User login
Think Gender, Chronic Bronchitis in COPD
KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.

KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.
KEYSTONE, COLO. – Chronic bronchitis and gender might provide more clinically meaningful clues to phenotyping patients with chronic obstructive pulmonary disease than does lung function, recent findings from the COPDGene study suggest.
"There are a lot of important features of COPD that we don’t capture by FEV1 [forced expiratory volume in 1 second], and we need additional clinical features and radiographic information so we can tailor our therapies even more in the future," COPDGene investigator Dr. Barry J. Make said at a meeting on allergy and respiratory diseases.
Researchers with the ongoing COPD genetic epidemiology study used the ATS (American Thoracic Society) questionnaire to identify chronic bronchitis in 1,061 patients with GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage 2-4 COPD. In all, 290 patients had chronic bronchitis, defined as cough and sputum for at least 3 months/year for at least 2 consecutive years, and 771 did not have chronic bronchitis.
The researchers found that chronic bronchitis is a predictor of future COPD exacerbations, said Dr. Make, codirector of the COPD program and medical director of respiratory care services at Denver’s National Jewish Health, which sponsored the meeting. The chronic bronchitis–positive group had 1.21 exacerbations/patient per year, compared with 0.63 exacerbations/patient per year in the chronic bronchitis–negative group (P less than .027). In addition, more patients in the chronic bronchitis–positive group reported severe exacerbations (26.6% vs. 20%; P = .024).
"We’re concerned about exacerbations, because if you’re hospitalized with an exacerbation of COPD, your mortality within the first year after you get out of the hospital is 20%," he said.
COPD patients with chronic bronchitis were younger, smoked more, were more often current smokers, and had more wheezing and nocturnal awakenings caused by cough and dyspnea. Dr. Make pointed out that the ATS questionnaire is validated to check for cough and sputum, but also emphasized the importance of using CT in assessing patients with COPD.
Notably, patients who have chronic bronchitis have thicker airways on chest CT, compared with the chronic bronchitis–negative group, as indicated by a higher mean segmental wall area percentage (63.2% vs. 62.6%; P = .013). Their percent gas trapping and lung emphysema were similar (Chest 2011;140:626-33).
A second COPDGene study in 1,002 COPD patients reported that each 1-mm increase in bronchial wall thickness on quantitative CT is associated with a 1.84-fold increase in annual COPD exacerbations after multivariate analysis that adjusted for lung function, Dr. Make said. The analysis also found that for patients with 35% or greater total emphysema, each 5% increase in emphysema was associated with a 1.18-fold increase in annual exacerbation rate (Radiology 2011;261:274-82).
Thus, COPD patients with chronic bronchitis and emphysema have more exacerbations, and "from CT exam, we can predict a patient’s future exacerbations," he said.
Dr. Make pointed out that a history of chronic bronchitis and at least one COPD exacerbation requiring systemic corticosteroids and/or hospitalization were among the inclusion criteria for two pivotal trials that led to the 2011 approval of the phosphodiesterase-4 inhibitor roflumilast (Daliresp). Pooled data from the multicenter trials demonstrated a significant 17% reduction with roflumilast in the rate of moderate or severe exacerbations per patient per year among adult outpatients with COPD (Lancet 2009;374:685-94).
"Here we have personalized medicine that has made it to the FDA [U.S. Food and Drug Administration], but in order to determine if this medication might be right for your patients, you need to collect the right information," he said.
Gender Differences
Women with COPD are known to have more exacerbations than men, to have lower lung function than men with the same cigarette exposure, and to have more symptoms than men with the same lung function. In addition, more women die of COPD, compared with men. Yet, data are limited regarding gender differences in lung anatomy that might explain this troubling paradox, at least in part. Dr. Make highlighted a recent study that identified gender differences in airway dimensions in 1,021 male and 1,026 female smokers in the COPDGene cohort (COPD 2011;8:285-92).
Multidetector CT scans of the chest revealed that in all airways measured, women smokers had higher wall area percentage but smaller luminal area, internal diameter, and airway wall thickness than did male smokers. Gender remained one of the most significant predictors for these differences on multivariate analysis, even after researchers adjusted for age, body size, and other confounders.
"So maybe we should look at women differently than men – think about why they’re different and how to treat them or prevent the disease differently," said Dr. Make, who coauthored the study.
To drive home the point, Dr. Make showed a slide depicting a rail-thin old man with emphysema alongside the rosy-cheeked model Christy Turlington, who revealed at age 31 that she had early-stage emphysema after maintaining a pack-a-day cigarette habit for nearly a decade.
Dr. Make reported having served as an advisory board member, speaker, or trial investigator for AstraZeneca, Boehringer-Ingelheim, Breathe, Forest, GlaxoSmithKline, Ikaria, MedImmune, Merck, Novartis, Pfizer, and Sunovion, as well as the National Heart, Lung, and Blood Institute.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Adult Phenotypes No Help in Severe Pediatric Asthma
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).

Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).
Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
KEYSTONE, COLO. – Adult asthma phenotypes offer little guidance in the identification and management of severe, therapy-resistant asthma in children.
Cluster analysis was recently used to identify two subgroups with discordance between symptom expression and eosinophilic airway inflammation specific to refractory adult asthma (Am. J. Respir. Crit. Care Med. 2008;178:218-24). In addition, a treatment strategy based on minimizing eosinophilic inflammation proved superior to standard care in reducing exacerbation frequency (Lancet 2002;360:1715-21).
Recent efforts to replicate the findings in severe pediatric asthma, however, met with disappointing results, study coauthor Dr. Andrew Bush said at a meeting on allergy and respiratory diseases. The ability to identify asthma phenotypes that exhibit differences in clinical response could enable more targeted therapy and spare children unlikely to benefit from exposure to powerful anti-inflammatories like methotrexate and cyclosporine. The pediatric study did include an unvalidated post hoc analysis showing that a sputum normalization strategy in the first month after changing treatment may reduce asthma exacerbations (Thorax 2012;67:193-8).
Persistent airflow limitation is also a hallmark of severe, therapy-resistant asthma (STRA) in adults, and is typically defined using a postcorticosteroid trial, postacute bronchodilator response in forced expiratory volume in 1 second (FEV1), and z scores. What is not known for children, however, is what dose, route of administration, and duration of steroids is best, or what dose of bronchodilator is most effective.
"There really is no good pediatric evidence," said Dr. Bush, professor of pediatric respirology at the Royal Brompton Hospital and Imperial College in London. "The point in finding this out is that if you really do have persistent airflow obstruction [in] a child, there is no point in flogging them with more and more medications, if in fact they’re not going to open their airways."
Corticosteroid response is another cornerstone for identifying and managing STRA in adults. However, when Dr. Bush and his colleagues looked at corticosteroid response in a group of 50 children who had severe asthma by American Thoracic Society and American College of Surgeons criteria, 50% of the children had such good lung function that the adult definition of response, based on an FEV1 of at least 80% or a 15% increase, could not be applied.
"The adult definition of corticosteroid response based on lung function does not work in kids," he said.
Clinical phenotypes such as female gender and obesity, which are associated with more severe asthma after childhood, have also proved unreliable. Another unpublished study by the group involving 40 boys and 36 girls (aged 6-19 years) with STRA found no sex differences; it also found that young people with STRA had an average body mass index of 19 kg/m2, which was identical to the average BMI of a cohort of age-matched children with mild asthma and was lower than the mean of 20.4 kg/m2 in age-matched controls.
The children with STRA had symptoms for an average of 2-6 years, an average of six steroid bursts (range, 1-30), and three hospital admissions (range, 0-21) in the previous year; 21% had ever been intubated because of their asthma.
Asthma Control Test scores were low in the children with STRA (average, 13.5), and lung function varied widely from an FEV1 of 33% to 121% of predicted (average, 70%).
The children with STRA had a strong positive history of atopy (82%) and family history of atopy (84% in a first-degree relative), Dr. Bush noted.
"Indeed, if I see a child with alleged severe, therapy-resistant asthma who is not atopic, I take another further good hard look at the diagnosis," he said.
Getting the Basics Right
One of the most important steps in managing children with genuine STRA is to distinguish them from those with difficult asthma, in whom biologic therapies are not justified.
"In really severe childhood asthmatics, potentially reversible factors will be found in more than half of those not responding to treatment," Dr. Bush said at the meeting, sponsored by National Jewish Health.
The most important factors to look for are adherence, cigarettes, allergens, and psychosocial issues. He suggested that nurse-led home visits are particularly beneficial in identifying these factors. When nurses from Royal Brompton visited 71 "hard-core asthmatics," potentially modifiable factors were identified in 79%, and only 32 patients were thought to need further invasive investigation. A quarter could not produce a complete set of medications, a third were picking up fewer than half of their prescriptions, 38% did not have good inhaler technique despite multiple attempts at testing, and medication issues contributed to poor control in 48%.
"These guys know the nurses are coming; it’s not like the nurses come at 3:00 in the morning and bang on the door and say show me your medications," he said.
Dr. Bush reported no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Quality of Dyspnea Directs Diagnosis, Management
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.

