, the incidence of nontuberculous mycobacterial pulmonary disease shot up to 112 cases/100,000 person-years.
The tuberculosis incidence followed a similar pattern: 2.8 cases/100,000 person-years among the general Kaiser membership, 5.2 in those aged 50 years or older, 8.7 in RA patients never exposed to a TNF inhibitor, jumping to 56 cases/100,000 person-years among RA patients on an anti-TNF biologic, according to Dr. Winthrop.
In light of these data, physicians need to be on the lookout for nontuberculous mycobacterial pulmonary disease arising in RA patients using a TNF inhibitor.
"You will have patients with this. It’s best to diagnose them early, if possible, and get them off their biologic and also limit or discontinue prednisone," said Dr. Winthrop, an infectious diseases specialist at Oregon Health and Science University, Portland.
It’s his clinical impression, as well as that of other physicians participating in the Infectious Diseases Society of America’s Emerging Infections Network, that people who develop nontuberculous mycobacterial lung disease while on a TNF inhibitor tend to experience more rapid progression of their lung disease, he said at the meeting.
He and his coinvestigators at Kaiser also examined the pulmonary disease rates associated with individual TNF inhibitors. The nontuberculous mycobacterial lung disease rate in patients on etanercept was 35 cases/100,000 person-years of exposure, significantly less than the 116 cases/100,000 person-years with infliximab or 122 with adalimumab.
Similarly, the tuberculosis rate was lowest with etanercept at 17 cases/100,000 person-years as compared to 83 with infliximab and 61 with adalimumab.
The Kaiser experience confirms a 2010 report from the British Society for Rheumatology biologic registry that provided the first solid epidemiologic data showing that TNF inhibitors carry an increased tuberculosis risk. In the U.K. study, etanercept use was associated with a tuberculosis incidence of 39 cases per 100,000 person-years, significantly lower than the 136 cases per 100,000 person-years with infliximab or 144 with adalimumab. In contrast, the tuberculosis rate among more than 3,200 RA patients on a conventional disease-modifying anti-rheumatic drug was zero. The background tuberculosis incidence in the United Kingdom during that time period was about 12 cases/100,000 person-years (Ann. Rheum. Dis. 2010;69:522-8).
"I’m convinced that the monoclonal antibody TNF inhibitors [infliximab and adalimumab] cause more tuberculosis than [does] etanercept. I’m not convinced I know why," Dr. Winthrop admitted.
Numerous potential mechanisms have been floated to explain this differential effect. The two he finds most plausible are that etanercept is less able to penetrate tuberculosis granulomas than are the monoclonal antibody TNF inhibitors, as shown in a mouse model, and the possibility – as yet unproven – that etanercept might also cause less downregulation of CD8 cells producing the antimicrobial peptides perforin and granulysin, which are directed against Mycobacterium tuberculosis.
Dr. Winthrop said the epidemiology of nontuberculous mycobacterial pulmonary disease is changing. Decades ago, it was viewed as a disease of elderly men. As the incidence has climbed during the past 2 decades, however, the disease has come to be recognized as mainly one of postmenopausal women, typically with no history of underlying lung disease or smoking. The phenotype is one of an elderly woman who is tall, slender, and underweight, often with mitral valve prolapse, scoliosis, or pectus defects.
In a large study conducted at four geographically diverse large health plans, the annual prevalence of nontuberculous mycobacterial lung disease among persons age 60 years or older rose from 19.6 cases/100,000 in 1994-1996 to 26.7 cases/100,000 person-years in 2004-2006, a rate two- to threefold greater than the prevalence of tuberculosis at those sites during 2004-2006 (Am. J. Respir. Crit. Care Med. 2010;182:970-6).
Nontuberculous mycobacteria are ubiquitous in tap water and soil. Unlike tuberculosis, which is spread from person to person by coughing, nontuberculous mycobacterial infections are acquired directly from the environment.
Dr. Winthrop said he is reluctant to recommend resuming biologic therapy after a RA patient has been treated for nontuberculous mycobacterial lung disease or coccidioidomycosis.
Dr. Winthrop reported having received consultant fees from Abbott, Amgen, and Pfizer as well as research funding from Pfizer.
EXPERT ANALYSIS FROM A SYMPOSIUM SPONSORED BY THE AMERICAN COLLEGE OF RHEUMATOLOGY
Frequent Respiratory Infections? Rule Out Bronchiectasis
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.

She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND PULMONARY DISEASES
Teach Insomniacs That Beds Are for Sleeping
PHOENIX – Reducing bedtime stimulation and, oddly enough, restricting sleep both have powerful, relatively fast effects on insomnia, especially when used in tandem.
Among cognitive-behavioral therapy approaches, they have the best supporting evidence and, "happily, are the easiest to do," said Allison Harvey, Ph.D., director of the University of California, Berkeley, Golden Bear Sleep and Mood Research Clinic.

The goal is to teach insomniacs that their beds are for sleeping, not watching TV, surfing the Net, eating potato chips, or fretting about not getting enough sleep.
Sleep restriction limits their time in bed to the time they actually sleep. The first step is to discover that ratio by having patients keep a sleep diary for a week or 2. Insomniacs are usually about 60% sleep efficient; for every 8 hours in bed, they’ll sleep about 5.
The next step is limiting bed time to sleep time. At first, that might cause a bit of sleep deprivation, but that’s a good thing because it builds homeostatic pressure to sleep, Dr. Harvey said.
The goal is 85% sleep efficiency; 4.25 hours of sleep, for instance, for every 5 hours in bed. As long as patients remain 85% efficient, time in bed can be increased by 15 minutes every 5 or so days. Within about 6 weeks, patients should be getting an efficient 7 or 8 hours of sleep per night.
At first, "we never go less than 5 hours a night" and "make the determination of how low we go dependent on safety issues. So, if someone’s a truck driver, we probably wouldn’t do this treatment. If someone has bipolar disorder, I wouldn’t go below 6½ hours because sleep deprivation can trigger a manic episode." Naps are okay if needed, so long as they are before 3 p.m. and are 30 minutes or less, Dr. Harvey said.
Stimulus control reinforces the bed-sleep connection. If patients aren’t asleep within 20 minutes, "Don’t let them clock watch. [Tell them to] get up and move to another room, and stay up until they are really sleepy," she said.
If they want to read, it shouldn’t be something that will keep them up all night. If they want to watch TV, it should be something relaxing, not channel surfing. If they’re anxious, writing in a journal can help.
"I had one patient who said, ‘Oh, I can get some housework done.’ No. Nothing productive. Other patients say, ‘I can get on my computer and do some e-mail.’ No; [they need] dim light conditions," Dr. Harvey said.
Flexibility is important. Some patients might want to restrict sleep in the evening, others in the morning. Both are fine. Some patients might worry that 5 hours is too little bedtime, so "start with 7½; it’s better than 8½. Sleep efficiency will pop up a bit, they’ll get confidence. They’ll come down to seven hours the next week. Just base it on what makes sense for the person," Dr. Harvey said.
It might take a few weeks for patients to see benefits, so support is important, too. Troubleshoot their routine for problems, and encourage them to continue the program, she said.
It’s uncertain what benefit sedative hypnotics such as zolpidem (Ambien) would add to the approach, she noted.
Dr. Harvey reported having no relevant financial disclosures.
PHOENIX – Reducing bedtime stimulation and, oddly enough, restricting sleep both have powerful, relatively fast effects on insomnia, especially when used in tandem.
Among cognitive-behavioral therapy approaches, they have the best supporting evidence and, "happily, are the easiest to do," said Allison Harvey, Ph.D., director of the University of California, Berkeley, Golden Bear Sleep and Mood Research Clinic.
The goal is to teach insomniacs that their beds are for sleeping, not watching TV, surfing the Net, eating potato chips, or fretting about not getting enough sleep.
Sleep restriction limits their time in bed to the time they actually sleep. The first step is to discover that ratio by having patients keep a sleep diary for a week or 2. Insomniacs are usually about 60% sleep efficient; for every 8 hours in bed, they’ll sleep about 5.
The next step is limiting bed time to sleep time. At first, that might cause a bit of sleep deprivation, but that’s a good thing because it builds homeostatic pressure to sleep, Dr. Harvey said.
The goal is 85% sleep efficiency; 4.25 hours of sleep, for instance, for every 5 hours in bed. As long as patients remain 85% efficient, time in bed can be increased by 15 minutes every 5 or so days. Within about 6 weeks, patients should be getting an efficient 7 or 8 hours of sleep per night.
At first, "we never go less than 5 hours a night" and "make the determination of how low we go dependent on safety issues. So, if someone’s a truck driver, we probably wouldn’t do this treatment. If someone has bipolar disorder, I wouldn’t go below 6½ hours because sleep deprivation can trigger a manic episode." Naps are okay if needed, so long as they are before 3 p.m. and are 30 minutes or less, Dr. Harvey said.
Stimulus control reinforces the bed-sleep connection. If patients aren’t asleep within 20 minutes, "Don’t let them clock watch. [Tell them to] get up and move to another room, and stay up until they are really sleepy," she said.
If they want to read, it shouldn’t be something that will keep them up all night. If they want to watch TV, it should be something relaxing, not channel surfing. If they’re anxious, writing in a journal can help.
"I had one patient who said, ‘Oh, I can get some housework done.’ No. Nothing productive. Other patients say, ‘I can get on my computer and do some e-mail.’ No; [they need] dim light conditions," Dr. Harvey said.
Flexibility is important. Some patients might want to restrict sleep in the evening, others in the morning. Both are fine. Some patients might worry that 5 hours is too little bedtime, so "start with 7½; it’s better than 8½. Sleep efficiency will pop up a bit, they’ll get confidence. They’ll come down to seven hours the next week. Just base it on what makes sense for the person," Dr. Harvey said.
It might take a few weeks for patients to see benefits, so support is important, too. Troubleshoot their routine for problems, and encourage them to continue the program, she said.
It’s uncertain what benefit sedative hypnotics such as zolpidem (Ambien) would add to the approach, she noted.
Dr. Harvey reported having no relevant financial disclosures.
PHOENIX – Reducing bedtime stimulation and, oddly enough, restricting sleep both have powerful, relatively fast effects on insomnia, especially when used in tandem.
Among cognitive-behavioral therapy approaches, they have the best supporting evidence and, "happily, are the easiest to do," said Allison Harvey, Ph.D., director of the University of California, Berkeley, Golden Bear Sleep and Mood Research Clinic.
The goal is to teach insomniacs that their beds are for sleeping, not watching TV, surfing the Net, eating potato chips, or fretting about not getting enough sleep.
Sleep restriction limits their time in bed to the time they actually sleep. The first step is to discover that ratio by having patients keep a sleep diary for a week or 2. Insomniacs are usually about 60% sleep efficient; for every 8 hours in bed, they’ll sleep about 5.
The next step is limiting bed time to sleep time. At first, that might cause a bit of sleep deprivation, but that’s a good thing because it builds homeostatic pressure to sleep, Dr. Harvey said.
The goal is 85% sleep efficiency; 4.25 hours of sleep, for instance, for every 5 hours in bed. As long as patients remain 85% efficient, time in bed can be increased by 15 minutes every 5 or so days. Within about 6 weeks, patients should be getting an efficient 7 or 8 hours of sleep per night.
At first, "we never go less than 5 hours a night" and "make the determination of how low we go dependent on safety issues. So, if someone’s a truck driver, we probably wouldn’t do this treatment. If someone has bipolar disorder, I wouldn’t go below 6½ hours because sleep deprivation can trigger a manic episode." Naps are okay if needed, so long as they are before 3 p.m. and are 30 minutes or less, Dr. Harvey said.
Stimulus control reinforces the bed-sleep connection. If patients aren’t asleep within 20 minutes, "Don’t let them clock watch. [Tell them to] get up and move to another room, and stay up until they are really sleepy," she said.
If they want to read, it shouldn’t be something that will keep them up all night. If they want to watch TV, it should be something relaxing, not channel surfing. If they’re anxious, writing in a journal can help.
"I had one patient who said, ‘Oh, I can get some housework done.’ No. Nothing productive. Other patients say, ‘I can get on my computer and do some e-mail.’ No; [they need] dim light conditions," Dr. Harvey said.
Flexibility is important. Some patients might want to restrict sleep in the evening, others in the morning. Both are fine. Some patients might worry that 5 hours is too little bedtime, so "start with 7½; it’s better than 8½. Sleep efficiency will pop up a bit, they’ll get confidence. They’ll come down to seven hours the next week. Just base it on what makes sense for the person," Dr. Harvey said.
It might take a few weeks for patients to see benefits, so support is important, too. Troubleshoot their routine for problems, and encourage them to continue the program, she said.
It’s uncertain what benefit sedative hypnotics such as zolpidem (Ambien) would add to the approach, she noted.
Dr. Harvey reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING ON SLEEP MEDICINE SPONSORED BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Melatonin May Normalize Night Owl Sleep Schedules
PHOENIX – When patients’ sleep cycles are out of synch with the rest of the world, melatonin and light therapy can help.
But for night owls – people who fall asleep at 5 a.m. and awake at noon, for instance – it’s important to use a low dose of melatonin, 0.5-1 mg, and it should be given around 7 p.m., 4-5 hours before their desired sleep time, according to Dr. Phyllis Zee, associate director of the Northwestern University Center for Sleep and Circadian Biology in Evanston, Ill.
Bedtime "is not when you give melatonin," she said. And a small dose is better than a larger one for moving internal sleep clocks forward and less likely to make people sleepy in the early evening.
Night owl patients are clinically described as having a delayed sleep phase disorder, a circadian rhythm problem. Bright light therapy in the early morning, around the time when they would like to wake up, also helps, sometimes in just a few sessions.
Light and melatonin have strong, but opposite, effects on the suprachiasmatic nucleus (SCN), thought to be the brain’s internal clock. Light, especially blue light, increases SCN firing, alerting the body. Melatonin, secreted by the pineal gland under SCN control on a 24-hour cycle, decreases SCN firing, promoting sleep.
Dim light triggers melatonin secretion; endogenous levels begin to rise about 2 hours before sleep, a phenomenon known as dim-light melatonin onset (DLMO). Melatonin supplements help the rise come earlier in night owls, who should also avoid bright light in the evening.
The role of melatonin is uncertain in people with an advanced sleep phase disorder – those who routinely fall asleep at 7 p.m., for instance, and awake at 4 a.m. – but bright light therapy early in the evening can push back their sleep schedule, also in just a few sessions. "In someone with advanced sleep phase, that’s what I would do first. Bright light therapy in the evening," Dr. Zee said
Patients with circadian sleep disorders don’t have insomnia. Once asleep, they get a full night’s rest.
Even so, being out of synch with the world can cause problems. People with delayed phase disorders can barely get out bed for work, and when they do, they’re sleepy all day. An advanced-phase person’s internal clock tells that person to go to bed when the rest of the world is still active. Such misalignments can trigger actual insomnia and lead to health problems. Delayed phase disorders also correlate with depression.
"Many people who we think have primary insomnia or psychological insomnia actually have delayed or advanced circadian phases. It isn’t so much they complain about insomnia; they really complain about excessive sleepiness," Dr. Zee said.
To make the right therapeutic call, it’s important to know the timing of patients’ internal clocks. History gives a clue. "I’ve never met a delayed person who is not an owl. I’ve never met an advance sleep phase disorder person who is not a lark," Dr. Zee said.
A sleep diary helps, too, along with actigraphy, which involves recording wrist activity with a watch-like device worn over several days. It gives a good idea of sleep/wake activity.
