User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Deep suctioning increases length of stay in infants with bronchiolitis
Deep suctioning and long lapses between suction treatments were associated with significantly increased lengths of stay in babies hospitalized with bronchiolitis.
Patients who never had deep suctioning stayed a little more than a day, but the length of stay was more than 2 days in patients for whom deep suctioning accounted for 60% or more of their treatments, Dr. Grant M. Mussman and his colleagues reported in the March 4 online issue of JAMA Pediatrics (2013[doi:10.1001/jamapediatrics.2013.36]).
Similarly, patients who experienced several lapses of 4 hours between treatments were hospitalized significantly longer than were those with no treatment lapses (mean of 2.3 days vs. 1.7 days).
Compared with a noninvasive nasal-type suction device, deep suctioning may aggravate the bronchial swelling and mucus sloughing that already causes breathing problems in these tiny patients, wrote Dr. Mussman of Cincinnati Children’s Hospital Medical Center.
"[It] may be that deep suctioning causes edema and irritation of the upper airway. Alternatively, noninvasive suctioning could be more effective in mobilizing nasal secretions through the larger caliber catheter."
Regular treatments with no lapses probably keep the airways open more consistently, they noted. "It is also possible that regular suctioning results in agitation of the patient, with resultant increased minute volume and secretion mobilization, resulting in shorter length of stay."
The study cohort consisted of 740 patients who were studied for device type (deep or noninvasive), 695 of which were studied for treatment timing. The patients were a mean of 6 months old, and all had been hospitalized for bronchiolitis.
Deep suction was defined as the insertion of a nasopharyngeal catheter, and noninvasive as the use of nasal-type aspirators, excluding bulb syringe. The exposure was the percentage of treatments that used deep suctioning (0%-35%; more than 35%-60%; and more then 60%).
The adjusted mean length of stay for infants who had no deep suctioning was 1.75 days. The stay was 1.91 days for those with up to 35% deep suctioning, 1.96 days for more than 35%-60% deep suctioning, and 2.35 days for more than 60% deep suctioning.
For the suction treatment timing group, a suctioning lapse was defined as two sequential suctioning events separated by more than 4 hours during the first 24 hours of admission. The investigators said that the 4-hour increment is the most common reassessment timing.
Infants with no treatment lapses had a mean adjusted hospital stay of 1.62 days. In contrast, the mean length of stay was 1.72 days for infants with one treatment lapse, 2.09 days for those with two lapses, and 2.64 days for those with three or four lapses.
"We believe the difference in geometric mean of up to 1 day between patients with no suctioning lapses and those with three or four lapses is clinically meaningful," the authors noted. However, "Because there is insufficient data to determine a causal relationship, we intend to continue to examine these associations as we incorporate these findings into clinical practice at our institution."
Dr. Mussman had no relevant financial disclosures.
Deep suctioning and long lapses between suction treatments were associated with significantly increased lengths of stay in babies hospitalized with bronchiolitis.
Patients who never had deep suctioning stayed a little more than a day, but the length of stay was more than 2 days in patients for whom deep suctioning accounted for 60% or more of their treatments, Dr. Grant M. Mussman and his colleagues reported in the March 4 online issue of JAMA Pediatrics (2013[doi:10.1001/jamapediatrics.2013.36]).
Similarly, patients who experienced several lapses of 4 hours between treatments were hospitalized significantly longer than were those with no treatment lapses (mean of 2.3 days vs. 1.7 days).
Compared with a noninvasive nasal-type suction device, deep suctioning may aggravate the bronchial swelling and mucus sloughing that already causes breathing problems in these tiny patients, wrote Dr. Mussman of Cincinnati Children’s Hospital Medical Center.
"[It] may be that deep suctioning causes edema and irritation of the upper airway. Alternatively, noninvasive suctioning could be more effective in mobilizing nasal secretions through the larger caliber catheter."
Regular treatments with no lapses probably keep the airways open more consistently, they noted. "It is also possible that regular suctioning results in agitation of the patient, with resultant increased minute volume and secretion mobilization, resulting in shorter length of stay."
The study cohort consisted of 740 patients who were studied for device type (deep or noninvasive), 695 of which were studied for treatment timing. The patients were a mean of 6 months old, and all had been hospitalized for bronchiolitis.
Deep suction was defined as the insertion of a nasopharyngeal catheter, and noninvasive as the use of nasal-type aspirators, excluding bulb syringe. The exposure was the percentage of treatments that used deep suctioning (0%-35%; more than 35%-60%; and more then 60%).
The adjusted mean length of stay for infants who had no deep suctioning was 1.75 days. The stay was 1.91 days for those with up to 35% deep suctioning, 1.96 days for more than 35%-60% deep suctioning, and 2.35 days for more than 60% deep suctioning.
For the suction treatment timing group, a suctioning lapse was defined as two sequential suctioning events separated by more than 4 hours during the first 24 hours of admission. The investigators said that the 4-hour increment is the most common reassessment timing.
Infants with no treatment lapses had a mean adjusted hospital stay of 1.62 days. In contrast, the mean length of stay was 1.72 days for infants with one treatment lapse, 2.09 days for those with two lapses, and 2.64 days for those with three or four lapses.
"We believe the difference in geometric mean of up to 1 day between patients with no suctioning lapses and those with three or four lapses is clinically meaningful," the authors noted. However, "Because there is insufficient data to determine a causal relationship, we intend to continue to examine these associations as we incorporate these findings into clinical practice at our institution."
Dr. Mussman had no relevant financial disclosures.
Deep suctioning and long lapses between suction treatments were associated with significantly increased lengths of stay in babies hospitalized with bronchiolitis.
Patients who never had deep suctioning stayed a little more than a day, but the length of stay was more than 2 days in patients for whom deep suctioning accounted for 60% or more of their treatments, Dr. Grant M. Mussman and his colleagues reported in the March 4 online issue of JAMA Pediatrics (2013[doi:10.1001/jamapediatrics.2013.36]).
Similarly, patients who experienced several lapses of 4 hours between treatments were hospitalized significantly longer than were those with no treatment lapses (mean of 2.3 days vs. 1.7 days).
Compared with a noninvasive nasal-type suction device, deep suctioning may aggravate the bronchial swelling and mucus sloughing that already causes breathing problems in these tiny patients, wrote Dr. Mussman of Cincinnati Children’s Hospital Medical Center.
"[It] may be that deep suctioning causes edema and irritation of the upper airway. Alternatively, noninvasive suctioning could be more effective in mobilizing nasal secretions through the larger caliber catheter."
Regular treatments with no lapses probably keep the airways open more consistently, they noted. "It is also possible that regular suctioning results in agitation of the patient, with resultant increased minute volume and secretion mobilization, resulting in shorter length of stay."
The study cohort consisted of 740 patients who were studied for device type (deep or noninvasive), 695 of which were studied for treatment timing. The patients were a mean of 6 months old, and all had been hospitalized for bronchiolitis.
Deep suction was defined as the insertion of a nasopharyngeal catheter, and noninvasive as the use of nasal-type aspirators, excluding bulb syringe. The exposure was the percentage of treatments that used deep suctioning (0%-35%; more than 35%-60%; and more then 60%).
The adjusted mean length of stay for infants who had no deep suctioning was 1.75 days. The stay was 1.91 days for those with up to 35% deep suctioning, 1.96 days for more than 35%-60% deep suctioning, and 2.35 days for more than 60% deep suctioning.
For the suction treatment timing group, a suctioning lapse was defined as two sequential suctioning events separated by more than 4 hours during the first 24 hours of admission. The investigators said that the 4-hour increment is the most common reassessment timing.
Infants with no treatment lapses had a mean adjusted hospital stay of 1.62 days. In contrast, the mean length of stay was 1.72 days for infants with one treatment lapse, 2.09 days for those with two lapses, and 2.64 days for those with three or four lapses.
"We believe the difference in geometric mean of up to 1 day between patients with no suctioning lapses and those with three or four lapses is clinically meaningful," the authors noted. However, "Because there is insufficient data to determine a causal relationship, we intend to continue to examine these associations as we incorporate these findings into clinical practice at our institution."
Dr. Mussman had no relevant financial disclosures.
FROM JAMA PEDIATRICS
Major Finding: The increasing use of deep suctioning increased length of stay by up to 1 day in infants hospitalized with bronchiolitis, while lapses in suction treatments increased the length of stay by almost 2 days.
Data Source: The retrospective study involved 1,435 patients.
Disclosures: Dr. Mussman had no relevant financial disclosures.
Early antibiotics may up food allergy risk
Antibiotic exposure during the first year of life is associated with an increased risk of food allergy in young children, according to findings from a large case-control study.
The risk is greatest among those exposed to multiple antibiotic courses, Bryan L. Love, Pharm.D., reported during a late-breaking abstract session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

The mean number of antibiotic courses received by 1,105 case patients with food allergy was 2.65, compared with 1.84 for 6,433 food allergy–free control patients. The mean time to first antibiotic course was 181.5 days for those with food allergies, compared with 190.1 days for controls. These differences were statistically significant, said Dr. Love of the South Carolina College of Pharmacy, Columbia.
Additionally, only 24% of case patients, compared with a third of controls, had never received an antibiotic.
Later vs. earlier antibiotic exposure (during months 7-12 vs. months 0-6) also was associated with greater likelihood of developing food allergy (odds ratio, 1.98).
"This makes sense, because [months 7-12] is typically when new foods are being introduced to children," Dr. Love said.
Furthermore, the risk increased in tandem with the number of antibiotic exposures. No significant increase in food allergy risk was seen with one or two antibiotic courses, but the odds ratio became significant with three or four courses, and was highest with five or more courses (odds ratio, 2.15), he noted.
Case patients in this study were children born between 2007 and 2009 with a diagnosis of food allergy made before Dec. 31, 2010 (and after first antibiotic exposure), based on South Carolina Medicaid billing data. Certain patients, such as those with asthma, atopic dermatitis, or eczema, were excluded, because they have an increased risk of food allergy and antibiotic exposure. Controls were matched to the case patients by birth year, sex, and race.
Penicillins were the most frequently prescribed type of antibiotic, followed by cephalosporins, Dr. Love said.
The findings support the hypothesis of this study, which is that alteration of normal gut flora that occurs after antibiotic exposure might contribute to the increasing prevalence of childhood food allergy. Normal gut immune response, including the interaction with a diverse microbiome, promotes the development of food tolerance, he explained.
Though limited by the study’s retrospective design and the reliance on ICD-9 coding for diagnoses, the findings do, indeed, suggest that early antibiotic exposures are problematic. The possibility that antibiotic exposures have a causative effect with respect to food allergy development in children deserves further study, particularly given the significant use of antibiotics in young children, who receive an average of 2.2 antibiotic prescriptions in the first year of life, and the increasing incidence of food allergy, he said.
Further analysis of the data will assess whether certain antibiotic drug classes confer greater risk of food allergy, he noted.
This study was funded by the Health Resources and Services Administration. Dr. Love reported having no other disclosures.
Antibiotic exposure during the first year of life is associated with an increased risk of food allergy in young children, according to findings from a large case-control study.
The risk is greatest among those exposed to multiple antibiotic courses, Bryan L. Love, Pharm.D., reported during a late-breaking abstract session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The mean number of antibiotic courses received by 1,105 case patients with food allergy was 2.65, compared with 1.84 for 6,433 food allergy–free control patients. The mean time to first antibiotic course was 181.5 days for those with food allergies, compared with 190.1 days for controls. These differences were statistically significant, said Dr. Love of the South Carolina College of Pharmacy, Columbia.
Additionally, only 24% of case patients, compared with a third of controls, had never received an antibiotic.
Later vs. earlier antibiotic exposure (during months 7-12 vs. months 0-6) also was associated with greater likelihood of developing food allergy (odds ratio, 1.98).
"This makes sense, because [months 7-12] is typically when new foods are being introduced to children," Dr. Love said.
Furthermore, the risk increased in tandem with the number of antibiotic exposures. No significant increase in food allergy risk was seen with one or two antibiotic courses, but the odds ratio became significant with three or four courses, and was highest with five or more courses (odds ratio, 2.15), he noted.
Case patients in this study were children born between 2007 and 2009 with a diagnosis of food allergy made before Dec. 31, 2010 (and after first antibiotic exposure), based on South Carolina Medicaid billing data. Certain patients, such as those with asthma, atopic dermatitis, or eczema, were excluded, because they have an increased risk of food allergy and antibiotic exposure. Controls were matched to the case patients by birth year, sex, and race.
Penicillins were the most frequently prescribed type of antibiotic, followed by cephalosporins, Dr. Love said.
The findings support the hypothesis of this study, which is that alteration of normal gut flora that occurs after antibiotic exposure might contribute to the increasing prevalence of childhood food allergy. Normal gut immune response, including the interaction with a diverse microbiome, promotes the development of food tolerance, he explained.
Though limited by the study’s retrospective design and the reliance on ICD-9 coding for diagnoses, the findings do, indeed, suggest that early antibiotic exposures are problematic. The possibility that antibiotic exposures have a causative effect with respect to food allergy development in children deserves further study, particularly given the significant use of antibiotics in young children, who receive an average of 2.2 antibiotic prescriptions in the first year of life, and the increasing incidence of food allergy, he said.
Further analysis of the data will assess whether certain antibiotic drug classes confer greater risk of food allergy, he noted.
This study was funded by the Health Resources and Services Administration. Dr. Love reported having no other disclosures.
Antibiotic exposure during the first year of life is associated with an increased risk of food allergy in young children, according to findings from a large case-control study.
The risk is greatest among those exposed to multiple antibiotic courses, Bryan L. Love, Pharm.D., reported during a late-breaking abstract session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The mean number of antibiotic courses received by 1,105 case patients with food allergy was 2.65, compared with 1.84 for 6,433 food allergy–free control patients. The mean time to first antibiotic course was 181.5 days for those with food allergies, compared with 190.1 days for controls. These differences were statistically significant, said Dr. Love of the South Carolina College of Pharmacy, Columbia.
Additionally, only 24% of case patients, compared with a third of controls, had never received an antibiotic.
Later vs. earlier antibiotic exposure (during months 7-12 vs. months 0-6) also was associated with greater likelihood of developing food allergy (odds ratio, 1.98).
"This makes sense, because [months 7-12] is typically when new foods are being introduced to children," Dr. Love said.
Furthermore, the risk increased in tandem with the number of antibiotic exposures. No significant increase in food allergy risk was seen with one or two antibiotic courses, but the odds ratio became significant with three or four courses, and was highest with five or more courses (odds ratio, 2.15), he noted.
Case patients in this study were children born between 2007 and 2009 with a diagnosis of food allergy made before Dec. 31, 2010 (and after first antibiotic exposure), based on South Carolina Medicaid billing data. Certain patients, such as those with asthma, atopic dermatitis, or eczema, were excluded, because they have an increased risk of food allergy and antibiotic exposure. Controls were matched to the case patients by birth year, sex, and race.
Penicillins were the most frequently prescribed type of antibiotic, followed by cephalosporins, Dr. Love said.
The findings support the hypothesis of this study, which is that alteration of normal gut flora that occurs after antibiotic exposure might contribute to the increasing prevalence of childhood food allergy. Normal gut immune response, including the interaction with a diverse microbiome, promotes the development of food tolerance, he explained.
Though limited by the study’s retrospective design and the reliance on ICD-9 coding for diagnoses, the findings do, indeed, suggest that early antibiotic exposures are problematic. The possibility that antibiotic exposures have a causative effect with respect to food allergy development in children deserves further study, particularly given the significant use of antibiotics in young children, who receive an average of 2.2 antibiotic prescriptions in the first year of life, and the increasing incidence of food allergy, he said.
Further analysis of the data will assess whether certain antibiotic drug classes confer greater risk of food allergy, he noted.
This study was funded by the Health Resources and Services Administration. Dr. Love reported having no other disclosures.
AT THE AAAAI ANNUAL MEETING
Major finding: The mean number of antibiotic exposures in the first year of life was 2.65 vs. 1.84 in cases vs. controls, respectively.
Data source: A retrospective case-control study.
Disclosures: This study was funded by the Health Resources and Services Administration. Dr. Love reported having no other disclosures.

Cat allergy vaccine effects persist at 2 years
A short course of treatment with an investigational synthetic cat-peptide antigen desensitizing vaccine, or Cat-PAD, results in a substantial and persistent reduction in cat allergy symptom scores, according to two-year findings from a randomized, placebo-controlled phase II clinical study involving 202 adult patients.
Study participants were initially randomized to receive either eight 3-nmol intradermal doses at 2-week intervals, four 6 nmol-doses at 4-week intervals, or placebo. At 1-year follow-up, the improvement in Total Rhinoconjunctivitis Symptom Score (TRSS) was significantly greater in the patients who received four doses of Cat-PAD (ToleroMune Cat, Circassia Limited, Oxford, England), compared with those who received placebo (–7.1 points vs. –2.99 points), according to findings published online in the Journal of Allergy and Clinical Immunology (doi:10.1016/j.jaci.2012.12.1185).
Data from a 2-year follow-up study were reported by Rod P. Hafner, Ph.D., and his colleagues in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Of 89 patients enrolled into the follow-up study, 50 returned at 2-years after the start of treatment, having received no additional treatment, for an environmental exposure chamber challenge. The magnitude of difference from baseline in TRSS seen at 1 year in those who received 4 doses and those who received placebo was maintained at 2 years (–5.87 vs. –2.02) among those who initially received the 4-dose regimen.
"Cat-PAD is the first in a new class of synthetic peptide immune-regulatory epitopes. The results from this study provide the first evidence that four doses of 6 nmol Cat-PAD over a 12-week period has a disease-modifying effect with subjects showing sustained improvement at 2 years," the investigators wrote.
Study participants were adults aged 18-65 years with cat allergy who underwent a baseline environmental exposure chamber (EEC) challenge, as well as follow-up EEC challenges at 18-22 weeks and at 100-104 weeks.
"Cat allergen was dispersed into the EEC to achieve a consistent mean level of approx. 50 ng Fel d1/m3, using a validated method," they explained, noting that TRSS was calculated at each EEC challenge based on self-scoring of four nasal symptoms (running nose, sneezing, blocked nose, itchy nose), and four ocular symptoms (itchy eyes, watery eyes, red eyes, sore eyes) on a scale of 0-3, every 30 minutes during the challenge.
Cat-PAD is a "potentially exciting new approach to cat allergy immunotherapy," the investigators said, noting that improvements in the TRSS seen in the initial phase II study and follow-up study represent a substantial improvement over numerous therapies investigated in the past, in some cases reaching a threefold improvement in symptom reduction.
"For example, studies of similar design in an EEC reported TRSS changes of approximately –1.5 units after 16 weeks treatment with a sublingual cat allergy tablet, while a single 180-mg dose of the antihistamine fexofenadine achieved a mean difference in TRSS of –1.3 in a cat allergen study. Moreover, the change in TRSS of –3.8 units reported here was observed after four administrations of Cat-PAD over a 12-week period and persisted 21 months after the end of treatment," they concluded.
In late 2012 the investigators began enrolling a phase III study, which will include individuals aged 12-65 years.
This study was funded by Circassia Limited. Dr. Hafner is employed by Circassia.
A short course of treatment with an investigational synthetic cat-peptide antigen desensitizing vaccine, or Cat-PAD, results in a substantial and persistent reduction in cat allergy symptom scores, according to two-year findings from a randomized, placebo-controlled phase II clinical study involving 202 adult patients.
Study participants were initially randomized to receive either eight 3-nmol intradermal doses at 2-week intervals, four 6 nmol-doses at 4-week intervals, or placebo. At 1-year follow-up, the improvement in Total Rhinoconjunctivitis Symptom Score (TRSS) was significantly greater in the patients who received four doses of Cat-PAD (ToleroMune Cat, Circassia Limited, Oxford, England), compared with those who received placebo (–7.1 points vs. –2.99 points), according to findings published online in the Journal of Allergy and Clinical Immunology (doi:10.1016/j.jaci.2012.12.1185).
Data from a 2-year follow-up study were reported by Rod P. Hafner, Ph.D., and his colleagues in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Of 89 patients enrolled into the follow-up study, 50 returned at 2-years after the start of treatment, having received no additional treatment, for an environmental exposure chamber challenge. The magnitude of difference from baseline in TRSS seen at 1 year in those who received 4 doses and those who received placebo was maintained at 2 years (–5.87 vs. –2.02) among those who initially received the 4-dose regimen.
"Cat-PAD is the first in a new class of synthetic peptide immune-regulatory epitopes. The results from this study provide the first evidence that four doses of 6 nmol Cat-PAD over a 12-week period has a disease-modifying effect with subjects showing sustained improvement at 2 years," the investigators wrote.
Study participants were adults aged 18-65 years with cat allergy who underwent a baseline environmental exposure chamber (EEC) challenge, as well as follow-up EEC challenges at 18-22 weeks and at 100-104 weeks.
"Cat allergen was dispersed into the EEC to achieve a consistent mean level of approx. 50 ng Fel d1/m3, using a validated method," they explained, noting that TRSS was calculated at each EEC challenge based on self-scoring of four nasal symptoms (running nose, sneezing, blocked nose, itchy nose), and four ocular symptoms (itchy eyes, watery eyes, red eyes, sore eyes) on a scale of 0-3, every 30 minutes during the challenge.
Cat-PAD is a "potentially exciting new approach to cat allergy immunotherapy," the investigators said, noting that improvements in the TRSS seen in the initial phase II study and follow-up study represent a substantial improvement over numerous therapies investigated in the past, in some cases reaching a threefold improvement in symptom reduction.
"For example, studies of similar design in an EEC reported TRSS changes of approximately –1.5 units after 16 weeks treatment with a sublingual cat allergy tablet, while a single 180-mg dose of the antihistamine fexofenadine achieved a mean difference in TRSS of –1.3 in a cat allergen study. Moreover, the change in TRSS of –3.8 units reported here was observed after four administrations of Cat-PAD over a 12-week period and persisted 21 months after the end of treatment," they concluded.
In late 2012 the investigators began enrolling a phase III study, which will include individuals aged 12-65 years.
This study was funded by Circassia Limited. Dr. Hafner is employed by Circassia.
A short course of treatment with an investigational synthetic cat-peptide antigen desensitizing vaccine, or Cat-PAD, results in a substantial and persistent reduction in cat allergy symptom scores, according to two-year findings from a randomized, placebo-controlled phase II clinical study involving 202 adult patients.
