User login
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."

Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
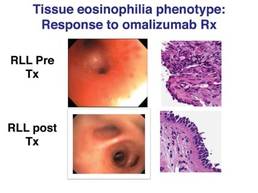
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Major Finding: Six phenotypes have been identified using bronchoscopy and a supraglottic index that can be used to evaluate and direct therapy for refractory asthma.
Data Source: Data were taken from an observational treatment study of 58 patients with difficult to treat, refractory asthma.
Disclosures: Dr. Martin and his coauthors reported no relevant conflicts of interest.