DLMO can be accessed directly as well, at least in a sleep lab. In dim light, patients are asked to chew a cotton ball every half hour for 24 hours. Melatonin concentrations are assessed from the saliva. DLMO usually comes at about 9 p.m. for someone on an 11 p.m.-7 a.m. sleep schedule.
Dr. Zee is a consultant for Sanofi-Aventis, Merck, Johnson & Johnson, UCB Pharma, Purdue Pharma, Jazz Pharmaceuticals, and Royal Philips Electronics/Respironics. She also disclosed stock options in Zeo.
PHOENIX – When patients’ sleep cycles are out of synch with the rest of the world, melatonin and light therapy can help.
But for night owls – people who fall asleep at 5 a.m. and awake at noon, for instance – it’s important to use a low dose of melatonin, 0.5-1 mg, and it should be given around 7 p.m., 4-5 hours before their desired sleep time, according to Dr. Phyllis Zee, associate director of the Northwestern University Center for Sleep and Circadian Biology in Evanston, Ill.
Bedtime "is not when you give melatonin," she said. And a small dose is better than a larger one for moving internal sleep clocks forward and less likely to make people sleepy in the early evening.
Night owl patients are clinically described as having a delayed sleep phase disorder, a circadian rhythm problem. Bright light therapy in the early morning, around the time when they would like to wake up, also helps, sometimes in just a few sessions.
Light and melatonin have strong, but opposite, effects on the suprachiasmatic nucleus (SCN), thought to be the brain’s internal clock. Light, especially blue light, increases SCN firing, alerting the body. Melatonin, secreted by the pineal gland under SCN control on a 24-hour cycle, decreases SCN firing, promoting sleep.
Dim light triggers melatonin secretion; endogenous levels begin to rise about 2 hours before sleep, a phenomenon known as dim-light melatonin onset (DLMO). Melatonin supplements help the rise come earlier in night owls, who should also avoid bright light in the evening.
The role of melatonin is uncertain in people with an advanced sleep phase disorder – those who routinely fall asleep at 7 p.m., for instance, and awake at 4 a.m. – but bright light therapy early in the evening can push back their sleep schedule, also in just a few sessions. "In someone with advanced sleep phase, that’s what I would do first. Bright light therapy in the evening," Dr. Zee said
Patients with circadian sleep disorders don’t have insomnia. Once asleep, they get a full night’s rest.
Even so, being out of synch with the world can cause problems. People with delayed phase disorders can barely get out bed for work, and when they do, they’re sleepy all day. An advanced-phase person’s internal clock tells that person to go to bed when the rest of the world is still active. Such misalignments can trigger actual insomnia and lead to health problems. Delayed phase disorders also correlate with depression.
"Many people who we think have primary insomnia or psychological insomnia actually have delayed or advanced circadian phases. It isn’t so much they complain about insomnia; they really complain about excessive sleepiness," Dr. Zee said.
To make the right therapeutic call, it’s important to know the timing of patients’ internal clocks. History gives a clue. "I’ve never met a delayed person who is not an owl. I’ve never met an advance sleep phase disorder person who is not a lark," Dr. Zee said.
A sleep diary helps, too, along with actigraphy, which involves recording wrist activity with a watch-like device worn over several days. It gives a good idea of sleep/wake activity.
DLMO can be accessed directly as well, at least in a sleep lab. In dim light, patients are asked to chew a cotton ball every half hour for 24 hours. Melatonin concentrations are assessed from the saliva. DLMO usually comes at about 9 p.m. for someone on an 11 p.m.-7 a.m. sleep schedule.
Dr. Zee is a consultant for Sanofi-Aventis, Merck, Johnson & Johnson, UCB Pharma, Purdue Pharma, Jazz Pharmaceuticals, and Royal Philips Electronics/Respironics. She also disclosed stock options in Zeo.
PHOENIX – When patients’ sleep cycles are out of synch with the rest of the world, melatonin and light therapy can help.
But for night owls – people who fall asleep at 5 a.m. and awake at noon, for instance – it’s important to use a low dose of melatonin, 0.5-1 mg, and it should be given around 7 p.m., 4-5 hours before their desired sleep time, according to Dr. Phyllis Zee, associate director of the Northwestern University Center for Sleep and Circadian Biology in Evanston, Ill.
Bedtime "is not when you give melatonin," she said. And a small dose is better than a larger one for moving internal sleep clocks forward and less likely to make people sleepy in the early evening.
Night owl patients are clinically described as having a delayed sleep phase disorder, a circadian rhythm problem. Bright light therapy in the early morning, around the time when they would like to wake up, also helps, sometimes in just a few sessions.
Light and melatonin have strong, but opposite, effects on the suprachiasmatic nucleus (SCN), thought to be the brain’s internal clock. Light, especially blue light, increases SCN firing, alerting the body. Melatonin, secreted by the pineal gland under SCN control on a 24-hour cycle, decreases SCN firing, promoting sleep.
Dim light triggers melatonin secretion; endogenous levels begin to rise about 2 hours before sleep, a phenomenon known as dim-light melatonin onset (DLMO). Melatonin supplements help the rise come earlier in night owls, who should also avoid bright light in the evening.
The role of melatonin is uncertain in people with an advanced sleep phase disorder – those who routinely fall asleep at 7 p.m., for instance, and awake at 4 a.m. – but bright light therapy early in the evening can push back their sleep schedule, also in just a few sessions. "In someone with advanced sleep phase, that’s what I would do first. Bright light therapy in the evening," Dr. Zee said
Patients with circadian sleep disorders don’t have insomnia. Once asleep, they get a full night’s rest.
Even so, being out of synch with the world can cause problems. People with delayed phase disorders can barely get out bed for work, and when they do, they’re sleepy all day. An advanced-phase person’s internal clock tells that person to go to bed when the rest of the world is still active. Such misalignments can trigger actual insomnia and lead to health problems. Delayed phase disorders also correlate with depression.
"Many people who we think have primary insomnia or psychological insomnia actually have delayed or advanced circadian phases. It isn’t so much they complain about insomnia; they really complain about excessive sleepiness," Dr. Zee said.
To make the right therapeutic call, it’s important to know the timing of patients’ internal clocks. History gives a clue. "I’ve never met a delayed person who is not an owl. I’ve never met an advance sleep phase disorder person who is not a lark," Dr. Zee said.
A sleep diary helps, too, along with actigraphy, which involves recording wrist activity with a watch-like device worn over several days. It gives a good idea of sleep/wake activity.
DLMO can be accessed directly as well, at least in a sleep lab. In dim light, patients are asked to chew a cotton ball every half hour for 24 hours. Melatonin concentrations are assessed from the saliva. DLMO usually comes at about 9 p.m. for someone on an 11 p.m.-7 a.m. sleep schedule.
Dr. Zee is a consultant for Sanofi-Aventis, Merck, Johnson & Johnson, UCB Pharma, Purdue Pharma, Jazz Pharmaceuticals, and Royal Philips Electronics/Respironics. She also disclosed stock options in Zeo.
EXPERT ANALYSIS FROM A MEETING ON SLEEP MEDICINE SPONSORED BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Would this long-acting bronchodilator be better for your patient?
Consider adding tiotropium to the medication regimen of patients with moderate to very severe chronic obstructive pulmonary disease (COPD), as a multinational study found it to be more effective than salmeterol in preventing exacerbations.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed randomized controlled trial.
Vogelmeier C, Hederer B, Glaab T, et al; POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
ILLUSTRATIVE CASE
A 60-year-old patient with moderate COPD and a history of frequent exacerbations comes in for a follow-up visit. She has been using albuterol and ipratropium intermittently. you want to add a longer-acting bronchodilator and wonder if tiotropium or salmeterol is more effective for reducing exacerbations.
COPD is the fourth leading cause of death in the United States.2 More than 12 million Americans have been diagnosed with COPD, and it is estimated that another 12 million would have a COPD diagnosis if all smokers older than 45 years underwent spirometry.2 The disorder accounts for some 16 million physician visits each year and costs the US health care system approximately $19 billion annually, with acute exacerbations and hospitalizations representing 58% of the total.2,3
Despite guidelines, COPD is often undertreated
One of the main goals of COPD treatment is to reduce the frequency and intensity of acute exacerbations, both to improve patients’ quality of life and reduce health care costs. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has developed guidelines for effective management of COPD, which recommend long-acting bronchodilators as first-line maintenance therapy for patients whose disease is moderate to very severe.4
Evidence suggests that physicians frequently undertreat moderate to severe COPD, however, following national guidelines only about a quarter of the time.5 This is, in part, because many clinicians doubt the efficacy of COPD treatment for improving symptoms or decreasing exacerbations.5,6 Yet studies have shown that the long-acting broncho dilators tiotropium (an anticholinergic agent) and salmeterol (a beta2-adrenergic agonist), used with or without inhaled corticosteroids, are effective in reducing the frequency of COPD exacerbations, improving quality of life and lung function, and reducing the number of hospitalizations.7-10
Long-acting bronchodilators are therefore clearly indicated but, until recently, there was little evidence as to which one is better.
STUDY SUMMARY: Tiotropium group had fewer exacerbations…
The Prevention Of Exacerbations with Tiotropium in COPD (POET-COPD) trial compared tiotropium with salmeterol for their ability to prevent exacerbations.1 This was a randomized double-blind trial of 7376 patients with moderate to very severe COPD diagnosed by spirometry. Participants were recruited from 725 medical centers in 25 countries. To be eligible, they had to be ≥40 years, with at least a 10 pack-year history of smoking, a forced expiratory volume in 1 second (FEV1) <70% predicted, an FEV1/forced vital capacity (FVC ) <70%, and at least one exacerbation in the previous year.
Patients were randomly assigned to either the tiotropium or the salmeterol group. Those on tiotropium received a daily dose of 18 mcg through a HandiHaler device, plus a placebo with a metered-dose inhaler twice a day. Patients in the other group received 50 mcg salmeterol through a metered-dose inhaler twice daily, plus a placebo with a HandiHaler once a day. These medications were in addition to patients’ current medication regimens, including inhaled corticosteroids, with this exception: Use of anticholinergics and long-acting beta-agonists was discontinued for the course of the trial.
All participants were followed for one year, with clinic visits at 2, 4, 8, and 12 months to assess for medication adherence and symptoms of exacerbation. The primary endpoint was the time to first exacerbation. This was defined as an increase in, or a new onset of, more than one symptom of COPD (ie, cough, sputum production, wheezing, dyspnea, and chest tightness), with at least one symptom lasting ≥3 days and leading to treatment with glucocorticoids and/or antibiotics, or hospitalization. Secondary outcomes were times to first moderate and severe exacerbations and use of steroids and antibiotics.
There were significant differences in several outcomes. The time to first exacerbation was 187 days for tiotropium vs 145 days for salmeterol, a difference of 42 days (hazard ratio [HR]=0.83; 95% confidence interval [CI], 0.77-0.90; P<.001). In addition, tiotropium reduced the annual number of exacerbations compared with salmeterol (rate ratio=0.89; 95% CI, 0.83-0.96; P=.002), with a number needed to treat (NNT) of 24 patients to prevent one moderate to severe exacerbation per year.
…and used fewer drugs
Compared with salmeterol, there was a 14% reduction in risk of a moderate exacerbation associated with tiotropium (HR=0.86; 95% CI, 0.79-0.93; P<.001; NNT=32) and a 28% reduction in risk of a severe exacerbation (HR=0.72; 95% CI, 0.61-0.85; P<.001; NNT=48). In addition, the tiotropium group had a 23% risk reduction in the use of systemic glucocorticoids (HR=0.77; 95% CI, 0.69-0.85; P<.001; NNT=26) compared with the salmeterol group, and a 15% risk reduction in the use of antibiotics (HR=0.85; 95% CI, 0.78-0.92; P<0.001; NNT=31). The difference in reduction in death rates between the 2 groups was not statistically significant.
The observed differences were consistent across all major subgroups (age, sex, smoking status, and severity of COPD) of patients studied. Interestingly, patients with low BMI or very severe COPD appeared to benefit the most from tiotropium.
WHAT’S NEW: The difference between 2 agents is clear
Although national guidelines recommend long-acting bronchodilators for COPD that is moderate or worse, there have been few data to guide clinicians in determining which one to use. The findings of this study suggest that tiotropium should be our first choice. Tiotropium’s once-a-day dosing is an additional benefit, as patients using it will likely have better compliance than those using twice-daily salmeterol. The data may also prompt development of a once-daily inhaled corticosteroid/ long-acting anticholinergic combination.
CAVEATS: Cost, funding source
Cost may be an issue. Spiriva and Serevent, the brand names for tiotropium and salmeterol, respectively, are second-tier medications on several formularies, and tiotropium is about 45% more expensive (tiotropium=$262, salmeterol=$181 for one month’s supply; www.drugstore.com, accessed January 19, 2012). There are also several long-acting beta-agonists in development that will be dosed once daily; once they’re approved, tiotropium’s once-a-day dosing may no longer be seen as an advantage.
It is also worth noting that this trial was supported by Boehringer Ingelheim and Pfizer, which jointly market Spiriva.
Finally, smoking must be addressed. Strongly encouraging patients to kick the habit is still the most important intervention we can make in helping to improve the quality of life, and survival, of patients with COPD.
CHALLENGES TO IMPLEMENTATION: COPD guidelines need updating
There are no major challenges to incorporating this recommendation into clinical practice; the key challenge lies in diagnosing COPD and adequately monitoring and helping patients manage the disease.
Current guidelines do not distinguish between the efficacy of long-acting bronchodilators, but findings from this study are important enough to change future versions of national guidelines. The GOLD committee is due to release a new guideline report soon, and will likely update its recommendations at that time.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Vogelmeier C, Hederer B, Glaab T, et al. POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
2. National Heart, Lung, and Blood Institute. Morbidity and mortality: 2009 chart book on cardiovascular, lung, and blood diseases. Available at: http://www.nhlbi.nih.gov/resources/docs/04chtbk.pdf. Accessed October 1, 2011.
3. Miravitlles M, Murio C, Guerrero T, et al. DAFNE Study Group. Pharmacoeconomic evaluation of acute exacerbations of chronic bronchitis and COPD. Chest. 2002;121:1449-1455.
4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Updated 2010. Available at: http://www.goldcopd.org. Accessed October 1, 2011.
5. Salinas GD, Williamson JC, Kalhan R, et al. Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians. Int J Chron Obstruct Pulmon Dis. 2011;6:171-179.
6. Yawn BP, Wollan PC. Knowledge and attitudes of family physicians coming to COPD continuing medical education. Int J Chron Obstruct Pulmon Dis. 2008;3:311-318.
7. Calverly PMA, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775-789.
8. Casaburi R, Mahler DA, Jones PW, et al. A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002;19:217-224.
9. Donahue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122:47-55.
10. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359:1543-1554.
Consider adding tiotropium to the medication regimen of patients with moderate to very severe chronic obstructive pulmonary disease (COPD), as a multinational study found it to be more effective than salmeterol in preventing exacerbations.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed randomized controlled trial.
Vogelmeier C, Hederer B, Glaab T, et al; POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
ILLUSTRATIVE CASE
A 60-year-old patient with moderate COPD and a history of frequent exacerbations comes in for a follow-up visit. She has been using albuterol and ipratropium intermittently. you want to add a longer-acting bronchodilator and wonder if tiotropium or salmeterol is more effective for reducing exacerbations.