Study participants were initially randomized to receive either eight 3-nmol intradermal doses at 2-week intervals, four 6 nmol-doses at 4-week intervals, or placebo. At 1-year follow-up, the improvement in Total Rhinoconjunctivitis Symptom Score (TRSS) was significantly greater in the patients who received four doses of Cat-PAD (ToleroMune Cat, Circassia Limited, Oxford, England), compared with those who received placebo (–7.1 points vs. –2.99 points), according to findings published online in the Journal of Allergy and Clinical Immunology (doi:10.1016/j.jaci.2012.12.1185).
Data from a 2-year follow-up study were reported by Rod P. Hafner, Ph.D., and his colleagues in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Of 89 patients enrolled into the follow-up study, 50 returned at 2-years after the start of treatment, having received no additional treatment, for an environmental exposure chamber challenge. The magnitude of difference from baseline in TRSS seen at 1 year in those who received 4 doses and those who received placebo was maintained at 2 years (–5.87 vs. –2.02) among those who initially received the 4-dose regimen.
"Cat-PAD is the first in a new class of synthetic peptide immune-regulatory epitopes. The results from this study provide the first evidence that four doses of 6 nmol Cat-PAD over a 12-week period has a disease-modifying effect with subjects showing sustained improvement at 2 years," the investigators wrote.
Study participants were adults aged 18-65 years with cat allergy who underwent a baseline environmental exposure chamber (EEC) challenge, as well as follow-up EEC challenges at 18-22 weeks and at 100-104 weeks.
"Cat allergen was dispersed into the EEC to achieve a consistent mean level of approx. 50 ng Fel d1/m3, using a validated method," they explained, noting that TRSS was calculated at each EEC challenge based on self-scoring of four nasal symptoms (running nose, sneezing, blocked nose, itchy nose), and four ocular symptoms (itchy eyes, watery eyes, red eyes, sore eyes) on a scale of 0-3, every 30 minutes during the challenge.
Cat-PAD is a "potentially exciting new approach to cat allergy immunotherapy," the investigators said, noting that improvements in the TRSS seen in the initial phase II study and follow-up study represent a substantial improvement over numerous therapies investigated in the past, in some cases reaching a threefold improvement in symptom reduction.
"For example, studies of similar design in an EEC reported TRSS changes of approximately –1.5 units after 16 weeks treatment with a sublingual cat allergy tablet, while a single 180-mg dose of the antihistamine fexofenadine achieved a mean difference in TRSS of –1.3 in a cat allergen study. Moreover, the change in TRSS of –3.8 units reported here was observed after four administrations of Cat-PAD over a 12-week period and persisted 21 months after the end of treatment," they concluded.
In late 2012 the investigators began enrolling a phase III study, which will include individuals aged 12-65 years.
This study was funded by Circassia Limited. Dr. Hafner is employed by Circassia.
AT THE AAAAI ANNUAL MEETING
Major finding: Improvements in TRSS in treated vs. placebo patients were similar at 1 year (–7.1 points vs. –2.99 points), and 2 years (–5.87 vs. –2.02) follow-up.
Data source: A randomized placebo-controlled study and follow-up study involving 202 adults.
Disclosures: This study was funded by Circassia Limited. Dr. Hafner is employed by Circassia.

Novel sublingual immunotherapy eased ragweed allergy symptoms
SAN ANTONIO – Once-daily use of an investigational sublingual allergy immunotherapy liquid extracted from ragweed pollen resulted in highly significant and clinically meaningful improvements in ragweed allergy symptoms in a pivotal phase III multicenter trial involving more than 400 patients.

Given that subcutaneous immunotherapy is the mainstay of therapy in North America for seasonal allergic rhinoconjunctivitis and mild asthma that is unresponsive to pharmacotherapy, this ragweed sublingual allergy immunotherapy liquid (RW-SAIL) extract could represent an important and more convenient option for the management of allergic respiratory disease. Sublingual immunotherapy (SLIT) is used off label in the United States, because it is not approved by the Food and Drug Administration. SLIT is more commonly used in Europe, where studies have demonstrated varying degrees of success.
The current randomized, double-blind, placebo-controlled trial involved 429 adults between the ages of 18-55 years who had ragweed-induced allergic rhinitis, which had necessitated the use of antiallergy medication for at least 2 years and who were positive for ragweed pollen extract on puncture skin test reactivity. They were randomized to self-administered RW-SAIL (Greer Laboratories Inc.) or placebo beginning 8-16 weeks prior to and continued through the 2011 ragweed season.
Of these, 218 adults who were randomized to receive RW-SAIL experienced a 43% reduction in the primary study endpoint of total combined symptom and medication score (TCS) for the entire ragweed pollen season that followed treatment initiation, compared with 211 patients randomized to receive placebo. Breaking that response down by time of ragweed season, the treatment group patients experienced a 42% reduction in TCS during the 3 peak weeks of the season, a 42% reduction in the daily-symptom score (DSS) for the entire season, and a 41% reduction in the DSS during the 3 peak weeks of the season, compared with the placebo group, Dr. Peter Creticos, an allergy and asthma specialist in Warrenton, Va., and his colleagues reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The RW-SAIL group also experienced a significantly greater increase from baseline in ragweed-specific IgG4 antibody, and in ragweed-specific IgE antibody, compared with the placebo group (0.99 vs. –0.1 mg/L, and 55.92 kU/L vs. 4.97 kU/L, respectively).
"Treatment with ragweed SAIL was well tolerated, with no deaths, systemic allergic reactions, or life-threatening events. No study subjects experienced anaphylaxis or required administration of epinephrine," the investigators wrote, noting that most adverse event were mild, and included headache, upper respiratory infection, and gastrointestinal effects. None of eight serious adverse events that occurred during the trial were attributable to the study drug.
The improvements achieved with RW-SAIL among the patients in the active-treatment group exceeded the criteria recently established by consensus panel reports, the investigators noted.
The findings have potentially important implications for the treatment of patients with ragweed allergy, the investigators said.
"Ragweed is the dominant seasonal aeroallergen for much of North America with observational studies showing sensitivity in about 25% of patients. It causes significant morbidity, is associated with disease sequelae and adversely impacts economic burden," they wrote.
The conventional subcutaneous approach to immunotherapy can also be burdensome, requiring a prolonged injection schedule that decreases compliance, discomfort associated with injections, and a recognized risk of anaphylaxis, they noted, concluding that RW-SAIL represents a safe and effective alternative treatment option for patients with ragweed allergy.
This study was funded by Greer Laboratories. Dr. Creticos disclosed relationships with Cercassia, Greer Laboratories, and Merck/Schering-Plough.
SAN ANTONIO – Once-daily use of an investigational sublingual allergy immunotherapy liquid extracted from ragweed pollen resulted in highly significant and clinically meaningful improvements in ragweed allergy symptoms in a pivotal phase III multicenter trial involving more than 400 patients.
Given that subcutaneous immunotherapy is the mainstay of therapy in North America for seasonal allergic rhinoconjunctivitis and mild asthma that is unresponsive to pharmacotherapy, this ragweed sublingual allergy immunotherapy liquid (RW-SAIL) extract could represent an important and more convenient option for the management of allergic respiratory disease. Sublingual immunotherapy (SLIT) is used off label in the United States, because it is not approved by the Food and Drug Administration. SLIT is more commonly used in Europe, where studies have demonstrated varying degrees of success.
The current randomized, double-blind, placebo-controlled trial involved 429 adults between the ages of 18-55 years who had ragweed-induced allergic rhinitis, which had necessitated the use of antiallergy medication for at least 2 years and who were positive for ragweed pollen extract on puncture skin test reactivity. They were randomized to self-administered RW-SAIL (Greer Laboratories Inc.) or placebo beginning 8-16 weeks prior to and continued through the 2011 ragweed season.
Of these, 218 adults who were randomized to receive RW-SAIL experienced a 43% reduction in the primary study endpoint of total combined symptom and medication score (TCS) for the entire ragweed pollen season that followed treatment initiation, compared with 211 patients randomized to receive placebo. Breaking that response down by time of ragweed season, the treatment group patients experienced a 42% reduction in TCS during the 3 peak weeks of the season, a 42% reduction in the daily-symptom score (DSS) for the entire season, and a 41% reduction in the DSS during the 3 peak weeks of the season, compared with the placebo group, Dr. Peter Creticos, an allergy and asthma specialist in Warrenton, Va., and his colleagues reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The RW-SAIL group also experienced a significantly greater increase from baseline in ragweed-specific IgG4 antibody, and in ragweed-specific IgE antibody, compared with the placebo group (0.99 vs. –0.1 mg/L, and 55.92 kU/L vs. 4.97 kU/L, respectively).
"Treatment with ragweed SAIL was well tolerated, with no deaths, systemic allergic reactions, or life-threatening events. No study subjects experienced anaphylaxis or required administration of epinephrine," the investigators wrote, noting that most adverse event were mild, and included headache, upper respiratory infection, and gastrointestinal effects. None of eight serious adverse events that occurred during the trial were attributable to the study drug.
The improvements achieved with RW-SAIL among the patients in the active-treatment group exceeded the criteria recently established by consensus panel reports, the investigators noted.
The findings have potentially important implications for the treatment of patients with ragweed allergy, the investigators said.
"Ragweed is the dominant seasonal aeroallergen for much of North America with observational studies showing sensitivity in about 25% of patients. It causes significant morbidity, is associated with disease sequelae and adversely impacts economic burden," they wrote.
The conventional subcutaneous approach to immunotherapy can also be burdensome, requiring a prolonged injection schedule that decreases compliance, discomfort associated with injections, and a recognized risk of anaphylaxis, they noted, concluding that RW-SAIL represents a safe and effective alternative treatment option for patients with ragweed allergy.
This study was funded by Greer Laboratories. Dr. Creticos disclosed relationships with Cercassia, Greer Laboratories, and Merck/Schering-Plough.
SAN ANTONIO – Once-daily use of an investigational sublingual allergy immunotherapy liquid extracted from ragweed pollen resulted in highly significant and clinically meaningful improvements in ragweed allergy symptoms in a pivotal phase III multicenter trial involving more than 400 patients.
Given that subcutaneous immunotherapy is the mainstay of therapy in North America for seasonal allergic rhinoconjunctivitis and mild asthma that is unresponsive to pharmacotherapy, this ragweed sublingual allergy immunotherapy liquid (RW-SAIL) extract could represent an important and more convenient option for the management of allergic respiratory disease. Sublingual immunotherapy (SLIT) is used off label in the United States, because it is not approved by the Food and Drug Administration. SLIT is more commonly used in Europe, where studies have demonstrated varying degrees of success.
The current randomized, double-blind, placebo-controlled trial involved 429 adults between the ages of 18-55 years who had ragweed-induced allergic rhinitis, which had necessitated the use of antiallergy medication for at least 2 years and who were positive for ragweed pollen extract on puncture skin test reactivity. They were randomized to self-administered RW-SAIL (Greer Laboratories Inc.) or placebo beginning 8-16 weeks prior to and continued through the 2011 ragweed season.
Of these, 218 adults who were randomized to receive RW-SAIL experienced a 43% reduction in the primary study endpoint of total combined symptom and medication score (TCS) for the entire ragweed pollen season that followed treatment initiation, compared with 211 patients randomized to receive placebo. Breaking that response down by time of ragweed season, the treatment group patients experienced a 42% reduction in TCS during the 3 peak weeks of the season, a 42% reduction in the daily-symptom score (DSS) for the entire season, and a 41% reduction in the DSS during the 3 peak weeks of the season, compared with the placebo group, Dr. Peter Creticos, an allergy and asthma specialist in Warrenton, Va., and his colleagues reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The RW-SAIL group also experienced a significantly greater increase from baseline in ragweed-specific IgG4 antibody, and in ragweed-specific IgE antibody, compared with the placebo group (0.99 vs. –0.1 mg/L, and 55.92 kU/L vs. 4.97 kU/L, respectively).
"Treatment with ragweed SAIL was well tolerated, with no deaths, systemic allergic reactions, or life-threatening events. No study subjects experienced anaphylaxis or required administration of epinephrine," the investigators wrote, noting that most adverse event were mild, and included headache, upper respiratory infection, and gastrointestinal effects. None of eight serious adverse events that occurred during the trial were attributable to the study drug.
The improvements achieved with RW-SAIL among the patients in the active-treatment group exceeded the criteria recently established by consensus panel reports, the investigators noted.
The findings have potentially important implications for the treatment of patients with ragweed allergy, the investigators said.
"Ragweed is the dominant seasonal aeroallergen for much of North America with observational studies showing sensitivity in about 25% of patients. It causes significant morbidity, is associated with disease sequelae and adversely impacts economic burden," they wrote.
The conventional subcutaneous approach to immunotherapy can also be burdensome, requiring a prolonged injection schedule that decreases compliance, discomfort associated with injections, and a recognized risk of anaphylaxis, they noted, concluding that RW-SAIL represents a safe and effective alternative treatment option for patients with ragweed allergy.
This study was funded by Greer Laboratories. Dr. Creticos disclosed relationships with Cercassia, Greer Laboratories, and Merck/Schering-Plough.
AT THE AAAAI ANNUAL MEETING
Major finding: RW-SAIL led to a 43% reduction in total combined symptom and medication score vs. placebo.
Data source: Randomized controlled phase III trial involving 429 patients.
Disclosures: This study was funded by Greer Laboratories, Inc. Dr. Creticos disclosed relationships with Cercassia, Greer Laboratories, and Merck/Schering-Plough.

CPAP vs. appliances for sleep apnea
Most likely I am not alone with the feeling that we spend a lot of resources diagnosing sleep apnea, meticulously titrating CPAP devices, and patiently listening to some of our patients as they list the reasons for not using it.
Many times, the patients have been back to the sleep specialists, who try in earnest to make it work because we all know the litany of potential adverse downstream effects if apnea is left untreated.
We all also know that frightening our patients ("untreated sleep apnea can increase the risk for sudden cardiac death and heart failure. ...") into CPAP compliance is ineffective. So, for the lucky patients whose insurance coverage facilitates the fitting of oral appliances, such as the mandibular advancement device (MAD), we can try these.
Although the reduction in overall apneic episodes is less with MAD than with CPAP devices, the adherence to the MAD may be higher.
So how do CPAP and oral appliances fare head-to-head?
Australian investigators conducted a randomized controlled clinical trial evaluating the health outcomes of patients using the MAD or CPAP for obstructive sleep apnea (Am. J. Respir. Crit. Care Med. Feb. 14, 2013 [doi:10.1164/rccm.201212-2223OC]).
In this study, 126 patients with moderate to severe OSA were randomly assigned to use of MAD or CPAP for 1 month. Patients were excluded if they had central sleep apnea, need for immediate treatment, a coexisting sleep disorder, regular use of sedatives or narcotics, or pre-existing lung or psychiatric disease.
The primary outcome was a difference in 24-hour mean arterial blood pressure. Secondary outcomes included cardiovascular events and arterial stiffness. Neurobehavioral function and quality of life also were measured.
CPAP was significantly more effective than MAD for reducing the apnea-hypopnea index (AHI), but compliance was significantly greater with MAD (6.5 hours per night vs. 5.2 hours per night). No differences in the 24-hour mean arterial pressure were observed, though neither treatment improved blood pressure. Sleepiness, driving stimulator performance, and disease-specific quality of life improved with both treatments by similar amounts. MAD was superior to CPAP on several quality-of-life domains.
This study is extremely informative for our practices in which we cannot consistently provide either motivational enhancement or interventions to improve adherence with CPAP. For CPAP-nonadherent patients for whom an appliance seems like an appropriate next step, this should be pursued. In the case of sleep apnea, we should not let perfect be the enemy of good.
Dr. Ebbert is professor of medicine and primary care clinician at the Mayo Clinic in Rochester, Minn. He reports having no conflicts of interest. The opinions expressed are those of the author. Reply via e-mail at imnews@elsevier.com.
Most likely I am not alone with the feeling that we spend a lot of resources diagnosing sleep apnea, meticulously titrating CPAP devices, and patiently listening to some of our patients as they list the reasons for not using it.
Many times, the patients have been back to the sleep specialists, who try in earnest to make it work because we all know the litany of potential adverse downstream effects if apnea is left untreated.
We all also know that frightening our patients ("untreated sleep apnea can increase the risk for sudden cardiac death and heart failure. ...") into CPAP compliance is ineffective. So, for the lucky patients whose insurance coverage facilitates the fitting of oral appliances, such as the mandibular advancement device (MAD), we can try these.
Although the reduction in overall apneic episodes is less with MAD than with CPAP devices, the adherence to the MAD may be higher.
So how do CPAP and oral appliances fare head-to-head?
Australian investigators conducted a randomized controlled clinical trial evaluating the health outcomes of patients using the MAD or CPAP for obstructive sleep apnea (Am. J. Respir. Crit. Care Med. Feb. 14, 2013 [doi:10.1164/rccm.201212-2223OC]).
In this study, 126 patients with moderate to severe OSA were randomly assigned to use of MAD or CPAP for 1 month. Patients were excluded if they had central sleep apnea, need for immediate treatment, a coexisting sleep disorder, regular use of sedatives or narcotics, or pre-existing lung or psychiatric disease.
The primary outcome was a difference in 24-hour mean arterial blood pressure. Secondary outcomes included cardiovascular events and arterial stiffness. Neurobehavioral function and quality of life also were measured.
CPAP was significantly more effective than MAD for reducing the apnea-hypopnea index (AHI), but compliance was significantly greater with MAD (6.5 hours per night vs. 5.2 hours per night). No differences in the 24-hour mean arterial pressure were observed, though neither treatment improved blood pressure. Sleepiness, driving stimulator performance, and disease-specific quality of life improved with both treatments by similar amounts. MAD was superior to CPAP on several quality-of-life domains.
This study is extremely informative for our practices in which we cannot consistently provide either motivational enhancement or interventions to improve adherence with CPAP. For CPAP-nonadherent patients for whom an appliance seems like an appropriate next step, this should be pursued. In the case of sleep apnea, we should not let perfect be the enemy of good.
Dr. Ebbert is professor of medicine and primary care clinician at the Mayo Clinic in Rochester, Minn. He reports having no conflicts of interest. The opinions expressed are those of the author. Reply via e-mail at imnews@elsevier.com.
Most likely I am not alone with the feeling that we spend a lot of resources diagnosing sleep apnea, meticulously titrating CPAP devices, and patiently listening to some of our patients as they list the reasons for not using it.
Many times, the patients have been back to the sleep specialists, who try in earnest to make it work because we all know the litany of potential adverse downstream effects if apnea is left untreated.
We all also know that frightening our patients ("untreated sleep apnea can increase the risk for sudden cardiac death and heart failure. ...") into CPAP compliance is ineffective. So, for the lucky patients whose insurance coverage facilitates the fitting of oral appliances, such as the mandibular advancement device (MAD), we can try these.
Although the reduction in overall apneic episodes is less with MAD than with CPAP devices, the adherence to the MAD may be higher.
So how do CPAP and oral appliances fare head-to-head?
Australian investigators conducted a randomized controlled clinical trial evaluating the health outcomes of patients using the MAD or CPAP for obstructive sleep apnea (Am. J. Respir. Crit. Care Med. Feb. 14, 2013 [doi:10.1164/rccm.201212-2223OC]).
In this study, 126 patients with moderate to severe OSA were randomly assigned to use of MAD or CPAP for 1 month. Patients were excluded if they had central sleep apnea, need for immediate treatment, a coexisting sleep disorder, regular use of sedatives or narcotics, or pre-existing lung or psychiatric disease.
The primary outcome was a difference in 24-hour mean arterial blood pressure. Secondary outcomes included cardiovascular events and arterial stiffness. Neurobehavioral function and quality of life also were measured.
CPAP was significantly more effective than MAD for reducing the apnea-hypopnea index (AHI), but compliance was significantly greater with MAD (6.5 hours per night vs. 5.2 hours per night). No differences in the 24-hour mean arterial pressure were observed, though neither treatment improved blood pressure. Sleepiness, driving stimulator performance, and disease-specific quality of life improved with both treatments by similar amounts. MAD was superior to CPAP on several quality-of-life domains.
This study is extremely informative for our practices in which we cannot consistently provide either motivational enhancement or interventions to improve adherence with CPAP. For CPAP-nonadherent patients for whom an appliance seems like an appropriate next step, this should be pursued. In the case of sleep apnea, we should not let perfect be the enemy of good.
Dr. Ebbert is professor of medicine and primary care clinician at the Mayo Clinic in Rochester, Minn. He reports having no conflicts of interest. The opinions expressed are those of the author. Reply via e-mail at imnews@elsevier.com.

Allergic rhinitis: What’s best for your patient?
• Use nasal steroids to treat allergic rhinitis (AR) in adults. A
• Recommend nasal saline irrigation to reduce symptoms in children and adults with seasonal rhinitis. A
• Consider immunotherapy for adults and children with severe AR that does not respond to conventional pharmacotherapy or allergen avoidance measures. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE A man in his 30s with allergic rhinitis (AR) at predictable times of the year with high pollen counts reports only modest symptom relief with a nasal steroid preparation after 3 weeks of use. He comes to see you because he’s “tired of feeling lousy all of the time.”
What management options would you consider?
There is a plethora of treatment options for patients like this one, and considerable variation in clinical practice when it comes to AR.1 The good news is that there are several recent guidelines for treating AR patients, whose symptoms (and underlying cause) can vary widely.
The following review—and accompanying algorithm—provides evidence-based recommendations that can help you refine your approach to AR.
Two guidelines, and several Cochrane reviews
Allergic Rhinitis and its Impact on Asthma (ARIA), a sentinel rhinitis treatment guideline, was published in 2001 and updated in 2008 and 2010.2-4 The British Society for Allergy and Clinical Immunology Standards of Care Committee (BSACI) published guidelines for rhinitis management in 2008 and guidelines for immunotherapy in 2011.5,6 In addition, several Cochrane reviews have been performed.7-12 The ALGORITHM1-6 combines these recommendations. The TABLE2-12 itemizes the recommendations made by each guideline.
ALGORITHM
An evidence-based approach to treating allergic rhinitis1-6
Based on recommendations from ARIA and BSACI guidelines and Cochrane reviews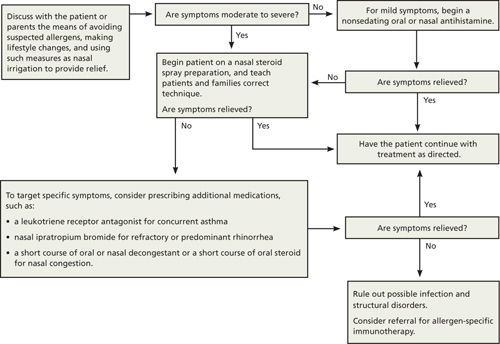
ARIA, Allergic Rhinitis and its Impact on Asthma; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee.