For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.
For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
KEYSTONE, COLO. – Understanding the quality of a patient’s dyspnea provides insights into the underlying physiologic mechanism and can guide management, according to Dr. James T. Good Jr., a pulmonologist at National Jewish Health in Denver.
Complaints that may represent dyspnea can be as vague as fatigue, lack of energy, or simply getting old, but most commonly are a sensation of air hunger, of work or effort to breathe, or of chest tightness. All three sensations are the result of a mismatch or neuromechanical dissociation between ongoing motor signals to the respiratory muscles and incoming afferent information from the lungs, chest wall, and upper airways, Dr. Good said at a meeting on allergy and respiratory diseases.
For the patient who describes air hunger, the sensation can be equated to being held underwater and is often so distressing that patients say they would prefer pain to air hunger. The sensation is mediated primarily through central and peripheral chemoreceptors and stimulated by hypercapnia or hypoxia in the presence of decreased arterial carbon dioxide (CO2) partial pressure and oxygen partial pressure, Dr. Good said.
In the patient who describes work or effort when breathing, the sensation is stimulated by respiratory motor muscle contraction and muscle fatigue and is mediated through a combination of central motor discharge, chest wall receptors, and metaboreceptors located within skeletal muscle, he said at the meeting, which was sponsored by National Jewish Health.
In patients with chest tightness, the sensation is stimulated by bronchoconstriction and tends to be mediated primary through rapidly adapting stretch receptors (RARs) and C-fiber receptors in the pulmonary and respiratory tract. Chest tightness can occur with other dyspneic sensations but is fairly specific to asthma and chronic obstructive pulmonary disease (COPD).
The first question to ask patients who present with complaints of an uncomfortable sensation associated with breathing is whether it occurs at rest or with exertion, Dr. Good suggested. Dyspnea at rest implies an acute illness or moderate to severe cardiopulmonary disease. It also is very common in patients with anxiety, with or without underlying disease, and in patients with alterations in the respiratory drive. Dyspnea with exertion is most common in patients with cardiac dysfunction, pulmonary diseases, metabolic disorders, deconditioning, obesity, and anemia.
The next important question to ask is whether the patient with dyspnea has normal oxygen saturation (SaO2), he said. A normal SaO2 implies a mild disorder such as exercise-induced bronchospasm, while an abnormal SaO2 implies moderate to severe cardiopulmonary disease if dyspnea occurs at rest, mild to moderate cardiopulmonary disease if dyspnea occurs during exercise, or sleep-disordered breathing if it occurs with sleep.
Dr. Good observed that many of his cardiology colleagues routinely obtain an electrocardiogram in their patients who are short of breath, which is an important part of the work-up, but that they overlook spirometry.
"If a patient has dyspnea they need to have spirometry," he said. "You have to start with that. It is absolutely key."
Dyspneic patients with normal spirometry are unlikely to have significant underlying COPD or interstitial lung disease (ILD), but they could have exercise-induced bronchospasm, mild or persistent asthma, or vocal cord dysfunction.
If an obstructive pattern is observed on spirometry, this could be a clue to evaluate for COPD or asthma. A restrictive pattern on spirometry should raise suspicion for ILD, neuromuscular disease, chest wall abnormalities, pleural effusion, or heart failure, he said.
Dr. Good presented several cases that highlighted the importance of a thorough work-up, including that of a 70-year-old retired engineer with increasing air hunger dyspnea on exertion. Spirometry revealed a normal forced expiratory volume in 1 second of 2.74 L, or 84% of predicted volume, and forced expiratory vital capacity of 4.91 L, or 111% of predicted volume. The FEV1/FVC ratio was 56%, which is low, but not enough to explain the amount of dyspnea the patient was experiencing. Cardiac evaluation proved uneventful, but pulmonary function tests revealed a diffusion capacity of 17.2, or just 53% of predicted value.
Dr. Good said that pulmonologists frequently rely on diffusion capacity when spirometry is normal, and when values are less than 50% of predicted, patients are frequently dyspneic.
"Once the dyspnea evaluation is complete, it is usually possible to determine all factors that are contributing to the patient’s breathlessness and direct specific therapy" to the underlying disease process, he said.
Other therapeutic approaches include conditioning, fitness, and weight loss in obese patients with dyspnea, as well as beta-agonists and anticholinergics, theophylline, opiates, anxiolytics, and selective serotonin reuptake inhibitors. Supplemental oxygen usually relieves dyspnea in hypoxemic patients, making vagal afferents unlikely contributors, he said.
Dr. Good disclosed serving as an investigator and speaker for Genentech and as a speaker for GlaxoSmithKline and Merck.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Early Strides Made in Personalized Refractory Asthma Care
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."

Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
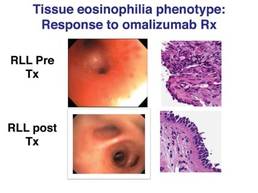
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Major Finding: Six phenotypes have been identified using bronchoscopy and a supraglottic index that can be used to evaluate and direct therapy for refractory asthma.
Data Source: Data were taken from an observational treatment study of 58 patients with difficult to treat, refractory asthma.
Disclosures: Dr. Martin and his coauthors reported no relevant conflicts of interest.
Frequent Respiratory Infections? Rule Out Bronchiectasis
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.

She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND PULMONARY DISEASES