COPD is the fourth leading cause of death in the United States.2 More than 12 million Americans have been diagnosed with COPD, and it is estimated that another 12 million would have a COPD diagnosis if all smokers older than 45 years underwent spirometry.2 The disorder accounts for some 16 million physician visits each year and costs the US health care system approximately $19 billion annually, with acute exacerbations and hospitalizations representing 58% of the total.2,3
Despite guidelines, COPD is often undertreated
One of the main goals of COPD treatment is to reduce the frequency and intensity of acute exacerbations, both to improve patients’ quality of life and reduce health care costs. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has developed guidelines for effective management of COPD, which recommend long-acting bronchodilators as first-line maintenance therapy for patients whose disease is moderate to very severe.4
Evidence suggests that physicians frequently undertreat moderate to severe COPD, however, following national guidelines only about a quarter of the time.5 This is, in part, because many clinicians doubt the efficacy of COPD treatment for improving symptoms or decreasing exacerbations.5,6 Yet studies have shown that the long-acting broncho dilators tiotropium (an anticholinergic agent) and salmeterol (a beta2-adrenergic agonist), used with or without inhaled corticosteroids, are effective in reducing the frequency of COPD exacerbations, improving quality of life and lung function, and reducing the number of hospitalizations.7-10
Long-acting bronchodilators are therefore clearly indicated but, until recently, there was little evidence as to which one is better.
STUDY SUMMARY: Tiotropium group had fewer exacerbations…
The Prevention Of Exacerbations with Tiotropium in COPD (POET-COPD) trial compared tiotropium with salmeterol for their ability to prevent exacerbations.1 This was a randomized double-blind trial of 7376 patients with moderate to very severe COPD diagnosed by spirometry. Participants were recruited from 725 medical centers in 25 countries. To be eligible, they had to be ≥40 years, with at least a 10 pack-year history of smoking, a forced expiratory volume in 1 second (FEV1) <70% predicted, an FEV1/forced vital capacity (FVC ) <70%, and at least one exacerbation in the previous year.
Patients were randomly assigned to either the tiotropium or the salmeterol group. Those on tiotropium received a daily dose of 18 mcg through a HandiHaler device, plus a placebo with a metered-dose inhaler twice a day. Patients in the other group received 50 mcg salmeterol through a metered-dose inhaler twice daily, plus a placebo with a HandiHaler once a day. These medications were in addition to patients’ current medication regimens, including inhaled corticosteroids, with this exception: Use of anticholinergics and long-acting beta-agonists was discontinued for the course of the trial.
All participants were followed for one year, with clinic visits at 2, 4, 8, and 12 months to assess for medication adherence and symptoms of exacerbation. The primary endpoint was the time to first exacerbation. This was defined as an increase in, or a new onset of, more than one symptom of COPD (ie, cough, sputum production, wheezing, dyspnea, and chest tightness), with at least one symptom lasting ≥3 days and leading to treatment with glucocorticoids and/or antibiotics, or hospitalization. Secondary outcomes were times to first moderate and severe exacerbations and use of steroids and antibiotics.
There were significant differences in several outcomes. The time to first exacerbation was 187 days for tiotropium vs 145 days for salmeterol, a difference of 42 days (hazard ratio [HR]=0.83; 95% confidence interval [CI], 0.77-0.90; P<.001). In addition, tiotropium reduced the annual number of exacerbations compared with salmeterol (rate ratio=0.89; 95% CI, 0.83-0.96; P=.002), with a number needed to treat (NNT) of 24 patients to prevent one moderate to severe exacerbation per year.
…and used fewer drugs
Compared with salmeterol, there was a 14% reduction in risk of a moderate exacerbation associated with tiotropium (HR=0.86; 95% CI, 0.79-0.93; P<.001; NNT=32) and a 28% reduction in risk of a severe exacerbation (HR=0.72; 95% CI, 0.61-0.85; P<.001; NNT=48). In addition, the tiotropium group had a 23% risk reduction in the use of systemic glucocorticoids (HR=0.77; 95% CI, 0.69-0.85; P<.001; NNT=26) compared with the salmeterol group, and a 15% risk reduction in the use of antibiotics (HR=0.85; 95% CI, 0.78-0.92; P<0.001; NNT=31). The difference in reduction in death rates between the 2 groups was not statistically significant.
The observed differences were consistent across all major subgroups (age, sex, smoking status, and severity of COPD) of patients studied. Interestingly, patients with low BMI or very severe COPD appeared to benefit the most from tiotropium.
WHAT’S NEW: The difference between 2 agents is clear
Although national guidelines recommend long-acting bronchodilators for COPD that is moderate or worse, there have been few data to guide clinicians in determining which one to use. The findings of this study suggest that tiotropium should be our first choice. Tiotropium’s once-a-day dosing is an additional benefit, as patients using it will likely have better compliance than those using twice-daily salmeterol. The data may also prompt development of a once-daily inhaled corticosteroid/ long-acting anticholinergic combination.
CAVEATS: Cost, funding source
Cost may be an issue. Spiriva and Serevent, the brand names for tiotropium and salmeterol, respectively, are second-tier medications on several formularies, and tiotropium is about 45% more expensive (tiotropium=$262, salmeterol=$181 for one month’s supply; www.drugstore.com, accessed January 19, 2012). There are also several long-acting beta-agonists in development that will be dosed once daily; once they’re approved, tiotropium’s once-a-day dosing may no longer be seen as an advantage.
It is also worth noting that this trial was supported by Boehringer Ingelheim and Pfizer, which jointly market Spiriva.
Finally, smoking must be addressed. Strongly encouraging patients to kick the habit is still the most important intervention we can make in helping to improve the quality of life, and survival, of patients with COPD.
CHALLENGES TO IMPLEMENTATION: COPD guidelines need updating
There are no major challenges to incorporating this recommendation into clinical practice; the key challenge lies in diagnosing COPD and adequately monitoring and helping patients manage the disease.
Current guidelines do not distinguish between the efficacy of long-acting bronchodilators, but findings from this study are important enough to change future versions of national guidelines. The GOLD committee is due to release a new guideline report soon, and will likely update its recommendations at that time.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Consider adding tiotropium to the medication regimen of patients with moderate to very severe chronic obstructive pulmonary disease (COPD), as a multinational study found it to be more effective than salmeterol in preventing exacerbations.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed randomized controlled trial.
Vogelmeier C, Hederer B, Glaab T, et al; POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
ILLUSTRATIVE CASE
A 60-year-old patient with moderate COPD and a history of frequent exacerbations comes in for a follow-up visit. She has been using albuterol and ipratropium intermittently. you want to add a longer-acting bronchodilator and wonder if tiotropium or salmeterol is more effective for reducing exacerbations.
COPD is the fourth leading cause of death in the United States.2 More than 12 million Americans have been diagnosed with COPD, and it is estimated that another 12 million would have a COPD diagnosis if all smokers older than 45 years underwent spirometry.2 The disorder accounts for some 16 million physician visits each year and costs the US health care system approximately $19 billion annually, with acute exacerbations and hospitalizations representing 58% of the total.2,3
Despite guidelines, COPD is often undertreated
One of the main goals of COPD treatment is to reduce the frequency and intensity of acute exacerbations, both to improve patients’ quality of life and reduce health care costs. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has developed guidelines for effective management of COPD, which recommend long-acting bronchodilators as first-line maintenance therapy for patients whose disease is moderate to very severe.4
Evidence suggests that physicians frequently undertreat moderate to severe COPD, however, following national guidelines only about a quarter of the time.5 This is, in part, because many clinicians doubt the efficacy of COPD treatment for improving symptoms or decreasing exacerbations.5,6 Yet studies have shown that the long-acting broncho dilators tiotropium (an anticholinergic agent) and salmeterol (a beta2-adrenergic agonist), used with or without inhaled corticosteroids, are effective in reducing the frequency of COPD exacerbations, improving quality of life and lung function, and reducing the number of hospitalizations.7-10
Long-acting bronchodilators are therefore clearly indicated but, until recently, there was little evidence as to which one is better.
STUDY SUMMARY: Tiotropium group had fewer exacerbations…
The Prevention Of Exacerbations with Tiotropium in COPD (POET-COPD) trial compared tiotropium with salmeterol for their ability to prevent exacerbations.1 This was a randomized double-blind trial of 7376 patients with moderate to very severe COPD diagnosed by spirometry. Participants were recruited from 725 medical centers in 25 countries. To be eligible, they had to be ≥40 years, with at least a 10 pack-year history of smoking, a forced expiratory volume in 1 second (FEV1) <70% predicted, an FEV1/forced vital capacity (FVC ) <70%, and at least one exacerbation in the previous year.
Patients were randomly assigned to either the tiotropium or the salmeterol group. Those on tiotropium received a daily dose of 18 mcg through a HandiHaler device, plus a placebo with a metered-dose inhaler twice a day. Patients in the other group received 50 mcg salmeterol through a metered-dose inhaler twice daily, plus a placebo with a HandiHaler once a day. These medications were in addition to patients’ current medication regimens, including inhaled corticosteroids, with this exception: Use of anticholinergics and long-acting beta-agonists was discontinued for the course of the trial.
All participants were followed for one year, with clinic visits at 2, 4, 8, and 12 months to assess for medication adherence and symptoms of exacerbation. The primary endpoint was the time to first exacerbation. This was defined as an increase in, or a new onset of, more than one symptom of COPD (ie, cough, sputum production, wheezing, dyspnea, and chest tightness), with at least one symptom lasting ≥3 days and leading to treatment with glucocorticoids and/or antibiotics, or hospitalization. Secondary outcomes were times to first moderate and severe exacerbations and use of steroids and antibiotics.
There were significant differences in several outcomes. The time to first exacerbation was 187 days for tiotropium vs 145 days for salmeterol, a difference of 42 days (hazard ratio [HR]=0.83; 95% confidence interval [CI], 0.77-0.90; P<.001). In addition, tiotropium reduced the annual number of exacerbations compared with salmeterol (rate ratio=0.89; 95% CI, 0.83-0.96; P=.002), with a number needed to treat (NNT) of 24 patients to prevent one moderate to severe exacerbation per year.
…and used fewer drugs
Compared with salmeterol, there was a 14% reduction in risk of a moderate exacerbation associated with tiotropium (HR=0.86; 95% CI, 0.79-0.93; P<.001; NNT=32) and a 28% reduction in risk of a severe exacerbation (HR=0.72; 95% CI, 0.61-0.85; P<.001; NNT=48). In addition, the tiotropium group had a 23% risk reduction in the use of systemic glucocorticoids (HR=0.77; 95% CI, 0.69-0.85; P<.001; NNT=26) compared with the salmeterol group, and a 15% risk reduction in the use of antibiotics (HR=0.85; 95% CI, 0.78-0.92; P<0.001; NNT=31). The difference in reduction in death rates between the 2 groups was not statistically significant.
The observed differences were consistent across all major subgroups (age, sex, smoking status, and severity of COPD) of patients studied. Interestingly, patients with low BMI or very severe COPD appeared to benefit the most from tiotropium.
WHAT’S NEW: The difference between 2 agents is clear
Although national guidelines recommend long-acting bronchodilators for COPD that is moderate or worse, there have been few data to guide clinicians in determining which one to use. The findings of this study suggest that tiotropium should be our first choice. Tiotropium’s once-a-day dosing is an additional benefit, as patients using it will likely have better compliance than those using twice-daily salmeterol. The data may also prompt development of a once-daily inhaled corticosteroid/ long-acting anticholinergic combination.
CAVEATS: Cost, funding source
Cost may be an issue. Spiriva and Serevent, the brand names for tiotropium and salmeterol, respectively, are second-tier medications on several formularies, and tiotropium is about 45% more expensive (tiotropium=$262, salmeterol=$181 for one month’s supply; www.drugstore.com, accessed January 19, 2012). There are also several long-acting beta-agonists in development that will be dosed once daily; once they’re approved, tiotropium’s once-a-day dosing may no longer be seen as an advantage.
It is also worth noting that this trial was supported by Boehringer Ingelheim and Pfizer, which jointly market Spiriva.
Finally, smoking must be addressed. Strongly encouraging patients to kick the habit is still the most important intervention we can make in helping to improve the quality of life, and survival, of patients with COPD.
CHALLENGES TO IMPLEMENTATION: COPD guidelines need updating
There are no major challenges to incorporating this recommendation into clinical practice; the key challenge lies in diagnosing COPD and adequately monitoring and helping patients manage the disease.
Current guidelines do not distinguish between the efficacy of long-acting bronchodilators, but findings from this study are important enough to change future versions of national guidelines. The GOLD committee is due to release a new guideline report soon, and will likely update its recommendations at that time.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Vogelmeier C, Hederer B, Glaab T, et al. POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
2. National Heart, Lung, and Blood Institute. Morbidity and mortality: 2009 chart book on cardiovascular, lung, and blood diseases. Available at: http://www.nhlbi.nih.gov/resources/docs/04chtbk.pdf. Accessed October 1, 2011.
3. Miravitlles M, Murio C, Guerrero T, et al. DAFNE Study Group. Pharmacoeconomic evaluation of acute exacerbations of chronic bronchitis and COPD. Chest. 2002;121:1449-1455.
4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Updated 2010. Available at: http://www.goldcopd.org. Accessed October 1, 2011.
5. Salinas GD, Williamson JC, Kalhan R, et al. Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians. Int J Chron Obstruct Pulmon Dis. 2011;6:171-179.
6. Yawn BP, Wollan PC. Knowledge and attitudes of family physicians coming to COPD continuing medical education. Int J Chron Obstruct Pulmon Dis. 2008;3:311-318.
7. Calverly PMA, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775-789.
8. Casaburi R, Mahler DA, Jones PW, et al. A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002;19:217-224.
9. Donahue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122:47-55.
10. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359:1543-1554.
1. Vogelmeier C, Hederer B, Glaab T, et al. POET-COPD investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093-1103.
2. National Heart, Lung, and Blood Institute. Morbidity and mortality: 2009 chart book on cardiovascular, lung, and blood diseases. Available at: http://www.nhlbi.nih.gov/resources/docs/04chtbk.pdf. Accessed October 1, 2011.
3. Miravitlles M, Murio C, Guerrero T, et al. DAFNE Study Group. Pharmacoeconomic evaluation of acute exacerbations of chronic bronchitis and COPD. Chest. 2002;121:1449-1455.
4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Updated 2010. Available at: http://www.goldcopd.org. Accessed October 1, 2011.
5. Salinas GD, Williamson JC, Kalhan R, et al. Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians. Int J Chron Obstruct Pulmon Dis. 2011;6:171-179.
6. Yawn BP, Wollan PC. Knowledge and attitudes of family physicians coming to COPD continuing medical education. Int J Chron Obstruct Pulmon Dis. 2008;3:311-318.
7. Calverly PMA, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775-789.
8. Casaburi R, Mahler DA, Jones PW, et al. A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002;19:217-224.
9. Donahue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122:47-55.
10. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359:1543-1554.
Copyright © 2012 The Family Physicians Inquiries Network.
All rights reserved.
Not your garden variety neck pain ... Untimely death blamed on undiagnosed PE ... More
Not your garden variety neck pain
PERSISTENT BILATERAL NECK PAIN so severe that he couldn’t sit down brought a man to the emergency department (ED), where he was given ketorolac and diazepam. About an hour later, he said that the pain was better and was discharged with a diagnosis of neck strain and spasm and instructions to see his primary care physician if the pain persisted or worsened.
Four days later, the patient went to his primary care physician complaining of neck pain radiating down both arms, numbness in the right thumb, fever, chills, dysuria, and myalgia in his legs. The doctor observed decreased range of motion of the neck in all directions and diagnosed likely prostatitis. He ordered co-trimoxazole (trimethoprim and sulfamethoxazole), a nonemergent magnetic resonance imaging (MRI) scan, and physical therapy.