TABLE
Treatment recommendations/suggestions for allergic rhinitis2-12
| TREATMENT RECOMMENDATIONS/SUGGESTIONS | ARIA 2001 | ARIA 2008 | ARIA 2010 | BSACI 2008 | BSACI 2011 | COCHRANE REVIEWS |
|---|---|---|---|---|---|---|
| General principles of treatment | ||||||
| Maintenance therapy is required for persistent AR as medications have little effect after cessation. | X | |||||
| Patient education | ||||||
| Standardized patient education improves disease-specific quality of life. | X | |||||
| Nasal steroids | ||||||
| NS are the most effective monotherapy for all symptoms of AR, seasonal and perennial,* including nasal congestion. | X | |||||
| NS are recommended for AR treatment in adults and suggested for children. | X | |||||
| NS are the treatment of choice for moderate to severe persistent* AR and for treatment failures with antihistamines alone. | X | |||||
| NS are suggested over oral antihistamines in adults and children for seasonal AR. | X | |||||
| NS are suggested over oral antihistamines for adults and children with persistent AR. | X | |||||
| NS are recommended rather than nasal antihistamines. | X | |||||
| NS are recommended over oral leukotriene receptor antagonists for seasonal AR. | X | |||||
| NS are the most effective treatment of AR for children. | X | |||||
| There is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR. | X (2010) | |||||
| Intermittent* NS use may be beneficial in children. | X | |||||
| Avoid NS with high bioavailability (betamethasone) in children, as regular use for >1 year may decrease growth rate. | X | |||||
| Antihistamines | ||||||
| New-generation oral nonsedating antihistamines that do not affect cytochrome P450 are recommended for the treatment of patients with AR. | X | |||||
| Oral or topical antihistamines are first-line treatment for mild to moderate intermittent and moderate persistent AR. | X | |||||
| When NS alone do not control moderate to severe persistent AR, may add oral or topical antihistamines. | X | |||||
| New-generation oral antihistamines are suggested over nasal antihistamines for children and adults, and for children with seasonal or persistent AR. | X | |||||
| Oral antihistamines are suggested over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR. | X | |||||
| Nasal antihistamines are suggested over nasal chromones (the need to use chromones 4 times daily may limit adherence). | X | |||||
| Nasal antihistamine use is suggested for children and adults with seasonal AR. | X | |||||
| Patients with persistent AR should avoid using nasal antihistamines until more data on efficacy and safety are available. | X | |||||
| In children, weigh adverse effects of antihistamines against the general malaise caused by AR. | X | |||||
| Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children. | X | |||||
| Continuous administration of antihistamines is optimal in children, rather than as needed. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for patients with ocular symptoms. | X | |||||
| Oral leukotriene receptor antagonists | ||||||
| Oral leukotriene receptor antagonists are suggested for children and adults with seasonal AR and for preschool children with persistent AR. | X | |||||
| Avoid oral leukotriene receptor antagonists in adults with persistent AR. | X | |||||
| Decongestants | ||||||
| For adults with severe nasal obstruction, a short course (<5 days) of a nasal decongestant, along with other drugs, is suggested. | X | |||||
| Nasal decongestants may be useful for eustachian tube dysfunction when flying, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency prior to NS use. | X | |||||
| Regular oral decongestant use is not suggested. | X | X | ||||
| Avoid decongestants in pregnant patients. | X | |||||
| Avoid using nasal decongestants in preschool children. | X | |||||
| Chromones | ||||||
| Limited use of chromones is recommended for children and adults with mild symptoms. | X | |||||
| Chromones are less effective than NS or antihistamines. | X | |||||
| Nasal antihistamines are suggested over nasal chromones. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for ocular symptoms. Due to the excellent safety of these agents, chromones may be tried before antihistamines. | X | |||||
| Nasal saline | ||||||
| Nasal saline irrigation reduces symptoms in children and adults with seasonal rhinitis. | X | |||||
| Oral, intramuscular steroids | ||||||
| A short course of oral glucocorticosteroids is suggested for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments. | X | |||||
| Oral steroids are rarely indicated, but a short course (5-10 days) may be used for severe nasal congestion, uncontrolled symptoms on conventional pharmacotherapy, or important social/work events. | X | |||||
| Avoid intramuscular steroids. | X | X | ||||
| Ipratropium | ||||||
| Nasal ipratropium is suggested for treatment of rhinorrhea for patients with persistent AR. | X | |||||
| Allergen-specific immunotherapy | ||||||
| Immunotherapy is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy or allergen avoidance measures. | X | |||||
| SCIT is suggested for adults with seasonal AR and those with persistent AR due to house dust mites. | X | |||||
| SCIT is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few severe adverse reactions. | X (2007) | |||||
| SLIT is suggested for adults with AR due to pollen, although other alternatives may be equally reasonable. | X | |||||
| SLIT is safe and efficacious for AR treatment, decreasing symptoms and medication requirements. | X (2003) | |||||
| Nasal immunotherapy is suggested for adults with AR due to pollens. | X | |||||
| For pregnant patients, maintenance ASI may be continued, but starting ASI or increasing the dose is contraindicated. | X | |||||
| SCIT is suggested for children with AR. | X | |||||
| SCIT should not be started before 5 years of age. | X | |||||
| Based on preliminary studies, SLIT is safe, but more studies are needed in children. | X | |||||
| SLIT and NIT are suggested for children with AR due to pollens, acknowledging that other alternatives may be equally reasonable. SLIT should not be given to children with AR due to HDM unless being done for research. | X | |||||
| Lifestyle changes | ||||||
| Avoid single chemical or physical preventive and combination preventive methods to reduce HDM exposure. | X | |||||
| Allergen avoidance may decrease AR symptoms, but more research is needed. | X (2010) | |||||
| Achieving substantial reductions in HDM load may decrease AR symptoms. | X (2012) | |||||
| Avoidance of mold or animal dander is recommended for patients who are allergic to them. | X | |||||
| Nasal filters can reduce symptoms of AR during ragweed and grass pollen seasons. | X | |||||
| Complementary and alternative medicine | ||||||
| Avoid homeopathy, acupuncture, butterbur, herbal medicines, and phototherapy. | X | |||||
| AR, allergic rhinitis; ARIA, Allergic Rhinitis and its Impact on Asthma; ASI, allergen-specific immunotherapy; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee; HDM, house dust mites; NIT, nasal immunotherapy; NS, nasal steroids; SCIT, subcutaneous immunotherapy; SLIT, sublingual immunotherapy. *ARIA 2008 recommended changing the classification of AR from seasonal and perennial (frequent nonseasonal nasal or ocular symptoms) to intermittent (symptoms lasting <4 days per week or <4 weeks per year) or persistent (symptoms >4 days per week and >4 weeks per year).3 AR severity is classified as mild or moderate to severe.2,3 | ||||||
The summary that follows provides a more detailed look at the recommendations, with a review of the pathophysiology of AR (“Phases of allergic rhinitis”2,3,5,8,13-15).
The early phase of allergic rhinitis (AR) occurs within minutes of allergen exposure. Mast cell degranulation releases histamine and other inflammatory mediators that cause sneezing, pruritus, rhinorrhea, and nasal congestion.3,8,13 The late phase, beginning at 4 hours and peaking 6 to 12 hours after exposure, is believed to be due to recruitment of circulating leukocytes—particularly eosinophils. Leukocyte activation causes additional inflammatory mediators to be released, which primarily causes nasal congestion—often the most bothersome symptom of AR.2,5,8,13,14 Other presenting symptoms may include feeling “fuzzy” or tired, chronic viral infections, sniffing, eye rubbing, blinking, congested voice, snoring, or dark skin beneath the eyes (allergic shiners).15
Of note: This summary preserves the terminology used in ARIA 2010. Specifically, the ARIA guideline uses the term suggest for conditional recommendations and recommend for strong recommendations.4 That same language is used here.
Nasal steroids: First-line Tx for moderate to severe symptoms
BSACI indicates that nasal steroids (NS) are the treatment of choice for moderate to severe persistent AR (symptoms lasting >4 days per week or >4 weeks per year).5 ARIA 2010 suggests NS as first-line treatment rather than oral antihistamines for adults and children with seasonal (related to outdoor allergens such as pollens or molds) and persistent AR.4 ARIA 2008 finds NS are the most effective treatment for children.3 Steroids reduce inflammation by decreasing inflammatory cell migration and inhibiting cytokine release.16 They are the most effective monotherapy for all symptoms of AR, including nasal congestion, which antihistamines do not treat effectively.13,16 NS also treat ocular symptoms of allergy effectively.15,17
The ARIA 2010 guideline also recommends using NS rather than nasal antihistamines and leukotriene receptor antagonists.4 Combination therapy (eg, NS with the addition of nasal antihistamines) is an option for severe or persistent AR, but it appears to be no more effective than monotherapy with NS.16 A 2010 Cochrane review determined there is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR.7 Intermittent steroid use may be beneficial in children.5
Steroids begin working 6 to 8 hours after the first dose, although symptom reduction may take days and maximal effect up to 2 weeks.5 Treatment failure may be due to poor technique that can cause local adverse effects (ie, dryness, irritation, epistaxis). Technique-related failure occurs in up to 10% of users.5,15 Educating patients and families about correct technique with steroid spray may decrease nonadherence due to irritation and epistaxis.18 Tell them to shake the bottle well, look down, aim the nozzle toward the outside wall of the nostril using the opposite hand, and spray while sniffing lightly.5
Any steroid is appropriate for adults. For children ≥2 years of age, consider fluticasone propionate, mometasone furoate, or triamcinolone acetonide.3 These medications have lower systemic bioavailability and a decreased risk of such adverse effects as hypothalamic-pituitary-adrenal axis suppression and growth retardation.15 Budesonide is appropriate for those ≥6 years.19-21 Avoid regular use of betamethasone, which has high bioavailability, for >1 year in children, as it may decrease their growth rate.3 Beclomethasone, fluticasone, and budesonide have been used widely and safely for pregnant women with asthma.5
Antihistamines are first-line Tx for mild symptoms
ARIA 2010 recommends new-generation oral nonsedating antihistamines that do not affect cytochrome P450 for mild AR,4 such as cetirizine, levocetirizine, loratadine, desloratadine, and fexofenadine. First-generation antihistamines can reduce symptoms, but are not first-line treatment as they cause sedation, fatigue, decreased cognitive function, and reduced academic and work performance.3-5 ARIA 2010 further suggests choosing oral antihistamines over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR.4
BSACI recommends oral or topical antihistamines as first-line treatment for mild to moderate symptoms lasting <4 days per week or <4 weeks per year and moderate persistent AR.5 When steroids alone do not control moderate to severe persistent AR, BSACI recommends adding oral or topical antihistamines.5 Oral and topical antihistamines decrease histamine-related symptoms of itching, rhinorrhea, and sneezing, but do not significantly decrease nasal congestion.15
Nasal antihistamines (levocabastine, azelastine) have a rapid onset of action and few adverse effects.3 ARIA 2010 suggests nasal antihistamines over nasal chromones (inhibitors of mast cell degranulation) and notes that the need to use chromones 4 times daily may limit adherence.4 The same guidelines suggest nasal antihistamine use for children and adults with seasonal AR and suggest not using nasal antihistamines for patients with persistent AR until more data on efficacy and safety are available.4
Alezastine is approved for individuals ≥5 years, and olopatadine is approved for individuals ≥6 years for the treatment of AR.16,22,23 A pediatric review article noted nasal antihistamine (azelastine) plus nasal fluticasone was more efficacious than NS alone.15
In children, weigh adverse effects of antihistamines against the general malaise caused by AR.3 Do not use first-generation antihistamines due to the sedation that may interfere with learning.15 Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children.5 Continuous administration, rather than as needed, is optimal treatment in children.5 Cetirizine, loratadine, and levocetirizine have been studied and are effective and safe in children.3 Levocetirizine has proven safe and efficacious for children ≥2 years.24 Fexofenadine was found to be effective and safe for those ≥6 years.25
For children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones.4 Due to the safety of these agents, chromones may be used first, then antihistamines.4 Just as with nasal chromones, the need to use intraocular chromones 4 times daily may limit their use in children.4
Pregnant patients. Antihistamines do cross the placenta.5 Agents that appear to be safe for pregnant patients are chlorphenamine (first-generation), loratadine, and cetirizine.5
Leukotriene receptor antagonists: Always pair with antihistamines
As adjunctive therapy for additional symptom control, ARIA 2010 suggests oral leukotriene receptor antagonists for children and adults with seasonal AR, and for preschool children with persistent AR. These agents may also be helpful in children with concurrent asthma.15 Always pair leukotriene receptor antagonists with antihistamines. Montelukast is approved for seasonal AR in children ≥2 years and for frequent nonseasonal nasal or ocular AR symptoms in children ≥6 months.26
ARIA 2010 recommends against the use of oral leukotriene receptor antagonists in adults with persistent AR.4
Decongestants are for limited use only
For adults with severe nasal obstruction, ARIA 2010 suggests a short course (<5 days) of nasal decongestant along with other drugs.4 Limiting use of nasal decongestants to <10 days helps prevent rhinitis medicamentosa.5,27 BSACI notes nasal decongestants may be useful for eustachian tube dysfunction experienced aboard airplanes, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency before NS use.5 Both guidelines suggest against regular oral decongestant use.4,5
Avoid decongestants in pregnant patients.5 ARIA 2010 suggests against nasal decongestant use in preschool children.4
Chromones may help, but require multiple daily dosing
Chromones inhibit mast cell degranulation, are weakly effective for reducing nasal obstruction in AR, and have a high safety profile.3-5,28 As noted earlier, they must be used 4 times daily, which may reduce adherence—particularly in children.4
ARIA 2008 notes that disodium cromoglycate is less effective than NS or antihistamines.3 The 2010 update suggests nasal antihistamines over nasal chromones.4 For adults as well as children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones. BSACI recommends limited use of chromones for children and adults with mild symptoms.5
Nasal saline helpful as adjunct to medication
Nasal saline irrigation improves symptoms of AR, clears nasal passages, and is helpful for pregnant patients, for whom medications should be used with caution.2,3,5 Nasal irrigation using a neti pot or squeeze bottle is efficacious for chronic rhinorrhea, as solo or complementary treatment, and for children.5,16,27
Oral steroids: Use only rarely
ARIA 2010 suggests a short course of oral glucocorticosteroids for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments.4 BSACI notes oral steroids are rarely indicated, but that their use over 5 to 10 days may help with severe nasal congestion, symptoms uncontrolled by conventional pharmacotherapy, or before important social or work events.5 Both guidelines recommend against intramuscular steroids.4 ARIA 2008 notes oral and depot preparations of steroids affect growth in young children.3
Ipratropium when rhinorrhea is severe
Nasal ipratropium bromide, a topical anticholinergic, is helpful for excessive or refractory rhinorrhea. Consider using ipratropium with NS for patients for whom rhinorrhea is the dominant symptom.5,16,28 ARIA 2010 suggests using nasal ipratropium to treat rhinorrhea in patients with persistent AR.4
Allergen-specific immunotherapy: When other treatments fail
Allergen-specific immunotherapy (ASI) consists of repeated exposure to an allergen to induce immunomodulation, which prevents or reduces allergy symptoms and actually changes the natural course of AR. (For more on identifying the offending agent, see “Time for allergen testing?”2,5,15,18,29.) This treatment process decreases medication needs, prevents new allergen sensitization, and results in long-lasting improvement.2,5,6,30 BSACI 2011 notes that ASI is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy and allergen avoidance measures.6
When a patient’s symptoms are poorly controlled or persist after treatment, consider allergen testing.29 Skin prick testing (SPT) is the best means of eliciting specific allergen sensitization. However, limit testing to allergens most likely causing the patient’s symptoms rather than ordering a random panel; 15% of those with a positive SPT to specific allergens do not have symptoms when exposed to those allergens in their environment.5 And always interpret results of allergy testing in light of the patient’s history.2,15,18
SPT has a high negative predictive value, which can prevent unnecessary lifestyle changes.29 However, keep in mind that SPT results may be suppressed if the patient is using antihistamines, tricyclic antidepressants, or topical steroids.29 If SPT is not feasible or the patient is taking medications that may suppress results, consider arranging for serum-specific IgE testing, also known as radioallergosorbent testing, or RAST.5 RAST and SPT have similar sensitivities for house dust mites, but RAST is not as sensitive as SPT for other inhalants (eg, cat epithelium, mold, grass pollen).5
ASI methods developed to date use subcutaneous, sublingual, or nasal routes of administration. However, the US Food and Drug Administration has yet to approve commercial sublingual or nasal products for use in the United States.16
Subcutaneous immunotherapy may cause local adverse reactions (pruritus and swelling) and systemic reactions that can be severe or life threatening (anaphylaxis) and thus must be given in a doctor’s office prepared to treat anaphylaxis.6,16,30 Adrenaline administration has been necessary in 0.13% of those being treated.9 Subcutaneous immunotherapy must be done for 3 to 5 years for sustained effective treatment.15
ARIA 2010 suggests subcutaneous immunotherapy for adults with seasonal AR and with persistent AR due to house dust mites.4 A 2007 Cochrane review found subcutaneous immunotherapy is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few significant severe adverse reactions.9 A meta-analysis showed subcutaneous immunotherapy is as potent as pharmacotherapy in controlling seasonal AR symptoms as early as the first season of treatment.31
What if the patient is pregnant—or a child? BSACI notes that maintenance ASI may be continued in a patient who becomes pregnant, but starting ASI or increasing the dose is contraindicated.5
Based on ARIA 2008 and 2010, consider subcutaneous immunotherapy for children—but not for those <5 years.3,4 Care must be used in selecting patients, as 3 to 5 years of treatment are necessary for sustained benefit.15
Lifestyle changes: Limited benefit may be achievable
ARIA 2010 recommends mold avoidance and animal dander avoidance for patients so affected.4 Allergens from pets can persist in homes for months after pet removal.15 BSACI found that commercially available nasal filters (filters or screens placed over or within both nares) reduced symptoms of AR during ragweed and grass pollen seasons.5 Allergen avoidance for children with persistent AR has not shown consistent benefit.15 A 2010 Cochrane review concluded that allergen avoidance may decrease AR symptoms, but more research is needed.11
House dust mites. The 2010 Cochrane review also reported on 2 trials that assessed high-efficiency particulate air (HEPA) filters specifically for patients allergic to house dust mites.11 The studies, which had methodological limitations (inconsistent randomization, small sample size, and short duration), concluded that HEPA filters alone will not likely reduce symptoms of house dust mite allergy. But HEPA filters may be beneficial as one component of an extensive bedroom-based environmental control program.11
Impermeable bedding has been shown to reduce dust mite load by 50% to 70%, leaving residual allergen that may still trigger symptoms.11 A 2012 Cochrane review concluded that achieving substantial reductions in house dust mite load using a combination approach of multiple interventions, including acaricides and extensive bedroom-based environmental control programs, may decrease AR symptoms.12 However, ARIA 2010 recommends against single chemical or physical preventive methods and against combination preventive methods to reduce house dust mite exposure.4
Total elimination of house dust mites may be impossible, and recommending use of impermeable covers and HEPA filters, removal of rugs and curtains, and frequent cleaning must take into account a patient’s symptoms and a family’s motivation and finances.11,18
Complementary and alternative medicine: Too little evidence
ARIA 2010 suggests against patients using homeopathy, acupuncture, butterbur, herbal medicines, or phototherapy for AR.4 While one systematic review of acupuncture for AR demonstrated mixed results with no specific effects for seasonal AR and some improvement of frequent nonseasonal symptoms,32 another review concluded evidence was insufficient to make any recommendation.32,33 The benefit of ear acupressure is unknown, as supporting studies are of low methodological quality, although it appeared to provide some benefit for AR.34
Due to lack of data, probiotics should not be recommended.27 A pediatric review article noted that probiotics may alter cytokine production in patients with seasonal AR and may be more helpful in AR than in asthma, although more research was needed.15 Another review showed that probiotics may reduce AR symptoms and medication use.35
CASE Since the nasal steroid you prescribed for your patient did not provide adequate relief, you opt to add cetirizine 10 mg to his NS regimen. This step relieved his symptoms within 2 to 3 days. Had his symptoms persisted, the patient would have been a candidate for a one-week course of oral decongestant, such as pseudoephedrine 120 mg orally every 12 hours, as needed; and then for allergen testing, specifically for pollens corresponding to the seasonality of his AR. Appropriate follow-up would be to monitor the patient until his symptoms resolved or became manageable.
1. Bousquet J, Schünemann HJ, Zuberbier T, et al. Development and implementation of guidelines in allergic rhinitis – an ARIA-GA2LEN paper. Allergy. 2010;65:1212-1221.
2. Bousquet J, Van-Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(suppl):S147-S334.
3. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008. Allergy. 2008;63(suppl 86):S8-S160.
4. Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) Guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466-476.
5. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin Exp Allergy. 2008;38:19-42.
6. Walker SM, Durham SR, Till SJ, et al. Immunotherapy for allergic rhinitis. Clin Exp Allergy. 2011;41:1177-1200.
7. Al Sayyad JJ, Fedorowicz Z, Alhashimi D, et al. Topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2007;(1):CD003163.-
8. Nasser M, Fedorowicz, Alijufairi H, et al. Antihistamines used in addition to topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2010;(7):CD006989.-
9. Calderon MA, Alves B, Jacobson M, et al. Allergen injection immunotherapy for seasonal allergic rhinitis. Cochrane Database Syst Rev. 2007;(1):CD001936.-
10. Wilson D, Torres-Lima M, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev. 2003;(2):CD002893.-
11. Sheikh A, Hurwitz B, Nurmatov U, et al. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. 2010;(7):CD001563.-
12. Nurmatov U, van Schayck CP, Hurwitz B, et al. House dust mite avoidance measures for perennial allergic rhinitis: an updated Cochrane systematic review. Allergy. 2012;67:158-165.
13. Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108(suppl):S2-S8.
14. Nathan RA. The pathophysiology, clinical impact, and management of nasal congestion in allergic rhinitis. Clin Ther. 2008;30:573-586.
15. Kemp AS. Allergic rhinitis. Paediatric Respir Rev. 2009;10:63-68.
16. Sur DK, Scandale S. Treatment of allergic rhinitis. Am Fam Physician. 2010;81:1440-1446.
17. Hong J, Bielory B, Rosenberg JL, et al. Efficacy of intranasal corticosteroids for the ocular symptoms of allergic rhinitis: a systematic review. Allergy Asthma Proc. 2011;32:22-35.