Fourteen hours after the doctor visit, the patient went back to the ED in a wheelchair. An emergency MRI showed epidural disease up and down the cervical spine and extending into the thoracic spine. An epidural abscess with spinal cord compression was diagnosed and decompression and evacuation surgery with spinal fusion was performed.
After several weeks in the hospital, the patient was referred to rehabilitation for partial quadriplegia. He has no use of his legs and very limited use of his hands and fingers. He’s confined to a wheelchair and needs help with most activities of daily living.
PLAINTIFF’S CLAIM When the patient visited his primary care physician, he had a classic presentation of a spinal abscess and should have undergone an emergent MRI, which would have revealed the abscess and allowed treatment with antibiotics and surgery before permanent damage occurred.
THE DEFENSE The patient’s symptoms weren’t a typical presentation of spinal abscess. There was no way the physician could have known what would happen the next day.
VERDICT $3 million Massachusetts settlement.
COMMENT Yes, there are zebras among the horses. We have to be vigilant to diagnose the rare serious cause of common problems such as neck pain. The combination of neck pain, patchy neurologic findings, signs of infection, and bladder symptoms should have raised red flags.
Untimely death blamed on undiagnosed PE
A 28-YEAR-OLD MAN went to the emergency department (ED) complaining of low-grade fever, nonproductive cough, and dizziness for 2 days. He also had tachycardia and significant hypoxia. An ED physician who saw the patient an hour after his arrival noted that he complained of weakness, shortness of breath, and light-headedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism.
After reviewing an electrocardiogram, chest radiograph, and laboratory studies, the ED doctor diagnosed pneumonia and renal insufficiency. The patient was admitted to the hospital, then transferred to another hospital about 8 hours later. He wasn’t evaluated by a physician when he was admitted to the second hospital.
About 5 hours after admission, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the patient never regained consciousness and died about an hour and a half later. An autopsy established a pulmonary embolism as the cause of death.
PLAINTIFF’S CLAIM The doctors were negligent in failing to diagnose and treat the pulmonary embolism. Proper treatment would have allowed the patient to survive.
THE DEFENSE There was no negligence; heparin therapy wouldn’t have prevented the patient’s death.
VERDICT $6.1 million Maryland verdict.
COMMENT It isn’t enough to think of pulmonary embolism; a prompt definitive diagnostic work-up and timely treatment are key to preventing such a catastrophic outcome.
Delayed herpes diagnosis leads to lifelong consequences
A 10-DAY-OLD INFANT was examined by a pediatrician, who noted vesicles dotting the baby’s tongue, a possible manifestation of herpes, and observed herpes labialis on the mother’s lips. The pediatrician concluded that the vesicles didn’t indicate herpes and discharged the baby, instructing the parents to have him reexamined if he developed a fever, irritability, or lethargy. The next day the pediatrician consulted a neonatologist, who advised immediate reexamination. The baby was taken to a hospital, but then was immediately transported to another hospital.
At the second hospital, a physician examined the baby and consulted an oral surgeon. The surgeon believed that the vesicles were caused by burns from a hot baby bottle. The baby was discharged.
Six days later, the mother brought the baby to his regular pediatrician. She reported that the infant had been feverish and lethargic. The pediatrician didn’t find vesicles or other abnormalities. She ordered a complete blood count and blood culture, gave antibiotics, and told the parents to bring the baby back to see her the next day.
Very early the next day, the parents brought the baby to a hospital with a temperature of 101.2°F. The examining physician contacted the child’s pediatrician, who said she wanted to see the baby at 8:00 AM. When the pediatrician examined him, the infant’s temperature was 100.5°F. She gave antibiotics and instructed the parents to bring the baby back the next day, when his test results would be available.
The next day, the parents told the pediatrician’s assistant who examined the baby that his arms and legs had been twitching the previous evening. The infant received antibiotics but began to exhibit jerky movements. The parents were told to take him to a hospital, where he was diagnosed with herpes simplex and residual brain damage.
The child has quadriparesis and can’t talk, walk, or feed himself. He can eat only pureed food.
PLAINTIFF’S CLAIM The herpes simplex infection should have been diagnosed earlier. The pediatrician who examined the infant initially should have cultured the vesicles (and made sure that acyclovir was given) or consulted with, or referred the child to, a specialist. The physician who saw the child at the second hospital should have consulted a specialist, which would have led to the administration of acyclovir.
THE DEFENSE Hospitalization wasn’t necessary and a culture wasn’t appropriate. The appearance of the vesicles when the baby was examined at the second hospital didn’t suggest herpes.
VERDICT Multiple New York settlements totaling $10.2 million.
COMMENT As with many malpractice cases, there were many opportunities to prevent an egregious outcome. I wonder whether anyone involved stopped to entertain a differential diagnosis and note the urgent conditions the presentation clearly suggested.
Not your garden variety neck pain
PERSISTENT BILATERAL NECK PAIN so severe that he couldn’t sit down brought a man to the emergency department (ED), where he was given ketorolac and diazepam. About an hour later, he said that the pain was better and was discharged with a diagnosis of neck strain and spasm and instructions to see his primary care physician if the pain persisted or worsened.
Four days later, the patient went to his primary care physician complaining of neck pain radiating down both arms, numbness in the right thumb, fever, chills, dysuria, and myalgia in his legs. The doctor observed decreased range of motion of the neck in all directions and diagnosed likely prostatitis. He ordered co-trimoxazole (trimethoprim and sulfamethoxazole), a nonemergent magnetic resonance imaging (MRI) scan, and physical therapy.
Fourteen hours after the doctor visit, the patient went back to the ED in a wheelchair. An emergency MRI showed epidural disease up and down the cervical spine and extending into the thoracic spine. An epidural abscess with spinal cord compression was diagnosed and decompression and evacuation surgery with spinal fusion was performed.
After several weeks in the hospital, the patient was referred to rehabilitation for partial quadriplegia. He has no use of his legs and very limited use of his hands and fingers. He’s confined to a wheelchair and needs help with most activities of daily living.
PLAINTIFF’S CLAIM When the patient visited his primary care physician, he had a classic presentation of a spinal abscess and should have undergone an emergent MRI, which would have revealed the abscess and allowed treatment with antibiotics and surgery before permanent damage occurred.
THE DEFENSE The patient’s symptoms weren’t a typical presentation of spinal abscess. There was no way the physician could have known what would happen the next day.
VERDICT $3 million Massachusetts settlement.
COMMENT Yes, there are zebras among the horses. We have to be vigilant to diagnose the rare serious cause of common problems such as neck pain. The combination of neck pain, patchy neurologic findings, signs of infection, and bladder symptoms should have raised red flags.
Untimely death blamed on undiagnosed PE
A 28-YEAR-OLD MAN went to the emergency department (ED) complaining of low-grade fever, nonproductive cough, and dizziness for 2 days. He also had tachycardia and significant hypoxia. An ED physician who saw the patient an hour after his arrival noted that he complained of weakness, shortness of breath, and light-headedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism.
After reviewing an electrocardiogram, chest radiograph, and laboratory studies, the ED doctor diagnosed pneumonia and renal insufficiency. The patient was admitted to the hospital, then transferred to another hospital about 8 hours later. He wasn’t evaluated by a physician when he was admitted to the second hospital.
About 5 hours after admission, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the patient never regained consciousness and died about an hour and a half later. An autopsy established a pulmonary embolism as the cause of death.
PLAINTIFF’S CLAIM The doctors were negligent in failing to diagnose and treat the pulmonary embolism. Proper treatment would have allowed the patient to survive.
THE DEFENSE There was no negligence; heparin therapy wouldn’t have prevented the patient’s death.
VERDICT $6.1 million Maryland verdict.
COMMENT It isn’t enough to think of pulmonary embolism; a prompt definitive diagnostic work-up and timely treatment are key to preventing such a catastrophic outcome.
Delayed herpes diagnosis leads to lifelong consequences
A 10-DAY-OLD INFANT was examined by a pediatrician, who noted vesicles dotting the baby’s tongue, a possible manifestation of herpes, and observed herpes labialis on the mother’s lips. The pediatrician concluded that the vesicles didn’t indicate herpes and discharged the baby, instructing the parents to have him reexamined if he developed a fever, irritability, or lethargy. The next day the pediatrician consulted a neonatologist, who advised immediate reexamination. The baby was taken to a hospital, but then was immediately transported to another hospital.
At the second hospital, a physician examined the baby and consulted an oral surgeon. The surgeon believed that the vesicles were caused by burns from a hot baby bottle. The baby was discharged.
Six days later, the mother brought the baby to his regular pediatrician. She reported that the infant had been feverish and lethargic. The pediatrician didn’t find vesicles or other abnormalities. She ordered a complete blood count and blood culture, gave antibiotics, and told the parents to bring the baby back to see her the next day.
Very early the next day, the parents brought the baby to a hospital with a temperature of 101.2°F. The examining physician contacted the child’s pediatrician, who said she wanted to see the baby at 8:00 AM. When the pediatrician examined him, the infant’s temperature was 100.5°F. She gave antibiotics and instructed the parents to bring the baby back the next day, when his test results would be available.
The next day, the parents told the pediatrician’s assistant who examined the baby that his arms and legs had been twitching the previous evening. The infant received antibiotics but began to exhibit jerky movements. The parents were told to take him to a hospital, where he was diagnosed with herpes simplex and residual brain damage.
The child has quadriparesis and can’t talk, walk, or feed himself. He can eat only pureed food.
PLAINTIFF’S CLAIM The herpes simplex infection should have been diagnosed earlier. The pediatrician who examined the infant initially should have cultured the vesicles (and made sure that acyclovir was given) or consulted with, or referred the child to, a specialist. The physician who saw the child at the second hospital should have consulted a specialist, which would have led to the administration of acyclovir.
THE DEFENSE Hospitalization wasn’t necessary and a culture wasn’t appropriate. The appearance of the vesicles when the baby was examined at the second hospital didn’t suggest herpes.
VERDICT Multiple New York settlements totaling $10.2 million.
COMMENT As with many malpractice cases, there were many opportunities to prevent an egregious outcome. I wonder whether anyone involved stopped to entertain a differential diagnosis and note the urgent conditions the presentation clearly suggested.
Not your garden variety neck pain
PERSISTENT BILATERAL NECK PAIN so severe that he couldn’t sit down brought a man to the emergency department (ED), where he was given ketorolac and diazepam. About an hour later, he said that the pain was better and was discharged with a diagnosis of neck strain and spasm and instructions to see his primary care physician if the pain persisted or worsened.
Four days later, the patient went to his primary care physician complaining of neck pain radiating down both arms, numbness in the right thumb, fever, chills, dysuria, and myalgia in his legs. The doctor observed decreased range of motion of the neck in all directions and diagnosed likely prostatitis. He ordered co-trimoxazole (trimethoprim and sulfamethoxazole), a nonemergent magnetic resonance imaging (MRI) scan, and physical therapy.
Fourteen hours after the doctor visit, the patient went back to the ED in a wheelchair. An emergency MRI showed epidural disease up and down the cervical spine and extending into the thoracic spine. An epidural abscess with spinal cord compression was diagnosed and decompression and evacuation surgery with spinal fusion was performed.
After several weeks in the hospital, the patient was referred to rehabilitation for partial quadriplegia. He has no use of his legs and very limited use of his hands and fingers. He’s confined to a wheelchair and needs help with most activities of daily living.
PLAINTIFF’S CLAIM When the patient visited his primary care physician, he had a classic presentation of a spinal abscess and should have undergone an emergent MRI, which would have revealed the abscess and allowed treatment with antibiotics and surgery before permanent damage occurred.
THE DEFENSE The patient’s symptoms weren’t a typical presentation of spinal abscess. There was no way the physician could have known what would happen the next day.
VERDICT $3 million Massachusetts settlement.
COMMENT Yes, there are zebras among the horses. We have to be vigilant to diagnose the rare serious cause of common problems such as neck pain. The combination of neck pain, patchy neurologic findings, signs of infection, and bladder symptoms should have raised red flags.
Untimely death blamed on undiagnosed PE
A 28-YEAR-OLD MAN went to the emergency department (ED) complaining of low-grade fever, nonproductive cough, and dizziness for 2 days. He also had tachycardia and significant hypoxia. An ED physician who saw the patient an hour after his arrival noted that he complained of weakness, shortness of breath, and light-headedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism.
After reviewing an electrocardiogram, chest radiograph, and laboratory studies, the ED doctor diagnosed pneumonia and renal insufficiency. The patient was admitted to the hospital, then transferred to another hospital about 8 hours later. He wasn’t evaluated by a physician when he was admitted to the second hospital.
About 5 hours after admission, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the patient never regained consciousness and died about an hour and a half later. An autopsy established a pulmonary embolism as the cause of death.
PLAINTIFF’S CLAIM The doctors were negligent in failing to diagnose and treat the pulmonary embolism. Proper treatment would have allowed the patient to survive.
THE DEFENSE There was no negligence; heparin therapy wouldn’t have prevented the patient’s death.
VERDICT $6.1 million Maryland verdict.
COMMENT It isn’t enough to think of pulmonary embolism; a prompt definitive diagnostic work-up and timely treatment are key to preventing such a catastrophic outcome.
Delayed herpes diagnosis leads to lifelong consequences
A 10-DAY-OLD INFANT was examined by a pediatrician, who noted vesicles dotting the baby’s tongue, a possible manifestation of herpes, and observed herpes labialis on the mother’s lips. The pediatrician concluded that the vesicles didn’t indicate herpes and discharged the baby, instructing the parents to have him reexamined if he developed a fever, irritability, or lethargy. The next day the pediatrician consulted a neonatologist, who advised immediate reexamination. The baby was taken to a hospital, but then was immediately transported to another hospital.
At the second hospital, a physician examined the baby and consulted an oral surgeon. The surgeon believed that the vesicles were caused by burns from a hot baby bottle. The baby was discharged.
Six days later, the mother brought the baby to his regular pediatrician. She reported that the infant had been feverish and lethargic. The pediatrician didn’t find vesicles or other abnormalities. She ordered a complete blood count and blood culture, gave antibiotics, and told the parents to bring the baby back to see her the next day.
Very early the next day, the parents brought the baby to a hospital with a temperature of 101.2°F. The examining physician contacted the child’s pediatrician, who said she wanted to see the baby at 8:00 AM. When the pediatrician examined him, the infant’s temperature was 100.5°F. She gave antibiotics and instructed the parents to bring the baby back the next day, when his test results would be available.
The next day, the parents told the pediatrician’s assistant who examined the baby that his arms and legs had been twitching the previous evening. The infant received antibiotics but began to exhibit jerky movements. The parents were told to take him to a hospital, where he was diagnosed with herpes simplex and residual brain damage.
The child has quadriparesis and can’t talk, walk, or feed himself. He can eat only pureed food.
PLAINTIFF’S CLAIM The herpes simplex infection should have been diagnosed earlier. The pediatrician who examined the infant initially should have cultured the vesicles (and made sure that acyclovir was given) or consulted with, or referred the child to, a specialist. The physician who saw the child at the second hospital should have consulted a specialist, which would have led to the administration of acyclovir.
THE DEFENSE Hospitalization wasn’t necessary and a culture wasn’t appropriate. The appearance of the vesicles when the baby was examined at the second hospital didn’t suggest herpes.
VERDICT Multiple New York settlements totaling $10.2 million.
COMMENT As with many malpractice cases, there were many opportunities to prevent an egregious outcome. I wonder whether anyone involved stopped to entertain a differential diagnosis and note the urgent conditions the presentation clearly suggested.