18. Hu W, Katelaris CH, Kemp AS. Allergic rhinitis – practical management strategies. Aust Fam Physician. 2008;37:214-220.
19. Veramyst (fluticasone furoate) nasal spray [prescribing information]. Research Triangle Park, NC: GlaxoSmithKline; August 2012. Available at: http://us.gsk.com/products/assets/us_veramyst.pdf. Accessed January 16, 2013.
20. Nasacort AQ (triamcinolone acetonide) nasal spray [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/nasacort_aq/nasacort_aq.html. Accessed January 16, 2013.
21. Rhinocort AQUA 32 mcg (budesonide) nasal spray [prescribing information]. Wilmington, Del: AstraZeneca; revised December 2010. Available at: http://www1.astrazeneca-us.com/pi/Rhinocort_Aqua.pdf. Accessed January 16, 2013.
22. Astelin (azelastine hydrochloride) spray, metered [prescribing information]. Somerset, NJ: Meda Pharmaceuticals; revised July 2011. Available at: http://www.astelin.com/pdf/astelin_pi.pdf. Accessed January 16, 2013.
23. Patanase (olopatadine hydrochloride) nasal spray [prescribing information]. Fort Worth, Tex: Alcon Laboratories; revised February 2012. Available at: http://ecatalog.alcon.com/PI/Patanase_us_en.pdf. Accessed January 16, 2013.
24. Xyzal (levocetirizine dihydrochloride) tablets and oral solution [prescribing information]. Smyrna, Ga: UCB and Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/xyzal/xyzal.pdf. Accessed January 16, 2013.
25. Allegra (fexofenadine hydrochloride) tablets, ODT, and oral suspension [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2007. Available at: http://products.sanofi.us/allegra/allegra.html. Accessed January 16, 2013.
26. Singulair (montelukast sodium) tablets, chewable tablets, and oral granules [prescribing information]. Whitehouse Station, NJ: Merck; revised November 2012. Available at: http://www.merck.com/product/usa/pi_circulars/s/singulair/singulair_pi.pdf. Accessed January 16, 2013.
27. Meltzer EO, Bukstein DA. The economic impact of allergic rhinitis and current guidelines for treatment. Ann Allergy Asthma Immunol. 2011;106(suppl):S12-S16.
28. Lim MY, Leong JM. Allergic rhinitis: evidence-based practice. Singapore Med J. 2010;51:542-550.
29. Angier E, Willington J, Scadding G, et al. Management of allergic and non-allergic rhinitis: a primary care summary of the BSACI guideline. Prim Care Respir J. 2010;19:217-222.
30. Radulovic S, Wilson D, Calderon M, et al. Systematic reviews of sublingual immunotherapy (SLIT). Allergy. 2011;66:740-752.
31. Matricardi PM, Kuna P, Panetta V, et al. Subcutaneous immunotherapy and pharmacology in seasonal allergic rhinitis: a comparison based on meta-analyses. J Allergy Clin Immunol. 2011;128:791-799.
32. Lee MS, Pittler MH, Shin B, et al. Acupuncture for allergic rhinitis: a systematic review. Ann Allergy Asthma Immunol. 2009;102:269-279.
33. Roberts J, Huissoon A, Dretzke J, et al. A systematic review of the clinical effectiveness of acupuncture for allergic rhinitis. BMC Complement Altern Med. 2008;8:13.-
34. Zhang CS, Yang AW, Zhang AL, et al. Ear-acupressure for allergic rhinitis: a systematic review. Clin Otolaryngol. 2010;35:6-12.
35. Vliagoftis H, Kouranos VD, Betsi GI, et al. Probiotics for the treatment of allergic rhinitis and asthma: systematic review of randomized controlled trials. Ann Allergy Asthma Immunol. 2008;101:570-579.
CORRESPONDENCE Suzanne Minor, MD, Florida International University Herbert Wertheim College of Medicine; 11200 SW 8th Street, AHC II 361A, Miami, FL 33199; seminor@fiu.edu
• Use nasal steroids to treat allergic rhinitis (AR) in adults. A
• Recommend nasal saline irrigation to reduce symptoms in children and adults with seasonal rhinitis. A
• Consider immunotherapy for adults and children with severe AR that does not respond to conventional pharmacotherapy or allergen avoidance measures. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE A man in his 30s with allergic rhinitis (AR) at predictable times of the year with high pollen counts reports only modest symptom relief with a nasal steroid preparation after 3 weeks of use. He comes to see you because he’s “tired of feeling lousy all of the time.”
What management options would you consider?
There is a plethora of treatment options for patients like this one, and considerable variation in clinical practice when it comes to AR.1 The good news is that there are several recent guidelines for treating AR patients, whose symptoms (and underlying cause) can vary widely.
The following review—and accompanying algorithm—provides evidence-based recommendations that can help you refine your approach to AR.
Two guidelines, and several Cochrane reviews
Allergic Rhinitis and its Impact on Asthma (ARIA), a sentinel rhinitis treatment guideline, was published in 2001 and updated in 2008 and 2010.2-4 The British Society for Allergy and Clinical Immunology Standards of Care Committee (BSACI) published guidelines for rhinitis management in 2008 and guidelines for immunotherapy in 2011.5,6 In addition, several Cochrane reviews have been performed.7-12 The ALGORITHM1-6 combines these recommendations. The TABLE2-12 itemizes the recommendations made by each guideline.
ALGORITHM
An evidence-based approach to treating allergic rhinitis1-6
Based on recommendations from ARIA and BSACI guidelines and Cochrane reviews
ARIA, Allergic Rhinitis and its Impact on Asthma; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee.
TABLE
Treatment recommendations/suggestions for allergic rhinitis2-12
| TREATMENT RECOMMENDATIONS/SUGGESTIONS | ARIA 2001 | ARIA 2008 | ARIA 2010 | BSACI 2008 | BSACI 2011 | COCHRANE REVIEWS |
|---|---|---|---|---|---|---|
| General principles of treatment | ||||||
| Maintenance therapy is required for persistent AR as medications have little effect after cessation. | X | |||||
| Patient education | ||||||
| Standardized patient education improves disease-specific quality of life. | X | |||||
| Nasal steroids | ||||||
| NS are the most effective monotherapy for all symptoms of AR, seasonal and perennial,* including nasal congestion. | X | |||||
| NS are recommended for AR treatment in adults and suggested for children. | X | |||||
| NS are the treatment of choice for moderate to severe persistent* AR and for treatment failures with antihistamines alone. | X | |||||
| NS are suggested over oral antihistamines in adults and children for seasonal AR. | X | |||||
| NS are suggested over oral antihistamines for adults and children with persistent AR. | X | |||||
| NS are recommended rather than nasal antihistamines. | X | |||||
| NS are recommended over oral leukotriene receptor antagonists for seasonal AR. | X | |||||
| NS are the most effective treatment of AR for children. | X | |||||
| There is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR. | X (2010) | |||||
| Intermittent* NS use may be beneficial in children. | X | |||||
| Avoid NS with high bioavailability (betamethasone) in children, as regular use for >1 year may decrease growth rate. | X | |||||
| Antihistamines | ||||||
| New-generation oral nonsedating antihistamines that do not affect cytochrome P450 are recommended for the treatment of patients with AR. | X | |||||
| Oral or topical antihistamines are first-line treatment for mild to moderate intermittent and moderate persistent AR. | X | |||||
| When NS alone do not control moderate to severe persistent AR, may add oral or topical antihistamines. | X | |||||
| New-generation oral antihistamines are suggested over nasal antihistamines for children and adults, and for children with seasonal or persistent AR. | X | |||||
| Oral antihistamines are suggested over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR. | X | |||||
| Nasal antihistamines are suggested over nasal chromones (the need to use chromones 4 times daily may limit adherence). | X | |||||
| Nasal antihistamine use is suggested for children and adults with seasonal AR. | X | |||||
| Patients with persistent AR should avoid using nasal antihistamines until more data on efficacy and safety are available. | X | |||||
| In children, weigh adverse effects of antihistamines against the general malaise caused by AR. | X | |||||
| Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children. | X | |||||
| Continuous administration of antihistamines is optimal in children, rather than as needed. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for patients with ocular symptoms. | X | |||||
| Oral leukotriene receptor antagonists | ||||||
| Oral leukotriene receptor antagonists are suggested for children and adults with seasonal AR and for preschool children with persistent AR. | X | |||||
| Avoid oral leukotriene receptor antagonists in adults with persistent AR. | X | |||||
| Decongestants | ||||||
| For adults with severe nasal obstruction, a short course (<5 days) of a nasal decongestant, along with other drugs, is suggested. | X | |||||
| Nasal decongestants may be useful for eustachian tube dysfunction when flying, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency prior to NS use. | X | |||||
| Regular oral decongestant use is not suggested. | X | X | ||||
| Avoid decongestants in pregnant patients. | X | |||||
| Avoid using nasal decongestants in preschool children. | X | |||||
| Chromones | ||||||
| Limited use of chromones is recommended for children and adults with mild symptoms. | X | |||||
| Chromones are less effective than NS or antihistamines. | X | |||||
| Nasal antihistamines are suggested over nasal chromones. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for ocular symptoms. Due to the excellent safety of these agents, chromones may be tried before antihistamines. | X | |||||
| Nasal saline | ||||||
| Nasal saline irrigation reduces symptoms in children and adults with seasonal rhinitis. | X | |||||
| Oral, intramuscular steroids | ||||||
| A short course of oral glucocorticosteroids is suggested for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments. | X | |||||
| Oral steroids are rarely indicated, but a short course (5-10 days) may be used for severe nasal congestion, uncontrolled symptoms on conventional pharmacotherapy, or important social/work events. | X | |||||
| Avoid intramuscular steroids. | X | X | ||||
| Ipratropium | ||||||
| Nasal ipratropium is suggested for treatment of rhinorrhea for patients with persistent AR. | X | |||||
| Allergen-specific immunotherapy | ||||||
| Immunotherapy is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy or allergen avoidance measures. | X | |||||
| SCIT is suggested for adults with seasonal AR and those with persistent AR due to house dust mites. | X | |||||
| SCIT is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few severe adverse reactions. | X (2007) | |||||
| SLIT is suggested for adults with AR due to pollen, although other alternatives may be equally reasonable. | X | |||||
| SLIT is safe and efficacious for AR treatment, decreasing symptoms and medication requirements. | X (2003) | |||||
| Nasal immunotherapy is suggested for adults with AR due to pollens. | X | |||||
| For pregnant patients, maintenance ASI may be continued, but starting ASI or increasing the dose is contraindicated. | X | |||||
| SCIT is suggested for children with AR. | X | |||||
| SCIT should not be started before 5 years of age. | X | |||||
| Based on preliminary studies, SLIT is safe, but more studies are needed in children. | X | |||||
| SLIT and NIT are suggested for children with AR due to pollens, acknowledging that other alternatives may be equally reasonable. SLIT should not be given to children with AR due to HDM unless being done for research. | X | |||||
| Lifestyle changes | ||||||
| Avoid single chemical or physical preventive and combination preventive methods to reduce HDM exposure. | X | |||||
| Allergen avoidance may decrease AR symptoms, but more research is needed. | X (2010) | |||||
| Achieving substantial reductions in HDM load may decrease AR symptoms. | X (2012) | |||||
| Avoidance of mold or animal dander is recommended for patients who are allergic to them. | X | |||||
| Nasal filters can reduce symptoms of AR during ragweed and grass pollen seasons. | X | |||||
| Complementary and alternative medicine | ||||||
| Avoid homeopathy, acupuncture, butterbur, herbal medicines, and phototherapy. | X | |||||
| AR, allergic rhinitis; ARIA, Allergic Rhinitis and its Impact on Asthma; ASI, allergen-specific immunotherapy; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee; HDM, house dust mites; NIT, nasal immunotherapy; NS, nasal steroids; SCIT, subcutaneous immunotherapy; SLIT, sublingual immunotherapy. *ARIA 2008 recommended changing the classification of AR from seasonal and perennial (frequent nonseasonal nasal or ocular symptoms) to intermittent (symptoms lasting <4 days per week or <4 weeks per year) or persistent (symptoms >4 days per week and >4 weeks per year).3 AR severity is classified as mild or moderate to severe.2,3 | ||||||
The summary that follows provides a more detailed look at the recommendations, with a review of the pathophysiology of AR (“Phases of allergic rhinitis”2,3,5,8,13-15).
The early phase of allergic rhinitis (AR) occurs within minutes of allergen exposure. Mast cell degranulation releases histamine and other inflammatory mediators that cause sneezing, pruritus, rhinorrhea, and nasal congestion.3,8,13 The late phase, beginning at 4 hours and peaking 6 to 12 hours after exposure, is believed to be due to recruitment of circulating leukocytes—particularly eosinophils. Leukocyte activation causes additional inflammatory mediators to be released, which primarily causes nasal congestion—often the most bothersome symptom of AR.2,5,8,13,14 Other presenting symptoms may include feeling “fuzzy” or tired, chronic viral infections, sniffing, eye rubbing, blinking, congested voice, snoring, or dark skin beneath the eyes (allergic shiners).15
Of note: This summary preserves the terminology used in ARIA 2010. Specifically, the ARIA guideline uses the term suggest for conditional recommendations and recommend for strong recommendations.4 That same language is used here.
Nasal steroids: First-line Tx for moderate to severe symptoms
BSACI indicates that nasal steroids (NS) are the treatment of choice for moderate to severe persistent AR (symptoms lasting >4 days per week or >4 weeks per year).5 ARIA 2010 suggests NS as first-line treatment rather than oral antihistamines for adults and children with seasonal (related to outdoor allergens such as pollens or molds) and persistent AR.4 ARIA 2008 finds NS are the most effective treatment for children.3 Steroids reduce inflammation by decreasing inflammatory cell migration and inhibiting cytokine release.16 They are the most effective monotherapy for all symptoms of AR, including nasal congestion, which antihistamines do not treat effectively.13,16 NS also treat ocular symptoms of allergy effectively.15,17
The ARIA 2010 guideline also recommends using NS rather than nasal antihistamines and leukotriene receptor antagonists.4 Combination therapy (eg, NS with the addition of nasal antihistamines) is an option for severe or persistent AR, but it appears to be no more effective than monotherapy with NS.16 A 2010 Cochrane review determined there is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR.7 Intermittent steroid use may be beneficial in children.5
Steroids begin working 6 to 8 hours after the first dose, although symptom reduction may take days and maximal effect up to 2 weeks.5 Treatment failure may be due to poor technique that can cause local adverse effects (ie, dryness, irritation, epistaxis). Technique-related failure occurs in up to 10% of users.5,15 Educating patients and families about correct technique with steroid spray may decrease nonadherence due to irritation and epistaxis.18 Tell them to shake the bottle well, look down, aim the nozzle toward the outside wall of the nostril using the opposite hand, and spray while sniffing lightly.5
Any steroid is appropriate for adults. For children ≥2 years of age, consider fluticasone propionate, mometasone furoate, or triamcinolone acetonide.3 These medications have lower systemic bioavailability and a decreased risk of such adverse effects as hypothalamic-pituitary-adrenal axis suppression and growth retardation.15 Budesonide is appropriate for those ≥6 years.19-21 Avoid regular use of betamethasone, which has high bioavailability, for >1 year in children, as it may decrease their growth rate.3 Beclomethasone, fluticasone, and budesonide have been used widely and safely for pregnant women with asthma.5
Antihistamines are first-line Tx for mild symptoms
ARIA 2010 recommends new-generation oral nonsedating antihistamines that do not affect cytochrome P450 for mild AR,4 such as cetirizine, levocetirizine, loratadine, desloratadine, and fexofenadine. First-generation antihistamines can reduce symptoms, but are not first-line treatment as they cause sedation, fatigue, decreased cognitive function, and reduced academic and work performance.3-5 ARIA 2010 further suggests choosing oral antihistamines over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR.4
BSACI recommends oral or topical antihistamines as first-line treatment for mild to moderate symptoms lasting <4 days per week or <4 weeks per year and moderate persistent AR.5 When steroids alone do not control moderate to severe persistent AR, BSACI recommends adding oral or topical antihistamines.5 Oral and topical antihistamines decrease histamine-related symptoms of itching, rhinorrhea, and sneezing, but do not significantly decrease nasal congestion.15
Nasal antihistamines (levocabastine, azelastine) have a rapid onset of action and few adverse effects.3 ARIA 2010 suggests nasal antihistamines over nasal chromones (inhibitors of mast cell degranulation) and notes that the need to use chromones 4 times daily may limit adherence.4 The same guidelines suggest nasal antihistamine use for children and adults with seasonal AR and suggest not using nasal antihistamines for patients with persistent AR until more data on efficacy and safety are available.4
Alezastine is approved for individuals ≥5 years, and olopatadine is approved for individuals ≥6 years for the treatment of AR.16,22,23 A pediatric review article noted nasal antihistamine (azelastine) plus nasal fluticasone was more efficacious than NS alone.15
In children, weigh adverse effects of antihistamines against the general malaise caused by AR.3 Do not use first-generation antihistamines due to the sedation that may interfere with learning.15 Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children.5 Continuous administration, rather than as needed, is optimal treatment in children.5 Cetirizine, loratadine, and levocetirizine have been studied and are effective and safe in children.3 Levocetirizine has proven safe and efficacious for children ≥2 years.24 Fexofenadine was found to be effective and safe for those ≥6 years.25
For children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones.4 Due to the safety of these agents, chromones may be used first, then antihistamines.4 Just as with nasal chromones, the need to use intraocular chromones 4 times daily may limit their use in children.4
Pregnant patients. Antihistamines do cross the placenta.5 Agents that appear to be safe for pregnant patients are chlorphenamine (first-generation), loratadine, and cetirizine.5
Leukotriene receptor antagonists: Always pair with antihistamines
As adjunctive therapy for additional symptom control, ARIA 2010 suggests oral leukotriene receptor antagonists for children and adults with seasonal AR, and for preschool children with persistent AR. These agents may also be helpful in children with concurrent asthma.15 Always pair leukotriene receptor antagonists with antihistamines. Montelukast is approved for seasonal AR in children ≥2 years and for frequent nonseasonal nasal or ocular AR symptoms in children ≥6 months.26
ARIA 2010 recommends against the use of oral leukotriene receptor antagonists in adults with persistent AR.4
Decongestants are for limited use only
For adults with severe nasal obstruction, ARIA 2010 suggests a short course (<5 days) of nasal decongestant along with other drugs.4 Limiting use of nasal decongestants to <10 days helps prevent rhinitis medicamentosa.5,27 BSACI notes nasal decongestants may be useful for eustachian tube dysfunction experienced aboard airplanes, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency before NS use.5 Both guidelines suggest against regular oral decongestant use.4,5
Avoid decongestants in pregnant patients.5 ARIA 2010 suggests against nasal decongestant use in preschool children.4
Chromones may help, but require multiple daily dosing
Chromones inhibit mast cell degranulation, are weakly effective for reducing nasal obstruction in AR, and have a high safety profile.3-5,28 As noted earlier, they must be used 4 times daily, which may reduce adherence—particularly in children.4
ARIA 2008 notes that disodium cromoglycate is less effective than NS or antihistamines.3 The 2010 update suggests nasal antihistamines over nasal chromones.4 For adults as well as children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones. BSACI recommends limited use of chromones for children and adults with mild symptoms.5
Nasal saline helpful as adjunct to medication
Nasal saline irrigation improves symptoms of AR, clears nasal passages, and is helpful for pregnant patients, for whom medications should be used with caution.2,3,5 Nasal irrigation using a neti pot or squeeze bottle is efficacious for chronic rhinorrhea, as solo or complementary treatment, and for children.5,16,27
Oral steroids: Use only rarely
ARIA 2010 suggests a short course of oral glucocorticosteroids for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments.4 BSACI notes oral steroids are rarely indicated, but that their use over 5 to 10 days may help with severe nasal congestion, symptoms uncontrolled by conventional pharmacotherapy, or before important social or work events.5 Both guidelines recommend against intramuscular steroids.4 ARIA 2008 notes oral and depot preparations of steroids affect growth in young children.3
Ipratropium when rhinorrhea is severe
Nasal ipratropium bromide, a topical anticholinergic, is helpful for excessive or refractory rhinorrhea. Consider using ipratropium with NS for patients for whom rhinorrhea is the dominant symptom.5,16,28 ARIA 2010 suggests using nasal ipratropium to treat rhinorrhea in patients with persistent AR.4
Allergen-specific immunotherapy: When other treatments fail
Allergen-specific immunotherapy (ASI) consists of repeated exposure to an allergen to induce immunomodulation, which prevents or reduces allergy symptoms and actually changes the natural course of AR. (For more on identifying the offending agent, see “Time for allergen testing?”2,5,15,18,29.) This treatment process decreases medication needs, prevents new allergen sensitization, and results in long-lasting improvement.2,5,6,30 BSACI 2011 notes that ASI is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy and allergen avoidance measures.6
When a patient’s symptoms are poorly controlled or persist after treatment, consider allergen testing.29 Skin prick testing (SPT) is the best means of eliciting specific allergen sensitization. However, limit testing to allergens most likely causing the patient’s symptoms rather than ordering a random panel; 15% of those with a positive SPT to specific allergens do not have symptoms when exposed to those allergens in their environment.5 And always interpret results of allergy testing in light of the patient’s history.2,15,18
SPT has a high negative predictive value, which can prevent unnecessary lifestyle changes.29 However, keep in mind that SPT results may be suppressed if the patient is using antihistamines, tricyclic antidepressants, or topical steroids.29 If SPT is not feasible or the patient is taking medications that may suppress results, consider arranging for serum-specific IgE testing, also known as radioallergosorbent testing, or RAST.5 RAST and SPT have similar sensitivities for house dust mites, but RAST is not as sensitive as SPT for other inhalants (eg, cat epithelium, mold, grass pollen).5
ASI methods developed to date use subcutaneous, sublingual, or nasal routes of administration. However, the US Food and Drug Administration has yet to approve commercial sublingual or nasal products for use in the United States.16
Subcutaneous immunotherapy may cause local adverse reactions (pruritus and swelling) and systemic reactions that can be severe or life threatening (anaphylaxis) and thus must be given in a doctor’s office prepared to treat anaphylaxis.6,16,30 Adrenaline administration has been necessary in 0.13% of those being treated.9 Subcutaneous immunotherapy must be done for 3 to 5 years for sustained effective treatment.15
ARIA 2010 suggests subcutaneous immunotherapy for adults with seasonal AR and with persistent AR due to house dust mites.4 A 2007 Cochrane review found subcutaneous immunotherapy is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few significant severe adverse reactions.9 A meta-analysis showed subcutaneous immunotherapy is as potent as pharmacotherapy in controlling seasonal AR symptoms as early as the first season of treatment.31
What if the patient is pregnant—or a child? BSACI notes that maintenance ASI may be continued in a patient who becomes pregnant, but starting ASI or increasing the dose is contraindicated.5
Based on ARIA 2008 and 2010, consider subcutaneous immunotherapy for children—but not for those <5 years.3,4 Care must be used in selecting patients, as 3 to 5 years of treatment are necessary for sustained benefit.15
Lifestyle changes: Limited benefit may be achievable
ARIA 2010 recommends mold avoidance and animal dander avoidance for patients so affected.4 Allergens from pets can persist in homes for months after pet removal.15 BSACI found that commercially available nasal filters (filters or screens placed over or within both nares) reduced symptoms of AR during ragweed and grass pollen seasons.5 Allergen avoidance for children with persistent AR has not shown consistent benefit.15 A 2010 Cochrane review concluded that allergen avoidance may decrease AR symptoms, but more research is needed.11
House dust mites. The 2010 Cochrane review also reported on 2 trials that assessed high-efficiency particulate air (HEPA) filters specifically for patients allergic to house dust mites.11 The studies, which had methodological limitations (inconsistent randomization, small sample size, and short duration), concluded that HEPA filters alone will not likely reduce symptoms of house dust mite allergy. But HEPA filters may be beneficial as one component of an extensive bedroom-based environmental control program.11
Impermeable bedding has been shown to reduce dust mite load by 50% to 70%, leaving residual allergen that may still trigger symptoms.11 A 2012 Cochrane review concluded that achieving substantial reductions in house dust mite load using a combination approach of multiple interventions, including acaricides and extensive bedroom-based environmental control programs, may decrease AR symptoms.12 However, ARIA 2010 recommends against single chemical or physical preventive methods and against combination preventive methods to reduce house dust mite exposure.4
Total elimination of house dust mites may be impossible, and recommending use of impermeable covers and HEPA filters, removal of rugs and curtains, and frequent cleaning must take into account a patient’s symptoms and a family’s motivation and finances.11,18
Complementary and alternative medicine: Too little evidence
ARIA 2010 suggests against patients using homeopathy, acupuncture, butterbur, herbal medicines, or phototherapy for AR.4 While one systematic review of acupuncture for AR demonstrated mixed results with no specific effects for seasonal AR and some improvement of frequent nonseasonal symptoms,32 another review concluded evidence was insufficient to make any recommendation.32,33 The benefit of ear acupressure is unknown, as supporting studies are of low methodological quality, although it appeared to provide some benefit for AR.34
Due to lack of data, probiotics should not be recommended.27 A pediatric review article noted that probiotics may alter cytokine production in patients with seasonal AR and may be more helpful in AR than in asthma, although more research was needed.15 Another review showed that probiotics may reduce AR symptoms and medication use.35
CASE Since the nasal steroid you prescribed for your patient did not provide adequate relief, you opt to add cetirizine 10 mg to his NS regimen. This step relieved his symptoms within 2 to 3 days. Had his symptoms persisted, the patient would have been a candidate for a one-week course of oral decongestant, such as pseudoephedrine 120 mg orally every 12 hours, as needed; and then for allergen testing, specifically for pollens corresponding to the seasonality of his AR. Appropriate follow-up would be to monitor the patient until his symptoms resolved or became manageable.