Combatting the cough that won’t quit
• Always include postnasal drip, asthma, and gastroesophageal reflux disease in the differential diagnosis for persistent cough, regardless of clinical signs and symptoms. B
• Do not rely on a patient’s description of the character and timing of the cough or the absence (or presence) of sputum to narrow down the differential diagnosis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Margaret M, a 52-year-old nonsmoker, came to our clinic because of a persistent cough that had started about 4 weeks earlier. She had tried multiple over-the-counter cough suppressants, including dextromethorphan and guaifenesin, as well as cough drops, but none had been effective.
Margaret denied having had a cold or respiratory infection in the past few months or being in close contact with anyone with a chronic cough, and she had never had an asthma diagnosis. In response to a question about previous coughing episodes, the patient recalled having had several bouts of chronic cough in the past, including one about a year ago.
While Margaret had no known allergies, she did have occasional heartburn, which an antacid—or, at times, a drink of water—always relieved. Thyroid medication and calcium were the only things she took on a regular basis, separated by several hours to avoid problems with absorption.
Patients like Margaret, who seek help from their primary care physician only after attempting to combat a persistent cough on their own, may be quite frustrated by the time they arrive in your office. They’re counting on you to provide a cure. Fortunately, you’re likely to find it, as the differential diagnosis for subacute cough (a cough of 3-8 weeks’ duration) is limited.
Nonetheless, finding the cause of a subacute or chronic cough (lasting >8 weeks) is sometimes a matter of trial and error. Postnasal drip (also known as upper airway cough syndrome, or UACS), asthma, and gastroesophageal reflux disease (GERD) are the most common causes,1,2 followed by postinfectious cough, nonasthmatic eosinophilic bronchitis (NAEB), and pertussis.3 Although these conditions are all relatively well known, they are not always easy to detect: Some disorders, including UACS, asthma, and GERD, may be “silent,” with persistent cough the only presenting sign or symptom.4 In other cases, more than one condition may be contributing to the cough.
Starting with trials of empiric therapy for the most common causes of persistent cough—with sequential therapy and diagnostic tests, as needed—is far more effective than searching for relatively uncommon or obscure conditions. Following such a protocol, as detailed in the algorithm (FIGURE)4-7 we’ve developed and in the text that follows, can help you combat subacute and chronic cough in a cost-effective, timely way.
FIGURE
Dx and treatment when persistent cough is the only symptom4-7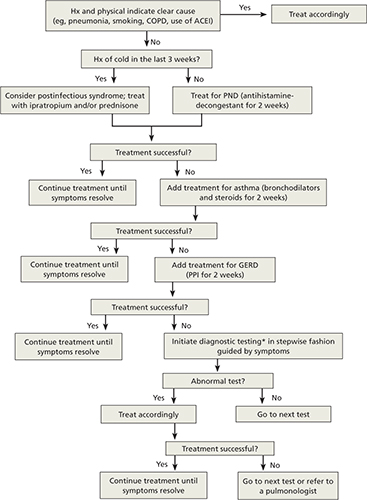
*May include CXR, PPD, B pertussis IgG or IgA, spirometry with methacholine inhalation challenge, barium swallow, prolonged pH monitoring, sinus CT, and sputum eosinophil count, excluding any tests that have already been performed.
ACEI, angiotensin-converting enzyme inhibitor; CT, computed tomography; COPD, chronic obstructive pulmonary disease; CXR, chest x-ray; GERD, gastroesophageal reflux disease; IgA, immunoglobulin A; IgG, immunoglobulin G; PND, postnasal drip; PPD, purified protein derivative; PPI, proton pump inhibitor.
Treat all patients for upper airway cough syndrome
Postnasal drip—renamed UACS by the guideline committee of the American Association of Chest Physicians because it isn’t clear whether the cough is caused by irritation from direct contact with postnasal drip or by inflammation of cough receptors in the upper airway—is the most common cause of chronic cough.6
The differential diagnosis for UACS, which is implicated in about 34% of cases of persistent cough, includes allergic, postinfectious, and occupational rhinitis; rhinitis due to anatomic abnormalities or physical or chemical irritants, rhinitis medicamentosa, and rhinitis of pregnancy; bacterial sinusitis; and allergic fungal sinusitis.8
The signs and symptoms of UACS are nonspecific, and a definitive diagnosis typically cannot be made from the medical history and physical examination alone. What’s more, the absence of any of the usual clinical findings—eg, rhinorrhea and excess sputum production—should not preclude an empiric trial with a first-generation antihistamine-decongestant combination such as brompheniramine/sustained-release pseudoephedrine. Second-and third-generation combination products, such as fexofenadine/pseudoephedrine, should not be used, as they are not effective in treating UACS.4
CASE Margaret’s physical exam was unremarkable. Her vital signs were stable, she had no cervical lymphadenopathy, and her chest was clear on auscultation. She had a dry cough that occurred twice during the exam, but not on inspiration.
The patient’s work-up included office spirometry, which was normal; a nasopharyngeal culture for Bordetella pertussis was negative. We prescribed a 2-week course of therapy with brompheniramine/sustained-release pseudoephedrine and scheduled a return visit shortly after it was completed.
There is no gold standard diagnostic test to confirm or rule out postnasal drip as the cause of cough. CT scanning of sinuses has a poor positive predictive value and is no longer recommended as part of an initial work-up,9 but may be useful for patients whose symptoms persist longer than 3 weeks.
Consider bronchodilator Tx when asthma is suspected
Cough-variant asthma is the second most common cause of persistent cough, and is responsible for an estimated 28% of cases.6 Asthma is the easiest of the conditions included in the differential diagnosis for persistent cough to establish in an office setting. The challenge is to remember to consider it in patients who present with cough but no sign of the classic expiratory wheezing. When you suspect that a patient has asthma, consider empiric bronchodilator therapy—or conduct spirometry testing.
Spirometric values of forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) <70% and a positive bronchodilator response (≥12%) are consistent with an asthma diagnosis. Management of asthma depends on severity, and patients should be evaluated based on the National Heart, Lung, and Blood Institute’s National Asthma Education and Prevention Program Guidelines for the Diagnosis and Management of Asthma.10
It is crucial to ask patients with asthma (and, indeed, to ask all patients with a persistent cough) about exposure to secondhand smoke, and to stress the importance of avoiding smoking and secondary exposure. Individuals who are regularly exposed to secondhand smoke report more nasal symptoms and greater use of nasal decongestants compared with people with no exposure to smoke;11 they also have poor control of asthma.12-14
Cough unresolved? Add therapy for GERD
Although GERD is primarily associated with heartburn and gastrointestinal distress, it is not unusual for cough to be its only sign or symptom.15 In fact, GERD is the third most common cause of subacute cough—affecting about 21% of patients who seek help for cough at primary care practices.3
CASE Margaret returned to the clinic shortly after completion of a 2-week course of brompheniramine/sustained-release pseudoephedrine, and reported that she was still coughing frequently—and that the medication had brought little improvement. Because of her history of heartburn, we added a 2-week trial with a proton pump inhibitor (PPI)—omeprazole 20 mg/d.
While there are diagnostic tests for GERD, including a pH probe of the esophagus, a barium esophagogram, and manometry testing, empiric therapy with a PPI—starting with a trial of at least 2 weeks—often eliminates the troublesome cough.16 If the patient responds to treatment, the medication can be continued. Risks associated with long-term PPI therapy include osteoporosis and interference with calcium and magnesium absorption,17 so it is important to monitor patients taking them and to discontinue treatment as soon as the cough symptoms resolve.
Have you ruled out postinfectious cough?
If a patient has a cough that has lingered for 3 to 8 weeks after his or her recovery from an acute upper respiratory infection (URI), postinfectious cough may be the reason.18,19 Such a cough is subacute and self-limiting. (If the cough lasts >8 weeks after an acute illness, other diagnoses, such as chronic infection, are more likely.)
The pathogenesis for postinfectious cough may be related to postviral airway inflammation or bronchial hyperresponsiveness, and antibiotics are not indicated.4 Patients may be treated with a bronchodilator such as ipratropium rather than a beta-agonist or inhaled corticosteroids; oral tapered prednisone can be prescribed, if needed, for severe paroxysms, although there is limited evidence of its efficacy.20 Central antitussive agents such as codeine and dextromethorphan can be used when other measures fail to bring relief.
Nonasthmatic eosinophilic bronchitis does not impede airflow
NAEB is less well known than the conditions discussed thus far, but it is a relatively common cause of persistent cough.21-23 In some studies, up to 13% of patients with subacute cough were diagnosed with NAEB.6
Unlike asthma, NAEB is not associated with abnormalities in airway function; patients have no dyspnea and no wheezing, and no obstruction of airflow.24 Patients will have FEV1 >80% and FEV1/FVC >75% on spirometric examination, a negative response to bronchoprovocation, and, typically, an elevated sputum eosinophil count of >3%. Because induced sputum or bronchoscopic washings are difficult, exhaled nitric oxide testing is another option. If these tests are not available, a trial of inhaled steroids is indicated, even if neither spirometry nor bronchoprovocation testing was abnormal.9
Patients with NAEB respond well to inhaled corticosteroids, and budesonide 400 mcg twice a day or prednisolone 30 mg daily may be prescribed. It is also important to remove airway irritants. Long-term follow-up studies of patients with NAEB have had conflicting results. One study found that most cases resolve completely;23 another showed a need for long-term treatment, and suggested that patients with NAEB may be at increased risk for asthma and chronic obstructive pulmonary disease. 25
Paroxysmal cough, whoops point to pertussis
When a patient has paroxysms of cough, posttussive vomiting, and/or an inspiratory whooping sound, B pertussis infection is the likely culprit.26-28 A definitive diagnosis of pertussis, or whooping cough, may be based on a positive culture from a nasopharyngeal aspirate swab.29 Suspected cases can be confirmed with a polymerase chain reaction test, and a presumptive diagnosis may be made as a result of a 4-fold increase in immunoglobulin G or immunoglobulin A antibodies for B pertussis.4
A macrolide antibiotic, usually azithromycin, is the standard treatment for pertussis.30-32 Patients should be isolated for 5 days from the start of treatment. Antibiotic therapy will reduce the risk of transmission, but will not affect the duration of the cough, which may be 6 to 8 weeks. Long-acting beta-agonists, antihistamines, and corticosteroids should not be used to treat pertussis.4
CASE After a 2-week course of omeprazole 20 mg daily, Margaret was coughing much less. We extended the prescription, and by the end of the next 4 weeks, she was no longer coughing. After 2 months, both the PPI and the antihistamine/decongestant were discontinued. We advised her to institute antireflux measures, such as elevating her head at night and not eating after 6 pm, and she has not had a relapse.
CORRESPONDENCE Rebecca H. Gladu, MD, FAAFP, San Jacinto Methodist Hospital, 4401 Garth Road, Baytown, TX 77521; Rgladu@tmhs.org
1. Corrao WM. Chronic persistent cough: diagnosis and treatment update. Pediatr Ann. 1996;25:162-168.
2. Holmes RL, Fadden CT. Evaluation of the patient with chronic cough. Am Fam Physician. 2004;69:2159-2166.
3. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990;141:640-647.
4. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough. Executive summary: ACCP evidence-based practice guideline. Chest. 2006;129(1 suppl):1S-23S.
5. Pratter MR, Bartter T, Akers S, et al. An algorithmic approach to chronic cough. Ann Intern Med. 1993;119:977-983.
6. Pratter MR, Brightling CE, Boulet LP, et al. An empiric integrative approach to the management of cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129 (1 suppl):222S-231S.
7. Irwin RS, Madison JM. Anatomical diagnostic protocol in evaluating chronic cough with specific reference to gastroesophageal reflux disease. Am J Med. 2000;108(suppl 4a):126S-130S.
8. Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981;123 (4 Pt 1):413-417.
9. Birring SS. Controversies in the evaluation and management of chronic cough. Am J Respir Crit Care Med. 2011;183:708-715.
10. National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
11. Reh DD, Lin SY, Clipp SL, et al. Secondhand tobacco smoke exposure and chronic rhinosinusitis: a population-based case-control study. Am J Rhinol Allergy. 2009;23:562-567.
12. Stapleton M, Howard-Thompson A, George C, et al. Smoking and asthma. J Am Board Fam Med. 2011;24:313-322.
13. Hersoug LG, Husemoen LL, Sigsgaard T, et al. Indoor exposure to environmental cigarette smoke, but not other inhaled particulates associates with respiratory symptoms and diminished lung function in adults. Respirology. 2010;15:993-1000.
14. Self TH, Wallace JL, Gray LA, et al. Are we failing to document adequate smoking histories? A brief review 1999-2009. Curr Med Res Opin. 2010;26:1691-1696.
15. Sontag SJ. The spectrum of pulmonary symptoms due to gastroesophageal reflux. Thorac Surg Clin. 2005;15:353-368.
16. Irwin RS. Chronic cough due to gastroesophageal reflux. ACCP evidence-based clinical practice guidelines. Chest. 2006;129(suppl 1):80S-94S.
17. Chen J, Yuan YC, Leontiadis GI, et al. Recent safety concerns with proton pump inhibitors. J Clin Gastroenterol. 2012;46:93-114.
18. Braman SS. Postinfectious cough: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):138S-146S.
19. Pratter MR. Cough and the common cold: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):72S-74S.
20. Chang AB, McKean M, Morris P. Inhaled anticholinergics for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2004;(1):CD004358.-
21. Brightling CE, Ward R, Goh KL, et al. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med. 1999;160:406-410.
22. Gonlugur U, Gonlugur TE. Eosinophilic bronchitis without asthma. Int Arch Allergy Immunol. 2008;147:1-5.
23. Brightling CE. Cough due to asthma and nonasthmatic eosinophilic bronchitis. Lung. 2010;188 (suppl 1):S13-S17.
24. Gibson PG, Hargreave FE, Girgis-Gabardo, et al. Chronic cough with eosinophilic bronchitis: examination for variable airflow obstruction and response to corticosteroid. Clin Exp Allergy. 1995;25:127-132.
25. Berry MA, Hargadon B, McKenna S, et al. Observational study of the natural history of eosinophilic bronchitis. Clin Exp Allergy. 2005;35:598-601.
26. Antico A, Fabozzi F, Scipiotti C. Pertussis in adults. A study in an Italian population with chronic cough. Monaldi Arch Chest Dis. 2002;57:247-252.
27. Birkebaek NH, Kristiansen M, Seefeldt T, et al. Bordetella pertussis and chronic cough in adults. Clin Infect Dis. 1999;29:1239-1242.
28. Kapaskelis AM, Vouloumanou EK, Rafailidis PI, et al. High prevalence of antibody titers against Bordetella pertussis in an adult population with prolonged cough. Respir Med. 2008;102:1586-1591.
29. Cornia PB, Hersh AL, Lipsky BA, et al. Does this coughing adolescent or adult patient have pertussis? JAMA. 2010;304:890-896.
30. Devasia RA, Jones TF, Collier B, et al. Compliance with azithromycin versus erythromycin in the setting of a pertussis outbreak. Am J Med Sci. 2009;337:176-178.
31. Poe RH, Harder RV, Israel RH, et al. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest. 1989;95:723-728.
32. Altunaji SM, Kukuruzovic RH, Curtis NC, et al. Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev. 2007;(3):CD004404.-
• Always include postnasal drip, asthma, and gastroesophageal reflux disease in the differential diagnosis for persistent cough, regardless of clinical signs and symptoms. B
• Do not rely on a patient’s description of the character and timing of the cough or the absence (or presence) of sputum to narrow down the differential diagnosis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Margaret M, a 52-year-old nonsmoker, came to our clinic because of a persistent cough that had started about 4 weeks earlier. She had tried multiple over-the-counter cough suppressants, including dextromethorphan and guaifenesin, as well as cough drops, but none had been effective.
Margaret denied having had a cold or respiratory infection in the past few months or being in close contact with anyone with a chronic cough, and she had never had an asthma diagnosis. In response to a question about previous coughing episodes, the patient recalled having had several bouts of chronic cough in the past, including one about a year ago.
While Margaret had no known allergies, she did have occasional heartburn, which an antacid—or, at times, a drink of water—always relieved. Thyroid medication and calcium were the only things she took on a regular basis, separated by several hours to avoid problems with absorption.
Patients like Margaret, who seek help from their primary care physician only after attempting to combat a persistent cough on their own, may be quite frustrated by the time they arrive in your office. They’re counting on you to provide a cure. Fortunately, you’re likely to find it, as the differential diagnosis for subacute cough (a cough of 3-8 weeks’ duration) is limited.
Nonetheless, finding the cause of a subacute or chronic cough (lasting >8 weeks) is sometimes a matter of trial and error. Postnasal drip (also known as upper airway cough syndrome, or UACS), asthma, and gastroesophageal reflux disease (GERD) are the most common causes,1,2 followed by postinfectious cough, nonasthmatic eosinophilic bronchitis (NAEB), and pertussis.3 Although these conditions are all relatively well known, they are not always easy to detect: Some disorders, including UACS, asthma, and GERD, may be “silent,” with persistent cough the only presenting sign or symptom.4 In other cases, more than one condition may be contributing to the cough.
Starting with trials of empiric therapy for the most common causes of persistent cough—with sequential therapy and diagnostic tests, as needed—is far more effective than searching for relatively uncommon or obscure conditions. Following such a protocol, as detailed in the algorithm (FIGURE)4-7 we’ve developed and in the text that follows, can help you combat subacute and chronic cough in a cost-effective, timely way.
FIGURE
Dx and treatment when persistent cough is the only symptom4-7
*May include CXR, PPD, B pertussis IgG or IgA, spirometry with methacholine inhalation challenge, barium swallow, prolonged pH monitoring, sinus CT, and sputum eosinophil count, excluding any tests that have already been performed.
ACEI, angiotensin-converting enzyme inhibitor; CT, computed tomography; COPD, chronic obstructive pulmonary disease; CXR, chest x-ray; GERD, gastroesophageal reflux disease; IgA, immunoglobulin A; IgG, immunoglobulin G; PND, postnasal drip; PPD, purified protein derivative; PPI, proton pump inhibitor.
Treat all patients for upper airway cough syndrome
Postnasal drip—renamed UACS by the guideline committee of the American Association of Chest Physicians because it isn’t clear whether the cough is caused by irritation from direct contact with postnasal drip or by inflammation of cough receptors in the upper airway—is the most common cause of chronic cough.6
The differential diagnosis for UACS, which is implicated in about 34% of cases of persistent cough, includes allergic, postinfectious, and occupational rhinitis; rhinitis due to anatomic abnormalities or physical or chemical irritants, rhinitis medicamentosa, and rhinitis of pregnancy; bacterial sinusitis; and allergic fungal sinusitis.8
The signs and symptoms of UACS are nonspecific, and a definitive diagnosis typically cannot be made from the medical history and physical examination alone. What’s more, the absence of any of the usual clinical findings—eg, rhinorrhea and excess sputum production—should not preclude an empiric trial with a first-generation antihistamine-decongestant combination such as brompheniramine/sustained-release pseudoephedrine. Second-and third-generation combination products, such as fexofenadine/pseudoephedrine, should not be used, as they are not effective in treating UACS.4
CASE Margaret’s physical exam was unremarkable. Her vital signs were stable, she had no cervical lymphadenopathy, and her chest was clear on auscultation. She had a dry cough that occurred twice during the exam, but not on inspiration.
The patient’s work-up included office spirometry, which was normal; a nasopharyngeal culture for Bordetella pertussis was negative. We prescribed a 2-week course of therapy with brompheniramine/sustained-release pseudoephedrine and scheduled a return visit shortly after it was completed.
There is no gold standard diagnostic test to confirm or rule out postnasal drip as the cause of cough. CT scanning of sinuses has a poor positive predictive value and is no longer recommended as part of an initial work-up,9 but may be useful for patients whose symptoms persist longer than 3 weeks.
Consider bronchodilator Tx when asthma is suspected
Cough-variant asthma is the second most common cause of persistent cough, and is responsible for an estimated 28% of cases.6 Asthma is the easiest of the conditions included in the differential diagnosis for persistent cough to establish in an office setting. The challenge is to remember to consider it in patients who present with cough but no sign of the classic expiratory wheezing. When you suspect that a patient has asthma, consider empiric bronchodilator therapy—or conduct spirometry testing.
Spirometric values of forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) <70% and a positive bronchodilator response (≥12%) are consistent with an asthma diagnosis. Management of asthma depends on severity, and patients should be evaluated based on the National Heart, Lung, and Blood Institute’s National Asthma Education and Prevention Program Guidelines for the Diagnosis and Management of Asthma.10
It is crucial to ask patients with asthma (and, indeed, to ask all patients with a persistent cough) about exposure to secondhand smoke, and to stress the importance of avoiding smoking and secondary exposure. Individuals who are regularly exposed to secondhand smoke report more nasal symptoms and greater use of nasal decongestants compared with people with no exposure to smoke;11 they also have poor control of asthma.12-14
Cough unresolved? Add therapy for GERD
Although GERD is primarily associated with heartburn and gastrointestinal distress, it is not unusual for cough to be its only sign or symptom.15 In fact, GERD is the third most common cause of subacute cough—affecting about 21% of patients who seek help for cough at primary care practices.3
CASE Margaret returned to the clinic shortly after completion of a 2-week course of brompheniramine/sustained-release pseudoephedrine, and reported that she was still coughing frequently—and that the medication had brought little improvement. Because of her history of heartburn, we added a 2-week trial with a proton pump inhibitor (PPI)—omeprazole 20 mg/d.
While there are diagnostic tests for GERD, including a pH probe of the esophagus, a barium esophagogram, and manometry testing, empiric therapy with a PPI—starting with a trial of at least 2 weeks—often eliminates the troublesome cough.16 If the patient responds to treatment, the medication can be continued. Risks associated with long-term PPI therapy include osteoporosis and interference with calcium and magnesium absorption,17 so it is important to monitor patients taking them and to discontinue treatment as soon as the cough symptoms resolve.
Have you ruled out postinfectious cough?
If a patient has a cough that has lingered for 3 to 8 weeks after his or her recovery from an acute upper respiratory infection (URI), postinfectious cough may be the reason.18,19 Such a cough is subacute and self-limiting. (If the cough lasts >8 weeks after an acute illness, other diagnoses, such as chronic infection, are more likely.)
The pathogenesis for postinfectious cough may be related to postviral airway inflammation or bronchial hyperresponsiveness, and antibiotics are not indicated.4 Patients may be treated with a bronchodilator such as ipratropium rather than a beta-agonist or inhaled corticosteroids; oral tapered prednisone can be prescribed, if needed, for severe paroxysms, although there is limited evidence of its efficacy.20 Central antitussive agents such as codeine and dextromethorphan can be used when other measures fail to bring relief.
Nonasthmatic eosinophilic bronchitis does not impede airflow
NAEB is less well known than the conditions discussed thus far, but it is a relatively common cause of persistent cough.21-23 In some studies, up to 13% of patients with subacute cough were diagnosed with NAEB.6
Unlike asthma, NAEB is not associated with abnormalities in airway function; patients have no dyspnea and no wheezing, and no obstruction of airflow.24 Patients will have FEV1 >80% and FEV1/FVC >75% on spirometric examination, a negative response to bronchoprovocation, and, typically, an elevated sputum eosinophil count of >3%. Because induced sputum or bronchoscopic washings are difficult, exhaled nitric oxide testing is another option. If these tests are not available, a trial of inhaled steroids is indicated, even if neither spirometry nor bronchoprovocation testing was abnormal.9
Patients with NAEB respond well to inhaled corticosteroids, and budesonide 400 mcg twice a day or prednisolone 30 mg daily may be prescribed. It is also important to remove airway irritants. Long-term follow-up studies of patients with NAEB have had conflicting results. One study found that most cases resolve completely;23 another showed a need for long-term treatment, and suggested that patients with NAEB may be at increased risk for asthma and chronic obstructive pulmonary disease. 25
Paroxysmal cough, whoops point to pertussis
When a patient has paroxysms of cough, posttussive vomiting, and/or an inspiratory whooping sound, B pertussis infection is the likely culprit.26-28 A definitive diagnosis of pertussis, or whooping cough, may be based on a positive culture from a nasopharyngeal aspirate swab.29 Suspected cases can be confirmed with a polymerase chain reaction test, and a presumptive diagnosis may be made as a result of a 4-fold increase in immunoglobulin G or immunoglobulin A antibodies for B pertussis.4
A macrolide antibiotic, usually azithromycin, is the standard treatment for pertussis.30-32 Patients should be isolated for 5 days from the start of treatment. Antibiotic therapy will reduce the risk of transmission, but will not affect the duration of the cough, which may be 6 to 8 weeks. Long-acting beta-agonists, antihistamines, and corticosteroids should not be used to treat pertussis.4
CASE After a 2-week course of omeprazole 20 mg daily, Margaret was coughing much less. We extended the prescription, and by the end of the next 4 weeks, she was no longer coughing. After 2 months, both the PPI and the antihistamine/decongestant were discontinued. We advised her to institute antireflux measures, such as elevating her head at night and not eating after 6 pm, and she has not had a relapse.
CORRESPONDENCE Rebecca H. Gladu, MD, FAAFP, San Jacinto Methodist Hospital, 4401 Garth Road, Baytown, TX 77521; Rgladu@tmhs.org
• Always include postnasal drip, asthma, and gastroesophageal reflux disease in the differential diagnosis for persistent cough, regardless of clinical signs and symptoms. B
• Do not rely on a patient’s description of the character and timing of the cough or the absence (or presence) of sputum to narrow down the differential diagnosis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Margaret M, a 52-year-old nonsmoker, came to our clinic because of a persistent cough that had started about 4 weeks earlier. She had tried multiple over-the-counter cough suppressants, including dextromethorphan and guaifenesin, as well as cough drops, but none had been effective.
Margaret denied having had a cold or respiratory infection in the past few months or being in close contact with anyone with a chronic cough, and she had never had an asthma diagnosis. In response to a question about previous coughing episodes, the patient recalled having had several bouts of chronic cough in the past, including one about a year ago.
While Margaret had no known allergies, she did have occasional heartburn, which an antacid—or, at times, a drink of water—always relieved. Thyroid medication and calcium were the only things she took on a regular basis, separated by several hours to avoid problems with absorption.
Patients like Margaret, who seek help from their primary care physician only after attempting to combat a persistent cough on their own, may be quite frustrated by the time they arrive in your office. They’re counting on you to provide a cure. Fortunately, you’re likely to find it, as the differential diagnosis for subacute cough (a cough of 3-8 weeks’ duration) is limited.
Nonetheless, finding the cause of a subacute or chronic cough (lasting >8 weeks) is sometimes a matter of trial and error. Postnasal drip (also known as upper airway cough syndrome, or UACS), asthma, and gastroesophageal reflux disease (GERD) are the most common causes,1,2 followed by postinfectious cough, nonasthmatic eosinophilic bronchitis (NAEB), and pertussis.3 Although these conditions are all relatively well known, they are not always easy to detect: Some disorders, including UACS, asthma, and GERD, may be “silent,” with persistent cough the only presenting sign or symptom.4 In other cases, more than one condition may be contributing to the cough.
Starting with trials of empiric therapy for the most common causes of persistent cough—with sequential therapy and diagnostic tests, as needed—is far more effective than searching for relatively uncommon or obscure conditions. Following such a protocol, as detailed in the algorithm (FIGURE)4-7 we’ve developed and in the text that follows, can help you combat subacute and chronic cough in a cost-effective, timely way.
FIGURE
Dx and treatment when persistent cough is the only symptom4-7
*May include CXR, PPD, B pertussis IgG or IgA, spirometry with methacholine inhalation challenge, barium swallow, prolonged pH monitoring, sinus CT, and sputum eosinophil count, excluding any tests that have already been performed.
ACEI, angiotensin-converting enzyme inhibitor; CT, computed tomography; COPD, chronic obstructive pulmonary disease; CXR, chest x-ray; GERD, gastroesophageal reflux disease; IgA, immunoglobulin A; IgG, immunoglobulin G; PND, postnasal drip; PPD, purified protein derivative; PPI, proton pump inhibitor.
Treat all patients for upper airway cough syndrome
Postnasal drip—renamed UACS by the guideline committee of the American Association of Chest Physicians because it isn’t clear whether the cough is caused by irritation from direct contact with postnasal drip or by inflammation of cough receptors in the upper airway—is the most common cause of chronic cough.6
The differential diagnosis for UACS, which is implicated in about 34% of cases of persistent cough, includes allergic, postinfectious, and occupational rhinitis; rhinitis due to anatomic abnormalities or physical or chemical irritants, rhinitis medicamentosa, and rhinitis of pregnancy; bacterial sinusitis; and allergic fungal sinusitis.8
The signs and symptoms of UACS are nonspecific, and a definitive diagnosis typically cannot be made from the medical history and physical examination alone. What’s more, the absence of any of the usual clinical findings—eg, rhinorrhea and excess sputum production—should not preclude an empiric trial with a first-generation antihistamine-decongestant combination such as brompheniramine/sustained-release pseudoephedrine. Second-and third-generation combination products, such as fexofenadine/pseudoephedrine, should not be used, as they are not effective in treating UACS.4
CASE Margaret’s physical exam was unremarkable. Her vital signs were stable, she had no cervical lymphadenopathy, and her chest was clear on auscultation. She had a dry cough that occurred twice during the exam, but not on inspiration.
The patient’s work-up included office spirometry, which was normal; a nasopharyngeal culture for Bordetella pertussis was negative. We prescribed a 2-week course of therapy with brompheniramine/sustained-release pseudoephedrine and scheduled a return visit shortly after it was completed.
There is no gold standard diagnostic test to confirm or rule out postnasal drip as the cause of cough. CT scanning of sinuses has a poor positive predictive value and is no longer recommended as part of an initial work-up,9 but may be useful for patients whose symptoms persist longer than 3 weeks.
Consider bronchodilator Tx when asthma is suspected
Cough-variant asthma is the second most common cause of persistent cough, and is responsible for an estimated 28% of cases.6 Asthma is the easiest of the conditions included in the differential diagnosis for persistent cough to establish in an office setting. The challenge is to remember to consider it in patients who present with cough but no sign of the classic expiratory wheezing. When you suspect that a patient has asthma, consider empiric bronchodilator therapy—or conduct spirometry testing.
Spirometric values of forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) <70% and a positive bronchodilator response (≥12%) are consistent with an asthma diagnosis. Management of asthma depends on severity, and patients should be evaluated based on the National Heart, Lung, and Blood Institute’s National Asthma Education and Prevention Program Guidelines for the Diagnosis and Management of Asthma.10
It is crucial to ask patients with asthma (and, indeed, to ask all patients with a persistent cough) about exposure to secondhand smoke, and to stress the importance of avoiding smoking and secondary exposure. Individuals who are regularly exposed to secondhand smoke report more nasal symptoms and greater use of nasal decongestants compared with people with no exposure to smoke;11 they also have poor control of asthma.12-14
Cough unresolved? Add therapy for GERD
Although GERD is primarily associated with heartburn and gastrointestinal distress, it is not unusual for cough to be its only sign or symptom.15 In fact, GERD is the third most common cause of subacute cough—affecting about 21% of patients who seek help for cough at primary care practices.3
CASE Margaret returned to the clinic shortly after completion of a 2-week course of brompheniramine/sustained-release pseudoephedrine, and reported that she was still coughing frequently—and that the medication had brought little improvement. Because of her history of heartburn, we added a 2-week trial with a proton pump inhibitor (PPI)—omeprazole 20 mg/d.