• Use nasal steroids to treat allergic rhinitis (AR) in adults. A
• Recommend nasal saline irrigation to reduce symptoms in children and adults with seasonal rhinitis. A
• Consider immunotherapy for adults and children with severe AR that does not respond to conventional pharmacotherapy or allergen avoidance measures. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE A man in his 30s with allergic rhinitis (AR) at predictable times of the year with high pollen counts reports only modest symptom relief with a nasal steroid preparation after 3 weeks of use. He comes to see you because he’s “tired of feeling lousy all of the time.”
What management options would you consider?
There is a plethora of treatment options for patients like this one, and considerable variation in clinical practice when it comes to AR.1 The good news is that there are several recent guidelines for treating AR patients, whose symptoms (and underlying cause) can vary widely.
The following review—and accompanying algorithm—provides evidence-based recommendations that can help you refine your approach to AR.
Two guidelines, and several Cochrane reviews
Allergic Rhinitis and its Impact on Asthma (ARIA), a sentinel rhinitis treatment guideline, was published in 2001 and updated in 2008 and 2010.2-4 The British Society for Allergy and Clinical Immunology Standards of Care Committee (BSACI) published guidelines for rhinitis management in 2008 and guidelines for immunotherapy in 2011.5,6 In addition, several Cochrane reviews have been performed.7-12 The ALGORITHM1-6 combines these recommendations. The TABLE2-12 itemizes the recommendations made by each guideline.
ALGORITHM
An evidence-based approach to treating allergic rhinitis1-6
Based on recommendations from ARIA and BSACI guidelines and Cochrane reviews
ARIA, Allergic Rhinitis and its Impact on Asthma; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee.
TABLE
Treatment recommendations/suggestions for allergic rhinitis2-12
| TREATMENT RECOMMENDATIONS/SUGGESTIONS | ARIA 2001 | ARIA 2008 | ARIA 2010 | BSACI 2008 | BSACI 2011 | COCHRANE REVIEWS |
|---|---|---|---|---|---|---|
| General principles of treatment | ||||||
| Maintenance therapy is required for persistent AR as medications have little effect after cessation. | X | |||||
| Patient education | ||||||
| Standardized patient education improves disease-specific quality of life. | X | |||||
| Nasal steroids | ||||||
| NS are the most effective monotherapy for all symptoms of AR, seasonal and perennial,* including nasal congestion. | X | |||||
| NS are recommended for AR treatment in adults and suggested for children. | X | |||||
| NS are the treatment of choice for moderate to severe persistent* AR and for treatment failures with antihistamines alone. | X | |||||
| NS are suggested over oral antihistamines in adults and children for seasonal AR. | X | |||||
| NS are suggested over oral antihistamines for adults and children with persistent AR. | X | |||||
| NS are recommended rather than nasal antihistamines. | X | |||||
| NS are recommended over oral leukotriene receptor antagonists for seasonal AR. | X | |||||
| NS are the most effective treatment of AR for children. | X | |||||
| There is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR. | X (2010) | |||||
| Intermittent* NS use may be beneficial in children. | X | |||||
| Avoid NS with high bioavailability (betamethasone) in children, as regular use for >1 year may decrease growth rate. | X | |||||
| Antihistamines | ||||||
| New-generation oral nonsedating antihistamines that do not affect cytochrome P450 are recommended for the treatment of patients with AR. | X | |||||
| Oral or topical antihistamines are first-line treatment for mild to moderate intermittent and moderate persistent AR. | X | |||||
| When NS alone do not control moderate to severe persistent AR, may add oral or topical antihistamines. | X | |||||
| New-generation oral antihistamines are suggested over nasal antihistamines for children and adults, and for children with seasonal or persistent AR. | X | |||||
| Oral antihistamines are suggested over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR. | X | |||||
| Nasal antihistamines are suggested over nasal chromones (the need to use chromones 4 times daily may limit adherence). | X | |||||
| Nasal antihistamine use is suggested for children and adults with seasonal AR. | X | |||||
| Patients with persistent AR should avoid using nasal antihistamines until more data on efficacy and safety are available. | X | |||||
| In children, weigh adverse effects of antihistamines against the general malaise caused by AR. | X | |||||
| Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children. | X | |||||
| Continuous administration of antihistamines is optimal in children, rather than as needed. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for patients with ocular symptoms. | X | |||||
| Oral leukotriene receptor antagonists | ||||||
| Oral leukotriene receptor antagonists are suggested for children and adults with seasonal AR and for preschool children with persistent AR. | X | |||||
| Avoid oral leukotriene receptor antagonists in adults with persistent AR. | X | |||||
| Decongestants | ||||||
| For adults with severe nasal obstruction, a short course (<5 days) of a nasal decongestant, along with other drugs, is suggested. | X | |||||
| Nasal decongestants may be useful for eustachian tube dysfunction when flying, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency prior to NS use. | X | |||||
| Regular oral decongestant use is not suggested. | X | X | ||||
| Avoid decongestants in pregnant patients. | X | |||||
| Avoid using nasal decongestants in preschool children. | X | |||||
| Chromones | ||||||
| Limited use of chromones is recommended for children and adults with mild symptoms. | X | |||||
| Chromones are less effective than NS or antihistamines. | X | |||||
| Nasal antihistamines are suggested over nasal chromones. | X | |||||
| Intraocular antihistamines or intraocular chromones are suggested for ocular symptoms. Due to the excellent safety of these agents, chromones may be tried before antihistamines. | X | |||||
| Nasal saline | ||||||
| Nasal saline irrigation reduces symptoms in children and adults with seasonal rhinitis. | X | |||||
| Oral, intramuscular steroids | ||||||
| A short course of oral glucocorticosteroids is suggested for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments. | X | |||||
| Oral steroids are rarely indicated, but a short course (5-10 days) may be used for severe nasal congestion, uncontrolled symptoms on conventional pharmacotherapy, or important social/work events. | X | |||||
| Avoid intramuscular steroids. | X | X | ||||
| Ipratropium | ||||||
| Nasal ipratropium is suggested for treatment of rhinorrhea for patients with persistent AR. | X | |||||
| Allergen-specific immunotherapy | ||||||
| Immunotherapy is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy or allergen avoidance measures. | X | |||||
| SCIT is suggested for adults with seasonal AR and those with persistent AR due to house dust mites. | X | |||||
| SCIT is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few severe adverse reactions. | X (2007) | |||||
| SLIT is suggested for adults with AR due to pollen, although other alternatives may be equally reasonable. | X | |||||
| SLIT is safe and efficacious for AR treatment, decreasing symptoms and medication requirements. | X (2003) | |||||
| Nasal immunotherapy is suggested for adults with AR due to pollens. | X | |||||
| For pregnant patients, maintenance ASI may be continued, but starting ASI or increasing the dose is contraindicated. | X | |||||
| SCIT is suggested for children with AR. | X | |||||
| SCIT should not be started before 5 years of age. | X | |||||
| Based on preliminary studies, SLIT is safe, but more studies are needed in children. | X | |||||
| SLIT and NIT are suggested for children with AR due to pollens, acknowledging that other alternatives may be equally reasonable. SLIT should not be given to children with AR due to HDM unless being done for research. | X | |||||
| Lifestyle changes | ||||||
| Avoid single chemical or physical preventive and combination preventive methods to reduce HDM exposure. | X | |||||
| Allergen avoidance may decrease AR symptoms, but more research is needed. | X (2010) | |||||
| Achieving substantial reductions in HDM load may decrease AR symptoms. | X (2012) | |||||
| Avoidance of mold or animal dander is recommended for patients who are allergic to them. | X | |||||
| Nasal filters can reduce symptoms of AR during ragweed and grass pollen seasons. | X | |||||
| Complementary and alternative medicine | ||||||
| Avoid homeopathy, acupuncture, butterbur, herbal medicines, and phototherapy. | X | |||||
| AR, allergic rhinitis; ARIA, Allergic Rhinitis and its Impact on Asthma; ASI, allergen-specific immunotherapy; BSACI, British Society for Allergy and Clinical Immunology Standards of Care Committee; HDM, house dust mites; NIT, nasal immunotherapy; NS, nasal steroids; SCIT, subcutaneous immunotherapy; SLIT, sublingual immunotherapy. *ARIA 2008 recommended changing the classification of AR from seasonal and perennial (frequent nonseasonal nasal or ocular symptoms) to intermittent (symptoms lasting <4 days per week or <4 weeks per year) or persistent (symptoms >4 days per week and >4 weeks per year).3 AR severity is classified as mild or moderate to severe.2,3 | ||||||
The summary that follows provides a more detailed look at the recommendations, with a review of the pathophysiology of AR (“Phases of allergic rhinitis”2,3,5,8,13-15).
The early phase of allergic rhinitis (AR) occurs within minutes of allergen exposure. Mast cell degranulation releases histamine and other inflammatory mediators that cause sneezing, pruritus, rhinorrhea, and nasal congestion.3,8,13 The late phase, beginning at 4 hours and peaking 6 to 12 hours after exposure, is believed to be due to recruitment of circulating leukocytes—particularly eosinophils. Leukocyte activation causes additional inflammatory mediators to be released, which primarily causes nasal congestion—often the most bothersome symptom of AR.2,5,8,13,14 Other presenting symptoms may include feeling “fuzzy” or tired, chronic viral infections, sniffing, eye rubbing, blinking, congested voice, snoring, or dark skin beneath the eyes (allergic shiners).15
Of note: This summary preserves the terminology used in ARIA 2010. Specifically, the ARIA guideline uses the term suggest for conditional recommendations and recommend for strong recommendations.4 That same language is used here.
Nasal steroids: First-line Tx for moderate to severe symptoms
BSACI indicates that nasal steroids (NS) are the treatment of choice for moderate to severe persistent AR (symptoms lasting >4 days per week or >4 weeks per year).5 ARIA 2010 suggests NS as first-line treatment rather than oral antihistamines for adults and children with seasonal (related to outdoor allergens such as pollens or molds) and persistent AR.4 ARIA 2008 finds NS are the most effective treatment for children.3 Steroids reduce inflammation by decreasing inflammatory cell migration and inhibiting cytokine release.16 They are the most effective monotherapy for all symptoms of AR, including nasal congestion, which antihistamines do not treat effectively.13,16 NS also treat ocular symptoms of allergy effectively.15,17
The ARIA 2010 guideline also recommends using NS rather than nasal antihistamines and leukotriene receptor antagonists.4 Combination therapy (eg, NS with the addition of nasal antihistamines) is an option for severe or persistent AR, but it appears to be no more effective than monotherapy with NS.16 A 2010 Cochrane review determined there is insufficient evidence for or against the use of oral antihistamines plus NS vs NS alone in children with AR.7 Intermittent steroid use may be beneficial in children.5
Steroids begin working 6 to 8 hours after the first dose, although symptom reduction may take days and maximal effect up to 2 weeks.5 Treatment failure may be due to poor technique that can cause local adverse effects (ie, dryness, irritation, epistaxis). Technique-related failure occurs in up to 10% of users.5,15 Educating patients and families about correct technique with steroid spray may decrease nonadherence due to irritation and epistaxis.18 Tell them to shake the bottle well, look down, aim the nozzle toward the outside wall of the nostril using the opposite hand, and spray while sniffing lightly.5
Any steroid is appropriate for adults. For children ≥2 years of age, consider fluticasone propionate, mometasone furoate, or triamcinolone acetonide.3 These medications have lower systemic bioavailability and a decreased risk of such adverse effects as hypothalamic-pituitary-adrenal axis suppression and growth retardation.15 Budesonide is appropriate for those ≥6 years.19-21 Avoid regular use of betamethasone, which has high bioavailability, for >1 year in children, as it may decrease their growth rate.3 Beclomethasone, fluticasone, and budesonide have been used widely and safely for pregnant women with asthma.5
Antihistamines are first-line Tx for mild symptoms
ARIA 2010 recommends new-generation oral nonsedating antihistamines that do not affect cytochrome P450 for mild AR,4 such as cetirizine, levocetirizine, loratadine, desloratadine, and fexofenadine. First-generation antihistamines can reduce symptoms, but are not first-line treatment as they cause sedation, fatigue, decreased cognitive function, and reduced academic and work performance.3-5 ARIA 2010 further suggests choosing oral antihistamines over oral leukotriene receptor antagonists in patients with seasonal AR and in preschool children with persistent AR.4
BSACI recommends oral or topical antihistamines as first-line treatment for mild to moderate symptoms lasting <4 days per week or <4 weeks per year and moderate persistent AR.5 When steroids alone do not control moderate to severe persistent AR, BSACI recommends adding oral or topical antihistamines.5 Oral and topical antihistamines decrease histamine-related symptoms of itching, rhinorrhea, and sneezing, but do not significantly decrease nasal congestion.15
Nasal antihistamines (levocabastine, azelastine) have a rapid onset of action and few adverse effects.3 ARIA 2010 suggests nasal antihistamines over nasal chromones (inhibitors of mast cell degranulation) and notes that the need to use chromones 4 times daily may limit adherence.4 The same guidelines suggest nasal antihistamine use for children and adults with seasonal AR and suggest not using nasal antihistamines for patients with persistent AR until more data on efficacy and safety are available.4
Alezastine is approved for individuals ≥5 years, and olopatadine is approved for individuals ≥6 years for the treatment of AR.16,22,23 A pediatric review article noted nasal antihistamine (azelastine) plus nasal fluticasone was more efficacious than NS alone.15
In children, weigh adverse effects of antihistamines against the general malaise caused by AR.3 Do not use first-generation antihistamines due to the sedation that may interfere with learning.15 Treatment with once-daily, long-acting antihistamines rather than multiple daily dosing may improve adherence in children.5 Continuous administration, rather than as needed, is optimal treatment in children.5 Cetirizine, loratadine, and levocetirizine have been studied and are effective and safe in children.3 Levocetirizine has proven safe and efficacious for children ≥2 years.24 Fexofenadine was found to be effective and safe for those ≥6 years.25
For children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones.4 Due to the safety of these agents, chromones may be used first, then antihistamines.4 Just as with nasal chromones, the need to use intraocular chromones 4 times daily may limit their use in children.4
Pregnant patients. Antihistamines do cross the placenta.5 Agents that appear to be safe for pregnant patients are chlorphenamine (first-generation), loratadine, and cetirizine.5
Leukotriene receptor antagonists: Always pair with antihistamines
As adjunctive therapy for additional symptom control, ARIA 2010 suggests oral leukotriene receptor antagonists for children and adults with seasonal AR, and for preschool children with persistent AR. These agents may also be helpful in children with concurrent asthma.15 Always pair leukotriene receptor antagonists with antihistamines. Montelukast is approved for seasonal AR in children ≥2 years and for frequent nonseasonal nasal or ocular AR symptoms in children ≥6 months.26
ARIA 2010 recommends against the use of oral leukotriene receptor antagonists in adults with persistent AR.4
Decongestants are for limited use only
For adults with severe nasal obstruction, ARIA 2010 suggests a short course (<5 days) of nasal decongestant along with other drugs.4 Limiting use of nasal decongestants to <10 days helps prevent rhinitis medicamentosa.5,27 BSACI notes nasal decongestants may be useful for eustachian tube dysfunction experienced aboard airplanes, for children with acute otitis media with middle ear pain, to relieve congestion after an upper respiratory infection, and to improve nasal patency before NS use.5 Both guidelines suggest against regular oral decongestant use.4,5
Avoid decongestants in pregnant patients.5 ARIA 2010 suggests against nasal decongestant use in preschool children.4
Chromones may help, but require multiple daily dosing
Chromones inhibit mast cell degranulation, are weakly effective for reducing nasal obstruction in AR, and have a high safety profile.3-5,28 As noted earlier, they must be used 4 times daily, which may reduce adherence—particularly in children.4
ARIA 2008 notes that disodium cromoglycate is less effective than NS or antihistamines.3 The 2010 update suggests nasal antihistamines over nasal chromones.4 For adults as well as children with ocular symptoms, ARIA 2010 suggests intraocular antihistamines or intraocular chromones. BSACI recommends limited use of chromones for children and adults with mild symptoms.5
Nasal saline helpful as adjunct to medication
Nasal saline irrigation improves symptoms of AR, clears nasal passages, and is helpful for pregnant patients, for whom medications should be used with caution.2,3,5 Nasal irrigation using a neti pot or squeeze bottle is efficacious for chronic rhinorrhea, as solo or complementary treatment, and for children.5,16,27
Oral steroids: Use only rarely
ARIA 2010 suggests a short course of oral glucocorticosteroids for patients with AR and moderate to severe nasal or ocular symptoms not controlled with other treatments.4 BSACI notes oral steroids are rarely indicated, but that their use over 5 to 10 days may help with severe nasal congestion, symptoms uncontrolled by conventional pharmacotherapy, or before important social or work events.5 Both guidelines recommend against intramuscular steroids.4 ARIA 2008 notes oral and depot preparations of steroids affect growth in young children.3
Ipratropium when rhinorrhea is severe
Nasal ipratropium bromide, a topical anticholinergic, is helpful for excessive or refractory rhinorrhea. Consider using ipratropium with NS for patients for whom rhinorrhea is the dominant symptom.5,16,28 ARIA 2010 suggests using nasal ipratropium to treat rhinorrhea in patients with persistent AR.4
Allergen-specific immunotherapy: When other treatments fail
Allergen-specific immunotherapy (ASI) consists of repeated exposure to an allergen to induce immunomodulation, which prevents or reduces allergy symptoms and actually changes the natural course of AR. (For more on identifying the offending agent, see “Time for allergen testing?”2,5,15,18,29.) This treatment process decreases medication needs, prevents new allergen sensitization, and results in long-lasting improvement.2,5,6,30 BSACI 2011 notes that ASI is effective for adults and children with severe AR who do not respond to conventional pharmacotherapy and allergen avoidance measures.6
When a patient’s symptoms are poorly controlled or persist after treatment, consider allergen testing.29 Skin prick testing (SPT) is the best means of eliciting specific allergen sensitization. However, limit testing to allergens most likely causing the patient’s symptoms rather than ordering a random panel; 15% of those with a positive SPT to specific allergens do not have symptoms when exposed to those allergens in their environment.5 And always interpret results of allergy testing in light of the patient’s history.2,15,18
SPT has a high negative predictive value, which can prevent unnecessary lifestyle changes.29 However, keep in mind that SPT results may be suppressed if the patient is using antihistamines, tricyclic antidepressants, or topical steroids.29 If SPT is not feasible or the patient is taking medications that may suppress results, consider arranging for serum-specific IgE testing, also known as radioallergosorbent testing, or RAST.5 RAST and SPT have similar sensitivities for house dust mites, but RAST is not as sensitive as SPT for other inhalants (eg, cat epithelium, mold, grass pollen).5
ASI methods developed to date use subcutaneous, sublingual, or nasal routes of administration. However, the US Food and Drug Administration has yet to approve commercial sublingual or nasal products for use in the United States.16
Subcutaneous immunotherapy may cause local adverse reactions (pruritus and swelling) and systemic reactions that can be severe or life threatening (anaphylaxis) and thus must be given in a doctor’s office prepared to treat anaphylaxis.6,16,30 Adrenaline administration has been necessary in 0.13% of those being treated.9 Subcutaneous immunotherapy must be done for 3 to 5 years for sustained effective treatment.15
ARIA 2010 suggests subcutaneous immunotherapy for adults with seasonal AR and with persistent AR due to house dust mites.4 A 2007 Cochrane review found subcutaneous immunotherapy is efficacious for patients with seasonal AR due to pollens, resulting in decreased symptoms and medication use with few significant severe adverse reactions.9 A meta-analysis showed subcutaneous immunotherapy is as potent as pharmacotherapy in controlling seasonal AR symptoms as early as the first season of treatment.31
What if the patient is pregnant—or a child? BSACI notes that maintenance ASI may be continued in a patient who becomes pregnant, but starting ASI or increasing the dose is contraindicated.5
Based on ARIA 2008 and 2010, consider subcutaneous immunotherapy for children—but not for those <5 years.3,4 Care must be used in selecting patients, as 3 to 5 years of treatment are necessary for sustained benefit.15
Lifestyle changes: Limited benefit may be achievable
ARIA 2010 recommends mold avoidance and animal dander avoidance for patients so affected.4 Allergens from pets can persist in homes for months after pet removal.15 BSACI found that commercially available nasal filters (filters or screens placed over or within both nares) reduced symptoms of AR during ragweed and grass pollen seasons.5 Allergen avoidance for children with persistent AR has not shown consistent benefit.15 A 2010 Cochrane review concluded that allergen avoidance may decrease AR symptoms, but more research is needed.11
House dust mites. The 2010 Cochrane review also reported on 2 trials that assessed high-efficiency particulate air (HEPA) filters specifically for patients allergic to house dust mites.11 The studies, which had methodological limitations (inconsistent randomization, small sample size, and short duration), concluded that HEPA filters alone will not likely reduce symptoms of house dust mite allergy. But HEPA filters may be beneficial as one component of an extensive bedroom-based environmental control program.11
Impermeable bedding has been shown to reduce dust mite load by 50% to 70%, leaving residual allergen that may still trigger symptoms.11 A 2012 Cochrane review concluded that achieving substantial reductions in house dust mite load using a combination approach of multiple interventions, including acaricides and extensive bedroom-based environmental control programs, may decrease AR symptoms.12 However, ARIA 2010 recommends against single chemical or physical preventive methods and against combination preventive methods to reduce house dust mite exposure.4
Total elimination of house dust mites may be impossible, and recommending use of impermeable covers and HEPA filters, removal of rugs and curtains, and frequent cleaning must take into account a patient’s symptoms and a family’s motivation and finances.11,18
Complementary and alternative medicine: Too little evidence
ARIA 2010 suggests against patients using homeopathy, acupuncture, butterbur, herbal medicines, or phototherapy for AR.4 While one systematic review of acupuncture for AR demonstrated mixed results with no specific effects for seasonal AR and some improvement of frequent nonseasonal symptoms,32 another review concluded evidence was insufficient to make any recommendation.32,33 The benefit of ear acupressure is unknown, as supporting studies are of low methodological quality, although it appeared to provide some benefit for AR.34
Due to lack of data, probiotics should not be recommended.27 A pediatric review article noted that probiotics may alter cytokine production in patients with seasonal AR and may be more helpful in AR than in asthma, although more research was needed.15 Another review showed that probiotics may reduce AR symptoms and medication use.35
CASE Since the nasal steroid you prescribed for your patient did not provide adequate relief, you opt to add cetirizine 10 mg to his NS regimen. This step relieved his symptoms within 2 to 3 days. Had his symptoms persisted, the patient would have been a candidate for a one-week course of oral decongestant, such as pseudoephedrine 120 mg orally every 12 hours, as needed; and then for allergen testing, specifically for pollens corresponding to the seasonality of his AR. Appropriate follow-up would be to monitor the patient until his symptoms resolved or became manageable.