While there are diagnostic tests for GERD, including a pH probe of the esophagus, a barium esophagogram, and manometry testing, empiric therapy with a PPI—starting with a trial of at least 2 weeks—often eliminates the troublesome cough.16 If the patient responds to treatment, the medication can be continued. Risks associated with long-term PPI therapy include osteoporosis and interference with calcium and magnesium absorption,17 so it is important to monitor patients taking them and to discontinue treatment as soon as the cough symptoms resolve.
Have you ruled out postinfectious cough?
If a patient has a cough that has lingered for 3 to 8 weeks after his or her recovery from an acute upper respiratory infection (URI), postinfectious cough may be the reason.18,19 Such a cough is subacute and self-limiting. (If the cough lasts >8 weeks after an acute illness, other diagnoses, such as chronic infection, are more likely.)
The pathogenesis for postinfectious cough may be related to postviral airway inflammation or bronchial hyperresponsiveness, and antibiotics are not indicated.4 Patients may be treated with a bronchodilator such as ipratropium rather than a beta-agonist or inhaled corticosteroids; oral tapered prednisone can be prescribed, if needed, for severe paroxysms, although there is limited evidence of its efficacy.20 Central antitussive agents such as codeine and dextromethorphan can be used when other measures fail to bring relief.
Nonasthmatic eosinophilic bronchitis does not impede airflow
NAEB is less well known than the conditions discussed thus far, but it is a relatively common cause of persistent cough.21-23 In some studies, up to 13% of patients with subacute cough were diagnosed with NAEB.6
Unlike asthma, NAEB is not associated with abnormalities in airway function; patients have no dyspnea and no wheezing, and no obstruction of airflow.24 Patients will have FEV1 >80% and FEV1/FVC >75% on spirometric examination, a negative response to bronchoprovocation, and, typically, an elevated sputum eosinophil count of >3%. Because induced sputum or bronchoscopic washings are difficult, exhaled nitric oxide testing is another option. If these tests are not available, a trial of inhaled steroids is indicated, even if neither spirometry nor bronchoprovocation testing was abnormal.9
Patients with NAEB respond well to inhaled corticosteroids, and budesonide 400 mcg twice a day or prednisolone 30 mg daily may be prescribed. It is also important to remove airway irritants. Long-term follow-up studies of patients with NAEB have had conflicting results. One study found that most cases resolve completely;23 another showed a need for long-term treatment, and suggested that patients with NAEB may be at increased risk for asthma and chronic obstructive pulmonary disease. 25
Paroxysmal cough, whoops point to pertussis
When a patient has paroxysms of cough, posttussive vomiting, and/or an inspiratory whooping sound, B pertussis infection is the likely culprit.26-28 A definitive diagnosis of pertussis, or whooping cough, may be based on a positive culture from a nasopharyngeal aspirate swab.29 Suspected cases can be confirmed with a polymerase chain reaction test, and a presumptive diagnosis may be made as a result of a 4-fold increase in immunoglobulin G or immunoglobulin A antibodies for B pertussis.4
A macrolide antibiotic, usually azithromycin, is the standard treatment for pertussis.30-32 Patients should be isolated for 5 days from the start of treatment. Antibiotic therapy will reduce the risk of transmission, but will not affect the duration of the cough, which may be 6 to 8 weeks. Long-acting beta-agonists, antihistamines, and corticosteroids should not be used to treat pertussis.4
CASE After a 2-week course of omeprazole 20 mg daily, Margaret was coughing much less. We extended the prescription, and by the end of the next 4 weeks, she was no longer coughing. After 2 months, both the PPI and the antihistamine/decongestant were discontinued. We advised her to institute antireflux measures, such as elevating her head at night and not eating after 6 pm, and she has not had a relapse.
CORRESPONDENCE Rebecca H. Gladu, MD, FAAFP, San Jacinto Methodist Hospital, 4401 Garth Road, Baytown, TX 77521; Rgladu@tmhs.org
1. Corrao WM. Chronic persistent cough: diagnosis and treatment update. Pediatr Ann. 1996;25:162-168.
2. Holmes RL, Fadden CT. Evaluation of the patient with chronic cough. Am Fam Physician. 2004;69:2159-2166.
3. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990;141:640-647.
4. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough. Executive summary: ACCP evidence-based practice guideline. Chest. 2006;129(1 suppl):1S-23S.
5. Pratter MR, Bartter T, Akers S, et al. An algorithmic approach to chronic cough. Ann Intern Med. 1993;119:977-983.
6. Pratter MR, Brightling CE, Boulet LP, et al. An empiric integrative approach to the management of cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129 (1 suppl):222S-231S.
7. Irwin RS, Madison JM. Anatomical diagnostic protocol in evaluating chronic cough with specific reference to gastroesophageal reflux disease. Am J Med. 2000;108(suppl 4a):126S-130S.
8. Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981;123 (4 Pt 1):413-417.
9. Birring SS. Controversies in the evaluation and management of chronic cough. Am J Respir Crit Care Med. 2011;183:708-715.
10. National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
11. Reh DD, Lin SY, Clipp SL, et al. Secondhand tobacco smoke exposure and chronic rhinosinusitis: a population-based case-control study. Am J Rhinol Allergy. 2009;23:562-567.
12. Stapleton M, Howard-Thompson A, George C, et al. Smoking and asthma. J Am Board Fam Med. 2011;24:313-322.
13. Hersoug LG, Husemoen LL, Sigsgaard T, et al. Indoor exposure to environmental cigarette smoke, but not other inhaled particulates associates with respiratory symptoms and diminished lung function in adults. Respirology. 2010;15:993-1000.
14. Self TH, Wallace JL, Gray LA, et al. Are we failing to document adequate smoking histories? A brief review 1999-2009. Curr Med Res Opin. 2010;26:1691-1696.
15. Sontag SJ. The spectrum of pulmonary symptoms due to gastroesophageal reflux. Thorac Surg Clin. 2005;15:353-368.
16. Irwin RS. Chronic cough due to gastroesophageal reflux. ACCP evidence-based clinical practice guidelines. Chest. 2006;129(suppl 1):80S-94S.
17. Chen J, Yuan YC, Leontiadis GI, et al. Recent safety concerns with proton pump inhibitors. J Clin Gastroenterol. 2012;46:93-114.
18. Braman SS. Postinfectious cough: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):138S-146S.
19. Pratter MR. Cough and the common cold: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):72S-74S.
20. Chang AB, McKean M, Morris P. Inhaled anticholinergics for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2004;(1):CD004358.-
21. Brightling CE, Ward R, Goh KL, et al. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med. 1999;160:406-410.
22. Gonlugur U, Gonlugur TE. Eosinophilic bronchitis without asthma. Int Arch Allergy Immunol. 2008;147:1-5.
23. Brightling CE. Cough due to asthma and nonasthmatic eosinophilic bronchitis. Lung. 2010;188 (suppl 1):S13-S17.
24. Gibson PG, Hargreave FE, Girgis-Gabardo, et al. Chronic cough with eosinophilic bronchitis: examination for variable airflow obstruction and response to corticosteroid. Clin Exp Allergy. 1995;25:127-132.
25. Berry MA, Hargadon B, McKenna S, et al. Observational study of the natural history of eosinophilic bronchitis. Clin Exp Allergy. 2005;35:598-601.
26. Antico A, Fabozzi F, Scipiotti C. Pertussis in adults. A study in an Italian population with chronic cough. Monaldi Arch Chest Dis. 2002;57:247-252.
27. Birkebaek NH, Kristiansen M, Seefeldt T, et al. Bordetella pertussis and chronic cough in adults. Clin Infect Dis. 1999;29:1239-1242.
28. Kapaskelis AM, Vouloumanou EK, Rafailidis PI, et al. High prevalence of antibody titers against Bordetella pertussis in an adult population with prolonged cough. Respir Med. 2008;102:1586-1591.
29. Cornia PB, Hersh AL, Lipsky BA, et al. Does this coughing adolescent or adult patient have pertussis? JAMA. 2010;304:890-896.
30. Devasia RA, Jones TF, Collier B, et al. Compliance with azithromycin versus erythromycin in the setting of a pertussis outbreak. Am J Med Sci. 2009;337:176-178.
31. Poe RH, Harder RV, Israel RH, et al. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest. 1989;95:723-728.
32. Altunaji SM, Kukuruzovic RH, Curtis NC, et al. Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev. 2007;(3):CD004404.-
1. Corrao WM. Chronic persistent cough: diagnosis and treatment update. Pediatr Ann. 1996;25:162-168.
2. Holmes RL, Fadden CT. Evaluation of the patient with chronic cough. Am Fam Physician. 2004;69:2159-2166.
3. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990;141:640-647.
4. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough. Executive summary: ACCP evidence-based practice guideline. Chest. 2006;129(1 suppl):1S-23S.
5. Pratter MR, Bartter T, Akers S, et al. An algorithmic approach to chronic cough. Ann Intern Med. 1993;119:977-983.
6. Pratter MR, Brightling CE, Boulet LP, et al. An empiric integrative approach to the management of cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129 (1 suppl):222S-231S.
7. Irwin RS, Madison JM. Anatomical diagnostic protocol in evaluating chronic cough with specific reference to gastroesophageal reflux disease. Am J Med. 2000;108(suppl 4a):126S-130S.
8. Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981;123 (4 Pt 1):413-417.
9. Birring SS. Controversies in the evaluation and management of chronic cough. Am J Respir Crit Care Med. 2011;183:708-715.
10. National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
11. Reh DD, Lin SY, Clipp SL, et al. Secondhand tobacco smoke exposure and chronic rhinosinusitis: a population-based case-control study. Am J Rhinol Allergy. 2009;23:562-567.
12. Stapleton M, Howard-Thompson A, George C, et al. Smoking and asthma. J Am Board Fam Med. 2011;24:313-322.
13. Hersoug LG, Husemoen LL, Sigsgaard T, et al. Indoor exposure to environmental cigarette smoke, but not other inhaled particulates associates with respiratory symptoms and diminished lung function in adults. Respirology. 2010;15:993-1000.
14. Self TH, Wallace JL, Gray LA, et al. Are we failing to document adequate smoking histories? A brief review 1999-2009. Curr Med Res Opin. 2010;26:1691-1696.
15. Sontag SJ. The spectrum of pulmonary symptoms due to gastroesophageal reflux. Thorac Surg Clin. 2005;15:353-368.
16. Irwin RS. Chronic cough due to gastroesophageal reflux. ACCP evidence-based clinical practice guidelines. Chest. 2006;129(suppl 1):80S-94S.
17. Chen J, Yuan YC, Leontiadis GI, et al. Recent safety concerns with proton pump inhibitors. J Clin Gastroenterol. 2012;46:93-114.
18. Braman SS. Postinfectious cough: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):138S-146S.
19. Pratter MR. Cough and the common cold: ACCP evidence-based practice guidelines. Chest. 2006;129(suppl 1):72S-74S.
20. Chang AB, McKean M, Morris P. Inhaled anticholinergics for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2004;(1):CD004358.-
21. Brightling CE, Ward R, Goh KL, et al. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med. 1999;160:406-410.
22. Gonlugur U, Gonlugur TE. Eosinophilic bronchitis without asthma. Int Arch Allergy Immunol. 2008;147:1-5.
23. Brightling CE. Cough due to asthma and nonasthmatic eosinophilic bronchitis. Lung. 2010;188 (suppl 1):S13-S17.
24. Gibson PG, Hargreave FE, Girgis-Gabardo, et al. Chronic cough with eosinophilic bronchitis: examination for variable airflow obstruction and response to corticosteroid. Clin Exp Allergy. 1995;25:127-132.
25. Berry MA, Hargadon B, McKenna S, et al. Observational study of the natural history of eosinophilic bronchitis. Clin Exp Allergy. 2005;35:598-601.
26. Antico A, Fabozzi F, Scipiotti C. Pertussis in adults. A study in an Italian population with chronic cough. Monaldi Arch Chest Dis. 2002;57:247-252.
27. Birkebaek NH, Kristiansen M, Seefeldt T, et al. Bordetella pertussis and chronic cough in adults. Clin Infect Dis. 1999;29:1239-1242.
28. Kapaskelis AM, Vouloumanou EK, Rafailidis PI, et al. High prevalence of antibody titers against Bordetella pertussis in an adult population with prolonged cough. Respir Med. 2008;102:1586-1591.
29. Cornia PB, Hersh AL, Lipsky BA, et al. Does this coughing adolescent or adult patient have pertussis? JAMA. 2010;304:890-896.
30. Devasia RA, Jones TF, Collier B, et al. Compliance with azithromycin versus erythromycin in the setting of a pertussis outbreak. Am J Med Sci. 2009;337:176-178.
31. Poe RH, Harder RV, Israel RH, et al. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest. 1989;95:723-728.
32. Altunaji SM, Kukuruzovic RH, Curtis NC, et al. Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev. 2007;(3):CD004404.-
Local and Regional Lung Allocation Systems Conflict
FT. LAUDERDALE, FLA. – More than a decade ago, the Department of Health and Human Services issued the "Final Rule on Organ Procurement and Transplantation Network Amendments," which was intended to ensure that "organs will be [allocated] based on medical criteria, not accidents of geography." Despite the introduction of this final rule, disparities in waiting list outcomes are known to be significantly influenced by where the transplantation candidate lives, and lower priority candidates are receiving organs at the expense of the more severely ill.
Although all candidates are ranked based on an objective priority score known as the Lung Allocation Score (LAS), lung allocation remains a locally based system. Organs are first allocated based on geography regardless of LAS score. Therefore, organs are initially offered only to the subset of matched lung transplant candidates (based on blood group and size) within the donor’s local Donor Service Area (DSA).
As a result, if an available organ is first accepted for a candidate within the local DSA, it is never offered to potentially more-severely ill candidates at the broader regional or national level – even if the regional or national candidate has a much higher priority score. There is evidence that this is a frequent occurrence, according to research presented by Dr. Mark J. Russo at the annual meeting of the Society of Thoracic Surgeons.

Dr. Russo and his colleagues analyzed data provided by the United Network for Organ Sharing to determine the frequency with which donor lungs were allocated to local candidates when blood group– and size-matched candidates with a higher LAS existed in the same region.
Their study cohort included all locally allocated organs for double lung transplantation in the United States in the year 2009. The researchers then identified all cases in which ABO blood group– and height-matched (within 10 cm) double-lung candidates in the same region had a higher LAS than did the local candidates who actually received the lung. They also calculated the number of these events in which the LAS difference was greater than 10 and greater than 25. The number of these bypassed regional candidates who then died on the waiting list was also determined.
Among the 580 locally allocated double-lung transplants analyzed, there was a mean of 6.0 blood group – and height-matched double-lung events per transplant (3,454 total, impacting 1,193 different candidates) in the same region where candidates had a higher LAS than did the local candidate who received the organ. A total of 24% (828) of the events involved skipping over a regional candidate with an LAS greater than 10 points higher than the local recipient, with 7.2% (250) of events involving a regional candidate with an LAS greater than 25 points higher than the local recipient. Overall, 185 of the bypassed regional candidates died on the waiting list.