1. Bousquet J, Schünemann HJ, Zuberbier T, et al. Development and implementation of guidelines in allergic rhinitis – an ARIA-GA2LEN paper. Allergy. 2010;65:1212-1221.
2. Bousquet J, Van-Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(suppl):S147-S334.
3. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008. Allergy. 2008;63(suppl 86):S8-S160.
4. Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) Guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466-476.
5. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin Exp Allergy. 2008;38:19-42.
6. Walker SM, Durham SR, Till SJ, et al. Immunotherapy for allergic rhinitis. Clin Exp Allergy. 2011;41:1177-1200.
7. Al Sayyad JJ, Fedorowicz Z, Alhashimi D, et al. Topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2007;(1):CD003163.-
8. Nasser M, Fedorowicz, Alijufairi H, et al. Antihistamines used in addition to topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2010;(7):CD006989.-
9. Calderon MA, Alves B, Jacobson M, et al. Allergen injection immunotherapy for seasonal allergic rhinitis. Cochrane Database Syst Rev. 2007;(1):CD001936.-
10. Wilson D, Torres-Lima M, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev. 2003;(2):CD002893.-
11. Sheikh A, Hurwitz B, Nurmatov U, et al. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. 2010;(7):CD001563.-
12. Nurmatov U, van Schayck CP, Hurwitz B, et al. House dust mite avoidance measures for perennial allergic rhinitis: an updated Cochrane systematic review. Allergy. 2012;67:158-165.
13. Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108(suppl):S2-S8.
14. Nathan RA. The pathophysiology, clinical impact, and management of nasal congestion in allergic rhinitis. Clin Ther. 2008;30:573-586.
15. Kemp AS. Allergic rhinitis. Paediatric Respir Rev. 2009;10:63-68.
16. Sur DK, Scandale S. Treatment of allergic rhinitis. Am Fam Physician. 2010;81:1440-1446.
17. Hong J, Bielory B, Rosenberg JL, et al. Efficacy of intranasal corticosteroids for the ocular symptoms of allergic rhinitis: a systematic review. Allergy Asthma Proc. 2011;32:22-35.
18. Hu W, Katelaris CH, Kemp AS. Allergic rhinitis – practical management strategies. Aust Fam Physician. 2008;37:214-220.
19. Veramyst (fluticasone furoate) nasal spray [prescribing information]. Research Triangle Park, NC: GlaxoSmithKline; August 2012. Available at: http://us.gsk.com/products/assets/us_veramyst.pdf. Accessed January 16, 2013.
20. Nasacort AQ (triamcinolone acetonide) nasal spray [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/nasacort_aq/nasacort_aq.html. Accessed January 16, 2013.
21. Rhinocort AQUA 32 mcg (budesonide) nasal spray [prescribing information]. Wilmington, Del: AstraZeneca; revised December 2010. Available at: http://www1.astrazeneca-us.com/pi/Rhinocort_Aqua.pdf. Accessed January 16, 2013.
22. Astelin (azelastine hydrochloride) spray, metered [prescribing information]. Somerset, NJ: Meda Pharmaceuticals; revised July 2011. Available at: http://www.astelin.com/pdf/astelin_pi.pdf. Accessed January 16, 2013.
23. Patanase (olopatadine hydrochloride) nasal spray [prescribing information]. Fort Worth, Tex: Alcon Laboratories; revised February 2012. Available at: http://ecatalog.alcon.com/PI/Patanase_us_en.pdf. Accessed January 16, 2013.
24. Xyzal (levocetirizine dihydrochloride) tablets and oral solution [prescribing information]. Smyrna, Ga: UCB and Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/xyzal/xyzal.pdf. Accessed January 16, 2013.
25. Allegra (fexofenadine hydrochloride) tablets, ODT, and oral suspension [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2007. Available at: http://products.sanofi.us/allegra/allegra.html. Accessed January 16, 2013.
26. Singulair (montelukast sodium) tablets, chewable tablets, and oral granules [prescribing information]. Whitehouse Station, NJ: Merck; revised November 2012. Available at: http://www.merck.com/product/usa/pi_circulars/s/singulair/singulair_pi.pdf. Accessed January 16, 2013.
27. Meltzer EO, Bukstein DA. The economic impact of allergic rhinitis and current guidelines for treatment. Ann Allergy Asthma Immunol. 2011;106(suppl):S12-S16.
28. Lim MY, Leong JM. Allergic rhinitis: evidence-based practice. Singapore Med J. 2010;51:542-550.
29. Angier E, Willington J, Scadding G, et al. Management of allergic and non-allergic rhinitis: a primary care summary of the BSACI guideline. Prim Care Respir J. 2010;19:217-222.
30. Radulovic S, Wilson D, Calderon M, et al. Systematic reviews of sublingual immunotherapy (SLIT). Allergy. 2011;66:740-752.
31. Matricardi PM, Kuna P, Panetta V, et al. Subcutaneous immunotherapy and pharmacology in seasonal allergic rhinitis: a comparison based on meta-analyses. J Allergy Clin Immunol. 2011;128:791-799.
32. Lee MS, Pittler MH, Shin B, et al. Acupuncture for allergic rhinitis: a systematic review. Ann Allergy Asthma Immunol. 2009;102:269-279.
33. Roberts J, Huissoon A, Dretzke J, et al. A systematic review of the clinical effectiveness of acupuncture for allergic rhinitis. BMC Complement Altern Med. 2008;8:13.-
34. Zhang CS, Yang AW, Zhang AL, et al. Ear-acupressure for allergic rhinitis: a systematic review. Clin Otolaryngol. 2010;35:6-12.
35. Vliagoftis H, Kouranos VD, Betsi GI, et al. Probiotics for the treatment of allergic rhinitis and asthma: systematic review of randomized controlled trials. Ann Allergy Asthma Immunol. 2008;101:570-579.
CORRESPONDENCE Suzanne Minor, MD, Florida International University Herbert Wertheim College of Medicine; 11200 SW 8th Street, AHC II 361A, Miami, FL 33199; seminor@fiu.edu
1. Bousquet J, Schünemann HJ, Zuberbier T, et al. Development and implementation of guidelines in allergic rhinitis – an ARIA-GA2LEN paper. Allergy. 2010;65:1212-1221.
2. Bousquet J, Van-Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(suppl):S147-S334.
3. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008. Allergy. 2008;63(suppl 86):S8-S160.
4. Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) Guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466-476.
5. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin Exp Allergy. 2008;38:19-42.
6. Walker SM, Durham SR, Till SJ, et al. Immunotherapy for allergic rhinitis. Clin Exp Allergy. 2011;41:1177-1200.
7. Al Sayyad JJ, Fedorowicz Z, Alhashimi D, et al. Topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2007;(1):CD003163.-
8. Nasser M, Fedorowicz, Alijufairi H, et al. Antihistamines used in addition to topical nasal steroids for intermittent and persistent allergic rhinitis in children. Cochrane Database Syst Rev. 2010;(7):CD006989.-
9. Calderon MA, Alves B, Jacobson M, et al. Allergen injection immunotherapy for seasonal allergic rhinitis. Cochrane Database Syst Rev. 2007;(1):CD001936.-
10. Wilson D, Torres-Lima M, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev. 2003;(2):CD002893.-
11. Sheikh A, Hurwitz B, Nurmatov U, et al. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. 2010;(7):CD001563.-
12. Nurmatov U, van Schayck CP, Hurwitz B, et al. House dust mite avoidance measures for perennial allergic rhinitis: an updated Cochrane systematic review. Allergy. 2012;67:158-165.
13. Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108(suppl):S2-S8.
14. Nathan RA. The pathophysiology, clinical impact, and management of nasal congestion in allergic rhinitis. Clin Ther. 2008;30:573-586.
15. Kemp AS. Allergic rhinitis. Paediatric Respir Rev. 2009;10:63-68.
16. Sur DK, Scandale S. Treatment of allergic rhinitis. Am Fam Physician. 2010;81:1440-1446.
17. Hong J, Bielory B, Rosenberg JL, et al. Efficacy of intranasal corticosteroids for the ocular symptoms of allergic rhinitis: a systematic review. Allergy Asthma Proc. 2011;32:22-35.
18. Hu W, Katelaris CH, Kemp AS. Allergic rhinitis – practical management strategies. Aust Fam Physician. 2008;37:214-220.
19. Veramyst (fluticasone furoate) nasal spray [prescribing information]. Research Triangle Park, NC: GlaxoSmithKline; August 2012. Available at: http://us.gsk.com/products/assets/us_veramyst.pdf. Accessed January 16, 2013.
20. Nasacort AQ (triamcinolone acetonide) nasal spray [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/nasacort_aq/nasacort_aq.html. Accessed January 16, 2013.
21. Rhinocort AQUA 32 mcg (budesonide) nasal spray [prescribing information]. Wilmington, Del: AstraZeneca; revised December 2010. Available at: http://www1.astrazeneca-us.com/pi/Rhinocort_Aqua.pdf. Accessed January 16, 2013.
22. Astelin (azelastine hydrochloride) spray, metered [prescribing information]. Somerset, NJ: Meda Pharmaceuticals; revised July 2011. Available at: http://www.astelin.com/pdf/astelin_pi.pdf. Accessed January 16, 2013.
23. Patanase (olopatadine hydrochloride) nasal spray [prescribing information]. Fort Worth, Tex: Alcon Laboratories; revised February 2012. Available at: http://ecatalog.alcon.com/PI/Patanase_us_en.pdf. Accessed January 16, 2013.
24. Xyzal (levocetirizine dihydrochloride) tablets and oral solution [prescribing information]. Smyrna, Ga: UCB and Bridgewater, NJ: sanofi-aventis; 2010. Available at: http://products.sanofi.us/xyzal/xyzal.pdf. Accessed January 16, 2013.
25. Allegra (fexofenadine hydrochloride) tablets, ODT, and oral suspension [prescribing information]. Bridgewater, NJ: sanofi-aventis; 2007. Available at: http://products.sanofi.us/allegra/allegra.html. Accessed January 16, 2013.
26. Singulair (montelukast sodium) tablets, chewable tablets, and oral granules [prescribing information]. Whitehouse Station, NJ: Merck; revised November 2012. Available at: http://www.merck.com/product/usa/pi_circulars/s/singulair/singulair_pi.pdf. Accessed January 16, 2013.
27. Meltzer EO, Bukstein DA. The economic impact of allergic rhinitis and current guidelines for treatment. Ann Allergy Asthma Immunol. 2011;106(suppl):S12-S16.
28. Lim MY, Leong JM. Allergic rhinitis: evidence-based practice. Singapore Med J. 2010;51:542-550.
29. Angier E, Willington J, Scadding G, et al. Management of allergic and non-allergic rhinitis: a primary care summary of the BSACI guideline. Prim Care Respir J. 2010;19:217-222.
30. Radulovic S, Wilson D, Calderon M, et al. Systematic reviews of sublingual immunotherapy (SLIT). Allergy. 2011;66:740-752.
31. Matricardi PM, Kuna P, Panetta V, et al. Subcutaneous immunotherapy and pharmacology in seasonal allergic rhinitis: a comparison based on meta-analyses. J Allergy Clin Immunol. 2011;128:791-799.
32. Lee MS, Pittler MH, Shin B, et al. Acupuncture for allergic rhinitis: a systematic review. Ann Allergy Asthma Immunol. 2009;102:269-279.
33. Roberts J, Huissoon A, Dretzke J, et al. A systematic review of the clinical effectiveness of acupuncture for allergic rhinitis. BMC Complement Altern Med. 2008;8:13.-
34. Zhang CS, Yang AW, Zhang AL, et al. Ear-acupressure for allergic rhinitis: a systematic review. Clin Otolaryngol. 2010;35:6-12.
35. Vliagoftis H, Kouranos VD, Betsi GI, et al. Probiotics for the treatment of allergic rhinitis and asthma: systematic review of randomized controlled trials. Ann Allergy Asthma Immunol. 2008;101:570-579.
CORRESPONDENCE Suzanne Minor, MD, Florida International University Herbert Wertheim College of Medicine; 11200 SW 8th Street, AHC II 361A, Miami, FL 33199; seminor@fiu.edu
A spoonful of honey helps a coughing child sleep
When a parent brings in a child (ages 1-5 years) with cough, runny nose, and other symptoms of a viral upper respiratory infection (URI), recommend that honey be given at bedtime.1
STRENGTH OF RECOMMENDATION
A: Based on a well-designed, randomized controlled trial (RCT)
Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
ILLUSTRATIVE CASE
A mother brings in her 18-month-old son because he’s had a runny nose and low-grade fever for the past 4 days—and a cough that kept them both up last night. You diagnose a viral URI, and she requests a strong cough medicine so he (and she) can get a good night’s sleep. What can you recommend that is both safe and effective for a child of this age?
For primary care physicians, office visits for coughing kids with URIs are commonplace. In addition to the cost of such visits, Americans spend some $3.5 billion a year on over-the-counter (OTC) cough and cold remedies, and often give them to young children.
It’s not enough to tell parents what not to do
As physicians (and parents), we understand the desire to give a coughing child something to ease the symptoms. We also know that OTC cough and cold medications can lead to serious complications, and even death. Between 1983 and 2007, 118 pediatric deaths were attributed to the misuse of such preparations.2 And, in a 3-year span (2005-2008), the American Association of Poison Control Centers received 64,658 calls for exposures to cough and cold remedies in children younger than 2 years of age, 28 of which resulted in a major adverse reaction or death.3
The US Food and Drug Administration recommends against the use of OTC cough and cold medications in children younger than 2 years,4 and the American Academy of Pediatrics has issued strict warnings about the use of OTC cough and cold preparations in children younger than 6 years.5 But warning parents of the dangers of giving them to young children without offering an alternative doesn’t satisfy anyone’s needs, and many parents continue to use these medications.
What about honey?
A study published in 2007 evaluated buckwheat honey and found it to be superior to no treatment and equal to honey-flavored dextromethorphan in reducing cough severity and improving sleep for children and their parents.6 Honey is known to have both antioxidant and antimicrobial properties—a possible scientific explanation for its effect. Before recommending honey for kids with URIs, however, more evidence of its efficacy was needed.
STUDY SUMMARY: Honey reduces cough frequency and severity
Cohen et al sought to determine whether honey, administered before bedtime, would decrease coughing in children between the ages of one and 5 years—and improve sleep for both the children and their caregivers.1 They enrolled 300 children with a nocturnal cough of <7 days’ duration and a diagnosis of URI in a one-night study.
Children were excluded if they had any signs or symptoms of asthma, pneumonia, sinusitis, allergic rhinitis, or laryngotracheobronchitis, or if they had been given any cough remedy, including honey, the night before. Parents completed a 5-question survey, using a 7-point Likert scale to assess the child’s cough and both the child’s and parents’ sleep the previous night. Only children whose parents rated their child’s cough severity ≥3 in 2 of the 3 questions related to cough were included in the trial.
The study had a double-blind randomized design, with 4 treatment arms. Three groups received 10 g (about 1.5 tsp) of one of 3 types of honey: eucalyptus, citrus, or labiatae (derived from plants including sage, mint, and thyme); the fourth group received a placebo of silan date extract, which is similar to honey in color, texture, and taste.
Children in all 4 groups received the preparation 30 minutes before bedtime. Neither the parents nor the physicians or study coordinators knew which preparation the children received. The following day, research assistants telephoned the parent who had completed the initial survey and asked the same 5 questions. The primary outcome measure was the change in cough frequency from the night before to the night after treatment. Secondary measures included cough severity and the effect on sleep for both the child and the parent.
Of the 300 children initially enrolled, 270 (90%) completed the trial, with an even distribution among the groups. While there were improvements across all outcomes for both the treatment and placebo groups, the changes were statistically significant only in the treatment groups. There were no significant differences in efficacy noted among the 3 types of honey. Adverse effects of stomachache, nausea, or vomiting were noted by 4 parents in the treatment groups and one in the placebo group, a difference that was not statistically significant.
WHAT’S NEW?: We have more evidence of honey’s efficacy
For children older than one year with a viral URI, we can now recommend 1.5 tsp honey to be given prior to bedtime as a cough remedy. This may reduce the use of potentially harmful and often ineffective OTC cough and cold remedies.
CAVEATS: Honey is unsafe for the youngest children
An obvious limitation of this study was its brevity. Although one night of improved cough and sleep is important, a study that showed honey’s sustained benefit as a cough suppressant would be more convincing. What’s more, there are safety concerns that are age-related.
Honey is considered unsafe for children younger than one year because of the risk of botulism. And honey has the potential to increase dental caries if it is given nightly for a prolonged period of time.
We do not know whether all varieties of honey will have the same benefit, and the source of store-bought honey is not always identified. The authors of this study received funding from the Honey Board of Israel.
CHALLENGES TO IMPLEMENTATION: Parents may be reluctant to abandon OTCs
Changing the behavior of parents and other caregivers who are accustomed to treating children with OTC cough and cold remedies is likely to be an uphill battle. Because honey is readily available, however—often as close as the pantry—and perceived to be safe and nutritious, a recommendation from a trusted physician could go a long way toward its implementation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
2. Dart RC, Paul IM, Bond GR, et al. Pediatric fatalities associated with over the counter (nonprescription) cough and cold medications. Ann Emerg Med. 2009;53:411-417.
3. Srinivasan A, Budnitz D, Shehab N, et al. Infant deaths associated with cough and cold medications—two states, 2005. JAMA. 2007;297:800-801.
4. US Food and Drug Administration. Public Health Advisory: FDA recommends that over-the-counter (OTC) cough and cold products not be used for Infants and children under 2 years of age. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/PublicHealthAdvisories/ucm051137.htm. Accessed February 14, 2013.
5. American Academy of Pediatrics. Withdrawal of cold medicines: addressing parent concerns. Available at: http://www.aap.org/en-us/professional-resources/practice-support/Pages/Withdrawal-of-Cold-Medicines-Addressing-Parent-Concerns.aspx. Accessed February 14, 2013.
6. Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Arch Pediatr Adolesc Med. 2007;161:1140-1146.
When a parent brings in a child (ages 1-5 years) with cough, runny nose, and other symptoms of a viral upper respiratory infection (URI), recommend that honey be given at bedtime.1
STRENGTH OF RECOMMENDATION
A: Based on a well-designed, randomized controlled trial (RCT)
Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
ILLUSTRATIVE CASE
A mother brings in her 18-month-old son because he’s had a runny nose and low-grade fever for the past 4 days—and a cough that kept them both up last night. You diagnose a viral URI, and she requests a strong cough medicine so he (and she) can get a good night’s sleep. What can you recommend that is both safe and effective for a child of this age?
For primary care physicians, office visits for coughing kids with URIs are commonplace. In addition to the cost of such visits, Americans spend some $3.5 billion a year on over-the-counter (OTC) cough and cold remedies, and often give them to young children.