Dr. Russo said that although the issue of transportation is important, generally the adverse impact of an additional hour or two of ischemic time due to transportation is not clinically significant, and should not be a major factor in the decision as to local vs. regional candidates. In addition, the regional candidate is often not far from the donor, he added.
"Ideally, a suitable donor organ would be available for every lung transplant candidate who could benefit from transplantation. Unfortunately, there remains a critical scarcity of donor organs available for transplantation. Therefore, efficient allocation of organs is necessary to ensure maximum benefit from the available organs," according to Dr. Russo, a cardiothoracic surgeon at the University of Chicago Medical Center.
"Locally-based allocation results in a high number of events in which a lung is allocated to a lower-priority candidate when an appropriately matched, higher-priority candidate exists in the same region. As a result, low-priority candidates, defined by an LAS less than 50, account for nearly 90% of lung transplant recipients, while candidates with higher LAS scores, defined by an LAS greater than 75, continue to die at extremely high rates while awaiting transplantation," Dr. Russo stated.
Dr. Russo said further that because this study considered only double-lung candidates, did not consider the possibility of national matching, and did not allow for blood groups to be crossed, it likely significantly underestimates the frequency of these events and lives lost.
"These findings suggest that further study of organ sharing over broader geographies should be pursued to determine if it would improve [waiting] list outcomes, including higher rates of organ allocation to higher-priority candidates, improved survival on the waiting list, and greater net benefit from the organs available for transplantation," he concluded.
Dr. Russo reported that he had no financial disclosures.
FT. LAUDERDALE, FLA. – More than a decade ago, the Department of Health and Human Services issued the "Final Rule on Organ Procurement and Transplantation Network Amendments," which was intended to ensure that "organs will be [allocated] based on medical criteria, not accidents of geography." Despite the introduction of this final rule, disparities in waiting list outcomes are known to be significantly influenced by where the transplantation candidate lives, and lower priority candidates are receiving organs at the expense of the more severely ill.
Although all candidates are ranked based on an objective priority score known as the Lung Allocation Score (LAS), lung allocation remains a locally based system. Organs are first allocated based on geography regardless of LAS score. Therefore, organs are initially offered only to the subset of matched lung transplant candidates (based on blood group and size) within the donor’s local Donor Service Area (DSA).
As a result, if an available organ is first accepted for a candidate within the local DSA, it is never offered to potentially more-severely ill candidates at the broader regional or national level – even if the regional or national candidate has a much higher priority score. There is evidence that this is a frequent occurrence, according to research presented by Dr. Mark J. Russo at the annual meeting of the Society of Thoracic Surgeons.
Dr. Russo and his colleagues analyzed data provided by the United Network for Organ Sharing to determine the frequency with which donor lungs were allocated to local candidates when blood group– and size-matched candidates with a higher LAS existed in the same region.
Their study cohort included all locally allocated organs for double lung transplantation in the United States in the year 2009. The researchers then identified all cases in which ABO blood group– and height-matched (within 10 cm) double-lung candidates in the same region had a higher LAS than did the local candidates who actually received the lung. They also calculated the number of these events in which the LAS difference was greater than 10 and greater than 25. The number of these bypassed regional candidates who then died on the waiting list was also determined.
Among the 580 locally allocated double-lung transplants analyzed, there was a mean of 6.0 blood group – and height-matched double-lung events per transplant (3,454 total, impacting 1,193 different candidates) in the same region where candidates had a higher LAS than did the local candidate who received the organ. A total of 24% (828) of the events involved skipping over a regional candidate with an LAS greater than 10 points higher than the local recipient, with 7.2% (250) of events involving a regional candidate with an LAS greater than 25 points higher than the local recipient. Overall, 185 of the bypassed regional candidates died on the waiting list.
Dr. Russo said that although the issue of transportation is important, generally the adverse impact of an additional hour or two of ischemic time due to transportation is not clinically significant, and should not be a major factor in the decision as to local vs. regional candidates. In addition, the regional candidate is often not far from the donor, he added.
"Ideally, a suitable donor organ would be available for every lung transplant candidate who could benefit from transplantation. Unfortunately, there remains a critical scarcity of donor organs available for transplantation. Therefore, efficient allocation of organs is necessary to ensure maximum benefit from the available organs," according to Dr. Russo, a cardiothoracic surgeon at the University of Chicago Medical Center.
"Locally-based allocation results in a high number of events in which a lung is allocated to a lower-priority candidate when an appropriately matched, higher-priority candidate exists in the same region. As a result, low-priority candidates, defined by an LAS less than 50, account for nearly 90% of lung transplant recipients, while candidates with higher LAS scores, defined by an LAS greater than 75, continue to die at extremely high rates while awaiting transplantation," Dr. Russo stated.
Dr. Russo said further that because this study considered only double-lung candidates, did not consider the possibility of national matching, and did not allow for blood groups to be crossed, it likely significantly underestimates the frequency of these events and lives lost.
"These findings suggest that further study of organ sharing over broader geographies should be pursued to determine if it would improve [waiting] list outcomes, including higher rates of organ allocation to higher-priority candidates, improved survival on the waiting list, and greater net benefit from the organs available for transplantation," he concluded.
Dr. Russo reported that he had no financial disclosures.
FT. LAUDERDALE, FLA. – More than a decade ago, the Department of Health and Human Services issued the "Final Rule on Organ Procurement and Transplantation Network Amendments," which was intended to ensure that "organs will be [allocated] based on medical criteria, not accidents of geography." Despite the introduction of this final rule, disparities in waiting list outcomes are known to be significantly influenced by where the transplantation candidate lives, and lower priority candidates are receiving organs at the expense of the more severely ill.
Although all candidates are ranked based on an objective priority score known as the Lung Allocation Score (LAS), lung allocation remains a locally based system. Organs are first allocated based on geography regardless of LAS score. Therefore, organs are initially offered only to the subset of matched lung transplant candidates (based on blood group and size) within the donor’s local Donor Service Area (DSA).
As a result, if an available organ is first accepted for a candidate within the local DSA, it is never offered to potentially more-severely ill candidates at the broader regional or national level – even if the regional or national candidate has a much higher priority score. There is evidence that this is a frequent occurrence, according to research presented by Dr. Mark J. Russo at the annual meeting of the Society of Thoracic Surgeons.
Dr. Russo and his colleagues analyzed data provided by the United Network for Organ Sharing to determine the frequency with which donor lungs were allocated to local candidates when blood group– and size-matched candidates with a higher LAS existed in the same region.
Their study cohort included all locally allocated organs for double lung transplantation in the United States in the year 2009. The researchers then identified all cases in which ABO blood group– and height-matched (within 10 cm) double-lung candidates in the same region had a higher LAS than did the local candidates who actually received the lung. They also calculated the number of these events in which the LAS difference was greater than 10 and greater than 25. The number of these bypassed regional candidates who then died on the waiting list was also determined.
Among the 580 locally allocated double-lung transplants analyzed, there was a mean of 6.0 blood group – and height-matched double-lung events per transplant (3,454 total, impacting 1,193 different candidates) in the same region where candidates had a higher LAS than did the local candidate who received the organ. A total of 24% (828) of the events involved skipping over a regional candidate with an LAS greater than 10 points higher than the local recipient, with 7.2% (250) of events involving a regional candidate with an LAS greater than 25 points higher than the local recipient. Overall, 185 of the bypassed regional candidates died on the waiting list.
Dr. Russo said that although the issue of transportation is important, generally the adverse impact of an additional hour or two of ischemic time due to transportation is not clinically significant, and should not be a major factor in the decision as to local vs. regional candidates. In addition, the regional candidate is often not far from the donor, he added.
"Ideally, a suitable donor organ would be available for every lung transplant candidate who could benefit from transplantation. Unfortunately, there remains a critical scarcity of donor organs available for transplantation. Therefore, efficient allocation of organs is necessary to ensure maximum benefit from the available organs," according to Dr. Russo, a cardiothoracic surgeon at the University of Chicago Medical Center.
"Locally-based allocation results in a high number of events in which a lung is allocated to a lower-priority candidate when an appropriately matched, higher-priority candidate exists in the same region. As a result, low-priority candidates, defined by an LAS less than 50, account for nearly 90% of lung transplant recipients, while candidates with higher LAS scores, defined by an LAS greater than 75, continue to die at extremely high rates while awaiting transplantation," Dr. Russo stated.
Dr. Russo said further that because this study considered only double-lung candidates, did not consider the possibility of national matching, and did not allow for blood groups to be crossed, it likely significantly underestimates the frequency of these events and lives lost.
"These findings suggest that further study of organ sharing over broader geographies should be pursued to determine if it would improve [waiting] list outcomes, including higher rates of organ allocation to higher-priority candidates, improved survival on the waiting list, and greater net benefit from the organs available for transplantation," he concluded.
Dr. Russo reported that he had no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: Low-priority candidates accounted for nearly 90% of lung recipients, while candidates with higher LAS scores continue to die at extremely high rates while awaiting transplantation.
Data Source: A cohort that included all locally allocated organs for double lung transplantation in the United States in the year 2009.
Disclosures: Dr. Russo reported that he had no financial disclosures.
FDA Quickly Approves 'Breakthrough' Cystic Fibrosis Drug
The Food and Drug Administration on Jan. 31 approved the drug ivacaftor (Kalydeco) for cystic fibrosis patients aged 6 years and older who have the G551D mutation.
According to ivacaftor maker Vertex Pharmaceuticals, the approval is one of the fastest ever at the FDA. It took only 3 months from submission of data to approval.
Ivacaftor targets the G551D mutation in the cystic fibrosis transmembrane regulator (CFTR) gene. CFTR proteins regulate the flow of salt and water across the cells. A defective CFTR protein causes thick, sticky mucus to build up in the lungs, digestive tract, and other parts of the body, which can lead to respiratory and digestive problems and other complications.
The Vertex drug, taken orally twice a day, is a CFTR potentiator. It targets abnormal CFTR protein channels and opens them to allow chloride ions to move into and out of the cell; that, in turn, thins the mucus and the airways become less clogged, according to Vertex.
The FDA said that about 1,200 people – 4% of the 30,000 with cystic fibrosis in the United States – have the G551D mutation. Ivacaftor can help only those with the mutation. The agency and Vertex recommend FDA-approved molecular diagnostic testing before starting the therapy.
"Kalydeco is an excellent example of the promise of personalized medicine – targeted drugs that treat patients with a specific genetic makeup," said Dr. Margaret A. Hamburg, FDA commissioner, in a statement.
Added Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, "Kalydeco is the first available treatment that targets the defective CFTR protein, which is the underlying cause of cystic fibrosis. This is a breakthrough therapy for the cystic fibrosis community because current therapies only treat the symptoms of this genetic disease."
The FDA’s approval was based on two 48-week, placebo-controlled clinical studies that enrolled 213 patients. One study was in patients aged 12 years and older, and the other was in patients aged 6-11 years.
They all had at least one copy of the G551D mutation. The ivacaftor-treated groups had significant and sustained improvements in lung function, as well as in weight gain and some quality of life measurements, compared with those who received placebo, according to Vertex. They also had fewer pulmonary exacerbations.
The most common side effects were upper respiratory tract infection, headache, stomach ache, rash, diarrhea, and dizziness.
Vertex said it would begin shipping ivacaftor to U.S. pharmacies this week.
The Food and Drug Administration on Jan. 31 approved the drug ivacaftor (Kalydeco) for cystic fibrosis patients aged 6 years and older who have the G551D mutation.
According to ivacaftor maker Vertex Pharmaceuticals, the approval is one of the fastest ever at the FDA. It took only 3 months from submission of data to approval.
Ivacaftor targets the G551D mutation in the cystic fibrosis transmembrane regulator (CFTR) gene. CFTR proteins regulate the flow of salt and water across the cells. A defective CFTR protein causes thick, sticky mucus to build up in the lungs, digestive tract, and other parts of the body, which can lead to respiratory and digestive problems and other complications.
The Vertex drug, taken orally twice a day, is a CFTR potentiator. It targets abnormal CFTR protein channels and opens them to allow chloride ions to move into and out of the cell; that, in turn, thins the mucus and the airways become less clogged, according to Vertex.
The FDA said that about 1,200 people – 4% of the 30,000 with cystic fibrosis in the United States – have the G551D mutation. Ivacaftor can help only those with the mutation. The agency and Vertex recommend FDA-approved molecular diagnostic testing before starting the therapy.
"Kalydeco is an excellent example of the promise of personalized medicine – targeted drugs that treat patients with a specific genetic makeup," said Dr. Margaret A. Hamburg, FDA commissioner, in a statement.
Added Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, "Kalydeco is the first available treatment that targets the defective CFTR protein, which is the underlying cause of cystic fibrosis. This is a breakthrough therapy for the cystic fibrosis community because current therapies only treat the symptoms of this genetic disease."
The FDA’s approval was based on two 48-week, placebo-controlled clinical studies that enrolled 213 patients. One study was in patients aged 12 years and older, and the other was in patients aged 6-11 years.
They all had at least one copy of the G551D mutation. The ivacaftor-treated groups had significant and sustained improvements in lung function, as well as in weight gain and some quality of life measurements, compared with those who received placebo, according to Vertex. They also had fewer pulmonary exacerbations.
The most common side effects were upper respiratory tract infection, headache, stomach ache, rash, diarrhea, and dizziness.
Vertex said it would begin shipping ivacaftor to U.S. pharmacies this week.
The Food and Drug Administration on Jan. 31 approved the drug ivacaftor (Kalydeco) for cystic fibrosis patients aged 6 years and older who have the G551D mutation.
According to ivacaftor maker Vertex Pharmaceuticals, the approval is one of the fastest ever at the FDA. It took only 3 months from submission of data to approval.
Ivacaftor targets the G551D mutation in the cystic fibrosis transmembrane regulator (CFTR) gene. CFTR proteins regulate the flow of salt and water across the cells. A defective CFTR protein causes thick, sticky mucus to build up in the lungs, digestive tract, and other parts of the body, which can lead to respiratory and digestive problems and other complications.
The Vertex drug, taken orally twice a day, is a CFTR potentiator. It targets abnormal CFTR protein channels and opens them to allow chloride ions to move into and out of the cell; that, in turn, thins the mucus and the airways become less clogged, according to Vertex.
The FDA said that about 1,200 people – 4% of the 30,000 with cystic fibrosis in the United States – have the G551D mutation. Ivacaftor can help only those with the mutation. The agency and Vertex recommend FDA-approved molecular diagnostic testing before starting the therapy.
"Kalydeco is an excellent example of the promise of personalized medicine – targeted drugs that treat patients with a specific genetic makeup," said Dr. Margaret A. Hamburg, FDA commissioner, in a statement.
Added Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, "Kalydeco is the first available treatment that targets the defective CFTR protein, which is the underlying cause of cystic fibrosis. This is a breakthrough therapy for the cystic fibrosis community because current therapies only treat the symptoms of this genetic disease."
The FDA’s approval was based on two 48-week, placebo-controlled clinical studies that enrolled 213 patients. One study was in patients aged 12 years and older, and the other was in patients aged 6-11 years.
They all had at least one copy of the G551D mutation. The ivacaftor-treated groups had significant and sustained improvements in lung function, as well as in weight gain and some quality of life measurements, compared with those who received placebo, according to Vertex. They also had fewer pulmonary exacerbations.
The most common side effects were upper respiratory tract infection, headache, stomach ache, rash, diarrhea, and dizziness.
Vertex said it would begin shipping ivacaftor to U.S. pharmacies this week.