It’s not enough to tell parents what not to do
As physicians (and parents), we understand the desire to give a coughing child something to ease the symptoms. We also know that OTC cough and cold medications can lead to serious complications, and even death. Between 1983 and 2007, 118 pediatric deaths were attributed to the misuse of such preparations.2 And, in a 3-year span (2005-2008), the American Association of Poison Control Centers received 64,658 calls for exposures to cough and cold remedies in children younger than 2 years of age, 28 of which resulted in a major adverse reaction or death.3
The US Food and Drug Administration recommends against the use of OTC cough and cold medications in children younger than 2 years,4 and the American Academy of Pediatrics has issued strict warnings about the use of OTC cough and cold preparations in children younger than 6 years.5 But warning parents of the dangers of giving them to young children without offering an alternative doesn’t satisfy anyone’s needs, and many parents continue to use these medications.
What about honey?
A study published in 2007 evaluated buckwheat honey and found it to be superior to no treatment and equal to honey-flavored dextromethorphan in reducing cough severity and improving sleep for children and their parents.6 Honey is known to have both antioxidant and antimicrobial properties—a possible scientific explanation for its effect. Before recommending honey for kids with URIs, however, more evidence of its efficacy was needed.
STUDY SUMMARY: Honey reduces cough frequency and severity
Cohen et al sought to determine whether honey, administered before bedtime, would decrease coughing in children between the ages of one and 5 years—and improve sleep for both the children and their caregivers.1 They enrolled 300 children with a nocturnal cough of <7 days’ duration and a diagnosis of URI in a one-night study.
Children were excluded if they had any signs or symptoms of asthma, pneumonia, sinusitis, allergic rhinitis, or laryngotracheobronchitis, or if they had been given any cough remedy, including honey, the night before. Parents completed a 5-question survey, using a 7-point Likert scale to assess the child’s cough and both the child’s and parents’ sleep the previous night. Only children whose parents rated their child’s cough severity ≥3 in 2 of the 3 questions related to cough were included in the trial.
The study had a double-blind randomized design, with 4 treatment arms. Three groups received 10 g (about 1.5 tsp) of one of 3 types of honey: eucalyptus, citrus, or labiatae (derived from plants including sage, mint, and thyme); the fourth group received a placebo of silan date extract, which is similar to honey in color, texture, and taste.
Children in all 4 groups received the preparation 30 minutes before bedtime. Neither the parents nor the physicians or study coordinators knew which preparation the children received. The following day, research assistants telephoned the parent who had completed the initial survey and asked the same 5 questions. The primary outcome measure was the change in cough frequency from the night before to the night after treatment. Secondary measures included cough severity and the effect on sleep for both the child and the parent.
Of the 300 children initially enrolled, 270 (90%) completed the trial, with an even distribution among the groups. While there were improvements across all outcomes for both the treatment and placebo groups, the changes were statistically significant only in the treatment groups. There were no significant differences in efficacy noted among the 3 types of honey. Adverse effects of stomachache, nausea, or vomiting were noted by 4 parents in the treatment groups and one in the placebo group, a difference that was not statistically significant.
WHAT’S NEW?: We have more evidence of honey’s efficacy
For children older than one year with a viral URI, we can now recommend 1.5 tsp honey to be given prior to bedtime as a cough remedy. This may reduce the use of potentially harmful and often ineffective OTC cough and cold remedies.
CAVEATS: Honey is unsafe for the youngest children
An obvious limitation of this study was its brevity. Although one night of improved cough and sleep is important, a study that showed honey’s sustained benefit as a cough suppressant would be more convincing. What’s more, there are safety concerns that are age-related.
Honey is considered unsafe for children younger than one year because of the risk of botulism. And honey has the potential to increase dental caries if it is given nightly for a prolonged period of time.
We do not know whether all varieties of honey will have the same benefit, and the source of store-bought honey is not always identified. The authors of this study received funding from the Honey Board of Israel.
CHALLENGES TO IMPLEMENTATION: Parents may be reluctant to abandon OTCs
Changing the behavior of parents and other caregivers who are accustomed to treating children with OTC cough and cold remedies is likely to be an uphill battle. Because honey is readily available, however—often as close as the pantry—and perceived to be safe and nutritious, a recommendation from a trusted physician could go a long way toward its implementation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
When a parent brings in a child (ages 1-5 years) with cough, runny nose, and other symptoms of a viral upper respiratory infection (URI), recommend that honey be given at bedtime.1
STRENGTH OF RECOMMENDATION
A: Based on a well-designed, randomized controlled trial (RCT)
Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
ILLUSTRATIVE CASE
A mother brings in her 18-month-old son because he’s had a runny nose and low-grade fever for the past 4 days—and a cough that kept them both up last night. You diagnose a viral URI, and she requests a strong cough medicine so he (and she) can get a good night’s sleep. What can you recommend that is both safe and effective for a child of this age?
For primary care physicians, office visits for coughing kids with URIs are commonplace. In addition to the cost of such visits, Americans spend some $3.5 billion a year on over-the-counter (OTC) cough and cold remedies, and often give them to young children.
It’s not enough to tell parents what not to do
As physicians (and parents), we understand the desire to give a coughing child something to ease the symptoms. We also know that OTC cough and cold medications can lead to serious complications, and even death. Between 1983 and 2007, 118 pediatric deaths were attributed to the misuse of such preparations.2 And, in a 3-year span (2005-2008), the American Association of Poison Control Centers received 64,658 calls for exposures to cough and cold remedies in children younger than 2 years of age, 28 of which resulted in a major adverse reaction or death.3
The US Food and Drug Administration recommends against the use of OTC cough and cold medications in children younger than 2 years,4 and the American Academy of Pediatrics has issued strict warnings about the use of OTC cough and cold preparations in children younger than 6 years.5 But warning parents of the dangers of giving them to young children without offering an alternative doesn’t satisfy anyone’s needs, and many parents continue to use these medications.
What about honey?
A study published in 2007 evaluated buckwheat honey and found it to be superior to no treatment and equal to honey-flavored dextromethorphan in reducing cough severity and improving sleep for children and their parents.6 Honey is known to have both antioxidant and antimicrobial properties—a possible scientific explanation for its effect. Before recommending honey for kids with URIs, however, more evidence of its efficacy was needed.
STUDY SUMMARY: Honey reduces cough frequency and severity
Cohen et al sought to determine whether honey, administered before bedtime, would decrease coughing in children between the ages of one and 5 years—and improve sleep for both the children and their caregivers.1 They enrolled 300 children with a nocturnal cough of <7 days’ duration and a diagnosis of URI in a one-night study.
Children were excluded if they had any signs or symptoms of asthma, pneumonia, sinusitis, allergic rhinitis, or laryngotracheobronchitis, or if they had been given any cough remedy, including honey, the night before. Parents completed a 5-question survey, using a 7-point Likert scale to assess the child’s cough and both the child’s and parents’ sleep the previous night. Only children whose parents rated their child’s cough severity ≥3 in 2 of the 3 questions related to cough were included in the trial.
The study had a double-blind randomized design, with 4 treatment arms. Three groups received 10 g (about 1.5 tsp) of one of 3 types of honey: eucalyptus, citrus, or labiatae (derived from plants including sage, mint, and thyme); the fourth group received a placebo of silan date extract, which is similar to honey in color, texture, and taste.
Children in all 4 groups received the preparation 30 minutes before bedtime. Neither the parents nor the physicians or study coordinators knew which preparation the children received. The following day, research assistants telephoned the parent who had completed the initial survey and asked the same 5 questions. The primary outcome measure was the change in cough frequency from the night before to the night after treatment. Secondary measures included cough severity and the effect on sleep for both the child and the parent.
Of the 300 children initially enrolled, 270 (90%) completed the trial, with an even distribution among the groups. While there were improvements across all outcomes for both the treatment and placebo groups, the changes were statistically significant only in the treatment groups. There were no significant differences in efficacy noted among the 3 types of honey. Adverse effects of stomachache, nausea, or vomiting were noted by 4 parents in the treatment groups and one in the placebo group, a difference that was not statistically significant.
WHAT’S NEW?: We have more evidence of honey’s efficacy
For children older than one year with a viral URI, we can now recommend 1.5 tsp honey to be given prior to bedtime as a cough remedy. This may reduce the use of potentially harmful and often ineffective OTC cough and cold remedies.
CAVEATS: Honey is unsafe for the youngest children
An obvious limitation of this study was its brevity. Although one night of improved cough and sleep is important, a study that showed honey’s sustained benefit as a cough suppressant would be more convincing. What’s more, there are safety concerns that are age-related.
Honey is considered unsafe for children younger than one year because of the risk of botulism. And honey has the potential to increase dental caries if it is given nightly for a prolonged period of time.
We do not know whether all varieties of honey will have the same benefit, and the source of store-bought honey is not always identified. The authors of this study received funding from the Honey Board of Israel.
CHALLENGES TO IMPLEMENTATION: Parents may be reluctant to abandon OTCs
Changing the behavior of parents and other caregivers who are accustomed to treating children with OTC cough and cold remedies is likely to be an uphill battle. Because honey is readily available, however—often as close as the pantry—and perceived to be safe and nutritious, a recommendation from a trusted physician could go a long way toward its implementation.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
2. Dart RC, Paul IM, Bond GR, et al. Pediatric fatalities associated with over the counter (nonprescription) cough and cold medications. Ann Emerg Med. 2009;53:411-417.
3. Srinivasan A, Budnitz D, Shehab N, et al. Infant deaths associated with cough and cold medications—two states, 2005. JAMA. 2007;297:800-801.
4. US Food and Drug Administration. Public Health Advisory: FDA recommends that over-the-counter (OTC) cough and cold products not be used for Infants and children under 2 years of age. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/PublicHealthAdvisories/ucm051137.htm. Accessed February 14, 2013.
5. American Academy of Pediatrics. Withdrawal of cold medicines: addressing parent concerns. Available at: http://www.aap.org/en-us/professional-resources/practice-support/Pages/Withdrawal-of-Cold-Medicines-Addressing-Parent-Concerns.aspx. Accessed February 14, 2013.
6. Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Arch Pediatr Adolesc Med. 2007;161:1140-1146.
1. Cohen HA, Rozen J, Kristal H, et al. Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. 2012;130:465-471.
2. Dart RC, Paul IM, Bond GR, et al. Pediatric fatalities associated with over the counter (nonprescription) cough and cold medications. Ann Emerg Med. 2009;53:411-417.
3. Srinivasan A, Budnitz D, Shehab N, et al. Infant deaths associated with cough and cold medications—two states, 2005. JAMA. 2007;297:800-801.
4. US Food and Drug Administration. Public Health Advisory: FDA recommends that over-the-counter (OTC) cough and cold products not be used for Infants and children under 2 years of age. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/PublicHealthAdvisories/ucm051137.htm. Accessed February 14, 2013.
5. American Academy of Pediatrics. Withdrawal of cold medicines: addressing parent concerns. Available at: http://www.aap.org/en-us/professional-resources/practice-support/Pages/Withdrawal-of-Cold-Medicines-Addressing-Parent-Concerns.aspx. Accessed February 14, 2013.
6. Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Arch Pediatr Adolesc Med. 2007;161:1140-1146.
Copyright © 2013 The Family Physicians Inquiries Network. All rights reserved.
Meta-analysis bolsters strength of tuberculosis assay
The sensitivity and specificity of a diagnostic test that rapidly detects tuberculosis support its use as an initial diagnostic test in adults suspected of having TB, including multidrug- resistant or HIV-associated disease, based on a meta-analysis of studies evaluating the test, researchers say.
In addition, the meta-analysis results suggest that the test, the Xpert assay, "may also be valuable as an add-on test following a negative smear microscopy result in patients suspected of having TB," said Karen Steingart, of the University of Washington School of Public Health, Seattle, and her associates. The researchers were from the Cochrane Infectious Diseases Group; McGill University, Montreal; and the Foundation for Innovative New Diagnostics (FIND), Geneva. The study was published in the Cochrane Database of Systematic Reviews (doi:10.1002/14651858.CD009593.pub2).
Xpert, manufactured by Cepheid Inc., is an automated polymerase chain reaction test that detects Mycobacterium tuberculosis complex and rifampin resistance within two hours using a sputum sample, used outside of a reference lab "with minimal hands-on technical time," as opposed to conventional sputum smear microscopy, which is cheaper, but requires a microscope in a lab and does not detect drug resistance.
In 2010, Xpert was endorsed by the World Health Organization for use as the initial diagnostic test on people suspected of having MDR-TB or HIV-associated TB. That year, WHO reported that there were 8.8 million new cases of TB worldwide; and that 1.1 million people who did not have HIV and 350,000 people with HIV died of TB.
The study reviewed 18 studies of more than 7,500 adults, mostly in low and middle-income countries, with a high burden of TB, which evaluated the test as an initial test used as a replacement for microscopy, and as an add-on test when a microscopy smear was negative, in adults suspected of having in pulmonary TB, or multidrug-resistant TB, with or without HIV infection.
The main results of the test are as follows:
• A "modest" sensitivity of 88% and a "high" specificity of 98% for detecting TB when used it as an initial test that replaced smear microscopy.
• A sensitivity of 67% and a specificity of 98% when used as an add-on follow-up test to detect TB, after a negative smear microscopy.
• A sensitivity of 80% for detecting TB in people with HIV and 89% in people without HIV.
•A sensitivity of 94% and a specificity of 98% for detecting rifampin resistance (an indicator of multidrug resistances) when used as a replacement for culture based-drug susceptibility testing
The rate of indeterminate results was a "very low" 1%, they said.
The results "lend support to the WHO recommendation on the use of Xpert as an initial diagnostic test for TB detection and rifampicin resistance detection in patients suspected of having MDR-TB or HIV-associated TB," the authors concluded. Future studies should include those that evaluate the results of the test in children, as those data are starting to accumulate, and result of the test in different settings, such as TB screening centers and antiretroviral clinics, they added.
The review "provides high quality evidence that reinforces WHO’s endorsement of this test," Dr. Karin Weyer, the coordinator of Diagnostics and Drug Resistance Laboratories at WHO, said in a written statement. "Recent price reductions have greatly facilitated roll-out of this technology," with 1.4 million test cartridges and the instruments needed to perform the test to be distributed in 21 countries with a high TB burden, she added.
In the United States, TB has been declining, since a peak in 1992, with 10,528 TB cases reported in 2011, almost a 6% drop from the number of reports in 2010, according to the Centers for Disease Control and Prevention. In 2009, the last year mortality data are available, there were 529 TB deaths, a 10% drop from 2008, when there were 590 deaths.
The editorial base of the Cochrane Infectious Diseases Group (CIDG), which provided part of the funding for the review, is funded by the U.K. Department for International Development "for the benefit of developing countries." One study author disclosed having conducted studies and published on the Xpert test in a project with FIND, Cepheid, and academic partners. Others reported having no relevant financial conflicts.
The sensitivity and specificity of a diagnostic test that rapidly detects tuberculosis support its use as an initial diagnostic test in adults suspected of having TB, including multidrug- resistant or HIV-associated disease, based on a meta-analysis of studies evaluating the test, researchers say.
In addition, the meta-analysis results suggest that the test, the Xpert assay, "may also be valuable as an add-on test following a negative smear microscopy result in patients suspected of having TB," said Karen Steingart, of the University of Washington School of Public Health, Seattle, and her associates. The researchers were from the Cochrane Infectious Diseases Group; McGill University, Montreal; and the Foundation for Innovative New Diagnostics (FIND), Geneva. The study was published in the Cochrane Database of Systematic Reviews (doi:10.1002/14651858.CD009593.pub2).
Xpert, manufactured by Cepheid Inc., is an automated polymerase chain reaction test that detects Mycobacterium tuberculosis complex and rifampin resistance within two hours using a sputum sample, used outside of a reference lab "with minimal hands-on technical time," as opposed to conventional sputum smear microscopy, which is cheaper, but requires a microscope in a lab and does not detect drug resistance.
In 2010, Xpert was endorsed by the World Health Organization for use as the initial diagnostic test on people suspected of having MDR-TB or HIV-associated TB. That year, WHO reported that there were 8.8 million new cases of TB worldwide; and that 1.1 million people who did not have HIV and 350,000 people with HIV died of TB.
The study reviewed 18 studies of more than 7,500 adults, mostly in low and middle-income countries, with a high burden of TB, which evaluated the test as an initial test used as a replacement for microscopy, and as an add-on test when a microscopy smear was negative, in adults suspected of having in pulmonary TB, or multidrug-resistant TB, with or without HIV infection.
The main results of the test are as follows:
• A "modest" sensitivity of 88% and a "high" specificity of 98% for detecting TB when used it as an initial test that replaced smear microscopy.
• A sensitivity of 67% and a specificity of 98% when used as an add-on follow-up test to detect TB, after a negative smear microscopy.
• A sensitivity of 80% for detecting TB in people with HIV and 89% in people without HIV.
•A sensitivity of 94% and a specificity of 98% for detecting rifampin resistance (an indicator of multidrug resistances) when used as a replacement for culture based-drug susceptibility testing
The rate of indeterminate results was a "very low" 1%, they said.
The results "lend support to the WHO recommendation on the use of Xpert as an initial diagnostic test for TB detection and rifampicin resistance detection in patients suspected of having MDR-TB or HIV-associated TB," the authors concluded. Future studies should include those that evaluate the results of the test in children, as those data are starting to accumulate, and result of the test in different settings, such as TB screening centers and antiretroviral clinics, they added.
The review "provides high quality evidence that reinforces WHO’s endorsement of this test," Dr. Karin Weyer, the coordinator of Diagnostics and Drug Resistance Laboratories at WHO, said in a written statement. "Recent price reductions have greatly facilitated roll-out of this technology," with 1.4 million test cartridges and the instruments needed to perform the test to be distributed in 21 countries with a high TB burden, she added.
In the United States, TB has been declining, since a peak in 1992, with 10,528 TB cases reported in 2011, almost a 6% drop from the number of reports in 2010, according to the Centers for Disease Control and Prevention. In 2009, the last year mortality data are available, there were 529 TB deaths, a 10% drop from 2008, when there were 590 deaths.
The editorial base of the Cochrane Infectious Diseases Group (CIDG), which provided part of the funding for the review, is funded by the U.K. Department for International Development "for the benefit of developing countries." One study author disclosed having conducted studies and published on the Xpert test in a project with FIND, Cepheid, and academic partners. Others reported having no relevant financial conflicts.
The sensitivity and specificity of a diagnostic test that rapidly detects tuberculosis support its use as an initial diagnostic test in adults suspected of having TB, including multidrug- resistant or HIV-associated disease, based on a meta-analysis of studies evaluating the test, researchers say.
In addition, the meta-analysis results suggest that the test, the Xpert assay, "may also be valuable as an add-on test following a negative smear microscopy result in patients suspected of having TB," said Karen Steingart, of the University of Washington School of Public Health, Seattle, and her associates. The researchers were from the Cochrane Infectious Diseases Group; McGill University, Montreal; and the Foundation for Innovative New Diagnostics (FIND), Geneva. The study was published in the Cochrane Database of Systematic Reviews (doi:10.1002/14651858.CD009593.pub2).
Xpert, manufactured by Cepheid Inc., is an automated polymerase chain reaction test that detects Mycobacterium tuberculosis complex and rifampin resistance within two hours using a sputum sample, used outside of a reference lab "with minimal hands-on technical time," as opposed to conventional sputum smear microscopy, which is cheaper, but requires a microscope in a lab and does not detect drug resistance.
In 2010, Xpert was endorsed by the World Health Organization for use as the initial diagnostic test on people suspected of having MDR-TB or HIV-associated TB. That year, WHO reported that there were 8.8 million new cases of TB worldwide; and that 1.1 million people who did not have HIV and 350,000 people with HIV died of TB.
The study reviewed 18 studies of more than 7,500 adults, mostly in low and middle-income countries, with a high burden of TB, which evaluated the test as an initial test used as a replacement for microscopy, and as an add-on test when a microscopy smear was negative, in adults suspected of having in pulmonary TB, or multidrug-resistant TB, with or without HIV infection.
The main results of the test are as follows:
• A "modest" sensitivity of 88% and a "high" specificity of 98% for detecting TB when used it as an initial test that replaced smear microscopy.
• A sensitivity of 67% and a specificity of 98% when used as an add-on follow-up test to detect TB, after a negative smear microscopy.
• A sensitivity of 80% for detecting TB in people with HIV and 89% in people without HIV.
•A sensitivity of 94% and a specificity of 98% for detecting rifampin resistance (an indicator of multidrug resistances) when used as a replacement for culture based-drug susceptibility testing
The rate of indeterminate results was a "very low" 1%, they said.
The results "lend support to the WHO recommendation on the use of Xpert as an initial diagnostic test for TB detection and rifampicin resistance detection in patients suspected of having MDR-TB or HIV-associated TB," the authors concluded. Future studies should include those that evaluate the results of the test in children, as those data are starting to accumulate, and result of the test in different settings, such as TB screening centers and antiretroviral clinics, they added.
The review "provides high quality evidence that reinforces WHO’s endorsement of this test," Dr. Karin Weyer, the coordinator of Diagnostics and Drug Resistance Laboratories at WHO, said in a written statement. "Recent price reductions have greatly facilitated roll-out of this technology," with 1.4 million test cartridges and the instruments needed to perform the test to be distributed in 21 countries with a high TB burden, she added.
In the United States, TB has been declining, since a peak in 1992, with 10,528 TB cases reported in 2011, almost a 6% drop from the number of reports in 2010, according to the Centers for Disease Control and Prevention. In 2009, the last year mortality data are available, there were 529 TB deaths, a 10% drop from 2008, when there were 590 deaths.
The editorial base of the Cochrane Infectious Diseases Group (CIDG), which provided part of the funding for the review, is funded by the U.K. Department for International Development "for the benefit of developing countries." One study author disclosed having conducted studies and published on the Xpert test in a project with FIND, Cepheid, and academic partners. Others reported having no relevant financial conflicts.
FROM THE COCHRANE LIBRARY
Major Finding: A rapid automated polymerase chain reaction test that detects Mycobacterium tuberculosis complex and rifampin resistance using a sputum sample had a "modest" sensitivity of 88% and a "high" specificity of 98% for detecting tuberculosis when used it as an initial test that replaced smear microscopy.
Data Source: A meta-analysis of 18 studies of more than 7,500 adults.
Disclosures: The editorial base of the Cochrane Infectious Diseases Group, funded by the U.K. Department for International Development, provided part of the funding. The authors had no financial disclosures.
Food and milk allergies increase growth impairment risk
SAN ANTONIO – Dietary restrictions prescribed for children with food allergies may lead to growth impairment, according to findings from a review of medical records for 245 food-allergic pediatric patients.
The risk of growth impairment was greatest for children whose dietary restrictions required elimination of more than two foods and/or elimination of cow’s milk, Dr. Brian P. Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

After age 2 years, the food-allergic children had lower mean percentiles for weight (67.5 vs. 72.5) and a lower body mass index (57.6 vs.68.0), than did 4,584 healthy age-matched controls.
Furthermore, the 52 patients with more than two food allergies (and thus more than two food restrictions), compared with 193 patients with one or two food allergies, had significantly lower mean percentiles for height (62.2 vs. 74.8) and weight (55.3 vs. 69.2). The 66 patients with milk allergy, compared with those with other food allergies, had lower mean percentiles for weight (54.5 vs. 70.6) and BMI (48.9 vs. 58.8), according to Dr. Vickery of the University of North Carolina at Chapel Hill.
Milk-allergic children younger than 2 years of age were particularly vulnerable to growth restriction, he said during a press briefing at the meeting.
The food-allergic children in this study, who were aged 1 month to 11 years and who presented to a University of North Carolina outpatient clinic between 2007 and 2011, also were compared with 205 "disease controls," consisting of children with either cystic fibrosis or celiac disease, two conditions that are associated with impaired growth. When children passed their second birthday, the effect of food allergy on growth was very similar to the effect of celiac disease on growth, Dr. Vickery said.
The findings of this study confirm those from a smaller study, conducted more than a decade ago, that also showed that milk allergy and multiple food allergies were associated with growth impairment.
That study is "the most commonly cited previous study to address the growth of food-allergic children in the United States," Dr. Vickery noted.
"The prevalence [of food allergy] has increased over the past 10 years, so we wanted to take another look in a bigger population to kind of reassess the impact of elimination diets on growth," he said.
The current findings demonstrate that a food allergy–associated elimination diet can place children at risk of impaired growth, compared with their healthy peers, regardless of whether they are under age 2 years, or are 2-11 years old, and that after age 2, the effect of food allergy on growth is very similar to that of chronic diseases known to affect growth, he said.
"While awareness of food allergy is increasing along with the prevalence of the disease, it is important to draw attention to the important consequences of elimination diets. We feel that providers should counsel patients and caregivers about the growth-related risks of the elimination diets that are used to treat food allergy, and ensure that families are excluding only the foods that are medically required or otherwise culturally indicated, that nutritional assessment and/or supplementation is provided as needed, and that subspecialty consultation is arranged, especially for children at highest risk," he said.
Dr. Vickery reported having no relevant financial disclosures.
SAN ANTONIO – Dietary restrictions prescribed for children with food allergies may lead to growth impairment, according to findings from a review of medical records for 245 food-allergic pediatric patients.
The risk of growth impairment was greatest for children whose dietary restrictions required elimination of more than two foods and/or elimination of cow’s milk, Dr. Brian P. Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
After age 2 years, the food-allergic children had lower mean percentiles for weight (67.5 vs. 72.5) and a lower body mass index (57.6 vs.68.0), than did 4,584 healthy age-matched controls.
Furthermore, the 52 patients with more than two food allergies (and thus more than two food restrictions), compared with 193 patients with one or two food allergies, had significantly lower mean percentiles for height (62.2 vs. 74.8) and weight (55.3 vs. 69.2). The 66 patients with milk allergy, compared with those with other food allergies, had lower mean percentiles for weight (54.5 vs. 70.6) and BMI (48.9 vs. 58.8), according to Dr. Vickery of the University of North Carolina at Chapel Hill.
Milk-allergic children younger than 2 years of age were particularly vulnerable to growth restriction, he said during a press briefing at the meeting.
The food-allergic children in this study, who were aged 1 month to 11 years and who presented to a University of North Carolina outpatient clinic between 2007 and 2011, also were compared with 205 "disease controls," consisting of children with either cystic fibrosis or celiac disease, two conditions that are associated with impaired growth. When children passed their second birthday, the effect of food allergy on growth was very similar to the effect of celiac disease on growth, Dr. Vickery said.
The findings of this study confirm those from a smaller study, conducted more than a decade ago, that also showed that milk allergy and multiple food allergies were associated with growth impairment.
That study is "the most commonly cited previous study to address the growth of food-allergic children in the United States," Dr. Vickery noted.
"The prevalence [of food allergy] has increased over the past 10 years, so we wanted to take another look in a bigger population to kind of reassess the impact of elimination diets on growth," he said.
The current findings demonstrate that a food allergy–associated elimination diet can place children at risk of impaired growth, compared with their healthy peers, regardless of whether they are under age 2 years, or are 2-11 years old, and that after age 2, the effect of food allergy on growth is very similar to that of chronic diseases known to affect growth, he said.
"While awareness of food allergy is increasing along with the prevalence of the disease, it is important to draw attention to the important consequences of elimination diets. We feel that providers should counsel patients and caregivers about the growth-related risks of the elimination diets that are used to treat food allergy, and ensure that families are excluding only the foods that are medically required or otherwise culturally indicated, that nutritional assessment and/or supplementation is provided as needed, and that subspecialty consultation is arranged, especially for children at highest risk," he said.
Dr. Vickery reported having no relevant financial disclosures.
SAN ANTONIO – Dietary restrictions prescribed for children with food allergies may lead to growth impairment, according to findings from a review of medical records for 245 food-allergic pediatric patients.
The risk of growth impairment was greatest for children whose dietary restrictions required elimination of more than two foods and/or elimination of cow’s milk, Dr. Brian P. Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
After age 2 years, the food-allergic children had lower mean percentiles for weight (67.5 vs. 72.5) and a lower body mass index (57.6 vs.68.0), than did 4,584 healthy age-matched controls.
Furthermore, the 52 patients with more than two food allergies (and thus more than two food restrictions), compared with 193 patients with one or two food allergies, had significantly lower mean percentiles for height (62.2 vs. 74.8) and weight (55.3 vs. 69.2). The 66 patients with milk allergy, compared with those with other food allergies, had lower mean percentiles for weight (54.5 vs. 70.6) and BMI (48.9 vs. 58.8), according to Dr. Vickery of the University of North Carolina at Chapel Hill.
Milk-allergic children younger than 2 years of age were particularly vulnerable to growth restriction, he said during a press briefing at the meeting.
The food-allergic children in this study, who were aged 1 month to 11 years and who presented to a University of North Carolina outpatient clinic between 2007 and 2011, also were compared with 205 "disease controls," consisting of children with either cystic fibrosis or celiac disease, two conditions that are associated with impaired growth. When children passed their second birthday, the effect of food allergy on growth was very similar to the effect of celiac disease on growth, Dr. Vickery said.
The findings of this study confirm those from a smaller study, conducted more than a decade ago, that also showed that milk allergy and multiple food allergies were associated with growth impairment.
That study is "the most commonly cited previous study to address the growth of food-allergic children in the United States," Dr. Vickery noted.
"The prevalence [of food allergy] has increased over the past 10 years, so we wanted to take another look in a bigger population to kind of reassess the impact of elimination diets on growth," he said.
The current findings demonstrate that a food allergy–associated elimination diet can place children at risk of impaired growth, compared with their healthy peers, regardless of whether they are under age 2 years, or are 2-11 years old, and that after age 2, the effect of food allergy on growth is very similar to that of chronic diseases known to affect growth, he said.
"While awareness of food allergy is increasing along with the prevalence of the disease, it is important to draw attention to the important consequences of elimination diets. We feel that providers should counsel patients and caregivers about the growth-related risks of the elimination diets that are used to treat food allergy, and ensure that families are excluding only the foods that are medically required or otherwise culturally indicated, that nutritional assessment and/or supplementation is provided as needed, and that subspecialty consultation is arranged, especially for children at highest risk," he said.
Dr. Vickery reported having no relevant financial disclosures.
AT THE AAAAI ANNUAL MEETING
Major finding: After age 2 years, 245 food-allergic children, compared with 4,584 healthy age-matched controls, had lower mean percentiles for weight (67.5 vs. 72.5) and body mass index (57.6 vs. 68).
Data source: A review of charts of a cohort of children with food allergies.
Disclosures: Dr. Vickery reported having no relevant financial disclosures.

New respiratory coronavirus shows concerning SARS echoes
The short-lived, worldwide epidemic of severe acute respiratory syndrome that began its streak across the globe 10 years ago, starting in February 2003, has been echoed over the past 8 months by what is so far a much more limited number of cases of a new, mysterious respiratory virus closely related to the SARS pathogen.
Mostly known so far as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus, and by late February the new virus had been identified in 13 patients worldwide – in Saudi Arabia, Jordan, the United Kingdom, and Qatar – causing seven deaths and severe illness in five of the other six patients.
Since the World Health Organization (WHO) and other epidemiology groups first became aware of the NCoV last September, and as the number of identified cases has inched up, researchers have scrambled to gather information about the novel virus and heighten surveillance for new cases. SARS left a legacy of just over 8,000 probable cases in 29 countries, including 29 probable U.S. cases, with an overall fatality rate of 10%. After bursting on the scene in early 2003, SARS quickly flamed out, with the last handful of clinical cases ever seen identified in China in early 2004.
"It’s likely we will see more" of the NCoV. "We’ll need to cast a wide net since we now know there are a dozen cases and different clinical presentations," Dr. Larry Madoff said at the International Meeting on Emerging Diseases and Surveillance. Although almost every patient with confirmed NCoV infection has had severe illness, one U.K. patient who acquired the infection from another household member had a mild, flulike illness. The milder case "calls into question the [WHO] established case definition for this illness," said Dr. Madoff, director of epidemiology and immunization at the Massachusetts Department of Public Health in Boston and chairman of the meeting’s program committee.
In the days after Dr. Madoff made that assessment at the meeting, the WHO on Feb. 21 reported the 13th case, a patient in Saudi Arabia first hospitalized in late January who died in mid-February.
An effort to track down the origin of the NCoV led to the area surrounding the Saudi Arabian city of Bisha, home of the first identified Saudi case. Suspecting a bat origin for the virus because the SARS-associated virus had been identified as a bat virus (although initial human transmission came via a civet), and because the human isolates of the NCoV could infect several bat-cell lines in the lab, U.S. epidemiologist Jonathan Epstein, D.V.M., led a team that surveyed bats from the Bisha area last fall to see if they could find coronaviruses similar to NCoV. Researchers previously reported finding NCoV-like viruses in bats from other locations that are related to the bats that live in the Bisha area, Dr. Epstein said at the meeting.*
"Everywhere you look in bats there seem to be one or two new coronaviruses, but most bat coronaviruses are not SARS-like. The novel coronavirus is the second bat coronavirus in addition to the SARS virus to cause a human infection," said Dr. Epstein, vice president for conservation medicine at EcoHealth Alliance, an environmental medical research organization based in New York.
"Based on published evidence, there is close relatedness between the novel coronavirus and the SARS virus, but SARS uses a receptor that is deep in the respiratory tract. The novel virus uses a different receptor. It’s not clear whether the novel virus can infect mucosa or the upper respiratory tract, but if it could it might be more transmissible," Dr. Epstein said in an interview.
A report from a team of Swiss researchers published on Feb. 19 (subsequent to Dr. Epstein’s comments) reported that the NCoV (which the Swiss researchers call human coronavirus [HCoV]-EMC) grew very efficiently in vitro on human bronchial epithelial cells, and that interferon treatment cut replication of the virus in these cells (mBio 2013;4:e00611-2).

The episodes of human infection by the NCoV so far that seem to be geographically disparate also have a precedent with SARS.
The pattern of cases "suggests that the source of the infection is common or widespread," Dr. Epstein said. "It’s a challenge to identify common environmental features in the case histories of the infected patients. But with SARS there were multiple spill-over events in different regions of southeast China" when the SARS virus moved from civets into people.
"There clearly are many unknowns about the epidemiology" of the NCoV, Dr. Marjorie R. Pollack, a consultant medical epidemiologist based in New York, wrote in a recent comment on the new coronavirus (ProMed Mail, 2013;Archive Number: 20130221.1554109). "Genetic studies on this NCoV place it related to coronaviruses found in bats. But how did the jump from bats to humans occur? Is there an intermediate host animal?"
According to recent guidance from the WHO, member states should "continue their surveillance for severe acute respiratory infections and to carefully review any unusual patterns. Testing for the NCoV should be considered in patients with unexplained pneumonias or in patients with unexplained severe, progressive or complicated respiratory illness not responding to treatment, particularly in persons traveling from or resident in areas of the world known to be affected."
Dr. Madoff, Dr. Epstein, and Dr. Pollack had no disclosures.
On Twitter @mitchelzoler
*Correction, 3/1/2013: In an earlier version of this story, the findings regarding the Saudi Arabian bats sampled by Dr. Jonathan Epstein and his associates were misstated. Dr. Epstein and his colleagues led a team that surveyed bats from the Bisha area last fall. They have not yet reported their findings.
The short-lived, worldwide epidemic of severe acute respiratory syndrome that began its streak across the globe 10 years ago, starting in February 2003, has been echoed over the past 8 months by what is so far a much more limited number of cases of a new, mysterious respiratory virus closely related to the SARS pathogen.
Mostly known so far as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus, and by late February the new virus had been identified in 13 patients worldwide – in Saudi Arabia, Jordan, the United Kingdom, and Qatar – causing seven deaths and severe illness in five of the other six patients.
Since the World Health Organization (WHO) and other epidemiology groups first became aware of the NCoV last September, and as the number of identified cases has inched up, researchers have scrambled to gather information about the novel virus and heighten surveillance for new cases. SARS left a legacy of just over 8,000 probable cases in 29 countries, including 29 probable U.S. cases, with an overall fatality rate of 10%. After bursting on the scene in early 2003, SARS quickly flamed out, with the last handful of clinical cases ever seen identified in China in early 2004.
"It’s likely we will see more" of the NCoV. "We’ll need to cast a wide net since we now know there are a dozen cases and different clinical presentations," Dr. Larry Madoff said at the International Meeting on Emerging Diseases and Surveillance. Although almost every patient with confirmed NCoV infection has had severe illness, one U.K. patient who acquired the infection from another household member had a mild, flulike illness. The milder case "calls into question the [WHO] established case definition for this illness," said Dr. Madoff, director of epidemiology and immunization at the Massachusetts Department of Public Health in Boston and chairman of the meeting’s program committee.
In the days after Dr. Madoff made that assessment at the meeting, the WHO on Feb. 21 reported the 13th case, a patient in Saudi Arabia first hospitalized in late January who died in mid-February.
An effort to track down the origin of the NCoV led to the area surrounding the Saudi Arabian city of Bisha, home of the first identified Saudi case. Suspecting a bat origin for the virus because the SARS-associated virus had been identified as a bat virus (although initial human transmission came via a civet), and because the human isolates of the NCoV could infect several bat-cell lines in the lab, U.S. epidemiologist Jonathan Epstein, D.V.M., led a team that surveyed bats from the Bisha area last fall to see if they could find coronaviruses similar to NCoV. Researchers previously reported finding NCoV-like viruses in bats from other locations that are related to the bats that live in the Bisha area, Dr. Epstein said at the meeting.*
"Everywhere you look in bats there seem to be one or two new coronaviruses, but most bat coronaviruses are not SARS-like. The novel coronavirus is the second bat coronavirus in addition to the SARS virus to cause a human infection," said Dr. Epstein, vice president for conservation medicine at EcoHealth Alliance, an environmental medical research organization based in New York.
"Based on published evidence, there is close relatedness between the novel coronavirus and the SARS virus, but SARS uses a receptor that is deep in the respiratory tract. The novel virus uses a different receptor. It’s not clear whether the novel virus can infect mucosa or the upper respiratory tract, but if it could it might be more transmissible," Dr. Epstein said in an interview.
A report from a team of Swiss researchers published on Feb. 19 (subsequent to Dr. Epstein’s comments) reported that the NCoV (which the Swiss researchers call human coronavirus [HCoV]-EMC) grew very efficiently in vitro on human bronchial epithelial cells, and that interferon treatment cut replication of the virus in these cells (mBio 2013;4:e00611-2).
The episodes of human infection by the NCoV so far that seem to be geographically disparate also have a precedent with SARS.
The pattern of cases "suggests that the source of the infection is common or widespread," Dr. Epstein said. "It’s a challenge to identify common environmental features in the case histories of the infected patients. But with SARS there were multiple spill-over events in different regions of southeast China" when the SARS virus moved from civets into people.
"There clearly are many unknowns about the epidemiology" of the NCoV, Dr. Marjorie R. Pollack, a consultant medical epidemiologist based in New York, wrote in a recent comment on the new coronavirus (ProMed Mail, 2013;Archive Number: 20130221.1554109). "Genetic studies on this NCoV place it related to coronaviruses found in bats. But how did the jump from bats to humans occur? Is there an intermediate host animal?"
According to recent guidance from the WHO, member states should "continue their surveillance for severe acute respiratory infections and to carefully review any unusual patterns. Testing for the NCoV should be considered in patients with unexplained pneumonias or in patients with unexplained severe, progressive or complicated respiratory illness not responding to treatment, particularly in persons traveling from or resident in areas of the world known to be affected."
Dr. Madoff, Dr. Epstein, and Dr. Pollack had no disclosures.
On Twitter @mitchelzoler
*Correction, 3/1/2013: In an earlier version of this story, the findings regarding the Saudi Arabian bats sampled by Dr. Jonathan Epstein and his associates were misstated. Dr. Epstein and his colleagues led a team that surveyed bats from the Bisha area last fall. They have not yet reported their findings.
The short-lived, worldwide epidemic of severe acute respiratory syndrome that began its streak across the globe 10 years ago, starting in February 2003, has been echoed over the past 8 months by what is so far a much more limited number of cases of a new, mysterious respiratory virus closely related to the SARS pathogen.
Mostly known so far as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus, and by late February the new virus had been identified in 13 patients worldwide – in Saudi Arabia, Jordan, the United Kingdom, and Qatar – causing seven deaths and severe illness in five of the other six patients.
Since the World Health Organization (WHO) and other epidemiology groups first became aware of the NCoV last September, and as the number of identified cases has inched up, researchers have scrambled to gather information about the novel virus and heighten surveillance for new cases. SARS left a legacy of just over 8,000 probable cases in 29 countries, including 29 probable U.S. cases, with an overall fatality rate of 10%. After bursting on the scene in early 2003, SARS quickly flamed out, with the last handful of clinical cases ever seen identified in China in early 2004.
"It’s likely we will see more" of the NCoV. "We’ll need to cast a wide net since we now know there are a dozen cases and different clinical presentations," Dr. Larry Madoff said at the International Meeting on Emerging Diseases and Surveillance. Although almost every patient with confirmed NCoV infection has had severe illness, one U.K. patient who acquired the infection from another household member had a mild, flulike illness. The milder case "calls into question the [WHO] established case definition for this illness," said Dr. Madoff, director of epidemiology and immunization at the Massachusetts Department of Public Health in Boston and chairman of the meeting’s program committee.
In the days after Dr. Madoff made that assessment at the meeting, the WHO on Feb. 21 reported the 13th case, a patient in Saudi Arabia first hospitalized in late January who died in mid-February.
An effort to track down the origin of the NCoV led to the area surrounding the Saudi Arabian city of Bisha, home of the first identified Saudi case. Suspecting a bat origin for the virus because the SARS-associated virus had been identified as a bat virus (although initial human transmission came via a civet), and because the human isolates of the NCoV could infect several bat-cell lines in the lab, U.S. epidemiologist Jonathan Epstein, D.V.M., led a team that surveyed bats from the Bisha area last fall to see if they could find coronaviruses similar to NCoV. Researchers previously reported finding NCoV-like viruses in bats from other locations that are related to the bats that live in the Bisha area, Dr. Epstein said at the meeting.*
"Everywhere you look in bats there seem to be one or two new coronaviruses, but most bat coronaviruses are not SARS-like. The novel coronavirus is the second bat coronavirus in addition to the SARS virus to cause a human infection," said Dr. Epstein, vice president for conservation medicine at EcoHealth Alliance, an environmental medical research organization based in New York.
"Based on published evidence, there is close relatedness between the novel coronavirus and the SARS virus, but SARS uses a receptor that is deep in the respiratory tract. The novel virus uses a different receptor. It’s not clear whether the novel virus can infect mucosa or the upper respiratory tract, but if it could it might be more transmissible," Dr. Epstein said in an interview.
A report from a team of Swiss researchers published on Feb. 19 (subsequent to Dr. Epstein’s comments) reported that the NCoV (which the Swiss researchers call human coronavirus [HCoV]-EMC) grew very efficiently in vitro on human bronchial epithelial cells, and that interferon treatment cut replication of the virus in these cells (mBio 2013;4:e00611-2).
The episodes of human infection by the NCoV so far that seem to be geographically disparate also have a precedent with SARS.
The pattern of cases "suggests that the source of the infection is common or widespread," Dr. Epstein said. "It’s a challenge to identify common environmental features in the case histories of the infected patients. But with SARS there were multiple spill-over events in different regions of southeast China" when the SARS virus moved from civets into people.
"There clearly are many unknowns about the epidemiology" of the NCoV, Dr. Marjorie R. Pollack, a consultant medical epidemiologist based in New York, wrote in a recent comment on the new coronavirus (ProMed Mail, 2013;Archive Number: 20130221.1554109). "Genetic studies on this NCoV place it related to coronaviruses found in bats. But how did the jump from bats to humans occur? Is there an intermediate host animal?"
According to recent guidance from the WHO, member states should "continue their surveillance for severe acute respiratory infections and to carefully review any unusual patterns. Testing for the NCoV should be considered in patients with unexplained pneumonias or in patients with unexplained severe, progressive or complicated respiratory illness not responding to treatment, particularly in persons traveling from or resident in areas of the world known to be affected."
Dr. Madoff, Dr. Epstein, and Dr. Pollack had no disclosures.
On Twitter @mitchelzoler
*Correction, 3/1/2013: In an earlier version of this story, the findings regarding the Saudi Arabian bats sampled by Dr. Jonathan Epstein and his associates were misstated. Dr. Epstein and his colleagues led a team that surveyed bats from the Bisha area last fall. They have not yet reported their findings.
AT IMED2013
Major Finding: As of Feb. 21, 13 people had been identified as infected with a novel coronavrius since July 2012, with seven deaths.
Data Source: World Health Organization.
Disclosures: Dr. Madoff, Dr. Epstein, and Dr. Pollack had no disclosures.
